User login
Larry Beresford is an Oakland, Calif.-based freelance medical journalist with a breadth of experience writing about the policy, financial, clinical, management and human aspects of hospice, palliative care, end-of-life care, death, and dying. He is a longtime contributor to The Hospitalist, for which he covers re-admissions, pain management, palliative care, physician stress and burnout, quality improvement, waste prevention, practice management, innovation, and technology. He also contributes to Medscape. Learn more about his work at www.larryberesford.com; follow him on Twitter @larryberesford.
Hospitalists Play Integral Roles in HHS-Funded Innovation Projects
In May and June, U.S. Department of Health and Human Services (HHS) Secretary Kathleen Sebelius in May and June announced 107 healthcare innovations grants to improve coordination of care and reduce costs. The grants, a provision of the Affordable Care Act (ACA), range from $1 million to $30 million. HHS anticipates that the projects will reduce healthcare spending by $254 million over the next three years and provide "new ideas on how to deliver better health, improved care, and lower costs to people enrolled in Medicare, Medicaid and [the] Children's Health Insurance Program (CHIP)."
Hospitalists played key roles in planning and developing several of the projects. Common themes include coordination and integration of services, promotion of community collaborations, integrating behavioral and physical care, and the use of telemedicine—many of the same approaches utilized by SHM's Project BOOST and other national initiatives for preventing unnecessary readmissions.
In Atlanta, Emory University's Center for Critical Care received a $10.7 million grant to deploy 40 nurse practitioners (NPs) and physician assistants (PAs) trained in critical care to underserved and rural ICUs in Georgia. In many of the targeted hospitals, hospitalists manage patients in the ICU, but this program brings an additional layer of staffing and expertise to the care, allowing patients to stay in their beds rather than having to be transferred, says Daniel Owens, MBA, the center’s director of operations and senior administrator of the division of hospital medicine at Emory.
The project will bring NPs and PAs from participating hospitals to Emory for an intensive, six-month, critical-care residency. "If they don't have these folks, we'll help to identify staff for the jobs," he adds.
At Vanderbilt University Medical Center in Nashville, Tenn., a $2.4 million project to reduce rehospitalizations for a high-risk geriatric patients aims to close the gaps in care transitions between hospital, outpatient, post-acute, and extended-care settings, says Vanderbilt hospitalist Eduard Vasilevskis, MD. The project will employ transition advocates or coordinators in the hospital to improve communication at both ends, with evidence-based protocols to improve discharge planning. Long-term care providers will be offered Web-based training and video conferencing.
"The goal is to break the cycle of rehospitalization," says Dr. Vasilevskis, "but if patients need to come back to the hospital, there will be someone involved in their care who is familiar with the settings where they’ve come from."
Beth Israel Deaconess Medical Center (BIDMC) in Boston received $4.9 million for its Post-Acute Care Transitions program (PACT), which links the hospital to six affiliated primary care practices using a bundle of post-acute care interventions, care-transition specialists, and dedicated clinical pharmacists. Nurses remain in contact with patients by telephone for 30 days post-hospital discharge and coordinate the services of extended-care facilities and visiting nurses. Pharmacists perform in-hospital medication reconciliation and patient education, says hospitalist Lauren Doctoroff, MD, FHM. She and Julius Yang, MD, BIDMC medical director of inpatient quality, helped develop the pilot program, which began in August 2011.
"These care-transitions specialists offer us an added level of patient support and a different level of integration focused on risk assessment of such issues as social supports and problems with medical compliance, which can be used by the inpatient team to come up with the most rational and ideal discharge plan," Dr. Doctoroff says. "One of my colleagues said to me, ‘I feel so much better knowing there is this added level of support for patients after discharge.'"
The HHS grants reflect an important recognition that what happens to patients following discharge partly reflects what happens in the hospital but also depends on collaborations with post-acute providers, Dr. Doctoroff says.
"Hospitalists can't do everything, but they need their eye out of the hospital on post-acute providers in order to deliver the best care," she adds.
In May and June, U.S. Department of Health and Human Services (HHS) Secretary Kathleen Sebelius in May and June announced 107 healthcare innovations grants to improve coordination of care and reduce costs. The grants, a provision of the Affordable Care Act (ACA), range from $1 million to $30 million. HHS anticipates that the projects will reduce healthcare spending by $254 million over the next three years and provide "new ideas on how to deliver better health, improved care, and lower costs to people enrolled in Medicare, Medicaid and [the] Children's Health Insurance Program (CHIP)."
Hospitalists played key roles in planning and developing several of the projects. Common themes include coordination and integration of services, promotion of community collaborations, integrating behavioral and physical care, and the use of telemedicine—many of the same approaches utilized by SHM's Project BOOST and other national initiatives for preventing unnecessary readmissions.
In Atlanta, Emory University's Center for Critical Care received a $10.7 million grant to deploy 40 nurse practitioners (NPs) and physician assistants (PAs) trained in critical care to underserved and rural ICUs in Georgia. In many of the targeted hospitals, hospitalists manage patients in the ICU, but this program brings an additional layer of staffing and expertise to the care, allowing patients to stay in their beds rather than having to be transferred, says Daniel Owens, MBA, the center’s director of operations and senior administrator of the division of hospital medicine at Emory.
The project will bring NPs and PAs from participating hospitals to Emory for an intensive, six-month, critical-care residency. "If they don't have these folks, we'll help to identify staff for the jobs," he adds.
At Vanderbilt University Medical Center in Nashville, Tenn., a $2.4 million project to reduce rehospitalizations for a high-risk geriatric patients aims to close the gaps in care transitions between hospital, outpatient, post-acute, and extended-care settings, says Vanderbilt hospitalist Eduard Vasilevskis, MD. The project will employ transition advocates or coordinators in the hospital to improve communication at both ends, with evidence-based protocols to improve discharge planning. Long-term care providers will be offered Web-based training and video conferencing.
"The goal is to break the cycle of rehospitalization," says Dr. Vasilevskis, "but if patients need to come back to the hospital, there will be someone involved in their care who is familiar with the settings where they’ve come from."
Beth Israel Deaconess Medical Center (BIDMC) in Boston received $4.9 million for its Post-Acute Care Transitions program (PACT), which links the hospital to six affiliated primary care practices using a bundle of post-acute care interventions, care-transition specialists, and dedicated clinical pharmacists. Nurses remain in contact with patients by telephone for 30 days post-hospital discharge and coordinate the services of extended-care facilities and visiting nurses. Pharmacists perform in-hospital medication reconciliation and patient education, says hospitalist Lauren Doctoroff, MD, FHM. She and Julius Yang, MD, BIDMC medical director of inpatient quality, helped develop the pilot program, which began in August 2011.
"These care-transitions specialists offer us an added level of patient support and a different level of integration focused on risk assessment of such issues as social supports and problems with medical compliance, which can be used by the inpatient team to come up with the most rational and ideal discharge plan," Dr. Doctoroff says. "One of my colleagues said to me, ‘I feel so much better knowing there is this added level of support for patients after discharge.'"
The HHS grants reflect an important recognition that what happens to patients following discharge partly reflects what happens in the hospital but also depends on collaborations with post-acute providers, Dr. Doctoroff says.
"Hospitalists can't do everything, but they need their eye out of the hospital on post-acute providers in order to deliver the best care," she adds.
In May and June, U.S. Department of Health and Human Services (HHS) Secretary Kathleen Sebelius in May and June announced 107 healthcare innovations grants to improve coordination of care and reduce costs. The grants, a provision of the Affordable Care Act (ACA), range from $1 million to $30 million. HHS anticipates that the projects will reduce healthcare spending by $254 million over the next three years and provide "new ideas on how to deliver better health, improved care, and lower costs to people enrolled in Medicare, Medicaid and [the] Children's Health Insurance Program (CHIP)."
Hospitalists played key roles in planning and developing several of the projects. Common themes include coordination and integration of services, promotion of community collaborations, integrating behavioral and physical care, and the use of telemedicine—many of the same approaches utilized by SHM's Project BOOST and other national initiatives for preventing unnecessary readmissions.
In Atlanta, Emory University's Center for Critical Care received a $10.7 million grant to deploy 40 nurse practitioners (NPs) and physician assistants (PAs) trained in critical care to underserved and rural ICUs in Georgia. In many of the targeted hospitals, hospitalists manage patients in the ICU, but this program brings an additional layer of staffing and expertise to the care, allowing patients to stay in their beds rather than having to be transferred, says Daniel Owens, MBA, the center’s director of operations and senior administrator of the division of hospital medicine at Emory.
The project will bring NPs and PAs from participating hospitals to Emory for an intensive, six-month, critical-care residency. "If they don't have these folks, we'll help to identify staff for the jobs," he adds.
At Vanderbilt University Medical Center in Nashville, Tenn., a $2.4 million project to reduce rehospitalizations for a high-risk geriatric patients aims to close the gaps in care transitions between hospital, outpatient, post-acute, and extended-care settings, says Vanderbilt hospitalist Eduard Vasilevskis, MD. The project will employ transition advocates or coordinators in the hospital to improve communication at both ends, with evidence-based protocols to improve discharge planning. Long-term care providers will be offered Web-based training and video conferencing.
"The goal is to break the cycle of rehospitalization," says Dr. Vasilevskis, "but if patients need to come back to the hospital, there will be someone involved in their care who is familiar with the settings where they’ve come from."
Beth Israel Deaconess Medical Center (BIDMC) in Boston received $4.9 million for its Post-Acute Care Transitions program (PACT), which links the hospital to six affiliated primary care practices using a bundle of post-acute care interventions, care-transition specialists, and dedicated clinical pharmacists. Nurses remain in contact with patients by telephone for 30 days post-hospital discharge and coordinate the services of extended-care facilities and visiting nurses. Pharmacists perform in-hospital medication reconciliation and patient education, says hospitalist Lauren Doctoroff, MD, FHM. She and Julius Yang, MD, BIDMC medical director of inpatient quality, helped develop the pilot program, which began in August 2011.
"These care-transitions specialists offer us an added level of patient support and a different level of integration focused on risk assessment of such issues as social supports and problems with medical compliance, which can be used by the inpatient team to come up with the most rational and ideal discharge plan," Dr. Doctoroff says. "One of my colleagues said to me, ‘I feel so much better knowing there is this added level of support for patients after discharge.'"
The HHS grants reflect an important recognition that what happens to patients following discharge partly reflects what happens in the hospital but also depends on collaborations with post-acute providers, Dr. Doctoroff says.
"Hospitalists can't do everything, but they need their eye out of the hospital on post-acute providers in order to deliver the best care," she adds.
Local Solutions Spark Readmission Reductions
Earlier this month CMS announced 17 additional awards under its Community-Based Care Transitions Program (CCTP), which now encompasses 200 acute-care hospitals and their hospitalists partnering with community agencies and coalitions to improve transitions of care in advance of the Oct. 1 start for excessive readmissions penalties. Innovative solutions to the readmissions dilemma are being tested at the local level by a variety of partnerships with hospitals and hospitalists.
For example, William C. Cook, DO, chief of hospital medicine for the Ohio Permanente Medical Group in Cleveland, is part of a community-wide quality coalition called Better Health Greater Cleveland, one of 17 such groups in the Robert Wood Johnson Foundation's Aligning Forces for Quality collaborative. The program includes 150 quality teams in 100 hospitals posting readmissions reductions and other quality metrics. Dr. Cook, who co-chairs Better Health's Steering Committee for Transitions of Care, is spearheading a transitions pilot with two local nursing homes.
"From the hospitalist perspective, our role is to make care transitions safe and predictable," Dr. Cook says. "The way I can contribute most to these transitions is by thinking ahead about what's going to happen next—and how do I prepare the patient and the next provider." One key step is taking time to complete the real-time discharge summary for each patient, he adds.
The idea, Dr. Cook explains, is to identify and communicate with collaborators across care settings so that the "coaching baton" can be passed in a manner that appears seamless to the patient.
Nearly a third of the 17 new CCTP sites participate in SHM's Project BOOST, including three hospitals in California and one each in Illinois and Pennsylvania. Project BOOST is accepting applications for its next round of sites through September.
Earlier this month CMS announced 17 additional awards under its Community-Based Care Transitions Program (CCTP), which now encompasses 200 acute-care hospitals and their hospitalists partnering with community agencies and coalitions to improve transitions of care in advance of the Oct. 1 start for excessive readmissions penalties. Innovative solutions to the readmissions dilemma are being tested at the local level by a variety of partnerships with hospitals and hospitalists.
For example, William C. Cook, DO, chief of hospital medicine for the Ohio Permanente Medical Group in Cleveland, is part of a community-wide quality coalition called Better Health Greater Cleveland, one of 17 such groups in the Robert Wood Johnson Foundation's Aligning Forces for Quality collaborative. The program includes 150 quality teams in 100 hospitals posting readmissions reductions and other quality metrics. Dr. Cook, who co-chairs Better Health's Steering Committee for Transitions of Care, is spearheading a transitions pilot with two local nursing homes.
"From the hospitalist perspective, our role is to make care transitions safe and predictable," Dr. Cook says. "The way I can contribute most to these transitions is by thinking ahead about what's going to happen next—and how do I prepare the patient and the next provider." One key step is taking time to complete the real-time discharge summary for each patient, he adds.
The idea, Dr. Cook explains, is to identify and communicate with collaborators across care settings so that the "coaching baton" can be passed in a manner that appears seamless to the patient.
Nearly a third of the 17 new CCTP sites participate in SHM's Project BOOST, including three hospitals in California and one each in Illinois and Pennsylvania. Project BOOST is accepting applications for its next round of sites through September.
Earlier this month CMS announced 17 additional awards under its Community-Based Care Transitions Program (CCTP), which now encompasses 200 acute-care hospitals and their hospitalists partnering with community agencies and coalitions to improve transitions of care in advance of the Oct. 1 start for excessive readmissions penalties. Innovative solutions to the readmissions dilemma are being tested at the local level by a variety of partnerships with hospitals and hospitalists.
For example, William C. Cook, DO, chief of hospital medicine for the Ohio Permanente Medical Group in Cleveland, is part of a community-wide quality coalition called Better Health Greater Cleveland, one of 17 such groups in the Robert Wood Johnson Foundation's Aligning Forces for Quality collaborative. The program includes 150 quality teams in 100 hospitals posting readmissions reductions and other quality metrics. Dr. Cook, who co-chairs Better Health's Steering Committee for Transitions of Care, is spearheading a transitions pilot with two local nursing homes.
"From the hospitalist perspective, our role is to make care transitions safe and predictable," Dr. Cook says. "The way I can contribute most to these transitions is by thinking ahead about what's going to happen next—and how do I prepare the patient and the next provider." One key step is taking time to complete the real-time discharge summary for each patient, he adds.
The idea, Dr. Cook explains, is to identify and communicate with collaborators across care settings so that the "coaching baton" can be passed in a manner that appears seamless to the patient.
Nearly a third of the 17 new CCTP sites participate in SHM's Project BOOST, including three hospitals in California and one each in Illinois and Pennsylvania. Project BOOST is accepting applications for its next round of sites through September.
OB/GYN Hospitalists Emerge as a Specialty
The OB/GYN hospitalist field is growing, with at least 164 identified programs and 1,500 to 2,500 practitioners who spend all or part of their workweek in hospital labor and delivery departments. SHM and the American College of Obstetricians and Gynecologists helped birth the 90-member Society of OB/GYN Hospitalists in 2011, but it is now independent, says founding president Rob Olson, MD, an OB/GYN hospitalist practicing in Bellingham, Wash. The fledgling society is planning its second annual conference, Sept. 27-29 in Denver, with obstetric emergency simulation training, clinical lectures, and pearls from the experience of general hospitalist practice by HM pioneer John Nelson, MD, MHM.
Also known as laborists, these board-certified OB/GYN docs’ dedicated presence affords rapid on-site response to changes in patients’ conditions, Dr. Olson says. Laborists might cover nights and weekends, pick up unassigned patients, or cover for private obstetricians who are fully engaged. Laborists do not supplant the private practitioner’s role in delivering babies in the hospital, Dr. Olson says, “unless the private physician asks them to,” which, he adds, is happening more often.
Laborists typically are limited to labor and delivery services, although some also address gynecological cases in the ED. Most of the programs provide coverage 24/7, and invariably they are in facilities with medical hospitalists who might consult on medical complications for expectant mothers. One to two new programs open every month, Dr. Olson says, and his website lists 120 job openings. For information, visit www.ObGynHospitalist.com.
The OB/GYN hospitalist field is growing, with at least 164 identified programs and 1,500 to 2,500 practitioners who spend all or part of their workweek in hospital labor and delivery departments. SHM and the American College of Obstetricians and Gynecologists helped birth the 90-member Society of OB/GYN Hospitalists in 2011, but it is now independent, says founding president Rob Olson, MD, an OB/GYN hospitalist practicing in Bellingham, Wash. The fledgling society is planning its second annual conference, Sept. 27-29 in Denver, with obstetric emergency simulation training, clinical lectures, and pearls from the experience of general hospitalist practice by HM pioneer John Nelson, MD, MHM.
Also known as laborists, these board-certified OB/GYN docs’ dedicated presence affords rapid on-site response to changes in patients’ conditions, Dr. Olson says. Laborists might cover nights and weekends, pick up unassigned patients, or cover for private obstetricians who are fully engaged. Laborists do not supplant the private practitioner’s role in delivering babies in the hospital, Dr. Olson says, “unless the private physician asks them to,” which, he adds, is happening more often.
Laborists typically are limited to labor and delivery services, although some also address gynecological cases in the ED. Most of the programs provide coverage 24/7, and invariably they are in facilities with medical hospitalists who might consult on medical complications for expectant mothers. One to two new programs open every month, Dr. Olson says, and his website lists 120 job openings. For information, visit www.ObGynHospitalist.com.
The OB/GYN hospitalist field is growing, with at least 164 identified programs and 1,500 to 2,500 practitioners who spend all or part of their workweek in hospital labor and delivery departments. SHM and the American College of Obstetricians and Gynecologists helped birth the 90-member Society of OB/GYN Hospitalists in 2011, but it is now independent, says founding president Rob Olson, MD, an OB/GYN hospitalist practicing in Bellingham, Wash. The fledgling society is planning its second annual conference, Sept. 27-29 in Denver, with obstetric emergency simulation training, clinical lectures, and pearls from the experience of general hospitalist practice by HM pioneer John Nelson, MD, MHM.
Also known as laborists, these board-certified OB/GYN docs’ dedicated presence affords rapid on-site response to changes in patients’ conditions, Dr. Olson says. Laborists might cover nights and weekends, pick up unassigned patients, or cover for private obstetricians who are fully engaged. Laborists do not supplant the private practitioner’s role in delivering babies in the hospital, Dr. Olson says, “unless the private physician asks them to,” which, he adds, is happening more often.
Laborists typically are limited to labor and delivery services, although some also address gynecological cases in the ED. Most of the programs provide coverage 24/7, and invariably they are in facilities with medical hospitalists who might consult on medical complications for expectant mothers. One to two new programs open every month, Dr. Olson says, and his website lists 120 job openings. For information, visit www.ObGynHospitalist.com.
Consumers Union Joins Hospital Safety Ratings Game
A new hospital patient-safety ranking system was released in July by Consumers Union (CU), an independent consumer advocacy organization in Yonkers, N.Y., and published in the August issue of its magazine Consumer Reports.1 CU rated 1,155 hospitals in six categories, including hospital-acquired infections, readmissions, and the quality of communication by physicians and nurses to patients. The highest-scoring hospital: Billings Clinic in Montana, which received a 72 on CU’s 100-point safety score.
“The new Consumer Reports hospital safety ratings add to a growing list of publicly reported performance rating schemes,” says SHM president Shaun Frost, MD, SFHM, FACP, associate medical director for care-delivery systems at HealthPartners in Minneapolis. Hospitalists should be aware of these ratings and review them “with an eye toward identifying improvement opportunities that are within their scope of influence....Hospitalists must embrace these issues as theirs to own and improve upon, as the ability to demonstrably improve the safety and care quality in the hospitals in which we practice is dependent on us.”
Reference
A new hospital patient-safety ranking system was released in July by Consumers Union (CU), an independent consumer advocacy organization in Yonkers, N.Y., and published in the August issue of its magazine Consumer Reports.1 CU rated 1,155 hospitals in six categories, including hospital-acquired infections, readmissions, and the quality of communication by physicians and nurses to patients. The highest-scoring hospital: Billings Clinic in Montana, which received a 72 on CU’s 100-point safety score.
“The new Consumer Reports hospital safety ratings add to a growing list of publicly reported performance rating schemes,” says SHM president Shaun Frost, MD, SFHM, FACP, associate medical director for care-delivery systems at HealthPartners in Minneapolis. Hospitalists should be aware of these ratings and review them “with an eye toward identifying improvement opportunities that are within their scope of influence....Hospitalists must embrace these issues as theirs to own and improve upon, as the ability to demonstrably improve the safety and care quality in the hospitals in which we practice is dependent on us.”
Reference
A new hospital patient-safety ranking system was released in July by Consumers Union (CU), an independent consumer advocacy organization in Yonkers, N.Y., and published in the August issue of its magazine Consumer Reports.1 CU rated 1,155 hospitals in six categories, including hospital-acquired infections, readmissions, and the quality of communication by physicians and nurses to patients. The highest-scoring hospital: Billings Clinic in Montana, which received a 72 on CU’s 100-point safety score.
“The new Consumer Reports hospital safety ratings add to a growing list of publicly reported performance rating schemes,” says SHM president Shaun Frost, MD, SFHM, FACP, associate medical director for care-delivery systems at HealthPartners in Minneapolis. Hospitalists should be aware of these ratings and review them “with an eye toward identifying improvement opportunities that are within their scope of influence....Hospitalists must embrace these issues as theirs to own and improve upon, as the ability to demonstrably improve the safety and care quality in the hospitals in which we practice is dependent on us.”
Reference
Ultrasound Joins Stethoscope as Portable Diagnostic Tool for Hospitalists
Prairie Business Magazine recently reported that hospitalist Neville Alberto, MD, FACP, of Sanford Health in Fargo, N.D., carries on his rounds not a stethoscope but “a portable ultrasound draped around his neck.”1 The article illustrates ultrasound’s increased portability, wider application at the hospital bedside, and increased use by trained hospitalists. It’s a topic also discussed in a recent post by Robert Wachter, MD, MHM, author of the blog Wachter’s World, professor, and chief of the division of hospital medicine at the University of California at San Francisco (UCSF). Dr. Wachter says “the time has come to—carefully and thoughtfully—add hospitalists” to the growing list of medical specialties that have staked a claim to a procedure previously reserved for radiologists.2
“The one I carry on me is no larger than my smartphone,” Dr. Alberto explains. “It’s well-placed, so nobody notices.”
A hospitalist since 2001, Dr. Alberto is often on the move in his seven-story hospital building. He uses the device to assist in determining whether a patient needs more fluids, or to examine an elderly patient’s bladder for urinary retention when a urinary tract infection is suspected. Only a few colleagues in Dr. Alberto’s 22-member hospitalist group are as comfortable with ultrasound technology, he says, but he has helped develop a curriculum to teach ultrasound techniques to physicians, residents, and medical students.
Diane Sliwka, MD, a UCSF hospitalist and advocate for more widespread ultrasound use by hospitalists, says most physicians have yet to adopt the technology as fully as Dr. Alberto has. “But they’ve seen it and they want it,” she adds.
Hospitalists first utilized portable ultrasound to guide such procedures as thoracentesis or paracentesis. Increasingly, it is being used to assess, for example, cardiac function, fluid buildup around the heart, or the location of a blood clot—“when decisions are needed quickly about what’s going on and how to treat it,” she says. Other growing targets include lung pathologies (pneumothorax) and differentiating between COPD and pulmonary edema, or pneumonia and gallstones, she says.
The technology is advancing faster than the speed of light, with an iPad/tablet application in the works, according to a recent Technology Review blog post from the Massachusetts Institute of Technology.3
References
- Doctors use technology to better diagnose and treat illnesses in a less invasive manner. Prairie Business website. Available at: www.prairiebizmag.com. Accessed July 31, 2012.
- Wachter RM. Bedside ultrasound for hospitalists: our time has come. Wachter’s World website. Available at: http://community.the-hospitalist.org/2012/05/16/bedside-ultrasound-for-hospitalists-our-time-has-come. Accessed July 31, 2012.
- Mims C. Patent hints at iPad-powered portable ultrasound machine. Technology Review website. Available at: www.technologyreview.com/view/427600/patent-hints-at-ipad-powered-portable-ultrasound. Accessed July 29, 2012.
Prairie Business Magazine recently reported that hospitalist Neville Alberto, MD, FACP, of Sanford Health in Fargo, N.D., carries on his rounds not a stethoscope but “a portable ultrasound draped around his neck.”1 The article illustrates ultrasound’s increased portability, wider application at the hospital bedside, and increased use by trained hospitalists. It’s a topic also discussed in a recent post by Robert Wachter, MD, MHM, author of the blog Wachter’s World, professor, and chief of the division of hospital medicine at the University of California at San Francisco (UCSF). Dr. Wachter says “the time has come to—carefully and thoughtfully—add hospitalists” to the growing list of medical specialties that have staked a claim to a procedure previously reserved for radiologists.2
“The one I carry on me is no larger than my smartphone,” Dr. Alberto explains. “It’s well-placed, so nobody notices.”
A hospitalist since 2001, Dr. Alberto is often on the move in his seven-story hospital building. He uses the device to assist in determining whether a patient needs more fluids, or to examine an elderly patient’s bladder for urinary retention when a urinary tract infection is suspected. Only a few colleagues in Dr. Alberto’s 22-member hospitalist group are as comfortable with ultrasound technology, he says, but he has helped develop a curriculum to teach ultrasound techniques to physicians, residents, and medical students.
Diane Sliwka, MD, a UCSF hospitalist and advocate for more widespread ultrasound use by hospitalists, says most physicians have yet to adopt the technology as fully as Dr. Alberto has. “But they’ve seen it and they want it,” she adds.
Hospitalists first utilized portable ultrasound to guide such procedures as thoracentesis or paracentesis. Increasingly, it is being used to assess, for example, cardiac function, fluid buildup around the heart, or the location of a blood clot—“when decisions are needed quickly about what’s going on and how to treat it,” she says. Other growing targets include lung pathologies (pneumothorax) and differentiating between COPD and pulmonary edema, or pneumonia and gallstones, she says.
The technology is advancing faster than the speed of light, with an iPad/tablet application in the works, according to a recent Technology Review blog post from the Massachusetts Institute of Technology.3
References
- Doctors use technology to better diagnose and treat illnesses in a less invasive manner. Prairie Business website. Available at: www.prairiebizmag.com. Accessed July 31, 2012.
- Wachter RM. Bedside ultrasound for hospitalists: our time has come. Wachter’s World website. Available at: http://community.the-hospitalist.org/2012/05/16/bedside-ultrasound-for-hospitalists-our-time-has-come. Accessed July 31, 2012.
- Mims C. Patent hints at iPad-powered portable ultrasound machine. Technology Review website. Available at: www.technologyreview.com/view/427600/patent-hints-at-ipad-powered-portable-ultrasound. Accessed July 29, 2012.
Prairie Business Magazine recently reported that hospitalist Neville Alberto, MD, FACP, of Sanford Health in Fargo, N.D., carries on his rounds not a stethoscope but “a portable ultrasound draped around his neck.”1 The article illustrates ultrasound’s increased portability, wider application at the hospital bedside, and increased use by trained hospitalists. It’s a topic also discussed in a recent post by Robert Wachter, MD, MHM, author of the blog Wachter’s World, professor, and chief of the division of hospital medicine at the University of California at San Francisco (UCSF). Dr. Wachter says “the time has come to—carefully and thoughtfully—add hospitalists” to the growing list of medical specialties that have staked a claim to a procedure previously reserved for radiologists.2
“The one I carry on me is no larger than my smartphone,” Dr. Alberto explains. “It’s well-placed, so nobody notices.”
A hospitalist since 2001, Dr. Alberto is often on the move in his seven-story hospital building. He uses the device to assist in determining whether a patient needs more fluids, or to examine an elderly patient’s bladder for urinary retention when a urinary tract infection is suspected. Only a few colleagues in Dr. Alberto’s 22-member hospitalist group are as comfortable with ultrasound technology, he says, but he has helped develop a curriculum to teach ultrasound techniques to physicians, residents, and medical students.
Diane Sliwka, MD, a UCSF hospitalist and advocate for more widespread ultrasound use by hospitalists, says most physicians have yet to adopt the technology as fully as Dr. Alberto has. “But they’ve seen it and they want it,” she adds.
Hospitalists first utilized portable ultrasound to guide such procedures as thoracentesis or paracentesis. Increasingly, it is being used to assess, for example, cardiac function, fluid buildup around the heart, or the location of a blood clot—“when decisions are needed quickly about what’s going on and how to treat it,” she says. Other growing targets include lung pathologies (pneumothorax) and differentiating between COPD and pulmonary edema, or pneumonia and gallstones, she says.
The technology is advancing faster than the speed of light, with an iPad/tablet application in the works, according to a recent Technology Review blog post from the Massachusetts Institute of Technology.3
References
- Doctors use technology to better diagnose and treat illnesses in a less invasive manner. Prairie Business website. Available at: www.prairiebizmag.com. Accessed July 31, 2012.
- Wachter RM. Bedside ultrasound for hospitalists: our time has come. Wachter’s World website. Available at: http://community.the-hospitalist.org/2012/05/16/bedside-ultrasound-for-hospitalists-our-time-has-come. Accessed July 31, 2012.
- Mims C. Patent hints at iPad-powered portable ultrasound machine. Technology Review website. Available at: www.technologyreview.com/view/427600/patent-hints-at-ipad-powered-portable-ultrasound. Accessed July 29, 2012.
By the Numbers: 1%
Share of physician job-search assignments conducted by Irving, Texas-based physician recruiting firm Merritt Hawkins from April 1, 2011, and March 31, 2012, that featured openings for independent, solo practitioners; the share was 17% in 2006.1 Merritt Hawkins’ 2012 Review of Physician Recruiting Incentives report concludes “the recruitment of physicians into solo practice settings has almost abated.” Conversely, 63% of the firm’s job searches were with hospitals, up from 56% the year before.
Reference
Share of physician job-search assignments conducted by Irving, Texas-based physician recruiting firm Merritt Hawkins from April 1, 2011, and March 31, 2012, that featured openings for independent, solo practitioners; the share was 17% in 2006.1 Merritt Hawkins’ 2012 Review of Physician Recruiting Incentives report concludes “the recruitment of physicians into solo practice settings has almost abated.” Conversely, 63% of the firm’s job searches were with hospitals, up from 56% the year before.
Reference
Share of physician job-search assignments conducted by Irving, Texas-based physician recruiting firm Merritt Hawkins from April 1, 2011, and March 31, 2012, that featured openings for independent, solo practitioners; the share was 17% in 2006.1 Merritt Hawkins’ 2012 Review of Physician Recruiting Incentives report concludes “the recruitment of physicians into solo practice settings has almost abated.” Conversely, 63% of the firm’s job searches were with hospitals, up from 56% the year before.
Reference
Interactive Quality, Leadership Lessons for Residents
An interactive program to teach quality and leadership skills to internal-medicine residents at Mount Sinai School of Medicine in New York City—described in an Research, Innovations and Clinical Vignettes (RIV) poster presented at HM12 in San Diego—found that medical trainees are eager and willing to learn the skills that will be required from hospitalists in a reformed healthcare system.1 Lead author Brian Markoff, MD, SFHM, associate chief of hospital medicine at Mount Sinai, says the Healthcare Leadership Track’s elective, one-month block in quality improvement (QI) and patient safety was established with four second-year residents in 2011-2012.
Along with didactic presentations, participants were offered novel structured learning exercises that included:
- Teaching a care-transitions module to interns;
- Proposing a new clinical pathway;
- Leading a conference on QI;
- Examining a hospital readmission for what went wrong;
- Pairing with a ward medical director;
- Conducting a mentored QI research project; and
- Participating in a book club.
All four participants from the first year “strongly agree that the block was highly relevant to their current and future careers,” Dr. Markoff says.
In their third year, the residents will have the opportunity to participate in one-month electives for leadership, teaching, and the business of medicine.
Six new second-year residents are joining the program, and longitudinal components span the program’s two years. “Most institutions that train residents have a lot of this activity going on,” he says. “Why not get house staff involved in experiential learning in these areas?”
Reference
An interactive program to teach quality and leadership skills to internal-medicine residents at Mount Sinai School of Medicine in New York City—described in an Research, Innovations and Clinical Vignettes (RIV) poster presented at HM12 in San Diego—found that medical trainees are eager and willing to learn the skills that will be required from hospitalists in a reformed healthcare system.1 Lead author Brian Markoff, MD, SFHM, associate chief of hospital medicine at Mount Sinai, says the Healthcare Leadership Track’s elective, one-month block in quality improvement (QI) and patient safety was established with four second-year residents in 2011-2012.
Along with didactic presentations, participants were offered novel structured learning exercises that included:
- Teaching a care-transitions module to interns;
- Proposing a new clinical pathway;
- Leading a conference on QI;
- Examining a hospital readmission for what went wrong;
- Pairing with a ward medical director;
- Conducting a mentored QI research project; and
- Participating in a book club.
All four participants from the first year “strongly agree that the block was highly relevant to their current and future careers,” Dr. Markoff says.
In their third year, the residents will have the opportunity to participate in one-month electives for leadership, teaching, and the business of medicine.
Six new second-year residents are joining the program, and longitudinal components span the program’s two years. “Most institutions that train residents have a lot of this activity going on,” he says. “Why not get house staff involved in experiential learning in these areas?”
Reference
An interactive program to teach quality and leadership skills to internal-medicine residents at Mount Sinai School of Medicine in New York City—described in an Research, Innovations and Clinical Vignettes (RIV) poster presented at HM12 in San Diego—found that medical trainees are eager and willing to learn the skills that will be required from hospitalists in a reformed healthcare system.1 Lead author Brian Markoff, MD, SFHM, associate chief of hospital medicine at Mount Sinai, says the Healthcare Leadership Track’s elective, one-month block in quality improvement (QI) and patient safety was established with four second-year residents in 2011-2012.
Along with didactic presentations, participants were offered novel structured learning exercises that included:
- Teaching a care-transitions module to interns;
- Proposing a new clinical pathway;
- Leading a conference on QI;
- Examining a hospital readmission for what went wrong;
- Pairing with a ward medical director;
- Conducting a mentored QI research project; and
- Participating in a book club.
All four participants from the first year “strongly agree that the block was highly relevant to their current and future careers,” Dr. Markoff says.
In their third year, the residents will have the opportunity to participate in one-month electives for leadership, teaching, and the business of medicine.
Six new second-year residents are joining the program, and longitudinal components span the program’s two years. “Most institutions that train residents have a lot of this activity going on,” he says. “Why not get house staff involved in experiential learning in these areas?”
Reference
Teach Back Communication Strategy Helps Healthcare Providers Help Their Patients
“Do you understand what I just told you?”
Hospitalists who are experts on communicating with patients say that this kind of simple, yes/no question can engender all sorts of confusion. This kind of query often results in unrealistic discharge plans, failed post-discharge treatments, and unnecessary rehospitalizations. And they happen all the time in hospitals across the country.
“Yes/no questions, unless they are very concrete—such as ‘Do you have a headache?’—have little relation to assessing a patient’s understanding of essential healthcare information,” says Jeffrey Greenwald, MD, SFHM, hospitalist and educator at Massachusetts General Hospital in Boston. Many times, he adds, patients say “yes” just to please the doctor or nurse, or to avoid looking ignorant.
A better approach to patient-provider communication, one that successfully addresses communication gaps, is teach-back, a strategy in which providers ask patients to repeat (or “teach back”), in their own words, what they have just learned about their medical condition, treatments, and self-care. For example, a physician using the teach-back method could ask, “Mr. Smith, can you tell me why you are in the hospital?”
The approach is an integral part of SHM’s Project BOOST (Better Outcomes for Older Adults through Safer Transitions) care-transitions quality initiative, says Dr. Greenwald, a BOOST coinvestigator. But too often, hospitalists fail to embrace the mandate of effective communication, he says, leaving responsibility to clarify the patient’s understanding to nurses and other members of the care team.
“Having taught this skill all over the country, I continue to find members of my own profession who feel that it is not their job to assess if patients understand self-care and medication instructions. To me, there’s no question that physicians have a role to play as teachers. We educate patients, whether we think we do or not,” Dr. Greenwald says, adding that some hospitalists do so with greater effectiveness than others.
In an era of accountable-care organizations, patient-centered care, and shared decision-making, hospitalists need to provide their patients the same core messages as the rest of the care team does. According to a recent report by the University of California San Francisco (UCSF) Center for Vulnerable Populations at San Francisco General Hospital, 77 million Americans have difficulty understanding even basic healthcare information.1
In addition to widespread language barriers, the Institute of Medicine in a 2004 report concluded that 90 million U.S. adults have literacy skills that test below the high-school level.2 As most hospitalists know, many inpatients go to great lengths to mask these limitations—appearing knowledgeable while failing to grasp essential health concepts. Medical jargon, acronyms, and instructions can be confusing, even for patients with a high level of education.
“First and foremost, we have to be able to communicate with our patients—to make sure that we understand their goals and that they understand our approach to treatment and the therapeutic goals we are proposing,” Dr. Greenwald says. “This process also helps to achieve true informed consent. We want to ensure that their questions are being answered, and that the options we are discussing are in line with their goals of care so that they are more likely to actually undertake them when they go home. And if they can’t, we need to know that in advance, so that we can intervene in other ways.”
Embracing the Method
One health system that has embraced teach-back as a patient-education strategy is the Lehigh Valley Health Network (LVHN), a 988-bed, three-hospital system based in Allentown, Pa. In an HM12 workshop, the Lehigh Valley team explained how its teach-back initiative grew out of quality initiatives to target patient flow and readmissions. Lehigh joined an Institute for Healthcare Improvement quality collaborative, implemented “Lean” quality-improvement (QI) methodologies, and adopted a patient-coaching program.3
“This process has shined a stark spotlight on how poorly we as physicians communicate with patients overall,” says Michael Pistoria, DO, SFHM, former hospitalist and president of medical staff at LVHN who was a member of the teach-back team.
“I’d like to think I’m a little above averagein this regard, but it has made me realize how much better I could be in checking in with patients, gauging their health literacy, and engaging them with the care plan. As hospitalists, we all have to rethink how we talk to patients and families.”
A multidisciplinary team, originally created to analyze care transitions, was divided into four work groups. One group, which focused on patient/family understanding of the disease process, quickly learned that care-team members often failed to identify the patient’s “key learner”—the patient, a family member, or someone else. If the information is given to the wrong person, breakdowns can result. Such breakdowns usually lead to readmissions. One instrumental change that came as a result of the QI team’s efforts is that LVHN care-team members now recognize it is their responsibility to ask who the key learner is and to put that person’s name on a whiteboard in the patient’s room.
In the workshop in at SHM’s annual meeting in San Diego, Kim Jordan, MHA, BSN, RN, NE-BC, LVHN’s administrator of patient-care services, described teach-back as an effective, easy-to-use communication strategy that improves patient learning outcomes. “We created a standard work process using teach-back strategies across the healthcare system,” with training offered to all professionals who provide education to patients and families, she said.
Starting with heart failure, prompts were written into the electronic health record (EHR) to provide four scripted teach-back questions, each focused on the patient’s knowledge, attitudes, and behavior, to be asked consecutively over three days. Information was “chunked” into manageable pieces, emphasizing what was most important for the patient to learn on that day.
Results from one of the pilot units showed 30-day readmission rates for heart failure patients were cut in half, from 28% to 14%.4 Teach-back scripts also are being developed for the anticoagulant clinic and for patients with stroke, myocardial infarction, chronic obstructive pulmonary disease (COPD), community-acquired pneumonia, and diabetes.
“Continued analysis continues to show reduced rehospitalizations, and we even find that for those who are readmitted, their second admissions have been shorter,” Dr. Pistoria says, noting LVHN nurses have reported higher satisfaction. “They say, ‘This is wonderful. This is what I love about nursing—I get to teach the patients.’”
A Quality Mandate
The importance of effective communication with hospitalized patients is recognized in the federal Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS)5 quality ratings and, more recently, by Consumers Union’s new hospital safety ratings,6 which include communication in its six categories of patient-safety measures. And a recent study from the University of Washington says patients place high value on verbal communication about their discharge care plans and how to improve their health, and personal communication between their inpatient and outpatient providers.7
Large volumes of important information often are “dumped” on hospitalized patients, and many times patients are provided insufficient time to assimilate the information or ask questions about it.8 Such situations are especially common at discharge. And although physicians and other care-team members might feel they can’t afford the time to assure themselves that the patient understands what they are saying, the alternative is a lot more time spent dealing with preventable crises, misunderstandings—and preventable readmissions.
“People say, ‘I don’t have time for this,’” says Laura Vento, MSN, RN, clinical nurse leader on an acute-care medical unit at the University of California at San Diego medical center, who spearheaded teach-back at her hospital. “I did some observations around discharge visits, and it took an average of six minutes. After we implemented teach-back, it took eight to nine minutes. Nurses and patients were both very satisfied with the results. I say to staff: ‘Give it a try, and see what a difference an extra two minutes can make.’”
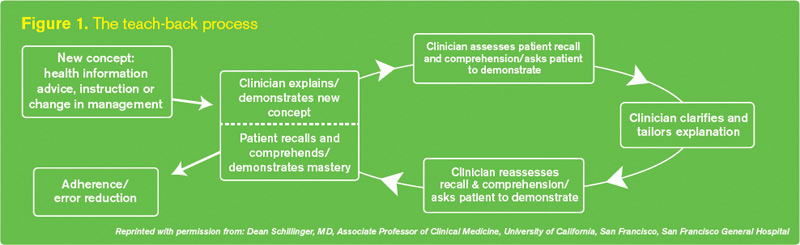
Dr. Pistoria describes teach-back as “humble inquiry...the simple need and ability to ask patients, ‘I know I’ve been throwing a lot of information at you. Can you tell me what I just said?’ Then, shut up and listen.” The goal is to have patients confirm that they understand fully what the provider thinks they need to know. The technique is presented as a test not of the patient’s learning ability, but of the provider’s communication effectiveness and success in explaining the information (see Figure 1). If the message has not been transmitted successfully, the professional reteaches, corrects misconceptions, and again asks the patient to teach back.
The theory is that physicians will then avoid the closed-ended questions (“Do you understand what I just told you?”) that make patients uncomfortable or inhibit the communication that needs to happen between patient and provider.
“We didn’t invent teach-back, which long predated Project BOOST,” Dr. Greenwald says. “But we use it and endorse it strongly, and believe it is an important part of communication with patients, particularly around care transitions.”
Dr. Greenwald thinks teach-back “is not a big stretch for hospitalists.” But he says it requires meaningful training and practice, ideally in a multidisciplinary team context. Participating Project BOOST ([email protected]) and Electronic Quality Improvement Programs (eQUIPS) sites receive a two-year license to post the “train-the-trainer” curriculum on their intranet systems.8 An instructional webinar, and the trainer curriculum and video, are available in the SHM store (www.hospitalmedicine.org/store). SHM also provides on-site training sessions for health systems or learning collaboratives (contact [email protected]).
‘Teach-Back on Steroids’
Teach-back, while a useful approach for improving patients’ understanding about hospital discharges, post-discharge care plans, and patient self-care, is just one of many teaching models that hospitalist groups can use to improve provider-to-patient communication. HM groups should assess health literacy in their regions and physician communication skills before deciding on one or more improvement tools.
LVHN, for example, has incorporated brief motivational interviewing techniques to its teach-back system, and the results are now being studied, says Paula Robinson, MSN, RN, BC, LVHN’s manager of patient, family, and consumer education.
“A lot of research out there emphasizes how patient education and knowledge alone don’t make a difference in adherence or compliance to treatment plans, even if they are getting the knowledge right 100% of the time,” Robinson says. “You also need to give patients permission to explore their feelings.”
One of Robinson’s colleagues, patient-care specialist Debra Peters, MSN, RN, BC, CMSRN, remembers using teach-back with a heart failure patient with recurrent rehospitalizations, exploring why it was important to control his salt intake. “The patient said, ‘Honey, I salt my ham, and I have no intention of changing that.’ This issue would not have come up if we had just addressed the knowledge component and told him: ‘You need to reduce your salt intake.’”
There might not be easy solutions to that kind of patient attitude, although in this case Peters made a referral to a dietitian who worked with the patient on food substitutions and other tools for managing his salt intake. “I don’t know if we made a big difference, but I haven’t seen him back in the hospital,” she says.
Motivational interviewing is a directive, client-centered counseling style for eliciting behavioral changes by helping clients to explore and resolve their ambivalence about making changes.9 Robinson calls it “the next step in our journey, with teach-back as a jumping-off place. We’ve worked on open-ended questions, getting patients to tell their stories, and our own reflective listening skills. I look at teach-back as a great communication tool and strategy—and motivational interviewing as ‘teach-back on steroids.’”
A number of similar, comparable, or complementary techniques and systems, with names like “Teach-to-Goal” and often paired with such resources as written materials, can help advance the same ends (visit the-hospitalist.org to learn about a technique for communicating bad news to patients).
The Flinders Program, developed at Flinders University in Adelaide, Australia, is a four-part structured motivational interview that asks patients to identify what they see as the biggest problem they face.10 LVHN medical educator Krista Hirschmann, MA, PhD, says this method was taught at LVHN by Australian experts and is now being used by its home-care department. “It is truly a patient-centered approach, and could be used by anybody in the health system,” she says.
Project RED (Re-Engineered Discharge), a care-transitions strategy developed by Brian Jack, MD, and colleagues at Boston University School of Medicine, was used to create a “virtual discharge advocate,” a computer avatar that simulates the face-to-face interaction between a patient and a nurse at the bedside.11 Patients interact with the avatar, named Louise, through a touch-screen display to review their after-hospital care packet and to answer her questions, confirming their understanding without being rushed for time.
Ultimately, Dr. Greenwald says, it doesn’t matter if physicians use teach-back or some other system to improve health literacy. “What matters is whether your patients understand what they need to know in order to go home and take care of themselves,” he says.
Larry Beresford is a freelance writer based in Oakland, Calif.
References
- Brach C, Keller D, Hernandez LM, et al. Ten attributes of health literate health care organizations. Institute of Medicine of the National Academies website. Available at: http://iom.edu/Global/Perspectives/2012/HealthLitAttributes.aspx. Accessed Aug. 9, 2012.
- Nielsen-Bohlman L, Panzer AM, Kindig DA, eds., Committee on Health Literacy. Health Literacy: A Prescription to End Confusion. Washington: Institute of Medicine; 2004.
- Care Transitions Program; University of Colorado School of Medicine, Division of Health Care Policy and Research. Available at: www.caretransitions.org. Accessed July 28, 2012.
- Healthcare Benchmarks and Quality Improvement. Teach-back program reduces readmissions. HighBeam Research website. Available at: http://www.highbeam.com/doc/1G1-269890846.html. Accessed Aug. 9, 2012.
- Hospital Consumer Assessment of Healthcare Providers and Systems. Centers for Medicare & Medicaid Services website. Available at: www.hcahpsonline.org. Accessed July 23, 2012.
- Consumer Reports. How safe is your hospital? Our new ratings find that some are riskier than others. Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/2012/08/how-safe-is-your-hospital/index.htm. Accessed Aug. 1, 2012.
- Shoeb M, Merel SE, Jackson MB, Anawalt BD. “Can’t we just stop and talk?” Patients value verbal communication about discharge care plans. J Hosp Med. 2012;7(6):504-7.
- Schillinger D, Piette J, Grumbach K, et al. Closing the loop: physician communication with diabetic patients who have low health literacy. Arch Intern Med. 2003;163:83-90.
- Borrelli B, Riekert KA, Weinstein W, Rathier L. Brief motivational interviewing as a clinical strategy to promote asthma medication adherence. J Allergy Clinical Immunol. 2007;120(5):1023-30.
- eQUIPS (Electronic Quality Improvement Programs). Society of Hospital Medicine website. Available at: http:// www.hospitalmedicine.org/equips. Accessed Aug. 1, 2012.
- Kelly J, Kubina N. Navigating self-management: a practical approach for Australian health agencies. Flinders University, Adelaide, Australia. Available at: www.flinders.edu.au/medicine/sites/fhbhru/self-management.cfm. Accessed Aug. 1, 2012.
- Project RED (Re-Engineered Discharge). Boston University Medical Center website. Available at: http:// www.bu.edu/fammed/projectred/publications.html. Accessed Aug. 1, 2012.
“Do you understand what I just told you?”
Hospitalists who are experts on communicating with patients say that this kind of simple, yes/no question can engender all sorts of confusion. This kind of query often results in unrealistic discharge plans, failed post-discharge treatments, and unnecessary rehospitalizations. And they happen all the time in hospitals across the country.
“Yes/no questions, unless they are very concrete—such as ‘Do you have a headache?’—have little relation to assessing a patient’s understanding of essential healthcare information,” says Jeffrey Greenwald, MD, SFHM, hospitalist and educator at Massachusetts General Hospital in Boston. Many times, he adds, patients say “yes” just to please the doctor or nurse, or to avoid looking ignorant.
A better approach to patient-provider communication, one that successfully addresses communication gaps, is teach-back, a strategy in which providers ask patients to repeat (or “teach back”), in their own words, what they have just learned about their medical condition, treatments, and self-care. For example, a physician using the teach-back method could ask, “Mr. Smith, can you tell me why you are in the hospital?”
The approach is an integral part of SHM’s Project BOOST (Better Outcomes for Older Adults through Safer Transitions) care-transitions quality initiative, says Dr. Greenwald, a BOOST coinvestigator. But too often, hospitalists fail to embrace the mandate of effective communication, he says, leaving responsibility to clarify the patient’s understanding to nurses and other members of the care team.
“Having taught this skill all over the country, I continue to find members of my own profession who feel that it is not their job to assess if patients understand self-care and medication instructions. To me, there’s no question that physicians have a role to play as teachers. We educate patients, whether we think we do or not,” Dr. Greenwald says, adding that some hospitalists do so with greater effectiveness than others.
In an era of accountable-care organizations, patient-centered care, and shared decision-making, hospitalists need to provide their patients the same core messages as the rest of the care team does. According to a recent report by the University of California San Francisco (UCSF) Center for Vulnerable Populations at San Francisco General Hospital, 77 million Americans have difficulty understanding even basic healthcare information.1
In addition to widespread language barriers, the Institute of Medicine in a 2004 report concluded that 90 million U.S. adults have literacy skills that test below the high-school level.2 As most hospitalists know, many inpatients go to great lengths to mask these limitations—appearing knowledgeable while failing to grasp essential health concepts. Medical jargon, acronyms, and instructions can be confusing, even for patients with a high level of education.
“First and foremost, we have to be able to communicate with our patients—to make sure that we understand their goals and that they understand our approach to treatment and the therapeutic goals we are proposing,” Dr. Greenwald says. “This process also helps to achieve true informed consent. We want to ensure that their questions are being answered, and that the options we are discussing are in line with their goals of care so that they are more likely to actually undertake them when they go home. And if they can’t, we need to know that in advance, so that we can intervene in other ways.”
Embracing the Method
One health system that has embraced teach-back as a patient-education strategy is the Lehigh Valley Health Network (LVHN), a 988-bed, three-hospital system based in Allentown, Pa. In an HM12 workshop, the Lehigh Valley team explained how its teach-back initiative grew out of quality initiatives to target patient flow and readmissions. Lehigh joined an Institute for Healthcare Improvement quality collaborative, implemented “Lean” quality-improvement (QI) methodologies, and adopted a patient-coaching program.3
“This process has shined a stark spotlight on how poorly we as physicians communicate with patients overall,” says Michael Pistoria, DO, SFHM, former hospitalist and president of medical staff at LVHN who was a member of the teach-back team.
“I’d like to think I’m a little above averagein this regard, but it has made me realize how much better I could be in checking in with patients, gauging their health literacy, and engaging them with the care plan. As hospitalists, we all have to rethink how we talk to patients and families.”
A multidisciplinary team, originally created to analyze care transitions, was divided into four work groups. One group, which focused on patient/family understanding of the disease process, quickly learned that care-team members often failed to identify the patient’s “key learner”—the patient, a family member, or someone else. If the information is given to the wrong person, breakdowns can result. Such breakdowns usually lead to readmissions. One instrumental change that came as a result of the QI team’s efforts is that LVHN care-team members now recognize it is their responsibility to ask who the key learner is and to put that person’s name on a whiteboard in the patient’s room.
In the workshop in at SHM’s annual meeting in San Diego, Kim Jordan, MHA, BSN, RN, NE-BC, LVHN’s administrator of patient-care services, described teach-back as an effective, easy-to-use communication strategy that improves patient learning outcomes. “We created a standard work process using teach-back strategies across the healthcare system,” with training offered to all professionals who provide education to patients and families, she said.
Starting with heart failure, prompts were written into the electronic health record (EHR) to provide four scripted teach-back questions, each focused on the patient’s knowledge, attitudes, and behavior, to be asked consecutively over three days. Information was “chunked” into manageable pieces, emphasizing what was most important for the patient to learn on that day.
Results from one of the pilot units showed 30-day readmission rates for heart failure patients were cut in half, from 28% to 14%.4 Teach-back scripts also are being developed for the anticoagulant clinic and for patients with stroke, myocardial infarction, chronic obstructive pulmonary disease (COPD), community-acquired pneumonia, and diabetes.
“Continued analysis continues to show reduced rehospitalizations, and we even find that for those who are readmitted, their second admissions have been shorter,” Dr. Pistoria says, noting LVHN nurses have reported higher satisfaction. “They say, ‘This is wonderful. This is what I love about nursing—I get to teach the patients.’”
A Quality Mandate
The importance of effective communication with hospitalized patients is recognized in the federal Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS)5 quality ratings and, more recently, by Consumers Union’s new hospital safety ratings,6 which include communication in its six categories of patient-safety measures. And a recent study from the University of Washington says patients place high value on verbal communication about their discharge care plans and how to improve their health, and personal communication between their inpatient and outpatient providers.7
Large volumes of important information often are “dumped” on hospitalized patients, and many times patients are provided insufficient time to assimilate the information or ask questions about it.8 Such situations are especially common at discharge. And although physicians and other care-team members might feel they can’t afford the time to assure themselves that the patient understands what they are saying, the alternative is a lot more time spent dealing with preventable crises, misunderstandings—and preventable readmissions.
“People say, ‘I don’t have time for this,’” says Laura Vento, MSN, RN, clinical nurse leader on an acute-care medical unit at the University of California at San Diego medical center, who spearheaded teach-back at her hospital. “I did some observations around discharge visits, and it took an average of six minutes. After we implemented teach-back, it took eight to nine minutes. Nurses and patients were both very satisfied with the results. I say to staff: ‘Give it a try, and see what a difference an extra two minutes can make.’”
Dr. Pistoria describes teach-back as “humble inquiry...the simple need and ability to ask patients, ‘I know I’ve been throwing a lot of information at you. Can you tell me what I just said?’ Then, shut up and listen.” The goal is to have patients confirm that they understand fully what the provider thinks they need to know. The technique is presented as a test not of the patient’s learning ability, but of the provider’s communication effectiveness and success in explaining the information (see Figure 1). If the message has not been transmitted successfully, the professional reteaches, corrects misconceptions, and again asks the patient to teach back.
The theory is that physicians will then avoid the closed-ended questions (“Do you understand what I just told you?”) that make patients uncomfortable or inhibit the communication that needs to happen between patient and provider.
“We didn’t invent teach-back, which long predated Project BOOST,” Dr. Greenwald says. “But we use it and endorse it strongly, and believe it is an important part of communication with patients, particularly around care transitions.”
Dr. Greenwald thinks teach-back “is not a big stretch for hospitalists.” But he says it requires meaningful training and practice, ideally in a multidisciplinary team context. Participating Project BOOST ([email protected]) and Electronic Quality Improvement Programs (eQUIPS) sites receive a two-year license to post the “train-the-trainer” curriculum on their intranet systems.8 An instructional webinar, and the trainer curriculum and video, are available in the SHM store (www.hospitalmedicine.org/store). SHM also provides on-site training sessions for health systems or learning collaboratives (contact [email protected]).
‘Teach-Back on Steroids’
Teach-back, while a useful approach for improving patients’ understanding about hospital discharges, post-discharge care plans, and patient self-care, is just one of many teaching models that hospitalist groups can use to improve provider-to-patient communication. HM groups should assess health literacy in their regions and physician communication skills before deciding on one or more improvement tools.
LVHN, for example, has incorporated brief motivational interviewing techniques to its teach-back system, and the results are now being studied, says Paula Robinson, MSN, RN, BC, LVHN’s manager of patient, family, and consumer education.
“A lot of research out there emphasizes how patient education and knowledge alone don’t make a difference in adherence or compliance to treatment plans, even if they are getting the knowledge right 100% of the time,” Robinson says. “You also need to give patients permission to explore their feelings.”
One of Robinson’s colleagues, patient-care specialist Debra Peters, MSN, RN, BC, CMSRN, remembers using teach-back with a heart failure patient with recurrent rehospitalizations, exploring why it was important to control his salt intake. “The patient said, ‘Honey, I salt my ham, and I have no intention of changing that.’ This issue would not have come up if we had just addressed the knowledge component and told him: ‘You need to reduce your salt intake.’”
There might not be easy solutions to that kind of patient attitude, although in this case Peters made a referral to a dietitian who worked with the patient on food substitutions and other tools for managing his salt intake. “I don’t know if we made a big difference, but I haven’t seen him back in the hospital,” she says.
Motivational interviewing is a directive, client-centered counseling style for eliciting behavioral changes by helping clients to explore and resolve their ambivalence about making changes.9 Robinson calls it “the next step in our journey, with teach-back as a jumping-off place. We’ve worked on open-ended questions, getting patients to tell their stories, and our own reflective listening skills. I look at teach-back as a great communication tool and strategy—and motivational interviewing as ‘teach-back on steroids.’”
A number of similar, comparable, or complementary techniques and systems, with names like “Teach-to-Goal” and often paired with such resources as written materials, can help advance the same ends (visit the-hospitalist.org to learn about a technique for communicating bad news to patients).
The Flinders Program, developed at Flinders University in Adelaide, Australia, is a four-part structured motivational interview that asks patients to identify what they see as the biggest problem they face.10 LVHN medical educator Krista Hirschmann, MA, PhD, says this method was taught at LVHN by Australian experts and is now being used by its home-care department. “It is truly a patient-centered approach, and could be used by anybody in the health system,” she says.
Project RED (Re-Engineered Discharge), a care-transitions strategy developed by Brian Jack, MD, and colleagues at Boston University School of Medicine, was used to create a “virtual discharge advocate,” a computer avatar that simulates the face-to-face interaction between a patient and a nurse at the bedside.11 Patients interact with the avatar, named Louise, through a touch-screen display to review their after-hospital care packet and to answer her questions, confirming their understanding without being rushed for time.
Ultimately, Dr. Greenwald says, it doesn’t matter if physicians use teach-back or some other system to improve health literacy. “What matters is whether your patients understand what they need to know in order to go home and take care of themselves,” he says.
Larry Beresford is a freelance writer based in Oakland, Calif.
References
- Brach C, Keller D, Hernandez LM, et al. Ten attributes of health literate health care organizations. Institute of Medicine of the National Academies website. Available at: http://iom.edu/Global/Perspectives/2012/HealthLitAttributes.aspx. Accessed Aug. 9, 2012.
- Nielsen-Bohlman L, Panzer AM, Kindig DA, eds., Committee on Health Literacy. Health Literacy: A Prescription to End Confusion. Washington: Institute of Medicine; 2004.
- Care Transitions Program; University of Colorado School of Medicine, Division of Health Care Policy and Research. Available at: www.caretransitions.org. Accessed July 28, 2012.
- Healthcare Benchmarks and Quality Improvement. Teach-back program reduces readmissions. HighBeam Research website. Available at: http://www.highbeam.com/doc/1G1-269890846.html. Accessed Aug. 9, 2012.
- Hospital Consumer Assessment of Healthcare Providers and Systems. Centers for Medicare & Medicaid Services website. Available at: www.hcahpsonline.org. Accessed July 23, 2012.
- Consumer Reports. How safe is your hospital? Our new ratings find that some are riskier than others. Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/2012/08/how-safe-is-your-hospital/index.htm. Accessed Aug. 1, 2012.
- Shoeb M, Merel SE, Jackson MB, Anawalt BD. “Can’t we just stop and talk?” Patients value verbal communication about discharge care plans. J Hosp Med. 2012;7(6):504-7.
- Schillinger D, Piette J, Grumbach K, et al. Closing the loop: physician communication with diabetic patients who have low health literacy. Arch Intern Med. 2003;163:83-90.
- Borrelli B, Riekert KA, Weinstein W, Rathier L. Brief motivational interviewing as a clinical strategy to promote asthma medication adherence. J Allergy Clinical Immunol. 2007;120(5):1023-30.
- eQUIPS (Electronic Quality Improvement Programs). Society of Hospital Medicine website. Available at: http:// www.hospitalmedicine.org/equips. Accessed Aug. 1, 2012.
- Kelly J, Kubina N. Navigating self-management: a practical approach for Australian health agencies. Flinders University, Adelaide, Australia. Available at: www.flinders.edu.au/medicine/sites/fhbhru/self-management.cfm. Accessed Aug. 1, 2012.
- Project RED (Re-Engineered Discharge). Boston University Medical Center website. Available at: http:// www.bu.edu/fammed/projectred/publications.html. Accessed Aug. 1, 2012.
“Do you understand what I just told you?”
Hospitalists who are experts on communicating with patients say that this kind of simple, yes/no question can engender all sorts of confusion. This kind of query often results in unrealistic discharge plans, failed post-discharge treatments, and unnecessary rehospitalizations. And they happen all the time in hospitals across the country.
“Yes/no questions, unless they are very concrete—such as ‘Do you have a headache?’—have little relation to assessing a patient’s understanding of essential healthcare information,” says Jeffrey Greenwald, MD, SFHM, hospitalist and educator at Massachusetts General Hospital in Boston. Many times, he adds, patients say “yes” just to please the doctor or nurse, or to avoid looking ignorant.
A better approach to patient-provider communication, one that successfully addresses communication gaps, is teach-back, a strategy in which providers ask patients to repeat (or “teach back”), in their own words, what they have just learned about their medical condition, treatments, and self-care. For example, a physician using the teach-back method could ask, “Mr. Smith, can you tell me why you are in the hospital?”
The approach is an integral part of SHM’s Project BOOST (Better Outcomes for Older Adults through Safer Transitions) care-transitions quality initiative, says Dr. Greenwald, a BOOST coinvestigator. But too often, hospitalists fail to embrace the mandate of effective communication, he says, leaving responsibility to clarify the patient’s understanding to nurses and other members of the care team.
“Having taught this skill all over the country, I continue to find members of my own profession who feel that it is not their job to assess if patients understand self-care and medication instructions. To me, there’s no question that physicians have a role to play as teachers. We educate patients, whether we think we do or not,” Dr. Greenwald says, adding that some hospitalists do so with greater effectiveness than others.
In an era of accountable-care organizations, patient-centered care, and shared decision-making, hospitalists need to provide their patients the same core messages as the rest of the care team does. According to a recent report by the University of California San Francisco (UCSF) Center for Vulnerable Populations at San Francisco General Hospital, 77 million Americans have difficulty understanding even basic healthcare information.1
In addition to widespread language barriers, the Institute of Medicine in a 2004 report concluded that 90 million U.S. adults have literacy skills that test below the high-school level.2 As most hospitalists know, many inpatients go to great lengths to mask these limitations—appearing knowledgeable while failing to grasp essential health concepts. Medical jargon, acronyms, and instructions can be confusing, even for patients with a high level of education.
“First and foremost, we have to be able to communicate with our patients—to make sure that we understand their goals and that they understand our approach to treatment and the therapeutic goals we are proposing,” Dr. Greenwald says. “This process also helps to achieve true informed consent. We want to ensure that their questions are being answered, and that the options we are discussing are in line with their goals of care so that they are more likely to actually undertake them when they go home. And if they can’t, we need to know that in advance, so that we can intervene in other ways.”
Embracing the Method
One health system that has embraced teach-back as a patient-education strategy is the Lehigh Valley Health Network (LVHN), a 988-bed, three-hospital system based in Allentown, Pa. In an HM12 workshop, the Lehigh Valley team explained how its teach-back initiative grew out of quality initiatives to target patient flow and readmissions. Lehigh joined an Institute for Healthcare Improvement quality collaborative, implemented “Lean” quality-improvement (QI) methodologies, and adopted a patient-coaching program.3
“This process has shined a stark spotlight on how poorly we as physicians communicate with patients overall,” says Michael Pistoria, DO, SFHM, former hospitalist and president of medical staff at LVHN who was a member of the teach-back team.
“I’d like to think I’m a little above averagein this regard, but it has made me realize how much better I could be in checking in with patients, gauging their health literacy, and engaging them with the care plan. As hospitalists, we all have to rethink how we talk to patients and families.”
A multidisciplinary team, originally created to analyze care transitions, was divided into four work groups. One group, which focused on patient/family understanding of the disease process, quickly learned that care-team members often failed to identify the patient’s “key learner”—the patient, a family member, or someone else. If the information is given to the wrong person, breakdowns can result. Such breakdowns usually lead to readmissions. One instrumental change that came as a result of the QI team’s efforts is that LVHN care-team members now recognize it is their responsibility to ask who the key learner is and to put that person’s name on a whiteboard in the patient’s room.
In the workshop in at SHM’s annual meeting in San Diego, Kim Jordan, MHA, BSN, RN, NE-BC, LVHN’s administrator of patient-care services, described teach-back as an effective, easy-to-use communication strategy that improves patient learning outcomes. “We created a standard work process using teach-back strategies across the healthcare system,” with training offered to all professionals who provide education to patients and families, she said.
Starting with heart failure, prompts were written into the electronic health record (EHR) to provide four scripted teach-back questions, each focused on the patient’s knowledge, attitudes, and behavior, to be asked consecutively over three days. Information was “chunked” into manageable pieces, emphasizing what was most important for the patient to learn on that day.
Results from one of the pilot units showed 30-day readmission rates for heart failure patients were cut in half, from 28% to 14%.4 Teach-back scripts also are being developed for the anticoagulant clinic and for patients with stroke, myocardial infarction, chronic obstructive pulmonary disease (COPD), community-acquired pneumonia, and diabetes.
“Continued analysis continues to show reduced rehospitalizations, and we even find that for those who are readmitted, their second admissions have been shorter,” Dr. Pistoria says, noting LVHN nurses have reported higher satisfaction. “They say, ‘This is wonderful. This is what I love about nursing—I get to teach the patients.’”
A Quality Mandate
The importance of effective communication with hospitalized patients is recognized in the federal Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS)5 quality ratings and, more recently, by Consumers Union’s new hospital safety ratings,6 which include communication in its six categories of patient-safety measures. And a recent study from the University of Washington says patients place high value on verbal communication about their discharge care plans and how to improve their health, and personal communication between their inpatient and outpatient providers.7
Large volumes of important information often are “dumped” on hospitalized patients, and many times patients are provided insufficient time to assimilate the information or ask questions about it.8 Such situations are especially common at discharge. And although physicians and other care-team members might feel they can’t afford the time to assure themselves that the patient understands what they are saying, the alternative is a lot more time spent dealing with preventable crises, misunderstandings—and preventable readmissions.
“People say, ‘I don’t have time for this,’” says Laura Vento, MSN, RN, clinical nurse leader on an acute-care medical unit at the University of California at San Diego medical center, who spearheaded teach-back at her hospital. “I did some observations around discharge visits, and it took an average of six minutes. After we implemented teach-back, it took eight to nine minutes. Nurses and patients were both very satisfied with the results. I say to staff: ‘Give it a try, and see what a difference an extra two minutes can make.’”
Dr. Pistoria describes teach-back as “humble inquiry...the simple need and ability to ask patients, ‘I know I’ve been throwing a lot of information at you. Can you tell me what I just said?’ Then, shut up and listen.” The goal is to have patients confirm that they understand fully what the provider thinks they need to know. The technique is presented as a test not of the patient’s learning ability, but of the provider’s communication effectiveness and success in explaining the information (see Figure 1). If the message has not been transmitted successfully, the professional reteaches, corrects misconceptions, and again asks the patient to teach back.
The theory is that physicians will then avoid the closed-ended questions (“Do you understand what I just told you?”) that make patients uncomfortable or inhibit the communication that needs to happen between patient and provider.
“We didn’t invent teach-back, which long predated Project BOOST,” Dr. Greenwald says. “But we use it and endorse it strongly, and believe it is an important part of communication with patients, particularly around care transitions.”
Dr. Greenwald thinks teach-back “is not a big stretch for hospitalists.” But he says it requires meaningful training and practice, ideally in a multidisciplinary team context. Participating Project BOOST ([email protected]) and Electronic Quality Improvement Programs (eQUIPS) sites receive a two-year license to post the “train-the-trainer” curriculum on their intranet systems.8 An instructional webinar, and the trainer curriculum and video, are available in the SHM store (www.hospitalmedicine.org/store). SHM also provides on-site training sessions for health systems or learning collaboratives (contact [email protected]).
‘Teach-Back on Steroids’
Teach-back, while a useful approach for improving patients’ understanding about hospital discharges, post-discharge care plans, and patient self-care, is just one of many teaching models that hospitalist groups can use to improve provider-to-patient communication. HM groups should assess health literacy in their regions and physician communication skills before deciding on one or more improvement tools.
LVHN, for example, has incorporated brief motivational interviewing techniques to its teach-back system, and the results are now being studied, says Paula Robinson, MSN, RN, BC, LVHN’s manager of patient, family, and consumer education.
“A lot of research out there emphasizes how patient education and knowledge alone don’t make a difference in adherence or compliance to treatment plans, even if they are getting the knowledge right 100% of the time,” Robinson says. “You also need to give patients permission to explore their feelings.”
One of Robinson’s colleagues, patient-care specialist Debra Peters, MSN, RN, BC, CMSRN, remembers using teach-back with a heart failure patient with recurrent rehospitalizations, exploring why it was important to control his salt intake. “The patient said, ‘Honey, I salt my ham, and I have no intention of changing that.’ This issue would not have come up if we had just addressed the knowledge component and told him: ‘You need to reduce your salt intake.’”
There might not be easy solutions to that kind of patient attitude, although in this case Peters made a referral to a dietitian who worked with the patient on food substitutions and other tools for managing his salt intake. “I don’t know if we made a big difference, but I haven’t seen him back in the hospital,” she says.
Motivational interviewing is a directive, client-centered counseling style for eliciting behavioral changes by helping clients to explore and resolve their ambivalence about making changes.9 Robinson calls it “the next step in our journey, with teach-back as a jumping-off place. We’ve worked on open-ended questions, getting patients to tell their stories, and our own reflective listening skills. I look at teach-back as a great communication tool and strategy—and motivational interviewing as ‘teach-back on steroids.’”
A number of similar, comparable, or complementary techniques and systems, with names like “Teach-to-Goal” and often paired with such resources as written materials, can help advance the same ends (visit the-hospitalist.org to learn about a technique for communicating bad news to patients).
The Flinders Program, developed at Flinders University in Adelaide, Australia, is a four-part structured motivational interview that asks patients to identify what they see as the biggest problem they face.10 LVHN medical educator Krista Hirschmann, MA, PhD, says this method was taught at LVHN by Australian experts and is now being used by its home-care department. “It is truly a patient-centered approach, and could be used by anybody in the health system,” she says.
Project RED (Re-Engineered Discharge), a care-transitions strategy developed by Brian Jack, MD, and colleagues at Boston University School of Medicine, was used to create a “virtual discharge advocate,” a computer avatar that simulates the face-to-face interaction between a patient and a nurse at the bedside.11 Patients interact with the avatar, named Louise, through a touch-screen display to review their after-hospital care packet and to answer her questions, confirming their understanding without being rushed for time.
Ultimately, Dr. Greenwald says, it doesn’t matter if physicians use teach-back or some other system to improve health literacy. “What matters is whether your patients understand what they need to know in order to go home and take care of themselves,” he says.
Larry Beresford is a freelance writer based in Oakland, Calif.
References
- Brach C, Keller D, Hernandez LM, et al. Ten attributes of health literate health care organizations. Institute of Medicine of the National Academies website. Available at: http://iom.edu/Global/Perspectives/2012/HealthLitAttributes.aspx. Accessed Aug. 9, 2012.
- Nielsen-Bohlman L, Panzer AM, Kindig DA, eds., Committee on Health Literacy. Health Literacy: A Prescription to End Confusion. Washington: Institute of Medicine; 2004.
- Care Transitions Program; University of Colorado School of Medicine, Division of Health Care Policy and Research. Available at: www.caretransitions.org. Accessed July 28, 2012.
- Healthcare Benchmarks and Quality Improvement. Teach-back program reduces readmissions. HighBeam Research website. Available at: http://www.highbeam.com/doc/1G1-269890846.html. Accessed Aug. 9, 2012.
- Hospital Consumer Assessment of Healthcare Providers and Systems. Centers for Medicare & Medicaid Services website. Available at: www.hcahpsonline.org. Accessed July 23, 2012.
- Consumer Reports. How safe is your hospital? Our new ratings find that some are riskier than others. Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/2012/08/how-safe-is-your-hospital/index.htm. Accessed Aug. 1, 2012.
- Shoeb M, Merel SE, Jackson MB, Anawalt BD. “Can’t we just stop and talk?” Patients value verbal communication about discharge care plans. J Hosp Med. 2012;7(6):504-7.
- Schillinger D, Piette J, Grumbach K, et al. Closing the loop: physician communication with diabetic patients who have low health literacy. Arch Intern Med. 2003;163:83-90.
- Borrelli B, Riekert KA, Weinstein W, Rathier L. Brief motivational interviewing as a clinical strategy to promote asthma medication adherence. J Allergy Clinical Immunol. 2007;120(5):1023-30.
- eQUIPS (Electronic Quality Improvement Programs). Society of Hospital Medicine website. Available at: http:// www.hospitalmedicine.org/equips. Accessed Aug. 1, 2012.
- Kelly J, Kubina N. Navigating self-management: a practical approach for Australian health agencies. Flinders University, Adelaide, Australia. Available at: www.flinders.edu.au/medicine/sites/fhbhru/self-management.cfm. Accessed Aug. 1, 2012.
- Project RED (Re-Engineered Discharge). Boston University Medical Center website. Available at: http:// www.bu.edu/fammed/projectred/publications.html. Accessed Aug. 1, 2012.
Enhanced Provider-Patient Communication Improves Discharge Process
Laura Vento, MSN, RN, first took an interest in the teach-back process when her father had a liver transplant. Following a prolonged hospitalization, Vento’s dad was sent home with little understanding of how to take care of himself; most notably, he had no wound-care education. And when she reviewed his medications, Vento found serious discrepancies with his anti-rejection drug prescriptions.
Her mind was filled with questions: “What kind of transition of care was this? How well am I as a nurse preparing my patients for discharge?” says Vento, a clinical nurse leader on an acute-care medical unit at the University of California at San Diego (UCSD) Medical Center. “I have since learned that shocking numbers of [hospitalized] patients receive little or no education about how to care for themselves.”
About the same time as her dad’s recovery, Vento’s nurse manager heard about SHM’s Project BOOST. They applied for a grant to support training hospital staff in the teach-back system, an integral Project BOOST strategy for educating patients about their post-discharge care needs.
At UCSD, teach-back was incorporated into a larger process of improving care transitions and preventing avoidable readmissions. In addition to the new communication techniques, the process also includes risk assessment, post-discharge follow-up phone calls, and other strategies, supported by a hospitalwide, multidisciplinary education council.
Following a four-hour teach-back curriculum presented to nursing staff, “we did role modeling and role plays,” Vento says. “We followed up with a teach-back coach, me, going to patients’ bedsides with the nurses, because the workshop content alone was not enough without the patient interaction. We needed to verify the nurses’ competency.”
From its initial piloting on two units, teach-back is being hard-wired into UCSD’s electronic health record, with guides to ask for five basic teach-back checks: reason for admission, self-care needs, when to call a physician or 9ll, scheduled follow-up appointments, and changes to the medication list. The education council is now rolling out teach-back to nurses across the system. For her efforts in disseminating the strategy the past two years, Vento was named the UCSD health system’s Nurse of the Year for 2011.
And yet, despite this systemwide recognition, “the focus up to this point has mostly been on the nurses, who are responsible for the bulk of patient education,” says UCSD hospitalist and Project BOOST mentor Jennifer Quartarolo, MD, SFHM. “It’s probably been underutilized by other members of the care team.”
Despite competing demands on physicians’ time, Dr. Quartarolo says hospitalists need to improve their patient education skills. “Teach-back can help us effectively communicate the key teaching points that we’d like our hospitalized patients and their caregivers to take home with them,” she says.
Laura Vento, MSN, RN, first took an interest in the teach-back process when her father had a liver transplant. Following a prolonged hospitalization, Vento’s dad was sent home with little understanding of how to take care of himself; most notably, he had no wound-care education. And when she reviewed his medications, Vento found serious discrepancies with his anti-rejection drug prescriptions.
Her mind was filled with questions: “What kind of transition of care was this? How well am I as a nurse preparing my patients for discharge?” says Vento, a clinical nurse leader on an acute-care medical unit at the University of California at San Diego (UCSD) Medical Center. “I have since learned that shocking numbers of [hospitalized] patients receive little or no education about how to care for themselves.”
About the same time as her dad’s recovery, Vento’s nurse manager heard about SHM’s Project BOOST. They applied for a grant to support training hospital staff in the teach-back system, an integral Project BOOST strategy for educating patients about their post-discharge care needs.
At UCSD, teach-back was incorporated into a larger process of improving care transitions and preventing avoidable readmissions. In addition to the new communication techniques, the process also includes risk assessment, post-discharge follow-up phone calls, and other strategies, supported by a hospitalwide, multidisciplinary education council.
Following a four-hour teach-back curriculum presented to nursing staff, “we did role modeling and role plays,” Vento says. “We followed up with a teach-back coach, me, going to patients’ bedsides with the nurses, because the workshop content alone was not enough without the patient interaction. We needed to verify the nurses’ competency.”
From its initial piloting on two units, teach-back is being hard-wired into UCSD’s electronic health record, with guides to ask for five basic teach-back checks: reason for admission, self-care needs, when to call a physician or 9ll, scheduled follow-up appointments, and changes to the medication list. The education council is now rolling out teach-back to nurses across the system. For her efforts in disseminating the strategy the past two years, Vento was named the UCSD health system’s Nurse of the Year for 2011.
And yet, despite this systemwide recognition, “the focus up to this point has mostly been on the nurses, who are responsible for the bulk of patient education,” says UCSD hospitalist and Project BOOST mentor Jennifer Quartarolo, MD, SFHM. “It’s probably been underutilized by other members of the care team.”
Despite competing demands on physicians’ time, Dr. Quartarolo says hospitalists need to improve their patient education skills. “Teach-back can help us effectively communicate the key teaching points that we’d like our hospitalized patients and their caregivers to take home with them,” she says.
Laura Vento, MSN, RN, first took an interest in the teach-back process when her father had a liver transplant. Following a prolonged hospitalization, Vento’s dad was sent home with little understanding of how to take care of himself; most notably, he had no wound-care education. And when she reviewed his medications, Vento found serious discrepancies with his anti-rejection drug prescriptions.
Her mind was filled with questions: “What kind of transition of care was this? How well am I as a nurse preparing my patients for discharge?” says Vento, a clinical nurse leader on an acute-care medical unit at the University of California at San Diego (UCSD) Medical Center. “I have since learned that shocking numbers of [hospitalized] patients receive little or no education about how to care for themselves.”
About the same time as her dad’s recovery, Vento’s nurse manager heard about SHM’s Project BOOST. They applied for a grant to support training hospital staff in the teach-back system, an integral Project BOOST strategy for educating patients about their post-discharge care needs.
At UCSD, teach-back was incorporated into a larger process of improving care transitions and preventing avoidable readmissions. In addition to the new communication techniques, the process also includes risk assessment, post-discharge follow-up phone calls, and other strategies, supported by a hospitalwide, multidisciplinary education council.
Following a four-hour teach-back curriculum presented to nursing staff, “we did role modeling and role plays,” Vento says. “We followed up with a teach-back coach, me, going to patients’ bedsides with the nurses, because the workshop content alone was not enough without the patient interaction. We needed to verify the nurses’ competency.”
From its initial piloting on two units, teach-back is being hard-wired into UCSD’s electronic health record, with guides to ask for five basic teach-back checks: reason for admission, self-care needs, when to call a physician or 9ll, scheduled follow-up appointments, and changes to the medication list. The education council is now rolling out teach-back to nurses across the system. For her efforts in disseminating the strategy the past two years, Vento was named the UCSD health system’s Nurse of the Year for 2011.
And yet, despite this systemwide recognition, “the focus up to this point has mostly been on the nurses, who are responsible for the bulk of patient education,” says UCSD hospitalist and Project BOOST mentor Jennifer Quartarolo, MD, SFHM. “It’s probably been underutilized by other members of the care team.”
Despite competing demands on physicians’ time, Dr. Quartarolo says hospitalists need to improve their patient education skills. “Teach-back can help us effectively communicate the key teaching points that we’d like our hospitalized patients and their caregivers to take home with them,” she says.
AHRQ's Director Looks to Hospitalists to Help Reduce Readmissions
Although a recently released study of Medicare data uncovers little progress in reducing hospital readmissions, and the Oct. 1 deadline to implement CMS’ Hospital Readmissions Reduction Program looms, Carolyn Clancy, MD, director of the Agency for Healthcare Research and Quality (AHRQ), says she's not worried about the ability of America’s hospitalists to rise to the occasion and get a handle on the problem.
Dr. Clancy recently wrote a commentary outlining the government's approach to controlling readmissions, stating that taking aim at readmissions is 1) an integral component of its value-based purchasing program and 2) is an opportunity for improving hospital quality and patient safety.
"Hospitalists are often on the receiving end of hospitalizations resulting from poor coordination of care. I think it would be very exciting to be part of the solution," Dr. Clancy says. She says she observed firsthand during a recent hospital stay how hospitalists helped her to think about how she should care for herself after returning home. But her father suffered a needless rehospitalization when important information (how much Coumadin to take) was miscommunicated in a post-discharge follow-up phone call, causing him to start bleeding.
"Hospitalists who want to embrace the challenge will find a phenomenal amount of information on Innovations Exchange, where people from all over America are sharing their clinical innovations."
Dr. Clancy says she hopes AHRQ-supported tools and studies "will make it easier for hospitals to do the right thing."
Although a recently released study of Medicare data uncovers little progress in reducing hospital readmissions, and the Oct. 1 deadline to implement CMS’ Hospital Readmissions Reduction Program looms, Carolyn Clancy, MD, director of the Agency for Healthcare Research and Quality (AHRQ), says she's not worried about the ability of America’s hospitalists to rise to the occasion and get a handle on the problem.
Dr. Clancy recently wrote a commentary outlining the government's approach to controlling readmissions, stating that taking aim at readmissions is 1) an integral component of its value-based purchasing program and 2) is an opportunity for improving hospital quality and patient safety.
"Hospitalists are often on the receiving end of hospitalizations resulting from poor coordination of care. I think it would be very exciting to be part of the solution," Dr. Clancy says. She says she observed firsthand during a recent hospital stay how hospitalists helped her to think about how she should care for herself after returning home. But her father suffered a needless rehospitalization when important information (how much Coumadin to take) was miscommunicated in a post-discharge follow-up phone call, causing him to start bleeding.
"Hospitalists who want to embrace the challenge will find a phenomenal amount of information on Innovations Exchange, where people from all over America are sharing their clinical innovations."
Dr. Clancy says she hopes AHRQ-supported tools and studies "will make it easier for hospitals to do the right thing."
Although a recently released study of Medicare data uncovers little progress in reducing hospital readmissions, and the Oct. 1 deadline to implement CMS’ Hospital Readmissions Reduction Program looms, Carolyn Clancy, MD, director of the Agency for Healthcare Research and Quality (AHRQ), says she's not worried about the ability of America’s hospitalists to rise to the occasion and get a handle on the problem.
Dr. Clancy recently wrote a commentary outlining the government's approach to controlling readmissions, stating that taking aim at readmissions is 1) an integral component of its value-based purchasing program and 2) is an opportunity for improving hospital quality and patient safety.
"Hospitalists are often on the receiving end of hospitalizations resulting from poor coordination of care. I think it would be very exciting to be part of the solution," Dr. Clancy says. She says she observed firsthand during a recent hospital stay how hospitalists helped her to think about how she should care for herself after returning home. But her father suffered a needless rehospitalization when important information (how much Coumadin to take) was miscommunicated in a post-discharge follow-up phone call, causing him to start bleeding.
"Hospitalists who want to embrace the challenge will find a phenomenal amount of information on Innovations Exchange, where people from all over America are sharing their clinical innovations."
Dr. Clancy says she hopes AHRQ-supported tools and studies "will make it easier for hospitals to do the right thing."