User login
Work-Hour Restrictions Impact Staffing, Education for Academic Hospital Medicine
Source: 2012 State of Hospital Medicine report


In July 2011, the Accreditation Council for Graduate Medical Education (ACGME) implemented new duty-hour restrictions on resident physicians. Among other changes, interns were restricted to a maximum of 16 hours of continuous duty. New rules also limited second-year residents and above to 24 hours of continuous duty, plus up to four additional hours for transition and educational activities. Recommendations were made for strategic napping, greater supervision requirements, and a minimum of eight to 10 hours off between shifts.
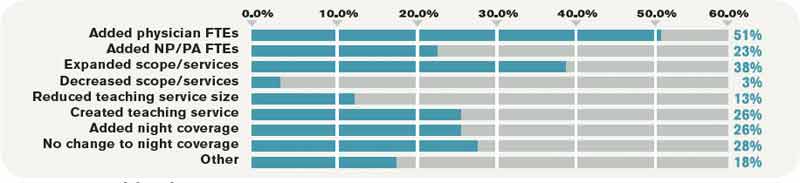
The 2012 State of Hospital Medicine report, which is based on 2011 data encompassing the period of these duty-hour changes, takes a systematic look at how academic HM practices have adjusted to the new resident rules. The most notable changes have been the addition of physician FTEs (51.3% of adult academic HM practices have done so) and nurse practitioners or physician assistants (23%). Additional common responses to resident work-hour limitations are listed in Table 1.
Source: 2012 State of Hospital Medicine report
These data underscore the immensity of changes academic HM groups have faced as a result of new work-hour limitations, as the majority of internal-medicine residents work with hospitalist attendings on inpatient medicine rotations. House staff no longer can be used as an inexpensive source of labor, given limitations on service and new expectations for resident education and supervision.
As others have commented on this topic in The Hospitalist, the role of the academic hospitalist is being redefined. No longer is academic HM synonymous with teaching alone; the clinical duties of many academic hospitalists now include a combination of teaching and non-teaching services, often with some night coverage. At our hospitals in San Diego and Boston, for instance, changes incurred due to work-hour restrictions include elimination of house staff coverage from one of the medical center’s hospitals and a significant increase in nonteaching service responsibilities across all hospitalists. An alternative approach that some programs have embraced is the recruitment of separate cadres of teaching and nonteaching hospitalists, which might result in markedly different professional expectations within the same group or institution.
Trends shifting clinical work from residents to hospitalists are likely to continue, no doubt increasing demand for hospitalists and physician extenders. In the past, the combination of less expensive resident labor and lower salaries in academia was financially favorable for hospitals. Due to resident duty-hour limitations, academic hospitalist groups have had to negotiate not only for additional hires, but, in many instances, also higher salaries commensurate with nonteaching work.
Given the impact on a hospital’s finances, academic HM practices have had to look more closely at clinical volumes and productivity, making protected time for nonclinical pursuits more difficult to come by. Alignment of hospitalists’ interests with those of hospital administrators through performance-improvement projects (e.g. reducing length of stay, readmissions, or nosocomial infections) will be crucial to the financial viability of the academic HM practice, and leadership in these areas will define and differentiate academic hospitalists in the future.
Dr. Bryan Huang, who works in Boston, and Dr. Grace Huang, who works in San Diego, both are members of SHM’s Practice Analysis Committee.
Source: 2012 State of Hospital Medicine report
In July 2011, the Accreditation Council for Graduate Medical Education (ACGME) implemented new duty-hour restrictions on resident physicians. Among other changes, interns were restricted to a maximum of 16 hours of continuous duty. New rules also limited second-year residents and above to 24 hours of continuous duty, plus up to four additional hours for transition and educational activities. Recommendations were made for strategic napping, greater supervision requirements, and a minimum of eight to 10 hours off between shifts.
The 2012 State of Hospital Medicine report, which is based on 2011 data encompassing the period of these duty-hour changes, takes a systematic look at how academic HM practices have adjusted to the new resident rules. The most notable changes have been the addition of physician FTEs (51.3% of adult academic HM practices have done so) and nurse practitioners or physician assistants (23%). Additional common responses to resident work-hour limitations are listed in Table 1.
Source: 2012 State of Hospital Medicine report
These data underscore the immensity of changes academic HM groups have faced as a result of new work-hour limitations, as the majority of internal-medicine residents work with hospitalist attendings on inpatient medicine rotations. House staff no longer can be used as an inexpensive source of labor, given limitations on service and new expectations for resident education and supervision.
As others have commented on this topic in The Hospitalist, the role of the academic hospitalist is being redefined. No longer is academic HM synonymous with teaching alone; the clinical duties of many academic hospitalists now include a combination of teaching and non-teaching services, often with some night coverage. At our hospitals in San Diego and Boston, for instance, changes incurred due to work-hour restrictions include elimination of house staff coverage from one of the medical center’s hospitals and a significant increase in nonteaching service responsibilities across all hospitalists. An alternative approach that some programs have embraced is the recruitment of separate cadres of teaching and nonteaching hospitalists, which might result in markedly different professional expectations within the same group or institution.
Trends shifting clinical work from residents to hospitalists are likely to continue, no doubt increasing demand for hospitalists and physician extenders. In the past, the combination of less expensive resident labor and lower salaries in academia was financially favorable for hospitals. Due to resident duty-hour limitations, academic hospitalist groups have had to negotiate not only for additional hires, but, in many instances, also higher salaries commensurate with nonteaching work.
Given the impact on a hospital’s finances, academic HM practices have had to look more closely at clinical volumes and productivity, making protected time for nonclinical pursuits more difficult to come by. Alignment of hospitalists’ interests with those of hospital administrators through performance-improvement projects (e.g. reducing length of stay, readmissions, or nosocomial infections) will be crucial to the financial viability of the academic HM practice, and leadership in these areas will define and differentiate academic hospitalists in the future.
Dr. Bryan Huang, who works in Boston, and Dr. Grace Huang, who works in San Diego, both are members of SHM’s Practice Analysis Committee.
Source: 2012 State of Hospital Medicine report
In July 2011, the Accreditation Council for Graduate Medical Education (ACGME) implemented new duty-hour restrictions on resident physicians. Among other changes, interns were restricted to a maximum of 16 hours of continuous duty. New rules also limited second-year residents and above to 24 hours of continuous duty, plus up to four additional hours for transition and educational activities. Recommendations were made for strategic napping, greater supervision requirements, and a minimum of eight to 10 hours off between shifts.
The 2012 State of Hospital Medicine report, which is based on 2011 data encompassing the period of these duty-hour changes, takes a systematic look at how academic HM practices have adjusted to the new resident rules. The most notable changes have been the addition of physician FTEs (51.3% of adult academic HM practices have done so) and nurse practitioners or physician assistants (23%). Additional common responses to resident work-hour limitations are listed in Table 1.
Source: 2012 State of Hospital Medicine report
These data underscore the immensity of changes academic HM groups have faced as a result of new work-hour limitations, as the majority of internal-medicine residents work with hospitalist attendings on inpatient medicine rotations. House staff no longer can be used as an inexpensive source of labor, given limitations on service and new expectations for resident education and supervision.
As others have commented on this topic in The Hospitalist, the role of the academic hospitalist is being redefined. No longer is academic HM synonymous with teaching alone; the clinical duties of many academic hospitalists now include a combination of teaching and non-teaching services, often with some night coverage. At our hospitals in San Diego and Boston, for instance, changes incurred due to work-hour restrictions include elimination of house staff coverage from one of the medical center’s hospitals and a significant increase in nonteaching service responsibilities across all hospitalists. An alternative approach that some programs have embraced is the recruitment of separate cadres of teaching and nonteaching hospitalists, which might result in markedly different professional expectations within the same group or institution.
Trends shifting clinical work from residents to hospitalists are likely to continue, no doubt increasing demand for hospitalists and physician extenders. In the past, the combination of less expensive resident labor and lower salaries in academia was financially favorable for hospitals. Due to resident duty-hour limitations, academic hospitalist groups have had to negotiate not only for additional hires, but, in many instances, also higher salaries commensurate with nonteaching work.
Given the impact on a hospital’s finances, academic HM practices have had to look more closely at clinical volumes and productivity, making protected time for nonclinical pursuits more difficult to come by. Alignment of hospitalists’ interests with those of hospital administrators through performance-improvement projects (e.g. reducing length of stay, readmissions, or nosocomial infections) will be crucial to the financial viability of the academic HM practice, and leadership in these areas will define and differentiate academic hospitalists in the future.
Dr. Bryan Huang, who works in Boston, and Dr. Grace Huang, who works in San Diego, both are members of SHM’s Practice Analysis Committee.
Transition Time
The light at the end of the tunnel has arrived—finally. The long hours, scut work, and call nights have paid off; you’re an attending. The transition to the “real world” can be intimidating, especially when you’ve been in training for so long. Here are some tips to ease the transition.
1. Cultivate relationships. Your interactions with nurses, house staff, case managers, social workers, and your colleagues are even more important as an attending and will serve as the building blocks of your reputation. Diplomacy during times of conflict is invaluable. Your approach to resolving situations can further your career—or be a barrier to success.
In the beginning, you might be misidentified as a resident, so it’s important to introduce yourself and have regular conversations with colleagues and consultants until you are recognized and are on a first-name basis with them. Effective communication will go a long way with your patients, their families, and primary-care physicians (PCPs). The benefits of good communication include good Press Ganey patient satisfaction scores, less liability from lawsuits, safer hospital transitions and discharges, and a successful HM practice.
2. Learn the business of practice. The first year of practice will feature a steep learning curve in the areas of billing and documentation. Effective and appropriate billing is essential to maintaining the financial viability of a hospitalist group. Most HM groups provide formal training in billing and documentation as well as chart audits by billing experts. You may find it helpful to review “Billing and Coding” articles in The Hospitalist (also available at www.the-hospitalist.org).
Take time to learn business goals and areas in need of improvement, as this will allow you to improve individual and group performance. This may include maximizing pay for performance, improving hospital throughput by prioritizing discharges early in the morning, and reducing length of stay and readmission rates.
3. Seek work-life balance. Expect to be presented with multiple opportunities to get involved outside of your clinical duties. You could have the chance to participate in quality-improvement (QI) projects, teaching, hospital committees, and research. These activities will add to the depth of your curriculum vitae and give you a voice in hospital operations.
It’s important, however, to remember to pace yourself when you add duties outside the realm of your primary job responsibilities. Avoid spreading yourself too thin. As an attending, your work hours will be fewer and your salary will be better, but your responsibility will be greater. Be sure to set aside personal time and make job satisfaction a priority. More information is available in “A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction” (www.hospitalmedicine.org/dashboard), which outlines the pillars of career satisfaction: autonomy/workflow, workload/schedule, reward/recognition, and community/ environment.
4. Stay current. In addition to reading prominent journals, such as the New England Journal of Medicine and the Journal of Hospital Medicine, look to newer resources that screen up-to-date literature for articles most relevant to hospitalists. American College of Physicians (ACP) members can sign up for ACP Journal Club Plus (acpjc.org), which provides periodic e-mail alerts when new articles meet customized quality and relevance filters. The Hospitalist has a monthly column, “In the Literature,” (see p. 9) that summarizes recent medical research. It also is important to understand how to find evidence-based information quickly. Familiarize yourself with Medline searches and pre-appraised literature resources, such as the Cochrane database, the print version of ACP Journal Club, and guidelines.gov.
5. Be efficient and thorough. Time-management skills are critical as an attending, especially when you’re being pulled in multiple directions. Develop a “to do” list to stay organized. When you are working with nurse practitioners, physician assistants, and residents, delegate certain duties to maximize your own efficiency. Their notes often can be used to assist with documentation, but remember to properly chart the clinical rationale for critical decisions and document medical stability on the day of patient discharge. Be sure you regularly review primary data, such as imaging, culture results, and consultant recommendations. Routinely communicate with PCPs—a prompt, real-time discharge summary is easiest when the information is fresh in your mind, and it ensures proper follow-up care.
6. Know help is available. Just because you’re not a trainee anymore doesn’t mean help isn’t available. Medicine is a constantly evolving field, and you will encounter novel disease states as well as changing diagnostics and therapeutics throughout your career. When you encounter a challenging case, use your colleagues as a sounding board for ideas. When you’re not sure what to do, consultants can be called to assist. Remember, you’re not there to impress others but to provide the best possible care for your patients. Sometimes that means obtaining the advice of a specialist.
If you practice with physician extenders or house staff, you’ll find it helpful to occasionally speak directly to the attending consultant. This helps promote collegial relationships, gives consultants a better understanding of your concerns, and improves your own base of knowledge.
7. Use supervisory skills. If you are practicing in an academic setting or one with physician extenders, you will want to be readily accessible to house staff, physician assistants, and nurse practitioners under your supervision. When you first greet a patient, be sure to clearly identify yourself as the attending physician. At the same time, afford trainees the opportunity to experience being the physician—allow them to actively participate in decision-making, reinforcing best-practice and evidence-based principles as you teach.
8. Understand licensing and certification. Understand your state’s policies and start the licensing process right away, especially if your first job is in a state other than where you completed residency. For most hospitalists, this means taking the medicine boards, then a recertification exam every 10 years, as well as regularly completing continuing medical education (CME). For those looking for a promotion down the line, familiarize yourself with the culture and selection criteria of your individual hospital or group. TH
Dr. Huang is assistant clinical professor in the department of hospital medicine at the University of California San Diego Department of Medicine. Dr. Patel is associate director of hospitalist services at Staten Island University Hospital and assistant clinical professor of medicine at SUNY-Brooklyn. Dr. Chacko is a member of SHM’s Young Physician Committee and medical director of the hospitalist program at Preferred Health Partners in New York City.
The light at the end of the tunnel has arrived—finally. The long hours, scut work, and call nights have paid off; you’re an attending. The transition to the “real world” can be intimidating, especially when you’ve been in training for so long. Here are some tips to ease the transition.
1. Cultivate relationships. Your interactions with nurses, house staff, case managers, social workers, and your colleagues are even more important as an attending and will serve as the building blocks of your reputation. Diplomacy during times of conflict is invaluable. Your approach to resolving situations can further your career—or be a barrier to success.
In the beginning, you might be misidentified as a resident, so it’s important to introduce yourself and have regular conversations with colleagues and consultants until you are recognized and are on a first-name basis with them. Effective communication will go a long way with your patients, their families, and primary-care physicians (PCPs). The benefits of good communication include good Press Ganey patient satisfaction scores, less liability from lawsuits, safer hospital transitions and discharges, and a successful HM practice.
2. Learn the business of practice. The first year of practice will feature a steep learning curve in the areas of billing and documentation. Effective and appropriate billing is essential to maintaining the financial viability of a hospitalist group. Most HM groups provide formal training in billing and documentation as well as chart audits by billing experts. You may find it helpful to review “Billing and Coding” articles in The Hospitalist (also available at www.the-hospitalist.org).
Take time to learn business goals and areas in need of improvement, as this will allow you to improve individual and group performance. This may include maximizing pay for performance, improving hospital throughput by prioritizing discharges early in the morning, and reducing length of stay and readmission rates.
3. Seek work-life balance. Expect to be presented with multiple opportunities to get involved outside of your clinical duties. You could have the chance to participate in quality-improvement (QI) projects, teaching, hospital committees, and research. These activities will add to the depth of your curriculum vitae and give you a voice in hospital operations.
It’s important, however, to remember to pace yourself when you add duties outside the realm of your primary job responsibilities. Avoid spreading yourself too thin. As an attending, your work hours will be fewer and your salary will be better, but your responsibility will be greater. Be sure to set aside personal time and make job satisfaction a priority. More information is available in “A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction” (www.hospitalmedicine.org/dashboard), which outlines the pillars of career satisfaction: autonomy/workflow, workload/schedule, reward/recognition, and community/ environment.
4. Stay current. In addition to reading prominent journals, such as the New England Journal of Medicine and the Journal of Hospital Medicine, look to newer resources that screen up-to-date literature for articles most relevant to hospitalists. American College of Physicians (ACP) members can sign up for ACP Journal Club Plus (acpjc.org), which provides periodic e-mail alerts when new articles meet customized quality and relevance filters. The Hospitalist has a monthly column, “In the Literature,” (see p. 9) that summarizes recent medical research. It also is important to understand how to find evidence-based information quickly. Familiarize yourself with Medline searches and pre-appraised literature resources, such as the Cochrane database, the print version of ACP Journal Club, and guidelines.gov.
5. Be efficient and thorough. Time-management skills are critical as an attending, especially when you’re being pulled in multiple directions. Develop a “to do” list to stay organized. When you are working with nurse practitioners, physician assistants, and residents, delegate certain duties to maximize your own efficiency. Their notes often can be used to assist with documentation, but remember to properly chart the clinical rationale for critical decisions and document medical stability on the day of patient discharge. Be sure you regularly review primary data, such as imaging, culture results, and consultant recommendations. Routinely communicate with PCPs—a prompt, real-time discharge summary is easiest when the information is fresh in your mind, and it ensures proper follow-up care.
6. Know help is available. Just because you’re not a trainee anymore doesn’t mean help isn’t available. Medicine is a constantly evolving field, and you will encounter novel disease states as well as changing diagnostics and therapeutics throughout your career. When you encounter a challenging case, use your colleagues as a sounding board for ideas. When you’re not sure what to do, consultants can be called to assist. Remember, you’re not there to impress others but to provide the best possible care for your patients. Sometimes that means obtaining the advice of a specialist.
If you practice with physician extenders or house staff, you’ll find it helpful to occasionally speak directly to the attending consultant. This helps promote collegial relationships, gives consultants a better understanding of your concerns, and improves your own base of knowledge.
7. Use supervisory skills. If you are practicing in an academic setting or one with physician extenders, you will want to be readily accessible to house staff, physician assistants, and nurse practitioners under your supervision. When you first greet a patient, be sure to clearly identify yourself as the attending physician. At the same time, afford trainees the opportunity to experience being the physician—allow them to actively participate in decision-making, reinforcing best-practice and evidence-based principles as you teach.
8. Understand licensing and certification. Understand your state’s policies and start the licensing process right away, especially if your first job is in a state other than where you completed residency. For most hospitalists, this means taking the medicine boards, then a recertification exam every 10 years, as well as regularly completing continuing medical education (CME). For those looking for a promotion down the line, familiarize yourself with the culture and selection criteria of your individual hospital or group. TH
Dr. Huang is assistant clinical professor in the department of hospital medicine at the University of California San Diego Department of Medicine. Dr. Patel is associate director of hospitalist services at Staten Island University Hospital and assistant clinical professor of medicine at SUNY-Brooklyn. Dr. Chacko is a member of SHM’s Young Physician Committee and medical director of the hospitalist program at Preferred Health Partners in New York City.
The light at the end of the tunnel has arrived—finally. The long hours, scut work, and call nights have paid off; you’re an attending. The transition to the “real world” can be intimidating, especially when you’ve been in training for so long. Here are some tips to ease the transition.
1. Cultivate relationships. Your interactions with nurses, house staff, case managers, social workers, and your colleagues are even more important as an attending and will serve as the building blocks of your reputation. Diplomacy during times of conflict is invaluable. Your approach to resolving situations can further your career—or be a barrier to success.
In the beginning, you might be misidentified as a resident, so it’s important to introduce yourself and have regular conversations with colleagues and consultants until you are recognized and are on a first-name basis with them. Effective communication will go a long way with your patients, their families, and primary-care physicians (PCPs). The benefits of good communication include good Press Ganey patient satisfaction scores, less liability from lawsuits, safer hospital transitions and discharges, and a successful HM practice.
2. Learn the business of practice. The first year of practice will feature a steep learning curve in the areas of billing and documentation. Effective and appropriate billing is essential to maintaining the financial viability of a hospitalist group. Most HM groups provide formal training in billing and documentation as well as chart audits by billing experts. You may find it helpful to review “Billing and Coding” articles in The Hospitalist (also available at www.the-hospitalist.org).
Take time to learn business goals and areas in need of improvement, as this will allow you to improve individual and group performance. This may include maximizing pay for performance, improving hospital throughput by prioritizing discharges early in the morning, and reducing length of stay and readmission rates.
3. Seek work-life balance. Expect to be presented with multiple opportunities to get involved outside of your clinical duties. You could have the chance to participate in quality-improvement (QI) projects, teaching, hospital committees, and research. These activities will add to the depth of your curriculum vitae and give you a voice in hospital operations.
It’s important, however, to remember to pace yourself when you add duties outside the realm of your primary job responsibilities. Avoid spreading yourself too thin. As an attending, your work hours will be fewer and your salary will be better, but your responsibility will be greater. Be sure to set aside personal time and make job satisfaction a priority. More information is available in “A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction” (www.hospitalmedicine.org/dashboard), which outlines the pillars of career satisfaction: autonomy/workflow, workload/schedule, reward/recognition, and community/ environment.
4. Stay current. In addition to reading prominent journals, such as the New England Journal of Medicine and the Journal of Hospital Medicine, look to newer resources that screen up-to-date literature for articles most relevant to hospitalists. American College of Physicians (ACP) members can sign up for ACP Journal Club Plus (acpjc.org), which provides periodic e-mail alerts when new articles meet customized quality and relevance filters. The Hospitalist has a monthly column, “In the Literature,” (see p. 9) that summarizes recent medical research. It also is important to understand how to find evidence-based information quickly. Familiarize yourself with Medline searches and pre-appraised literature resources, such as the Cochrane database, the print version of ACP Journal Club, and guidelines.gov.
5. Be efficient and thorough. Time-management skills are critical as an attending, especially when you’re being pulled in multiple directions. Develop a “to do” list to stay organized. When you are working with nurse practitioners, physician assistants, and residents, delegate certain duties to maximize your own efficiency. Their notes often can be used to assist with documentation, but remember to properly chart the clinical rationale for critical decisions and document medical stability on the day of patient discharge. Be sure you regularly review primary data, such as imaging, culture results, and consultant recommendations. Routinely communicate with PCPs—a prompt, real-time discharge summary is easiest when the information is fresh in your mind, and it ensures proper follow-up care.
6. Know help is available. Just because you’re not a trainee anymore doesn’t mean help isn’t available. Medicine is a constantly evolving field, and you will encounter novel disease states as well as changing diagnostics and therapeutics throughout your career. When you encounter a challenging case, use your colleagues as a sounding board for ideas. When you’re not sure what to do, consultants can be called to assist. Remember, you’re not there to impress others but to provide the best possible care for your patients. Sometimes that means obtaining the advice of a specialist.
If you practice with physician extenders or house staff, you’ll find it helpful to occasionally speak directly to the attending consultant. This helps promote collegial relationships, gives consultants a better understanding of your concerns, and improves your own base of knowledge.
7. Use supervisory skills. If you are practicing in an academic setting or one with physician extenders, you will want to be readily accessible to house staff, physician assistants, and nurse practitioners under your supervision. When you first greet a patient, be sure to clearly identify yourself as the attending physician. At the same time, afford trainees the opportunity to experience being the physician—allow them to actively participate in decision-making, reinforcing best-practice and evidence-based principles as you teach.
8. Understand licensing and certification. Understand your state’s policies and start the licensing process right away, especially if your first job is in a state other than where you completed residency. For most hospitalists, this means taking the medicine boards, then a recertification exam every 10 years, as well as regularly completing continuing medical education (CME). For those looking for a promotion down the line, familiarize yourself with the culture and selection criteria of your individual hospital or group. TH
Dr. Huang is assistant clinical professor in the department of hospital medicine at the University of California San Diego Department of Medicine. Dr. Patel is associate director of hospitalist services at Staten Island University Hospital and assistant clinical professor of medicine at SUNY-Brooklyn. Dr. Chacko is a member of SHM’s Young Physician Committee and medical director of the hospitalist program at Preferred Health Partners in New York City.
The Art of Negotiation
Got a job offer? Congratulations! The hard part of finding your first job after residency is complete. This also is a time to sit down and think about what’s important to you, as you want the details of your job to be stated in a contract. Here are some tips about contract negotiation.
Get It in Writing
Just as in practice, where we are always told, “it didn’t happen if it’s not documented in the chart,” the same holds true for your workplace contract. This is the time to prioritize what elements are important to you in order to have a satisfying and rewarding career, both professionally and financially. If a particular aspect of your employment agreement is important to you, be it salary, schedule, or malpractice insurance coverage, be sure its stated in writing in your contract. Verbal statements from your employer, such as “we’ll discuss this after you start your job,” should raise a red flag.
Know What Is Negotiable
Some residents are relieved just to secure their first job offer and they immediately accept the initial offer as-is, without attempting to negotiate. Although it’s probably unreasonable to negotiate everything, after you read the initial contract, if anything important is not to your satisfaction, it is practical to have a discussion with your employer. Employers expect this of their hires and, if done politely and professionally, this is a time to build bridges with your future supervisor. Moreover, they begin to better understand your needs and you theirs.
You may find it helpful to talk to associates in the group about what parts of their contracts were negotiable. For example, particularly in academic settings, you may find salary and benefits are not negotiable; however, other benefits, such as office space or protected research time, may be negotiable. Basically, the best time to negotiate is the “honeymoon” period, right after a job offer has been made, as the employer will be doing its best to entice a prospective employee.
Consider a Legal Opinion
In general, the more complex your contract, the more important it will be to solicit the help of an attorney experienced in healthcare. Even if your contract is very simple, contains a standardized salary and benefit structure, has no restrictive covenants, and partnership is not an issue, it may be helpful to have your contract reviewed by an attorney. Understand what is written in your contract and, if there is any doubt, hire a lawyer.
Ultimately, you will be signing the contract, not your lawyer, so be sure you understand what is in it and don’t get mired in “legalese.” Some firms offer third-party contract negotiation; they will assign an attorney to step in as an intermediary. Then again, most experts recommend against hiring a third-party negotiator, as this may increase the distance between you and your employer at a time probably best spent getting to know each other.
Maintain a Keen Eye
Specifics to look for in your new contract:
Work requirements. The employment agreement should visibly define your job responsibilities. Things to look for in your contract include the obligations of the physician, number of shifts or hours or weeks per year you are expected to work, call responsibilities, a census cap (if applicable), allotted vacation time, and continuing medical education time.
Compensation. The contract clearly should delineate how you will be paid. Some hospitalists are compensated solely via a salary; others are paid based on billing/productivity, while the majority are paid based on a combination of these methods (a base salary plus incentives). Be sure you understand the incentive and/or bonus structure of your salary. Practices basing incentives on physician productivity will incorporate your own billing practices and often is measured in relative value units (RVUs). In some settings, group incentives are based on quality targets set by the administration, such as the Joint Commission on the Accreditation of Healthcare Organi-zations (JCAHO) core measure compliance, dictation timeliness, or patient/primary care physician satisfaction.
Benefits. In addition to your salary, you should see that your benefits are spelled out. The obvious benefits include medical, dental, and vision insurance, as well as a retirement savings plan. As discussed in the July 2008 issue of The Hospitalist, as demand for hospitalists continues to exceed supply, look for signing bonuses, coverage of relocation expenses, and the possibility of student loan payoff. Other important benefits include coverage of professional dues, CME allocation, and licensing and board examination fees.
Malpractice Insurance. This can be a complicated topic. In general, there are two major classes of malpractice insurance: an occurrence policy and a claims-made policy. In respect to an occurrence policy, any malpractice incident arising while the coverage was in place, regardless of when the claim was filed, will be covered even after you have stopped practicing under that policy. A claims-made policy, on the other hand, protects physicians for any covered claim, if they are insured when the claim is made. It does not cover malpractice claims filed after the physician cancels the malpractice policy, even if the claim is about an event that occurred while the physician was insured.
If you are offered a claims-made policy, require your employer to add tail coverage, which covers you after leaving the practice for any events occurred during employment. If you are unclear about any part of the group’s malpractice coverage, consider seeking legal advice.
Restrictive covenants. These are non-compete clauses often setting geographic and time restrictions of where and when a physician can practice in the event they leave the group. Though you never know what the future holds, this becomes relevant if you were to change jobs and work at an adjacent local facility or one in a nearby county. In general, hospitalists rarely carry a panel of patients, so an employer probably should not be concerned about hospitalists taking patients with them if/when they leave the practice. Be cautious of restrictive covenants found in your contract.
Ownership/Partnership. In some private groups, partnership will be offered after a preliminary employment period, usually one to two years. Look for your contract to state when and how partnership might be offered, and what the criteria to join are. This also is the time to ask others in the group to get a sense of how many associates are offered partnership and when this might happen.
Allowable Activities. Look for any restrictions regarding your activities outside normal clinical duties, such as teaching, research, or consulting for other firms. If such restrictions are in your contract, there may be specifications about whether income from such activities is yours or whether it is shared with the rest of the practice. TH
Bryan Huang, MD, assistant clinical professor, division of hospital medicine, University of California-San Diego Department of Medicine, Bhavin Patel, MD, hospitalist at Regions Hospital, HealthPartners Medical Group, St. Paul, Minn., Bijo Chacko, MD, hospitalist program medical director, Preferred Health Partners, New York City, and chair of SHM’s Young Physician Committee.
Got a job offer? Congratulations! The hard part of finding your first job after residency is complete. This also is a time to sit down and think about what’s important to you, as you want the details of your job to be stated in a contract. Here are some tips about contract negotiation.
Get It in Writing
Just as in practice, where we are always told, “it didn’t happen if it’s not documented in the chart,” the same holds true for your workplace contract. This is the time to prioritize what elements are important to you in order to have a satisfying and rewarding career, both professionally and financially. If a particular aspect of your employment agreement is important to you, be it salary, schedule, or malpractice insurance coverage, be sure its stated in writing in your contract. Verbal statements from your employer, such as “we’ll discuss this after you start your job,” should raise a red flag.
Know What Is Negotiable
Some residents are relieved just to secure their first job offer and they immediately accept the initial offer as-is, without attempting to negotiate. Although it’s probably unreasonable to negotiate everything, after you read the initial contract, if anything important is not to your satisfaction, it is practical to have a discussion with your employer. Employers expect this of their hires and, if done politely and professionally, this is a time to build bridges with your future supervisor. Moreover, they begin to better understand your needs and you theirs.
You may find it helpful to talk to associates in the group about what parts of their contracts were negotiable. For example, particularly in academic settings, you may find salary and benefits are not negotiable; however, other benefits, such as office space or protected research time, may be negotiable. Basically, the best time to negotiate is the “honeymoon” period, right after a job offer has been made, as the employer will be doing its best to entice a prospective employee.
Consider a Legal Opinion
In general, the more complex your contract, the more important it will be to solicit the help of an attorney experienced in healthcare. Even if your contract is very simple, contains a standardized salary and benefit structure, has no restrictive covenants, and partnership is not an issue, it may be helpful to have your contract reviewed by an attorney. Understand what is written in your contract and, if there is any doubt, hire a lawyer.
Ultimately, you will be signing the contract, not your lawyer, so be sure you understand what is in it and don’t get mired in “legalese.” Some firms offer third-party contract negotiation; they will assign an attorney to step in as an intermediary. Then again, most experts recommend against hiring a third-party negotiator, as this may increase the distance between you and your employer at a time probably best spent getting to know each other.
Maintain a Keen Eye
Specifics to look for in your new contract:
Work requirements. The employment agreement should visibly define your job responsibilities. Things to look for in your contract include the obligations of the physician, number of shifts or hours or weeks per year you are expected to work, call responsibilities, a census cap (if applicable), allotted vacation time, and continuing medical education time.
Compensation. The contract clearly should delineate how you will be paid. Some hospitalists are compensated solely via a salary; others are paid based on billing/productivity, while the majority are paid based on a combination of these methods (a base salary plus incentives). Be sure you understand the incentive and/or bonus structure of your salary. Practices basing incentives on physician productivity will incorporate your own billing practices and often is measured in relative value units (RVUs). In some settings, group incentives are based on quality targets set by the administration, such as the Joint Commission on the Accreditation of Healthcare Organi-zations (JCAHO) core measure compliance, dictation timeliness, or patient/primary care physician satisfaction.
Benefits. In addition to your salary, you should see that your benefits are spelled out. The obvious benefits include medical, dental, and vision insurance, as well as a retirement savings plan. As discussed in the July 2008 issue of The Hospitalist, as demand for hospitalists continues to exceed supply, look for signing bonuses, coverage of relocation expenses, and the possibility of student loan payoff. Other important benefits include coverage of professional dues, CME allocation, and licensing and board examination fees.
Malpractice Insurance. This can be a complicated topic. In general, there are two major classes of malpractice insurance: an occurrence policy and a claims-made policy. In respect to an occurrence policy, any malpractice incident arising while the coverage was in place, regardless of when the claim was filed, will be covered even after you have stopped practicing under that policy. A claims-made policy, on the other hand, protects physicians for any covered claim, if they are insured when the claim is made. It does not cover malpractice claims filed after the physician cancels the malpractice policy, even if the claim is about an event that occurred while the physician was insured.
If you are offered a claims-made policy, require your employer to add tail coverage, which covers you after leaving the practice for any events occurred during employment. If you are unclear about any part of the group’s malpractice coverage, consider seeking legal advice.
Restrictive covenants. These are non-compete clauses often setting geographic and time restrictions of where and when a physician can practice in the event they leave the group. Though you never know what the future holds, this becomes relevant if you were to change jobs and work at an adjacent local facility or one in a nearby county. In general, hospitalists rarely carry a panel of patients, so an employer probably should not be concerned about hospitalists taking patients with them if/when they leave the practice. Be cautious of restrictive covenants found in your contract.
Ownership/Partnership. In some private groups, partnership will be offered after a preliminary employment period, usually one to two years. Look for your contract to state when and how partnership might be offered, and what the criteria to join are. This also is the time to ask others in the group to get a sense of how many associates are offered partnership and when this might happen.
Allowable Activities. Look for any restrictions regarding your activities outside normal clinical duties, such as teaching, research, or consulting for other firms. If such restrictions are in your contract, there may be specifications about whether income from such activities is yours or whether it is shared with the rest of the practice. TH
Bryan Huang, MD, assistant clinical professor, division of hospital medicine, University of California-San Diego Department of Medicine, Bhavin Patel, MD, hospitalist at Regions Hospital, HealthPartners Medical Group, St. Paul, Minn., Bijo Chacko, MD, hospitalist program medical director, Preferred Health Partners, New York City, and chair of SHM’s Young Physician Committee.
Got a job offer? Congratulations! The hard part of finding your first job after residency is complete. This also is a time to sit down and think about what’s important to you, as you want the details of your job to be stated in a contract. Here are some tips about contract negotiation.
Get It in Writing
Just as in practice, where we are always told, “it didn’t happen if it’s not documented in the chart,” the same holds true for your workplace contract. This is the time to prioritize what elements are important to you in order to have a satisfying and rewarding career, both professionally and financially. If a particular aspect of your employment agreement is important to you, be it salary, schedule, or malpractice insurance coverage, be sure its stated in writing in your contract. Verbal statements from your employer, such as “we’ll discuss this after you start your job,” should raise a red flag.
Know What Is Negotiable
Some residents are relieved just to secure their first job offer and they immediately accept the initial offer as-is, without attempting to negotiate. Although it’s probably unreasonable to negotiate everything, after you read the initial contract, if anything important is not to your satisfaction, it is practical to have a discussion with your employer. Employers expect this of their hires and, if done politely and professionally, this is a time to build bridges with your future supervisor. Moreover, they begin to better understand your needs and you theirs.
You may find it helpful to talk to associates in the group about what parts of their contracts were negotiable. For example, particularly in academic settings, you may find salary and benefits are not negotiable; however, other benefits, such as office space or protected research time, may be negotiable. Basically, the best time to negotiate is the “honeymoon” period, right after a job offer has been made, as the employer will be doing its best to entice a prospective employee.
Consider a Legal Opinion
In general, the more complex your contract, the more important it will be to solicit the help of an attorney experienced in healthcare. Even if your contract is very simple, contains a standardized salary and benefit structure, has no restrictive covenants, and partnership is not an issue, it may be helpful to have your contract reviewed by an attorney. Understand what is written in your contract and, if there is any doubt, hire a lawyer.
Ultimately, you will be signing the contract, not your lawyer, so be sure you understand what is in it and don’t get mired in “legalese.” Some firms offer third-party contract negotiation; they will assign an attorney to step in as an intermediary. Then again, most experts recommend against hiring a third-party negotiator, as this may increase the distance between you and your employer at a time probably best spent getting to know each other.
Maintain a Keen Eye
Specifics to look for in your new contract:
Work requirements. The employment agreement should visibly define your job responsibilities. Things to look for in your contract include the obligations of the physician, number of shifts or hours or weeks per year you are expected to work, call responsibilities, a census cap (if applicable), allotted vacation time, and continuing medical education time.
Compensation. The contract clearly should delineate how you will be paid. Some hospitalists are compensated solely via a salary; others are paid based on billing/productivity, while the majority are paid based on a combination of these methods (a base salary plus incentives). Be sure you understand the incentive and/or bonus structure of your salary. Practices basing incentives on physician productivity will incorporate your own billing practices and often is measured in relative value units (RVUs). In some settings, group incentives are based on quality targets set by the administration, such as the Joint Commission on the Accreditation of Healthcare Organi-zations (JCAHO) core measure compliance, dictation timeliness, or patient/primary care physician satisfaction.
Benefits. In addition to your salary, you should see that your benefits are spelled out. The obvious benefits include medical, dental, and vision insurance, as well as a retirement savings plan. As discussed in the July 2008 issue of The Hospitalist, as demand for hospitalists continues to exceed supply, look for signing bonuses, coverage of relocation expenses, and the possibility of student loan payoff. Other important benefits include coverage of professional dues, CME allocation, and licensing and board examination fees.
Malpractice Insurance. This can be a complicated topic. In general, there are two major classes of malpractice insurance: an occurrence policy and a claims-made policy. In respect to an occurrence policy, any malpractice incident arising while the coverage was in place, regardless of when the claim was filed, will be covered even after you have stopped practicing under that policy. A claims-made policy, on the other hand, protects physicians for any covered claim, if they are insured when the claim is made. It does not cover malpractice claims filed after the physician cancels the malpractice policy, even if the claim is about an event that occurred while the physician was insured.
If you are offered a claims-made policy, require your employer to add tail coverage, which covers you after leaving the practice for any events occurred during employment. If you are unclear about any part of the group’s malpractice coverage, consider seeking legal advice.
Restrictive covenants. These are non-compete clauses often setting geographic and time restrictions of where and when a physician can practice in the event they leave the group. Though you never know what the future holds, this becomes relevant if you were to change jobs and work at an adjacent local facility or one in a nearby county. In general, hospitalists rarely carry a panel of patients, so an employer probably should not be concerned about hospitalists taking patients with them if/when they leave the practice. Be cautious of restrictive covenants found in your contract.
Ownership/Partnership. In some private groups, partnership will be offered after a preliminary employment period, usually one to two years. Look for your contract to state when and how partnership might be offered, and what the criteria to join are. This also is the time to ask others in the group to get a sense of how many associates are offered partnership and when this might happen.
Allowable Activities. Look for any restrictions regarding your activities outside normal clinical duties, such as teaching, research, or consulting for other firms. If such restrictions are in your contract, there may be specifications about whether income from such activities is yours or whether it is shared with the rest of the practice. TH
Bryan Huang, MD, assistant clinical professor, division of hospital medicine, University of California-San Diego Department of Medicine, Bhavin Patel, MD, hospitalist at Regions Hospital, HealthPartners Medical Group, St. Paul, Minn., Bijo Chacko, MD, hospitalist program medical director, Preferred Health Partners, New York City, and chair of SHM’s Young Physician Committee.