User login
Lost in Transition

It’s been nearly two decades since I graduated from medical school. I think back and I honestly do not remember any lectures about transitions of care.
During residency, I remember some attending physicians would insist that when I discharged patients from the hospital, the patients had to leave with post-discharge appointments in hand. Like any diligent intern, I did as I was told. I telephoned the administrative assistants in clinic and booked follow-up appointments for my patients. I always asked for the first available appointment. Why? Because that was what my senior resident told me to do. I suspect he learned that from his resident as well.
Sometimes the appointment was scheduled for the week following discharge; other times it was six months later. I honestly didn’t give it much thought. There was a blank on the discharge paperwork and I filled it in with a date and time. I was doing my job—or so I thought.
Can you imagine if someone just gave you a slip of paper today telling you when to show up to get your teeth cleaned without consulting your schedule? How about scheduling the oil change for your car at a garage 100 miles away? Seems pretty silly, doesn’t it? Nothing about it seems customer-centric or cost-efficient.
With such a system in place, why are we surprised when patients do not show up for their follow-up appointments? When the patient presents to the ED later and is readmitted to the hospital, we label them as “non-compliant” because they failed to show up for their follow-up appointment.
Inefficient, Ineffective, Inappropriate
There are multiple problems with the above situation. The first problem: Why are doctors calling to schedule follow-up appointments in the first place? Do we ask airline pilots to serve refreshments? I suppose they could, but I’d rather they concentrate on flying the plane. It also seems like an awful waste of money and resources when we could accomplish the same feat with less-expensive airline attendants who are better trained to interact with passengers.
At most teaching hospitals across the country, I suspect we still rely on trainees to book follow-up appointments for patients. At hospitals without trainees, I suspect some of this responsibility falls on nurses and unit coordinators. Again, I wonder how often these people are actually in a position to schedule an appointment that the patient is likely to keep—or whether they are filling in a box on a checklist like I used to do.
Common Problem?
How do other industries address this issue? Well, many utilize customer service representatives to help consumers book their appointments. Some industries have advanced software, which allows consumers to book their own appointment online. I have to tell you that I am chuckling as I write this. I’m chuckling not because this is funny—I am just amazed that something that is so common sense is not utilized consistently across the hospital industry. When was the last time you actually called a hotel to book a room? Most of us find it so much more convenient to book airline tickets or hotel rooms online.
If we were to create a system with the consumer’s satisfaction and cost in mind, would you rely on trainees, nurses, or unit coordinators to book follow-up appointments? I suppose Hypothetical System 2.0 would include consumer representatives speaking with patients to book appointments. Hypothetical System 3.0 would allow patients and/or a family member to book the appointment online.
I can tell you that folks at Beth Israel Deaconess Medical Center in Boston, where I work, have given this some thought. We are nowhere near a 3.0 version, but we do rely on professional appointment-makers to work with our hospitalized patients to book follow-up appointments. Inpatient providers put in the order online requesting follow-up appointments for their hospitalized patients. The online application asks the provider to specify the requests. Does the patient need follow-up with specialists, as well as their primary outpatient provider? The inpatient provider can specify the window of time in which they recommend follow-up for the patient. If I want my patient to follow up with their primary-care physician (PCP) within one week and with their cardiologist within two weeks, the appointment-maker will work with the patient and the respective doctors’ offices to make this happen. I am contacted only if any issues arise.
All of this information is provided to the patient with their other discharge paperwork. Some of you might be asking: How can the hospital afford to pay for this software and for the cadre of professional appointment-makers? I am wondering how hospitals can afford not to. It’s like worrying about the cost of a college degree until you realize how difficult it is trying to get a job without one.
Part of the PCP “access” problem we have in this country is due to the fact that not every patient shows up for scheduled appointments. Our appointment-makers minimize the “no show” rate because, by speaking with patients about their schedules, they are providing appointments to patients with knowledge that they are likely to make the appointment. One of the things we learned at Beth Israel was that our trainees were sometimes requesting appointments for patients within one week of discharge when I knew darn well that the patient was unlikely to make that appointment because the patient most likely would still be at rehab.
Prior to this system, we also had the occasional PCP who was upset because we booked their patient’s follow-up with a specialist who was outside that PCP’s “inner circle” of specialists. How in the world are any of us supposed to remember this information?
Well, our professional appointment-makers utilize this information as part of the algorithm they follow when booking appointments for patients. As our nation moves towards a value-based purchasing system for healthcare, we don’t need to recreate the wheel; we can adopt proven practices from other cost-effective industries—and we can improve customer satisfaction.
I am interested in hearing how appointments are arranged for your hospitalized patients. Send me your thoughts at [email protected].
Dr. Li is president of SHM.
It’s been nearly two decades since I graduated from medical school. I think back and I honestly do not remember any lectures about transitions of care.
During residency, I remember some attending physicians would insist that when I discharged patients from the hospital, the patients had to leave with post-discharge appointments in hand. Like any diligent intern, I did as I was told. I telephoned the administrative assistants in clinic and booked follow-up appointments for my patients. I always asked for the first available appointment. Why? Because that was what my senior resident told me to do. I suspect he learned that from his resident as well.
Sometimes the appointment was scheduled for the week following discharge; other times it was six months later. I honestly didn’t give it much thought. There was a blank on the discharge paperwork and I filled it in with a date and time. I was doing my job—or so I thought.
Can you imagine if someone just gave you a slip of paper today telling you when to show up to get your teeth cleaned without consulting your schedule? How about scheduling the oil change for your car at a garage 100 miles away? Seems pretty silly, doesn’t it? Nothing about it seems customer-centric or cost-efficient.
With such a system in place, why are we surprised when patients do not show up for their follow-up appointments? When the patient presents to the ED later and is readmitted to the hospital, we label them as “non-compliant” because they failed to show up for their follow-up appointment.
Inefficient, Ineffective, Inappropriate
There are multiple problems with the above situation. The first problem: Why are doctors calling to schedule follow-up appointments in the first place? Do we ask airline pilots to serve refreshments? I suppose they could, but I’d rather they concentrate on flying the plane. It also seems like an awful waste of money and resources when we could accomplish the same feat with less-expensive airline attendants who are better trained to interact with passengers.
At most teaching hospitals across the country, I suspect we still rely on trainees to book follow-up appointments for patients. At hospitals without trainees, I suspect some of this responsibility falls on nurses and unit coordinators. Again, I wonder how often these people are actually in a position to schedule an appointment that the patient is likely to keep—or whether they are filling in a box on a checklist like I used to do.
Common Problem?
How do other industries address this issue? Well, many utilize customer service representatives to help consumers book their appointments. Some industries have advanced software, which allows consumers to book their own appointment online. I have to tell you that I am chuckling as I write this. I’m chuckling not because this is funny—I am just amazed that something that is so common sense is not utilized consistently across the hospital industry. When was the last time you actually called a hotel to book a room? Most of us find it so much more convenient to book airline tickets or hotel rooms online.
If we were to create a system with the consumer’s satisfaction and cost in mind, would you rely on trainees, nurses, or unit coordinators to book follow-up appointments? I suppose Hypothetical System 2.0 would include consumer representatives speaking with patients to book appointments. Hypothetical System 3.0 would allow patients and/or a family member to book the appointment online.
I can tell you that folks at Beth Israel Deaconess Medical Center in Boston, where I work, have given this some thought. We are nowhere near a 3.0 version, but we do rely on professional appointment-makers to work with our hospitalized patients to book follow-up appointments. Inpatient providers put in the order online requesting follow-up appointments for their hospitalized patients. The online application asks the provider to specify the requests. Does the patient need follow-up with specialists, as well as their primary outpatient provider? The inpatient provider can specify the window of time in which they recommend follow-up for the patient. If I want my patient to follow up with their primary-care physician (PCP) within one week and with their cardiologist within two weeks, the appointment-maker will work with the patient and the respective doctors’ offices to make this happen. I am contacted only if any issues arise.
All of this information is provided to the patient with their other discharge paperwork. Some of you might be asking: How can the hospital afford to pay for this software and for the cadre of professional appointment-makers? I am wondering how hospitals can afford not to. It’s like worrying about the cost of a college degree until you realize how difficult it is trying to get a job without one.
Part of the PCP “access” problem we have in this country is due to the fact that not every patient shows up for scheduled appointments. Our appointment-makers minimize the “no show” rate because, by speaking with patients about their schedules, they are providing appointments to patients with knowledge that they are likely to make the appointment. One of the things we learned at Beth Israel was that our trainees were sometimes requesting appointments for patients within one week of discharge when I knew darn well that the patient was unlikely to make that appointment because the patient most likely would still be at rehab.
Prior to this system, we also had the occasional PCP who was upset because we booked their patient’s follow-up with a specialist who was outside that PCP’s “inner circle” of specialists. How in the world are any of us supposed to remember this information?
Well, our professional appointment-makers utilize this information as part of the algorithm they follow when booking appointments for patients. As our nation moves towards a value-based purchasing system for healthcare, we don’t need to recreate the wheel; we can adopt proven practices from other cost-effective industries—and we can improve customer satisfaction.
I am interested in hearing how appointments are arranged for your hospitalized patients. Send me your thoughts at [email protected].
Dr. Li is president of SHM.
It’s been nearly two decades since I graduated from medical school. I think back and I honestly do not remember any lectures about transitions of care.
During residency, I remember some attending physicians would insist that when I discharged patients from the hospital, the patients had to leave with post-discharge appointments in hand. Like any diligent intern, I did as I was told. I telephoned the administrative assistants in clinic and booked follow-up appointments for my patients. I always asked for the first available appointment. Why? Because that was what my senior resident told me to do. I suspect he learned that from his resident as well.
Sometimes the appointment was scheduled for the week following discharge; other times it was six months later. I honestly didn’t give it much thought. There was a blank on the discharge paperwork and I filled it in with a date and time. I was doing my job—or so I thought.
Can you imagine if someone just gave you a slip of paper today telling you when to show up to get your teeth cleaned without consulting your schedule? How about scheduling the oil change for your car at a garage 100 miles away? Seems pretty silly, doesn’t it? Nothing about it seems customer-centric or cost-efficient.
With such a system in place, why are we surprised when patients do not show up for their follow-up appointments? When the patient presents to the ED later and is readmitted to the hospital, we label them as “non-compliant” because they failed to show up for their follow-up appointment.
Inefficient, Ineffective, Inappropriate
There are multiple problems with the above situation. The first problem: Why are doctors calling to schedule follow-up appointments in the first place? Do we ask airline pilots to serve refreshments? I suppose they could, but I’d rather they concentrate on flying the plane. It also seems like an awful waste of money and resources when we could accomplish the same feat with less-expensive airline attendants who are better trained to interact with passengers.
At most teaching hospitals across the country, I suspect we still rely on trainees to book follow-up appointments for patients. At hospitals without trainees, I suspect some of this responsibility falls on nurses and unit coordinators. Again, I wonder how often these people are actually in a position to schedule an appointment that the patient is likely to keep—or whether they are filling in a box on a checklist like I used to do.
Common Problem?
How do other industries address this issue? Well, many utilize customer service representatives to help consumers book their appointments. Some industries have advanced software, which allows consumers to book their own appointment online. I have to tell you that I am chuckling as I write this. I’m chuckling not because this is funny—I am just amazed that something that is so common sense is not utilized consistently across the hospital industry. When was the last time you actually called a hotel to book a room? Most of us find it so much more convenient to book airline tickets or hotel rooms online.
If we were to create a system with the consumer’s satisfaction and cost in mind, would you rely on trainees, nurses, or unit coordinators to book follow-up appointments? I suppose Hypothetical System 2.0 would include consumer representatives speaking with patients to book appointments. Hypothetical System 3.0 would allow patients and/or a family member to book the appointment online.
I can tell you that folks at Beth Israel Deaconess Medical Center in Boston, where I work, have given this some thought. We are nowhere near a 3.0 version, but we do rely on professional appointment-makers to work with our hospitalized patients to book follow-up appointments. Inpatient providers put in the order online requesting follow-up appointments for their hospitalized patients. The online application asks the provider to specify the requests. Does the patient need follow-up with specialists, as well as their primary outpatient provider? The inpatient provider can specify the window of time in which they recommend follow-up for the patient. If I want my patient to follow up with their primary-care physician (PCP) within one week and with their cardiologist within two weeks, the appointment-maker will work with the patient and the respective doctors’ offices to make this happen. I am contacted only if any issues arise.
All of this information is provided to the patient with their other discharge paperwork. Some of you might be asking: How can the hospital afford to pay for this software and for the cadre of professional appointment-makers? I am wondering how hospitals can afford not to. It’s like worrying about the cost of a college degree until you realize how difficult it is trying to get a job without one.
Part of the PCP “access” problem we have in this country is due to the fact that not every patient shows up for scheduled appointments. Our appointment-makers minimize the “no show” rate because, by speaking with patients about their schedules, they are providing appointments to patients with knowledge that they are likely to make the appointment. One of the things we learned at Beth Israel was that our trainees were sometimes requesting appointments for patients within one week of discharge when I knew darn well that the patient was unlikely to make that appointment because the patient most likely would still be at rehab.
Prior to this system, we also had the occasional PCP who was upset because we booked their patient’s follow-up with a specialist who was outside that PCP’s “inner circle” of specialists. How in the world are any of us supposed to remember this information?
Well, our professional appointment-makers utilize this information as part of the algorithm they follow when booking appointments for patients. As our nation moves towards a value-based purchasing system for healthcare, we don’t need to recreate the wheel; we can adopt proven practices from other cost-effective industries—and we can improve customer satisfaction.
I am interested in hearing how appointments are arranged for your hospitalized patients. Send me your thoughts at [email protected].
Dr. Li is president of SHM.
New Jersey Hospital Funds Care-Transitions “Coach”
Robert Wood Johnson University Hospital in Hamilton, N.J., has partnered with Jewish Family and Children’s Services of Greater Mercer County to support care transitions for 350 chronically ill older patients. Patients will receive a transitions coach following hospital discharge for education, support, and encouragement to keep appointments with their physicians. This “coach” will develop a plan of care for the patient, making one hospital visit, one home visit, and three phone calls, says Joyce Schwarz, the hospital’s vice president of quality and the project’s director.
The hospital received a $300,000 grant under the New Jersey Health Initiative from the Robert Wood Johnson Foundation to use an evidence-based intervention to improve care transitions and reduce readmissions, acting as a bridge between hospital personnel and community physicians.
Robert Wood Johnson University Hospital in Hamilton, N.J., has partnered with Jewish Family and Children’s Services of Greater Mercer County to support care transitions for 350 chronically ill older patients. Patients will receive a transitions coach following hospital discharge for education, support, and encouragement to keep appointments with their physicians. This “coach” will develop a plan of care for the patient, making one hospital visit, one home visit, and three phone calls, says Joyce Schwarz, the hospital’s vice president of quality and the project’s director.
The hospital received a $300,000 grant under the New Jersey Health Initiative from the Robert Wood Johnson Foundation to use an evidence-based intervention to improve care transitions and reduce readmissions, acting as a bridge between hospital personnel and community physicians.
Robert Wood Johnson University Hospital in Hamilton, N.J., has partnered with Jewish Family and Children’s Services of Greater Mercer County to support care transitions for 350 chronically ill older patients. Patients will receive a transitions coach following hospital discharge for education, support, and encouragement to keep appointments with their physicians. This “coach” will develop a plan of care for the patient, making one hospital visit, one home visit, and three phone calls, says Joyce Schwarz, the hospital’s vice president of quality and the project’s director.
The hospital received a $300,000 grant under the New Jersey Health Initiative from the Robert Wood Johnson Foundation to use an evidence-based intervention to improve care transitions and reduce readmissions, acting as a bridge between hospital personnel and community physicians.
Joint Commission Launches Certification for Hospital Palliative Care
A new Joint Commission program offering advanced certification for hospital-based palliative-care services is accepting applications and conducting daylong surveys through the end of this month. As with the Joint Commission’s reviews of other specialty services (e.g. primary stroke centers), certification is narrower in scope, with service-specific evaluation of care and outcomes, than a full accreditation survey—which is an organizationwide evaluation of core processes and functions.
Advanced certification in palliative care is voluntary for the steadily growing number of acute-care hospitals offering palliative-care services (1,568, according to the latest count by the American Hospital Association), but the hospital seeking it must be accredited by the Joint Commission.1 Certification is intended for formal, defined, inpatient palliative care, whether dedicated units or consultation services, with the ability to direct clinical management of patients.
The core palliative-care team includes “licensed independent practitioners” (typically physicians), registered nurses, chaplains, and social workers.2 The service should follow palliative-care guidelines and evidence-based practice, and it must collect quality data on four performance measures—two of them clinical—and use these data to improve performance.
According to Michelle Sacco, the Joint Commission’s executive director for palliative care, evidence-based practice includes ensuring appropriate transitions to other community resources, such as hospices. She thinks the program is perfect for hospitalists, as HM increasingly is participating in palliative care in their hospitals. “This is also an opportunity to change the mindset that palliative care is for the end-stage only,” Sacco says.
Two-year certification costs $9,655, including the onsite review. For more information, visit the Joint Commission website (www.jointcommission.org/certification) or the Center to Advance Palliative Care’s site (www.capc.org).
References
- Palliative care in hospitals continues rapid growth for 10th straight year, according to latest analysis. Center to Advance Palliative Care website. Available at: www.capc.org/news-and-events/releases/07-14-11. Accessed Aug. 30, 2011.
- The National Consensus Project’s Clinical Practice Guidelines for Quality Palliative Care. The National Consensus Project website. Available at: www.nationalconsensusproject.org/. Accessed Aug. 31, 2011.
A new Joint Commission program offering advanced certification for hospital-based palliative-care services is accepting applications and conducting daylong surveys through the end of this month. As with the Joint Commission’s reviews of other specialty services (e.g. primary stroke centers), certification is narrower in scope, with service-specific evaluation of care and outcomes, than a full accreditation survey—which is an organizationwide evaluation of core processes and functions.
Advanced certification in palliative care is voluntary for the steadily growing number of acute-care hospitals offering palliative-care services (1,568, according to the latest count by the American Hospital Association), but the hospital seeking it must be accredited by the Joint Commission.1 Certification is intended for formal, defined, inpatient palliative care, whether dedicated units or consultation services, with the ability to direct clinical management of patients.
The core palliative-care team includes “licensed independent practitioners” (typically physicians), registered nurses, chaplains, and social workers.2 The service should follow palliative-care guidelines and evidence-based practice, and it must collect quality data on four performance measures—two of them clinical—and use these data to improve performance.
According to Michelle Sacco, the Joint Commission’s executive director for palliative care, evidence-based practice includes ensuring appropriate transitions to other community resources, such as hospices. She thinks the program is perfect for hospitalists, as HM increasingly is participating in palliative care in their hospitals. “This is also an opportunity to change the mindset that palliative care is for the end-stage only,” Sacco says.
Two-year certification costs $9,655, including the onsite review. For more information, visit the Joint Commission website (www.jointcommission.org/certification) or the Center to Advance Palliative Care’s site (www.capc.org).
References
- Palliative care in hospitals continues rapid growth for 10th straight year, according to latest analysis. Center to Advance Palliative Care website. Available at: www.capc.org/news-and-events/releases/07-14-11. Accessed Aug. 30, 2011.
- The National Consensus Project’s Clinical Practice Guidelines for Quality Palliative Care. The National Consensus Project website. Available at: www.nationalconsensusproject.org/. Accessed Aug. 31, 2011.
A new Joint Commission program offering advanced certification for hospital-based palliative-care services is accepting applications and conducting daylong surveys through the end of this month. As with the Joint Commission’s reviews of other specialty services (e.g. primary stroke centers), certification is narrower in scope, with service-specific evaluation of care and outcomes, than a full accreditation survey—which is an organizationwide evaluation of core processes and functions.
Advanced certification in palliative care is voluntary for the steadily growing number of acute-care hospitals offering palliative-care services (1,568, according to the latest count by the American Hospital Association), but the hospital seeking it must be accredited by the Joint Commission.1 Certification is intended for formal, defined, inpatient palliative care, whether dedicated units or consultation services, with the ability to direct clinical management of patients.
The core palliative-care team includes “licensed independent practitioners” (typically physicians), registered nurses, chaplains, and social workers.2 The service should follow palliative-care guidelines and evidence-based practice, and it must collect quality data on four performance measures—two of them clinical—and use these data to improve performance.
According to Michelle Sacco, the Joint Commission’s executive director for palliative care, evidence-based practice includes ensuring appropriate transitions to other community resources, such as hospices. She thinks the program is perfect for hospitalists, as HM increasingly is participating in palliative care in their hospitals. “This is also an opportunity to change the mindset that palliative care is for the end-stage only,” Sacco says.
Two-year certification costs $9,655, including the onsite review. For more information, visit the Joint Commission website (www.jointcommission.org/certification) or the Center to Advance Palliative Care’s site (www.capc.org).
References
- Palliative care in hospitals continues rapid growth for 10th straight year, according to latest analysis. Center to Advance Palliative Care website. Available at: www.capc.org/news-and-events/releases/07-14-11. Accessed Aug. 30, 2011.
- The National Consensus Project’s Clinical Practice Guidelines for Quality Palliative Care. The National Consensus Project website. Available at: www.nationalconsensusproject.org/. Accessed Aug. 31, 2011.
ONLINE EXCLUSIVE: A Discharge Solution—or Problem?
In a bit of counterintuition, an empty discharge lounge might be the most successful kind.
Christine Collins, executive director of patient access services at Brigham and Women’s Hospital in Boston, says that the lounge should be a service for discharged patients who have completed medical treatment, but who for some reason remain unable to leave the institution. Such cases can include waiting on a prescription from the pharmacy, or simply waiting on a relative or friend to arrive with transportation.
—Christine Collins, executive director, patient access services, Brigham and Women’s Hospital, Boston
She does not view Brigham’s discharge lounge, a room with lounge chairs and light meals that is staffed by a registered nurse, as the answer to the throughput conundrum hospitals across the country face each and every day. So when the lounge is empty, it means patients have been discharged without any hang-ups.
“It’s not a patient-care area,” Collins says. “They’re people that should be home.”
Some view discharge lounges as a potential aid in smoothing out the discharge process. In theory, patients ready to be medically discharged but unable to leave the hospital have a place to go. But keeping the patients in the building, and under the eye of a nurse, could create liability issues, says Ken Simone, DO, SFHM, president of Hospitalist and Practice Solutions in Veazie, Maine, and a member of Team Hospitalist. Dr. Simone also wonders how the lounge concept impacts patient satisfaction, as some could view it negatively if they’re told they have to sit in what could be construed as a back-end waiting room.
“People need to assess what they’re doing it for and is it really accomplishing what they want it to accomplish,” Collins says.
Discharge lounges “can’t be another nursing unit because a patient is supposed to be discharged. ... Whether you have a discharge lounge or not, you need to improve your systems so that the patients leave when they leave.”
Richard Quinn is a freelance writer based in New Jersey.
In a bit of counterintuition, an empty discharge lounge might be the most successful kind.
Christine Collins, executive director of patient access services at Brigham and Women’s Hospital in Boston, says that the lounge should be a service for discharged patients who have completed medical treatment, but who for some reason remain unable to leave the institution. Such cases can include waiting on a prescription from the pharmacy, or simply waiting on a relative or friend to arrive with transportation.
—Christine Collins, executive director, patient access services, Brigham and Women’s Hospital, Boston
She does not view Brigham’s discharge lounge, a room with lounge chairs and light meals that is staffed by a registered nurse, as the answer to the throughput conundrum hospitals across the country face each and every day. So when the lounge is empty, it means patients have been discharged without any hang-ups.
“It’s not a patient-care area,” Collins says. “They’re people that should be home.”
Some view discharge lounges as a potential aid in smoothing out the discharge process. In theory, patients ready to be medically discharged but unable to leave the hospital have a place to go. But keeping the patients in the building, and under the eye of a nurse, could create liability issues, says Ken Simone, DO, SFHM, president of Hospitalist and Practice Solutions in Veazie, Maine, and a member of Team Hospitalist. Dr. Simone also wonders how the lounge concept impacts patient satisfaction, as some could view it negatively if they’re told they have to sit in what could be construed as a back-end waiting room.
“People need to assess what they’re doing it for and is it really accomplishing what they want it to accomplish,” Collins says.
Discharge lounges “can’t be another nursing unit because a patient is supposed to be discharged. ... Whether you have a discharge lounge or not, you need to improve your systems so that the patients leave when they leave.”
Richard Quinn is a freelance writer based in New Jersey.
In a bit of counterintuition, an empty discharge lounge might be the most successful kind.
Christine Collins, executive director of patient access services at Brigham and Women’s Hospital in Boston, says that the lounge should be a service for discharged patients who have completed medical treatment, but who for some reason remain unable to leave the institution. Such cases can include waiting on a prescription from the pharmacy, or simply waiting on a relative or friend to arrive with transportation.
—Christine Collins, executive director, patient access services, Brigham and Women’s Hospital, Boston
She does not view Brigham’s discharge lounge, a room with lounge chairs and light meals that is staffed by a registered nurse, as the answer to the throughput conundrum hospitals across the country face each and every day. So when the lounge is empty, it means patients have been discharged without any hang-ups.
“It’s not a patient-care area,” Collins says. “They’re people that should be home.”
Some view discharge lounges as a potential aid in smoothing out the discharge process. In theory, patients ready to be medically discharged but unable to leave the hospital have a place to go. But keeping the patients in the building, and under the eye of a nurse, could create liability issues, says Ken Simone, DO, SFHM, president of Hospitalist and Practice Solutions in Veazie, Maine, and a member of Team Hospitalist. Dr. Simone also wonders how the lounge concept impacts patient satisfaction, as some could view it negatively if they’re told they have to sit in what could be construed as a back-end waiting room.
“People need to assess what they’re doing it for and is it really accomplishing what they want it to accomplish,” Collins says.
Discharge lounges “can’t be another nursing unit because a patient is supposed to be discharged. ... Whether you have a discharge lounge or not, you need to improve your systems so that the patients leave when they leave.”
Richard Quinn is a freelance writer based in New Jersey.
ONLINE EXCLUSIVE: Experts discuss strategies to improve early discharges
ONLINE EXCLUSIVE: The “Weak Link” in Patient Handoffs
Increased handoffs are often viewed as a byproduct of the growth in hospital medicine, with heightened scrutiny on the quality of communication that accompanies these transfers of care. As research suggests, though, finding and fixing the weak links can require persistence.
A study led by Siddhartha Singh, MD, MS, associate chief medical officer of Medical College Physicians, the adult practice for Medical College of Wisconsin in Milwaukee, compared a traditional, resident-based model of care to one involving a hospitalist-physician assistant team. Initially, his study found a 6% higher length of stay (LOS) for the hospitalist-physician assistant teams, with no differences in costs or readmission rates.1
But when the researchers pored over their results, they discovered that the increased LOS was limited to patients admitted overnight. Those patients, Dr. Singh says, were admitted by other providers—a night-float resident or faculty hospitalist—and then transferred to the hospitalist-physician assistant teams when they arrived in the morning. These “overflow patients” also were admitted only during busy periods, when limits on the number of admissions by house staff required other arrangements.
To make a direct comparison, Dr. Singh focused on a window from 11 a.m. to 4 p.m., when patients would have an equal probability of being admitted by a resident team or a hospitalist-physician assistant team. From a pool of about 3,000 admitted patients, the study found no significant difference in LOS, cost, readmission rates, or mortality. Instead of highlighting significant differences in models of care, then, Dr. Singh says, his study highlighted a potential weak link in the “treacherous” overnight-to-morning handoffs during busy periods that should be addressed.
“There have been a lot of studies implicating poor communication as a cause of patient-safety issues,” notes Sunil Kripalani, MD, MSc, FHM, chief of the section of hospital medicine and an associate professor of medicine at Vanderbilt University Medical Center in Nashville, Tenn. But fewer studies, he says, have shown how to effectively improve communication in a way that improves patient safety.
One focal point is the often incomplete and inadequate nature of discharge summaries. Several models are emerging on how to build a better discharge summary, Dr. Kripalani says, with researchers offering solid recommendations (as multiple presentations at SHM’s annual meeting suggest). The trick is ensuring that those plans can be implemented into practice on a consistent and timely basis.
Dr. Kripalani says at least one straightforward strategy might help improve handoffs, however: building time into the schedule for them, such as 15-minute overlaps between shifts.—BN
Increased handoffs are often viewed as a byproduct of the growth in hospital medicine, with heightened scrutiny on the quality of communication that accompanies these transfers of care. As research suggests, though, finding and fixing the weak links can require persistence.
A study led by Siddhartha Singh, MD, MS, associate chief medical officer of Medical College Physicians, the adult practice for Medical College of Wisconsin in Milwaukee, compared a traditional, resident-based model of care to one involving a hospitalist-physician assistant team. Initially, his study found a 6% higher length of stay (LOS) for the hospitalist-physician assistant teams, with no differences in costs or readmission rates.1
But when the researchers pored over their results, they discovered that the increased LOS was limited to patients admitted overnight. Those patients, Dr. Singh says, were admitted by other providers—a night-float resident or faculty hospitalist—and then transferred to the hospitalist-physician assistant teams when they arrived in the morning. These “overflow patients” also were admitted only during busy periods, when limits on the number of admissions by house staff required other arrangements.
To make a direct comparison, Dr. Singh focused on a window from 11 a.m. to 4 p.m., when patients would have an equal probability of being admitted by a resident team or a hospitalist-physician assistant team. From a pool of about 3,000 admitted patients, the study found no significant difference in LOS, cost, readmission rates, or mortality. Instead of highlighting significant differences in models of care, then, Dr. Singh says, his study highlighted a potential weak link in the “treacherous” overnight-to-morning handoffs during busy periods that should be addressed.
“There have been a lot of studies implicating poor communication as a cause of patient-safety issues,” notes Sunil Kripalani, MD, MSc, FHM, chief of the section of hospital medicine and an associate professor of medicine at Vanderbilt University Medical Center in Nashville, Tenn. But fewer studies, he says, have shown how to effectively improve communication in a way that improves patient safety.
One focal point is the often incomplete and inadequate nature of discharge summaries. Several models are emerging on how to build a better discharge summary, Dr. Kripalani says, with researchers offering solid recommendations (as multiple presentations at SHM’s annual meeting suggest). The trick is ensuring that those plans can be implemented into practice on a consistent and timely basis.
Dr. Kripalani says at least one straightforward strategy might help improve handoffs, however: building time into the schedule for them, such as 15-minute overlaps between shifts.—BN
Increased handoffs are often viewed as a byproduct of the growth in hospital medicine, with heightened scrutiny on the quality of communication that accompanies these transfers of care. As research suggests, though, finding and fixing the weak links can require persistence.
A study led by Siddhartha Singh, MD, MS, associate chief medical officer of Medical College Physicians, the adult practice for Medical College of Wisconsin in Milwaukee, compared a traditional, resident-based model of care to one involving a hospitalist-physician assistant team. Initially, his study found a 6% higher length of stay (LOS) for the hospitalist-physician assistant teams, with no differences in costs or readmission rates.1
But when the researchers pored over their results, they discovered that the increased LOS was limited to patients admitted overnight. Those patients, Dr. Singh says, were admitted by other providers—a night-float resident or faculty hospitalist—and then transferred to the hospitalist-physician assistant teams when they arrived in the morning. These “overflow patients” also were admitted only during busy periods, when limits on the number of admissions by house staff required other arrangements.
To make a direct comparison, Dr. Singh focused on a window from 11 a.m. to 4 p.m., when patients would have an equal probability of being admitted by a resident team or a hospitalist-physician assistant team. From a pool of about 3,000 admitted patients, the study found no significant difference in LOS, cost, readmission rates, or mortality. Instead of highlighting significant differences in models of care, then, Dr. Singh says, his study highlighted a potential weak link in the “treacherous” overnight-to-morning handoffs during busy periods that should be addressed.
“There have been a lot of studies implicating poor communication as a cause of patient-safety issues,” notes Sunil Kripalani, MD, MSc, FHM, chief of the section of hospital medicine and an associate professor of medicine at Vanderbilt University Medical Center in Nashville, Tenn. But fewer studies, he says, have shown how to effectively improve communication in a way that improves patient safety.
One focal point is the often incomplete and inadequate nature of discharge summaries. Several models are emerging on how to build a better discharge summary, Dr. Kripalani says, with researchers offering solid recommendations (as multiple presentations at SHM’s annual meeting suggest). The trick is ensuring that those plans can be implemented into practice on a consistent and timely basis.
Dr. Kripalani says at least one straightforward strategy might help improve handoffs, however: building time into the schedule for them, such as 15-minute overlaps between shifts.—BN
It Takes a Village
Gregory Misky, MD, has been a hospitalist for 12 years, first at a community hospital and for the past seven years at the University of Colorado Denver. In recent years, his frustration has grown over the challenges of discharge planning, care transitions, and preventing readmissions for vulnerable, disadvantaged patients, including the uninsured, underinsured, and medically indigent.
“There’s a big elephant in the room that we’re not talking about, and that elephant is having babies,” he says. “Access is such a big problem for these patients and, as a hospitalist, it’s just not OK to me anymore. I need to be proactive about finding solutions.”
Dr. Misky’s concerns led him to do research with mentor Eric Coleman, MD, the university’s creator of the Care Transitions Program (www.caretransitions.org), studying patients who lacked primary-care physicians (PCPs) or timely PCP follow-up, and their resulting higher rates of readmissions.1 Dr. Misky also helped develop care pathways, including post-discharge care, for VTE patients, a “common, costly, and dangerous” condition. He is working with a hospitalist colleague to explore how electronic health records (EHR) might be used to help trigger post-discharge follow-up for at-risk patients.
University of Colorado Hospital (UCH), a 425-bed urban academic tertiary-care center, is not the designated safety net hospital for metro Denver, yet 28% to 32% of patients discharged from its medical services are uninsured, Dr. Misky says. He finds that academic physicians at UCH are not always able to take on large numbers of uninsured patients in their clinics, given the productivity demands they face, while the hospital has not been able to participate in systemwide, comprehensive national models for improving care transitions, such as SHM’s Project BOOST (www.hospitalmedicine.org/boost) or Boston Medical Center’s Project RED (www.bu.edu/fammed/projectred/).
Dr. Misky is in discussions with local community services, such as the Metro Community Provider Network (MCPN) of clinics for underserved patients, and exploring the development of a collaborative model for integrating post-hospital care between UCH and MCPN. “A lot of our ideas are still very exploratory—trying to get the key providers to the table to talk about what these approaches might look like,” Dr. Misky explains. “I’ve been part of ongoing meetings, and I think similar kinds of conversations are happening at many levels at UCH, but there’s not a unified, consensus approach to care transitions—and that’s a problem. But I’m in the midst of it all, trying to highlight the issues and explore solutions.”
—Patricia Rutherford, RN, MS, vice president, Institute for Healthcare Improvement
Dr. Misky says every hospital-based provider—hospitalist, nurses, social workers—feels the same frustration and worry about the level of care when indigent patients are discharged to the community. Uninsured patients can run into problems post-hospitalization and return to the ED for their primary care because they lack other options, he says. “Without established liaisons to the community clinics,” he notes, “it can take three or four months for a new indigent patient to get seen at one.”
Disproportional Issues of the Uninsured
Hospitalists at San Francisco General Hospital, which is the safety-net provider for the Bay Area, are looking at similar issues, says Jeff Critchfield, MD, division chief of hospital medicine. “What we know about the uninsured is that they have a wealth of other challenges and barriers that they bring to the table,” he says. “First of all, un- and underinsured patients are more likely to have chronic illnesses, to be hospitalized for those illnesses, and then to be rehospitalized after discharge.”
Other issues disproportionally impacting uninsured or indigent patients include low literacy, low healthcare literacy, language barriers, cross-cultural barriers, substance abuse and mental health issues, homelessness or marginal housing, transportation barriers, and “social isolation, which also plagues our population and, I believe, places patients at risk, as does depression,” says Dr. Critchfield’s colleague Michelle Schneidermann, MD.
One-third of San Francisco General’s patients are uninsured and 40% have Medi-Cal (California’s version of Medicaid), which basically means they are underinsured.
“California has 19 safety-net hospitals, with 6% of the state’s inpatient beds but 50% of its uninsured population. So that’s what we do,” Dr. Critchfield says. But almost any hospital or hospitalist will see many of the same issues and problems, just not in the same proportions. “These are patients who can be most frustrating to hospitalists, requiring a disproportionate amount of our time,” he says, adding the greatest difficulty is helping these patients understand and follow post-discharge care plans. But if someone is ill enough to need acute hospitalization and is later discharged back to the street, readmission should not be a surprise. “We’ve done that experiment for many years, and we know how it turns out,” he says.
Dr. Schneidermann serves as medical director of San Francisco General’s medical respite program, a 45-bed emergency shelter that accepts homeless or marginally housed patients in need of follow-up care following discharge from any of the city’s acute-care hospitals. Research has shown that the programs can have a major effect on keeping discharged patients off the street, reducing their rates of rehospitalization by as much as 50%.2,3
“We know that homeless patients have longer lengths of hospital stay because their discharges are fraught with problems,” she says. A homeless patient hospitalized with a blood clot potentially could be kept in the hospital for a week while transitioning from heparin to Coumadin, while similar patients with community support might get discharged in a day.
“We are also fortunate to have a program called Healthy San Francisco,” which isn’t a health insurance program per se but since 2007 has provided access to outpatient, inpatient, and preventive care and medications for indigent patients, Dr. Schneidermann says. Sponsored by the city’s Department of Public Health, it is accessed through 32 medical homes located in both public and private clinics. The hospitalists’ goal is to have a follow-up appointment set with a receiving provider at the time of discharge. “It doesn’t always happen, but that’s the goal,” she explains. “Someone, by name, who has accepted the referral.”
Dr. Critchfield is running a randomized controlled trial of the hospital’s interventions to stem the tide of readmissions in patients 60 and older; many of these patients share the same indigent demographics of the rest of San Francisco General’s caseload, although most patients 65 and older qualify for Medicare. He describes the program as a hybrid of Project RED and Dr. Coleman’s Care Transitions Program, although it targets patients who speak English, Spanish, Cantonese, and Mandarin.
How many Americans are uninsured today is a moving target in the context of healthcare reform and its uncertain future, but the number increased to 53 million in 2007 from 42 million in 1998.4 The number of hospitalizations of uninsured patients also grew to 2.3 million from 1.8 million in the same time period, an increase of 31%, while total hospitalizations were increasing by 13%. A May 2011 research brief from the U.S. Department of Health and Human Services estimates that uncompensated costs of hospital care incurred for uninsured patients total $73 billion per year.5
The homeless in shelters or on the street number about 630,000 on any given evening, and 1.5 million Americans experienced homelessness last year, says Sabrina Edgington, MSSW, program and policy specialist at the National Health Care for the Homeless Council in Nashville, Tenn. That said, 30% of the U.S. homeless have health insurance. Uninsured patients are less likely to receive necessary diagnostic tests and labs while in the hospital, and they face limited access and longer wait times—even in the facilities that are willing to take them.7 Research published in the Journal of Hospital Medicine finds that uninsured or Medicaid patients with three common conditions are more likely to die in the hospital than insured patients.8 A 2008 national sample survey of physicians found that “most U.S. physicians limit their care of medically indigent patients.”9 Other recent research suggests that readmission rates are affected by race and by site of care—with hospitals serving a higher proportion of black patients also having higher readmission rates.10
“This is not a hospital problem—it’s a communitywide problem. So there’s not just a hospital solution; it will take the whole village,” says Patricia Rutherford, RN, MS, vice president of the Institute for Healthcare Improvement (IHI), which sponsors initiatives targeting care transitions.
The major national care-transitions programs that assist hospitals with addressing rehospitalizations all share similar objectives, Rutherford says, and all could be helpful in improving hospitals’ responses to indigent patients. The recognized programs include IHI’s STAAR (State Action on Avoidable Rehospitalizations: www.ihi.org/IHI/Programs), a multistate, multistakeholder quality improvement (QI) program; Project BOOST; Project RED; Dr. Coleman’s Care Transitions Project; the nursing-based Transitional Care Model (www.transitionalcare.info); and the American College of Cardiology’s Hospital to Home (www.cardiosource.org).

—Amy Boutwell, MD, MPP, hospitalist, Newton (Mass.) Wellesley Hospital, president, Collaborative Healthcare Strategies
Most of these “well-established, evidence-based interventions,” including BOOST, will be given preference in applications for grants from the federal Community-Based Care Transitions Program (CCTP). The program recently committed $500 million to support community-based coalitions that include hospitals that are working with community partners to create seamless care transitions. “It’s most important that hospitalists are integrally involved with these care-transition teams—if not leading them,” Rutherford says.
BOOST’s approach is built on a major change-management strategy to reconstruct hospitals’ care transitions and discharge processes from the ground up, says Tina Budnitz, MPH, the project’s director at SHM (see “Discharge Improvement,” p. 7.) “The first thing we do, we literally get out pens and paper and chart what happens before patients get into the hospital and what happens after they are discharged, all of the services that touch them—or should,” she says. “The planning process occurs on many levels, with all of the stakeholders in the community looking at the process map and seeing where people fall off and end up readmitted.”
—Jeff Critchfield, MD, division chief of hospital medicine, San Francisco General Hospital
SHM is planning to launch several new BOOST cohorts for participating hospitals this fall, along with a wider range of technical support, Budnitz says.
The Cross-Setting Team
Research on care transitions for uninsured or indigent patients “is not very robust,” observes Amy Boutwell, MD, MPP, a hospitalist at Newton Wellesley Hospital in Newton, Mass., former director of health policy at IHI and president of Collaborative Healthcare Strategies. “We don’t have the information we need, but there are great opportunities to improve our research base,” she explains.
Dr. Boutwell is a big fan of the “cross-setting team,” which brings together around a conference table professionals who work in different care settings, including the hospital, long-term care, and home-based care. She says it’s her job “to make sure patients are safe upon discharge, but if the community is under-resourced for primary-care physicians, if the patient is uninsured and we can’t find a PCP, the hospitalist and cross-setting team need to say, ‘We just can’t accept that.’ ”
What Do HM’s Community Partners Think About the Problem?

Lori J. Heim, MD, FAAFP, board chair of the American Academy of Family Physicians, a family physician in Vass, N.C., and hospitalist at Scotland Memorial Hospital in Laurinburg, N.C., says the unassigned patient who lacks a PCP might be the hardest issue to overcome in improving care transitions.
“We have a lot of members who volunteer at free clinics. Others are part of revolving lists of physicians willing to take unassigned call and accept referrals of indigent patients from the hospital,” Dr. Heim says. “If you look at the number of primary-care practices that are barely surviving, most hospitalists I know are very cognizant of how financially strapped family practice and general internist physicians are these days.”
It isn’t always clear who benefits financially from improved care transitions, particularly for indigent patients, Dr. Heim says. But the growth of patient-centered medical homes through the rollout of national healthcare reform, opportunities for community clinics to become those medical homes, and the wider dissemination of electronic medical records are all important components of the changes that need to take place.
“I would encourage hospitalists to be involved with their hospital leadership on these issues and have ongoing communication with community physicians. Both sides need to think more in terms of the systemic demands,” she says. “Often the ED doctor or the hospitalist knows about these issues and can help hospital leaders understand potential solutions for uninsured patients.–LB
A proper handoff should be done in a way that helps the patient and the physician providing the follow-up care. “But you won’t know what that is unless you ask the people you’re sending patients to how you’re doing,” she explains. “When we routinely review readmitted patients in cross-setting groups, it quickly breaks down the mindset that we in the hospital did everything we could have done to make the discharge successful.”
Dr. Boutwell recommends that hospitalists avoid thinking of these issues in a vacuum, as medical-clinical issues that only doctors can fix. “Because you can’t,” she says. “I would never ask an individual hospitalist to reduce readmissions. It requires a multidisciplinary, all-hands-on-deck approach by the hospital. This is different and more exciting than other quality-improvement efforts.” What’s more, she says, the day is coming—and soon—when failing to manage these readmissions will be a bad business proposition for the hospital (see “Value-Based Purchasing Raises the Stakes,” May 2011, p. 1).
IHI’s STAAR Initiative is working with coalitions of providers in Massachusetts, Michigan, Ohio, and Washington. One of those coalitions, Detroit CARR (Community Action to Reduce Rehospitalizations), convened by MPRO, a Michigan-based quality-improvement organization, is a great example of a cross-continuum team involving five inner-city hospitals, Dr. Boutwell says.
“CARR has really dug deeply into the needs of vulnerable patients in one of America’s most economically challenged communities, with a high proportion of Medicaid, uninsured, and disabled patients” and a shrinking population, she says. Many rehospitalizations are related to socio-economics. “The CARR coalition is meeting with the homeless shelters, the food pantries, and the faith-based agencies,” she says. “They’re really getting at the root of significant issues in their community.”
Nancy Vecchioni, RN, MSN, CPHQ, vice present of Medicare operations at MPRO, says CARR involves more than just healthcare providers; it also brings community agencies together with them to take ownership of the patient. Organizations that a year ago weren’t talking to each other are now meeting regularly to focus on the most vulnerable patients, reviewing cases of rehospitalized homeless patients, and sharing their experiences. Rehospitalized patients are being interviewed, using a prepared script (see Figure 1, p. 34), which allows the patient to tell their story. The information is shared within the coalition.
Each hospital has its own transition team, with post-acute providers, physicians, home health agencies, and community service providers, Vecchioni says. For patients who can’t get in to see a PCP within five days of discharge, some hospitals are opening continuity clinics. Others give patients three- to 30-day supplies of needed medications. “There’s no magic bullet—it’s just a different way of looking at how we do this work,” she adds. “Every day we see new barriers. But we’ve already seen a 5% overall reduction in readmissions. And I think hospitalists can be the champions and leaders of these efforts.”
Hospitalists have to raise the bar for themselves, Dr. Schneidermann says, “doing our best while recognizing we can only do so much. There is a lot we can learn from geriatrics, starting with truly embracing the multidisciplinary team.” If hospitalists feel like they are functioning in isolation, she says, they need to look around. “Are these kinds of interdisciplinary meetings happening? If so, join them. If not, light a fire. Convert your frustrating experiences with patients into action.” TH
Larry Beresford is a freelance medical writer based in California.
References
- Misky GJ, Wald HL, Coleman EA. Post-hospitalization transitions: Examining the effects of timing of primary care provider follow-up. J Hosp Med. 2010;5:392-397.
- Buchanan D, Doblin B, Sai T, Garcia P. The effects of respite care for homeless patients: a cohort study. Am J Public Health. 2006;96:1278-1281.
- Kertesz SG, Posner MA, O’Connell JJ, et al. Post-hospital medical respite care and hospital readmission of homeless persons. J Prev Inter Community. 2009;37:129-142.
- Nagamine M, Stocks C, Merrill C. Trends in uninsured hospital stays, 1998-2007. Health Care Cost & Utilization Project (HCUP) Statistical Brief #88. May 2010.
- U.S. Department of Health and Human Services. ASPE Research Brief. The value of health insurance: few of the uninsured have adequate resources to pay potential hospital bills. May 2011.
- U.S. Department of Housing and Urban Development. The Annual Housing Assessment Report to Congress, 2009.
- Kellerman A, Coleman M. Care without Coverage: Too Little, Too Late. Report by Institute of Medicine, May 2002.
- Hasan O, Orav EJ, Hicks LS. Insurance status and hospital care for myocardial infarction, stroke, and pneumonia. J Hosp Med. 2010;5(8):452-459.
- Chirayath HT, Wentworth AL. Constraints to caring: Service to medically indigent patients by allopathic and osteopathic physicians. J Health Care Poor Underserved. 2008;19:500-511.
- Joynt KE, Orav EJ, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305:675-681.
- Buchanan D, Rohr L, Kehoe L, Glick SB, Jain S. Changing attitudes toward homeless people. J Gen Intern Med. 2004;19(5 Pt 2):566-568.
Liability and Compliance Issues

Hospitalists and other experts say medical/legal liability for indigent patients resulting from readmissions has not been a major focus of their care-transitions initiatives. Even as bundled care models will give hospitals greater financial responsibility for episodes of care across settings, getting sued by patients is not said to be a major concern.
“What we try to do is put together the most robust plan of care that we can for patients, whether insured or not,” says Jeff Critchfield, MD, chief of hospital medicine and medical director of risk management at San Francisco General Hospital. “The tone of the conversation for patients without insurance is different—because the options are fewer. We may have to keep these patients longer because of the absence of options. But rarely does risk management come into it. We don’t get sued by these patients, so that’s not a driving force.”
State and local regulations and Medicare conditions of participation also define expectations for hospitals regarding the care of indigent patients who present at the hospital with acute medical needs. In Los Angeles, a controversy emerged in 2005 when several hospitals were accused of dumping homeless patients on skid row. Local governments responded by approving a $100 million plan to provide homeless shelters across Los Angeles County; in 2008, the same public officials passed an ordinance making it illegal for hospitals to discharge homeless patients to the streets without their consent.
There can be liability issues for any patient who gets transferred out of the hospital and the transition is not a good one, Dr. Critchfield adds, “but I try to think about this population the same as any other.”—LB
Gregory Misky, MD, has been a hospitalist for 12 years, first at a community hospital and for the past seven years at the University of Colorado Denver. In recent years, his frustration has grown over the challenges of discharge planning, care transitions, and preventing readmissions for vulnerable, disadvantaged patients, including the uninsured, underinsured, and medically indigent.
“There’s a big elephant in the room that we’re not talking about, and that elephant is having babies,” he says. “Access is such a big problem for these patients and, as a hospitalist, it’s just not OK to me anymore. I need to be proactive about finding solutions.”
Dr. Misky’s concerns led him to do research with mentor Eric Coleman, MD, the university’s creator of the Care Transitions Program (www.caretransitions.org), studying patients who lacked primary-care physicians (PCPs) or timely PCP follow-up, and their resulting higher rates of readmissions.1 Dr. Misky also helped develop care pathways, including post-discharge care, for VTE patients, a “common, costly, and dangerous” condition. He is working with a hospitalist colleague to explore how electronic health records (EHR) might be used to help trigger post-discharge follow-up for at-risk patients.
University of Colorado Hospital (UCH), a 425-bed urban academic tertiary-care center, is not the designated safety net hospital for metro Denver, yet 28% to 32% of patients discharged from its medical services are uninsured, Dr. Misky says. He finds that academic physicians at UCH are not always able to take on large numbers of uninsured patients in their clinics, given the productivity demands they face, while the hospital has not been able to participate in systemwide, comprehensive national models for improving care transitions, such as SHM’s Project BOOST (www.hospitalmedicine.org/boost) or Boston Medical Center’s Project RED (www.bu.edu/fammed/projectred/).
Dr. Misky is in discussions with local community services, such as the Metro Community Provider Network (MCPN) of clinics for underserved patients, and exploring the development of a collaborative model for integrating post-hospital care between UCH and MCPN. “A lot of our ideas are still very exploratory—trying to get the key providers to the table to talk about what these approaches might look like,” Dr. Misky explains. “I’ve been part of ongoing meetings, and I think similar kinds of conversations are happening at many levels at UCH, but there’s not a unified, consensus approach to care transitions—and that’s a problem. But I’m in the midst of it all, trying to highlight the issues and explore solutions.”
—Patricia Rutherford, RN, MS, vice president, Institute for Healthcare Improvement
Dr. Misky says every hospital-based provider—hospitalist, nurses, social workers—feels the same frustration and worry about the level of care when indigent patients are discharged to the community. Uninsured patients can run into problems post-hospitalization and return to the ED for their primary care because they lack other options, he says. “Without established liaisons to the community clinics,” he notes, “it can take three or four months for a new indigent patient to get seen at one.”
Disproportional Issues of the Uninsured
Hospitalists at San Francisco General Hospital, which is the safety-net provider for the Bay Area, are looking at similar issues, says Jeff Critchfield, MD, division chief of hospital medicine. “What we know about the uninsured is that they have a wealth of other challenges and barriers that they bring to the table,” he says. “First of all, un- and underinsured patients are more likely to have chronic illnesses, to be hospitalized for those illnesses, and then to be rehospitalized after discharge.”
Other issues disproportionally impacting uninsured or indigent patients include low literacy, low healthcare literacy, language barriers, cross-cultural barriers, substance abuse and mental health issues, homelessness or marginal housing, transportation barriers, and “social isolation, which also plagues our population and, I believe, places patients at risk, as does depression,” says Dr. Critchfield’s colleague Michelle Schneidermann, MD.
One-third of San Francisco General’s patients are uninsured and 40% have Medi-Cal (California’s version of Medicaid), which basically means they are underinsured.
“California has 19 safety-net hospitals, with 6% of the state’s inpatient beds but 50% of its uninsured population. So that’s what we do,” Dr. Critchfield says. But almost any hospital or hospitalist will see many of the same issues and problems, just not in the same proportions. “These are patients who can be most frustrating to hospitalists, requiring a disproportionate amount of our time,” he says, adding the greatest difficulty is helping these patients understand and follow post-discharge care plans. But if someone is ill enough to need acute hospitalization and is later discharged back to the street, readmission should not be a surprise. “We’ve done that experiment for many years, and we know how it turns out,” he says.
Dr. Schneidermann serves as medical director of San Francisco General’s medical respite program, a 45-bed emergency shelter that accepts homeless or marginally housed patients in need of follow-up care following discharge from any of the city’s acute-care hospitals. Research has shown that the programs can have a major effect on keeping discharged patients off the street, reducing their rates of rehospitalization by as much as 50%.2,3
“We know that homeless patients have longer lengths of hospital stay because their discharges are fraught with problems,” she says. A homeless patient hospitalized with a blood clot potentially could be kept in the hospital for a week while transitioning from heparin to Coumadin, while similar patients with community support might get discharged in a day.
“We are also fortunate to have a program called Healthy San Francisco,” which isn’t a health insurance program per se but since 2007 has provided access to outpatient, inpatient, and preventive care and medications for indigent patients, Dr. Schneidermann says. Sponsored by the city’s Department of Public Health, it is accessed through 32 medical homes located in both public and private clinics. The hospitalists’ goal is to have a follow-up appointment set with a receiving provider at the time of discharge. “It doesn’t always happen, but that’s the goal,” she explains. “Someone, by name, who has accepted the referral.”
Dr. Critchfield is running a randomized controlled trial of the hospital’s interventions to stem the tide of readmissions in patients 60 and older; many of these patients share the same indigent demographics of the rest of San Francisco General’s caseload, although most patients 65 and older qualify for Medicare. He describes the program as a hybrid of Project RED and Dr. Coleman’s Care Transitions Program, although it targets patients who speak English, Spanish, Cantonese, and Mandarin.
How many Americans are uninsured today is a moving target in the context of healthcare reform and its uncertain future, but the number increased to 53 million in 2007 from 42 million in 1998.4 The number of hospitalizations of uninsured patients also grew to 2.3 million from 1.8 million in the same time period, an increase of 31%, while total hospitalizations were increasing by 13%. A May 2011 research brief from the U.S. Department of Health and Human Services estimates that uncompensated costs of hospital care incurred for uninsured patients total $73 billion per year.5
The homeless in shelters or on the street number about 630,000 on any given evening, and 1.5 million Americans experienced homelessness last year, says Sabrina Edgington, MSSW, program and policy specialist at the National Health Care for the Homeless Council in Nashville, Tenn. That said, 30% of the U.S. homeless have health insurance. Uninsured patients are less likely to receive necessary diagnostic tests and labs while in the hospital, and they face limited access and longer wait times—even in the facilities that are willing to take them.7 Research published in the Journal of Hospital Medicine finds that uninsured or Medicaid patients with three common conditions are more likely to die in the hospital than insured patients.8 A 2008 national sample survey of physicians found that “most U.S. physicians limit their care of medically indigent patients.”9 Other recent research suggests that readmission rates are affected by race and by site of care—with hospitals serving a higher proportion of black patients also having higher readmission rates.10
“This is not a hospital problem—it’s a communitywide problem. So there’s not just a hospital solution; it will take the whole village,” says Patricia Rutherford, RN, MS, vice president of the Institute for Healthcare Improvement (IHI), which sponsors initiatives targeting care transitions.
The major national care-transitions programs that assist hospitals with addressing rehospitalizations all share similar objectives, Rutherford says, and all could be helpful in improving hospitals’ responses to indigent patients. The recognized programs include IHI’s STAAR (State Action on Avoidable Rehospitalizations: www.ihi.org/IHI/Programs), a multistate, multistakeholder quality improvement (QI) program; Project BOOST; Project RED; Dr. Coleman’s Care Transitions Project; the nursing-based Transitional Care Model (www.transitionalcare.info); and the American College of Cardiology’s Hospital to Home (www.cardiosource.org).
—Amy Boutwell, MD, MPP, hospitalist, Newton (Mass.) Wellesley Hospital, president, Collaborative Healthcare Strategies
Most of these “well-established, evidence-based interventions,” including BOOST, will be given preference in applications for grants from the federal Community-Based Care Transitions Program (CCTP). The program recently committed $500 million to support community-based coalitions that include hospitals that are working with community partners to create seamless care transitions. “It’s most important that hospitalists are integrally involved with these care-transition teams—if not leading them,” Rutherford says.
BOOST’s approach is built on a major change-management strategy to reconstruct hospitals’ care transitions and discharge processes from the ground up, says Tina Budnitz, MPH, the project’s director at SHM (see “Discharge Improvement,” p. 7.) “The first thing we do, we literally get out pens and paper and chart what happens before patients get into the hospital and what happens after they are discharged, all of the services that touch them—or should,” she says. “The planning process occurs on many levels, with all of the stakeholders in the community looking at the process map and seeing where people fall off and end up readmitted.”
—Jeff Critchfield, MD, division chief of hospital medicine, San Francisco General Hospital
SHM is planning to launch several new BOOST cohorts for participating hospitals this fall, along with a wider range of technical support, Budnitz says.
The Cross-Setting Team
Research on care transitions for uninsured or indigent patients “is not very robust,” observes Amy Boutwell, MD, MPP, a hospitalist at Newton Wellesley Hospital in Newton, Mass., former director of health policy at IHI and president of Collaborative Healthcare Strategies. “We don’t have the information we need, but there are great opportunities to improve our research base,” she explains.
Dr. Boutwell is a big fan of the “cross-setting team,” which brings together around a conference table professionals who work in different care settings, including the hospital, long-term care, and home-based care. She says it’s her job “to make sure patients are safe upon discharge, but if the community is under-resourced for primary-care physicians, if the patient is uninsured and we can’t find a PCP, the hospitalist and cross-setting team need to say, ‘We just can’t accept that.’ ”
What Do HM’s Community Partners Think About the Problem?
Lori J. Heim, MD, FAAFP, board chair of the American Academy of Family Physicians, a family physician in Vass, N.C., and hospitalist at Scotland Memorial Hospital in Laurinburg, N.C., says the unassigned patient who lacks a PCP might be the hardest issue to overcome in improving care transitions.
“We have a lot of members who volunteer at free clinics. Others are part of revolving lists of physicians willing to take unassigned call and accept referrals of indigent patients from the hospital,” Dr. Heim says. “If you look at the number of primary-care practices that are barely surviving, most hospitalists I know are very cognizant of how financially strapped family practice and general internist physicians are these days.”
It isn’t always clear who benefits financially from improved care transitions, particularly for indigent patients, Dr. Heim says. But the growth of patient-centered medical homes through the rollout of national healthcare reform, opportunities for community clinics to become those medical homes, and the wider dissemination of electronic medical records are all important components of the changes that need to take place.
“I would encourage hospitalists to be involved with their hospital leadership on these issues and have ongoing communication with community physicians. Both sides need to think more in terms of the systemic demands,” she says. “Often the ED doctor or the hospitalist knows about these issues and can help hospital leaders understand potential solutions for uninsured patients.–LB
A proper handoff should be done in a way that helps the patient and the physician providing the follow-up care. “But you won’t know what that is unless you ask the people you’re sending patients to how you’re doing,” she explains. “When we routinely review readmitted patients in cross-setting groups, it quickly breaks down the mindset that we in the hospital did everything we could have done to make the discharge successful.”
Dr. Boutwell recommends that hospitalists avoid thinking of these issues in a vacuum, as medical-clinical issues that only doctors can fix. “Because you can’t,” she says. “I would never ask an individual hospitalist to reduce readmissions. It requires a multidisciplinary, all-hands-on-deck approach by the hospital. This is different and more exciting than other quality-improvement efforts.” What’s more, she says, the day is coming—and soon—when failing to manage these readmissions will be a bad business proposition for the hospital (see “Value-Based Purchasing Raises the Stakes,” May 2011, p. 1).
IHI’s STAAR Initiative is working with coalitions of providers in Massachusetts, Michigan, Ohio, and Washington. One of those coalitions, Detroit CARR (Community Action to Reduce Rehospitalizations), convened by MPRO, a Michigan-based quality-improvement organization, is a great example of a cross-continuum team involving five inner-city hospitals, Dr. Boutwell says.
“CARR has really dug deeply into the needs of vulnerable patients in one of America’s most economically challenged communities, with a high proportion of Medicaid, uninsured, and disabled patients” and a shrinking population, she says. Many rehospitalizations are related to socio-economics. “The CARR coalition is meeting with the homeless shelters, the food pantries, and the faith-based agencies,” she says. “They’re really getting at the root of significant issues in their community.”
Nancy Vecchioni, RN, MSN, CPHQ, vice present of Medicare operations at MPRO, says CARR involves more than just healthcare providers; it also brings community agencies together with them to take ownership of the patient. Organizations that a year ago weren’t talking to each other are now meeting regularly to focus on the most vulnerable patients, reviewing cases of rehospitalized homeless patients, and sharing their experiences. Rehospitalized patients are being interviewed, using a prepared script (see Figure 1, p. 34), which allows the patient to tell their story. The information is shared within the coalition.
Each hospital has its own transition team, with post-acute providers, physicians, home health agencies, and community service providers, Vecchioni says. For patients who can’t get in to see a PCP within five days of discharge, some hospitals are opening continuity clinics. Others give patients three- to 30-day supplies of needed medications. “There’s no magic bullet—it’s just a different way of looking at how we do this work,” she adds. “Every day we see new barriers. But we’ve already seen a 5% overall reduction in readmissions. And I think hospitalists can be the champions and leaders of these efforts.”
Hospitalists have to raise the bar for themselves, Dr. Schneidermann says, “doing our best while recognizing we can only do so much. There is a lot we can learn from geriatrics, starting with truly embracing the multidisciplinary team.” If hospitalists feel like they are functioning in isolation, she says, they need to look around. “Are these kinds of interdisciplinary meetings happening? If so, join them. If not, light a fire. Convert your frustrating experiences with patients into action.” TH
Larry Beresford is a freelance medical writer based in California.
References
- Misky GJ, Wald HL, Coleman EA. Post-hospitalization transitions: Examining the effects of timing of primary care provider follow-up. J Hosp Med. 2010;5:392-397.
- Buchanan D, Doblin B, Sai T, Garcia P. The effects of respite care for homeless patients: a cohort study. Am J Public Health. 2006;96:1278-1281.
- Kertesz SG, Posner MA, O’Connell JJ, et al. Post-hospital medical respite care and hospital readmission of homeless persons. J Prev Inter Community. 2009;37:129-142.
- Nagamine M, Stocks C, Merrill C. Trends in uninsured hospital stays, 1998-2007. Health Care Cost & Utilization Project (HCUP) Statistical Brief #88. May 2010.
- U.S. Department of Health and Human Services. ASPE Research Brief. The value of health insurance: few of the uninsured have adequate resources to pay potential hospital bills. May 2011.
- U.S. Department of Housing and Urban Development. The Annual Housing Assessment Report to Congress, 2009.
- Kellerman A, Coleman M. Care without Coverage: Too Little, Too Late. Report by Institute of Medicine, May 2002.
- Hasan O, Orav EJ, Hicks LS. Insurance status and hospital care for myocardial infarction, stroke, and pneumonia. J Hosp Med. 2010;5(8):452-459.
- Chirayath HT, Wentworth AL. Constraints to caring: Service to medically indigent patients by allopathic and osteopathic physicians. J Health Care Poor Underserved. 2008;19:500-511.
- Joynt KE, Orav EJ, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305:675-681.
- Buchanan D, Rohr L, Kehoe L, Glick SB, Jain S. Changing attitudes toward homeless people. J Gen Intern Med. 2004;19(5 Pt 2):566-568.
Liability and Compliance Issues
Hospitalists and other experts say medical/legal liability for indigent patients resulting from readmissions has not been a major focus of their care-transitions initiatives. Even as bundled care models will give hospitals greater financial responsibility for episodes of care across settings, getting sued by patients is not said to be a major concern.
“What we try to do is put together the most robust plan of care that we can for patients, whether insured or not,” says Jeff Critchfield, MD, chief of hospital medicine and medical director of risk management at San Francisco General Hospital. “The tone of the conversation for patients without insurance is different—because the options are fewer. We may have to keep these patients longer because of the absence of options. But rarely does risk management come into it. We don’t get sued by these patients, so that’s not a driving force.”
State and local regulations and Medicare conditions of participation also define expectations for hospitals regarding the care of indigent patients who present at the hospital with acute medical needs. In Los Angeles, a controversy emerged in 2005 when several hospitals were accused of dumping homeless patients on skid row. Local governments responded by approving a $100 million plan to provide homeless shelters across Los Angeles County; in 2008, the same public officials passed an ordinance making it illegal for hospitals to discharge homeless patients to the streets without their consent.
There can be liability issues for any patient who gets transferred out of the hospital and the transition is not a good one, Dr. Critchfield adds, “but I try to think about this population the same as any other.”—LB
Gregory Misky, MD, has been a hospitalist for 12 years, first at a community hospital and for the past seven years at the University of Colorado Denver. In recent years, his frustration has grown over the challenges of discharge planning, care transitions, and preventing readmissions for vulnerable, disadvantaged patients, including the uninsured, underinsured, and medically indigent.
“There’s a big elephant in the room that we’re not talking about, and that elephant is having babies,” he says. “Access is such a big problem for these patients and, as a hospitalist, it’s just not OK to me anymore. I need to be proactive about finding solutions.”
Dr. Misky’s concerns led him to do research with mentor Eric Coleman, MD, the university’s creator of the Care Transitions Program (www.caretransitions.org), studying patients who lacked primary-care physicians (PCPs) or timely PCP follow-up, and their resulting higher rates of readmissions.1 Dr. Misky also helped develop care pathways, including post-discharge care, for VTE patients, a “common, costly, and dangerous” condition. He is working with a hospitalist colleague to explore how electronic health records (EHR) might be used to help trigger post-discharge follow-up for at-risk patients.
University of Colorado Hospital (UCH), a 425-bed urban academic tertiary-care center, is not the designated safety net hospital for metro Denver, yet 28% to 32% of patients discharged from its medical services are uninsured, Dr. Misky says. He finds that academic physicians at UCH are not always able to take on large numbers of uninsured patients in their clinics, given the productivity demands they face, while the hospital has not been able to participate in systemwide, comprehensive national models for improving care transitions, such as SHM’s Project BOOST (www.hospitalmedicine.org/boost) or Boston Medical Center’s Project RED (www.bu.edu/fammed/projectred/).
Dr. Misky is in discussions with local community services, such as the Metro Community Provider Network (MCPN) of clinics for underserved patients, and exploring the development of a collaborative model for integrating post-hospital care between UCH and MCPN. “A lot of our ideas are still very exploratory—trying to get the key providers to the table to talk about what these approaches might look like,” Dr. Misky explains. “I’ve been part of ongoing meetings, and I think similar kinds of conversations are happening at many levels at UCH, but there’s not a unified, consensus approach to care transitions—and that’s a problem. But I’m in the midst of it all, trying to highlight the issues and explore solutions.”
—Patricia Rutherford, RN, MS, vice president, Institute for Healthcare Improvement
Dr. Misky says every hospital-based provider—hospitalist, nurses, social workers—feels the same frustration and worry about the level of care when indigent patients are discharged to the community. Uninsured patients can run into problems post-hospitalization and return to the ED for their primary care because they lack other options, he says. “Without established liaisons to the community clinics,” he notes, “it can take three or four months for a new indigent patient to get seen at one.”
Disproportional Issues of the Uninsured
Hospitalists at San Francisco General Hospital, which is the safety-net provider for the Bay Area, are looking at similar issues, says Jeff Critchfield, MD, division chief of hospital medicine. “What we know about the uninsured is that they have a wealth of other challenges and barriers that they bring to the table,” he says. “First of all, un- and underinsured patients are more likely to have chronic illnesses, to be hospitalized for those illnesses, and then to be rehospitalized after discharge.”
Other issues disproportionally impacting uninsured or indigent patients include low literacy, low healthcare literacy, language barriers, cross-cultural barriers, substance abuse and mental health issues, homelessness or marginal housing, transportation barriers, and “social isolation, which also plagues our population and, I believe, places patients at risk, as does depression,” says Dr. Critchfield’s colleague Michelle Schneidermann, MD.
One-third of San Francisco General’s patients are uninsured and 40% have Medi-Cal (California’s version of Medicaid), which basically means they are underinsured.
“California has 19 safety-net hospitals, with 6% of the state’s inpatient beds but 50% of its uninsured population. So that’s what we do,” Dr. Critchfield says. But almost any hospital or hospitalist will see many of the same issues and problems, just not in the same proportions. “These are patients who can be most frustrating to hospitalists, requiring a disproportionate amount of our time,” he says, adding the greatest difficulty is helping these patients understand and follow post-discharge care plans. But if someone is ill enough to need acute hospitalization and is later discharged back to the street, readmission should not be a surprise. “We’ve done that experiment for many years, and we know how it turns out,” he says.
Dr. Schneidermann serves as medical director of San Francisco General’s medical respite program, a 45-bed emergency shelter that accepts homeless or marginally housed patients in need of follow-up care following discharge from any of the city’s acute-care hospitals. Research has shown that the programs can have a major effect on keeping discharged patients off the street, reducing their rates of rehospitalization by as much as 50%.2,3
“We know that homeless patients have longer lengths of hospital stay because their discharges are fraught with problems,” she says. A homeless patient hospitalized with a blood clot potentially could be kept in the hospital for a week while transitioning from heparin to Coumadin, while similar patients with community support might get discharged in a day.
“We are also fortunate to have a program called Healthy San Francisco,” which isn’t a health insurance program per se but since 2007 has provided access to outpatient, inpatient, and preventive care and medications for indigent patients, Dr. Schneidermann says. Sponsored by the city’s Department of Public Health, it is accessed through 32 medical homes located in both public and private clinics. The hospitalists’ goal is to have a follow-up appointment set with a receiving provider at the time of discharge. “It doesn’t always happen, but that’s the goal,” she explains. “Someone, by name, who has accepted the referral.”
Dr. Critchfield is running a randomized controlled trial of the hospital’s interventions to stem the tide of readmissions in patients 60 and older; many of these patients share the same indigent demographics of the rest of San Francisco General’s caseload, although most patients 65 and older qualify for Medicare. He describes the program as a hybrid of Project RED and Dr. Coleman’s Care Transitions Program, although it targets patients who speak English, Spanish, Cantonese, and Mandarin.
How many Americans are uninsured today is a moving target in the context of healthcare reform and its uncertain future, but the number increased to 53 million in 2007 from 42 million in 1998.4 The number of hospitalizations of uninsured patients also grew to 2.3 million from 1.8 million in the same time period, an increase of 31%, while total hospitalizations were increasing by 13%. A May 2011 research brief from the U.S. Department of Health and Human Services estimates that uncompensated costs of hospital care incurred for uninsured patients total $73 billion per year.5
The homeless in shelters or on the street number about 630,000 on any given evening, and 1.5 million Americans experienced homelessness last year, says Sabrina Edgington, MSSW, program and policy specialist at the National Health Care for the Homeless Council in Nashville, Tenn. That said, 30% of the U.S. homeless have health insurance. Uninsured patients are less likely to receive necessary diagnostic tests and labs while in the hospital, and they face limited access and longer wait times—even in the facilities that are willing to take them.7 Research published in the Journal of Hospital Medicine finds that uninsured or Medicaid patients with three common conditions are more likely to die in the hospital than insured patients.8 A 2008 national sample survey of physicians found that “most U.S. physicians limit their care of medically indigent patients.”9 Other recent research suggests that readmission rates are affected by race and by site of care—with hospitals serving a higher proportion of black patients also having higher readmission rates.10
“This is not a hospital problem—it’s a communitywide problem. So there’s not just a hospital solution; it will take the whole village,” says Patricia Rutherford, RN, MS, vice president of the Institute for Healthcare Improvement (IHI), which sponsors initiatives targeting care transitions.
The major national care-transitions programs that assist hospitals with addressing rehospitalizations all share similar objectives, Rutherford says, and all could be helpful in improving hospitals’ responses to indigent patients. The recognized programs include IHI’s STAAR (State Action on Avoidable Rehospitalizations: www.ihi.org/IHI/Programs), a multistate, multistakeholder quality improvement (QI) program; Project BOOST; Project RED; Dr. Coleman’s Care Transitions Project; the nursing-based Transitional Care Model (www.transitionalcare.info); and the American College of Cardiology’s Hospital to Home (www.cardiosource.org).
—Amy Boutwell, MD, MPP, hospitalist, Newton (Mass.) Wellesley Hospital, president, Collaborative Healthcare Strategies
Most of these “well-established, evidence-based interventions,” including BOOST, will be given preference in applications for grants from the federal Community-Based Care Transitions Program (CCTP). The program recently committed $500 million to support community-based coalitions that include hospitals that are working with community partners to create seamless care transitions. “It’s most important that hospitalists are integrally involved with these care-transition teams—if not leading them,” Rutherford says.
BOOST’s approach is built on a major change-management strategy to reconstruct hospitals’ care transitions and discharge processes from the ground up, says Tina Budnitz, MPH, the project’s director at SHM (see “Discharge Improvement,” p. 7.) “The first thing we do, we literally get out pens and paper and chart what happens before patients get into the hospital and what happens after they are discharged, all of the services that touch them—or should,” she says. “The planning process occurs on many levels, with all of the stakeholders in the community looking at the process map and seeing where people fall off and end up readmitted.”
—Jeff Critchfield, MD, division chief of hospital medicine, San Francisco General Hospital
SHM is planning to launch several new BOOST cohorts for participating hospitals this fall, along with a wider range of technical support, Budnitz says.
The Cross-Setting Team
Research on care transitions for uninsured or indigent patients “is not very robust,” observes Amy Boutwell, MD, MPP, a hospitalist at Newton Wellesley Hospital in Newton, Mass., former director of health policy at IHI and president of Collaborative Healthcare Strategies. “We don’t have the information we need, but there are great opportunities to improve our research base,” she explains.
Dr. Boutwell is a big fan of the “cross-setting team,” which brings together around a conference table professionals who work in different care settings, including the hospital, long-term care, and home-based care. She says it’s her job “to make sure patients are safe upon discharge, but if the community is under-resourced for primary-care physicians, if the patient is uninsured and we can’t find a PCP, the hospitalist and cross-setting team need to say, ‘We just can’t accept that.’ ”
What Do HM’s Community Partners Think About the Problem?
Lori J. Heim, MD, FAAFP, board chair of the American Academy of Family Physicians, a family physician in Vass, N.C., and hospitalist at Scotland Memorial Hospital in Laurinburg, N.C., says the unassigned patient who lacks a PCP might be the hardest issue to overcome in improving care transitions.
“We have a lot of members who volunteer at free clinics. Others are part of revolving lists of physicians willing to take unassigned call and accept referrals of indigent patients from the hospital,” Dr. Heim says. “If you look at the number of primary-care practices that are barely surviving, most hospitalists I know are very cognizant of how financially strapped family practice and general internist physicians are these days.”
It isn’t always clear who benefits financially from improved care transitions, particularly for indigent patients, Dr. Heim says. But the growth of patient-centered medical homes through the rollout of national healthcare reform, opportunities for community clinics to become those medical homes, and the wider dissemination of electronic medical records are all important components of the changes that need to take place.
“I would encourage hospitalists to be involved with their hospital leadership on these issues and have ongoing communication with community physicians. Both sides need to think more in terms of the systemic demands,” she says. “Often the ED doctor or the hospitalist knows about these issues and can help hospital leaders understand potential solutions for uninsured patients.–LB
A proper handoff should be done in a way that helps the patient and the physician providing the follow-up care. “But you won’t know what that is unless you ask the people you’re sending patients to how you’re doing,” she explains. “When we routinely review readmitted patients in cross-setting groups, it quickly breaks down the mindset that we in the hospital did everything we could have done to make the discharge successful.”
Dr. Boutwell recommends that hospitalists avoid thinking of these issues in a vacuum, as medical-clinical issues that only doctors can fix. “Because you can’t,” she says. “I would never ask an individual hospitalist to reduce readmissions. It requires a multidisciplinary, all-hands-on-deck approach by the hospital. This is different and more exciting than other quality-improvement efforts.” What’s more, she says, the day is coming—and soon—when failing to manage these readmissions will be a bad business proposition for the hospital (see “Value-Based Purchasing Raises the Stakes,” May 2011, p. 1).
IHI’s STAAR Initiative is working with coalitions of providers in Massachusetts, Michigan, Ohio, and Washington. One of those coalitions, Detroit CARR (Community Action to Reduce Rehospitalizations), convened by MPRO, a Michigan-based quality-improvement organization, is a great example of a cross-continuum team involving five inner-city hospitals, Dr. Boutwell says.
“CARR has really dug deeply into the needs of vulnerable patients in one of America’s most economically challenged communities, with a high proportion of Medicaid, uninsured, and disabled patients” and a shrinking population, she says. Many rehospitalizations are related to socio-economics. “The CARR coalition is meeting with the homeless shelters, the food pantries, and the faith-based agencies,” she says. “They’re really getting at the root of significant issues in their community.”
Nancy Vecchioni, RN, MSN, CPHQ, vice present of Medicare operations at MPRO, says CARR involves more than just healthcare providers; it also brings community agencies together with them to take ownership of the patient. Organizations that a year ago weren’t talking to each other are now meeting regularly to focus on the most vulnerable patients, reviewing cases of rehospitalized homeless patients, and sharing their experiences. Rehospitalized patients are being interviewed, using a prepared script (see Figure 1, p. 34), which allows the patient to tell their story. The information is shared within the coalition.
Each hospital has its own transition team, with post-acute providers, physicians, home health agencies, and community service providers, Vecchioni says. For patients who can’t get in to see a PCP within five days of discharge, some hospitals are opening continuity clinics. Others give patients three- to 30-day supplies of needed medications. “There’s no magic bullet—it’s just a different way of looking at how we do this work,” she adds. “Every day we see new barriers. But we’ve already seen a 5% overall reduction in readmissions. And I think hospitalists can be the champions and leaders of these efforts.”
Hospitalists have to raise the bar for themselves, Dr. Schneidermann says, “doing our best while recognizing we can only do so much. There is a lot we can learn from geriatrics, starting with truly embracing the multidisciplinary team.” If hospitalists feel like they are functioning in isolation, she says, they need to look around. “Are these kinds of interdisciplinary meetings happening? If so, join them. If not, light a fire. Convert your frustrating experiences with patients into action.” TH
Larry Beresford is a freelance medical writer based in California.
References
- Misky GJ, Wald HL, Coleman EA. Post-hospitalization transitions: Examining the effects of timing of primary care provider follow-up. J Hosp Med. 2010;5:392-397.
- Buchanan D, Doblin B, Sai T, Garcia P. The effects of respite care for homeless patients: a cohort study. Am J Public Health. 2006;96:1278-1281.
- Kertesz SG, Posner MA, O’Connell JJ, et al. Post-hospital medical respite care and hospital readmission of homeless persons. J Prev Inter Community. 2009;37:129-142.
- Nagamine M, Stocks C, Merrill C. Trends in uninsured hospital stays, 1998-2007. Health Care Cost & Utilization Project (HCUP) Statistical Brief #88. May 2010.
- U.S. Department of Health and Human Services. ASPE Research Brief. The value of health insurance: few of the uninsured have adequate resources to pay potential hospital bills. May 2011.
- U.S. Department of Housing and Urban Development. The Annual Housing Assessment Report to Congress, 2009.
- Kellerman A, Coleman M. Care without Coverage: Too Little, Too Late. Report by Institute of Medicine, May 2002.
- Hasan O, Orav EJ, Hicks LS. Insurance status and hospital care for myocardial infarction, stroke, and pneumonia. J Hosp Med. 2010;5(8):452-459.
- Chirayath HT, Wentworth AL. Constraints to caring: Service to medically indigent patients by allopathic and osteopathic physicians. J Health Care Poor Underserved. 2008;19:500-511.
- Joynt KE, Orav EJ, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305:675-681.
- Buchanan D, Rohr L, Kehoe L, Glick SB, Jain S. Changing attitudes toward homeless people. J Gen Intern Med. 2004;19(5 Pt 2):566-568.
Liability and Compliance Issues
Hospitalists and other experts say medical/legal liability for indigent patients resulting from readmissions has not been a major focus of their care-transitions initiatives. Even as bundled care models will give hospitals greater financial responsibility for episodes of care across settings, getting sued by patients is not said to be a major concern.
“What we try to do is put together the most robust plan of care that we can for patients, whether insured or not,” says Jeff Critchfield, MD, chief of hospital medicine and medical director of risk management at San Francisco General Hospital. “The tone of the conversation for patients without insurance is different—because the options are fewer. We may have to keep these patients longer because of the absence of options. But rarely does risk management come into it. We don’t get sued by these patients, so that’s not a driving force.”
State and local regulations and Medicare conditions of participation also define expectations for hospitals regarding the care of indigent patients who present at the hospital with acute medical needs. In Los Angeles, a controversy emerged in 2005 when several hospitals were accused of dumping homeless patients on skid row. Local governments responded by approving a $100 million plan to provide homeless shelters across Los Angeles County; in 2008, the same public officials passed an ordinance making it illegal for hospitals to discharge homeless patients to the streets without their consent.
There can be liability issues for any patient who gets transferred out of the hospital and the transition is not a good one, Dr. Critchfield adds, “but I try to think about this population the same as any other.”—LB
Marriage of Necessity
Doctors and hospitals need each other. Healthcare reform is requiring hospitals to rely more heavily on physicians to help them meet quality, safety, and efficiency goals. But in return, doctors are demanding more financial security and a larger role in hospital leadership.
Just how far are they willing to take their mutual relationship to meet their individual needs? A new report by professional services company PwC (formerly PricewaterhouseCoopers) examines the mindsets of potential partners, including an online survey of more than 1,000 doctors and in-depth interviews with 28 healthcare executives. The results suggest plenty of opportunities for alignment, though perhaps also the need for serious pre-marriage counseling.
“From Courtship to Marriage Part II” (www.PwC.com/us/PhysicianHospitalAlignment) follows an initial report that emphasizes the element of trust that’s necessary for any doctor-hospital alignment to succeed. This time around, the sequel is focusing on more concrete steps needed to take the budding relationship to the next level and sustain it. In particular, the new report focuses on sharing power (governance), sharing resources (compensation), and sharing outcomes (guidelines).
The PwC report preempts the naysayers by acknowledging at the outset that “hospitals and physicians have been to the altar before, but many of those marriages ended in divorce.” So what’s different from the 1990s, that decade of broken marriages doomed by the irreconcilable differences over capitation?
“Number one is that back in the ’90s, there wasn’t a clear consensus in defining and determining what is quality,” says Warren Skea, a director in the PwC Health Enterprise Growth Practice. In the intervening years, he says, membership societies—SHM among them—and nonprofit organizations, such as the National Quality Forum, have helped address the need to define and measure healthcare quality. The Centers for Medicare & Medicaid Services (CMS) followed up by adopting and implementing some of those measures in programs, including hospital value-based purchasing (see “Value-Based Purchasing Raises the Stakes,” May 2011, p. 1).
Another missing component in the ’90s, Skea says, was an adequate set of tools for gauging quality. “Even if we did agree what quality was, we couldn’t go back in there and measure it in a valid way,” he explains. “We just didn’t have that capacity.”
A third lesson learned the hard way is that decision-making should involve all physicians, from primary-care doctors to specialists. That power-sharing will be critical, Skea says, as reimbursement models move away from fee-for-service, transaction-based compensation methods and toward paying for outcomes and quality. Silos of care are out, and transitioning patients across a continuum of care is definitely in.
Sound familiar? It should, and the similarity to the hospitalist job description isn’t lost on Skea. “I think hospitalists have served as a very good illustrative example of how physicians can add value to that efficiency equation, improve quality, increase [good] outcomes—all of those things,” he says. In fact, Skea says, the question now is how the quarterback role assumed by hospitalists can be translated or projected to the larger industry and other settings (e.g. outpatient clinics, home care rehabilitation, and continuing care facilities).
Accountable-care organizations (ACOs) are a hot topic in any discussion of better patient transitions and closer doctor-hospital alignments, but they’re hardly the only wedding chapels in town. The new report sketches out the corresponding amenities of a comanagement model and provider-owned plan, and Skea notes that part of the new Center for Medicare & Medicaid Innovation’s mandate will be to investigate other promising methods for encouraging providers to work together.
Leaders, Partners
For most doctors, according to the survey, working together means making joint decisions. More than 90% said they should be involved in “hospital governance activities such as serving on boards, being in management, and taking part in performance.”
“That didn’t surprise me at all; there’s a huge appetite for physicians to be involved in strategic governance and oversight,” Skea says. “That’s where hospitalists have been really good: taking it to that next level of strategy and leadership.”
Next to compensation, he says, governance is the biggest issue for many hospital-affiliated physicians. One wrinkle, however, is what the report’s authors heard from hospital executives. “There’s a recognition by hospital executives that they need those physicians in those governance roles,” Skea says. But the executives felt that more physicians should be trained and educated in business and financial decision-making.
Some of the training strategies, he says, are homegrown. One hospital client, for example, is providing its physicians with courses in statistical analysis, financial modeling, and change management, and referring to the educational package as “MBA in a box.” Other hospitals are steering their physicians toward outside sources of instruction. SHM’s four-day Leadership Academy (www.hospitalmedicine.org/leadership) offers another resource for hospitalists seeking more prominent roles within their institutions.
Along with a desire for more power-sharing, doctors looking to a hospital setting have clearly indicated that they expect to hold their own financially. According to the survey, 83% of doctors considering hospital employment expect to be paid as much as or more than they are currently earning.
And therein lies another potential sticking point. Based on past experience, doctors might expect that hospitals’ financial resources will still allow them to maximize their compensation. But as health reform plays out, Skea cautions, “everybody is going to have to do more with less.”
Compromise Ahead
But other survey results hint at the potential for compromise. According to the report, physicians agreed that half of their compensation should be a fixed salary, while the remaining half could be based on meeting productivity, quality, patient satisfaction, and cost-of-care goals, with the potential for performance rewards. “This shows that physicians realize the health system is changing to track and reward performance and that they can influence the quality and cost of care delivery at the institutional level,” the report states.
And as for the guidelines doctors follow while delivering healthcare, 62% of those surveyed believe nationally accepted guidelines should guide the way they practice medicine; 30% prefer local guidelines.
Skea says he was a bit surprised that nearly 1 in 3 doctors are still resistant to national guidelines, though he believes that number is on the wane. After an initial pushback, he says, doctors seem to be gravitating toward the national standards, due in part to physician societies taking active roles in the discussions.
So what should hospitalists take away from all of this? Skea says they should continue to highlight and demonstrate the value they provide in standardizing care, measuring quality, and improving efficiencies in the four walls of the hospital. “They’ve had a track record, I think they have the mindset, and they’ve had the relationship with hospital executives,” he says.
Hospitalists likely will be called upon to help educate their physician colleagues in other specialties. Because of their background and history of success, Skea says, “they could be one of the real leaders and catalysts for change within an ACO or some of these other more integrated and aligned delivery models, and then move into governance.”
With a little assistance, perhaps this marriage might work after all. TH
Bryn Nelson is a freelance medical writer based in Seattle.
Doctors and hospitals need each other. Healthcare reform is requiring hospitals to rely more heavily on physicians to help them meet quality, safety, and efficiency goals. But in return, doctors are demanding more financial security and a larger role in hospital leadership.
Just how far are they willing to take their mutual relationship to meet their individual needs? A new report by professional services company PwC (formerly PricewaterhouseCoopers) examines the mindsets of potential partners, including an online survey of more than 1,000 doctors and in-depth interviews with 28 healthcare executives. The results suggest plenty of opportunities for alignment, though perhaps also the need for serious pre-marriage counseling.
“From Courtship to Marriage Part II” (www.PwC.com/us/PhysicianHospitalAlignment) follows an initial report that emphasizes the element of trust that’s necessary for any doctor-hospital alignment to succeed. This time around, the sequel is focusing on more concrete steps needed to take the budding relationship to the next level and sustain it. In particular, the new report focuses on sharing power (governance), sharing resources (compensation), and sharing outcomes (guidelines).
The PwC report preempts the naysayers by acknowledging at the outset that “hospitals and physicians have been to the altar before, but many of those marriages ended in divorce.” So what’s different from the 1990s, that decade of broken marriages doomed by the irreconcilable differences over capitation?
“Number one is that back in the ’90s, there wasn’t a clear consensus in defining and determining what is quality,” says Warren Skea, a director in the PwC Health Enterprise Growth Practice. In the intervening years, he says, membership societies—SHM among them—and nonprofit organizations, such as the National Quality Forum, have helped address the need to define and measure healthcare quality. The Centers for Medicare & Medicaid Services (CMS) followed up by adopting and implementing some of those measures in programs, including hospital value-based purchasing (see “Value-Based Purchasing Raises the Stakes,” May 2011, p. 1).
Another missing component in the ’90s, Skea says, was an adequate set of tools for gauging quality. “Even if we did agree what quality was, we couldn’t go back in there and measure it in a valid way,” he explains. “We just didn’t have that capacity.”
A third lesson learned the hard way is that decision-making should involve all physicians, from primary-care doctors to specialists. That power-sharing will be critical, Skea says, as reimbursement models move away from fee-for-service, transaction-based compensation methods and toward paying for outcomes and quality. Silos of care are out, and transitioning patients across a continuum of care is definitely in.
Sound familiar? It should, and the similarity to the hospitalist job description isn’t lost on Skea. “I think hospitalists have served as a very good illustrative example of how physicians can add value to that efficiency equation, improve quality, increase [good] outcomes—all of those things,” he says. In fact, Skea says, the question now is how the quarterback role assumed by hospitalists can be translated or projected to the larger industry and other settings (e.g. outpatient clinics, home care rehabilitation, and continuing care facilities).
Accountable-care organizations (ACOs) are a hot topic in any discussion of better patient transitions and closer doctor-hospital alignments, but they’re hardly the only wedding chapels in town. The new report sketches out the corresponding amenities of a comanagement model and provider-owned plan, and Skea notes that part of the new Center for Medicare & Medicaid Innovation’s mandate will be to investigate other promising methods for encouraging providers to work together.
Leaders, Partners
For most doctors, according to the survey, working together means making joint decisions. More than 90% said they should be involved in “hospital governance activities such as serving on boards, being in management, and taking part in performance.”
“That didn’t surprise me at all; there’s a huge appetite for physicians to be involved in strategic governance and oversight,” Skea says. “That’s where hospitalists have been really good: taking it to that next level of strategy and leadership.”
Next to compensation, he says, governance is the biggest issue for many hospital-affiliated physicians. One wrinkle, however, is what the report’s authors heard from hospital executives. “There’s a recognition by hospital executives that they need those physicians in those governance roles,” Skea says. But the executives felt that more physicians should be trained and educated in business and financial decision-making.
Some of the training strategies, he says, are homegrown. One hospital client, for example, is providing its physicians with courses in statistical analysis, financial modeling, and change management, and referring to the educational package as “MBA in a box.” Other hospitals are steering their physicians toward outside sources of instruction. SHM’s four-day Leadership Academy (www.hospitalmedicine.org/leadership) offers another resource for hospitalists seeking more prominent roles within their institutions.
Along with a desire for more power-sharing, doctors looking to a hospital setting have clearly indicated that they expect to hold their own financially. According to the survey, 83% of doctors considering hospital employment expect to be paid as much as or more than they are currently earning.
And therein lies another potential sticking point. Based on past experience, doctors might expect that hospitals’ financial resources will still allow them to maximize their compensation. But as health reform plays out, Skea cautions, “everybody is going to have to do more with less.”
Compromise Ahead
But other survey results hint at the potential for compromise. According to the report, physicians agreed that half of their compensation should be a fixed salary, while the remaining half could be based on meeting productivity, quality, patient satisfaction, and cost-of-care goals, with the potential for performance rewards. “This shows that physicians realize the health system is changing to track and reward performance and that they can influence the quality and cost of care delivery at the institutional level,” the report states.
And as for the guidelines doctors follow while delivering healthcare, 62% of those surveyed believe nationally accepted guidelines should guide the way they practice medicine; 30% prefer local guidelines.
Skea says he was a bit surprised that nearly 1 in 3 doctors are still resistant to national guidelines, though he believes that number is on the wane. After an initial pushback, he says, doctors seem to be gravitating toward the national standards, due in part to physician societies taking active roles in the discussions.
So what should hospitalists take away from all of this? Skea says they should continue to highlight and demonstrate the value they provide in standardizing care, measuring quality, and improving efficiencies in the four walls of the hospital. “They’ve had a track record, I think they have the mindset, and they’ve had the relationship with hospital executives,” he says.
Hospitalists likely will be called upon to help educate their physician colleagues in other specialties. Because of their background and history of success, Skea says, “they could be one of the real leaders and catalysts for change within an ACO or some of these other more integrated and aligned delivery models, and then move into governance.”
With a little assistance, perhaps this marriage might work after all. TH
Bryn Nelson is a freelance medical writer based in Seattle.
Doctors and hospitals need each other. Healthcare reform is requiring hospitals to rely more heavily on physicians to help them meet quality, safety, and efficiency goals. But in return, doctors are demanding more financial security and a larger role in hospital leadership.
Just how far are they willing to take their mutual relationship to meet their individual needs? A new report by professional services company PwC (formerly PricewaterhouseCoopers) examines the mindsets of potential partners, including an online survey of more than 1,000 doctors and in-depth interviews with 28 healthcare executives. The results suggest plenty of opportunities for alignment, though perhaps also the need for serious pre-marriage counseling.
“From Courtship to Marriage Part II” (www.PwC.com/us/PhysicianHospitalAlignment) follows an initial report that emphasizes the element of trust that’s necessary for any doctor-hospital alignment to succeed. This time around, the sequel is focusing on more concrete steps needed to take the budding relationship to the next level and sustain it. In particular, the new report focuses on sharing power (governance), sharing resources (compensation), and sharing outcomes (guidelines).
The PwC report preempts the naysayers by acknowledging at the outset that “hospitals and physicians have been to the altar before, but many of those marriages ended in divorce.” So what’s different from the 1990s, that decade of broken marriages doomed by the irreconcilable differences over capitation?
“Number one is that back in the ’90s, there wasn’t a clear consensus in defining and determining what is quality,” says Warren Skea, a director in the PwC Health Enterprise Growth Practice. In the intervening years, he says, membership societies—SHM among them—and nonprofit organizations, such as the National Quality Forum, have helped address the need to define and measure healthcare quality. The Centers for Medicare & Medicaid Services (CMS) followed up by adopting and implementing some of those measures in programs, including hospital value-based purchasing (see “Value-Based Purchasing Raises the Stakes,” May 2011, p. 1).
Another missing component in the ’90s, Skea says, was an adequate set of tools for gauging quality. “Even if we did agree what quality was, we couldn’t go back in there and measure it in a valid way,” he explains. “We just didn’t have that capacity.”
A third lesson learned the hard way is that decision-making should involve all physicians, from primary-care doctors to specialists. That power-sharing will be critical, Skea says, as reimbursement models move away from fee-for-service, transaction-based compensation methods and toward paying for outcomes and quality. Silos of care are out, and transitioning patients across a continuum of care is definitely in.
Sound familiar? It should, and the similarity to the hospitalist job description isn’t lost on Skea. “I think hospitalists have served as a very good illustrative example of how physicians can add value to that efficiency equation, improve quality, increase [good] outcomes—all of those things,” he says. In fact, Skea says, the question now is how the quarterback role assumed by hospitalists can be translated or projected to the larger industry and other settings (e.g. outpatient clinics, home care rehabilitation, and continuing care facilities).
Accountable-care organizations (ACOs) are a hot topic in any discussion of better patient transitions and closer doctor-hospital alignments, but they’re hardly the only wedding chapels in town. The new report sketches out the corresponding amenities of a comanagement model and provider-owned plan, and Skea notes that part of the new Center for Medicare & Medicaid Innovation’s mandate will be to investigate other promising methods for encouraging providers to work together.
Leaders, Partners
For most doctors, according to the survey, working together means making joint decisions. More than 90% said they should be involved in “hospital governance activities such as serving on boards, being in management, and taking part in performance.”
“That didn’t surprise me at all; there’s a huge appetite for physicians to be involved in strategic governance and oversight,” Skea says. “That’s where hospitalists have been really good: taking it to that next level of strategy and leadership.”
Next to compensation, he says, governance is the biggest issue for many hospital-affiliated physicians. One wrinkle, however, is what the report’s authors heard from hospital executives. “There’s a recognition by hospital executives that they need those physicians in those governance roles,” Skea says. But the executives felt that more physicians should be trained and educated in business and financial decision-making.
Some of the training strategies, he says, are homegrown. One hospital client, for example, is providing its physicians with courses in statistical analysis, financial modeling, and change management, and referring to the educational package as “MBA in a box.” Other hospitals are steering their physicians toward outside sources of instruction. SHM’s four-day Leadership Academy (www.hospitalmedicine.org/leadership) offers another resource for hospitalists seeking more prominent roles within their institutions.
Along with a desire for more power-sharing, doctors looking to a hospital setting have clearly indicated that they expect to hold their own financially. According to the survey, 83% of doctors considering hospital employment expect to be paid as much as or more than they are currently earning.
And therein lies another potential sticking point. Based on past experience, doctors might expect that hospitals’ financial resources will still allow them to maximize their compensation. But as health reform plays out, Skea cautions, “everybody is going to have to do more with less.”
Compromise Ahead
But other survey results hint at the potential for compromise. According to the report, physicians agreed that half of their compensation should be a fixed salary, while the remaining half could be based on meeting productivity, quality, patient satisfaction, and cost-of-care goals, with the potential for performance rewards. “This shows that physicians realize the health system is changing to track and reward performance and that they can influence the quality and cost of care delivery at the institutional level,” the report states.
And as for the guidelines doctors follow while delivering healthcare, 62% of those surveyed believe nationally accepted guidelines should guide the way they practice medicine; 30% prefer local guidelines.
Skea says he was a bit surprised that nearly 1 in 3 doctors are still resistant to national guidelines, though he believes that number is on the wane. After an initial pushback, he says, doctors seem to be gravitating toward the national standards, due in part to physician societies taking active roles in the discussions.
So what should hospitalists take away from all of this? Skea says they should continue to highlight and demonstrate the value they provide in standardizing care, measuring quality, and improving efficiencies in the four walls of the hospital. “They’ve had a track record, I think they have the mindset, and they’ve had the relationship with hospital executives,” he says.
Hospitalists likely will be called upon to help educate their physician colleagues in other specialties. Because of their background and history of success, Skea says, “they could be one of the real leaders and catalysts for change within an ACO or some of these other more integrated and aligned delivery models, and then move into governance.”
With a little assistance, perhaps this marriage might work after all. TH
Bryn Nelson is a freelance medical writer based in Seattle.
All Aboard
Ten years ago, Stephen Jencks, MD, MPH, was hospitalized after taking a nasty spill and rupturing a kidney, breaking two ribs, and fracturing two transverse processes. The independent healthcare safety and quality consultant based in Baltimore still laughs ruefully at what happened next.
Dr. Jencks was stabilized and given OxyContin to treat his considerable pain, and then he was discharged—without his wife or another caregiver present, with a prescription for nothing more than Tylenol, and without any instructions on what to do if his condition worsened. Twelve hours after returning home, his pain re-emerged with such a vengeance that he experienced severe muscle spasms.
Dr. Jencks suspects his doctor was so focused on his ruptured kidney that pain management and follow-up fell by the wayside. “I am not an unassertive individual, so why didn’t I say something?” he asks. “The simple answer is that, at least for me, if I’m taking OxyContin, there are no problems. People tend not to be at the very top of their game when they’re on opioids and traumatized.”
He made it through the night at home and received better pain medication in the morning, but his experience, he says, “beautifully illustrates” the chronic problem of less-than-graceful transfers of care that can lead to unnecessary hospital readmissions. If it nearly happened to him, it can happen to anyone.
And, based on his research, it often does. In an influential 2009 New England Journal of Medicine study coauthored with Mark Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, and principal investigator of SHM’s Project BOOST, and Eric Coleman, MD, MPH, FACP, associate professor of medicine and director of the care transitions program at the University of Colorado Denver, Dr. Jencks helped uncover some startling statistics: During a 15-month period from 2003 to 2004, nearly 20% of the roughly 12 million Medicare beneficiaries discharged from hospitals were readmitted within 30 days (see “State-by-State Breakdown of 30-Day Rehospitalizations of Medicare Beneficiaries,” p. 7).1 Of those patients discharged to the community and then rehospitalized, half had not seen their own primary-care physician (PCP) in the interim. In all, the authors estimated Medicare’s financial toll from unplanned rehospitalizations at $17.4 billion for 2004 alone.

Surprisingly, Dr. Jencks’ study and a 2007 Medicare Payment Advisory Commission report to Congress provided the first estimates of the overall burden of rehospitalization in nearly a quarter-century. Since then, however, the topic has been a mainstay in conversations about the kinds of interventions that could yield major improvements in healthcare.
“The thing that has propelled this to the front is the recognition that we really can do better,” Dr. Jencks says. “What had tended to be seen as just an evitable consequence of people being sick is now increasingly seen as often being the consequence of not having done as good a job as we should have.”
Beyond the potential for poor patient outcomes and wasted money, healthcare experts say excessive readmissions have the potential to undermine the reputations of hospitalists just as they are moving to center stage in national quality-improvement (QI) efforts.
“I see, basically every day, patients that come back to the hospital because the discharge process is broken,” says Eric Howell, MD, SFHM, director of the hospitalist division at Johns Hopkins Bayview Medical Center in Baltimore. Dr. Howell says communication difficulties between the hospital and a nursing home have plagued one “revolving door” case involving a patient with a stomach ulcer that requires surgical resection. Hospital surgeons have repeatedly arranged to see her as an outpatient and schedule the surgery, but before the surgery can take place, the patient vomits up blood and is rehospitalized.
Another contributing factor, Dr. Howell argues, is the lack of incentives for both hospitals and hospitalists to work hard at preventing the next readmission. Although Dr. Jencks’ study suggests readmissions might not always be profitable, Dr. Howell and others say the sizeable contribution of rehospitalizations to overall admission numbers and the single-digit profit margins of most hospitals offer little motivation to change the status quo. “I think there are good people who want to fix it,” says Dr. Howell, an SHM board member and Project BOOST mentor. But changing the reimbursement system so that hospitalists can better focus on reducing readmissions, he adds, “will really go a long way.”
A New Landscape
Change is in the air. As part of the federal Affordable Care Act of 2010, the Centers for Medicare & Medicaid Services (CMS) is expanding a pilot project on bundling payments to doctors and hospitals around episodes of care. Starting Jan. 1, 2013, the bundling pilot will define “episodes” as all medical services administered three days before a hospital admission until 30 days after discharge. A rehospitalization within that timeframe would net reduced reimbursements.
CMS also has begun accepting applications for what’s known as the Community-Based Care Transitions Program, with $500 million over five years authorized by the healthcare reform act to fund collaborative, readmission-reducing efforts between hospitals and community-based organizations. Linda Magno, CMS director of the Medicare Demonstrations Program Group (www.cms.gov/CMSLeadership/19_Office_ORDI.asp), says program participants will form a learning network so the agency can quickly deliver information about who’s doing well and what approaches are working better than others. The participating organizations, she says, can then help teach best practices to other hospitals around the country.
CMS has adopted public reporting requirements as another tactic. The “Hospital Compare” website (www.hospitalcompare.hhs.gov/) set up by CMS, for example, uses discharge data to publish rehospitalization rates for heart failure, acute myocardial infarction, and pneumonia. More published rates will be added soon. More importantly, Medicare will begin penalizing poorly performing institutions in October 2012 by withholding a percentage of their payments, starting at 1% and rising to 3% within three years, as part of the value-based purchasing initiative.
For hospitals, the looming deadline has prompted widespread concern about the potential financial impact. With a growing number of models and projects springing up around the country, however, hospitalists and other healthcare providers are finding encouraging signs that even relatively simple interventions might help profoundly change the trajectory of care transitions.
Rachel George, MD, MBA, FHM, regional medical director and vice president of operations for West Cogent Healthcare Inc., says Cogent has found success with one tactic—ensuring that all patients are called after being discharged. The call helps to verify that prescribed medications have been picked up and that other care-related questions have been answered. Even before discharge, Dr. George says, Cogent also tries to ensure that a follow-up appointment with every patient’s PCP is on the calendar.
Debbie White, project coordinator for the Little Rock, Ark.-based National Transitions of Care Coalition (NTOCC), says it helps to frame the entire process as a transition plan rather than a discharge. White says patients—and often their family caregivers—are the one constant in every transition. “Some older Americans, including the baby boomers, came from a culture where you don’t question your physician or even an RN,” White says. “So they’ve had a hard time speaking up and learning to ask for a list of their medications, or who’s going to make their next follow-up appointment.” Among its tools, NTOCC offers resources to teach patients how to take more responsibility for their own care (see “Patient Interaction,” p. 5).

On the other side of the equation, the most downloaded tool on the coalition’s website is an evaluation and implementation plan that helps healthcare professionals find the gaps in care transitions. Other tools, including case scenarios and checklists, help healthcare providers consider specific steps, and a compendium of evidence offers a look at successful models and projects.
Dr. Bradley M. Sherman, MD, FHM, chairman of the department of medicine at Glen Cove Hospital/North Shore-LIJ University Health System in New York, led one such project, sponsored by the Greater New York Hospital Association. Dr. Sherman targeted heart failure, the condition with the highest readmission rate for both Glen Cove Hospital and the North Shore/LIJ system. By placing special emphasis on medication compliance, dietary adherence, and physician follow-up, Dr. Sherman says, the hospital cut its readmission rates by more than half, to well below the national average.
Another effort led by Johns Hopkins’ Dr. Howell, known as Safe and Successful Transition of Elderly Patients (Safe STEP), used a collaborative staff approach in general medicine wards overseen by hospitalists to reduce 30-day readmission rates from 22% to 14%. The encouraging results, first reported at SHM’s annual meeting in 2008, provided the impetus for a project called Better Outcomes for Older Adults through Safe Transitions, or Project BOOST (www.hospitalmedicine.org/BOOST).
Developed by SHM, BOOST features a yearlong mentoring program to help sites implement the QI project. It began at six hospitals and has since spread to 62 active mentor sites. Enrollment may swell to between 100 and 120 sites by the end of 2011, according to project director Tina Budnitz, MPH. Data from the first phase revealed a 21% reduction in 30-day readmission rates at the six pilot sites, to 11.2% from 14.2%. Follow-up data from the larger cohort are expected this spring.
Eric Siegal, MD, SFHM, an SHM board member, past chair of SHM’s Public Policy Committee, and a clinical assistant professor of medicine at the University of Wisconsin School of Medicine and Public Health, says BOOST has benefited from being solidly in place at the right time, gaining momentum and garnering significant national attention as the focus on better care transitions has intensified.

“If BOOST demonstrates substantial and reproducible decreases in rehospitalizations, improvements in quality, and presumed projected cost reductions, I think that it’s going to go off like a bomb,” he says, “in a good way.”
Lakshmi Halasyamani, MD, SFHM, vice president for medical affairs for the Saint Joseph Mercy Health System in Michigan and an SHM board member, says BOOST encourages hospitalists to think about ways in which a discharge might fail. “And then we need to actively mitigate those risks,” she says.
National Collaborations
CMS has tapped a network of technical assistance and QI contractors in all 50 states, known as quality-improvement organizations (QIOs), for its own project addressing rehospitalizations. In 2008, these QIOs began working with communities in 14 states to implement what’s known as the Care Transitions Program.
The program has helped community leaders highlight three root causes of high readmission rates: patients’ lack of knowledge and understanding about their chronic conditions, lack of communication among providers, and the healthcare system’s lack of known standards.
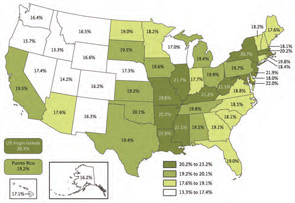
The 14 communities, 70 hospitals, and 1.25 million Medicare beneficiaries being followed to date suggest that 30-day readmission rates can be significantly decreased, says Paul McGann, MD, CMS deputy chief medical officer. Preliminary data based on the number of readmissions per 1,000 Medicare beneficiaries, he says, show that participating communities have improved by an average of 4.7% over the first two years of the project, with the top performer improving 14% (for more information, visit www.cfmc.org/caretransitions).
Dr. Halasyamani says no single program has necessarily found the “secret sauce” to improve readmission rates across the board. “And we definitely haven’t figured out how to implement that in as cost-effective a way as possible,” she says.
But optimism is clearly building. With the initial focus on coaching low-performing institutions to improve their rates, Medicare could tap programs that demonstrate early promise as the main go-to teaching aids.
More importantly, hospitals around the country are finding what it takes to help their own patients.
“The question isn’t, ‘Is our number better than St. Elsewhere’s down the street?’ ” Dr. Jencks concludes. “The real question is, ‘Are there things we could reasonably have done for this patient and could do for the next patient that will keep this from happening to them?’ ” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Jencks SJ, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418-1428.
Ten years ago, Stephen Jencks, MD, MPH, was hospitalized after taking a nasty spill and rupturing a kidney, breaking two ribs, and fracturing two transverse processes. The independent healthcare safety and quality consultant based in Baltimore still laughs ruefully at what happened next.
Dr. Jencks was stabilized and given OxyContin to treat his considerable pain, and then he was discharged—without his wife or another caregiver present, with a prescription for nothing more than Tylenol, and without any instructions on what to do if his condition worsened. Twelve hours after returning home, his pain re-emerged with such a vengeance that he experienced severe muscle spasms.
Dr. Jencks suspects his doctor was so focused on his ruptured kidney that pain management and follow-up fell by the wayside. “I am not an unassertive individual, so why didn’t I say something?” he asks. “The simple answer is that, at least for me, if I’m taking OxyContin, there are no problems. People tend not to be at the very top of their game when they’re on opioids and traumatized.”
He made it through the night at home and received better pain medication in the morning, but his experience, he says, “beautifully illustrates” the chronic problem of less-than-graceful transfers of care that can lead to unnecessary hospital readmissions. If it nearly happened to him, it can happen to anyone.
And, based on his research, it often does. In an influential 2009 New England Journal of Medicine study coauthored with Mark Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, and principal investigator of SHM’s Project BOOST, and Eric Coleman, MD, MPH, FACP, associate professor of medicine and director of the care transitions program at the University of Colorado Denver, Dr. Jencks helped uncover some startling statistics: During a 15-month period from 2003 to 2004, nearly 20% of the roughly 12 million Medicare beneficiaries discharged from hospitals were readmitted within 30 days (see “State-by-State Breakdown of 30-Day Rehospitalizations of Medicare Beneficiaries,” p. 7).1 Of those patients discharged to the community and then rehospitalized, half had not seen their own primary-care physician (PCP) in the interim. In all, the authors estimated Medicare’s financial toll from unplanned rehospitalizations at $17.4 billion for 2004 alone.
Surprisingly, Dr. Jencks’ study and a 2007 Medicare Payment Advisory Commission report to Congress provided the first estimates of the overall burden of rehospitalization in nearly a quarter-century. Since then, however, the topic has been a mainstay in conversations about the kinds of interventions that could yield major improvements in healthcare.
“The thing that has propelled this to the front is the recognition that we really can do better,” Dr. Jencks says. “What had tended to be seen as just an evitable consequence of people being sick is now increasingly seen as often being the consequence of not having done as good a job as we should have.”
Beyond the potential for poor patient outcomes and wasted money, healthcare experts say excessive readmissions have the potential to undermine the reputations of hospitalists just as they are moving to center stage in national quality-improvement (QI) efforts.
“I see, basically every day, patients that come back to the hospital because the discharge process is broken,” says Eric Howell, MD, SFHM, director of the hospitalist division at Johns Hopkins Bayview Medical Center in Baltimore. Dr. Howell says communication difficulties between the hospital and a nursing home have plagued one “revolving door” case involving a patient with a stomach ulcer that requires surgical resection. Hospital surgeons have repeatedly arranged to see her as an outpatient and schedule the surgery, but before the surgery can take place, the patient vomits up blood and is rehospitalized.
Another contributing factor, Dr. Howell argues, is the lack of incentives for both hospitals and hospitalists to work hard at preventing the next readmission. Although Dr. Jencks’ study suggests readmissions might not always be profitable, Dr. Howell and others say the sizeable contribution of rehospitalizations to overall admission numbers and the single-digit profit margins of most hospitals offer little motivation to change the status quo. “I think there are good people who want to fix it,” says Dr. Howell, an SHM board member and Project BOOST mentor. But changing the reimbursement system so that hospitalists can better focus on reducing readmissions, he adds, “will really go a long way.”
A New Landscape
Change is in the air. As part of the federal Affordable Care Act of 2010, the Centers for Medicare & Medicaid Services (CMS) is expanding a pilot project on bundling payments to doctors and hospitals around episodes of care. Starting Jan. 1, 2013, the bundling pilot will define “episodes” as all medical services administered three days before a hospital admission until 30 days after discharge. A rehospitalization within that timeframe would net reduced reimbursements.
CMS also has begun accepting applications for what’s known as the Community-Based Care Transitions Program, with $500 million over five years authorized by the healthcare reform act to fund collaborative, readmission-reducing efforts between hospitals and community-based organizations. Linda Magno, CMS director of the Medicare Demonstrations Program Group (www.cms.gov/CMSLeadership/19_Office_ORDI.asp), says program participants will form a learning network so the agency can quickly deliver information about who’s doing well and what approaches are working better than others. The participating organizations, she says, can then help teach best practices to other hospitals around the country.
CMS has adopted public reporting requirements as another tactic. The “Hospital Compare” website (www.hospitalcompare.hhs.gov/) set up by CMS, for example, uses discharge data to publish rehospitalization rates for heart failure, acute myocardial infarction, and pneumonia. More published rates will be added soon. More importantly, Medicare will begin penalizing poorly performing institutions in October 2012 by withholding a percentage of their payments, starting at 1% and rising to 3% within three years, as part of the value-based purchasing initiative.
For hospitals, the looming deadline has prompted widespread concern about the potential financial impact. With a growing number of models and projects springing up around the country, however, hospitalists and other healthcare providers are finding encouraging signs that even relatively simple interventions might help profoundly change the trajectory of care transitions.
Rachel George, MD, MBA, FHM, regional medical director and vice president of operations for West Cogent Healthcare Inc., says Cogent has found success with one tactic—ensuring that all patients are called after being discharged. The call helps to verify that prescribed medications have been picked up and that other care-related questions have been answered. Even before discharge, Dr. George says, Cogent also tries to ensure that a follow-up appointment with every patient’s PCP is on the calendar.
Debbie White, project coordinator for the Little Rock, Ark.-based National Transitions of Care Coalition (NTOCC), says it helps to frame the entire process as a transition plan rather than a discharge. White says patients—and often their family caregivers—are the one constant in every transition. “Some older Americans, including the baby boomers, came from a culture where you don’t question your physician or even an RN,” White says. “So they’ve had a hard time speaking up and learning to ask for a list of their medications, or who’s going to make their next follow-up appointment.” Among its tools, NTOCC offers resources to teach patients how to take more responsibility for their own care (see “Patient Interaction,” p. 5).
On the other side of the equation, the most downloaded tool on the coalition’s website is an evaluation and implementation plan that helps healthcare professionals find the gaps in care transitions. Other tools, including case scenarios and checklists, help healthcare providers consider specific steps, and a compendium of evidence offers a look at successful models and projects.
Dr. Bradley M. Sherman, MD, FHM, chairman of the department of medicine at Glen Cove Hospital/North Shore-LIJ University Health System in New York, led one such project, sponsored by the Greater New York Hospital Association. Dr. Sherman targeted heart failure, the condition with the highest readmission rate for both Glen Cove Hospital and the North Shore/LIJ system. By placing special emphasis on medication compliance, dietary adherence, and physician follow-up, Dr. Sherman says, the hospital cut its readmission rates by more than half, to well below the national average.
Another effort led by Johns Hopkins’ Dr. Howell, known as Safe and Successful Transition of Elderly Patients (Safe STEP), used a collaborative staff approach in general medicine wards overseen by hospitalists to reduce 30-day readmission rates from 22% to 14%. The encouraging results, first reported at SHM’s annual meeting in 2008, provided the impetus for a project called Better Outcomes for Older Adults through Safe Transitions, or Project BOOST (www.hospitalmedicine.org/BOOST).
Developed by SHM, BOOST features a yearlong mentoring program to help sites implement the QI project. It began at six hospitals and has since spread to 62 active mentor sites. Enrollment may swell to between 100 and 120 sites by the end of 2011, according to project director Tina Budnitz, MPH. Data from the first phase revealed a 21% reduction in 30-day readmission rates at the six pilot sites, to 11.2% from 14.2%. Follow-up data from the larger cohort are expected this spring.
Eric Siegal, MD, SFHM, an SHM board member, past chair of SHM’s Public Policy Committee, and a clinical assistant professor of medicine at the University of Wisconsin School of Medicine and Public Health, says BOOST has benefited from being solidly in place at the right time, gaining momentum and garnering significant national attention as the focus on better care transitions has intensified.
“If BOOST demonstrates substantial and reproducible decreases in rehospitalizations, improvements in quality, and presumed projected cost reductions, I think that it’s going to go off like a bomb,” he says, “in a good way.”
Lakshmi Halasyamani, MD, SFHM, vice president for medical affairs for the Saint Joseph Mercy Health System in Michigan and an SHM board member, says BOOST encourages hospitalists to think about ways in which a discharge might fail. “And then we need to actively mitigate those risks,” she says.
National Collaborations
CMS has tapped a network of technical assistance and QI contractors in all 50 states, known as quality-improvement organizations (QIOs), for its own project addressing rehospitalizations. In 2008, these QIOs began working with communities in 14 states to implement what’s known as the Care Transitions Program.
The program has helped community leaders highlight three root causes of high readmission rates: patients’ lack of knowledge and understanding about their chronic conditions, lack of communication among providers, and the healthcare system’s lack of known standards.
The 14 communities, 70 hospitals, and 1.25 million Medicare beneficiaries being followed to date suggest that 30-day readmission rates can be significantly decreased, says Paul McGann, MD, CMS deputy chief medical officer. Preliminary data based on the number of readmissions per 1,000 Medicare beneficiaries, he says, show that participating communities have improved by an average of 4.7% over the first two years of the project, with the top performer improving 14% (for more information, visit www.cfmc.org/caretransitions).
Dr. Halasyamani says no single program has necessarily found the “secret sauce” to improve readmission rates across the board. “And we definitely haven’t figured out how to implement that in as cost-effective a way as possible,” she says.
But optimism is clearly building. With the initial focus on coaching low-performing institutions to improve their rates, Medicare could tap programs that demonstrate early promise as the main go-to teaching aids.
More importantly, hospitals around the country are finding what it takes to help their own patients.
“The question isn’t, ‘Is our number better than St. Elsewhere’s down the street?’ ” Dr. Jencks concludes. “The real question is, ‘Are there things we could reasonably have done for this patient and could do for the next patient that will keep this from happening to them?’ ” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Jencks SJ, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418-1428.
Ten years ago, Stephen Jencks, MD, MPH, was hospitalized after taking a nasty spill and rupturing a kidney, breaking two ribs, and fracturing two transverse processes. The independent healthcare safety and quality consultant based in Baltimore still laughs ruefully at what happened next.
Dr. Jencks was stabilized and given OxyContin to treat his considerable pain, and then he was discharged—without his wife or another caregiver present, with a prescription for nothing more than Tylenol, and without any instructions on what to do if his condition worsened. Twelve hours after returning home, his pain re-emerged with such a vengeance that he experienced severe muscle spasms.
Dr. Jencks suspects his doctor was so focused on his ruptured kidney that pain management and follow-up fell by the wayside. “I am not an unassertive individual, so why didn’t I say something?” he asks. “The simple answer is that, at least for me, if I’m taking OxyContin, there are no problems. People tend not to be at the very top of their game when they’re on opioids and traumatized.”
He made it through the night at home and received better pain medication in the morning, but his experience, he says, “beautifully illustrates” the chronic problem of less-than-graceful transfers of care that can lead to unnecessary hospital readmissions. If it nearly happened to him, it can happen to anyone.
And, based on his research, it often does. In an influential 2009 New England Journal of Medicine study coauthored with Mark Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, and principal investigator of SHM’s Project BOOST, and Eric Coleman, MD, MPH, FACP, associate professor of medicine and director of the care transitions program at the University of Colorado Denver, Dr. Jencks helped uncover some startling statistics: During a 15-month period from 2003 to 2004, nearly 20% of the roughly 12 million Medicare beneficiaries discharged from hospitals were readmitted within 30 days (see “State-by-State Breakdown of 30-Day Rehospitalizations of Medicare Beneficiaries,” p. 7).1 Of those patients discharged to the community and then rehospitalized, half had not seen their own primary-care physician (PCP) in the interim. In all, the authors estimated Medicare’s financial toll from unplanned rehospitalizations at $17.4 billion for 2004 alone.
Surprisingly, Dr. Jencks’ study and a 2007 Medicare Payment Advisory Commission report to Congress provided the first estimates of the overall burden of rehospitalization in nearly a quarter-century. Since then, however, the topic has been a mainstay in conversations about the kinds of interventions that could yield major improvements in healthcare.
“The thing that has propelled this to the front is the recognition that we really can do better,” Dr. Jencks says. “What had tended to be seen as just an evitable consequence of people being sick is now increasingly seen as often being the consequence of not having done as good a job as we should have.”
Beyond the potential for poor patient outcomes and wasted money, healthcare experts say excessive readmissions have the potential to undermine the reputations of hospitalists just as they are moving to center stage in national quality-improvement (QI) efforts.
“I see, basically every day, patients that come back to the hospital because the discharge process is broken,” says Eric Howell, MD, SFHM, director of the hospitalist division at Johns Hopkins Bayview Medical Center in Baltimore. Dr. Howell says communication difficulties between the hospital and a nursing home have plagued one “revolving door” case involving a patient with a stomach ulcer that requires surgical resection. Hospital surgeons have repeatedly arranged to see her as an outpatient and schedule the surgery, but before the surgery can take place, the patient vomits up blood and is rehospitalized.
Another contributing factor, Dr. Howell argues, is the lack of incentives for both hospitals and hospitalists to work hard at preventing the next readmission. Although Dr. Jencks’ study suggests readmissions might not always be profitable, Dr. Howell and others say the sizeable contribution of rehospitalizations to overall admission numbers and the single-digit profit margins of most hospitals offer little motivation to change the status quo. “I think there are good people who want to fix it,” says Dr. Howell, an SHM board member and Project BOOST mentor. But changing the reimbursement system so that hospitalists can better focus on reducing readmissions, he adds, “will really go a long way.”
A New Landscape
Change is in the air. As part of the federal Affordable Care Act of 2010, the Centers for Medicare & Medicaid Services (CMS) is expanding a pilot project on bundling payments to doctors and hospitals around episodes of care. Starting Jan. 1, 2013, the bundling pilot will define “episodes” as all medical services administered three days before a hospital admission until 30 days after discharge. A rehospitalization within that timeframe would net reduced reimbursements.
CMS also has begun accepting applications for what’s known as the Community-Based Care Transitions Program, with $500 million over five years authorized by the healthcare reform act to fund collaborative, readmission-reducing efforts between hospitals and community-based organizations. Linda Magno, CMS director of the Medicare Demonstrations Program Group (www.cms.gov/CMSLeadership/19_Office_ORDI.asp), says program participants will form a learning network so the agency can quickly deliver information about who’s doing well and what approaches are working better than others. The participating organizations, she says, can then help teach best practices to other hospitals around the country.
CMS has adopted public reporting requirements as another tactic. The “Hospital Compare” website (www.hospitalcompare.hhs.gov/) set up by CMS, for example, uses discharge data to publish rehospitalization rates for heart failure, acute myocardial infarction, and pneumonia. More published rates will be added soon. More importantly, Medicare will begin penalizing poorly performing institutions in October 2012 by withholding a percentage of their payments, starting at 1% and rising to 3% within three years, as part of the value-based purchasing initiative.
For hospitals, the looming deadline has prompted widespread concern about the potential financial impact. With a growing number of models and projects springing up around the country, however, hospitalists and other healthcare providers are finding encouraging signs that even relatively simple interventions might help profoundly change the trajectory of care transitions.
Rachel George, MD, MBA, FHM, regional medical director and vice president of operations for West Cogent Healthcare Inc., says Cogent has found success with one tactic—ensuring that all patients are called after being discharged. The call helps to verify that prescribed medications have been picked up and that other care-related questions have been answered. Even before discharge, Dr. George says, Cogent also tries to ensure that a follow-up appointment with every patient’s PCP is on the calendar.
Debbie White, project coordinator for the Little Rock, Ark.-based National Transitions of Care Coalition (NTOCC), says it helps to frame the entire process as a transition plan rather than a discharge. White says patients—and often their family caregivers—are the one constant in every transition. “Some older Americans, including the baby boomers, came from a culture where you don’t question your physician or even an RN,” White says. “So they’ve had a hard time speaking up and learning to ask for a list of their medications, or who’s going to make their next follow-up appointment.” Among its tools, NTOCC offers resources to teach patients how to take more responsibility for their own care (see “Patient Interaction,” p. 5).
On the other side of the equation, the most downloaded tool on the coalition’s website is an evaluation and implementation plan that helps healthcare professionals find the gaps in care transitions. Other tools, including case scenarios and checklists, help healthcare providers consider specific steps, and a compendium of evidence offers a look at successful models and projects.
Dr. Bradley M. Sherman, MD, FHM, chairman of the department of medicine at Glen Cove Hospital/North Shore-LIJ University Health System in New York, led one such project, sponsored by the Greater New York Hospital Association. Dr. Sherman targeted heart failure, the condition with the highest readmission rate for both Glen Cove Hospital and the North Shore/LIJ system. By placing special emphasis on medication compliance, dietary adherence, and physician follow-up, Dr. Sherman says, the hospital cut its readmission rates by more than half, to well below the national average.
Another effort led by Johns Hopkins’ Dr. Howell, known as Safe and Successful Transition of Elderly Patients (Safe STEP), used a collaborative staff approach in general medicine wards overseen by hospitalists to reduce 30-day readmission rates from 22% to 14%. The encouraging results, first reported at SHM’s annual meeting in 2008, provided the impetus for a project called Better Outcomes for Older Adults through Safe Transitions, or Project BOOST (www.hospitalmedicine.org/BOOST).
Developed by SHM, BOOST features a yearlong mentoring program to help sites implement the QI project. It began at six hospitals and has since spread to 62 active mentor sites. Enrollment may swell to between 100 and 120 sites by the end of 2011, according to project director Tina Budnitz, MPH. Data from the first phase revealed a 21% reduction in 30-day readmission rates at the six pilot sites, to 11.2% from 14.2%. Follow-up data from the larger cohort are expected this spring.
Eric Siegal, MD, SFHM, an SHM board member, past chair of SHM’s Public Policy Committee, and a clinical assistant professor of medicine at the University of Wisconsin School of Medicine and Public Health, says BOOST has benefited from being solidly in place at the right time, gaining momentum and garnering significant national attention as the focus on better care transitions has intensified.
“If BOOST demonstrates substantial and reproducible decreases in rehospitalizations, improvements in quality, and presumed projected cost reductions, I think that it’s going to go off like a bomb,” he says, “in a good way.”
Lakshmi Halasyamani, MD, SFHM, vice president for medical affairs for the Saint Joseph Mercy Health System in Michigan and an SHM board member, says BOOST encourages hospitalists to think about ways in which a discharge might fail. “And then we need to actively mitigate those risks,” she says.
National Collaborations
CMS has tapped a network of technical assistance and QI contractors in all 50 states, known as quality-improvement organizations (QIOs), for its own project addressing rehospitalizations. In 2008, these QIOs began working with communities in 14 states to implement what’s known as the Care Transitions Program.
The program has helped community leaders highlight three root causes of high readmission rates: patients’ lack of knowledge and understanding about their chronic conditions, lack of communication among providers, and the healthcare system’s lack of known standards.
The 14 communities, 70 hospitals, and 1.25 million Medicare beneficiaries being followed to date suggest that 30-day readmission rates can be significantly decreased, says Paul McGann, MD, CMS deputy chief medical officer. Preliminary data based on the number of readmissions per 1,000 Medicare beneficiaries, he says, show that participating communities have improved by an average of 4.7% over the first two years of the project, with the top performer improving 14% (for more information, visit www.cfmc.org/caretransitions).
Dr. Halasyamani says no single program has necessarily found the “secret sauce” to improve readmission rates across the board. “And we definitely haven’t figured out how to implement that in as cost-effective a way as possible,” she says.
But optimism is clearly building. With the initial focus on coaching low-performing institutions to improve their rates, Medicare could tap programs that demonstrate early promise as the main go-to teaching aids.
More importantly, hospitals around the country are finding what it takes to help their own patients.
“The question isn’t, ‘Is our number better than St. Elsewhere’s down the street?’ ” Dr. Jencks concludes. “The real question is, ‘Are there things we could reasonably have done for this patient and could do for the next patient that will keep this from happening to them?’ ” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Jencks SJ, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418-1428.
Change You Should Believe In
Christina Payne, MD, is a third-year resident at Emory University Hospital in Atlanta who will begin her first hospitalist job, with Emory in September. In spite of her dearth of practical experience, she already has experience researching one of the most vexing problems confronting HM: how to improve transitions of care.
Dr. Payne has been studying the benefits of a structured electronic tool that generates a standardized sign-out list of a hospital team’s full census at the time of shift change, compared with the usual, highly variable sign-out practices of medical residents. At a poster presentation at Internal Medicine 2010 in April in Toronto, Dr. Payne and colleagues reported that residents using the tool were twice as confident at performing handoffs, had lower rates of perceived near-miss events, and were happier.1
“Hospitalists everywhere are starting to realize the importance of trying to reduce opportunities for human error that occur during care transitions,” Dr. Payne says. “The biggest thing I learned from this research is the importance of standardizing the handoff process [with information communicated consistently].
“It is essential to keep communication lines open,” Dr. Payne adds. “No tool can replace the importance of communication between doctors and the need to sit down and talk. The ideal signout happens in a quiet room where the two of you can talk about active patients and achieve rapport. But, realistically, how often does that happen?”
Standardization is one of a handful of strategies hospitalists, researchers, and policymakers are using to tackle transitions—both in-hospital handoffs and post-discharge transitions—with outpatient care. Some hospitalists are using practice simulations and training strategies; others have implemented medication reconciliation checks at every discharge, checklists and other communication strategies, team-based quality-improvement (QI) initiatives, and new technologies to enhance and streamline communication. Some interventions follow the patient from the hospital to the community physician with a phone call, follow-up clinic, or other contact; others aim to empower the patient to be a better self-advocate. But for hospitalists, the challenge is to communicate the right amount of transfer information to the right receiver at the right time.
No matter the technique, the goal is the same: Improve the handoff and discharge process in a way that promotes efficiency and patient safety. And hospitalists are at the forefront of the changing landscape of care transitions.
Under the Microscope
Care transitions of all kinds are under the magnifying glass of national healthcare reform, with growing recognition of the need to make care safer and reduce the preventable, costly hospital readmissions caused by incomplete handoffs. Care transitions for hospitalists include internal handoffs, both at daily shift changes and at service changes when an outgoing provider is leaving after a period of consecutive daily shifts. These typically involve a sign-out process and face-to-face encounter, with some kind of written backup. One teaching institution reported that such handoffs take place 4,000 times per day in the hospital, or 1.6 million times per year.2

—Arpana Vidyarthi, MD, University of California at San Francisco
Geographical transitions can be from one floor or department to another, or out the hospital door to another facility or home. Transitions typically involve a discharge process and a written discharge summary. Care transitions also include hospital admissions, which put the hospitalist in the role of handoff receiver rather than initiator, plus a variety of other transitions involving nurses, physician extenders, and other practitioners.
Each transition is a major decision point in the course of a patient’s hospitalization; each transition also presents a time of heightened vulnerability (e.g., potential communication breakdowns, medication errors, patient anxiety or confusion, etc.). In fact, according to a Transitions of Care Consensus Policy Statement published in 2009 by SHM and five other medical societies, handoffs are ubiquitous in HM, with significant patient safety and quality deficiencies in handoffs existing in the current system.3
Poor communication at the time of handoff has been implicated in near-misses and adverse events in a variety of healthcare contexts, including 70% of hospital sentinel events studied by The Joint Commission, which named standardized handoffs (with an opportunity for interactive communication) as a National Patient Safety Goal in 2006.4 The federal government is studying care transitions, supporting demonstration projects for Medicare enrollees, and including readmission rates in national hospital report card data.

“Transitions of care and handoffs are a huge focus right now because of the increased fragmentation of care in the United States. Hospitalists are in charge of a greater percentage of hospitalized patients, which means more coordination of care is needed,” says Vineet Arora, MD, MA, FHM, assistant professor of medicine and associate director of the internal-medicine residency at the University of Chicago, and chair of the SHM task force on handoffs.
Inadequate communication and poor care transitions can undermine hospitalists’ best care-planning efforts, erode patients’ and families’ confidence and satisfaction with hospital care, and leave primary-care physicians (PCPs) feeling unsatisfied with the relationship. As many as 1 in 5 Medicare beneficiary hospitalizations result in a readmission within 30 days, and while not all of these are preventable, far too many are.5 Another prospective cohort study found that 1 in 5 patients discharged from the hospital to the home experienced an adverse event within three weeks of discharge.6 Complex comorbidities, advanced age, unknown PCP, and limited healthcare literacy present hospitalists with extremely difficult transitions.
Patient safety and cost control are the linchpins to national efforts to improve transitions of care. Dr. Arora recently coauthored an original research paper, which will be published in the Journal of Hospital Medicine in September, showing older hospitalized patients are twice as likely to report problems after discharge if their PCPs were not aware they were hospitalized.
“With escalating healthcare costs, people are looking at ways to save money and reduce redundant care,” Dr. Arora explains, pointing out, as an example, repeated tests resulting from inadequate communication between healthcare providers.
The System Must Change
“All of the effort we put into saving someone’s life—the years of experience, training, medical school, and residency—all of it comes to bear on that hospitalized patient. And it can all be unraveled at the time of discharge if it’s not handled properly,” says Arpana Vidyarthi, MD, a hospitalist and director of quality at the University of California at San Francisco.
Dr. Vidyarthi views in-hospital and discharge transitions as integrally related. “The analysis is similar, even if different techniques may be needed,” she says, adding that, fundamentally, it involves having a system that allows people—or forces them—to do the “right thing.”
That’s why achieving effective care transitions will require more than just a standardized tool or process, Dr. Vidyarthi says. “This is about understanding the ways people communicate and finding ways to train them to communicate better,” she says. “The problem we have is not a lack of information, but how to communicate what, to whom, and when.”
What’s really needed, Dr. Vidyarthi says, is a hospital’s commitment to more effective transitions and its hospitalists’ leadership in driving a comprehensive, multidisciplinary, team- and evidence-based QI process. The new process should be a QI-based solution to a hospital’s care-transitions issues. “Before you can standardize your process, you need to understand it,” she says. “This is a complex problem, and it needs a multifaceted solution. But this lies squarely within the hospitalist arena. We’re part of everything that happens in the hospital.

—Anuj Dalal, MD, Brigham and Women’s Hospital, Boston
Hospital administrators are looking to HM to solve transition and readmission problems now, says Tina Budnitz, MPH, BOOST Project Director (Better Outcomes for Older Adults through Safe Transitions). She expects the scrutiny from the C-suite, legislators, and watchdog groups to increase as the spotlight continues to shine on the healthcare system.
“Any hospitalist can act as a leader in their institution,” Budnitz says. “Be a change agent, pull a group together, and start asking questions: Do we have safe care-transitions practices and processes in place? Just by asking the right question, you can be a catalyst for the system.”
Budnitz also emphasizes the importance of teamwork in the hospital setting. “How can I help my teammates? What am I communicating to the nurses on rounds?” she says. “Can you initiate dialogue with your outpatient medical groups: ‘These faxes we’re sending you—is that information getting to you in ways and times that are helpful? And, by the way, when your patient is admitted, this information would really help me.’ ”

Innovative Strategies
One of the most important initiatives responding to concerns about care transitions is Project BOOST (www.hos pitalmedicine.org/BOOST), a comprehensive toolkit for improving a hospital’s transitions of care. The project aims to build a national consensus for best practices in transitions; collaborate with representatives from the Agency for Healthcare Research and Quality (AHRQ), the Centers for Medicare and Medicaid Services (CMS), and the Joint Commission; and develop a national resource library, Budnitz says.
“Project BOOST not only puts forth best practices for admitting patients, planning for discharge, and then doing the discharge, it also helps show facilities how to change their systems, with resources and tools for analyzing and re-engineering the system,” she says. “Sites get one-to-one assistance from a mentor.”
Six hospitals signed on to the pilot program in 2008; 24 more joined last year. In January, SHM announced a collaborative with the University of Michigan and Blue Cross Blue Shield of Michigan for 15 Michigan hospitals to receive training and mentorship starting in May. And last month, SHM and the California HealthCare Foundation announced a Project BOOST initiative for 20 of the health system’s hospitals (see “California Dreamin’”, p. 6). Other free resources offered on the BOOST Web portal include clinical, data collection, and project management tools. SHM also has a DVD that explains how to use the “teachback” method to improve communication with patients.
Jennifer Myers, MD, FHM, assistant professor of clinical medicine and patient-safety officer at the Hospital of the University of Pennsylvania in Philadelphia, is a Project BOOST participant who spearheaded a process change to improve the quality of her facility’s discharge summary, along with accompanying resident education.7 The discharge summary recently was integrated with the hospital’s electronic health record (EHR) system.
“We’ve gone from dictating the discharge summary to an electronic version completed by the hospitalist, with prompts for key components of the summary, which allows us to create summaries more efficiently—ideally on the day of discharge, but usually within 48 hours,” Dr. Myers says. “We previously researched whether teaching made a difference in the quality of discharges; we found that it did. So we look forward to standardizing our teaching approach around this important topic for all residents.”
Another care-transitions innovation receiving a lot of attention from the government and the private sector is Project RED (Re-Engineered Discharge), led by Brian Jack, MD, vice chair of the department of family medicine at Boston Medical Center. The Project RED research group develops and tests strategies to improve the hospital discharge process to promote patient safety and reduce rehospitalization rates.
“We used re-engineering tools borrowed from other fields, brought together experts from all over the hospital, divided up the whole discharge process, and identified key principles,” Dr. Jack explains. The resulting discharge strategy is reflected in an 11-item checklist of discrete, mutually reinforcing components, which have been shown to reduce rehospitalization rates by 32% while raising patient satisfaction.8 It includes comprehensive discharge and after-hospital plans, a nurse discharge advocate, and a medication reconciliation phone call to the patient. A virtual “patient advocate,” a computerized avatar named Louise, is now being tested. If successful, it will allow patients to interact with a touch-screen teacher of the after-care plan who has time to work at the patient’s pace.
Technology and Transitions

Informatics can be a key player in facilitating care transitions, says Anuj Dalal, MD, a hospitalist and instructor in medicine at Brigham and Women’s Hospital in Boston. He is using one of his hospital’s technological strengths—a well-established, firewall-protected e-mail system—to help improve the discharge process.
“We decided to try to improve awareness of test results pending at the time of discharge,” Dr. Dalal explains. “We created an intervention that automatically triggers an e-mail with the finalized test results to the responsible providers. The intervention creates a loop of communication between the inpatient attending and the PCP. What we hope to show in our research over the next year or two is whether the intervention actually increases awareness of test results by providers.”
One thing to remember is that “all kinds of things can go wrong with care transitions,” no matter the size of the institution, the experience of the staff, or technological limitations, says Vineet Chopra, MD, FACP, a hospitalist at the University of Michigan Health System in Ann Arbor. “The problems of transitions vary from place to place, day to day, time of day, shift changes; and let’s not forget physician extenders and the other members of the healthcare team,” he says. “The more complicated the team, the more complicated the information needing to be handed off becomes.”
Who Else Is Looking at Transitions of Care?

SHM convened the Handoffs Task Force in 2006. The team systematically reviewed the literature and published recommendations in the September 2009 Journal of Hospital Medicine.9 The recommendations are aimed at both community and academic hospitals, as well as hospitalists and other healthcare providers. A new collaborative designed to supplement Project BOOST for hospitalist group handoffs and help put the guidelines into practice is in the works, says Dr. Arora, the task force’s chair.
SHM and five medical groups, including the American College of Physicians, issued a Transitions of Care Consensus Statement, published in the July 2009 issue of the Journal of Hospital Medicine.5 Guiding principles relate to education, measurement, accountability, timely interchange of information, inclusion of patient and family, respect for the medical home, and the need for national standards.
The Joint Commission’s Center for Transforming Health Care, established in 2009 to solve healthcare’s most critical safety and quality problems, has made handoff communications its second major target, and is now working with 10 healthcare systems. Standardized handoff processes and communications were the subject of the Joint Commission’s 2006 National Patient Safety Goal, while the Comprehensive Accreditation Manual for Hospitals also specifies that before a hospital discharges or transfers a patient, it should inform and educate the patient about his or her follow-up care and services.
“We now have a safety goal under review dealing with medication reconciliation, and there are relevant standards related to culturally sensitive communication and low-literacy-level communication,” says Deborah Zadzam, PhD, RN, FAAN, director of international quality and performance measures for Joint Commission Resources. “The essential message the Joint Commission has for hospitalists is to communicate clearly, effectively and thoroughly; don’t assume you are understood or that you understand.”—LB
Before he joined the group at the university, Dr. Chopra worked at a community hospital, St. Joseph’s Mercy Hospital in Hot Springs, Ark. “It’s hard to come up with a one-size-fits-all solution when there are so many variables,” he says. At the community hospital, “we mandated that the hospitalist call the PCP at the time of discharge. At the academic medical center, we share an EHR with the PCPs and can reach them electronically. We are required to have the discharge summary in the computer before the patient leaves the hospital, and we mandate that hospitalists are reachable by e-mail or phone when they are off.
“I’m not a believer in throwing more technology at problems and just adding more layers of information tools,” Dr. Chopra adds. “Hospitalists who used to carry stethoscopes now also have a clipboard, phone, pager, PDA, and nine different signouts in their pockets. What we want to do is make their life easier. Here, we are looking at technology as a means to do that.”
Dr. Chopra and hospitalist colleague Prasanth Gosineni, MD, have been working with an Ann Arbor tech company called Synaptin to develop a lightweight, mobile client application designed to work on smartphones. Still in pilot testing, it would allow for task-oriented and priority-based messaging in real time and the systematic transfer of important information for the next hospitalist shift.
“You need to be able to share information in a systematic way, but that’s only half of the answer. The other half is the ability to ask specific questions,” Dr. Chopra says. “Technology doesn’t take away from the face-to-face encounter that needs to happen. Nothing will replace face time, but part of the solution is to provide data efficiently and in a way that is easily accessible.”
Dr. Chopra admits that EHR presents both positives and negatives to improved transitions and patient care, “depending on how well it works and what smart features it offers,” he says, “but also recognizing that EHR and other technologies have also taken us farther away from face-to-face exchanges. Some would say that’s part of the problem.”
Handoffs, discharges, and other transitions are ubiquitous in HM—and fraught with the potential for costly and harmful errors. The ideal of an interactive, face-to-face handoff simply is not available for many care transitions. However, hospitalists are challenged to find solutions that will work in their hospitals, with their teams, and their types of patients. Patients and policymakers expect nothing less. TH
Larry Beresford is a freelance writer based in Oakland, Calif.
References
- Payne C, Stein J, Dressler D. Implementation of a structured electronic tool to improve patient handoffs and resident satisfaction. Poster abstract: Internal Medicine 2010, April 21-24, 2010, Toronto.
- Vidyarthi AR. Triple Handoff. AHRQ WebM&M website. Available at: webmm.ahrq.gov/case.aspx? caseID=134. Published May 2006. Accessed May 29, 2010.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement: American College of Physicians, Society of General Internal Medicine, Society of Hospital Medicine, American Geriatrics Society, American College of Emergency Physicians, and Society for Academic Emergency Medicine. J Hosp Med. 2009;4(6):364-370.
- 2006 National Patient Safety Goals. The Joint Commission website. Available at: www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/06_npsgs.htm. Accessed June 8, 2010.
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009; 2:360:1418-1428.
- Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161-167.
- Myers JS, Jaipaul CK, Kogan JR, Krekun S, Bellini LM, Shea JA. Are discharge summaries teachable? The effects of a discharge summary curriculum on the quality of discharge summaries in an internal medicine residency program. Acad Med. 2006; 81(10):S5-S8.
- Jack BW, Chetty VK, Anthony D, et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009;150(3):178-187.
- Arora VM, Manjarrez E, Dressler DD, Basaviah P, Halasyamani L, Kripalani S. Hospitalist handoffs: a systematic review and task force recommendations. J Hosp Med. 2009;4(7): 433-440.
- Halasyamani L, Kripalani S, Coleman E, et al. Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists. J Hosp Med. 2006;1(6):354-360.
- Schnipper JL, Kirwin JL, Cotugno MC, et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Int Med. 2006;166(5):565-571.
- Dudas V, Bookwalter T, Kerr KM, Pantilat SZ. The impact of follow-up telephone calls to patients after hospitalization. Am J Med. 2001;111(9B): 26S-30S.
Care Transition Tips for Hospitalists and Groups

One recognized key to effective internal handoffs is the face-to-face verbal update, with opportunities to ask questions, priority given to sicker patients, and a written backup filling in the blanks with information that might become important as the patient’s condition changes. But if that is not practical for your HM group, what tools and processes will come closest to the ideal?
A key to effective discharge from the hospital is connection with the PCP, although face-to-face encounters with PCPs are highly unlikely. Hospitalists say there are levels of connection with PCPs, from the urgent (“I need to talk to someone right now”) to the routine (“It’s OK if they get this information tomorrow”). Many often wonder if there should be two levels of discharge communication with PCPs: an immediate message relaying crucial information and a formal discharge summary coming later.
For HM groups, the following is a list of suggestions from transitions-of-care researchers:
- Keep accurate and up-to-date contact information, including preferred communication medium, on referring physicians; survey them on their satisfaction with the discharge communications they receive from hospitalists.
- Partner with hospital administrators and with patient-safety and quality officers to address handoff issues.
- Partner with IT staff to help bridge the divide between clinicians and information technology.
- Track such outcomes as rehospitalization rates.
- Offer formal training on handoffs, discharges, and effective communication to physicians and other providers.
- Standardize the signout process, with computerized tools when appropriate, and create automated systems for following up on tests and lab results that come back after discharge.
- Structure shifts and their overlaps to help facilitate signouts.
- Consider implementing a discharge checklist.10
- Develop a strategy for medication reconciliation, with someone assigned to the process, be that a hospitalist, pharmacist or nurse.11
- Advocate for a post-discharge call-back policy by assigned staff at defined intervals, either for every patient discharged or for those targeted as higher-risk.12
- Consider creating a post-discharge clinic and/or a phone number that discharged patients can call to clarify post-discharge questions and concerns.
For individual hospitalists:
- Understand the transition process, where it fails, and why.
- Be open to changing the way you do things. Be accountable for transitions, and a role model for others.
- Focus on the present—today’s baseline, current to-do items, and what to expect next in the patient’s care.
- Track patients and their future discharge needs from the day of admission. What’s the likely date for going home? What does the patient need to learn in the meantime? Help nurses focus on achieving those needs and, if possible, schedule the initial outpatient clinic appointment before the patient leaves the hospital.
- Take time to talk your patients, listen to their concerns and confirm their understanding of what lies ahead.
For hospitalists on the receiving end of transition messages:
- Actively listen—stay focused, limit interruptions, take notes.
- Ask questions to ensure your understanding and read back what you understand to be the communication.
- Have a system for keeping track of to-do items requiring follow-up.—LB
Christina Payne, MD, is a third-year resident at Emory University Hospital in Atlanta who will begin her first hospitalist job, with Emory in September. In spite of her dearth of practical experience, she already has experience researching one of the most vexing problems confronting HM: how to improve transitions of care.
Dr. Payne has been studying the benefits of a structured electronic tool that generates a standardized sign-out list of a hospital team’s full census at the time of shift change, compared with the usual, highly variable sign-out practices of medical residents. At a poster presentation at Internal Medicine 2010 in April in Toronto, Dr. Payne and colleagues reported that residents using the tool were twice as confident at performing handoffs, had lower rates of perceived near-miss events, and were happier.1
“Hospitalists everywhere are starting to realize the importance of trying to reduce opportunities for human error that occur during care transitions,” Dr. Payne says. “The biggest thing I learned from this research is the importance of standardizing the handoff process [with information communicated consistently].
“It is essential to keep communication lines open,” Dr. Payne adds. “No tool can replace the importance of communication between doctors and the need to sit down and talk. The ideal signout happens in a quiet room where the two of you can talk about active patients and achieve rapport. But, realistically, how often does that happen?”
Standardization is one of a handful of strategies hospitalists, researchers, and policymakers are using to tackle transitions—both in-hospital handoffs and post-discharge transitions—with outpatient care. Some hospitalists are using practice simulations and training strategies; others have implemented medication reconciliation checks at every discharge, checklists and other communication strategies, team-based quality-improvement (QI) initiatives, and new technologies to enhance and streamline communication. Some interventions follow the patient from the hospital to the community physician with a phone call, follow-up clinic, or other contact; others aim to empower the patient to be a better self-advocate. But for hospitalists, the challenge is to communicate the right amount of transfer information to the right receiver at the right time.
No matter the technique, the goal is the same: Improve the handoff and discharge process in a way that promotes efficiency and patient safety. And hospitalists are at the forefront of the changing landscape of care transitions.
Under the Microscope
Care transitions of all kinds are under the magnifying glass of national healthcare reform, with growing recognition of the need to make care safer and reduce the preventable, costly hospital readmissions caused by incomplete handoffs. Care transitions for hospitalists include internal handoffs, both at daily shift changes and at service changes when an outgoing provider is leaving after a period of consecutive daily shifts. These typically involve a sign-out process and face-to-face encounter, with some kind of written backup. One teaching institution reported that such handoffs take place 4,000 times per day in the hospital, or 1.6 million times per year.2
—Arpana Vidyarthi, MD, University of California at San Francisco
Geographical transitions can be from one floor or department to another, or out the hospital door to another facility or home. Transitions typically involve a discharge process and a written discharge summary. Care transitions also include hospital admissions, which put the hospitalist in the role of handoff receiver rather than initiator, plus a variety of other transitions involving nurses, physician extenders, and other practitioners.
Each transition is a major decision point in the course of a patient’s hospitalization; each transition also presents a time of heightened vulnerability (e.g., potential communication breakdowns, medication errors, patient anxiety or confusion, etc.). In fact, according to a Transitions of Care Consensus Policy Statement published in 2009 by SHM and five other medical societies, handoffs are ubiquitous in HM, with significant patient safety and quality deficiencies in handoffs existing in the current system.3
Poor communication at the time of handoff has been implicated in near-misses and adverse events in a variety of healthcare contexts, including 70% of hospital sentinel events studied by The Joint Commission, which named standardized handoffs (with an opportunity for interactive communication) as a National Patient Safety Goal in 2006.4 The federal government is studying care transitions, supporting demonstration projects for Medicare enrollees, and including readmission rates in national hospital report card data.
“Transitions of care and handoffs are a huge focus right now because of the increased fragmentation of care in the United States. Hospitalists are in charge of a greater percentage of hospitalized patients, which means more coordination of care is needed,” says Vineet Arora, MD, MA, FHM, assistant professor of medicine and associate director of the internal-medicine residency at the University of Chicago, and chair of the SHM task force on handoffs.
Inadequate communication and poor care transitions can undermine hospitalists’ best care-planning efforts, erode patients’ and families’ confidence and satisfaction with hospital care, and leave primary-care physicians (PCPs) feeling unsatisfied with the relationship. As many as 1 in 5 Medicare beneficiary hospitalizations result in a readmission within 30 days, and while not all of these are preventable, far too many are.5 Another prospective cohort study found that 1 in 5 patients discharged from the hospital to the home experienced an adverse event within three weeks of discharge.6 Complex comorbidities, advanced age, unknown PCP, and limited healthcare literacy present hospitalists with extremely difficult transitions.
Patient safety and cost control are the linchpins to national efforts to improve transitions of care. Dr. Arora recently coauthored an original research paper, which will be published in the Journal of Hospital Medicine in September, showing older hospitalized patients are twice as likely to report problems after discharge if their PCPs were not aware they were hospitalized.
“With escalating healthcare costs, people are looking at ways to save money and reduce redundant care,” Dr. Arora explains, pointing out, as an example, repeated tests resulting from inadequate communication between healthcare providers.
The System Must Change
“All of the effort we put into saving someone’s life—the years of experience, training, medical school, and residency—all of it comes to bear on that hospitalized patient. And it can all be unraveled at the time of discharge if it’s not handled properly,” says Arpana Vidyarthi, MD, a hospitalist and director of quality at the University of California at San Francisco.
Dr. Vidyarthi views in-hospital and discharge transitions as integrally related. “The analysis is similar, even if different techniques may be needed,” she says, adding that, fundamentally, it involves having a system that allows people—or forces them—to do the “right thing.”
That’s why achieving effective care transitions will require more than just a standardized tool or process, Dr. Vidyarthi says. “This is about understanding the ways people communicate and finding ways to train them to communicate better,” she says. “The problem we have is not a lack of information, but how to communicate what, to whom, and when.”
What’s really needed, Dr. Vidyarthi says, is a hospital’s commitment to more effective transitions and its hospitalists’ leadership in driving a comprehensive, multidisciplinary, team- and evidence-based QI process. The new process should be a QI-based solution to a hospital’s care-transitions issues. “Before you can standardize your process, you need to understand it,” she says. “This is a complex problem, and it needs a multifaceted solution. But this lies squarely within the hospitalist arena. We’re part of everything that happens in the hospital.
—Anuj Dalal, MD, Brigham and Women’s Hospital, Boston
Hospital administrators are looking to HM to solve transition and readmission problems now, says Tina Budnitz, MPH, BOOST Project Director (Better Outcomes for Older Adults through Safe Transitions). She expects the scrutiny from the C-suite, legislators, and watchdog groups to increase as the spotlight continues to shine on the healthcare system.
“Any hospitalist can act as a leader in their institution,” Budnitz says. “Be a change agent, pull a group together, and start asking questions: Do we have safe care-transitions practices and processes in place? Just by asking the right question, you can be a catalyst for the system.”
Budnitz also emphasizes the importance of teamwork in the hospital setting. “How can I help my teammates? What am I communicating to the nurses on rounds?” she says. “Can you initiate dialogue with your outpatient medical groups: ‘These faxes we’re sending you—is that information getting to you in ways and times that are helpful? And, by the way, when your patient is admitted, this information would really help me.’ ”
Innovative Strategies
One of the most important initiatives responding to concerns about care transitions is Project BOOST (www.hos pitalmedicine.org/BOOST), a comprehensive toolkit for improving a hospital’s transitions of care. The project aims to build a national consensus for best practices in transitions; collaborate with representatives from the Agency for Healthcare Research and Quality (AHRQ), the Centers for Medicare and Medicaid Services (CMS), and the Joint Commission; and develop a national resource library, Budnitz says.
“Project BOOST not only puts forth best practices for admitting patients, planning for discharge, and then doing the discharge, it also helps show facilities how to change their systems, with resources and tools for analyzing and re-engineering the system,” she says. “Sites get one-to-one assistance from a mentor.”
Six hospitals signed on to the pilot program in 2008; 24 more joined last year. In January, SHM announced a collaborative with the University of Michigan and Blue Cross Blue Shield of Michigan for 15 Michigan hospitals to receive training and mentorship starting in May. And last month, SHM and the California HealthCare Foundation announced a Project BOOST initiative for 20 of the health system’s hospitals (see “California Dreamin’”, p. 6). Other free resources offered on the BOOST Web portal include clinical, data collection, and project management tools. SHM also has a DVD that explains how to use the “teachback” method to improve communication with patients.
Jennifer Myers, MD, FHM, assistant professor of clinical medicine and patient-safety officer at the Hospital of the University of Pennsylvania in Philadelphia, is a Project BOOST participant who spearheaded a process change to improve the quality of her facility’s discharge summary, along with accompanying resident education.7 The discharge summary recently was integrated with the hospital’s electronic health record (EHR) system.
“We’ve gone from dictating the discharge summary to an electronic version completed by the hospitalist, with prompts for key components of the summary, which allows us to create summaries more efficiently—ideally on the day of discharge, but usually within 48 hours,” Dr. Myers says. “We previously researched whether teaching made a difference in the quality of discharges; we found that it did. So we look forward to standardizing our teaching approach around this important topic for all residents.”
Another care-transitions innovation receiving a lot of attention from the government and the private sector is Project RED (Re-Engineered Discharge), led by Brian Jack, MD, vice chair of the department of family medicine at Boston Medical Center. The Project RED research group develops and tests strategies to improve the hospital discharge process to promote patient safety and reduce rehospitalization rates.
“We used re-engineering tools borrowed from other fields, brought together experts from all over the hospital, divided up the whole discharge process, and identified key principles,” Dr. Jack explains. The resulting discharge strategy is reflected in an 11-item checklist of discrete, mutually reinforcing components, which have been shown to reduce rehospitalization rates by 32% while raising patient satisfaction.8 It includes comprehensive discharge and after-hospital plans, a nurse discharge advocate, and a medication reconciliation phone call to the patient. A virtual “patient advocate,” a computerized avatar named Louise, is now being tested. If successful, it will allow patients to interact with a touch-screen teacher of the after-care plan who has time to work at the patient’s pace.
Technology and Transitions
Informatics can be a key player in facilitating care transitions, says Anuj Dalal, MD, a hospitalist and instructor in medicine at Brigham and Women’s Hospital in Boston. He is using one of his hospital’s technological strengths—a well-established, firewall-protected e-mail system—to help improve the discharge process.
“We decided to try to improve awareness of test results pending at the time of discharge,” Dr. Dalal explains. “We created an intervention that automatically triggers an e-mail with the finalized test results to the responsible providers. The intervention creates a loop of communication between the inpatient attending and the PCP. What we hope to show in our research over the next year or two is whether the intervention actually increases awareness of test results by providers.”
One thing to remember is that “all kinds of things can go wrong with care transitions,” no matter the size of the institution, the experience of the staff, or technological limitations, says Vineet Chopra, MD, FACP, a hospitalist at the University of Michigan Health System in Ann Arbor. “The problems of transitions vary from place to place, day to day, time of day, shift changes; and let’s not forget physician extenders and the other members of the healthcare team,” he says. “The more complicated the team, the more complicated the information needing to be handed off becomes.”
Who Else Is Looking at Transitions of Care?
SHM convened the Handoffs Task Force in 2006. The team systematically reviewed the literature and published recommendations in the September 2009 Journal of Hospital Medicine.9 The recommendations are aimed at both community and academic hospitals, as well as hospitalists and other healthcare providers. A new collaborative designed to supplement Project BOOST for hospitalist group handoffs and help put the guidelines into practice is in the works, says Dr. Arora, the task force’s chair.
SHM and five medical groups, including the American College of Physicians, issued a Transitions of Care Consensus Statement, published in the July 2009 issue of the Journal of Hospital Medicine.5 Guiding principles relate to education, measurement, accountability, timely interchange of information, inclusion of patient and family, respect for the medical home, and the need for national standards.
The Joint Commission’s Center for Transforming Health Care, established in 2009 to solve healthcare’s most critical safety and quality problems, has made handoff communications its second major target, and is now working with 10 healthcare systems. Standardized handoff processes and communications were the subject of the Joint Commission’s 2006 National Patient Safety Goal, while the Comprehensive Accreditation Manual for Hospitals also specifies that before a hospital discharges or transfers a patient, it should inform and educate the patient about his or her follow-up care and services.
“We now have a safety goal under review dealing with medication reconciliation, and there are relevant standards related to culturally sensitive communication and low-literacy-level communication,” says Deborah Zadzam, PhD, RN, FAAN, director of international quality and performance measures for Joint Commission Resources. “The essential message the Joint Commission has for hospitalists is to communicate clearly, effectively and thoroughly; don’t assume you are understood or that you understand.”—LB
Before he joined the group at the university, Dr. Chopra worked at a community hospital, St. Joseph’s Mercy Hospital in Hot Springs, Ark. “It’s hard to come up with a one-size-fits-all solution when there are so many variables,” he says. At the community hospital, “we mandated that the hospitalist call the PCP at the time of discharge. At the academic medical center, we share an EHR with the PCPs and can reach them electronically. We are required to have the discharge summary in the computer before the patient leaves the hospital, and we mandate that hospitalists are reachable by e-mail or phone when they are off.
“I’m not a believer in throwing more technology at problems and just adding more layers of information tools,” Dr. Chopra adds. “Hospitalists who used to carry stethoscopes now also have a clipboard, phone, pager, PDA, and nine different signouts in their pockets. What we want to do is make their life easier. Here, we are looking at technology as a means to do that.”
Dr. Chopra and hospitalist colleague Prasanth Gosineni, MD, have been working with an Ann Arbor tech company called Synaptin to develop a lightweight, mobile client application designed to work on smartphones. Still in pilot testing, it would allow for task-oriented and priority-based messaging in real time and the systematic transfer of important information for the next hospitalist shift.
“You need to be able to share information in a systematic way, but that’s only half of the answer. The other half is the ability to ask specific questions,” Dr. Chopra says. “Technology doesn’t take away from the face-to-face encounter that needs to happen. Nothing will replace face time, but part of the solution is to provide data efficiently and in a way that is easily accessible.”
Dr. Chopra admits that EHR presents both positives and negatives to improved transitions and patient care, “depending on how well it works and what smart features it offers,” he says, “but also recognizing that EHR and other technologies have also taken us farther away from face-to-face exchanges. Some would say that’s part of the problem.”
Handoffs, discharges, and other transitions are ubiquitous in HM—and fraught with the potential for costly and harmful errors. The ideal of an interactive, face-to-face handoff simply is not available for many care transitions. However, hospitalists are challenged to find solutions that will work in their hospitals, with their teams, and their types of patients. Patients and policymakers expect nothing less. TH
Larry Beresford is a freelance writer based in Oakland, Calif.
References
- Payne C, Stein J, Dressler D. Implementation of a structured electronic tool to improve patient handoffs and resident satisfaction. Poster abstract: Internal Medicine 2010, April 21-24, 2010, Toronto.
- Vidyarthi AR. Triple Handoff. AHRQ WebM&M website. Available at: webmm.ahrq.gov/case.aspx? caseID=134. Published May 2006. Accessed May 29, 2010.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement: American College of Physicians, Society of General Internal Medicine, Society of Hospital Medicine, American Geriatrics Society, American College of Emergency Physicians, and Society for Academic Emergency Medicine. J Hosp Med. 2009;4(6):364-370.
- 2006 National Patient Safety Goals. The Joint Commission website. Available at: www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/06_npsgs.htm. Accessed June 8, 2010.
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009; 2:360:1418-1428.
- Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161-167.
- Myers JS, Jaipaul CK, Kogan JR, Krekun S, Bellini LM, Shea JA. Are discharge summaries teachable? The effects of a discharge summary curriculum on the quality of discharge summaries in an internal medicine residency program. Acad Med. 2006; 81(10):S5-S8.
- Jack BW, Chetty VK, Anthony D, et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009;150(3):178-187.
- Arora VM, Manjarrez E, Dressler DD, Basaviah P, Halasyamani L, Kripalani S. Hospitalist handoffs: a systematic review and task force recommendations. J Hosp Med. 2009;4(7): 433-440.
- Halasyamani L, Kripalani S, Coleman E, et al. Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists. J Hosp Med. 2006;1(6):354-360.
- Schnipper JL, Kirwin JL, Cotugno MC, et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Int Med. 2006;166(5):565-571.
- Dudas V, Bookwalter T, Kerr KM, Pantilat SZ. The impact of follow-up telephone calls to patients after hospitalization. Am J Med. 2001;111(9B): 26S-30S.
Care Transition Tips for Hospitalists and Groups
One recognized key to effective internal handoffs is the face-to-face verbal update, with opportunities to ask questions, priority given to sicker patients, and a written backup filling in the blanks with information that might become important as the patient’s condition changes. But if that is not practical for your HM group, what tools and processes will come closest to the ideal?
A key to effective discharge from the hospital is connection with the PCP, although face-to-face encounters with PCPs are highly unlikely. Hospitalists say there are levels of connection with PCPs, from the urgent (“I need to talk to someone right now”) to the routine (“It’s OK if they get this information tomorrow”). Many often wonder if there should be two levels of discharge communication with PCPs: an immediate message relaying crucial information and a formal discharge summary coming later.
For HM groups, the following is a list of suggestions from transitions-of-care researchers:
- Keep accurate and up-to-date contact information, including preferred communication medium, on referring physicians; survey them on their satisfaction with the discharge communications they receive from hospitalists.
- Partner with hospital administrators and with patient-safety and quality officers to address handoff issues.
- Partner with IT staff to help bridge the divide between clinicians and information technology.
- Track such outcomes as rehospitalization rates.
- Offer formal training on handoffs, discharges, and effective communication to physicians and other providers.
- Standardize the signout process, with computerized tools when appropriate, and create automated systems for following up on tests and lab results that come back after discharge.
- Structure shifts and their overlaps to help facilitate signouts.
- Consider implementing a discharge checklist.10
- Develop a strategy for medication reconciliation, with someone assigned to the process, be that a hospitalist, pharmacist or nurse.11
- Advocate for a post-discharge call-back policy by assigned staff at defined intervals, either for every patient discharged or for those targeted as higher-risk.12
- Consider creating a post-discharge clinic and/or a phone number that discharged patients can call to clarify post-discharge questions and concerns.
For individual hospitalists:
- Understand the transition process, where it fails, and why.
- Be open to changing the way you do things. Be accountable for transitions, and a role model for others.
- Focus on the present—today’s baseline, current to-do items, and what to expect next in the patient’s care.
- Track patients and their future discharge needs from the day of admission. What’s the likely date for going home? What does the patient need to learn in the meantime? Help nurses focus on achieving those needs and, if possible, schedule the initial outpatient clinic appointment before the patient leaves the hospital.
- Take time to talk your patients, listen to their concerns and confirm their understanding of what lies ahead.
For hospitalists on the receiving end of transition messages:
- Actively listen—stay focused, limit interruptions, take notes.
- Ask questions to ensure your understanding and read back what you understand to be the communication.
- Have a system for keeping track of to-do items requiring follow-up.—LB
Christina Payne, MD, is a third-year resident at Emory University Hospital in Atlanta who will begin her first hospitalist job, with Emory in September. In spite of her dearth of practical experience, she already has experience researching one of the most vexing problems confronting HM: how to improve transitions of care.
Dr. Payne has been studying the benefits of a structured electronic tool that generates a standardized sign-out list of a hospital team’s full census at the time of shift change, compared with the usual, highly variable sign-out practices of medical residents. At a poster presentation at Internal Medicine 2010 in April in Toronto, Dr. Payne and colleagues reported that residents using the tool were twice as confident at performing handoffs, had lower rates of perceived near-miss events, and were happier.1
“Hospitalists everywhere are starting to realize the importance of trying to reduce opportunities for human error that occur during care transitions,” Dr. Payne says. “The biggest thing I learned from this research is the importance of standardizing the handoff process [with information communicated consistently].
“It is essential to keep communication lines open,” Dr. Payne adds. “No tool can replace the importance of communication between doctors and the need to sit down and talk. The ideal signout happens in a quiet room where the two of you can talk about active patients and achieve rapport. But, realistically, how often does that happen?”
Standardization is one of a handful of strategies hospitalists, researchers, and policymakers are using to tackle transitions—both in-hospital handoffs and post-discharge transitions—with outpatient care. Some hospitalists are using practice simulations and training strategies; others have implemented medication reconciliation checks at every discharge, checklists and other communication strategies, team-based quality-improvement (QI) initiatives, and new technologies to enhance and streamline communication. Some interventions follow the patient from the hospital to the community physician with a phone call, follow-up clinic, or other contact; others aim to empower the patient to be a better self-advocate. But for hospitalists, the challenge is to communicate the right amount of transfer information to the right receiver at the right time.
No matter the technique, the goal is the same: Improve the handoff and discharge process in a way that promotes efficiency and patient safety. And hospitalists are at the forefront of the changing landscape of care transitions.
Under the Microscope
Care transitions of all kinds are under the magnifying glass of national healthcare reform, with growing recognition of the need to make care safer and reduce the preventable, costly hospital readmissions caused by incomplete handoffs. Care transitions for hospitalists include internal handoffs, both at daily shift changes and at service changes when an outgoing provider is leaving after a period of consecutive daily shifts. These typically involve a sign-out process and face-to-face encounter, with some kind of written backup. One teaching institution reported that such handoffs take place 4,000 times per day in the hospital, or 1.6 million times per year.2
—Arpana Vidyarthi, MD, University of California at San Francisco
Geographical transitions can be from one floor or department to another, or out the hospital door to another facility or home. Transitions typically involve a discharge process and a written discharge summary. Care transitions also include hospital admissions, which put the hospitalist in the role of handoff receiver rather than initiator, plus a variety of other transitions involving nurses, physician extenders, and other practitioners.
Each transition is a major decision point in the course of a patient’s hospitalization; each transition also presents a time of heightened vulnerability (e.g., potential communication breakdowns, medication errors, patient anxiety or confusion, etc.). In fact, according to a Transitions of Care Consensus Policy Statement published in 2009 by SHM and five other medical societies, handoffs are ubiquitous in HM, with significant patient safety and quality deficiencies in handoffs existing in the current system.3
Poor communication at the time of handoff has been implicated in near-misses and adverse events in a variety of healthcare contexts, including 70% of hospital sentinel events studied by The Joint Commission, which named standardized handoffs (with an opportunity for interactive communication) as a National Patient Safety Goal in 2006.4 The federal government is studying care transitions, supporting demonstration projects for Medicare enrollees, and including readmission rates in national hospital report card data.
“Transitions of care and handoffs are a huge focus right now because of the increased fragmentation of care in the United States. Hospitalists are in charge of a greater percentage of hospitalized patients, which means more coordination of care is needed,” says Vineet Arora, MD, MA, FHM, assistant professor of medicine and associate director of the internal-medicine residency at the University of Chicago, and chair of the SHM task force on handoffs.
Inadequate communication and poor care transitions can undermine hospitalists’ best care-planning efforts, erode patients’ and families’ confidence and satisfaction with hospital care, and leave primary-care physicians (PCPs) feeling unsatisfied with the relationship. As many as 1 in 5 Medicare beneficiary hospitalizations result in a readmission within 30 days, and while not all of these are preventable, far too many are.5 Another prospective cohort study found that 1 in 5 patients discharged from the hospital to the home experienced an adverse event within three weeks of discharge.6 Complex comorbidities, advanced age, unknown PCP, and limited healthcare literacy present hospitalists with extremely difficult transitions.
Patient safety and cost control are the linchpins to national efforts to improve transitions of care. Dr. Arora recently coauthored an original research paper, which will be published in the Journal of Hospital Medicine in September, showing older hospitalized patients are twice as likely to report problems after discharge if their PCPs were not aware they were hospitalized.
“With escalating healthcare costs, people are looking at ways to save money and reduce redundant care,” Dr. Arora explains, pointing out, as an example, repeated tests resulting from inadequate communication between healthcare providers.
The System Must Change
“All of the effort we put into saving someone’s life—the years of experience, training, medical school, and residency—all of it comes to bear on that hospitalized patient. And it can all be unraveled at the time of discharge if it’s not handled properly,” says Arpana Vidyarthi, MD, a hospitalist and director of quality at the University of California at San Francisco.
Dr. Vidyarthi views in-hospital and discharge transitions as integrally related. “The analysis is similar, even if different techniques may be needed,” she says, adding that, fundamentally, it involves having a system that allows people—or forces them—to do the “right thing.”
That’s why achieving effective care transitions will require more than just a standardized tool or process, Dr. Vidyarthi says. “This is about understanding the ways people communicate and finding ways to train them to communicate better,” she says. “The problem we have is not a lack of information, but how to communicate what, to whom, and when.”
What’s really needed, Dr. Vidyarthi says, is a hospital’s commitment to more effective transitions and its hospitalists’ leadership in driving a comprehensive, multidisciplinary, team- and evidence-based QI process. The new process should be a QI-based solution to a hospital’s care-transitions issues. “Before you can standardize your process, you need to understand it,” she says. “This is a complex problem, and it needs a multifaceted solution. But this lies squarely within the hospitalist arena. We’re part of everything that happens in the hospital.
—Anuj Dalal, MD, Brigham and Women’s Hospital, Boston
Hospital administrators are looking to HM to solve transition and readmission problems now, says Tina Budnitz, MPH, BOOST Project Director (Better Outcomes for Older Adults through Safe Transitions). She expects the scrutiny from the C-suite, legislators, and watchdog groups to increase as the spotlight continues to shine on the healthcare system.
“Any hospitalist can act as a leader in their institution,” Budnitz says. “Be a change agent, pull a group together, and start asking questions: Do we have safe care-transitions practices and processes in place? Just by asking the right question, you can be a catalyst for the system.”
Budnitz also emphasizes the importance of teamwork in the hospital setting. “How can I help my teammates? What am I communicating to the nurses on rounds?” she says. “Can you initiate dialogue with your outpatient medical groups: ‘These faxes we’re sending you—is that information getting to you in ways and times that are helpful? And, by the way, when your patient is admitted, this information would really help me.’ ”
Innovative Strategies
One of the most important initiatives responding to concerns about care transitions is Project BOOST (www.hos pitalmedicine.org/BOOST), a comprehensive toolkit for improving a hospital’s transitions of care. The project aims to build a national consensus for best practices in transitions; collaborate with representatives from the Agency for Healthcare Research and Quality (AHRQ), the Centers for Medicare and Medicaid Services (CMS), and the Joint Commission; and develop a national resource library, Budnitz says.
“Project BOOST not only puts forth best practices for admitting patients, planning for discharge, and then doing the discharge, it also helps show facilities how to change their systems, with resources and tools for analyzing and re-engineering the system,” she says. “Sites get one-to-one assistance from a mentor.”
Six hospitals signed on to the pilot program in 2008; 24 more joined last year. In January, SHM announced a collaborative with the University of Michigan and Blue Cross Blue Shield of Michigan for 15 Michigan hospitals to receive training and mentorship starting in May. And last month, SHM and the California HealthCare Foundation announced a Project BOOST initiative for 20 of the health system’s hospitals (see “California Dreamin’”, p. 6). Other free resources offered on the BOOST Web portal include clinical, data collection, and project management tools. SHM also has a DVD that explains how to use the “teachback” method to improve communication with patients.
Jennifer Myers, MD, FHM, assistant professor of clinical medicine and patient-safety officer at the Hospital of the University of Pennsylvania in Philadelphia, is a Project BOOST participant who spearheaded a process change to improve the quality of her facility’s discharge summary, along with accompanying resident education.7 The discharge summary recently was integrated with the hospital’s electronic health record (EHR) system.
“We’ve gone from dictating the discharge summary to an electronic version completed by the hospitalist, with prompts for key components of the summary, which allows us to create summaries more efficiently—ideally on the day of discharge, but usually within 48 hours,” Dr. Myers says. “We previously researched whether teaching made a difference in the quality of discharges; we found that it did. So we look forward to standardizing our teaching approach around this important topic for all residents.”
Another care-transitions innovation receiving a lot of attention from the government and the private sector is Project RED (Re-Engineered Discharge), led by Brian Jack, MD, vice chair of the department of family medicine at Boston Medical Center. The Project RED research group develops and tests strategies to improve the hospital discharge process to promote patient safety and reduce rehospitalization rates.
“We used re-engineering tools borrowed from other fields, brought together experts from all over the hospital, divided up the whole discharge process, and identified key principles,” Dr. Jack explains. The resulting discharge strategy is reflected in an 11-item checklist of discrete, mutually reinforcing components, which have been shown to reduce rehospitalization rates by 32% while raising patient satisfaction.8 It includes comprehensive discharge and after-hospital plans, a nurse discharge advocate, and a medication reconciliation phone call to the patient. A virtual “patient advocate,” a computerized avatar named Louise, is now being tested. If successful, it will allow patients to interact with a touch-screen teacher of the after-care plan who has time to work at the patient’s pace.
Technology and Transitions
Informatics can be a key player in facilitating care transitions, says Anuj Dalal, MD, a hospitalist and instructor in medicine at Brigham and Women’s Hospital in Boston. He is using one of his hospital’s technological strengths—a well-established, firewall-protected e-mail system—to help improve the discharge process.
“We decided to try to improve awareness of test results pending at the time of discharge,” Dr. Dalal explains. “We created an intervention that automatically triggers an e-mail with the finalized test results to the responsible providers. The intervention creates a loop of communication between the inpatient attending and the PCP. What we hope to show in our research over the next year or two is whether the intervention actually increases awareness of test results by providers.”
One thing to remember is that “all kinds of things can go wrong with care transitions,” no matter the size of the institution, the experience of the staff, or technological limitations, says Vineet Chopra, MD, FACP, a hospitalist at the University of Michigan Health System in Ann Arbor. “The problems of transitions vary from place to place, day to day, time of day, shift changes; and let’s not forget physician extenders and the other members of the healthcare team,” he says. “The more complicated the team, the more complicated the information needing to be handed off becomes.”
Who Else Is Looking at Transitions of Care?
SHM convened the Handoffs Task Force in 2006. The team systematically reviewed the literature and published recommendations in the September 2009 Journal of Hospital Medicine.9 The recommendations are aimed at both community and academic hospitals, as well as hospitalists and other healthcare providers. A new collaborative designed to supplement Project BOOST for hospitalist group handoffs and help put the guidelines into practice is in the works, says Dr. Arora, the task force’s chair.
SHM and five medical groups, including the American College of Physicians, issued a Transitions of Care Consensus Statement, published in the July 2009 issue of the Journal of Hospital Medicine.5 Guiding principles relate to education, measurement, accountability, timely interchange of information, inclusion of patient and family, respect for the medical home, and the need for national standards.
The Joint Commission’s Center for Transforming Health Care, established in 2009 to solve healthcare’s most critical safety and quality problems, has made handoff communications its second major target, and is now working with 10 healthcare systems. Standardized handoff processes and communications were the subject of the Joint Commission’s 2006 National Patient Safety Goal, while the Comprehensive Accreditation Manual for Hospitals also specifies that before a hospital discharges or transfers a patient, it should inform and educate the patient about his or her follow-up care and services.
“We now have a safety goal under review dealing with medication reconciliation, and there are relevant standards related to culturally sensitive communication and low-literacy-level communication,” says Deborah Zadzam, PhD, RN, FAAN, director of international quality and performance measures for Joint Commission Resources. “The essential message the Joint Commission has for hospitalists is to communicate clearly, effectively and thoroughly; don’t assume you are understood or that you understand.”—LB
Before he joined the group at the university, Dr. Chopra worked at a community hospital, St. Joseph’s Mercy Hospital in Hot Springs, Ark. “It’s hard to come up with a one-size-fits-all solution when there are so many variables,” he says. At the community hospital, “we mandated that the hospitalist call the PCP at the time of discharge. At the academic medical center, we share an EHR with the PCPs and can reach them electronically. We are required to have the discharge summary in the computer before the patient leaves the hospital, and we mandate that hospitalists are reachable by e-mail or phone when they are off.
“I’m not a believer in throwing more technology at problems and just adding more layers of information tools,” Dr. Chopra adds. “Hospitalists who used to carry stethoscopes now also have a clipboard, phone, pager, PDA, and nine different signouts in their pockets. What we want to do is make their life easier. Here, we are looking at technology as a means to do that.”
Dr. Chopra and hospitalist colleague Prasanth Gosineni, MD, have been working with an Ann Arbor tech company called Synaptin to develop a lightweight, mobile client application designed to work on smartphones. Still in pilot testing, it would allow for task-oriented and priority-based messaging in real time and the systematic transfer of important information for the next hospitalist shift.
“You need to be able to share information in a systematic way, but that’s only half of the answer. The other half is the ability to ask specific questions,” Dr. Chopra says. “Technology doesn’t take away from the face-to-face encounter that needs to happen. Nothing will replace face time, but part of the solution is to provide data efficiently and in a way that is easily accessible.”
Dr. Chopra admits that EHR presents both positives and negatives to improved transitions and patient care, “depending on how well it works and what smart features it offers,” he says, “but also recognizing that EHR and other technologies have also taken us farther away from face-to-face exchanges. Some would say that’s part of the problem.”
Handoffs, discharges, and other transitions are ubiquitous in HM—and fraught with the potential for costly and harmful errors. The ideal of an interactive, face-to-face handoff simply is not available for many care transitions. However, hospitalists are challenged to find solutions that will work in their hospitals, with their teams, and their types of patients. Patients and policymakers expect nothing less. TH
Larry Beresford is a freelance writer based in Oakland, Calif.
References
- Payne C, Stein J, Dressler D. Implementation of a structured electronic tool to improve patient handoffs and resident satisfaction. Poster abstract: Internal Medicine 2010, April 21-24, 2010, Toronto.
- Vidyarthi AR. Triple Handoff. AHRQ WebM&M website. Available at: webmm.ahrq.gov/case.aspx? caseID=134. Published May 2006. Accessed May 29, 2010.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement: American College of Physicians, Society of General Internal Medicine, Society of Hospital Medicine, American Geriatrics Society, American College of Emergency Physicians, and Society for Academic Emergency Medicine. J Hosp Med. 2009;4(6):364-370.
- 2006 National Patient Safety Goals. The Joint Commission website. Available at: www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/06_npsgs.htm. Accessed June 8, 2010.
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009; 2:360:1418-1428.
- Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161-167.
- Myers JS, Jaipaul CK, Kogan JR, Krekun S, Bellini LM, Shea JA. Are discharge summaries teachable? The effects of a discharge summary curriculum on the quality of discharge summaries in an internal medicine residency program. Acad Med. 2006; 81(10):S5-S8.
- Jack BW, Chetty VK, Anthony D, et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009;150(3):178-187.
- Arora VM, Manjarrez E, Dressler DD, Basaviah P, Halasyamani L, Kripalani S. Hospitalist handoffs: a systematic review and task force recommendations. J Hosp Med. 2009;4(7): 433-440.
- Halasyamani L, Kripalani S, Coleman E, et al. Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists. J Hosp Med. 2006;1(6):354-360.
- Schnipper JL, Kirwin JL, Cotugno MC, et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Int Med. 2006;166(5):565-571.
- Dudas V, Bookwalter T, Kerr KM, Pantilat SZ. The impact of follow-up telephone calls to patients after hospitalization. Am J Med. 2001;111(9B): 26S-30S.
Care Transition Tips for Hospitalists and Groups
One recognized key to effective internal handoffs is the face-to-face verbal update, with opportunities to ask questions, priority given to sicker patients, and a written backup filling in the blanks with information that might become important as the patient’s condition changes. But if that is not practical for your HM group, what tools and processes will come closest to the ideal?
A key to effective discharge from the hospital is connection with the PCP, although face-to-face encounters with PCPs are highly unlikely. Hospitalists say there are levels of connection with PCPs, from the urgent (“I need to talk to someone right now”) to the routine (“It’s OK if they get this information tomorrow”). Many often wonder if there should be two levels of discharge communication with PCPs: an immediate message relaying crucial information and a formal discharge summary coming later.
For HM groups, the following is a list of suggestions from transitions-of-care researchers:
- Keep accurate and up-to-date contact information, including preferred communication medium, on referring physicians; survey them on their satisfaction with the discharge communications they receive from hospitalists.
- Partner with hospital administrators and with patient-safety and quality officers to address handoff issues.
- Partner with IT staff to help bridge the divide between clinicians and information technology.
- Track such outcomes as rehospitalization rates.
- Offer formal training on handoffs, discharges, and effective communication to physicians and other providers.
- Standardize the signout process, with computerized tools when appropriate, and create automated systems for following up on tests and lab results that come back after discharge.
- Structure shifts and their overlaps to help facilitate signouts.
- Consider implementing a discharge checklist.10
- Develop a strategy for medication reconciliation, with someone assigned to the process, be that a hospitalist, pharmacist or nurse.11
- Advocate for a post-discharge call-back policy by assigned staff at defined intervals, either for every patient discharged or for those targeted as higher-risk.12
- Consider creating a post-discharge clinic and/or a phone number that discharged patients can call to clarify post-discharge questions and concerns.
For individual hospitalists:
- Understand the transition process, where it fails, and why.
- Be open to changing the way you do things. Be accountable for transitions, and a role model for others.
- Focus on the present—today’s baseline, current to-do items, and what to expect next in the patient’s care.
- Track patients and their future discharge needs from the day of admission. What’s the likely date for going home? What does the patient need to learn in the meantime? Help nurses focus on achieving those needs and, if possible, schedule the initial outpatient clinic appointment before the patient leaves the hospital.
- Take time to talk your patients, listen to their concerns and confirm their understanding of what lies ahead.
For hospitalists on the receiving end of transition messages:
- Actively listen—stay focused, limit interruptions, take notes.
- Ask questions to ensure your understanding and read back what you understand to be the communication.
- Have a system for keeping track of to-do items requiring follow-up.—LB