User login
The Hospitalist only
Town & Gown
Centers of academia and learning have been physically located within urban communities since the time of the ancient Greeks. During the Middle Ages, church-supported universities were established in Italian cities, in Paris, and in Britain at Oxford. Typically, the university community resided in a sequestered segment of the city. As a result of financial endowment and protection granted by the Church, they were largely independent of civil laws and regulations.
In the Middle Ages, students and teachers wore gowns over their attire for warmth in the drafty libraries as well as to identify themselves as scholars; hence the distinction of “town,” a term referring to the townspeople, from “gown,” the people associated with the university.1 For a host of reasons, the traditional relationship between the local community and associated centers of academia has been one of suspicion and hostility.
Establishing Alliances
Over the years, better communication and cooperation between the academic communities and their host cities has eased some of these tensions and—in some cases—has resulted in positive and cordial relationships. Some academic institutions endeavor to contribute to the general community by providing access to evening study events and lectures and by inviting the community to participate in fine arts performances.
These overtures are welcome, but it is important to recognize the potential for universities to exert a dominating influence within a community. The impact of a university on the local community can vary, depending on the size and reputation of the university as well as the size of the town. A large, powerful university has a more profound influence when it is located in a moderate-size city (one with a population less than 250,000) than if it is located in a major metropolitan community. In this situation, the onus is upon the university to recognize its position with respect to the local community and its obligation to contribute to the general societal good.
Most universities recognize the value of establishing strong alliances and trusting relationships with their host communities. Located in Gainesville, Fla., a city with a population of 186,000, the University of Florida is a large university with a major medical school and a 576-bed teaching hospital. In response to community concerns about neighborhood issues, the university’s president appointed a University of Florida Town/Gown Task Force to identify problems and make recommendations to initiate change.2 The task force members included individuals representing the student body, the university faculty, and various representatives of the local community.
Other universities also recognize the importance of working together for the common good. Situated in a town of 13,000, South Carolina’s Clemson University, which has 17,100 students, developed a town-and-gown symposium in 2006 called Community Is a Contact Sport: Universities and Cities Reaching Common Ground. Designed to address neighborhood issues, it also provided a forum for concerns, as well as an opportunity for conflict resolution (www.clemson.edu/town-gown).
From Concern to Conflict
The conflict escalates on multiple levels when town-and-gown issues are set in the context of academic versus private practice medicine. University physicians and community doctors compete for the same patient population. Primary care physicians across the country have complained that when they refer their patients to academic teaching hospitals for specialized care, the patients are absorbed by the university hospitals. They complain that they are not afforded the courtesy of a follow-up letter, nor does the patient return to their care when the acute event is resolved.3 Private practice physicians and community-based hospitals provide important services and are necessary within any community. When the local, private medical community becomes concerned that a university-based medical center seeks to usurp their patients and their livelihood, a heated conflict may ensue.
University-based, research-oriented academic medical centers, with training programs involved in cutting edge technology and highly specialized patient care services, are clearly a positive adjunct to any local community’s—or state’s, for that matter—capability to provide top-notch patient care and services. No one can deny the benefits afforded by this level of expertise. Problems arise when university-based medical centers set a powerful and lustful gaze upon the medical community at large.
During the 1990s, large medical centers across the country bought up community hospitals and medical practices. At that time, and continuing into the present, office overhead—building costs, liability insurance, personnel costs—for private practice groups has often exceeded the ability of these primary care groups to survive. Not unexpectedly, once incorporated into the system, these practices are used to support the subspecialty services at the university medical center, bypassing the community-based subspecialty physicians.
Additionally, large, academic medical centers set up funded and university-supported subspecialty groups that compete head-on with independent practitioners. Private practitioners view these circumstances as stacked competition. The primary-care doctor’s decision in selecting a subspecialty doctor for a patient is no longer based on service, timeliness, and competence, but is instead a result of proscribed referral patterns delineated by the academic institution. Discriminatory referral patterns—not based on merit—result in local discontent, frustration, and unhealthy competition.
Short-Term Savings, Long-Term Loss
These issues are complex. A case can always be made to consolidate resources at the university hospital and avoid duplication of services by stripping away departments in the community hospitals. If pursued to its logical end, this operational model effectively starves community hospitals until they evolve into low acuity, “feeder” stations for the main academic hospital facility. On paper, this plan presents economic advantages. In practice, it not only deprives the metropolitan area of community-based hospital options, but it also results in a dwindling population base and the general decline and disenchantment of the local medical community. As the medical community contracts, so does the patient-base referral radius.
University-owned community hospitals are subject to the discretion of the university medical center. Decision making is attributed to maximum utilization of resources and certification of need, but most observers see the basic principle as economic: ways of garnering a larger portion of the healthcare dollar in the university coffers. Services and even departments provided by community hospitals are likewise subject to the benevolence of the university medical system. Hospitals function like living organisms: If a department such as pediatrics is withdrawn, the hospital continues—but with a limp. Few children can be seen and evaluated in the emergency department; likewise, high-risk obstetrics must be transferred to a major university hospital because the patient may need a neonatal intensive care unit. Hospitalists and internists who happen to be double boarded in medicine and pediatrics steer away from hospitals without a pediatric department. The changes are subtle but, over time, the effects of the loss are apparent.
Hospitalists need to be cognizant of these issues when pursuing employment opportunities. Many career-minded hospitalists seek employment in community-based, full-service hospitals with university medical center affiliations. This combination can provide the best of both worlds: autonomy, opportunities for growth and development, and opportunities for working with house staff and teaching. Checking the status of the relationship between the community hospital and the affiliated university medical center may be an important factor in pre-contract negotiations and decision-making for career hospitalists.
The Bottom Line
The turf battle between community medicine and academic medicine is primarily one of economics. Interesting parallels may be drawn between this conflict and the teachings of Adam Smith. Prior to Smith, economic theory was based on the idea that every dollar you have is one less dollar for me. Smith proposed an entirely different concept: If I help you earn dollars, the economic house will grow, and I, too, will make more dollars, and then you will make more dollars. In this way, the entire system generates more than anyone could have previously imagined. This economic concept extrapolates well to the present discussion of the university medical center versus community medicine.
University health systems do not seem to realize that real growth happens when communities grow together. A robust and vibrant community hospital supports a university medical center with more vigor than an anemic, waning, and disenchanted community hospital that perceives its woes as a result of the powerful—and perhaps dogmatic—university health system. There are enough patients to grow both systems together—the patient base radius grows wider with cooperation and growth—but this cannot happen if the university engenders distrust among local practitioners and the local community. This is a situation that will either be win-win or lose-lose.
Although the crux of the conflict is economic, other aspects of town-and-gown medicine can contribute to better cooperation and understanding. Some academic medical centers have explored ways to incorporate local physicians in university-based clinical trials. These programs offer cutting edge medicine and an opportunity to participate in intellectually stimulating work; at the same time, physicians retain their private practices.
This research opportunity is being offered and supported by a number of academic institutions, including Columbia-Presbyterian in New York City, Duke in Durham, N.C., Partners HealthCare in Boston, the University of Pittsburgh, the University of Rochester (N.Y.), and Washington University (St. Louis, Mo.).4 This is a good-faith start in mending the relationship between the academic and private medical sectors. To achieve a lasting positive relationship, community physicians must trust the academic community to respect their autonomy and to recognize that they have the right to provide full-service care to their patients and to serve their patients without the fear of being unfairly disenfranchised.
The lack of integration of the academic medical community and private practitioners of medicine—the proverbial town and gown—is an old dilemma. It is time to lay it to rest. The solutions are straightforward. Empowering community hospitals and physicians will not diminish the influence of university-based hospitals, nor will there be loss of reimbursement. Just the opposite will occur. In the end, with cooperation, everyone wins; with adversarial actions, all parties lose, especially the patients. TH
Dr. Brezina is a member of the consulting clinical faculty at Duke University, Durham, N.C.
References
- Town and gown in the Middle Ages. Available at: http://en.wikipedia.org/wiki/Town_and_gown. Last accessed March 29, 2007.
- University of Florida Web site. Town/gown task force. Available at: www.facilities.ufl.edu/cp/towngown.htm. Last accessed March 29, 2007.
- Adams D, Croasdale M. Town and gown: turning rivalries into relationships [American Medical News Web site]. January 13, 2003. Available at: www.ama-assn.org/amednews/2003/01/13/prsa0113.htm. Last accessed March 20, 2007.
- Maguire P. Marriage of town and gown brings clinical research to busy practices [ACP-ASIM Observer Web site]. February 2001. Available at: www.acponline.org/journals/news/feb01/clinresearch.htm. Last accessed March 20, 2007.
Centers of academia and learning have been physically located within urban communities since the time of the ancient Greeks. During the Middle Ages, church-supported universities were established in Italian cities, in Paris, and in Britain at Oxford. Typically, the university community resided in a sequestered segment of the city. As a result of financial endowment and protection granted by the Church, they were largely independent of civil laws and regulations.
In the Middle Ages, students and teachers wore gowns over their attire for warmth in the drafty libraries as well as to identify themselves as scholars; hence the distinction of “town,” a term referring to the townspeople, from “gown,” the people associated with the university.1 For a host of reasons, the traditional relationship between the local community and associated centers of academia has been one of suspicion and hostility.
Establishing Alliances
Over the years, better communication and cooperation between the academic communities and their host cities has eased some of these tensions and—in some cases—has resulted in positive and cordial relationships. Some academic institutions endeavor to contribute to the general community by providing access to evening study events and lectures and by inviting the community to participate in fine arts performances.
These overtures are welcome, but it is important to recognize the potential for universities to exert a dominating influence within a community. The impact of a university on the local community can vary, depending on the size and reputation of the university as well as the size of the town. A large, powerful university has a more profound influence when it is located in a moderate-size city (one with a population less than 250,000) than if it is located in a major metropolitan community. In this situation, the onus is upon the university to recognize its position with respect to the local community and its obligation to contribute to the general societal good.
Most universities recognize the value of establishing strong alliances and trusting relationships with their host communities. Located in Gainesville, Fla., a city with a population of 186,000, the University of Florida is a large university with a major medical school and a 576-bed teaching hospital. In response to community concerns about neighborhood issues, the university’s president appointed a University of Florida Town/Gown Task Force to identify problems and make recommendations to initiate change.2 The task force members included individuals representing the student body, the university faculty, and various representatives of the local community.
Other universities also recognize the importance of working together for the common good. Situated in a town of 13,000, South Carolina’s Clemson University, which has 17,100 students, developed a town-and-gown symposium in 2006 called Community Is a Contact Sport: Universities and Cities Reaching Common Ground. Designed to address neighborhood issues, it also provided a forum for concerns, as well as an opportunity for conflict resolution (www.clemson.edu/town-gown).
From Concern to Conflict
The conflict escalates on multiple levels when town-and-gown issues are set in the context of academic versus private practice medicine. University physicians and community doctors compete for the same patient population. Primary care physicians across the country have complained that when they refer their patients to academic teaching hospitals for specialized care, the patients are absorbed by the university hospitals. They complain that they are not afforded the courtesy of a follow-up letter, nor does the patient return to their care when the acute event is resolved.3 Private practice physicians and community-based hospitals provide important services and are necessary within any community. When the local, private medical community becomes concerned that a university-based medical center seeks to usurp their patients and their livelihood, a heated conflict may ensue.
University-based, research-oriented academic medical centers, with training programs involved in cutting edge technology and highly specialized patient care services, are clearly a positive adjunct to any local community’s—or state’s, for that matter—capability to provide top-notch patient care and services. No one can deny the benefits afforded by this level of expertise. Problems arise when university-based medical centers set a powerful and lustful gaze upon the medical community at large.
During the 1990s, large medical centers across the country bought up community hospitals and medical practices. At that time, and continuing into the present, office overhead—building costs, liability insurance, personnel costs—for private practice groups has often exceeded the ability of these primary care groups to survive. Not unexpectedly, once incorporated into the system, these practices are used to support the subspecialty services at the university medical center, bypassing the community-based subspecialty physicians.
Additionally, large, academic medical centers set up funded and university-supported subspecialty groups that compete head-on with independent practitioners. Private practitioners view these circumstances as stacked competition. The primary-care doctor’s decision in selecting a subspecialty doctor for a patient is no longer based on service, timeliness, and competence, but is instead a result of proscribed referral patterns delineated by the academic institution. Discriminatory referral patterns—not based on merit—result in local discontent, frustration, and unhealthy competition.
Short-Term Savings, Long-Term Loss
These issues are complex. A case can always be made to consolidate resources at the university hospital and avoid duplication of services by stripping away departments in the community hospitals. If pursued to its logical end, this operational model effectively starves community hospitals until they evolve into low acuity, “feeder” stations for the main academic hospital facility. On paper, this plan presents economic advantages. In practice, it not only deprives the metropolitan area of community-based hospital options, but it also results in a dwindling population base and the general decline and disenchantment of the local medical community. As the medical community contracts, so does the patient-base referral radius.
University-owned community hospitals are subject to the discretion of the university medical center. Decision making is attributed to maximum utilization of resources and certification of need, but most observers see the basic principle as economic: ways of garnering a larger portion of the healthcare dollar in the university coffers. Services and even departments provided by community hospitals are likewise subject to the benevolence of the university medical system. Hospitals function like living organisms: If a department such as pediatrics is withdrawn, the hospital continues—but with a limp. Few children can be seen and evaluated in the emergency department; likewise, high-risk obstetrics must be transferred to a major university hospital because the patient may need a neonatal intensive care unit. Hospitalists and internists who happen to be double boarded in medicine and pediatrics steer away from hospitals without a pediatric department. The changes are subtle but, over time, the effects of the loss are apparent.
Hospitalists need to be cognizant of these issues when pursuing employment opportunities. Many career-minded hospitalists seek employment in community-based, full-service hospitals with university medical center affiliations. This combination can provide the best of both worlds: autonomy, opportunities for growth and development, and opportunities for working with house staff and teaching. Checking the status of the relationship between the community hospital and the affiliated university medical center may be an important factor in pre-contract negotiations and decision-making for career hospitalists.
The Bottom Line
The turf battle between community medicine and academic medicine is primarily one of economics. Interesting parallels may be drawn between this conflict and the teachings of Adam Smith. Prior to Smith, economic theory was based on the idea that every dollar you have is one less dollar for me. Smith proposed an entirely different concept: If I help you earn dollars, the economic house will grow, and I, too, will make more dollars, and then you will make more dollars. In this way, the entire system generates more than anyone could have previously imagined. This economic concept extrapolates well to the present discussion of the university medical center versus community medicine.
University health systems do not seem to realize that real growth happens when communities grow together. A robust and vibrant community hospital supports a university medical center with more vigor than an anemic, waning, and disenchanted community hospital that perceives its woes as a result of the powerful—and perhaps dogmatic—university health system. There are enough patients to grow both systems together—the patient base radius grows wider with cooperation and growth—but this cannot happen if the university engenders distrust among local practitioners and the local community. This is a situation that will either be win-win or lose-lose.
Although the crux of the conflict is economic, other aspects of town-and-gown medicine can contribute to better cooperation and understanding. Some academic medical centers have explored ways to incorporate local physicians in university-based clinical trials. These programs offer cutting edge medicine and an opportunity to participate in intellectually stimulating work; at the same time, physicians retain their private practices.
This research opportunity is being offered and supported by a number of academic institutions, including Columbia-Presbyterian in New York City, Duke in Durham, N.C., Partners HealthCare in Boston, the University of Pittsburgh, the University of Rochester (N.Y.), and Washington University (St. Louis, Mo.).4 This is a good-faith start in mending the relationship between the academic and private medical sectors. To achieve a lasting positive relationship, community physicians must trust the academic community to respect their autonomy and to recognize that they have the right to provide full-service care to their patients and to serve their patients without the fear of being unfairly disenfranchised.
The lack of integration of the academic medical community and private practitioners of medicine—the proverbial town and gown—is an old dilemma. It is time to lay it to rest. The solutions are straightforward. Empowering community hospitals and physicians will not diminish the influence of university-based hospitals, nor will there be loss of reimbursement. Just the opposite will occur. In the end, with cooperation, everyone wins; with adversarial actions, all parties lose, especially the patients. TH
Dr. Brezina is a member of the consulting clinical faculty at Duke University, Durham, N.C.
References
- Town and gown in the Middle Ages. Available at: http://en.wikipedia.org/wiki/Town_and_gown. Last accessed March 29, 2007.
- University of Florida Web site. Town/gown task force. Available at: www.facilities.ufl.edu/cp/towngown.htm. Last accessed March 29, 2007.
- Adams D, Croasdale M. Town and gown: turning rivalries into relationships [American Medical News Web site]. January 13, 2003. Available at: www.ama-assn.org/amednews/2003/01/13/prsa0113.htm. Last accessed March 20, 2007.
- Maguire P. Marriage of town and gown brings clinical research to busy practices [ACP-ASIM Observer Web site]. February 2001. Available at: www.acponline.org/journals/news/feb01/clinresearch.htm. Last accessed March 20, 2007.
Centers of academia and learning have been physically located within urban communities since the time of the ancient Greeks. During the Middle Ages, church-supported universities were established in Italian cities, in Paris, and in Britain at Oxford. Typically, the university community resided in a sequestered segment of the city. As a result of financial endowment and protection granted by the Church, they were largely independent of civil laws and regulations.
In the Middle Ages, students and teachers wore gowns over their attire for warmth in the drafty libraries as well as to identify themselves as scholars; hence the distinction of “town,” a term referring to the townspeople, from “gown,” the people associated with the university.1 For a host of reasons, the traditional relationship between the local community and associated centers of academia has been one of suspicion and hostility.
Establishing Alliances
Over the years, better communication and cooperation between the academic communities and their host cities has eased some of these tensions and—in some cases—has resulted in positive and cordial relationships. Some academic institutions endeavor to contribute to the general community by providing access to evening study events and lectures and by inviting the community to participate in fine arts performances.
These overtures are welcome, but it is important to recognize the potential for universities to exert a dominating influence within a community. The impact of a university on the local community can vary, depending on the size and reputation of the university as well as the size of the town. A large, powerful university has a more profound influence when it is located in a moderate-size city (one with a population less than 250,000) than if it is located in a major metropolitan community. In this situation, the onus is upon the university to recognize its position with respect to the local community and its obligation to contribute to the general societal good.
Most universities recognize the value of establishing strong alliances and trusting relationships with their host communities. Located in Gainesville, Fla., a city with a population of 186,000, the University of Florida is a large university with a major medical school and a 576-bed teaching hospital. In response to community concerns about neighborhood issues, the university’s president appointed a University of Florida Town/Gown Task Force to identify problems and make recommendations to initiate change.2 The task force members included individuals representing the student body, the university faculty, and various representatives of the local community.
Other universities also recognize the importance of working together for the common good. Situated in a town of 13,000, South Carolina’s Clemson University, which has 17,100 students, developed a town-and-gown symposium in 2006 called Community Is a Contact Sport: Universities and Cities Reaching Common Ground. Designed to address neighborhood issues, it also provided a forum for concerns, as well as an opportunity for conflict resolution (www.clemson.edu/town-gown).
From Concern to Conflict
The conflict escalates on multiple levels when town-and-gown issues are set in the context of academic versus private practice medicine. University physicians and community doctors compete for the same patient population. Primary care physicians across the country have complained that when they refer their patients to academic teaching hospitals for specialized care, the patients are absorbed by the university hospitals. They complain that they are not afforded the courtesy of a follow-up letter, nor does the patient return to their care when the acute event is resolved.3 Private practice physicians and community-based hospitals provide important services and are necessary within any community. When the local, private medical community becomes concerned that a university-based medical center seeks to usurp their patients and their livelihood, a heated conflict may ensue.
University-based, research-oriented academic medical centers, with training programs involved in cutting edge technology and highly specialized patient care services, are clearly a positive adjunct to any local community’s—or state’s, for that matter—capability to provide top-notch patient care and services. No one can deny the benefits afforded by this level of expertise. Problems arise when university-based medical centers set a powerful and lustful gaze upon the medical community at large.
During the 1990s, large medical centers across the country bought up community hospitals and medical practices. At that time, and continuing into the present, office overhead—building costs, liability insurance, personnel costs—for private practice groups has often exceeded the ability of these primary care groups to survive. Not unexpectedly, once incorporated into the system, these practices are used to support the subspecialty services at the university medical center, bypassing the community-based subspecialty physicians.
Additionally, large, academic medical centers set up funded and university-supported subspecialty groups that compete head-on with independent practitioners. Private practitioners view these circumstances as stacked competition. The primary-care doctor’s decision in selecting a subspecialty doctor for a patient is no longer based on service, timeliness, and competence, but is instead a result of proscribed referral patterns delineated by the academic institution. Discriminatory referral patterns—not based on merit—result in local discontent, frustration, and unhealthy competition.
Short-Term Savings, Long-Term Loss
These issues are complex. A case can always be made to consolidate resources at the university hospital and avoid duplication of services by stripping away departments in the community hospitals. If pursued to its logical end, this operational model effectively starves community hospitals until they evolve into low acuity, “feeder” stations for the main academic hospital facility. On paper, this plan presents economic advantages. In practice, it not only deprives the metropolitan area of community-based hospital options, but it also results in a dwindling population base and the general decline and disenchantment of the local medical community. As the medical community contracts, so does the patient-base referral radius.
University-owned community hospitals are subject to the discretion of the university medical center. Decision making is attributed to maximum utilization of resources and certification of need, but most observers see the basic principle as economic: ways of garnering a larger portion of the healthcare dollar in the university coffers. Services and even departments provided by community hospitals are likewise subject to the benevolence of the university medical system. Hospitals function like living organisms: If a department such as pediatrics is withdrawn, the hospital continues—but with a limp. Few children can be seen and evaluated in the emergency department; likewise, high-risk obstetrics must be transferred to a major university hospital because the patient may need a neonatal intensive care unit. Hospitalists and internists who happen to be double boarded in medicine and pediatrics steer away from hospitals without a pediatric department. The changes are subtle but, over time, the effects of the loss are apparent.
Hospitalists need to be cognizant of these issues when pursuing employment opportunities. Many career-minded hospitalists seek employment in community-based, full-service hospitals with university medical center affiliations. This combination can provide the best of both worlds: autonomy, opportunities for growth and development, and opportunities for working with house staff and teaching. Checking the status of the relationship between the community hospital and the affiliated university medical center may be an important factor in pre-contract negotiations and decision-making for career hospitalists.
The Bottom Line
The turf battle between community medicine and academic medicine is primarily one of economics. Interesting parallels may be drawn between this conflict and the teachings of Adam Smith. Prior to Smith, economic theory was based on the idea that every dollar you have is one less dollar for me. Smith proposed an entirely different concept: If I help you earn dollars, the economic house will grow, and I, too, will make more dollars, and then you will make more dollars. In this way, the entire system generates more than anyone could have previously imagined. This economic concept extrapolates well to the present discussion of the university medical center versus community medicine.
University health systems do not seem to realize that real growth happens when communities grow together. A robust and vibrant community hospital supports a university medical center with more vigor than an anemic, waning, and disenchanted community hospital that perceives its woes as a result of the powerful—and perhaps dogmatic—university health system. There are enough patients to grow both systems together—the patient base radius grows wider with cooperation and growth—but this cannot happen if the university engenders distrust among local practitioners and the local community. This is a situation that will either be win-win or lose-lose.
Although the crux of the conflict is economic, other aspects of town-and-gown medicine can contribute to better cooperation and understanding. Some academic medical centers have explored ways to incorporate local physicians in university-based clinical trials. These programs offer cutting edge medicine and an opportunity to participate in intellectually stimulating work; at the same time, physicians retain their private practices.
This research opportunity is being offered and supported by a number of academic institutions, including Columbia-Presbyterian in New York City, Duke in Durham, N.C., Partners HealthCare in Boston, the University of Pittsburgh, the University of Rochester (N.Y.), and Washington University (St. Louis, Mo.).4 This is a good-faith start in mending the relationship between the academic and private medical sectors. To achieve a lasting positive relationship, community physicians must trust the academic community to respect their autonomy and to recognize that they have the right to provide full-service care to their patients and to serve their patients without the fear of being unfairly disenfranchised.
The lack of integration of the academic medical community and private practitioners of medicine—the proverbial town and gown—is an old dilemma. It is time to lay it to rest. The solutions are straightforward. Empowering community hospitals and physicians will not diminish the influence of university-based hospitals, nor will there be loss of reimbursement. Just the opposite will occur. In the end, with cooperation, everyone wins; with adversarial actions, all parties lose, especially the patients. TH
Dr. Brezina is a member of the consulting clinical faculty at Duke University, Durham, N.C.
References
- Town and gown in the Middle Ages. Available at: http://en.wikipedia.org/wiki/Town_and_gown. Last accessed March 29, 2007.
- University of Florida Web site. Town/gown task force. Available at: www.facilities.ufl.edu/cp/towngown.htm. Last accessed March 29, 2007.
- Adams D, Croasdale M. Town and gown: turning rivalries into relationships [American Medical News Web site]. January 13, 2003. Available at: www.ama-assn.org/amednews/2003/01/13/prsa0113.htm. Last accessed March 20, 2007.
- Maguire P. Marriage of town and gown brings clinical research to busy practices [ACP-ASIM Observer Web site]. February 2001. Available at: www.acponline.org/journals/news/feb01/clinresearch.htm. Last accessed March 20, 2007.
Scapular Pain
Case
A 67-year-old female was referred for two weeks of left shoulder pain that kept her from sleeping and moving her arm and interfered with her job as a typist. The pain was located in the posterior shoulder just medial to the scapula, radiated down her left arm, and was positional. She had not noticed a decreased range of motion.
After failure of steroids and NSAIDs, she was referred to a chiropractor, who did not improve her shoulder pain. When she got up from the table, she noticed that she was having crushing chest pain bilaterally on each side of the sternum at the level of the first and second ribs. Since then, she had been on significant doses of opiates and oral steroids without pain resolution.
Physical Exam
A shoulder exam revealed bilateral normal range of motion with no crepitus. The patient’s head was slightly tilted, her back laterally rotated. There was a palpable tender mass over the medial aspect of her left scapula. Palpation of the rhomboid muscle caused intense acute pain that radiated down her arm and reproduced her symptoms (See sample photos 1 & 2).

Rhomboid Spasm
Etiology: A rhomboid muscle strain or spasm is usually caused by overuse of the shoulder and arm, especially during repetitive overhead activities like serving a tennis ball or reaching to put objects on a high shelf. It can also result from activities such as the prolonged use of a computer, the problem experienced by this patient.
Anatomy: The rhomboids originate on the last (seventh) cervical and first five thoracic vertebrae and insert on the medial border of the scapula. They work with the levator scapulae and the upper trapezius to elevate and retract the scapula. Spasms of the rhomboids refer pain to a local and limited area, as well as down the lateral aspect of the arm, and are often accompanied by trigger points in levator scapulae, trapezius, and pectoralis major and minor. (See photos 3a, 3b, and 4).
Treatment
Rhomboid spasm should be treated by local lidocaine injection and a depot corticosteroid into the rhomboid muscle. The lidocaine provides the direct effect of reducing the current spasm, and the anti-inflammatory effect of the steroid reduces recurrence.


Rhomboid Injection
To administer a rhomboid injection, first locate the rhomboid muscle just medial to the scapula on the posterior shoulder. A rhomboid muscle in spasm often presents as a painful, palpable mass. Next, identify an area of point tenderness. Inject lidocaine and a corticosteroid. The correct location will be confirmed by immediate pain relief; the steroid, however, may take up to a week to provide pain relief.
Three-Month Follow-Up
The patient returned three months after her rhomboid muscle was injected with lidocaine and a depo-steroid preparation. She has resumed her job as a typist and performs rhomboid spasm prevention exercises. She sleeps well and can move her arm without pain. She is active in her daily activities and enjoys shopping with her friends.

Prevention
Prevention can be achieved through the following rhomboid exercises:
- Sit with your legs stretched in front of you. Bend your right knee and place your right foot on the left/outside of your left knee. With your right hand, grab and hold on to your right ankle. Holding on to your right ankle, lean back. (See 5A.)
- The key: Press your right elbow into your right knee and point/push your right shoulder toward the floor in front of you. (See 5B.)
- Stand with your arms at your sides. Stretch one arm across your body and pull it in toward your body with your other hand. (See 5C.)
- Sit on a chair firmly planted on the floor. Lift your right leg and put the right ankle onto the knee of the left leg. Grab your right ankle with your right hand and rest your right elbow on your right knee. With your left hand, grasp the chair back behind you and rotate your torso to the left to look over your left hand. (See 5D.)




Dr. Ficalora is an associate professor of medicine at the Mayo Clinic College of Medicine, and Gerhart is a third-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.
Case
A 67-year-old female was referred for two weeks of left shoulder pain that kept her from sleeping and moving her arm and interfered with her job as a typist. The pain was located in the posterior shoulder just medial to the scapula, radiated down her left arm, and was positional. She had not noticed a decreased range of motion.
After failure of steroids and NSAIDs, she was referred to a chiropractor, who did not improve her shoulder pain. When she got up from the table, she noticed that she was having crushing chest pain bilaterally on each side of the sternum at the level of the first and second ribs. Since then, she had been on significant doses of opiates and oral steroids without pain resolution.
Physical Exam
A shoulder exam revealed bilateral normal range of motion with no crepitus. The patient’s head was slightly tilted, her back laterally rotated. There was a palpable tender mass over the medial aspect of her left scapula. Palpation of the rhomboid muscle caused intense acute pain that radiated down her arm and reproduced her symptoms (See sample photos 1 & 2).
Rhomboid Spasm
Etiology: A rhomboid muscle strain or spasm is usually caused by overuse of the shoulder and arm, especially during repetitive overhead activities like serving a tennis ball or reaching to put objects on a high shelf. It can also result from activities such as the prolonged use of a computer, the problem experienced by this patient.
Anatomy: The rhomboids originate on the last (seventh) cervical and first five thoracic vertebrae and insert on the medial border of the scapula. They work with the levator scapulae and the upper trapezius to elevate and retract the scapula. Spasms of the rhomboids refer pain to a local and limited area, as well as down the lateral aspect of the arm, and are often accompanied by trigger points in levator scapulae, trapezius, and pectoralis major and minor. (See photos 3a, 3b, and 4).
Treatment
Rhomboid spasm should be treated by local lidocaine injection and a depot corticosteroid into the rhomboid muscle. The lidocaine provides the direct effect of reducing the current spasm, and the anti-inflammatory effect of the steroid reduces recurrence.
Rhomboid Injection
To administer a rhomboid injection, first locate the rhomboid muscle just medial to the scapula on the posterior shoulder. A rhomboid muscle in spasm often presents as a painful, palpable mass. Next, identify an area of point tenderness. Inject lidocaine and a corticosteroid. The correct location will be confirmed by immediate pain relief; the steroid, however, may take up to a week to provide pain relief.
Three-Month Follow-Up
The patient returned three months after her rhomboid muscle was injected with lidocaine and a depo-steroid preparation. She has resumed her job as a typist and performs rhomboid spasm prevention exercises. She sleeps well and can move her arm without pain. She is active in her daily activities and enjoys shopping with her friends.
Prevention
Prevention can be achieved through the following rhomboid exercises:
- Sit with your legs stretched in front of you. Bend your right knee and place your right foot on the left/outside of your left knee. With your right hand, grab and hold on to your right ankle. Holding on to your right ankle, lean back. (See 5A.)
- The key: Press your right elbow into your right knee and point/push your right shoulder toward the floor in front of you. (See 5B.)
- Stand with your arms at your sides. Stretch one arm across your body and pull it in toward your body with your other hand. (See 5C.)
- Sit on a chair firmly planted on the floor. Lift your right leg and put the right ankle onto the knee of the left leg. Grab your right ankle with your right hand and rest your right elbow on your right knee. With your left hand, grasp the chair back behind you and rotate your torso to the left to look over your left hand. (See 5D.)
Dr. Ficalora is an associate professor of medicine at the Mayo Clinic College of Medicine, and Gerhart is a third-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.
Case
A 67-year-old female was referred for two weeks of left shoulder pain that kept her from sleeping and moving her arm and interfered with her job as a typist. The pain was located in the posterior shoulder just medial to the scapula, radiated down her left arm, and was positional. She had not noticed a decreased range of motion.
After failure of steroids and NSAIDs, she was referred to a chiropractor, who did not improve her shoulder pain. When she got up from the table, she noticed that she was having crushing chest pain bilaterally on each side of the sternum at the level of the first and second ribs. Since then, she had been on significant doses of opiates and oral steroids without pain resolution.
Physical Exam
A shoulder exam revealed bilateral normal range of motion with no crepitus. The patient’s head was slightly tilted, her back laterally rotated. There was a palpable tender mass over the medial aspect of her left scapula. Palpation of the rhomboid muscle caused intense acute pain that radiated down her arm and reproduced her symptoms (See sample photos 1 & 2).
Rhomboid Spasm
Etiology: A rhomboid muscle strain or spasm is usually caused by overuse of the shoulder and arm, especially during repetitive overhead activities like serving a tennis ball or reaching to put objects on a high shelf. It can also result from activities such as the prolonged use of a computer, the problem experienced by this patient.
Anatomy: The rhomboids originate on the last (seventh) cervical and first five thoracic vertebrae and insert on the medial border of the scapula. They work with the levator scapulae and the upper trapezius to elevate and retract the scapula. Spasms of the rhomboids refer pain to a local and limited area, as well as down the lateral aspect of the arm, and are often accompanied by trigger points in levator scapulae, trapezius, and pectoralis major and minor. (See photos 3a, 3b, and 4).
Treatment
Rhomboid spasm should be treated by local lidocaine injection and a depot corticosteroid into the rhomboid muscle. The lidocaine provides the direct effect of reducing the current spasm, and the anti-inflammatory effect of the steroid reduces recurrence.
Rhomboid Injection
To administer a rhomboid injection, first locate the rhomboid muscle just medial to the scapula on the posterior shoulder. A rhomboid muscle in spasm often presents as a painful, palpable mass. Next, identify an area of point tenderness. Inject lidocaine and a corticosteroid. The correct location will be confirmed by immediate pain relief; the steroid, however, may take up to a week to provide pain relief.
Three-Month Follow-Up
The patient returned three months after her rhomboid muscle was injected with lidocaine and a depo-steroid preparation. She has resumed her job as a typist and performs rhomboid spasm prevention exercises. She sleeps well and can move her arm without pain. She is active in her daily activities and enjoys shopping with her friends.
Prevention
Prevention can be achieved through the following rhomboid exercises:
- Sit with your legs stretched in front of you. Bend your right knee and place your right foot on the left/outside of your left knee. With your right hand, grab and hold on to your right ankle. Holding on to your right ankle, lean back. (See 5A.)
- The key: Press your right elbow into your right knee and point/push your right shoulder toward the floor in front of you. (See 5B.)
- Stand with your arms at your sides. Stretch one arm across your body and pull it in toward your body with your other hand. (See 5C.)
- Sit on a chair firmly planted on the floor. Lift your right leg and put the right ankle onto the knee of the left leg. Grab your right ankle with your right hand and rest your right elbow on your right knee. With your left hand, grasp the chair back behind you and rotate your torso to the left to look over your left hand. (See 5D.)
Dr. Ficalora is an associate professor of medicine at the Mayo Clinic College of Medicine, and Gerhart is a third-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.
SHM Behind the Scenes

Remember the classic episod-es of “Star Trek” where a new cast member went on a mission? Chances were that guy would be the one to fall off a cliff or get zapped with a laser gun and would not make it back safely to the starship Enterprise.
Recently I was in a meeting focused on what happens when older adults are discharged from the hospital. I thought to myself: “Those are the patients wearing the red uniforms. But what if we could make the experience of older adults more like that of Spock and Captain Kirk, where luck and good preparation are on their side and the data to make informed decisions follow them everywhere?”
The transition of patients in and out of the hospital has become a key patient-safety concern. Patients frequently arrive at the hospital with incomplete medical histories and uncertain or missing medication lists. During a typical hospitalization, patients receive less than optimal preparation before their discharge and often leave the hospital without a clear understanding of how to care for themselves, identify new symptoms that require immediate medical attention, or take their medications. Further, it is often unclear whom patients should call with questions while they are in “the white space”—that time period between hospital discharge and follow-up care. Do they call the hospital? The hospitalist? Their primary care physician? Their cardiologist?
Safety related to transitions of care is a concern frequently raised about the hospital medicine movement. The use of hospitalists forces physician discontinuity at admission and discharge. However, SHM plans to make discharge planning an issue that brings hospitalists and hospital medicine the greatest praise. SHM is taking a clear, proactive leadership role to define safe transitions, create toolkits for hospitals to improve their current transition practices, and develop technical assistance programs to build quality improvement capacity at local institutions.
Safe Transitions
SHM is participating in two major initiatives to define safe transitions. As a member of the American Board of Internal Medicine (ABIM) Foundation Stepping Up To The Plate Initiative (SUTTP), we are helping to develop sets of principles of and standards for safe and effective transitions.
SHM also co-chaired a Transitions of Care Consensus Conference (TOCCC) in partnership with the American College of Physicians and Society of General Internal Medicine. The TOCCC further reviewed the work of the SUTTP conference and focused more specifically on issues that arise as patients transfer in and out of the hospital.
In these meetings and others, SHM’s messages were clear:
- Improvements in transitions are needed now, and shouldn’t wait for other movements such as creation of medical homes or national electronic medical records to become a reality;
- Safe transitions require teams of medical professionals on both sides of the transfer and patients and their families working together;
- Patients and their families/ caregivers must be included and prepared for transfers of care;
- Better information on patient history and medications needs to follow patients into the hospital; and
- A small subset of information from the care plan, or transition record, should follow patients through each transfer, and be made available to them in lay terms.
Both the SUTTP and TOCCC documents are under review for endorsement by multiple medical professional societies. SHM is pursuing the development of related performance measures for safe care transitions.
Technical Assistance
SHM has for years distinguished its educational offerings by offering “implementation education.” We focus on translating best practices into actual practices. To that end, with generous support from the John A. Hartford Foundation, we are developing a discharge planning toolkit.
The toolkit will provide a step-wise approach to plan, implement, and evaluate interventions to improve discharge planning. The toolkit will help quality teams establish goals, garner internal support for interventions, educate support staff, and evaluate their results.
The interventional approaches and tools are focused on:
- Improving communication among sending and receiving physicians;
- Better preparing patients for post-discharge medication management and other self-care; and
- Facilitating follow-up care and transfer of patient information.
On Sept. 7, SHM convened an advisory board in Chicago to review and provide feedback on our proposed interventional strategies, technical support offerings, and evaluation plan. An impressive group of key stakeholders attended, including:
- Representatives from major payer groups such as the Centers for Medicare and Medicaid Services, Blue Cross Blue Shield, and Kaiser Permanente;
- Professional societies including the American Geriatrics Society, the Society of General Internal Medicine, the Case Management Society of America, and the American Society of Health System Pharmacists.
- Representation from the John A. Hartford Foundation, patient advocates from The Families and Health Care Project, and leaders and practicing professionals in nursing, social work, case management, patient advocacy, geriatrics, primary care, quality improvement and, of course, hospital medicine.
While not at the September meeting, the advisory board also includes representatives from the Agency for Healthcare Research and Quality and the Joint Commission.
The advisory board provided valuable feedback on SHM’s proposed toolkit and applauded our efforts to lead teams to make substantial local hospital improvements. Participants also had the opportunity to share existing resources and strategize opportunities to encourage wide-scale adoption of the toolkit. In February the advisory board plans to reconvene to review the completed toolkit.
SHM is developing training opportunities for institutions adopting the toolkit, designed to meet the full spectrum of technical assistance needs. The full toolkit will be available free on SHM’s Web site in the spring. At the April 2008 SHM Annual Meeting in San Diego, quality teams can participate in a daylong pre-course on general quality improvement principles and hands-on application of the toolkit.
In May, SHM will begin reviewing applications for sites wishing to participate in the yearlong mentoring program or a more intensive short-term, on-site consultant service. For more information on these technical assistance programs, visit the SHM Web site at www.hospitalmedicine.org and select the “Quality Improvement” link, then “Current Initiatives.”
We hope you and your institution will join our journey into the white space to improve discharge planning and help our patients “live long and prosper.” TH
Remember the classic episod-es of “Star Trek” where a new cast member went on a mission? Chances were that guy would be the one to fall off a cliff or get zapped with a laser gun and would not make it back safely to the starship Enterprise.
Recently I was in a meeting focused on what happens when older adults are discharged from the hospital. I thought to myself: “Those are the patients wearing the red uniforms. But what if we could make the experience of older adults more like that of Spock and Captain Kirk, where luck and good preparation are on their side and the data to make informed decisions follow them everywhere?”
The transition of patients in and out of the hospital has become a key patient-safety concern. Patients frequently arrive at the hospital with incomplete medical histories and uncertain or missing medication lists. During a typical hospitalization, patients receive less than optimal preparation before their discharge and often leave the hospital without a clear understanding of how to care for themselves, identify new symptoms that require immediate medical attention, or take their medications. Further, it is often unclear whom patients should call with questions while they are in “the white space”—that time period between hospital discharge and follow-up care. Do they call the hospital? The hospitalist? Their primary care physician? Their cardiologist?
Safety related to transitions of care is a concern frequently raised about the hospital medicine movement. The use of hospitalists forces physician discontinuity at admission and discharge. However, SHM plans to make discharge planning an issue that brings hospitalists and hospital medicine the greatest praise. SHM is taking a clear, proactive leadership role to define safe transitions, create toolkits for hospitals to improve their current transition practices, and develop technical assistance programs to build quality improvement capacity at local institutions.
Safe Transitions
SHM is participating in two major initiatives to define safe transitions. As a member of the American Board of Internal Medicine (ABIM) Foundation Stepping Up To The Plate Initiative (SUTTP), we are helping to develop sets of principles of and standards for safe and effective transitions.
SHM also co-chaired a Transitions of Care Consensus Conference (TOCCC) in partnership with the American College of Physicians and Society of General Internal Medicine. The TOCCC further reviewed the work of the SUTTP conference and focused more specifically on issues that arise as patients transfer in and out of the hospital.
In these meetings and others, SHM’s messages were clear:
- Improvements in transitions are needed now, and shouldn’t wait for other movements such as creation of medical homes or national electronic medical records to become a reality;
- Safe transitions require teams of medical professionals on both sides of the transfer and patients and their families working together;
- Patients and their families/ caregivers must be included and prepared for transfers of care;
- Better information on patient history and medications needs to follow patients into the hospital; and
- A small subset of information from the care plan, or transition record, should follow patients through each transfer, and be made available to them in lay terms.
Both the SUTTP and TOCCC documents are under review for endorsement by multiple medical professional societies. SHM is pursuing the development of related performance measures for safe care transitions.
Technical Assistance
SHM has for years distinguished its educational offerings by offering “implementation education.” We focus on translating best practices into actual practices. To that end, with generous support from the John A. Hartford Foundation, we are developing a discharge planning toolkit.
The toolkit will provide a step-wise approach to plan, implement, and evaluate interventions to improve discharge planning. The toolkit will help quality teams establish goals, garner internal support for interventions, educate support staff, and evaluate their results.
The interventional approaches and tools are focused on:
- Improving communication among sending and receiving physicians;
- Better preparing patients for post-discharge medication management and other self-care; and
- Facilitating follow-up care and transfer of patient information.
On Sept. 7, SHM convened an advisory board in Chicago to review and provide feedback on our proposed interventional strategies, technical support offerings, and evaluation plan. An impressive group of key stakeholders attended, including:
- Representatives from major payer groups such as the Centers for Medicare and Medicaid Services, Blue Cross Blue Shield, and Kaiser Permanente;
- Professional societies including the American Geriatrics Society, the Society of General Internal Medicine, the Case Management Society of America, and the American Society of Health System Pharmacists.
- Representation from the John A. Hartford Foundation, patient advocates from The Families and Health Care Project, and leaders and practicing professionals in nursing, social work, case management, patient advocacy, geriatrics, primary care, quality improvement and, of course, hospital medicine.
While not at the September meeting, the advisory board also includes representatives from the Agency for Healthcare Research and Quality and the Joint Commission.
The advisory board provided valuable feedback on SHM’s proposed toolkit and applauded our efforts to lead teams to make substantial local hospital improvements. Participants also had the opportunity to share existing resources and strategize opportunities to encourage wide-scale adoption of the toolkit. In February the advisory board plans to reconvene to review the completed toolkit.
SHM is developing training opportunities for institutions adopting the toolkit, designed to meet the full spectrum of technical assistance needs. The full toolkit will be available free on SHM’s Web site in the spring. At the April 2008 SHM Annual Meeting in San Diego, quality teams can participate in a daylong pre-course on general quality improvement principles and hands-on application of the toolkit.
In May, SHM will begin reviewing applications for sites wishing to participate in the yearlong mentoring program or a more intensive short-term, on-site consultant service. For more information on these technical assistance programs, visit the SHM Web site at www.hospitalmedicine.org and select the “Quality Improvement” link, then “Current Initiatives.”
We hope you and your institution will join our journey into the white space to improve discharge planning and help our patients “live long and prosper.” TH
Remember the classic episod-es of “Star Trek” where a new cast member went on a mission? Chances were that guy would be the one to fall off a cliff or get zapped with a laser gun and would not make it back safely to the starship Enterprise.
Recently I was in a meeting focused on what happens when older adults are discharged from the hospital. I thought to myself: “Those are the patients wearing the red uniforms. But what if we could make the experience of older adults more like that of Spock and Captain Kirk, where luck and good preparation are on their side and the data to make informed decisions follow them everywhere?”
The transition of patients in and out of the hospital has become a key patient-safety concern. Patients frequently arrive at the hospital with incomplete medical histories and uncertain or missing medication lists. During a typical hospitalization, patients receive less than optimal preparation before their discharge and often leave the hospital without a clear understanding of how to care for themselves, identify new symptoms that require immediate medical attention, or take their medications. Further, it is often unclear whom patients should call with questions while they are in “the white space”—that time period between hospital discharge and follow-up care. Do they call the hospital? The hospitalist? Their primary care physician? Their cardiologist?
Safety related to transitions of care is a concern frequently raised about the hospital medicine movement. The use of hospitalists forces physician discontinuity at admission and discharge. However, SHM plans to make discharge planning an issue that brings hospitalists and hospital medicine the greatest praise. SHM is taking a clear, proactive leadership role to define safe transitions, create toolkits for hospitals to improve their current transition practices, and develop technical assistance programs to build quality improvement capacity at local institutions.
Safe Transitions
SHM is participating in two major initiatives to define safe transitions. As a member of the American Board of Internal Medicine (ABIM) Foundation Stepping Up To The Plate Initiative (SUTTP), we are helping to develop sets of principles of and standards for safe and effective transitions.
SHM also co-chaired a Transitions of Care Consensus Conference (TOCCC) in partnership with the American College of Physicians and Society of General Internal Medicine. The TOCCC further reviewed the work of the SUTTP conference and focused more specifically on issues that arise as patients transfer in and out of the hospital.
In these meetings and others, SHM’s messages were clear:
- Improvements in transitions are needed now, and shouldn’t wait for other movements such as creation of medical homes or national electronic medical records to become a reality;
- Safe transitions require teams of medical professionals on both sides of the transfer and patients and their families working together;
- Patients and their families/ caregivers must be included and prepared for transfers of care;
- Better information on patient history and medications needs to follow patients into the hospital; and
- A small subset of information from the care plan, or transition record, should follow patients through each transfer, and be made available to them in lay terms.
Both the SUTTP and TOCCC documents are under review for endorsement by multiple medical professional societies. SHM is pursuing the development of related performance measures for safe care transitions.
Technical Assistance
SHM has for years distinguished its educational offerings by offering “implementation education.” We focus on translating best practices into actual practices. To that end, with generous support from the John A. Hartford Foundation, we are developing a discharge planning toolkit.
The toolkit will provide a step-wise approach to plan, implement, and evaluate interventions to improve discharge planning. The toolkit will help quality teams establish goals, garner internal support for interventions, educate support staff, and evaluate their results.
The interventional approaches and tools are focused on:
- Improving communication among sending and receiving physicians;
- Better preparing patients for post-discharge medication management and other self-care; and
- Facilitating follow-up care and transfer of patient information.
On Sept. 7, SHM convened an advisory board in Chicago to review and provide feedback on our proposed interventional strategies, technical support offerings, and evaluation plan. An impressive group of key stakeholders attended, including:
- Representatives from major payer groups such as the Centers for Medicare and Medicaid Services, Blue Cross Blue Shield, and Kaiser Permanente;
- Professional societies including the American Geriatrics Society, the Society of General Internal Medicine, the Case Management Society of America, and the American Society of Health System Pharmacists.
- Representation from the John A. Hartford Foundation, patient advocates from The Families and Health Care Project, and leaders and practicing professionals in nursing, social work, case management, patient advocacy, geriatrics, primary care, quality improvement and, of course, hospital medicine.
While not at the September meeting, the advisory board also includes representatives from the Agency for Healthcare Research and Quality and the Joint Commission.
The advisory board provided valuable feedback on SHM’s proposed toolkit and applauded our efforts to lead teams to make substantial local hospital improvements. Participants also had the opportunity to share existing resources and strategize opportunities to encourage wide-scale adoption of the toolkit. In February the advisory board plans to reconvene to review the completed toolkit.
SHM is developing training opportunities for institutions adopting the toolkit, designed to meet the full spectrum of technical assistance needs. The full toolkit will be available free on SHM’s Web site in the spring. At the April 2008 SHM Annual Meeting in San Diego, quality teams can participate in a daylong pre-course on general quality improvement principles and hands-on application of the toolkit.
In May, SHM will begin reviewing applications for sites wishing to participate in the yearlong mentoring program or a more intensive short-term, on-site consultant service. For more information on these technical assistance programs, visit the SHM Web site at www.hospitalmedicine.org and select the “Quality Improvement” link, then “Current Initiatives.”
We hope you and your institution will join our journey into the white space to improve discharge planning and help our patients “live long and prosper.” TH
SHM Launches Geriatric Special Interest Group

At the 2006 SHM Annual Meeting Geriatrics Special Interest Forum, participants asked, “Can we create an area on the SHM Web site focused on our unique interests and needs?” Last month, SHM answered with a resounding “Yes!” as we launched the Geriatrics Special Interest Group on www.hospitalmedicine.org.
The SHM Geriatrics Special Interest Group provides a portal for SHM members to access relevant, timely information about and resources for geriatric medicine. The Community Forums provide a mechanism for participants to communicate with each other about issues in geriatric medicine and other areas of interest. In particular, the Geriatrics Special Interest Group allows users to post information about training and career development opportunities, professional meetings and forums, and funding opportunities. Users can access a wealth of geriatric-medicine resources, including breaking medical news, clinical and quality improvement tools, key publications, and archived SHM Annual Meeting presentations. The Geriatrics Special Interest Group will serve as a template for future member-requested special interest groups, including palliative care, pediatrics, and others.
The Geriatrics Special Interest Group was developed by SHM members, other experts from the community of geriatric medicine, and a team of SHM staffers. SHM member Melissa Mattison, MD, (Beth Israel Deaconess) serves as medical editor for the site and helped shape its vision, along with members Param Dedhia, MD, (Johns Hopkins, Bayview) and Jason Stein, MD (Emory University). The group also benefited from reviews and contributions made by John Degelau, MD, at HealthPartners Medical Group, Gavin W. Hougham, MD, PhD, at The John A. Hartford Foundation, Nancy Lundebjerg, MPA, and Jane Potter, MD, at the American Geriatrics Society, Odette van der Willik at the American Federation for Aging Research, and Paula M. Podrazik, MD, at the Case Management Society of America. The internal SHM development team was led by Shannon Roach and included Bruce Hanson, Travis Kamps, and Tina Budnitz.
To view the Geriatrics Special Interest Group, go to SHM’s Web site or type the address into your browser: www.hospitalmedicine.org/AM/Template.cfm?Section=Home&Template=/CM/HTMLDisplay.cfm&ContentID=12369.
We hope SHM members will utilize the Geriatrics Special Interest Group to share ideas and resources, to network, and to improve inpatient geriatric medicine. Let us know if the site meets your needs by sending your comments and suggestions to Shannon Roach at [email protected]. Have an idea for another special interest group? E-mail us that suggestion, too.
SHM: BEHIND THE SCENES
Education and quality improvement: Reflections of a New Staff Member
By Kristin Beck

It’s nice to come to work every day and focus on education and quality improvement. Ensuring that hospitalists have the most up to date information as well as support and encouragement for implementing positive change are good reasons for leaving the house in the morning.
Only three weeks into my role as senior project manager, I have had the sincere pleasure of being involved with updating quality improvement resource rooms (common Web site areas that house tools for implementing quality improvement programs) by initiating a grant-supported program for examining observation units as they relate to treating the number one reason people are hospitalized. I have also accomplished writing and submitting a grant for the Quality Improvement Pre-Course, as well as, working with a committee that looks at patient quality care and projects to enhance it.
Our work here focuses on examining what has been done, how we can improve it, and how we can institute best practices. Not bad for three weeks’ work!
Conversations in our department focus on whether members get what they need and want. People meet regularly to discuss how we can refine and improve the services we offer. Strategies for securing funding and developing programs are reviewed, not for this calendar or fiscal year but for years to come. In one of my final interviews for this job, I was reminded that we don’t deliver here—we over-deliver. Looking through The Hospitalist, titles that stand out include the words unforgettable, safety, expert, leader, admire, and smart.
When people ask what I do in my new job, I tell them that hospital medicine looks at the total experience of being a doctor. It focuses not only on medical care but also on the complete experience of being a working professional: the arts of research, negotiation, best practices, team-focused care, conflict resolution, and systems change. I explain that we do life-saving work, for it is far more than the practice of just day-to-day medicine that improves all of our lives. I tell people that it is work that makes sense.
When you come to work every day and are surrounded by a dynamic, positive energy, the work you produce is likely to mirror the hospital medicine movement: You will reflect, revise, and grow stronger. Sincere, well-planned initiatives are infectious. Continually participating in an environment that asks the questions, “Where can we take this?” and “What can we do better?” is a pretty good reason to get out of bed in the morning.
Beck is the senior project manager at SHM.
VTE Prevention Collaborative off to a Great Start
The VTE Prevention Collaborative (VTE PC) is the latest SHM initiative to support hospitalist-led efforts to reduce the incidence of preventable, hospital-acquired VTE. Launched in January 2007, the program offers individualized assistance to hospitalists who want to take the lead on this critical quality and patient safety issue.
Hospital-Acquired Venous Thromboembolism
The problem of hospital-acquired VTE is huge. More than 2 million Americans suffer from VTE each year. Most hospitalized patients have at least one risk factor for VTE. In a large registry trial capturing more than 5,451 patients at 183 sites in a six-month period, 50% (2,726) developed their VTE during hospitalization.1 A 400-bed hospital with an average rate of VTE prophylaxis can expect that 200 patients will suffer from hospital-acquired VTE each year; around half of these cases are potentially preventable.1,2
The good news is that effective and safe measures to prevent hospital-acquired VTE exist. Pharmacologic prophylaxis reduces the incidence of asymptomatic and symptomatic DVT and pulmonary embolism (PE) by 50%-65%.3, 4-11 Prevention of DVT also prevents PE and fatalities from PE. The chief concern of prophylaxis is bleeding, but bleeding risk secondary to pharmacologic prophylaxis is a rare event, as is shown in abundant data from meta-analyses and placebo-controlled, randomized controlled trials.3,4
Close the Gap
Reliably preventing VTE in the hospital is inherently complex. VTE risk and bleeding risks vary within patient populations, and these risks may change for an individual patient several times in the course of the hospital stay. Weight, age, renal function, medication changes, and recent or impending invasive interventions may all influence decisions about the best VTE prevention options. Transitions across care providers and locations translate into multiple opportunities for breakdown in the delivery of optimal VTE prophylaxis. Thoughtful, evidence-based protocols, multidisciplinary system changes, and comprehensive educational efforts are required to achieve optimal VTE prophylaxis in the complex hospital setting.
How the VTE PC Can Help
The VTE PC program builds on and complements the VTE prevention materials and educational resources that SHM has produced in recent years. “Our Quality Improvement Resource Rooms have the information and resources needed to tackle a number of key quality issues,” says SHM CEO Larry Wellikson. “The VTE PC project takes this one step further by providing individualized mentorship. SHM is committed to supporting these forward-thinking, unique strategies that will allow hospitalists to lead their hospitals into a better future.”
VTE PC participants can choose the type of support that best fits their needs: a full year of distance mentoring or a one-day evaluation and consultation visit to their site.
The mentoring program presents a perfect option for individuals interested in ongoing support for their planned or active VTE prevention projects. Through the project, SHM mentors with VTE and QI experts who work with participants during eight telephone calls scheduled throughout a yearlong mentoring period. During the calls, mentors offer individualized assistance on any topics, tasks, and barriers that are encountered in the course of designing, implementing, and evaluating a VTE prevention project. Instruction and assistance are tailored to participant needs and commonly focus on:
- Working with medical center administration;
- Using practical methods to assess institutional performance in VTE prophylaxis;
- Identifying and tracking patients with hospital-acquired VTE;
- Constructing a VTE risk-assessment model and integrating it into workflow, order sets, and protocols;
- Enhancing selection of appropriate prophylaxis by linking the VTE risk assessment to a corresponding menu of proven options; and
- Bolstering your chances of success by utilizing high-reliability design features and effective implementation techniques.
The on-site consultation program is a good option for individuals interested in securing expert evaluation and input on a VTE prevention program but who don’t need ongoing support. Through the on-site consultation program, SHM consultants with VTE and QI expertise visit applicants’ hospitals to evaluate active or planned VTE prevention programs. The visits are especially helpful to participants with existing VTE prevention programs that they wish to expand or improve upon.
The consultation visits feature a structured evaluation of the site’s strengths and resources, barriers to improvement, and the design and functioning of active or proposed VTE prevention interventions. Specific consultation-visit activities vary according to participant goals and needs but may include meeting with the local project team, QI leaders, hospital administrators, and hospital medicine group leaders, as well as reviewing project documents—order sets, policies, and procedures—data, and data collection/management tools. Following the visits, SHM consultants provide participants with a written report of findings and recommendations. Participants also receive one follow-up telephone consultation.
Collaborative Members
SHM membership has responded enthusiastically to the VTE PC project. Early enrollees have a wide range of experience with VTE prevention and QI in general. Some fill QI leadership roles in their hospitals or hospital medicine groups; for others, the VTE prevention project is their first experience leading a QI effort. Enrollees represent a range of hospital types (academic centers, community teaching hospitals, community hospitals) and sizes (staffed beds range from 135 to 650) and are located in every U.S. geographic region in multiple hospital systems.
Several participants represent hospitals where VTE prevention programs have been implemented, while most have active projects in which no intervention has yet been implemented; a handful are still in the planning/initial exploration phase of work. Nearly half of the enrolled sites have a history of failed QI efforts in VTE prevention.
Many enrollees are looking to their VTE prevention efforts as a means of positioning their hospital medicine group as a local QI force. “This is the first large project the hospitalist group has undertaken since getting up and running,” reports one attendee. “I would really like to make a positive impact on patient care and lay the groundwork with this project that would allow us to be successful with future undertakings.”
Applying to the Programs
Participation in both the mentoring and on-site consultation programs is open to hospitalists who lead proposed or active VTE prevention projects. Participation is free, but enrollment is limited, so interested individuals are encouraged to apply early. SHM members can apply to either program by completing the online application available on the VTE Prevention Collaborative Web site: www.hospitalmedicine.org/vte-pc.
Direct your questions about VTE Prevention Collaborative programs to [email protected].
Bibliography
- Goldhaber SZ, Tapson VF; DVT FREE Steering Committee. A prospective registry of 5,451 patients with ultrasound-confirmed deep vein thrombosis. Am J Cardiol. 2004 Jan;93(2):259-262.
- Maynard G. Workbook for Improvement: optimize prevention of venous thromboembolism at your medical center [SHM Web site, VTE Quality Improvement Resource Room]. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms&Template=/CM/ContentDisplay.cfm&ContentID=6092. Last accessed March 19, 2007.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):338S-400S. Review. Comment in Chest. 2005 Jun;127(6):2297-2298.
- Shojania KG, Duncan BW, McDonald KM, et al. Making health care safer: a critical analysis of patient safety practices. Evidence Report/Technology Assessment No. 43 [Agency for Healthcare Research and Quality Web site]. July 2001;332–346;AHRQ Publication No. 01-E058. Available at: www.ahrq.gov/clinic/ptsafety/. Last accessed March 19, 2007.
- Belch JJ, Lowe GD, Ward AG, et al. Prevention of deep vein thrombosis in medical patients by low-dose heparin. Scott Med J. 1981 Apr;26(2):115–117.
- Gardlund B. Randomised, controlled trial of low-dose heparin for prevention of fatal pulmonary embolism in patients with infectious diseases. The Heparin Prophylaxis Study Group. Lancet. 1996 May 18;347(9021):1357–1361. Comment in: ACP J Club. 1996 Nov-Dec;125(3):64 & Lancet. 1996 Jul 20; 348(9021):205-206.
- Samama MM, Cohen AT, Darmon JY, et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in Medical Patients with Enoxaparin Study Group. N Engl J Med. 1999 Sep 9;341(11):793–800.
- Leizorovicz A, Cohen AT, Turpie AG, et al. Randomized, placebo-controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients. Circulation. 2004 Aug 17;110(7):874-879.
- Kleber FX, Witt C, Vogel G, et al. Randomized comparison of enoxaparin with unfractionated heparin for the prevention of venous thromboembolism in medical patients with heart failure or severe respiratory disease. Am Heart J. 2003 Apr;145(4):614–621.
- Lechler E, Schramm W, Flosbach CW. The venous thrombotic risk in non-surgical patients: epidemiological data and efficacy/safety profile of a low-molecular-weight heparin (enoxaparin). The Prime Study Group. Haemostasis. 1996;26(Suppl):49–56.
- Cohen AT, Davidson BL, Gallus AS, et al. Fondaparinux for the prevention of VTE in acutely ill medical patients (abstract 42). Blood. 2003;102:15a.
Awards Ceremony Preview
SHM created the Awards of Excellence program to honor members whose contributions to the hospital medicine movement deserve acknowledgment and respect. Award winners will receive complimentary registration and paid airfare to SHM’s Annual Meeting, which is being held this month in Dallas and will be presented during the President’s luncheon. Any physician member whose focus is the general medical care of hospitalized patients is eligible for nomination of the four awards. Award winners have been selected for the following categories: Clinical Excellence, Excellence in Teaching, Outstanding Service, and Research.
The SHM Award for Clinical Excellence will be presented to an individual for recognition of exemplary clinical service in hospital medicine. The Awards Committee has evaluated the candidates according to their outstanding contributions to patient care, their advancement of clinical knowledge, including their leadership and professionalism in medicine, as well as personal excellence in practice management.
The SHM Award for Excellence in Teaching is presented in recognition of outstanding teaching and mentorship in hospital medicine, most specifically within the academic and community practice settings. Consideration was given to those nominees who demonstrated outstanding teaching ability and who served as role models and mentored other hospitalists, residents, medical students, or other healthcare professionals.
The SHM Award for Outstanding Service in Hospital Medicine is presented in recognition of exceptional service to the discipline of hospital medicine. The winning candidate has displayed exemplary organizational and leadership activities within organized medicine and has shown contributing support in public policy.
The SHM Excellence in Research Award is presented in recognition of outstanding achievement by a researcher in the discipline of hospital medicine. The candidate selected presented peer-reviewed publications and continued education with additional research and training that provided for both intra- and extramural funding for research.
For additional information regarding SHM’s Awards Program, please e-mail [email protected]. TH
At the 2006 SHM Annual Meeting Geriatrics Special Interest Forum, participants asked, “Can we create an area on the SHM Web site focused on our unique interests and needs?” Last month, SHM answered with a resounding “Yes!” as we launched the Geriatrics Special Interest Group on www.hospitalmedicine.org.
The SHM Geriatrics Special Interest Group provides a portal for SHM members to access relevant, timely information about and resources for geriatric medicine. The Community Forums provide a mechanism for participants to communicate with each other about issues in geriatric medicine and other areas of interest. In particular, the Geriatrics Special Interest Group allows users to post information about training and career development opportunities, professional meetings and forums, and funding opportunities. Users can access a wealth of geriatric-medicine resources, including breaking medical news, clinical and quality improvement tools, key publications, and archived SHM Annual Meeting presentations. The Geriatrics Special Interest Group will serve as a template for future member-requested special interest groups, including palliative care, pediatrics, and others.
The Geriatrics Special Interest Group was developed by SHM members, other experts from the community of geriatric medicine, and a team of SHM staffers. SHM member Melissa Mattison, MD, (Beth Israel Deaconess) serves as medical editor for the site and helped shape its vision, along with members Param Dedhia, MD, (Johns Hopkins, Bayview) and Jason Stein, MD (Emory University). The group also benefited from reviews and contributions made by John Degelau, MD, at HealthPartners Medical Group, Gavin W. Hougham, MD, PhD, at The John A. Hartford Foundation, Nancy Lundebjerg, MPA, and Jane Potter, MD, at the American Geriatrics Society, Odette van der Willik at the American Federation for Aging Research, and Paula M. Podrazik, MD, at the Case Management Society of America. The internal SHM development team was led by Shannon Roach and included Bruce Hanson, Travis Kamps, and Tina Budnitz.
To view the Geriatrics Special Interest Group, go to SHM’s Web site or type the address into your browser: www.hospitalmedicine.org/AM/Template.cfm?Section=Home&Template=/CM/HTMLDisplay.cfm&ContentID=12369.
We hope SHM members will utilize the Geriatrics Special Interest Group to share ideas and resources, to network, and to improve inpatient geriatric medicine. Let us know if the site meets your needs by sending your comments and suggestions to Shannon Roach at [email protected]. Have an idea for another special interest group? E-mail us that suggestion, too.
SHM: BEHIND THE SCENES
Education and quality improvement: Reflections of a New Staff Member
By Kristin Beck
It’s nice to come to work every day and focus on education and quality improvement. Ensuring that hospitalists have the most up to date information as well as support and encouragement for implementing positive change are good reasons for leaving the house in the morning.
Only three weeks into my role as senior project manager, I have had the sincere pleasure of being involved with updating quality improvement resource rooms (common Web site areas that house tools for implementing quality improvement programs) by initiating a grant-supported program for examining observation units as they relate to treating the number one reason people are hospitalized. I have also accomplished writing and submitting a grant for the Quality Improvement Pre-Course, as well as, working with a committee that looks at patient quality care and projects to enhance it.
Our work here focuses on examining what has been done, how we can improve it, and how we can institute best practices. Not bad for three weeks’ work!
Conversations in our department focus on whether members get what they need and want. People meet regularly to discuss how we can refine and improve the services we offer. Strategies for securing funding and developing programs are reviewed, not for this calendar or fiscal year but for years to come. In one of my final interviews for this job, I was reminded that we don’t deliver here—we over-deliver. Looking through The Hospitalist, titles that stand out include the words unforgettable, safety, expert, leader, admire, and smart.
When people ask what I do in my new job, I tell them that hospital medicine looks at the total experience of being a doctor. It focuses not only on medical care but also on the complete experience of being a working professional: the arts of research, negotiation, best practices, team-focused care, conflict resolution, and systems change. I explain that we do life-saving work, for it is far more than the practice of just day-to-day medicine that improves all of our lives. I tell people that it is work that makes sense.
When you come to work every day and are surrounded by a dynamic, positive energy, the work you produce is likely to mirror the hospital medicine movement: You will reflect, revise, and grow stronger. Sincere, well-planned initiatives are infectious. Continually participating in an environment that asks the questions, “Where can we take this?” and “What can we do better?” is a pretty good reason to get out of bed in the morning.
Beck is the senior project manager at SHM.
VTE Prevention Collaborative off to a Great Start
The VTE Prevention Collaborative (VTE PC) is the latest SHM initiative to support hospitalist-led efforts to reduce the incidence of preventable, hospital-acquired VTE. Launched in January 2007, the program offers individualized assistance to hospitalists who want to take the lead on this critical quality and patient safety issue.
Hospital-Acquired Venous Thromboembolism
The problem of hospital-acquired VTE is huge. More than 2 million Americans suffer from VTE each year. Most hospitalized patients have at least one risk factor for VTE. In a large registry trial capturing more than 5,451 patients at 183 sites in a six-month period, 50% (2,726) developed their VTE during hospitalization.1 A 400-bed hospital with an average rate of VTE prophylaxis can expect that 200 patients will suffer from hospital-acquired VTE each year; around half of these cases are potentially preventable.1,2
The good news is that effective and safe measures to prevent hospital-acquired VTE exist. Pharmacologic prophylaxis reduces the incidence of asymptomatic and symptomatic DVT and pulmonary embolism (PE) by 50%-65%.3, 4-11 Prevention of DVT also prevents PE and fatalities from PE. The chief concern of prophylaxis is bleeding, but bleeding risk secondary to pharmacologic prophylaxis is a rare event, as is shown in abundant data from meta-analyses and placebo-controlled, randomized controlled trials.3,4
Close the Gap
Reliably preventing VTE in the hospital is inherently complex. VTE risk and bleeding risks vary within patient populations, and these risks may change for an individual patient several times in the course of the hospital stay. Weight, age, renal function, medication changes, and recent or impending invasive interventions may all influence decisions about the best VTE prevention options. Transitions across care providers and locations translate into multiple opportunities for breakdown in the delivery of optimal VTE prophylaxis. Thoughtful, evidence-based protocols, multidisciplinary system changes, and comprehensive educational efforts are required to achieve optimal VTE prophylaxis in the complex hospital setting.
How the VTE PC Can Help
The VTE PC program builds on and complements the VTE prevention materials and educational resources that SHM has produced in recent years. “Our Quality Improvement Resource Rooms have the information and resources needed to tackle a number of key quality issues,” says SHM CEO Larry Wellikson. “The VTE PC project takes this one step further by providing individualized mentorship. SHM is committed to supporting these forward-thinking, unique strategies that will allow hospitalists to lead their hospitals into a better future.”
VTE PC participants can choose the type of support that best fits their needs: a full year of distance mentoring or a one-day evaluation and consultation visit to their site.
The mentoring program presents a perfect option for individuals interested in ongoing support for their planned or active VTE prevention projects. Through the project, SHM mentors with VTE and QI experts who work with participants during eight telephone calls scheduled throughout a yearlong mentoring period. During the calls, mentors offer individualized assistance on any topics, tasks, and barriers that are encountered in the course of designing, implementing, and evaluating a VTE prevention project. Instruction and assistance are tailored to participant needs and commonly focus on:
- Working with medical center administration;
- Using practical methods to assess institutional performance in VTE prophylaxis;
- Identifying and tracking patients with hospital-acquired VTE;
- Constructing a VTE risk-assessment model and integrating it into workflow, order sets, and protocols;
- Enhancing selection of appropriate prophylaxis by linking the VTE risk assessment to a corresponding menu of proven options; and
- Bolstering your chances of success by utilizing high-reliability design features and effective implementation techniques.
The on-site consultation program is a good option for individuals interested in securing expert evaluation and input on a VTE prevention program but who don’t need ongoing support. Through the on-site consultation program, SHM consultants with VTE and QI expertise visit applicants’ hospitals to evaluate active or planned VTE prevention programs. The visits are especially helpful to participants with existing VTE prevention programs that they wish to expand or improve upon.
The consultation visits feature a structured evaluation of the site’s strengths and resources, barriers to improvement, and the design and functioning of active or proposed VTE prevention interventions. Specific consultation-visit activities vary according to participant goals and needs but may include meeting with the local project team, QI leaders, hospital administrators, and hospital medicine group leaders, as well as reviewing project documents—order sets, policies, and procedures—data, and data collection/management tools. Following the visits, SHM consultants provide participants with a written report of findings and recommendations. Participants also receive one follow-up telephone consultation.
Collaborative Members
SHM membership has responded enthusiastically to the VTE PC project. Early enrollees have a wide range of experience with VTE prevention and QI in general. Some fill QI leadership roles in their hospitals or hospital medicine groups; for others, the VTE prevention project is their first experience leading a QI effort. Enrollees represent a range of hospital types (academic centers, community teaching hospitals, community hospitals) and sizes (staffed beds range from 135 to 650) and are located in every U.S. geographic region in multiple hospital systems.
Several participants represent hospitals where VTE prevention programs have been implemented, while most have active projects in which no intervention has yet been implemented; a handful are still in the planning/initial exploration phase of work. Nearly half of the enrolled sites have a history of failed QI efforts in VTE prevention.
Many enrollees are looking to their VTE prevention efforts as a means of positioning their hospital medicine group as a local QI force. “This is the first large project the hospitalist group has undertaken since getting up and running,” reports one attendee. “I would really like to make a positive impact on patient care and lay the groundwork with this project that would allow us to be successful with future undertakings.”
Applying to the Programs
Participation in both the mentoring and on-site consultation programs is open to hospitalists who lead proposed or active VTE prevention projects. Participation is free, but enrollment is limited, so interested individuals are encouraged to apply early. SHM members can apply to either program by completing the online application available on the VTE Prevention Collaborative Web site: www.hospitalmedicine.org/vte-pc.
Direct your questions about VTE Prevention Collaborative programs to [email protected].
Bibliography
- Goldhaber SZ, Tapson VF; DVT FREE Steering Committee. A prospective registry of 5,451 patients with ultrasound-confirmed deep vein thrombosis. Am J Cardiol. 2004 Jan;93(2):259-262.
- Maynard G. Workbook for Improvement: optimize prevention of venous thromboembolism at your medical center [SHM Web site, VTE Quality Improvement Resource Room]. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms&Template=/CM/ContentDisplay.cfm&ContentID=6092. Last accessed March 19, 2007.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):338S-400S. Review. Comment in Chest. 2005 Jun;127(6):2297-2298.
- Shojania KG, Duncan BW, McDonald KM, et al. Making health care safer: a critical analysis of patient safety practices. Evidence Report/Technology Assessment No. 43 [Agency for Healthcare Research and Quality Web site]. July 2001;332–346;AHRQ Publication No. 01-E058. Available at: www.ahrq.gov/clinic/ptsafety/. Last accessed March 19, 2007.
- Belch JJ, Lowe GD, Ward AG, et al. Prevention of deep vein thrombosis in medical patients by low-dose heparin. Scott Med J. 1981 Apr;26(2):115–117.
- Gardlund B. Randomised, controlled trial of low-dose heparin for prevention of fatal pulmonary embolism in patients with infectious diseases. The Heparin Prophylaxis Study Group. Lancet. 1996 May 18;347(9021):1357–1361. Comment in: ACP J Club. 1996 Nov-Dec;125(3):64 & Lancet. 1996 Jul 20; 348(9021):205-206.
- Samama MM, Cohen AT, Darmon JY, et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in Medical Patients with Enoxaparin Study Group. N Engl J Med. 1999 Sep 9;341(11):793–800.
- Leizorovicz A, Cohen AT, Turpie AG, et al. Randomized, placebo-controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients. Circulation. 2004 Aug 17;110(7):874-879.
- Kleber FX, Witt C, Vogel G, et al. Randomized comparison of enoxaparin with unfractionated heparin for the prevention of venous thromboembolism in medical patients with heart failure or severe respiratory disease. Am Heart J. 2003 Apr;145(4):614–621.
- Lechler E, Schramm W, Flosbach CW. The venous thrombotic risk in non-surgical patients: epidemiological data and efficacy/safety profile of a low-molecular-weight heparin (enoxaparin). The Prime Study Group. Haemostasis. 1996;26(Suppl):49–56.
- Cohen AT, Davidson BL, Gallus AS, et al. Fondaparinux for the prevention of VTE in acutely ill medical patients (abstract 42). Blood. 2003;102:15a.
Awards Ceremony Preview
SHM created the Awards of Excellence program to honor members whose contributions to the hospital medicine movement deserve acknowledgment and respect. Award winners will receive complimentary registration and paid airfare to SHM’s Annual Meeting, which is being held this month in Dallas and will be presented during the President’s luncheon. Any physician member whose focus is the general medical care of hospitalized patients is eligible for nomination of the four awards. Award winners have been selected for the following categories: Clinical Excellence, Excellence in Teaching, Outstanding Service, and Research.
The SHM Award for Clinical Excellence will be presented to an individual for recognition of exemplary clinical service in hospital medicine. The Awards Committee has evaluated the candidates according to their outstanding contributions to patient care, their advancement of clinical knowledge, including their leadership and professionalism in medicine, as well as personal excellence in practice management.
The SHM Award for Excellence in Teaching is presented in recognition of outstanding teaching and mentorship in hospital medicine, most specifically within the academic and community practice settings. Consideration was given to those nominees who demonstrated outstanding teaching ability and who served as role models and mentored other hospitalists, residents, medical students, or other healthcare professionals.
The SHM Award for Outstanding Service in Hospital Medicine is presented in recognition of exceptional service to the discipline of hospital medicine. The winning candidate has displayed exemplary organizational and leadership activities within organized medicine and has shown contributing support in public policy.
The SHM Excellence in Research Award is presented in recognition of outstanding achievement by a researcher in the discipline of hospital medicine. The candidate selected presented peer-reviewed publications and continued education with additional research and training that provided for both intra- and extramural funding for research.
For additional information regarding SHM’s Awards Program, please e-mail [email protected]. TH
At the 2006 SHM Annual Meeting Geriatrics Special Interest Forum, participants asked, “Can we create an area on the SHM Web site focused on our unique interests and needs?” Last month, SHM answered with a resounding “Yes!” as we launched the Geriatrics Special Interest Group on www.hospitalmedicine.org.
The SHM Geriatrics Special Interest Group provides a portal for SHM members to access relevant, timely information about and resources for geriatric medicine. The Community Forums provide a mechanism for participants to communicate with each other about issues in geriatric medicine and other areas of interest. In particular, the Geriatrics Special Interest Group allows users to post information about training and career development opportunities, professional meetings and forums, and funding opportunities. Users can access a wealth of geriatric-medicine resources, including breaking medical news, clinical and quality improvement tools, key publications, and archived SHM Annual Meeting presentations. The Geriatrics Special Interest Group will serve as a template for future member-requested special interest groups, including palliative care, pediatrics, and others.
The Geriatrics Special Interest Group was developed by SHM members, other experts from the community of geriatric medicine, and a team of SHM staffers. SHM member Melissa Mattison, MD, (Beth Israel Deaconess) serves as medical editor for the site and helped shape its vision, along with members Param Dedhia, MD, (Johns Hopkins, Bayview) and Jason Stein, MD (Emory University). The group also benefited from reviews and contributions made by John Degelau, MD, at HealthPartners Medical Group, Gavin W. Hougham, MD, PhD, at The John A. Hartford Foundation, Nancy Lundebjerg, MPA, and Jane Potter, MD, at the American Geriatrics Society, Odette van der Willik at the American Federation for Aging Research, and Paula M. Podrazik, MD, at the Case Management Society of America. The internal SHM development team was led by Shannon Roach and included Bruce Hanson, Travis Kamps, and Tina Budnitz.
To view the Geriatrics Special Interest Group, go to SHM’s Web site or type the address into your browser: www.hospitalmedicine.org/AM/Template.cfm?Section=Home&Template=/CM/HTMLDisplay.cfm&ContentID=12369.
We hope SHM members will utilize the Geriatrics Special Interest Group to share ideas and resources, to network, and to improve inpatient geriatric medicine. Let us know if the site meets your needs by sending your comments and suggestions to Shannon Roach at [email protected]. Have an idea for another special interest group? E-mail us that suggestion, too.
SHM: BEHIND THE SCENES
Education and quality improvement: Reflections of a New Staff Member
By Kristin Beck
It’s nice to come to work every day and focus on education and quality improvement. Ensuring that hospitalists have the most up to date information as well as support and encouragement for implementing positive change are good reasons for leaving the house in the morning.
Only three weeks into my role as senior project manager, I have had the sincere pleasure of being involved with updating quality improvement resource rooms (common Web site areas that house tools for implementing quality improvement programs) by initiating a grant-supported program for examining observation units as they relate to treating the number one reason people are hospitalized. I have also accomplished writing and submitting a grant for the Quality Improvement Pre-Course, as well as, working with a committee that looks at patient quality care and projects to enhance it.
Our work here focuses on examining what has been done, how we can improve it, and how we can institute best practices. Not bad for three weeks’ work!
Conversations in our department focus on whether members get what they need and want. People meet regularly to discuss how we can refine and improve the services we offer. Strategies for securing funding and developing programs are reviewed, not for this calendar or fiscal year but for years to come. In one of my final interviews for this job, I was reminded that we don’t deliver here—we over-deliver. Looking through The Hospitalist, titles that stand out include the words unforgettable, safety, expert, leader, admire, and smart.
When people ask what I do in my new job, I tell them that hospital medicine looks at the total experience of being a doctor. It focuses not only on medical care but also on the complete experience of being a working professional: the arts of research, negotiation, best practices, team-focused care, conflict resolution, and systems change. I explain that we do life-saving work, for it is far more than the practice of just day-to-day medicine that improves all of our lives. I tell people that it is work that makes sense.
When you come to work every day and are surrounded by a dynamic, positive energy, the work you produce is likely to mirror the hospital medicine movement: You will reflect, revise, and grow stronger. Sincere, well-planned initiatives are infectious. Continually participating in an environment that asks the questions, “Where can we take this?” and “What can we do better?” is a pretty good reason to get out of bed in the morning.
Beck is the senior project manager at SHM.
VTE Prevention Collaborative off to a Great Start
The VTE Prevention Collaborative (VTE PC) is the latest SHM initiative to support hospitalist-led efforts to reduce the incidence of preventable, hospital-acquired VTE. Launched in January 2007, the program offers individualized assistance to hospitalists who want to take the lead on this critical quality and patient safety issue.
Hospital-Acquired Venous Thromboembolism
The problem of hospital-acquired VTE is huge. More than 2 million Americans suffer from VTE each year. Most hospitalized patients have at least one risk factor for VTE. In a large registry trial capturing more than 5,451 patients at 183 sites in a six-month period, 50% (2,726) developed their VTE during hospitalization.1 A 400-bed hospital with an average rate of VTE prophylaxis can expect that 200 patients will suffer from hospital-acquired VTE each year; around half of these cases are potentially preventable.1,2
The good news is that effective and safe measures to prevent hospital-acquired VTE exist. Pharmacologic prophylaxis reduces the incidence of asymptomatic and symptomatic DVT and pulmonary embolism (PE) by 50%-65%.3, 4-11 Prevention of DVT also prevents PE and fatalities from PE. The chief concern of prophylaxis is bleeding, but bleeding risk secondary to pharmacologic prophylaxis is a rare event, as is shown in abundant data from meta-analyses and placebo-controlled, randomized controlled trials.3,4
Close the Gap
Reliably preventing VTE in the hospital is inherently complex. VTE risk and bleeding risks vary within patient populations, and these risks may change for an individual patient several times in the course of the hospital stay. Weight, age, renal function, medication changes, and recent or impending invasive interventions may all influence decisions about the best VTE prevention options. Transitions across care providers and locations translate into multiple opportunities for breakdown in the delivery of optimal VTE prophylaxis. Thoughtful, evidence-based protocols, multidisciplinary system changes, and comprehensive educational efforts are required to achieve optimal VTE prophylaxis in the complex hospital setting.
How the VTE PC Can Help
The VTE PC program builds on and complements the VTE prevention materials and educational resources that SHM has produced in recent years. “Our Quality Improvement Resource Rooms have the information and resources needed to tackle a number of key quality issues,” says SHM CEO Larry Wellikson. “The VTE PC project takes this one step further by providing individualized mentorship. SHM is committed to supporting these forward-thinking, unique strategies that will allow hospitalists to lead their hospitals into a better future.”
VTE PC participants can choose the type of support that best fits their needs: a full year of distance mentoring or a one-day evaluation and consultation visit to their site.
The mentoring program presents a perfect option for individuals interested in ongoing support for their planned or active VTE prevention projects. Through the project, SHM mentors with VTE and QI experts who work with participants during eight telephone calls scheduled throughout a yearlong mentoring period. During the calls, mentors offer individualized assistance on any topics, tasks, and barriers that are encountered in the course of designing, implementing, and evaluating a VTE prevention project. Instruction and assistance are tailored to participant needs and commonly focus on:
- Working with medical center administration;
- Using practical methods to assess institutional performance in VTE prophylaxis;
- Identifying and tracking patients with hospital-acquired VTE;
- Constructing a VTE risk-assessment model and integrating it into workflow, order sets, and protocols;
- Enhancing selection of appropriate prophylaxis by linking the VTE risk assessment to a corresponding menu of proven options; and
- Bolstering your chances of success by utilizing high-reliability design features and effective implementation techniques.
The on-site consultation program is a good option for individuals interested in securing expert evaluation and input on a VTE prevention program but who don’t need ongoing support. Through the on-site consultation program, SHM consultants with VTE and QI expertise visit applicants’ hospitals to evaluate active or planned VTE prevention programs. The visits are especially helpful to participants with existing VTE prevention programs that they wish to expand or improve upon.
The consultation visits feature a structured evaluation of the site’s strengths and resources, barriers to improvement, and the design and functioning of active or proposed VTE prevention interventions. Specific consultation-visit activities vary according to participant goals and needs but may include meeting with the local project team, QI leaders, hospital administrators, and hospital medicine group leaders, as well as reviewing project documents—order sets, policies, and procedures—data, and data collection/management tools. Following the visits, SHM consultants provide participants with a written report of findings and recommendations. Participants also receive one follow-up telephone consultation.
Collaborative Members
SHM membership has responded enthusiastically to the VTE PC project. Early enrollees have a wide range of experience with VTE prevention and QI in general. Some fill QI leadership roles in their hospitals or hospital medicine groups; for others, the VTE prevention project is their first experience leading a QI effort. Enrollees represent a range of hospital types (academic centers, community teaching hospitals, community hospitals) and sizes (staffed beds range from 135 to 650) and are located in every U.S. geographic region in multiple hospital systems.
Several participants represent hospitals where VTE prevention programs have been implemented, while most have active projects in which no intervention has yet been implemented; a handful are still in the planning/initial exploration phase of work. Nearly half of the enrolled sites have a history of failed QI efforts in VTE prevention.
Many enrollees are looking to their VTE prevention efforts as a means of positioning their hospital medicine group as a local QI force. “This is the first large project the hospitalist group has undertaken since getting up and running,” reports one attendee. “I would really like to make a positive impact on patient care and lay the groundwork with this project that would allow us to be successful with future undertakings.”
Applying to the Programs
Participation in both the mentoring and on-site consultation programs is open to hospitalists who lead proposed or active VTE prevention projects. Participation is free, but enrollment is limited, so interested individuals are encouraged to apply early. SHM members can apply to either program by completing the online application available on the VTE Prevention Collaborative Web site: www.hospitalmedicine.org/vte-pc.
Direct your questions about VTE Prevention Collaborative programs to [email protected].
Bibliography
- Goldhaber SZ, Tapson VF; DVT FREE Steering Committee. A prospective registry of 5,451 patients with ultrasound-confirmed deep vein thrombosis. Am J Cardiol. 2004 Jan;93(2):259-262.
- Maynard G. Workbook for Improvement: optimize prevention of venous thromboembolism at your medical center [SHM Web site, VTE Quality Improvement Resource Room]. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms&Template=/CM/ContentDisplay.cfm&ContentID=6092. Last accessed March 19, 2007.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):338S-400S. Review. Comment in Chest. 2005 Jun;127(6):2297-2298.
- Shojania KG, Duncan BW, McDonald KM, et al. Making health care safer: a critical analysis of patient safety practices. Evidence Report/Technology Assessment No. 43 [Agency for Healthcare Research and Quality Web site]. July 2001;332–346;AHRQ Publication No. 01-E058. Available at: www.ahrq.gov/clinic/ptsafety/. Last accessed March 19, 2007.
- Belch JJ, Lowe GD, Ward AG, et al. Prevention of deep vein thrombosis in medical patients by low-dose heparin. Scott Med J. 1981 Apr;26(2):115–117.
- Gardlund B. Randomised, controlled trial of low-dose heparin for prevention of fatal pulmonary embolism in patients with infectious diseases. The Heparin Prophylaxis Study Group. Lancet. 1996 May 18;347(9021):1357–1361. Comment in: ACP J Club. 1996 Nov-Dec;125(3):64 & Lancet. 1996 Jul 20; 348(9021):205-206.
- Samama MM, Cohen AT, Darmon JY, et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in Medical Patients with Enoxaparin Study Group. N Engl J Med. 1999 Sep 9;341(11):793–800.
- Leizorovicz A, Cohen AT, Turpie AG, et al. Randomized, placebo-controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients. Circulation. 2004 Aug 17;110(7):874-879.
- Kleber FX, Witt C, Vogel G, et al. Randomized comparison of enoxaparin with unfractionated heparin for the prevention of venous thromboembolism in medical patients with heart failure or severe respiratory disease. Am Heart J. 2003 Apr;145(4):614–621.
- Lechler E, Schramm W, Flosbach CW. The venous thrombotic risk in non-surgical patients: epidemiological data and efficacy/safety profile of a low-molecular-weight heparin (enoxaparin). The Prime Study Group. Haemostasis. 1996;26(Suppl):49–56.
- Cohen AT, Davidson BL, Gallus AS, et al. Fondaparinux for the prevention of VTE in acutely ill medical patients (abstract 42). Blood. 2003;102:15a.
Awards Ceremony Preview
SHM created the Awards of Excellence program to honor members whose contributions to the hospital medicine movement deserve acknowledgment and respect. Award winners will receive complimentary registration and paid airfare to SHM’s Annual Meeting, which is being held this month in Dallas and will be presented during the President’s luncheon. Any physician member whose focus is the general medical care of hospitalized patients is eligible for nomination of the four awards. Award winners have been selected for the following categories: Clinical Excellence, Excellence in Teaching, Outstanding Service, and Research.
The SHM Award for Clinical Excellence will be presented to an individual for recognition of exemplary clinical service in hospital medicine. The Awards Committee has evaluated the candidates according to their outstanding contributions to patient care, their advancement of clinical knowledge, including their leadership and professionalism in medicine, as well as personal excellence in practice management.
The SHM Award for Excellence in Teaching is presented in recognition of outstanding teaching and mentorship in hospital medicine, most specifically within the academic and community practice settings. Consideration was given to those nominees who demonstrated outstanding teaching ability and who served as role models and mentored other hospitalists, residents, medical students, or other healthcare professionals.
The SHM Award for Outstanding Service in Hospital Medicine is presented in recognition of exceptional service to the discipline of hospital medicine. The winning candidate has displayed exemplary organizational and leadership activities within organized medicine and has shown contributing support in public policy.
The SHM Excellence in Research Award is presented in recognition of outstanding achievement by a researcher in the discipline of hospital medicine. The candidate selected presented peer-reviewed publications and continued education with additional research and training that provided for both intra- and extramural funding for research.
For additional information regarding SHM’s Awards Program, please e-mail [email protected]. TH
Dysphagia, Dizziness, and Dysarthria

Brief history: A 32-year-old female presents with dysphagia, dizziness, and dysarthria.
Salient findings: Chest X-ray demonstrates many embolization coils within both lungs. Photographs demonstrate superficial telangiectasias of the tongue and distal phalanx. These findings indicate the patient’s diagnosis: hereditary hemorrhagic telangiectasia (HHT), previously known as Osler-Weber-Rendu syndrome.



Patient population/natural history of disease: HHT is an autosomal dominant trait, so family members should be counseled on the implications of having a relative with the disease. HHT patients have abnormal vessels prone to bleeding and often develop arteriovenous malformations (AVMs). Diagnosis is made with 75% of the following symptoms:
- Epistaxis;
- Mucocutaneous telangiectasias;
- GI, pulmonary, or hepatic AVMs; and/or
- A first-degree relative with HHT.
Patients often present with dyspnea and hemoptysis. With pulmonary AVMs, the oxygenation and filtration functions of the lungs are bypassed, placing the patient at risk for hypoxia, polycythemia, paradoxical strokes, and brain abscesses.
Management: AVMs can be diagnosed and treated with angiography and embolization. In this patient the coils had been placed elsewhere. The use of coils larger than 3 mm in AVMs should be treated because they are associated with significantly increased morbidity and mortality. Steel coils are covered with thrombogenic fibers that induce clotting and sealing of the AVM; blood is no longer shunted through the right-to-left shunt. Unfortunately, a long-term complication of pulmonary AVMs treated by embolization therapy is the development of new pulmonary AVMs.
The patient in this case had many metallic coils visible on chest X-ray and because she had required multiple pulmonary angiograms and embolizations over the years.
It’s important to administer an ECG to all HHT patients prior to treatment; those with a left bundle branch block must have pacing mechanisms in place or at hand because catheter placement and manipulation within the right heart can induce right heart blockage. Take care to avoid air emboli in all lines due to right-to-left shunting in these patients.
Take-Home Points:
- Untreated pulmonary AVMs are associated with paradoxical strokes, brain abscesses, and hypoxia;
- HHT is associated with pulmonary AVMs;
- Coil embolization of pulmonary AVMs has been shown to improve dyspnea and oxygen saturation while decreasing right-to-left shunt fraction in HHT patients.
- Complications of embolization therapy may include development of new pulmonary AVMs; and
- All patients should undergo ECG prior to pulmonary angiography to screen for left bundle branch block. TH
Helena Summers is a radiology resident and Erik Summers is a hospitalist at the Mayo Clinic College of Medicine, Rochester, Minn.
References
- Swanson KL, Prakash UB, Stanson AW. Pulmonary arteriovenous fistulas: Mayo Clinic experience, 1982-1997. Mayo Clin Proc. 1999 Jul;74(7):671-680.
- Cottin V, Plauchu H, Bayle JY, et al. Pulmonary arteriovenous malformations in patients with hereditary hemorrhagic telangiectasia. Am J Respir Crit Care Med. 2004 May 1;169(9):994-1000. Epub 2004 Jan 23.
Brief history: A 32-year-old female presents with dysphagia, dizziness, and dysarthria.
Salient findings: Chest X-ray demonstrates many embolization coils within both lungs. Photographs demonstrate superficial telangiectasias of the tongue and distal phalanx. These findings indicate the patient’s diagnosis: hereditary hemorrhagic telangiectasia (HHT), previously known as Osler-Weber-Rendu syndrome.
Patient population/natural history of disease: HHT is an autosomal dominant trait, so family members should be counseled on the implications of having a relative with the disease. HHT patients have abnormal vessels prone to bleeding and often develop arteriovenous malformations (AVMs). Diagnosis is made with 75% of the following symptoms:
- Epistaxis;
- Mucocutaneous telangiectasias;
- GI, pulmonary, or hepatic AVMs; and/or
- A first-degree relative with HHT.
Patients often present with dyspnea and hemoptysis. With pulmonary AVMs, the oxygenation and filtration functions of the lungs are bypassed, placing the patient at risk for hypoxia, polycythemia, paradoxical strokes, and brain abscesses.
Management: AVMs can be diagnosed and treated with angiography and embolization. In this patient the coils had been placed elsewhere. The use of coils larger than 3 mm in AVMs should be treated because they are associated with significantly increased morbidity and mortality. Steel coils are covered with thrombogenic fibers that induce clotting and sealing of the AVM; blood is no longer shunted through the right-to-left shunt. Unfortunately, a long-term complication of pulmonary AVMs treated by embolization therapy is the development of new pulmonary AVMs.
The patient in this case had many metallic coils visible on chest X-ray and because she had required multiple pulmonary angiograms and embolizations over the years.
It’s important to administer an ECG to all HHT patients prior to treatment; those with a left bundle branch block must have pacing mechanisms in place or at hand because catheter placement and manipulation within the right heart can induce right heart blockage. Take care to avoid air emboli in all lines due to right-to-left shunting in these patients.
Take-Home Points:
- Untreated pulmonary AVMs are associated with paradoxical strokes, brain abscesses, and hypoxia;
- HHT is associated with pulmonary AVMs;
- Coil embolization of pulmonary AVMs has been shown to improve dyspnea and oxygen saturation while decreasing right-to-left shunt fraction in HHT patients.
- Complications of embolization therapy may include development of new pulmonary AVMs; and
- All patients should undergo ECG prior to pulmonary angiography to screen for left bundle branch block. TH
Helena Summers is a radiology resident and Erik Summers is a hospitalist at the Mayo Clinic College of Medicine, Rochester, Minn.
References
- Swanson KL, Prakash UB, Stanson AW. Pulmonary arteriovenous fistulas: Mayo Clinic experience, 1982-1997. Mayo Clin Proc. 1999 Jul;74(7):671-680.
- Cottin V, Plauchu H, Bayle JY, et al. Pulmonary arteriovenous malformations in patients with hereditary hemorrhagic telangiectasia. Am J Respir Crit Care Med. 2004 May 1;169(9):994-1000. Epub 2004 Jan 23.
Brief history: A 32-year-old female presents with dysphagia, dizziness, and dysarthria.
Salient findings: Chest X-ray demonstrates many embolization coils within both lungs. Photographs demonstrate superficial telangiectasias of the tongue and distal phalanx. These findings indicate the patient’s diagnosis: hereditary hemorrhagic telangiectasia (HHT), previously known as Osler-Weber-Rendu syndrome.
Patient population/natural history of disease: HHT is an autosomal dominant trait, so family members should be counseled on the implications of having a relative with the disease. HHT patients have abnormal vessels prone to bleeding and often develop arteriovenous malformations (AVMs). Diagnosis is made with 75% of the following symptoms:
- Epistaxis;
- Mucocutaneous telangiectasias;
- GI, pulmonary, or hepatic AVMs; and/or
- A first-degree relative with HHT.
Patients often present with dyspnea and hemoptysis. With pulmonary AVMs, the oxygenation and filtration functions of the lungs are bypassed, placing the patient at risk for hypoxia, polycythemia, paradoxical strokes, and brain abscesses.
Management: AVMs can be diagnosed and treated with angiography and embolization. In this patient the coils had been placed elsewhere. The use of coils larger than 3 mm in AVMs should be treated because they are associated with significantly increased morbidity and mortality. Steel coils are covered with thrombogenic fibers that induce clotting and sealing of the AVM; blood is no longer shunted through the right-to-left shunt. Unfortunately, a long-term complication of pulmonary AVMs treated by embolization therapy is the development of new pulmonary AVMs.
The patient in this case had many metallic coils visible on chest X-ray and because she had required multiple pulmonary angiograms and embolizations over the years.
It’s important to administer an ECG to all HHT patients prior to treatment; those with a left bundle branch block must have pacing mechanisms in place or at hand because catheter placement and manipulation within the right heart can induce right heart blockage. Take care to avoid air emboli in all lines due to right-to-left shunting in these patients.
Take-Home Points:
- Untreated pulmonary AVMs are associated with paradoxical strokes, brain abscesses, and hypoxia;
- HHT is associated with pulmonary AVMs;
- Coil embolization of pulmonary AVMs has been shown to improve dyspnea and oxygen saturation while decreasing right-to-left shunt fraction in HHT patients.
- Complications of embolization therapy may include development of new pulmonary AVMs; and
- All patients should undergo ECG prior to pulmonary angiography to screen for left bundle branch block. TH
Helena Summers is a radiology resident and Erik Summers is a hospitalist at the Mayo Clinic College of Medicine, Rochester, Minn.
References
- Swanson KL, Prakash UB, Stanson AW. Pulmonary arteriovenous fistulas: Mayo Clinic experience, 1982-1997. Mayo Clin Proc. 1999 Jul;74(7):671-680.
- Cottin V, Plauchu H, Bayle JY, et al. Pulmonary arteriovenous malformations in patients with hereditary hemorrhagic telangiectasia. Am J Respir Crit Care Med. 2004 May 1;169(9):994-1000. Epub 2004 Jan 23.
In the Literature

Hospital Quality for AMI: Process Measures and Their Relationship with Short-term Mortality
Bradley EH, Herrin J, Elbel B, et al. Hospital quality for acute myocardial infarction: correlation among process measures and relationship with short-term mortality. JAMA. 2006 Jul 5;296(1):72-78.
Background
The Centers for Medicare and Medicaid Services (CMS) and the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) monitor and publicly report hospital performance in the treatment of acute myocardial infarction (AMI). Core process measures are considered an indicator of quality of care, but little is known about how these measures affect outcomes (mortality). Five of the seven core measures for AMI assess medication prescription practices; the other two measures are counseling on smoking cessation and timely reperfusion therapy.
Inferences about a hospital’s quality of care for AMI are created by measuring the hospital’s success at performing these measures. No previous study had evaluated a possible correlation between performance on these measures and short-term mortality. The authors of this study used National Registry of Myocardial Infarction (NRMI) and CMS databases to determine the association between hospital performance on AMI process measures and hospital-specific, risk-standardized, 30-day mortality rates.
Methods
A cross-sectional study was performed using hospitals that reported AMI discharges to the NRMI from January 2002 through March 2003. Hospitals had to report a minimum of 10 eligible patients. Hospital performance on core measures was recorded: beta-blocker on admission, beta-blocker on dismissal, aspirin on admission, aspirin on dismissal, angiotensin-converting enzyme inhibitor (ACE) prescription on dismissal, smoking cessation counseling for smokers during admission, and time to reperfusion therapy. Risk-standardized, 30-day, all-cause mortality rates were calculated for each hospital using CMS Medicare claims for patients ages 66 and older with AMI. The primary analysis determined the association of hospital-specific, risk-standardized, 30-day mortality rates with hospital performance on the core process measures.
Results
The most successfully completed core process measure for AMI was aspirin on admission. A mean of 86.4% of participating hospitals completed this measure. The core process measure for AMI that was the least frequently documented was smoking cessation counseling; a mean of 13.9% of participating hospitals completed this measure. Notably, timely reperfusion therapy for AMI—fibrinolytic therapy within 30 minutes of arrival or percutaneous intervention within 120 minutes of arrival—was completed by only 54.5% (mean) of participating hospitals.
Each core process measure had a statistically significant but small correlation with the risk-standardized, 30-day mortality rate (explaining between 0.1% and 3.3% of variance in mortality). Of the 180 hospitals in the top quintile of risk-standardized, 30-day mortality rates, only 31% were in the top quintile of the core process measures. A composite model of all seven core process measures determined that these measures could only explain 6% of the hospital-level variation in risk-standardized, 30-day mortality rates. Secondary analyses did not differ substantially.
Conclusions
In this study, each core process measure for AMI showed a modest correlation with 30-day mortality, but accounted for only 6% of 30-day mortality. This finding highlights the fact that continued measurement of these processes is valuable, but a hospital’s short-term mortality rates for AMI cannot be reliably inferred from performance on publicly reported process measures. These measures are weighted more toward long-term outcome measures. There is a need for new research to define and study new AMI process measures that can explain more of the variance in both short- and long-term outcomes.
Clopidogrel and Aspirin versus Aspirin Alone for the Prevention of Atherothrombotic Events
Bhatt DL, Fox KA, Hacke W, et al. Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events. N Engl J Med. 2006 Apr 20;354(16):1706-1717.
Background
Atherothrombotic disorders of the circulatory system are the leading cause of death and disability in the world. Low-dose aspirin has been shown to reduce ischemic event in populations above a certain risk threshold; however, aspirin alone may be insufficient treatment to prevent ischemic events in high-risk patients. Dual antiplatelet therapy with aspirin and clopidogrel has been shown to reduce ischemic events in patients with unstable angina, non-ST segment elevation and ST segment elevation myocardial infarction, as well as in those undergoing angioplasty and stenting.
Methods
This was a prospective, multicenter, randomized, double-blind, placebo-controlled study of the efficacy and safety of aspirin plus clopidogrel in comparison with aspirin plus placebo in patients at high risk for a cardiovascular event. Patients included in the study were 45 or older and had one of the following: multiple atherothrombotic risk factors, documented coronary artery disease, documented cerebrovascular disease, or documented symptomatic peripheral vascular disease. The primary efficacy endpoint was the first occurrence of myocardial infarction (MI), stroke, or death from cardiovascular causes. The primary safety endpoint was severe bleeding.
Results
A total of 15,603 patients were enrolled in the study. Treatment was permanently discontinued by 20.4% in the clopidogrel group as compared with 18.2% in the placebo group (P<0.001). A total of 4.8% of patients in the clopidogrel group and 4.9% in the placebo group discontinued treatment because of an adverse event (P=0.67). Other than the treatment medications, concomitant medication use was similar in both groups. A median follow-up of 28 months revealed that the rates of primary efficacy events in the clopidogrel and placebo group were similar (6.8% versus 7.3%, P=0.22, respectively). The rate of primary safety events was 1.7% in the clopidogrel group and 1.3% in the placebo group, P=0.09.
Conclusions
This trial enrolled patients who either had established atherothrombotic disease or were at high risk for such disease and found that there was no significant benefit associated with the use of clopidogrel plus aspirin compared to aspirin alone in reducing myocardial infarction, stroke, or cardiovascular death. The risk of moderate or severe bleeding in symptomatic patients was higher in the clopidogrel plus aspirin group than in the aspirin plus placebo group. Overall, these findings do not support the use of dual antiplatelet therapy across this broad patient population.
D-Dimer in the Diagnosis of Pulmonary Embolism
Kearon C, Ginsberg JS, Douketis J, et al. An evaluation of D-dimer in the diagnosis of pulmonary embolism: a randomized trial. Ann Intern Med. 2006 Jun 6;144(11):812-821.
Background
The clinical usefulness of the D-dimer test in the diagnosis of pulmonary embolism (PE) has been previously studied. In patients with suspected PE, it may be safe to omit additional diagnostic testing if a patient has a negative D-dimer test; however, this approach has never been evaluated in a randomized, controlled trial.
The investigators in this trial studied two subgroups of patients with suspected PE and a negative D-dimer: patients with a low clinical probability of PE and those with a moderate or high clinical probability of PE who had a non-diagnostic ventilation perfusion scan (VQ scan) and no proximal deep vein thrombosis on venous ultrasonography. The hypothesis was that patients with a negative D-dimer who do not have further testing for PE won’t have a higher frequency of venous thromboembolism during follow-up than patients who undergo routine diagnostic testing.
Methods
Before any diagnostic testing, patients were assigned a probability score, using the Wells Criteria, to categorize the probability of PE as low or moderate to high.
Patients with low probability Wells scores: D-dimer testing was done on all patients with a low clinical probability of PE. Patients with a negative D-dimer were randomly assigned either to no additional diagnostic testing and no anticoagulation treatment or to additional diagnostic testing with an initial VQ scan. If the VQ scan was negative, then PE was excluded. If the VQ scan showed one or more segmental perfusion defects that were normally ventilated, then the scan was considered diagnostic for PE. If there were perfusion defects that did not meet the criteria for a high probability scan, then the scan was considered non-diagnostic. Patients with non-diagnostic scans underwent ultrasonography of the proximal veins of the legs. If deep vein thrombosis was present, PE was diagnosed. If ultrasonography was normal, the test was repeated after seven and 14 days. In all patients with a positive D-dimer, a VQ scan was performed.
Patients with moderate to high probability Wells scores: A VQ scan was performed on all patients with a moderate to high probability for PE. Patients with high probability scans were treated; patients with normal scans were not treated. Patients with non-diagnostic scans and normal venous ultrasonography were randomly assigned to receive either no additional testing or serial ultrasonography.
Outcomes: All patients were followed for six months for the development of venous thromboembolism after initial diagnostic testing.
Results
The study enrolled 1,126 patients. Overall, 160 patients (14.2%) had PE diagnosed at initial presentation or by venous ultrasonography. Of 952 patients who did not receive an initial diagnosis of PE, 11 (1.2%) had PE diagnosed at follow-up.
Patients with low probability Wells scores: Low clinical probability was present in 670 patients (60%). In patients with low clinical probability of PE, 373 (56%) had negative D-dimer tests and 297 (44%) had positive D-dimer tests. Of the 373 patients with low probability and negative D-dimer results, 187 were randomized to no additional testing and 186 received a VQ scan. The frequency of venous thromboembolism at six-month follow-up was similar in these two groups (-0.5% [CI, -3.0% to 1.6%]). Three patients with negative D-dimer tests were diagnosed with PE by VQ scan. Results were fairly complete (five patients without a six-month follow-up in the no additional testing group and one without a follow-up in the VQ scan group).
Twenty-four patients with low clinical probability and positive D-dimer results (n=297) were diagnosed with PE. Three patients did not complete the six-month follow-up. Of the remaining 294 patients, five patients had venous thromboembolism at six months.
Patients with moderate to high probability Wells scores: There were 456 patients (40%) had moderate or high clinical probability for PE. Each of these patients had a VQ scan. Non-diagnostic VQ scans and normal venous ultrasonography were performed on 226 patients. Of these 226 patients, 86 had a negative D-dimer and 140 had a positive D-dimer. Of the 86 patients with negative VQ scans, normal venous ultrasonography, and a negative D-dimer, 83 were randomly assigned to no additional testing or serial venous ultrasonography (42 and 41 respectively). At six months follow-up, one patient assigned to no additional testing had venous thromboembolism, and no patients in the additional testing group had venous thromboembolism.
Conclusions
The results of this trial suggest that it is safe to withhold additional diagnostic testing in patients with suspected PE, low pretest clinical probability, and a negative D-dimer test. Even in patients with moderate to high pretest clinical probability, a non-diagnostic VQ scan, and normal venous ultrasonography, only one patient with a negative D-dimer had a venous thromboembolic event at six months follow-up. The assay used for this study was an erythrocyte agglutination SimpliRED assay. Reported sensitivity is approximately 90%, and specificity is approximately 75%. To the readers, it should be noted that the authors defined a low probability Wells score as 4 rather than 1.5 or lower.
Efficacy and Safety of Inhaled Insulin Therapy in Adults with Diabetes Mellitus
Ceglia L, Lau J, Pittas AG. Meta-analysis: efficacy and safety of inhaled insulin therapy in adults with diabetes mellitus. Ann Intern Med. 2006 Nov 7;145(9):665-675.
Background
Despite its effectiveness in attaining glycemic control, there is considerable resistance to insulin use by patients and healthcare providers, primarily because of the need for subcutaneous injection. In January 2006, the U.S. Food and Drug Administration (FDA) approved the first formulation of inhaled insulin for clinical use in nonsmoking adults with type 1 or type 2 diabetes and no pulmonary disease. The authors of this paper present a systematic review to examine the efficacy, safety, and patient acceptability of inhaled insulin.
Methods
The authors conducted a search of MEDLINE to find English-language, randomized, controlled trials of inhaled insulin in nonpregnant adults with diabetes. To find unpublished studies, the authors reviewed the briefing document on Exubera powder for oral inhalation (Pfizer Inc., New York). An abstract was included if it reported original data from controlled trials in patients with type 1 or 2 diabetes and hemoglobin A1C outcomes for patients receiving inhaled insulin versus outcomes for a comparison group (subcutaneous insulin or oral hypoglycemics). Studies with less than 12 weeks duration were excluded because no comparison could be made regarding glycemic efficacy. For glycemic efficacy, the primary outcome was the treatment group difference in hemoglobin A1C from baseline. Secondary outcome was the proportion of patients with hemoglobin A1C levels less than 7%. To evaluate safety, the primary outcomes were severe hypoglycemia (glucose ≤36 mg/dL), cough, and treatment group difference in pulmonary function variables.
Results
Sixteen trials involving a total of 4,023 patients met inclusion criteria. Seven trials compared inhaled insulin with various subcutaneous insulin regimens in patients with type 1 diabetes. Nine trials compared inhaled insulin with subcutaneous insulin or oral hypoglycemic agents in patients with type 2 diabetes. Inhaled insulin was given with meals and titrated according to study-specific glucose goals. Subcutaneous insulin was titrated to the same specific goals. Doses of oral hypoglycemic agents were adjusted for glycemic targets in only two of the nine trials. The combined data from the studies demonstrated a small but statistically significant decrease in the levels of baseline hemoglobin A1C levels in favor of subcutaneous insulin (weighted mean difference 0.08%, [CI 0.03% to 0.14%]) in patients with type 1 or type 2 diabetes. The greatest advantage of subcutaneous insulin was noted in the study with the longest duration (104 weeks). There was no difference between the study groups in studies with duration of 24 weeks or less. Patients with type 1 or type 2 diabetes taking inhaled insulin were no more likely to achieve hemoglobin A1C levels less than 7% than those using subcutaneous insulin.
The combined data from studies comparing inhaled insulin to oral hypoglycemic agents in patients with type 2 diabetes showed that inhaled insulin lowered hemoglobin A1C levels more effectively (weighted mean difference -1.04%, [CI -1.59% to -0.49%]). In studies in which the oral hypoglycemic agents were titrated, inhaled insulin still lowered baseline hemoglobin A1C levels but to a lesser degree (weighted mean difference -0.20%, [CI - 0.34% to -0.07%]). Patients with type 2 diabetes taking inhaled insulin were more likely to achieve hemoglobin A1C levels less than 7% than those taking oral agents.
There was no difference in episodes of severe hypoglycemia in patients using inhaled insulin compared to those using subcutaneous insulin. A higher proportion of patients using inhaled insulin reported at least one episode of severe hypoglycemia compared to those using oral agents (risk ratio, 3.06 [CI 1.03 to 9.07]; 9.4% versus 3.5%, respectively).
With respect to pulmonary safety, all trials selected patients without histories of pulmonary problems and with at least six months of nonsmoking status. Pulmonary safety was assessed by self-reported symptoms and by pulmonary function tests. The most common pulmonary symptom associated with inhaled insulin was nonproductive cough. This symptom was reported more frequently compared to patients using subcutaneous insulin or oral agents (risk ratio, 3.52 [CI 2.23 to 5.56]; 16.9% versus 5.0%). Cough was noted early in the treatment course and diminished in frequency over time. Patients receiving inhaled insulin had a greater decrease in FEV1 (forced expiratory volume in the first second) from baseline than the comparator group (weighted mean difference, -0.031 L [CI-0.043 L to -0.020 L]). This decrease progressed slowly over the first six months but stabilized in studies of up to two years’ duration.
Only four trials reported data on overall patient satisfaction for inhaled insulin versus subcutaneous insulin. All trials reported a statistically significant increase in overall patient satisfaction with inhaled insulin over subcutaneous insulin. Patients randomly assigned to inhaled insulin were more likely to continue taking inhaled insulin than to switch back to subcutaneous insulin.
Conclusions
This meta-analysis showed that inhaled insulin is comparable to subcutaneous insulin in lowering hemoglobin A1C levels in patients with type 1 or type 2 diabetes. The proportion of patients reaching a target hemoglobin A1C of less than 7% was much lower in the studies in this meta-analysis as compared to levels in trials of intensive subcutaneous insulin therapy.
It’s more difficult to compare inhaled insulin with oral hypoglycemic agents because most studies involving oral agents used fixed dosing with different types of oral agents. There was a three-fold risk of severe hypoglycemia in patients using inhaled insulin compared to those using oral hypoglycemic agents. This is probably due to overall improved glycemic control in the inhaled insulin group. Cough was more common in the inhaled insulin groups, and there were small decreases in FEV1, but these did not progress over two years. The potential for pulmonary toxicity with long-term administration has not been evaluated and deserves further study.
Hospital Quality for AMI: Process Measures and Their Relationship with Short-term Mortality
Bradley EH, Herrin J, Elbel B, et al. Hospital quality for acute myocardial infarction: correlation among process measures and relationship with short-term mortality. JAMA. 2006 Jul 5;296(1):72-78.
Background
The Centers for Medicare and Medicaid Services (CMS) and the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) monitor and publicly report hospital performance in the treatment of acute myocardial infarction (AMI). Core process measures are considered an indicator of quality of care, but little is known about how these measures affect outcomes (mortality). Five of the seven core measures for AMI assess medication prescription practices; the other two measures are counseling on smoking cessation and timely reperfusion therapy.
Inferences about a hospital’s quality of care for AMI are created by measuring the hospital’s success at performing these measures. No previous study had evaluated a possible correlation between performance on these measures and short-term mortality. The authors of this study used National Registry of Myocardial Infarction (NRMI) and CMS databases to determine the association between hospital performance on AMI process measures and hospital-specific, risk-standardized, 30-day mortality rates.
Methods
A cross-sectional study was performed using hospitals that reported AMI discharges to the NRMI from January 2002 through March 2003. Hospitals had to report a minimum of 10 eligible patients. Hospital performance on core measures was recorded: beta-blocker on admission, beta-blocker on dismissal, aspirin on admission, aspirin on dismissal, angiotensin-converting enzyme inhibitor (ACE) prescription on dismissal, smoking cessation counseling for smokers during admission, and time to reperfusion therapy. Risk-standardized, 30-day, all-cause mortality rates were calculated for each hospital using CMS Medicare claims for patients ages 66 and older with AMI. The primary analysis determined the association of hospital-specific, risk-standardized, 30-day mortality rates with hospital performance on the core process measures.
Results
The most successfully completed core process measure for AMI was aspirin on admission. A mean of 86.4% of participating hospitals completed this measure. The core process measure for AMI that was the least frequently documented was smoking cessation counseling; a mean of 13.9% of participating hospitals completed this measure. Notably, timely reperfusion therapy for AMI—fibrinolytic therapy within 30 minutes of arrival or percutaneous intervention within 120 minutes of arrival—was completed by only 54.5% (mean) of participating hospitals.
Each core process measure had a statistically significant but small correlation with the risk-standardized, 30-day mortality rate (explaining between 0.1% and 3.3% of variance in mortality). Of the 180 hospitals in the top quintile of risk-standardized, 30-day mortality rates, only 31% were in the top quintile of the core process measures. A composite model of all seven core process measures determined that these measures could only explain 6% of the hospital-level variation in risk-standardized, 30-day mortality rates. Secondary analyses did not differ substantially.
Conclusions
In this study, each core process measure for AMI showed a modest correlation with 30-day mortality, but accounted for only 6% of 30-day mortality. This finding highlights the fact that continued measurement of these processes is valuable, but a hospital’s short-term mortality rates for AMI cannot be reliably inferred from performance on publicly reported process measures. These measures are weighted more toward long-term outcome measures. There is a need for new research to define and study new AMI process measures that can explain more of the variance in both short- and long-term outcomes.
Clopidogrel and Aspirin versus Aspirin Alone for the Prevention of Atherothrombotic Events
Bhatt DL, Fox KA, Hacke W, et al. Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events. N Engl J Med. 2006 Apr 20;354(16):1706-1717.
Background
Atherothrombotic disorders of the circulatory system are the leading cause of death and disability in the world. Low-dose aspirin has been shown to reduce ischemic event in populations above a certain risk threshold; however, aspirin alone may be insufficient treatment to prevent ischemic events in high-risk patients. Dual antiplatelet therapy with aspirin and clopidogrel has been shown to reduce ischemic events in patients with unstable angina, non-ST segment elevation and ST segment elevation myocardial infarction, as well as in those undergoing angioplasty and stenting.
Methods
This was a prospective, multicenter, randomized, double-blind, placebo-controlled study of the efficacy and safety of aspirin plus clopidogrel in comparison with aspirin plus placebo in patients at high risk for a cardiovascular event. Patients included in the study were 45 or older and had one of the following: multiple atherothrombotic risk factors, documented coronary artery disease, documented cerebrovascular disease, or documented symptomatic peripheral vascular disease. The primary efficacy endpoint was the first occurrence of myocardial infarction (MI), stroke, or death from cardiovascular causes. The primary safety endpoint was severe bleeding.
Results
A total of 15,603 patients were enrolled in the study. Treatment was permanently discontinued by 20.4% in the clopidogrel group as compared with 18.2% in the placebo group (P<0.001). A total of 4.8% of patients in the clopidogrel group and 4.9% in the placebo group discontinued treatment because of an adverse event (P=0.67). Other than the treatment medications, concomitant medication use was similar in both groups. A median follow-up of 28 months revealed that the rates of primary efficacy events in the clopidogrel and placebo group were similar (6.8% versus 7.3%, P=0.22, respectively). The rate of primary safety events was 1.7% in the clopidogrel group and 1.3% in the placebo group, P=0.09.
Conclusions
This trial enrolled patients who either had established atherothrombotic disease or were at high risk for such disease and found that there was no significant benefit associated with the use of clopidogrel plus aspirin compared to aspirin alone in reducing myocardial infarction, stroke, or cardiovascular death. The risk of moderate or severe bleeding in symptomatic patients was higher in the clopidogrel plus aspirin group than in the aspirin plus placebo group. Overall, these findings do not support the use of dual antiplatelet therapy across this broad patient population.
D-Dimer in the Diagnosis of Pulmonary Embolism
Kearon C, Ginsberg JS, Douketis J, et al. An evaluation of D-dimer in the diagnosis of pulmonary embolism: a randomized trial. Ann Intern Med. 2006 Jun 6;144(11):812-821.
Background
The clinical usefulness of the D-dimer test in the diagnosis of pulmonary embolism (PE) has been previously studied. In patients with suspected PE, it may be safe to omit additional diagnostic testing if a patient has a negative D-dimer test; however, this approach has never been evaluated in a randomized, controlled trial.
The investigators in this trial studied two subgroups of patients with suspected PE and a negative D-dimer: patients with a low clinical probability of PE and those with a moderate or high clinical probability of PE who had a non-diagnostic ventilation perfusion scan (VQ scan) and no proximal deep vein thrombosis on venous ultrasonography. The hypothesis was that patients with a negative D-dimer who do not have further testing for PE won’t have a higher frequency of venous thromboembolism during follow-up than patients who undergo routine diagnostic testing.
Methods
Before any diagnostic testing, patients were assigned a probability score, using the Wells Criteria, to categorize the probability of PE as low or moderate to high.
Patients with low probability Wells scores: D-dimer testing was done on all patients with a low clinical probability of PE. Patients with a negative D-dimer were randomly assigned either to no additional diagnostic testing and no anticoagulation treatment or to additional diagnostic testing with an initial VQ scan. If the VQ scan was negative, then PE was excluded. If the VQ scan showed one or more segmental perfusion defects that were normally ventilated, then the scan was considered diagnostic for PE. If there were perfusion defects that did not meet the criteria for a high probability scan, then the scan was considered non-diagnostic. Patients with non-diagnostic scans underwent ultrasonography of the proximal veins of the legs. If deep vein thrombosis was present, PE was diagnosed. If ultrasonography was normal, the test was repeated after seven and 14 days. In all patients with a positive D-dimer, a VQ scan was performed.
Patients with moderate to high probability Wells scores: A VQ scan was performed on all patients with a moderate to high probability for PE. Patients with high probability scans were treated; patients with normal scans were not treated. Patients with non-diagnostic scans and normal venous ultrasonography were randomly assigned to receive either no additional testing or serial ultrasonography.
Outcomes: All patients were followed for six months for the development of venous thromboembolism after initial diagnostic testing.
Results
The study enrolled 1,126 patients. Overall, 160 patients (14.2%) had PE diagnosed at initial presentation or by venous ultrasonography. Of 952 patients who did not receive an initial diagnosis of PE, 11 (1.2%) had PE diagnosed at follow-up.
Patients with low probability Wells scores: Low clinical probability was present in 670 patients (60%). In patients with low clinical probability of PE, 373 (56%) had negative D-dimer tests and 297 (44%) had positive D-dimer tests. Of the 373 patients with low probability and negative D-dimer results, 187 were randomized to no additional testing and 186 received a VQ scan. The frequency of venous thromboembolism at six-month follow-up was similar in these two groups (-0.5% [CI, -3.0% to 1.6%]). Three patients with negative D-dimer tests were diagnosed with PE by VQ scan. Results were fairly complete (five patients without a six-month follow-up in the no additional testing group and one without a follow-up in the VQ scan group).
Twenty-four patients with low clinical probability and positive D-dimer results (n=297) were diagnosed with PE. Three patients did not complete the six-month follow-up. Of the remaining 294 patients, five patients had venous thromboembolism at six months.
Patients with moderate to high probability Wells scores: There were 456 patients (40%) had moderate or high clinical probability for PE. Each of these patients had a VQ scan. Non-diagnostic VQ scans and normal venous ultrasonography were performed on 226 patients. Of these 226 patients, 86 had a negative D-dimer and 140 had a positive D-dimer. Of the 86 patients with negative VQ scans, normal venous ultrasonography, and a negative D-dimer, 83 were randomly assigned to no additional testing or serial venous ultrasonography (42 and 41 respectively). At six months follow-up, one patient assigned to no additional testing had venous thromboembolism, and no patients in the additional testing group had venous thromboembolism.
Conclusions
The results of this trial suggest that it is safe to withhold additional diagnostic testing in patients with suspected PE, low pretest clinical probability, and a negative D-dimer test. Even in patients with moderate to high pretest clinical probability, a non-diagnostic VQ scan, and normal venous ultrasonography, only one patient with a negative D-dimer had a venous thromboembolic event at six months follow-up. The assay used for this study was an erythrocyte agglutination SimpliRED assay. Reported sensitivity is approximately 90%, and specificity is approximately 75%. To the readers, it should be noted that the authors defined a low probability Wells score as 4 rather than 1.5 or lower.
Efficacy and Safety of Inhaled Insulin Therapy in Adults with Diabetes Mellitus
Ceglia L, Lau J, Pittas AG. Meta-analysis: efficacy and safety of inhaled insulin therapy in adults with diabetes mellitus. Ann Intern Med. 2006 Nov 7;145(9):665-675.
Background
Despite its effectiveness in attaining glycemic control, there is considerable resistance to insulin use by patients and healthcare providers, primarily because of the need for subcutaneous injection. In January 2006, the U.S. Food and Drug Administration (FDA) approved the first formulation of inhaled insulin for clinical use in nonsmoking adults with type 1 or type 2 diabetes and no pulmonary disease. The authors of this paper present a systematic review to examine the efficacy, safety, and patient acceptability of inhaled insulin.
Methods
The authors conducted a search of MEDLINE to find English-language, randomized, controlled trials of inhaled insulin in nonpregnant adults with diabetes. To find unpublished studies, the authors reviewed the briefing document on Exubera powder for oral inhalation (Pfizer Inc., New York). An abstract was included if it reported original data from controlled trials in patients with type 1 or 2 diabetes and hemoglobin A1C outcomes for patients receiving inhaled insulin versus outcomes for a comparison group (subcutaneous insulin or oral hypoglycemics). Studies with less than 12 weeks duration were excluded because no comparison could be made regarding glycemic efficacy. For glycemic efficacy, the primary outcome was the treatment group difference in hemoglobin A1C from baseline. Secondary outcome was the proportion of patients with hemoglobin A1C levels less than 7%. To evaluate safety, the primary outcomes were severe hypoglycemia (glucose ≤36 mg/dL), cough, and treatment group difference in pulmonary function variables.
Results
Sixteen trials involving a total of 4,023 patients met inclusion criteria. Seven trials compared inhaled insulin with various subcutaneous insulin regimens in patients with type 1 diabetes. Nine trials compared inhaled insulin with subcutaneous insulin or oral hypoglycemic agents in patients with type 2 diabetes. Inhaled insulin was given with meals and titrated according to study-specific glucose goals. Subcutaneous insulin was titrated to the same specific goals. Doses of oral hypoglycemic agents were adjusted for glycemic targets in only two of the nine trials. The combined data from the studies demonstrated a small but statistically significant decrease in the levels of baseline hemoglobin A1C levels in favor of subcutaneous insulin (weighted mean difference 0.08%, [CI 0.03% to 0.14%]) in patients with type 1 or type 2 diabetes. The greatest advantage of subcutaneous insulin was noted in the study with the longest duration (104 weeks). There was no difference between the study groups in studies with duration of 24 weeks or less. Patients with type 1 or type 2 diabetes taking inhaled insulin were no more likely to achieve hemoglobin A1C levels less than 7% than those using subcutaneous insulin.
The combined data from studies comparing inhaled insulin to oral hypoglycemic agents in patients with type 2 diabetes showed that inhaled insulin lowered hemoglobin A1C levels more effectively (weighted mean difference -1.04%, [CI -1.59% to -0.49%]). In studies in which the oral hypoglycemic agents were titrated, inhaled insulin still lowered baseline hemoglobin A1C levels but to a lesser degree (weighted mean difference -0.20%, [CI - 0.34% to -0.07%]). Patients with type 2 diabetes taking inhaled insulin were more likely to achieve hemoglobin A1C levels less than 7% than those taking oral agents.
There was no difference in episodes of severe hypoglycemia in patients using inhaled insulin compared to those using subcutaneous insulin. A higher proportion of patients using inhaled insulin reported at least one episode of severe hypoglycemia compared to those using oral agents (risk ratio, 3.06 [CI 1.03 to 9.07]; 9.4% versus 3.5%, respectively).
With respect to pulmonary safety, all trials selected patients without histories of pulmonary problems and with at least six months of nonsmoking status. Pulmonary safety was assessed by self-reported symptoms and by pulmonary function tests. The most common pulmonary symptom associated with inhaled insulin was nonproductive cough. This symptom was reported more frequently compared to patients using subcutaneous insulin or oral agents (risk ratio, 3.52 [CI 2.23 to 5.56]; 16.9% versus 5.0%). Cough was noted early in the treatment course and diminished in frequency over time. Patients receiving inhaled insulin had a greater decrease in FEV1 (forced expiratory volume in the first second) from baseline than the comparator group (weighted mean difference, -0.031 L [CI-0.043 L to -0.020 L]). This decrease progressed slowly over the first six months but stabilized in studies of up to two years’ duration.
Only four trials reported data on overall patient satisfaction for inhaled insulin versus subcutaneous insulin. All trials reported a statistically significant increase in overall patient satisfaction with inhaled insulin over subcutaneous insulin. Patients randomly assigned to inhaled insulin were more likely to continue taking inhaled insulin than to switch back to subcutaneous insulin.
Conclusions
This meta-analysis showed that inhaled insulin is comparable to subcutaneous insulin in lowering hemoglobin A1C levels in patients with type 1 or type 2 diabetes. The proportion of patients reaching a target hemoglobin A1C of less than 7% was much lower in the studies in this meta-analysis as compared to levels in trials of intensive subcutaneous insulin therapy.
It’s more difficult to compare inhaled insulin with oral hypoglycemic agents because most studies involving oral agents used fixed dosing with different types of oral agents. There was a three-fold risk of severe hypoglycemia in patients using inhaled insulin compared to those using oral hypoglycemic agents. This is probably due to overall improved glycemic control in the inhaled insulin group. Cough was more common in the inhaled insulin groups, and there were small decreases in FEV1, but these did not progress over two years. The potential for pulmonary toxicity with long-term administration has not been evaluated and deserves further study.
Hospital Quality for AMI: Process Measures and Their Relationship with Short-term Mortality
Bradley EH, Herrin J, Elbel B, et al. Hospital quality for acute myocardial infarction: correlation among process measures and relationship with short-term mortality. JAMA. 2006 Jul 5;296(1):72-78.
Background
The Centers for Medicare and Medicaid Services (CMS) and the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) monitor and publicly report hospital performance in the treatment of acute myocardial infarction (AMI). Core process measures are considered an indicator of quality of care, but little is known about how these measures affect outcomes (mortality). Five of the seven core measures for AMI assess medication prescription practices; the other two measures are counseling on smoking cessation and timely reperfusion therapy.
Inferences about a hospital’s quality of care for AMI are created by measuring the hospital’s success at performing these measures. No previous study had evaluated a possible correlation between performance on these measures and short-term mortality. The authors of this study used National Registry of Myocardial Infarction (NRMI) and CMS databases to determine the association between hospital performance on AMI process measures and hospital-specific, risk-standardized, 30-day mortality rates.
Methods
A cross-sectional study was performed using hospitals that reported AMI discharges to the NRMI from January 2002 through March 2003. Hospitals had to report a minimum of 10 eligible patients. Hospital performance on core measures was recorded: beta-blocker on admission, beta-blocker on dismissal, aspirin on admission, aspirin on dismissal, angiotensin-converting enzyme inhibitor (ACE) prescription on dismissal, smoking cessation counseling for smokers during admission, and time to reperfusion therapy. Risk-standardized, 30-day, all-cause mortality rates were calculated for each hospital using CMS Medicare claims for patients ages 66 and older with AMI. The primary analysis determined the association of hospital-specific, risk-standardized, 30-day mortality rates with hospital performance on the core process measures.
Results
The most successfully completed core process measure for AMI was aspirin on admission. A mean of 86.4% of participating hospitals completed this measure. The core process measure for AMI that was the least frequently documented was smoking cessation counseling; a mean of 13.9% of participating hospitals completed this measure. Notably, timely reperfusion therapy for AMI—fibrinolytic therapy within 30 minutes of arrival or percutaneous intervention within 120 minutes of arrival—was completed by only 54.5% (mean) of participating hospitals.
Each core process measure had a statistically significant but small correlation with the risk-standardized, 30-day mortality rate (explaining between 0.1% and 3.3% of variance in mortality). Of the 180 hospitals in the top quintile of risk-standardized, 30-day mortality rates, only 31% were in the top quintile of the core process measures. A composite model of all seven core process measures determined that these measures could only explain 6% of the hospital-level variation in risk-standardized, 30-day mortality rates. Secondary analyses did not differ substantially.
Conclusions
In this study, each core process measure for AMI showed a modest correlation with 30-day mortality, but accounted for only 6% of 30-day mortality. This finding highlights the fact that continued measurement of these processes is valuable, but a hospital’s short-term mortality rates for AMI cannot be reliably inferred from performance on publicly reported process measures. These measures are weighted more toward long-term outcome measures. There is a need for new research to define and study new AMI process measures that can explain more of the variance in both short- and long-term outcomes.
Clopidogrel and Aspirin versus Aspirin Alone for the Prevention of Atherothrombotic Events
Bhatt DL, Fox KA, Hacke W, et al. Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events. N Engl J Med. 2006 Apr 20;354(16):1706-1717.
Background
Atherothrombotic disorders of the circulatory system are the leading cause of death and disability in the world. Low-dose aspirin has been shown to reduce ischemic event in populations above a certain risk threshold; however, aspirin alone may be insufficient treatment to prevent ischemic events in high-risk patients. Dual antiplatelet therapy with aspirin and clopidogrel has been shown to reduce ischemic events in patients with unstable angina, non-ST segment elevation and ST segment elevation myocardial infarction, as well as in those undergoing angioplasty and stenting.
Methods
This was a prospective, multicenter, randomized, double-blind, placebo-controlled study of the efficacy and safety of aspirin plus clopidogrel in comparison with aspirin plus placebo in patients at high risk for a cardiovascular event. Patients included in the study were 45 or older and had one of the following: multiple atherothrombotic risk factors, documented coronary artery disease, documented cerebrovascular disease, or documented symptomatic peripheral vascular disease. The primary efficacy endpoint was the first occurrence of myocardial infarction (MI), stroke, or death from cardiovascular causes. The primary safety endpoint was severe bleeding.
Results
A total of 15,603 patients were enrolled in the study. Treatment was permanently discontinued by 20.4% in the clopidogrel group as compared with 18.2% in the placebo group (P<0.001). A total of 4.8% of patients in the clopidogrel group and 4.9% in the placebo group discontinued treatment because of an adverse event (P=0.67). Other than the treatment medications, concomitant medication use was similar in both groups. A median follow-up of 28 months revealed that the rates of primary efficacy events in the clopidogrel and placebo group were similar (6.8% versus 7.3%, P=0.22, respectively). The rate of primary safety events was 1.7% in the clopidogrel group and 1.3% in the placebo group, P=0.09.
Conclusions
This trial enrolled patients who either had established atherothrombotic disease or were at high risk for such disease and found that there was no significant benefit associated with the use of clopidogrel plus aspirin compared to aspirin alone in reducing myocardial infarction, stroke, or cardiovascular death. The risk of moderate or severe bleeding in symptomatic patients was higher in the clopidogrel plus aspirin group than in the aspirin plus placebo group. Overall, these findings do not support the use of dual antiplatelet therapy across this broad patient population.
D-Dimer in the Diagnosis of Pulmonary Embolism
Kearon C, Ginsberg JS, Douketis J, et al. An evaluation of D-dimer in the diagnosis of pulmonary embolism: a randomized trial. Ann Intern Med. 2006 Jun 6;144(11):812-821.
Background
The clinical usefulness of the D-dimer test in the diagnosis of pulmonary embolism (PE) has been previously studied. In patients with suspected PE, it may be safe to omit additional diagnostic testing if a patient has a negative D-dimer test; however, this approach has never been evaluated in a randomized, controlled trial.
The investigators in this trial studied two subgroups of patients with suspected PE and a negative D-dimer: patients with a low clinical probability of PE and those with a moderate or high clinical probability of PE who had a non-diagnostic ventilation perfusion scan (VQ scan) and no proximal deep vein thrombosis on venous ultrasonography. The hypothesis was that patients with a negative D-dimer who do not have further testing for PE won’t have a higher frequency of venous thromboembolism during follow-up than patients who undergo routine diagnostic testing.
Methods
Before any diagnostic testing, patients were assigned a probability score, using the Wells Criteria, to categorize the probability of PE as low or moderate to high.
Patients with low probability Wells scores: D-dimer testing was done on all patients with a low clinical probability of PE. Patients with a negative D-dimer were randomly assigned either to no additional diagnostic testing and no anticoagulation treatment or to additional diagnostic testing with an initial VQ scan. If the VQ scan was negative, then PE was excluded. If the VQ scan showed one or more segmental perfusion defects that were normally ventilated, then the scan was considered diagnostic for PE. If there were perfusion defects that did not meet the criteria for a high probability scan, then the scan was considered non-diagnostic. Patients with non-diagnostic scans underwent ultrasonography of the proximal veins of the legs. If deep vein thrombosis was present, PE was diagnosed. If ultrasonography was normal, the test was repeated after seven and 14 days. In all patients with a positive D-dimer, a VQ scan was performed.
Patients with moderate to high probability Wells scores: A VQ scan was performed on all patients with a moderate to high probability for PE. Patients with high probability scans were treated; patients with normal scans were not treated. Patients with non-diagnostic scans and normal venous ultrasonography were randomly assigned to receive either no additional testing or serial ultrasonography.
Outcomes: All patients were followed for six months for the development of venous thromboembolism after initial diagnostic testing.
Results
The study enrolled 1,126 patients. Overall, 160 patients (14.2%) had PE diagnosed at initial presentation or by venous ultrasonography. Of 952 patients who did not receive an initial diagnosis of PE, 11 (1.2%) had PE diagnosed at follow-up.
Patients with low probability Wells scores: Low clinical probability was present in 670 patients (60%). In patients with low clinical probability of PE, 373 (56%) had negative D-dimer tests and 297 (44%) had positive D-dimer tests. Of the 373 patients with low probability and negative D-dimer results, 187 were randomized to no additional testing and 186 received a VQ scan. The frequency of venous thromboembolism at six-month follow-up was similar in these two groups (-0.5% [CI, -3.0% to 1.6%]). Three patients with negative D-dimer tests were diagnosed with PE by VQ scan. Results were fairly complete (five patients without a six-month follow-up in the no additional testing group and one without a follow-up in the VQ scan group).
Twenty-four patients with low clinical probability and positive D-dimer results (n=297) were diagnosed with PE. Three patients did not complete the six-month follow-up. Of the remaining 294 patients, five patients had venous thromboembolism at six months.
Patients with moderate to high probability Wells scores: There were 456 patients (40%) had moderate or high clinical probability for PE. Each of these patients had a VQ scan. Non-diagnostic VQ scans and normal venous ultrasonography were performed on 226 patients. Of these 226 patients, 86 had a negative D-dimer and 140 had a positive D-dimer. Of the 86 patients with negative VQ scans, normal venous ultrasonography, and a negative D-dimer, 83 were randomly assigned to no additional testing or serial venous ultrasonography (42 and 41 respectively). At six months follow-up, one patient assigned to no additional testing had venous thromboembolism, and no patients in the additional testing group had venous thromboembolism.
Conclusions
The results of this trial suggest that it is safe to withhold additional diagnostic testing in patients with suspected PE, low pretest clinical probability, and a negative D-dimer test. Even in patients with moderate to high pretest clinical probability, a non-diagnostic VQ scan, and normal venous ultrasonography, only one patient with a negative D-dimer had a venous thromboembolic event at six months follow-up. The assay used for this study was an erythrocyte agglutination SimpliRED assay. Reported sensitivity is approximately 90%, and specificity is approximately 75%. To the readers, it should be noted that the authors defined a low probability Wells score as 4 rather than 1.5 or lower.
Efficacy and Safety of Inhaled Insulin Therapy in Adults with Diabetes Mellitus
Ceglia L, Lau J, Pittas AG. Meta-analysis: efficacy and safety of inhaled insulin therapy in adults with diabetes mellitus. Ann Intern Med. 2006 Nov 7;145(9):665-675.
Background
Despite its effectiveness in attaining glycemic control, there is considerable resistance to insulin use by patients and healthcare providers, primarily because of the need for subcutaneous injection. In January 2006, the U.S. Food and Drug Administration (FDA) approved the first formulation of inhaled insulin for clinical use in nonsmoking adults with type 1 or type 2 diabetes and no pulmonary disease. The authors of this paper present a systematic review to examine the efficacy, safety, and patient acceptability of inhaled insulin.
Methods
The authors conducted a search of MEDLINE to find English-language, randomized, controlled trials of inhaled insulin in nonpregnant adults with diabetes. To find unpublished studies, the authors reviewed the briefing document on Exubera powder for oral inhalation (Pfizer Inc., New York). An abstract was included if it reported original data from controlled trials in patients with type 1 or 2 diabetes and hemoglobin A1C outcomes for patients receiving inhaled insulin versus outcomes for a comparison group (subcutaneous insulin or oral hypoglycemics). Studies with less than 12 weeks duration were excluded because no comparison could be made regarding glycemic efficacy. For glycemic efficacy, the primary outcome was the treatment group difference in hemoglobin A1C from baseline. Secondary outcome was the proportion of patients with hemoglobin A1C levels less than 7%. To evaluate safety, the primary outcomes were severe hypoglycemia (glucose ≤36 mg/dL), cough, and treatment group difference in pulmonary function variables.
Results
Sixteen trials involving a total of 4,023 patients met inclusion criteria. Seven trials compared inhaled insulin with various subcutaneous insulin regimens in patients with type 1 diabetes. Nine trials compared inhaled insulin with subcutaneous insulin or oral hypoglycemic agents in patients with type 2 diabetes. Inhaled insulin was given with meals and titrated according to study-specific glucose goals. Subcutaneous insulin was titrated to the same specific goals. Doses of oral hypoglycemic agents were adjusted for glycemic targets in only two of the nine trials. The combined data from the studies demonstrated a small but statistically significant decrease in the levels of baseline hemoglobin A1C levels in favor of subcutaneous insulin (weighted mean difference 0.08%, [CI 0.03% to 0.14%]) in patients with type 1 or type 2 diabetes. The greatest advantage of subcutaneous insulin was noted in the study with the longest duration (104 weeks). There was no difference between the study groups in studies with duration of 24 weeks or less. Patients with type 1 or type 2 diabetes taking inhaled insulin were no more likely to achieve hemoglobin A1C levels less than 7% than those using subcutaneous insulin.
The combined data from studies comparing inhaled insulin to oral hypoglycemic agents in patients with type 2 diabetes showed that inhaled insulin lowered hemoglobin A1C levels more effectively (weighted mean difference -1.04%, [CI -1.59% to -0.49%]). In studies in which the oral hypoglycemic agents were titrated, inhaled insulin still lowered baseline hemoglobin A1C levels but to a lesser degree (weighted mean difference -0.20%, [CI - 0.34% to -0.07%]). Patients with type 2 diabetes taking inhaled insulin were more likely to achieve hemoglobin A1C levels less than 7% than those taking oral agents.
There was no difference in episodes of severe hypoglycemia in patients using inhaled insulin compared to those using subcutaneous insulin. A higher proportion of patients using inhaled insulin reported at least one episode of severe hypoglycemia compared to those using oral agents (risk ratio, 3.06 [CI 1.03 to 9.07]; 9.4% versus 3.5%, respectively).
With respect to pulmonary safety, all trials selected patients without histories of pulmonary problems and with at least six months of nonsmoking status. Pulmonary safety was assessed by self-reported symptoms and by pulmonary function tests. The most common pulmonary symptom associated with inhaled insulin was nonproductive cough. This symptom was reported more frequently compared to patients using subcutaneous insulin or oral agents (risk ratio, 3.52 [CI 2.23 to 5.56]; 16.9% versus 5.0%). Cough was noted early in the treatment course and diminished in frequency over time. Patients receiving inhaled insulin had a greater decrease in FEV1 (forced expiratory volume in the first second) from baseline than the comparator group (weighted mean difference, -0.031 L [CI-0.043 L to -0.020 L]). This decrease progressed slowly over the first six months but stabilized in studies of up to two years’ duration.
Only four trials reported data on overall patient satisfaction for inhaled insulin versus subcutaneous insulin. All trials reported a statistically significant increase in overall patient satisfaction with inhaled insulin over subcutaneous insulin. Patients randomly assigned to inhaled insulin were more likely to continue taking inhaled insulin than to switch back to subcutaneous insulin.
Conclusions
This meta-analysis showed that inhaled insulin is comparable to subcutaneous insulin in lowering hemoglobin A1C levels in patients with type 1 or type 2 diabetes. The proportion of patients reaching a target hemoglobin A1C of less than 7% was much lower in the studies in this meta-analysis as compared to levels in trials of intensive subcutaneous insulin therapy.
It’s more difficult to compare inhaled insulin with oral hypoglycemic agents because most studies involving oral agents used fixed dosing with different types of oral agents. There was a three-fold risk of severe hypoglycemia in patients using inhaled insulin compared to those using oral hypoglycemic agents. This is probably due to overall improved glycemic control in the inhaled insulin group. Cough was more common in the inhaled insulin groups, and there were small decreases in FEV1, but these did not progress over two years. The potential for pulmonary toxicity with long-term administration has not been evaluated and deserves further study.
From Weapon to Wonder Drug

Gas! Gas! Quick, boys! An ecstasy of fumbling, Fitting the clumsy helmets just in time; But someone still was yelling out and stumbling And flound’ring like a man in fire or lime.
—Wilfred Owen, Dulce et Decorum Est (1917)
In virtually every hospital around the world, oncology patients are treated with constantly evolving life- and limb-saving protocols. Cancer has plagued mankind for thousands of years. Records of cancer exist from as early as the ancient Egyptian era. The famous Edwin Smith Surgical Papyrus, dating to 1,600 B.C., describes a man with “bulging tumors on his breast.” The translation of the treatment for this case simply reads: “There is no treatment.” Unfortunately, the history of chemotherapy lags behind that of the disease it treats by at least 4,000 years. And ironically, the first modern day anticancer drug was spawned from a deadly World War I weapon.
Sulfur mustard, or mustard gas, has the dubious distinction of being one of the original chemical weapons. Bis-(2-chloroethyl) sulfide was first synthesized by London Institute of Physics Co-founder Frederick Guthrie in 1860. Guthrie, a profound believer in the advancement of science through experimentation rather than discussion, first documented the toxic effects of mustard gas by applying his mixture of ethylene and sulfur dichloride to his own skin, thus joining other notables in the halls of self-experimentation.
Mustard gas was mass-produced under the name LOST (an acronym fashioned from the names of its developers) for the German company Bayer AG during the first decade of the 20th century. Unfortunately, this proved to be perfect timing for the introduction of chemical warfare by the German army in 1917. The first strike was against Canadian troops. One year later the British used the same agent to destroy the “impregnable” Hindenburg Line. This culmination of the storied allied forces’ 100 Days Offensive ultimately led to the end of the First World War.
Various permutations of this compound were used sporadically by numerous world powers over the next 25 years. The malevolent use of mustard gas may be responsible for nearly 100,000 deaths and approximately five times as many wartime injuries. In fact, sulfur mustard gas—not a gas or a mustard, but rather a yellowish-brown vaporized liquid with a mustard seed-like odor—is known primarily as an incapacitant rather than as a lethal weapon. The effects of this poison may remain hidden for two to 24 hours after exposure.
Sulfur mustard is a vesicant. It exerts its effects on the body’s mucous membranes. The skin and the eyes are among the first organs to be affected. The toxicity of this agent is dose-dependent. While lower concentrations can cause symptoms as minor as skin irritation and conjunctivitis, higher titers can lead to morbid consequences such as necrotic ulcerations of the skin and blindness. At still higher concentrations, inhaled vapors can damage the mucous membrane lining of the respiratory tract, leading to hemorrhagic pulmonary edema.
Sulfur mustard also causes chronic sequelae. After exposure, surviving victims might exhibit nausea, vomiting, alopecia, and increased vulnerability to infection. These later symptoms are the result of the poison’s ability to act as an alkylating agent, cross-linking DNA and preventing the normal sequence of DNA replication. The organs primarily affected are the lining of the gastrointestinal tract and the bone marrow, due to their inherent high mitotic activity.
Despite its sinister history, mustard gas has played a key role in the development of anti-cancer chemotherapeutic agents and may justly be referred to as the egg from which medical oncology has hatched. The history of medicine contains many tales of accidental discovery, but how did a deadly gas become the first effective chemotherapeutic agent?
Fast forward 30 years to the Second World War. The interwar period resulted in numerous provisions—including the Geneva Protocol of 1929—to ban the use of chemical weapons. It was also a time during which many nations—both purposefully and accidentally—developed and stockpiled chemical agents. Thankfully, chemical weapons, including mustard gas, were not used extensively by either side during World War II. This was a period of intense—and justified—paranoia, however. General Dwight D. Eisenhower had made provisions for a stockpile of 100 tons of mustard gas on the S.S. John Harvey, which was stationed in Italy’s Bari Harbor. In December 1943, Nazi air strikes destroyed the John Harvey, among other ships, resulting in surprisingly few casualties despite the impressive amount of fire and destruction.
In the days and weeks following this catastrophe, however, survivors began to develop the familiar signs of mustard gas exposure. Lt. Col. Stewart Francis Alexander, an expert in chemical warfare, suspected exposure to the famous vapor. Autopsies of the victims reported profound lymphopenia as well as suppression of myeloid cell lines. This prompted the United States to lift the Office of Scientific Research and Development publication ban in 1946. At this time, numerous accounts were uncovered of mustard gas and its derivatives in experimental trials involving humans and cloned mice.
The first clinical trial, conducted by Louis Goodman and Alfred Gilman, involved the use of nitrogen mustard on a patient with advanced lymphosarcoma. After just four days of therapy, the patient’s tumor mass receded remarkably. Unfortunately, withdrawal of the medication due to profound neutropenia resulted in an abrupt return of the tumors. A second, shorter course resulted in a less profound reduction in tumor bulk, and a third try had no effect at all.

Interestingly, this temporary miracle with its subsequent failure illustrates two paradigms faced by medical oncologists today. Chemotherapeutic agents exert a toxic toll on the host, and tumor cells eventually develop resistance to circumvent the effects of these same medications. This is exactly why complicated protocols are used to treat patients with cancer.
Goodman and Gilman, authors of the famous medical pharmacology textbook The Pharmacological Basis of Therapeutics, used nitrogen mustard, a derivative of sulfur mustard, for their experiment. This compound, also known as mechlorethamine, is the first in-class alkylating agent, and is still used as a topical ointment in the treatment of cutaneous lymphomas. Other alkylating agents, such as cyclophosphamide, ifosfamide, and cisplatin, are used in cancer protocols worldwide.
We have not seen the last of mustard gas, which made its last acknowledged appearance in the Iran-Iraq war. Frequently, those things that are most destructive can be tamed for medical use.
The next time you have a patient receiving chemotherapy, think back to the roots of the cure. TH
References
- Pratt WB, Ruddon RW, Ensminger WD, et al. The Anticancer Drugs. 2nd ed. New York: Oxford University Press; 1994.
- Faguet GB. The War on Cancer: An Anatomy of Failure, a Blueprint for the Future. Dordrecht, Netherlands: Springer Press; 2005.
- Baguley BC, Kerr DJ, eds. Anticancer Drug Development. New York: Academic Press; 2002.
- Goodman LS, Wintrobe MM, Dameshek W, et al. Landmark article Sept. 21, 1946: Nitrogen mustard therapy. Use of methyl-bis(beta-chloroethyl)amine hydrochloride and tris(beta-chloroethyl)amine hydrochloride for Hodgkin’s disease, lymphosarcoma, leukemia and certain allied and miscellaneous disorders. JAMA. 1984;251:2255-2261.
- Kazin RA, Lowitt NR, Lowitt MH. Update in dermatology. Ann Intern Med. 2001;135:124-132.
Gas! Gas! Quick, boys! An ecstasy of fumbling, Fitting the clumsy helmets just in time; But someone still was yelling out and stumbling And flound’ring like a man in fire or lime.
—Wilfred Owen, Dulce et Decorum Est (1917)
In virtually every hospital around the world, oncology patients are treated with constantly evolving life- and limb-saving protocols. Cancer has plagued mankind for thousands of years. Records of cancer exist from as early as the ancient Egyptian era. The famous Edwin Smith Surgical Papyrus, dating to 1,600 B.C., describes a man with “bulging tumors on his breast.” The translation of the treatment for this case simply reads: “There is no treatment.” Unfortunately, the history of chemotherapy lags behind that of the disease it treats by at least 4,000 years. And ironically, the first modern day anticancer drug was spawned from a deadly World War I weapon.
Sulfur mustard, or mustard gas, has the dubious distinction of being one of the original chemical weapons. Bis-(2-chloroethyl) sulfide was first synthesized by London Institute of Physics Co-founder Frederick Guthrie in 1860. Guthrie, a profound believer in the advancement of science through experimentation rather than discussion, first documented the toxic effects of mustard gas by applying his mixture of ethylene and sulfur dichloride to his own skin, thus joining other notables in the halls of self-experimentation.
Mustard gas was mass-produced under the name LOST (an acronym fashioned from the names of its developers) for the German company Bayer AG during the first decade of the 20th century. Unfortunately, this proved to be perfect timing for the introduction of chemical warfare by the German army in 1917. The first strike was against Canadian troops. One year later the British used the same agent to destroy the “impregnable” Hindenburg Line. This culmination of the storied allied forces’ 100 Days Offensive ultimately led to the end of the First World War.
Various permutations of this compound were used sporadically by numerous world powers over the next 25 years. The malevolent use of mustard gas may be responsible for nearly 100,000 deaths and approximately five times as many wartime injuries. In fact, sulfur mustard gas—not a gas or a mustard, but rather a yellowish-brown vaporized liquid with a mustard seed-like odor—is known primarily as an incapacitant rather than as a lethal weapon. The effects of this poison may remain hidden for two to 24 hours after exposure.
Sulfur mustard is a vesicant. It exerts its effects on the body’s mucous membranes. The skin and the eyes are among the first organs to be affected. The toxicity of this agent is dose-dependent. While lower concentrations can cause symptoms as minor as skin irritation and conjunctivitis, higher titers can lead to morbid consequences such as necrotic ulcerations of the skin and blindness. At still higher concentrations, inhaled vapors can damage the mucous membrane lining of the respiratory tract, leading to hemorrhagic pulmonary edema.
Sulfur mustard also causes chronic sequelae. After exposure, surviving victims might exhibit nausea, vomiting, alopecia, and increased vulnerability to infection. These later symptoms are the result of the poison’s ability to act as an alkylating agent, cross-linking DNA and preventing the normal sequence of DNA replication. The organs primarily affected are the lining of the gastrointestinal tract and the bone marrow, due to their inherent high mitotic activity.
Despite its sinister history, mustard gas has played a key role in the development of anti-cancer chemotherapeutic agents and may justly be referred to as the egg from which medical oncology has hatched. The history of medicine contains many tales of accidental discovery, but how did a deadly gas become the first effective chemotherapeutic agent?
Fast forward 30 years to the Second World War. The interwar period resulted in numerous provisions—including the Geneva Protocol of 1929—to ban the use of chemical weapons. It was also a time during which many nations—both purposefully and accidentally—developed and stockpiled chemical agents. Thankfully, chemical weapons, including mustard gas, were not used extensively by either side during World War II. This was a period of intense—and justified—paranoia, however. General Dwight D. Eisenhower had made provisions for a stockpile of 100 tons of mustard gas on the S.S. John Harvey, which was stationed in Italy’s Bari Harbor. In December 1943, Nazi air strikes destroyed the John Harvey, among other ships, resulting in surprisingly few casualties despite the impressive amount of fire and destruction.
In the days and weeks following this catastrophe, however, survivors began to develop the familiar signs of mustard gas exposure. Lt. Col. Stewart Francis Alexander, an expert in chemical warfare, suspected exposure to the famous vapor. Autopsies of the victims reported profound lymphopenia as well as suppression of myeloid cell lines. This prompted the United States to lift the Office of Scientific Research and Development publication ban in 1946. At this time, numerous accounts were uncovered of mustard gas and its derivatives in experimental trials involving humans and cloned mice.
The first clinical trial, conducted by Louis Goodman and Alfred Gilman, involved the use of nitrogen mustard on a patient with advanced lymphosarcoma. After just four days of therapy, the patient’s tumor mass receded remarkably. Unfortunately, withdrawal of the medication due to profound neutropenia resulted in an abrupt return of the tumors. A second, shorter course resulted in a less profound reduction in tumor bulk, and a third try had no effect at all.
Interestingly, this temporary miracle with its subsequent failure illustrates two paradigms faced by medical oncologists today. Chemotherapeutic agents exert a toxic toll on the host, and tumor cells eventually develop resistance to circumvent the effects of these same medications. This is exactly why complicated protocols are used to treat patients with cancer.
Goodman and Gilman, authors of the famous medical pharmacology textbook The Pharmacological Basis of Therapeutics, used nitrogen mustard, a derivative of sulfur mustard, for their experiment. This compound, also known as mechlorethamine, is the first in-class alkylating agent, and is still used as a topical ointment in the treatment of cutaneous lymphomas. Other alkylating agents, such as cyclophosphamide, ifosfamide, and cisplatin, are used in cancer protocols worldwide.
We have not seen the last of mustard gas, which made its last acknowledged appearance in the Iran-Iraq war. Frequently, those things that are most destructive can be tamed for medical use.
The next time you have a patient receiving chemotherapy, think back to the roots of the cure. TH
References
- Pratt WB, Ruddon RW, Ensminger WD, et al. The Anticancer Drugs. 2nd ed. New York: Oxford University Press; 1994.
- Faguet GB. The War on Cancer: An Anatomy of Failure, a Blueprint for the Future. Dordrecht, Netherlands: Springer Press; 2005.
- Baguley BC, Kerr DJ, eds. Anticancer Drug Development. New York: Academic Press; 2002.
- Goodman LS, Wintrobe MM, Dameshek W, et al. Landmark article Sept. 21, 1946: Nitrogen mustard therapy. Use of methyl-bis(beta-chloroethyl)amine hydrochloride and tris(beta-chloroethyl)amine hydrochloride for Hodgkin’s disease, lymphosarcoma, leukemia and certain allied and miscellaneous disorders. JAMA. 1984;251:2255-2261.
- Kazin RA, Lowitt NR, Lowitt MH. Update in dermatology. Ann Intern Med. 2001;135:124-132.
Gas! Gas! Quick, boys! An ecstasy of fumbling, Fitting the clumsy helmets just in time; But someone still was yelling out and stumbling And flound’ring like a man in fire or lime.
—Wilfred Owen, Dulce et Decorum Est (1917)
In virtually every hospital around the world, oncology patients are treated with constantly evolving life- and limb-saving protocols. Cancer has plagued mankind for thousands of years. Records of cancer exist from as early as the ancient Egyptian era. The famous Edwin Smith Surgical Papyrus, dating to 1,600 B.C., describes a man with “bulging tumors on his breast.” The translation of the treatment for this case simply reads: “There is no treatment.” Unfortunately, the history of chemotherapy lags behind that of the disease it treats by at least 4,000 years. And ironically, the first modern day anticancer drug was spawned from a deadly World War I weapon.
Sulfur mustard, or mustard gas, has the dubious distinction of being one of the original chemical weapons. Bis-(2-chloroethyl) sulfide was first synthesized by London Institute of Physics Co-founder Frederick Guthrie in 1860. Guthrie, a profound believer in the advancement of science through experimentation rather than discussion, first documented the toxic effects of mustard gas by applying his mixture of ethylene and sulfur dichloride to his own skin, thus joining other notables in the halls of self-experimentation.
Mustard gas was mass-produced under the name LOST (an acronym fashioned from the names of its developers) for the German company Bayer AG during the first decade of the 20th century. Unfortunately, this proved to be perfect timing for the introduction of chemical warfare by the German army in 1917. The first strike was against Canadian troops. One year later the British used the same agent to destroy the “impregnable” Hindenburg Line. This culmination of the storied allied forces’ 100 Days Offensive ultimately led to the end of the First World War.
Various permutations of this compound were used sporadically by numerous world powers over the next 25 years. The malevolent use of mustard gas may be responsible for nearly 100,000 deaths and approximately five times as many wartime injuries. In fact, sulfur mustard gas—not a gas or a mustard, but rather a yellowish-brown vaporized liquid with a mustard seed-like odor—is known primarily as an incapacitant rather than as a lethal weapon. The effects of this poison may remain hidden for two to 24 hours after exposure.
Sulfur mustard is a vesicant. It exerts its effects on the body’s mucous membranes. The skin and the eyes are among the first organs to be affected. The toxicity of this agent is dose-dependent. While lower concentrations can cause symptoms as minor as skin irritation and conjunctivitis, higher titers can lead to morbid consequences such as necrotic ulcerations of the skin and blindness. At still higher concentrations, inhaled vapors can damage the mucous membrane lining of the respiratory tract, leading to hemorrhagic pulmonary edema.
Sulfur mustard also causes chronic sequelae. After exposure, surviving victims might exhibit nausea, vomiting, alopecia, and increased vulnerability to infection. These later symptoms are the result of the poison’s ability to act as an alkylating agent, cross-linking DNA and preventing the normal sequence of DNA replication. The organs primarily affected are the lining of the gastrointestinal tract and the bone marrow, due to their inherent high mitotic activity.
Despite its sinister history, mustard gas has played a key role in the development of anti-cancer chemotherapeutic agents and may justly be referred to as the egg from which medical oncology has hatched. The history of medicine contains many tales of accidental discovery, but how did a deadly gas become the first effective chemotherapeutic agent?
Fast forward 30 years to the Second World War. The interwar period resulted in numerous provisions—including the Geneva Protocol of 1929—to ban the use of chemical weapons. It was also a time during which many nations—both purposefully and accidentally—developed and stockpiled chemical agents. Thankfully, chemical weapons, including mustard gas, were not used extensively by either side during World War II. This was a period of intense—and justified—paranoia, however. General Dwight D. Eisenhower had made provisions for a stockpile of 100 tons of mustard gas on the S.S. John Harvey, which was stationed in Italy’s Bari Harbor. In December 1943, Nazi air strikes destroyed the John Harvey, among other ships, resulting in surprisingly few casualties despite the impressive amount of fire and destruction.
In the days and weeks following this catastrophe, however, survivors began to develop the familiar signs of mustard gas exposure. Lt. Col. Stewart Francis Alexander, an expert in chemical warfare, suspected exposure to the famous vapor. Autopsies of the victims reported profound lymphopenia as well as suppression of myeloid cell lines. This prompted the United States to lift the Office of Scientific Research and Development publication ban in 1946. At this time, numerous accounts were uncovered of mustard gas and its derivatives in experimental trials involving humans and cloned mice.
The first clinical trial, conducted by Louis Goodman and Alfred Gilman, involved the use of nitrogen mustard on a patient with advanced lymphosarcoma. After just four days of therapy, the patient’s tumor mass receded remarkably. Unfortunately, withdrawal of the medication due to profound neutropenia resulted in an abrupt return of the tumors. A second, shorter course resulted in a less profound reduction in tumor bulk, and a third try had no effect at all.
Interestingly, this temporary miracle with its subsequent failure illustrates two paradigms faced by medical oncologists today. Chemotherapeutic agents exert a toxic toll on the host, and tumor cells eventually develop resistance to circumvent the effects of these same medications. This is exactly why complicated protocols are used to treat patients with cancer.
Goodman and Gilman, authors of the famous medical pharmacology textbook The Pharmacological Basis of Therapeutics, used nitrogen mustard, a derivative of sulfur mustard, for their experiment. This compound, also known as mechlorethamine, is the first in-class alkylating agent, and is still used as a topical ointment in the treatment of cutaneous lymphomas. Other alkylating agents, such as cyclophosphamide, ifosfamide, and cisplatin, are used in cancer protocols worldwide.
We have not seen the last of mustard gas, which made its last acknowledged appearance in the Iran-Iraq war. Frequently, those things that are most destructive can be tamed for medical use.
The next time you have a patient receiving chemotherapy, think back to the roots of the cure. TH
References
- Pratt WB, Ruddon RW, Ensminger WD, et al. The Anticancer Drugs. 2nd ed. New York: Oxford University Press; 1994.
- Faguet GB. The War on Cancer: An Anatomy of Failure, a Blueprint for the Future. Dordrecht, Netherlands: Springer Press; 2005.
- Baguley BC, Kerr DJ, eds. Anticancer Drug Development. New York: Academic Press; 2002.
- Goodman LS, Wintrobe MM, Dameshek W, et al. Landmark article Sept. 21, 1946: Nitrogen mustard therapy. Use of methyl-bis(beta-chloroethyl)amine hydrochloride and tris(beta-chloroethyl)amine hydrochloride for Hodgkin’s disease, lymphosarcoma, leukemia and certain allied and miscellaneous disorders. JAMA. 1984;251:2255-2261.
- Kazin RA, Lowitt NR, Lowitt MH. Update in dermatology. Ann Intern Med. 2001;135:124-132.
Constructive Criticism

This is the first in a two-part series about how to provide constructive criticism to your hospitalist peers.
Part of improving your performance is learning from other hospitalists on a regular basis. You can do this through observation or discussion, and—when appropriate—by offering or receiving constructive criticism.
There are two types of physician-to-physician constructive criticism: When discussing perceived poor handling of a patient’s case, comments should take place within a formal peer review. Concerns about a physician’s non-clinical performance, such as communications problems or lack of availability, can be handled in a one-on-one conversation. Herein we’ll examine the peer review process; next month we’ll take a look at how and when to give constructive criticism to a peer informally.
Why Use Peer Review?
When a hospitalist notices a colleague’s clinical error or lack of judgment, it should be addressed in the program’s next peer review meeting, both for legal and procedural reasons.
“The key thing to understand is that ‘peer review’ offers certain protections for physicians and their colleagues,” explains Richard Rohr, MD, director, Hospitalist Service, Milford Hospital, Milford, Conn. “Ordinarily, if I discuss [another physician’s] case and render my opinion, then—in principle—if that patient were to file a lawsuit, they could subpoena me to testify about what I thought about their case. In the past, this had a chilling effect on peer review.”
Due to state laws passed years ago, peer review meetings now offer protection against subpoena. “Peer review meetings are protected,” says Dr. Rohr. “They can’t be used in court, and this makes it possible to have an organized peer review where you look at physicians’ work and provide an opinion about that work without fear of being drawn into a legal situation.”
The bottom line: “If you want to talk to another physician about their case, do so within [the peer review structure] so you’re legally protected,” says Dr. Rohr.
Focus on Improvement
When discussing a specific case or physician, remember that the reason for doing so is to improve quality of care. “Every practice should sit down, look at specific cases, and talk about possible areas of improvement,” says Dr. Rohr. “You need to take minutes of these meetings that are marked as confidential.”
The key to improvement is having an open discussion in each peer review meeting. “A good meeting is educational,” says Dr. Rohr. “The objective is to support each other and improve performance. A lot depends on the attitude that people bring to it. You have to not be afraid to say something; you must be willing to express opinions, or you’ll have a wasted meeting.”
Sometimes you may find that the problem goes beyond a single physician’s actions on a case. “If there is a problem with a case, find out whether it’s an aberration or if the problem needs to be addressed,” says Dr. Rohr. “Some things are not a physician’s fault, so much as [they are] signs that a medical system doesn’t work as effectively as it should or [that there is] a general lack of training. For example, an ER [emergency room] doctor misses a fracture. Was finding that fracture outside his competency? Does he need training reading X-rays, or can you manage to get radiologists in to check X-rays fast enough to become part of the process?”
Use a Set Structure
It’s up to the hospital medicine program director to set up a peer review process, which should be done within the structure established by the hospital. Peer review meetings “should be done on a regular basis,” advises Dr. Rohr. “How often depends on the volume of the program, but a typical group should meet monthly. You’ll probably look at three or four cases, which is a reasonable number to cover in one meeting. Look at unexpected mortalities or complications—you have a responsibility to the public to examine these.”
You might do best by bringing in an outside facilitator for the meetings. This creates an impartial atmosphere for discussions. “We bring in an external facilitator from a local teaching hospital,” says Dr. Rohr. “It’s good to have an educator lead the meeting; someone from academia will have a greater fund of knowledge and [a stronger] grasp of the medical literature, which helps bring the discussion to a more educational level. Everyone respects medical science.”
Note that the facilitator may need to be credentialed as a member of the medical staff in order for the proceedings to be protected from legal discovery.
“Peer review is difficult in smaller practices, because everyone knows everyone and they may be uncomfortable addressing problems,” explains Dr. Rohr. “Here, it’s especially helpful to have a leader from the outside who can render opinions and get everyone to chime in and render their own opinions.”
Remember that your peer review system is reportable. “As part of the hospital’s peer review structure, you’ll have to report findings from the meetings,” adds Dr. Rohr. “If someone is showing a pattern, these things have to be trended. Do they need training, or should they be dismissed?”
Giving Feedback through Peer Review
When you participate in a peer review discussion, don’t let your comments get too personal or subjective. “The most important thing is to keep it professional and make it educational to the greatest extent possible,” says Dr. Rohr. “Reference facts in the medical literature as often as possible. Point to something that’s been published to support your opinion. Base your comments on what’s known, and apply that to your analysis of the case.”
An evidence-based opinion doesn’t have to cite specific details; as long as you’re aware of major papers on the topic, you should have a grounded opinion.
Finally, as a physician participating in a peer review discussion, think before you speak. “Peer review works best when you have a basic respect for each other, as well as basic humility,” he says. TH
Jane Jerrard has written for The Hospitalist since 2005.
This is the first in a two-part series about how to provide constructive criticism to your hospitalist peers.
Part of improving your performance is learning from other hospitalists on a regular basis. You can do this through observation or discussion, and—when appropriate—by offering or receiving constructive criticism.
There are two types of physician-to-physician constructive criticism: When discussing perceived poor handling of a patient’s case, comments should take place within a formal peer review. Concerns about a physician’s non-clinical performance, such as communications problems or lack of availability, can be handled in a one-on-one conversation. Herein we’ll examine the peer review process; next month we’ll take a look at how and when to give constructive criticism to a peer informally.
Why Use Peer Review?
When a hospitalist notices a colleague’s clinical error or lack of judgment, it should be addressed in the program’s next peer review meeting, both for legal and procedural reasons.
“The key thing to understand is that ‘peer review’ offers certain protections for physicians and their colleagues,” explains Richard Rohr, MD, director, Hospitalist Service, Milford Hospital, Milford, Conn. “Ordinarily, if I discuss [another physician’s] case and render my opinion, then—in principle—if that patient were to file a lawsuit, they could subpoena me to testify about what I thought about their case. In the past, this had a chilling effect on peer review.”
Due to state laws passed years ago, peer review meetings now offer protection against subpoena. “Peer review meetings are protected,” says Dr. Rohr. “They can’t be used in court, and this makes it possible to have an organized peer review where you look at physicians’ work and provide an opinion about that work without fear of being drawn into a legal situation.”
The bottom line: “If you want to talk to another physician about their case, do so within [the peer review structure] so you’re legally protected,” says Dr. Rohr.
Focus on Improvement
When discussing a specific case or physician, remember that the reason for doing so is to improve quality of care. “Every practice should sit down, look at specific cases, and talk about possible areas of improvement,” says Dr. Rohr. “You need to take minutes of these meetings that are marked as confidential.”
The key to improvement is having an open discussion in each peer review meeting. “A good meeting is educational,” says Dr. Rohr. “The objective is to support each other and improve performance. A lot depends on the attitude that people bring to it. You have to not be afraid to say something; you must be willing to express opinions, or you’ll have a wasted meeting.”
Sometimes you may find that the problem goes beyond a single physician’s actions on a case. “If there is a problem with a case, find out whether it’s an aberration or if the problem needs to be addressed,” says Dr. Rohr. “Some things are not a physician’s fault, so much as [they are] signs that a medical system doesn’t work as effectively as it should or [that there is] a general lack of training. For example, an ER [emergency room] doctor misses a fracture. Was finding that fracture outside his competency? Does he need training reading X-rays, or can you manage to get radiologists in to check X-rays fast enough to become part of the process?”
Use a Set Structure
It’s up to the hospital medicine program director to set up a peer review process, which should be done within the structure established by the hospital. Peer review meetings “should be done on a regular basis,” advises Dr. Rohr. “How often depends on the volume of the program, but a typical group should meet monthly. You’ll probably look at three or four cases, which is a reasonable number to cover in one meeting. Look at unexpected mortalities or complications—you have a responsibility to the public to examine these.”
You might do best by bringing in an outside facilitator for the meetings. This creates an impartial atmosphere for discussions. “We bring in an external facilitator from a local teaching hospital,” says Dr. Rohr. “It’s good to have an educator lead the meeting; someone from academia will have a greater fund of knowledge and [a stronger] grasp of the medical literature, which helps bring the discussion to a more educational level. Everyone respects medical science.”
Note that the facilitator may need to be credentialed as a member of the medical staff in order for the proceedings to be protected from legal discovery.
“Peer review is difficult in smaller practices, because everyone knows everyone and they may be uncomfortable addressing problems,” explains Dr. Rohr. “Here, it’s especially helpful to have a leader from the outside who can render opinions and get everyone to chime in and render their own opinions.”
Remember that your peer review system is reportable. “As part of the hospital’s peer review structure, you’ll have to report findings from the meetings,” adds Dr. Rohr. “If someone is showing a pattern, these things have to be trended. Do they need training, or should they be dismissed?”
Giving Feedback through Peer Review
When you participate in a peer review discussion, don’t let your comments get too personal or subjective. “The most important thing is to keep it professional and make it educational to the greatest extent possible,” says Dr. Rohr. “Reference facts in the medical literature as often as possible. Point to something that’s been published to support your opinion. Base your comments on what’s known, and apply that to your analysis of the case.”
An evidence-based opinion doesn’t have to cite specific details; as long as you’re aware of major papers on the topic, you should have a grounded opinion.
Finally, as a physician participating in a peer review discussion, think before you speak. “Peer review works best when you have a basic respect for each other, as well as basic humility,” he says. TH
Jane Jerrard has written for The Hospitalist since 2005.
This is the first in a two-part series about how to provide constructive criticism to your hospitalist peers.
Part of improving your performance is learning from other hospitalists on a regular basis. You can do this through observation or discussion, and—when appropriate—by offering or receiving constructive criticism.
There are two types of physician-to-physician constructive criticism: When discussing perceived poor handling of a patient’s case, comments should take place within a formal peer review. Concerns about a physician’s non-clinical performance, such as communications problems or lack of availability, can be handled in a one-on-one conversation. Herein we’ll examine the peer review process; next month we’ll take a look at how and when to give constructive criticism to a peer informally.
Why Use Peer Review?
When a hospitalist notices a colleague’s clinical error or lack of judgment, it should be addressed in the program’s next peer review meeting, both for legal and procedural reasons.
“The key thing to understand is that ‘peer review’ offers certain protections for physicians and their colleagues,” explains Richard Rohr, MD, director, Hospitalist Service, Milford Hospital, Milford, Conn. “Ordinarily, if I discuss [another physician’s] case and render my opinion, then—in principle—if that patient were to file a lawsuit, they could subpoena me to testify about what I thought about their case. In the past, this had a chilling effect on peer review.”
Due to state laws passed years ago, peer review meetings now offer protection against subpoena. “Peer review meetings are protected,” says Dr. Rohr. “They can’t be used in court, and this makes it possible to have an organized peer review where you look at physicians’ work and provide an opinion about that work without fear of being drawn into a legal situation.”
The bottom line: “If you want to talk to another physician about their case, do so within [the peer review structure] so you’re legally protected,” says Dr. Rohr.
Focus on Improvement
When discussing a specific case or physician, remember that the reason for doing so is to improve quality of care. “Every practice should sit down, look at specific cases, and talk about possible areas of improvement,” says Dr. Rohr. “You need to take minutes of these meetings that are marked as confidential.”
The key to improvement is having an open discussion in each peer review meeting. “A good meeting is educational,” says Dr. Rohr. “The objective is to support each other and improve performance. A lot depends on the attitude that people bring to it. You have to not be afraid to say something; you must be willing to express opinions, or you’ll have a wasted meeting.”
Sometimes you may find that the problem goes beyond a single physician’s actions on a case. “If there is a problem with a case, find out whether it’s an aberration or if the problem needs to be addressed,” says Dr. Rohr. “Some things are not a physician’s fault, so much as [they are] signs that a medical system doesn’t work as effectively as it should or [that there is] a general lack of training. For example, an ER [emergency room] doctor misses a fracture. Was finding that fracture outside his competency? Does he need training reading X-rays, or can you manage to get radiologists in to check X-rays fast enough to become part of the process?”
Use a Set Structure
It’s up to the hospital medicine program director to set up a peer review process, which should be done within the structure established by the hospital. Peer review meetings “should be done on a regular basis,” advises Dr. Rohr. “How often depends on the volume of the program, but a typical group should meet monthly. You’ll probably look at three or four cases, which is a reasonable number to cover in one meeting. Look at unexpected mortalities or complications—you have a responsibility to the public to examine these.”
You might do best by bringing in an outside facilitator for the meetings. This creates an impartial atmosphere for discussions. “We bring in an external facilitator from a local teaching hospital,” says Dr. Rohr. “It’s good to have an educator lead the meeting; someone from academia will have a greater fund of knowledge and [a stronger] grasp of the medical literature, which helps bring the discussion to a more educational level. Everyone respects medical science.”
Note that the facilitator may need to be credentialed as a member of the medical staff in order for the proceedings to be protected from legal discovery.
“Peer review is difficult in smaller practices, because everyone knows everyone and they may be uncomfortable addressing problems,” explains Dr. Rohr. “Here, it’s especially helpful to have a leader from the outside who can render opinions and get everyone to chime in and render their own opinions.”
Remember that your peer review system is reportable. “As part of the hospital’s peer review structure, you’ll have to report findings from the meetings,” adds Dr. Rohr. “If someone is showing a pattern, these things have to be trended. Do they need training, or should they be dismissed?”
Giving Feedback through Peer Review
When you participate in a peer review discussion, don’t let your comments get too personal or subjective. “The most important thing is to keep it professional and make it educational to the greatest extent possible,” says Dr. Rohr. “Reference facts in the medical literature as often as possible. Point to something that’s been published to support your opinion. Base your comments on what’s known, and apply that to your analysis of the case.”
An evidence-based opinion doesn’t have to cite specific details; as long as you’re aware of major papers on the topic, you should have a grounded opinion.
Finally, as a physician participating in a peer review discussion, think before you speak. “Peer review works best when you have a basic respect for each other, as well as basic humility,” he says. TH
Jane Jerrard has written for The Hospitalist since 2005.
Fibromuscular Dysplasia

Brief history: 52-year-old female with uncontrolled hypertension.
Salient findings: The middle third of the arteries are involved with a “string of pearls” appearance of alternating webs and stenoses. This appearance is classic for fibromuscular dysplasia (FMD) (white arrow, above). The patient also has a 1.8-cm right renal artery aneurysm at the trifurcation of her first order renal artery branches (black arrow, above).
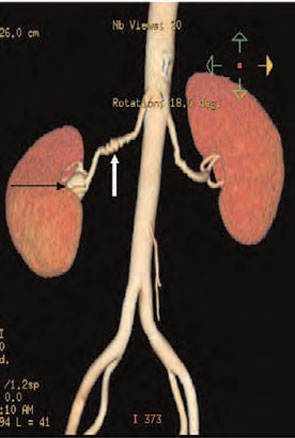
Patient population and natural history of disease: FMD is most common in young adult females, and its etiology is unknown. An association with alpha-1 antitrypsin deficiency has been reported in the literature. FMD is a leading cause of curable hypertension. Clinical manifestations of FMD include distal embolization of thrombus formed in small aneurysms, hypertension/ischemia due to obstruction by webs, and occlusion/infarct via spontaneous dissection. The natural prevalence of renal artery aneurysms is low—0.1% in all angiography patients—and its natural course is not well established. Renal artery aneurysms are most common in FMD, vasculitides, neoplasm, trauma, and Ehlers-Danlos Syndrome; they may be iatrogenic or idiopathic.
Management: Symptomatic medial fibroplasia-type FMD responds well to balloon angioplasty. Renal artery aneurysms may be managed medically or surgically, depending on risk factors. Indications for repair of renal artery aneurysms include a size of 2 cm or greater, pregnancy, expansion, renovascular hypertension, distal embolization, and rupture. Mortality from ruptured renal artery aneurysms is 10% in nonpregnant patients and 55% during pregnancy.
This patient had a good response to balloon angioplasty of the left renal artery. The right renal artery could not be angioplastied secondary to increased risk of aneurysm rupture with restoration of arterial blood flow due to increased pressure on the walls of the aneurysm. Hence, physicians surgically resected the right renal artery aneurysm and performed a bypass to the aorta.

Take Home Points
- FMD is most common in young or middle-age women;
- FMD is a type of curable hypertension, treated by renal artery angioplasty;
- FMD is diagnosed by an angiographic study—in classic cases, the involved artery has a string of pearls appearance; and
- FMD is associated with renal artery aneurysms. Consider surgical intervention in aneurysms greater than 2 cm. TH
Helena Summers is a radiology resident and Erik Summers is a hospitalist at the Mayo Clinic College of Medicine, Rochester, Minn.
Bibliography
- Kaufman JA, Lee MJ. Vascular and Interventional Radiology: The Requisites. Philadelphia: Mosby; 2004.
- Bisschops RH, Popma JJ, Meyerovitz MF. Treatment of fibromuscular dysplasia and renal artery aneurysm with use of a stent-graft. J Vasc Interv Radiol. 2001 Jun;12(6):757-760.
- Luscher TF, Lie JT, Stanson AW, et al. Arterial fibromuscular dysplasia. Mayo Clin Proc. 1987;62:931-952.
Brief history: 52-year-old female with uncontrolled hypertension.
Salient findings: The middle third of the arteries are involved with a “string of pearls” appearance of alternating webs and stenoses. This appearance is classic for fibromuscular dysplasia (FMD) (white arrow, above). The patient also has a 1.8-cm right renal artery aneurysm at the trifurcation of her first order renal artery branches (black arrow, above).
Patient population and natural history of disease: FMD is most common in young adult females, and its etiology is unknown. An association with alpha-1 antitrypsin deficiency has been reported in the literature. FMD is a leading cause of curable hypertension. Clinical manifestations of FMD include distal embolization of thrombus formed in small aneurysms, hypertension/ischemia due to obstruction by webs, and occlusion/infarct via spontaneous dissection. The natural prevalence of renal artery aneurysms is low—0.1% in all angiography patients—and its natural course is not well established. Renal artery aneurysms are most common in FMD, vasculitides, neoplasm, trauma, and Ehlers-Danlos Syndrome; they may be iatrogenic or idiopathic.
Management: Symptomatic medial fibroplasia-type FMD responds well to balloon angioplasty. Renal artery aneurysms may be managed medically or surgically, depending on risk factors. Indications for repair of renal artery aneurysms include a size of 2 cm or greater, pregnancy, expansion, renovascular hypertension, distal embolization, and rupture. Mortality from ruptured renal artery aneurysms is 10% in nonpregnant patients and 55% during pregnancy.
This patient had a good response to balloon angioplasty of the left renal artery. The right renal artery could not be angioplastied secondary to increased risk of aneurysm rupture with restoration of arterial blood flow due to increased pressure on the walls of the aneurysm. Hence, physicians surgically resected the right renal artery aneurysm and performed a bypass to the aorta.
Take Home Points
- FMD is most common in young or middle-age women;
- FMD is a type of curable hypertension, treated by renal artery angioplasty;
- FMD is diagnosed by an angiographic study—in classic cases, the involved artery has a string of pearls appearance; and
- FMD is associated with renal artery aneurysms. Consider surgical intervention in aneurysms greater than 2 cm. TH
Helena Summers is a radiology resident and Erik Summers is a hospitalist at the Mayo Clinic College of Medicine, Rochester, Minn.
Bibliography
- Kaufman JA, Lee MJ. Vascular and Interventional Radiology: The Requisites. Philadelphia: Mosby; 2004.
- Bisschops RH, Popma JJ, Meyerovitz MF. Treatment of fibromuscular dysplasia and renal artery aneurysm with use of a stent-graft. J Vasc Interv Radiol. 2001 Jun;12(6):757-760.
- Luscher TF, Lie JT, Stanson AW, et al. Arterial fibromuscular dysplasia. Mayo Clin Proc. 1987;62:931-952.
Brief history: 52-year-old female with uncontrolled hypertension.
Salient findings: The middle third of the arteries are involved with a “string of pearls” appearance of alternating webs and stenoses. This appearance is classic for fibromuscular dysplasia (FMD) (white arrow, above). The patient also has a 1.8-cm right renal artery aneurysm at the trifurcation of her first order renal artery branches (black arrow, above).
Patient population and natural history of disease: FMD is most common in young adult females, and its etiology is unknown. An association with alpha-1 antitrypsin deficiency has been reported in the literature. FMD is a leading cause of curable hypertension. Clinical manifestations of FMD include distal embolization of thrombus formed in small aneurysms, hypertension/ischemia due to obstruction by webs, and occlusion/infarct via spontaneous dissection. The natural prevalence of renal artery aneurysms is low—0.1% in all angiography patients—and its natural course is not well established. Renal artery aneurysms are most common in FMD, vasculitides, neoplasm, trauma, and Ehlers-Danlos Syndrome; they may be iatrogenic or idiopathic.
Management: Symptomatic medial fibroplasia-type FMD responds well to balloon angioplasty. Renal artery aneurysms may be managed medically or surgically, depending on risk factors. Indications for repair of renal artery aneurysms include a size of 2 cm or greater, pregnancy, expansion, renovascular hypertension, distal embolization, and rupture. Mortality from ruptured renal artery aneurysms is 10% in nonpregnant patients and 55% during pregnancy.
This patient had a good response to balloon angioplasty of the left renal artery. The right renal artery could not be angioplastied secondary to increased risk of aneurysm rupture with restoration of arterial blood flow due to increased pressure on the walls of the aneurysm. Hence, physicians surgically resected the right renal artery aneurysm and performed a bypass to the aorta.
Take Home Points
- FMD is most common in young or middle-age women;
- FMD is a type of curable hypertension, treated by renal artery angioplasty;
- FMD is diagnosed by an angiographic study—in classic cases, the involved artery has a string of pearls appearance; and
- FMD is associated with renal artery aneurysms. Consider surgical intervention in aneurysms greater than 2 cm. TH
Helena Summers is a radiology resident and Erik Summers is a hospitalist at the Mayo Clinic College of Medicine, Rochester, Minn.
Bibliography
- Kaufman JA, Lee MJ. Vascular and Interventional Radiology: The Requisites. Philadelphia: Mosby; 2004.
- Bisschops RH, Popma JJ, Meyerovitz MF. Treatment of fibromuscular dysplasia and renal artery aneurysm with use of a stent-graft. J Vasc Interv Radiol. 2001 Jun;12(6):757-760.
- Luscher TF, Lie JT, Stanson AW, et al. Arterial fibromuscular dysplasia. Mayo Clin Proc. 1987;62:931-952.
New Party in Power

Due to an overwhelming number of Democratic victories in last November’s midterm elections, the 110th Congress, which took office early this year, has new leaders and a new agenda that could bode well for healthcare legislation.
In this article, Laura Allendorf, SHM’s senior advisor for advocacy and government affairs, explains what the changes in Congress could mean for the near future of healthcare and for the legislation and issues that SHM strongly supports. Based in Washington, D.C., Allendorf is responsible for providing government relations services for SHM. She advises the organization on key legislative and regulatory healthcare issues before Congress and the Bush administration, and she works with SHM leaders and staff on policy development and advocacy strategies.
Majority Rules
The midterm elections brought about a shift in power that goes deeper than numbers of bodies on each side of the aisle. “The Democrats are now the majority in both chambers. This is significant, because they’ve been the minority since 1994, says Allendorf. “As the majority, they control the agenda now—on healthcare and other issues—and they also head the key committees.”
What can we expect to see from the Democratic Congress? “We should expect to see a more expansionist agenda” in general, according to Allendorf. “We’re going to see more activism in the area of healthcare, but whether anything gets done remains to be seen. There’s only a slim majority in the Senate, and President Bush can wield his veto pen. For example, the Democrats would like to give [the Department of] Health and Human Services the power to negotiate drug prices with pharmaceutical companies, specifically on Medicare Part D, but Bush won’t like that.”
Much depends on the issues at hand, as well as on how much bipartisan support exists for each specific bill.
Changing of the Guard
Anyone who glances at the newspaper knows that Democrat Nancy Pelosi (Calif.) is now the Speaker of the House. But Democratic leadership goes much deeper than that because the ruling party has also taken over leadership of Congressional committees. These committees shape the legislation introduced in the House and Senate.
As of press time, Congressional committee assignments had not been formally decided—at least not in the Senate—but many assignments were certain. “Typically, the highest-ranking Democrat [House or Senate] on a committee will become the new head, though Nancy Pelosi isn’t sticking to that,” explains Allendorf. “Pete Stark (D-Calif.) will likely chair the Ways and Means Committee’s Subcommittee on Health, and Charles Rangel (D-N.Y.) will head the House Ways and Means Committee. John Dingell (D-Mich.) will chair the House Energy and Commerce Committee.” (For more on committee chairs, visit http://media-newswire.com/release_1040623.html.)
For a complete list of committee members, visit SHM’s new Legislative Action Center at http://capwiz.com/hospitalmedicine/home/. See “New Advocacy Tool Available,” for more information on the Legislative Action Center, above.)
Starting Over on Key Issues
Many of the bills introduced in 2006—particularly spending bills—were not voted on by the end of the lame duck session last fall. That means that these bills must be reintroduced in the new year. Bills that recommend funding changes are frozen, so agencies continue to receive 2006 funding until the new Congress votes to change their budget.
“All bills have to be reintroduced in the 110th,” stresses Allendorf. “It will take some time—how much depends on the issue. The Democrats may want to hold hearings on legislation, or they may simply dust off legislation that was introduced last year.”
The Democrats are expected to move on many of the issues that SHM has been lobbying for. “They’ve said that they want to reform the healthcare system,” says Allendorf. “Top issues include providing coverage to the uninsured, reforming Medicare Part D, and resolving the physician payment issue.”
Allendorf believes that there will be a bipartisan effort to push through physician payment reform. “There are some 265 members of Congress who requested action on this issue this year [in 2006],” she points out. “There’s a genuine interest and desire to address physician payment reform and pay-for-performance as well. They may differ on how quickly they want to move on some of these.”
The news is not so good on the issue of gainsharing, where physicians are allowed to share the profits realized by a hospital’s cost reductions when linked to specific best practices. “Representative Nancy Johnson (R-Conn.) was a big proponent of this issue in the House, and she was not re-elected,” says Allendorf. “Stark is an opponent of gainsharing, so there may not be the same Congressional push behind it—at least in the House.”
However, the unexpected gainsharing demonstration projects approved in 2006 are underway, and Congress will hear reports on those in several years, once the projects have been analyzed.
Another issue that may not be addressed is liability. “Medical liability reform will be on the back burner,” warns Allendorf. “It’s generally not supported by the Democrats.”
In 2006, SHM supported increased funding for the Agency for Healthcare Research and Quality (AHRQ)—this was one of the major issues addressed by members during Legislative Advocacy Day during the Annual Meeting in Washington, D.C. Whether the next budget includes more money for the agency remains to be seen. “The Democrats support increased funding for NIH (National Institutes of Health), AHRQ, and other healthcare agencies,” says Allendorf. “There’s certainly political will, but where is the money going to come from?”
New Congress, New Issues
What about new issues? “Democrats have signaled that healthcare access for the uninsured will be a priority,” says Allendorf. “I think that we’ll see new legislation with a renewed emphasis on access to care.”
SHM’s Public Policy Committee will be waiting for the first legislation to be introduced regarding coverage for uninsured Americans. “This is an issue that SHM is strongly in favor of,” explains Allendorf. “SHM will look at any bills that come out on this issue and then form a policy.”
Regardless of which healthcare issues come to the forefront first, SHM’s Public Policy Committee, staff, and members are likely to be more active than ever. “I see a very busy year legislatively for SHM,” says Allendorf. TH
Jane Jerrard regularly writes “Public Policy” for The Hospitalist.
Due to an overwhelming number of Democratic victories in last November’s midterm elections, the 110th Congress, which took office early this year, has new leaders and a new agenda that could bode well for healthcare legislation.
In this article, Laura Allendorf, SHM’s senior advisor for advocacy and government affairs, explains what the changes in Congress could mean for the near future of healthcare and for the legislation and issues that SHM strongly supports. Based in Washington, D.C., Allendorf is responsible for providing government relations services for SHM. She advises the organization on key legislative and regulatory healthcare issues before Congress and the Bush administration, and she works with SHM leaders and staff on policy development and advocacy strategies.
Majority Rules
The midterm elections brought about a shift in power that goes deeper than numbers of bodies on each side of the aisle. “The Democrats are now the majority in both chambers. This is significant, because they’ve been the minority since 1994, says Allendorf. “As the majority, they control the agenda now—on healthcare and other issues—and they also head the key committees.”
What can we expect to see from the Democratic Congress? “We should expect to see a more expansionist agenda” in general, according to Allendorf. “We’re going to see more activism in the area of healthcare, but whether anything gets done remains to be seen. There’s only a slim majority in the Senate, and President Bush can wield his veto pen. For example, the Democrats would like to give [the Department of] Health and Human Services the power to negotiate drug prices with pharmaceutical companies, specifically on Medicare Part D, but Bush won’t like that.”
Much depends on the issues at hand, as well as on how much bipartisan support exists for each specific bill.
Changing of the Guard
Anyone who glances at the newspaper knows that Democrat Nancy Pelosi (Calif.) is now the Speaker of the House. But Democratic leadership goes much deeper than that because the ruling party has also taken over leadership of Congressional committees. These committees shape the legislation introduced in the House and Senate.
As of press time, Congressional committee assignments had not been formally decided—at least not in the Senate—but many assignments were certain. “Typically, the highest-ranking Democrat [House or Senate] on a committee will become the new head, though Nancy Pelosi isn’t sticking to that,” explains Allendorf. “Pete Stark (D-Calif.) will likely chair the Ways and Means Committee’s Subcommittee on Health, and Charles Rangel (D-N.Y.) will head the House Ways and Means Committee. John Dingell (D-Mich.) will chair the House Energy and Commerce Committee.” (For more on committee chairs, visit http://media-newswire.com/release_1040623.html.)
For a complete list of committee members, visit SHM’s new Legislative Action Center at http://capwiz.com/hospitalmedicine/home/. See “New Advocacy Tool Available,” for more information on the Legislative Action Center, above.)
Starting Over on Key Issues
Many of the bills introduced in 2006—particularly spending bills—were not voted on by the end of the lame duck session last fall. That means that these bills must be reintroduced in the new year. Bills that recommend funding changes are frozen, so agencies continue to receive 2006 funding until the new Congress votes to change their budget.
“All bills have to be reintroduced in the 110th,” stresses Allendorf. “It will take some time—how much depends on the issue. The Democrats may want to hold hearings on legislation, or they may simply dust off legislation that was introduced last year.”
The Democrats are expected to move on many of the issues that SHM has been lobbying for. “They’ve said that they want to reform the healthcare system,” says Allendorf. “Top issues include providing coverage to the uninsured, reforming Medicare Part D, and resolving the physician payment issue.”
Allendorf believes that there will be a bipartisan effort to push through physician payment reform. “There are some 265 members of Congress who requested action on this issue this year [in 2006],” she points out. “There’s a genuine interest and desire to address physician payment reform and pay-for-performance as well. They may differ on how quickly they want to move on some of these.”
The news is not so good on the issue of gainsharing, where physicians are allowed to share the profits realized by a hospital’s cost reductions when linked to specific best practices. “Representative Nancy Johnson (R-Conn.) was a big proponent of this issue in the House, and she was not re-elected,” says Allendorf. “Stark is an opponent of gainsharing, so there may not be the same Congressional push behind it—at least in the House.”
However, the unexpected gainsharing demonstration projects approved in 2006 are underway, and Congress will hear reports on those in several years, once the projects have been analyzed.
Another issue that may not be addressed is liability. “Medical liability reform will be on the back burner,” warns Allendorf. “It’s generally not supported by the Democrats.”
In 2006, SHM supported increased funding for the Agency for Healthcare Research and Quality (AHRQ)—this was one of the major issues addressed by members during Legislative Advocacy Day during the Annual Meeting in Washington, D.C. Whether the next budget includes more money for the agency remains to be seen. “The Democrats support increased funding for NIH (National Institutes of Health), AHRQ, and other healthcare agencies,” says Allendorf. “There’s certainly political will, but where is the money going to come from?”
New Congress, New Issues
What about new issues? “Democrats have signaled that healthcare access for the uninsured will be a priority,” says Allendorf. “I think that we’ll see new legislation with a renewed emphasis on access to care.”
SHM’s Public Policy Committee will be waiting for the first legislation to be introduced regarding coverage for uninsured Americans. “This is an issue that SHM is strongly in favor of,” explains Allendorf. “SHM will look at any bills that come out on this issue and then form a policy.”
Regardless of which healthcare issues come to the forefront first, SHM’s Public Policy Committee, staff, and members are likely to be more active than ever. “I see a very busy year legislatively for SHM,” says Allendorf. TH
Jane Jerrard regularly writes “Public Policy” for The Hospitalist.
Due to an overwhelming number of Democratic victories in last November’s midterm elections, the 110th Congress, which took office early this year, has new leaders and a new agenda that could bode well for healthcare legislation.
In this article, Laura Allendorf, SHM’s senior advisor for advocacy and government affairs, explains what the changes in Congress could mean for the near future of healthcare and for the legislation and issues that SHM strongly supports. Based in Washington, D.C., Allendorf is responsible for providing government relations services for SHM. She advises the organization on key legislative and regulatory healthcare issues before Congress and the Bush administration, and she works with SHM leaders and staff on policy development and advocacy strategies.
Majority Rules
The midterm elections brought about a shift in power that goes deeper than numbers of bodies on each side of the aisle. “The Democrats are now the majority in both chambers. This is significant, because they’ve been the minority since 1994, says Allendorf. “As the majority, they control the agenda now—on healthcare and other issues—and they also head the key committees.”
What can we expect to see from the Democratic Congress? “We should expect to see a more expansionist agenda” in general, according to Allendorf. “We’re going to see more activism in the area of healthcare, but whether anything gets done remains to be seen. There’s only a slim majority in the Senate, and President Bush can wield his veto pen. For example, the Democrats would like to give [the Department of] Health and Human Services the power to negotiate drug prices with pharmaceutical companies, specifically on Medicare Part D, but Bush won’t like that.”
Much depends on the issues at hand, as well as on how much bipartisan support exists for each specific bill.
Changing of the Guard
Anyone who glances at the newspaper knows that Democrat Nancy Pelosi (Calif.) is now the Speaker of the House. But Democratic leadership goes much deeper than that because the ruling party has also taken over leadership of Congressional committees. These committees shape the legislation introduced in the House and Senate.
As of press time, Congressional committee assignments had not been formally decided—at least not in the Senate—but many assignments were certain. “Typically, the highest-ranking Democrat [House or Senate] on a committee will become the new head, though Nancy Pelosi isn’t sticking to that,” explains Allendorf. “Pete Stark (D-Calif.) will likely chair the Ways and Means Committee’s Subcommittee on Health, and Charles Rangel (D-N.Y.) will head the House Ways and Means Committee. John Dingell (D-Mich.) will chair the House Energy and Commerce Committee.” (For more on committee chairs, visit http://media-newswire.com/release_1040623.html.)
For a complete list of committee members, visit SHM’s new Legislative Action Center at http://capwiz.com/hospitalmedicine/home/. See “New Advocacy Tool Available,” for more information on the Legislative Action Center, above.)
Starting Over on Key Issues
Many of the bills introduced in 2006—particularly spending bills—were not voted on by the end of the lame duck session last fall. That means that these bills must be reintroduced in the new year. Bills that recommend funding changes are frozen, so agencies continue to receive 2006 funding until the new Congress votes to change their budget.
“All bills have to be reintroduced in the 110th,” stresses Allendorf. “It will take some time—how much depends on the issue. The Democrats may want to hold hearings on legislation, or they may simply dust off legislation that was introduced last year.”
The Democrats are expected to move on many of the issues that SHM has been lobbying for. “They’ve said that they want to reform the healthcare system,” says Allendorf. “Top issues include providing coverage to the uninsured, reforming Medicare Part D, and resolving the physician payment issue.”
Allendorf believes that there will be a bipartisan effort to push through physician payment reform. “There are some 265 members of Congress who requested action on this issue this year [in 2006],” she points out. “There’s a genuine interest and desire to address physician payment reform and pay-for-performance as well. They may differ on how quickly they want to move on some of these.”
The news is not so good on the issue of gainsharing, where physicians are allowed to share the profits realized by a hospital’s cost reductions when linked to specific best practices. “Representative Nancy Johnson (R-Conn.) was a big proponent of this issue in the House, and she was not re-elected,” says Allendorf. “Stark is an opponent of gainsharing, so there may not be the same Congressional push behind it—at least in the House.”
However, the unexpected gainsharing demonstration projects approved in 2006 are underway, and Congress will hear reports on those in several years, once the projects have been analyzed.
Another issue that may not be addressed is liability. “Medical liability reform will be on the back burner,” warns Allendorf. “It’s generally not supported by the Democrats.”
In 2006, SHM supported increased funding for the Agency for Healthcare Research and Quality (AHRQ)—this was one of the major issues addressed by members during Legislative Advocacy Day during the Annual Meeting in Washington, D.C. Whether the next budget includes more money for the agency remains to be seen. “The Democrats support increased funding for NIH (National Institutes of Health), AHRQ, and other healthcare agencies,” says Allendorf. “There’s certainly political will, but where is the money going to come from?”
New Congress, New Issues
What about new issues? “Democrats have signaled that healthcare access for the uninsured will be a priority,” says Allendorf. “I think that we’ll see new legislation with a renewed emphasis on access to care.”
SHM’s Public Policy Committee will be waiting for the first legislation to be introduced regarding coverage for uninsured Americans. “This is an issue that SHM is strongly in favor of,” explains Allendorf. “SHM will look at any bills that come out on this issue and then form a policy.”
Regardless of which healthcare issues come to the forefront first, SHM’s Public Policy Committee, staff, and members are likely to be more active than ever. “I see a very busy year legislatively for SHM,” says Allendorf. TH
Jane Jerrard regularly writes “Public Policy” for The Hospitalist.