User login
Jason Carris is director, Digital Media and Strategy, Society Partners, at Frontline Medical Communications. He previously worked in the newspaper industry as a writer and editor. He resides in Central New Jersey with his wife and three children. Email him at [email protected].
Hospitalists on the Move: June 2011


Robert Harrington Jr., MD, SFHM, and Erin Stucky Fisher, MD, MHM, have been elected to SHM’s board of directors. Dr. Harrington, chief medical officer for Locum Leaders, serves as chair of SHM’s Family Medicine Task Force and board liaison to the IT Core Committee. Dr. Fisher, professor of clinical pediatrics at the University of California at San Diego, is actively involved with quality initiatives for the American Academy of Pediatrics, the Institute for Healthcare Improvement, and the National Association of Children’s Hospitals.
Jasen W. Gundersen, MD, MBA, CPE, SFHM, has been appointed chief medical officer for TeamHealth Hospital Medicine.
IPC: The Hospitalist Company Inc. has appointed Kerry Weiner, MD, to the newly created position of chief clinical officer. Dr. Weiner will lead the clinical functions of the company and continue the development of hospitalist leaders throughout IPC.

Steven Pantilat, MD, FACP, SFHM, has received a 2011 James Irvine Foundation Leadership Award. Dr. Pantilat, one of five recipients, is professor of clinical medicine, the Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care, and director of the Palliative Care Leadership Center at UCSF. Now in its sixth year, the award celebrates extraordinary leaders who are applying innovative and effective solutions to significant state issues. Dr. Pantilat, a past SHM president, will receive $125,000 in organizational support.
Hospitalist Patrick O’Neil, DO, has been named Lake Regional Health System’s 2011 Physician of the Year. The 116-bed health system serves 1,300 employees in the Land of the Ozarks, Mo., area.
Hospitalist Wiley Robinson, MD, has been named president-elect of the Tennessee Medical Association and will head the organization for 2012-2013. An internal-medicine specialist, Dr. Robinson is cofounder and president of Inpatient Physicians of the Mid-South, a Memphis-based hospitalist group.

The Association of Specialty Professors announced Robert M. Wachter, MD, MHM, will receive the 2011 ASP Eric G. Neilson, MD, Distinguished Professor Award. Dr. Wachter is professor of medicine and the Marc and Lynne Benioff Endowed Chair in Hospital Medicine at the University of California at San Francisco (UCSF) School of Medicine, and a past president of SHM. The Neilson Award is presented annually to a leader who has shaped the internal-medicine landscape and promotes the work of leaders who bring about change for specialty medicine. TH
Robert Harrington Jr., MD, SFHM, and Erin Stucky Fisher, MD, MHM, have been elected to SHM’s board of directors. Dr. Harrington, chief medical officer for Locum Leaders, serves as chair of SHM’s Family Medicine Task Force and board liaison to the IT Core Committee. Dr. Fisher, professor of clinical pediatrics at the University of California at San Diego, is actively involved with quality initiatives for the American Academy of Pediatrics, the Institute for Healthcare Improvement, and the National Association of Children’s Hospitals.
Jasen W. Gundersen, MD, MBA, CPE, SFHM, has been appointed chief medical officer for TeamHealth Hospital Medicine.
IPC: The Hospitalist Company Inc. has appointed Kerry Weiner, MD, to the newly created position of chief clinical officer. Dr. Weiner will lead the clinical functions of the company and continue the development of hospitalist leaders throughout IPC.
Steven Pantilat, MD, FACP, SFHM, has received a 2011 James Irvine Foundation Leadership Award. Dr. Pantilat, one of five recipients, is professor of clinical medicine, the Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care, and director of the Palliative Care Leadership Center at UCSF. Now in its sixth year, the award celebrates extraordinary leaders who are applying innovative and effective solutions to significant state issues. Dr. Pantilat, a past SHM president, will receive $125,000 in organizational support.
Hospitalist Patrick O’Neil, DO, has been named Lake Regional Health System’s 2011 Physician of the Year. The 116-bed health system serves 1,300 employees in the Land of the Ozarks, Mo., area.
Hospitalist Wiley Robinson, MD, has been named president-elect of the Tennessee Medical Association and will head the organization for 2012-2013. An internal-medicine specialist, Dr. Robinson is cofounder and president of Inpatient Physicians of the Mid-South, a Memphis-based hospitalist group.
The Association of Specialty Professors announced Robert M. Wachter, MD, MHM, will receive the 2011 ASP Eric G. Neilson, MD, Distinguished Professor Award. Dr. Wachter is professor of medicine and the Marc and Lynne Benioff Endowed Chair in Hospital Medicine at the University of California at San Francisco (UCSF) School of Medicine, and a past president of SHM. The Neilson Award is presented annually to a leader who has shaped the internal-medicine landscape and promotes the work of leaders who bring about change for specialty medicine. TH
Robert Harrington Jr., MD, SFHM, and Erin Stucky Fisher, MD, MHM, have been elected to SHM’s board of directors. Dr. Harrington, chief medical officer for Locum Leaders, serves as chair of SHM’s Family Medicine Task Force and board liaison to the IT Core Committee. Dr. Fisher, professor of clinical pediatrics at the University of California at San Diego, is actively involved with quality initiatives for the American Academy of Pediatrics, the Institute for Healthcare Improvement, and the National Association of Children’s Hospitals.
Jasen W. Gundersen, MD, MBA, CPE, SFHM, has been appointed chief medical officer for TeamHealth Hospital Medicine.
IPC: The Hospitalist Company Inc. has appointed Kerry Weiner, MD, to the newly created position of chief clinical officer. Dr. Weiner will lead the clinical functions of the company and continue the development of hospitalist leaders throughout IPC.
Steven Pantilat, MD, FACP, SFHM, has received a 2011 James Irvine Foundation Leadership Award. Dr. Pantilat, one of five recipients, is professor of clinical medicine, the Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care, and director of the Palliative Care Leadership Center at UCSF. Now in its sixth year, the award celebrates extraordinary leaders who are applying innovative and effective solutions to significant state issues. Dr. Pantilat, a past SHM president, will receive $125,000 in organizational support.
Hospitalist Patrick O’Neil, DO, has been named Lake Regional Health System’s 2011 Physician of the Year. The 116-bed health system serves 1,300 employees in the Land of the Ozarks, Mo., area.
Hospitalist Wiley Robinson, MD, has been named president-elect of the Tennessee Medical Association and will head the organization for 2012-2013. An internal-medicine specialist, Dr. Robinson is cofounder and president of Inpatient Physicians of the Mid-South, a Memphis-based hospitalist group.
The Association of Specialty Professors announced Robert M. Wachter, MD, MHM, will receive the 2011 ASP Eric G. Neilson, MD, Distinguished Professor Award. Dr. Wachter is professor of medicine and the Marc and Lynne Benioff Endowed Chair in Hospital Medicine at the University of California at San Francisco (UCSF) School of Medicine, and a past president of SHM. The Neilson Award is presented annually to a leader who has shaped the internal-medicine landscape and promotes the work of leaders who bring about change for specialty medicine. TH
The Suggestions Box: SHM's Special Interest Forums
It was only natural when SHM started hosting Special Interest Forums a few meetings ago that a chat devoted to quality would emerge. So it was no surprise when some 60 HM11 attendees crowded into a room to talk about just that. But part of preaching the value of quality is knowing how to preach.
To that end, Mangla Gulati, MD, FACP, assistant professor in the Department of Medicine at the University of Maryland School of Medicine in Baltimore, wants resources to teach her how to talk with administrators on their level. “We need to know the language to parlay with our CFO or CEO,” she says. “That’s what’s helpful for us.”
Joe Miller, SHM’s senior vice president and chief solutions officer, suggested the society could create a microsite within www.hospitalmedicine.org dedicated to the topic. He says there are online toolkits the society has developed in the past, and will continue to develop, that will help introduce hospitalists to already-existing quality initiatives they simply don’t know about. He particularly noted SQUINT, SHM’s searchable database for quality projects that is just getting off the ground.
“The stuff that’s there, I use and I love it,” says Dorothy Pusateri, MD, of Allegheny Hospitalist Service in Pittsburgh. “The stuff on Project BOOST [Better Outcomes for Older Adults through Safer Transitions] was enough to teach me.”
Rural Hospitalists
Small-town hospitalists from every corner of the country discussed recruiting issues, scheduling solutions, advocacy concerns, and more. A group of 15 rural hospitalists shared concerns about brutal, “72-hour” shifts and potential solutions to hiring and staffing issues, including growing your own hospitalists and hiring nonphysician providers (NPPs) to supplement 24/7 coverage.
“You can’t sustain mentally if you are doing all of it by yourself all day, all night,” said Martin Johns, MD, a hospitalist at 25-bed Gifford Medical Center in Randolph, Vt. Dr. Johns suggested rural groups think about utilizing NPPs and physician assistants (PAs) to fill coverage gaps; however, the opinions varied widely in what was considered proper compensation and responsibilities for nonphysicians.
“Our PAs make almost as much as our docs,” said Dale Vizcarra, MD, medical director of the hospitalist group at St. Mary’s Healthcare, a 68-bed critical-care hospital in Pierre, S.D.
The group also discussed at length the difficulties in bringing doctors to small towns. Although compensation can be higher than in large urban centers, the group agreed that the “one-man show” aspect of working as a small-town hospitalist is a detractor.
“I hear it all the time,” said forum moderator Alan Himmelstein, a regional vice president for Sound Physicians. “I can take care of gunshot wounds, but I forgot everything I know about community-acquired pneumonia. You aren’t surrounded by 23 specialists; in rural communities, you guys are the top of the heap. Your skill set, by definition, has to make you comfortable to take care of everything that comes through the door. You don’t have another facility a half-hour away; a lot of your geography doesn’t allow helicopters to fly 365 days.”
Rural hospitalists, who as a group admit nearly 40% of all hospital admissions nationwide, also are looking for a voice. “We’re a huge constituency,” Dr. Johns said, “and we are under-represented.”
Jason Carris, editor of The Hospitalist, contributed to this report.
It was only natural when SHM started hosting Special Interest Forums a few meetings ago that a chat devoted to quality would emerge. So it was no surprise when some 60 HM11 attendees crowded into a room to talk about just that. But part of preaching the value of quality is knowing how to preach.
To that end, Mangla Gulati, MD, FACP, assistant professor in the Department of Medicine at the University of Maryland School of Medicine in Baltimore, wants resources to teach her how to talk with administrators on their level. “We need to know the language to parlay with our CFO or CEO,” she says. “That’s what’s helpful for us.”
Joe Miller, SHM’s senior vice president and chief solutions officer, suggested the society could create a microsite within www.hospitalmedicine.org dedicated to the topic. He says there are online toolkits the society has developed in the past, and will continue to develop, that will help introduce hospitalists to already-existing quality initiatives they simply don’t know about. He particularly noted SQUINT, SHM’s searchable database for quality projects that is just getting off the ground.
“The stuff that’s there, I use and I love it,” says Dorothy Pusateri, MD, of Allegheny Hospitalist Service in Pittsburgh. “The stuff on Project BOOST [Better Outcomes for Older Adults through Safer Transitions] was enough to teach me.”
Rural Hospitalists
Small-town hospitalists from every corner of the country discussed recruiting issues, scheduling solutions, advocacy concerns, and more. A group of 15 rural hospitalists shared concerns about brutal, “72-hour” shifts and potential solutions to hiring and staffing issues, including growing your own hospitalists and hiring nonphysician providers (NPPs) to supplement 24/7 coverage.
“You can’t sustain mentally if you are doing all of it by yourself all day, all night,” said Martin Johns, MD, a hospitalist at 25-bed Gifford Medical Center in Randolph, Vt. Dr. Johns suggested rural groups think about utilizing NPPs and physician assistants (PAs) to fill coverage gaps; however, the opinions varied widely in what was considered proper compensation and responsibilities for nonphysicians.
“Our PAs make almost as much as our docs,” said Dale Vizcarra, MD, medical director of the hospitalist group at St. Mary’s Healthcare, a 68-bed critical-care hospital in Pierre, S.D.
The group also discussed at length the difficulties in bringing doctors to small towns. Although compensation can be higher than in large urban centers, the group agreed that the “one-man show” aspect of working as a small-town hospitalist is a detractor.
“I hear it all the time,” said forum moderator Alan Himmelstein, a regional vice president for Sound Physicians. “I can take care of gunshot wounds, but I forgot everything I know about community-acquired pneumonia. You aren’t surrounded by 23 specialists; in rural communities, you guys are the top of the heap. Your skill set, by definition, has to make you comfortable to take care of everything that comes through the door. You don’t have another facility a half-hour away; a lot of your geography doesn’t allow helicopters to fly 365 days.”
Rural hospitalists, who as a group admit nearly 40% of all hospital admissions nationwide, also are looking for a voice. “We’re a huge constituency,” Dr. Johns said, “and we are under-represented.”
Jason Carris, editor of The Hospitalist, contributed to this report.
It was only natural when SHM started hosting Special Interest Forums a few meetings ago that a chat devoted to quality would emerge. So it was no surprise when some 60 HM11 attendees crowded into a room to talk about just that. But part of preaching the value of quality is knowing how to preach.
To that end, Mangla Gulati, MD, FACP, assistant professor in the Department of Medicine at the University of Maryland School of Medicine in Baltimore, wants resources to teach her how to talk with administrators on their level. “We need to know the language to parlay with our CFO or CEO,” she says. “That’s what’s helpful for us.”
Joe Miller, SHM’s senior vice president and chief solutions officer, suggested the society could create a microsite within www.hospitalmedicine.org dedicated to the topic. He says there are online toolkits the society has developed in the past, and will continue to develop, that will help introduce hospitalists to already-existing quality initiatives they simply don’t know about. He particularly noted SQUINT, SHM’s searchable database for quality projects that is just getting off the ground.
“The stuff that’s there, I use and I love it,” says Dorothy Pusateri, MD, of Allegheny Hospitalist Service in Pittsburgh. “The stuff on Project BOOST [Better Outcomes for Older Adults through Safer Transitions] was enough to teach me.”
Rural Hospitalists
Small-town hospitalists from every corner of the country discussed recruiting issues, scheduling solutions, advocacy concerns, and more. A group of 15 rural hospitalists shared concerns about brutal, “72-hour” shifts and potential solutions to hiring and staffing issues, including growing your own hospitalists and hiring nonphysician providers (NPPs) to supplement 24/7 coverage.
“You can’t sustain mentally if you are doing all of it by yourself all day, all night,” said Martin Johns, MD, a hospitalist at 25-bed Gifford Medical Center in Randolph, Vt. Dr. Johns suggested rural groups think about utilizing NPPs and physician assistants (PAs) to fill coverage gaps; however, the opinions varied widely in what was considered proper compensation and responsibilities for nonphysicians.
“Our PAs make almost as much as our docs,” said Dale Vizcarra, MD, medical director of the hospitalist group at St. Mary’s Healthcare, a 68-bed critical-care hospital in Pierre, S.D.
The group also discussed at length the difficulties in bringing doctors to small towns. Although compensation can be higher than in large urban centers, the group agreed that the “one-man show” aspect of working as a small-town hospitalist is a detractor.
“I hear it all the time,” said forum moderator Alan Himmelstein, a regional vice president for Sound Physicians. “I can take care of gunshot wounds, but I forgot everything I know about community-acquired pneumonia. You aren’t surrounded by 23 specialists; in rural communities, you guys are the top of the heap. Your skill set, by definition, has to make you comfortable to take care of everything that comes through the door. You don’t have another facility a half-hour away; a lot of your geography doesn’t allow helicopters to fly 365 days.”
Rural hospitalists, who as a group admit nearly 40% of all hospital admissions nationwide, also are looking for a voice. “We’re a huge constituency,” Dr. Johns said, “and we are under-represented.”
Jason Carris, editor of The Hospitalist, contributed to this report.
Infectious-Disease Cases Require Patience
Take your time, gather pertinent data, and know what you are dealing with before making kneejerk decisions, a national infectious-disease expert told hundreds of hospitalists this morning at HM11.
Shanta Zimmer, MD, associate professor of medicine and director of the internal-medicine residency program at the University of Pittsburgh Medical School walked hospitalists through a half dozen common and uncommon patients, cases ranging from Staphylococcus aureus to Candida albicans to zygomycosis.
Her main message to hospitalists:
- Not all fevers are infectious.
- Get or repeat blood cultures before starting antibiotics, because although administering antibiotics might be the right thing to do, the effects of the drugs makes it difficult to determine the origin. “Then you have to play the guessing game whether or not to treat,” she said. “There also is a lot of morbidity associated with long-term antibiotic therapy.”
- Remove lines when you are able to do so.
- Hold off on antibiotics when a patient is stable and infectious ediology is unknown.
- Take your time, as “very few things in medicine are an emergency; we often have time to think and make a decision,” she said.
- Narrow antibiotic coverage, when possible.
Dr. Zimmer also warned hospitalists to respect S. aureus, which she says remains a large percentage of her caseload. “It never ceases to amaze me how virulent and aggressive it can be,” she said. “It frightens me."
Take your time, gather pertinent data, and know what you are dealing with before making kneejerk decisions, a national infectious-disease expert told hundreds of hospitalists this morning at HM11.
Shanta Zimmer, MD, associate professor of medicine and director of the internal-medicine residency program at the University of Pittsburgh Medical School walked hospitalists through a half dozen common and uncommon patients, cases ranging from Staphylococcus aureus to Candida albicans to zygomycosis.
Her main message to hospitalists:
- Not all fevers are infectious.
- Get or repeat blood cultures before starting antibiotics, because although administering antibiotics might be the right thing to do, the effects of the drugs makes it difficult to determine the origin. “Then you have to play the guessing game whether or not to treat,” she said. “There also is a lot of morbidity associated with long-term antibiotic therapy.”
- Remove lines when you are able to do so.
- Hold off on antibiotics when a patient is stable and infectious ediology is unknown.
- Take your time, as “very few things in medicine are an emergency; we often have time to think and make a decision,” she said.
- Narrow antibiotic coverage, when possible.
Dr. Zimmer also warned hospitalists to respect S. aureus, which she says remains a large percentage of her caseload. “It never ceases to amaze me how virulent and aggressive it can be,” she said. “It frightens me."
Take your time, gather pertinent data, and know what you are dealing with before making kneejerk decisions, a national infectious-disease expert told hundreds of hospitalists this morning at HM11.
Shanta Zimmer, MD, associate professor of medicine and director of the internal-medicine residency program at the University of Pittsburgh Medical School walked hospitalists through a half dozen common and uncommon patients, cases ranging from Staphylococcus aureus to Candida albicans to zygomycosis.
Her main message to hospitalists:
- Not all fevers are infectious.
- Get or repeat blood cultures before starting antibiotics, because although administering antibiotics might be the right thing to do, the effects of the drugs makes it difficult to determine the origin. “Then you have to play the guessing game whether or not to treat,” she said. “There also is a lot of morbidity associated with long-term antibiotic therapy.”
- Remove lines when you are able to do so.
- Hold off on antibiotics when a patient is stable and infectious ediology is unknown.
- Take your time, as “very few things in medicine are an emergency; we often have time to think and make a decision,” she said.
- Narrow antibiotic coverage, when possible.
Dr. Zimmer also warned hospitalists to respect S. aureus, which she says remains a large percentage of her caseload. “It never ceases to amaze me how virulent and aggressive it can be,” she said. “It frightens me."
Project BOOST Shows Significant LOS Reduction
GRAPEVINE, Texas—Preliminary data released today shows SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) quality improvement (QI) program offers statistically significant decreases in patient length of stay, according to the principal investigator of SHM’s quality improvement project targeting transitions of care.
“When we deliver a coordinated approach to the discharge process, LOS went down,” Mark Williams, MD, SFHM, told more than 150 hospitalists at HM11. He also said that the data from 12 BOOST sites shows no reduction in 30-day readmissions, which is similar to previously published national data.
Dr. Williams, CMS’ Linda Magno, and Jeffrey Greenwald, MD, SFHM, of Massachusetts General Hospital in Boston, agreed that implementing QI is “difficult” and barriers to national initiatives to improve those quality issues still exist, however, “we’re noticing a significant change,” Dr. Williams says. “I think healthcare reform is changing that.”
With CMS looking to reduce readmissions by 20% in 10 years and the pool of hospitalized patients expected to grow exponentially in the next decade, Magno detailed how HM groups can partner with hospitals and community organizations to take part in the recently announced Community-Based Care Transitions Program, a $500 million project to incentivize continuity of care. She said the application process has no deadline, that CMS is interested in quality applications, and that 300-500 hospitals will participate.
”Many organizations will be interested in this, but some will need to take some time to prepare and work toward organizational readiness,” she says.
Dr. Greenwald explained Project BOOST is one of the select QI programs on the CCTP short list, and that BOOST mentors can help HM groups with the CCTP application process.
For more information on Project BOOST, check out the SHM website.
GRAPEVINE, Texas—Preliminary data released today shows SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) quality improvement (QI) program offers statistically significant decreases in patient length of stay, according to the principal investigator of SHM’s quality improvement project targeting transitions of care.
“When we deliver a coordinated approach to the discharge process, LOS went down,” Mark Williams, MD, SFHM, told more than 150 hospitalists at HM11. He also said that the data from 12 BOOST sites shows no reduction in 30-day readmissions, which is similar to previously published national data.
Dr. Williams, CMS’ Linda Magno, and Jeffrey Greenwald, MD, SFHM, of Massachusetts General Hospital in Boston, agreed that implementing QI is “difficult” and barriers to national initiatives to improve those quality issues still exist, however, “we’re noticing a significant change,” Dr. Williams says. “I think healthcare reform is changing that.”
With CMS looking to reduce readmissions by 20% in 10 years and the pool of hospitalized patients expected to grow exponentially in the next decade, Magno detailed how HM groups can partner with hospitals and community organizations to take part in the recently announced Community-Based Care Transitions Program, a $500 million project to incentivize continuity of care. She said the application process has no deadline, that CMS is interested in quality applications, and that 300-500 hospitals will participate.
”Many organizations will be interested in this, but some will need to take some time to prepare and work toward organizational readiness,” she says.
Dr. Greenwald explained Project BOOST is one of the select QI programs on the CCTP short list, and that BOOST mentors can help HM groups with the CCTP application process.
For more information on Project BOOST, check out the SHM website.
GRAPEVINE, Texas—Preliminary data released today shows SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) quality improvement (QI) program offers statistically significant decreases in patient length of stay, according to the principal investigator of SHM’s quality improvement project targeting transitions of care.
“When we deliver a coordinated approach to the discharge process, LOS went down,” Mark Williams, MD, SFHM, told more than 150 hospitalists at HM11. He also said that the data from 12 BOOST sites shows no reduction in 30-day readmissions, which is similar to previously published national data.
Dr. Williams, CMS’ Linda Magno, and Jeffrey Greenwald, MD, SFHM, of Massachusetts General Hospital in Boston, agreed that implementing QI is “difficult” and barriers to national initiatives to improve those quality issues still exist, however, “we’re noticing a significant change,” Dr. Williams says. “I think healthcare reform is changing that.”
With CMS looking to reduce readmissions by 20% in 10 years and the pool of hospitalized patients expected to grow exponentially in the next decade, Magno detailed how HM groups can partner with hospitals and community organizations to take part in the recently announced Community-Based Care Transitions Program, a $500 million project to incentivize continuity of care. She said the application process has no deadline, that CMS is interested in quality applications, and that 300-500 hospitals will participate.
”Many organizations will be interested in this, but some will need to take some time to prepare and work toward organizational readiness,” she says.
Dr. Greenwald explained Project BOOST is one of the select QI programs on the CCTP short list, and that BOOST mentors can help HM groups with the CCTP application process.
For more information on Project BOOST, check out the SHM website.
Learning to Share
GRAPEVINE, Texas — Sitting in the third row of a large meeting room, Robin Buckley, MD, FHM, was soaking in the morning portion of the "ABIM Maintenance of Certification (MOC) Learning Session" pre-course, clicking her keypad with answers to questions and making mental notes this morning at HM11.
Dr. Buckley, medical director of hospitalist services at 72-bed Scott & White Healthcare in Round Rock, Texas, has to recertify in 2012, so she is getting an early start. One of nine pre-courses held annually, the learning session offers 6.5 CME credits.
"I'm really excited about sharing the information with my group, especially the questions focused on quality," says Dr. Buckley, who has been a hospitalist since 2004 and joined her expanding HM group in 2008. "I want to apply the information to our clinical practice, because I think it’s going to make us better."
She's also considering the Focused Practice in Hospital Medicine (FPHM) pathway, and used the pre-course to understand the specialized MOC pathway better. The main concerns, she says, are the added cost and the every-three-year requirement of the Performance Improvement Modules (PIM).
"The three-year PIM cycle makes a lot of sense," Dr. Buckley says, noting she is "encouraged" to learn ABIM has approved three of SHM's quality projects to count toward the MOC requirement. Although she might still recertify through the traditional internal-medicine MOC next year, she definitely has the FPHM on the radar.
"Maybe in a couple years," Dr. Buckley says. "The PIM templates will be extremely helpful and encourage me to do it even more. The FPHM shows dedication to the field."
GRAPEVINE, Texas — Sitting in the third row of a large meeting room, Robin Buckley, MD, FHM, was soaking in the morning portion of the "ABIM Maintenance of Certification (MOC) Learning Session" pre-course, clicking her keypad with answers to questions and making mental notes this morning at HM11.
Dr. Buckley, medical director of hospitalist services at 72-bed Scott & White Healthcare in Round Rock, Texas, has to recertify in 2012, so she is getting an early start. One of nine pre-courses held annually, the learning session offers 6.5 CME credits.
"I'm really excited about sharing the information with my group, especially the questions focused on quality," says Dr. Buckley, who has been a hospitalist since 2004 and joined her expanding HM group in 2008. "I want to apply the information to our clinical practice, because I think it’s going to make us better."
She's also considering the Focused Practice in Hospital Medicine (FPHM) pathway, and used the pre-course to understand the specialized MOC pathway better. The main concerns, she says, are the added cost and the every-three-year requirement of the Performance Improvement Modules (PIM).
"The three-year PIM cycle makes a lot of sense," Dr. Buckley says, noting she is "encouraged" to learn ABIM has approved three of SHM's quality projects to count toward the MOC requirement. Although she might still recertify through the traditional internal-medicine MOC next year, she definitely has the FPHM on the radar.
"Maybe in a couple years," Dr. Buckley says. "The PIM templates will be extremely helpful and encourage me to do it even more. The FPHM shows dedication to the field."
GRAPEVINE, Texas — Sitting in the third row of a large meeting room, Robin Buckley, MD, FHM, was soaking in the morning portion of the "ABIM Maintenance of Certification (MOC) Learning Session" pre-course, clicking her keypad with answers to questions and making mental notes this morning at HM11.
Dr. Buckley, medical director of hospitalist services at 72-bed Scott & White Healthcare in Round Rock, Texas, has to recertify in 2012, so she is getting an early start. One of nine pre-courses held annually, the learning session offers 6.5 CME credits.
"I'm really excited about sharing the information with my group, especially the questions focused on quality," says Dr. Buckley, who has been a hospitalist since 2004 and joined her expanding HM group in 2008. "I want to apply the information to our clinical practice, because I think it’s going to make us better."
She's also considering the Focused Practice in Hospital Medicine (FPHM) pathway, and used the pre-course to understand the specialized MOC pathway better. The main concerns, she says, are the added cost and the every-three-year requirement of the Performance Improvement Modules (PIM).
"The three-year PIM cycle makes a lot of sense," Dr. Buckley says, noting she is "encouraged" to learn ABIM has approved three of SHM's quality projects to count toward the MOC requirement. Although she might still recertify through the traditional internal-medicine MOC next year, she definitely has the FPHM on the radar.
"Maybe in a couple years," Dr. Buckley says. "The PIM templates will be extremely helpful and encourage me to do it even more. The FPHM shows dedication to the field."
Tablet technology benefits HM efficiency, patient satisfaction
During my training in the 1990s, my white coat pockets were stuffed with books. The Internet, in its relative infancy, was not easily accessible in the hospital and contained a tiny fraction of its current knowledge. Back then, information was only at your fingertips when it was committed to memory or in your pocket.
Now, the Internet is at every workstation in the hospital, and all orders are entered electronically. Questions about any clinical situation are answered online in a matter of seconds. As a result, I spend much of my time not with my patients but in front of a computer—entering orders, reviewing labs, writing notes, and reading and sending email.
There is tremendous interest in increasing quality of care, patient satisfaction, and improving communication between doctors, patients, and caregivers.
However, our reliance on technology encourages physicians to spend time at computers that might be better spent with the patient. It seems like we could do a better job of integrating technology into a patient-centric hospital environment.
A few years ago, our hospital installed wireless access to our internal computer network and the Internet. To provide computers to the staff on the wards, the hospital now provides two or three COWs (computers on wheels) to each ward. Unfortunately, their physical design leaves a lot to be desired. They are large and bulky, and they can be hard to move around. The physician must stand with these machines between them and the patient, and even taking a few minutes to find one can feel like a burden during a busy day.
In stark contrast, many patients bring their own laptops into the hospital. They are able to research their condition online, and can be more connected at times than the doctor who is expected to know all the answers.
Because I only have been able to access our hospital network while at a COW, nurses’ station, or my desk, I keep a “to do” list on a piece of paper. My desire to keep a short list and promptly enter orders encourages me to get to a computer as often as possible. While entering my username and password dozens of time each day or waiting in line for a workstation, I can't help but think how nice it would be to spend more time on direct patient care and less time dealing with IT logistics.
Recently, I heard about the value of the iPad in a hospital setting from one of my colleagues. Last week, I set off for my first stint on the wards with an iPad, my stethoscope, a pen, and some business cards. My white coat pockets were empty.
I carried this new lightweight computer like a clipboard. Because of its onscreen keyboard and other characteristics (lightweight, small size, lightning-quick Web browsing), I found that I was naturally sitting alongside each patient as I listened to their concerns. When we determined that a switch of medication or diet was appropriate, I made the change quickly and easily without getting up from my seat—never leaving the patient’s side. Email was available to update the patient’s PCP, social worker, or other care team member.
I spent more time with each patient than I could remember. I did not feel the pressure to hurry out of the room to enter orders as soon as possible. Although I did spend time at a computer during the visit, my patients were able to watch me modify their orders and communicate with their outpatient care team.
Much of the mystery that often surrounds the physician/patient relationship was discarded as we sat side by side. I was able to reconcile medications on the computer with the patient watching and helping make sure that no errors were made. Errors might have been prevented since I no longer had to write down the medications on a piece of paper, carry it down the hall, and enter it on to a computer. It certainly saved me time, enabled the correct list to be entered, and could have provided the patient some confidence that it was done right.
My view of the hospital bed is no longer at the foot, standing up, with weighted pockets. It’s seated, in a chair, at the bedside. I hope to soon master the art of maximizing the benefit of my time with the patient with technology more as a collaborative tool and less as an obstacle.
Melissa L.P. Mattison, MD, SFHM, FACP,
associate director of hospital medicine,
Beth Israel Deaconess Medical Center, Boston
During my training in the 1990s, my white coat pockets were stuffed with books. The Internet, in its relative infancy, was not easily accessible in the hospital and contained a tiny fraction of its current knowledge. Back then, information was only at your fingertips when it was committed to memory or in your pocket.
Now, the Internet is at every workstation in the hospital, and all orders are entered electronically. Questions about any clinical situation are answered online in a matter of seconds. As a result, I spend much of my time not with my patients but in front of a computer—entering orders, reviewing labs, writing notes, and reading and sending email.
There is tremendous interest in increasing quality of care, patient satisfaction, and improving communication between doctors, patients, and caregivers.
However, our reliance on technology encourages physicians to spend time at computers that might be better spent with the patient. It seems like we could do a better job of integrating technology into a patient-centric hospital environment.
A few years ago, our hospital installed wireless access to our internal computer network and the Internet. To provide computers to the staff on the wards, the hospital now provides two or three COWs (computers on wheels) to each ward. Unfortunately, their physical design leaves a lot to be desired. They are large and bulky, and they can be hard to move around. The physician must stand with these machines between them and the patient, and even taking a few minutes to find one can feel like a burden during a busy day.
In stark contrast, many patients bring their own laptops into the hospital. They are able to research their condition online, and can be more connected at times than the doctor who is expected to know all the answers.
Because I only have been able to access our hospital network while at a COW, nurses’ station, or my desk, I keep a “to do” list on a piece of paper. My desire to keep a short list and promptly enter orders encourages me to get to a computer as often as possible. While entering my username and password dozens of time each day or waiting in line for a workstation, I can't help but think how nice it would be to spend more time on direct patient care and less time dealing with IT logistics.
Recently, I heard about the value of the iPad in a hospital setting from one of my colleagues. Last week, I set off for my first stint on the wards with an iPad, my stethoscope, a pen, and some business cards. My white coat pockets were empty.
I carried this new lightweight computer like a clipboard. Because of its onscreen keyboard and other characteristics (lightweight, small size, lightning-quick Web browsing), I found that I was naturally sitting alongside each patient as I listened to their concerns. When we determined that a switch of medication or diet was appropriate, I made the change quickly and easily without getting up from my seat—never leaving the patient’s side. Email was available to update the patient’s PCP, social worker, or other care team member.
I spent more time with each patient than I could remember. I did not feel the pressure to hurry out of the room to enter orders as soon as possible. Although I did spend time at a computer during the visit, my patients were able to watch me modify their orders and communicate with their outpatient care team.
Much of the mystery that often surrounds the physician/patient relationship was discarded as we sat side by side. I was able to reconcile medications on the computer with the patient watching and helping make sure that no errors were made. Errors might have been prevented since I no longer had to write down the medications on a piece of paper, carry it down the hall, and enter it on to a computer. It certainly saved me time, enabled the correct list to be entered, and could have provided the patient some confidence that it was done right.
My view of the hospital bed is no longer at the foot, standing up, with weighted pockets. It’s seated, in a chair, at the bedside. I hope to soon master the art of maximizing the benefit of my time with the patient with technology more as a collaborative tool and less as an obstacle.
Melissa L.P. Mattison, MD, SFHM, FACP,
associate director of hospital medicine,
Beth Israel Deaconess Medical Center, Boston
During my training in the 1990s, my white coat pockets were stuffed with books. The Internet, in its relative infancy, was not easily accessible in the hospital and contained a tiny fraction of its current knowledge. Back then, information was only at your fingertips when it was committed to memory or in your pocket.
Now, the Internet is at every workstation in the hospital, and all orders are entered electronically. Questions about any clinical situation are answered online in a matter of seconds. As a result, I spend much of my time not with my patients but in front of a computer—entering orders, reviewing labs, writing notes, and reading and sending email.
There is tremendous interest in increasing quality of care, patient satisfaction, and improving communication between doctors, patients, and caregivers.
However, our reliance on technology encourages physicians to spend time at computers that might be better spent with the patient. It seems like we could do a better job of integrating technology into a patient-centric hospital environment.
A few years ago, our hospital installed wireless access to our internal computer network and the Internet. To provide computers to the staff on the wards, the hospital now provides two or three COWs (computers on wheels) to each ward. Unfortunately, their physical design leaves a lot to be desired. They are large and bulky, and they can be hard to move around. The physician must stand with these machines between them and the patient, and even taking a few minutes to find one can feel like a burden during a busy day.
In stark contrast, many patients bring their own laptops into the hospital. They are able to research their condition online, and can be more connected at times than the doctor who is expected to know all the answers.
Because I only have been able to access our hospital network while at a COW, nurses’ station, or my desk, I keep a “to do” list on a piece of paper. My desire to keep a short list and promptly enter orders encourages me to get to a computer as often as possible. While entering my username and password dozens of time each day or waiting in line for a workstation, I can't help but think how nice it would be to spend more time on direct patient care and less time dealing with IT logistics.
Recently, I heard about the value of the iPad in a hospital setting from one of my colleagues. Last week, I set off for my first stint on the wards with an iPad, my stethoscope, a pen, and some business cards. My white coat pockets were empty.
I carried this new lightweight computer like a clipboard. Because of its onscreen keyboard and other characteristics (lightweight, small size, lightning-quick Web browsing), I found that I was naturally sitting alongside each patient as I listened to their concerns. When we determined that a switch of medication or diet was appropriate, I made the change quickly and easily without getting up from my seat—never leaving the patient’s side. Email was available to update the patient’s PCP, social worker, or other care team member.
I spent more time with each patient than I could remember. I did not feel the pressure to hurry out of the room to enter orders as soon as possible. Although I did spend time at a computer during the visit, my patients were able to watch me modify their orders and communicate with their outpatient care team.
Much of the mystery that often surrounds the physician/patient relationship was discarded as we sat side by side. I was able to reconcile medications on the computer with the patient watching and helping make sure that no errors were made. Errors might have been prevented since I no longer had to write down the medications on a piece of paper, carry it down the hall, and enter it on to a computer. It certainly saved me time, enabled the correct list to be entered, and could have provided the patient some confidence that it was done right.
My view of the hospital bed is no longer at the foot, standing up, with weighted pockets. It’s seated, in a chair, at the bedside. I hope to soon master the art of maximizing the benefit of my time with the patient with technology more as a collaborative tool and less as an obstacle.
Melissa L.P. Mattison, MD, SFHM, FACP,
associate director of hospital medicine,
Beth Israel Deaconess Medical Center, Boston
ABIM Recognizes Hospitalists via Focused Practice Re-Certification

Congratulations are in order for the dozens of hospitalists who formally have been recognized by the American Board of Internal Medicine (ABIM) in the Recognition of Focused Practice in Hospital Medicine (FPHM) program.
“This is a monumental career step for any hospitalist and a significant move forward for the hospital medicine specialty,” says Jeff Wiese, MD, SFHM, SHM president. “We applaud all of the hospitalists who satisfied the requirements for this new program and encourage more hospitalists to begin this year’s application process now.”
Registration for the next FPHM exam ends Aug. 1. For more information, visit www.abim.org.
Among those hospitalists who have earned the Focused Practice in Hospital Medicine recognition:
- William Campbell, MD, SFHM, Pembroke Pines, Fla.
- Patrick Torcson, MD, MMM, FACP, SFHM, director of hospital medicine, St. Tammy Parish Hospital, Covington, La.
- Weston Chandler, MD, FACP, SFHM, president, CEO, Pacific Hospitalists Associates, Newport Beach, Calif.
- Natarajan Ravi, MD, Ellis Hospital Inpatient Medical Services, Schenectady, N.Y.
- Ilya Bilik, MD, director of community medicine, Beth Israel Medical Center, Brooklyn, N.Y., St. John’s Medical Center, Jackson Hole, Wy.
- Karim Godamunne, MD, MBA, FHM, medical director, Eagle Hospital Physicians, Roswell, Ga.
- Le Roi Hicks, MD, MPH, Saint Vincent Hospital, Boston
- Charles Knight, MD
- Anand Kartha, MD, VA, Boston Healthcare System, West Roxbury, Mass.
- Christine Lum Lung, MD, SFHM, medical director, Northern Colorado Hospitalists, Fort Collins
- Alokananda Bhattacharya, MD, New York Presbyterian Hospital, New York City
- Cathleen Ammann, MD, Director, Wentworth Douglas Hospital, Dover, N.H.
- Melinda Johnson, MD, associate professor, University of Iowa Hospitals & Clinics, Iowa City
- Michael Pistoria, DO, SFHM, medical director of hospitalist services, Lehigh Valley Health Network, Allentown, Pa.
- David Lauver, MD, Central Maine Inpatient Physicians, Lewistown
“This program also represents a groundbreaking partnership between SHM and ABIM,” Dr. Wiese says. “We look forward to working with ABIM to maintain public accountability for hospitalists, and to continually recognize hospitalists who choose to enhance their careers with this designation.”—BS
Congratulations are in order for the dozens of hospitalists who formally have been recognized by the American Board of Internal Medicine (ABIM) in the Recognition of Focused Practice in Hospital Medicine (FPHM) program.
“This is a monumental career step for any hospitalist and a significant move forward for the hospital medicine specialty,” says Jeff Wiese, MD, SFHM, SHM president. “We applaud all of the hospitalists who satisfied the requirements for this new program and encourage more hospitalists to begin this year’s application process now.”
Registration for the next FPHM exam ends Aug. 1. For more information, visit www.abim.org.
Among those hospitalists who have earned the Focused Practice in Hospital Medicine recognition:
- William Campbell, MD, SFHM, Pembroke Pines, Fla.
- Patrick Torcson, MD, MMM, FACP, SFHM, director of hospital medicine, St. Tammy Parish Hospital, Covington, La.
- Weston Chandler, MD, FACP, SFHM, president, CEO, Pacific Hospitalists Associates, Newport Beach, Calif.
- Natarajan Ravi, MD, Ellis Hospital Inpatient Medical Services, Schenectady, N.Y.
- Ilya Bilik, MD, director of community medicine, Beth Israel Medical Center, Brooklyn, N.Y., St. John’s Medical Center, Jackson Hole, Wy.
- Karim Godamunne, MD, MBA, FHM, medical director, Eagle Hospital Physicians, Roswell, Ga.
- Le Roi Hicks, MD, MPH, Saint Vincent Hospital, Boston
- Charles Knight, MD
- Anand Kartha, MD, VA, Boston Healthcare System, West Roxbury, Mass.
- Christine Lum Lung, MD, SFHM, medical director, Northern Colorado Hospitalists, Fort Collins
- Alokananda Bhattacharya, MD, New York Presbyterian Hospital, New York City
- Cathleen Ammann, MD, Director, Wentworth Douglas Hospital, Dover, N.H.
- Melinda Johnson, MD, associate professor, University of Iowa Hospitals & Clinics, Iowa City
- Michael Pistoria, DO, SFHM, medical director of hospitalist services, Lehigh Valley Health Network, Allentown, Pa.
- David Lauver, MD, Central Maine Inpatient Physicians, Lewistown
“This program also represents a groundbreaking partnership between SHM and ABIM,” Dr. Wiese says. “We look forward to working with ABIM to maintain public accountability for hospitalists, and to continually recognize hospitalists who choose to enhance their careers with this designation.”—BS
Congratulations are in order for the dozens of hospitalists who formally have been recognized by the American Board of Internal Medicine (ABIM) in the Recognition of Focused Practice in Hospital Medicine (FPHM) program.
“This is a monumental career step for any hospitalist and a significant move forward for the hospital medicine specialty,” says Jeff Wiese, MD, SFHM, SHM president. “We applaud all of the hospitalists who satisfied the requirements for this new program and encourage more hospitalists to begin this year’s application process now.”
Registration for the next FPHM exam ends Aug. 1. For more information, visit www.abim.org.
Among those hospitalists who have earned the Focused Practice in Hospital Medicine recognition:
- William Campbell, MD, SFHM, Pembroke Pines, Fla.
- Patrick Torcson, MD, MMM, FACP, SFHM, director of hospital medicine, St. Tammy Parish Hospital, Covington, La.
- Weston Chandler, MD, FACP, SFHM, president, CEO, Pacific Hospitalists Associates, Newport Beach, Calif.
- Natarajan Ravi, MD, Ellis Hospital Inpatient Medical Services, Schenectady, N.Y.
- Ilya Bilik, MD, director of community medicine, Beth Israel Medical Center, Brooklyn, N.Y., St. John’s Medical Center, Jackson Hole, Wy.
- Karim Godamunne, MD, MBA, FHM, medical director, Eagle Hospital Physicians, Roswell, Ga.
- Le Roi Hicks, MD, MPH, Saint Vincent Hospital, Boston
- Charles Knight, MD
- Anand Kartha, MD, VA, Boston Healthcare System, West Roxbury, Mass.
- Christine Lum Lung, MD, SFHM, medical director, Northern Colorado Hospitalists, Fort Collins
- Alokananda Bhattacharya, MD, New York Presbyterian Hospital, New York City
- Cathleen Ammann, MD, Director, Wentworth Douglas Hospital, Dover, N.H.
- Melinda Johnson, MD, associate professor, University of Iowa Hospitals & Clinics, Iowa City
- Michael Pistoria, DO, SFHM, medical director of hospitalist services, Lehigh Valley Health Network, Allentown, Pa.
- David Lauver, MD, Central Maine Inpatient Physicians, Lewistown
“This program also represents a groundbreaking partnership between SHM and ABIM,” Dr. Wiese says. “We look forward to working with ABIM to maintain public accountability for hospitalists, and to continually recognize hospitalists who choose to enhance their careers with this designation.”—BS
Under the Microscope: Medication Reconciliation



Boston hospitalist Jeffrey Schnipper, MD, MPH, FHM, is no stranger to quality initiatives aimed at medication reconciliation (MR). His research at Brigham and Women’s Hospital and Massachusetts General Hospital revealed a potential reduction of serious medical errors per patient to 0.3 from 1.4 in the past four years.
“I think those are achievable results,” he says. “This is all about doing those things better than we were always doing before.”
Now Dr. Schnipper will work to bring similar results to hospitals across America as principal investigator for SHM’s three-year, multicenter, MR quality-improvement study. The study, funded by a $1.5 million grant from the Agency for Healthcare Research and Quality (AHRQ), will develop a database to research the best practices in MR and provide a mentored implementation model for other hospitals to use.
The project also will include a package of materials and tools adaptable for any hospital, as well as an implementation guide with the mentored implementation model. “It really should be everything a site needs to improve its MR process,” says Dr. Schnipper, director of clinical research at the Brigham and Women’s Hospital Hospitalist Service and assistant professor at Harvard Medical School.
According to The Institute for Safe Medication Practices, MR is the process of comparing a patient’s medication orders with their previously prescribed medication regimen and communicating any necessary changes to patients and their next providers of care. More than 1.3 million medication errors occur annually in the U.S.; MR has been shown to eliminate as many as half of those errors and 20% of adverse medical events.
JoAnne Resnic, MBA, BSN, RN, senior project manager at SHM, says SHM will use the grant to fund research investigators, SHM’s project staff, and the development of a database for each of the study’s six sites to house their data collection and provide site-specific progress reports throughout the course of the study. SHM is working with consultants and physician co-investigators, a steering committee of nationally recognized thought leaders in medication reconciliation, a research pharmacist, and others to “help us take a pretty deep dive into the process and, hopefully, explain why some interventions work in some places and why they may not in others,” Resnic says.
According to Dr. Schnipper, SHM will conduct an interrupted time series at the sites, collecting baseline data for six months at each, then for 21 months after interventions begin. The study specifically will address 13 facets of medication reconciliation, scoring the facets based on their effectiveness (see Table 1, p. 6).
Each facet will be re-evaluated when different parts of the intervention are turned on, which should reveal “the most active ingredients that correspond to improved outcomes,” he says.
Dr. Schnipper emphasizes that there are two integral facets for improving MR: patient education and access to preadmission medication sources. Technology could be an answer to advancing these components, but it is not the sole link. “There may be ways to serve up the discharged medication list in a patient-friendly way using some IT or an image library of medications to help patients,” he says. “I do not foresee a medication reconciliation IT application, unfortunately.”
AHRQ selected SHM for the grant after a “peer review process [that] evaluates the merit of the applications against very rigorous criteria,” an AHRQ representative says. SHM was chosen “based upon its leadership and previous experience in medication reconciliation.” TH
Kevin Stevens is a staff writer based in New Jersey.
Boston hospitalist Jeffrey Schnipper, MD, MPH, FHM, is no stranger to quality initiatives aimed at medication reconciliation (MR). His research at Brigham and Women’s Hospital and Massachusetts General Hospital revealed a potential reduction of serious medical errors per patient to 0.3 from 1.4 in the past four years.
“I think those are achievable results,” he says. “This is all about doing those things better than we were always doing before.”
Now Dr. Schnipper will work to bring similar results to hospitals across America as principal investigator for SHM’s three-year, multicenter, MR quality-improvement study. The study, funded by a $1.5 million grant from the Agency for Healthcare Research and Quality (AHRQ), will develop a database to research the best practices in MR and provide a mentored implementation model for other hospitals to use.
The project also will include a package of materials and tools adaptable for any hospital, as well as an implementation guide with the mentored implementation model. “It really should be everything a site needs to improve its MR process,” says Dr. Schnipper, director of clinical research at the Brigham and Women’s Hospital Hospitalist Service and assistant professor at Harvard Medical School.
According to The Institute for Safe Medication Practices, MR is the process of comparing a patient’s medication orders with their previously prescribed medication regimen and communicating any necessary changes to patients and their next providers of care. More than 1.3 million medication errors occur annually in the U.S.; MR has been shown to eliminate as many as half of those errors and 20% of adverse medical events.
JoAnne Resnic, MBA, BSN, RN, senior project manager at SHM, says SHM will use the grant to fund research investigators, SHM’s project staff, and the development of a database for each of the study’s six sites to house their data collection and provide site-specific progress reports throughout the course of the study. SHM is working with consultants and physician co-investigators, a steering committee of nationally recognized thought leaders in medication reconciliation, a research pharmacist, and others to “help us take a pretty deep dive into the process and, hopefully, explain why some interventions work in some places and why they may not in others,” Resnic says.
According to Dr. Schnipper, SHM will conduct an interrupted time series at the sites, collecting baseline data for six months at each, then for 21 months after interventions begin. The study specifically will address 13 facets of medication reconciliation, scoring the facets based on their effectiveness (see Table 1, p. 6).
Each facet will be re-evaluated when different parts of the intervention are turned on, which should reveal “the most active ingredients that correspond to improved outcomes,” he says.
Dr. Schnipper emphasizes that there are two integral facets for improving MR: patient education and access to preadmission medication sources. Technology could be an answer to advancing these components, but it is not the sole link. “There may be ways to serve up the discharged medication list in a patient-friendly way using some IT or an image library of medications to help patients,” he says. “I do not foresee a medication reconciliation IT application, unfortunately.”
AHRQ selected SHM for the grant after a “peer review process [that] evaluates the merit of the applications against very rigorous criteria,” an AHRQ representative says. SHM was chosen “based upon its leadership and previous experience in medication reconciliation.” TH
Kevin Stevens is a staff writer based in New Jersey.
Boston hospitalist Jeffrey Schnipper, MD, MPH, FHM, is no stranger to quality initiatives aimed at medication reconciliation (MR). His research at Brigham and Women’s Hospital and Massachusetts General Hospital revealed a potential reduction of serious medical errors per patient to 0.3 from 1.4 in the past four years.
“I think those are achievable results,” he says. “This is all about doing those things better than we were always doing before.”
Now Dr. Schnipper will work to bring similar results to hospitals across America as principal investigator for SHM’s three-year, multicenter, MR quality-improvement study. The study, funded by a $1.5 million grant from the Agency for Healthcare Research and Quality (AHRQ), will develop a database to research the best practices in MR and provide a mentored implementation model for other hospitals to use.
The project also will include a package of materials and tools adaptable for any hospital, as well as an implementation guide with the mentored implementation model. “It really should be everything a site needs to improve its MR process,” says Dr. Schnipper, director of clinical research at the Brigham and Women’s Hospital Hospitalist Service and assistant professor at Harvard Medical School.
According to The Institute for Safe Medication Practices, MR is the process of comparing a patient’s medication orders with their previously prescribed medication regimen and communicating any necessary changes to patients and their next providers of care. More than 1.3 million medication errors occur annually in the U.S.; MR has been shown to eliminate as many as half of those errors and 20% of adverse medical events.
JoAnne Resnic, MBA, BSN, RN, senior project manager at SHM, says SHM will use the grant to fund research investigators, SHM’s project staff, and the development of a database for each of the study’s six sites to house their data collection and provide site-specific progress reports throughout the course of the study. SHM is working with consultants and physician co-investigators, a steering committee of nationally recognized thought leaders in medication reconciliation, a research pharmacist, and others to “help us take a pretty deep dive into the process and, hopefully, explain why some interventions work in some places and why they may not in others,” Resnic says.
According to Dr. Schnipper, SHM will conduct an interrupted time series at the sites, collecting baseline data for six months at each, then for 21 months after interventions begin. The study specifically will address 13 facets of medication reconciliation, scoring the facets based on their effectiveness (see Table 1, p. 6).
Each facet will be re-evaluated when different parts of the intervention are turned on, which should reveal “the most active ingredients that correspond to improved outcomes,” he says.
Dr. Schnipper emphasizes that there are two integral facets for improving MR: patient education and access to preadmission medication sources. Technology could be an answer to advancing these components, but it is not the sole link. “There may be ways to serve up the discharged medication list in a patient-friendly way using some IT or an image library of medications to help patients,” he says. “I do not foresee a medication reconciliation IT application, unfortunately.”
AHRQ selected SHM for the grant after a “peer review process [that] evaluates the merit of the applications against very rigorous criteria,” an AHRQ representative says. SHM was chosen “based upon its leadership and previous experience in medication reconciliation.” TH
Kevin Stevens is a staff writer based in New Jersey.
FDA Mandates Enrollment for Erythropoesis Stimulating Agents

I heard from my hospital’s pharmacist director that soon I will not be able to prescribe Epogen unless I get some additional certification. Is this true? Can you explain what is going on?
Ritesh Magge, MD,
Detroit
Dr. Hospitalist responds: Your pharmacist is referring to the new FDA-mandated requirements, which went into effect in February, that will affect who can prescribe erythropoesis-stimulating agents (ESAs), including epoetin (Epogen, Procrit) and darbepoetin (Aranesp). This is part of a broader FDA strategy to improve patient safety as it relates to medications.
According to the FDA website, “The Food and Drug Administration Amendments Act of 2007 gave FDA the authority to require a Risk Evaluation and Mitigation Strategy (REMS) from manufacturers to ensure that the benefits of a drug or biological product outweigh its risks.”
The ESAs are not the only class of drug that will require a REM. More than 150 drugs already have varying requirements. For a complete list of these medications, please visit the FDA website (www.fda.gov) and search “drug safety.” The FDA plans to create additional REMs for additional drugs and biologic agents.
If you are a provider who will prescribe a medication with a REM, you will be obligated to adhere to the FDA REM associated with that medication. The drug manufacturers are working with the FDA to set up REMs for their drugs. For example, if you plan to prescribe an ESA for a patient with cancer, you will first need to enroll in the ESA APPRISE (Assisting Providers and Cancer Patients with Risk Information for the Safe Use of ESAs) Oncology Program, which was established by ESA drug manufacturers. Once enrolled in the program, you will be assigned a unique ESA APPRISE ID number. ESA prescribers will be required to provide and review the ESA Medication Guide and counsel each patient on the risks and benefits of ESAs before each course of therapy. This counseling must be done no more than every 30 days after the first dose. (At the same time, prescribing ESAs to non-cancer patients basically only entails patient education.)
Providers also will be required to fill out the ESA APPRISE Oncology Program Patient and Healthcare Professional Acknowledgment form, which documents that the risk-benefit discussion occurred. This form is in triplicate and includes both the patient and the provider signature. One copy is given to the patient, another copy placed in the chart, and the third copy is stored for potential future audit.
For more information about the ESA APPRISE Oncology Program, please visit www.esaapprise.com/ESAAppriseUI/ESAAppriseUI/default.jsp. TH
I heard from my hospital’s pharmacist director that soon I will not be able to prescribe Epogen unless I get some additional certification. Is this true? Can you explain what is going on?
Ritesh Magge, MD,
Detroit
Dr. Hospitalist responds: Your pharmacist is referring to the new FDA-mandated requirements, which went into effect in February, that will affect who can prescribe erythropoesis-stimulating agents (ESAs), including epoetin (Epogen, Procrit) and darbepoetin (Aranesp). This is part of a broader FDA strategy to improve patient safety as it relates to medications.
According to the FDA website, “The Food and Drug Administration Amendments Act of 2007 gave FDA the authority to require a Risk Evaluation and Mitigation Strategy (REMS) from manufacturers to ensure that the benefits of a drug or biological product outweigh its risks.”
The ESAs are not the only class of drug that will require a REM. More than 150 drugs already have varying requirements. For a complete list of these medications, please visit the FDA website (www.fda.gov) and search “drug safety.” The FDA plans to create additional REMs for additional drugs and biologic agents.
If you are a provider who will prescribe a medication with a REM, you will be obligated to adhere to the FDA REM associated with that medication. The drug manufacturers are working with the FDA to set up REMs for their drugs. For example, if you plan to prescribe an ESA for a patient with cancer, you will first need to enroll in the ESA APPRISE (Assisting Providers and Cancer Patients with Risk Information for the Safe Use of ESAs) Oncology Program, which was established by ESA drug manufacturers. Once enrolled in the program, you will be assigned a unique ESA APPRISE ID number. ESA prescribers will be required to provide and review the ESA Medication Guide and counsel each patient on the risks and benefits of ESAs before each course of therapy. This counseling must be done no more than every 30 days after the first dose. (At the same time, prescribing ESAs to non-cancer patients basically only entails patient education.)
Providers also will be required to fill out the ESA APPRISE Oncology Program Patient and Healthcare Professional Acknowledgment form, which documents that the risk-benefit discussion occurred. This form is in triplicate and includes both the patient and the provider signature. One copy is given to the patient, another copy placed in the chart, and the third copy is stored for potential future audit.
For more information about the ESA APPRISE Oncology Program, please visit www.esaapprise.com/ESAAppriseUI/ESAAppriseUI/default.jsp. TH
I heard from my hospital’s pharmacist director that soon I will not be able to prescribe Epogen unless I get some additional certification. Is this true? Can you explain what is going on?
Ritesh Magge, MD,
Detroit
Dr. Hospitalist responds: Your pharmacist is referring to the new FDA-mandated requirements, which went into effect in February, that will affect who can prescribe erythropoesis-stimulating agents (ESAs), including epoetin (Epogen, Procrit) and darbepoetin (Aranesp). This is part of a broader FDA strategy to improve patient safety as it relates to medications.
According to the FDA website, “The Food and Drug Administration Amendments Act of 2007 gave FDA the authority to require a Risk Evaluation and Mitigation Strategy (REMS) from manufacturers to ensure that the benefits of a drug or biological product outweigh its risks.”
The ESAs are not the only class of drug that will require a REM. More than 150 drugs already have varying requirements. For a complete list of these medications, please visit the FDA website (www.fda.gov) and search “drug safety.” The FDA plans to create additional REMs for additional drugs and biologic agents.
If you are a provider who will prescribe a medication with a REM, you will be obligated to adhere to the FDA REM associated with that medication. The drug manufacturers are working with the FDA to set up REMs for their drugs. For example, if you plan to prescribe an ESA for a patient with cancer, you will first need to enroll in the ESA APPRISE (Assisting Providers and Cancer Patients with Risk Information for the Safe Use of ESAs) Oncology Program, which was established by ESA drug manufacturers. Once enrolled in the program, you will be assigned a unique ESA APPRISE ID number. ESA prescribers will be required to provide and review the ESA Medication Guide and counsel each patient on the risks and benefits of ESAs before each course of therapy. This counseling must be done no more than every 30 days after the first dose. (At the same time, prescribing ESAs to non-cancer patients basically only entails patient education.)
Providers also will be required to fill out the ESA APPRISE Oncology Program Patient and Healthcare Professional Acknowledgment form, which documents that the risk-benefit discussion occurred. This form is in triplicate and includes both the patient and the provider signature. One copy is given to the patient, another copy placed in the chart, and the third copy is stored for potential future audit.
For more information about the ESA APPRISE Oncology Program, please visit www.esaapprise.com/ESAAppriseUI/ESAAppriseUI/default.jsp. TH
Call of Duty
Dave Bowman, MD, doesn’t run anywhere anymore; it’s more of a fast walk. He doesn’t consider himself political, yet he does his civic duty and votes in every election. He’s not a big fan of vegetables, but he eats them to appease his wife and his conscience. Most important, Dr. Bowman doesn’t consider himself a hero. In fact, he doesn’t consider what he did that day any different from what he does every day in the hospital.
On the morning of Jan. 8, Dr. Bowman and his wife, Nancy, were thrust into the epicenter of one of the worst shooting rampages in American history. Dr. Bowman, a hospitalist, was the first physician on the scene outside the Tucson, Ariz., grocery store where a lone gunman killed six people and injured 13 others, including U.S. Representative Gabrielle Giffords (D-Ariz.).
“A hero is somebody, to me, who steps out of their element, steps up to the task that is needed, a task that is completely foreign to them, and steps up and helps people,” says Dr. Bowman, 61, executive director for IPC The Hospitalist Co.’s Tucson region. “A hero is not somebody who should be able to help in some manner and should be expected to help. … I don’t think nurses, doctors, firemen, EMTs get to be labeled as heroes. It’s what we should do, and gladly do, and in many cases took an oath to do.”
Even so, Dr. Bowman’s recollection of that frightful morning is a story laced with tragedy, courage, and hope. He remembers those who are “no longer with us.” He remembers his wife administering CPR and calling victims’ loved ones on their cellphones. And he remembers the brave men and women who not only subdued the shooter, but who worked together, selflessly, and in many cases with no medical training, to assist their injured neighbors.

“It was a pretty traumatic scene. More for others than for me; I am supposed to be the doctor and can handle all that,” he says, pausing. “But they don’t teach this course in medical school.”
Shots Ring Out, First Thought Is Help
Born and raised 100 miles south of Tucson and internal-medicine-trained at the University of Arizona, Dr. Bowman became a hospitalist in 1998 and began working with IPC in 2000. He supervises a staff of about 90 providers, including more than 50 full-time hospitalists, serving two large community hospitals, rehabilitations centers, and skilled nursing facilities in the Tucson area.
Yet he knows who the real boss is in the Bowman household. He and Nancy, an ICU nurse, had just finished a brisk walk, eaten breakfast at McDonald’s, and stopped at Safeway to pick up some vegetables on the morning of Jan. 8. “I had the oatmeal. I was so proud of myself,” Dr. Bowman says. “And, as wives will want to do, she pushes the envelope and says she wants to stop by and get some Brussels sprouts. She hadn’t had them in 20 years, and I hadn’t had them in 45 years—since my mom stunk up the house with them. So we ended up at the Safeway, because the two things that keeps a marriage together are those two words: ‘Yes, dear.’ ”
The Bowmans passed by Rep. Giffords, her staff, and about 25 people in front of the grocery store entrance. They went to the produce department and had not been in the store for more than three or four minutes before shots rang out.
“I was 150 percent sure they were gunshots,” Dr. Bowman says. “I said to my wife, ‘Let’s go, Nancy,’ and she didn’t hear me. I thought she was right behind me. But she had gone over to the Brussels sprouts and I was still in mushrooms.”
Walking to the door, Dr. Bowman saw a woman rushing in and shouting, “They shot her. They shot Congresswoman Giffords.”
“I stepped out and stood behind a pillar until no more gunshots,” he says. “They’d actually already taken down the shooter as soon as he ran out of bullets. I looked around the corner to the carnage, as you’d expect, with Congresswoman Giffords the first person I saw right at the head of the line near the front door.
“Quite frankly, I stepped over people who were no longer with us to get to her. I got her turned around and moved off to the window; she wasn’t breathing real well. I worked on her airway, cleaning her airway with the young man [Rep. Giffords’ intern, Daniel Hernandez], who then held her for the next 15 to 20 minutes until the paramedics got her ready to go to the hospital.”
From that moment, Dr. Bowman says his training and instincts took over. More important, he went into field-triage mode, “which means you can’t do anything for that one. Can’t do anything there, this one is breathing and talking, not bleeding bad, good; still breathing, good, stay right there, I will be back. You go all the way up the line from person to person, seeing who you can and can’t help.
“The problem with field triage is that you really can’t stop and do a lot, like CPR, because then the rest of the people don’t have anybody looking at them. So you just keep moving,” he explains.
He says that while it was only minutes from the first gunshot to the time police arrived and secured the scene to the time paramedics were allowed to assist with the injured, it seemed like hours. Additionally, in his haste to help, Dr. Bowman had lost track of Nancy.
“I looked back and she was not there,” he says, adding she’d been swept to the back of the grocery store. “I kept working and I looked back and she had pushed [aside] the 17-year-old sacker who was acting as a security guard. … She came outside and started doing CPR on the first person she saw. I got up the line and there was a doctor doing CPR on the young girl [Christina-Taylor Green]. He was in the parking lot when the shots rang out; he threw his wife in the car and ran up to the little girl.”
Instinct and Autopilot
In a little more than 10 seconds, the gunman had fired more than 30 rounds and killed or injured nearly 20 people.
After he’d checked on all of the wounded, Dr. Bowman says he came upon four people holding the suspected shooter down. “One of them, I didn’t know it, was one of my colleagues, Dr. Stephen Rayle,” Dr. Bowman says. “I said, ‘Hold him, and I will send the first officer over here.’ ”
From there, Dr. Bowman says, he went back up the line of injured, checking for breathing sounds and bleeding, making sure every injured person was being attended to.
“People shot in the leg were holding a hand over a chest wound on the man or woman next to them,” he says. “It was one of those chaotic scenes that you try to make some kind of order to, by deciding who you can help and who you can’t.”
When the first paramedics arrived, Dr. Bowman directed them to Rep. Giffords and the 9-year-old girl. Soon after, there were enough EMTs on scene to attend to each of the victims.
“You are just on automatic,” Dr. Bowman explains. “Actually, after I dealt with the first two victims pretty quickly, Giffords taking the most time to just get her situated, I did stop and look out in the parking lot just to see if anybody was aiming anything at us.”
The most difficult part of field triage, Dr. Bowman says, is staying calm, organized, and “not losing it emotionally.” In fact, he ushered some shell-shocked bystanders away from the scene. “Some people will step right forward and say, ‘Can I help? I know CPR.’ Other people will just stand there and scream.”
Even tougher, he says, was watching his wife try to save the life of U.S. District Judge John Roll (see “Remembering the Dead,” above). “I finally had to go to my wife, pull her off of him, and say, ‘Honey, he’s gone. I need help with this lady who has been shot in the chest laying in the street,’ ” Dr. Bowman says. “Pulling them away is pretty hard. ... It was harder for her and the bystanders, because they were the ones getting right down close with the patient, talking to them, telling patients to ‘keep looking at me.’ That is a very close bond that develops. Field triage, you just keep moving.”
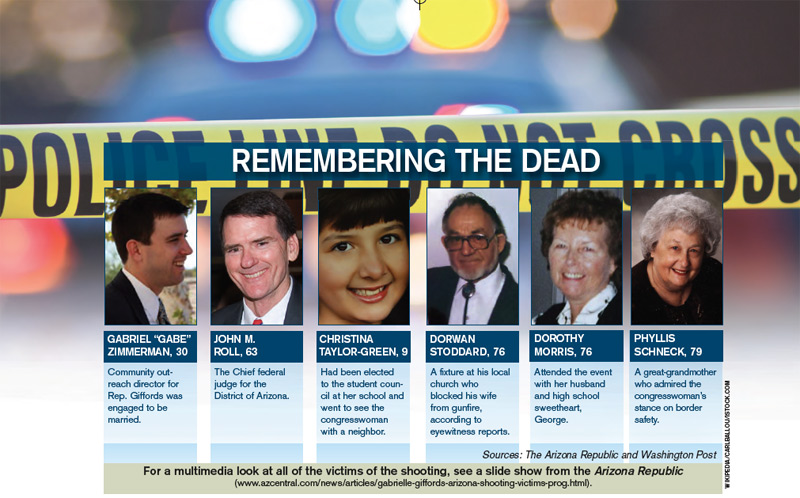
Human Spirit, Cooperation, and Hope
One month after the shooting, Rep. Giffords was moving, talking, thinking, and recuperating at what her doctors at Houston’s TIRR Hermann Memorial deemed “lightning speed.” For Dr. Bowman, such news brings more than a sigh of relief.
“In truth, when I was first with her, she wasn’t responding,” he says. “She was breathing, although with a compromised airway. We got that straightened away and she had a good pulse. Daniel Hernandez, the young man with her, had some nursing training and was comfortable being with her.
“It was amazing to me, the second or third time down the line, just to look over to this guy, and he was watching for me, and he would nod and say, ‘We’re OK. She’s breathing, pulse is OK.’ I didn’t have to go back, and the third time down he said, ‘She’s moving, she’s squeezing my hand.’ ”
It was at that moment that Dr. Bowman felt the congresswoman, in spite of her severe head trauma, had a fighting chance. Others miracles were happening all around him. Each memory ceases to amaze the veteran physician.
“People who were injured holding somebody’s head in their lap because they were hit in the head and this person was hit in the chest,” he says. “It gives you hope for the human race. Those people, to me, were the heroes.”
Looking back, Dr. Bowman says, he’s played back the moment in his mind more than a few times, wondering if he did the right thing for every victim. He wonders how much he and his wife, the other doctors at the scene, and the bystanders really helped. Then, after a brief moment, he has the answer.
“It really took two weeks to really say that, when all the victims that had expired were dead at the scene, and everybody that got taken away made it and out of the hospital, it sunk in that we had made the right decisions,” he says. “Nobody died on the operating table because we didn’t pick up the gunshot wound to the back. It took two weeks to realize we did the right thing.”
Some of those answers will take many more weeks. Rep. Giffords, although she is on a positive path, still has a long road to a full recovery, and doctors are making no promises. “I don’t know how far she will make it or how long it is going to take, but there are some miracles out there,” Dr. Bowman says.
You’re a Hospitalist? You’re Ready
As a physician in the middle of a mass-casualty event, the media called upon Dr. Bowman to recount the events of the Tucson shooting. In more than a dozen interviews with local and national media, not once was Dr. Bowman referred to as a hospitalist.
“At the scene, when I kneel down, I am a doctor. Can you tell me what’s going on, can you talk to me? It goes no farther than that,” he says. “In talking with one of the interviewers, she asked, ‘What kind of doctor are you?’ I said, ‘I am an internist and a hospitalist, which is a doctor who works just in the hospital.’ They weren’t interested in that. When the cameras rolled, she said, ‘I understand you are an intern?’ I said, ‘No, I am an internist. Turn that thing off and start again.’
“That’s the level of knowledge you are dealing with, and that was a national anchorperson I was dealing with.”
It’s an all-too-common refrain for hospitalists around the country, but one Dr. Bowman and others like him have endured for years. It doesn’t bother him, and he says it shouldn’t bother others.
“Doctor or nurse was as far as it got. I can certainly understand that,” he says. “We explain what a hospitalist is every day. We’ve been doing it for 12, 13, 14 years, and people still don’t understand. It’s OK.”
What isn’t OK is hospitalist unpreparedness. In fact, Dr. Bowman says, his training as an internist and his years of HM experience played a pivotal role in managing the scene of the Tucson shooting. The first thing to do, in addition to remaining calm, is to keep your priorities straight and remember your ABCs.

“It’s airway, airway, airway,” he says. “Without an airway, people don’t live. Then you are looking for bleeding, bleeding, bleeding. Then if they are talking, not a lot of bleeding and have a pulse, that is good enough for right now. So, it’s ‘Lady, just keep pushing on the chest right there on that wound.’ … I think, if you remember your ABCs, that’s all you can do in a field triage situation.”
Although the circumstances are less stressful, hospitalists are faced with make-or-break decisions every day, Dr. Bowman says. For example, it’s 4 p.m. and the day shift physician in the ED calls and says he has six admissions he’s been working on for the past three hours. “You, based on the info given to you, have to decide, Well, who is sickest, who do I have to get to first, who is going to the ICU?” Dr. Bowman says. “You do this triage thing in your mind as you walk to the ED. If there is any corollary, it’s the fact that you, as the hospitalist, get hit with a slew of patients all at once. They don’t come in one every 15 minutes like in your office for a blood-pressure check.
“Be ready. And, by the way, you are ready,” he adds. “You take care of a stroke patient in room one, take care of a gangrenous leg in room two, a diabetic with ketoacidosis in room three. The broadness, the generality of your training, you are ready to take care of a variety of things. You’re going to be able to help. Just be ready.” TH
Jason Carris is editor of The Hospitalist.
Dave Bowman, MD, doesn’t run anywhere anymore; it’s more of a fast walk. He doesn’t consider himself political, yet he does his civic duty and votes in every election. He’s not a big fan of vegetables, but he eats them to appease his wife and his conscience. Most important, Dr. Bowman doesn’t consider himself a hero. In fact, he doesn’t consider what he did that day any different from what he does every day in the hospital.
On the morning of Jan. 8, Dr. Bowman and his wife, Nancy, were thrust into the epicenter of one of the worst shooting rampages in American history. Dr. Bowman, a hospitalist, was the first physician on the scene outside the Tucson, Ariz., grocery store where a lone gunman killed six people and injured 13 others, including U.S. Representative Gabrielle Giffords (D-Ariz.).
“A hero is somebody, to me, who steps out of their element, steps up to the task that is needed, a task that is completely foreign to them, and steps up and helps people,” says Dr. Bowman, 61, executive director for IPC The Hospitalist Co.’s Tucson region. “A hero is not somebody who should be able to help in some manner and should be expected to help. … I don’t think nurses, doctors, firemen, EMTs get to be labeled as heroes. It’s what we should do, and gladly do, and in many cases took an oath to do.”
Even so, Dr. Bowman’s recollection of that frightful morning is a story laced with tragedy, courage, and hope. He remembers those who are “no longer with us.” He remembers his wife administering CPR and calling victims’ loved ones on their cellphones. And he remembers the brave men and women who not only subdued the shooter, but who worked together, selflessly, and in many cases with no medical training, to assist their injured neighbors.
“It was a pretty traumatic scene. More for others than for me; I am supposed to be the doctor and can handle all that,” he says, pausing. “But they don’t teach this course in medical school.”
Shots Ring Out, First Thought Is Help
Born and raised 100 miles south of Tucson and internal-medicine-trained at the University of Arizona, Dr. Bowman became a hospitalist in 1998 and began working with IPC in 2000. He supervises a staff of about 90 providers, including more than 50 full-time hospitalists, serving two large community hospitals, rehabilitations centers, and skilled nursing facilities in the Tucson area.
Yet he knows who the real boss is in the Bowman household. He and Nancy, an ICU nurse, had just finished a brisk walk, eaten breakfast at McDonald’s, and stopped at Safeway to pick up some vegetables on the morning of Jan. 8. “I had the oatmeal. I was so proud of myself,” Dr. Bowman says. “And, as wives will want to do, she pushes the envelope and says she wants to stop by and get some Brussels sprouts. She hadn’t had them in 20 years, and I hadn’t had them in 45 years—since my mom stunk up the house with them. So we ended up at the Safeway, because the two things that keeps a marriage together are those two words: ‘Yes, dear.’ ”
The Bowmans passed by Rep. Giffords, her staff, and about 25 people in front of the grocery store entrance. They went to the produce department and had not been in the store for more than three or four minutes before shots rang out.
“I was 150 percent sure they were gunshots,” Dr. Bowman says. “I said to my wife, ‘Let’s go, Nancy,’ and she didn’t hear me. I thought she was right behind me. But she had gone over to the Brussels sprouts and I was still in mushrooms.”
Walking to the door, Dr. Bowman saw a woman rushing in and shouting, “They shot her. They shot Congresswoman Giffords.”
“I stepped out and stood behind a pillar until no more gunshots,” he says. “They’d actually already taken down the shooter as soon as he ran out of bullets. I looked around the corner to the carnage, as you’d expect, with Congresswoman Giffords the first person I saw right at the head of the line near the front door.
“Quite frankly, I stepped over people who were no longer with us to get to her. I got her turned around and moved off to the window; she wasn’t breathing real well. I worked on her airway, cleaning her airway with the young man [Rep. Giffords’ intern, Daniel Hernandez], who then held her for the next 15 to 20 minutes until the paramedics got her ready to go to the hospital.”
From that moment, Dr. Bowman says his training and instincts took over. More important, he went into field-triage mode, “which means you can’t do anything for that one. Can’t do anything there, this one is breathing and talking, not bleeding bad, good; still breathing, good, stay right there, I will be back. You go all the way up the line from person to person, seeing who you can and can’t help.
“The problem with field triage is that you really can’t stop and do a lot, like CPR, because then the rest of the people don’t have anybody looking at them. So you just keep moving,” he explains.
He says that while it was only minutes from the first gunshot to the time police arrived and secured the scene to the time paramedics were allowed to assist with the injured, it seemed like hours. Additionally, in his haste to help, Dr. Bowman had lost track of Nancy.
“I looked back and she was not there,” he says, adding she’d been swept to the back of the grocery store. “I kept working and I looked back and she had pushed [aside] the 17-year-old sacker who was acting as a security guard. … She came outside and started doing CPR on the first person she saw. I got up the line and there was a doctor doing CPR on the young girl [Christina-Taylor Green]. He was in the parking lot when the shots rang out; he threw his wife in the car and ran up to the little girl.”
Instinct and Autopilot
In a little more than 10 seconds, the gunman had fired more than 30 rounds and killed or injured nearly 20 people.
After he’d checked on all of the wounded, Dr. Bowman says he came upon four people holding the suspected shooter down. “One of them, I didn’t know it, was one of my colleagues, Dr. Stephen Rayle,” Dr. Bowman says. “I said, ‘Hold him, and I will send the first officer over here.’ ”
From there, Dr. Bowman says, he went back up the line of injured, checking for breathing sounds and bleeding, making sure every injured person was being attended to.
“People shot in the leg were holding a hand over a chest wound on the man or woman next to them,” he says. “It was one of those chaotic scenes that you try to make some kind of order to, by deciding who you can help and who you can’t.”
When the first paramedics arrived, Dr. Bowman directed them to Rep. Giffords and the 9-year-old girl. Soon after, there were enough EMTs on scene to attend to each of the victims.
“You are just on automatic,” Dr. Bowman explains. “Actually, after I dealt with the first two victims pretty quickly, Giffords taking the most time to just get her situated, I did stop and look out in the parking lot just to see if anybody was aiming anything at us.”
The most difficult part of field triage, Dr. Bowman says, is staying calm, organized, and “not losing it emotionally.” In fact, he ushered some shell-shocked bystanders away from the scene. “Some people will step right forward and say, ‘Can I help? I know CPR.’ Other people will just stand there and scream.”
Even tougher, he says, was watching his wife try to save the life of U.S. District Judge John Roll (see “Remembering the Dead,” above). “I finally had to go to my wife, pull her off of him, and say, ‘Honey, he’s gone. I need help with this lady who has been shot in the chest laying in the street,’ ” Dr. Bowman says. “Pulling them away is pretty hard. ... It was harder for her and the bystanders, because they were the ones getting right down close with the patient, talking to them, telling patients to ‘keep looking at me.’ That is a very close bond that develops. Field triage, you just keep moving.”
Human Spirit, Cooperation, and Hope
One month after the shooting, Rep. Giffords was moving, talking, thinking, and recuperating at what her doctors at Houston’s TIRR Hermann Memorial deemed “lightning speed.” For Dr. Bowman, such news brings more than a sigh of relief.
“In truth, when I was first with her, she wasn’t responding,” he says. “She was breathing, although with a compromised airway. We got that straightened away and she had a good pulse. Daniel Hernandez, the young man with her, had some nursing training and was comfortable being with her.
“It was amazing to me, the second or third time down the line, just to look over to this guy, and he was watching for me, and he would nod and say, ‘We’re OK. She’s breathing, pulse is OK.’ I didn’t have to go back, and the third time down he said, ‘She’s moving, she’s squeezing my hand.’ ”
It was at that moment that Dr. Bowman felt the congresswoman, in spite of her severe head trauma, had a fighting chance. Others miracles were happening all around him. Each memory ceases to amaze the veteran physician.
“People who were injured holding somebody’s head in their lap because they were hit in the head and this person was hit in the chest,” he says. “It gives you hope for the human race. Those people, to me, were the heroes.”
Looking back, Dr. Bowman says, he’s played back the moment in his mind more than a few times, wondering if he did the right thing for every victim. He wonders how much he and his wife, the other doctors at the scene, and the bystanders really helped. Then, after a brief moment, he has the answer.
“It really took two weeks to really say that, when all the victims that had expired were dead at the scene, and everybody that got taken away made it and out of the hospital, it sunk in that we had made the right decisions,” he says. “Nobody died on the operating table because we didn’t pick up the gunshot wound to the back. It took two weeks to realize we did the right thing.”
Some of those answers will take many more weeks. Rep. Giffords, although she is on a positive path, still has a long road to a full recovery, and doctors are making no promises. “I don’t know how far she will make it or how long it is going to take, but there are some miracles out there,” Dr. Bowman says.
You’re a Hospitalist? You’re Ready
As a physician in the middle of a mass-casualty event, the media called upon Dr. Bowman to recount the events of the Tucson shooting. In more than a dozen interviews with local and national media, not once was Dr. Bowman referred to as a hospitalist.
“At the scene, when I kneel down, I am a doctor. Can you tell me what’s going on, can you talk to me? It goes no farther than that,” he says. “In talking with one of the interviewers, she asked, ‘What kind of doctor are you?’ I said, ‘I am an internist and a hospitalist, which is a doctor who works just in the hospital.’ They weren’t interested in that. When the cameras rolled, she said, ‘I understand you are an intern?’ I said, ‘No, I am an internist. Turn that thing off and start again.’
“That’s the level of knowledge you are dealing with, and that was a national anchorperson I was dealing with.”
It’s an all-too-common refrain for hospitalists around the country, but one Dr. Bowman and others like him have endured for years. It doesn’t bother him, and he says it shouldn’t bother others.
“Doctor or nurse was as far as it got. I can certainly understand that,” he says. “We explain what a hospitalist is every day. We’ve been doing it for 12, 13, 14 years, and people still don’t understand. It’s OK.”
What isn’t OK is hospitalist unpreparedness. In fact, Dr. Bowman says, his training as an internist and his years of HM experience played a pivotal role in managing the scene of the Tucson shooting. The first thing to do, in addition to remaining calm, is to keep your priorities straight and remember your ABCs.
“It’s airway, airway, airway,” he says. “Without an airway, people don’t live. Then you are looking for bleeding, bleeding, bleeding. Then if they are talking, not a lot of bleeding and have a pulse, that is good enough for right now. So, it’s ‘Lady, just keep pushing on the chest right there on that wound.’ … I think, if you remember your ABCs, that’s all you can do in a field triage situation.”
Although the circumstances are less stressful, hospitalists are faced with make-or-break decisions every day, Dr. Bowman says. For example, it’s 4 p.m. and the day shift physician in the ED calls and says he has six admissions he’s been working on for the past three hours. “You, based on the info given to you, have to decide, Well, who is sickest, who do I have to get to first, who is going to the ICU?” Dr. Bowman says. “You do this triage thing in your mind as you walk to the ED. If there is any corollary, it’s the fact that you, as the hospitalist, get hit with a slew of patients all at once. They don’t come in one every 15 minutes like in your office for a blood-pressure check.
“Be ready. And, by the way, you are ready,” he adds. “You take care of a stroke patient in room one, take care of a gangrenous leg in room two, a diabetic with ketoacidosis in room three. The broadness, the generality of your training, you are ready to take care of a variety of things. You’re going to be able to help. Just be ready.” TH
Jason Carris is editor of The Hospitalist.
Dave Bowman, MD, doesn’t run anywhere anymore; it’s more of a fast walk. He doesn’t consider himself political, yet he does his civic duty and votes in every election. He’s not a big fan of vegetables, but he eats them to appease his wife and his conscience. Most important, Dr. Bowman doesn’t consider himself a hero. In fact, he doesn’t consider what he did that day any different from what he does every day in the hospital.
On the morning of Jan. 8, Dr. Bowman and his wife, Nancy, were thrust into the epicenter of one of the worst shooting rampages in American history. Dr. Bowman, a hospitalist, was the first physician on the scene outside the Tucson, Ariz., grocery store where a lone gunman killed six people and injured 13 others, including U.S. Representative Gabrielle Giffords (D-Ariz.).
“A hero is somebody, to me, who steps out of their element, steps up to the task that is needed, a task that is completely foreign to them, and steps up and helps people,” says Dr. Bowman, 61, executive director for IPC The Hospitalist Co.’s Tucson region. “A hero is not somebody who should be able to help in some manner and should be expected to help. … I don’t think nurses, doctors, firemen, EMTs get to be labeled as heroes. It’s what we should do, and gladly do, and in many cases took an oath to do.”
Even so, Dr. Bowman’s recollection of that frightful morning is a story laced with tragedy, courage, and hope. He remembers those who are “no longer with us.” He remembers his wife administering CPR and calling victims’ loved ones on their cellphones. And he remembers the brave men and women who not only subdued the shooter, but who worked together, selflessly, and in many cases with no medical training, to assist their injured neighbors.
“It was a pretty traumatic scene. More for others than for me; I am supposed to be the doctor and can handle all that,” he says, pausing. “But they don’t teach this course in medical school.”
Shots Ring Out, First Thought Is Help
Born and raised 100 miles south of Tucson and internal-medicine-trained at the University of Arizona, Dr. Bowman became a hospitalist in 1998 and began working with IPC in 2000. He supervises a staff of about 90 providers, including more than 50 full-time hospitalists, serving two large community hospitals, rehabilitations centers, and skilled nursing facilities in the Tucson area.
Yet he knows who the real boss is in the Bowman household. He and Nancy, an ICU nurse, had just finished a brisk walk, eaten breakfast at McDonald’s, and stopped at Safeway to pick up some vegetables on the morning of Jan. 8. “I had the oatmeal. I was so proud of myself,” Dr. Bowman says. “And, as wives will want to do, she pushes the envelope and says she wants to stop by and get some Brussels sprouts. She hadn’t had them in 20 years, and I hadn’t had them in 45 years—since my mom stunk up the house with them. So we ended up at the Safeway, because the two things that keeps a marriage together are those two words: ‘Yes, dear.’ ”
The Bowmans passed by Rep. Giffords, her staff, and about 25 people in front of the grocery store entrance. They went to the produce department and had not been in the store for more than three or four minutes before shots rang out.
“I was 150 percent sure they were gunshots,” Dr. Bowman says. “I said to my wife, ‘Let’s go, Nancy,’ and she didn’t hear me. I thought she was right behind me. But she had gone over to the Brussels sprouts and I was still in mushrooms.”
Walking to the door, Dr. Bowman saw a woman rushing in and shouting, “They shot her. They shot Congresswoman Giffords.”
“I stepped out and stood behind a pillar until no more gunshots,” he says. “They’d actually already taken down the shooter as soon as he ran out of bullets. I looked around the corner to the carnage, as you’d expect, with Congresswoman Giffords the first person I saw right at the head of the line near the front door.
“Quite frankly, I stepped over people who were no longer with us to get to her. I got her turned around and moved off to the window; she wasn’t breathing real well. I worked on her airway, cleaning her airway with the young man [Rep. Giffords’ intern, Daniel Hernandez], who then held her for the next 15 to 20 minutes until the paramedics got her ready to go to the hospital.”
From that moment, Dr. Bowman says his training and instincts took over. More important, he went into field-triage mode, “which means you can’t do anything for that one. Can’t do anything there, this one is breathing and talking, not bleeding bad, good; still breathing, good, stay right there, I will be back. You go all the way up the line from person to person, seeing who you can and can’t help.
“The problem with field triage is that you really can’t stop and do a lot, like CPR, because then the rest of the people don’t have anybody looking at them. So you just keep moving,” he explains.
He says that while it was only minutes from the first gunshot to the time police arrived and secured the scene to the time paramedics were allowed to assist with the injured, it seemed like hours. Additionally, in his haste to help, Dr. Bowman had lost track of Nancy.
“I looked back and she was not there,” he says, adding she’d been swept to the back of the grocery store. “I kept working and I looked back and she had pushed [aside] the 17-year-old sacker who was acting as a security guard. … She came outside and started doing CPR on the first person she saw. I got up the line and there was a doctor doing CPR on the young girl [Christina-Taylor Green]. He was in the parking lot when the shots rang out; he threw his wife in the car and ran up to the little girl.”
Instinct and Autopilot
In a little more than 10 seconds, the gunman had fired more than 30 rounds and killed or injured nearly 20 people.
After he’d checked on all of the wounded, Dr. Bowman says he came upon four people holding the suspected shooter down. “One of them, I didn’t know it, was one of my colleagues, Dr. Stephen Rayle,” Dr. Bowman says. “I said, ‘Hold him, and I will send the first officer over here.’ ”
From there, Dr. Bowman says, he went back up the line of injured, checking for breathing sounds and bleeding, making sure every injured person was being attended to.
“People shot in the leg were holding a hand over a chest wound on the man or woman next to them,” he says. “It was one of those chaotic scenes that you try to make some kind of order to, by deciding who you can help and who you can’t.”
When the first paramedics arrived, Dr. Bowman directed them to Rep. Giffords and the 9-year-old girl. Soon after, there were enough EMTs on scene to attend to each of the victims.
“You are just on automatic,” Dr. Bowman explains. “Actually, after I dealt with the first two victims pretty quickly, Giffords taking the most time to just get her situated, I did stop and look out in the parking lot just to see if anybody was aiming anything at us.”
The most difficult part of field triage, Dr. Bowman says, is staying calm, organized, and “not losing it emotionally.” In fact, he ushered some shell-shocked bystanders away from the scene. “Some people will step right forward and say, ‘Can I help? I know CPR.’ Other people will just stand there and scream.”
Even tougher, he says, was watching his wife try to save the life of U.S. District Judge John Roll (see “Remembering the Dead,” above). “I finally had to go to my wife, pull her off of him, and say, ‘Honey, he’s gone. I need help with this lady who has been shot in the chest laying in the street,’ ” Dr. Bowman says. “Pulling them away is pretty hard. ... It was harder for her and the bystanders, because they were the ones getting right down close with the patient, talking to them, telling patients to ‘keep looking at me.’ That is a very close bond that develops. Field triage, you just keep moving.”
Human Spirit, Cooperation, and Hope
One month after the shooting, Rep. Giffords was moving, talking, thinking, and recuperating at what her doctors at Houston’s TIRR Hermann Memorial deemed “lightning speed.” For Dr. Bowman, such news brings more than a sigh of relief.
“In truth, when I was first with her, she wasn’t responding,” he says. “She was breathing, although with a compromised airway. We got that straightened away and she had a good pulse. Daniel Hernandez, the young man with her, had some nursing training and was comfortable being with her.
“It was amazing to me, the second or third time down the line, just to look over to this guy, and he was watching for me, and he would nod and say, ‘We’re OK. She’s breathing, pulse is OK.’ I didn’t have to go back, and the third time down he said, ‘She’s moving, she’s squeezing my hand.’ ”
It was at that moment that Dr. Bowman felt the congresswoman, in spite of her severe head trauma, had a fighting chance. Others miracles were happening all around him. Each memory ceases to amaze the veteran physician.
“People who were injured holding somebody’s head in their lap because they were hit in the head and this person was hit in the chest,” he says. “It gives you hope for the human race. Those people, to me, were the heroes.”
Looking back, Dr. Bowman says, he’s played back the moment in his mind more than a few times, wondering if he did the right thing for every victim. He wonders how much he and his wife, the other doctors at the scene, and the bystanders really helped. Then, after a brief moment, he has the answer.
“It really took two weeks to really say that, when all the victims that had expired were dead at the scene, and everybody that got taken away made it and out of the hospital, it sunk in that we had made the right decisions,” he says. “Nobody died on the operating table because we didn’t pick up the gunshot wound to the back. It took two weeks to realize we did the right thing.”
Some of those answers will take many more weeks. Rep. Giffords, although she is on a positive path, still has a long road to a full recovery, and doctors are making no promises. “I don’t know how far she will make it or how long it is going to take, but there are some miracles out there,” Dr. Bowman says.
You’re a Hospitalist? You’re Ready
As a physician in the middle of a mass-casualty event, the media called upon Dr. Bowman to recount the events of the Tucson shooting. In more than a dozen interviews with local and national media, not once was Dr. Bowman referred to as a hospitalist.
“At the scene, when I kneel down, I am a doctor. Can you tell me what’s going on, can you talk to me? It goes no farther than that,” he says. “In talking with one of the interviewers, she asked, ‘What kind of doctor are you?’ I said, ‘I am an internist and a hospitalist, which is a doctor who works just in the hospital.’ They weren’t interested in that. When the cameras rolled, she said, ‘I understand you are an intern?’ I said, ‘No, I am an internist. Turn that thing off and start again.’
“That’s the level of knowledge you are dealing with, and that was a national anchorperson I was dealing with.”
It’s an all-too-common refrain for hospitalists around the country, but one Dr. Bowman and others like him have endured for years. It doesn’t bother him, and he says it shouldn’t bother others.
“Doctor or nurse was as far as it got. I can certainly understand that,” he says. “We explain what a hospitalist is every day. We’ve been doing it for 12, 13, 14 years, and people still don’t understand. It’s OK.”
What isn’t OK is hospitalist unpreparedness. In fact, Dr. Bowman says, his training as an internist and his years of HM experience played a pivotal role in managing the scene of the Tucson shooting. The first thing to do, in addition to remaining calm, is to keep your priorities straight and remember your ABCs.
“It’s airway, airway, airway,” he says. “Without an airway, people don’t live. Then you are looking for bleeding, bleeding, bleeding. Then if they are talking, not a lot of bleeding and have a pulse, that is good enough for right now. So, it’s ‘Lady, just keep pushing on the chest right there on that wound.’ … I think, if you remember your ABCs, that’s all you can do in a field triage situation.”
Although the circumstances are less stressful, hospitalists are faced with make-or-break decisions every day, Dr. Bowman says. For example, it’s 4 p.m. and the day shift physician in the ED calls and says he has six admissions he’s been working on for the past three hours. “You, based on the info given to you, have to decide, Well, who is sickest, who do I have to get to first, who is going to the ICU?” Dr. Bowman says. “You do this triage thing in your mind as you walk to the ED. If there is any corollary, it’s the fact that you, as the hospitalist, get hit with a slew of patients all at once. They don’t come in one every 15 minutes like in your office for a blood-pressure check.
“Be ready. And, by the way, you are ready,” he adds. “You take care of a stroke patient in room one, take care of a gangrenous leg in room two, a diabetic with ketoacidosis in room three. The broadness, the generality of your training, you are ready to take care of a variety of things. You’re going to be able to help. Just be ready.” TH
Jason Carris is editor of The Hospitalist.