User login
Welcome to Current Psychiatry, a leading source of information, online and in print, for practitioners of psychiatry and its related subspecialties, including addiction psychiatry, child and adolescent psychiatry, and geriatric psychiatry. This Web site contains evidence-based reviews of the prevention, diagnosis, and treatment of mental illness and psychological disorders; case reports; updates on psychopharmacology; news about the specialty of psychiatry; pearls for practice; and other topics of interest and use to this audience.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-current-psychiatry')]
div[contains(@class, 'pane-pub-home-current-psychiatry')]
div[contains(@class, 'pane-pub-topic-current-psychiatry')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
7 ways to improve ‘cultural competence’
As this nation’s population becomes increasingly diverse, tailoring your practice to your area’s demographics is crucial to providing effective treatment.
Here’s how to improve your “cultural competence.”
- Recognize that culture extends beyond skin color. Although darker-skinned persons are commonly identified as “black” or African-American, some identify themselves as Hispanic, Jamaican, or white. Others may identify with their religion, gender, sexual preference, age, geography, socioeconomic status, or occupation. For example, the “tough-it-out” ethos of firefighters can breed denial of depression or trauma that limits their desire to seek or stay in treatment.
- Find out each patient’s cultural background. On your intake forms, include questions about race, ethnicity, language(s), religion, and age, or ask the patient to discuss his or her cultural background during the initial interview.
- Determine your cultural effectiveness. A sample breakdown of your patients can help you analyze treatment, compliance, progress, and outcomes among cultural groups.
- Make your patients feel “at home.” If possible, your staff should reflect your area’s cultural makeup.
- Conduct culturally sensitive evaluations. Cultural identification often leads to misdiagnosis.1 For example, African-American men tend to be over-diagnosed with paranoid schizophrenia or antisocial personality disorder.2
- Elicit patient expectations and preferences. Some cultures distrust modern drug therapy, while some patients think medication should magically resolve their disorders. Still others think psychotherapy works only for whites.
- Understand your cultural identity. Do a “cultural self-analysis” and see how your values apply to psychiatry. For example, if your culture values independence and individuality, you may underestimate the effectiveness of family therapy for patients whose cultures value interdependence.
1. Moffic HS, Kinzie JD. The history and future of cross-cultural psychiatric services. Comm Mental Health J 1996;32(6):581-92.
2. Whaley A. Cultural mistrust of white mental health clinicians among African Americans with severe mental illness. Am J Orthopsychiatry 2001;7(2):252-6.
Dr. Moffic is professor of psychiatry, Medical College of Wisconsin, Milwaukee.
As this nation’s population becomes increasingly diverse, tailoring your practice to your area’s demographics is crucial to providing effective treatment.
Here’s how to improve your “cultural competence.”
- Recognize that culture extends beyond skin color. Although darker-skinned persons are commonly identified as “black” or African-American, some identify themselves as Hispanic, Jamaican, or white. Others may identify with their religion, gender, sexual preference, age, geography, socioeconomic status, or occupation. For example, the “tough-it-out” ethos of firefighters can breed denial of depression or trauma that limits their desire to seek or stay in treatment.
- Find out each patient’s cultural background. On your intake forms, include questions about race, ethnicity, language(s), religion, and age, or ask the patient to discuss his or her cultural background during the initial interview.
- Determine your cultural effectiveness. A sample breakdown of your patients can help you analyze treatment, compliance, progress, and outcomes among cultural groups.
- Make your patients feel “at home.” If possible, your staff should reflect your area’s cultural makeup.
- Conduct culturally sensitive evaluations. Cultural identification often leads to misdiagnosis.1 For example, African-American men tend to be over-diagnosed with paranoid schizophrenia or antisocial personality disorder.2
- Elicit patient expectations and preferences. Some cultures distrust modern drug therapy, while some patients think medication should magically resolve their disorders. Still others think psychotherapy works only for whites.
- Understand your cultural identity. Do a “cultural self-analysis” and see how your values apply to psychiatry. For example, if your culture values independence and individuality, you may underestimate the effectiveness of family therapy for patients whose cultures value interdependence.
As this nation’s population becomes increasingly diverse, tailoring your practice to your area’s demographics is crucial to providing effective treatment.
Here’s how to improve your “cultural competence.”
- Recognize that culture extends beyond skin color. Although darker-skinned persons are commonly identified as “black” or African-American, some identify themselves as Hispanic, Jamaican, or white. Others may identify with their religion, gender, sexual preference, age, geography, socioeconomic status, or occupation. For example, the “tough-it-out” ethos of firefighters can breed denial of depression or trauma that limits their desire to seek or stay in treatment.
- Find out each patient’s cultural background. On your intake forms, include questions about race, ethnicity, language(s), religion, and age, or ask the patient to discuss his or her cultural background during the initial interview.
- Determine your cultural effectiveness. A sample breakdown of your patients can help you analyze treatment, compliance, progress, and outcomes among cultural groups.
- Make your patients feel “at home.” If possible, your staff should reflect your area’s cultural makeup.
- Conduct culturally sensitive evaluations. Cultural identification often leads to misdiagnosis.1 For example, African-American men tend to be over-diagnosed with paranoid schizophrenia or antisocial personality disorder.2
- Elicit patient expectations and preferences. Some cultures distrust modern drug therapy, while some patients think medication should magically resolve their disorders. Still others think psychotherapy works only for whites.
- Understand your cultural identity. Do a “cultural self-analysis” and see how your values apply to psychiatry. For example, if your culture values independence and individuality, you may underestimate the effectiveness of family therapy for patients whose cultures value interdependence.
1. Moffic HS, Kinzie JD. The history and future of cross-cultural psychiatric services. Comm Mental Health J 1996;32(6):581-92.
2. Whaley A. Cultural mistrust of white mental health clinicians among African Americans with severe mental illness. Am J Orthopsychiatry 2001;7(2):252-6.
Dr. Moffic is professor of psychiatry, Medical College of Wisconsin, Milwaukee.
1. Moffic HS, Kinzie JD. The history and future of cross-cultural psychiatric services. Comm Mental Health J 1996;32(6):581-92.
2. Whaley A. Cultural mistrust of white mental health clinicians among African Americans with severe mental illness. Am J Orthopsychiatry 2001;7(2):252-6.
Dr. Moffic is professor of psychiatry, Medical College of Wisconsin, Milwaukee.
Why are hospitals so stupid?
I’m sure we’ve all asked ourselves that question. Psychiatrists spend a lot of time observing hospitals. Our training requires us to work in hospitals, and many of us practice in hospitals after training.
You probably have ideas that could save your hospital thousands—even millions—of dollars, but the powers that be are not interested. You also, undoubtedly, have ideas to improve patient safety and satisfaction, but they are not interested in those, either.
Before anyone takes offense, I want to distinguish between hospitals—which tend to be stupid—and hospital administrators—who tend to be bright. I would guess that hospital administrators are even more frustrated than we are about how difficult it is for hospitals to make good decisions. Hospitals have this problem because they are big, complex systems with nobody in charge.
Years of “cost-based pricing”—when insurers paid whatever hospitals reported as t heir costs—contributed to hospital stupidity. This free-lunch reimbursement system may well have caused hospitals irreversible brain damage. It certainly made it difficult for them to adjust to “price-based costing”—having to bring costs in line with predetermined prices dictated by the payer.
I think, though, that the main reason hospitals became stupid was because they could get away with it. Hospitals had so much money and power that they did not need to be rational or responsive. Increased competition has eroded hospitals’ supremacy in the health-care market, but old habits die hard.
What can psychiatry learn from hospitals’ mistakes? If our profession could become more powerful without becoming stupid, we could rule the world—or, at least, the mental health care delivery system.

James Randolph Hillard, MD
Editor-in-Chief
James Randolph Hillard, MD
Editor-in-Chief
James Randolph Hillard, MD
Editor-in-Chief
I’m sure we’ve all asked ourselves that question. Psychiatrists spend a lot of time observing hospitals. Our training requires us to work in hospitals, and many of us practice in hospitals after training.
You probably have ideas that could save your hospital thousands—even millions—of dollars, but the powers that be are not interested. You also, undoubtedly, have ideas to improve patient safety and satisfaction, but they are not interested in those, either.
Before anyone takes offense, I want to distinguish between hospitals—which tend to be stupid—and hospital administrators—who tend to be bright. I would guess that hospital administrators are even more frustrated than we are about how difficult it is for hospitals to make good decisions. Hospitals have this problem because they are big, complex systems with nobody in charge.
Years of “cost-based pricing”—when insurers paid whatever hospitals reported as t heir costs—contributed to hospital stupidity. This free-lunch reimbursement system may well have caused hospitals irreversible brain damage. It certainly made it difficult for them to adjust to “price-based costing”—having to bring costs in line with predetermined prices dictated by the payer.
I think, though, that the main reason hospitals became stupid was because they could get away with it. Hospitals had so much money and power that they did not need to be rational or responsive. Increased competition has eroded hospitals’ supremacy in the health-care market, but old habits die hard.
What can psychiatry learn from hospitals’ mistakes? If our profession could become more powerful without becoming stupid, we could rule the world—or, at least, the mental health care delivery system.
I’m sure we’ve all asked ourselves that question. Psychiatrists spend a lot of time observing hospitals. Our training requires us to work in hospitals, and many of us practice in hospitals after training.
You probably have ideas that could save your hospital thousands—even millions—of dollars, but the powers that be are not interested. You also, undoubtedly, have ideas to improve patient safety and satisfaction, but they are not interested in those, either.
Before anyone takes offense, I want to distinguish between hospitals—which tend to be stupid—and hospital administrators—who tend to be bright. I would guess that hospital administrators are even more frustrated than we are about how difficult it is for hospitals to make good decisions. Hospitals have this problem because they are big, complex systems with nobody in charge.
Years of “cost-based pricing”—when insurers paid whatever hospitals reported as t heir costs—contributed to hospital stupidity. This free-lunch reimbursement system may well have caused hospitals irreversible brain damage. It certainly made it difficult for them to adjust to “price-based costing”—having to bring costs in line with predetermined prices dictated by the payer.
I think, though, that the main reason hospitals became stupid was because they could get away with it. Hospitals had so much money and power that they did not need to be rational or responsive. Increased competition has eroded hospitals’ supremacy in the health-care market, but old habits die hard.
What can psychiatry learn from hospitals’ mistakes? If our profession could become more powerful without becoming stupid, we could rule the world—or, at least, the mental health care delivery system.
First psychotic episode—a window of opportunity: Seize the moment to build a therapeutic alliance
A first psychotic episode offers the opportunity to build a therapeutic alliance at a teachable moment—while patients and their families are dealing with a devastating diagnosis. With a proactive approach, you can influence how patients view themselves and their experience, including psychotic illness, your efforts to treat its symptoms, and the costs and benefits of interventions.
Unfortunately, the typical first psychotic episode goes undiagnosed and untreated for 1 to 2 years, which some studies suggest may allow schizophrenia to progress. Although controversial, evidence links a prolonged duration of untreated psychosis to poorer outcome.1 Interventions during a prodromal (ie, pre-psychotic but already symptomatic) phase of schizophrenia also is being investigated, with the goal of attenuating—or perhaps even preventing—progression to frank psychosis.2-6
The implication for clinicians: timely identification and treatment may improve response, reduce relapse rates, and ultimately improve schizophrenic patients’ quality of life.
High rates of response—and relapse
Patients with a first psychotic episode show a higher response rate to antipsychotics—up to 87% within 1 year7 —and are more sensitive to side effects than are multi-episode patients.8 Yet despite their high response rate, new-onset patients often suffer from residual symptoms, even when treated in controlled settings. They also have a high rate of relapse—82% within 5 years.9
The strongest modifiable predictor of relapse is medication non-adherence, which has been shown to increase the risk of relapse five-fold.7 The first treatment experience provides a window of opportunity to help the patient accept taking medications as a normal part of life.
Mr. C, a 19-year-old college student, was brought for psychiatric admission after he told his roommates he was a new messiah who “needed to starve himself during the sunlight to enhance his holiness.” Approximately 7 months earlier he had become socially withdrawn and less able to do his college work. Two months later, he started using cannabis frequently. About 5 weeks prior to admission, he developed paranoid ideas involving his roommates and immersed himself in Eastern religions.
History and work-up. Mr. C was overweight and presented with mild dehydration. He did not report relevant signs of depression or mania and had no history of medical or psychiatric problems. Admission work-up included physical and neurologic exams, head CT, and blood work, which were unremarkable except for a positive cannabis toxicology. Family history was significant for one grandfather with alcohol abuse and one uncle who required psychiatric hospitalization in his 20s and never recovered functionally.
Family concerns. Mr. C’s parents were convinced a new diet was causing his symptoms and demanded that he be admitted to a medical ward. His brother insisted the symptoms were secondary to some “bad weed” and that everything would clear up in a few days. Although a brief medication-free observation period was considered to rule out substance-induced psychosis, the prodromal pattern of functional decline for more than 6 months and the bizarre quality of his delusions led to the diagnosis of a first episode of schizophrenia.
Treatment strategy. The treatment team met with Mr. C and his family to educate them about psychotic illness, the risks and benefits of novel antipsychotics, and the need to begin immediate treatment. With the patient’s and family’s consent, risperidone was initiated at 0.5 mg at bedtime and slowly increased over 1 week to 3 mg/d, with only mild and transient sedation. Within 3 weeks, Mr. C responded robustly and was discharged back to his family. Over the next 7 months, he continued taking risperidone, 3 mg/d, with some residual negative symptoms (social isolation without depression) and full remission of positive symptoms, which enabled him to return to college.
Therapeutic alliance. Your approach is key to building a therapeutic alliance with a person whose reality often is clouded by paranoia and referential thinking. Trust begins with the first clinical contact—during history-taking, ordering of tests, answering questions about the diagnosis, and discussing treatment options. Patients and their families must be informed about:
- target symptoms
- medication side effects
- predictors of response and relapse
- lack of certainty about how or when a patient will respond to any antipsychotic
- and the importance of rapid and uninterrupted treatment.
Supportive therapy. Support groups for the patient and family can help destigmatize the illness and reduce stress. Information about schizophrenia’s nature and course is available from the National Alliance for the Mentally Ill, National Mental Health Association, and other sources (see “Related resources”).10
CBT. Adjunctive cognitive-behavioral therapy (CBT) may speed up acute symptom response,11,12 reduce rates of nonresponse, and shorten hospital stays13 by helping patients deal with uncertainty about outer and inner realities. CBT approaches are understudied but so far have not been found to reduce relapse rates.
A moving target. As treatment moves from acute to consolidation and maintenance, target symptoms may change, side effects can limit the preferred approach, and partial or nonresponse may require drug or dosing adjustments. It is prudent to be prepared to re-evaluate the initial diagnosis as new symptoms emerge, response patterns develop, additional test or historical data become available, or as the illness’ course becomes more clear. To improve outcome, address comorbid or concurrent diseases—such as substance abuse or dependence, mood disorders, anxiety and obsessive-compulsive symptoms, or eating disorders.
Diagnostic work-up
As in Mr. C’s case (Box), a first psychotic episode is characterized by DSM-IV diagnostic criteria for schizophrenia, including hallucinations, delusions, disorganized thoughts or speech, disorganized behavior(s), or negative symptoms (such as anhedonia, amotivation, asociality, alogia, or affective flattening). The work-up is more comprehensive than that for subsequent episodes and includes a thorough history, complete physical examination, and brain imaging (Table 1) to explore other possible medical and psychiatric diagnoses (Table 2).
Table 1
WORK-UP OF PATIENTS PRESENTING WITHA FIRST EPISODE OF PSYCHOSIS
| Priority | Mode of evaluation |
|---|---|
| Routine | History Symptoms, time course, medical conditions, current/previous medications, herbs, drugs Medical and neurologic exam Blood work: CBC with differential, complete metabolic panel, thyroid and liver function tests, syphilis serology, pregnancy test, toxicology Urinalysis, toxicology ECG |
| Recommended | Fasting glucose and lipid profile (ideally before starting atypical antipsychotic) Head CT (especially if history of recent trauma) or brain MRI |
| Optional | Erythrocyte sedimentation rate, antinuclear antibodies, lumbar puncture, sleep-deprived EEG |
The history—ideally gathered from the patient and others—includes:
- medical and psychiatric diagnoses
- medications (prescribed and over-the-counter remedies)
- presence of stressors/triggers
- chronology of symptoms
- potential for the episode to endanger the patient or others.
Imaging. Despite a relatively low yield, we recommend that every patient with a first psychotic episode undergo a brain CT or MRI to rule out a potentially treatable organic cause for the psychosis.14
Other tests. Because of the increased risk of hyperglycemia, dyslipidemia, and possible cardiac conduction abnormalities with atypical antipsychotics, obtain a baseline fasting blood glucose, lipid profile, and ECG. A sleep-deprived EEG is recommended for patients with unclear motor movements or family history of epilepsy.
Choosing medications
Medication choices for the patient with first-episode schizophrenia are influenced by:
- target symptoms
- whether the symptoms endanger the patient or others
- the patient’s personal or family history of medication response or side effects
- a generally increased sensitivity to side effects in patients who have never been exposed to antipsychotics
- concurrent medical and/or psychiatric disorders
- prescriber, patient, and family preferences.
Psychiatrists generally select psychotropic classes by symptom domains (Table 3) and individual agents in each class by side effect profile. Except for clozapine’s superior effectiveness in patients with refractory psychosis, controlled studies have shown no clinically significant differences in efficacy among the drugs in each class—including the antipsychotics. Individual patients, however, may respond differently to different agents.
Principles of prescribing antipsychotics
Antipsychotics are effective in treating most psychotic core symptoms, such as hallucinations, delusions, agitation, aggression, and disorganized thinking and behavior. Other medications can be added to speed up or enhance treatment response or to target other domains.
Dosages. First-episode patients often require lower dosages and slower titration than multi-episode patients. As a rule, antipsychotics are started at about one-half the dosage given to patients with a chronic treatment history, although symptom severity and absence of side effects at lower dosages can help individualize titration.
Side effects. Atypical antipsychotics are preferred because of their reduced risk of extrapyramidal symptoms (EPS), positive effects on depressive and cognitive symptoms, and improved patient satisfaction and adherence, compared with the older antipsychotics.15-17 Atypicals’ potential side effects include weight gain, hyperglycemia, and dyslipidemia,18 as well as often-overlooked sexual side effects.19
Table 2
DIFFERENTIAL DIAGNOSIS OF FIRST-EPISODE PSYCHOSIS
| Possible diagnosis | Key points for differentiation |
|---|---|
| Schizophrenia | 6 months of psychosis* (including prodromal symptoms); total duration of mood episodes brief relative to active and residual psychotic phases; not directly caused by medical condition or substance |
| Schizophreniform disorder | Same as above, except symptoms are present 1 to 6 months |
| Brief psychotic disorder | Same as above, except symptoms are present 1 day to 1 month |
| Delusional disorder | Apart from non-bizarre delusions, functioning not markedly impaired; total duration of mood episodes brief relative to active and residual psychotic phases; not caused by direct physiologic effects of medical condition or substance |
| Psychotic disorder NOS | Psychotic symptoms insufficient to make a specific diagnosis |
| Schizoaffective disorder | Like schizophrenia for at least 2 weeks, but with mania or major depression present for much of the active and residual psychotic periods |
| Mood disorder with psychosis | Psychotic symptoms occur exclusively during mood disorder episodes |
| Psychosis due to general medical condition | Psychotic symptoms caused by direct physiologic effects of a general medical condition |
| Delirium due to general medical condition | Psychotic symptoms associated with a disturbance in consciousness and other cognitive deficits; characterized by a fluctuating course |
| Dementia due to general medical condition | Psychotic symptoms associated with memory impairment and other cognitive deficits |
| Substance-induced psychotic disorder | Psychotic symptoms caused by direct physiologic effects of a substance; reaction exceeds that usually encountered with intoxication or withdrawal |
| Substance-induced psychotic delirium | Similar to above, but associated with a disturbance in consciousness and other cognitive deficits; characterized by a fluctuating course |
| Substance intoxication or withdrawal | Caused by direct physiologic effects of a substance; reaction is typically encountered with intoxication or withdrawal |
| Conversion disorder | Contradictory and inconsistent history and presentation; secondary gain |
| Malingering | Contradictory and inconsistent history and presentation; primary gain |
| * Psychotic symptoms must interfere with functioning, and at least two of the following are required: delusions, hallucinations, disorganized thoughts or speech, disorganized behavior, or negative symptoms (avolition, alogia, affective flattening, asociality, or anhedonia), unless delusions are bizarre (impossible), or hallucinations consist of a running commentary or of two or more voices conversing with each other. | |
| Source: Adapted from DSM-IV handbook of differential diagnosis. Washington, DC: American Psychiatric Press, 1995. | |
Consider the patient’s risk for side effects when choosing an atypical antipsychotic, as each drug has strengths and weaknesses. For example, it may be reasonable to consider:
- risperidone, ziprasidone, or aripiprazole—rather than olanzapine or quetiapine—for patients at high risk for weight gain or with a family history of diabetes
- avoiding risperidone for patients with an early indication of sensitivity to EPS or prolactin-related side effects
- an agent that can be loaded rapidly, such as olanzapine or aripiprazole—rather than an agent that requires titration, such as quetiapine—for a patient presenting with severe agitation.
Clozapine—because of its side effect potential—is generally reserved for patients who have not responded to at least two antipsychotic trials of at least 4 to 6 weeks duration and have a steady-state clozapine level >350 ng/dl.
Acute agitation. Short-acting IM formulations can be used effectively for acute agitation and impulsivity or for patients who refuse oral antipsychotics. Until recently, only first-generation antipsychotics such as haloperidol and fluphenazine were available in IM formulations. Injectable ziprasidone mesylate is now available for acute agitation and has been found to be as safe and effective as haloperidol. Lorazepam may be used to treat agitation or as an adjunct to a patient’s antipsychotic agent.
Adjunctive therapies
When antipsychotic monotherapy is inadequate, adjunctive medications may be considered:
- to treat catatonia, obsessive-compulsive disorder, or depression
- to resolve agitation or mania more quickly
- to control agitation or anxiety while an antipsychotic dosage is being titrated
- when side effects emerge or residual symptoms remain despite adequate dosage and duration of antipsychotic treatment.
Deciding if and when to add another drug depends on the nature and severity of target symptoms, the degree and time course of response, and whether side effects appear. If you use adjunctive therapies during acute stabilization, attempt to taper and discontinue them after the patient’s symptoms have improved. Avoid combining antipsychotics, as no clinical data support the effectiveness and safety of this practice.20
Benzodiazepines are often used adjunctively for agitation, anxiety, or temporary insomnia in patients with schizophrenia. Common dosages are:
- for agitation or anxiety, lorazepam, 0.5 to 2 mg bid or tid, or clonazepam, 0.5 mg bid to 2 mg tid
- for insomnia, lorazepam or clonazepam, 1 to 2 mg at bedtime, or zolpidem, 5 to 10 mg at bedtime.
Benzodiazepines also are effective for catatonia, which may be misdiagnosed as negative symptoms or depression when it presents as marked psychomotor retardation, staring, selective mutism, negativism, mild posturing, or stereotypies. If undiagnosed, catatonia may worsen during antipsychotic titration. Symptoms usually respond to high-dose lorazepam, 1 mg bid or tid, with increases up to a maximum dosage of 12 mg/d.
Mood stabilizers are often used adjunctively to treat acute agitation and disinhibition21 or as add-on agents for residual psychotic or affective symptoms. Recommended dosages and blood levels, as tolerated, are:
- valproic acid, starting at 10 to 20 mg/kg bid, with a target serum level of 60 to 120 μg/ml. A once-daily, extended-release formulation may improve compliance.
- lithium, starting at 300 mg bid to tid, aiming for a serum level of 0.8 to 1.2 mEq/L.
Manic symptoms in a schizoaffective presentation may require one or even two mood stabilizers.
Lamotrigine may be the treatment of choice for depressed patients with schizoaffective disorder, bipolar type.22 However, it must be started at 25 mg/d and titrated extremely slowly—by 25 mg every other week, up to a target 200 to 400 mg/d—to avoid the risk of potentially fatal Stevens-Johnson syndrome.
Gabapentin, 300 mg tid to 1,500 mg tid, may help treat anxiety—particularly in patients with comorbid substance abuse, in whom benzodiazepines should be used sparingly after stabilization.
Table 3
SYMPTOM-BASED DRUG TREATMENT OF FIRST-EPISODE SCHIZOPHRENIA
| Target symptom | Medication choices | Dosage range | Comments |
|---|---|---|---|
| Agitation | Atypical antipsychotic Mood stabilizer Benzodiazepine ECT | Depends on level of agitation and individual agent | Ziprasidone IM may be useful for acute agitation |
| Psychosis | Atypical antipsychotic ECT | =50% of dosage used for multiple episode patients | Start low/go slow, monitor side effects |
| Catatonia | Lorazepam ECT | 1 mg/d bid to4 mg/d tid | Use sedation, symptom resolution as threshold |
| Negative symptoms | Atypical antipsychotic Glycine, cycloserine may help | Dictated by positive symptom response | Effect on functioning, quality of life unclear |
| Cognitive symptoms | Atypical antipsychotic | Same as above for negative symptoms | Same as above |
| Insomnia | Lorazepam Zolpidem Trazodone Mirtazapine | 1 to 2 mg HS 5 to 10 mg HS 50 to 200 mg HS 7.5 to 15 mg HS | Short-term treatment preferred |
| Depression, obsessive-compulsive symptoms, anxiety/panic | SSRI, SNDRI, NDRI, SARI, NASA | As per individual agent Possible interference with | antipsychotic blood levels* |
| Parkinsonism | Benztropine Trihexyphenidyl | 0.5 to 2 mg/d 1 to 15 mg/d | Possible effect of decreased cognition |
| Akathisia | Propranolol | 20 to 160 mg/d | Monitor blood pressure |
| Weight gain | Ziprasidone Aripiprazole | Dictated by positive symptom response | Prevention more effective than remediation |
| Non-adherence | Olanzapine oral disintegrating tablets Risperidone liquid Risperidone microspheres | 5 to 20 mg/d 1 to 4 mg/d IM injections every 2 weeks | Dissolves instantly Can be mixed with water, coffee, orange juice, or low-fat milk Not yet available |
| * Fluoxetine and paroxetine increase risperidone levels by CYP-P450 2D6 inhibition; fluvoxamine increases clozapine and olanzapine levels by CYP-P450 1A2 inhibition; fluvoxamine and nefazodone increase quetiapine and may increase ziprasidone levels by CYP-P450 3A4 inhibition; all three CYP-P450 inhibitors may increase aripiprazole levels, but the extent is not known. | |||
| ECT: electroconvulsive therapy; SSRI: selective serotonin reuptake inhibitor; SNDRI: serotonin-norepinephrine-dopamine reuptake inhibitor; NDRI: norepinephrinedopamine reuptake inhibitor; SARI: serotonin antagonist and reuptake inhibitor; NASA: norepinephrine-antagonist and serotonin antagonist. | |||
Antidepressants. Patients with schizophrenia can develop depression, even if they do not meet diagnostic criteria for schizoaffective disorder. Untreated depression can lead to non-adherence, self-medication with alcohol or illicit substances, and increased risk of suicide.
Differentiating depression from negative symptoms may be difficult, but there are subtle distinctions:
- Patients with negative symptoms appear more emotionally flat and unconcerned about their lack of motivation and diminished social and role functioning.
- Depressed persons often verbalize their demoralization, hopelessness, and desire to feel and behave differently.
Treat depression with any selective serotonin reuptake inhibitor or other newer-generation antidepressant such as mirtazapine, nefazodone, or venlafaxine at usual doses, as tolerated.
Miscellaneous medications. Use anticholinergic medications such as benztropine, 0.5 to 2 mg bid, or trihexyphenidyl, 1 to 5 mg bid, if parkinsonian symptoms occur and changing to an antipsychotic with a lower EPS potential is not feasible.
For akathisia, propranolol (10 mg bid or tid; titrate up to 160 mg/d if pulse rate and blood pressure remain stable) or benzodiazepines may be useful. Amantadine may also be used at dosages between 50 and 150 mg bid.
Insomnia may be treated with low dosages of sedating antidepressants, such as trazodone, 50 to 200 mg HS, or mirtazapine, 7.5 to 15 mg HS.
Preventing relapse during maintenance
Medication adherence depends on patient insight and attitude towards medications.23 Once you start a first-episode patient on drug therapy, encourage adherence by monitoring symptoms and anticipating side effects. Every 3 months after the acute phase:
- Use a structured evaluation, such as the Brief Psychiatric Rating Scale,24 to plot symptom severity, response, and risk for relapse.
- Rate EPS with the Simpson-Angus Scale25 and tardive dyskinesia (TD) with the Abnormal Involuntary Movement Scale26 because EPS and TD are associated with poor symptom response, adherence, and outcome.7
Reinforce information about the chronic nature of schizophrenia, especially when the patient or family question why treatment is needed if symptoms have resolved. Continue to counsel them about the patient’s need for:
- regular sleep of sufficient duration and without sleep-wake reversal
- gradual return to premorbid social, educational, and vocational activities/responsibilities
- ongoing treatment.
Encourage vigilance for relapse warning signs, including insomnia, social withdrawal, anxiety, refusal to eat or take medications, suspiciousness, agitation, disorganization, preoccupation with overvalued ideas, or responses to internal stimuli.
If the patient is noncompliant with antipsychotics in tablets or capsules, options include:
- liquid risperidone or olanzapine in a rapidly dissolving form that the patient cannot hide and spit out later
- long-acting depot formulations if the patient cannot be supervised and monitored daily. Older antipsychotics (such as haloperidol decanoate and fluphenazine decanoate) are available in depot formulations, and the FDA is considering risperidone in a microsphere formulation that would allow biweekly injections.
Medication withdrawal
Although the ideal duration of maintenance treatment after a first psychotic episode is debatable, we recommend that antipsychotics be continued at the full dosage that achieved symptom remission for at least 1 year.27 Then, if the patient has returned to the premorbid baseline, you can attempt a gradual medication withdrawal across 2 to 4 months, ideally when the patient’s environment is stable.
Be cautious when withdrawing antipsychotics from patients with a family history of psychosis. Consider a more gradual dose reduction, ongoing group and/or individual psychotherapy, and at least monthly monitoring. When possible, involve people who are significant in the patient’s life and educate them to look for deterioration’s warning signs, such as insomnia, irritability, anxiety, social withdrawal, preoccupation with overvalued ideas, or pacing.
If relapse occurs, carefully assess how well the patient has adhered to medication. Once a second psychotic episode occurs, his or her medication probably should be continued indefinitely.
- National Alliance for the Mentally Ill (800) 950-NAMI (6264); www.nami.org
- National Mental Health Association (800) 969-NMHA (6642); www.nmha.org
- National Alliance for Research on Schizophrenia and Depression (516) 829-0091; www.narsad.org/index.html
- Miller R, Mason SE. Diagnosis schizophrenia. A comprehensive resource. New York: Columbia University Press, 2002.
Drug brand names
- Aripiprazole • Abilify
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Clozapine • Clozaril
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Lorazepam • Ativan
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Trazodone • Desyrel
- Venlafaxine • Effexor
- Ziprasidone • Geodon
- Zolpidem • Ambien
Disclosure
Dr. Correll reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Mendelowitz receives grant/research support from, is a consultant to, and/or is a speaker for Pfizer Inc., Bristol-Myers Squibb Co.; and AstraZeneca Pharmaceuticals.
Acknowledgments
Research for this article was supported by grant 5P30MH60575 to The Zucker Hillside Hospital Intervention Research Center for Schizophrenia from the National Institute of Mental Health, Bethesda, MD.
1. Norman RM, Malla AK. Duration of untreated psychosis: a critical examination of the concept and its importance. Psychol Med 2001;31:381-400.
2. Cornblatt B, Lencz T, Obuchowski M. The schizophrenia prodrome: treatment and high-risk perspectives. Schizophr Res 2002;54(1-2):177-86.
3. McGorry PD, Yung AR, Phillips LJ, et al. Randomized controlled trial of interventions designed to reduce the risk of progression to first-episode psychosis in a clinical sample with subthreshold symptoms. Arch Gen Psychiatry 2002;59(10):921-8.
4. Heinssen RK, Perkins DO, Appelbaum PS, et al. Informed consent in early psychosis research: National Institute of Mental Health workshop, November 15, 2000. Schizophr Bull 2001;27(4):571-83.
5. Miller TJ, McGlashan TH, Rosen JL, et al. Prospective diagnosis of the initial prodrome for schizophrenia based on the Structured Interview for Prodromal Syndromes: preliminary evidence of interrater reliability and predictive validity. Am J Psychiatry 2002;159(5):863-5.
6. Young LT, Bakish D, Beaulieu S. The neurobiology of treatment response to antidepressants and mood stabilizing medications. J Psychiatry Neurosci 2002;27(4):260-5.
7. Robinson D, Woerner MG, Alvir JM, et al. Predictors of relapse following response from a first episode of schizophrenia or schizoaffective disorder. Arch Gen Psychiatry 1999;56(3):241-7.
8. Tauscher J, Kapur S. Choosing the right dose of antipsychotics in schizophrenia: lessons from neuroimaging studies. CNS Drugs 2001;15:671-8.
9. Robinson D, Woerner MG, Alvir JM, et al. Predictors of relapse following response from a first episode of schizophrenia or schizoaffective disorder. Arch Gen Psychiatry 1999;56(3):241-7.
10. Miller R, Mason SE. Diagnosis schizophrenia. A comprehensive resource, New York: Columbia University Press, 2002.
11. Lewis S, Tarrier N, Haddock G, et al. Randomised controlled trial of cognitivebehavioural therapy in early schizophrenia: acute-phase outcomes. Br J Psychiatry Suppl 2002;43:S91-7.
12. Turkington D, Kingdon D, Turner T. Effectiveness of a brief cognitive-behavioural therapy intervention in the treatment of schizophrenia. Br J Psychiatry 2002;180:523-7.
13. Cormac I, Jones C, Campbell C. Cognitive behaviour therapy for schizophrenia. Cochrane Database Syst Rev 2002;(1):CD000524.-
14. Smith GN, Flynn SW, Kopala LC, et al. A comprehensive method of assessing routine CT scans in schizophrenia. Acta Psychiatr Scand 1997;96:395-401.
15. Leucht S, Pitschel-Walz G, Abraham D, et al. Efficacy and extrapyramidal sideeffects of the new antipsychotics olanzapine, quetiapine, risperidone, and sertindole compared to conventional antipsychotics and placebo. A meta-analysis of randomized controlled trials. Schizophr Res 1999;35(1):51-68.
16. Keefe RS, Silva SG, Perkins DO, Lieberman JA. The effects of atypical antipsychotic drugs on neurocognitive impairment in schizophrenia: A review and meta-analysis. Schizophr Bull 1999;25(2):201-22.
17. Dolder CR, Lacro JP, Dunn LB, Jeste DV. Antipsychotic medication adherence: is there a difference between typical and atypical agents? Am J Psychiatry 2002;159(1):103-8.
18. Vieweg WVR, Adler RA, Fernandez A. Weight control and antipsychotics: How to tip the scale away from diabetes and heart disease. Current Psychiatry 2002;1(5):10-19.
19. Compton MT, Miller AH. Sexual side effects associated with conventional and atypical antipsychotics. Psychopharmacol Bull 2001;35:89-108.
20. Stahl SM. Antipsychotic polypharmacy: squandering precious resources? J Clin Psychiatry 2002;63(2):93-4.
21. Casey DE, Daniel DG, Wassef AA, Tracy KA, Wozniak P, Sommerville KW. Effect of divalproex combined with olanzapine or risperidone in patients with an acute exacerbation of schizophrenia. Neuropsychopharmacology 2003;28(1):182-92.
22. Calabrese JR, Shelton MD, Rapport DJ, Kimmel SE. Bipolar disorders and the effectiveness of novel anticonvulsants. J Clin Psychiatry. 2002;63(Suppl 3):5-9.
23. Kampman O, Laippala P, Vaananen J, et al. Indicators of medication compliance in first-episode psychosis. Psychiatry Res 2002;110:39-48.
24. Overall JE, Gorham DR. Brief psychiatric rating scale. Psychol Rep 1962;10:799-812.
25. Simpson GM, Angus JW. A rating scale for extrapyramidal side effects. Acta Psychiatr Scand 1970(suppl);212:11-19.
26. Guy W (ed). ECDEU assessment manual for psychopharmacology. Publication ABM 76-338. Washington, DC: U.S. Department of Health, Education, and Welfare, 1976;534-7.
27. Bosveld-van Haandel LJ, Slooff CJ, van den Bosch RJ. Reasoning about the optimal duration of prophylactic antipsychotic medication in schizophrenia: evidence and arguments. Acta Psychiatr Scand 2001;103(5):335-46.
A first psychotic episode offers the opportunity to build a therapeutic alliance at a teachable moment—while patients and their families are dealing with a devastating diagnosis. With a proactive approach, you can influence how patients view themselves and their experience, including psychotic illness, your efforts to treat its symptoms, and the costs and benefits of interventions.
Unfortunately, the typical first psychotic episode goes undiagnosed and untreated for 1 to 2 years, which some studies suggest may allow schizophrenia to progress. Although controversial, evidence links a prolonged duration of untreated psychosis to poorer outcome.1 Interventions during a prodromal (ie, pre-psychotic but already symptomatic) phase of schizophrenia also is being investigated, with the goal of attenuating—or perhaps even preventing—progression to frank psychosis.2-6
The implication for clinicians: timely identification and treatment may improve response, reduce relapse rates, and ultimately improve schizophrenic patients’ quality of life.
High rates of response—and relapse
Patients with a first psychotic episode show a higher response rate to antipsychotics—up to 87% within 1 year7 —and are more sensitive to side effects than are multi-episode patients.8 Yet despite their high response rate, new-onset patients often suffer from residual symptoms, even when treated in controlled settings. They also have a high rate of relapse—82% within 5 years.9
The strongest modifiable predictor of relapse is medication non-adherence, which has been shown to increase the risk of relapse five-fold.7 The first treatment experience provides a window of opportunity to help the patient accept taking medications as a normal part of life.
Mr. C, a 19-year-old college student, was brought for psychiatric admission after he told his roommates he was a new messiah who “needed to starve himself during the sunlight to enhance his holiness.” Approximately 7 months earlier he had become socially withdrawn and less able to do his college work. Two months later, he started using cannabis frequently. About 5 weeks prior to admission, he developed paranoid ideas involving his roommates and immersed himself in Eastern religions.
History and work-up. Mr. C was overweight and presented with mild dehydration. He did not report relevant signs of depression or mania and had no history of medical or psychiatric problems. Admission work-up included physical and neurologic exams, head CT, and blood work, which were unremarkable except for a positive cannabis toxicology. Family history was significant for one grandfather with alcohol abuse and one uncle who required psychiatric hospitalization in his 20s and never recovered functionally.
Family concerns. Mr. C’s parents were convinced a new diet was causing his symptoms and demanded that he be admitted to a medical ward. His brother insisted the symptoms were secondary to some “bad weed” and that everything would clear up in a few days. Although a brief medication-free observation period was considered to rule out substance-induced psychosis, the prodromal pattern of functional decline for more than 6 months and the bizarre quality of his delusions led to the diagnosis of a first episode of schizophrenia.
Treatment strategy. The treatment team met with Mr. C and his family to educate them about psychotic illness, the risks and benefits of novel antipsychotics, and the need to begin immediate treatment. With the patient’s and family’s consent, risperidone was initiated at 0.5 mg at bedtime and slowly increased over 1 week to 3 mg/d, with only mild and transient sedation. Within 3 weeks, Mr. C responded robustly and was discharged back to his family. Over the next 7 months, he continued taking risperidone, 3 mg/d, with some residual negative symptoms (social isolation without depression) and full remission of positive symptoms, which enabled him to return to college.
Therapeutic alliance. Your approach is key to building a therapeutic alliance with a person whose reality often is clouded by paranoia and referential thinking. Trust begins with the first clinical contact—during history-taking, ordering of tests, answering questions about the diagnosis, and discussing treatment options. Patients and their families must be informed about:
- target symptoms
- medication side effects
- predictors of response and relapse
- lack of certainty about how or when a patient will respond to any antipsychotic
- and the importance of rapid and uninterrupted treatment.
Supportive therapy. Support groups for the patient and family can help destigmatize the illness and reduce stress. Information about schizophrenia’s nature and course is available from the National Alliance for the Mentally Ill, National Mental Health Association, and other sources (see “Related resources”).10
CBT. Adjunctive cognitive-behavioral therapy (CBT) may speed up acute symptom response,11,12 reduce rates of nonresponse, and shorten hospital stays13 by helping patients deal with uncertainty about outer and inner realities. CBT approaches are understudied but so far have not been found to reduce relapse rates.
A moving target. As treatment moves from acute to consolidation and maintenance, target symptoms may change, side effects can limit the preferred approach, and partial or nonresponse may require drug or dosing adjustments. It is prudent to be prepared to re-evaluate the initial diagnosis as new symptoms emerge, response patterns develop, additional test or historical data become available, or as the illness’ course becomes more clear. To improve outcome, address comorbid or concurrent diseases—such as substance abuse or dependence, mood disorders, anxiety and obsessive-compulsive symptoms, or eating disorders.
Diagnostic work-up
As in Mr. C’s case (Box), a first psychotic episode is characterized by DSM-IV diagnostic criteria for schizophrenia, including hallucinations, delusions, disorganized thoughts or speech, disorganized behavior(s), or negative symptoms (such as anhedonia, amotivation, asociality, alogia, or affective flattening). The work-up is more comprehensive than that for subsequent episodes and includes a thorough history, complete physical examination, and brain imaging (Table 1) to explore other possible medical and psychiatric diagnoses (Table 2).
Table 1
WORK-UP OF PATIENTS PRESENTING WITHA FIRST EPISODE OF PSYCHOSIS
| Priority | Mode of evaluation |
|---|---|
| Routine | History Symptoms, time course, medical conditions, current/previous medications, herbs, drugs Medical and neurologic exam Blood work: CBC with differential, complete metabolic panel, thyroid and liver function tests, syphilis serology, pregnancy test, toxicology Urinalysis, toxicology ECG |
| Recommended | Fasting glucose and lipid profile (ideally before starting atypical antipsychotic) Head CT (especially if history of recent trauma) or brain MRI |
| Optional | Erythrocyte sedimentation rate, antinuclear antibodies, lumbar puncture, sleep-deprived EEG |
The history—ideally gathered from the patient and others—includes:
- medical and psychiatric diagnoses
- medications (prescribed and over-the-counter remedies)
- presence of stressors/triggers
- chronology of symptoms
- potential for the episode to endanger the patient or others.
Imaging. Despite a relatively low yield, we recommend that every patient with a first psychotic episode undergo a brain CT or MRI to rule out a potentially treatable organic cause for the psychosis.14
Other tests. Because of the increased risk of hyperglycemia, dyslipidemia, and possible cardiac conduction abnormalities with atypical antipsychotics, obtain a baseline fasting blood glucose, lipid profile, and ECG. A sleep-deprived EEG is recommended for patients with unclear motor movements or family history of epilepsy.
Choosing medications
Medication choices for the patient with first-episode schizophrenia are influenced by:
- target symptoms
- whether the symptoms endanger the patient or others
- the patient’s personal or family history of medication response or side effects
- a generally increased sensitivity to side effects in patients who have never been exposed to antipsychotics
- concurrent medical and/or psychiatric disorders
- prescriber, patient, and family preferences.
Psychiatrists generally select psychotropic classes by symptom domains (Table 3) and individual agents in each class by side effect profile. Except for clozapine’s superior effectiveness in patients with refractory psychosis, controlled studies have shown no clinically significant differences in efficacy among the drugs in each class—including the antipsychotics. Individual patients, however, may respond differently to different agents.
Principles of prescribing antipsychotics
Antipsychotics are effective in treating most psychotic core symptoms, such as hallucinations, delusions, agitation, aggression, and disorganized thinking and behavior. Other medications can be added to speed up or enhance treatment response or to target other domains.
Dosages. First-episode patients often require lower dosages and slower titration than multi-episode patients. As a rule, antipsychotics are started at about one-half the dosage given to patients with a chronic treatment history, although symptom severity and absence of side effects at lower dosages can help individualize titration.
Side effects. Atypical antipsychotics are preferred because of their reduced risk of extrapyramidal symptoms (EPS), positive effects on depressive and cognitive symptoms, and improved patient satisfaction and adherence, compared with the older antipsychotics.15-17 Atypicals’ potential side effects include weight gain, hyperglycemia, and dyslipidemia,18 as well as often-overlooked sexual side effects.19
Table 2
DIFFERENTIAL DIAGNOSIS OF FIRST-EPISODE PSYCHOSIS
| Possible diagnosis | Key points for differentiation |
|---|---|
| Schizophrenia | 6 months of psychosis* (including prodromal symptoms); total duration of mood episodes brief relative to active and residual psychotic phases; not directly caused by medical condition or substance |
| Schizophreniform disorder | Same as above, except symptoms are present 1 to 6 months |
| Brief psychotic disorder | Same as above, except symptoms are present 1 day to 1 month |
| Delusional disorder | Apart from non-bizarre delusions, functioning not markedly impaired; total duration of mood episodes brief relative to active and residual psychotic phases; not caused by direct physiologic effects of medical condition or substance |
| Psychotic disorder NOS | Psychotic symptoms insufficient to make a specific diagnosis |
| Schizoaffective disorder | Like schizophrenia for at least 2 weeks, but with mania or major depression present for much of the active and residual psychotic periods |
| Mood disorder with psychosis | Psychotic symptoms occur exclusively during mood disorder episodes |
| Psychosis due to general medical condition | Psychotic symptoms caused by direct physiologic effects of a general medical condition |
| Delirium due to general medical condition | Psychotic symptoms associated with a disturbance in consciousness and other cognitive deficits; characterized by a fluctuating course |
| Dementia due to general medical condition | Psychotic symptoms associated with memory impairment and other cognitive deficits |
| Substance-induced psychotic disorder | Psychotic symptoms caused by direct physiologic effects of a substance; reaction exceeds that usually encountered with intoxication or withdrawal |
| Substance-induced psychotic delirium | Similar to above, but associated with a disturbance in consciousness and other cognitive deficits; characterized by a fluctuating course |
| Substance intoxication or withdrawal | Caused by direct physiologic effects of a substance; reaction is typically encountered with intoxication or withdrawal |
| Conversion disorder | Contradictory and inconsistent history and presentation; secondary gain |
| Malingering | Contradictory and inconsistent history and presentation; primary gain |
| * Psychotic symptoms must interfere with functioning, and at least two of the following are required: delusions, hallucinations, disorganized thoughts or speech, disorganized behavior, or negative symptoms (avolition, alogia, affective flattening, asociality, or anhedonia), unless delusions are bizarre (impossible), or hallucinations consist of a running commentary or of two or more voices conversing with each other. | |
| Source: Adapted from DSM-IV handbook of differential diagnosis. Washington, DC: American Psychiatric Press, 1995. | |
Consider the patient’s risk for side effects when choosing an atypical antipsychotic, as each drug has strengths and weaknesses. For example, it may be reasonable to consider:
- risperidone, ziprasidone, or aripiprazole—rather than olanzapine or quetiapine—for patients at high risk for weight gain or with a family history of diabetes
- avoiding risperidone for patients with an early indication of sensitivity to EPS or prolactin-related side effects
- an agent that can be loaded rapidly, such as olanzapine or aripiprazole—rather than an agent that requires titration, such as quetiapine—for a patient presenting with severe agitation.
Clozapine—because of its side effect potential—is generally reserved for patients who have not responded to at least two antipsychotic trials of at least 4 to 6 weeks duration and have a steady-state clozapine level >350 ng/dl.
Acute agitation. Short-acting IM formulations can be used effectively for acute agitation and impulsivity or for patients who refuse oral antipsychotics. Until recently, only first-generation antipsychotics such as haloperidol and fluphenazine were available in IM formulations. Injectable ziprasidone mesylate is now available for acute agitation and has been found to be as safe and effective as haloperidol. Lorazepam may be used to treat agitation or as an adjunct to a patient’s antipsychotic agent.
Adjunctive therapies
When antipsychotic monotherapy is inadequate, adjunctive medications may be considered:
- to treat catatonia, obsessive-compulsive disorder, or depression
- to resolve agitation or mania more quickly
- to control agitation or anxiety while an antipsychotic dosage is being titrated
- when side effects emerge or residual symptoms remain despite adequate dosage and duration of antipsychotic treatment.
Deciding if and when to add another drug depends on the nature and severity of target symptoms, the degree and time course of response, and whether side effects appear. If you use adjunctive therapies during acute stabilization, attempt to taper and discontinue them after the patient’s symptoms have improved. Avoid combining antipsychotics, as no clinical data support the effectiveness and safety of this practice.20
Benzodiazepines are often used adjunctively for agitation, anxiety, or temporary insomnia in patients with schizophrenia. Common dosages are:
- for agitation or anxiety, lorazepam, 0.5 to 2 mg bid or tid, or clonazepam, 0.5 mg bid to 2 mg tid
- for insomnia, lorazepam or clonazepam, 1 to 2 mg at bedtime, or zolpidem, 5 to 10 mg at bedtime.
Benzodiazepines also are effective for catatonia, which may be misdiagnosed as negative symptoms or depression when it presents as marked psychomotor retardation, staring, selective mutism, negativism, mild posturing, or stereotypies. If undiagnosed, catatonia may worsen during antipsychotic titration. Symptoms usually respond to high-dose lorazepam, 1 mg bid or tid, with increases up to a maximum dosage of 12 mg/d.
Mood stabilizers are often used adjunctively to treat acute agitation and disinhibition21 or as add-on agents for residual psychotic or affective symptoms. Recommended dosages and blood levels, as tolerated, are:
- valproic acid, starting at 10 to 20 mg/kg bid, with a target serum level of 60 to 120 μg/ml. A once-daily, extended-release formulation may improve compliance.
- lithium, starting at 300 mg bid to tid, aiming for a serum level of 0.8 to 1.2 mEq/L.
Manic symptoms in a schizoaffective presentation may require one or even two mood stabilizers.
Lamotrigine may be the treatment of choice for depressed patients with schizoaffective disorder, bipolar type.22 However, it must be started at 25 mg/d and titrated extremely slowly—by 25 mg every other week, up to a target 200 to 400 mg/d—to avoid the risk of potentially fatal Stevens-Johnson syndrome.
Gabapentin, 300 mg tid to 1,500 mg tid, may help treat anxiety—particularly in patients with comorbid substance abuse, in whom benzodiazepines should be used sparingly after stabilization.
Table 3
SYMPTOM-BASED DRUG TREATMENT OF FIRST-EPISODE SCHIZOPHRENIA
| Target symptom | Medication choices | Dosage range | Comments |
|---|---|---|---|
| Agitation | Atypical antipsychotic Mood stabilizer Benzodiazepine ECT | Depends on level of agitation and individual agent | Ziprasidone IM may be useful for acute agitation |
| Psychosis | Atypical antipsychotic ECT | =50% of dosage used for multiple episode patients | Start low/go slow, monitor side effects |
| Catatonia | Lorazepam ECT | 1 mg/d bid to4 mg/d tid | Use sedation, symptom resolution as threshold |
| Negative symptoms | Atypical antipsychotic Glycine, cycloserine may help | Dictated by positive symptom response | Effect on functioning, quality of life unclear |
| Cognitive symptoms | Atypical antipsychotic | Same as above for negative symptoms | Same as above |
| Insomnia | Lorazepam Zolpidem Trazodone Mirtazapine | 1 to 2 mg HS 5 to 10 mg HS 50 to 200 mg HS 7.5 to 15 mg HS | Short-term treatment preferred |
| Depression, obsessive-compulsive symptoms, anxiety/panic | SSRI, SNDRI, NDRI, SARI, NASA | As per individual agent Possible interference with | antipsychotic blood levels* |
| Parkinsonism | Benztropine Trihexyphenidyl | 0.5 to 2 mg/d 1 to 15 mg/d | Possible effect of decreased cognition |
| Akathisia | Propranolol | 20 to 160 mg/d | Monitor blood pressure |
| Weight gain | Ziprasidone Aripiprazole | Dictated by positive symptom response | Prevention more effective than remediation |
| Non-adherence | Olanzapine oral disintegrating tablets Risperidone liquid Risperidone microspheres | 5 to 20 mg/d 1 to 4 mg/d IM injections every 2 weeks | Dissolves instantly Can be mixed with water, coffee, orange juice, or low-fat milk Not yet available |
| * Fluoxetine and paroxetine increase risperidone levels by CYP-P450 2D6 inhibition; fluvoxamine increases clozapine and olanzapine levels by CYP-P450 1A2 inhibition; fluvoxamine and nefazodone increase quetiapine and may increase ziprasidone levels by CYP-P450 3A4 inhibition; all three CYP-P450 inhibitors may increase aripiprazole levels, but the extent is not known. | |||
| ECT: electroconvulsive therapy; SSRI: selective serotonin reuptake inhibitor; SNDRI: serotonin-norepinephrine-dopamine reuptake inhibitor; NDRI: norepinephrinedopamine reuptake inhibitor; SARI: serotonin antagonist and reuptake inhibitor; NASA: norepinephrine-antagonist and serotonin antagonist. | |||
Antidepressants. Patients with schizophrenia can develop depression, even if they do not meet diagnostic criteria for schizoaffective disorder. Untreated depression can lead to non-adherence, self-medication with alcohol or illicit substances, and increased risk of suicide.
Differentiating depression from negative symptoms may be difficult, but there are subtle distinctions:
- Patients with negative symptoms appear more emotionally flat and unconcerned about their lack of motivation and diminished social and role functioning.
- Depressed persons often verbalize their demoralization, hopelessness, and desire to feel and behave differently.
Treat depression with any selective serotonin reuptake inhibitor or other newer-generation antidepressant such as mirtazapine, nefazodone, or venlafaxine at usual doses, as tolerated.
Miscellaneous medications. Use anticholinergic medications such as benztropine, 0.5 to 2 mg bid, or trihexyphenidyl, 1 to 5 mg bid, if parkinsonian symptoms occur and changing to an antipsychotic with a lower EPS potential is not feasible.
For akathisia, propranolol (10 mg bid or tid; titrate up to 160 mg/d if pulse rate and blood pressure remain stable) or benzodiazepines may be useful. Amantadine may also be used at dosages between 50 and 150 mg bid.
Insomnia may be treated with low dosages of sedating antidepressants, such as trazodone, 50 to 200 mg HS, or mirtazapine, 7.5 to 15 mg HS.
Preventing relapse during maintenance
Medication adherence depends on patient insight and attitude towards medications.23 Once you start a first-episode patient on drug therapy, encourage adherence by monitoring symptoms and anticipating side effects. Every 3 months after the acute phase:
- Use a structured evaluation, such as the Brief Psychiatric Rating Scale,24 to plot symptom severity, response, and risk for relapse.
- Rate EPS with the Simpson-Angus Scale25 and tardive dyskinesia (TD) with the Abnormal Involuntary Movement Scale26 because EPS and TD are associated with poor symptom response, adherence, and outcome.7
Reinforce information about the chronic nature of schizophrenia, especially when the patient or family question why treatment is needed if symptoms have resolved. Continue to counsel them about the patient’s need for:
- regular sleep of sufficient duration and without sleep-wake reversal
- gradual return to premorbid social, educational, and vocational activities/responsibilities
- ongoing treatment.
Encourage vigilance for relapse warning signs, including insomnia, social withdrawal, anxiety, refusal to eat or take medications, suspiciousness, agitation, disorganization, preoccupation with overvalued ideas, or responses to internal stimuli.
If the patient is noncompliant with antipsychotics in tablets or capsules, options include:
- liquid risperidone or olanzapine in a rapidly dissolving form that the patient cannot hide and spit out later
- long-acting depot formulations if the patient cannot be supervised and monitored daily. Older antipsychotics (such as haloperidol decanoate and fluphenazine decanoate) are available in depot formulations, and the FDA is considering risperidone in a microsphere formulation that would allow biweekly injections.
Medication withdrawal
Although the ideal duration of maintenance treatment after a first psychotic episode is debatable, we recommend that antipsychotics be continued at the full dosage that achieved symptom remission for at least 1 year.27 Then, if the patient has returned to the premorbid baseline, you can attempt a gradual medication withdrawal across 2 to 4 months, ideally when the patient’s environment is stable.
Be cautious when withdrawing antipsychotics from patients with a family history of psychosis. Consider a more gradual dose reduction, ongoing group and/or individual psychotherapy, and at least monthly monitoring. When possible, involve people who are significant in the patient’s life and educate them to look for deterioration’s warning signs, such as insomnia, irritability, anxiety, social withdrawal, preoccupation with overvalued ideas, or pacing.
If relapse occurs, carefully assess how well the patient has adhered to medication. Once a second psychotic episode occurs, his or her medication probably should be continued indefinitely.
- National Alliance for the Mentally Ill (800) 950-NAMI (6264); www.nami.org
- National Mental Health Association (800) 969-NMHA (6642); www.nmha.org
- National Alliance for Research on Schizophrenia and Depression (516) 829-0091; www.narsad.org/index.html
- Miller R, Mason SE. Diagnosis schizophrenia. A comprehensive resource. New York: Columbia University Press, 2002.
Drug brand names
- Aripiprazole • Abilify
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Clozapine • Clozaril
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Lorazepam • Ativan
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Trazodone • Desyrel
- Venlafaxine • Effexor
- Ziprasidone • Geodon
- Zolpidem • Ambien
Disclosure
Dr. Correll reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Mendelowitz receives grant/research support from, is a consultant to, and/or is a speaker for Pfizer Inc., Bristol-Myers Squibb Co.; and AstraZeneca Pharmaceuticals.
Acknowledgments
Research for this article was supported by grant 5P30MH60575 to The Zucker Hillside Hospital Intervention Research Center for Schizophrenia from the National Institute of Mental Health, Bethesda, MD.
A first psychotic episode offers the opportunity to build a therapeutic alliance at a teachable moment—while patients and their families are dealing with a devastating diagnosis. With a proactive approach, you can influence how patients view themselves and their experience, including psychotic illness, your efforts to treat its symptoms, and the costs and benefits of interventions.
Unfortunately, the typical first psychotic episode goes undiagnosed and untreated for 1 to 2 years, which some studies suggest may allow schizophrenia to progress. Although controversial, evidence links a prolonged duration of untreated psychosis to poorer outcome.1 Interventions during a prodromal (ie, pre-psychotic but already symptomatic) phase of schizophrenia also is being investigated, with the goal of attenuating—or perhaps even preventing—progression to frank psychosis.2-6
The implication for clinicians: timely identification and treatment may improve response, reduce relapse rates, and ultimately improve schizophrenic patients’ quality of life.
High rates of response—and relapse
Patients with a first psychotic episode show a higher response rate to antipsychotics—up to 87% within 1 year7 —and are more sensitive to side effects than are multi-episode patients.8 Yet despite their high response rate, new-onset patients often suffer from residual symptoms, even when treated in controlled settings. They also have a high rate of relapse—82% within 5 years.9
The strongest modifiable predictor of relapse is medication non-adherence, which has been shown to increase the risk of relapse five-fold.7 The first treatment experience provides a window of opportunity to help the patient accept taking medications as a normal part of life.
Mr. C, a 19-year-old college student, was brought for psychiatric admission after he told his roommates he was a new messiah who “needed to starve himself during the sunlight to enhance his holiness.” Approximately 7 months earlier he had become socially withdrawn and less able to do his college work. Two months later, he started using cannabis frequently. About 5 weeks prior to admission, he developed paranoid ideas involving his roommates and immersed himself in Eastern religions.
History and work-up. Mr. C was overweight and presented with mild dehydration. He did not report relevant signs of depression or mania and had no history of medical or psychiatric problems. Admission work-up included physical and neurologic exams, head CT, and blood work, which were unremarkable except for a positive cannabis toxicology. Family history was significant for one grandfather with alcohol abuse and one uncle who required psychiatric hospitalization in his 20s and never recovered functionally.
Family concerns. Mr. C’s parents were convinced a new diet was causing his symptoms and demanded that he be admitted to a medical ward. His brother insisted the symptoms were secondary to some “bad weed” and that everything would clear up in a few days. Although a brief medication-free observation period was considered to rule out substance-induced psychosis, the prodromal pattern of functional decline for more than 6 months and the bizarre quality of his delusions led to the diagnosis of a first episode of schizophrenia.
Treatment strategy. The treatment team met with Mr. C and his family to educate them about psychotic illness, the risks and benefits of novel antipsychotics, and the need to begin immediate treatment. With the patient’s and family’s consent, risperidone was initiated at 0.5 mg at bedtime and slowly increased over 1 week to 3 mg/d, with only mild and transient sedation. Within 3 weeks, Mr. C responded robustly and was discharged back to his family. Over the next 7 months, he continued taking risperidone, 3 mg/d, with some residual negative symptoms (social isolation without depression) and full remission of positive symptoms, which enabled him to return to college.
Therapeutic alliance. Your approach is key to building a therapeutic alliance with a person whose reality often is clouded by paranoia and referential thinking. Trust begins with the first clinical contact—during history-taking, ordering of tests, answering questions about the diagnosis, and discussing treatment options. Patients and their families must be informed about:
- target symptoms
- medication side effects
- predictors of response and relapse
- lack of certainty about how or when a patient will respond to any antipsychotic
- and the importance of rapid and uninterrupted treatment.
Supportive therapy. Support groups for the patient and family can help destigmatize the illness and reduce stress. Information about schizophrenia’s nature and course is available from the National Alliance for the Mentally Ill, National Mental Health Association, and other sources (see “Related resources”).10
CBT. Adjunctive cognitive-behavioral therapy (CBT) may speed up acute symptom response,11,12 reduce rates of nonresponse, and shorten hospital stays13 by helping patients deal with uncertainty about outer and inner realities. CBT approaches are understudied but so far have not been found to reduce relapse rates.
A moving target. As treatment moves from acute to consolidation and maintenance, target symptoms may change, side effects can limit the preferred approach, and partial or nonresponse may require drug or dosing adjustments. It is prudent to be prepared to re-evaluate the initial diagnosis as new symptoms emerge, response patterns develop, additional test or historical data become available, or as the illness’ course becomes more clear. To improve outcome, address comorbid or concurrent diseases—such as substance abuse or dependence, mood disorders, anxiety and obsessive-compulsive symptoms, or eating disorders.
Diagnostic work-up
As in Mr. C’s case (Box), a first psychotic episode is characterized by DSM-IV diagnostic criteria for schizophrenia, including hallucinations, delusions, disorganized thoughts or speech, disorganized behavior(s), or negative symptoms (such as anhedonia, amotivation, asociality, alogia, or affective flattening). The work-up is more comprehensive than that for subsequent episodes and includes a thorough history, complete physical examination, and brain imaging (Table 1) to explore other possible medical and psychiatric diagnoses (Table 2).
Table 1
WORK-UP OF PATIENTS PRESENTING WITHA FIRST EPISODE OF PSYCHOSIS
| Priority | Mode of evaluation |
|---|---|
| Routine | History Symptoms, time course, medical conditions, current/previous medications, herbs, drugs Medical and neurologic exam Blood work: CBC with differential, complete metabolic panel, thyroid and liver function tests, syphilis serology, pregnancy test, toxicology Urinalysis, toxicology ECG |
| Recommended | Fasting glucose and lipid profile (ideally before starting atypical antipsychotic) Head CT (especially if history of recent trauma) or brain MRI |
| Optional | Erythrocyte sedimentation rate, antinuclear antibodies, lumbar puncture, sleep-deprived EEG |
The history—ideally gathered from the patient and others—includes:
- medical and psychiatric diagnoses
- medications (prescribed and over-the-counter remedies)
- presence of stressors/triggers
- chronology of symptoms
- potential for the episode to endanger the patient or others.
Imaging. Despite a relatively low yield, we recommend that every patient with a first psychotic episode undergo a brain CT or MRI to rule out a potentially treatable organic cause for the psychosis.14
Other tests. Because of the increased risk of hyperglycemia, dyslipidemia, and possible cardiac conduction abnormalities with atypical antipsychotics, obtain a baseline fasting blood glucose, lipid profile, and ECG. A sleep-deprived EEG is recommended for patients with unclear motor movements or family history of epilepsy.
Choosing medications
Medication choices for the patient with first-episode schizophrenia are influenced by:
- target symptoms
- whether the symptoms endanger the patient or others
- the patient’s personal or family history of medication response or side effects
- a generally increased sensitivity to side effects in patients who have never been exposed to antipsychotics
- concurrent medical and/or psychiatric disorders
- prescriber, patient, and family preferences.
Psychiatrists generally select psychotropic classes by symptom domains (Table 3) and individual agents in each class by side effect profile. Except for clozapine’s superior effectiveness in patients with refractory psychosis, controlled studies have shown no clinically significant differences in efficacy among the drugs in each class—including the antipsychotics. Individual patients, however, may respond differently to different agents.
Principles of prescribing antipsychotics
Antipsychotics are effective in treating most psychotic core symptoms, such as hallucinations, delusions, agitation, aggression, and disorganized thinking and behavior. Other medications can be added to speed up or enhance treatment response or to target other domains.
Dosages. First-episode patients often require lower dosages and slower titration than multi-episode patients. As a rule, antipsychotics are started at about one-half the dosage given to patients with a chronic treatment history, although symptom severity and absence of side effects at lower dosages can help individualize titration.
Side effects. Atypical antipsychotics are preferred because of their reduced risk of extrapyramidal symptoms (EPS), positive effects on depressive and cognitive symptoms, and improved patient satisfaction and adherence, compared with the older antipsychotics.15-17 Atypicals’ potential side effects include weight gain, hyperglycemia, and dyslipidemia,18 as well as often-overlooked sexual side effects.19
Table 2
DIFFERENTIAL DIAGNOSIS OF FIRST-EPISODE PSYCHOSIS
| Possible diagnosis | Key points for differentiation |
|---|---|
| Schizophrenia | 6 months of psychosis* (including prodromal symptoms); total duration of mood episodes brief relative to active and residual psychotic phases; not directly caused by medical condition or substance |
| Schizophreniform disorder | Same as above, except symptoms are present 1 to 6 months |
| Brief psychotic disorder | Same as above, except symptoms are present 1 day to 1 month |
| Delusional disorder | Apart from non-bizarre delusions, functioning not markedly impaired; total duration of mood episodes brief relative to active and residual psychotic phases; not caused by direct physiologic effects of medical condition or substance |
| Psychotic disorder NOS | Psychotic symptoms insufficient to make a specific diagnosis |
| Schizoaffective disorder | Like schizophrenia for at least 2 weeks, but with mania or major depression present for much of the active and residual psychotic periods |
| Mood disorder with psychosis | Psychotic symptoms occur exclusively during mood disorder episodes |
| Psychosis due to general medical condition | Psychotic symptoms caused by direct physiologic effects of a general medical condition |
| Delirium due to general medical condition | Psychotic symptoms associated with a disturbance in consciousness and other cognitive deficits; characterized by a fluctuating course |
| Dementia due to general medical condition | Psychotic symptoms associated with memory impairment and other cognitive deficits |
| Substance-induced psychotic disorder | Psychotic symptoms caused by direct physiologic effects of a substance; reaction exceeds that usually encountered with intoxication or withdrawal |
| Substance-induced psychotic delirium | Similar to above, but associated with a disturbance in consciousness and other cognitive deficits; characterized by a fluctuating course |
| Substance intoxication or withdrawal | Caused by direct physiologic effects of a substance; reaction is typically encountered with intoxication or withdrawal |
| Conversion disorder | Contradictory and inconsistent history and presentation; secondary gain |
| Malingering | Contradictory and inconsistent history and presentation; primary gain |
| * Psychotic symptoms must interfere with functioning, and at least two of the following are required: delusions, hallucinations, disorganized thoughts or speech, disorganized behavior, or negative symptoms (avolition, alogia, affective flattening, asociality, or anhedonia), unless delusions are bizarre (impossible), or hallucinations consist of a running commentary or of two or more voices conversing with each other. | |
| Source: Adapted from DSM-IV handbook of differential diagnosis. Washington, DC: American Psychiatric Press, 1995. | |
Consider the patient’s risk for side effects when choosing an atypical antipsychotic, as each drug has strengths and weaknesses. For example, it may be reasonable to consider:
- risperidone, ziprasidone, or aripiprazole—rather than olanzapine or quetiapine—for patients at high risk for weight gain or with a family history of diabetes
- avoiding risperidone for patients with an early indication of sensitivity to EPS or prolactin-related side effects
- an agent that can be loaded rapidly, such as olanzapine or aripiprazole—rather than an agent that requires titration, such as quetiapine—for a patient presenting with severe agitation.
Clozapine—because of its side effect potential—is generally reserved for patients who have not responded to at least two antipsychotic trials of at least 4 to 6 weeks duration and have a steady-state clozapine level >350 ng/dl.
Acute agitation. Short-acting IM formulations can be used effectively for acute agitation and impulsivity or for patients who refuse oral antipsychotics. Until recently, only first-generation antipsychotics such as haloperidol and fluphenazine were available in IM formulations. Injectable ziprasidone mesylate is now available for acute agitation and has been found to be as safe and effective as haloperidol. Lorazepam may be used to treat agitation or as an adjunct to a patient’s antipsychotic agent.
Adjunctive therapies
When antipsychotic monotherapy is inadequate, adjunctive medications may be considered:
- to treat catatonia, obsessive-compulsive disorder, or depression
- to resolve agitation or mania more quickly
- to control agitation or anxiety while an antipsychotic dosage is being titrated
- when side effects emerge or residual symptoms remain despite adequate dosage and duration of antipsychotic treatment.
Deciding if and when to add another drug depends on the nature and severity of target symptoms, the degree and time course of response, and whether side effects appear. If you use adjunctive therapies during acute stabilization, attempt to taper and discontinue them after the patient’s symptoms have improved. Avoid combining antipsychotics, as no clinical data support the effectiveness and safety of this practice.20
Benzodiazepines are often used adjunctively for agitation, anxiety, or temporary insomnia in patients with schizophrenia. Common dosages are:
- for agitation or anxiety, lorazepam, 0.5 to 2 mg bid or tid, or clonazepam, 0.5 mg bid to 2 mg tid
- for insomnia, lorazepam or clonazepam, 1 to 2 mg at bedtime, or zolpidem, 5 to 10 mg at bedtime.
Benzodiazepines also are effective for catatonia, which may be misdiagnosed as negative symptoms or depression when it presents as marked psychomotor retardation, staring, selective mutism, negativism, mild posturing, or stereotypies. If undiagnosed, catatonia may worsen during antipsychotic titration. Symptoms usually respond to high-dose lorazepam, 1 mg bid or tid, with increases up to a maximum dosage of 12 mg/d.
Mood stabilizers are often used adjunctively to treat acute agitation and disinhibition21 or as add-on agents for residual psychotic or affective symptoms. Recommended dosages and blood levels, as tolerated, are:
- valproic acid, starting at 10 to 20 mg/kg bid, with a target serum level of 60 to 120 μg/ml. A once-daily, extended-release formulation may improve compliance.
- lithium, starting at 300 mg bid to tid, aiming for a serum level of 0.8 to 1.2 mEq/L.
Manic symptoms in a schizoaffective presentation may require one or even two mood stabilizers.
Lamotrigine may be the treatment of choice for depressed patients with schizoaffective disorder, bipolar type.22 However, it must be started at 25 mg/d and titrated extremely slowly—by 25 mg every other week, up to a target 200 to 400 mg/d—to avoid the risk of potentially fatal Stevens-Johnson syndrome.
Gabapentin, 300 mg tid to 1,500 mg tid, may help treat anxiety—particularly in patients with comorbid substance abuse, in whom benzodiazepines should be used sparingly after stabilization.
Table 3
SYMPTOM-BASED DRUG TREATMENT OF FIRST-EPISODE SCHIZOPHRENIA
| Target symptom | Medication choices | Dosage range | Comments |
|---|---|---|---|
| Agitation | Atypical antipsychotic Mood stabilizer Benzodiazepine ECT | Depends on level of agitation and individual agent | Ziprasidone IM may be useful for acute agitation |
| Psychosis | Atypical antipsychotic ECT | =50% of dosage used for multiple episode patients | Start low/go slow, monitor side effects |
| Catatonia | Lorazepam ECT | 1 mg/d bid to4 mg/d tid | Use sedation, symptom resolution as threshold |
| Negative symptoms | Atypical antipsychotic Glycine, cycloserine may help | Dictated by positive symptom response | Effect on functioning, quality of life unclear |
| Cognitive symptoms | Atypical antipsychotic | Same as above for negative symptoms | Same as above |
| Insomnia | Lorazepam Zolpidem Trazodone Mirtazapine | 1 to 2 mg HS 5 to 10 mg HS 50 to 200 mg HS 7.5 to 15 mg HS | Short-term treatment preferred |
| Depression, obsessive-compulsive symptoms, anxiety/panic | SSRI, SNDRI, NDRI, SARI, NASA | As per individual agent Possible interference with | antipsychotic blood levels* |
| Parkinsonism | Benztropine Trihexyphenidyl | 0.5 to 2 mg/d 1 to 15 mg/d | Possible effect of decreased cognition |
| Akathisia | Propranolol | 20 to 160 mg/d | Monitor blood pressure |
| Weight gain | Ziprasidone Aripiprazole | Dictated by positive symptom response | Prevention more effective than remediation |
| Non-adherence | Olanzapine oral disintegrating tablets Risperidone liquid Risperidone microspheres | 5 to 20 mg/d 1 to 4 mg/d IM injections every 2 weeks | Dissolves instantly Can be mixed with water, coffee, orange juice, or low-fat milk Not yet available |
| * Fluoxetine and paroxetine increase risperidone levels by CYP-P450 2D6 inhibition; fluvoxamine increases clozapine and olanzapine levels by CYP-P450 1A2 inhibition; fluvoxamine and nefazodone increase quetiapine and may increase ziprasidone levels by CYP-P450 3A4 inhibition; all three CYP-P450 inhibitors may increase aripiprazole levels, but the extent is not known. | |||
| ECT: electroconvulsive therapy; SSRI: selective serotonin reuptake inhibitor; SNDRI: serotonin-norepinephrine-dopamine reuptake inhibitor; NDRI: norepinephrinedopamine reuptake inhibitor; SARI: serotonin antagonist and reuptake inhibitor; NASA: norepinephrine-antagonist and serotonin antagonist. | |||
Antidepressants. Patients with schizophrenia can develop depression, even if they do not meet diagnostic criteria for schizoaffective disorder. Untreated depression can lead to non-adherence, self-medication with alcohol or illicit substances, and increased risk of suicide.
Differentiating depression from negative symptoms may be difficult, but there are subtle distinctions:
- Patients with negative symptoms appear more emotionally flat and unconcerned about their lack of motivation and diminished social and role functioning.
- Depressed persons often verbalize their demoralization, hopelessness, and desire to feel and behave differently.
Treat depression with any selective serotonin reuptake inhibitor or other newer-generation antidepressant such as mirtazapine, nefazodone, or venlafaxine at usual doses, as tolerated.
Miscellaneous medications. Use anticholinergic medications such as benztropine, 0.5 to 2 mg bid, or trihexyphenidyl, 1 to 5 mg bid, if parkinsonian symptoms occur and changing to an antipsychotic with a lower EPS potential is not feasible.
For akathisia, propranolol (10 mg bid or tid; titrate up to 160 mg/d if pulse rate and blood pressure remain stable) or benzodiazepines may be useful. Amantadine may also be used at dosages between 50 and 150 mg bid.
Insomnia may be treated with low dosages of sedating antidepressants, such as trazodone, 50 to 200 mg HS, or mirtazapine, 7.5 to 15 mg HS.
Preventing relapse during maintenance
Medication adherence depends on patient insight and attitude towards medications.23 Once you start a first-episode patient on drug therapy, encourage adherence by monitoring symptoms and anticipating side effects. Every 3 months after the acute phase:
- Use a structured evaluation, such as the Brief Psychiatric Rating Scale,24 to plot symptom severity, response, and risk for relapse.
- Rate EPS with the Simpson-Angus Scale25 and tardive dyskinesia (TD) with the Abnormal Involuntary Movement Scale26 because EPS and TD are associated with poor symptom response, adherence, and outcome.7
Reinforce information about the chronic nature of schizophrenia, especially when the patient or family question why treatment is needed if symptoms have resolved. Continue to counsel them about the patient’s need for:
- regular sleep of sufficient duration and without sleep-wake reversal
- gradual return to premorbid social, educational, and vocational activities/responsibilities
- ongoing treatment.
Encourage vigilance for relapse warning signs, including insomnia, social withdrawal, anxiety, refusal to eat or take medications, suspiciousness, agitation, disorganization, preoccupation with overvalued ideas, or responses to internal stimuli.
If the patient is noncompliant with antipsychotics in tablets or capsules, options include:
- liquid risperidone or olanzapine in a rapidly dissolving form that the patient cannot hide and spit out later
- long-acting depot formulations if the patient cannot be supervised and monitored daily. Older antipsychotics (such as haloperidol decanoate and fluphenazine decanoate) are available in depot formulations, and the FDA is considering risperidone in a microsphere formulation that would allow biweekly injections.
Medication withdrawal
Although the ideal duration of maintenance treatment after a first psychotic episode is debatable, we recommend that antipsychotics be continued at the full dosage that achieved symptom remission for at least 1 year.27 Then, if the patient has returned to the premorbid baseline, you can attempt a gradual medication withdrawal across 2 to 4 months, ideally when the patient’s environment is stable.
Be cautious when withdrawing antipsychotics from patients with a family history of psychosis. Consider a more gradual dose reduction, ongoing group and/or individual psychotherapy, and at least monthly monitoring. When possible, involve people who are significant in the patient’s life and educate them to look for deterioration’s warning signs, such as insomnia, irritability, anxiety, social withdrawal, preoccupation with overvalued ideas, or pacing.
If relapse occurs, carefully assess how well the patient has adhered to medication. Once a second psychotic episode occurs, his or her medication probably should be continued indefinitely.
- National Alliance for the Mentally Ill (800) 950-NAMI (6264); www.nami.org
- National Mental Health Association (800) 969-NMHA (6642); www.nmha.org
- National Alliance for Research on Schizophrenia and Depression (516) 829-0091; www.narsad.org/index.html
- Miller R, Mason SE. Diagnosis schizophrenia. A comprehensive resource. New York: Columbia University Press, 2002.
Drug brand names
- Aripiprazole • Abilify
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Clozapine • Clozaril
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Lorazepam • Ativan
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Trazodone • Desyrel
- Venlafaxine • Effexor
- Ziprasidone • Geodon
- Zolpidem • Ambien
Disclosure
Dr. Correll reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Mendelowitz receives grant/research support from, is a consultant to, and/or is a speaker for Pfizer Inc., Bristol-Myers Squibb Co.; and AstraZeneca Pharmaceuticals.
Acknowledgments
Research for this article was supported by grant 5P30MH60575 to The Zucker Hillside Hospital Intervention Research Center for Schizophrenia from the National Institute of Mental Health, Bethesda, MD.
1. Norman RM, Malla AK. Duration of untreated psychosis: a critical examination of the concept and its importance. Psychol Med 2001;31:381-400.
2. Cornblatt B, Lencz T, Obuchowski M. The schizophrenia prodrome: treatment and high-risk perspectives. Schizophr Res 2002;54(1-2):177-86.
3. McGorry PD, Yung AR, Phillips LJ, et al. Randomized controlled trial of interventions designed to reduce the risk of progression to first-episode psychosis in a clinical sample with subthreshold symptoms. Arch Gen Psychiatry 2002;59(10):921-8.
4. Heinssen RK, Perkins DO, Appelbaum PS, et al. Informed consent in early psychosis research: National Institute of Mental Health workshop, November 15, 2000. Schizophr Bull 2001;27(4):571-83.
5. Miller TJ, McGlashan TH, Rosen JL, et al. Prospective diagnosis of the initial prodrome for schizophrenia based on the Structured Interview for Prodromal Syndromes: preliminary evidence of interrater reliability and predictive validity. Am J Psychiatry 2002;159(5):863-5.
6. Young LT, Bakish D, Beaulieu S. The neurobiology of treatment response to antidepressants and mood stabilizing medications. J Psychiatry Neurosci 2002;27(4):260-5.
7. Robinson D, Woerner MG, Alvir JM, et al. Predictors of relapse following response from a first episode of schizophrenia or schizoaffective disorder. Arch Gen Psychiatry 1999;56(3):241-7.
8. Tauscher J, Kapur S. Choosing the right dose of antipsychotics in schizophrenia: lessons from neuroimaging studies. CNS Drugs 2001;15:671-8.
9. Robinson D, Woerner MG, Alvir JM, et al. Predictors of relapse following response from a first episode of schizophrenia or schizoaffective disorder. Arch Gen Psychiatry 1999;56(3):241-7.
10. Miller R, Mason SE. Diagnosis schizophrenia. A comprehensive resource, New York: Columbia University Press, 2002.
11. Lewis S, Tarrier N, Haddock G, et al. Randomised controlled trial of cognitivebehavioural therapy in early schizophrenia: acute-phase outcomes. Br J Psychiatry Suppl 2002;43:S91-7.
12. Turkington D, Kingdon D, Turner T. Effectiveness of a brief cognitive-behavioural therapy intervention in the treatment of schizophrenia. Br J Psychiatry 2002;180:523-7.
13. Cormac I, Jones C, Campbell C. Cognitive behaviour therapy for schizophrenia. Cochrane Database Syst Rev 2002;(1):CD000524.-
14. Smith GN, Flynn SW, Kopala LC, et al. A comprehensive method of assessing routine CT scans in schizophrenia. Acta Psychiatr Scand 1997;96:395-401.
15. Leucht S, Pitschel-Walz G, Abraham D, et al. Efficacy and extrapyramidal sideeffects of the new antipsychotics olanzapine, quetiapine, risperidone, and sertindole compared to conventional antipsychotics and placebo. A meta-analysis of randomized controlled trials. Schizophr Res 1999;35(1):51-68.
16. Keefe RS, Silva SG, Perkins DO, Lieberman JA. The effects of atypical antipsychotic drugs on neurocognitive impairment in schizophrenia: A review and meta-analysis. Schizophr Bull 1999;25(2):201-22.
17. Dolder CR, Lacro JP, Dunn LB, Jeste DV. Antipsychotic medication adherence: is there a difference between typical and atypical agents? Am J Psychiatry 2002;159(1):103-8.
18. Vieweg WVR, Adler RA, Fernandez A. Weight control and antipsychotics: How to tip the scale away from diabetes and heart disease. Current Psychiatry 2002;1(5):10-19.
19. Compton MT, Miller AH. Sexual side effects associated with conventional and atypical antipsychotics. Psychopharmacol Bull 2001;35:89-108.
20. Stahl SM. Antipsychotic polypharmacy: squandering precious resources? J Clin Psychiatry 2002;63(2):93-4.
21. Casey DE, Daniel DG, Wassef AA, Tracy KA, Wozniak P, Sommerville KW. Effect of divalproex combined with olanzapine or risperidone in patients with an acute exacerbation of schizophrenia. Neuropsychopharmacology 2003;28(1):182-92.
22. Calabrese JR, Shelton MD, Rapport DJ, Kimmel SE. Bipolar disorders and the effectiveness of novel anticonvulsants. J Clin Psychiatry. 2002;63(Suppl 3):5-9.
23. Kampman O, Laippala P, Vaananen J, et al. Indicators of medication compliance in first-episode psychosis. Psychiatry Res 2002;110:39-48.
24. Overall JE, Gorham DR. Brief psychiatric rating scale. Psychol Rep 1962;10:799-812.
25. Simpson GM, Angus JW. A rating scale for extrapyramidal side effects. Acta Psychiatr Scand 1970(suppl);212:11-19.
26. Guy W (ed). ECDEU assessment manual for psychopharmacology. Publication ABM 76-338. Washington, DC: U.S. Department of Health, Education, and Welfare, 1976;534-7.
27. Bosveld-van Haandel LJ, Slooff CJ, van den Bosch RJ. Reasoning about the optimal duration of prophylactic antipsychotic medication in schizophrenia: evidence and arguments. Acta Psychiatr Scand 2001;103(5):335-46.
1. Norman RM, Malla AK. Duration of untreated psychosis: a critical examination of the concept and its importance. Psychol Med 2001;31:381-400.
2. Cornblatt B, Lencz T, Obuchowski M. The schizophrenia prodrome: treatment and high-risk perspectives. Schizophr Res 2002;54(1-2):177-86.
3. McGorry PD, Yung AR, Phillips LJ, et al. Randomized controlled trial of interventions designed to reduce the risk of progression to first-episode psychosis in a clinical sample with subthreshold symptoms. Arch Gen Psychiatry 2002;59(10):921-8.
4. Heinssen RK, Perkins DO, Appelbaum PS, et al. Informed consent in early psychosis research: National Institute of Mental Health workshop, November 15, 2000. Schizophr Bull 2001;27(4):571-83.
5. Miller TJ, McGlashan TH, Rosen JL, et al. Prospective diagnosis of the initial prodrome for schizophrenia based on the Structured Interview for Prodromal Syndromes: preliminary evidence of interrater reliability and predictive validity. Am J Psychiatry 2002;159(5):863-5.
6. Young LT, Bakish D, Beaulieu S. The neurobiology of treatment response to antidepressants and mood stabilizing medications. J Psychiatry Neurosci 2002;27(4):260-5.
7. Robinson D, Woerner MG, Alvir JM, et al. Predictors of relapse following response from a first episode of schizophrenia or schizoaffective disorder. Arch Gen Psychiatry 1999;56(3):241-7.
8. Tauscher J, Kapur S. Choosing the right dose of antipsychotics in schizophrenia: lessons from neuroimaging studies. CNS Drugs 2001;15:671-8.
9. Robinson D, Woerner MG, Alvir JM, et al. Predictors of relapse following response from a first episode of schizophrenia or schizoaffective disorder. Arch Gen Psychiatry 1999;56(3):241-7.
10. Miller R, Mason SE. Diagnosis schizophrenia. A comprehensive resource, New York: Columbia University Press, 2002.
11. Lewis S, Tarrier N, Haddock G, et al. Randomised controlled trial of cognitivebehavioural therapy in early schizophrenia: acute-phase outcomes. Br J Psychiatry Suppl 2002;43:S91-7.
12. Turkington D, Kingdon D, Turner T. Effectiveness of a brief cognitive-behavioural therapy intervention in the treatment of schizophrenia. Br J Psychiatry 2002;180:523-7.
13. Cormac I, Jones C, Campbell C. Cognitive behaviour therapy for schizophrenia. Cochrane Database Syst Rev 2002;(1):CD000524.-
14. Smith GN, Flynn SW, Kopala LC, et al. A comprehensive method of assessing routine CT scans in schizophrenia. Acta Psychiatr Scand 1997;96:395-401.
15. Leucht S, Pitschel-Walz G, Abraham D, et al. Efficacy and extrapyramidal sideeffects of the new antipsychotics olanzapine, quetiapine, risperidone, and sertindole compared to conventional antipsychotics and placebo. A meta-analysis of randomized controlled trials. Schizophr Res 1999;35(1):51-68.
16. Keefe RS, Silva SG, Perkins DO, Lieberman JA. The effects of atypical antipsychotic drugs on neurocognitive impairment in schizophrenia: A review and meta-analysis. Schizophr Bull 1999;25(2):201-22.
17. Dolder CR, Lacro JP, Dunn LB, Jeste DV. Antipsychotic medication adherence: is there a difference between typical and atypical agents? Am J Psychiatry 2002;159(1):103-8.
18. Vieweg WVR, Adler RA, Fernandez A. Weight control and antipsychotics: How to tip the scale away from diabetes and heart disease. Current Psychiatry 2002;1(5):10-19.
19. Compton MT, Miller AH. Sexual side effects associated with conventional and atypical antipsychotics. Psychopharmacol Bull 2001;35:89-108.
20. Stahl SM. Antipsychotic polypharmacy: squandering precious resources? J Clin Psychiatry 2002;63(2):93-4.
21. Casey DE, Daniel DG, Wassef AA, Tracy KA, Wozniak P, Sommerville KW. Effect of divalproex combined with olanzapine or risperidone in patients with an acute exacerbation of schizophrenia. Neuropsychopharmacology 2003;28(1):182-92.
22. Calabrese JR, Shelton MD, Rapport DJ, Kimmel SE. Bipolar disorders and the effectiveness of novel anticonvulsants. J Clin Psychiatry. 2002;63(Suppl 3):5-9.
23. Kampman O, Laippala P, Vaananen J, et al. Indicators of medication compliance in first-episode psychosis. Psychiatry Res 2002;110:39-48.
24. Overall JE, Gorham DR. Brief psychiatric rating scale. Psychol Rep 1962;10:799-812.
25. Simpson GM, Angus JW. A rating scale for extrapyramidal side effects. Acta Psychiatr Scand 1970(suppl);212:11-19.
26. Guy W (ed). ECDEU assessment manual for psychopharmacology. Publication ABM 76-338. Washington, DC: U.S. Department of Health, Education, and Welfare, 1976;534-7.
27. Bosveld-van Haandel LJ, Slooff CJ, van den Bosch RJ. Reasoning about the optimal duration of prophylactic antipsychotic medication in schizophrenia: evidence and arguments. Acta Psychiatr Scand 2001;103(5):335-46.
Managing a distraught patient during psychotherapy
When a patient revisits past trauma during psychotherapy, strong reactions may surface. There is no single best way to confront emotions such as anger or despair, nor does the patient warn you before an outburst happens. The emotional reaction could be part of the healing process or could signal the need for additional treatment. You must decide on the spot whether to move up the next session, check on the patient the next day, or hospitalize the patient for his or her protection.
Keys to assessment
Before gauging a distraught patient’s needs, consider:
- How well do you know the patient? An established patient can be appraised fairly quickly. Assessing a new patient with confidence may take more time, however.
- Can the patient set emotional boundaries? Can he or she make sound choices and consider their consequences?
- Does the patient have adequate support? Is the patient going home to an empty room, a loving family or significant other, or a situation between the two?
- What therapy model are you employing? For example, cognitive therapy might address the meaning a patient places on a situation or reaction.
Dealing with emotional reaction
When a patient becomes overwrought:
- Encourage the patient to talk about the issue. This allows the patient to problem-solve and gives you time to think and plan.
- Extend the therapy session, especially if you fear a prompt discharge would endanger the patient. Consider the patient’s cognitive and emotional state. If you are uneasy with his or her degree of self-control, don’t discharge that patient.
- Formulate a plan to address the trauma. You might say: “It seems clear that this is troubling you. How can we work together to ease the burden? Can you comfortably think it through so that we can work it out next week? Would writing down your feelings and thoughts help?”
- Move up the patient’s next appointment. If the patient typically reacts badly to a certain issue or cannot handle feeling distraught, bringing him or her back sooner can be reassuring.
- Call the patient that evening or the next day. A distraught patient who does not need immediate hospitalization may benefit from extra contact. Decide whether to call the patient at a set time or to arrange for the patient to contact you. These usually brief calls reassure you that the patient has gained some perspective toward the problem and convey to the patient that you care.
Arrange to admit the patient to the hospital until the acute situation is resolved or perspective restored. Consider a brief hospitalization:
- when a situation or issue seriously challenges the patient’s coping mechanisms
- for patients with a history of self-harm when stressed
- for a patient who is psychotic and whose response to the emotional state is unpredictable
- when drugs or alcohol cloud the patient’s sensorium
- for a patient who lives alone.
Dr. Schuyler, a cognitive therapist, is clinical associate professor of psychiatry, Medical University of South Carolina, Charleston.
When a patient revisits past trauma during psychotherapy, strong reactions may surface. There is no single best way to confront emotions such as anger or despair, nor does the patient warn you before an outburst happens. The emotional reaction could be part of the healing process or could signal the need for additional treatment. You must decide on the spot whether to move up the next session, check on the patient the next day, or hospitalize the patient for his or her protection.
Keys to assessment
Before gauging a distraught patient’s needs, consider:
- How well do you know the patient? An established patient can be appraised fairly quickly. Assessing a new patient with confidence may take more time, however.
- Can the patient set emotional boundaries? Can he or she make sound choices and consider their consequences?
- Does the patient have adequate support? Is the patient going home to an empty room, a loving family or significant other, or a situation between the two?
- What therapy model are you employing? For example, cognitive therapy might address the meaning a patient places on a situation or reaction.
Dealing with emotional reaction
When a patient becomes overwrought:
- Encourage the patient to talk about the issue. This allows the patient to problem-solve and gives you time to think and plan.
- Extend the therapy session, especially if you fear a prompt discharge would endanger the patient. Consider the patient’s cognitive and emotional state. If you are uneasy with his or her degree of self-control, don’t discharge that patient.
- Formulate a plan to address the trauma. You might say: “It seems clear that this is troubling you. How can we work together to ease the burden? Can you comfortably think it through so that we can work it out next week? Would writing down your feelings and thoughts help?”
- Move up the patient’s next appointment. If the patient typically reacts badly to a certain issue or cannot handle feeling distraught, bringing him or her back sooner can be reassuring.
- Call the patient that evening or the next day. A distraught patient who does not need immediate hospitalization may benefit from extra contact. Decide whether to call the patient at a set time or to arrange for the patient to contact you. These usually brief calls reassure you that the patient has gained some perspective toward the problem and convey to the patient that you care.
Arrange to admit the patient to the hospital until the acute situation is resolved or perspective restored. Consider a brief hospitalization:
- when a situation or issue seriously challenges the patient’s coping mechanisms
- for patients with a history of self-harm when stressed
- for a patient who is psychotic and whose response to the emotional state is unpredictable
- when drugs or alcohol cloud the patient’s sensorium
- for a patient who lives alone.
When a patient revisits past trauma during psychotherapy, strong reactions may surface. There is no single best way to confront emotions such as anger or despair, nor does the patient warn you before an outburst happens. The emotional reaction could be part of the healing process or could signal the need for additional treatment. You must decide on the spot whether to move up the next session, check on the patient the next day, or hospitalize the patient for his or her protection.
Keys to assessment
Before gauging a distraught patient’s needs, consider:
- How well do you know the patient? An established patient can be appraised fairly quickly. Assessing a new patient with confidence may take more time, however.
- Can the patient set emotional boundaries? Can he or she make sound choices and consider their consequences?
- Does the patient have adequate support? Is the patient going home to an empty room, a loving family or significant other, or a situation between the two?
- What therapy model are you employing? For example, cognitive therapy might address the meaning a patient places on a situation or reaction.
Dealing with emotional reaction
When a patient becomes overwrought:
- Encourage the patient to talk about the issue. This allows the patient to problem-solve and gives you time to think and plan.
- Extend the therapy session, especially if you fear a prompt discharge would endanger the patient. Consider the patient’s cognitive and emotional state. If you are uneasy with his or her degree of self-control, don’t discharge that patient.
- Formulate a plan to address the trauma. You might say: “It seems clear that this is troubling you. How can we work together to ease the burden? Can you comfortably think it through so that we can work it out next week? Would writing down your feelings and thoughts help?”
- Move up the patient’s next appointment. If the patient typically reacts badly to a certain issue or cannot handle feeling distraught, bringing him or her back sooner can be reassuring.
- Call the patient that evening or the next day. A distraught patient who does not need immediate hospitalization may benefit from extra contact. Decide whether to call the patient at a set time or to arrange for the patient to contact you. These usually brief calls reassure you that the patient has gained some perspective toward the problem and convey to the patient that you care.
Arrange to admit the patient to the hospital until the acute situation is resolved or perspective restored. Consider a brief hospitalization:
- when a situation or issue seriously challenges the patient’s coping mechanisms
- for patients with a history of self-harm when stressed
- for a patient who is psychotic and whose response to the emotional state is unpredictable
- when drugs or alcohol cloud the patient’s sensorium
- for a patient who lives alone.
Dr. Schuyler, a cognitive therapist, is clinical associate professor of psychiatry, Medical University of South Carolina, Charleston.
Dr. Schuyler, a cognitive therapist, is clinical associate professor of psychiatry, Medical University of South Carolina, Charleston.
Aripiprazole: What the researchers say
A typical antipsychotics have enhanced outcomes in schizophrenia while helping patients avert the troublesome motor effects associated with older agents. Some side effects, such as weight gain and prolactin elevation, have remained a concern, however.
Aripiprazole, a novel antipsychotic recently FDA-approved for treating schizophrenia, exhibited efficacy and tolerability in preclinical and clinical trials.
How aripiprazole works
Aripiprazole’s mechanism of action is important to our understanding of the dopamine hypothesis of antipsychotic effect.1
The dopamine hypothesis remains the predominant explanation of how antipsychotics work.2 However, the evolution of antipsychotic therapy has led to further refinement of the dopamine hypothesis, including selective dopamine (D4) antagonism, rapid dissociation from dopamine receptors, dopamine-serotonin receptor system interactions, dopamine-GABA system interactions, and now (with aripiprazole) partial agonist effects at dopamine (and selective serotonin) receptors.1,2
Table
ARIPIPRAZOLE: FASTFACTS
| Drug brand name: Abilify |
| Class: Atypical antipsychotic |
| FDA-approved indication: Schizophrenia |
| Approval date: Nov. 15, 2002 |
| Manufacturer: Bristol-Myers Squibb Co. & Otsuka America Pharmaceutical |
| Dosing forms: 10 mg, 15 mg, 20 mg, and 30 mg tablets |
| Recommended dosage: Start at 10 to 15 mg/d for all age groups. Maintenance dosage may be the same as initial dosage or may increase over time. Maximum recommended dosage is 30 mg/d. Cross-titration with prior treatment is recommended. |
Table 1
ARIPIPRAZOLE’S RECEPTOR-BINDING PROFILE
| Receptor type | Effect |
|---|---|
| Dopamine D2 | Partial agonism |
| Serotonin 5HT1A | Partial agonism |
| Serotonin 5HT2A | Antagonism |
| Alpha 1A | Minimal antagonism |
| Muscarinic | Minimal antagonism |
| Histaminergic | Minimal antagonism |
Table 2
POTENTIAL DRUG-DRUG INTERACTIONS WITH ARIPIPRAZOLE
| Drug | Effect on plasma concentration of aripiprazole |
|---|---|
| Quinidine | Increase |
| Ketoconazole | Increase |
| Carbamazepine | Decrease |
| Fluoxetine | Increase |
| Paroxetine | Increase |
Unlike other antipsychotics, which appear to act through dopamine receptor antagonism, aripiprazole is a potent partial agonist at both the dopamine (D2) and serotonin (5HT1A) receptors.1,2Table 1 describes the agent’s receptor-binding profile.
The agent offers 78% bioavailability. It is metabolized through the hepatic microenzyme system, specifically the cytochrome P450 enzymes 2D6 and 3A4. Use of nicotine does not alter the agent’s plasma levels. Its active moiety is aripiprazole with minor contributions from the derivative dehydro-aripiprazole.
Aripiprazole therapy can be started at 10 or 15 mg/d; the starting dosage—15 mg/d in most cases—may also suffice as maintenance therapy for many patients. If the patient does not respond, it is prudent to wait several weeks before increasing the dosage beyond 15 mg/d.
The FDA-approved maximum dosage for aripiprazole is 30 mg/d. However, information from clinical trials indicates that increasing the dosage from 15 to 30 mg/d does not enhance the antipsychotic’s efficacy.3,4 Because of its absorption properties, the agent can be taken with or without food.
Aripiprazole has a relatively long half-life (75 hours), so it can be administered once daily. This provides an advantage when switching treatments. Some information suggests that patients may be switched directly to aripiprazole,5 although cross-titration is recommended.3
Although data in clinical populations are insufficient, studies in normal volunteers suggest that aripiprazole can be given at regular dosages to older patients and to those with renal or hepatic impairment.3Table 2 highlights potential drug-drug interactions with agents that can influence the hepatic microenzyme system.
Efficacy
Aripiprazole has demonstrated efficacy in clinical studies of patients with schizophrenia and schizoaffective disorder.3-8
- In a placebo-controlled, 4-week trial, patients who received aripiprazole, 15 to 30 mg/d, or haloperidol, 10 mg/d, reported similar improvements in positive and negative symptoms, psychopathology, and overall function.6
- A placebo-controlled, 4-week trial of aripiprazole, 20 and 30 mg/d, compared with risperidone, 6 mg/d, revealed similar efficacy with respect to symptom improvement and overall functioning.7
- Aripiprazole and olanzapine demonstrated comparable efficacy in a 28-week study. However, patients in the aripiprazole group showed greater improvement at 8 weeks and sustained improvement through 28 weeks in a measure of verbal memory.8
Researchers have not yet compared aripiprazole with clozapine, quetiapine, or ziprasidone. Also, information on the dosing, efficacy, and tolerability of aripiprazole in patients with first-episode or treatment-refractory schizophrenia is limited. According to the manufacturers’ prescription information, aripiprazole’s long-term efficacy in schizophrenia treatment has not been established. Data on 1-year treatment with aripiprazole appear encouraging.3
Preliminary data suggest that aripiprazole may help treat nonpsychotic conditions, although which ones has yet to be determined. A 3-week, placebo-controlled study demonstrated that aripiprazole, 30 mg/d, helped ameliorate symptoms of mania.9
Tolerability
Aripiprazole’s side-effect profile, revealed in preclinical and clinical trials, suggests that the drug could be well tolerated among a broad range of patients.10
In the 4-week, placebo-controlled comparison with haloperidol, rates of extrapyramidal symptoms (EPS) among aripiprazole-treated patients were much lower than those in the haloperidol group and similar to those in the placebo group.6 There is no evidence that higher dosages of aripiprazole lead to increased EPS. It is also not known whether aripiprazole will cause EPS in children and in patients older than 65, who are more susceptible than other age groups to antipsychotic-induced motor side effects.
Aripiprazole is believed to be less likely than typical antipsychotics to induce tardive dyskinesia, but more long-term information is needed.3
Studies have associated aripiprazole use with some weight gain, but (marginally) less than risperidone,7 less than haloperidol,6 and substantially less than olanzapine.8 Direct comparisons with other atypicals are not yet available.
Aripiprazole’s effect on glucose metabolism has not been determined, but early information suggests a favorable profile with respect to metabolic indices. Aripiprazole does not appear to elevate prolactin or cause cardiac QTc prolongation. Sedation appears to be the most pronounced side effect; this effect also appears to increase with higher dosages.
As has happened with the other atypicals, the pattern of use for aripiprazole will unfold over time as clinicians gain experience with using this agent in distinct patient groups.
Related resources
- Jordan S, Koprivica V, Chen R, et al. The antipsychotic aripiprazole is a potent, partial agonist at the human 5HT(1A) receptor. Eur J Pharmacol 2002;50:873-83.
- Kane JM, Carson WH, Saha AR, et al. Efficacy and safety of aripiprazole and haloperidol versus placebo in patients with schizophrenia and schizoaffective disorder. J Clin Psychiatry 2002;63:763-71.
Drug brand names
- Carbamazepine • Tegretol
- Clozapine • Clozaril
- Fluoxetine • Prozac
- Haloperidol • Haldol
- Ketoconazole • Nizoral
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosure
Dr. Buckley receives grant support from, is a consultant to, and is a speaker for AstraZeneca Pharmaceuticals, Bristol-Myers Squibb Co., Eli Lilly and Co., Janssen Pharmaceutica, and Novartis Pharmaceuticals Corp.
Dr. Sinha is a consultant to Bristol-Myers Squibb Co.
Dr. Sebastian is a consultant to Eli Lilly and Co.
Ms. Stirewalt reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Stahl SM. Dopamine system stabilizers, aripiprazole, and the next generation of antipsychotics, part 1: “Goldilocks” actions at dopamine receptors. J Clin Psychiatry 2001;62:841-2.
2. Kapur S, Remington G. Dopamine D2 receptors and their role in atypical antipsychotic action: still necessary and maybe even sufficient. Biol Psychiatry 2001;50:873-83.
3. Buckley PF. Aripiprazole: efficacy and tolerability profile of a novel-acting atypical antipsychotic. Drugs of Today 2003 (in press).
4. Kujawa M, Carson WH, Stock E, et al. Meta-analysis of the efficacy of aripiprazole (abstract). Schizophr Res 2002;53.:
5. Casey D, Kujawa M, et al. Switching from other antipsychotics to aripiprazole (abstract). Int J Neuropsychopharmacol 2002;5(1):S187.-
6. Kane JM, Carson WH, Saha AR, et al. Efficacy and safety of aripiprazole and haloperidol versus placebo in patients with schizophrenia and schizoaffective disorder. J Clin Psychiatry 2002;63:763-71.
7. Potkin SG, et al. A comparison of aripiprazole versus risperidone in patients with schizophrenia. Arch Gen Psychiatry (in press)
8. Cornblatt B, Creen MF, et al. A comparison of cognitive performance on aripiprazole versus olanzapine (abstract). Int J Neuropsychopharmacol 2002;5(1):S185.-
9. Kujawa M, et al. A 52 week comparison of aripiprazole versus haloperidol in the treatment of schizophrenia (abstract). Int J Neuropsychopharmacol 2002;5(1):S186-
10. Keck P, Carson WH, Saha AR. A placebo controlled trial of aripiprazole for the treatment of mania. American Psychiatric Association annual meeting, Philadelphia, May 2002.
A typical antipsychotics have enhanced outcomes in schizophrenia while helping patients avert the troublesome motor effects associated with older agents. Some side effects, such as weight gain and prolactin elevation, have remained a concern, however.
Aripiprazole, a novel antipsychotic recently FDA-approved for treating schizophrenia, exhibited efficacy and tolerability in preclinical and clinical trials.
How aripiprazole works
Aripiprazole’s mechanism of action is important to our understanding of the dopamine hypothesis of antipsychotic effect.1
The dopamine hypothesis remains the predominant explanation of how antipsychotics work.2 However, the evolution of antipsychotic therapy has led to further refinement of the dopamine hypothesis, including selective dopamine (D4) antagonism, rapid dissociation from dopamine receptors, dopamine-serotonin receptor system interactions, dopamine-GABA system interactions, and now (with aripiprazole) partial agonist effects at dopamine (and selective serotonin) receptors.1,2
Table
ARIPIPRAZOLE: FASTFACTS
| Drug brand name: Abilify |
| Class: Atypical antipsychotic |
| FDA-approved indication: Schizophrenia |
| Approval date: Nov. 15, 2002 |
| Manufacturer: Bristol-Myers Squibb Co. & Otsuka America Pharmaceutical |
| Dosing forms: 10 mg, 15 mg, 20 mg, and 30 mg tablets |
| Recommended dosage: Start at 10 to 15 mg/d for all age groups. Maintenance dosage may be the same as initial dosage or may increase over time. Maximum recommended dosage is 30 mg/d. Cross-titration with prior treatment is recommended. |
Table 1
ARIPIPRAZOLE’S RECEPTOR-BINDING PROFILE
| Receptor type | Effect |
|---|---|
| Dopamine D2 | Partial agonism |
| Serotonin 5HT1A | Partial agonism |
| Serotonin 5HT2A | Antagonism |
| Alpha 1A | Minimal antagonism |
| Muscarinic | Minimal antagonism |
| Histaminergic | Minimal antagonism |
Table 2
POTENTIAL DRUG-DRUG INTERACTIONS WITH ARIPIPRAZOLE
| Drug | Effect on plasma concentration of aripiprazole |
|---|---|
| Quinidine | Increase |
| Ketoconazole | Increase |
| Carbamazepine | Decrease |
| Fluoxetine | Increase |
| Paroxetine | Increase |
Unlike other antipsychotics, which appear to act through dopamine receptor antagonism, aripiprazole is a potent partial agonist at both the dopamine (D2) and serotonin (5HT1A) receptors.1,2Table 1 describes the agent’s receptor-binding profile.
The agent offers 78% bioavailability. It is metabolized through the hepatic microenzyme system, specifically the cytochrome P450 enzymes 2D6 and 3A4. Use of nicotine does not alter the agent’s plasma levels. Its active moiety is aripiprazole with minor contributions from the derivative dehydro-aripiprazole.
Aripiprazole therapy can be started at 10 or 15 mg/d; the starting dosage—15 mg/d in most cases—may also suffice as maintenance therapy for many patients. If the patient does not respond, it is prudent to wait several weeks before increasing the dosage beyond 15 mg/d.
The FDA-approved maximum dosage for aripiprazole is 30 mg/d. However, information from clinical trials indicates that increasing the dosage from 15 to 30 mg/d does not enhance the antipsychotic’s efficacy.3,4 Because of its absorption properties, the agent can be taken with or without food.
Aripiprazole has a relatively long half-life (75 hours), so it can be administered once daily. This provides an advantage when switching treatments. Some information suggests that patients may be switched directly to aripiprazole,5 although cross-titration is recommended.3
Although data in clinical populations are insufficient, studies in normal volunteers suggest that aripiprazole can be given at regular dosages to older patients and to those with renal or hepatic impairment.3Table 2 highlights potential drug-drug interactions with agents that can influence the hepatic microenzyme system.
Efficacy
Aripiprazole has demonstrated efficacy in clinical studies of patients with schizophrenia and schizoaffective disorder.3-8
- In a placebo-controlled, 4-week trial, patients who received aripiprazole, 15 to 30 mg/d, or haloperidol, 10 mg/d, reported similar improvements in positive and negative symptoms, psychopathology, and overall function.6
- A placebo-controlled, 4-week trial of aripiprazole, 20 and 30 mg/d, compared with risperidone, 6 mg/d, revealed similar efficacy with respect to symptom improvement and overall functioning.7
- Aripiprazole and olanzapine demonstrated comparable efficacy in a 28-week study. However, patients in the aripiprazole group showed greater improvement at 8 weeks and sustained improvement through 28 weeks in a measure of verbal memory.8
Researchers have not yet compared aripiprazole with clozapine, quetiapine, or ziprasidone. Also, information on the dosing, efficacy, and tolerability of aripiprazole in patients with first-episode or treatment-refractory schizophrenia is limited. According to the manufacturers’ prescription information, aripiprazole’s long-term efficacy in schizophrenia treatment has not been established. Data on 1-year treatment with aripiprazole appear encouraging.3
Preliminary data suggest that aripiprazole may help treat nonpsychotic conditions, although which ones has yet to be determined. A 3-week, placebo-controlled study demonstrated that aripiprazole, 30 mg/d, helped ameliorate symptoms of mania.9
Tolerability
Aripiprazole’s side-effect profile, revealed in preclinical and clinical trials, suggests that the drug could be well tolerated among a broad range of patients.10
In the 4-week, placebo-controlled comparison with haloperidol, rates of extrapyramidal symptoms (EPS) among aripiprazole-treated patients were much lower than those in the haloperidol group and similar to those in the placebo group.6 There is no evidence that higher dosages of aripiprazole lead to increased EPS. It is also not known whether aripiprazole will cause EPS in children and in patients older than 65, who are more susceptible than other age groups to antipsychotic-induced motor side effects.
Aripiprazole is believed to be less likely than typical antipsychotics to induce tardive dyskinesia, but more long-term information is needed.3
Studies have associated aripiprazole use with some weight gain, but (marginally) less than risperidone,7 less than haloperidol,6 and substantially less than olanzapine.8 Direct comparisons with other atypicals are not yet available.
Aripiprazole’s effect on glucose metabolism has not been determined, but early information suggests a favorable profile with respect to metabolic indices. Aripiprazole does not appear to elevate prolactin or cause cardiac QTc prolongation. Sedation appears to be the most pronounced side effect; this effect also appears to increase with higher dosages.
As has happened with the other atypicals, the pattern of use for aripiprazole will unfold over time as clinicians gain experience with using this agent in distinct patient groups.
Related resources
- Jordan S, Koprivica V, Chen R, et al. The antipsychotic aripiprazole is a potent, partial agonist at the human 5HT(1A) receptor. Eur J Pharmacol 2002;50:873-83.
- Kane JM, Carson WH, Saha AR, et al. Efficacy and safety of aripiprazole and haloperidol versus placebo in patients with schizophrenia and schizoaffective disorder. J Clin Psychiatry 2002;63:763-71.
Drug brand names
- Carbamazepine • Tegretol
- Clozapine • Clozaril
- Fluoxetine • Prozac
- Haloperidol • Haldol
- Ketoconazole • Nizoral
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosure
Dr. Buckley receives grant support from, is a consultant to, and is a speaker for AstraZeneca Pharmaceuticals, Bristol-Myers Squibb Co., Eli Lilly and Co., Janssen Pharmaceutica, and Novartis Pharmaceuticals Corp.
Dr. Sinha is a consultant to Bristol-Myers Squibb Co.
Dr. Sebastian is a consultant to Eli Lilly and Co.
Ms. Stirewalt reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
A typical antipsychotics have enhanced outcomes in schizophrenia while helping patients avert the troublesome motor effects associated with older agents. Some side effects, such as weight gain and prolactin elevation, have remained a concern, however.
Aripiprazole, a novel antipsychotic recently FDA-approved for treating schizophrenia, exhibited efficacy and tolerability in preclinical and clinical trials.
How aripiprazole works
Aripiprazole’s mechanism of action is important to our understanding of the dopamine hypothesis of antipsychotic effect.1
The dopamine hypothesis remains the predominant explanation of how antipsychotics work.2 However, the evolution of antipsychotic therapy has led to further refinement of the dopamine hypothesis, including selective dopamine (D4) antagonism, rapid dissociation from dopamine receptors, dopamine-serotonin receptor system interactions, dopamine-GABA system interactions, and now (with aripiprazole) partial agonist effects at dopamine (and selective serotonin) receptors.1,2
Table
ARIPIPRAZOLE: FASTFACTS
| Drug brand name: Abilify |
| Class: Atypical antipsychotic |
| FDA-approved indication: Schizophrenia |
| Approval date: Nov. 15, 2002 |
| Manufacturer: Bristol-Myers Squibb Co. & Otsuka America Pharmaceutical |
| Dosing forms: 10 mg, 15 mg, 20 mg, and 30 mg tablets |
| Recommended dosage: Start at 10 to 15 mg/d for all age groups. Maintenance dosage may be the same as initial dosage or may increase over time. Maximum recommended dosage is 30 mg/d. Cross-titration with prior treatment is recommended. |
Table 1
ARIPIPRAZOLE’S RECEPTOR-BINDING PROFILE
| Receptor type | Effect |
|---|---|
| Dopamine D2 | Partial agonism |
| Serotonin 5HT1A | Partial agonism |
| Serotonin 5HT2A | Antagonism |
| Alpha 1A | Minimal antagonism |
| Muscarinic | Minimal antagonism |
| Histaminergic | Minimal antagonism |
Table 2
POTENTIAL DRUG-DRUG INTERACTIONS WITH ARIPIPRAZOLE
| Drug | Effect on plasma concentration of aripiprazole |
|---|---|
| Quinidine | Increase |
| Ketoconazole | Increase |
| Carbamazepine | Decrease |
| Fluoxetine | Increase |
| Paroxetine | Increase |
Unlike other antipsychotics, which appear to act through dopamine receptor antagonism, aripiprazole is a potent partial agonist at both the dopamine (D2) and serotonin (5HT1A) receptors.1,2Table 1 describes the agent’s receptor-binding profile.
The agent offers 78% bioavailability. It is metabolized through the hepatic microenzyme system, specifically the cytochrome P450 enzymes 2D6 and 3A4. Use of nicotine does not alter the agent’s plasma levels. Its active moiety is aripiprazole with minor contributions from the derivative dehydro-aripiprazole.
Aripiprazole therapy can be started at 10 or 15 mg/d; the starting dosage—15 mg/d in most cases—may also suffice as maintenance therapy for many patients. If the patient does not respond, it is prudent to wait several weeks before increasing the dosage beyond 15 mg/d.
The FDA-approved maximum dosage for aripiprazole is 30 mg/d. However, information from clinical trials indicates that increasing the dosage from 15 to 30 mg/d does not enhance the antipsychotic’s efficacy.3,4 Because of its absorption properties, the agent can be taken with or without food.
Aripiprazole has a relatively long half-life (75 hours), so it can be administered once daily. This provides an advantage when switching treatments. Some information suggests that patients may be switched directly to aripiprazole,5 although cross-titration is recommended.3
Although data in clinical populations are insufficient, studies in normal volunteers suggest that aripiprazole can be given at regular dosages to older patients and to those with renal or hepatic impairment.3Table 2 highlights potential drug-drug interactions with agents that can influence the hepatic microenzyme system.
Efficacy
Aripiprazole has demonstrated efficacy in clinical studies of patients with schizophrenia and schizoaffective disorder.3-8
- In a placebo-controlled, 4-week trial, patients who received aripiprazole, 15 to 30 mg/d, or haloperidol, 10 mg/d, reported similar improvements in positive and negative symptoms, psychopathology, and overall function.6
- A placebo-controlled, 4-week trial of aripiprazole, 20 and 30 mg/d, compared with risperidone, 6 mg/d, revealed similar efficacy with respect to symptom improvement and overall functioning.7
- Aripiprazole and olanzapine demonstrated comparable efficacy in a 28-week study. However, patients in the aripiprazole group showed greater improvement at 8 weeks and sustained improvement through 28 weeks in a measure of verbal memory.8
Researchers have not yet compared aripiprazole with clozapine, quetiapine, or ziprasidone. Also, information on the dosing, efficacy, and tolerability of aripiprazole in patients with first-episode or treatment-refractory schizophrenia is limited. According to the manufacturers’ prescription information, aripiprazole’s long-term efficacy in schizophrenia treatment has not been established. Data on 1-year treatment with aripiprazole appear encouraging.3
Preliminary data suggest that aripiprazole may help treat nonpsychotic conditions, although which ones has yet to be determined. A 3-week, placebo-controlled study demonstrated that aripiprazole, 30 mg/d, helped ameliorate symptoms of mania.9
Tolerability
Aripiprazole’s side-effect profile, revealed in preclinical and clinical trials, suggests that the drug could be well tolerated among a broad range of patients.10
In the 4-week, placebo-controlled comparison with haloperidol, rates of extrapyramidal symptoms (EPS) among aripiprazole-treated patients were much lower than those in the haloperidol group and similar to those in the placebo group.6 There is no evidence that higher dosages of aripiprazole lead to increased EPS. It is also not known whether aripiprazole will cause EPS in children and in patients older than 65, who are more susceptible than other age groups to antipsychotic-induced motor side effects.
Aripiprazole is believed to be less likely than typical antipsychotics to induce tardive dyskinesia, but more long-term information is needed.3
Studies have associated aripiprazole use with some weight gain, but (marginally) less than risperidone,7 less than haloperidol,6 and substantially less than olanzapine.8 Direct comparisons with other atypicals are not yet available.
Aripiprazole’s effect on glucose metabolism has not been determined, but early information suggests a favorable profile with respect to metabolic indices. Aripiprazole does not appear to elevate prolactin or cause cardiac QTc prolongation. Sedation appears to be the most pronounced side effect; this effect also appears to increase with higher dosages.
As has happened with the other atypicals, the pattern of use for aripiprazole will unfold over time as clinicians gain experience with using this agent in distinct patient groups.
Related resources
- Jordan S, Koprivica V, Chen R, et al. The antipsychotic aripiprazole is a potent, partial agonist at the human 5HT(1A) receptor. Eur J Pharmacol 2002;50:873-83.
- Kane JM, Carson WH, Saha AR, et al. Efficacy and safety of aripiprazole and haloperidol versus placebo in patients with schizophrenia and schizoaffective disorder. J Clin Psychiatry 2002;63:763-71.
Drug brand names
- Carbamazepine • Tegretol
- Clozapine • Clozaril
- Fluoxetine • Prozac
- Haloperidol • Haldol
- Ketoconazole • Nizoral
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosure
Dr. Buckley receives grant support from, is a consultant to, and is a speaker for AstraZeneca Pharmaceuticals, Bristol-Myers Squibb Co., Eli Lilly and Co., Janssen Pharmaceutica, and Novartis Pharmaceuticals Corp.
Dr. Sinha is a consultant to Bristol-Myers Squibb Co.
Dr. Sebastian is a consultant to Eli Lilly and Co.
Ms. Stirewalt reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Stahl SM. Dopamine system stabilizers, aripiprazole, and the next generation of antipsychotics, part 1: “Goldilocks” actions at dopamine receptors. J Clin Psychiatry 2001;62:841-2.
2. Kapur S, Remington G. Dopamine D2 receptors and their role in atypical antipsychotic action: still necessary and maybe even sufficient. Biol Psychiatry 2001;50:873-83.
3. Buckley PF. Aripiprazole: efficacy and tolerability profile of a novel-acting atypical antipsychotic. Drugs of Today 2003 (in press).
4. Kujawa M, Carson WH, Stock E, et al. Meta-analysis of the efficacy of aripiprazole (abstract). Schizophr Res 2002;53.:
5. Casey D, Kujawa M, et al. Switching from other antipsychotics to aripiprazole (abstract). Int J Neuropsychopharmacol 2002;5(1):S187.-
6. Kane JM, Carson WH, Saha AR, et al. Efficacy and safety of aripiprazole and haloperidol versus placebo in patients with schizophrenia and schizoaffective disorder. J Clin Psychiatry 2002;63:763-71.
7. Potkin SG, et al. A comparison of aripiprazole versus risperidone in patients with schizophrenia. Arch Gen Psychiatry (in press)
8. Cornblatt B, Creen MF, et al. A comparison of cognitive performance on aripiprazole versus olanzapine (abstract). Int J Neuropsychopharmacol 2002;5(1):S185.-
9. Kujawa M, et al. A 52 week comparison of aripiprazole versus haloperidol in the treatment of schizophrenia (abstract). Int J Neuropsychopharmacol 2002;5(1):S186-
10. Keck P, Carson WH, Saha AR. A placebo controlled trial of aripiprazole for the treatment of mania. American Psychiatric Association annual meeting, Philadelphia, May 2002.
1. Stahl SM. Dopamine system stabilizers, aripiprazole, and the next generation of antipsychotics, part 1: “Goldilocks” actions at dopamine receptors. J Clin Psychiatry 2001;62:841-2.
2. Kapur S, Remington G. Dopamine D2 receptors and their role in atypical antipsychotic action: still necessary and maybe even sufficient. Biol Psychiatry 2001;50:873-83.
3. Buckley PF. Aripiprazole: efficacy and tolerability profile of a novel-acting atypical antipsychotic. Drugs of Today 2003 (in press).
4. Kujawa M, Carson WH, Stock E, et al. Meta-analysis of the efficacy of aripiprazole (abstract). Schizophr Res 2002;53.:
5. Casey D, Kujawa M, et al. Switching from other antipsychotics to aripiprazole (abstract). Int J Neuropsychopharmacol 2002;5(1):S187.-
6. Kane JM, Carson WH, Saha AR, et al. Efficacy and safety of aripiprazole and haloperidol versus placebo in patients with schizophrenia and schizoaffective disorder. J Clin Psychiatry 2002;63:763-71.
7. Potkin SG, et al. A comparison of aripiprazole versus risperidone in patients with schizophrenia. Arch Gen Psychiatry (in press)
8. Cornblatt B, Creen MF, et al. A comparison of cognitive performance on aripiprazole versus olanzapine (abstract). Int J Neuropsychopharmacol 2002;5(1):S185.-
9. Kujawa M, et al. A 52 week comparison of aripiprazole versus haloperidol in the treatment of schizophrenia (abstract). Int J Neuropsychopharmacol 2002;5(1):S186-
10. Keck P, Carson WH, Saha AR. A placebo controlled trial of aripiprazole for the treatment of mania. American Psychiatric Association annual meeting, Philadelphia, May 2002.
Shedding light on SAD therapy
Dr. Hillard states that “light therapy should not be used without pharmacotherapy to treat a major depressive episode” in seasonal affective disorder, or SAD (Current Psychiatry, December 2002).
It is well supported that both full syndromal and sub-syndromal winter depression can be successfully treated with light therapy alone.1,2 Response rates have varied between 60 and 90%. Many—if not most—SAD specialists consider light therapy the treatment of choice.1 Antidepressant medication can be added later if light therapy does not achieve an optimal result.
An error appeared in Figure 1 of the Current Psychiatry supplement, “Foundational treatment for bipolar disorder” (March 2003). The correct figure is printed here.
Figure 1 Antimanic efficacy of olanzapine, 15 mg/d, in acute bipolar mania and mixed episodes
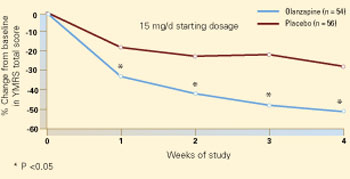
Patients with acute bipolar mania or a mixed episode were treated with olanzapine or placebo for 4 weeks in a randomized, double-blind trial. Compared with placebo, olanzapine at a starting dosage of 15 mg/d was associated with significant symptom improvement in the first week (50% change from baseline in Young Mania Rating Scale total score). This trend continued throughout the trial.
Source: Reprinted with permission from Tohen M et al. Arch Gen Psychiatry 2002; 57(9):841-9. Copyright 2002. American Medical Association
Psychotropics are first-line therapy only for severely depressed inpatients with SAD.2 This occurs infrequently, however, and even in these rare cases the efficacy of drug vs. light therapy or combined treatment has not been definitively studied.
J. Daniel Kanofsky MD, MPH; Assistant professor of psychiatry
Albert Einstein College of Medicine of Yeshiva University; Bronx, NY
Brenda Byrne, PhD; Margolis Berman Byrne Health Psychology Philadelphia, PA
- Wirz-Justice A. Beginning to see the light. Arch Gen Psychiatry 1998;55(10):861–2.
- Lam RW. Seasonal affective disorder: diagnosis and management. Primary Care Psychiatry 1998;4:63-74.
Your article on SAD indicates that “Light therapy can be used alone or in addition to pharmacotherapy in patients whose previously well-controlled depressive symptoms worsen in the fall or winter.”
However, Philips Electronics states on its Web site: “Do not take antidepressants in combination with light therapy—this may damage your eyes.”1
I would like an authoritative, reliable resolution. Can light therapy be used concurrently with antidepressants without resulting in eye damage?
Martin Schwartz; New York, NY
- Philips Bright Light Energy: Alternatives to light baths. Available at: www.brightlight.philips.co.uk/b/4.html. Accessed Feb. 25, 2003.
Dr. Hillard responds
I thank Drs. Kanofsky and Byrne and Mr. Schwartz for their insights.
After an extensive search of the literature and the Philips Electronics Web site, we can find no justification for not using drug therapy in SAD.
J. Randolph Hillard, MD
Editor-in-chief
Dr. Hillard states that “light therapy should not be used without pharmacotherapy to treat a major depressive episode” in seasonal affective disorder, or SAD (Current Psychiatry, December 2002).
It is well supported that both full syndromal and sub-syndromal winter depression can be successfully treated with light therapy alone.1,2 Response rates have varied between 60 and 90%. Many—if not most—SAD specialists consider light therapy the treatment of choice.1 Antidepressant medication can be added later if light therapy does not achieve an optimal result.
An error appeared in Figure 1 of the Current Psychiatry supplement, “Foundational treatment for bipolar disorder” (March 2003). The correct figure is printed here.
Figure 1 Antimanic efficacy of olanzapine, 15 mg/d, in acute bipolar mania and mixed episodes
Patients with acute bipolar mania or a mixed episode were treated with olanzapine or placebo for 4 weeks in a randomized, double-blind trial. Compared with placebo, olanzapine at a starting dosage of 15 mg/d was associated with significant symptom improvement in the first week (50% change from baseline in Young Mania Rating Scale total score). This trend continued throughout the trial.
Source: Reprinted with permission from Tohen M et al. Arch Gen Psychiatry 2002; 57(9):841-9. Copyright 2002. American Medical Association
Psychotropics are first-line therapy only for severely depressed inpatients with SAD.2 This occurs infrequently, however, and even in these rare cases the efficacy of drug vs. light therapy or combined treatment has not been definitively studied.
J. Daniel Kanofsky MD, MPH; Assistant professor of psychiatry
Albert Einstein College of Medicine of Yeshiva University; Bronx, NY
Brenda Byrne, PhD; Margolis Berman Byrne Health Psychology Philadelphia, PA
- Wirz-Justice A. Beginning to see the light. Arch Gen Psychiatry 1998;55(10):861–2.
- Lam RW. Seasonal affective disorder: diagnosis and management. Primary Care Psychiatry 1998;4:63-74.
Your article on SAD indicates that “Light therapy can be used alone or in addition to pharmacotherapy in patients whose previously well-controlled depressive symptoms worsen in the fall or winter.”
However, Philips Electronics states on its Web site: “Do not take antidepressants in combination with light therapy—this may damage your eyes.”1
I would like an authoritative, reliable resolution. Can light therapy be used concurrently with antidepressants without resulting in eye damage?
Martin Schwartz; New York, NY
- Philips Bright Light Energy: Alternatives to light baths. Available at: www.brightlight.philips.co.uk/b/4.html. Accessed Feb. 25, 2003.
Dr. Hillard responds
I thank Drs. Kanofsky and Byrne and Mr. Schwartz for their insights.
After an extensive search of the literature and the Philips Electronics Web site, we can find no justification for not using drug therapy in SAD.
J. Randolph Hillard, MD
Editor-in-chief
Dr. Hillard states that “light therapy should not be used without pharmacotherapy to treat a major depressive episode” in seasonal affective disorder, or SAD (Current Psychiatry, December 2002).
It is well supported that both full syndromal and sub-syndromal winter depression can be successfully treated with light therapy alone.1,2 Response rates have varied between 60 and 90%. Many—if not most—SAD specialists consider light therapy the treatment of choice.1 Antidepressant medication can be added later if light therapy does not achieve an optimal result.
An error appeared in Figure 1 of the Current Psychiatry supplement, “Foundational treatment for bipolar disorder” (March 2003). The correct figure is printed here.
Figure 1 Antimanic efficacy of olanzapine, 15 mg/d, in acute bipolar mania and mixed episodes
Patients with acute bipolar mania or a mixed episode were treated with olanzapine or placebo for 4 weeks in a randomized, double-blind trial. Compared with placebo, olanzapine at a starting dosage of 15 mg/d was associated with significant symptom improvement in the first week (50% change from baseline in Young Mania Rating Scale total score). This trend continued throughout the trial.
Source: Reprinted with permission from Tohen M et al. Arch Gen Psychiatry 2002; 57(9):841-9. Copyright 2002. American Medical Association
Psychotropics are first-line therapy only for severely depressed inpatients with SAD.2 This occurs infrequently, however, and even in these rare cases the efficacy of drug vs. light therapy or combined treatment has not been definitively studied.
J. Daniel Kanofsky MD, MPH; Assistant professor of psychiatry
Albert Einstein College of Medicine of Yeshiva University; Bronx, NY
Brenda Byrne, PhD; Margolis Berman Byrne Health Psychology Philadelphia, PA
- Wirz-Justice A. Beginning to see the light. Arch Gen Psychiatry 1998;55(10):861–2.
- Lam RW. Seasonal affective disorder: diagnosis and management. Primary Care Psychiatry 1998;4:63-74.
Your article on SAD indicates that “Light therapy can be used alone or in addition to pharmacotherapy in patients whose previously well-controlled depressive symptoms worsen in the fall or winter.”
However, Philips Electronics states on its Web site: “Do not take antidepressants in combination with light therapy—this may damage your eyes.”1
I would like an authoritative, reliable resolution. Can light therapy be used concurrently with antidepressants without resulting in eye damage?
Martin Schwartz; New York, NY
- Philips Bright Light Energy: Alternatives to light baths. Available at: www.brightlight.philips.co.uk/b/4.html. Accessed Feb. 25, 2003.
Dr. Hillard responds
I thank Drs. Kanofsky and Byrne and Mr. Schwartz for their insights.
After an extensive search of the literature and the Philips Electronics Web site, we can find no justification for not using drug therapy in SAD.
J. Randolph Hillard, MD
Editor-in-chief
Time to log off: New diagnostic criteria for problematic Internet use
Many psychiatrists diagnose problematic Internet use with schemas based on substance use disorders and pathologic gambling. These predefined diagnoses, however, may lead to premature conclusions and prevent you from fully exploring other treatable diagnoses.
We propose a screening tool called “MOUSE” and diagnostic criteria for problematic Internet use, which we developed from research by our group and others. This article discusses the new criteria and answers three questions:
- How does problematic Internet use present?
- Is it an addiction or an impulse control disorder?
- How can we help those afflicted with this problem?
When Internet use goes over the line
Recognizing problematic Internet use is difficult because the Internet can serve as a tool in nearly every aspect of our lives—communication, shopping, business, travel, research, entertainment, and more. The evidence suggests that Internet use becomes a behavior disorder when:
- an individual loses the ability to control his or her use and begins to suffer distress and impaired daily function1
- and employment and relationships are jeopardized by the hours spent online2 (Box).
Relationships—particularly marriages but also parent-child relationships, dating relationships, and close friendships—appear to suffer the greatest harm. At least one-half of “Internet addicts” (53%) report that their Internet use has caused serious relationship problems.
School. Academic problems are common; one study showed 58% of students blamed Internet use for a drop in grades, missed classes, declining study habits, or being placed on probation.
Workplace. Many executives—55% in one study—complain that time spent on the Internet for non-business purposes reduces their employees’ effectiveness.
Health. Some users spend 40 to 80 hours per week online, and single sessions can last up to 20 hours. Lack of sleep results in fatigue, decreased exercise, and decreased immunity. Sitting in front of the computer for hours also increases the risk of carpal tunnel syndrome, eye strain, and back pain.
Other addictions. The more time spent on the Internet, the greater the user’s risk of exposure to other addictive activities, such as online gambling and sexual solicitations. This risk is particularly concerning in children and adolescents.
Source: Young KS. Innovations in Clin Pract 1999;17:19-31.
Case: Computer gamer out of control
Mr. A is 32 and in his fourth year of college. His psychiatric history includes obsessive-compulsive disorder (OCD), paraphilia not otherwise specified, and bipolar disorder, most recently depressed in partial remission. He has had only one manic episode 10 years ago and took lithium briefly. He experienced pleasure from masturbating in public, but his paraphilia did not meet criteria for voyeurism as he did not want to be seen. He engaged in this behavior from ages 16 to 18 and found it distressing.
He is taking no medications. The only clinically significant family history is his father’s apparent OCD, undiagnosed and untreated.
Mr. A’s excessive computer use started in high school, when he played computer games to the point where his grades suffered. He began using the Internet at age 28, just before starting college, and spent most of his time online playing multi-player, video/strategy games.
Mr. A underestimates the time he spends online at 24 hours per week, including 21 hours in nonessential use and 3 hours in essential use (required for job or school). His actual average is 35.9 hours per week—nearly equivalent to a full-time job. He divides his nonessential use among various online activities, mostly related to playing computer games:
- 35% in chat forums, communicating with gaming partners he has never met
- 25% in multi-player, video/strategy games
- 15% using e-mail
- and lesser times surfing the Web (5%), transferring files (5%), viewing pornography (5%), shopping (5%), listening to music (3%), and selling (2%).
He reports rising tension before logging on and relief after doing so. He admits to using the Internet for longer periods than intended and especially when emotionally stressed. He knows his behavior has hurt him academically, and he has tried unsuccessfully to cut down or stop his Internet use.
Internet overuse: An ‘addiction’?
Ivan Goldberg introduced the idea of Internet addiction in 1995 by posting factitious “diagnostic criteria” on a Web site as a joke.3 He was surprised at the overwhelming response he received from persons whose Internet use was interfering with their lives. The first case reports were soon published.4,5
Initially, excessive Internet use was called an “addiction”—implying a disorder similar to substance dependence. Recently, however, Internet overuse has come to be viewed as more closely resembling an impulse control disorder.5-8 Shapira et al studied 20 subjects with problematic Internet use, and all met DSM-IV criteria for an impulse control disorder, not otherwise specified. Three also met criteria for obsessive-compulsive disorder.1
As with other impulse control disorders (such as eating disorders and pathologic gambling), researchers have noticed increased depression associated with pathologic Internet use.8
Diagnostic criteria. Although Mr. A’s comorbid psychiatric illnesses complicate his presentation, his behavior clearly could be described as representing an impulse control disorder. His case also meets our proposed criteria for problematic Internet use (Table 1),9 which we define as:
- uncontrollable
- markedly distressing, time-consuming, or resulting in social, occupational, or financial difficulties
- and not solely present during mania or hypomania.
Teasing out comorbid disorders
As in Mr. A’s case, Internet overuse can serve as an expression of and a conduit for other psychiatric illnesses. Studies have found high rates of comorbidity with mood and anxiety disorders, social phobias, attention-deficit disorder with or without hyperactivity, paraphilias, insomnia, pathologic gambling, and substance use disorders.10-12
Although some researchers feel that the many comorbid and complicating factors cannot be teased out,13 most agree that compulsive Internet use or overuse can have adverse consequences and that more research is needed.
A predisposition? Are “Internet addicts” predisposed to or susceptible to Internet overuse? Researchers are exploring whether Internet overuse causes or is an effect of psychiatric illness.
Shapira et al1,14 found at least one psychiatric condition that predated the development of Internet overuse in 20 subjects. In a similar study of 21 subjects with excessive computer use, Black11 found:
- 33% had a mood disorder
- 38% had a substance use disorder
- 19% had an anxiety disorder
- 52% met criteria for at least one personality disorder.
On average, these 41 subjects were in their 20s and 30s and reported having problems with Internet use for about 3 years. They spent an average of 28 hours per week online for pleasure or recreation, and many experienced emotional distress, social impairment, and social, occupational, or financial difficulties.1,11
Table 1
PROPOSED DIAGNOSTIC CRITERIA FOR PROBLEMATIC INTERNET USE
| Maladaptive preoccupation with Internet use, as indicated by at least one of the following: |
|
|
| Source: Reprinted with permission from an article by Shapira et al9 that has been accepted for publication in Depression and Anxiety. © Copyright 2003 John Wiley & Sons. |
Isolation and depression. Increasing Internet use and withdrawal from family activities has been associated with increased depression and loneliness; Kraut et al15 hypothesized that the Internet use caused the depression. Pratarelli et al16 noted a maladaptive cycle in some persons; the more isolated they feel, the more they use the Internet and increase their social withdrawal.
In a survey of college students, individuals with “Internet addiction” were found to:
- have obsessive characteristics
- prefer online interactions to real-life interactions
- use the Internet “to feel better,” alleviate depression, and become sexually aroused.16
Personality traits. In another study, Orzack12 found that subjects viewed the computer as a means to satisfy, induce excitement, and reduce tension or induce relief. Six personality traits were identified as strong predictors of “Internet addiction disorder:”
- boredom
- private self-consciousness
- loneliness
- social anxiety
- shyness
- and low self-esteem.
Table 2
5 SCREENING QUESTIONS FOR PROBLEMATIC INTERNET USE
| More than intended time spent online? |
| Other responsibilities or activities neglected? |
| Unsuccessful attempts to cut down? |
| Significant relationship discord due to use? |
| Excessive thoughts or anxiety when not online? |
Diagnosing Internet overuse
Screening. During any psychiatric interview, ask patients how they spend their free time or what they most enjoy doing. If patients say they spend hours on the Internet or their use appears to usurp other activities, five questions—easily recalled by the mnemonic MOUSE—can help you screen for problematic Internet use (Table 2).
History. Typically, persons with problematic Internet use spend time in one Internet domain, such as chat rooms, interactive games, news groups, or search engines.17 Ask which application they use, how many hours they use it, how they rank the importance of various applications, and what they like about their preferred application.
To determine how the Internet may alter the patient’s moods, ask how he or she feels while online as opposed to offline. Keeping an hourly log and a “feelings diary” may help the patient sort through his or her emotions.17
Often patients use the Internet to escape from dissatisfaction or disappointment or to counteract a sense of personal inadequacy.17 They tend to take pride in their computer skills2 and incorporate them into their daily lives in many ways, allowing them to rationalize their excessive Internet use (“I’m using it for work, academics, travel, research, etc.”).
Chomorbidities. Given the high incidence of psychiatric comorbidity,1 it is important to complete a thorough psychiatric evaluation and treat any underlying illness. Whether the illness is primary or comorbid, it is likely exacerbating the symptoms of problematic Internet use.
Changing problematic behaviors
Psychotherapy. Once you find the motives and possible causes of Internet overuse, what is the best form of treatment? This question warrants further study, but cognitive-behavioral therapy (CBT) is the primary treatment at this time.
The goal of CBT is for patients to disrupt their problematic computer use and reconstruct their routines with other activities. They can:
- use external timers to keep track of time online
- set goals of brief, frequent sessions online
- carry cards listing the destructive effects of their Internet use and ranking other activities they have neglected.17
Using emotion journals or mood monitoring forms may help the patient discover which dysfunctional thoughts and feelings are triggering excessive Internet use.12 Support groups and family therapy can help repair damaged relationships and engage friends and family in the treatment plan.
Drug therapy. No studies have looked at drug therapy for problematic Internet use, beyond treating comorbid psychiatric illnesses.
Treatment declined. Mr. A declined treatment for his problematic Internet use. As in many other psychiatric illnesses, insight into impulse control disorders tends to be limited. We can address the problem directly and offer to help patients change their online behaviors, but we cannot force them into treatment if they are not endangering themselves or others.
Related resources
- Computer Addiction Services. Maressa Hecht Orzack, PhD. www.computeraddiction.com; (617) 855-2908.
- Center for Online Addiction. Kimberly S. Young, PhD. www.netaddiction.com; (877) 292-3737.
1. Shapira NA, Goldsmith TG, Keck PE, Jr, Khosla UM, McElroy SL. Psychiatric features of individuals with problematic Internet use. J Affect Disord 2000;57:267-72.
2. Beard KW, Wolf EM. Modification in the proposed diagnostic criteria for Internet addiction. Cyberpsychol Behav 2001;4:377-83.
3. Goldberg I. Internet addiction. Available at http://www.cybernothing.org/jdfalk/media-coverage/archive/msg01305.html. Accessed Feb. 26, 2003.
4. Griffiths MD. Internet addiction: an issue for clinical psychology? Clin Psychol Forum 1996;97:32-6.
5. Young KS. Psychology of computer use: XL. Addictive use of the Internet: a case that breaks the stereotype. Psychol Rep 1996;79:899-902.
6. Treuer T, Fábián Z, Füredi J. Internet addiction associated with features of impulse control disorder: is it a real psychiatric disorder? J Affect Disord 2001;66:283.-
7. Young KS. Caught in the net: how to recognize the signs of Internet addiction-and a winning strategy for recovery. New York: John Wiley & Sons, Inc. 1998;8.-
8. Young KS, Rogers RC. The relationship between depression and Internet addiction. Cyberpsychol Behav 1998;1:25-8.
9. Shapira NA, Lessig MC, Goldsmith TD, et al. Problematic Internet use: proposed classification and diagnostic criteria. Depress Anxiety (in press).
10. Griffiths MD. Internet addiction: Fact or fiction? Psychologist 1999;12:246-50.
11. Black DW, Belsare G, Schlosser S. Clinical features, psychiatric comorbidity, and health-related quality of life in persons reporting compulsive computer use behavior. J Clin Psychiatry 1999;60:839-44.
12. Orzack MH. How to recognize and treat computer.com addictions. Directions in Mental Health Counseling 1999;9:13-20.
13. Stein DJ. Internet addiction, Internet psychotherapy (letter; comment). Am J Psychiatry 1997;154(6):890.-
14. Shapira NA. Unpublished data, 2000.
15. Kraut R, Lundmark V, Patterson M, Kiesler S, Mukopadhyay T, Scherlis W. Internet paradox: A social technology that reduces social involvement and psychological wellbeing? Am Psychol 1998;53:1017-31.
16. Pratarelli ME, Browne BL. Confirmatory factor analysis of Internet use and addiction. Cyberpsychol Behav 2002;5:53-64.
17. Young KS. Internet addiction: symptoms, evaluation and treatment. Innovations in Clin Pract 1999;17:19-31.
Many psychiatrists diagnose problematic Internet use with schemas based on substance use disorders and pathologic gambling. These predefined diagnoses, however, may lead to premature conclusions and prevent you from fully exploring other treatable diagnoses.
We propose a screening tool called “MOUSE” and diagnostic criteria for problematic Internet use, which we developed from research by our group and others. This article discusses the new criteria and answers three questions:
- How does problematic Internet use present?
- Is it an addiction or an impulse control disorder?
- How can we help those afflicted with this problem?
When Internet use goes over the line
Recognizing problematic Internet use is difficult because the Internet can serve as a tool in nearly every aspect of our lives—communication, shopping, business, travel, research, entertainment, and more. The evidence suggests that Internet use becomes a behavior disorder when:
- an individual loses the ability to control his or her use and begins to suffer distress and impaired daily function1
- and employment and relationships are jeopardized by the hours spent online2 (Box).
Relationships—particularly marriages but also parent-child relationships, dating relationships, and close friendships—appear to suffer the greatest harm. At least one-half of “Internet addicts” (53%) report that their Internet use has caused serious relationship problems.
School. Academic problems are common; one study showed 58% of students blamed Internet use for a drop in grades, missed classes, declining study habits, or being placed on probation.
Workplace. Many executives—55% in one study—complain that time spent on the Internet for non-business purposes reduces their employees’ effectiveness.
Health. Some users spend 40 to 80 hours per week online, and single sessions can last up to 20 hours. Lack of sleep results in fatigue, decreased exercise, and decreased immunity. Sitting in front of the computer for hours also increases the risk of carpal tunnel syndrome, eye strain, and back pain.
Other addictions. The more time spent on the Internet, the greater the user’s risk of exposure to other addictive activities, such as online gambling and sexual solicitations. This risk is particularly concerning in children and adolescents.
Source: Young KS. Innovations in Clin Pract 1999;17:19-31.
Case: Computer gamer out of control
Mr. A is 32 and in his fourth year of college. His psychiatric history includes obsessive-compulsive disorder (OCD), paraphilia not otherwise specified, and bipolar disorder, most recently depressed in partial remission. He has had only one manic episode 10 years ago and took lithium briefly. He experienced pleasure from masturbating in public, but his paraphilia did not meet criteria for voyeurism as he did not want to be seen. He engaged in this behavior from ages 16 to 18 and found it distressing.
He is taking no medications. The only clinically significant family history is his father’s apparent OCD, undiagnosed and untreated.
Mr. A’s excessive computer use started in high school, when he played computer games to the point where his grades suffered. He began using the Internet at age 28, just before starting college, and spent most of his time online playing multi-player, video/strategy games.
Mr. A underestimates the time he spends online at 24 hours per week, including 21 hours in nonessential use and 3 hours in essential use (required for job or school). His actual average is 35.9 hours per week—nearly equivalent to a full-time job. He divides his nonessential use among various online activities, mostly related to playing computer games:
- 35% in chat forums, communicating with gaming partners he has never met
- 25% in multi-player, video/strategy games
- 15% using e-mail
- and lesser times surfing the Web (5%), transferring files (5%), viewing pornography (5%), shopping (5%), listening to music (3%), and selling (2%).
He reports rising tension before logging on and relief after doing so. He admits to using the Internet for longer periods than intended and especially when emotionally stressed. He knows his behavior has hurt him academically, and he has tried unsuccessfully to cut down or stop his Internet use.
Internet overuse: An ‘addiction’?
Ivan Goldberg introduced the idea of Internet addiction in 1995 by posting factitious “diagnostic criteria” on a Web site as a joke.3 He was surprised at the overwhelming response he received from persons whose Internet use was interfering with their lives. The first case reports were soon published.4,5
Initially, excessive Internet use was called an “addiction”—implying a disorder similar to substance dependence. Recently, however, Internet overuse has come to be viewed as more closely resembling an impulse control disorder.5-8 Shapira et al studied 20 subjects with problematic Internet use, and all met DSM-IV criteria for an impulse control disorder, not otherwise specified. Three also met criteria for obsessive-compulsive disorder.1
As with other impulse control disorders (such as eating disorders and pathologic gambling), researchers have noticed increased depression associated with pathologic Internet use.8
Diagnostic criteria. Although Mr. A’s comorbid psychiatric illnesses complicate his presentation, his behavior clearly could be described as representing an impulse control disorder. His case also meets our proposed criteria for problematic Internet use (Table 1),9 which we define as:
- uncontrollable
- markedly distressing, time-consuming, or resulting in social, occupational, or financial difficulties
- and not solely present during mania or hypomania.
Teasing out comorbid disorders
As in Mr. A’s case, Internet overuse can serve as an expression of and a conduit for other psychiatric illnesses. Studies have found high rates of comorbidity with mood and anxiety disorders, social phobias, attention-deficit disorder with or without hyperactivity, paraphilias, insomnia, pathologic gambling, and substance use disorders.10-12
Although some researchers feel that the many comorbid and complicating factors cannot be teased out,13 most agree that compulsive Internet use or overuse can have adverse consequences and that more research is needed.
A predisposition? Are “Internet addicts” predisposed to or susceptible to Internet overuse? Researchers are exploring whether Internet overuse causes or is an effect of psychiatric illness.
Shapira et al1,14 found at least one psychiatric condition that predated the development of Internet overuse in 20 subjects. In a similar study of 21 subjects with excessive computer use, Black11 found:
- 33% had a mood disorder
- 38% had a substance use disorder
- 19% had an anxiety disorder
- 52% met criteria for at least one personality disorder.
On average, these 41 subjects were in their 20s and 30s and reported having problems with Internet use for about 3 years. They spent an average of 28 hours per week online for pleasure or recreation, and many experienced emotional distress, social impairment, and social, occupational, or financial difficulties.1,11
Table 1
PROPOSED DIAGNOSTIC CRITERIA FOR PROBLEMATIC INTERNET USE
| Maladaptive preoccupation with Internet use, as indicated by at least one of the following: |
|
|
| Source: Reprinted with permission from an article by Shapira et al9 that has been accepted for publication in Depression and Anxiety. © Copyright 2003 John Wiley & Sons. |
Isolation and depression. Increasing Internet use and withdrawal from family activities has been associated with increased depression and loneliness; Kraut et al15 hypothesized that the Internet use caused the depression. Pratarelli et al16 noted a maladaptive cycle in some persons; the more isolated they feel, the more they use the Internet and increase their social withdrawal.
In a survey of college students, individuals with “Internet addiction” were found to:
- have obsessive characteristics
- prefer online interactions to real-life interactions
- use the Internet “to feel better,” alleviate depression, and become sexually aroused.16
Personality traits. In another study, Orzack12 found that subjects viewed the computer as a means to satisfy, induce excitement, and reduce tension or induce relief. Six personality traits were identified as strong predictors of “Internet addiction disorder:”
- boredom
- private self-consciousness
- loneliness
- social anxiety
- shyness
- and low self-esteem.
Table 2
5 SCREENING QUESTIONS FOR PROBLEMATIC INTERNET USE
| More than intended time spent online? |
| Other responsibilities or activities neglected? |
| Unsuccessful attempts to cut down? |
| Significant relationship discord due to use? |
| Excessive thoughts or anxiety when not online? |
Diagnosing Internet overuse
Screening. During any psychiatric interview, ask patients how they spend their free time or what they most enjoy doing. If patients say they spend hours on the Internet or their use appears to usurp other activities, five questions—easily recalled by the mnemonic MOUSE—can help you screen for problematic Internet use (Table 2).
History. Typically, persons with problematic Internet use spend time in one Internet domain, such as chat rooms, interactive games, news groups, or search engines.17 Ask which application they use, how many hours they use it, how they rank the importance of various applications, and what they like about their preferred application.
To determine how the Internet may alter the patient’s moods, ask how he or she feels while online as opposed to offline. Keeping an hourly log and a “feelings diary” may help the patient sort through his or her emotions.17
Often patients use the Internet to escape from dissatisfaction or disappointment or to counteract a sense of personal inadequacy.17 They tend to take pride in their computer skills2 and incorporate them into their daily lives in many ways, allowing them to rationalize their excessive Internet use (“I’m using it for work, academics, travel, research, etc.”).
Chomorbidities. Given the high incidence of psychiatric comorbidity,1 it is important to complete a thorough psychiatric evaluation and treat any underlying illness. Whether the illness is primary or comorbid, it is likely exacerbating the symptoms of problematic Internet use.
Changing problematic behaviors
Psychotherapy. Once you find the motives and possible causes of Internet overuse, what is the best form of treatment? This question warrants further study, but cognitive-behavioral therapy (CBT) is the primary treatment at this time.
The goal of CBT is for patients to disrupt their problematic computer use and reconstruct their routines with other activities. They can:
- use external timers to keep track of time online
- set goals of brief, frequent sessions online
- carry cards listing the destructive effects of their Internet use and ranking other activities they have neglected.17
Using emotion journals or mood monitoring forms may help the patient discover which dysfunctional thoughts and feelings are triggering excessive Internet use.12 Support groups and family therapy can help repair damaged relationships and engage friends and family in the treatment plan.
Drug therapy. No studies have looked at drug therapy for problematic Internet use, beyond treating comorbid psychiatric illnesses.
Treatment declined. Mr. A declined treatment for his problematic Internet use. As in many other psychiatric illnesses, insight into impulse control disorders tends to be limited. We can address the problem directly and offer to help patients change their online behaviors, but we cannot force them into treatment if they are not endangering themselves or others.
Related resources
- Computer Addiction Services. Maressa Hecht Orzack, PhD. www.computeraddiction.com; (617) 855-2908.
- Center for Online Addiction. Kimberly S. Young, PhD. www.netaddiction.com; (877) 292-3737.
Many psychiatrists diagnose problematic Internet use with schemas based on substance use disorders and pathologic gambling. These predefined diagnoses, however, may lead to premature conclusions and prevent you from fully exploring other treatable diagnoses.
We propose a screening tool called “MOUSE” and diagnostic criteria for problematic Internet use, which we developed from research by our group and others. This article discusses the new criteria and answers three questions:
- How does problematic Internet use present?
- Is it an addiction or an impulse control disorder?
- How can we help those afflicted with this problem?
When Internet use goes over the line
Recognizing problematic Internet use is difficult because the Internet can serve as a tool in nearly every aspect of our lives—communication, shopping, business, travel, research, entertainment, and more. The evidence suggests that Internet use becomes a behavior disorder when:
- an individual loses the ability to control his or her use and begins to suffer distress and impaired daily function1
- and employment and relationships are jeopardized by the hours spent online2 (Box).
Relationships—particularly marriages but also parent-child relationships, dating relationships, and close friendships—appear to suffer the greatest harm. At least one-half of “Internet addicts” (53%) report that their Internet use has caused serious relationship problems.
School. Academic problems are common; one study showed 58% of students blamed Internet use for a drop in grades, missed classes, declining study habits, or being placed on probation.
Workplace. Many executives—55% in one study—complain that time spent on the Internet for non-business purposes reduces their employees’ effectiveness.
Health. Some users spend 40 to 80 hours per week online, and single sessions can last up to 20 hours. Lack of sleep results in fatigue, decreased exercise, and decreased immunity. Sitting in front of the computer for hours also increases the risk of carpal tunnel syndrome, eye strain, and back pain.
Other addictions. The more time spent on the Internet, the greater the user’s risk of exposure to other addictive activities, such as online gambling and sexual solicitations. This risk is particularly concerning in children and adolescents.
Source: Young KS. Innovations in Clin Pract 1999;17:19-31.
Case: Computer gamer out of control
Mr. A is 32 and in his fourth year of college. His psychiatric history includes obsessive-compulsive disorder (OCD), paraphilia not otherwise specified, and bipolar disorder, most recently depressed in partial remission. He has had only one manic episode 10 years ago and took lithium briefly. He experienced pleasure from masturbating in public, but his paraphilia did not meet criteria for voyeurism as he did not want to be seen. He engaged in this behavior from ages 16 to 18 and found it distressing.
He is taking no medications. The only clinically significant family history is his father’s apparent OCD, undiagnosed and untreated.
Mr. A’s excessive computer use started in high school, when he played computer games to the point where his grades suffered. He began using the Internet at age 28, just before starting college, and spent most of his time online playing multi-player, video/strategy games.
Mr. A underestimates the time he spends online at 24 hours per week, including 21 hours in nonessential use and 3 hours in essential use (required for job or school). His actual average is 35.9 hours per week—nearly equivalent to a full-time job. He divides his nonessential use among various online activities, mostly related to playing computer games:
- 35% in chat forums, communicating with gaming partners he has never met
- 25% in multi-player, video/strategy games
- 15% using e-mail
- and lesser times surfing the Web (5%), transferring files (5%), viewing pornography (5%), shopping (5%), listening to music (3%), and selling (2%).
He reports rising tension before logging on and relief after doing so. He admits to using the Internet for longer periods than intended and especially when emotionally stressed. He knows his behavior has hurt him academically, and he has tried unsuccessfully to cut down or stop his Internet use.
Internet overuse: An ‘addiction’?
Ivan Goldberg introduced the idea of Internet addiction in 1995 by posting factitious “diagnostic criteria” on a Web site as a joke.3 He was surprised at the overwhelming response he received from persons whose Internet use was interfering with their lives. The first case reports were soon published.4,5
Initially, excessive Internet use was called an “addiction”—implying a disorder similar to substance dependence. Recently, however, Internet overuse has come to be viewed as more closely resembling an impulse control disorder.5-8 Shapira et al studied 20 subjects with problematic Internet use, and all met DSM-IV criteria for an impulse control disorder, not otherwise specified. Three also met criteria for obsessive-compulsive disorder.1
As with other impulse control disorders (such as eating disorders and pathologic gambling), researchers have noticed increased depression associated with pathologic Internet use.8
Diagnostic criteria. Although Mr. A’s comorbid psychiatric illnesses complicate his presentation, his behavior clearly could be described as representing an impulse control disorder. His case also meets our proposed criteria for problematic Internet use (Table 1),9 which we define as:
- uncontrollable
- markedly distressing, time-consuming, or resulting in social, occupational, or financial difficulties
- and not solely present during mania or hypomania.
Teasing out comorbid disorders
As in Mr. A’s case, Internet overuse can serve as an expression of and a conduit for other psychiatric illnesses. Studies have found high rates of comorbidity with mood and anxiety disorders, social phobias, attention-deficit disorder with or without hyperactivity, paraphilias, insomnia, pathologic gambling, and substance use disorders.10-12
Although some researchers feel that the many comorbid and complicating factors cannot be teased out,13 most agree that compulsive Internet use or overuse can have adverse consequences and that more research is needed.
A predisposition? Are “Internet addicts” predisposed to or susceptible to Internet overuse? Researchers are exploring whether Internet overuse causes or is an effect of psychiatric illness.
Shapira et al1,14 found at least one psychiatric condition that predated the development of Internet overuse in 20 subjects. In a similar study of 21 subjects with excessive computer use, Black11 found:
- 33% had a mood disorder
- 38% had a substance use disorder
- 19% had an anxiety disorder
- 52% met criteria for at least one personality disorder.
On average, these 41 subjects were in their 20s and 30s and reported having problems with Internet use for about 3 years. They spent an average of 28 hours per week online for pleasure or recreation, and many experienced emotional distress, social impairment, and social, occupational, or financial difficulties.1,11
Table 1
PROPOSED DIAGNOSTIC CRITERIA FOR PROBLEMATIC INTERNET USE
| Maladaptive preoccupation with Internet use, as indicated by at least one of the following: |
|
|
| Source: Reprinted with permission from an article by Shapira et al9 that has been accepted for publication in Depression and Anxiety. © Copyright 2003 John Wiley & Sons. |
Isolation and depression. Increasing Internet use and withdrawal from family activities has been associated with increased depression and loneliness; Kraut et al15 hypothesized that the Internet use caused the depression. Pratarelli et al16 noted a maladaptive cycle in some persons; the more isolated they feel, the more they use the Internet and increase their social withdrawal.
In a survey of college students, individuals with “Internet addiction” were found to:
- have obsessive characteristics
- prefer online interactions to real-life interactions
- use the Internet “to feel better,” alleviate depression, and become sexually aroused.16
Personality traits. In another study, Orzack12 found that subjects viewed the computer as a means to satisfy, induce excitement, and reduce tension or induce relief. Six personality traits were identified as strong predictors of “Internet addiction disorder:”
- boredom
- private self-consciousness
- loneliness
- social anxiety
- shyness
- and low self-esteem.
Table 2
5 SCREENING QUESTIONS FOR PROBLEMATIC INTERNET USE
| More than intended time spent online? |
| Other responsibilities or activities neglected? |
| Unsuccessful attempts to cut down? |
| Significant relationship discord due to use? |
| Excessive thoughts or anxiety when not online? |
Diagnosing Internet overuse
Screening. During any psychiatric interview, ask patients how they spend their free time or what they most enjoy doing. If patients say they spend hours on the Internet or their use appears to usurp other activities, five questions—easily recalled by the mnemonic MOUSE—can help you screen for problematic Internet use (Table 2).
History. Typically, persons with problematic Internet use spend time in one Internet domain, such as chat rooms, interactive games, news groups, or search engines.17 Ask which application they use, how many hours they use it, how they rank the importance of various applications, and what they like about their preferred application.
To determine how the Internet may alter the patient’s moods, ask how he or she feels while online as opposed to offline. Keeping an hourly log and a “feelings diary” may help the patient sort through his or her emotions.17
Often patients use the Internet to escape from dissatisfaction or disappointment or to counteract a sense of personal inadequacy.17 They tend to take pride in their computer skills2 and incorporate them into their daily lives in many ways, allowing them to rationalize their excessive Internet use (“I’m using it for work, academics, travel, research, etc.”).
Chomorbidities. Given the high incidence of psychiatric comorbidity,1 it is important to complete a thorough psychiatric evaluation and treat any underlying illness. Whether the illness is primary or comorbid, it is likely exacerbating the symptoms of problematic Internet use.
Changing problematic behaviors
Psychotherapy. Once you find the motives and possible causes of Internet overuse, what is the best form of treatment? This question warrants further study, but cognitive-behavioral therapy (CBT) is the primary treatment at this time.
The goal of CBT is for patients to disrupt their problematic computer use and reconstruct their routines with other activities. They can:
- use external timers to keep track of time online
- set goals of brief, frequent sessions online
- carry cards listing the destructive effects of their Internet use and ranking other activities they have neglected.17
Using emotion journals or mood monitoring forms may help the patient discover which dysfunctional thoughts and feelings are triggering excessive Internet use.12 Support groups and family therapy can help repair damaged relationships and engage friends and family in the treatment plan.
Drug therapy. No studies have looked at drug therapy for problematic Internet use, beyond treating comorbid psychiatric illnesses.
Treatment declined. Mr. A declined treatment for his problematic Internet use. As in many other psychiatric illnesses, insight into impulse control disorders tends to be limited. We can address the problem directly and offer to help patients change their online behaviors, but we cannot force them into treatment if they are not endangering themselves or others.
Related resources
- Computer Addiction Services. Maressa Hecht Orzack, PhD. www.computeraddiction.com; (617) 855-2908.
- Center for Online Addiction. Kimberly S. Young, PhD. www.netaddiction.com; (877) 292-3737.
1. Shapira NA, Goldsmith TG, Keck PE, Jr, Khosla UM, McElroy SL. Psychiatric features of individuals with problematic Internet use. J Affect Disord 2000;57:267-72.
2. Beard KW, Wolf EM. Modification in the proposed diagnostic criteria for Internet addiction. Cyberpsychol Behav 2001;4:377-83.
3. Goldberg I. Internet addiction. Available at http://www.cybernothing.org/jdfalk/media-coverage/archive/msg01305.html. Accessed Feb. 26, 2003.
4. Griffiths MD. Internet addiction: an issue for clinical psychology? Clin Psychol Forum 1996;97:32-6.
5. Young KS. Psychology of computer use: XL. Addictive use of the Internet: a case that breaks the stereotype. Psychol Rep 1996;79:899-902.
6. Treuer T, Fábián Z, Füredi J. Internet addiction associated with features of impulse control disorder: is it a real psychiatric disorder? J Affect Disord 2001;66:283.-
7. Young KS. Caught in the net: how to recognize the signs of Internet addiction-and a winning strategy for recovery. New York: John Wiley & Sons, Inc. 1998;8.-
8. Young KS, Rogers RC. The relationship between depression and Internet addiction. Cyberpsychol Behav 1998;1:25-8.
9. Shapira NA, Lessig MC, Goldsmith TD, et al. Problematic Internet use: proposed classification and diagnostic criteria. Depress Anxiety (in press).
10. Griffiths MD. Internet addiction: Fact or fiction? Psychologist 1999;12:246-50.
11. Black DW, Belsare G, Schlosser S. Clinical features, psychiatric comorbidity, and health-related quality of life in persons reporting compulsive computer use behavior. J Clin Psychiatry 1999;60:839-44.
12. Orzack MH. How to recognize and treat computer.com addictions. Directions in Mental Health Counseling 1999;9:13-20.
13. Stein DJ. Internet addiction, Internet psychotherapy (letter; comment). Am J Psychiatry 1997;154(6):890.-
14. Shapira NA. Unpublished data, 2000.
15. Kraut R, Lundmark V, Patterson M, Kiesler S, Mukopadhyay T, Scherlis W. Internet paradox: A social technology that reduces social involvement and psychological wellbeing? Am Psychol 1998;53:1017-31.
16. Pratarelli ME, Browne BL. Confirmatory factor analysis of Internet use and addiction. Cyberpsychol Behav 2002;5:53-64.
17. Young KS. Internet addiction: symptoms, evaluation and treatment. Innovations in Clin Pract 1999;17:19-31.
1. Shapira NA, Goldsmith TG, Keck PE, Jr, Khosla UM, McElroy SL. Psychiatric features of individuals with problematic Internet use. J Affect Disord 2000;57:267-72.
2. Beard KW, Wolf EM. Modification in the proposed diagnostic criteria for Internet addiction. Cyberpsychol Behav 2001;4:377-83.
3. Goldberg I. Internet addiction. Available at http://www.cybernothing.org/jdfalk/media-coverage/archive/msg01305.html. Accessed Feb. 26, 2003.
4. Griffiths MD. Internet addiction: an issue for clinical psychology? Clin Psychol Forum 1996;97:32-6.
5. Young KS. Psychology of computer use: XL. Addictive use of the Internet: a case that breaks the stereotype. Psychol Rep 1996;79:899-902.
6. Treuer T, Fábián Z, Füredi J. Internet addiction associated with features of impulse control disorder: is it a real psychiatric disorder? J Affect Disord 2001;66:283.-
7. Young KS. Caught in the net: how to recognize the signs of Internet addiction-and a winning strategy for recovery. New York: John Wiley & Sons, Inc. 1998;8.-
8. Young KS, Rogers RC. The relationship between depression and Internet addiction. Cyberpsychol Behav 1998;1:25-8.
9. Shapira NA, Lessig MC, Goldsmith TD, et al. Problematic Internet use: proposed classification and diagnostic criteria. Depress Anxiety (in press).
10. Griffiths MD. Internet addiction: Fact or fiction? Psychologist 1999;12:246-50.
11. Black DW, Belsare G, Schlosser S. Clinical features, psychiatric comorbidity, and health-related quality of life in persons reporting compulsive computer use behavior. J Clin Psychiatry 1999;60:839-44.
12. Orzack MH. How to recognize and treat computer.com addictions. Directions in Mental Health Counseling 1999;9:13-20.
13. Stein DJ. Internet addiction, Internet psychotherapy (letter; comment). Am J Psychiatry 1997;154(6):890.-
14. Shapira NA. Unpublished data, 2000.
15. Kraut R, Lundmark V, Patterson M, Kiesler S, Mukopadhyay T, Scherlis W. Internet paradox: A social technology that reduces social involvement and psychological wellbeing? Am Psychol 1998;53:1017-31.
16. Pratarelli ME, Browne BL. Confirmatory factor analysis of Internet use and addiction. Cyberpsychol Behav 2002;5:53-64.
17. Young KS. Internet addiction: symptoms, evaluation and treatment. Innovations in Clin Pract 1999;17:19-31.
First-episode psychosis: our greatest challenge
“If I’m ever angry at a psychiatrist, I will refer that doctor a patient with a first episode of psychosis.”
A psychiatrist whose brother suffers from a psychotic disorder once said this to me. She was joking, but—in a way—she was totally serious. The serious part relates to her experience as the loving family member of someone who suddenly and inexplicably became devastatingly ill. She and her family wanted to know the diagnosis, yet were afraid to find out. They alternately wanted to—and didn’t want to—discover a physical cause behind the illness. They blamed themselves, then resolved not to blame themselves.
They were educated and reasonably well informed; they thought they understood what serious mental illness was about. But when it came to confronting it in a loved one, they ultimately realized they knew nothing. In retrospect, they viewed their psychiatrist as pretty good, but at the time they had nothing good to say about him. Patients and their families often feel unhappy with the psychiatrist who treats a first episode of psychosis.
All physicians have the burden of helping patients and families come to terms with terrible, unexpected, and incomprehensible illnesses. That task is doubly difficult for psychiatrists, because of:
- the stigma attached to the illnesses we treat
- the subtlety of some early symptoms
- and peoples’ belief that a psychiatric illness cannot happen to them or to their loved ones.
First-episode psychoses may pose our greatest challenge as clinicians. In “First psychotic episode—a window of opportunity”, Christoph Correll, MD, and Alan Mendelowitz, MD, adeptly describe the many challenges we face in this clinical scenario: differential diagnosis, communicating the diagnosis, encouraging the family and patient to engage constructively in treatment, and getting the patient, attendants, and externals on the same page.
Nowhere in medicine is Hippocrates’ first aphorism more relevant: “Life is short, the art is long; the occasion is fleeting; experience fallacious, and judgment difficult.” I would probably say “help the patient … cooperate,” rather than “make the patient … cooperate,” but other than that, despite everything we have learned in medicine in the last few millennia, I would not change a thing.

Randy Hillard, MD
Editor-in-chief
Randy Hillard, MD
Editor-in-chief
Randy Hillard, MD
Editor-in-chief
“If I’m ever angry at a psychiatrist, I will refer that doctor a patient with a first episode of psychosis.”
A psychiatrist whose brother suffers from a psychotic disorder once said this to me. She was joking, but—in a way—she was totally serious. The serious part relates to her experience as the loving family member of someone who suddenly and inexplicably became devastatingly ill. She and her family wanted to know the diagnosis, yet were afraid to find out. They alternately wanted to—and didn’t want to—discover a physical cause behind the illness. They blamed themselves, then resolved not to blame themselves.
They were educated and reasonably well informed; they thought they understood what serious mental illness was about. But when it came to confronting it in a loved one, they ultimately realized they knew nothing. In retrospect, they viewed their psychiatrist as pretty good, but at the time they had nothing good to say about him. Patients and their families often feel unhappy with the psychiatrist who treats a first episode of psychosis.
All physicians have the burden of helping patients and families come to terms with terrible, unexpected, and incomprehensible illnesses. That task is doubly difficult for psychiatrists, because of:
- the stigma attached to the illnesses we treat
- the subtlety of some early symptoms
- and peoples’ belief that a psychiatric illness cannot happen to them or to their loved ones.
First-episode psychoses may pose our greatest challenge as clinicians. In “First psychotic episode—a window of opportunity”, Christoph Correll, MD, and Alan Mendelowitz, MD, adeptly describe the many challenges we face in this clinical scenario: differential diagnosis, communicating the diagnosis, encouraging the family and patient to engage constructively in treatment, and getting the patient, attendants, and externals on the same page.
Nowhere in medicine is Hippocrates’ first aphorism more relevant: “Life is short, the art is long; the occasion is fleeting; experience fallacious, and judgment difficult.” I would probably say “help the patient … cooperate,” rather than “make the patient … cooperate,” but other than that, despite everything we have learned in medicine in the last few millennia, I would not change a thing.
“If I’m ever angry at a psychiatrist, I will refer that doctor a patient with a first episode of psychosis.”
A psychiatrist whose brother suffers from a psychotic disorder once said this to me. She was joking, but—in a way—she was totally serious. The serious part relates to her experience as the loving family member of someone who suddenly and inexplicably became devastatingly ill. She and her family wanted to know the diagnosis, yet were afraid to find out. They alternately wanted to—and didn’t want to—discover a physical cause behind the illness. They blamed themselves, then resolved not to blame themselves.
They were educated and reasonably well informed; they thought they understood what serious mental illness was about. But when it came to confronting it in a loved one, they ultimately realized they knew nothing. In retrospect, they viewed their psychiatrist as pretty good, but at the time they had nothing good to say about him. Patients and their families often feel unhappy with the psychiatrist who treats a first episode of psychosis.
All physicians have the burden of helping patients and families come to terms with terrible, unexpected, and incomprehensible illnesses. That task is doubly difficult for psychiatrists, because of:
- the stigma attached to the illnesses we treat
- the subtlety of some early symptoms
- and peoples’ belief that a psychiatric illness cannot happen to them or to their loved ones.
First-episode psychoses may pose our greatest challenge as clinicians. In “First psychotic episode—a window of opportunity”, Christoph Correll, MD, and Alan Mendelowitz, MD, adeptly describe the many challenges we face in this clinical scenario: differential diagnosis, communicating the diagnosis, encouraging the family and patient to engage constructively in treatment, and getting the patient, attendants, and externals on the same page.
Nowhere in medicine is Hippocrates’ first aphorism more relevant: “Life is short, the art is long; the occasion is fleeting; experience fallacious, and judgment difficult.” I would probably say “help the patient … cooperate,” rather than “make the patient … cooperate,” but other than that, despite everything we have learned in medicine in the last few millennia, I would not change a thing.
Atypical depression Puzzled? How to piece together symptoms and treatments
Deciding if a patient’s depressive episodes are “atypical” can be difficult because key pieces of the diagnostic puzzle are missing. Notwithstanding DSM-IV criteria, atypical depression’s definition remains unclear. This creates a therapeutic dilemma because we know that patients with atypical depression respond differently to antidepressants:
- Monoamine oxidase inhibitors (MAOIs) may be most effective, but their side effects can be troublesome.
- Tricyclics are clearly less effective than MAOIs, but the newer antidepressants’ role in treating atypical depressive symptoms has not been adequately explored.
We offer recommendations for diagnosing and treating atypical depression and address issues that may affect your clinical approach. These include possible overemphasis on mood reactivity in DSM-IV, shortcomings in studies defining the atypical depressive syndrome, and the potential role of biological markers in clarifying this challenging diagnosis.
Features of atypical depression
Atypical depression, as defined in DSM-IV,1 is characterized by mood reactivity and two or more of the following criteria:
- hypersomnia
- increased appetite or weight gain
- leaden paralysis (heavy, leaden feeling in arms or legs)
- longstanding sensitivity to interpersonal rejection that results in significant social or occupational impairment (Table 1 ).
An estimated 16 to 23% of patients with unipolar depression present with atypical features.2 These rates are higher among patients with bipolar disorder.2,3
Distinctive features. Studies comparing atypical depression with typical or melancholic depression suggest that atypical depression may be distinct in epidemiology, family history, comorbidity, and course of illness (Table 2). Specifically, atypical depression has a higher female-to-male ratio and earlier age of onset.4 Patients with atypical depression have higher rates of comorbid panic disorder,4,5 social phobia,4,5 bipolar II disorder,5 and bulimia6 than do those with typical depression.
Family members of patients with atypical depression are more likely to have atypical features during a depressive episode than are family members of patients with melancholic depression.7 These findings suggest a genetic component to atypical depression. Atypical depressive episodes also may be more likely to become chronic.4,8
Not all patients are alike. Studies of the diagnostic stability of atypical depression over time suggest that patients exhibiting atypical features are heterogeneous.9 Some longitudinal studies report reasonable diagnostic stability, with 59% to 100% of patients with an index episode of atypical depression exhibiting atypical features 12 to 24 months later.9,10 In a follow-up study of patients in remission from an episode of atypical depression, 64% of patients suffering a relapse were again found to have atypical features.11
Table 1
MOOD EPISODES: DSM-IV CRITERIA FOR ATYPICAL FEATURES SPECIFIER
| The following criteria must be present in the last 2 weeks of the episode |
| Criterion A. Mood reactivity (ie, mood brightens in response to positive events) |
| Criterion B. Two or more of the following: Increased appetite or weight gain Hypersomnia Leaden paralysis Longstanding sensitivity to interpersonal rejection |
Although numerous studies have failed to replicate one or more of these findings,4,8 several investigators have concluded that atypical depression is a distinct and valid sub-type of major depression.4,7,8
Antidepressant dilemmas
Unlike typical or melancholic depression, atypical depression responds more robustly to MAOIs than to tricyclic antidepressants (TCAs).12 MAOIs are roughly twice as effective as TCAs (response rate 72% vs. 44%, respectively), according to a meta-analysis of six studies comparing MAOIs and TCAs in patients with atypical depression.13
Clinicians rarely use MAOIs as first-line antidepressants, however, because of side effects and potential dietary and drug interactions. A depressed patient is thus unlikely to receive MAOIs unless the clinician strongly suspects that the presentation is atypical.
SSRIs. Few studies have evaluated how patients with atypical depression respond to newer antidepressants, particularly selective serotonin reuptake inhibitors (SSRIs). This lack of evidence creates a dilemma when treating atypical depression, as SSRIs are widely used in depressed patients, including those with atypical features.
One study found fluoxetine and phenelzine comparably effective in atypical depression,14 while another found sertraline works as well as moclobe-mide.15 However, the fluoxetine study was limited by a relatively small sample size (n=42), and both studies lacked placebo controls.
Some studies have suggested that SSRIs are less effective than MAOIs16 or as effective as TCAs in depressed patients with atypical features.17,18 However, one of these trials was limited by a small sample size (n=28),18 and only one was placebo-controlled.17
Bupropion. Studies of other antidepressants in atypical depression also are limited. In two separate trials, depressed patients with atypical features showed a greater response to bupropion than did depressed patients with typical features.19,20
Bupropion—a combined dopaminergic-noradrenergic antidepressant—appears to have stimulating properties that may help patients with hypersomnia and hyperphagia. Like MAOIs, bupropion also appears to have a greater effect on dopaminergic systems than either TCAs or SSRIs.
Recommendation. The most prudent approach appears to be using SSRIs or bupropion as first-line treatment for atypical depression and reserving MAOIs for patients who do not respond.
Attempts to define atypical depression
Although atypical depression responds differently to MAOIs than to TCAs, it is unclear which patients will respond preferentially to MAOIs. Early attempts to classify this subgroup recognized that these patients display symptom clusters, including:
- anxious depression (prominent anxiety symptoms)
- anergic depression (prominent fatigue and/or psychomotor retardation)
- and depression with reversed vegetative symptoms (hypersomnia and increased weight/appetite).7,21
Researchers have focused on patients with different combinations of these symptom profiles when defining the atypical depressive syndrome. Some have defined atypical depression as anxious temperament and reactive mood; others, as depression with reversed vegetative symptoms and severe fatigue; still others employ aspects of both profiles, as does DSM-IV.21 As a result of this confusion, investigators have demonstrated the preferential response to MAOIs in groups that exhibit different “atypical” symptoms.
Mood reactivity. The importance of mood reactivity in the diagnosis of atypical depression has been debated. DSM-IV requires mood reactivity for the diagnosis, perhaps to clearly differentiate melancholia from atypical depression.7 Yet some studies have demonstrated the preferential MAOI response in patients without this symptom.
Table 2
HOW ATYPICAL DEPRESSION COMPARES WITH MELANCHOLIC OR ‘TYPICAL’ DEPRESSION
| Feature | Atypical depression | Melancholic (MEL)/typical (TYP) depression |
|---|---|---|
| Symptom | ||
| Sleep | Increased | Decreased |
| Appetite | Increased | Decreased |
| Age of onset | Late teens to early 20s | Mid to late 30s |
| Female:male ratio | > 2:1 | Between 1:1 and 2:1 |
| Frequency of bipolar II disorder | Increased compared with MEL/TYP | |
| Duration of episodes | Increased compared with MEL/TYP | |
| Biology | ||
| HPA axis activity | Low to normal | High |
| Comorbidity | ||
| Panic disorder, social phobia, bulimia | Frequency increased compared with MEL/TYP | |
The Columbia group, from whose work the DSM-IV definition was adopted, performed several convincing studies showing clear superiority of MAOIs in patients who had reactive mood and displayed at least two additional atypical features, such as reversed vegetative symptoms and anergia.22 Patients with reactive mood and only one additional atypical symptom (classified as “probable” atypical depression) also displayed the preferential response to MAOIs, whereas patients who displayed mood reactivity alone did not.12
Thase et al,23 however, reported that reversed vegetative symptoms were more common with nonreactive mood (48%) than with reactive mood (16%) in patients with highly recurrent depression. Moreover, patients who displayed reversed vegetative symptoms without mood reactivity showed the same preferential response to MAOIs as the mood-reactive group. Patients with typical vegetative symptoms did not show this differential response.
Table 3
HOW ANTIDEPRESSANTS COMPARE IN CLINICAL TRIALS OF ATYPICAL DEPRESSION
| MAOIs | 8 controlled trials found MAOI > placebo 6 controlled trials found MAOI > TCA |
| TCAs | 6 controlled trials found MAOI > TCA |
| SSRIs | 2 controlled trials found SSRI = MAOI 1 trial found MAOI > SSRI 2 trials found SSRI = TCA |
| Bupropion | 1 open-label trial found bupropion more effective in atypical depression than in typical depression 1 open-label trial found bupropion effective in depression with hypersomnia 1 retrospective study found bupropion > fluoxetine in atypical depression |
| > more effective than | |
| = as effective as | |
More evidence suggests that mood reactivity should not be given the hierarchical importance it holds in the DSM-IV definition of atypical depression. In studies using latent class and cluster analyses, mood reactivity did not correlate with any other atypical feature,4,21 whereas hyperphagia, hypersomnia, leaden paralysis, and rejection sensitivity appear to be associated with one another.
Recommendation. Mood reactivity’s uncertain status in atypical depression’s definition makes it difficult to predict which patients may respond preferentially to MAOIs, as many patients present with other atypical features and nonreactive mood. Most recently, it has been suggested that atypical depression’s diagnostic criteria should be modified so that mood reactivity is not required but is one of five atypical features, of which three must be present for the diagnosis.24
Biological markers of depression
Atypical depression’s definition might be clarified if specific depressive symptoms could be linked to any biological markers. One proposed marker is decreased HPA axis activity, possibly caused by a central deficiency of corticotropin-releasing hormone (CRH),25 a potent HPA axis stimulator.
- HPA axis hyperactivity—presumably caused by increased CRH activity in the central nervous system—has been linked to melancholic depressive symptoms—particularly insomnia and reduced appetite.26
- Normal or diminished HPA axis activity—suggested by normal cortisol levels, low levels of CRH in cerebrospinal fluid, and increased frequency of dexamethasone suppression—has been associated with some atypical depressive features—specifically reversed vegetative symptoms.27-29
However, no studies have examined whether low HPA axis activity is associated with other atypical symptoms listed in DSM-IV. Research is needed to determine whether HPA axis hypoactivity is associated only with reversed vegetative symptoms or with atypical depression per se.
Obesity and eating disorders. Depressed patients who are obese or present with eating disorders may overlap with the atypical subtype and may respond better to some drug interventions than to others. Evidence suggests that depression—particularly the atypical subtype—is associated with increased rates of obesity8,29 and eating disorders.8,30
In our clinical experience, the combination of venlafaxine and bupropion can be effective for both depression and excessive eating in these patients, many of whom also exhibit other atypical features. A possible explanation is that the combined pharmacologic effect of venlafaxine and bupropion resembles that of the MAOIs (increased synaptic availability of serotonin, norepinephrine, and dopamine) without many MAOI side effects, such as weight gain.
We have, however, also observed treatment-emergent hypomania when using this drug combination, which is consistent with:
- the idea that mood reactivity and rejection sensitivity may be markers for bipolar disorder
- the often-reported high rate of bipolar II disorder among patients with atypical depression.5
In obese patients with bipolar II disorder, we have found that adding topiramate to mood stabilizer therapy can help treat both mood instability and overeating.31,32 same preferential response to MAOIs as the mood-reactive group. Patients with typical vegetative symptoms did not show this differential response.
Related resources
- Parker G, Roy K, Mitchell P, Wilhelm K, Malhi G, Hadzi-Pavlovic D. Atypical depression: a reappraisal. Am J Psychiatry 2002;159(9):1470-9.
- Gold PW, Chrousos GP. Organization of the stress system and its dysregulation in melancholic and atypical depression: high vs. low CRH/NE states. Mol Psychiatry 2002;7(3):254-75.
- Nierenberg AA, Alpert JE, Pava J, Rosenbaum JF, Fava M. Course and treatment of atypical depression. J Clin Psychiatry 1998;59(suppl 18):5-9.
Drug brand names
- Bupropion • Wellbutrin
- Fluoxetine • Prozac
- Moclobemide • Manerix
- Phenelzine • Nardil
- Sertraline • Zoloft
- Topiramate • Topamax
- Venlafaxine • Effexor
Disclosure
Dr. Nelson receives grant/research support from Eli Lilly & Co. and Wyeth Pharmaceuticals and is on the speakers bureau of Wyeth Pharmaceuticals.
Dr. McElroy is a consultant or scientific advisor to Abbott Laboratories, Bristol-Myers Squibb Co., Elan Corp., GlaxoSmithKline, Janssen Pharmaceutica, Eli Lilly & Co., Novartis Pharmaceuticals Corp., Ortho-McNeil Pharmaceutical, UCB Pharma, and Wyeth Pharmaceuticals. She receives research support from Forest Laboratories, GlaxoSmithKline, Elan Corp., Eli Lilly & Co., Merck & Co., Ortho-McNeil Pharmaceutical, Pfizer Inc., Sanofi-Synthelabo, and UCB Pharma.
1. American Psychiatric Association. Diagnostic and statistical manual of mentab disorders (4th ed). Washington DC: American Psychiatric Association, 2000.
2. Benazzi F. Prevalence and clinical features of atypical depression in depressed outpatients: a 467-case study. Psychiatry Res 1999;86(3):259-65.
3. Benazzi F. Is atypical depression a moderate severity depression? A 536-case study. J Psychiatry Neurosci 1999;24(3):244-7.
4. Posternak MA, Zimmerman M. Partial validation of the atypical features subtype of major depressive disorder. Arch Gen Psychiatry 2002;59(1):70-6.
5. Perugi G, Akiskal HS, Lattanzi L, et al. The high prevalence of “soft” bipolar (II) features in atypical depression. Compr Psychiatry 1998;39(2):63-71.
6. Levitan RD, Kaplan AS, Brown GM, et al. Low plasma cortisol in bulimia nervosa patients with reversed neurovegetative symptoms of depression. Biol Psychiatry 1997;41(3):366-8.
7. Stewart JW, McGrath PJ, Rabkin JG, Quitkin FM. Atypical depression. A valid clinical entity? Psychiatr Clin North Am 1993;16(3):479-95.
8. Kendler KS, Eaves LJ, Walters EE, Neale MC, Heath AC, Kessler RC. The identification and validation of distinct depressive syndromes in a population-based sample of female twins. Arch Gen Psychiatry 1996;53(5):391-9.
9. Ebert D, Barocka A. The early course of atypical depression. Eur Arch Psychiatry Clin Neurosci 1991;241(2):131-2.
10. Zubieta JK, Pande AC, Demitrack MA. Two-year follow-up of atypical depression. J Psychiatr Res 1999;33(1):23-9.
11. Nierenberg AA, Pava JA, Clancy K, Rosenbaum JF, Fava M. Are neurovegetative symptoms stable in relapsing or recurrent atypical depressive episodes? Biol Psychiatry 1996;40(8):691-6.
12. Quitkin FM, McGrath PJ, Stewart JW, et al. Phenelzine and imipramine in mood reactive depressives. Further delineation of the syndrome of atypical depression. Arch Gen Psychiatry 1989;46(9):787-93.
13. Pande AC, Birkett M, Fechner-Bates S, Haskett RF, Greden JF. Fluoxetine versus phenelzine in atypical depression. Biol Psychiatry 1996;40(10):1017-20.
14. Sogaard J, Lane R, Latimer P, et al. A 12-week study comparing moclobemide and sertraline in the treatment of outpatients with atypical depression. J Psychopharmacol 1999;13(4):406-14.
15. Lonnqvist J, Sihvo S, Syvalahti E, Kiviruusu O. Moclobemide and fluoxetine in atypical depression: a double-blind trial. J Affect Disord 1994;32(3):169-77.
16. McGrath PJ, Stewart JW, Janal MN, Petkova E, Quitkin FM, Klein DF. A placebo-controlled study of fluoxetine versus imipramine in the acute treatment of atypical depression. Am J Psychiatry 2000;157(3):344-50.
17. Stratta P, Bolino F, Cupillari M, Casacchia M. A double-blind parallel study comparing fluoxetine with imipramine in the treatment of atypical depression. Int Clin Psychopharmacol 1991;6(3):193-6.
18. Goodnick PJ, Dominguez RA, DeVane CL, Bowden CL. Bupropion slow-release response in depression: diagnosis and biochemistry. Biol Psychiatry 1998;44(7):629-32.
19. Goodnick PJ, Extein I. Bupropion and fluoxetine in depressive subtypes. Ann Clin Psychiatry 1989;1:119-22.
20. Rye DB, Dihenia B, Bliwise DL. Reversal of atypical depression, sleepiness, and REM-sleep propensity in narcolepsy with bupropion. Depress Anxiety 1998;7(2):92-5.
21. Parker G, Roy K, Mitchell P, Wilhelm K, Malhi G, Hadzi-Pavlovic D. Atypical depression: a reappraisal. Am J Psychiatry 2002;159(9):1470-9.
22. Liebowitz MR, Quitkin FM, Stewart JW, et al. Phenelzine v imipramine in atypical depression. A preliminary report. Arch Gen Psychiatry 1984;41(7):669-77.
23. Thase ME, Carpenter L, Kupfer DJ, Frank E. Clinical significance of reversed vegetative subtypes of recurrent major depression. Psychopharmacol Bull 1991;27(1):17-22.
24. Angst J, Gamma A, Sellaro R, Zhang H, Merikangas K. Toward validation of atypical depression in the community: results of the Zurich cohort study. J Affect Disord 2002;72(2):125-38.
25. Gold PW, Chrousos GP. The endocrinology of melancholic and atypical depression: relation to neurocircuitry and somatic consequences. Proc Assoc Am Physicians 1999;111(1):22-34.
26. Garvey MJ, Schaffer C, Schaffer L, Perry PJ. Is DST status associated with depression characteristics? J Affect Disord 1989;16(2-3):159-65.
27. Geracioti TD, Jr, Loosen PT, Orth DN. Low cerebrospinal fluid corticotropin-releasing hormone concentrations in eucortisolemic depression. Biol Psychiatry 1997;42(3):165-74.
28. Casper RC, Kocsis J, Dysken M, et al. Cortisol measures in primary major depressive disorder with hypersomnia or appetite increase. J Affect Disord 1988;15(2):131-40.
29. Sullivan PF, Kessler RC, Kendler KS. Latent class analysis of lifetime depressive symptoms in the national comorbidity survey. Am J Psychiatry 1998;155(10):1398-406.
30. Levitan RD, Lesage A, Parikh SV, Goering P, Kennedy SH. Reversed neurovegetative symptoms of depression: a community study of Ontario. Am J Psychiatry 1997;154(7):934-40.
31. McElroy SL, Suppes T, Keck PE, Jr, et al. Open-label adjunctive topiramate in the treatment of bipolar disorders. Biol Psychiatry 2000;47(12):1025-33.
32. Shapira NA, Goldsmith TD, McElroy SL. Treatment of binge-eating disorder with topiramate: a clinical case series. J Clin Psychiatry 2000;61(5):368-72.
Deciding if a patient’s depressive episodes are “atypical” can be difficult because key pieces of the diagnostic puzzle are missing. Notwithstanding DSM-IV criteria, atypical depression’s definition remains unclear. This creates a therapeutic dilemma because we know that patients with atypical depression respond differently to antidepressants:
- Monoamine oxidase inhibitors (MAOIs) may be most effective, but their side effects can be troublesome.
- Tricyclics are clearly less effective than MAOIs, but the newer antidepressants’ role in treating atypical depressive symptoms has not been adequately explored.
We offer recommendations for diagnosing and treating atypical depression and address issues that may affect your clinical approach. These include possible overemphasis on mood reactivity in DSM-IV, shortcomings in studies defining the atypical depressive syndrome, and the potential role of biological markers in clarifying this challenging diagnosis.
Features of atypical depression
Atypical depression, as defined in DSM-IV,1 is characterized by mood reactivity and two or more of the following criteria:
- hypersomnia
- increased appetite or weight gain
- leaden paralysis (heavy, leaden feeling in arms or legs)
- longstanding sensitivity to interpersonal rejection that results in significant social or occupational impairment (Table 1 ).
An estimated 16 to 23% of patients with unipolar depression present with atypical features.2 These rates are higher among patients with bipolar disorder.2,3
Distinctive features. Studies comparing atypical depression with typical or melancholic depression suggest that atypical depression may be distinct in epidemiology, family history, comorbidity, and course of illness (Table 2). Specifically, atypical depression has a higher female-to-male ratio and earlier age of onset.4 Patients with atypical depression have higher rates of comorbid panic disorder,4,5 social phobia,4,5 bipolar II disorder,5 and bulimia6 than do those with typical depression.
Family members of patients with atypical depression are more likely to have atypical features during a depressive episode than are family members of patients with melancholic depression.7 These findings suggest a genetic component to atypical depression. Atypical depressive episodes also may be more likely to become chronic.4,8
Not all patients are alike. Studies of the diagnostic stability of atypical depression over time suggest that patients exhibiting atypical features are heterogeneous.9 Some longitudinal studies report reasonable diagnostic stability, with 59% to 100% of patients with an index episode of atypical depression exhibiting atypical features 12 to 24 months later.9,10 In a follow-up study of patients in remission from an episode of atypical depression, 64% of patients suffering a relapse were again found to have atypical features.11
Table 1
MOOD EPISODES: DSM-IV CRITERIA FOR ATYPICAL FEATURES SPECIFIER
| The following criteria must be present in the last 2 weeks of the episode |
| Criterion A. Mood reactivity (ie, mood brightens in response to positive events) |
| Criterion B. Two or more of the following: Increased appetite or weight gain Hypersomnia Leaden paralysis Longstanding sensitivity to interpersonal rejection |
Although numerous studies have failed to replicate one or more of these findings,4,8 several investigators have concluded that atypical depression is a distinct and valid sub-type of major depression.4,7,8
Antidepressant dilemmas
Unlike typical or melancholic depression, atypical depression responds more robustly to MAOIs than to tricyclic antidepressants (TCAs).12 MAOIs are roughly twice as effective as TCAs (response rate 72% vs. 44%, respectively), according to a meta-analysis of six studies comparing MAOIs and TCAs in patients with atypical depression.13
Clinicians rarely use MAOIs as first-line antidepressants, however, because of side effects and potential dietary and drug interactions. A depressed patient is thus unlikely to receive MAOIs unless the clinician strongly suspects that the presentation is atypical.
SSRIs. Few studies have evaluated how patients with atypical depression respond to newer antidepressants, particularly selective serotonin reuptake inhibitors (SSRIs). This lack of evidence creates a dilemma when treating atypical depression, as SSRIs are widely used in depressed patients, including those with atypical features.
One study found fluoxetine and phenelzine comparably effective in atypical depression,14 while another found sertraline works as well as moclobe-mide.15 However, the fluoxetine study was limited by a relatively small sample size (n=42), and both studies lacked placebo controls.
Some studies have suggested that SSRIs are less effective than MAOIs16 or as effective as TCAs in depressed patients with atypical features.17,18 However, one of these trials was limited by a small sample size (n=28),18 and only one was placebo-controlled.17
Bupropion. Studies of other antidepressants in atypical depression also are limited. In two separate trials, depressed patients with atypical features showed a greater response to bupropion than did depressed patients with typical features.19,20
Bupropion—a combined dopaminergic-noradrenergic antidepressant—appears to have stimulating properties that may help patients with hypersomnia and hyperphagia. Like MAOIs, bupropion also appears to have a greater effect on dopaminergic systems than either TCAs or SSRIs.
Recommendation. The most prudent approach appears to be using SSRIs or bupropion as first-line treatment for atypical depression and reserving MAOIs for patients who do not respond.
Attempts to define atypical depression
Although atypical depression responds differently to MAOIs than to TCAs, it is unclear which patients will respond preferentially to MAOIs. Early attempts to classify this subgroup recognized that these patients display symptom clusters, including:
- anxious depression (prominent anxiety symptoms)
- anergic depression (prominent fatigue and/or psychomotor retardation)
- and depression with reversed vegetative symptoms (hypersomnia and increased weight/appetite).7,21
Researchers have focused on patients with different combinations of these symptom profiles when defining the atypical depressive syndrome. Some have defined atypical depression as anxious temperament and reactive mood; others, as depression with reversed vegetative symptoms and severe fatigue; still others employ aspects of both profiles, as does DSM-IV.21 As a result of this confusion, investigators have demonstrated the preferential response to MAOIs in groups that exhibit different “atypical” symptoms.
Mood reactivity. The importance of mood reactivity in the diagnosis of atypical depression has been debated. DSM-IV requires mood reactivity for the diagnosis, perhaps to clearly differentiate melancholia from atypical depression.7 Yet some studies have demonstrated the preferential MAOI response in patients without this symptom.
Table 2
HOW ATYPICAL DEPRESSION COMPARES WITH MELANCHOLIC OR ‘TYPICAL’ DEPRESSION
| Feature | Atypical depression | Melancholic (MEL)/typical (TYP) depression |
|---|---|---|
| Symptom | ||
| Sleep | Increased | Decreased |
| Appetite | Increased | Decreased |
| Age of onset | Late teens to early 20s | Mid to late 30s |
| Female:male ratio | > 2:1 | Between 1:1 and 2:1 |
| Frequency of bipolar II disorder | Increased compared with MEL/TYP | |
| Duration of episodes | Increased compared with MEL/TYP | |
| Biology | ||
| HPA axis activity | Low to normal | High |
| Comorbidity | ||
| Panic disorder, social phobia, bulimia | Frequency increased compared with MEL/TYP | |
The Columbia group, from whose work the DSM-IV definition was adopted, performed several convincing studies showing clear superiority of MAOIs in patients who had reactive mood and displayed at least two additional atypical features, such as reversed vegetative symptoms and anergia.22 Patients with reactive mood and only one additional atypical symptom (classified as “probable” atypical depression) also displayed the preferential response to MAOIs, whereas patients who displayed mood reactivity alone did not.12
Thase et al,23 however, reported that reversed vegetative symptoms were more common with nonreactive mood (48%) than with reactive mood (16%) in patients with highly recurrent depression. Moreover, patients who displayed reversed vegetative symptoms without mood reactivity showed the same preferential response to MAOIs as the mood-reactive group. Patients with typical vegetative symptoms did not show this differential response.
Table 3
HOW ANTIDEPRESSANTS COMPARE IN CLINICAL TRIALS OF ATYPICAL DEPRESSION
| MAOIs | 8 controlled trials found MAOI > placebo 6 controlled trials found MAOI > TCA |
| TCAs | 6 controlled trials found MAOI > TCA |
| SSRIs | 2 controlled trials found SSRI = MAOI 1 trial found MAOI > SSRI 2 trials found SSRI = TCA |
| Bupropion | 1 open-label trial found bupropion more effective in atypical depression than in typical depression 1 open-label trial found bupropion effective in depression with hypersomnia 1 retrospective study found bupropion > fluoxetine in atypical depression |
| > more effective than | |
| = as effective as | |
More evidence suggests that mood reactivity should not be given the hierarchical importance it holds in the DSM-IV definition of atypical depression. In studies using latent class and cluster analyses, mood reactivity did not correlate with any other atypical feature,4,21 whereas hyperphagia, hypersomnia, leaden paralysis, and rejection sensitivity appear to be associated with one another.
Recommendation. Mood reactivity’s uncertain status in atypical depression’s definition makes it difficult to predict which patients may respond preferentially to MAOIs, as many patients present with other atypical features and nonreactive mood. Most recently, it has been suggested that atypical depression’s diagnostic criteria should be modified so that mood reactivity is not required but is one of five atypical features, of which three must be present for the diagnosis.24
Biological markers of depression
Atypical depression’s definition might be clarified if specific depressive symptoms could be linked to any biological markers. One proposed marker is decreased HPA axis activity, possibly caused by a central deficiency of corticotropin-releasing hormone (CRH),25 a potent HPA axis stimulator.
- HPA axis hyperactivity—presumably caused by increased CRH activity in the central nervous system—has been linked to melancholic depressive symptoms—particularly insomnia and reduced appetite.26
- Normal or diminished HPA axis activity—suggested by normal cortisol levels, low levels of CRH in cerebrospinal fluid, and increased frequency of dexamethasone suppression—has been associated with some atypical depressive features—specifically reversed vegetative symptoms.27-29
However, no studies have examined whether low HPA axis activity is associated with other atypical symptoms listed in DSM-IV. Research is needed to determine whether HPA axis hypoactivity is associated only with reversed vegetative symptoms or with atypical depression per se.
Obesity and eating disorders. Depressed patients who are obese or present with eating disorders may overlap with the atypical subtype and may respond better to some drug interventions than to others. Evidence suggests that depression—particularly the atypical subtype—is associated with increased rates of obesity8,29 and eating disorders.8,30
In our clinical experience, the combination of venlafaxine and bupropion can be effective for both depression and excessive eating in these patients, many of whom also exhibit other atypical features. A possible explanation is that the combined pharmacologic effect of venlafaxine and bupropion resembles that of the MAOIs (increased synaptic availability of serotonin, norepinephrine, and dopamine) without many MAOI side effects, such as weight gain.
We have, however, also observed treatment-emergent hypomania when using this drug combination, which is consistent with:
- the idea that mood reactivity and rejection sensitivity may be markers for bipolar disorder
- the often-reported high rate of bipolar II disorder among patients with atypical depression.5
In obese patients with bipolar II disorder, we have found that adding topiramate to mood stabilizer therapy can help treat both mood instability and overeating.31,32 same preferential response to MAOIs as the mood-reactive group. Patients with typical vegetative symptoms did not show this differential response.
Related resources
- Parker G, Roy K, Mitchell P, Wilhelm K, Malhi G, Hadzi-Pavlovic D. Atypical depression: a reappraisal. Am J Psychiatry 2002;159(9):1470-9.
- Gold PW, Chrousos GP. Organization of the stress system and its dysregulation in melancholic and atypical depression: high vs. low CRH/NE states. Mol Psychiatry 2002;7(3):254-75.
- Nierenberg AA, Alpert JE, Pava J, Rosenbaum JF, Fava M. Course and treatment of atypical depression. J Clin Psychiatry 1998;59(suppl 18):5-9.
Drug brand names
- Bupropion • Wellbutrin
- Fluoxetine • Prozac
- Moclobemide • Manerix
- Phenelzine • Nardil
- Sertraline • Zoloft
- Topiramate • Topamax
- Venlafaxine • Effexor
Disclosure
Dr. Nelson receives grant/research support from Eli Lilly & Co. and Wyeth Pharmaceuticals and is on the speakers bureau of Wyeth Pharmaceuticals.
Dr. McElroy is a consultant or scientific advisor to Abbott Laboratories, Bristol-Myers Squibb Co., Elan Corp., GlaxoSmithKline, Janssen Pharmaceutica, Eli Lilly & Co., Novartis Pharmaceuticals Corp., Ortho-McNeil Pharmaceutical, UCB Pharma, and Wyeth Pharmaceuticals. She receives research support from Forest Laboratories, GlaxoSmithKline, Elan Corp., Eli Lilly & Co., Merck & Co., Ortho-McNeil Pharmaceutical, Pfizer Inc., Sanofi-Synthelabo, and UCB Pharma.
Deciding if a patient’s depressive episodes are “atypical” can be difficult because key pieces of the diagnostic puzzle are missing. Notwithstanding DSM-IV criteria, atypical depression’s definition remains unclear. This creates a therapeutic dilemma because we know that patients with atypical depression respond differently to antidepressants:
- Monoamine oxidase inhibitors (MAOIs) may be most effective, but their side effects can be troublesome.
- Tricyclics are clearly less effective than MAOIs, but the newer antidepressants’ role in treating atypical depressive symptoms has not been adequately explored.
We offer recommendations for diagnosing and treating atypical depression and address issues that may affect your clinical approach. These include possible overemphasis on mood reactivity in DSM-IV, shortcomings in studies defining the atypical depressive syndrome, and the potential role of biological markers in clarifying this challenging diagnosis.
Features of atypical depression
Atypical depression, as defined in DSM-IV,1 is characterized by mood reactivity and two or more of the following criteria:
- hypersomnia
- increased appetite or weight gain
- leaden paralysis (heavy, leaden feeling in arms or legs)
- longstanding sensitivity to interpersonal rejection that results in significant social or occupational impairment (Table 1 ).
An estimated 16 to 23% of patients with unipolar depression present with atypical features.2 These rates are higher among patients with bipolar disorder.2,3
Distinctive features. Studies comparing atypical depression with typical or melancholic depression suggest that atypical depression may be distinct in epidemiology, family history, comorbidity, and course of illness (Table 2). Specifically, atypical depression has a higher female-to-male ratio and earlier age of onset.4 Patients with atypical depression have higher rates of comorbid panic disorder,4,5 social phobia,4,5 bipolar II disorder,5 and bulimia6 than do those with typical depression.
Family members of patients with atypical depression are more likely to have atypical features during a depressive episode than are family members of patients with melancholic depression.7 These findings suggest a genetic component to atypical depression. Atypical depressive episodes also may be more likely to become chronic.4,8
Not all patients are alike. Studies of the diagnostic stability of atypical depression over time suggest that patients exhibiting atypical features are heterogeneous.9 Some longitudinal studies report reasonable diagnostic stability, with 59% to 100% of patients with an index episode of atypical depression exhibiting atypical features 12 to 24 months later.9,10 In a follow-up study of patients in remission from an episode of atypical depression, 64% of patients suffering a relapse were again found to have atypical features.11
Table 1
MOOD EPISODES: DSM-IV CRITERIA FOR ATYPICAL FEATURES SPECIFIER
| The following criteria must be present in the last 2 weeks of the episode |
| Criterion A. Mood reactivity (ie, mood brightens in response to positive events) |
| Criterion B. Two or more of the following: Increased appetite or weight gain Hypersomnia Leaden paralysis Longstanding sensitivity to interpersonal rejection |
Although numerous studies have failed to replicate one or more of these findings,4,8 several investigators have concluded that atypical depression is a distinct and valid sub-type of major depression.4,7,8
Antidepressant dilemmas
Unlike typical or melancholic depression, atypical depression responds more robustly to MAOIs than to tricyclic antidepressants (TCAs).12 MAOIs are roughly twice as effective as TCAs (response rate 72% vs. 44%, respectively), according to a meta-analysis of six studies comparing MAOIs and TCAs in patients with atypical depression.13
Clinicians rarely use MAOIs as first-line antidepressants, however, because of side effects and potential dietary and drug interactions. A depressed patient is thus unlikely to receive MAOIs unless the clinician strongly suspects that the presentation is atypical.
SSRIs. Few studies have evaluated how patients with atypical depression respond to newer antidepressants, particularly selective serotonin reuptake inhibitors (SSRIs). This lack of evidence creates a dilemma when treating atypical depression, as SSRIs are widely used in depressed patients, including those with atypical features.
One study found fluoxetine and phenelzine comparably effective in atypical depression,14 while another found sertraline works as well as moclobe-mide.15 However, the fluoxetine study was limited by a relatively small sample size (n=42), and both studies lacked placebo controls.
Some studies have suggested that SSRIs are less effective than MAOIs16 or as effective as TCAs in depressed patients with atypical features.17,18 However, one of these trials was limited by a small sample size (n=28),18 and only one was placebo-controlled.17
Bupropion. Studies of other antidepressants in atypical depression also are limited. In two separate trials, depressed patients with atypical features showed a greater response to bupropion than did depressed patients with typical features.19,20
Bupropion—a combined dopaminergic-noradrenergic antidepressant—appears to have stimulating properties that may help patients with hypersomnia and hyperphagia. Like MAOIs, bupropion also appears to have a greater effect on dopaminergic systems than either TCAs or SSRIs.
Recommendation. The most prudent approach appears to be using SSRIs or bupropion as first-line treatment for atypical depression and reserving MAOIs for patients who do not respond.
Attempts to define atypical depression
Although atypical depression responds differently to MAOIs than to TCAs, it is unclear which patients will respond preferentially to MAOIs. Early attempts to classify this subgroup recognized that these patients display symptom clusters, including:
- anxious depression (prominent anxiety symptoms)
- anergic depression (prominent fatigue and/or psychomotor retardation)
- and depression with reversed vegetative symptoms (hypersomnia and increased weight/appetite).7,21
Researchers have focused on patients with different combinations of these symptom profiles when defining the atypical depressive syndrome. Some have defined atypical depression as anxious temperament and reactive mood; others, as depression with reversed vegetative symptoms and severe fatigue; still others employ aspects of both profiles, as does DSM-IV.21 As a result of this confusion, investigators have demonstrated the preferential response to MAOIs in groups that exhibit different “atypical” symptoms.
Mood reactivity. The importance of mood reactivity in the diagnosis of atypical depression has been debated. DSM-IV requires mood reactivity for the diagnosis, perhaps to clearly differentiate melancholia from atypical depression.7 Yet some studies have demonstrated the preferential MAOI response in patients without this symptom.
Table 2
HOW ATYPICAL DEPRESSION COMPARES WITH MELANCHOLIC OR ‘TYPICAL’ DEPRESSION
| Feature | Atypical depression | Melancholic (MEL)/typical (TYP) depression |
|---|---|---|
| Symptom | ||
| Sleep | Increased | Decreased |
| Appetite | Increased | Decreased |
| Age of onset | Late teens to early 20s | Mid to late 30s |
| Female:male ratio | > 2:1 | Between 1:1 and 2:1 |
| Frequency of bipolar II disorder | Increased compared with MEL/TYP | |
| Duration of episodes | Increased compared with MEL/TYP | |
| Biology | ||
| HPA axis activity | Low to normal | High |
| Comorbidity | ||
| Panic disorder, social phobia, bulimia | Frequency increased compared with MEL/TYP | |
The Columbia group, from whose work the DSM-IV definition was adopted, performed several convincing studies showing clear superiority of MAOIs in patients who had reactive mood and displayed at least two additional atypical features, such as reversed vegetative symptoms and anergia.22 Patients with reactive mood and only one additional atypical symptom (classified as “probable” atypical depression) also displayed the preferential response to MAOIs, whereas patients who displayed mood reactivity alone did not.12
Thase et al,23 however, reported that reversed vegetative symptoms were more common with nonreactive mood (48%) than with reactive mood (16%) in patients with highly recurrent depression. Moreover, patients who displayed reversed vegetative symptoms without mood reactivity showed the same preferential response to MAOIs as the mood-reactive group. Patients with typical vegetative symptoms did not show this differential response.
Table 3
HOW ANTIDEPRESSANTS COMPARE IN CLINICAL TRIALS OF ATYPICAL DEPRESSION
| MAOIs | 8 controlled trials found MAOI > placebo 6 controlled trials found MAOI > TCA |
| TCAs | 6 controlled trials found MAOI > TCA |
| SSRIs | 2 controlled trials found SSRI = MAOI 1 trial found MAOI > SSRI 2 trials found SSRI = TCA |
| Bupropion | 1 open-label trial found bupropion more effective in atypical depression than in typical depression 1 open-label trial found bupropion effective in depression with hypersomnia 1 retrospective study found bupropion > fluoxetine in atypical depression |
| > more effective than | |
| = as effective as | |
More evidence suggests that mood reactivity should not be given the hierarchical importance it holds in the DSM-IV definition of atypical depression. In studies using latent class and cluster analyses, mood reactivity did not correlate with any other atypical feature,4,21 whereas hyperphagia, hypersomnia, leaden paralysis, and rejection sensitivity appear to be associated with one another.
Recommendation. Mood reactivity’s uncertain status in atypical depression’s definition makes it difficult to predict which patients may respond preferentially to MAOIs, as many patients present with other atypical features and nonreactive mood. Most recently, it has been suggested that atypical depression’s diagnostic criteria should be modified so that mood reactivity is not required but is one of five atypical features, of which three must be present for the diagnosis.24
Biological markers of depression
Atypical depression’s definition might be clarified if specific depressive symptoms could be linked to any biological markers. One proposed marker is decreased HPA axis activity, possibly caused by a central deficiency of corticotropin-releasing hormone (CRH),25 a potent HPA axis stimulator.
- HPA axis hyperactivity—presumably caused by increased CRH activity in the central nervous system—has been linked to melancholic depressive symptoms—particularly insomnia and reduced appetite.26
- Normal or diminished HPA axis activity—suggested by normal cortisol levels, low levels of CRH in cerebrospinal fluid, and increased frequency of dexamethasone suppression—has been associated with some atypical depressive features—specifically reversed vegetative symptoms.27-29
However, no studies have examined whether low HPA axis activity is associated with other atypical symptoms listed in DSM-IV. Research is needed to determine whether HPA axis hypoactivity is associated only with reversed vegetative symptoms or with atypical depression per se.
Obesity and eating disorders. Depressed patients who are obese or present with eating disorders may overlap with the atypical subtype and may respond better to some drug interventions than to others. Evidence suggests that depression—particularly the atypical subtype—is associated with increased rates of obesity8,29 and eating disorders.8,30
In our clinical experience, the combination of venlafaxine and bupropion can be effective for both depression and excessive eating in these patients, many of whom also exhibit other atypical features. A possible explanation is that the combined pharmacologic effect of venlafaxine and bupropion resembles that of the MAOIs (increased synaptic availability of serotonin, norepinephrine, and dopamine) without many MAOI side effects, such as weight gain.
We have, however, also observed treatment-emergent hypomania when using this drug combination, which is consistent with:
- the idea that mood reactivity and rejection sensitivity may be markers for bipolar disorder
- the often-reported high rate of bipolar II disorder among patients with atypical depression.5
In obese patients with bipolar II disorder, we have found that adding topiramate to mood stabilizer therapy can help treat both mood instability and overeating.31,32 same preferential response to MAOIs as the mood-reactive group. Patients with typical vegetative symptoms did not show this differential response.
Related resources
- Parker G, Roy K, Mitchell P, Wilhelm K, Malhi G, Hadzi-Pavlovic D. Atypical depression: a reappraisal. Am J Psychiatry 2002;159(9):1470-9.
- Gold PW, Chrousos GP. Organization of the stress system and its dysregulation in melancholic and atypical depression: high vs. low CRH/NE states. Mol Psychiatry 2002;7(3):254-75.
- Nierenberg AA, Alpert JE, Pava J, Rosenbaum JF, Fava M. Course and treatment of atypical depression. J Clin Psychiatry 1998;59(suppl 18):5-9.
Drug brand names
- Bupropion • Wellbutrin
- Fluoxetine • Prozac
- Moclobemide • Manerix
- Phenelzine • Nardil
- Sertraline • Zoloft
- Topiramate • Topamax
- Venlafaxine • Effexor
Disclosure
Dr. Nelson receives grant/research support from Eli Lilly & Co. and Wyeth Pharmaceuticals and is on the speakers bureau of Wyeth Pharmaceuticals.
Dr. McElroy is a consultant or scientific advisor to Abbott Laboratories, Bristol-Myers Squibb Co., Elan Corp., GlaxoSmithKline, Janssen Pharmaceutica, Eli Lilly & Co., Novartis Pharmaceuticals Corp., Ortho-McNeil Pharmaceutical, UCB Pharma, and Wyeth Pharmaceuticals. She receives research support from Forest Laboratories, GlaxoSmithKline, Elan Corp., Eli Lilly & Co., Merck & Co., Ortho-McNeil Pharmaceutical, Pfizer Inc., Sanofi-Synthelabo, and UCB Pharma.
1. American Psychiatric Association. Diagnostic and statistical manual of mentab disorders (4th ed). Washington DC: American Psychiatric Association, 2000.
2. Benazzi F. Prevalence and clinical features of atypical depression in depressed outpatients: a 467-case study. Psychiatry Res 1999;86(3):259-65.
3. Benazzi F. Is atypical depression a moderate severity depression? A 536-case study. J Psychiatry Neurosci 1999;24(3):244-7.
4. Posternak MA, Zimmerman M. Partial validation of the atypical features subtype of major depressive disorder. Arch Gen Psychiatry 2002;59(1):70-6.
5. Perugi G, Akiskal HS, Lattanzi L, et al. The high prevalence of “soft” bipolar (II) features in atypical depression. Compr Psychiatry 1998;39(2):63-71.
6. Levitan RD, Kaplan AS, Brown GM, et al. Low plasma cortisol in bulimia nervosa patients with reversed neurovegetative symptoms of depression. Biol Psychiatry 1997;41(3):366-8.
7. Stewart JW, McGrath PJ, Rabkin JG, Quitkin FM. Atypical depression. A valid clinical entity? Psychiatr Clin North Am 1993;16(3):479-95.
8. Kendler KS, Eaves LJ, Walters EE, Neale MC, Heath AC, Kessler RC. The identification and validation of distinct depressive syndromes in a population-based sample of female twins. Arch Gen Psychiatry 1996;53(5):391-9.
9. Ebert D, Barocka A. The early course of atypical depression. Eur Arch Psychiatry Clin Neurosci 1991;241(2):131-2.
10. Zubieta JK, Pande AC, Demitrack MA. Two-year follow-up of atypical depression. J Psychiatr Res 1999;33(1):23-9.
11. Nierenberg AA, Pava JA, Clancy K, Rosenbaum JF, Fava M. Are neurovegetative symptoms stable in relapsing or recurrent atypical depressive episodes? Biol Psychiatry 1996;40(8):691-6.
12. Quitkin FM, McGrath PJ, Stewart JW, et al. Phenelzine and imipramine in mood reactive depressives. Further delineation of the syndrome of atypical depression. Arch Gen Psychiatry 1989;46(9):787-93.
13. Pande AC, Birkett M, Fechner-Bates S, Haskett RF, Greden JF. Fluoxetine versus phenelzine in atypical depression. Biol Psychiatry 1996;40(10):1017-20.
14. Sogaard J, Lane R, Latimer P, et al. A 12-week study comparing moclobemide and sertraline in the treatment of outpatients with atypical depression. J Psychopharmacol 1999;13(4):406-14.
15. Lonnqvist J, Sihvo S, Syvalahti E, Kiviruusu O. Moclobemide and fluoxetine in atypical depression: a double-blind trial. J Affect Disord 1994;32(3):169-77.
16. McGrath PJ, Stewart JW, Janal MN, Petkova E, Quitkin FM, Klein DF. A placebo-controlled study of fluoxetine versus imipramine in the acute treatment of atypical depression. Am J Psychiatry 2000;157(3):344-50.
17. Stratta P, Bolino F, Cupillari M, Casacchia M. A double-blind parallel study comparing fluoxetine with imipramine in the treatment of atypical depression. Int Clin Psychopharmacol 1991;6(3):193-6.
18. Goodnick PJ, Dominguez RA, DeVane CL, Bowden CL. Bupropion slow-release response in depression: diagnosis and biochemistry. Biol Psychiatry 1998;44(7):629-32.
19. Goodnick PJ, Extein I. Bupropion and fluoxetine in depressive subtypes. Ann Clin Psychiatry 1989;1:119-22.
20. Rye DB, Dihenia B, Bliwise DL. Reversal of atypical depression, sleepiness, and REM-sleep propensity in narcolepsy with bupropion. Depress Anxiety 1998;7(2):92-5.
21. Parker G, Roy K, Mitchell P, Wilhelm K, Malhi G, Hadzi-Pavlovic D. Atypical depression: a reappraisal. Am J Psychiatry 2002;159(9):1470-9.
22. Liebowitz MR, Quitkin FM, Stewart JW, et al. Phenelzine v imipramine in atypical depression. A preliminary report. Arch Gen Psychiatry 1984;41(7):669-77.
23. Thase ME, Carpenter L, Kupfer DJ, Frank E. Clinical significance of reversed vegetative subtypes of recurrent major depression. Psychopharmacol Bull 1991;27(1):17-22.
24. Angst J, Gamma A, Sellaro R, Zhang H, Merikangas K. Toward validation of atypical depression in the community: results of the Zurich cohort study. J Affect Disord 2002;72(2):125-38.
25. Gold PW, Chrousos GP. The endocrinology of melancholic and atypical depression: relation to neurocircuitry and somatic consequences. Proc Assoc Am Physicians 1999;111(1):22-34.
26. Garvey MJ, Schaffer C, Schaffer L, Perry PJ. Is DST status associated with depression characteristics? J Affect Disord 1989;16(2-3):159-65.
27. Geracioti TD, Jr, Loosen PT, Orth DN. Low cerebrospinal fluid corticotropin-releasing hormone concentrations in eucortisolemic depression. Biol Psychiatry 1997;42(3):165-74.
28. Casper RC, Kocsis J, Dysken M, et al. Cortisol measures in primary major depressive disorder with hypersomnia or appetite increase. J Affect Disord 1988;15(2):131-40.
29. Sullivan PF, Kessler RC, Kendler KS. Latent class analysis of lifetime depressive symptoms in the national comorbidity survey. Am J Psychiatry 1998;155(10):1398-406.
30. Levitan RD, Lesage A, Parikh SV, Goering P, Kennedy SH. Reversed neurovegetative symptoms of depression: a community study of Ontario. Am J Psychiatry 1997;154(7):934-40.
31. McElroy SL, Suppes T, Keck PE, Jr, et al. Open-label adjunctive topiramate in the treatment of bipolar disorders. Biol Psychiatry 2000;47(12):1025-33.
32. Shapira NA, Goldsmith TD, McElroy SL. Treatment of binge-eating disorder with topiramate: a clinical case series. J Clin Psychiatry 2000;61(5):368-72.
1. American Psychiatric Association. Diagnostic and statistical manual of mentab disorders (4th ed). Washington DC: American Psychiatric Association, 2000.
2. Benazzi F. Prevalence and clinical features of atypical depression in depressed outpatients: a 467-case study. Psychiatry Res 1999;86(3):259-65.
3. Benazzi F. Is atypical depression a moderate severity depression? A 536-case study. J Psychiatry Neurosci 1999;24(3):244-7.
4. Posternak MA, Zimmerman M. Partial validation of the atypical features subtype of major depressive disorder. Arch Gen Psychiatry 2002;59(1):70-6.
5. Perugi G, Akiskal HS, Lattanzi L, et al. The high prevalence of “soft” bipolar (II) features in atypical depression. Compr Psychiatry 1998;39(2):63-71.
6. Levitan RD, Kaplan AS, Brown GM, et al. Low plasma cortisol in bulimia nervosa patients with reversed neurovegetative symptoms of depression. Biol Psychiatry 1997;41(3):366-8.
7. Stewart JW, McGrath PJ, Rabkin JG, Quitkin FM. Atypical depression. A valid clinical entity? Psychiatr Clin North Am 1993;16(3):479-95.
8. Kendler KS, Eaves LJ, Walters EE, Neale MC, Heath AC, Kessler RC. The identification and validation of distinct depressive syndromes in a population-based sample of female twins. Arch Gen Psychiatry 1996;53(5):391-9.
9. Ebert D, Barocka A. The early course of atypical depression. Eur Arch Psychiatry Clin Neurosci 1991;241(2):131-2.
10. Zubieta JK, Pande AC, Demitrack MA. Two-year follow-up of atypical depression. J Psychiatr Res 1999;33(1):23-9.
11. Nierenberg AA, Pava JA, Clancy K, Rosenbaum JF, Fava M. Are neurovegetative symptoms stable in relapsing or recurrent atypical depressive episodes? Biol Psychiatry 1996;40(8):691-6.
12. Quitkin FM, McGrath PJ, Stewart JW, et al. Phenelzine and imipramine in mood reactive depressives. Further delineation of the syndrome of atypical depression. Arch Gen Psychiatry 1989;46(9):787-93.
13. Pande AC, Birkett M, Fechner-Bates S, Haskett RF, Greden JF. Fluoxetine versus phenelzine in atypical depression. Biol Psychiatry 1996;40(10):1017-20.
14. Sogaard J, Lane R, Latimer P, et al. A 12-week study comparing moclobemide and sertraline in the treatment of outpatients with atypical depression. J Psychopharmacol 1999;13(4):406-14.
15. Lonnqvist J, Sihvo S, Syvalahti E, Kiviruusu O. Moclobemide and fluoxetine in atypical depression: a double-blind trial. J Affect Disord 1994;32(3):169-77.
16. McGrath PJ, Stewart JW, Janal MN, Petkova E, Quitkin FM, Klein DF. A placebo-controlled study of fluoxetine versus imipramine in the acute treatment of atypical depression. Am J Psychiatry 2000;157(3):344-50.
17. Stratta P, Bolino F, Cupillari M, Casacchia M. A double-blind parallel study comparing fluoxetine with imipramine in the treatment of atypical depression. Int Clin Psychopharmacol 1991;6(3):193-6.
18. Goodnick PJ, Dominguez RA, DeVane CL, Bowden CL. Bupropion slow-release response in depression: diagnosis and biochemistry. Biol Psychiatry 1998;44(7):629-32.
19. Goodnick PJ, Extein I. Bupropion and fluoxetine in depressive subtypes. Ann Clin Psychiatry 1989;1:119-22.
20. Rye DB, Dihenia B, Bliwise DL. Reversal of atypical depression, sleepiness, and REM-sleep propensity in narcolepsy with bupropion. Depress Anxiety 1998;7(2):92-5.
21. Parker G, Roy K, Mitchell P, Wilhelm K, Malhi G, Hadzi-Pavlovic D. Atypical depression: a reappraisal. Am J Psychiatry 2002;159(9):1470-9.
22. Liebowitz MR, Quitkin FM, Stewart JW, et al. Phenelzine v imipramine in atypical depression. A preliminary report. Arch Gen Psychiatry 1984;41(7):669-77.
23. Thase ME, Carpenter L, Kupfer DJ, Frank E. Clinical significance of reversed vegetative subtypes of recurrent major depression. Psychopharmacol Bull 1991;27(1):17-22.
24. Angst J, Gamma A, Sellaro R, Zhang H, Merikangas K. Toward validation of atypical depression in the community: results of the Zurich cohort study. J Affect Disord 2002;72(2):125-38.
25. Gold PW, Chrousos GP. The endocrinology of melancholic and atypical depression: relation to neurocircuitry and somatic consequences. Proc Assoc Am Physicians 1999;111(1):22-34.
26. Garvey MJ, Schaffer C, Schaffer L, Perry PJ. Is DST status associated with depression characteristics? J Affect Disord 1989;16(2-3):159-65.
27. Geracioti TD, Jr, Loosen PT, Orth DN. Low cerebrospinal fluid corticotropin-releasing hormone concentrations in eucortisolemic depression. Biol Psychiatry 1997;42(3):165-74.
28. Casper RC, Kocsis J, Dysken M, et al. Cortisol measures in primary major depressive disorder with hypersomnia or appetite increase. J Affect Disord 1988;15(2):131-40.
29. Sullivan PF, Kessler RC, Kendler KS. Latent class analysis of lifetime depressive symptoms in the national comorbidity survey. Am J Psychiatry 1998;155(10):1398-406.
30. Levitan RD, Lesage A, Parikh SV, Goering P, Kennedy SH. Reversed neurovegetative symptoms of depression: a community study of Ontario. Am J Psychiatry 1997;154(7):934-40.
31. McElroy SL, Suppes T, Keck PE, Jr, et al. Open-label adjunctive topiramate in the treatment of bipolar disorders. Biol Psychiatry 2000;47(12):1025-33.
32. Shapira NA, Goldsmith TD, McElroy SL. Treatment of binge-eating disorder with topiramate: a clinical case series. J Clin Psychiatry 2000;61(5):368-72.
The search for the hidden depressant
History: Initial symptoms
Ms. G, 17, has battled attention-deficit/hyperactivity disorder (ADHD) since age 6, and within the past 2 years was also diagnosed as having schizoaffective disorder, bipolar type. An outpatient child psychiatrist and a therapist have helped keep her symptoms in control through much of her life.
During one recent visit to her psychiatrist, however, she complained of decreased energy, increased crying spells, broken sleep, and a depressed mood. She reported that these symptoms began approximately 2 months before the visit, and neither she nor her parents could identify a clear-cut cause.
Throughout her life she has complied with her drug regimens. For 2 years she has been taking divalproex sodium, 500 mg twice daily to manage her manic and depressive episodes, dextroamphetamine sulfate, 30 mg in the morning for her ADHD; risperidone, 2 mg at bedtime for her psychotic symptoms; and mestranol, 60 mcg/d, plus norethindrone, 1 mg/d, for contraception. A recent valproic acid reading of 62 μg/ml is consistent with levels over the last 2 years.
During previous psychotic episodes, Ms. G often became delusional and paranoid with command-type hallucinations. She destroyed her room during her most recent episode.
Ms. G’s adoptive mother accompanied her during this visit. She is concerned for her daughter, especially with the start of school about 1 month away.
Which would you address first: the depression or the psychosis? Would you change Ms. G’s medication and if so, how?
Figure 1 DEPRESSION IN SCHIZOPHRENIA: IMPROVING OUTCOMES
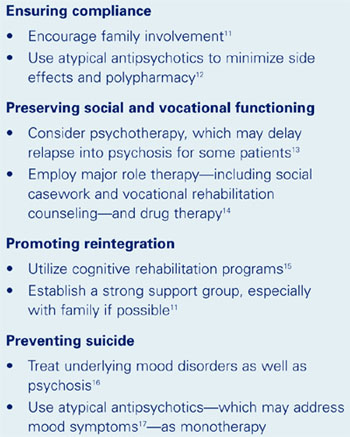
Drs. Yu’s and Maguire’s observations
Complaints of depression in a patient with schizoaffective disorder are especially concerning because multiple domains could be affected (Figure 1). For patients with schizophrenia, the 60% lifetime incidence of major depressive disorder substantially exceeds the 8 to 26% risk in the general population. Ms. G’s comorbid depression also may predispose her to an increased rate of relapse into schizoaffective psychosis, poor treatment response, and a longer duration of psychotic illness that could require hospitalization.1
Although Ms. G’s divalproex level was therapeutic (between 50 and 100 μg/ml), some data indicate that valproic acid may be less effective in schizoaffective disorder than in bipolar I disorder. Still, treatment of schizoaffective disorder often follows antimanic and antidepressant protocols.2
Treatment: An agent is added
The outpatient psychiatrist adds fluoxetine, 20 mg each morning, to address Ms. G’s depressive symptoms. She reports no improvement after 1 month, and her fluoxetine is increased to 30 mg/d.
Three weeks later, Ms. G’s parents bring her to the psychiatrist for an emergency visit. She reports suicidal ideation over the previous month. Rolling up both sleeves, she reveals several superficial cuts on her forearms and wrists that she inflicted after breaking up with her boyfriend.
Her mother, appearing anxious and overwhelmed, reports that her daughter pushed her because she had refused to give Ms. G her calling card. She had told her mother that she wanted to call a boy in Utah that she had met over the Internet.
Ms. G’s speech is noticeably pressured and she is extremely distractible. Her mother notes that her daughter is sleeping only 2 to 3 hours a night, yet exhibits no decrease in energy. Still depressed, her affect is markedly labile, crying at one moment when discussing her suicidality, then railing at her mother when she tries to explain Ms. G’s aggressiveness. When the psychiatrist recommends hospitalization to stabilize her symptoms, she vehemently demands to be let out so that she can run in front of a moving car. The police are called, and she is restrained and brought into the hospital.
What caused Ms. G’s sudden decline? How would you address it?
Drs. Yu’s and Maguire’s observations
Although antidepressants can effectively treat depression in schizoaffective disorder, many of these medications can trigger a manic episode,3 which can include mania, mixed mania with depression, or rapid cycling every few days or hours. In Ms. G’s case, an increase in serotonin due to the fluoxetine may have caused her mania.
We would stop the fluoxetine and see if her manic symptoms resolve. Fluoxetine’s long half-life (4 to 16 days) cuts down the odds of a serotonin-discontinuation syndrome, making immediate discontinuation feasible.
Still, the cause of Ms. G’s depressive symptoms remains unknown. At this stage, observation in the adolescent inpatient ward holds our best hope of reaching a definitive diagnosis.
Treatment: A diagnostic clue surfaces
Blood tests on admission (including a negative drug screen for narcotics or other depressogenic substances) are normal, and her valproic acid level is 61 μg/ml. Her divalproex is increased to 500 mg in the morning and 750 mg at bedtime, and she is tapered off fluoxetine. Her symptoms gradually improve with the change in the medications and her attendance in milieu and group therapy on the ward. A second valproic acid reading on day three of hospitalization is 67 μg/ml.
That day, a nurse informs the inpatient child/adolescent psychiatrist that Ms. G has requested extra hospital gowns. Ms. G later reveals that for about 4 months she has been producing a milky discharge from both breasts, and that the flow has been increasing in frequency and quantity. She adds that she has not menstruated for almost 5 months and complains of breast tenderness.
What do Ms. G’s latest symptoms suggest? How will your response to these symptoms affect treatment?
Drs. Yu’s and Maguire’s observations
Complaints of menstrual irregularities, breast tenderness, and galactorrhea should arouse suspicions of hyperprolactinemia. Because tumors that raise prolactin levels are rare, medications are the most likely culprit in Ms. G’s case. Dopamine blockade within the tuberoinfundibular tract is the mechanism of action behind prolactin elevation.4
Prolactin levels in patients with schizophrenia are generally normal (1 to 25 mg/L) prior to treatment,5 but have been known to increase with use of typical antipsychotics. The atypical antipsychotic risperidone has been associated with dose-related increases in plasma prolactin concentration, although Kleinberg et al found no correlation between risperidone-induced plasma prolactin concentrations and adverse events.6
Figure 2 POSSIBLE ADVERSE EFFECTS OF HYPERPROLACTINEMIA8
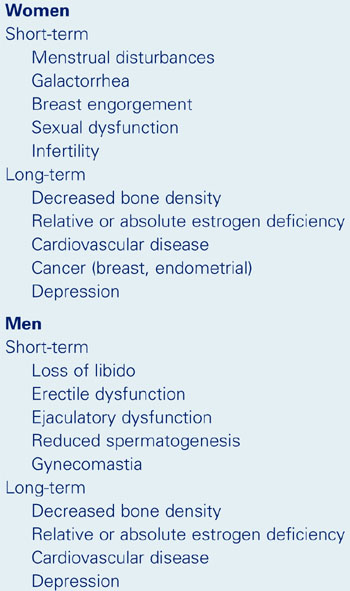
Prolactin-sparing atypical antipsychotics such as olanzapine, quetiapine, ziprasidone, and aripiprazole may cause a transient prolactin increase in the first few weeks of use. These levels tend to remain within the normal range before decreasing to baseline levels or lower.7,8
Prolactin elevation in women may lead to an estrogen deficiency, causing changes in mood and cognition and psychopathology9 that can manifest as increased depression, anxiety, and hostility.10 Hyperprolactinemia can also cause depression in men, though the mechanism of action is unknown.
Prolactin elevation can lead to numerous other health disturbances (Figure 2). When screening women who are taking antipsychotics, ask about menstrual irregularities, sexual dysfunction, breast tenderness, and galactorrhea. Ask male patients about a loss of libido, erectile dysfunction, ejaculatory dysfunction, and gynecomastia.
When hyperprolactinemia becomes apparent, we suggest discontinuing the offending drug and, if necessary:
- switching to a prolactin-sparing atypical antipsychotic
- or trying another agent, such as bromocriptine or pergolide, if switching to another antipsychotic is infeasible.10,11
Baseline prolactin levels should be measured before starting any prolactin-elevating antipsychotic. Because prolactin levels may not correlate with severity of clinical symptoms, the net change in these levels may be a better indicator.4 If prolactin levels exceed 100 mg/L, consider an MRI with fine cuts though the sellae to check for a primary adenoma.4
Conclusion: A cause is found
An MRI of Ms. G’s head is normal, but her serum prolactin level is 125 μg/L. Her risperidone is tapered off, and olanzapine, 10 mg at bedtime, is started with her mother’s consent. Two days later, her prolactin level drops to 85 μg/L. Notable improvement is reported on day seven of hospitalization; she is sleeping and eating well with no suicidal or homicidal ideations and notes no psychotic symptoms. She is discharged that day.
Two weeks later, Ms. G’s improvement continues. Lab tests reveal normal prolactin levels. Over the next few months, she remains stable, attends school, and takes her medications with no adverse effects.
Related resources
- Maguire GA. Prolactin elevation with antipsychotic medications: mechanisms of action and clinical consequences. J Clin Psychiatry 2002; 63(suppl 4):56-62. Available at: www.psychiatrist.com/supplenet/v63s04/v63s0408.pdf. Accessed March 11, 2003.
Drug brand names
- Aripiprazole • Abilify
- Dextroamphetamine sulfate • Dexadrine
- Divalproex sodium • Depakote
- Fluoxetine • Prozac
- Mestranol • Necon 1/50
- Norethindrone • Activella
- Pergolide • Permax
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosure
Dr. Yu receives research/grant support from, is a consultant to, and/or is a speaker for Cephalon Inc., Eli Lilly and Co., Novartis Pharmaceuticals Corp., and Pfizer Inc.
Dr. Maguire receives research/grant support from, is a consultant to, and/or is a speaker for Eli Lilly and Co., Pfizer Inc., Forest Laboratories, and GlaxoSmithKline.
1. Bartels SJ, Drake RE. Depressive symptoms in schizophrenia: comprehensive differential diagnosis. Compr Psychiatry 1988;29(5):467-83.
2. Sadock BJ, Sadock VA. Kaplan and Sadock’s comprehensive textbook of psychiatry (7th ed). Philadelphia Lippincott Williams & Wilkins, 2000.
3. Stahl SM. Essential psychopharmacology: neuroscientific basis and practical application (2nd ed). Cambridge, UK: Cambridge University Press, 2000:chap 5.
4. Maguire GA. Prolactin elevation with antipsychotic medications: mechanisms of action and clinical consequences. J Clin Psychiatry 2002;63(suppl 4):56-62.
5. Kuruvilla A, Srikrishna G, Peedicayil J, et al. A study on serum prolactin levels in schizophrenia: correlation with positive and negative symptoms. Int Clin Psychopharmacol 1993;8:177-9.
6. Kleinberg DL, Davis JM, De Coster R, et al. Prolactin levels and adverse events in patients treated with risperidone. J Clin Psychopharmacol 1999;19:57-61.
7. Petty RG. Prolactin and antipsychotic medications: mechanisms of actions. Schizophr Res 1999;35(suppl):S67-S73.
8. Tran PV, Hamilton SH, Kuntz AJ, et al. Double-blind comparison of olanzapine versus risperidone in the treatment of schizophrenia and other psychotic disorders. J Clin Psychopharmacology 1997;17:407-18.
9. Panay N, Studd JW. The psychotherapeutic effects of estrogens. Gynecol Endocrinol 1998;12:353-65.
10. Kellner R, Buckman MT, Fava M, et al. Prolactin, aggression and hostility: a discussion of recent studies. Psychiatry Dev 1984;2:131-8.
11. Pharoah FM, Mari JJ, Streiner D. Family intervention for schizophrenia. Cochrane Database Syst Rev 2000;(2):CD000088.-
12. Weiden PJ, Aquila R, Emanuel M, Zygmunt A. Long-term considerations after switching antipsychotics. J Clin Psychiatry 1998;59(suppl 19):36-49.
13. Goldberg SC, Schooler NR, Hogarty GE, et al. Prediction of relapse in schizophrenic outpatients treated by drug and sociotherapy. Arch Gen Psychiatry 1977;34:171-84.
14. Hogarty GE, Ulrich RF. The limitations of antipsychotic medication on schizophrenia relapse and adjustment and the contributions of psychosocial treatment. J Psychiatr Res 1998;32:243-50.
15. Bellack AS, Gold JM, Buchanan RW. Cognitive rehabilitation for schizophrenia: problems, prospects, and strategies. Schizophr Bull 1999;25:257-75.
16. Siris SG. Assessment and treatment of secondary depression in schizophrenia. Psychiatr Ann 1994;24:463-7.
17. Keck PE, Jr, Strakowski SM, McElroy SL. The efficacy of atypical antipsychotics in the treatment of depressive symptoms, hostility and suicidality in patients with schizophrenia. J Clin Psychiatry 2000;61(suppl 3):4-9.
18. Mattox JH, Buckman MT, Bernstein J, et al. Dopamine agonists for reducing depression associated with hyperprolactinemia. J Reprod Med 1986;31:694-8.
History: Initial symptoms
Ms. G, 17, has battled attention-deficit/hyperactivity disorder (ADHD) since age 6, and within the past 2 years was also diagnosed as having schizoaffective disorder, bipolar type. An outpatient child psychiatrist and a therapist have helped keep her symptoms in control through much of her life.
During one recent visit to her psychiatrist, however, she complained of decreased energy, increased crying spells, broken sleep, and a depressed mood. She reported that these symptoms began approximately 2 months before the visit, and neither she nor her parents could identify a clear-cut cause.
Throughout her life she has complied with her drug regimens. For 2 years she has been taking divalproex sodium, 500 mg twice daily to manage her manic and depressive episodes, dextroamphetamine sulfate, 30 mg in the morning for her ADHD; risperidone, 2 mg at bedtime for her psychotic symptoms; and mestranol, 60 mcg/d, plus norethindrone, 1 mg/d, for contraception. A recent valproic acid reading of 62 μg/ml is consistent with levels over the last 2 years.
During previous psychotic episodes, Ms. G often became delusional and paranoid with command-type hallucinations. She destroyed her room during her most recent episode.
Ms. G’s adoptive mother accompanied her during this visit. She is concerned for her daughter, especially with the start of school about 1 month away.
Which would you address first: the depression or the psychosis? Would you change Ms. G’s medication and if so, how?
Figure 1 DEPRESSION IN SCHIZOPHRENIA: IMPROVING OUTCOMES
Drs. Yu’s and Maguire’s observations
Complaints of depression in a patient with schizoaffective disorder are especially concerning because multiple domains could be affected (Figure 1). For patients with schizophrenia, the 60% lifetime incidence of major depressive disorder substantially exceeds the 8 to 26% risk in the general population. Ms. G’s comorbid depression also may predispose her to an increased rate of relapse into schizoaffective psychosis, poor treatment response, and a longer duration of psychotic illness that could require hospitalization.1
Although Ms. G’s divalproex level was therapeutic (between 50 and 100 μg/ml), some data indicate that valproic acid may be less effective in schizoaffective disorder than in bipolar I disorder. Still, treatment of schizoaffective disorder often follows antimanic and antidepressant protocols.2
Treatment: An agent is added
The outpatient psychiatrist adds fluoxetine, 20 mg each morning, to address Ms. G’s depressive symptoms. She reports no improvement after 1 month, and her fluoxetine is increased to 30 mg/d.
Three weeks later, Ms. G’s parents bring her to the psychiatrist for an emergency visit. She reports suicidal ideation over the previous month. Rolling up both sleeves, she reveals several superficial cuts on her forearms and wrists that she inflicted after breaking up with her boyfriend.
Her mother, appearing anxious and overwhelmed, reports that her daughter pushed her because she had refused to give Ms. G her calling card. She had told her mother that she wanted to call a boy in Utah that she had met over the Internet.
Ms. G’s speech is noticeably pressured and she is extremely distractible. Her mother notes that her daughter is sleeping only 2 to 3 hours a night, yet exhibits no decrease in energy. Still depressed, her affect is markedly labile, crying at one moment when discussing her suicidality, then railing at her mother when she tries to explain Ms. G’s aggressiveness. When the psychiatrist recommends hospitalization to stabilize her symptoms, she vehemently demands to be let out so that she can run in front of a moving car. The police are called, and she is restrained and brought into the hospital.
What caused Ms. G’s sudden decline? How would you address it?
Drs. Yu’s and Maguire’s observations
Although antidepressants can effectively treat depression in schizoaffective disorder, many of these medications can trigger a manic episode,3 which can include mania, mixed mania with depression, or rapid cycling every few days or hours. In Ms. G’s case, an increase in serotonin due to the fluoxetine may have caused her mania.
We would stop the fluoxetine and see if her manic symptoms resolve. Fluoxetine’s long half-life (4 to 16 days) cuts down the odds of a serotonin-discontinuation syndrome, making immediate discontinuation feasible.
Still, the cause of Ms. G’s depressive symptoms remains unknown. At this stage, observation in the adolescent inpatient ward holds our best hope of reaching a definitive diagnosis.
Treatment: A diagnostic clue surfaces
Blood tests on admission (including a negative drug screen for narcotics or other depressogenic substances) are normal, and her valproic acid level is 61 μg/ml. Her divalproex is increased to 500 mg in the morning and 750 mg at bedtime, and she is tapered off fluoxetine. Her symptoms gradually improve with the change in the medications and her attendance in milieu and group therapy on the ward. A second valproic acid reading on day three of hospitalization is 67 μg/ml.
That day, a nurse informs the inpatient child/adolescent psychiatrist that Ms. G has requested extra hospital gowns. Ms. G later reveals that for about 4 months she has been producing a milky discharge from both breasts, and that the flow has been increasing in frequency and quantity. She adds that she has not menstruated for almost 5 months and complains of breast tenderness.
What do Ms. G’s latest symptoms suggest? How will your response to these symptoms affect treatment?
Drs. Yu’s and Maguire’s observations
Complaints of menstrual irregularities, breast tenderness, and galactorrhea should arouse suspicions of hyperprolactinemia. Because tumors that raise prolactin levels are rare, medications are the most likely culprit in Ms. G’s case. Dopamine blockade within the tuberoinfundibular tract is the mechanism of action behind prolactin elevation.4
Prolactin levels in patients with schizophrenia are generally normal (1 to 25 mg/L) prior to treatment,5 but have been known to increase with use of typical antipsychotics. The atypical antipsychotic risperidone has been associated with dose-related increases in plasma prolactin concentration, although Kleinberg et al found no correlation between risperidone-induced plasma prolactin concentrations and adverse events.6
Figure 2 POSSIBLE ADVERSE EFFECTS OF HYPERPROLACTINEMIA8
Prolactin-sparing atypical antipsychotics such as olanzapine, quetiapine, ziprasidone, and aripiprazole may cause a transient prolactin increase in the first few weeks of use. These levels tend to remain within the normal range before decreasing to baseline levels or lower.7,8
Prolactin elevation in women may lead to an estrogen deficiency, causing changes in mood and cognition and psychopathology9 that can manifest as increased depression, anxiety, and hostility.10 Hyperprolactinemia can also cause depression in men, though the mechanism of action is unknown.
Prolactin elevation can lead to numerous other health disturbances (Figure 2). When screening women who are taking antipsychotics, ask about menstrual irregularities, sexual dysfunction, breast tenderness, and galactorrhea. Ask male patients about a loss of libido, erectile dysfunction, ejaculatory dysfunction, and gynecomastia.
When hyperprolactinemia becomes apparent, we suggest discontinuing the offending drug and, if necessary:
- switching to a prolactin-sparing atypical antipsychotic
- or trying another agent, such as bromocriptine or pergolide, if switching to another antipsychotic is infeasible.10,11
Baseline prolactin levels should be measured before starting any prolactin-elevating antipsychotic. Because prolactin levels may not correlate with severity of clinical symptoms, the net change in these levels may be a better indicator.4 If prolactin levels exceed 100 mg/L, consider an MRI with fine cuts though the sellae to check for a primary adenoma.4
Conclusion: A cause is found
An MRI of Ms. G’s head is normal, but her serum prolactin level is 125 μg/L. Her risperidone is tapered off, and olanzapine, 10 mg at bedtime, is started with her mother’s consent. Two days later, her prolactin level drops to 85 μg/L. Notable improvement is reported on day seven of hospitalization; she is sleeping and eating well with no suicidal or homicidal ideations and notes no psychotic symptoms. She is discharged that day.
Two weeks later, Ms. G’s improvement continues. Lab tests reveal normal prolactin levels. Over the next few months, she remains stable, attends school, and takes her medications with no adverse effects.
Related resources
- Maguire GA. Prolactin elevation with antipsychotic medications: mechanisms of action and clinical consequences. J Clin Psychiatry 2002; 63(suppl 4):56-62. Available at: www.psychiatrist.com/supplenet/v63s04/v63s0408.pdf. Accessed March 11, 2003.
Drug brand names
- Aripiprazole • Abilify
- Dextroamphetamine sulfate • Dexadrine
- Divalproex sodium • Depakote
- Fluoxetine • Prozac
- Mestranol • Necon 1/50
- Norethindrone • Activella
- Pergolide • Permax
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosure
Dr. Yu receives research/grant support from, is a consultant to, and/or is a speaker for Cephalon Inc., Eli Lilly and Co., Novartis Pharmaceuticals Corp., and Pfizer Inc.
Dr. Maguire receives research/grant support from, is a consultant to, and/or is a speaker for Eli Lilly and Co., Pfizer Inc., Forest Laboratories, and GlaxoSmithKline.
History: Initial symptoms
Ms. G, 17, has battled attention-deficit/hyperactivity disorder (ADHD) since age 6, and within the past 2 years was also diagnosed as having schizoaffective disorder, bipolar type. An outpatient child psychiatrist and a therapist have helped keep her symptoms in control through much of her life.
During one recent visit to her psychiatrist, however, she complained of decreased energy, increased crying spells, broken sleep, and a depressed mood. She reported that these symptoms began approximately 2 months before the visit, and neither she nor her parents could identify a clear-cut cause.
Throughout her life she has complied with her drug regimens. For 2 years she has been taking divalproex sodium, 500 mg twice daily to manage her manic and depressive episodes, dextroamphetamine sulfate, 30 mg in the morning for her ADHD; risperidone, 2 mg at bedtime for her psychotic symptoms; and mestranol, 60 mcg/d, plus norethindrone, 1 mg/d, for contraception. A recent valproic acid reading of 62 μg/ml is consistent with levels over the last 2 years.
During previous psychotic episodes, Ms. G often became delusional and paranoid with command-type hallucinations. She destroyed her room during her most recent episode.
Ms. G’s adoptive mother accompanied her during this visit. She is concerned for her daughter, especially with the start of school about 1 month away.
Which would you address first: the depression or the psychosis? Would you change Ms. G’s medication and if so, how?
Figure 1 DEPRESSION IN SCHIZOPHRENIA: IMPROVING OUTCOMES
Drs. Yu’s and Maguire’s observations
Complaints of depression in a patient with schizoaffective disorder are especially concerning because multiple domains could be affected (Figure 1). For patients with schizophrenia, the 60% lifetime incidence of major depressive disorder substantially exceeds the 8 to 26% risk in the general population. Ms. G’s comorbid depression also may predispose her to an increased rate of relapse into schizoaffective psychosis, poor treatment response, and a longer duration of psychotic illness that could require hospitalization.1
Although Ms. G’s divalproex level was therapeutic (between 50 and 100 μg/ml), some data indicate that valproic acid may be less effective in schizoaffective disorder than in bipolar I disorder. Still, treatment of schizoaffective disorder often follows antimanic and antidepressant protocols.2
Treatment: An agent is added
The outpatient psychiatrist adds fluoxetine, 20 mg each morning, to address Ms. G’s depressive symptoms. She reports no improvement after 1 month, and her fluoxetine is increased to 30 mg/d.
Three weeks later, Ms. G’s parents bring her to the psychiatrist for an emergency visit. She reports suicidal ideation over the previous month. Rolling up both sleeves, she reveals several superficial cuts on her forearms and wrists that she inflicted after breaking up with her boyfriend.
Her mother, appearing anxious and overwhelmed, reports that her daughter pushed her because she had refused to give Ms. G her calling card. She had told her mother that she wanted to call a boy in Utah that she had met over the Internet.
Ms. G’s speech is noticeably pressured and she is extremely distractible. Her mother notes that her daughter is sleeping only 2 to 3 hours a night, yet exhibits no decrease in energy. Still depressed, her affect is markedly labile, crying at one moment when discussing her suicidality, then railing at her mother when she tries to explain Ms. G’s aggressiveness. When the psychiatrist recommends hospitalization to stabilize her symptoms, she vehemently demands to be let out so that she can run in front of a moving car. The police are called, and she is restrained and brought into the hospital.
What caused Ms. G’s sudden decline? How would you address it?
Drs. Yu’s and Maguire’s observations
Although antidepressants can effectively treat depression in schizoaffective disorder, many of these medications can trigger a manic episode,3 which can include mania, mixed mania with depression, or rapid cycling every few days or hours. In Ms. G’s case, an increase in serotonin due to the fluoxetine may have caused her mania.
We would stop the fluoxetine and see if her manic symptoms resolve. Fluoxetine’s long half-life (4 to 16 days) cuts down the odds of a serotonin-discontinuation syndrome, making immediate discontinuation feasible.
Still, the cause of Ms. G’s depressive symptoms remains unknown. At this stage, observation in the adolescent inpatient ward holds our best hope of reaching a definitive diagnosis.
Treatment: A diagnostic clue surfaces
Blood tests on admission (including a negative drug screen for narcotics or other depressogenic substances) are normal, and her valproic acid level is 61 μg/ml. Her divalproex is increased to 500 mg in the morning and 750 mg at bedtime, and she is tapered off fluoxetine. Her symptoms gradually improve with the change in the medications and her attendance in milieu and group therapy on the ward. A second valproic acid reading on day three of hospitalization is 67 μg/ml.
That day, a nurse informs the inpatient child/adolescent psychiatrist that Ms. G has requested extra hospital gowns. Ms. G later reveals that for about 4 months she has been producing a milky discharge from both breasts, and that the flow has been increasing in frequency and quantity. She adds that she has not menstruated for almost 5 months and complains of breast tenderness.
What do Ms. G’s latest symptoms suggest? How will your response to these symptoms affect treatment?
Drs. Yu’s and Maguire’s observations
Complaints of menstrual irregularities, breast tenderness, and galactorrhea should arouse suspicions of hyperprolactinemia. Because tumors that raise prolactin levels are rare, medications are the most likely culprit in Ms. G’s case. Dopamine blockade within the tuberoinfundibular tract is the mechanism of action behind prolactin elevation.4
Prolactin levels in patients with schizophrenia are generally normal (1 to 25 mg/L) prior to treatment,5 but have been known to increase with use of typical antipsychotics. The atypical antipsychotic risperidone has been associated with dose-related increases in plasma prolactin concentration, although Kleinberg et al found no correlation between risperidone-induced plasma prolactin concentrations and adverse events.6
Figure 2 POSSIBLE ADVERSE EFFECTS OF HYPERPROLACTINEMIA8
Prolactin-sparing atypical antipsychotics such as olanzapine, quetiapine, ziprasidone, and aripiprazole may cause a transient prolactin increase in the first few weeks of use. These levels tend to remain within the normal range before decreasing to baseline levels or lower.7,8
Prolactin elevation in women may lead to an estrogen deficiency, causing changes in mood and cognition and psychopathology9 that can manifest as increased depression, anxiety, and hostility.10 Hyperprolactinemia can also cause depression in men, though the mechanism of action is unknown.
Prolactin elevation can lead to numerous other health disturbances (Figure 2). When screening women who are taking antipsychotics, ask about menstrual irregularities, sexual dysfunction, breast tenderness, and galactorrhea. Ask male patients about a loss of libido, erectile dysfunction, ejaculatory dysfunction, and gynecomastia.
When hyperprolactinemia becomes apparent, we suggest discontinuing the offending drug and, if necessary:
- switching to a prolactin-sparing atypical antipsychotic
- or trying another agent, such as bromocriptine or pergolide, if switching to another antipsychotic is infeasible.10,11
Baseline prolactin levels should be measured before starting any prolactin-elevating antipsychotic. Because prolactin levels may not correlate with severity of clinical symptoms, the net change in these levels may be a better indicator.4 If prolactin levels exceed 100 mg/L, consider an MRI with fine cuts though the sellae to check for a primary adenoma.4
Conclusion: A cause is found
An MRI of Ms. G’s head is normal, but her serum prolactin level is 125 μg/L. Her risperidone is tapered off, and olanzapine, 10 mg at bedtime, is started with her mother’s consent. Two days later, her prolactin level drops to 85 μg/L. Notable improvement is reported on day seven of hospitalization; she is sleeping and eating well with no suicidal or homicidal ideations and notes no psychotic symptoms. She is discharged that day.
Two weeks later, Ms. G’s improvement continues. Lab tests reveal normal prolactin levels. Over the next few months, she remains stable, attends school, and takes her medications with no adverse effects.
Related resources
- Maguire GA. Prolactin elevation with antipsychotic medications: mechanisms of action and clinical consequences. J Clin Psychiatry 2002; 63(suppl 4):56-62. Available at: www.psychiatrist.com/supplenet/v63s04/v63s0408.pdf. Accessed March 11, 2003.
Drug brand names
- Aripiprazole • Abilify
- Dextroamphetamine sulfate • Dexadrine
- Divalproex sodium • Depakote
- Fluoxetine • Prozac
- Mestranol • Necon 1/50
- Norethindrone • Activella
- Pergolide • Permax
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosure
Dr. Yu receives research/grant support from, is a consultant to, and/or is a speaker for Cephalon Inc., Eli Lilly and Co., Novartis Pharmaceuticals Corp., and Pfizer Inc.
Dr. Maguire receives research/grant support from, is a consultant to, and/or is a speaker for Eli Lilly and Co., Pfizer Inc., Forest Laboratories, and GlaxoSmithKline.
1. Bartels SJ, Drake RE. Depressive symptoms in schizophrenia: comprehensive differential diagnosis. Compr Psychiatry 1988;29(5):467-83.
2. Sadock BJ, Sadock VA. Kaplan and Sadock’s comprehensive textbook of psychiatry (7th ed). Philadelphia Lippincott Williams & Wilkins, 2000.
3. Stahl SM. Essential psychopharmacology: neuroscientific basis and practical application (2nd ed). Cambridge, UK: Cambridge University Press, 2000:chap 5.
4. Maguire GA. Prolactin elevation with antipsychotic medications: mechanisms of action and clinical consequences. J Clin Psychiatry 2002;63(suppl 4):56-62.
5. Kuruvilla A, Srikrishna G, Peedicayil J, et al. A study on serum prolactin levels in schizophrenia: correlation with positive and negative symptoms. Int Clin Psychopharmacol 1993;8:177-9.
6. Kleinberg DL, Davis JM, De Coster R, et al. Prolactin levels and adverse events in patients treated with risperidone. J Clin Psychopharmacol 1999;19:57-61.
7. Petty RG. Prolactin and antipsychotic medications: mechanisms of actions. Schizophr Res 1999;35(suppl):S67-S73.
8. Tran PV, Hamilton SH, Kuntz AJ, et al. Double-blind comparison of olanzapine versus risperidone in the treatment of schizophrenia and other psychotic disorders. J Clin Psychopharmacology 1997;17:407-18.
9. Panay N, Studd JW. The psychotherapeutic effects of estrogens. Gynecol Endocrinol 1998;12:353-65.
10. Kellner R, Buckman MT, Fava M, et al. Prolactin, aggression and hostility: a discussion of recent studies. Psychiatry Dev 1984;2:131-8.
11. Pharoah FM, Mari JJ, Streiner D. Family intervention for schizophrenia. Cochrane Database Syst Rev 2000;(2):CD000088.-
12. Weiden PJ, Aquila R, Emanuel M, Zygmunt A. Long-term considerations after switching antipsychotics. J Clin Psychiatry 1998;59(suppl 19):36-49.
13. Goldberg SC, Schooler NR, Hogarty GE, et al. Prediction of relapse in schizophrenic outpatients treated by drug and sociotherapy. Arch Gen Psychiatry 1977;34:171-84.
14. Hogarty GE, Ulrich RF. The limitations of antipsychotic medication on schizophrenia relapse and adjustment and the contributions of psychosocial treatment. J Psychiatr Res 1998;32:243-50.
15. Bellack AS, Gold JM, Buchanan RW. Cognitive rehabilitation for schizophrenia: problems, prospects, and strategies. Schizophr Bull 1999;25:257-75.
16. Siris SG. Assessment and treatment of secondary depression in schizophrenia. Psychiatr Ann 1994;24:463-7.
17. Keck PE, Jr, Strakowski SM, McElroy SL. The efficacy of atypical antipsychotics in the treatment of depressive symptoms, hostility and suicidality in patients with schizophrenia. J Clin Psychiatry 2000;61(suppl 3):4-9.
18. Mattox JH, Buckman MT, Bernstein J, et al. Dopamine agonists for reducing depression associated with hyperprolactinemia. J Reprod Med 1986;31:694-8.
1. Bartels SJ, Drake RE. Depressive symptoms in schizophrenia: comprehensive differential diagnosis. Compr Psychiatry 1988;29(5):467-83.
2. Sadock BJ, Sadock VA. Kaplan and Sadock’s comprehensive textbook of psychiatry (7th ed). Philadelphia Lippincott Williams & Wilkins, 2000.
3. Stahl SM. Essential psychopharmacology: neuroscientific basis and practical application (2nd ed). Cambridge, UK: Cambridge University Press, 2000:chap 5.
4. Maguire GA. Prolactin elevation with antipsychotic medications: mechanisms of action and clinical consequences. J Clin Psychiatry 2002;63(suppl 4):56-62.
5. Kuruvilla A, Srikrishna G, Peedicayil J, et al. A study on serum prolactin levels in schizophrenia: correlation with positive and negative symptoms. Int Clin Psychopharmacol 1993;8:177-9.
6. Kleinberg DL, Davis JM, De Coster R, et al. Prolactin levels and adverse events in patients treated with risperidone. J Clin Psychopharmacol 1999;19:57-61.
7. Petty RG. Prolactin and antipsychotic medications: mechanisms of actions. Schizophr Res 1999;35(suppl):S67-S73.
8. Tran PV, Hamilton SH, Kuntz AJ, et al. Double-blind comparison of olanzapine versus risperidone in the treatment of schizophrenia and other psychotic disorders. J Clin Psychopharmacology 1997;17:407-18.
9. Panay N, Studd JW. The psychotherapeutic effects of estrogens. Gynecol Endocrinol 1998;12:353-65.
10. Kellner R, Buckman MT, Fava M, et al. Prolactin, aggression and hostility: a discussion of recent studies. Psychiatry Dev 1984;2:131-8.
11. Pharoah FM, Mari JJ, Streiner D. Family intervention for schizophrenia. Cochrane Database Syst Rev 2000;(2):CD000088.-
12. Weiden PJ, Aquila R, Emanuel M, Zygmunt A. Long-term considerations after switching antipsychotics. J Clin Psychiatry 1998;59(suppl 19):36-49.
13. Goldberg SC, Schooler NR, Hogarty GE, et al. Prediction of relapse in schizophrenic outpatients treated by drug and sociotherapy. Arch Gen Psychiatry 1977;34:171-84.
14. Hogarty GE, Ulrich RF. The limitations of antipsychotic medication on schizophrenia relapse and adjustment and the contributions of psychosocial treatment. J Psychiatr Res 1998;32:243-50.
15. Bellack AS, Gold JM, Buchanan RW. Cognitive rehabilitation for schizophrenia: problems, prospects, and strategies. Schizophr Bull 1999;25:257-75.
16. Siris SG. Assessment and treatment of secondary depression in schizophrenia. Psychiatr Ann 1994;24:463-7.
17. Keck PE, Jr, Strakowski SM, McElroy SL. The efficacy of atypical antipsychotics in the treatment of depressive symptoms, hostility and suicidality in patients with schizophrenia. J Clin Psychiatry 2000;61(suppl 3):4-9.
18. Mattox JH, Buckman MT, Bernstein J, et al. Dopamine agonists for reducing depression associated with hyperprolactinemia. J Reprod Med 1986;31:694-8.