User login
Safety, Salary, and Saints

I just returned from the SHM annual meeting, and I am brimming with new knowledge. While we’ve tried to capture the essence of the meeting in this edition of The Hospitalist, it’s hard to describe in print the excitement, energy, and edification I encountered during those three days in San Diego.
Nearly 1,600 hospitalists descended on the Grand Hyatt on the San Diego Harbor for the six pre-courses April 3 and the two-day meeting April 4-5, marking the biggest and widest-reaching hospitalist meeting to date. Here’s just a smattering of what I learned in southern California.
I learned that Don Berwick, MD, is a healthcare visionary. In his plenary address the founder of the Institute for Healthcare Improvement and national leader of the patient safety movement gave his insights on the quality of the healthcare system and offered a challenge for hospitalists. He started by deftly outlining how Americans pay $3,000 more per capita for healthcare than other industrialized countries only to receive less access, worse care, and higher mortality rates. Clearly, more money does not equate to better care.
After noting that every system is perfectly designed to achieve the results it gets, Dr. Berwick challenged hospitalists to debunk the romantic view of the “individual as the cause of excellence” in favor of creating multidisciplinary teams and systems of care whose results do not depend on the heroism of the individual.
I learned that hospitalists are getting paid more today for the same amount of work they provided in 2005. At the same time that the average salary is up 13% to $193,300 (compared with 2005) the average number of annual encounters per hospitalist is down 4% from 2,558 in 2005 to 2,447 in 2007.
I’ve seen several interpretations of these data. The most cynical take, generally from non-hospitalists, is that this is further proof that hospitalists are overpaid compared with our non-hospitalist generalist colleagues in internal and family medicine. While these changes obviously represent a free-market response to a shortage of hospitalists, I firmly believe these higher salaries are a more accurate valuation of the work hospitalists do—and the more appropriate interpretation is that we’ve been underpaid in previous years. Now it’s time for our healthcare system to more appropriately reward our outpatient colleagues as well.
I also learned that academic hospitalists are struggling with similar issues across the country. Drs. Adrienne Bennett, Brian Lucas, and Bob Wachter, led an enthralling but sobering session surveying the challenges facing academic hospitalist groups. In many cases the vision of developing a sustainable academic model around the core tenets of research, scholarly activity, and education is being undermined by the service mandate of non-teaching clinical work.
These tensions lead to profound challenges come promotion time, a topic that Drs. Scott Flanders, David Meltzer, and Sankey Williams covered in an afternoon session.
As a director of an academic program who recently went through the promotion process, I view these two issues as critical to the health of all segments of hospital medicine, not just academics. Community hospitalist groups will encounter even larger workforce deficiencies if future hospitalists (i.e., current residents) shy away from the field because they see academic hospitalists devalued as unpromotable resident extenders and academic second-class citizens.
Speaking of workforce shortages, I learned that several highly respect leaders in hospital medicine believe this to be one of the most significant factors threatening the field. In a plenary panel discussion, Drs. Ron Greeno, John Nelson, Mike Guthrie, and John Laverty, commented that overcoming the current and future hospitalist shortage requires rethinking the current model. Dr. Greeno highlighted the need to build more efficient care models whereby hospitalists could see more patients in the same time by reducing the high levels of busy work and administrative minutiae.
Other ideas centered on the development of midlevel provider hospitalists and limiting our scope of practice. To the latter point, there was a lively debate about just how much of the traditionally “non-medical” piece of the pie hospitalists should bite off. Eric Siegal, MD, tackled this issue in a later session challenging hospitalist groups to rethink the value of further expanding the co-management model to more surgical patients while we struggle to care for the patients for whom we currently care.
I learned that Drs. Nelson and Win Whitcomb, co-founders of SHM, showed tremendous vision in their founding of this society. I had the chance to have lunch with John, and I asked him if he ever imagined that the tiny group he brought together in San Diego 11 years ago would ever grow to this—20,000 hospitalists, 6,000 SHM members, an annual meeting with 1,600 people, and a hospitalist (Russell Holman, MD, past president of SHM) seated at the table of the most influential healthcare policy meetings in Washington, D.C.
Rather than being awestruck by the development of this field and SHM, he simply noted this is exactly what he and Win foresaw more than a decade ago; this is the reason they founded SHM. That’s the kind of vision that explains why the field of hospital medicine is the fastest-growing medical specialty.
I learned that the future of hospital medicine is being defined today. Nearly 200 posters were presented at the Research, Innovations and Clinical Vignettes (RIV) Competition. When we look back 10 years from now, we will see a mature field and wonder how we got there so quickly.
That future is being constructed today by folks like Ken Epstein, MD, who presented fascinating data on the effects of fragmentation of hospitalist care, and Param Dedhia, MD, who showed that a formalized discharge toolkit could reduce emergency visits and hospital readmissions in elderly patients.
Finally, while I was away in the city named after a saint, I learned that my wife, too, is a saint. Unable to travel with me, she was landlocked in Denver with our 6-month-old son. I, like many attendees, acknowledge the families who sacrificed so their loved ones could attend the meeting. While I was socializing, learning, networking, and teaching a session, my wife was home soothing tears, changing diapers, cleaning chinfuls of cereal, and answering 3 a.m. wakeup calls. On behalf of all attendees I say thanks to all the saints who enabled us to be away charting the course of hospital medicine at Hospital Medicine 2008. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
I just returned from the SHM annual meeting, and I am brimming with new knowledge. While we’ve tried to capture the essence of the meeting in this edition of The Hospitalist, it’s hard to describe in print the excitement, energy, and edification I encountered during those three days in San Diego.
Nearly 1,600 hospitalists descended on the Grand Hyatt on the San Diego Harbor for the six pre-courses April 3 and the two-day meeting April 4-5, marking the biggest and widest-reaching hospitalist meeting to date. Here’s just a smattering of what I learned in southern California.
I learned that Don Berwick, MD, is a healthcare visionary. In his plenary address the founder of the Institute for Healthcare Improvement and national leader of the patient safety movement gave his insights on the quality of the healthcare system and offered a challenge for hospitalists. He started by deftly outlining how Americans pay $3,000 more per capita for healthcare than other industrialized countries only to receive less access, worse care, and higher mortality rates. Clearly, more money does not equate to better care.
After noting that every system is perfectly designed to achieve the results it gets, Dr. Berwick challenged hospitalists to debunk the romantic view of the “individual as the cause of excellence” in favor of creating multidisciplinary teams and systems of care whose results do not depend on the heroism of the individual.
I learned that hospitalists are getting paid more today for the same amount of work they provided in 2005. At the same time that the average salary is up 13% to $193,300 (compared with 2005) the average number of annual encounters per hospitalist is down 4% from 2,558 in 2005 to 2,447 in 2007.
I’ve seen several interpretations of these data. The most cynical take, generally from non-hospitalists, is that this is further proof that hospitalists are overpaid compared with our non-hospitalist generalist colleagues in internal and family medicine. While these changes obviously represent a free-market response to a shortage of hospitalists, I firmly believe these higher salaries are a more accurate valuation of the work hospitalists do—and the more appropriate interpretation is that we’ve been underpaid in previous years. Now it’s time for our healthcare system to more appropriately reward our outpatient colleagues as well.
I also learned that academic hospitalists are struggling with similar issues across the country. Drs. Adrienne Bennett, Brian Lucas, and Bob Wachter, led an enthralling but sobering session surveying the challenges facing academic hospitalist groups. In many cases the vision of developing a sustainable academic model around the core tenets of research, scholarly activity, and education is being undermined by the service mandate of non-teaching clinical work.
These tensions lead to profound challenges come promotion time, a topic that Drs. Scott Flanders, David Meltzer, and Sankey Williams covered in an afternoon session.
As a director of an academic program who recently went through the promotion process, I view these two issues as critical to the health of all segments of hospital medicine, not just academics. Community hospitalist groups will encounter even larger workforce deficiencies if future hospitalists (i.e., current residents) shy away from the field because they see academic hospitalists devalued as unpromotable resident extenders and academic second-class citizens.
Speaking of workforce shortages, I learned that several highly respect leaders in hospital medicine believe this to be one of the most significant factors threatening the field. In a plenary panel discussion, Drs. Ron Greeno, John Nelson, Mike Guthrie, and John Laverty, commented that overcoming the current and future hospitalist shortage requires rethinking the current model. Dr. Greeno highlighted the need to build more efficient care models whereby hospitalists could see more patients in the same time by reducing the high levels of busy work and administrative minutiae.
Other ideas centered on the development of midlevel provider hospitalists and limiting our scope of practice. To the latter point, there was a lively debate about just how much of the traditionally “non-medical” piece of the pie hospitalists should bite off. Eric Siegal, MD, tackled this issue in a later session challenging hospitalist groups to rethink the value of further expanding the co-management model to more surgical patients while we struggle to care for the patients for whom we currently care.
I learned that Drs. Nelson and Win Whitcomb, co-founders of SHM, showed tremendous vision in their founding of this society. I had the chance to have lunch with John, and I asked him if he ever imagined that the tiny group he brought together in San Diego 11 years ago would ever grow to this—20,000 hospitalists, 6,000 SHM members, an annual meeting with 1,600 people, and a hospitalist (Russell Holman, MD, past president of SHM) seated at the table of the most influential healthcare policy meetings in Washington, D.C.
Rather than being awestruck by the development of this field and SHM, he simply noted this is exactly what he and Win foresaw more than a decade ago; this is the reason they founded SHM. That’s the kind of vision that explains why the field of hospital medicine is the fastest-growing medical specialty.
I learned that the future of hospital medicine is being defined today. Nearly 200 posters were presented at the Research, Innovations and Clinical Vignettes (RIV) Competition. When we look back 10 years from now, we will see a mature field and wonder how we got there so quickly.
That future is being constructed today by folks like Ken Epstein, MD, who presented fascinating data on the effects of fragmentation of hospitalist care, and Param Dedhia, MD, who showed that a formalized discharge toolkit could reduce emergency visits and hospital readmissions in elderly patients.
Finally, while I was away in the city named after a saint, I learned that my wife, too, is a saint. Unable to travel with me, she was landlocked in Denver with our 6-month-old son. I, like many attendees, acknowledge the families who sacrificed so their loved ones could attend the meeting. While I was socializing, learning, networking, and teaching a session, my wife was home soothing tears, changing diapers, cleaning chinfuls of cereal, and answering 3 a.m. wakeup calls. On behalf of all attendees I say thanks to all the saints who enabled us to be away charting the course of hospital medicine at Hospital Medicine 2008. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
I just returned from the SHM annual meeting, and I am brimming with new knowledge. While we’ve tried to capture the essence of the meeting in this edition of The Hospitalist, it’s hard to describe in print the excitement, energy, and edification I encountered during those three days in San Diego.
Nearly 1,600 hospitalists descended on the Grand Hyatt on the San Diego Harbor for the six pre-courses April 3 and the two-day meeting April 4-5, marking the biggest and widest-reaching hospitalist meeting to date. Here’s just a smattering of what I learned in southern California.
I learned that Don Berwick, MD, is a healthcare visionary. In his plenary address the founder of the Institute for Healthcare Improvement and national leader of the patient safety movement gave his insights on the quality of the healthcare system and offered a challenge for hospitalists. He started by deftly outlining how Americans pay $3,000 more per capita for healthcare than other industrialized countries only to receive less access, worse care, and higher mortality rates. Clearly, more money does not equate to better care.
After noting that every system is perfectly designed to achieve the results it gets, Dr. Berwick challenged hospitalists to debunk the romantic view of the “individual as the cause of excellence” in favor of creating multidisciplinary teams and systems of care whose results do not depend on the heroism of the individual.
I learned that hospitalists are getting paid more today for the same amount of work they provided in 2005. At the same time that the average salary is up 13% to $193,300 (compared with 2005) the average number of annual encounters per hospitalist is down 4% from 2,558 in 2005 to 2,447 in 2007.
I’ve seen several interpretations of these data. The most cynical take, generally from non-hospitalists, is that this is further proof that hospitalists are overpaid compared with our non-hospitalist generalist colleagues in internal and family medicine. While these changes obviously represent a free-market response to a shortage of hospitalists, I firmly believe these higher salaries are a more accurate valuation of the work hospitalists do—and the more appropriate interpretation is that we’ve been underpaid in previous years. Now it’s time for our healthcare system to more appropriately reward our outpatient colleagues as well.
I also learned that academic hospitalists are struggling with similar issues across the country. Drs. Adrienne Bennett, Brian Lucas, and Bob Wachter, led an enthralling but sobering session surveying the challenges facing academic hospitalist groups. In many cases the vision of developing a sustainable academic model around the core tenets of research, scholarly activity, and education is being undermined by the service mandate of non-teaching clinical work.
These tensions lead to profound challenges come promotion time, a topic that Drs. Scott Flanders, David Meltzer, and Sankey Williams covered in an afternoon session.
As a director of an academic program who recently went through the promotion process, I view these two issues as critical to the health of all segments of hospital medicine, not just academics. Community hospitalist groups will encounter even larger workforce deficiencies if future hospitalists (i.e., current residents) shy away from the field because they see academic hospitalists devalued as unpromotable resident extenders and academic second-class citizens.
Speaking of workforce shortages, I learned that several highly respect leaders in hospital medicine believe this to be one of the most significant factors threatening the field. In a plenary panel discussion, Drs. Ron Greeno, John Nelson, Mike Guthrie, and John Laverty, commented that overcoming the current and future hospitalist shortage requires rethinking the current model. Dr. Greeno highlighted the need to build more efficient care models whereby hospitalists could see more patients in the same time by reducing the high levels of busy work and administrative minutiae.
Other ideas centered on the development of midlevel provider hospitalists and limiting our scope of practice. To the latter point, there was a lively debate about just how much of the traditionally “non-medical” piece of the pie hospitalists should bite off. Eric Siegal, MD, tackled this issue in a later session challenging hospitalist groups to rethink the value of further expanding the co-management model to more surgical patients while we struggle to care for the patients for whom we currently care.
I learned that Drs. Nelson and Win Whitcomb, co-founders of SHM, showed tremendous vision in their founding of this society. I had the chance to have lunch with John, and I asked him if he ever imagined that the tiny group he brought together in San Diego 11 years ago would ever grow to this—20,000 hospitalists, 6,000 SHM members, an annual meeting with 1,600 people, and a hospitalist (Russell Holman, MD, past president of SHM) seated at the table of the most influential healthcare policy meetings in Washington, D.C.
Rather than being awestruck by the development of this field and SHM, he simply noted this is exactly what he and Win foresaw more than a decade ago; this is the reason they founded SHM. That’s the kind of vision that explains why the field of hospital medicine is the fastest-growing medical specialty.
I learned that the future of hospital medicine is being defined today. Nearly 200 posters were presented at the Research, Innovations and Clinical Vignettes (RIV) Competition. When we look back 10 years from now, we will see a mature field and wonder how we got there so quickly.
That future is being constructed today by folks like Ken Epstein, MD, who presented fascinating data on the effects of fragmentation of hospitalist care, and Param Dedhia, MD, who showed that a formalized discharge toolkit could reduce emergency visits and hospital readmissions in elderly patients.
Finally, while I was away in the city named after a saint, I learned that my wife, too, is a saint. Unable to travel with me, she was landlocked in Denver with our 6-month-old son. I, like many attendees, acknowledge the families who sacrificed so their loved ones could attend the meeting. While I was socializing, learning, networking, and teaching a session, my wife was home soothing tears, changing diapers, cleaning chinfuls of cereal, and answering 3 a.m. wakeup calls. On behalf of all attendees I say thanks to all the saints who enabled us to be away charting the course of hospital medicine at Hospital Medicine 2008. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
MySpace For Hospitalists

As I stared down the length of a limp, moderately deflated breakfast burrito, my thoughts meandered. I doubted about the ability of my little chylomicron-infused buddy to dust the cobwebs from a night in the Gaslamp Quarter that overemphasized wine and underemphasized sleep. I pondered the merit of showing up at 6:30 in the morning for this meeting.
I was shaken from my musings by a voice introducing himself as Bob Wachter. Clearly this apparition parading as one of the luminaries of the hospital medicine movement must be another manifestation of a night of overabundant revelry—and not my adviser for this SHM mentorship breakfast.
It turns out it was the real Dr. Wachter, and indeed he was there to provide an hour and a half of his undivided attention to mentor me as an early-career academic hospitalist. The year was 2003, the location San Diego, the event the sixth SHM Annual Meeting. The significance: This was my first SHM meeting.
Descending on San Diego five years later, I’ve had the chance to reflect on my growth as a hospitalist and the enzymatic role the society’s annual meeting has played in my development.
At the time I had been an academic hospitalist at the Denver Veterans Affairs Medical Center for three years. I’d come to San Diego to learn more about this group that was—until a name change announced at this meeting—calling itself the NAIP, or the National Association of Inpatient Physicians. I also came to present, for the first time, a research abstract.
The annual meeting represents many things to many people. For some it is a time to expand their clinical horizons. Indeed, the clinical content is top-notch and ensures that attendees stay current. The meeting also offers opportunities to learn a new skill such as how to build a hospital medicine program, become a top-notch educator, or develop procedural skills.
Others look to the meeting to present their research data to their peers. Still others attend to get away from the grind of their daily job and bathe in the rejuvenating energy of the annual meeting. Some even look to the meeting location as a vehicle to visit distant family or explore a new or favorite city.
I came to my first annual meeting to sample many of these offerings. What I found was something unexpected and powerful—a professional and social network.
This brings me back to my encounter with Bob. I had seen him speak the day prior at the “Building and Improving Hospitalist Programs” pre-course. Bob gave a rousing and edifying discourse about documenting the value of your hospitalist group. Our early morning gathering was part of the SHM mentorship breakfast, where an early-career hospitalist is paired with a more senior hospitalist in his/her area of interest for career counseling.
Meeting the man who coined the word “hospitalist” was, needless to say, a little nerve-wracking. However, Bob was disarming, engaging, and truly interested in helping me advance. We talked about the development of a hospitalist group at the University of Colorado, a new group I was to direct in three short months. Subsequent to our meeting, Bob was instrumental in helping me develop our group’s business plan, connecting frequently via e-mail and phone.
Later that morning as I was setting up my abstract poster, I looked up to find one of my medical school colleagues, Thomas McIlriath, perusing the aisles of posters.
Thomas, who directs the Mercy Medical Group’s hospitalist program in Sacramento, and I had been good friends in medical school but found our friendship sidetracked by the grind of residency training at different institutions. I had not seen or heard from him in seven years. I later stumbled upon another medical school colleague and quite enjoyed the opportunity to reconnect with such important figures from my past.
Over lunch I attended my first SHM research committee meeting. Not knowing what to expect, I found a group of early-career hospitalists interested in developing academic careers and a burgeoning SHM research infrastructure. I also met Andy Auerbach, MD, at the time a slightly younger but no less talented clinician-researcher at the University of California, San Francisco. Over the years I’ve had the chance to get to know Andy much better and have found him an inspiration, a collaborator, and an enjoyable person to reconnect with whenever serendipity offers us the chance.
Toward the end of the first day’s sessions I attended an innovations workshop that featured a presentation of an online billing tool I thought might be the answer to a research question that I had. Unbeknownst to me the presenter was Eric Siegal, MD, who had graduated from my residency the year before I started and had been a passing acquaintance.
In the end, the presentation was not the answer to my question. But connecting with Eric, now a regional director at Cogent Healthcare, was not only pleasurable but has led to a burgeoning professional bond and personal friendship that has resulted in a couple of co-written publications, hikes through the mountains of Montana, and too numerous to count phone calls seeking professional advice.
That evening I presented my data to my peers at the abstract session and found the feedback to be interesting and enlightening. I also found it another opportunity to discover like-minded people with common interests.
One of them was Ken Epstein, MD, with IPC-The Hospitalist Company. It turned out that Ken had access to data that could answer the research question that had brought me to the innovations session earlier in the day.
Since this encounter, Ken and I have published the answer to our research question and formed a friendship and collaboration that continues to grow today.
While I didn’t recognize it at the time, that span of 24 hours in early April 2003 was arguably the most important and productive day of my working career. I reconnected with old friends, developed new professional acquaintances, and, most important, forged several new and lasting friendships.
As I ready myself for another annual meeting in San Diego I excitedly ponder the opportunities that await me—not least of which is another go in the Gaslamp Quarter! TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
As I stared down the length of a limp, moderately deflated breakfast burrito, my thoughts meandered. I doubted about the ability of my little chylomicron-infused buddy to dust the cobwebs from a night in the Gaslamp Quarter that overemphasized wine and underemphasized sleep. I pondered the merit of showing up at 6:30 in the morning for this meeting.
I was shaken from my musings by a voice introducing himself as Bob Wachter. Clearly this apparition parading as one of the luminaries of the hospital medicine movement must be another manifestation of a night of overabundant revelry—and not my adviser for this SHM mentorship breakfast.
It turns out it was the real Dr. Wachter, and indeed he was there to provide an hour and a half of his undivided attention to mentor me as an early-career academic hospitalist. The year was 2003, the location San Diego, the event the sixth SHM Annual Meeting. The significance: This was my first SHM meeting.
Descending on San Diego five years later, I’ve had the chance to reflect on my growth as a hospitalist and the enzymatic role the society’s annual meeting has played in my development.
At the time I had been an academic hospitalist at the Denver Veterans Affairs Medical Center for three years. I’d come to San Diego to learn more about this group that was—until a name change announced at this meeting—calling itself the NAIP, or the National Association of Inpatient Physicians. I also came to present, for the first time, a research abstract.
The annual meeting represents many things to many people. For some it is a time to expand their clinical horizons. Indeed, the clinical content is top-notch and ensures that attendees stay current. The meeting also offers opportunities to learn a new skill such as how to build a hospital medicine program, become a top-notch educator, or develop procedural skills.
Others look to the meeting to present their research data to their peers. Still others attend to get away from the grind of their daily job and bathe in the rejuvenating energy of the annual meeting. Some even look to the meeting location as a vehicle to visit distant family or explore a new or favorite city.
I came to my first annual meeting to sample many of these offerings. What I found was something unexpected and powerful—a professional and social network.
This brings me back to my encounter with Bob. I had seen him speak the day prior at the “Building and Improving Hospitalist Programs” pre-course. Bob gave a rousing and edifying discourse about documenting the value of your hospitalist group. Our early morning gathering was part of the SHM mentorship breakfast, where an early-career hospitalist is paired with a more senior hospitalist in his/her area of interest for career counseling.
Meeting the man who coined the word “hospitalist” was, needless to say, a little nerve-wracking. However, Bob was disarming, engaging, and truly interested in helping me advance. We talked about the development of a hospitalist group at the University of Colorado, a new group I was to direct in three short months. Subsequent to our meeting, Bob was instrumental in helping me develop our group’s business plan, connecting frequently via e-mail and phone.
Later that morning as I was setting up my abstract poster, I looked up to find one of my medical school colleagues, Thomas McIlriath, perusing the aisles of posters.
Thomas, who directs the Mercy Medical Group’s hospitalist program in Sacramento, and I had been good friends in medical school but found our friendship sidetracked by the grind of residency training at different institutions. I had not seen or heard from him in seven years. I later stumbled upon another medical school colleague and quite enjoyed the opportunity to reconnect with such important figures from my past.
Over lunch I attended my first SHM research committee meeting. Not knowing what to expect, I found a group of early-career hospitalists interested in developing academic careers and a burgeoning SHM research infrastructure. I also met Andy Auerbach, MD, at the time a slightly younger but no less talented clinician-researcher at the University of California, San Francisco. Over the years I’ve had the chance to get to know Andy much better and have found him an inspiration, a collaborator, and an enjoyable person to reconnect with whenever serendipity offers us the chance.
Toward the end of the first day’s sessions I attended an innovations workshop that featured a presentation of an online billing tool I thought might be the answer to a research question that I had. Unbeknownst to me the presenter was Eric Siegal, MD, who had graduated from my residency the year before I started and had been a passing acquaintance.
In the end, the presentation was not the answer to my question. But connecting with Eric, now a regional director at Cogent Healthcare, was not only pleasurable but has led to a burgeoning professional bond and personal friendship that has resulted in a couple of co-written publications, hikes through the mountains of Montana, and too numerous to count phone calls seeking professional advice.
That evening I presented my data to my peers at the abstract session and found the feedback to be interesting and enlightening. I also found it another opportunity to discover like-minded people with common interests.
One of them was Ken Epstein, MD, with IPC-The Hospitalist Company. It turned out that Ken had access to data that could answer the research question that had brought me to the innovations session earlier in the day.
Since this encounter, Ken and I have published the answer to our research question and formed a friendship and collaboration that continues to grow today.
While I didn’t recognize it at the time, that span of 24 hours in early April 2003 was arguably the most important and productive day of my working career. I reconnected with old friends, developed new professional acquaintances, and, most important, forged several new and lasting friendships.
As I ready myself for another annual meeting in San Diego I excitedly ponder the opportunities that await me—not least of which is another go in the Gaslamp Quarter! TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
As I stared down the length of a limp, moderately deflated breakfast burrito, my thoughts meandered. I doubted about the ability of my little chylomicron-infused buddy to dust the cobwebs from a night in the Gaslamp Quarter that overemphasized wine and underemphasized sleep. I pondered the merit of showing up at 6:30 in the morning for this meeting.
I was shaken from my musings by a voice introducing himself as Bob Wachter. Clearly this apparition parading as one of the luminaries of the hospital medicine movement must be another manifestation of a night of overabundant revelry—and not my adviser for this SHM mentorship breakfast.
It turns out it was the real Dr. Wachter, and indeed he was there to provide an hour and a half of his undivided attention to mentor me as an early-career academic hospitalist. The year was 2003, the location San Diego, the event the sixth SHM Annual Meeting. The significance: This was my first SHM meeting.
Descending on San Diego five years later, I’ve had the chance to reflect on my growth as a hospitalist and the enzymatic role the society’s annual meeting has played in my development.
At the time I had been an academic hospitalist at the Denver Veterans Affairs Medical Center for three years. I’d come to San Diego to learn more about this group that was—until a name change announced at this meeting—calling itself the NAIP, or the National Association of Inpatient Physicians. I also came to present, for the first time, a research abstract.
The annual meeting represents many things to many people. For some it is a time to expand their clinical horizons. Indeed, the clinical content is top-notch and ensures that attendees stay current. The meeting also offers opportunities to learn a new skill such as how to build a hospital medicine program, become a top-notch educator, or develop procedural skills.
Others look to the meeting to present their research data to their peers. Still others attend to get away from the grind of their daily job and bathe in the rejuvenating energy of the annual meeting. Some even look to the meeting location as a vehicle to visit distant family or explore a new or favorite city.
I came to my first annual meeting to sample many of these offerings. What I found was something unexpected and powerful—a professional and social network.
This brings me back to my encounter with Bob. I had seen him speak the day prior at the “Building and Improving Hospitalist Programs” pre-course. Bob gave a rousing and edifying discourse about documenting the value of your hospitalist group. Our early morning gathering was part of the SHM mentorship breakfast, where an early-career hospitalist is paired with a more senior hospitalist in his/her area of interest for career counseling.
Meeting the man who coined the word “hospitalist” was, needless to say, a little nerve-wracking. However, Bob was disarming, engaging, and truly interested in helping me advance. We talked about the development of a hospitalist group at the University of Colorado, a new group I was to direct in three short months. Subsequent to our meeting, Bob was instrumental in helping me develop our group’s business plan, connecting frequently via e-mail and phone.
Later that morning as I was setting up my abstract poster, I looked up to find one of my medical school colleagues, Thomas McIlriath, perusing the aisles of posters.
Thomas, who directs the Mercy Medical Group’s hospitalist program in Sacramento, and I had been good friends in medical school but found our friendship sidetracked by the grind of residency training at different institutions. I had not seen or heard from him in seven years. I later stumbled upon another medical school colleague and quite enjoyed the opportunity to reconnect with such important figures from my past.
Over lunch I attended my first SHM research committee meeting. Not knowing what to expect, I found a group of early-career hospitalists interested in developing academic careers and a burgeoning SHM research infrastructure. I also met Andy Auerbach, MD, at the time a slightly younger but no less talented clinician-researcher at the University of California, San Francisco. Over the years I’ve had the chance to get to know Andy much better and have found him an inspiration, a collaborator, and an enjoyable person to reconnect with whenever serendipity offers us the chance.
Toward the end of the first day’s sessions I attended an innovations workshop that featured a presentation of an online billing tool I thought might be the answer to a research question that I had. Unbeknownst to me the presenter was Eric Siegal, MD, who had graduated from my residency the year before I started and had been a passing acquaintance.
In the end, the presentation was not the answer to my question. But connecting with Eric, now a regional director at Cogent Healthcare, was not only pleasurable but has led to a burgeoning professional bond and personal friendship that has resulted in a couple of co-written publications, hikes through the mountains of Montana, and too numerous to count phone calls seeking professional advice.
That evening I presented my data to my peers at the abstract session and found the feedback to be interesting and enlightening. I also found it another opportunity to discover like-minded people with common interests.
One of them was Ken Epstein, MD, with IPC-The Hospitalist Company. It turned out that Ken had access to data that could answer the research question that had brought me to the innovations session earlier in the day.
Since this encounter, Ken and I have published the answer to our research question and formed a friendship and collaboration that continues to grow today.
While I didn’t recognize it at the time, that span of 24 hours in early April 2003 was arguably the most important and productive day of my working career. I reconnected with old friends, developed new professional acquaintances, and, most important, forged several new and lasting friendships.
As I ready myself for another annual meeting in San Diego I excitedly ponder the opportunities that await me—not least of which is another go in the Gaslamp Quarter! TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Lessons of the Deposed

Recently I served as an expert witness in two cases; in each a hospitalist was being sued. While I can’t share details of these confidential cases, I can share my insights using a couple of hypothetical cases that illustrate the key lessons I learned:
- A 75-year-old woman was admitted by orthopedics after a fall requiring hip fracture repair. A hospitalist automatically saw her per the standing agreement. The hospitalist adjusted her diabetes regimen and held her aspirin because of bleeding. On the evening prior to discharge she developed right lower-extremity pain. The on-call orthopedist ordered a lower-extremity ultrasound from home.
The patient felt better the next morning and was discharged with hospitalist recommendations to increase her basal insulin, restart her aspirin, and follow up with her primary care provider (PCP). Three days later the patient presented in respiratory extremis and died in the emergency department. Post-mortem chart review noted a sonographic venous thrombosis in the right femoral vein that went unnoticed during her hospital stay.
- A 58-year-old woman was admitted after an uncomplicated appendectomy. On post-op day two, the surgeon asked the hospitalist to see the patient for a depressed mood. The hospitalist recommended starting an antidepressant and following up with her PCP after discharge. She also noted that the patient had right lower-extremity pain and swelling and recommended an ultrasound for workup of a deep venous thrombosis (DVT). The hospitalist did not see the patient again, and the ultrasound was not completed. Two days after discharge, the patient died at home after complaining of chest pain. Post-mortem autopsy revealed massive pulmonary embolism.
Two difficult cases, indeed. And I learned plenty from them:
Lesson one: Most lawsuits do not stem from deficiencies of medical knowledge.
In both cases, the hospitalists’ clinical reasoning was sound. In the first he was unaware of the patient’s overnight symptoms, which were not documented in the chart because the patient was not seen by the on-call orthopedist—a major systems error and lack of professionalism. This was compounded by a system that did not alert providers that an ultrasound was ordered or read as abnormal.
In the second case, the hospitalist got it right and made the correct recommendation—but the surgeon didn’t follow through.
Lesson two: Clarify your role—consultant or co-manager.
The differences between consultant and co-manager are subtle but crucial.
A consult is a request to answer a specific question: “Is this patient depressed, and how would you manage this problem?” This results in a detailed, focused appraisal of that issue, culminating in a note listing recommendations for further evaluation and management. It is the primary team’s responsibility to follow up on recommendations as they deem appropriate.
With this decision-making capacity, the primary team accepts near-full clinical and medical legal responsibility. As long as the consultant does due diligence and makes sound recommendations, it is unlikely he/she will be successfully sued for a bad outcome if the recommendations are not followed.
However, the hospitalist movement has changed this landscape considerably. We often function in a co-management model with our consulting colleagues, each of us caring for the issues within our respective scope of expertise.
This paradigm demands a level of responsibility sharing and communication that differs significantly from the traditional consultative model.
Knowing which model you are functioning under and who is responsible for which problems can be tricky. In the first case, who owned the decision-making for the patient’s DVT work-up?
The orthopedist may assume his role is focused on the care of the hip fracture surgery, while all else is the hospitalist’s purview. The hospitalist may assume DVT is a complication of the hip fracture surgery and is the orthopedist’s responsibility.
The second case seems easier as the hospitalist was clearly functioning as a consultant and therefore his obligation ends with his recommendation to further evaluate for DVT.
Or does it?
Lesson three: Communication is imperative.
The role we are functioning in—consultant versus co-manager—is not always intuitive. This perplexity can be further exacerbated by poor communication.
In both cases the hospitalists’ role was not established up front. Further, the hospitalists and their colleagues never spoke directly about the case or the management decisions.
In the second case the surgeon saw the recommendation but presumed the hospitalist would write the order for the ultrasound because they were co-managing the patient. He argued that he is not expert in the care of DVT and could not determine if the recommendation was sound. He assumed the hospitalist would appropriately evaluate this situation and complete the work-up if warranted. Because the hospitalist did not, the surgeon assumed the hospitalist was no longer concerned about DVT.
The hospitalist countered that she was specifically consulted to answer a question about depression. The recommendations regarding the swollen calf were also done in a consultative fashion, and the decision to obtain the ultrasound would fall to the surgeon.
The hospitalist argued that because the surgeon did not consult her again for this specific issue, she assumed he was comfortable evaluating and managing DVT.
This foray into the legal system reminded me that our patients trust we will give them the best care. When system and communication inadequacies get in the way of this, we can get sued—but our patients can lose their lives. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Recently I served as an expert witness in two cases; in each a hospitalist was being sued. While I can’t share details of these confidential cases, I can share my insights using a couple of hypothetical cases that illustrate the key lessons I learned:
- A 75-year-old woman was admitted by orthopedics after a fall requiring hip fracture repair. A hospitalist automatically saw her per the standing agreement. The hospitalist adjusted her diabetes regimen and held her aspirin because of bleeding. On the evening prior to discharge she developed right lower-extremity pain. The on-call orthopedist ordered a lower-extremity ultrasound from home.
The patient felt better the next morning and was discharged with hospitalist recommendations to increase her basal insulin, restart her aspirin, and follow up with her primary care provider (PCP). Three days later the patient presented in respiratory extremis and died in the emergency department. Post-mortem chart review noted a sonographic venous thrombosis in the right femoral vein that went unnoticed during her hospital stay.
- A 58-year-old woman was admitted after an uncomplicated appendectomy. On post-op day two, the surgeon asked the hospitalist to see the patient for a depressed mood. The hospitalist recommended starting an antidepressant and following up with her PCP after discharge. She also noted that the patient had right lower-extremity pain and swelling and recommended an ultrasound for workup of a deep venous thrombosis (DVT). The hospitalist did not see the patient again, and the ultrasound was not completed. Two days after discharge, the patient died at home after complaining of chest pain. Post-mortem autopsy revealed massive pulmonary embolism.
Two difficult cases, indeed. And I learned plenty from them:
Lesson one: Most lawsuits do not stem from deficiencies of medical knowledge.
In both cases, the hospitalists’ clinical reasoning was sound. In the first he was unaware of the patient’s overnight symptoms, which were not documented in the chart because the patient was not seen by the on-call orthopedist—a major systems error and lack of professionalism. This was compounded by a system that did not alert providers that an ultrasound was ordered or read as abnormal.
In the second case, the hospitalist got it right and made the correct recommendation—but the surgeon didn’t follow through.
Lesson two: Clarify your role—consultant or co-manager.
The differences between consultant and co-manager are subtle but crucial.
A consult is a request to answer a specific question: “Is this patient depressed, and how would you manage this problem?” This results in a detailed, focused appraisal of that issue, culminating in a note listing recommendations for further evaluation and management. It is the primary team’s responsibility to follow up on recommendations as they deem appropriate.
With this decision-making capacity, the primary team accepts near-full clinical and medical legal responsibility. As long as the consultant does due diligence and makes sound recommendations, it is unlikely he/she will be successfully sued for a bad outcome if the recommendations are not followed.
However, the hospitalist movement has changed this landscape considerably. We often function in a co-management model with our consulting colleagues, each of us caring for the issues within our respective scope of expertise.
This paradigm demands a level of responsibility sharing and communication that differs significantly from the traditional consultative model.
Knowing which model you are functioning under and who is responsible for which problems can be tricky. In the first case, who owned the decision-making for the patient’s DVT work-up?
The orthopedist may assume his role is focused on the care of the hip fracture surgery, while all else is the hospitalist’s purview. The hospitalist may assume DVT is a complication of the hip fracture surgery and is the orthopedist’s responsibility.
The second case seems easier as the hospitalist was clearly functioning as a consultant and therefore his obligation ends with his recommendation to further evaluate for DVT.
Or does it?
Lesson three: Communication is imperative.
The role we are functioning in—consultant versus co-manager—is not always intuitive. This perplexity can be further exacerbated by poor communication.
In both cases the hospitalists’ role was not established up front. Further, the hospitalists and their colleagues never spoke directly about the case or the management decisions.
In the second case the surgeon saw the recommendation but presumed the hospitalist would write the order for the ultrasound because they were co-managing the patient. He argued that he is not expert in the care of DVT and could not determine if the recommendation was sound. He assumed the hospitalist would appropriately evaluate this situation and complete the work-up if warranted. Because the hospitalist did not, the surgeon assumed the hospitalist was no longer concerned about DVT.
The hospitalist countered that she was specifically consulted to answer a question about depression. The recommendations regarding the swollen calf were also done in a consultative fashion, and the decision to obtain the ultrasound would fall to the surgeon.
The hospitalist argued that because the surgeon did not consult her again for this specific issue, she assumed he was comfortable evaluating and managing DVT.
This foray into the legal system reminded me that our patients trust we will give them the best care. When system and communication inadequacies get in the way of this, we can get sued—but our patients can lose their lives. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Recently I served as an expert witness in two cases; in each a hospitalist was being sued. While I can’t share details of these confidential cases, I can share my insights using a couple of hypothetical cases that illustrate the key lessons I learned:
- A 75-year-old woman was admitted by orthopedics after a fall requiring hip fracture repair. A hospitalist automatically saw her per the standing agreement. The hospitalist adjusted her diabetes regimen and held her aspirin because of bleeding. On the evening prior to discharge she developed right lower-extremity pain. The on-call orthopedist ordered a lower-extremity ultrasound from home.
The patient felt better the next morning and was discharged with hospitalist recommendations to increase her basal insulin, restart her aspirin, and follow up with her primary care provider (PCP). Three days later the patient presented in respiratory extremis and died in the emergency department. Post-mortem chart review noted a sonographic venous thrombosis in the right femoral vein that went unnoticed during her hospital stay.
- A 58-year-old woman was admitted after an uncomplicated appendectomy. On post-op day two, the surgeon asked the hospitalist to see the patient for a depressed mood. The hospitalist recommended starting an antidepressant and following up with her PCP after discharge. She also noted that the patient had right lower-extremity pain and swelling and recommended an ultrasound for workup of a deep venous thrombosis (DVT). The hospitalist did not see the patient again, and the ultrasound was not completed. Two days after discharge, the patient died at home after complaining of chest pain. Post-mortem autopsy revealed massive pulmonary embolism.
Two difficult cases, indeed. And I learned plenty from them:
Lesson one: Most lawsuits do not stem from deficiencies of medical knowledge.
In both cases, the hospitalists’ clinical reasoning was sound. In the first he was unaware of the patient’s overnight symptoms, which were not documented in the chart because the patient was not seen by the on-call orthopedist—a major systems error and lack of professionalism. This was compounded by a system that did not alert providers that an ultrasound was ordered or read as abnormal.
In the second case, the hospitalist got it right and made the correct recommendation—but the surgeon didn’t follow through.
Lesson two: Clarify your role—consultant or co-manager.
The differences between consultant and co-manager are subtle but crucial.
A consult is a request to answer a specific question: “Is this patient depressed, and how would you manage this problem?” This results in a detailed, focused appraisal of that issue, culminating in a note listing recommendations for further evaluation and management. It is the primary team’s responsibility to follow up on recommendations as they deem appropriate.
With this decision-making capacity, the primary team accepts near-full clinical and medical legal responsibility. As long as the consultant does due diligence and makes sound recommendations, it is unlikely he/she will be successfully sued for a bad outcome if the recommendations are not followed.
However, the hospitalist movement has changed this landscape considerably. We often function in a co-management model with our consulting colleagues, each of us caring for the issues within our respective scope of expertise.
This paradigm demands a level of responsibility sharing and communication that differs significantly from the traditional consultative model.
Knowing which model you are functioning under and who is responsible for which problems can be tricky. In the first case, who owned the decision-making for the patient’s DVT work-up?
The orthopedist may assume his role is focused on the care of the hip fracture surgery, while all else is the hospitalist’s purview. The hospitalist may assume DVT is a complication of the hip fracture surgery and is the orthopedist’s responsibility.
The second case seems easier as the hospitalist was clearly functioning as a consultant and therefore his obligation ends with his recommendation to further evaluate for DVT.
Or does it?
Lesson three: Communication is imperative.
The role we are functioning in—consultant versus co-manager—is not always intuitive. This perplexity can be further exacerbated by poor communication.
In both cases the hospitalists’ role was not established up front. Further, the hospitalists and their colleagues never spoke directly about the case or the management decisions.
In the second case the surgeon saw the recommendation but presumed the hospitalist would write the order for the ultrasound because they were co-managing the patient. He argued that he is not expert in the care of DVT and could not determine if the recommendation was sound. He assumed the hospitalist would appropriately evaluate this situation and complete the work-up if warranted. Because the hospitalist did not, the surgeon assumed the hospitalist was no longer concerned about DVT.
The hospitalist countered that she was specifically consulted to answer a question about depression. The recommendations regarding the swollen calf were also done in a consultative fashion, and the decision to obtain the ultrasound would fall to the surgeon.
The hospitalist argued that because the surgeon did not consult her again for this specific issue, she assumed he was comfortable evaluating and managing DVT.
This foray into the legal system reminded me that our patients trust we will give them the best care. When system and communication inadequacies get in the way of this, we can get sued—but our patients can lose their lives. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Exceed Acceptable

Armed with a cup of coffee, with my dogs walked and fed and the sun rising into view, I eased into my home office chair and contentedly folded open the pages of The Wall Street Journal.
My ritual early-morning glance at the local and national papers usually provides little more than a glum outlook for my favorite sports teams, a glummer view of my financial investments, and a few seeds to cultivate into elevator small talk.
This morning, however, I was struck by this headline: “‘Hospitalists’ Are Seen as Help.”1 I happily noted the subheading, which referred to us as “specialists.” I reveled in the general tone of the article, which indicated that we reduce hospital length of stay and costs.
The article reported the findings of a New England Journal of Medicine paper by Lindenauer, et al., that showed a 0.4-day reduction in length of stay (LOS) and a net savings of $268 per patient compared with non-hospitalist general internist providers.2 Good news for the field, indeed.
Or was it? What was not highlighted in The Wall Street Journal was that while hospitalists also reduced LOS 0.4 days versus non-hospitalist family physicians, there was no statistically significant reduction in cost versus this cohort. Further, there was no difference in hospital mortality or 14-day readmission rate versus either non-hospitalist set of providers.
While not the greatest markers of quality, mortality and readmission rate are two of the easiest and most recognized markers of effective care. Dr. Lindenauer’s paper found no benefit from the hospitalist model.
Granted, other studies have shown a benefit of the hospitalist model in areas such as co-management of orthopedic patients. But these effects were modest and primarily limited to process measures, not quality-of-care outcomes.
Another recent paper by Auerbach, et al., reported that general medical consultation by hospitalists on surgical patients did not result in better glycemic control, use of perioperative beta blockade, or venous thromboembolism prophylaxis versus surgical care alone.
In a healthcare system that the Institute of Medicine claims is responsible for unfathomable rates of medication errors and upward of 100,000 avoidable inpatient deaths every year, it sounds as though hospitalists are missing the chance to fulfill their promise.
The promise of the hospital medicine movement is that hospitalists will do it better: cheaper, faster, and safer. If we accept this, then these new data appear to paint a picture of a movement that is chugging off course.
I don’t think it’s that simple. Rather, this speaks to two key elements in the maturation process of the hospitalist field.
First, changing the fundamentals of healthcare delivery is difficult work. This is especially true for a young group of providers, who struggle with overwhelming growth, constant understaffing, and a business model that favors patient encounters over process improvement.
On top of this, we are asked to change behavior in a complex system where instituting change often involves altering the practice of others outside your group, such as nurses or other physician groups.
Add to this significant undertraining in patient safety and process improvement, and a lack of time for quality improvement work or rewards to encourage it.
It’s little wonder we haven’t moved the quality needle much. Viewed through this lens, the fact that we have accomplished even modest improvements is impressive.
Second, we need to do a better job of measuring our benefit. Mortality and readmission are important outcomes, and we should always aim to improve these quality indicators. However, they’re both downstream markers that are easy to measure but difficult to budge.
We must acknowledge, however, that we haven’t done a good job of measuring our effect on the value-added aspects of hospital medicine: nursing happiness, hospital leadership, team work, staff education, patient satisfaction, protocol development, and our willingness to take on work others are not keen to do, such as unassigned emergency department call.
How do we put a price on the value of being available for a patient in extremis, a nurse with a question, a committee chairpersonship? How do we measure the downstream benefit of offloading our surgical and medical subspecialty colleagues so they can perform more procedures while we care for their recently proceduralized patients?
This is difficult material to measure, especially in a scientific manner. In this regard, it is incumbent on local leaders to ensure these data are collected and available for presentation to those who subsidize our practices.
Short of this, groups are exposed to a serious threat from a hospital chief financial officer armed with a directive to cut costs and the Dec. 20 edition of The Wall Street Journal.
Hospital medicine is a work in progress. We need to do a better job of measuring our value-added benefits. However, we should strive to exceed what is acceptable. While it is reasonable to accept little documented improvement in quality indicators today, it should not be acceptable in the near future.
The field will need to move toward improving, documenting, and rewarding improvements in clinical outcomes. This means elemental change toward developing practice standards and models of care for common disease states, standardizing care throughout the hospital and actively engaging in improving quality at every turn.
Hospitalists will need to agree to be measured, participate in measurement, and be held accountable for achieving quality benchmarks.
This transformation necessitates that hospitalist educators (both residency and post-residency) better prepare hospitalists to lead change in areas of quality improvement.
These educators must impart the basic tenets of change management, process improvement, and patient safety.
These changes will take provider time—time that will need to be supported by hospitals and group leaders in the form of accepting less revenue per provider, which will in turn require inspired leadership to negotiate this time and build a new sustainable business model centered around quality.
As the field matures it is becoming clearer that our business can no longer be predicated on cost savings and efficiency alone.
While we need to be ever mindful of these metrics, we need to evolve beyond this model to one with quality at its core.
We should expect and reward superior patient outcomes at the expense of quantity. Anything short of this squanders one of the purest opportunities to positively affect the U.S. healthcare system for generations to come. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Levitz J. Hospitalists are seen as help. The Wall Street Journal. Dec. 20, 2007:D7.
- Lindenauer PK, Rothberg MB, Pekow PS, Kenwood C, Benjamin EM, Auerbach AD et al. Outcomes of care by hospitalists, general internists, and family physicians. N Engl J Med. 2007 Dec 20; 357(25):2589-2600.
- Auerbach AD, Rasic MA, Sehgal N, Ide B, Stone B, Maselli Jet al. Opportunity missed: medical consultation, resource use, and quality of care of patients undergoing major surgery. Arch Intern Med. 2007 Nov. 26;167(21): 2338-2344.
Armed with a cup of coffee, with my dogs walked and fed and the sun rising into view, I eased into my home office chair and contentedly folded open the pages of The Wall Street Journal.
My ritual early-morning glance at the local and national papers usually provides little more than a glum outlook for my favorite sports teams, a glummer view of my financial investments, and a few seeds to cultivate into elevator small talk.
This morning, however, I was struck by this headline: “‘Hospitalists’ Are Seen as Help.”1 I happily noted the subheading, which referred to us as “specialists.” I reveled in the general tone of the article, which indicated that we reduce hospital length of stay and costs.
The article reported the findings of a New England Journal of Medicine paper by Lindenauer, et al., that showed a 0.4-day reduction in length of stay (LOS) and a net savings of $268 per patient compared with non-hospitalist general internist providers.2 Good news for the field, indeed.
Or was it? What was not highlighted in The Wall Street Journal was that while hospitalists also reduced LOS 0.4 days versus non-hospitalist family physicians, there was no statistically significant reduction in cost versus this cohort. Further, there was no difference in hospital mortality or 14-day readmission rate versus either non-hospitalist set of providers.
While not the greatest markers of quality, mortality and readmission rate are two of the easiest and most recognized markers of effective care. Dr. Lindenauer’s paper found no benefit from the hospitalist model.
Granted, other studies have shown a benefit of the hospitalist model in areas such as co-management of orthopedic patients. But these effects were modest and primarily limited to process measures, not quality-of-care outcomes.
Another recent paper by Auerbach, et al., reported that general medical consultation by hospitalists on surgical patients did not result in better glycemic control, use of perioperative beta blockade, or venous thromboembolism prophylaxis versus surgical care alone.
In a healthcare system that the Institute of Medicine claims is responsible for unfathomable rates of medication errors and upward of 100,000 avoidable inpatient deaths every year, it sounds as though hospitalists are missing the chance to fulfill their promise.
The promise of the hospital medicine movement is that hospitalists will do it better: cheaper, faster, and safer. If we accept this, then these new data appear to paint a picture of a movement that is chugging off course.
I don’t think it’s that simple. Rather, this speaks to two key elements in the maturation process of the hospitalist field.
First, changing the fundamentals of healthcare delivery is difficult work. This is especially true for a young group of providers, who struggle with overwhelming growth, constant understaffing, and a business model that favors patient encounters over process improvement.
On top of this, we are asked to change behavior in a complex system where instituting change often involves altering the practice of others outside your group, such as nurses or other physician groups.
Add to this significant undertraining in patient safety and process improvement, and a lack of time for quality improvement work or rewards to encourage it.
It’s little wonder we haven’t moved the quality needle much. Viewed through this lens, the fact that we have accomplished even modest improvements is impressive.
Second, we need to do a better job of measuring our benefit. Mortality and readmission are important outcomes, and we should always aim to improve these quality indicators. However, they’re both downstream markers that are easy to measure but difficult to budge.
We must acknowledge, however, that we haven’t done a good job of measuring our effect on the value-added aspects of hospital medicine: nursing happiness, hospital leadership, team work, staff education, patient satisfaction, protocol development, and our willingness to take on work others are not keen to do, such as unassigned emergency department call.
How do we put a price on the value of being available for a patient in extremis, a nurse with a question, a committee chairpersonship? How do we measure the downstream benefit of offloading our surgical and medical subspecialty colleagues so they can perform more procedures while we care for their recently proceduralized patients?
This is difficult material to measure, especially in a scientific manner. In this regard, it is incumbent on local leaders to ensure these data are collected and available for presentation to those who subsidize our practices.
Short of this, groups are exposed to a serious threat from a hospital chief financial officer armed with a directive to cut costs and the Dec. 20 edition of The Wall Street Journal.
Hospital medicine is a work in progress. We need to do a better job of measuring our value-added benefits. However, we should strive to exceed what is acceptable. While it is reasonable to accept little documented improvement in quality indicators today, it should not be acceptable in the near future.
The field will need to move toward improving, documenting, and rewarding improvements in clinical outcomes. This means elemental change toward developing practice standards and models of care for common disease states, standardizing care throughout the hospital and actively engaging in improving quality at every turn.
Hospitalists will need to agree to be measured, participate in measurement, and be held accountable for achieving quality benchmarks.
This transformation necessitates that hospitalist educators (both residency and post-residency) better prepare hospitalists to lead change in areas of quality improvement.
These educators must impart the basic tenets of change management, process improvement, and patient safety.
These changes will take provider time—time that will need to be supported by hospitals and group leaders in the form of accepting less revenue per provider, which will in turn require inspired leadership to negotiate this time and build a new sustainable business model centered around quality.
As the field matures it is becoming clearer that our business can no longer be predicated on cost savings and efficiency alone.
While we need to be ever mindful of these metrics, we need to evolve beyond this model to one with quality at its core.
We should expect and reward superior patient outcomes at the expense of quantity. Anything short of this squanders one of the purest opportunities to positively affect the U.S. healthcare system for generations to come. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Levitz J. Hospitalists are seen as help. The Wall Street Journal. Dec. 20, 2007:D7.
- Lindenauer PK, Rothberg MB, Pekow PS, Kenwood C, Benjamin EM, Auerbach AD et al. Outcomes of care by hospitalists, general internists, and family physicians. N Engl J Med. 2007 Dec 20; 357(25):2589-2600.
- Auerbach AD, Rasic MA, Sehgal N, Ide B, Stone B, Maselli Jet al. Opportunity missed: medical consultation, resource use, and quality of care of patients undergoing major surgery. Arch Intern Med. 2007 Nov. 26;167(21): 2338-2344.
Armed with a cup of coffee, with my dogs walked and fed and the sun rising into view, I eased into my home office chair and contentedly folded open the pages of The Wall Street Journal.
My ritual early-morning glance at the local and national papers usually provides little more than a glum outlook for my favorite sports teams, a glummer view of my financial investments, and a few seeds to cultivate into elevator small talk.
This morning, however, I was struck by this headline: “‘Hospitalists’ Are Seen as Help.”1 I happily noted the subheading, which referred to us as “specialists.” I reveled in the general tone of the article, which indicated that we reduce hospital length of stay and costs.
The article reported the findings of a New England Journal of Medicine paper by Lindenauer, et al., that showed a 0.4-day reduction in length of stay (LOS) and a net savings of $268 per patient compared with non-hospitalist general internist providers.2 Good news for the field, indeed.
Or was it? What was not highlighted in The Wall Street Journal was that while hospitalists also reduced LOS 0.4 days versus non-hospitalist family physicians, there was no statistically significant reduction in cost versus this cohort. Further, there was no difference in hospital mortality or 14-day readmission rate versus either non-hospitalist set of providers.
While not the greatest markers of quality, mortality and readmission rate are two of the easiest and most recognized markers of effective care. Dr. Lindenauer’s paper found no benefit from the hospitalist model.
Granted, other studies have shown a benefit of the hospitalist model in areas such as co-management of orthopedic patients. But these effects were modest and primarily limited to process measures, not quality-of-care outcomes.
Another recent paper by Auerbach, et al., reported that general medical consultation by hospitalists on surgical patients did not result in better glycemic control, use of perioperative beta blockade, or venous thromboembolism prophylaxis versus surgical care alone.
In a healthcare system that the Institute of Medicine claims is responsible for unfathomable rates of medication errors and upward of 100,000 avoidable inpatient deaths every year, it sounds as though hospitalists are missing the chance to fulfill their promise.
The promise of the hospital medicine movement is that hospitalists will do it better: cheaper, faster, and safer. If we accept this, then these new data appear to paint a picture of a movement that is chugging off course.
I don’t think it’s that simple. Rather, this speaks to two key elements in the maturation process of the hospitalist field.
First, changing the fundamentals of healthcare delivery is difficult work. This is especially true for a young group of providers, who struggle with overwhelming growth, constant understaffing, and a business model that favors patient encounters over process improvement.
On top of this, we are asked to change behavior in a complex system where instituting change often involves altering the practice of others outside your group, such as nurses or other physician groups.
Add to this significant undertraining in patient safety and process improvement, and a lack of time for quality improvement work or rewards to encourage it.
It’s little wonder we haven’t moved the quality needle much. Viewed through this lens, the fact that we have accomplished even modest improvements is impressive.
Second, we need to do a better job of measuring our benefit. Mortality and readmission are important outcomes, and we should always aim to improve these quality indicators. However, they’re both downstream markers that are easy to measure but difficult to budge.
We must acknowledge, however, that we haven’t done a good job of measuring our effect on the value-added aspects of hospital medicine: nursing happiness, hospital leadership, team work, staff education, patient satisfaction, protocol development, and our willingness to take on work others are not keen to do, such as unassigned emergency department call.
How do we put a price on the value of being available for a patient in extremis, a nurse with a question, a committee chairpersonship? How do we measure the downstream benefit of offloading our surgical and medical subspecialty colleagues so they can perform more procedures while we care for their recently proceduralized patients?
This is difficult material to measure, especially in a scientific manner. In this regard, it is incumbent on local leaders to ensure these data are collected and available for presentation to those who subsidize our practices.
Short of this, groups are exposed to a serious threat from a hospital chief financial officer armed with a directive to cut costs and the Dec. 20 edition of The Wall Street Journal.
Hospital medicine is a work in progress. We need to do a better job of measuring our value-added benefits. However, we should strive to exceed what is acceptable. While it is reasonable to accept little documented improvement in quality indicators today, it should not be acceptable in the near future.
The field will need to move toward improving, documenting, and rewarding improvements in clinical outcomes. This means elemental change toward developing practice standards and models of care for common disease states, standardizing care throughout the hospital and actively engaging in improving quality at every turn.
Hospitalists will need to agree to be measured, participate in measurement, and be held accountable for achieving quality benchmarks.
This transformation necessitates that hospitalist educators (both residency and post-residency) better prepare hospitalists to lead change in areas of quality improvement.
These educators must impart the basic tenets of change management, process improvement, and patient safety.
These changes will take provider time—time that will need to be supported by hospitals and group leaders in the form of accepting less revenue per provider, which will in turn require inspired leadership to negotiate this time and build a new sustainable business model centered around quality.
As the field matures it is becoming clearer that our business can no longer be predicated on cost savings and efficiency alone.
While we need to be ever mindful of these metrics, we need to evolve beyond this model to one with quality at its core.
We should expect and reward superior patient outcomes at the expense of quantity. Anything short of this squanders one of the purest opportunities to positively affect the U.S. healthcare system for generations to come. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Levitz J. Hospitalists are seen as help. The Wall Street Journal. Dec. 20, 2007:D7.
- Lindenauer PK, Rothberg MB, Pekow PS, Kenwood C, Benjamin EM, Auerbach AD et al. Outcomes of care by hospitalists, general internists, and family physicians. N Engl J Med. 2007 Dec 20; 357(25):2589-2600.
- Auerbach AD, Rasic MA, Sehgal N, Ide B, Stone B, Maselli Jet al. Opportunity missed: medical consultation, resource use, and quality of care of patients undergoing major surgery. Arch Intern Med. 2007 Nov. 26;167(21): 2338-2344.
Fight the Losing Battle

With shirt buttons bulging and my panniculus spilling like the top of an oversized muffin over my belt—which was essentially a tourniquet strangling my lower extremities—I examined my options.
After hours of grazing through the snack food pyramid and consuming significant portions of a dinosaur-size turkey, an acromegalic dollop of dressing, a bog of cranberries, and a field of mashed potatoes, I was faced with the proposition of shoveling in another 500 calories cleverly disguised as a heaping slice of pumpkin pie.
The intensity of the situation was palpable. My in-laws sat mouths agape, stunned by the amount and rate at which I forked thousands of calories into my gullet. They fidgeted as I stared with steely, miotic pupils and furrowed, sweat-beaded brow at my prospective ingestion.
The tension heightened as my lower two shirt buttons gave up the cause, careening across the table and striking, respectively, a deserted bowl of creamed corn and the forehead of a comatose relative who had long ago lost interest in watching my acute food intoxication. As my cousins brokered bets over the likelihood of my impending demise, I sat and deliberated, fork hovering over my sugary prey.
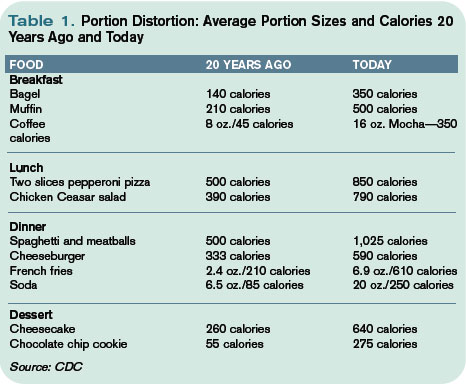
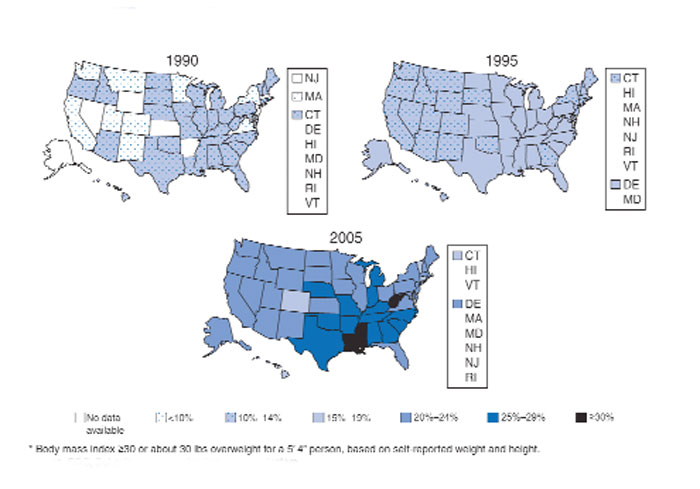
Obesity Epidemic
As healthcare practitioners, we are well aware of the dangers of obesity, yet seem paralyzed to make change. However, hospitalists are perfectly positioned to help patients resolve to lose their weight.
A body mass index (BMI) of 30 or more indicates obesity; its slimmer overweight cousin weighs in with a BMI of 25-29.
Overweight or obese people are at increased risk of osteoarthritis, dyslipidemia, obstructive sleep apnea, hypertension, coronary artery disease, stroke, cancer, and diabetes. Obesity accounts for 300,000 excess deaths per year in the U.S., along with about 10% of all healthcare expenditures, according to the Centers for Disease Control and Prevention (CDC). It affects all ages, races, and professions—including physicians. It is perhaps the most significant health issue facing our nation.
Despite this awareness, we keep getting bigger. In the past 20 years we have seen an epic swelling of American waistlines. In 1990 the CDC reported that among adult residents, 10 states had a prevalence rate of obesity less than 10%, and no states had a rate more than 15% (see Fig. 1, above). By 2006, no state had a prevalence of obesity less than 10%, while only four states clocked in with a rate less than 20%. A whopping 22 states found at least 25% of their inhabitants obese. Since 2005 we’ve become so big the CDC had to create a new category for states with more than 30% of their residents being obese. When the BMI cutoff is dropped to 25 or more, 66% meet of U.S. adults meet this definition for being overweight or obese.
Recent CDC data reveal a glimmer of hope. There was no statistically significant increase in the prevalence of obesity in 2005-2006, compared with 2003-2004. In the earlier time period, 31.1% of men and 33.2% of women were obese, compared with 33.3% of men and 35.3% of women in the most recent time period.
Still, one of every three U.S. adults is obese. That’s 100 million Americans. More than 50% of non-Hispanic black and Mexican-American women age 40-59 are obese. Sixty-one percent of non-Hispanic black women older than 60 are obese.
A complex mix of components, including environment and genetics, determines weight gain. The rapid rate of weight gain in recent years is unlikely to be explained by genetics alone—the population’s genetic composition cannot change that quickly. Thus the bulk of the recent increase in obesity is likely related to cultural and environmental determinants. A 2007 paper by Christakis, et al., found that social networks play a large role in the spread of obesity.1 The study followed 12,067 people for more than 30 years. Those with a friend, sibling, or spouse who became obese over that period were 57%, 40%, and 37% more likely, respectively, to become obese. The authors hypothesize that obesity may become less stigmatized and more tolerable for those surrounded by obese associates. Another theory is that peer groups tend to adopt similar behaviors, such as smoking, eating fast food, and inactivity.
The average person gains about one to two pounds a year.2 When distilled to its simplest form, weight gain occurs anytime calories in exceed calories out—that is, a positive energy balance or gap.
The six weeks from Thanksgiving to New Year’s is an especially vulnerable time for weight gain. In a 2000 study of 195 subjects, the average person gained about one pound during the holiday season. When these subjects were followed up with six months later, there was no statistically significant loss of peri-holiday weight gain. This holiday pound may seem trivial (and keep in mind these subjects gained weight despite being closely watched in a weight-gain study). But this weight appears hard to shed and results in much of the weight gained during adulthood.
However, unlike my Thanksgiving gorging, the hallmark of obesity is the small but frequent positive energy gaps, that is, days of 50 to 100 calories of intake greater than use. Over the course of the year, these small daily caloric gaps are anabolically transformed into pounds.
Resolve to Lose
By now, like me, many of you may have added a holiday pound or two. This may be in addition to a nefarious pound or two added throughout the rest of the year. As you ponder scribing your annual resolutions, consider making weight loss a top priority for your patients and yourself, if appropriate.
Unfortunately no magic bullet will turn your New Year’s resolution into reality, just hard work. The key is to tilt the energy balance toward weight loss by reducing caloric intake and increasing activity. Fortunately this can be done in non-Draconian ways. Just as weight gain can snowball from small daily caloric overdoses, it can be removed the same way. Instead of setting or recommending insurmountable goals to your patients—like reducing intake to 1,000 calories a day or adhering to a triathletic training regimen—the CDC suggests a simpler, more sustainable approach to shedding those pounds, namely tipping your energy balance to a negative 150 calories per day.
A net negative energy balance of 150 calories per day will at worst stabilize your weight (depending on your current energy balance) and at best net five to 10 pounds of weight loss per year. For most this can result from something as simple as switching your daily Coke to a Diet Coke. Even more ground can be gained by reducing portion size. The super-sizing of the American menu over the past 20 years is one of the prime drivers of the obesity epidemic (see Table 1, p. 64). Consider cutting back in small ways. For example, continue to enjoy that gourmet chocolate chip cookie but downsize it to a smaller version and reduce your intake by 150 to 200 calories.
As important as reducing caloric intake is the need for activity. Adding moderate amounts of exercise five days a week can burn an additional 150 calories per day, reducing overall weight by another five to 10 pounds in a year. This can include things like walking for 30 minutes, swimming for 20 minutes, or biking for 15 minutes. More adventurous (dancing for 30 minutes), parental (pushing a stroller for 30 minutes), agricultural (gardening for 30 minutes), or chore-oriented (shoveling 15 minutes) options also help.
Much to the dismay of my cousin Mike, who bet that I’d eat at least half the piece of Thanksgiving pie, I put down my fork. After packing away a winter’s worth of calories I was feeling diaphoretic and pathetic. I wobbled away from the table and began charting my course to redemption. It would begin the next day with an apple instead of a bagel, an extra hour at the gym—and a trip to the cleaners to get those buttons replaced. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Editor’s note: The author’s driver license claims a weight of 165 pounds. Physical evidence, as well as his wife’s report, paints a substantially different picture.
References
- Christakis NA, Fowler JH. The spread of obesity in a large social network over 32 years. N Engl J Med. 2007;357:370-379.
- Yanovksi JA, Yanovski SZ, Sovik KN, et al. A prospective study of holiday weight gain. N Engl J Med. 2000;342:861-867.
With shirt buttons bulging and my panniculus spilling like the top of an oversized muffin over my belt—which was essentially a tourniquet strangling my lower extremities—I examined my options.
After hours of grazing through the snack food pyramid and consuming significant portions of a dinosaur-size turkey, an acromegalic dollop of dressing, a bog of cranberries, and a field of mashed potatoes, I was faced with the proposition of shoveling in another 500 calories cleverly disguised as a heaping slice of pumpkin pie.
The intensity of the situation was palpable. My in-laws sat mouths agape, stunned by the amount and rate at which I forked thousands of calories into my gullet. They fidgeted as I stared with steely, miotic pupils and furrowed, sweat-beaded brow at my prospective ingestion.
The tension heightened as my lower two shirt buttons gave up the cause, careening across the table and striking, respectively, a deserted bowl of creamed corn and the forehead of a comatose relative who had long ago lost interest in watching my acute food intoxication. As my cousins brokered bets over the likelihood of my impending demise, I sat and deliberated, fork hovering over my sugary prey.
Obesity Epidemic
As healthcare practitioners, we are well aware of the dangers of obesity, yet seem paralyzed to make change. However, hospitalists are perfectly positioned to help patients resolve to lose their weight.
A body mass index (BMI) of 30 or more indicates obesity; its slimmer overweight cousin weighs in with a BMI of 25-29.
Overweight or obese people are at increased risk of osteoarthritis, dyslipidemia, obstructive sleep apnea, hypertension, coronary artery disease, stroke, cancer, and diabetes. Obesity accounts for 300,000 excess deaths per year in the U.S., along with about 10% of all healthcare expenditures, according to the Centers for Disease Control and Prevention (CDC). It affects all ages, races, and professions—including physicians. It is perhaps the most significant health issue facing our nation.
Despite this awareness, we keep getting bigger. In the past 20 years we have seen an epic swelling of American waistlines. In 1990 the CDC reported that among adult residents, 10 states had a prevalence rate of obesity less than 10%, and no states had a rate more than 15% (see Fig. 1, above). By 2006, no state had a prevalence of obesity less than 10%, while only four states clocked in with a rate less than 20%. A whopping 22 states found at least 25% of their inhabitants obese. Since 2005 we’ve become so big the CDC had to create a new category for states with more than 30% of their residents being obese. When the BMI cutoff is dropped to 25 or more, 66% meet of U.S. adults meet this definition for being overweight or obese.
Recent CDC data reveal a glimmer of hope. There was no statistically significant increase in the prevalence of obesity in 2005-2006, compared with 2003-2004. In the earlier time period, 31.1% of men and 33.2% of women were obese, compared with 33.3% of men and 35.3% of women in the most recent time period.
Still, one of every three U.S. adults is obese. That’s 100 million Americans. More than 50% of non-Hispanic black and Mexican-American women age 40-59 are obese. Sixty-one percent of non-Hispanic black women older than 60 are obese.
A complex mix of components, including environment and genetics, determines weight gain. The rapid rate of weight gain in recent years is unlikely to be explained by genetics alone—the population’s genetic composition cannot change that quickly. Thus the bulk of the recent increase in obesity is likely related to cultural and environmental determinants. A 2007 paper by Christakis, et al., found that social networks play a large role in the spread of obesity.1 The study followed 12,067 people for more than 30 years. Those with a friend, sibling, or spouse who became obese over that period were 57%, 40%, and 37% more likely, respectively, to become obese. The authors hypothesize that obesity may become less stigmatized and more tolerable for those surrounded by obese associates. Another theory is that peer groups tend to adopt similar behaviors, such as smoking, eating fast food, and inactivity.
The average person gains about one to two pounds a year.2 When distilled to its simplest form, weight gain occurs anytime calories in exceed calories out—that is, a positive energy balance or gap.
The six weeks from Thanksgiving to New Year’s is an especially vulnerable time for weight gain. In a 2000 study of 195 subjects, the average person gained about one pound during the holiday season. When these subjects were followed up with six months later, there was no statistically significant loss of peri-holiday weight gain. This holiday pound may seem trivial (and keep in mind these subjects gained weight despite being closely watched in a weight-gain study). But this weight appears hard to shed and results in much of the weight gained during adulthood.
However, unlike my Thanksgiving gorging, the hallmark of obesity is the small but frequent positive energy gaps, that is, days of 50 to 100 calories of intake greater than use. Over the course of the year, these small daily caloric gaps are anabolically transformed into pounds.
Resolve to Lose
By now, like me, many of you may have added a holiday pound or two. This may be in addition to a nefarious pound or two added throughout the rest of the year. As you ponder scribing your annual resolutions, consider making weight loss a top priority for your patients and yourself, if appropriate.
Unfortunately no magic bullet will turn your New Year’s resolution into reality, just hard work. The key is to tilt the energy balance toward weight loss by reducing caloric intake and increasing activity. Fortunately this can be done in non-Draconian ways. Just as weight gain can snowball from small daily caloric overdoses, it can be removed the same way. Instead of setting or recommending insurmountable goals to your patients—like reducing intake to 1,000 calories a day or adhering to a triathletic training regimen—the CDC suggests a simpler, more sustainable approach to shedding those pounds, namely tipping your energy balance to a negative 150 calories per day.
A net negative energy balance of 150 calories per day will at worst stabilize your weight (depending on your current energy balance) and at best net five to 10 pounds of weight loss per year. For most this can result from something as simple as switching your daily Coke to a Diet Coke. Even more ground can be gained by reducing portion size. The super-sizing of the American menu over the past 20 years is one of the prime drivers of the obesity epidemic (see Table 1, p. 64). Consider cutting back in small ways. For example, continue to enjoy that gourmet chocolate chip cookie but downsize it to a smaller version and reduce your intake by 150 to 200 calories.
As important as reducing caloric intake is the need for activity. Adding moderate amounts of exercise five days a week can burn an additional 150 calories per day, reducing overall weight by another five to 10 pounds in a year. This can include things like walking for 30 minutes, swimming for 20 minutes, or biking for 15 minutes. More adventurous (dancing for 30 minutes), parental (pushing a stroller for 30 minutes), agricultural (gardening for 30 minutes), or chore-oriented (shoveling 15 minutes) options also help.
Much to the dismay of my cousin Mike, who bet that I’d eat at least half the piece of Thanksgiving pie, I put down my fork. After packing away a winter’s worth of calories I was feeling diaphoretic and pathetic. I wobbled away from the table and began charting my course to redemption. It would begin the next day with an apple instead of a bagel, an extra hour at the gym—and a trip to the cleaners to get those buttons replaced. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Editor’s note: The author’s driver license claims a weight of 165 pounds. Physical evidence, as well as his wife’s report, paints a substantially different picture.
References
- Christakis NA, Fowler JH. The spread of obesity in a large social network over 32 years. N Engl J Med. 2007;357:370-379.
- Yanovksi JA, Yanovski SZ, Sovik KN, et al. A prospective study of holiday weight gain. N Engl J Med. 2000;342:861-867.
With shirt buttons bulging and my panniculus spilling like the top of an oversized muffin over my belt—which was essentially a tourniquet strangling my lower extremities—I examined my options.
After hours of grazing through the snack food pyramid and consuming significant portions of a dinosaur-size turkey, an acromegalic dollop of dressing, a bog of cranberries, and a field of mashed potatoes, I was faced with the proposition of shoveling in another 500 calories cleverly disguised as a heaping slice of pumpkin pie.
The intensity of the situation was palpable. My in-laws sat mouths agape, stunned by the amount and rate at which I forked thousands of calories into my gullet. They fidgeted as I stared with steely, miotic pupils and furrowed, sweat-beaded brow at my prospective ingestion.
The tension heightened as my lower two shirt buttons gave up the cause, careening across the table and striking, respectively, a deserted bowl of creamed corn and the forehead of a comatose relative who had long ago lost interest in watching my acute food intoxication. As my cousins brokered bets over the likelihood of my impending demise, I sat and deliberated, fork hovering over my sugary prey.
Obesity Epidemic
As healthcare practitioners, we are well aware of the dangers of obesity, yet seem paralyzed to make change. However, hospitalists are perfectly positioned to help patients resolve to lose their weight.
A body mass index (BMI) of 30 or more indicates obesity; its slimmer overweight cousin weighs in with a BMI of 25-29.
Overweight or obese people are at increased risk of osteoarthritis, dyslipidemia, obstructive sleep apnea, hypertension, coronary artery disease, stroke, cancer, and diabetes. Obesity accounts for 300,000 excess deaths per year in the U.S., along with about 10% of all healthcare expenditures, according to the Centers for Disease Control and Prevention (CDC). It affects all ages, races, and professions—including physicians. It is perhaps the most significant health issue facing our nation.
Despite this awareness, we keep getting bigger. In the past 20 years we have seen an epic swelling of American waistlines. In 1990 the CDC reported that among adult residents, 10 states had a prevalence rate of obesity less than 10%, and no states had a rate more than 15% (see Fig. 1, above). By 2006, no state had a prevalence of obesity less than 10%, while only four states clocked in with a rate less than 20%. A whopping 22 states found at least 25% of their inhabitants obese. Since 2005 we’ve become so big the CDC had to create a new category for states with more than 30% of their residents being obese. When the BMI cutoff is dropped to 25 or more, 66% meet of U.S. adults meet this definition for being overweight or obese.
Recent CDC data reveal a glimmer of hope. There was no statistically significant increase in the prevalence of obesity in 2005-2006, compared with 2003-2004. In the earlier time period, 31.1% of men and 33.2% of women were obese, compared with 33.3% of men and 35.3% of women in the most recent time period.
Still, one of every three U.S. adults is obese. That’s 100 million Americans. More than 50% of non-Hispanic black and Mexican-American women age 40-59 are obese. Sixty-one percent of non-Hispanic black women older than 60 are obese.
A complex mix of components, including environment and genetics, determines weight gain. The rapid rate of weight gain in recent years is unlikely to be explained by genetics alone—the population’s genetic composition cannot change that quickly. Thus the bulk of the recent increase in obesity is likely related to cultural and environmental determinants. A 2007 paper by Christakis, et al., found that social networks play a large role in the spread of obesity.1 The study followed 12,067 people for more than 30 years. Those with a friend, sibling, or spouse who became obese over that period were 57%, 40%, and 37% more likely, respectively, to become obese. The authors hypothesize that obesity may become less stigmatized and more tolerable for those surrounded by obese associates. Another theory is that peer groups tend to adopt similar behaviors, such as smoking, eating fast food, and inactivity.
The average person gains about one to two pounds a year.2 When distilled to its simplest form, weight gain occurs anytime calories in exceed calories out—that is, a positive energy balance or gap.
The six weeks from Thanksgiving to New Year’s is an especially vulnerable time for weight gain. In a 2000 study of 195 subjects, the average person gained about one pound during the holiday season. When these subjects were followed up with six months later, there was no statistically significant loss of peri-holiday weight gain. This holiday pound may seem trivial (and keep in mind these subjects gained weight despite being closely watched in a weight-gain study). But this weight appears hard to shed and results in much of the weight gained during adulthood.
However, unlike my Thanksgiving gorging, the hallmark of obesity is the small but frequent positive energy gaps, that is, days of 50 to 100 calories of intake greater than use. Over the course of the year, these small daily caloric gaps are anabolically transformed into pounds.
Resolve to Lose
By now, like me, many of you may have added a holiday pound or two. This may be in addition to a nefarious pound or two added throughout the rest of the year. As you ponder scribing your annual resolutions, consider making weight loss a top priority for your patients and yourself, if appropriate.
Unfortunately no magic bullet will turn your New Year’s resolution into reality, just hard work. The key is to tilt the energy balance toward weight loss by reducing caloric intake and increasing activity. Fortunately this can be done in non-Draconian ways. Just as weight gain can snowball from small daily caloric overdoses, it can be removed the same way. Instead of setting or recommending insurmountable goals to your patients—like reducing intake to 1,000 calories a day or adhering to a triathletic training regimen—the CDC suggests a simpler, more sustainable approach to shedding those pounds, namely tipping your energy balance to a negative 150 calories per day.
A net negative energy balance of 150 calories per day will at worst stabilize your weight (depending on your current energy balance) and at best net five to 10 pounds of weight loss per year. For most this can result from something as simple as switching your daily Coke to a Diet Coke. Even more ground can be gained by reducing portion size. The super-sizing of the American menu over the past 20 years is one of the prime drivers of the obesity epidemic (see Table 1, p. 64). Consider cutting back in small ways. For example, continue to enjoy that gourmet chocolate chip cookie but downsize it to a smaller version and reduce your intake by 150 to 200 calories.
As important as reducing caloric intake is the need for activity. Adding moderate amounts of exercise five days a week can burn an additional 150 calories per day, reducing overall weight by another five to 10 pounds in a year. This can include things like walking for 30 minutes, swimming for 20 minutes, or biking for 15 minutes. More adventurous (dancing for 30 minutes), parental (pushing a stroller for 30 minutes), agricultural (gardening for 30 minutes), or chore-oriented (shoveling 15 minutes) options also help.
Much to the dismay of my cousin Mike, who bet that I’d eat at least half the piece of Thanksgiving pie, I put down my fork. After packing away a winter’s worth of calories I was feeling diaphoretic and pathetic. I wobbled away from the table and began charting my course to redemption. It would begin the next day with an apple instead of a bagel, an extra hour at the gym—and a trip to the cleaners to get those buttons replaced. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Editor’s note: The author’s driver license claims a weight of 165 pounds. Physical evidence, as well as his wife’s report, paints a substantially different picture.
References
- Christakis NA, Fowler JH. The spread of obesity in a large social network over 32 years. N Engl J Med. 2007;357:370-379.
- Yanovksi JA, Yanovski SZ, Sovik KN, et al. A prospective study of holiday weight gain. N Engl J Med. 2000;342:861-867.
Hours to Expertise

Glass of wine in one hand and the Sept. 30 copy of Wine Spectator in the other, I intended to relax a bit—the future of hospital medicine not necessarily uppermost in my mind. But then I was struck by an article by Matt Kramer titled “10,000 hours.” In it he discusses the implications Daniel Levitin’s new book This Is Your Brain on Music: The Science of a Human Obsession (Dutton) may have for the field of wine tasting.
Levitin notes that “ten thousand hours of practice is required to achieve the level of mastery associated with being a world-class expert—in anything.” It turns out it doesn’t matter what you are trying to master.
“In study after study of composers, basketball players, fiction writers, ice skaters, concert pianists, chess players, master criminals, and what have you, this number comes up again and again,” he says. “No one has yet found a case in which true world-class expertise was accomplished in less time.” This is consistent with how we learn. “Learning requires the assimilation and consolidation of information in neural tissue,” writes Levitin. “The more experiences we have with something the stronger the memory/learning trace for the experience becomes.”
Ten thousand hours. Are you an expert in hospital medicine? Have you compiled the requisite 10,000 hours? The average hospitalist working approximately 200 shifts a year of 10 to 12 hours each would take four to five years to master the practice of hospital medicine. On the other hand, a provider spending 10 hours a week in the hospital would require 20 years to achieve the numeric equivalent of expert status.
While Levitin was discussing the impact of this calculation on music and Kramer on wine expertise, it struck me as applicable to one of the great debates surrounding hospital medicine. Early in the days of the hospitalist movement, many inside and outside the field opined as to whether hospitals should be the domain of hospitalists and clinics the domain of primary care doctors, without overlap. SHM and I proclaimed hospitals should be open to all providers, regardless of primary practice site.
Over time the argument has died down as the threat of a hospitalist takeover has given way to the realization that many primary care doctors prefer a practice without inpatient obligations.
Recently the American Board of Internal Medicine (ABIM) has decided to move forward with a Recognition of Focused Practice in hospital medicine (RFP-HM) certification. This designation will utilize the structure of the ABIM Maintenance of Certification (MOC) program. It will be available to those who have practiced hospital medicine at least three years, meet inpatient volume requirements, and successfully complete hospital medicine-specific Self-Evaluation Process (SEP) modules, Practice Improvement Modules (PIM) and a secure exam.
This has again raised concerns about the growth and direction of hospital medicine and the implications for internal medicine. Would this confer specialty status to hospitalists while leaving primary care doctors as the remaining generalists? Would this further fracture the field of internal medicine? Would this allow hospital-credentialing boards to preferentially allow only those with RFP-HM to practice within their walls, effectively outlawing the primary care doctor?
Having been a member of the task force that worked on RFP-HM, I can say emphatically that it is not intended to confer specialty status to hospitalists or exalt them above other general internists. Rather, it is meant to recognize that a practitioner has focused his or her practice in a manner that demonstrates greater proficiency in the practice of hospital medicine. While this denotes a presumably higher level of proficiency by RFP-HM providers, it does not mean those without it are not capable providers.
How then should we define who is a capable provider in the hospital setting? According to the Dreyfus Model of Skills Acquisition, as learners develop along the continuum from novice to beginner to competent to proficient to expert, their skills become more developed, letting them tackle more complex issues and tasks more efficiently.
For example, the novice knows that a patient with dyspnea might have pneumonia and orders a chest X-ray but little more. The competent provider realizes many other disease states can cause dyspnea and would assess for those as well, often getting bogged down in extraneous details. The proficient provider immediately focuses on the important details and determines pneumonia as the cause of the dyspnea, applying the proper treatment algorithms with a level of efficiency beyond that of the competent peer.
The expert intuitively diagnoses the pneumonia and prescribes the proper diagnostic and therapeutic evaluation. He does so while considering the patient’s immune status, the impact of the hospital’s antimicrobial resistance patterns, and the potential risks and benefits of short-course antimicrobial therapy—all through the prism of quality core measures, cost, and throughput.
In a healthcare system at best strained and by most evidence severely fractured, we can no longer accept competence as the determinant of a capable provider. Rather, we should use proficiency moving toward expertise as the measuring stick for caring for increasingly more complex patients.
The designation “hospitalist” or even RFP-HM should not determine if one is proficient to practice hospital medicine, just as the designation of primary care provider should not exclude one from practicing in the hospital. Certainly, there are practitioners able to seamlessly cross the inpatient/outpatient boundary without losing a step. However, I suspect the more likely scenario is expertise in one and at best proficiency in the other.
Levitin’s 10,000-hour threshold supports this assumption, as it would take at least 10 years to amass 10,000 hours in each practice setting. Most likely, development of expertise in one arena means mere competence in another. As exhibit A, I tremble at the thought of the mischief I would cause if I took my stethoscope to the primary care clinic.
Instead, the ethical standards of our profession should dictate that each provider determines if they meet this pursuit-of-expertise standard. Employers and credentialing boards need to raise the bar toward expertise, ensuring these thresholds are met.
In the end, hospital or clinic sites should be the domain of capable providers, regardless of their primary practice site. However, we need to recalibrate how we define a capable provider who is moving away from competence toward proficiency verging on expertise. Experience as a surrogate for expertise, more than primary practice setting or RFP-HM status, should be the major determinant for who cares for hospitalized patients. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Glass of wine in one hand and the Sept. 30 copy of Wine Spectator in the other, I intended to relax a bit—the future of hospital medicine not necessarily uppermost in my mind. But then I was struck by an article by Matt Kramer titled “10,000 hours.” In it he discusses the implications Daniel Levitin’s new book This Is Your Brain on Music: The Science of a Human Obsession (Dutton) may have for the field of wine tasting.
Levitin notes that “ten thousand hours of practice is required to achieve the level of mastery associated with being a world-class expert—in anything.” It turns out it doesn’t matter what you are trying to master.
“In study after study of composers, basketball players, fiction writers, ice skaters, concert pianists, chess players, master criminals, and what have you, this number comes up again and again,” he says. “No one has yet found a case in which true world-class expertise was accomplished in less time.” This is consistent with how we learn. “Learning requires the assimilation and consolidation of information in neural tissue,” writes Levitin. “The more experiences we have with something the stronger the memory/learning trace for the experience becomes.”
Ten thousand hours. Are you an expert in hospital medicine? Have you compiled the requisite 10,000 hours? The average hospitalist working approximately 200 shifts a year of 10 to 12 hours each would take four to five years to master the practice of hospital medicine. On the other hand, a provider spending 10 hours a week in the hospital would require 20 years to achieve the numeric equivalent of expert status.
While Levitin was discussing the impact of this calculation on music and Kramer on wine expertise, it struck me as applicable to one of the great debates surrounding hospital medicine. Early in the days of the hospitalist movement, many inside and outside the field opined as to whether hospitals should be the domain of hospitalists and clinics the domain of primary care doctors, without overlap. SHM and I proclaimed hospitals should be open to all providers, regardless of primary practice site.
Over time the argument has died down as the threat of a hospitalist takeover has given way to the realization that many primary care doctors prefer a practice without inpatient obligations.
Recently the American Board of Internal Medicine (ABIM) has decided to move forward with a Recognition of Focused Practice in hospital medicine (RFP-HM) certification. This designation will utilize the structure of the ABIM Maintenance of Certification (MOC) program. It will be available to those who have practiced hospital medicine at least three years, meet inpatient volume requirements, and successfully complete hospital medicine-specific Self-Evaluation Process (SEP) modules, Practice Improvement Modules (PIM) and a secure exam.
This has again raised concerns about the growth and direction of hospital medicine and the implications for internal medicine. Would this confer specialty status to hospitalists while leaving primary care doctors as the remaining generalists? Would this further fracture the field of internal medicine? Would this allow hospital-credentialing boards to preferentially allow only those with RFP-HM to practice within their walls, effectively outlawing the primary care doctor?
Having been a member of the task force that worked on RFP-HM, I can say emphatically that it is not intended to confer specialty status to hospitalists or exalt them above other general internists. Rather, it is meant to recognize that a practitioner has focused his or her practice in a manner that demonstrates greater proficiency in the practice of hospital medicine. While this denotes a presumably higher level of proficiency by RFP-HM providers, it does not mean those without it are not capable providers.
How then should we define who is a capable provider in the hospital setting? According to the Dreyfus Model of Skills Acquisition, as learners develop along the continuum from novice to beginner to competent to proficient to expert, their skills become more developed, letting them tackle more complex issues and tasks more efficiently.
For example, the novice knows that a patient with dyspnea might have pneumonia and orders a chest X-ray but little more. The competent provider realizes many other disease states can cause dyspnea and would assess for those as well, often getting bogged down in extraneous details. The proficient provider immediately focuses on the important details and determines pneumonia as the cause of the dyspnea, applying the proper treatment algorithms with a level of efficiency beyond that of the competent peer.
The expert intuitively diagnoses the pneumonia and prescribes the proper diagnostic and therapeutic evaluation. He does so while considering the patient’s immune status, the impact of the hospital’s antimicrobial resistance patterns, and the potential risks and benefits of short-course antimicrobial therapy—all through the prism of quality core measures, cost, and throughput.
In a healthcare system at best strained and by most evidence severely fractured, we can no longer accept competence as the determinant of a capable provider. Rather, we should use proficiency moving toward expertise as the measuring stick for caring for increasingly more complex patients.
The designation “hospitalist” or even RFP-HM should not determine if one is proficient to practice hospital medicine, just as the designation of primary care provider should not exclude one from practicing in the hospital. Certainly, there are practitioners able to seamlessly cross the inpatient/outpatient boundary without losing a step. However, I suspect the more likely scenario is expertise in one and at best proficiency in the other.
Levitin’s 10,000-hour threshold supports this assumption, as it would take at least 10 years to amass 10,000 hours in each practice setting. Most likely, development of expertise in one arena means mere competence in another. As exhibit A, I tremble at the thought of the mischief I would cause if I took my stethoscope to the primary care clinic.
Instead, the ethical standards of our profession should dictate that each provider determines if they meet this pursuit-of-expertise standard. Employers and credentialing boards need to raise the bar toward expertise, ensuring these thresholds are met.
In the end, hospital or clinic sites should be the domain of capable providers, regardless of their primary practice site. However, we need to recalibrate how we define a capable provider who is moving away from competence toward proficiency verging on expertise. Experience as a surrogate for expertise, more than primary practice setting or RFP-HM status, should be the major determinant for who cares for hospitalized patients. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Glass of wine in one hand and the Sept. 30 copy of Wine Spectator in the other, I intended to relax a bit—the future of hospital medicine not necessarily uppermost in my mind. But then I was struck by an article by Matt Kramer titled “10,000 hours.” In it he discusses the implications Daniel Levitin’s new book This Is Your Brain on Music: The Science of a Human Obsession (Dutton) may have for the field of wine tasting.
Levitin notes that “ten thousand hours of practice is required to achieve the level of mastery associated with being a world-class expert—in anything.” It turns out it doesn’t matter what you are trying to master.
“In study after study of composers, basketball players, fiction writers, ice skaters, concert pianists, chess players, master criminals, and what have you, this number comes up again and again,” he says. “No one has yet found a case in which true world-class expertise was accomplished in less time.” This is consistent with how we learn. “Learning requires the assimilation and consolidation of information in neural tissue,” writes Levitin. “The more experiences we have with something the stronger the memory/learning trace for the experience becomes.”
Ten thousand hours. Are you an expert in hospital medicine? Have you compiled the requisite 10,000 hours? The average hospitalist working approximately 200 shifts a year of 10 to 12 hours each would take four to five years to master the practice of hospital medicine. On the other hand, a provider spending 10 hours a week in the hospital would require 20 years to achieve the numeric equivalent of expert status.
While Levitin was discussing the impact of this calculation on music and Kramer on wine expertise, it struck me as applicable to one of the great debates surrounding hospital medicine. Early in the days of the hospitalist movement, many inside and outside the field opined as to whether hospitals should be the domain of hospitalists and clinics the domain of primary care doctors, without overlap. SHM and I proclaimed hospitals should be open to all providers, regardless of primary practice site.
Over time the argument has died down as the threat of a hospitalist takeover has given way to the realization that many primary care doctors prefer a practice without inpatient obligations.
Recently the American Board of Internal Medicine (ABIM) has decided to move forward with a Recognition of Focused Practice in hospital medicine (RFP-HM) certification. This designation will utilize the structure of the ABIM Maintenance of Certification (MOC) program. It will be available to those who have practiced hospital medicine at least three years, meet inpatient volume requirements, and successfully complete hospital medicine-specific Self-Evaluation Process (SEP) modules, Practice Improvement Modules (PIM) and a secure exam.
This has again raised concerns about the growth and direction of hospital medicine and the implications for internal medicine. Would this confer specialty status to hospitalists while leaving primary care doctors as the remaining generalists? Would this further fracture the field of internal medicine? Would this allow hospital-credentialing boards to preferentially allow only those with RFP-HM to practice within their walls, effectively outlawing the primary care doctor?
Having been a member of the task force that worked on RFP-HM, I can say emphatically that it is not intended to confer specialty status to hospitalists or exalt them above other general internists. Rather, it is meant to recognize that a practitioner has focused his or her practice in a manner that demonstrates greater proficiency in the practice of hospital medicine. While this denotes a presumably higher level of proficiency by RFP-HM providers, it does not mean those without it are not capable providers.
How then should we define who is a capable provider in the hospital setting? According to the Dreyfus Model of Skills Acquisition, as learners develop along the continuum from novice to beginner to competent to proficient to expert, their skills become more developed, letting them tackle more complex issues and tasks more efficiently.
For example, the novice knows that a patient with dyspnea might have pneumonia and orders a chest X-ray but little more. The competent provider realizes many other disease states can cause dyspnea and would assess for those as well, often getting bogged down in extraneous details. The proficient provider immediately focuses on the important details and determines pneumonia as the cause of the dyspnea, applying the proper treatment algorithms with a level of efficiency beyond that of the competent peer.
The expert intuitively diagnoses the pneumonia and prescribes the proper diagnostic and therapeutic evaluation. He does so while considering the patient’s immune status, the impact of the hospital’s antimicrobial resistance patterns, and the potential risks and benefits of short-course antimicrobial therapy—all through the prism of quality core measures, cost, and throughput.
In a healthcare system at best strained and by most evidence severely fractured, we can no longer accept competence as the determinant of a capable provider. Rather, we should use proficiency moving toward expertise as the measuring stick for caring for increasingly more complex patients.
The designation “hospitalist” or even RFP-HM should not determine if one is proficient to practice hospital medicine, just as the designation of primary care provider should not exclude one from practicing in the hospital. Certainly, there are practitioners able to seamlessly cross the inpatient/outpatient boundary without losing a step. However, I suspect the more likely scenario is expertise in one and at best proficiency in the other.
Levitin’s 10,000-hour threshold supports this assumption, as it would take at least 10 years to amass 10,000 hours in each practice setting. Most likely, development of expertise in one arena means mere competence in another. As exhibit A, I tremble at the thought of the mischief I would cause if I took my stethoscope to the primary care clinic.
Instead, the ethical standards of our profession should dictate that each provider determines if they meet this pursuit-of-expertise standard. Employers and credentialing boards need to raise the bar toward expertise, ensuring these thresholds are met.
In the end, hospital or clinic sites should be the domain of capable providers, regardless of their primary practice site. However, we need to recalibrate how we define a capable provider who is moving away from competence toward proficiency verging on expertise. Experience as a surrogate for expertise, more than primary practice setting or RFP-HM status, should be the major determinant for who cares for hospitalized patients. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Lesson of the Titanic

Author’s note: More than 1,500 passengers died in the Titanic, a disaster that resonates nearly a hundred years later. The equivalent of about 50 Titanics capsize annually in U.S. hospitals, nearly one every week (based on the Institute of Medicine’s estimate of 44,000-98,000 deaths per year from hospital adverse events). As hospitalists, it is our obligation to ensure the hull is solid, the crow’s nest properly manned, and the ship is turning in the right direction.
I’m the Rev. John Harper, and it’s April 10, 1912.
As I grasp my boarding pass I can’t contain my awe and excitement. Imagine me aboard the world’s most luxurious cruise liner heading to America. Granted, I’m booked in second class. But as everyone knows, second class on the Titanic outstrips first class on most liners these days. It should—for $66 this is an expensive way to travel. Still, it’s less than the cheapest first-class ticket of $125 and much less than a $4,500 booking in the millionaire’s suite. I could buy several houses for $4,500.
Walking along the gangway I recall hearing that this ship—the largest ever built—weighs nearly 47,000 tons and cost $7.5 million. Outside my cabin door I encounter a fellow passenger who exults over the ship’s amenities. The liner has a heated indoor swimming pool, four electric elevators, two libraries, a Turkish bath, a squash court and gymnasium, and ample room to move about. The White Star Line has thoughtfully limited the amount of lifeboats to 20 to preserve precious deck space for passengers.
I’m Jeff Glasheen, and it’s Sept. 15, 2007.
As my wife prepares to deliver our first child in the coming weeks, we visit the labor and delivery deck of the hospital.
It will be our first major interaction with the healthcare system as patients. It’s the largest healthcare system ever and costs nearly $2 trillion a year to operate. We have chosen a new hospital that features an amazing array of amenities, including a birthing center with private suites, in-room baths with oversize soaking tubs, an in-room sleeping area for family and friends, and a DVD player and flat-screen television. There are even Internet connections.
Room service is available 24 hours a day, and the staff is top-notch. I’m told some choose to stay in the VIP suites for an extra $1,000 a night. This restricted-access area offers 600-square-foot rooms with original art on the walls, luxury mattresses and 350-thread count linens, complimentary robes and slippers, and an office area supplied with newspapers, a printer, fax, voicemail, and teleconferencing capabilities. There is a family room as well as a private refrigerator, an assortment of beverages and a dedicated chef. Unfortunately the cost is too steep, so we’ll spend this voyage in second class. However, as everyone knows, second class on this vessel outstrips first class in most hospitals these days.
Midnight, April 14, 1912
Something has gone wrong; the ship just hiccupped a bit. From my cabin I clearly hear a grinding that could happen only when two large objects come into contact. It’s strange, but I assure my bunkmates there is nothing to worry about. The Titanic is unsinkable, built with every feasible safety feature. The ship’s hull is made of inch-thick steel and held together with nearly 3 million steel rivets. In the unlikely event the hull is breached, the ship contains 15 watertight bulkheads to contain the leakage. Further, 3,560 life vests, 48 life buoys, and the aforementioned 20 lifeboats (four more than required by British law) allay my concerns.
On the off chance something should go wrong, the ship is outfitted with the recently developed Marconi wireless telegraph capable of communicating with any ship or shore within 500 miles.
5 p.m., Sept. 17, 2007
As I write this column I consider that something could go wrong during our hospital stay. The Institute of Medicine reports that medications harm 1.5 million people annually (400,000 incidents occur in the hospital) and that nearly 100,000 die annually in adverse hospital events.
I assure myself there is nothing to worry about. The hospital of today is unsinkable, built with every feasible safety measure. Today’s hospitals require two patient identifiers, time-outs before procedures, read-backs, standardized abbreviations, rules for reporting of critical results, standardized approaches to hand-offs, awareness of look-alike/sound-alike medications, hand-hygiene guidelines, medication reconciliation, core measures, quality and patient safety committees—and, on the off chance that something should go wrong, requirements for communicating sentinel event reviews with regulatory agencies.
1:30 a.m., April 14, 1912
The scuttlebutt is that the Titanic has hit an iceberg, tearing open the hull, flooding the bulkheads, and overcoming the ship’s pumps. Apparently the crow’s nest spotted the iceberg only 30 seconds before the impact. The crew tried to change course immediately. But the unprecedented size and speed of the ship (there is a rumor that the captain may have been trying to set a new trans-Atlantic crossing record) made it impossible to avoid our destiny.
We are clearly sinking. As I anxiously pace the deck waiting for a spot on a lifeboat, I chat with a crew member who assures me help is coming. The ship’s band plays on deck, the music soothing in the night air.
1 p.m., Aug. 26, 2007
I’m about halfway through the Titanic exhibit at the local museum of nature and science. The display is designed to give you the experience of being a passenger aboard the RMS Titanic.
Prior to entering, visitors receive a boarding pass with information about one of the actual passengers. I am the Rev. John Harper, traveling to America with my young daughter to begin a series of revival meetings in Chicago. At the end of the tour I’ll view the passenger manifest to discover my outcome.
Reluctantly, I board the ship, anxiously awaiting my fate. I gaze upon thousands of trinkets and treasures rescued from the Titanic since its remains were discovered 2.5 miles below the ocean’s surface 900 miles off the coast of New York in 1985.
I marvel at dioramas of first- and third-class cabins with recovered china settings, uncorked and still-full bottles of champagne, toiletries, jewelry, and clothing.
One of the most fascinating pieces is a chunk of ice the size and shape of a small whale. The display represents the iceberg that doomed the Titanic and simulates the temperature of the water that fateful night. At approximately 28 degrees Fahrenheit, the average person would survive less than 15 minutes in the water. I was able to hold my hand on the ice only a few moments, quickly understanding the horrific way most passengers would die.
As I complete the tour and nervously approach the passenger manifest I am struck by how many lessons from the Titanic can be applied to modern medicine.
We operate in a system surrounded by perilous obstacles in a huge vessel that is slow to change course even in the face of extreme danger and poor outcomes.
We steam along at unparalleled speed embracing new, relatively untested technologies, procedures, and medications. Modern healthcare, like the Titanic, values building technologically advanced, well-adorned vessels rather than investing in the basic infrastructure to make it safer. We eschew quality for appearance.
We spend money on heated indoor pools, squash courts, and Turkish baths rather than computerized provider order entry, bar code administration, and hand-off improvements. Despite all of this, our passengers trust the vessel is safe. They trust that we will protect them—that we have enough lifeboats.
The Rev. John Harper perished on April 14, 1912; unlike him, as I cross the threshold of the healthcare Titanic I am not filled with awe and excitement. I feel fear and dread. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver and Health Sciences Center, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Author’s note: More than 1,500 passengers died in the Titanic, a disaster that resonates nearly a hundred years later. The equivalent of about 50 Titanics capsize annually in U.S. hospitals, nearly one every week (based on the Institute of Medicine’s estimate of 44,000-98,000 deaths per year from hospital adverse events). As hospitalists, it is our obligation to ensure the hull is solid, the crow’s nest properly manned, and the ship is turning in the right direction.
I’m the Rev. John Harper, and it’s April 10, 1912.
As I grasp my boarding pass I can’t contain my awe and excitement. Imagine me aboard the world’s most luxurious cruise liner heading to America. Granted, I’m booked in second class. But as everyone knows, second class on the Titanic outstrips first class on most liners these days. It should—for $66 this is an expensive way to travel. Still, it’s less than the cheapest first-class ticket of $125 and much less than a $4,500 booking in the millionaire’s suite. I could buy several houses for $4,500.
Walking along the gangway I recall hearing that this ship—the largest ever built—weighs nearly 47,000 tons and cost $7.5 million. Outside my cabin door I encounter a fellow passenger who exults over the ship’s amenities. The liner has a heated indoor swimming pool, four electric elevators, two libraries, a Turkish bath, a squash court and gymnasium, and ample room to move about. The White Star Line has thoughtfully limited the amount of lifeboats to 20 to preserve precious deck space for passengers.
I’m Jeff Glasheen, and it’s Sept. 15, 2007.
As my wife prepares to deliver our first child in the coming weeks, we visit the labor and delivery deck of the hospital.
It will be our first major interaction with the healthcare system as patients. It’s the largest healthcare system ever and costs nearly $2 trillion a year to operate. We have chosen a new hospital that features an amazing array of amenities, including a birthing center with private suites, in-room baths with oversize soaking tubs, an in-room sleeping area for family and friends, and a DVD player and flat-screen television. There are even Internet connections.
Room service is available 24 hours a day, and the staff is top-notch. I’m told some choose to stay in the VIP suites for an extra $1,000 a night. This restricted-access area offers 600-square-foot rooms with original art on the walls, luxury mattresses and 350-thread count linens, complimentary robes and slippers, and an office area supplied with newspapers, a printer, fax, voicemail, and teleconferencing capabilities. There is a family room as well as a private refrigerator, an assortment of beverages and a dedicated chef. Unfortunately the cost is too steep, so we’ll spend this voyage in second class. However, as everyone knows, second class on this vessel outstrips first class in most hospitals these days.
Midnight, April 14, 1912
Something has gone wrong; the ship just hiccupped a bit. From my cabin I clearly hear a grinding that could happen only when two large objects come into contact. It’s strange, but I assure my bunkmates there is nothing to worry about. The Titanic is unsinkable, built with every feasible safety feature. The ship’s hull is made of inch-thick steel and held together with nearly 3 million steel rivets. In the unlikely event the hull is breached, the ship contains 15 watertight bulkheads to contain the leakage. Further, 3,560 life vests, 48 life buoys, and the aforementioned 20 lifeboats (four more than required by British law) allay my concerns.
On the off chance something should go wrong, the ship is outfitted with the recently developed Marconi wireless telegraph capable of communicating with any ship or shore within 500 miles.
5 p.m., Sept. 17, 2007
As I write this column I consider that something could go wrong during our hospital stay. The Institute of Medicine reports that medications harm 1.5 million people annually (400,000 incidents occur in the hospital) and that nearly 100,000 die annually in adverse hospital events.
I assure myself there is nothing to worry about. The hospital of today is unsinkable, built with every feasible safety measure. Today’s hospitals require two patient identifiers, time-outs before procedures, read-backs, standardized abbreviations, rules for reporting of critical results, standardized approaches to hand-offs, awareness of look-alike/sound-alike medications, hand-hygiene guidelines, medication reconciliation, core measures, quality and patient safety committees—and, on the off chance that something should go wrong, requirements for communicating sentinel event reviews with regulatory agencies.
1:30 a.m., April 14, 1912
The scuttlebutt is that the Titanic has hit an iceberg, tearing open the hull, flooding the bulkheads, and overcoming the ship’s pumps. Apparently the crow’s nest spotted the iceberg only 30 seconds before the impact. The crew tried to change course immediately. But the unprecedented size and speed of the ship (there is a rumor that the captain may have been trying to set a new trans-Atlantic crossing record) made it impossible to avoid our destiny.
We are clearly sinking. As I anxiously pace the deck waiting for a spot on a lifeboat, I chat with a crew member who assures me help is coming. The ship’s band plays on deck, the music soothing in the night air.
1 p.m., Aug. 26, 2007
I’m about halfway through the Titanic exhibit at the local museum of nature and science. The display is designed to give you the experience of being a passenger aboard the RMS Titanic.
Prior to entering, visitors receive a boarding pass with information about one of the actual passengers. I am the Rev. John Harper, traveling to America with my young daughter to begin a series of revival meetings in Chicago. At the end of the tour I’ll view the passenger manifest to discover my outcome.
Reluctantly, I board the ship, anxiously awaiting my fate. I gaze upon thousands of trinkets and treasures rescued from the Titanic since its remains were discovered 2.5 miles below the ocean’s surface 900 miles off the coast of New York in 1985.
I marvel at dioramas of first- and third-class cabins with recovered china settings, uncorked and still-full bottles of champagne, toiletries, jewelry, and clothing.
One of the most fascinating pieces is a chunk of ice the size and shape of a small whale. The display represents the iceberg that doomed the Titanic and simulates the temperature of the water that fateful night. At approximately 28 degrees Fahrenheit, the average person would survive less than 15 minutes in the water. I was able to hold my hand on the ice only a few moments, quickly understanding the horrific way most passengers would die.
As I complete the tour and nervously approach the passenger manifest I am struck by how many lessons from the Titanic can be applied to modern medicine.
We operate in a system surrounded by perilous obstacles in a huge vessel that is slow to change course even in the face of extreme danger and poor outcomes.
We steam along at unparalleled speed embracing new, relatively untested technologies, procedures, and medications. Modern healthcare, like the Titanic, values building technologically advanced, well-adorned vessels rather than investing in the basic infrastructure to make it safer. We eschew quality for appearance.
We spend money on heated indoor pools, squash courts, and Turkish baths rather than computerized provider order entry, bar code administration, and hand-off improvements. Despite all of this, our passengers trust the vessel is safe. They trust that we will protect them—that we have enough lifeboats.
The Rev. John Harper perished on April 14, 1912; unlike him, as I cross the threshold of the healthcare Titanic I am not filled with awe and excitement. I feel fear and dread. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver and Health Sciences Center, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Author’s note: More than 1,500 passengers died in the Titanic, a disaster that resonates nearly a hundred years later. The equivalent of about 50 Titanics capsize annually in U.S. hospitals, nearly one every week (based on the Institute of Medicine’s estimate of 44,000-98,000 deaths per year from hospital adverse events). As hospitalists, it is our obligation to ensure the hull is solid, the crow’s nest properly manned, and the ship is turning in the right direction.
I’m the Rev. John Harper, and it’s April 10, 1912.
As I grasp my boarding pass I can’t contain my awe and excitement. Imagine me aboard the world’s most luxurious cruise liner heading to America. Granted, I’m booked in second class. But as everyone knows, second class on the Titanic outstrips first class on most liners these days. It should—for $66 this is an expensive way to travel. Still, it’s less than the cheapest first-class ticket of $125 and much less than a $4,500 booking in the millionaire’s suite. I could buy several houses for $4,500.
Walking along the gangway I recall hearing that this ship—the largest ever built—weighs nearly 47,000 tons and cost $7.5 million. Outside my cabin door I encounter a fellow passenger who exults over the ship’s amenities. The liner has a heated indoor swimming pool, four electric elevators, two libraries, a Turkish bath, a squash court and gymnasium, and ample room to move about. The White Star Line has thoughtfully limited the amount of lifeboats to 20 to preserve precious deck space for passengers.
I’m Jeff Glasheen, and it’s Sept. 15, 2007.
As my wife prepares to deliver our first child in the coming weeks, we visit the labor and delivery deck of the hospital.
It will be our first major interaction with the healthcare system as patients. It’s the largest healthcare system ever and costs nearly $2 trillion a year to operate. We have chosen a new hospital that features an amazing array of amenities, including a birthing center with private suites, in-room baths with oversize soaking tubs, an in-room sleeping area for family and friends, and a DVD player and flat-screen television. There are even Internet connections.
Room service is available 24 hours a day, and the staff is top-notch. I’m told some choose to stay in the VIP suites for an extra $1,000 a night. This restricted-access area offers 600-square-foot rooms with original art on the walls, luxury mattresses and 350-thread count linens, complimentary robes and slippers, and an office area supplied with newspapers, a printer, fax, voicemail, and teleconferencing capabilities. There is a family room as well as a private refrigerator, an assortment of beverages and a dedicated chef. Unfortunately the cost is too steep, so we’ll spend this voyage in second class. However, as everyone knows, second class on this vessel outstrips first class in most hospitals these days.
Midnight, April 14, 1912
Something has gone wrong; the ship just hiccupped a bit. From my cabin I clearly hear a grinding that could happen only when two large objects come into contact. It’s strange, but I assure my bunkmates there is nothing to worry about. The Titanic is unsinkable, built with every feasible safety feature. The ship’s hull is made of inch-thick steel and held together with nearly 3 million steel rivets. In the unlikely event the hull is breached, the ship contains 15 watertight bulkheads to contain the leakage. Further, 3,560 life vests, 48 life buoys, and the aforementioned 20 lifeboats (four more than required by British law) allay my concerns.
On the off chance something should go wrong, the ship is outfitted with the recently developed Marconi wireless telegraph capable of communicating with any ship or shore within 500 miles.
5 p.m., Sept. 17, 2007
As I write this column I consider that something could go wrong during our hospital stay. The Institute of Medicine reports that medications harm 1.5 million people annually (400,000 incidents occur in the hospital) and that nearly 100,000 die annually in adverse hospital events.
I assure myself there is nothing to worry about. The hospital of today is unsinkable, built with every feasible safety measure. Today’s hospitals require two patient identifiers, time-outs before procedures, read-backs, standardized abbreviations, rules for reporting of critical results, standardized approaches to hand-offs, awareness of look-alike/sound-alike medications, hand-hygiene guidelines, medication reconciliation, core measures, quality and patient safety committees—and, on the off chance that something should go wrong, requirements for communicating sentinel event reviews with regulatory agencies.
1:30 a.m., April 14, 1912
The scuttlebutt is that the Titanic has hit an iceberg, tearing open the hull, flooding the bulkheads, and overcoming the ship’s pumps. Apparently the crow’s nest spotted the iceberg only 30 seconds before the impact. The crew tried to change course immediately. But the unprecedented size and speed of the ship (there is a rumor that the captain may have been trying to set a new trans-Atlantic crossing record) made it impossible to avoid our destiny.
We are clearly sinking. As I anxiously pace the deck waiting for a spot on a lifeboat, I chat with a crew member who assures me help is coming. The ship’s band plays on deck, the music soothing in the night air.
1 p.m., Aug. 26, 2007
I’m about halfway through the Titanic exhibit at the local museum of nature and science. The display is designed to give you the experience of being a passenger aboard the RMS Titanic.
Prior to entering, visitors receive a boarding pass with information about one of the actual passengers. I am the Rev. John Harper, traveling to America with my young daughter to begin a series of revival meetings in Chicago. At the end of the tour I’ll view the passenger manifest to discover my outcome.
Reluctantly, I board the ship, anxiously awaiting my fate. I gaze upon thousands of trinkets and treasures rescued from the Titanic since its remains were discovered 2.5 miles below the ocean’s surface 900 miles off the coast of New York in 1985.
I marvel at dioramas of first- and third-class cabins with recovered china settings, uncorked and still-full bottles of champagne, toiletries, jewelry, and clothing.
One of the most fascinating pieces is a chunk of ice the size and shape of a small whale. The display represents the iceberg that doomed the Titanic and simulates the temperature of the water that fateful night. At approximately 28 degrees Fahrenheit, the average person would survive less than 15 minutes in the water. I was able to hold my hand on the ice only a few moments, quickly understanding the horrific way most passengers would die.
As I complete the tour and nervously approach the passenger manifest I am struck by how many lessons from the Titanic can be applied to modern medicine.
We operate in a system surrounded by perilous obstacles in a huge vessel that is slow to change course even in the face of extreme danger and poor outcomes.
We steam along at unparalleled speed embracing new, relatively untested technologies, procedures, and medications. Modern healthcare, like the Titanic, values building technologically advanced, well-adorned vessels rather than investing in the basic infrastructure to make it safer. We eschew quality for appearance.
We spend money on heated indoor pools, squash courts, and Turkish baths rather than computerized provider order entry, bar code administration, and hand-off improvements. Despite all of this, our passengers trust the vessel is safe. They trust that we will protect them—that we have enough lifeboats.
The Rev. John Harper perished on April 14, 1912; unlike him, as I cross the threshold of the healthcare Titanic I am not filled with awe and excitement. I feel fear and dread. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver and Health Sciences Center, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
End-of-Life Predictions

The July 26 New England Journal of Medicine contained several articles of interest for hospitalists: A trial of steroids for bronchiolitis, mortality associated with type B aortic dissections, cardiovascular outcomes in patients using rofecoxib, implications of our social networks on obesity, and a terrific review of methicillin-resistant Staph aureus in soft-tissue infections.
But all these were trumped in the media by Oscar the cat.1
National Public Radio, CNN, Fox, and the BBC all covered the story about the cantankerous cat that could predict death in a community nursing home’s third-floor dementia unit with Grim Reaper-like proficiency. The 2-year-old cat was adopted and raised from kittenhood by staff members at the Steere House Nursing and Rehabilitation Center in Providence, R.I.
Nursing staff began noticing that Oscar would curl up in bed next to patients who had only hours to live. Oscar was so adept at predicting death that the nursing staff began using his prophesies to alert family members of an impending demise. Oscar rounds daily, waiting for closed doors to open when necessary and employing somewhat less-sophisticated methods than his human colleagues—namely observing and sniffing. However, this “cat scan” appears to serve as an unprecedented augur, accurately predicting the death of 25 nursing home residents.
Why all the fuss about this predictive puss in boots? To be sure it’s an intriguing story. But why does the public care so much that Oscar the cat can now be found in Wikipedia—and why should the average hospitalist care about a prognosticating cat?
The answer lies in the medical profession’s dreadful lack of ability to predict patients’ survival at the end of life. Multiple studies have shown physicians are terrible at predicting survival, most often in an overly optimistic manner. A paper in the British Medical Journal examined the ability of 343 doctors to estimate the survival of 468 patients at the time of referral to hospice.2 Only 20% of physicians were able to accurately prognosticate the time of death to within 33% of the actual survival. While median survival was 24 days doctors, on average, predicted patients would live 5.3 times longer than they did. Interestingly, the longer the doctor knew the patient the more likely they were to predict wrongly.
Most seriously ill patients value prognostic information more than they do information about therapeutic options. It is a central determinant in how patients and families make end-of-life decisions. The fact that we seem to systematically provide overly optimistic predictions has several important downstream effects.
Unduly optimistic predictions likely delay referral to palliative care providers and hospice. Doctors generally believe patients should receive hospice care for several months before death. However, patients typically receive this care for less than a month and in many cases only a few hours. Our inability to realistically predict survival most likely plays into this discrepancy and negatively affects our patients’ quality of life.
Second, our consistently overestimated predictions likely translate into patients making inappropriate or counterproductive end-of-life decisions.
We’ve all experienced the patient who continues to push for obviously futile care despite our attempts to nudge them toward a palliative approach. Yet it’s easy to see why patients who believe they have six months to live would push for more aggressive treatments. If they knew they had six weeks to live, they might choose more palliative options.
Finally, hospitalists are increasingly under the gun to decrease length of stay (LOS) and contain costs. It is estimated that more than 25% of Medicare costs (approximately $88 billion a year) are associated with care in the last year of life, much of it in the hospital. While several studies have shown that early palliative care intervention reduces LOS and cost of care, overly optimistic predictions make it less likely these timely referrals will be made.
The development of the hospitalist model, with its fractured approach to care, might provide an opportunity to improve end-of-life prognostication. Having a strong, long-lasting relationship with a patient appears to be an important predictor of inaccurate prognosis. It isn’t hard to imagine that a provider with a long relationship with a patient might have a more difficult time acknowledging a patient’s poor outcome or unwittingly be less likely to squelch a patient’s hope with a poor prognosis.
We can take advantage of the inherent discontinuities of the hospitalist model as well as the severity and immediacy of the patient’s acute illness to not only proffer an end-of-life prediction but contextualize it for the patient. This, of course, needs to be done in a sensitive manner that recognizes our brief role in their care and, as such, is most often best managed in concert with the patient’s primary care provider.
The promise of the hospital medicine movement is that we can do it better and cheaper. This is a tall order indeed. While the hospitalist model has improved efficiency and quality, future improvements will require us to adopt and develop new efficiencies and better systems of care.
It is in this vein that I believe we can and should be able to improve end-of-life care. An early salvo in this front can be a dedicated and systematic push to improve end-of-life prognostication and its myriad downstream effects. This will require a conscientious effort, more formal education, and better predictive tools. As hospitalists, we are perfectly positioned to lead these efforts. The other alternative may be to adopt more cats into our multidisciplinary team. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver and Health Sciences Center, where he serves as director of the Hospital Medicine Program, Inpatient Clinical Services in the Department of Medicine, and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Dosa DA. A day in the life of Oscar the cat. N Engl J Med. 2007;357(4):328-329.
- Christakis NA, Lamont EB. Extent and determinants of error in doctors’ prognoses in terminally ill patients: prospective cohort study. BMJ. 2000;320:469-472.
The July 26 New England Journal of Medicine contained several articles of interest for hospitalists: A trial of steroids for bronchiolitis, mortality associated with type B aortic dissections, cardiovascular outcomes in patients using rofecoxib, implications of our social networks on obesity, and a terrific review of methicillin-resistant Staph aureus in soft-tissue infections.
But all these were trumped in the media by Oscar the cat.1
National Public Radio, CNN, Fox, and the BBC all covered the story about the cantankerous cat that could predict death in a community nursing home’s third-floor dementia unit with Grim Reaper-like proficiency. The 2-year-old cat was adopted and raised from kittenhood by staff members at the Steere House Nursing and Rehabilitation Center in Providence, R.I.
Nursing staff began noticing that Oscar would curl up in bed next to patients who had only hours to live. Oscar was so adept at predicting death that the nursing staff began using his prophesies to alert family members of an impending demise. Oscar rounds daily, waiting for closed doors to open when necessary and employing somewhat less-sophisticated methods than his human colleagues—namely observing and sniffing. However, this “cat scan” appears to serve as an unprecedented augur, accurately predicting the death of 25 nursing home residents.
Why all the fuss about this predictive puss in boots? To be sure it’s an intriguing story. But why does the public care so much that Oscar the cat can now be found in Wikipedia—and why should the average hospitalist care about a prognosticating cat?
The answer lies in the medical profession’s dreadful lack of ability to predict patients’ survival at the end of life. Multiple studies have shown physicians are terrible at predicting survival, most often in an overly optimistic manner. A paper in the British Medical Journal examined the ability of 343 doctors to estimate the survival of 468 patients at the time of referral to hospice.2 Only 20% of physicians were able to accurately prognosticate the time of death to within 33% of the actual survival. While median survival was 24 days doctors, on average, predicted patients would live 5.3 times longer than they did. Interestingly, the longer the doctor knew the patient the more likely they were to predict wrongly.
Most seriously ill patients value prognostic information more than they do information about therapeutic options. It is a central determinant in how patients and families make end-of-life decisions. The fact that we seem to systematically provide overly optimistic predictions has several important downstream effects.
Unduly optimistic predictions likely delay referral to palliative care providers and hospice. Doctors generally believe patients should receive hospice care for several months before death. However, patients typically receive this care for less than a month and in many cases only a few hours. Our inability to realistically predict survival most likely plays into this discrepancy and negatively affects our patients’ quality of life.
Second, our consistently overestimated predictions likely translate into patients making inappropriate or counterproductive end-of-life decisions.
We’ve all experienced the patient who continues to push for obviously futile care despite our attempts to nudge them toward a palliative approach. Yet it’s easy to see why patients who believe they have six months to live would push for more aggressive treatments. If they knew they had six weeks to live, they might choose more palliative options.
Finally, hospitalists are increasingly under the gun to decrease length of stay (LOS) and contain costs. It is estimated that more than 25% of Medicare costs (approximately $88 billion a year) are associated with care in the last year of life, much of it in the hospital. While several studies have shown that early palliative care intervention reduces LOS and cost of care, overly optimistic predictions make it less likely these timely referrals will be made.
The development of the hospitalist model, with its fractured approach to care, might provide an opportunity to improve end-of-life prognostication. Having a strong, long-lasting relationship with a patient appears to be an important predictor of inaccurate prognosis. It isn’t hard to imagine that a provider with a long relationship with a patient might have a more difficult time acknowledging a patient’s poor outcome or unwittingly be less likely to squelch a patient’s hope with a poor prognosis.
We can take advantage of the inherent discontinuities of the hospitalist model as well as the severity and immediacy of the patient’s acute illness to not only proffer an end-of-life prediction but contextualize it for the patient. This, of course, needs to be done in a sensitive manner that recognizes our brief role in their care and, as such, is most often best managed in concert with the patient’s primary care provider.
The promise of the hospital medicine movement is that we can do it better and cheaper. This is a tall order indeed. While the hospitalist model has improved efficiency and quality, future improvements will require us to adopt and develop new efficiencies and better systems of care.
It is in this vein that I believe we can and should be able to improve end-of-life care. An early salvo in this front can be a dedicated and systematic push to improve end-of-life prognostication and its myriad downstream effects. This will require a conscientious effort, more formal education, and better predictive tools. As hospitalists, we are perfectly positioned to lead these efforts. The other alternative may be to adopt more cats into our multidisciplinary team. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver and Health Sciences Center, where he serves as director of the Hospital Medicine Program, Inpatient Clinical Services in the Department of Medicine, and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Dosa DA. A day in the life of Oscar the cat. N Engl J Med. 2007;357(4):328-329.
- Christakis NA, Lamont EB. Extent and determinants of error in doctors’ prognoses in terminally ill patients: prospective cohort study. BMJ. 2000;320:469-472.
The July 26 New England Journal of Medicine contained several articles of interest for hospitalists: A trial of steroids for bronchiolitis, mortality associated with type B aortic dissections, cardiovascular outcomes in patients using rofecoxib, implications of our social networks on obesity, and a terrific review of methicillin-resistant Staph aureus in soft-tissue infections.
But all these were trumped in the media by Oscar the cat.1
National Public Radio, CNN, Fox, and the BBC all covered the story about the cantankerous cat that could predict death in a community nursing home’s third-floor dementia unit with Grim Reaper-like proficiency. The 2-year-old cat was adopted and raised from kittenhood by staff members at the Steere House Nursing and Rehabilitation Center in Providence, R.I.
Nursing staff began noticing that Oscar would curl up in bed next to patients who had only hours to live. Oscar was so adept at predicting death that the nursing staff began using his prophesies to alert family members of an impending demise. Oscar rounds daily, waiting for closed doors to open when necessary and employing somewhat less-sophisticated methods than his human colleagues—namely observing and sniffing. However, this “cat scan” appears to serve as an unprecedented augur, accurately predicting the death of 25 nursing home residents.
Why all the fuss about this predictive puss in boots? To be sure it’s an intriguing story. But why does the public care so much that Oscar the cat can now be found in Wikipedia—and why should the average hospitalist care about a prognosticating cat?
The answer lies in the medical profession’s dreadful lack of ability to predict patients’ survival at the end of life. Multiple studies have shown physicians are terrible at predicting survival, most often in an overly optimistic manner. A paper in the British Medical Journal examined the ability of 343 doctors to estimate the survival of 468 patients at the time of referral to hospice.2 Only 20% of physicians were able to accurately prognosticate the time of death to within 33% of the actual survival. While median survival was 24 days doctors, on average, predicted patients would live 5.3 times longer than they did. Interestingly, the longer the doctor knew the patient the more likely they were to predict wrongly.
Most seriously ill patients value prognostic information more than they do information about therapeutic options. It is a central determinant in how patients and families make end-of-life decisions. The fact that we seem to systematically provide overly optimistic predictions has several important downstream effects.
Unduly optimistic predictions likely delay referral to palliative care providers and hospice. Doctors generally believe patients should receive hospice care for several months before death. However, patients typically receive this care for less than a month and in many cases only a few hours. Our inability to realistically predict survival most likely plays into this discrepancy and negatively affects our patients’ quality of life.
Second, our consistently overestimated predictions likely translate into patients making inappropriate or counterproductive end-of-life decisions.
We’ve all experienced the patient who continues to push for obviously futile care despite our attempts to nudge them toward a palliative approach. Yet it’s easy to see why patients who believe they have six months to live would push for more aggressive treatments. If they knew they had six weeks to live, they might choose more palliative options.
Finally, hospitalists are increasingly under the gun to decrease length of stay (LOS) and contain costs. It is estimated that more than 25% of Medicare costs (approximately $88 billion a year) are associated with care in the last year of life, much of it in the hospital. While several studies have shown that early palliative care intervention reduces LOS and cost of care, overly optimistic predictions make it less likely these timely referrals will be made.
The development of the hospitalist model, with its fractured approach to care, might provide an opportunity to improve end-of-life prognostication. Having a strong, long-lasting relationship with a patient appears to be an important predictor of inaccurate prognosis. It isn’t hard to imagine that a provider with a long relationship with a patient might have a more difficult time acknowledging a patient’s poor outcome or unwittingly be less likely to squelch a patient’s hope with a poor prognosis.
We can take advantage of the inherent discontinuities of the hospitalist model as well as the severity and immediacy of the patient’s acute illness to not only proffer an end-of-life prediction but contextualize it for the patient. This, of course, needs to be done in a sensitive manner that recognizes our brief role in their care and, as such, is most often best managed in concert with the patient’s primary care provider.
The promise of the hospital medicine movement is that we can do it better and cheaper. This is a tall order indeed. While the hospitalist model has improved efficiency and quality, future improvements will require us to adopt and develop new efficiencies and better systems of care.
It is in this vein that I believe we can and should be able to improve end-of-life care. An early salvo in this front can be a dedicated and systematic push to improve end-of-life prognostication and its myriad downstream effects. This will require a conscientious effort, more formal education, and better predictive tools. As hospitalists, we are perfectly positioned to lead these efforts. The other alternative may be to adopt more cats into our multidisciplinary team. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver and Health Sciences Center, where he serves as director of the Hospital Medicine Program, Inpatient Clinical Services in the Department of Medicine, and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Dosa DA. A day in the life of Oscar the cat. N Engl J Med. 2007;357(4):328-329.
- Christakis NA, Lamont EB. Extent and determinants of error in doctors’ prognoses in terminally ill patients: prospective cohort study. BMJ. 2000;320:469-472.
Transitions of Care

As I embark on my tenure as physician editor of The Hospitalist, I am struck by the similarities between the editor transition and the transitions of care that happen as part of the daily backdrop of our hospitalist lives.
Both scenarios depend on open communication, a multidisciplinary team approach, a well-considered plan, and constituent feedback.
Similar to the communication between providers in patient handoffs, the previous editor, Jamie Newman, MD, and I talked about the history, course, and plan for the publication. Unlike most of my hospital handoffs, this patient is in great condition.
Jamie took over 24 months ago during a major transition for the publication and masterfully shepherded it to the place of prominence it holds today. For this he deserves a ton of credit. The content is top-notch, the reporting timely and noteworthy, and the design compelling.
As a consequence the readership is strong; so strong, it has played an influential role in our transitional communication. Several months ago we asked you to submit feedback about the publication in the form of a reader survey. From that data it was clear The Hospitalist was headed in the right direction but could use a slight “rehab” consult to make it even stronger. You provided several inputs instrumental to enhancing the publication. In short, you clearly desired more clinical content, an easier-to-use “In the Literature” section, and more concise material. These ideas formed the cornerstone of the upcoming changes in the publication.
More Clinical Content
In the near future we will begin to run more articles about the topics that induce the most angina in hospitalists. In general, we will de-emphasize comprehensive topic reviews (e.g., “Congestive heart failure from A to Z: genomics, pathogenesis, presentation, diagnostics, therapeutics and beyond”).
In its place we will introduce shorter articles centered on controversial questions in hospital medicine, the type and scope of questions that by their very nature are common, contentious, and stress-inducing (e.g.,
When should nesiritide therapy be initiated in acute decompensated CHF?).
New “In the Lit”
While this is one of the most well-read sections, many noted it can be difficult to navigate and sometimes seems bloated. To remedy this, we will increase the number of articles reviewed while decreasing the amount of detail per article. What we lose in depth we hope to gain in breadth.
We feel this will provide a general overview of all the pertinent literature so you can be confident you are up to date on take-home points of the most current studies. The department will also be reformatted so it is much easier to find the most crucial information. Look for these changes in the next month or two.
New Departments
The “Legal Eagle” and “Billing and Coding” departments will provide important information on medical malpractice and reimbursement documentation, while the “Hospital Pharmacy” department will offer up-to-the minute highlights of advances in therapeutics.
Finally, an advice column will give you the opportunity to ask experts your questions about the practice of hospital medicine.
Of course, much of The Hospitalist will remain unchanged. We will preserve your favorite features such John Nelson’s “Practice Management” column, Larry Wellikson’s “SHM Point of View” column, and the “Society Pages” and “Public Policy” departments. All this will happen against the backdrop of timely, in-depth reporting that keeps you abreast of the world of hospital medicine.
In all this transitioning it is important to recognize the team effort this publication requires. Indeed, the success of this publication is multidisciplinary and includes the expertise of the many folks at Wiley, notably Lisa Dionne (editorial director), Geoff Giordano (editor), and our colleagues at SHM—Larry Wellikson (CEO of SHM) and Todd Von Deak (director of membership and marketing) as well as the entire editorial and publishing staff at Wiley.
Most importantly, the success of this transition—and indeed the publication itself—depends on feedback from you, the reader. My e-mail box is always open to suggestions on how to improve the publication, including feedback on what we’re doing right and what we need to change. I’m also interested in hearing your ideas about clinical content areas that need to be covered. Just shoot me an e-mail saying, “I’d like to learn more about … .” And, we always welcome offers to contribute content to the publication.
To all of you: Thanks for helping make this transition such a successful one. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver and Health Sciences Center, where he serves as director of the Hospital Medicine Program, Inpatient Clinical Services in the Department of Medicine, and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
As I embark on my tenure as physician editor of The Hospitalist, I am struck by the similarities between the editor transition and the transitions of care that happen as part of the daily backdrop of our hospitalist lives.
Both scenarios depend on open communication, a multidisciplinary team approach, a well-considered plan, and constituent feedback.
Similar to the communication between providers in patient handoffs, the previous editor, Jamie Newman, MD, and I talked about the history, course, and plan for the publication. Unlike most of my hospital handoffs, this patient is in great condition.
Jamie took over 24 months ago during a major transition for the publication and masterfully shepherded it to the place of prominence it holds today. For this he deserves a ton of credit. The content is top-notch, the reporting timely and noteworthy, and the design compelling.
As a consequence the readership is strong; so strong, it has played an influential role in our transitional communication. Several months ago we asked you to submit feedback about the publication in the form of a reader survey. From that data it was clear The Hospitalist was headed in the right direction but could use a slight “rehab” consult to make it even stronger. You provided several inputs instrumental to enhancing the publication. In short, you clearly desired more clinical content, an easier-to-use “In the Literature” section, and more concise material. These ideas formed the cornerstone of the upcoming changes in the publication.
More Clinical Content
In the near future we will begin to run more articles about the topics that induce the most angina in hospitalists. In general, we will de-emphasize comprehensive topic reviews (e.g., “Congestive heart failure from A to Z: genomics, pathogenesis, presentation, diagnostics, therapeutics and beyond”).
In its place we will introduce shorter articles centered on controversial questions in hospital medicine, the type and scope of questions that by their very nature are common, contentious, and stress-inducing (e.g.,
When should nesiritide therapy be initiated in acute decompensated CHF?).
New “In the Lit”
While this is one of the most well-read sections, many noted it can be difficult to navigate and sometimes seems bloated. To remedy this, we will increase the number of articles reviewed while decreasing the amount of detail per article. What we lose in depth we hope to gain in breadth.
We feel this will provide a general overview of all the pertinent literature so you can be confident you are up to date on take-home points of the most current studies. The department will also be reformatted so it is much easier to find the most crucial information. Look for these changes in the next month or two.
New Departments
The “Legal Eagle” and “Billing and Coding” departments will provide important information on medical malpractice and reimbursement documentation, while the “Hospital Pharmacy” department will offer up-to-the minute highlights of advances in therapeutics.
Finally, an advice column will give you the opportunity to ask experts your questions about the practice of hospital medicine.
Of course, much of The Hospitalist will remain unchanged. We will preserve your favorite features such John Nelson’s “Practice Management” column, Larry Wellikson’s “SHM Point of View” column, and the “Society Pages” and “Public Policy” departments. All this will happen against the backdrop of timely, in-depth reporting that keeps you abreast of the world of hospital medicine.
In all this transitioning it is important to recognize the team effort this publication requires. Indeed, the success of this publication is multidisciplinary and includes the expertise of the many folks at Wiley, notably Lisa Dionne (editorial director), Geoff Giordano (editor), and our colleagues at SHM—Larry Wellikson (CEO of SHM) and Todd Von Deak (director of membership and marketing) as well as the entire editorial and publishing staff at Wiley.
Most importantly, the success of this transition—and indeed the publication itself—depends on feedback from you, the reader. My e-mail box is always open to suggestions on how to improve the publication, including feedback on what we’re doing right and what we need to change. I’m also interested in hearing your ideas about clinical content areas that need to be covered. Just shoot me an e-mail saying, “I’d like to learn more about … .” And, we always welcome offers to contribute content to the publication.
To all of you: Thanks for helping make this transition such a successful one. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver and Health Sciences Center, where he serves as director of the Hospital Medicine Program, Inpatient Clinical Services in the Department of Medicine, and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
As I embark on my tenure as physician editor of The Hospitalist, I am struck by the similarities between the editor transition and the transitions of care that happen as part of the daily backdrop of our hospitalist lives.
Both scenarios depend on open communication, a multidisciplinary team approach, a well-considered plan, and constituent feedback.
Similar to the communication between providers in patient handoffs, the previous editor, Jamie Newman, MD, and I talked about the history, course, and plan for the publication. Unlike most of my hospital handoffs, this patient is in great condition.
Jamie took over 24 months ago during a major transition for the publication and masterfully shepherded it to the place of prominence it holds today. For this he deserves a ton of credit. The content is top-notch, the reporting timely and noteworthy, and the design compelling.
As a consequence the readership is strong; so strong, it has played an influential role in our transitional communication. Several months ago we asked you to submit feedback about the publication in the form of a reader survey. From that data it was clear The Hospitalist was headed in the right direction but could use a slight “rehab” consult to make it even stronger. You provided several inputs instrumental to enhancing the publication. In short, you clearly desired more clinical content, an easier-to-use “In the Literature” section, and more concise material. These ideas formed the cornerstone of the upcoming changes in the publication.
More Clinical Content
In the near future we will begin to run more articles about the topics that induce the most angina in hospitalists. In general, we will de-emphasize comprehensive topic reviews (e.g., “Congestive heart failure from A to Z: genomics, pathogenesis, presentation, diagnostics, therapeutics and beyond”).
In its place we will introduce shorter articles centered on controversial questions in hospital medicine, the type and scope of questions that by their very nature are common, contentious, and stress-inducing (e.g.,
When should nesiritide therapy be initiated in acute decompensated CHF?).
New “In the Lit”
While this is one of the most well-read sections, many noted it can be difficult to navigate and sometimes seems bloated. To remedy this, we will increase the number of articles reviewed while decreasing the amount of detail per article. What we lose in depth we hope to gain in breadth.
We feel this will provide a general overview of all the pertinent literature so you can be confident you are up to date on take-home points of the most current studies. The department will also be reformatted so it is much easier to find the most crucial information. Look for these changes in the next month or two.
New Departments
The “Legal Eagle” and “Billing and Coding” departments will provide important information on medical malpractice and reimbursement documentation, while the “Hospital Pharmacy” department will offer up-to-the minute highlights of advances in therapeutics.
Finally, an advice column will give you the opportunity to ask experts your questions about the practice of hospital medicine.
Of course, much of The Hospitalist will remain unchanged. We will preserve your favorite features such John Nelson’s “Practice Management” column, Larry Wellikson’s “SHM Point of View” column, and the “Society Pages” and “Public Policy” departments. All this will happen against the backdrop of timely, in-depth reporting that keeps you abreast of the world of hospital medicine.
In all this transitioning it is important to recognize the team effort this publication requires. Indeed, the success of this publication is multidisciplinary and includes the expertise of the many folks at Wiley, notably Lisa Dionne (editorial director), Geoff Giordano (editor), and our colleagues at SHM—Larry Wellikson (CEO of SHM) and Todd Von Deak (director of membership and marketing) as well as the entire editorial and publishing staff at Wiley.
Most importantly, the success of this transition—and indeed the publication itself—depends on feedback from you, the reader. My e-mail box is always open to suggestions on how to improve the publication, including feedback on what we’re doing right and what we need to change. I’m also interested in hearing your ideas about clinical content areas that need to be covered. Just shoot me an e-mail saying, “I’d like to learn more about … .” And, we always welcome offers to contribute content to the publication.
To all of you: Thanks for helping make this transition such a successful one. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver and Health Sciences Center, where he serves as director of the Hospital Medicine Program, Inpatient Clinical Services in the Department of Medicine, and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
In the Literature
Repeat Testing for C. Diff?
By Jeff Glasheen, MD
Mohan SS, McDermott BP, Parchuri S, et al. Lack of value of repeat stool testing for Clostridium difficile toxin. Am J Med. 2006 Apr;119(4):356.e7-356.e8
Clostridium difficile is a common complication of antibiotic and chemotherapeutic use, especially in hospitalized patients. Yet most nosocomial diarrhea is not caused by C. difficile. Most antibiotics can cause loose stools through changes in the gastrointestinal flora that result in inadequate digestion and absorption of carbohydrates and a resultant osmotic diarrhea. Further, antibiotics such as erythromycin and amoxicillin/clavulanate may result in diarrhea via increases in GI tract motility. While osmotic and motility causes of diarrhea tend to improve with antibiotic discontinuation, C. difficile-associated diarrhea is associated with significant morbidity that often continues until adequately treated.
Thus having a test that differentiates between C. difficile and non-clostridial diarrhea is essential. The most commonly used test is the enzyme immunoassay (EIA) that detects toxins A and B. The sensitivity and specificity of this test has been reported to range between 50%-90% and 70%-95%, respectively. The authors of this paper evaluated the utility of repeat EIA testing in patients with a one negative test in the setting of nosocomial diarrhea associated with antibiotic use.
The authors reviewed 474 sequential EIA tests for C. difficile in 396 patients over a 10-month period at a large university-affiliated community hospital with an EIA sensitivity and specificity of 80%-90% and 80%-95%, respectively. Tests were considered to be “repeat” if they occurred within seven days of the original negative test. Of the 78 repeat tests (16.5% of all tests), only one was positive, resulting in a 0.8% conversion rate. At an institutional cost of $128 per test the total cost of EIA testing over the 10-month period was $60,672. The cost of repeat testing alone was $9,984. The authors conclude that there is limited value—and high cost—in repeat EIA testing and that alternative sources of diarrhea should be sought or we should repeat EIA testing in patients with continued nosocomial diarrhea and a negative EIA test.
While prior studies have shown incremental benefit of retesting for C. difficile with the EIA assay, this study’s authors conclude that repeat “C. difficile testing is not clinically justified and is economically wasteful.” Unfortunately, the authors did not utilize a strong enough research design to defend this statement. From the data presented, all we can conclude is that repeat testing with an EIA assay did not add significant value to the diagnostic workup. The lack of a negative gold standard test, such as the cytotoxin assay or follow up outcomes, such as resolution of diarrhea, leaves the reader pondering if the repeat EIA assays were negative because the patients did not have C. difficile or because the test was not sensitive enough to detect the toxin. The reported sensitivity for the EIA assay used was 80-90%, meaning that 10%-20% of patients with C. difficile disease would have had a false negative test. While a second negative test would lower the likelihood of true disease, it would not lower it enough in a patient with a high pre-test probability of disease to sufficiently rule out the disease such that further testing is indicated.
Additionally, while we can extrapolate that the EIA test was of little utility to the patients studied here, no patient-specific data is presented. Thus it is difficult to determine if our patient population is represented in the study. More knowledge about the patients would allow the reader to use published prediction rules to better delineate how likely it was that this cohort was at high risk for having toxin-mediated diarrhea. Perhaps a more reasonable approach to this clinical conundrum would be to send the repeat stool test for a cytotoxin assay or to treat the patient empirically in situations where either the likelihood of disease or the disease burden is high.
Stroke after MI
By Ethan Cumbler, MD
Witt BJ, Ballman KV, Brown RD Jr, et al. The incidence of stroke after myocardial infarction: a meta-analysis. Am J Med. 2006 Apr;119(4):354.e1-9.
Stroke and myocardial infarction (MI) share many of the risk factors leading to atherosclerosis, including hypertension, hyperlipidemia, diabetes, tobacco abuse, and age. Logically, patients at risk for one event would also be at risk for the other, yet this interaction appears to be more complex. The study by Witt, et al., aims to elucidate the rate of in-hospital stroke in patients initially admitted with an MI.
The authors analyzed 22 observational studies of myocardial infarction that recorded the incidence of cerebrovascular accidents after acute MI. Clinical trials were excluded from the analysis in order to provide representation of an unselected population. Of the trials reviewed, 11 were included in the analysis of in-hospital strokes, three for the 30-day time point, and two for the one-year time point. The other trials used different time points and were not included in the analysis. The patients had a mean age ranging between 59 and 72.7 years, and all had a predominance of males. The rate of in-hospital stroke was 11.1 events per 1,000 hospitalizations. This incidence rose to 12.2/1,000 at 30 days and 21.4/1,000 at one year.
Plausible hypotheses for why the rate of cerebrovascular accident would be particularly high in the post-MI period include the potential for localized wall motion dysmotility or low flow leading to intracardiac thrombosis, event-related arrhythmia, or procedure-related embolic events. The studies from which this meta-analysis was derived were not designed in such a way for a causal relationship to be identified. However, age, diabetes, hypertension, prior stroke, anterior location of MI, atrial fibrillation, heart failure, and nonwhite race were all found to have an association with increased risk for stroke. Interestingly, angina on presentation was associated with an apparent decreased risk, theorized to potentially be due to ischemic preconditioning.
While this study shares the usual limitations of meta-analyses of observational studies, the authors have done an excellent summation of the data available including both English and non-English language articles in the analysis. Notably, the review included studies spanning more than 25 years and, thus, included data from studies done in the era prior to modern therapy for cardiac ischemia including potent antiplatelet and statin therapy. The three studies with in-hospital time points started in the 1990s had a lower average rate of stroke, which may reflect the effect of more potent anti-platelet agents used in today’s therapy for acute coronary syndromes.
The implication for the hospitalist is to recognize that patients admitted for MI are at high risk for stroke during the index hospitalization. A low threshold for suspicion of a cerebrovascular event needs to be maintained for post-MI patients with new neurologic symptoms. Future studies will be needed to address the risk/benefit of anticoagulation in high-risk patients for stroke following a myocardial infarction.
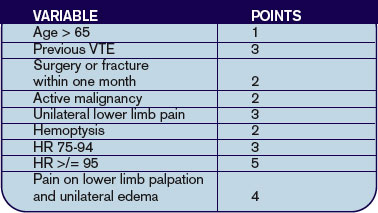
Predicting PE in the ED Using Revised Geneva Score
By Jeffrey Carter, MD
Le Gal G, Righini M, Roy PM, et al. Prediction of pulmonary embolism in the emergency department: the revised Geneva score. Ann Intern Med. 2006 Feb 7;144(3):165-171.
Introduction: Pulmonary embolism remains a common life-threatening disorder with imperfect diagnostic modalities and strategies. Much of the current literature focuses on the development and validation of clinical probability assessments that identify low-risk patients who can be safely managed without invasive testing or lung scanning.
Two common scoring systems include the Geneva and Wells criteria, which employ a combination of historical information, clinical and laboratory data to stratify patients into three risk groups.1,2 It has recently been shown that a single negative D-dimer test safely excludes patients with suspected VTE in a large cohort, with a three-month follow-up rate of VTE of 0%.3 Criticism of current clinical probability assessment strategies include the inclusion of subjective criteria or the need for blood gas values.1,2 In this paper, the authors sought to derive and validate a scoring system based on readily available objective clinical data.
Methods: The cohort evaluated in this study consists of the same 965 patients used to prospectively evaluate an emergency department diagnostic strategy of VTE.3 Patients presenting to the emergency ward with complaints of chest pain or shortness of breath were evaluated with a standard diagnostic workup that included a checklist of demographic and historical information, signs and symptoms possibly consistent with VTE, ABG, chest X-ray, and EKG results, as well as the likelihood of another diagnosis. However, the goal was to create a scoring system based on readily available objective data, so ABG, chest X-ray and electrocardiogram results were not evaluated as possible components of the score. Clinical variables associated with pulmonary embolism were evaluated for statistical significance in both a univariate and multivariate model. These variables were then validated both internally and with an external cohort.
Results: The incidence of VTE was 23% (222/965). Ten clinical variables were found to be statistically significantly associated with VTE; these comprise the Revised Geneva Score.
Clinical probability is based on points: 0-3 is low probability; 4-10 is intermediate probability, and >10 is high probability. Low, intermediate, and high clinical probabilities had respective rates of VTE of 8%, 28%, and 74%. These percentages were found in the validation cohort and were similar to those in the derivation cohort.
Discussion: This study focuses on the derivation and validation of a clinical scoring system that can provide a numerical estimate of likelihood of VTE. The diagnostic strategy by which VTE is confirmed or excluded is from derivation cohort and is published elsewhere.3 In that study patients classified as no VTE and not treated had a 90-day risk of VTE of 1%. The nine-point revised Geneva score does indeed provide an accurate assessment of risk of VTE, and can thus help guide clinical decision-making. However it is not clear that the revised Geneva score will help decrease invasive diagnostic tests. In the low-risk group, 8% is too great a risk of a life-threatening illness to forego further diagnostic evaluation. Coupled with a negative ELISA D-dimer, exclusion of these patients is safe, but these patients cannot be safely excluded without risk stratification.3
References
- Wells PS, Anderson DR, Rodger M, et al. Derivation of a simple clinical model to categorize patients’ probability of pulmonary embolism: increasing the model’s utility with the SimpliRED D-dimer. Thromb Haemost. 2000 Mar;83:416-420.
- Wicki J, Perneger TV, Junof AF, et al. Assessing clinical probability of pulmonary embolism in the emergency ward: a simple score. Arch Intern Med. 2001 Jan 8;161(1):92-97.
- Perrier A, Roy PM, Aujesky D, et al. Diagnosing pulmonary embolism in outpatients with clinical assessment, D-dimer measurement, venous ultrasound and helical computed tomography: a multicenter management study. Am J Med. 2004 Mar 1;116(5):291-299.
LMWH for Inpatient Palliative Care
By Jeanie Youngwerth, MD
Noble SI, Nelson A, Turner C, et al. Acceptability of low molecular weight heparin thromboprophylaxis for patients receiving palliative care: qualitative study. BMJ. 2006 Mar 11:332(7541);577-580.ePub 2006 Feb 3.
Venous thromboembolism is a major risk factor for patients with malignancy. VTE may reduce survival time in patients receiving palliative care, with one in seven inpatients with cancer dying from pulmonary embolism. The American College of Chest Physicians recommend low molecular weight heparin (LMWH) in hospitalized patients with cancer as level 1A evidence in their 2004 consensus statement on VTE. There are no thromboprophylaxis guidelines in the United Kingdom. Many physicians view daily injections of LMWH as unnecessary distress for palliative care patients. This study focused on what inpatients with advanced cancer receiving palliative care thought about the effect of thromboprophylaxis on overall quality of life.
This was a qualitative study of 28 inpatients receiving palliative care who had advanced metastatic cancer and who were in a regional cancer center in Wales. The patients had received LMWH for at least five consecutive days. The patients were audiotaped and then had semi-structured interviews transcribed regarding cancer treatments they had received. These interviews covered the patients’ insight into prognosis, their understanding of thromboprophylaxis, their beliefs concerning the effects of thromboprophylaxis on overall quality of life, and the negative aspects of heparin treatment.
The main outcome measures were recurring themes of the effect of thromboprophylaxis on overall quality of life. Major themes identified were insight into prognosis, knowledge and understanding of thromboprophylaxis, acceptability of heparin thromboprophylaxis, reassurance, and optimism. Minor themes identified were bruising, negative impact of antiembolic stockings, and anger at paternalistic views toward terminally ill patients.
Most patients showed clear insight into the nature of their condition and understood heparin prophylaxis for VTE. Many patients identified immobility and surgery as VTE risk factors, with little understanding of cancer as a risk factor. All knew that VTE could cause death, but none were aware of the common symptoms. All patients found LMWH thromboprophylaxis acceptable. Patients believed taking measures to prevent symptoms might improve their quality of life and felt that the medical team had not given up on them.
The only negative experiences of LMWH thromboprophylaxis was bruising. All of the patients who wore antiembolic stockings during previous admissions found them uncomfortable. Patients expressed their need to be involved in decision-making, particularly with respect to withdrawal or non-administration of treatment.
This small, qualitative study showed that, contrary to many physicians’ beliefs, patients in palliative care units believe that LMWH injections are acceptable as thromboprophylaxis, but antiembolic stockings are not. The effect of daily injections had little or no effect on the quality of life, with many patients having positive feelings that things were being done to prevent new problems from occurring.
This study was limited by the small sample size, the qualitative nature that could introduce interpretation bias, and the fact that only patients using LMWH were included. Additionally, the United Kingdom has aggressively educated the public on the risks of VTE associated with long flights such that baseline knowledge may differ in other parts of the world. Resource utilization, including drug costs and length of stay, as well as effect on mortality were not studied.
The implications for hospitalists are that many inpatients with advanced cancer receiving palliative care may find LMWH thromboprophylaxis acceptable therapy, and that discussions with the patient regarding this option should be explored together.
Cost Analysis: Intensive Glycemic Control in Critically Ill Adults
By Whitney Woodmansee, MD
Krinsley JS, Jones, RL. Cost analysis of intensive glycemic control in critically ill adult patients. Chest. 2006;129:644-650.
Several studies have demonstrated improved outcomes and decreased mortality in ICU patients treated with intensive control of blood glucose levels. This study sought to identify the costs associated with intensive glycemic control in the ICU.
An ICU patient database was analyzed for cost data related to intensive glycemic control. A baseline group of 800 consecutive ICU patients admitted prior to initiation (baseline) of an intensive glucose management (blood glucose levels between 80-140 mg/dl protocol were compared with a treatment group of 800 consecutive patients admitted after initiation of the protocol). Previously reported outcomes of these patients demonstrated significant improvement in mortality with tight glycemic control. Costs related to ICU and non-ICU length of stay; duration of mechanical ventilation; and all laboratory, pharmacy, and radiology services were analyzed between groups. Resource utilization was determined by assessing charges from the database and adjusting for inflation and applying Medicare cost, charge ratios for each category, and fiscal year. Costs associated with the intensive glycemic control protocol were determined. Unfortunately, only cost estimates for insulin and associated disposable supplies for each group were available for analysis.
Baseline and treatment populations did not differ significantly regarding demographics such as age, gender, race, admitting diagnosis, diabetes prevalence, or APACHE II scores. There were fewer patients in the treatment group that required mechanical ventilation during their ICU stay (40.6% versus 33.6%). Intensive glucose management was associated with a 13.9% reduction in total ICU days and duration of mechanical ventilation (median of two days decreased to 1.7 days p=0.045). There was a $1,580 adjusted cost savings per patient in the intensive treatment group compared with the baseline group (p<0.001). This reduction in cost was primarily driven by a decrease in laboratory and radiology costs in the ventilated patients. There were nonsignificant cost reductions in the unventilated patients.
Intensive control of hyperglycemia in the hospitalized ICU patient appears to be associated with reduction of morbidity and mortality. This suggests that tight glycemic control also leads to reductions in overall patient care costs—particularly in the ventilated ICU patient. Although not a randomized control trial, database analysis of costs and resource utilization demonstrated an overall cost savings in the treatment group (after initiation of an intensive glycemic control protocol) compared with the baseline group (before protocol initiation). One caveat is that the authors used estimates when determining the costs associated with the implementation of the intensive glucose management protocol. Nevertheless, intensive glycemic control was associated with an overall reduction in patient costs related to decreased ICU days and mechanical ventilation as well as resource utilization in a patient population already shown to have improved mortality. These results, if confirmed, suggest that tight glycemic control in the ICU is cost effective and should become standard medical practice. TH
Repeat Testing for C. Diff?
By Jeff Glasheen, MD
Mohan SS, McDermott BP, Parchuri S, et al. Lack of value of repeat stool testing for Clostridium difficile toxin. Am J Med. 2006 Apr;119(4):356.e7-356.e8
Clostridium difficile is a common complication of antibiotic and chemotherapeutic use, especially in hospitalized patients. Yet most nosocomial diarrhea is not caused by C. difficile. Most antibiotics can cause loose stools through changes in the gastrointestinal flora that result in inadequate digestion and absorption of carbohydrates and a resultant osmotic diarrhea. Further, antibiotics such as erythromycin and amoxicillin/clavulanate may result in diarrhea via increases in GI tract motility. While osmotic and motility causes of diarrhea tend to improve with antibiotic discontinuation, C. difficile-associated diarrhea is associated with significant morbidity that often continues until adequately treated.
Thus having a test that differentiates between C. difficile and non-clostridial diarrhea is essential. The most commonly used test is the enzyme immunoassay (EIA) that detects toxins A and B. The sensitivity and specificity of this test has been reported to range between 50%-90% and 70%-95%, respectively. The authors of this paper evaluated the utility of repeat EIA testing in patients with a one negative test in the setting of nosocomial diarrhea associated with antibiotic use.
The authors reviewed 474 sequential EIA tests for C. difficile in 396 patients over a 10-month period at a large university-affiliated community hospital with an EIA sensitivity and specificity of 80%-90% and 80%-95%, respectively. Tests were considered to be “repeat” if they occurred within seven days of the original negative test. Of the 78 repeat tests (16.5% of all tests), only one was positive, resulting in a 0.8% conversion rate. At an institutional cost of $128 per test the total cost of EIA testing over the 10-month period was $60,672. The cost of repeat testing alone was $9,984. The authors conclude that there is limited value—and high cost—in repeat EIA testing and that alternative sources of diarrhea should be sought or we should repeat EIA testing in patients with continued nosocomial diarrhea and a negative EIA test.
While prior studies have shown incremental benefit of retesting for C. difficile with the EIA assay, this study’s authors conclude that repeat “C. difficile testing is not clinically justified and is economically wasteful.” Unfortunately, the authors did not utilize a strong enough research design to defend this statement. From the data presented, all we can conclude is that repeat testing with an EIA assay did not add significant value to the diagnostic workup. The lack of a negative gold standard test, such as the cytotoxin assay or follow up outcomes, such as resolution of diarrhea, leaves the reader pondering if the repeat EIA assays were negative because the patients did not have C. difficile or because the test was not sensitive enough to detect the toxin. The reported sensitivity for the EIA assay used was 80-90%, meaning that 10%-20% of patients with C. difficile disease would have had a false negative test. While a second negative test would lower the likelihood of true disease, it would not lower it enough in a patient with a high pre-test probability of disease to sufficiently rule out the disease such that further testing is indicated.
Additionally, while we can extrapolate that the EIA test was of little utility to the patients studied here, no patient-specific data is presented. Thus it is difficult to determine if our patient population is represented in the study. More knowledge about the patients would allow the reader to use published prediction rules to better delineate how likely it was that this cohort was at high risk for having toxin-mediated diarrhea. Perhaps a more reasonable approach to this clinical conundrum would be to send the repeat stool test for a cytotoxin assay or to treat the patient empirically in situations where either the likelihood of disease or the disease burden is high.
Stroke after MI
By Ethan Cumbler, MD
Witt BJ, Ballman KV, Brown RD Jr, et al. The incidence of stroke after myocardial infarction: a meta-analysis. Am J Med. 2006 Apr;119(4):354.e1-9.
Stroke and myocardial infarction (MI) share many of the risk factors leading to atherosclerosis, including hypertension, hyperlipidemia, diabetes, tobacco abuse, and age. Logically, patients at risk for one event would also be at risk for the other, yet this interaction appears to be more complex. The study by Witt, et al., aims to elucidate the rate of in-hospital stroke in patients initially admitted with an MI.
The authors analyzed 22 observational studies of myocardial infarction that recorded the incidence of cerebrovascular accidents after acute MI. Clinical trials were excluded from the analysis in order to provide representation of an unselected population. Of the trials reviewed, 11 were included in the analysis of in-hospital strokes, three for the 30-day time point, and two for the one-year time point. The other trials used different time points and were not included in the analysis. The patients had a mean age ranging between 59 and 72.7 years, and all had a predominance of males. The rate of in-hospital stroke was 11.1 events per 1,000 hospitalizations. This incidence rose to 12.2/1,000 at 30 days and 21.4/1,000 at one year.
Plausible hypotheses for why the rate of cerebrovascular accident would be particularly high in the post-MI period include the potential for localized wall motion dysmotility or low flow leading to intracardiac thrombosis, event-related arrhythmia, or procedure-related embolic events. The studies from which this meta-analysis was derived were not designed in such a way for a causal relationship to be identified. However, age, diabetes, hypertension, prior stroke, anterior location of MI, atrial fibrillation, heart failure, and nonwhite race were all found to have an association with increased risk for stroke. Interestingly, angina on presentation was associated with an apparent decreased risk, theorized to potentially be due to ischemic preconditioning.
While this study shares the usual limitations of meta-analyses of observational studies, the authors have done an excellent summation of the data available including both English and non-English language articles in the analysis. Notably, the review included studies spanning more than 25 years and, thus, included data from studies done in the era prior to modern therapy for cardiac ischemia including potent antiplatelet and statin therapy. The three studies with in-hospital time points started in the 1990s had a lower average rate of stroke, which may reflect the effect of more potent anti-platelet agents used in today’s therapy for acute coronary syndromes.
The implication for the hospitalist is to recognize that patients admitted for MI are at high risk for stroke during the index hospitalization. A low threshold for suspicion of a cerebrovascular event needs to be maintained for post-MI patients with new neurologic symptoms. Future studies will be needed to address the risk/benefit of anticoagulation in high-risk patients for stroke following a myocardial infarction.
Predicting PE in the ED Using Revised Geneva Score
By Jeffrey Carter, MD
Le Gal G, Righini M, Roy PM, et al. Prediction of pulmonary embolism in the emergency department: the revised Geneva score. Ann Intern Med. 2006 Feb 7;144(3):165-171.
Introduction: Pulmonary embolism remains a common life-threatening disorder with imperfect diagnostic modalities and strategies. Much of the current literature focuses on the development and validation of clinical probability assessments that identify low-risk patients who can be safely managed without invasive testing or lung scanning.
Two common scoring systems include the Geneva and Wells criteria, which employ a combination of historical information, clinical and laboratory data to stratify patients into three risk groups.1,2 It has recently been shown that a single negative D-dimer test safely excludes patients with suspected VTE in a large cohort, with a three-month follow-up rate of VTE of 0%.3 Criticism of current clinical probability assessment strategies include the inclusion of subjective criteria or the need for blood gas values.1,2 In this paper, the authors sought to derive and validate a scoring system based on readily available objective clinical data.
Methods: The cohort evaluated in this study consists of the same 965 patients used to prospectively evaluate an emergency department diagnostic strategy of VTE.3 Patients presenting to the emergency ward with complaints of chest pain or shortness of breath were evaluated with a standard diagnostic workup that included a checklist of demographic and historical information, signs and symptoms possibly consistent with VTE, ABG, chest X-ray, and EKG results, as well as the likelihood of another diagnosis. However, the goal was to create a scoring system based on readily available objective data, so ABG, chest X-ray and electrocardiogram results were not evaluated as possible components of the score. Clinical variables associated with pulmonary embolism were evaluated for statistical significance in both a univariate and multivariate model. These variables were then validated both internally and with an external cohort.
Results: The incidence of VTE was 23% (222/965). Ten clinical variables were found to be statistically significantly associated with VTE; these comprise the Revised Geneva Score.
Clinical probability is based on points: 0-3 is low probability; 4-10 is intermediate probability, and >10 is high probability. Low, intermediate, and high clinical probabilities had respective rates of VTE of 8%, 28%, and 74%. These percentages were found in the validation cohort and were similar to those in the derivation cohort.
Discussion: This study focuses on the derivation and validation of a clinical scoring system that can provide a numerical estimate of likelihood of VTE. The diagnostic strategy by which VTE is confirmed or excluded is from derivation cohort and is published elsewhere.3 In that study patients classified as no VTE and not treated had a 90-day risk of VTE of 1%. The nine-point revised Geneva score does indeed provide an accurate assessment of risk of VTE, and can thus help guide clinical decision-making. However it is not clear that the revised Geneva score will help decrease invasive diagnostic tests. In the low-risk group, 8% is too great a risk of a life-threatening illness to forego further diagnostic evaluation. Coupled with a negative ELISA D-dimer, exclusion of these patients is safe, but these patients cannot be safely excluded without risk stratification.3
References
- Wells PS, Anderson DR, Rodger M, et al. Derivation of a simple clinical model to categorize patients’ probability of pulmonary embolism: increasing the model’s utility with the SimpliRED D-dimer. Thromb Haemost. 2000 Mar;83:416-420.
- Wicki J, Perneger TV, Junof AF, et al. Assessing clinical probability of pulmonary embolism in the emergency ward: a simple score. Arch Intern Med. 2001 Jan 8;161(1):92-97.
- Perrier A, Roy PM, Aujesky D, et al. Diagnosing pulmonary embolism in outpatients with clinical assessment, D-dimer measurement, venous ultrasound and helical computed tomography: a multicenter management study. Am J Med. 2004 Mar 1;116(5):291-299.
LMWH for Inpatient Palliative Care
By Jeanie Youngwerth, MD
Noble SI, Nelson A, Turner C, et al. Acceptability of low molecular weight heparin thromboprophylaxis for patients receiving palliative care: qualitative study. BMJ. 2006 Mar 11:332(7541);577-580.ePub 2006 Feb 3.
Venous thromboembolism is a major risk factor for patients with malignancy. VTE may reduce survival time in patients receiving palliative care, with one in seven inpatients with cancer dying from pulmonary embolism. The American College of Chest Physicians recommend low molecular weight heparin (LMWH) in hospitalized patients with cancer as level 1A evidence in their 2004 consensus statement on VTE. There are no thromboprophylaxis guidelines in the United Kingdom. Many physicians view daily injections of LMWH as unnecessary distress for palliative care patients. This study focused on what inpatients with advanced cancer receiving palliative care thought about the effect of thromboprophylaxis on overall quality of life.
This was a qualitative study of 28 inpatients receiving palliative care who had advanced metastatic cancer and who were in a regional cancer center in Wales. The patients had received LMWH for at least five consecutive days. The patients were audiotaped and then had semi-structured interviews transcribed regarding cancer treatments they had received. These interviews covered the patients’ insight into prognosis, their understanding of thromboprophylaxis, their beliefs concerning the effects of thromboprophylaxis on overall quality of life, and the negative aspects of heparin treatment.
The main outcome measures were recurring themes of the effect of thromboprophylaxis on overall quality of life. Major themes identified were insight into prognosis, knowledge and understanding of thromboprophylaxis, acceptability of heparin thromboprophylaxis, reassurance, and optimism. Minor themes identified were bruising, negative impact of antiembolic stockings, and anger at paternalistic views toward terminally ill patients.
Most patients showed clear insight into the nature of their condition and understood heparin prophylaxis for VTE. Many patients identified immobility and surgery as VTE risk factors, with little understanding of cancer as a risk factor. All knew that VTE could cause death, but none were aware of the common symptoms. All patients found LMWH thromboprophylaxis acceptable. Patients believed taking measures to prevent symptoms might improve their quality of life and felt that the medical team had not given up on them.
The only negative experiences of LMWH thromboprophylaxis was bruising. All of the patients who wore antiembolic stockings during previous admissions found them uncomfortable. Patients expressed their need to be involved in decision-making, particularly with respect to withdrawal or non-administration of treatment.
This small, qualitative study showed that, contrary to many physicians’ beliefs, patients in palliative care units believe that LMWH injections are acceptable as thromboprophylaxis, but antiembolic stockings are not. The effect of daily injections had little or no effect on the quality of life, with many patients having positive feelings that things were being done to prevent new problems from occurring.
This study was limited by the small sample size, the qualitative nature that could introduce interpretation bias, and the fact that only patients using LMWH were included. Additionally, the United Kingdom has aggressively educated the public on the risks of VTE associated with long flights such that baseline knowledge may differ in other parts of the world. Resource utilization, including drug costs and length of stay, as well as effect on mortality were not studied.
The implications for hospitalists are that many inpatients with advanced cancer receiving palliative care may find LMWH thromboprophylaxis acceptable therapy, and that discussions with the patient regarding this option should be explored together.
Cost Analysis: Intensive Glycemic Control in Critically Ill Adults
By Whitney Woodmansee, MD
Krinsley JS, Jones, RL. Cost analysis of intensive glycemic control in critically ill adult patients. Chest. 2006;129:644-650.
Several studies have demonstrated improved outcomes and decreased mortality in ICU patients treated with intensive control of blood glucose levels. This study sought to identify the costs associated with intensive glycemic control in the ICU.
An ICU patient database was analyzed for cost data related to intensive glycemic control. A baseline group of 800 consecutive ICU patients admitted prior to initiation (baseline) of an intensive glucose management (blood glucose levels between 80-140 mg/dl protocol were compared with a treatment group of 800 consecutive patients admitted after initiation of the protocol). Previously reported outcomes of these patients demonstrated significant improvement in mortality with tight glycemic control. Costs related to ICU and non-ICU length of stay; duration of mechanical ventilation; and all laboratory, pharmacy, and radiology services were analyzed between groups. Resource utilization was determined by assessing charges from the database and adjusting for inflation and applying Medicare cost, charge ratios for each category, and fiscal year. Costs associated with the intensive glycemic control protocol were determined. Unfortunately, only cost estimates for insulin and associated disposable supplies for each group were available for analysis.
Baseline and treatment populations did not differ significantly regarding demographics such as age, gender, race, admitting diagnosis, diabetes prevalence, or APACHE II scores. There were fewer patients in the treatment group that required mechanical ventilation during their ICU stay (40.6% versus 33.6%). Intensive glucose management was associated with a 13.9% reduction in total ICU days and duration of mechanical ventilation (median of two days decreased to 1.7 days p=0.045). There was a $1,580 adjusted cost savings per patient in the intensive treatment group compared with the baseline group (p<0.001). This reduction in cost was primarily driven by a decrease in laboratory and radiology costs in the ventilated patients. There were nonsignificant cost reductions in the unventilated patients.
Intensive control of hyperglycemia in the hospitalized ICU patient appears to be associated with reduction of morbidity and mortality. This suggests that tight glycemic control also leads to reductions in overall patient care costs—particularly in the ventilated ICU patient. Although not a randomized control trial, database analysis of costs and resource utilization demonstrated an overall cost savings in the treatment group (after initiation of an intensive glycemic control protocol) compared with the baseline group (before protocol initiation). One caveat is that the authors used estimates when determining the costs associated with the implementation of the intensive glucose management protocol. Nevertheless, intensive glycemic control was associated with an overall reduction in patient costs related to decreased ICU days and mechanical ventilation as well as resource utilization in a patient population already shown to have improved mortality. These results, if confirmed, suggest that tight glycemic control in the ICU is cost effective and should become standard medical practice. TH
Repeat Testing for C. Diff?
By Jeff Glasheen, MD
Mohan SS, McDermott BP, Parchuri S, et al. Lack of value of repeat stool testing for Clostridium difficile toxin. Am J Med. 2006 Apr;119(4):356.e7-356.e8
Clostridium difficile is a common complication of antibiotic and chemotherapeutic use, especially in hospitalized patients. Yet most nosocomial diarrhea is not caused by C. difficile. Most antibiotics can cause loose stools through changes in the gastrointestinal flora that result in inadequate digestion and absorption of carbohydrates and a resultant osmotic diarrhea. Further, antibiotics such as erythromycin and amoxicillin/clavulanate may result in diarrhea via increases in GI tract motility. While osmotic and motility causes of diarrhea tend to improve with antibiotic discontinuation, C. difficile-associated diarrhea is associated with significant morbidity that often continues until adequately treated.
Thus having a test that differentiates between C. difficile and non-clostridial diarrhea is essential. The most commonly used test is the enzyme immunoassay (EIA) that detects toxins A and B. The sensitivity and specificity of this test has been reported to range between 50%-90% and 70%-95%, respectively. The authors of this paper evaluated the utility of repeat EIA testing in patients with a one negative test in the setting of nosocomial diarrhea associated with antibiotic use.
The authors reviewed 474 sequential EIA tests for C. difficile in 396 patients over a 10-month period at a large university-affiliated community hospital with an EIA sensitivity and specificity of 80%-90% and 80%-95%, respectively. Tests were considered to be “repeat” if they occurred within seven days of the original negative test. Of the 78 repeat tests (16.5% of all tests), only one was positive, resulting in a 0.8% conversion rate. At an institutional cost of $128 per test the total cost of EIA testing over the 10-month period was $60,672. The cost of repeat testing alone was $9,984. The authors conclude that there is limited value—and high cost—in repeat EIA testing and that alternative sources of diarrhea should be sought or we should repeat EIA testing in patients with continued nosocomial diarrhea and a negative EIA test.
While prior studies have shown incremental benefit of retesting for C. difficile with the EIA assay, this study’s authors conclude that repeat “C. difficile testing is not clinically justified and is economically wasteful.” Unfortunately, the authors did not utilize a strong enough research design to defend this statement. From the data presented, all we can conclude is that repeat testing with an EIA assay did not add significant value to the diagnostic workup. The lack of a negative gold standard test, such as the cytotoxin assay or follow up outcomes, such as resolution of diarrhea, leaves the reader pondering if the repeat EIA assays were negative because the patients did not have C. difficile or because the test was not sensitive enough to detect the toxin. The reported sensitivity for the EIA assay used was 80-90%, meaning that 10%-20% of patients with C. difficile disease would have had a false negative test. While a second negative test would lower the likelihood of true disease, it would not lower it enough in a patient with a high pre-test probability of disease to sufficiently rule out the disease such that further testing is indicated.
Additionally, while we can extrapolate that the EIA test was of little utility to the patients studied here, no patient-specific data is presented. Thus it is difficult to determine if our patient population is represented in the study. More knowledge about the patients would allow the reader to use published prediction rules to better delineate how likely it was that this cohort was at high risk for having toxin-mediated diarrhea. Perhaps a more reasonable approach to this clinical conundrum would be to send the repeat stool test for a cytotoxin assay or to treat the patient empirically in situations where either the likelihood of disease or the disease burden is high.
Stroke after MI
By Ethan Cumbler, MD
Witt BJ, Ballman KV, Brown RD Jr, et al. The incidence of stroke after myocardial infarction: a meta-analysis. Am J Med. 2006 Apr;119(4):354.e1-9.
Stroke and myocardial infarction (MI) share many of the risk factors leading to atherosclerosis, including hypertension, hyperlipidemia, diabetes, tobacco abuse, and age. Logically, patients at risk for one event would also be at risk for the other, yet this interaction appears to be more complex. The study by Witt, et al., aims to elucidate the rate of in-hospital stroke in patients initially admitted with an MI.
The authors analyzed 22 observational studies of myocardial infarction that recorded the incidence of cerebrovascular accidents after acute MI. Clinical trials were excluded from the analysis in order to provide representation of an unselected population. Of the trials reviewed, 11 were included in the analysis of in-hospital strokes, three for the 30-day time point, and two for the one-year time point. The other trials used different time points and were not included in the analysis. The patients had a mean age ranging between 59 and 72.7 years, and all had a predominance of males. The rate of in-hospital stroke was 11.1 events per 1,000 hospitalizations. This incidence rose to 12.2/1,000 at 30 days and 21.4/1,000 at one year.
Plausible hypotheses for why the rate of cerebrovascular accident would be particularly high in the post-MI period include the potential for localized wall motion dysmotility or low flow leading to intracardiac thrombosis, event-related arrhythmia, or procedure-related embolic events. The studies from which this meta-analysis was derived were not designed in such a way for a causal relationship to be identified. However, age, diabetes, hypertension, prior stroke, anterior location of MI, atrial fibrillation, heart failure, and nonwhite race were all found to have an association with increased risk for stroke. Interestingly, angina on presentation was associated with an apparent decreased risk, theorized to potentially be due to ischemic preconditioning.
While this study shares the usual limitations of meta-analyses of observational studies, the authors have done an excellent summation of the data available including both English and non-English language articles in the analysis. Notably, the review included studies spanning more than 25 years and, thus, included data from studies done in the era prior to modern therapy for cardiac ischemia including potent antiplatelet and statin therapy. The three studies with in-hospital time points started in the 1990s had a lower average rate of stroke, which may reflect the effect of more potent anti-platelet agents used in today’s therapy for acute coronary syndromes.
The implication for the hospitalist is to recognize that patients admitted for MI are at high risk for stroke during the index hospitalization. A low threshold for suspicion of a cerebrovascular event needs to be maintained for post-MI patients with new neurologic symptoms. Future studies will be needed to address the risk/benefit of anticoagulation in high-risk patients for stroke following a myocardial infarction.
Predicting PE in the ED Using Revised Geneva Score
By Jeffrey Carter, MD
Le Gal G, Righini M, Roy PM, et al. Prediction of pulmonary embolism in the emergency department: the revised Geneva score. Ann Intern Med. 2006 Feb 7;144(3):165-171.
Introduction: Pulmonary embolism remains a common life-threatening disorder with imperfect diagnostic modalities and strategies. Much of the current literature focuses on the development and validation of clinical probability assessments that identify low-risk patients who can be safely managed without invasive testing or lung scanning.
Two common scoring systems include the Geneva and Wells criteria, which employ a combination of historical information, clinical and laboratory data to stratify patients into three risk groups.1,2 It has recently been shown that a single negative D-dimer test safely excludes patients with suspected VTE in a large cohort, with a three-month follow-up rate of VTE of 0%.3 Criticism of current clinical probability assessment strategies include the inclusion of subjective criteria or the need for blood gas values.1,2 In this paper, the authors sought to derive and validate a scoring system based on readily available objective clinical data.
Methods: The cohort evaluated in this study consists of the same 965 patients used to prospectively evaluate an emergency department diagnostic strategy of VTE.3 Patients presenting to the emergency ward with complaints of chest pain or shortness of breath were evaluated with a standard diagnostic workup that included a checklist of demographic and historical information, signs and symptoms possibly consistent with VTE, ABG, chest X-ray, and EKG results, as well as the likelihood of another diagnosis. However, the goal was to create a scoring system based on readily available objective data, so ABG, chest X-ray and electrocardiogram results were not evaluated as possible components of the score. Clinical variables associated with pulmonary embolism were evaluated for statistical significance in both a univariate and multivariate model. These variables were then validated both internally and with an external cohort.
Results: The incidence of VTE was 23% (222/965). Ten clinical variables were found to be statistically significantly associated with VTE; these comprise the Revised Geneva Score.
Clinical probability is based on points: 0-3 is low probability; 4-10 is intermediate probability, and >10 is high probability. Low, intermediate, and high clinical probabilities had respective rates of VTE of 8%, 28%, and 74%. These percentages were found in the validation cohort and were similar to those in the derivation cohort.
Discussion: This study focuses on the derivation and validation of a clinical scoring system that can provide a numerical estimate of likelihood of VTE. The diagnostic strategy by which VTE is confirmed or excluded is from derivation cohort and is published elsewhere.3 In that study patients classified as no VTE and not treated had a 90-day risk of VTE of 1%. The nine-point revised Geneva score does indeed provide an accurate assessment of risk of VTE, and can thus help guide clinical decision-making. However it is not clear that the revised Geneva score will help decrease invasive diagnostic tests. In the low-risk group, 8% is too great a risk of a life-threatening illness to forego further diagnostic evaluation. Coupled with a negative ELISA D-dimer, exclusion of these patients is safe, but these patients cannot be safely excluded without risk stratification.3
References
- Wells PS, Anderson DR, Rodger M, et al. Derivation of a simple clinical model to categorize patients’ probability of pulmonary embolism: increasing the model’s utility with the SimpliRED D-dimer. Thromb Haemost. 2000 Mar;83:416-420.
- Wicki J, Perneger TV, Junof AF, et al. Assessing clinical probability of pulmonary embolism in the emergency ward: a simple score. Arch Intern Med. 2001 Jan 8;161(1):92-97.
- Perrier A, Roy PM, Aujesky D, et al. Diagnosing pulmonary embolism in outpatients with clinical assessment, D-dimer measurement, venous ultrasound and helical computed tomography: a multicenter management study. Am J Med. 2004 Mar 1;116(5):291-299.
LMWH for Inpatient Palliative Care
By Jeanie Youngwerth, MD
Noble SI, Nelson A, Turner C, et al. Acceptability of low molecular weight heparin thromboprophylaxis for patients receiving palliative care: qualitative study. BMJ. 2006 Mar 11:332(7541);577-580.ePub 2006 Feb 3.
Venous thromboembolism is a major risk factor for patients with malignancy. VTE may reduce survival time in patients receiving palliative care, with one in seven inpatients with cancer dying from pulmonary embolism. The American College of Chest Physicians recommend low molecular weight heparin (LMWH) in hospitalized patients with cancer as level 1A evidence in their 2004 consensus statement on VTE. There are no thromboprophylaxis guidelines in the United Kingdom. Many physicians view daily injections of LMWH as unnecessary distress for palliative care patients. This study focused on what inpatients with advanced cancer receiving palliative care thought about the effect of thromboprophylaxis on overall quality of life.
This was a qualitative study of 28 inpatients receiving palliative care who had advanced metastatic cancer and who were in a regional cancer center in Wales. The patients had received LMWH for at least five consecutive days. The patients were audiotaped and then had semi-structured interviews transcribed regarding cancer treatments they had received. These interviews covered the patients’ insight into prognosis, their understanding of thromboprophylaxis, their beliefs concerning the effects of thromboprophylaxis on overall quality of life, and the negative aspects of heparin treatment.
The main outcome measures were recurring themes of the effect of thromboprophylaxis on overall quality of life. Major themes identified were insight into prognosis, knowledge and understanding of thromboprophylaxis, acceptability of heparin thromboprophylaxis, reassurance, and optimism. Minor themes identified were bruising, negative impact of antiembolic stockings, and anger at paternalistic views toward terminally ill patients.
Most patients showed clear insight into the nature of their condition and understood heparin prophylaxis for VTE. Many patients identified immobility and surgery as VTE risk factors, with little understanding of cancer as a risk factor. All knew that VTE could cause death, but none were aware of the common symptoms. All patients found LMWH thromboprophylaxis acceptable. Patients believed taking measures to prevent symptoms might improve their quality of life and felt that the medical team had not given up on them.
The only negative experiences of LMWH thromboprophylaxis was bruising. All of the patients who wore antiembolic stockings during previous admissions found them uncomfortable. Patients expressed their need to be involved in decision-making, particularly with respect to withdrawal or non-administration of treatment.
This small, qualitative study showed that, contrary to many physicians’ beliefs, patients in palliative care units believe that LMWH injections are acceptable as thromboprophylaxis, but antiembolic stockings are not. The effect of daily injections had little or no effect on the quality of life, with many patients having positive feelings that things were being done to prevent new problems from occurring.
This study was limited by the small sample size, the qualitative nature that could introduce interpretation bias, and the fact that only patients using LMWH were included. Additionally, the United Kingdom has aggressively educated the public on the risks of VTE associated with long flights such that baseline knowledge may differ in other parts of the world. Resource utilization, including drug costs and length of stay, as well as effect on mortality were not studied.
The implications for hospitalists are that many inpatients with advanced cancer receiving palliative care may find LMWH thromboprophylaxis acceptable therapy, and that discussions with the patient regarding this option should be explored together.
Cost Analysis: Intensive Glycemic Control in Critically Ill Adults
By Whitney Woodmansee, MD
Krinsley JS, Jones, RL. Cost analysis of intensive glycemic control in critically ill adult patients. Chest. 2006;129:644-650.
Several studies have demonstrated improved outcomes and decreased mortality in ICU patients treated with intensive control of blood glucose levels. This study sought to identify the costs associated with intensive glycemic control in the ICU.
An ICU patient database was analyzed for cost data related to intensive glycemic control. A baseline group of 800 consecutive ICU patients admitted prior to initiation (baseline) of an intensive glucose management (blood glucose levels between 80-140 mg/dl protocol were compared with a treatment group of 800 consecutive patients admitted after initiation of the protocol). Previously reported outcomes of these patients demonstrated significant improvement in mortality with tight glycemic control. Costs related to ICU and non-ICU length of stay; duration of mechanical ventilation; and all laboratory, pharmacy, and radiology services were analyzed between groups. Resource utilization was determined by assessing charges from the database and adjusting for inflation and applying Medicare cost, charge ratios for each category, and fiscal year. Costs associated with the intensive glycemic control protocol were determined. Unfortunately, only cost estimates for insulin and associated disposable supplies for each group were available for analysis.
Baseline and treatment populations did not differ significantly regarding demographics such as age, gender, race, admitting diagnosis, diabetes prevalence, or APACHE II scores. There were fewer patients in the treatment group that required mechanical ventilation during their ICU stay (40.6% versus 33.6%). Intensive glucose management was associated with a 13.9% reduction in total ICU days and duration of mechanical ventilation (median of two days decreased to 1.7 days p=0.045). There was a $1,580 adjusted cost savings per patient in the intensive treatment group compared with the baseline group (p<0.001). This reduction in cost was primarily driven by a decrease in laboratory and radiology costs in the ventilated patients. There were nonsignificant cost reductions in the unventilated patients.
Intensive control of hyperglycemia in the hospitalized ICU patient appears to be associated with reduction of morbidity and mortality. This suggests that tight glycemic control also leads to reductions in overall patient care costs—particularly in the ventilated ICU patient. Although not a randomized control trial, database analysis of costs and resource utilization demonstrated an overall cost savings in the treatment group (after initiation of an intensive glycemic control protocol) compared with the baseline group (before protocol initiation). One caveat is that the authors used estimates when determining the costs associated with the implementation of the intensive glucose management protocol. Nevertheless, intensive glycemic control was associated with an overall reduction in patient costs related to decreased ICU days and mechanical ventilation as well as resource utilization in a patient population already shown to have improved mortality. These results, if confirmed, suggest that tight glycemic control in the ICU is cost effective and should become standard medical practice. TH