User login
AVAHO
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Simpler Screening Criteria Could Catch More Lung Cancers
Simpler Screening Criteria Could Catch More Lung Cancers
Offering lung cancer screening to everyone with a 20-year smoking history could expand access to screening, identify more cancers, and reduce disparities, new research suggests.
In an analysis of nearly 1 million US veterans, researchers estimated that a simplified approach to lung cancer screening — based on smoking duration rather than pack-years — would expand screening eligibility by nearly 30% and reduce potentially missed lung cancers by over 70%.
Those shifts would be especially pronounced among women and Black individuals — 2 groups that are underserved by current screening criteria.
The results, presented at the American Society of Clinical Oncology (ASCO) 2026, come at a time when some groups are revisiting their lung cancer screening guidelines.
And they support smoking duration as a “simpler, more sensitive, and more equitable metric for screening eligibility,” researcher Brendan T. Heiden, MD, MPHS, Washington University School of Medicine in St. Louis, St. Louis, told meeting attendees.
Toward a Better Metric
Current guidelines from the US Preventive Services Task Force (USPSTF) recommend annual lung cancer screening with low-dose CT for adults aged 50-80 years who have at least a 20 pack-year smoking history and either currently smoke or quit within the past 15 years.
The 20 pack-year metric is equivalent to smoking a pack of cigarettes per day for 20 years. Because it requires patients to remember their smoking intensity over decades, it can be challenging to calculate and translate into care, Heiden said.
As it stands, few Americans who are eligible under current USPSTF guidelines actually undergo lung cancer screening, at about 15%-20%, Heiden noted. Meanwhile, mounting evidence suggests that many lung cancers occur in individuals who never meet those eligibility criteria.
Boosting screening uptake, Heiden said, is not enough: There’s a need to revisit eligibility itself to reach more high-risk individuals.
Some groups are already taking steps in that direction. Recently updated guidelines from the National Comprehensive Cancer Network (NCCN) added a category 2B recommendation supporting screening for individuals with at least a 20-year smoking history, regardless of pack-years. (The guidelines also say former smokers are eligible no matter how long ago they quit.)
For their study, Heiden’s team sought to estimate the performance of that smoking-duration metric against current USPSTF pack-year criteria. They used Veterans Health Administration data on over 980,000 veterans whose smoking histories were prospectively collected; lung cancer diagnoses were identified through the Veterans Affairs Central Cancer Registry.
Most of the included veterans (67%) had a smoking history; their mean age was 64 years, and 21% were Black.
Overall, the researchers found that basing eligibility on 20-year smoking duration would substantially expand access to screening: Among veterans with a smoking history, 68% qualified for screening under current USPSTF criteria compared with 87% using the smoking-duration approach.
The gains were especially pronounced among women and Black individuals (who, based on prior research, typically smoke less intensely than White males). Under USPSTF criteria, only about 55% of female and Black veterans qualified for screening compared with 83% for both groups under the smoking-duration criterion.
Importantly, Heiden said, people meeting the smoking-duration threshold remained at substantially elevated risk for lung cancer, suggesting the broader screening criteria were not merely capturing low-risk smokers.
The 5-year lung cancer incidence among veterans eligible under the smoking-duration approach was 1.59% — 11 times the rate of 0.14% among never smokers.
Perhaps most striking, Heiden said, the proportion of potentially missed cancers dropped from 13% with the pack-year metric to just 4% using the smoking-duration metric — a relative reduction of more than 70%.
Again, women and Black individuals would see the largest gains: Among Black veterans, potentially missed cancers fell from 25% to 6%, whereas among female veterans they declined from 22% to 7%.
Optimal Approach Still Unclear
The analysis had limitations, including a predominantly male veteran population whose smoking exposure was far greater than that of the general US population, indicating high inherent lung cancer risk.
But the results support what the NCCN has already done, according to Mary Reid, PhD, MSPH, BSN, a member of the group’s lung cancer screening guideline panel and chief of cancer screening, survivorship and mentorship at Roswell Park Comprehensive Cancer Center in Buffalo, New York.
“Doing the calculation for pack-years can be difficult,” Reid told Medscape Medical News. “Smoking duration is easier to calculate and really the way to go.”
The USPSTF does not comment on individual studies outside of its recommendation development process.
At the meeting, study discussant Katharine A. Rendle, PhD, called the work “impressive,” citing the size of the cohort and strength of the data.
It’s particularly noteworthy that the simpler screening criteria improved sensitivity for all veterans, while largely eliminating disparities, according to Rendle, of the Abramson Cancer Center at the University of Pennsylvania in Philadelphia.
Still, she said, further research could better define the optimal screening strategy.
“Smoking duration is a promising approach, but in my opinion, guidelines likely need to account for the underlying risk in the population,” Rendle said, noting that current smoking prevalence in the US population is about 10%.
She suggested future studies consider other smoking-duration thresholds, such as 30 or 40 years, and look at other outcomes, including life-years gained.
“It’s critical that we prioritize strategies that maximize potential benefit from screening — not just identify those at lung cancer risk — given downstream costs and burden on populations and health care systems,” Rendle said.
The study had no commercial funding. Heiden, Rendle, and Reid had no relevant disclosures.
A version of this article first appeared on Medscape.com.
Offering lung cancer screening to everyone with a 20-year smoking history could expand access to screening, identify more cancers, and reduce disparities, new research suggests.
In an analysis of nearly 1 million US veterans, researchers estimated that a simplified approach to lung cancer screening — based on smoking duration rather than pack-years — would expand screening eligibility by nearly 30% and reduce potentially missed lung cancers by over 70%.
Those shifts would be especially pronounced among women and Black individuals — 2 groups that are underserved by current screening criteria.
The results, presented at the American Society of Clinical Oncology (ASCO) 2026, come at a time when some groups are revisiting their lung cancer screening guidelines.
And they support smoking duration as a “simpler, more sensitive, and more equitable metric for screening eligibility,” researcher Brendan T. Heiden, MD, MPHS, Washington University School of Medicine in St. Louis, St. Louis, told meeting attendees.
Toward a Better Metric
Current guidelines from the US Preventive Services Task Force (USPSTF) recommend annual lung cancer screening with low-dose CT for adults aged 50-80 years who have at least a 20 pack-year smoking history and either currently smoke or quit within the past 15 years.
The 20 pack-year metric is equivalent to smoking a pack of cigarettes per day for 20 years. Because it requires patients to remember their smoking intensity over decades, it can be challenging to calculate and translate into care, Heiden said.
As it stands, few Americans who are eligible under current USPSTF guidelines actually undergo lung cancer screening, at about 15%-20%, Heiden noted. Meanwhile, mounting evidence suggests that many lung cancers occur in individuals who never meet those eligibility criteria.
Boosting screening uptake, Heiden said, is not enough: There’s a need to revisit eligibility itself to reach more high-risk individuals.
Some groups are already taking steps in that direction. Recently updated guidelines from the National Comprehensive Cancer Network (NCCN) added a category 2B recommendation supporting screening for individuals with at least a 20-year smoking history, regardless of pack-years. (The guidelines also say former smokers are eligible no matter how long ago they quit.)
For their study, Heiden’s team sought to estimate the performance of that smoking-duration metric against current USPSTF pack-year criteria. They used Veterans Health Administration data on over 980,000 veterans whose smoking histories were prospectively collected; lung cancer diagnoses were identified through the Veterans Affairs Central Cancer Registry.
Most of the included veterans (67%) had a smoking history; their mean age was 64 years, and 21% were Black.
Overall, the researchers found that basing eligibility on 20-year smoking duration would substantially expand access to screening: Among veterans with a smoking history, 68% qualified for screening under current USPSTF criteria compared with 87% using the smoking-duration approach.
The gains were especially pronounced among women and Black individuals (who, based on prior research, typically smoke less intensely than White males). Under USPSTF criteria, only about 55% of female and Black veterans qualified for screening compared with 83% for both groups under the smoking-duration criterion.
Importantly, Heiden said, people meeting the smoking-duration threshold remained at substantially elevated risk for lung cancer, suggesting the broader screening criteria were not merely capturing low-risk smokers.
The 5-year lung cancer incidence among veterans eligible under the smoking-duration approach was 1.59% — 11 times the rate of 0.14% among never smokers.
Perhaps most striking, Heiden said, the proportion of potentially missed cancers dropped from 13% with the pack-year metric to just 4% using the smoking-duration metric — a relative reduction of more than 70%.
Again, women and Black individuals would see the largest gains: Among Black veterans, potentially missed cancers fell from 25% to 6%, whereas among female veterans they declined from 22% to 7%.
Optimal Approach Still Unclear
The analysis had limitations, including a predominantly male veteran population whose smoking exposure was far greater than that of the general US population, indicating high inherent lung cancer risk.
But the results support what the NCCN has already done, according to Mary Reid, PhD, MSPH, BSN, a member of the group’s lung cancer screening guideline panel and chief of cancer screening, survivorship and mentorship at Roswell Park Comprehensive Cancer Center in Buffalo, New York.
“Doing the calculation for pack-years can be difficult,” Reid told Medscape Medical News. “Smoking duration is easier to calculate and really the way to go.”
The USPSTF does not comment on individual studies outside of its recommendation development process.
At the meeting, study discussant Katharine A. Rendle, PhD, called the work “impressive,” citing the size of the cohort and strength of the data.
It’s particularly noteworthy that the simpler screening criteria improved sensitivity for all veterans, while largely eliminating disparities, according to Rendle, of the Abramson Cancer Center at the University of Pennsylvania in Philadelphia.
Still, she said, further research could better define the optimal screening strategy.
“Smoking duration is a promising approach, but in my opinion, guidelines likely need to account for the underlying risk in the population,” Rendle said, noting that current smoking prevalence in the US population is about 10%.
She suggested future studies consider other smoking-duration thresholds, such as 30 or 40 years, and look at other outcomes, including life-years gained.
“It’s critical that we prioritize strategies that maximize potential benefit from screening — not just identify those at lung cancer risk — given downstream costs and burden on populations and health care systems,” Rendle said.
The study had no commercial funding. Heiden, Rendle, and Reid had no relevant disclosures.
A version of this article first appeared on Medscape.com.
Offering lung cancer screening to everyone with a 20-year smoking history could expand access to screening, identify more cancers, and reduce disparities, new research suggests.
In an analysis of nearly 1 million US veterans, researchers estimated that a simplified approach to lung cancer screening — based on smoking duration rather than pack-years — would expand screening eligibility by nearly 30% and reduce potentially missed lung cancers by over 70%.
Those shifts would be especially pronounced among women and Black individuals — 2 groups that are underserved by current screening criteria.
The results, presented at the American Society of Clinical Oncology (ASCO) 2026, come at a time when some groups are revisiting their lung cancer screening guidelines.
And they support smoking duration as a “simpler, more sensitive, and more equitable metric for screening eligibility,” researcher Brendan T. Heiden, MD, MPHS, Washington University School of Medicine in St. Louis, St. Louis, told meeting attendees.
Toward a Better Metric
Current guidelines from the US Preventive Services Task Force (USPSTF) recommend annual lung cancer screening with low-dose CT for adults aged 50-80 years who have at least a 20 pack-year smoking history and either currently smoke or quit within the past 15 years.
The 20 pack-year metric is equivalent to smoking a pack of cigarettes per day for 20 years. Because it requires patients to remember their smoking intensity over decades, it can be challenging to calculate and translate into care, Heiden said.
As it stands, few Americans who are eligible under current USPSTF guidelines actually undergo lung cancer screening, at about 15%-20%, Heiden noted. Meanwhile, mounting evidence suggests that many lung cancers occur in individuals who never meet those eligibility criteria.
Boosting screening uptake, Heiden said, is not enough: There’s a need to revisit eligibility itself to reach more high-risk individuals.
Some groups are already taking steps in that direction. Recently updated guidelines from the National Comprehensive Cancer Network (NCCN) added a category 2B recommendation supporting screening for individuals with at least a 20-year smoking history, regardless of pack-years. (The guidelines also say former smokers are eligible no matter how long ago they quit.)
For their study, Heiden’s team sought to estimate the performance of that smoking-duration metric against current USPSTF pack-year criteria. They used Veterans Health Administration data on over 980,000 veterans whose smoking histories were prospectively collected; lung cancer diagnoses were identified through the Veterans Affairs Central Cancer Registry.
Most of the included veterans (67%) had a smoking history; their mean age was 64 years, and 21% were Black.
Overall, the researchers found that basing eligibility on 20-year smoking duration would substantially expand access to screening: Among veterans with a smoking history, 68% qualified for screening under current USPSTF criteria compared with 87% using the smoking-duration approach.
The gains were especially pronounced among women and Black individuals (who, based on prior research, typically smoke less intensely than White males). Under USPSTF criteria, only about 55% of female and Black veterans qualified for screening compared with 83% for both groups under the smoking-duration criterion.
Importantly, Heiden said, people meeting the smoking-duration threshold remained at substantially elevated risk for lung cancer, suggesting the broader screening criteria were not merely capturing low-risk smokers.
The 5-year lung cancer incidence among veterans eligible under the smoking-duration approach was 1.59% — 11 times the rate of 0.14% among never smokers.
Perhaps most striking, Heiden said, the proportion of potentially missed cancers dropped from 13% with the pack-year metric to just 4% using the smoking-duration metric — a relative reduction of more than 70%.
Again, women and Black individuals would see the largest gains: Among Black veterans, potentially missed cancers fell from 25% to 6%, whereas among female veterans they declined from 22% to 7%.
Optimal Approach Still Unclear
The analysis had limitations, including a predominantly male veteran population whose smoking exposure was far greater than that of the general US population, indicating high inherent lung cancer risk.
But the results support what the NCCN has already done, according to Mary Reid, PhD, MSPH, BSN, a member of the group’s lung cancer screening guideline panel and chief of cancer screening, survivorship and mentorship at Roswell Park Comprehensive Cancer Center in Buffalo, New York.
“Doing the calculation for pack-years can be difficult,” Reid told Medscape Medical News. “Smoking duration is easier to calculate and really the way to go.”
The USPSTF does not comment on individual studies outside of its recommendation development process.
At the meeting, study discussant Katharine A. Rendle, PhD, called the work “impressive,” citing the size of the cohort and strength of the data.
It’s particularly noteworthy that the simpler screening criteria improved sensitivity for all veterans, while largely eliminating disparities, according to Rendle, of the Abramson Cancer Center at the University of Pennsylvania in Philadelphia.
Still, she said, further research could better define the optimal screening strategy.
“Smoking duration is a promising approach, but in my opinion, guidelines likely need to account for the underlying risk in the population,” Rendle said, noting that current smoking prevalence in the US population is about 10%.
She suggested future studies consider other smoking-duration thresholds, such as 30 or 40 years, and look at other outcomes, including life-years gained.
“It’s critical that we prioritize strategies that maximize potential benefit from screening — not just identify those at lung cancer risk — given downstream costs and burden on populations and health care systems,” Rendle said.
The study had no commercial funding. Heiden, Rendle, and Reid had no relevant disclosures.
A version of this article first appeared on Medscape.com.
Simpler Screening Criteria Could Catch More Lung Cancers
Simpler Screening Criteria Could Catch More Lung Cancers
Alcohol Intake Tied to Increased Colorectal Cancer Risk
Alcohol Intake Tied to Increased Colorectal Cancer Risk
Transcript generated from video captions.
Hello. I’m Dr Maurie Markman, from City of Hope. I’d like to discuss a very interesting paper that appeared in Cancer, entitled, “Association of alcohol intake over the lifetime with colorectal adenoma and colorectal cancer risk in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial.”
This is an important paper. It is very clear, certainly to those in the public health community and cancer doctors, that there is an association with alcohol intake and the risk of cancer. However, in population-based surveys, there is a very large percentage of individuals who do not appear to see the risk of alcohol intake, particularly excessive alcohol intake, related to cancer, or an even larger segment of population simply doesn’t know. This analysis is important to help address this question.
The investigators looked at adults in the United States who were enrolled in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial, which is a very important study that had been ongoing for many years. Individuals in this study reported at several timepoints during their participation what their current and past alcohol intake was.
What these investigators found is as follows. Among the 88,092 participants, there were a total of 1679 incident colorectal cancers that developed over 20 years of follow-up. Investigators demonstrated that current drinkers with an average lifetime alcohol intake of 14 or more drinks per week, or approximately 2 drinks per day, had a higher risk of colorectal cancer with a hazard ratio of 1.25, a 25% increase, compared to those individuals who had ≤ 1 drink per week.
Very importantly, individuals were characterized by their own information that they provided as consistent heavy drinking versus light drinking. This was associated with almost a doubling of the risk of the development of colorectal cancer over that 20-year period.
Clearly, heavy drinking and higher lifetime alcohol intake is associated with an increased risk of colorectal cancer. This is relevant information for public health officials, primary care doctors, and the public in general to understand that there is a risk if you drink often, particularly heavy drinking, with increased development of cancer in general — but in this case, we’re talking specifically about colorectal cancer.
I thank you for your attention.
A version of this article first appeared on Medscape.com.
Transcript generated from video captions.
Hello. I’m Dr Maurie Markman, from City of Hope. I’d like to discuss a very interesting paper that appeared in Cancer, entitled, “Association of alcohol intake over the lifetime with colorectal adenoma and colorectal cancer risk in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial.”
This is an important paper. It is very clear, certainly to those in the public health community and cancer doctors, that there is an association with alcohol intake and the risk of cancer. However, in population-based surveys, there is a very large percentage of individuals who do not appear to see the risk of alcohol intake, particularly excessive alcohol intake, related to cancer, or an even larger segment of population simply doesn’t know. This analysis is important to help address this question.
The investigators looked at adults in the United States who were enrolled in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial, which is a very important study that had been ongoing for many years. Individuals in this study reported at several timepoints during their participation what their current and past alcohol intake was.
What these investigators found is as follows. Among the 88,092 participants, there were a total of 1679 incident colorectal cancers that developed over 20 years of follow-up. Investigators demonstrated that current drinkers with an average lifetime alcohol intake of 14 or more drinks per week, or approximately 2 drinks per day, had a higher risk of colorectal cancer with a hazard ratio of 1.25, a 25% increase, compared to those individuals who had ≤ 1 drink per week.
Very importantly, individuals were characterized by their own information that they provided as consistent heavy drinking versus light drinking. This was associated with almost a doubling of the risk of the development of colorectal cancer over that 20-year period.
Clearly, heavy drinking and higher lifetime alcohol intake is associated with an increased risk of colorectal cancer. This is relevant information for public health officials, primary care doctors, and the public in general to understand that there is a risk if you drink often, particularly heavy drinking, with increased development of cancer in general — but in this case, we’re talking specifically about colorectal cancer.
I thank you for your attention.
A version of this article first appeared on Medscape.com.
Transcript generated from video captions.
Hello. I’m Dr Maurie Markman, from City of Hope. I’d like to discuss a very interesting paper that appeared in Cancer, entitled, “Association of alcohol intake over the lifetime with colorectal adenoma and colorectal cancer risk in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial.”
This is an important paper. It is very clear, certainly to those in the public health community and cancer doctors, that there is an association with alcohol intake and the risk of cancer. However, in population-based surveys, there is a very large percentage of individuals who do not appear to see the risk of alcohol intake, particularly excessive alcohol intake, related to cancer, or an even larger segment of population simply doesn’t know. This analysis is important to help address this question.
The investigators looked at adults in the United States who were enrolled in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial, which is a very important study that had been ongoing for many years. Individuals in this study reported at several timepoints during their participation what their current and past alcohol intake was.
What these investigators found is as follows. Among the 88,092 participants, there were a total of 1679 incident colorectal cancers that developed over 20 years of follow-up. Investigators demonstrated that current drinkers with an average lifetime alcohol intake of 14 or more drinks per week, or approximately 2 drinks per day, had a higher risk of colorectal cancer with a hazard ratio of 1.25, a 25% increase, compared to those individuals who had ≤ 1 drink per week.
Very importantly, individuals were characterized by their own information that they provided as consistent heavy drinking versus light drinking. This was associated with almost a doubling of the risk of the development of colorectal cancer over that 20-year period.
Clearly, heavy drinking and higher lifetime alcohol intake is associated with an increased risk of colorectal cancer. This is relevant information for public health officials, primary care doctors, and the public in general to understand that there is a risk if you drink often, particularly heavy drinking, with increased development of cancer in general — but in this case, we’re talking specifically about colorectal cancer.
I thank you for your attention.
A version of this article first appeared on Medscape.com.
Alcohol Intake Tied to Increased Colorectal Cancer Risk
Alcohol Intake Tied to Increased Colorectal Cancer Risk
GLP-1s Tied to Lower Cancer Risk in Patients With Obesity
GLP-1s Tied to Lower Cancer Risk in Patients With Obesity
Individuals with obesity without diabetes taking GLP-1 receptor agonists (RAs) may have a reduced risk for certain cancers, a new study suggests.
The target trial emulation of more than 160,000 patients found that individuals receiving the medications had a 41% lower risk for obesity-associated cancers (OACs), with an even more substantial 68% risk reduction among men.
“If confirmed in prospective studies, GLP-1 RAs may be associated with a broader clinical profile that extends beyond obesity management to include potential effects on cancer risk,” wrote lead author A.H.-C. Hsu, of Houston Methodist Neal Cancer Center, Houston, and colleagues in Annals of Oncology.
How Are GLP-1 RAs Linked to Reduced Cancer Risk?
According to the investigators, obesity is a recognized risk factor for 13 malignancies: breast, colorectal, endometrial, kidney, pancreatic, thyroid, ovarian, esophageal, gastric, liver, and gallbladder cancers, as well as multiple myeloma and meningioma. These conditions account for about 40% of cancers diagnosed in high-income countries, with incidence rising fastest among younger adults.
Preclinical work suggests GLP-1 receptor activation can suppress proliferation in cancer cells that express the receptor, although these mechanisms remain poorly understood. Observational clinical data have linked GLP-1 RAs to lower cancer risk, mainly in people with type 2 diabetes, but it has remained unclear whether the same association would hold among patients with obesity without diabetes.
How Was the New Study Designed?
The investigators first identified 229,467 adults with obesity without diabetes or a prior OAC in the TriNetX federated database. These patients were entered into a target trial emulation framework, which uses trial-like eligibility, treatment, and follow-up rules to approximate a randomized comparison from observational data.
The population was divided into two cohorts; the first comprised patients who filled at least two prescriptions for a GLP-1 RA and the second included patients who received only diet or exercise counseling. Groups were balanced using 1:1 propensity score matching, yielding 80,899 patients per group. The mean age was 47 years, and about 72% of the population were women.
The primary outcome was the cumulative incidence of OACs over 2 years. Further analyses characterized the same outcome based on sex, BMI, race, and the two most-used drugs, semaglutide and tirzepatide.
What Were the Key Findings?
GLP-1 RA use was associated with a 41% lower incidence of OACs overall (hazard ratio [HR], 0.59). The association held across most subgroups, with a more pronounced benefit among men (HR, 0.32) compared with women (HR, 0.65).
Taking tirzepatide (HR, 0.31) was also associated with a greater risk reduction than taking semaglutide (HR, 0.80); however, the investigators encouraged a cautious interpretation of these findings because the study was not designed for a head-to-head comparison between the agents.
In contrast with the above positive findings, no significant risk reduction was observed among Black patients (HR, 0.77; 95% CI, 0.58-1.03) vs a roughly 50% risk reduction among White patients (HR, 0.54; 95% CI, 0.47-0.62).
The reason for the lack of benefit among Black patients is unclear.
Among specific OACs, greatest risk reductions were reported for multiple myeloma (HR, 0.37), pancreatic cancer (HR, 0.40), endometrial cancer (HR, 0.42), and colorectal cancer (HR, 0.49).
No significant risk reductions were observed for breast cancer, ovarian cancer, or meningioma.
What Are the Clinical Implications?
The investigators emphasized that the study, being observational, is insufficient to confirm that GLP-1 RAs prevent cancer in this patient population. Still, the findings may be worth mentioning to patients considering GLP-1 RAs.
While using GLP-1 RAs specifically to lower cancer risk is “not ready for prime time yet,” the data may offer some reassurance for patients concerned about OACs who already have reason to be prescribed GLP-1 RAs, Michael D. Iglesia, MD, PhD, told Medscape Medical News.
Iglesia, who was not involved in the study, took a more cautious stance on the subgroup findings, first pointing out that women report higher rates of gastrointestinal side effects with GLP-1 RAs, so “the men in this study may have received more consistent GLP-1 RA exposure.”
Commenting on the negative findings among Black patients in the study, Iglesia, who is a medical oncologist at the UNC Lineberger Comprehensive Cancer Center pointed out that this subgroup comprised only 82 GLP-1 RA users and 106 people on diet or exercise.
“Issues related to structural inequality and access to care often affect this kind of study,” he said, adding that further work on social and structural factors is needed “before we posit any biological underpinnings for this observed difference.”
What Questions Remain?
Hsu and colleagues called for long-term prospective trials and postmarketing surveillance to track cancer outcomes among GLP-1 RA users, particularly younger patients.
Underlying mechanisms remain a key unknown, the investigators noted, as it remains unclear whether GLP-1 RAs lower cancer risk through weight loss, direct effects on cancer cells, or some combination thereof.
“Knowing the mechanism behind the association shown in this paper would be important for understanding which cancer types may be treated best with GLP-1 RAs,” Iglesia said.
The investigators and Iglesia reported having no conflicts of interest.
A version of this article first appeared on Medscape.com.
Individuals with obesity without diabetes taking GLP-1 receptor agonists (RAs) may have a reduced risk for certain cancers, a new study suggests.
The target trial emulation of more than 160,000 patients found that individuals receiving the medications had a 41% lower risk for obesity-associated cancers (OACs), with an even more substantial 68% risk reduction among men.
“If confirmed in prospective studies, GLP-1 RAs may be associated with a broader clinical profile that extends beyond obesity management to include potential effects on cancer risk,” wrote lead author A.H.-C. Hsu, of Houston Methodist Neal Cancer Center, Houston, and colleagues in Annals of Oncology.
How Are GLP-1 RAs Linked to Reduced Cancer Risk?
According to the investigators, obesity is a recognized risk factor for 13 malignancies: breast, colorectal, endometrial, kidney, pancreatic, thyroid, ovarian, esophageal, gastric, liver, and gallbladder cancers, as well as multiple myeloma and meningioma. These conditions account for about 40% of cancers diagnosed in high-income countries, with incidence rising fastest among younger adults.
Preclinical work suggests GLP-1 receptor activation can suppress proliferation in cancer cells that express the receptor, although these mechanisms remain poorly understood. Observational clinical data have linked GLP-1 RAs to lower cancer risk, mainly in people with type 2 diabetes, but it has remained unclear whether the same association would hold among patients with obesity without diabetes.
How Was the New Study Designed?
The investigators first identified 229,467 adults with obesity without diabetes or a prior OAC in the TriNetX federated database. These patients were entered into a target trial emulation framework, which uses trial-like eligibility, treatment, and follow-up rules to approximate a randomized comparison from observational data.
The population was divided into two cohorts; the first comprised patients who filled at least two prescriptions for a GLP-1 RA and the second included patients who received only diet or exercise counseling. Groups were balanced using 1:1 propensity score matching, yielding 80,899 patients per group. The mean age was 47 years, and about 72% of the population were women.
The primary outcome was the cumulative incidence of OACs over 2 years. Further analyses characterized the same outcome based on sex, BMI, race, and the two most-used drugs, semaglutide and tirzepatide.
What Were the Key Findings?
GLP-1 RA use was associated with a 41% lower incidence of OACs overall (hazard ratio [HR], 0.59). The association held across most subgroups, with a more pronounced benefit among men (HR, 0.32) compared with women (HR, 0.65).
Taking tirzepatide (HR, 0.31) was also associated with a greater risk reduction than taking semaglutide (HR, 0.80); however, the investigators encouraged a cautious interpretation of these findings because the study was not designed for a head-to-head comparison between the agents.
In contrast with the above positive findings, no significant risk reduction was observed among Black patients (HR, 0.77; 95% CI, 0.58-1.03) vs a roughly 50% risk reduction among White patients (HR, 0.54; 95% CI, 0.47-0.62).
The reason for the lack of benefit among Black patients is unclear.
Among specific OACs, greatest risk reductions were reported for multiple myeloma (HR, 0.37), pancreatic cancer (HR, 0.40), endometrial cancer (HR, 0.42), and colorectal cancer (HR, 0.49).
No significant risk reductions were observed for breast cancer, ovarian cancer, or meningioma.
What Are the Clinical Implications?
The investigators emphasized that the study, being observational, is insufficient to confirm that GLP-1 RAs prevent cancer in this patient population. Still, the findings may be worth mentioning to patients considering GLP-1 RAs.
While using GLP-1 RAs specifically to lower cancer risk is “not ready for prime time yet,” the data may offer some reassurance for patients concerned about OACs who already have reason to be prescribed GLP-1 RAs, Michael D. Iglesia, MD, PhD, told Medscape Medical News.
Iglesia, who was not involved in the study, took a more cautious stance on the subgroup findings, first pointing out that women report higher rates of gastrointestinal side effects with GLP-1 RAs, so “the men in this study may have received more consistent GLP-1 RA exposure.”
Commenting on the negative findings among Black patients in the study, Iglesia, who is a medical oncologist at the UNC Lineberger Comprehensive Cancer Center pointed out that this subgroup comprised only 82 GLP-1 RA users and 106 people on diet or exercise.
“Issues related to structural inequality and access to care often affect this kind of study,” he said, adding that further work on social and structural factors is needed “before we posit any biological underpinnings for this observed difference.”
What Questions Remain?
Hsu and colleagues called for long-term prospective trials and postmarketing surveillance to track cancer outcomes among GLP-1 RA users, particularly younger patients.
Underlying mechanisms remain a key unknown, the investigators noted, as it remains unclear whether GLP-1 RAs lower cancer risk through weight loss, direct effects on cancer cells, or some combination thereof.
“Knowing the mechanism behind the association shown in this paper would be important for understanding which cancer types may be treated best with GLP-1 RAs,” Iglesia said.
The investigators and Iglesia reported having no conflicts of interest.
A version of this article first appeared on Medscape.com.
Individuals with obesity without diabetes taking GLP-1 receptor agonists (RAs) may have a reduced risk for certain cancers, a new study suggests.
The target trial emulation of more than 160,000 patients found that individuals receiving the medications had a 41% lower risk for obesity-associated cancers (OACs), with an even more substantial 68% risk reduction among men.
“If confirmed in prospective studies, GLP-1 RAs may be associated with a broader clinical profile that extends beyond obesity management to include potential effects on cancer risk,” wrote lead author A.H.-C. Hsu, of Houston Methodist Neal Cancer Center, Houston, and colleagues in Annals of Oncology.
How Are GLP-1 RAs Linked to Reduced Cancer Risk?
According to the investigators, obesity is a recognized risk factor for 13 malignancies: breast, colorectal, endometrial, kidney, pancreatic, thyroid, ovarian, esophageal, gastric, liver, and gallbladder cancers, as well as multiple myeloma and meningioma. These conditions account for about 40% of cancers diagnosed in high-income countries, with incidence rising fastest among younger adults.
Preclinical work suggests GLP-1 receptor activation can suppress proliferation in cancer cells that express the receptor, although these mechanisms remain poorly understood. Observational clinical data have linked GLP-1 RAs to lower cancer risk, mainly in people with type 2 diabetes, but it has remained unclear whether the same association would hold among patients with obesity without diabetes.
How Was the New Study Designed?
The investigators first identified 229,467 adults with obesity without diabetes or a prior OAC in the TriNetX federated database. These patients were entered into a target trial emulation framework, which uses trial-like eligibility, treatment, and follow-up rules to approximate a randomized comparison from observational data.
The population was divided into two cohorts; the first comprised patients who filled at least two prescriptions for a GLP-1 RA and the second included patients who received only diet or exercise counseling. Groups were balanced using 1:1 propensity score matching, yielding 80,899 patients per group. The mean age was 47 years, and about 72% of the population were women.
The primary outcome was the cumulative incidence of OACs over 2 years. Further analyses characterized the same outcome based on sex, BMI, race, and the two most-used drugs, semaglutide and tirzepatide.
What Were the Key Findings?
GLP-1 RA use was associated with a 41% lower incidence of OACs overall (hazard ratio [HR], 0.59). The association held across most subgroups, with a more pronounced benefit among men (HR, 0.32) compared with women (HR, 0.65).
Taking tirzepatide (HR, 0.31) was also associated with a greater risk reduction than taking semaglutide (HR, 0.80); however, the investigators encouraged a cautious interpretation of these findings because the study was not designed for a head-to-head comparison between the agents.
In contrast with the above positive findings, no significant risk reduction was observed among Black patients (HR, 0.77; 95% CI, 0.58-1.03) vs a roughly 50% risk reduction among White patients (HR, 0.54; 95% CI, 0.47-0.62).
The reason for the lack of benefit among Black patients is unclear.
Among specific OACs, greatest risk reductions were reported for multiple myeloma (HR, 0.37), pancreatic cancer (HR, 0.40), endometrial cancer (HR, 0.42), and colorectal cancer (HR, 0.49).
No significant risk reductions were observed for breast cancer, ovarian cancer, or meningioma.
What Are the Clinical Implications?
The investigators emphasized that the study, being observational, is insufficient to confirm that GLP-1 RAs prevent cancer in this patient population. Still, the findings may be worth mentioning to patients considering GLP-1 RAs.
While using GLP-1 RAs specifically to lower cancer risk is “not ready for prime time yet,” the data may offer some reassurance for patients concerned about OACs who already have reason to be prescribed GLP-1 RAs, Michael D. Iglesia, MD, PhD, told Medscape Medical News.
Iglesia, who was not involved in the study, took a more cautious stance on the subgroup findings, first pointing out that women report higher rates of gastrointestinal side effects with GLP-1 RAs, so “the men in this study may have received more consistent GLP-1 RA exposure.”
Commenting on the negative findings among Black patients in the study, Iglesia, who is a medical oncologist at the UNC Lineberger Comprehensive Cancer Center pointed out that this subgroup comprised only 82 GLP-1 RA users and 106 people on diet or exercise.
“Issues related to structural inequality and access to care often affect this kind of study,” he said, adding that further work on social and structural factors is needed “before we posit any biological underpinnings for this observed difference.”
What Questions Remain?
Hsu and colleagues called for long-term prospective trials and postmarketing surveillance to track cancer outcomes among GLP-1 RA users, particularly younger patients.
Underlying mechanisms remain a key unknown, the investigators noted, as it remains unclear whether GLP-1 RAs lower cancer risk through weight loss, direct effects on cancer cells, or some combination thereof.
“Knowing the mechanism behind the association shown in this paper would be important for understanding which cancer types may be treated best with GLP-1 RAs,” Iglesia said.
The investigators and Iglesia reported having no conflicts of interest.
A version of this article first appeared on Medscape.com.
GLP-1s Tied to Lower Cancer Risk in Patients With Obesity
GLP-1s Tied to Lower Cancer Risk in Patients With Obesity
RAS Drug Nearly Doubles Survival in Metastatic Pancreatic Cancer
RAS Drug Nearly Doubles Survival in Metastatic Pancreatic Cancer
An investigational oral drug that targets RAS, the dominant oncogenic driver in pancreatic cancer, nearly doubled overall survival compared with common second-line chemotherapy regimens in patients with previously treated metastatic disease.
In the 500-patient phase 3 RASolute 302 trial, patients who received daraxonrasib, a RAS(ON) multi-selective inhibitor, lived a median of 13.2 months compared with 6.7 months for those who received chemotherapy. The drug also doubled progression-free survival, tripled the response rate, and delayed deterioration in both pain and quality of life.
“Results from RASolute 302 support daraxonrasib as a new standard of care for patients with previously treated metastatic pancreatic cancer,” said lead investigator Brian Wolpin, MD, MPH, director of the Hale Family Center for Pancreatic Cancer Research, Dana-Farber Cancer Institute in Boston, who presented the findings at the American Society of Clinical Oncology (ASCO) 2026. The study was also published simultaneously on May 31 in The New England Journal of Medicine.
Pancreatic ductal adenocarcinoma is one of the most lethal cancers, with most patients presenting with advanced disease at diagnosis. For those whose cancer progresses after first-line chemotherapy, no single standard second-line treatment has been established. Available regimens typically produce median progression-free survival of 3-4 months and a median overall survival of 6-7 months.
More than 90% of pancreatic cancers harbor activating RAS mutations — most commonly KRAS G12D and G12V — that drive tumor growth. The first approved KRAS inhibitors — sotorasib and adagrasib for certain lung and colorectal cancers — target KRAS G12C, which is rare in pancreatic cancer. So far, no RAS-targeted therapy has been approved for pancreatic cancer.
Daraxonrasib takes a broader approach. The oral agent can target a range of RAS variants, including mutant and wild-type RAS, by binding the active form of RAS and blocking downstream signaling.
In the phase 3 open-label RASolute 302 trial, researchers randomized 500 patients with previously treated metastatic pancreatic cancer 1:1 to receive daraxonrasib 300 mg orally once daily or investigator’s choice of chemotherapy. The most used regimens in the control arm were gemcitabine plus nab-paclitaxel (56.5%) and liposomal irinotecan plus fluorouracil and leucovorin (32.7%).
Patients were required to have an Eastern Cooperative Oncology Group performance status of 0 or 1. Documented RAS mutational status was required, and nearly 92% of patients had RAS G12 mutations.
The dual primary endpoints were overall survival and progression-free survival in the RAS G12 population. Key secondary endpoints included the same measures in the overall population as well as objective response rate and patient-reported quality of life. The median follow-up was 8.5 months.
In the RAS G12 population, daraxonrasib reduced the risk for death by 60% (hazard ratio [HR], 0.40; P < .001). The median overall survival was 13.2 months with daraxonrasib vs 6.6 months with chemotherapy. Results were nearly identical in the overall population: 13.2 vs 6.7 months (HR, 0.40; P < .001).
Progression-free survival in the RAS G12 population was 7.3 vs 3.5 months (HR, 0.45; P < .001). The objective response rate was 33.2% vs 11.8%.
Daraxonrasib significantly delayed deterioration in pain (median, 9.0 vs 3.7 months; HR, 0.51; P < .001) and global quality of life (5.6 vs 2.4 months; HR, 0.60; P < .001).
Treatment-related adverse events of grade ≥ 3 occurred in 43.6% of patients on daraxonrasib vs 57.5% of patients on chemotherapy. The most common high-grade events with daraxonrasib were rash (13.7%) and stomatitis (12.0%), whereas neutropenia (27.6%) and anemia (16.4%) were most common with chemotherapy.
One patient in the daraxonrasib arm died from treatment-related pneumonitis. Discontinuation due to adverse events occurred in 1.2% of patients on daraxonrasib vs 11.2% of patients on chemotherapy.
The median duration of treatment was 6.2 months with daraxonrasib vs 1.5-3.2 months across chemotherapy regimens, and 42% of patients on daraxonrasib remained on treatment at data cutoff, Wolpin said.
The open-label design is a limitation. About 15% of patients randomized to chemotherapy never received treatment, largely after learning their treatment assignment, although all were included in the intention-to-treat analysis.
Invited discussant Jennifer Knox, MD, a medical oncologist at Princess Margaret Cancer Center and professor of medicine at the University of Toronto in Toronto, Ontario, Canada, called daraxonrasib a game changer, describing the drug as “probably the most exciting strategy in five decades” for pancreatic cancer.
“It is an absolutely beautiful curve,” Knox said of the overall survival data, noting that the Kaplan-Meier curves separated early and continued to widen over time — a pattern rarely seen in pancreatic cancer trials where initial separation between treatment arms typically narrows as patients in both groups deteriorate.
Knox highlighted the pain and quality-of-life data as “the most important endpoints for our patients,” given the severity of the disease.
She pointed out, however, that the combination of rash and stomatitis will be “challenging” in practice, and called for improved supportive care and closer collaboration with dermatology as oncologists gain experience with this first-in-class drug.
Knox said RAS-targeted therapy “should dominate trials across the full spectrum of pancreatic cancer clinical presentations,” pointing to first-line combination trials already underway and noting that treating a larger, earlier population would have the greatest impact.
“This is the first glimpse at the real power of targeting RAS in pancreas cancer,” Knox said.
The study was funded by Revolution Medicines. Wolpin reported consulting or advisory roles with Revolution Medicines, Mirati Therapeutics, Ipsen, and others, and institutional research funding from Revolution Medicines, Agios, Amgen, AstraZeneca, Lilly, and Novartis. Knox reported receiving honoraria from Astellas Pharma, AstraZeneca, Incyte, and Ipsen, and consulting or advisory roles with AstraZeneca/MedImmune, Incyte, and Ipsen.
A version of this article was previously published on Medscape.com.
An investigational oral drug that targets RAS, the dominant oncogenic driver in pancreatic cancer, nearly doubled overall survival compared with common second-line chemotherapy regimens in patients with previously treated metastatic disease.
In the 500-patient phase 3 RASolute 302 trial, patients who received daraxonrasib, a RAS(ON) multi-selective inhibitor, lived a median of 13.2 months compared with 6.7 months for those who received chemotherapy. The drug also doubled progression-free survival, tripled the response rate, and delayed deterioration in both pain and quality of life.
“Results from RASolute 302 support daraxonrasib as a new standard of care for patients with previously treated metastatic pancreatic cancer,” said lead investigator Brian Wolpin, MD, MPH, director of the Hale Family Center for Pancreatic Cancer Research, Dana-Farber Cancer Institute in Boston, who presented the findings at the American Society of Clinical Oncology (ASCO) 2026. The study was also published simultaneously on May 31 in The New England Journal of Medicine.
Pancreatic ductal adenocarcinoma is one of the most lethal cancers, with most patients presenting with advanced disease at diagnosis. For those whose cancer progresses after first-line chemotherapy, no single standard second-line treatment has been established. Available regimens typically produce median progression-free survival of 3-4 months and a median overall survival of 6-7 months.
More than 90% of pancreatic cancers harbor activating RAS mutations — most commonly KRAS G12D and G12V — that drive tumor growth. The first approved KRAS inhibitors — sotorasib and adagrasib for certain lung and colorectal cancers — target KRAS G12C, which is rare in pancreatic cancer. So far, no RAS-targeted therapy has been approved for pancreatic cancer.
Daraxonrasib takes a broader approach. The oral agent can target a range of RAS variants, including mutant and wild-type RAS, by binding the active form of RAS and blocking downstream signaling.
In the phase 3 open-label RASolute 302 trial, researchers randomized 500 patients with previously treated metastatic pancreatic cancer 1:1 to receive daraxonrasib 300 mg orally once daily or investigator’s choice of chemotherapy. The most used regimens in the control arm were gemcitabine plus nab-paclitaxel (56.5%) and liposomal irinotecan plus fluorouracil and leucovorin (32.7%).
Patients were required to have an Eastern Cooperative Oncology Group performance status of 0 or 1. Documented RAS mutational status was required, and nearly 92% of patients had RAS G12 mutations.
The dual primary endpoints were overall survival and progression-free survival in the RAS G12 population. Key secondary endpoints included the same measures in the overall population as well as objective response rate and patient-reported quality of life. The median follow-up was 8.5 months.
In the RAS G12 population, daraxonrasib reduced the risk for death by 60% (hazard ratio [HR], 0.40; P < .001). The median overall survival was 13.2 months with daraxonrasib vs 6.6 months with chemotherapy. Results were nearly identical in the overall population: 13.2 vs 6.7 months (HR, 0.40; P < .001).
Progression-free survival in the RAS G12 population was 7.3 vs 3.5 months (HR, 0.45; P < .001). The objective response rate was 33.2% vs 11.8%.
Daraxonrasib significantly delayed deterioration in pain (median, 9.0 vs 3.7 months; HR, 0.51; P < .001) and global quality of life (5.6 vs 2.4 months; HR, 0.60; P < .001).
Treatment-related adverse events of grade ≥ 3 occurred in 43.6% of patients on daraxonrasib vs 57.5% of patients on chemotherapy. The most common high-grade events with daraxonrasib were rash (13.7%) and stomatitis (12.0%), whereas neutropenia (27.6%) and anemia (16.4%) were most common with chemotherapy.
One patient in the daraxonrasib arm died from treatment-related pneumonitis. Discontinuation due to adverse events occurred in 1.2% of patients on daraxonrasib vs 11.2% of patients on chemotherapy.
The median duration of treatment was 6.2 months with daraxonrasib vs 1.5-3.2 months across chemotherapy regimens, and 42% of patients on daraxonrasib remained on treatment at data cutoff, Wolpin said.
The open-label design is a limitation. About 15% of patients randomized to chemotherapy never received treatment, largely after learning their treatment assignment, although all were included in the intention-to-treat analysis.
Invited discussant Jennifer Knox, MD, a medical oncologist at Princess Margaret Cancer Center and professor of medicine at the University of Toronto in Toronto, Ontario, Canada, called daraxonrasib a game changer, describing the drug as “probably the most exciting strategy in five decades” for pancreatic cancer.
“It is an absolutely beautiful curve,” Knox said of the overall survival data, noting that the Kaplan-Meier curves separated early and continued to widen over time — a pattern rarely seen in pancreatic cancer trials where initial separation between treatment arms typically narrows as patients in both groups deteriorate.
Knox highlighted the pain and quality-of-life data as “the most important endpoints for our patients,” given the severity of the disease.
She pointed out, however, that the combination of rash and stomatitis will be “challenging” in practice, and called for improved supportive care and closer collaboration with dermatology as oncologists gain experience with this first-in-class drug.
Knox said RAS-targeted therapy “should dominate trials across the full spectrum of pancreatic cancer clinical presentations,” pointing to first-line combination trials already underway and noting that treating a larger, earlier population would have the greatest impact.
“This is the first glimpse at the real power of targeting RAS in pancreas cancer,” Knox said.
The study was funded by Revolution Medicines. Wolpin reported consulting or advisory roles with Revolution Medicines, Mirati Therapeutics, Ipsen, and others, and institutional research funding from Revolution Medicines, Agios, Amgen, AstraZeneca, Lilly, and Novartis. Knox reported receiving honoraria from Astellas Pharma, AstraZeneca, Incyte, and Ipsen, and consulting or advisory roles with AstraZeneca/MedImmune, Incyte, and Ipsen.
A version of this article was previously published on Medscape.com.
An investigational oral drug that targets RAS, the dominant oncogenic driver in pancreatic cancer, nearly doubled overall survival compared with common second-line chemotherapy regimens in patients with previously treated metastatic disease.
In the 500-patient phase 3 RASolute 302 trial, patients who received daraxonrasib, a RAS(ON) multi-selective inhibitor, lived a median of 13.2 months compared with 6.7 months for those who received chemotherapy. The drug also doubled progression-free survival, tripled the response rate, and delayed deterioration in both pain and quality of life.
“Results from RASolute 302 support daraxonrasib as a new standard of care for patients with previously treated metastatic pancreatic cancer,” said lead investigator Brian Wolpin, MD, MPH, director of the Hale Family Center for Pancreatic Cancer Research, Dana-Farber Cancer Institute in Boston, who presented the findings at the American Society of Clinical Oncology (ASCO) 2026. The study was also published simultaneously on May 31 in The New England Journal of Medicine.
Pancreatic ductal adenocarcinoma is one of the most lethal cancers, with most patients presenting with advanced disease at diagnosis. For those whose cancer progresses after first-line chemotherapy, no single standard second-line treatment has been established. Available regimens typically produce median progression-free survival of 3-4 months and a median overall survival of 6-7 months.
More than 90% of pancreatic cancers harbor activating RAS mutations — most commonly KRAS G12D and G12V — that drive tumor growth. The first approved KRAS inhibitors — sotorasib and adagrasib for certain lung and colorectal cancers — target KRAS G12C, which is rare in pancreatic cancer. So far, no RAS-targeted therapy has been approved for pancreatic cancer.
Daraxonrasib takes a broader approach. The oral agent can target a range of RAS variants, including mutant and wild-type RAS, by binding the active form of RAS and blocking downstream signaling.
In the phase 3 open-label RASolute 302 trial, researchers randomized 500 patients with previously treated metastatic pancreatic cancer 1:1 to receive daraxonrasib 300 mg orally once daily or investigator’s choice of chemotherapy. The most used regimens in the control arm were gemcitabine plus nab-paclitaxel (56.5%) and liposomal irinotecan plus fluorouracil and leucovorin (32.7%).
Patients were required to have an Eastern Cooperative Oncology Group performance status of 0 or 1. Documented RAS mutational status was required, and nearly 92% of patients had RAS G12 mutations.
The dual primary endpoints were overall survival and progression-free survival in the RAS G12 population. Key secondary endpoints included the same measures in the overall population as well as objective response rate and patient-reported quality of life. The median follow-up was 8.5 months.
In the RAS G12 population, daraxonrasib reduced the risk for death by 60% (hazard ratio [HR], 0.40; P < .001). The median overall survival was 13.2 months with daraxonrasib vs 6.6 months with chemotherapy. Results were nearly identical in the overall population: 13.2 vs 6.7 months (HR, 0.40; P < .001).
Progression-free survival in the RAS G12 population was 7.3 vs 3.5 months (HR, 0.45; P < .001). The objective response rate was 33.2% vs 11.8%.
Daraxonrasib significantly delayed deterioration in pain (median, 9.0 vs 3.7 months; HR, 0.51; P < .001) and global quality of life (5.6 vs 2.4 months; HR, 0.60; P < .001).
Treatment-related adverse events of grade ≥ 3 occurred in 43.6% of patients on daraxonrasib vs 57.5% of patients on chemotherapy. The most common high-grade events with daraxonrasib were rash (13.7%) and stomatitis (12.0%), whereas neutropenia (27.6%) and anemia (16.4%) were most common with chemotherapy.
One patient in the daraxonrasib arm died from treatment-related pneumonitis. Discontinuation due to adverse events occurred in 1.2% of patients on daraxonrasib vs 11.2% of patients on chemotherapy.
The median duration of treatment was 6.2 months with daraxonrasib vs 1.5-3.2 months across chemotherapy regimens, and 42% of patients on daraxonrasib remained on treatment at data cutoff, Wolpin said.
The open-label design is a limitation. About 15% of patients randomized to chemotherapy never received treatment, largely after learning their treatment assignment, although all were included in the intention-to-treat analysis.
Invited discussant Jennifer Knox, MD, a medical oncologist at Princess Margaret Cancer Center and professor of medicine at the University of Toronto in Toronto, Ontario, Canada, called daraxonrasib a game changer, describing the drug as “probably the most exciting strategy in five decades” for pancreatic cancer.
“It is an absolutely beautiful curve,” Knox said of the overall survival data, noting that the Kaplan-Meier curves separated early and continued to widen over time — a pattern rarely seen in pancreatic cancer trials where initial separation between treatment arms typically narrows as patients in both groups deteriorate.
Knox highlighted the pain and quality-of-life data as “the most important endpoints for our patients,” given the severity of the disease.
She pointed out, however, that the combination of rash and stomatitis will be “challenging” in practice, and called for improved supportive care and closer collaboration with dermatology as oncologists gain experience with this first-in-class drug.
Knox said RAS-targeted therapy “should dominate trials across the full spectrum of pancreatic cancer clinical presentations,” pointing to first-line combination trials already underway and noting that treating a larger, earlier population would have the greatest impact.
“This is the first glimpse at the real power of targeting RAS in pancreas cancer,” Knox said.
The study was funded by Revolution Medicines. Wolpin reported consulting or advisory roles with Revolution Medicines, Mirati Therapeutics, Ipsen, and others, and institutional research funding from Revolution Medicines, Agios, Amgen, AstraZeneca, Lilly, and Novartis. Knox reported receiving honoraria from Astellas Pharma, AstraZeneca, Incyte, and Ipsen, and consulting or advisory roles with AstraZeneca/MedImmune, Incyte, and Ipsen.
A version of this article was previously published on Medscape.com.
RAS Drug Nearly Doubles Survival in Metastatic Pancreatic Cancer
RAS Drug Nearly Doubles Survival in Metastatic Pancreatic Cancer
Rare Blood Diseases the Focus of AVAHO Virtual Session
The Association of Veterans Affairs Hematology/Oncology (AVAHO) will provide more than education during a special virtual session on July 18 devoted to 4 rare and ultra-rare disorders in classical hematology. The program includes 2.25 free continuing education credits and the organization hopes it will spur hematology pathways within the US Department of Veterans Affairs (VA) National Oncology Program, according to AVAHO President Nicholas Burwick, MD.
“Guidance on hematology disorders lag far behind oncologic disorders at the national level,” said Burwick, who specializes in hematology and bone marrow transplant at the Veterans Affairs Puget Sound Health Care System in Seattle.
“Providers are facing real diagnostic and treatment decisions, and there are more and more treatment options available, some with significant cost implications,” Burwick said.
Burwick He is optimistic the session will have a lasting impact. He expanded on the 4 disorders slated for discussion at the meeting: aplastic anemia, thrombotic thrombocytopenic purpura (TTP), hereditary hemorrhagic telangiectasia (HHT), and acquired hemophilia A in a discussion with Federal Practitioner. The interview transcript has been edited for length and clarity.
What is aplastic anemia?
Aplastic anemia is a true bone marrow failure. The marrow stops producing cells. At a referral center like Seattle, we might see a few [cases] a year because we also do bone marrow transplant. Most facilities are probably seeing 1 or 2 a year at most.
Different mechanisms are behind it: immune-mediated causes, genetic predispositions, and acquired toxic injury. In the military population, aplastic anemia due to toxic exposure is a significant concern.
Who tends to develop aplastic anemia?
The age spectrum is broader than people think. We do see it in patients in their 40s and 50s, not just seniors. The general rule has been, if a patient is under 40, pursue transplant; over 40, pursue immunosuppressive therapy. However, that cutoff is somewhat arbitrary.
What are some things clinicians should understand about this disease?
Clinicians need to know the diagnostic criteria, what tests to run, how to put in transplant referral requests, and how to get a case on the radar at a transplant center like Nashville or Seattle.
Patients need referral quickly. They often don’t respond to standard treatments like growth factors, so they end up requiring a lot of transfusions. You don’t want to sit around.
Even if the transplant happens outside the VA, it usually runs through a transplant center for review first. There’s also the question of whether a condition qualifies as a service-connected disability or if the diagnosis is a presumptive condition for certain exposures.
How often do you see TTP, which produces small blood clots in blood vessels?
Some clinicians may see 1 case every 3 to 4 years, or possibly 1 case in an entire career. There is an inherited form and an acquired form. We’re primarily focused on the acquired autoimmune form, which can present in young adulthood or later.
What should clinicians know?
These patients come in needing urgent treatment. Recognizing the diagnosis quickly, ordering the right tests, and acting fast are all critical. This can be life-threatening within days without treatment.
Treatment involves plasma exchange, which not every facility is equipped to perform. There are also medications: steroids are standard, but there’s also caplacizumab, which is highly specific to TTP and unlikely to be stocked in a VA pharmacy because of how rarely it’s needed. Pharmacies often have to procure it on demand once the diagnosis is made, which can delay care. A key part of managing these cases is knowing who to reach out to and when to transfer a patient to an academic or community partner that has plasma exchange capability.
Are VA clinicians likely to see HHT, an inherited disorder that causes bleeding due to malformed blood vessels?
There’s a misconception that veterans don’t have inherited bleeding disorders, the assumption being that they wouldn’t have gotten into the military (had they had them). But many of these conditions don’t get diagnosed until later in life: symptoms can be mild initially or not present until young adulthood or later.
Patients might come in with recurrent nosebleeds or unexplained [gastrointestinal] bleeding. We probably all have patients with HHT in our practices without knowing it because we’re not always doing appropriate diagnostic testing.
How are treatments evolving?
Recent developments include both local options like laser treatment and systemic medications such as pomalidomide, which was approved recently, and bevacizumab. [The virtual session] speaker has been involved in clinical trials for pomalidomide and will speak to when to use these medications and how to choose between them now that there are options, both of which are expensive.
What is acquired hemophilia A?
It occurs when someone without a genetic predisposition loses their factor VIII activity due to an autoimmune process. It presents quickly, often with bleeding or bruising, and patients frequently show up in the [emergency department].
The treatment challenge is distinct from inherited hemophilia. Standard factor VIII replacement doesn’t work here because the autoantibody breaks it down. Treatment requires bypassing factor VIII—options include factor VIIa and emicizumab.
Emicizumab is FDA-approved for inherited hemophilia A and used off-label for the acquired form. Procuring it in a VA facility can be difficult, and that is exactly where a VA clinical pathway would help.
The VA doesn’t currently have strong hemophilia expertise internally. So, engaging with hemophilia treatment centers is important, as is developing subject matter experts within VA hematology who can serve as go-to resources for less-resourced facilities.
What unites these 4 rare hematology conditions?
There are common threads: rare presentations requiring urgent decision-making, diagnostic criteria that aren’t always familiar, and treatments that may be hard to procure quickly. VA-specific resources—pathways, referral contacts, teleoncology consults—can make the difference in patient outcomes.
A centralized virtual hematology hub, where providers could reach a knowledgeable hematologist for consultation, would go a long way. That’s what we’re ultimately trying to build toward.
The AVAHO Virtual Session on Rare and Ultra-Rare Hematologic Disorders will be held on July 18, 2026, from 12-2:30 p.m. EST.
The program is available to any health care professional who wants to learn more about the diagnosis and management of these hematologic disorders; 2.25 free continuing education credits are available.
The speakers are:
• Aplastic anemia: Emma Groarke, MB, BCh, BAO, MD, National Institutes of Health
• Thrombotic thrombocytopenic purpura: Yazan Abou-Ismail, MD, University of Utah
• Hereditary hemorrhagic telangiectasia: Hanny Al-Samkari, MD, Massachusetts General Hospital/Harvard Medical School; and
• Acquired hemophilia A, Aaron Boothby, MD, University of Washington/Fred Hutchinson Cancer Center.
The Association of Veterans Affairs Hematology/Oncology (AVAHO) will provide more than education during a special virtual session on July 18 devoted to 4 rare and ultra-rare disorders in classical hematology. The program includes 2.25 free continuing education credits and the organization hopes it will spur hematology pathways within the US Department of Veterans Affairs (VA) National Oncology Program, according to AVAHO President Nicholas Burwick, MD.
“Guidance on hematology disorders lag far behind oncologic disorders at the national level,” said Burwick, who specializes in hematology and bone marrow transplant at the Veterans Affairs Puget Sound Health Care System in Seattle.
“Providers are facing real diagnostic and treatment decisions, and there are more and more treatment options available, some with significant cost implications,” Burwick said.
Burwick He is optimistic the session will have a lasting impact. He expanded on the 4 disorders slated for discussion at the meeting: aplastic anemia, thrombotic thrombocytopenic purpura (TTP), hereditary hemorrhagic telangiectasia (HHT), and acquired hemophilia A in a discussion with Federal Practitioner. The interview transcript has been edited for length and clarity.
What is aplastic anemia?
Aplastic anemia is a true bone marrow failure. The marrow stops producing cells. At a referral center like Seattle, we might see a few [cases] a year because we also do bone marrow transplant. Most facilities are probably seeing 1 or 2 a year at most.
Different mechanisms are behind it: immune-mediated causes, genetic predispositions, and acquired toxic injury. In the military population, aplastic anemia due to toxic exposure is a significant concern.
Who tends to develop aplastic anemia?
The age spectrum is broader than people think. We do see it in patients in their 40s and 50s, not just seniors. The general rule has been, if a patient is under 40, pursue transplant; over 40, pursue immunosuppressive therapy. However, that cutoff is somewhat arbitrary.
What are some things clinicians should understand about this disease?
Clinicians need to know the diagnostic criteria, what tests to run, how to put in transplant referral requests, and how to get a case on the radar at a transplant center like Nashville or Seattle.
Patients need referral quickly. They often don’t respond to standard treatments like growth factors, so they end up requiring a lot of transfusions. You don’t want to sit around.
Even if the transplant happens outside the VA, it usually runs through a transplant center for review first. There’s also the question of whether a condition qualifies as a service-connected disability or if the diagnosis is a presumptive condition for certain exposures.
How often do you see TTP, which produces small blood clots in blood vessels?
Some clinicians may see 1 case every 3 to 4 years, or possibly 1 case in an entire career. There is an inherited form and an acquired form. We’re primarily focused on the acquired autoimmune form, which can present in young adulthood or later.
What should clinicians know?
These patients come in needing urgent treatment. Recognizing the diagnosis quickly, ordering the right tests, and acting fast are all critical. This can be life-threatening within days without treatment.
Treatment involves plasma exchange, which not every facility is equipped to perform. There are also medications: steroids are standard, but there’s also caplacizumab, which is highly specific to TTP and unlikely to be stocked in a VA pharmacy because of how rarely it’s needed. Pharmacies often have to procure it on demand once the diagnosis is made, which can delay care. A key part of managing these cases is knowing who to reach out to and when to transfer a patient to an academic or community partner that has plasma exchange capability.
Are VA clinicians likely to see HHT, an inherited disorder that causes bleeding due to malformed blood vessels?
There’s a misconception that veterans don’t have inherited bleeding disorders, the assumption being that they wouldn’t have gotten into the military (had they had them). But many of these conditions don’t get diagnosed until later in life: symptoms can be mild initially or not present until young adulthood or later.
Patients might come in with recurrent nosebleeds or unexplained [gastrointestinal] bleeding. We probably all have patients with HHT in our practices without knowing it because we’re not always doing appropriate diagnostic testing.
How are treatments evolving?
Recent developments include both local options like laser treatment and systemic medications such as pomalidomide, which was approved recently, and bevacizumab. [The virtual session] speaker has been involved in clinical trials for pomalidomide and will speak to when to use these medications and how to choose between them now that there are options, both of which are expensive.
What is acquired hemophilia A?
It occurs when someone without a genetic predisposition loses their factor VIII activity due to an autoimmune process. It presents quickly, often with bleeding or bruising, and patients frequently show up in the [emergency department].
The treatment challenge is distinct from inherited hemophilia. Standard factor VIII replacement doesn’t work here because the autoantibody breaks it down. Treatment requires bypassing factor VIII—options include factor VIIa and emicizumab.
Emicizumab is FDA-approved for inherited hemophilia A and used off-label for the acquired form. Procuring it in a VA facility can be difficult, and that is exactly where a VA clinical pathway would help.
The VA doesn’t currently have strong hemophilia expertise internally. So, engaging with hemophilia treatment centers is important, as is developing subject matter experts within VA hematology who can serve as go-to resources for less-resourced facilities.
What unites these 4 rare hematology conditions?
There are common threads: rare presentations requiring urgent decision-making, diagnostic criteria that aren’t always familiar, and treatments that may be hard to procure quickly. VA-specific resources—pathways, referral contacts, teleoncology consults—can make the difference in patient outcomes.
A centralized virtual hematology hub, where providers could reach a knowledgeable hematologist for consultation, would go a long way. That’s what we’re ultimately trying to build toward.
The AVAHO Virtual Session on Rare and Ultra-Rare Hematologic Disorders will be held on July 18, 2026, from 12-2:30 p.m. EST.
The program is available to any health care professional who wants to learn more about the diagnosis and management of these hematologic disorders; 2.25 free continuing education credits are available.
The speakers are:
• Aplastic anemia: Emma Groarke, MB, BCh, BAO, MD, National Institutes of Health
• Thrombotic thrombocytopenic purpura: Yazan Abou-Ismail, MD, University of Utah
• Hereditary hemorrhagic telangiectasia: Hanny Al-Samkari, MD, Massachusetts General Hospital/Harvard Medical School; and
• Acquired hemophilia A, Aaron Boothby, MD, University of Washington/Fred Hutchinson Cancer Center.
The Association of Veterans Affairs Hematology/Oncology (AVAHO) will provide more than education during a special virtual session on July 18 devoted to 4 rare and ultra-rare disorders in classical hematology. The program includes 2.25 free continuing education credits and the organization hopes it will spur hematology pathways within the US Department of Veterans Affairs (VA) National Oncology Program, according to AVAHO President Nicholas Burwick, MD.
“Guidance on hematology disorders lag far behind oncologic disorders at the national level,” said Burwick, who specializes in hematology and bone marrow transplant at the Veterans Affairs Puget Sound Health Care System in Seattle.
“Providers are facing real diagnostic and treatment decisions, and there are more and more treatment options available, some with significant cost implications,” Burwick said.
Burwick He is optimistic the session will have a lasting impact. He expanded on the 4 disorders slated for discussion at the meeting: aplastic anemia, thrombotic thrombocytopenic purpura (TTP), hereditary hemorrhagic telangiectasia (HHT), and acquired hemophilia A in a discussion with Federal Practitioner. The interview transcript has been edited for length and clarity.
What is aplastic anemia?
Aplastic anemia is a true bone marrow failure. The marrow stops producing cells. At a referral center like Seattle, we might see a few [cases] a year because we also do bone marrow transplant. Most facilities are probably seeing 1 or 2 a year at most.
Different mechanisms are behind it: immune-mediated causes, genetic predispositions, and acquired toxic injury. In the military population, aplastic anemia due to toxic exposure is a significant concern.
Who tends to develop aplastic anemia?
The age spectrum is broader than people think. We do see it in patients in their 40s and 50s, not just seniors. The general rule has been, if a patient is under 40, pursue transplant; over 40, pursue immunosuppressive therapy. However, that cutoff is somewhat arbitrary.
What are some things clinicians should understand about this disease?
Clinicians need to know the diagnostic criteria, what tests to run, how to put in transplant referral requests, and how to get a case on the radar at a transplant center like Nashville or Seattle.
Patients need referral quickly. They often don’t respond to standard treatments like growth factors, so they end up requiring a lot of transfusions. You don’t want to sit around.
Even if the transplant happens outside the VA, it usually runs through a transplant center for review first. There’s also the question of whether a condition qualifies as a service-connected disability or if the diagnosis is a presumptive condition for certain exposures.
How often do you see TTP, which produces small blood clots in blood vessels?
Some clinicians may see 1 case every 3 to 4 years, or possibly 1 case in an entire career. There is an inherited form and an acquired form. We’re primarily focused on the acquired autoimmune form, which can present in young adulthood or later.
What should clinicians know?
These patients come in needing urgent treatment. Recognizing the diagnosis quickly, ordering the right tests, and acting fast are all critical. This can be life-threatening within days without treatment.
Treatment involves plasma exchange, which not every facility is equipped to perform. There are also medications: steroids are standard, but there’s also caplacizumab, which is highly specific to TTP and unlikely to be stocked in a VA pharmacy because of how rarely it’s needed. Pharmacies often have to procure it on demand once the diagnosis is made, which can delay care. A key part of managing these cases is knowing who to reach out to and when to transfer a patient to an academic or community partner that has plasma exchange capability.
Are VA clinicians likely to see HHT, an inherited disorder that causes bleeding due to malformed blood vessels?
There’s a misconception that veterans don’t have inherited bleeding disorders, the assumption being that they wouldn’t have gotten into the military (had they had them). But many of these conditions don’t get diagnosed until later in life: symptoms can be mild initially or not present until young adulthood or later.
Patients might come in with recurrent nosebleeds or unexplained [gastrointestinal] bleeding. We probably all have patients with HHT in our practices without knowing it because we’re not always doing appropriate diagnostic testing.
How are treatments evolving?
Recent developments include both local options like laser treatment and systemic medications such as pomalidomide, which was approved recently, and bevacizumab. [The virtual session] speaker has been involved in clinical trials for pomalidomide and will speak to when to use these medications and how to choose between them now that there are options, both of which are expensive.
What is acquired hemophilia A?
It occurs when someone without a genetic predisposition loses their factor VIII activity due to an autoimmune process. It presents quickly, often with bleeding or bruising, and patients frequently show up in the [emergency department].
The treatment challenge is distinct from inherited hemophilia. Standard factor VIII replacement doesn’t work here because the autoantibody breaks it down. Treatment requires bypassing factor VIII—options include factor VIIa and emicizumab.
Emicizumab is FDA-approved for inherited hemophilia A and used off-label for the acquired form. Procuring it in a VA facility can be difficult, and that is exactly where a VA clinical pathway would help.
The VA doesn’t currently have strong hemophilia expertise internally. So, engaging with hemophilia treatment centers is important, as is developing subject matter experts within VA hematology who can serve as go-to resources for less-resourced facilities.
What unites these 4 rare hematology conditions?
There are common threads: rare presentations requiring urgent decision-making, diagnostic criteria that aren’t always familiar, and treatments that may be hard to procure quickly. VA-specific resources—pathways, referral contacts, teleoncology consults—can make the difference in patient outcomes.
A centralized virtual hematology hub, where providers could reach a knowledgeable hematologist for consultation, would go a long way. That’s what we’re ultimately trying to build toward.
The AVAHO Virtual Session on Rare and Ultra-Rare Hematologic Disorders will be held on July 18, 2026, from 12-2:30 p.m. EST.
The program is available to any health care professional who wants to learn more about the diagnosis and management of these hematologic disorders; 2.25 free continuing education credits are available.
The speakers are:
• Aplastic anemia: Emma Groarke, MB, BCh, BAO, MD, National Institutes of Health
• Thrombotic thrombocytopenic purpura: Yazan Abou-Ismail, MD, University of Utah
• Hereditary hemorrhagic telangiectasia: Hanny Al-Samkari, MD, Massachusetts General Hospital/Harvard Medical School; and
• Acquired hemophilia A, Aaron Boothby, MD, University of Washington/Fred Hutchinson Cancer Center.
Fact vs Fallacy: Challenging the Norms of Cancer Care Fallacies in Medicine
Fact vs Fallacy: Challenging the Norms of Cancer Care Fallacies in Medicine
This transcript has been edited for clarity.
Hello, everyone. This is Dr Bishal Gyawali, from Queens University, Kingston, Canada. Today, I’m back with you to talk about some of the fallacies that I have seen in medicine, oncology, and the drug regulatory space. I wanted to clarify some of these fallacies.
In my last video, I talked about the FDA denying the approval of a new cancer drug. Let me start with one of the fallacies that is pertinent to that, which is that some people make an argument that patients are dying from a certain condition, such as cancer, or even any other disease besides cancer. That is an absolutely true statement, but that does not necessarily mean there should be a lower bar for drug approvals or we should be approving any drug that has a hint of benefit.
In fact, if we have increased mortality rates and our patients are dying from a certain condition, that means we actually need to have good drugs. We need to have drugs that prevent mortality. We need to have drugs that improve outcomes. Just having any drug out there, if we lower our threshold and are letting any drug be used in these patients because the argument is that people are dying, then in fact, it can have negative consequences.
First, there will be opportunity costs. If you can get any lousy drug into the market and make billions of dollars out of it, then there is no strong motivation to produce drugs that actually remarkably improve outcomes.
Second, patients will also be misled. It’s the patient’s opportunity cost in that they will use whatever time they have remaining to pursue these treatments that were not going to improve their outcomes anyway. This is time they could have better spent either in pursuing better treatments, if those treatments are out there, or to prioritize their time accordingly. This rather gives them a false hope, which can be harmful in the long term.
The first fallacy is that just because people are dying does not necessarily mean we should have more new drugs with a lower bar for approval.
The second fallacy I want to talk about, which is also related to this, is that if a certain cancer is rare, the bar for new drug approval should be quite low.
Of course, rare cancers are a special category, and rare cancers should be treated differently from a regulatory perspective. Absolutely. If the cancer is rare, we cannot have trials with large sample sizes to generate evidence. That problem is there, but that does not necessarily translate to the decision that we should approve anything, even something with a small hint of benefit.
There are other methods to make sure that, even in rare cancers, we can generate good-quality evidence. In fact, from an equity perspective, why should patients with rare cancer not deserve drugs that have good-quality evidence?
We can’t tell someone that, “Your cancer is rare, so you should get drugs that only have a benefit in terms of response rate whereas other cancers that are not rare will have drugs based on survival.”
Going back to the point about the difficulty in doing big trials in patients with rare cancers, that is absolutely true and there should be regulatory flexibility in this. I think accelerated approval is a pathway that allows for this regulatory flexibility, which allows access to these drugs early on based on earlier signals of benefit. You can continue to generate evidence in the future and confirm the clinical benefit.
There are also other nuances to this. One is that we should also make sure that this regulatory flexibility with rare cancers should not be misused. What do I mean by that? First, all rare cancers are not the same. There are some cancers that are ultra rare, and then there are some cancers that technically might fit the definition of rare, but trials are possible. Case in point: adrenocortical cancer. It is considered to be a very rare cancer, but there have been randomized trials in adrenocortical cancer.
Our efforts should be to maximize our collaboration globally so that a cancer that is rare locally will still not be so rare globally when we collect all these patients.
In certain situations, like let’s say, based on the molecular subtypes, any common cancer can be sliced and diced into a rare subtype: MSI-high, BRAF-negative, HER2-positive, right-sided colon cancer. If you start to slice cancers into these smaller and smaller molecular subtypes, you can consider anything as a rare cancer. That should not be misused as an excuse to get away from doing proper trials and generating adequate evidence for our patients.
The third fallacy I want to talk about is that increasing cancer incidence in a certain subgroup of population does not automatically translate into, “We should start screening this subgroup of population.”
A certain cancer — let’s say cancer X or cancer Y — is increasing in a young population, so therefore, we should lower the age of the screening of young populations. This cancer is increasing in this ethnic population, so therefore we should start screening this ethnic population more frequently. This cancer is increasing in this type of minority, so therefore, we should start screening this minority more.
No, it does not work like that. Increasing incidence will make us concerned, of course, but that does not necessarily translate into, “We should start screening them.” In order for a screening test to be useful, it has to fulfill a number of criteria.
The goal is not to detect cancers. The goal is to detect cancers that are not indolent enough that they would have never caused problems, nor speed up the diagnosis of aggressive cancers that are going to be lethal pretty soon anyway. The goal is to detect those cancers in the middle, so that by detecting early, we can intervene and improve the outcomes and improve the mortality from that cancer.
This type of intervention requires a thoughtful consideration of the increasing incidence of the cancer, of course, but also the utility of the screening test in that subgroup of population; the life expectancy of this subgroup of patients with and without cancer; the interventions available to address that increasing burden of cancer; and whether by intervening we are going to reduce the mortality rates.
Just because we can detect cancers does not mean we should detect cancers. That’s the third fallacy I wanted to talk about.
The fourth fallacy is related to when someone is asking for more evidence for anything. There is a new drug for this cancer,so what is the evidence? Or there is this new intervention that will detect ctDNA or whatever before the cancer relapses, or before the cancer even shows up as a screening test.
Whenever there is any treatment that is being promoted and someone asks for evidence, people sometimes try to make personal attacks by saying, “Oh, so, you’re okay with patients dying. You don’t want to save lives.”
Absolutely we want to save lives. That’s why we’re in this field, and that’s why we’re asking for more evidence. You should not consider someone who is asking for evidence as evil or that this person does not want this new drug, or this person does not want this innovation. No, that person actually wants to make sure that that innovation actually helps people. That’s why that person is asking for more evidence.
If we stop asking for evidence, then our whole practice becomes based on emotions, faith, and trust rather than science. You could extrapolate it to the other extreme, like if you are not asking for evidence. If it is interpreted as someone who is asking for evidence is evil, or someone who does not want patients to get new drugs, then you could extrapolate these to people also making claims about alternative medicines or ivermectin nowadays, and claiming that this cures cancer.
Science is science. You need to be the same no matter the circumstances. If you are asking for data for ivermectin, you should also be asking data for your cancer drug that you think is going to work. We should always ask for evidence.
Asking for evidence is not a sign that whoever is asking for evidence does not want the patient to have access to the drug. It is showing that the person who is asking for evidence actually wants to make sure that the patients who get this drug are actually being helped by the drug rather than being harmed.
I’m talking about 5 fallacies today. The final, fifth fallacy is that clinical expertise does not equal expertise in making public health decisions or even expertise in critical appraisal. Someone can be a fantastic breast cancer doctor, the best oncologist for breast cancer. That does not automatically make that person the best person to evaluate clinical trials of breast cancer drugs.
Someone can be a fantastic colon cancer doctor. That does not make that person automatically the best person to evaluate whether or not colonoscopy or colon cancer screening is indicated in a certain patient population.
These population-level decisions — including should this drug be approved, should this drug be funded, and should this screening test be made a public health measure, all of these public health decisions that are done at a population level — require different expertise in critical appraisal, clinical epidemiology, and public health.
Just because someone is a fantastic clinician does not make that person a fantastic public health expert. I see on social media often that a famous doctor with expertise in their domain, let’s say a famous neurosurgeon, might say, “I think brain tumors are increasing in incidence in young persons, so we should be targeting an MRI screening for everyone over the age of 30.”
I’m just making this up, but we see examples of things not dissimilar to this. Just because someone is a neurosurgeon does not make them an expert on brain tumor epidemiology, surveillance, or screening. We should separate clinical expertise from public health expertise.
Thank you.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello, everyone. This is Dr Bishal Gyawali, from Queens University, Kingston, Canada. Today, I’m back with you to talk about some of the fallacies that I have seen in medicine, oncology, and the drug regulatory space. I wanted to clarify some of these fallacies.
In my last video, I talked about the FDA denying the approval of a new cancer drug. Let me start with one of the fallacies that is pertinent to that, which is that some people make an argument that patients are dying from a certain condition, such as cancer, or even any other disease besides cancer. That is an absolutely true statement, but that does not necessarily mean there should be a lower bar for drug approvals or we should be approving any drug that has a hint of benefit.
In fact, if we have increased mortality rates and our patients are dying from a certain condition, that means we actually need to have good drugs. We need to have drugs that prevent mortality. We need to have drugs that improve outcomes. Just having any drug out there, if we lower our threshold and are letting any drug be used in these patients because the argument is that people are dying, then in fact, it can have negative consequences.
First, there will be opportunity costs. If you can get any lousy drug into the market and make billions of dollars out of it, then there is no strong motivation to produce drugs that actually remarkably improve outcomes.
Second, patients will also be misled. It’s the patient’s opportunity cost in that they will use whatever time they have remaining to pursue these treatments that were not going to improve their outcomes anyway. This is time they could have better spent either in pursuing better treatments, if those treatments are out there, or to prioritize their time accordingly. This rather gives them a false hope, which can be harmful in the long term.
The first fallacy is that just because people are dying does not necessarily mean we should have more new drugs with a lower bar for approval.
The second fallacy I want to talk about, which is also related to this, is that if a certain cancer is rare, the bar for new drug approval should be quite low.
Of course, rare cancers are a special category, and rare cancers should be treated differently from a regulatory perspective. Absolutely. If the cancer is rare, we cannot have trials with large sample sizes to generate evidence. That problem is there, but that does not necessarily translate to the decision that we should approve anything, even something with a small hint of benefit.
There are other methods to make sure that, even in rare cancers, we can generate good-quality evidence. In fact, from an equity perspective, why should patients with rare cancer not deserve drugs that have good-quality evidence?
We can’t tell someone that, “Your cancer is rare, so you should get drugs that only have a benefit in terms of response rate whereas other cancers that are not rare will have drugs based on survival.”
Going back to the point about the difficulty in doing big trials in patients with rare cancers, that is absolutely true and there should be regulatory flexibility in this. I think accelerated approval is a pathway that allows for this regulatory flexibility, which allows access to these drugs early on based on earlier signals of benefit. You can continue to generate evidence in the future and confirm the clinical benefit.
There are also other nuances to this. One is that we should also make sure that this regulatory flexibility with rare cancers should not be misused. What do I mean by that? First, all rare cancers are not the same. There are some cancers that are ultra rare, and then there are some cancers that technically might fit the definition of rare, but trials are possible. Case in point: adrenocortical cancer. It is considered to be a very rare cancer, but there have been randomized trials in adrenocortical cancer.
Our efforts should be to maximize our collaboration globally so that a cancer that is rare locally will still not be so rare globally when we collect all these patients.
In certain situations, like let’s say, based on the molecular subtypes, any common cancer can be sliced and diced into a rare subtype: MSI-high, BRAF-negative, HER2-positive, right-sided colon cancer. If you start to slice cancers into these smaller and smaller molecular subtypes, you can consider anything as a rare cancer. That should not be misused as an excuse to get away from doing proper trials and generating adequate evidence for our patients.
The third fallacy I want to talk about is that increasing cancer incidence in a certain subgroup of population does not automatically translate into, “We should start screening this subgroup of population.”
A certain cancer — let’s say cancer X or cancer Y — is increasing in a young population, so therefore, we should lower the age of the screening of young populations. This cancer is increasing in this ethnic population, so therefore we should start screening this ethnic population more frequently. This cancer is increasing in this type of minority, so therefore, we should start screening this minority more.
No, it does not work like that. Increasing incidence will make us concerned, of course, but that does not necessarily translate into, “We should start screening them.” In order for a screening test to be useful, it has to fulfill a number of criteria.
The goal is not to detect cancers. The goal is to detect cancers that are not indolent enough that they would have never caused problems, nor speed up the diagnosis of aggressive cancers that are going to be lethal pretty soon anyway. The goal is to detect those cancers in the middle, so that by detecting early, we can intervene and improve the outcomes and improve the mortality from that cancer.
This type of intervention requires a thoughtful consideration of the increasing incidence of the cancer, of course, but also the utility of the screening test in that subgroup of population; the life expectancy of this subgroup of patients with and without cancer; the interventions available to address that increasing burden of cancer; and whether by intervening we are going to reduce the mortality rates.
Just because we can detect cancers does not mean we should detect cancers. That’s the third fallacy I wanted to talk about.
The fourth fallacy is related to when someone is asking for more evidence for anything. There is a new drug for this cancer,so what is the evidence? Or there is this new intervention that will detect ctDNA or whatever before the cancer relapses, or before the cancer even shows up as a screening test.
Whenever there is any treatment that is being promoted and someone asks for evidence, people sometimes try to make personal attacks by saying, “Oh, so, you’re okay with patients dying. You don’t want to save lives.”
Absolutely we want to save lives. That’s why we’re in this field, and that’s why we’re asking for more evidence. You should not consider someone who is asking for evidence as evil or that this person does not want this new drug, or this person does not want this innovation. No, that person actually wants to make sure that that innovation actually helps people. That’s why that person is asking for more evidence.
If we stop asking for evidence, then our whole practice becomes based on emotions, faith, and trust rather than science. You could extrapolate it to the other extreme, like if you are not asking for evidence. If it is interpreted as someone who is asking for evidence is evil, or someone who does not want patients to get new drugs, then you could extrapolate these to people also making claims about alternative medicines or ivermectin nowadays, and claiming that this cures cancer.
Science is science. You need to be the same no matter the circumstances. If you are asking for data for ivermectin, you should also be asking data for your cancer drug that you think is going to work. We should always ask for evidence.
Asking for evidence is not a sign that whoever is asking for evidence does not want the patient to have access to the drug. It is showing that the person who is asking for evidence actually wants to make sure that the patients who get this drug are actually being helped by the drug rather than being harmed.
I’m talking about 5 fallacies today. The final, fifth fallacy is that clinical expertise does not equal expertise in making public health decisions or even expertise in critical appraisal. Someone can be a fantastic breast cancer doctor, the best oncologist for breast cancer. That does not automatically make that person the best person to evaluate clinical trials of breast cancer drugs.
Someone can be a fantastic colon cancer doctor. That does not make that person automatically the best person to evaluate whether or not colonoscopy or colon cancer screening is indicated in a certain patient population.
These population-level decisions — including should this drug be approved, should this drug be funded, and should this screening test be made a public health measure, all of these public health decisions that are done at a population level — require different expertise in critical appraisal, clinical epidemiology, and public health.
Just because someone is a fantastic clinician does not make that person a fantastic public health expert. I see on social media often that a famous doctor with expertise in their domain, let’s say a famous neurosurgeon, might say, “I think brain tumors are increasing in incidence in young persons, so we should be targeting an MRI screening for everyone over the age of 30.”
I’m just making this up, but we see examples of things not dissimilar to this. Just because someone is a neurosurgeon does not make them an expert on brain tumor epidemiology, surveillance, or screening. We should separate clinical expertise from public health expertise.
Thank you.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello, everyone. This is Dr Bishal Gyawali, from Queens University, Kingston, Canada. Today, I’m back with you to talk about some of the fallacies that I have seen in medicine, oncology, and the drug regulatory space. I wanted to clarify some of these fallacies.
In my last video, I talked about the FDA denying the approval of a new cancer drug. Let me start with one of the fallacies that is pertinent to that, which is that some people make an argument that patients are dying from a certain condition, such as cancer, or even any other disease besides cancer. That is an absolutely true statement, but that does not necessarily mean there should be a lower bar for drug approvals or we should be approving any drug that has a hint of benefit.
In fact, if we have increased mortality rates and our patients are dying from a certain condition, that means we actually need to have good drugs. We need to have drugs that prevent mortality. We need to have drugs that improve outcomes. Just having any drug out there, if we lower our threshold and are letting any drug be used in these patients because the argument is that people are dying, then in fact, it can have negative consequences.
First, there will be opportunity costs. If you can get any lousy drug into the market and make billions of dollars out of it, then there is no strong motivation to produce drugs that actually remarkably improve outcomes.
Second, patients will also be misled. It’s the patient’s opportunity cost in that they will use whatever time they have remaining to pursue these treatments that were not going to improve their outcomes anyway. This is time they could have better spent either in pursuing better treatments, if those treatments are out there, or to prioritize their time accordingly. This rather gives them a false hope, which can be harmful in the long term.
The first fallacy is that just because people are dying does not necessarily mean we should have more new drugs with a lower bar for approval.
The second fallacy I want to talk about, which is also related to this, is that if a certain cancer is rare, the bar for new drug approval should be quite low.
Of course, rare cancers are a special category, and rare cancers should be treated differently from a regulatory perspective. Absolutely. If the cancer is rare, we cannot have trials with large sample sizes to generate evidence. That problem is there, but that does not necessarily translate to the decision that we should approve anything, even something with a small hint of benefit.
There are other methods to make sure that, even in rare cancers, we can generate good-quality evidence. In fact, from an equity perspective, why should patients with rare cancer not deserve drugs that have good-quality evidence?
We can’t tell someone that, “Your cancer is rare, so you should get drugs that only have a benefit in terms of response rate whereas other cancers that are not rare will have drugs based on survival.”
Going back to the point about the difficulty in doing big trials in patients with rare cancers, that is absolutely true and there should be regulatory flexibility in this. I think accelerated approval is a pathway that allows for this regulatory flexibility, which allows access to these drugs early on based on earlier signals of benefit. You can continue to generate evidence in the future and confirm the clinical benefit.
There are also other nuances to this. One is that we should also make sure that this regulatory flexibility with rare cancers should not be misused. What do I mean by that? First, all rare cancers are not the same. There are some cancers that are ultra rare, and then there are some cancers that technically might fit the definition of rare, but trials are possible. Case in point: adrenocortical cancer. It is considered to be a very rare cancer, but there have been randomized trials in adrenocortical cancer.
Our efforts should be to maximize our collaboration globally so that a cancer that is rare locally will still not be so rare globally when we collect all these patients.
In certain situations, like let’s say, based on the molecular subtypes, any common cancer can be sliced and diced into a rare subtype: MSI-high, BRAF-negative, HER2-positive, right-sided colon cancer. If you start to slice cancers into these smaller and smaller molecular subtypes, you can consider anything as a rare cancer. That should not be misused as an excuse to get away from doing proper trials and generating adequate evidence for our patients.
The third fallacy I want to talk about is that increasing cancer incidence in a certain subgroup of population does not automatically translate into, “We should start screening this subgroup of population.”
A certain cancer — let’s say cancer X or cancer Y — is increasing in a young population, so therefore, we should lower the age of the screening of young populations. This cancer is increasing in this ethnic population, so therefore we should start screening this ethnic population more frequently. This cancer is increasing in this type of minority, so therefore, we should start screening this minority more.
No, it does not work like that. Increasing incidence will make us concerned, of course, but that does not necessarily translate into, “We should start screening them.” In order for a screening test to be useful, it has to fulfill a number of criteria.
The goal is not to detect cancers. The goal is to detect cancers that are not indolent enough that they would have never caused problems, nor speed up the diagnosis of aggressive cancers that are going to be lethal pretty soon anyway. The goal is to detect those cancers in the middle, so that by detecting early, we can intervene and improve the outcomes and improve the mortality from that cancer.
This type of intervention requires a thoughtful consideration of the increasing incidence of the cancer, of course, but also the utility of the screening test in that subgroup of population; the life expectancy of this subgroup of patients with and without cancer; the interventions available to address that increasing burden of cancer; and whether by intervening we are going to reduce the mortality rates.
Just because we can detect cancers does not mean we should detect cancers. That’s the third fallacy I wanted to talk about.
The fourth fallacy is related to when someone is asking for more evidence for anything. There is a new drug for this cancer,so what is the evidence? Or there is this new intervention that will detect ctDNA or whatever before the cancer relapses, or before the cancer even shows up as a screening test.
Whenever there is any treatment that is being promoted and someone asks for evidence, people sometimes try to make personal attacks by saying, “Oh, so, you’re okay with patients dying. You don’t want to save lives.”
Absolutely we want to save lives. That’s why we’re in this field, and that’s why we’re asking for more evidence. You should not consider someone who is asking for evidence as evil or that this person does not want this new drug, or this person does not want this innovation. No, that person actually wants to make sure that that innovation actually helps people. That’s why that person is asking for more evidence.
If we stop asking for evidence, then our whole practice becomes based on emotions, faith, and trust rather than science. You could extrapolate it to the other extreme, like if you are not asking for evidence. If it is interpreted as someone who is asking for evidence is evil, or someone who does not want patients to get new drugs, then you could extrapolate these to people also making claims about alternative medicines or ivermectin nowadays, and claiming that this cures cancer.
Science is science. You need to be the same no matter the circumstances. If you are asking for data for ivermectin, you should also be asking data for your cancer drug that you think is going to work. We should always ask for evidence.
Asking for evidence is not a sign that whoever is asking for evidence does not want the patient to have access to the drug. It is showing that the person who is asking for evidence actually wants to make sure that the patients who get this drug are actually being helped by the drug rather than being harmed.
I’m talking about 5 fallacies today. The final, fifth fallacy is that clinical expertise does not equal expertise in making public health decisions or even expertise in critical appraisal. Someone can be a fantastic breast cancer doctor, the best oncologist for breast cancer. That does not automatically make that person the best person to evaluate clinical trials of breast cancer drugs.
Someone can be a fantastic colon cancer doctor. That does not make that person automatically the best person to evaluate whether or not colonoscopy or colon cancer screening is indicated in a certain patient population.
These population-level decisions — including should this drug be approved, should this drug be funded, and should this screening test be made a public health measure, all of these public health decisions that are done at a population level — require different expertise in critical appraisal, clinical epidemiology, and public health.
Just because someone is a fantastic clinician does not make that person a fantastic public health expert. I see on social media often that a famous doctor with expertise in their domain, let’s say a famous neurosurgeon, might say, “I think brain tumors are increasing in incidence in young persons, so we should be targeting an MRI screening for everyone over the age of 30.”
I’m just making this up, but we see examples of things not dissimilar to this. Just because someone is a neurosurgeon does not make them an expert on brain tumor epidemiology, surveillance, or screening. We should separate clinical expertise from public health expertise.
Thank you.
A version of this article first appeared on Medscape.com.
Fact vs Fallacy: Challenging the Norms of Cancer Care Fallacies in Medicine
Fact vs Fallacy: Challenging the Norms of Cancer Care Fallacies in Medicine
The Fastest Way to Better Anticoagulants May Be a Land Snail
The Fastest Way to Better Anticoagulants May Be a Land Snail
The fastest way to a new anticoagulation therapy that prevents blood clots without prolonging bleeding or healing time may be a land snail.
A recent preclinical study in ACS Central Science investigating bioactive molecules derived from the land snail Camaena cicatricosa identified a compound that significantly reduced clot formation without prolonging bleeding time and wound healing in rodent models, directly challenging the assumption that effective anticoagulant therapy must inherently disrupt physiologic repair processes.
“I was quite excited,” said Lisha Lin, PhD, lead author on the study and research assistant at the State Key Laboratory of Phytochemistry and Natural Medicines at the Kunming Institute of Botany, Chinese Academy of Sciences, in Kunming, China. “A novel polysaccharide was identified, and more importantly, it showed anticoagulant activity by inhibiting a novel target, with different action mechanism from heparins.”
What Led to the Land Snail?
The choice of C cicatricosa reflects a shift in thinking. The team screened a range of mollusk-derived biomolecules in search of safer anticoagulation strategies, ultimately isolating a novel galactosylated glycosaminoglycan (CCG) from this terrestrial species.
“We compared the anticoagulant activity of glycosaminoglycans from three snail species,” said Lin. They initially studied polysaccharides from C cicatricosa, Achatina fulica, and Helix lucorum — all sulfated glycosaminoglycans with similar structures. “However, we only found CCG from [C cicatricosa] showed anticoagulant activity but not other snail polysaccharides.”
This unexpected selectivity proved crucial. “The result indicated that the galactose branches and special sulfate substitution were important,” she explained, helping to explain why this particular species stood out among structurally similar compounds.
While CCG shares some similarities with heparin-like molecules, it notably lacks the specific pentasaccharide sequence required for antithrombin binding. Researchers hypothesized that this absence could reduce bleeding risk while maintaining antithrombotic activity.
Rather than broadly inhibiting coagulation, the compound selectively disrupts the intrinsic tenase complex, a pathway more closely associated with pathologic thrombosis than with physiologic hemostasis. This mechanism’s selectivity is central to the study’s findings and helps explain why normal wound healing remained intact in preclinical models.
The isolated compound demonstrated a rare combination in anticoagulant research: potent inhibition of pathologic thrombosis with no significant increase in bleeding time and intact wound healing across multiple experimental models. The compound did not act as a broad-spectrum anticoagulant, instead selectively targeting pathways more relevant to disease-associated clot formation.
The Hope of Lowering Bleeding Risk
For decades, anticoagulation therapy has been built on the assumption that inhibiting clot formation inevitably increases bleeding risk. For physicians treating patients with deep vein thrombosis or atrial fibrillation or those requiring postsurgical attention, the balancing act is constant. Prevent clot formation aggressively enough and the bleeding risk rises. Reduce intensity and thrombosis risk returns.
Current therapies, including heparin and direct oral anticoagulants (DOACs), function by broadly targeting the coagulation cascade. This lack of specialty is precisely what limits them. Even when carefully dosed, the treatments interfere with both pathologic clot formation and physiologic hemostasis.
Physicians managing patients on heparin and DOACs frequently encounter recurrent epistaxis, gastrointestinal bleeding ranging from occult to clinically significant, and urogenital bleeding. A degree of mild bleeding after surgery is often expected and usually resolves on its own. However, it’s crucial to evaluate in the context of ongoing anticoagulation to rule out early signs of clinically significant complications.
“There is definitely a lot of interest in the concept of ‘uncoupling’ thrombosis from hemostasis,” said Yazan Abou-Ismail, MD, hematologist and associate professor of medicine at the University of Utah Health in Salt Lake City, who was not involved in the research. “This concept highlights the differences in pathways essential for normal hemostasis at sites of vessel injury, in contrast with those needed for clot propagation and blood vessel lumen occlusion.”
Abou-Ismail noted that this approach has been explored with Factor XI (FXI) inhibitors currently in clinical trials. However, he raised an important mechanistic concern.
“This mechanism may not necessarily accomplish that goal of uncoupling thrombosis from hemostasis, although it might at narrow therapeutic windows,” Abou-Ismail said. “The tenase complex is a central component of coagulation whose deficiency underlies hemophilia A and B, diseases that cause significant bleeding in humans, and it is more essential to hemostasis than [FXI inhibitors]. Tenase inhibition seems like it may pose a higher bleeding risk in humans.”
He explained that FXI inhibitors have a strong mechanistic rationale because they target the feedback loop that amplifies clot propagation, which is less essential for hemostasis. “FXI inhibitors have clinical trial data demonstrating that FXI inhibition is in fact associated with less bleeding compared to current established anticoagulants,” he said. “However, CCG disrupts the FIXa/FVIIIa intrinsic tenase complex itself, which is considered essential for hemostasis.”
Surprises and Confirmations
The researchers were not anticipating such a clear separation between antithrombotic activity and bleeding risk. The preservation of normal wound healing was equally surprising, directly challenging the belief that interfering with clot formation inevitably disrupts tissue repair.
However, the path to these conclusions was not straightforward. “The structural definition of complex macromolecules like sulfated polysaccharides is a common challenge in the research field,” Lin said. “We spent a lot of time to analyze the structure of CCG.”
Even after identifying the candidate compound, the team had to rigorously confirm that its effects were truly anticoagulant in nature, rather than secondary to anti-inflammatory or vascular remodeling properties. Mechanistic studies were essential in demonstrating its targeted disruption of the intrinsic tenase complex, helping to explain how thrombosis could be reduced without broadly impairing coagulation.
Lin is excited but knows patience and skepticism are needed. “Our research is still at the basic stage, but based on the available data, we may provide a potential anticoagulant option with low bleeding risk,” she said. “In the discussion section of our paper, we also stated that ‘the data suggest a wide therapeutic window of CCG, which may offer therapeutic advantages for patients with bleeding contraindication, such as elderly patients and those with renal failure, as well as for safer long-term anticoagulation.’”
A New Direction for Heparin Alternatives?
Despite these concerns, Abou-Ismail acknowledged that the research has genuinely noteworthy aspects. “A future anticoagulant with a novel mechanism of action may be useful in patients who have experienced anticoagulant failure or breakthrough thrombosis from currently established anticoagulants,” he said. “Having another option might be useful when all other options have failed or are not feasible.”
However, he added a note of caution: “If a therapeutic window exists where partial tenase disruption has antithrombotic effect that does not impair hemostasis, then that would definitely be a promising future finding, but it is too early to arrive at that conclusion with this study.”
The search for safer heparin alternatives has been ongoing for decades, but most candidates still operate within the same fundamental paradigm of broad coagulation inhibition. This snail can’t move fast enough.
Abou-Ismail reported having no relevant conflicts. Disclosure information for study authors is available in the original study publication.
A version of this article first appeared on Medscape.com.
The fastest way to a new anticoagulation therapy that prevents blood clots without prolonging bleeding or healing time may be a land snail.
A recent preclinical study in ACS Central Science investigating bioactive molecules derived from the land snail Camaena cicatricosa identified a compound that significantly reduced clot formation without prolonging bleeding time and wound healing in rodent models, directly challenging the assumption that effective anticoagulant therapy must inherently disrupt physiologic repair processes.
“I was quite excited,” said Lisha Lin, PhD, lead author on the study and research assistant at the State Key Laboratory of Phytochemistry and Natural Medicines at the Kunming Institute of Botany, Chinese Academy of Sciences, in Kunming, China. “A novel polysaccharide was identified, and more importantly, it showed anticoagulant activity by inhibiting a novel target, with different action mechanism from heparins.”
What Led to the Land Snail?
The choice of C cicatricosa reflects a shift in thinking. The team screened a range of mollusk-derived biomolecules in search of safer anticoagulation strategies, ultimately isolating a novel galactosylated glycosaminoglycan (CCG) from this terrestrial species.
“We compared the anticoagulant activity of glycosaminoglycans from three snail species,” said Lin. They initially studied polysaccharides from C cicatricosa, Achatina fulica, and Helix lucorum — all sulfated glycosaminoglycans with similar structures. “However, we only found CCG from [C cicatricosa] showed anticoagulant activity but not other snail polysaccharides.”
This unexpected selectivity proved crucial. “The result indicated that the galactose branches and special sulfate substitution were important,” she explained, helping to explain why this particular species stood out among structurally similar compounds.
While CCG shares some similarities with heparin-like molecules, it notably lacks the specific pentasaccharide sequence required for antithrombin binding. Researchers hypothesized that this absence could reduce bleeding risk while maintaining antithrombotic activity.
Rather than broadly inhibiting coagulation, the compound selectively disrupts the intrinsic tenase complex, a pathway more closely associated with pathologic thrombosis than with physiologic hemostasis. This mechanism’s selectivity is central to the study’s findings and helps explain why normal wound healing remained intact in preclinical models.
The isolated compound demonstrated a rare combination in anticoagulant research: potent inhibition of pathologic thrombosis with no significant increase in bleeding time and intact wound healing across multiple experimental models. The compound did not act as a broad-spectrum anticoagulant, instead selectively targeting pathways more relevant to disease-associated clot formation.
The Hope of Lowering Bleeding Risk
For decades, anticoagulation therapy has been built on the assumption that inhibiting clot formation inevitably increases bleeding risk. For physicians treating patients with deep vein thrombosis or atrial fibrillation or those requiring postsurgical attention, the balancing act is constant. Prevent clot formation aggressively enough and the bleeding risk rises. Reduce intensity and thrombosis risk returns.
Current therapies, including heparin and direct oral anticoagulants (DOACs), function by broadly targeting the coagulation cascade. This lack of specialty is precisely what limits them. Even when carefully dosed, the treatments interfere with both pathologic clot formation and physiologic hemostasis.
Physicians managing patients on heparin and DOACs frequently encounter recurrent epistaxis, gastrointestinal bleeding ranging from occult to clinically significant, and urogenital bleeding. A degree of mild bleeding after surgery is often expected and usually resolves on its own. However, it’s crucial to evaluate in the context of ongoing anticoagulation to rule out early signs of clinically significant complications.
“There is definitely a lot of interest in the concept of ‘uncoupling’ thrombosis from hemostasis,” said Yazan Abou-Ismail, MD, hematologist and associate professor of medicine at the University of Utah Health in Salt Lake City, who was not involved in the research. “This concept highlights the differences in pathways essential for normal hemostasis at sites of vessel injury, in contrast with those needed for clot propagation and blood vessel lumen occlusion.”
Abou-Ismail noted that this approach has been explored with Factor XI (FXI) inhibitors currently in clinical trials. However, he raised an important mechanistic concern.
“This mechanism may not necessarily accomplish that goal of uncoupling thrombosis from hemostasis, although it might at narrow therapeutic windows,” Abou-Ismail said. “The tenase complex is a central component of coagulation whose deficiency underlies hemophilia A and B, diseases that cause significant bleeding in humans, and it is more essential to hemostasis than [FXI inhibitors]. Tenase inhibition seems like it may pose a higher bleeding risk in humans.”
He explained that FXI inhibitors have a strong mechanistic rationale because they target the feedback loop that amplifies clot propagation, which is less essential for hemostasis. “FXI inhibitors have clinical trial data demonstrating that FXI inhibition is in fact associated with less bleeding compared to current established anticoagulants,” he said. “However, CCG disrupts the FIXa/FVIIIa intrinsic tenase complex itself, which is considered essential for hemostasis.”
Surprises and Confirmations
The researchers were not anticipating such a clear separation between antithrombotic activity and bleeding risk. The preservation of normal wound healing was equally surprising, directly challenging the belief that interfering with clot formation inevitably disrupts tissue repair.
However, the path to these conclusions was not straightforward. “The structural definition of complex macromolecules like sulfated polysaccharides is a common challenge in the research field,” Lin said. “We spent a lot of time to analyze the structure of CCG.”
Even after identifying the candidate compound, the team had to rigorously confirm that its effects were truly anticoagulant in nature, rather than secondary to anti-inflammatory or vascular remodeling properties. Mechanistic studies were essential in demonstrating its targeted disruption of the intrinsic tenase complex, helping to explain how thrombosis could be reduced without broadly impairing coagulation.
Lin is excited but knows patience and skepticism are needed. “Our research is still at the basic stage, but based on the available data, we may provide a potential anticoagulant option with low bleeding risk,” she said. “In the discussion section of our paper, we also stated that ‘the data suggest a wide therapeutic window of CCG, which may offer therapeutic advantages for patients with bleeding contraindication, such as elderly patients and those with renal failure, as well as for safer long-term anticoagulation.’”
A New Direction for Heparin Alternatives?
Despite these concerns, Abou-Ismail acknowledged that the research has genuinely noteworthy aspects. “A future anticoagulant with a novel mechanism of action may be useful in patients who have experienced anticoagulant failure or breakthrough thrombosis from currently established anticoagulants,” he said. “Having another option might be useful when all other options have failed or are not feasible.”
However, he added a note of caution: “If a therapeutic window exists where partial tenase disruption has antithrombotic effect that does not impair hemostasis, then that would definitely be a promising future finding, but it is too early to arrive at that conclusion with this study.”
The search for safer heparin alternatives has been ongoing for decades, but most candidates still operate within the same fundamental paradigm of broad coagulation inhibition. This snail can’t move fast enough.
Abou-Ismail reported having no relevant conflicts. Disclosure information for study authors is available in the original study publication.
A version of this article first appeared on Medscape.com.
The fastest way to a new anticoagulation therapy that prevents blood clots without prolonging bleeding or healing time may be a land snail.
A recent preclinical study in ACS Central Science investigating bioactive molecules derived from the land snail Camaena cicatricosa identified a compound that significantly reduced clot formation without prolonging bleeding time and wound healing in rodent models, directly challenging the assumption that effective anticoagulant therapy must inherently disrupt physiologic repair processes.
“I was quite excited,” said Lisha Lin, PhD, lead author on the study and research assistant at the State Key Laboratory of Phytochemistry and Natural Medicines at the Kunming Institute of Botany, Chinese Academy of Sciences, in Kunming, China. “A novel polysaccharide was identified, and more importantly, it showed anticoagulant activity by inhibiting a novel target, with different action mechanism from heparins.”
What Led to the Land Snail?
The choice of C cicatricosa reflects a shift in thinking. The team screened a range of mollusk-derived biomolecules in search of safer anticoagulation strategies, ultimately isolating a novel galactosylated glycosaminoglycan (CCG) from this terrestrial species.
“We compared the anticoagulant activity of glycosaminoglycans from three snail species,” said Lin. They initially studied polysaccharides from C cicatricosa, Achatina fulica, and Helix lucorum — all sulfated glycosaminoglycans with similar structures. “However, we only found CCG from [C cicatricosa] showed anticoagulant activity but not other snail polysaccharides.”
This unexpected selectivity proved crucial. “The result indicated that the galactose branches and special sulfate substitution were important,” she explained, helping to explain why this particular species stood out among structurally similar compounds.
While CCG shares some similarities with heparin-like molecules, it notably lacks the specific pentasaccharide sequence required for antithrombin binding. Researchers hypothesized that this absence could reduce bleeding risk while maintaining antithrombotic activity.
Rather than broadly inhibiting coagulation, the compound selectively disrupts the intrinsic tenase complex, a pathway more closely associated with pathologic thrombosis than with physiologic hemostasis. This mechanism’s selectivity is central to the study’s findings and helps explain why normal wound healing remained intact in preclinical models.
The isolated compound demonstrated a rare combination in anticoagulant research: potent inhibition of pathologic thrombosis with no significant increase in bleeding time and intact wound healing across multiple experimental models. The compound did not act as a broad-spectrum anticoagulant, instead selectively targeting pathways more relevant to disease-associated clot formation.
The Hope of Lowering Bleeding Risk
For decades, anticoagulation therapy has been built on the assumption that inhibiting clot formation inevitably increases bleeding risk. For physicians treating patients with deep vein thrombosis or atrial fibrillation or those requiring postsurgical attention, the balancing act is constant. Prevent clot formation aggressively enough and the bleeding risk rises. Reduce intensity and thrombosis risk returns.
Current therapies, including heparin and direct oral anticoagulants (DOACs), function by broadly targeting the coagulation cascade. This lack of specialty is precisely what limits them. Even when carefully dosed, the treatments interfere with both pathologic clot formation and physiologic hemostasis.
Physicians managing patients on heparin and DOACs frequently encounter recurrent epistaxis, gastrointestinal bleeding ranging from occult to clinically significant, and urogenital bleeding. A degree of mild bleeding after surgery is often expected and usually resolves on its own. However, it’s crucial to evaluate in the context of ongoing anticoagulation to rule out early signs of clinically significant complications.
“There is definitely a lot of interest in the concept of ‘uncoupling’ thrombosis from hemostasis,” said Yazan Abou-Ismail, MD, hematologist and associate professor of medicine at the University of Utah Health in Salt Lake City, who was not involved in the research. “This concept highlights the differences in pathways essential for normal hemostasis at sites of vessel injury, in contrast with those needed for clot propagation and blood vessel lumen occlusion.”
Abou-Ismail noted that this approach has been explored with Factor XI (FXI) inhibitors currently in clinical trials. However, he raised an important mechanistic concern.
“This mechanism may not necessarily accomplish that goal of uncoupling thrombosis from hemostasis, although it might at narrow therapeutic windows,” Abou-Ismail said. “The tenase complex is a central component of coagulation whose deficiency underlies hemophilia A and B, diseases that cause significant bleeding in humans, and it is more essential to hemostasis than [FXI inhibitors]. Tenase inhibition seems like it may pose a higher bleeding risk in humans.”
He explained that FXI inhibitors have a strong mechanistic rationale because they target the feedback loop that amplifies clot propagation, which is less essential for hemostasis. “FXI inhibitors have clinical trial data demonstrating that FXI inhibition is in fact associated with less bleeding compared to current established anticoagulants,” he said. “However, CCG disrupts the FIXa/FVIIIa intrinsic tenase complex itself, which is considered essential for hemostasis.”
Surprises and Confirmations
The researchers were not anticipating such a clear separation between antithrombotic activity and bleeding risk. The preservation of normal wound healing was equally surprising, directly challenging the belief that interfering with clot formation inevitably disrupts tissue repair.
However, the path to these conclusions was not straightforward. “The structural definition of complex macromolecules like sulfated polysaccharides is a common challenge in the research field,” Lin said. “We spent a lot of time to analyze the structure of CCG.”
Even after identifying the candidate compound, the team had to rigorously confirm that its effects were truly anticoagulant in nature, rather than secondary to anti-inflammatory or vascular remodeling properties. Mechanistic studies were essential in demonstrating its targeted disruption of the intrinsic tenase complex, helping to explain how thrombosis could be reduced without broadly impairing coagulation.
Lin is excited but knows patience and skepticism are needed. “Our research is still at the basic stage, but based on the available data, we may provide a potential anticoagulant option with low bleeding risk,” she said. “In the discussion section of our paper, we also stated that ‘the data suggest a wide therapeutic window of CCG, which may offer therapeutic advantages for patients with bleeding contraindication, such as elderly patients and those with renal failure, as well as for safer long-term anticoagulation.’”
A New Direction for Heparin Alternatives?
Despite these concerns, Abou-Ismail acknowledged that the research has genuinely noteworthy aspects. “A future anticoagulant with a novel mechanism of action may be useful in patients who have experienced anticoagulant failure or breakthrough thrombosis from currently established anticoagulants,” he said. “Having another option might be useful when all other options have failed or are not feasible.”
However, he added a note of caution: “If a therapeutic window exists where partial tenase disruption has antithrombotic effect that does not impair hemostasis, then that would definitely be a promising future finding, but it is too early to arrive at that conclusion with this study.”
The search for safer heparin alternatives has been ongoing for decades, but most candidates still operate within the same fundamental paradigm of broad coagulation inhibition. This snail can’t move fast enough.
Abou-Ismail reported having no relevant conflicts. Disclosure information for study authors is available in the original study publication.
A version of this article first appeared on Medscape.com.
The Fastest Way to Better Anticoagulants May Be a Land Snail
The Fastest Way to Better Anticoagulants May Be a Land Snail
Can Fasting Around Chemo Improve Ovarian Cancer Outcomes?
Can Fasting Around Chemo Improve Ovarian Cancer Outcomes?
A few days of fasting around chemotherapy sessions may improve treatment response and outcomes for some patients with advanced ovarian cancer, a small phase 2 trial suggests.
The study, of 36 patients with stage III or IV high-grade ovarian cancer, found that those randomly assigned to fast for 36 hours before chemotherapy and 24 hours afterward had stronger pathologic responses to chemotherapy and longer progression-free survival than patients who ate normally during treatment.
The findings, reported at a press briefing ahead the American Society of Clinical Oncology (ASCO) 2026, hint at a straightforward measure to potentially improve patients’ outcomes.
The working theory is that short-term fasting boosts chemotherapy response by lowering insulin and IGF-1 levels, both of which are implicated in tumor growth and chemotherapy resistance, said study presenter Claudia Marchetti, MD, of Agostino Gemelli University in Rome, Italy.
Speaking at the briefing, ASCO President Eric Small, MD, of the University of California San Francisco, called the study “a great example of a very simple intervention that has benefit and can be undertaken and implemented anywhere in the world.”
“It’s not an expensive new drug,” he said, “and yet it has the potential to really have an impact on this cancer.”
Ovarian cancer affects more than 324,000 women worldwide each year and causes more than 206,000 deaths annually. Around 80% of patients are diagnosed at an advanced stage, and up to 60% receive neoadjuvant chemotherapy to reduce tumor size and facilitate surgery.
Despite advances in surgery and chemotherapy, patients with advanced disease still face poor outcomes. There is, Marchetti said, “an urgent need for safe, low-cost, and easily implementable strategies that can enhance treatment efficacy and improve patient prognosis.”
Given evidence on the role of insulin in tumor growth and chemotherapy response, her team hypothesized that short bouts of fasting around the time of treatment might have benefits.
To test that idea, the researchers recruited 36 patients with newly diagnosed stage III or IV high-grade serous ovarian carcinoma who were not candidates for primary cytoreduction. All were in good general health, with a mean age of 62 years.
All patients received 3 rounds of carboplatin and paclitaxel before surgery. Prior to starting chemotherapy, half were randomly assigned to fast for 36 hours before and 24 hours after chemotherapy, whereas the other half ate normally throughout treatment.
Patients in the fasting group consumed no more than 350 calories per day during the fasting window. They were allowed to have unrestricted water, herbal tea, limited vegetable juice, and small amounts of light vegetable broth. (A ketogenic diet group had initially been planned but was closed early because of poor patient compliance.)
The study met its primary endpoint of change in insulin levels during chemotherapy, Marchetti reported. Baseline insulin levels were comparable between the 2 groups, but after 3 rounds of chemotherapy, they’d dipped by an average of 1.12 µIU/mL in the fasting group and increased by 9.76 µIU/mL in the control group (P = .01).
Fasting also improved clinical outcomes. Specifically, Marchetti said, 59% of fasting patients achieved a chemotherapy response score of 3 — indicating complete or near-complete tumor response before surgery — compared with 17% of patients in the control group.
Median progression-free survival was significantly longer in the fasting group, at 38 vs 24 months.
Importantly, Marchetti said, the fasting protocol was feasible, well tolerated, and safe: All patients assigned to the fasting group completed treatment, and rates of chemotherapy-related toxicities were similar between the 2 groups.
Additional analyses shed more light on the possible mechanisms underlying the fasting group’s improved outcomes: The researchers found that those patients tended to have lower levels of circulating suppressor granulocyte and monocyte populations that have been linked to tumor immune escape, which suggests, Marchetti said, fasting may have set the stage for a “more favorable immune environment” during chemotherapy.
However, she cautioned that much more research is needed. Her team is planning a larger multicenter trial to validate the current findings, and longer-term follow-up is necessary to see whether fasting ultimately impacts patients’ survival, Marchetti said.
In a statement, Eleonora Teplinsky, MD, an ASCO expert in gynecologic cancers, said these early findings are “encouraging, support earlier data, and highlight a promising area of cancer research.”
But she, too, emphasized the need for larger clinical trials to build on the results.
The study had no commercial funding. Marchetti disclosed having relationships with Arquer Diagnostics, AstraZeneca, Clovis Oncology, and other companies. Small disclosed having relationships with Janssen, Johnson & Johnson, and others. Teplinsky had no disclosures.
A version of this article first appeared on Medscape.com.
A few days of fasting around chemotherapy sessions may improve treatment response and outcomes for some patients with advanced ovarian cancer, a small phase 2 trial suggests.
The study, of 36 patients with stage III or IV high-grade ovarian cancer, found that those randomly assigned to fast for 36 hours before chemotherapy and 24 hours afterward had stronger pathologic responses to chemotherapy and longer progression-free survival than patients who ate normally during treatment.
The findings, reported at a press briefing ahead the American Society of Clinical Oncology (ASCO) 2026, hint at a straightforward measure to potentially improve patients’ outcomes.
The working theory is that short-term fasting boosts chemotherapy response by lowering insulin and IGF-1 levels, both of which are implicated in tumor growth and chemotherapy resistance, said study presenter Claudia Marchetti, MD, of Agostino Gemelli University in Rome, Italy.
Speaking at the briefing, ASCO President Eric Small, MD, of the University of California San Francisco, called the study “a great example of a very simple intervention that has benefit and can be undertaken and implemented anywhere in the world.”
“It’s not an expensive new drug,” he said, “and yet it has the potential to really have an impact on this cancer.”
Ovarian cancer affects more than 324,000 women worldwide each year and causes more than 206,000 deaths annually. Around 80% of patients are diagnosed at an advanced stage, and up to 60% receive neoadjuvant chemotherapy to reduce tumor size and facilitate surgery.
Despite advances in surgery and chemotherapy, patients with advanced disease still face poor outcomes. There is, Marchetti said, “an urgent need for safe, low-cost, and easily implementable strategies that can enhance treatment efficacy and improve patient prognosis.”
Given evidence on the role of insulin in tumor growth and chemotherapy response, her team hypothesized that short bouts of fasting around the time of treatment might have benefits.
To test that idea, the researchers recruited 36 patients with newly diagnosed stage III or IV high-grade serous ovarian carcinoma who were not candidates for primary cytoreduction. All were in good general health, with a mean age of 62 years.
All patients received 3 rounds of carboplatin and paclitaxel before surgery. Prior to starting chemotherapy, half were randomly assigned to fast for 36 hours before and 24 hours after chemotherapy, whereas the other half ate normally throughout treatment.
Patients in the fasting group consumed no more than 350 calories per day during the fasting window. They were allowed to have unrestricted water, herbal tea, limited vegetable juice, and small amounts of light vegetable broth. (A ketogenic diet group had initially been planned but was closed early because of poor patient compliance.)
The study met its primary endpoint of change in insulin levels during chemotherapy, Marchetti reported. Baseline insulin levels were comparable between the 2 groups, but after 3 rounds of chemotherapy, they’d dipped by an average of 1.12 µIU/mL in the fasting group and increased by 9.76 µIU/mL in the control group (P = .01).
Fasting also improved clinical outcomes. Specifically, Marchetti said, 59% of fasting patients achieved a chemotherapy response score of 3 — indicating complete or near-complete tumor response before surgery — compared with 17% of patients in the control group.
Median progression-free survival was significantly longer in the fasting group, at 38 vs 24 months.
Importantly, Marchetti said, the fasting protocol was feasible, well tolerated, and safe: All patients assigned to the fasting group completed treatment, and rates of chemotherapy-related toxicities were similar between the 2 groups.
Additional analyses shed more light on the possible mechanisms underlying the fasting group’s improved outcomes: The researchers found that those patients tended to have lower levels of circulating suppressor granulocyte and monocyte populations that have been linked to tumor immune escape, which suggests, Marchetti said, fasting may have set the stage for a “more favorable immune environment” during chemotherapy.
However, she cautioned that much more research is needed. Her team is planning a larger multicenter trial to validate the current findings, and longer-term follow-up is necessary to see whether fasting ultimately impacts patients’ survival, Marchetti said.
In a statement, Eleonora Teplinsky, MD, an ASCO expert in gynecologic cancers, said these early findings are “encouraging, support earlier data, and highlight a promising area of cancer research.”
But she, too, emphasized the need for larger clinical trials to build on the results.
The study had no commercial funding. Marchetti disclosed having relationships with Arquer Diagnostics, AstraZeneca, Clovis Oncology, and other companies. Small disclosed having relationships with Janssen, Johnson & Johnson, and others. Teplinsky had no disclosures.
A version of this article first appeared on Medscape.com.
A few days of fasting around chemotherapy sessions may improve treatment response and outcomes for some patients with advanced ovarian cancer, a small phase 2 trial suggests.
The study, of 36 patients with stage III or IV high-grade ovarian cancer, found that those randomly assigned to fast for 36 hours before chemotherapy and 24 hours afterward had stronger pathologic responses to chemotherapy and longer progression-free survival than patients who ate normally during treatment.
The findings, reported at a press briefing ahead the American Society of Clinical Oncology (ASCO) 2026, hint at a straightforward measure to potentially improve patients’ outcomes.
The working theory is that short-term fasting boosts chemotherapy response by lowering insulin and IGF-1 levels, both of which are implicated in tumor growth and chemotherapy resistance, said study presenter Claudia Marchetti, MD, of Agostino Gemelli University in Rome, Italy.
Speaking at the briefing, ASCO President Eric Small, MD, of the University of California San Francisco, called the study “a great example of a very simple intervention that has benefit and can be undertaken and implemented anywhere in the world.”
“It’s not an expensive new drug,” he said, “and yet it has the potential to really have an impact on this cancer.”
Ovarian cancer affects more than 324,000 women worldwide each year and causes more than 206,000 deaths annually. Around 80% of patients are diagnosed at an advanced stage, and up to 60% receive neoadjuvant chemotherapy to reduce tumor size and facilitate surgery.
Despite advances in surgery and chemotherapy, patients with advanced disease still face poor outcomes. There is, Marchetti said, “an urgent need for safe, low-cost, and easily implementable strategies that can enhance treatment efficacy and improve patient prognosis.”
Given evidence on the role of insulin in tumor growth and chemotherapy response, her team hypothesized that short bouts of fasting around the time of treatment might have benefits.
To test that idea, the researchers recruited 36 patients with newly diagnosed stage III or IV high-grade serous ovarian carcinoma who were not candidates for primary cytoreduction. All were in good general health, with a mean age of 62 years.
All patients received 3 rounds of carboplatin and paclitaxel before surgery. Prior to starting chemotherapy, half were randomly assigned to fast for 36 hours before and 24 hours after chemotherapy, whereas the other half ate normally throughout treatment.
Patients in the fasting group consumed no more than 350 calories per day during the fasting window. They were allowed to have unrestricted water, herbal tea, limited vegetable juice, and small amounts of light vegetable broth. (A ketogenic diet group had initially been planned but was closed early because of poor patient compliance.)
The study met its primary endpoint of change in insulin levels during chemotherapy, Marchetti reported. Baseline insulin levels were comparable between the 2 groups, but after 3 rounds of chemotherapy, they’d dipped by an average of 1.12 µIU/mL in the fasting group and increased by 9.76 µIU/mL in the control group (P = .01).
Fasting also improved clinical outcomes. Specifically, Marchetti said, 59% of fasting patients achieved a chemotherapy response score of 3 — indicating complete or near-complete tumor response before surgery — compared with 17% of patients in the control group.
Median progression-free survival was significantly longer in the fasting group, at 38 vs 24 months.
Importantly, Marchetti said, the fasting protocol was feasible, well tolerated, and safe: All patients assigned to the fasting group completed treatment, and rates of chemotherapy-related toxicities were similar between the 2 groups.
Additional analyses shed more light on the possible mechanisms underlying the fasting group’s improved outcomes: The researchers found that those patients tended to have lower levels of circulating suppressor granulocyte and monocyte populations that have been linked to tumor immune escape, which suggests, Marchetti said, fasting may have set the stage for a “more favorable immune environment” during chemotherapy.
However, she cautioned that much more research is needed. Her team is planning a larger multicenter trial to validate the current findings, and longer-term follow-up is necessary to see whether fasting ultimately impacts patients’ survival, Marchetti said.
In a statement, Eleonora Teplinsky, MD, an ASCO expert in gynecologic cancers, said these early findings are “encouraging, support earlier data, and highlight a promising area of cancer research.”
But she, too, emphasized the need for larger clinical trials to build on the results.
The study had no commercial funding. Marchetti disclosed having relationships with Arquer Diagnostics, AstraZeneca, Clovis Oncology, and other companies. Small disclosed having relationships with Janssen, Johnson & Johnson, and others. Teplinsky had no disclosures.
A version of this article first appeared on Medscape.com.
Can Fasting Around Chemo Improve Ovarian Cancer Outcomes?
Can Fasting Around Chemo Improve Ovarian Cancer Outcomes?
Nurse Practitioner-Led Outreach Boosts Cancer Screening Rates Among Women Veterans in Rural Settings
Nurse Practitioner-Led Outreach Boosts Cancer Screening Rates Among Women Veterans in Rural Settings
TOPLINE:
Telephone outreach by a nurse practitioner (NP) providing counseling and care coordination reduced the gaps in breast and cervical cancer screenings among women veterans in rural areas, according to a retrospective study.
METHODOLOGY:
- Researchers conducted a retrospective chart review of 55 women veterans who received interventions related to breast or cervical cancer screening at a rural Veterans Health Administration health care system.
- A Boost team, including an NP, a medical director, a program coordinator, and a program evaluation team, was established to provide care coordination and counseling for these participants.
- The NP conducted outreach by telephone to these participants receiving care at five community-based outpatient clinics located in rural counties and helped coordinate access to screening appointments through the Office of Community Care.
- Outcomes included the number of veterans due for breast or cervical cancer screening at the time of outreach and the number of mammograms and Pap smears completed in the 12-month period following the intervention.
TAKEAWAY:
- Of the 55 veterans who received Boost interventions related to cancer screening, 35 (64%) were due for breast cancer screening and 27 (49%) were due for cervical cancer screening before the intervention.
- Following the Boost intervention, the number of veterans due for breast cancer and cervical cancer screenings decreased to 18 (32%) and 16 (29%), respectively.
- Among veterans due for breast cancer screening, 29 (83%) received counseling regarding screening and 17 (59%) of counseled participants completed mammography; however, among those due for cervical cancer screening, 22 (81%) received counseling and 11 (50%) completed screening.
- None of the veterans who were due for screening but did not receive counseling completed their screening, demonstrating the critical role of clinician-provided education and counseling.
IN PRACTICE:
“We hope to expand Boost outreach from one NP working part-time across two health systems to a national partnership of licensed independent providers conducting clinician-initiated outreach to a broader and geographically more diverse group of veterans,” the authors wrote.
SOURCE:
This study was led by Lina Vadlamani, MD, MBA, San Francisco Internal Medicine Residency Program, University of California, San Francisco. It was published online on April 24, 2026, in Military Medicine.
LIMITATIONS:
This study was a secondary analysis in which participants were not randomly assigned, limiting causal inferences. Veterans who answered the phone and engaged with the NP were likely easier to reach and potentially more proactive about their health than those who did not engage, and this selection bias may have limited the generalizability of the findings.
DISCLOSURES:
This study was funded by the Department of Veterans Affairs, Veterans Health Administration, and Office of Rural Health. The authors reported having no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Telephone outreach by a nurse practitioner (NP) providing counseling and care coordination reduced the gaps in breast and cervical cancer screenings among women veterans in rural areas, according to a retrospective study.
METHODOLOGY:
- Researchers conducted a retrospective chart review of 55 women veterans who received interventions related to breast or cervical cancer screening at a rural Veterans Health Administration health care system.
- A Boost team, including an NP, a medical director, a program coordinator, and a program evaluation team, was established to provide care coordination and counseling for these participants.
- The NP conducted outreach by telephone to these participants receiving care at five community-based outpatient clinics located in rural counties and helped coordinate access to screening appointments through the Office of Community Care.
- Outcomes included the number of veterans due for breast or cervical cancer screening at the time of outreach and the number of mammograms and Pap smears completed in the 12-month period following the intervention.
TAKEAWAY:
- Of the 55 veterans who received Boost interventions related to cancer screening, 35 (64%) were due for breast cancer screening and 27 (49%) were due for cervical cancer screening before the intervention.
- Following the Boost intervention, the number of veterans due for breast cancer and cervical cancer screenings decreased to 18 (32%) and 16 (29%), respectively.
- Among veterans due for breast cancer screening, 29 (83%) received counseling regarding screening and 17 (59%) of counseled participants completed mammography; however, among those due for cervical cancer screening, 22 (81%) received counseling and 11 (50%) completed screening.
- None of the veterans who were due for screening but did not receive counseling completed their screening, demonstrating the critical role of clinician-provided education and counseling.
IN PRACTICE:
“We hope to expand Boost outreach from one NP working part-time across two health systems to a national partnership of licensed independent providers conducting clinician-initiated outreach to a broader and geographically more diverse group of veterans,” the authors wrote.
SOURCE:
This study was led by Lina Vadlamani, MD, MBA, San Francisco Internal Medicine Residency Program, University of California, San Francisco. It was published online on April 24, 2026, in Military Medicine.
LIMITATIONS:
This study was a secondary analysis in which participants were not randomly assigned, limiting causal inferences. Veterans who answered the phone and engaged with the NP were likely easier to reach and potentially more proactive about their health than those who did not engage, and this selection bias may have limited the generalizability of the findings.
DISCLOSURES:
This study was funded by the Department of Veterans Affairs, Veterans Health Administration, and Office of Rural Health. The authors reported having no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Telephone outreach by a nurse practitioner (NP) providing counseling and care coordination reduced the gaps in breast and cervical cancer screenings among women veterans in rural areas, according to a retrospective study.
METHODOLOGY:
- Researchers conducted a retrospective chart review of 55 women veterans who received interventions related to breast or cervical cancer screening at a rural Veterans Health Administration health care system.
- A Boost team, including an NP, a medical director, a program coordinator, and a program evaluation team, was established to provide care coordination and counseling for these participants.
- The NP conducted outreach by telephone to these participants receiving care at five community-based outpatient clinics located in rural counties and helped coordinate access to screening appointments through the Office of Community Care.
- Outcomes included the number of veterans due for breast or cervical cancer screening at the time of outreach and the number of mammograms and Pap smears completed in the 12-month period following the intervention.
TAKEAWAY:
- Of the 55 veterans who received Boost interventions related to cancer screening, 35 (64%) were due for breast cancer screening and 27 (49%) were due for cervical cancer screening before the intervention.
- Following the Boost intervention, the number of veterans due for breast cancer and cervical cancer screenings decreased to 18 (32%) and 16 (29%), respectively.
- Among veterans due for breast cancer screening, 29 (83%) received counseling regarding screening and 17 (59%) of counseled participants completed mammography; however, among those due for cervical cancer screening, 22 (81%) received counseling and 11 (50%) completed screening.
- None of the veterans who were due for screening but did not receive counseling completed their screening, demonstrating the critical role of clinician-provided education and counseling.
IN PRACTICE:
“We hope to expand Boost outreach from one NP working part-time across two health systems to a national partnership of licensed independent providers conducting clinician-initiated outreach to a broader and geographically more diverse group of veterans,” the authors wrote.
SOURCE:
This study was led by Lina Vadlamani, MD, MBA, San Francisco Internal Medicine Residency Program, University of California, San Francisco. It was published online on April 24, 2026, in Military Medicine.
LIMITATIONS:
This study was a secondary analysis in which participants were not randomly assigned, limiting causal inferences. Veterans who answered the phone and engaged with the NP were likely easier to reach and potentially more proactive about their health than those who did not engage, and this selection bias may have limited the generalizability of the findings.
DISCLOSURES:
This study was funded by the Department of Veterans Affairs, Veterans Health Administration, and Office of Rural Health. The authors reported having no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
Nurse Practitioner-Led Outreach Boosts Cancer Screening Rates Among Women Veterans in Rural Settings
Nurse Practitioner-Led Outreach Boosts Cancer Screening Rates Among Women Veterans in Rural Settings
Diagnostic Challenge of Immune Checkpoint Inhibitor-Induced Hypophysitis in a Patient With Advanced Melanoma
Diagnostic Challenge of Immune Checkpoint Inhibitor-Induced Hypophysitis in a Patient With Advanced Melanoma
Immune checkpoint inhibitors (ICIs) have become important in oncology and represent an evolving area of therapeutics. Since their approval by the US Food and Drug Administration (FDA) in 2011, ICIs have been increasingly used as modalities in neoadjuvant and adjuvant treatment for resectable solid malignancies and in unresectable disease, such as advanced melanoma, and are associated with improved survival.1
Immune checkpoints are present on the cell surface of activated T cells as well as other immune cells like B cells and natural killer cells. By regulating the length and amplitude of the body’s innate immune response, they maintain immune homeostasis and prevent its overactivation. Immune checkpoints are often thought of as the brakes on the immune system.2
Two glycoproteins that act as immune checkpoints and are targeted by ICIs are cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) and programmed cell death protein 1 (PD-1). CTLA-4 is upregulated on activated T cells. PD-1 is also expressed on activated T cells, as well as macrophages, B cells, and dendritic cells. Cancer cells can evade immune surveillance by exploiting immune checkpoint pathways. Inhibition of these checkpoints with ICIs reactivates T cells and enables the immune system to recognize and attack cancer cells more effectively. Ipilimumab blocks the activity of CTLA-4 on T cells. Nivolumab and pembrolizumab block the interaction between PD-1 on T cells and its ligand PD-L1 on cancer cells.3,4
Inhibition of these checkpoints is often effective in cancer treatment but can result in the loss of immunologic tolerance with resultant immune-related adverse events (irAEs) and potentially permanent autoimmune disorders. Autoreactive T cells can damage host cell tissues including the colon, lungs, liver, pituitary gland, thyroid, and skin. Severe irAEs include type 1 diabetes mellitus, myositis, nephritis, colitis, pneumonitis, hepatitis, uveitis, hypophysitis, and adrenalitis.4
Hypophysitis is inflammation of the pituitary gland, often with thickening of the pituitary stalk, resulting in dysfunction and hormone deficiencies. While primary hypophysitis is idiopathic, secondary hypophysitis is the result of an underlying condition such as exposure to an ICI. Immune-mediated inflammation of the pituitary gland in hypophysitis may disrupt corticotroph function, leading to adrenocorticotropic hormone (ACTH) deficiency. Early warning features are often vague and nonspecific, such as headache, fatigue, and weakness, which makes diagnosis challenging.3,5
CASE PRESENTATION
A 73-year-old male veteran with a history of metastatic melanoma on ipilimumab 3 mg/kg and nivolumab 1 mg/kg every 3 weeks (a standard combination regimen for advanced melanoma) presented to the emergency department (ED) with 2 weeks of cough, nausea, and severe headache 3 weeks after cycle 2 of combination ICI therapy. The patient had undergone excision of multiple sites of melanoma in situ with recurrence and disease progression after 5 cycles of pembrolizumab. He was subsequently started on combination ICI therapy.
On ED arrival, the patient was afebrile and saturating well on room air. He was normotensive but found to have orthostatic blood pressure. Physical examination was remarkable for dry oral mucosa and decreased skin turgor. Initial laboratory results were significant for hyponatremia of 123 mmol/L (reference range, 136-145 mmol/L), low-normal free thyroxine (T4) level of 0.5 ng/dL (reference range, 0.6-1.2 ng/dL), a low total triiodothyronine level of 32.14 ng/dL (reference range, 85-178 ng/dL), and a low thyrotropin level of 0.19 mIU/L (reference range, 0.35-5.50 mIU/L). Serum osmolarity was low at 259 mOsm/kg (reference range, 285-315 mOsm/kg), urine sodium was high at 168 mEq/L (reference, 20 mEq/L), and urine osmolarity was inappropriately concentrated at 726 mOsm/kg (reference range, 250-1000 mOsm/kg). The patient was admitted for additional testing. His morning cortisol level was within normal limits at 15 mcg/dL (reference range, 6.7-22.5 mcg/dL).
Computed tomography (CT) of the patient’s head revealed no acute findings. Chest CT revealed posterior right lower lobe mild ground-glass opacities, with possible ICI-induced pneumonitis. The patient received fluid resuscitation. Given concern for syndrome of inappropriate antidiuretic hormone secretion, the patient was started on 3 g salt tablets 3 times a day and urea 30 g powder daily. The etiology of the abnormal thyroid levels was unclear to endocrinology at that time. The differential diagnosis included a nonthyroidal illness or central hypothyroidism.
The patient started levothyroxine 75 mcg due to abnormal thyroid levels and persistent fatigue and fludrocortisone 0.1 mg daily to manage orthostatic hypotension. His sodium levels improved to 132 mmol/L over 6 days and he was discharged with levothyroxine 75 mcg daily, fludrocortisone 0.1 mg daily, 3 g salt tabs 3 times a day, urea 30 g powder daily, as well as oral cefpodoxime 500 mg twice daily for 3 days and azithromycin 500 mg once daily for 2 days (for a total of 10 days of antibiotic therapy) to treat potential occult pneumonia.
The patient returned to the ED 3 days after discharge following an outpatient oncology appointment with ongoing severe headaches and persistent nausea. There was concern for recurrent hyponatremia. His sodium level was within normal limits at 133 mmol/L. Repeat morning cortisol was low-normal at 9 mcg/dL. Magnetic resonance imaging (MRI) of the brain was negative for metastatic disease, but showed a slight interval increase in size of the pituitary gland compared with an MRI from 6 months prior, with mild fullness and a slightly convex superior margin near homogeneous enhancement, raising concern for infection or hypophysitis (Figure 1).
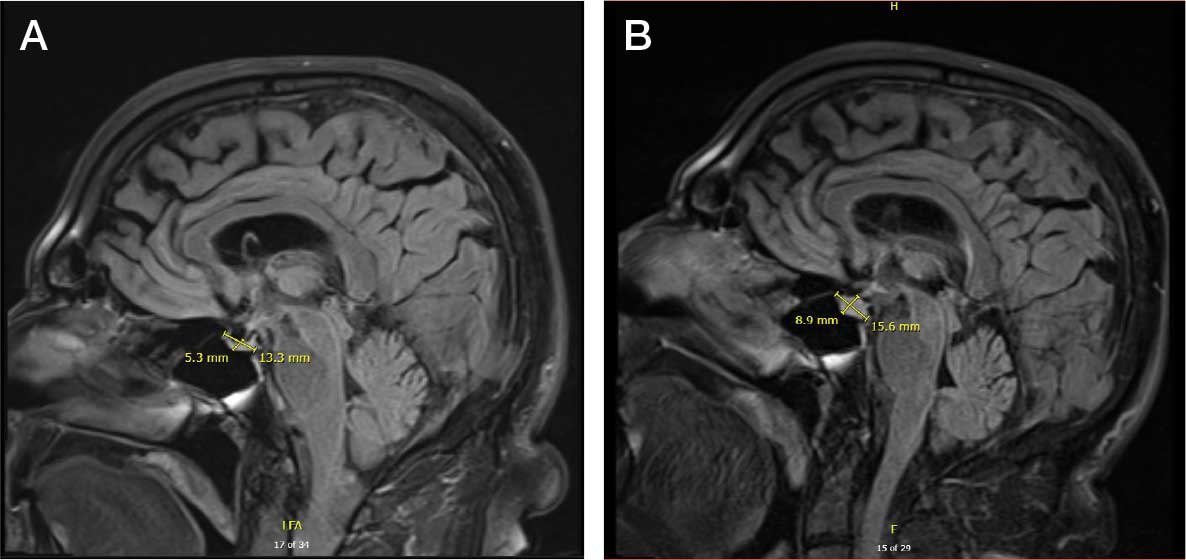
The patient was readmitted to the general medicine service and was given intravenous hydrocortisone 100 mg every 8 hours because of concern for central adrenal insufficiency due to grade 3 hypophysitis in the setting of MRI imaging and severe headaches (Table 1). He was not hypotensive at the time of hydrocortisone initiation and other vital signs were stable. A cosyntropin stimulation test—a standard diagnostic test for central adrenal insufficiency—was not performed because the patient had already started high-dose hydrocortisone. The patient’s free T4 on this admission remained low at 0.6 ng/dL.

No adjustments were made to his levothyroxine dose given that he recently began the medication and levels may lag after initiation. After a 4-day hospitalization, the decision was made to continue with the steroid taper and follow up with outpatient endocrinology to obtain a cosyntropin stimulation test to complete a full assessment of his pituitary axis (Figure 2). Repeat thyroid function testing for levothyroxine titration was arranged. The levothyroxine dosage was later increased to 88 mcg daily, but the patient discontinued the medication and remained euthyroid. Endocrinology attributed a nonthyroidal illness as the etiology of his hypothyroidism, likely euthyroid sick syndrome in the setting of illness. His hydrocortisone was tapered during outpatient care and fludrocortisone was discontinued due to hypertension.
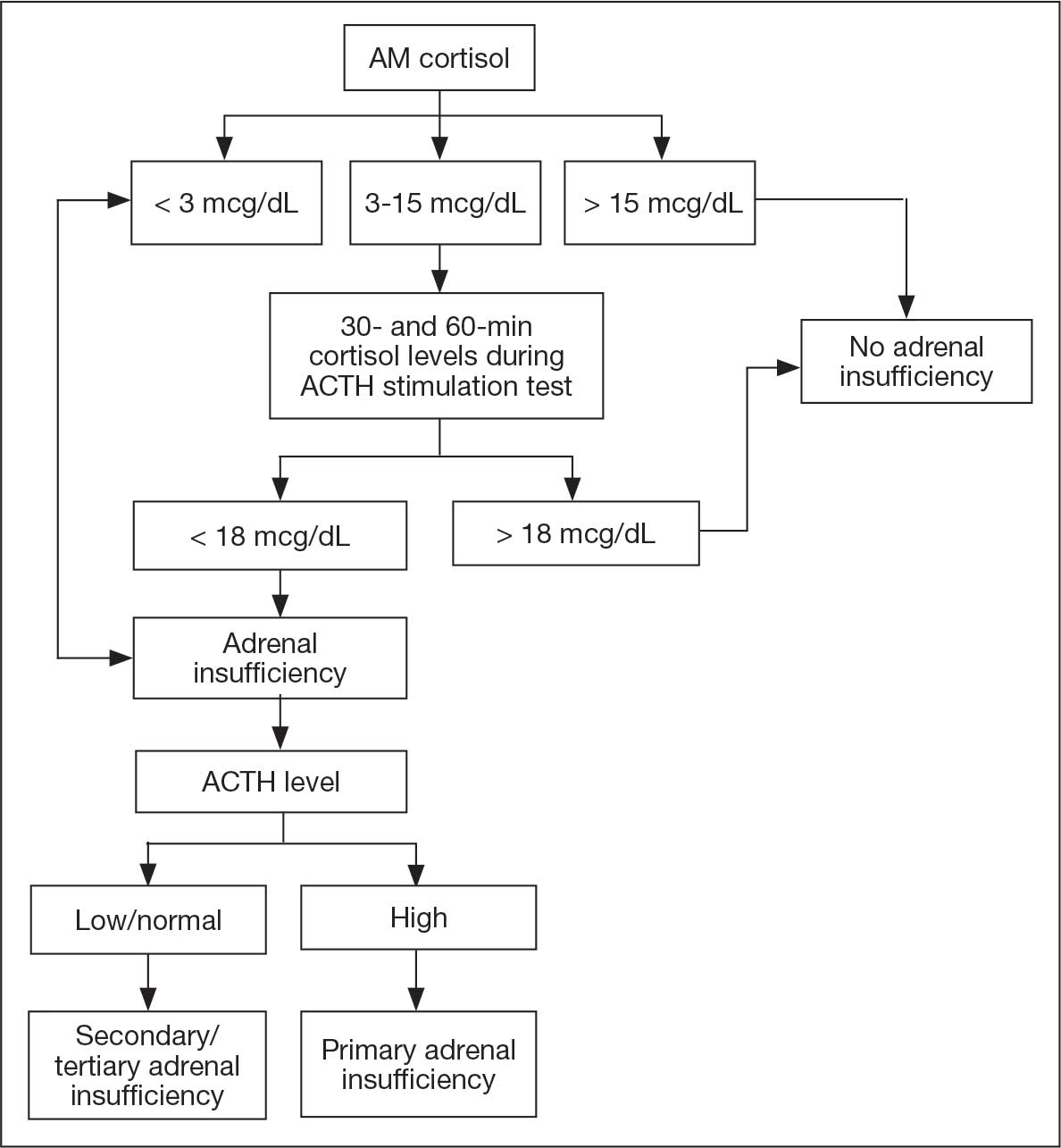
One month after his second discharge, the patient presented to the ED with 2 weeks of dizziness, associated lightheadedness, and blurred vision when standing from a sitting position. Upon assessment, symptoms were attributed to poor oral intake. The patient’s vital signs were again positive for orthostatic hypotension, though refractory to adequate fluid replacement. Laboratory testing was significant for a low ACTH level of 3.0 pg/mL (reference range, 7.2-63.3 pg/mL). Given that the patient had not received steroids for 1 week, he underwent a cosyntropin stimulation test, which revealed a blunted response supporting a diagnosis of central adrenal insufficiency secondary to ICI-induced hypophysitis (Table 2).
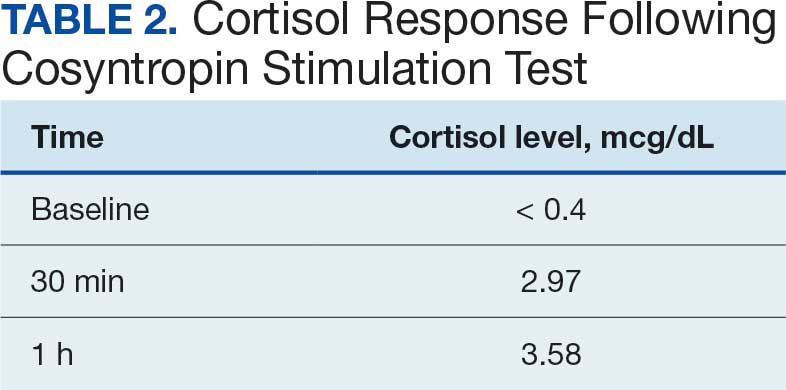
The patient was again readmitted to the general medicine service. A brain MRI showed interval shrinkage of the pituitary gland compared to imaging one month prior, which was attributed to hydrocortisone treatment during this month. CT of the patient’s abdomen demonstrated normal-sized adrenal glands. Positron emission tomography (PET)/CT showed no evidence of pituitary or adrenal metastases. Endocrinology recommended reinitiating oral hydrocortisone 50 mg in the morning and 50 mg around 3 pm daily with fludrocortisone 0.2 mg once daily, which resulted in near resolution of the patient’s symptoms. He was discharged after a 14-day hospitalization with home physical therapy services and endocrinology, nephrology, and oncology follow-up appointments.
The patient was readmitted twice to the general medicine service over the next 6 months for complications from hydrocortisone and fludrocortisone treatment including hypokalemia. He followed up with outpatient clinicians until his death 14 months later. He did not restart ICI therapy, and eventually joined a clinical trial for other advanced melanoma treatments at another institution. The patient’s family consented to the publication of this case report with the accompanying images.
DISCUSSION
The combination of ipilimumab (anti-CTLA-4 monoclonal antibody) and nivolumab (anti-PD-1 monoclonal antibody) is FDA-approved for treatment of advanced melanoma with the goal of harnessing complementary and synergistic mechanisms of dual therapy.6-8 Combination therapy, however, can increase the incidence of irAEs, which are often endocrine-related and more common in patients treated with dual immunotherapy than with monotherapy.9 Hypophysitis has the lowest reported fatality rate among ICI-related irAEs (< 1%), compared with higher mortality rates seen in myocarditis (25%-50%) and pneumonitis (10%-20%).4,10
The patient initially presented with ICI-related hypothyroidism, later identified as secondary (central) hypothyroidism. He was treated with levothyroxine until central hypothyroidism was confirmed. Subsequently, the patient developed headache, poor appetite, and lightheadedness, with MRI findings suggestive of hypophysitis, for which he was started on hydrocortisone. A component of primary adrenal insufficiency was initially considered, given the low ACTH level and blunted response to cosyntropin stimulation following prior high-dose steroid therapy. However, CT imaging demonstrated normal adrenal morphology without atrophy, supporting a diagnosis of central adrenal insufficiency secondary to ICI-induced hypophysitis.
The estimated incidence of ICI-induced hypophysitis is 1.5% to 13.3% with anti-CTLA-4 agents, 0.3% to 3.0% with anti-PD-1 agents, and can be as high as 12.8% with combination therapy.1 ICI-induced hypophysitis is believed to arise from the direct binding of ICI antibodies to their targets on anterior pituitary cells, such as corticotrophs, thyrotrophs, and gonadotrophs, triggering an immune response. One theory for targeting these cells is high CTLA-4 expression in the anterior pituitary gland.11 PD-1 therapies tend to manifest as either hypothyroidism, hyperthyroidism, Graves’ disease, diabetes, or adrenal insufficiency.10
A concern in patients with advanced melanoma is metastasis. Melanoma has a high propensity for brain metastasis.12 There was moderate suspicion for pituitary gland metastasis in this case, though pituitary metastasis more often manifests with symptoms of posterior pituitary gland deficiency, such as polyuria and polydipsia.13 The adrenal gland is the fourth-most common site for melanoma metastases, after the lung, liver, and bone.14 This patient had no evidence of pituitary or adrenal metastases on PET/CT. Therefore, his symptoms were most likely due to ICI therapy. Cases of ≥ 1 endocrine dysfunction have been reported as an ICI therapy irAE.15 In these situations, diagnosing primary and central adrenal insufficiency in the same patient is complex because hormone profiles are intertwined.
Many patients who develop hypophysitis from ICI therapy will require permanent replacement therapy. It is unclear whether low-dose replacement steroids have a significant effect on the efficacy of ICIs. Given that ICI treatment works by enhancing the immune system, medications that suppress the body’s immune system, such as steroids, could interfere with treatment efficacy. However, there are speculations that the development of irAEs is an indicator of effective treatment. In a phase 1 trial of a CTLA-4 blocker in patients with metastatic melanoma, there was a correlation between reduced CTLA-4 expression as well as low rates of melanoma recurrence and a higher incidence of irAEs.16
When assessing patients on ICI treatment, clinicians must remain vigilant for all potential irAEs, especially in patients receiving combination therapy. ICI-induced irAEs can present with vague and nonspecific symptoms. Concurrent endocrine irAEs, such as hypophysitis with thyroiditis or adrenalitis, are not uncommon in combination therapy and can complicate interpretation of hormone profiles. It is prudent for clinicians to review known risk factors. Hypophysitis is typically associated with older adult male patients.17,18
The irAEs of ICI therapy deeply affected the quality of life of the patient in this case, as he was often experiencing many of the clinical symptoms of his hormone insufficiencies as well as the treatment modalities, thus requiring repeated hospital admissions. The risks and benefits of continuing ICI therapy should be an ongoing discussion between the physician and patient and should take into account the acuity and severity of irAEs and oncological disease burden, among other variables. Given the severity of his AEs, the patient stopped ICI therapy and instead opted to enroll in a clinical trial at another institution for continued alternative treatments.
CONCLUSIONS
This case offers a lesson in the diagnostic challenges of vague symptoms in patients with cancer who are receiving ICI therapy. ICI therapy is widely used in the treatment of solid malignancies, and as its use increases, it is expected that clinicians will likely see more cases of irAEs in hospitalized patients. The vague presentation of irAEs can often lead to treatment delays, especially when > 1 irAE presents concurrently. There are ongoing studies researching potential ways to predict the likelihood of developing these irAEs. It is imperative that clinicians are aware of these ICI-related complications and that more research be conducted to understand patient quality of life and treatment guidance based on irAE severity and disease burden.
- Villani A, Potestio L, Fabbrocini G, et al. The treatment of advanced melanoma: therapeutic update. Int J Mol Sci. 2022;23:6388. doi:10.3390/ijms23126388
- Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer. 2012;12:252-264. doi:10.1038/nrc3239
- Chang LS, Barroso-Sousa R, Tolaney SM, et al. Endocrine toxicity of cancer immunotherapy targeting immune checkpoints. Endocr Rev. 2019;40:17-65. doi:10.1210/er.2018-00006
- June CH, Warshauer JT, Bluestone JA. Is autoimmunity the Achilles’ heel of cancer immunotherapy? Nat Med. 2017;23:540-547. doi:10.1038/nm.4321
- Jessel S, Weiss SA, Austin M, et al. Immune checkpoint inhibitor-induced hypophysitis and patterns of loss of pituitary function. Front Oncol. 2022;12:836859. doi:10.3389/fonc.2022.836859
- Betof AS, Nipp RD, Giobbie-Hurder A, et al. Impact of age on outcomes with immunotherapy for patients with melanoma. Oncologist. 2017;22:963-971. doi:10.1634/theoncologist.2016-0450
- Wolchok JD, Kluger H, Callahan MK, et al. Nivolumab plus ipilimumab in advanced melanoma. N Engl J Med. 2013;369:122-133. doi:10.1056/NEJMoa1302369
- Hodi FS, O’Day SJ, McDermott DF, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363:711-723. doi:10.1056/NEJMoa1003466
- Benhima N, Belbaraka R, Langouo Fontsa MD. Single agent vs combination immunotherapy in advanced melanoma: a review of the evidence. Curr Opin Oncol. 2024;36:69-73. doi:10.1097/CCO.0000000000001014
- Tong J, Kartolo A, Yeung C, et al. Long-term toxicities of immune checkpoint inhibitor (ICI) in melanoma patients. Curr Oncol. 2022;29:7953-7963. doi:10.3390/curroncol29100629
- Grouthier V, Lebrun-Vignes B, Moey M, et al. Immune checkpoint inhibitor-associated primary adrenal insufficiency: WHO VigiBase report analysis. Oncologist. 2020;25:696-701. doi:10.1634/theoncologist.2019-0555
- Park BC, Jung S, Wright JJ, et al. Recurrence of hypophysitis after immune checkpoint inhibitor rechallenge. Oncologist. 2022;27:e967-e969. doi:10.1093/oncolo/oyac220
- Zhang D, Wang Z, Shang D, et al. Incidence and prognosis of brain metastases in cutaneous melanoma patients: a population-based study. Melanoma Res. 2019;29:77-84. doi:10.1097/CMR.0000000000000538
- Barnabei A, Carpano S, Chiefari A, et al. Case report: ipilimumab-induced panhypophysitis: an infrequent occurrence and literature review. Front Oncol. 2020;10:582394. doi:10.3389/fonc.2020.582394
- Shortreed H, Burute N, Aseyev O. Management of undifferentiated adrenal gland metastases from malignant melanoma: case report. Front Oncol. 2024;14:1419827. doi:10.3389/fonc.2024.1419827
- Rossi S, Silvetti F, Bordoni M, et al. Pembrolizumab-induced thyroiditis, hypophysitis and adrenalitis: a case of triple endocrine dysfunction. JCEM Case Rep. 2024;2:luae200. doi:10.1210/jcemcr/luae200
- Sanderson K, Scotland R, Lee P, et al. Autoimmunity in a phase I trial of a fully human anti-cytotoxic T-lymphocyte antigen-4 monoclonal antibody with multiple melanoma peptides and Montanide ISA 51 for patients with resected stages III and IV melanoma. J Clin Oncol. 2005;23:741-750. doi:10.1200/JCO.2005.01.128
- de Filette J, Andreescu CE, Cools F, Bravenboer B, Velkeniers B. A systematic review and meta-analysis of endocrine-related adverse events associated with immune checkpoint inhibitors. Horm Metab Res. 2019;51:145-156. doi:10.1055/a-0843-3366
Immune checkpoint inhibitors (ICIs) have become important in oncology and represent an evolving area of therapeutics. Since their approval by the US Food and Drug Administration (FDA) in 2011, ICIs have been increasingly used as modalities in neoadjuvant and adjuvant treatment for resectable solid malignancies and in unresectable disease, such as advanced melanoma, and are associated with improved survival.1
Immune checkpoints are present on the cell surface of activated T cells as well as other immune cells like B cells and natural killer cells. By regulating the length and amplitude of the body’s innate immune response, they maintain immune homeostasis and prevent its overactivation. Immune checkpoints are often thought of as the brakes on the immune system.2
Two glycoproteins that act as immune checkpoints and are targeted by ICIs are cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) and programmed cell death protein 1 (PD-1). CTLA-4 is upregulated on activated T cells. PD-1 is also expressed on activated T cells, as well as macrophages, B cells, and dendritic cells. Cancer cells can evade immune surveillance by exploiting immune checkpoint pathways. Inhibition of these checkpoints with ICIs reactivates T cells and enables the immune system to recognize and attack cancer cells more effectively. Ipilimumab blocks the activity of CTLA-4 on T cells. Nivolumab and pembrolizumab block the interaction between PD-1 on T cells and its ligand PD-L1 on cancer cells.3,4
Inhibition of these checkpoints is often effective in cancer treatment but can result in the loss of immunologic tolerance with resultant immune-related adverse events (irAEs) and potentially permanent autoimmune disorders. Autoreactive T cells can damage host cell tissues including the colon, lungs, liver, pituitary gland, thyroid, and skin. Severe irAEs include type 1 diabetes mellitus, myositis, nephritis, colitis, pneumonitis, hepatitis, uveitis, hypophysitis, and adrenalitis.4
Hypophysitis is inflammation of the pituitary gland, often with thickening of the pituitary stalk, resulting in dysfunction and hormone deficiencies. While primary hypophysitis is idiopathic, secondary hypophysitis is the result of an underlying condition such as exposure to an ICI. Immune-mediated inflammation of the pituitary gland in hypophysitis may disrupt corticotroph function, leading to adrenocorticotropic hormone (ACTH) deficiency. Early warning features are often vague and nonspecific, such as headache, fatigue, and weakness, which makes diagnosis challenging.3,5
CASE PRESENTATION
A 73-year-old male veteran with a history of metastatic melanoma on ipilimumab 3 mg/kg and nivolumab 1 mg/kg every 3 weeks (a standard combination regimen for advanced melanoma) presented to the emergency department (ED) with 2 weeks of cough, nausea, and severe headache 3 weeks after cycle 2 of combination ICI therapy. The patient had undergone excision of multiple sites of melanoma in situ with recurrence and disease progression after 5 cycles of pembrolizumab. He was subsequently started on combination ICI therapy.
On ED arrival, the patient was afebrile and saturating well on room air. He was normotensive but found to have orthostatic blood pressure. Physical examination was remarkable for dry oral mucosa and decreased skin turgor. Initial laboratory results were significant for hyponatremia of 123 mmol/L (reference range, 136-145 mmol/L), low-normal free thyroxine (T4) level of 0.5 ng/dL (reference range, 0.6-1.2 ng/dL), a low total triiodothyronine level of 32.14 ng/dL (reference range, 85-178 ng/dL), and a low thyrotropin level of 0.19 mIU/L (reference range, 0.35-5.50 mIU/L). Serum osmolarity was low at 259 mOsm/kg (reference range, 285-315 mOsm/kg), urine sodium was high at 168 mEq/L (reference, 20 mEq/L), and urine osmolarity was inappropriately concentrated at 726 mOsm/kg (reference range, 250-1000 mOsm/kg). The patient was admitted for additional testing. His morning cortisol level was within normal limits at 15 mcg/dL (reference range, 6.7-22.5 mcg/dL).
Computed tomography (CT) of the patient’s head revealed no acute findings. Chest CT revealed posterior right lower lobe mild ground-glass opacities, with possible ICI-induced pneumonitis. The patient received fluid resuscitation. Given concern for syndrome of inappropriate antidiuretic hormone secretion, the patient was started on 3 g salt tablets 3 times a day and urea 30 g powder daily. The etiology of the abnormal thyroid levels was unclear to endocrinology at that time. The differential diagnosis included a nonthyroidal illness or central hypothyroidism.
The patient started levothyroxine 75 mcg due to abnormal thyroid levels and persistent fatigue and fludrocortisone 0.1 mg daily to manage orthostatic hypotension. His sodium levels improved to 132 mmol/L over 6 days and he was discharged with levothyroxine 75 mcg daily, fludrocortisone 0.1 mg daily, 3 g salt tabs 3 times a day, urea 30 g powder daily, as well as oral cefpodoxime 500 mg twice daily for 3 days and azithromycin 500 mg once daily for 2 days (for a total of 10 days of antibiotic therapy) to treat potential occult pneumonia.
The patient returned to the ED 3 days after discharge following an outpatient oncology appointment with ongoing severe headaches and persistent nausea. There was concern for recurrent hyponatremia. His sodium level was within normal limits at 133 mmol/L. Repeat morning cortisol was low-normal at 9 mcg/dL. Magnetic resonance imaging (MRI) of the brain was negative for metastatic disease, but showed a slight interval increase in size of the pituitary gland compared with an MRI from 6 months prior, with mild fullness and a slightly convex superior margin near homogeneous enhancement, raising concern for infection or hypophysitis (Figure 1).
The patient was readmitted to the general medicine service and was given intravenous hydrocortisone 100 mg every 8 hours because of concern for central adrenal insufficiency due to grade 3 hypophysitis in the setting of MRI imaging and severe headaches (Table 1). He was not hypotensive at the time of hydrocortisone initiation and other vital signs were stable. A cosyntropin stimulation test—a standard diagnostic test for central adrenal insufficiency—was not performed because the patient had already started high-dose hydrocortisone. The patient’s free T4 on this admission remained low at 0.6 ng/dL.
No adjustments were made to his levothyroxine dose given that he recently began the medication and levels may lag after initiation. After a 4-day hospitalization, the decision was made to continue with the steroid taper and follow up with outpatient endocrinology to obtain a cosyntropin stimulation test to complete a full assessment of his pituitary axis (Figure 2). Repeat thyroid function testing for levothyroxine titration was arranged. The levothyroxine dosage was later increased to 88 mcg daily, but the patient discontinued the medication and remained euthyroid. Endocrinology attributed a nonthyroidal illness as the etiology of his hypothyroidism, likely euthyroid sick syndrome in the setting of illness. His hydrocortisone was tapered during outpatient care and fludrocortisone was discontinued due to hypertension.
One month after his second discharge, the patient presented to the ED with 2 weeks of dizziness, associated lightheadedness, and blurred vision when standing from a sitting position. Upon assessment, symptoms were attributed to poor oral intake. The patient’s vital signs were again positive for orthostatic hypotension, though refractory to adequate fluid replacement. Laboratory testing was significant for a low ACTH level of 3.0 pg/mL (reference range, 7.2-63.3 pg/mL). Given that the patient had not received steroids for 1 week, he underwent a cosyntropin stimulation test, which revealed a blunted response supporting a diagnosis of central adrenal insufficiency secondary to ICI-induced hypophysitis (Table 2).
The patient was again readmitted to the general medicine service. A brain MRI showed interval shrinkage of the pituitary gland compared to imaging one month prior, which was attributed to hydrocortisone treatment during this month. CT of the patient’s abdomen demonstrated normal-sized adrenal glands. Positron emission tomography (PET)/CT showed no evidence of pituitary or adrenal metastases. Endocrinology recommended reinitiating oral hydrocortisone 50 mg in the morning and 50 mg around 3 pm daily with fludrocortisone 0.2 mg once daily, which resulted in near resolution of the patient’s symptoms. He was discharged after a 14-day hospitalization with home physical therapy services and endocrinology, nephrology, and oncology follow-up appointments.
The patient was readmitted twice to the general medicine service over the next 6 months for complications from hydrocortisone and fludrocortisone treatment including hypokalemia. He followed up with outpatient clinicians until his death 14 months later. He did not restart ICI therapy, and eventually joined a clinical trial for other advanced melanoma treatments at another institution. The patient’s family consented to the publication of this case report with the accompanying images.
DISCUSSION
The combination of ipilimumab (anti-CTLA-4 monoclonal antibody) and nivolumab (anti-PD-1 monoclonal antibody) is FDA-approved for treatment of advanced melanoma with the goal of harnessing complementary and synergistic mechanisms of dual therapy.6-8 Combination therapy, however, can increase the incidence of irAEs, which are often endocrine-related and more common in patients treated with dual immunotherapy than with monotherapy.9 Hypophysitis has the lowest reported fatality rate among ICI-related irAEs (< 1%), compared with higher mortality rates seen in myocarditis (25%-50%) and pneumonitis (10%-20%).4,10
The patient initially presented with ICI-related hypothyroidism, later identified as secondary (central) hypothyroidism. He was treated with levothyroxine until central hypothyroidism was confirmed. Subsequently, the patient developed headache, poor appetite, and lightheadedness, with MRI findings suggestive of hypophysitis, for which he was started on hydrocortisone. A component of primary adrenal insufficiency was initially considered, given the low ACTH level and blunted response to cosyntropin stimulation following prior high-dose steroid therapy. However, CT imaging demonstrated normal adrenal morphology without atrophy, supporting a diagnosis of central adrenal insufficiency secondary to ICI-induced hypophysitis.
The estimated incidence of ICI-induced hypophysitis is 1.5% to 13.3% with anti-CTLA-4 agents, 0.3% to 3.0% with anti-PD-1 agents, and can be as high as 12.8% with combination therapy.1 ICI-induced hypophysitis is believed to arise from the direct binding of ICI antibodies to their targets on anterior pituitary cells, such as corticotrophs, thyrotrophs, and gonadotrophs, triggering an immune response. One theory for targeting these cells is high CTLA-4 expression in the anterior pituitary gland.11 PD-1 therapies tend to manifest as either hypothyroidism, hyperthyroidism, Graves’ disease, diabetes, or adrenal insufficiency.10
A concern in patients with advanced melanoma is metastasis. Melanoma has a high propensity for brain metastasis.12 There was moderate suspicion for pituitary gland metastasis in this case, though pituitary metastasis more often manifests with symptoms of posterior pituitary gland deficiency, such as polyuria and polydipsia.13 The adrenal gland is the fourth-most common site for melanoma metastases, after the lung, liver, and bone.14 This patient had no evidence of pituitary or adrenal metastases on PET/CT. Therefore, his symptoms were most likely due to ICI therapy. Cases of ≥ 1 endocrine dysfunction have been reported as an ICI therapy irAE.15 In these situations, diagnosing primary and central adrenal insufficiency in the same patient is complex because hormone profiles are intertwined.
Many patients who develop hypophysitis from ICI therapy will require permanent replacement therapy. It is unclear whether low-dose replacement steroids have a significant effect on the efficacy of ICIs. Given that ICI treatment works by enhancing the immune system, medications that suppress the body’s immune system, such as steroids, could interfere with treatment efficacy. However, there are speculations that the development of irAEs is an indicator of effective treatment. In a phase 1 trial of a CTLA-4 blocker in patients with metastatic melanoma, there was a correlation between reduced CTLA-4 expression as well as low rates of melanoma recurrence and a higher incidence of irAEs.16
When assessing patients on ICI treatment, clinicians must remain vigilant for all potential irAEs, especially in patients receiving combination therapy. ICI-induced irAEs can present with vague and nonspecific symptoms. Concurrent endocrine irAEs, such as hypophysitis with thyroiditis or adrenalitis, are not uncommon in combination therapy and can complicate interpretation of hormone profiles. It is prudent for clinicians to review known risk factors. Hypophysitis is typically associated with older adult male patients.17,18
The irAEs of ICI therapy deeply affected the quality of life of the patient in this case, as he was often experiencing many of the clinical symptoms of his hormone insufficiencies as well as the treatment modalities, thus requiring repeated hospital admissions. The risks and benefits of continuing ICI therapy should be an ongoing discussion between the physician and patient and should take into account the acuity and severity of irAEs and oncological disease burden, among other variables. Given the severity of his AEs, the patient stopped ICI therapy and instead opted to enroll in a clinical trial at another institution for continued alternative treatments.
CONCLUSIONS
This case offers a lesson in the diagnostic challenges of vague symptoms in patients with cancer who are receiving ICI therapy. ICI therapy is widely used in the treatment of solid malignancies, and as its use increases, it is expected that clinicians will likely see more cases of irAEs in hospitalized patients. The vague presentation of irAEs can often lead to treatment delays, especially when > 1 irAE presents concurrently. There are ongoing studies researching potential ways to predict the likelihood of developing these irAEs. It is imperative that clinicians are aware of these ICI-related complications and that more research be conducted to understand patient quality of life and treatment guidance based on irAE severity and disease burden.
Immune checkpoint inhibitors (ICIs) have become important in oncology and represent an evolving area of therapeutics. Since their approval by the US Food and Drug Administration (FDA) in 2011, ICIs have been increasingly used as modalities in neoadjuvant and adjuvant treatment for resectable solid malignancies and in unresectable disease, such as advanced melanoma, and are associated with improved survival.1
Immune checkpoints are present on the cell surface of activated T cells as well as other immune cells like B cells and natural killer cells. By regulating the length and amplitude of the body’s innate immune response, they maintain immune homeostasis and prevent its overactivation. Immune checkpoints are often thought of as the brakes on the immune system.2
Two glycoproteins that act as immune checkpoints and are targeted by ICIs are cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) and programmed cell death protein 1 (PD-1). CTLA-4 is upregulated on activated T cells. PD-1 is also expressed on activated T cells, as well as macrophages, B cells, and dendritic cells. Cancer cells can evade immune surveillance by exploiting immune checkpoint pathways. Inhibition of these checkpoints with ICIs reactivates T cells and enables the immune system to recognize and attack cancer cells more effectively. Ipilimumab blocks the activity of CTLA-4 on T cells. Nivolumab and pembrolizumab block the interaction between PD-1 on T cells and its ligand PD-L1 on cancer cells.3,4
Inhibition of these checkpoints is often effective in cancer treatment but can result in the loss of immunologic tolerance with resultant immune-related adverse events (irAEs) and potentially permanent autoimmune disorders. Autoreactive T cells can damage host cell tissues including the colon, lungs, liver, pituitary gland, thyroid, and skin. Severe irAEs include type 1 diabetes mellitus, myositis, nephritis, colitis, pneumonitis, hepatitis, uveitis, hypophysitis, and adrenalitis.4
Hypophysitis is inflammation of the pituitary gland, often with thickening of the pituitary stalk, resulting in dysfunction and hormone deficiencies. While primary hypophysitis is idiopathic, secondary hypophysitis is the result of an underlying condition such as exposure to an ICI. Immune-mediated inflammation of the pituitary gland in hypophysitis may disrupt corticotroph function, leading to adrenocorticotropic hormone (ACTH) deficiency. Early warning features are often vague and nonspecific, such as headache, fatigue, and weakness, which makes diagnosis challenging.3,5
CASE PRESENTATION
A 73-year-old male veteran with a history of metastatic melanoma on ipilimumab 3 mg/kg and nivolumab 1 mg/kg every 3 weeks (a standard combination regimen for advanced melanoma) presented to the emergency department (ED) with 2 weeks of cough, nausea, and severe headache 3 weeks after cycle 2 of combination ICI therapy. The patient had undergone excision of multiple sites of melanoma in situ with recurrence and disease progression after 5 cycles of pembrolizumab. He was subsequently started on combination ICI therapy.
On ED arrival, the patient was afebrile and saturating well on room air. He was normotensive but found to have orthostatic blood pressure. Physical examination was remarkable for dry oral mucosa and decreased skin turgor. Initial laboratory results were significant for hyponatremia of 123 mmol/L (reference range, 136-145 mmol/L), low-normal free thyroxine (T4) level of 0.5 ng/dL (reference range, 0.6-1.2 ng/dL), a low total triiodothyronine level of 32.14 ng/dL (reference range, 85-178 ng/dL), and a low thyrotropin level of 0.19 mIU/L (reference range, 0.35-5.50 mIU/L). Serum osmolarity was low at 259 mOsm/kg (reference range, 285-315 mOsm/kg), urine sodium was high at 168 mEq/L (reference, 20 mEq/L), and urine osmolarity was inappropriately concentrated at 726 mOsm/kg (reference range, 250-1000 mOsm/kg). The patient was admitted for additional testing. His morning cortisol level was within normal limits at 15 mcg/dL (reference range, 6.7-22.5 mcg/dL).
Computed tomography (CT) of the patient’s head revealed no acute findings. Chest CT revealed posterior right lower lobe mild ground-glass opacities, with possible ICI-induced pneumonitis. The patient received fluid resuscitation. Given concern for syndrome of inappropriate antidiuretic hormone secretion, the patient was started on 3 g salt tablets 3 times a day and urea 30 g powder daily. The etiology of the abnormal thyroid levels was unclear to endocrinology at that time. The differential diagnosis included a nonthyroidal illness or central hypothyroidism.
The patient started levothyroxine 75 mcg due to abnormal thyroid levels and persistent fatigue and fludrocortisone 0.1 mg daily to manage orthostatic hypotension. His sodium levels improved to 132 mmol/L over 6 days and he was discharged with levothyroxine 75 mcg daily, fludrocortisone 0.1 mg daily, 3 g salt tabs 3 times a day, urea 30 g powder daily, as well as oral cefpodoxime 500 mg twice daily for 3 days and azithromycin 500 mg once daily for 2 days (for a total of 10 days of antibiotic therapy) to treat potential occult pneumonia.
The patient returned to the ED 3 days after discharge following an outpatient oncology appointment with ongoing severe headaches and persistent nausea. There was concern for recurrent hyponatremia. His sodium level was within normal limits at 133 mmol/L. Repeat morning cortisol was low-normal at 9 mcg/dL. Magnetic resonance imaging (MRI) of the brain was negative for metastatic disease, but showed a slight interval increase in size of the pituitary gland compared with an MRI from 6 months prior, with mild fullness and a slightly convex superior margin near homogeneous enhancement, raising concern for infection or hypophysitis (Figure 1).
The patient was readmitted to the general medicine service and was given intravenous hydrocortisone 100 mg every 8 hours because of concern for central adrenal insufficiency due to grade 3 hypophysitis in the setting of MRI imaging and severe headaches (Table 1). He was not hypotensive at the time of hydrocortisone initiation and other vital signs were stable. A cosyntropin stimulation test—a standard diagnostic test for central adrenal insufficiency—was not performed because the patient had already started high-dose hydrocortisone. The patient’s free T4 on this admission remained low at 0.6 ng/dL.
No adjustments were made to his levothyroxine dose given that he recently began the medication and levels may lag after initiation. After a 4-day hospitalization, the decision was made to continue with the steroid taper and follow up with outpatient endocrinology to obtain a cosyntropin stimulation test to complete a full assessment of his pituitary axis (Figure 2). Repeat thyroid function testing for levothyroxine titration was arranged. The levothyroxine dosage was later increased to 88 mcg daily, but the patient discontinued the medication and remained euthyroid. Endocrinology attributed a nonthyroidal illness as the etiology of his hypothyroidism, likely euthyroid sick syndrome in the setting of illness. His hydrocortisone was tapered during outpatient care and fludrocortisone was discontinued due to hypertension.
One month after his second discharge, the patient presented to the ED with 2 weeks of dizziness, associated lightheadedness, and blurred vision when standing from a sitting position. Upon assessment, symptoms were attributed to poor oral intake. The patient’s vital signs were again positive for orthostatic hypotension, though refractory to adequate fluid replacement. Laboratory testing was significant for a low ACTH level of 3.0 pg/mL (reference range, 7.2-63.3 pg/mL). Given that the patient had not received steroids for 1 week, he underwent a cosyntropin stimulation test, which revealed a blunted response supporting a diagnosis of central adrenal insufficiency secondary to ICI-induced hypophysitis (Table 2).
The patient was again readmitted to the general medicine service. A brain MRI showed interval shrinkage of the pituitary gland compared to imaging one month prior, which was attributed to hydrocortisone treatment during this month. CT of the patient’s abdomen demonstrated normal-sized adrenal glands. Positron emission tomography (PET)/CT showed no evidence of pituitary or adrenal metastases. Endocrinology recommended reinitiating oral hydrocortisone 50 mg in the morning and 50 mg around 3 pm daily with fludrocortisone 0.2 mg once daily, which resulted in near resolution of the patient’s symptoms. He was discharged after a 14-day hospitalization with home physical therapy services and endocrinology, nephrology, and oncology follow-up appointments.
The patient was readmitted twice to the general medicine service over the next 6 months for complications from hydrocortisone and fludrocortisone treatment including hypokalemia. He followed up with outpatient clinicians until his death 14 months later. He did not restart ICI therapy, and eventually joined a clinical trial for other advanced melanoma treatments at another institution. The patient’s family consented to the publication of this case report with the accompanying images.
DISCUSSION
The combination of ipilimumab (anti-CTLA-4 monoclonal antibody) and nivolumab (anti-PD-1 monoclonal antibody) is FDA-approved for treatment of advanced melanoma with the goal of harnessing complementary and synergistic mechanisms of dual therapy.6-8 Combination therapy, however, can increase the incidence of irAEs, which are often endocrine-related and more common in patients treated with dual immunotherapy than with monotherapy.9 Hypophysitis has the lowest reported fatality rate among ICI-related irAEs (< 1%), compared with higher mortality rates seen in myocarditis (25%-50%) and pneumonitis (10%-20%).4,10
The patient initially presented with ICI-related hypothyroidism, later identified as secondary (central) hypothyroidism. He was treated with levothyroxine until central hypothyroidism was confirmed. Subsequently, the patient developed headache, poor appetite, and lightheadedness, with MRI findings suggestive of hypophysitis, for which he was started on hydrocortisone. A component of primary adrenal insufficiency was initially considered, given the low ACTH level and blunted response to cosyntropin stimulation following prior high-dose steroid therapy. However, CT imaging demonstrated normal adrenal morphology without atrophy, supporting a diagnosis of central adrenal insufficiency secondary to ICI-induced hypophysitis.
The estimated incidence of ICI-induced hypophysitis is 1.5% to 13.3% with anti-CTLA-4 agents, 0.3% to 3.0% with anti-PD-1 agents, and can be as high as 12.8% with combination therapy.1 ICI-induced hypophysitis is believed to arise from the direct binding of ICI antibodies to their targets on anterior pituitary cells, such as corticotrophs, thyrotrophs, and gonadotrophs, triggering an immune response. One theory for targeting these cells is high CTLA-4 expression in the anterior pituitary gland.11 PD-1 therapies tend to manifest as either hypothyroidism, hyperthyroidism, Graves’ disease, diabetes, or adrenal insufficiency.10
A concern in patients with advanced melanoma is metastasis. Melanoma has a high propensity for brain metastasis.12 There was moderate suspicion for pituitary gland metastasis in this case, though pituitary metastasis more often manifests with symptoms of posterior pituitary gland deficiency, such as polyuria and polydipsia.13 The adrenal gland is the fourth-most common site for melanoma metastases, after the lung, liver, and bone.14 This patient had no evidence of pituitary or adrenal metastases on PET/CT. Therefore, his symptoms were most likely due to ICI therapy. Cases of ≥ 1 endocrine dysfunction have been reported as an ICI therapy irAE.15 In these situations, diagnosing primary and central adrenal insufficiency in the same patient is complex because hormone profiles are intertwined.
Many patients who develop hypophysitis from ICI therapy will require permanent replacement therapy. It is unclear whether low-dose replacement steroids have a significant effect on the efficacy of ICIs. Given that ICI treatment works by enhancing the immune system, medications that suppress the body’s immune system, such as steroids, could interfere with treatment efficacy. However, there are speculations that the development of irAEs is an indicator of effective treatment. In a phase 1 trial of a CTLA-4 blocker in patients with metastatic melanoma, there was a correlation between reduced CTLA-4 expression as well as low rates of melanoma recurrence and a higher incidence of irAEs.16
When assessing patients on ICI treatment, clinicians must remain vigilant for all potential irAEs, especially in patients receiving combination therapy. ICI-induced irAEs can present with vague and nonspecific symptoms. Concurrent endocrine irAEs, such as hypophysitis with thyroiditis or adrenalitis, are not uncommon in combination therapy and can complicate interpretation of hormone profiles. It is prudent for clinicians to review known risk factors. Hypophysitis is typically associated with older adult male patients.17,18
The irAEs of ICI therapy deeply affected the quality of life of the patient in this case, as he was often experiencing many of the clinical symptoms of his hormone insufficiencies as well as the treatment modalities, thus requiring repeated hospital admissions. The risks and benefits of continuing ICI therapy should be an ongoing discussion between the physician and patient and should take into account the acuity and severity of irAEs and oncological disease burden, among other variables. Given the severity of his AEs, the patient stopped ICI therapy and instead opted to enroll in a clinical trial at another institution for continued alternative treatments.
CONCLUSIONS
This case offers a lesson in the diagnostic challenges of vague symptoms in patients with cancer who are receiving ICI therapy. ICI therapy is widely used in the treatment of solid malignancies, and as its use increases, it is expected that clinicians will likely see more cases of irAEs in hospitalized patients. The vague presentation of irAEs can often lead to treatment delays, especially when > 1 irAE presents concurrently. There are ongoing studies researching potential ways to predict the likelihood of developing these irAEs. It is imperative that clinicians are aware of these ICI-related complications and that more research be conducted to understand patient quality of life and treatment guidance based on irAE severity and disease burden.
- Villani A, Potestio L, Fabbrocini G, et al. The treatment of advanced melanoma: therapeutic update. Int J Mol Sci. 2022;23:6388. doi:10.3390/ijms23126388
- Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer. 2012;12:252-264. doi:10.1038/nrc3239
- Chang LS, Barroso-Sousa R, Tolaney SM, et al. Endocrine toxicity of cancer immunotherapy targeting immune checkpoints. Endocr Rev. 2019;40:17-65. doi:10.1210/er.2018-00006
- June CH, Warshauer JT, Bluestone JA. Is autoimmunity the Achilles’ heel of cancer immunotherapy? Nat Med. 2017;23:540-547. doi:10.1038/nm.4321
- Jessel S, Weiss SA, Austin M, et al. Immune checkpoint inhibitor-induced hypophysitis and patterns of loss of pituitary function. Front Oncol. 2022;12:836859. doi:10.3389/fonc.2022.836859
- Betof AS, Nipp RD, Giobbie-Hurder A, et al. Impact of age on outcomes with immunotherapy for patients with melanoma. Oncologist. 2017;22:963-971. doi:10.1634/theoncologist.2016-0450
- Wolchok JD, Kluger H, Callahan MK, et al. Nivolumab plus ipilimumab in advanced melanoma. N Engl J Med. 2013;369:122-133. doi:10.1056/NEJMoa1302369
- Hodi FS, O’Day SJ, McDermott DF, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363:711-723. doi:10.1056/NEJMoa1003466
- Benhima N, Belbaraka R, Langouo Fontsa MD. Single agent vs combination immunotherapy in advanced melanoma: a review of the evidence. Curr Opin Oncol. 2024;36:69-73. doi:10.1097/CCO.0000000000001014
- Tong J, Kartolo A, Yeung C, et al. Long-term toxicities of immune checkpoint inhibitor (ICI) in melanoma patients. Curr Oncol. 2022;29:7953-7963. doi:10.3390/curroncol29100629
- Grouthier V, Lebrun-Vignes B, Moey M, et al. Immune checkpoint inhibitor-associated primary adrenal insufficiency: WHO VigiBase report analysis. Oncologist. 2020;25:696-701. doi:10.1634/theoncologist.2019-0555
- Park BC, Jung S, Wright JJ, et al. Recurrence of hypophysitis after immune checkpoint inhibitor rechallenge. Oncologist. 2022;27:e967-e969. doi:10.1093/oncolo/oyac220
- Zhang D, Wang Z, Shang D, et al. Incidence and prognosis of brain metastases in cutaneous melanoma patients: a population-based study. Melanoma Res. 2019;29:77-84. doi:10.1097/CMR.0000000000000538
- Barnabei A, Carpano S, Chiefari A, et al. Case report: ipilimumab-induced panhypophysitis: an infrequent occurrence and literature review. Front Oncol. 2020;10:582394. doi:10.3389/fonc.2020.582394
- Shortreed H, Burute N, Aseyev O. Management of undifferentiated adrenal gland metastases from malignant melanoma: case report. Front Oncol. 2024;14:1419827. doi:10.3389/fonc.2024.1419827
- Rossi S, Silvetti F, Bordoni M, et al. Pembrolizumab-induced thyroiditis, hypophysitis and adrenalitis: a case of triple endocrine dysfunction. JCEM Case Rep. 2024;2:luae200. doi:10.1210/jcemcr/luae200
- Sanderson K, Scotland R, Lee P, et al. Autoimmunity in a phase I trial of a fully human anti-cytotoxic T-lymphocyte antigen-4 monoclonal antibody with multiple melanoma peptides and Montanide ISA 51 for patients with resected stages III and IV melanoma. J Clin Oncol. 2005;23:741-750. doi:10.1200/JCO.2005.01.128
- de Filette J, Andreescu CE, Cools F, Bravenboer B, Velkeniers B. A systematic review and meta-analysis of endocrine-related adverse events associated with immune checkpoint inhibitors. Horm Metab Res. 2019;51:145-156. doi:10.1055/a-0843-3366
- Villani A, Potestio L, Fabbrocini G, et al. The treatment of advanced melanoma: therapeutic update. Int J Mol Sci. 2022;23:6388. doi:10.3390/ijms23126388
- Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer. 2012;12:252-264. doi:10.1038/nrc3239
- Chang LS, Barroso-Sousa R, Tolaney SM, et al. Endocrine toxicity of cancer immunotherapy targeting immune checkpoints. Endocr Rev. 2019;40:17-65. doi:10.1210/er.2018-00006
- June CH, Warshauer JT, Bluestone JA. Is autoimmunity the Achilles’ heel of cancer immunotherapy? Nat Med. 2017;23:540-547. doi:10.1038/nm.4321
- Jessel S, Weiss SA, Austin M, et al. Immune checkpoint inhibitor-induced hypophysitis and patterns of loss of pituitary function. Front Oncol. 2022;12:836859. doi:10.3389/fonc.2022.836859
- Betof AS, Nipp RD, Giobbie-Hurder A, et al. Impact of age on outcomes with immunotherapy for patients with melanoma. Oncologist. 2017;22:963-971. doi:10.1634/theoncologist.2016-0450
- Wolchok JD, Kluger H, Callahan MK, et al. Nivolumab plus ipilimumab in advanced melanoma. N Engl J Med. 2013;369:122-133. doi:10.1056/NEJMoa1302369
- Hodi FS, O’Day SJ, McDermott DF, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363:711-723. doi:10.1056/NEJMoa1003466
- Benhima N, Belbaraka R, Langouo Fontsa MD. Single agent vs combination immunotherapy in advanced melanoma: a review of the evidence. Curr Opin Oncol. 2024;36:69-73. doi:10.1097/CCO.0000000000001014
- Tong J, Kartolo A, Yeung C, et al. Long-term toxicities of immune checkpoint inhibitor (ICI) in melanoma patients. Curr Oncol. 2022;29:7953-7963. doi:10.3390/curroncol29100629
- Grouthier V, Lebrun-Vignes B, Moey M, et al. Immune checkpoint inhibitor-associated primary adrenal insufficiency: WHO VigiBase report analysis. Oncologist. 2020;25:696-701. doi:10.1634/theoncologist.2019-0555
- Park BC, Jung S, Wright JJ, et al. Recurrence of hypophysitis after immune checkpoint inhibitor rechallenge. Oncologist. 2022;27:e967-e969. doi:10.1093/oncolo/oyac220
- Zhang D, Wang Z, Shang D, et al. Incidence and prognosis of brain metastases in cutaneous melanoma patients: a population-based study. Melanoma Res. 2019;29:77-84. doi:10.1097/CMR.0000000000000538
- Barnabei A, Carpano S, Chiefari A, et al. Case report: ipilimumab-induced panhypophysitis: an infrequent occurrence and literature review. Front Oncol. 2020;10:582394. doi:10.3389/fonc.2020.582394
- Shortreed H, Burute N, Aseyev O. Management of undifferentiated adrenal gland metastases from malignant melanoma: case report. Front Oncol. 2024;14:1419827. doi:10.3389/fonc.2024.1419827
- Rossi S, Silvetti F, Bordoni M, et al. Pembrolizumab-induced thyroiditis, hypophysitis and adrenalitis: a case of triple endocrine dysfunction. JCEM Case Rep. 2024;2:luae200. doi:10.1210/jcemcr/luae200
- Sanderson K, Scotland R, Lee P, et al. Autoimmunity in a phase I trial of a fully human anti-cytotoxic T-lymphocyte antigen-4 monoclonal antibody with multiple melanoma peptides and Montanide ISA 51 for patients with resected stages III and IV melanoma. J Clin Oncol. 2005;23:741-750. doi:10.1200/JCO.2005.01.128
- de Filette J, Andreescu CE, Cools F, Bravenboer B, Velkeniers B. A systematic review and meta-analysis of endocrine-related adverse events associated with immune checkpoint inhibitors. Horm Metab Res. 2019;51:145-156. doi:10.1055/a-0843-3366
Diagnostic Challenge of Immune Checkpoint Inhibitor-Induced Hypophysitis in a Patient With Advanced Melanoma
Diagnostic Challenge of Immune Checkpoint Inhibitor-Induced Hypophysitis in a Patient With Advanced Melanoma