User login
Society of Hospital Medicine Membership Ambassador Program Offers Perks
Do you know someone who should be a part of the hospital medicine movement but hasn’t joined SHM? Now you can both win: Your colleague can enjoy all the benefits of SHM membership, and you can receive credits against your future dues. Plus, you’ll get the chance to win free registration to HM15.
Now through December 31, all active SHM members can earn dues credits and special recognition for recruiting new physician, allied health, or affiliate members. Active members will be eligible for:
- A $35 credit toward 2015-2016 dues when recruiting one new member;
- A $50 credit toward 2015-2016 dues when recruiting two to four new members;
- A $75 credit toward 2015-2016 dues when recruiting five to nine new members; or
- A $125 credit toward 2015-2016 dues when recruiting 10+ new members.
For EVERY member recruited, individuals will receive one entry into a grand prize drawing to receive complimentary registration to Hospital Medicine 2015 in National Harbor, Md.
For details, visit www.hospitalmedicine.org/membership.
Do you know someone who should be a part of the hospital medicine movement but hasn’t joined SHM? Now you can both win: Your colleague can enjoy all the benefits of SHM membership, and you can receive credits against your future dues. Plus, you’ll get the chance to win free registration to HM15.
Now through December 31, all active SHM members can earn dues credits and special recognition for recruiting new physician, allied health, or affiliate members. Active members will be eligible for:
- A $35 credit toward 2015-2016 dues when recruiting one new member;
- A $50 credit toward 2015-2016 dues when recruiting two to four new members;
- A $75 credit toward 2015-2016 dues when recruiting five to nine new members; or
- A $125 credit toward 2015-2016 dues when recruiting 10+ new members.
For EVERY member recruited, individuals will receive one entry into a grand prize drawing to receive complimentary registration to Hospital Medicine 2015 in National Harbor, Md.
For details, visit www.hospitalmedicine.org/membership.
Do you know someone who should be a part of the hospital medicine movement but hasn’t joined SHM? Now you can both win: Your colleague can enjoy all the benefits of SHM membership, and you can receive credits against your future dues. Plus, you’ll get the chance to win free registration to HM15.
Now through December 31, all active SHM members can earn dues credits and special recognition for recruiting new physician, allied health, or affiliate members. Active members will be eligible for:
- A $35 credit toward 2015-2016 dues when recruiting one new member;
- A $50 credit toward 2015-2016 dues when recruiting two to four new members;
- A $75 credit toward 2015-2016 dues when recruiting five to nine new members; or
- A $125 credit toward 2015-2016 dues when recruiting 10+ new members.
For EVERY member recruited, individuals will receive one entry into a grand prize drawing to receive complimentary registration to Hospital Medicine 2015 in National Harbor, Md.
For details, visit www.hospitalmedicine.org/membership.
Get Involved in Hospital Medicine Movement
As the hospital medicine specialty continues to grow, hospitalists often ask: “How can I get involved?”
Getting involved in the hospital medicine movement and contributing to SHM’s goal of helping hospitalists provide exceptional care to hospitalized patients is easy—and it can start today.
A: Awards

Nominating a colleague—or yourself—for one of SHM’s seven awards is a great way to share your successes with the rest of the specialty. It also generates national recognition for the people and practices that make hospital medicine great.
This year, SHM will be awarding seven awards:
- Excellence in Teamwork in Quality Improvement;
- Excellence in Research;
- Excellence in Hospital Medicine for Non-Physicians;
- Excellence in Teaching;
- Outstanding Service in Hospital Medicine;
- Clinical Excellence; and
- Excellence in Humanitarian Services.
Award winners will be recognized onstage at HM15 in National Harbor, Md.
For more information or to nominate yourself or someone else for an award, visit www.hospitalmedicine.org/awards. But don’t wait. The deadline for award submissions is Oct. 13.
B: Board

Are you ready to take a national leadership position within hospital medicine? SHM’s board of directors guides the specialty and helps ensure that SHM provides hospitalists with the tools and education they need to be the best caregivers possible.
Any SHM member in good standing is eligible to become a board member. Four seats are open for the three-year term starting in 2015.
Recently, the SHM Board of Directors oversaw the creation and publication of the “Key Principles and Characteristics of an Effective Hospital Medicine Group,” a formative set of principles that were published in the Journal of Hospital Medicine and now help hospital medicine groups across the country evaluate their performance.
The board will continue to take on major projects like the key characteristics; if you would like to nominate yourself or someone else, visit the “Board of Directors” section of “About SHM” on www.hospitalmedicine.org.
But don’t wait long. Nominations are due Oct. 22.
C: Committees

Committees are the engines of change for hospital medicine. They guide SHM’s policy initiatives, address pressing quality improvement issues for hospitalists, and serve as the point of engagement for many of SHM’s important audiences, including nurse practitioners, physician assistants, family medicine practitioners, and physicians in training.
With more than 20 committees ranging in topics from information technology to support for SHM’s local chapters, there is bound to be one that could benefit from your passion and expertise.
For more information, visit www.hospitalmedicine.org/committees.
Brendon Shank is SHM’s associate vice president for communications.
As the hospital medicine specialty continues to grow, hospitalists often ask: “How can I get involved?”
Getting involved in the hospital medicine movement and contributing to SHM’s goal of helping hospitalists provide exceptional care to hospitalized patients is easy—and it can start today.
A: Awards
Nominating a colleague—or yourself—for one of SHM’s seven awards is a great way to share your successes with the rest of the specialty. It also generates national recognition for the people and practices that make hospital medicine great.
This year, SHM will be awarding seven awards:
- Excellence in Teamwork in Quality Improvement;
- Excellence in Research;
- Excellence in Hospital Medicine for Non-Physicians;
- Excellence in Teaching;
- Outstanding Service in Hospital Medicine;
- Clinical Excellence; and
- Excellence in Humanitarian Services.
Award winners will be recognized onstage at HM15 in National Harbor, Md.
For more information or to nominate yourself or someone else for an award, visit www.hospitalmedicine.org/awards. But don’t wait. The deadline for award submissions is Oct. 13.
B: Board
Are you ready to take a national leadership position within hospital medicine? SHM’s board of directors guides the specialty and helps ensure that SHM provides hospitalists with the tools and education they need to be the best caregivers possible.
Any SHM member in good standing is eligible to become a board member. Four seats are open for the three-year term starting in 2015.
Recently, the SHM Board of Directors oversaw the creation and publication of the “Key Principles and Characteristics of an Effective Hospital Medicine Group,” a formative set of principles that were published in the Journal of Hospital Medicine and now help hospital medicine groups across the country evaluate their performance.
The board will continue to take on major projects like the key characteristics; if you would like to nominate yourself or someone else, visit the “Board of Directors” section of “About SHM” on www.hospitalmedicine.org.
But don’t wait long. Nominations are due Oct. 22.
C: Committees
Committees are the engines of change for hospital medicine. They guide SHM’s policy initiatives, address pressing quality improvement issues for hospitalists, and serve as the point of engagement for many of SHM’s important audiences, including nurse practitioners, physician assistants, family medicine practitioners, and physicians in training.
With more than 20 committees ranging in topics from information technology to support for SHM’s local chapters, there is bound to be one that could benefit from your passion and expertise.
For more information, visit www.hospitalmedicine.org/committees.
Brendon Shank is SHM’s associate vice president for communications.
As the hospital medicine specialty continues to grow, hospitalists often ask: “How can I get involved?”
Getting involved in the hospital medicine movement and contributing to SHM’s goal of helping hospitalists provide exceptional care to hospitalized patients is easy—and it can start today.
A: Awards
Nominating a colleague—or yourself—for one of SHM’s seven awards is a great way to share your successes with the rest of the specialty. It also generates national recognition for the people and practices that make hospital medicine great.
This year, SHM will be awarding seven awards:
- Excellence in Teamwork in Quality Improvement;
- Excellence in Research;
- Excellence in Hospital Medicine for Non-Physicians;
- Excellence in Teaching;
- Outstanding Service in Hospital Medicine;
- Clinical Excellence; and
- Excellence in Humanitarian Services.
Award winners will be recognized onstage at HM15 in National Harbor, Md.
For more information or to nominate yourself or someone else for an award, visit www.hospitalmedicine.org/awards. But don’t wait. The deadline for award submissions is Oct. 13.
B: Board
Are you ready to take a national leadership position within hospital medicine? SHM’s board of directors guides the specialty and helps ensure that SHM provides hospitalists with the tools and education they need to be the best caregivers possible.
Any SHM member in good standing is eligible to become a board member. Four seats are open for the three-year term starting in 2015.
Recently, the SHM Board of Directors oversaw the creation and publication of the “Key Principles and Characteristics of an Effective Hospital Medicine Group,” a formative set of principles that were published in the Journal of Hospital Medicine and now help hospital medicine groups across the country evaluate their performance.
The board will continue to take on major projects like the key characteristics; if you would like to nominate yourself or someone else, visit the “Board of Directors” section of “About SHM” on www.hospitalmedicine.org.
But don’t wait long. Nominations are due Oct. 22.
C: Committees
Committees are the engines of change for hospital medicine. They guide SHM’s policy initiatives, address pressing quality improvement issues for hospitalists, and serve as the point of engagement for many of SHM’s important audiences, including nurse practitioners, physician assistants, family medicine practitioners, and physicians in training.
With more than 20 committees ranging in topics from information technology to support for SHM’s local chapters, there is bound to be one that could benefit from your passion and expertise.
For more information, visit www.hospitalmedicine.org/committees.
Brendon Shank is SHM’s associate vice president for communications.
Better Prescription Practices Can Curb Antibiotic Resistance
Overuse of antibiotics is fueling antimicrobial resistance, posing a threat to people around the world and prompting increased attention to antibiotic stewardship practices. Good stewardship requires hospitals and clinicians to adopt coordinated interventions that focus on reducing inappropriate antibiotic prescribing while remaining focused on the health of patients.
Although it can seem overwhelming to physicians with busy workloads and sick patients to engage in these practices, not addressing the issue of responsible antibiotic prescribing is putting patients at risk.
“We know development of resistance is complicated,” says Arjun Srinivasan, MD, FSHEA, associate director for the CDC’s Healthcare Associated Infection Prevention Program and medical director of Get Smart for Healthcare in the CDC’s division of Healthcare Quality Promotion. Dr. Srinivasan is one of the authors of a recent CDC report on antibiotic prescribing practices across the U.S. “Nonetheless, we know that overuse of antibiotics leads to increases in resistance. We also know that if we can improve the way we prescribe them, we can reduce antibiotic resistance.”
The CDC recommends that hospitals adopt, at a minimum, the following antibiotic stewardship checklist:
- Commit leadership: Dedicate necessary human, financial, and information technology resources.
- Create accountability: Appoint a single leader responsible for program outcomes. Physicians have proven successful in this role.
- Provide drug expertise: Appoint a single pharmacist leader to support improved prescribing.
- Act: Take at least one prescribing improvement action, such as requiring reassessment within 48 hours to check drug choice, dose, and duration.
- Track: Monitor prescribing and antibiotic resistance patterns.
- Report: Regularly report to staff on prescribing and resistance patterns, as well as steps to improve.
- Educate: Offer education about antibiotic resistance and improving prescribing practices.
- Work with other healthcare facilities to prevent infections, transmission, and resistance.
These practices are not just the domain of infectious disease clinicians, either, says Neil Fishman, MD, chief patient safety officer and associate chief medical officer at the University of Pennsylvania Health System and past president of the Society for Healthcare Epidemiology of America. In 1992, Dr. Fishman helped establish an antibiotic stewardship program at Penn, working with infectious disease staff to identify and adopt best practices tailored to their needs.
Their efforts have shown promise in improving the health of their patients, he says, and many institutions that adopt stewardship programs typically see cost savings, too.
“These programs do usually end up decreasing drug costs but also increasing the quality of care,”
Dr. Fishman says. “If you can cut out 30% of unnecessary drugs, you cut drug costs. To me, that meets the true definition of value in healthcare.”
In one study that looked at stewardship-related cost reduction, primarily among larger healthcare settings, the average annual savings from reduced inappropriate antibiotic prescribing ranged from $200,000 to $900,000.
The recent CDC report, to which Dr. Srinivasan contributed, was published March 4 in Vital Signs. The study found that as many as a third of antibiotics prescribed are done so inappropriately. According to experts, hospitals and other healthcare institutions need to develop processes and standards to assist physicians in efforts to be responsible antibiotic prescribers.
“Sometimes, when you’re focusing on other issues, antibiotics are a bit of an afterthought,” says Scott Flanders, MD, FACP, MHM, professor of internal medicine and director of hospital medicine at University of Michigan Medical School in Ann Arbor.
“If there is not a checklist of processes [and] things are not accounted for in a systematic way, it doesn’t happen.”
Dr. Flanders and colleague Sanjay Saint, MD, MPH, the University of Michigan George Dock Collegiate professor of internal medicine and associate chief of medicine at the VA Ann Arbor Healthcare System, recently published an article in the Journal of the American Medical Association Internal Medicine in which they recommend the following:
- Antimicrobial stewardship programs, which aim to develop guidelines and implement programs that help optimize antibiotic use among hospitalized patients, should partner with front-line clinicians to tackle the problem.
- Clinicians should better document aspects of antibiotic use that can be shared with other providers caring for the same patient throughout his or her hospital stay and after discharge.
- Clinicians should take an “antibiotic time-out” after 48-72 hours of a patient’s use of antibiotics to reassess the use of these drugs.
- Treatment and its duration should be in line with evidence-based guidelines, and institutions should work to clearly identify appropriate treatment duration.
- Improved diagnostic tests should be available to physicians.
- Target diagnostic error by working to improve how physicians think when considering whether to provide antibiotics.
- Develop performance measures that highlight common conditions in which antibiotics are overprescribed, to shine a brighter light on the problem.
“I think we can make a lot of progress,” Dr. Flanders says. “The problem is complex; it developed over decades, and any solutions are unlikely to solve the problem immediately. But there are several examples of institutions and hospitals making significant inroads in a short period of time.” —KAT
Overuse of antibiotics is fueling antimicrobial resistance, posing a threat to people around the world and prompting increased attention to antibiotic stewardship practices. Good stewardship requires hospitals and clinicians to adopt coordinated interventions that focus on reducing inappropriate antibiotic prescribing while remaining focused on the health of patients.
Although it can seem overwhelming to physicians with busy workloads and sick patients to engage in these practices, not addressing the issue of responsible antibiotic prescribing is putting patients at risk.
“We know development of resistance is complicated,” says Arjun Srinivasan, MD, FSHEA, associate director for the CDC’s Healthcare Associated Infection Prevention Program and medical director of Get Smart for Healthcare in the CDC’s division of Healthcare Quality Promotion. Dr. Srinivasan is one of the authors of a recent CDC report on antibiotic prescribing practices across the U.S. “Nonetheless, we know that overuse of antibiotics leads to increases in resistance. We also know that if we can improve the way we prescribe them, we can reduce antibiotic resistance.”
The CDC recommends that hospitals adopt, at a minimum, the following antibiotic stewardship checklist:
- Commit leadership: Dedicate necessary human, financial, and information technology resources.
- Create accountability: Appoint a single leader responsible for program outcomes. Physicians have proven successful in this role.
- Provide drug expertise: Appoint a single pharmacist leader to support improved prescribing.
- Act: Take at least one prescribing improvement action, such as requiring reassessment within 48 hours to check drug choice, dose, and duration.
- Track: Monitor prescribing and antibiotic resistance patterns.
- Report: Regularly report to staff on prescribing and resistance patterns, as well as steps to improve.
- Educate: Offer education about antibiotic resistance and improving prescribing practices.
- Work with other healthcare facilities to prevent infections, transmission, and resistance.
These practices are not just the domain of infectious disease clinicians, either, says Neil Fishman, MD, chief patient safety officer and associate chief medical officer at the University of Pennsylvania Health System and past president of the Society for Healthcare Epidemiology of America. In 1992, Dr. Fishman helped establish an antibiotic stewardship program at Penn, working with infectious disease staff to identify and adopt best practices tailored to their needs.
Their efforts have shown promise in improving the health of their patients, he says, and many institutions that adopt stewardship programs typically see cost savings, too.
“These programs do usually end up decreasing drug costs but also increasing the quality of care,”
Dr. Fishman says. “If you can cut out 30% of unnecessary drugs, you cut drug costs. To me, that meets the true definition of value in healthcare.”
In one study that looked at stewardship-related cost reduction, primarily among larger healthcare settings, the average annual savings from reduced inappropriate antibiotic prescribing ranged from $200,000 to $900,000.
The recent CDC report, to which Dr. Srinivasan contributed, was published March 4 in Vital Signs. The study found that as many as a third of antibiotics prescribed are done so inappropriately. According to experts, hospitals and other healthcare institutions need to develop processes and standards to assist physicians in efforts to be responsible antibiotic prescribers.
“Sometimes, when you’re focusing on other issues, antibiotics are a bit of an afterthought,” says Scott Flanders, MD, FACP, MHM, professor of internal medicine and director of hospital medicine at University of Michigan Medical School in Ann Arbor.
“If there is not a checklist of processes [and] things are not accounted for in a systematic way, it doesn’t happen.”
Dr. Flanders and colleague Sanjay Saint, MD, MPH, the University of Michigan George Dock Collegiate professor of internal medicine and associate chief of medicine at the VA Ann Arbor Healthcare System, recently published an article in the Journal of the American Medical Association Internal Medicine in which they recommend the following:
- Antimicrobial stewardship programs, which aim to develop guidelines and implement programs that help optimize antibiotic use among hospitalized patients, should partner with front-line clinicians to tackle the problem.
- Clinicians should better document aspects of antibiotic use that can be shared with other providers caring for the same patient throughout his or her hospital stay and after discharge.
- Clinicians should take an “antibiotic time-out” after 48-72 hours of a patient’s use of antibiotics to reassess the use of these drugs.
- Treatment and its duration should be in line with evidence-based guidelines, and institutions should work to clearly identify appropriate treatment duration.
- Improved diagnostic tests should be available to physicians.
- Target diagnostic error by working to improve how physicians think when considering whether to provide antibiotics.
- Develop performance measures that highlight common conditions in which antibiotics are overprescribed, to shine a brighter light on the problem.
“I think we can make a lot of progress,” Dr. Flanders says. “The problem is complex; it developed over decades, and any solutions are unlikely to solve the problem immediately. But there are several examples of institutions and hospitals making significant inroads in a short period of time.” —KAT
Overuse of antibiotics is fueling antimicrobial resistance, posing a threat to people around the world and prompting increased attention to antibiotic stewardship practices. Good stewardship requires hospitals and clinicians to adopt coordinated interventions that focus on reducing inappropriate antibiotic prescribing while remaining focused on the health of patients.
Although it can seem overwhelming to physicians with busy workloads and sick patients to engage in these practices, not addressing the issue of responsible antibiotic prescribing is putting patients at risk.
“We know development of resistance is complicated,” says Arjun Srinivasan, MD, FSHEA, associate director for the CDC’s Healthcare Associated Infection Prevention Program and medical director of Get Smart for Healthcare in the CDC’s division of Healthcare Quality Promotion. Dr. Srinivasan is one of the authors of a recent CDC report on antibiotic prescribing practices across the U.S. “Nonetheless, we know that overuse of antibiotics leads to increases in resistance. We also know that if we can improve the way we prescribe them, we can reduce antibiotic resistance.”
The CDC recommends that hospitals adopt, at a minimum, the following antibiotic stewardship checklist:
- Commit leadership: Dedicate necessary human, financial, and information technology resources.
- Create accountability: Appoint a single leader responsible for program outcomes. Physicians have proven successful in this role.
- Provide drug expertise: Appoint a single pharmacist leader to support improved prescribing.
- Act: Take at least one prescribing improvement action, such as requiring reassessment within 48 hours to check drug choice, dose, and duration.
- Track: Monitor prescribing and antibiotic resistance patterns.
- Report: Regularly report to staff on prescribing and resistance patterns, as well as steps to improve.
- Educate: Offer education about antibiotic resistance and improving prescribing practices.
- Work with other healthcare facilities to prevent infections, transmission, and resistance.
These practices are not just the domain of infectious disease clinicians, either, says Neil Fishman, MD, chief patient safety officer and associate chief medical officer at the University of Pennsylvania Health System and past president of the Society for Healthcare Epidemiology of America. In 1992, Dr. Fishman helped establish an antibiotic stewardship program at Penn, working with infectious disease staff to identify and adopt best practices tailored to their needs.
Their efforts have shown promise in improving the health of their patients, he says, and many institutions that adopt stewardship programs typically see cost savings, too.
“These programs do usually end up decreasing drug costs but also increasing the quality of care,”
Dr. Fishman says. “If you can cut out 30% of unnecessary drugs, you cut drug costs. To me, that meets the true definition of value in healthcare.”
In one study that looked at stewardship-related cost reduction, primarily among larger healthcare settings, the average annual savings from reduced inappropriate antibiotic prescribing ranged from $200,000 to $900,000.
The recent CDC report, to which Dr. Srinivasan contributed, was published March 4 in Vital Signs. The study found that as many as a third of antibiotics prescribed are done so inappropriately. According to experts, hospitals and other healthcare institutions need to develop processes and standards to assist physicians in efforts to be responsible antibiotic prescribers.
“Sometimes, when you’re focusing on other issues, antibiotics are a bit of an afterthought,” says Scott Flanders, MD, FACP, MHM, professor of internal medicine and director of hospital medicine at University of Michigan Medical School in Ann Arbor.
“If there is not a checklist of processes [and] things are not accounted for in a systematic way, it doesn’t happen.”
Dr. Flanders and colleague Sanjay Saint, MD, MPH, the University of Michigan George Dock Collegiate professor of internal medicine and associate chief of medicine at the VA Ann Arbor Healthcare System, recently published an article in the Journal of the American Medical Association Internal Medicine in which they recommend the following:
- Antimicrobial stewardship programs, which aim to develop guidelines and implement programs that help optimize antibiotic use among hospitalized patients, should partner with front-line clinicians to tackle the problem.
- Clinicians should better document aspects of antibiotic use that can be shared with other providers caring for the same patient throughout his or her hospital stay and after discharge.
- Clinicians should take an “antibiotic time-out” after 48-72 hours of a patient’s use of antibiotics to reassess the use of these drugs.
- Treatment and its duration should be in line with evidence-based guidelines, and institutions should work to clearly identify appropriate treatment duration.
- Improved diagnostic tests should be available to physicians.
- Target diagnostic error by working to improve how physicians think when considering whether to provide antibiotics.
- Develop performance measures that highlight common conditions in which antibiotics are overprescribed, to shine a brighter light on the problem.
“I think we can make a lot of progress,” Dr. Flanders says. “The problem is complex; it developed over decades, and any solutions are unlikely to solve the problem immediately. But there are several examples of institutions and hospitals making significant inroads in a short period of time.” —KAT
Hospitalists Adopt Strategies to Become More Responsible Prescribers of Antibiotics
A recent CDC study found that nearly a third of antibiotics might be inappropriately prescribed.1 The report also found wide variation in antibiotic prescribing practices for patients in similar treatment areas in hospitals across the country.
Across the globe, antibiotic resistance has become a daunting threat. Some public health officials have labeled it a crisis, and improper prescribing and use of antibiotics is at least partly to blame, experts say.
“We’re dangerously close to a pre-antibiotic era where we don’t have antibiotics to treat common infections,” says Neil Fishman, MD, chief patient safety officer and associate chief medical officer at the University of Pennsylvania Health System and past president of the Society for Healthcare Epidemiology of America. “We are seeing more and more infections, usually hospital-based, caused by bacterial resistance to most, if not all, of the antibiotics that we have.”
It’s an issue hospitalists around the country are championing.
“I think for a long time there’s been a misperception that antibiotic stewardship is at odds with hospitalists, who are managing very busy patient loads and managing inpatient prescribing,” says Arjun Srinivasan, MD, FSHEA, associate director for the CDC’s Healthcare Associated Infection Prevention Program and medical director of Get Smart for Healthcare in the division of Healthcare Quality Promotion at the CDC. Dr. Srinivasan is one of the authors of the new CDC study.
But “they have taken that ball and run with it,” says Dr. Srinivasan, who has worked with the Society of Hospital Medicine to address antibiotic resistance issues.
The goals of the study, published in the CDC’s Vital Signs on March 4, 2014, were to evaluate the extent and rationale for the prescribing of antibiotics in U.S. hospitals, while demonstrating opportunities for improvement in prescribing practices.
—Neil Fishman, MD, chief patient safety officer and associate chief medical officer at the University of Pennsylvania Health System
Study authors analyzed data from the Truven Health MarketScan Hospital Drug Database and the CDC’s Emerging Infection Program and, using a model based on the data, demonstrated that a 30% reduction in broad-spectrum antibiotics use would decrease Clostridium difficile infection (CDI) by 26%. Overall antibiotic use would drop by 5%.
According to the CDC, antibiotics are among the most frequent causes of adverse drug events among hospitalized patients in the U.S., and complications like CDI can be deadly. In fact, 250,000 hospitalized patients are infected with CDI each year, resulting in 14,000 deaths.
“We’re really at a critical juncture in healthcare now,” Dr. Fishman says. “The field of stewardship has evolved mainly in academic tertiary care settings. The CDC report is timely because it highlights the necessity of making sure antibiotics are used appropriately in all healthcare settings.”
Take a Break
One of the ways in which hospitalists have addressed the need for more appropriate antibiotic prescribing in their institutions is the practice of an “antibiotic time-out.”
“After some point, when the dust settles at about 48-72 hours, you can evaluate the patient’s progress, evaluate their studies, [and] you may have culture results,” says Scott Flanders, MD, FACP, MHM, professor of internal medicine and director of hospital medicine at the University of Michigan Medical School in Ann Arbor. At that point, physicians can decide whether to maintain a patient on the original antibiotic, alter the duration of treatment, or take them off the treatment altogether.
Dr. Flanders and a colleague published an editorial in the Journal of the American Medical Association Internal Medicine that coincided with the CDC report.2 A 2007 study published in Clinical Infectious Diseases found that the choice of antibiotic agent or duration of treatment can be incorrect in as many as half of all cases in which antibiotics are prescribed.3
Dr. Flanders, a past president of SHM who has worked extensively with the CDC and the Institute for Healthcare Improvement, was behind the development of the time-out strategy. Dr. Srinivasan says the clinical utility of the method was “eye-opening.”
The strategy, which has taken hold among hospital groups the CDC has worked with, has demonstrated that stewardship and patient management are not at odds, Dr. Srinivasan says. Despite patient sign-outs and hand-offs, the time-out strategy allows any clinician to track a patient’s antibiotic status and reevaluate the treatment plan.
Having a process is critical to more responsible prescribing practices, Dr. Flanders says. He attributes much of the variability in antibiotics prescribing among similar departments at hospitals across the country to a lack of standards, though he noted that variability in patient populations undoubtedly plays a role.
Lack of Stats
The CDC report showed up to a threefold difference in the number of antibiotics prescribed to patients in similar hospital settings at hospitals across the country. The reasons for this are not known, Dr. Fishman says.
“The main reason we don’t know is we don’t have a good mechanism in the U.S. right now to monitor antibiotics use,” he explains. “We don’t have a way for healthcare facilities to benchmark their use.”
Without good strategies to monitor and develop more responsible antibiotics prescription practices, Dr. Flanders believes many physicians find themselves trapped by the “chagrin” of not prescribing.
“Patients often enter the hospital without a clear diagnosis,” he says. “They are quite ill. They may have a serious bacterial infection, and, in diagnosing them, we can’t guess wrong and make the decision to withhold antibiotics, only to find out later the patient is infected.
“We know delays increase mortality, and that’s not an acceptable option.”

—Scott Flanders, MD, FACP, MHM, professor of internal medicine, director of hospital medicine, University of Michigan Medical School, Ann Arbor, past president, SHM
Beyond the Bedside
Many physicians fail to consider the bigger societal implications when prescribing antibiotics for sick patients in their charge, because their responsibility is, first and foremost, to that individual. But, Dr. Srinivasan says, “good antibiotic stewardship is beneficial to the patient lying in the bed in front of you, because every day we are confronted with C. diff. infections, adverse drug events, all of these issues.”
Strategies and processes help hospitalists make the best decision for their patients at the time they require care, while providing room for adaptation and the improvements that serve all patients.
Some institutions use interventions like prospective audit and feedback monitoring to help physicians become more responsible antibiotic prescribers, says Dr. Fishman, who worked with infectious disease specialists at the University of Pennsylvania in the early 1990s to develop a stewardship program there.
“In our institution, we see better outcomes—lower complications—usually associated with a decreased length of stay, at least in the ICU for critically ill patients—and increased cure rates,” he says.
Stewardship efforts take investment on the part of the hospital. Dr. Fishman cited a recent study at the Children’s Hospital of Pennsylvania that looked at whether a particular education strategy the hospital implemented actually led to improvements.4
“It was successful in intervening in this problem [of inappropriate prescribing] in pediatricians, but it did take ongoing education of both healthcare providers and patients,” he says, noting that large financial and time investments are necessary for the ongoing training and follow-up that is necessary.
And patients need to be educated, too.
“It takes a minute to write that prescription and probably 15 or 20 minutes not to write it,” Dr. Fishman says. “We need to educate patients about potential complications of antibiotics use, as well as the signs and symptoms of infection.”
The CDC report is a call to action for all healthcare providers to consider how they can become better antibiotic stewards. There are very few new antibiotics on the market and little in the pipeline. All providers must do what they can to preserve the antibiotics we currently have, Dr. Fishman says.
“There is opportunity, and I think hospitalists are up to the challenge,” Dr. Flanders says. “They are doing lots of work to improve quality across lots of domains in their hospitals. I think this is an area where attention is deserved.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
References
- Centers for Disease Control and Prevention. Morbidity and Mortality Weekly Report. Vital signs: improving antibiotic use among hospitalized patients. Available at: www.cdc.gov/mmwr/preview/mmwrhtml/mm6309a4.htm?s_cid=mm6309a4_w. Accessed August 31, 2014.
- Flanders SA, Saint S. Why does antrimicrobial overuse in hospitalized patients persist? JAMA Internal Medicine online. Available at: http://archinte.jamanetwork.com/article.aspx?articleid=1838720. Accessed August 31, 2014.
- Dellit TH, Owens RC, McGowan JE, et al. Clinical Infectious Diseases online. Available at: http://cid.oxfordjournals.org/content/44/2/159.full. Accessed August 31, 2014.
- Gerber JS, Prasad PA, Fiks A, et al. Effect of an outpatient antimicrobial stewardship intervention on broad-spectrum antibiotic prescribing by primary care pediatricians. JAMA. 2013;309(22):2345-2352.
A recent CDC study found that nearly a third of antibiotics might be inappropriately prescribed.1 The report also found wide variation in antibiotic prescribing practices for patients in similar treatment areas in hospitals across the country.
Across the globe, antibiotic resistance has become a daunting threat. Some public health officials have labeled it a crisis, and improper prescribing and use of antibiotics is at least partly to blame, experts say.
“We’re dangerously close to a pre-antibiotic era where we don’t have antibiotics to treat common infections,” says Neil Fishman, MD, chief patient safety officer and associate chief medical officer at the University of Pennsylvania Health System and past president of the Society for Healthcare Epidemiology of America. “We are seeing more and more infections, usually hospital-based, caused by bacterial resistance to most, if not all, of the antibiotics that we have.”
It’s an issue hospitalists around the country are championing.
“I think for a long time there’s been a misperception that antibiotic stewardship is at odds with hospitalists, who are managing very busy patient loads and managing inpatient prescribing,” says Arjun Srinivasan, MD, FSHEA, associate director for the CDC’s Healthcare Associated Infection Prevention Program and medical director of Get Smart for Healthcare in the division of Healthcare Quality Promotion at the CDC. Dr. Srinivasan is one of the authors of the new CDC study.
But “they have taken that ball and run with it,” says Dr. Srinivasan, who has worked with the Society of Hospital Medicine to address antibiotic resistance issues.
The goals of the study, published in the CDC’s Vital Signs on March 4, 2014, were to evaluate the extent and rationale for the prescribing of antibiotics in U.S. hospitals, while demonstrating opportunities for improvement in prescribing practices.
—Neil Fishman, MD, chief patient safety officer and associate chief medical officer at the University of Pennsylvania Health System
Study authors analyzed data from the Truven Health MarketScan Hospital Drug Database and the CDC’s Emerging Infection Program and, using a model based on the data, demonstrated that a 30% reduction in broad-spectrum antibiotics use would decrease Clostridium difficile infection (CDI) by 26%. Overall antibiotic use would drop by 5%.
According to the CDC, antibiotics are among the most frequent causes of adverse drug events among hospitalized patients in the U.S., and complications like CDI can be deadly. In fact, 250,000 hospitalized patients are infected with CDI each year, resulting in 14,000 deaths.
“We’re really at a critical juncture in healthcare now,” Dr. Fishman says. “The field of stewardship has evolved mainly in academic tertiary care settings. The CDC report is timely because it highlights the necessity of making sure antibiotics are used appropriately in all healthcare settings.”
Take a Break
One of the ways in which hospitalists have addressed the need for more appropriate antibiotic prescribing in their institutions is the practice of an “antibiotic time-out.”
“After some point, when the dust settles at about 48-72 hours, you can evaluate the patient’s progress, evaluate their studies, [and] you may have culture results,” says Scott Flanders, MD, FACP, MHM, professor of internal medicine and director of hospital medicine at the University of Michigan Medical School in Ann Arbor. At that point, physicians can decide whether to maintain a patient on the original antibiotic, alter the duration of treatment, or take them off the treatment altogether.
Dr. Flanders and a colleague published an editorial in the Journal of the American Medical Association Internal Medicine that coincided with the CDC report.2 A 2007 study published in Clinical Infectious Diseases found that the choice of antibiotic agent or duration of treatment can be incorrect in as many as half of all cases in which antibiotics are prescribed.3
Dr. Flanders, a past president of SHM who has worked extensively with the CDC and the Institute for Healthcare Improvement, was behind the development of the time-out strategy. Dr. Srinivasan says the clinical utility of the method was “eye-opening.”
The strategy, which has taken hold among hospital groups the CDC has worked with, has demonstrated that stewardship and patient management are not at odds, Dr. Srinivasan says. Despite patient sign-outs and hand-offs, the time-out strategy allows any clinician to track a patient’s antibiotic status and reevaluate the treatment plan.
Having a process is critical to more responsible prescribing practices, Dr. Flanders says. He attributes much of the variability in antibiotics prescribing among similar departments at hospitals across the country to a lack of standards, though he noted that variability in patient populations undoubtedly plays a role.
Lack of Stats
The CDC report showed up to a threefold difference in the number of antibiotics prescribed to patients in similar hospital settings at hospitals across the country. The reasons for this are not known, Dr. Fishman says.
“The main reason we don’t know is we don’t have a good mechanism in the U.S. right now to monitor antibiotics use,” he explains. “We don’t have a way for healthcare facilities to benchmark their use.”
Without good strategies to monitor and develop more responsible antibiotics prescription practices, Dr. Flanders believes many physicians find themselves trapped by the “chagrin” of not prescribing.
“Patients often enter the hospital without a clear diagnosis,” he says. “They are quite ill. They may have a serious bacterial infection, and, in diagnosing them, we can’t guess wrong and make the decision to withhold antibiotics, only to find out later the patient is infected.
“We know delays increase mortality, and that’s not an acceptable option.”
—Scott Flanders, MD, FACP, MHM, professor of internal medicine, director of hospital medicine, University of Michigan Medical School, Ann Arbor, past president, SHM
Beyond the Bedside
Many physicians fail to consider the bigger societal implications when prescribing antibiotics for sick patients in their charge, because their responsibility is, first and foremost, to that individual. But, Dr. Srinivasan says, “good antibiotic stewardship is beneficial to the patient lying in the bed in front of you, because every day we are confronted with C. diff. infections, adverse drug events, all of these issues.”
Strategies and processes help hospitalists make the best decision for their patients at the time they require care, while providing room for adaptation and the improvements that serve all patients.
Some institutions use interventions like prospective audit and feedback monitoring to help physicians become more responsible antibiotic prescribers, says Dr. Fishman, who worked with infectious disease specialists at the University of Pennsylvania in the early 1990s to develop a stewardship program there.
“In our institution, we see better outcomes—lower complications—usually associated with a decreased length of stay, at least in the ICU for critically ill patients—and increased cure rates,” he says.
Stewardship efforts take investment on the part of the hospital. Dr. Fishman cited a recent study at the Children’s Hospital of Pennsylvania that looked at whether a particular education strategy the hospital implemented actually led to improvements.4
“It was successful in intervening in this problem [of inappropriate prescribing] in pediatricians, but it did take ongoing education of both healthcare providers and patients,” he says, noting that large financial and time investments are necessary for the ongoing training and follow-up that is necessary.
And patients need to be educated, too.
“It takes a minute to write that prescription and probably 15 or 20 minutes not to write it,” Dr. Fishman says. “We need to educate patients about potential complications of antibiotics use, as well as the signs and symptoms of infection.”
The CDC report is a call to action for all healthcare providers to consider how they can become better antibiotic stewards. There are very few new antibiotics on the market and little in the pipeline. All providers must do what they can to preserve the antibiotics we currently have, Dr. Fishman says.
“There is opportunity, and I think hospitalists are up to the challenge,” Dr. Flanders says. “They are doing lots of work to improve quality across lots of domains in their hospitals. I think this is an area where attention is deserved.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
References
- Centers for Disease Control and Prevention. Morbidity and Mortality Weekly Report. Vital signs: improving antibiotic use among hospitalized patients. Available at: www.cdc.gov/mmwr/preview/mmwrhtml/mm6309a4.htm?s_cid=mm6309a4_w. Accessed August 31, 2014.
- Flanders SA, Saint S. Why does antrimicrobial overuse in hospitalized patients persist? JAMA Internal Medicine online. Available at: http://archinte.jamanetwork.com/article.aspx?articleid=1838720. Accessed August 31, 2014.
- Dellit TH, Owens RC, McGowan JE, et al. Clinical Infectious Diseases online. Available at: http://cid.oxfordjournals.org/content/44/2/159.full. Accessed August 31, 2014.
- Gerber JS, Prasad PA, Fiks A, et al. Effect of an outpatient antimicrobial stewardship intervention on broad-spectrum antibiotic prescribing by primary care pediatricians. JAMA. 2013;309(22):2345-2352.
A recent CDC study found that nearly a third of antibiotics might be inappropriately prescribed.1 The report also found wide variation in antibiotic prescribing practices for patients in similar treatment areas in hospitals across the country.
Across the globe, antibiotic resistance has become a daunting threat. Some public health officials have labeled it a crisis, and improper prescribing and use of antibiotics is at least partly to blame, experts say.
“We’re dangerously close to a pre-antibiotic era where we don’t have antibiotics to treat common infections,” says Neil Fishman, MD, chief patient safety officer and associate chief medical officer at the University of Pennsylvania Health System and past president of the Society for Healthcare Epidemiology of America. “We are seeing more and more infections, usually hospital-based, caused by bacterial resistance to most, if not all, of the antibiotics that we have.”
It’s an issue hospitalists around the country are championing.
“I think for a long time there’s been a misperception that antibiotic stewardship is at odds with hospitalists, who are managing very busy patient loads and managing inpatient prescribing,” says Arjun Srinivasan, MD, FSHEA, associate director for the CDC’s Healthcare Associated Infection Prevention Program and medical director of Get Smart for Healthcare in the division of Healthcare Quality Promotion at the CDC. Dr. Srinivasan is one of the authors of the new CDC study.
But “they have taken that ball and run with it,” says Dr. Srinivasan, who has worked with the Society of Hospital Medicine to address antibiotic resistance issues.
The goals of the study, published in the CDC’s Vital Signs on March 4, 2014, were to evaluate the extent and rationale for the prescribing of antibiotics in U.S. hospitals, while demonstrating opportunities for improvement in prescribing practices.
—Neil Fishman, MD, chief patient safety officer and associate chief medical officer at the University of Pennsylvania Health System
Study authors analyzed data from the Truven Health MarketScan Hospital Drug Database and the CDC’s Emerging Infection Program and, using a model based on the data, demonstrated that a 30% reduction in broad-spectrum antibiotics use would decrease Clostridium difficile infection (CDI) by 26%. Overall antibiotic use would drop by 5%.
According to the CDC, antibiotics are among the most frequent causes of adverse drug events among hospitalized patients in the U.S., and complications like CDI can be deadly. In fact, 250,000 hospitalized patients are infected with CDI each year, resulting in 14,000 deaths.
“We’re really at a critical juncture in healthcare now,” Dr. Fishman says. “The field of stewardship has evolved mainly in academic tertiary care settings. The CDC report is timely because it highlights the necessity of making sure antibiotics are used appropriately in all healthcare settings.”
Take a Break
One of the ways in which hospitalists have addressed the need for more appropriate antibiotic prescribing in their institutions is the practice of an “antibiotic time-out.”
“After some point, when the dust settles at about 48-72 hours, you can evaluate the patient’s progress, evaluate their studies, [and] you may have culture results,” says Scott Flanders, MD, FACP, MHM, professor of internal medicine and director of hospital medicine at the University of Michigan Medical School in Ann Arbor. At that point, physicians can decide whether to maintain a patient on the original antibiotic, alter the duration of treatment, or take them off the treatment altogether.
Dr. Flanders and a colleague published an editorial in the Journal of the American Medical Association Internal Medicine that coincided with the CDC report.2 A 2007 study published in Clinical Infectious Diseases found that the choice of antibiotic agent or duration of treatment can be incorrect in as many as half of all cases in which antibiotics are prescribed.3
Dr. Flanders, a past president of SHM who has worked extensively with the CDC and the Institute for Healthcare Improvement, was behind the development of the time-out strategy. Dr. Srinivasan says the clinical utility of the method was “eye-opening.”
The strategy, which has taken hold among hospital groups the CDC has worked with, has demonstrated that stewardship and patient management are not at odds, Dr. Srinivasan says. Despite patient sign-outs and hand-offs, the time-out strategy allows any clinician to track a patient’s antibiotic status and reevaluate the treatment plan.
Having a process is critical to more responsible prescribing practices, Dr. Flanders says. He attributes much of the variability in antibiotics prescribing among similar departments at hospitals across the country to a lack of standards, though he noted that variability in patient populations undoubtedly plays a role.
Lack of Stats
The CDC report showed up to a threefold difference in the number of antibiotics prescribed to patients in similar hospital settings at hospitals across the country. The reasons for this are not known, Dr. Fishman says.
“The main reason we don’t know is we don’t have a good mechanism in the U.S. right now to monitor antibiotics use,” he explains. “We don’t have a way for healthcare facilities to benchmark their use.”
Without good strategies to monitor and develop more responsible antibiotics prescription practices, Dr. Flanders believes many physicians find themselves trapped by the “chagrin” of not prescribing.
“Patients often enter the hospital without a clear diagnosis,” he says. “They are quite ill. They may have a serious bacterial infection, and, in diagnosing them, we can’t guess wrong and make the decision to withhold antibiotics, only to find out later the patient is infected.
“We know delays increase mortality, and that’s not an acceptable option.”
—Scott Flanders, MD, FACP, MHM, professor of internal medicine, director of hospital medicine, University of Michigan Medical School, Ann Arbor, past president, SHM
Beyond the Bedside
Many physicians fail to consider the bigger societal implications when prescribing antibiotics for sick patients in their charge, because their responsibility is, first and foremost, to that individual. But, Dr. Srinivasan says, “good antibiotic stewardship is beneficial to the patient lying in the bed in front of you, because every day we are confronted with C. diff. infections, adverse drug events, all of these issues.”
Strategies and processes help hospitalists make the best decision for their patients at the time they require care, while providing room for adaptation and the improvements that serve all patients.
Some institutions use interventions like prospective audit and feedback monitoring to help physicians become more responsible antibiotic prescribers, says Dr. Fishman, who worked with infectious disease specialists at the University of Pennsylvania in the early 1990s to develop a stewardship program there.
“In our institution, we see better outcomes—lower complications—usually associated with a decreased length of stay, at least in the ICU for critically ill patients—and increased cure rates,” he says.
Stewardship efforts take investment on the part of the hospital. Dr. Fishman cited a recent study at the Children’s Hospital of Pennsylvania that looked at whether a particular education strategy the hospital implemented actually led to improvements.4
“It was successful in intervening in this problem [of inappropriate prescribing] in pediatricians, but it did take ongoing education of both healthcare providers and patients,” he says, noting that large financial and time investments are necessary for the ongoing training and follow-up that is necessary.
And patients need to be educated, too.
“It takes a minute to write that prescription and probably 15 or 20 minutes not to write it,” Dr. Fishman says. “We need to educate patients about potential complications of antibiotics use, as well as the signs and symptoms of infection.”
The CDC report is a call to action for all healthcare providers to consider how they can become better antibiotic stewards. There are very few new antibiotics on the market and little in the pipeline. All providers must do what they can to preserve the antibiotics we currently have, Dr. Fishman says.
“There is opportunity, and I think hospitalists are up to the challenge,” Dr. Flanders says. “They are doing lots of work to improve quality across lots of domains in their hospitals. I think this is an area where attention is deserved.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
References
- Centers for Disease Control and Prevention. Morbidity and Mortality Weekly Report. Vital signs: improving antibiotic use among hospitalized patients. Available at: www.cdc.gov/mmwr/preview/mmwrhtml/mm6309a4.htm?s_cid=mm6309a4_w. Accessed August 31, 2014.
- Flanders SA, Saint S. Why does antrimicrobial overuse in hospitalized patients persist? JAMA Internal Medicine online. Available at: http://archinte.jamanetwork.com/article.aspx?articleid=1838720. Accessed August 31, 2014.
- Dellit TH, Owens RC, McGowan JE, et al. Clinical Infectious Diseases online. Available at: http://cid.oxfordjournals.org/content/44/2/159.full. Accessed August 31, 2014.
- Gerber JS, Prasad PA, Fiks A, et al. Effect of an outpatient antimicrobial stewardship intervention on broad-spectrum antibiotic prescribing by primary care pediatricians. JAMA. 2013;309(22):2345-2352.
New State of Hospital Medicine Report Offers Insight to Trends in Hospitalist Compensation, Productivity

The highlight of SHM’s biennial State of Hospital Medicine (SOHM) report is how much hospitalists earn. So it’s to be expected that rank-and-file practitioners and group leaders who read this year’s edition will first notice that median compensation for adult hospitalists rose 8% to $252,996 in 2013, according to data from the Medical Group Management Association (MGMA). The compensation data from MGMA is wrapped into the SOHM 2014 report this year.
But to stop there would be a wasted opportunity, says William “Tex” Landis, MD, FHM, medical director of Wellspan Hospitalists in York, Pa., and a member and former chair of SHM’s Practice Analysis Committee. Along with compensation, the report (available at www.hospitalmedicine.org/survey) delves into scheduling, productivity, staffing, how compensation is broken down, practice models, and dozens of other topics that hospital medicine group (HMG) leaders will find useful.
“Scope of services is a big one,” Dr. Landis adds. “What other things are hospital medicine groups around the country being held responsible for? Are we morphing into universal admitters? How involved in palliative care are we? What about transitions of care? How many hospital medicine groups are becoming involved in managing nursing home patients? What’s the relationship with surgical co-management? How much ICU work are we doing?”
Dr. Landis’ laundry list of unanswered questions might seem daunting, but that’s the point of the research SHM has been collecting and reporting for years. The society surveyed 499 groups, representing some 6,300 providers, to give the specialty’s most detailed list of most popular, if not best, practices.
“It has the usual limitations of any survey; however, it is the very best survey, quantity and quality, of hospital medicine groups,” Dr. Landis says. “And so it becomes the best source of information to make important decisions about resourcing and operating hospital medicine groups.”
Earnings Up
And, like it or not, compensation for providers typically is a HMG’s largest budget line. In that regard, the specialty appears to be doing well. Median compensation for adult hospitalists rose to a record high last year, according to the MGMA Physician Compensation and Production Survey: 2014 Report Based on 2013 Data. Half of respondents work in practices owned by hospitals/integrated delivery systems, down from 56% in SOHM 2012.
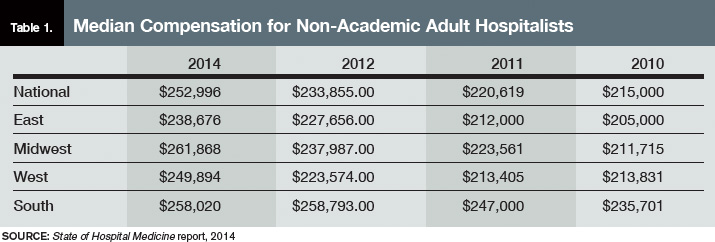
Although hospitalists in the South region continue to earn the most (median compensation $258,020, essentially static with the $258,793 figure reported in 2012), the region was the only one to report a decrease (see Table 1 for historical data). The largest percentage jump (11.8%) was for hospitalists in the West region ($249,894). Hospitalists in the Midwest saw a 10% increase ($261,868), while those in the East had both the smallest increase (4.8%) and the lowest median compensation ($238,676).

—R. Jeffrey Taylor, president and COO, IPC The Hospitalist Co., North Hollywood, Calif.
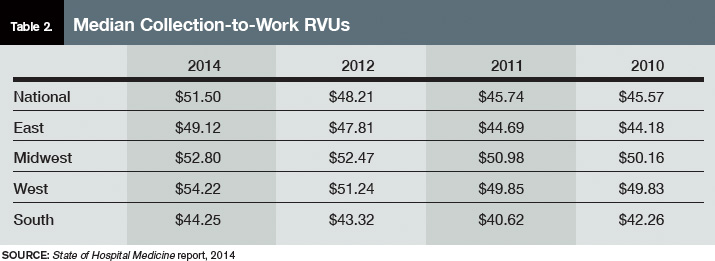
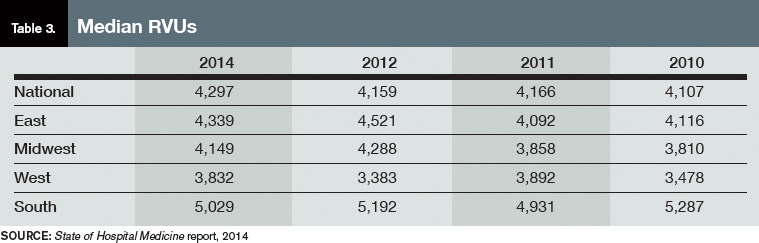
Part of the compensation increase is tied to upward pressure on productivity. Nationwide, median relative value units (RVUs) rose 3.3%, to 4,297 from 4,159. Median collection-to-work RVUs ticked up 6.8%, to 51.5 from 48.21 (see Table 2 for regional breakdowns). Production (10.5%) and performance (6.6%) are also slightly larger portions of mean compensation than they were in 2012, a figure many expect to increase further in future reports. The report also noted that academic/university hospitalists receive more in base pay, while hospitalists in private practice receive less.
Compensation and work volume will be intrinsically tied in the coming years, says R. Jeffrey Taylor, president and chief operating officer of IPC The Hospitalist Co., based in North Hollywood, Calif. And if pay outpaces productivity, “then it’s a bit concerning for the system at large,” he says.
“Particularly for whoever is subsidizing that shortfall, whether it’s a hospital employing doctors or an outsourced group employing the doctors but requiring a large subsidy from the hospital because the doctors are not seeing enough patient flow to pay their salary and benefits,” Taylor says.
More than 89% of HMGs rely on their host hospitals for financial support, according to the new data. The median support is $156,063 per full-time employee (FTE), which would total $1 million at just over seven FTEs. As healthcare reform progresses and hospitals’ budgets are increasingly burdened, Taylor says that pressure for hospitalists to generate enough revenue to cover their own salaries will grow. That sets up a likely showdown between hospitalists and their institutions; SOHM 2014 reported that just 6% of HMGs received enough income from professional fee revenue to cover expenses.
SOURCE: State of Hospital Medicine report, 2014
SOURCE: State of Hospital Medicine report, 2014
“Some productivity element in compensation plans, we believe, and I believe personally, is important,” Taylor says, later adding: “We already have a physician shortage and a shortage of people to see all these patients. It’s exacerbated by two things: lack of productivity and shift-model scheduling.”
To wit, IPC pays lower base salaries but provides bonuses tied to productivity and quality metrics. The average IPC hospitalist, Taylor says, earned more than $290,000 last year, nearly 15% above the median figure in the SOHM report. Between 30%-40% of that compensation, however, was earned via bonus tied to both “productivity and clinical achievement.”
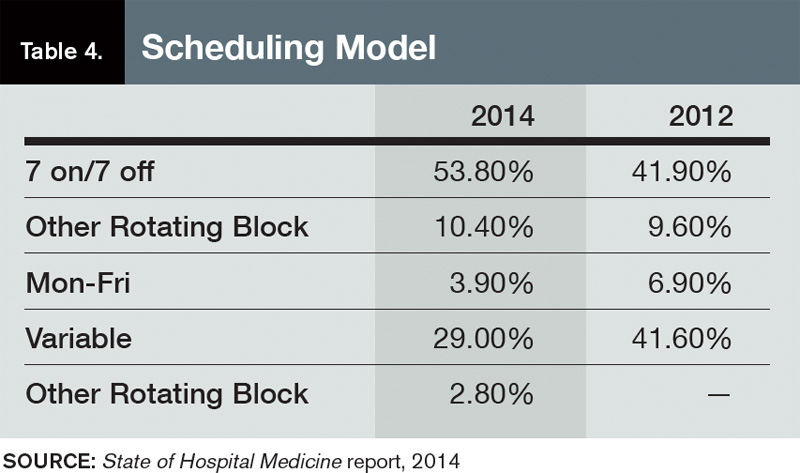
Taylor, an outspoken advocate for moving away from the seven-on/seven-off scheduling model popular throughout hospital medicine, ties some of his doctors’ higher compensation to his firm’s preference for avoiding that schedule. But he’s not surprised the new report shows that 53.8% of responding HMGs use the model, up from 41.9% in 2012.
“It will be interesting to see what the data shows over the next three or four years,” he says, “if stipends, as we believe we are seeing, come under pressure and hospitals are doing more outsourcing.”
SOURCE: State of Hospital Medicine report, 2014
The PCP Link
Industry leaders use the information in the biennial reports to gauge where the specialty stands in the overall healthcare spectrum. Dea Robinson, MA, FACMPE, CPC, director of consulting for MGMA Health Care Consulting Group, says that the growth of hospital medicine (HM) compensation is tied to that of primary care physicians (PCPs).
“I don’t think we can look at hospitalists without looking at primary care, because it’s really an extension of primary care,” says Robinson, a member of SHM’s Practice Management Committee. “As primary care compensation increases, hospitalists’ compensation might increase as well. And with the focus on patient-centered medical homes, which is basically primary care centered, that might very well be part of the driver in the future of seeing hospitalists grow.”
While facing a well-known physician shortage, primary care’s compensation growth also lags behind HM. For example, median compensation for hospitalists rose 8%; it increased 5.5% for PCPs.
“When it comes to growth of the two individual industries, I think they are connected in some way,” she adds. “But in terms of the compensation, now we’re starting to see different codes that hospitalists are able to use but that primary care used to use exclusively. So, you really see more of an extension and a collaboration between true primary care and hospitalists.”
Bryan Weiss, MBA, FHM, managing director of the consulting services practice at Irving, Texas-based MedSynergies, agrees that hospitalists and PCPs are connected. He believes the higher compensation figures are a sign of how young HM is as a specialty. He fears compensation “is probably growing too fast.”
“This takes me back to the 1990s, with the private [physician practice management]-type model, where it just grew so fast that the bottom fell out,” says Weiss, a member of Team Hospitalist. “Not that I think the bottom is going to fall out of hospital medicine, but a lot of this is reminiscent of that, and I think there’s going to be a ceiling, or at least a slowing down.”

—Stuart Guterman, vice president, Medicare and cost control, The Commonwealth Fund
In contrast, one good sign for the specialty’s compensation and financial support is that “hospitals are still the hub of the healthcare system and need to be an important part of healthcare reform,” says Stuart Guterman, vice president for Medicare and cost control at The Commonwealth Fund, a New York foundation focused on improving healthcare delivery. Guterman says that while President Obama and congressional leaders are looking to cut the rate of growth in healthcare spending, the figure is already so high that there should still be plenty of resources in the system.
“If you took today’s spending and you increased it at the [GDP] growth rate for 10 years, I think we’re talking about something over $30 trillion over 10 years,” Guterman says. “And remember that we’re starting at a point that’s over 50% higher than any other country in the world. So, we’re talking about plenty of resources still in this healthcare system.”
With accountable care organizations, the specter of bundled payments, and penalties for readmitted patients, Guterman says that the pending issue for the specialty isn’t whether hospitalists—or other hospital-based practitioners—are going to get paid more or less, but rather what their compensation will be based on.
“Things like better coordination of care, sending the patients to the right place, having the patients in the right place, having them in the hospital if they need to be, or keeping them out of the hospital if they don’t need to be in the hospital,” he explains. “But the hospital is certainly a big part of that health system.”
In fact, physicians who play to the strengths of the new healthcare metrics—quality, value, lower-cost care—can probably earn as much compensation as, if not more than, they could in the traditional fee-for-service model hospitalists, Guterman says.
“The big point is to remind people that when we’re talking about controlling health spending growth, we’re still talking about a growing industry,” he notes. “We’re not talking about disenfranchising healthcare or providers. We’re talking about more reasonable growth and about, more than anything, paying for the right things. Folks ought to be able to do quite well if they do the right things.”
SOURCE: State of Hospital Medicine report, 2014
Multiple Uses
The SOHM report can be used as a measuring stick to compare against national and regional competitors and to provide data points for discussions with hospital administrators, says Team Hospitalist’s Weiss.
“This is vital in terms of recruiting physicians,” he says, “as well as negotiating with the hospital, as far as what the average investment is.”
Dr. Landis of SHM’s Practice Analysis Committee believes that having data points to make “resourcing decisions” with is particularly helpful, both in hiring and scheduling and in “right-sizing” hospital support for groups that are not self-sufficient.
“It is critical for physicians and their administrative partners to get the resourcing right, as inappropriately resourced groups [too much or too little] can quickly become unsustainable and/or unstable,” Dr. Landis says.
Take his group’s compensation.
“When we look at what we want to incent physicians, we’ll look at what other groups are doing,” Dr. Landis adds. “Are they using core measures? Are they using patient satisfaction? What about good citizenship? It’s one thing to say, ‘A hospital down the road is doing it.’ It’s another thing to take this book and say, ‘Let’s look the numbers up.’”
Of course, the wrinkle in benchmarking against national or regional figures is that HMGs can be “very particular,” says MGMA’s Robinson.
“We use benchmarks to give us an idea of what the pulse is, but we don’t use it as the only number,” she adds. “It’s very individualistic to the practice and to the program.”
Dr. Landis understands that point of view. Take his group’s policy on how much of hospitalists’ compensation is based on performance. The median component of compensation tied to performance for hospitalists nationwide is 6.6%, according to SOHM 2014. Dr. Landis’ group is at 15%. In meetings with his C-suite executives, he says he thinks in the back of his mind about how far outside the mean his group is in that regard. But he tempers that thought with the view that many hospitalists believe that performance and other metrics will continue to grow into a larger portion of hospitalists’ overall compensation.
“You have to be careful,” he says. “The first person to do an innovative, valuable thing isn’t going to be the 85%. You have to be careful not to stifle innovation. One of the cautions is not to use ‘just because everyone else is doing it means it’s the best way.’”
Weiss calls on an old adage in the industry: “If you’ve seen one hospitalist program, you’ve seen exactly one hospitalist program,” he says. “Because while they can be part of a large health system or a management company, while they try to have some commonality or some typical procedures, there’s still going to be individuality.”
Richard Quinn is a freelance writer in New Jersey.
The highlight of SHM’s biennial State of Hospital Medicine (SOHM) report is how much hospitalists earn. So it’s to be expected that rank-and-file practitioners and group leaders who read this year’s edition will first notice that median compensation for adult hospitalists rose 8% to $252,996 in 2013, according to data from the Medical Group Management Association (MGMA). The compensation data from MGMA is wrapped into the SOHM 2014 report this year.
But to stop there would be a wasted opportunity, says William “Tex” Landis, MD, FHM, medical director of Wellspan Hospitalists in York, Pa., and a member and former chair of SHM’s Practice Analysis Committee. Along with compensation, the report (available at www.hospitalmedicine.org/survey) delves into scheduling, productivity, staffing, how compensation is broken down, practice models, and dozens of other topics that hospital medicine group (HMG) leaders will find useful.
“Scope of services is a big one,” Dr. Landis adds. “What other things are hospital medicine groups around the country being held responsible for? Are we morphing into universal admitters? How involved in palliative care are we? What about transitions of care? How many hospital medicine groups are becoming involved in managing nursing home patients? What’s the relationship with surgical co-management? How much ICU work are we doing?”
Dr. Landis’ laundry list of unanswered questions might seem daunting, but that’s the point of the research SHM has been collecting and reporting for years. The society surveyed 499 groups, representing some 6,300 providers, to give the specialty’s most detailed list of most popular, if not best, practices.
“It has the usual limitations of any survey; however, it is the very best survey, quantity and quality, of hospital medicine groups,” Dr. Landis says. “And so it becomes the best source of information to make important decisions about resourcing and operating hospital medicine groups.”
Earnings Up
And, like it or not, compensation for providers typically is a HMG’s largest budget line. In that regard, the specialty appears to be doing well. Median compensation for adult hospitalists rose to a record high last year, according to the MGMA Physician Compensation and Production Survey: 2014 Report Based on 2013 Data. Half of respondents work in practices owned by hospitals/integrated delivery systems, down from 56% in SOHM 2012.
Although hospitalists in the South region continue to earn the most (median compensation $258,020, essentially static with the $258,793 figure reported in 2012), the region was the only one to report a decrease (see Table 1 for historical data). The largest percentage jump (11.8%) was for hospitalists in the West region ($249,894). Hospitalists in the Midwest saw a 10% increase ($261,868), while those in the East had both the smallest increase (4.8%) and the lowest median compensation ($238,676).
—R. Jeffrey Taylor, president and COO, IPC The Hospitalist Co., North Hollywood, Calif.
Part of the compensation increase is tied to upward pressure on productivity. Nationwide, median relative value units (RVUs) rose 3.3%, to 4,297 from 4,159. Median collection-to-work RVUs ticked up 6.8%, to 51.5 from 48.21 (see Table 2 for regional breakdowns). Production (10.5%) and performance (6.6%) are also slightly larger portions of mean compensation than they were in 2012, a figure many expect to increase further in future reports. The report also noted that academic/university hospitalists receive more in base pay, while hospitalists in private practice receive less.
Compensation and work volume will be intrinsically tied in the coming years, says R. Jeffrey Taylor, president and chief operating officer of IPC The Hospitalist Co., based in North Hollywood, Calif. And if pay outpaces productivity, “then it’s a bit concerning for the system at large,” he says.
“Particularly for whoever is subsidizing that shortfall, whether it’s a hospital employing doctors or an outsourced group employing the doctors but requiring a large subsidy from the hospital because the doctors are not seeing enough patient flow to pay their salary and benefits,” Taylor says.
More than 89% of HMGs rely on their host hospitals for financial support, according to the new data. The median support is $156,063 per full-time employee (FTE), which would total $1 million at just over seven FTEs. As healthcare reform progresses and hospitals’ budgets are increasingly burdened, Taylor says that pressure for hospitalists to generate enough revenue to cover their own salaries will grow. That sets up a likely showdown between hospitalists and their institutions; SOHM 2014 reported that just 6% of HMGs received enough income from professional fee revenue to cover expenses.
SOURCE: State of Hospital Medicine report, 2014
SOURCE: State of Hospital Medicine report, 2014
“Some productivity element in compensation plans, we believe, and I believe personally, is important,” Taylor says, later adding: “We already have a physician shortage and a shortage of people to see all these patients. It’s exacerbated by two things: lack of productivity and shift-model scheduling.”
To wit, IPC pays lower base salaries but provides bonuses tied to productivity and quality metrics. The average IPC hospitalist, Taylor says, earned more than $290,000 last year, nearly 15% above the median figure in the SOHM report. Between 30%-40% of that compensation, however, was earned via bonus tied to both “productivity and clinical achievement.”
Taylor, an outspoken advocate for moving away from the seven-on/seven-off scheduling model popular throughout hospital medicine, ties some of his doctors’ higher compensation to his firm’s preference for avoiding that schedule. But he’s not surprised the new report shows that 53.8% of responding HMGs use the model, up from 41.9% in 2012.
“It will be interesting to see what the data shows over the next three or four years,” he says, “if stipends, as we believe we are seeing, come under pressure and hospitals are doing more outsourcing.”
SOURCE: State of Hospital Medicine report, 2014
The PCP Link
Industry leaders use the information in the biennial reports to gauge where the specialty stands in the overall healthcare spectrum. Dea Robinson, MA, FACMPE, CPC, director of consulting for MGMA Health Care Consulting Group, says that the growth of hospital medicine (HM) compensation is tied to that of primary care physicians (PCPs).
“I don’t think we can look at hospitalists without looking at primary care, because it’s really an extension of primary care,” says Robinson, a member of SHM’s Practice Management Committee. “As primary care compensation increases, hospitalists’ compensation might increase as well. And with the focus on patient-centered medical homes, which is basically primary care centered, that might very well be part of the driver in the future of seeing hospitalists grow.”
While facing a well-known physician shortage, primary care’s compensation growth also lags behind HM. For example, median compensation for hospitalists rose 8%; it increased 5.5% for PCPs.
“When it comes to growth of the two individual industries, I think they are connected in some way,” she adds. “But in terms of the compensation, now we’re starting to see different codes that hospitalists are able to use but that primary care used to use exclusively. So, you really see more of an extension and a collaboration between true primary care and hospitalists.”
Bryan Weiss, MBA, FHM, managing director of the consulting services practice at Irving, Texas-based MedSynergies, agrees that hospitalists and PCPs are connected. He believes the higher compensation figures are a sign of how young HM is as a specialty. He fears compensation “is probably growing too fast.”
“This takes me back to the 1990s, with the private [physician practice management]-type model, where it just grew so fast that the bottom fell out,” says Weiss, a member of Team Hospitalist. “Not that I think the bottom is going to fall out of hospital medicine, but a lot of this is reminiscent of that, and I think there’s going to be a ceiling, or at least a slowing down.”
—Stuart Guterman, vice president, Medicare and cost control, The Commonwealth Fund
In contrast, one good sign for the specialty’s compensation and financial support is that “hospitals are still the hub of the healthcare system and need to be an important part of healthcare reform,” says Stuart Guterman, vice president for Medicare and cost control at The Commonwealth Fund, a New York foundation focused on improving healthcare delivery. Guterman says that while President Obama and congressional leaders are looking to cut the rate of growth in healthcare spending, the figure is already so high that there should still be plenty of resources in the system.
“If you took today’s spending and you increased it at the [GDP] growth rate for 10 years, I think we’re talking about something over $30 trillion over 10 years,” Guterman says. “And remember that we’re starting at a point that’s over 50% higher than any other country in the world. So, we’re talking about plenty of resources still in this healthcare system.”
With accountable care organizations, the specter of bundled payments, and penalties for readmitted patients, Guterman says that the pending issue for the specialty isn’t whether hospitalists—or other hospital-based practitioners—are going to get paid more or less, but rather what their compensation will be based on.
“Things like better coordination of care, sending the patients to the right place, having the patients in the right place, having them in the hospital if they need to be, or keeping them out of the hospital if they don’t need to be in the hospital,” he explains. “But the hospital is certainly a big part of that health system.”
In fact, physicians who play to the strengths of the new healthcare metrics—quality, value, lower-cost care—can probably earn as much compensation as, if not more than, they could in the traditional fee-for-service model hospitalists, Guterman says.
“The big point is to remind people that when we’re talking about controlling health spending growth, we’re still talking about a growing industry,” he notes. “We’re not talking about disenfranchising healthcare or providers. We’re talking about more reasonable growth and about, more than anything, paying for the right things. Folks ought to be able to do quite well if they do the right things.”
SOURCE: State of Hospital Medicine report, 2014
Multiple Uses
The SOHM report can be used as a measuring stick to compare against national and regional competitors and to provide data points for discussions with hospital administrators, says Team Hospitalist’s Weiss.
“This is vital in terms of recruiting physicians,” he says, “as well as negotiating with the hospital, as far as what the average investment is.”
Dr. Landis of SHM’s Practice Analysis Committee believes that having data points to make “resourcing decisions” with is particularly helpful, both in hiring and scheduling and in “right-sizing” hospital support for groups that are not self-sufficient.
“It is critical for physicians and their administrative partners to get the resourcing right, as inappropriately resourced groups [too much or too little] can quickly become unsustainable and/or unstable,” Dr. Landis says.
Take his group’s compensation.
“When we look at what we want to incent physicians, we’ll look at what other groups are doing,” Dr. Landis adds. “Are they using core measures? Are they using patient satisfaction? What about good citizenship? It’s one thing to say, ‘A hospital down the road is doing it.’ It’s another thing to take this book and say, ‘Let’s look the numbers up.’”
Of course, the wrinkle in benchmarking against national or regional figures is that HMGs can be “very particular,” says MGMA’s Robinson.
“We use benchmarks to give us an idea of what the pulse is, but we don’t use it as the only number,” she adds. “It’s very individualistic to the practice and to the program.”
Dr. Landis understands that point of view. Take his group’s policy on how much of hospitalists’ compensation is based on performance. The median component of compensation tied to performance for hospitalists nationwide is 6.6%, according to SOHM 2014. Dr. Landis’ group is at 15%. In meetings with his C-suite executives, he says he thinks in the back of his mind about how far outside the mean his group is in that regard. But he tempers that thought with the view that many hospitalists believe that performance and other metrics will continue to grow into a larger portion of hospitalists’ overall compensation.
“You have to be careful,” he says. “The first person to do an innovative, valuable thing isn’t going to be the 85%. You have to be careful not to stifle innovation. One of the cautions is not to use ‘just because everyone else is doing it means it’s the best way.’”
Weiss calls on an old adage in the industry: “If you’ve seen one hospitalist program, you’ve seen exactly one hospitalist program,” he says. “Because while they can be part of a large health system or a management company, while they try to have some commonality or some typical procedures, there’s still going to be individuality.”
Richard Quinn is a freelance writer in New Jersey.
The highlight of SHM’s biennial State of Hospital Medicine (SOHM) report is how much hospitalists earn. So it’s to be expected that rank-and-file practitioners and group leaders who read this year’s edition will first notice that median compensation for adult hospitalists rose 8% to $252,996 in 2013, according to data from the Medical Group Management Association (MGMA). The compensation data from MGMA is wrapped into the SOHM 2014 report this year.
But to stop there would be a wasted opportunity, says William “Tex” Landis, MD, FHM, medical director of Wellspan Hospitalists in York, Pa., and a member and former chair of SHM’s Practice Analysis Committee. Along with compensation, the report (available at www.hospitalmedicine.org/survey) delves into scheduling, productivity, staffing, how compensation is broken down, practice models, and dozens of other topics that hospital medicine group (HMG) leaders will find useful.
“Scope of services is a big one,” Dr. Landis adds. “What other things are hospital medicine groups around the country being held responsible for? Are we morphing into universal admitters? How involved in palliative care are we? What about transitions of care? How many hospital medicine groups are becoming involved in managing nursing home patients? What’s the relationship with surgical co-management? How much ICU work are we doing?”
Dr. Landis’ laundry list of unanswered questions might seem daunting, but that’s the point of the research SHM has been collecting and reporting for years. The society surveyed 499 groups, representing some 6,300 providers, to give the specialty’s most detailed list of most popular, if not best, practices.
“It has the usual limitations of any survey; however, it is the very best survey, quantity and quality, of hospital medicine groups,” Dr. Landis says. “And so it becomes the best source of information to make important decisions about resourcing and operating hospital medicine groups.”
Earnings Up
And, like it or not, compensation for providers typically is a HMG’s largest budget line. In that regard, the specialty appears to be doing well. Median compensation for adult hospitalists rose to a record high last year, according to the MGMA Physician Compensation and Production Survey: 2014 Report Based on 2013 Data. Half of respondents work in practices owned by hospitals/integrated delivery systems, down from 56% in SOHM 2012.
Although hospitalists in the South region continue to earn the most (median compensation $258,020, essentially static with the $258,793 figure reported in 2012), the region was the only one to report a decrease (see Table 1 for historical data). The largest percentage jump (11.8%) was for hospitalists in the West region ($249,894). Hospitalists in the Midwest saw a 10% increase ($261,868), while those in the East had both the smallest increase (4.8%) and the lowest median compensation ($238,676).
—R. Jeffrey Taylor, president and COO, IPC The Hospitalist Co., North Hollywood, Calif.
Part of the compensation increase is tied to upward pressure on productivity. Nationwide, median relative value units (RVUs) rose 3.3%, to 4,297 from 4,159. Median collection-to-work RVUs ticked up 6.8%, to 51.5 from 48.21 (see Table 2 for regional breakdowns). Production (10.5%) and performance (6.6%) are also slightly larger portions of mean compensation than they were in 2012, a figure many expect to increase further in future reports. The report also noted that academic/university hospitalists receive more in base pay, while hospitalists in private practice receive less.
Compensation and work volume will be intrinsically tied in the coming years, says R. Jeffrey Taylor, president and chief operating officer of IPC The Hospitalist Co., based in North Hollywood, Calif. And if pay outpaces productivity, “then it’s a bit concerning for the system at large,” he says.
“Particularly for whoever is subsidizing that shortfall, whether it’s a hospital employing doctors or an outsourced group employing the doctors but requiring a large subsidy from the hospital because the doctors are not seeing enough patient flow to pay their salary and benefits,” Taylor says.
More than 89% of HMGs rely on their host hospitals for financial support, according to the new data. The median support is $156,063 per full-time employee (FTE), which would total $1 million at just over seven FTEs. As healthcare reform progresses and hospitals’ budgets are increasingly burdened, Taylor says that pressure for hospitalists to generate enough revenue to cover their own salaries will grow. That sets up a likely showdown between hospitalists and their institutions; SOHM 2014 reported that just 6% of HMGs received enough income from professional fee revenue to cover expenses.
SOURCE: State of Hospital Medicine report, 2014
SOURCE: State of Hospital Medicine report, 2014
“Some productivity element in compensation plans, we believe, and I believe personally, is important,” Taylor says, later adding: “We already have a physician shortage and a shortage of people to see all these patients. It’s exacerbated by two things: lack of productivity and shift-model scheduling.”
To wit, IPC pays lower base salaries but provides bonuses tied to productivity and quality metrics. The average IPC hospitalist, Taylor says, earned more than $290,000 last year, nearly 15% above the median figure in the SOHM report. Between 30%-40% of that compensation, however, was earned via bonus tied to both “productivity and clinical achievement.”
Taylor, an outspoken advocate for moving away from the seven-on/seven-off scheduling model popular throughout hospital medicine, ties some of his doctors’ higher compensation to his firm’s preference for avoiding that schedule. But he’s not surprised the new report shows that 53.8% of responding HMGs use the model, up from 41.9% in 2012.
“It will be interesting to see what the data shows over the next three or four years,” he says, “if stipends, as we believe we are seeing, come under pressure and hospitals are doing more outsourcing.”
SOURCE: State of Hospital Medicine report, 2014
The PCP Link
Industry leaders use the information in the biennial reports to gauge where the specialty stands in the overall healthcare spectrum. Dea Robinson, MA, FACMPE, CPC, director of consulting for MGMA Health Care Consulting Group, says that the growth of hospital medicine (HM) compensation is tied to that of primary care physicians (PCPs).
“I don’t think we can look at hospitalists without looking at primary care, because it’s really an extension of primary care,” says Robinson, a member of SHM’s Practice Management Committee. “As primary care compensation increases, hospitalists’ compensation might increase as well. And with the focus on patient-centered medical homes, which is basically primary care centered, that might very well be part of the driver in the future of seeing hospitalists grow.”
While facing a well-known physician shortage, primary care’s compensation growth also lags behind HM. For example, median compensation for hospitalists rose 8%; it increased 5.5% for PCPs.
“When it comes to growth of the two individual industries, I think they are connected in some way,” she adds. “But in terms of the compensation, now we’re starting to see different codes that hospitalists are able to use but that primary care used to use exclusively. So, you really see more of an extension and a collaboration between true primary care and hospitalists.”
Bryan Weiss, MBA, FHM, managing director of the consulting services practice at Irving, Texas-based MedSynergies, agrees that hospitalists and PCPs are connected. He believes the higher compensation figures are a sign of how young HM is as a specialty. He fears compensation “is probably growing too fast.”
“This takes me back to the 1990s, with the private [physician practice management]-type model, where it just grew so fast that the bottom fell out,” says Weiss, a member of Team Hospitalist. “Not that I think the bottom is going to fall out of hospital medicine, but a lot of this is reminiscent of that, and I think there’s going to be a ceiling, or at least a slowing down.”
—Stuart Guterman, vice president, Medicare and cost control, The Commonwealth Fund
In contrast, one good sign for the specialty’s compensation and financial support is that “hospitals are still the hub of the healthcare system and need to be an important part of healthcare reform,” says Stuart Guterman, vice president for Medicare and cost control at The Commonwealth Fund, a New York foundation focused on improving healthcare delivery. Guterman says that while President Obama and congressional leaders are looking to cut the rate of growth in healthcare spending, the figure is already so high that there should still be plenty of resources in the system.
“If you took today’s spending and you increased it at the [GDP] growth rate for 10 years, I think we’re talking about something over $30 trillion over 10 years,” Guterman says. “And remember that we’re starting at a point that’s over 50% higher than any other country in the world. So, we’re talking about plenty of resources still in this healthcare system.”
With accountable care organizations, the specter of bundled payments, and penalties for readmitted patients, Guterman says that the pending issue for the specialty isn’t whether hospitalists—or other hospital-based practitioners—are going to get paid more or less, but rather what their compensation will be based on.
“Things like better coordination of care, sending the patients to the right place, having the patients in the right place, having them in the hospital if they need to be, or keeping them out of the hospital if they don’t need to be in the hospital,” he explains. “But the hospital is certainly a big part of that health system.”
In fact, physicians who play to the strengths of the new healthcare metrics—quality, value, lower-cost care—can probably earn as much compensation as, if not more than, they could in the traditional fee-for-service model hospitalists, Guterman says.
“The big point is to remind people that when we’re talking about controlling health spending growth, we’re still talking about a growing industry,” he notes. “We’re not talking about disenfranchising healthcare or providers. We’re talking about more reasonable growth and about, more than anything, paying for the right things. Folks ought to be able to do quite well if they do the right things.”
SOURCE: State of Hospital Medicine report, 2014
Multiple Uses
The SOHM report can be used as a measuring stick to compare against national and regional competitors and to provide data points for discussions with hospital administrators, says Team Hospitalist’s Weiss.
“This is vital in terms of recruiting physicians,” he says, “as well as negotiating with the hospital, as far as what the average investment is.”
Dr. Landis of SHM’s Practice Analysis Committee believes that having data points to make “resourcing decisions” with is particularly helpful, both in hiring and scheduling and in “right-sizing” hospital support for groups that are not self-sufficient.
“It is critical for physicians and their administrative partners to get the resourcing right, as inappropriately resourced groups [too much or too little] can quickly become unsustainable and/or unstable,” Dr. Landis says.
Take his group’s compensation.
“When we look at what we want to incent physicians, we’ll look at what other groups are doing,” Dr. Landis adds. “Are they using core measures? Are they using patient satisfaction? What about good citizenship? It’s one thing to say, ‘A hospital down the road is doing it.’ It’s another thing to take this book and say, ‘Let’s look the numbers up.’”
Of course, the wrinkle in benchmarking against national or regional figures is that HMGs can be “very particular,” says MGMA’s Robinson.
“We use benchmarks to give us an idea of what the pulse is, but we don’t use it as the only number,” she adds. “It’s very individualistic to the practice and to the program.”
Dr. Landis understands that point of view. Take his group’s policy on how much of hospitalists’ compensation is based on performance. The median component of compensation tied to performance for hospitalists nationwide is 6.6%, according to SOHM 2014. Dr. Landis’ group is at 15%. In meetings with his C-suite executives, he says he thinks in the back of his mind about how far outside the mean his group is in that regard. But he tempers that thought with the view that many hospitalists believe that performance and other metrics will continue to grow into a larger portion of hospitalists’ overall compensation.
“You have to be careful,” he says. “The first person to do an innovative, valuable thing isn’t going to be the 85%. You have to be careful not to stifle innovation. One of the cautions is not to use ‘just because everyone else is doing it means it’s the best way.’”
Weiss calls on an old adage in the industry: “If you’ve seen one hospitalist program, you’ve seen exactly one hospitalist program,” he says. “Because while they can be part of a large health system or a management company, while they try to have some commonality or some typical procedures, there’s still going to be individuality.”
Richard Quinn is a freelance writer in New Jersey.
Shorter Stay, Fewer Interventions With Initial Cholecystectomy for Choledocholithiasis
Clinical question
Which strategy — initial cholecystectomy or common duct endoscopic investigation followed by cholecystectomy — leads to better outcomes in the treatment of suspected common duct stones?
Bottom line
As compared with a strategy of sequential common duct endoscopy followed by surgery, the use of initial cholecystectomy with intraoperative cholangiogram for patients at intermediate risk of choledocholithiasis leads to shorter hospital length of stay and fewer interventions with otherwise comparable outcomes. (LOE = 1b)
Reference
Iranmanesh P, Frossard J, Mugnier-Konrad B, et al. Initial cholecystectomy vs. sequential common duct endoscopic assessment and subsequent cholecystectomy for suspected gallstone migration. JAMA 2014;312(2):137-144.
Study design
Randomized controlled trial (nonblinded)
Funding source
Unknown/not stated
Allocation
Concealed
Setting
Inpatient (any location) with outpatient follow-up
Synopsis
The role of common duct endoscopic investigation prior to cholecystectomy for patients at intermediate risk of choledocholithiasis is questionable as stones often migrate into the duodenum without such intervention. Using concealed allocation, investigators randomized 100 patients who presented to an emergency department with clinical suspicion of choledocholithiasis (right upper quadrant or epigastric abdominal pain with elevated liver function test results and ultrasound-confirmed gallstone) to 1 of 2 groups. The study group underwent primary cholecystectomy with intraoperative cholangiogram, while the classical treatment group first had common duct exploration with magnetic resonance cholangiopancreatography (MRCP), endoscopic ultrasound (EUS), and endoscopic retrograde cholangiopancreatography (ERCP), if needed, followed by cholecystectomy. The authors excluded patients with severe sepsis, pancreatitis, bilirubinemia greater than 4 mg/dL, or proven common duct stones on admission. The 2 groups had similar baseline characteristics, including similar preoperative health status scores. Overall, the number of confirmed common duct stones in each group was approximately 20%. Patients in the cholecystectomy-first group had a significantly shorter hospital length of stay than the classical treatment group (5 days vs 8 days; P < .001) and also had fewer common duct investigations (MRCP, EUS, or ERCP; 25 vs 71; P < .001). There were no significant differences detected between the 2 groups in quality-of-life assessments or in surgical or medical complications within 6 months.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question
Which strategy — initial cholecystectomy or common duct endoscopic investigation followed by cholecystectomy — leads to better outcomes in the treatment of suspected common duct stones?
Bottom line
As compared with a strategy of sequential common duct endoscopy followed by surgery, the use of initial cholecystectomy with intraoperative cholangiogram for patients at intermediate risk of choledocholithiasis leads to shorter hospital length of stay and fewer interventions with otherwise comparable outcomes. (LOE = 1b)
Reference
Iranmanesh P, Frossard J, Mugnier-Konrad B, et al. Initial cholecystectomy vs. sequential common duct endoscopic assessment and subsequent cholecystectomy for suspected gallstone migration. JAMA 2014;312(2):137-144.
Study design
Randomized controlled trial (nonblinded)
Funding source
Unknown/not stated
Allocation
Concealed
Setting
Inpatient (any location) with outpatient follow-up
Synopsis
The role of common duct endoscopic investigation prior to cholecystectomy for patients at intermediate risk of choledocholithiasis is questionable as stones often migrate into the duodenum without such intervention. Using concealed allocation, investigators randomized 100 patients who presented to an emergency department with clinical suspicion of choledocholithiasis (right upper quadrant or epigastric abdominal pain with elevated liver function test results and ultrasound-confirmed gallstone) to 1 of 2 groups. The study group underwent primary cholecystectomy with intraoperative cholangiogram, while the classical treatment group first had common duct exploration with magnetic resonance cholangiopancreatography (MRCP), endoscopic ultrasound (EUS), and endoscopic retrograde cholangiopancreatography (ERCP), if needed, followed by cholecystectomy. The authors excluded patients with severe sepsis, pancreatitis, bilirubinemia greater than 4 mg/dL, or proven common duct stones on admission. The 2 groups had similar baseline characteristics, including similar preoperative health status scores. Overall, the number of confirmed common duct stones in each group was approximately 20%. Patients in the cholecystectomy-first group had a significantly shorter hospital length of stay than the classical treatment group (5 days vs 8 days; P < .001) and also had fewer common duct investigations (MRCP, EUS, or ERCP; 25 vs 71; P < .001). There were no significant differences detected between the 2 groups in quality-of-life assessments or in surgical or medical complications within 6 months.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question
Which strategy — initial cholecystectomy or common duct endoscopic investigation followed by cholecystectomy — leads to better outcomes in the treatment of suspected common duct stones?
Bottom line
As compared with a strategy of sequential common duct endoscopy followed by surgery, the use of initial cholecystectomy with intraoperative cholangiogram for patients at intermediate risk of choledocholithiasis leads to shorter hospital length of stay and fewer interventions with otherwise comparable outcomes. (LOE = 1b)
Reference
Iranmanesh P, Frossard J, Mugnier-Konrad B, et al. Initial cholecystectomy vs. sequential common duct endoscopic assessment and subsequent cholecystectomy for suspected gallstone migration. JAMA 2014;312(2):137-144.
Study design
Randomized controlled trial (nonblinded)
Funding source
Unknown/not stated
Allocation
Concealed
Setting
Inpatient (any location) with outpatient follow-up
Synopsis
The role of common duct endoscopic investigation prior to cholecystectomy for patients at intermediate risk of choledocholithiasis is questionable as stones often migrate into the duodenum without such intervention. Using concealed allocation, investigators randomized 100 patients who presented to an emergency department with clinical suspicion of choledocholithiasis (right upper quadrant or epigastric abdominal pain with elevated liver function test results and ultrasound-confirmed gallstone) to 1 of 2 groups. The study group underwent primary cholecystectomy with intraoperative cholangiogram, while the classical treatment group first had common duct exploration with magnetic resonance cholangiopancreatography (MRCP), endoscopic ultrasound (EUS), and endoscopic retrograde cholangiopancreatography (ERCP), if needed, followed by cholecystectomy. The authors excluded patients with severe sepsis, pancreatitis, bilirubinemia greater than 4 mg/dL, or proven common duct stones on admission. The 2 groups had similar baseline characteristics, including similar preoperative health status scores. Overall, the number of confirmed common duct stones in each group was approximately 20%. Patients in the cholecystectomy-first group had a significantly shorter hospital length of stay than the classical treatment group (5 days vs 8 days; P < .001) and also had fewer common duct investigations (MRCP, EUS, or ERCP; 25 vs 71; P < .001). There were no significant differences detected between the 2 groups in quality-of-life assessments or in surgical or medical complications within 6 months.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
No Harm in Stopping Antibiotics After Cholecystectomy for Acute Cholecystitis
Clinical question
Does stopping antibiotic treatment after cholecystectomy for mild to moderate acute calculous cholecystitis affect outcomes?
Bottom line
Stopping antibiotic treatment after cholecystectomy for mild to moderate acute cholecystitis does not increase postoperative infection rates compared with a strategy of 5 days of postoperative antibiotics. (LOE = 1b)
Reference
Regimbeau JM, Fuks D, Pautrat K, et al, for the FRENCH Study Group. Effect of postoperative antibiotic administration on postoperative infection following cholecystectomy for acute calculous cholecystitis. JAMA 2014;312(2):145-154.
Study design
Randomized controlled trial (nonblinded)
Funding source
Government
Allocation
Concealed
Setting
Inpatient (any location) with outpatient follow-up
Synopsis
Using concealed allocation, these investigators randomized 414 adult patients who presented to an emergency department with mild or moderate acute calculous cholecystitis requiring cholecystectomy into 2 groups: (1) continue taking antibiotics or (2) stop taking antibiotics during the postoperative period. Those with severe cholecystitis, defined as concomitant dysfunction of other organ systems, were excluded, as were those with acute pancreatitis, cholangitis, biliary peritonitis, or cirrhosis. All study patients received amoxicillin plus clavulanic acid 3 times a day from admission to day of surgery. The treatment group continued the same antibiotic regimen for 5 days after surgery, while the nontreatment group received no further antibiotics. The 2 groups were well balanced, with a mean age of 56 years and mean duration of preoperative antibiotics of 2 days. Approximately half the patients in each group had mild cholecystitis. For the primary outcome of postoperative surgical site or distant site infections at 4 weeks, there was no significant difference detected between the 2 groups in either the intention-to-treat or per-protocol analyses (intention-to-treat: 17% for nontreatment vs 15% for antibiotic group; per-protocol: 13% for both groups). This held true when the outcomes were analyzed according to severity of cholecystitis or duration of preoperative antibiotic use.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question
Does stopping antibiotic treatment after cholecystectomy for mild to moderate acute calculous cholecystitis affect outcomes?
Bottom line
Stopping antibiotic treatment after cholecystectomy for mild to moderate acute cholecystitis does not increase postoperative infection rates compared with a strategy of 5 days of postoperative antibiotics. (LOE = 1b)
Reference
Regimbeau JM, Fuks D, Pautrat K, et al, for the FRENCH Study Group. Effect of postoperative antibiotic administration on postoperative infection following cholecystectomy for acute calculous cholecystitis. JAMA 2014;312(2):145-154.
Study design
Randomized controlled trial (nonblinded)
Funding source
Government
Allocation
Concealed
Setting
Inpatient (any location) with outpatient follow-up
Synopsis
Using concealed allocation, these investigators randomized 414 adult patients who presented to an emergency department with mild or moderate acute calculous cholecystitis requiring cholecystectomy into 2 groups: (1) continue taking antibiotics or (2) stop taking antibiotics during the postoperative period. Those with severe cholecystitis, defined as concomitant dysfunction of other organ systems, were excluded, as were those with acute pancreatitis, cholangitis, biliary peritonitis, or cirrhosis. All study patients received amoxicillin plus clavulanic acid 3 times a day from admission to day of surgery. The treatment group continued the same antibiotic regimen for 5 days after surgery, while the nontreatment group received no further antibiotics. The 2 groups were well balanced, with a mean age of 56 years and mean duration of preoperative antibiotics of 2 days. Approximately half the patients in each group had mild cholecystitis. For the primary outcome of postoperative surgical site or distant site infections at 4 weeks, there was no significant difference detected between the 2 groups in either the intention-to-treat or per-protocol analyses (intention-to-treat: 17% for nontreatment vs 15% for antibiotic group; per-protocol: 13% for both groups). This held true when the outcomes were analyzed according to severity of cholecystitis or duration of preoperative antibiotic use.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question
Does stopping antibiotic treatment after cholecystectomy for mild to moderate acute calculous cholecystitis affect outcomes?
Bottom line
Stopping antibiotic treatment after cholecystectomy for mild to moderate acute cholecystitis does not increase postoperative infection rates compared with a strategy of 5 days of postoperative antibiotics. (LOE = 1b)
Reference
Regimbeau JM, Fuks D, Pautrat K, et al, for the FRENCH Study Group. Effect of postoperative antibiotic administration on postoperative infection following cholecystectomy for acute calculous cholecystitis. JAMA 2014;312(2):145-154.
Study design
Randomized controlled trial (nonblinded)
Funding source
Government
Allocation
Concealed
Setting
Inpatient (any location) with outpatient follow-up
Synopsis
Using concealed allocation, these investigators randomized 414 adult patients who presented to an emergency department with mild or moderate acute calculous cholecystitis requiring cholecystectomy into 2 groups: (1) continue taking antibiotics or (2) stop taking antibiotics during the postoperative period. Those with severe cholecystitis, defined as concomitant dysfunction of other organ systems, were excluded, as were those with acute pancreatitis, cholangitis, biliary peritonitis, or cirrhosis. All study patients received amoxicillin plus clavulanic acid 3 times a day from admission to day of surgery. The treatment group continued the same antibiotic regimen for 5 days after surgery, while the nontreatment group received no further antibiotics. The 2 groups were well balanced, with a mean age of 56 years and mean duration of preoperative antibiotics of 2 days. Approximately half the patients in each group had mild cholecystitis. For the primary outcome of postoperative surgical site or distant site infections at 4 weeks, there was no significant difference detected between the 2 groups in either the intention-to-treat or per-protocol analyses (intention-to-treat: 17% for nontreatment vs 15% for antibiotic group; per-protocol: 13% for both groups). This held true when the outcomes were analyzed according to severity of cholecystitis or duration of preoperative antibiotic use.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Hospitalist Compensation Up 8% in Latest Survey
Annual median compensation for adult hospitalists in the U.S. rose 8% to a record high $252,996 in 2013, according to SHM's newly released 2014 State of Hospital Medicine (SOHM) report.
Hospitalists in the South region continue to earn the most, with a median compensation of $258,020—essentially static with $258,793 reported in 2012—according to data from the Medical Group Management Association Physician Compensation and Production Survey: 2014 Report Based on 2013 Data. The MGMA compensation and productivity data are wrapped into the biennial SOHM, whose 2014 edition debuted last week.
The largest compensation jump was for hospitalists in the West region, who logged an 11.8% gain in annual median compensation to $249,894 for 2013, up from $223,574 reported in 2012. Hospitalists in the Midwest saw a 10% increase, up to $261,868 from $237,987. Practitioners in the East had both the smallest increase, 4.8%, and the lowest median compensation, $238,676 in 2013, which is up slightly from $227,656. Part of the compensation push is tied to upward pressure on productivity. Nationwide, median relative value units (RVUs) ticked up 3.3% to 4,297 in 2013 from 4,159 in the 2012 report.
Median collection-to-work RVUs rose 6.8% to 51.5 from 48.21. Production (10.5%) and performance (6.6%) in 2013 were also slightly larger portions of mean compensation than in 2012, figures many industry experts expect will increase in the future. The 2014 SOHM report also notes that academic/university hospitalists typically receive more in base pay, while hospitalists in private practice receive less.
"It is the very best survey, quantity and quality, of hospital medicine [HM] groups," says William "Tex" Landis, MD, FHM, medical director of WellSpan Hospitalists in York, Pa., and a member and former chair of SHM's Practice Analysis Committee. "And so it becomes the best source of information to make important decisions about resourcing and operating hospital medicine groups."
Beyond analyzing hospitalists' median compensation, the SOHM report delves into scheduling, productivity, staffing, a breakdown of payment allocations, practice models, and dozens of other topics that HM group leaders find useful. In all, 499 groups representing some 6,300 providers were included in the survey. TH
SHM will also be hosting a free webinar Oct. 14 to discuss the specifics of the report.
Visit our website for more information about SHM's 2014 State of Hospital Medicine.
Annual median compensation for adult hospitalists in the U.S. rose 8% to a record high $252,996 in 2013, according to SHM's newly released 2014 State of Hospital Medicine (SOHM) report.
Hospitalists in the South region continue to earn the most, with a median compensation of $258,020—essentially static with $258,793 reported in 2012—according to data from the Medical Group Management Association Physician Compensation and Production Survey: 2014 Report Based on 2013 Data. The MGMA compensation and productivity data are wrapped into the biennial SOHM, whose 2014 edition debuted last week.
The largest compensation jump was for hospitalists in the West region, who logged an 11.8% gain in annual median compensation to $249,894 for 2013, up from $223,574 reported in 2012. Hospitalists in the Midwest saw a 10% increase, up to $261,868 from $237,987. Practitioners in the East had both the smallest increase, 4.8%, and the lowest median compensation, $238,676 in 2013, which is up slightly from $227,656. Part of the compensation push is tied to upward pressure on productivity. Nationwide, median relative value units (RVUs) ticked up 3.3% to 4,297 in 2013 from 4,159 in the 2012 report.
Median collection-to-work RVUs rose 6.8% to 51.5 from 48.21. Production (10.5%) and performance (6.6%) in 2013 were also slightly larger portions of mean compensation than in 2012, figures many industry experts expect will increase in the future. The 2014 SOHM report also notes that academic/university hospitalists typically receive more in base pay, while hospitalists in private practice receive less.
"It is the very best survey, quantity and quality, of hospital medicine [HM] groups," says William "Tex" Landis, MD, FHM, medical director of WellSpan Hospitalists in York, Pa., and a member and former chair of SHM's Practice Analysis Committee. "And so it becomes the best source of information to make important decisions about resourcing and operating hospital medicine groups."
Beyond analyzing hospitalists' median compensation, the SOHM report delves into scheduling, productivity, staffing, a breakdown of payment allocations, practice models, and dozens of other topics that HM group leaders find useful. In all, 499 groups representing some 6,300 providers were included in the survey. TH
SHM will also be hosting a free webinar Oct. 14 to discuss the specifics of the report.
Visit our website for more information about SHM's 2014 State of Hospital Medicine.
Annual median compensation for adult hospitalists in the U.S. rose 8% to a record high $252,996 in 2013, according to SHM's newly released 2014 State of Hospital Medicine (SOHM) report.
Hospitalists in the South region continue to earn the most, with a median compensation of $258,020—essentially static with $258,793 reported in 2012—according to data from the Medical Group Management Association Physician Compensation and Production Survey: 2014 Report Based on 2013 Data. The MGMA compensation and productivity data are wrapped into the biennial SOHM, whose 2014 edition debuted last week.
The largest compensation jump was for hospitalists in the West region, who logged an 11.8% gain in annual median compensation to $249,894 for 2013, up from $223,574 reported in 2012. Hospitalists in the Midwest saw a 10% increase, up to $261,868 from $237,987. Practitioners in the East had both the smallest increase, 4.8%, and the lowest median compensation, $238,676 in 2013, which is up slightly from $227,656. Part of the compensation push is tied to upward pressure on productivity. Nationwide, median relative value units (RVUs) ticked up 3.3% to 4,297 in 2013 from 4,159 in the 2012 report.
Median collection-to-work RVUs rose 6.8% to 51.5 from 48.21. Production (10.5%) and performance (6.6%) in 2013 were also slightly larger portions of mean compensation than in 2012, figures many industry experts expect will increase in the future. The 2014 SOHM report also notes that academic/university hospitalists typically receive more in base pay, while hospitalists in private practice receive less.
"It is the very best survey, quantity and quality, of hospital medicine [HM] groups," says William "Tex" Landis, MD, FHM, medical director of WellSpan Hospitalists in York, Pa., and a member and former chair of SHM's Practice Analysis Committee. "And so it becomes the best source of information to make important decisions about resourcing and operating hospital medicine groups."
Beyond analyzing hospitalists' median compensation, the SOHM report delves into scheduling, productivity, staffing, a breakdown of payment allocations, practice models, and dozens of other topics that HM group leaders find useful. In all, 499 groups representing some 6,300 providers were included in the survey. TH
SHM will also be hosting a free webinar Oct. 14 to discuss the specifics of the report.
Visit our website for more information about SHM's 2014 State of Hospital Medicine.
Improved Diet Is Recipe for Improved Inpatient Outcomes
How well is your patient eating?
How often you ask this question could improve your hospital's readmission and length-of-stay rates, says Melissa Parkhurst, MD, FHM, medical director of hospital medicine and nutrition support at the University of Kansas Hospital in Kansas City.
A recent report from the Alliance to Advance Patient Nutrition [PDF]—a partnership of four organizations, including SHM, organized to improve nutrition screening and intervention among hospitalized patients—notes that about one in three patients admitted to a hospital meets the criteria for being malnourished. If left untreated, two-thirds of these patients will become more malnourished in the hospital.
"Often patients aren't eating because of testing or because their appetites are depressed because they're ill and not feeling well," says Dr. Parkhurst, an Alliance representative. "Sometimes their medications can alter their tastes, make them nauseated, or give them diarrhea."
Released last month, the findings are included in the partnership's first progress report. It describes the group's efforts in raising awareness about hospital nutrition, such as through info booths at medical meetings and via an online resource center on SHM's Center for Hospital Innovation & Improvement website.
Dr. Parkhurst points to studies that show inpatient malnutrition can lead to higher costs and more complications, as well as make patients more prone to surgical site infections, pressure ulcers, and falls.
"Malnourished patients are more apt to come back to the hospitals and to come in with complications," she says. "That is something we all should be concerned about as clinicians and at the hospital-administration level as well."
Here are Dr. Parkhurst's tips for improving nutrition among your patients:
- Ensure that every patient is getting a nutritional assessment upon admission and that staff is available to follow up with the results;
- Incorporate nutrition into the daily scope of patient care, for example, regularly ask staff whether your patients are eating or not;
- Include information about nutrition in the discharge plan and educate the patient’s family about nutritional interventions; and
- Work with hospital leadership to see how policies and procedures compare with the patient-care models put forth by the Alliance and note areas for improvement.
TH
Visit our website for more information about the importance of inpatient nutrition.
How well is your patient eating?
How often you ask this question could improve your hospital's readmission and length-of-stay rates, says Melissa Parkhurst, MD, FHM, medical director of hospital medicine and nutrition support at the University of Kansas Hospital in Kansas City.
A recent report from the Alliance to Advance Patient Nutrition [PDF]—a partnership of four organizations, including SHM, organized to improve nutrition screening and intervention among hospitalized patients—notes that about one in three patients admitted to a hospital meets the criteria for being malnourished. If left untreated, two-thirds of these patients will become more malnourished in the hospital.
"Often patients aren't eating because of testing or because their appetites are depressed because they're ill and not feeling well," says Dr. Parkhurst, an Alliance representative. "Sometimes their medications can alter their tastes, make them nauseated, or give them diarrhea."
Released last month, the findings are included in the partnership's first progress report. It describes the group's efforts in raising awareness about hospital nutrition, such as through info booths at medical meetings and via an online resource center on SHM's Center for Hospital Innovation & Improvement website.
Dr. Parkhurst points to studies that show inpatient malnutrition can lead to higher costs and more complications, as well as make patients more prone to surgical site infections, pressure ulcers, and falls.
"Malnourished patients are more apt to come back to the hospitals and to come in with complications," she says. "That is something we all should be concerned about as clinicians and at the hospital-administration level as well."
Here are Dr. Parkhurst's tips for improving nutrition among your patients:
- Ensure that every patient is getting a nutritional assessment upon admission and that staff is available to follow up with the results;
- Incorporate nutrition into the daily scope of patient care, for example, regularly ask staff whether your patients are eating or not;
- Include information about nutrition in the discharge plan and educate the patient’s family about nutritional interventions; and
- Work with hospital leadership to see how policies and procedures compare with the patient-care models put forth by the Alliance and note areas for improvement.
TH
Visit our website for more information about the importance of inpatient nutrition.
How well is your patient eating?
How often you ask this question could improve your hospital's readmission and length-of-stay rates, says Melissa Parkhurst, MD, FHM, medical director of hospital medicine and nutrition support at the University of Kansas Hospital in Kansas City.
A recent report from the Alliance to Advance Patient Nutrition [PDF]—a partnership of four organizations, including SHM, organized to improve nutrition screening and intervention among hospitalized patients—notes that about one in three patients admitted to a hospital meets the criteria for being malnourished. If left untreated, two-thirds of these patients will become more malnourished in the hospital.
"Often patients aren't eating because of testing or because their appetites are depressed because they're ill and not feeling well," says Dr. Parkhurst, an Alliance representative. "Sometimes their medications can alter their tastes, make them nauseated, or give them diarrhea."
Released last month, the findings are included in the partnership's first progress report. It describes the group's efforts in raising awareness about hospital nutrition, such as through info booths at medical meetings and via an online resource center on SHM's Center for Hospital Innovation & Improvement website.
Dr. Parkhurst points to studies that show inpatient malnutrition can lead to higher costs and more complications, as well as make patients more prone to surgical site infections, pressure ulcers, and falls.
"Malnourished patients are more apt to come back to the hospitals and to come in with complications," she says. "That is something we all should be concerned about as clinicians and at the hospital-administration level as well."
Here are Dr. Parkhurst's tips for improving nutrition among your patients:
- Ensure that every patient is getting a nutritional assessment upon admission and that staff is available to follow up with the results;
- Incorporate nutrition into the daily scope of patient care, for example, regularly ask staff whether your patients are eating or not;
- Include information about nutrition in the discharge plan and educate the patient’s family about nutritional interventions; and
- Work with hospital leadership to see how policies and procedures compare with the patient-care models put forth by the Alliance and note areas for improvement.
TH
Visit our website for more information about the importance of inpatient nutrition.
LISTEN NOW: Greg Maynard, MD, SFHM, Chats about SHM's Mentored Implementation Programs
Click here to listen to excerpts of our interview with Dr. Maynard
Click here to listen to excerpts of our interview with Dr. Maynard
Click here to listen to excerpts of our interview with Dr. Maynard