User login
ONLINE EXCLUSIVE: Listen to a senior research scholar Mary Gatta, PhD, discuss why gender pay gaps continue to exist
Click here to listen to Dr. Gatta
Click here to listen to Dr. Gatta
Click here to listen to Dr. Gatta
Gender Pay Gaps in Hospital Medicine

Roberta Gebhard, DO, thought that her 20 years of experience as a physician in the U.S., 10 of them as a hospitalist, would mean she would get paid more than a new graduate just out of residency would.
She was wrong.
Dr. Gebhard was working at a hospital run by the U.S. Department of Veterans Affairs when she learned that the less experienced doctor—a man—was making $10,000 more a year than she was.
“After that, the job was no longer interesting to me,” says Dr. Gebhard, who left the hospital over the pay discrepancy and now works as a hospitalist at WCA Hospital in Jamestown, N.Y. “Women think that things should be fair, so they assume that they are. I’m a good negotiator, and when that happened to me, I was like, ‘Wait a minute! I didn’t just take what they offered me.’ I pushed a few times and was basically told it was a government position, there was no wiggle room, and I couldn’t get more salary.
“It happens, and women need to know that it happens,” she says.
Earnings data and research show that the gender pay gap lingers. More problematic is pinpointing why the gap won’t close. Explanations range from ignorance of the issue and trading in compensation for other job benefits to women’s lack of negotiating skills to subtle gender discrimination.
Because gender pay discrepancies persist and because theories abound as to the cause, the issue will be addressed during a “Women in Hospital Medicine” session at HM12 next month in San Diego, along with such topics as leadership challenges and work-life balance, says Patience Reich, MD, SFHM, a hospitalist and assistant professor of medicine at Wake Forest University School of Medicine in Winston-Salem, N.C.
“When we conceived the session, we were actually thinking about women in leadership, but decided to go for more general topics that affect women hospitalists, whether they are in leadership or not,” says Dr. Reich, a member of SHM’s Leadership Committee who helped coordinate the HM12 session.
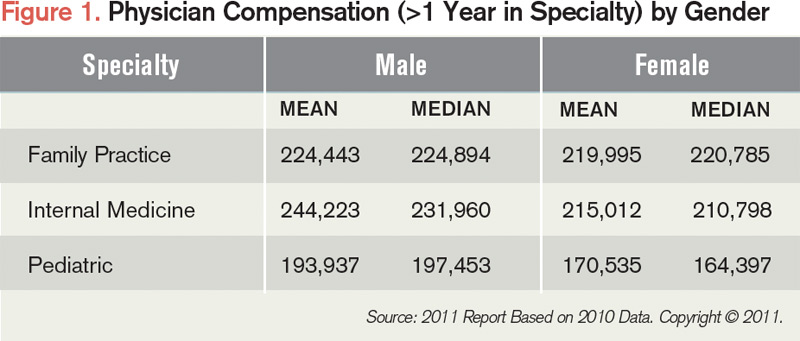
According to the 2011 SHM-MGMA compensation and productivity survey, mean annual compensation for female hospitalists in family practice, internal medicine, and pediatrics is lower than that of their male counterparts. For example, female hospitalists in family practice, internal medicine, and pediatrics have mean annual compensations of $219,995, $215,012, and $170,535, respectively, or $4,448, $29,211, and $23,402 less than male counterparts in similar positions (see Figure 1). Such factors as practice location, practice ownership, and productivity have an effect on compensation and could be the reason behind the disparity, says Liz Boten, a spokeswoman for Englewood, Colo.-based Medical Group Management Association (MGMA).
But research that is controlled for numerous observable factors has shown that the gender earnings gap continues to exist among physicians.1,2,3,4 Of particular note are two studies, including one focused on hospital medicine.
In 2004, a study authored by Timothy J. Hoff, PhD, an associate professor at State University of New York at Albany, controlled for a wide range of work and non-work variables, including clinical workload, compensation type, employer type, tenure, marital status, and tenure in hospital medicine.5 The data show that female hospitalists earned approximately $22,000 less per year than male hospitalists, despite similar work patterns. Additional study results showed that married female hospitalists with children worked just as much and carried as heavy a clinical workload as married male hospitalists who had children.
—Roberta Gebhard, DO, hospitalist, WCA Hospital, Jamestown, N.Y., American Medical Women’s Association’s Gender Equity Task Force co-chair
Last year, a study in Health Affairs generated considerable interest when it found that male physicians newly trained in New York state made on average $16,819 more than newly trained female physicians in 2008, compared with a $3,600 difference in 1999.6 The authors controlled for specialty type, hours worked, designation of hours, immigration status, age, and practice location. And by focusing on starting salaries, factors such as job tenure, institutional rank, and job productivity didn’t come into play, signifying that the experiences of married female and male hospitalists with children differed less than one might presume based upon perceptions that women with families sacrifice work commitments to take care of their spouses and children.
“It is studies like this that are going to be critically important for us to move forward,” says Janet Nagamine, RN, MD, SFHM, a hospitalist at Kaiser Permanente Medical Center in Santa Clara, Calif., and an SHM board member who is assisting with the “Women in Hospital Medicine” session at HM12. “As we talk about a pay gap, we need to be more evidence-based.”
Studies that show a gender earnings gap even among highly skilled professionals don’t surprise researchers. The U.S. Bureau of Labor Statistics collects earnings data on hundreds of occupations, including physicians, and men outearn women across the board, regardless of educational requirements, says Mary Gatta, PhD, past director of gender and workforce policy at the Center for Women and Work at Rutgers University in New Brunswick, N.J., and current senior research scholar at Wider Opportunities for Women, a Washington, D.C.-based organization that focuses on opportunity equality for women.
The Gap that Won’t Close
So why, in 2012, do gender-based pay discrepancies remain?
How much people earn typically is not public information, so women often don’t know they aren’t being paid equally and, therefore, don’t have information on which to act, Dr. Gatta says.
“My opinion on it is women don’t know about the pay gap,” says Dr. Gebhard, co-chair of the American Medical Women’s Association’s (AMWA) Gender Equity Task Force. She recalls a salary negotiation lecture she helped lead after which a woman finishing residency raised her hand to say she was joining a faculty where everyone was paid the same. “The entire room just groaned,” she says. “Clearly, women out there think everything is fair and people are paid the same. They don’t know they’re being paid less.”
In trying to explain the widening pay gap, authors of the 2011 Health Affairs study posited that the influx of women into the physician workforce is reshaping the practice and business of medicine.6
“The notion we suggest is that the increasing gender gap can be explained by new women physicians increasingly demanding non-pecuniary aspects of their jobs, and because of the greater aggregate presence of women in the physician labor market, being able to get it,” says lead author Anthony Lo Sasso, a professor and senior research scientist at the School of Public Health at the University of Illinois at Chicago. “Remember, cash wages are but one part of the compensation package in any job.”
Hoff’s study also uncovered gender differences in employment preferences, with men attracted to HM for the compensation possibilities and women for the predictable hours and lifestyle flexibility. For this reason, Hoff suggested, hospitalist employers can use different recruiting pitches for women than men and, to the extent they hire female hospitalists, save money (see “Negotiating Strategies for Better Compensation,” below).
“The Hoff paper is a goldmine,” says Linda Brodsky, MD, a pediatric otolaryngologist in Buffalo, N.Y., who co-chairs AMWA’s Gender Equity Task Force and whose organization, Expediting the Inevitable, advocates for gender equity in healthcare. “How is it that when you have shift work, women are getting paid less per shift? Because Hoff tells you at the end, employers can get away with it. Even if they know they are underpaying women, they will take the chance because it’s so hard for anybody to take legal action.”
Women also find themselves in a double bind when it comes to negotiating higher compensation, says Barbara Gault, PhD, executive director of the Institute for Women’s Policy Research in Washington, D.C. Some suggest a pay gap exists because women are not negotiating for themselves, but research shows women tend to be perceived as less likable when they are more assertive about higher wages, she says.
Erin Stucky Fisher, MD, MHM, has seen this phenomena play out in her roles as medical director for quality at Rady Children’s Hospital in San Diego and associate program director for the University of California at San Diego Pediatric Residency Program.
“I do a lot of interviewing for the hospital, and it does seem, in general, that women are less likely to promote themselves than men in the same situation,” says Dr. Fisher, an SHM board member who is also assisting with the HM12 “Women in Hospital Medicine” session. “There are reasons behind it that might have to do with women not wanting to be perceived as self-serving or arrogant.”

—Erin Stucky Fisher, MD, FAAP, MHM, medical director for quality, Rady Children’s Hospital, associate program director, University of California at San Diego Pediatric Residency Program, SHM board member
Dr. Brodsky agrees with the perception issues facing physicians.
“Women are supposed to be grateful, accommodating, and get along, which are excellent qualities,” she says. “But when you’re expected to do that and you instead negotiate with any kind of spirit, it’s perceived as troublemaking, whereas in men, it’s perceived as strength.”
Subtle forms of gender discrimination continue to exist in workplaces, Dr. Gatta says. Beliefs remain that men have a family to support, so they should be paid more, and that women are in the workforce just for extra money, even though recent data show that women’s income is key to families’ well-being, she notes.
Common patterns of gender bias will be discussed at the HM12 session, says Dr. Reich, who was a victim of gender pay disparity when she worked a locum tenens job earlier in her career.
“There was no logical explanation. The men did less work by all measures, and the other woman and I didn’t have young children at home, so explanations of women trading in money for time with family didn’t apply,” she explains. “Why did they think I should be paid less? I didn’t understand, and I never got a logical reason.”
Potential Solutions
Shortly after arriving at Wake Forest in 2004, Dr. Reich had the opportunity to build the hospitalist program. A set of thorough, transparent criteria for determining compensation were established almost immediately to help prevent pay discrepancies.
“We tried to be as objective as we could, and we involved the group in talking about it because we felt it was important,” she says.

—Linda Brodsky, MD, pediatric otolaryngologist, Buffalo, N.Y., co-chair, AMWA Gender Equity Task Force
Organizations can conduct self-audits to assess whether men and women are being compensated equitably, then make adjustments when necessary, Dr. Gault says. Policies can be adopted to promote pay transparency and allow employees to discuss compensation and suggest ways it can be improved, she adds. In workplaces where compensation discussions are discouraged, women can try to informally speak with their male friends to gather information and determine if there’s a pay gap problem.
Equal pay laws, such as the Lily Ledbetter Fair Pay Act, exist at the federal level. But Dr. Gatta says work must be done on the enforcement end to make a real difference. Similarly, Dr. Brodsky describes the Equal Employment Opportunity Commission as a toothless oversight agency with limited power to investigate complaints and assess fines.
“It’s on women to go and be the whistleblower, the policeman, and pay for legal action. It’s impossible,” she says. “When you utter the words ‘gender discrimination,’ immediately, retaliation goes into high gear.”
While employers and enforcement agencies have a significant role in closing the pay gap, women themselves must collectively advocate for equal pay, Dr. Gault says.
“Any woman physician who is in the senior ranks must be obligated to start changing the culture and making sure the fairness issue gets raised and is an important part of their agenda,” Dr. Brodsky says. “Enough women are now part of the physician population. They have to start saying, ‘We are a group to be reckoned with, and we are going to make changes.’”
Lisa Ryan is a freelance writer based in New Jersey.
References
- Wright AL, Schwindt LA, Bassford TL, et al. Gender differences in academic advancement: patterns, causes, and potential solutions in one US College of Medicine. Acad Med. 2003;78(5):500-508.
- Ash AS, Carr PL, Goldstein R, et al. Compensation and advancement of women in academic medicine: is there equity? Ann Intern Med. 2004;141(3):205-212.
- Ness RB, Ukoli F, Hunt S, et al. Salary equity among male and female internists in Pennsylvania. Ann Intern Med. 2000;133(2):104-110.
- Weeks WB, Wallace TA, Wallace AE. How do race and sex affect the earnings of primary care physicians? Health Aff (Millwood). 2009;28(2):557-566.
- Hoff TJ. Doing the same and earning less: male and female physicians in a new medical specialty. Inquiry. 2004;41:301-315.
- Lo Sasso AT, Richards MR, Chou C, Gerber SE. The $16,819 pay gap for newly trained physicians: the unexplained trend of men earning more than women. Health Aff (Millwood). 2011;30:193-201.
Roberta Gebhard, DO, thought that her 20 years of experience as a physician in the U.S., 10 of them as a hospitalist, would mean she would get paid more than a new graduate just out of residency would.
She was wrong.
Dr. Gebhard was working at a hospital run by the U.S. Department of Veterans Affairs when she learned that the less experienced doctor—a man—was making $10,000 more a year than she was.
“After that, the job was no longer interesting to me,” says Dr. Gebhard, who left the hospital over the pay discrepancy and now works as a hospitalist at WCA Hospital in Jamestown, N.Y. “Women think that things should be fair, so they assume that they are. I’m a good negotiator, and when that happened to me, I was like, ‘Wait a minute! I didn’t just take what they offered me.’ I pushed a few times and was basically told it was a government position, there was no wiggle room, and I couldn’t get more salary.
“It happens, and women need to know that it happens,” she says.
Earnings data and research show that the gender pay gap lingers. More problematic is pinpointing why the gap won’t close. Explanations range from ignorance of the issue and trading in compensation for other job benefits to women’s lack of negotiating skills to subtle gender discrimination.
Because gender pay discrepancies persist and because theories abound as to the cause, the issue will be addressed during a “Women in Hospital Medicine” session at HM12 next month in San Diego, along with such topics as leadership challenges and work-life balance, says Patience Reich, MD, SFHM, a hospitalist and assistant professor of medicine at Wake Forest University School of Medicine in Winston-Salem, N.C.
“When we conceived the session, we were actually thinking about women in leadership, but decided to go for more general topics that affect women hospitalists, whether they are in leadership or not,” says Dr. Reich, a member of SHM’s Leadership Committee who helped coordinate the HM12 session.
According to the 2011 SHM-MGMA compensation and productivity survey, mean annual compensation for female hospitalists in family practice, internal medicine, and pediatrics is lower than that of their male counterparts. For example, female hospitalists in family practice, internal medicine, and pediatrics have mean annual compensations of $219,995, $215,012, and $170,535, respectively, or $4,448, $29,211, and $23,402 less than male counterparts in similar positions (see Figure 1). Such factors as practice location, practice ownership, and productivity have an effect on compensation and could be the reason behind the disparity, says Liz Boten, a spokeswoman for Englewood, Colo.-based Medical Group Management Association (MGMA).
But research that is controlled for numerous observable factors has shown that the gender earnings gap continues to exist among physicians.1,2,3,4 Of particular note are two studies, including one focused on hospital medicine.
In 2004, a study authored by Timothy J. Hoff, PhD, an associate professor at State University of New York at Albany, controlled for a wide range of work and non-work variables, including clinical workload, compensation type, employer type, tenure, marital status, and tenure in hospital medicine.5 The data show that female hospitalists earned approximately $22,000 less per year than male hospitalists, despite similar work patterns. Additional study results showed that married female hospitalists with children worked just as much and carried as heavy a clinical workload as married male hospitalists who had children.
—Roberta Gebhard, DO, hospitalist, WCA Hospital, Jamestown, N.Y., American Medical Women’s Association’s Gender Equity Task Force co-chair
Last year, a study in Health Affairs generated considerable interest when it found that male physicians newly trained in New York state made on average $16,819 more than newly trained female physicians in 2008, compared with a $3,600 difference in 1999.6 The authors controlled for specialty type, hours worked, designation of hours, immigration status, age, and practice location. And by focusing on starting salaries, factors such as job tenure, institutional rank, and job productivity didn’t come into play, signifying that the experiences of married female and male hospitalists with children differed less than one might presume based upon perceptions that women with families sacrifice work commitments to take care of their spouses and children.
“It is studies like this that are going to be critically important for us to move forward,” says Janet Nagamine, RN, MD, SFHM, a hospitalist at Kaiser Permanente Medical Center in Santa Clara, Calif., and an SHM board member who is assisting with the “Women in Hospital Medicine” session at HM12. “As we talk about a pay gap, we need to be more evidence-based.”
Studies that show a gender earnings gap even among highly skilled professionals don’t surprise researchers. The U.S. Bureau of Labor Statistics collects earnings data on hundreds of occupations, including physicians, and men outearn women across the board, regardless of educational requirements, says Mary Gatta, PhD, past director of gender and workforce policy at the Center for Women and Work at Rutgers University in New Brunswick, N.J., and current senior research scholar at Wider Opportunities for Women, a Washington, D.C.-based organization that focuses on opportunity equality for women.
The Gap that Won’t Close
So why, in 2012, do gender-based pay discrepancies remain?
How much people earn typically is not public information, so women often don’t know they aren’t being paid equally and, therefore, don’t have information on which to act, Dr. Gatta says.
“My opinion on it is women don’t know about the pay gap,” says Dr. Gebhard, co-chair of the American Medical Women’s Association’s (AMWA) Gender Equity Task Force. She recalls a salary negotiation lecture she helped lead after which a woman finishing residency raised her hand to say she was joining a faculty where everyone was paid the same. “The entire room just groaned,” she says. “Clearly, women out there think everything is fair and people are paid the same. They don’t know they’re being paid less.”
In trying to explain the widening pay gap, authors of the 2011 Health Affairs study posited that the influx of women into the physician workforce is reshaping the practice and business of medicine.6
“The notion we suggest is that the increasing gender gap can be explained by new women physicians increasingly demanding non-pecuniary aspects of their jobs, and because of the greater aggregate presence of women in the physician labor market, being able to get it,” says lead author Anthony Lo Sasso, a professor and senior research scientist at the School of Public Health at the University of Illinois at Chicago. “Remember, cash wages are but one part of the compensation package in any job.”
Hoff’s study also uncovered gender differences in employment preferences, with men attracted to HM for the compensation possibilities and women for the predictable hours and lifestyle flexibility. For this reason, Hoff suggested, hospitalist employers can use different recruiting pitches for women than men and, to the extent they hire female hospitalists, save money (see “Negotiating Strategies for Better Compensation,” below).
“The Hoff paper is a goldmine,” says Linda Brodsky, MD, a pediatric otolaryngologist in Buffalo, N.Y., who co-chairs AMWA’s Gender Equity Task Force and whose organization, Expediting the Inevitable, advocates for gender equity in healthcare. “How is it that when you have shift work, women are getting paid less per shift? Because Hoff tells you at the end, employers can get away with it. Even if they know they are underpaying women, they will take the chance because it’s so hard for anybody to take legal action.”
Women also find themselves in a double bind when it comes to negotiating higher compensation, says Barbara Gault, PhD, executive director of the Institute for Women’s Policy Research in Washington, D.C. Some suggest a pay gap exists because women are not negotiating for themselves, but research shows women tend to be perceived as less likable when they are more assertive about higher wages, she says.
Erin Stucky Fisher, MD, MHM, has seen this phenomena play out in her roles as medical director for quality at Rady Children’s Hospital in San Diego and associate program director for the University of California at San Diego Pediatric Residency Program.
“I do a lot of interviewing for the hospital, and it does seem, in general, that women are less likely to promote themselves than men in the same situation,” says Dr. Fisher, an SHM board member who is also assisting with the HM12 “Women in Hospital Medicine” session. “There are reasons behind it that might have to do with women not wanting to be perceived as self-serving or arrogant.”
—Erin Stucky Fisher, MD, FAAP, MHM, medical director for quality, Rady Children’s Hospital, associate program director, University of California at San Diego Pediatric Residency Program, SHM board member
Dr. Brodsky agrees with the perception issues facing physicians.
“Women are supposed to be grateful, accommodating, and get along, which are excellent qualities,” she says. “But when you’re expected to do that and you instead negotiate with any kind of spirit, it’s perceived as troublemaking, whereas in men, it’s perceived as strength.”
Subtle forms of gender discrimination continue to exist in workplaces, Dr. Gatta says. Beliefs remain that men have a family to support, so they should be paid more, and that women are in the workforce just for extra money, even though recent data show that women’s income is key to families’ well-being, she notes.
Common patterns of gender bias will be discussed at the HM12 session, says Dr. Reich, who was a victim of gender pay disparity when she worked a locum tenens job earlier in her career.
“There was no logical explanation. The men did less work by all measures, and the other woman and I didn’t have young children at home, so explanations of women trading in money for time with family didn’t apply,” she explains. “Why did they think I should be paid less? I didn’t understand, and I never got a logical reason.”
Potential Solutions
Shortly after arriving at Wake Forest in 2004, Dr. Reich had the opportunity to build the hospitalist program. A set of thorough, transparent criteria for determining compensation were established almost immediately to help prevent pay discrepancies.
“We tried to be as objective as we could, and we involved the group in talking about it because we felt it was important,” she says.
—Linda Brodsky, MD, pediatric otolaryngologist, Buffalo, N.Y., co-chair, AMWA Gender Equity Task Force
Organizations can conduct self-audits to assess whether men and women are being compensated equitably, then make adjustments when necessary, Dr. Gault says. Policies can be adopted to promote pay transparency and allow employees to discuss compensation and suggest ways it can be improved, she adds. In workplaces where compensation discussions are discouraged, women can try to informally speak with their male friends to gather information and determine if there’s a pay gap problem.
Equal pay laws, such as the Lily Ledbetter Fair Pay Act, exist at the federal level. But Dr. Gatta says work must be done on the enforcement end to make a real difference. Similarly, Dr. Brodsky describes the Equal Employment Opportunity Commission as a toothless oversight agency with limited power to investigate complaints and assess fines.
“It’s on women to go and be the whistleblower, the policeman, and pay for legal action. It’s impossible,” she says. “When you utter the words ‘gender discrimination,’ immediately, retaliation goes into high gear.”
While employers and enforcement agencies have a significant role in closing the pay gap, women themselves must collectively advocate for equal pay, Dr. Gault says.
“Any woman physician who is in the senior ranks must be obligated to start changing the culture and making sure the fairness issue gets raised and is an important part of their agenda,” Dr. Brodsky says. “Enough women are now part of the physician population. They have to start saying, ‘We are a group to be reckoned with, and we are going to make changes.’”
Lisa Ryan is a freelance writer based in New Jersey.
References
- Wright AL, Schwindt LA, Bassford TL, et al. Gender differences in academic advancement: patterns, causes, and potential solutions in one US College of Medicine. Acad Med. 2003;78(5):500-508.
- Ash AS, Carr PL, Goldstein R, et al. Compensation and advancement of women in academic medicine: is there equity? Ann Intern Med. 2004;141(3):205-212.
- Ness RB, Ukoli F, Hunt S, et al. Salary equity among male and female internists in Pennsylvania. Ann Intern Med. 2000;133(2):104-110.
- Weeks WB, Wallace TA, Wallace AE. How do race and sex affect the earnings of primary care physicians? Health Aff (Millwood). 2009;28(2):557-566.
- Hoff TJ. Doing the same and earning less: male and female physicians in a new medical specialty. Inquiry. 2004;41:301-315.
- Lo Sasso AT, Richards MR, Chou C, Gerber SE. The $16,819 pay gap for newly trained physicians: the unexplained trend of men earning more than women. Health Aff (Millwood). 2011;30:193-201.
Roberta Gebhard, DO, thought that her 20 years of experience as a physician in the U.S., 10 of them as a hospitalist, would mean she would get paid more than a new graduate just out of residency would.
She was wrong.
Dr. Gebhard was working at a hospital run by the U.S. Department of Veterans Affairs when she learned that the less experienced doctor—a man—was making $10,000 more a year than she was.
“After that, the job was no longer interesting to me,” says Dr. Gebhard, who left the hospital over the pay discrepancy and now works as a hospitalist at WCA Hospital in Jamestown, N.Y. “Women think that things should be fair, so they assume that they are. I’m a good negotiator, and when that happened to me, I was like, ‘Wait a minute! I didn’t just take what they offered me.’ I pushed a few times and was basically told it was a government position, there was no wiggle room, and I couldn’t get more salary.
“It happens, and women need to know that it happens,” she says.
Earnings data and research show that the gender pay gap lingers. More problematic is pinpointing why the gap won’t close. Explanations range from ignorance of the issue and trading in compensation for other job benefits to women’s lack of negotiating skills to subtle gender discrimination.
Because gender pay discrepancies persist and because theories abound as to the cause, the issue will be addressed during a “Women in Hospital Medicine” session at HM12 next month in San Diego, along with such topics as leadership challenges and work-life balance, says Patience Reich, MD, SFHM, a hospitalist and assistant professor of medicine at Wake Forest University School of Medicine in Winston-Salem, N.C.
“When we conceived the session, we were actually thinking about women in leadership, but decided to go for more general topics that affect women hospitalists, whether they are in leadership or not,” says Dr. Reich, a member of SHM’s Leadership Committee who helped coordinate the HM12 session.
According to the 2011 SHM-MGMA compensation and productivity survey, mean annual compensation for female hospitalists in family practice, internal medicine, and pediatrics is lower than that of their male counterparts. For example, female hospitalists in family practice, internal medicine, and pediatrics have mean annual compensations of $219,995, $215,012, and $170,535, respectively, or $4,448, $29,211, and $23,402 less than male counterparts in similar positions (see Figure 1). Such factors as practice location, practice ownership, and productivity have an effect on compensation and could be the reason behind the disparity, says Liz Boten, a spokeswoman for Englewood, Colo.-based Medical Group Management Association (MGMA).
But research that is controlled for numerous observable factors has shown that the gender earnings gap continues to exist among physicians.1,2,3,4 Of particular note are two studies, including one focused on hospital medicine.
In 2004, a study authored by Timothy J. Hoff, PhD, an associate professor at State University of New York at Albany, controlled for a wide range of work and non-work variables, including clinical workload, compensation type, employer type, tenure, marital status, and tenure in hospital medicine.5 The data show that female hospitalists earned approximately $22,000 less per year than male hospitalists, despite similar work patterns. Additional study results showed that married female hospitalists with children worked just as much and carried as heavy a clinical workload as married male hospitalists who had children.
—Roberta Gebhard, DO, hospitalist, WCA Hospital, Jamestown, N.Y., American Medical Women’s Association’s Gender Equity Task Force co-chair
Last year, a study in Health Affairs generated considerable interest when it found that male physicians newly trained in New York state made on average $16,819 more than newly trained female physicians in 2008, compared with a $3,600 difference in 1999.6 The authors controlled for specialty type, hours worked, designation of hours, immigration status, age, and practice location. And by focusing on starting salaries, factors such as job tenure, institutional rank, and job productivity didn’t come into play, signifying that the experiences of married female and male hospitalists with children differed less than one might presume based upon perceptions that women with families sacrifice work commitments to take care of their spouses and children.
“It is studies like this that are going to be critically important for us to move forward,” says Janet Nagamine, RN, MD, SFHM, a hospitalist at Kaiser Permanente Medical Center in Santa Clara, Calif., and an SHM board member who is assisting with the “Women in Hospital Medicine” session at HM12. “As we talk about a pay gap, we need to be more evidence-based.”
Studies that show a gender earnings gap even among highly skilled professionals don’t surprise researchers. The U.S. Bureau of Labor Statistics collects earnings data on hundreds of occupations, including physicians, and men outearn women across the board, regardless of educational requirements, says Mary Gatta, PhD, past director of gender and workforce policy at the Center for Women and Work at Rutgers University in New Brunswick, N.J., and current senior research scholar at Wider Opportunities for Women, a Washington, D.C.-based organization that focuses on opportunity equality for women.
The Gap that Won’t Close
So why, in 2012, do gender-based pay discrepancies remain?
How much people earn typically is not public information, so women often don’t know they aren’t being paid equally and, therefore, don’t have information on which to act, Dr. Gatta says.
“My opinion on it is women don’t know about the pay gap,” says Dr. Gebhard, co-chair of the American Medical Women’s Association’s (AMWA) Gender Equity Task Force. She recalls a salary negotiation lecture she helped lead after which a woman finishing residency raised her hand to say she was joining a faculty where everyone was paid the same. “The entire room just groaned,” she says. “Clearly, women out there think everything is fair and people are paid the same. They don’t know they’re being paid less.”
In trying to explain the widening pay gap, authors of the 2011 Health Affairs study posited that the influx of women into the physician workforce is reshaping the practice and business of medicine.6
“The notion we suggest is that the increasing gender gap can be explained by new women physicians increasingly demanding non-pecuniary aspects of their jobs, and because of the greater aggregate presence of women in the physician labor market, being able to get it,” says lead author Anthony Lo Sasso, a professor and senior research scientist at the School of Public Health at the University of Illinois at Chicago. “Remember, cash wages are but one part of the compensation package in any job.”
Hoff’s study also uncovered gender differences in employment preferences, with men attracted to HM for the compensation possibilities and women for the predictable hours and lifestyle flexibility. For this reason, Hoff suggested, hospitalist employers can use different recruiting pitches for women than men and, to the extent they hire female hospitalists, save money (see “Negotiating Strategies for Better Compensation,” below).
“The Hoff paper is a goldmine,” says Linda Brodsky, MD, a pediatric otolaryngologist in Buffalo, N.Y., who co-chairs AMWA’s Gender Equity Task Force and whose organization, Expediting the Inevitable, advocates for gender equity in healthcare. “How is it that when you have shift work, women are getting paid less per shift? Because Hoff tells you at the end, employers can get away with it. Even if they know they are underpaying women, they will take the chance because it’s so hard for anybody to take legal action.”
Women also find themselves in a double bind when it comes to negotiating higher compensation, says Barbara Gault, PhD, executive director of the Institute for Women’s Policy Research in Washington, D.C. Some suggest a pay gap exists because women are not negotiating for themselves, but research shows women tend to be perceived as less likable when they are more assertive about higher wages, she says.
Erin Stucky Fisher, MD, MHM, has seen this phenomena play out in her roles as medical director for quality at Rady Children’s Hospital in San Diego and associate program director for the University of California at San Diego Pediatric Residency Program.
“I do a lot of interviewing for the hospital, and it does seem, in general, that women are less likely to promote themselves than men in the same situation,” says Dr. Fisher, an SHM board member who is also assisting with the HM12 “Women in Hospital Medicine” session. “There are reasons behind it that might have to do with women not wanting to be perceived as self-serving or arrogant.”
—Erin Stucky Fisher, MD, FAAP, MHM, medical director for quality, Rady Children’s Hospital, associate program director, University of California at San Diego Pediatric Residency Program, SHM board member
Dr. Brodsky agrees with the perception issues facing physicians.
“Women are supposed to be grateful, accommodating, and get along, which are excellent qualities,” she says. “But when you’re expected to do that and you instead negotiate with any kind of spirit, it’s perceived as troublemaking, whereas in men, it’s perceived as strength.”
Subtle forms of gender discrimination continue to exist in workplaces, Dr. Gatta says. Beliefs remain that men have a family to support, so they should be paid more, and that women are in the workforce just for extra money, even though recent data show that women’s income is key to families’ well-being, she notes.
Common patterns of gender bias will be discussed at the HM12 session, says Dr. Reich, who was a victim of gender pay disparity when she worked a locum tenens job earlier in her career.
“There was no logical explanation. The men did less work by all measures, and the other woman and I didn’t have young children at home, so explanations of women trading in money for time with family didn’t apply,” she explains. “Why did they think I should be paid less? I didn’t understand, and I never got a logical reason.”
Potential Solutions
Shortly after arriving at Wake Forest in 2004, Dr. Reich had the opportunity to build the hospitalist program. A set of thorough, transparent criteria for determining compensation were established almost immediately to help prevent pay discrepancies.
“We tried to be as objective as we could, and we involved the group in talking about it because we felt it was important,” she says.
—Linda Brodsky, MD, pediatric otolaryngologist, Buffalo, N.Y., co-chair, AMWA Gender Equity Task Force
Organizations can conduct self-audits to assess whether men and women are being compensated equitably, then make adjustments when necessary, Dr. Gault says. Policies can be adopted to promote pay transparency and allow employees to discuss compensation and suggest ways it can be improved, she adds. In workplaces where compensation discussions are discouraged, women can try to informally speak with their male friends to gather information and determine if there’s a pay gap problem.
Equal pay laws, such as the Lily Ledbetter Fair Pay Act, exist at the federal level. But Dr. Gatta says work must be done on the enforcement end to make a real difference. Similarly, Dr. Brodsky describes the Equal Employment Opportunity Commission as a toothless oversight agency with limited power to investigate complaints and assess fines.
“It’s on women to go and be the whistleblower, the policeman, and pay for legal action. It’s impossible,” she says. “When you utter the words ‘gender discrimination,’ immediately, retaliation goes into high gear.”
While employers and enforcement agencies have a significant role in closing the pay gap, women themselves must collectively advocate for equal pay, Dr. Gault says.
“Any woman physician who is in the senior ranks must be obligated to start changing the culture and making sure the fairness issue gets raised and is an important part of their agenda,” Dr. Brodsky says. “Enough women are now part of the physician population. They have to start saying, ‘We are a group to be reckoned with, and we are going to make changes.’”
Lisa Ryan is a freelance writer based in New Jersey.
References
- Wright AL, Schwindt LA, Bassford TL, et al. Gender differences in academic advancement: patterns, causes, and potential solutions in one US College of Medicine. Acad Med. 2003;78(5):500-508.
- Ash AS, Carr PL, Goldstein R, et al. Compensation and advancement of women in academic medicine: is there equity? Ann Intern Med. 2004;141(3):205-212.
- Ness RB, Ukoli F, Hunt S, et al. Salary equity among male and female internists in Pennsylvania. Ann Intern Med. 2000;133(2):104-110.
- Weeks WB, Wallace TA, Wallace AE. How do race and sex affect the earnings of primary care physicians? Health Aff (Millwood). 2009;28(2):557-566.
- Hoff TJ. Doing the same and earning less: male and female physicians in a new medical specialty. Inquiry. 2004;41:301-315.
- Lo Sasso AT, Richards MR, Chou C, Gerber SE. The $16,819 pay gap for newly trained physicians: the unexplained trend of men earning more than women. Health Aff (Millwood). 2011;30:193-201.
Negotiation Strategies for Better Compensation

The first step in negotiating is deciding to negotiate at all, Dr. Gebhard says. You must also recognize that many employers initially offer a lower compensation package because they expect negotiation to occur.
“You should have the mindset that everything is negotiable,” she says. “You have things to offer them and they have things to offer you, and it’s usually somewhere in between where you land.”
To prepare, a hospitalist should at minimum know what the local expectations are in pay, Dr. Fisher says. You might want to consider hiring a physician coach to learn effective negotiating strategies, Dr. Gebhard adds. Role-playing negotiation situations with a more experienced hospitalist can help, Dr. Reich says, as can attending negotiation skills workshops offered by SHM, the American Medical Women’s Association, and the American College of Physician Executives.
“It’s a matter of training people to feel negotiating is not self-serving or asking for more than what you’re valued at,” Dr. Fisher says. “It’s instead placing a value that’s appropriate and feeling confident that you’re asking for something that others in your same position would be asking for.”
Compensation isn’t the only negotiating point. “How much you’re worth is how many resources they’re going to invest in you so you can do the best job possible,” Dr. Brodsky says. “If you have adequate resources, then it’s much easier to bring yourself into a flexible situation because you’re getting what you need fairly. You can make the job look the way you want it to look while giving your employer fair value.”
Because people expect women to be communally interested rather than self-interested, a female hospitalist might want to approach negotiating from the standpoint of the common good of her family or the company, Dr. Gault says. “These sorts of requests aren’t met with surprise or negative judgment as much,” she says.
Nonetheless, women must be prepared for defeat.
“I think women should negotiate more. Not so much because it will be a successful strategy, but because in order to support one another, women have to get used to doing it,” Dr. Gault says. “We have to be willing to take the risk so that our perceptions and our ideas about what women should or shouldn’t do gradually shift over time.”
The first step in negotiating is deciding to negotiate at all, Dr. Gebhard says. You must also recognize that many employers initially offer a lower compensation package because they expect negotiation to occur.
“You should have the mindset that everything is negotiable,” she says. “You have things to offer them and they have things to offer you, and it’s usually somewhere in between where you land.”
To prepare, a hospitalist should at minimum know what the local expectations are in pay, Dr. Fisher says. You might want to consider hiring a physician coach to learn effective negotiating strategies, Dr. Gebhard adds. Role-playing negotiation situations with a more experienced hospitalist can help, Dr. Reich says, as can attending negotiation skills workshops offered by SHM, the American Medical Women’s Association, and the American College of Physician Executives.
“It’s a matter of training people to feel negotiating is not self-serving or asking for more than what you’re valued at,” Dr. Fisher says. “It’s instead placing a value that’s appropriate and feeling confident that you’re asking for something that others in your same position would be asking for.”
Compensation isn’t the only negotiating point. “How much you’re worth is how many resources they’re going to invest in you so you can do the best job possible,” Dr. Brodsky says. “If you have adequate resources, then it’s much easier to bring yourself into a flexible situation because you’re getting what you need fairly. You can make the job look the way you want it to look while giving your employer fair value.”
Because people expect women to be communally interested rather than self-interested, a female hospitalist might want to approach negotiating from the standpoint of the common good of her family or the company, Dr. Gault says. “These sorts of requests aren’t met with surprise or negative judgment as much,” she says.
Nonetheless, women must be prepared for defeat.
“I think women should negotiate more. Not so much because it will be a successful strategy, but because in order to support one another, women have to get used to doing it,” Dr. Gault says. “We have to be willing to take the risk so that our perceptions and our ideas about what women should or shouldn’t do gradually shift over time.”
The first step in negotiating is deciding to negotiate at all, Dr. Gebhard says. You must also recognize that many employers initially offer a lower compensation package because they expect negotiation to occur.
“You should have the mindset that everything is negotiable,” she says. “You have things to offer them and they have things to offer you, and it’s usually somewhere in between where you land.”
To prepare, a hospitalist should at minimum know what the local expectations are in pay, Dr. Fisher says. You might want to consider hiring a physician coach to learn effective negotiating strategies, Dr. Gebhard adds. Role-playing negotiation situations with a more experienced hospitalist can help, Dr. Reich says, as can attending negotiation skills workshops offered by SHM, the American Medical Women’s Association, and the American College of Physician Executives.
“It’s a matter of training people to feel negotiating is not self-serving or asking for more than what you’re valued at,” Dr. Fisher says. “It’s instead placing a value that’s appropriate and feeling confident that you’re asking for something that others in your same position would be asking for.”
Compensation isn’t the only negotiating point. “How much you’re worth is how many resources they’re going to invest in you so you can do the best job possible,” Dr. Brodsky says. “If you have adequate resources, then it’s much easier to bring yourself into a flexible situation because you’re getting what you need fairly. You can make the job look the way you want it to look while giving your employer fair value.”
Because people expect women to be communally interested rather than self-interested, a female hospitalist might want to approach negotiating from the standpoint of the common good of her family or the company, Dr. Gault says. “These sorts of requests aren’t met with surprise or negative judgment as much,” she says.
Nonetheless, women must be prepared for defeat.
“I think women should negotiate more. Not so much because it will be a successful strategy, but because in order to support one another, women have to get used to doing it,” Dr. Gault says. “We have to be willing to take the risk so that our perceptions and our ideas about what women should or shouldn’t do gradually shift over time.”
Resume Red Flags
Fifteen seconds: That’s approximately how long an employer looks at a CV. Recruiters and employers know what they want; they skim even the best resumes. They are on the lookout for applicants who meet their requirements; sometimes they’ll take a chance on a long shot whose pitch catches their eye.
So what happens when a resume stands out for the wrong reasons? Work histories aren’t always perfect, and recruiters and prospective employers will notice any blemishes.
“The thing about red flags is they’re just an indicator that the applicant is an outlier,” says Kim Bell, MD, FACP, SFHM, regional medical director of the Pacific West Region for EmCare, a Dallas-based company that provides outsourced physician services to more than 500 hospitals in 40 states. “It doesn’t necessarily rule them out.”
Preempt Suspicion
For hospitalists, resume imperfections that attract attention include:
- Gaps in employment;
- Frequent changes in employment;
- Changes in residency;
- Medical board sanctions or probation;
- Failures on the board exam; and
- Forced resignations or firings.
—Cheryl O’Malley, MD, FACP, program director, Department of Internal Medicine and Pediatrics, Banner Good Samaritan Medical Center, Phoenix
When recruiters or employers notice a red flag, they look for other problems to see if patterns emerge and to discern if the applicant exhibited bad judgment, has character flaws, or shows an inability to learn from a mistake, says Jeff Kaplan, PhD, MBA, MCC, a licensed psychologist and Philadelphia-based executive coach whose clients include healthcare industry executives. If such signs exist, the applicant is generally eliminated from consideration. Therefore, it’s critical that applicants explain clearly and succinctly the reason for any resume shortcoming.
“A good way is to actually write a cover letter to explain some uniqueness in their CV that they want [recruiters] to understand,” says Alpesh Amin, MD, MBA, FACP, SFHM, professor and chairman of the Department of Medicine and executive director of the hospitalist program at the University of California at Irvine.
By explaining the situation, Dr. Bell says, the hospitalist doesn’t give the employer a chance to guess a reason for the red flag—and potentially guess wrong.
“There’s a big difference between there’s been some sort of serious censure and they’ve been driven out, versus they thought another setting might be more interesting or they just wanted to make a geographic move,” says Thomas E. Thorsheim, PhD, a licensed psychologist and physician leadership coach based in Greenville, S.C. “It’s important to preempt any concerns about how reliable or stable they’re going to be.”
Applicants with resume red flags should show that they’ve taken responsibility for what happened and grown from the experience, say Dr. Thorsheim and Cheryl O’Malley, MD, FACP, program director in the department of internal medicine and pediatrics at Banner Good Samaritan Medical Center in Phoenix.
“Everyone wants to know that you have learned from your mistakes. Try to have a demonstrated remediation of the concern and go above and beyond the minimum requirements,” Dr. O’Malley says. “For example, if the red flag is academic concerns or not passing your board exams, then bring in documentation of your schedule for reading daily and all of the CME and MKSAP you complete. If it is interpersonal issues, then give examples of recent successes that show how you have improved.”
Brand Recognition
Physicians with a resume blemish should concentrate on highlighting their strengths and “branding” themselves as a workplace contributor, says Bernadette Norz, MBA, ACC, a certified physician development coach. While this advice applies to all applicants, it is particularly critical for those with resume problems, as it will demonstrate they have skills that set them apart from others.
“What people are really looking for is what did you do and what was the result,” Norz says. “Things that one accomplished as a volunteer or on a committee count, too, because that’s where people gain a lot of leadership skills.”
Resumes should not be recitations of job descriptions, she advises. They should be lists of achievements described with action verbs that give the applicant a clear identity and brand. “When you read a resume, you should walk away from it knowing who this person is,” says Dr. Kaplan. “If you don’t see that on their resume, then you’ve got to question it.”
The best applicants network. The more you can develop a relationship and rapport with peers and potential employers, the more likely you will be given a greater chance to sell your strengths and explain weaknesses, says career strategist Ellen Dunagan, president of Traverse Management Solutions in Arlington, Va. “You really want to step it up and be much more active with your own pitch,” she says.
Attitude Matters
But before a hospitalist or any applicant with a resume shortcoming begins to look for a job, they must resolve the issue internally, Dr. Kaplan notes. Taking responsibility will allow you to speak clearly and comfortably about what happened, without negativity or blame.
“If you don’t, you will fumble,” he says. “The prospective employer will start seeing those red flags and they will ask you about it, and you thought you had your pitch ready. Then they ask you two more questions, and before you know it, they’re not going to feel a sense of transparency with you.”
More and more, what employers are looking for is positivity, Dunagan says. It’s a trait applicants won’t have if they still harbor negative feelings toward a previous employer. “It’s just very important to be not only a team player, but to have a really good attitude,” she says. “So present yourself in the best possible light.”
Lisa Ryan is a freelance writer based in New Jersey.
Fifteen seconds: That’s approximately how long an employer looks at a CV. Recruiters and employers know what they want; they skim even the best resumes. They are on the lookout for applicants who meet their requirements; sometimes they’ll take a chance on a long shot whose pitch catches their eye.
So what happens when a resume stands out for the wrong reasons? Work histories aren’t always perfect, and recruiters and prospective employers will notice any blemishes.
“The thing about red flags is they’re just an indicator that the applicant is an outlier,” says Kim Bell, MD, FACP, SFHM, regional medical director of the Pacific West Region for EmCare, a Dallas-based company that provides outsourced physician services to more than 500 hospitals in 40 states. “It doesn’t necessarily rule them out.”
Preempt Suspicion
For hospitalists, resume imperfections that attract attention include:
- Gaps in employment;
- Frequent changes in employment;
- Changes in residency;
- Medical board sanctions or probation;
- Failures on the board exam; and
- Forced resignations or firings.
—Cheryl O’Malley, MD, FACP, program director, Department of Internal Medicine and Pediatrics, Banner Good Samaritan Medical Center, Phoenix
When recruiters or employers notice a red flag, they look for other problems to see if patterns emerge and to discern if the applicant exhibited bad judgment, has character flaws, or shows an inability to learn from a mistake, says Jeff Kaplan, PhD, MBA, MCC, a licensed psychologist and Philadelphia-based executive coach whose clients include healthcare industry executives. If such signs exist, the applicant is generally eliminated from consideration. Therefore, it’s critical that applicants explain clearly and succinctly the reason for any resume shortcoming.
“A good way is to actually write a cover letter to explain some uniqueness in their CV that they want [recruiters] to understand,” says Alpesh Amin, MD, MBA, FACP, SFHM, professor and chairman of the Department of Medicine and executive director of the hospitalist program at the University of California at Irvine.
By explaining the situation, Dr. Bell says, the hospitalist doesn’t give the employer a chance to guess a reason for the red flag—and potentially guess wrong.
“There’s a big difference between there’s been some sort of serious censure and they’ve been driven out, versus they thought another setting might be more interesting or they just wanted to make a geographic move,” says Thomas E. Thorsheim, PhD, a licensed psychologist and physician leadership coach based in Greenville, S.C. “It’s important to preempt any concerns about how reliable or stable they’re going to be.”
Applicants with resume red flags should show that they’ve taken responsibility for what happened and grown from the experience, say Dr. Thorsheim and Cheryl O’Malley, MD, FACP, program director in the department of internal medicine and pediatrics at Banner Good Samaritan Medical Center in Phoenix.
“Everyone wants to know that you have learned from your mistakes. Try to have a demonstrated remediation of the concern and go above and beyond the minimum requirements,” Dr. O’Malley says. “For example, if the red flag is academic concerns or not passing your board exams, then bring in documentation of your schedule for reading daily and all of the CME and MKSAP you complete. If it is interpersonal issues, then give examples of recent successes that show how you have improved.”
Brand Recognition
Physicians with a resume blemish should concentrate on highlighting their strengths and “branding” themselves as a workplace contributor, says Bernadette Norz, MBA, ACC, a certified physician development coach. While this advice applies to all applicants, it is particularly critical for those with resume problems, as it will demonstrate they have skills that set them apart from others.
“What people are really looking for is what did you do and what was the result,” Norz says. “Things that one accomplished as a volunteer or on a committee count, too, because that’s where people gain a lot of leadership skills.”
Resumes should not be recitations of job descriptions, she advises. They should be lists of achievements described with action verbs that give the applicant a clear identity and brand. “When you read a resume, you should walk away from it knowing who this person is,” says Dr. Kaplan. “If you don’t see that on their resume, then you’ve got to question it.”
The best applicants network. The more you can develop a relationship and rapport with peers and potential employers, the more likely you will be given a greater chance to sell your strengths and explain weaknesses, says career strategist Ellen Dunagan, president of Traverse Management Solutions in Arlington, Va. “You really want to step it up and be much more active with your own pitch,” she says.
Attitude Matters
But before a hospitalist or any applicant with a resume shortcoming begins to look for a job, they must resolve the issue internally, Dr. Kaplan notes. Taking responsibility will allow you to speak clearly and comfortably about what happened, without negativity or blame.
“If you don’t, you will fumble,” he says. “The prospective employer will start seeing those red flags and they will ask you about it, and you thought you had your pitch ready. Then they ask you two more questions, and before you know it, they’re not going to feel a sense of transparency with you.”
More and more, what employers are looking for is positivity, Dunagan says. It’s a trait applicants won’t have if they still harbor negative feelings toward a previous employer. “It’s just very important to be not only a team player, but to have a really good attitude,” she says. “So present yourself in the best possible light.”
Lisa Ryan is a freelance writer based in New Jersey.
Fifteen seconds: That’s approximately how long an employer looks at a CV. Recruiters and employers know what they want; they skim even the best resumes. They are on the lookout for applicants who meet their requirements; sometimes they’ll take a chance on a long shot whose pitch catches their eye.
So what happens when a resume stands out for the wrong reasons? Work histories aren’t always perfect, and recruiters and prospective employers will notice any blemishes.
“The thing about red flags is they’re just an indicator that the applicant is an outlier,” says Kim Bell, MD, FACP, SFHM, regional medical director of the Pacific West Region for EmCare, a Dallas-based company that provides outsourced physician services to more than 500 hospitals in 40 states. “It doesn’t necessarily rule them out.”
Preempt Suspicion
For hospitalists, resume imperfections that attract attention include:
- Gaps in employment;
- Frequent changes in employment;
- Changes in residency;
- Medical board sanctions or probation;
- Failures on the board exam; and
- Forced resignations or firings.
—Cheryl O’Malley, MD, FACP, program director, Department of Internal Medicine and Pediatrics, Banner Good Samaritan Medical Center, Phoenix
When recruiters or employers notice a red flag, they look for other problems to see if patterns emerge and to discern if the applicant exhibited bad judgment, has character flaws, or shows an inability to learn from a mistake, says Jeff Kaplan, PhD, MBA, MCC, a licensed psychologist and Philadelphia-based executive coach whose clients include healthcare industry executives. If such signs exist, the applicant is generally eliminated from consideration. Therefore, it’s critical that applicants explain clearly and succinctly the reason for any resume shortcoming.
“A good way is to actually write a cover letter to explain some uniqueness in their CV that they want [recruiters] to understand,” says Alpesh Amin, MD, MBA, FACP, SFHM, professor and chairman of the Department of Medicine and executive director of the hospitalist program at the University of California at Irvine.
By explaining the situation, Dr. Bell says, the hospitalist doesn’t give the employer a chance to guess a reason for the red flag—and potentially guess wrong.
“There’s a big difference between there’s been some sort of serious censure and they’ve been driven out, versus they thought another setting might be more interesting or they just wanted to make a geographic move,” says Thomas E. Thorsheim, PhD, a licensed psychologist and physician leadership coach based in Greenville, S.C. “It’s important to preempt any concerns about how reliable or stable they’re going to be.”
Applicants with resume red flags should show that they’ve taken responsibility for what happened and grown from the experience, say Dr. Thorsheim and Cheryl O’Malley, MD, FACP, program director in the department of internal medicine and pediatrics at Banner Good Samaritan Medical Center in Phoenix.
“Everyone wants to know that you have learned from your mistakes. Try to have a demonstrated remediation of the concern and go above and beyond the minimum requirements,” Dr. O’Malley says. “For example, if the red flag is academic concerns or not passing your board exams, then bring in documentation of your schedule for reading daily and all of the CME and MKSAP you complete. If it is interpersonal issues, then give examples of recent successes that show how you have improved.”
Brand Recognition
Physicians with a resume blemish should concentrate on highlighting their strengths and “branding” themselves as a workplace contributor, says Bernadette Norz, MBA, ACC, a certified physician development coach. While this advice applies to all applicants, it is particularly critical for those with resume problems, as it will demonstrate they have skills that set them apart from others.
“What people are really looking for is what did you do and what was the result,” Norz says. “Things that one accomplished as a volunteer or on a committee count, too, because that’s where people gain a lot of leadership skills.”
Resumes should not be recitations of job descriptions, she advises. They should be lists of achievements described with action verbs that give the applicant a clear identity and brand. “When you read a resume, you should walk away from it knowing who this person is,” says Dr. Kaplan. “If you don’t see that on their resume, then you’ve got to question it.”
The best applicants network. The more you can develop a relationship and rapport with peers and potential employers, the more likely you will be given a greater chance to sell your strengths and explain weaknesses, says career strategist Ellen Dunagan, president of Traverse Management Solutions in Arlington, Va. “You really want to step it up and be much more active with your own pitch,” she says.
Attitude Matters
But before a hospitalist or any applicant with a resume shortcoming begins to look for a job, they must resolve the issue internally, Dr. Kaplan notes. Taking responsibility will allow you to speak clearly and comfortably about what happened, without negativity or blame.
“If you don’t, you will fumble,” he says. “The prospective employer will start seeing those red flags and they will ask you about it, and you thought you had your pitch ready. Then they ask you two more questions, and before you know it, they’re not going to feel a sense of transparency with you.”
More and more, what employers are looking for is positivity, Dunagan says. It’s a trait applicants won’t have if they still harbor negative feelings toward a previous employer. “It’s just very important to be not only a team player, but to have a really good attitude,” she says. “So present yourself in the best possible light.”
Lisa Ryan is a freelance writer based in New Jersey.
Professional-Growth Planning Is Essential to HM Group Success
In the changing healthcare landscape, hospitalists are being asked to be leaders and managers in their day-to-day activities. Often, the HM director will need to help provide hospitalists in their groups with the skills they need to succeed, says Bryce Gartland, MD, FHM, associate director of the hospital medicine division and medical director of care coordination at Emory Healthcare in Atlanta.
“Critical to that is making sure you’ve got a standardized structure in place for ensuring their professional growth and development,” he says.
HM group directors can invite experts to conduct feedback sessions on particular areas of concern or send their hospitalists to outside training, he says. For example, SHM hosts a Leadership Academy that offers a “Foundation for Effective Leadership” course, along with two more advanced leadership seminars.
The American College of Physicians offers the “Leadership Enhancement and Development” (LEAD) program, and the Center for the Health Professions at the University of California at San Francisco offers several leadership initiatives.

—John Bulger, DO, FACP, FHM, chief quality officer, director, HM service line, Geisinger Health System, Danville, Pa.
It also is incumbent on HM directors to get their physicians training in quality improvement (QI), asserts John Bulger, DO, FACP, FHM, chief quality officer and director of the HM service line for Geisinger Health System in Danville, Pa. “In my view, quality improvement is really where hospitalists make their hay in being a value added to the hospital,” he says.
SHM’s Center for Hospital Innovation and Improvement offers a wide variety of tools and resources to educate hospitalists on QI. SHM also has a Quality Improvement Skills pre-course at its annual meeting in April in San Diego.
The Institute for Healthcare Improvement, a nonprofit organization based in Cambridge, Mass., that focuses on healthcare best practices, and the Institute for Health Care Delivery Research at InterMountain Healthcare in Salt Lake City, Utah, have respected QI training programs.
QI training also comes from mentorship and putting hospitalists on QI-related committees. “That really has a twofold benefit for the hospital medicine group, because you are also able to stretch your reach,” Dr. Bulger says. “Now you’ve got a hospitalist on that committee who can report back to you and tell you what’s going on, and help you be involved in the changes going on in the hospital.”
Lisa Ryan is a freelance writer based in New Jersey.
In the changing healthcare landscape, hospitalists are being asked to be leaders and managers in their day-to-day activities. Often, the HM director will need to help provide hospitalists in their groups with the skills they need to succeed, says Bryce Gartland, MD, FHM, associate director of the hospital medicine division and medical director of care coordination at Emory Healthcare in Atlanta.
“Critical to that is making sure you’ve got a standardized structure in place for ensuring their professional growth and development,” he says.
HM group directors can invite experts to conduct feedback sessions on particular areas of concern or send their hospitalists to outside training, he says. For example, SHM hosts a Leadership Academy that offers a “Foundation for Effective Leadership” course, along with two more advanced leadership seminars.
The American College of Physicians offers the “Leadership Enhancement and Development” (LEAD) program, and the Center for the Health Professions at the University of California at San Francisco offers several leadership initiatives.
—John Bulger, DO, FACP, FHM, chief quality officer, director, HM service line, Geisinger Health System, Danville, Pa.
It also is incumbent on HM directors to get their physicians training in quality improvement (QI), asserts John Bulger, DO, FACP, FHM, chief quality officer and director of the HM service line for Geisinger Health System in Danville, Pa. “In my view, quality improvement is really where hospitalists make their hay in being a value added to the hospital,” he says.
SHM’s Center for Hospital Innovation and Improvement offers a wide variety of tools and resources to educate hospitalists on QI. SHM also has a Quality Improvement Skills pre-course at its annual meeting in April in San Diego.
The Institute for Healthcare Improvement, a nonprofit organization based in Cambridge, Mass., that focuses on healthcare best practices, and the Institute for Health Care Delivery Research at InterMountain Healthcare in Salt Lake City, Utah, have respected QI training programs.
QI training also comes from mentorship and putting hospitalists on QI-related committees. “That really has a twofold benefit for the hospital medicine group, because you are also able to stretch your reach,” Dr. Bulger says. “Now you’ve got a hospitalist on that committee who can report back to you and tell you what’s going on, and help you be involved in the changes going on in the hospital.”
Lisa Ryan is a freelance writer based in New Jersey.
In the changing healthcare landscape, hospitalists are being asked to be leaders and managers in their day-to-day activities. Often, the HM director will need to help provide hospitalists in their groups with the skills they need to succeed, says Bryce Gartland, MD, FHM, associate director of the hospital medicine division and medical director of care coordination at Emory Healthcare in Atlanta.
“Critical to that is making sure you’ve got a standardized structure in place for ensuring their professional growth and development,” he says.
HM group directors can invite experts to conduct feedback sessions on particular areas of concern or send their hospitalists to outside training, he says. For example, SHM hosts a Leadership Academy that offers a “Foundation for Effective Leadership” course, along with two more advanced leadership seminars.
The American College of Physicians offers the “Leadership Enhancement and Development” (LEAD) program, and the Center for the Health Professions at the University of California at San Francisco offers several leadership initiatives.
—John Bulger, DO, FACP, FHM, chief quality officer, director, HM service line, Geisinger Health System, Danville, Pa.
It also is incumbent on HM directors to get their physicians training in quality improvement (QI), asserts John Bulger, DO, FACP, FHM, chief quality officer and director of the HM service line for Geisinger Health System in Danville, Pa. “In my view, quality improvement is really where hospitalists make their hay in being a value added to the hospital,” he says.
SHM’s Center for Hospital Innovation and Improvement offers a wide variety of tools and resources to educate hospitalists on QI. SHM also has a Quality Improvement Skills pre-course at its annual meeting in April in San Diego.
The Institute for Healthcare Improvement, a nonprofit organization based in Cambridge, Mass., that focuses on healthcare best practices, and the Institute for Health Care Delivery Research at InterMountain Healthcare in Salt Lake City, Utah, have respected QI training programs.
QI training also comes from mentorship and putting hospitalists on QI-related committees. “That really has a twofold benefit for the hospital medicine group, because you are also able to stretch your reach,” Dr. Bulger says. “Now you’ve got a hospitalist on that committee who can report back to you and tell you what’s going on, and help you be involved in the changes going on in the hospital.”
Lisa Ryan is a freelance writer based in New Jersey.
ONLINE EXCLUSIVE: Listen to Martin Buser and Bryce Gartland discuss directors' impact on HM program success
Click here to listen to Martin Buser
Click here to listen to Dr. Gartland
Click here to listen to Martin Buser
Click here to listen to Dr. Gartland
Click here to listen to Martin Buser
Click here to listen to Dr. Gartland
The Buck Starts Here
Some of the best companies in America started in a garage or a basement with an individual who had a great idea and the ability to grow it into a progressively larger business.
“It takes a leader with different capabilities to take a company to the next level,” says Martin Buser, MPH, FACHE, a partner with Hospitalist Management Resources LLC in San Diego, which has helped more than 350 HM programs nationwide in the past 15 years. “It’s an attitude of never stop learning, an ability to look at issues from 30,000 feet instead of ground zero so you can see the whole picture.”
Similarly, the most important predictor of an HM program’s success is its director, Buser says. If directors know how to communicate, innovate, facilitate, problem-solve, and inspire, they are much more likely to run a high-performing hospitalist program, says David Lee, MD, MBA, FACP, FHM, vice chairman of the Hospital Medicine Department at Ochsner Health System in New Orleans.
If group directors lack the skills and fail to adapt to change, the program’s outlook is far from certain. “We unfortunately get involved with these programs,” Buser says. “It’s painful to see.” Bad behavior is nothing new to the hospital setting, and HM is not immune to poor management. The following are common examples of bad behaviors and how groups can avoid the mishaps.
Scenario No. 1 : Great Clinician, Nice Person, Weak Advocate

—Martin Buser, MPH, FACHE, partner, Hospitalist Management Resources LLC, San Diego
The case: Earlier this year, medical center administrators asked the hospitalist program to do more with less, explaining the hospital was having a bad financial year. Administration approached the HM director, an exceptional, gregarious clinician who was named to the position years ago to help the program gain acceptance. The director agreed to indefinitely postpone two much-needed hirings, deciding it was better to share in the sacrifice than protest the cuts to the program’s budget. Hospitalists have since been working more shifts without a pay increase, and burnout symptoms have emerged with no signs of a thaw in the hiring freeze.
Expert advice: Buser says the “weak advocate” is a common issue among hospitalist groups, many of which he says are “going to hell” when he gets a rescue call. When a hospital is facing financial hardship, it is imperative that the HM director stand up for the program by explaining in detail the ramifications of each level of budget cuts. That’s because administrators might not realize the long-term damage that would result from such actions, he says. Being a strong, savvy advocate is even more important now since the financial future of many hospitals is ominous.
“With all of our hospitalist clients, we ask the CFO what is happening in the future…and the numbers are phenomenal,” says Buser. “They are seeing reductions of $10 million to $30 million off their bottom line.”
Administrators’ knee-jerk reaction is to cut costs. But there is another option: Grow the hospital out of its financial difficulties. It is up to the HM director to show administrators how the HM group has strategically gained them market share and how it will continue to do so. Good directors are in near constant contact with administrators, demonstrating the value their hospitalist program brings to the hospital, Buser says.
“You’re having regular meetings with the administrator, you’re producing the dashboard on a regular basis, you’re giving him trends that are going on,” he explains. “Show that you understand the hospital’s issues. Certain things you want to compromise on, but other things you have to say, ‘If we do that, the ramifications are such that it’s just not going to work.’”
Scenario No. 2 : Recruiting Roulette

—David Friar, MD, SFHM, CEO, Hospitalists of Northern Michigan, Traverse City
The case: The HM director felt pressure to hire. The program’s hospitalists were seeing two to three patients a day more than they should have been, and hospital administrators were worried the program was losing ground to the other hospitalist group in the community. Using an outside recruiter, the director hired two adept physicians with stellar CVs after an expedited review process that included a background check, a few phone interviews, and day of in-person interviews with some administrators and a hospitalist on the team. Now, nearly a year later, one of the physicians is about to leave because her family doesn’t like the community, and the other new hire’s abrasive personality has caused considerable damage to the team’s cohesion.
Expert advice: A big part of an HM program’s value is how it practices as a unified team, and directors need to recognize how vital the “team fit” is to hospitalists, says David Friar, MD, SFHM, CEO of Hospitalists of Northern Michigan in Traverse City.
“A bad team fit is often worse than being short-staffed because it can literally destroy the team spirit,” he says.
Directors should have a standardized recruitment process that includes a comprehensive background screening where references are closely checked, a round of interviews by people outside the HM program (nurses and referring physicians), and substantial time spent with hospitalists in the program, says Bryce Gartland, MD, FHM, associate director of the hospital medicine division and medical director of care coordination at Emory Healthcare in Atlanta.
“We put [candidates] with one of our physicians to actually go around the hospital,” he says. “It’s amazing to me the number of things you can pick up by that broader exposure that you may not pick up sitting in a room with a candidate across the table for an hour.”
If a recruitment service is used, the director must describe the HM program in detail to the recruiter and even have them meet hospitalists on the staff, Dr. Friar says.
“Sending them a memo saying ‘We need three new hospitalists ASAP’ isn’t helping them find you the perfect candidate,” he says. “Even the best recruiter can only do a great job for you if they really know your team and what it is you need in a candidate.”
A director also is well served to make recruiting a family event where spouses and even children are part of the interview process.
“By including the entire family and then supporting them after the move, we are much more likely to recruit providers that will stay good members of our team for years to come,” Dr. Friar says.
Scenario No. 3 : Amitte Diem

—John Bulger, DO, FACP, FHM, chief quality officer, director, hospital medicine service line, Geisinger Health System, Danville, Pa.
The case: For months, the medical center has been receiving an increased number of referrals from outlying hospitals, and no end is in sight. The extra patient load, much of it involving complex cases, has agitated the medical center’s staff, particularly the specialists, and they’ve begun to complain to hospital administrators. Seeking an ally, the specialists reach out to the HM director to present their case. Without doing independent analysis, the HM director sides with the specialists. Hospital administrators, facing growing resistance, work to decrease the referrals and are successful.
Expert advice: Consider working in the opposite direction, one that might turn a referral challenge into a profitable opportunity, Buser says. One of his firm’s clients, after thorough research, established a transfer center and set up an activation fee for the specialists who took the referrals. Hospitalists admitted about 90% of the cases, called consults, and named specialists so they received full fee-for-service at Medicare rates if they saw uninsured patients.
“That hospital is now making about $78 million a year, and the medical staff is saying, ‘How can we grow this?’” Buser says. “Here’s an example of how the hospital medicine director was key to turning the bad into something good.”
Because physicians tend to be reticent to change, it’s critical for hospitalist directors who want to seize an opportunity to thoroughly plan out how the change will occur and to prepare for potential obstacles along the way, says John Bulger, DO, FACP, FHM, chief quality officer and director of the hospital medicine service line for Geisinger Health System in Danville, Pa.
“You really need to be prepared with your rationale of why you’re doing it, if there’s data behind why you’re doing it, what the data is that’s driving it, and really what you hope to do with that change,” he says. “If you don’t get buy in from your staff, the change is doomed to fail from the beginning.”
Directors must embrace being a change agent if they want their HM programs to continue to be successful. In the minds of many hospital administrators, a program is only as good as its last achievement.
“It’s kind of like, ‘What have you done for me lately?’” Buser says. “You want to stay ahead of the curve and be alert to what’s going on and not be caught keeping your eyes off the ball and, as a result, not moving your program forward.”
Scenario No. 4 : Fumbling the Handoff

—Daniel Cusator, MD, MBA, vice president, Camden Group, El Segundo, Calif.
The case: The medical center’s monthly data for the past year has shown that hospitalists are taking care of their patients efficiently and getting them out of the hospital more quickly. However, mixed in with the positive numbers is a stubbornly high 30-day readmission rate. Indeed, some primary care groups and referring geriatricians have begun to grouse to the HM director about the discharge notes, complaining they aren’t as comprehensive as they would like.
Plus, the notes always arrive via office fax, which makes them more likely to get misplaced and harder to receive when doctors are out of the office.
Expert advice: Handoffs from discharge to pickup are where a lot of complications, errors, and safety issues arise, and poor handoffs are one of the largest drivers of readmission rates, especially in the elderly patient population, says Daniel Cusator, MD, MBA, vice president of the Camden Group, a healthcare consulting firm in El Segundo, Calif.
If the hospitalist director doesn’t provide the leadership and resources to help the HM team better coordinate with patients’ regular doctors, handoffs won’t be a priority throughout the group.
The HM director must recognize that the term “discharge note” is a misnomer.
What referring physicians really want is a care plan, which includes information about testing done in the hospital, testing that might be needed in the outpatient setting, medications the patient is on, complications the patient had in the hospital, potential problems to monitor, and any necessary follow-up, says Dr. Cusator, formerly the chief medical officer of clinical integration at Providence Health & Services in Southern California.
PCPs also want the care plan transmitted in their preferred method, whether that is text messaging, HIPAA-compliant email messaging, secure messaging, or fax.
“What I’ve seen some hospitalist groups do is create a menu capability for each of the physicians to choose their preferred method of notification of discharge of their patient,” Dr. Cusator says. Results suggest such a menu leads to improved physician satisfaction and reduced patient complications after discharge, he adds.
With today’s technological innovations, HM directors are unlimited in their ability to improve handoffs between their team and patients’ PCPs and specialists, Dr. Cusator says. Some HM directors, for example, are leading efforts to link electronic medical records systems to hospital-based health information exchange hubs that are accessible to physicians in the community.
“Notes and clinical information are submitted to this health information exchange and made available to any of the physicians who are caring for the patient almost immediately upon dictation and notation,” he says.
Scenario No. 5 : Protect Your Assets

—David Lee, MD, MBA, FACP, FHM, vice chairman, Hospital Medicine Department, Ochsner Health System, New Orleans.
The case: A physician isn’t sure she wants a career in hospital medicine. She finds the specialty rewarding but is looking for a different challenge, something beyond exclusively seeing patients. The HM director notices the physician has an aptitude for finding ways to do tasks more efficiently.
The director privately thinks the physician would be a good fit for a quality improvement project that’s about to start but doesn’t pursue it. The HM team just added a primary care group, and its patient census is quickly rising, requiring the hospitalists to devote their entire shifts to patient care. Within the year, the physician leaves the team for a fellowship program outside hospital medicine.
Expert advice: There are three communities in hospital medicine, Dr. Bulger says: people who want to be hospitalists, people who are passing through on their way to something else, and people who sit somewhere in the middle.
HM directors, he says, should do everything they can to develop not only the career hospitalists but also those on the fence.
“A lot of them you can turn into people who are going to be hospitalists if they are doing something that is rewarding for them,” Dr. Bulger says. “Many times rewarding for them is being involved more in the leadership of the group, being involved in quality improvement projects, really seeing how they can impact the care for populations of patients—and not just the patient who happens to be sitting in front of them.”
It’s incumbent on HM group leaders to link hospitalists with mentors and help them find a niche, Dr. Lee says. It keeps people interested and makes them feel part of a group.
“They need to feel they belong,” he says. “There has to be a cohesiveness in order for your department to excel. You have to protect your assets in the group, which is your physicians.”
Sending hospitalists to professional development training, such as SHM’s Leadership Academy (see “Leadership Academy Adds ‘Women in HM Issues’ to Schedule,” p. 9) or QI-focused webinars offered by SHM or the Institute of Healthcare Improvement, and following up with day-to-day coaching is a solid physician-development strategy, Dr. Gartland says. By virtue of their job, hospitalists are expected to lead and manage people in interactions with the ED, primary care, non-physician providers, nursing staff, and beyond, he says.
Directors also have to stop assuming that competent physicians are competent managers. “A lot of physicians don’t have those core skill sets, and we’ve got to pay conscious attention toward spending time dedicated to developing those,” Dr. Gartland says.
If directors don’t make professional development a priority or provide hospitalists with the flexibility to do non-clinical activities, retention may become an issue, Dr. Bulger says. “They could leave and go somewhere else,” he says, yet perhaps the more significant danger is losing hospitalists to programs and specialties outside hospital medicine.
Lisa Ryan is a freelance writer based in New Jersey.
THE FUNDAMENTALS
As hospitals position themselves for healthcare reform, they increasingly will turn to HM for strategies on how to provide high-quality patient care at a lower cost, Buser says. To meet hospitals’ needs and enhance the value of their programs, hospitalist directors should consider adopting these strategies recommended by HM leaders:
- Align compensation with the HM program’s goals. For example, if quality improvement is the priority, directors should financially reward hospitalists on quality performance, Dr. Lee says.
- Boost support staff and functions. For example, directors should ensure their team has access to the hospital’s case managers, who can handle discharge logistics so the hospitalist can focus on clinical issues, Dr. Cusator says.
- Control program growth. To borrow a popular line from the movie Field of Dreams: “If you build it, they will come.” Directors should be deliberate with group expansion and ensure enough staff is in place before adding to their referral base or adding a new service line, Dr. Bulger says. This reduces hospitalist burnout and preserves the group’s quality of patient care.
- Define two to three targets for success in the upcoming year and concentrate on accomplishing them. Start by consolidating what your team is working on, says Steven Deitelzweig, MD, SFHM, chairman of the Department of Hospital Medicine at Ochsner Health System in New Orleans. Pick too many things to master, and you end up excelling in none, he adds.
- Evaluate performance beyond a scorecard. Using constructive criticism grounded with examples, HM directors should provide feedback about what a physician is doing well and what can be done better so they can improve, Dr. Gartland says.
- Foster creative problem solving by including hospitalists in decisions. Directors should encourage the expression of different opinions and ideas, which helps the program avoid “group think” and allows innovation to occur, Dr. Lee says.
- Galvanize the new generation. To retain young physicians and make them feel part of the program, directors should learn how they communicate, how they work, and how they view work, Dr. Lee says.
- Help your hospital accurately measure reimbursement and mortality rates. Directors should make coding a priority and provide hospitalists with the tools they need to capture correct ICD-9 and CPT codes for their patients, Dr. Cusator says.
- Identify missing core capabilities and dedicate resources for it. For example, if HM programs have a high census of chronically ill and end-of-life patients, directors should assist the hospital in establishing a palliative care or hospice program, Dr. Cusator says.
Some of the best companies in America started in a garage or a basement with an individual who had a great idea and the ability to grow it into a progressively larger business.
“It takes a leader with different capabilities to take a company to the next level,” says Martin Buser, MPH, FACHE, a partner with Hospitalist Management Resources LLC in San Diego, which has helped more than 350 HM programs nationwide in the past 15 years. “It’s an attitude of never stop learning, an ability to look at issues from 30,000 feet instead of ground zero so you can see the whole picture.”
Similarly, the most important predictor of an HM program’s success is its director, Buser says. If directors know how to communicate, innovate, facilitate, problem-solve, and inspire, they are much more likely to run a high-performing hospitalist program, says David Lee, MD, MBA, FACP, FHM, vice chairman of the Hospital Medicine Department at Ochsner Health System in New Orleans.
If group directors lack the skills and fail to adapt to change, the program’s outlook is far from certain. “We unfortunately get involved with these programs,” Buser says. “It’s painful to see.” Bad behavior is nothing new to the hospital setting, and HM is not immune to poor management. The following are common examples of bad behaviors and how groups can avoid the mishaps.
Scenario No. 1 : Great Clinician, Nice Person, Weak Advocate
—Martin Buser, MPH, FACHE, partner, Hospitalist Management Resources LLC, San Diego
The case: Earlier this year, medical center administrators asked the hospitalist program to do more with less, explaining the hospital was having a bad financial year. Administration approached the HM director, an exceptional, gregarious clinician who was named to the position years ago to help the program gain acceptance. The director agreed to indefinitely postpone two much-needed hirings, deciding it was better to share in the sacrifice than protest the cuts to the program’s budget. Hospitalists have since been working more shifts without a pay increase, and burnout symptoms have emerged with no signs of a thaw in the hiring freeze.
Expert advice: Buser says the “weak advocate” is a common issue among hospitalist groups, many of which he says are “going to hell” when he gets a rescue call. When a hospital is facing financial hardship, it is imperative that the HM director stand up for the program by explaining in detail the ramifications of each level of budget cuts. That’s because administrators might not realize the long-term damage that would result from such actions, he says. Being a strong, savvy advocate is even more important now since the financial future of many hospitals is ominous.
“With all of our hospitalist clients, we ask the CFO what is happening in the future…and the numbers are phenomenal,” says Buser. “They are seeing reductions of $10 million to $30 million off their bottom line.”
Administrators’ knee-jerk reaction is to cut costs. But there is another option: Grow the hospital out of its financial difficulties. It is up to the HM director to show administrators how the HM group has strategically gained them market share and how it will continue to do so. Good directors are in near constant contact with administrators, demonstrating the value their hospitalist program brings to the hospital, Buser says.
“You’re having regular meetings with the administrator, you’re producing the dashboard on a regular basis, you’re giving him trends that are going on,” he explains. “Show that you understand the hospital’s issues. Certain things you want to compromise on, but other things you have to say, ‘If we do that, the ramifications are such that it’s just not going to work.’”
Scenario No. 2 : Recruiting Roulette
—David Friar, MD, SFHM, CEO, Hospitalists of Northern Michigan, Traverse City
The case: The HM director felt pressure to hire. The program’s hospitalists were seeing two to three patients a day more than they should have been, and hospital administrators were worried the program was losing ground to the other hospitalist group in the community. Using an outside recruiter, the director hired two adept physicians with stellar CVs after an expedited review process that included a background check, a few phone interviews, and day of in-person interviews with some administrators and a hospitalist on the team. Now, nearly a year later, one of the physicians is about to leave because her family doesn’t like the community, and the other new hire’s abrasive personality has caused considerable damage to the team’s cohesion.
Expert advice: A big part of an HM program’s value is how it practices as a unified team, and directors need to recognize how vital the “team fit” is to hospitalists, says David Friar, MD, SFHM, CEO of Hospitalists of Northern Michigan in Traverse City.
“A bad team fit is often worse than being short-staffed because it can literally destroy the team spirit,” he says.
Directors should have a standardized recruitment process that includes a comprehensive background screening where references are closely checked, a round of interviews by people outside the HM program (nurses and referring physicians), and substantial time spent with hospitalists in the program, says Bryce Gartland, MD, FHM, associate director of the hospital medicine division and medical director of care coordination at Emory Healthcare in Atlanta.
“We put [candidates] with one of our physicians to actually go around the hospital,” he says. “It’s amazing to me the number of things you can pick up by that broader exposure that you may not pick up sitting in a room with a candidate across the table for an hour.”
If a recruitment service is used, the director must describe the HM program in detail to the recruiter and even have them meet hospitalists on the staff, Dr. Friar says.
“Sending them a memo saying ‘We need three new hospitalists ASAP’ isn’t helping them find you the perfect candidate,” he says. “Even the best recruiter can only do a great job for you if they really know your team and what it is you need in a candidate.”
A director also is well served to make recruiting a family event where spouses and even children are part of the interview process.
“By including the entire family and then supporting them after the move, we are much more likely to recruit providers that will stay good members of our team for years to come,” Dr. Friar says.
Scenario No. 3 : Amitte Diem
—John Bulger, DO, FACP, FHM, chief quality officer, director, hospital medicine service line, Geisinger Health System, Danville, Pa.
The case: For months, the medical center has been receiving an increased number of referrals from outlying hospitals, and no end is in sight. The extra patient load, much of it involving complex cases, has agitated the medical center’s staff, particularly the specialists, and they’ve begun to complain to hospital administrators. Seeking an ally, the specialists reach out to the HM director to present their case. Without doing independent analysis, the HM director sides with the specialists. Hospital administrators, facing growing resistance, work to decrease the referrals and are successful.
Expert advice: Consider working in the opposite direction, one that might turn a referral challenge into a profitable opportunity, Buser says. One of his firm’s clients, after thorough research, established a transfer center and set up an activation fee for the specialists who took the referrals. Hospitalists admitted about 90% of the cases, called consults, and named specialists so they received full fee-for-service at Medicare rates if they saw uninsured patients.
“That hospital is now making about $78 million a year, and the medical staff is saying, ‘How can we grow this?’” Buser says. “Here’s an example of how the hospital medicine director was key to turning the bad into something good.”
Because physicians tend to be reticent to change, it’s critical for hospitalist directors who want to seize an opportunity to thoroughly plan out how the change will occur and to prepare for potential obstacles along the way, says John Bulger, DO, FACP, FHM, chief quality officer and director of the hospital medicine service line for Geisinger Health System in Danville, Pa.
“You really need to be prepared with your rationale of why you’re doing it, if there’s data behind why you’re doing it, what the data is that’s driving it, and really what you hope to do with that change,” he says. “If you don’t get buy in from your staff, the change is doomed to fail from the beginning.”
Directors must embrace being a change agent if they want their HM programs to continue to be successful. In the minds of many hospital administrators, a program is only as good as its last achievement.
“It’s kind of like, ‘What have you done for me lately?’” Buser says. “You want to stay ahead of the curve and be alert to what’s going on and not be caught keeping your eyes off the ball and, as a result, not moving your program forward.”
Scenario No. 4 : Fumbling the Handoff
—Daniel Cusator, MD, MBA, vice president, Camden Group, El Segundo, Calif.
The case: The medical center’s monthly data for the past year has shown that hospitalists are taking care of their patients efficiently and getting them out of the hospital more quickly. However, mixed in with the positive numbers is a stubbornly high 30-day readmission rate. Indeed, some primary care groups and referring geriatricians have begun to grouse to the HM director about the discharge notes, complaining they aren’t as comprehensive as they would like.
Plus, the notes always arrive via office fax, which makes them more likely to get misplaced and harder to receive when doctors are out of the office.
Expert advice: Handoffs from discharge to pickup are where a lot of complications, errors, and safety issues arise, and poor handoffs are one of the largest drivers of readmission rates, especially in the elderly patient population, says Daniel Cusator, MD, MBA, vice president of the Camden Group, a healthcare consulting firm in El Segundo, Calif.
If the hospitalist director doesn’t provide the leadership and resources to help the HM team better coordinate with patients’ regular doctors, handoffs won’t be a priority throughout the group.
The HM director must recognize that the term “discharge note” is a misnomer.
What referring physicians really want is a care plan, which includes information about testing done in the hospital, testing that might be needed in the outpatient setting, medications the patient is on, complications the patient had in the hospital, potential problems to monitor, and any necessary follow-up, says Dr. Cusator, formerly the chief medical officer of clinical integration at Providence Health & Services in Southern California.
PCPs also want the care plan transmitted in their preferred method, whether that is text messaging, HIPAA-compliant email messaging, secure messaging, or fax.
“What I’ve seen some hospitalist groups do is create a menu capability for each of the physicians to choose their preferred method of notification of discharge of their patient,” Dr. Cusator says. Results suggest such a menu leads to improved physician satisfaction and reduced patient complications after discharge, he adds.
With today’s technological innovations, HM directors are unlimited in their ability to improve handoffs between their team and patients’ PCPs and specialists, Dr. Cusator says. Some HM directors, for example, are leading efforts to link electronic medical records systems to hospital-based health information exchange hubs that are accessible to physicians in the community.
“Notes and clinical information are submitted to this health information exchange and made available to any of the physicians who are caring for the patient almost immediately upon dictation and notation,” he says.
Scenario No. 5 : Protect Your Assets
—David Lee, MD, MBA, FACP, FHM, vice chairman, Hospital Medicine Department, Ochsner Health System, New Orleans.
The case: A physician isn’t sure she wants a career in hospital medicine. She finds the specialty rewarding but is looking for a different challenge, something beyond exclusively seeing patients. The HM director notices the physician has an aptitude for finding ways to do tasks more efficiently.
The director privately thinks the physician would be a good fit for a quality improvement project that’s about to start but doesn’t pursue it. The HM team just added a primary care group, and its patient census is quickly rising, requiring the hospitalists to devote their entire shifts to patient care. Within the year, the physician leaves the team for a fellowship program outside hospital medicine.
Expert advice: There are three communities in hospital medicine, Dr. Bulger says: people who want to be hospitalists, people who are passing through on their way to something else, and people who sit somewhere in the middle.
HM directors, he says, should do everything they can to develop not only the career hospitalists but also those on the fence.
“A lot of them you can turn into people who are going to be hospitalists if they are doing something that is rewarding for them,” Dr. Bulger says. “Many times rewarding for them is being involved more in the leadership of the group, being involved in quality improvement projects, really seeing how they can impact the care for populations of patients—and not just the patient who happens to be sitting in front of them.”
It’s incumbent on HM group leaders to link hospitalists with mentors and help them find a niche, Dr. Lee says. It keeps people interested and makes them feel part of a group.
“They need to feel they belong,” he says. “There has to be a cohesiveness in order for your department to excel. You have to protect your assets in the group, which is your physicians.”
Sending hospitalists to professional development training, such as SHM’s Leadership Academy (see “Leadership Academy Adds ‘Women in HM Issues’ to Schedule,” p. 9) or QI-focused webinars offered by SHM or the Institute of Healthcare Improvement, and following up with day-to-day coaching is a solid physician-development strategy, Dr. Gartland says. By virtue of their job, hospitalists are expected to lead and manage people in interactions with the ED, primary care, non-physician providers, nursing staff, and beyond, he says.
Directors also have to stop assuming that competent physicians are competent managers. “A lot of physicians don’t have those core skill sets, and we’ve got to pay conscious attention toward spending time dedicated to developing those,” Dr. Gartland says.
If directors don’t make professional development a priority or provide hospitalists with the flexibility to do non-clinical activities, retention may become an issue, Dr. Bulger says. “They could leave and go somewhere else,” he says, yet perhaps the more significant danger is losing hospitalists to programs and specialties outside hospital medicine.
Lisa Ryan is a freelance writer based in New Jersey.
THE FUNDAMENTALS
As hospitals position themselves for healthcare reform, they increasingly will turn to HM for strategies on how to provide high-quality patient care at a lower cost, Buser says. To meet hospitals’ needs and enhance the value of their programs, hospitalist directors should consider adopting these strategies recommended by HM leaders:
- Align compensation with the HM program’s goals. For example, if quality improvement is the priority, directors should financially reward hospitalists on quality performance, Dr. Lee says.
- Boost support staff and functions. For example, directors should ensure their team has access to the hospital’s case managers, who can handle discharge logistics so the hospitalist can focus on clinical issues, Dr. Cusator says.
- Control program growth. To borrow a popular line from the movie Field of Dreams: “If you build it, they will come.” Directors should be deliberate with group expansion and ensure enough staff is in place before adding to their referral base or adding a new service line, Dr. Bulger says. This reduces hospitalist burnout and preserves the group’s quality of patient care.
- Define two to three targets for success in the upcoming year and concentrate on accomplishing them. Start by consolidating what your team is working on, says Steven Deitelzweig, MD, SFHM, chairman of the Department of Hospital Medicine at Ochsner Health System in New Orleans. Pick too many things to master, and you end up excelling in none, he adds.
- Evaluate performance beyond a scorecard. Using constructive criticism grounded with examples, HM directors should provide feedback about what a physician is doing well and what can be done better so they can improve, Dr. Gartland says.
- Foster creative problem solving by including hospitalists in decisions. Directors should encourage the expression of different opinions and ideas, which helps the program avoid “group think” and allows innovation to occur, Dr. Lee says.
- Galvanize the new generation. To retain young physicians and make them feel part of the program, directors should learn how they communicate, how they work, and how they view work, Dr. Lee says.
- Help your hospital accurately measure reimbursement and mortality rates. Directors should make coding a priority and provide hospitalists with the tools they need to capture correct ICD-9 and CPT codes for their patients, Dr. Cusator says.
- Identify missing core capabilities and dedicate resources for it. For example, if HM programs have a high census of chronically ill and end-of-life patients, directors should assist the hospital in establishing a palliative care or hospice program, Dr. Cusator says.
Some of the best companies in America started in a garage or a basement with an individual who had a great idea and the ability to grow it into a progressively larger business.
“It takes a leader with different capabilities to take a company to the next level,” says Martin Buser, MPH, FACHE, a partner with Hospitalist Management Resources LLC in San Diego, which has helped more than 350 HM programs nationwide in the past 15 years. “It’s an attitude of never stop learning, an ability to look at issues from 30,000 feet instead of ground zero so you can see the whole picture.”
Similarly, the most important predictor of an HM program’s success is its director, Buser says. If directors know how to communicate, innovate, facilitate, problem-solve, and inspire, they are much more likely to run a high-performing hospitalist program, says David Lee, MD, MBA, FACP, FHM, vice chairman of the Hospital Medicine Department at Ochsner Health System in New Orleans.
If group directors lack the skills and fail to adapt to change, the program’s outlook is far from certain. “We unfortunately get involved with these programs,” Buser says. “It’s painful to see.” Bad behavior is nothing new to the hospital setting, and HM is not immune to poor management. The following are common examples of bad behaviors and how groups can avoid the mishaps.
Scenario No. 1 : Great Clinician, Nice Person, Weak Advocate
—Martin Buser, MPH, FACHE, partner, Hospitalist Management Resources LLC, San Diego
The case: Earlier this year, medical center administrators asked the hospitalist program to do more with less, explaining the hospital was having a bad financial year. Administration approached the HM director, an exceptional, gregarious clinician who was named to the position years ago to help the program gain acceptance. The director agreed to indefinitely postpone two much-needed hirings, deciding it was better to share in the sacrifice than protest the cuts to the program’s budget. Hospitalists have since been working more shifts without a pay increase, and burnout symptoms have emerged with no signs of a thaw in the hiring freeze.
Expert advice: Buser says the “weak advocate” is a common issue among hospitalist groups, many of which he says are “going to hell” when he gets a rescue call. When a hospital is facing financial hardship, it is imperative that the HM director stand up for the program by explaining in detail the ramifications of each level of budget cuts. That’s because administrators might not realize the long-term damage that would result from such actions, he says. Being a strong, savvy advocate is even more important now since the financial future of many hospitals is ominous.
“With all of our hospitalist clients, we ask the CFO what is happening in the future…and the numbers are phenomenal,” says Buser. “They are seeing reductions of $10 million to $30 million off their bottom line.”
Administrators’ knee-jerk reaction is to cut costs. But there is another option: Grow the hospital out of its financial difficulties. It is up to the HM director to show administrators how the HM group has strategically gained them market share and how it will continue to do so. Good directors are in near constant contact with administrators, demonstrating the value their hospitalist program brings to the hospital, Buser says.
“You’re having regular meetings with the administrator, you’re producing the dashboard on a regular basis, you’re giving him trends that are going on,” he explains. “Show that you understand the hospital’s issues. Certain things you want to compromise on, but other things you have to say, ‘If we do that, the ramifications are such that it’s just not going to work.’”
Scenario No. 2 : Recruiting Roulette
—David Friar, MD, SFHM, CEO, Hospitalists of Northern Michigan, Traverse City
The case: The HM director felt pressure to hire. The program’s hospitalists were seeing two to three patients a day more than they should have been, and hospital administrators were worried the program was losing ground to the other hospitalist group in the community. Using an outside recruiter, the director hired two adept physicians with stellar CVs after an expedited review process that included a background check, a few phone interviews, and day of in-person interviews with some administrators and a hospitalist on the team. Now, nearly a year later, one of the physicians is about to leave because her family doesn’t like the community, and the other new hire’s abrasive personality has caused considerable damage to the team’s cohesion.
Expert advice: A big part of an HM program’s value is how it practices as a unified team, and directors need to recognize how vital the “team fit” is to hospitalists, says David Friar, MD, SFHM, CEO of Hospitalists of Northern Michigan in Traverse City.
“A bad team fit is often worse than being short-staffed because it can literally destroy the team spirit,” he says.
Directors should have a standardized recruitment process that includes a comprehensive background screening where references are closely checked, a round of interviews by people outside the HM program (nurses and referring physicians), and substantial time spent with hospitalists in the program, says Bryce Gartland, MD, FHM, associate director of the hospital medicine division and medical director of care coordination at Emory Healthcare in Atlanta.
“We put [candidates] with one of our physicians to actually go around the hospital,” he says. “It’s amazing to me the number of things you can pick up by that broader exposure that you may not pick up sitting in a room with a candidate across the table for an hour.”
If a recruitment service is used, the director must describe the HM program in detail to the recruiter and even have them meet hospitalists on the staff, Dr. Friar says.
“Sending them a memo saying ‘We need three new hospitalists ASAP’ isn’t helping them find you the perfect candidate,” he says. “Even the best recruiter can only do a great job for you if they really know your team and what it is you need in a candidate.”
A director also is well served to make recruiting a family event where spouses and even children are part of the interview process.
“By including the entire family and then supporting them after the move, we are much more likely to recruit providers that will stay good members of our team for years to come,” Dr. Friar says.
Scenario No. 3 : Amitte Diem
—John Bulger, DO, FACP, FHM, chief quality officer, director, hospital medicine service line, Geisinger Health System, Danville, Pa.
The case: For months, the medical center has been receiving an increased number of referrals from outlying hospitals, and no end is in sight. The extra patient load, much of it involving complex cases, has agitated the medical center’s staff, particularly the specialists, and they’ve begun to complain to hospital administrators. Seeking an ally, the specialists reach out to the HM director to present their case. Without doing independent analysis, the HM director sides with the specialists. Hospital administrators, facing growing resistance, work to decrease the referrals and are successful.
Expert advice: Consider working in the opposite direction, one that might turn a referral challenge into a profitable opportunity, Buser says. One of his firm’s clients, after thorough research, established a transfer center and set up an activation fee for the specialists who took the referrals. Hospitalists admitted about 90% of the cases, called consults, and named specialists so they received full fee-for-service at Medicare rates if they saw uninsured patients.
“That hospital is now making about $78 million a year, and the medical staff is saying, ‘How can we grow this?’” Buser says. “Here’s an example of how the hospital medicine director was key to turning the bad into something good.”
Because physicians tend to be reticent to change, it’s critical for hospitalist directors who want to seize an opportunity to thoroughly plan out how the change will occur and to prepare for potential obstacles along the way, says John Bulger, DO, FACP, FHM, chief quality officer and director of the hospital medicine service line for Geisinger Health System in Danville, Pa.
“You really need to be prepared with your rationale of why you’re doing it, if there’s data behind why you’re doing it, what the data is that’s driving it, and really what you hope to do with that change,” he says. “If you don’t get buy in from your staff, the change is doomed to fail from the beginning.”
Directors must embrace being a change agent if they want their HM programs to continue to be successful. In the minds of many hospital administrators, a program is only as good as its last achievement.
“It’s kind of like, ‘What have you done for me lately?’” Buser says. “You want to stay ahead of the curve and be alert to what’s going on and not be caught keeping your eyes off the ball and, as a result, not moving your program forward.”
Scenario No. 4 : Fumbling the Handoff
—Daniel Cusator, MD, MBA, vice president, Camden Group, El Segundo, Calif.
The case: The medical center’s monthly data for the past year has shown that hospitalists are taking care of their patients efficiently and getting them out of the hospital more quickly. However, mixed in with the positive numbers is a stubbornly high 30-day readmission rate. Indeed, some primary care groups and referring geriatricians have begun to grouse to the HM director about the discharge notes, complaining they aren’t as comprehensive as they would like.
Plus, the notes always arrive via office fax, which makes them more likely to get misplaced and harder to receive when doctors are out of the office.
Expert advice: Handoffs from discharge to pickup are where a lot of complications, errors, and safety issues arise, and poor handoffs are one of the largest drivers of readmission rates, especially in the elderly patient population, says Daniel Cusator, MD, MBA, vice president of the Camden Group, a healthcare consulting firm in El Segundo, Calif.
If the hospitalist director doesn’t provide the leadership and resources to help the HM team better coordinate with patients’ regular doctors, handoffs won’t be a priority throughout the group.
The HM director must recognize that the term “discharge note” is a misnomer.
What referring physicians really want is a care plan, which includes information about testing done in the hospital, testing that might be needed in the outpatient setting, medications the patient is on, complications the patient had in the hospital, potential problems to monitor, and any necessary follow-up, says Dr. Cusator, formerly the chief medical officer of clinical integration at Providence Health & Services in Southern California.
PCPs also want the care plan transmitted in their preferred method, whether that is text messaging, HIPAA-compliant email messaging, secure messaging, or fax.
“What I’ve seen some hospitalist groups do is create a menu capability for each of the physicians to choose their preferred method of notification of discharge of their patient,” Dr. Cusator says. Results suggest such a menu leads to improved physician satisfaction and reduced patient complications after discharge, he adds.
With today’s technological innovations, HM directors are unlimited in their ability to improve handoffs between their team and patients’ PCPs and specialists, Dr. Cusator says. Some HM directors, for example, are leading efforts to link electronic medical records systems to hospital-based health information exchange hubs that are accessible to physicians in the community.
“Notes and clinical information are submitted to this health information exchange and made available to any of the physicians who are caring for the patient almost immediately upon dictation and notation,” he says.
Scenario No. 5 : Protect Your Assets
—David Lee, MD, MBA, FACP, FHM, vice chairman, Hospital Medicine Department, Ochsner Health System, New Orleans.
The case: A physician isn’t sure she wants a career in hospital medicine. She finds the specialty rewarding but is looking for a different challenge, something beyond exclusively seeing patients. The HM director notices the physician has an aptitude for finding ways to do tasks more efficiently.
The director privately thinks the physician would be a good fit for a quality improvement project that’s about to start but doesn’t pursue it. The HM team just added a primary care group, and its patient census is quickly rising, requiring the hospitalists to devote their entire shifts to patient care. Within the year, the physician leaves the team for a fellowship program outside hospital medicine.
Expert advice: There are three communities in hospital medicine, Dr. Bulger says: people who want to be hospitalists, people who are passing through on their way to something else, and people who sit somewhere in the middle.
HM directors, he says, should do everything they can to develop not only the career hospitalists but also those on the fence.
“A lot of them you can turn into people who are going to be hospitalists if they are doing something that is rewarding for them,” Dr. Bulger says. “Many times rewarding for them is being involved more in the leadership of the group, being involved in quality improvement projects, really seeing how they can impact the care for populations of patients—and not just the patient who happens to be sitting in front of them.”
It’s incumbent on HM group leaders to link hospitalists with mentors and help them find a niche, Dr. Lee says. It keeps people interested and makes them feel part of a group.
“They need to feel they belong,” he says. “There has to be a cohesiveness in order for your department to excel. You have to protect your assets in the group, which is your physicians.”
Sending hospitalists to professional development training, such as SHM’s Leadership Academy (see “Leadership Academy Adds ‘Women in HM Issues’ to Schedule,” p. 9) or QI-focused webinars offered by SHM or the Institute of Healthcare Improvement, and following up with day-to-day coaching is a solid physician-development strategy, Dr. Gartland says. By virtue of their job, hospitalists are expected to lead and manage people in interactions with the ED, primary care, non-physician providers, nursing staff, and beyond, he says.
Directors also have to stop assuming that competent physicians are competent managers. “A lot of physicians don’t have those core skill sets, and we’ve got to pay conscious attention toward spending time dedicated to developing those,” Dr. Gartland says.
If directors don’t make professional development a priority or provide hospitalists with the flexibility to do non-clinical activities, retention may become an issue, Dr. Bulger says. “They could leave and go somewhere else,” he says, yet perhaps the more significant danger is losing hospitalists to programs and specialties outside hospital medicine.
Lisa Ryan is a freelance writer based in New Jersey.
THE FUNDAMENTALS
As hospitals position themselves for healthcare reform, they increasingly will turn to HM for strategies on how to provide high-quality patient care at a lower cost, Buser says. To meet hospitals’ needs and enhance the value of their programs, hospitalist directors should consider adopting these strategies recommended by HM leaders:
- Align compensation with the HM program’s goals. For example, if quality improvement is the priority, directors should financially reward hospitalists on quality performance, Dr. Lee says.
- Boost support staff and functions. For example, directors should ensure their team has access to the hospital’s case managers, who can handle discharge logistics so the hospitalist can focus on clinical issues, Dr. Cusator says.
- Control program growth. To borrow a popular line from the movie Field of Dreams: “If you build it, they will come.” Directors should be deliberate with group expansion and ensure enough staff is in place before adding to their referral base or adding a new service line, Dr. Bulger says. This reduces hospitalist burnout and preserves the group’s quality of patient care.
- Define two to three targets for success in the upcoming year and concentrate on accomplishing them. Start by consolidating what your team is working on, says Steven Deitelzweig, MD, SFHM, chairman of the Department of Hospital Medicine at Ochsner Health System in New Orleans. Pick too many things to master, and you end up excelling in none, he adds.
- Evaluate performance beyond a scorecard. Using constructive criticism grounded with examples, HM directors should provide feedback about what a physician is doing well and what can be done better so they can improve, Dr. Gartland says.
- Foster creative problem solving by including hospitalists in decisions. Directors should encourage the expression of different opinions and ideas, which helps the program avoid “group think” and allows innovation to occur, Dr. Lee says.
- Galvanize the new generation. To retain young physicians and make them feel part of the program, directors should learn how they communicate, how they work, and how they view work, Dr. Lee says.
- Help your hospital accurately measure reimbursement and mortality rates. Directors should make coding a priority and provide hospitalists with the tools they need to capture correct ICD-9 and CPT codes for their patients, Dr. Cusator says.
- Identify missing core capabilities and dedicate resources for it. For example, if HM programs have a high census of chronically ill and end-of-life patients, directors should assist the hospital in establishing a palliative care or hospice program, Dr. Cusator says.
Career Checkup
Hospitalists need only look at their inboxes to see the demand they command. Messages beckon from recruiters, professional acquaintances, even prospective employers, pitching job openings as the next big gig. The constant barrage of opportunities can leave hospitalists wondering if there really is something better out there, and if they’re getting the most out of their current jobs.
One way to answer these types of questions is to conduct a formal career assessment, which inventories what is working and what isn’t working in a career and examines how a career fits into a person’s overall life at that point in time, says Cezanne Allen, MD, a certified physician development coach based in Bainbridge Island, Wash.
“Any time a hospitalist finds themselves in a situation where they are dissatisfied or unhappy in their job, they’re not feeling that their current job is very rewarding, or maybe they have career goals they don’t feel they are achieving yet, that would be a good time to do a career assessment,” says Leslie Flores, MHA, a partner at Nelson Flores Hospital Medicine Consultants. “Sometimes you just have to step back and say, ‘What do I really want and is this going to get me there, and if not, what do I need to do about it?’”
—Thomas Frederickson, MD, MBA, FACP, FHM, medical director of hospital medicine service, Alegent Health, Omaha, Neb.
You’ve Got Personality
Career assessments are as unique as the person conducting them, but there are some elements that hospitalists should consider. A behavioral profile or personality test is extremely helpful for physicians in understanding what their natural “hard-wiring” is when it comes to learning, problem-solving, and communication, says Francine Gaillour, MD, FACPE, MBA, executive director of the Physician Coaching Institute in Bellevue, Wash., which links doctors and healthcare teams with certified career coaches.
A number of personality tests are available for physicians (see “What’s My Personality?,” at right), but a career expert can help interpret the results and best use the information. Along with behavioral style and personality traits, hospitalists should consider their strengths and weaknesses, skills, interests, and criteria for the right job, Flores says. This introspection falls within a career assessment’s self-awareness component, she explains.
Hospitalists can add a situation component, in which they examine their current job and what “can” and “can’t” be changed, or an options component, in which they evaluate staying in the same organization versus leaving, Flores says.
If a physician is dissatisfied with their job, they should seek out the source of their frustration, Dr. Allen says. For example, is it the quality of work, workload, types of patients, patient interaction, practice development, medical knowledge limitations, lack of enjoyment, staff support, reimbursement, or work environment?
“It’s asking myself where I see the problem and then following it up with, ‘What does that tell me about what I really want?’” Dr. Allen says.
A mentor, who can provide objective and critical insight, can help in the assessment process, says Thomas Frederickson, MD, MBA, FACP, FHM, medical director of hospital medicine service at Alegent Health in Omaha, Neb. “There are often mentors within your group who have developed skills and expertise, and have learned to do different things in their careers that you might find exciting,” he explains.
Hospitalists should consult at least one “blind-spot buddy”—be it a mentor, colleague, or some other person—who can pinpoint their weaknesses, Flores says. “It’s somebody who knows you in your work world, who is close enough to be able to observe how you’re functioning in your work world, who can give you good feedback, and who cares enough about you to give you honest feedback, even when it’s not something you want to hear,” she says.
SHM can be a resource for hospitalists to find ways and people to help them assess their careers, say Dr. Frederickson.
“The Society of Hospital Medicine and their annual meetings and chapter meetings are a great place to do networking and a good place to find out different ways and different people you can align yourself with to start looking at your career in an objective way and a critical way,” he says.
Career coaches can be a good option, particularly for hospitalists who are struggling with significant change. Coaches do more than assist with resumes and interview strategies, says Dr. Gaillour. They help people align their careers with their values, strengths, passions, and goals so that they reach their full potential as a professional and a person, she says.
Coaches also advise on how to strategically plan a career and help physicians build career resilience.
“By resilience, I mean that there is always going to be some relevance to what you’re doing and you’re going to be able to weather some of the [healthcare] changes,” Dr. Gaillour says. “With a lot of physician groups and hospitals coming together and the stress of new initiatives, mergers, integrations, electronic medical records, and accountable-care organizations, all of that has a direct impact on physicians.”
The Time Is Right
Recommendations vary on how often career assessments should be conducted. Flores suggests hospitalists conduct a career checkup every two to three years “to see if they’re still on track and if their interests and goals have changed.”
Two years ago, William Atchley Jr., MD, FACP, SFHM, assessed his career while chief of the division of hospital medicine for Sentara Healthcare, a nonprofit healthcare system based in Norfolk, Va. The assessment was illuminating, he says, because it helped him to crystallize his strengths and weaknesses and determine “what I wanted to be doing,” he says.
In July, Dr. Atchley joined Atlanta-based Eagle Hospital Physicians, a physician-led company that develops and manages hospitalist practices for client hospitals. He is now regional senior medical director and is overseeing clinical services and medical affairs in South Carolina, North Carolina, and Virginia.
The more often physicians examine their career, the better they become at understanding themselves and using that understanding to their advantage, Dr. Gaillour says, who advocates annual assessments. Others suggest a daily dose of assessment.
“Daily, a physician can create a ritual to just check in with themselves, have a space where they can ask themselves questions of what went well today, what do I want more of, if there are complaints that are arising,” Dr. Allen says. “It’s an important way of preventing ourselves from getting in a place where we are really dissatisfied.”
Lisa Ryan is a freelance writer based in New Jersey.
Hospitalists need only look at their inboxes to see the demand they command. Messages beckon from recruiters, professional acquaintances, even prospective employers, pitching job openings as the next big gig. The constant barrage of opportunities can leave hospitalists wondering if there really is something better out there, and if they’re getting the most out of their current jobs.
One way to answer these types of questions is to conduct a formal career assessment, which inventories what is working and what isn’t working in a career and examines how a career fits into a person’s overall life at that point in time, says Cezanne Allen, MD, a certified physician development coach based in Bainbridge Island, Wash.
“Any time a hospitalist finds themselves in a situation where they are dissatisfied or unhappy in their job, they’re not feeling that their current job is very rewarding, or maybe they have career goals they don’t feel they are achieving yet, that would be a good time to do a career assessment,” says Leslie Flores, MHA, a partner at Nelson Flores Hospital Medicine Consultants. “Sometimes you just have to step back and say, ‘What do I really want and is this going to get me there, and if not, what do I need to do about it?’”
—Thomas Frederickson, MD, MBA, FACP, FHM, medical director of hospital medicine service, Alegent Health, Omaha, Neb.
You’ve Got Personality
Career assessments are as unique as the person conducting them, but there are some elements that hospitalists should consider. A behavioral profile or personality test is extremely helpful for physicians in understanding what their natural “hard-wiring” is when it comes to learning, problem-solving, and communication, says Francine Gaillour, MD, FACPE, MBA, executive director of the Physician Coaching Institute in Bellevue, Wash., which links doctors and healthcare teams with certified career coaches.
A number of personality tests are available for physicians (see “What’s My Personality?,” at right), but a career expert can help interpret the results and best use the information. Along with behavioral style and personality traits, hospitalists should consider their strengths and weaknesses, skills, interests, and criteria for the right job, Flores says. This introspection falls within a career assessment’s self-awareness component, she explains.
Hospitalists can add a situation component, in which they examine their current job and what “can” and “can’t” be changed, or an options component, in which they evaluate staying in the same organization versus leaving, Flores says.
If a physician is dissatisfied with their job, they should seek out the source of their frustration, Dr. Allen says. For example, is it the quality of work, workload, types of patients, patient interaction, practice development, medical knowledge limitations, lack of enjoyment, staff support, reimbursement, or work environment?
“It’s asking myself where I see the problem and then following it up with, ‘What does that tell me about what I really want?’” Dr. Allen says.
A mentor, who can provide objective and critical insight, can help in the assessment process, says Thomas Frederickson, MD, MBA, FACP, FHM, medical director of hospital medicine service at Alegent Health in Omaha, Neb. “There are often mentors within your group who have developed skills and expertise, and have learned to do different things in their careers that you might find exciting,” he explains.
Hospitalists should consult at least one “blind-spot buddy”—be it a mentor, colleague, or some other person—who can pinpoint their weaknesses, Flores says. “It’s somebody who knows you in your work world, who is close enough to be able to observe how you’re functioning in your work world, who can give you good feedback, and who cares enough about you to give you honest feedback, even when it’s not something you want to hear,” she says.
SHM can be a resource for hospitalists to find ways and people to help them assess their careers, say Dr. Frederickson.
“The Society of Hospital Medicine and their annual meetings and chapter meetings are a great place to do networking and a good place to find out different ways and different people you can align yourself with to start looking at your career in an objective way and a critical way,” he says.
Career coaches can be a good option, particularly for hospitalists who are struggling with significant change. Coaches do more than assist with resumes and interview strategies, says Dr. Gaillour. They help people align their careers with their values, strengths, passions, and goals so that they reach their full potential as a professional and a person, she says.
Coaches also advise on how to strategically plan a career and help physicians build career resilience.
“By resilience, I mean that there is always going to be some relevance to what you’re doing and you’re going to be able to weather some of the [healthcare] changes,” Dr. Gaillour says. “With a lot of physician groups and hospitals coming together and the stress of new initiatives, mergers, integrations, electronic medical records, and accountable-care organizations, all of that has a direct impact on physicians.”
The Time Is Right
Recommendations vary on how often career assessments should be conducted. Flores suggests hospitalists conduct a career checkup every two to three years “to see if they’re still on track and if their interests and goals have changed.”
Two years ago, William Atchley Jr., MD, FACP, SFHM, assessed his career while chief of the division of hospital medicine for Sentara Healthcare, a nonprofit healthcare system based in Norfolk, Va. The assessment was illuminating, he says, because it helped him to crystallize his strengths and weaknesses and determine “what I wanted to be doing,” he says.
In July, Dr. Atchley joined Atlanta-based Eagle Hospital Physicians, a physician-led company that develops and manages hospitalist practices for client hospitals. He is now regional senior medical director and is overseeing clinical services and medical affairs in South Carolina, North Carolina, and Virginia.
The more often physicians examine their career, the better they become at understanding themselves and using that understanding to their advantage, Dr. Gaillour says, who advocates annual assessments. Others suggest a daily dose of assessment.
“Daily, a physician can create a ritual to just check in with themselves, have a space where they can ask themselves questions of what went well today, what do I want more of, if there are complaints that are arising,” Dr. Allen says. “It’s an important way of preventing ourselves from getting in a place where we are really dissatisfied.”
Lisa Ryan is a freelance writer based in New Jersey.
Hospitalists need only look at their inboxes to see the demand they command. Messages beckon from recruiters, professional acquaintances, even prospective employers, pitching job openings as the next big gig. The constant barrage of opportunities can leave hospitalists wondering if there really is something better out there, and if they’re getting the most out of their current jobs.
One way to answer these types of questions is to conduct a formal career assessment, which inventories what is working and what isn’t working in a career and examines how a career fits into a person’s overall life at that point in time, says Cezanne Allen, MD, a certified physician development coach based in Bainbridge Island, Wash.
“Any time a hospitalist finds themselves in a situation where they are dissatisfied or unhappy in their job, they’re not feeling that their current job is very rewarding, or maybe they have career goals they don’t feel they are achieving yet, that would be a good time to do a career assessment,” says Leslie Flores, MHA, a partner at Nelson Flores Hospital Medicine Consultants. “Sometimes you just have to step back and say, ‘What do I really want and is this going to get me there, and if not, what do I need to do about it?’”
—Thomas Frederickson, MD, MBA, FACP, FHM, medical director of hospital medicine service, Alegent Health, Omaha, Neb.
You’ve Got Personality
Career assessments are as unique as the person conducting them, but there are some elements that hospitalists should consider. A behavioral profile or personality test is extremely helpful for physicians in understanding what their natural “hard-wiring” is when it comes to learning, problem-solving, and communication, says Francine Gaillour, MD, FACPE, MBA, executive director of the Physician Coaching Institute in Bellevue, Wash., which links doctors and healthcare teams with certified career coaches.
A number of personality tests are available for physicians (see “What’s My Personality?,” at right), but a career expert can help interpret the results and best use the information. Along with behavioral style and personality traits, hospitalists should consider their strengths and weaknesses, skills, interests, and criteria for the right job, Flores says. This introspection falls within a career assessment’s self-awareness component, she explains.
Hospitalists can add a situation component, in which they examine their current job and what “can” and “can’t” be changed, or an options component, in which they evaluate staying in the same organization versus leaving, Flores says.
If a physician is dissatisfied with their job, they should seek out the source of their frustration, Dr. Allen says. For example, is it the quality of work, workload, types of patients, patient interaction, practice development, medical knowledge limitations, lack of enjoyment, staff support, reimbursement, or work environment?
“It’s asking myself where I see the problem and then following it up with, ‘What does that tell me about what I really want?’” Dr. Allen says.
A mentor, who can provide objective and critical insight, can help in the assessment process, says Thomas Frederickson, MD, MBA, FACP, FHM, medical director of hospital medicine service at Alegent Health in Omaha, Neb. “There are often mentors within your group who have developed skills and expertise, and have learned to do different things in their careers that you might find exciting,” he explains.
Hospitalists should consult at least one “blind-spot buddy”—be it a mentor, colleague, or some other person—who can pinpoint their weaknesses, Flores says. “It’s somebody who knows you in your work world, who is close enough to be able to observe how you’re functioning in your work world, who can give you good feedback, and who cares enough about you to give you honest feedback, even when it’s not something you want to hear,” she says.
SHM can be a resource for hospitalists to find ways and people to help them assess their careers, say Dr. Frederickson.
“The Society of Hospital Medicine and their annual meetings and chapter meetings are a great place to do networking and a good place to find out different ways and different people you can align yourself with to start looking at your career in an objective way and a critical way,” he says.
Career coaches can be a good option, particularly for hospitalists who are struggling with significant change. Coaches do more than assist with resumes and interview strategies, says Dr. Gaillour. They help people align their careers with their values, strengths, passions, and goals so that they reach their full potential as a professional and a person, she says.
Coaches also advise on how to strategically plan a career and help physicians build career resilience.
“By resilience, I mean that there is always going to be some relevance to what you’re doing and you’re going to be able to weather some of the [healthcare] changes,” Dr. Gaillour says. “With a lot of physician groups and hospitals coming together and the stress of new initiatives, mergers, integrations, electronic medical records, and accountable-care organizations, all of that has a direct impact on physicians.”
The Time Is Right
Recommendations vary on how often career assessments should be conducted. Flores suggests hospitalists conduct a career checkup every two to three years “to see if they’re still on track and if their interests and goals have changed.”
Two years ago, William Atchley Jr., MD, FACP, SFHM, assessed his career while chief of the division of hospital medicine for Sentara Healthcare, a nonprofit healthcare system based in Norfolk, Va. The assessment was illuminating, he says, because it helped him to crystallize his strengths and weaknesses and determine “what I wanted to be doing,” he says.
In July, Dr. Atchley joined Atlanta-based Eagle Hospital Physicians, a physician-led company that develops and manages hospitalist practices for client hospitals. He is now regional senior medical director and is overseeing clinical services and medical affairs in South Carolina, North Carolina, and Virginia.
The more often physicians examine their career, the better they become at understanding themselves and using that understanding to their advantage, Dr. Gaillour says, who advocates annual assessments. Others suggest a daily dose of assessment.
“Daily, a physician can create a ritual to just check in with themselves, have a space where they can ask themselves questions of what went well today, what do I want more of, if there are complaints that are arising,” Dr. Allen says. “It’s an important way of preventing ourselves from getting in a place where we are really dissatisfied.”
Lisa Ryan is a freelance writer based in New Jersey.
The Burden of Burnout
SHM’s Career Satisfaction Task Force is no longer active, but its mission—to help hospitalists and groups improve job and career satisfaction—continues with a small group of former members. Working behind the scenes, the group surveyed hospitalists across the nation and began analyzing the data, all with the goal of finding maximal approaches to preventing burnout among their peers and colleagues.
“It’s one thing to describe burnout as a problem, and it’s a second thing to say, ‘How do we minimize the risk of burnout for the individual and for the program?’ ” says Chad Whelan, MD, FHM, director of the division of hospital medicine at Loyola University Health System in Maywood, Ill.
Dr. Whelan is one of three people working on the Hospital Medicine Physician Worklife Survey project. The others are Keiki Hinami, MD, assistant professor in the division of hospital medicine at Northwestern Memorial Hospital in Chicago, and Tosha Wetterneck, MD, FACP, associate professor of medicine at the University of Wisconsin School of Medicine and Public Health in Madison.
They surveyed nearly 3,800 potential hospitalists, ultimately analyzing more than 800 responses, and Dr. Wetterneck presented results and analysis through two research abstracts at HM11. The first abstract was translated into a paper and published online in July by the Journal of General Internal Medicine.1
What they found was while 62.6% of respondents reported high satisfaction with their job and 69% with the HM specialty, there were certain satisfaction domains—such as organizational climate and personal time availability—that rated low. The authors suspect those low ratings could lead to burnout, but they also note the results provide a roadmap for HM groups looking to address the issue.
“Now we have a lot more needs and demands put upon us as a profession,” Dr. Wetterneck says. “We wanted to know what people were doing nowadays, what kind of work were they doing, and were they happy with it.”
One revealing result, she notes, is that some hospitalists are “not happy” with some of the reasons they initially chose a career in HM. For example, many physicians turn to HM because of the flexibility in scheduling and team approach to patient care and QI. Yet, survey results suggest hospitalists are unhappy with the amount of personal time they have and don’t feel like they are part of a team, she says.

—Tosha Wetterneck, MD, FACP, associate professor of medicine, University of Wisconsin School of Medicine and Public Health, Madison
Workload Worries
The JGIM article, which assessed hospitalists’ satisfaction with such aspects as workload, compensation, patient-care quality, organizational fairness, autonomy, availability of personal time, and work relationships, showed that while hospitalists rated care quality and relationships with staff and colleagues high, they ranked compensation, organizational climate, autonomy, and availability of personal time low.
“To have such low satisfaction scores with their climate and their organization is concerning,” Dr. Wetterneck says. “It’s very important for [hospitalists] to be able to feel like they’re part of a team, that they’re part of an organization, and that the work they do really matters within that organization.”
Dr. Wetterneck acknowledges schedule flexibility is a key factor in hospitalist career choice, and it worries her that a majority of hospitalists surveyed are unhappy with the amount of personal time they had.
“When I presented these findings at the meeting, I had a lot of people telling me that the field has grown so quickly and the demands on the hospitalist group have grown so much that they haven’t been able to keep pace with hiring hospitalists to meet the demands in the workplace,” she says. “So people have to work more than they thought they would in the beginning, and that’s impinging on their personal time. … The flexibility piece is lost.”
Most hospitalists asked to work more are resilient and adapt. But over time, Dr. Wetterneck says, they begin to lose the ability to balance the demands and rewards of the job, and burnout develops.
“The study that we’ve been conducting suggests that the rate of burnout among practicing hospitalists is about 30 percent, which is a significant proportion of us,” Dr. Hinami says. “[It appears] that the rate of burnout symptoms of practicing hospitalists has remained stable, or may have increased, since the last time the publication of a nationwide survey was done.”
The last time a large survey measuring satisfaction among hospitalists was published was in 2001.2 It found that about 13% of hospitalists were burned out and about 25% were at risk of burnout, says Winthrop Whitcomb, MD, MHM, medical director of healthcare quality at Baystate Medical Center in Springfield, Mass., and one of the authors of the 2001 study. Without question, burnout continues to be a major challenge for the entire field of HM, he says.
“Growth has always and will continue to fuel burnout,” says Dr. Whitcomb, cofounder and past president of SHM. “It’s a hard job, and as long as you’re growing, you’re not really getting your feet underneath you.”
The task force study found that hospitalists with burnout symptoms were much more likely to reduce work effort, leave their clinical situation, leave HM, and abandon direct patient care altogether than those without burnout symptoms.
Whereas the task force survey used a single-item question to ask hospitalists their level of burnout on a scale of 1 to 5, the 2001 study used a different scale and asked multiple questions to determine if respondents were burned out or at risk of burnout, Dr. Wetterneck explains.
“Even though it’s not a fair comparison, could it be that more hospitalists are burned out now than they were 10 years ago? I happen to think it probably is real … because of some of the satisfaction data we’re looking at,” she says.
Dr. Wetterneck’s group hasn’t analyzed if the reasons for burnout among hospitalists have changed over the years, but, anecdotally, Dr. Whelan has noticed a difference. Early hospitalists often burned out because they had to work day shifts and take night call. Today, far fewer hospitalists are always on. However, there are more hospitalists than ever before working in the hospital at off hours, which comes with different stressors, he says.
Greater Responsibility, Greater Dissatisfaction
As hospitalists’ roles expand, unpredictable interruptions are more frequent, says Sylvia McKean, MD, SFHM, FACP, a senior hospitalist at Brigham and Women’s Hospital in Boston, associate professor of medicine at Harvard Medical School, and former co-chair of the Career Satisfaction Task Force.
“For example, if you’re [scheduled] to admit patients to the hospital and you’re also on the rapid-response team and someone happens to need a rapid assessment, you can be interrupted,” she says. “If you’re a hospitalist taking care of someone who has had a subarachnoid hemorrhage and the neurosurgeon is going to come in the next morning but you’re uncertain about what to do or even to recognize a problem in that patient, those are the kinds of things that cause people to get anxious and feel more fatigued.”
As more subspecialists focus on consultations in the hospital, hospitalists are tending to see more specialty patients and, as a result, could feel overwhelmed, Dr. McKean says.
The new survey group is not yet in a position to be prescriptive about burnout, Dr. Hinami says. However, he and his colleagues hope to shed some light on possible solutions in the near future.
“What we understand about burnout is that it depends on both individual characteristics and characteristics of the work environment,” Dr. Hinami says. “We’re exploring the kind of ways in which job designs can be altered to help hospitalists—whatever their personal endowments are—to cope better with the stresses of the work.”
According to the research group, one thing is clear: Compensation is not a cure-all. One of the HM11 abstracts showed that satisfaction with compensation was correlated the least with both. “There’s only so much you can be paid more to do before it’s not enough anymore,” Dr. Wetterneck says. “There are some people who take money over a happy job, and that’s what they want to do for a couple of years. That’s not really going to grow our profession in the long run.”
Lisa Ryan is a freelance writer based in New Jersey.
Reference
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. July 2011 [epub ahead of print].
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.
SHM’s Career Satisfaction Task Force is no longer active, but its mission—to help hospitalists and groups improve job and career satisfaction—continues with a small group of former members. Working behind the scenes, the group surveyed hospitalists across the nation and began analyzing the data, all with the goal of finding maximal approaches to preventing burnout among their peers and colleagues.
“It’s one thing to describe burnout as a problem, and it’s a second thing to say, ‘How do we minimize the risk of burnout for the individual and for the program?’ ” says Chad Whelan, MD, FHM, director of the division of hospital medicine at Loyola University Health System in Maywood, Ill.
Dr. Whelan is one of three people working on the Hospital Medicine Physician Worklife Survey project. The others are Keiki Hinami, MD, assistant professor in the division of hospital medicine at Northwestern Memorial Hospital in Chicago, and Tosha Wetterneck, MD, FACP, associate professor of medicine at the University of Wisconsin School of Medicine and Public Health in Madison.
They surveyed nearly 3,800 potential hospitalists, ultimately analyzing more than 800 responses, and Dr. Wetterneck presented results and analysis through two research abstracts at HM11. The first abstract was translated into a paper and published online in July by the Journal of General Internal Medicine.1
What they found was while 62.6% of respondents reported high satisfaction with their job and 69% with the HM specialty, there were certain satisfaction domains—such as organizational climate and personal time availability—that rated low. The authors suspect those low ratings could lead to burnout, but they also note the results provide a roadmap for HM groups looking to address the issue.
“Now we have a lot more needs and demands put upon us as a profession,” Dr. Wetterneck says. “We wanted to know what people were doing nowadays, what kind of work were they doing, and were they happy with it.”
One revealing result, she notes, is that some hospitalists are “not happy” with some of the reasons they initially chose a career in HM. For example, many physicians turn to HM because of the flexibility in scheduling and team approach to patient care and QI. Yet, survey results suggest hospitalists are unhappy with the amount of personal time they have and don’t feel like they are part of a team, she says.
—Tosha Wetterneck, MD, FACP, associate professor of medicine, University of Wisconsin School of Medicine and Public Health, Madison
Workload Worries
The JGIM article, which assessed hospitalists’ satisfaction with such aspects as workload, compensation, patient-care quality, organizational fairness, autonomy, availability of personal time, and work relationships, showed that while hospitalists rated care quality and relationships with staff and colleagues high, they ranked compensation, organizational climate, autonomy, and availability of personal time low.
“To have such low satisfaction scores with their climate and their organization is concerning,” Dr. Wetterneck says. “It’s very important for [hospitalists] to be able to feel like they’re part of a team, that they’re part of an organization, and that the work they do really matters within that organization.”
Dr. Wetterneck acknowledges schedule flexibility is a key factor in hospitalist career choice, and it worries her that a majority of hospitalists surveyed are unhappy with the amount of personal time they had.
“When I presented these findings at the meeting, I had a lot of people telling me that the field has grown so quickly and the demands on the hospitalist group have grown so much that they haven’t been able to keep pace with hiring hospitalists to meet the demands in the workplace,” she says. “So people have to work more than they thought they would in the beginning, and that’s impinging on their personal time. … The flexibility piece is lost.”
Most hospitalists asked to work more are resilient and adapt. But over time, Dr. Wetterneck says, they begin to lose the ability to balance the demands and rewards of the job, and burnout develops.
“The study that we’ve been conducting suggests that the rate of burnout among practicing hospitalists is about 30 percent, which is a significant proportion of us,” Dr. Hinami says. “[It appears] that the rate of burnout symptoms of practicing hospitalists has remained stable, or may have increased, since the last time the publication of a nationwide survey was done.”
The last time a large survey measuring satisfaction among hospitalists was published was in 2001.2 It found that about 13% of hospitalists were burned out and about 25% were at risk of burnout, says Winthrop Whitcomb, MD, MHM, medical director of healthcare quality at Baystate Medical Center in Springfield, Mass., and one of the authors of the 2001 study. Without question, burnout continues to be a major challenge for the entire field of HM, he says.
“Growth has always and will continue to fuel burnout,” says Dr. Whitcomb, cofounder and past president of SHM. “It’s a hard job, and as long as you’re growing, you’re not really getting your feet underneath you.”
The task force study found that hospitalists with burnout symptoms were much more likely to reduce work effort, leave their clinical situation, leave HM, and abandon direct patient care altogether than those without burnout symptoms.
Whereas the task force survey used a single-item question to ask hospitalists their level of burnout on a scale of 1 to 5, the 2001 study used a different scale and asked multiple questions to determine if respondents were burned out or at risk of burnout, Dr. Wetterneck explains.
“Even though it’s not a fair comparison, could it be that more hospitalists are burned out now than they were 10 years ago? I happen to think it probably is real … because of some of the satisfaction data we’re looking at,” she says.
Dr. Wetterneck’s group hasn’t analyzed if the reasons for burnout among hospitalists have changed over the years, but, anecdotally, Dr. Whelan has noticed a difference. Early hospitalists often burned out because they had to work day shifts and take night call. Today, far fewer hospitalists are always on. However, there are more hospitalists than ever before working in the hospital at off hours, which comes with different stressors, he says.
Greater Responsibility, Greater Dissatisfaction
As hospitalists’ roles expand, unpredictable interruptions are more frequent, says Sylvia McKean, MD, SFHM, FACP, a senior hospitalist at Brigham and Women’s Hospital in Boston, associate professor of medicine at Harvard Medical School, and former co-chair of the Career Satisfaction Task Force.
“For example, if you’re [scheduled] to admit patients to the hospital and you’re also on the rapid-response team and someone happens to need a rapid assessment, you can be interrupted,” she says. “If you’re a hospitalist taking care of someone who has had a subarachnoid hemorrhage and the neurosurgeon is going to come in the next morning but you’re uncertain about what to do or even to recognize a problem in that patient, those are the kinds of things that cause people to get anxious and feel more fatigued.”
As more subspecialists focus on consultations in the hospital, hospitalists are tending to see more specialty patients and, as a result, could feel overwhelmed, Dr. McKean says.
The new survey group is not yet in a position to be prescriptive about burnout, Dr. Hinami says. However, he and his colleagues hope to shed some light on possible solutions in the near future.
“What we understand about burnout is that it depends on both individual characteristics and characteristics of the work environment,” Dr. Hinami says. “We’re exploring the kind of ways in which job designs can be altered to help hospitalists—whatever their personal endowments are—to cope better with the stresses of the work.”
According to the research group, one thing is clear: Compensation is not a cure-all. One of the HM11 abstracts showed that satisfaction with compensation was correlated the least with both. “There’s only so much you can be paid more to do before it’s not enough anymore,” Dr. Wetterneck says. “There are some people who take money over a happy job, and that’s what they want to do for a couple of years. That’s not really going to grow our profession in the long run.”
Lisa Ryan is a freelance writer based in New Jersey.
Reference
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. July 2011 [epub ahead of print].
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.
SHM’s Career Satisfaction Task Force is no longer active, but its mission—to help hospitalists and groups improve job and career satisfaction—continues with a small group of former members. Working behind the scenes, the group surveyed hospitalists across the nation and began analyzing the data, all with the goal of finding maximal approaches to preventing burnout among their peers and colleagues.
“It’s one thing to describe burnout as a problem, and it’s a second thing to say, ‘How do we minimize the risk of burnout for the individual and for the program?’ ” says Chad Whelan, MD, FHM, director of the division of hospital medicine at Loyola University Health System in Maywood, Ill.
Dr. Whelan is one of three people working on the Hospital Medicine Physician Worklife Survey project. The others are Keiki Hinami, MD, assistant professor in the division of hospital medicine at Northwestern Memorial Hospital in Chicago, and Tosha Wetterneck, MD, FACP, associate professor of medicine at the University of Wisconsin School of Medicine and Public Health in Madison.
They surveyed nearly 3,800 potential hospitalists, ultimately analyzing more than 800 responses, and Dr. Wetterneck presented results and analysis through two research abstracts at HM11. The first abstract was translated into a paper and published online in July by the Journal of General Internal Medicine.1
What they found was while 62.6% of respondents reported high satisfaction with their job and 69% with the HM specialty, there were certain satisfaction domains—such as organizational climate and personal time availability—that rated low. The authors suspect those low ratings could lead to burnout, but they also note the results provide a roadmap for HM groups looking to address the issue.
“Now we have a lot more needs and demands put upon us as a profession,” Dr. Wetterneck says. “We wanted to know what people were doing nowadays, what kind of work were they doing, and were they happy with it.”
One revealing result, she notes, is that some hospitalists are “not happy” with some of the reasons they initially chose a career in HM. For example, many physicians turn to HM because of the flexibility in scheduling and team approach to patient care and QI. Yet, survey results suggest hospitalists are unhappy with the amount of personal time they have and don’t feel like they are part of a team, she says.
—Tosha Wetterneck, MD, FACP, associate professor of medicine, University of Wisconsin School of Medicine and Public Health, Madison
Workload Worries
The JGIM article, which assessed hospitalists’ satisfaction with such aspects as workload, compensation, patient-care quality, organizational fairness, autonomy, availability of personal time, and work relationships, showed that while hospitalists rated care quality and relationships with staff and colleagues high, they ranked compensation, organizational climate, autonomy, and availability of personal time low.
“To have such low satisfaction scores with their climate and their organization is concerning,” Dr. Wetterneck says. “It’s very important for [hospitalists] to be able to feel like they’re part of a team, that they’re part of an organization, and that the work they do really matters within that organization.”
Dr. Wetterneck acknowledges schedule flexibility is a key factor in hospitalist career choice, and it worries her that a majority of hospitalists surveyed are unhappy with the amount of personal time they had.
“When I presented these findings at the meeting, I had a lot of people telling me that the field has grown so quickly and the demands on the hospitalist group have grown so much that they haven’t been able to keep pace with hiring hospitalists to meet the demands in the workplace,” she says. “So people have to work more than they thought they would in the beginning, and that’s impinging on their personal time. … The flexibility piece is lost.”
Most hospitalists asked to work more are resilient and adapt. But over time, Dr. Wetterneck says, they begin to lose the ability to balance the demands and rewards of the job, and burnout develops.
“The study that we’ve been conducting suggests that the rate of burnout among practicing hospitalists is about 30 percent, which is a significant proportion of us,” Dr. Hinami says. “[It appears] that the rate of burnout symptoms of practicing hospitalists has remained stable, or may have increased, since the last time the publication of a nationwide survey was done.”
The last time a large survey measuring satisfaction among hospitalists was published was in 2001.2 It found that about 13% of hospitalists were burned out and about 25% were at risk of burnout, says Winthrop Whitcomb, MD, MHM, medical director of healthcare quality at Baystate Medical Center in Springfield, Mass., and one of the authors of the 2001 study. Without question, burnout continues to be a major challenge for the entire field of HM, he says.
“Growth has always and will continue to fuel burnout,” says Dr. Whitcomb, cofounder and past president of SHM. “It’s a hard job, and as long as you’re growing, you’re not really getting your feet underneath you.”
The task force study found that hospitalists with burnout symptoms were much more likely to reduce work effort, leave their clinical situation, leave HM, and abandon direct patient care altogether than those without burnout symptoms.
Whereas the task force survey used a single-item question to ask hospitalists their level of burnout on a scale of 1 to 5, the 2001 study used a different scale and asked multiple questions to determine if respondents were burned out or at risk of burnout, Dr. Wetterneck explains.
“Even though it’s not a fair comparison, could it be that more hospitalists are burned out now than they were 10 years ago? I happen to think it probably is real … because of some of the satisfaction data we’re looking at,” she says.
Dr. Wetterneck’s group hasn’t analyzed if the reasons for burnout among hospitalists have changed over the years, but, anecdotally, Dr. Whelan has noticed a difference. Early hospitalists often burned out because they had to work day shifts and take night call. Today, far fewer hospitalists are always on. However, there are more hospitalists than ever before working in the hospital at off hours, which comes with different stressors, he says.
Greater Responsibility, Greater Dissatisfaction
As hospitalists’ roles expand, unpredictable interruptions are more frequent, says Sylvia McKean, MD, SFHM, FACP, a senior hospitalist at Brigham and Women’s Hospital in Boston, associate professor of medicine at Harvard Medical School, and former co-chair of the Career Satisfaction Task Force.
“For example, if you’re [scheduled] to admit patients to the hospital and you’re also on the rapid-response team and someone happens to need a rapid assessment, you can be interrupted,” she says. “If you’re a hospitalist taking care of someone who has had a subarachnoid hemorrhage and the neurosurgeon is going to come in the next morning but you’re uncertain about what to do or even to recognize a problem in that patient, those are the kinds of things that cause people to get anxious and feel more fatigued.”
As more subspecialists focus on consultations in the hospital, hospitalists are tending to see more specialty patients and, as a result, could feel overwhelmed, Dr. McKean says.
The new survey group is not yet in a position to be prescriptive about burnout, Dr. Hinami says. However, he and his colleagues hope to shed some light on possible solutions in the near future.
“What we understand about burnout is that it depends on both individual characteristics and characteristics of the work environment,” Dr. Hinami says. “We’re exploring the kind of ways in which job designs can be altered to help hospitalists—whatever their personal endowments are—to cope better with the stresses of the work.”
According to the research group, one thing is clear: Compensation is not a cure-all. One of the HM11 abstracts showed that satisfaction with compensation was correlated the least with both. “There’s only so much you can be paid more to do before it’s not enough anymore,” Dr. Wetterneck says. “There are some people who take money over a happy job, and that’s what they want to do for a couple of years. That’s not really going to grow our profession in the long run.”
Lisa Ryan is a freelance writer based in New Jersey.
Reference
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. July 2011 [epub ahead of print].
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.