User login
The Medicaid Gap
Amid the recent focus on Medicare’s spiraling costs and efforts to rein in government spending, media accounts have painted a grim picture of Medicaid financing as well:
- With record enrollment, Kentucky’s Medicaid program is facing a budget shortfall of nearly $500 million. In Arizona, the gap is expected to be $1 billion.
- In September, Washington state announced $112.8 million in Medicaid cuts, a reduction that the state’s Medicaid director described as “devastating.”
- According to the Kaiser Family Foundation, Louisiana cut Medicaid inpatient hospital rates 3.5% in fiscal year 2009, 12.1% in 2010, and an additional 4.6% for 2011 to help close budget gaps.
- Maine politicians are facing off over a $380 million state debt owed to hospitals providing Medicaid services.
Safety-net hospitals that care for a disproportionate share of uninsured and Medicaid patients are likely to feel the most pain. So what does that mean for hospitalists? Experts say they will be increasingly looked to for guidance and leadership in identifying cost-saving measures and in helping hospitals avoid further penalties by focusing on such critical metrics as readmission rates.
Political ‘Hot Potato’
The pressure isn’t likely to ease anytime soon. The American Recovery and Reinvestment Act provided $87 billion to help states pay for Medicaid costs from October 2008 through the end of this year by temporarily boosting the federal Medicaid matching rate, officially known as the Federal Medical Assistance Percentages (FMAP). In August, Congress passed legislation that provided an additional $16.1 billion to provide six more months of scaled-back relief through June, when the fiscal year ends in most states.
That’s when things could get really sticky. According to an annual survey conducted by the Kaiser Family Foundation, average state spending on Medicaid jumped 8.8% last year, the biggest increase in eight years and higher than the initial prediction of 6.3%. State Medicaid officials reported swelling ranks of eligible families due to the recession as a main reason for the rise. The pace is expected to cool slightly next year, but states that had relied heavily on federal aid to meet budget shortfalls are now facing the prospect of doing without amid a continued expansion of Medicaid enrollees.
“That’s the catch-22 that you’re in right now,” says Ellen Kugler, executive director of the National Association of Urban Hospitals, based in Sterling, Va. “There is increased demand and increasing numbers of uninsured. States are still in fiscal crisis, and there’s a delay before new dollars become available.”
New federal funds become available in 2014 to help pay for insuring those who currently lack insurance. That money will flow either through subsidies to state-administered exchanges or through direct Medicaid payments. But that same year, Kugler says, safety-net hospitals will begin seeing hefty reductions in Medicare disproportionate share (DSH) payments and possibly Medicaid DSH payments, too.
In theory, more people will have some form of health insurance by then, lessening the need to pay hospitals to help them recoup the cost of treating uninsured and underinsured patients. However, Kugler is urging caution on the DSH pay cuts, warning that it’s not clear what the ranks of the newly insured will be. Current projections, she says, suggest that half of those insured patients will fall under Medicaid programs, meaning that significant cuts could pose a financial hardship to hospitals that serve those populations.
Beyond reductions in services and reimbursement rates to doctors and hospitals, few politicians have had the stomach to propose major overhauls in how Medicaid is managed and financed. In New York state, however, a suite of proposals by Lt. Gov. Richard Ravitch has earned praise from The New York Times.1 One would streamline management of the program, now administered by 58 local governments and multiple state agencies. Ravitch also supports reducing the political wrangling over how reimbursement fees are calculated by wresting that power away from the state legislature and giving it to the state’s Medicaid director, who would be advised by an expert panel.
Another unresolved issue is how to pay for the long-term care of chronically ill patients, which in New York accounts for nearly half of its Medicaid spending. Kugler says the high incidence of chronic conditions, including mental illness, among patients in urban settings can contribute to the high readmission rates the new law is set to begin penalizing in 2012. Other studies have found that among Medicaid patients at high risk for frequent hospital admissions, substance abuse can be a major contributor.2
The difficult task, then, is to ensure that the hospitals serving these populations don’t lose even more resources through penalties due to subpar quality metrics. “Do the legwork now. Get your IT systems in place to be able to provide the coordinated care,” Kugler advises. Identifying efficiencies while maintaining the appropriate level of care will be key, whether in appropriate reductions in length of stay or in increased focus on communication with outpatient providers and other forms of outreach.
Hope for the Safety Net
Despite the financial and logistical challenges, Lenny Lopez, MD, MPH, a hospitalist at Brigham and Women’s Hospital and an assistant in health policy at Massachusetts General Hospital, both in Boston, says the situation is far from hopeless for safety-net hospitals. “The idea that if you’re a DSH hospital you’re somehow pegged and destined to provide low-quality care—that does not have to be the case,” he says. Nor do problems such as disparities in how patients are treated necessarily require expensive solutions.
In a recent paper in Academic Emergency Medicine, Dr. Lopez and his colleagues found that among patients with chest pain admitted to EDs, blacks, Hispanics, and those who lacked insurance or were on Medicare were less likely to receive urgent triage care.3 “These are problems that are fixable in a low-cost way,” he argues. “We don’t need another fancy machine to diagnose chest pain.” Rather, he suggests, the problem is really one of quality improvement that centers on boosting guidelines, not buying more equipment or involving more personnel.
Properly defining the problem, Dr. Lopez says, can lead to effective measures to boost quality. Amid the continuing budget crunch, pinpointing where interventions could provide the biggest bang for the buck also might prove enormously helpful.
Of the roughly 4,200 acute-care hospitals in the country, Dr. Lopez and his colleagues found that less than 10% care for the bulk of minority patients, and those on Medicaid or lacking insurance. That means such care is concentrated in about 400 hospitals, “which is a huge opportunity for intervention options for this kind of an issue,” he says. TH
Bryn Nelson is a freelance medical writer based in Seattle.
References
- 1. Benefits and burdens of Medicaid. The New York Times website. Available at: www.nytimes.com/2010/09/22/opinion/22wed2.html?_r=2&hp. Accessed Oct. 23, 2010.
- 2. Raven MC, Billings JC, Goldfrank LR, Manheimer ED, Gourevitch MN. Medicaid patients at high risk for frequent hospital admission: real-time identification and remediable risks. J Urban Health. 2009;86(2):230-241.
- 3. López L, Wilper AP, Cervantes MC, Betancourt JR, Green AR. Racial and sex differences in emergency department triage assessment and test ordering for chest pain, 1997-2006. Acad Emerg Med. 2010:17 (8):801-810.
Amid the recent focus on Medicare’s spiraling costs and efforts to rein in government spending, media accounts have painted a grim picture of Medicaid financing as well:
- With record enrollment, Kentucky’s Medicaid program is facing a budget shortfall of nearly $500 million. In Arizona, the gap is expected to be $1 billion.
- In September, Washington state announced $112.8 million in Medicaid cuts, a reduction that the state’s Medicaid director described as “devastating.”
- According to the Kaiser Family Foundation, Louisiana cut Medicaid inpatient hospital rates 3.5% in fiscal year 2009, 12.1% in 2010, and an additional 4.6% for 2011 to help close budget gaps.
- Maine politicians are facing off over a $380 million state debt owed to hospitals providing Medicaid services.
Safety-net hospitals that care for a disproportionate share of uninsured and Medicaid patients are likely to feel the most pain. So what does that mean for hospitalists? Experts say they will be increasingly looked to for guidance and leadership in identifying cost-saving measures and in helping hospitals avoid further penalties by focusing on such critical metrics as readmission rates.
Political ‘Hot Potato’
The pressure isn’t likely to ease anytime soon. The American Recovery and Reinvestment Act provided $87 billion to help states pay for Medicaid costs from October 2008 through the end of this year by temporarily boosting the federal Medicaid matching rate, officially known as the Federal Medical Assistance Percentages (FMAP). In August, Congress passed legislation that provided an additional $16.1 billion to provide six more months of scaled-back relief through June, when the fiscal year ends in most states.
That’s when things could get really sticky. According to an annual survey conducted by the Kaiser Family Foundation, average state spending on Medicaid jumped 8.8% last year, the biggest increase in eight years and higher than the initial prediction of 6.3%. State Medicaid officials reported swelling ranks of eligible families due to the recession as a main reason for the rise. The pace is expected to cool slightly next year, but states that had relied heavily on federal aid to meet budget shortfalls are now facing the prospect of doing without amid a continued expansion of Medicaid enrollees.
“That’s the catch-22 that you’re in right now,” says Ellen Kugler, executive director of the National Association of Urban Hospitals, based in Sterling, Va. “There is increased demand and increasing numbers of uninsured. States are still in fiscal crisis, and there’s a delay before new dollars become available.”
New federal funds become available in 2014 to help pay for insuring those who currently lack insurance. That money will flow either through subsidies to state-administered exchanges or through direct Medicaid payments. But that same year, Kugler says, safety-net hospitals will begin seeing hefty reductions in Medicare disproportionate share (DSH) payments and possibly Medicaid DSH payments, too.
In theory, more people will have some form of health insurance by then, lessening the need to pay hospitals to help them recoup the cost of treating uninsured and underinsured patients. However, Kugler is urging caution on the DSH pay cuts, warning that it’s not clear what the ranks of the newly insured will be. Current projections, she says, suggest that half of those insured patients will fall under Medicaid programs, meaning that significant cuts could pose a financial hardship to hospitals that serve those populations.
Beyond reductions in services and reimbursement rates to doctors and hospitals, few politicians have had the stomach to propose major overhauls in how Medicaid is managed and financed. In New York state, however, a suite of proposals by Lt. Gov. Richard Ravitch has earned praise from The New York Times.1 One would streamline management of the program, now administered by 58 local governments and multiple state agencies. Ravitch also supports reducing the political wrangling over how reimbursement fees are calculated by wresting that power away from the state legislature and giving it to the state’s Medicaid director, who would be advised by an expert panel.
Another unresolved issue is how to pay for the long-term care of chronically ill patients, which in New York accounts for nearly half of its Medicaid spending. Kugler says the high incidence of chronic conditions, including mental illness, among patients in urban settings can contribute to the high readmission rates the new law is set to begin penalizing in 2012. Other studies have found that among Medicaid patients at high risk for frequent hospital admissions, substance abuse can be a major contributor.2
The difficult task, then, is to ensure that the hospitals serving these populations don’t lose even more resources through penalties due to subpar quality metrics. “Do the legwork now. Get your IT systems in place to be able to provide the coordinated care,” Kugler advises. Identifying efficiencies while maintaining the appropriate level of care will be key, whether in appropriate reductions in length of stay or in increased focus on communication with outpatient providers and other forms of outreach.
Hope for the Safety Net
Despite the financial and logistical challenges, Lenny Lopez, MD, MPH, a hospitalist at Brigham and Women’s Hospital and an assistant in health policy at Massachusetts General Hospital, both in Boston, says the situation is far from hopeless for safety-net hospitals. “The idea that if you’re a DSH hospital you’re somehow pegged and destined to provide low-quality care—that does not have to be the case,” he says. Nor do problems such as disparities in how patients are treated necessarily require expensive solutions.
In a recent paper in Academic Emergency Medicine, Dr. Lopez and his colleagues found that among patients with chest pain admitted to EDs, blacks, Hispanics, and those who lacked insurance or were on Medicare were less likely to receive urgent triage care.3 “These are problems that are fixable in a low-cost way,” he argues. “We don’t need another fancy machine to diagnose chest pain.” Rather, he suggests, the problem is really one of quality improvement that centers on boosting guidelines, not buying more equipment or involving more personnel.
Properly defining the problem, Dr. Lopez says, can lead to effective measures to boost quality. Amid the continuing budget crunch, pinpointing where interventions could provide the biggest bang for the buck also might prove enormously helpful.
Of the roughly 4,200 acute-care hospitals in the country, Dr. Lopez and his colleagues found that less than 10% care for the bulk of minority patients, and those on Medicaid or lacking insurance. That means such care is concentrated in about 400 hospitals, “which is a huge opportunity for intervention options for this kind of an issue,” he says. TH
Bryn Nelson is a freelance medical writer based in Seattle.
References
- 1. Benefits and burdens of Medicaid. The New York Times website. Available at: www.nytimes.com/2010/09/22/opinion/22wed2.html?_r=2&hp. Accessed Oct. 23, 2010.
- 2. Raven MC, Billings JC, Goldfrank LR, Manheimer ED, Gourevitch MN. Medicaid patients at high risk for frequent hospital admission: real-time identification and remediable risks. J Urban Health. 2009;86(2):230-241.
- 3. López L, Wilper AP, Cervantes MC, Betancourt JR, Green AR. Racial and sex differences in emergency department triage assessment and test ordering for chest pain, 1997-2006. Acad Emerg Med. 2010:17 (8):801-810.
Amid the recent focus on Medicare’s spiraling costs and efforts to rein in government spending, media accounts have painted a grim picture of Medicaid financing as well:
- With record enrollment, Kentucky’s Medicaid program is facing a budget shortfall of nearly $500 million. In Arizona, the gap is expected to be $1 billion.
- In September, Washington state announced $112.8 million in Medicaid cuts, a reduction that the state’s Medicaid director described as “devastating.”
- According to the Kaiser Family Foundation, Louisiana cut Medicaid inpatient hospital rates 3.5% in fiscal year 2009, 12.1% in 2010, and an additional 4.6% for 2011 to help close budget gaps.
- Maine politicians are facing off over a $380 million state debt owed to hospitals providing Medicaid services.
Safety-net hospitals that care for a disproportionate share of uninsured and Medicaid patients are likely to feel the most pain. So what does that mean for hospitalists? Experts say they will be increasingly looked to for guidance and leadership in identifying cost-saving measures and in helping hospitals avoid further penalties by focusing on such critical metrics as readmission rates.
Political ‘Hot Potato’
The pressure isn’t likely to ease anytime soon. The American Recovery and Reinvestment Act provided $87 billion to help states pay for Medicaid costs from October 2008 through the end of this year by temporarily boosting the federal Medicaid matching rate, officially known as the Federal Medical Assistance Percentages (FMAP). In August, Congress passed legislation that provided an additional $16.1 billion to provide six more months of scaled-back relief through June, when the fiscal year ends in most states.
That’s when things could get really sticky. According to an annual survey conducted by the Kaiser Family Foundation, average state spending on Medicaid jumped 8.8% last year, the biggest increase in eight years and higher than the initial prediction of 6.3%. State Medicaid officials reported swelling ranks of eligible families due to the recession as a main reason for the rise. The pace is expected to cool slightly next year, but states that had relied heavily on federal aid to meet budget shortfalls are now facing the prospect of doing without amid a continued expansion of Medicaid enrollees.
“That’s the catch-22 that you’re in right now,” says Ellen Kugler, executive director of the National Association of Urban Hospitals, based in Sterling, Va. “There is increased demand and increasing numbers of uninsured. States are still in fiscal crisis, and there’s a delay before new dollars become available.”
New federal funds become available in 2014 to help pay for insuring those who currently lack insurance. That money will flow either through subsidies to state-administered exchanges or through direct Medicaid payments. But that same year, Kugler says, safety-net hospitals will begin seeing hefty reductions in Medicare disproportionate share (DSH) payments and possibly Medicaid DSH payments, too.
In theory, more people will have some form of health insurance by then, lessening the need to pay hospitals to help them recoup the cost of treating uninsured and underinsured patients. However, Kugler is urging caution on the DSH pay cuts, warning that it’s not clear what the ranks of the newly insured will be. Current projections, she says, suggest that half of those insured patients will fall under Medicaid programs, meaning that significant cuts could pose a financial hardship to hospitals that serve those populations.
Beyond reductions in services and reimbursement rates to doctors and hospitals, few politicians have had the stomach to propose major overhauls in how Medicaid is managed and financed. In New York state, however, a suite of proposals by Lt. Gov. Richard Ravitch has earned praise from The New York Times.1 One would streamline management of the program, now administered by 58 local governments and multiple state agencies. Ravitch also supports reducing the political wrangling over how reimbursement fees are calculated by wresting that power away from the state legislature and giving it to the state’s Medicaid director, who would be advised by an expert panel.
Another unresolved issue is how to pay for the long-term care of chronically ill patients, which in New York accounts for nearly half of its Medicaid spending. Kugler says the high incidence of chronic conditions, including mental illness, among patients in urban settings can contribute to the high readmission rates the new law is set to begin penalizing in 2012. Other studies have found that among Medicaid patients at high risk for frequent hospital admissions, substance abuse can be a major contributor.2
The difficult task, then, is to ensure that the hospitals serving these populations don’t lose even more resources through penalties due to subpar quality metrics. “Do the legwork now. Get your IT systems in place to be able to provide the coordinated care,” Kugler advises. Identifying efficiencies while maintaining the appropriate level of care will be key, whether in appropriate reductions in length of stay or in increased focus on communication with outpatient providers and other forms of outreach.
Hope for the Safety Net
Despite the financial and logistical challenges, Lenny Lopez, MD, MPH, a hospitalist at Brigham and Women’s Hospital and an assistant in health policy at Massachusetts General Hospital, both in Boston, says the situation is far from hopeless for safety-net hospitals. “The idea that if you’re a DSH hospital you’re somehow pegged and destined to provide low-quality care—that does not have to be the case,” he says. Nor do problems such as disparities in how patients are treated necessarily require expensive solutions.
In a recent paper in Academic Emergency Medicine, Dr. Lopez and his colleagues found that among patients with chest pain admitted to EDs, blacks, Hispanics, and those who lacked insurance or were on Medicare were less likely to receive urgent triage care.3 “These are problems that are fixable in a low-cost way,” he argues. “We don’t need another fancy machine to diagnose chest pain.” Rather, he suggests, the problem is really one of quality improvement that centers on boosting guidelines, not buying more equipment or involving more personnel.
Properly defining the problem, Dr. Lopez says, can lead to effective measures to boost quality. Amid the continuing budget crunch, pinpointing where interventions could provide the biggest bang for the buck also might prove enormously helpful.
Of the roughly 4,200 acute-care hospitals in the country, Dr. Lopez and his colleagues found that less than 10% care for the bulk of minority patients, and those on Medicaid or lacking insurance. That means such care is concentrated in about 400 hospitals, “which is a huge opportunity for intervention options for this kind of an issue,” he says. TH
Bryn Nelson is a freelance medical writer based in Seattle.
References
- 1. Benefits and burdens of Medicaid. The New York Times website. Available at: www.nytimes.com/2010/09/22/opinion/22wed2.html?_r=2&hp. Accessed Oct. 23, 2010.
- 2. Raven MC, Billings JC, Goldfrank LR, Manheimer ED, Gourevitch MN. Medicaid patients at high risk for frequent hospital admission: real-time identification and remediable risks. J Urban Health. 2009;86(2):230-241.
- 3. López L, Wilper AP, Cervantes MC, Betancourt JR, Green AR. Racial and sex differences in emergency department triage assessment and test ordering for chest pain, 1997-2006. Acad Emerg Med. 2010:17 (8):801-810.
A Bundle of Nerves
In a single year, one health system saved itself more than $2 million on orthopedic, cardiology, and cardiovascular surgery procedures. Another hospital saved Medicare an estimated $750,000. Supply costs dropped, scores on quality metrics rose, and bonus payments were distributed to participating doctors.
A runaway success? Not so fast.
Encouraging, if early, results from Medicare’s Acute Care Episode (ACE) Demonstration might have strengthened the case for bundling payments around episodes of care as an effective way to rein in spiraling healthcare costs and transition from a volume-based to a value-based payment system. But broad skepticism persists over the wisdom of binding together the fates of hospitals and doctors, and critics are far from ready to drop their argument that bundling will be unworkable across wider, less-well-defined swaths of healthcare.
The current bundling and gain-sharing duo differs only superficially from the despised capitation model of the 1990s, argues Adam Singer, MD, CEO of North Hollywood, Calif.-based IPC: The Hospitalist Company. “It’s capitation in a different dress, except that instead of over a patient population, it’s done over an individual patient’s case,” he says.
Not so, says Lisa Kettering, MD, SFHM, vice president of medical affairs and CMO at Exempla St. Joseph Hospital in Denver.
“I’ve been around in medicine long enough to have been around when there was capitation,” she says. “I think the current bundling project is a vast improvement and I think it’s a very different animal from old capitation … and pivots absolutely critically on the physician involvement at the heart of quality, at the heart of decision-making. That’s never happened before.”
Amid the swirling expectations and apprehensions, what has the ACE demo taught us so far about bundling, and what does it mean for the future of hospital medicine? In essence, bundling lumps Medicare Part A and Part B reimbursements into a single payment aimed at encouraging hospitals and doctors to work together to improve efficiency, maintain high-quality care, and reduce overall expenses. Hospitals participating in the ACE Demonstration provide a roughly 5% discount to Medicare for a specific list of diagnosis-related groups (DRGs), and the Centers for Medicare & Medicaid Services (CMS) passes on half of the savings to beneficiaries who use participating hospitals for the covered procedures.
After submitting their claims, the hospitals receive a bundled Medicare payment, from which they pay doctors 100% of their Part B fees. As an incentive, some providers are eligible for bonus payments in the form of gain-sharing. CMS rules preclude any payments for referrals, cap all payments at 25% of the physician fee schedule, and mandate that any payment be based on reductions in patient care costs due to ACE activities. But participating hospitals are otherwise free to devise their own formulas and specific quality metrics that doctors must meet to gain the bonus.
SHM repeatedly has signaled its support for exploring bundling as a way to better align financial incentives among providers and reward them for quality and efficiency instead of quantity. The 10,000-member society strongly supports further testing of payment bundling methodologies prior to a national rollout, however, and has called for the integral involvement of hospitalists in developing and implementing bundling projects.
With its main focus on cardiologists, orthopedic surgeons, and cardiovascular surgeons, the ACE Demonstration has had little direct impact on hospitalists’ jobs or bank accounts—so far. That could change with an expanded pilot mandated by healthcare reform legislation. Slated to begin by Jan. 1, 2013, the project will redefine covered episodes of care to include all medical services administered three days before a hospital admission through 30 days after discharge.
CMS hasn’t yet decided which procedures will be covered, but officials say they’ve learned from past experience to begin with well-defined episodes of care. “Back in the ’90s, we did a bundled demonstration for bypass procedures and also for cataract procedures,” says Cynthia Mason, project manager with the CMS Medicare Demonstrations Group. “What we learned from that is obviously it’s easier both for Medicare, as well as for the providers, to predict utilization when you have a more standardized package of services. You also need a variety and large number of services in order to give you opportunities for looking at efficiencies and improvements in the system.”
Upfront Investment, Immediate Savings, Improved Quality
Early opinions have been mostly positive among the ACE participants. Hillcrest Medical Center in Tulsa, Okla., was first out of the gate in May 2009. Over the project’s first year, Hillcrest CEO Steve Dobbs estimates that the 490-bed hospital has saved CMS about $750,000; half of that sum has been passed along to patients. The hospital itself has spent about $550,000 in marketing, start-up costs, corporate support, and paying third-party claims. But recent investments have led to double-digit gains in patient volume (24% in cardiology and cardiovascular surgery, and a whopping 37% in orthopedics), margins in orthopedics are up, and direct negotiations between participating doctors and national vendors have netted additional savings. As a reward for help with cost-cutting, Hillcrest recently passed along two gain-sharing checks totaling $130,000 to be split among six independent orthopedists.
“What’s actually driving this program is the supply cost savings from all of our national partners,” Dobbs says. A big question is whether the negotiated savings—and hence the gain-sharing—could be maintained over a greatly expanded pilot project. “If this goes nationwide and everybody’s in it, do you get the same benefit? I don’t know the answer to that right now,” he says.
Dobbs is careful to point out that success is not measured by patient volume and supply costs alone. Hillcrest’s gain-sharing plan stipulates that physicians must reach the 90% threshold for a range of quality metrics. For one previously problematic category—stopping antibiotics 24 hours post-surgery—Dobbs says both the orthopedics and cardiovascular surgery departments have dramatically increased their compliance rates.
Baptist Health System in San Antonio, which began its own demonstration in June 2009, has reported savings of $2.2 million for its 1,275-bed, four-campus health system. So far, the roughly 20 hospitalists employed by IPC: The Hospitalist Company who work within the Baptist Health System have not directly participated in the project. But Felix Aguirre, MD, FHM, IPC’s vice president of medical affairs in San Antonio, says the demonstration has had a definite impact on efficiency.

“Since the demonstration project has come up, it seems like everybody is obeying the evidence-based guidelines now,” says Dr. Aguirre, a member of SHM’s Public Policy Committee and Team Hospitalist. “So it’s not keeping the hip replacement patient in for five days, it’s what the guidelines say: three days.”
Some kinks still need to be worked out. Baptist has had trouble with double payments and other claims-related issues, Dr. Aguirre says. Hillcrest’s Dobbs complains that he has heard virtually no feedback from CMS. Medicare’s Mason says officials have been “very pleased” with the project’s progress so far, but concedes that a delay in updating a claims processing system has pushed back the launch at two other demonstration sites until Nov. 1.
At one of those sites, 361-bed Exempla St. Joseph Hospital, the three-year demonstration will encompass only cardiology and cardiovascular surgery. Dr. Kettering, a former SHM board member who serves as executive sponsor and director of St. Joseph Hospital’s ACE demo, says the shared-savings program will be limited to cardiovascular surgery for the first year to ensure the system is running smoothly. In the second or third year, however, hospitalists who care for eligible patients could theoretically benefit from a similar gain-sharing agreement, if they meet certain agreed-upon, evidence-based metrics. In that circumstance, she says, hospitalists would begin to learn the ropes and become directly involved in quality outcomes. Extending the model beyond ACE, their primary role could expand dramatically to that of learning how to operate bundling across the continuum of care.
The eventual bundling experiences at all five demonstration sites will likely be positive, Dr. Aguirre says, given that they were carefully chosen to maximize the likelihood of success. “Where the rubber will hit the road is, how do you translate where you’re obviously going to be successful at five sites to implementing it across maybe a thousand sites and making it successful?” he asks.

All Eggs in One Basket?
One thing is certain: For bundling to expand, it will have to convince some fierce critics of its staying power. IPC’s Dr. Singer says so much emphasis has been placed on bundling that it has drowned out any discussion of other alternatives. “It seems like we as a society are hell-bent on putting this in as the method of payment, but I don’t really see all the elements that really would promote a higher-quality product that would reduce cost, which is what it should be about,” he says.
If not bundling, what? For some observers, payment-reform options follow a continuum arcing away from the fee-for-service system, though not everyone agrees on just how widely each might—or should—depart from the status quo. Some healthcare leaders, for example, contend that it would be easiest to simply devise new DRG categories for hospitalists or primary-care physicians (PCPs) to replace the existing fee-for-service CPT codes. “It’s a very simple way of aligning the doctor and the hospital without combining the doctor and the hospital into one entity, which is what bundling does,” Dr. Singer says.
Even some bundling advocates say the solution might ease some anxiety over who controls the purse strings, though such a system would need to account for critical-access hospitals, which currently don’t use the DRG system at all. Alternatively, some analysts see broadened gain-sharing rules as a good way to align incentives toward more efficient care, regardless of whether the incentive system accompanies bundling.
Although still in their formative stages, accountable-care organizations (ACOs) and patient-centered medical homes (PCMHs)—and the implicit bundling of medical services across patient populations—are being advanced as longer-term reforms. Even then, analysts argue over whether such models will be sufficiently free from a fee-for-service foundation. Despite the vigorous debate, most observers agree that Medicare officials are keen to offload more of the risk, whether onto physicians or onto hospitals. “They’re saying, ‘Here’s the dollar. You administer it. And if you end up in the negative, you do, but if it’s in the positive, you get a share of everything,’ ” Dr. Aguirre says.
HM: Front and Center
Hospitalists might be uniquely well positioned to bring more efficiency and value, as well as help hospitals manage that risk. With bundling, though, the big question is how they’ll be paid for their services amid the demands of multiple providers. “I’ve heard it described as a big potential food fight,” says Kirk Mathews, CEO of St. Louis-based Inpatient Management Inc. and a member of SHM’s Workforce Summit Committee.
In the scenario relayed to him by fearful hospitalists, a hospital administrator is seated at the table with pie in hand, with the various providers clamoring for a slice. “Everyone will be sitting there saying, ‘Here’s why we deserve this percent of the bundled payment,’” Mathews says. “Whether that’s an accurate portrayal or not, that’s the fear.”
Taken a step further, the scenario envisions hospitalists struggling to hold their own at the table against high-powered and higher-paid specialists. Some of the ACE Demonstration sites, however, have used physician-hospital organizations, or PHOs, to help decentralize the decision-making and ensure that stakeholders are represented. Similarly, if patient referrals to hospitalists from other providers drop—as they did for some of the ACE Demonstration bundles at Baptist and Hillcrest—could hospitalists lose their bargaining power through an erosion of recouped professional fees?
If bundling expands, Hillcrest’s CEO says hospitalists are instead likely to assume a more central role (see “Six Pieces of Bundling-Related Advice for Hospitalists,” right). “If we truly go to bundled payments on everything,” Dobbs says, “then I think everybody’s got to be at the table and contributing, and especially the hospitalist, because the medical DRGs, that’s going to be where the hospitalists drive the equation, and that’s going to be a huge part of this.”
As SHM’s CEO Larry Wellikson, MD, SFHM, wrote in The Hospitalist last year (see “Bundling Bedlam,” July 2009, p. 46), the bundling of Medicare Part A dollars that subsidize HM with Part B physicians’ payments might actually pave the way for a more professional discussion of the value that hospitalists deliver. With bundling, he wrote, “the need for subsidies or support could diminish or vanish.”

But that doesn’t resolve the issue of how to fairly size each bundle. Stuart Guterman, vice president of the Washington, D.C.-based Common-wealth Fund’s Program on Payment and System Reform, says one lesson from the capitation scheme of the ’90s is that an overemphasis on cost savings can lead to payments that are frequently insufficient to cover the costs of appropriate care.
“So there’s got to be more collaboration on what an appropriate amount is, and that’s a very important feature,” Guterman says. “Clearly, if you don’t pay enough, it doesn’t bode well for the success of any kind of payment approach. If you pay too much, it means you’re wasting money.”
The size and complexity of healthcare networks will influence how those bundle-related payments are negotiated. And in this case, several analysts say bigger isn’t necessarily better. “My own view is that it’s easier for a handful of hospitalists and a few community doctors in the hospital to come to an agreement on how they’re going to work within a bundle,” says Robert Berenson, MD, a senior fellow in the Urban Institute’s Health Policy Center and vice chair of the Medicare Payment Advisory Commission (MedPAC).

“My experience is that in rural communities, there’s a greater alliance of interests between the doctors and the hospitals, whereas in big urban areas they’re often competing with each other. So I don’t see that as the problem, frankly. I think this is probably better designed for smaller places where there’s already reasonably good relationships.”
L. Scott Sussman, MD, a hospitalist at Mt. Ascutney Hospital and Health Center in Windsor, Vt., agrees that bundling likely wouldn’t negatively affect the day-to-day operations of the 25-bed critical-access hospital. Almost all admitted patients have PCPs in the affiliated Mt. Ascutney Physicians Practice, aiding communication during hospitalizations and care transitions. Dr. Sussman thinks bundling fits well with the mission of hospitalists to provide quality care and help smooth their patients’ transition back to community providers. “From the reading that I’ve done on bundling, it does seem to me that if implemented properly, it really could achieve cost savings while maintaining quality care,” he says.
Nevertheless, he has plenty of questions and concerns. Bundling would be more complicated, he concedes, if most admissions were referred from private-practice physicians in the community. And because Mt. Ascutney is a critical-access hospital, patients who develop complications or require a higher level of care are transferred to a tertiary-care facility—in this case, a 22-mile drive over the state line to Dartmouth-Hitchcock Medical Center in Lebanon, N.H. “How would the payment be divided up at that point?” he asks.
To make bundling work, healthcare leaders will clearly need to blaze a trail through uncharted territory.
But if the goal is getting more from the trillions spent annually on healthcare, advocates like Guterman say it provides an important step toward a better-functioning system.
Among hospitalists, at least some observers are betting that bundling will ultimately find its way. “I think bundled payments are here to stay,” Dr. Aguirre says. “I think our goal now is to see how we can modify it or create it so it can have the best impact for us and we can have the best impact for it.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
In a single year, one health system saved itself more than $2 million on orthopedic, cardiology, and cardiovascular surgery procedures. Another hospital saved Medicare an estimated $750,000. Supply costs dropped, scores on quality metrics rose, and bonus payments were distributed to participating doctors.
A runaway success? Not so fast.
Encouraging, if early, results from Medicare’s Acute Care Episode (ACE) Demonstration might have strengthened the case for bundling payments around episodes of care as an effective way to rein in spiraling healthcare costs and transition from a volume-based to a value-based payment system. But broad skepticism persists over the wisdom of binding together the fates of hospitals and doctors, and critics are far from ready to drop their argument that bundling will be unworkable across wider, less-well-defined swaths of healthcare.
The current bundling and gain-sharing duo differs only superficially from the despised capitation model of the 1990s, argues Adam Singer, MD, CEO of North Hollywood, Calif.-based IPC: The Hospitalist Company. “It’s capitation in a different dress, except that instead of over a patient population, it’s done over an individual patient’s case,” he says.
Not so, says Lisa Kettering, MD, SFHM, vice president of medical affairs and CMO at Exempla St. Joseph Hospital in Denver.
“I’ve been around in medicine long enough to have been around when there was capitation,” she says. “I think the current bundling project is a vast improvement and I think it’s a very different animal from old capitation … and pivots absolutely critically on the physician involvement at the heart of quality, at the heart of decision-making. That’s never happened before.”
Amid the swirling expectations and apprehensions, what has the ACE demo taught us so far about bundling, and what does it mean for the future of hospital medicine? In essence, bundling lumps Medicare Part A and Part B reimbursements into a single payment aimed at encouraging hospitals and doctors to work together to improve efficiency, maintain high-quality care, and reduce overall expenses. Hospitals participating in the ACE Demonstration provide a roughly 5% discount to Medicare for a specific list of diagnosis-related groups (DRGs), and the Centers for Medicare & Medicaid Services (CMS) passes on half of the savings to beneficiaries who use participating hospitals for the covered procedures.
After submitting their claims, the hospitals receive a bundled Medicare payment, from which they pay doctors 100% of their Part B fees. As an incentive, some providers are eligible for bonus payments in the form of gain-sharing. CMS rules preclude any payments for referrals, cap all payments at 25% of the physician fee schedule, and mandate that any payment be based on reductions in patient care costs due to ACE activities. But participating hospitals are otherwise free to devise their own formulas and specific quality metrics that doctors must meet to gain the bonus.
SHM repeatedly has signaled its support for exploring bundling as a way to better align financial incentives among providers and reward them for quality and efficiency instead of quantity. The 10,000-member society strongly supports further testing of payment bundling methodologies prior to a national rollout, however, and has called for the integral involvement of hospitalists in developing and implementing bundling projects.
With its main focus on cardiologists, orthopedic surgeons, and cardiovascular surgeons, the ACE Demonstration has had little direct impact on hospitalists’ jobs or bank accounts—so far. That could change with an expanded pilot mandated by healthcare reform legislation. Slated to begin by Jan. 1, 2013, the project will redefine covered episodes of care to include all medical services administered three days before a hospital admission through 30 days after discharge.
CMS hasn’t yet decided which procedures will be covered, but officials say they’ve learned from past experience to begin with well-defined episodes of care. “Back in the ’90s, we did a bundled demonstration for bypass procedures and also for cataract procedures,” says Cynthia Mason, project manager with the CMS Medicare Demonstrations Group. “What we learned from that is obviously it’s easier both for Medicare, as well as for the providers, to predict utilization when you have a more standardized package of services. You also need a variety and large number of services in order to give you opportunities for looking at efficiencies and improvements in the system.”
Upfront Investment, Immediate Savings, Improved Quality
Early opinions have been mostly positive among the ACE participants. Hillcrest Medical Center in Tulsa, Okla., was first out of the gate in May 2009. Over the project’s first year, Hillcrest CEO Steve Dobbs estimates that the 490-bed hospital has saved CMS about $750,000; half of that sum has been passed along to patients. The hospital itself has spent about $550,000 in marketing, start-up costs, corporate support, and paying third-party claims. But recent investments have led to double-digit gains in patient volume (24% in cardiology and cardiovascular surgery, and a whopping 37% in orthopedics), margins in orthopedics are up, and direct negotiations between participating doctors and national vendors have netted additional savings. As a reward for help with cost-cutting, Hillcrest recently passed along two gain-sharing checks totaling $130,000 to be split among six independent orthopedists.
“What’s actually driving this program is the supply cost savings from all of our national partners,” Dobbs says. A big question is whether the negotiated savings—and hence the gain-sharing—could be maintained over a greatly expanded pilot project. “If this goes nationwide and everybody’s in it, do you get the same benefit? I don’t know the answer to that right now,” he says.
Dobbs is careful to point out that success is not measured by patient volume and supply costs alone. Hillcrest’s gain-sharing plan stipulates that physicians must reach the 90% threshold for a range of quality metrics. For one previously problematic category—stopping antibiotics 24 hours post-surgery—Dobbs says both the orthopedics and cardiovascular surgery departments have dramatically increased their compliance rates.
Baptist Health System in San Antonio, which began its own demonstration in June 2009, has reported savings of $2.2 million for its 1,275-bed, four-campus health system. So far, the roughly 20 hospitalists employed by IPC: The Hospitalist Company who work within the Baptist Health System have not directly participated in the project. But Felix Aguirre, MD, FHM, IPC’s vice president of medical affairs in San Antonio, says the demonstration has had a definite impact on efficiency.
“Since the demonstration project has come up, it seems like everybody is obeying the evidence-based guidelines now,” says Dr. Aguirre, a member of SHM’s Public Policy Committee and Team Hospitalist. “So it’s not keeping the hip replacement patient in for five days, it’s what the guidelines say: three days.”
Some kinks still need to be worked out. Baptist has had trouble with double payments and other claims-related issues, Dr. Aguirre says. Hillcrest’s Dobbs complains that he has heard virtually no feedback from CMS. Medicare’s Mason says officials have been “very pleased” with the project’s progress so far, but concedes that a delay in updating a claims processing system has pushed back the launch at two other demonstration sites until Nov. 1.
At one of those sites, 361-bed Exempla St. Joseph Hospital, the three-year demonstration will encompass only cardiology and cardiovascular surgery. Dr. Kettering, a former SHM board member who serves as executive sponsor and director of St. Joseph Hospital’s ACE demo, says the shared-savings program will be limited to cardiovascular surgery for the first year to ensure the system is running smoothly. In the second or third year, however, hospitalists who care for eligible patients could theoretically benefit from a similar gain-sharing agreement, if they meet certain agreed-upon, evidence-based metrics. In that circumstance, she says, hospitalists would begin to learn the ropes and become directly involved in quality outcomes. Extending the model beyond ACE, their primary role could expand dramatically to that of learning how to operate bundling across the continuum of care.
The eventual bundling experiences at all five demonstration sites will likely be positive, Dr. Aguirre says, given that they were carefully chosen to maximize the likelihood of success. “Where the rubber will hit the road is, how do you translate where you’re obviously going to be successful at five sites to implementing it across maybe a thousand sites and making it successful?” he asks.
All Eggs in One Basket?
One thing is certain: For bundling to expand, it will have to convince some fierce critics of its staying power. IPC’s Dr. Singer says so much emphasis has been placed on bundling that it has drowned out any discussion of other alternatives. “It seems like we as a society are hell-bent on putting this in as the method of payment, but I don’t really see all the elements that really would promote a higher-quality product that would reduce cost, which is what it should be about,” he says.
If not bundling, what? For some observers, payment-reform options follow a continuum arcing away from the fee-for-service system, though not everyone agrees on just how widely each might—or should—depart from the status quo. Some healthcare leaders, for example, contend that it would be easiest to simply devise new DRG categories for hospitalists or primary-care physicians (PCPs) to replace the existing fee-for-service CPT codes. “It’s a very simple way of aligning the doctor and the hospital without combining the doctor and the hospital into one entity, which is what bundling does,” Dr. Singer says.
Even some bundling advocates say the solution might ease some anxiety over who controls the purse strings, though such a system would need to account for critical-access hospitals, which currently don’t use the DRG system at all. Alternatively, some analysts see broadened gain-sharing rules as a good way to align incentives toward more efficient care, regardless of whether the incentive system accompanies bundling.
Although still in their formative stages, accountable-care organizations (ACOs) and patient-centered medical homes (PCMHs)—and the implicit bundling of medical services across patient populations—are being advanced as longer-term reforms. Even then, analysts argue over whether such models will be sufficiently free from a fee-for-service foundation. Despite the vigorous debate, most observers agree that Medicare officials are keen to offload more of the risk, whether onto physicians or onto hospitals. “They’re saying, ‘Here’s the dollar. You administer it. And if you end up in the negative, you do, but if it’s in the positive, you get a share of everything,’ ” Dr. Aguirre says.
HM: Front and Center
Hospitalists might be uniquely well positioned to bring more efficiency and value, as well as help hospitals manage that risk. With bundling, though, the big question is how they’ll be paid for their services amid the demands of multiple providers. “I’ve heard it described as a big potential food fight,” says Kirk Mathews, CEO of St. Louis-based Inpatient Management Inc. and a member of SHM’s Workforce Summit Committee.
In the scenario relayed to him by fearful hospitalists, a hospital administrator is seated at the table with pie in hand, with the various providers clamoring for a slice. “Everyone will be sitting there saying, ‘Here’s why we deserve this percent of the bundled payment,’” Mathews says. “Whether that’s an accurate portrayal or not, that’s the fear.”
Taken a step further, the scenario envisions hospitalists struggling to hold their own at the table against high-powered and higher-paid specialists. Some of the ACE Demonstration sites, however, have used physician-hospital organizations, or PHOs, to help decentralize the decision-making and ensure that stakeholders are represented. Similarly, if patient referrals to hospitalists from other providers drop—as they did for some of the ACE Demonstration bundles at Baptist and Hillcrest—could hospitalists lose their bargaining power through an erosion of recouped professional fees?
If bundling expands, Hillcrest’s CEO says hospitalists are instead likely to assume a more central role (see “Six Pieces of Bundling-Related Advice for Hospitalists,” right). “If we truly go to bundled payments on everything,” Dobbs says, “then I think everybody’s got to be at the table and contributing, and especially the hospitalist, because the medical DRGs, that’s going to be where the hospitalists drive the equation, and that’s going to be a huge part of this.”
As SHM’s CEO Larry Wellikson, MD, SFHM, wrote in The Hospitalist last year (see “Bundling Bedlam,” July 2009, p. 46), the bundling of Medicare Part A dollars that subsidize HM with Part B physicians’ payments might actually pave the way for a more professional discussion of the value that hospitalists deliver. With bundling, he wrote, “the need for subsidies or support could diminish or vanish.”
But that doesn’t resolve the issue of how to fairly size each bundle. Stuart Guterman, vice president of the Washington, D.C.-based Common-wealth Fund’s Program on Payment and System Reform, says one lesson from the capitation scheme of the ’90s is that an overemphasis on cost savings can lead to payments that are frequently insufficient to cover the costs of appropriate care.
“So there’s got to be more collaboration on what an appropriate amount is, and that’s a very important feature,” Guterman says. “Clearly, if you don’t pay enough, it doesn’t bode well for the success of any kind of payment approach. If you pay too much, it means you’re wasting money.”
The size and complexity of healthcare networks will influence how those bundle-related payments are negotiated. And in this case, several analysts say bigger isn’t necessarily better. “My own view is that it’s easier for a handful of hospitalists and a few community doctors in the hospital to come to an agreement on how they’re going to work within a bundle,” says Robert Berenson, MD, a senior fellow in the Urban Institute’s Health Policy Center and vice chair of the Medicare Payment Advisory Commission (MedPAC).
“My experience is that in rural communities, there’s a greater alliance of interests between the doctors and the hospitals, whereas in big urban areas they’re often competing with each other. So I don’t see that as the problem, frankly. I think this is probably better designed for smaller places where there’s already reasonably good relationships.”
L. Scott Sussman, MD, a hospitalist at Mt. Ascutney Hospital and Health Center in Windsor, Vt., agrees that bundling likely wouldn’t negatively affect the day-to-day operations of the 25-bed critical-access hospital. Almost all admitted patients have PCPs in the affiliated Mt. Ascutney Physicians Practice, aiding communication during hospitalizations and care transitions. Dr. Sussman thinks bundling fits well with the mission of hospitalists to provide quality care and help smooth their patients’ transition back to community providers. “From the reading that I’ve done on bundling, it does seem to me that if implemented properly, it really could achieve cost savings while maintaining quality care,” he says.
Nevertheless, he has plenty of questions and concerns. Bundling would be more complicated, he concedes, if most admissions were referred from private-practice physicians in the community. And because Mt. Ascutney is a critical-access hospital, patients who develop complications or require a higher level of care are transferred to a tertiary-care facility—in this case, a 22-mile drive over the state line to Dartmouth-Hitchcock Medical Center in Lebanon, N.H. “How would the payment be divided up at that point?” he asks.
To make bundling work, healthcare leaders will clearly need to blaze a trail through uncharted territory.
But if the goal is getting more from the trillions spent annually on healthcare, advocates like Guterman say it provides an important step toward a better-functioning system.
Among hospitalists, at least some observers are betting that bundling will ultimately find its way. “I think bundled payments are here to stay,” Dr. Aguirre says. “I think our goal now is to see how we can modify it or create it so it can have the best impact for us and we can have the best impact for it.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
In a single year, one health system saved itself more than $2 million on orthopedic, cardiology, and cardiovascular surgery procedures. Another hospital saved Medicare an estimated $750,000. Supply costs dropped, scores on quality metrics rose, and bonus payments were distributed to participating doctors.
A runaway success? Not so fast.
Encouraging, if early, results from Medicare’s Acute Care Episode (ACE) Demonstration might have strengthened the case for bundling payments around episodes of care as an effective way to rein in spiraling healthcare costs and transition from a volume-based to a value-based payment system. But broad skepticism persists over the wisdom of binding together the fates of hospitals and doctors, and critics are far from ready to drop their argument that bundling will be unworkable across wider, less-well-defined swaths of healthcare.
The current bundling and gain-sharing duo differs only superficially from the despised capitation model of the 1990s, argues Adam Singer, MD, CEO of North Hollywood, Calif.-based IPC: The Hospitalist Company. “It’s capitation in a different dress, except that instead of over a patient population, it’s done over an individual patient’s case,” he says.
Not so, says Lisa Kettering, MD, SFHM, vice president of medical affairs and CMO at Exempla St. Joseph Hospital in Denver.
“I’ve been around in medicine long enough to have been around when there was capitation,” she says. “I think the current bundling project is a vast improvement and I think it’s a very different animal from old capitation … and pivots absolutely critically on the physician involvement at the heart of quality, at the heart of decision-making. That’s never happened before.”
Amid the swirling expectations and apprehensions, what has the ACE demo taught us so far about bundling, and what does it mean for the future of hospital medicine? In essence, bundling lumps Medicare Part A and Part B reimbursements into a single payment aimed at encouraging hospitals and doctors to work together to improve efficiency, maintain high-quality care, and reduce overall expenses. Hospitals participating in the ACE Demonstration provide a roughly 5% discount to Medicare for a specific list of diagnosis-related groups (DRGs), and the Centers for Medicare & Medicaid Services (CMS) passes on half of the savings to beneficiaries who use participating hospitals for the covered procedures.
After submitting their claims, the hospitals receive a bundled Medicare payment, from which they pay doctors 100% of their Part B fees. As an incentive, some providers are eligible for bonus payments in the form of gain-sharing. CMS rules preclude any payments for referrals, cap all payments at 25% of the physician fee schedule, and mandate that any payment be based on reductions in patient care costs due to ACE activities. But participating hospitals are otherwise free to devise their own formulas and specific quality metrics that doctors must meet to gain the bonus.
SHM repeatedly has signaled its support for exploring bundling as a way to better align financial incentives among providers and reward them for quality and efficiency instead of quantity. The 10,000-member society strongly supports further testing of payment bundling methodologies prior to a national rollout, however, and has called for the integral involvement of hospitalists in developing and implementing bundling projects.
With its main focus on cardiologists, orthopedic surgeons, and cardiovascular surgeons, the ACE Demonstration has had little direct impact on hospitalists’ jobs or bank accounts—so far. That could change with an expanded pilot mandated by healthcare reform legislation. Slated to begin by Jan. 1, 2013, the project will redefine covered episodes of care to include all medical services administered three days before a hospital admission through 30 days after discharge.
CMS hasn’t yet decided which procedures will be covered, but officials say they’ve learned from past experience to begin with well-defined episodes of care. “Back in the ’90s, we did a bundled demonstration for bypass procedures and also for cataract procedures,” says Cynthia Mason, project manager with the CMS Medicare Demonstrations Group. “What we learned from that is obviously it’s easier both for Medicare, as well as for the providers, to predict utilization when you have a more standardized package of services. You also need a variety and large number of services in order to give you opportunities for looking at efficiencies and improvements in the system.”
Upfront Investment, Immediate Savings, Improved Quality
Early opinions have been mostly positive among the ACE participants. Hillcrest Medical Center in Tulsa, Okla., was first out of the gate in May 2009. Over the project’s first year, Hillcrest CEO Steve Dobbs estimates that the 490-bed hospital has saved CMS about $750,000; half of that sum has been passed along to patients. The hospital itself has spent about $550,000 in marketing, start-up costs, corporate support, and paying third-party claims. But recent investments have led to double-digit gains in patient volume (24% in cardiology and cardiovascular surgery, and a whopping 37% in orthopedics), margins in orthopedics are up, and direct negotiations between participating doctors and national vendors have netted additional savings. As a reward for help with cost-cutting, Hillcrest recently passed along two gain-sharing checks totaling $130,000 to be split among six independent orthopedists.
“What’s actually driving this program is the supply cost savings from all of our national partners,” Dobbs says. A big question is whether the negotiated savings—and hence the gain-sharing—could be maintained over a greatly expanded pilot project. “If this goes nationwide and everybody’s in it, do you get the same benefit? I don’t know the answer to that right now,” he says.
Dobbs is careful to point out that success is not measured by patient volume and supply costs alone. Hillcrest’s gain-sharing plan stipulates that physicians must reach the 90% threshold for a range of quality metrics. For one previously problematic category—stopping antibiotics 24 hours post-surgery—Dobbs says both the orthopedics and cardiovascular surgery departments have dramatically increased their compliance rates.
Baptist Health System in San Antonio, which began its own demonstration in June 2009, has reported savings of $2.2 million for its 1,275-bed, four-campus health system. So far, the roughly 20 hospitalists employed by IPC: The Hospitalist Company who work within the Baptist Health System have not directly participated in the project. But Felix Aguirre, MD, FHM, IPC’s vice president of medical affairs in San Antonio, says the demonstration has had a definite impact on efficiency.
“Since the demonstration project has come up, it seems like everybody is obeying the evidence-based guidelines now,” says Dr. Aguirre, a member of SHM’s Public Policy Committee and Team Hospitalist. “So it’s not keeping the hip replacement patient in for five days, it’s what the guidelines say: three days.”
Some kinks still need to be worked out. Baptist has had trouble with double payments and other claims-related issues, Dr. Aguirre says. Hillcrest’s Dobbs complains that he has heard virtually no feedback from CMS. Medicare’s Mason says officials have been “very pleased” with the project’s progress so far, but concedes that a delay in updating a claims processing system has pushed back the launch at two other demonstration sites until Nov. 1.
At one of those sites, 361-bed Exempla St. Joseph Hospital, the three-year demonstration will encompass only cardiology and cardiovascular surgery. Dr. Kettering, a former SHM board member who serves as executive sponsor and director of St. Joseph Hospital’s ACE demo, says the shared-savings program will be limited to cardiovascular surgery for the first year to ensure the system is running smoothly. In the second or third year, however, hospitalists who care for eligible patients could theoretically benefit from a similar gain-sharing agreement, if they meet certain agreed-upon, evidence-based metrics. In that circumstance, she says, hospitalists would begin to learn the ropes and become directly involved in quality outcomes. Extending the model beyond ACE, their primary role could expand dramatically to that of learning how to operate bundling across the continuum of care.
The eventual bundling experiences at all five demonstration sites will likely be positive, Dr. Aguirre says, given that they were carefully chosen to maximize the likelihood of success. “Where the rubber will hit the road is, how do you translate where you’re obviously going to be successful at five sites to implementing it across maybe a thousand sites and making it successful?” he asks.
All Eggs in One Basket?
One thing is certain: For bundling to expand, it will have to convince some fierce critics of its staying power. IPC’s Dr. Singer says so much emphasis has been placed on bundling that it has drowned out any discussion of other alternatives. “It seems like we as a society are hell-bent on putting this in as the method of payment, but I don’t really see all the elements that really would promote a higher-quality product that would reduce cost, which is what it should be about,” he says.
If not bundling, what? For some observers, payment-reform options follow a continuum arcing away from the fee-for-service system, though not everyone agrees on just how widely each might—or should—depart from the status quo. Some healthcare leaders, for example, contend that it would be easiest to simply devise new DRG categories for hospitalists or primary-care physicians (PCPs) to replace the existing fee-for-service CPT codes. “It’s a very simple way of aligning the doctor and the hospital without combining the doctor and the hospital into one entity, which is what bundling does,” Dr. Singer says.
Even some bundling advocates say the solution might ease some anxiety over who controls the purse strings, though such a system would need to account for critical-access hospitals, which currently don’t use the DRG system at all. Alternatively, some analysts see broadened gain-sharing rules as a good way to align incentives toward more efficient care, regardless of whether the incentive system accompanies bundling.
Although still in their formative stages, accountable-care organizations (ACOs) and patient-centered medical homes (PCMHs)—and the implicit bundling of medical services across patient populations—are being advanced as longer-term reforms. Even then, analysts argue over whether such models will be sufficiently free from a fee-for-service foundation. Despite the vigorous debate, most observers agree that Medicare officials are keen to offload more of the risk, whether onto physicians or onto hospitals. “They’re saying, ‘Here’s the dollar. You administer it. And if you end up in the negative, you do, but if it’s in the positive, you get a share of everything,’ ” Dr. Aguirre says.
HM: Front and Center
Hospitalists might be uniquely well positioned to bring more efficiency and value, as well as help hospitals manage that risk. With bundling, though, the big question is how they’ll be paid for their services amid the demands of multiple providers. “I’ve heard it described as a big potential food fight,” says Kirk Mathews, CEO of St. Louis-based Inpatient Management Inc. and a member of SHM’s Workforce Summit Committee.
In the scenario relayed to him by fearful hospitalists, a hospital administrator is seated at the table with pie in hand, with the various providers clamoring for a slice. “Everyone will be sitting there saying, ‘Here’s why we deserve this percent of the bundled payment,’” Mathews says. “Whether that’s an accurate portrayal or not, that’s the fear.”
Taken a step further, the scenario envisions hospitalists struggling to hold their own at the table against high-powered and higher-paid specialists. Some of the ACE Demonstration sites, however, have used physician-hospital organizations, or PHOs, to help decentralize the decision-making and ensure that stakeholders are represented. Similarly, if patient referrals to hospitalists from other providers drop—as they did for some of the ACE Demonstration bundles at Baptist and Hillcrest—could hospitalists lose their bargaining power through an erosion of recouped professional fees?
If bundling expands, Hillcrest’s CEO says hospitalists are instead likely to assume a more central role (see “Six Pieces of Bundling-Related Advice for Hospitalists,” right). “If we truly go to bundled payments on everything,” Dobbs says, “then I think everybody’s got to be at the table and contributing, and especially the hospitalist, because the medical DRGs, that’s going to be where the hospitalists drive the equation, and that’s going to be a huge part of this.”
As SHM’s CEO Larry Wellikson, MD, SFHM, wrote in The Hospitalist last year (see “Bundling Bedlam,” July 2009, p. 46), the bundling of Medicare Part A dollars that subsidize HM with Part B physicians’ payments might actually pave the way for a more professional discussion of the value that hospitalists deliver. With bundling, he wrote, “the need for subsidies or support could diminish or vanish.”
But that doesn’t resolve the issue of how to fairly size each bundle. Stuart Guterman, vice president of the Washington, D.C.-based Common-wealth Fund’s Program on Payment and System Reform, says one lesson from the capitation scheme of the ’90s is that an overemphasis on cost savings can lead to payments that are frequently insufficient to cover the costs of appropriate care.
“So there’s got to be more collaboration on what an appropriate amount is, and that’s a very important feature,” Guterman says. “Clearly, if you don’t pay enough, it doesn’t bode well for the success of any kind of payment approach. If you pay too much, it means you’re wasting money.”
The size and complexity of healthcare networks will influence how those bundle-related payments are negotiated. And in this case, several analysts say bigger isn’t necessarily better. “My own view is that it’s easier for a handful of hospitalists and a few community doctors in the hospital to come to an agreement on how they’re going to work within a bundle,” says Robert Berenson, MD, a senior fellow in the Urban Institute’s Health Policy Center and vice chair of the Medicare Payment Advisory Commission (MedPAC).
“My experience is that in rural communities, there’s a greater alliance of interests between the doctors and the hospitals, whereas in big urban areas they’re often competing with each other. So I don’t see that as the problem, frankly. I think this is probably better designed for smaller places where there’s already reasonably good relationships.”
L. Scott Sussman, MD, a hospitalist at Mt. Ascutney Hospital and Health Center in Windsor, Vt., agrees that bundling likely wouldn’t negatively affect the day-to-day operations of the 25-bed critical-access hospital. Almost all admitted patients have PCPs in the affiliated Mt. Ascutney Physicians Practice, aiding communication during hospitalizations and care transitions. Dr. Sussman thinks bundling fits well with the mission of hospitalists to provide quality care and help smooth their patients’ transition back to community providers. “From the reading that I’ve done on bundling, it does seem to me that if implemented properly, it really could achieve cost savings while maintaining quality care,” he says.
Nevertheless, he has plenty of questions and concerns. Bundling would be more complicated, he concedes, if most admissions were referred from private-practice physicians in the community. And because Mt. Ascutney is a critical-access hospital, patients who develop complications or require a higher level of care are transferred to a tertiary-care facility—in this case, a 22-mile drive over the state line to Dartmouth-Hitchcock Medical Center in Lebanon, N.H. “How would the payment be divided up at that point?” he asks.
To make bundling work, healthcare leaders will clearly need to blaze a trail through uncharted territory.
But if the goal is getting more from the trillions spent annually on healthcare, advocates like Guterman say it provides an important step toward a better-functioning system.
Among hospitalists, at least some observers are betting that bundling will ultimately find its way. “I think bundled payments are here to stay,” Dr. Aguirre says. “I think our goal now is to see how we can modify it or create it so it can have the best impact for us and we can have the best impact for it.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
A Taxing Future for HM?
When Congress returns for a likely lame-duck session after the midterm elections, the biggest battle might be fought over whether to extend the 2001 and 2003 tax cuts to everyone or only to those earning less than $200,000 annually ($250,000 for families). And depending on the makeup of the 112th Congress, which will be seated in January, Republicans might try to make good on a campaign pledge to repeal all or most of the healthcare reform legislation.
The expected flashpoints are being teased endlessly with media sound bites featuring phrases that most of us love to hate: higher taxes, spiraling medical bills, soaring insurance premiums. Insurance companies already are blaming a spike in premiums on the healthcare legislation, claiming that new provisions and mandates are forcing them to further hike their rates.
Closer to home, the high-profile frays could put hospitalists in the awkward position of supporting political positions that sock them in the wallet. After all, doctors are workers and healthcare consumers, too. So what impact could higher taxes and higher insurance premiums really have? Let’s start with health insurance.
Insurance Cost Increases
Signed into law in March, the Affordable Care Act includes tax credits for small businesses to help defray the costs of health insurance coverage. But in 2013, it also raises the threshold for medical expense deductions for most taxpayers, to 10% from 7.5% of adjusted gross income. In other words, families can claim tax deductions only after having spent 10% or more of their adjusted gross income on medical bills. For families with hefty medical bills, that 2.5% difference could translate into a significant shortfall.
CMS was able to negotiate with insurers to achieve a slight drop in Medicare Advantage premiums, but many individual states have had less luck in preventing rate increases from private insurers who blame their higher premiums on new mandates. The Wall Street Journal has documented rate increases of 18% in states like Wisconsin and North Carolina—about 9% of which insurance company officials pinned on the new law.1 Such increases are hardly inevitable, however. The Obama administration’s White House blog, for instance, has cited the example of North Carolina Blue Cross and Blue Shield, which announced Sept. 20 that it will provide $156 million in refunds to more than 215,000 customers after state regulators found an overcharge that should be reversed due to new rules in the reform law.2 WellPoint will similarly refund $20 million to its health insurance customers in Colorado.2
The requested premium increases and identified overcharges have contributed to plenty of finger-pointing among insurers, state regulators, and the Obama administration, which has assailed insurers for using the law as a convenient excuse to raise rates. Highlighting the unease of many consumers, however, is the verdict that the proposed increases—if approved—would hit small businesses and individuals hardest.
According to the State of Hospital Medicine: 2010 Report Based on 2009 Data, released in September by SHM and the Medical Group Management Association, participating hospitalist groups have a median of 10 physician full-time equivalents. Roughly 25% of respondents are in physician-owned groups, while 14% are in a management services organization (MSO) or physician practice management company (PPMC). Smaller HM groups wouldn’t be alone in feeling the pinch, but they might need to consider some serious comparison-shopping to avoid costly premium increases.
Cherilyn Murer, president and CEO of Joliet, Ill.-based Murer Consultants Inc., has worked with healthcare systems and providers in 42 states, but even her company has not been immune to having to contend with rising premiums. “Our managing partner just renegotiated our health benefits [premiums] that were supposed to have gone up 30% by our previous carrier,” Murer says. “Through protracted negotiations and diligence, he was able to find a plan that did not increase our costs, and retained pretty much the same benefits.”
For at least the next three to five years, Murer says, niche firms will need to be diligent about shopping around and managing their expenses in a volatile insurance marketplace. Healthcare reform, she says, is certainly not a panacea for reining in costs, but “just the beginning.”
Concerns over healthcare costs, in fact, could be among the factors driving what Robert Zipper, MD, FHM, regional chief medical officer for Tacoma, Wash.-based Sound Physicians, sees as continuing consolidation among hospitalist groups. “By that, I mean that either groups are swallowed up by the hospital in which they work or they become part of a regional or national company,” he says. Sound Physicians, with about 400 hospitalists in seven states, offers health insurance policies that don’t vary by state, easing its negotiations.
Eyes on the Bottom Line
What about the dreaded “T” word? Dr. Zipper says he hasn’t heard that many concerns about the potential tax increase just yet. “I think it’s not an issue to hospitalists in a broad sense yet,” he says, “but if you look at the salary trajectory and where things have been over the past 10 years, it’s pretty easy to predict that it will be an issue for single-income [households] where the hospitalist is the sole breadwinner.”
The 2010 State of Hospital Medicine report, which surveyed 4,211 nonacademic hospitalists from 443 groups, found a median annual income of $215,000. Calculating trends from past income surveys is difficult due to very different respondent populations, but many hospitalists are clearly near or above the $200,000 threshold for individuals and near the $250,000 threshold for families already, even before considering spousal income. The survey, for example, found median salaries of about $235,700 in the 13 states that make up the Southern region.
Even if higher-earning hospitalists are subjected to a higher tax rate next year—if the current rates expire, a climb of 4.6 percentage points, to 39.6% from 35%—not all of them are necessarily opposed to it. Political polling on the issue isn’t broken down by specific professions, but a number of blogs have pointed to a Quinnipiac University poll conducted back in March that suggested nearly two-thirds of upper-income Americans were prepared to sacrifice some of their take-home pay to help reduce the deficit. In that poll (www.quinnipiac.edu/x1295.xml?ReleaseID=1438), some 64% of respondents earning more than $250,000 agreed that raising income taxes on themselves and other households making more than $250,000 should be a main part of any government approach to the deficit.
If taxes and insurance premiums are more immediate concerns, some HM observers are eyeing longer trends that could impact the pre-tax pay of the profession. Most hospitalists still earn far less than their specialist counterparts, of course, but increasing demand for hospitalist services has helped fuel a rise in median salaries. Last year, some observers predicted that after an impressive run, annual pay would plateau or even fall, given the current economic uncertainty, tightening profit margins, and assessment that many hospitals run HM programs at a loss.3 And in the current RVU-driven system, the “What have you done for me lately?” mentality can indeed make it difficult for hospitalists to demonstrate a solid return on the investment.
The State of Hospital Medicine report suggests that respondent HM groups have been subsidized by an average of $111,486 per physician FTE (median is $98,253), with the highest numbers in hospital-owned practices. But many experts see a window of a few years in which new healthcare delivery and payment experiments will be trotted out, whether modeled on a bundled system, accountable-care organization (ACO), or other vehicle. Under these models, payment incentives to physicians—and to hospitalists especially—could be fundamentally restructured to better reflect their true contributions as the emphasis on quality and efficiency increases.
Within the next three years, Murer says, hospitalists need to continue to infiltrate inpatient medical services, demonstrate their worth, and show the cost efficiencies that arise from their profession. “I think they’ve got a window of three years to really decide how much of that [inpatient physician] market they will retain,” she says.
Despite the current volatility, both Murer and Dr. Zipper agree that hospitalists are well positioned to take advantage of the coming changes in the healthcare delivery system. But to seize the opportunity, hospitalists must clearly demonstrate the necessity of their services in the emerging models of care and claim an early seat at the table where decisions will be made about how the pot of money is dispersed. Doing so could help resolve one of the most important financial considerations of all: job security. TH
Bryn Nelson is a freelance medical writer based in Seattle.
References
- Adamy J. Health insurers plan hikes. Wall Street Journal website. Available at: http://online.wsj.com/article/SB10001424052748703720004575478200948908976.html. Accessed Sept. 21, 2010.
- Cutter S. Look you in the eye. The White House website. Available at: www.whitehouse.gov/blog/2010/09/23/look-you-eye. Accessed Sept. 27, 2010.
- How will the economy affect hospitalist salaries? MedPage Today website. Available at: www.kevinmd .com/blog/2009/03/how-will-economy-affect-hospitalist-2.html. Accessed Sept. 27, 2010.
When Congress returns for a likely lame-duck session after the midterm elections, the biggest battle might be fought over whether to extend the 2001 and 2003 tax cuts to everyone or only to those earning less than $200,000 annually ($250,000 for families). And depending on the makeup of the 112th Congress, which will be seated in January, Republicans might try to make good on a campaign pledge to repeal all or most of the healthcare reform legislation.
The expected flashpoints are being teased endlessly with media sound bites featuring phrases that most of us love to hate: higher taxes, spiraling medical bills, soaring insurance premiums. Insurance companies already are blaming a spike in premiums on the healthcare legislation, claiming that new provisions and mandates are forcing them to further hike their rates.
Closer to home, the high-profile frays could put hospitalists in the awkward position of supporting political positions that sock them in the wallet. After all, doctors are workers and healthcare consumers, too. So what impact could higher taxes and higher insurance premiums really have? Let’s start with health insurance.
Insurance Cost Increases
Signed into law in March, the Affordable Care Act includes tax credits for small businesses to help defray the costs of health insurance coverage. But in 2013, it also raises the threshold for medical expense deductions for most taxpayers, to 10% from 7.5% of adjusted gross income. In other words, families can claim tax deductions only after having spent 10% or more of their adjusted gross income on medical bills. For families with hefty medical bills, that 2.5% difference could translate into a significant shortfall.
CMS was able to negotiate with insurers to achieve a slight drop in Medicare Advantage premiums, but many individual states have had less luck in preventing rate increases from private insurers who blame their higher premiums on new mandates. The Wall Street Journal has documented rate increases of 18% in states like Wisconsin and North Carolina—about 9% of which insurance company officials pinned on the new law.1 Such increases are hardly inevitable, however. The Obama administration’s White House blog, for instance, has cited the example of North Carolina Blue Cross and Blue Shield, which announced Sept. 20 that it will provide $156 million in refunds to more than 215,000 customers after state regulators found an overcharge that should be reversed due to new rules in the reform law.2 WellPoint will similarly refund $20 million to its health insurance customers in Colorado.2
The requested premium increases and identified overcharges have contributed to plenty of finger-pointing among insurers, state regulators, and the Obama administration, which has assailed insurers for using the law as a convenient excuse to raise rates. Highlighting the unease of many consumers, however, is the verdict that the proposed increases—if approved—would hit small businesses and individuals hardest.
According to the State of Hospital Medicine: 2010 Report Based on 2009 Data, released in September by SHM and the Medical Group Management Association, participating hospitalist groups have a median of 10 physician full-time equivalents. Roughly 25% of respondents are in physician-owned groups, while 14% are in a management services organization (MSO) or physician practice management company (PPMC). Smaller HM groups wouldn’t be alone in feeling the pinch, but they might need to consider some serious comparison-shopping to avoid costly premium increases.
Cherilyn Murer, president and CEO of Joliet, Ill.-based Murer Consultants Inc., has worked with healthcare systems and providers in 42 states, but even her company has not been immune to having to contend with rising premiums. “Our managing partner just renegotiated our health benefits [premiums] that were supposed to have gone up 30% by our previous carrier,” Murer says. “Through protracted negotiations and diligence, he was able to find a plan that did not increase our costs, and retained pretty much the same benefits.”
For at least the next three to five years, Murer says, niche firms will need to be diligent about shopping around and managing their expenses in a volatile insurance marketplace. Healthcare reform, she says, is certainly not a panacea for reining in costs, but “just the beginning.”
Concerns over healthcare costs, in fact, could be among the factors driving what Robert Zipper, MD, FHM, regional chief medical officer for Tacoma, Wash.-based Sound Physicians, sees as continuing consolidation among hospitalist groups. “By that, I mean that either groups are swallowed up by the hospital in which they work or they become part of a regional or national company,” he says. Sound Physicians, with about 400 hospitalists in seven states, offers health insurance policies that don’t vary by state, easing its negotiations.
Eyes on the Bottom Line
What about the dreaded “T” word? Dr. Zipper says he hasn’t heard that many concerns about the potential tax increase just yet. “I think it’s not an issue to hospitalists in a broad sense yet,” he says, “but if you look at the salary trajectory and where things have been over the past 10 years, it’s pretty easy to predict that it will be an issue for single-income [households] where the hospitalist is the sole breadwinner.”
The 2010 State of Hospital Medicine report, which surveyed 4,211 nonacademic hospitalists from 443 groups, found a median annual income of $215,000. Calculating trends from past income surveys is difficult due to very different respondent populations, but many hospitalists are clearly near or above the $200,000 threshold for individuals and near the $250,000 threshold for families already, even before considering spousal income. The survey, for example, found median salaries of about $235,700 in the 13 states that make up the Southern region.
Even if higher-earning hospitalists are subjected to a higher tax rate next year—if the current rates expire, a climb of 4.6 percentage points, to 39.6% from 35%—not all of them are necessarily opposed to it. Political polling on the issue isn’t broken down by specific professions, but a number of blogs have pointed to a Quinnipiac University poll conducted back in March that suggested nearly two-thirds of upper-income Americans were prepared to sacrifice some of their take-home pay to help reduce the deficit. In that poll (www.quinnipiac.edu/x1295.xml?ReleaseID=1438), some 64% of respondents earning more than $250,000 agreed that raising income taxes on themselves and other households making more than $250,000 should be a main part of any government approach to the deficit.
If taxes and insurance premiums are more immediate concerns, some HM observers are eyeing longer trends that could impact the pre-tax pay of the profession. Most hospitalists still earn far less than their specialist counterparts, of course, but increasing demand for hospitalist services has helped fuel a rise in median salaries. Last year, some observers predicted that after an impressive run, annual pay would plateau or even fall, given the current economic uncertainty, tightening profit margins, and assessment that many hospitals run HM programs at a loss.3 And in the current RVU-driven system, the “What have you done for me lately?” mentality can indeed make it difficult for hospitalists to demonstrate a solid return on the investment.
The State of Hospital Medicine report suggests that respondent HM groups have been subsidized by an average of $111,486 per physician FTE (median is $98,253), with the highest numbers in hospital-owned practices. But many experts see a window of a few years in which new healthcare delivery and payment experiments will be trotted out, whether modeled on a bundled system, accountable-care organization (ACO), or other vehicle. Under these models, payment incentives to physicians—and to hospitalists especially—could be fundamentally restructured to better reflect their true contributions as the emphasis on quality and efficiency increases.
Within the next three years, Murer says, hospitalists need to continue to infiltrate inpatient medical services, demonstrate their worth, and show the cost efficiencies that arise from their profession. “I think they’ve got a window of three years to really decide how much of that [inpatient physician] market they will retain,” she says.
Despite the current volatility, both Murer and Dr. Zipper agree that hospitalists are well positioned to take advantage of the coming changes in the healthcare delivery system. But to seize the opportunity, hospitalists must clearly demonstrate the necessity of their services in the emerging models of care and claim an early seat at the table where decisions will be made about how the pot of money is dispersed. Doing so could help resolve one of the most important financial considerations of all: job security. TH
Bryn Nelson is a freelance medical writer based in Seattle.
References
- Adamy J. Health insurers plan hikes. Wall Street Journal website. Available at: http://online.wsj.com/article/SB10001424052748703720004575478200948908976.html. Accessed Sept. 21, 2010.
- Cutter S. Look you in the eye. The White House website. Available at: www.whitehouse.gov/blog/2010/09/23/look-you-eye. Accessed Sept. 27, 2010.
- How will the economy affect hospitalist salaries? MedPage Today website. Available at: www.kevinmd .com/blog/2009/03/how-will-economy-affect-hospitalist-2.html. Accessed Sept. 27, 2010.
When Congress returns for a likely lame-duck session after the midterm elections, the biggest battle might be fought over whether to extend the 2001 and 2003 tax cuts to everyone or only to those earning less than $200,000 annually ($250,000 for families). And depending on the makeup of the 112th Congress, which will be seated in January, Republicans might try to make good on a campaign pledge to repeal all or most of the healthcare reform legislation.
The expected flashpoints are being teased endlessly with media sound bites featuring phrases that most of us love to hate: higher taxes, spiraling medical bills, soaring insurance premiums. Insurance companies already are blaming a spike in premiums on the healthcare legislation, claiming that new provisions and mandates are forcing them to further hike their rates.
Closer to home, the high-profile frays could put hospitalists in the awkward position of supporting political positions that sock them in the wallet. After all, doctors are workers and healthcare consumers, too. So what impact could higher taxes and higher insurance premiums really have? Let’s start with health insurance.
Insurance Cost Increases
Signed into law in March, the Affordable Care Act includes tax credits for small businesses to help defray the costs of health insurance coverage. But in 2013, it also raises the threshold for medical expense deductions for most taxpayers, to 10% from 7.5% of adjusted gross income. In other words, families can claim tax deductions only after having spent 10% or more of their adjusted gross income on medical bills. For families with hefty medical bills, that 2.5% difference could translate into a significant shortfall.
CMS was able to negotiate with insurers to achieve a slight drop in Medicare Advantage premiums, but many individual states have had less luck in preventing rate increases from private insurers who blame their higher premiums on new mandates. The Wall Street Journal has documented rate increases of 18% in states like Wisconsin and North Carolina—about 9% of which insurance company officials pinned on the new law.1 Such increases are hardly inevitable, however. The Obama administration’s White House blog, for instance, has cited the example of North Carolina Blue Cross and Blue Shield, which announced Sept. 20 that it will provide $156 million in refunds to more than 215,000 customers after state regulators found an overcharge that should be reversed due to new rules in the reform law.2 WellPoint will similarly refund $20 million to its health insurance customers in Colorado.2
The requested premium increases and identified overcharges have contributed to plenty of finger-pointing among insurers, state regulators, and the Obama administration, which has assailed insurers for using the law as a convenient excuse to raise rates. Highlighting the unease of many consumers, however, is the verdict that the proposed increases—if approved—would hit small businesses and individuals hardest.
According to the State of Hospital Medicine: 2010 Report Based on 2009 Data, released in September by SHM and the Medical Group Management Association, participating hospitalist groups have a median of 10 physician full-time equivalents. Roughly 25% of respondents are in physician-owned groups, while 14% are in a management services organization (MSO) or physician practice management company (PPMC). Smaller HM groups wouldn’t be alone in feeling the pinch, but they might need to consider some serious comparison-shopping to avoid costly premium increases.
Cherilyn Murer, president and CEO of Joliet, Ill.-based Murer Consultants Inc., has worked with healthcare systems and providers in 42 states, but even her company has not been immune to having to contend with rising premiums. “Our managing partner just renegotiated our health benefits [premiums] that were supposed to have gone up 30% by our previous carrier,” Murer says. “Through protracted negotiations and diligence, he was able to find a plan that did not increase our costs, and retained pretty much the same benefits.”
For at least the next three to five years, Murer says, niche firms will need to be diligent about shopping around and managing their expenses in a volatile insurance marketplace. Healthcare reform, she says, is certainly not a panacea for reining in costs, but “just the beginning.”
Concerns over healthcare costs, in fact, could be among the factors driving what Robert Zipper, MD, FHM, regional chief medical officer for Tacoma, Wash.-based Sound Physicians, sees as continuing consolidation among hospitalist groups. “By that, I mean that either groups are swallowed up by the hospital in which they work or they become part of a regional or national company,” he says. Sound Physicians, with about 400 hospitalists in seven states, offers health insurance policies that don’t vary by state, easing its negotiations.
Eyes on the Bottom Line
What about the dreaded “T” word? Dr. Zipper says he hasn’t heard that many concerns about the potential tax increase just yet. “I think it’s not an issue to hospitalists in a broad sense yet,” he says, “but if you look at the salary trajectory and where things have been over the past 10 years, it’s pretty easy to predict that it will be an issue for single-income [households] where the hospitalist is the sole breadwinner.”
The 2010 State of Hospital Medicine report, which surveyed 4,211 nonacademic hospitalists from 443 groups, found a median annual income of $215,000. Calculating trends from past income surveys is difficult due to very different respondent populations, but many hospitalists are clearly near or above the $200,000 threshold for individuals and near the $250,000 threshold for families already, even before considering spousal income. The survey, for example, found median salaries of about $235,700 in the 13 states that make up the Southern region.
Even if higher-earning hospitalists are subjected to a higher tax rate next year—if the current rates expire, a climb of 4.6 percentage points, to 39.6% from 35%—not all of them are necessarily opposed to it. Political polling on the issue isn’t broken down by specific professions, but a number of blogs have pointed to a Quinnipiac University poll conducted back in March that suggested nearly two-thirds of upper-income Americans were prepared to sacrifice some of their take-home pay to help reduce the deficit. In that poll (www.quinnipiac.edu/x1295.xml?ReleaseID=1438), some 64% of respondents earning more than $250,000 agreed that raising income taxes on themselves and other households making more than $250,000 should be a main part of any government approach to the deficit.
If taxes and insurance premiums are more immediate concerns, some HM observers are eyeing longer trends that could impact the pre-tax pay of the profession. Most hospitalists still earn far less than their specialist counterparts, of course, but increasing demand for hospitalist services has helped fuel a rise in median salaries. Last year, some observers predicted that after an impressive run, annual pay would plateau or even fall, given the current economic uncertainty, tightening profit margins, and assessment that many hospitals run HM programs at a loss.3 And in the current RVU-driven system, the “What have you done for me lately?” mentality can indeed make it difficult for hospitalists to demonstrate a solid return on the investment.
The State of Hospital Medicine report suggests that respondent HM groups have been subsidized by an average of $111,486 per physician FTE (median is $98,253), with the highest numbers in hospital-owned practices. But many experts see a window of a few years in which new healthcare delivery and payment experiments will be trotted out, whether modeled on a bundled system, accountable-care organization (ACO), or other vehicle. Under these models, payment incentives to physicians—and to hospitalists especially—could be fundamentally restructured to better reflect their true contributions as the emphasis on quality and efficiency increases.
Within the next three years, Murer says, hospitalists need to continue to infiltrate inpatient medical services, demonstrate their worth, and show the cost efficiencies that arise from their profession. “I think they’ve got a window of three years to really decide how much of that [inpatient physician] market they will retain,” she says.
Despite the current volatility, both Murer and Dr. Zipper agree that hospitalists are well positioned to take advantage of the coming changes in the healthcare delivery system. But to seize the opportunity, hospitalists must clearly demonstrate the necessity of their services in the emerging models of care and claim an early seat at the table where decisions will be made about how the pot of money is dispersed. Doing so could help resolve one of the most important financial considerations of all: job security. TH
Bryn Nelson is a freelance medical writer based in Seattle.
References
- Adamy J. Health insurers plan hikes. Wall Street Journal website. Available at: http://online.wsj.com/article/SB10001424052748703720004575478200948908976.html. Accessed Sept. 21, 2010.
- Cutter S. Look you in the eye. The White House website. Available at: www.whitehouse.gov/blog/2010/09/23/look-you-eye. Accessed Sept. 27, 2010.
- How will the economy affect hospitalist salaries? MedPage Today website. Available at: www.kevinmd .com/blog/2009/03/how-will-economy-affect-hospitalist-2.html. Accessed Sept. 27, 2010.
ONLINE EXCLUSIVE: Trial by Error: An Oklahoma Hospital’s Bundling Experience
Hillcrest Medical Center in Tulsa, Okla., went live with its ACE Demonstration on May 1, 2009. Over the next 15 months, scores on several quality metrics soared, supply costs plunged, patient volumes shot up, and the hospital saved Medicare $750,000 on 37 diagnosis-related groups (DRGs).
So what’s the problem?
For one thing, handling the bundled payment system required “massive” computer conversions, says Hillcrest CEO Steve Dobbs, and cash payments from CMS were significantly delayed, in part due to glitches over how discharges were handled. And then there was the confusion over processing supplemental Medicare plans.
Hillcrest’s first-year experience with bundled payments for orthopedics, cardiology, and cardiovascular surgery provides an illuminating window into what other hospitals might encounter as the concept of bundling expands beyond the first few pilot sites.
Because Hillcrest didn’t have a way to pay physician claims, it hired a third-party vendor, Texas-based Trailblazer, to manage them. Then Hillcrest set up two LLCs—one for orthopedics and one for cardiology—to receive the bundled payments. CMS required the hospital to establish a quality committee, finance committee, and board within each LLC, and report quarterly about the program. But Dobbs says the hospital has received no written feedback from CMS or any indications of how the ACE Demonstration has worked at two other sites that also started last year.
Through “trial by error,” the hospital has had to learn many of its lessons on its own, he says, explaining that “you just had to go make some mistakes and try something.” For example, the hospital began posting the Medicare rate for each of the demonstration’s 37 DRGs on its website after frequent updates to the rates led to widespread confusion among area physicians. Hillcrest also learned that it needed to set up a dedicated toll-free call center for people to get information about the program.
There have been triumphs, too. Scores on such metrics as antibiotics administered one hour prior to surgical start and antibiotics stopped 24 hours post-surgery have climbed significantly, perhaps by linking them to gainsharing incentives. When one heart valve vendor “wouldn’t play,” Dobbs says, the hospital switched to another, less expensive vendor. By involving its open-heart surgeons in scrutinizing supplies, the hospital saved 10% of the cost of sterile packs in the operating room.
Hillcrest’s orthopedic surgeons—an independent group—also combed through instruments and drugs to look for savings. For their efforts, the six orthopedists netted a combined $130,000 in incentive checks. For the hospital’s own cardiologists and cardiovascular surgeons, the bonus money went back into the practice.
Early in the demonstration project, Dobbs says, hospitalists saw a dip in the number of cases they were getting pulled in on. “Early on they called me and said, ‘What’s up, because we’re not getting as many referrals from orthopedics?’” Dobbs says. “I think it’s leveled out over time, and they really haven’t seen that big of a change.”
The hospital also is reaping the rewards of recent investments, including a new heart hospital, heavy investment in cardiology, and a three-year-old orthopedics unit. In the first year of its demonstration, the hospital saw a 24% gain in its cardiology and cardiovascular surgery volume, and a whopping 37% gain in orthopedics volume.
One facet of the project that has been less fruitful is the Medicare discount given to patients who have their orthopedic or cardiology procedure done at Hillcrest. “People are saying it’s nice to have, but that’s not why they chose the program, especially in cardiology,” Dobbs says. “You don’t have a heart attack and tell the ambulance driver, ‘Oh, by the way, I want to get my incentive check.’ ”
Hillcrest Medical Center in Tulsa, Okla., went live with its ACE Demonstration on May 1, 2009. Over the next 15 months, scores on several quality metrics soared, supply costs plunged, patient volumes shot up, and the hospital saved Medicare $750,000 on 37 diagnosis-related groups (DRGs).
So what’s the problem?
For one thing, handling the bundled payment system required “massive” computer conversions, says Hillcrest CEO Steve Dobbs, and cash payments from CMS were significantly delayed, in part due to glitches over how discharges were handled. And then there was the confusion over processing supplemental Medicare plans.
Hillcrest’s first-year experience with bundled payments for orthopedics, cardiology, and cardiovascular surgery provides an illuminating window into what other hospitals might encounter as the concept of bundling expands beyond the first few pilot sites.
Because Hillcrest didn’t have a way to pay physician claims, it hired a third-party vendor, Texas-based Trailblazer, to manage them. Then Hillcrest set up two LLCs—one for orthopedics and one for cardiology—to receive the bundled payments. CMS required the hospital to establish a quality committee, finance committee, and board within each LLC, and report quarterly about the program. But Dobbs says the hospital has received no written feedback from CMS or any indications of how the ACE Demonstration has worked at two other sites that also started last year.
Through “trial by error,” the hospital has had to learn many of its lessons on its own, he says, explaining that “you just had to go make some mistakes and try something.” For example, the hospital began posting the Medicare rate for each of the demonstration’s 37 DRGs on its website after frequent updates to the rates led to widespread confusion among area physicians. Hillcrest also learned that it needed to set up a dedicated toll-free call center for people to get information about the program.
There have been triumphs, too. Scores on such metrics as antibiotics administered one hour prior to surgical start and antibiotics stopped 24 hours post-surgery have climbed significantly, perhaps by linking them to gainsharing incentives. When one heart valve vendor “wouldn’t play,” Dobbs says, the hospital switched to another, less expensive vendor. By involving its open-heart surgeons in scrutinizing supplies, the hospital saved 10% of the cost of sterile packs in the operating room.
Hillcrest’s orthopedic surgeons—an independent group—also combed through instruments and drugs to look for savings. For their efforts, the six orthopedists netted a combined $130,000 in incentive checks. For the hospital’s own cardiologists and cardiovascular surgeons, the bonus money went back into the practice.
Early in the demonstration project, Dobbs says, hospitalists saw a dip in the number of cases they were getting pulled in on. “Early on they called me and said, ‘What’s up, because we’re not getting as many referrals from orthopedics?’” Dobbs says. “I think it’s leveled out over time, and they really haven’t seen that big of a change.”
The hospital also is reaping the rewards of recent investments, including a new heart hospital, heavy investment in cardiology, and a three-year-old orthopedics unit. In the first year of its demonstration, the hospital saw a 24% gain in its cardiology and cardiovascular surgery volume, and a whopping 37% gain in orthopedics volume.
One facet of the project that has been less fruitful is the Medicare discount given to patients who have their orthopedic or cardiology procedure done at Hillcrest. “People are saying it’s nice to have, but that’s not why they chose the program, especially in cardiology,” Dobbs says. “You don’t have a heart attack and tell the ambulance driver, ‘Oh, by the way, I want to get my incentive check.’ ”
Hillcrest Medical Center in Tulsa, Okla., went live with its ACE Demonstration on May 1, 2009. Over the next 15 months, scores on several quality metrics soared, supply costs plunged, patient volumes shot up, and the hospital saved Medicare $750,000 on 37 diagnosis-related groups (DRGs).
So what’s the problem?
For one thing, handling the bundled payment system required “massive” computer conversions, says Hillcrest CEO Steve Dobbs, and cash payments from CMS were significantly delayed, in part due to glitches over how discharges were handled. And then there was the confusion over processing supplemental Medicare plans.
Hillcrest’s first-year experience with bundled payments for orthopedics, cardiology, and cardiovascular surgery provides an illuminating window into what other hospitals might encounter as the concept of bundling expands beyond the first few pilot sites.
Because Hillcrest didn’t have a way to pay physician claims, it hired a third-party vendor, Texas-based Trailblazer, to manage them. Then Hillcrest set up two LLCs—one for orthopedics and one for cardiology—to receive the bundled payments. CMS required the hospital to establish a quality committee, finance committee, and board within each LLC, and report quarterly about the program. But Dobbs says the hospital has received no written feedback from CMS or any indications of how the ACE Demonstration has worked at two other sites that also started last year.
Through “trial by error,” the hospital has had to learn many of its lessons on its own, he says, explaining that “you just had to go make some mistakes and try something.” For example, the hospital began posting the Medicare rate for each of the demonstration’s 37 DRGs on its website after frequent updates to the rates led to widespread confusion among area physicians. Hillcrest also learned that it needed to set up a dedicated toll-free call center for people to get information about the program.
There have been triumphs, too. Scores on such metrics as antibiotics administered one hour prior to surgical start and antibiotics stopped 24 hours post-surgery have climbed significantly, perhaps by linking them to gainsharing incentives. When one heart valve vendor “wouldn’t play,” Dobbs says, the hospital switched to another, less expensive vendor. By involving its open-heart surgeons in scrutinizing supplies, the hospital saved 10% of the cost of sterile packs in the operating room.
Hillcrest’s orthopedic surgeons—an independent group—also combed through instruments and drugs to look for savings. For their efforts, the six orthopedists netted a combined $130,000 in incentive checks. For the hospital’s own cardiologists and cardiovascular surgeons, the bonus money went back into the practice.
Early in the demonstration project, Dobbs says, hospitalists saw a dip in the number of cases they were getting pulled in on. “Early on they called me and said, ‘What’s up, because we’re not getting as many referrals from orthopedics?’” Dobbs says. “I think it’s leveled out over time, and they really haven’t seen that big of a change.”
The hospital also is reaping the rewards of recent investments, including a new heart hospital, heavy investment in cardiology, and a three-year-old orthopedics unit. In the first year of its demonstration, the hospital saw a 24% gain in its cardiology and cardiovascular surgery volume, and a whopping 37% gain in orthopedics volume.
One facet of the project that has been less fruitful is the Medicare discount given to patients who have their orthopedic or cardiology procedure done at Hillcrest. “People are saying it’s nice to have, but that’s not why they chose the program, especially in cardiology,” Dobbs says. “You don’t have a heart attack and tell the ambulance driver, ‘Oh, by the way, I want to get my incentive check.’ ”
Medical Tourism
David Dupray, a 60-year-old uninsured coffee shop owner from Bar Harbor, Maine, had been having left leg pain on ambulation for four years. His cardiologist recommended stent placement for left iliac artery stenosis. The estimated bill: approximately $35,000.
Unable to afford the procedure, Dupray began searching the Web for affordable medical care overseas. His physician suggested Thailand. Within days, Dupray had an appointment with a cardiologist halfway around the world—at Bumrungrad Hospital in Bangkok, Thailand. Dupray spent two days in the hotel-like hospital, had three stents placed in his leg arteries, and completed a cardiac stress test. The total bill: $18,000.
“I will never go to a hospital in the U.S.,” says Dupray, who represents a growing number of Americans searching for affordable healthcare in the global marketplace.
With rising U.S. healthcare costs and millions of Americans uninsured or underinsured, more American patients are seeking affordable, high-quality medical care abroad—known as “medical tourism.” In 2007, an estimated 750,000 Americans traveled abroad for medical care; the number is expected to increase to 6 million by the end of this year.1 On the flip side, only a little more than 400,000 nonresidents visited the U.S. in 2008 for the latest medical care.1 Globally, the medical tourism industry is estimated to grow into a $21 billion-a-year industry by 2012, with much of the growth expected from Western patients traveling overseas for affordable care.2
“As hospitalists, we have been seeing increasing numbers of patients going overseas for urgent and elective procedures, as it is a general perception the medical treatment overseas is less expensive,” says Joseph Ming Wah Li, MD, SFHM, director of hospital medicine at Beth Israel Deaconess Medical Center in Boston and SHM president-elect.
Physicians in U.S. hospitals encounter potential medical tourists all the time. Some are uninsured or underinsured. Some have insurance carriers that limit or exclude coverage for certain procedures and treatments. Even those with insurance sometimes struggle to pay deductibles, copays, and their costs after insurance has paid its part. Others are uncomfortable with the language barriers and cultural differences of U.S. hospitals and physicians.
Medical tourism also lures patients who are citizens of countries (e.g. Canada, the United Kingdom) that offer universal healthcare, Dr. Li says.3 For example, more expatriates from India and Malaysia are traveling to their native countries for medical care, as they receive affordable and quicker medical care while visiting family.
Hospitalists routinely care for patients requiring essential cardiac or orthopedic surgeries—conditions that are common in the medical tourism trade. With medical tourism growing in scope and popularity, it is essential that hospitalists are prepared to discuss with their patients the pros and cons of traveling for medical care. Hospitalists should be able to:
- Identify patients who might benefit from medical tourism;
- Know where and how to look for an accredited overseas facility; and
- Explain to patients the potential travel risks and complications, including insurance coverage and legal restrictions in destination countries.
A basic understanding of the industry and the issues can help guide your patients through medical decisions and help you care for those who have returned from a medical trip.
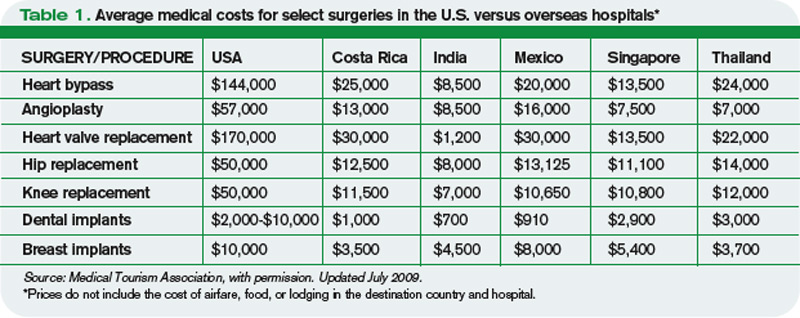
Big Menu, Discount Prices
Medical tourism offers a wide range of medical services performed in hospitals on nearly every continent, with a wide range of costs for certain procedures (Table 1, p. 26). Most surgeries cost 50% to 90% less than the average cost of the same surgery at a U.S. hospital. Many in the medical tourism industry say these types of savings have brought once-unaffordable surgery within the reach of most Americans, regardless of insurance status. For example, cardiac bypass surgery on average costs $144,000 in the U.S.; it costs about $8,500 in India.
The reasons the costs are so much less at overseas hospitals, as compared with U.S. costs, are many:
- Lower wages for providers;
- Less expensive medical devices and pharmaceutical products;
- Less involvement by third-party payors; and
- Lower malpractice premiums.4
For example, the annual liability insurance premium for a surgeon in India is $4,000; the average cost of a New York City surgeon’s liability insurance premium is $100,000.5
Brazil, Costa Rica, and Mexico are attractive destinations for cosmetic and dental surgeries; Singapore, Malaysia, Thailand, and India have emerged as hubs for cardiac and orthopedic surgeries (Table 1, above).6
The growth in medical tourism led the Joint Commission in 1999 to launch Joint Commission International (JCI), which ensures that offshore hospitals provide the highest-quality care to international patients (see “Ultra-Affordable Prices and No Decline in Quality of Care,” p. 28). JCI has accredited 120 overseas hospitals that meet these standards.
“Overseas hospitals are always keen in partnering with U.S. hospitals,” Dr. Li says. Collaborations, such as Johns Hopkins International Medical Center’s partnership with International Medical Clinic Singapore, and Partners Harvard Medical International’s affiliation with Wockhardt Hospitals in Mumbai, India, have helped facilitate the accreditation process and alleviate U.S. patient concerns.
Overseas hospitals not only offer greatly discounted rates than insurer-negotiated U.S. prices, but many of the international hospitals also report quality scores equal to or better than the average U.S. hospital’s.7
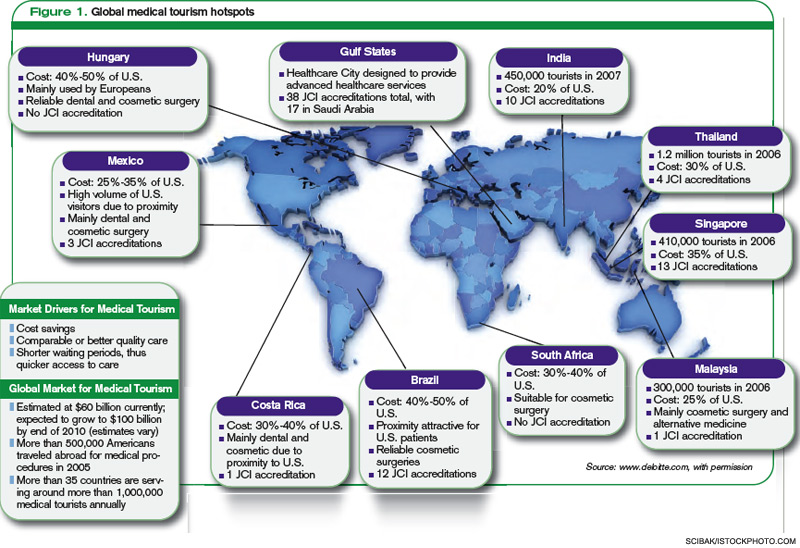
Before You Book a Trip …
How do patients find overseas facilities? It’s as easy as a click of the mouse.
“Our survey shows 75 percent of patients located offshore hospitals through the Internet,” says Renee-Marie Stephano, president of the Medical Tourism Association, a nonprofit group based in West Palm Beach, Fla., that was established in 2007 to promote education, transparency, and communication in the medical tourism community. Patients use overseas hospital websites, international medical coordinators, and medical tourism companies, such as PlanetHospital.com and MedRetreat.com, to find facilities and providers, and to coordinate medical travel.
“Medical tourism is currently unregulated,” Stephano says. “One of our goals is to certify medical tourism facilitators to create the best standard of practice.”
In 2007, the American Medical Association (AMA) published medical tourism guidelines to help healthcare entities engaged in overseas medical care.8 (Download a PDF of the guidelines at www.ama-assn.org/ama1/pub/upload/mm/31/medicaltourism.pdf.) The AMA suggests that:
- Medical care outside the U.S. should be voluntary, and patients should be informed of their legal rights and recourses before agreeing to travel outside the U.S.;
- Before traveling, local follow-up care should be arranged to ensure continuity of care;
- Patients should have access to physician licensing, facility accreditation, and outcomes data for both;
- Medical record transfers should follow HIPAA guidelines; and
- Patients should be informed of the potential risks of combining surgical procedures with long flights and vacation activities.
—Kenneth Mays, senior director, marketing and business development, Bumrungrad Hospital, Bangkok, Thailand
Patient Concerns
Hospitalists are highly focused on a patient’s quality of care; the same can be said of some overseas hospitals that attract large numbers of medical tourists. “I think the service and quality of care provided at our hospital compares favorably with the very best American hospitals,” says Kenneth Mays, senior director of hospital marketing and business development at Bumrungrad Hospital in Bangkok.
That might be so, but the growth of medical tourism also raises concerns stateside. With sleek websites making it easy for U.S. patients to schedule procedure vacations from their kitchen tables, many U.S. physician and watchdog groups worry about patient safety, privacy, liability, and continuity of care. Although most international hospitals and physicians provide outcomes data, rarely do the benchmarks compare directly with U.S. hospital quality and safety data.
“Quality comparisons are difficult, even within U.S. hospitals, as hospitals use different methodologies to collect data,” says Stephano. “Patients have to rely on JCI accreditation, surgeon experience, volume, and outcomes to decide.”
Recent studies echo the Medical Tourism Association’s claim: Increased cardiac surgery volume at Apollo Hospitals—an 8,500-bed healthcare system with 50 locations throughout India—and Narayana Hospital in Bommasandra, India, has lowered costs, with similar, or even lower, mortality rates compared with the average U.S. hospital.7,9 Other challenges like getting medical records exist even within U.S. hospitals, so emerging platforms like Google Health and Microsoft Vault, where medical records can be uploaded at the touch of a button, “will benefit patients and providers,” Dr. Li says.
The Medical Tourism Association envisions U.S.-based physicians offering follow-up care to medical tourism patients. “Currently, we encourage patients to follow up with their primary-care physician,” Stephano says.
Dr. Li says malpractice is always a concern when traveling overseas; however, he also notes the legal system in the U.S. is strong enough “to handle any medical malpractice.” That said, a patient who experiences a poor medical outcome as the result of overseas treatment might seek legal remedies, but the reality is that malpractice laws are either nonexistent or not well implemented in some destination countries. That makes malpractice claims on overseas procedures a dicey proposition.
“Patients receiving overseas treatment need to realize that they are agreeing to the jurisdiction of the destination country,” Stephano says. Other risks associated with extended travel include exposure to regional infectious diseases and poor infrastructure in the destination country, which could undermine the benefits of medical travel.
Cost-saving benefits have led some U.S. insurance companies to begin integrating overseas medical coverage. For example, Blue Cross Blue Shield of South Carolina offers incentives for patients willing to obtain medical care overseas at JCI-approved hospitals. BCBS then waives deductibles and copays, and several other insurers have launched similar pilot programs.10 “We will see more of these changes,” Stephano says, “to cut costs and remain competitive.”
Immediate Impact
In 2008, U.S. healthcare spending was $2.3 trillion.11 A 2005 Institute of Medicine report suggests that 30% to 40% of current U.S. healthcare expenditure is wasted.12 U.S. lawmakers, employers, hospitals, and consumers are scrambling to find ways to reduce healthcare costs and improve efficiency. Medical tourism seems to benefit a select few Americans, only lowering U.S. healthcare spending by 1% to 2%.12
Medical tourism revenue generated in destination countries currently is limited to the private sector, but that might change soon. Government funding for healthcare initiatives in such countries as India, Brazil, and Thailand is declining. Some entrepreneurial physicians and hospitals are looking to medical tourism to fill the funding gap.
Medical tourism likely will continue to grow; so too will the legal, quality, and insurance protections for patients. Efficient resource utilization might help reduce U.S. healthcare costs, and improved distribution of destination-country resources might help improve infrastructure and access to better healthcare for their own citizens.
With their leadership skills and expertise, hospitalists can play a major role in reducing healthcare costs.
However, what actual reforms healthcare legislation brings to medical tourism remain to be seen. TH
Dr. Thakkar is a hospitalist and assistant professor in the division of hospital medicine at Johns Hopkins University School of Medicine in Baltimore.
References
- Medical tourism: Consumers in search of value. Deloitte Consulting LLP website. Available at: www.deloitte.com/dtt/cda/doc/content/us%5Fchs%5FMedicalTourismStudy(1).pdf. Accessed Sept. 13, 2010.
- Pafford B. The third wave—medical tourism in the 21st century. South Med J. 2009;102(8):810-813.
- Kher U. Outsourcing your heart. Available at: http://proquest.umi.com/pqdweb?did=1041533291&Fmt=7&clientId=5241&RQT=309&VName=PQD. Accessed Sept. 13, 2010.
- Forgione DA, Smith PC. Medical tourism and its impact on the US health care system. J Health Care Finance. 2007;34(1):27-35.
- Lancaster J. Surgeries, side trips for “medical tourists.” The Washington Post website. Available at: www.washingtonpost.com/wp-dyn/articles/A497432004Oct20.html. Accessed Sept. 13, 2010.
- Horowitz MD, Rosensweig JA, Jones CA. Medical tourism: Globaliz-ation of the healthcare marketplace. MedGenMed. 2007;9(4):33.
- Milstein A, Smith M. Will the surgical world become flat? Health Aff (Millwood). 2007;26(1):137-141.
- New AMA guidelines on medical tourism. AMA website. Available at: www.ama-assn.org/ama1/pub/upload/mm/31/medicaltourism.pdf. Accessed March 26, 2010.
- Anand G. The Henry Ford of heart surgery. Wall Street Journal website. Available at: online.wsj.com/article/SB12587589288795811.html.
- Einhorn B. Outsourcing the patients. Business Week website. Available at: www.businessweek.com/magazine/content/08_12/b40760367 77780.htm. Accessed Sept. 13, 2010.
- . Hartman M, Martin A, Nuccio O, Catlin A, et al. Health spending growth at a historic low in 2008. Health Aff (Millwood). 2010;29(1): 147-155.
- Milstein A, Smith M. America’s new refugees—seeking affordable surgery offshore. N Engl J Med. 2006;355(16):1637-1640.
David Dupray, a 60-year-old uninsured coffee shop owner from Bar Harbor, Maine, had been having left leg pain on ambulation for four years. His cardiologist recommended stent placement for left iliac artery stenosis. The estimated bill: approximately $35,000.
Unable to afford the procedure, Dupray began searching the Web for affordable medical care overseas. His physician suggested Thailand. Within days, Dupray had an appointment with a cardiologist halfway around the world—at Bumrungrad Hospital in Bangkok, Thailand. Dupray spent two days in the hotel-like hospital, had three stents placed in his leg arteries, and completed a cardiac stress test. The total bill: $18,000.
“I will never go to a hospital in the U.S.,” says Dupray, who represents a growing number of Americans searching for affordable healthcare in the global marketplace.
With rising U.S. healthcare costs and millions of Americans uninsured or underinsured, more American patients are seeking affordable, high-quality medical care abroad—known as “medical tourism.” In 2007, an estimated 750,000 Americans traveled abroad for medical care; the number is expected to increase to 6 million by the end of this year.1 On the flip side, only a little more than 400,000 nonresidents visited the U.S. in 2008 for the latest medical care.1 Globally, the medical tourism industry is estimated to grow into a $21 billion-a-year industry by 2012, with much of the growth expected from Western patients traveling overseas for affordable care.2
“As hospitalists, we have been seeing increasing numbers of patients going overseas for urgent and elective procedures, as it is a general perception the medical treatment overseas is less expensive,” says Joseph Ming Wah Li, MD, SFHM, director of hospital medicine at Beth Israel Deaconess Medical Center in Boston and SHM president-elect.
Physicians in U.S. hospitals encounter potential medical tourists all the time. Some are uninsured or underinsured. Some have insurance carriers that limit or exclude coverage for certain procedures and treatments. Even those with insurance sometimes struggle to pay deductibles, copays, and their costs after insurance has paid its part. Others are uncomfortable with the language barriers and cultural differences of U.S. hospitals and physicians.
Medical tourism also lures patients who are citizens of countries (e.g. Canada, the United Kingdom) that offer universal healthcare, Dr. Li says.3 For example, more expatriates from India and Malaysia are traveling to their native countries for medical care, as they receive affordable and quicker medical care while visiting family.
Hospitalists routinely care for patients requiring essential cardiac or orthopedic surgeries—conditions that are common in the medical tourism trade. With medical tourism growing in scope and popularity, it is essential that hospitalists are prepared to discuss with their patients the pros and cons of traveling for medical care. Hospitalists should be able to:
- Identify patients who might benefit from medical tourism;
- Know where and how to look for an accredited overseas facility; and
- Explain to patients the potential travel risks and complications, including insurance coverage and legal restrictions in destination countries.
A basic understanding of the industry and the issues can help guide your patients through medical decisions and help you care for those who have returned from a medical trip.
Big Menu, Discount Prices
Medical tourism offers a wide range of medical services performed in hospitals on nearly every continent, with a wide range of costs for certain procedures (Table 1, p. 26). Most surgeries cost 50% to 90% less than the average cost of the same surgery at a U.S. hospital. Many in the medical tourism industry say these types of savings have brought once-unaffordable surgery within the reach of most Americans, regardless of insurance status. For example, cardiac bypass surgery on average costs $144,000 in the U.S.; it costs about $8,500 in India.
The reasons the costs are so much less at overseas hospitals, as compared with U.S. costs, are many:
- Lower wages for providers;
- Less expensive medical devices and pharmaceutical products;
- Less involvement by third-party payors; and
- Lower malpractice premiums.4
For example, the annual liability insurance premium for a surgeon in India is $4,000; the average cost of a New York City surgeon’s liability insurance premium is $100,000.5
Brazil, Costa Rica, and Mexico are attractive destinations for cosmetic and dental surgeries; Singapore, Malaysia, Thailand, and India have emerged as hubs for cardiac and orthopedic surgeries (Table 1, above).6
The growth in medical tourism led the Joint Commission in 1999 to launch Joint Commission International (JCI), which ensures that offshore hospitals provide the highest-quality care to international patients (see “Ultra-Affordable Prices and No Decline in Quality of Care,” p. 28). JCI has accredited 120 overseas hospitals that meet these standards.
“Overseas hospitals are always keen in partnering with U.S. hospitals,” Dr. Li says. Collaborations, such as Johns Hopkins International Medical Center’s partnership with International Medical Clinic Singapore, and Partners Harvard Medical International’s affiliation with Wockhardt Hospitals in Mumbai, India, have helped facilitate the accreditation process and alleviate U.S. patient concerns.
Overseas hospitals not only offer greatly discounted rates than insurer-negotiated U.S. prices, but many of the international hospitals also report quality scores equal to or better than the average U.S. hospital’s.7
Before You Book a Trip …
How do patients find overseas facilities? It’s as easy as a click of the mouse.
“Our survey shows 75 percent of patients located offshore hospitals through the Internet,” says Renee-Marie Stephano, president of the Medical Tourism Association, a nonprofit group based in West Palm Beach, Fla., that was established in 2007 to promote education, transparency, and communication in the medical tourism community. Patients use overseas hospital websites, international medical coordinators, and medical tourism companies, such as PlanetHospital.com and MedRetreat.com, to find facilities and providers, and to coordinate medical travel.
“Medical tourism is currently unregulated,” Stephano says. “One of our goals is to certify medical tourism facilitators to create the best standard of practice.”
In 2007, the American Medical Association (AMA) published medical tourism guidelines to help healthcare entities engaged in overseas medical care.8 (Download a PDF of the guidelines at www.ama-assn.org/ama1/pub/upload/mm/31/medicaltourism.pdf.) The AMA suggests that:
- Medical care outside the U.S. should be voluntary, and patients should be informed of their legal rights and recourses before agreeing to travel outside the U.S.;
- Before traveling, local follow-up care should be arranged to ensure continuity of care;
- Patients should have access to physician licensing, facility accreditation, and outcomes data for both;
- Medical record transfers should follow HIPAA guidelines; and
- Patients should be informed of the potential risks of combining surgical procedures with long flights and vacation activities.
—Kenneth Mays, senior director, marketing and business development, Bumrungrad Hospital, Bangkok, Thailand
Patient Concerns
Hospitalists are highly focused on a patient’s quality of care; the same can be said of some overseas hospitals that attract large numbers of medical tourists. “I think the service and quality of care provided at our hospital compares favorably with the very best American hospitals,” says Kenneth Mays, senior director of hospital marketing and business development at Bumrungrad Hospital in Bangkok.
That might be so, but the growth of medical tourism also raises concerns stateside. With sleek websites making it easy for U.S. patients to schedule procedure vacations from their kitchen tables, many U.S. physician and watchdog groups worry about patient safety, privacy, liability, and continuity of care. Although most international hospitals and physicians provide outcomes data, rarely do the benchmarks compare directly with U.S. hospital quality and safety data.
“Quality comparisons are difficult, even within U.S. hospitals, as hospitals use different methodologies to collect data,” says Stephano. “Patients have to rely on JCI accreditation, surgeon experience, volume, and outcomes to decide.”
Recent studies echo the Medical Tourism Association’s claim: Increased cardiac surgery volume at Apollo Hospitals—an 8,500-bed healthcare system with 50 locations throughout India—and Narayana Hospital in Bommasandra, India, has lowered costs, with similar, or even lower, mortality rates compared with the average U.S. hospital.7,9 Other challenges like getting medical records exist even within U.S. hospitals, so emerging platforms like Google Health and Microsoft Vault, where medical records can be uploaded at the touch of a button, “will benefit patients and providers,” Dr. Li says.
The Medical Tourism Association envisions U.S.-based physicians offering follow-up care to medical tourism patients. “Currently, we encourage patients to follow up with their primary-care physician,” Stephano says.
Dr. Li says malpractice is always a concern when traveling overseas; however, he also notes the legal system in the U.S. is strong enough “to handle any medical malpractice.” That said, a patient who experiences a poor medical outcome as the result of overseas treatment might seek legal remedies, but the reality is that malpractice laws are either nonexistent or not well implemented in some destination countries. That makes malpractice claims on overseas procedures a dicey proposition.
“Patients receiving overseas treatment need to realize that they are agreeing to the jurisdiction of the destination country,” Stephano says. Other risks associated with extended travel include exposure to regional infectious diseases and poor infrastructure in the destination country, which could undermine the benefits of medical travel.
Cost-saving benefits have led some U.S. insurance companies to begin integrating overseas medical coverage. For example, Blue Cross Blue Shield of South Carolina offers incentives for patients willing to obtain medical care overseas at JCI-approved hospitals. BCBS then waives deductibles and copays, and several other insurers have launched similar pilot programs.10 “We will see more of these changes,” Stephano says, “to cut costs and remain competitive.”
Immediate Impact
In 2008, U.S. healthcare spending was $2.3 trillion.11 A 2005 Institute of Medicine report suggests that 30% to 40% of current U.S. healthcare expenditure is wasted.12 U.S. lawmakers, employers, hospitals, and consumers are scrambling to find ways to reduce healthcare costs and improve efficiency. Medical tourism seems to benefit a select few Americans, only lowering U.S. healthcare spending by 1% to 2%.12
Medical tourism revenue generated in destination countries currently is limited to the private sector, but that might change soon. Government funding for healthcare initiatives in such countries as India, Brazil, and Thailand is declining. Some entrepreneurial physicians and hospitals are looking to medical tourism to fill the funding gap.
Medical tourism likely will continue to grow; so too will the legal, quality, and insurance protections for patients. Efficient resource utilization might help reduce U.S. healthcare costs, and improved distribution of destination-country resources might help improve infrastructure and access to better healthcare for their own citizens.
With their leadership skills and expertise, hospitalists can play a major role in reducing healthcare costs.
However, what actual reforms healthcare legislation brings to medical tourism remain to be seen. TH
Dr. Thakkar is a hospitalist and assistant professor in the division of hospital medicine at Johns Hopkins University School of Medicine in Baltimore.
References
- Medical tourism: Consumers in search of value. Deloitte Consulting LLP website. Available at: www.deloitte.com/dtt/cda/doc/content/us%5Fchs%5FMedicalTourismStudy(1).pdf. Accessed Sept. 13, 2010.
- Pafford B. The third wave—medical tourism in the 21st century. South Med J. 2009;102(8):810-813.
- Kher U. Outsourcing your heart. Available at: http://proquest.umi.com/pqdweb?did=1041533291&Fmt=7&clientId=5241&RQT=309&VName=PQD. Accessed Sept. 13, 2010.
- Forgione DA, Smith PC. Medical tourism and its impact on the US health care system. J Health Care Finance. 2007;34(1):27-35.
- Lancaster J. Surgeries, side trips for “medical tourists.” The Washington Post website. Available at: www.washingtonpost.com/wp-dyn/articles/A497432004Oct20.html. Accessed Sept. 13, 2010.
- Horowitz MD, Rosensweig JA, Jones CA. Medical tourism: Globaliz-ation of the healthcare marketplace. MedGenMed. 2007;9(4):33.
- Milstein A, Smith M. Will the surgical world become flat? Health Aff (Millwood). 2007;26(1):137-141.
- New AMA guidelines on medical tourism. AMA website. Available at: www.ama-assn.org/ama1/pub/upload/mm/31/medicaltourism.pdf. Accessed March 26, 2010.
- Anand G. The Henry Ford of heart surgery. Wall Street Journal website. Available at: online.wsj.com/article/SB12587589288795811.html.
- Einhorn B. Outsourcing the patients. Business Week website. Available at: www.businessweek.com/magazine/content/08_12/b40760367 77780.htm. Accessed Sept. 13, 2010.
- . Hartman M, Martin A, Nuccio O, Catlin A, et al. Health spending growth at a historic low in 2008. Health Aff (Millwood). 2010;29(1): 147-155.
- Milstein A, Smith M. America’s new refugees—seeking affordable surgery offshore. N Engl J Med. 2006;355(16):1637-1640.
David Dupray, a 60-year-old uninsured coffee shop owner from Bar Harbor, Maine, had been having left leg pain on ambulation for four years. His cardiologist recommended stent placement for left iliac artery stenosis. The estimated bill: approximately $35,000.
Unable to afford the procedure, Dupray began searching the Web for affordable medical care overseas. His physician suggested Thailand. Within days, Dupray had an appointment with a cardiologist halfway around the world—at Bumrungrad Hospital in Bangkok, Thailand. Dupray spent two days in the hotel-like hospital, had three stents placed in his leg arteries, and completed a cardiac stress test. The total bill: $18,000.
“I will never go to a hospital in the U.S.,” says Dupray, who represents a growing number of Americans searching for affordable healthcare in the global marketplace.
With rising U.S. healthcare costs and millions of Americans uninsured or underinsured, more American patients are seeking affordable, high-quality medical care abroad—known as “medical tourism.” In 2007, an estimated 750,000 Americans traveled abroad for medical care; the number is expected to increase to 6 million by the end of this year.1 On the flip side, only a little more than 400,000 nonresidents visited the U.S. in 2008 for the latest medical care.1 Globally, the medical tourism industry is estimated to grow into a $21 billion-a-year industry by 2012, with much of the growth expected from Western patients traveling overseas for affordable care.2
“As hospitalists, we have been seeing increasing numbers of patients going overseas for urgent and elective procedures, as it is a general perception the medical treatment overseas is less expensive,” says Joseph Ming Wah Li, MD, SFHM, director of hospital medicine at Beth Israel Deaconess Medical Center in Boston and SHM president-elect.
Physicians in U.S. hospitals encounter potential medical tourists all the time. Some are uninsured or underinsured. Some have insurance carriers that limit or exclude coverage for certain procedures and treatments. Even those with insurance sometimes struggle to pay deductibles, copays, and their costs after insurance has paid its part. Others are uncomfortable with the language barriers and cultural differences of U.S. hospitals and physicians.
Medical tourism also lures patients who are citizens of countries (e.g. Canada, the United Kingdom) that offer universal healthcare, Dr. Li says.3 For example, more expatriates from India and Malaysia are traveling to their native countries for medical care, as they receive affordable and quicker medical care while visiting family.
Hospitalists routinely care for patients requiring essential cardiac or orthopedic surgeries—conditions that are common in the medical tourism trade. With medical tourism growing in scope and popularity, it is essential that hospitalists are prepared to discuss with their patients the pros and cons of traveling for medical care. Hospitalists should be able to:
- Identify patients who might benefit from medical tourism;
- Know where and how to look for an accredited overseas facility; and
- Explain to patients the potential travel risks and complications, including insurance coverage and legal restrictions in destination countries.
A basic understanding of the industry and the issues can help guide your patients through medical decisions and help you care for those who have returned from a medical trip.
Big Menu, Discount Prices
Medical tourism offers a wide range of medical services performed in hospitals on nearly every continent, with a wide range of costs for certain procedures (Table 1, p. 26). Most surgeries cost 50% to 90% less than the average cost of the same surgery at a U.S. hospital. Many in the medical tourism industry say these types of savings have brought once-unaffordable surgery within the reach of most Americans, regardless of insurance status. For example, cardiac bypass surgery on average costs $144,000 in the U.S.; it costs about $8,500 in India.
The reasons the costs are so much less at overseas hospitals, as compared with U.S. costs, are many:
- Lower wages for providers;
- Less expensive medical devices and pharmaceutical products;
- Less involvement by third-party payors; and
- Lower malpractice premiums.4
For example, the annual liability insurance premium for a surgeon in India is $4,000; the average cost of a New York City surgeon’s liability insurance premium is $100,000.5
Brazil, Costa Rica, and Mexico are attractive destinations for cosmetic and dental surgeries; Singapore, Malaysia, Thailand, and India have emerged as hubs for cardiac and orthopedic surgeries (Table 1, above).6
The growth in medical tourism led the Joint Commission in 1999 to launch Joint Commission International (JCI), which ensures that offshore hospitals provide the highest-quality care to international patients (see “Ultra-Affordable Prices and No Decline in Quality of Care,” p. 28). JCI has accredited 120 overseas hospitals that meet these standards.
“Overseas hospitals are always keen in partnering with U.S. hospitals,” Dr. Li says. Collaborations, such as Johns Hopkins International Medical Center’s partnership with International Medical Clinic Singapore, and Partners Harvard Medical International’s affiliation with Wockhardt Hospitals in Mumbai, India, have helped facilitate the accreditation process and alleviate U.S. patient concerns.
Overseas hospitals not only offer greatly discounted rates than insurer-negotiated U.S. prices, but many of the international hospitals also report quality scores equal to or better than the average U.S. hospital’s.7
Before You Book a Trip …
How do patients find overseas facilities? It’s as easy as a click of the mouse.
“Our survey shows 75 percent of patients located offshore hospitals through the Internet,” says Renee-Marie Stephano, president of the Medical Tourism Association, a nonprofit group based in West Palm Beach, Fla., that was established in 2007 to promote education, transparency, and communication in the medical tourism community. Patients use overseas hospital websites, international medical coordinators, and medical tourism companies, such as PlanetHospital.com and MedRetreat.com, to find facilities and providers, and to coordinate medical travel.
“Medical tourism is currently unregulated,” Stephano says. “One of our goals is to certify medical tourism facilitators to create the best standard of practice.”
In 2007, the American Medical Association (AMA) published medical tourism guidelines to help healthcare entities engaged in overseas medical care.8 (Download a PDF of the guidelines at www.ama-assn.org/ama1/pub/upload/mm/31/medicaltourism.pdf.) The AMA suggests that:
- Medical care outside the U.S. should be voluntary, and patients should be informed of their legal rights and recourses before agreeing to travel outside the U.S.;
- Before traveling, local follow-up care should be arranged to ensure continuity of care;
- Patients should have access to physician licensing, facility accreditation, and outcomes data for both;
- Medical record transfers should follow HIPAA guidelines; and
- Patients should be informed of the potential risks of combining surgical procedures with long flights and vacation activities.
—Kenneth Mays, senior director, marketing and business development, Bumrungrad Hospital, Bangkok, Thailand
Patient Concerns
Hospitalists are highly focused on a patient’s quality of care; the same can be said of some overseas hospitals that attract large numbers of medical tourists. “I think the service and quality of care provided at our hospital compares favorably with the very best American hospitals,” says Kenneth Mays, senior director of hospital marketing and business development at Bumrungrad Hospital in Bangkok.
That might be so, but the growth of medical tourism also raises concerns stateside. With sleek websites making it easy for U.S. patients to schedule procedure vacations from their kitchen tables, many U.S. physician and watchdog groups worry about patient safety, privacy, liability, and continuity of care. Although most international hospitals and physicians provide outcomes data, rarely do the benchmarks compare directly with U.S. hospital quality and safety data.
“Quality comparisons are difficult, even within U.S. hospitals, as hospitals use different methodologies to collect data,” says Stephano. “Patients have to rely on JCI accreditation, surgeon experience, volume, and outcomes to decide.”
Recent studies echo the Medical Tourism Association’s claim: Increased cardiac surgery volume at Apollo Hospitals—an 8,500-bed healthcare system with 50 locations throughout India—and Narayana Hospital in Bommasandra, India, has lowered costs, with similar, or even lower, mortality rates compared with the average U.S. hospital.7,9 Other challenges like getting medical records exist even within U.S. hospitals, so emerging platforms like Google Health and Microsoft Vault, where medical records can be uploaded at the touch of a button, “will benefit patients and providers,” Dr. Li says.
The Medical Tourism Association envisions U.S.-based physicians offering follow-up care to medical tourism patients. “Currently, we encourage patients to follow up with their primary-care physician,” Stephano says.
Dr. Li says malpractice is always a concern when traveling overseas; however, he also notes the legal system in the U.S. is strong enough “to handle any medical malpractice.” That said, a patient who experiences a poor medical outcome as the result of overseas treatment might seek legal remedies, but the reality is that malpractice laws are either nonexistent or not well implemented in some destination countries. That makes malpractice claims on overseas procedures a dicey proposition.
“Patients receiving overseas treatment need to realize that they are agreeing to the jurisdiction of the destination country,” Stephano says. Other risks associated with extended travel include exposure to regional infectious diseases and poor infrastructure in the destination country, which could undermine the benefits of medical travel.
Cost-saving benefits have led some U.S. insurance companies to begin integrating overseas medical coverage. For example, Blue Cross Blue Shield of South Carolina offers incentives for patients willing to obtain medical care overseas at JCI-approved hospitals. BCBS then waives deductibles and copays, and several other insurers have launched similar pilot programs.10 “We will see more of these changes,” Stephano says, “to cut costs and remain competitive.”
Immediate Impact
In 2008, U.S. healthcare spending was $2.3 trillion.11 A 2005 Institute of Medicine report suggests that 30% to 40% of current U.S. healthcare expenditure is wasted.12 U.S. lawmakers, employers, hospitals, and consumers are scrambling to find ways to reduce healthcare costs and improve efficiency. Medical tourism seems to benefit a select few Americans, only lowering U.S. healthcare spending by 1% to 2%.12
Medical tourism revenue generated in destination countries currently is limited to the private sector, but that might change soon. Government funding for healthcare initiatives in such countries as India, Brazil, and Thailand is declining. Some entrepreneurial physicians and hospitals are looking to medical tourism to fill the funding gap.
Medical tourism likely will continue to grow; so too will the legal, quality, and insurance protections for patients. Efficient resource utilization might help reduce U.S. healthcare costs, and improved distribution of destination-country resources might help improve infrastructure and access to better healthcare for their own citizens.
With their leadership skills and expertise, hospitalists can play a major role in reducing healthcare costs.
However, what actual reforms healthcare legislation brings to medical tourism remain to be seen. TH
Dr. Thakkar is a hospitalist and assistant professor in the division of hospital medicine at Johns Hopkins University School of Medicine in Baltimore.
References
- Medical tourism: Consumers in search of value. Deloitte Consulting LLP website. Available at: www.deloitte.com/dtt/cda/doc/content/us%5Fchs%5FMedicalTourismStudy(1).pdf. Accessed Sept. 13, 2010.
- Pafford B. The third wave—medical tourism in the 21st century. South Med J. 2009;102(8):810-813.
- Kher U. Outsourcing your heart. Available at: http://proquest.umi.com/pqdweb?did=1041533291&Fmt=7&clientId=5241&RQT=309&VName=PQD. Accessed Sept. 13, 2010.
- Forgione DA, Smith PC. Medical tourism and its impact on the US health care system. J Health Care Finance. 2007;34(1):27-35.
- Lancaster J. Surgeries, side trips for “medical tourists.” The Washington Post website. Available at: www.washingtonpost.com/wp-dyn/articles/A497432004Oct20.html. Accessed Sept. 13, 2010.
- Horowitz MD, Rosensweig JA, Jones CA. Medical tourism: Globaliz-ation of the healthcare marketplace. MedGenMed. 2007;9(4):33.
- Milstein A, Smith M. Will the surgical world become flat? Health Aff (Millwood). 2007;26(1):137-141.
- New AMA guidelines on medical tourism. AMA website. Available at: www.ama-assn.org/ama1/pub/upload/mm/31/medicaltourism.pdf. Accessed March 26, 2010.
- Anand G. The Henry Ford of heart surgery. Wall Street Journal website. Available at: online.wsj.com/article/SB12587589288795811.html.
- Einhorn B. Outsourcing the patients. Business Week website. Available at: www.businessweek.com/magazine/content/08_12/b40760367 77780.htm. Accessed Sept. 13, 2010.
- . Hartman M, Martin A, Nuccio O, Catlin A, et al. Health spending growth at a historic low in 2008. Health Aff (Millwood). 2010;29(1): 147-155.
- Milstein A, Smith M. America’s new refugees—seeking affordable surgery offshore. N Engl J Med. 2006;355(16):1637-1640.
Endangered Species?
The 1961 classic “The Ecology of Medical Care,” published in the New England Journal of Medicine, mapped out the broad features of the American healthcare landscape.1 For every 1,000 adult, the study suggested, 750 reported an illness, 250 consulted a doctor, and nine were admitted to a hospital in any given month. The subsequent arrival of Medicare and Medicaid fundamentally changed the U.S. healthcare system. And yet an updated version of the study, released in 2001, yielded surprisingly similar numbers, with 800 residents experiencing symptoms, 217 visiting a physician’s office, and eight being hospitalized in an average month.2
“It helps kind of put in perspective where the bulk of care really occurs,” says Ann O’Malley, MD, a senior researcher at the Washington, D.C.-based Center for Studying Health System Change. “It’s in outpatient provider offices, mostly primary-care provider offices.”
Dr. O’Malley and a host of other observers, however, are warning that the keystone members of this healthcare ecosystem are in serious trouble. As organizations such as SHM have likewise made clear, the accelerating shortage of general internists, family practitioners, and other PCPs has created sizable cracks in the supports of the entire healthcare infrastructure.
How big are the cracks? The number of medical school students pursuing a primary-care career has dropped by more than half since 1997, according to the American Academy of Family Physicians. And with the number of medical students entering the field unable to keep up with attrition, the remaining doctors are facing increasingly difficult working conditions. “Overloaded primary-care practices, whose doctors are aptly compared to hamsters on a treadmill, struggle to provide prompt access and high-quality care,” asserted a 2009 op-ed in the New England Journal of Medicine.3 The result: a vicious circle of decline leading to an anticipated shortfall of roughly 21,000 PCPs by 2015, according to the Association of American Medical Colleges.
Many primary-care providers had already stopped taking new patients when June’s Medicare reimbursement rate fiasco allowed the sustainable growth rate (SGR) formula’s mandated 21.2 percent rate cut to temporarily go into effect. Legislators eventually plugged the hole, but not before a new round of jitters seized the nation’s physicians, and reports proliferated throughout the summer about Medicare beneficiaries being unable to find a doctor willing to see them. The recession hasn’t helped, with more privately insured patients waiting longer to see their doctors to avoid copays, and with hospital emergency departments becoming de facto primary-care centers for those patients who have waited too long or have no other alternatives.
Uneven Challenges
Not only is there an acute shortage of primary-care physicians, Dr. O’Malley says, but there is also a distinctly uneven distribution throughout the country. For hospitalists, she says, the implications could be profound. “Hospitalists are increasingly going to be evaluated around issues such as avoiding hospital readmissions and [reducing] length of stay,” she says, “and if they want to improve both of those things, one of the keys is improving chronic care management in the outpatient setting, and improving follow-up post discharge.”
Both metrics will require the involvement of outpatient care providers, underscoring the importance of good communication and mutual respect. Despite the longstanding support of hospitalists for their primary-care counterparts, however, leaders are still being forced to address the perception that HM is somehow bad for what ails PCPs.
In a recent online article posted on the Becker’s Hospital Review website, SHM President Jeff Wiese, MD, SFHM, responded to one such criticism: that hospitalists make primary care less attractive for physicians. Hospitalists are not to blame for the decrease in interest, he asserted, but are actually complementary to the PCP role. And with millions more Americans about to be newly insured, that complementary relationship will be even more important. “It’s a tremendous waste of resources to use a primary-care provider for [a hospital visit]. We need to move into proactive mode, not reactive mode,” Dr. Wiese said. “More PCPs are going to need even more time in the clinic to handle the increased number of patients, and you lose the luxury to run back and forth between the clinic and the hospital. For those that can develop a trusting relationship with a hospitalist, you can work together to see more patients and provide more care.”
So what’s the real root of the problem? Money. According to recent surveys, PCPs earn about half the salary of dermatologists and an even smaller fraction of an average cardiologist’s pay. With medical school debt routinely reaching $200,000, Dr. O’Malley and other analysts say, many doctors simply can’t afford to go into primary care.
“It all comes down to payment, basically,” she says. “At present, our payment system for physician services and for medical procedures is quite skewed. It overcompensates for certain types of diagnostics and procedures, and it undercompensates for the more cognitive type of care that primary-care providers provide.”
The Road Ahead
Fortunately, some relief is trickling in. One measure strongly supported by SHM and included in the Affordable Care Act is a 10% Medicare reimbursement bonus for primary care delivered by qualified doctors, slated to begin next year. In June, U.S. Department of Health and Human Services Secretary Kathleen Sebelius announced a separate, $250 million initiative to boost the primary-care workforce. The money would help train PCPs by creating more residency slots, and offer new support for physician assistants, nurses, and nurse practitioners. Among the measures included in last year’s stimulus package, an expansion of the National Health Service Corps will provide more debt-relief opportunities for PCPs. And in mid-September, HHS tapped stimulus funds to award another $50.3 million for primary care training programs and loan repayment.
The Obama administration has claimed its combined actions “will support the training and development of more than 16,000 new primary-care providers over the next five years,” according to a June 16 HHS press release.
Observers say those measures alone are unlikely to be enough to stem the tide, however. “It’s definitely a step in the right direction,” Dr. O’Malley says of the Medicare bonus. “I don’t think it’s going to solve the primary-care workforce issue, because a 10% bonus, given how low primary-care physician salaries are compared to their specialist counterparts, is not going to be that much of an increase. Among the physicians that I’ve talked to and other healthcare providers, few feel that that’s sufficient enough to really encourage a lot of people to pursue primary care.”
Several other efforts now underway might help:
- Texas Tech University Health Sciences Center unveiled a new Family Medicine Accelerated Track program, which will allow primary-care medical students to complete a degree in three years. Certain students will receive a one-year scholarship, meaning that overall debt for some could be half that of the standard four-year program.
- Reid Hospital and Health Care Services in Richmond, Ind., successfully reversed a downward trend in primary-care referrals by forming its own nonprofit subsidiary corporation, Reid Physician Associates. The nonprofit will include about 50 employed outpatient providers by year’s end to complement the 233-bed hospital’s inpatient staff.
- Danville, Pa.-based Geisinger Health System has begun paying the salaries of extra nurses for both in-network and independent primary-care practices. The nurses manage patients’ chronic conditions, ensure that they are following prescribed treatments, and communicate with hospitalists and other providers about transitions of care. Although still in its early stages, the experiment suggests the nurses are helping to spot problems, prevent unnecessary hospitalizations, and save money.
The Geisinger experiment is among the first steps toward a patient-centered medical home model of care. An eventual Medicare-led expansion of such medical homes and accountable-care organizations, now in the early experimental stages, could provide even more direct support to PCPs. To be successful, though, Dr. O’Malley says the models will need to focus on paying providers fairly for the value they bring to the system. “Obviously, payment reform is what we need if we’re ever going to develop a sustainable primary-care workforce in this country,” she says. TH
Bryn Nelson is a freelance medical writer based in Seattle.
References
- White KL, Williams TF, Greenberg BG. The ecology of medical care. N Engl J Med. 1961;265:885-992.
- Green LA, Fryer GE Jr., Yawn BP, Lanier D, Dovey SM. The ecology of medical care revisited. N Engl J Med. 2001;344(26):2021-2025.
- Bodenheimer T, Grumbach K, Berenson RA. A lifeline for primary care. N Engl J Med. 2009;360(26):2693-2696.
The 1961 classic “The Ecology of Medical Care,” published in the New England Journal of Medicine, mapped out the broad features of the American healthcare landscape.1 For every 1,000 adult, the study suggested, 750 reported an illness, 250 consulted a doctor, and nine were admitted to a hospital in any given month. The subsequent arrival of Medicare and Medicaid fundamentally changed the U.S. healthcare system. And yet an updated version of the study, released in 2001, yielded surprisingly similar numbers, with 800 residents experiencing symptoms, 217 visiting a physician’s office, and eight being hospitalized in an average month.2
“It helps kind of put in perspective where the bulk of care really occurs,” says Ann O’Malley, MD, a senior researcher at the Washington, D.C.-based Center for Studying Health System Change. “It’s in outpatient provider offices, mostly primary-care provider offices.”
Dr. O’Malley and a host of other observers, however, are warning that the keystone members of this healthcare ecosystem are in serious trouble. As organizations such as SHM have likewise made clear, the accelerating shortage of general internists, family practitioners, and other PCPs has created sizable cracks in the supports of the entire healthcare infrastructure.
How big are the cracks? The number of medical school students pursuing a primary-care career has dropped by more than half since 1997, according to the American Academy of Family Physicians. And with the number of medical students entering the field unable to keep up with attrition, the remaining doctors are facing increasingly difficult working conditions. “Overloaded primary-care practices, whose doctors are aptly compared to hamsters on a treadmill, struggle to provide prompt access and high-quality care,” asserted a 2009 op-ed in the New England Journal of Medicine.3 The result: a vicious circle of decline leading to an anticipated shortfall of roughly 21,000 PCPs by 2015, according to the Association of American Medical Colleges.
Many primary-care providers had already stopped taking new patients when June’s Medicare reimbursement rate fiasco allowed the sustainable growth rate (SGR) formula’s mandated 21.2 percent rate cut to temporarily go into effect. Legislators eventually plugged the hole, but not before a new round of jitters seized the nation’s physicians, and reports proliferated throughout the summer about Medicare beneficiaries being unable to find a doctor willing to see them. The recession hasn’t helped, with more privately insured patients waiting longer to see their doctors to avoid copays, and with hospital emergency departments becoming de facto primary-care centers for those patients who have waited too long or have no other alternatives.
Uneven Challenges
Not only is there an acute shortage of primary-care physicians, Dr. O’Malley says, but there is also a distinctly uneven distribution throughout the country. For hospitalists, she says, the implications could be profound. “Hospitalists are increasingly going to be evaluated around issues such as avoiding hospital readmissions and [reducing] length of stay,” she says, “and if they want to improve both of those things, one of the keys is improving chronic care management in the outpatient setting, and improving follow-up post discharge.”
Both metrics will require the involvement of outpatient care providers, underscoring the importance of good communication and mutual respect. Despite the longstanding support of hospitalists for their primary-care counterparts, however, leaders are still being forced to address the perception that HM is somehow bad for what ails PCPs.
In a recent online article posted on the Becker’s Hospital Review website, SHM President Jeff Wiese, MD, SFHM, responded to one such criticism: that hospitalists make primary care less attractive for physicians. Hospitalists are not to blame for the decrease in interest, he asserted, but are actually complementary to the PCP role. And with millions more Americans about to be newly insured, that complementary relationship will be even more important. “It’s a tremendous waste of resources to use a primary-care provider for [a hospital visit]. We need to move into proactive mode, not reactive mode,” Dr. Wiese said. “More PCPs are going to need even more time in the clinic to handle the increased number of patients, and you lose the luxury to run back and forth between the clinic and the hospital. For those that can develop a trusting relationship with a hospitalist, you can work together to see more patients and provide more care.”
So what’s the real root of the problem? Money. According to recent surveys, PCPs earn about half the salary of dermatologists and an even smaller fraction of an average cardiologist’s pay. With medical school debt routinely reaching $200,000, Dr. O’Malley and other analysts say, many doctors simply can’t afford to go into primary care.
“It all comes down to payment, basically,” she says. “At present, our payment system for physician services and for medical procedures is quite skewed. It overcompensates for certain types of diagnostics and procedures, and it undercompensates for the more cognitive type of care that primary-care providers provide.”
The Road Ahead
Fortunately, some relief is trickling in. One measure strongly supported by SHM and included in the Affordable Care Act is a 10% Medicare reimbursement bonus for primary care delivered by qualified doctors, slated to begin next year. In June, U.S. Department of Health and Human Services Secretary Kathleen Sebelius announced a separate, $250 million initiative to boost the primary-care workforce. The money would help train PCPs by creating more residency slots, and offer new support for physician assistants, nurses, and nurse practitioners. Among the measures included in last year’s stimulus package, an expansion of the National Health Service Corps will provide more debt-relief opportunities for PCPs. And in mid-September, HHS tapped stimulus funds to award another $50.3 million for primary care training programs and loan repayment.
The Obama administration has claimed its combined actions “will support the training and development of more than 16,000 new primary-care providers over the next five years,” according to a June 16 HHS press release.
Observers say those measures alone are unlikely to be enough to stem the tide, however. “It’s definitely a step in the right direction,” Dr. O’Malley says of the Medicare bonus. “I don’t think it’s going to solve the primary-care workforce issue, because a 10% bonus, given how low primary-care physician salaries are compared to their specialist counterparts, is not going to be that much of an increase. Among the physicians that I’ve talked to and other healthcare providers, few feel that that’s sufficient enough to really encourage a lot of people to pursue primary care.”
Several other efforts now underway might help:
- Texas Tech University Health Sciences Center unveiled a new Family Medicine Accelerated Track program, which will allow primary-care medical students to complete a degree in three years. Certain students will receive a one-year scholarship, meaning that overall debt for some could be half that of the standard four-year program.
- Reid Hospital and Health Care Services in Richmond, Ind., successfully reversed a downward trend in primary-care referrals by forming its own nonprofit subsidiary corporation, Reid Physician Associates. The nonprofit will include about 50 employed outpatient providers by year’s end to complement the 233-bed hospital’s inpatient staff.
- Danville, Pa.-based Geisinger Health System has begun paying the salaries of extra nurses for both in-network and independent primary-care practices. The nurses manage patients’ chronic conditions, ensure that they are following prescribed treatments, and communicate with hospitalists and other providers about transitions of care. Although still in its early stages, the experiment suggests the nurses are helping to spot problems, prevent unnecessary hospitalizations, and save money.
The Geisinger experiment is among the first steps toward a patient-centered medical home model of care. An eventual Medicare-led expansion of such medical homes and accountable-care organizations, now in the early experimental stages, could provide even more direct support to PCPs. To be successful, though, Dr. O’Malley says the models will need to focus on paying providers fairly for the value they bring to the system. “Obviously, payment reform is what we need if we’re ever going to develop a sustainable primary-care workforce in this country,” she says. TH
Bryn Nelson is a freelance medical writer based in Seattle.
References
- White KL, Williams TF, Greenberg BG. The ecology of medical care. N Engl J Med. 1961;265:885-992.
- Green LA, Fryer GE Jr., Yawn BP, Lanier D, Dovey SM. The ecology of medical care revisited. N Engl J Med. 2001;344(26):2021-2025.
- Bodenheimer T, Grumbach K, Berenson RA. A lifeline for primary care. N Engl J Med. 2009;360(26):2693-2696.
The 1961 classic “The Ecology of Medical Care,” published in the New England Journal of Medicine, mapped out the broad features of the American healthcare landscape.1 For every 1,000 adult, the study suggested, 750 reported an illness, 250 consulted a doctor, and nine were admitted to a hospital in any given month. The subsequent arrival of Medicare and Medicaid fundamentally changed the U.S. healthcare system. And yet an updated version of the study, released in 2001, yielded surprisingly similar numbers, with 800 residents experiencing symptoms, 217 visiting a physician’s office, and eight being hospitalized in an average month.2
“It helps kind of put in perspective where the bulk of care really occurs,” says Ann O’Malley, MD, a senior researcher at the Washington, D.C.-based Center for Studying Health System Change. “It’s in outpatient provider offices, mostly primary-care provider offices.”
Dr. O’Malley and a host of other observers, however, are warning that the keystone members of this healthcare ecosystem are in serious trouble. As organizations such as SHM have likewise made clear, the accelerating shortage of general internists, family practitioners, and other PCPs has created sizable cracks in the supports of the entire healthcare infrastructure.
How big are the cracks? The number of medical school students pursuing a primary-care career has dropped by more than half since 1997, according to the American Academy of Family Physicians. And with the number of medical students entering the field unable to keep up with attrition, the remaining doctors are facing increasingly difficult working conditions. “Overloaded primary-care practices, whose doctors are aptly compared to hamsters on a treadmill, struggle to provide prompt access and high-quality care,” asserted a 2009 op-ed in the New England Journal of Medicine.3 The result: a vicious circle of decline leading to an anticipated shortfall of roughly 21,000 PCPs by 2015, according to the Association of American Medical Colleges.
Many primary-care providers had already stopped taking new patients when June’s Medicare reimbursement rate fiasco allowed the sustainable growth rate (SGR) formula’s mandated 21.2 percent rate cut to temporarily go into effect. Legislators eventually plugged the hole, but not before a new round of jitters seized the nation’s physicians, and reports proliferated throughout the summer about Medicare beneficiaries being unable to find a doctor willing to see them. The recession hasn’t helped, with more privately insured patients waiting longer to see their doctors to avoid copays, and with hospital emergency departments becoming de facto primary-care centers for those patients who have waited too long or have no other alternatives.
Uneven Challenges
Not only is there an acute shortage of primary-care physicians, Dr. O’Malley says, but there is also a distinctly uneven distribution throughout the country. For hospitalists, she says, the implications could be profound. “Hospitalists are increasingly going to be evaluated around issues such as avoiding hospital readmissions and [reducing] length of stay,” she says, “and if they want to improve both of those things, one of the keys is improving chronic care management in the outpatient setting, and improving follow-up post discharge.”
Both metrics will require the involvement of outpatient care providers, underscoring the importance of good communication and mutual respect. Despite the longstanding support of hospitalists for their primary-care counterparts, however, leaders are still being forced to address the perception that HM is somehow bad for what ails PCPs.
In a recent online article posted on the Becker’s Hospital Review website, SHM President Jeff Wiese, MD, SFHM, responded to one such criticism: that hospitalists make primary care less attractive for physicians. Hospitalists are not to blame for the decrease in interest, he asserted, but are actually complementary to the PCP role. And with millions more Americans about to be newly insured, that complementary relationship will be even more important. “It’s a tremendous waste of resources to use a primary-care provider for [a hospital visit]. We need to move into proactive mode, not reactive mode,” Dr. Wiese said. “More PCPs are going to need even more time in the clinic to handle the increased number of patients, and you lose the luxury to run back and forth between the clinic and the hospital. For those that can develop a trusting relationship with a hospitalist, you can work together to see more patients and provide more care.”
So what’s the real root of the problem? Money. According to recent surveys, PCPs earn about half the salary of dermatologists and an even smaller fraction of an average cardiologist’s pay. With medical school debt routinely reaching $200,000, Dr. O’Malley and other analysts say, many doctors simply can’t afford to go into primary care.
“It all comes down to payment, basically,” she says. “At present, our payment system for physician services and for medical procedures is quite skewed. It overcompensates for certain types of diagnostics and procedures, and it undercompensates for the more cognitive type of care that primary-care providers provide.”
The Road Ahead
Fortunately, some relief is trickling in. One measure strongly supported by SHM and included in the Affordable Care Act is a 10% Medicare reimbursement bonus for primary care delivered by qualified doctors, slated to begin next year. In June, U.S. Department of Health and Human Services Secretary Kathleen Sebelius announced a separate, $250 million initiative to boost the primary-care workforce. The money would help train PCPs by creating more residency slots, and offer new support for physician assistants, nurses, and nurse practitioners. Among the measures included in last year’s stimulus package, an expansion of the National Health Service Corps will provide more debt-relief opportunities for PCPs. And in mid-September, HHS tapped stimulus funds to award another $50.3 million for primary care training programs and loan repayment.
The Obama administration has claimed its combined actions “will support the training and development of more than 16,000 new primary-care providers over the next five years,” according to a June 16 HHS press release.
Observers say those measures alone are unlikely to be enough to stem the tide, however. “It’s definitely a step in the right direction,” Dr. O’Malley says of the Medicare bonus. “I don’t think it’s going to solve the primary-care workforce issue, because a 10% bonus, given how low primary-care physician salaries are compared to their specialist counterparts, is not going to be that much of an increase. Among the physicians that I’ve talked to and other healthcare providers, few feel that that’s sufficient enough to really encourage a lot of people to pursue primary care.”
Several other efforts now underway might help:
- Texas Tech University Health Sciences Center unveiled a new Family Medicine Accelerated Track program, which will allow primary-care medical students to complete a degree in three years. Certain students will receive a one-year scholarship, meaning that overall debt for some could be half that of the standard four-year program.
- Reid Hospital and Health Care Services in Richmond, Ind., successfully reversed a downward trend in primary-care referrals by forming its own nonprofit subsidiary corporation, Reid Physician Associates. The nonprofit will include about 50 employed outpatient providers by year’s end to complement the 233-bed hospital’s inpatient staff.
- Danville, Pa.-based Geisinger Health System has begun paying the salaries of extra nurses for both in-network and independent primary-care practices. The nurses manage patients’ chronic conditions, ensure that they are following prescribed treatments, and communicate with hospitalists and other providers about transitions of care. Although still in its early stages, the experiment suggests the nurses are helping to spot problems, prevent unnecessary hospitalizations, and save money.
The Geisinger experiment is among the first steps toward a patient-centered medical home model of care. An eventual Medicare-led expansion of such medical homes and accountable-care organizations, now in the early experimental stages, could provide even more direct support to PCPs. To be successful, though, Dr. O’Malley says the models will need to focus on paying providers fairly for the value they bring to the system. “Obviously, payment reform is what we need if we’re ever going to develop a sustainable primary-care workforce in this country,” she says. TH
Bryn Nelson is a freelance medical writer based in Seattle.
References
- White KL, Williams TF, Greenberg BG. The ecology of medical care. N Engl J Med. 1961;265:885-992.
- Green LA, Fryer GE Jr., Yawn BP, Lanier D, Dovey SM. The ecology of medical care revisited. N Engl J Med. 2001;344(26):2021-2025.
- Bodenheimer T, Grumbach K, Berenson RA. A lifeline for primary care. N Engl J Med. 2009;360(26):2693-2696.
Playground Politics
Baseball, kick the can, Russian roulette—pick your game. Chances are good that it has worked its way into a metaphor to illustrate the infuriating, perplexing, and altogether frustrating inability of Congress to step up to the plate and pass a long-term fix to the broken sustainable growth rate (SGR) formula used to determine Medicare reimbursement rates.
On June 24, legislators avoided catastrophe by temporarily rescinding a 21.3% rate cut that went into effect June 1. The after-the-fact patch meant that some Medicare claims had to be reprocessed to recoup the full value, creating an administrative mess. The accompanying 2.2% rate increase expires Nov. 30. The reimbursement cut could reach nearly 30% next year unless Congress intervenes again.
“Obviously, there’s a lot of frustration around the issue, especially on the membership side,” says Ron Greeno, MD, FACP, SFHM, a member of SHM’s Public Policy and Leadership committees, and chief medical officer for Brentwood, Tenn.-based Cogent Healthcare. For hospitalists in many small private practices, he says, a major percentage of income comes from Medicare. “It’s a tremendous headache,” he says of the uncertainty. “It’s very hard to plan for. You’re trying to budget and you don’t know what the policy is going to be literally from week to week.”
The Blame Game
Despite the widespread sentiment among doctors that a permanent reimbursement rate fix should have been included in the healthcare reform legislation, skittishness over the price tag led legislators to drop it from the package. Based on last fall’s estimates, the total cost of a reform bill that scrapped the SGR would have ballooned by roughly $250 billion over 10 years, which would have threatened the bill’s passage.
But Congress has since been unable to pass a permanent fix as standalone legislation amid mounting concern over the national debt, and the price of inaction continues to rise. On April 30, the Congressional Budget Office (CBO) estimated that the cost of jettisoning the SGR formula and freezing rates at current levels had grown to $276 billion over 10 years.
Any serious consideration of lasting alternatives has now been pushed back to the lame-duck session, after the midterm elections. The can has been kicked down the road so many times, Dr. Greeno and others say, that most Congressional members have boot marks all over them. “So now you have a bigger problem at a more crucial time, when money is tighter than ever in a poor economy,” Dr. Greeno says. “And I just think it’s been a failure of our politicians.”
Other healthcare industry leaders have been just as critical. “Delaying the problem is not a solution,” said AMA President Cecil B. Wilson, MD, in a prepared statement after Congress passed the latest six-month reprieve in June. “It doesn’t solve the Medicare mess Congress has created with a long series of short-term Medicare patches over the last decade—including four to avert the 2010 cut alone.”
AMA-sponsored print ads have reminded legislators that delaying a fix until 2013 will again increase its cost, to $396 billion over 10 years. And the association’s June press release asserted that “Congress is playing a dangerous game of Russian roulette with seniors’ healthcare.”
Perhaps a game of “chicken” would be more apt.
Republicans have dared Democrats to spend the billions for a more lasting solution—in the absence of any cuts elsewhere in the healthcare delivery system—and be labeled as fiscally irresponsible. In turn, Democrats have dared Republicans to let the rate cut take effect and be labeled heartless as Medicare beneficiaries lose access to their healthcare providers.
Both parties blinked, resorting to almost unanimous short-term fixes that have allowed legislators to save face while putting off politically risky votes until after the November elections.
Lynne M. Allen, MN, ARNP, who works as a part-time hospitalist in hematology-oncology at 188-bed Kadlec Regional Medical Center in Richland, Wash., says she and other colleagues were initially hopeful that the Obama administration would make Congress work together to find a lasting solution. “There’s a sense of frustration because instead of that happening from our legislators, they’re playing a lot of games with the funding,” says Allen, a member of Team Hospitalist. “They’re not willing to step up to the plate, as they say, and make a decision that will allow us to go forward smoothly.”
The result, Allen says, has been a “roller-coaster ride” of uncertainty over reimbursements. Because Washington’s Tri-Cities region has a relatively high percentage of patients with private insurance, her hospital is somewhat cushioned from a precipitous drop in Medicare fees. But if CMS is ever forced to cut back on its rates, she fully expects private insurers to follow the same downward track.
Practical Concerns
Barbara Hartley, MD, a part-time hospitalist at 22-bed Benson Hospital in Benson, Ariz., says the town’s healthcare facility is somewhat protected from potential Medicare rate cuts through its official status as a Critical Access Hospital. Instead of being reimbursed through diagnosis-related group (DRG) codes, the rural hospital is repaid by Medicare for its total cost per day per patient.
The arrangement is a stable one at the moment, but not enough to dispel Dr. Hartley’s uneasy question: If the economy worsens, will Medicare be able to retain its commitment to rural hospitals? If not, the pain might be felt acutely in communities like Benson, where Dr. Hartley estimates that as much as 75% of the hospital’s in-patient business is through either Medicare or a Medicare Advantage plan.
Kirk Mathews, CEO of St. Louis-based Inpatient Management Inc. and a member of SHM’s Public Policy and Practice Management committees, says Medicare rate cuts also could significantly reduce the leverage of hospitalists during contract negotiations.
“Even if we’re employed by the hospital, but our professional fees that the hospital can recoup for our services are dramatically affected, it will affect how those future contracts go,” Mathews says. “We might be insulated temporarily by the strength of our current contract. But if the formula—however that works out—dramatically impacts the hospitalist reimbursement on the professional fee side, the hospital will feel that, and then hospitalists will eventually feel that as well.” In other words, it could strengthen the bargaining hand of the hospital at the expense of the hospitalist. “Therein lies the long-term threat,” he points out.
Independent Solution?
Some of the authority over physician payments might eventually be depoliticized via language in the reform legislation that empowers a new entity, the Independent Payment Advisory Board, to create policy on such critical monetary issues as reimbursement rates. Congress could still override the board’s policy decisions, but only if the Congressional alternative saves just as much money.
In the meantime, the money for a fix still has to come from somewhere, and no consensus has emerged. Advocates likewise refuse to coalesce around any single alternative. Some experts favor a new formula based on the Medicare economic index, which measures inflation in healthcare delivery costs. But the CBO estimates that per-beneficiary spending under such a formula would be 30% more by 2016 than under the current formula. Other proposals call for temporarily increasing rates, then reverting to annual GDP growth, plus a bit more to cover physician costs.
No matter how the crisis is resolved, experts say, doctors almost certainly will have to make do with less. “When healthcare reform is finally fully implemented, there are going to be less dollars to pay for more services. It’s inevitable,” Mathews says. “And whether it takes the form of SGR or some other form, I’m afraid physicians are going to have to get used to having less money in the pool of money that’s allocated to pay providers.”
It could be a whole new ballgame. TH
Bryn Nelson, PhD, is a freelance medical writer based in Seattle.
Baseball, kick the can, Russian roulette—pick your game. Chances are good that it has worked its way into a metaphor to illustrate the infuriating, perplexing, and altogether frustrating inability of Congress to step up to the plate and pass a long-term fix to the broken sustainable growth rate (SGR) formula used to determine Medicare reimbursement rates.
On June 24, legislators avoided catastrophe by temporarily rescinding a 21.3% rate cut that went into effect June 1. The after-the-fact patch meant that some Medicare claims had to be reprocessed to recoup the full value, creating an administrative mess. The accompanying 2.2% rate increase expires Nov. 30. The reimbursement cut could reach nearly 30% next year unless Congress intervenes again.
“Obviously, there’s a lot of frustration around the issue, especially on the membership side,” says Ron Greeno, MD, FACP, SFHM, a member of SHM’s Public Policy and Leadership committees, and chief medical officer for Brentwood, Tenn.-based Cogent Healthcare. For hospitalists in many small private practices, he says, a major percentage of income comes from Medicare. “It’s a tremendous headache,” he says of the uncertainty. “It’s very hard to plan for. You’re trying to budget and you don’t know what the policy is going to be literally from week to week.”
The Blame Game
Despite the widespread sentiment among doctors that a permanent reimbursement rate fix should have been included in the healthcare reform legislation, skittishness over the price tag led legislators to drop it from the package. Based on last fall’s estimates, the total cost of a reform bill that scrapped the SGR would have ballooned by roughly $250 billion over 10 years, which would have threatened the bill’s passage.
But Congress has since been unable to pass a permanent fix as standalone legislation amid mounting concern over the national debt, and the price of inaction continues to rise. On April 30, the Congressional Budget Office (CBO) estimated that the cost of jettisoning the SGR formula and freezing rates at current levels had grown to $276 billion over 10 years.
Any serious consideration of lasting alternatives has now been pushed back to the lame-duck session, after the midterm elections. The can has been kicked down the road so many times, Dr. Greeno and others say, that most Congressional members have boot marks all over them. “So now you have a bigger problem at a more crucial time, when money is tighter than ever in a poor economy,” Dr. Greeno says. “And I just think it’s been a failure of our politicians.”
Other healthcare industry leaders have been just as critical. “Delaying the problem is not a solution,” said AMA President Cecil B. Wilson, MD, in a prepared statement after Congress passed the latest six-month reprieve in June. “It doesn’t solve the Medicare mess Congress has created with a long series of short-term Medicare patches over the last decade—including four to avert the 2010 cut alone.”
AMA-sponsored print ads have reminded legislators that delaying a fix until 2013 will again increase its cost, to $396 billion over 10 years. And the association’s June press release asserted that “Congress is playing a dangerous game of Russian roulette with seniors’ healthcare.”
Perhaps a game of “chicken” would be more apt.
Republicans have dared Democrats to spend the billions for a more lasting solution—in the absence of any cuts elsewhere in the healthcare delivery system—and be labeled as fiscally irresponsible. In turn, Democrats have dared Republicans to let the rate cut take effect and be labeled heartless as Medicare beneficiaries lose access to their healthcare providers.
Both parties blinked, resorting to almost unanimous short-term fixes that have allowed legislators to save face while putting off politically risky votes until after the November elections.
Lynne M. Allen, MN, ARNP, who works as a part-time hospitalist in hematology-oncology at 188-bed Kadlec Regional Medical Center in Richland, Wash., says she and other colleagues were initially hopeful that the Obama administration would make Congress work together to find a lasting solution. “There’s a sense of frustration because instead of that happening from our legislators, they’re playing a lot of games with the funding,” says Allen, a member of Team Hospitalist. “They’re not willing to step up to the plate, as they say, and make a decision that will allow us to go forward smoothly.”
The result, Allen says, has been a “roller-coaster ride” of uncertainty over reimbursements. Because Washington’s Tri-Cities region has a relatively high percentage of patients with private insurance, her hospital is somewhat cushioned from a precipitous drop in Medicare fees. But if CMS is ever forced to cut back on its rates, she fully expects private insurers to follow the same downward track.
Practical Concerns
Barbara Hartley, MD, a part-time hospitalist at 22-bed Benson Hospital in Benson, Ariz., says the town’s healthcare facility is somewhat protected from potential Medicare rate cuts through its official status as a Critical Access Hospital. Instead of being reimbursed through diagnosis-related group (DRG) codes, the rural hospital is repaid by Medicare for its total cost per day per patient.
The arrangement is a stable one at the moment, but not enough to dispel Dr. Hartley’s uneasy question: If the economy worsens, will Medicare be able to retain its commitment to rural hospitals? If not, the pain might be felt acutely in communities like Benson, where Dr. Hartley estimates that as much as 75% of the hospital’s in-patient business is through either Medicare or a Medicare Advantage plan.
Kirk Mathews, CEO of St. Louis-based Inpatient Management Inc. and a member of SHM’s Public Policy and Practice Management committees, says Medicare rate cuts also could significantly reduce the leverage of hospitalists during contract negotiations.
“Even if we’re employed by the hospital, but our professional fees that the hospital can recoup for our services are dramatically affected, it will affect how those future contracts go,” Mathews says. “We might be insulated temporarily by the strength of our current contract. But if the formula—however that works out—dramatically impacts the hospitalist reimbursement on the professional fee side, the hospital will feel that, and then hospitalists will eventually feel that as well.” In other words, it could strengthen the bargaining hand of the hospital at the expense of the hospitalist. “Therein lies the long-term threat,” he points out.
Independent Solution?
Some of the authority over physician payments might eventually be depoliticized via language in the reform legislation that empowers a new entity, the Independent Payment Advisory Board, to create policy on such critical monetary issues as reimbursement rates. Congress could still override the board’s policy decisions, but only if the Congressional alternative saves just as much money.
In the meantime, the money for a fix still has to come from somewhere, and no consensus has emerged. Advocates likewise refuse to coalesce around any single alternative. Some experts favor a new formula based on the Medicare economic index, which measures inflation in healthcare delivery costs. But the CBO estimates that per-beneficiary spending under such a formula would be 30% more by 2016 than under the current formula. Other proposals call for temporarily increasing rates, then reverting to annual GDP growth, plus a bit more to cover physician costs.
No matter how the crisis is resolved, experts say, doctors almost certainly will have to make do with less. “When healthcare reform is finally fully implemented, there are going to be less dollars to pay for more services. It’s inevitable,” Mathews says. “And whether it takes the form of SGR or some other form, I’m afraid physicians are going to have to get used to having less money in the pool of money that’s allocated to pay providers.”
It could be a whole new ballgame. TH
Bryn Nelson, PhD, is a freelance medical writer based in Seattle.
Baseball, kick the can, Russian roulette—pick your game. Chances are good that it has worked its way into a metaphor to illustrate the infuriating, perplexing, and altogether frustrating inability of Congress to step up to the plate and pass a long-term fix to the broken sustainable growth rate (SGR) formula used to determine Medicare reimbursement rates.
On June 24, legislators avoided catastrophe by temporarily rescinding a 21.3% rate cut that went into effect June 1. The after-the-fact patch meant that some Medicare claims had to be reprocessed to recoup the full value, creating an administrative mess. The accompanying 2.2% rate increase expires Nov. 30. The reimbursement cut could reach nearly 30% next year unless Congress intervenes again.
“Obviously, there’s a lot of frustration around the issue, especially on the membership side,” says Ron Greeno, MD, FACP, SFHM, a member of SHM’s Public Policy and Leadership committees, and chief medical officer for Brentwood, Tenn.-based Cogent Healthcare. For hospitalists in many small private practices, he says, a major percentage of income comes from Medicare. “It’s a tremendous headache,” he says of the uncertainty. “It’s very hard to plan for. You’re trying to budget and you don’t know what the policy is going to be literally from week to week.”
The Blame Game
Despite the widespread sentiment among doctors that a permanent reimbursement rate fix should have been included in the healthcare reform legislation, skittishness over the price tag led legislators to drop it from the package. Based on last fall’s estimates, the total cost of a reform bill that scrapped the SGR would have ballooned by roughly $250 billion over 10 years, which would have threatened the bill’s passage.
But Congress has since been unable to pass a permanent fix as standalone legislation amid mounting concern over the national debt, and the price of inaction continues to rise. On April 30, the Congressional Budget Office (CBO) estimated that the cost of jettisoning the SGR formula and freezing rates at current levels had grown to $276 billion over 10 years.
Any serious consideration of lasting alternatives has now been pushed back to the lame-duck session, after the midterm elections. The can has been kicked down the road so many times, Dr. Greeno and others say, that most Congressional members have boot marks all over them. “So now you have a bigger problem at a more crucial time, when money is tighter than ever in a poor economy,” Dr. Greeno says. “And I just think it’s been a failure of our politicians.”
Other healthcare industry leaders have been just as critical. “Delaying the problem is not a solution,” said AMA President Cecil B. Wilson, MD, in a prepared statement after Congress passed the latest six-month reprieve in June. “It doesn’t solve the Medicare mess Congress has created with a long series of short-term Medicare patches over the last decade—including four to avert the 2010 cut alone.”
AMA-sponsored print ads have reminded legislators that delaying a fix until 2013 will again increase its cost, to $396 billion over 10 years. And the association’s June press release asserted that “Congress is playing a dangerous game of Russian roulette with seniors’ healthcare.”
Perhaps a game of “chicken” would be more apt.
Republicans have dared Democrats to spend the billions for a more lasting solution—in the absence of any cuts elsewhere in the healthcare delivery system—and be labeled as fiscally irresponsible. In turn, Democrats have dared Republicans to let the rate cut take effect and be labeled heartless as Medicare beneficiaries lose access to their healthcare providers.
Both parties blinked, resorting to almost unanimous short-term fixes that have allowed legislators to save face while putting off politically risky votes until after the November elections.
Lynne M. Allen, MN, ARNP, who works as a part-time hospitalist in hematology-oncology at 188-bed Kadlec Regional Medical Center in Richland, Wash., says she and other colleagues were initially hopeful that the Obama administration would make Congress work together to find a lasting solution. “There’s a sense of frustration because instead of that happening from our legislators, they’re playing a lot of games with the funding,” says Allen, a member of Team Hospitalist. “They’re not willing to step up to the plate, as they say, and make a decision that will allow us to go forward smoothly.”
The result, Allen says, has been a “roller-coaster ride” of uncertainty over reimbursements. Because Washington’s Tri-Cities region has a relatively high percentage of patients with private insurance, her hospital is somewhat cushioned from a precipitous drop in Medicare fees. But if CMS is ever forced to cut back on its rates, she fully expects private insurers to follow the same downward track.
Practical Concerns
Barbara Hartley, MD, a part-time hospitalist at 22-bed Benson Hospital in Benson, Ariz., says the town’s healthcare facility is somewhat protected from potential Medicare rate cuts through its official status as a Critical Access Hospital. Instead of being reimbursed through diagnosis-related group (DRG) codes, the rural hospital is repaid by Medicare for its total cost per day per patient.
The arrangement is a stable one at the moment, but not enough to dispel Dr. Hartley’s uneasy question: If the economy worsens, will Medicare be able to retain its commitment to rural hospitals? If not, the pain might be felt acutely in communities like Benson, where Dr. Hartley estimates that as much as 75% of the hospital’s in-patient business is through either Medicare or a Medicare Advantage plan.
Kirk Mathews, CEO of St. Louis-based Inpatient Management Inc. and a member of SHM’s Public Policy and Practice Management committees, says Medicare rate cuts also could significantly reduce the leverage of hospitalists during contract negotiations.
“Even if we’re employed by the hospital, but our professional fees that the hospital can recoup for our services are dramatically affected, it will affect how those future contracts go,” Mathews says. “We might be insulated temporarily by the strength of our current contract. But if the formula—however that works out—dramatically impacts the hospitalist reimbursement on the professional fee side, the hospital will feel that, and then hospitalists will eventually feel that as well.” In other words, it could strengthen the bargaining hand of the hospital at the expense of the hospitalist. “Therein lies the long-term threat,” he points out.
Independent Solution?
Some of the authority over physician payments might eventually be depoliticized via language in the reform legislation that empowers a new entity, the Independent Payment Advisory Board, to create policy on such critical monetary issues as reimbursement rates. Congress could still override the board’s policy decisions, but only if the Congressional alternative saves just as much money.
In the meantime, the money for a fix still has to come from somewhere, and no consensus has emerged. Advocates likewise refuse to coalesce around any single alternative. Some experts favor a new formula based on the Medicare economic index, which measures inflation in healthcare delivery costs. But the CBO estimates that per-beneficiary spending under such a formula would be 30% more by 2016 than under the current formula. Other proposals call for temporarily increasing rates, then reverting to annual GDP growth, plus a bit more to cover physician costs.
No matter how the crisis is resolved, experts say, doctors almost certainly will have to make do with less. “When healthcare reform is finally fully implemented, there are going to be less dollars to pay for more services. It’s inevitable,” Mathews says. “And whether it takes the form of SGR or some other form, I’m afraid physicians are going to have to get used to having less money in the pool of money that’s allocated to pay providers.”
It could be a whole new ballgame. TH
Bryn Nelson, PhD, is a freelance medical writer based in Seattle.
Hospital-Acquired Condition (HAC) Guidelines Produce $20M in Medicare Savings

How much has Medicare saved by not paying hospitals when patients get infections?
Hugh Black, DO
Charlotte, N.C.
Dr. Hospitalist responds: Since 2007, the Centers for Medicare and Medicaid Services (CMS) has tried to reduce the number of high-cost, hospital-acquired conditions (HACs), including infections, by encouraging providers to adhere to evidence-based guidelines. Some examples of these hospital-acquired conditions include:
- Catheter-associated urinary tract infections;
- Foreign objects retained after surgery; and
- Stage III and IV pressure ulcers.
CMS requires that acute-care hospitals, “effective with discharges occurring on or after Oct. 1, 2007, submit information on Medicare claims specifying whether diagnoses were present on admission.” Effective Oct. 1, 2008, Medicare no longer pays for charges associated with these HACs. So, if a Medicare beneficiary developed a Stage III pressure ulcer during his stay at an acute-care hospital, CMS would not pay for the incremental cost of the care associated with the “HAC.”
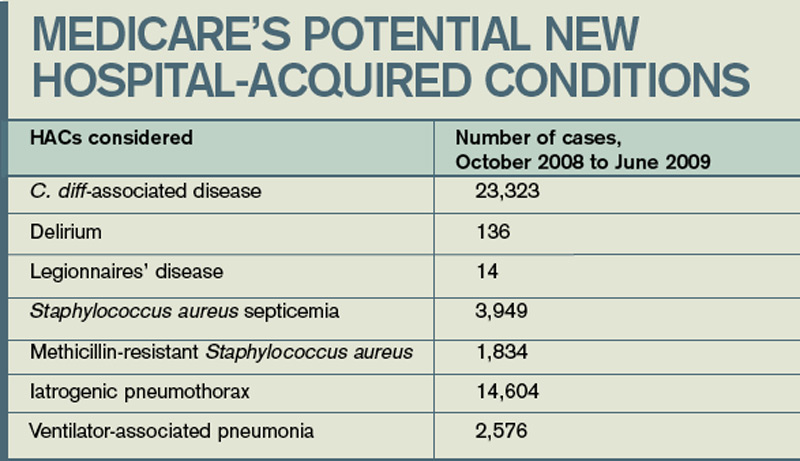
The U.S. government, in the May 4, 2010, edition of the Federal Register, reviewed the impact of this program. The data are based on Medicare claims data from October 2008 to June 2009. During this period of time, there were approximately 7.17 million acute-care hospital Medicare discharges.
The total net savings during this nine-month period for all HACs was $16.4 million. Three HACs (Stage III and IV pressure ulcers, DVT/PE after orthopedic procedure, and falls and trauma) accounted for more than $15.1 million in savings. Pro-rated for a 12-month period, the total net savings for all HACs would exceed $20 million.
Falls and trauma accounted for 34% of all HACs reported (11,253), followed by vascular catheter-associated infection (16%) and catheter-associated UTIs (16%). Air embolism and mediastinitis after CABG were the least recorded HACs; both were less than .01% if the total.
The goal is that, over time, with improvement in care, there would be a decrease in the number of hospital discharges where these conditions would be present. Therefore, the net savings would be expected to decline.
Medicare has considered a number of other HACs for this program, and reviewed the numbers of these conditions over the same nine-month period (see “Medicare’s Potential New Hospital-Acquired Conditions,” above). Despite some large numbers, CMS has stated it’s not proposing to add or remove HAC categories at this time. If you are interested in reviewing the entire report, visit http://edocket.access.gpo.gov/2010/pdf/ 2010-9163.pdf. TH
How much has Medicare saved by not paying hospitals when patients get infections?
Hugh Black, DO
Charlotte, N.C.
Dr. Hospitalist responds: Since 2007, the Centers for Medicare and Medicaid Services (CMS) has tried to reduce the number of high-cost, hospital-acquired conditions (HACs), including infections, by encouraging providers to adhere to evidence-based guidelines. Some examples of these hospital-acquired conditions include:
- Catheter-associated urinary tract infections;
- Foreign objects retained after surgery; and
- Stage III and IV pressure ulcers.
CMS requires that acute-care hospitals, “effective with discharges occurring on or after Oct. 1, 2007, submit information on Medicare claims specifying whether diagnoses were present on admission.” Effective Oct. 1, 2008, Medicare no longer pays for charges associated with these HACs. So, if a Medicare beneficiary developed a Stage III pressure ulcer during his stay at an acute-care hospital, CMS would not pay for the incremental cost of the care associated with the “HAC.”
The U.S. government, in the May 4, 2010, edition of the Federal Register, reviewed the impact of this program. The data are based on Medicare claims data from October 2008 to June 2009. During this period of time, there were approximately 7.17 million acute-care hospital Medicare discharges.
The total net savings during this nine-month period for all HACs was $16.4 million. Three HACs (Stage III and IV pressure ulcers, DVT/PE after orthopedic procedure, and falls and trauma) accounted for more than $15.1 million in savings. Pro-rated for a 12-month period, the total net savings for all HACs would exceed $20 million.
Falls and trauma accounted for 34% of all HACs reported (11,253), followed by vascular catheter-associated infection (16%) and catheter-associated UTIs (16%). Air embolism and mediastinitis after CABG were the least recorded HACs; both were less than .01% if the total.
The goal is that, over time, with improvement in care, there would be a decrease in the number of hospital discharges where these conditions would be present. Therefore, the net savings would be expected to decline.
Medicare has considered a number of other HACs for this program, and reviewed the numbers of these conditions over the same nine-month period (see “Medicare’s Potential New Hospital-Acquired Conditions,” above). Despite some large numbers, CMS has stated it’s not proposing to add or remove HAC categories at this time. If you are interested in reviewing the entire report, visit http://edocket.access.gpo.gov/2010/pdf/ 2010-9163.pdf. TH
How much has Medicare saved by not paying hospitals when patients get infections?
Hugh Black, DO
Charlotte, N.C.
Dr. Hospitalist responds: Since 2007, the Centers for Medicare and Medicaid Services (CMS) has tried to reduce the number of high-cost, hospital-acquired conditions (HACs), including infections, by encouraging providers to adhere to evidence-based guidelines. Some examples of these hospital-acquired conditions include:
- Catheter-associated urinary tract infections;
- Foreign objects retained after surgery; and
- Stage III and IV pressure ulcers.
CMS requires that acute-care hospitals, “effective with discharges occurring on or after Oct. 1, 2007, submit information on Medicare claims specifying whether diagnoses were present on admission.” Effective Oct. 1, 2008, Medicare no longer pays for charges associated with these HACs. So, if a Medicare beneficiary developed a Stage III pressure ulcer during his stay at an acute-care hospital, CMS would not pay for the incremental cost of the care associated with the “HAC.”
The U.S. government, in the May 4, 2010, edition of the Federal Register, reviewed the impact of this program. The data are based on Medicare claims data from October 2008 to June 2009. During this period of time, there were approximately 7.17 million acute-care hospital Medicare discharges.
The total net savings during this nine-month period for all HACs was $16.4 million. Three HACs (Stage III and IV pressure ulcers, DVT/PE after orthopedic procedure, and falls and trauma) accounted for more than $15.1 million in savings. Pro-rated for a 12-month period, the total net savings for all HACs would exceed $20 million.
Falls and trauma accounted for 34% of all HACs reported (11,253), followed by vascular catheter-associated infection (16%) and catheter-associated UTIs (16%). Air embolism and mediastinitis after CABG were the least recorded HACs; both were less than .01% if the total.
The goal is that, over time, with improvement in care, there would be a decrease in the number of hospital discharges where these conditions would be present. Therefore, the net savings would be expected to decline.
Medicare has considered a number of other HACs for this program, and reviewed the numbers of these conditions over the same nine-month period (see “Medicare’s Potential New Hospital-Acquired Conditions,” above). Despite some large numbers, CMS has stated it’s not proposing to add or remove HAC categories at this time. If you are interested in reviewing the entire report, visit http://edocket.access.gpo.gov/2010/pdf/ 2010-9163.pdf. TH
The Coming Challenges—and Opportunities—of Value-Based Purchasing
The Coming Challenges—and Opportunities—of Value-Based Purchasing
The Patient Protection and Affordable Care Act was signed into law in March, furthering the federal government’s commitment to increasing the efficiency of the U.S. healthcare system by decreasing cost and improving quality. An expansion of the “value-based purchasing” model, this law mandates that ratings and reimbursements to physicians and hospitals be increasingly tied to measured quality of care.
In this system, a physician’s quality profile will be determined by a variety of factors, including reported quality data, severity-adjusted clinical outcome measures, patient-safety indicators, and hospital-acquired conditions (HACs). Since all of these are, to a large extent, documentation issues, physicians are now forced to pay close attention to how they identify and describe diagnoses and procedures.
Medicare will, in effect, attempt to determine: “Did the clinical team correctly identify and appropriately treat all relevant patient conditions—without causing any adverse conditions—and do so safely, efficiently, and with good outcomes?”
The patient chart must “tell the story” of the episode of care in the hospital. It must accurately describe all of the patient’s conditions and demonstrate the complexity of medical decision-making and establishment of risk. Upon discharge, this risk must “match up” with the diagnoses that are being coded and the Medicare Severity Diagnostic Related Group (MS-DRGs) being assigned. Often, the information is present in the chart but is inconsistent from provider to provider, or documented in a way that is misunderstood by hospital coders.
If successful in improving our documentation skills, the reward will be a higher rating and increased reimbursement.
Medicare also is ramping up its claims denial and recovery business to help “clean up” the system. This includes the national rollout of the Recovery Audit Contactor (RAC) initiative (see “Attention to Detail,” April 2010, p. 1), as well as the new Medicare administrative contractors (MACs). Both rely on accurate documentation. The RACs will penalize hospitals and physicians financially for documentation lacking in specificity and accuracy; the MACs will deny payment for claims erroneously submitted (technical errors) or lacking documentation of medical necessity.
What makes many physicians even more uncomfortable in this new environment is that Medicare is striving to better align the priorities and financial incentives of hospitals and physicians. Alliances between the two are strongly encouraged through such programs as the Acute Care Episode (ACE) Demonstration Project (the precursor to hospital-physician bundled payments), and the establishment of accountable care organizations (ACOs).
This emerging environment presents a unique set of challenges and opportunities to HM groups. Hospitalists are historically more aligned with hospital administrations, as compared with most other specialties. Hospitalists also are asked to participate in the care of an increasingly large percentage of patients across all specialties. This could well be an opportunity to be rewarded for embracing both of these trends.
Hospitalists are uniquely positioned to function as the documentation improvement clinical team leaders, working closely with other physicians across all specialties and the administration to fulfill all documentation requirements—and to be rewarded for doing so. Though hospitalists should have a general understanding of the language and rules of documentation, a system must be in place that helps them identify and capture all the pertinent aspects of the medical record without the need to become coders themselves. To this end, a clinical documentation improvement (CDI) program is critical.
But it might not be enough.
What is needed is a clinical integration program, an enhancement of traditional CDI. This approach requires participation from ED physicians, along with clinical integration specialists, to document accurately and completely from the start. The clinical integration specialist ensures that medical necessity for inpatient admission and patient risk is being addressed and established, conditions are appropriately identified as being present on admission (POA), and all diagnoses are properly recognized and documented thoroughly and accurately. Clinical integration through collaborative documentation then continues throughout the hospitalization, with diagnostic authority and oversight from the hospitalist, all the way through discharge.
Hospitalists should welcome and champion this type of program. As documentation becomes the key to survival, a complete medical record will stand up to any and all scrutiny by Medicare or others.
As for the negatives, there are none.
Andrew H. Dombro, MD, national medical director, and Paul Weygandt, MD, JD, vice president of physician services, J.A. Thomas & Associates, Atlanta
The Coming Challenges—and Opportunities—of Value-Based Purchasing
The Patient Protection and Affordable Care Act was signed into law in March, furthering the federal government’s commitment to increasing the efficiency of the U.S. healthcare system by decreasing cost and improving quality. An expansion of the “value-based purchasing” model, this law mandates that ratings and reimbursements to physicians and hospitals be increasingly tied to measured quality of care.
In this system, a physician’s quality profile will be determined by a variety of factors, including reported quality data, severity-adjusted clinical outcome measures, patient-safety indicators, and hospital-acquired conditions (HACs). Since all of these are, to a large extent, documentation issues, physicians are now forced to pay close attention to how they identify and describe diagnoses and procedures.
Medicare will, in effect, attempt to determine: “Did the clinical team correctly identify and appropriately treat all relevant patient conditions—without causing any adverse conditions—and do so safely, efficiently, and with good outcomes?”
The patient chart must “tell the story” of the episode of care in the hospital. It must accurately describe all of the patient’s conditions and demonstrate the complexity of medical decision-making and establishment of risk. Upon discharge, this risk must “match up” with the diagnoses that are being coded and the Medicare Severity Diagnostic Related Group (MS-DRGs) being assigned. Often, the information is present in the chart but is inconsistent from provider to provider, or documented in a way that is misunderstood by hospital coders.
If successful in improving our documentation skills, the reward will be a higher rating and increased reimbursement.
Medicare also is ramping up its claims denial and recovery business to help “clean up” the system. This includes the national rollout of the Recovery Audit Contactor (RAC) initiative (see “Attention to Detail,” April 2010, p. 1), as well as the new Medicare administrative contractors (MACs). Both rely on accurate documentation. The RACs will penalize hospitals and physicians financially for documentation lacking in specificity and accuracy; the MACs will deny payment for claims erroneously submitted (technical errors) or lacking documentation of medical necessity.
What makes many physicians even more uncomfortable in this new environment is that Medicare is striving to better align the priorities and financial incentives of hospitals and physicians. Alliances between the two are strongly encouraged through such programs as the Acute Care Episode (ACE) Demonstration Project (the precursor to hospital-physician bundled payments), and the establishment of accountable care organizations (ACOs).
This emerging environment presents a unique set of challenges and opportunities to HM groups. Hospitalists are historically more aligned with hospital administrations, as compared with most other specialties. Hospitalists also are asked to participate in the care of an increasingly large percentage of patients across all specialties. This could well be an opportunity to be rewarded for embracing both of these trends.
Hospitalists are uniquely positioned to function as the documentation improvement clinical team leaders, working closely with other physicians across all specialties and the administration to fulfill all documentation requirements—and to be rewarded for doing so. Though hospitalists should have a general understanding of the language and rules of documentation, a system must be in place that helps them identify and capture all the pertinent aspects of the medical record without the need to become coders themselves. To this end, a clinical documentation improvement (CDI) program is critical.
But it might not be enough.
What is needed is a clinical integration program, an enhancement of traditional CDI. This approach requires participation from ED physicians, along with clinical integration specialists, to document accurately and completely from the start. The clinical integration specialist ensures that medical necessity for inpatient admission and patient risk is being addressed and established, conditions are appropriately identified as being present on admission (POA), and all diagnoses are properly recognized and documented thoroughly and accurately. Clinical integration through collaborative documentation then continues throughout the hospitalization, with diagnostic authority and oversight from the hospitalist, all the way through discharge.
Hospitalists should welcome and champion this type of program. As documentation becomes the key to survival, a complete medical record will stand up to any and all scrutiny by Medicare or others.
As for the negatives, there are none.
Andrew H. Dombro, MD, national medical director, and Paul Weygandt, MD, JD, vice president of physician services, J.A. Thomas & Associates, Atlanta
The Coming Challenges—and Opportunities—of Value-Based Purchasing
The Patient Protection and Affordable Care Act was signed into law in March, furthering the federal government’s commitment to increasing the efficiency of the U.S. healthcare system by decreasing cost and improving quality. An expansion of the “value-based purchasing” model, this law mandates that ratings and reimbursements to physicians and hospitals be increasingly tied to measured quality of care.
In this system, a physician’s quality profile will be determined by a variety of factors, including reported quality data, severity-adjusted clinical outcome measures, patient-safety indicators, and hospital-acquired conditions (HACs). Since all of these are, to a large extent, documentation issues, physicians are now forced to pay close attention to how they identify and describe diagnoses and procedures.
Medicare will, in effect, attempt to determine: “Did the clinical team correctly identify and appropriately treat all relevant patient conditions—without causing any adverse conditions—and do so safely, efficiently, and with good outcomes?”
The patient chart must “tell the story” of the episode of care in the hospital. It must accurately describe all of the patient’s conditions and demonstrate the complexity of medical decision-making and establishment of risk. Upon discharge, this risk must “match up” with the diagnoses that are being coded and the Medicare Severity Diagnostic Related Group (MS-DRGs) being assigned. Often, the information is present in the chart but is inconsistent from provider to provider, or documented in a way that is misunderstood by hospital coders.
If successful in improving our documentation skills, the reward will be a higher rating and increased reimbursement.
Medicare also is ramping up its claims denial and recovery business to help “clean up” the system. This includes the national rollout of the Recovery Audit Contactor (RAC) initiative (see “Attention to Detail,” April 2010, p. 1), as well as the new Medicare administrative contractors (MACs). Both rely on accurate documentation. The RACs will penalize hospitals and physicians financially for documentation lacking in specificity and accuracy; the MACs will deny payment for claims erroneously submitted (technical errors) or lacking documentation of medical necessity.
What makes many physicians even more uncomfortable in this new environment is that Medicare is striving to better align the priorities and financial incentives of hospitals and physicians. Alliances between the two are strongly encouraged through such programs as the Acute Care Episode (ACE) Demonstration Project (the precursor to hospital-physician bundled payments), and the establishment of accountable care organizations (ACOs).
This emerging environment presents a unique set of challenges and opportunities to HM groups. Hospitalists are historically more aligned with hospital administrations, as compared with most other specialties. Hospitalists also are asked to participate in the care of an increasingly large percentage of patients across all specialties. This could well be an opportunity to be rewarded for embracing both of these trends.
Hospitalists are uniquely positioned to function as the documentation improvement clinical team leaders, working closely with other physicians across all specialties and the administration to fulfill all documentation requirements—and to be rewarded for doing so. Though hospitalists should have a general understanding of the language and rules of documentation, a system must be in place that helps them identify and capture all the pertinent aspects of the medical record without the need to become coders themselves. To this end, a clinical documentation improvement (CDI) program is critical.
But it might not be enough.
What is needed is a clinical integration program, an enhancement of traditional CDI. This approach requires participation from ED physicians, along with clinical integration specialists, to document accurately and completely from the start. The clinical integration specialist ensures that medical necessity for inpatient admission and patient risk is being addressed and established, conditions are appropriately identified as being present on admission (POA), and all diagnoses are properly recognized and documented thoroughly and accurately. Clinical integration through collaborative documentation then continues throughout the hospitalization, with diagnostic authority and oversight from the hospitalist, all the way through discharge.
Hospitalists should welcome and champion this type of program. As documentation becomes the key to survival, a complete medical record will stand up to any and all scrutiny by Medicare or others.
As for the negatives, there are none.
Andrew H. Dombro, MD, national medical director, and Paul Weygandt, MD, JD, vice president of physician services, J.A. Thomas & Associates, Atlanta
Radical vs. Sensible

Hospital medicine had grown rapidly and provided the platform for change in our nation’s hospitals long before there was any meaningful healthcare legislation in Washington. With President Obama’s appointment of an innovator—Don Berwick—to head the Centers for Medicare and Medicaid Services (CMS), there is increased opportunity to ramp up revisions, large and small, to provide the incentives and the impetus to create a healthcare system for the 21st century.
With that in mind, I thought I’d offer a few ideas that Don could institute on Day 1, which could start us in the right direction, or throw us all into chaos, depending on how it plays out. While most of my attention is directed to the Medicare population, all of these ideas would be equally applicable to the commercially insured population.
Advanced Directives
We all know that too few people in this country have taken the opportunity to discuss with their families and their personal physicians how they want their care managed at critical junctures, whether it comes on suddenly with an accident or with aging. The suggestion that Medicare would pay for an office visit with your doctor to discuss this imploded with the news media’s fanning of the “death panel” flames first stoked by Sarah Palin, which sidetracked all rational discussion.
Besides setting up people for unwarranted and unwanted assaults and protracted misery, mismanaging the end stages of life leads to an enormous misallocation of physicians’ focus at a time when we all need to be mindful stewards of our limited healthcare resources.
It is acceptable if, after careful consideration, anyone chooses to not have any advanced directive, but it should be a cognitive directed choice, not just a failure to engage.
Therefore, I am proposing that Medicare offer an incentive (e.g., waiving co-payments or deductibles) to have all Medicare beneficiaries complete an advanced directive annually, or sign a form indicating they were offered an advanced directive and declined to have one invoked. In addition, Medicare could set up a system that would allow physicians (or facilities) who would manage the patient’s healthcare to have access to the conditions of the advance directives. The forms could be attached to individual Medicare profiles, possibly on the Web, in addition to being held by a patient’s PCP or medical home, if they have one.
Personal Health Records
Most people in this country can access most of the information about their personal financial status in real time from any computer in the world. Less than 10% of Americans can retrieve meaningful personal medical information. This is in spite of the prevalence of Web-based personal health record (PHR) software from Microsoft, Revolution Health, and other software vendors, along with Kaiser Permanente and a handful of insurance companies.
PHRs allow for an initial baseline set of data to be recorded and updated as new tests, diagnoses, and medications are employed. It allows for a composite knowledge of what has been tried in the past and what is being utilized in the present. This can be under patients’ control, but it would allow for appropriate access at times of acute need (e.g., an ED visit or a hospital admission).
Too often, patients with a long-term relationship with a local PCP present to the hospital and all of the healthcare professionals are forced to make critical decisions in the first few hours with insufficient or inaccurate information. This leads to needless repetition of tests or inability to compare current data with previous data (wouldn’t it be nice to have the last EKG or labs?), or in retrying a treatment regimen that hasn’t worked in the past.
And if you are in another city or if you don’t have a local physician with all of your old records, the information gap is far worse.
Once again, we could incentivize patients to have an up-to-date PHR with reduced premiums, or lower deductibles or copayments. We could look for ways to incentivize PCPs and hospitals to help patients build and maintain their PHR. We could make it a matter of course that a patient’s PHR would be updated at each intersection with healthcare information (e.g., the pharmacy or the lab or each office visit).
Physician Accountability
Somehow, we have evolved into a fragmented health system. We need to repair the disconnect between patients and physicians. The professional pact between the patient and their primary physician needs to be in place until the patient and the “next” physician agree to the handoff of responsibility. As hospitalists, we see this at both ends of the continuum. Patients shouldn’t just be “sent” to the ED or the hospital, especially not when they are acutely ill. Their personal physician, their medical home, should “arrange” for an orderly transfer of care. This would involve a transfer of information (possibly facilitated by an updated PHR), but as much by the assurance that the accepting physician or institution is prepared for the handoff, acknowledges this to the PCP, and that the patient understands the handoff has taken place.
In the same way, patients would not be just “sent out” from the hospital. The treating physician (it could be the hospitalist, but also the surgeon or cardiologist) would remain the doctor of record—the first resource for patients’ question and issues—until another “receiving” physician has accepted the handoff, acknowledges this role, and the patient agrees.
We could rapidly shift this process by allowing the patient to decide when the hospitalization has ended. We could change the system overnight by making one of the conditions for payment for a hospitalization (to the physicians and the hospital) that the patient has signed off that indeed the hospitalization has ended.
This might include a discussion of chronic medications to continue, acute therapies to complete, understanding by the patient of where and when to receive follow-up testing and evaluation, and a clear understanding of which physician is now accountable for future issues and questions as patients travel from acute illness to normal function.
There certainly are economic and societal issues. Not everyone has a PCP or can pay for their outpatient care, and this could be a full-employment plan for liability attorneys, but in the end I am confident medical professionals would create the linkages that would minimize the deep white space patients find themselves in once they are wheeled to the front door of their hospitals.
Creatively Complete the Hospitalization
In a perfect world, everyone would have a functional, robust medical home to return to after an acute hospitalization. Unfortunately, a patient-centered medical home (PCMH) is much more of a hope than a reality for most Americans. While we are working to create a better “horizontal” hospitalization, there are clear gaps in the vertical-care world.
If we are going to be responsible for bundled care that encompasses pre-admit and post-discharge care (e.g., 30 days after discharge), then we must beef up our outpatient capabilities.
Hopefully in the long run, this can be supplied by a reinvigorated and reinvented medical home, but it is still a long way off. If payment and accountability continue to blur just when the hospitalization ends, then hospitals (and hospitalists) and Medicare and insurers will need to be creative in how and who will manage the patient. We’ll need to solve the issues around patients who are no longer sick enough to require a hospital bed but clearly are not back to their steady state.
This ties in with the accountability gap that vexes our patients every day. Very likely, hospitalists will have to assume a role in managing the patients after hospital discharge. This might take the form of a few follow-up visits and continued support systems via the Web and telephone. It will probably require a new class of hospitalist—the ambulist or the subacutist—supported by dedicated ancillary staff and systems.
Once again, Medicare and insurers can drive to a better system of post-acute care by supplying incentives: a more robust discharge payment or rewarding successful completion of a hospitalization, possibly by bundled payment incentives. In addition, there could be clear standards set that would define when this is done well with associated rewards.
I know some of these ideas are radical and make us uncomfortable. They seem to assign more responsibilities to an already overburdened profession. To be successful, these innovations require an active participation and accountability of our patients. We as the providers of healthcare cannot do this alone. It also requires the evolution of the hospital as an institution from just the healthcare provider for the acutely ill, horizontal patient, but as more a part of a continuum from acute illness to return to function. And it cries out for a robust, capable, outpatient partner in a medical home or accountable care organization (ACO) that is equally dedicated, incentivized, and accountable.
We won’t get there tomorrow, even if Dr. Berwick reads this and acts on all of the ideas on his first day at CMS.
But if we don’t get started, we know we definitely won’t get there at any time in our future. TH
Dr. Wellikson is CEO of SHM.
Hospital medicine had grown rapidly and provided the platform for change in our nation’s hospitals long before there was any meaningful healthcare legislation in Washington. With President Obama’s appointment of an innovator—Don Berwick—to head the Centers for Medicare and Medicaid Services (CMS), there is increased opportunity to ramp up revisions, large and small, to provide the incentives and the impetus to create a healthcare system for the 21st century.
With that in mind, I thought I’d offer a few ideas that Don could institute on Day 1, which could start us in the right direction, or throw us all into chaos, depending on how it plays out. While most of my attention is directed to the Medicare population, all of these ideas would be equally applicable to the commercially insured population.
Advanced Directives
We all know that too few people in this country have taken the opportunity to discuss with their families and their personal physicians how they want their care managed at critical junctures, whether it comes on suddenly with an accident or with aging. The suggestion that Medicare would pay for an office visit with your doctor to discuss this imploded with the news media’s fanning of the “death panel” flames first stoked by Sarah Palin, which sidetracked all rational discussion.
Besides setting up people for unwarranted and unwanted assaults and protracted misery, mismanaging the end stages of life leads to an enormous misallocation of physicians’ focus at a time when we all need to be mindful stewards of our limited healthcare resources.
It is acceptable if, after careful consideration, anyone chooses to not have any advanced directive, but it should be a cognitive directed choice, not just a failure to engage.
Therefore, I am proposing that Medicare offer an incentive (e.g., waiving co-payments or deductibles) to have all Medicare beneficiaries complete an advanced directive annually, or sign a form indicating they were offered an advanced directive and declined to have one invoked. In addition, Medicare could set up a system that would allow physicians (or facilities) who would manage the patient’s healthcare to have access to the conditions of the advance directives. The forms could be attached to individual Medicare profiles, possibly on the Web, in addition to being held by a patient’s PCP or medical home, if they have one.
Personal Health Records
Most people in this country can access most of the information about their personal financial status in real time from any computer in the world. Less than 10% of Americans can retrieve meaningful personal medical information. This is in spite of the prevalence of Web-based personal health record (PHR) software from Microsoft, Revolution Health, and other software vendors, along with Kaiser Permanente and a handful of insurance companies.
PHRs allow for an initial baseline set of data to be recorded and updated as new tests, diagnoses, and medications are employed. It allows for a composite knowledge of what has been tried in the past and what is being utilized in the present. This can be under patients’ control, but it would allow for appropriate access at times of acute need (e.g., an ED visit or a hospital admission).
Too often, patients with a long-term relationship with a local PCP present to the hospital and all of the healthcare professionals are forced to make critical decisions in the first few hours with insufficient or inaccurate information. This leads to needless repetition of tests or inability to compare current data with previous data (wouldn’t it be nice to have the last EKG or labs?), or in retrying a treatment regimen that hasn’t worked in the past.
And if you are in another city or if you don’t have a local physician with all of your old records, the information gap is far worse.
Once again, we could incentivize patients to have an up-to-date PHR with reduced premiums, or lower deductibles or copayments. We could look for ways to incentivize PCPs and hospitals to help patients build and maintain their PHR. We could make it a matter of course that a patient’s PHR would be updated at each intersection with healthcare information (e.g., the pharmacy or the lab or each office visit).
Physician Accountability
Somehow, we have evolved into a fragmented health system. We need to repair the disconnect between patients and physicians. The professional pact between the patient and their primary physician needs to be in place until the patient and the “next” physician agree to the handoff of responsibility. As hospitalists, we see this at both ends of the continuum. Patients shouldn’t just be “sent” to the ED or the hospital, especially not when they are acutely ill. Their personal physician, their medical home, should “arrange” for an orderly transfer of care. This would involve a transfer of information (possibly facilitated by an updated PHR), but as much by the assurance that the accepting physician or institution is prepared for the handoff, acknowledges this to the PCP, and that the patient understands the handoff has taken place.
In the same way, patients would not be just “sent out” from the hospital. The treating physician (it could be the hospitalist, but also the surgeon or cardiologist) would remain the doctor of record—the first resource for patients’ question and issues—until another “receiving” physician has accepted the handoff, acknowledges this role, and the patient agrees.
We could rapidly shift this process by allowing the patient to decide when the hospitalization has ended. We could change the system overnight by making one of the conditions for payment for a hospitalization (to the physicians and the hospital) that the patient has signed off that indeed the hospitalization has ended.
This might include a discussion of chronic medications to continue, acute therapies to complete, understanding by the patient of where and when to receive follow-up testing and evaluation, and a clear understanding of which physician is now accountable for future issues and questions as patients travel from acute illness to normal function.
There certainly are economic and societal issues. Not everyone has a PCP or can pay for their outpatient care, and this could be a full-employment plan for liability attorneys, but in the end I am confident medical professionals would create the linkages that would minimize the deep white space patients find themselves in once they are wheeled to the front door of their hospitals.
Creatively Complete the Hospitalization
In a perfect world, everyone would have a functional, robust medical home to return to after an acute hospitalization. Unfortunately, a patient-centered medical home (PCMH) is much more of a hope than a reality for most Americans. While we are working to create a better “horizontal” hospitalization, there are clear gaps in the vertical-care world.
If we are going to be responsible for bundled care that encompasses pre-admit and post-discharge care (e.g., 30 days after discharge), then we must beef up our outpatient capabilities.
Hopefully in the long run, this can be supplied by a reinvigorated and reinvented medical home, but it is still a long way off. If payment and accountability continue to blur just when the hospitalization ends, then hospitals (and hospitalists) and Medicare and insurers will need to be creative in how and who will manage the patient. We’ll need to solve the issues around patients who are no longer sick enough to require a hospital bed but clearly are not back to their steady state.
This ties in with the accountability gap that vexes our patients every day. Very likely, hospitalists will have to assume a role in managing the patients after hospital discharge. This might take the form of a few follow-up visits and continued support systems via the Web and telephone. It will probably require a new class of hospitalist—the ambulist or the subacutist—supported by dedicated ancillary staff and systems.
Once again, Medicare and insurers can drive to a better system of post-acute care by supplying incentives: a more robust discharge payment or rewarding successful completion of a hospitalization, possibly by bundled payment incentives. In addition, there could be clear standards set that would define when this is done well with associated rewards.
I know some of these ideas are radical and make us uncomfortable. They seem to assign more responsibilities to an already overburdened profession. To be successful, these innovations require an active participation and accountability of our patients. We as the providers of healthcare cannot do this alone. It also requires the evolution of the hospital as an institution from just the healthcare provider for the acutely ill, horizontal patient, but as more a part of a continuum from acute illness to return to function. And it cries out for a robust, capable, outpatient partner in a medical home or accountable care organization (ACO) that is equally dedicated, incentivized, and accountable.
We won’t get there tomorrow, even if Dr. Berwick reads this and acts on all of the ideas on his first day at CMS.
But if we don’t get started, we know we definitely won’t get there at any time in our future. TH
Dr. Wellikson is CEO of SHM.
Hospital medicine had grown rapidly and provided the platform for change in our nation’s hospitals long before there was any meaningful healthcare legislation in Washington. With President Obama’s appointment of an innovator—Don Berwick—to head the Centers for Medicare and Medicaid Services (CMS), there is increased opportunity to ramp up revisions, large and small, to provide the incentives and the impetus to create a healthcare system for the 21st century.
With that in mind, I thought I’d offer a few ideas that Don could institute on Day 1, which could start us in the right direction, or throw us all into chaos, depending on how it plays out. While most of my attention is directed to the Medicare population, all of these ideas would be equally applicable to the commercially insured population.
Advanced Directives
We all know that too few people in this country have taken the opportunity to discuss with their families and their personal physicians how they want their care managed at critical junctures, whether it comes on suddenly with an accident or with aging. The suggestion that Medicare would pay for an office visit with your doctor to discuss this imploded with the news media’s fanning of the “death panel” flames first stoked by Sarah Palin, which sidetracked all rational discussion.
Besides setting up people for unwarranted and unwanted assaults and protracted misery, mismanaging the end stages of life leads to an enormous misallocation of physicians’ focus at a time when we all need to be mindful stewards of our limited healthcare resources.
It is acceptable if, after careful consideration, anyone chooses to not have any advanced directive, but it should be a cognitive directed choice, not just a failure to engage.
Therefore, I am proposing that Medicare offer an incentive (e.g., waiving co-payments or deductibles) to have all Medicare beneficiaries complete an advanced directive annually, or sign a form indicating they were offered an advanced directive and declined to have one invoked. In addition, Medicare could set up a system that would allow physicians (or facilities) who would manage the patient’s healthcare to have access to the conditions of the advance directives. The forms could be attached to individual Medicare profiles, possibly on the Web, in addition to being held by a patient’s PCP or medical home, if they have one.
Personal Health Records
Most people in this country can access most of the information about their personal financial status in real time from any computer in the world. Less than 10% of Americans can retrieve meaningful personal medical information. This is in spite of the prevalence of Web-based personal health record (PHR) software from Microsoft, Revolution Health, and other software vendors, along with Kaiser Permanente and a handful of insurance companies.
PHRs allow for an initial baseline set of data to be recorded and updated as new tests, diagnoses, and medications are employed. It allows for a composite knowledge of what has been tried in the past and what is being utilized in the present. This can be under patients’ control, but it would allow for appropriate access at times of acute need (e.g., an ED visit or a hospital admission).
Too often, patients with a long-term relationship with a local PCP present to the hospital and all of the healthcare professionals are forced to make critical decisions in the first few hours with insufficient or inaccurate information. This leads to needless repetition of tests or inability to compare current data with previous data (wouldn’t it be nice to have the last EKG or labs?), or in retrying a treatment regimen that hasn’t worked in the past.
And if you are in another city or if you don’t have a local physician with all of your old records, the information gap is far worse.
Once again, we could incentivize patients to have an up-to-date PHR with reduced premiums, or lower deductibles or copayments. We could look for ways to incentivize PCPs and hospitals to help patients build and maintain their PHR. We could make it a matter of course that a patient’s PHR would be updated at each intersection with healthcare information (e.g., the pharmacy or the lab or each office visit).
Physician Accountability
Somehow, we have evolved into a fragmented health system. We need to repair the disconnect between patients and physicians. The professional pact between the patient and their primary physician needs to be in place until the patient and the “next” physician agree to the handoff of responsibility. As hospitalists, we see this at both ends of the continuum. Patients shouldn’t just be “sent” to the ED or the hospital, especially not when they are acutely ill. Their personal physician, their medical home, should “arrange” for an orderly transfer of care. This would involve a transfer of information (possibly facilitated by an updated PHR), but as much by the assurance that the accepting physician or institution is prepared for the handoff, acknowledges this to the PCP, and that the patient understands the handoff has taken place.
In the same way, patients would not be just “sent out” from the hospital. The treating physician (it could be the hospitalist, but also the surgeon or cardiologist) would remain the doctor of record—the first resource for patients’ question and issues—until another “receiving” physician has accepted the handoff, acknowledges this role, and the patient agrees.
We could rapidly shift this process by allowing the patient to decide when the hospitalization has ended. We could change the system overnight by making one of the conditions for payment for a hospitalization (to the physicians and the hospital) that the patient has signed off that indeed the hospitalization has ended.
This might include a discussion of chronic medications to continue, acute therapies to complete, understanding by the patient of where and when to receive follow-up testing and evaluation, and a clear understanding of which physician is now accountable for future issues and questions as patients travel from acute illness to normal function.
There certainly are economic and societal issues. Not everyone has a PCP or can pay for their outpatient care, and this could be a full-employment plan for liability attorneys, but in the end I am confident medical professionals would create the linkages that would minimize the deep white space patients find themselves in once they are wheeled to the front door of their hospitals.
Creatively Complete the Hospitalization
In a perfect world, everyone would have a functional, robust medical home to return to after an acute hospitalization. Unfortunately, a patient-centered medical home (PCMH) is much more of a hope than a reality for most Americans. While we are working to create a better “horizontal” hospitalization, there are clear gaps in the vertical-care world.
If we are going to be responsible for bundled care that encompasses pre-admit and post-discharge care (e.g., 30 days after discharge), then we must beef up our outpatient capabilities.
Hopefully in the long run, this can be supplied by a reinvigorated and reinvented medical home, but it is still a long way off. If payment and accountability continue to blur just when the hospitalization ends, then hospitals (and hospitalists) and Medicare and insurers will need to be creative in how and who will manage the patient. We’ll need to solve the issues around patients who are no longer sick enough to require a hospital bed but clearly are not back to their steady state.
This ties in with the accountability gap that vexes our patients every day. Very likely, hospitalists will have to assume a role in managing the patients after hospital discharge. This might take the form of a few follow-up visits and continued support systems via the Web and telephone. It will probably require a new class of hospitalist—the ambulist or the subacutist—supported by dedicated ancillary staff and systems.
Once again, Medicare and insurers can drive to a better system of post-acute care by supplying incentives: a more robust discharge payment or rewarding successful completion of a hospitalization, possibly by bundled payment incentives. In addition, there could be clear standards set that would define when this is done well with associated rewards.
I know some of these ideas are radical and make us uncomfortable. They seem to assign more responsibilities to an already overburdened profession. To be successful, these innovations require an active participation and accountability of our patients. We as the providers of healthcare cannot do this alone. It also requires the evolution of the hospital as an institution from just the healthcare provider for the acutely ill, horizontal patient, but as more a part of a continuum from acute illness to return to function. And it cries out for a robust, capable, outpatient partner in a medical home or accountable care organization (ACO) that is equally dedicated, incentivized, and accountable.
We won’t get there tomorrow, even if Dr. Berwick reads this and acts on all of the ideas on his first day at CMS.
But if we don’t get started, we know we definitely won’t get there at any time in our future. TH
Dr. Wellikson is CEO of SHM.