User login
Case: Patient becomes a liability when nonadherant to prescribed tests
MC, a 42-year-old woman (G1P1001), presents for an office visit. As the medical assistant hands you the chart, she says, “Good luck with this one. She yelled at me because you were 20 minutes behind schedule. She didn’t like sitting in the waiting room.” You greet the patient, obtain her medical history, proceed with a physical examination, and outline a management plan. You recall from the chart that you operated on her 8 months ago and there was a complication/maloccurrence in which postoperative bleeding necessitated return to the operating room (OR) for a laparotomy to control bleeding. The patient has not brought this up since being discharged from the hospital.
During the current office visit, the esprit de corps in the consultation room is a bit uncomfortable, and you sense the patient is not happy. You leave the examination room and discuss the management plan with the nurse, who then returns to the patient to review the plan. The patient is unhappy with the battery of tests you have ordered but tells the nurse that she will comply.
One week later the nurse follows up with the patient by phone because she has not obtained the requested lab tests. The nurse reports to you, “She read me the riot act: ‘Why do I need all these tests? They are expensive.’ The patient indicated that she has no understanding as to why the tests were ordered in the first place.” After a discussion with you, the nurse calls the patient back in an effort to clarify her understanding of the need for the tests. The patient hangs up on her in the middle of the conversation.
The office manager tracks you down to discuss this patient. “Enough is enough,” she exclaims. “This patient is harassing the staff. She told the nurse what tests she herself believes are best and that those are the only ones she will comply with.” Your office manager states that this patient is “a liability.”
What are your choices at this point? You have thought about picking up the phone and calling her. You have considered ending her relationship with your practice. You ask yourself again, what is the best approach?
Patients have the legal right to “dismiss” or change health care providers at any time and for almost any reason without notice. But that right is not reciprocal—clinicians have a legal duty not to abandon a patient and an ethical duty to promote continuity of patient care. A clinician may dismiss a patient from his or her practice (other than for a discriminatory reason that violates ethical or legal limitations), but it must be done in the proper way.
We examine the legal, practical, and ethical issues in dismissing a patient, and how to do it without unnecessary risk. In addition, we will look at a new issue that sometimes arises in these circumstances—managed care limitations.
Physicians’ ethical obligations
The American Medical Association suggests the following ethical consideration:
Reference
- American Medical Association Council on Ethical and Judicial Affairs. Opinion 10.015. The Patient-Physician Relationship. Code of Medical Ethics. American Medical Association. http://www.ama-assn.org/ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion10015.page. Issued December 2001. Accessed May 8, 2015.
Legal and medical issues
Why would you end a clinician−patient relationship?
There are a number of reasons for dismissing a patient, including1,2:
- the patient’s failure to comply with a treatment plan (probably the most frequent reason)
- persistent, inappropriate, rude, or disruptive behavior
- falsifying medical history
- seductive behavior toward health care professionals or staff
- Sentinel incident (verbal threat, violence, or criminal activity—as when a patient threatens or inappropriately touches or hits your staff)
- failure to pay billed charges (this can raise special legal issues).
The legal details vary from state to state, but fortunately there is sufficient similarity that best practices can be determined. The law starts with the proposition that ordinarily professionals may choose their patients or clients. There are limits, however, in state and federal law. A clinician may not discriminate based, for example, on ethnicity, religion, gender, or sexual orientation. In addition, the Americans with Disabilities Act limits the basis for not providing care to a patient.3
Limiting factors when dismissing a patient
Once a patient has been accepted and a professional relationship has begun, the clinician has a duty of continued care and must act reasonably to end the relationship in a way that protects the patient’s well-being.
Other recognized limitations to the ending of a treatment relationship exist. These are:
- In an emergency situation or during ongoing care in which it proves unfeasible to find another physician. At the extreme, a surgeon may not leave in the middle of surgery. Less clear, but still problematic, is the obstetrician who wants to dismiss a patient 1 or 2 weeks before an expected delivery. In any event, a clinician should not leave a patient at a critical stage without giving reasonable notice or making suitable arrangements for the attendance of another equally competent substitute.
- When there is no other health care provider available who could provide the continuity of care the clinician has begun. This limitation probably arises from the frontier days (when it was much more common for no other health care professional to be available who could provide the continuity of care the clinician began). A modern version of this might be a patient in an HMO who does not have other physicians of the same subspecialty available who are taking patients. This, of course, requires consultation with the managed care organization.
Abandonment
The legal and ethical issues are essentially related to “abandonment”—dismissing a patient improperly. Technically, abandonment is a form of negligence (the clinician does not act reasonably to protect the patient’s interests). The Oklahoma Supreme Court put it clearly: “When further medical and/or surgical attention is needed, a physician may terminate the doctor−patient relationship only after giving reasonable notice and affording an ample opportunity for the patient to secure other medical attention from other physicians” (emphasis added).4–6
How to end a patient relationship
Always send a letter
Two elements must be taken into account when dismissing a patient:
- reasonable notice
- reasonable opportunity to find another clinician.
Together, these elements mean that the intention of ending the clinician−patient relationship and the importance of finding an alternative care provider must be clearly communicated to the patient. That communication needs to be in writing—both to get the patient’s attention and as clear proof of what was said.
Some experts suggest that the best process is to have a face-to-face meeting with the patient followed by a letter. A goal of such a meeting is to make the parting as amicable as possible. It may seem more professional for a clinician to communicate such an important matter in person. The risk is that it may become a confrontation that exacerbates the situation because one or both parties may have some built-up emotion. It, therefore, depends on the circumstances as to whether such a meeting is desirable. Even if there is an oral conversation, it must be followed up with a letter to the patient.
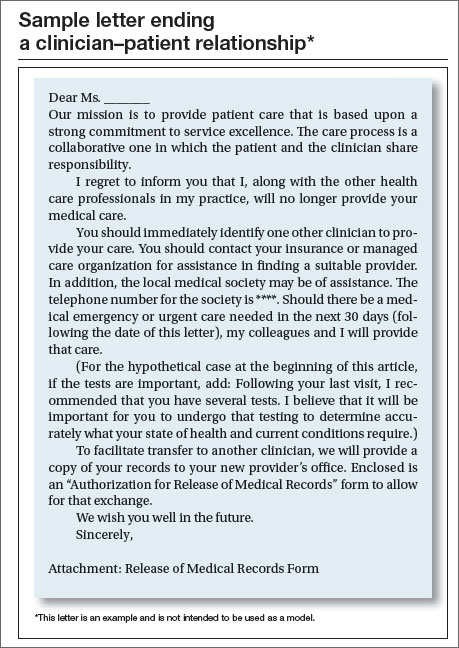
A reasonable time frame to give the patient to find another clinician is commonly a maximum of 30 days of follow-up and emergency care. A set period of time may be a legitimate starting point but it needs to be adjusted in lieu of special circumstances, such as the availability of other similar specialists in the vicinity who are taking new patients or managed care complications. A specific time period should be indicated, along with an agreement to provide care during that time period in “emergency” or “urgent” circumstances. Of course, ongoing care also should be continued for a reasonable time (30 days is often reasonable, as mentioned). It may be best to also discuss any specific ongoing issues that should be attended to (such as the recommended tests in our opening case).
There is disagreement among experts as to whether a general statement of the reasons for ending the care relationship should be included in the letter. The argument for doing so is that, without a stated reason, the patient may call to ask why. The other side of the argument is that it adds an element of accusation; the patient undoubtedly knows what the problem is. Not writing down the reasons seems the better part of valor, especially if there has been an oral conversation.7,8
The box above provides an example of a letter to a patient (but not a model). Experts agree that the letter should be sent by certified mail with return receipt. Should the patient reject the letter, a regular delivery letter should be sent with full documentation kept in the file of the time and place it was mailed.
Managed care considerations
A consideration of increasing importance is managed care. Before taking any action, ensure that the managed care contract(s) (including federal or state government programs) have provisions concerning patient dismissals. These may be as simple as notifying the organization as to any time limits for care or of the process of dismissal.
Make sure your staff knows
Your scheduling staff needs to know with clarity the rules for scheduling (or not scheduling) this patient in the future. As a general matter, the better course of action is to allow an appointment if the patient reports that it is an emergency, whether the staff believes it is or not. In such cases it may be good to document to the patient that the emergency care does not constitute reestablishing a regular clinician−patient relationship.
Document everything
The patient’s record, at a minimum, should contain a copy of the letter sent to the patient and a log of any conversations with her about ending the relationship. Keep your own notes concerning the disruption or problems with the patient over time.
Are there risks of a malpractice lawsuit?
The abandonment claim is, of course, one possibility for a malpractice lawsuit. That is why documentation and careful communication are so important. This is one area in which having legal advice when developing a letter template should be part of the ongoing relationship with a health law attorney.
There is another malpractice risk illustrated in our hypothetical case. The physician “operated on her 8 months ago and there was a complication/maloccurrence in which postoperative bleeding necessitated return to the OR and laparotomy to control bleeding.” Malpractice claims (as opposed to actual malpractice occurrences) most often arise because of bad communication with patients or when patients feel ignored. The clinician is thus between a rock and a hard place. On one hand, by ending this relationship, the clinician could well precipitate a claim based primarily on the earlier “maloccurrence.” On the other hand, continuing to treat a patient who is resisting care and creating problems with the staff has its own difficulties. It may be time for the health care professional to discuss the matter with an attorney.
Although not present in this hypothetical case, ending a patient relationship because of nonpayment of professional fees is also a touchy situation. It can be one of the other precipitating events for malpractice claims, and calls for special care.
Tread with care
Having to dismiss a patient is almost always a difficult process. The decision neither can be made lightly nor implemented sloppily. Because it is difficult, it calls on professionals to be particularly careful to not cut essential corners.9
Case: Resolved
You ask the nurse to note the details of her follow-up phone conversation with the patient in the chart. You then call MC to explain the importance of the tests. She says she is unavailable to talk right now, so you ask her to come in for an appointment, free of charge. The patient makes an appointment but does not show.
You send a letter by certified mail describing the medical necessity for the tests and that her lack of adherence and refusal to come to the office have compelled you to end your clinician−patient relationship. You write that she should immediately identify another health care professional and suggest that she contact her managed care organization for assistance. You note that, should there be a medical emergency or urgent care needed in the next 30 days, you will provide that care. You enclose a release of medical records form in the letter.
In the patient’s record you note the details of the phone conversation and ask the office manager to add that the patient was a no show for her appointment. You include a copy of the certified letter and proof of mailing in the chart.
Two weeks later, the office manager reports that she is sending the patient’s records to another physician upon receipt of the release of medical records form from the patient.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
1. Kodner C. Challenging physician-patient interactions. FP Essentials. ed 354. AAFP home study. Leawood, KS: American Academy of Family Physicians; November 2008.
2. Harris SM. Take care when firing a patient. Am Med News. http://www.ama-assn.org/amed- news/2008/02/04/bica0204 .htm. Published February 4, 2008. Accessed May 8, 2015.
3. Lynch HF. Discrimination at the doctor’s office. N Engl J Med. 2013;386(18):1668–1670.
4. Jackson v Oklahoma Memorial Hospital, 909 P.2d 765 (OK 1995). http://law.justia.com/cases/oklahoma/supreme-court/1995/4226-1.html. Accessed May 8, 2015.
5. Randolph DS, Burkett TM. When physicians fire patients: avoiding patient “abandonment” lawsuits. J Okla State Med Assoc. 2009;102(11):356–358.
6. Crauman R, Baruch J. Abandonment in the physician-patient relationship. Med Health R I. 2004;87(5):154–156.
7. Cepelewicz BB. Firing a patient: when its needed and how to handle it correctly. Med Econ. 2014;91(2):42–43.
8. Santalucia C, Michota F. When and how is it appropriate to terminate the physician-patient relationship? Cleve Clin J Med. 2004;71(3):179–183.
9. Lippman H, Davenport J. Patient dismissal: the right way to do it. J Fam Pract. 2011;60(3):135–140. http://www.jfponline.com/specialty-focus/practice-management/article/patient-dismissal-the-right-way-to-do-it/30f9501e8b3eb6ddaf6dd67ce88e0d16.html. Accessed May 8, 2015.
Joseph S. Sanfilippo, MD, MBA, and Steven R. Smith, JD
| Joseph S. Sanfilippo, MD, MBA is Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility, at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
|
Steven R. Smith, JD, is Professor of Law and Dean Emeritus at California Western School of Law, San Diego, California. |
|
Shirley M. Pruitt, BSN, JD, is a Partner in the firm of Yates, McLamb & Weyher, LLP, in Raleigh, North Carolina. She is an OBG Management Contributing Editor. |


The authors report no financial relationships relevant to this article.
*The “facts” of this case are based on actual cases but are a composite of several events and do not reflect a specific case.
Joseph S. Sanfilippo, MD, MBA, and Steven R. Smith, JD
|
| Joseph S. Sanfilippo, MD, MBA is Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility, at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
|
Steven R. Smith, JD, is Professor of Law and Dean Emeritus at California Western School of Law, San Diego, California. |
|
Shirley M. Pruitt, BSN, JD, is a Partner in the firm of Yates, McLamb & Weyher, LLP, in Raleigh, North Carolina. She is an OBG Management Contributing Editor. |
The authors report no financial relationships relevant to this article.
*The “facts” of this case are based on actual cases but are a composite of several events and do not reflect a specific case.
Joseph S. Sanfilippo, MD, MBA, and Steven R. Smith, JD
|
| Joseph S. Sanfilippo, MD, MBA is Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility, at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
|
Steven R. Smith, JD, is Professor of Law and Dean Emeritus at California Western School of Law, San Diego, California. |
|
Shirley M. Pruitt, BSN, JD, is a Partner in the firm of Yates, McLamb & Weyher, LLP, in Raleigh, North Carolina. She is an OBG Management Contributing Editor. |
The authors report no financial relationships relevant to this article.
*The “facts” of this case are based on actual cases but are a composite of several events and do not reflect a specific case.
Case: Patient becomes a liability when nonadherant to prescribed tests
MC, a 42-year-old woman (G1P1001), presents for an office visit. As the medical assistant hands you the chart, she says, “Good luck with this one. She yelled at me because you were 20 minutes behind schedule. She didn’t like sitting in the waiting room.” You greet the patient, obtain her medical history, proceed with a physical examination, and outline a management plan. You recall from the chart that you operated on her 8 months ago and there was a complication/maloccurrence in which postoperative bleeding necessitated return to the operating room (OR) for a laparotomy to control bleeding. The patient has not brought this up since being discharged from the hospital.
During the current office visit, the esprit de corps in the consultation room is a bit uncomfortable, and you sense the patient is not happy. You leave the examination room and discuss the management plan with the nurse, who then returns to the patient to review the plan. The patient is unhappy with the battery of tests you have ordered but tells the nurse that she will comply.
One week later the nurse follows up with the patient by phone because she has not obtained the requested lab tests. The nurse reports to you, “She read me the riot act: ‘Why do I need all these tests? They are expensive.’ The patient indicated that she has no understanding as to why the tests were ordered in the first place.” After a discussion with you, the nurse calls the patient back in an effort to clarify her understanding of the need for the tests. The patient hangs up on her in the middle of the conversation.
The office manager tracks you down to discuss this patient. “Enough is enough,” she exclaims. “This patient is harassing the staff. She told the nurse what tests she herself believes are best and that those are the only ones she will comply with.” Your office manager states that this patient is “a liability.”
What are your choices at this point? You have thought about picking up the phone and calling her. You have considered ending her relationship with your practice. You ask yourself again, what is the best approach?
Patients have the legal right to “dismiss” or change health care providers at any time and for almost any reason without notice. But that right is not reciprocal—clinicians have a legal duty not to abandon a patient and an ethical duty to promote continuity of patient care. A clinician may dismiss a patient from his or her practice (other than for a discriminatory reason that violates ethical or legal limitations), but it must be done in the proper way.
We examine the legal, practical, and ethical issues in dismissing a patient, and how to do it without unnecessary risk. In addition, we will look at a new issue that sometimes arises in these circumstances—managed care limitations.
Physicians’ ethical obligations
The American Medical Association suggests the following ethical consideration:
Reference
- American Medical Association Council on Ethical and Judicial Affairs. Opinion 10.015. The Patient-Physician Relationship. Code of Medical Ethics. American Medical Association. http://www.ama-assn.org/ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion10015.page. Issued December 2001. Accessed May 8, 2015.
Legal and medical issues
Why would you end a clinician−patient relationship?
There are a number of reasons for dismissing a patient, including1,2:
- the patient’s failure to comply with a treatment plan (probably the most frequent reason)
- persistent, inappropriate, rude, or disruptive behavior
- falsifying medical history
- seductive behavior toward health care professionals or staff
- Sentinel incident (verbal threat, violence, or criminal activity—as when a patient threatens or inappropriately touches or hits your staff)
- failure to pay billed charges (this can raise special legal issues).
The legal details vary from state to state, but fortunately there is sufficient similarity that best practices can be determined. The law starts with the proposition that ordinarily professionals may choose their patients or clients. There are limits, however, in state and federal law. A clinician may not discriminate based, for example, on ethnicity, religion, gender, or sexual orientation. In addition, the Americans with Disabilities Act limits the basis for not providing care to a patient.3
Limiting factors when dismissing a patient
Once a patient has been accepted and a professional relationship has begun, the clinician has a duty of continued care and must act reasonably to end the relationship in a way that protects the patient’s well-being.
Other recognized limitations to the ending of a treatment relationship exist. These are:
- In an emergency situation or during ongoing care in which it proves unfeasible to find another physician. At the extreme, a surgeon may not leave in the middle of surgery. Less clear, but still problematic, is the obstetrician who wants to dismiss a patient 1 or 2 weeks before an expected delivery. In any event, a clinician should not leave a patient at a critical stage without giving reasonable notice or making suitable arrangements for the attendance of another equally competent substitute.
- When there is no other health care provider available who could provide the continuity of care the clinician has begun. This limitation probably arises from the frontier days (when it was much more common for no other health care professional to be available who could provide the continuity of care the clinician began). A modern version of this might be a patient in an HMO who does not have other physicians of the same subspecialty available who are taking patients. This, of course, requires consultation with the managed care organization.
Abandonment
The legal and ethical issues are essentially related to “abandonment”—dismissing a patient improperly. Technically, abandonment is a form of negligence (the clinician does not act reasonably to protect the patient’s interests). The Oklahoma Supreme Court put it clearly: “When further medical and/or surgical attention is needed, a physician may terminate the doctor−patient relationship only after giving reasonable notice and affording an ample opportunity for the patient to secure other medical attention from other physicians” (emphasis added).4–6
How to end a patient relationship
Always send a letter
Two elements must be taken into account when dismissing a patient:
- reasonable notice
- reasonable opportunity to find another clinician.
Together, these elements mean that the intention of ending the clinician−patient relationship and the importance of finding an alternative care provider must be clearly communicated to the patient. That communication needs to be in writing—both to get the patient’s attention and as clear proof of what was said.
Some experts suggest that the best process is to have a face-to-face meeting with the patient followed by a letter. A goal of such a meeting is to make the parting as amicable as possible. It may seem more professional for a clinician to communicate such an important matter in person. The risk is that it may become a confrontation that exacerbates the situation because one or both parties may have some built-up emotion. It, therefore, depends on the circumstances as to whether such a meeting is desirable. Even if there is an oral conversation, it must be followed up with a letter to the patient.
A reasonable time frame to give the patient to find another clinician is commonly a maximum of 30 days of follow-up and emergency care. A set period of time may be a legitimate starting point but it needs to be adjusted in lieu of special circumstances, such as the availability of other similar specialists in the vicinity who are taking new patients or managed care complications. A specific time period should be indicated, along with an agreement to provide care during that time period in “emergency” or “urgent” circumstances. Of course, ongoing care also should be continued for a reasonable time (30 days is often reasonable, as mentioned). It may be best to also discuss any specific ongoing issues that should be attended to (such as the recommended tests in our opening case).
There is disagreement among experts as to whether a general statement of the reasons for ending the care relationship should be included in the letter. The argument for doing so is that, without a stated reason, the patient may call to ask why. The other side of the argument is that it adds an element of accusation; the patient undoubtedly knows what the problem is. Not writing down the reasons seems the better part of valor, especially if there has been an oral conversation.7,8
The box above provides an example of a letter to a patient (but not a model). Experts agree that the letter should be sent by certified mail with return receipt. Should the patient reject the letter, a regular delivery letter should be sent with full documentation kept in the file of the time and place it was mailed.
Managed care considerations
A consideration of increasing importance is managed care. Before taking any action, ensure that the managed care contract(s) (including federal or state government programs) have provisions concerning patient dismissals. These may be as simple as notifying the organization as to any time limits for care or of the process of dismissal.
Make sure your staff knows
Your scheduling staff needs to know with clarity the rules for scheduling (or not scheduling) this patient in the future. As a general matter, the better course of action is to allow an appointment if the patient reports that it is an emergency, whether the staff believes it is or not. In such cases it may be good to document to the patient that the emergency care does not constitute reestablishing a regular clinician−patient relationship.
Document everything
The patient’s record, at a minimum, should contain a copy of the letter sent to the patient and a log of any conversations with her about ending the relationship. Keep your own notes concerning the disruption or problems with the patient over time.
Are there risks of a malpractice lawsuit?
The abandonment claim is, of course, one possibility for a malpractice lawsuit. That is why documentation and careful communication are so important. This is one area in which having legal advice when developing a letter template should be part of the ongoing relationship with a health law attorney.
There is another malpractice risk illustrated in our hypothetical case. The physician “operated on her 8 months ago and there was a complication/maloccurrence in which postoperative bleeding necessitated return to the OR and laparotomy to control bleeding.” Malpractice claims (as opposed to actual malpractice occurrences) most often arise because of bad communication with patients or when patients feel ignored. The clinician is thus between a rock and a hard place. On one hand, by ending this relationship, the clinician could well precipitate a claim based primarily on the earlier “maloccurrence.” On the other hand, continuing to treat a patient who is resisting care and creating problems with the staff has its own difficulties. It may be time for the health care professional to discuss the matter with an attorney.
Although not present in this hypothetical case, ending a patient relationship because of nonpayment of professional fees is also a touchy situation. It can be one of the other precipitating events for malpractice claims, and calls for special care.
Tread with care
Having to dismiss a patient is almost always a difficult process. The decision neither can be made lightly nor implemented sloppily. Because it is difficult, it calls on professionals to be particularly careful to not cut essential corners.9
Case: Resolved
You ask the nurse to note the details of her follow-up phone conversation with the patient in the chart. You then call MC to explain the importance of the tests. She says she is unavailable to talk right now, so you ask her to come in for an appointment, free of charge. The patient makes an appointment but does not show.
You send a letter by certified mail describing the medical necessity for the tests and that her lack of adherence and refusal to come to the office have compelled you to end your clinician−patient relationship. You write that she should immediately identify another health care professional and suggest that she contact her managed care organization for assistance. You note that, should there be a medical emergency or urgent care needed in the next 30 days, you will provide that care. You enclose a release of medical records form in the letter.
In the patient’s record you note the details of the phone conversation and ask the office manager to add that the patient was a no show for her appointment. You include a copy of the certified letter and proof of mailing in the chart.
Two weeks later, the office manager reports that she is sending the patient’s records to another physician upon receipt of the release of medical records form from the patient.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Case: Patient becomes a liability when nonadherant to prescribed tests
MC, a 42-year-old woman (G1P1001), presents for an office visit. As the medical assistant hands you the chart, she says, “Good luck with this one. She yelled at me because you were 20 minutes behind schedule. She didn’t like sitting in the waiting room.” You greet the patient, obtain her medical history, proceed with a physical examination, and outline a management plan. You recall from the chart that you operated on her 8 months ago and there was a complication/maloccurrence in which postoperative bleeding necessitated return to the operating room (OR) for a laparotomy to control bleeding. The patient has not brought this up since being discharged from the hospital.
During the current office visit, the esprit de corps in the consultation room is a bit uncomfortable, and you sense the patient is not happy. You leave the examination room and discuss the management plan with the nurse, who then returns to the patient to review the plan. The patient is unhappy with the battery of tests you have ordered but tells the nurse that she will comply.
One week later the nurse follows up with the patient by phone because she has not obtained the requested lab tests. The nurse reports to you, “She read me the riot act: ‘Why do I need all these tests? They are expensive.’ The patient indicated that she has no understanding as to why the tests were ordered in the first place.” After a discussion with you, the nurse calls the patient back in an effort to clarify her understanding of the need for the tests. The patient hangs up on her in the middle of the conversation.
The office manager tracks you down to discuss this patient. “Enough is enough,” she exclaims. “This patient is harassing the staff. She told the nurse what tests she herself believes are best and that those are the only ones she will comply with.” Your office manager states that this patient is “a liability.”
What are your choices at this point? You have thought about picking up the phone and calling her. You have considered ending her relationship with your practice. You ask yourself again, what is the best approach?
Patients have the legal right to “dismiss” or change health care providers at any time and for almost any reason without notice. But that right is not reciprocal—clinicians have a legal duty not to abandon a patient and an ethical duty to promote continuity of patient care. A clinician may dismiss a patient from his or her practice (other than for a discriminatory reason that violates ethical or legal limitations), but it must be done in the proper way.
We examine the legal, practical, and ethical issues in dismissing a patient, and how to do it without unnecessary risk. In addition, we will look at a new issue that sometimes arises in these circumstances—managed care limitations.
Physicians’ ethical obligations
The American Medical Association suggests the following ethical consideration:
Reference
- American Medical Association Council on Ethical and Judicial Affairs. Opinion 10.015. The Patient-Physician Relationship. Code of Medical Ethics. American Medical Association. http://www.ama-assn.org/ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion10015.page. Issued December 2001. Accessed May 8, 2015.
Legal and medical issues
Why would you end a clinician−patient relationship?
There are a number of reasons for dismissing a patient, including1,2:
- the patient’s failure to comply with a treatment plan (probably the most frequent reason)
- persistent, inappropriate, rude, or disruptive behavior
- falsifying medical history
- seductive behavior toward health care professionals or staff
- Sentinel incident (verbal threat, violence, or criminal activity—as when a patient threatens or inappropriately touches or hits your staff)
- failure to pay billed charges (this can raise special legal issues).
The legal details vary from state to state, but fortunately there is sufficient similarity that best practices can be determined. The law starts with the proposition that ordinarily professionals may choose their patients or clients. There are limits, however, in state and federal law. A clinician may not discriminate based, for example, on ethnicity, religion, gender, or sexual orientation. In addition, the Americans with Disabilities Act limits the basis for not providing care to a patient.3
Limiting factors when dismissing a patient
Once a patient has been accepted and a professional relationship has begun, the clinician has a duty of continued care and must act reasonably to end the relationship in a way that protects the patient’s well-being.
Other recognized limitations to the ending of a treatment relationship exist. These are:
- In an emergency situation or during ongoing care in which it proves unfeasible to find another physician. At the extreme, a surgeon may not leave in the middle of surgery. Less clear, but still problematic, is the obstetrician who wants to dismiss a patient 1 or 2 weeks before an expected delivery. In any event, a clinician should not leave a patient at a critical stage without giving reasonable notice or making suitable arrangements for the attendance of another equally competent substitute.
- When there is no other health care provider available who could provide the continuity of care the clinician has begun. This limitation probably arises from the frontier days (when it was much more common for no other health care professional to be available who could provide the continuity of care the clinician began). A modern version of this might be a patient in an HMO who does not have other physicians of the same subspecialty available who are taking patients. This, of course, requires consultation with the managed care organization.
Abandonment
The legal and ethical issues are essentially related to “abandonment”—dismissing a patient improperly. Technically, abandonment is a form of negligence (the clinician does not act reasonably to protect the patient’s interests). The Oklahoma Supreme Court put it clearly: “When further medical and/or surgical attention is needed, a physician may terminate the doctor−patient relationship only after giving reasonable notice and affording an ample opportunity for the patient to secure other medical attention from other physicians” (emphasis added).4–6
How to end a patient relationship
Always send a letter
Two elements must be taken into account when dismissing a patient:
- reasonable notice
- reasonable opportunity to find another clinician.
Together, these elements mean that the intention of ending the clinician−patient relationship and the importance of finding an alternative care provider must be clearly communicated to the patient. That communication needs to be in writing—both to get the patient’s attention and as clear proof of what was said.
Some experts suggest that the best process is to have a face-to-face meeting with the patient followed by a letter. A goal of such a meeting is to make the parting as amicable as possible. It may seem more professional for a clinician to communicate such an important matter in person. The risk is that it may become a confrontation that exacerbates the situation because one or both parties may have some built-up emotion. It, therefore, depends on the circumstances as to whether such a meeting is desirable. Even if there is an oral conversation, it must be followed up with a letter to the patient.
A reasonable time frame to give the patient to find another clinician is commonly a maximum of 30 days of follow-up and emergency care. A set period of time may be a legitimate starting point but it needs to be adjusted in lieu of special circumstances, such as the availability of other similar specialists in the vicinity who are taking new patients or managed care complications. A specific time period should be indicated, along with an agreement to provide care during that time period in “emergency” or “urgent” circumstances. Of course, ongoing care also should be continued for a reasonable time (30 days is often reasonable, as mentioned). It may be best to also discuss any specific ongoing issues that should be attended to (such as the recommended tests in our opening case).
There is disagreement among experts as to whether a general statement of the reasons for ending the care relationship should be included in the letter. The argument for doing so is that, without a stated reason, the patient may call to ask why. The other side of the argument is that it adds an element of accusation; the patient undoubtedly knows what the problem is. Not writing down the reasons seems the better part of valor, especially if there has been an oral conversation.7,8
The box above provides an example of a letter to a patient (but not a model). Experts agree that the letter should be sent by certified mail with return receipt. Should the patient reject the letter, a regular delivery letter should be sent with full documentation kept in the file of the time and place it was mailed.
Managed care considerations
A consideration of increasing importance is managed care. Before taking any action, ensure that the managed care contract(s) (including federal or state government programs) have provisions concerning patient dismissals. These may be as simple as notifying the organization as to any time limits for care or of the process of dismissal.
Make sure your staff knows
Your scheduling staff needs to know with clarity the rules for scheduling (or not scheduling) this patient in the future. As a general matter, the better course of action is to allow an appointment if the patient reports that it is an emergency, whether the staff believes it is or not. In such cases it may be good to document to the patient that the emergency care does not constitute reestablishing a regular clinician−patient relationship.
Document everything
The patient’s record, at a minimum, should contain a copy of the letter sent to the patient and a log of any conversations with her about ending the relationship. Keep your own notes concerning the disruption or problems with the patient over time.
Are there risks of a malpractice lawsuit?
The abandonment claim is, of course, one possibility for a malpractice lawsuit. That is why documentation and careful communication are so important. This is one area in which having legal advice when developing a letter template should be part of the ongoing relationship with a health law attorney.
There is another malpractice risk illustrated in our hypothetical case. The physician “operated on her 8 months ago and there was a complication/maloccurrence in which postoperative bleeding necessitated return to the OR and laparotomy to control bleeding.” Malpractice claims (as opposed to actual malpractice occurrences) most often arise because of bad communication with patients or when patients feel ignored. The clinician is thus between a rock and a hard place. On one hand, by ending this relationship, the clinician could well precipitate a claim based primarily on the earlier “maloccurrence.” On the other hand, continuing to treat a patient who is resisting care and creating problems with the staff has its own difficulties. It may be time for the health care professional to discuss the matter with an attorney.
Although not present in this hypothetical case, ending a patient relationship because of nonpayment of professional fees is also a touchy situation. It can be one of the other precipitating events for malpractice claims, and calls for special care.
Tread with care
Having to dismiss a patient is almost always a difficult process. The decision neither can be made lightly nor implemented sloppily. Because it is difficult, it calls on professionals to be particularly careful to not cut essential corners.9
Case: Resolved
You ask the nurse to note the details of her follow-up phone conversation with the patient in the chart. You then call MC to explain the importance of the tests. She says she is unavailable to talk right now, so you ask her to come in for an appointment, free of charge. The patient makes an appointment but does not show.
You send a letter by certified mail describing the medical necessity for the tests and that her lack of adherence and refusal to come to the office have compelled you to end your clinician−patient relationship. You write that she should immediately identify another health care professional and suggest that she contact her managed care organization for assistance. You note that, should there be a medical emergency or urgent care needed in the next 30 days, you will provide that care. You enclose a release of medical records form in the letter.
In the patient’s record you note the details of the phone conversation and ask the office manager to add that the patient was a no show for her appointment. You include a copy of the certified letter and proof of mailing in the chart.
Two weeks later, the office manager reports that she is sending the patient’s records to another physician upon receipt of the release of medical records form from the patient.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
1. Kodner C. Challenging physician-patient interactions. FP Essentials. ed 354. AAFP home study. Leawood, KS: American Academy of Family Physicians; November 2008.
2. Harris SM. Take care when firing a patient. Am Med News. http://www.ama-assn.org/amed- news/2008/02/04/bica0204 .htm. Published February 4, 2008. Accessed May 8, 2015.
3. Lynch HF. Discrimination at the doctor’s office. N Engl J Med. 2013;386(18):1668–1670.
4. Jackson v Oklahoma Memorial Hospital, 909 P.2d 765 (OK 1995). http://law.justia.com/cases/oklahoma/supreme-court/1995/4226-1.html. Accessed May 8, 2015.
5. Randolph DS, Burkett TM. When physicians fire patients: avoiding patient “abandonment” lawsuits. J Okla State Med Assoc. 2009;102(11):356–358.
6. Crauman R, Baruch J. Abandonment in the physician-patient relationship. Med Health R I. 2004;87(5):154–156.
7. Cepelewicz BB. Firing a patient: when its needed and how to handle it correctly. Med Econ. 2014;91(2):42–43.
8. Santalucia C, Michota F. When and how is it appropriate to terminate the physician-patient relationship? Cleve Clin J Med. 2004;71(3):179–183.
9. Lippman H, Davenport J. Patient dismissal: the right way to do it. J Fam Pract. 2011;60(3):135–140. http://www.jfponline.com/specialty-focus/practice-management/article/patient-dismissal-the-right-way-to-do-it/30f9501e8b3eb6ddaf6dd67ce88e0d16.html. Accessed May 8, 2015.
1. Kodner C. Challenging physician-patient interactions. FP Essentials. ed 354. AAFP home study. Leawood, KS: American Academy of Family Physicians; November 2008.
2. Harris SM. Take care when firing a patient. Am Med News. http://www.ama-assn.org/amed- news/2008/02/04/bica0204 .htm. Published February 4, 2008. Accessed May 8, 2015.
3. Lynch HF. Discrimination at the doctor’s office. N Engl J Med. 2013;386(18):1668–1670.
4. Jackson v Oklahoma Memorial Hospital, 909 P.2d 765 (OK 1995). http://law.justia.com/cases/oklahoma/supreme-court/1995/4226-1.html. Accessed May 8, 2015.
5. Randolph DS, Burkett TM. When physicians fire patients: avoiding patient “abandonment” lawsuits. J Okla State Med Assoc. 2009;102(11):356–358.
6. Crauman R, Baruch J. Abandonment in the physician-patient relationship. Med Health R I. 2004;87(5):154–156.
7. Cepelewicz BB. Firing a patient: when its needed and how to handle it correctly. Med Econ. 2014;91(2):42–43.
8. Santalucia C, Michota F. When and how is it appropriate to terminate the physician-patient relationship? Cleve Clin J Med. 2004;71(3):179–183.
9. Lippman H, Davenport J. Patient dismissal: the right way to do it. J Fam Pract. 2011;60(3):135–140. http://www.jfponline.com/specialty-focus/practice-management/article/patient-dismissal-the-right-way-to-do-it/30f9501e8b3eb6ddaf6dd67ce88e0d16.html. Accessed May 8, 2015.
In this article
- Physicians’ ethical obligations
- Sample letter ending a clinician–patient relationship
