User login
CASE Diagnosis precedes sentinel episode of bleeding
“G.A.” is a 39-year-old gravida 6, para 1041 who was diagnosed with complete placenta previa during a target ultrasound exam performed at 18 weeks for advanced maternal age. She had a sentinel episode of vaginal bleeding at 29 weeks and was hospitalized for close monitoring.
Management strategy
One course of steroid was given, vaginal bleeding subsided, and she was discharged for outpatient conservative management, including iron and folic acid supplementation.
The outcome
The patient progressed to 36 weeks’ gestation, when she underwent amniocentesis to assess fetal lung maturity. When the results were reassuring, a cesarean section was scheduled. Intraoperative blood loss was diminished using pelvic vessel embolization. Surgery was uncomplicated, and a healthy infant was delivered.
Placenta previa is a leading and potentially life-threatening cause of third-trimester bleeding.1 Although the overall incidence is about 0.4% in pregnancies exceeding 20 weeks’ gestation,2 that figure rises with the number of cesarean sections and may reach 10% among women who have undergone 4 or more cesarean deliveries.3 Since more women are requesting elective and repeat cesarean deliveries, we are increasingly likely to encounter this condition.
Fortunately, technological advances have improved maternal and neonatal outcomes after placenta previa:
Nevertheless, the condition necessitates cesarean delivery and can cause serious maternal and perinatal morbidity, including:
It can also occur in association with vasa previa, which, though rare, carries a very high perinatal mortality rate.5
Risk factors
An enlarged placenta or endometrial disruption or scarring in the upper uterine segment due to 1 or more of the factors listed below may increase the likelihood of abnormal placental implantation in the unscarred lower uterine segment:3,6,7
Previa often begins with painless vaginal bleeding
The condition often presents as painless, bright red, vaginal bleeding in the third trimester. It is usually distinguished from abruptio placenta by the absence of abdominal pain and uterine contractions.5 However, approximately 20% of women have uterine activity associated with the first episode of vaginal bleeding.13,14 Moreover, in some cases, painful contractions and labor may precipitate vaginal bleeding from placenta previa.5 Therefore, ultrasound examination is strongly recommended for all women with vaginal bleeding during pregnancy.
Ultrasound for other reasons uncovers many cases
With greater routine use of ultrasonography in obstetrics, a large percentage of women with placenta previa are diagnosed prior to the onset of the characteristic painless vaginal bleeding. In a 2003 study by Dola and colleagues,15 approximately 43% of placenta previa cases were diagnosed by ultrasonography performed for other obstetrical indications prior to the onset of vaginal bleeding.
Look for “warning hemorrhage”
The first episode of vaginal bleeding is rarely profuse or life-threatening to the mother or fetus. The bleeding usually subsides spontaneously, although it could recur and become more severe with subsequent episodes. Pregnancy typically continues after the initial bleeding episode.
The mean gestational age at the time of the first bleeding is 29 to 32 weeks.13,14 However, a third of cases have vaginal bleeding before the 30th week of gestation, a third between 30 and 36 weeks, and a third after 36 weeks’ gestation.13-15 Ten percent of women with the condition may be completely asymptomatic and progress to 38 weeks’ gestation without vaginal bleeding.13,14
Which form of ultrasound is most accurate?
With the advanced technology available today, ultrasound has become the standard means of diagnosing placenta previa.16,17
Transabdominal ultrasound has accuracy as high as 95% and a false-negative rate of 7% in the diagnosis of placenta previa.13,19 However, its accuracy may be adversely affected by maternal obesity, acoustic shadowing of the fetal head in a cephalic presentation, inability to locate the internal cervical os (which is critical for correct diagnosis), and difficulty imaging a posterior placenta and the lateral uterine walls. In addition, a full maternal bladder—usually helpful in transabdominal ultrasound imaging—may cause a false-positive diagnosis if the bladder is overly distended. In this situation, the cervix would appear artificially elongated and give a normally implanted placenta the appearance of encroachment into the internal cervical os.
Transvaginal ultrasound is superior for diagnosis of previa
Leerentveld et al20 reported false-positive and false-negative rates of 1% and 2%, respectively—a striking improvement over transabdominal ultrasound, which has rates of 2% to 6% and 7%, respectively.
Transvaginal sonography has several advantages over transabdominal imaging in localization of the placenta. The shorter distance from the vaginal probe transducer to the cervix and lower uterine segment allows the use of higher-frequency ultrasound waves, with improved resolution; therefore, the relationship between the placental edge and the internal os can be determined more accurately.
Some clinicians may worry that the probe used in transvaginal sonography will disrupt the placenta and provoke significant maternal hemorrhage, but this concern is unfounded. Multiple studies have attested to the safety of transvaginal sonography in localization of the placenta.5,20-22 The probe is introduced and positioned under direct ultrasound guidance at all times, and inadvertent insertion of the endovaginal probe into the internal cervical os is virtually impossible due to the anatomical relationship of the vagina and cervix.21
Transperineal ultrasound is another option. Several investigators have found it to be superior to transabdominal and similarly advantageous to transvaginal sonography in the diagnosis and exclusion of placenta previa.18
Start with transabdominal imaging
In current practice, transabdominal ultrasound is usually performed first to localize the placenta. If there is reason to suspect placenta previa, transvaginal or transperineal sonography is then used to confirm the location of the placenta.
Contractions may hinder imaging
Accurate diagnosis or exclusion of placenta previa may be difficult if uterine contractions are present during ultrasound evaluation. Myometrial contractions shorten the distance between the internal cervical os and the placental edge, altering measurement of this distance. In addition, the ultrasound appearance of a contraction may simulate placental tissue, making it difficult to exclude placenta previa.
The trouble with tradition
The 4 types of placenta previa in the traditional classification system—complete, partial, marginal, and low-lying—predate the era of ultrasound diagnosis and are based on digital palpation of the placenta through a partly dilated cervical os during labor.
A new system of 3 types
Along with other authors,5,15-18 we propose a new system with 3 categories—complete, incomplete, and low-lying—because ultrasound may not distinguish a placenta partially covering the internal os (a discrete point) from one that is merely encroaching on it.
Complete previa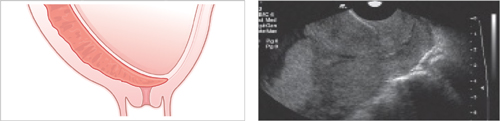
The placenta completely covers the internal cervical os
Incomplete previa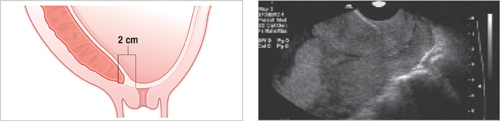
The placental edge is within 2 cm of the internal cervical os, but does not cover the os
Low-lying previa
The distance from the internal cervical os to the placental edge is between 2 and 3.5 cm
Look for placenta accreta
When placenta previa is diagnosed by ultrasound examination, further diagnostic measures are needed to determine whether placenta accreta is present.5,23 In placenta accreta, neither the normal plane of separation between the placental villi and uterine wall, nor the intervening fibrinoid layer of Nitabuch, is present.5,23
Degrees of abnormal placental implantation
Risk of accreta can reach 67%
There are varying reports on the incidence of placenta accreta, but women with placenta previa and previous cesarean deliveries appear to have the highest incidence.3,23,24 In women with placenta previa and 1 previous cesarean section, the risk of placenta accreta has been estimated at 24%, but it increases to 67% for women with placenta previa and 4 previous cesarean sections.3
Sonographic appearance of placenta accreta
Certain characteristics are suggestive of placenta accreta25,26:
Unfortunately, diagnosis of placenta accreta is difficult prior to delivery, although transvaginal sonography and adjunctive color flow/power Doppler imaging with 2- and 3-dimensional techniques offer improved resolution and have yielded promising results in prenatal diagnosis.27-30
Magnetic resonance imaging (MRI) may also prove useful in detecting placental tissue invasion and evaluating the degree of invasion, especially in a posterior or lateral placenta previa or when there is invasion into the bladder.31-33
Gestational age, symptoms determine management
The management of women with placenta previa in the third trimester depends on the extent of maternal hemorrhage and the fetal gestational age. Clinical categories include:
Some asymptomatic cases resolve
Outpatient management is possible for women who have never bled after diagnosis in the second trimester. These women should abstain from intercourse, avoid digital examination after 20 weeks’ gestation, and immediately present to the hospital if there is any evidence of vaginal bleeding.34
Monthly ultrasound evaluations are necessary to determine whether placenta previa has resolved,34-37 since 90% of cases detected in the second trimester resolve by the third trimester.34 However, if placenta previa persists beyond 24 weeks’ gestation, there is a 50% risk that delivery will be complicated by it.35 If placenta previa persists after 32 weeks, that risk approaches 75%.35
2-fold risk of congenital malformations
Most investigators report a 2-fold increased risk of fetal congenital malformations in cases of placenta previa.5 These malformations include anomalies of the central nervous system, cardiovascular system, respiratory tract, and gastrointestinal tract. Therefore, a target ultrasound examination for fetal anatomy is recommended at the initial ultrasound diagnosis of placenta previa.
Risk of fetal growth restriction warrants heightened surveillance
Some controversy surrounds the incidence of fetal growth restriction in pregnancies complicated by placenta previa. Varma38 reported that fetal growth restriction occurs in 16% of women with placenta previa and is correlated with the number of antepartum bleeding episodes. Other investigators have reported normal fetal growth in women with placenta previa.39 Given this uncertainty, serial follow-up ultrasound evaluations are usually advised for fetal growth assessment.
When patient remains asymptomatic, perform amniocentesis at 36 weeks
Some women progress to the late third trimester without any vaginal bleeding. In these women, amniocentesis is recommended at approximately 36 weeks’ gestation to assess fetal lung maturity.34,40 Elective cesarean delivery can then be planned if pulmonary maturity is documented.
The benefits of elective delivery include a stable patient and an optimally prepared surgical team, as well as the avoidance of emergent surgery, which increases the risk for maternal complications. Emergent surgery also places the fetus at greater risk for anemia, compared with elective procedures(27.7% vs 2.9%, respectively).13
Vaginal bleeding requires inpatient evaluation
Any woman with placenta previa who presents with vaginal bleeding should be admitted to the labor and delivery unit for immediate evaluation of maternal and fetal status, including an estimation of gestational age.
Initial acute care and assessment necessitate34:
If hemorrhage is life-threatening, deliver immediately
During initial evaluation, if the hemorrhage is judged to be massive and life-threatening, resuscitative measures and immediate delivery are necessary to avoid serious maternal morbidity. Recommended measures include constant monitoring of maternal status, aggressive IV fluid resuscitation, transfusion of blood and blood products, assessment of fetal status, and immediate delivery without regard to the maturity of the fetus.
A woman at term or near term (with documented fetal lung maturity) who presents with mild or moderate vaginal bleeding should be delivered via cesarean section.
Conservative management may be appropriate for mild preterm bleeding
If vaginal bleeding is not threatening to the life of the mother, and the fetus is preterm, a conservative approach with aggressive expectant management is appropriate, since most first episodes of vaginal bleeding are self-limited and rarely life-threatening to mother or fetus. Expectant management allows fetal maturation in utero without jeopardizing maternal health. If maternal and fetal health remain stable, the expectant approach allows a safe delay of delivery until the fetus matures.
Hospitalization is recommended. Candidates for expectant management should be hospitalized after the initial episode of vaginal bleeding. Once maternal and fetal conditions stabilize, the woman should be transferred to the antepartum ward for hospital bed rest with bathroom privileges. For expectant management:
Delivery is warranted for life-threatening hemorrhage, fetal lung maturity, and/or the usual maternal and fetal indications.
The question of tocolysis
Third-trimester tocolytic therapy in a woman with vaginal bleeding is controversial. In placenta previa, vaginal bleeding appears to arise from disruption of the placental implantation site as the lower uterine segment develops.41,42 It is unclear whether uterine contractions play a role, as only 20% of women with placenta previa have uterine activity at the time of vaginal bleeding.13,14,42 It is difficult to determine whether these women have true preterm labor, because digital examination of the cervix to document cervical dilatation is impossible.
Does uterine activity precipitate bleeding?
Some investigators believe uterine activity is a predisposing factor for the vaginal bleeding associated with placenta previa, and would consider tocolytic therapy in a stable patient at a premature gestational age. However, further evidence of its safety is needed.
In particular, beta-mimetics should be avoided in hemorrhaging women because their vasodilatory effects can precipitate maternal hypotension. Another side effect of beta-mimetics: maternal tachycardia,43 which may mask the hypovolemic state in women with significant hemorrhage.
Magnesium sulfate has less effect on the maternal cardiovascular system and could be a better choice in symptomatic placenta previa.41 Also consider indomethacin, which appears to have fewer adverse maternal effects.
Inpatient vs outpatient management
Because 2 to 3 weeks of maternal hospitalization can pass between the initial warning hemorrhage and delivery of the fetus, outpatient care has become an option. Several retrospective studies have demonstrated the cost-effectiveness and safety of outpatient management of symptomatic placenta previa.44,45 These studies emphasized careful patient section.
Wing and associates46 conducted a prospective, randomized, controlled trial that reinforces the need for judicious use of outpatient management. In their study, fewer than half the patients diagnosed with placenta previa prior to 37 weeks were candidates. The authors point out the small number of patients in their study, and the fact that vaginal bleeding recurred in approximately 60% of patients. Because of the difficulty of predicting which patients will have recurrent bleeding and when, outpatient management should be reserved for those judged to be compliant with home bed rest who can rapidly return to the hospital, if necessary.
Women with recurrent vaginal bleeding during outpatient management should be rehospitalized.
In the event of massive hemorrhage, immediate compression of the aorta below the level of the renal arteries will reduce the bleeding enough to allow time to evaluate the situation.56 At the same time, aggressive IV fluid resuscitation and blood transfusion should begin. Reevaluate coagulation status after every 5 to 10 U of blood.57
Focused repair may be effective. In some situations, the hemorrhage may be controlled by oversewing and repairing the focal placental site defects.40
Bracketing the bleeding area. Another measure is a circular suture technique in which interrupted sutures are placed on the serosal surface of the anterior and posterior aspects of the uterus and as deeply as possible into the endometrium in a circumferential manner, bracketing the bleeding area.58
The argon beam coagulator can be used to achieve hemostasis; it is more effective than traditional bipolar cautery at ensuring hemostasis in extensive areas.56,57
Stepwise devascularization was effective in 100% of 103 women with postpartum hemorrhage who did not respond to traditional management.59 It involves 5 procedures to be performed in sequence until hemostasis is achieved: unilateral uterine vessel ligation, bilateral uterine vessel ligation, low uterine vessel ligation, unilateral ovarian vessel ligation, and bilateral ovarian vessel ligation.
Hypogastric artery ligation is another option, but it is technically challenging and successful in less than 50% of cases.57 In fact, the time spent on this technique may actually lead to increased blood loss.
Components of safe delivery
A detailed plan is necessary when major hemorrhage is anticipated at the time of elective cesarean delivery for placenta previa, including consultation with experts in different disciplines such as radiology, anesthesiology, urology, pathology, blood bank, neonatology, and gynecologic oncology.
Also pay attention to the maternal red blood cell reserve. Iron and folic acid should be administered to prevent and treat anemia, and antepartum erythropoietin should be considered as a way of increasing the hemoglobin level in women with placenta previa. Autologous blood transfusion, including acute normovolemic hemodilution, is another option.
Pelvic vessel embolization
Elective embolization or occlusion of the hypogastric or uterine arteries has proved to be safe and effective for postpartum hemorrhage, with a success rate of more than 90% in women with normal coagulation.47
In addition, elective catheterization with a balloon-tipped catheter can be used prophylactically to reduce blood flow to the placenta. Prophylactic catheterization of the anterior division of the internal iliac arteries can be performed right before the scheduled cesarean section. An axillary approach is technically easier for fluoroscopically guided catheterization of the internal iliac.48 The actual fluoroscopy time is minutes, so the risk of fetal exposure to radiation and irreversible ovarian damage is minimal.
The fetus is monitored during the procedure, and the balloons are left in the deflated state until after delivery, reducing the risk of uteroplacental insufficiency. Balloon inflation after delivery occludes the hypogastric arteries and diminishes uterine arterial blood flow during surgery. In some cases, the temporary occlusive effect of the balloons may control intraoperative bleeding completely. If substantial bleeding persists, subsequent embolization of the uterine arteries is advised, using absorbable Gelfoam particles, which are temporary and do not damage pelvic organs. Menstruation is not impaired, and normal pregnancies have been reported after this procedure.49,50
In women who undergo cesarean delivery under regional anesthesia, placement of a dry epidural catheter for later dosing of anesthetic agents should be considered prior to balloon catheterization, since the patient’s mobility is restricted after placement of the balloon-tipped catheter.
This therapy is especially useful when there is a high index of suspicion for placenta accreta.
Recommendations at the time of delivery
Hysterectomy for placenta previa, placenta accreta
This procedure is technically challenging when there is a markedly enlarged uterus with engorged collateral vessels. One useful method, delayed ligation technique, was originally described by Dyer et al on the Tulane obstetrics service at Charity Hospital of New Orleans.53 This technique facilitates quick control of all uterine vasculature with rapid hemostasis. Later modification of this method involves successive clamping and severing of all vascular pedicles supplying the uterus, prior to their suture ligation, for quick control of bleeding.
Close follow-up continues even after surgery
Immediately after surgery, close monitoring of hemodynamic status is required, ideally in a critical care setting. Because women with placenta previa/placenta accreta have often received massive transfusions of blood and blood products along with large volumes of crystalloid fluids, pulmonary edema may develop. Conversely, hypovolemia can result from inadequate replacement of blood or persistent intra-abdominal bleeding. Thus, close attention to urinary output allows early detection of pulmonary edema, acute respiratory distress syndrome, hypovolemia, or persistent intra-abdominal bleeding. Patients who undergo peripartum hysterectomy should also be monitored closely for possible ureteral injury.
Thromboprophylaxis should continue until the patient is ambulatory.
Recommended laboratory tests
Get a complete blood count with platelets and fibrinogen immediately after surgery and at frequent intervals as needed. A chemistry panel with calcium, albumin, electrolytes, and creatinine also is helpful.
Serious morbidity in 3% to 5% of women after emergent hysterectomy
Conditions such as acute respiratory distress syndrome from massive blood transfusion and pulmonary capillary leakage, acute tubular necrosis from renal failure, and pulmonary embolism may complicate 3% to 5% of cases.54
Reoperation for persistent intra-abdominal bleeding may be necessary, and 9% of women will have urologic injury. Unfortunately, the maternal mortality rate associated with this procedure is 0.8%, so meticulous postoperative care is mandated.55
The authors report no financial relationships with any company whose products are mentioned in this article.
1. Ananth CV, Savitz DA, Luther ER. Maternal cigarette smoking as a risk factor for placental abruption, placenta previa, and uterine bleeding in pregnancy. Am J Epidemiol. 1996;144:881-889.
2. Faiz AS, Ananth CV. Etiology and risk factors for placenta previa: an overview and meta-analysis of observational studies. J Matern Fetal Neonatal Med. 2003;13:175.-
3. Clark SL, Koonings PP, et al. Placenta previa/accreta and prior cesarean section. Obstet Gynecol. 1985;66:89-92.
4. Neri A, Manor Y, Matityahu A, Blieden L. Placenta previa and congenital cardiac anomalies. Fetal Ther. 1989;4:138-140.
5. Clark SL. Placenta previa and abruptio placenta. In: Creasy RK, Resnik R. Maternal-Fetal Medicine, Principles and Practice. 4th ed. Philadelphia: W.B. Saunders; 1999:616–631.
6. Miller DA, Chollet J, Goodwin TM. Clinical risks factors for placenta previa-placenta accreta. Am J Obstet Gynecol. 1997;177:210-214.
7. Ananth CV, Demissie K, Smulian JC, Vintzileos AM. Placenta previa in singleton and twin births in the United States, 1989 through 1998: a comparison of risk factor profiles and associated conditions. Am J Obstet Gynecol. 2003;188:275-281.
8. Gilbert WM, Nesbitt TS, Danielsen B. Childbearing beyond age 40: pregnancy outcome in 24,032 cases. Obstet Gynecol. 1999;93:9-14.
9. Lavery JP. Placenta previa. Clin Obstet Gynecol. 1990;33:414-421.
10. Taylor VM, Kramer MD, Vaughan TL, Peacock S. Placenta previa in relation to induced and spontaneous abortion: a population- based study. Obstet Gynecol. 1993;82:88-91.
11. Williams MA, Mittendorf R, Lieberman E, Monson RR, Schoenbaum SC, Genest DR. Cigarette smoking during pregnancy in relation to placenta previa. Am J Obstet Gynecol. 1991;165:28-32.
12. Handler AS, Mason ED, Rosenberg DL, Davis FG. The relationship between exposure during pregnancy to cigarette smoking and cocaine use and placenta previa. Am J Obstet Gynecol. 1994;170:884-889.
13. Cotton DB, Read JA, Paul RH, Quilligan EJ. The conservative aggressive management of placenta previa. Am J Obstet Gynecol. 1980;137:687-695.
14. Silver R, Depp R, Sabbagha RE, Dooley SL. Placenta previa: aggressive expectant management. Am J Obstet Gynecol. 1984;150:15-22.
15. Dola CP, Garite TJ, Dowling DD, Friend D, Ahdoot D, Asrat T. Placenta previa: does its type affect pregnancy outcome? Am J Perinatol. 2003;20:353-360.
16. Oppenheimer LW, Farine D, Ritchie JWK, Lewinsky RM, Telford J, Fairbanks LA. What is low-lying placenta? Am J Obstet Gynecol. 1991;165:1036-1038.
17. Bhide A, Thilaganathan B. Recent advances in the management of placenta previa. Curr Opin Obstet Gynecol. 2004;16:447-451.
18. Dawson WB, Dumas MD, Romano WM, Gagnon R, Gratton RJ, Mowbray RD. Translabial ultrasonography and placenta previa: does measurement of the os-placenta distance predict outcome? J Ultrasound Med. 1996;15:44-46.
19. Egley CC. Abruptio placentae and placenta previa. In: Winn HN, Hobbins JC. Clinical Maternal-Fetal Medicine.1st ed. Pearl River, NY: Parthenon Publishing; 2000:47–53.
20. Leerentveld RA, Gilberts E, Arnold M, Wladimiroff JW. Accuracy and safety of transvaginal sonographic placental localization. Obstet Gynecol. 1990;76:759-762.
21. Timor-Tritsch I, Yunis R. Confirming the safety of transvaginal sonography in patients suspected of placenta previa. Obstet Gynecol. 1993;81:742-744.
22. Tan NH, Abu M, Woo JLS, Tahir H. The role of transvaginal sonography in the diagnosis of placenta previa. Aust NZ J Obstet Gynaecol. 1995;35:42-45.
23. Miller DA, Cholleet JA, Goodwin TM. Clinical risk factors for placenta previa-placenta accreta. Am J Obstet Gynecol. 1997;177:210-214.
24. Chattopadhyay SK, Kharif H, Sherbeeni MM. Placenta previa and accreta after previous cesarean section. Eur J Obstet Gynecol Reprod Biol. 1993;52:151.-
25. Comstock CH, Love JJ, Jr, Bronsteen RA, et al. Sonographic detection of placenta accreta in the second and third trimesters of pregnancy. Am J Obstet Gynecol. 2004;190:1135-1140.
26. Comstock CH, Lee W, Vettraino IM, Bronsteen RA. The early sonographic appearance of placenta accreta. J Ultrasound Med. 2003;22:19-23.
27. Chou MM, Ho ES. Prenatal diagnosis of placenta previa accreta with power amplitude ultrasonic agiography. Am J Obstet Gynecol. 1997;177:1523-1525.
28. Levine D, Hulka CA, Ludmir J, Li W, Edelman RR. Placenta accreta: evaluation with color Doppler US, power Doppler US, and MR imaging. Radiology. 1997;205:773-776.
29. Taipale P, Orden MR, Berg M, Manninen H, Alafuzoff I. Prenatal diagnosis of placenta accreta and percreta with ultrasonography, color Doppler, and magnetic resonance imaging. Obstet Gynecol. 2004;104:537-540.
30. Chou MM, Tseng JJ, Ho ES, Hwang JI. Three-dimensional color power Doppler imaging in the assessment of uteroplacental neovascularization in placenta previa increta/percreta. Am J Obstet Gynecol. 2001;185:1257-1260.
31. Maldjian C, Adam R, Pelosi M, II, Pelosi M III, Rudelli RD, Maldjian J. MRI appearance of placenta percreta and placenta accreta. Magnetic Resonance Imaging. 1999;17:965-971.
32. Thorp JM, Councell RB, Sandridge DA, Wiest HH. Antepartum diagnosis of placenta previa percreta by magnetic resonance imaging. Obstet Gynecol. 1992;80:506-508.
33. Kay HH, Spritzer CE. Preliminary experience with magnetic resonance imaging in patients with third-trimester bleeding. Obstet Gynecol. 1991;78:424-429.
34. Russo-Stieglitz K, Lockwood CJ. Placenta previa and vasa previa. Up To Date. 2005. Available at: www.uptodate.com.
35. Dashe JS, McIntire DD, Ramus RM, Santos-Ramos R, Twickler DM. Persistence of placenta previa according to gestational age at ultrasound detection. Obstet Gynecol. 2002;99:692-697.
36. Taipale P, Hiilesmaa V, Ylostalo P. Transvaginal ultrasonography at 18-23 weeks in predicting placenta previa at delivery. Ultrasound Obstet Gynecol. 1998;12:422.-
37. Rosati P, Guariglia L. Clinical significance of placenta previa detected at early routine transvaginal scan. J Ultrasound Med. 2000;19:581-585.
38. Varma TR. Fetal growth and placental function in patients with placenta previa. J Obstet Gynaecol Br Commonw. 1973;80:311-315.
39. Crane JM, Van Den Hof MC, et al. Neonatal outcomes with placenta previa. Obstet Gynecol. 1999;93:541-544.
40. Benedetti TJ. Obstetric hemorrhage. In: Gabbe SG, Niebyl, JR, Simpson JL. Obstetrics: Normal and Problem Pregnancies. 4th ed. Philadelphia: Churchill Livingstone; 2002:503–538.
41. Besinger RE, Moniak CW, Paskiewicz LS, et al. The effects of tocolytic use in the management of symptomatic placenta previa. Am J Obstet Gynecol. 1995;172:1770-1778.
42. Magann EF, Johnson CA, Gookin KS, Roberts WE, Martin RW, Morrison JC. Placenta praevia: does uterine activity cause bleeding? Aust NZ J Obstet Gynaecol. 1993;33:22-24
43. Benedetti TJ. Maternal complication of parenteral B-sympathomimetic therapy for premature labor. Am J Obstet Gynecol. 1983;145:1-6.
44. Mouer JR. Placenta previa: Antepartum conservative management, inpatient versus outpatient. Am J Obstet Gynecol. 1994;170:1683-1686.
45. Droste S, Keil K. Expectant management of placenta previa: cost-benefit analysis of outpatient treatment. Am J Obstet Gynecol. 1994;170:1254-1257.
46. Wing D, Paul RH, Millar LK. Management of the symptomatic placenta previa: a randomized, controlled trial of inpatient versus outpatient expectant management. Am J Obstet Gynecol. 1996;175:806-811.
47. Hansch E, Chitkara U, McAlpine J, El-Sayed Y, Dake MD, Razavi MK. Pelvic arterial embolization for control of obstetric hemorrhage: a five-year experience. Am J Obstet Gynecol. 1999;180:1454-1460.
48. Dubois J, Garel L, Grignon A, Lemay M, Leduc L. Placenta percreta: balloon occlusion and embolization of the internal iliac arteries to reduce intraoperative blood losses. Am J Obstet Gynecol. 1997;176:723-726.
49. Suresh V, Goodwin SC, McLucas B, Mohr G. Uterine artery embolization: an underused method of controlling pelvic hemorrhage. Am J Obstet Gynecol. 1997;176:938-948.
50. Salomon LJ, deTayrac R, Castaigne-Meary V, et al. Fertility and pregnancy outcome following pelvic arterial embolization for severe postpartum haemorrhage. A cohort study. Hum Reprod. 2003;18:849-852.
51. Frederiksen MC, Glassenberg R, Stika CS. Placenta previa: a 22-year analysis. Am J Obstet Gynecol. 1999;180:1432-1437.
52. Lockwood CJ, Artal R. Placenta accreta. Obstet Gynecol. 2002;99:1133-1134.
53. Dyer I, Nix GF, Weed JC. Total hysterectomy at cesarean section and the immediate puerperal period. Am J Obstet Gynecol. 1953;65:517-527.
54. Catanzarite VA, Stanco L, Schrimmer D, Conroy C. Managing placenta previa/accreta. Contemporary OB/GYN. 1996;4(5):66-95.
55. Stanco L, Schrimmer D, Paul D, Mishell D. Emergency peripartum hysterectomy and associated risk factors. Am J Obstet Gynecol. 1993;168:879-883.
56. Hudon L, Belfort MA, Broome DR. Diagnosis and management of placenta percreta: a review. Obstet Gynecol Surv. 1998;53:509-517.
57. Shevell T, Malone FD. Management of obstetric hemorrhage. Sem Perinatol. 2003;27:86-104.
58. Cho J, Kim S, Cha K, et al. Interrupted circular suture: bleeding control during cesarean delivery in placenta previa accreta. Obstet Gynecol. 1991;78:876-879.
59. AbdRabbo SA. Stepwise uterine devascularization: a novel technique for management of uncontrollable postpartum hemorrhage with preservation of the uterus. Am J Obstet Gynecol. 1994;171:694-700.
CASE Diagnosis precedes sentinel episode of bleeding
“G.A.” is a 39-year-old gravida 6, para 1041 who was diagnosed with complete placenta previa during a target ultrasound exam performed at 18 weeks for advanced maternal age. She had a sentinel episode of vaginal bleeding at 29 weeks and was hospitalized for close monitoring.
Management strategy
One course of steroid was given, vaginal bleeding subsided, and she was discharged for outpatient conservative management, including iron and folic acid supplementation.
The outcome
The patient progressed to 36 weeks’ gestation, when she underwent amniocentesis to assess fetal lung maturity. When the results were reassuring, a cesarean section was scheduled. Intraoperative blood loss was diminished using pelvic vessel embolization. Surgery was uncomplicated, and a healthy infant was delivered.
Placenta previa is a leading and potentially life-threatening cause of third-trimester bleeding.1 Although the overall incidence is about 0.4% in pregnancies exceeding 20 weeks’ gestation,2 that figure rises with the number of cesarean sections and may reach 10% among women who have undergone 4 or more cesarean deliveries.3 Since more women are requesting elective and repeat cesarean deliveries, we are increasingly likely to encounter this condition.
Fortunately, technological advances have improved maternal and neonatal outcomes after placenta previa:
Nevertheless, the condition necessitates cesarean delivery and can cause serious maternal and perinatal morbidity, including:
It can also occur in association with vasa previa, which, though rare, carries a very high perinatal mortality rate.5
Risk factors
An enlarged placenta or endometrial disruption or scarring in the upper uterine segment due to 1 or more of the factors listed below may increase the likelihood of abnormal placental implantation in the unscarred lower uterine segment:3,6,7
Previa often begins with painless vaginal bleeding
The condition often presents as painless, bright red, vaginal bleeding in the third trimester. It is usually distinguished from abruptio placenta by the absence of abdominal pain and uterine contractions.5 However, approximately 20% of women have uterine activity associated with the first episode of vaginal bleeding.13,14 Moreover, in some cases, painful contractions and labor may precipitate vaginal bleeding from placenta previa.5 Therefore, ultrasound examination is strongly recommended for all women with vaginal bleeding during pregnancy.
Ultrasound for other reasons uncovers many cases
With greater routine use of ultrasonography in obstetrics, a large percentage of women with placenta previa are diagnosed prior to the onset of the characteristic painless vaginal bleeding. In a 2003 study by Dola and colleagues,15 approximately 43% of placenta previa cases were diagnosed by ultrasonography performed for other obstetrical indications prior to the onset of vaginal bleeding.
Look for “warning hemorrhage”
The first episode of vaginal bleeding is rarely profuse or life-threatening to the mother or fetus. The bleeding usually subsides spontaneously, although it could recur and become more severe with subsequent episodes. Pregnancy typically continues after the initial bleeding episode.
The mean gestational age at the time of the first bleeding is 29 to 32 weeks.13,14 However, a third of cases have vaginal bleeding before the 30th week of gestation, a third between 30 and 36 weeks, and a third after 36 weeks’ gestation.13-15 Ten percent of women with the condition may be completely asymptomatic and progress to 38 weeks’ gestation without vaginal bleeding.13,14
Which form of ultrasound is most accurate?
With the advanced technology available today, ultrasound has become the standard means of diagnosing placenta previa.16,17
Transabdominal ultrasound has accuracy as high as 95% and a false-negative rate of 7% in the diagnosis of placenta previa.13,19 However, its accuracy may be adversely affected by maternal obesity, acoustic shadowing of the fetal head in a cephalic presentation, inability to locate the internal cervical os (which is critical for correct diagnosis), and difficulty imaging a posterior placenta and the lateral uterine walls. In addition, a full maternal bladder—usually helpful in transabdominal ultrasound imaging—may cause a false-positive diagnosis if the bladder is overly distended. In this situation, the cervix would appear artificially elongated and give a normally implanted placenta the appearance of encroachment into the internal cervical os.
Transvaginal ultrasound is superior for diagnosis of previa
Leerentveld et al20 reported false-positive and false-negative rates of 1% and 2%, respectively—a striking improvement over transabdominal ultrasound, which has rates of 2% to 6% and 7%, respectively.
Transvaginal sonography has several advantages over transabdominal imaging in localization of the placenta. The shorter distance from the vaginal probe transducer to the cervix and lower uterine segment allows the use of higher-frequency ultrasound waves, with improved resolution; therefore, the relationship between the placental edge and the internal os can be determined more accurately.
Some clinicians may worry that the probe used in transvaginal sonography will disrupt the placenta and provoke significant maternal hemorrhage, but this concern is unfounded. Multiple studies have attested to the safety of transvaginal sonography in localization of the placenta.5,20-22 The probe is introduced and positioned under direct ultrasound guidance at all times, and inadvertent insertion of the endovaginal probe into the internal cervical os is virtually impossible due to the anatomical relationship of the vagina and cervix.21
Transperineal ultrasound is another option. Several investigators have found it to be superior to transabdominal and similarly advantageous to transvaginal sonography in the diagnosis and exclusion of placenta previa.18
Start with transabdominal imaging
In current practice, transabdominal ultrasound is usually performed first to localize the placenta. If there is reason to suspect placenta previa, transvaginal or transperineal sonography is then used to confirm the location of the placenta.
Contractions may hinder imaging
Accurate diagnosis or exclusion of placenta previa may be difficult if uterine contractions are present during ultrasound evaluation. Myometrial contractions shorten the distance between the internal cervical os and the placental edge, altering measurement of this distance. In addition, the ultrasound appearance of a contraction may simulate placental tissue, making it difficult to exclude placenta previa.
The trouble with tradition
The 4 types of placenta previa in the traditional classification system—complete, partial, marginal, and low-lying—predate the era of ultrasound diagnosis and are based on digital palpation of the placenta through a partly dilated cervical os during labor.
A new system of 3 types
Along with other authors,5,15-18 we propose a new system with 3 categories—complete, incomplete, and low-lying—because ultrasound may not distinguish a placenta partially covering the internal os (a discrete point) from one that is merely encroaching on it.
Complete previa
The placenta completely covers the internal cervical os
Incomplete previa
The placental edge is within 2 cm of the internal cervical os, but does not cover the os
Low-lying previa
The distance from the internal cervical os to the placental edge is between 2 and 3.5 cm
Look for placenta accreta
When placenta previa is diagnosed by ultrasound examination, further diagnostic measures are needed to determine whether placenta accreta is present.5,23 In placenta accreta, neither the normal plane of separation between the placental villi and uterine wall, nor the intervening fibrinoid layer of Nitabuch, is present.5,23
Degrees of abnormal placental implantation
Risk of accreta can reach 67%
There are varying reports on the incidence of placenta accreta, but women with placenta previa and previous cesarean deliveries appear to have the highest incidence.3,23,24 In women with placenta previa and 1 previous cesarean section, the risk of placenta accreta has been estimated at 24%, but it increases to 67% for women with placenta previa and 4 previous cesarean sections.3
Sonographic appearance of placenta accreta
Certain characteristics are suggestive of placenta accreta25,26:
Unfortunately, diagnosis of placenta accreta is difficult prior to delivery, although transvaginal sonography and adjunctive color flow/power Doppler imaging with 2- and 3-dimensional techniques offer improved resolution and have yielded promising results in prenatal diagnosis.27-30
Magnetic resonance imaging (MRI) may also prove useful in detecting placental tissue invasion and evaluating the degree of invasion, especially in a posterior or lateral placenta previa or when there is invasion into the bladder.31-33
Gestational age, symptoms determine management
The management of women with placenta previa in the third trimester depends on the extent of maternal hemorrhage and the fetal gestational age. Clinical categories include:
Some asymptomatic cases resolve
Outpatient management is possible for women who have never bled after diagnosis in the second trimester. These women should abstain from intercourse, avoid digital examination after 20 weeks’ gestation, and immediately present to the hospital if there is any evidence of vaginal bleeding.34
Monthly ultrasound evaluations are necessary to determine whether placenta previa has resolved,34-37 since 90% of cases detected in the second trimester resolve by the third trimester.34 However, if placenta previa persists beyond 24 weeks’ gestation, there is a 50% risk that delivery will be complicated by it.35 If placenta previa persists after 32 weeks, that risk approaches 75%.35
2-fold risk of congenital malformations
Most investigators report a 2-fold increased risk of fetal congenital malformations in cases of placenta previa.5 These malformations include anomalies of the central nervous system, cardiovascular system, respiratory tract, and gastrointestinal tract. Therefore, a target ultrasound examination for fetal anatomy is recommended at the initial ultrasound diagnosis of placenta previa.
Risk of fetal growth restriction warrants heightened surveillance
Some controversy surrounds the incidence of fetal growth restriction in pregnancies complicated by placenta previa. Varma38 reported that fetal growth restriction occurs in 16% of women with placenta previa and is correlated with the number of antepartum bleeding episodes. Other investigators have reported normal fetal growth in women with placenta previa.39 Given this uncertainty, serial follow-up ultrasound evaluations are usually advised for fetal growth assessment.
When patient remains asymptomatic, perform amniocentesis at 36 weeks
Some women progress to the late third trimester without any vaginal bleeding. In these women, amniocentesis is recommended at approximately 36 weeks’ gestation to assess fetal lung maturity.34,40 Elective cesarean delivery can then be planned if pulmonary maturity is documented.
The benefits of elective delivery include a stable patient and an optimally prepared surgical team, as well as the avoidance of emergent surgery, which increases the risk for maternal complications. Emergent surgery also places the fetus at greater risk for anemia, compared with elective procedures(27.7% vs 2.9%, respectively).13
Vaginal bleeding requires inpatient evaluation
Any woman with placenta previa who presents with vaginal bleeding should be admitted to the labor and delivery unit for immediate evaluation of maternal and fetal status, including an estimation of gestational age.
Initial acute care and assessment necessitate34:
If hemorrhage is life-threatening, deliver immediately
During initial evaluation, if the hemorrhage is judged to be massive and life-threatening, resuscitative measures and immediate delivery are necessary to avoid serious maternal morbidity. Recommended measures include constant monitoring of maternal status, aggressive IV fluid resuscitation, transfusion of blood and blood products, assessment of fetal status, and immediate delivery without regard to the maturity of the fetus.
A woman at term or near term (with documented fetal lung maturity) who presents with mild or moderate vaginal bleeding should be delivered via cesarean section.
Conservative management may be appropriate for mild preterm bleeding
If vaginal bleeding is not threatening to the life of the mother, and the fetus is preterm, a conservative approach with aggressive expectant management is appropriate, since most first episodes of vaginal bleeding are self-limited and rarely life-threatening to mother or fetus. Expectant management allows fetal maturation in utero without jeopardizing maternal health. If maternal and fetal health remain stable, the expectant approach allows a safe delay of delivery until the fetus matures.
Hospitalization is recommended. Candidates for expectant management should be hospitalized after the initial episode of vaginal bleeding. Once maternal and fetal conditions stabilize, the woman should be transferred to the antepartum ward for hospital bed rest with bathroom privileges. For expectant management:
Delivery is warranted for life-threatening hemorrhage, fetal lung maturity, and/or the usual maternal and fetal indications.
The question of tocolysis
Third-trimester tocolytic therapy in a woman with vaginal bleeding is controversial. In placenta previa, vaginal bleeding appears to arise from disruption of the placental implantation site as the lower uterine segment develops.41,42 It is unclear whether uterine contractions play a role, as only 20% of women with placenta previa have uterine activity at the time of vaginal bleeding.13,14,42 It is difficult to determine whether these women have true preterm labor, because digital examination of the cervix to document cervical dilatation is impossible.
Does uterine activity precipitate bleeding?
Some investigators believe uterine activity is a predisposing factor for the vaginal bleeding associated with placenta previa, and would consider tocolytic therapy in a stable patient at a premature gestational age. However, further evidence of its safety is needed.
In particular, beta-mimetics should be avoided in hemorrhaging women because their vasodilatory effects can precipitate maternal hypotension. Another side effect of beta-mimetics: maternal tachycardia,43 which may mask the hypovolemic state in women with significant hemorrhage.
Magnesium sulfate has less effect on the maternal cardiovascular system and could be a better choice in symptomatic placenta previa.41 Also consider indomethacin, which appears to have fewer adverse maternal effects.
Inpatient vs outpatient management
Because 2 to 3 weeks of maternal hospitalization can pass between the initial warning hemorrhage and delivery of the fetus, outpatient care has become an option. Several retrospective studies have demonstrated the cost-effectiveness and safety of outpatient management of symptomatic placenta previa.44,45 These studies emphasized careful patient section.
Wing and associates46 conducted a prospective, randomized, controlled trial that reinforces the need for judicious use of outpatient management. In their study, fewer than half the patients diagnosed with placenta previa prior to 37 weeks were candidates. The authors point out the small number of patients in their study, and the fact that vaginal bleeding recurred in approximately 60% of patients. Because of the difficulty of predicting which patients will have recurrent bleeding and when, outpatient management should be reserved for those judged to be compliant with home bed rest who can rapidly return to the hospital, if necessary.
Women with recurrent vaginal bleeding during outpatient management should be rehospitalized.
In the event of massive hemorrhage, immediate compression of the aorta below the level of the renal arteries will reduce the bleeding enough to allow time to evaluate the situation.56 At the same time, aggressive IV fluid resuscitation and blood transfusion should begin. Reevaluate coagulation status after every 5 to 10 U of blood.57
Focused repair may be effective. In some situations, the hemorrhage may be controlled by oversewing and repairing the focal placental site defects.40
Bracketing the bleeding area. Another measure is a circular suture technique in which interrupted sutures are placed on the serosal surface of the anterior and posterior aspects of the uterus and as deeply as possible into the endometrium in a circumferential manner, bracketing the bleeding area.58
The argon beam coagulator can be used to achieve hemostasis; it is more effective than traditional bipolar cautery at ensuring hemostasis in extensive areas.56,57
Stepwise devascularization was effective in 100% of 103 women with postpartum hemorrhage who did not respond to traditional management.59 It involves 5 procedures to be performed in sequence until hemostasis is achieved: unilateral uterine vessel ligation, bilateral uterine vessel ligation, low uterine vessel ligation, unilateral ovarian vessel ligation, and bilateral ovarian vessel ligation.
Hypogastric artery ligation is another option, but it is technically challenging and successful in less than 50% of cases.57 In fact, the time spent on this technique may actually lead to increased blood loss.
Components of safe delivery
A detailed plan is necessary when major hemorrhage is anticipated at the time of elective cesarean delivery for placenta previa, including consultation with experts in different disciplines such as radiology, anesthesiology, urology, pathology, blood bank, neonatology, and gynecologic oncology.
Also pay attention to the maternal red blood cell reserve. Iron and folic acid should be administered to prevent and treat anemia, and antepartum erythropoietin should be considered as a way of increasing the hemoglobin level in women with placenta previa. Autologous blood transfusion, including acute normovolemic hemodilution, is another option.
Pelvic vessel embolization
Elective embolization or occlusion of the hypogastric or uterine arteries has proved to be safe and effective for postpartum hemorrhage, with a success rate of more than 90% in women with normal coagulation.47
In addition, elective catheterization with a balloon-tipped catheter can be used prophylactically to reduce blood flow to the placenta. Prophylactic catheterization of the anterior division of the internal iliac arteries can be performed right before the scheduled cesarean section. An axillary approach is technically easier for fluoroscopically guided catheterization of the internal iliac.48 The actual fluoroscopy time is minutes, so the risk of fetal exposure to radiation and irreversible ovarian damage is minimal.
The fetus is monitored during the procedure, and the balloons are left in the deflated state until after delivery, reducing the risk of uteroplacental insufficiency. Balloon inflation after delivery occludes the hypogastric arteries and diminishes uterine arterial blood flow during surgery. In some cases, the temporary occlusive effect of the balloons may control intraoperative bleeding completely. If substantial bleeding persists, subsequent embolization of the uterine arteries is advised, using absorbable Gelfoam particles, which are temporary and do not damage pelvic organs. Menstruation is not impaired, and normal pregnancies have been reported after this procedure.49,50
In women who undergo cesarean delivery under regional anesthesia, placement of a dry epidural catheter for later dosing of anesthetic agents should be considered prior to balloon catheterization, since the patient’s mobility is restricted after placement of the balloon-tipped catheter.
This therapy is especially useful when there is a high index of suspicion for placenta accreta.
Recommendations at the time of delivery
Hysterectomy for placenta previa, placenta accreta
This procedure is technically challenging when there is a markedly enlarged uterus with engorged collateral vessels. One useful method, delayed ligation technique, was originally described by Dyer et al on the Tulane obstetrics service at Charity Hospital of New Orleans.53 This technique facilitates quick control of all uterine vasculature with rapid hemostasis. Later modification of this method involves successive clamping and severing of all vascular pedicles supplying the uterus, prior to their suture ligation, for quick control of bleeding.
Close follow-up continues even after surgery
Immediately after surgery, close monitoring of hemodynamic status is required, ideally in a critical care setting. Because women with placenta previa/placenta accreta have often received massive transfusions of blood and blood products along with large volumes of crystalloid fluids, pulmonary edema may develop. Conversely, hypovolemia can result from inadequate replacement of blood or persistent intra-abdominal bleeding. Thus, close attention to urinary output allows early detection of pulmonary edema, acute respiratory distress syndrome, hypovolemia, or persistent intra-abdominal bleeding. Patients who undergo peripartum hysterectomy should also be monitored closely for possible ureteral injury.
Thromboprophylaxis should continue until the patient is ambulatory.
Recommended laboratory tests
Get a complete blood count with platelets and fibrinogen immediately after surgery and at frequent intervals as needed. A chemistry panel with calcium, albumin, electrolytes, and creatinine also is helpful.
Serious morbidity in 3% to 5% of women after emergent hysterectomy
Conditions such as acute respiratory distress syndrome from massive blood transfusion and pulmonary capillary leakage, acute tubular necrosis from renal failure, and pulmonary embolism may complicate 3% to 5% of cases.54
Reoperation for persistent intra-abdominal bleeding may be necessary, and 9% of women will have urologic injury. Unfortunately, the maternal mortality rate associated with this procedure is 0.8%, so meticulous postoperative care is mandated.55
The authors report no financial relationships with any company whose products are mentioned in this article.
CASE Diagnosis precedes sentinel episode of bleeding
“G.A.” is a 39-year-old gravida 6, para 1041 who was diagnosed with complete placenta previa during a target ultrasound exam performed at 18 weeks for advanced maternal age. She had a sentinel episode of vaginal bleeding at 29 weeks and was hospitalized for close monitoring.
Management strategy
One course of steroid was given, vaginal bleeding subsided, and she was discharged for outpatient conservative management, including iron and folic acid supplementation.
The outcome
The patient progressed to 36 weeks’ gestation, when she underwent amniocentesis to assess fetal lung maturity. When the results were reassuring, a cesarean section was scheduled. Intraoperative blood loss was diminished using pelvic vessel embolization. Surgery was uncomplicated, and a healthy infant was delivered.
Placenta previa is a leading and potentially life-threatening cause of third-trimester bleeding.1 Although the overall incidence is about 0.4% in pregnancies exceeding 20 weeks’ gestation,2 that figure rises with the number of cesarean sections and may reach 10% among women who have undergone 4 or more cesarean deliveries.3 Since more women are requesting elective and repeat cesarean deliveries, we are increasingly likely to encounter this condition.
Fortunately, technological advances have improved maternal and neonatal outcomes after placenta previa:
Nevertheless, the condition necessitates cesarean delivery and can cause serious maternal and perinatal morbidity, including:
It can also occur in association with vasa previa, which, though rare, carries a very high perinatal mortality rate.5
Risk factors
An enlarged placenta or endometrial disruption or scarring in the upper uterine segment due to 1 or more of the factors listed below may increase the likelihood of abnormal placental implantation in the unscarred lower uterine segment:3,6,7
Previa often begins with painless vaginal bleeding
The condition often presents as painless, bright red, vaginal bleeding in the third trimester. It is usually distinguished from abruptio placenta by the absence of abdominal pain and uterine contractions.5 However, approximately 20% of women have uterine activity associated with the first episode of vaginal bleeding.13,14 Moreover, in some cases, painful contractions and labor may precipitate vaginal bleeding from placenta previa.5 Therefore, ultrasound examination is strongly recommended for all women with vaginal bleeding during pregnancy.
Ultrasound for other reasons uncovers many cases
With greater routine use of ultrasonography in obstetrics, a large percentage of women with placenta previa are diagnosed prior to the onset of the characteristic painless vaginal bleeding. In a 2003 study by Dola and colleagues,15 approximately 43% of placenta previa cases were diagnosed by ultrasonography performed for other obstetrical indications prior to the onset of vaginal bleeding.
Look for “warning hemorrhage”
The first episode of vaginal bleeding is rarely profuse or life-threatening to the mother or fetus. The bleeding usually subsides spontaneously, although it could recur and become more severe with subsequent episodes. Pregnancy typically continues after the initial bleeding episode.
The mean gestational age at the time of the first bleeding is 29 to 32 weeks.13,14 However, a third of cases have vaginal bleeding before the 30th week of gestation, a third between 30 and 36 weeks, and a third after 36 weeks’ gestation.13-15 Ten percent of women with the condition may be completely asymptomatic and progress to 38 weeks’ gestation without vaginal bleeding.13,14
Which form of ultrasound is most accurate?
With the advanced technology available today, ultrasound has become the standard means of diagnosing placenta previa.16,17
Transabdominal ultrasound has accuracy as high as 95% and a false-negative rate of 7% in the diagnosis of placenta previa.13,19 However, its accuracy may be adversely affected by maternal obesity, acoustic shadowing of the fetal head in a cephalic presentation, inability to locate the internal cervical os (which is critical for correct diagnosis), and difficulty imaging a posterior placenta and the lateral uterine walls. In addition, a full maternal bladder—usually helpful in transabdominal ultrasound imaging—may cause a false-positive diagnosis if the bladder is overly distended. In this situation, the cervix would appear artificially elongated and give a normally implanted placenta the appearance of encroachment into the internal cervical os.
Transvaginal ultrasound is superior for diagnosis of previa
Leerentveld et al20 reported false-positive and false-negative rates of 1% and 2%, respectively—a striking improvement over transabdominal ultrasound, which has rates of 2% to 6% and 7%, respectively.
Transvaginal sonography has several advantages over transabdominal imaging in localization of the placenta. The shorter distance from the vaginal probe transducer to the cervix and lower uterine segment allows the use of higher-frequency ultrasound waves, with improved resolution; therefore, the relationship between the placental edge and the internal os can be determined more accurately.
Some clinicians may worry that the probe used in transvaginal sonography will disrupt the placenta and provoke significant maternal hemorrhage, but this concern is unfounded. Multiple studies have attested to the safety of transvaginal sonography in localization of the placenta.5,20-22 The probe is introduced and positioned under direct ultrasound guidance at all times, and inadvertent insertion of the endovaginal probe into the internal cervical os is virtually impossible due to the anatomical relationship of the vagina and cervix.21
Transperineal ultrasound is another option. Several investigators have found it to be superior to transabdominal and similarly advantageous to transvaginal sonography in the diagnosis and exclusion of placenta previa.18
Start with transabdominal imaging
In current practice, transabdominal ultrasound is usually performed first to localize the placenta. If there is reason to suspect placenta previa, transvaginal or transperineal sonography is then used to confirm the location of the placenta.
Contractions may hinder imaging
Accurate diagnosis or exclusion of placenta previa may be difficult if uterine contractions are present during ultrasound evaluation. Myometrial contractions shorten the distance between the internal cervical os and the placental edge, altering measurement of this distance. In addition, the ultrasound appearance of a contraction may simulate placental tissue, making it difficult to exclude placenta previa.
The trouble with tradition
The 4 types of placenta previa in the traditional classification system—complete, partial, marginal, and low-lying—predate the era of ultrasound diagnosis and are based on digital palpation of the placenta through a partly dilated cervical os during labor.
A new system of 3 types
Along with other authors,5,15-18 we propose a new system with 3 categories—complete, incomplete, and low-lying—because ultrasound may not distinguish a placenta partially covering the internal os (a discrete point) from one that is merely encroaching on it.
Complete previa
The placenta completely covers the internal cervical os
Incomplete previa
The placental edge is within 2 cm of the internal cervical os, but does not cover the os
Low-lying previa
The distance from the internal cervical os to the placental edge is between 2 and 3.5 cm
Look for placenta accreta
When placenta previa is diagnosed by ultrasound examination, further diagnostic measures are needed to determine whether placenta accreta is present.5,23 In placenta accreta, neither the normal plane of separation between the placental villi and uterine wall, nor the intervening fibrinoid layer of Nitabuch, is present.5,23
Degrees of abnormal placental implantation
Risk of accreta can reach 67%
There are varying reports on the incidence of placenta accreta, but women with placenta previa and previous cesarean deliveries appear to have the highest incidence.3,23,24 In women with placenta previa and 1 previous cesarean section, the risk of placenta accreta has been estimated at 24%, but it increases to 67% for women with placenta previa and 4 previous cesarean sections.3
Sonographic appearance of placenta accreta
Certain characteristics are suggestive of placenta accreta25,26:
Unfortunately, diagnosis of placenta accreta is difficult prior to delivery, although transvaginal sonography and adjunctive color flow/power Doppler imaging with 2- and 3-dimensional techniques offer improved resolution and have yielded promising results in prenatal diagnosis.27-30
Magnetic resonance imaging (MRI) may also prove useful in detecting placental tissue invasion and evaluating the degree of invasion, especially in a posterior or lateral placenta previa or when there is invasion into the bladder.31-33
Gestational age, symptoms determine management
The management of women with placenta previa in the third trimester depends on the extent of maternal hemorrhage and the fetal gestational age. Clinical categories include:
Some asymptomatic cases resolve
Outpatient management is possible for women who have never bled after diagnosis in the second trimester. These women should abstain from intercourse, avoid digital examination after 20 weeks’ gestation, and immediately present to the hospital if there is any evidence of vaginal bleeding.34
Monthly ultrasound evaluations are necessary to determine whether placenta previa has resolved,34-37 since 90% of cases detected in the second trimester resolve by the third trimester.34 However, if placenta previa persists beyond 24 weeks’ gestation, there is a 50% risk that delivery will be complicated by it.35 If placenta previa persists after 32 weeks, that risk approaches 75%.35
2-fold risk of congenital malformations
Most investigators report a 2-fold increased risk of fetal congenital malformations in cases of placenta previa.5 These malformations include anomalies of the central nervous system, cardiovascular system, respiratory tract, and gastrointestinal tract. Therefore, a target ultrasound examination for fetal anatomy is recommended at the initial ultrasound diagnosis of placenta previa.
Risk of fetal growth restriction warrants heightened surveillance
Some controversy surrounds the incidence of fetal growth restriction in pregnancies complicated by placenta previa. Varma38 reported that fetal growth restriction occurs in 16% of women with placenta previa and is correlated with the number of antepartum bleeding episodes. Other investigators have reported normal fetal growth in women with placenta previa.39 Given this uncertainty, serial follow-up ultrasound evaluations are usually advised for fetal growth assessment.
When patient remains asymptomatic, perform amniocentesis at 36 weeks
Some women progress to the late third trimester without any vaginal bleeding. In these women, amniocentesis is recommended at approximately 36 weeks’ gestation to assess fetal lung maturity.34,40 Elective cesarean delivery can then be planned if pulmonary maturity is documented.
The benefits of elective delivery include a stable patient and an optimally prepared surgical team, as well as the avoidance of emergent surgery, which increases the risk for maternal complications. Emergent surgery also places the fetus at greater risk for anemia, compared with elective procedures(27.7% vs 2.9%, respectively).13
Vaginal bleeding requires inpatient evaluation
Any woman with placenta previa who presents with vaginal bleeding should be admitted to the labor and delivery unit for immediate evaluation of maternal and fetal status, including an estimation of gestational age.
Initial acute care and assessment necessitate34:
If hemorrhage is life-threatening, deliver immediately
During initial evaluation, if the hemorrhage is judged to be massive and life-threatening, resuscitative measures and immediate delivery are necessary to avoid serious maternal morbidity. Recommended measures include constant monitoring of maternal status, aggressive IV fluid resuscitation, transfusion of blood and blood products, assessment of fetal status, and immediate delivery without regard to the maturity of the fetus.
A woman at term or near term (with documented fetal lung maturity) who presents with mild or moderate vaginal bleeding should be delivered via cesarean section.
Conservative management may be appropriate for mild preterm bleeding
If vaginal bleeding is not threatening to the life of the mother, and the fetus is preterm, a conservative approach with aggressive expectant management is appropriate, since most first episodes of vaginal bleeding are self-limited and rarely life-threatening to mother or fetus. Expectant management allows fetal maturation in utero without jeopardizing maternal health. If maternal and fetal health remain stable, the expectant approach allows a safe delay of delivery until the fetus matures.
Hospitalization is recommended. Candidates for expectant management should be hospitalized after the initial episode of vaginal bleeding. Once maternal and fetal conditions stabilize, the woman should be transferred to the antepartum ward for hospital bed rest with bathroom privileges. For expectant management:
Delivery is warranted for life-threatening hemorrhage, fetal lung maturity, and/or the usual maternal and fetal indications.
The question of tocolysis
Third-trimester tocolytic therapy in a woman with vaginal bleeding is controversial. In placenta previa, vaginal bleeding appears to arise from disruption of the placental implantation site as the lower uterine segment develops.41,42 It is unclear whether uterine contractions play a role, as only 20% of women with placenta previa have uterine activity at the time of vaginal bleeding.13,14,42 It is difficult to determine whether these women have true preterm labor, because digital examination of the cervix to document cervical dilatation is impossible.
Does uterine activity precipitate bleeding?
Some investigators believe uterine activity is a predisposing factor for the vaginal bleeding associated with placenta previa, and would consider tocolytic therapy in a stable patient at a premature gestational age. However, further evidence of its safety is needed.
In particular, beta-mimetics should be avoided in hemorrhaging women because their vasodilatory effects can precipitate maternal hypotension. Another side effect of beta-mimetics: maternal tachycardia,43 which may mask the hypovolemic state in women with significant hemorrhage.
Magnesium sulfate has less effect on the maternal cardiovascular system and could be a better choice in symptomatic placenta previa.41 Also consider indomethacin, which appears to have fewer adverse maternal effects.
Inpatient vs outpatient management
Because 2 to 3 weeks of maternal hospitalization can pass between the initial warning hemorrhage and delivery of the fetus, outpatient care has become an option. Several retrospective studies have demonstrated the cost-effectiveness and safety of outpatient management of symptomatic placenta previa.44,45 These studies emphasized careful patient section.
Wing and associates46 conducted a prospective, randomized, controlled trial that reinforces the need for judicious use of outpatient management. In their study, fewer than half the patients diagnosed with placenta previa prior to 37 weeks were candidates. The authors point out the small number of patients in their study, and the fact that vaginal bleeding recurred in approximately 60% of patients. Because of the difficulty of predicting which patients will have recurrent bleeding and when, outpatient management should be reserved for those judged to be compliant with home bed rest who can rapidly return to the hospital, if necessary.
Women with recurrent vaginal bleeding during outpatient management should be rehospitalized.
In the event of massive hemorrhage, immediate compression of the aorta below the level of the renal arteries will reduce the bleeding enough to allow time to evaluate the situation.56 At the same time, aggressive IV fluid resuscitation and blood transfusion should begin. Reevaluate coagulation status after every 5 to 10 U of blood.57
Focused repair may be effective. In some situations, the hemorrhage may be controlled by oversewing and repairing the focal placental site defects.40
Bracketing the bleeding area. Another measure is a circular suture technique in which interrupted sutures are placed on the serosal surface of the anterior and posterior aspects of the uterus and as deeply as possible into the endometrium in a circumferential manner, bracketing the bleeding area.58
The argon beam coagulator can be used to achieve hemostasis; it is more effective than traditional bipolar cautery at ensuring hemostasis in extensive areas.56,57
Stepwise devascularization was effective in 100% of 103 women with postpartum hemorrhage who did not respond to traditional management.59 It involves 5 procedures to be performed in sequence until hemostasis is achieved: unilateral uterine vessel ligation, bilateral uterine vessel ligation, low uterine vessel ligation, unilateral ovarian vessel ligation, and bilateral ovarian vessel ligation.
Hypogastric artery ligation is another option, but it is technically challenging and successful in less than 50% of cases.57 In fact, the time spent on this technique may actually lead to increased blood loss.
Components of safe delivery
A detailed plan is necessary when major hemorrhage is anticipated at the time of elective cesarean delivery for placenta previa, including consultation with experts in different disciplines such as radiology, anesthesiology, urology, pathology, blood bank, neonatology, and gynecologic oncology.
Also pay attention to the maternal red blood cell reserve. Iron and folic acid should be administered to prevent and treat anemia, and antepartum erythropoietin should be considered as a way of increasing the hemoglobin level in women with placenta previa. Autologous blood transfusion, including acute normovolemic hemodilution, is another option.
Pelvic vessel embolization
Elective embolization or occlusion of the hypogastric or uterine arteries has proved to be safe and effective for postpartum hemorrhage, with a success rate of more than 90% in women with normal coagulation.47
In addition, elective catheterization with a balloon-tipped catheter can be used prophylactically to reduce blood flow to the placenta. Prophylactic catheterization of the anterior division of the internal iliac arteries can be performed right before the scheduled cesarean section. An axillary approach is technically easier for fluoroscopically guided catheterization of the internal iliac.48 The actual fluoroscopy time is minutes, so the risk of fetal exposure to radiation and irreversible ovarian damage is minimal.
The fetus is monitored during the procedure, and the balloons are left in the deflated state until after delivery, reducing the risk of uteroplacental insufficiency. Balloon inflation after delivery occludes the hypogastric arteries and diminishes uterine arterial blood flow during surgery. In some cases, the temporary occlusive effect of the balloons may control intraoperative bleeding completely. If substantial bleeding persists, subsequent embolization of the uterine arteries is advised, using absorbable Gelfoam particles, which are temporary and do not damage pelvic organs. Menstruation is not impaired, and normal pregnancies have been reported after this procedure.49,50
In women who undergo cesarean delivery under regional anesthesia, placement of a dry epidural catheter for later dosing of anesthetic agents should be considered prior to balloon catheterization, since the patient’s mobility is restricted after placement of the balloon-tipped catheter.
This therapy is especially useful when there is a high index of suspicion for placenta accreta.
Recommendations at the time of delivery
Hysterectomy for placenta previa, placenta accreta
This procedure is technically challenging when there is a markedly enlarged uterus with engorged collateral vessels. One useful method, delayed ligation technique, was originally described by Dyer et al on the Tulane obstetrics service at Charity Hospital of New Orleans.53 This technique facilitates quick control of all uterine vasculature with rapid hemostasis. Later modification of this method involves successive clamping and severing of all vascular pedicles supplying the uterus, prior to their suture ligation, for quick control of bleeding.
Close follow-up continues even after surgery
Immediately after surgery, close monitoring of hemodynamic status is required, ideally in a critical care setting. Because women with placenta previa/placenta accreta have often received massive transfusions of blood and blood products along with large volumes of crystalloid fluids, pulmonary edema may develop. Conversely, hypovolemia can result from inadequate replacement of blood or persistent intra-abdominal bleeding. Thus, close attention to urinary output allows early detection of pulmonary edema, acute respiratory distress syndrome, hypovolemia, or persistent intra-abdominal bleeding. Patients who undergo peripartum hysterectomy should also be monitored closely for possible ureteral injury.
Thromboprophylaxis should continue until the patient is ambulatory.
Recommended laboratory tests
Get a complete blood count with platelets and fibrinogen immediately after surgery and at frequent intervals as needed. A chemistry panel with calcium, albumin, electrolytes, and creatinine also is helpful.
Serious morbidity in 3% to 5% of women after emergent hysterectomy
Conditions such as acute respiratory distress syndrome from massive blood transfusion and pulmonary capillary leakage, acute tubular necrosis from renal failure, and pulmonary embolism may complicate 3% to 5% of cases.54
Reoperation for persistent intra-abdominal bleeding may be necessary, and 9% of women will have urologic injury. Unfortunately, the maternal mortality rate associated with this procedure is 0.8%, so meticulous postoperative care is mandated.55
The authors report no financial relationships with any company whose products are mentioned in this article.
1. Ananth CV, Savitz DA, Luther ER. Maternal cigarette smoking as a risk factor for placental abruption, placenta previa, and uterine bleeding in pregnancy. Am J Epidemiol. 1996;144:881-889.
2. Faiz AS, Ananth CV. Etiology and risk factors for placenta previa: an overview and meta-analysis of observational studies. J Matern Fetal Neonatal Med. 2003;13:175.-
3. Clark SL, Koonings PP, et al. Placenta previa/accreta and prior cesarean section. Obstet Gynecol. 1985;66:89-92.
4. Neri A, Manor Y, Matityahu A, Blieden L. Placenta previa and congenital cardiac anomalies. Fetal Ther. 1989;4:138-140.
5. Clark SL. Placenta previa and abruptio placenta. In: Creasy RK, Resnik R. Maternal-Fetal Medicine, Principles and Practice. 4th ed. Philadelphia: W.B. Saunders; 1999:616–631.
6. Miller DA, Chollet J, Goodwin TM. Clinical risks factors for placenta previa-placenta accreta. Am J Obstet Gynecol. 1997;177:210-214.
7. Ananth CV, Demissie K, Smulian JC, Vintzileos AM. Placenta previa in singleton and twin births in the United States, 1989 through 1998: a comparison of risk factor profiles and associated conditions. Am J Obstet Gynecol. 2003;188:275-281.
8. Gilbert WM, Nesbitt TS, Danielsen B. Childbearing beyond age 40: pregnancy outcome in 24,032 cases. Obstet Gynecol. 1999;93:9-14.
9. Lavery JP. Placenta previa. Clin Obstet Gynecol. 1990;33:414-421.
10. Taylor VM, Kramer MD, Vaughan TL, Peacock S. Placenta previa in relation to induced and spontaneous abortion: a population- based study. Obstet Gynecol. 1993;82:88-91.
11. Williams MA, Mittendorf R, Lieberman E, Monson RR, Schoenbaum SC, Genest DR. Cigarette smoking during pregnancy in relation to placenta previa. Am J Obstet Gynecol. 1991;165:28-32.
12. Handler AS, Mason ED, Rosenberg DL, Davis FG. The relationship between exposure during pregnancy to cigarette smoking and cocaine use and placenta previa. Am J Obstet Gynecol. 1994;170:884-889.
13. Cotton DB, Read JA, Paul RH, Quilligan EJ. The conservative aggressive management of placenta previa. Am J Obstet Gynecol. 1980;137:687-695.
14. Silver R, Depp R, Sabbagha RE, Dooley SL. Placenta previa: aggressive expectant management. Am J Obstet Gynecol. 1984;150:15-22.
15. Dola CP, Garite TJ, Dowling DD, Friend D, Ahdoot D, Asrat T. Placenta previa: does its type affect pregnancy outcome? Am J Perinatol. 2003;20:353-360.
16. Oppenheimer LW, Farine D, Ritchie JWK, Lewinsky RM, Telford J, Fairbanks LA. What is low-lying placenta? Am J Obstet Gynecol. 1991;165:1036-1038.
17. Bhide A, Thilaganathan B. Recent advances in the management of placenta previa. Curr Opin Obstet Gynecol. 2004;16:447-451.
18. Dawson WB, Dumas MD, Romano WM, Gagnon R, Gratton RJ, Mowbray RD. Translabial ultrasonography and placenta previa: does measurement of the os-placenta distance predict outcome? J Ultrasound Med. 1996;15:44-46.
19. Egley CC. Abruptio placentae and placenta previa. In: Winn HN, Hobbins JC. Clinical Maternal-Fetal Medicine.1st ed. Pearl River, NY: Parthenon Publishing; 2000:47–53.
20. Leerentveld RA, Gilberts E, Arnold M, Wladimiroff JW. Accuracy and safety of transvaginal sonographic placental localization. Obstet Gynecol. 1990;76:759-762.
21. Timor-Tritsch I, Yunis R. Confirming the safety of transvaginal sonography in patients suspected of placenta previa. Obstet Gynecol. 1993;81:742-744.
22. Tan NH, Abu M, Woo JLS, Tahir H. The role of transvaginal sonography in the diagnosis of placenta previa. Aust NZ J Obstet Gynaecol. 1995;35:42-45.
23. Miller DA, Cholleet JA, Goodwin TM. Clinical risk factors for placenta previa-placenta accreta. Am J Obstet Gynecol. 1997;177:210-214.
24. Chattopadhyay SK, Kharif H, Sherbeeni MM. Placenta previa and accreta after previous cesarean section. Eur J Obstet Gynecol Reprod Biol. 1993;52:151.-
25. Comstock CH, Love JJ, Jr, Bronsteen RA, et al. Sonographic detection of placenta accreta in the second and third trimesters of pregnancy. Am J Obstet Gynecol. 2004;190:1135-1140.
26. Comstock CH, Lee W, Vettraino IM, Bronsteen RA. The early sonographic appearance of placenta accreta. J Ultrasound Med. 2003;22:19-23.
27. Chou MM, Ho ES. Prenatal diagnosis of placenta previa accreta with power amplitude ultrasonic agiography. Am J Obstet Gynecol. 1997;177:1523-1525.
28. Levine D, Hulka CA, Ludmir J, Li W, Edelman RR. Placenta accreta: evaluation with color Doppler US, power Doppler US, and MR imaging. Radiology. 1997;205:773-776.
29. Taipale P, Orden MR, Berg M, Manninen H, Alafuzoff I. Prenatal diagnosis of placenta accreta and percreta with ultrasonography, color Doppler, and magnetic resonance imaging. Obstet Gynecol. 2004;104:537-540.
30. Chou MM, Tseng JJ, Ho ES, Hwang JI. Three-dimensional color power Doppler imaging in the assessment of uteroplacental neovascularization in placenta previa increta/percreta. Am J Obstet Gynecol. 2001;185:1257-1260.
31. Maldjian C, Adam R, Pelosi M, II, Pelosi M III, Rudelli RD, Maldjian J. MRI appearance of placenta percreta and placenta accreta. Magnetic Resonance Imaging. 1999;17:965-971.
32. Thorp JM, Councell RB, Sandridge DA, Wiest HH. Antepartum diagnosis of placenta previa percreta by magnetic resonance imaging. Obstet Gynecol. 1992;80:506-508.
33. Kay HH, Spritzer CE. Preliminary experience with magnetic resonance imaging in patients with third-trimester bleeding. Obstet Gynecol. 1991;78:424-429.
34. Russo-Stieglitz K, Lockwood CJ. Placenta previa and vasa previa. Up To Date. 2005. Available at: www.uptodate.com.
35. Dashe JS, McIntire DD, Ramus RM, Santos-Ramos R, Twickler DM. Persistence of placenta previa according to gestational age at ultrasound detection. Obstet Gynecol. 2002;99:692-697.
36. Taipale P, Hiilesmaa V, Ylostalo P. Transvaginal ultrasonography at 18-23 weeks in predicting placenta previa at delivery. Ultrasound Obstet Gynecol. 1998;12:422.-
37. Rosati P, Guariglia L. Clinical significance of placenta previa detected at early routine transvaginal scan. J Ultrasound Med. 2000;19:581-585.
38. Varma TR. Fetal growth and placental function in patients with placenta previa. J Obstet Gynaecol Br Commonw. 1973;80:311-315.
39. Crane JM, Van Den Hof MC, et al. Neonatal outcomes with placenta previa. Obstet Gynecol. 1999;93:541-544.
40. Benedetti TJ. Obstetric hemorrhage. In: Gabbe SG, Niebyl, JR, Simpson JL. Obstetrics: Normal and Problem Pregnancies. 4th ed. Philadelphia: Churchill Livingstone; 2002:503–538.
41. Besinger RE, Moniak CW, Paskiewicz LS, et al. The effects of tocolytic use in the management of symptomatic placenta previa. Am J Obstet Gynecol. 1995;172:1770-1778.
42. Magann EF, Johnson CA, Gookin KS, Roberts WE, Martin RW, Morrison JC. Placenta praevia: does uterine activity cause bleeding? Aust NZ J Obstet Gynaecol. 1993;33:22-24
43. Benedetti TJ. Maternal complication of parenteral B-sympathomimetic therapy for premature labor. Am J Obstet Gynecol. 1983;145:1-6.
44. Mouer JR. Placenta previa: Antepartum conservative management, inpatient versus outpatient. Am J Obstet Gynecol. 1994;170:1683-1686.
45. Droste S, Keil K. Expectant management of placenta previa: cost-benefit analysis of outpatient treatment. Am J Obstet Gynecol. 1994;170:1254-1257.
46. Wing D, Paul RH, Millar LK. Management of the symptomatic placenta previa: a randomized, controlled trial of inpatient versus outpatient expectant management. Am J Obstet Gynecol. 1996;175:806-811.
47. Hansch E, Chitkara U, McAlpine J, El-Sayed Y, Dake MD, Razavi MK. Pelvic arterial embolization for control of obstetric hemorrhage: a five-year experience. Am J Obstet Gynecol. 1999;180:1454-1460.
48. Dubois J, Garel L, Grignon A, Lemay M, Leduc L. Placenta percreta: balloon occlusion and embolization of the internal iliac arteries to reduce intraoperative blood losses. Am J Obstet Gynecol. 1997;176:723-726.
49. Suresh V, Goodwin SC, McLucas B, Mohr G. Uterine artery embolization: an underused method of controlling pelvic hemorrhage. Am J Obstet Gynecol. 1997;176:938-948.
50. Salomon LJ, deTayrac R, Castaigne-Meary V, et al. Fertility and pregnancy outcome following pelvic arterial embolization for severe postpartum haemorrhage. A cohort study. Hum Reprod. 2003;18:849-852.
51. Frederiksen MC, Glassenberg R, Stika CS. Placenta previa: a 22-year analysis. Am J Obstet Gynecol. 1999;180:1432-1437.
52. Lockwood CJ, Artal R. Placenta accreta. Obstet Gynecol. 2002;99:1133-1134.
53. Dyer I, Nix GF, Weed JC. Total hysterectomy at cesarean section and the immediate puerperal period. Am J Obstet Gynecol. 1953;65:517-527.
54. Catanzarite VA, Stanco L, Schrimmer D, Conroy C. Managing placenta previa/accreta. Contemporary OB/GYN. 1996;4(5):66-95.
55. Stanco L, Schrimmer D, Paul D, Mishell D. Emergency peripartum hysterectomy and associated risk factors. Am J Obstet Gynecol. 1993;168:879-883.
56. Hudon L, Belfort MA, Broome DR. Diagnosis and management of placenta percreta: a review. Obstet Gynecol Surv. 1998;53:509-517.
57. Shevell T, Malone FD. Management of obstetric hemorrhage. Sem Perinatol. 2003;27:86-104.
58. Cho J, Kim S, Cha K, et al. Interrupted circular suture: bleeding control during cesarean delivery in placenta previa accreta. Obstet Gynecol. 1991;78:876-879.
59. AbdRabbo SA. Stepwise uterine devascularization: a novel technique for management of uncontrollable postpartum hemorrhage with preservation of the uterus. Am J Obstet Gynecol. 1994;171:694-700.
1. Ananth CV, Savitz DA, Luther ER. Maternal cigarette smoking as a risk factor for placental abruption, placenta previa, and uterine bleeding in pregnancy. Am J Epidemiol. 1996;144:881-889.
2. Faiz AS, Ananth CV. Etiology and risk factors for placenta previa: an overview and meta-analysis of observational studies. J Matern Fetal Neonatal Med. 2003;13:175.-
3. Clark SL, Koonings PP, et al. Placenta previa/accreta and prior cesarean section. Obstet Gynecol. 1985;66:89-92.
4. Neri A, Manor Y, Matityahu A, Blieden L. Placenta previa and congenital cardiac anomalies. Fetal Ther. 1989;4:138-140.
5. Clark SL. Placenta previa and abruptio placenta. In: Creasy RK, Resnik R. Maternal-Fetal Medicine, Principles and Practice. 4th ed. Philadelphia: W.B. Saunders; 1999:616–631.
6. Miller DA, Chollet J, Goodwin TM. Clinical risks factors for placenta previa-placenta accreta. Am J Obstet Gynecol. 1997;177:210-214.
7. Ananth CV, Demissie K, Smulian JC, Vintzileos AM. Placenta previa in singleton and twin births in the United States, 1989 through 1998: a comparison of risk factor profiles and associated conditions. Am J Obstet Gynecol. 2003;188:275-281.
8. Gilbert WM, Nesbitt TS, Danielsen B. Childbearing beyond age 40: pregnancy outcome in 24,032 cases. Obstet Gynecol. 1999;93:9-14.
9. Lavery JP. Placenta previa. Clin Obstet Gynecol. 1990;33:414-421.
10. Taylor VM, Kramer MD, Vaughan TL, Peacock S. Placenta previa in relation to induced and spontaneous abortion: a population- based study. Obstet Gynecol. 1993;82:88-91.
11. Williams MA, Mittendorf R, Lieberman E, Monson RR, Schoenbaum SC, Genest DR. Cigarette smoking during pregnancy in relation to placenta previa. Am J Obstet Gynecol. 1991;165:28-32.
12. Handler AS, Mason ED, Rosenberg DL, Davis FG. The relationship between exposure during pregnancy to cigarette smoking and cocaine use and placenta previa. Am J Obstet Gynecol. 1994;170:884-889.
13. Cotton DB, Read JA, Paul RH, Quilligan EJ. The conservative aggressive management of placenta previa. Am J Obstet Gynecol. 1980;137:687-695.
14. Silver R, Depp R, Sabbagha RE, Dooley SL. Placenta previa: aggressive expectant management. Am J Obstet Gynecol. 1984;150:15-22.
15. Dola CP, Garite TJ, Dowling DD, Friend D, Ahdoot D, Asrat T. Placenta previa: does its type affect pregnancy outcome? Am J Perinatol. 2003;20:353-360.
16. Oppenheimer LW, Farine D, Ritchie JWK, Lewinsky RM, Telford J, Fairbanks LA. What is low-lying placenta? Am J Obstet Gynecol. 1991;165:1036-1038.
17. Bhide A, Thilaganathan B. Recent advances in the management of placenta previa. Curr Opin Obstet Gynecol. 2004;16:447-451.
18. Dawson WB, Dumas MD, Romano WM, Gagnon R, Gratton RJ, Mowbray RD. Translabial ultrasonography and placenta previa: does measurement of the os-placenta distance predict outcome? J Ultrasound Med. 1996;15:44-46.
19. Egley CC. Abruptio placentae and placenta previa. In: Winn HN, Hobbins JC. Clinical Maternal-Fetal Medicine.1st ed. Pearl River, NY: Parthenon Publishing; 2000:47–53.
20. Leerentveld RA, Gilberts E, Arnold M, Wladimiroff JW. Accuracy and safety of transvaginal sonographic placental localization. Obstet Gynecol. 1990;76:759-762.
21. Timor-Tritsch I, Yunis R. Confirming the safety of transvaginal sonography in patients suspected of placenta previa. Obstet Gynecol. 1993;81:742-744.
22. Tan NH, Abu M, Woo JLS, Tahir H. The role of transvaginal sonography in the diagnosis of placenta previa. Aust NZ J Obstet Gynaecol. 1995;35:42-45.
23. Miller DA, Cholleet JA, Goodwin TM. Clinical risk factors for placenta previa-placenta accreta. Am J Obstet Gynecol. 1997;177:210-214.
24. Chattopadhyay SK, Kharif H, Sherbeeni MM. Placenta previa and accreta after previous cesarean section. Eur J Obstet Gynecol Reprod Biol. 1993;52:151.-
25. Comstock CH, Love JJ, Jr, Bronsteen RA, et al. Sonographic detection of placenta accreta in the second and third trimesters of pregnancy. Am J Obstet Gynecol. 2004;190:1135-1140.
26. Comstock CH, Lee W, Vettraino IM, Bronsteen RA. The early sonographic appearance of placenta accreta. J Ultrasound Med. 2003;22:19-23.
27. Chou MM, Ho ES. Prenatal diagnosis of placenta previa accreta with power amplitude ultrasonic agiography. Am J Obstet Gynecol. 1997;177:1523-1525.
28. Levine D, Hulka CA, Ludmir J, Li W, Edelman RR. Placenta accreta: evaluation with color Doppler US, power Doppler US, and MR imaging. Radiology. 1997;205:773-776.
29. Taipale P, Orden MR, Berg M, Manninen H, Alafuzoff I. Prenatal diagnosis of placenta accreta and percreta with ultrasonography, color Doppler, and magnetic resonance imaging. Obstet Gynecol. 2004;104:537-540.
30. Chou MM, Tseng JJ, Ho ES, Hwang JI. Three-dimensional color power Doppler imaging in the assessment of uteroplacental neovascularization in placenta previa increta/percreta. Am J Obstet Gynecol. 2001;185:1257-1260.
31. Maldjian C, Adam R, Pelosi M, II, Pelosi M III, Rudelli RD, Maldjian J. MRI appearance of placenta percreta and placenta accreta. Magnetic Resonance Imaging. 1999;17:965-971.
32. Thorp JM, Councell RB, Sandridge DA, Wiest HH. Antepartum diagnosis of placenta previa percreta by magnetic resonance imaging. Obstet Gynecol. 1992;80:506-508.
33. Kay HH, Spritzer CE. Preliminary experience with magnetic resonance imaging in patients with third-trimester bleeding. Obstet Gynecol. 1991;78:424-429.
34. Russo-Stieglitz K, Lockwood CJ. Placenta previa and vasa previa. Up To Date. 2005. Available at: www.uptodate.com.
35. Dashe JS, McIntire DD, Ramus RM, Santos-Ramos R, Twickler DM. Persistence of placenta previa according to gestational age at ultrasound detection. Obstet Gynecol. 2002;99:692-697.
36. Taipale P, Hiilesmaa V, Ylostalo P. Transvaginal ultrasonography at 18-23 weeks in predicting placenta previa at delivery. Ultrasound Obstet Gynecol. 1998;12:422.-
37. Rosati P, Guariglia L. Clinical significance of placenta previa detected at early routine transvaginal scan. J Ultrasound Med. 2000;19:581-585.
38. Varma TR. Fetal growth and placental function in patients with placenta previa. J Obstet Gynaecol Br Commonw. 1973;80:311-315.
39. Crane JM, Van Den Hof MC, et al. Neonatal outcomes with placenta previa. Obstet Gynecol. 1999;93:541-544.
40. Benedetti TJ. Obstetric hemorrhage. In: Gabbe SG, Niebyl, JR, Simpson JL. Obstetrics: Normal and Problem Pregnancies. 4th ed. Philadelphia: Churchill Livingstone; 2002:503–538.
41. Besinger RE, Moniak CW, Paskiewicz LS, et al. The effects of tocolytic use in the management of symptomatic placenta previa. Am J Obstet Gynecol. 1995;172:1770-1778.
42. Magann EF, Johnson CA, Gookin KS, Roberts WE, Martin RW, Morrison JC. Placenta praevia: does uterine activity cause bleeding? Aust NZ J Obstet Gynaecol. 1993;33:22-24
43. Benedetti TJ. Maternal complication of parenteral B-sympathomimetic therapy for premature labor. Am J Obstet Gynecol. 1983;145:1-6.
44. Mouer JR. Placenta previa: Antepartum conservative management, inpatient versus outpatient. Am J Obstet Gynecol. 1994;170:1683-1686.
45. Droste S, Keil K. Expectant management of placenta previa: cost-benefit analysis of outpatient treatment. Am J Obstet Gynecol. 1994;170:1254-1257.
46. Wing D, Paul RH, Millar LK. Management of the symptomatic placenta previa: a randomized, controlled trial of inpatient versus outpatient expectant management. Am J Obstet Gynecol. 1996;175:806-811.
47. Hansch E, Chitkara U, McAlpine J, El-Sayed Y, Dake MD, Razavi MK. Pelvic arterial embolization for control of obstetric hemorrhage: a five-year experience. Am J Obstet Gynecol. 1999;180:1454-1460.
48. Dubois J, Garel L, Grignon A, Lemay M, Leduc L. Placenta percreta: balloon occlusion and embolization of the internal iliac arteries to reduce intraoperative blood losses. Am J Obstet Gynecol. 1997;176:723-726.
49. Suresh V, Goodwin SC, McLucas B, Mohr G. Uterine artery embolization: an underused method of controlling pelvic hemorrhage. Am J Obstet Gynecol. 1997;176:938-948.
50. Salomon LJ, deTayrac R, Castaigne-Meary V, et al. Fertility and pregnancy outcome following pelvic arterial embolization for severe postpartum haemorrhage. A cohort study. Hum Reprod. 2003;18:849-852.
51. Frederiksen MC, Glassenberg R, Stika CS. Placenta previa: a 22-year analysis. Am J Obstet Gynecol. 1999;180:1432-1437.
52. Lockwood CJ, Artal R. Placenta accreta. Obstet Gynecol. 2002;99:1133-1134.
53. Dyer I, Nix GF, Weed JC. Total hysterectomy at cesarean section and the immediate puerperal period. Am J Obstet Gynecol. 1953;65:517-527.
54. Catanzarite VA, Stanco L, Schrimmer D, Conroy C. Managing placenta previa/accreta. Contemporary OB/GYN. 1996;4(5):66-95.
55. Stanco L, Schrimmer D, Paul D, Mishell D. Emergency peripartum hysterectomy and associated risk factors. Am J Obstet Gynecol. 1993;168:879-883.
56. Hudon L, Belfort MA, Broome DR. Diagnosis and management of placenta percreta: a review. Obstet Gynecol Surv. 1998;53:509-517.
57. Shevell T, Malone FD. Management of obstetric hemorrhage. Sem Perinatol. 2003;27:86-104.
58. Cho J, Kim S, Cha K, et al. Interrupted circular suture: bleeding control during cesarean delivery in placenta previa accreta. Obstet Gynecol. 1991;78:876-879.
59. AbdRabbo SA. Stepwise uterine devascularization: a novel technique for management of uncontrollable postpartum hemorrhage with preservation of the uterus. Am J Obstet Gynecol. 1994;171:694-700.