User login
Chronotherapeutics Corrects Circadian Rhythm Abnormalities in Many Psychiatric Disorders
AMSTERDAM – Circadian dysfunction can greatly affect brain function – impairing behavior, cognition, and affect – and can be improved with a “chronotherapeutic” approach, according to one of the leading researchers in the field. Anna Wirz-Justice, Ph.D., professor emeritus at the center for chronobiology at Psychiatric University Clinics in Basel, Switzerland, who is one of the leading researchers in this field. She coauthored the treatment manual, “Chronotherapeutics for Affective Disorders: A Clinician’s Manual for Light and Wake Therapy” (Basel: Karger, 2009).

“In the treatment of affective disorders, chronotherapeutics offers a new synthesis of nonpharmacologic interventions designed to accelerate remission. Combining it with concomitant or follow-up medications shows great promise,” said Dr. Wirz-Justice, who has led numerous investigative studies in the field and lectured on the role of circadian rhythms in affective disorders at the annual congress of the European College if Neuropsychopharmacology.
Circadian rhythms are directed by a master biological block in the suprachiasmatic nucleus (SCN) as well as circadian oscillators in all brain regions and peripheral tissues. The SCN is synchronized daily by environmental signals, mainly light. Receiving information on lighting conditions directly from the retina, the SCN drives secretion of melatonin and regulates peripheral “clocks,” whose outputs modulate the SCN through feedback or feed-forward effects.
Specific circadian genes such as CLOCK, BMAL1, and PER are responsible for the main SCN “clock-working” machinery. New interest in the role of circadian dysregulation in psychiatric disorders has arisen from the finding that a mutation in a core circadian clock gene induces hyperactivity, decreased sleep, and manialike behavior in mice.
“Animal studies were the key development that brought the field to its present exciting position, by suggesting that ‘clock genes’ are directing the circadian rhythms in all physiological processes,” she said.
Clinical Impact on Affective Disorders
In healthy individuals, physiological, and biochemical variables such as body temperature, cortisol and melatonin, thyroid stimulating hormone, norepinephrine and serotonin exhibit circadian rhythms. However, in patients with affective disorders, many of these rhythms are disturbed in phase and amplitude.
For instance, in major depressive disorder (MDD), most patients present with sleep disturbances and altered circadian rhythms, including hormonal secretion, cardiac function, and body temperature. Sleep disruption is a major symptom in depression and is often the factor prompting depressed persons to seek medical help.
Synchronizing impaired circadian rhythms through “chronotherapeutics” – improving sleep or paradoxically staying awake most of the night – can be extremely helpful in treating patients with MDD and bipolar disorder, but the approach is not limited to depression. In addition to major depression (seasonal and nonseasonal), chronotherapeutics indications include bipolar disorder, premenstrual dysphoric disorder and depression during pregnancy, bulimia nervosa, attention-deficit/hyperactivity disorder, dementia, Parkinson’s disease and shift work and jet-lag disturbances, according to Dr. Wirz-Justice.
“Light therapy has been used to resynchronize disturbed sleep schedules back to a more normal pattern. Light is also an effective antidepressant, acting on many of the same neurotransmitter systems and brain structures as antidepressant drugs,” she said.
“The new message is that light therapy is not just for seasonal affective disorder but for all forms of depression and for many other disorders,” she added. “As an adjuvant to antidepressants in unipolar depressive patients or to lithium in bipolar patients, morning light hastens and potentiates the antidepressant response. Light therapy shows benefit even for patients with chronic depression of 2 years or more and provides a viable alternative for patients who refuse, resist, or cannot tolerate medication.”
Elements of chronotherapy include light therapy, dark therapy or blue-blocking sunglasses, wake therapy (total or partial sleep deprivation in the second half of the night), phase advance of the sleep-wake cycle, and exogenously administered melatonin.
Sleep Deprivation and Dark Therapy
A 1-night sleep deprivation, or “wake therapy,” is the most rapid antidepressant known, according to Dr. Wirz-Justice. A single night’s sleep deprivation induces similar brain changes as many weeks of antidepressant drugs (Curr. Pharm. Des. 2009;15:2637-49).
“Approximately 60% of patients, independent of diagnostic subtypes, respond with marked improvement within hours,” she said. “Mostly, however, they relapse after recovery sleep, which indicates how important wakefulness must be. We have found you can prevent relapse by combining daily light therapy with antidepressants or lithium or a short phase advance of sleep over 3 days.”
Dark therapy (defined as keeping patients in a dark setting and extending rest-sleep for periods of 10-14 hours) has yielded positive results in controlling symptoms in acute mania and calming rapid-cycling bipolar patients in the manic phase, she said. Because this approach is impractical, an alternative being investigated is the use of blue-blocking sunglasses. Blue is the wavelength to which the circadian system is particularly sensitive, thus by blocking this range in the light spectrum one can induce “circadian darkness” while not impairing vision, she explained.
Dr. Wirz-Justice is advocating wider use of these techniques in psychiatry and their incorporation into residency programs. “In clinical practice, there is still rather widespread ignorance about circadian sleep disturbances and chronotherapeutics in spite of the significant evidence base,” she said. “Enterprising doctors should try this out, and the techniques should be taught in residency programs.”
Disclosures: Dr. Wirz-Justice reported no potential conflicts of interest.
For more information on chronotherapeutics, check out the Center for Environmental Therapeutics.
AMSTERDAM – Circadian dysfunction can greatly affect brain function – impairing behavior, cognition, and affect – and can be improved with a “chronotherapeutic” approach, according to one of the leading researchers in the field. Anna Wirz-Justice, Ph.D., professor emeritus at the center for chronobiology at Psychiatric University Clinics in Basel, Switzerland, who is one of the leading researchers in this field. She coauthored the treatment manual, “Chronotherapeutics for Affective Disorders: A Clinician’s Manual for Light and Wake Therapy” (Basel: Karger, 2009).
“In the treatment of affective disorders, chronotherapeutics offers a new synthesis of nonpharmacologic interventions designed to accelerate remission. Combining it with concomitant or follow-up medications shows great promise,” said Dr. Wirz-Justice, who has led numerous investigative studies in the field and lectured on the role of circadian rhythms in affective disorders at the annual congress of the European College if Neuropsychopharmacology.
Circadian rhythms are directed by a master biological block in the suprachiasmatic nucleus (SCN) as well as circadian oscillators in all brain regions and peripheral tissues. The SCN is synchronized daily by environmental signals, mainly light. Receiving information on lighting conditions directly from the retina, the SCN drives secretion of melatonin and regulates peripheral “clocks,” whose outputs modulate the SCN through feedback or feed-forward effects.
Specific circadian genes such as CLOCK, BMAL1, and PER are responsible for the main SCN “clock-working” machinery. New interest in the role of circadian dysregulation in psychiatric disorders has arisen from the finding that a mutation in a core circadian clock gene induces hyperactivity, decreased sleep, and manialike behavior in mice.
“Animal studies were the key development that brought the field to its present exciting position, by suggesting that ‘clock genes’ are directing the circadian rhythms in all physiological processes,” she said.
Clinical Impact on Affective Disorders
In healthy individuals, physiological, and biochemical variables such as body temperature, cortisol and melatonin, thyroid stimulating hormone, norepinephrine and serotonin exhibit circadian rhythms. However, in patients with affective disorders, many of these rhythms are disturbed in phase and amplitude.
For instance, in major depressive disorder (MDD), most patients present with sleep disturbances and altered circadian rhythms, including hormonal secretion, cardiac function, and body temperature. Sleep disruption is a major symptom in depression and is often the factor prompting depressed persons to seek medical help.
Synchronizing impaired circadian rhythms through “chronotherapeutics” – improving sleep or paradoxically staying awake most of the night – can be extremely helpful in treating patients with MDD and bipolar disorder, but the approach is not limited to depression. In addition to major depression (seasonal and nonseasonal), chronotherapeutics indications include bipolar disorder, premenstrual dysphoric disorder and depression during pregnancy, bulimia nervosa, attention-deficit/hyperactivity disorder, dementia, Parkinson’s disease and shift work and jet-lag disturbances, according to Dr. Wirz-Justice.
“Light therapy has been used to resynchronize disturbed sleep schedules back to a more normal pattern. Light is also an effective antidepressant, acting on many of the same neurotransmitter systems and brain structures as antidepressant drugs,” she said.
“The new message is that light therapy is not just for seasonal affective disorder but for all forms of depression and for many other disorders,” she added. “As an adjuvant to antidepressants in unipolar depressive patients or to lithium in bipolar patients, morning light hastens and potentiates the antidepressant response. Light therapy shows benefit even for patients with chronic depression of 2 years or more and provides a viable alternative for patients who refuse, resist, or cannot tolerate medication.”
Elements of chronotherapy include light therapy, dark therapy or blue-blocking sunglasses, wake therapy (total or partial sleep deprivation in the second half of the night), phase advance of the sleep-wake cycle, and exogenously administered melatonin.
Sleep Deprivation and Dark Therapy
A 1-night sleep deprivation, or “wake therapy,” is the most rapid antidepressant known, according to Dr. Wirz-Justice. A single night’s sleep deprivation induces similar brain changes as many weeks of antidepressant drugs (Curr. Pharm. Des. 2009;15:2637-49).
“Approximately 60% of patients, independent of diagnostic subtypes, respond with marked improvement within hours,” she said. “Mostly, however, they relapse after recovery sleep, which indicates how important wakefulness must be. We have found you can prevent relapse by combining daily light therapy with antidepressants or lithium or a short phase advance of sleep over 3 days.”
Dark therapy (defined as keeping patients in a dark setting and extending rest-sleep for periods of 10-14 hours) has yielded positive results in controlling symptoms in acute mania and calming rapid-cycling bipolar patients in the manic phase, she said. Because this approach is impractical, an alternative being investigated is the use of blue-blocking sunglasses. Blue is the wavelength to which the circadian system is particularly sensitive, thus by blocking this range in the light spectrum one can induce “circadian darkness” while not impairing vision, she explained.
Dr. Wirz-Justice is advocating wider use of these techniques in psychiatry and their incorporation into residency programs. “In clinical practice, there is still rather widespread ignorance about circadian sleep disturbances and chronotherapeutics in spite of the significant evidence base,” she said. “Enterprising doctors should try this out, and the techniques should be taught in residency programs.”
Disclosures: Dr. Wirz-Justice reported no potential conflicts of interest.
For more information on chronotherapeutics, check out the Center for Environmental Therapeutics.
AMSTERDAM – Circadian dysfunction can greatly affect brain function – impairing behavior, cognition, and affect – and can be improved with a “chronotherapeutic” approach, according to one of the leading researchers in the field. Anna Wirz-Justice, Ph.D., professor emeritus at the center for chronobiology at Psychiatric University Clinics in Basel, Switzerland, who is one of the leading researchers in this field. She coauthored the treatment manual, “Chronotherapeutics for Affective Disorders: A Clinician’s Manual for Light and Wake Therapy” (Basel: Karger, 2009).
“In the treatment of affective disorders, chronotherapeutics offers a new synthesis of nonpharmacologic interventions designed to accelerate remission. Combining it with concomitant or follow-up medications shows great promise,” said Dr. Wirz-Justice, who has led numerous investigative studies in the field and lectured on the role of circadian rhythms in affective disorders at the annual congress of the European College if Neuropsychopharmacology.
Circadian rhythms are directed by a master biological block in the suprachiasmatic nucleus (SCN) as well as circadian oscillators in all brain regions and peripheral tissues. The SCN is synchronized daily by environmental signals, mainly light. Receiving information on lighting conditions directly from the retina, the SCN drives secretion of melatonin and regulates peripheral “clocks,” whose outputs modulate the SCN through feedback or feed-forward effects.
Specific circadian genes such as CLOCK, BMAL1, and PER are responsible for the main SCN “clock-working” machinery. New interest in the role of circadian dysregulation in psychiatric disorders has arisen from the finding that a mutation in a core circadian clock gene induces hyperactivity, decreased sleep, and manialike behavior in mice.
“Animal studies were the key development that brought the field to its present exciting position, by suggesting that ‘clock genes’ are directing the circadian rhythms in all physiological processes,” she said.
Clinical Impact on Affective Disorders
In healthy individuals, physiological, and biochemical variables such as body temperature, cortisol and melatonin, thyroid stimulating hormone, norepinephrine and serotonin exhibit circadian rhythms. However, in patients with affective disorders, many of these rhythms are disturbed in phase and amplitude.
For instance, in major depressive disorder (MDD), most patients present with sleep disturbances and altered circadian rhythms, including hormonal secretion, cardiac function, and body temperature. Sleep disruption is a major symptom in depression and is often the factor prompting depressed persons to seek medical help.
Synchronizing impaired circadian rhythms through “chronotherapeutics” – improving sleep or paradoxically staying awake most of the night – can be extremely helpful in treating patients with MDD and bipolar disorder, but the approach is not limited to depression. In addition to major depression (seasonal and nonseasonal), chronotherapeutics indications include bipolar disorder, premenstrual dysphoric disorder and depression during pregnancy, bulimia nervosa, attention-deficit/hyperactivity disorder, dementia, Parkinson’s disease and shift work and jet-lag disturbances, according to Dr. Wirz-Justice.
“Light therapy has been used to resynchronize disturbed sleep schedules back to a more normal pattern. Light is also an effective antidepressant, acting on many of the same neurotransmitter systems and brain structures as antidepressant drugs,” she said.
“The new message is that light therapy is not just for seasonal affective disorder but for all forms of depression and for many other disorders,” she added. “As an adjuvant to antidepressants in unipolar depressive patients or to lithium in bipolar patients, morning light hastens and potentiates the antidepressant response. Light therapy shows benefit even for patients with chronic depression of 2 years or more and provides a viable alternative for patients who refuse, resist, or cannot tolerate medication.”
Elements of chronotherapy include light therapy, dark therapy or blue-blocking sunglasses, wake therapy (total or partial sleep deprivation in the second half of the night), phase advance of the sleep-wake cycle, and exogenously administered melatonin.
Sleep Deprivation and Dark Therapy
A 1-night sleep deprivation, or “wake therapy,” is the most rapid antidepressant known, according to Dr. Wirz-Justice. A single night’s sleep deprivation induces similar brain changes as many weeks of antidepressant drugs (Curr. Pharm. Des. 2009;15:2637-49).
“Approximately 60% of patients, independent of diagnostic subtypes, respond with marked improvement within hours,” she said. “Mostly, however, they relapse after recovery sleep, which indicates how important wakefulness must be. We have found you can prevent relapse by combining daily light therapy with antidepressants or lithium or a short phase advance of sleep over 3 days.”
Dark therapy (defined as keeping patients in a dark setting and extending rest-sleep for periods of 10-14 hours) has yielded positive results in controlling symptoms in acute mania and calming rapid-cycling bipolar patients in the manic phase, she said. Because this approach is impractical, an alternative being investigated is the use of blue-blocking sunglasses. Blue is the wavelength to which the circadian system is particularly sensitive, thus by blocking this range in the light spectrum one can induce “circadian darkness” while not impairing vision, she explained.
Dr. Wirz-Justice is advocating wider use of these techniques in psychiatry and their incorporation into residency programs. “In clinical practice, there is still rather widespread ignorance about circadian sleep disturbances and chronotherapeutics in spite of the significant evidence base,” she said. “Enterprising doctors should try this out, and the techniques should be taught in residency programs.”
Disclosures: Dr. Wirz-Justice reported no potential conflicts of interest.
For more information on chronotherapeutics, check out the Center for Environmental Therapeutics.
Disclosures: Dr. Wirz-Justice reported no potential conflicts of interest.
International Study Finds Frequent Switching of Antipsychotics
AMSTERDAM – A large multinational study found that one in five adult patients with schizophrenia switched medications within the previous 12 weeks, mostly because of inadequate symptom control as one-third reported a relapse on the initial drug.
Tolerability issues also were important and differed between first- and second-generation antipsychotics, reported Dr. Beata Galinska-Skok of the Medical University of Bialystok in Choroszcz, Poland.
“In the long-term management of schizophrenia, around one-third of patients treated with antipsychotic drugs change their medication every year. There is a need to better understand the dynamics of switching in real-world conditions. We performed a naturalistic multinational observational survey to evaluate the parameters of treatment discontinuation and substitutions in the management of schizophrenia in every day clinical practice,” Dr. Galinska-Skok said.
The primary objective of the cross-sectional observational study conducted in 11 countries was to identify the frequency of and reasons for switching antipsychotic treatments in patients with schizophrenia. Participating physicians were community- or hospital-based psychiatrists who reflected local psychiatric practices and patient management.
The countries represented were Algeria, Greece, India, Jordan, Lithuania, Mexico, Philippines, Poland, Slovakia, Ukraine, and Vietnam.
The registry population included 23,441 adult patients (mean age 41), of whom 22,126 were analyzable. Of those, 5,128 patients (23.2%) reported a treatment switch in the previous 12 weeks and thus constituted the switch population; 3,130 consented to the study and constitute the analysis population.
The medication that was discontinued in the previous 12 weeks was a second-generation antipsychotic for 55.6% of patients and a first-generation agent for 41.8%, while 2.6% discontinued both types. After the switch, most patients received a second-generation agent (90%) either alone (72.4%) or in combination with a first-generation agent (18.3%). The remainder received a first-generation agent as monotherapy, Dr. Galinska-Skok reported.
Main Reason for Switching: Lack of Efficacy
Physicians could report more than one reason for switching. The survey found the main reason to be inadequate symptom control (79.4%), while the occurrence of adverse events was also common (55.3%). Other reasons frequently cited included poor quality of life (31.7%), relapse on medication (30.1%), poor compliance (25.3%), and patient request (18.3%). Two to six percent reported problems with drug availability, financial or life events, and comorbid medical conditions.
“Over half the changes were motivated by an adverse event,” Dr. Galinska-Skok noted. “The nature of the adverse events differed depending on the class of antipsychotic the patient was taking before the switch. Extrapyramidal symptoms and sedation were the two adverse events that most frequently motivated switching from a first-generation agent. Sedation and weight gain were the two most frequent adverse events motivating switching from a second-generation agent.”
Extrapyramidal symptoms were observed in 36% on a first-generation agent, 12% on a second-generation agent and 28% on the combination. Sedation was observed in 20%, 25% and 23%, respectively. Weight gain was problematic for 10%, 26%, and 23%, respectively. Tardive dyskinesia was observed in 15% receiving combination therapy. Less common were abnormal glucose tolerance, dyslipidemia, and sexual dysfunction.
The study was funded by Sanofi-Aventis.
Dr. Galinska-Skok reported no conflicts relevant to this study.
AMSTERDAM – A large multinational study found that one in five adult patients with schizophrenia switched medications within the previous 12 weeks, mostly because of inadequate symptom control as one-third reported a relapse on the initial drug.
Tolerability issues also were important and differed between first- and second-generation antipsychotics, reported Dr. Beata Galinska-Skok of the Medical University of Bialystok in Choroszcz, Poland.
“In the long-term management of schizophrenia, around one-third of patients treated with antipsychotic drugs change their medication every year. There is a need to better understand the dynamics of switching in real-world conditions. We performed a naturalistic multinational observational survey to evaluate the parameters of treatment discontinuation and substitutions in the management of schizophrenia in every day clinical practice,” Dr. Galinska-Skok said.
The primary objective of the cross-sectional observational study conducted in 11 countries was to identify the frequency of and reasons for switching antipsychotic treatments in patients with schizophrenia. Participating physicians were community- or hospital-based psychiatrists who reflected local psychiatric practices and patient management.
The countries represented were Algeria, Greece, India, Jordan, Lithuania, Mexico, Philippines, Poland, Slovakia, Ukraine, and Vietnam.
The registry population included 23,441 adult patients (mean age 41), of whom 22,126 were analyzable. Of those, 5,128 patients (23.2%) reported a treatment switch in the previous 12 weeks and thus constituted the switch population; 3,130 consented to the study and constitute the analysis population.
The medication that was discontinued in the previous 12 weeks was a second-generation antipsychotic for 55.6% of patients and a first-generation agent for 41.8%, while 2.6% discontinued both types. After the switch, most patients received a second-generation agent (90%) either alone (72.4%) or in combination with a first-generation agent (18.3%). The remainder received a first-generation agent as monotherapy, Dr. Galinska-Skok reported.
Main Reason for Switching: Lack of Efficacy
Physicians could report more than one reason for switching. The survey found the main reason to be inadequate symptom control (79.4%), while the occurrence of adverse events was also common (55.3%). Other reasons frequently cited included poor quality of life (31.7%), relapse on medication (30.1%), poor compliance (25.3%), and patient request (18.3%). Two to six percent reported problems with drug availability, financial or life events, and comorbid medical conditions.
“Over half the changes were motivated by an adverse event,” Dr. Galinska-Skok noted. “The nature of the adverse events differed depending on the class of antipsychotic the patient was taking before the switch. Extrapyramidal symptoms and sedation were the two adverse events that most frequently motivated switching from a first-generation agent. Sedation and weight gain were the two most frequent adverse events motivating switching from a second-generation agent.”
Extrapyramidal symptoms were observed in 36% on a first-generation agent, 12% on a second-generation agent and 28% on the combination. Sedation was observed in 20%, 25% and 23%, respectively. Weight gain was problematic for 10%, 26%, and 23%, respectively. Tardive dyskinesia was observed in 15% receiving combination therapy. Less common were abnormal glucose tolerance, dyslipidemia, and sexual dysfunction.
The study was funded by Sanofi-Aventis.
Dr. Galinska-Skok reported no conflicts relevant to this study.
AMSTERDAM – A large multinational study found that one in five adult patients with schizophrenia switched medications within the previous 12 weeks, mostly because of inadequate symptom control as one-third reported a relapse on the initial drug.
Tolerability issues also were important and differed between first- and second-generation antipsychotics, reported Dr. Beata Galinska-Skok of the Medical University of Bialystok in Choroszcz, Poland.
“In the long-term management of schizophrenia, around one-third of patients treated with antipsychotic drugs change their medication every year. There is a need to better understand the dynamics of switching in real-world conditions. We performed a naturalistic multinational observational survey to evaluate the parameters of treatment discontinuation and substitutions in the management of schizophrenia in every day clinical practice,” Dr. Galinska-Skok said.
The primary objective of the cross-sectional observational study conducted in 11 countries was to identify the frequency of and reasons for switching antipsychotic treatments in patients with schizophrenia. Participating physicians were community- or hospital-based psychiatrists who reflected local psychiatric practices and patient management.
The countries represented were Algeria, Greece, India, Jordan, Lithuania, Mexico, Philippines, Poland, Slovakia, Ukraine, and Vietnam.
The registry population included 23,441 adult patients (mean age 41), of whom 22,126 were analyzable. Of those, 5,128 patients (23.2%) reported a treatment switch in the previous 12 weeks and thus constituted the switch population; 3,130 consented to the study and constitute the analysis population.
The medication that was discontinued in the previous 12 weeks was a second-generation antipsychotic for 55.6% of patients and a first-generation agent for 41.8%, while 2.6% discontinued both types. After the switch, most patients received a second-generation agent (90%) either alone (72.4%) or in combination with a first-generation agent (18.3%). The remainder received a first-generation agent as monotherapy, Dr. Galinska-Skok reported.
Main Reason for Switching: Lack of Efficacy
Physicians could report more than one reason for switching. The survey found the main reason to be inadequate symptom control (79.4%), while the occurrence of adverse events was also common (55.3%). Other reasons frequently cited included poor quality of life (31.7%), relapse on medication (30.1%), poor compliance (25.3%), and patient request (18.3%). Two to six percent reported problems with drug availability, financial or life events, and comorbid medical conditions.
“Over half the changes were motivated by an adverse event,” Dr. Galinska-Skok noted. “The nature of the adverse events differed depending on the class of antipsychotic the patient was taking before the switch. Extrapyramidal symptoms and sedation were the two adverse events that most frequently motivated switching from a first-generation agent. Sedation and weight gain were the two most frequent adverse events motivating switching from a second-generation agent.”
Extrapyramidal symptoms were observed in 36% on a first-generation agent, 12% on a second-generation agent and 28% on the combination. Sedation was observed in 20%, 25% and 23%, respectively. Weight gain was problematic for 10%, 26%, and 23%, respectively. Tardive dyskinesia was observed in 15% receiving combination therapy. Less common were abnormal glucose tolerance, dyslipidemia, and sexual dysfunction.
The study was funded by Sanofi-Aventis.
Dr. Galinska-Skok reported no conflicts relevant to this study.
Major Finding: One in five adult patients with schizophrenia switched antipsychotic medications in the previous 12 weeks, mostly because of lack of efficacy and secondarily because of side effects.
Data Source: Observational study of over 23,000 patients from 11 countries.
Disclosures: The study was funded by Sanofi-Aventis.
Baclofen May Effectively Treat Alcohol Dependence
AMSTERDAM – The gamma-aminobutryric acid (GABA) receptor agonist baclofen, which is indicated for the treatment of spasticity, might represent a novel and effective drug treatment for alcohol dependence, according to an addiction specialist who presented evidence for this at the annual congress of the European College of Neuropsychopharmacology.
“Activation of the GABAB receptor by means of agonists or positive allosteric modulators of the GABAB receptor produces suppressive effects on alcohol intake, alcohol reinforcement, and motivation to seek for and consume alcohol,” said Dr. Giancarlo Colombo, of the Institute of Neuroscience at the Consiglio Nazionale delle Ricerche in Cagliari, Italy. “These data support the hypothesis of the involvement of the GABAB receptor in the neural substrate controlling alcohol drinking and seeking behaviors.”
In rodents, acutely or repeatedly administered baclofen suppressed several alcohol-related behaviors, including acquisition and maintenance of alcohol drinking behavior, relapselike drinking, bingelike drinking, and cannabinoid- or opioid-induced increases in alcohol intake under a variety of test conditions. Most of these findings were replicated by baclofen infusion into the ventral tegmental area of rats and mice, pointing to the likely involvement of the mesolimbic dopamine system, or the brain “reward” circuit, in alcohol dependence, Dr. Colombo explained.
Additionally, baclofen administration has been found to suppress the intensity of different signs of alcohol withdrawal syndrome, including anxiety-related behaviors, tremors and seizures, in rats made physically dependent on alcohol.
Preliminary clinical studies and accumulating case-reports have extended most of these findings to human alcoholics, as baclofen has been found to promote abstinence and suppress alcohol consumption, craving for alcohol, and severity of alcohol withdrawal symptoms, including delirium tremens, he said.
In case reports evaluating high doses of baclofen (75-270 mg/day), significant improvements have been observed in the achievement of complete abstinence, control over drinking, relapse prevention, and suppression of craving.
One physician who battled alcoholism, in fact, credits baclofen for his recovery in his book, “The End of My Addiction” (New York: Farrar, Straus and Giroux, 2008). The book cover asserts, “Olivier Ameisen was a renowned cardiologist until alcoholism took over his life. This is the story of how he cured himself.”
In open-label and double-blind clinical studies of low-to-moderate doses (30 mg/day), reductions have been observed in the number of daily drinks, days of heavy drinking, days of abstinence, and alcohol craving scores. However, in the most recent study (Alcohol Clin. Exp. Res. 2010 July 21 [doi: 10.1111/j.1530-0277.2010.01273.x]) baclofen showed no effective over placebo on alcohol drinking in alcohol-dependent patients treated for 12 weeks, he noted.
Possible reasons for the negative study might be that, compared with pivotal data from earlier Italian studies, the baseline number of drinks per day was lower, withdrawal symptoms were less severe, patients were recruited via U.S. newspaper ads rather than treatment centers, and patients had less severe dependence characteristics or different treatment goals.
Examining these discrepancies, Dr. Colombo speculated, “Baclofen may be more effective in the presence of more severe physical dependence.”
The newer positive allosteric modulators of the GABA receptor are showing promise for alcohol dependence in animal models, he added.
Dr. Colombo reported no potential conflicts of interest.
AMSTERDAM – The gamma-aminobutryric acid (GABA) receptor agonist baclofen, which is indicated for the treatment of spasticity, might represent a novel and effective drug treatment for alcohol dependence, according to an addiction specialist who presented evidence for this at the annual congress of the European College of Neuropsychopharmacology.
“Activation of the GABAB receptor by means of agonists or positive allosteric modulators of the GABAB receptor produces suppressive effects on alcohol intake, alcohol reinforcement, and motivation to seek for and consume alcohol,” said Dr. Giancarlo Colombo, of the Institute of Neuroscience at the Consiglio Nazionale delle Ricerche in Cagliari, Italy. “These data support the hypothesis of the involvement of the GABAB receptor in the neural substrate controlling alcohol drinking and seeking behaviors.”
In rodents, acutely or repeatedly administered baclofen suppressed several alcohol-related behaviors, including acquisition and maintenance of alcohol drinking behavior, relapselike drinking, bingelike drinking, and cannabinoid- or opioid-induced increases in alcohol intake under a variety of test conditions. Most of these findings were replicated by baclofen infusion into the ventral tegmental area of rats and mice, pointing to the likely involvement of the mesolimbic dopamine system, or the brain “reward” circuit, in alcohol dependence, Dr. Colombo explained.
Additionally, baclofen administration has been found to suppress the intensity of different signs of alcohol withdrawal syndrome, including anxiety-related behaviors, tremors and seizures, in rats made physically dependent on alcohol.
Preliminary clinical studies and accumulating case-reports have extended most of these findings to human alcoholics, as baclofen has been found to promote abstinence and suppress alcohol consumption, craving for alcohol, and severity of alcohol withdrawal symptoms, including delirium tremens, he said.
In case reports evaluating high doses of baclofen (75-270 mg/day), significant improvements have been observed in the achievement of complete abstinence, control over drinking, relapse prevention, and suppression of craving.
One physician who battled alcoholism, in fact, credits baclofen for his recovery in his book, “The End of My Addiction” (New York: Farrar, Straus and Giroux, 2008). The book cover asserts, “Olivier Ameisen was a renowned cardiologist until alcoholism took over his life. This is the story of how he cured himself.”
In open-label and double-blind clinical studies of low-to-moderate doses (30 mg/day), reductions have been observed in the number of daily drinks, days of heavy drinking, days of abstinence, and alcohol craving scores. However, in the most recent study (Alcohol Clin. Exp. Res. 2010 July 21 [doi: 10.1111/j.1530-0277.2010.01273.x]) baclofen showed no effective over placebo on alcohol drinking in alcohol-dependent patients treated for 12 weeks, he noted.
Possible reasons for the negative study might be that, compared with pivotal data from earlier Italian studies, the baseline number of drinks per day was lower, withdrawal symptoms were less severe, patients were recruited via U.S. newspaper ads rather than treatment centers, and patients had less severe dependence characteristics or different treatment goals.
Examining these discrepancies, Dr. Colombo speculated, “Baclofen may be more effective in the presence of more severe physical dependence.”
The newer positive allosteric modulators of the GABA receptor are showing promise for alcohol dependence in animal models, he added.
Dr. Colombo reported no potential conflicts of interest.
AMSTERDAM – The gamma-aminobutryric acid (GABA) receptor agonist baclofen, which is indicated for the treatment of spasticity, might represent a novel and effective drug treatment for alcohol dependence, according to an addiction specialist who presented evidence for this at the annual congress of the European College of Neuropsychopharmacology.
“Activation of the GABAB receptor by means of agonists or positive allosteric modulators of the GABAB receptor produces suppressive effects on alcohol intake, alcohol reinforcement, and motivation to seek for and consume alcohol,” said Dr. Giancarlo Colombo, of the Institute of Neuroscience at the Consiglio Nazionale delle Ricerche in Cagliari, Italy. “These data support the hypothesis of the involvement of the GABAB receptor in the neural substrate controlling alcohol drinking and seeking behaviors.”
In rodents, acutely or repeatedly administered baclofen suppressed several alcohol-related behaviors, including acquisition and maintenance of alcohol drinking behavior, relapselike drinking, bingelike drinking, and cannabinoid- or opioid-induced increases in alcohol intake under a variety of test conditions. Most of these findings were replicated by baclofen infusion into the ventral tegmental area of rats and mice, pointing to the likely involvement of the mesolimbic dopamine system, or the brain “reward” circuit, in alcohol dependence, Dr. Colombo explained.
Additionally, baclofen administration has been found to suppress the intensity of different signs of alcohol withdrawal syndrome, including anxiety-related behaviors, tremors and seizures, in rats made physically dependent on alcohol.
Preliminary clinical studies and accumulating case-reports have extended most of these findings to human alcoholics, as baclofen has been found to promote abstinence and suppress alcohol consumption, craving for alcohol, and severity of alcohol withdrawal symptoms, including delirium tremens, he said.
In case reports evaluating high doses of baclofen (75-270 mg/day), significant improvements have been observed in the achievement of complete abstinence, control over drinking, relapse prevention, and suppression of craving.
One physician who battled alcoholism, in fact, credits baclofen for his recovery in his book, “The End of My Addiction” (New York: Farrar, Straus and Giroux, 2008). The book cover asserts, “Olivier Ameisen was a renowned cardiologist until alcoholism took over his life. This is the story of how he cured himself.”
In open-label and double-blind clinical studies of low-to-moderate doses (30 mg/day), reductions have been observed in the number of daily drinks, days of heavy drinking, days of abstinence, and alcohol craving scores. However, in the most recent study (Alcohol Clin. Exp. Res. 2010 July 21 [doi: 10.1111/j.1530-0277.2010.01273.x]) baclofen showed no effective over placebo on alcohol drinking in alcohol-dependent patients treated for 12 weeks, he noted.
Possible reasons for the negative study might be that, compared with pivotal data from earlier Italian studies, the baseline number of drinks per day was lower, withdrawal symptoms were less severe, patients were recruited via U.S. newspaper ads rather than treatment centers, and patients had less severe dependence characteristics or different treatment goals.
Examining these discrepancies, Dr. Colombo speculated, “Baclofen may be more effective in the presence of more severe physical dependence.”
The newer positive allosteric modulators of the GABA receptor are showing promise for alcohol dependence in animal models, he added.
Dr. Colombo reported no potential conflicts of interest.
D-Cycloserine Enhances the Effects of Exposure Therapy
AMSTERDAM – The N-methyl-d-aspartate partial agonist d-cycloserine might enhance the results of exposure therapy, especially when it is properly timed and dosed, according to a leading researcher in this field.
Barbara O. Rothbaum, Ph.D., professor of psychiatry at Emory University, Atlanta, discussed the application of d-cycloserine (DCS) to exposure therapy for fear-related conditions at the annual congress of the European College of Neuropsychopharmacology.
DCS has been shown to facilitate exposure therapy in the treatment of obsessive-compulsive disorder, panic disorder, and social phobia, whereas adding “traditional medications” such as alprazolam, imipramine, and fluvoxamine to exposure therapy have shown no advantage over cognitive-behavioral therapy (CBT) alone for these anxiety disorders, according to Dr. Rothbaum.
Pharmacotherapy is aimed at improving the learning that takes place during exposure-based therapy and not at treating the symptoms of anxiety. The glutamatergic N-methyl-d-aspartate (NMDA) receptor is critically involved in learning and memory, and this learning might be augmented by the NMDA partial agonist DCS. In other words, DCS accelerates the associative learning processes that contribute to correcting the psychopathology, she said.
“The use of DCS is a direct attempt to stimulate chemically the NMDA synapses that are thought to be the critical nerve cell mechanisms that support short-term learning and memory at the same moment that CBT is being used to help the patient learn new behaviors,” he said. “DCS is a unique partial agonist for this purpose, because it is thought to work cooperatively with the glutamate that is presumably being released through synaptic activity associated with the patient’s participation in CBT.”
In a double-blind, placebo-controlled study of patients undergoing virtual reality exposure for the treatment of fear of heights, exposure therapy combined with DCS resulted in significantly larger reductions of acrophobia symptoms on all main outcome measures (Arch. Gen. Psych. 2004;61:1136-44). Differences were observed within the virtual environment 1 week and 3 months after treatment. Subjects also showed significantly greater decreases in posttreatment skin conductance fluctuations during the virtual exposure, and had significantly greater improvements on general measures of real world acrophobia symptoms.
The drug did not, however, work by decreasing anxiety during exposure, but it did reduce anxiety, compared with placebo, post treatment (P less than .001) and at 3 months’ follow-up (P less than .05). Its use also was associated with a doubling in the number of height exposures post treatment (P less than .01).
Dr. Rothbaum is now conducting a study in which Iraq war veterans with posttraumatic stress disorder (PTSD) are treated with five sessions of virtual reality exposure therapy plus DCS, alprazolam, or placebo (one pill before each session). Virtual reality exposure therapy (minus the medication) has shown strong efficacy in case studies, one of which showed that PTSD symptoms score dropped from 35 to 10 after four sessions. Currently, 76 subjects have been enrolled in the study, which is still blinded.
Studies in several disorders have evaluated various doses and schedules of DCS when it is given with the exposure therapy. Dr. Rothbaum noted that negative studies have tended to use higher doses administered several hours ahead of the exposure, and she has concluded that dose and timing are critical for this combined approach.
In particular, dosing too early might lead to the peak drug effect’s not being coincident with the emotional learning processes that take place during and immediately after psychotherapy sessions, she maintained. Similarly, too high a dose might activate the antagonist properties of the NMDA partial agonist and the floor effect of subjects improving from a full course of therapy, which could obscure the effects of the drug.
She has concluded – based on these observations and the mechanism of action – that “less d-cycloserine is better than more d-cycloserine, and the timing of the dosing is critical.” She advocates a lower dose that is given approximately once per week and is administered just an hour or so ahead of the exposure therapy session.
Dr. Rothbaum is a consultant to and owns equity in Virtually Better Inc., which is developing products related to virtual reality research.
AMSTERDAM – The N-methyl-d-aspartate partial agonist d-cycloserine might enhance the results of exposure therapy, especially when it is properly timed and dosed, according to a leading researcher in this field.
Barbara O. Rothbaum, Ph.D., professor of psychiatry at Emory University, Atlanta, discussed the application of d-cycloserine (DCS) to exposure therapy for fear-related conditions at the annual congress of the European College of Neuropsychopharmacology.
DCS has been shown to facilitate exposure therapy in the treatment of obsessive-compulsive disorder, panic disorder, and social phobia, whereas adding “traditional medications” such as alprazolam, imipramine, and fluvoxamine to exposure therapy have shown no advantage over cognitive-behavioral therapy (CBT) alone for these anxiety disorders, according to Dr. Rothbaum.
Pharmacotherapy is aimed at improving the learning that takes place during exposure-based therapy and not at treating the symptoms of anxiety. The glutamatergic N-methyl-d-aspartate (NMDA) receptor is critically involved in learning and memory, and this learning might be augmented by the NMDA partial agonist DCS. In other words, DCS accelerates the associative learning processes that contribute to correcting the psychopathology, she said.
“The use of DCS is a direct attempt to stimulate chemically the NMDA synapses that are thought to be the critical nerve cell mechanisms that support short-term learning and memory at the same moment that CBT is being used to help the patient learn new behaviors,” he said. “DCS is a unique partial agonist for this purpose, because it is thought to work cooperatively with the glutamate that is presumably being released through synaptic activity associated with the patient’s participation in CBT.”
In a double-blind, placebo-controlled study of patients undergoing virtual reality exposure for the treatment of fear of heights, exposure therapy combined with DCS resulted in significantly larger reductions of acrophobia symptoms on all main outcome measures (Arch. Gen. Psych. 2004;61:1136-44). Differences were observed within the virtual environment 1 week and 3 months after treatment. Subjects also showed significantly greater decreases in posttreatment skin conductance fluctuations during the virtual exposure, and had significantly greater improvements on general measures of real world acrophobia symptoms.
The drug did not, however, work by decreasing anxiety during exposure, but it did reduce anxiety, compared with placebo, post treatment (P less than .001) and at 3 months’ follow-up (P less than .05). Its use also was associated with a doubling in the number of height exposures post treatment (P less than .01).
Dr. Rothbaum is now conducting a study in which Iraq war veterans with posttraumatic stress disorder (PTSD) are treated with five sessions of virtual reality exposure therapy plus DCS, alprazolam, or placebo (one pill before each session). Virtual reality exposure therapy (minus the medication) has shown strong efficacy in case studies, one of which showed that PTSD symptoms score dropped from 35 to 10 after four sessions. Currently, 76 subjects have been enrolled in the study, which is still blinded.
Studies in several disorders have evaluated various doses and schedules of DCS when it is given with the exposure therapy. Dr. Rothbaum noted that negative studies have tended to use higher doses administered several hours ahead of the exposure, and she has concluded that dose and timing are critical for this combined approach.
In particular, dosing too early might lead to the peak drug effect’s not being coincident with the emotional learning processes that take place during and immediately after psychotherapy sessions, she maintained. Similarly, too high a dose might activate the antagonist properties of the NMDA partial agonist and the floor effect of subjects improving from a full course of therapy, which could obscure the effects of the drug.
She has concluded – based on these observations and the mechanism of action – that “less d-cycloserine is better than more d-cycloserine, and the timing of the dosing is critical.” She advocates a lower dose that is given approximately once per week and is administered just an hour or so ahead of the exposure therapy session.
Dr. Rothbaum is a consultant to and owns equity in Virtually Better Inc., which is developing products related to virtual reality research.
AMSTERDAM – The N-methyl-d-aspartate partial agonist d-cycloserine might enhance the results of exposure therapy, especially when it is properly timed and dosed, according to a leading researcher in this field.
Barbara O. Rothbaum, Ph.D., professor of psychiatry at Emory University, Atlanta, discussed the application of d-cycloserine (DCS) to exposure therapy for fear-related conditions at the annual congress of the European College of Neuropsychopharmacology.
DCS has been shown to facilitate exposure therapy in the treatment of obsessive-compulsive disorder, panic disorder, and social phobia, whereas adding “traditional medications” such as alprazolam, imipramine, and fluvoxamine to exposure therapy have shown no advantage over cognitive-behavioral therapy (CBT) alone for these anxiety disorders, according to Dr. Rothbaum.
Pharmacotherapy is aimed at improving the learning that takes place during exposure-based therapy and not at treating the symptoms of anxiety. The glutamatergic N-methyl-d-aspartate (NMDA) receptor is critically involved in learning and memory, and this learning might be augmented by the NMDA partial agonist DCS. In other words, DCS accelerates the associative learning processes that contribute to correcting the psychopathology, she said.
“The use of DCS is a direct attempt to stimulate chemically the NMDA synapses that are thought to be the critical nerve cell mechanisms that support short-term learning and memory at the same moment that CBT is being used to help the patient learn new behaviors,” he said. “DCS is a unique partial agonist for this purpose, because it is thought to work cooperatively with the glutamate that is presumably being released through synaptic activity associated with the patient’s participation in CBT.”
In a double-blind, placebo-controlled study of patients undergoing virtual reality exposure for the treatment of fear of heights, exposure therapy combined with DCS resulted in significantly larger reductions of acrophobia symptoms on all main outcome measures (Arch. Gen. Psych. 2004;61:1136-44). Differences were observed within the virtual environment 1 week and 3 months after treatment. Subjects also showed significantly greater decreases in posttreatment skin conductance fluctuations during the virtual exposure, and had significantly greater improvements on general measures of real world acrophobia symptoms.
The drug did not, however, work by decreasing anxiety during exposure, but it did reduce anxiety, compared with placebo, post treatment (P less than .001) and at 3 months’ follow-up (P less than .05). Its use also was associated with a doubling in the number of height exposures post treatment (P less than .01).
Dr. Rothbaum is now conducting a study in which Iraq war veterans with posttraumatic stress disorder (PTSD) are treated with five sessions of virtual reality exposure therapy plus DCS, alprazolam, or placebo (one pill before each session). Virtual reality exposure therapy (minus the medication) has shown strong efficacy in case studies, one of which showed that PTSD symptoms score dropped from 35 to 10 after four sessions. Currently, 76 subjects have been enrolled in the study, which is still blinded.
Studies in several disorders have evaluated various doses and schedules of DCS when it is given with the exposure therapy. Dr. Rothbaum noted that negative studies have tended to use higher doses administered several hours ahead of the exposure, and she has concluded that dose and timing are critical for this combined approach.
In particular, dosing too early might lead to the peak drug effect’s not being coincident with the emotional learning processes that take place during and immediately after psychotherapy sessions, she maintained. Similarly, too high a dose might activate the antagonist properties of the NMDA partial agonist and the floor effect of subjects improving from a full course of therapy, which could obscure the effects of the drug.
She has concluded – based on these observations and the mechanism of action – that “less d-cycloserine is better than more d-cycloserine, and the timing of the dosing is critical.” She advocates a lower dose that is given approximately once per week and is administered just an hour or so ahead of the exposure therapy session.
Dr. Rothbaum is a consultant to and owns equity in Virtually Better Inc., which is developing products related to virtual reality research.
Major Finding: Augmenting exposure therapy for fear-related conditions with this NMDA partial agonist can result in greater extinction effects.
Data Source: A double-blind, placebo controlled study in patients with fear of heights, and reference to studies of other disorders.
Disclosures: Dr. Rothbaum is a consultant to and owns equity in Virtually Better Inc., which is developing products related to virtual reality research.
Serotonin Transporter Occupancy Predicts Treatment Response to SSRIs
AMSTERDAM – A significant relationship was observed between treatment response to selective serotonin reuptake inhibitors and serotonin transporter availability and occupancy in a study that used positron emission tomography in patients with major depressive disorder. Dr. Elena Akimova of the Medical University of Vienna presented the findings at the annual congress of the European College of Neuropsychopharmacology.
“We found no correlation between plasma drug level and clinical improvement, but we found that the higher the plasma level, the higher the SERT occupancy, and that lower availability and higher occupancy in the raphe and midbrain regions were related to treatment response,” Dr. Akimova said in an interview.
Impaired serotonin neurotransmission is implicated in the pathophysiology of affective disorders. As an underlying mechanism involved in the effects of selective serotonin reuptake inhibitors (SSRIs), evidence points to a key role for the serotonin transporter (SERT) in high concentrations in the raphe nuclei. The SSRIs bind to SERT, thereby blocking the reuptake of serotonin from the synaptic cleft.
The predictive value of SERT availability in the clinical response to antidepressants is a new research interest. Looking into this question, these investigators conducted a double-blind, randomized longitudinal study with two parallel treatment groups of 18 patients with MDD receiving 10 mg/day escitalopram or 20 mg/day citalopram (which are equivalent doses). Patients underwent PET scanning with [11C] DASB, a new, highly selective PET radiotracer that shows high affinity for SERT. Superior to other PET radioligands for SERT, [11C] DASB permits reliable quantification of subcortical and cortical SERT binding, according to the investigators, whose study earned them a “travel award” to the meeting.
Patients were measured three times to assess SERT availability in the unmedicated state and SERT occupancy 4 hours after a single dose and after the first 3 weeks of treatment with SSRIs. The Hamilton Depression Rating Scale (HAM-D, 17 items) was administered at the screening visit and before each PET scan. SERT availability at baseline and SSRI treatment-induced occupancies of SERT were quantified in 10 brain regions in which high to medium SERT availability might be expected: nucleus caudatus, putamen, midbrain, thalamus, dorsal raphe nucleus, median raphe nucleus, nucleus accumbens, amygdala, anterior cingulated cortex insula. This was correlated with treatment response assessed by the HAM-D.
There were 10 responders and 8 nonresponders to 3 weeks of SSRI treatment. The study found no significant interaction between drug plasma levels and treatment response after either the single dose or prolonged treatment but did find that lower pretreatment SERT availability in raphe regions and midbrain indicated improved treatment responses 3 weeks later, Dr. Akimova reported.
“Our results show that lower availability of SERT before treatment in the midbrain and raphe regions may indicate better treatment outcome in response to SSRIs,” she said.
In the brain regions, pretreatment SERT availability significantly explained the variability in the proportional decrease of HAM-D scores in the midbrain and raphe regions only. Significant correlations between the decrease in HAM-D scores and SERT availability were found in the midbrain (P = .004), median raphe nucleus (P = .002) and dorsal raphe nucleus (P = .011).
“In other words, lower pretreatment SERT availability in these regions indicated improved treatment response 3 weeks later,” she said.
A significant relationship between treatment response and transporter occupancy (second PET) was also observed in the median raphe nucleus (P = .012).
A single dose of SSRIs led to a considerable transporter blockage, resulting in relatively high mean brain occupancy of 74.8%. Continuous SSRI treatment over 3 weeks raised the occupancy to 84.0%, she added.
“To our knowledge, this is the first PET study with [11C] DASB demonstrating a significant relationship between treatment response and SERT availability and occupancy,” she said. “Some investigators suggest that availability and occupancy of SERT may be a key component in the response to SSRIs. In our sample, we were able to show this for the raphe and midbrain regions. With our study, we aim to contribute to the controversial research topic of biological markers.”
Dr. Akimova reported no conflicts of interest.
AMSTERDAM – A significant relationship was observed between treatment response to selective serotonin reuptake inhibitors and serotonin transporter availability and occupancy in a study that used positron emission tomography in patients with major depressive disorder. Dr. Elena Akimova of the Medical University of Vienna presented the findings at the annual congress of the European College of Neuropsychopharmacology.
“We found no correlation between plasma drug level and clinical improvement, but we found that the higher the plasma level, the higher the SERT occupancy, and that lower availability and higher occupancy in the raphe and midbrain regions were related to treatment response,” Dr. Akimova said in an interview.
Impaired serotonin neurotransmission is implicated in the pathophysiology of affective disorders. As an underlying mechanism involved in the effects of selective serotonin reuptake inhibitors (SSRIs), evidence points to a key role for the serotonin transporter (SERT) in high concentrations in the raphe nuclei. The SSRIs bind to SERT, thereby blocking the reuptake of serotonin from the synaptic cleft.
The predictive value of SERT availability in the clinical response to antidepressants is a new research interest. Looking into this question, these investigators conducted a double-blind, randomized longitudinal study with two parallel treatment groups of 18 patients with MDD receiving 10 mg/day escitalopram or 20 mg/day citalopram (which are equivalent doses). Patients underwent PET scanning with [11C] DASB, a new, highly selective PET radiotracer that shows high affinity for SERT. Superior to other PET radioligands for SERT, [11C] DASB permits reliable quantification of subcortical and cortical SERT binding, according to the investigators, whose study earned them a “travel award” to the meeting.
Patients were measured three times to assess SERT availability in the unmedicated state and SERT occupancy 4 hours after a single dose and after the first 3 weeks of treatment with SSRIs. The Hamilton Depression Rating Scale (HAM-D, 17 items) was administered at the screening visit and before each PET scan. SERT availability at baseline and SSRI treatment-induced occupancies of SERT were quantified in 10 brain regions in which high to medium SERT availability might be expected: nucleus caudatus, putamen, midbrain, thalamus, dorsal raphe nucleus, median raphe nucleus, nucleus accumbens, amygdala, anterior cingulated cortex insula. This was correlated with treatment response assessed by the HAM-D.
There were 10 responders and 8 nonresponders to 3 weeks of SSRI treatment. The study found no significant interaction between drug plasma levels and treatment response after either the single dose or prolonged treatment but did find that lower pretreatment SERT availability in raphe regions and midbrain indicated improved treatment responses 3 weeks later, Dr. Akimova reported.
“Our results show that lower availability of SERT before treatment in the midbrain and raphe regions may indicate better treatment outcome in response to SSRIs,” she said.
In the brain regions, pretreatment SERT availability significantly explained the variability in the proportional decrease of HAM-D scores in the midbrain and raphe regions only. Significant correlations between the decrease in HAM-D scores and SERT availability were found in the midbrain (P = .004), median raphe nucleus (P = .002) and dorsal raphe nucleus (P = .011).
“In other words, lower pretreatment SERT availability in these regions indicated improved treatment response 3 weeks later,” she said.
A significant relationship between treatment response and transporter occupancy (second PET) was also observed in the median raphe nucleus (P = .012).
A single dose of SSRIs led to a considerable transporter blockage, resulting in relatively high mean brain occupancy of 74.8%. Continuous SSRI treatment over 3 weeks raised the occupancy to 84.0%, she added.
“To our knowledge, this is the first PET study with [11C] DASB demonstrating a significant relationship between treatment response and SERT availability and occupancy,” she said. “Some investigators suggest that availability and occupancy of SERT may be a key component in the response to SSRIs. In our sample, we were able to show this for the raphe and midbrain regions. With our study, we aim to contribute to the controversial research topic of biological markers.”
Dr. Akimova reported no conflicts of interest.
AMSTERDAM – A significant relationship was observed between treatment response to selective serotonin reuptake inhibitors and serotonin transporter availability and occupancy in a study that used positron emission tomography in patients with major depressive disorder. Dr. Elena Akimova of the Medical University of Vienna presented the findings at the annual congress of the European College of Neuropsychopharmacology.
“We found no correlation between plasma drug level and clinical improvement, but we found that the higher the plasma level, the higher the SERT occupancy, and that lower availability and higher occupancy in the raphe and midbrain regions were related to treatment response,” Dr. Akimova said in an interview.
Impaired serotonin neurotransmission is implicated in the pathophysiology of affective disorders. As an underlying mechanism involved in the effects of selective serotonin reuptake inhibitors (SSRIs), evidence points to a key role for the serotonin transporter (SERT) in high concentrations in the raphe nuclei. The SSRIs bind to SERT, thereby blocking the reuptake of serotonin from the synaptic cleft.
The predictive value of SERT availability in the clinical response to antidepressants is a new research interest. Looking into this question, these investigators conducted a double-blind, randomized longitudinal study with two parallel treatment groups of 18 patients with MDD receiving 10 mg/day escitalopram or 20 mg/day citalopram (which are equivalent doses). Patients underwent PET scanning with [11C] DASB, a new, highly selective PET radiotracer that shows high affinity for SERT. Superior to other PET radioligands for SERT, [11C] DASB permits reliable quantification of subcortical and cortical SERT binding, according to the investigators, whose study earned them a “travel award” to the meeting.
Patients were measured three times to assess SERT availability in the unmedicated state and SERT occupancy 4 hours after a single dose and after the first 3 weeks of treatment with SSRIs. The Hamilton Depression Rating Scale (HAM-D, 17 items) was administered at the screening visit and before each PET scan. SERT availability at baseline and SSRI treatment-induced occupancies of SERT were quantified in 10 brain regions in which high to medium SERT availability might be expected: nucleus caudatus, putamen, midbrain, thalamus, dorsal raphe nucleus, median raphe nucleus, nucleus accumbens, amygdala, anterior cingulated cortex insula. This was correlated with treatment response assessed by the HAM-D.
There were 10 responders and 8 nonresponders to 3 weeks of SSRI treatment. The study found no significant interaction between drug plasma levels and treatment response after either the single dose or prolonged treatment but did find that lower pretreatment SERT availability in raphe regions and midbrain indicated improved treatment responses 3 weeks later, Dr. Akimova reported.
“Our results show that lower availability of SERT before treatment in the midbrain and raphe regions may indicate better treatment outcome in response to SSRIs,” she said.
In the brain regions, pretreatment SERT availability significantly explained the variability in the proportional decrease of HAM-D scores in the midbrain and raphe regions only. Significant correlations between the decrease in HAM-D scores and SERT availability were found in the midbrain (P = .004), median raphe nucleus (P = .002) and dorsal raphe nucleus (P = .011).
“In other words, lower pretreatment SERT availability in these regions indicated improved treatment response 3 weeks later,” she said.
A significant relationship between treatment response and transporter occupancy (second PET) was also observed in the median raphe nucleus (P = .012).
A single dose of SSRIs led to a considerable transporter blockage, resulting in relatively high mean brain occupancy of 74.8%. Continuous SSRI treatment over 3 weeks raised the occupancy to 84.0%, she added.
“To our knowledge, this is the first PET study with [11C] DASB demonstrating a significant relationship between treatment response and SERT availability and occupancy,” she said. “Some investigators suggest that availability and occupancy of SERT may be a key component in the response to SSRIs. In our sample, we were able to show this for the raphe and midbrain regions. With our study, we aim to contribute to the controversial research topic of biological markers.”
Dr. Akimova reported no conflicts of interest.
Major Finding: A significant relationship was found between clinical response to SSRIs and low serotonin transporter availability pretreatment and high occupancy post treatment in the median raphe nucleus, quantified by PET.
Data Source: Double-blind, randomized, longitudinal PET study of two parallel groups of 18 patients using a highly selective radiotracer, [11C] DASB.
Disclosures: Dr. Akimova reported no conflicts of interest.
Magnetic Seizure Therapy for Depression Has Faster Recovery Than ECT
AMSTERDAM – In one of the few clinical trials conducted to date, magnetic seizure therapy yielded outcomes similar to electroconvulsive therapy for the treatment of resistant depression but had the advantage of faster recovery, German investigators reported at the annual congress of the European College of Neuropsychopharmacology.
“For treatment-resistant depression, electroconvulsive therapy [ECT] is often the treatment of last resort. It has been applied for 75 years and is effective, but has cognitive side effects, relapse rates as high as 50%, and it carries a stigma,” said Dr. Sarah Kayser of the University Hospital of Bonn (Germany), who presented the findings.
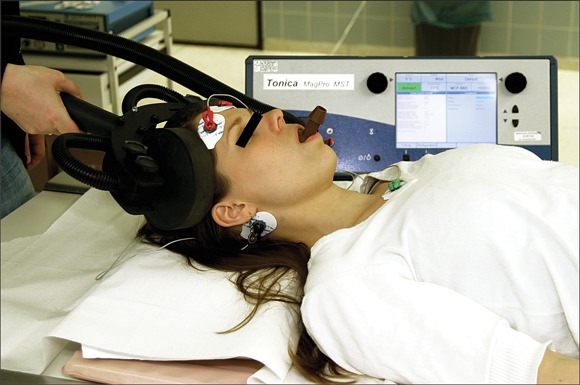
Magnetic seizure therapy [MST], performed under general anesthesia, is a more focal form of convulsive therapy that uses a strong magnetic field to evoke a seizure. It provides greater control over sites of seizure onset and patterns of seizure spread, she said.
Preliminary studies on small groups of patients have suggested that MST is a successful antidepressant approach, with less potential for cognitive side effects, compared with ECT. Although the initial prototype machine was large and unwieldy with multiple components, the newer MagPro MST, which is made in Denmark, is much smaller and easier to work with, she noted.
The prospective study included 20 patients: 16 with a DSM-IV diagnosis of major depressive disorder and 4 with bipolar disorder. The average patient was a 50-year-old female who had had six lifetime episodes of illness, been treated with 18 medications, and been hospitalized four times. The average duration of the most recent episode of illness was 6 years in the MST group and 3.5 years in the ECT group. One out of five patients had attempted suicide.
Ten patients received ECT, and the other 10 received a full course (up to 12 treatments) of MST. The outcome measure of effectiveness was remission or a 50% reduction in depressive symptom severity according to the Hamilton Depression Rating Scale (HDRS28) and the Montgomery-?sberg Depression Rating Scale (MADRS).
The two treatment groups both demonstrated significant improvement over baseline. Response criteria were met by 65% of the patients, whereas 53% met the criteria for remission, Dr. Kayser reported. Mean scores on the HDRS28 declined by approximately 12 points in each treatment arm (P less than .001), and on the MADRS they dropped approximately 12 points after ECT and 15 points after MST (P less than .001).
Several aspects of recovery from the procedure were significantly better in the MST arm, compared with ECT, she reported. “Patients were quicker to breathe independently after anesthesia, and their reorientation time was faster, based on their answers to biographical questions such as name, date, and so forth,” she said.
Mean recovery time (defined as independent breathing) was nearly 4 minutes after ECT, compared with approximately 1.5 minutes with MST (P less than .01). Reorientation time was 8 minutes vs. 2 minutes (P less than .01). EEG showed no effects on brain structure with either approach.
Neither arm showed significant changes in cognitive outcomes, including learning and memory (verbal and visual), abstract knowledge, executive functions (verbal fluency) and speed of processing.
This is an emerging treatment for severe depression that is being studied in only four clinical trials that are centered in New York/Dallas; Australia; Bonn, Germany; and Berlin.
The authors had no relevant financial conflicts of interest.
AMSTERDAM – In one of the few clinical trials conducted to date, magnetic seizure therapy yielded outcomes similar to electroconvulsive therapy for the treatment of resistant depression but had the advantage of faster recovery, German investigators reported at the annual congress of the European College of Neuropsychopharmacology.
“For treatment-resistant depression, electroconvulsive therapy [ECT] is often the treatment of last resort. It has been applied for 75 years and is effective, but has cognitive side effects, relapse rates as high as 50%, and it carries a stigma,” said Dr. Sarah Kayser of the University Hospital of Bonn (Germany), who presented the findings.
Magnetic seizure therapy [MST], performed under general anesthesia, is a more focal form of convulsive therapy that uses a strong magnetic field to evoke a seizure. It provides greater control over sites of seizure onset and patterns of seizure spread, she said.
Preliminary studies on small groups of patients have suggested that MST is a successful antidepressant approach, with less potential for cognitive side effects, compared with ECT. Although the initial prototype machine was large and unwieldy with multiple components, the newer MagPro MST, which is made in Denmark, is much smaller and easier to work with, she noted.
The prospective study included 20 patients: 16 with a DSM-IV diagnosis of major depressive disorder and 4 with bipolar disorder. The average patient was a 50-year-old female who had had six lifetime episodes of illness, been treated with 18 medications, and been hospitalized four times. The average duration of the most recent episode of illness was 6 years in the MST group and 3.5 years in the ECT group. One out of five patients had attempted suicide.
Ten patients received ECT, and the other 10 received a full course (up to 12 treatments) of MST. The outcome measure of effectiveness was remission or a 50% reduction in depressive symptom severity according to the Hamilton Depression Rating Scale (HDRS28) and the Montgomery-?sberg Depression Rating Scale (MADRS).
The two treatment groups both demonstrated significant improvement over baseline. Response criteria were met by 65% of the patients, whereas 53% met the criteria for remission, Dr. Kayser reported. Mean scores on the HDRS28 declined by approximately 12 points in each treatment arm (P less than .001), and on the MADRS they dropped approximately 12 points after ECT and 15 points after MST (P less than .001).
Several aspects of recovery from the procedure were significantly better in the MST arm, compared with ECT, she reported. “Patients were quicker to breathe independently after anesthesia, and their reorientation time was faster, based on their answers to biographical questions such as name, date, and so forth,” she said.
Mean recovery time (defined as independent breathing) was nearly 4 minutes after ECT, compared with approximately 1.5 minutes with MST (P less than .01). Reorientation time was 8 minutes vs. 2 minutes (P less than .01). EEG showed no effects on brain structure with either approach.
Neither arm showed significant changes in cognitive outcomes, including learning and memory (verbal and visual), abstract knowledge, executive functions (verbal fluency) and speed of processing.
This is an emerging treatment for severe depression that is being studied in only four clinical trials that are centered in New York/Dallas; Australia; Bonn, Germany; and Berlin.
The authors had no relevant financial conflicts of interest.
AMSTERDAM – In one of the few clinical trials conducted to date, magnetic seizure therapy yielded outcomes similar to electroconvulsive therapy for the treatment of resistant depression but had the advantage of faster recovery, German investigators reported at the annual congress of the European College of Neuropsychopharmacology.
“For treatment-resistant depression, electroconvulsive therapy [ECT] is often the treatment of last resort. It has been applied for 75 years and is effective, but has cognitive side effects, relapse rates as high as 50%, and it carries a stigma,” said Dr. Sarah Kayser of the University Hospital of Bonn (Germany), who presented the findings.
Magnetic seizure therapy [MST], performed under general anesthesia, is a more focal form of convulsive therapy that uses a strong magnetic field to evoke a seizure. It provides greater control over sites of seizure onset and patterns of seizure spread, she said.
Preliminary studies on small groups of patients have suggested that MST is a successful antidepressant approach, with less potential for cognitive side effects, compared with ECT. Although the initial prototype machine was large and unwieldy with multiple components, the newer MagPro MST, which is made in Denmark, is much smaller and easier to work with, she noted.
The prospective study included 20 patients: 16 with a DSM-IV diagnosis of major depressive disorder and 4 with bipolar disorder. The average patient was a 50-year-old female who had had six lifetime episodes of illness, been treated with 18 medications, and been hospitalized four times. The average duration of the most recent episode of illness was 6 years in the MST group and 3.5 years in the ECT group. One out of five patients had attempted suicide.
Ten patients received ECT, and the other 10 received a full course (up to 12 treatments) of MST. The outcome measure of effectiveness was remission or a 50% reduction in depressive symptom severity according to the Hamilton Depression Rating Scale (HDRS28) and the Montgomery-?sberg Depression Rating Scale (MADRS).
The two treatment groups both demonstrated significant improvement over baseline. Response criteria were met by 65% of the patients, whereas 53% met the criteria for remission, Dr. Kayser reported. Mean scores on the HDRS28 declined by approximately 12 points in each treatment arm (P less than .001), and on the MADRS they dropped approximately 12 points after ECT and 15 points after MST (P less than .001).
Several aspects of recovery from the procedure were significantly better in the MST arm, compared with ECT, she reported. “Patients were quicker to breathe independently after anesthesia, and their reorientation time was faster, based on their answers to biographical questions such as name, date, and so forth,” she said.
Mean recovery time (defined as independent breathing) was nearly 4 minutes after ECT, compared with approximately 1.5 minutes with MST (P less than .01). Reorientation time was 8 minutes vs. 2 minutes (P less than .01). EEG showed no effects on brain structure with either approach.
Neither arm showed significant changes in cognitive outcomes, including learning and memory (verbal and visual), abstract knowledge, executive functions (verbal fluency) and speed of processing.
This is an emerging treatment for severe depression that is being studied in only four clinical trials that are centered in New York/Dallas; Australia; Bonn, Germany; and Berlin.
The authors had no relevant financial conflicts of interest.
Major Finding: This was one of only a few clinical studies of MST. It found comparable outcome to ECT but quicker recovery and reorientation.
Data Source: Prospective study of 20 patients: 16 with major depressive disorder and 4 with bipolar disorder.
Disclosures: The authors had no relevant financial conflicts of interest.
Intensive Group CBT May Be Effective in Body Dysmorphic Disorder
AMSTERDAM – An intensive cognitive-behavioral therapy group treatment program proved very effective for body dysmorphic disorder, with 75% of participants responding, in a study reported by researchers from the Netherlands at the annual congress of the European College of Neuropsychopharmacology.
“We found that our intensive group CBT [cognitive-behavioral therapy] program was an effective strategy in treating severe BDD [body dysmorphic disorder] and symptoms associated with BDD, which can be quite disabling,” said C.A. Molenaar, a doctoral candidate at the University of Amsterdam.
BDD affects approximately 1%-2% of the general population. CBT is currently the treatment of choice, based on altering negative appraisals of body imaging and core beliefs as well as extinction of conditioned fear. But BDD is a complex disorder that can involve delusional beliefs, extensive rituals, and widespread avoidance behaviors. The investigators hypothesized that a more intensive treatment program would be more effective than standard CBT and designed a pilot study to test this approach.
The study involved 12 patients (mean age 30 years) with severe BDD who were enrolled in an 18-week program that included four group sessions per day for one day per week. All but two patients had received medication, without sufficient effects on BDD symptoms, and most had received individual therapy. Global Assessment of Functioning scores varied from 30 to 60, with a mean of 48 points.
The sessions provided psychoeducation about BDD, exposure and response prevention, cognitive therapy, and mirror retraining and refocusing. Assessments were made at baseline, midpoint, and post treatment for BDD symptoms, delusional beliefs, and symptoms of depression and anxiety. Response was measured by the BDD-Yale Brown Obsessive Compulsive Scale (YBOCS).
Significant improvements were observed in all symptoms. Nine of the 12 patients were classified as responders on the BDD-YBOCS (greater than 25% reduction from baseline levels). After treatment, BDD symptoms of preoccupation and compulsive behavior, as measured by the BDD-YBOCS, decreased significantly by a mean of 10.17 points (P less than .005), which was a 36% reduction.
In addition, delusionality as measured by the Brown Assessment of Beliefs Scale decreased by a mean of 5.4 points (P less than .015), a 40% reduction. Depressive symptoms decreased by a mean of 5.0 points on the Hamilton Rating Scale for Depression (HAM-D) (P less than .005), a 27% reduction, and anxiety symptoms decreased by 7.1 points on the Hamilton Anxiety Rating Scale (P less than .044), a 23% reduction.
“We feel these are very good results, based not only on the main scale of severity but also on scales of depression and anxiety,” Ms. Molinaar said in an interview.
She said the program is not only efficacious but probably more cost effective than individual therapy, which will be evaluated in a future study. Furthermore, the group experience might contribute to the success of the program, she maintained.
“Patients were very anxious at the start, but after a few sessions their anxiety diminished and they were very open to each other,” she said. “We believe this is one reason why group therapy works.”
No disclosures were reported.
AMSTERDAM – An intensive cognitive-behavioral therapy group treatment program proved very effective for body dysmorphic disorder, with 75% of participants responding, in a study reported by researchers from the Netherlands at the annual congress of the European College of Neuropsychopharmacology.
“We found that our intensive group CBT [cognitive-behavioral therapy] program was an effective strategy in treating severe BDD [body dysmorphic disorder] and symptoms associated with BDD, which can be quite disabling,” said C.A. Molenaar, a doctoral candidate at the University of Amsterdam.
BDD affects approximately 1%-2% of the general population. CBT is currently the treatment of choice, based on altering negative appraisals of body imaging and core beliefs as well as extinction of conditioned fear. But BDD is a complex disorder that can involve delusional beliefs, extensive rituals, and widespread avoidance behaviors. The investigators hypothesized that a more intensive treatment program would be more effective than standard CBT and designed a pilot study to test this approach.
The study involved 12 patients (mean age 30 years) with severe BDD who were enrolled in an 18-week program that included four group sessions per day for one day per week. All but two patients had received medication, without sufficient effects on BDD symptoms, and most had received individual therapy. Global Assessment of Functioning scores varied from 30 to 60, with a mean of 48 points.
The sessions provided psychoeducation about BDD, exposure and response prevention, cognitive therapy, and mirror retraining and refocusing. Assessments were made at baseline, midpoint, and post treatment for BDD symptoms, delusional beliefs, and symptoms of depression and anxiety. Response was measured by the BDD-Yale Brown Obsessive Compulsive Scale (YBOCS).
Significant improvements were observed in all symptoms. Nine of the 12 patients were classified as responders on the BDD-YBOCS (greater than 25% reduction from baseline levels). After treatment, BDD symptoms of preoccupation and compulsive behavior, as measured by the BDD-YBOCS, decreased significantly by a mean of 10.17 points (P less than .005), which was a 36% reduction.
In addition, delusionality as measured by the Brown Assessment of Beliefs Scale decreased by a mean of 5.4 points (P less than .015), a 40% reduction. Depressive symptoms decreased by a mean of 5.0 points on the Hamilton Rating Scale for Depression (HAM-D) (P less than .005), a 27% reduction, and anxiety symptoms decreased by 7.1 points on the Hamilton Anxiety Rating Scale (P less than .044), a 23% reduction.
“We feel these are very good results, based not only on the main scale of severity but also on scales of depression and anxiety,” Ms. Molinaar said in an interview.
She said the program is not only efficacious but probably more cost effective than individual therapy, which will be evaluated in a future study. Furthermore, the group experience might contribute to the success of the program, she maintained.
“Patients were very anxious at the start, but after a few sessions their anxiety diminished and they were very open to each other,” she said. “We believe this is one reason why group therapy works.”
No disclosures were reported.
AMSTERDAM – An intensive cognitive-behavioral therapy group treatment program proved very effective for body dysmorphic disorder, with 75% of participants responding, in a study reported by researchers from the Netherlands at the annual congress of the European College of Neuropsychopharmacology.
“We found that our intensive group CBT [cognitive-behavioral therapy] program was an effective strategy in treating severe BDD [body dysmorphic disorder] and symptoms associated with BDD, which can be quite disabling,” said C.A. Molenaar, a doctoral candidate at the University of Amsterdam.
BDD affects approximately 1%-2% of the general population. CBT is currently the treatment of choice, based on altering negative appraisals of body imaging and core beliefs as well as extinction of conditioned fear. But BDD is a complex disorder that can involve delusional beliefs, extensive rituals, and widespread avoidance behaviors. The investigators hypothesized that a more intensive treatment program would be more effective than standard CBT and designed a pilot study to test this approach.
The study involved 12 patients (mean age 30 years) with severe BDD who were enrolled in an 18-week program that included four group sessions per day for one day per week. All but two patients had received medication, without sufficient effects on BDD symptoms, and most had received individual therapy. Global Assessment of Functioning scores varied from 30 to 60, with a mean of 48 points.
The sessions provided psychoeducation about BDD, exposure and response prevention, cognitive therapy, and mirror retraining and refocusing. Assessments were made at baseline, midpoint, and post treatment for BDD symptoms, delusional beliefs, and symptoms of depression and anxiety. Response was measured by the BDD-Yale Brown Obsessive Compulsive Scale (YBOCS).
Significant improvements were observed in all symptoms. Nine of the 12 patients were classified as responders on the BDD-YBOCS (greater than 25% reduction from baseline levels). After treatment, BDD symptoms of preoccupation and compulsive behavior, as measured by the BDD-YBOCS, decreased significantly by a mean of 10.17 points (P less than .005), which was a 36% reduction.
In addition, delusionality as measured by the Brown Assessment of Beliefs Scale decreased by a mean of 5.4 points (P less than .015), a 40% reduction. Depressive symptoms decreased by a mean of 5.0 points on the Hamilton Rating Scale for Depression (HAM-D) (P less than .005), a 27% reduction, and anxiety symptoms decreased by 7.1 points on the Hamilton Anxiety Rating Scale (P less than .044), a 23% reduction.
“We feel these are very good results, based not only on the main scale of severity but also on scales of depression and anxiety,” Ms. Molinaar said in an interview.
She said the program is not only efficacious but probably more cost effective than individual therapy, which will be evaluated in a future study. Furthermore, the group experience might contribute to the success of the program, she maintained.
“Patients were very anxious at the start, but after a few sessions their anxiety diminished and they were very open to each other,” she said. “We believe this is one reason why group therapy works.”
No disclosures were reported.
From the annual congress of the European College of Neuropsychopharmacology
Major Finding: An intensive group approach using CBT produced responses in 75% of individuals with BDD.
Data Source: Pilot study of 12 patients with severe BDD who were enrolled in an 18-week program
Disclosures: The researchers reported no conflicts.
Patients Accompanied by Therapists During Exposure Sessions Have Better Outcomes
AMSTERDAM – Cognitive-behavioral therapy for panic disorder and agoraphobia seems to work better when the therapist accompanies the patient during the in vivo exposure sessions.
Investigators from Technische Universität in Dresden, Germany, made this finding, and, additionally, found that therapists need not adhere strongly to a CBT manual to produce symptomatic changes.
The two studies were reported at the annual congress of the European College of Neuropsychopharmacology by Andrew T. Gloster, Ph.D., and Christina Hauke of the Institute of Clinical Psychology and Psychotherapy.
The first was a multicenter study of 369 patients with panic disorder and agoraphobia as well as a high rate of comorbid disorders (41%-73%). The study’s primary aim was to determine whether variations in treatment delivery affect outcomes of CBT.
The patients were randomized to two active variations of CBT. In one, the therapist was present during in vivo exposure exercises (n = 163); in the other, the therapist planned and discussed the exercises but did not accompany the patient (n = 138). A third group (control) was assigned to a wait list (n = 68).
“Leaving the room is crucial for the patient, and we explored whether there is a benefit for the therapist being with the patient for these exposures. Data suggest you can do the therapy both ways, but you absolutely must prepare the patient as to what will occur,” Dr. Gloster said. “We have this conversation many times with the patient. If the therapist is going with the patient, then the conversation can occur as it is needed.”
Attaining Better Response Rates
At the end of treatment, both active treatment groups were superior to the wait list group, but the therapist-present group obtained more favorable results on nearly every index. The largest differences were noted on agoraphobic avoidance and global functioning, he reported.
“We found there are additive effects when the therapist goes with the patient on all five exposure sessions,” Dr. Gloster said.
On global functioning, the mean baseline value was 5.4 for the therapist-present group, and 5.2 for both the therapist-not-present and the wait-list groups. From baseline to end of treatment (last observation carried forward), scores were reduced by nearly 2.5 points with the therapist present and 2.0 points without the therapist present (P less than .05). Patients continued to improve over time, and at the 6-month follow-up, these scores were further reduced (nonsignificantly) by another 1.0 and 0.75 points, respectively.
These numbers represented response rates post treatment of 49.7% for the therapist-present condition and 39.1% for therapist-not-present condition. At the 6-month follow-up, response rates rose to 68.7% and 60.9%, respectively.
The wait-list group showed little change post treatment, with scores reduced by a mean of less than 0.5, corresponding with a response rate of 7.4%, Dr. Gloster reported.
For agoraphobic avoidance, mean scores were approximately 3.0 at baseline for all groups and were reduced by approximately 1.2 points in the therapist-present arm and 0.75 in the therapist-not-present arm (P less than .05). Slight additional improvements were seen at 6 months. Wait-list patients showed little improvement.
Similarly, the percentage of patients panic free after treatment was 49.4% with the therapist present and 45.7% without, and at 6 months it was 66.3% and 60.9%, respectively. In the wait-list arm, just 25% became panic free. The number of panic attacks also was reduced, with statistical significance observed between the active treatment groups at 6 months. General anxiety similarly improved.
The rate of decrease in agoraphobic avoidance accelerated after the introduction of in vivo exposure, he added. Patients who exposed themselves to more anxiety-provoking situations had better outcomes.
“When the therapist accompanied the patient, at 6 months we saw a significantly greater reduction in panic attacks,” Dr. Gloster said. “Patients are having more spontaneous exposures, and this is the most important factor in the therapy.”
Strict Adherence Not Essential
The same investigators also reported a minimal inverse relationship between adherence to the CBT manual and outcome. “Overall, at a global level, adherence was not relevant to treatment outcome,” Ms. Hauke reported.
The finding could be biased, she acknowledged, by the fact that 80% of sessions were rated as “good adherence” or “highly adherent” so there was little room for improvement.
The study included 275 of the same patients as in the first study, treated by 62 therapists in the two exposure-based models described above. Investigators looked at the sample of completers (n = 230) who finished 12 twice-weekly sessions, and drop-outs (n = 45), who terminated before session 12. Therapist adherence ratings were generated by analysis of randomly selected videotapes of the sessions using the Therapist Adherence and Competency Rating Scales (TACRS) developed by Dr. Gloster and colleagues. Outcome measures were changes on scores on standard instruments.
Rates of adherence were similar for therapists of completers and drop-outs, approximately 5.5 on an 8-point scale, and higher level of adherence was associated minimally with worse outcomes, Ms. Hauke reported.
The therapists of the completers were significantly less likely to adhere to the protocol if they were assigned to the therapist-present exposure situation, compared with standard CBT (P = .025). Adherence was not, however, associated with outcomes for patients who dropped out. Therapists of patients who dropped out for exposure-related reasons (for example, anxious, not motivated) versus other reasons (for example, organizational problems, symptom improvement, or deterioration) had a strong trend toward lower levels of adherence (P = .05), which became significant after the researchers controlled for years of therapist experience (P = .036).
The findings might suggest “that levels of adherence should be matched with individual patient requirements before implementing a manualized therapy,” she said.
The main point, Ms. Hauke said, is that robust adherence to the CBT manual is not the only important factor in treatment outcome, and other modifiers should be examined.
The authors reported no potential conflicts of interest. The work was funded by the German Federal Ministry of Education and Research.
AMSTERDAM – Cognitive-behavioral therapy for panic disorder and agoraphobia seems to work better when the therapist accompanies the patient during the in vivo exposure sessions.
Investigators from Technische Universität in Dresden, Germany, made this finding, and, additionally, found that therapists need not adhere strongly to a CBT manual to produce symptomatic changes.
The two studies were reported at the annual congress of the European College of Neuropsychopharmacology by Andrew T. Gloster, Ph.D., and Christina Hauke of the Institute of Clinical Psychology and Psychotherapy.
The first was a multicenter study of 369 patients with panic disorder and agoraphobia as well as a high rate of comorbid disorders (41%-73%). The study’s primary aim was to determine whether variations in treatment delivery affect outcomes of CBT.
The patients were randomized to two active variations of CBT. In one, the therapist was present during in vivo exposure exercises (n = 163); in the other, the therapist planned and discussed the exercises but did not accompany the patient (n = 138). A third group (control) was assigned to a wait list (n = 68).
“Leaving the room is crucial for the patient, and we explored whether there is a benefit for the therapist being with the patient for these exposures. Data suggest you can do the therapy both ways, but you absolutely must prepare the patient as to what will occur,” Dr. Gloster said. “We have this conversation many times with the patient. If the therapist is going with the patient, then the conversation can occur as it is needed.”
Attaining Better Response Rates
At the end of treatment, both active treatment groups were superior to the wait list group, but the therapist-present group obtained more favorable results on nearly every index. The largest differences were noted on agoraphobic avoidance and global functioning, he reported.
“We found there are additive effects when the therapist goes with the patient on all five exposure sessions,” Dr. Gloster said.
On global functioning, the mean baseline value was 5.4 for the therapist-present group, and 5.2 for both the therapist-not-present and the wait-list groups. From baseline to end of treatment (last observation carried forward), scores were reduced by nearly 2.5 points with the therapist present and 2.0 points without the therapist present (P less than .05). Patients continued to improve over time, and at the 6-month follow-up, these scores were further reduced (nonsignificantly) by another 1.0 and 0.75 points, respectively.
These numbers represented response rates post treatment of 49.7% for the therapist-present condition and 39.1% for therapist-not-present condition. At the 6-month follow-up, response rates rose to 68.7% and 60.9%, respectively.
The wait-list group showed little change post treatment, with scores reduced by a mean of less than 0.5, corresponding with a response rate of 7.4%, Dr. Gloster reported.
For agoraphobic avoidance, mean scores were approximately 3.0 at baseline for all groups and were reduced by approximately 1.2 points in the therapist-present arm and 0.75 in the therapist-not-present arm (P less than .05). Slight additional improvements were seen at 6 months. Wait-list patients showed little improvement.
Similarly, the percentage of patients panic free after treatment was 49.4% with the therapist present and 45.7% without, and at 6 months it was 66.3% and 60.9%, respectively. In the wait-list arm, just 25% became panic free. The number of panic attacks also was reduced, with statistical significance observed between the active treatment groups at 6 months. General anxiety similarly improved.
The rate of decrease in agoraphobic avoidance accelerated after the introduction of in vivo exposure, he added. Patients who exposed themselves to more anxiety-provoking situations had better outcomes.
“When the therapist accompanied the patient, at 6 months we saw a significantly greater reduction in panic attacks,” Dr. Gloster said. “Patients are having more spontaneous exposures, and this is the most important factor in the therapy.”
Strict Adherence Not Essential
The same investigators also reported a minimal inverse relationship between adherence to the CBT manual and outcome. “Overall, at a global level, adherence was not relevant to treatment outcome,” Ms. Hauke reported.
The finding could be biased, she acknowledged, by the fact that 80% of sessions were rated as “good adherence” or “highly adherent” so there was little room for improvement.
The study included 275 of the same patients as in the first study, treated by 62 therapists in the two exposure-based models described above. Investigators looked at the sample of completers (n = 230) who finished 12 twice-weekly sessions, and drop-outs (n = 45), who terminated before session 12. Therapist adherence ratings were generated by analysis of randomly selected videotapes of the sessions using the Therapist Adherence and Competency Rating Scales (TACRS) developed by Dr. Gloster and colleagues. Outcome measures were changes on scores on standard instruments.
Rates of adherence were similar for therapists of completers and drop-outs, approximately 5.5 on an 8-point scale, and higher level of adherence was associated minimally with worse outcomes, Ms. Hauke reported.
The therapists of the completers were significantly less likely to adhere to the protocol if they were assigned to the therapist-present exposure situation, compared with standard CBT (P = .025). Adherence was not, however, associated with outcomes for patients who dropped out. Therapists of patients who dropped out for exposure-related reasons (for example, anxious, not motivated) versus other reasons (for example, organizational problems, symptom improvement, or deterioration) had a strong trend toward lower levels of adherence (P = .05), which became significant after the researchers controlled for years of therapist experience (P = .036).
The findings might suggest “that levels of adherence should be matched with individual patient requirements before implementing a manualized therapy,” she said.
The main point, Ms. Hauke said, is that robust adherence to the CBT manual is not the only important factor in treatment outcome, and other modifiers should be examined.
The authors reported no potential conflicts of interest. The work was funded by the German Federal Ministry of Education and Research.
AMSTERDAM – Cognitive-behavioral therapy for panic disorder and agoraphobia seems to work better when the therapist accompanies the patient during the in vivo exposure sessions.
Investigators from Technische Universität in Dresden, Germany, made this finding, and, additionally, found that therapists need not adhere strongly to a CBT manual to produce symptomatic changes.
The two studies were reported at the annual congress of the European College of Neuropsychopharmacology by Andrew T. Gloster, Ph.D., and Christina Hauke of the Institute of Clinical Psychology and Psychotherapy.
The first was a multicenter study of 369 patients with panic disorder and agoraphobia as well as a high rate of comorbid disorders (41%-73%). The study’s primary aim was to determine whether variations in treatment delivery affect outcomes of CBT.
The patients were randomized to two active variations of CBT. In one, the therapist was present during in vivo exposure exercises (n = 163); in the other, the therapist planned and discussed the exercises but did not accompany the patient (n = 138). A third group (control) was assigned to a wait list (n = 68).
“Leaving the room is crucial for the patient, and we explored whether there is a benefit for the therapist being with the patient for these exposures. Data suggest you can do the therapy both ways, but you absolutely must prepare the patient as to what will occur,” Dr. Gloster said. “We have this conversation many times with the patient. If the therapist is going with the patient, then the conversation can occur as it is needed.”
Attaining Better Response Rates
At the end of treatment, both active treatment groups were superior to the wait list group, but the therapist-present group obtained more favorable results on nearly every index. The largest differences were noted on agoraphobic avoidance and global functioning, he reported.
“We found there are additive effects when the therapist goes with the patient on all five exposure sessions,” Dr. Gloster said.
On global functioning, the mean baseline value was 5.4 for the therapist-present group, and 5.2 for both the therapist-not-present and the wait-list groups. From baseline to end of treatment (last observation carried forward), scores were reduced by nearly 2.5 points with the therapist present and 2.0 points without the therapist present (P less than .05). Patients continued to improve over time, and at the 6-month follow-up, these scores were further reduced (nonsignificantly) by another 1.0 and 0.75 points, respectively.
These numbers represented response rates post treatment of 49.7% for the therapist-present condition and 39.1% for therapist-not-present condition. At the 6-month follow-up, response rates rose to 68.7% and 60.9%, respectively.
The wait-list group showed little change post treatment, with scores reduced by a mean of less than 0.5, corresponding with a response rate of 7.4%, Dr. Gloster reported.
For agoraphobic avoidance, mean scores were approximately 3.0 at baseline for all groups and were reduced by approximately 1.2 points in the therapist-present arm and 0.75 in the therapist-not-present arm (P less than .05). Slight additional improvements were seen at 6 months. Wait-list patients showed little improvement.
Similarly, the percentage of patients panic free after treatment was 49.4% with the therapist present and 45.7% without, and at 6 months it was 66.3% and 60.9%, respectively. In the wait-list arm, just 25% became panic free. The number of panic attacks also was reduced, with statistical significance observed between the active treatment groups at 6 months. General anxiety similarly improved.
The rate of decrease in agoraphobic avoidance accelerated after the introduction of in vivo exposure, he added. Patients who exposed themselves to more anxiety-provoking situations had better outcomes.
“When the therapist accompanied the patient, at 6 months we saw a significantly greater reduction in panic attacks,” Dr. Gloster said. “Patients are having more spontaneous exposures, and this is the most important factor in the therapy.”
Strict Adherence Not Essential
The same investigators also reported a minimal inverse relationship between adherence to the CBT manual and outcome. “Overall, at a global level, adherence was not relevant to treatment outcome,” Ms. Hauke reported.
The finding could be biased, she acknowledged, by the fact that 80% of sessions were rated as “good adherence” or “highly adherent” so there was little room for improvement.
The study included 275 of the same patients as in the first study, treated by 62 therapists in the two exposure-based models described above. Investigators looked at the sample of completers (n = 230) who finished 12 twice-weekly sessions, and drop-outs (n = 45), who terminated before session 12. Therapist adherence ratings were generated by analysis of randomly selected videotapes of the sessions using the Therapist Adherence and Competency Rating Scales (TACRS) developed by Dr. Gloster and colleagues. Outcome measures were changes on scores on standard instruments.
Rates of adherence were similar for therapists of completers and drop-outs, approximately 5.5 on an 8-point scale, and higher level of adherence was associated minimally with worse outcomes, Ms. Hauke reported.
The therapists of the completers were significantly less likely to adhere to the protocol if they were assigned to the therapist-present exposure situation, compared with standard CBT (P = .025). Adherence was not, however, associated with outcomes for patients who dropped out. Therapists of patients who dropped out for exposure-related reasons (for example, anxious, not motivated) versus other reasons (for example, organizational problems, symptom improvement, or deterioration) had a strong trend toward lower levels of adherence (P = .05), which became significant after the researchers controlled for years of therapist experience (P = .036).
The findings might suggest “that levels of adherence should be matched with individual patient requirements before implementing a manualized therapy,” she said.
The main point, Ms. Hauke said, is that robust adherence to the CBT manual is not the only important factor in treatment outcome, and other modifiers should be examined.
The authors reported no potential conflicts of interest. The work was funded by the German Federal Ministry of Education and Research.
From the annual congress of the European College of Neuropsychopharmacology
Major Finding: Patients with panic disorder and agoraphobia had better outcomes on global functioning, agoraphobic avoidance, and numbers of panic attacks when accompanied by the therapist during exposure sessions, versus preparing the patient for a solo experience. An accompanying study found no need for therapists to strictly adhere to the CBT manual when treating these patients.
Data Source: A large prospective multicenter study conducted in Germany.
Disclosures: The authors reported no conflicts of interest. The work was funded by the German Federal Ministry of Education and Research.
Targeted CBT-Based Program for Cannabis Dependence Proves Effective
AMSTERDAM – A targeted cognitive-behavioral treatment program designed by German addiction specialists for cannabis use disorder promoted abstinence in 50% of subjects and significantly reduced global addiction severity and psychopathological symptoms.

The approach was described by Hans-Ulrich Wittchen, Ph.D., director of the Institute of Clinical Psychology and Psychotherapy at Technische Universit?t Dresden at the annual congress of the European College of Neuropsychopharmacology.
“The majority [of participants] are abstinent 6 months after treatment,” even when urine tests are done. “This is a remarkable finding that we did not expect at the beginning,” he said.
For many individuals, cannabis is the primary drug of abuse. Regular heavy cannabis use is associated with a substantial risk of a cannabis dependence syndrome and, when this is combined with other substance abuse and internalizing disorders, the result is often psychosocial, cognitive, and mental health problems.
“Cannabis use is regularly associated with a wide range of psychological symptoms, and the largest group has anxiety and depression. Patients with primary CUD [cannabis use disorder] have become the largest group in substance-abuse centers in many European countries. These individuals have different profiles and treatment needs that are not being met in the current health care system. No clear interventional strategies have been developed,” he said. “The patients tell us they do not feel well placed, sitting next to heroin users. In fact, that’s how impressionable young people learn how to use other drugs.”
CBT as the Foundation
Dr. Wittchen and his colleagues designed a treatment program (10 individual sessions of 90 minutes each) specifically related to CUD. Based on evidence that types of cognitive-behavioral therapy (CBT) can be effective (via motivational enhancement, cognitive restructuring, psychosocial problem solving), they used CBT as a foundation. Modular components include CBT, motivational enhancement, and psychosocial problem solving. Patients develop an individual change concept and set goals. There is “quit day” preparation and training in relapse prevention, cannabis refusal skills, and so forth.
A randomized, controlled trial was designed to assess the effect of the program, compared with a delayed-treatment group, which included individuals seeking help but who were asked to wait until there was availability within the program. Two approaches were evaluated: a standardized approach and a variant tailored to the individual’s specific needs that minimized components deemed unnecessary (such as less motivational work in patients who express high motivation at baseline).
Participants were aged 16-45 years old with substantial current cannabis use and meeting criteria for DSM-IV CUD. They also had significant CUD-associated psychosocial problems and could have comorbid mental disorders (though no history of psychotic disorder, suicidal ideation, or phobias) as well as concomitant other drug use (though no other dependencies).
“Our entry criteria was meant to correspond to the most frequent and typical characteristics of this population,” he said. “And our general campaign message was for ‘everyone who wants to stop, reduce, or think about his or her cannabis use.’?”
The typical patient was a male who used cannabis more than 20 times per week. Seventy percent met criteria for cannabis dependence, 78% reported life-time use of other illicit drugs, and 38% had signs of dependency for those. Anxiety disorders were diagnosed in 40% and mood disorders in 38%. “We concluded that a severe chronic CUD sample of patients was included in the study,” he said.
There were 51 subjects in the standardized treatment group, 39 in the targeted standardized treatment group and 32 in the delayed treatment group, which served as controls. Assessments were made after 3 and 6 months to test the stability of the effects. The primary outcome measure was abstinence as measured by self-report and negative urine screen, cannabis use, addiction severity total score and domains, and severity of psychopathological symptoms. The tailored treatment was found not to be superior to the standardized treatment; therefore, these two groups were combined for the analysis.
Randomized Trial Showed Robust Effect
At the end of treatment, approximately 50% of participants reported complete abstinence for at least 7 days and this remained stable at 3 months, dropping to approximately 40% at 6 months. At all time points, urine screens were negative for approximately 40% of persons. In contrast, abstinence was reported by approximately 10% of the control group at the end of treatment.
Similarly, mean number of cannabis-use episodes per week was substantially decreased, according to the last-observation-carried-forward analysis. Mean use (past 7 days) at baseline was 27 for the active treatment group and 21 for the delayed treatment group. After the intervention, this dropped to 7.4/week with treatment but rose to 25/week for the control group. At 6 months’ follow-up, mean weekly use was 12 in the treatment group and 20 in the control group.
Scores on the Addiction Severity Index were significantly improved in all domains except for “satisfaction,” which Dr. Wittchen attributed to the requirement that participants alter their social network, which in turn, affected their quality of life. Psychopathological symptoms also were significantly improved, but a reduction in alcohol use was not found.
Altogether, at 6 months, vs. baseline, stable continued abstinence was observed in 49%, and marked reduction or temporal abstinence was observed in 38%, while 11% had no change and 3% progressed to heavier use of cannabis.
More than 80% of participants reported that the therapy as “very helpful,” he added. “They particularly liked the character of the program,” for example, it was not a typical substance abuse setting. In addition, they appreciated the limited number of “dense” sessions and the short-term duration of treatment.
The investigators have prepared a manual describing the program, which has procedural specifications of all elements, including diagnostic assessments. It is modular (to identify the core active components of the therapy) and highly structured (with scripts and verbatim descriptions of critical procedures). Specification and standardization are meant to enhance the ease of training, transfer, consistency of use, and reproducibility. The program also has just been evaluated in a 15-site translational study involving 450 persons, “with similarly impressive findings,” Dr. Wittchen added.
Dr. Wittchen reported no conflicts relevant to the study. It was funded by the German Federal Ministry of Education and Research.
AMSTERDAM – A targeted cognitive-behavioral treatment program designed by German addiction specialists for cannabis use disorder promoted abstinence in 50% of subjects and significantly reduced global addiction severity and psychopathological symptoms.
The approach was described by Hans-Ulrich Wittchen, Ph.D., director of the Institute of Clinical Psychology and Psychotherapy at Technische Universit?t Dresden at the annual congress of the European College of Neuropsychopharmacology.
“The majority [of participants] are abstinent 6 months after treatment,” even when urine tests are done. “This is a remarkable finding that we did not expect at the beginning,” he said.
For many individuals, cannabis is the primary drug of abuse. Regular heavy cannabis use is associated with a substantial risk of a cannabis dependence syndrome and, when this is combined with other substance abuse and internalizing disorders, the result is often psychosocial, cognitive, and mental health problems.
“Cannabis use is regularly associated with a wide range of psychological symptoms, and the largest group has anxiety and depression. Patients with primary CUD [cannabis use disorder] have become the largest group in substance-abuse centers in many European countries. These individuals have different profiles and treatment needs that are not being met in the current health care system. No clear interventional strategies have been developed,” he said. “The patients tell us they do not feel well placed, sitting next to heroin users. In fact, that’s how impressionable young people learn how to use other drugs.”
CBT as the Foundation
Dr. Wittchen and his colleagues designed a treatment program (10 individual sessions of 90 minutes each) specifically related to CUD. Based on evidence that types of cognitive-behavioral therapy (CBT) can be effective (via motivational enhancement, cognitive restructuring, psychosocial problem solving), they used CBT as a foundation. Modular components include CBT, motivational enhancement, and psychosocial problem solving. Patients develop an individual change concept and set goals. There is “quit day” preparation and training in relapse prevention, cannabis refusal skills, and so forth.
A randomized, controlled trial was designed to assess the effect of the program, compared with a delayed-treatment group, which included individuals seeking help but who were asked to wait until there was availability within the program. Two approaches were evaluated: a standardized approach and a variant tailored to the individual’s specific needs that minimized components deemed unnecessary (such as less motivational work in patients who express high motivation at baseline).
Participants were aged 16-45 years old with substantial current cannabis use and meeting criteria for DSM-IV CUD. They also had significant CUD-associated psychosocial problems and could have comorbid mental disorders (though no history of psychotic disorder, suicidal ideation, or phobias) as well as concomitant other drug use (though no other dependencies).
“Our entry criteria was meant to correspond to the most frequent and typical characteristics of this population,” he said. “And our general campaign message was for ‘everyone who wants to stop, reduce, or think about his or her cannabis use.’?”
The typical patient was a male who used cannabis more than 20 times per week. Seventy percent met criteria for cannabis dependence, 78% reported life-time use of other illicit drugs, and 38% had signs of dependency for those. Anxiety disorders were diagnosed in 40% and mood disorders in 38%. “We concluded that a severe chronic CUD sample of patients was included in the study,” he said.
There were 51 subjects in the standardized treatment group, 39 in the targeted standardized treatment group and 32 in the delayed treatment group, which served as controls. Assessments were made after 3 and 6 months to test the stability of the effects. The primary outcome measure was abstinence as measured by self-report and negative urine screen, cannabis use, addiction severity total score and domains, and severity of psychopathological symptoms. The tailored treatment was found not to be superior to the standardized treatment; therefore, these two groups were combined for the analysis.
Randomized Trial Showed Robust Effect
At the end of treatment, approximately 50% of participants reported complete abstinence for at least 7 days and this remained stable at 3 months, dropping to approximately 40% at 6 months. At all time points, urine screens were negative for approximately 40% of persons. In contrast, abstinence was reported by approximately 10% of the control group at the end of treatment.
Similarly, mean number of cannabis-use episodes per week was substantially decreased, according to the last-observation-carried-forward analysis. Mean use (past 7 days) at baseline was 27 for the active treatment group and 21 for the delayed treatment group. After the intervention, this dropped to 7.4/week with treatment but rose to 25/week for the control group. At 6 months’ follow-up, mean weekly use was 12 in the treatment group and 20 in the control group.
Scores on the Addiction Severity Index were significantly improved in all domains except for “satisfaction,” which Dr. Wittchen attributed to the requirement that participants alter their social network, which in turn, affected their quality of life. Psychopathological symptoms also were significantly improved, but a reduction in alcohol use was not found.
Altogether, at 6 months, vs. baseline, stable continued abstinence was observed in 49%, and marked reduction or temporal abstinence was observed in 38%, while 11% had no change and 3% progressed to heavier use of cannabis.
More than 80% of participants reported that the therapy as “very helpful,” he added. “They particularly liked the character of the program,” for example, it was not a typical substance abuse setting. In addition, they appreciated the limited number of “dense” sessions and the short-term duration of treatment.
The investigators have prepared a manual describing the program, which has procedural specifications of all elements, including diagnostic assessments. It is modular (to identify the core active components of the therapy) and highly structured (with scripts and verbatim descriptions of critical procedures). Specification and standardization are meant to enhance the ease of training, transfer, consistency of use, and reproducibility. The program also has just been evaluated in a 15-site translational study involving 450 persons, “with similarly impressive findings,” Dr. Wittchen added.
Dr. Wittchen reported no conflicts relevant to the study. It was funded by the German Federal Ministry of Education and Research.
AMSTERDAM – A targeted cognitive-behavioral treatment program designed by German addiction specialists for cannabis use disorder promoted abstinence in 50% of subjects and significantly reduced global addiction severity and psychopathological symptoms.
The approach was described by Hans-Ulrich Wittchen, Ph.D., director of the Institute of Clinical Psychology and Psychotherapy at Technische Universit?t Dresden at the annual congress of the European College of Neuropsychopharmacology.
“The majority [of participants] are abstinent 6 months after treatment,” even when urine tests are done. “This is a remarkable finding that we did not expect at the beginning,” he said.
For many individuals, cannabis is the primary drug of abuse. Regular heavy cannabis use is associated with a substantial risk of a cannabis dependence syndrome and, when this is combined with other substance abuse and internalizing disorders, the result is often psychosocial, cognitive, and mental health problems.
“Cannabis use is regularly associated with a wide range of psychological symptoms, and the largest group has anxiety and depression. Patients with primary CUD [cannabis use disorder] have become the largest group in substance-abuse centers in many European countries. These individuals have different profiles and treatment needs that are not being met in the current health care system. No clear interventional strategies have been developed,” he said. “The patients tell us they do not feel well placed, sitting next to heroin users. In fact, that’s how impressionable young people learn how to use other drugs.”
CBT as the Foundation
Dr. Wittchen and his colleagues designed a treatment program (10 individual sessions of 90 minutes each) specifically related to CUD. Based on evidence that types of cognitive-behavioral therapy (CBT) can be effective (via motivational enhancement, cognitive restructuring, psychosocial problem solving), they used CBT as a foundation. Modular components include CBT, motivational enhancement, and psychosocial problem solving. Patients develop an individual change concept and set goals. There is “quit day” preparation and training in relapse prevention, cannabis refusal skills, and so forth.
A randomized, controlled trial was designed to assess the effect of the program, compared with a delayed-treatment group, which included individuals seeking help but who were asked to wait until there was availability within the program. Two approaches were evaluated: a standardized approach and a variant tailored to the individual’s specific needs that minimized components deemed unnecessary (such as less motivational work in patients who express high motivation at baseline).
Participants were aged 16-45 years old with substantial current cannabis use and meeting criteria for DSM-IV CUD. They also had significant CUD-associated psychosocial problems and could have comorbid mental disorders (though no history of psychotic disorder, suicidal ideation, or phobias) as well as concomitant other drug use (though no other dependencies).
“Our entry criteria was meant to correspond to the most frequent and typical characteristics of this population,” he said. “And our general campaign message was for ‘everyone who wants to stop, reduce, or think about his or her cannabis use.’?”
The typical patient was a male who used cannabis more than 20 times per week. Seventy percent met criteria for cannabis dependence, 78% reported life-time use of other illicit drugs, and 38% had signs of dependency for those. Anxiety disorders were diagnosed in 40% and mood disorders in 38%. “We concluded that a severe chronic CUD sample of patients was included in the study,” he said.
There were 51 subjects in the standardized treatment group, 39 in the targeted standardized treatment group and 32 in the delayed treatment group, which served as controls. Assessments were made after 3 and 6 months to test the stability of the effects. The primary outcome measure was abstinence as measured by self-report and negative urine screen, cannabis use, addiction severity total score and domains, and severity of psychopathological symptoms. The tailored treatment was found not to be superior to the standardized treatment; therefore, these two groups were combined for the analysis.
Randomized Trial Showed Robust Effect
At the end of treatment, approximately 50% of participants reported complete abstinence for at least 7 days and this remained stable at 3 months, dropping to approximately 40% at 6 months. At all time points, urine screens were negative for approximately 40% of persons. In contrast, abstinence was reported by approximately 10% of the control group at the end of treatment.
Similarly, mean number of cannabis-use episodes per week was substantially decreased, according to the last-observation-carried-forward analysis. Mean use (past 7 days) at baseline was 27 for the active treatment group and 21 for the delayed treatment group. After the intervention, this dropped to 7.4/week with treatment but rose to 25/week for the control group. At 6 months’ follow-up, mean weekly use was 12 in the treatment group and 20 in the control group.
Scores on the Addiction Severity Index were significantly improved in all domains except for “satisfaction,” which Dr. Wittchen attributed to the requirement that participants alter their social network, which in turn, affected their quality of life. Psychopathological symptoms also were significantly improved, but a reduction in alcohol use was not found.
Altogether, at 6 months, vs. baseline, stable continued abstinence was observed in 49%, and marked reduction or temporal abstinence was observed in 38%, while 11% had no change and 3% progressed to heavier use of cannabis.
More than 80% of participants reported that the therapy as “very helpful,” he added. “They particularly liked the character of the program,” for example, it was not a typical substance abuse setting. In addition, they appreciated the limited number of “dense” sessions and the short-term duration of treatment.
The investigators have prepared a manual describing the program, which has procedural specifications of all elements, including diagnostic assessments. It is modular (to identify the core active components of the therapy) and highly structured (with scripts and verbatim descriptions of critical procedures). Specification and standardization are meant to enhance the ease of training, transfer, consistency of use, and reproducibility. The program also has just been evaluated in a 15-site translational study involving 450 persons, “with similarly impressive findings,” Dr. Wittchen added.
Dr. Wittchen reported no conflicts relevant to the study. It was funded by the German Federal Ministry of Education and Research.
Major Finding: An intervention for cannabis dependency was highly effective, producing complete abstinence rates of 50% that lasted at least 6 months.
Data Source: Randomized trial of 51 subjects in the standardized treatment group, 39 in the targeted standardized treatment group, and 32 in the delayed treatment group, which served as controls.
Disclosures: Dr. Wittchen reported no conflicts relevant to this study. It was funded by the German Federal Ministry of Education and Research.
Flexible Approach Advised for Constipation-Predominant IBS
NEW ORLEANS — When patients with constipation-predominant irritable bowel syndrome do not respond to standard treatments, good communication is essential for defining the multiple factors likely to be causing symptoms, Dr. Lin Chang said.
“Use 'brain' and 'gut' signs to help guide centrally versus peripherally acting therapy,” advised Dr. Chang, of the Center for Neurobiology of Stress at the University of California, Los Angeles.
The standard treatment, fiber, may not be sufficient for C-IBS because the dose may be insufficient, the side effects intolerable, or the patient's symptoms too severe or not responsive to fiber. Some patients may have dyssynergic defecation, which will not be helped with fiber.
Dr. Chang defined key areas in managing C-IBS:
▸ Establish a good provider/patient relationship.
First, determine the reason for the current visit. For example, is it worsening pain, lack of treatment response, or concern about cancer? Next, assess the severity of gastrointestinal and non-GI symptoms and any stress-related or comorbid psychological symptoms. Finally, conduct a patient-centered interview to determine whether the patient understands the illness. This is an opportunity for patient education and involvement of the patient in treatment decisions.
Dr. Chang said she incorporates her own form of counseling in sessions with severe symptoms, especially when there is a strong emotional component, but she does not hesitate to refer patients for psychological treatment. Frequent follow-up is important for moderately and severely affected patients.
▸ Rely on evidence-based pharmacotherapy.
The use of fiber and polyethylene glycol laxatives have only grade 2C recommendations in specialty guidelines since they improve constipation but have little to no effect on pain, which is key in IBS.
Lubiprostone and antidepressants, on the other hand, improve global symptoms and pain. Lubiprostone activates chloride channel-2, increases liquidity in the intestinal lumen, and improves stool consistency. These two approaches carry a grade 1B recommendation. While tegaserod improves global symptoms, bloating, stool frequency, stool consistency, and pain in some patients, the risk/benefit ratio is not favorable and therefore it has a grade 2A recommendation.
Probiotics can also help, as there is a physiological basis for their benefit. At least for Bifidobacterium infantis, clinical trials have shown positive results.
▸ Consider psychological treatment.
GI distress is multifactorial. It affects, and is affected by, emotions such as visceral and general anxiety, depression, devitalization, and somatization, and by cognitive factors, including locus of control, catastrophizing, anticipatory concerns, embarrassment, and stigma.
Tricyclic antidepressants are effective in some patients, especially patients with enhanced sensory perception, according to nine randomized controlled trials. Dr. Chang said she favors desipramine, since it has fewer anticholinergic effects, and starts with a low dose and titrates slowly. Selective serotonin receptor inhibitors (SSRIs) have also shown efficacy in at least five trials, though the study populations were smaller. She considers them when psychological symptoms seem to be driving the IBS symptoms or there is a coexistent somatic pain syndrome. SSRIs may be better for somatic than for visceral pain, and their effects can be additive with tricyclics.
▸ Anticipate new treatments.
Emerging therapies include linaclotide, a chloride channel activator that boosts intestinal fluid secretion, and prucalopride, a 5-HT4 agonist.
At DDW, investigators presented the phase III results for linaclotide. In two nearly identical 12-week trials involving 1,272 patients, linaclotide significantly increased the percentage of patients having at least three complete spontaneous bowel movements (CSBMs) per week, and increased the weekly CSBM count by at least one from baseline. Response rates were 21.3% and 19.4% for high-dose linaclotide in the two studies, compared with 6.0% and 3.3% for placebo, reported Dr. Anthony Lembo of Beth Israel Deaconess Medical Center, Boston.
In patients with chronic constipation, prucalopride has also been shown to significantly increase CSBMs, versus placebo (N. Engl. J. Med. 2008;358:2344-54).
Finally, Dr. Chang reminded clinicians that patients who are refractory to all treatments may have dyssynergic defecation. Biofeedback has been shown to significantly improve constipation in these patients, according to a study in which 80% responded to biofeedback versus 20% to laxatives (Gastroenterology 2006;130:657-64).
Disclosures: Dr. Chang has received consulting fees from Albireo, GlaxoSmithKline, McNeil Pharmaceuticals, Ocera Therapeutics, Prometheus Laboratories, Rose Pharmaceuticals, Salix Pharmaceuticals, and Takeda Pharmaceutical Co., as well as salary and grant/research support from Prometheus, Rose, and Takeda.
{kind=link}
'Use “brain” and “gut” signs to help guide centrally versus peripherally acting therapy.'
Source DR. CHANG
NEW ORLEANS — When patients with constipation-predominant irritable bowel syndrome do not respond to standard treatments, good communication is essential for defining the multiple factors likely to be causing symptoms, Dr. Lin Chang said.
“Use 'brain' and 'gut' signs to help guide centrally versus peripherally acting therapy,” advised Dr. Chang, of the Center for Neurobiology of Stress at the University of California, Los Angeles.
The standard treatment, fiber, may not be sufficient for C-IBS because the dose may be insufficient, the side effects intolerable, or the patient's symptoms too severe or not responsive to fiber. Some patients may have dyssynergic defecation, which will not be helped with fiber.
Dr. Chang defined key areas in managing C-IBS:
▸ Establish a good provider/patient relationship.
First, determine the reason for the current visit. For example, is it worsening pain, lack of treatment response, or concern about cancer? Next, assess the severity of gastrointestinal and non-GI symptoms and any stress-related or comorbid psychological symptoms. Finally, conduct a patient-centered interview to determine whether the patient understands the illness. This is an opportunity for patient education and involvement of the patient in treatment decisions.
Dr. Chang said she incorporates her own form of counseling in sessions with severe symptoms, especially when there is a strong emotional component, but she does not hesitate to refer patients for psychological treatment. Frequent follow-up is important for moderately and severely affected patients.
▸ Rely on evidence-based pharmacotherapy.
The use of fiber and polyethylene glycol laxatives have only grade 2C recommendations in specialty guidelines since they improve constipation but have little to no effect on pain, which is key in IBS.
Lubiprostone and antidepressants, on the other hand, improve global symptoms and pain. Lubiprostone activates chloride channel-2, increases liquidity in the intestinal lumen, and improves stool consistency. These two approaches carry a grade 1B recommendation. While tegaserod improves global symptoms, bloating, stool frequency, stool consistency, and pain in some patients, the risk/benefit ratio is not favorable and therefore it has a grade 2A recommendation.
Probiotics can also help, as there is a physiological basis for their benefit. At least for Bifidobacterium infantis, clinical trials have shown positive results.
▸ Consider psychological treatment.
GI distress is multifactorial. It affects, and is affected by, emotions such as visceral and general anxiety, depression, devitalization, and somatization, and by cognitive factors, including locus of control, catastrophizing, anticipatory concerns, embarrassment, and stigma.
Tricyclic antidepressants are effective in some patients, especially patients with enhanced sensory perception, according to nine randomized controlled trials. Dr. Chang said she favors desipramine, since it has fewer anticholinergic effects, and starts with a low dose and titrates slowly. Selective serotonin receptor inhibitors (SSRIs) have also shown efficacy in at least five trials, though the study populations were smaller. She considers them when psychological symptoms seem to be driving the IBS symptoms or there is a coexistent somatic pain syndrome. SSRIs may be better for somatic than for visceral pain, and their effects can be additive with tricyclics.
▸ Anticipate new treatments.
Emerging therapies include linaclotide, a chloride channel activator that boosts intestinal fluid secretion, and prucalopride, a 5-HT4 agonist.
At DDW, investigators presented the phase III results for linaclotide. In two nearly identical 12-week trials involving 1,272 patients, linaclotide significantly increased the percentage of patients having at least three complete spontaneous bowel movements (CSBMs) per week, and increased the weekly CSBM count by at least one from baseline. Response rates were 21.3% and 19.4% for high-dose linaclotide in the two studies, compared with 6.0% and 3.3% for placebo, reported Dr. Anthony Lembo of Beth Israel Deaconess Medical Center, Boston.
In patients with chronic constipation, prucalopride has also been shown to significantly increase CSBMs, versus placebo (N. Engl. J. Med. 2008;358:2344-54).
Finally, Dr. Chang reminded clinicians that patients who are refractory to all treatments may have dyssynergic defecation. Biofeedback has been shown to significantly improve constipation in these patients, according to a study in which 80% responded to biofeedback versus 20% to laxatives (Gastroenterology 2006;130:657-64).
Disclosures: Dr. Chang has received consulting fees from Albireo, GlaxoSmithKline, McNeil Pharmaceuticals, Ocera Therapeutics, Prometheus Laboratories, Rose Pharmaceuticals, Salix Pharmaceuticals, and Takeda Pharmaceutical Co., as well as salary and grant/research support from Prometheus, Rose, and Takeda.
'Use “brain” and “gut” signs to help guide centrally versus peripherally acting therapy.'
Source DR. CHANG
NEW ORLEANS — When patients with constipation-predominant irritable bowel syndrome do not respond to standard treatments, good communication is essential for defining the multiple factors likely to be causing symptoms, Dr. Lin Chang said.
“Use 'brain' and 'gut' signs to help guide centrally versus peripherally acting therapy,” advised Dr. Chang, of the Center for Neurobiology of Stress at the University of California, Los Angeles.
The standard treatment, fiber, may not be sufficient for C-IBS because the dose may be insufficient, the side effects intolerable, or the patient's symptoms too severe or not responsive to fiber. Some patients may have dyssynergic defecation, which will not be helped with fiber.
Dr. Chang defined key areas in managing C-IBS:
▸ Establish a good provider/patient relationship.
First, determine the reason for the current visit. For example, is it worsening pain, lack of treatment response, or concern about cancer? Next, assess the severity of gastrointestinal and non-GI symptoms and any stress-related or comorbid psychological symptoms. Finally, conduct a patient-centered interview to determine whether the patient understands the illness. This is an opportunity for patient education and involvement of the patient in treatment decisions.
Dr. Chang said she incorporates her own form of counseling in sessions with severe symptoms, especially when there is a strong emotional component, but she does not hesitate to refer patients for psychological treatment. Frequent follow-up is important for moderately and severely affected patients.
▸ Rely on evidence-based pharmacotherapy.
The use of fiber and polyethylene glycol laxatives have only grade 2C recommendations in specialty guidelines since they improve constipation but have little to no effect on pain, which is key in IBS.
Lubiprostone and antidepressants, on the other hand, improve global symptoms and pain. Lubiprostone activates chloride channel-2, increases liquidity in the intestinal lumen, and improves stool consistency. These two approaches carry a grade 1B recommendation. While tegaserod improves global symptoms, bloating, stool frequency, stool consistency, and pain in some patients, the risk/benefit ratio is not favorable and therefore it has a grade 2A recommendation.
Probiotics can also help, as there is a physiological basis for their benefit. At least for Bifidobacterium infantis, clinical trials have shown positive results.
▸ Consider psychological treatment.
GI distress is multifactorial. It affects, and is affected by, emotions such as visceral and general anxiety, depression, devitalization, and somatization, and by cognitive factors, including locus of control, catastrophizing, anticipatory concerns, embarrassment, and stigma.
Tricyclic antidepressants are effective in some patients, especially patients with enhanced sensory perception, according to nine randomized controlled trials. Dr. Chang said she favors desipramine, since it has fewer anticholinergic effects, and starts with a low dose and titrates slowly. Selective serotonin receptor inhibitors (SSRIs) have also shown efficacy in at least five trials, though the study populations were smaller. She considers them when psychological symptoms seem to be driving the IBS symptoms or there is a coexistent somatic pain syndrome. SSRIs may be better for somatic than for visceral pain, and their effects can be additive with tricyclics.
▸ Anticipate new treatments.
Emerging therapies include linaclotide, a chloride channel activator that boosts intestinal fluid secretion, and prucalopride, a 5-HT4 agonist.
At DDW, investigators presented the phase III results for linaclotide. In two nearly identical 12-week trials involving 1,272 patients, linaclotide significantly increased the percentage of patients having at least three complete spontaneous bowel movements (CSBMs) per week, and increased the weekly CSBM count by at least one from baseline. Response rates were 21.3% and 19.4% for high-dose linaclotide in the two studies, compared with 6.0% and 3.3% for placebo, reported Dr. Anthony Lembo of Beth Israel Deaconess Medical Center, Boston.
In patients with chronic constipation, prucalopride has also been shown to significantly increase CSBMs, versus placebo (N. Engl. J. Med. 2008;358:2344-54).
Finally, Dr. Chang reminded clinicians that patients who are refractory to all treatments may have dyssynergic defecation. Biofeedback has been shown to significantly improve constipation in these patients, according to a study in which 80% responded to biofeedback versus 20% to laxatives (Gastroenterology 2006;130:657-64).
Disclosures: Dr. Chang has received consulting fees from Albireo, GlaxoSmithKline, McNeil Pharmaceuticals, Ocera Therapeutics, Prometheus Laboratories, Rose Pharmaceuticals, Salix Pharmaceuticals, and Takeda Pharmaceutical Co., as well as salary and grant/research support from Prometheus, Rose, and Takeda.
'Use “brain” and “gut” signs to help guide centrally versus peripherally acting therapy.'
Source DR. CHANG