User login
MRI Reveals Lymphatic Vessels in Dura
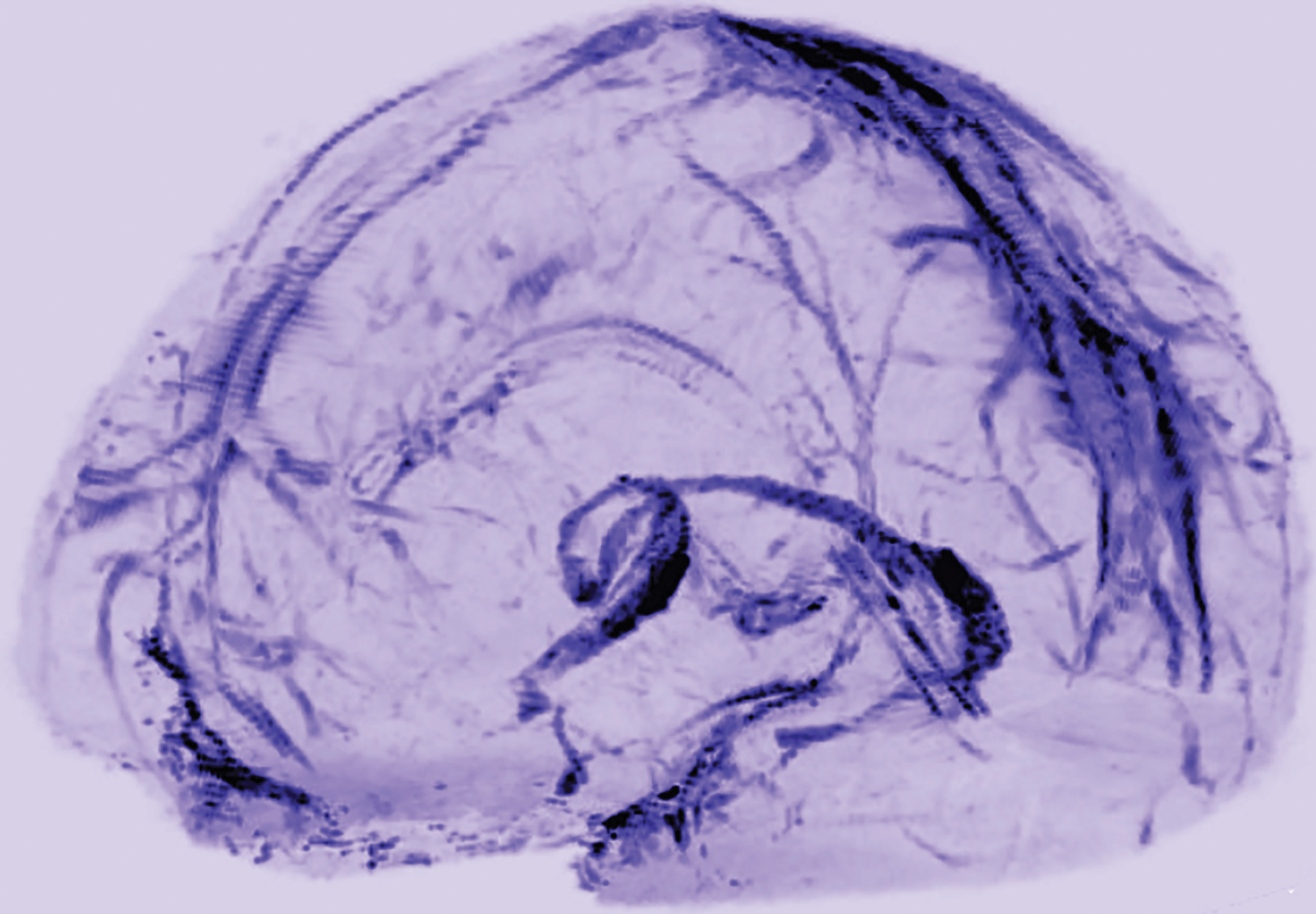
Researchers have visualized lymphatic vessels in the dura mater of humans on MRI, according to a short report published October 3, 2017, in eLife. They also have identified lymphatic vessels in brain tissue samples using immunostaining. The results suggest that the vessels could act as a pipeline between the brain and the immune system.
“Overall, our data clearly and consistently demonstrate the existence of lymphatic vessels within the dura mater of human and nonhuman primates,” said Daniel S. Reich, MD, PhD, Senior Investigator at the NINDS, and colleagues. “The ability to image the meningeal lymphatics noninvasively immediately suggests the possibility of studying potential abnormalities” in neurologic disorders, they said.

A Fundamental Shift
In most of the body, lymphatic vessels transport immune cells and waste products from organs to the bloodstream, but the brain was thought not to have lymphatic vessels. In 2015, however, researchers found evidence of the brain’s lymphatic system in the dura of mice. Dr. Reich saw a presentation by an author of one the mouse studies, Jonathan Kipnis, PhD, Chair of the Department of Neuroscience at the University of Virginia in Charlottesville, and “was completely surprised.”
“In medical school, we were taught that the brain has no lymphatic system,” Dr. Reich said. “After Dr. Kipnis’s talk, I thought maybe we could find it in human brains.”
Dr. Reich and colleagues scanned the brains of five healthy volunteers who had been injected with gadobutrol, a dye used during MRI scans to visualize brain blood vessels. Gadobutrol that had leaked out of blood vessels in the dura as part of a normal process collected inside lymphatic vessels in the dura and showed up as bright white lines on MRI. “We watched people’s brains drain fluid into these vessels,” said Dr. Reich. When they repeated the experiment using a different dye that leaks much less out of blood vessels (ie, gadofosveset), the lymphatic vessels did not appear on imaging.
Similar findings were observed in monkeys.
The lymphatic vessels had been difficult to identify because they resemble blood vessels, which are far more numerous, the researchers said.
“These results could fundamentally change the way we think about how the brain and immune system interrelate,” said Walter J. Koroshetz, MD, NINDS director.
Meningeal Lymphatic Network
MRI showed collection of interstitial gadolinium within dural lymphatic vessels in all five of the healthy volunteers (ages 28 to 53, three women) and all three of the common marmoset monkeys studied. The vessels had a maximum apparent diameter of approximately 1 mm. “Our results suggest that in the dura, similar to many other organs throughout the body, small intravascular molecules extravasate into the interstitium and then, under a hydrostatic pressure gradient, collect into lymphatic capillaries through a loose lymphatic endothelium,” the researchers said. “On 3D rendering of subtraction MRI images, dural lymphatics are seen running parallel to the dural venous sinuses, especially the superior sagittal and straight sinuses, and alongside branches of the middle meningeal artery. The topography of the meningeal lymphatics fits with the previously described network in rodents.”
Although MRI shows large, slow-flow lymphatic ducts, “blind-ending and small lymphatic capillaries, clearly seen by histopathology, are unlikely to be revealed by MRI,” the researchers noted. In addition, they “could not prove whether dural lymphatic vessels drain immune cells, CSF, or other substances from the brain to deep cervical lymph nodes” or assess any link with the glymphatic system. “A comprehensive map of the meningeal lymphatic network would have implications for unraveling the ways in which the meningeal lymphatics participate in waste clearance and in immune cell trafficking within the CNS,” the researchers said.
Neuropathologic evaluation focused on dura samples from two formalin-fixed brains (from patients ages 60 and 77 with longstanding progressive multiple sclerosis) and from a 33-year-old patient with refractory epilepsy undergoing anterior temporal lobectomy.
Future studies may examine the role that dural lymphatics play in inflammatory pathologic conditions. The researchers have observed “clusters of extravascular CD3+ lymphocytes and CD68+ phagocytic meningeal macrophages … in the dura of several multiple sclerosis autopsies, confirming intense immune cell trafficking and communication.” Furthermore, “lymphatic dysfunction might impair waste clearance in neurodegenerative diseases and aging, in line with the recently captured deposition of β-amyloid in human dura in elderly people,” the researchers said.
—Jake Remaly
Suggested Reading
Absinta M, Ha SK, Nair G, et al. Human and nonhuman primate meninges harbor lymphatic vessels that can be visualized noninvasively by MRI. Elife. 2017 Oct 3;6:e29738.
Researchers have visualized lymphatic vessels in the dura mater of humans on MRI, according to a short report published October 3, 2017, in eLife. They also have identified lymphatic vessels in brain tissue samples using immunostaining. The results suggest that the vessels could act as a pipeline between the brain and the immune system.
“Overall, our data clearly and consistently demonstrate the existence of lymphatic vessels within the dura mater of human and nonhuman primates,” said Daniel S. Reich, MD, PhD, Senior Investigator at the NINDS, and colleagues. “The ability to image the meningeal lymphatics noninvasively immediately suggests the possibility of studying potential abnormalities” in neurologic disorders, they said.
A Fundamental Shift
In most of the body, lymphatic vessels transport immune cells and waste products from organs to the bloodstream, but the brain was thought not to have lymphatic vessels. In 2015, however, researchers found evidence of the brain’s lymphatic system in the dura of mice. Dr. Reich saw a presentation by an author of one the mouse studies, Jonathan Kipnis, PhD, Chair of the Department of Neuroscience at the University of Virginia in Charlottesville, and “was completely surprised.”
“In medical school, we were taught that the brain has no lymphatic system,” Dr. Reich said. “After Dr. Kipnis’s talk, I thought maybe we could find it in human brains.”
Dr. Reich and colleagues scanned the brains of five healthy volunteers who had been injected with gadobutrol, a dye used during MRI scans to visualize brain blood vessels. Gadobutrol that had leaked out of blood vessels in the dura as part of a normal process collected inside lymphatic vessels in the dura and showed up as bright white lines on MRI. “We watched people’s brains drain fluid into these vessels,” said Dr. Reich. When they repeated the experiment using a different dye that leaks much less out of blood vessels (ie, gadofosveset), the lymphatic vessels did not appear on imaging.
Similar findings were observed in monkeys.
The lymphatic vessels had been difficult to identify because they resemble blood vessels, which are far more numerous, the researchers said.
“These results could fundamentally change the way we think about how the brain and immune system interrelate,” said Walter J. Koroshetz, MD, NINDS director.
Meningeal Lymphatic Network
MRI showed collection of interstitial gadolinium within dural lymphatic vessels in all five of the healthy volunteers (ages 28 to 53, three women) and all three of the common marmoset monkeys studied. The vessels had a maximum apparent diameter of approximately 1 mm. “Our results suggest that in the dura, similar to many other organs throughout the body, small intravascular molecules extravasate into the interstitium and then, under a hydrostatic pressure gradient, collect into lymphatic capillaries through a loose lymphatic endothelium,” the researchers said. “On 3D rendering of subtraction MRI images, dural lymphatics are seen running parallel to the dural venous sinuses, especially the superior sagittal and straight sinuses, and alongside branches of the middle meningeal artery. The topography of the meningeal lymphatics fits with the previously described network in rodents.”
Although MRI shows large, slow-flow lymphatic ducts, “blind-ending and small lymphatic capillaries, clearly seen by histopathology, are unlikely to be revealed by MRI,” the researchers noted. In addition, they “could not prove whether dural lymphatic vessels drain immune cells, CSF, or other substances from the brain to deep cervical lymph nodes” or assess any link with the glymphatic system. “A comprehensive map of the meningeal lymphatic network would have implications for unraveling the ways in which the meningeal lymphatics participate in waste clearance and in immune cell trafficking within the CNS,” the researchers said.
Neuropathologic evaluation focused on dura samples from two formalin-fixed brains (from patients ages 60 and 77 with longstanding progressive multiple sclerosis) and from a 33-year-old patient with refractory epilepsy undergoing anterior temporal lobectomy.
Future studies may examine the role that dural lymphatics play in inflammatory pathologic conditions. The researchers have observed “clusters of extravascular CD3+ lymphocytes and CD68+ phagocytic meningeal macrophages … in the dura of several multiple sclerosis autopsies, confirming intense immune cell trafficking and communication.” Furthermore, “lymphatic dysfunction might impair waste clearance in neurodegenerative diseases and aging, in line with the recently captured deposition of β-amyloid in human dura in elderly people,” the researchers said.
—Jake Remaly
Suggested Reading
Absinta M, Ha SK, Nair G, et al. Human and nonhuman primate meninges harbor lymphatic vessels that can be visualized noninvasively by MRI. Elife. 2017 Oct 3;6:e29738.
Researchers have visualized lymphatic vessels in the dura mater of humans on MRI, according to a short report published October 3, 2017, in eLife. They also have identified lymphatic vessels in brain tissue samples using immunostaining. The results suggest that the vessels could act as a pipeline between the brain and the immune system.
“Overall, our data clearly and consistently demonstrate the existence of lymphatic vessels within the dura mater of human and nonhuman primates,” said Daniel S. Reich, MD, PhD, Senior Investigator at the NINDS, and colleagues. “The ability to image the meningeal lymphatics noninvasively immediately suggests the possibility of studying potential abnormalities” in neurologic disorders, they said.
A Fundamental Shift
In most of the body, lymphatic vessels transport immune cells and waste products from organs to the bloodstream, but the brain was thought not to have lymphatic vessels. In 2015, however, researchers found evidence of the brain’s lymphatic system in the dura of mice. Dr. Reich saw a presentation by an author of one the mouse studies, Jonathan Kipnis, PhD, Chair of the Department of Neuroscience at the University of Virginia in Charlottesville, and “was completely surprised.”
“In medical school, we were taught that the brain has no lymphatic system,” Dr. Reich said. “After Dr. Kipnis’s talk, I thought maybe we could find it in human brains.”
Dr. Reich and colleagues scanned the brains of five healthy volunteers who had been injected with gadobutrol, a dye used during MRI scans to visualize brain blood vessels. Gadobutrol that had leaked out of blood vessels in the dura as part of a normal process collected inside lymphatic vessels in the dura and showed up as bright white lines on MRI. “We watched people’s brains drain fluid into these vessels,” said Dr. Reich. When they repeated the experiment using a different dye that leaks much less out of blood vessels (ie, gadofosveset), the lymphatic vessels did not appear on imaging.
Similar findings were observed in monkeys.
The lymphatic vessels had been difficult to identify because they resemble blood vessels, which are far more numerous, the researchers said.
“These results could fundamentally change the way we think about how the brain and immune system interrelate,” said Walter J. Koroshetz, MD, NINDS director.
Meningeal Lymphatic Network
MRI showed collection of interstitial gadolinium within dural lymphatic vessels in all five of the healthy volunteers (ages 28 to 53, three women) and all three of the common marmoset monkeys studied. The vessels had a maximum apparent diameter of approximately 1 mm. “Our results suggest that in the dura, similar to many other organs throughout the body, small intravascular molecules extravasate into the interstitium and then, under a hydrostatic pressure gradient, collect into lymphatic capillaries through a loose lymphatic endothelium,” the researchers said. “On 3D rendering of subtraction MRI images, dural lymphatics are seen running parallel to the dural venous sinuses, especially the superior sagittal and straight sinuses, and alongside branches of the middle meningeal artery. The topography of the meningeal lymphatics fits with the previously described network in rodents.”
Although MRI shows large, slow-flow lymphatic ducts, “blind-ending and small lymphatic capillaries, clearly seen by histopathology, are unlikely to be revealed by MRI,” the researchers noted. In addition, they “could not prove whether dural lymphatic vessels drain immune cells, CSF, or other substances from the brain to deep cervical lymph nodes” or assess any link with the glymphatic system. “A comprehensive map of the meningeal lymphatic network would have implications for unraveling the ways in which the meningeal lymphatics participate in waste clearance and in immune cell trafficking within the CNS,” the researchers said.
Neuropathologic evaluation focused on dura samples from two formalin-fixed brains (from patients ages 60 and 77 with longstanding progressive multiple sclerosis) and from a 33-year-old patient with refractory epilepsy undergoing anterior temporal lobectomy.
Future studies may examine the role that dural lymphatics play in inflammatory pathologic conditions. The researchers have observed “clusters of extravascular CD3+ lymphocytes and CD68+ phagocytic meningeal macrophages … in the dura of several multiple sclerosis autopsies, confirming intense immune cell trafficking and communication.” Furthermore, “lymphatic dysfunction might impair waste clearance in neurodegenerative diseases and aging, in line with the recently captured deposition of β-amyloid in human dura in elderly people,” the researchers said.
—Jake Remaly
Suggested Reading
Absinta M, Ha SK, Nair G, et al. Human and nonhuman primate meninges harbor lymphatic vessels that can be visualized noninvasively by MRI. Elife. 2017 Oct 3;6:e29738.
Sodium Oxybate Reduces Daytime Sleepiness in Parkinson’s Disease
Sodium oxybate effectively treats excessive daytime sleepiness and nocturnal sleep disturbance in patients with Parkinson’s disease, according to research published in the January issue of JAMA Neurology. Patients receiving this therapy should be monitored with follow-up polysomnography to rule out treatment-related complications, the investigators said.
Many patients with Parkinson’s disease have excessive daytime sleepiness and disturbed sleep, but few treatments are available for them. An open-label study found that sodium oxybate, a first-line therapy for narcolepsy type 1, improved sleep and reduced daytime sleepiness in Parkinson’s disease.
A Phase II Crossover Study
To investigate this treatment further, Christian Baumann, MD, Senior Physician at University Hospital Zürich, and colleagues enrolled 18 patients into a double-blind, placebo-controlled, crossover phase IIa study. Eligible participants had Parkinson’s disease and regularly took dopaminergic medication. People with sleep apnea, cognitive problems, or depression, and those who took hypnotics, were excluded from the study.

The researchers randomized participants in equal groups to sodium oxybate or placebo. Study medications were taken daily at bedtime and 2.5 to four hours later for six weeks. Doses were titrated between 3 g/night and 9 g/night according to efficacy and tolerability. After a two- to four-week washout period, participants crossed over to the opposite treatment arm for six weeks.
The trial’s primary efficacy end point was treatment effect on mean sleep latency (MSL), as measured by the Multiple Sleep Latency Test (MSLT). Secondary end points included change in subjective excessive daytime sleepiness (as measured by the Epworth Sleepiness Scale [ESS]), sleep quality, and objective sleep parameters. The investigators measured outcomes in the sleep laboratory at baseline and after six weeks of therapy.
Adverse Events Were Mild or Moderate
Five patients were excluded because of sleep apnea, and one patient withdrew consent. Of the 12 patients randomized, two were women. At baseline, participants’ mean age was 62, and mean disease duration was 8.4 years. Two patients developed de novo sleep apnea during sodium oxybate treatment, and one of them dropped out.
In the intention-to-treat analysis, sodium oxybate increased MSL by 2.9 minutes and reduced ESS score by 4.2 points. In the per-protocol analysis, sodium oxybate increased MSL by 3.5 minutes and reduced ESS score by 5.2 points. The responder rate for sodium oxybate (ie, the percentage of patients who had an improvement in MSL of more than 50%) was 67%. ESS score normalized for half of patients.
Every patient who received sodium oxybate had adverse events of mild or moderate intensity. The majority of these adverse events resolved after dose adjustment. Four patients continued to have adverse events until the end of the study, but none dropped out because of them.
Sodium oxybate had a treatment effect “that, to our knowledge, is unmatched by any other intervention reported so far,” said Dr. Baumann and colleagues. Although the sample size was large enough to provide class I evidence of efficacy, it was insufficient to support conclusions about safety, said the researchers. Larger follow-up trials thus are necessary, they concluded.
—Erik Greb
Suggested Reading
Büchele F, Hackius M, Schreglmann SR, et al. Sodium oxybate for excessive daytime sleepiness and sleep disturbance in Parkinson disease: a randomized clinical trial. JAMA Neurol. 2018;75(1):114-118.
Sodium oxybate effectively treats excessive daytime sleepiness and nocturnal sleep disturbance in patients with Parkinson’s disease, according to research published in the January issue of JAMA Neurology. Patients receiving this therapy should be monitored with follow-up polysomnography to rule out treatment-related complications, the investigators said.
Many patients with Parkinson’s disease have excessive daytime sleepiness and disturbed sleep, but few treatments are available for them. An open-label study found that sodium oxybate, a first-line therapy for narcolepsy type 1, improved sleep and reduced daytime sleepiness in Parkinson’s disease.
A Phase II Crossover Study
To investigate this treatment further, Christian Baumann, MD, Senior Physician at University Hospital Zürich, and colleagues enrolled 18 patients into a double-blind, placebo-controlled, crossover phase IIa study. Eligible participants had Parkinson’s disease and regularly took dopaminergic medication. People with sleep apnea, cognitive problems, or depression, and those who took hypnotics, were excluded from the study.
The researchers randomized participants in equal groups to sodium oxybate or placebo. Study medications were taken daily at bedtime and 2.5 to four hours later for six weeks. Doses were titrated between 3 g/night and 9 g/night according to efficacy and tolerability. After a two- to four-week washout period, participants crossed over to the opposite treatment arm for six weeks.
The trial’s primary efficacy end point was treatment effect on mean sleep latency (MSL), as measured by the Multiple Sleep Latency Test (MSLT). Secondary end points included change in subjective excessive daytime sleepiness (as measured by the Epworth Sleepiness Scale [ESS]), sleep quality, and objective sleep parameters. The investigators measured outcomes in the sleep laboratory at baseline and after six weeks of therapy.
Adverse Events Were Mild or Moderate
Five patients were excluded because of sleep apnea, and one patient withdrew consent. Of the 12 patients randomized, two were women. At baseline, participants’ mean age was 62, and mean disease duration was 8.4 years. Two patients developed de novo sleep apnea during sodium oxybate treatment, and one of them dropped out.
In the intention-to-treat analysis, sodium oxybate increased MSL by 2.9 minutes and reduced ESS score by 4.2 points. In the per-protocol analysis, sodium oxybate increased MSL by 3.5 minutes and reduced ESS score by 5.2 points. The responder rate for sodium oxybate (ie, the percentage of patients who had an improvement in MSL of more than 50%) was 67%. ESS score normalized for half of patients.
Every patient who received sodium oxybate had adverse events of mild or moderate intensity. The majority of these adverse events resolved after dose adjustment. Four patients continued to have adverse events until the end of the study, but none dropped out because of them.
Sodium oxybate had a treatment effect “that, to our knowledge, is unmatched by any other intervention reported so far,” said Dr. Baumann and colleagues. Although the sample size was large enough to provide class I evidence of efficacy, it was insufficient to support conclusions about safety, said the researchers. Larger follow-up trials thus are necessary, they concluded.
—Erik Greb
Suggested Reading
Büchele F, Hackius M, Schreglmann SR, et al. Sodium oxybate for excessive daytime sleepiness and sleep disturbance in Parkinson disease: a randomized clinical trial. JAMA Neurol. 2018;75(1):114-118.
Sodium oxybate effectively treats excessive daytime sleepiness and nocturnal sleep disturbance in patients with Parkinson’s disease, according to research published in the January issue of JAMA Neurology. Patients receiving this therapy should be monitored with follow-up polysomnography to rule out treatment-related complications, the investigators said.
Many patients with Parkinson’s disease have excessive daytime sleepiness and disturbed sleep, but few treatments are available for them. An open-label study found that sodium oxybate, a first-line therapy for narcolepsy type 1, improved sleep and reduced daytime sleepiness in Parkinson’s disease.
A Phase II Crossover Study
To investigate this treatment further, Christian Baumann, MD, Senior Physician at University Hospital Zürich, and colleagues enrolled 18 patients into a double-blind, placebo-controlled, crossover phase IIa study. Eligible participants had Parkinson’s disease and regularly took dopaminergic medication. People with sleep apnea, cognitive problems, or depression, and those who took hypnotics, were excluded from the study.
The researchers randomized participants in equal groups to sodium oxybate or placebo. Study medications were taken daily at bedtime and 2.5 to four hours later for six weeks. Doses were titrated between 3 g/night and 9 g/night according to efficacy and tolerability. After a two- to four-week washout period, participants crossed over to the opposite treatment arm for six weeks.
The trial’s primary efficacy end point was treatment effect on mean sleep latency (MSL), as measured by the Multiple Sleep Latency Test (MSLT). Secondary end points included change in subjective excessive daytime sleepiness (as measured by the Epworth Sleepiness Scale [ESS]), sleep quality, and objective sleep parameters. The investigators measured outcomes in the sleep laboratory at baseline and after six weeks of therapy.
Adverse Events Were Mild or Moderate
Five patients were excluded because of sleep apnea, and one patient withdrew consent. Of the 12 patients randomized, two were women. At baseline, participants’ mean age was 62, and mean disease duration was 8.4 years. Two patients developed de novo sleep apnea during sodium oxybate treatment, and one of them dropped out.
In the intention-to-treat analysis, sodium oxybate increased MSL by 2.9 minutes and reduced ESS score by 4.2 points. In the per-protocol analysis, sodium oxybate increased MSL by 3.5 minutes and reduced ESS score by 5.2 points. The responder rate for sodium oxybate (ie, the percentage of patients who had an improvement in MSL of more than 50%) was 67%. ESS score normalized for half of patients.
Every patient who received sodium oxybate had adverse events of mild or moderate intensity. The majority of these adverse events resolved after dose adjustment. Four patients continued to have adverse events until the end of the study, but none dropped out because of them.
Sodium oxybate had a treatment effect “that, to our knowledge, is unmatched by any other intervention reported so far,” said Dr. Baumann and colleagues. Although the sample size was large enough to provide class I evidence of efficacy, it was insufficient to support conclusions about safety, said the researchers. Larger follow-up trials thus are necessary, they concluded.
—Erik Greb
Suggested Reading
Büchele F, Hackius M, Schreglmann SR, et al. Sodium oxybate for excessive daytime sleepiness and sleep disturbance in Parkinson disease: a randomized clinical trial. JAMA Neurol. 2018;75(1):114-118.
Gene Replacement Improves Survival in Spinal Muscular Atrophy
A single IV infusion to replace the gene encoding survival motor neuron 1 (SMN1) increases survival among infants with spinal muscular atrophy type 1 (SMA1), according to research published in the November 2, 2017, issue of the New England Journal of Medicine. The treatment also improves motor function, and its effects are maintained for two years, the researchers said.
The loss or dysfunction of SMN1 causes SMA, a progressive disease characterized by the degeneration and loss of lower motor neurons. Onset of SMA1 typically occurs at one month of age. Children with the disease usually are weak, fail to achieve motor milestones, and have declines in respiration and swallowing. At a median age of 10.5 months, patients die or need permanent ventilatory assistance.
In December 2016, the FDA approved nusinersen for the treatment of SMA. A phase III study found that patients treated with nusinersen were more likely than controls to have improved motor function and event-free survival. The trial was stopped early because of the treatment’s efficacy.
A Small, Open-Label Trial
A mouse study indicated that IV administration of an adenoassociated viral vector (ie, AAV9) containing SMN1 reduced the effects of SMA and extended survival. Jerry R. Mendell, MD, Principal Investigator at Nationwide Children’s Hospital’s Center for Gene Therapy in Columbus, Ohio, and colleagues studied this therapeutic technique in humans.
They enrolled 15 patients with a genetically confirmed diagnosis of SMA1 into two cohorts. The first cohort received a low dose (6.7×1013 vg/kg) of treatment, and the second cohort received a high dose (2.0×1014 vg/kg). Because the first patient in cohort one had serum aminotransferase elevations, the investigators gave 1 mg/kg/day of oral prednisolone to all subsequent patients for 30 days, starting 24 hours before gene therapy.
The study’s primary outcome was treatment-related adverse events of grade 3 or higher. The secondary outcome was time until death or the need for permanent ventilatory assistance, which was defined as at least 16 hours/day of continuous respiratory assistance for at least 14 days. The achievement of motor milestones and Children’s Hospital of Philadelphia Infant Test of Neuromuscular Disorders (CHOP INTEND) scores were exploratory outcomes.
Motor Scores Improved
Three patients entered the low-dose cohort, and 12 were enrolled in the high-dose cohort. Patients’ mean age at treatment was 6.3 months in cohort 1 and 3.4 months in cohort 2. At the last follow-up, all patients had reached age 20 months, and none required permanent mechanical ventilation. Approximately 8% of patients in a historical cohort met these criteria.
All patients had increases from baseline in CHOP INTEND score and maintained these increases throughout the study. Patients in cohort 2 had mean increases of 9.8 points at one month and 15.4 points at three months. Eleven patients achieved and sustained scores greater than 40 points, which is considered clinically meaningful in SMA.
Of the patients in cohort 2, 11 sat unassisted, nine rolled over, 11 fed orally and could speak, and two walked independently. No patients in the historical cohorts achieved any of these milestones, and they rarely became able to speak.
Dr. Mendell and colleagues observed two treatment-related grade 4 adverse events. Both were elevations in serum aminotransferase levels that were attenuated after treatment with prednisolone. The researchers also noted three treatment-related nonserious adverse events (ie, asymptomatic elevations in serum aminotransferase levels that were resolved without additional prednisolone treatment).
The study results were consistent with those of the preclinical mouse study. During a follow-up period of as long as two years, Dr. Mendell and colleagues did not observe any decrease in treatment effect or regression in motor function among the study participants. The presence of antibodies to AAV9 could be a potential limitation of the therapy, however. Further research to assess the treatment’s safety and the durability of its effect are needed, according to the authors.
Comparing Two Treatments
It is difficult to compare the results of Dr. Mendell and colleagues with those of the phase III nusinersen study, because of the two trials’ different designs, said Ans T. van der Ploeg, MD, PhD, Chair of the Center for Lysosomal and Metabolic Diseases at the Erasmus MC University in Rotterdam, the Netherlands, in an accompanying editorial. One potential advantage of AAV9 gene therapy is that it might require a single IV infusion. Nusinersen, on the other hand, may require lifelong intrathecal treatment.
“The durability of the effects is uncertain for both treatments,” said Dr. van der Ploeg. “If the expression of the scAAV9 gene therapy declines over time, the same treatment may not be able to be repeated, because antibodies against AAV capsid proteins are anticipated to form.”
In addition, neither of the two therapies cures SMA type 1. Earlier treatment could be beneficial, as could a combination of both treatments, said Dr. van der Ploeg. But the high expected cost of nusinersen is “an important constraint,” she concluded.
—Erik Greb
Suggested Reading
Mendell JR, Al-Zaidy S, Shell R, et al. Single-dose gene-replacement therapy for spinal muscular atrophy. N Engl J Med. 2017;377(18):1713-1722.
van der Ploeg AT. The dilemma of two innovative therapies for spinal muscular atrophy. N Engl J Med. 2017;377(18):1786-1787.
A single IV infusion to replace the gene encoding survival motor neuron 1 (SMN1) increases survival among infants with spinal muscular atrophy type 1 (SMA1), according to research published in the November 2, 2017, issue of the New England Journal of Medicine. The treatment also improves motor function, and its effects are maintained for two years, the researchers said.
The loss or dysfunction of SMN1 causes SMA, a progressive disease characterized by the degeneration and loss of lower motor neurons. Onset of SMA1 typically occurs at one month of age. Children with the disease usually are weak, fail to achieve motor milestones, and have declines in respiration and swallowing. At a median age of 10.5 months, patients die or need permanent ventilatory assistance.
In December 2016, the FDA approved nusinersen for the treatment of SMA. A phase III study found that patients treated with nusinersen were more likely than controls to have improved motor function and event-free survival. The trial was stopped early because of the treatment’s efficacy.
A Small, Open-Label Trial
A mouse study indicated that IV administration of an adenoassociated viral vector (ie, AAV9) containing SMN1 reduced the effects of SMA and extended survival. Jerry R. Mendell, MD, Principal Investigator at Nationwide Children’s Hospital’s Center for Gene Therapy in Columbus, Ohio, and colleagues studied this therapeutic technique in humans.
They enrolled 15 patients with a genetically confirmed diagnosis of SMA1 into two cohorts. The first cohort received a low dose (6.7×1013 vg/kg) of treatment, and the second cohort received a high dose (2.0×1014 vg/kg). Because the first patient in cohort one had serum aminotransferase elevations, the investigators gave 1 mg/kg/day of oral prednisolone to all subsequent patients for 30 days, starting 24 hours before gene therapy.
The study’s primary outcome was treatment-related adverse events of grade 3 or higher. The secondary outcome was time until death or the need for permanent ventilatory assistance, which was defined as at least 16 hours/day of continuous respiratory assistance for at least 14 days. The achievement of motor milestones and Children’s Hospital of Philadelphia Infant Test of Neuromuscular Disorders (CHOP INTEND) scores were exploratory outcomes.
Motor Scores Improved
Three patients entered the low-dose cohort, and 12 were enrolled in the high-dose cohort. Patients’ mean age at treatment was 6.3 months in cohort 1 and 3.4 months in cohort 2. At the last follow-up, all patients had reached age 20 months, and none required permanent mechanical ventilation. Approximately 8% of patients in a historical cohort met these criteria.
All patients had increases from baseline in CHOP INTEND score and maintained these increases throughout the study. Patients in cohort 2 had mean increases of 9.8 points at one month and 15.4 points at three months. Eleven patients achieved and sustained scores greater than 40 points, which is considered clinically meaningful in SMA.
Of the patients in cohort 2, 11 sat unassisted, nine rolled over, 11 fed orally and could speak, and two walked independently. No patients in the historical cohorts achieved any of these milestones, and they rarely became able to speak.
Dr. Mendell and colleagues observed two treatment-related grade 4 adverse events. Both were elevations in serum aminotransferase levels that were attenuated after treatment with prednisolone. The researchers also noted three treatment-related nonserious adverse events (ie, asymptomatic elevations in serum aminotransferase levels that were resolved without additional prednisolone treatment).
The study results were consistent with those of the preclinical mouse study. During a follow-up period of as long as two years, Dr. Mendell and colleagues did not observe any decrease in treatment effect or regression in motor function among the study participants. The presence of antibodies to AAV9 could be a potential limitation of the therapy, however. Further research to assess the treatment’s safety and the durability of its effect are needed, according to the authors.
Comparing Two Treatments
It is difficult to compare the results of Dr. Mendell and colleagues with those of the phase III nusinersen study, because of the two trials’ different designs, said Ans T. van der Ploeg, MD, PhD, Chair of the Center for Lysosomal and Metabolic Diseases at the Erasmus MC University in Rotterdam, the Netherlands, in an accompanying editorial. One potential advantage of AAV9 gene therapy is that it might require a single IV infusion. Nusinersen, on the other hand, may require lifelong intrathecal treatment.
“The durability of the effects is uncertain for both treatments,” said Dr. van der Ploeg. “If the expression of the scAAV9 gene therapy declines over time, the same treatment may not be able to be repeated, because antibodies against AAV capsid proteins are anticipated to form.”
In addition, neither of the two therapies cures SMA type 1. Earlier treatment could be beneficial, as could a combination of both treatments, said Dr. van der Ploeg. But the high expected cost of nusinersen is “an important constraint,” she concluded.
—Erik Greb
Suggested Reading
Mendell JR, Al-Zaidy S, Shell R, et al. Single-dose gene-replacement therapy for spinal muscular atrophy. N Engl J Med. 2017;377(18):1713-1722.
van der Ploeg AT. The dilemma of two innovative therapies for spinal muscular atrophy. N Engl J Med. 2017;377(18):1786-1787.
A single IV infusion to replace the gene encoding survival motor neuron 1 (SMN1) increases survival among infants with spinal muscular atrophy type 1 (SMA1), according to research published in the November 2, 2017, issue of the New England Journal of Medicine. The treatment also improves motor function, and its effects are maintained for two years, the researchers said.
The loss or dysfunction of SMN1 causes SMA, a progressive disease characterized by the degeneration and loss of lower motor neurons. Onset of SMA1 typically occurs at one month of age. Children with the disease usually are weak, fail to achieve motor milestones, and have declines in respiration and swallowing. At a median age of 10.5 months, patients die or need permanent ventilatory assistance.
In December 2016, the FDA approved nusinersen for the treatment of SMA. A phase III study found that patients treated with nusinersen were more likely than controls to have improved motor function and event-free survival. The trial was stopped early because of the treatment’s efficacy.
A Small, Open-Label Trial
A mouse study indicated that IV administration of an adenoassociated viral vector (ie, AAV9) containing SMN1 reduced the effects of SMA and extended survival. Jerry R. Mendell, MD, Principal Investigator at Nationwide Children’s Hospital’s Center for Gene Therapy in Columbus, Ohio, and colleagues studied this therapeutic technique in humans.
They enrolled 15 patients with a genetically confirmed diagnosis of SMA1 into two cohorts. The first cohort received a low dose (6.7×1013 vg/kg) of treatment, and the second cohort received a high dose (2.0×1014 vg/kg). Because the first patient in cohort one had serum aminotransferase elevations, the investigators gave 1 mg/kg/day of oral prednisolone to all subsequent patients for 30 days, starting 24 hours before gene therapy.
The study’s primary outcome was treatment-related adverse events of grade 3 or higher. The secondary outcome was time until death or the need for permanent ventilatory assistance, which was defined as at least 16 hours/day of continuous respiratory assistance for at least 14 days. The achievement of motor milestones and Children’s Hospital of Philadelphia Infant Test of Neuromuscular Disorders (CHOP INTEND) scores were exploratory outcomes.
Motor Scores Improved
Three patients entered the low-dose cohort, and 12 were enrolled in the high-dose cohort. Patients’ mean age at treatment was 6.3 months in cohort 1 and 3.4 months in cohort 2. At the last follow-up, all patients had reached age 20 months, and none required permanent mechanical ventilation. Approximately 8% of patients in a historical cohort met these criteria.
All patients had increases from baseline in CHOP INTEND score and maintained these increases throughout the study. Patients in cohort 2 had mean increases of 9.8 points at one month and 15.4 points at three months. Eleven patients achieved and sustained scores greater than 40 points, which is considered clinically meaningful in SMA.
Of the patients in cohort 2, 11 sat unassisted, nine rolled over, 11 fed orally and could speak, and two walked independently. No patients in the historical cohorts achieved any of these milestones, and they rarely became able to speak.
Dr. Mendell and colleagues observed two treatment-related grade 4 adverse events. Both were elevations in serum aminotransferase levels that were attenuated after treatment with prednisolone. The researchers also noted three treatment-related nonserious adverse events (ie, asymptomatic elevations in serum aminotransferase levels that were resolved without additional prednisolone treatment).
The study results were consistent with those of the preclinical mouse study. During a follow-up period of as long as two years, Dr. Mendell and colleagues did not observe any decrease in treatment effect or regression in motor function among the study participants. The presence of antibodies to AAV9 could be a potential limitation of the therapy, however. Further research to assess the treatment’s safety and the durability of its effect are needed, according to the authors.
Comparing Two Treatments
It is difficult to compare the results of Dr. Mendell and colleagues with those of the phase III nusinersen study, because of the two trials’ different designs, said Ans T. van der Ploeg, MD, PhD, Chair of the Center for Lysosomal and Metabolic Diseases at the Erasmus MC University in Rotterdam, the Netherlands, in an accompanying editorial. One potential advantage of AAV9 gene therapy is that it might require a single IV infusion. Nusinersen, on the other hand, may require lifelong intrathecal treatment.
“The durability of the effects is uncertain for both treatments,” said Dr. van der Ploeg. “If the expression of the scAAV9 gene therapy declines over time, the same treatment may not be able to be repeated, because antibodies against AAV capsid proteins are anticipated to form.”
In addition, neither of the two therapies cures SMA type 1. Earlier treatment could be beneficial, as could a combination of both treatments, said Dr. van der Ploeg. But the high expected cost of nusinersen is “an important constraint,” she concluded.
—Erik Greb
Suggested Reading
Mendell JR, Al-Zaidy S, Shell R, et al. Single-dose gene-replacement therapy for spinal muscular atrophy. N Engl J Med. 2017;377(18):1713-1722.
van der Ploeg AT. The dilemma of two innovative therapies for spinal muscular atrophy. N Engl J Med. 2017;377(18):1786-1787.
Thrombectomy at Six to 24 Hours After Stroke May Improve Outcomes
Compared with standard care alone, standard care plus endovascular thrombectomy at six to 24 hours after stroke onset appears to reduce disability and increase functional independence among patients with a mismatch between clinical deficit and infarct. These findings, which were published online ahead of print November 11 in the New England Journal of Medicine, could benefit patients with stroke who arrive at the hospital after the current six-hour treatment window has closed, said the authors.
“When the irreversibly damaged brain area affected by the stroke is small, we see that clot removal can make a significant positive difference, even if performed outside the six-hour window,” said Tudor Jovin, MD, Director of the University of Pittsburgh Medical Center Stroke Institute. “However, this does not diminish the urgency with which patients must be rushed to the emergency room in the event of a stroke. The mantra ‘time is brain’ still holds true.”

The DAWN Trial Examined Late Thrombectomy
Previous research has indicated that thrombectomy provides clinical benefits for patients with acute ischemic stroke when it is performed within six hours of symptom onset. The benefit of treatment appeared to decrease as the time to treatment increased. Nonrandomized studies, however, have shown that reperfusion of occluded proximal anterior cerebral vessels improves outcomes in patients with a mismatch between the volume of brain tissue that may be salvaged and the volume of infarcted tissue, even if performed more than six hours after the patient was last known to be well.
Dr. Jovin and colleagues conducted the DAWN trial, a multicenter, prospective, randomized, open-label study, to evaluate the effects of late thrombectomy. Eligible patients had an occlusion of the intracranial internal carotid artery or proximal middle cerebral artery and had last been known to be well six to 24 hours earlier. Patients either did not meet criteria for treatment with IV alteplase because of late presentation, or had persistent vessel occlusion despite treatment with IV alteplase.
Participants also had a mismatch between the severity of the clinical deficit and the infarct volume, which was assessed using diffusion-weighted MRI or perfusion CT. The investigators sorted mismatches into three groups. Group A included patients age 80 or older with an NIH Stroke Scale (NIHSS) score of 10 or higher and an infarct volume of less than 21 mL. Group B included patients younger than 80 with an NIHSS score of 10 or higher and an infarct volume of less than 31 mL. Group C included patients younger than 80 with an NIHSS score of 20 or higher and had an infarct volume between 31 mL and 51 mL.
The investigators randomized participants to thrombectomy plus standard care or standard care alone. The first primary end point was the mean score for disability on the utility-weighted modified Rankin scale, which ranges from 0 (ie, death) to 10 (ie, no symptoms or disability). The second was the rate of functional independence (ie, a score of 0–2 on the modified Rankin scale) at 90 days. The main safety end point was stroke-related death at 90 days.
Enrollment Was Halted Early
Dr. Jovin and colleagues enrolled 206 patients in the trial. Enrollment was stopped at 31 months, because an interim analysis found that thrombectomy plus standard care was 95% likely to be superior to standard care alone for the first primary end point. In all, 107 patients received thrombectomy plus standard care, and 99 received standard care alone.
Participants’ mean age was 70, and approximately 46% of participants were men. Median NIHSS score was 17, and median infarct volume was 8.25 mL. The treatment arms were generally balanced, except for three factors. History of atrial fibrillation and wake-up stroke were more common in the thrombectomy group, and treatment with IV alteplase was more common in the control group.
The mean utility-weighted modified Rankin scale score at 90 days was 5.5 in the thrombectomy group and 3.4 in the control group. The rate of functional independence at 90 days was 49% in the thrombectomy group and 13% in the control group. The superiority of thrombectomy plus standard treatment to standard treatment alone for both end points remained significant in post hoc sensitivity analyses that adjusted for between-group differences in baseline characteristics.
The rate of stroke-related death at 90 days did not differ significantly between the treatment groups. Nor did the rate of death from any cause at 90 days or the rate of symptomatic intracerebral hemorrhage differ significantly between groups. The rate of neurologic deterioration was lower in the thrombectomy group than in the control group.
Should the Time Window Be Expanded?
By selecting patients who had a region of brain that was poorly perfused, but not yet infarcted, Dr. Jovin and colleagues replaced the conventional six-hour time window for stroke treatment with a “tissue window,” said Werner Hacke, MD, PhD, Chair of the Department of Neurology at the University of Heidelberg in Germany, in an accompanying editorial. The rate of functional independence at 90 days in the DAWN trial (49%) was similar to that in a previous meta-analysis of several trials of mechanical thrombectomy (46%). “These similar findings suggest that the use of a ‘tissue window’ in choosing patients for thrombectomy is as good as the use of a time window,” said Dr. Hacke. “However, it is also worth emphasizing that the 13% rate of functional independence in the control group in the DAWN trial was lower than the 26% rate in the control group in the pooled analysis.” This low rate of functional independence “is probably the best we can expect” for patients who have not had recanalization by 24 hours after stroke onset.
The DAWN trial provides reason to expect that trials investigating late IV thrombolysis that require the presence of ischemic tissue might have positive outcomes. But “the results of the DAWN trial do not support a general liberalization of the time window for thrombectomy or thrombolysis,” Dr. Hacke continued. “Reducing the time from the onset of stroke to treatment remains essential and results in the best outcomes.”
—Erik Greb
Suggested Reading
Nogueira RG, Jadhav AP, Haussen DC, et al. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N Engl J Med. 2017 Nov 11 [Epub ahead of print].
Hacke W. A new DAWN for imaging-based selection in the treatment of acute stroke. N Engl J Med. 2017 Nov 11 [Epub ahead of print].
Compared with standard care alone, standard care plus endovascular thrombectomy at six to 24 hours after stroke onset appears to reduce disability and increase functional independence among patients with a mismatch between clinical deficit and infarct. These findings, which were published online ahead of print November 11 in the New England Journal of Medicine, could benefit patients with stroke who arrive at the hospital after the current six-hour treatment window has closed, said the authors.
“When the irreversibly damaged brain area affected by the stroke is small, we see that clot removal can make a significant positive difference, even if performed outside the six-hour window,” said Tudor Jovin, MD, Director of the University of Pittsburgh Medical Center Stroke Institute. “However, this does not diminish the urgency with which patients must be rushed to the emergency room in the event of a stroke. The mantra ‘time is brain’ still holds true.”
The DAWN Trial Examined Late Thrombectomy
Previous research has indicated that thrombectomy provides clinical benefits for patients with acute ischemic stroke when it is performed within six hours of symptom onset. The benefit of treatment appeared to decrease as the time to treatment increased. Nonrandomized studies, however, have shown that reperfusion of occluded proximal anterior cerebral vessels improves outcomes in patients with a mismatch between the volume of brain tissue that may be salvaged and the volume of infarcted tissue, even if performed more than six hours after the patient was last known to be well.
Dr. Jovin and colleagues conducted the DAWN trial, a multicenter, prospective, randomized, open-label study, to evaluate the effects of late thrombectomy. Eligible patients had an occlusion of the intracranial internal carotid artery or proximal middle cerebral artery and had last been known to be well six to 24 hours earlier. Patients either did not meet criteria for treatment with IV alteplase because of late presentation, or had persistent vessel occlusion despite treatment with IV alteplase.
Participants also had a mismatch between the severity of the clinical deficit and the infarct volume, which was assessed using diffusion-weighted MRI or perfusion CT. The investigators sorted mismatches into three groups. Group A included patients age 80 or older with an NIH Stroke Scale (NIHSS) score of 10 or higher and an infarct volume of less than 21 mL. Group B included patients younger than 80 with an NIHSS score of 10 or higher and an infarct volume of less than 31 mL. Group C included patients younger than 80 with an NIHSS score of 20 or higher and had an infarct volume between 31 mL and 51 mL.
The investigators randomized participants to thrombectomy plus standard care or standard care alone. The first primary end point was the mean score for disability on the utility-weighted modified Rankin scale, which ranges from 0 (ie, death) to 10 (ie, no symptoms or disability). The second was the rate of functional independence (ie, a score of 0–2 on the modified Rankin scale) at 90 days. The main safety end point was stroke-related death at 90 days.
Enrollment Was Halted Early
Dr. Jovin and colleagues enrolled 206 patients in the trial. Enrollment was stopped at 31 months, because an interim analysis found that thrombectomy plus standard care was 95% likely to be superior to standard care alone for the first primary end point. In all, 107 patients received thrombectomy plus standard care, and 99 received standard care alone.
Participants’ mean age was 70, and approximately 46% of participants were men. Median NIHSS score was 17, and median infarct volume was 8.25 mL. The treatment arms were generally balanced, except for three factors. History of atrial fibrillation and wake-up stroke were more common in the thrombectomy group, and treatment with IV alteplase was more common in the control group.
The mean utility-weighted modified Rankin scale score at 90 days was 5.5 in the thrombectomy group and 3.4 in the control group. The rate of functional independence at 90 days was 49% in the thrombectomy group and 13% in the control group. The superiority of thrombectomy plus standard treatment to standard treatment alone for both end points remained significant in post hoc sensitivity analyses that adjusted for between-group differences in baseline characteristics.
The rate of stroke-related death at 90 days did not differ significantly between the treatment groups. Nor did the rate of death from any cause at 90 days or the rate of symptomatic intracerebral hemorrhage differ significantly between groups. The rate of neurologic deterioration was lower in the thrombectomy group than in the control group.
Should the Time Window Be Expanded?
By selecting patients who had a region of brain that was poorly perfused, but not yet infarcted, Dr. Jovin and colleagues replaced the conventional six-hour time window for stroke treatment with a “tissue window,” said Werner Hacke, MD, PhD, Chair of the Department of Neurology at the University of Heidelberg in Germany, in an accompanying editorial. The rate of functional independence at 90 days in the DAWN trial (49%) was similar to that in a previous meta-analysis of several trials of mechanical thrombectomy (46%). “These similar findings suggest that the use of a ‘tissue window’ in choosing patients for thrombectomy is as good as the use of a time window,” said Dr. Hacke. “However, it is also worth emphasizing that the 13% rate of functional independence in the control group in the DAWN trial was lower than the 26% rate in the control group in the pooled analysis.” This low rate of functional independence “is probably the best we can expect” for patients who have not had recanalization by 24 hours after stroke onset.
The DAWN trial provides reason to expect that trials investigating late IV thrombolysis that require the presence of ischemic tissue might have positive outcomes. But “the results of the DAWN trial do not support a general liberalization of the time window for thrombectomy or thrombolysis,” Dr. Hacke continued. “Reducing the time from the onset of stroke to treatment remains essential and results in the best outcomes.”
—Erik Greb
Suggested Reading
Nogueira RG, Jadhav AP, Haussen DC, et al. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N Engl J Med. 2017 Nov 11 [Epub ahead of print].
Hacke W. A new DAWN for imaging-based selection in the treatment of acute stroke. N Engl J Med. 2017 Nov 11 [Epub ahead of print].
Compared with standard care alone, standard care plus endovascular thrombectomy at six to 24 hours after stroke onset appears to reduce disability and increase functional independence among patients with a mismatch between clinical deficit and infarct. These findings, which were published online ahead of print November 11 in the New England Journal of Medicine, could benefit patients with stroke who arrive at the hospital after the current six-hour treatment window has closed, said the authors.
“When the irreversibly damaged brain area affected by the stroke is small, we see that clot removal can make a significant positive difference, even if performed outside the six-hour window,” said Tudor Jovin, MD, Director of the University of Pittsburgh Medical Center Stroke Institute. “However, this does not diminish the urgency with which patients must be rushed to the emergency room in the event of a stroke. The mantra ‘time is brain’ still holds true.”
The DAWN Trial Examined Late Thrombectomy
Previous research has indicated that thrombectomy provides clinical benefits for patients with acute ischemic stroke when it is performed within six hours of symptom onset. The benefit of treatment appeared to decrease as the time to treatment increased. Nonrandomized studies, however, have shown that reperfusion of occluded proximal anterior cerebral vessels improves outcomes in patients with a mismatch between the volume of brain tissue that may be salvaged and the volume of infarcted tissue, even if performed more than six hours after the patient was last known to be well.
Dr. Jovin and colleagues conducted the DAWN trial, a multicenter, prospective, randomized, open-label study, to evaluate the effects of late thrombectomy. Eligible patients had an occlusion of the intracranial internal carotid artery or proximal middle cerebral artery and had last been known to be well six to 24 hours earlier. Patients either did not meet criteria for treatment with IV alteplase because of late presentation, or had persistent vessel occlusion despite treatment with IV alteplase.
Participants also had a mismatch between the severity of the clinical deficit and the infarct volume, which was assessed using diffusion-weighted MRI or perfusion CT. The investigators sorted mismatches into three groups. Group A included patients age 80 or older with an NIH Stroke Scale (NIHSS) score of 10 or higher and an infarct volume of less than 21 mL. Group B included patients younger than 80 with an NIHSS score of 10 or higher and an infarct volume of less than 31 mL. Group C included patients younger than 80 with an NIHSS score of 20 or higher and had an infarct volume between 31 mL and 51 mL.
The investigators randomized participants to thrombectomy plus standard care or standard care alone. The first primary end point was the mean score for disability on the utility-weighted modified Rankin scale, which ranges from 0 (ie, death) to 10 (ie, no symptoms or disability). The second was the rate of functional independence (ie, a score of 0–2 on the modified Rankin scale) at 90 days. The main safety end point was stroke-related death at 90 days.
Enrollment Was Halted Early
Dr. Jovin and colleagues enrolled 206 patients in the trial. Enrollment was stopped at 31 months, because an interim analysis found that thrombectomy plus standard care was 95% likely to be superior to standard care alone for the first primary end point. In all, 107 patients received thrombectomy plus standard care, and 99 received standard care alone.
Participants’ mean age was 70, and approximately 46% of participants were men. Median NIHSS score was 17, and median infarct volume was 8.25 mL. The treatment arms were generally balanced, except for three factors. History of atrial fibrillation and wake-up stroke were more common in the thrombectomy group, and treatment with IV alteplase was more common in the control group.
The mean utility-weighted modified Rankin scale score at 90 days was 5.5 in the thrombectomy group and 3.4 in the control group. The rate of functional independence at 90 days was 49% in the thrombectomy group and 13% in the control group. The superiority of thrombectomy plus standard treatment to standard treatment alone for both end points remained significant in post hoc sensitivity analyses that adjusted for between-group differences in baseline characteristics.
The rate of stroke-related death at 90 days did not differ significantly between the treatment groups. Nor did the rate of death from any cause at 90 days or the rate of symptomatic intracerebral hemorrhage differ significantly between groups. The rate of neurologic deterioration was lower in the thrombectomy group than in the control group.
Should the Time Window Be Expanded?
By selecting patients who had a region of brain that was poorly perfused, but not yet infarcted, Dr. Jovin and colleagues replaced the conventional six-hour time window for stroke treatment with a “tissue window,” said Werner Hacke, MD, PhD, Chair of the Department of Neurology at the University of Heidelberg in Germany, in an accompanying editorial. The rate of functional independence at 90 days in the DAWN trial (49%) was similar to that in a previous meta-analysis of several trials of mechanical thrombectomy (46%). “These similar findings suggest that the use of a ‘tissue window’ in choosing patients for thrombectomy is as good as the use of a time window,” said Dr. Hacke. “However, it is also worth emphasizing that the 13% rate of functional independence in the control group in the DAWN trial was lower than the 26% rate in the control group in the pooled analysis.” This low rate of functional independence “is probably the best we can expect” for patients who have not had recanalization by 24 hours after stroke onset.
The DAWN trial provides reason to expect that trials investigating late IV thrombolysis that require the presence of ischemic tissue might have positive outcomes. But “the results of the DAWN trial do not support a general liberalization of the time window for thrombectomy or thrombolysis,” Dr. Hacke continued. “Reducing the time from the onset of stroke to treatment remains essential and results in the best outcomes.”
—Erik Greb
Suggested Reading
Nogueira RG, Jadhav AP, Haussen DC, et al. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N Engl J Med. 2017 Nov 11 [Epub ahead of print].
Hacke W. A new DAWN for imaging-based selection in the treatment of acute stroke. N Engl J Med. 2017 Nov 11 [Epub ahead of print].
Is the Estrogen–CGRP Relationship Relevant to Migraine?
Calcitonin gene-related peptide (CGRP) plays a key role in migraine pathophysiology, and recent studies have identified interactions between ovarian steroid hormones, CGRP, and the trigeminovascular system, according to a review published online ahead of print October 30, 2017, in Cephalalgia.
“Numerous animal and human studies have shown that cyclic fluctuations of ovarian hormones (mainly estrogen) modulate CGRP in the peripheral and central trigeminovascular system; this [effect] is especially relevant now that novel antibodies directed against CGRP or its receptor are currently in clinical trials,” said Alejandro Labastida-Ramírez of the Division of Vascular Medicine and Pharmacology at Erasmus University Medical Center in Rotterdam, the Netherlands, and colleagues.
The relationship between estrogen and CGRP seems to be “a key factor involved in the higher prevalence of migraine in women,” the authors said. “Future studies should focus on how fluctuations of gonadal hormones influence migraine pathophysiology in both genders…. Hopefully, these sex-related differences may contribute to the development of gender-specific therapies.”
Interplay of Hormones and CGRP
A clinical study by Stevenson et al in 1986 was one of the first to discover a relationship between female sex hormones and CGRP. In this study, concentrations of immunoreactive plasma CGRP in healthy women were significantly increased throughout pregnancy and decreased after delivery. A 1990 study by Valdemarsson et al found that in healthy subjects, immunoreactive plasma CGRP levels were significantly higher in females than in males. “The use of combined contraceptive pills was associated with even higher levels of immunoreactive CGRP in plasma,” said the review authors. “Accordingly, in postmenopausal women, decreased estradiol serum levels were positively correlated with decreased plasma immunoreactive CGRP concentrations, [suggesting] that the CGRP system could be influenced directly by endogenous or exogenous ovarian steroid hormones.”
Ibrahimi et al in 2017 used an experimental model to explore gender differences in CGRP-dependent dermal blood flow in healthy subjects and migraineurs. Dermal blood flow in males did not vary over time and was comparable between healthy subjects and migraineurs. In healthy women, fluctuations of ovarian steroid hormones influenced CGRP-dependent dermal blood flow. “Interestingly, in female migraine patients, dermal blood flow responses were elevated, compared to healthy subjects, but these responses were independent of the menstrual cycle,” the review authors noted.
Therapeutic Trials
Three humanized monoclonal antibodies targeting CGRP and one fully human monoclonal antibody targeting the CGRP receptor are in development.
While trials indicate that CGRP blockade is effective for treating migraine, further studies are needed to “elucidate whether these novel drugs are safe in individuals with cardiovascular risk factors, if there are any consequences of chronic CGRP inhibition in young reproductive women with a normal menstrual cycle, and whether efficacy depends on the phase of the menstrual cycle,” the authors said.
—Jake Remaly
Suggested Reading
Ibrahimi K, Vermeersch S, Frederiks P, et al. The influence of migraine and female hormones on capsaicin-induced dermal blood flow. Cephalalgia. 2017;37(12):1164-1172.
Labastida-Ramírez A, Rubio-Beltrán E, Villalón CM, MaassenVanDenBrink A. Gender aspects of CGRP in migraine. Cephalalgia. 2017 Oct 30 [Epub ahead of print].
Stevenson JC, Macdonald DW, Warren RC, et al. Increased concentration of circulating calcitonin gene related peptide during normal human pregnancy. Br Med J (Clin Res Ed). 1986;293(6558):1329-1330.
Valdemarsson S, Edvinsson L, Hedner P, Ekman R. Hormonal influence on calcitonin gene-related peptide in man: effects of sex difference and contraceptive pills. Scand J Clin Lab Invest. 1990;50(4):385-388.
Calcitonin gene-related peptide (CGRP) plays a key role in migraine pathophysiology, and recent studies have identified interactions between ovarian steroid hormones, CGRP, and the trigeminovascular system, according to a review published online ahead of print October 30, 2017, in Cephalalgia.
“Numerous animal and human studies have shown that cyclic fluctuations of ovarian hormones (mainly estrogen) modulate CGRP in the peripheral and central trigeminovascular system; this [effect] is especially relevant now that novel antibodies directed against CGRP or its receptor are currently in clinical trials,” said Alejandro Labastida-Ramírez of the Division of Vascular Medicine and Pharmacology at Erasmus University Medical Center in Rotterdam, the Netherlands, and colleagues.
The relationship between estrogen and CGRP seems to be “a key factor involved in the higher prevalence of migraine in women,” the authors said. “Future studies should focus on how fluctuations of gonadal hormones influence migraine pathophysiology in both genders…. Hopefully, these sex-related differences may contribute to the development of gender-specific therapies.”
Interplay of Hormones and CGRP
A clinical study by Stevenson et al in 1986 was one of the first to discover a relationship between female sex hormones and CGRP. In this study, concentrations of immunoreactive plasma CGRP in healthy women were significantly increased throughout pregnancy and decreased after delivery. A 1990 study by Valdemarsson et al found that in healthy subjects, immunoreactive plasma CGRP levels were significantly higher in females than in males. “The use of combined contraceptive pills was associated with even higher levels of immunoreactive CGRP in plasma,” said the review authors. “Accordingly, in postmenopausal women, decreased estradiol serum levels were positively correlated with decreased plasma immunoreactive CGRP concentrations, [suggesting] that the CGRP system could be influenced directly by endogenous or exogenous ovarian steroid hormones.”
Ibrahimi et al in 2017 used an experimental model to explore gender differences in CGRP-dependent dermal blood flow in healthy subjects and migraineurs. Dermal blood flow in males did not vary over time and was comparable between healthy subjects and migraineurs. In healthy women, fluctuations of ovarian steroid hormones influenced CGRP-dependent dermal blood flow. “Interestingly, in female migraine patients, dermal blood flow responses were elevated, compared to healthy subjects, but these responses were independent of the menstrual cycle,” the review authors noted.
Therapeutic Trials
Three humanized monoclonal antibodies targeting CGRP and one fully human monoclonal antibody targeting the CGRP receptor are in development.
While trials indicate that CGRP blockade is effective for treating migraine, further studies are needed to “elucidate whether these novel drugs are safe in individuals with cardiovascular risk factors, if there are any consequences of chronic CGRP inhibition in young reproductive women with a normal menstrual cycle, and whether efficacy depends on the phase of the menstrual cycle,” the authors said.
—Jake Remaly
Suggested Reading
Ibrahimi K, Vermeersch S, Frederiks P, et al. The influence of migraine and female hormones on capsaicin-induced dermal blood flow. Cephalalgia. 2017;37(12):1164-1172.
Labastida-Ramírez A, Rubio-Beltrán E, Villalón CM, MaassenVanDenBrink A. Gender aspects of CGRP in migraine. Cephalalgia. 2017 Oct 30 [Epub ahead of print].
Stevenson JC, Macdonald DW, Warren RC, et al. Increased concentration of circulating calcitonin gene related peptide during normal human pregnancy. Br Med J (Clin Res Ed). 1986;293(6558):1329-1330.
Valdemarsson S, Edvinsson L, Hedner P, Ekman R. Hormonal influence on calcitonin gene-related peptide in man: effects of sex difference and contraceptive pills. Scand J Clin Lab Invest. 1990;50(4):385-388.
Calcitonin gene-related peptide (CGRP) plays a key role in migraine pathophysiology, and recent studies have identified interactions between ovarian steroid hormones, CGRP, and the trigeminovascular system, according to a review published online ahead of print October 30, 2017, in Cephalalgia.
“Numerous animal and human studies have shown that cyclic fluctuations of ovarian hormones (mainly estrogen) modulate CGRP in the peripheral and central trigeminovascular system; this [effect] is especially relevant now that novel antibodies directed against CGRP or its receptor are currently in clinical trials,” said Alejandro Labastida-Ramírez of the Division of Vascular Medicine and Pharmacology at Erasmus University Medical Center in Rotterdam, the Netherlands, and colleagues.
The relationship between estrogen and CGRP seems to be “a key factor involved in the higher prevalence of migraine in women,” the authors said. “Future studies should focus on how fluctuations of gonadal hormones influence migraine pathophysiology in both genders…. Hopefully, these sex-related differences may contribute to the development of gender-specific therapies.”
Interplay of Hormones and CGRP
A clinical study by Stevenson et al in 1986 was one of the first to discover a relationship between female sex hormones and CGRP. In this study, concentrations of immunoreactive plasma CGRP in healthy women were significantly increased throughout pregnancy and decreased after delivery. A 1990 study by Valdemarsson et al found that in healthy subjects, immunoreactive plasma CGRP levels were significantly higher in females than in males. “The use of combined contraceptive pills was associated with even higher levels of immunoreactive CGRP in plasma,” said the review authors. “Accordingly, in postmenopausal women, decreased estradiol serum levels were positively correlated with decreased plasma immunoreactive CGRP concentrations, [suggesting] that the CGRP system could be influenced directly by endogenous or exogenous ovarian steroid hormones.”
Ibrahimi et al in 2017 used an experimental model to explore gender differences in CGRP-dependent dermal blood flow in healthy subjects and migraineurs. Dermal blood flow in males did not vary over time and was comparable between healthy subjects and migraineurs. In healthy women, fluctuations of ovarian steroid hormones influenced CGRP-dependent dermal blood flow. “Interestingly, in female migraine patients, dermal blood flow responses were elevated, compared to healthy subjects, but these responses were independent of the menstrual cycle,” the review authors noted.
Therapeutic Trials
Three humanized monoclonal antibodies targeting CGRP and one fully human monoclonal antibody targeting the CGRP receptor are in development.
While trials indicate that CGRP blockade is effective for treating migraine, further studies are needed to “elucidate whether these novel drugs are safe in individuals with cardiovascular risk factors, if there are any consequences of chronic CGRP inhibition in young reproductive women with a normal menstrual cycle, and whether efficacy depends on the phase of the menstrual cycle,” the authors said.
—Jake Remaly
Suggested Reading
Ibrahimi K, Vermeersch S, Frederiks P, et al. The influence of migraine and female hormones on capsaicin-induced dermal blood flow. Cephalalgia. 2017;37(12):1164-1172.
Labastida-Ramírez A, Rubio-Beltrán E, Villalón CM, MaassenVanDenBrink A. Gender aspects of CGRP in migraine. Cephalalgia. 2017 Oct 30 [Epub ahead of print].
Stevenson JC, Macdonald DW, Warren RC, et al. Increased concentration of circulating calcitonin gene related peptide during normal human pregnancy. Br Med J (Clin Res Ed). 1986;293(6558):1329-1330.
Valdemarsson S, Edvinsson L, Hedner P, Ekman R. Hormonal influence on calcitonin gene-related peptide in man: effects of sex difference and contraceptive pills. Scand J Clin Lab Invest. 1990;50(4):385-388.
Does Midlife Physical Activity Affect Cognitive Health in Later Life?
In contrast with previous research, a study published in the Journal of Alzheimer’s Disease indicates that exercise in midlife is not associated with cognitive fitness in late life. The data suggest that physical activity may not help maintain cognitive function or prevent the onset of Alzheimer’s disease. Physical activity in late life, however, is associated with high cognitive function two years later, according to the researchers.
The literature contains few prospective data on the relationship between midlife and late-life physical activity and late-life cognitive performance. Cross-sectional study designs and short durations of follow-up have made several studies of this relationship unsatisfactory, according to Alden L. Gross, PhD, Assistant Professor of Epidemiology at Johns Hopkins Bloomberg School of Public Health in Baltimore, and colleagues.
A Prospective Study of Medical Graduates
To conduct a prospective analysis of the possible association between exercise in midlife and cognitive performance in later life, Dr. Gross and colleagues examined 30 years of longitudinal data from the Johns Hopkins Precursors study. This study enrolled medical graduates from 1948 to 1964 and followed them annually with health questionnaires. Surveys of physical activity were mailed in 1978, 1986, 1989, 1993, 1995, 1997, 2003, and 2006. Participants underwent cognitive testing in 2005 and 2008.
An adjudication committee consisting of physicians assigned diagnoses of dementia and dates of onset based on participants’ medical records. The investigators assigned a metabolic equivalent value (MET) to each category of activity (ie, vigorous, moderate, light, and sleep). They used linear regression for cognitive tests and Cox proportional hazards models for dementia onset to characterize associations with midlife physical activity. Models were adjusted for age, sex, smoking, diabetes, and hypertension.
Exercise Had No Long-Term Cognitive Effects
The study sample included 646 participants (48 women). In 1978, participants’ mean age was 47, mean BMI was 23.7 kg/m2, the prevalence of hypertension was 8.8%, and the prevalence of diabetes was 0.8%. Approximately 74% of participants reported regular exercise. In 2006, 54% of participants had hypertension, and 12% had diabetes. The incidence of dementia was 4.3%, and mean age at onset was 77.
No measure of activity in 1978, including MET h/day, decile of physical activity, and engagement in regular exercise, was associated with cognitive performance in demographic-adjusted or fully adjusted models. Regular exercise in 2006 and MET h/day expended in 2006, however, were associated with better cognitive performance. In addition, no physical activity exposure in 1978 was associated with onset of dementia. Greater physical activity in 2006, however, had a modest inverse association with risk of dementia.
The strength of the association between cognitive outcomes and physical activity in 1978 did not vary by gender. In 2006, however, greater MET h/day in a typical week and regular exercise were significantly associated with better cognitive performance in women, but not in men.
Homogeneous Sample Reduced Confounders
Previous studies included diverse cross sections of people and thus may have been susceptible to residual confounding by factors such as years of education, said the investigators. The Precursors study represents a highly homogeneous sample, however, which reduces the likelihood of such confounding. Nevertheless, the homogenous sample may limit the results’ generalizability, particularly to women.
“The prevailing notion that higher levels of physical activity protect against cognitive impairment in later life may result from the artifact of reverse causation,” said the authors. “While physical activity is strongly recommended for many reasons, our data suggest cognitive health may not be one of those reasons.”
“These findings have implications for intervention work moving forward,” said Dr. Gross. “We still need to focus on causes and mechanisms of Alzheimer’s [disease] and dementia, since we do not yet know which preventive measures may or may not work. For now, when I speak in the community about Alzheimer’s [disease], I find that people take some relief in understanding that there was not anything that anyone might have done to avoid a loved one developing Alzheimer’s [disease]. Of course, the goal for researchers is to identify factors that may help older people maintain their cognitive function into their later years. More long-term studies like the Precursors study are needed.”
—Erik Greb
Suggested Reading
Gross AL, Lu H, Meoni L, et al. Physical activity in midlife is not associated with cognitive health in later life among cognitively normal older adults. J Alzheimers Dis. 2017;59(4):1349-1358.
In contrast with previous research, a study published in the Journal of Alzheimer’s Disease indicates that exercise in midlife is not associated with cognitive fitness in late life. The data suggest that physical activity may not help maintain cognitive function or prevent the onset of Alzheimer’s disease. Physical activity in late life, however, is associated with high cognitive function two years later, according to the researchers.
The literature contains few prospective data on the relationship between midlife and late-life physical activity and late-life cognitive performance. Cross-sectional study designs and short durations of follow-up have made several studies of this relationship unsatisfactory, according to Alden L. Gross, PhD, Assistant Professor of Epidemiology at Johns Hopkins Bloomberg School of Public Health in Baltimore, and colleagues.
A Prospective Study of Medical Graduates
To conduct a prospective analysis of the possible association between exercise in midlife and cognitive performance in later life, Dr. Gross and colleagues examined 30 years of longitudinal data from the Johns Hopkins Precursors study. This study enrolled medical graduates from 1948 to 1964 and followed them annually with health questionnaires. Surveys of physical activity were mailed in 1978, 1986, 1989, 1993, 1995, 1997, 2003, and 2006. Participants underwent cognitive testing in 2005 and 2008.
An adjudication committee consisting of physicians assigned diagnoses of dementia and dates of onset based on participants’ medical records. The investigators assigned a metabolic equivalent value (MET) to each category of activity (ie, vigorous, moderate, light, and sleep). They used linear regression for cognitive tests and Cox proportional hazards models for dementia onset to characterize associations with midlife physical activity. Models were adjusted for age, sex, smoking, diabetes, and hypertension.
Exercise Had No Long-Term Cognitive Effects
The study sample included 646 participants (48 women). In 1978, participants’ mean age was 47, mean BMI was 23.7 kg/m2, the prevalence of hypertension was 8.8%, and the prevalence of diabetes was 0.8%. Approximately 74% of participants reported regular exercise. In 2006, 54% of participants had hypertension, and 12% had diabetes. The incidence of dementia was 4.3%, and mean age at onset was 77.
No measure of activity in 1978, including MET h/day, decile of physical activity, and engagement in regular exercise, was associated with cognitive performance in demographic-adjusted or fully adjusted models. Regular exercise in 2006 and MET h/day expended in 2006, however, were associated with better cognitive performance. In addition, no physical activity exposure in 1978 was associated with onset of dementia. Greater physical activity in 2006, however, had a modest inverse association with risk of dementia.
The strength of the association between cognitive outcomes and physical activity in 1978 did not vary by gender. In 2006, however, greater MET h/day in a typical week and regular exercise were significantly associated with better cognitive performance in women, but not in men.
Homogeneous Sample Reduced Confounders
Previous studies included diverse cross sections of people and thus may have been susceptible to residual confounding by factors such as years of education, said the investigators. The Precursors study represents a highly homogeneous sample, however, which reduces the likelihood of such confounding. Nevertheless, the homogenous sample may limit the results’ generalizability, particularly to women.
“The prevailing notion that higher levels of physical activity protect against cognitive impairment in later life may result from the artifact of reverse causation,” said the authors. “While physical activity is strongly recommended for many reasons, our data suggest cognitive health may not be one of those reasons.”
“These findings have implications for intervention work moving forward,” said Dr. Gross. “We still need to focus on causes and mechanisms of Alzheimer’s [disease] and dementia, since we do not yet know which preventive measures may or may not work. For now, when I speak in the community about Alzheimer’s [disease], I find that people take some relief in understanding that there was not anything that anyone might have done to avoid a loved one developing Alzheimer’s [disease]. Of course, the goal for researchers is to identify factors that may help older people maintain their cognitive function into their later years. More long-term studies like the Precursors study are needed.”
—Erik Greb
Suggested Reading
Gross AL, Lu H, Meoni L, et al. Physical activity in midlife is not associated with cognitive health in later life among cognitively normal older adults. J Alzheimers Dis. 2017;59(4):1349-1358.
In contrast with previous research, a study published in the Journal of Alzheimer’s Disease indicates that exercise in midlife is not associated with cognitive fitness in late life. The data suggest that physical activity may not help maintain cognitive function or prevent the onset of Alzheimer’s disease. Physical activity in late life, however, is associated with high cognitive function two years later, according to the researchers.
The literature contains few prospective data on the relationship between midlife and late-life physical activity and late-life cognitive performance. Cross-sectional study designs and short durations of follow-up have made several studies of this relationship unsatisfactory, according to Alden L. Gross, PhD, Assistant Professor of Epidemiology at Johns Hopkins Bloomberg School of Public Health in Baltimore, and colleagues.
A Prospective Study of Medical Graduates
To conduct a prospective analysis of the possible association between exercise in midlife and cognitive performance in later life, Dr. Gross and colleagues examined 30 years of longitudinal data from the Johns Hopkins Precursors study. This study enrolled medical graduates from 1948 to 1964 and followed them annually with health questionnaires. Surveys of physical activity were mailed in 1978, 1986, 1989, 1993, 1995, 1997, 2003, and 2006. Participants underwent cognitive testing in 2005 and 2008.
An adjudication committee consisting of physicians assigned diagnoses of dementia and dates of onset based on participants’ medical records. The investigators assigned a metabolic equivalent value (MET) to each category of activity (ie, vigorous, moderate, light, and sleep). They used linear regression for cognitive tests and Cox proportional hazards models for dementia onset to characterize associations with midlife physical activity. Models were adjusted for age, sex, smoking, diabetes, and hypertension.
Exercise Had No Long-Term Cognitive Effects
The study sample included 646 participants (48 women). In 1978, participants’ mean age was 47, mean BMI was 23.7 kg/m2, the prevalence of hypertension was 8.8%, and the prevalence of diabetes was 0.8%. Approximately 74% of participants reported regular exercise. In 2006, 54% of participants had hypertension, and 12% had diabetes. The incidence of dementia was 4.3%, and mean age at onset was 77.
No measure of activity in 1978, including MET h/day, decile of physical activity, and engagement in regular exercise, was associated with cognitive performance in demographic-adjusted or fully adjusted models. Regular exercise in 2006 and MET h/day expended in 2006, however, were associated with better cognitive performance. In addition, no physical activity exposure in 1978 was associated with onset of dementia. Greater physical activity in 2006, however, had a modest inverse association with risk of dementia.
The strength of the association between cognitive outcomes and physical activity in 1978 did not vary by gender. In 2006, however, greater MET h/day in a typical week and regular exercise were significantly associated with better cognitive performance in women, but not in men.
Homogeneous Sample Reduced Confounders
Previous studies included diverse cross sections of people and thus may have been susceptible to residual confounding by factors such as years of education, said the investigators. The Precursors study represents a highly homogeneous sample, however, which reduces the likelihood of such confounding. Nevertheless, the homogenous sample may limit the results’ generalizability, particularly to women.
“The prevailing notion that higher levels of physical activity protect against cognitive impairment in later life may result from the artifact of reverse causation,” said the authors. “While physical activity is strongly recommended for many reasons, our data suggest cognitive health may not be one of those reasons.”
“These findings have implications for intervention work moving forward,” said Dr. Gross. “We still need to focus on causes and mechanisms of Alzheimer’s [disease] and dementia, since we do not yet know which preventive measures may or may not work. For now, when I speak in the community about Alzheimer’s [disease], I find that people take some relief in understanding that there was not anything that anyone might have done to avoid a loved one developing Alzheimer’s [disease]. Of course, the goal for researchers is to identify factors that may help older people maintain their cognitive function into their later years. More long-term studies like the Precursors study are needed.”
—Erik Greb
Suggested Reading
Gross AL, Lu H, Meoni L, et al. Physical activity in midlife is not associated with cognitive health in later life among cognitively normal older adults. J Alzheimers Dis. 2017;59(4):1349-1358.
Is Change in Personality an Early Sign of Dementia?
Evidence does not support the hypothesis that change in personality is a marker for preclinical mild cognitive impairment or dementia, according to research published online ahead of print September 20 in JAMA Psychiatry. Patients who subsequently develop dementia, however, appear to score higher on neuroticism and lower on conscientiousness and extraversion than people who remain cognitively healthy.
“These findings suggest that tracking change in self-rated personality as an early indicator of dementia is unlikely to be fruitful, while a single assessment provides reliable information on the personality traits that increase resilience (eg, conscientiousness) or vulnerability (eg, neuroticism) to clinical dementia,” said Antonio Terracciano, PhD, Associate Professor of Geriatrics at Florida State University College of Medicine in Tallahassee.

Changes in behavior and personality are one criterion for the diagnosis of dementia. It is uncertain whether such changes begin before the clinical onset of the disease, however. Prospective studies of this question have either not assessed all five major dimensions of personality or administered assessments too close in time to the diagnosis of dementia.
Examining Change in Personality Traits
Dr. Terracciano and colleagues conducted a study to determine whether increases in neuroticism, declines in conscientiousness, and changes in other personality traits occur before the onset of mild cognitive impairment or dementia. They examined data for a cohort of 2,046 community-dwelling older adults who participated in the Baltimore Longitudinal Study of Aging. In the latter study, participants with no cognitive impairment underwent periodic personality and clinical assessments between 1980 and July 13, 2016. Follow-up lasted for as long as 36 years.
Participants completed the self-report version of the Revised NEO Personality Inventory (NEO-PI-R), or an earlier version, in 1980 and 1986. The NEO-PI-R is a 240-item questionnaire that assesses 30 facets of personality, including six for each of the following five major dimensions: neuroticism, extraversion, openness, agreeableness, and conscientiousness. In addition, participants were evaluated at enrollment for history of neurologic or cerebrovascular disease and for impairment of cognitive or behavioral functioning. Follow-up evaluations included a neuropsychologic battery and clinical examination, including an informant-and-participant-structured interview.
Patients With Dementia Had Higher Neuroticism Scores
Participants’ mean age at baseline was 62. In all, 931 participants (46%) were women. The population sample included 374 blacks (18%), 1,582 whites (77%), and 55 Asians or Pacific Islanders (3%). During the study, 104 participants (5%) developed mild cognitive impairment, and 255 (13%) developed all-cause dementia, including 194 (10%) who developed Alzheimer’s disease.
Change in personality before the onset of mild cognitive impairment or dementia was not significantly different between participants who remained unimpaired and those who developed Alzheimer’s disease. Change in personality for participants who developed mild cognitive impairment and all-cause dementia also was similar to that in unimpaired participants. Neuroticism and conscientiousness did not change significantly as disease onset approached.
One limitation of this study was that the population sample was selective and highly educated, said the authors. Another limitation was that the unimpaired participants were relatively young and could develop dementia in the future. “More research is needed on personality and Alzheimer’s disease biomarkers and how personality may increase resilience against neuropathology and forestall the emergence of clinical dementia,” said Dr. Terracciano.
—Erica Tricarico
Suggested Reading
Terracciano A, An Y, Sutin AR, et al. Personality change in the preclinical phase of Alzheimer disease. JAMA Psychiatry. 2017 Sep 20 [Epub ahead of print].
Evidence does not support the hypothesis that change in personality is a marker for preclinical mild cognitive impairment or dementia, according to research published online ahead of print September 20 in JAMA Psychiatry. Patients who subsequently develop dementia, however, appear to score higher on neuroticism and lower on conscientiousness and extraversion than people who remain cognitively healthy.
“These findings suggest that tracking change in self-rated personality as an early indicator of dementia is unlikely to be fruitful, while a single assessment provides reliable information on the personality traits that increase resilience (eg, conscientiousness) or vulnerability (eg, neuroticism) to clinical dementia,” said Antonio Terracciano, PhD, Associate Professor of Geriatrics at Florida State University College of Medicine in Tallahassee.
Changes in behavior and personality are one criterion for the diagnosis of dementia. It is uncertain whether such changes begin before the clinical onset of the disease, however. Prospective studies of this question have either not assessed all five major dimensions of personality or administered assessments too close in time to the diagnosis of dementia.
Examining Change in Personality Traits
Dr. Terracciano and colleagues conducted a study to determine whether increases in neuroticism, declines in conscientiousness, and changes in other personality traits occur before the onset of mild cognitive impairment or dementia. They examined data for a cohort of 2,046 community-dwelling older adults who participated in the Baltimore Longitudinal Study of Aging. In the latter study, participants with no cognitive impairment underwent periodic personality and clinical assessments between 1980 and July 13, 2016. Follow-up lasted for as long as 36 years.
Participants completed the self-report version of the Revised NEO Personality Inventory (NEO-PI-R), or an earlier version, in 1980 and 1986. The NEO-PI-R is a 240-item questionnaire that assesses 30 facets of personality, including six for each of the following five major dimensions: neuroticism, extraversion, openness, agreeableness, and conscientiousness. In addition, participants were evaluated at enrollment for history of neurologic or cerebrovascular disease and for impairment of cognitive or behavioral functioning. Follow-up evaluations included a neuropsychologic battery and clinical examination, including an informant-and-participant-structured interview.
Patients With Dementia Had Higher Neuroticism Scores
Participants’ mean age at baseline was 62. In all, 931 participants (46%) were women. The population sample included 374 blacks (18%), 1,582 whites (77%), and 55 Asians or Pacific Islanders (3%). During the study, 104 participants (5%) developed mild cognitive impairment, and 255 (13%) developed all-cause dementia, including 194 (10%) who developed Alzheimer’s disease.
Change in personality before the onset of mild cognitive impairment or dementia was not significantly different between participants who remained unimpaired and those who developed Alzheimer’s disease. Change in personality for participants who developed mild cognitive impairment and all-cause dementia also was similar to that in unimpaired participants. Neuroticism and conscientiousness did not change significantly as disease onset approached.
One limitation of this study was that the population sample was selective and highly educated, said the authors. Another limitation was that the unimpaired participants were relatively young and could develop dementia in the future. “More research is needed on personality and Alzheimer’s disease biomarkers and how personality may increase resilience against neuropathology and forestall the emergence of clinical dementia,” said Dr. Terracciano.
—Erica Tricarico
Suggested Reading
Terracciano A, An Y, Sutin AR, et al. Personality change in the preclinical phase of Alzheimer disease. JAMA Psychiatry. 2017 Sep 20 [Epub ahead of print].
Evidence does not support the hypothesis that change in personality is a marker for preclinical mild cognitive impairment or dementia, according to research published online ahead of print September 20 in JAMA Psychiatry. Patients who subsequently develop dementia, however, appear to score higher on neuroticism and lower on conscientiousness and extraversion than people who remain cognitively healthy.
“These findings suggest that tracking change in self-rated personality as an early indicator of dementia is unlikely to be fruitful, while a single assessment provides reliable information on the personality traits that increase resilience (eg, conscientiousness) or vulnerability (eg, neuroticism) to clinical dementia,” said Antonio Terracciano, PhD, Associate Professor of Geriatrics at Florida State University College of Medicine in Tallahassee.
Changes in behavior and personality are one criterion for the diagnosis of dementia. It is uncertain whether such changes begin before the clinical onset of the disease, however. Prospective studies of this question have either not assessed all five major dimensions of personality or administered assessments too close in time to the diagnosis of dementia.
Examining Change in Personality Traits
Dr. Terracciano and colleagues conducted a study to determine whether increases in neuroticism, declines in conscientiousness, and changes in other personality traits occur before the onset of mild cognitive impairment or dementia. They examined data for a cohort of 2,046 community-dwelling older adults who participated in the Baltimore Longitudinal Study of Aging. In the latter study, participants with no cognitive impairment underwent periodic personality and clinical assessments between 1980 and July 13, 2016. Follow-up lasted for as long as 36 years.
Participants completed the self-report version of the Revised NEO Personality Inventory (NEO-PI-R), or an earlier version, in 1980 and 1986. The NEO-PI-R is a 240-item questionnaire that assesses 30 facets of personality, including six for each of the following five major dimensions: neuroticism, extraversion, openness, agreeableness, and conscientiousness. In addition, participants were evaluated at enrollment for history of neurologic or cerebrovascular disease and for impairment of cognitive or behavioral functioning. Follow-up evaluations included a neuropsychologic battery and clinical examination, including an informant-and-participant-structured interview.
Patients With Dementia Had Higher Neuroticism Scores
Participants’ mean age at baseline was 62. In all, 931 participants (46%) were women. The population sample included 374 blacks (18%), 1,582 whites (77%), and 55 Asians or Pacific Islanders (3%). During the study, 104 participants (5%) developed mild cognitive impairment, and 255 (13%) developed all-cause dementia, including 194 (10%) who developed Alzheimer’s disease.
Change in personality before the onset of mild cognitive impairment or dementia was not significantly different between participants who remained unimpaired and those who developed Alzheimer’s disease. Change in personality for participants who developed mild cognitive impairment and all-cause dementia also was similar to that in unimpaired participants. Neuroticism and conscientiousness did not change significantly as disease onset approached.
One limitation of this study was that the population sample was selective and highly educated, said the authors. Another limitation was that the unimpaired participants were relatively young and could develop dementia in the future. “More research is needed on personality and Alzheimer’s disease biomarkers and how personality may increase resilience against neuropathology and forestall the emergence of clinical dementia,” said Dr. Terracciano.
—Erica Tricarico
Suggested Reading
Terracciano A, An Y, Sutin AR, et al. Personality change in the preclinical phase of Alzheimer disease. JAMA Psychiatry. 2017 Sep 20 [Epub ahead of print].
CDC Updates Guidance on Infants With Possible Zika Infection
Infants with possible prenatal exposure to Zika who test positive for the virus should receive an in-depth ophthalmologic exam, intensified hearing testing, and a thorough neurologic evaluation with brain imaging within one month of birth, according to new interim guidance from the Centers for Disease Control and Prevention (CDC).
The new clinical management guidelines, published in the October 20 issue of Morbidity and Mortality Weekly Report, supersede the CDC guidance issued in August 2016. The update was the product of a forum on the diagnosis, evaluation, and management of Zika in infants that the centers convened with the American Academy of Pediatrics and the American College of Obstetricians and Gynecologists. Practicing clinicians and federal agency representatives reviewed the evolving body of knowledge on how best to care for these infants. Since Zika emerged as a public health concern, clinicians have reported postnatal onset of some symptoms, including eye abnormalities, incident microcephaly in infants with a normal head circumference at birth, EEG abnormalities, and diaphragmatic paralysis.

Infants With Clinical Findings Consistent With Zika Syndrome
Infants with clinical findings consistent with congenital Zika syndrome who are born to mothers with possible Zika virus exposure in pregnancy should be tested for Zika virus with serum and urine tests. If those tests are negative, and there is no other apparent cause of the symptoms, they should have a CSF sample tested for Zika RNA and IgM Zika antibodies.
By one month, these infants should undergo a head ultrasound and a detailed ophthalmologic exam. The eye exam should pick up any anomalies of the anterior and posterior eye, including microphthalmia, coloboma, intraocular calcifications, optic nerve hypoplasia and atrophy, and macular scarring with focal pigmentary retinal mottling.
By one month, these infants also should undergo auditory brainstem response (ABR) audiometry, especially if the initial newborn hearing screen was done by otoacoustic emissions alone. Zika syndrome can include sensorineural hearing loss, although late-onset hearing loss has not been seen. Therefore, the follow-up ABR previously recommended at four to six months is no longer deemed necessary.
A comprehensive neurologic exam also is recommended. Seizures are sometimes part of Zika syndrome, but infants can also have subclinical EEG abnormalities. Advanced neuroimaging can identify obvious and subtle brain abnormalities, such as cortical thinning, corpus callosum abnormalities, calcifications at the junction of white and gray matter, and ventricular enlargement.
As infants grow, clinicians should be alert for signs of increased intracranial pressure that could signal postnatal hydrocephalus. Diaphragmatic paralysis also has been seen; it manifests as respiratory distress. Dysphagia that interferes with feeding can develop as well.
“The follow-up care of [these infants] requires a multidisciplinary team and an established medical home to facilitate the coordination of care and ensure that abnormal findings are addressed,” said Dr. Adebanjo and colleagues.
Asymptomatic Infants of Mothers With Possible Infection
Infants without clinical findings born to mothers with laboratory evidence of possible Zika virus infection during pregnancy should have the same early head ultrasound, hearing, and eye exams as those with clinical findings. All of these infants also should be tested for Zika virus just as those with clinical findings should be.
If tests are positive, these infants should have all the investigations and follow-up recommended for babies with clinical findings. If laboratory testing is negative, and clinical findings are normal, Zika infection is highly unlikely, and the infants can receive routine care. Clinicians and parents should be on the lookout, however, for new symptoms that might suggest postnatal Zika syndrome.
Asymptomatic Infants Whose Mothers Had Unconfirmed Zika Exposure
Infants without clinical findings consistent with congenital Zika syndrome born to mothers with possible Zika virus exposure in pregnancy, but without laboratory evidence of possible Zika virus infection during pregnancy, constitute a large group. Some women, for example, are never tested during pregnancy, and others have false negative test results. “Because the latter issues are not easily discerned, all mothers with possible exposure to Zika virus during pregnancy who do not have laboratory evidence of possible Zika virus infection, including those who tested negative with currently available technology, should be considered in this group,” said Dr. Adebanjo and colleagues.
The CDC do not recommend further Zika evaluation for these infants unless additional testing confirms maternal infection. For older infants, parents and clinicians should decide together whether further evaluations would be helpful. “If findings consistent with congenital Zika syndrome are identified at any time, referrals to the appropriate specialists should be made, and subsequent evaluation should follow recommendations for infants with clinical findings consistent with congenital Zika syndrome,” said the authors.
The CDC also reiterated their special recommendations for infants who had a prenatal diagnosis of Zika infection. For now, these recommendations remain unchanged, although “as more data become available, understanding of the diagnostic role of prenatal ultrasound and amniocentesis … will improve, and guidance will be updated.”
The optimal timing for a Zika diagnostic ultrasound is uncertain. The CDC recommend that serial ultrasounds be performed every three to four weeks for women with laboratory-confirmed prenatal Zika exposure. Women with possible exposure need only routine ultrasound screenings.
While Zika RNA has been identified in amniotic fluid, there is no consensus on the value of amniocentesis as a prenatal diagnostic tool. Investigations of serial amniocentesis suggest that viral shedding into the amniotic fluid might be transient. If amniocentesis is performed for other reasons, Zika nucleic acid testing can be incorporated.
A shared decision-making process about screening is key, said Dr. Adebanjo and colleagues. “For example, serial ultrasound examinations might be inconvenient, unpleasant, and expensive, and might prompt unnecessary interventions; amniocentesis carries additional known risks such as fetal loss. These potential harms of prenatal screening for congenital Zika syndrome might outweigh the clinical benefits for some patients; therefore, these decisions should be individualized.”
—Michele G. Sullivan
Suggested Reading
Adebanjo T, Godfred-Cato S, Viens L, et al. Update: Interim guidance for the diagnosis, evaluation, and management of infants with possible congenital Zika virus infection - United States, October 2017. MMWR Morb Mortal Wkly Rep. 2017;66(41):1089-1099.
Infants with possible prenatal exposure to Zika who test positive for the virus should receive an in-depth ophthalmologic exam, intensified hearing testing, and a thorough neurologic evaluation with brain imaging within one month of birth, according to new interim guidance from the Centers for Disease Control and Prevention (CDC).
The new clinical management guidelines, published in the October 20 issue of Morbidity and Mortality Weekly Report, supersede the CDC guidance issued in August 2016. The update was the product of a forum on the diagnosis, evaluation, and management of Zika in infants that the centers convened with the American Academy of Pediatrics and the American College of Obstetricians and Gynecologists. Practicing clinicians and federal agency representatives reviewed the evolving body of knowledge on how best to care for these infants. Since Zika emerged as a public health concern, clinicians have reported postnatal onset of some symptoms, including eye abnormalities, incident microcephaly in infants with a normal head circumference at birth, EEG abnormalities, and diaphragmatic paralysis.
Infants With Clinical Findings Consistent With Zika Syndrome
Infants with clinical findings consistent with congenital Zika syndrome who are born to mothers with possible Zika virus exposure in pregnancy should be tested for Zika virus with serum and urine tests. If those tests are negative, and there is no other apparent cause of the symptoms, they should have a CSF sample tested for Zika RNA and IgM Zika antibodies.
By one month, these infants should undergo a head ultrasound and a detailed ophthalmologic exam. The eye exam should pick up any anomalies of the anterior and posterior eye, including microphthalmia, coloboma, intraocular calcifications, optic nerve hypoplasia and atrophy, and macular scarring with focal pigmentary retinal mottling.
By one month, these infants also should undergo auditory brainstem response (ABR) audiometry, especially if the initial newborn hearing screen was done by otoacoustic emissions alone. Zika syndrome can include sensorineural hearing loss, although late-onset hearing loss has not been seen. Therefore, the follow-up ABR previously recommended at four to six months is no longer deemed necessary.
A comprehensive neurologic exam also is recommended. Seizures are sometimes part of Zika syndrome, but infants can also have subclinical EEG abnormalities. Advanced neuroimaging can identify obvious and subtle brain abnormalities, such as cortical thinning, corpus callosum abnormalities, calcifications at the junction of white and gray matter, and ventricular enlargement.
As infants grow, clinicians should be alert for signs of increased intracranial pressure that could signal postnatal hydrocephalus. Diaphragmatic paralysis also has been seen; it manifests as respiratory distress. Dysphagia that interferes with feeding can develop as well.
“The follow-up care of [these infants] requires a multidisciplinary team and an established medical home to facilitate the coordination of care and ensure that abnormal findings are addressed,” said Dr. Adebanjo and colleagues.
Asymptomatic Infants of Mothers With Possible Infection
Infants without clinical findings born to mothers with laboratory evidence of possible Zika virus infection during pregnancy should have the same early head ultrasound, hearing, and eye exams as those with clinical findings. All of these infants also should be tested for Zika virus just as those with clinical findings should be.
If tests are positive, these infants should have all the investigations and follow-up recommended for babies with clinical findings. If laboratory testing is negative, and clinical findings are normal, Zika infection is highly unlikely, and the infants can receive routine care. Clinicians and parents should be on the lookout, however, for new symptoms that might suggest postnatal Zika syndrome.
Asymptomatic Infants Whose Mothers Had Unconfirmed Zika Exposure
Infants without clinical findings consistent with congenital Zika syndrome born to mothers with possible Zika virus exposure in pregnancy, but without laboratory evidence of possible Zika virus infection during pregnancy, constitute a large group. Some women, for example, are never tested during pregnancy, and others have false negative test results. “Because the latter issues are not easily discerned, all mothers with possible exposure to Zika virus during pregnancy who do not have laboratory evidence of possible Zika virus infection, including those who tested negative with currently available technology, should be considered in this group,” said Dr. Adebanjo and colleagues.
The CDC do not recommend further Zika evaluation for these infants unless additional testing confirms maternal infection. For older infants, parents and clinicians should decide together whether further evaluations would be helpful. “If findings consistent with congenital Zika syndrome are identified at any time, referrals to the appropriate specialists should be made, and subsequent evaluation should follow recommendations for infants with clinical findings consistent with congenital Zika syndrome,” said the authors.
The CDC also reiterated their special recommendations for infants who had a prenatal diagnosis of Zika infection. For now, these recommendations remain unchanged, although “as more data become available, understanding of the diagnostic role of prenatal ultrasound and amniocentesis … will improve, and guidance will be updated.”
The optimal timing for a Zika diagnostic ultrasound is uncertain. The CDC recommend that serial ultrasounds be performed every three to four weeks for women with laboratory-confirmed prenatal Zika exposure. Women with possible exposure need only routine ultrasound screenings.
While Zika RNA has been identified in amniotic fluid, there is no consensus on the value of amniocentesis as a prenatal diagnostic tool. Investigations of serial amniocentesis suggest that viral shedding into the amniotic fluid might be transient. If amniocentesis is performed for other reasons, Zika nucleic acid testing can be incorporated.
A shared decision-making process about screening is key, said Dr. Adebanjo and colleagues. “For example, serial ultrasound examinations might be inconvenient, unpleasant, and expensive, and might prompt unnecessary interventions; amniocentesis carries additional known risks such as fetal loss. These potential harms of prenatal screening for congenital Zika syndrome might outweigh the clinical benefits for some patients; therefore, these decisions should be individualized.”
—Michele G. Sullivan
Suggested Reading
Adebanjo T, Godfred-Cato S, Viens L, et al. Update: Interim guidance for the diagnosis, evaluation, and management of infants with possible congenital Zika virus infection - United States, October 2017. MMWR Morb Mortal Wkly Rep. 2017;66(41):1089-1099.
Infants with possible prenatal exposure to Zika who test positive for the virus should receive an in-depth ophthalmologic exam, intensified hearing testing, and a thorough neurologic evaluation with brain imaging within one month of birth, according to new interim guidance from the Centers for Disease Control and Prevention (CDC).
The new clinical management guidelines, published in the October 20 issue of Morbidity and Mortality Weekly Report, supersede the CDC guidance issued in August 2016. The update was the product of a forum on the diagnosis, evaluation, and management of Zika in infants that the centers convened with the American Academy of Pediatrics and the American College of Obstetricians and Gynecologists. Practicing clinicians and federal agency representatives reviewed the evolving body of knowledge on how best to care for these infants. Since Zika emerged as a public health concern, clinicians have reported postnatal onset of some symptoms, including eye abnormalities, incident microcephaly in infants with a normal head circumference at birth, EEG abnormalities, and diaphragmatic paralysis.
Infants With Clinical Findings Consistent With Zika Syndrome
Infants with clinical findings consistent with congenital Zika syndrome who are born to mothers with possible Zika virus exposure in pregnancy should be tested for Zika virus with serum and urine tests. If those tests are negative, and there is no other apparent cause of the symptoms, they should have a CSF sample tested for Zika RNA and IgM Zika antibodies.
By one month, these infants should undergo a head ultrasound and a detailed ophthalmologic exam. The eye exam should pick up any anomalies of the anterior and posterior eye, including microphthalmia, coloboma, intraocular calcifications, optic nerve hypoplasia and atrophy, and macular scarring with focal pigmentary retinal mottling.
By one month, these infants also should undergo auditory brainstem response (ABR) audiometry, especially if the initial newborn hearing screen was done by otoacoustic emissions alone. Zika syndrome can include sensorineural hearing loss, although late-onset hearing loss has not been seen. Therefore, the follow-up ABR previously recommended at four to six months is no longer deemed necessary.
A comprehensive neurologic exam also is recommended. Seizures are sometimes part of Zika syndrome, but infants can also have subclinical EEG abnormalities. Advanced neuroimaging can identify obvious and subtle brain abnormalities, such as cortical thinning, corpus callosum abnormalities, calcifications at the junction of white and gray matter, and ventricular enlargement.
As infants grow, clinicians should be alert for signs of increased intracranial pressure that could signal postnatal hydrocephalus. Diaphragmatic paralysis also has been seen; it manifests as respiratory distress. Dysphagia that interferes with feeding can develop as well.
“The follow-up care of [these infants] requires a multidisciplinary team and an established medical home to facilitate the coordination of care and ensure that abnormal findings are addressed,” said Dr. Adebanjo and colleagues.
Asymptomatic Infants of Mothers With Possible Infection
Infants without clinical findings born to mothers with laboratory evidence of possible Zika virus infection during pregnancy should have the same early head ultrasound, hearing, and eye exams as those with clinical findings. All of these infants also should be tested for Zika virus just as those with clinical findings should be.
If tests are positive, these infants should have all the investigations and follow-up recommended for babies with clinical findings. If laboratory testing is negative, and clinical findings are normal, Zika infection is highly unlikely, and the infants can receive routine care. Clinicians and parents should be on the lookout, however, for new symptoms that might suggest postnatal Zika syndrome.
Asymptomatic Infants Whose Mothers Had Unconfirmed Zika Exposure
Infants without clinical findings consistent with congenital Zika syndrome born to mothers with possible Zika virus exposure in pregnancy, but without laboratory evidence of possible Zika virus infection during pregnancy, constitute a large group. Some women, for example, are never tested during pregnancy, and others have false negative test results. “Because the latter issues are not easily discerned, all mothers with possible exposure to Zika virus during pregnancy who do not have laboratory evidence of possible Zika virus infection, including those who tested negative with currently available technology, should be considered in this group,” said Dr. Adebanjo and colleagues.
The CDC do not recommend further Zika evaluation for these infants unless additional testing confirms maternal infection. For older infants, parents and clinicians should decide together whether further evaluations would be helpful. “If findings consistent with congenital Zika syndrome are identified at any time, referrals to the appropriate specialists should be made, and subsequent evaluation should follow recommendations for infants with clinical findings consistent with congenital Zika syndrome,” said the authors.
The CDC also reiterated their special recommendations for infants who had a prenatal diagnosis of Zika infection. For now, these recommendations remain unchanged, although “as more data become available, understanding of the diagnostic role of prenatal ultrasound and amniocentesis … will improve, and guidance will be updated.”
The optimal timing for a Zika diagnostic ultrasound is uncertain. The CDC recommend that serial ultrasounds be performed every three to four weeks for women with laboratory-confirmed prenatal Zika exposure. Women with possible exposure need only routine ultrasound screenings.
While Zika RNA has been identified in amniotic fluid, there is no consensus on the value of amniocentesis as a prenatal diagnostic tool. Investigations of serial amniocentesis suggest that viral shedding into the amniotic fluid might be transient. If amniocentesis is performed for other reasons, Zika nucleic acid testing can be incorporated.
A shared decision-making process about screening is key, said Dr. Adebanjo and colleagues. “For example, serial ultrasound examinations might be inconvenient, unpleasant, and expensive, and might prompt unnecessary interventions; amniocentesis carries additional known risks such as fetal loss. These potential harms of prenatal screening for congenital Zika syndrome might outweigh the clinical benefits for some patients; therefore, these decisions should be individualized.”
—Michele G. Sullivan
Suggested Reading
Adebanjo T, Godfred-Cato S, Viens L, et al. Update: Interim guidance for the diagnosis, evaluation, and management of infants with possible congenital Zika virus infection - United States, October 2017. MMWR Morb Mortal Wkly Rep. 2017;66(41):1089-1099.
Epilepsy and Increased Risk of Adverse Pregnancy Outcomes: What Is the Real Risk?
Epilepsy during pregnancy is associated with a moderately increased risk of adverse pregnancy, delivery, and perinatal outcomes, according to research published in the August issue of JAMA Neurology. The use of antiepileptic drugs (AEDs), however, is not associated with adverse outcomes, according to the researchers.

Information From National Registries
Data suggesting associations between AEDs and the risk of congenital malformations have received much attention in recent years. But population-based evidence about the association between maternal epilepsy itself and risks of adverse outcomes has been scarce.
Dr. Razaz and colleagues conducted a retrospective study of all singleton births in Sweden from 1997 through 2011. The investigators obtained information from the country’s Medical Birth Register, the National Patient Register, and the Prescribed Drug Registry. They included information about 1,429,652 pregnancies (869,947 mothers without epilepsy and 3,586 mothers with epilepsy). Mean age at first delivery for women with epilepsy was 31. Data on AED exposure were available for offspring born between July 1, 2005, and December 31, 2011. Lamotrigine and carbamazepine were the most commonly used AEDs.
Relative Risks
Pregnancies in women with epilepsy were associated with increased risks of pre-eclampsia (adjusted risk ratio [aRR], 1.24), infection (aRR, 1.85), placental abruption (aRR, 1.68), induction (aRR, 1.31), elective cesarean section (aRR, 1.58), and emergency cesarean section (aRR, 1.09), compared with pregnancies in women without epilepsy. After adjustment for potential confounders, neonates of women with epilepsy had significantly higher risks of stillbirth, being born small for gestational age, medically indicated and spontaneous preterm births, any and major congenital malformations, neonatal infections, asphyxia-related complications, low five-minute Apgar scores, and neonatal hypoglycemia and respiratory distress, compared with neonates of women without epilepsy.
Among women with epilepsy, the rate of pre-eclampsia was higher in those who received AEDs, compared with women who did not receive AEDs (aRR, 1.39). In the propensity score-adjusted analyses, however, increased risk of induced labor (aRR, 1.30) was the only pregnancy and delivery outcome significantly associated with use of AEDs.
Offspring of women exposed to AEDs had a higher frequency of major malformation (6.7% vs 4.7%), respiratory distress (6.0% vs 4.5%), and being small for gestational age (9.5% vs 6.9%) at birth, compared with nonexposed offspring. Propensity score-adjusted analyses, however, showed no significantly increased risk of adverse neonatal outcomes.
Women with epilepsy who receive AEDs during pregnancy “may receive extra surveillance ... from their clinicians that may have contributed to the comparable outcomes observed in our study,” said the researchers. The study results may improve counseling for pregnant women with epilepsy who contemplate discontinuing treatment.
—Erik Greb
Suggested Reading
Razaz N, Tomson T, Wikström AK, Cnattingius S. Association between pregnancy and perinatal outcomes among women with epilepsy. JAMA Neurol. 2017;74(8):983-991.
Epilepsy during pregnancy is associated with a moderately increased risk of adverse pregnancy, delivery, and perinatal outcomes, according to research published in the August issue of JAMA Neurology. The use of antiepileptic drugs (AEDs), however, is not associated with adverse outcomes, according to the researchers.
Information From National Registries
Data suggesting associations between AEDs and the risk of congenital malformations have received much attention in recent years. But population-based evidence about the association between maternal epilepsy itself and risks of adverse outcomes has been scarce.
Dr. Razaz and colleagues conducted a retrospective study of all singleton births in Sweden from 1997 through 2011. The investigators obtained information from the country’s Medical Birth Register, the National Patient Register, and the Prescribed Drug Registry. They included information about 1,429,652 pregnancies (869,947 mothers without epilepsy and 3,586 mothers with epilepsy). Mean age at first delivery for women with epilepsy was 31. Data on AED exposure were available for offspring born between July 1, 2005, and December 31, 2011. Lamotrigine and carbamazepine were the most commonly used AEDs.
Relative Risks
Pregnancies in women with epilepsy were associated with increased risks of pre-eclampsia (adjusted risk ratio [aRR], 1.24), infection (aRR, 1.85), placental abruption (aRR, 1.68), induction (aRR, 1.31), elective cesarean section (aRR, 1.58), and emergency cesarean section (aRR, 1.09), compared with pregnancies in women without epilepsy. After adjustment for potential confounders, neonates of women with epilepsy had significantly higher risks of stillbirth, being born small for gestational age, medically indicated and spontaneous preterm births, any and major congenital malformations, neonatal infections, asphyxia-related complications, low five-minute Apgar scores, and neonatal hypoglycemia and respiratory distress, compared with neonates of women without epilepsy.
Among women with epilepsy, the rate of pre-eclampsia was higher in those who received AEDs, compared with women who did not receive AEDs (aRR, 1.39). In the propensity score-adjusted analyses, however, increased risk of induced labor (aRR, 1.30) was the only pregnancy and delivery outcome significantly associated with use of AEDs.
Offspring of women exposed to AEDs had a higher frequency of major malformation (6.7% vs 4.7%), respiratory distress (6.0% vs 4.5%), and being small for gestational age (9.5% vs 6.9%) at birth, compared with nonexposed offspring. Propensity score-adjusted analyses, however, showed no significantly increased risk of adverse neonatal outcomes.
Women with epilepsy who receive AEDs during pregnancy “may receive extra surveillance ... from their clinicians that may have contributed to the comparable outcomes observed in our study,” said the researchers. The study results may improve counseling for pregnant women with epilepsy who contemplate discontinuing treatment.
—Erik Greb
Suggested Reading
Razaz N, Tomson T, Wikström AK, Cnattingius S. Association between pregnancy and perinatal outcomes among women with epilepsy. JAMA Neurol. 2017;74(8):983-991.
Epilepsy during pregnancy is associated with a moderately increased risk of adverse pregnancy, delivery, and perinatal outcomes, according to research published in the August issue of JAMA Neurology. The use of antiepileptic drugs (AEDs), however, is not associated with adverse outcomes, according to the researchers.
Information From National Registries
Data suggesting associations between AEDs and the risk of congenital malformations have received much attention in recent years. But population-based evidence about the association between maternal epilepsy itself and risks of adverse outcomes has been scarce.
Dr. Razaz and colleagues conducted a retrospective study of all singleton births in Sweden from 1997 through 2011. The investigators obtained information from the country’s Medical Birth Register, the National Patient Register, and the Prescribed Drug Registry. They included information about 1,429,652 pregnancies (869,947 mothers without epilepsy and 3,586 mothers with epilepsy). Mean age at first delivery for women with epilepsy was 31. Data on AED exposure were available for offspring born between July 1, 2005, and December 31, 2011. Lamotrigine and carbamazepine were the most commonly used AEDs.
Relative Risks
Pregnancies in women with epilepsy were associated with increased risks of pre-eclampsia (adjusted risk ratio [aRR], 1.24), infection (aRR, 1.85), placental abruption (aRR, 1.68), induction (aRR, 1.31), elective cesarean section (aRR, 1.58), and emergency cesarean section (aRR, 1.09), compared with pregnancies in women without epilepsy. After adjustment for potential confounders, neonates of women with epilepsy had significantly higher risks of stillbirth, being born small for gestational age, medically indicated and spontaneous preterm births, any and major congenital malformations, neonatal infections, asphyxia-related complications, low five-minute Apgar scores, and neonatal hypoglycemia and respiratory distress, compared with neonates of women without epilepsy.
Among women with epilepsy, the rate of pre-eclampsia was higher in those who received AEDs, compared with women who did not receive AEDs (aRR, 1.39). In the propensity score-adjusted analyses, however, increased risk of induced labor (aRR, 1.30) was the only pregnancy and delivery outcome significantly associated with use of AEDs.
Offspring of women exposed to AEDs had a higher frequency of major malformation (6.7% vs 4.7%), respiratory distress (6.0% vs 4.5%), and being small for gestational age (9.5% vs 6.9%) at birth, compared with nonexposed offspring. Propensity score-adjusted analyses, however, showed no significantly increased risk of adverse neonatal outcomes.
Women with epilepsy who receive AEDs during pregnancy “may receive extra surveillance ... from their clinicians that may have contributed to the comparable outcomes observed in our study,” said the researchers. The study results may improve counseling for pregnant women with epilepsy who contemplate discontinuing treatment.
—Erik Greb
Suggested Reading
Razaz N, Tomson T, Wikström AK, Cnattingius S. Association between pregnancy and perinatal outcomes among women with epilepsy. JAMA Neurol. 2017;74(8):983-991.
Virtual House Calls Are Feasible for Patients With Parkinson’s Disease
Providing remote neurologic care directly into the homes of patients with Parkinson’s disease is feasible and is neither more nor less efficacious than usual in-person care, according to research published in the September 12 issue of

Virtual house calls are becoming increasingly common for episodic conditions, but limited evidence supports their use for chronic conditions, according to the researchers. Approximately 40% of patients with Parkinson’s disease never receive care from a neurologist. These patients are more likely to have increased morbidity, to lose independence, and to die prematurely, they said.
Standard Care Versus Virtual House Calls
To determine whether providing virtual house calls is feasible, valuable, and beneficial, Dr. Beck and colleagues conducted a one-year randomized controlled study. Eligible participants had a clinical diagnosis of Parkinson’s disease; had a private, Internet-enabled device; and lived in a state where a site investigator was licensed to practice. Patients currently hospitalized, who had a condition that would preclude study participation in the judgment of the site investigator, or who were currently enrolled in another telemedicine study were excluded.
Investigators compared usual care to usual care supplemented with four virtual visits via video conferencing from a remote specialist into patients’ homes. Primary outcome measures were feasibility, measured by the proportion of participants who completed at least one virtual visit and the proportion of virtual visits completed on time, and efficacy, measured by change in the Parkinson’s Disease Questionnaire-39, a quality of life scale. Secondary outcomes included quality of care, caregiver burden, and time and travel savings.
Most Participants Were Satisfied With Virtual Visits
A total of 927 patients indicated interest in the study. Of these, 732 were excluded because they did not meet eligibility requirements, did not consent, or withdrew prior to randomization. A total of 210 patients were enrolled, and 195 were randomized. In all, 73% of participants had recently visited a specialist, 73% were college-educated, and 96% were white. The mean age of participants was 66. Ninety-eight percent of participants randomized to the intervention arm completed at least one virtual visit; 91% of 388 virtual visits were completed.
Quality of life did not improve for patients who received virtual house calls, nor did quality of care or caregiver burden. However, each virtual house call saved patients a median of 88 minutes per visit and 38 miles per visit. Ninety-seven percent of patients and 86% of physicians were satisfied or very satisfied with virtual visits.
One limitation of this study was that the majority of participants were white, well educated, and more familiar with the Internet than the general population. “Dedicated outreach to underserved populations, including those with advanced disease and from underserved demographic groups, especially women, rural residents, minorities, the homebound, or those in assisted living facilities, will help determine if the results are more generalizable and whether the benefits are potentially greater for those with historically less access to care,” said Dr. Beck and colleagues.
“Virtual house calls generated great interest and provided substantial convenience,” the researchers said. “Future efforts must address the digital divide and policy barriers to ensure that this new care model can address inequities in access to care.”
—Erica Tricarico
Suggested Reading
Beck CA, Beran DB, Biglan KM, et al. National randomized controlled trial of virtual house calls for Parkinson disease. Neurology. 2017;89(11):1152-1161.
Providing remote neurologic care directly into the homes of patients with Parkinson’s disease is feasible and is neither more nor less efficacious than usual in-person care, according to research published in the September 12 issue of
Virtual house calls are becoming increasingly common for episodic conditions, but limited evidence supports their use for chronic conditions, according to the researchers. Approximately 40% of patients with Parkinson’s disease never receive care from a neurologist. These patients are more likely to have increased morbidity, to lose independence, and to die prematurely, they said.
Standard Care Versus Virtual House Calls
To determine whether providing virtual house calls is feasible, valuable, and beneficial, Dr. Beck and colleagues conducted a one-year randomized controlled study. Eligible participants had a clinical diagnosis of Parkinson’s disease; had a private, Internet-enabled device; and lived in a state where a site investigator was licensed to practice. Patients currently hospitalized, who had a condition that would preclude study participation in the judgment of the site investigator, or who were currently enrolled in another telemedicine study were excluded.
Investigators compared usual care to usual care supplemented with four virtual visits via video conferencing from a remote specialist into patients’ homes. Primary outcome measures were feasibility, measured by the proportion of participants who completed at least one virtual visit and the proportion of virtual visits completed on time, and efficacy, measured by change in the Parkinson’s Disease Questionnaire-39, a quality of life scale. Secondary outcomes included quality of care, caregiver burden, and time and travel savings.
Most Participants Were Satisfied With Virtual Visits
A total of 927 patients indicated interest in the study. Of these, 732 were excluded because they did not meet eligibility requirements, did not consent, or withdrew prior to randomization. A total of 210 patients were enrolled, and 195 were randomized. In all, 73% of participants had recently visited a specialist, 73% were college-educated, and 96% were white. The mean age of participants was 66. Ninety-eight percent of participants randomized to the intervention arm completed at least one virtual visit; 91% of 388 virtual visits were completed.
Quality of life did not improve for patients who received virtual house calls, nor did quality of care or caregiver burden. However, each virtual house call saved patients a median of 88 minutes per visit and 38 miles per visit. Ninety-seven percent of patients and 86% of physicians were satisfied or very satisfied with virtual visits.
One limitation of this study was that the majority of participants were white, well educated, and more familiar with the Internet than the general population. “Dedicated outreach to underserved populations, including those with advanced disease and from underserved demographic groups, especially women, rural residents, minorities, the homebound, or those in assisted living facilities, will help determine if the results are more generalizable and whether the benefits are potentially greater for those with historically less access to care,” said Dr. Beck and colleagues.
“Virtual house calls generated great interest and provided substantial convenience,” the researchers said. “Future efforts must address the digital divide and policy barriers to ensure that this new care model can address inequities in access to care.”
—Erica Tricarico
Suggested Reading
Beck CA, Beran DB, Biglan KM, et al. National randomized controlled trial of virtual house calls for Parkinson disease. Neurology. 2017;89(11):1152-1161.
Providing remote neurologic care directly into the homes of patients with Parkinson’s disease is feasible and is neither more nor less efficacious than usual in-person care, according to research published in the September 12 issue of
Virtual house calls are becoming increasingly common for episodic conditions, but limited evidence supports their use for chronic conditions, according to the researchers. Approximately 40% of patients with Parkinson’s disease never receive care from a neurologist. These patients are more likely to have increased morbidity, to lose independence, and to die prematurely, they said.
Standard Care Versus Virtual House Calls
To determine whether providing virtual house calls is feasible, valuable, and beneficial, Dr. Beck and colleagues conducted a one-year randomized controlled study. Eligible participants had a clinical diagnosis of Parkinson’s disease; had a private, Internet-enabled device; and lived in a state where a site investigator was licensed to practice. Patients currently hospitalized, who had a condition that would preclude study participation in the judgment of the site investigator, or who were currently enrolled in another telemedicine study were excluded.
Investigators compared usual care to usual care supplemented with four virtual visits via video conferencing from a remote specialist into patients’ homes. Primary outcome measures were feasibility, measured by the proportion of participants who completed at least one virtual visit and the proportion of virtual visits completed on time, and efficacy, measured by change in the Parkinson’s Disease Questionnaire-39, a quality of life scale. Secondary outcomes included quality of care, caregiver burden, and time and travel savings.
Most Participants Were Satisfied With Virtual Visits
A total of 927 patients indicated interest in the study. Of these, 732 were excluded because they did not meet eligibility requirements, did not consent, or withdrew prior to randomization. A total of 210 patients were enrolled, and 195 were randomized. In all, 73% of participants had recently visited a specialist, 73% were college-educated, and 96% were white. The mean age of participants was 66. Ninety-eight percent of participants randomized to the intervention arm completed at least one virtual visit; 91% of 388 virtual visits were completed.
Quality of life did not improve for patients who received virtual house calls, nor did quality of care or caregiver burden. However, each virtual house call saved patients a median of 88 minutes per visit and 38 miles per visit. Ninety-seven percent of patients and 86% of physicians were satisfied or very satisfied with virtual visits.
One limitation of this study was that the majority of participants were white, well educated, and more familiar with the Internet than the general population. “Dedicated outreach to underserved populations, including those with advanced disease and from underserved demographic groups, especially women, rural residents, minorities, the homebound, or those in assisted living facilities, will help determine if the results are more generalizable and whether the benefits are potentially greater for those with historically less access to care,” said Dr. Beck and colleagues.
“Virtual house calls generated great interest and provided substantial convenience,” the researchers said. “Future efforts must address the digital divide and policy barriers to ensure that this new care model can address inequities in access to care.”
—Erica Tricarico
Suggested Reading
Beck CA, Beran DB, Biglan KM, et al. National randomized controlled trial of virtual house calls for Parkinson disease. Neurology. 2017;89(11):1152-1161.