User login
Guselkumab safe and effective for early PsA in real-life setting
Key clinical point: Findings from this real-life cohort of patients with early psoriatic arthritis (PsA) confirm the safety and efficacy of guselkumab on peripheral and axial manifestations.
Major finding: After 12 months of guselkumab treatment, the mean Patient Global Assessment (P less than .0001), Visual Analogue Scale of Pain (P less than .001), and Disease Activity Score of PsA (P less than .0001) decreased significantly. Inflammatory low back pain disappeared as early as 24 weeks in all patients with concomitant axial disease. Low disease activity and remission were achieved by 65% and 35% of patients, respectively. No adverse events were reported.
Study details: The data come from an observational study involving 24 patients with early PsA who initiated therapy with guselkumab for severe skin involvement.
Disclosures: No specific funding was received for this study. The authors declared no conflicts of interest.
Source: Pantano I et al. Rheumatology (Oxford). 2021 Jun 21. doi: 10.1093/rheumatology/keab509.
Key clinical point: Findings from this real-life cohort of patients with early psoriatic arthritis (PsA) confirm the safety and efficacy of guselkumab on peripheral and axial manifestations.
Major finding: After 12 months of guselkumab treatment, the mean Patient Global Assessment (P less than .0001), Visual Analogue Scale of Pain (P less than .001), and Disease Activity Score of PsA (P less than .0001) decreased significantly. Inflammatory low back pain disappeared as early as 24 weeks in all patients with concomitant axial disease. Low disease activity and remission were achieved by 65% and 35% of patients, respectively. No adverse events were reported.
Study details: The data come from an observational study involving 24 patients with early PsA who initiated therapy with guselkumab for severe skin involvement.
Disclosures: No specific funding was received for this study. The authors declared no conflicts of interest.
Source: Pantano I et al. Rheumatology (Oxford). 2021 Jun 21. doi: 10.1093/rheumatology/keab509.
Key clinical point: Findings from this real-life cohort of patients with early psoriatic arthritis (PsA) confirm the safety and efficacy of guselkumab on peripheral and axial manifestations.
Major finding: After 12 months of guselkumab treatment, the mean Patient Global Assessment (P less than .0001), Visual Analogue Scale of Pain (P less than .001), and Disease Activity Score of PsA (P less than .0001) decreased significantly. Inflammatory low back pain disappeared as early as 24 weeks in all patients with concomitant axial disease. Low disease activity and remission were achieved by 65% and 35% of patients, respectively. No adverse events were reported.
Study details: The data come from an observational study involving 24 patients with early PsA who initiated therapy with guselkumab for severe skin involvement.
Disclosures: No specific funding was received for this study. The authors declared no conflicts of interest.
Source: Pantano I et al. Rheumatology (Oxford). 2021 Jun 21. doi: 10.1093/rheumatology/keab509.
Nail involvement in PsA may help identify patients at high risk
Key clinical point: Patients with psoriatic arthritis (PsA) with vs without nail involvement had higher rates of carotid plaque (CP) and carotid intima-media thickness (cIMT). Additionally, nail involvement in PsA was independently associated with CP risk.
Major finding: Patients with vs without nail involvement showed a higher prevalence of CP (53.1% vs 25.0%; P = .021) and cIMT (0.85 vs 0.59 mm; P = .026). The nail involvement was an independent risk factor for the presence of CP (odds ratio, 6.64; P = .006).
Study details: Findings are from a cross-sectional, observational study involving 64 patients with PsA. Patients with nail involvement were matched by age, gender, and type 2 diabetes mellitus diagnosis to those without nail involvement.
Disclosures: No specific funding or conflicts of interest were declared.
Source: Colunga-Pedraza IJ et al. Ann Rheum Dis. 2021 Jun 24. doi: 10.1136/annrheumdis-2021-220782.
Key clinical point: Patients with psoriatic arthritis (PsA) with vs without nail involvement had higher rates of carotid plaque (CP) and carotid intima-media thickness (cIMT). Additionally, nail involvement in PsA was independently associated with CP risk.
Major finding: Patients with vs without nail involvement showed a higher prevalence of CP (53.1% vs 25.0%; P = .021) and cIMT (0.85 vs 0.59 mm; P = .026). The nail involvement was an independent risk factor for the presence of CP (odds ratio, 6.64; P = .006).
Study details: Findings are from a cross-sectional, observational study involving 64 patients with PsA. Patients with nail involvement were matched by age, gender, and type 2 diabetes mellitus diagnosis to those without nail involvement.
Disclosures: No specific funding or conflicts of interest were declared.
Source: Colunga-Pedraza IJ et al. Ann Rheum Dis. 2021 Jun 24. doi: 10.1136/annrheumdis-2021-220782.
Key clinical point: Patients with psoriatic arthritis (PsA) with vs without nail involvement had higher rates of carotid plaque (CP) and carotid intima-media thickness (cIMT). Additionally, nail involvement in PsA was independently associated with CP risk.
Major finding: Patients with vs without nail involvement showed a higher prevalence of CP (53.1% vs 25.0%; P = .021) and cIMT (0.85 vs 0.59 mm; P = .026). The nail involvement was an independent risk factor for the presence of CP (odds ratio, 6.64; P = .006).
Study details: Findings are from a cross-sectional, observational study involving 64 patients with PsA. Patients with nail involvement were matched by age, gender, and type 2 diabetes mellitus diagnosis to those without nail involvement.
Disclosures: No specific funding or conflicts of interest were declared.
Source: Colunga-Pedraza IJ et al. Ann Rheum Dis. 2021 Jun 24. doi: 10.1136/annrheumdis-2021-220782.
Guselkumab effective for PsA patients having axial symptoms
Key clinical point: Patients with active psoriatic arthritis (PsA) and imaging-confirmed sacroiliitis treated with guselkumab every 4 weeks (Q4) or every 8 weeks (Q8) had greater mean improvements in Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and Ankylosing Spondylitis Disease Activity Score (ASDAS) score than placebo.
Major finding: At week 24, guselkumab Q4 and Q8 groups vs placebo showed higher least-squares mean changes in BASDAI (−2.7 and −2.7 vs −1.3; P less than .0001) and ASDAS (−1.4 and −1.4 vs −0.7; P less than .0001) scores, which were maintained until week 52.
Study details: This was a post hoc analysis of 2 DISCOVER studies including 312 patients with PsA with imaging-confirmed sacroiliitis who were randomly assigned to either placebo (n=118), guselkumab Q4 (n=103), or Q8 (n=91).
Disclosures: This study was funded by Janssen Research & Development LLC. The authors including the lead author reported grants and/or personal fees from various sources. Some of the authors declared being employees of Janssen Scientific Affairs LLC and Janssen Global Services LLC. Ten authors owned shares/stock options in Johnson & Johnson.
Source: Mease PJ et al. Lancet Rheumatol. 2021 Jun 29. doi: 10.1016/S2665-9913(21)00105-3.
Key clinical point: Patients with active psoriatic arthritis (PsA) and imaging-confirmed sacroiliitis treated with guselkumab every 4 weeks (Q4) or every 8 weeks (Q8) had greater mean improvements in Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and Ankylosing Spondylitis Disease Activity Score (ASDAS) score than placebo.
Major finding: At week 24, guselkumab Q4 and Q8 groups vs placebo showed higher least-squares mean changes in BASDAI (−2.7 and −2.7 vs −1.3; P less than .0001) and ASDAS (−1.4 and −1.4 vs −0.7; P less than .0001) scores, which were maintained until week 52.
Study details: This was a post hoc analysis of 2 DISCOVER studies including 312 patients with PsA with imaging-confirmed sacroiliitis who were randomly assigned to either placebo (n=118), guselkumab Q4 (n=103), or Q8 (n=91).
Disclosures: This study was funded by Janssen Research & Development LLC. The authors including the lead author reported grants and/or personal fees from various sources. Some of the authors declared being employees of Janssen Scientific Affairs LLC and Janssen Global Services LLC. Ten authors owned shares/stock options in Johnson & Johnson.
Source: Mease PJ et al. Lancet Rheumatol. 2021 Jun 29. doi: 10.1016/S2665-9913(21)00105-3.
Key clinical point: Patients with active psoriatic arthritis (PsA) and imaging-confirmed sacroiliitis treated with guselkumab every 4 weeks (Q4) or every 8 weeks (Q8) had greater mean improvements in Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and Ankylosing Spondylitis Disease Activity Score (ASDAS) score than placebo.
Major finding: At week 24, guselkumab Q4 and Q8 groups vs placebo showed higher least-squares mean changes in BASDAI (−2.7 and −2.7 vs −1.3; P less than .0001) and ASDAS (−1.4 and −1.4 vs −0.7; P less than .0001) scores, which were maintained until week 52.
Study details: This was a post hoc analysis of 2 DISCOVER studies including 312 patients with PsA with imaging-confirmed sacroiliitis who were randomly assigned to either placebo (n=118), guselkumab Q4 (n=103), or Q8 (n=91).
Disclosures: This study was funded by Janssen Research & Development LLC. The authors including the lead author reported grants and/or personal fees from various sources. Some of the authors declared being employees of Janssen Scientific Affairs LLC and Janssen Global Services LLC. Ten authors owned shares/stock options in Johnson & Johnson.
Source: Mease PJ et al. Lancet Rheumatol. 2021 Jun 29. doi: 10.1016/S2665-9913(21)00105-3.
COVID-19 vaccine hesitancy still weighs heavy for some rheumatic disease patients
With 49% of the U.S. population fully vaccinated against SARS-CoV-2, a new study highlights the degree of vaccine hesitancy among patients with rheumatic disease to get the vaccine.

The international study, published in May 2021 in Rheumatology, suggests that, of 1,258 patients surveyed worldwide, approximately 40% of patients said they would decline the vaccine.
“Sometimes it’s helpful to talk through their concerns,” said Jeffrey Curtis, MD, MPH, a University of Alabama at Birmingham rheumatologist who leads the American College of Rheumatology COVID-19 vaccine task force. Dr. Curtis recently reviewed the current literature on COVID-19 vaccination in patients with rheumatic and musculoskeletal diseases (RMDs) at the annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis.
COVID-19 vaccinations for patients with autoimmune inflammatory rheumatic disease (AIIRD) is not straightforward. The immune response can be blunted by existing treatments and disease flares can occur.

The latest version of COVID-19 vaccination guidance for patients with RMDs from the ACR addresses vaccine use and implementation strategies. The guidance was issued as conditional or provisional because of the lack of evidence. Its principals are largely based on accepted practice for other vaccines. The guidance is routinely updated as new evidence becomes available. In his presentation at GRAPPA, Dr. Curtis reviewed the latest version of the guidance, which he emphasized is a guidance only and not meant to replace clinical judgment or shared decision-making with patients.
“This is a platform for you to start from as you are thinking about and discussing with your patient what might be best for him or her,” he said.
Concerns about impact of disease activity, treatments on effectiveness
Dr. Curtis highlighted some controversial aspects of COVID-19 vaccines, including heterogeneity of rheumatic diseases and treatment. Patients with AIIRD, including psoriatic arthritis, spondyloarthritis, RA, and lupus, are at higher risk for hospitalized COVID-19 and worse outcomes, and as such, they are prioritized for vaccination by the Centers for Disease Control and Prevention.
However, for AIIRD patients, the immune response to COVID-19 vaccination can be “blunted,” according to one study. This may be because of glucocorticoid use or high disease activity. Immunomodulatory therapies, such as methotrexate, rituximab, and abatacept, are known to diminish vaccine response in general. The evidence is less clear for tumor necrosis factor and Janus kinase inhibitors, but they are thought to have the same impact on vaccine effectiveness, Dr. Curtis said. But in these cases, if the effect of a COVID-19 vaccine drops from 90% to 70%, the benefits of vaccination still far outweighs the risk of contracting COVID-19.
“Although we don’t have strong data with clinical outcomes for autoimmune disease or inflammatory disease patients, I’ll run a hypothetical and say: ‘Look, if this vaccine starts 90%-95% effective, even if it’s only 70% effective in somebody with lupus or vasculitis or someone who is taking a higher dose of steroids, I’ll take 70% over nothing if you chose to be vaccinated,’ ” he said.
The benefit of vaccination also outweighs the potential risk of disease flare, he said. The risk is real, but to date, no studies have pointed to a significant risk of disease flare or worsening. However, there have been reported cases of myocardial infarction.
Autoimmune manifestations after vaccination vs. after infection
Researchers writing in the June 29, 2021, issue of JAMA Cardiology described case reports of acute myocarditis in 23 people who received the BNT162b2-mRNA (Pfizer-BioNTech) or mRNA-1273 (Moderna) messenger RNA (mRNA) COVID-19 vaccines. Plus, there been subsequent reports of myocarditis in other patients, wrote David K. Shay, MD, MPH, in an accompanying editorial. Dr. Shay is a member of the CDC COVID-19 Response Team.
“What do we know about this possible association between myocarditis and immunization with mRNA-based COVID-19 vaccines, and what remains unclear? Acute onset of chest pain 3-5 days after vaccine administration, usually after a second dose, is a typical feature of reported cases and suggests an immune-mediated mechanism,” he said.
The cases of myocarditis are concerning, Dr. Curtis said, but the risk is very low with relatively few cases reported among 161 million fully vaccinated people in the United States.
“Certainly, we’re not seeking to minimize that, but the risk of getting COVID and some of the downstream sequelae (autoimmune manifestations) almost certainly outweigh the risks for some of the autoimmune manifestations or worsening [condition],” he said.
A nationwide cohort study from Denmark of 58,052 patients with inflammatory rheumatic disease published in December 2020 in Rheumatology, found that patients with COVID-19 who had an inflammatory rheumatic disease were more likely to be admitted to the hospital, compared with COVID-19 patients without rheumatic disease. Patients with rheumatic disease had a higher risk of a severe COVID-19 outcome, but it was not a statistically significant difference, said Dr. Curtis, adding that the individual factors such as age and treatment currently received largely determines the risk. The strongest associations between hospitalization for COVID-19 and rheumatic disease were found among patients with RA, vasculitis, and connective tissue disease. Dr. Curtis noted that his own new study results show that risk of death from a COVID-19 infection is higher for patients who have RA or psoriatic arthritis.
There have been published case reports of patients who have developed new-onset lupus, vasculitis, Kawasaki disease, multiple sclerosis, autoimmune cytopenias, and other manifestations after a COVID-19 infection. “These authors suggest that perhaps there is a transient influence on the immune system that leads to a loss of self-tolerance to antigens,” Dr. Curtis said. “Some patients may have an underlying predisposition to autoimmunity in which infections just unmask as we sometimes see with other infections – chronic hepatitis for example.”
Antibody tests not recommended
In its COVID-19 guidance, the ACR, like the Food and Drug Administration, recommends health care providers not to routinely order antibody tests for IgM or IgG to assess immunity after a person has been vaccinated or to assess the need for vaccination in an unvaccinated person. More research is needed to determine if antibodies provide protection, and if so, for how long and how much. Plus, the antibody testing process is not clear cut, so ordering the wrong test is possible, Dr. Curtis said. The tests should clearly differentiate between spike proteins or nucleocapsid proteins.
“The bottom line is that you might be ordering the wrong lab test. Even if you’re ordering the right lab test, I would assert that you probably don’t know what to do with the result. I would then ask you, ‘Does it mean they are protected? Does it mean they are not protected? What are you going to do with the results?’ ” he asked.

Kevin Winthrop, MD, MPH, a specialist in infectious diseases at Oregon Health & Science University, Portland, said that, at this point, it’s too early to know what antibody tests mean. “I think it is tempting to test some people, especially patients on B-cell depletion therapy and those on mycophenolate mofetil (MMF). Outside of those two types of [disease-modifying antirheumatic drug] users, I wouldn’t be tempted to test. We don’t know how well protected they are, but we assume they are protected to some extent,” he said. “They’re probably partially protected and as such, they should take the same precautions they were taking a year ago: masking and avoidance. I think that’s just how it’s going to be for those folks for another year until we get this thing sorted out.”
Modifications to existing rheumatic disease therapies
In its COVID-19 vaccine guidance, the ACR issued recommendations for some common rheumatic disease therapeutics before and/or after the COVID-19 vaccine is administered. The modifications are limited to MMF, methotrexate, JAK inhibitors, subcutaneous abatacept, acetaminophen, and NSAIDs. The recommendations include: hold mycophenolate for 1 week after vaccination if disease is stable; for patients with well-controlled disease, hold methotrexate for 1 week after each of the two mRNA vaccine doses; for patients with well-controlled disease receiving the Johnson & Johnson vaccine, hold methotrexate for 2 weeks after receiving the vaccine; hold JAK inhibitors for 1 week after each dose; for abatacept subcutaneous, hold treatment for 1 week before and after the first dose; and in patients with stable disease, hold acetaminophen and NSAIDs for 24 hours before vaccination, because taking either before vaccination could blunt the vaccine response, Dr. Curtis said.
Holding medication, such as methotrexate, could risk having a flare-up of disease. One study showed the rate of disease flare-up because of withholding standard treatment may be up to 11%, compared with 5.1% in patients who did not hold treatment, he said.
“The point is, if you hold some of these therapies, whether methotrexate or tofacitinib, arthritis will get a little bit worse,” Dr. Curtis said.
A study published on the preprint server medRxiv found that immunosuppressive therapies blunted the response of SARS-CoV-2 vaccines in patients with chronic inflammatory diseases, most significantly with glucocorticoids and B-cell therapies.
“That’s what’s led to a lot of the guidance statements about holding treatments for a week or 2 for rituximab. If you’re giving it at 6-month intervals, you want to schedule the vaccine dose or series at about month 5, or a month before the next cycle,” he said.
Talking with patients about COVID-19 vaccination
In talking with patients about vaccine safety, Dr. Curtis recommends addressing a few common misperceptions. First, COVID-19 viruses were not created with a live-attenuated virus (which would be contraindicated for immunosuppressed patients). “You can put patients’ mind at ease that none of the vaccine candidates or platforms – even those that say viral vector – put patients at risk for contracting the infection. These are nonreplicating. So, it’s like you extracted the engine that would allow this virus to replicate,” he said.
Of three COVID-19 vaccinations available in the United States, is one better than the other? The ACR COVID-19 vaccine task force did not reach a consensus on safety profiles of the vaccines because, without head-to-head comparisons, it’s impossible to know, he said.
In talking with patients, review the protocol for continuing with prescribed treatment modalities before the patient receives a COVID-19 vaccine. Safety concerns and concerns about the possibility of having a disease flare-up should be addressed, he said.
With 49% of the U.S. population fully vaccinated against SARS-CoV-2, a new study highlights the degree of vaccine hesitancy among patients with rheumatic disease to get the vaccine.
The international study, published in May 2021 in Rheumatology, suggests that, of 1,258 patients surveyed worldwide, approximately 40% of patients said they would decline the vaccine.
“Sometimes it’s helpful to talk through their concerns,” said Jeffrey Curtis, MD, MPH, a University of Alabama at Birmingham rheumatologist who leads the American College of Rheumatology COVID-19 vaccine task force. Dr. Curtis recently reviewed the current literature on COVID-19 vaccination in patients with rheumatic and musculoskeletal diseases (RMDs) at the annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis.
COVID-19 vaccinations for patients with autoimmune inflammatory rheumatic disease (AIIRD) is not straightforward. The immune response can be blunted by existing treatments and disease flares can occur.
The latest version of COVID-19 vaccination guidance for patients with RMDs from the ACR addresses vaccine use and implementation strategies. The guidance was issued as conditional or provisional because of the lack of evidence. Its principals are largely based on accepted practice for other vaccines. The guidance is routinely updated as new evidence becomes available. In his presentation at GRAPPA, Dr. Curtis reviewed the latest version of the guidance, which he emphasized is a guidance only and not meant to replace clinical judgment or shared decision-making with patients.
“This is a platform for you to start from as you are thinking about and discussing with your patient what might be best for him or her,” he said.
Concerns about impact of disease activity, treatments on effectiveness
Dr. Curtis highlighted some controversial aspects of COVID-19 vaccines, including heterogeneity of rheumatic diseases and treatment. Patients with AIIRD, including psoriatic arthritis, spondyloarthritis, RA, and lupus, are at higher risk for hospitalized COVID-19 and worse outcomes, and as such, they are prioritized for vaccination by the Centers for Disease Control and Prevention.
However, for AIIRD patients, the immune response to COVID-19 vaccination can be “blunted,” according to one study. This may be because of glucocorticoid use or high disease activity. Immunomodulatory therapies, such as methotrexate, rituximab, and abatacept, are known to diminish vaccine response in general. The evidence is less clear for tumor necrosis factor and Janus kinase inhibitors, but they are thought to have the same impact on vaccine effectiveness, Dr. Curtis said. But in these cases, if the effect of a COVID-19 vaccine drops from 90% to 70%, the benefits of vaccination still far outweighs the risk of contracting COVID-19.
“Although we don’t have strong data with clinical outcomes for autoimmune disease or inflammatory disease patients, I’ll run a hypothetical and say: ‘Look, if this vaccine starts 90%-95% effective, even if it’s only 70% effective in somebody with lupus or vasculitis or someone who is taking a higher dose of steroids, I’ll take 70% over nothing if you chose to be vaccinated,’ ” he said.
The benefit of vaccination also outweighs the potential risk of disease flare, he said. The risk is real, but to date, no studies have pointed to a significant risk of disease flare or worsening. However, there have been reported cases of myocardial infarction.
Autoimmune manifestations after vaccination vs. after infection
Researchers writing in the June 29, 2021, issue of JAMA Cardiology described case reports of acute myocarditis in 23 people who received the BNT162b2-mRNA (Pfizer-BioNTech) or mRNA-1273 (Moderna) messenger RNA (mRNA) COVID-19 vaccines. Plus, there been subsequent reports of myocarditis in other patients, wrote David K. Shay, MD, MPH, in an accompanying editorial. Dr. Shay is a member of the CDC COVID-19 Response Team.
“What do we know about this possible association between myocarditis and immunization with mRNA-based COVID-19 vaccines, and what remains unclear? Acute onset of chest pain 3-5 days after vaccine administration, usually after a second dose, is a typical feature of reported cases and suggests an immune-mediated mechanism,” he said.
The cases of myocarditis are concerning, Dr. Curtis said, but the risk is very low with relatively few cases reported among 161 million fully vaccinated people in the United States.
“Certainly, we’re not seeking to minimize that, but the risk of getting COVID and some of the downstream sequelae (autoimmune manifestations) almost certainly outweigh the risks for some of the autoimmune manifestations or worsening [condition],” he said.
A nationwide cohort study from Denmark of 58,052 patients with inflammatory rheumatic disease published in December 2020 in Rheumatology, found that patients with COVID-19 who had an inflammatory rheumatic disease were more likely to be admitted to the hospital, compared with COVID-19 patients without rheumatic disease. Patients with rheumatic disease had a higher risk of a severe COVID-19 outcome, but it was not a statistically significant difference, said Dr. Curtis, adding that the individual factors such as age and treatment currently received largely determines the risk. The strongest associations between hospitalization for COVID-19 and rheumatic disease were found among patients with RA, vasculitis, and connective tissue disease. Dr. Curtis noted that his own new study results show that risk of death from a COVID-19 infection is higher for patients who have RA or psoriatic arthritis.
There have been published case reports of patients who have developed new-onset lupus, vasculitis, Kawasaki disease, multiple sclerosis, autoimmune cytopenias, and other manifestations after a COVID-19 infection. “These authors suggest that perhaps there is a transient influence on the immune system that leads to a loss of self-tolerance to antigens,” Dr. Curtis said. “Some patients may have an underlying predisposition to autoimmunity in which infections just unmask as we sometimes see with other infections – chronic hepatitis for example.”
Antibody tests not recommended
In its COVID-19 guidance, the ACR, like the Food and Drug Administration, recommends health care providers not to routinely order antibody tests for IgM or IgG to assess immunity after a person has been vaccinated or to assess the need for vaccination in an unvaccinated person. More research is needed to determine if antibodies provide protection, and if so, for how long and how much. Plus, the antibody testing process is not clear cut, so ordering the wrong test is possible, Dr. Curtis said. The tests should clearly differentiate between spike proteins or nucleocapsid proteins.
“The bottom line is that you might be ordering the wrong lab test. Even if you’re ordering the right lab test, I would assert that you probably don’t know what to do with the result. I would then ask you, ‘Does it mean they are protected? Does it mean they are not protected? What are you going to do with the results?’ ” he asked.
Kevin Winthrop, MD, MPH, a specialist in infectious diseases at Oregon Health & Science University, Portland, said that, at this point, it’s too early to know what antibody tests mean. “I think it is tempting to test some people, especially patients on B-cell depletion therapy and those on mycophenolate mofetil (MMF). Outside of those two types of [disease-modifying antirheumatic drug] users, I wouldn’t be tempted to test. We don’t know how well protected they are, but we assume they are protected to some extent,” he said. “They’re probably partially protected and as such, they should take the same precautions they were taking a year ago: masking and avoidance. I think that’s just how it’s going to be for those folks for another year until we get this thing sorted out.”
Modifications to existing rheumatic disease therapies
In its COVID-19 vaccine guidance, the ACR issued recommendations for some common rheumatic disease therapeutics before and/or after the COVID-19 vaccine is administered. The modifications are limited to MMF, methotrexate, JAK inhibitors, subcutaneous abatacept, acetaminophen, and NSAIDs. The recommendations include: hold mycophenolate for 1 week after vaccination if disease is stable; for patients with well-controlled disease, hold methotrexate for 1 week after each of the two mRNA vaccine doses; for patients with well-controlled disease receiving the Johnson & Johnson vaccine, hold methotrexate for 2 weeks after receiving the vaccine; hold JAK inhibitors for 1 week after each dose; for abatacept subcutaneous, hold treatment for 1 week before and after the first dose; and in patients with stable disease, hold acetaminophen and NSAIDs for 24 hours before vaccination, because taking either before vaccination could blunt the vaccine response, Dr. Curtis said.
Holding medication, such as methotrexate, could risk having a flare-up of disease. One study showed the rate of disease flare-up because of withholding standard treatment may be up to 11%, compared with 5.1% in patients who did not hold treatment, he said.
“The point is, if you hold some of these therapies, whether methotrexate or tofacitinib, arthritis will get a little bit worse,” Dr. Curtis said.
A study published on the preprint server medRxiv found that immunosuppressive therapies blunted the response of SARS-CoV-2 vaccines in patients with chronic inflammatory diseases, most significantly with glucocorticoids and B-cell therapies.
“That’s what’s led to a lot of the guidance statements about holding treatments for a week or 2 for rituximab. If you’re giving it at 6-month intervals, you want to schedule the vaccine dose or series at about month 5, or a month before the next cycle,” he said.
Talking with patients about COVID-19 vaccination
In talking with patients about vaccine safety, Dr. Curtis recommends addressing a few common misperceptions. First, COVID-19 viruses were not created with a live-attenuated virus (which would be contraindicated for immunosuppressed patients). “You can put patients’ mind at ease that none of the vaccine candidates or platforms – even those that say viral vector – put patients at risk for contracting the infection. These are nonreplicating. So, it’s like you extracted the engine that would allow this virus to replicate,” he said.
Of three COVID-19 vaccinations available in the United States, is one better than the other? The ACR COVID-19 vaccine task force did not reach a consensus on safety profiles of the vaccines because, without head-to-head comparisons, it’s impossible to know, he said.
In talking with patients, review the protocol for continuing with prescribed treatment modalities before the patient receives a COVID-19 vaccine. Safety concerns and concerns about the possibility of having a disease flare-up should be addressed, he said.
With 49% of the U.S. population fully vaccinated against SARS-CoV-2, a new study highlights the degree of vaccine hesitancy among patients with rheumatic disease to get the vaccine.
The international study, published in May 2021 in Rheumatology, suggests that, of 1,258 patients surveyed worldwide, approximately 40% of patients said they would decline the vaccine.
“Sometimes it’s helpful to talk through their concerns,” said Jeffrey Curtis, MD, MPH, a University of Alabama at Birmingham rheumatologist who leads the American College of Rheumatology COVID-19 vaccine task force. Dr. Curtis recently reviewed the current literature on COVID-19 vaccination in patients with rheumatic and musculoskeletal diseases (RMDs) at the annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis.
COVID-19 vaccinations for patients with autoimmune inflammatory rheumatic disease (AIIRD) is not straightforward. The immune response can be blunted by existing treatments and disease flares can occur.
The latest version of COVID-19 vaccination guidance for patients with RMDs from the ACR addresses vaccine use and implementation strategies. The guidance was issued as conditional or provisional because of the lack of evidence. Its principals are largely based on accepted practice for other vaccines. The guidance is routinely updated as new evidence becomes available. In his presentation at GRAPPA, Dr. Curtis reviewed the latest version of the guidance, which he emphasized is a guidance only and not meant to replace clinical judgment or shared decision-making with patients.
“This is a platform for you to start from as you are thinking about and discussing with your patient what might be best for him or her,” he said.
Concerns about impact of disease activity, treatments on effectiveness
Dr. Curtis highlighted some controversial aspects of COVID-19 vaccines, including heterogeneity of rheumatic diseases and treatment. Patients with AIIRD, including psoriatic arthritis, spondyloarthritis, RA, and lupus, are at higher risk for hospitalized COVID-19 and worse outcomes, and as such, they are prioritized for vaccination by the Centers for Disease Control and Prevention.
However, for AIIRD patients, the immune response to COVID-19 vaccination can be “blunted,” according to one study. This may be because of glucocorticoid use or high disease activity. Immunomodulatory therapies, such as methotrexate, rituximab, and abatacept, are known to diminish vaccine response in general. The evidence is less clear for tumor necrosis factor and Janus kinase inhibitors, but they are thought to have the same impact on vaccine effectiveness, Dr. Curtis said. But in these cases, if the effect of a COVID-19 vaccine drops from 90% to 70%, the benefits of vaccination still far outweighs the risk of contracting COVID-19.
“Although we don’t have strong data with clinical outcomes for autoimmune disease or inflammatory disease patients, I’ll run a hypothetical and say: ‘Look, if this vaccine starts 90%-95% effective, even if it’s only 70% effective in somebody with lupus or vasculitis or someone who is taking a higher dose of steroids, I’ll take 70% over nothing if you chose to be vaccinated,’ ” he said.
The benefit of vaccination also outweighs the potential risk of disease flare, he said. The risk is real, but to date, no studies have pointed to a significant risk of disease flare or worsening. However, there have been reported cases of myocardial infarction.
Autoimmune manifestations after vaccination vs. after infection
Researchers writing in the June 29, 2021, issue of JAMA Cardiology described case reports of acute myocarditis in 23 people who received the BNT162b2-mRNA (Pfizer-BioNTech) or mRNA-1273 (Moderna) messenger RNA (mRNA) COVID-19 vaccines. Plus, there been subsequent reports of myocarditis in other patients, wrote David K. Shay, MD, MPH, in an accompanying editorial. Dr. Shay is a member of the CDC COVID-19 Response Team.
“What do we know about this possible association between myocarditis and immunization with mRNA-based COVID-19 vaccines, and what remains unclear? Acute onset of chest pain 3-5 days after vaccine administration, usually after a second dose, is a typical feature of reported cases and suggests an immune-mediated mechanism,” he said.
The cases of myocarditis are concerning, Dr. Curtis said, but the risk is very low with relatively few cases reported among 161 million fully vaccinated people in the United States.
“Certainly, we’re not seeking to minimize that, but the risk of getting COVID and some of the downstream sequelae (autoimmune manifestations) almost certainly outweigh the risks for some of the autoimmune manifestations or worsening [condition],” he said.
A nationwide cohort study from Denmark of 58,052 patients with inflammatory rheumatic disease published in December 2020 in Rheumatology, found that patients with COVID-19 who had an inflammatory rheumatic disease were more likely to be admitted to the hospital, compared with COVID-19 patients without rheumatic disease. Patients with rheumatic disease had a higher risk of a severe COVID-19 outcome, but it was not a statistically significant difference, said Dr. Curtis, adding that the individual factors such as age and treatment currently received largely determines the risk. The strongest associations between hospitalization for COVID-19 and rheumatic disease were found among patients with RA, vasculitis, and connective tissue disease. Dr. Curtis noted that his own new study results show that risk of death from a COVID-19 infection is higher for patients who have RA or psoriatic arthritis.
There have been published case reports of patients who have developed new-onset lupus, vasculitis, Kawasaki disease, multiple sclerosis, autoimmune cytopenias, and other manifestations after a COVID-19 infection. “These authors suggest that perhaps there is a transient influence on the immune system that leads to a loss of self-tolerance to antigens,” Dr. Curtis said. “Some patients may have an underlying predisposition to autoimmunity in which infections just unmask as we sometimes see with other infections – chronic hepatitis for example.”
Antibody tests not recommended
In its COVID-19 guidance, the ACR, like the Food and Drug Administration, recommends health care providers not to routinely order antibody tests for IgM or IgG to assess immunity after a person has been vaccinated or to assess the need for vaccination in an unvaccinated person. More research is needed to determine if antibodies provide protection, and if so, for how long and how much. Plus, the antibody testing process is not clear cut, so ordering the wrong test is possible, Dr. Curtis said. The tests should clearly differentiate between spike proteins or nucleocapsid proteins.
“The bottom line is that you might be ordering the wrong lab test. Even if you’re ordering the right lab test, I would assert that you probably don’t know what to do with the result. I would then ask you, ‘Does it mean they are protected? Does it mean they are not protected? What are you going to do with the results?’ ” he asked.
Kevin Winthrop, MD, MPH, a specialist in infectious diseases at Oregon Health & Science University, Portland, said that, at this point, it’s too early to know what antibody tests mean. “I think it is tempting to test some people, especially patients on B-cell depletion therapy and those on mycophenolate mofetil (MMF). Outside of those two types of [disease-modifying antirheumatic drug] users, I wouldn’t be tempted to test. We don’t know how well protected they are, but we assume they are protected to some extent,” he said. “They’re probably partially protected and as such, they should take the same precautions they were taking a year ago: masking and avoidance. I think that’s just how it’s going to be for those folks for another year until we get this thing sorted out.”
Modifications to existing rheumatic disease therapies
In its COVID-19 vaccine guidance, the ACR issued recommendations for some common rheumatic disease therapeutics before and/or after the COVID-19 vaccine is administered. The modifications are limited to MMF, methotrexate, JAK inhibitors, subcutaneous abatacept, acetaminophen, and NSAIDs. The recommendations include: hold mycophenolate for 1 week after vaccination if disease is stable; for patients with well-controlled disease, hold methotrexate for 1 week after each of the two mRNA vaccine doses; for patients with well-controlled disease receiving the Johnson & Johnson vaccine, hold methotrexate for 2 weeks after receiving the vaccine; hold JAK inhibitors for 1 week after each dose; for abatacept subcutaneous, hold treatment for 1 week before and after the first dose; and in patients with stable disease, hold acetaminophen and NSAIDs for 24 hours before vaccination, because taking either before vaccination could blunt the vaccine response, Dr. Curtis said.
Holding medication, such as methotrexate, could risk having a flare-up of disease. One study showed the rate of disease flare-up because of withholding standard treatment may be up to 11%, compared with 5.1% in patients who did not hold treatment, he said.
“The point is, if you hold some of these therapies, whether methotrexate or tofacitinib, arthritis will get a little bit worse,” Dr. Curtis said.
A study published on the preprint server medRxiv found that immunosuppressive therapies blunted the response of SARS-CoV-2 vaccines in patients with chronic inflammatory diseases, most significantly with glucocorticoids and B-cell therapies.
“That’s what’s led to a lot of the guidance statements about holding treatments for a week or 2 for rituximab. If you’re giving it at 6-month intervals, you want to schedule the vaccine dose or series at about month 5, or a month before the next cycle,” he said.
Talking with patients about COVID-19 vaccination
In talking with patients about vaccine safety, Dr. Curtis recommends addressing a few common misperceptions. First, COVID-19 viruses were not created with a live-attenuated virus (which would be contraindicated for immunosuppressed patients). “You can put patients’ mind at ease that none of the vaccine candidates or platforms – even those that say viral vector – put patients at risk for contracting the infection. These are nonreplicating. So, it’s like you extracted the engine that would allow this virus to replicate,” he said.
Of three COVID-19 vaccinations available in the United States, is one better than the other? The ACR COVID-19 vaccine task force did not reach a consensus on safety profiles of the vaccines because, without head-to-head comparisons, it’s impossible to know, he said.
In talking with patients, review the protocol for continuing with prescribed treatment modalities before the patient receives a COVID-19 vaccine. Safety concerns and concerns about the possibility of having a disease flare-up should be addressed, he said.
FROM THE GRAPPA 2021 ANNUAL MEETING
‘Gold cards’ allow Texas docs to skip prior authorizations
The law was passed in June and will take effect in September. It excuses physicians from having to obtain prior authorization if, during the previous 6 months, 90% of their treatments met medical necessity criteria by the health insurer. Through this law, doctors in the state will spend less time getting approvals for treatments for their patients.
Automatic approval of authorizations for treatments – or what the Texas Medical Association (TMA) calls a “gold card” – “allows patients to get the care they need in a more timely fashion,” says Debra Patt, MD, an Austin, Tex.–based oncologist and former chair of the council on legislation for the TMA.
Eighty-seven percent of Texas physicians reported a “drastic increase over the past five years in the burden of prior authorization on their patients and their practices,” per a 2020 survey by the TMA. Nearly half (48%) of Texas physicians have hired staff whose work focuses on processing requests for prior authorization, according to the survey.

Jack Resneck Jr., MD, a San Francisco–based dermatologist and president-elect of the American Medical Association (AMA), said other states have investigated ways to ease the impact of prior authorizations on physicians, but no other state has passed such a law.
Administrative burdens plague physicians around the country. The Medscape Physician Compensation Report 2021 found that physicians spend on average 15.6 hours per week on paperwork and administrative duties.
Better outcomes, less anxiety for patients
Dr. Patt, who testified in support of the law’s passage in the Texas legislature, says automatic approval of authorizations “is better for patients because it reduces their anxiety about whether they’re able to get the treatments they need now, and they will have better outcomes if they’re able to receive more timely care.”
Recently, a chemotherapy treatment Dr. Patt prescribed for one of her patients was not authorized by an insurer. The result is “a lot of anxiety and potentially health problems” for the patient, said Dr. Patt.
She expects that automatic approval for treatments will be based on prescribing patterns during the preceding 6 months. “It means that when I order a test today, the [health insurer] looks back at my record 6 months previously,” she said. Still, Dr. Patt awaits guidance from the Texas Department of Insurance, which regulates health insurers in the state, regarding the law.
Dr. Resneck said the pharmacy counter is where most patients encounter prior authorization delays. “That’s when the pharmacist looks at them and says, ‘Actually, this isn’t covered by your health insurer’s formulary,’ or it isn’t covered fully on their formulary.”
One of Dr. Resneck’s patients had a life-altering case of eczema that lasted many years. Because of the condition, the patient couldn’t work or maintain meaningful bonds with family members. A biologic treatment transformed his patient’s life. The patient was able to return to work and to re-engage with family, said Dr. Resneck. But a year after his patient started the treatment, the health insurer wouldn’t authorize the treatment because the patient wasn’t experiencing the same symptoms.
The patient didn’t have the same symptoms because the biologic treatment worked, said Dr. Resneck.
Kristine Grow, a spokesperson for America’s Health Insurance Plans, a national association for health insurers, said, “The use of prior authorization is relatively small – typically, less than 15% – and can help ensure safer opioid prescribing, help prevent dangerous drug interactions, and help protect patients from unnecessary exposure to potentially harmful radiation for inappropriate diagnostic imaging. Numerous studies show that Americans frequently receive inappropriate care, and 25% of unnecessary treatments are associated with complications or adverse events.”
Medical management tools, such as prior authorization, are an “an important way” to deliver “safe, high-quality care” to patients, she added.
State and federal efforts to curb prior authorization
In addition to efforts to curb prior authorization in other states, the AMA supports the Improving Seniors’ Timely Access to Care Act (HR 3173). The act includes a provision related to “gold-carding,” said Robert Mills, an AMA spokesperson.
The bill establishes requirements and standards for prior authorization processes related to Medicare Advantage (MA) plans. The requirements and standards for MA plans include the following:
- Establishing an electronic prior authorization program that meets specific standards, such as the ability to provide real-time decisions in response to requests for items and services that are routinely approved.
- Publishing on an annual basis specific prior authorization information, including the percentage of requests approved and the average response time.
- Meeting standards set by the Centers for Medicare & Medicaid Services related to the quality and timeliness of prior authorization determinations.
The act was introduced to the U.S. House of Representatives in May, after which it was referred to two committees for consideration.
A version of this article first appeared on Medscape.com.
The law was passed in June and will take effect in September. It excuses physicians from having to obtain prior authorization if, during the previous 6 months, 90% of their treatments met medical necessity criteria by the health insurer. Through this law, doctors in the state will spend less time getting approvals for treatments for their patients.
Automatic approval of authorizations for treatments – or what the Texas Medical Association (TMA) calls a “gold card” – “allows patients to get the care they need in a more timely fashion,” says Debra Patt, MD, an Austin, Tex.–based oncologist and former chair of the council on legislation for the TMA.
Eighty-seven percent of Texas physicians reported a “drastic increase over the past five years in the burden of prior authorization on their patients and their practices,” per a 2020 survey by the TMA. Nearly half (48%) of Texas physicians have hired staff whose work focuses on processing requests for prior authorization, according to the survey.
Jack Resneck Jr., MD, a San Francisco–based dermatologist and president-elect of the American Medical Association (AMA), said other states have investigated ways to ease the impact of prior authorizations on physicians, but no other state has passed such a law.
Administrative burdens plague physicians around the country. The Medscape Physician Compensation Report 2021 found that physicians spend on average 15.6 hours per week on paperwork and administrative duties.
Better outcomes, less anxiety for patients
Dr. Patt, who testified in support of the law’s passage in the Texas legislature, says automatic approval of authorizations “is better for patients because it reduces their anxiety about whether they’re able to get the treatments they need now, and they will have better outcomes if they’re able to receive more timely care.”
Recently, a chemotherapy treatment Dr. Patt prescribed for one of her patients was not authorized by an insurer. The result is “a lot of anxiety and potentially health problems” for the patient, said Dr. Patt.
She expects that automatic approval for treatments will be based on prescribing patterns during the preceding 6 months. “It means that when I order a test today, the [health insurer] looks back at my record 6 months previously,” she said. Still, Dr. Patt awaits guidance from the Texas Department of Insurance, which regulates health insurers in the state, regarding the law.
Dr. Resneck said the pharmacy counter is where most patients encounter prior authorization delays. “That’s when the pharmacist looks at them and says, ‘Actually, this isn’t covered by your health insurer’s formulary,’ or it isn’t covered fully on their formulary.”
One of Dr. Resneck’s patients had a life-altering case of eczema that lasted many years. Because of the condition, the patient couldn’t work or maintain meaningful bonds with family members. A biologic treatment transformed his patient’s life. The patient was able to return to work and to re-engage with family, said Dr. Resneck. But a year after his patient started the treatment, the health insurer wouldn’t authorize the treatment because the patient wasn’t experiencing the same symptoms.
The patient didn’t have the same symptoms because the biologic treatment worked, said Dr. Resneck.
Kristine Grow, a spokesperson for America’s Health Insurance Plans, a national association for health insurers, said, “The use of prior authorization is relatively small – typically, less than 15% – and can help ensure safer opioid prescribing, help prevent dangerous drug interactions, and help protect patients from unnecessary exposure to potentially harmful radiation for inappropriate diagnostic imaging. Numerous studies show that Americans frequently receive inappropriate care, and 25% of unnecessary treatments are associated with complications or adverse events.”
Medical management tools, such as prior authorization, are an “an important way” to deliver “safe, high-quality care” to patients, she added.
State and federal efforts to curb prior authorization
In addition to efforts to curb prior authorization in other states, the AMA supports the Improving Seniors’ Timely Access to Care Act (HR 3173). The act includes a provision related to “gold-carding,” said Robert Mills, an AMA spokesperson.
The bill establishes requirements and standards for prior authorization processes related to Medicare Advantage (MA) plans. The requirements and standards for MA plans include the following:
- Establishing an electronic prior authorization program that meets specific standards, such as the ability to provide real-time decisions in response to requests for items and services that are routinely approved.
- Publishing on an annual basis specific prior authorization information, including the percentage of requests approved and the average response time.
- Meeting standards set by the Centers for Medicare & Medicaid Services related to the quality and timeliness of prior authorization determinations.
The act was introduced to the U.S. House of Representatives in May, after which it was referred to two committees for consideration.
A version of this article first appeared on Medscape.com.
The law was passed in June and will take effect in September. It excuses physicians from having to obtain prior authorization if, during the previous 6 months, 90% of their treatments met medical necessity criteria by the health insurer. Through this law, doctors in the state will spend less time getting approvals for treatments for their patients.
Automatic approval of authorizations for treatments – or what the Texas Medical Association (TMA) calls a “gold card” – “allows patients to get the care they need in a more timely fashion,” says Debra Patt, MD, an Austin, Tex.–based oncologist and former chair of the council on legislation for the TMA.
Eighty-seven percent of Texas physicians reported a “drastic increase over the past five years in the burden of prior authorization on their patients and their practices,” per a 2020 survey by the TMA. Nearly half (48%) of Texas physicians have hired staff whose work focuses on processing requests for prior authorization, according to the survey.
Jack Resneck Jr., MD, a San Francisco–based dermatologist and president-elect of the American Medical Association (AMA), said other states have investigated ways to ease the impact of prior authorizations on physicians, but no other state has passed such a law.
Administrative burdens plague physicians around the country. The Medscape Physician Compensation Report 2021 found that physicians spend on average 15.6 hours per week on paperwork and administrative duties.
Better outcomes, less anxiety for patients
Dr. Patt, who testified in support of the law’s passage in the Texas legislature, says automatic approval of authorizations “is better for patients because it reduces their anxiety about whether they’re able to get the treatments they need now, and they will have better outcomes if they’re able to receive more timely care.”
Recently, a chemotherapy treatment Dr. Patt prescribed for one of her patients was not authorized by an insurer. The result is “a lot of anxiety and potentially health problems” for the patient, said Dr. Patt.
She expects that automatic approval for treatments will be based on prescribing patterns during the preceding 6 months. “It means that when I order a test today, the [health insurer] looks back at my record 6 months previously,” she said. Still, Dr. Patt awaits guidance from the Texas Department of Insurance, which regulates health insurers in the state, regarding the law.
Dr. Resneck said the pharmacy counter is where most patients encounter prior authorization delays. “That’s when the pharmacist looks at them and says, ‘Actually, this isn’t covered by your health insurer’s formulary,’ or it isn’t covered fully on their formulary.”
One of Dr. Resneck’s patients had a life-altering case of eczema that lasted many years. Because of the condition, the patient couldn’t work or maintain meaningful bonds with family members. A biologic treatment transformed his patient’s life. The patient was able to return to work and to re-engage with family, said Dr. Resneck. But a year after his patient started the treatment, the health insurer wouldn’t authorize the treatment because the patient wasn’t experiencing the same symptoms.
The patient didn’t have the same symptoms because the biologic treatment worked, said Dr. Resneck.
Kristine Grow, a spokesperson for America’s Health Insurance Plans, a national association for health insurers, said, “The use of prior authorization is relatively small – typically, less than 15% – and can help ensure safer opioid prescribing, help prevent dangerous drug interactions, and help protect patients from unnecessary exposure to potentially harmful radiation for inappropriate diagnostic imaging. Numerous studies show that Americans frequently receive inappropriate care, and 25% of unnecessary treatments are associated with complications or adverse events.”
Medical management tools, such as prior authorization, are an “an important way” to deliver “safe, high-quality care” to patients, she added.
State and federal efforts to curb prior authorization
In addition to efforts to curb prior authorization in other states, the AMA supports the Improving Seniors’ Timely Access to Care Act (HR 3173). The act includes a provision related to “gold-carding,” said Robert Mills, an AMA spokesperson.
The bill establishes requirements and standards for prior authorization processes related to Medicare Advantage (MA) plans. The requirements and standards for MA plans include the following:
- Establishing an electronic prior authorization program that meets specific standards, such as the ability to provide real-time decisions in response to requests for items and services that are routinely approved.
- Publishing on an annual basis specific prior authorization information, including the percentage of requests approved and the average response time.
- Meeting standards set by the Centers for Medicare & Medicaid Services related to the quality and timeliness of prior authorization determinations.
The act was introduced to the U.S. House of Representatives in May, after which it was referred to two committees for consideration.
A version of this article first appeared on Medscape.com.
Patients on methotrexate show T-cell response to Pfizer vaccine
People taking methotrexate had low antibody responses after the first dose of the Pfizer-BioNTech mRNA COVID-19 vaccine, but did show evidence of T-cell–mediated immune responses, findings from a small study show.
The common immunosuppressant has previously been linked to poor antibody responses to mRNA COVID-19 vaccines, but this appears to be the first study to look at T-cell responses in people taking methotrexate.
The study findings were presented online July 11 at the 31st European Congress of Clinical Microbiology & Infectious Diseases and published in The Lancet Rheumatology.
“These findings indicate that seroconversion alone might not adequately reflect vaccine immunogenicity in individuals with immune-mediated inflammatory diseases receiving therapeutic immunosuppression, and caution against routine use of seroconversion data in isolation in clinical practice,” Satveer K. Mahil, MBBChir, PhD, from St. John’s Institute of Dermatology, Guy’s and St. Thomas’ NHS Foundation Trust, London, and colleagues wrote.
“When taking into account functional humoral immunity and T-cell responses, our data suggest that targeted biologics do not impair vaccine responses and provide some reassurance to this vulnerable population,” they wrote. “Notably, although methotrexate attenuated humoral immunity, cellular responses were preserved.”
Dr. Mahil and colleagues assessed 84 consecutive patients from a psoriasis specialist clinic that serves London and southeast England. Median age of the cohort was 43 years, and 85% were White. All had a confirmed psoriasis diagnosis, received the first dose of the Pfizer-BioNTech COVID-19 vaccine, and were taking either methotrexate (17 patients) or a targeted biologic (27 were taking a tumor necrosis factor inhibitor, 15 an interleukin-17 inhibitor, and 25 an IL-23 inhibitor). In addition, 17 healthy patients not receiving immunosuppression therapy who received the Pfizer-BioNTech vaccine served as the control group.
Four weeks after the study participants received their first dose of the vaccine, 78% of the immunosuppressed patients underwent seroconversion – producing measurable antibodies – as did 100% of the control group. Patients taking methotrexate had the lowest seroconversion rate at 47%, compared with 79% with TNF inhibitors, 83% with IL-23 inhibitors, and 100% with IL-17 inhibitors.
Participants taking methotrexate also had lower neutralizing activity against SARS-CoV-2 than control subjects and those taking a targeted biologic, who had similar levels of neutralizing activity.
All participants had low neutralizing titers against the alpha (B.1.1.7) variant.
The researchers also assessed cellular immunity, “defined as the presence of T cells secreting interferon-gamma, IL-2, or IL-21 in response to stimulation with two peptide pools spanning the entire length of the SARS-CoV-2 spike glycoprotein.”
A T-cell response was seen in 84% of participants taking immunosuppressants, including 93% of those in the methotrexate group and 69% of control subjects.
‘Some protection is better than none’
These findings regarding antibodies match what has been seen in other research, said Ignacio Sanz, MD, director of the Lowance Center for Human Immunology at Emory University, Atlanta.
It would be helpful to see antibody responses after the second doses, he added. Those data will be reported later, according to Dr. Mahil and colleagues.
“The authors make the valid point that T-cell immunity should also be measured. The information is meaningful and supports the idea that there could be protection still provided,” Dr. Sanz said in an interview, adding that it would have been helpful to see CD8 T-cell response as well.
“My message to patients, still, is that some protection is better than none, and that, indeed, protection may be afforded in different ways, including T-cell immunity, which, to the extent tested, seems to be induced,” he said. But discussion of B cells independent of their role in producing antibodies is missing.
“When it comes to B-cell responses, antibodies are the easier and more direct measurement. However, it is perfectly possible that the vaccine may fail to induce high antibody titers and still generate good B-cell immunity,” in the same way virus-specific memory B cells do, he explained. “They would not directly produce antibodies, yet they would be available for a good and quick response in the case of subsequent encounter with the virus and, incidentally, in the case of a booster dose. It is possible that the generation of antibody-producing plasma cells might be uncoupled from the generation of memory B cells.”
Temporarily stopping methotrexate
It is well known that methotrexate impairs humoral responses to influenza and pneumococcal vaccines, write Caoilfhionn M. Connolly, MD, and Julie J. Paik, MD, both from the Johns Hopkins University, Baltimore, in an accompanying comment.
Research has also shown that temporarily stopping methotrexate therapy for 2 weeks enhances response to the flu vaccine in patients with rheumatoid arthritis, which prompted the American College of Rheumatology to recommended temporary interruption of methotrexate for 1 week after each dose of the COVID-19 vaccine, the pair notes.
“Although it is encouraging that cellular responses appear to be preserved even in patients with poor humoral responses, these findings are not consistent across study groups,” Dr. Connolly and Dr. Paik explained. “During this period of clinical uncertainty, patients might remain vulnerable, especially after the first dose, and should engage in risk mitigation strategies.”
Mild adverse events after vaccination were reported by 75% of the immunosuppressed patients – most commonly injection-site pain, headache, and fatigue – and by 94% of control subjects. No participants reported moderate or severe adverse effects.
However, 11% of immunosuppressed patients reported a worsening of psoriasis symptoms after vaccination.
This research was funded by the U.K. National Institute for Health Research. Dr. Mahil has received departmental income from AbbVie, Celgene, Eli Lilly, Janssen-Cilag, Novartis, Sano, and UCB unrelated to this study. Seven other authors have relationships with a wide range of pharmaceutical and other companies. Dr. Sanz, Dr. Connolly, and Dr. Paik disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
People taking methotrexate had low antibody responses after the first dose of the Pfizer-BioNTech mRNA COVID-19 vaccine, but did show evidence of T-cell–mediated immune responses, findings from a small study show.
The common immunosuppressant has previously been linked to poor antibody responses to mRNA COVID-19 vaccines, but this appears to be the first study to look at T-cell responses in people taking methotrexate.
The study findings were presented online July 11 at the 31st European Congress of Clinical Microbiology & Infectious Diseases and published in The Lancet Rheumatology.
“These findings indicate that seroconversion alone might not adequately reflect vaccine immunogenicity in individuals with immune-mediated inflammatory diseases receiving therapeutic immunosuppression, and caution against routine use of seroconversion data in isolation in clinical practice,” Satveer K. Mahil, MBBChir, PhD, from St. John’s Institute of Dermatology, Guy’s and St. Thomas’ NHS Foundation Trust, London, and colleagues wrote.
“When taking into account functional humoral immunity and T-cell responses, our data suggest that targeted biologics do not impair vaccine responses and provide some reassurance to this vulnerable population,” they wrote. “Notably, although methotrexate attenuated humoral immunity, cellular responses were preserved.”
Dr. Mahil and colleagues assessed 84 consecutive patients from a psoriasis specialist clinic that serves London and southeast England. Median age of the cohort was 43 years, and 85% were White. All had a confirmed psoriasis diagnosis, received the first dose of the Pfizer-BioNTech COVID-19 vaccine, and were taking either methotrexate (17 patients) or a targeted biologic (27 were taking a tumor necrosis factor inhibitor, 15 an interleukin-17 inhibitor, and 25 an IL-23 inhibitor). In addition, 17 healthy patients not receiving immunosuppression therapy who received the Pfizer-BioNTech vaccine served as the control group.
Four weeks after the study participants received their first dose of the vaccine, 78% of the immunosuppressed patients underwent seroconversion – producing measurable antibodies – as did 100% of the control group. Patients taking methotrexate had the lowest seroconversion rate at 47%, compared with 79% with TNF inhibitors, 83% with IL-23 inhibitors, and 100% with IL-17 inhibitors.
Participants taking methotrexate also had lower neutralizing activity against SARS-CoV-2 than control subjects and those taking a targeted biologic, who had similar levels of neutralizing activity.
All participants had low neutralizing titers against the alpha (B.1.1.7) variant.
The researchers also assessed cellular immunity, “defined as the presence of T cells secreting interferon-gamma, IL-2, or IL-21 in response to stimulation with two peptide pools spanning the entire length of the SARS-CoV-2 spike glycoprotein.”
A T-cell response was seen in 84% of participants taking immunosuppressants, including 93% of those in the methotrexate group and 69% of control subjects.
‘Some protection is better than none’
These findings regarding antibodies match what has been seen in other research, said Ignacio Sanz, MD, director of the Lowance Center for Human Immunology at Emory University, Atlanta.
It would be helpful to see antibody responses after the second doses, he added. Those data will be reported later, according to Dr. Mahil and colleagues.
“The authors make the valid point that T-cell immunity should also be measured. The information is meaningful and supports the idea that there could be protection still provided,” Dr. Sanz said in an interview, adding that it would have been helpful to see CD8 T-cell response as well.
“My message to patients, still, is that some protection is better than none, and that, indeed, protection may be afforded in different ways, including T-cell immunity, which, to the extent tested, seems to be induced,” he said. But discussion of B cells independent of their role in producing antibodies is missing.
“When it comes to B-cell responses, antibodies are the easier and more direct measurement. However, it is perfectly possible that the vaccine may fail to induce high antibody titers and still generate good B-cell immunity,” in the same way virus-specific memory B cells do, he explained. “They would not directly produce antibodies, yet they would be available for a good and quick response in the case of subsequent encounter with the virus and, incidentally, in the case of a booster dose. It is possible that the generation of antibody-producing plasma cells might be uncoupled from the generation of memory B cells.”
Temporarily stopping methotrexate
It is well known that methotrexate impairs humoral responses to influenza and pneumococcal vaccines, write Caoilfhionn M. Connolly, MD, and Julie J. Paik, MD, both from the Johns Hopkins University, Baltimore, in an accompanying comment.
Research has also shown that temporarily stopping methotrexate therapy for 2 weeks enhances response to the flu vaccine in patients with rheumatoid arthritis, which prompted the American College of Rheumatology to recommended temporary interruption of methotrexate for 1 week after each dose of the COVID-19 vaccine, the pair notes.
“Although it is encouraging that cellular responses appear to be preserved even in patients with poor humoral responses, these findings are not consistent across study groups,” Dr. Connolly and Dr. Paik explained. “During this period of clinical uncertainty, patients might remain vulnerable, especially after the first dose, and should engage in risk mitigation strategies.”
Mild adverse events after vaccination were reported by 75% of the immunosuppressed patients – most commonly injection-site pain, headache, and fatigue – and by 94% of control subjects. No participants reported moderate or severe adverse effects.
However, 11% of immunosuppressed patients reported a worsening of psoriasis symptoms after vaccination.
This research was funded by the U.K. National Institute for Health Research. Dr. Mahil has received departmental income from AbbVie, Celgene, Eli Lilly, Janssen-Cilag, Novartis, Sano, and UCB unrelated to this study. Seven other authors have relationships with a wide range of pharmaceutical and other companies. Dr. Sanz, Dr. Connolly, and Dr. Paik disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
People taking methotrexate had low antibody responses after the first dose of the Pfizer-BioNTech mRNA COVID-19 vaccine, but did show evidence of T-cell–mediated immune responses, findings from a small study show.
The common immunosuppressant has previously been linked to poor antibody responses to mRNA COVID-19 vaccines, but this appears to be the first study to look at T-cell responses in people taking methotrexate.
The study findings were presented online July 11 at the 31st European Congress of Clinical Microbiology & Infectious Diseases and published in The Lancet Rheumatology.
“These findings indicate that seroconversion alone might not adequately reflect vaccine immunogenicity in individuals with immune-mediated inflammatory diseases receiving therapeutic immunosuppression, and caution against routine use of seroconversion data in isolation in clinical practice,” Satveer K. Mahil, MBBChir, PhD, from St. John’s Institute of Dermatology, Guy’s and St. Thomas’ NHS Foundation Trust, London, and colleagues wrote.
“When taking into account functional humoral immunity and T-cell responses, our data suggest that targeted biologics do not impair vaccine responses and provide some reassurance to this vulnerable population,” they wrote. “Notably, although methotrexate attenuated humoral immunity, cellular responses were preserved.”
Dr. Mahil and colleagues assessed 84 consecutive patients from a psoriasis specialist clinic that serves London and southeast England. Median age of the cohort was 43 years, and 85% were White. All had a confirmed psoriasis diagnosis, received the first dose of the Pfizer-BioNTech COVID-19 vaccine, and were taking either methotrexate (17 patients) or a targeted biologic (27 were taking a tumor necrosis factor inhibitor, 15 an interleukin-17 inhibitor, and 25 an IL-23 inhibitor). In addition, 17 healthy patients not receiving immunosuppression therapy who received the Pfizer-BioNTech vaccine served as the control group.
Four weeks after the study participants received their first dose of the vaccine, 78% of the immunosuppressed patients underwent seroconversion – producing measurable antibodies – as did 100% of the control group. Patients taking methotrexate had the lowest seroconversion rate at 47%, compared with 79% with TNF inhibitors, 83% with IL-23 inhibitors, and 100% with IL-17 inhibitors.
Participants taking methotrexate also had lower neutralizing activity against SARS-CoV-2 than control subjects and those taking a targeted biologic, who had similar levels of neutralizing activity.
All participants had low neutralizing titers against the alpha (B.1.1.7) variant.
The researchers also assessed cellular immunity, “defined as the presence of T cells secreting interferon-gamma, IL-2, or IL-21 in response to stimulation with two peptide pools spanning the entire length of the SARS-CoV-2 spike glycoprotein.”
A T-cell response was seen in 84% of participants taking immunosuppressants, including 93% of those in the methotrexate group and 69% of control subjects.
‘Some protection is better than none’
These findings regarding antibodies match what has been seen in other research, said Ignacio Sanz, MD, director of the Lowance Center for Human Immunology at Emory University, Atlanta.
It would be helpful to see antibody responses after the second doses, he added. Those data will be reported later, according to Dr. Mahil and colleagues.
“The authors make the valid point that T-cell immunity should also be measured. The information is meaningful and supports the idea that there could be protection still provided,” Dr. Sanz said in an interview, adding that it would have been helpful to see CD8 T-cell response as well.
“My message to patients, still, is that some protection is better than none, and that, indeed, protection may be afforded in different ways, including T-cell immunity, which, to the extent tested, seems to be induced,” he said. But discussion of B cells independent of their role in producing antibodies is missing.
“When it comes to B-cell responses, antibodies are the easier and more direct measurement. However, it is perfectly possible that the vaccine may fail to induce high antibody titers and still generate good B-cell immunity,” in the same way virus-specific memory B cells do, he explained. “They would not directly produce antibodies, yet they would be available for a good and quick response in the case of subsequent encounter with the virus and, incidentally, in the case of a booster dose. It is possible that the generation of antibody-producing plasma cells might be uncoupled from the generation of memory B cells.”
Temporarily stopping methotrexate
It is well known that methotrexate impairs humoral responses to influenza and pneumococcal vaccines, write Caoilfhionn M. Connolly, MD, and Julie J. Paik, MD, both from the Johns Hopkins University, Baltimore, in an accompanying comment.
Research has also shown that temporarily stopping methotrexate therapy for 2 weeks enhances response to the flu vaccine in patients with rheumatoid arthritis, which prompted the American College of Rheumatology to recommended temporary interruption of methotrexate for 1 week after each dose of the COVID-19 vaccine, the pair notes.
“Although it is encouraging that cellular responses appear to be preserved even in patients with poor humoral responses, these findings are not consistent across study groups,” Dr. Connolly and Dr. Paik explained. “During this period of clinical uncertainty, patients might remain vulnerable, especially after the first dose, and should engage in risk mitigation strategies.”
Mild adverse events after vaccination were reported by 75% of the immunosuppressed patients – most commonly injection-site pain, headache, and fatigue – and by 94% of control subjects. No participants reported moderate or severe adverse effects.
However, 11% of immunosuppressed patients reported a worsening of psoriasis symptoms after vaccination.
This research was funded by the U.K. National Institute for Health Research. Dr. Mahil has received departmental income from AbbVie, Celgene, Eli Lilly, Janssen-Cilag, Novartis, Sano, and UCB unrelated to this study. Seven other authors have relationships with a wide range of pharmaceutical and other companies. Dr. Sanz, Dr. Connolly, and Dr. Paik disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Study spanning 2 decades offers insights into pediatric psoriasis trends
, while predictors of moderate to severe disease include morphology, non-White race, and culture-confirmed infection.

Those are among the key findings from a retrospective analysis of pediatric psoriasis patients who were seen at the University of California, San Francisco, over a 24-year period.
“Overall, our data support prior findings of age- and sex-based differences in location and morphology and presents new information demonstrating associations with severity,” presenting study author Carmel Aghdasi said during the annual meeting of the Society for Pediatric Dermatology. “We provide evidence of the increased use of systemic and biologic therapies over time, an important step in ensuring pediatric patients are adequately treated.”
To characterize the demographics, clinical features, comorbidities, and treatments, and to determine predictors of severity and changes in treatment patterns over 2 decades in a large cohort of pediatric psoriasis patients, Ms. Aghdasi, a 4th-year medical student at the University of California, San Francisco, and colleagues retrospectively evaluated the records of 754 pediatric patients up to 18 years of age who were seen at UCSF for psoriasis from 1997 to 2021. They collected demographic, clinical, familial, comorbidity, and treatment data and divided the cohort into two groups by date of last visit.
Group 1 consisted of 332 patients whose last visit was between 2001 and 2011, while the second group included 422 patients whose last visit was between 2012 and 2021. The researchers also divided the cohort into three age groups: infants (0-2 years of age), children (3-12 years of age), and adolescents (13-18 years of age).
Slightly more than half of the patients (55%) were female and 67% presented between ages 3 and 12. (Seventy-four patients were in the youngest category, 0-2 years, when they presented.) The average age of disease onset was 7 years, the average age at presentation to pediatric dermatology was 8.8 years, and 37% of the total cohort were overweight or obese. The top four comorbidities were being overweight or obese (37%), followed by atopic dermatitis (19%), psychiatric disease (7%), and arthritis (4%).
Plaque was the most common morphology (56%), while the most common sites of involvement were the head and neck (69%), extremities (61%), and trunk (44%). About half of the cohort (51%) had mild disease, 15% had culture-confirmed infections (9% had Streptococcal infections), and 66% of patients reported itch as a symptom.
The researchers observed that inverse psoriasis was significantly more common in infants and decreased with age. Anogenital involvement was more common in males and in those aged 0-2, while head and neck involvement was more common in females. Nail involvement was more common in childhood.
Topical therapy was the most common treatment overall and by far the most common among those in the 0-2 age category. “Overall, phototherapy was used in childhood and adolescents but almost never in infancy,” Ms. Aghdasi said. “Looking at changes in systemic treatment over time, conventional systemic use increased in infants and children and decreased in adolescents. Biologic use increased in all ages, most notably in children aged 3-12 years old.”
Multivariate regression analyses revealed that the following independent variables predicted moderate to severe psoriasis: adolescent age (adjusted odds ratio, 1.9; P = .03), guttate morphology (aOR, 2.2; P = .006), plaque and guttate morphology (aOR, 7.6; P less than .001), pustular or erythrodermic morphology (aOR, 5; P = .003), culture-confirmed infection (aOR, 2; P = .007), Black race (aOR, 3.3; P = .007), Asian race (aOR, 1.8; P = .04, and Hispanic race (aOR, 1.9; P = .03).
“Further analysis is needed to elucidate the influence of race on severity and of the clinical utility of infection as a marker of severity,” Ms. Aghdasi said. “Interestingly, we did not find that obesity was a marker of severity in our cohort.”
In an interview, senior study author Kelly M. Cordoro, MD, professor of dermatology and pediatrics at UCSF, noted that this finding conflicts with prior studies showing an association between obesity and severe psoriasis in children.

“Though methodologies and patient populations differ among studies, what is striking,” she said, is the percentage of overweight/obese patients (37%; defined as a body mass index ≥ 85th percentile) “in our 2-decade single institution dataset.” This “is nearly identical” to the percentage of patients with excess adiposity – 37.9% (also defined as BMI ≥ 85th percentile) – in an international cross-sectional study, which also identified an association between obesity (BMI ≥ 95th percentile) and psoriasis severity in children, she noted.
“What is clear is the strong association between obesity and childhood psoriasis, as multiple studies, including ours, confirm obesity as a major comorbidity of pediatric psoriasis,” Dr. Cordoro said. “Both conditions must be adequately managed to reduce the risk of adverse health outcomes for obese patients with psoriasis.”
The other study coauthors were Dana Feigenbaum, MD, and Alana Ju, MD. The work was supported by the UCSF Yearlong Inquiry Program. The researchers reported having no relevant financial disclosures.
, while predictors of moderate to severe disease include morphology, non-White race, and culture-confirmed infection.
Those are among the key findings from a retrospective analysis of pediatric psoriasis patients who were seen at the University of California, San Francisco, over a 24-year period.
“Overall, our data support prior findings of age- and sex-based differences in location and morphology and presents new information demonstrating associations with severity,” presenting study author Carmel Aghdasi said during the annual meeting of the Society for Pediatric Dermatology. “We provide evidence of the increased use of systemic and biologic therapies over time, an important step in ensuring pediatric patients are adequately treated.”
To characterize the demographics, clinical features, comorbidities, and treatments, and to determine predictors of severity and changes in treatment patterns over 2 decades in a large cohort of pediatric psoriasis patients, Ms. Aghdasi, a 4th-year medical student at the University of California, San Francisco, and colleagues retrospectively evaluated the records of 754 pediatric patients up to 18 years of age who were seen at UCSF for psoriasis from 1997 to 2021. They collected demographic, clinical, familial, comorbidity, and treatment data and divided the cohort into two groups by date of last visit.
Group 1 consisted of 332 patients whose last visit was between 2001 and 2011, while the second group included 422 patients whose last visit was between 2012 and 2021. The researchers also divided the cohort into three age groups: infants (0-2 years of age), children (3-12 years of age), and adolescents (13-18 years of age).
Slightly more than half of the patients (55%) were female and 67% presented between ages 3 and 12. (Seventy-four patients were in the youngest category, 0-2 years, when they presented.) The average age of disease onset was 7 years, the average age at presentation to pediatric dermatology was 8.8 years, and 37% of the total cohort were overweight or obese. The top four comorbidities were being overweight or obese (37%), followed by atopic dermatitis (19%), psychiatric disease (7%), and arthritis (4%).
Plaque was the most common morphology (56%), while the most common sites of involvement were the head and neck (69%), extremities (61%), and trunk (44%). About half of the cohort (51%) had mild disease, 15% had culture-confirmed infections (9% had Streptococcal infections), and 66% of patients reported itch as a symptom.
The researchers observed that inverse psoriasis was significantly more common in infants and decreased with age. Anogenital involvement was more common in males and in those aged 0-2, while head and neck involvement was more common in females. Nail involvement was more common in childhood.
Topical therapy was the most common treatment overall and by far the most common among those in the 0-2 age category. “Overall, phototherapy was used in childhood and adolescents but almost never in infancy,” Ms. Aghdasi said. “Looking at changes in systemic treatment over time, conventional systemic use increased in infants and children and decreased in adolescents. Biologic use increased in all ages, most notably in children aged 3-12 years old.”
Multivariate regression analyses revealed that the following independent variables predicted moderate to severe psoriasis: adolescent age (adjusted odds ratio, 1.9; P = .03), guttate morphology (aOR, 2.2; P = .006), plaque and guttate morphology (aOR, 7.6; P less than .001), pustular or erythrodermic morphology (aOR, 5; P = .003), culture-confirmed infection (aOR, 2; P = .007), Black race (aOR, 3.3; P = .007), Asian race (aOR, 1.8; P = .04, and Hispanic race (aOR, 1.9; P = .03).
“Further analysis is needed to elucidate the influence of race on severity and of the clinical utility of infection as a marker of severity,” Ms. Aghdasi said. “Interestingly, we did not find that obesity was a marker of severity in our cohort.”
In an interview, senior study author Kelly M. Cordoro, MD, professor of dermatology and pediatrics at UCSF, noted that this finding conflicts with prior studies showing an association between obesity and severe psoriasis in children.
“Though methodologies and patient populations differ among studies, what is striking,” she said, is the percentage of overweight/obese patients (37%; defined as a body mass index ≥ 85th percentile) “in our 2-decade single institution dataset.” This “is nearly identical” to the percentage of patients with excess adiposity – 37.9% (also defined as BMI ≥ 85th percentile) – in an international cross-sectional study, which also identified an association between obesity (BMI ≥ 95th percentile) and psoriasis severity in children, she noted.
“What is clear is the strong association between obesity and childhood psoriasis, as multiple studies, including ours, confirm obesity as a major comorbidity of pediatric psoriasis,” Dr. Cordoro said. “Both conditions must be adequately managed to reduce the risk of adverse health outcomes for obese patients with psoriasis.”
The other study coauthors were Dana Feigenbaum, MD, and Alana Ju, MD. The work was supported by the UCSF Yearlong Inquiry Program. The researchers reported having no relevant financial disclosures.
, while predictors of moderate to severe disease include morphology, non-White race, and culture-confirmed infection.
Those are among the key findings from a retrospective analysis of pediatric psoriasis patients who were seen at the University of California, San Francisco, over a 24-year period.
“Overall, our data support prior findings of age- and sex-based differences in location and morphology and presents new information demonstrating associations with severity,” presenting study author Carmel Aghdasi said during the annual meeting of the Society for Pediatric Dermatology. “We provide evidence of the increased use of systemic and biologic therapies over time, an important step in ensuring pediatric patients are adequately treated.”
To characterize the demographics, clinical features, comorbidities, and treatments, and to determine predictors of severity and changes in treatment patterns over 2 decades in a large cohort of pediatric psoriasis patients, Ms. Aghdasi, a 4th-year medical student at the University of California, San Francisco, and colleagues retrospectively evaluated the records of 754 pediatric patients up to 18 years of age who were seen at UCSF for psoriasis from 1997 to 2021. They collected demographic, clinical, familial, comorbidity, and treatment data and divided the cohort into two groups by date of last visit.
Group 1 consisted of 332 patients whose last visit was between 2001 and 2011, while the second group included 422 patients whose last visit was between 2012 and 2021. The researchers also divided the cohort into three age groups: infants (0-2 years of age), children (3-12 years of age), and adolescents (13-18 years of age).
Slightly more than half of the patients (55%) were female and 67% presented between ages 3 and 12. (Seventy-four patients were in the youngest category, 0-2 years, when they presented.) The average age of disease onset was 7 years, the average age at presentation to pediatric dermatology was 8.8 years, and 37% of the total cohort were overweight or obese. The top four comorbidities were being overweight or obese (37%), followed by atopic dermatitis (19%), psychiatric disease (7%), and arthritis (4%).
Plaque was the most common morphology (56%), while the most common sites of involvement were the head and neck (69%), extremities (61%), and trunk (44%). About half of the cohort (51%) had mild disease, 15% had culture-confirmed infections (9% had Streptococcal infections), and 66% of patients reported itch as a symptom.
The researchers observed that inverse psoriasis was significantly more common in infants and decreased with age. Anogenital involvement was more common in males and in those aged 0-2, while head and neck involvement was more common in females. Nail involvement was more common in childhood.
Topical therapy was the most common treatment overall and by far the most common among those in the 0-2 age category. “Overall, phototherapy was used in childhood and adolescents but almost never in infancy,” Ms. Aghdasi said. “Looking at changes in systemic treatment over time, conventional systemic use increased in infants and children and decreased in adolescents. Biologic use increased in all ages, most notably in children aged 3-12 years old.”
Multivariate regression analyses revealed that the following independent variables predicted moderate to severe psoriasis: adolescent age (adjusted odds ratio, 1.9; P = .03), guttate morphology (aOR, 2.2; P = .006), plaque and guttate morphology (aOR, 7.6; P less than .001), pustular or erythrodermic morphology (aOR, 5; P = .003), culture-confirmed infection (aOR, 2; P = .007), Black race (aOR, 3.3; P = .007), Asian race (aOR, 1.8; P = .04, and Hispanic race (aOR, 1.9; P = .03).
“Further analysis is needed to elucidate the influence of race on severity and of the clinical utility of infection as a marker of severity,” Ms. Aghdasi said. “Interestingly, we did not find that obesity was a marker of severity in our cohort.”
In an interview, senior study author Kelly M. Cordoro, MD, professor of dermatology and pediatrics at UCSF, noted that this finding conflicts with prior studies showing an association between obesity and severe psoriasis in children.
“Though methodologies and patient populations differ among studies, what is striking,” she said, is the percentage of overweight/obese patients (37%; defined as a body mass index ≥ 85th percentile) “in our 2-decade single institution dataset.” This “is nearly identical” to the percentage of patients with excess adiposity – 37.9% (also defined as BMI ≥ 85th percentile) – in an international cross-sectional study, which also identified an association between obesity (BMI ≥ 95th percentile) and psoriasis severity in children, she noted.
“What is clear is the strong association between obesity and childhood psoriasis, as multiple studies, including ours, confirm obesity as a major comorbidity of pediatric psoriasis,” Dr. Cordoro said. “Both conditions must be adequately managed to reduce the risk of adverse health outcomes for obese patients with psoriasis.”
The other study coauthors were Dana Feigenbaum, MD, and Alana Ju, MD. The work was supported by the UCSF Yearlong Inquiry Program. The researchers reported having no relevant financial disclosures.
FROM SPD 2021
New analysis puts U.S. psoriasis prevalence at 3%
, according to an analysis of national survey data from 2011 to 2014.
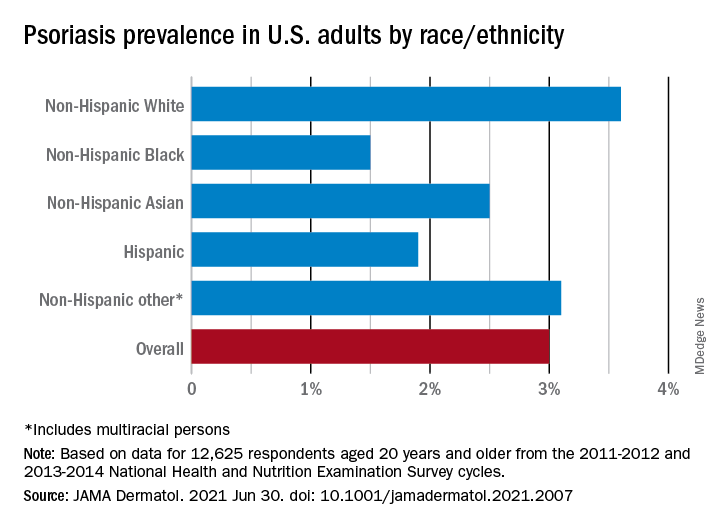
“The adult prevalence rate of 3.0% continues to place psoriasis as one of the most common immune-mediated diseases affecting adults” in the United States, April W. Armstrong, MD, MPH, and associates said in a report published in JAMA Dermatology. At that rate, approximately 7,560,000 Americans aged 20 years or older have psoriasis.
That overall rate among adults aged 20 years and older, based on data from the 2011-2012 and 2013-2014 cycles of the National Health and Nutrition Examination Survey (NHANES), did not change significantly when compared with the 2003-2004 NHANES, when it was 3.15% among those aged 20-59, said Dr. Armstrong, professor of dermatology, University of Southern California, Los Angeles, and associates.
For the 2011-2014 period, psoriasis prevalence was similar between women (3.2%) and men (2.8%) but was significantly associated with older age and White/non-White status. Those aged 50-59 years had the highest prevalence of any age group at 4.3% and those aged 70 and older had a rate of 3.9%, while those aged 20-29 were the lowest at 1.6%, the investigators reported.
The prevalence in non-Hispanic Whites in the United States was 3.6% over the study period, and their odds ratio for having psoriasis was 1.92, compared with non-White individuals. Asian respondents had a prevalence of 2.5%, with the Hispanic population at 1.9%, non-Hispanic Black respondents at 1.5%, and those identifying as other (including multiracial persons) at 3.1%, they said.
The NHANES sample consisted of 12,638 people who had participated in the question that asked if they had ever been diagnosed with psoriasis by a physician or other health care professional, of whom 12,625 gave a definitive yes or no answer, the investigators noted.
A much smaller number, 329, also answered a question about the severity of their disease: Fifty-six percent had little or no psoriasis, almost 22% reported 1-2 palms of involvement, 16% had 3-10 palms of involvement, and 5.5% said the coverage was more than 10 palms. Since the survey did not distinguish between treated and untreated patients, however, some “of those reporting low body surface area involvement may be receiving treatments that are controlling their otherwise more extensive disease,” they wrote.
Dr. Armstrong and another investigator said that they have received grants, personal fees, and honoraria from a number of pharmaceutical companies; two other investigators are employees of the National Psoriasis Foundation.
, according to an analysis of national survey data from 2011 to 2014.
“The adult prevalence rate of 3.0% continues to place psoriasis as one of the most common immune-mediated diseases affecting adults” in the United States, April W. Armstrong, MD, MPH, and associates said in a report published in JAMA Dermatology. At that rate, approximately 7,560,000 Americans aged 20 years or older have psoriasis.
That overall rate among adults aged 20 years and older, based on data from the 2011-2012 and 2013-2014 cycles of the National Health and Nutrition Examination Survey (NHANES), did not change significantly when compared with the 2003-2004 NHANES, when it was 3.15% among those aged 20-59, said Dr. Armstrong, professor of dermatology, University of Southern California, Los Angeles, and associates.
For the 2011-2014 period, psoriasis prevalence was similar between women (3.2%) and men (2.8%) but was significantly associated with older age and White/non-White status. Those aged 50-59 years had the highest prevalence of any age group at 4.3% and those aged 70 and older had a rate of 3.9%, while those aged 20-29 were the lowest at 1.6%, the investigators reported.
The prevalence in non-Hispanic Whites in the United States was 3.6% over the study period, and their odds ratio for having psoriasis was 1.92, compared with non-White individuals. Asian respondents had a prevalence of 2.5%, with the Hispanic population at 1.9%, non-Hispanic Black respondents at 1.5%, and those identifying as other (including multiracial persons) at 3.1%, they said.
The NHANES sample consisted of 12,638 people who had participated in the question that asked if they had ever been diagnosed with psoriasis by a physician or other health care professional, of whom 12,625 gave a definitive yes or no answer, the investigators noted.
A much smaller number, 329, also answered a question about the severity of their disease: Fifty-six percent had little or no psoriasis, almost 22% reported 1-2 palms of involvement, 16% had 3-10 palms of involvement, and 5.5% said the coverage was more than 10 palms. Since the survey did not distinguish between treated and untreated patients, however, some “of those reporting low body surface area involvement may be receiving treatments that are controlling their otherwise more extensive disease,” they wrote.
Dr. Armstrong and another investigator said that they have received grants, personal fees, and honoraria from a number of pharmaceutical companies; two other investigators are employees of the National Psoriasis Foundation.
, according to an analysis of national survey data from 2011 to 2014.
“The adult prevalence rate of 3.0% continues to place psoriasis as one of the most common immune-mediated diseases affecting adults” in the United States, April W. Armstrong, MD, MPH, and associates said in a report published in JAMA Dermatology. At that rate, approximately 7,560,000 Americans aged 20 years or older have psoriasis.
That overall rate among adults aged 20 years and older, based on data from the 2011-2012 and 2013-2014 cycles of the National Health and Nutrition Examination Survey (NHANES), did not change significantly when compared with the 2003-2004 NHANES, when it was 3.15% among those aged 20-59, said Dr. Armstrong, professor of dermatology, University of Southern California, Los Angeles, and associates.
For the 2011-2014 period, psoriasis prevalence was similar between women (3.2%) and men (2.8%) but was significantly associated with older age and White/non-White status. Those aged 50-59 years had the highest prevalence of any age group at 4.3% and those aged 70 and older had a rate of 3.9%, while those aged 20-29 were the lowest at 1.6%, the investigators reported.
The prevalence in non-Hispanic Whites in the United States was 3.6% over the study period, and their odds ratio for having psoriasis was 1.92, compared with non-White individuals. Asian respondents had a prevalence of 2.5%, with the Hispanic population at 1.9%, non-Hispanic Black respondents at 1.5%, and those identifying as other (including multiracial persons) at 3.1%, they said.
The NHANES sample consisted of 12,638 people who had participated in the question that asked if they had ever been diagnosed with psoriasis by a physician or other health care professional, of whom 12,625 gave a definitive yes or no answer, the investigators noted.
A much smaller number, 329, also answered a question about the severity of their disease: Fifty-six percent had little or no psoriasis, almost 22% reported 1-2 palms of involvement, 16% had 3-10 palms of involvement, and 5.5% said the coverage was more than 10 palms. Since the survey did not distinguish between treated and untreated patients, however, some “of those reporting low body surface area involvement may be receiving treatments that are controlling their otherwise more extensive disease,” they wrote.
Dr. Armstrong and another investigator said that they have received grants, personal fees, and honoraria from a number of pharmaceutical companies; two other investigators are employees of the National Psoriasis Foundation.
FROM JAMA DERMATOLOGY
Malignancy risk: Secukinumab shows long-term safety for psoriasis, PsA, ankylosing spondylitis
that included 49 clinical trials.

Secukinumab (Cosentyx), an interleukin-17A antagonist, is approved for several conditions: moderate to severe psoriasis in children and adults, PsA, ankylosing spondylitis (AS), and nonradiographic axial spondyloarthritis.
Although secukinumab has demonstrated safety and tolerability, data on long-term malignancy rates are limited, wrote Mark Lebwohl, MD, professor of dermatology at the Icahn School of Medicine at Mount Sinai, New York, and coauthors.
In a study published in the British Journal of Dermatology, they analyzed the combined safety data from clinical trials and postmarketing surveillance. The study population included 10,685 patients with psoriasis, 2,523 patients with PsA, and 1,311 patients with ankylosing spondylitis who received at least one approved dose of secukinumab (300 mg or 150 mg). The maximum follow-up was 5 years. The exposure-adjusted incidence rate was defined as the incidence rates per 100 patient treatment-years (PTY). The cumulative exposure for patients with psoriasis, PsA, and AS was 16,482, 4,944, and 2,668 PTY, respectively, with average follow-up times of 1.54, 1.96, and 2.03 years, respectively.
The observed and the expected number of malignancies were comparable, with a standardized incidence ratio (SIR) for malignancy of 0.99 across all treatment indications, the researchers said. In further analysis of malignancy by indication, the SIR was 0.87, 1.16, and 1.61 for psoriasis, PsA, and AS, respectively.
Data from postmarketing surveillance showed similar results: The estimated crude cumulative incidence reporting rate per 100 PTY was 0.27 for malignancy across all indications. The cumulative exposure was 285,811 PTY.
The study findings were limited by several factors including the post hoc design, differences in clinical trial methodologies, and lack of controlling for confounding variables, such as smoking status and previous exposure to systemic and biologic treatments, the researchers noted. In addition, the analysis did not include postexposure follow-up data, or data on patients who discontinued clinical trials, they said.
Overall, the analysis is the largest to date and supports the low risk of malignancy in patients with psoriasis, PsA, and AS treated with secukinumab, the researchers noted.
However, “while this assessment provides a broader understanding of the safety of secukinumab and supports its long-term use in these chronic systemic inflammatory conditions, registry data are further warranted to fully understand the real-world effect of biologics on malignancy risk,” they concluded.
“Secukinumab is a relatively newer biologic, approved in 2015, and there is currently a lack of longer-term data on the incidence of malignancy in secukinumab-treated patients, so it’s important to look at the data we have so far on this topic so we can better understand the long-term risks and counsel our psoriasis and psoriatic arthritis patients,” Flavia Fedeles, MD, of the department of dermatology at Massachusetts General Hospital, Boston, said in an interview.
Dr. Fedeles, who was not involved with the study, said that she was not surprised by the study results. “Data reported in the past from phase 3 clinical trials of secukinumab compared with placebo did not show an increase in risk of malignancy, though at that time no long-term safety data or data from patients with history of malignancy was available,” she said. “This study is reassuring in that there wasn’t a signal of increased malignancy events up to 5 years of secukinumab treatment,” said Dr. Fedeles.

However, she noted that the study has a number of limitations, including the use of clinical trials data, which have stringent inclusion/exclusion criteria that can lead to selection bias, the use of postmarketing surveillance data, the post hoc nature of the analysis, and the fact that the sponsor of the trial was the manufacturer of secukinumab, which “potentially can lead to bias to this study.”
She added that “registry data are needed to fully understand the real-world long-term effect of secukinumab on malignancy risk.”
The study was funded by Novartis. Lead author Dr. Lebwohl disclosed participating in advisory boards and/or as an investigator and/or speaker and receiving grants and/or honoraria from multiple companies including Novartis. Several study coauthors are employees of Novartis.
Dr. Fedeles had no financial conflicts to disclose.
that included 49 clinical trials.
Secukinumab (Cosentyx), an interleukin-17A antagonist, is approved for several conditions: moderate to severe psoriasis in children and adults, PsA, ankylosing spondylitis (AS), and nonradiographic axial spondyloarthritis.
Although secukinumab has demonstrated safety and tolerability, data on long-term malignancy rates are limited, wrote Mark Lebwohl, MD, professor of dermatology at the Icahn School of Medicine at Mount Sinai, New York, and coauthors.
In a study published in the British Journal of Dermatology, they analyzed the combined safety data from clinical trials and postmarketing surveillance. The study population included 10,685 patients with psoriasis, 2,523 patients with PsA, and 1,311 patients with ankylosing spondylitis who received at least one approved dose of secukinumab (300 mg or 150 mg). The maximum follow-up was 5 years. The exposure-adjusted incidence rate was defined as the incidence rates per 100 patient treatment-years (PTY). The cumulative exposure for patients with psoriasis, PsA, and AS was 16,482, 4,944, and 2,668 PTY, respectively, with average follow-up times of 1.54, 1.96, and 2.03 years, respectively.
The observed and the expected number of malignancies were comparable, with a standardized incidence ratio (SIR) for malignancy of 0.99 across all treatment indications, the researchers said. In further analysis of malignancy by indication, the SIR was 0.87, 1.16, and 1.61 for psoriasis, PsA, and AS, respectively.
Data from postmarketing surveillance showed similar results: The estimated crude cumulative incidence reporting rate per 100 PTY was 0.27 for malignancy across all indications. The cumulative exposure was 285,811 PTY.
The study findings were limited by several factors including the post hoc design, differences in clinical trial methodologies, and lack of controlling for confounding variables, such as smoking status and previous exposure to systemic and biologic treatments, the researchers noted. In addition, the analysis did not include postexposure follow-up data, or data on patients who discontinued clinical trials, they said.
Overall, the analysis is the largest to date and supports the low risk of malignancy in patients with psoriasis, PsA, and AS treated with secukinumab, the researchers noted.
However, “while this assessment provides a broader understanding of the safety of secukinumab and supports its long-term use in these chronic systemic inflammatory conditions, registry data are further warranted to fully understand the real-world effect of biologics on malignancy risk,” they concluded.
“Secukinumab is a relatively newer biologic, approved in 2015, and there is currently a lack of longer-term data on the incidence of malignancy in secukinumab-treated patients, so it’s important to look at the data we have so far on this topic so we can better understand the long-term risks and counsel our psoriasis and psoriatic arthritis patients,” Flavia Fedeles, MD, of the department of dermatology at Massachusetts General Hospital, Boston, said in an interview.
Dr. Fedeles, who was not involved with the study, said that she was not surprised by the study results. “Data reported in the past from phase 3 clinical trials of secukinumab compared with placebo did not show an increase in risk of malignancy, though at that time no long-term safety data or data from patients with history of malignancy was available,” she said. “This study is reassuring in that there wasn’t a signal of increased malignancy events up to 5 years of secukinumab treatment,” said Dr. Fedeles.
However, she noted that the study has a number of limitations, including the use of clinical trials data, which have stringent inclusion/exclusion criteria that can lead to selection bias, the use of postmarketing surveillance data, the post hoc nature of the analysis, and the fact that the sponsor of the trial was the manufacturer of secukinumab, which “potentially can lead to bias to this study.”
She added that “registry data are needed to fully understand the real-world long-term effect of secukinumab on malignancy risk.”
The study was funded by Novartis. Lead author Dr. Lebwohl disclosed participating in advisory boards and/or as an investigator and/or speaker and receiving grants and/or honoraria from multiple companies including Novartis. Several study coauthors are employees of Novartis.
Dr. Fedeles had no financial conflicts to disclose.
that included 49 clinical trials.
Secukinumab (Cosentyx), an interleukin-17A antagonist, is approved for several conditions: moderate to severe psoriasis in children and adults, PsA, ankylosing spondylitis (AS), and nonradiographic axial spondyloarthritis.
Although secukinumab has demonstrated safety and tolerability, data on long-term malignancy rates are limited, wrote Mark Lebwohl, MD, professor of dermatology at the Icahn School of Medicine at Mount Sinai, New York, and coauthors.
In a study published in the British Journal of Dermatology, they analyzed the combined safety data from clinical trials and postmarketing surveillance. The study population included 10,685 patients with psoriasis, 2,523 patients with PsA, and 1,311 patients with ankylosing spondylitis who received at least one approved dose of secukinumab (300 mg or 150 mg). The maximum follow-up was 5 years. The exposure-adjusted incidence rate was defined as the incidence rates per 100 patient treatment-years (PTY). The cumulative exposure for patients with psoriasis, PsA, and AS was 16,482, 4,944, and 2,668 PTY, respectively, with average follow-up times of 1.54, 1.96, and 2.03 years, respectively.
The observed and the expected number of malignancies were comparable, with a standardized incidence ratio (SIR) for malignancy of 0.99 across all treatment indications, the researchers said. In further analysis of malignancy by indication, the SIR was 0.87, 1.16, and 1.61 for psoriasis, PsA, and AS, respectively.
Data from postmarketing surveillance showed similar results: The estimated crude cumulative incidence reporting rate per 100 PTY was 0.27 for malignancy across all indications. The cumulative exposure was 285,811 PTY.
The study findings were limited by several factors including the post hoc design, differences in clinical trial methodologies, and lack of controlling for confounding variables, such as smoking status and previous exposure to systemic and biologic treatments, the researchers noted. In addition, the analysis did not include postexposure follow-up data, or data on patients who discontinued clinical trials, they said.
Overall, the analysis is the largest to date and supports the low risk of malignancy in patients with psoriasis, PsA, and AS treated with secukinumab, the researchers noted.
However, “while this assessment provides a broader understanding of the safety of secukinumab and supports its long-term use in these chronic systemic inflammatory conditions, registry data are further warranted to fully understand the real-world effect of biologics on malignancy risk,” they concluded.
“Secukinumab is a relatively newer biologic, approved in 2015, and there is currently a lack of longer-term data on the incidence of malignancy in secukinumab-treated patients, so it’s important to look at the data we have so far on this topic so we can better understand the long-term risks and counsel our psoriasis and psoriatic arthritis patients,” Flavia Fedeles, MD, of the department of dermatology at Massachusetts General Hospital, Boston, said in an interview.
Dr. Fedeles, who was not involved with the study, said that she was not surprised by the study results. “Data reported in the past from phase 3 clinical trials of secukinumab compared with placebo did not show an increase in risk of malignancy, though at that time no long-term safety data or data from patients with history of malignancy was available,” she said. “This study is reassuring in that there wasn’t a signal of increased malignancy events up to 5 years of secukinumab treatment,” said Dr. Fedeles.
However, she noted that the study has a number of limitations, including the use of clinical trials data, which have stringent inclusion/exclusion criteria that can lead to selection bias, the use of postmarketing surveillance data, the post hoc nature of the analysis, and the fact that the sponsor of the trial was the manufacturer of secukinumab, which “potentially can lead to bias to this study.”
She added that “registry data are needed to fully understand the real-world long-term effect of secukinumab on malignancy risk.”
The study was funded by Novartis. Lead author Dr. Lebwohl disclosed participating in advisory boards and/or as an investigator and/or speaker and receiving grants and/or honoraria from multiple companies including Novartis. Several study coauthors are employees of Novartis.
Dr. Fedeles had no financial conflicts to disclose.
FROM THE BRITISH JOURNAL OF DERMATOLOGY

Predictive factors for development of axial involvement in PsA
Key clinical point: Axial involvement in psoriatic arthritis (axPsA) is a unique phenotype with characteristics lying between axial spondyloarthritis and pure peripheral PsA. Male gender, elevated C-reactive protein (CRP), and absence of psoriasis were associated with axPsA.
Major finding: Axial involvement was observed in 35.5% of patients with PsA, and they were thus classified as axPsA. Being male (odds ratio [OR], 1.68; 95% confidence interval [CI], 1.09-2.61), having elevated CRP (OR, 2.87; 95% CI, 1.80-4.60), and absence of psoriasis (OR, 0.33; 95% CI, 0.15-0.72) were independently associated with axPsA.
Study details: The data come from an observational, cross-sectional ASAS-perSpA study of 3,684 patients with axial spondyloarthritis or PsA.
Disclosures: The ASAS-PerSpA study was funded by Pfizer, Lilly, AbbVie, Novartis, UCB, Janssen, and Merck. The authors including the lead author reported receiving consulting fees, speaking fees, and/or honoraria from various sources including AbbVie. Three authors reported no conflicts of interest.
Source: Benavent D et al. Semin Arthritis Rheum. 2021 May 5. doi: 10.1016/j.semarthrit.2021.04.018.
Key clinical point: Axial involvement in psoriatic arthritis (axPsA) is a unique phenotype with characteristics lying between axial spondyloarthritis and pure peripheral PsA. Male gender, elevated C-reactive protein (CRP), and absence of psoriasis were associated with axPsA.
Major finding: Axial involvement was observed in 35.5% of patients with PsA, and they were thus classified as axPsA. Being male (odds ratio [OR], 1.68; 95% confidence interval [CI], 1.09-2.61), having elevated CRP (OR, 2.87; 95% CI, 1.80-4.60), and absence of psoriasis (OR, 0.33; 95% CI, 0.15-0.72) were independently associated with axPsA.
Study details: The data come from an observational, cross-sectional ASAS-perSpA study of 3,684 patients with axial spondyloarthritis or PsA.
Disclosures: The ASAS-PerSpA study was funded by Pfizer, Lilly, AbbVie, Novartis, UCB, Janssen, and Merck. The authors including the lead author reported receiving consulting fees, speaking fees, and/or honoraria from various sources including AbbVie. Three authors reported no conflicts of interest.
Source: Benavent D et al. Semin Arthritis Rheum. 2021 May 5. doi: 10.1016/j.semarthrit.2021.04.018.
Key clinical point: Axial involvement in psoriatic arthritis (axPsA) is a unique phenotype with characteristics lying between axial spondyloarthritis and pure peripheral PsA. Male gender, elevated C-reactive protein (CRP), and absence of psoriasis were associated with axPsA.
Major finding: Axial involvement was observed in 35.5% of patients with PsA, and they were thus classified as axPsA. Being male (odds ratio [OR], 1.68; 95% confidence interval [CI], 1.09-2.61), having elevated CRP (OR, 2.87; 95% CI, 1.80-4.60), and absence of psoriasis (OR, 0.33; 95% CI, 0.15-0.72) were independently associated with axPsA.
Study details: The data come from an observational, cross-sectional ASAS-perSpA study of 3,684 patients with axial spondyloarthritis or PsA.
Disclosures: The ASAS-PerSpA study was funded by Pfizer, Lilly, AbbVie, Novartis, UCB, Janssen, and Merck. The authors including the lead author reported receiving consulting fees, speaking fees, and/or honoraria from various sources including AbbVie. Three authors reported no conflicts of interest.
Source: Benavent D et al. Semin Arthritis Rheum. 2021 May 5. doi: 10.1016/j.semarthrit.2021.04.018.