User login
The Society of Hospital Medicine’s 2012 State of Hospital Medicine report (SOHM) offers new insights about physician practice leaders.
Physician Leader Presence
“Choose a hospitalist leader with the right skills and experience. Selecting the right leader is fundamental to a successful hospitalist practice. These individuals are hard to find. They must be excellent clinically and have superb communication skills.”1
The SOHM survey shows that the vast majority (97%) of hospital medicine groups (HMGs) in the U.S. now have a designated physician leader (see Figure 1). Given this high percentage, examining the outliers is intriguing. Of the 13 adult medicine HMGs that reported not having a physician leader, the large majority were hospital-owned, located in the South region, and situated in non-teaching hospitals. The size of the HMG impacted the presence of a physician leader: 100% of groups with 20 or more full-time equivalents had physician leaders.
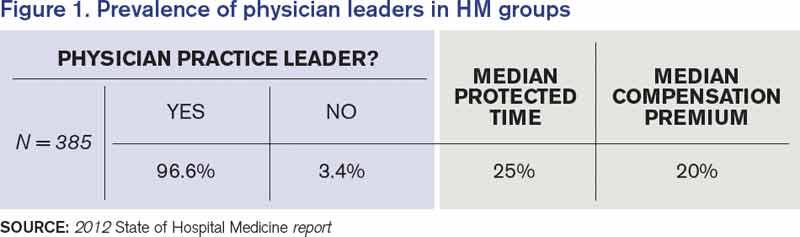
Source: 2012 State of Hospital Medicine report
Dedicated Leadership Time
“The medical director of the hospitalist program needs sufficient, non-clinical time to address administrative and leadership issues.”1
The 2007/2008 SOHM survey reported a median of 20% administrative time for physician leaders. In the 2012 survey, the median amount of time was 25% for adult medicine HMGs. The percentages were higher in the East and West regions, in hospital-owned programs, and in non- academic programs. The percentage of protected time also went up with group size.

Compensation
The 2012 SOHM shows median compensation premiums for physician leaders of 20%; that is, leader compensation is 120% of the average salary in their group. The numbers across regions and sizes were remarkably consistent. Overall, it seems that a 15% to 20% compensation premium for hospitalist leaders is standard.
Key Takeaways
No. 1, hospitalist groups need physician hospitalist leaders with protected leadership, but who also work clinically as a hospitalist. Why? Because hospitalists need a leader they respect, someone that they believe understands their specific issues. Unless the physician in charge has worked those 12-hour overnight shifts, argued with the consultants, tried to discharge an ornery patient, received 20 pages in an hour about medication reconciliation, or disagreed with an ED doc about the appropriateness of an admission, it would be hard for that leader to fully understand the stresses hospitalists encounter on a daily basis.
Hospitalist leaders are taking on increasingly important roles to help their organizations realize key performance improvement goals.
Additionally, the roles of outpatient doctors are changing: “Many physicians are no longer able or willing to serve on hospital committees or play a leadership role for the medical staff. Hospitalists have the potential to step in and help address these key issues”1
No. 2, size matters. Given increased responsibilities that include handling focused and ongoing professional practice evaluations, designing pathways to reduce adverse events, counseling, mentoring, disciplining, conducting yearly reviews, and investigating patient and staff complaints, it makes sense that larger programs also have leaders with more protected time and commensurate compensation.
As our healthcare systems ask hospitalists to offer higher reliability and to champion more administrative, safety, and quality projects, HM leaders—who are perfectly placed to organize and manage those projects—need the time and the compensation to do so. To borrow from hospitalist pioneer Bob Wachter, MD, MHM, our future C-suite leaders are percolating in hospitalist programs, learning the skills we will need to participate in the high reliability hospitals of our present and future.
Dr. Lovins is chief of hospital medicine at Middlesex Hospital in Middletown, Conn., and assistant clinical professor of medicine at Yale University School of Medicine. She is a member of SHM’s Practice Analysis Committee.
Reference
The Society of Hospital Medicine’s 2012 State of Hospital Medicine report (SOHM) offers new insights about physician practice leaders.
Physician Leader Presence
“Choose a hospitalist leader with the right skills and experience. Selecting the right leader is fundamental to a successful hospitalist practice. These individuals are hard to find. They must be excellent clinically and have superb communication skills.”1
The SOHM survey shows that the vast majority (97%) of hospital medicine groups (HMGs) in the U.S. now have a designated physician leader (see Figure 1). Given this high percentage, examining the outliers is intriguing. Of the 13 adult medicine HMGs that reported not having a physician leader, the large majority were hospital-owned, located in the South region, and situated in non-teaching hospitals. The size of the HMG impacted the presence of a physician leader: 100% of groups with 20 or more full-time equivalents had physician leaders.
Source: 2012 State of Hospital Medicine report
Dedicated Leadership Time
“The medical director of the hospitalist program needs sufficient, non-clinical time to address administrative and leadership issues.”1
The 2007/2008 SOHM survey reported a median of 20% administrative time for physician leaders. In the 2012 survey, the median amount of time was 25% for adult medicine HMGs. The percentages were higher in the East and West regions, in hospital-owned programs, and in non- academic programs. The percentage of protected time also went up with group size.
Compensation
The 2012 SOHM shows median compensation premiums for physician leaders of 20%; that is, leader compensation is 120% of the average salary in their group. The numbers across regions and sizes were remarkably consistent. Overall, it seems that a 15% to 20% compensation premium for hospitalist leaders is standard.
Key Takeaways
No. 1, hospitalist groups need physician hospitalist leaders with protected leadership, but who also work clinically as a hospitalist. Why? Because hospitalists need a leader they respect, someone that they believe understands their specific issues. Unless the physician in charge has worked those 12-hour overnight shifts, argued with the consultants, tried to discharge an ornery patient, received 20 pages in an hour about medication reconciliation, or disagreed with an ED doc about the appropriateness of an admission, it would be hard for that leader to fully understand the stresses hospitalists encounter on a daily basis.
Hospitalist leaders are taking on increasingly important roles to help their organizations realize key performance improvement goals.
Additionally, the roles of outpatient doctors are changing: “Many physicians are no longer able or willing to serve on hospital committees or play a leadership role for the medical staff. Hospitalists have the potential to step in and help address these key issues”1
No. 2, size matters. Given increased responsibilities that include handling focused and ongoing professional practice evaluations, designing pathways to reduce adverse events, counseling, mentoring, disciplining, conducting yearly reviews, and investigating patient and staff complaints, it makes sense that larger programs also have leaders with more protected time and commensurate compensation.
As our healthcare systems ask hospitalists to offer higher reliability and to champion more administrative, safety, and quality projects, HM leaders—who are perfectly placed to organize and manage those projects—need the time and the compensation to do so. To borrow from hospitalist pioneer Bob Wachter, MD, MHM, our future C-suite leaders are percolating in hospitalist programs, learning the skills we will need to participate in the high reliability hospitals of our present and future.
Dr. Lovins is chief of hospital medicine at Middlesex Hospital in Middletown, Conn., and assistant clinical professor of medicine at Yale University School of Medicine. She is a member of SHM’s Practice Analysis Committee.
Reference
The Society of Hospital Medicine’s 2012 State of Hospital Medicine report (SOHM) offers new insights about physician practice leaders.
Physician Leader Presence
“Choose a hospitalist leader with the right skills and experience. Selecting the right leader is fundamental to a successful hospitalist practice. These individuals are hard to find. They must be excellent clinically and have superb communication skills.”1
The SOHM survey shows that the vast majority (97%) of hospital medicine groups (HMGs) in the U.S. now have a designated physician leader (see Figure 1). Given this high percentage, examining the outliers is intriguing. Of the 13 adult medicine HMGs that reported not having a physician leader, the large majority were hospital-owned, located in the South region, and situated in non-teaching hospitals. The size of the HMG impacted the presence of a physician leader: 100% of groups with 20 or more full-time equivalents had physician leaders.
Source: 2012 State of Hospital Medicine report
Dedicated Leadership Time
“The medical director of the hospitalist program needs sufficient, non-clinical time to address administrative and leadership issues.”1
The 2007/2008 SOHM survey reported a median of 20% administrative time for physician leaders. In the 2012 survey, the median amount of time was 25% for adult medicine HMGs. The percentages were higher in the East and West regions, in hospital-owned programs, and in non- academic programs. The percentage of protected time also went up with group size.
Compensation
The 2012 SOHM shows median compensation premiums for physician leaders of 20%; that is, leader compensation is 120% of the average salary in their group. The numbers across regions and sizes were remarkably consistent. Overall, it seems that a 15% to 20% compensation premium for hospitalist leaders is standard.
Key Takeaways
No. 1, hospitalist groups need physician hospitalist leaders with protected leadership, but who also work clinically as a hospitalist. Why? Because hospitalists need a leader they respect, someone that they believe understands their specific issues. Unless the physician in charge has worked those 12-hour overnight shifts, argued with the consultants, tried to discharge an ornery patient, received 20 pages in an hour about medication reconciliation, or disagreed with an ED doc about the appropriateness of an admission, it would be hard for that leader to fully understand the stresses hospitalists encounter on a daily basis.
Hospitalist leaders are taking on increasingly important roles to help their organizations realize key performance improvement goals.
Additionally, the roles of outpatient doctors are changing: “Many physicians are no longer able or willing to serve on hospital committees or play a leadership role for the medical staff. Hospitalists have the potential to step in and help address these key issues”1
No. 2, size matters. Given increased responsibilities that include handling focused and ongoing professional practice evaluations, designing pathways to reduce adverse events, counseling, mentoring, disciplining, conducting yearly reviews, and investigating patient and staff complaints, it makes sense that larger programs also have leaders with more protected time and commensurate compensation.
As our healthcare systems ask hospitalists to offer higher reliability and to champion more administrative, safety, and quality projects, HM leaders—who are perfectly placed to organize and manage those projects—need the time and the compensation to do so. To borrow from hospitalist pioneer Bob Wachter, MD, MHM, our future C-suite leaders are percolating in hospitalist programs, learning the skills we will need to participate in the high reliability hospitals of our present and future.
Dr. Lovins is chief of hospital medicine at Middlesex Hospital in Middletown, Conn., and assistant clinical professor of medicine at Yale University School of Medicine. She is a member of SHM’s Practice Analysis Committee.