User login
Bronchoscopy and tracheostomy in the COVID-19 era
The coronavirus disease 2019 (COVID-19) pandemic has changed the way we deliver healthcare for the foreseeable future. Not only have we had to rapidly learn how to evaluate, diagnose, and treat this new disease, we have also had to shift how we screen, triage, and care for other patients for both their safety and ours. As the virus is primarily spread via respiratory droplets, aerosol-generating procedures (AGP), such as bronchoscopy and tracheostomy, are high-risk for viral transmission. We have therefore had to reassess the risk/benefit ratio of performing these procedures – what is the risk to the patient by procedure postponement vs the risk to the health-care personnel (HCP) involved by moving ahead with the procedure? And, if proceeding, how should we protect ourselves? How do we screen patients to help us stratify risk? In order to answer these questions, we generally divide patients into three categories: the asymptomatic outpatient, the symptomatic patient, and the critically ill patient.

The asymptomatic outpatient
Early in the pandemic as cases began to spike in the US, many hospitals decided to postpone all elective procedures and surgeries. Guidelines quickly emerged stratifying bronchoscopic procedures into emergent, urgent, acute, subacute, and truly elective with recommendations on the subsequent timing of those procedures (Pritchett MA, et al. J Thorac Dis. 2020 May;12[5]:1781-1798). As we have obtained further data and our infrastructure has been bolstered, many physicians have begun performing more routine procedures. Preprocedural screening, both with symptom questionnaires and nasopharyngeal swabs, has been enacted as a measure to prevent inadvertent exposure to infected patients. While there are limited data regarding the reliability of this measure, emerging data have shown good concordance between nasopharyngeal SARS-CoV-2 polymerase chain reaction (PCR) swabs and bronchoalveolar lavage (BAL) samples in low-risk patients (Oberg, et al. Personal communication, Sept 2020). Emergency procedures, such as foreign body aspiration, critical airway obstruction, and massive hemoptysis, were generally performed without delay throughout the pandemic. More recently, emphasis has been placed on prioritizing procedures for acute clinical diagnoses, such as biopsies for concerning lung nodules or masses in potentially early-stage patients, in those where staging is needed and in those where disease progression is suspected. Subacute procedures, such as inspection bronchoscopy for cough, minor hemoptysis, or airway stent surveillance, have generally been reintroduced while elective procedures, such as bronchial thermoplasty and bronchoscopic lung volume reduction, are considered elective, and their frequency and timing is determined mostly by the number of new cases of COVID-19 in the local community.
For all procedures, general modifications have been made. High-efficiency particulate air (HEPA) filters should be placed on all ventilatory circuits. When equivalent, flexible bronchoscopy is preferred over rigid bronchoscopy due to the closed circuit. Enhanced personal protective equipment (PPE) for all procedures is recommended – this typically includes a gown, gloves, hair bonnet, N-95 mask, and a face shield. Strict adherence to the Centers for Disease Control and Prevention (CDC) guidelines for postprocedure cleaning and sterilization is strongly recommended. In some cases, single-use bronchoscopes are being preferentially used, though no strong recommendations exist for this.
The symptomatic COVID-19 patient
In patients who have been diagnosed with SARS-CoV-2, we generally recommend postponing all procedures other than for life-threatening indications. For outpatients, we generally wait for two negative nasopharyngeal swabs prior to performing any nonemergent procedure. In inpatients, similar recommendations exist. Potential inpatient indications for bronchoscopy include diagnostic evaluation for alternate or coinfections, and therapeutic aspiration of clinically significant secretions. These should be carefully considered and performed only if deemed absolutely necessary. If bronchoscopy is needed in a patient with suspected or confirmed COVID-19, at a minimum, gown, gloves, head cover, face shield, and an N-95 mask should be worn. A powered air purifying respirator (PAPR) can be used and may provide increased protection. Proper donning and doffing techniques should be reviewed prior to any procedure. Personnel involved in the case should be limited to the minimum required. The procedure should be performed by experienced operators and limited in length. Removal and reinsertion of the bronchoscope should be minimized.

The critically ill COVID-19 patient
While the majority of patients infected with SARS-CoV-2 will have only mild symptoms, we know that a subset of patients will develop respiratory failure. Of those, a small but significant number will require prolonged mechanical ventilation during their clinical course. Thus, the consideration for tracheostomy comes into play.
Multiple issues arise when discussing tracheostomy placement in the COVID-19 world. Should it be done at all? If yes, what is the best technique and who should do it? When and where should it be done? Importantly – how do we care for patients once it is in place to facilitate recovery and, hopefully, decannulation?
Tracheostomy tubes are used in the ICU for patients who require prolonged mechanical ventilation for many reasons – patient comfort, decreased need for sedation, and to facilitate transfer out of the ICU to less acute care areas. These reasons are just as important in patients afflicted with respiratory failure from COVID-19, if not more so. As the patient volumes surge, health-care systems can quickly become overwhelmed. The ability to safely move patients out of the ICU frees up those resources for others who are more acutely ill.
The optimal technique for tracheostomy placement largely depends on the technological and human capital of each institution. Emphasis should be placed on procedural experience, efficiency, safety, and minimizing risk to HCP. While mortality rates do not differ between the surgical and percutaneous techniques, the percutaneous approach has been shown to require less procedural time (Iftikhar IH, et al. Lung. 2019[Jun];197[3]:267-275), an important infection control advantage in COVID-19 patients. Additionally, percutaneous tracheostomies are typically performed at the bedside, which offers the immediate benefit of minimizing patient transfer. This decreases exposure to multiple HCP, as well as contamination of other health-care areas. If performing a bronchoscopic-guided percutaneous tracheostomy, apnea should be maintained from insertion of the guiding catheter to tracheostomy insertion in order to minimize aerosolization. A novel technique involving placing the bronchoscope beside the endotracheal tube instead of through it has also been described (Angel L, et al. Ann Thorac Surg. 2020[Sep];110[3]:1006–1011).

Timing of tracheostomy placement in COVID-19 patients has varied widely. Initially, concern for the safety of HCP performing these procedures led to recommendations of waiting at least 21 days of intubation or until COVID-19 testing became negative. However, more recently, multiple recommendations have been made for tracheostomy placement after day 10 of intubation (McGrath, et al. Lancet Respir Med. 2020[Jul];8[7]:717-725).
Finally, once a tracheostomy tube has been placed, the care does not stop there. As patients are transitioned to rehabilitation centers or skilled nursing facilities and are assessed for weaning, downsizing, and decannulation, care should be taken to avoid virus aerosolization during key high-risk steps. Modifications such as performing spontaneous breathing trials using pressure support (a closed circuit) rather than tracheostomy mask, bypassing speaking valve trials in favor of direct tracheostomy capping, and avoiding routine tracheostomy downsizing are examples of simple steps that can be taken to facilitate patient progress while minimizing HCP risk (Divo, et al. Respir Care. 2020[Aug]5;respcare.08157).
What’s ahead?
As we move forward, we will continue to balance caring for patients effectively and efficiently while minimizing risk to ourselves and others. Ultimately until a vaccine exists, we will have to focus on prevention of infection and spread; therefore, the core principles of hand hygiene, mask wearing, and social distancing have never been more important. We encourage continued study, scrutiny, and collaboration in order to optimize procedural techniques as more information becomes available.
Dr. Oberg is with the Section of Interventional Pulmonology, David Geffen School of Medicine at UCLA; Dr. Beattie is with the Section of Interventional Pulmonology, Memorial Sloan Kettering Cancer Center, New York; and Dr. Folch is with the Section of Interventional Pulmonology, Massachusetts General Hospital, Harvard Medical School.
The coronavirus disease 2019 (COVID-19) pandemic has changed the way we deliver healthcare for the foreseeable future. Not only have we had to rapidly learn how to evaluate, diagnose, and treat this new disease, we have also had to shift how we screen, triage, and care for other patients for both their safety and ours. As the virus is primarily spread via respiratory droplets, aerosol-generating procedures (AGP), such as bronchoscopy and tracheostomy, are high-risk for viral transmission. We have therefore had to reassess the risk/benefit ratio of performing these procedures – what is the risk to the patient by procedure postponement vs the risk to the health-care personnel (HCP) involved by moving ahead with the procedure? And, if proceeding, how should we protect ourselves? How do we screen patients to help us stratify risk? In order to answer these questions, we generally divide patients into three categories: the asymptomatic outpatient, the symptomatic patient, and the critically ill patient.
The asymptomatic outpatient
Early in the pandemic as cases began to spike in the US, many hospitals decided to postpone all elective procedures and surgeries. Guidelines quickly emerged stratifying bronchoscopic procedures into emergent, urgent, acute, subacute, and truly elective with recommendations on the subsequent timing of those procedures (Pritchett MA, et al. J Thorac Dis. 2020 May;12[5]:1781-1798). As we have obtained further data and our infrastructure has been bolstered, many physicians have begun performing more routine procedures. Preprocedural screening, both with symptom questionnaires and nasopharyngeal swabs, has been enacted as a measure to prevent inadvertent exposure to infected patients. While there are limited data regarding the reliability of this measure, emerging data have shown good concordance between nasopharyngeal SARS-CoV-2 polymerase chain reaction (PCR) swabs and bronchoalveolar lavage (BAL) samples in low-risk patients (Oberg, et al. Personal communication, Sept 2020). Emergency procedures, such as foreign body aspiration, critical airway obstruction, and massive hemoptysis, were generally performed without delay throughout the pandemic. More recently, emphasis has been placed on prioritizing procedures for acute clinical diagnoses, such as biopsies for concerning lung nodules or masses in potentially early-stage patients, in those where staging is needed and in those where disease progression is suspected. Subacute procedures, such as inspection bronchoscopy for cough, minor hemoptysis, or airway stent surveillance, have generally been reintroduced while elective procedures, such as bronchial thermoplasty and bronchoscopic lung volume reduction, are considered elective, and their frequency and timing is determined mostly by the number of new cases of COVID-19 in the local community.
For all procedures, general modifications have been made. High-efficiency particulate air (HEPA) filters should be placed on all ventilatory circuits. When equivalent, flexible bronchoscopy is preferred over rigid bronchoscopy due to the closed circuit. Enhanced personal protective equipment (PPE) for all procedures is recommended – this typically includes a gown, gloves, hair bonnet, N-95 mask, and a face shield. Strict adherence to the Centers for Disease Control and Prevention (CDC) guidelines for postprocedure cleaning and sterilization is strongly recommended. In some cases, single-use bronchoscopes are being preferentially used, though no strong recommendations exist for this.
The symptomatic COVID-19 patient
In patients who have been diagnosed with SARS-CoV-2, we generally recommend postponing all procedures other than for life-threatening indications. For outpatients, we generally wait for two negative nasopharyngeal swabs prior to performing any nonemergent procedure. In inpatients, similar recommendations exist. Potential inpatient indications for bronchoscopy include diagnostic evaluation for alternate or coinfections, and therapeutic aspiration of clinically significant secretions. These should be carefully considered and performed only if deemed absolutely necessary. If bronchoscopy is needed in a patient with suspected or confirmed COVID-19, at a minimum, gown, gloves, head cover, face shield, and an N-95 mask should be worn. A powered air purifying respirator (PAPR) can be used and may provide increased protection. Proper donning and doffing techniques should be reviewed prior to any procedure. Personnel involved in the case should be limited to the minimum required. The procedure should be performed by experienced operators and limited in length. Removal and reinsertion of the bronchoscope should be minimized.
The critically ill COVID-19 patient
While the majority of patients infected with SARS-CoV-2 will have only mild symptoms, we know that a subset of patients will develop respiratory failure. Of those, a small but significant number will require prolonged mechanical ventilation during their clinical course. Thus, the consideration for tracheostomy comes into play.
Multiple issues arise when discussing tracheostomy placement in the COVID-19 world. Should it be done at all? If yes, what is the best technique and who should do it? When and where should it be done? Importantly – how do we care for patients once it is in place to facilitate recovery and, hopefully, decannulation?
Tracheostomy tubes are used in the ICU for patients who require prolonged mechanical ventilation for many reasons – patient comfort, decreased need for sedation, and to facilitate transfer out of the ICU to less acute care areas. These reasons are just as important in patients afflicted with respiratory failure from COVID-19, if not more so. As the patient volumes surge, health-care systems can quickly become overwhelmed. The ability to safely move patients out of the ICU frees up those resources for others who are more acutely ill.
The optimal technique for tracheostomy placement largely depends on the technological and human capital of each institution. Emphasis should be placed on procedural experience, efficiency, safety, and minimizing risk to HCP. While mortality rates do not differ between the surgical and percutaneous techniques, the percutaneous approach has been shown to require less procedural time (Iftikhar IH, et al. Lung. 2019[Jun];197[3]:267-275), an important infection control advantage in COVID-19 patients. Additionally, percutaneous tracheostomies are typically performed at the bedside, which offers the immediate benefit of minimizing patient transfer. This decreases exposure to multiple HCP, as well as contamination of other health-care areas. If performing a bronchoscopic-guided percutaneous tracheostomy, apnea should be maintained from insertion of the guiding catheter to tracheostomy insertion in order to minimize aerosolization. A novel technique involving placing the bronchoscope beside the endotracheal tube instead of through it has also been described (Angel L, et al. Ann Thorac Surg. 2020[Sep];110[3]:1006–1011).
Timing of tracheostomy placement in COVID-19 patients has varied widely. Initially, concern for the safety of HCP performing these procedures led to recommendations of waiting at least 21 days of intubation or until COVID-19 testing became negative. However, more recently, multiple recommendations have been made for tracheostomy placement after day 10 of intubation (McGrath, et al. Lancet Respir Med. 2020[Jul];8[7]:717-725).
Finally, once a tracheostomy tube has been placed, the care does not stop there. As patients are transitioned to rehabilitation centers or skilled nursing facilities and are assessed for weaning, downsizing, and decannulation, care should be taken to avoid virus aerosolization during key high-risk steps. Modifications such as performing spontaneous breathing trials using pressure support (a closed circuit) rather than tracheostomy mask, bypassing speaking valve trials in favor of direct tracheostomy capping, and avoiding routine tracheostomy downsizing are examples of simple steps that can be taken to facilitate patient progress while minimizing HCP risk (Divo, et al. Respir Care. 2020[Aug]5;respcare.08157).
What’s ahead?
As we move forward, we will continue to balance caring for patients effectively and efficiently while minimizing risk to ourselves and others. Ultimately until a vaccine exists, we will have to focus on prevention of infection and spread; therefore, the core principles of hand hygiene, mask wearing, and social distancing have never been more important. We encourage continued study, scrutiny, and collaboration in order to optimize procedural techniques as more information becomes available.
Dr. Oberg is with the Section of Interventional Pulmonology, David Geffen School of Medicine at UCLA; Dr. Beattie is with the Section of Interventional Pulmonology, Memorial Sloan Kettering Cancer Center, New York; and Dr. Folch is with the Section of Interventional Pulmonology, Massachusetts General Hospital, Harvard Medical School.
The coronavirus disease 2019 (COVID-19) pandemic has changed the way we deliver healthcare for the foreseeable future. Not only have we had to rapidly learn how to evaluate, diagnose, and treat this new disease, we have also had to shift how we screen, triage, and care for other patients for both their safety and ours. As the virus is primarily spread via respiratory droplets, aerosol-generating procedures (AGP), such as bronchoscopy and tracheostomy, are high-risk for viral transmission. We have therefore had to reassess the risk/benefit ratio of performing these procedures – what is the risk to the patient by procedure postponement vs the risk to the health-care personnel (HCP) involved by moving ahead with the procedure? And, if proceeding, how should we protect ourselves? How do we screen patients to help us stratify risk? In order to answer these questions, we generally divide patients into three categories: the asymptomatic outpatient, the symptomatic patient, and the critically ill patient.
The asymptomatic outpatient
Early in the pandemic as cases began to spike in the US, many hospitals decided to postpone all elective procedures and surgeries. Guidelines quickly emerged stratifying bronchoscopic procedures into emergent, urgent, acute, subacute, and truly elective with recommendations on the subsequent timing of those procedures (Pritchett MA, et al. J Thorac Dis. 2020 May;12[5]:1781-1798). As we have obtained further data and our infrastructure has been bolstered, many physicians have begun performing more routine procedures. Preprocedural screening, both with symptom questionnaires and nasopharyngeal swabs, has been enacted as a measure to prevent inadvertent exposure to infected patients. While there are limited data regarding the reliability of this measure, emerging data have shown good concordance between nasopharyngeal SARS-CoV-2 polymerase chain reaction (PCR) swabs and bronchoalveolar lavage (BAL) samples in low-risk patients (Oberg, et al. Personal communication, Sept 2020). Emergency procedures, such as foreign body aspiration, critical airway obstruction, and massive hemoptysis, were generally performed without delay throughout the pandemic. More recently, emphasis has been placed on prioritizing procedures for acute clinical diagnoses, such as biopsies for concerning lung nodules or masses in potentially early-stage patients, in those where staging is needed and in those where disease progression is suspected. Subacute procedures, such as inspection bronchoscopy for cough, minor hemoptysis, or airway stent surveillance, have generally been reintroduced while elective procedures, such as bronchial thermoplasty and bronchoscopic lung volume reduction, are considered elective, and their frequency and timing is determined mostly by the number of new cases of COVID-19 in the local community.
For all procedures, general modifications have been made. High-efficiency particulate air (HEPA) filters should be placed on all ventilatory circuits. When equivalent, flexible bronchoscopy is preferred over rigid bronchoscopy due to the closed circuit. Enhanced personal protective equipment (PPE) for all procedures is recommended – this typically includes a gown, gloves, hair bonnet, N-95 mask, and a face shield. Strict adherence to the Centers for Disease Control and Prevention (CDC) guidelines for postprocedure cleaning and sterilization is strongly recommended. In some cases, single-use bronchoscopes are being preferentially used, though no strong recommendations exist for this.
The symptomatic COVID-19 patient
In patients who have been diagnosed with SARS-CoV-2, we generally recommend postponing all procedures other than for life-threatening indications. For outpatients, we generally wait for two negative nasopharyngeal swabs prior to performing any nonemergent procedure. In inpatients, similar recommendations exist. Potential inpatient indications for bronchoscopy include diagnostic evaluation for alternate or coinfections, and therapeutic aspiration of clinically significant secretions. These should be carefully considered and performed only if deemed absolutely necessary. If bronchoscopy is needed in a patient with suspected or confirmed COVID-19, at a minimum, gown, gloves, head cover, face shield, and an N-95 mask should be worn. A powered air purifying respirator (PAPR) can be used and may provide increased protection. Proper donning and doffing techniques should be reviewed prior to any procedure. Personnel involved in the case should be limited to the minimum required. The procedure should be performed by experienced operators and limited in length. Removal and reinsertion of the bronchoscope should be minimized.
The critically ill COVID-19 patient
While the majority of patients infected with SARS-CoV-2 will have only mild symptoms, we know that a subset of patients will develop respiratory failure. Of those, a small but significant number will require prolonged mechanical ventilation during their clinical course. Thus, the consideration for tracheostomy comes into play.
Multiple issues arise when discussing tracheostomy placement in the COVID-19 world. Should it be done at all? If yes, what is the best technique and who should do it? When and where should it be done? Importantly – how do we care for patients once it is in place to facilitate recovery and, hopefully, decannulation?
Tracheostomy tubes are used in the ICU for patients who require prolonged mechanical ventilation for many reasons – patient comfort, decreased need for sedation, and to facilitate transfer out of the ICU to less acute care areas. These reasons are just as important in patients afflicted with respiratory failure from COVID-19, if not more so. As the patient volumes surge, health-care systems can quickly become overwhelmed. The ability to safely move patients out of the ICU frees up those resources for others who are more acutely ill.
The optimal technique for tracheostomy placement largely depends on the technological and human capital of each institution. Emphasis should be placed on procedural experience, efficiency, safety, and minimizing risk to HCP. While mortality rates do not differ between the surgical and percutaneous techniques, the percutaneous approach has been shown to require less procedural time (Iftikhar IH, et al. Lung. 2019[Jun];197[3]:267-275), an important infection control advantage in COVID-19 patients. Additionally, percutaneous tracheostomies are typically performed at the bedside, which offers the immediate benefit of minimizing patient transfer. This decreases exposure to multiple HCP, as well as contamination of other health-care areas. If performing a bronchoscopic-guided percutaneous tracheostomy, apnea should be maintained from insertion of the guiding catheter to tracheostomy insertion in order to minimize aerosolization. A novel technique involving placing the bronchoscope beside the endotracheal tube instead of through it has also been described (Angel L, et al. Ann Thorac Surg. 2020[Sep];110[3]:1006–1011).
Timing of tracheostomy placement in COVID-19 patients has varied widely. Initially, concern for the safety of HCP performing these procedures led to recommendations of waiting at least 21 days of intubation or until COVID-19 testing became negative. However, more recently, multiple recommendations have been made for tracheostomy placement after day 10 of intubation (McGrath, et al. Lancet Respir Med. 2020[Jul];8[7]:717-725).
Finally, once a tracheostomy tube has been placed, the care does not stop there. As patients are transitioned to rehabilitation centers or skilled nursing facilities and are assessed for weaning, downsizing, and decannulation, care should be taken to avoid virus aerosolization during key high-risk steps. Modifications such as performing spontaneous breathing trials using pressure support (a closed circuit) rather than tracheostomy mask, bypassing speaking valve trials in favor of direct tracheostomy capping, and avoiding routine tracheostomy downsizing are examples of simple steps that can be taken to facilitate patient progress while minimizing HCP risk (Divo, et al. Respir Care. 2020[Aug]5;respcare.08157).
What’s ahead?
As we move forward, we will continue to balance caring for patients effectively and efficiently while minimizing risk to ourselves and others. Ultimately until a vaccine exists, we will have to focus on prevention of infection and spread; therefore, the core principles of hand hygiene, mask wearing, and social distancing have never been more important. We encourage continued study, scrutiny, and collaboration in order to optimize procedural techniques as more information becomes available.
Dr. Oberg is with the Section of Interventional Pulmonology, David Geffen School of Medicine at UCLA; Dr. Beattie is with the Section of Interventional Pulmonology, Memorial Sloan Kettering Cancer Center, New York; and Dr. Folch is with the Section of Interventional Pulmonology, Massachusetts General Hospital, Harvard Medical School.
Endobronchial valves for lung volume reduction: What can we offer patients with advanced emphysema?
The global burden COPD is considerable. In the United States, it is the third most common cause of death and is associated with over $50 billion in annual direct and indirect health-care expenditures (Guarascio AJ, et al. Clinicoecon Outcomes Res. 2013;5:235). For patients with severe emphysema with hyperinflation, dyspnea is often a quality of life (QOL)-limiting symptom (O’Donnell DE, et al. Ann Am Thorac Soc. 2017;14:S30). Few proven palliation options exist, particularly for patients with dyspnea refractory to smoking cessation, medical management with bronchodilators, and pulmonary rehabilitation. The recent Food and Drug Administration (FDA) approval of two endobronchial valves for lung volume reduction has established the increasing importance of bronchoscopy as a management tool in advanced COPD.
Why were these valves developed?
For decades, lung volume reduction has been investigated as a mechanical approach to counter-act the physiologic effects of emphysematous hyperinflation. Its goal is to improve lung elastic recoil, respiratory muscle mechanical advantage and efficiency, and ventilation/perfusion matching. The landmark National Emphysema Treatment Trial (NETT), published in 2001 and 2003, demonstrated that in a select patient population (upper lobe-predominant emphysema and low exercise capacity), lung volume reduction surgery (LVRS) lowers mortality and improves QOL and exercise tolerance (Fishman A et al. N Engl J Med. 2003;348:2059). Despite the encouraging results in this study subpopulation, LVRS is per-formed infrequently (Decker MR, et al. J Thorac Cardiovasc Surg. 2014;148:2651). Concern about its morbidity and the specialized nature of the procedure has hindered widespread adoption. Subsequently, endobronchial techniques have been developed as an alternative to surgical lung volume reduction.
How does bronchoscopic lung volume reduction (BLVR) benefit patients with emphysema?
Valves used for ELVR are removable one-way flow devices placed by flexible bronchoscopy into selected airways supplying emphysematous lung. The valves block air entry but allow the exit of secretions and trapped air. This results in atelectasis of the targeted lobe and a decrease in lung volume.
Which endobronchial valves are available in the United States?
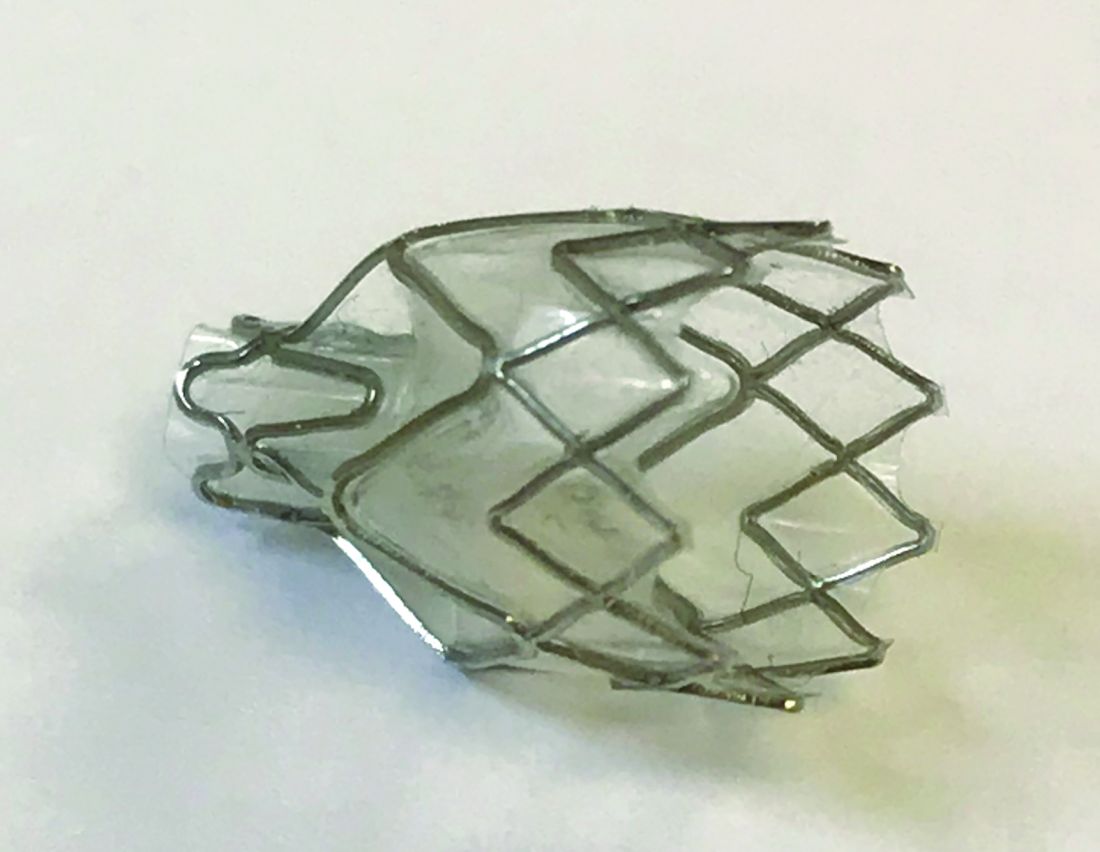
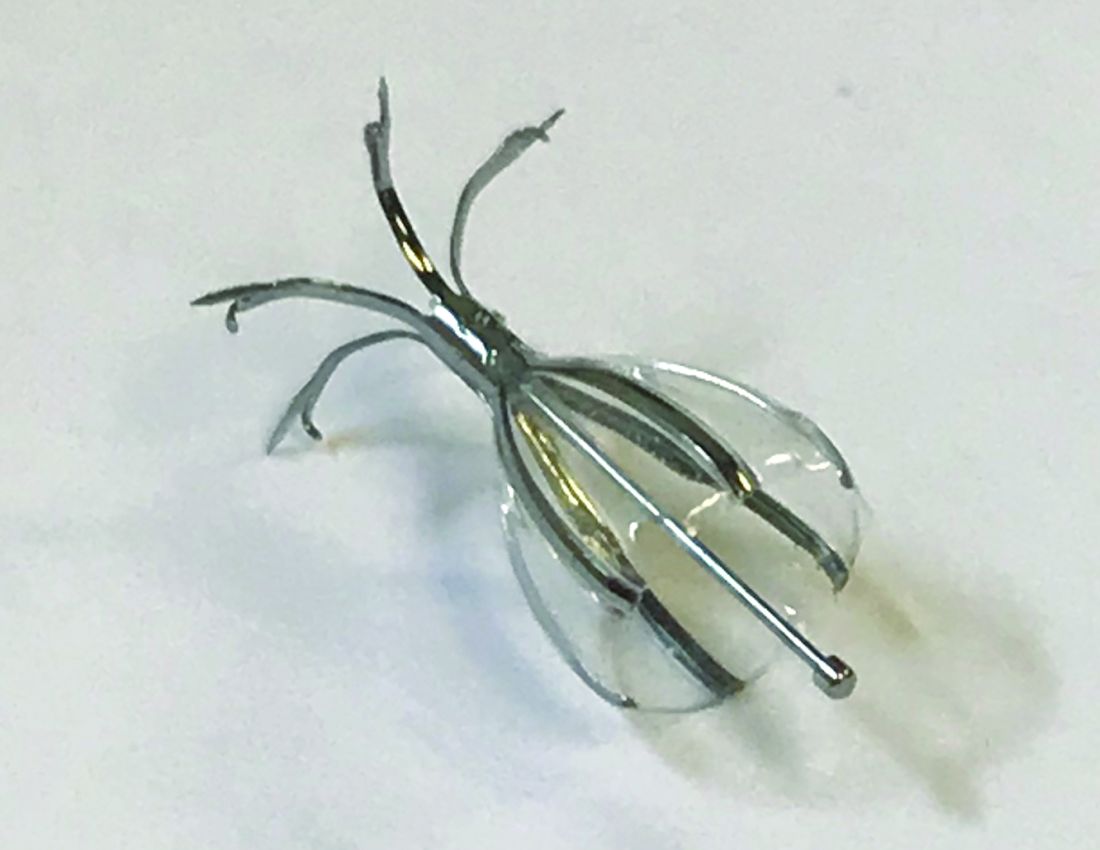
In 2018, two valves were approved by the FDA for bronchoscopic lung volume reduction (BLVR) – the Zephyr® EBV (Pulmonx) ( (Fig 1) and the Spiration® Valve System (Olympus) (IBV) (Fig 2). The Zephyr® EBV is a duckbill-shaped silicone valve mounted within a self-expanding nitinol (nickel titanium alloy) stent. It comes in three sizes for airways with a diameter 4 - 8.5 mm. The Spiration® IBV umbrella-shaped valve is com-posed of six nitinol struts surfaced with polyurethane. Its four sizes accommodate airway diameters 5 - 9 mm.
What’s the evidence behind BLVR?
Zephyr® Valves
The Endobronchial Valve for Emphysema Palliation Trial (VENT), the largest valve trial thus far, randomized patients with severe heterogeneous emphysema to receive unilateral Zephyr® valve placement or standard medical care (Sciurba FC, et al. N Engl J Med. 2010;363:1233). Overall improvement in spirometry and dyspnea scores was modest in the valve group. Post-hoc analysis identified an important subgroup of patients with significant clinical benefit, those with a complete fissure. This finding gave guidance to further EBV studies on patients with severe emphysema and absent collateral ventilation (CV).
Identifying a complete fissure on imaging is now used as a surrogate for assessing CV and is an integral part of the initial profiling of patients for EBV therapy (Koster TD, et al. Respiration. 2016;92(3):150).
In the STELVIO trial, 68 patients were randomized to Zephyr ® EBV placement or standard medical care (Klooster K, et al. N Engl J Med. 2015;373:2325). Those with EBV placement had significantly improved lung function and exercise capacity. TRANSFORM, a multicenter trial evaluating Zephyr® EBV placement in heterogeneous emphysema, showed similar results (Kemp SV, et al. Am J Respir Crit Care Med. 2017;196:1535).
The IMPACT trial compared patients with homogenous emphysema without CV to standard medical therapy alone. It showed improvement in FEV1, QOL scores, and exercise tolerance in the EBV group. This study affirmed that the absence of CV, rather than the pattern of emphysema, correlates with the clinical benefit from EBV therapy (Valipour A, et al. Am J Respir Crit Care Med. 2016;194(9):1073). Finally, LIBERATE, a multicenter study on the Zephyr® EBV, examined its placement in patients with heterogenous emphysema. This study demonstrated improvement in spirometry, QOL, and 6-minute walk test (6-MWT) distance (Criner GJ, et al. Am J Respir Crit Care Med. 2018;198:1151) over a longer period, 12 months, bolstering the findings of prior studies. These results prompted the Zephyr® valve’s FDA approval.
Spiration® Valves
Small trials have shown favorable results with the Spiration® IBV for BLVR, including a pilot multicenter cohort study of 30 patients with heterogeneous, upper-lobe emphysema who underwent valve placement (Wood DE, et al. J Thorac Cardiovasc Surg. 2007;133:65). In this trial, investigators found significant improvement in QOL scores, but no change in FEV1 or other physiologic parameters.
The EMPROVE trial is a multicenter, prospective, randomized, controlled study assessing BLVR with the Spiration® IBV. Six- and twelve-month data from the trial were presented in 2018 at the American Thoracic Society Conference and at the European Respiratory Society International Conference.
Collateral Ventilation
Identifying patients in whom there is no CV between lobes is critical to success with BLVR. Collateral ventilation allows air to bypass the valve occlusion distally, thereby negating the desired effect of valve placement, lobar atelectasis. High-resolution computed tomography (HRCT) scanning combined with quantitative software can be used to assess emphysema distribution and fissure integrity. Additionally, a proprietary technology, the Chartis System®, can be employed intra-procedure to estimate CV by measuring airway flow, resistance, and pressure in targeted balloon-occluded segments. Absence of CV based on Chartis evaluation was an inclusion criterion in the aforementioned valve studies.
Which patients with emphysema should be referred for consideration of valve placement?
The following criteria should be used in selecting patients for referral for BLVR:
• FEV1 15% - 45% of predicted value at baseline
• Evidence of hyperinflation: TLC greater than or equal to 100% and RV greater than or equal to 175%
• Baseline postpulmonary rehabilitation 6-MWT distance of 100 - 500 meters
• Clinically stable on < 20 mg prednisone (or equivalent) daily
• Nonsmoking for at least 4 months
• Integrity of one or both major fissures at least 75%
• Ability to provide informed consent and to tolerate bronchoscopy
Complications
The most common complication after valve placement is pneumothorax – a double-edged sword in that it typically indicates the achievement of atelectasis. In published trials, the frequency of pneumothorax varies. Some studies document rates below 10%. Others report rates of nearly 30% (Gompelmann D, et al. Respiration. 2014;87:485). In landmark trials, death related to pneumothorax occurred rarely. Most severe pneumothoraces occur within the first 72 hours after valve placement. This has prompted many centers to observe postprocedure patients in hospital for an extended period. Pneumonia and COPD exacerbations have also been reported after EBV placement. Therefore, in some trials, patients received prophylactic prednisolone and azithromycin. Other less common complications are hemoptysis, granulation tissue formation, and valve migration.
What’s ahead for ELVR?
Overall, valve technology for BLVR is an exciting option in the management of patients with severe emphysema and is now a staple for any advanced emphysema program. Key areas of future interest include management of patients with partial fissures, minimizing adverse procedural effects, and developing programs to optimize and streamline a multidisciplinary approach to timely and efficient referral, assessment, and intervention. As more patients with COPD undergo ELVR, one goal should be to create multi-institution prospective studies as well as registries to delineate further the optimal use of endobronchial valves for lung volume reduction.
Zephyr® Endobronchial Valve (Pulmonx)
Spiration® Valve System (Olympus)
The American College of Chest Physicians (CHEST) does not endorse or supp
The global burden COPD is considerable. In the United States, it is the third most common cause of death and is associated with over $50 billion in annual direct and indirect health-care expenditures (Guarascio AJ, et al. Clinicoecon Outcomes Res. 2013;5:235). For patients with severe emphysema with hyperinflation, dyspnea is often a quality of life (QOL)-limiting symptom (O’Donnell DE, et al. Ann Am Thorac Soc. 2017;14:S30). Few proven palliation options exist, particularly for patients with dyspnea refractory to smoking cessation, medical management with bronchodilators, and pulmonary rehabilitation. The recent Food and Drug Administration (FDA) approval of two endobronchial valves for lung volume reduction has established the increasing importance of bronchoscopy as a management tool in advanced COPD.
Why were these valves developed?
For decades, lung volume reduction has been investigated as a mechanical approach to counter-act the physiologic effects of emphysematous hyperinflation. Its goal is to improve lung elastic recoil, respiratory muscle mechanical advantage and efficiency, and ventilation/perfusion matching. The landmark National Emphysema Treatment Trial (NETT), published in 2001 and 2003, demonstrated that in a select patient population (upper lobe-predominant emphysema and low exercise capacity), lung volume reduction surgery (LVRS) lowers mortality and improves QOL and exercise tolerance (Fishman A et al. N Engl J Med. 2003;348:2059). Despite the encouraging results in this study subpopulation, LVRS is per-formed infrequently (Decker MR, et al. J Thorac Cardiovasc Surg. 2014;148:2651). Concern about its morbidity and the specialized nature of the procedure has hindered widespread adoption. Subsequently, endobronchial techniques have been developed as an alternative to surgical lung volume reduction.
How does bronchoscopic lung volume reduction (BLVR) benefit patients with emphysema?
Valves used for ELVR are removable one-way flow devices placed by flexible bronchoscopy into selected airways supplying emphysematous lung. The valves block air entry but allow the exit of secretions and trapped air. This results in atelectasis of the targeted lobe and a decrease in lung volume.
Which endobronchial valves are available in the United States?
In 2018, two valves were approved by the FDA for bronchoscopic lung volume reduction (BLVR) – the Zephyr® EBV (Pulmonx) ( (Fig 1) and the Spiration® Valve System (Olympus) (IBV) (Fig 2). The Zephyr® EBV is a duckbill-shaped silicone valve mounted within a self-expanding nitinol (nickel titanium alloy) stent. It comes in three sizes for airways with a diameter 4 - 8.5 mm. The Spiration® IBV umbrella-shaped valve is com-posed of six nitinol struts surfaced with polyurethane. Its four sizes accommodate airway diameters 5 - 9 mm.
What’s the evidence behind BLVR?
Zephyr® Valves
The Endobronchial Valve for Emphysema Palliation Trial (VENT), the largest valve trial thus far, randomized patients with severe heterogeneous emphysema to receive unilateral Zephyr® valve placement or standard medical care (Sciurba FC, et al. N Engl J Med. 2010;363:1233). Overall improvement in spirometry and dyspnea scores was modest in the valve group. Post-hoc analysis identified an important subgroup of patients with significant clinical benefit, those with a complete fissure. This finding gave guidance to further EBV studies on patients with severe emphysema and absent collateral ventilation (CV).
Identifying a complete fissure on imaging is now used as a surrogate for assessing CV and is an integral part of the initial profiling of patients for EBV therapy (Koster TD, et al. Respiration. 2016;92(3):150).
In the STELVIO trial, 68 patients were randomized to Zephyr ® EBV placement or standard medical care (Klooster K, et al. N Engl J Med. 2015;373:2325). Those with EBV placement had significantly improved lung function and exercise capacity. TRANSFORM, a multicenter trial evaluating Zephyr® EBV placement in heterogeneous emphysema, showed similar results (Kemp SV, et al. Am J Respir Crit Care Med. 2017;196:1535).
The IMPACT trial compared patients with homogenous emphysema without CV to standard medical therapy alone. It showed improvement in FEV1, QOL scores, and exercise tolerance in the EBV group. This study affirmed that the absence of CV, rather than the pattern of emphysema, correlates with the clinical benefit from EBV therapy (Valipour A, et al. Am J Respir Crit Care Med. 2016;194(9):1073). Finally, LIBERATE, a multicenter study on the Zephyr® EBV, examined its placement in patients with heterogenous emphysema. This study demonstrated improvement in spirometry, QOL, and 6-minute walk test (6-MWT) distance (Criner GJ, et al. Am J Respir Crit Care Med. 2018;198:1151) over a longer period, 12 months, bolstering the findings of prior studies. These results prompted the Zephyr® valve’s FDA approval.
Spiration® Valves
Small trials have shown favorable results with the Spiration® IBV for BLVR, including a pilot multicenter cohort study of 30 patients with heterogeneous, upper-lobe emphysema who underwent valve placement (Wood DE, et al. J Thorac Cardiovasc Surg. 2007;133:65). In this trial, investigators found significant improvement in QOL scores, but no change in FEV1 or other physiologic parameters.
The EMPROVE trial is a multicenter, prospective, randomized, controlled study assessing BLVR with the Spiration® IBV. Six- and twelve-month data from the trial were presented in 2018 at the American Thoracic Society Conference and at the European Respiratory Society International Conference.
Collateral Ventilation
Identifying patients in whom there is no CV between lobes is critical to success with BLVR. Collateral ventilation allows air to bypass the valve occlusion distally, thereby negating the desired effect of valve placement, lobar atelectasis. High-resolution computed tomography (HRCT) scanning combined with quantitative software can be used to assess emphysema distribution and fissure integrity. Additionally, a proprietary technology, the Chartis System®, can be employed intra-procedure to estimate CV by measuring airway flow, resistance, and pressure in targeted balloon-occluded segments. Absence of CV based on Chartis evaluation was an inclusion criterion in the aforementioned valve studies.
Which patients with emphysema should be referred for consideration of valve placement?
The following criteria should be used in selecting patients for referral for BLVR:
• FEV1 15% - 45% of predicted value at baseline
• Evidence of hyperinflation: TLC greater than or equal to 100% and RV greater than or equal to 175%
• Baseline postpulmonary rehabilitation 6-MWT distance of 100 - 500 meters
• Clinically stable on < 20 mg prednisone (or equivalent) daily
• Nonsmoking for at least 4 months
• Integrity of one or both major fissures at least 75%
• Ability to provide informed consent and to tolerate bronchoscopy
Complications
The most common complication after valve placement is pneumothorax – a double-edged sword in that it typically indicates the achievement of atelectasis. In published trials, the frequency of pneumothorax varies. Some studies document rates below 10%. Others report rates of nearly 30% (Gompelmann D, et al. Respiration. 2014;87:485). In landmark trials, death related to pneumothorax occurred rarely. Most severe pneumothoraces occur within the first 72 hours after valve placement. This has prompted many centers to observe postprocedure patients in hospital for an extended period. Pneumonia and COPD exacerbations have also been reported after EBV placement. Therefore, in some trials, patients received prophylactic prednisolone and azithromycin. Other less common complications are hemoptysis, granulation tissue formation, and valve migration.
What’s ahead for ELVR?
Overall, valve technology for BLVR is an exciting option in the management of patients with severe emphysema and is now a staple for any advanced emphysema program. Key areas of future interest include management of patients with partial fissures, minimizing adverse procedural effects, and developing programs to optimize and streamline a multidisciplinary approach to timely and efficient referral, assessment, and intervention. As more patients with COPD undergo ELVR, one goal should be to create multi-institution prospective studies as well as registries to delineate further the optimal use of endobronchial valves for lung volume reduction.
Zephyr® Endobronchial Valve (Pulmonx)
Spiration® Valve System (Olympus)
The American College of Chest Physicians (CHEST) does not endorse or supp
The global burden COPD is considerable. In the United States, it is the third most common cause of death and is associated with over $50 billion in annual direct and indirect health-care expenditures (Guarascio AJ, et al. Clinicoecon Outcomes Res. 2013;5:235). For patients with severe emphysema with hyperinflation, dyspnea is often a quality of life (QOL)-limiting symptom (O’Donnell DE, et al. Ann Am Thorac Soc. 2017;14:S30). Few proven palliation options exist, particularly for patients with dyspnea refractory to smoking cessation, medical management with bronchodilators, and pulmonary rehabilitation. The recent Food and Drug Administration (FDA) approval of two endobronchial valves for lung volume reduction has established the increasing importance of bronchoscopy as a management tool in advanced COPD.
Why were these valves developed?
For decades, lung volume reduction has been investigated as a mechanical approach to counter-act the physiologic effects of emphysematous hyperinflation. Its goal is to improve lung elastic recoil, respiratory muscle mechanical advantage and efficiency, and ventilation/perfusion matching. The landmark National Emphysema Treatment Trial (NETT), published in 2001 and 2003, demonstrated that in a select patient population (upper lobe-predominant emphysema and low exercise capacity), lung volume reduction surgery (LVRS) lowers mortality and improves QOL and exercise tolerance (Fishman A et al. N Engl J Med. 2003;348:2059). Despite the encouraging results in this study subpopulation, LVRS is per-formed infrequently (Decker MR, et al. J Thorac Cardiovasc Surg. 2014;148:2651). Concern about its morbidity and the specialized nature of the procedure has hindered widespread adoption. Subsequently, endobronchial techniques have been developed as an alternative to surgical lung volume reduction.
How does bronchoscopic lung volume reduction (BLVR) benefit patients with emphysema?
Valves used for ELVR are removable one-way flow devices placed by flexible bronchoscopy into selected airways supplying emphysematous lung. The valves block air entry but allow the exit of secretions and trapped air. This results in atelectasis of the targeted lobe and a decrease in lung volume.
Which endobronchial valves are available in the United States?
In 2018, two valves were approved by the FDA for bronchoscopic lung volume reduction (BLVR) – the Zephyr® EBV (Pulmonx) ( (Fig 1) and the Spiration® Valve System (Olympus) (IBV) (Fig 2). The Zephyr® EBV is a duckbill-shaped silicone valve mounted within a self-expanding nitinol (nickel titanium alloy) stent. It comes in three sizes for airways with a diameter 4 - 8.5 mm. The Spiration® IBV umbrella-shaped valve is com-posed of six nitinol struts surfaced with polyurethane. Its four sizes accommodate airway diameters 5 - 9 mm.
What’s the evidence behind BLVR?
Zephyr® Valves
The Endobronchial Valve for Emphysema Palliation Trial (VENT), the largest valve trial thus far, randomized patients with severe heterogeneous emphysema to receive unilateral Zephyr® valve placement or standard medical care (Sciurba FC, et al. N Engl J Med. 2010;363:1233). Overall improvement in spirometry and dyspnea scores was modest in the valve group. Post-hoc analysis identified an important subgroup of patients with significant clinical benefit, those with a complete fissure. This finding gave guidance to further EBV studies on patients with severe emphysema and absent collateral ventilation (CV).
Identifying a complete fissure on imaging is now used as a surrogate for assessing CV and is an integral part of the initial profiling of patients for EBV therapy (Koster TD, et al. Respiration. 2016;92(3):150).
In the STELVIO trial, 68 patients were randomized to Zephyr ® EBV placement or standard medical care (Klooster K, et al. N Engl J Med. 2015;373:2325). Those with EBV placement had significantly improved lung function and exercise capacity. TRANSFORM, a multicenter trial evaluating Zephyr® EBV placement in heterogeneous emphysema, showed similar results (Kemp SV, et al. Am J Respir Crit Care Med. 2017;196:1535).
The IMPACT trial compared patients with homogenous emphysema without CV to standard medical therapy alone. It showed improvement in FEV1, QOL scores, and exercise tolerance in the EBV group. This study affirmed that the absence of CV, rather than the pattern of emphysema, correlates with the clinical benefit from EBV therapy (Valipour A, et al. Am J Respir Crit Care Med. 2016;194(9):1073). Finally, LIBERATE, a multicenter study on the Zephyr® EBV, examined its placement in patients with heterogenous emphysema. This study demonstrated improvement in spirometry, QOL, and 6-minute walk test (6-MWT) distance (Criner GJ, et al. Am J Respir Crit Care Med. 2018;198:1151) over a longer period, 12 months, bolstering the findings of prior studies. These results prompted the Zephyr® valve’s FDA approval.
Spiration® Valves
Small trials have shown favorable results with the Spiration® IBV for BLVR, including a pilot multicenter cohort study of 30 patients with heterogeneous, upper-lobe emphysema who underwent valve placement (Wood DE, et al. J Thorac Cardiovasc Surg. 2007;133:65). In this trial, investigators found significant improvement in QOL scores, but no change in FEV1 or other physiologic parameters.
The EMPROVE trial is a multicenter, prospective, randomized, controlled study assessing BLVR with the Spiration® IBV. Six- and twelve-month data from the trial were presented in 2018 at the American Thoracic Society Conference and at the European Respiratory Society International Conference.
Collateral Ventilation
Identifying patients in whom there is no CV between lobes is critical to success with BLVR. Collateral ventilation allows air to bypass the valve occlusion distally, thereby negating the desired effect of valve placement, lobar atelectasis. High-resolution computed tomography (HRCT) scanning combined with quantitative software can be used to assess emphysema distribution and fissure integrity. Additionally, a proprietary technology, the Chartis System®, can be employed intra-procedure to estimate CV by measuring airway flow, resistance, and pressure in targeted balloon-occluded segments. Absence of CV based on Chartis evaluation was an inclusion criterion in the aforementioned valve studies.
Which patients with emphysema should be referred for consideration of valve placement?
The following criteria should be used in selecting patients for referral for BLVR:
• FEV1 15% - 45% of predicted value at baseline
• Evidence of hyperinflation: TLC greater than or equal to 100% and RV greater than or equal to 175%
• Baseline postpulmonary rehabilitation 6-MWT distance of 100 - 500 meters
• Clinically stable on < 20 mg prednisone (or equivalent) daily
• Nonsmoking for at least 4 months
• Integrity of one or both major fissures at least 75%
• Ability to provide informed consent and to tolerate bronchoscopy
Complications
The most common complication after valve placement is pneumothorax – a double-edged sword in that it typically indicates the achievement of atelectasis. In published trials, the frequency of pneumothorax varies. Some studies document rates below 10%. Others report rates of nearly 30% (Gompelmann D, et al. Respiration. 2014;87:485). In landmark trials, death related to pneumothorax occurred rarely. Most severe pneumothoraces occur within the first 72 hours after valve placement. This has prompted many centers to observe postprocedure patients in hospital for an extended period. Pneumonia and COPD exacerbations have also been reported after EBV placement. Therefore, in some trials, patients received prophylactic prednisolone and azithromycin. Other less common complications are hemoptysis, granulation tissue formation, and valve migration.
What’s ahead for ELVR?
Overall, valve technology for BLVR is an exciting option in the management of patients with severe emphysema and is now a staple for any advanced emphysema program. Key areas of future interest include management of patients with partial fissures, minimizing adverse procedural effects, and developing programs to optimize and streamline a multidisciplinary approach to timely and efficient referral, assessment, and intervention. As more patients with COPD undergo ELVR, one goal should be to create multi-institution prospective studies as well as registries to delineate further the optimal use of endobronchial valves for lung volume reduction.
Zephyr® Endobronchial Valve (Pulmonx)
Spiration® Valve System (Olympus)
The American College of Chest Physicians (CHEST) does not endorse or supp