User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
The effect of smoking lingers
Lung function appears to continue to decline even decades after smoking cessation, according to new data from the National Heart, Lung, and Blood Institute Pooled Cohort Study. Compared with never-smokers, former smokers had a decline in forced expiratory volume in 1 second (FEV1) about 20% as severe as current smokers, but nevertheless higher than never-smokers. Low-intensity smokers also fared worse than never-smokers, suggesting that no amount of smoke exposure should be considered safe.

The increased decline occurred even decades after smoking cessation, according to the study published in Lancet Respiratory Medicine, which was led by Elizabeth Oelsner, MD, MPH, of Columbia University, New York. Smoking prevalence has decreased from 42% to 16% in the past 50 years, and many smokers report that they smoke fewer cigarettes per day, from an average of 21 to 14, according to the authors. Despite those trends, the prevalence of chronic obstructive pulmonary disease has continued to increase, and is now the third-leading cause of death worldwide.
A meta-analysis of 47 studies and 88,887 adults found no association between smoking and FEV1 decline, but many of the studies were small or focused on nonrepresentative populations, and they used variably standardized spirometry.
The study pooled data from nine individual U.S. cohorts, with 25,352 participants recruited during 1983-2016. Subjects included those who underwent at least two prebronchodilator spirometry tests following American Thoracic Society standards. After adjustment, former smokers had increased FEV1 decline of 1.82 mL/year (P less than .0001), compared with never-smokers. Current smokers had an increased decline of 9.21 mL/year (P less than .0001).
Even after decades of abstinence, the effects of smoking appeared to linger: 20-30 years later, FEV1 loss was accelerated by 2.50 mL/year (P less than .0001), and by 0.93 mL/year (P = .0104) after 30 years, compared with never-smokers.
Even low-intensity smokers (cumulative less than 10 pack-years) had an significantly accelerated FEV1 decline (0.87 mL; P = .0153).
The researchers also found a relationship between FEV1 decline and intensity of current smoking: Those smoking fewer than 5 cigarettes per day had a lower decline than those smoking 30 or more (7.65 mL; 95% confidence interval, 6.21-9.09 vs. 11.24 mL; 95% CI, 9.86-12.62).
The study is limited by the fact that smoking status and daily tobacco reporting were self-reported, which could result in information bias.
The study was funded by the National Institutes of Health, National Heart Lung and Blood Institute, and U.S. Environmental Protection Agency. The authors report personal fees, consultancy fees, or grants from a wide variety of pharmaceutical companies.
SOURCE: Oelsner EC et al. Lancet Respir Med. 2019 Oct 9. doi: 10.1016/S2213-2600(19)30276-0.
It is unclear whether the small increase in FEV1 decline (1.82 mL) seen among former smokers is clinically significant, though it suggests lasting damage from smoking. The increased decline in low-intensity smokers is an important observation confirming accumulating evidence that no amount of smoking is free of harm. This is a key message because some physicians and members of the public believe that low-intensity smoking and use of low-dose tobacco products can reduce or eliminate risk, according to Yunus Çolak, MD, and Peter Lange, MD, in their accompanying commentary (Lancet Respir Med. 2019 Oct 9. doi. org/10.1016/S2213-2600[19]30349-2). “More information is needed to manage patients with COPD [chronic obstructive pulmonary disease] in an era with decreasing smoking prevalence and an increasing proportion of smokers with low,” they added. “We should begin by questioning the arbitrary cutoff of 10 pack-years of cumulated tobacco exposure, which is currently the rule in most clinical trials of COPD. Additionally, we should not promote low-intensity smoking and use of low-dose tobacco products as a means of harm reduction but instead promote early smoking cessation,” they concluded.
Dr. Çolak and Dr. Lange are at the University of Copenhagen. The remarks are from their online commentary to the article. The reported receiving fees and grants from a variety of pharmaceutical companies.
It is unclear whether the small increase in FEV1 decline (1.82 mL) seen among former smokers is clinically significant, though it suggests lasting damage from smoking. The increased decline in low-intensity smokers is an important observation confirming accumulating evidence that no amount of smoking is free of harm. This is a key message because some physicians and members of the public believe that low-intensity smoking and use of low-dose tobacco products can reduce or eliminate risk, according to Yunus Çolak, MD, and Peter Lange, MD, in their accompanying commentary (Lancet Respir Med. 2019 Oct 9. doi. org/10.1016/S2213-2600[19]30349-2). “More information is needed to manage patients with COPD [chronic obstructive pulmonary disease] in an era with decreasing smoking prevalence and an increasing proportion of smokers with low,” they added. “We should begin by questioning the arbitrary cutoff of 10 pack-years of cumulated tobacco exposure, which is currently the rule in most clinical trials of COPD. Additionally, we should not promote low-intensity smoking and use of low-dose tobacco products as a means of harm reduction but instead promote early smoking cessation,” they concluded.
Dr. Çolak and Dr. Lange are at the University of Copenhagen. The remarks are from their online commentary to the article. The reported receiving fees and grants from a variety of pharmaceutical companies.
It is unclear whether the small increase in FEV1 decline (1.82 mL) seen among former smokers is clinically significant, though it suggests lasting damage from smoking. The increased decline in low-intensity smokers is an important observation confirming accumulating evidence that no amount of smoking is free of harm. This is a key message because some physicians and members of the public believe that low-intensity smoking and use of low-dose tobacco products can reduce or eliminate risk, according to Yunus Çolak, MD, and Peter Lange, MD, in their accompanying commentary (Lancet Respir Med. 2019 Oct 9. doi. org/10.1016/S2213-2600[19]30349-2). “More information is needed to manage patients with COPD [chronic obstructive pulmonary disease] in an era with decreasing smoking prevalence and an increasing proportion of smokers with low,” they added. “We should begin by questioning the arbitrary cutoff of 10 pack-years of cumulated tobacco exposure, which is currently the rule in most clinical trials of COPD. Additionally, we should not promote low-intensity smoking and use of low-dose tobacco products as a means of harm reduction but instead promote early smoking cessation,” they concluded.
Dr. Çolak and Dr. Lange are at the University of Copenhagen. The remarks are from their online commentary to the article. The reported receiving fees and grants from a variety of pharmaceutical companies.
Lung function appears to continue to decline even decades after smoking cessation, according to new data from the National Heart, Lung, and Blood Institute Pooled Cohort Study. Compared with never-smokers, former smokers had a decline in forced expiratory volume in 1 second (FEV1) about 20% as severe as current smokers, but nevertheless higher than never-smokers. Low-intensity smokers also fared worse than never-smokers, suggesting that no amount of smoke exposure should be considered safe.
The increased decline occurred even decades after smoking cessation, according to the study published in Lancet Respiratory Medicine, which was led by Elizabeth Oelsner, MD, MPH, of Columbia University, New York. Smoking prevalence has decreased from 42% to 16% in the past 50 years, and many smokers report that they smoke fewer cigarettes per day, from an average of 21 to 14, according to the authors. Despite those trends, the prevalence of chronic obstructive pulmonary disease has continued to increase, and is now the third-leading cause of death worldwide.
A meta-analysis of 47 studies and 88,887 adults found no association between smoking and FEV1 decline, but many of the studies were small or focused on nonrepresentative populations, and they used variably standardized spirometry.
The study pooled data from nine individual U.S. cohorts, with 25,352 participants recruited during 1983-2016. Subjects included those who underwent at least two prebronchodilator spirometry tests following American Thoracic Society standards. After adjustment, former smokers had increased FEV1 decline of 1.82 mL/year (P less than .0001), compared with never-smokers. Current smokers had an increased decline of 9.21 mL/year (P less than .0001).
Even after decades of abstinence, the effects of smoking appeared to linger: 20-30 years later, FEV1 loss was accelerated by 2.50 mL/year (P less than .0001), and by 0.93 mL/year (P = .0104) after 30 years, compared with never-smokers.
Even low-intensity smokers (cumulative less than 10 pack-years) had an significantly accelerated FEV1 decline (0.87 mL; P = .0153).
The researchers also found a relationship between FEV1 decline and intensity of current smoking: Those smoking fewer than 5 cigarettes per day had a lower decline than those smoking 30 or more (7.65 mL; 95% confidence interval, 6.21-9.09 vs. 11.24 mL; 95% CI, 9.86-12.62).
The study is limited by the fact that smoking status and daily tobacco reporting were self-reported, which could result in information bias.
The study was funded by the National Institutes of Health, National Heart Lung and Blood Institute, and U.S. Environmental Protection Agency. The authors report personal fees, consultancy fees, or grants from a wide variety of pharmaceutical companies.
SOURCE: Oelsner EC et al. Lancet Respir Med. 2019 Oct 9. doi: 10.1016/S2213-2600(19)30276-0.
Lung function appears to continue to decline even decades after smoking cessation, according to new data from the National Heart, Lung, and Blood Institute Pooled Cohort Study. Compared with never-smokers, former smokers had a decline in forced expiratory volume in 1 second (FEV1) about 20% as severe as current smokers, but nevertheless higher than never-smokers. Low-intensity smokers also fared worse than never-smokers, suggesting that no amount of smoke exposure should be considered safe.
The increased decline occurred even decades after smoking cessation, according to the study published in Lancet Respiratory Medicine, which was led by Elizabeth Oelsner, MD, MPH, of Columbia University, New York. Smoking prevalence has decreased from 42% to 16% in the past 50 years, and many smokers report that they smoke fewer cigarettes per day, from an average of 21 to 14, according to the authors. Despite those trends, the prevalence of chronic obstructive pulmonary disease has continued to increase, and is now the third-leading cause of death worldwide.
A meta-analysis of 47 studies and 88,887 adults found no association between smoking and FEV1 decline, but many of the studies were small or focused on nonrepresentative populations, and they used variably standardized spirometry.
The study pooled data from nine individual U.S. cohorts, with 25,352 participants recruited during 1983-2016. Subjects included those who underwent at least two prebronchodilator spirometry tests following American Thoracic Society standards. After adjustment, former smokers had increased FEV1 decline of 1.82 mL/year (P less than .0001), compared with never-smokers. Current smokers had an increased decline of 9.21 mL/year (P less than .0001).
Even after decades of abstinence, the effects of smoking appeared to linger: 20-30 years later, FEV1 loss was accelerated by 2.50 mL/year (P less than .0001), and by 0.93 mL/year (P = .0104) after 30 years, compared with never-smokers.
Even low-intensity smokers (cumulative less than 10 pack-years) had an significantly accelerated FEV1 decline (0.87 mL; P = .0153).
The researchers also found a relationship between FEV1 decline and intensity of current smoking: Those smoking fewer than 5 cigarettes per day had a lower decline than those smoking 30 or more (7.65 mL; 95% confidence interval, 6.21-9.09 vs. 11.24 mL; 95% CI, 9.86-12.62).
The study is limited by the fact that smoking status and daily tobacco reporting were self-reported, which could result in information bias.
The study was funded by the National Institutes of Health, National Heart Lung and Blood Institute, and U.S. Environmental Protection Agency. The authors report personal fees, consultancy fees, or grants from a wide variety of pharmaceutical companies.
SOURCE: Oelsner EC et al. Lancet Respir Med. 2019 Oct 9. doi: 10.1016/S2213-2600(19)30276-0.
REPORTING FROM LANCET RESPIRATORY MEDICINE
One monoclonal dose gives preterm neonates season-long RSV protection
WASHINGTON – A single dose of a novel monoclonal antibody against a respiratory syncytial virus surface protein safely protected preterm infants against severe infections for 150 days during their first winter season in a randomized trial with more than 1,400 children.

One intramuscular injection of nirsevimab (also known as MEDI8897) administered to infants born at 29-35 weeks’ gestation at the start of the local respiratory syncytial virus (RSV) season (November in the Northern hemisphere) led to a 70% relative reduction in the rate of medically attended lower respiratory tract infections with RSV during the subsequent 150 days, compared with placebo, the study’s primary efficacy outcome, M. Pamela Griffin, MD, said at an annual scientific meeting on infectious diseases.
In a secondary efficacy measure, the rate of hospitalizations for RSV-caused lower respiratory tract infections, a single injection of nirsevimab dropped the incidence by 78%, relative to placebo. Both effects were statistically significant. The rate of total adverse events and serious adverse events was similar in the two treatment arms, reported Dr. Griffin, a clinical development lead with AstraZeneca.
These positive results for a single intramuscular injection of nirsevimab are the first findings from a series of studies aimed at getting the monoclonal antibody onto the U.S. market as a superior alternative to palivizumab (Synagis), which acts in a similar way to block RSV infection (albeit by targeting a different viral surface protein) but which requires administration every 30 days. This need for serial dosing of palivizumab in children younger than 1 year old for complete seasonal protection against RSV is probably a reason why the American Academy of Pediatrics, as well as other medical societies, have targeted using palivizumab only on certain types of high-risk infants: those born before 29 weeks’ gestational age, with chronic lung disease of prematurity, or with hemodynamically significant congenital heart disease (Pediatrics. 2014 Aug;134[2]:415-20). “It’s not feasible for most infants to come for five treatments during RSV season,” Dr. Griffin noted. A tweak in the structure of nirsevimab gives it a much longer blood half-life than palivizumab and allows a single dose to maintain efficacy for 5 months, the duration of RSV season.
“The big advantage of nirsevimab is one dose instead of five,” she said in an interview.
The study randomized 969 preterm infants to nirsevimab and 484 to placebo when the children averaged 3 months old and 4.5 kg. The incidence of the primary endpoint was 2.6% in the nirsevimab-treated infants and 9.5% in those who received placebo. The incidence of hospitalizations associated with an RSV lower respiratory tract infection was 0.8% in the nirsevimab group and 4.1% on placebo. Nirsevimab was equally effective regardless of RSV subtype, infant age, or sex. The rate of hypersensitivity reactions was low, less than 1%, and similar in the two treatment arms, as was the rate of detection of antidrug antibody, 3.8% with placebo and 5.6% with nirsevimab.
Two other large trials are underway to document the performance of nirsevimab in other types of infants. One study is examining the drug’s performance compared with placebo in term infants with a gestational age of at least 36 weeks, while another is comparing nirsevimab against a five-dose regimen of palivizumab in high-risk infants who are recommended to receive palivizumab by local medical societies. In the United States, this would be infants born at less than 29 weeks’ gestation, and those with either hemodynamically significant congenital heart disease or chronic lung disease of prematurity. In these studies, the researchers also will assess the cost effectiveness of nirsevimab relative to the costs for medical care needed by infants who receive comparator treatments, Dr. Griffin said.
The study was funded by AstraZeneca, the company developing nirsevimab. Dr. Griffin is an employee of and shareholder in AstraZeneca.
SOURCE: ClinicalTrials.gov identifier: NCT02878330.
WASHINGTON – A single dose of a novel monoclonal antibody against a respiratory syncytial virus surface protein safely protected preterm infants against severe infections for 150 days during their first winter season in a randomized trial with more than 1,400 children.
One intramuscular injection of nirsevimab (also known as MEDI8897) administered to infants born at 29-35 weeks’ gestation at the start of the local respiratory syncytial virus (RSV) season (November in the Northern hemisphere) led to a 70% relative reduction in the rate of medically attended lower respiratory tract infections with RSV during the subsequent 150 days, compared with placebo, the study’s primary efficacy outcome, M. Pamela Griffin, MD, said at an annual scientific meeting on infectious diseases.
In a secondary efficacy measure, the rate of hospitalizations for RSV-caused lower respiratory tract infections, a single injection of nirsevimab dropped the incidence by 78%, relative to placebo. Both effects were statistically significant. The rate of total adverse events and serious adverse events was similar in the two treatment arms, reported Dr. Griffin, a clinical development lead with AstraZeneca.
These positive results for a single intramuscular injection of nirsevimab are the first findings from a series of studies aimed at getting the monoclonal antibody onto the U.S. market as a superior alternative to palivizumab (Synagis), which acts in a similar way to block RSV infection (albeit by targeting a different viral surface protein) but which requires administration every 30 days. This need for serial dosing of palivizumab in children younger than 1 year old for complete seasonal protection against RSV is probably a reason why the American Academy of Pediatrics, as well as other medical societies, have targeted using palivizumab only on certain types of high-risk infants: those born before 29 weeks’ gestational age, with chronic lung disease of prematurity, or with hemodynamically significant congenital heart disease (Pediatrics. 2014 Aug;134[2]:415-20). “It’s not feasible for most infants to come for five treatments during RSV season,” Dr. Griffin noted. A tweak in the structure of nirsevimab gives it a much longer blood half-life than palivizumab and allows a single dose to maintain efficacy for 5 months, the duration of RSV season.
“The big advantage of nirsevimab is one dose instead of five,” she said in an interview.
The study randomized 969 preterm infants to nirsevimab and 484 to placebo when the children averaged 3 months old and 4.5 kg. The incidence of the primary endpoint was 2.6% in the nirsevimab-treated infants and 9.5% in those who received placebo. The incidence of hospitalizations associated with an RSV lower respiratory tract infection was 0.8% in the nirsevimab group and 4.1% on placebo. Nirsevimab was equally effective regardless of RSV subtype, infant age, or sex. The rate of hypersensitivity reactions was low, less than 1%, and similar in the two treatment arms, as was the rate of detection of antidrug antibody, 3.8% with placebo and 5.6% with nirsevimab.
Two other large trials are underway to document the performance of nirsevimab in other types of infants. One study is examining the drug’s performance compared with placebo in term infants with a gestational age of at least 36 weeks, while another is comparing nirsevimab against a five-dose regimen of palivizumab in high-risk infants who are recommended to receive palivizumab by local medical societies. In the United States, this would be infants born at less than 29 weeks’ gestation, and those with either hemodynamically significant congenital heart disease or chronic lung disease of prematurity. In these studies, the researchers also will assess the cost effectiveness of nirsevimab relative to the costs for medical care needed by infants who receive comparator treatments, Dr. Griffin said.
The study was funded by AstraZeneca, the company developing nirsevimab. Dr. Griffin is an employee of and shareholder in AstraZeneca.
SOURCE: ClinicalTrials.gov identifier: NCT02878330.
WASHINGTON – A single dose of a novel monoclonal antibody against a respiratory syncytial virus surface protein safely protected preterm infants against severe infections for 150 days during their first winter season in a randomized trial with more than 1,400 children.
One intramuscular injection of nirsevimab (also known as MEDI8897) administered to infants born at 29-35 weeks’ gestation at the start of the local respiratory syncytial virus (RSV) season (November in the Northern hemisphere) led to a 70% relative reduction in the rate of medically attended lower respiratory tract infections with RSV during the subsequent 150 days, compared with placebo, the study’s primary efficacy outcome, M. Pamela Griffin, MD, said at an annual scientific meeting on infectious diseases.
In a secondary efficacy measure, the rate of hospitalizations for RSV-caused lower respiratory tract infections, a single injection of nirsevimab dropped the incidence by 78%, relative to placebo. Both effects were statistically significant. The rate of total adverse events and serious adverse events was similar in the two treatment arms, reported Dr. Griffin, a clinical development lead with AstraZeneca.
These positive results for a single intramuscular injection of nirsevimab are the first findings from a series of studies aimed at getting the monoclonal antibody onto the U.S. market as a superior alternative to palivizumab (Synagis), which acts in a similar way to block RSV infection (albeit by targeting a different viral surface protein) but which requires administration every 30 days. This need for serial dosing of palivizumab in children younger than 1 year old for complete seasonal protection against RSV is probably a reason why the American Academy of Pediatrics, as well as other medical societies, have targeted using palivizumab only on certain types of high-risk infants: those born before 29 weeks’ gestational age, with chronic lung disease of prematurity, or with hemodynamically significant congenital heart disease (Pediatrics. 2014 Aug;134[2]:415-20). “It’s not feasible for most infants to come for five treatments during RSV season,” Dr. Griffin noted. A tweak in the structure of nirsevimab gives it a much longer blood half-life than palivizumab and allows a single dose to maintain efficacy for 5 months, the duration of RSV season.
“The big advantage of nirsevimab is one dose instead of five,” she said in an interview.
The study randomized 969 preterm infants to nirsevimab and 484 to placebo when the children averaged 3 months old and 4.5 kg. The incidence of the primary endpoint was 2.6% in the nirsevimab-treated infants and 9.5% in those who received placebo. The incidence of hospitalizations associated with an RSV lower respiratory tract infection was 0.8% in the nirsevimab group and 4.1% on placebo. Nirsevimab was equally effective regardless of RSV subtype, infant age, or sex. The rate of hypersensitivity reactions was low, less than 1%, and similar in the two treatment arms, as was the rate of detection of antidrug antibody, 3.8% with placebo and 5.6% with nirsevimab.
Two other large trials are underway to document the performance of nirsevimab in other types of infants. One study is examining the drug’s performance compared with placebo in term infants with a gestational age of at least 36 weeks, while another is comparing nirsevimab against a five-dose regimen of palivizumab in high-risk infants who are recommended to receive palivizumab by local medical societies. In the United States, this would be infants born at less than 29 weeks’ gestation, and those with either hemodynamically significant congenital heart disease or chronic lung disease of prematurity. In these studies, the researchers also will assess the cost effectiveness of nirsevimab relative to the costs for medical care needed by infants who receive comparator treatments, Dr. Griffin said.
The study was funded by AstraZeneca, the company developing nirsevimab. Dr. Griffin is an employee of and shareholder in AstraZeneca.
SOURCE: ClinicalTrials.gov identifier: NCT02878330.
REPORTING FROM ID WEEK 2019
Guidelines updated for treating community-acquired pneumonia
An update to the 2007 guidelines on the treatment of community-acquired pneumonia (CAP) was published by two medical societies, based upon the work of a multidisciplinary panel that “conducted pragmatic systematic reviews of the relevant research and applied Grading of Recommendations, Assessment, Development, and Evaluation methodology for clinical recommendations.”

The panel addressed 16 questions in the areas including diagnostic testing, determination of site of care, selection of initial empiric antibiotic therapy, and subsequent management decisions. Some of their recommendations remained unchanged from the 2007 guideline, but others were updated based upon more-recent clinical trials and epidemiological studies, according to Joshua P. Metlay, MD, of Massachusetts General Hospital, Boston, and colleagues on behalf of the Infectious Diseases Society of America and the American Thoracic Society.
Among the key recommendations differing from the previous guidelines, the 2019 guidelines include the following:
- Sputum and blood culture samples are recommended in patients with severe disease, as well as in all inpatients empirically treated for methicillin-resistant Staphylococcus aureus (MRSA) or Pseudomonas aeruginosa.
- Macrolide monotherapy is only conditionally recommended for outpatients based on resistance levels.
- Procalcitonin assessment, not covered in the 2007 guidelines, is not recommended in order to determine initial antibiotic therapy.
- Corticosteroid use, not covered in the 2007 guidelines, is not recommended, though it may be considered in patients with refractory septic shock.
- The use of health care–associated pneumonia (HCAP) as a category should be dropped, with a switch to an emphasis on local epidemiology and validated risk factors to determine the need for MRSA or P. aeruginosa treatment.
- Standard empiric therapy for severe CAP should be beta-lactam/macrolide and beta-lactam/fluoroquinolone combinations, but with stronger evidence in favor of the beta-lactam/macrolide combination.
The updated guidelines also include a number of other recommendations, such as those dealing with the management of patients with comorbidities, and were published in the American Journal of Respiratory and Critical Care Medicine.
“A difference between this guideline and previous ones is that we have significantly increased the proportion of patients in whom we recommend routinely obtaining respiratory tract samples for microbiologic studies. This decision is largely based on a desire to correct the overuse of anti-MRSA and antipseudomonal therapy that has occurred since the introduction of the HCAP classification (which we recommend abandoning) rather than high-quality evidence,” the authors stated in their conclusions. They added that they “expect our move against endorsing monotherapy with macrolides, which is based on population resistance data rather than high-quality clinical studies, will generate future outcomes studies comparing different treatment strategies.”
Many of the authors reported relationships with a variety of pharmaceutical companies; full disclosures are detailed at the end of the guideline publication.
SOURCE: Metlay JP et al. Am J Respir Crit Med. 2019;200(7):e45-67.
“Ever since we wrote the first CAP [community-acquired pneumonia] guidelines in 1993, we’ve heard good and bad things, and I agree with both,” Michael S. Niederman, MD, FCCP, said in a presentation at IDWeek 2019. “For good or for bad, [guidelines] are a standard against which care can be evaluated.” He discussed how, as guidelines have become more evidence based, they have often become “more wishy washy,” that when the evidence is weak, the recommendation is weak, and the guidelines merely advise doctors: “You figure it out.”
However, he pointed out that, since CAP guidelines were developed, there have been overall improvements in patient care and antibiotic stewardship. But he saw several weaknesses in the new guidelines, including the fact that they did not update minor criteria for determining severe CAP from the 2007 guidelines, despite several studies indicating that there were other criteria to consider. In addition, the updated guidelines held a negative view of the use of serum procalcitonin to guide site-of-care decisions, which Dr. Niederman argued went against an analysis of the Etiology of Pneumonia in the Community (EPIC) study (CHEST. 2016; 150[4]:819-28) and other studies that showed its utility. He referred to his own editorial, in which he discussed the subject extensively (Lancet Resp Med. 2016;4[12]:956).
“Similarly, to me, the macrolide issue is not resolved,” he added, citing several studies that, in contrast to the guideline recommendations, used outpatient macrolide monotherapy to good results, and one study showed that “there was a much better patient outcome for patients who got macrolide monotherapy than for those who got quinolones” (Resp Med. 2012;106[3]:451-8).
Dr. Niederman is clinical director of the division of pulmonary and critical care medicine at New York Presbyterian Hospital/Weill Cornell Medical Center, and professor of clinical medicine at Weill Cornell Medical College, New York. He disclosed that he is a consultant for and has received grants from a variety of pharmaceutical companies, including Bayer and Merck.
“Ever since we wrote the first CAP [community-acquired pneumonia] guidelines in 1993, we’ve heard good and bad things, and I agree with both,” Michael S. Niederman, MD, FCCP, said in a presentation at IDWeek 2019. “For good or for bad, [guidelines] are a standard against which care can be evaluated.” He discussed how, as guidelines have become more evidence based, they have often become “more wishy washy,” that when the evidence is weak, the recommendation is weak, and the guidelines merely advise doctors: “You figure it out.”
However, he pointed out that, since CAP guidelines were developed, there have been overall improvements in patient care and antibiotic stewardship. But he saw several weaknesses in the new guidelines, including the fact that they did not update minor criteria for determining severe CAP from the 2007 guidelines, despite several studies indicating that there were other criteria to consider. In addition, the updated guidelines held a negative view of the use of serum procalcitonin to guide site-of-care decisions, which Dr. Niederman argued went against an analysis of the Etiology of Pneumonia in the Community (EPIC) study (CHEST. 2016; 150[4]:819-28) and other studies that showed its utility. He referred to his own editorial, in which he discussed the subject extensively (Lancet Resp Med. 2016;4[12]:956).
“Similarly, to me, the macrolide issue is not resolved,” he added, citing several studies that, in contrast to the guideline recommendations, used outpatient macrolide monotherapy to good results, and one study showed that “there was a much better patient outcome for patients who got macrolide monotherapy than for those who got quinolones” (Resp Med. 2012;106[3]:451-8).
Dr. Niederman is clinical director of the division of pulmonary and critical care medicine at New York Presbyterian Hospital/Weill Cornell Medical Center, and professor of clinical medicine at Weill Cornell Medical College, New York. He disclosed that he is a consultant for and has received grants from a variety of pharmaceutical companies, including Bayer and Merck.
“Ever since we wrote the first CAP [community-acquired pneumonia] guidelines in 1993, we’ve heard good and bad things, and I agree with both,” Michael S. Niederman, MD, FCCP, said in a presentation at IDWeek 2019. “For good or for bad, [guidelines] are a standard against which care can be evaluated.” He discussed how, as guidelines have become more evidence based, they have often become “more wishy washy,” that when the evidence is weak, the recommendation is weak, and the guidelines merely advise doctors: “You figure it out.”
However, he pointed out that, since CAP guidelines were developed, there have been overall improvements in patient care and antibiotic stewardship. But he saw several weaknesses in the new guidelines, including the fact that they did not update minor criteria for determining severe CAP from the 2007 guidelines, despite several studies indicating that there were other criteria to consider. In addition, the updated guidelines held a negative view of the use of serum procalcitonin to guide site-of-care decisions, which Dr. Niederman argued went against an analysis of the Etiology of Pneumonia in the Community (EPIC) study (CHEST. 2016; 150[4]:819-28) and other studies that showed its utility. He referred to his own editorial, in which he discussed the subject extensively (Lancet Resp Med. 2016;4[12]:956).
“Similarly, to me, the macrolide issue is not resolved,” he added, citing several studies that, in contrast to the guideline recommendations, used outpatient macrolide monotherapy to good results, and one study showed that “there was a much better patient outcome for patients who got macrolide monotherapy than for those who got quinolones” (Resp Med. 2012;106[3]:451-8).
Dr. Niederman is clinical director of the division of pulmonary and critical care medicine at New York Presbyterian Hospital/Weill Cornell Medical Center, and professor of clinical medicine at Weill Cornell Medical College, New York. He disclosed that he is a consultant for and has received grants from a variety of pharmaceutical companies, including Bayer and Merck.
An update to the 2007 guidelines on the treatment of community-acquired pneumonia (CAP) was published by two medical societies, based upon the work of a multidisciplinary panel that “conducted pragmatic systematic reviews of the relevant research and applied Grading of Recommendations, Assessment, Development, and Evaluation methodology for clinical recommendations.”
The panel addressed 16 questions in the areas including diagnostic testing, determination of site of care, selection of initial empiric antibiotic therapy, and subsequent management decisions. Some of their recommendations remained unchanged from the 2007 guideline, but others were updated based upon more-recent clinical trials and epidemiological studies, according to Joshua P. Metlay, MD, of Massachusetts General Hospital, Boston, and colleagues on behalf of the Infectious Diseases Society of America and the American Thoracic Society.
Among the key recommendations differing from the previous guidelines, the 2019 guidelines include the following:
- Sputum and blood culture samples are recommended in patients with severe disease, as well as in all inpatients empirically treated for methicillin-resistant Staphylococcus aureus (MRSA) or Pseudomonas aeruginosa.
- Macrolide monotherapy is only conditionally recommended for outpatients based on resistance levels.
- Procalcitonin assessment, not covered in the 2007 guidelines, is not recommended in order to determine initial antibiotic therapy.
- Corticosteroid use, not covered in the 2007 guidelines, is not recommended, though it may be considered in patients with refractory septic shock.
- The use of health care–associated pneumonia (HCAP) as a category should be dropped, with a switch to an emphasis on local epidemiology and validated risk factors to determine the need for MRSA or P. aeruginosa treatment.
- Standard empiric therapy for severe CAP should be beta-lactam/macrolide and beta-lactam/fluoroquinolone combinations, but with stronger evidence in favor of the beta-lactam/macrolide combination.
The updated guidelines also include a number of other recommendations, such as those dealing with the management of patients with comorbidities, and were published in the American Journal of Respiratory and Critical Care Medicine.
“A difference between this guideline and previous ones is that we have significantly increased the proportion of patients in whom we recommend routinely obtaining respiratory tract samples for microbiologic studies. This decision is largely based on a desire to correct the overuse of anti-MRSA and antipseudomonal therapy that has occurred since the introduction of the HCAP classification (which we recommend abandoning) rather than high-quality evidence,” the authors stated in their conclusions. They added that they “expect our move against endorsing monotherapy with macrolides, which is based on population resistance data rather than high-quality clinical studies, will generate future outcomes studies comparing different treatment strategies.”
Many of the authors reported relationships with a variety of pharmaceutical companies; full disclosures are detailed at the end of the guideline publication.
SOURCE: Metlay JP et al. Am J Respir Crit Med. 2019;200(7):e45-67.
An update to the 2007 guidelines on the treatment of community-acquired pneumonia (CAP) was published by two medical societies, based upon the work of a multidisciplinary panel that “conducted pragmatic systematic reviews of the relevant research and applied Grading of Recommendations, Assessment, Development, and Evaluation methodology for clinical recommendations.”
The panel addressed 16 questions in the areas including diagnostic testing, determination of site of care, selection of initial empiric antibiotic therapy, and subsequent management decisions. Some of their recommendations remained unchanged from the 2007 guideline, but others were updated based upon more-recent clinical trials and epidemiological studies, according to Joshua P. Metlay, MD, of Massachusetts General Hospital, Boston, and colleagues on behalf of the Infectious Diseases Society of America and the American Thoracic Society.
Among the key recommendations differing from the previous guidelines, the 2019 guidelines include the following:
- Sputum and blood culture samples are recommended in patients with severe disease, as well as in all inpatients empirically treated for methicillin-resistant Staphylococcus aureus (MRSA) or Pseudomonas aeruginosa.
- Macrolide monotherapy is only conditionally recommended for outpatients based on resistance levels.
- Procalcitonin assessment, not covered in the 2007 guidelines, is not recommended in order to determine initial antibiotic therapy.
- Corticosteroid use, not covered in the 2007 guidelines, is not recommended, though it may be considered in patients with refractory septic shock.
- The use of health care–associated pneumonia (HCAP) as a category should be dropped, with a switch to an emphasis on local epidemiology and validated risk factors to determine the need for MRSA or P. aeruginosa treatment.
- Standard empiric therapy for severe CAP should be beta-lactam/macrolide and beta-lactam/fluoroquinolone combinations, but with stronger evidence in favor of the beta-lactam/macrolide combination.
The updated guidelines also include a number of other recommendations, such as those dealing with the management of patients with comorbidities, and were published in the American Journal of Respiratory and Critical Care Medicine.
“A difference between this guideline and previous ones is that we have significantly increased the proportion of patients in whom we recommend routinely obtaining respiratory tract samples for microbiologic studies. This decision is largely based on a desire to correct the overuse of anti-MRSA and antipseudomonal therapy that has occurred since the introduction of the HCAP classification (which we recommend abandoning) rather than high-quality evidence,” the authors stated in their conclusions. They added that they “expect our move against endorsing monotherapy with macrolides, which is based on population resistance data rather than high-quality clinical studies, will generate future outcomes studies comparing different treatment strategies.”
Many of the authors reported relationships with a variety of pharmaceutical companies; full disclosures are detailed at the end of the guideline publication.
SOURCE: Metlay JP et al. Am J Respir Crit Med. 2019;200(7):e45-67.
FROM THE AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
Amoxicillin/clavulanate emerges as best antibiotic for childhood bronchiectasis
MADRID – A placebo-controlled trial has confirmed that amoxicillin/clavulanate is beneficial for resolution of acute exacerbations in nonsevere bronchiectasis while also demonstrating a greater relative effect than azithromycin, based on data presented at the annual congress of the European Respiratory Society.

“We now have robust data with which to support our guidelines,” reported Vikas Goyal, MD, of the Children’s Health Clinical Unit, University of Queensland, Brisbane, Australia.
The study addresses a knowledge gap. Antibiotics are already recommended by many guidelines for treatment of acute exacerbations in children with bronchiectasis, but Dr. Goyal said that no controlled trials have ever been performed in this age group to confirm superiority to placebo.
In this multicenter study, called BEST-1, 197 children with bronchiectasis were randomized at the start of an exacerbation to placebo, 45 mg/kg per day of amoxicillin/clavulanate, or 5 mg/kg per day of azithromycin. To maintain blinding, patients in the active treatment groups received a dummy for the opposite antibiotic while patients on placebo received dummies for both active agents.
For the primary outcome, 65% of children randomized to amoxicillin/clavulanate had resolution of their exacerbation by day 14 versus 61% of those randomized to azithromycin and 43% of those randomized to placebo. On the basis of relative risk for reaching this end point, the outcome was superior to placebo for amoxicillin/clavulanate (RR, 1.5; P = .015).
Although the relative risk for azithromycin (RR, 1.4; P = .042) was only slightly lower, it did not reach a prespecified level of significance set at P = .025. Dr. Goyal did report that the resolution rate at 14 days in the placebo group was “higher than expected.”
In this trial, 53% of the 154 children who were tested for respiratory viruses with nasal swabs on day 1 of the exacerbation were found to have respiratory viruses. Of these viruses, rhinovirus was the most common, according to Dr. Goyal, whose data were published just prior to his presentation (Lancet Respir Med. 2019;7:791-801).
The median durations of the exacerbations were 7 days, 8 days, and 10 days for those treated with amoxicillin/clavulanate, azithromycin, and placebo, respectively. The difference between amoxicillin/clavulanate and placebo, but not that between azithromycin and placebo, reached statistical significance, Dr. Goyal said.
There were no between group differences in the time to next exacerbation.
In discussing limitations of this study, Dr. Goyal pointed out that the optimal doses of amoxicillin/clavulanate or azithromycin have never been established for the treatment of exacerbations in children with bronchiectasis. He noted that some infectious disease specialists have advocated higher doses of both than those employed in this trial, but dose-ranging studies have never been conducted in this age group.
In this study, adverse events were less common on azithromycin than amoxicillin/clavulanate (21% vs. 30%), but none were severe, according to Dr. Goyal. He said treatment with azithromycin was associated with increased macrolide-resistant bacteria.
On the basis of these data, Dr. Goyal concluded that amoxicillin/clavulanate should remain, as already specified in some guidelines, the standard first-line therapy for nonsevere exacerbations in nonhospitalized children with bronchiectasis. He recommended reserving azithromycin as an alternative therapy.
Dr. Goyal reports no potential conflicts of interest.
SOURCE: Goyal V et al. Lancet Respir Med. 2019;7:791-801.
MADRID – A placebo-controlled trial has confirmed that amoxicillin/clavulanate is beneficial for resolution of acute exacerbations in nonsevere bronchiectasis while also demonstrating a greater relative effect than azithromycin, based on data presented at the annual congress of the European Respiratory Society.
“We now have robust data with which to support our guidelines,” reported Vikas Goyal, MD, of the Children’s Health Clinical Unit, University of Queensland, Brisbane, Australia.
The study addresses a knowledge gap. Antibiotics are already recommended by many guidelines for treatment of acute exacerbations in children with bronchiectasis, but Dr. Goyal said that no controlled trials have ever been performed in this age group to confirm superiority to placebo.
In this multicenter study, called BEST-1, 197 children with bronchiectasis were randomized at the start of an exacerbation to placebo, 45 mg/kg per day of amoxicillin/clavulanate, or 5 mg/kg per day of azithromycin. To maintain blinding, patients in the active treatment groups received a dummy for the opposite antibiotic while patients on placebo received dummies for both active agents.
For the primary outcome, 65% of children randomized to amoxicillin/clavulanate had resolution of their exacerbation by day 14 versus 61% of those randomized to azithromycin and 43% of those randomized to placebo. On the basis of relative risk for reaching this end point, the outcome was superior to placebo for amoxicillin/clavulanate (RR, 1.5; P = .015).
Although the relative risk for azithromycin (RR, 1.4; P = .042) was only slightly lower, it did not reach a prespecified level of significance set at P = .025. Dr. Goyal did report that the resolution rate at 14 days in the placebo group was “higher than expected.”
In this trial, 53% of the 154 children who were tested for respiratory viruses with nasal swabs on day 1 of the exacerbation were found to have respiratory viruses. Of these viruses, rhinovirus was the most common, according to Dr. Goyal, whose data were published just prior to his presentation (Lancet Respir Med. 2019;7:791-801).
The median durations of the exacerbations were 7 days, 8 days, and 10 days for those treated with amoxicillin/clavulanate, azithromycin, and placebo, respectively. The difference between amoxicillin/clavulanate and placebo, but not that between azithromycin and placebo, reached statistical significance, Dr. Goyal said.
There were no between group differences in the time to next exacerbation.
In discussing limitations of this study, Dr. Goyal pointed out that the optimal doses of amoxicillin/clavulanate or azithromycin have never been established for the treatment of exacerbations in children with bronchiectasis. He noted that some infectious disease specialists have advocated higher doses of both than those employed in this trial, but dose-ranging studies have never been conducted in this age group.
In this study, adverse events were less common on azithromycin than amoxicillin/clavulanate (21% vs. 30%), but none were severe, according to Dr. Goyal. He said treatment with azithromycin was associated with increased macrolide-resistant bacteria.
On the basis of these data, Dr. Goyal concluded that amoxicillin/clavulanate should remain, as already specified in some guidelines, the standard first-line therapy for nonsevere exacerbations in nonhospitalized children with bronchiectasis. He recommended reserving azithromycin as an alternative therapy.
Dr. Goyal reports no potential conflicts of interest.
SOURCE: Goyal V et al. Lancet Respir Med. 2019;7:791-801.
MADRID – A placebo-controlled trial has confirmed that amoxicillin/clavulanate is beneficial for resolution of acute exacerbations in nonsevere bronchiectasis while also demonstrating a greater relative effect than azithromycin, based on data presented at the annual congress of the European Respiratory Society.
“We now have robust data with which to support our guidelines,” reported Vikas Goyal, MD, of the Children’s Health Clinical Unit, University of Queensland, Brisbane, Australia.
The study addresses a knowledge gap. Antibiotics are already recommended by many guidelines for treatment of acute exacerbations in children with bronchiectasis, but Dr. Goyal said that no controlled trials have ever been performed in this age group to confirm superiority to placebo.
In this multicenter study, called BEST-1, 197 children with bronchiectasis were randomized at the start of an exacerbation to placebo, 45 mg/kg per day of amoxicillin/clavulanate, or 5 mg/kg per day of azithromycin. To maintain blinding, patients in the active treatment groups received a dummy for the opposite antibiotic while patients on placebo received dummies for both active agents.
For the primary outcome, 65% of children randomized to amoxicillin/clavulanate had resolution of their exacerbation by day 14 versus 61% of those randomized to azithromycin and 43% of those randomized to placebo. On the basis of relative risk for reaching this end point, the outcome was superior to placebo for amoxicillin/clavulanate (RR, 1.5; P = .015).
Although the relative risk for azithromycin (RR, 1.4; P = .042) was only slightly lower, it did not reach a prespecified level of significance set at P = .025. Dr. Goyal did report that the resolution rate at 14 days in the placebo group was “higher than expected.”
In this trial, 53% of the 154 children who were tested for respiratory viruses with nasal swabs on day 1 of the exacerbation were found to have respiratory viruses. Of these viruses, rhinovirus was the most common, according to Dr. Goyal, whose data were published just prior to his presentation (Lancet Respir Med. 2019;7:791-801).
The median durations of the exacerbations were 7 days, 8 days, and 10 days for those treated with amoxicillin/clavulanate, azithromycin, and placebo, respectively. The difference between amoxicillin/clavulanate and placebo, but not that between azithromycin and placebo, reached statistical significance, Dr. Goyal said.
There were no between group differences in the time to next exacerbation.
In discussing limitations of this study, Dr. Goyal pointed out that the optimal doses of amoxicillin/clavulanate or azithromycin have never been established for the treatment of exacerbations in children with bronchiectasis. He noted that some infectious disease specialists have advocated higher doses of both than those employed in this trial, but dose-ranging studies have never been conducted in this age group.
In this study, adverse events were less common on azithromycin than amoxicillin/clavulanate (21% vs. 30%), but none were severe, according to Dr. Goyal. He said treatment with azithromycin was associated with increased macrolide-resistant bacteria.
On the basis of these data, Dr. Goyal concluded that amoxicillin/clavulanate should remain, as already specified in some guidelines, the standard first-line therapy for nonsevere exacerbations in nonhospitalized children with bronchiectasis. He recommended reserving azithromycin as an alternative therapy.
Dr. Goyal reports no potential conflicts of interest.
SOURCE: Goyal V et al. Lancet Respir Med. 2019;7:791-801.
REPORTING FROM ERS 2019
Physician: The nicotine, not the flavors, needs regulation
While most of the recent legislative action on e-cigarettes and other electronic nicotine delivery systems are focusing on the flavors that are appealing, especially to children,
Michael B. Siegel, MD, MPH, a physician and professor at Boston University School of Public Health, said the turning point in the spike in youth e-cigarettes occurred when products like Juul, Sourin, Smok, and Phix were introduced into the market.
Prior to that, he noted that, in 2014, citing that year’s National Youth Tobacco Survey from the Centers for Disease Control and Prevention, 74% of nonsmoking youth e-cigarette users reported using e-cigarettes no more than once per week, while only 4% reported daily use. By 2018, 12% of nonsmoking youth e-cigarette users were using e-cigarettes daily, while 42% of nonsmoking e-cigarette use was no more than once a week, according to that year’s CDC survey.
“All of these brands use a different nicotine formulation from virtually all other e-cigarettes,” Dr. Siegel testified Oct. 16 at a House Energy and Commerce Health Subcommittee hearing. “They use a nicotine salt at very high concentrations.”
His written testimony notes that Juul and similar products use nicotine salt at concentrations of 50 mg/mL, whereas most other e-cigarette products have nicotine concentrations that are less than 25 mg/mL.
“The use of nicotine salts allows nicotine to be absorbed into the bloodstream much more quickly, simulating the pattern you get with a real cigarette,” he continued. “That is why so many youth are now addicted to vaping. It is not the flavors. It’s the nicotine.”
Susanne Tanski, MD, testifying on behalf of the American Academy of Pediatrics agreed with Dr. Siegel that the Food and Drug Administration needs to be doing more to regulate the amount of nicotine that these products are releasing and that the introduction of nicotine salt was a significant cause of addiction.
However, she also targeted flavors as a key issue.
“There is reasonable concern that flavors may also modify the addictiveness of e-cigarettes, but with the thousands of flavor combinations on the market, there has not been specific research yet to test this hypothesis,” Dr. Tanksi, a pediatrician at Dartmouth-Hitchcock Medical Center in Lebanon, N.H., noted in her written testimony. “We know that flavors unto themselves are pleasurable. If you link a pleasurable flavor with a buzz of nicotine from a powerful nicotine delivery system such as the newer e-cigarettes, perhaps this is even more behaviorally and biologically reinforcing to drive the addictiveness of this new generation of products.”
Other panelists also expressed concern about the flavoring of e-cigarettes.
Subcommittee Chair Anna Eshoo (D-Calif.) noted that “flavor is very attractive. It really drives our eating habits and other habits.” She then asked whether “e-cigarettes’ sweet flavors have contributed to youth tobacco use.”
Matthew L. Myers, president of the Campaign for Tobacco-Free Kids, responded by saying that all “of the evidence is that they are the driving force of that and that it has gotten worse over the last 4 years.”
He also noted that while youth use of flavored products has spiked in the last 4 years, there really has not been any growth in adult usage of flavored tobacco.
“What it shows is the introduction of all these flavors has fueled a youth epidemic, but it has had no impact whatsoever” on adults. “Indeed, before Juul was introduced, the most popular e-cigarette flavor was tobacco. So, for smokers who want to quit, that was a viable option until Juul changed the market.”
The subcommittee hearing was held to solicit opinions on H.R. 2339, the “Reversing the Youth Tobacco Epidemic Act of 2019.” Among the provisions in the bill are raising the minimum age of purchasing all tobacco and nicotine products to age 21 years, requiring health warning labels on e-cigarette products, placing restrictions on advertising that are similar to those on smoking products, and prohibiting Internet sales of e-cigarettes.
Dr. Siegel voiced his approval for the bill, providing the provision that bans all flavored tobacco products was removed.
He noted that the current epidemic of vaping illness and deaths recently has not been caused primarily from legit e-cigarette and other vaping products, but rather from black market, THC-laced vaping cartridges.
“A ban on flavored e-cigarettes would create a public health disaster because it would create a new black market for flavored e-liquids,” he testified. “It is nearly certain that we would see more outbreaks similar to what we are seeing now with these tainted THC vape cartridges.”
He continued: “Banning flavored e-liquids is not going to do anything to curtail this respiratory disease outbreak, but it may make the outbreak worse. Why? Because the supply of e-liquids that youth are vaping is going to transition from one dominated by nicotine products to one dominated by THC products, exactly the products that are causing this outbreak.”
Dr. Siegel also spoke to the potential effect it might have on adult smokers who have abandoned combustible tobacco products in favor of e-cigarettes.
“More than 2 million adult smokers in the U.S. have quit smoking completely by switching to flavored electronic cigarettes,” he said. “If these products are banned, many of these ex-smokers will return to cigarette smoking. Most of those who don’t will turn to a new potentially dangerous black market that will be created by this legislation.”
Dr. Tanski, on the other hand, called the provision banning all flavored tobacco products, including menthol, “the single most important policy that Congress can pass to address the youth tobacco epidemic, and a step that Congress took years ago for other flavored cigarettes.”
While most of the recent legislative action on e-cigarettes and other electronic nicotine delivery systems are focusing on the flavors that are appealing, especially to children,
Michael B. Siegel, MD, MPH, a physician and professor at Boston University School of Public Health, said the turning point in the spike in youth e-cigarettes occurred when products like Juul, Sourin, Smok, and Phix were introduced into the market.
Prior to that, he noted that, in 2014, citing that year’s National Youth Tobacco Survey from the Centers for Disease Control and Prevention, 74% of nonsmoking youth e-cigarette users reported using e-cigarettes no more than once per week, while only 4% reported daily use. By 2018, 12% of nonsmoking youth e-cigarette users were using e-cigarettes daily, while 42% of nonsmoking e-cigarette use was no more than once a week, according to that year’s CDC survey.
“All of these brands use a different nicotine formulation from virtually all other e-cigarettes,” Dr. Siegel testified Oct. 16 at a House Energy and Commerce Health Subcommittee hearing. “They use a nicotine salt at very high concentrations.”
His written testimony notes that Juul and similar products use nicotine salt at concentrations of 50 mg/mL, whereas most other e-cigarette products have nicotine concentrations that are less than 25 mg/mL.
“The use of nicotine salts allows nicotine to be absorbed into the bloodstream much more quickly, simulating the pattern you get with a real cigarette,” he continued. “That is why so many youth are now addicted to vaping. It is not the flavors. It’s the nicotine.”
Susanne Tanski, MD, testifying on behalf of the American Academy of Pediatrics agreed with Dr. Siegel that the Food and Drug Administration needs to be doing more to regulate the amount of nicotine that these products are releasing and that the introduction of nicotine salt was a significant cause of addiction.
However, she also targeted flavors as a key issue.
“There is reasonable concern that flavors may also modify the addictiveness of e-cigarettes, but with the thousands of flavor combinations on the market, there has not been specific research yet to test this hypothesis,” Dr. Tanksi, a pediatrician at Dartmouth-Hitchcock Medical Center in Lebanon, N.H., noted in her written testimony. “We know that flavors unto themselves are pleasurable. If you link a pleasurable flavor with a buzz of nicotine from a powerful nicotine delivery system such as the newer e-cigarettes, perhaps this is even more behaviorally and biologically reinforcing to drive the addictiveness of this new generation of products.”
Other panelists also expressed concern about the flavoring of e-cigarettes.
Subcommittee Chair Anna Eshoo (D-Calif.) noted that “flavor is very attractive. It really drives our eating habits and other habits.” She then asked whether “e-cigarettes’ sweet flavors have contributed to youth tobacco use.”
Matthew L. Myers, president of the Campaign for Tobacco-Free Kids, responded by saying that all “of the evidence is that they are the driving force of that and that it has gotten worse over the last 4 years.”
He also noted that while youth use of flavored products has spiked in the last 4 years, there really has not been any growth in adult usage of flavored tobacco.
“What it shows is the introduction of all these flavors has fueled a youth epidemic, but it has had no impact whatsoever” on adults. “Indeed, before Juul was introduced, the most popular e-cigarette flavor was tobacco. So, for smokers who want to quit, that was a viable option until Juul changed the market.”
The subcommittee hearing was held to solicit opinions on H.R. 2339, the “Reversing the Youth Tobacco Epidemic Act of 2019.” Among the provisions in the bill are raising the minimum age of purchasing all tobacco and nicotine products to age 21 years, requiring health warning labels on e-cigarette products, placing restrictions on advertising that are similar to those on smoking products, and prohibiting Internet sales of e-cigarettes.
Dr. Siegel voiced his approval for the bill, providing the provision that bans all flavored tobacco products was removed.
He noted that the current epidemic of vaping illness and deaths recently has not been caused primarily from legit e-cigarette and other vaping products, but rather from black market, THC-laced vaping cartridges.
“A ban on flavored e-cigarettes would create a public health disaster because it would create a new black market for flavored e-liquids,” he testified. “It is nearly certain that we would see more outbreaks similar to what we are seeing now with these tainted THC vape cartridges.”
He continued: “Banning flavored e-liquids is not going to do anything to curtail this respiratory disease outbreak, but it may make the outbreak worse. Why? Because the supply of e-liquids that youth are vaping is going to transition from one dominated by nicotine products to one dominated by THC products, exactly the products that are causing this outbreak.”
Dr. Siegel also spoke to the potential effect it might have on adult smokers who have abandoned combustible tobacco products in favor of e-cigarettes.
“More than 2 million adult smokers in the U.S. have quit smoking completely by switching to flavored electronic cigarettes,” he said. “If these products are banned, many of these ex-smokers will return to cigarette smoking. Most of those who don’t will turn to a new potentially dangerous black market that will be created by this legislation.”
Dr. Tanski, on the other hand, called the provision banning all flavored tobacco products, including menthol, “the single most important policy that Congress can pass to address the youth tobacco epidemic, and a step that Congress took years ago for other flavored cigarettes.”
While most of the recent legislative action on e-cigarettes and other electronic nicotine delivery systems are focusing on the flavors that are appealing, especially to children,
Michael B. Siegel, MD, MPH, a physician and professor at Boston University School of Public Health, said the turning point in the spike in youth e-cigarettes occurred when products like Juul, Sourin, Smok, and Phix were introduced into the market.
Prior to that, he noted that, in 2014, citing that year’s National Youth Tobacco Survey from the Centers for Disease Control and Prevention, 74% of nonsmoking youth e-cigarette users reported using e-cigarettes no more than once per week, while only 4% reported daily use. By 2018, 12% of nonsmoking youth e-cigarette users were using e-cigarettes daily, while 42% of nonsmoking e-cigarette use was no more than once a week, according to that year’s CDC survey.
“All of these brands use a different nicotine formulation from virtually all other e-cigarettes,” Dr. Siegel testified Oct. 16 at a House Energy and Commerce Health Subcommittee hearing. “They use a nicotine salt at very high concentrations.”
His written testimony notes that Juul and similar products use nicotine salt at concentrations of 50 mg/mL, whereas most other e-cigarette products have nicotine concentrations that are less than 25 mg/mL.
“The use of nicotine salts allows nicotine to be absorbed into the bloodstream much more quickly, simulating the pattern you get with a real cigarette,” he continued. “That is why so many youth are now addicted to vaping. It is not the flavors. It’s the nicotine.”
Susanne Tanski, MD, testifying on behalf of the American Academy of Pediatrics agreed with Dr. Siegel that the Food and Drug Administration needs to be doing more to regulate the amount of nicotine that these products are releasing and that the introduction of nicotine salt was a significant cause of addiction.
However, she also targeted flavors as a key issue.
“There is reasonable concern that flavors may also modify the addictiveness of e-cigarettes, but with the thousands of flavor combinations on the market, there has not been specific research yet to test this hypothesis,” Dr. Tanksi, a pediatrician at Dartmouth-Hitchcock Medical Center in Lebanon, N.H., noted in her written testimony. “We know that flavors unto themselves are pleasurable. If you link a pleasurable flavor with a buzz of nicotine from a powerful nicotine delivery system such as the newer e-cigarettes, perhaps this is even more behaviorally and biologically reinforcing to drive the addictiveness of this new generation of products.”
Other panelists also expressed concern about the flavoring of e-cigarettes.
Subcommittee Chair Anna Eshoo (D-Calif.) noted that “flavor is very attractive. It really drives our eating habits and other habits.” She then asked whether “e-cigarettes’ sweet flavors have contributed to youth tobacco use.”
Matthew L. Myers, president of the Campaign for Tobacco-Free Kids, responded by saying that all “of the evidence is that they are the driving force of that and that it has gotten worse over the last 4 years.”
He also noted that while youth use of flavored products has spiked in the last 4 years, there really has not been any growth in adult usage of flavored tobacco.
“What it shows is the introduction of all these flavors has fueled a youth epidemic, but it has had no impact whatsoever” on adults. “Indeed, before Juul was introduced, the most popular e-cigarette flavor was tobacco. So, for smokers who want to quit, that was a viable option until Juul changed the market.”
The subcommittee hearing was held to solicit opinions on H.R. 2339, the “Reversing the Youth Tobacco Epidemic Act of 2019.” Among the provisions in the bill are raising the minimum age of purchasing all tobacco and nicotine products to age 21 years, requiring health warning labels on e-cigarette products, placing restrictions on advertising that are similar to those on smoking products, and prohibiting Internet sales of e-cigarettes.
Dr. Siegel voiced his approval for the bill, providing the provision that bans all flavored tobacco products was removed.
He noted that the current epidemic of vaping illness and deaths recently has not been caused primarily from legit e-cigarette and other vaping products, but rather from black market, THC-laced vaping cartridges.
“A ban on flavored e-cigarettes would create a public health disaster because it would create a new black market for flavored e-liquids,” he testified. “It is nearly certain that we would see more outbreaks similar to what we are seeing now with these tainted THC vape cartridges.”
He continued: “Banning flavored e-liquids is not going to do anything to curtail this respiratory disease outbreak, but it may make the outbreak worse. Why? Because the supply of e-liquids that youth are vaping is going to transition from one dominated by nicotine products to one dominated by THC products, exactly the products that are causing this outbreak.”
Dr. Siegel also spoke to the potential effect it might have on adult smokers who have abandoned combustible tobacco products in favor of e-cigarettes.
“More than 2 million adult smokers in the U.S. have quit smoking completely by switching to flavored electronic cigarettes,” he said. “If these products are banned, many of these ex-smokers will return to cigarette smoking. Most of those who don’t will turn to a new potentially dangerous black market that will be created by this legislation.”
Dr. Tanski, on the other hand, called the provision banning all flavored tobacco products, including menthol, “the single most important policy that Congress can pass to address the youth tobacco epidemic, and a step that Congress took years ago for other flavored cigarettes.”
REPORTING FROM A HOUSE ENERGY AND COMMERCE HEALTH SUBCOMMITTEE HEARING
Vaping-linked lung injuries near 1,500
according to the latest update provided by the Centers for Disease Control and Prevention. Thirty-three deaths have been confirmed.

E-cigarette–linked lung injuries, now called EVALI, occurred in all U.S. states (except Alaska), the District of Columbia, and the U.S. Virgin Islands. Seventy percent of patients are male, and 79% are under age 35 years.
Information on the substances used over the previous 3 months before symptom onset was available for 849 patients and included the following:
- 78% reported using THC-containing products, with or without nicotine-containing products;
- 31% reported exclusive use of THC-containing products;
- 58% reported using nicotine-containing products, with or without THC-containing products; and
- 10% reported exclusive use of nicotine-containing products.
CDC is now doing additional testing on available samples for chemical in the bronchoalveolar lavage fluid, blood, or urine, as well as lung biopsy or autopsy specimens. CDC is also validating methods for aerosol emission testing of case-associated product samples from vaping products and e-liquids.
In a related development, JUUL, maker of e-cigarette products, has announced that it will suspend the sale of nontobacco, nonmenthol flavors (mango, creme, fruit, and cucumber) in the United States, pending review by the Food and Drug Administration. The JUUL announcement comes in advance of an expected FDA ban on flavored e-cigarettes.
The CDC continues its investigation into EVALI but stated, “Since the specific cause or causes of lung injury are not yet known, the only way to assure that you are not at risk while the investigation continues is to consider refraining from use of all e-cigarette, or vaping, products.”
For more information and resources visit For the Public, For Healthcare Providers, and For State and Local Health Departments pages, as well as the CDC’s Publications and Resources page.
according to the latest update provided by the Centers for Disease Control and Prevention. Thirty-three deaths have been confirmed.
E-cigarette–linked lung injuries, now called EVALI, occurred in all U.S. states (except Alaska), the District of Columbia, and the U.S. Virgin Islands. Seventy percent of patients are male, and 79% are under age 35 years.
Information on the substances used over the previous 3 months before symptom onset was available for 849 patients and included the following:
- 78% reported using THC-containing products, with or without nicotine-containing products;
- 31% reported exclusive use of THC-containing products;
- 58% reported using nicotine-containing products, with or without THC-containing products; and
- 10% reported exclusive use of nicotine-containing products.
CDC is now doing additional testing on available samples for chemical in the bronchoalveolar lavage fluid, blood, or urine, as well as lung biopsy or autopsy specimens. CDC is also validating methods for aerosol emission testing of case-associated product samples from vaping products and e-liquids.
In a related development, JUUL, maker of e-cigarette products, has announced that it will suspend the sale of nontobacco, nonmenthol flavors (mango, creme, fruit, and cucumber) in the United States, pending review by the Food and Drug Administration. The JUUL announcement comes in advance of an expected FDA ban on flavored e-cigarettes.
The CDC continues its investigation into EVALI but stated, “Since the specific cause or causes of lung injury are not yet known, the only way to assure that you are not at risk while the investigation continues is to consider refraining from use of all e-cigarette, or vaping, products.”
For more information and resources visit For the Public, For Healthcare Providers, and For State and Local Health Departments pages, as well as the CDC’s Publications and Resources page.
according to the latest update provided by the Centers for Disease Control and Prevention. Thirty-three deaths have been confirmed.
E-cigarette–linked lung injuries, now called EVALI, occurred in all U.S. states (except Alaska), the District of Columbia, and the U.S. Virgin Islands. Seventy percent of patients are male, and 79% are under age 35 years.
Information on the substances used over the previous 3 months before symptom onset was available for 849 patients and included the following:
- 78% reported using THC-containing products, with or without nicotine-containing products;
- 31% reported exclusive use of THC-containing products;
- 58% reported using nicotine-containing products, with or without THC-containing products; and
- 10% reported exclusive use of nicotine-containing products.
CDC is now doing additional testing on available samples for chemical in the bronchoalveolar lavage fluid, blood, or urine, as well as lung biopsy or autopsy specimens. CDC is also validating methods for aerosol emission testing of case-associated product samples from vaping products and e-liquids.
In a related development, JUUL, maker of e-cigarette products, has announced that it will suspend the sale of nontobacco, nonmenthol flavors (mango, creme, fruit, and cucumber) in the United States, pending review by the Food and Drug Administration. The JUUL announcement comes in advance of an expected FDA ban on flavored e-cigarettes.
The CDC continues its investigation into EVALI but stated, “Since the specific cause or causes of lung injury are not yet known, the only way to assure that you are not at risk while the investigation continues is to consider refraining from use of all e-cigarette, or vaping, products.”
For more information and resources visit For the Public, For Healthcare Providers, and For State and Local Health Departments pages, as well as the CDC’s Publications and Resources page.
No clear benefit from conservative oxygen in mechanical ventilation
More conservative oxygen therapy during mechanical ventilation in intensive care does not appear to increase the number of ventilator-free days or reduce mortality, according to a study published online in the New England Journal of Medicine.
Diane Mackle of the Medical Research Institute of New Zealand and her co-authors wrote that hyperoxemia in adults undergoing mechanical ventilation has been associated with increased mortality, as well as fewer days free of ventilation, but there was a lack of data to guide oxygen administration.
In a parallel-group trial, 1,000 adults who were expected to require mechanical ventilation – with an intention-to-treat population of 965 – were randomized either to conservative oxygen therapy or usual therapy. For the conservative therapy, the upper limit of the pulse oximetry alarm would sound when levels reached 97% and the F102 was decreased to 0.21 if the pulse oximetry was above the acceptable lower limit, while usual therapy involved no specific limiting measures. In both groups, the default lower limit for oxygen saturation was 90%.
At day 28 after ventilation, there was no significant difference between the conservative and usual care groups in the number of ventilator-free days (21.3 days vs. 22.1 days). The patients in the conservative oxygen group spent a median of 29 hours receiving an F102 level of 0.21, compared with 1 hour in the usual care group.
The mortality rate at day 180 was 35.7% in the conservative oxygen group, and 34.5% in the usual-oxygen group (HR 1.05, 95% CI 0.85 – 1.30). Researchers also saw no differences between the two groups in paid employment and cognitive function.
In patients with suspected hypoxic-ischemic encephalopathy between-group differences were apparent; At day 28, those in the conservative-oxygen group had a median of 21.1 ventilator-free days, compared with none in the usual-oxygen group. The usual-oxygen group also had a higher 180-day mortality rate than those in the conservative-oxygen group (43% vs. 59%).
“Our data are suggestive of a possible benefit of conservative oxygen therapy in patients with suspected hypoxic-ischemic encephalopathy,” the authors wrote. “It is biologically plausible that conservative oxygen therapy reduces the incidence of secondary brain damage after resuscitation from cardiac arrest, and observational data suggest that exposure to hyperoxemia in such patients may be harmful.”
The authors noted that their trial did not rule out the possibility of benefit or harm had they used a more liberal oxygen regimen in their usual-care group, and that different conservative regimens might also have achieved different outcomes.
The study was funded by the New Zealand Health Research Council. Six authors declared research support for the trial from the study funder, and two declared unrelated research grants from private industry. No other conflicts of interest were declared.
SOURCE: Mackle D et al. NJEM 2019, October 14. DOI:10.1056/NEJMoa1903297.
More conservative oxygen therapy during mechanical ventilation in intensive care does not appear to increase the number of ventilator-free days or reduce mortality, according to a study published online in the New England Journal of Medicine.
Diane Mackle of the Medical Research Institute of New Zealand and her co-authors wrote that hyperoxemia in adults undergoing mechanical ventilation has been associated with increased mortality, as well as fewer days free of ventilation, but there was a lack of data to guide oxygen administration.
In a parallel-group trial, 1,000 adults who were expected to require mechanical ventilation – with an intention-to-treat population of 965 – were randomized either to conservative oxygen therapy or usual therapy. For the conservative therapy, the upper limit of the pulse oximetry alarm would sound when levels reached 97% and the F102 was decreased to 0.21 if the pulse oximetry was above the acceptable lower limit, while usual therapy involved no specific limiting measures. In both groups, the default lower limit for oxygen saturation was 90%.
At day 28 after ventilation, there was no significant difference between the conservative and usual care groups in the number of ventilator-free days (21.3 days vs. 22.1 days). The patients in the conservative oxygen group spent a median of 29 hours receiving an F102 level of 0.21, compared with 1 hour in the usual care group.
The mortality rate at day 180 was 35.7% in the conservative oxygen group, and 34.5% in the usual-oxygen group (HR 1.05, 95% CI 0.85 – 1.30). Researchers also saw no differences between the two groups in paid employment and cognitive function.
In patients with suspected hypoxic-ischemic encephalopathy between-group differences were apparent; At day 28, those in the conservative-oxygen group had a median of 21.1 ventilator-free days, compared with none in the usual-oxygen group. The usual-oxygen group also had a higher 180-day mortality rate than those in the conservative-oxygen group (43% vs. 59%).
“Our data are suggestive of a possible benefit of conservative oxygen therapy in patients with suspected hypoxic-ischemic encephalopathy,” the authors wrote. “It is biologically plausible that conservative oxygen therapy reduces the incidence of secondary brain damage after resuscitation from cardiac arrest, and observational data suggest that exposure to hyperoxemia in such patients may be harmful.”
The authors noted that their trial did not rule out the possibility of benefit or harm had they used a more liberal oxygen regimen in their usual-care group, and that different conservative regimens might also have achieved different outcomes.
The study was funded by the New Zealand Health Research Council. Six authors declared research support for the trial from the study funder, and two declared unrelated research grants from private industry. No other conflicts of interest were declared.
SOURCE: Mackle D et al. NJEM 2019, October 14. DOI:10.1056/NEJMoa1903297.
More conservative oxygen therapy during mechanical ventilation in intensive care does not appear to increase the number of ventilator-free days or reduce mortality, according to a study published online in the New England Journal of Medicine.
Diane Mackle of the Medical Research Institute of New Zealand and her co-authors wrote that hyperoxemia in adults undergoing mechanical ventilation has been associated with increased mortality, as well as fewer days free of ventilation, but there was a lack of data to guide oxygen administration.
In a parallel-group trial, 1,000 adults who were expected to require mechanical ventilation – with an intention-to-treat population of 965 – were randomized either to conservative oxygen therapy or usual therapy. For the conservative therapy, the upper limit of the pulse oximetry alarm would sound when levels reached 97% and the F102 was decreased to 0.21 if the pulse oximetry was above the acceptable lower limit, while usual therapy involved no specific limiting measures. In both groups, the default lower limit for oxygen saturation was 90%.
At day 28 after ventilation, there was no significant difference between the conservative and usual care groups in the number of ventilator-free days (21.3 days vs. 22.1 days). The patients in the conservative oxygen group spent a median of 29 hours receiving an F102 level of 0.21, compared with 1 hour in the usual care group.
The mortality rate at day 180 was 35.7% in the conservative oxygen group, and 34.5% in the usual-oxygen group (HR 1.05, 95% CI 0.85 – 1.30). Researchers also saw no differences between the two groups in paid employment and cognitive function.
In patients with suspected hypoxic-ischemic encephalopathy between-group differences were apparent; At day 28, those in the conservative-oxygen group had a median of 21.1 ventilator-free days, compared with none in the usual-oxygen group. The usual-oxygen group also had a higher 180-day mortality rate than those in the conservative-oxygen group (43% vs. 59%).
“Our data are suggestive of a possible benefit of conservative oxygen therapy in patients with suspected hypoxic-ischemic encephalopathy,” the authors wrote. “It is biologically plausible that conservative oxygen therapy reduces the incidence of secondary brain damage after resuscitation from cardiac arrest, and observational data suggest that exposure to hyperoxemia in such patients may be harmful.”
The authors noted that their trial did not rule out the possibility of benefit or harm had they used a more liberal oxygen regimen in their usual-care group, and that different conservative regimens might also have achieved different outcomes.
The study was funded by the New Zealand Health Research Council. Six authors declared research support for the trial from the study funder, and two declared unrelated research grants from private industry. No other conflicts of interest were declared.
SOURCE: Mackle D et al. NJEM 2019, October 14. DOI:10.1056/NEJMoa1903297.
FROM NEJM
Key clinical point: Conservative oxygen therapy during mechanical ventilation does not increase ventilation-free days.
Major finding: The number of ventilation-free days was similar in adults on conservative oxygen therapy and those on usual care.
Study details: Parallel-group randomized controlled trial in 965 adults undergoing mechanical ventilation.
Disclosures: The study was funded by the New Zealand Health Research Council. Six authors declared research support for the trial from the study funder, and two declared unrelated research grants from private industry. No other conflicts of interest were declared.
Source: Mackle D et al. NJEM 2019, October 14. DOI: 10.1056/NEJMoa1903297.
Wildfire smoke impact, part 2: Resources, advice for patients
Wildfires are on the move in California and communities from the Bay Area to Los Angeles County are once again coping with evacuation, possible destruction of homes, and health concerns related to poor air quality and smoke.

What can doctors tell their patients with cardiovascular and pulmonary conditions about the risks of smoke from wildfires?
EPA resources online
AirNow, a website managed by the Environmental Protection Agency, provides a variety of resources for the public and for health providers, including links to online tutorials, printable health fact sheets, and the newly updated document “Wildfire Smoke: Guide for Public Health Officials 2019.” When wildfire smoke generates an Air Quality Index (AQI) from 101-150, at-risk subgroups like people with asthma, chronic obstructive pulmonary disease (COPD), or heart disease should take precautions.
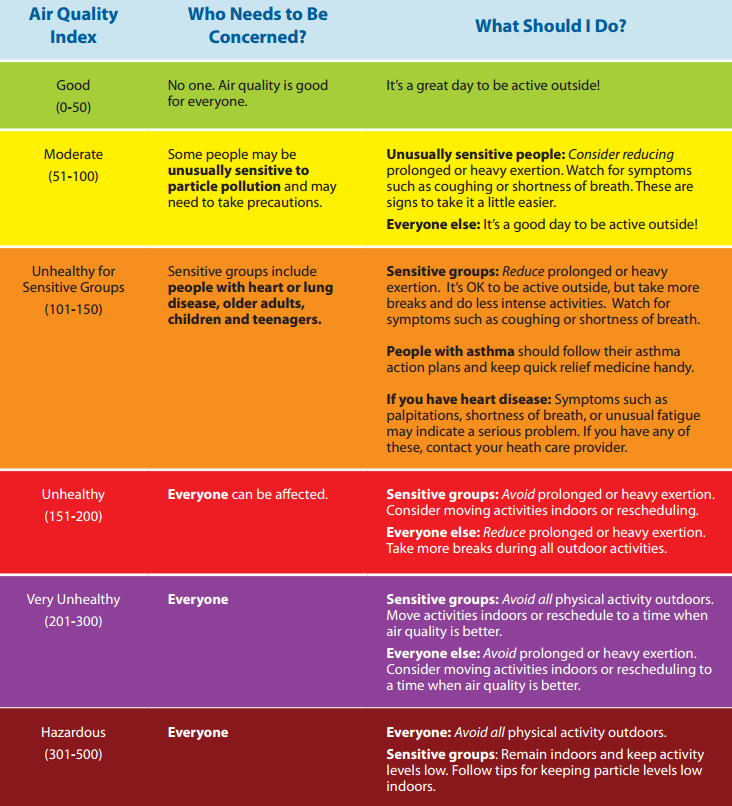
“An AQI of 151-200 is unhealthy for everyone, and an AQI above 200 is very unhealthy,” John R. Balmes, MD, a pulmonologist at the University of California, San Francisco, and an expert on the respiratory and cardiovascular effects of air pollutants, said in an interview. “That does not mean that everybody is going to die, though. You’re going to have some symptoms of scratchy throat, and you may cough once or twice an hour [from exposure to wildfire smoke], but people who don’t have any preexisting health problems are probably going to be fine and don’t necessarily have to wear an N95 mask. People should wear one if they need to feel comfortable.”
Masks – How much protection?

Wayne Cascio, MD, who directs the EPA’s National Health and Environmental Effects Research Laboratory, notes that some public health officials don’t recommend wearing N95 masks during wildfire smoke events. “There’s a lot of concern that people won’t use them correctly and will therefore feel like they’re protected and will spend more time outdoors than they should and still not get the benefit,” he said. “The masks also pose a challenge for children and for people with severe asthma and COPD.”
Masks also have to fit properly, which can be problematic for kids, added Dr. Balmes, one of the authors of “Wildfires Disaster Guidance: Tips for Staying Healthy During Wildfires” (Am J Respir Crit Care Med. 2019;199[2]:3-4).
“Even the small versions don’t necessarily fit kids well, so they’re not recommended for kids,” he said. “It doesn’t mean a kid couldn’t wear them, but it’s not officially recommended. The actual physiologic work of breathing isn’t much increased by using the N95 mask, but if you’re already struggling to get your breath, or experience dyspnea, then it might be hard to wear one. People with milder COPD can wear an N95 mask just like people with mild asthma if they have to go out.”
The EPA published a tip sheet about where and when to use an N95 or P100 mask, with warnings about the limited protection these devices offer, especially if not used correctly. Most masks do not protect the wearer from harmful gases that can be in wildfire smoke.
Ventilation systems
The EPA also recommends that people with more severe disease should stay indoors and avoid using air conditioning units that only draw in air from the outside or do not have a recirculating option. “If you have to bring in outside air because that’s how your system works, you should have a MERV 13 or better filter to filter out the fine particles,” Dr. Balmes said. “Not every ventilation system can handle it, but most can. That will help the house.”
Dr. Cascio pointed out that the instruction to close all windows and doors is a difficult proposition for people who live in states with moderate weather climates such as Montana and Colorado, where few homes have central air conditioning. “The treatment may be worse than the disease in this case, because it may exacerbate heat stress,” he said. “Try to find a place that has cleaner air. That might be a public building, a school, a fitness center, or a library. Yet we don’t know a lot about whether those areas are cleaner or not. That is currently the subject of some research on our part.”
Traveling away from an area affected by wildfire smoke to ride out the conditions is one option, but that can backfire. One weekend when smoke from the 2008 North Carolina peat fire was particularly troublesome, Dr. Cascio and his family drove about 60 miles west of Greenville to the town of Zebulon, where a minor league baseball game was being played and the air quality was good.
“My thought was to get the family to a better environment for at least a few hours,” Dr. Cascio recalled. “When we arrived in Zebulon the air quality was good as advertised. However, the direction of the wind shifted and the smoke started to move due west and within a short time you could barely see the players on the field. This experience also pointed out one of the lessons of wildfire smoke. That is, in the short term, it is sometimes difficult to predict where it will be present because of the nature of changes in weather and wind.”
Consumer tools to monitor air quality

Colleen E. Reid, PhD, of the department of geography at the University of Colorado, Boulder, an expert on the impact of wildfire smoke on human health, has observed in increase in consumer action to counter smoke inhalation during wildfire events. She said that consumers are buying personal laser particle counters, like the ones made by PurpleAir, to provide a real-time assessment of air quality.
“There is a lot of error with these smaller, cheaper monitors, but I think they give you a sense of trends over time,” Dr. Reid said. “People are trying to figure out how we can work with this sort of real-time data along with the high-quality EPA monitors. If everybody has their own monitor, or ways to better calibrate them to the high-quality data, that would be amazing. Researchers are trying to see how they can use that data to inform our understanding of the spatial and temporal patterning of air pollution.”

The EPA’s Smoke Sense app also holds promise. Characterized on its website as “a citizen science project,” the study uses a free mobile app to engage people living in affected communities to monitor their air quality and their cardiorespiratory symptoms. “Through engagement over time, you learn what the effects on your body are and what the expected effects are, so you can recognize the hazards and change the behavior when you’re experiencing it,” said Ana G. Rappold, PhD, who is the app’s principal investigator at the National Health and Environmental Effects Research Laboratory. One component of the app is time of last measurement of fine particulate matter and ozone based on the user’s location. Another is a module called Be Smoke Smart, which tests the user’s knowledge of wildfire smoke exposure. For example, one question is: “How likely are you to reduce your exposure on an Orange AQI alert day?” (which indicates that sensitive populations may experience health effects).
“Through gamification, they’re engaging with the issue,” Dr. Rappold said. “Then they learn about what others are reporting. In that part we also study how different messages change individuals’ perspective on how likely they are to make a change the next time they’re impacted by smoke.”
Wildfires are on the move in California and communities from the Bay Area to Los Angeles County are once again coping with evacuation, possible destruction of homes, and health concerns related to poor air quality and smoke.
What can doctors tell their patients with cardiovascular and pulmonary conditions about the risks of smoke from wildfires?
EPA resources online
AirNow, a website managed by the Environmental Protection Agency, provides a variety of resources for the public and for health providers, including links to online tutorials, printable health fact sheets, and the newly updated document “Wildfire Smoke: Guide for Public Health Officials 2019.” When wildfire smoke generates an Air Quality Index (AQI) from 101-150, at-risk subgroups like people with asthma, chronic obstructive pulmonary disease (COPD), or heart disease should take precautions.
“An AQI of 151-200 is unhealthy for everyone, and an AQI above 200 is very unhealthy,” John R. Balmes, MD, a pulmonologist at the University of California, San Francisco, and an expert on the respiratory and cardiovascular effects of air pollutants, said in an interview. “That does not mean that everybody is going to die, though. You’re going to have some symptoms of scratchy throat, and you may cough once or twice an hour [from exposure to wildfire smoke], but people who don’t have any preexisting health problems are probably going to be fine and don’t necessarily have to wear an N95 mask. People should wear one if they need to feel comfortable.”
Masks – How much protection?
Wayne Cascio, MD, who directs the EPA’s National Health and Environmental Effects Research Laboratory, notes that some public health officials don’t recommend wearing N95 masks during wildfire smoke events. “There’s a lot of concern that people won’t use them correctly and will therefore feel like they’re protected and will spend more time outdoors than they should and still not get the benefit,” he said. “The masks also pose a challenge for children and for people with severe asthma and COPD.”
Masks also have to fit properly, which can be problematic for kids, added Dr. Balmes, one of the authors of “Wildfires Disaster Guidance: Tips for Staying Healthy During Wildfires” (Am J Respir Crit Care Med. 2019;199[2]:3-4).
“Even the small versions don’t necessarily fit kids well, so they’re not recommended for kids,” he said. “It doesn’t mean a kid couldn’t wear them, but it’s not officially recommended. The actual physiologic work of breathing isn’t much increased by using the N95 mask, but if you’re already struggling to get your breath, or experience dyspnea, then it might be hard to wear one. People with milder COPD can wear an N95 mask just like people with mild asthma if they have to go out.”
The EPA published a tip sheet about where and when to use an N95 or P100 mask, with warnings about the limited protection these devices offer, especially if not used correctly. Most masks do not protect the wearer from harmful gases that can be in wildfire smoke.
Ventilation systems
The EPA also recommends that people with more severe disease should stay indoors and avoid using air conditioning units that only draw in air from the outside or do not have a recirculating option. “If you have to bring in outside air because that’s how your system works, you should have a MERV 13 or better filter to filter out the fine particles,” Dr. Balmes said. “Not every ventilation system can handle it, but most can. That will help the house.”
Dr. Cascio pointed out that the instruction to close all windows and doors is a difficult proposition for people who live in states with moderate weather climates such as Montana and Colorado, where few homes have central air conditioning. “The treatment may be worse than the disease in this case, because it may exacerbate heat stress,” he said. “Try to find a place that has cleaner air. That might be a public building, a school, a fitness center, or a library. Yet we don’t know a lot about whether those areas are cleaner or not. That is currently the subject of some research on our part.”
Traveling away from an area affected by wildfire smoke to ride out the conditions is one option, but that can backfire. One weekend when smoke from the 2008 North Carolina peat fire was particularly troublesome, Dr. Cascio and his family drove about 60 miles west of Greenville to the town of Zebulon, where a minor league baseball game was being played and the air quality was good.
“My thought was to get the family to a better environment for at least a few hours,” Dr. Cascio recalled. “When we arrived in Zebulon the air quality was good as advertised. However, the direction of the wind shifted and the smoke started to move due west and within a short time you could barely see the players on the field. This experience also pointed out one of the lessons of wildfire smoke. That is, in the short term, it is sometimes difficult to predict where it will be present because of the nature of changes in weather and wind.”
Consumer tools to monitor air quality
Colleen E. Reid, PhD, of the department of geography at the University of Colorado, Boulder, an expert on the impact of wildfire smoke on human health, has observed in increase in consumer action to counter smoke inhalation during wildfire events. She said that consumers are buying personal laser particle counters, like the ones made by PurpleAir, to provide a real-time assessment of air quality.
“There is a lot of error with these smaller, cheaper monitors, but I think they give you a sense of trends over time,” Dr. Reid said. “People are trying to figure out how we can work with this sort of real-time data along with the high-quality EPA monitors. If everybody has their own monitor, or ways to better calibrate them to the high-quality data, that would be amazing. Researchers are trying to see how they can use that data to inform our understanding of the spatial and temporal patterning of air pollution.”
The EPA’s Smoke Sense app also holds promise. Characterized on its website as “a citizen science project,” the study uses a free mobile app to engage people living in affected communities to monitor their air quality and their cardiorespiratory symptoms. “Through engagement over time, you learn what the effects on your body are and what the expected effects are, so you can recognize the hazards and change the behavior when you’re experiencing it,” said Ana G. Rappold, PhD, who is the app’s principal investigator at the National Health and Environmental Effects Research Laboratory. One component of the app is time of last measurement of fine particulate matter and ozone based on the user’s location. Another is a module called Be Smoke Smart, which tests the user’s knowledge of wildfire smoke exposure. For example, one question is: “How likely are you to reduce your exposure on an Orange AQI alert day?” (which indicates that sensitive populations may experience health effects).
“Through gamification, they’re engaging with the issue,” Dr. Rappold said. “Then they learn about what others are reporting. In that part we also study how different messages change individuals’ perspective on how likely they are to make a change the next time they’re impacted by smoke.”
Wildfires are on the move in California and communities from the Bay Area to Los Angeles County are once again coping with evacuation, possible destruction of homes, and health concerns related to poor air quality and smoke.
What can doctors tell their patients with cardiovascular and pulmonary conditions about the risks of smoke from wildfires?
EPA resources online
AirNow, a website managed by the Environmental Protection Agency, provides a variety of resources for the public and for health providers, including links to online tutorials, printable health fact sheets, and the newly updated document “Wildfire Smoke: Guide for Public Health Officials 2019.” When wildfire smoke generates an Air Quality Index (AQI) from 101-150, at-risk subgroups like people with asthma, chronic obstructive pulmonary disease (COPD), or heart disease should take precautions.
“An AQI of 151-200 is unhealthy for everyone, and an AQI above 200 is very unhealthy,” John R. Balmes, MD, a pulmonologist at the University of California, San Francisco, and an expert on the respiratory and cardiovascular effects of air pollutants, said in an interview. “That does not mean that everybody is going to die, though. You’re going to have some symptoms of scratchy throat, and you may cough once or twice an hour [from exposure to wildfire smoke], but people who don’t have any preexisting health problems are probably going to be fine and don’t necessarily have to wear an N95 mask. People should wear one if they need to feel comfortable.”
Masks – How much protection?
Wayne Cascio, MD, who directs the EPA’s National Health and Environmental Effects Research Laboratory, notes that some public health officials don’t recommend wearing N95 masks during wildfire smoke events. “There’s a lot of concern that people won’t use them correctly and will therefore feel like they’re protected and will spend more time outdoors than they should and still not get the benefit,” he said. “The masks also pose a challenge for children and for people with severe asthma and COPD.”
Masks also have to fit properly, which can be problematic for kids, added Dr. Balmes, one of the authors of “Wildfires Disaster Guidance: Tips for Staying Healthy During Wildfires” (Am J Respir Crit Care Med. 2019;199[2]:3-4).
“Even the small versions don’t necessarily fit kids well, so they’re not recommended for kids,” he said. “It doesn’t mean a kid couldn’t wear them, but it’s not officially recommended. The actual physiologic work of breathing isn’t much increased by using the N95 mask, but if you’re already struggling to get your breath, or experience dyspnea, then it might be hard to wear one. People with milder COPD can wear an N95 mask just like people with mild asthma if they have to go out.”
The EPA published a tip sheet about where and when to use an N95 or P100 mask, with warnings about the limited protection these devices offer, especially if not used correctly. Most masks do not protect the wearer from harmful gases that can be in wildfire smoke.
Ventilation systems
The EPA also recommends that people with more severe disease should stay indoors and avoid using air conditioning units that only draw in air from the outside or do not have a recirculating option. “If you have to bring in outside air because that’s how your system works, you should have a MERV 13 or better filter to filter out the fine particles,” Dr. Balmes said. “Not every ventilation system can handle it, but most can. That will help the house.”
Dr. Cascio pointed out that the instruction to close all windows and doors is a difficult proposition for people who live in states with moderate weather climates such as Montana and Colorado, where few homes have central air conditioning. “The treatment may be worse than the disease in this case, because it may exacerbate heat stress,” he said. “Try to find a place that has cleaner air. That might be a public building, a school, a fitness center, or a library. Yet we don’t know a lot about whether those areas are cleaner or not. That is currently the subject of some research on our part.”
Traveling away from an area affected by wildfire smoke to ride out the conditions is one option, but that can backfire. One weekend when smoke from the 2008 North Carolina peat fire was particularly troublesome, Dr. Cascio and his family drove about 60 miles west of Greenville to the town of Zebulon, where a minor league baseball game was being played and the air quality was good.
“My thought was to get the family to a better environment for at least a few hours,” Dr. Cascio recalled. “When we arrived in Zebulon the air quality was good as advertised. However, the direction of the wind shifted and the smoke started to move due west and within a short time you could barely see the players on the field. This experience also pointed out one of the lessons of wildfire smoke. That is, in the short term, it is sometimes difficult to predict where it will be present because of the nature of changes in weather and wind.”
Consumer tools to monitor air quality
Colleen E. Reid, PhD, of the department of geography at the University of Colorado, Boulder, an expert on the impact of wildfire smoke on human health, has observed in increase in consumer action to counter smoke inhalation during wildfire events. She said that consumers are buying personal laser particle counters, like the ones made by PurpleAir, to provide a real-time assessment of air quality.
“There is a lot of error with these smaller, cheaper monitors, but I think they give you a sense of trends over time,” Dr. Reid said. “People are trying to figure out how we can work with this sort of real-time data along with the high-quality EPA monitors. If everybody has their own monitor, or ways to better calibrate them to the high-quality data, that would be amazing. Researchers are trying to see how they can use that data to inform our understanding of the spatial and temporal patterning of air pollution.”
The EPA’s Smoke Sense app also holds promise. Characterized on its website as “a citizen science project,” the study uses a free mobile app to engage people living in affected communities to monitor their air quality and their cardiorespiratory symptoms. “Through engagement over time, you learn what the effects on your body are and what the expected effects are, so you can recognize the hazards and change the behavior when you’re experiencing it,” said Ana G. Rappold, PhD, who is the app’s principal investigator at the National Health and Environmental Effects Research Laboratory. One component of the app is time of last measurement of fine particulate matter and ozone based on the user’s location. Another is a module called Be Smoke Smart, which tests the user’s knowledge of wildfire smoke exposure. For example, one question is: “How likely are you to reduce your exposure on an Orange AQI alert day?” (which indicates that sensitive populations may experience health effects).
“Through gamification, they’re engaging with the issue,” Dr. Rappold said. “Then they learn about what others are reporting. In that part we also study how different messages change individuals’ perspective on how likely they are to make a change the next time they’re impacted by smoke.”
Azithromycin prevents airway complications of antibody deficiency
MADRID – Low-dose azithromycin prophylaxis significantly reduced exacerbations and hospitalizations in patients with primary antibody deficiency relative to placebo, according to a randomized multicenter phase 2 trial.

The study results support routine use of low-dose azithromycin in patients with primary antibody deficiency, according to Cinzia Milito, MD, PhD, department of molecular medicine, Sapienza University, Rome. Perhaps more importantly, the long-term benefits might be even greater.
“In patients with primary antibody deficiency, the respiratory tract is the major target of acute infections, leading to inflammation, increased airway reactivity, and over time to tissue remodeling and chronic lung disease,” Dr. Milito said at the annual congress of the European Respiratory Society. “Chronic lung disease is a major cause of death in this population.”
In this study 89 patients with primary antibody deficiency were randomized at seven centers in Italy to 250 mg per day of azithromycin or placebo administered on three consecutive days of each week for three years. Patients were maintained on other treatments, such as IgG replacement.
At the end of study, 33 of the 44 patients randomized to azithromycin and 34 of the 45 patients randomized to placebo remained on therapy. When compared for the primary endpoint of exacerbations, the median incidence rates were 3.6 episodes in the azithromycin group and 5.2 episodes in the placebo group, providing a 1.6 episode or 31% relative reduction (P=0.02).
The median number of hospitalizations for any cause, which was a secondary endpoint, was also significantly lower in the azithromycin arm (0.1 vs. 0.3 episodes).
In addition, the number of additional courses of antibiotics was significantly lower (2.3 vs. 3.6), and the time to the first course of antibiotic course was significantly longer (181.5 vs. 122.4 days) in the azithromycin group, reported Dr. Milito, whose study is now published (Milito C et al. J Allergy Clin Immunol 2019;144: 584-593).
“In a six-month washout at the end of the study, the relative advantages seen for azithromycin were lost,” Dr. Milito said.
Quality of life measured with the St. George’s Respiratory Questionnaire showed an association between low-dose azithromycin prophylaxis and significant improvement in the symptom domain when evaluated during and at the end of the study. Improvement on the Short-Form 36, which was observed one year into the study, was no longer significant at the end of the study.
Azithromycin was well tolerated with no significant differences in the rate of serious adverse events observed between the experimental and control arms of the study. Over the course of the study, however, azithromycin was associated with a significant protective effect against diarrhea (13% vs. 53%) and acute rhinosinusitus (4% vs. 27%).
There was no observed increase in macrolide resistance associated with azithromycin prophylaxis.
Macrolides have been evaluated for preventing progression of several chronic lung diseases, including chronic obstructive pulmonary disease, bronchiectasis, and cystic fibrosis. Like other drugs in its class, “azithromycin, in addition to its antimicrobial effect, has anti-inflammatory properties,” Dr. Milito said. This increases its potential to slow the time to airway damage in patients with primary antibiotic deficiency.
“Chronic lung disease is the result of a vicious cycle that begins with the inflammatory response to infection,” Dr. Milito explained. On the basis of these data, she believes azithromycin “should be considered a valuable addition to usual treatment” for primary antibody deficiencies.
SOURCE: EUROPEAN RESPIRATORY SOCIETY 2019 INTERNATIONAL CONGRESS
MADRID – Low-dose azithromycin prophylaxis significantly reduced exacerbations and hospitalizations in patients with primary antibody deficiency relative to placebo, according to a randomized multicenter phase 2 trial.
The study results support routine use of low-dose azithromycin in patients with primary antibody deficiency, according to Cinzia Milito, MD, PhD, department of molecular medicine, Sapienza University, Rome. Perhaps more importantly, the long-term benefits might be even greater.
“In patients with primary antibody deficiency, the respiratory tract is the major target of acute infections, leading to inflammation, increased airway reactivity, and over time to tissue remodeling and chronic lung disease,” Dr. Milito said at the annual congress of the European Respiratory Society. “Chronic lung disease is a major cause of death in this population.”
In this study 89 patients with primary antibody deficiency were randomized at seven centers in Italy to 250 mg per day of azithromycin or placebo administered on three consecutive days of each week for three years. Patients were maintained on other treatments, such as IgG replacement.
At the end of study, 33 of the 44 patients randomized to azithromycin and 34 of the 45 patients randomized to placebo remained on therapy. When compared for the primary endpoint of exacerbations, the median incidence rates were 3.6 episodes in the azithromycin group and 5.2 episodes in the placebo group, providing a 1.6 episode or 31% relative reduction (P=0.02).
The median number of hospitalizations for any cause, which was a secondary endpoint, was also significantly lower in the azithromycin arm (0.1 vs. 0.3 episodes).
In addition, the number of additional courses of antibiotics was significantly lower (2.3 vs. 3.6), and the time to the first course of antibiotic course was significantly longer (181.5 vs. 122.4 days) in the azithromycin group, reported Dr. Milito, whose study is now published (Milito C et al. J Allergy Clin Immunol 2019;144: 584-593).
“In a six-month washout at the end of the study, the relative advantages seen for azithromycin were lost,” Dr. Milito said.
Quality of life measured with the St. George’s Respiratory Questionnaire showed an association between low-dose azithromycin prophylaxis and significant improvement in the symptom domain when evaluated during and at the end of the study. Improvement on the Short-Form 36, which was observed one year into the study, was no longer significant at the end of the study.
Azithromycin was well tolerated with no significant differences in the rate of serious adverse events observed between the experimental and control arms of the study. Over the course of the study, however, azithromycin was associated with a significant protective effect against diarrhea (13% vs. 53%) and acute rhinosinusitus (4% vs. 27%).
There was no observed increase in macrolide resistance associated with azithromycin prophylaxis.
Macrolides have been evaluated for preventing progression of several chronic lung diseases, including chronic obstructive pulmonary disease, bronchiectasis, and cystic fibrosis. Like other drugs in its class, “azithromycin, in addition to its antimicrobial effect, has anti-inflammatory properties,” Dr. Milito said. This increases its potential to slow the time to airway damage in patients with primary antibiotic deficiency.
“Chronic lung disease is the result of a vicious cycle that begins with the inflammatory response to infection,” Dr. Milito explained. On the basis of these data, she believes azithromycin “should be considered a valuable addition to usual treatment” for primary antibody deficiencies.
SOURCE: EUROPEAN RESPIRATORY SOCIETY 2019 INTERNATIONAL CONGRESS
MADRID – Low-dose azithromycin prophylaxis significantly reduced exacerbations and hospitalizations in patients with primary antibody deficiency relative to placebo, according to a randomized multicenter phase 2 trial.
The study results support routine use of low-dose azithromycin in patients with primary antibody deficiency, according to Cinzia Milito, MD, PhD, department of molecular medicine, Sapienza University, Rome. Perhaps more importantly, the long-term benefits might be even greater.
“In patients with primary antibody deficiency, the respiratory tract is the major target of acute infections, leading to inflammation, increased airway reactivity, and over time to tissue remodeling and chronic lung disease,” Dr. Milito said at the annual congress of the European Respiratory Society. “Chronic lung disease is a major cause of death in this population.”
In this study 89 patients with primary antibody deficiency were randomized at seven centers in Italy to 250 mg per day of azithromycin or placebo administered on three consecutive days of each week for three years. Patients were maintained on other treatments, such as IgG replacement.
At the end of study, 33 of the 44 patients randomized to azithromycin and 34 of the 45 patients randomized to placebo remained on therapy. When compared for the primary endpoint of exacerbations, the median incidence rates were 3.6 episodes in the azithromycin group and 5.2 episodes in the placebo group, providing a 1.6 episode or 31% relative reduction (P=0.02).
The median number of hospitalizations for any cause, which was a secondary endpoint, was also significantly lower in the azithromycin arm (0.1 vs. 0.3 episodes).
In addition, the number of additional courses of antibiotics was significantly lower (2.3 vs. 3.6), and the time to the first course of antibiotic course was significantly longer (181.5 vs. 122.4 days) in the azithromycin group, reported Dr. Milito, whose study is now published (Milito C et al. J Allergy Clin Immunol 2019;144: 584-593).
“In a six-month washout at the end of the study, the relative advantages seen for azithromycin were lost,” Dr. Milito said.
Quality of life measured with the St. George’s Respiratory Questionnaire showed an association between low-dose azithromycin prophylaxis and significant improvement in the symptom domain when evaluated during and at the end of the study. Improvement on the Short-Form 36, which was observed one year into the study, was no longer significant at the end of the study.
Azithromycin was well tolerated with no significant differences in the rate of serious adverse events observed between the experimental and control arms of the study. Over the course of the study, however, azithromycin was associated with a significant protective effect against diarrhea (13% vs. 53%) and acute rhinosinusitus (4% vs. 27%).
There was no observed increase in macrolide resistance associated with azithromycin prophylaxis.
Macrolides have been evaluated for preventing progression of several chronic lung diseases, including chronic obstructive pulmonary disease, bronchiectasis, and cystic fibrosis. Like other drugs in its class, “azithromycin, in addition to its antimicrobial effect, has anti-inflammatory properties,” Dr. Milito said. This increases its potential to slow the time to airway damage in patients with primary antibiotic deficiency.
“Chronic lung disease is the result of a vicious cycle that begins with the inflammatory response to infection,” Dr. Milito explained. On the basis of these data, she believes azithromycin “should be considered a valuable addition to usual treatment” for primary antibody deficiencies.
SOURCE: EUROPEAN RESPIRATORY SOCIETY 2019 INTERNATIONAL CONGRESS
REPORTING FROM ERS 2019
CDC updates guidance on vaping-associated lung injury
The Centers for Disease Control and Prevention has released an updated interim clinical guidance for health providers for evaluating and treating patients with lung injury associated with e-cigarette use or vaping.
In a telebriefing, Anne Schuchat, MD, CDC principal deputy director, and her colleagues answered questions about the current investigation into the source of this lung injury outbreak and the updated clinical guidance. Dr. Schuchat said, “I can’t stress enough the seriousness of these injuries.” She added, “We are not seeing a drop in cases” but a continuation of the trend of hospitalization and deaths that started in August 2019.
Investigation update
The investigation to date has yielded some information about current cases of lung injury related to vaping:
• The acronym EVALI has been developed to refer to e-cigarette, or vaping products use associated lung injury;
• 1,299 EVALI cases have been reported as of Oct. 8;
• No single compound or ingredient has emerged as the cause of these injuries, and more than one substance may be involved;
• Among the 573 patients for whom data are available on vaping products used in the previous 90 days, 76% reported using THC-containing products; 58% reported using nicotine-containing products; 32% reported exclusive use of THC-containing products, and 13% reported exclusive use of nicotine-containing products;
• Of the 700+ samples sent to the CDC for analysis, most had little or no liquid remaining in the device, limiting content analysis. In 28 THC-containing samples, THC concentrations were found to be 13% - 77% (mean 41%).
• A “handful” of cases of readmission have been reported and the CDC is currently investigating whether these cases included patients who took up vaping again or had some other possible contributing factor.
• The CDC is currently developing an ICD-10 code relevant to EVALI.
Clinical guidance update
The CDC provided detailed guidance on evaluating and caring for patients with EVALI. The recommendations focus on patient history, lab testing, criteria for hospitalization, and follow-up of these patients.
Detailed history of patients presenting with suspected EVALI is especially important for this patient population, given the many unknowns surrounding this condition. The updated guidance states, “All health care providers evaluating patients for EVALI should ask about the use of e-cigarette, or vaping, products and ideally should ask about types of substances used (e.g.,THC, cannabis [oil, dabs], nicotine, modified products or the addition of substances not intended by the manufacturer); product source, specific product brand and name; duration and frequency of use, time of last use; product delivery system, and method of use (aerosolization, dabbing, or dripping).” The approach recommended for soliciting accurate information is “empathetic, nonjudgmental” and, the guidelines say, patients should be questioned in private regarding sensitive information to assure confidentiality.
A respiratory virus panel is recommended for all suspected EVALI patients, although at this time, these tests cannot be used to distinguish EVALI from infectious etiologies. All patients should be considered for urine toxicology testing, including testing for THC.
Imaging guidance for suspected EVALI patients includes chest x-ray, with additional CT scan when the x-ray result does not correlate with clinical findings or to evaluate severe or worsening disease.
Recommended criteria for hospitalization of patients with suspected EVALI are those patients with decreased O2 saturation (less than 95%) on room air, are in respiratory distress, or have comorbidities that compromise pulmonary reserve. As of Oct. 8, 96% of patients with suspected EVALI reported to CDC have been hospitalized.
As for medical treatment of these patients, corticosteroids have been found helpful. The statement noted, “Among 140 cases reported nationally to CDC that received corticosteroids, 82% of patients improved
The natural progression of this injury is not known, however, and it is possible that patients might recover without corticosteroids. Given the unknown etiology of the disease and “because the diagnosis remains one of exclusion, aggressive empiric therapy with corticosteroids, antimicrobial, and antiviral therapy might be warranted for patients with severe illness. A range of corticosteroid doses, durations, and taper plans might be considered on a case-by-case basis.”
The report concludes with a strong recommendation that patients hospitalized with EVALI are followed closely with a visit 1-2 weeks after discharge and again with additional testing 1-2 months later. Health care providers are also advised to consult medical specialists, in particular pulmonologists, who can offer further evaluation, recommend empiric treatment, and review indications for bronchoscopy.
Mitch Zeller, JD, director, Center for Tobacco Products with the Food and Drug Administration emphasized the extraordinary complexity of the EVALI problem but noted that the FDA and CDC “will leave no stone unturned until we get to the bottom of it.”
The Centers for Disease Control and Prevention has released an updated interim clinical guidance for health providers for evaluating and treating patients with lung injury associated with e-cigarette use or vaping.
In a telebriefing, Anne Schuchat, MD, CDC principal deputy director, and her colleagues answered questions about the current investigation into the source of this lung injury outbreak and the updated clinical guidance. Dr. Schuchat said, “I can’t stress enough the seriousness of these injuries.” She added, “We are not seeing a drop in cases” but a continuation of the trend of hospitalization and deaths that started in August 2019.
Investigation update
The investigation to date has yielded some information about current cases of lung injury related to vaping:
• The acronym EVALI has been developed to refer to e-cigarette, or vaping products use associated lung injury;
• 1,299 EVALI cases have been reported as of Oct. 8;
• No single compound or ingredient has emerged as the cause of these injuries, and more than one substance may be involved;
• Among the 573 patients for whom data are available on vaping products used in the previous 90 days, 76% reported using THC-containing products; 58% reported using nicotine-containing products; 32% reported exclusive use of THC-containing products, and 13% reported exclusive use of nicotine-containing products;
• Of the 700+ samples sent to the CDC for analysis, most had little or no liquid remaining in the device, limiting content analysis. In 28 THC-containing samples, THC concentrations were found to be 13% - 77% (mean 41%).
• A “handful” of cases of readmission have been reported and the CDC is currently investigating whether these cases included patients who took up vaping again or had some other possible contributing factor.
• The CDC is currently developing an ICD-10 code relevant to EVALI.
Clinical guidance update
The CDC provided detailed guidance on evaluating and caring for patients with EVALI. The recommendations focus on patient history, lab testing, criteria for hospitalization, and follow-up of these patients.
Detailed history of patients presenting with suspected EVALI is especially important for this patient population, given the many unknowns surrounding this condition. The updated guidance states, “All health care providers evaluating patients for EVALI should ask about the use of e-cigarette, or vaping, products and ideally should ask about types of substances used (e.g.,THC, cannabis [oil, dabs], nicotine, modified products or the addition of substances not intended by the manufacturer); product source, specific product brand and name; duration and frequency of use, time of last use; product delivery system, and method of use (aerosolization, dabbing, or dripping).” The approach recommended for soliciting accurate information is “empathetic, nonjudgmental” and, the guidelines say, patients should be questioned in private regarding sensitive information to assure confidentiality.
A respiratory virus panel is recommended for all suspected EVALI patients, although at this time, these tests cannot be used to distinguish EVALI from infectious etiologies. All patients should be considered for urine toxicology testing, including testing for THC.
Imaging guidance for suspected EVALI patients includes chest x-ray, with additional CT scan when the x-ray result does not correlate with clinical findings or to evaluate severe or worsening disease.
Recommended criteria for hospitalization of patients with suspected EVALI are those patients with decreased O2 saturation (less than 95%) on room air, are in respiratory distress, or have comorbidities that compromise pulmonary reserve. As of Oct. 8, 96% of patients with suspected EVALI reported to CDC have been hospitalized.
As for medical treatment of these patients, corticosteroids have been found helpful. The statement noted, “Among 140 cases reported nationally to CDC that received corticosteroids, 82% of patients improved
The natural progression of this injury is not known, however, and it is possible that patients might recover without corticosteroids. Given the unknown etiology of the disease and “because the diagnosis remains one of exclusion, aggressive empiric therapy with corticosteroids, antimicrobial, and antiviral therapy might be warranted for patients with severe illness. A range of corticosteroid doses, durations, and taper plans might be considered on a case-by-case basis.”
The report concludes with a strong recommendation that patients hospitalized with EVALI are followed closely with a visit 1-2 weeks after discharge and again with additional testing 1-2 months later. Health care providers are also advised to consult medical specialists, in particular pulmonologists, who can offer further evaluation, recommend empiric treatment, and review indications for bronchoscopy.
Mitch Zeller, JD, director, Center for Tobacco Products with the Food and Drug Administration emphasized the extraordinary complexity of the EVALI problem but noted that the FDA and CDC “will leave no stone unturned until we get to the bottom of it.”
The Centers for Disease Control and Prevention has released an updated interim clinical guidance for health providers for evaluating and treating patients with lung injury associated with e-cigarette use or vaping.
In a telebriefing, Anne Schuchat, MD, CDC principal deputy director, and her colleagues answered questions about the current investigation into the source of this lung injury outbreak and the updated clinical guidance. Dr. Schuchat said, “I can’t stress enough the seriousness of these injuries.” She added, “We are not seeing a drop in cases” but a continuation of the trend of hospitalization and deaths that started in August 2019.
Investigation update
The investigation to date has yielded some information about current cases of lung injury related to vaping:
• The acronym EVALI has been developed to refer to e-cigarette, or vaping products use associated lung injury;
• 1,299 EVALI cases have been reported as of Oct. 8;
• No single compound or ingredient has emerged as the cause of these injuries, and more than one substance may be involved;
• Among the 573 patients for whom data are available on vaping products used in the previous 90 days, 76% reported using THC-containing products; 58% reported using nicotine-containing products; 32% reported exclusive use of THC-containing products, and 13% reported exclusive use of nicotine-containing products;
• Of the 700+ samples sent to the CDC for analysis, most had little or no liquid remaining in the device, limiting content analysis. In 28 THC-containing samples, THC concentrations were found to be 13% - 77% (mean 41%).
• A “handful” of cases of readmission have been reported and the CDC is currently investigating whether these cases included patients who took up vaping again or had some other possible contributing factor.
• The CDC is currently developing an ICD-10 code relevant to EVALI.
Clinical guidance update
The CDC provided detailed guidance on evaluating and caring for patients with EVALI. The recommendations focus on patient history, lab testing, criteria for hospitalization, and follow-up of these patients.
Detailed history of patients presenting with suspected EVALI is especially important for this patient population, given the many unknowns surrounding this condition. The updated guidance states, “All health care providers evaluating patients for EVALI should ask about the use of e-cigarette, or vaping, products and ideally should ask about types of substances used (e.g.,THC, cannabis [oil, dabs], nicotine, modified products or the addition of substances not intended by the manufacturer); product source, specific product brand and name; duration and frequency of use, time of last use; product delivery system, and method of use (aerosolization, dabbing, or dripping).” The approach recommended for soliciting accurate information is “empathetic, nonjudgmental” and, the guidelines say, patients should be questioned in private regarding sensitive information to assure confidentiality.
A respiratory virus panel is recommended for all suspected EVALI patients, although at this time, these tests cannot be used to distinguish EVALI from infectious etiologies. All patients should be considered for urine toxicology testing, including testing for THC.
Imaging guidance for suspected EVALI patients includes chest x-ray, with additional CT scan when the x-ray result does not correlate with clinical findings or to evaluate severe or worsening disease.
Recommended criteria for hospitalization of patients with suspected EVALI are those patients with decreased O2 saturation (less than 95%) on room air, are in respiratory distress, or have comorbidities that compromise pulmonary reserve. As of Oct. 8, 96% of patients with suspected EVALI reported to CDC have been hospitalized.
As for medical treatment of these patients, corticosteroids have been found helpful. The statement noted, “Among 140 cases reported nationally to CDC that received corticosteroids, 82% of patients improved
The natural progression of this injury is not known, however, and it is possible that patients might recover without corticosteroids. Given the unknown etiology of the disease and “because the diagnosis remains one of exclusion, aggressive empiric therapy with corticosteroids, antimicrobial, and antiviral therapy might be warranted for patients with severe illness. A range of corticosteroid doses, durations, and taper plans might be considered on a case-by-case basis.”
The report concludes with a strong recommendation that patients hospitalized with EVALI are followed closely with a visit 1-2 weeks after discharge and again with additional testing 1-2 months later. Health care providers are also advised to consult medical specialists, in particular pulmonologists, who can offer further evaluation, recommend empiric treatment, and review indications for bronchoscopy.
Mitch Zeller, JD, director, Center for Tobacco Products with the Food and Drug Administration emphasized the extraordinary complexity of the EVALI problem but noted that the FDA and CDC “will leave no stone unturned until we get to the bottom of it.”
REPORTING FROM A CDC TELEBRIEFING
