User login
How to help nicotine-dependent adolescents quit smoking
Many adolescent psychiatric patients who smoke are not getting the help they need to quit. When we asked 120 teen inpatients if they smoked and then checked their charts, we found only 6 of 47 smokers had been diagnosed as nicotine-dependent.1
Adolescents who cannot quit on their own may benefit from smoking cessation therapies. Based on evidence and our experience, we offer a practical approach to treating nicotine dependence in adolescents, using drug and behavioral therapies.
PSYCHIATRIC COMORBIDITY
Psychiatric comorbidity is highly associated with cigarette smoking in adults and adolescents. In the United States:
- 44% of cigarettes smoked are sold to someone with a mental illness.2
- Persons with mental illness are 2.7 times more likely to smoke than are those without mental illness.2
- Most smokers start before age 18,3 and starting before age 13 is linked to psychopathology in later adolescence.4
Table
Smoking likelihood by age and comorbidity among adolescent psychiatric inpatients
| Significant variable | Logistic regression odds ratio | 95% confidence interval | Significance (P value) |
|---|---|---|---|
| Age | 1.30 | 1.03, 1.64 | 0.03 |
| Depressive disorders | 4.02 | 1.267, 12.734 | 0.018 |
| Conduct disorder | 12.96 | 1.678, 100.07 | 0.014 |
| Cannabis use disorder | 24.60 | 3.7, 163.42 | 0.0009 |
| Source: Data from 120 patients admitted to an inpatient child and adolescent psychiatry program. | |||
| Adapted with permission from reference 1. | |||
Disruptive behavior disorders in adolescent smokers include oppositional defiant disorder, conduct disorder, and attention-deficit/hyperactivity disorder (ADHD). Among psychiatric disorders, conduct disorder has the strongest association with smoking in adolescents.1 ADHD is associated with smoking and perhaps with increased difficulty in quitting.5,6
Mood disorders. Major depressive disorders have a strong, consistent, bidirectional association with smoking in the young. Depression may lead to smoking, and smoking to depression.7
Substance use disorders. Alcohol use disorders are strongly associated with smoking among adolescents, and the association is both bidirectional and dosedependent.8 Cannabis use disorder is also associated with cigarette smoking among adolescents (Table).9
Anxiety disorders. Evidence is emerging that anxiety disorders—especially social phobia—may be linked to smoking among adolescents.10
Nicotine withdrawal symptoms—irritability, anxiety, decreased concentration, increased appetite, craving for cigarettes—can mimic those of other psychiatric disorders. Adolescent smokers admitted to locked psychiatric units may experience withdrawal symptoms that require nicotine replacement treatment (Box).
Effect on quit rates. Psychiatric comorbidity may reduce quit rates during smoking cessation treatment.6 When smokers are trying to quit, watch for remission, worsening, or emergence of psychiatric conditions.
ASSESSING ADOLESCENT SMOKING
Adolescents with psychiatric diagnoses can be assessed for nicotine dependence—and vice versa—although accurately gauging their smoking habits is more difficult than in adults. For example:
- Rating scales for nicotine dependence severity—such as the modified Fagerstrom Tolerance Questionnaire11—lack standard cutoff scores for adolescents.
- Unlike adults, many adolescents cannot reliably report use in “packs per day” because the number of cigarettes they smoke varies widely from day to day.
Biological markers commonly used to assess smoking in adults include expired-air carbon monoxide (CO), cotinine (nicotine metabolite), and thiocynate levels. Preliminary evidence indicates that cotinine may be a more sensitive and specific biological marker for smoking among adolescents than CO levels.12 Thiocynate has not been evaluated as a marker for smoking in adolescents.
CO levels typically reflect smoking in the previous few hours, whereas the half-life of cotinine is longer (1 day or more). Also, factors such as environmental pollution or marijuana use can inflate CO levels. Thus, cotinine levels have greater accuracy and specificity, reflecting only the amount of nicotine consumed.
Unfortunately, most laboratories do not measure cotinine levels, and the expired-air CO test (CO Breathalyzer) is relatively expensive for most clinicians. Commercially available single-use cotinine test kits are modestly priced and provide semi-quantitative (a range instead of an exact number) urine cotinine levels. These tests, however, might not be covered by third-party insurers.
Until cotinine testing becomes widely available, we recommend a combination of self-report and expired-air CO level to monitor abstinence.
Self-report monitoring. Most clinicians rely on self-report rate of smoking among adolescents, as no screening assessment has been validated in this age group. As initial prompts, we recommend asking all adolescents if they smoke cigarettes, if they smoke regularly, and if they smoke daily.
We recommend using the “time line follow-back” method13 to monitor the self-reported smoking rate. Begin by providing the patient with a 30-day calendar, starting backwards from the day of assessment. Cite anchor points, such as special holidays and school or family events, to help the patient recall his or her cigarette use. Then have the patient fill in the number of cigarettes smoked each day for 30 days.
This assessment method appears more reliable than asking an adolescent “how many cigarettes do you smoke per day?”. After the initial time line follow-back assessment, encourage adolescent smokers to keep a daily diary of how many cigarettes they smoke, and monitor the diary at each visit.
Beth, age 15, was admitted overnight to an inpatient psychiatric unit after running away from home and being taken into police custody. Her primary diagnosis was conduct disorder.
At morning rounds, the nurse reported that Beth was very irritable, had threatened the staff, and had been moved to seclusion. During routine examination, the psychiatrist discovered that Beth was a half-pack/day smoker and “really” wanted a cigarette. The psychiatrist told her hospital policy did not allow smoking, but she could try a transdermal nicotine patch (TNP) to help reduce her nicotine withdrawal symptoms. She agreed and received a 14 mg/d nicotine patch.
Beth’s irritability improved substantially with TNP, and she moved back to her regular room within 2 hours without incident.
We have found daily smoking to be a good indicator of nicotine dependence, and anyone who smokes daily would receive significant health benefits from quitting. Hence, any daily smoker who wants to quit, regardless of DSM-IV nicotine dependence status, is a candidate for treatment.
BEHAVIORAL THERAPY
Unlike adults, adolescents usually lack smoking-related medical consequences, such as heart or lung disease. Even so, most adolescent smokers report that they would like to quit but face barriers such as:
- having to inform parents they smoke
- not knowing how to get help for smoking cessation
- lack of transportation for treatment
- lack of third-party reimbursement for smoking cessation treatment.
To help adolescents, we recommend following the U.S. Public Health Service guideline for smoking cessation.14 At least provide and discuss smoking cessation brochures developed specifically for adolescents. For example, one Centers for Disease Control and Prevention brochure describes what symptoms to expect when quitting, how to cope with craving, and other topics (see Related resources).
To manage peer pressure, we counsel teens to let their friends know they are trying to quit so that friends do not smoke in front of them. If that does not work, we ask patients to avoid being around friends who smoke at least for the first 2 weeks and preferably 2 months.
Many states have free telephone quit lines that provide support and advice on how to stop smoking. Several Web sites also are available for smokers (including adolescents) wanting to quit (see Related resources).
PHARMACOLOGIC TREATMENT
For adults, first-line FDA-approved medications for smoking cessation include nicotine replacement therapies (NRT)in transdermal, gum, inhaler, and lozenge forms and sustained-release bupropion. Nortriptyline, doxapine, and clonidine have shown effectiveness for smoking cessation but are not FDA-approved for this indication.15 Selegiline and mecamylamine have shown initial efficacy and are being examined in larger clinical trials.
For adolescents, little is known about what medications might help them stop smoking. Nicotine replacement therapies and bupropion SR have been most explored in adolescent smokers. The effect of psychiatric comorbidity on the quit rate is not well-studied in adolescents.
The transdermal nicotine patch (TNP) has shown modest results in preliminary trials among adolescents. One study found 11% abstinence at 6 weeks,16 and another found a <5% quit rate.17 A third study reported an 18% abstinence rate with a combination of TNP and contingency management therapy.18 Discussion of contingency management and other behavioral therapies is beyond the scope of this article.
A recent study comparing TNP, nicotine gum, and placebo in adolescent smokers found the lowest drop-out rate and highest compliance among the TNP group. Three-month abstinence rates were 17.6% for TNP, 6.5% for nicotine gum, and 2.5% for placebo. The difference between the TNP and placebo groups’ abstinence rates was statistically significant.19
Bupropion SR. In an open-label pilot study, our group treated 16 adolescent smokers weighing >90 lbs with bupropion SR, 150 mg bid. Average age was 18, and two-thirds of patients had ADHD. The endpoint abstinence rate—as measured by self-report and CO levels—was 31%, which is similar to rates reported in adult smokers treated with this dosage of bupropion SR.20
The adolescents did not gain weight during the study, which may be important to this age group. Reported side effects were similar to those in adults, with one adolescent reporting an allergic reaction (urticaria). We are conducting a larger follow-up study using bupropion SR with and without behavioral therapy.
A PRACTICAL CLINICAL APPROACH
Smoking behavior. For treatment, we propose two categories of adolescent smokers: regular (daily) and nonregular (nondaily) (see Algorithm). We recognize that many nondaily smokers smoke frequently and may benefit from aggressive treatment. However, we propose this two-track approach as a starting point because of limited data and medication risks, such as possible seizures with bupropion SR. We suggest:
- using behavioral therapy and patient education as first-line treatment for nonregular adolescent smokers
- using medication and behavioral therapy as first-line treatment for regular smokers and medication as second-line treatment for nonregular smokers who do not respond to behavior therapy/patient education.
Algorithm Suggested smoking cessation approaches for adolescents
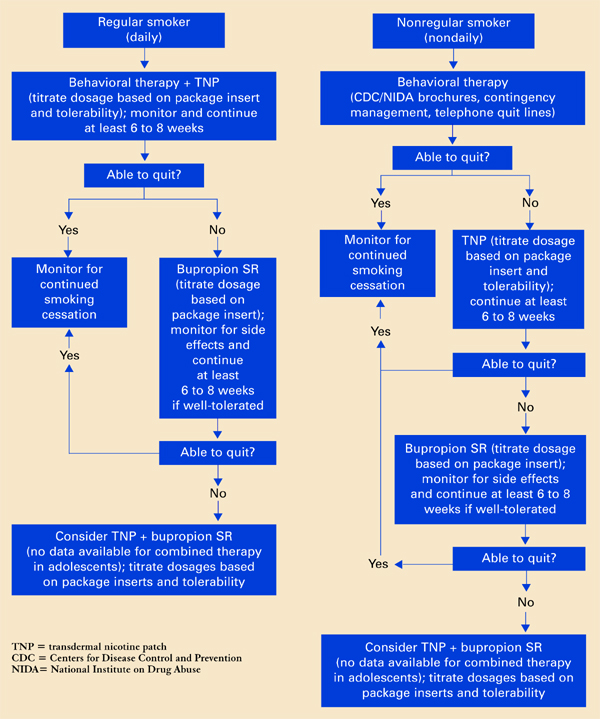
Offer a treatment for at least 6 to 8 weeks before considering a change in therapy. One definition of initial success is no tobacco use in a 7-day period by self-report and biological verification (such as CO levels).
Behavioral therapy is relatively low-risk and helps many adult smokers. Despite a lack of evidence, some sort of behavioral therapy in combination with pharmacologic therapy might also help adolescent smokers.
When adolescents get disheartened by a slip or relapse to smoking, be patient and encourage them to try again. Inform them that smokers often require multiple attempts before they can quit completely.
Medication. Based on the limited published evidence, we consider TNP and bupropion SR first-line medications for adolescent smokers who want to quit.
For adult smokers, clinicians often combine medication and NRT to increase success rates.15 No data suggest that combining TNP and bupropion SR may be more effective than monotherapy in adolescents, but the combination might help those who do not respond to either agent alone.
We recommend starting bupropion SR treatment at least 1 week before the patient’s quit date. Titrate the dosage based on the package insert and patient tolerance.
Start NRT according to package instructions, and titrate dosages based on response:
- increase if the patient reports substantial craving and withdrawal symptoms, such as irritability and anxiety.
- decrease in case of toxicity (such as nausea).
In our experience, adolescent smokers require slightly lower NRT dosages than adults, although this varies among individuals.
- Centers for Disease Control and Prevention. Tobacco Information and Prevention Source (TIPS). www.cdc.gov/tobacco/quit/iquit.htm
- National Institute of Drug Abuse. NIDA for Teens. The Science Behind Drug Abuse. http://teens.drugabuse.gov/index.asp
- Society for Research on Nicotine and Tobacco. www.srnt.org
Drug brand names
- Bupropion SR • Zyban
- Clonidine • Catapres
- Doxapine • Sinequan
- Mecamylamine • Inversine
- Nortriptyline • Pamelor
- Selegiline • Eldepryl
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Upadhyaya HP, Brady KT, Wharton M, Liao J. Psychiatric disorders and cigarette smoking among child and adolescent psychiatry inpatients. Am J Addict 2003;12:144-52.
2. Lasser K, Boyd JW, Woolhandler S, et al. Smoking and mental illness. A population-based prevalence study. JAMA 2000;284(20):2606-10.
3. Johnston LD, O’Malley PM, Bachman JG. Teen smoking continues to decline in 2003, but declines are slowing. Ann Arbor, MI: University of Michigan News and Information Services, Dec. 19, 2003. Available at: www.monitoringthefuture.org/press.html. Accessed 08/13/04.
4. Upadhyaya HP, Deas D, Brady KT, Kruesi M. Cigarette smoking and psychiatric comorbidity in children and adolescents. J Am Acad Child Adolesc Psychiatry 2002;41(11):1294-1305.
5. Molina BS, Pelham WE. Childhood predictors of adolescent substance use in a longitudinal study of children with ADHD. J Abnorm Psychol 2003;112(3):497-507.
6. Pomerleau OF, Downey KK, Stelson FW, Pomerleau CS. Cigarette smoking in adult patients diagnosed with attention-deficit/hyperactivity disorder. J Subst Abuse 1995;7:373-8.
7. Dierker LC, Avenevoli S, Merikangas KR, et al. Association between psychiatric disorders and the progression of tobacco use behaviors. J Am Acad Child Adolesc Psychiatry 2001;40(10):1159-67.
8. Zacny J. Behavioral aspects of alcohol-tobacco interactions. Recent Dev Alcohol 1990;8:205-19.
9. Rohde P, Lewinsohn P, Kahler C, et al. Natural course of alcohol use disorders from adolescence to young adulthood. J Am Acad Child Adolesc Psychiatry 2001;40(1):83-90.
10. Sonntag H, Wittchen HU, Hofler M, et al. Are social fears and DSM-IV social anxiety disorder associated with smoking and nicotine dependence in adolescents and young adults? Eur Psychiatry 2000;15:67-74.
11. Prokhorov AV, Pallonen UE, Fava JL, et al. Measuring nicotine dependence among high-risk adolescent smokers. Addict Behav 1996;21:117-27.
12. McDonald P, Colwell B, Backinger CL, et al. Better practices for youth tobacco cessation: evidence of review panel. Am J Health Behav 2003;27(suppl 2):S144-S158.
13. Sobell LC, Sobell MB, Leo GI, Cancilla A. Reliability of a timeline method: assessing normal drinkers’ reports of recent drinking and a comparative evaluation across several populations. Br J Addict 1988;83(4):393-402.
14. Fiore M, Bailey W, Cohen S. Treating tobacco use and dependence: Clinical practice guideline. Rockville, MD: US Public Health Service, 2000.
15. George TP, O’Malley SS. Current pharmacological treatments for nicotine dependence. Trends Pharmacol Sci 2004;25(1):42-8.
16. Hurt RD, Croghan GA, Beede SD, et al. Nicotine patch therapy in 101 adolescent smokers. Efficacy, withdrawal symptom relief, and carbon monoxide and plasma cotinine levels. Arch Pediatr Adolesc Med 2000;154:31-7.
17. Smith TA, House RF, Jr, Croghan IT, et al. Nicotine patch therapy in adolescent smokers. Pediatrics 1996;98:659-67.
18. Hanson K, Allen S, Jensen S, Hatsukami D. Treatment of adolescent smokers with the nicotine patch. Nicotine Tob Res 2003;5(4):515-26.
19. Moolchan ET. Efficacy of the nicotine patch and gum for the treatment of adolescent tobacco dependence. Scottsdale, AZ: Society for Research on Nicotine and Tobacco Research annual meeting, 2004.
20. Upadhyaya HP, Brady KT, Wang W. Bupropion SR in adolescents with comorbid ADHD and nicotine dependence: a pilot study. J Am Acad Child Adolesc Psychiatry 2004;43(2):199-205.
Many adolescent psychiatric patients who smoke are not getting the help they need to quit. When we asked 120 teen inpatients if they smoked and then checked their charts, we found only 6 of 47 smokers had been diagnosed as nicotine-dependent.1
Adolescents who cannot quit on their own may benefit from smoking cessation therapies. Based on evidence and our experience, we offer a practical approach to treating nicotine dependence in adolescents, using drug and behavioral therapies.
PSYCHIATRIC COMORBIDITY
Psychiatric comorbidity is highly associated with cigarette smoking in adults and adolescents. In the United States:
- 44% of cigarettes smoked are sold to someone with a mental illness.2
- Persons with mental illness are 2.7 times more likely to smoke than are those without mental illness.2
- Most smokers start before age 18,3 and starting before age 13 is linked to psychopathology in later adolescence.4
Table
Smoking likelihood by age and comorbidity among adolescent psychiatric inpatients
| Significant variable | Logistic regression odds ratio | 95% confidence interval | Significance (P value) |
|---|---|---|---|
| Age | 1.30 | 1.03, 1.64 | 0.03 |
| Depressive disorders | 4.02 | 1.267, 12.734 | 0.018 |
| Conduct disorder | 12.96 | 1.678, 100.07 | 0.014 |
| Cannabis use disorder | 24.60 | 3.7, 163.42 | 0.0009 |
| Source: Data from 120 patients admitted to an inpatient child and adolescent psychiatry program. | |||
| Adapted with permission from reference 1. | |||
Disruptive behavior disorders in adolescent smokers include oppositional defiant disorder, conduct disorder, and attention-deficit/hyperactivity disorder (ADHD). Among psychiatric disorders, conduct disorder has the strongest association with smoking in adolescents.1 ADHD is associated with smoking and perhaps with increased difficulty in quitting.5,6
Mood disorders. Major depressive disorders have a strong, consistent, bidirectional association with smoking in the young. Depression may lead to smoking, and smoking to depression.7
Substance use disorders. Alcohol use disorders are strongly associated with smoking among adolescents, and the association is both bidirectional and dosedependent.8 Cannabis use disorder is also associated with cigarette smoking among adolescents (Table).9
Anxiety disorders. Evidence is emerging that anxiety disorders—especially social phobia—may be linked to smoking among adolescents.10
Nicotine withdrawal symptoms—irritability, anxiety, decreased concentration, increased appetite, craving for cigarettes—can mimic those of other psychiatric disorders. Adolescent smokers admitted to locked psychiatric units may experience withdrawal symptoms that require nicotine replacement treatment (Box).
Effect on quit rates. Psychiatric comorbidity may reduce quit rates during smoking cessation treatment.6 When smokers are trying to quit, watch for remission, worsening, or emergence of psychiatric conditions.
ASSESSING ADOLESCENT SMOKING
Adolescents with psychiatric diagnoses can be assessed for nicotine dependence—and vice versa—although accurately gauging their smoking habits is more difficult than in adults. For example:
- Rating scales for nicotine dependence severity—such as the modified Fagerstrom Tolerance Questionnaire11—lack standard cutoff scores for adolescents.
- Unlike adults, many adolescents cannot reliably report use in “packs per day” because the number of cigarettes they smoke varies widely from day to day.
Biological markers commonly used to assess smoking in adults include expired-air carbon monoxide (CO), cotinine (nicotine metabolite), and thiocynate levels. Preliminary evidence indicates that cotinine may be a more sensitive and specific biological marker for smoking among adolescents than CO levels.12 Thiocynate has not been evaluated as a marker for smoking in adolescents.
CO levels typically reflect smoking in the previous few hours, whereas the half-life of cotinine is longer (1 day or more). Also, factors such as environmental pollution or marijuana use can inflate CO levels. Thus, cotinine levels have greater accuracy and specificity, reflecting only the amount of nicotine consumed.
Unfortunately, most laboratories do not measure cotinine levels, and the expired-air CO test (CO Breathalyzer) is relatively expensive for most clinicians. Commercially available single-use cotinine test kits are modestly priced and provide semi-quantitative (a range instead of an exact number) urine cotinine levels. These tests, however, might not be covered by third-party insurers.
Until cotinine testing becomes widely available, we recommend a combination of self-report and expired-air CO level to monitor abstinence.
Self-report monitoring. Most clinicians rely on self-report rate of smoking among adolescents, as no screening assessment has been validated in this age group. As initial prompts, we recommend asking all adolescents if they smoke cigarettes, if they smoke regularly, and if they smoke daily.
We recommend using the “time line follow-back” method13 to monitor the self-reported smoking rate. Begin by providing the patient with a 30-day calendar, starting backwards from the day of assessment. Cite anchor points, such as special holidays and school or family events, to help the patient recall his or her cigarette use. Then have the patient fill in the number of cigarettes smoked each day for 30 days.
This assessment method appears more reliable than asking an adolescent “how many cigarettes do you smoke per day?”. After the initial time line follow-back assessment, encourage adolescent smokers to keep a daily diary of how many cigarettes they smoke, and monitor the diary at each visit.
Beth, age 15, was admitted overnight to an inpatient psychiatric unit after running away from home and being taken into police custody. Her primary diagnosis was conduct disorder.
At morning rounds, the nurse reported that Beth was very irritable, had threatened the staff, and had been moved to seclusion. During routine examination, the psychiatrist discovered that Beth was a half-pack/day smoker and “really” wanted a cigarette. The psychiatrist told her hospital policy did not allow smoking, but she could try a transdermal nicotine patch (TNP) to help reduce her nicotine withdrawal symptoms. She agreed and received a 14 mg/d nicotine patch.
Beth’s irritability improved substantially with TNP, and she moved back to her regular room within 2 hours without incident.
We have found daily smoking to be a good indicator of nicotine dependence, and anyone who smokes daily would receive significant health benefits from quitting. Hence, any daily smoker who wants to quit, regardless of DSM-IV nicotine dependence status, is a candidate for treatment.
BEHAVIORAL THERAPY
Unlike adults, adolescents usually lack smoking-related medical consequences, such as heart or lung disease. Even so, most adolescent smokers report that they would like to quit but face barriers such as:
- having to inform parents they smoke
- not knowing how to get help for smoking cessation
- lack of transportation for treatment
- lack of third-party reimbursement for smoking cessation treatment.
To help adolescents, we recommend following the U.S. Public Health Service guideline for smoking cessation.14 At least provide and discuss smoking cessation brochures developed specifically for adolescents. For example, one Centers for Disease Control and Prevention brochure describes what symptoms to expect when quitting, how to cope with craving, and other topics (see Related resources).
To manage peer pressure, we counsel teens to let their friends know they are trying to quit so that friends do not smoke in front of them. If that does not work, we ask patients to avoid being around friends who smoke at least for the first 2 weeks and preferably 2 months.
Many states have free telephone quit lines that provide support and advice on how to stop smoking. Several Web sites also are available for smokers (including adolescents) wanting to quit (see Related resources).
PHARMACOLOGIC TREATMENT
For adults, first-line FDA-approved medications for smoking cessation include nicotine replacement therapies (NRT)in transdermal, gum, inhaler, and lozenge forms and sustained-release bupropion. Nortriptyline, doxapine, and clonidine have shown effectiveness for smoking cessation but are not FDA-approved for this indication.15 Selegiline and mecamylamine have shown initial efficacy and are being examined in larger clinical trials.
For adolescents, little is known about what medications might help them stop smoking. Nicotine replacement therapies and bupropion SR have been most explored in adolescent smokers. The effect of psychiatric comorbidity on the quit rate is not well-studied in adolescents.
The transdermal nicotine patch (TNP) has shown modest results in preliminary trials among adolescents. One study found 11% abstinence at 6 weeks,16 and another found a <5% quit rate.17 A third study reported an 18% abstinence rate with a combination of TNP and contingency management therapy.18 Discussion of contingency management and other behavioral therapies is beyond the scope of this article.
A recent study comparing TNP, nicotine gum, and placebo in adolescent smokers found the lowest drop-out rate and highest compliance among the TNP group. Three-month abstinence rates were 17.6% for TNP, 6.5% for nicotine gum, and 2.5% for placebo. The difference between the TNP and placebo groups’ abstinence rates was statistically significant.19
Bupropion SR. In an open-label pilot study, our group treated 16 adolescent smokers weighing >90 lbs with bupropion SR, 150 mg bid. Average age was 18, and two-thirds of patients had ADHD. The endpoint abstinence rate—as measured by self-report and CO levels—was 31%, which is similar to rates reported in adult smokers treated with this dosage of bupropion SR.20
The adolescents did not gain weight during the study, which may be important to this age group. Reported side effects were similar to those in adults, with one adolescent reporting an allergic reaction (urticaria). We are conducting a larger follow-up study using bupropion SR with and without behavioral therapy.
A PRACTICAL CLINICAL APPROACH
Smoking behavior. For treatment, we propose two categories of adolescent smokers: regular (daily) and nonregular (nondaily) (see Algorithm). We recognize that many nondaily smokers smoke frequently and may benefit from aggressive treatment. However, we propose this two-track approach as a starting point because of limited data and medication risks, such as possible seizures with bupropion SR. We suggest:
- using behavioral therapy and patient education as first-line treatment for nonregular adolescent smokers
- using medication and behavioral therapy as first-line treatment for regular smokers and medication as second-line treatment for nonregular smokers who do not respond to behavior therapy/patient education.
Algorithm Suggested smoking cessation approaches for adolescents
Offer a treatment for at least 6 to 8 weeks before considering a change in therapy. One definition of initial success is no tobacco use in a 7-day period by self-report and biological verification (such as CO levels).
Behavioral therapy is relatively low-risk and helps many adult smokers. Despite a lack of evidence, some sort of behavioral therapy in combination with pharmacologic therapy might also help adolescent smokers.
When adolescents get disheartened by a slip or relapse to smoking, be patient and encourage them to try again. Inform them that smokers often require multiple attempts before they can quit completely.
Medication. Based on the limited published evidence, we consider TNP and bupropion SR first-line medications for adolescent smokers who want to quit.
For adult smokers, clinicians often combine medication and NRT to increase success rates.15 No data suggest that combining TNP and bupropion SR may be more effective than monotherapy in adolescents, but the combination might help those who do not respond to either agent alone.
We recommend starting bupropion SR treatment at least 1 week before the patient’s quit date. Titrate the dosage based on the package insert and patient tolerance.
Start NRT according to package instructions, and titrate dosages based on response:
- increase if the patient reports substantial craving and withdrawal symptoms, such as irritability and anxiety.
- decrease in case of toxicity (such as nausea).
In our experience, adolescent smokers require slightly lower NRT dosages than adults, although this varies among individuals.
- Centers for Disease Control and Prevention. Tobacco Information and Prevention Source (TIPS). www.cdc.gov/tobacco/quit/iquit.htm
- National Institute of Drug Abuse. NIDA for Teens. The Science Behind Drug Abuse. http://teens.drugabuse.gov/index.asp
- Society for Research on Nicotine and Tobacco. www.srnt.org
Drug brand names
- Bupropion SR • Zyban
- Clonidine • Catapres
- Doxapine • Sinequan
- Mecamylamine • Inversine
- Nortriptyline • Pamelor
- Selegiline • Eldepryl
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Many adolescent psychiatric patients who smoke are not getting the help they need to quit. When we asked 120 teen inpatients if they smoked and then checked their charts, we found only 6 of 47 smokers had been diagnosed as nicotine-dependent.1
Adolescents who cannot quit on their own may benefit from smoking cessation therapies. Based on evidence and our experience, we offer a practical approach to treating nicotine dependence in adolescents, using drug and behavioral therapies.
PSYCHIATRIC COMORBIDITY
Psychiatric comorbidity is highly associated with cigarette smoking in adults and adolescents. In the United States:
- 44% of cigarettes smoked are sold to someone with a mental illness.2
- Persons with mental illness are 2.7 times more likely to smoke than are those without mental illness.2
- Most smokers start before age 18,3 and starting before age 13 is linked to psychopathology in later adolescence.4
Table
Smoking likelihood by age and comorbidity among adolescent psychiatric inpatients
| Significant variable | Logistic regression odds ratio | 95% confidence interval | Significance (P value) |
|---|---|---|---|
| Age | 1.30 | 1.03, 1.64 | 0.03 |
| Depressive disorders | 4.02 | 1.267, 12.734 | 0.018 |
| Conduct disorder | 12.96 | 1.678, 100.07 | 0.014 |
| Cannabis use disorder | 24.60 | 3.7, 163.42 | 0.0009 |
| Source: Data from 120 patients admitted to an inpatient child and adolescent psychiatry program. | |||
| Adapted with permission from reference 1. | |||
Disruptive behavior disorders in adolescent smokers include oppositional defiant disorder, conduct disorder, and attention-deficit/hyperactivity disorder (ADHD). Among psychiatric disorders, conduct disorder has the strongest association with smoking in adolescents.1 ADHD is associated with smoking and perhaps with increased difficulty in quitting.5,6
Mood disorders. Major depressive disorders have a strong, consistent, bidirectional association with smoking in the young. Depression may lead to smoking, and smoking to depression.7
Substance use disorders. Alcohol use disorders are strongly associated with smoking among adolescents, and the association is both bidirectional and dosedependent.8 Cannabis use disorder is also associated with cigarette smoking among adolescents (Table).9
Anxiety disorders. Evidence is emerging that anxiety disorders—especially social phobia—may be linked to smoking among adolescents.10
Nicotine withdrawal symptoms—irritability, anxiety, decreased concentration, increased appetite, craving for cigarettes—can mimic those of other psychiatric disorders. Adolescent smokers admitted to locked psychiatric units may experience withdrawal symptoms that require nicotine replacement treatment (Box).
Effect on quit rates. Psychiatric comorbidity may reduce quit rates during smoking cessation treatment.6 When smokers are trying to quit, watch for remission, worsening, or emergence of psychiatric conditions.
ASSESSING ADOLESCENT SMOKING
Adolescents with psychiatric diagnoses can be assessed for nicotine dependence—and vice versa—although accurately gauging their smoking habits is more difficult than in adults. For example:
- Rating scales for nicotine dependence severity—such as the modified Fagerstrom Tolerance Questionnaire11—lack standard cutoff scores for adolescents.
- Unlike adults, many adolescents cannot reliably report use in “packs per day” because the number of cigarettes they smoke varies widely from day to day.
Biological markers commonly used to assess smoking in adults include expired-air carbon monoxide (CO), cotinine (nicotine metabolite), and thiocynate levels. Preliminary evidence indicates that cotinine may be a more sensitive and specific biological marker for smoking among adolescents than CO levels.12 Thiocynate has not been evaluated as a marker for smoking in adolescents.
CO levels typically reflect smoking in the previous few hours, whereas the half-life of cotinine is longer (1 day or more). Also, factors such as environmental pollution or marijuana use can inflate CO levels. Thus, cotinine levels have greater accuracy and specificity, reflecting only the amount of nicotine consumed.
Unfortunately, most laboratories do not measure cotinine levels, and the expired-air CO test (CO Breathalyzer) is relatively expensive for most clinicians. Commercially available single-use cotinine test kits are modestly priced and provide semi-quantitative (a range instead of an exact number) urine cotinine levels. These tests, however, might not be covered by third-party insurers.
Until cotinine testing becomes widely available, we recommend a combination of self-report and expired-air CO level to monitor abstinence.
Self-report monitoring. Most clinicians rely on self-report rate of smoking among adolescents, as no screening assessment has been validated in this age group. As initial prompts, we recommend asking all adolescents if they smoke cigarettes, if they smoke regularly, and if they smoke daily.
We recommend using the “time line follow-back” method13 to monitor the self-reported smoking rate. Begin by providing the patient with a 30-day calendar, starting backwards from the day of assessment. Cite anchor points, such as special holidays and school or family events, to help the patient recall his or her cigarette use. Then have the patient fill in the number of cigarettes smoked each day for 30 days.
This assessment method appears more reliable than asking an adolescent “how many cigarettes do you smoke per day?”. After the initial time line follow-back assessment, encourage adolescent smokers to keep a daily diary of how many cigarettes they smoke, and monitor the diary at each visit.
Beth, age 15, was admitted overnight to an inpatient psychiatric unit after running away from home and being taken into police custody. Her primary diagnosis was conduct disorder.
At morning rounds, the nurse reported that Beth was very irritable, had threatened the staff, and had been moved to seclusion. During routine examination, the psychiatrist discovered that Beth was a half-pack/day smoker and “really” wanted a cigarette. The psychiatrist told her hospital policy did not allow smoking, but she could try a transdermal nicotine patch (TNP) to help reduce her nicotine withdrawal symptoms. She agreed and received a 14 mg/d nicotine patch.
Beth’s irritability improved substantially with TNP, and she moved back to her regular room within 2 hours without incident.
We have found daily smoking to be a good indicator of nicotine dependence, and anyone who smokes daily would receive significant health benefits from quitting. Hence, any daily smoker who wants to quit, regardless of DSM-IV nicotine dependence status, is a candidate for treatment.
BEHAVIORAL THERAPY
Unlike adults, adolescents usually lack smoking-related medical consequences, such as heart or lung disease. Even so, most adolescent smokers report that they would like to quit but face barriers such as:
- having to inform parents they smoke
- not knowing how to get help for smoking cessation
- lack of transportation for treatment
- lack of third-party reimbursement for smoking cessation treatment.
To help adolescents, we recommend following the U.S. Public Health Service guideline for smoking cessation.14 At least provide and discuss smoking cessation brochures developed specifically for adolescents. For example, one Centers for Disease Control and Prevention brochure describes what symptoms to expect when quitting, how to cope with craving, and other topics (see Related resources).
To manage peer pressure, we counsel teens to let their friends know they are trying to quit so that friends do not smoke in front of them. If that does not work, we ask patients to avoid being around friends who smoke at least for the first 2 weeks and preferably 2 months.
Many states have free telephone quit lines that provide support and advice on how to stop smoking. Several Web sites also are available for smokers (including adolescents) wanting to quit (see Related resources).
PHARMACOLOGIC TREATMENT
For adults, first-line FDA-approved medications for smoking cessation include nicotine replacement therapies (NRT)in transdermal, gum, inhaler, and lozenge forms and sustained-release bupropion. Nortriptyline, doxapine, and clonidine have shown effectiveness for smoking cessation but are not FDA-approved for this indication.15 Selegiline and mecamylamine have shown initial efficacy and are being examined in larger clinical trials.
For adolescents, little is known about what medications might help them stop smoking. Nicotine replacement therapies and bupropion SR have been most explored in adolescent smokers. The effect of psychiatric comorbidity on the quit rate is not well-studied in adolescents.
The transdermal nicotine patch (TNP) has shown modest results in preliminary trials among adolescents. One study found 11% abstinence at 6 weeks,16 and another found a <5% quit rate.17 A third study reported an 18% abstinence rate with a combination of TNP and contingency management therapy.18 Discussion of contingency management and other behavioral therapies is beyond the scope of this article.
A recent study comparing TNP, nicotine gum, and placebo in adolescent smokers found the lowest drop-out rate and highest compliance among the TNP group. Three-month abstinence rates were 17.6% for TNP, 6.5% for nicotine gum, and 2.5% for placebo. The difference between the TNP and placebo groups’ abstinence rates was statistically significant.19
Bupropion SR. In an open-label pilot study, our group treated 16 adolescent smokers weighing >90 lbs with bupropion SR, 150 mg bid. Average age was 18, and two-thirds of patients had ADHD. The endpoint abstinence rate—as measured by self-report and CO levels—was 31%, which is similar to rates reported in adult smokers treated with this dosage of bupropion SR.20
The adolescents did not gain weight during the study, which may be important to this age group. Reported side effects were similar to those in adults, with one adolescent reporting an allergic reaction (urticaria). We are conducting a larger follow-up study using bupropion SR with and without behavioral therapy.
A PRACTICAL CLINICAL APPROACH
Smoking behavior. For treatment, we propose two categories of adolescent smokers: regular (daily) and nonregular (nondaily) (see Algorithm). We recognize that many nondaily smokers smoke frequently and may benefit from aggressive treatment. However, we propose this two-track approach as a starting point because of limited data and medication risks, such as possible seizures with bupropion SR. We suggest:
- using behavioral therapy and patient education as first-line treatment for nonregular adolescent smokers
- using medication and behavioral therapy as first-line treatment for regular smokers and medication as second-line treatment for nonregular smokers who do not respond to behavior therapy/patient education.
Algorithm Suggested smoking cessation approaches for adolescents
Offer a treatment for at least 6 to 8 weeks before considering a change in therapy. One definition of initial success is no tobacco use in a 7-day period by self-report and biological verification (such as CO levels).
Behavioral therapy is relatively low-risk and helps many adult smokers. Despite a lack of evidence, some sort of behavioral therapy in combination with pharmacologic therapy might also help adolescent smokers.
When adolescents get disheartened by a slip or relapse to smoking, be patient and encourage them to try again. Inform them that smokers often require multiple attempts before they can quit completely.
Medication. Based on the limited published evidence, we consider TNP and bupropion SR first-line medications for adolescent smokers who want to quit.
For adult smokers, clinicians often combine medication and NRT to increase success rates.15 No data suggest that combining TNP and bupropion SR may be more effective than monotherapy in adolescents, but the combination might help those who do not respond to either agent alone.
We recommend starting bupropion SR treatment at least 1 week before the patient’s quit date. Titrate the dosage based on the package insert and patient tolerance.
Start NRT according to package instructions, and titrate dosages based on response:
- increase if the patient reports substantial craving and withdrawal symptoms, such as irritability and anxiety.
- decrease in case of toxicity (such as nausea).
In our experience, adolescent smokers require slightly lower NRT dosages than adults, although this varies among individuals.
- Centers for Disease Control and Prevention. Tobacco Information and Prevention Source (TIPS). www.cdc.gov/tobacco/quit/iquit.htm
- National Institute of Drug Abuse. NIDA for Teens. The Science Behind Drug Abuse. http://teens.drugabuse.gov/index.asp
- Society for Research on Nicotine and Tobacco. www.srnt.org
Drug brand names
- Bupropion SR • Zyban
- Clonidine • Catapres
- Doxapine • Sinequan
- Mecamylamine • Inversine
- Nortriptyline • Pamelor
- Selegiline • Eldepryl
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Upadhyaya HP, Brady KT, Wharton M, Liao J. Psychiatric disorders and cigarette smoking among child and adolescent psychiatry inpatients. Am J Addict 2003;12:144-52.
2. Lasser K, Boyd JW, Woolhandler S, et al. Smoking and mental illness. A population-based prevalence study. JAMA 2000;284(20):2606-10.
3. Johnston LD, O’Malley PM, Bachman JG. Teen smoking continues to decline in 2003, but declines are slowing. Ann Arbor, MI: University of Michigan News and Information Services, Dec. 19, 2003. Available at: www.monitoringthefuture.org/press.html. Accessed 08/13/04.
4. Upadhyaya HP, Deas D, Brady KT, Kruesi M. Cigarette smoking and psychiatric comorbidity in children and adolescents. J Am Acad Child Adolesc Psychiatry 2002;41(11):1294-1305.
5. Molina BS, Pelham WE. Childhood predictors of adolescent substance use in a longitudinal study of children with ADHD. J Abnorm Psychol 2003;112(3):497-507.
6. Pomerleau OF, Downey KK, Stelson FW, Pomerleau CS. Cigarette smoking in adult patients diagnosed with attention-deficit/hyperactivity disorder. J Subst Abuse 1995;7:373-8.
7. Dierker LC, Avenevoli S, Merikangas KR, et al. Association between psychiatric disorders and the progression of tobacco use behaviors. J Am Acad Child Adolesc Psychiatry 2001;40(10):1159-67.
8. Zacny J. Behavioral aspects of alcohol-tobacco interactions. Recent Dev Alcohol 1990;8:205-19.
9. Rohde P, Lewinsohn P, Kahler C, et al. Natural course of alcohol use disorders from adolescence to young adulthood. J Am Acad Child Adolesc Psychiatry 2001;40(1):83-90.
10. Sonntag H, Wittchen HU, Hofler M, et al. Are social fears and DSM-IV social anxiety disorder associated with smoking and nicotine dependence in adolescents and young adults? Eur Psychiatry 2000;15:67-74.
11. Prokhorov AV, Pallonen UE, Fava JL, et al. Measuring nicotine dependence among high-risk adolescent smokers. Addict Behav 1996;21:117-27.
12. McDonald P, Colwell B, Backinger CL, et al. Better practices for youth tobacco cessation: evidence of review panel. Am J Health Behav 2003;27(suppl 2):S144-S158.
13. Sobell LC, Sobell MB, Leo GI, Cancilla A. Reliability of a timeline method: assessing normal drinkers’ reports of recent drinking and a comparative evaluation across several populations. Br J Addict 1988;83(4):393-402.
14. Fiore M, Bailey W, Cohen S. Treating tobacco use and dependence: Clinical practice guideline. Rockville, MD: US Public Health Service, 2000.
15. George TP, O’Malley SS. Current pharmacological treatments for nicotine dependence. Trends Pharmacol Sci 2004;25(1):42-8.
16. Hurt RD, Croghan GA, Beede SD, et al. Nicotine patch therapy in 101 adolescent smokers. Efficacy, withdrawal symptom relief, and carbon monoxide and plasma cotinine levels. Arch Pediatr Adolesc Med 2000;154:31-7.
17. Smith TA, House RF, Jr, Croghan IT, et al. Nicotine patch therapy in adolescent smokers. Pediatrics 1996;98:659-67.
18. Hanson K, Allen S, Jensen S, Hatsukami D. Treatment of adolescent smokers with the nicotine patch. Nicotine Tob Res 2003;5(4):515-26.
19. Moolchan ET. Efficacy of the nicotine patch and gum for the treatment of adolescent tobacco dependence. Scottsdale, AZ: Society for Research on Nicotine and Tobacco Research annual meeting, 2004.
20. Upadhyaya HP, Brady KT, Wang W. Bupropion SR in adolescents with comorbid ADHD and nicotine dependence: a pilot study. J Am Acad Child Adolesc Psychiatry 2004;43(2):199-205.
1. Upadhyaya HP, Brady KT, Wharton M, Liao J. Psychiatric disorders and cigarette smoking among child and adolescent psychiatry inpatients. Am J Addict 2003;12:144-52.
2. Lasser K, Boyd JW, Woolhandler S, et al. Smoking and mental illness. A population-based prevalence study. JAMA 2000;284(20):2606-10.
3. Johnston LD, O’Malley PM, Bachman JG. Teen smoking continues to decline in 2003, but declines are slowing. Ann Arbor, MI: University of Michigan News and Information Services, Dec. 19, 2003. Available at: www.monitoringthefuture.org/press.html. Accessed 08/13/04.
4. Upadhyaya HP, Deas D, Brady KT, Kruesi M. Cigarette smoking and psychiatric comorbidity in children and adolescents. J Am Acad Child Adolesc Psychiatry 2002;41(11):1294-1305.
5. Molina BS, Pelham WE. Childhood predictors of adolescent substance use in a longitudinal study of children with ADHD. J Abnorm Psychol 2003;112(3):497-507.
6. Pomerleau OF, Downey KK, Stelson FW, Pomerleau CS. Cigarette smoking in adult patients diagnosed with attention-deficit/hyperactivity disorder. J Subst Abuse 1995;7:373-8.
7. Dierker LC, Avenevoli S, Merikangas KR, et al. Association between psychiatric disorders and the progression of tobacco use behaviors. J Am Acad Child Adolesc Psychiatry 2001;40(10):1159-67.
8. Zacny J. Behavioral aspects of alcohol-tobacco interactions. Recent Dev Alcohol 1990;8:205-19.
9. Rohde P, Lewinsohn P, Kahler C, et al. Natural course of alcohol use disorders from adolescence to young adulthood. J Am Acad Child Adolesc Psychiatry 2001;40(1):83-90.
10. Sonntag H, Wittchen HU, Hofler M, et al. Are social fears and DSM-IV social anxiety disorder associated with smoking and nicotine dependence in adolescents and young adults? Eur Psychiatry 2000;15:67-74.
11. Prokhorov AV, Pallonen UE, Fava JL, et al. Measuring nicotine dependence among high-risk adolescent smokers. Addict Behav 1996;21:117-27.
12. McDonald P, Colwell B, Backinger CL, et al. Better practices for youth tobacco cessation: evidence of review panel. Am J Health Behav 2003;27(suppl 2):S144-S158.
13. Sobell LC, Sobell MB, Leo GI, Cancilla A. Reliability of a timeline method: assessing normal drinkers’ reports of recent drinking and a comparative evaluation across several populations. Br J Addict 1988;83(4):393-402.
14. Fiore M, Bailey W, Cohen S. Treating tobacco use and dependence: Clinical practice guideline. Rockville, MD: US Public Health Service, 2000.
15. George TP, O’Malley SS. Current pharmacological treatments for nicotine dependence. Trends Pharmacol Sci 2004;25(1):42-8.
16. Hurt RD, Croghan GA, Beede SD, et al. Nicotine patch therapy in 101 adolescent smokers. Efficacy, withdrawal symptom relief, and carbon monoxide and plasma cotinine levels. Arch Pediatr Adolesc Med 2000;154:31-7.
17. Smith TA, House RF, Jr, Croghan IT, et al. Nicotine patch therapy in adolescent smokers. Pediatrics 1996;98:659-67.
18. Hanson K, Allen S, Jensen S, Hatsukami D. Treatment of adolescent smokers with the nicotine patch. Nicotine Tob Res 2003;5(4):515-26.
19. Moolchan ET. Efficacy of the nicotine patch and gum for the treatment of adolescent tobacco dependence. Scottsdale, AZ: Society for Research on Nicotine and Tobacco Research annual meeting, 2004.
20. Upadhyaya HP, Brady KT, Wang W. Bupropion SR in adolescents with comorbid ADHD and nicotine dependence: a pilot study. J Am Acad Child Adolesc Psychiatry 2004;43(2):199-205.
Crossing the line: When does teen substance use become abuse or dependence?
Assessing an adolescent for a possible substance use disorder can be streamlined by choosing age-appropriate screening tools and asking targeted questions. Based on our experience, we offer a 4-step approach to these at-risk patients1 (Box) that focuses on:
- quantifying alcohol or drug abuse and/or dependence
- identifying and treating psychiatric comorbidity
- evaluating and addressing social influences that contribute to substance use
- assessing negative consequences associated with substance abuse.
Adolescent substance use increases the risk of motor vehicle accidents, suicide, transmission of HIV and other sexual diseases, criminal behaviors, and psychological problems. Alcohol and marijuana are the substances most commonly abused by adolescents.
In 2002, the University of Michigan Institute for Social Research’s annual “Monitoring the Future” study reported:
- drunkenness in 7% of 8th graders, 18% of 10th graders, and 30% of 12th graders at least once in the previous 30 days.
- illicit drug use by 18% of 8th graders, 35% of 10th graders, and 41% of 12th graders in the previous 12 months.
Boys used substances more frequently than girls, and boys’ use was more severe. Within the previous month, boys reported greater alcohol use, binge drinking (five or more drinks in one sitting), and heavy drinking, as well as greater illicit drug use in the past year.1
INITIAL EVALUATION
Adolescents generally do not seek substance abuse treatment but are referred because of alcohol- or drug-related legal, school, or family problems. Thus, most present for evaluation with their parents, legal guardians, or officers of the court.
We begin by finding out from parents or guardians the reasons for the evaluation, their perspectives on the adolescent’s behavior, and their expectations of treatment. Then we interview the adolescent alone, assessing for substance use and evaluating peer relationships.
Components. A typical initial evaluation takes 90 minutes to 2 hours and includes:
- psychiatric history and symptoms
- medical history
- previous hospitalizations (medical and psychiatric)
- family history
- social history.
Specifically, the assessment focuses on the reason for the evaluation, with attention to diagnostic criteria for substance use/dependence.
STEP 1: QUANTIFYING DEPENDENCE
As with adults, clinical diagnosis of substance abuse or dependence in adolescents is based on DSM-IV diagnostic criteria (Table 1). Adolescents, however, differ from adults in diagnostic presentation, risk of dependence, and patterns of substance use.
Diagnostic ‘orphans.’ DSM-IV criteria for alcohol use disorders have limitations in adolescents.2 Teens who report one or two dependence symptoms and no abuse symptoms have been described as “diagnostic orphans”3—they fall short of criteria for dependence or abuse but clearly demonstrate substance use patterns. This presentation is common; in a survey of 74,008 high school students, almost 10% of 12th graders reported one or two dependence symptoms and no abuse symptoms.4
Risk of dependence. Adolescents who begin using alcohol or drugs develop dependence more rapidly than adults do.5
Patterns of use. Adolescents are more likely than adults to binge with alcohol and drugs, which may conceal the severity of their abuse. DSM-IV diagnostic criteria for substance abuse or dependence do not consider quantity of use, such as number of drinks or percent of days drinking or using drugs.
Assessment instruments. Many assessment instruments are available to explore adolescent substance use and its associated consequences. Some are described in detail and are available on the Internet. Common screening instruments that can be used for adolescent substance use are compared in Table 2.
DUSI-A and POSIT. Two self-report instruments—Drug Use Screening Inventory-Adolescents (DUSI-A)6 and Problem Oriented Screening Instrument for Teenagers (POSIT)7—can help explore alcohol or drug use in teens who admit to substance use. Anyone who endorses at least one DSM-IV abuse or dependence criterion requires further evaluation. Either test is a good starting point, and both have a built-in “lie” scale.
T-ASI and CASI. The Teen Addiction Severity Index (T-ASI)8 and Comprehensive Adolescent Severity Inventory (CASI)9 are more labor-intensive and require training to administer. These assessments are more appropriate for adolescents with extensive alcohol or drug abuse.
A-OCDS and Deas-MOCS. Our group recently developed the Adolescent Obsessive Compulsive Drinking Scale (A-OCDS)10 and the Deas-Marijuana Obsessive Compulsive Scale (Deas-MOCS).11
These self-report instruments have been validated in treatment- and nontreatment-seeking adolescents and young adults in inpatient and outpatient populations. They are sensitive and specific in identifying problem drinkers and marijuana users, respectively, and are quick, useful screens to determine need for further assessment.
Toxicology is useful for initial assessment and to monitor substance use patterns during treatment.
Urine samples are used to assess marijuana, sedative/hypnotic, amphetamine, cocaine, opiate, and phencyclidine use. Alcohol may be detected in urine, but alcohol levels detected by blood and breath testing are more accurate.
Table 1
Diagnostic criteria for substance abuse and dependence
| Substance abuse | 1 of these 4 symptoms in a 12-month period: Role impairment Hazardous use Legal problems associated with use Social problems |
| Substance dependence | At least 3 of the following: Tolerance Withdrawal Using more or longer than intended Attempting to quit or cut down Much time spent using Activities given up to use Psychological/physical problems resulting from use Subtyped as with or without physiologic features (tolerance or withdrawal symptoms) |
| Source: DSM-IV-TR | |
Marijuana may be detected in the urine for 3 days to 4 weeks, depending on level of use. Cocaine can be detected for 2 to 4 days in urine and longer in hair analysis.
Random screening. Adolescents who use drugs usually know how long substances can be detected, so random urine drug screening is important to treatment progress. We inform adolescents at the beginning of treatment that random screening will be performed to corroborate self-report of substance use. To ensure a reliable urine sample, same-gender staff observe while the adolescent gives the sample.
Table 2
Common screening instruments for alcohol and drug use in adolescents
| Instrument | Items (#) | How administered | Administration time |
|---|---|---|---|
| Drug Use Screening Inventory (DUSI-R), Revised | 159 | Self-report | 20 to 40 minutes |
| Problem-Oriented Screening Instrument for Teenagers (POSIT) | 139 | Self-report | 20 to 30 minutes |
| Teen Addiction Severity Index (T-ASI) | 133 | Clinician | 20 to 45 minutes |
| Comprehensive Adolescent Severity Inventory (CASI) | 245 | Clinician | Varies with experience of administrator |
| Adolescent Obsessive-Compulsive Drinking Scale (A-OCDS) | 14 | Self-report | About 5 minutes |
| Deas-Marijuana Obsessive-Compulsive Scale (Deas-MOCS) | 14 | Self-report | About 5 minutes |
STEP 2: IDENTIFYING PSYCHIATRIC COMORBIDITY
In adolescents, substance use disorder frequently goes hand-in-hand with psychiatric disorders, particularly:
- mood and anxiety disorders
- disruptive disorders (attention-deficit/hyperactivity, oppositional defiant, and conduct disorders)12
- and posttraumatic stress disorder.13
Uncontrolled psychiatric disorders may sabotage substance abuse treatment. Therefore, assess any adolescent presenting with substance use for psychiatric illness.
Did psychiatric symptoms predate or postdate substance use? The answer may suggest self-medication or a substance-induced phenomenon. This assumption does not always apply, however, as many factors affect the relationship between substance use and psychiatric disorders.
Adolescents who meet DSM-IV criteria for conduct disorder—especially those who are highly aggressive—tend to initiate substance use much earlier than adolescents without conduct disorder, and they continue their use longer.
Most adolescents with comorbid psychiatric and substance use disorders develop the psychiatric disorder first. Some report using various substances to medicate their psychiatric symptoms. Early diagnosis and treatment of the psychiatric disorder may prevent or decrease the adolescent’s substance use.
STEPS 3 AND 4: EVALUATING SOCIAL INFLUENCES AND CONSEQUENCES
Social influences that contribute to adolescent alcohol and drug abuse include family dynamics and peer relationships. Consequences include educational and legal problems. We explore these areas with the adolescents and their parents/guardians. In most cases, adolescents are honest when reporting how their alcohol or drug use has affected their lives.
What is his family like? Assess the adolescent’s family, including its structure and history of substance abuse, psychiatric illness, or trauma (Table 3). Adolescents whose parents or siblings use alcohol or drugs are at increased risk for substance use.14 To what extent this association is genetic, environmental, or both is undetermined, but the genetic influence increases as adolescents age.15
Who are her friends? Adolescents who try alcohol or drugs and continue to use them tend to have peers who use these substances.16 Moreover, the severity of adolescents’ substance use is correlated with the number of substance-using peers. To explore peer relationships, ask about:
- peer group composition, including whether peers use alcohol or drugs
- peer interactions, including the adolescent’s ability to assert him- or herself in the peer group
- markers for risky sexual behaviors related to substance use, including infection with HIV and other sexually transmitted diseases.
How is she doing in school? Inquire about the teen’s academic performance, attendance, disciplinary problems, and motivation. Even a small decline in school performance or an increase in disciplinary problems that result in suspension or expulsion can indicate substance use or other at-risk behaviors.
Poor grades or attendance problems suggest but are not the only clues to substance use. Some adolescents with good school performance engage in substance use and may be impaired in other life domains.
Has he been arrested? Substance-abusing adolescents tend to engage in delinquent behaviors, including shoplifting, vandalism, curfew violations, disorderly conduct, and drunken driving. When assessing for delinquency, ask about behaviors that did or did not result in arrest. The teen who avoided arrest for illegal activities may perceive his/her behaviors as less severe than those involving arrest, and it may help to address this denial in individual or group therapy.
Table 3
Questions to assess family influence on an adolescent’s substance use
| Family structure |
|
| Parenting styles |
|
| Substance abuse |
|
| Psychiatric disorders |
|
| Trauma |
|
TREATMENT
We consider any adolescent with dependence symptoms—whether or not the presentation meets full DSM-IV diagnostic criteria—to be a candidate for further assessment and treatment. Early intervention may prevent progression to substance dependence.
Effective treatments:
- are intensive and of sufficient duration to change attitude and behaviors
- are comprehensive and target multiple domains of the adolescent’s life
- are sensitive to cultural and socioeconomic realities
- involve the family
- emphasize pro-social recreational activities, such as playing sports, attending movies, camping, having lunch or dinner with peers, etc.
Inpatient or outpatient? Managed care and insurance restrictions limit many patients’ eligibility for inpatient or residential treatment, so partial hospitalization and outpatient settings have become standard for substance abuse treatment. Partial hospitalization programs vary but may entail several hours, several days per week. Outpatient treatment may encompass individual, group, and family therapy, including after-school programs.
Inpatient treatment is usually reserved for adolescents:
- who need detoxification
- with comorbid psychiatric disorders
- or who may harm themselves or others.
PSYCHOTHERAPIES
Behavioral therapy, family-based therapy, multisystematic therapy (MST), and 12-step approaches have shown efficacy in treating adolescents with substance use disorders.
Behavioral therapy. Behavioral therapy is recommended as initial treatment because substance use plays a functional role in the adolescent’s life and is learned and reinforced in the adolescent’s environment. Homework assignments and role-play are commonly used in therapy.
Three central ingredients are:
- functional analysis (identifying internal and external triggers for starting and continuing substance use)
- skills training (targeting problems identified in the functional analysis)
- and relapse prevention.
Behavioral therapy is more effective than supportive therapy in improving family relationships and school and work attendance and in decreasing substance use, as indicated by fewer positive urine toxicology screens.17
Cognitive-behavioral therapy (CBT) approaches substance use as a maladaptive response to life problems. Its goal is to teach new skills to help the adolescent recognize and avoid high-risk situations and cope with associated problems and behaviors.
In a recent study, Kaminer et al randomly assigned 82 adolescents with psychiatric and substance use disorders to 8 weeks of CBT or psychoeducational therapy (didactic or videotaped presentations of ways to address problems associated with substance use). Substance use was reduced in both treatment groups, but:
- adolescents receiving CBT had significantly fewer positive urine toxicology tests
- adolescents with comorbid conduct disorder were least likely to complete treatment or return for follow-up
- those with depressive and anxiety disorders were most likely to complete treatment.18
Family-based therapy. Two detailed reviews19,20 demonstrate that the adolescent’s family, community, and school relationships affect his or her perceptions and behaviors. Maladaptive relationships in any of these systems may lead to high-risk behaviors. Therefore, family therapy is core to the adolescent’s treatment, regardless of what modality is chosen.
Goals of family therapy may be:
- to help the adolescent abstain from substance use
- to engage in pro-social activities
- to decrease parental denial of the adolescent’s substance use
- to decrease resistance to treatment
- treatment maintenance
- to establish or re-establish structure in the adolescent’s environment
- to improve communication in the family.
Multisystemic therapy is comprehensive and involves all systems that relate to the adolescent’s substance use, including the family, school, community, and legal system. MST requires special training and intensive supervision, so it is usually reserved for adolescents who have not benefited from other forms of treatment.21
12-step approaches. For adolescents, 12-step programs usually augment other treatments and are rarely used alone. Alcoholics Anonymous, Narcotics Anonymous, and other 12-step programs have been studied more extensively in adults than in adolescents.
Adolescents, who often feel invulnerable, may have difficulty accepting the 12-step doctrine of lack of control. A modified 12-step program and workbook for adolescents are available through the American Academy of Child and Adolescent Psychiatry.22
Referral tips. If possible, refer an adolescent to a 12-step group specifically for adolescents. Teens who attend adult groups often perceive their substance use as normal, compared with the more severe and chronic patterns of some adults. Most adolescents relate better to peers with similar problems and may benefit from reminders of the negative consequences of substance use and the benefits of abstinence.
DRUG THERAPY
Drug therapy for adolescents with substance use disorders is usually considered in the context of detoxification, treating withdrawal symptoms, and treating comorbid psychiatric disorders. The same detoxification and withdrawal treatment principles used in adults apply to adolescents.
Clinical withdrawal symptoms are less common in adolescents than adults, probably because of adolescents’ binge patterns of substance use. Even so, some adolescents do experience withdrawal and may be at risk for complications if improperly treated.
Psychiatric comorbidity. To our knowledge, only two double-blind, placebo-controlled studies of drug therapy in treating adolescent substance use disorders have been published.
Depression. Deas et al23 randomized 10 adolescents with alcohol use disorders and depression to 12 weeks of group CBT plus sertraline or placebo. Sertraline was started at 25 mg/d and titrated to a maximum of 100 mg/d. Drinks per drinking day, percent of days drinking, and Hamilton Rating Scale for Depression scores declined similarly in both groups.
Drinking decreased significantly from baseline (by an average 4.7 drinks), and adolescents in both groups no longer met DSM-IV criteria for depression at the end of treatment. CBT’s effectiveness in treating alcohol use disorders and depression might have concealed any difference in effect between sertaline and placebo.
Bipolar disorder. Geller et al24 randomly assigned 25 adolescents with bipolar disorder and substance dependence to lithium or placebo for 6 weeks. Lithium was started as an evening dose of 600 mg and titrated to achieve a lithium blood level of 0.9 to 1.3 mEq/L. Among the 21 adolescents who completed the trial, those receiving lithium had significantly fewer positive urine toxicology screens and higher clinical global assessment of function scores.
Related resources
- National Clearinghouse for Alcohol and Drug Information, Substance Abuse and Mental Health Services Administration, U.S. Department of Health and Human Services. www.health.org/govpubs/bkd306/31k.aspx
- National Institute on Alcohol Abuse and Alcoholism (assessment instruments). www.niaaa.nih.gov/publications/instable.htm
- Deas D, Thomas SE. An overview of controlled studies of adolescent substance abuse treatment. Am J Addict 2001;10:178-89.
Drug brand names
- Sertraline • Zoloft
Disclosure
Dr. Deas receives grant support from Pfizer, Inc. and the National Institute of Alcohol Abuse and Alcoholism.
Dr. Upadhyaya receives grant support from the National Institute of Drug Abuse and GlaxoSmithKline.
Acknowledgment
The authors wish to thank Alva Blair for assistance with preparing this manuscript and Natalie Johnson, MA, Kess Mughelli, BS, and Lakeleia Middleton-Robinson, MA, for technical support.
1. Johnston LD, O’Malley PM, Bachman JG. Monitoring the Future: national results on adolescent drug use. Overview of key findings, 2002. Bethesda, MD: National Institute on Drug Abuse, 2003 (in press).
2. Martin CS, Kaczynski NA, Maisto SA, et al. Patterns of DSM-IV alcohol abuse and dependence symptoms in adolescent drinkers. J Stud Alcohol 1995;56:672-80.
3. Pollock NK, Martin CS. Diagnostic orphans: adolescents with alcohol symptoms who do not qualify for DSM-IV abuse or dependence diagnoses. Am J Psychiatry 1999;156:897-901.
4. Harrison PA, Fulkerson JA, Beebe TJ. DSM-IV substance use disorder criteria for adolescents: a critical examination based on a statewide school survey. Am J Psychiatry 1998;155:486-92.
5. Grant BF, Dawson DA. Age at onset of alcohol use and its association with DSM-IV alcohol abuse/dependence: results from the National Longitudinal Alcohol Epidemiological Survey. J Subst Abuse 1997;9:103-10.
6. Tarter RE, Laird SB, Bukstein O, Kaminer Y. Validation of the adolescent drug use screening inventory: preliminary findings. Psychol Addict Behav 1992;6:322-6.
7. Rahdert E (ed). The adolescent assessment/referral system manual. DHHS pub. no. (ADM) 91-1735. Rockville, MD: U.S. Department of Health and Human Services, 1991.
8. Kaminer Y, Bukstein OG, Tarter RE. The teen addiction severity index (T-ASI): rationale and reliability. Int J Addict 1991;26:219-26.
9. Meyers K, McLellan AT, Jaeger JL, Pettinati A. The development of the Comprehensive Addiction Severity Index for Adolescents (CASI-A): an interview for assessing multiple problems of adolescents. J Subst Abuse Treat 1995;12:181-93.
10. Deas DV, Roberts JS, Randall CL, Anton RF. Adolescent Obsessive-Compulsive Drinking Scale (A-OCDS): an assessment tool for problem drinking. J Natl Med Assoc 2001;93:92-103.
11. Deas D, Randall CL, Thomas S. The utility of the Deas-Marijuana Obsessive-Compulsive Scale (Deas-MOCS) in an inpatient adolescent substance abusing sample. Drug Alcohol Depend 2002;66(June):S43.-
12. Deas-Nesmith D, Campbell S, Brady KT. Substance use disorders in an adolescent inpatient psychiatric population. JAMA 1998;90:233-8.
13. Clark DB, Lesnick L, Hegedus AM. Traumas and other adverse life events in adolescents with alcohol abuse and dependence. Am Acad Child Adolesc Psychiatry 1997;36:1744-51.
14. Kilpatrick DG, Acierno R, Saunders B, et al. Risk factors for adolescent substance abuse and dependence: data from a national sample. J Consult Clin Psychol 2000;68:19-30.
15. Rose RJ. A developmental behavioral-genetic perspective on alcoholism risk. Alcohol Health Res World 1998;22:131-43.
16. Swadi H. Individual risk factors for adolescent substance use. Drug Alcohol Depend 1999;55:209-24.
17. Azrin N, McMahon P, Donohue B, et al. Behavior therapy for drug abuse: a controlled treatment outcome study. Behav Res Ther 1994;32:857-66.
18. Kaminer Y, Burleson JA, Goldberger R. Cognitive-behavioral coping skills and psychoeducation therapies for adolescent substance abuse. J Nerv Ment Dis 2002;190:737-45.
19. Liddle H, Dakof G. Efficacy of family therapy for drug abuse: promising but not definitive. J Marital Fam Ther 1995;21:511-43.
20. Waldron HB. Adolescent substance abuse and family therapy outcome: a review of randomized trials. Adv Clin Child Psychol 1997;19:199-234.
21. Henggeler SW, Melton LA. Effects of multisystemic therapy on drug use and abuse in serious juvenile offenders: a progress report from two outcome studies. Family Dynamics of Addiction Quarterly 1991;1:40-51.
22. Jaffe S. Step workbook for adolescent chemical dependency recovery. Washington, DC: American Academy of Child and Adolescent Psychiatry, 1990.
23. Deas DV, Randall C, Roberts J, Anton R. A double-blind, placebo-controlled trial of sertraline in depressed adolescent alcoholics: a pilot study. Human Psychopharmacology Clinical and Experimental 2000;15:461-9.
24. Geller B, Cooper T, Sun K, et al. Double-blind and placebo-controlled study of lithium for adolescent bipolar disorders with secondary substance dependency. J Am Acad Child Adolesc Psychiatry 1998;37:171-8.
Assessing an adolescent for a possible substance use disorder can be streamlined by choosing age-appropriate screening tools and asking targeted questions. Based on our experience, we offer a 4-step approach to these at-risk patients1 (Box) that focuses on:
- quantifying alcohol or drug abuse and/or dependence
- identifying and treating psychiatric comorbidity
- evaluating and addressing social influences that contribute to substance use
- assessing negative consequences associated with substance abuse.
Adolescent substance use increases the risk of motor vehicle accidents, suicide, transmission of HIV and other sexual diseases, criminal behaviors, and psychological problems. Alcohol and marijuana are the substances most commonly abused by adolescents.
In 2002, the University of Michigan Institute for Social Research’s annual “Monitoring the Future” study reported:
- drunkenness in 7% of 8th graders, 18% of 10th graders, and 30% of 12th graders at least once in the previous 30 days.
- illicit drug use by 18% of 8th graders, 35% of 10th graders, and 41% of 12th graders in the previous 12 months.
Boys used substances more frequently than girls, and boys’ use was more severe. Within the previous month, boys reported greater alcohol use, binge drinking (five or more drinks in one sitting), and heavy drinking, as well as greater illicit drug use in the past year.1
INITIAL EVALUATION
Adolescents generally do not seek substance abuse treatment but are referred because of alcohol- or drug-related legal, school, or family problems. Thus, most present for evaluation with their parents, legal guardians, or officers of the court.
We begin by finding out from parents or guardians the reasons for the evaluation, their perspectives on the adolescent’s behavior, and their expectations of treatment. Then we interview the adolescent alone, assessing for substance use and evaluating peer relationships.
Components. A typical initial evaluation takes 90 minutes to 2 hours and includes:
- psychiatric history and symptoms
- medical history
- previous hospitalizations (medical and psychiatric)
- family history
- social history.
Specifically, the assessment focuses on the reason for the evaluation, with attention to diagnostic criteria for substance use/dependence.
STEP 1: QUANTIFYING DEPENDENCE
As with adults, clinical diagnosis of substance abuse or dependence in adolescents is based on DSM-IV diagnostic criteria (Table 1). Adolescents, however, differ from adults in diagnostic presentation, risk of dependence, and patterns of substance use.
Diagnostic ‘orphans.’ DSM-IV criteria for alcohol use disorders have limitations in adolescents.2 Teens who report one or two dependence symptoms and no abuse symptoms have been described as “diagnostic orphans”3—they fall short of criteria for dependence or abuse but clearly demonstrate substance use patterns. This presentation is common; in a survey of 74,008 high school students, almost 10% of 12th graders reported one or two dependence symptoms and no abuse symptoms.4
Risk of dependence. Adolescents who begin using alcohol or drugs develop dependence more rapidly than adults do.5
Patterns of use. Adolescents are more likely than adults to binge with alcohol and drugs, which may conceal the severity of their abuse. DSM-IV diagnostic criteria for substance abuse or dependence do not consider quantity of use, such as number of drinks or percent of days drinking or using drugs.
Assessment instruments. Many assessment instruments are available to explore adolescent substance use and its associated consequences. Some are described in detail and are available on the Internet. Common screening instruments that can be used for adolescent substance use are compared in Table 2.
DUSI-A and POSIT. Two self-report instruments—Drug Use Screening Inventory-Adolescents (DUSI-A)6 and Problem Oriented Screening Instrument for Teenagers (POSIT)7—can help explore alcohol or drug use in teens who admit to substance use. Anyone who endorses at least one DSM-IV abuse or dependence criterion requires further evaluation. Either test is a good starting point, and both have a built-in “lie” scale.
T-ASI and CASI. The Teen Addiction Severity Index (T-ASI)8 and Comprehensive Adolescent Severity Inventory (CASI)9 are more labor-intensive and require training to administer. These assessments are more appropriate for adolescents with extensive alcohol or drug abuse.
A-OCDS and Deas-MOCS. Our group recently developed the Adolescent Obsessive Compulsive Drinking Scale (A-OCDS)10 and the Deas-Marijuana Obsessive Compulsive Scale (Deas-MOCS).11
These self-report instruments have been validated in treatment- and nontreatment-seeking adolescents and young adults in inpatient and outpatient populations. They are sensitive and specific in identifying problem drinkers and marijuana users, respectively, and are quick, useful screens to determine need for further assessment.
Toxicology is useful for initial assessment and to monitor substance use patterns during treatment.
Urine samples are used to assess marijuana, sedative/hypnotic, amphetamine, cocaine, opiate, and phencyclidine use. Alcohol may be detected in urine, but alcohol levels detected by blood and breath testing are more accurate.
Table 1
Diagnostic criteria for substance abuse and dependence
| Substance abuse | 1 of these 4 symptoms in a 12-month period: Role impairment Hazardous use Legal problems associated with use Social problems |
| Substance dependence | At least 3 of the following: Tolerance Withdrawal Using more or longer than intended Attempting to quit or cut down Much time spent using Activities given up to use Psychological/physical problems resulting from use Subtyped as with or without physiologic features (tolerance or withdrawal symptoms) |
| Source: DSM-IV-TR | |
Marijuana may be detected in the urine for 3 days to 4 weeks, depending on level of use. Cocaine can be detected for 2 to 4 days in urine and longer in hair analysis.
Random screening. Adolescents who use drugs usually know how long substances can be detected, so random urine drug screening is important to treatment progress. We inform adolescents at the beginning of treatment that random screening will be performed to corroborate self-report of substance use. To ensure a reliable urine sample, same-gender staff observe while the adolescent gives the sample.
Table 2
Common screening instruments for alcohol and drug use in adolescents
| Instrument | Items (#) | How administered | Administration time |
|---|---|---|---|
| Drug Use Screening Inventory (DUSI-R), Revised | 159 | Self-report | 20 to 40 minutes |
| Problem-Oriented Screening Instrument for Teenagers (POSIT) | 139 | Self-report | 20 to 30 minutes |
| Teen Addiction Severity Index (T-ASI) | 133 | Clinician | 20 to 45 minutes |
| Comprehensive Adolescent Severity Inventory (CASI) | 245 | Clinician | Varies with experience of administrator |
| Adolescent Obsessive-Compulsive Drinking Scale (A-OCDS) | 14 | Self-report | About 5 minutes |
| Deas-Marijuana Obsessive-Compulsive Scale (Deas-MOCS) | 14 | Self-report | About 5 minutes |
STEP 2: IDENTIFYING PSYCHIATRIC COMORBIDITY
In adolescents, substance use disorder frequently goes hand-in-hand with psychiatric disorders, particularly:
- mood and anxiety disorders
- disruptive disorders (attention-deficit/hyperactivity, oppositional defiant, and conduct disorders)12
- and posttraumatic stress disorder.13
Uncontrolled psychiatric disorders may sabotage substance abuse treatment. Therefore, assess any adolescent presenting with substance use for psychiatric illness.
Did psychiatric symptoms predate or postdate substance use? The answer may suggest self-medication or a substance-induced phenomenon. This assumption does not always apply, however, as many factors affect the relationship between substance use and psychiatric disorders.
Adolescents who meet DSM-IV criteria for conduct disorder—especially those who are highly aggressive—tend to initiate substance use much earlier than adolescents without conduct disorder, and they continue their use longer.
Most adolescents with comorbid psychiatric and substance use disorders develop the psychiatric disorder first. Some report using various substances to medicate their psychiatric symptoms. Early diagnosis and treatment of the psychiatric disorder may prevent or decrease the adolescent’s substance use.
STEPS 3 AND 4: EVALUATING SOCIAL INFLUENCES AND CONSEQUENCES
Social influences that contribute to adolescent alcohol and drug abuse include family dynamics and peer relationships. Consequences include educational and legal problems. We explore these areas with the adolescents and their parents/guardians. In most cases, adolescents are honest when reporting how their alcohol or drug use has affected their lives.
What is his family like? Assess the adolescent’s family, including its structure and history of substance abuse, psychiatric illness, or trauma (Table 3). Adolescents whose parents or siblings use alcohol or drugs are at increased risk for substance use.14 To what extent this association is genetic, environmental, or both is undetermined, but the genetic influence increases as adolescents age.15
Who are her friends? Adolescents who try alcohol or drugs and continue to use them tend to have peers who use these substances.16 Moreover, the severity of adolescents’ substance use is correlated with the number of substance-using peers. To explore peer relationships, ask about:
- peer group composition, including whether peers use alcohol or drugs
- peer interactions, including the adolescent’s ability to assert him- or herself in the peer group
- markers for risky sexual behaviors related to substance use, including infection with HIV and other sexually transmitted diseases.
How is she doing in school? Inquire about the teen’s academic performance, attendance, disciplinary problems, and motivation. Even a small decline in school performance or an increase in disciplinary problems that result in suspension or expulsion can indicate substance use or other at-risk behaviors.
Poor grades or attendance problems suggest but are not the only clues to substance use. Some adolescents with good school performance engage in substance use and may be impaired in other life domains.
Has he been arrested? Substance-abusing adolescents tend to engage in delinquent behaviors, including shoplifting, vandalism, curfew violations, disorderly conduct, and drunken driving. When assessing for delinquency, ask about behaviors that did or did not result in arrest. The teen who avoided arrest for illegal activities may perceive his/her behaviors as less severe than those involving arrest, and it may help to address this denial in individual or group therapy.
Table 3
Questions to assess family influence on an adolescent’s substance use
| Family structure |
|
| Parenting styles |
|
| Substance abuse |
|
| Psychiatric disorders |
|
| Trauma |
|
TREATMENT
We consider any adolescent with dependence symptoms—whether or not the presentation meets full DSM-IV diagnostic criteria—to be a candidate for further assessment and treatment. Early intervention may prevent progression to substance dependence.
Effective treatments:
- are intensive and of sufficient duration to change attitude and behaviors
- are comprehensive and target multiple domains of the adolescent’s life
- are sensitive to cultural and socioeconomic realities
- involve the family
- emphasize pro-social recreational activities, such as playing sports, attending movies, camping, having lunch or dinner with peers, etc.
Inpatient or outpatient? Managed care and insurance restrictions limit many patients’ eligibility for inpatient or residential treatment, so partial hospitalization and outpatient settings have become standard for substance abuse treatment. Partial hospitalization programs vary but may entail several hours, several days per week. Outpatient treatment may encompass individual, group, and family therapy, including after-school programs.
Inpatient treatment is usually reserved for adolescents:
- who need detoxification
- with comorbid psychiatric disorders
- or who may harm themselves or others.
PSYCHOTHERAPIES
Behavioral therapy, family-based therapy, multisystematic therapy (MST), and 12-step approaches have shown efficacy in treating adolescents with substance use disorders.
Behavioral therapy. Behavioral therapy is recommended as initial treatment because substance use plays a functional role in the adolescent’s life and is learned and reinforced in the adolescent’s environment. Homework assignments and role-play are commonly used in therapy.
Three central ingredients are:
- functional analysis (identifying internal and external triggers for starting and continuing substance use)
- skills training (targeting problems identified in the functional analysis)
- and relapse prevention.
Behavioral therapy is more effective than supportive therapy in improving family relationships and school and work attendance and in decreasing substance use, as indicated by fewer positive urine toxicology screens.17
Cognitive-behavioral therapy (CBT) approaches substance use as a maladaptive response to life problems. Its goal is to teach new skills to help the adolescent recognize and avoid high-risk situations and cope with associated problems and behaviors.
In a recent study, Kaminer et al randomly assigned 82 adolescents with psychiatric and substance use disorders to 8 weeks of CBT or psychoeducational therapy (didactic or videotaped presentations of ways to address problems associated with substance use). Substance use was reduced in both treatment groups, but:
- adolescents receiving CBT had significantly fewer positive urine toxicology tests
- adolescents with comorbid conduct disorder were least likely to complete treatment or return for follow-up
- those with depressive and anxiety disorders were most likely to complete treatment.18
Family-based therapy. Two detailed reviews19,20 demonstrate that the adolescent’s family, community, and school relationships affect his or her perceptions and behaviors. Maladaptive relationships in any of these systems may lead to high-risk behaviors. Therefore, family therapy is core to the adolescent’s treatment, regardless of what modality is chosen.
Goals of family therapy may be:
- to help the adolescent abstain from substance use
- to engage in pro-social activities
- to decrease parental denial of the adolescent’s substance use
- to decrease resistance to treatment
- treatment maintenance
- to establish or re-establish structure in the adolescent’s environment
- to improve communication in the family.
Multisystemic therapy is comprehensive and involves all systems that relate to the adolescent’s substance use, including the family, school, community, and legal system. MST requires special training and intensive supervision, so it is usually reserved for adolescents who have not benefited from other forms of treatment.21
12-step approaches. For adolescents, 12-step programs usually augment other treatments and are rarely used alone. Alcoholics Anonymous, Narcotics Anonymous, and other 12-step programs have been studied more extensively in adults than in adolescents.
Adolescents, who often feel invulnerable, may have difficulty accepting the 12-step doctrine of lack of control. A modified 12-step program and workbook for adolescents are available through the American Academy of Child and Adolescent Psychiatry.22
Referral tips. If possible, refer an adolescent to a 12-step group specifically for adolescents. Teens who attend adult groups often perceive their substance use as normal, compared with the more severe and chronic patterns of some adults. Most adolescents relate better to peers with similar problems and may benefit from reminders of the negative consequences of substance use and the benefits of abstinence.
DRUG THERAPY
Drug therapy for adolescents with substance use disorders is usually considered in the context of detoxification, treating withdrawal symptoms, and treating comorbid psychiatric disorders. The same detoxification and withdrawal treatment principles used in adults apply to adolescents.
Clinical withdrawal symptoms are less common in adolescents than adults, probably because of adolescents’ binge patterns of substance use. Even so, some adolescents do experience withdrawal and may be at risk for complications if improperly treated.
Psychiatric comorbidity. To our knowledge, only two double-blind, placebo-controlled studies of drug therapy in treating adolescent substance use disorders have been published.
Depression. Deas et al23 randomized 10 adolescents with alcohol use disorders and depression to 12 weeks of group CBT plus sertraline or placebo. Sertraline was started at 25 mg/d and titrated to a maximum of 100 mg/d. Drinks per drinking day, percent of days drinking, and Hamilton Rating Scale for Depression scores declined similarly in both groups.
Drinking decreased significantly from baseline (by an average 4.7 drinks), and adolescents in both groups no longer met DSM-IV criteria for depression at the end of treatment. CBT’s effectiveness in treating alcohol use disorders and depression might have concealed any difference in effect between sertaline and placebo.
Bipolar disorder. Geller et al24 randomly assigned 25 adolescents with bipolar disorder and substance dependence to lithium or placebo for 6 weeks. Lithium was started as an evening dose of 600 mg and titrated to achieve a lithium blood level of 0.9 to 1.3 mEq/L. Among the 21 adolescents who completed the trial, those receiving lithium had significantly fewer positive urine toxicology screens and higher clinical global assessment of function scores.
Related resources
- National Clearinghouse for Alcohol and Drug Information, Substance Abuse and Mental Health Services Administration, U.S. Department of Health and Human Services. www.health.org/govpubs/bkd306/31k.aspx
- National Institute on Alcohol Abuse and Alcoholism (assessment instruments). www.niaaa.nih.gov/publications/instable.htm
- Deas D, Thomas SE. An overview of controlled studies of adolescent substance abuse treatment. Am J Addict 2001;10:178-89.
Drug brand names
- Sertraline • Zoloft
Disclosure
Dr. Deas receives grant support from Pfizer, Inc. and the National Institute of Alcohol Abuse and Alcoholism.
Dr. Upadhyaya receives grant support from the National Institute of Drug Abuse and GlaxoSmithKline.
Acknowledgment
The authors wish to thank Alva Blair for assistance with preparing this manuscript and Natalie Johnson, MA, Kess Mughelli, BS, and Lakeleia Middleton-Robinson, MA, for technical support.
Assessing an adolescent for a possible substance use disorder can be streamlined by choosing age-appropriate screening tools and asking targeted questions. Based on our experience, we offer a 4-step approach to these at-risk patients1 (Box) that focuses on:
- quantifying alcohol or drug abuse and/or dependence
- identifying and treating psychiatric comorbidity
- evaluating and addressing social influences that contribute to substance use
- assessing negative consequences associated with substance abuse.
Adolescent substance use increases the risk of motor vehicle accidents, suicide, transmission of HIV and other sexual diseases, criminal behaviors, and psychological problems. Alcohol and marijuana are the substances most commonly abused by adolescents.
In 2002, the University of Michigan Institute for Social Research’s annual “Monitoring the Future” study reported:
- drunkenness in 7% of 8th graders, 18% of 10th graders, and 30% of 12th graders at least once in the previous 30 days.
- illicit drug use by 18% of 8th graders, 35% of 10th graders, and 41% of 12th graders in the previous 12 months.
Boys used substances more frequently than girls, and boys’ use was more severe. Within the previous month, boys reported greater alcohol use, binge drinking (five or more drinks in one sitting), and heavy drinking, as well as greater illicit drug use in the past year.1
INITIAL EVALUATION
Adolescents generally do not seek substance abuse treatment but are referred because of alcohol- or drug-related legal, school, or family problems. Thus, most present for evaluation with their parents, legal guardians, or officers of the court.
We begin by finding out from parents or guardians the reasons for the evaluation, their perspectives on the adolescent’s behavior, and their expectations of treatment. Then we interview the adolescent alone, assessing for substance use and evaluating peer relationships.
Components. A typical initial evaluation takes 90 minutes to 2 hours and includes:
- psychiatric history and symptoms
- medical history
- previous hospitalizations (medical and psychiatric)
- family history
- social history.
Specifically, the assessment focuses on the reason for the evaluation, with attention to diagnostic criteria for substance use/dependence.
STEP 1: QUANTIFYING DEPENDENCE
As with adults, clinical diagnosis of substance abuse or dependence in adolescents is based on DSM-IV diagnostic criteria (Table 1). Adolescents, however, differ from adults in diagnostic presentation, risk of dependence, and patterns of substance use.
Diagnostic ‘orphans.’ DSM-IV criteria for alcohol use disorders have limitations in adolescents.2 Teens who report one or two dependence symptoms and no abuse symptoms have been described as “diagnostic orphans”3—they fall short of criteria for dependence or abuse but clearly demonstrate substance use patterns. This presentation is common; in a survey of 74,008 high school students, almost 10% of 12th graders reported one or two dependence symptoms and no abuse symptoms.4
Risk of dependence. Adolescents who begin using alcohol or drugs develop dependence more rapidly than adults do.5
Patterns of use. Adolescents are more likely than adults to binge with alcohol and drugs, which may conceal the severity of their abuse. DSM-IV diagnostic criteria for substance abuse or dependence do not consider quantity of use, such as number of drinks or percent of days drinking or using drugs.
Assessment instruments. Many assessment instruments are available to explore adolescent substance use and its associated consequences. Some are described in detail and are available on the Internet. Common screening instruments that can be used for adolescent substance use are compared in Table 2.
DUSI-A and POSIT. Two self-report instruments—Drug Use Screening Inventory-Adolescents (DUSI-A)6 and Problem Oriented Screening Instrument for Teenagers (POSIT)7—can help explore alcohol or drug use in teens who admit to substance use. Anyone who endorses at least one DSM-IV abuse or dependence criterion requires further evaluation. Either test is a good starting point, and both have a built-in “lie” scale.
T-ASI and CASI. The Teen Addiction Severity Index (T-ASI)8 and Comprehensive Adolescent Severity Inventory (CASI)9 are more labor-intensive and require training to administer. These assessments are more appropriate for adolescents with extensive alcohol or drug abuse.
A-OCDS and Deas-MOCS. Our group recently developed the Adolescent Obsessive Compulsive Drinking Scale (A-OCDS)10 and the Deas-Marijuana Obsessive Compulsive Scale (Deas-MOCS).11
These self-report instruments have been validated in treatment- and nontreatment-seeking adolescents and young adults in inpatient and outpatient populations. They are sensitive and specific in identifying problem drinkers and marijuana users, respectively, and are quick, useful screens to determine need for further assessment.
Toxicology is useful for initial assessment and to monitor substance use patterns during treatment.
Urine samples are used to assess marijuana, sedative/hypnotic, amphetamine, cocaine, opiate, and phencyclidine use. Alcohol may be detected in urine, but alcohol levels detected by blood and breath testing are more accurate.
Table 1
Diagnostic criteria for substance abuse and dependence
| Substance abuse | 1 of these 4 symptoms in a 12-month period: Role impairment Hazardous use Legal problems associated with use Social problems |
| Substance dependence | At least 3 of the following: Tolerance Withdrawal Using more or longer than intended Attempting to quit or cut down Much time spent using Activities given up to use Psychological/physical problems resulting from use Subtyped as with or without physiologic features (tolerance or withdrawal symptoms) |
| Source: DSM-IV-TR | |
Marijuana may be detected in the urine for 3 days to 4 weeks, depending on level of use. Cocaine can be detected for 2 to 4 days in urine and longer in hair analysis.
Random screening. Adolescents who use drugs usually know how long substances can be detected, so random urine drug screening is important to treatment progress. We inform adolescents at the beginning of treatment that random screening will be performed to corroborate self-report of substance use. To ensure a reliable urine sample, same-gender staff observe while the adolescent gives the sample.
Table 2
Common screening instruments for alcohol and drug use in adolescents
| Instrument | Items (#) | How administered | Administration time |
|---|---|---|---|
| Drug Use Screening Inventory (DUSI-R), Revised | 159 | Self-report | 20 to 40 minutes |
| Problem-Oriented Screening Instrument for Teenagers (POSIT) | 139 | Self-report | 20 to 30 minutes |
| Teen Addiction Severity Index (T-ASI) | 133 | Clinician | 20 to 45 minutes |
| Comprehensive Adolescent Severity Inventory (CASI) | 245 | Clinician | Varies with experience of administrator |
| Adolescent Obsessive-Compulsive Drinking Scale (A-OCDS) | 14 | Self-report | About 5 minutes |
| Deas-Marijuana Obsessive-Compulsive Scale (Deas-MOCS) | 14 | Self-report | About 5 minutes |
STEP 2: IDENTIFYING PSYCHIATRIC COMORBIDITY
In adolescents, substance use disorder frequently goes hand-in-hand with psychiatric disorders, particularly:
- mood and anxiety disorders
- disruptive disorders (attention-deficit/hyperactivity, oppositional defiant, and conduct disorders)12
- and posttraumatic stress disorder.13
Uncontrolled psychiatric disorders may sabotage substance abuse treatment. Therefore, assess any adolescent presenting with substance use for psychiatric illness.
Did psychiatric symptoms predate or postdate substance use? The answer may suggest self-medication or a substance-induced phenomenon. This assumption does not always apply, however, as many factors affect the relationship between substance use and psychiatric disorders.
Adolescents who meet DSM-IV criteria for conduct disorder—especially those who are highly aggressive—tend to initiate substance use much earlier than adolescents without conduct disorder, and they continue their use longer.
Most adolescents with comorbid psychiatric and substance use disorders develop the psychiatric disorder first. Some report using various substances to medicate their psychiatric symptoms. Early diagnosis and treatment of the psychiatric disorder may prevent or decrease the adolescent’s substance use.
STEPS 3 AND 4: EVALUATING SOCIAL INFLUENCES AND CONSEQUENCES
Social influences that contribute to adolescent alcohol and drug abuse include family dynamics and peer relationships. Consequences include educational and legal problems. We explore these areas with the adolescents and their parents/guardians. In most cases, adolescents are honest when reporting how their alcohol or drug use has affected their lives.
What is his family like? Assess the adolescent’s family, including its structure and history of substance abuse, psychiatric illness, or trauma (Table 3). Adolescents whose parents or siblings use alcohol or drugs are at increased risk for substance use.14 To what extent this association is genetic, environmental, or both is undetermined, but the genetic influence increases as adolescents age.15
Who are her friends? Adolescents who try alcohol or drugs and continue to use them tend to have peers who use these substances.16 Moreover, the severity of adolescents’ substance use is correlated with the number of substance-using peers. To explore peer relationships, ask about:
- peer group composition, including whether peers use alcohol or drugs
- peer interactions, including the adolescent’s ability to assert him- or herself in the peer group
- markers for risky sexual behaviors related to substance use, including infection with HIV and other sexually transmitted diseases.
How is she doing in school? Inquire about the teen’s academic performance, attendance, disciplinary problems, and motivation. Even a small decline in school performance or an increase in disciplinary problems that result in suspension or expulsion can indicate substance use or other at-risk behaviors.
Poor grades or attendance problems suggest but are not the only clues to substance use. Some adolescents with good school performance engage in substance use and may be impaired in other life domains.
Has he been arrested? Substance-abusing adolescents tend to engage in delinquent behaviors, including shoplifting, vandalism, curfew violations, disorderly conduct, and drunken driving. When assessing for delinquency, ask about behaviors that did or did not result in arrest. The teen who avoided arrest for illegal activities may perceive his/her behaviors as less severe than those involving arrest, and it may help to address this denial in individual or group therapy.
Table 3
Questions to assess family influence on an adolescent’s substance use
| Family structure |
|
| Parenting styles |
|
| Substance abuse |
|
| Psychiatric disorders |
|
| Trauma |
|
TREATMENT
We consider any adolescent with dependence symptoms—whether or not the presentation meets full DSM-IV diagnostic criteria—to be a candidate for further assessment and treatment. Early intervention may prevent progression to substance dependence.
Effective treatments:
- are intensive and of sufficient duration to change attitude and behaviors
- are comprehensive and target multiple domains of the adolescent’s life
- are sensitive to cultural and socioeconomic realities
- involve the family
- emphasize pro-social recreational activities, such as playing sports, attending movies, camping, having lunch or dinner with peers, etc.
Inpatient or outpatient? Managed care and insurance restrictions limit many patients’ eligibility for inpatient or residential treatment, so partial hospitalization and outpatient settings have become standard for substance abuse treatment. Partial hospitalization programs vary but may entail several hours, several days per week. Outpatient treatment may encompass individual, group, and family therapy, including after-school programs.
Inpatient treatment is usually reserved for adolescents:
- who need detoxification
- with comorbid psychiatric disorders
- or who may harm themselves or others.
PSYCHOTHERAPIES
Behavioral therapy, family-based therapy, multisystematic therapy (MST), and 12-step approaches have shown efficacy in treating adolescents with substance use disorders.
Behavioral therapy. Behavioral therapy is recommended as initial treatment because substance use plays a functional role in the adolescent’s life and is learned and reinforced in the adolescent’s environment. Homework assignments and role-play are commonly used in therapy.
Three central ingredients are:
- functional analysis (identifying internal and external triggers for starting and continuing substance use)
- skills training (targeting problems identified in the functional analysis)
- and relapse prevention.
Behavioral therapy is more effective than supportive therapy in improving family relationships and school and work attendance and in decreasing substance use, as indicated by fewer positive urine toxicology screens.17
Cognitive-behavioral therapy (CBT) approaches substance use as a maladaptive response to life problems. Its goal is to teach new skills to help the adolescent recognize and avoid high-risk situations and cope with associated problems and behaviors.
In a recent study, Kaminer et al randomly assigned 82 adolescents with psychiatric and substance use disorders to 8 weeks of CBT or psychoeducational therapy (didactic or videotaped presentations of ways to address problems associated with substance use). Substance use was reduced in both treatment groups, but:
- adolescents receiving CBT had significantly fewer positive urine toxicology tests
- adolescents with comorbid conduct disorder were least likely to complete treatment or return for follow-up
- those with depressive and anxiety disorders were most likely to complete treatment.18
Family-based therapy. Two detailed reviews19,20 demonstrate that the adolescent’s family, community, and school relationships affect his or her perceptions and behaviors. Maladaptive relationships in any of these systems may lead to high-risk behaviors. Therefore, family therapy is core to the adolescent’s treatment, regardless of what modality is chosen.
Goals of family therapy may be:
- to help the adolescent abstain from substance use
- to engage in pro-social activities
- to decrease parental denial of the adolescent’s substance use
- to decrease resistance to treatment
- treatment maintenance
- to establish or re-establish structure in the adolescent’s environment
- to improve communication in the family.
Multisystemic therapy is comprehensive and involves all systems that relate to the adolescent’s substance use, including the family, school, community, and legal system. MST requires special training and intensive supervision, so it is usually reserved for adolescents who have not benefited from other forms of treatment.21
12-step approaches. For adolescents, 12-step programs usually augment other treatments and are rarely used alone. Alcoholics Anonymous, Narcotics Anonymous, and other 12-step programs have been studied more extensively in adults than in adolescents.
Adolescents, who often feel invulnerable, may have difficulty accepting the 12-step doctrine of lack of control. A modified 12-step program and workbook for adolescents are available through the American Academy of Child and Adolescent Psychiatry.22
Referral tips. If possible, refer an adolescent to a 12-step group specifically for adolescents. Teens who attend adult groups often perceive their substance use as normal, compared with the more severe and chronic patterns of some adults. Most adolescents relate better to peers with similar problems and may benefit from reminders of the negative consequences of substance use and the benefits of abstinence.
DRUG THERAPY
Drug therapy for adolescents with substance use disorders is usually considered in the context of detoxification, treating withdrawal symptoms, and treating comorbid psychiatric disorders. The same detoxification and withdrawal treatment principles used in adults apply to adolescents.
Clinical withdrawal symptoms are less common in adolescents than adults, probably because of adolescents’ binge patterns of substance use. Even so, some adolescents do experience withdrawal and may be at risk for complications if improperly treated.
Psychiatric comorbidity. To our knowledge, only two double-blind, placebo-controlled studies of drug therapy in treating adolescent substance use disorders have been published.
Depression. Deas et al23 randomized 10 adolescents with alcohol use disorders and depression to 12 weeks of group CBT plus sertraline or placebo. Sertraline was started at 25 mg/d and titrated to a maximum of 100 mg/d. Drinks per drinking day, percent of days drinking, and Hamilton Rating Scale for Depression scores declined similarly in both groups.
Drinking decreased significantly from baseline (by an average 4.7 drinks), and adolescents in both groups no longer met DSM-IV criteria for depression at the end of treatment. CBT’s effectiveness in treating alcohol use disorders and depression might have concealed any difference in effect between sertaline and placebo.
Bipolar disorder. Geller et al24 randomly assigned 25 adolescents with bipolar disorder and substance dependence to lithium or placebo for 6 weeks. Lithium was started as an evening dose of 600 mg and titrated to achieve a lithium blood level of 0.9 to 1.3 mEq/L. Among the 21 adolescents who completed the trial, those receiving lithium had significantly fewer positive urine toxicology screens and higher clinical global assessment of function scores.
Related resources
- National Clearinghouse for Alcohol and Drug Information, Substance Abuse and Mental Health Services Administration, U.S. Department of Health and Human Services. www.health.org/govpubs/bkd306/31k.aspx
- National Institute on Alcohol Abuse and Alcoholism (assessment instruments). www.niaaa.nih.gov/publications/instable.htm
- Deas D, Thomas SE. An overview of controlled studies of adolescent substance abuse treatment. Am J Addict 2001;10:178-89.
Drug brand names
- Sertraline • Zoloft
Disclosure
Dr. Deas receives grant support from Pfizer, Inc. and the National Institute of Alcohol Abuse and Alcoholism.
Dr. Upadhyaya receives grant support from the National Institute of Drug Abuse and GlaxoSmithKline.
Acknowledgment
The authors wish to thank Alva Blair for assistance with preparing this manuscript and Natalie Johnson, MA, Kess Mughelli, BS, and Lakeleia Middleton-Robinson, MA, for technical support.
1. Johnston LD, O’Malley PM, Bachman JG. Monitoring the Future: national results on adolescent drug use. Overview of key findings, 2002. Bethesda, MD: National Institute on Drug Abuse, 2003 (in press).
2. Martin CS, Kaczynski NA, Maisto SA, et al. Patterns of DSM-IV alcohol abuse and dependence symptoms in adolescent drinkers. J Stud Alcohol 1995;56:672-80.
3. Pollock NK, Martin CS. Diagnostic orphans: adolescents with alcohol symptoms who do not qualify for DSM-IV abuse or dependence diagnoses. Am J Psychiatry 1999;156:897-901.
4. Harrison PA, Fulkerson JA, Beebe TJ. DSM-IV substance use disorder criteria for adolescents: a critical examination based on a statewide school survey. Am J Psychiatry 1998;155:486-92.
5. Grant BF, Dawson DA. Age at onset of alcohol use and its association with DSM-IV alcohol abuse/dependence: results from the National Longitudinal Alcohol Epidemiological Survey. J Subst Abuse 1997;9:103-10.
6. Tarter RE, Laird SB, Bukstein O, Kaminer Y. Validation of the adolescent drug use screening inventory: preliminary findings. Psychol Addict Behav 1992;6:322-6.
7. Rahdert E (ed). The adolescent assessment/referral system manual. DHHS pub. no. (ADM) 91-1735. Rockville, MD: U.S. Department of Health and Human Services, 1991.
8. Kaminer Y, Bukstein OG, Tarter RE. The teen addiction severity index (T-ASI): rationale and reliability. Int J Addict 1991;26:219-26.
9. Meyers K, McLellan AT, Jaeger JL, Pettinati A. The development of the Comprehensive Addiction Severity Index for Adolescents (CASI-A): an interview for assessing multiple problems of adolescents. J Subst Abuse Treat 1995;12:181-93.
10. Deas DV, Roberts JS, Randall CL, Anton RF. Adolescent Obsessive-Compulsive Drinking Scale (A-OCDS): an assessment tool for problem drinking. J Natl Med Assoc 2001;93:92-103.
11. Deas D, Randall CL, Thomas S. The utility of the Deas-Marijuana Obsessive-Compulsive Scale (Deas-MOCS) in an inpatient adolescent substance abusing sample. Drug Alcohol Depend 2002;66(June):S43.-
12. Deas-Nesmith D, Campbell S, Brady KT. Substance use disorders in an adolescent inpatient psychiatric population. JAMA 1998;90:233-8.
13. Clark DB, Lesnick L, Hegedus AM. Traumas and other adverse life events in adolescents with alcohol abuse and dependence. Am Acad Child Adolesc Psychiatry 1997;36:1744-51.
14. Kilpatrick DG, Acierno R, Saunders B, et al. Risk factors for adolescent substance abuse and dependence: data from a national sample. J Consult Clin Psychol 2000;68:19-30.
15. Rose RJ. A developmental behavioral-genetic perspective on alcoholism risk. Alcohol Health Res World 1998;22:131-43.
16. Swadi H. Individual risk factors for adolescent substance use. Drug Alcohol Depend 1999;55:209-24.
17. Azrin N, McMahon P, Donohue B, et al. Behavior therapy for drug abuse: a controlled treatment outcome study. Behav Res Ther 1994;32:857-66.
18. Kaminer Y, Burleson JA, Goldberger R. Cognitive-behavioral coping skills and psychoeducation therapies for adolescent substance abuse. J Nerv Ment Dis 2002;190:737-45.
19. Liddle H, Dakof G. Efficacy of family therapy for drug abuse: promising but not definitive. J Marital Fam Ther 1995;21:511-43.
20. Waldron HB. Adolescent substance abuse and family therapy outcome: a review of randomized trials. Adv Clin Child Psychol 1997;19:199-234.
21. Henggeler SW, Melton LA. Effects of multisystemic therapy on drug use and abuse in serious juvenile offenders: a progress report from two outcome studies. Family Dynamics of Addiction Quarterly 1991;1:40-51.
22. Jaffe S. Step workbook for adolescent chemical dependency recovery. Washington, DC: American Academy of Child and Adolescent Psychiatry, 1990.
23. Deas DV, Randall C, Roberts J, Anton R. A double-blind, placebo-controlled trial of sertraline in depressed adolescent alcoholics: a pilot study. Human Psychopharmacology Clinical and Experimental 2000;15:461-9.
24. Geller B, Cooper T, Sun K, et al. Double-blind and placebo-controlled study of lithium for adolescent bipolar disorders with secondary substance dependency. J Am Acad Child Adolesc Psychiatry 1998;37:171-8.
1. Johnston LD, O’Malley PM, Bachman JG. Monitoring the Future: national results on adolescent drug use. Overview of key findings, 2002. Bethesda, MD: National Institute on Drug Abuse, 2003 (in press).
2. Martin CS, Kaczynski NA, Maisto SA, et al. Patterns of DSM-IV alcohol abuse and dependence symptoms in adolescent drinkers. J Stud Alcohol 1995;56:672-80.
3. Pollock NK, Martin CS. Diagnostic orphans: adolescents with alcohol symptoms who do not qualify for DSM-IV abuse or dependence diagnoses. Am J Psychiatry 1999;156:897-901.
4. Harrison PA, Fulkerson JA, Beebe TJ. DSM-IV substance use disorder criteria for adolescents: a critical examination based on a statewide school survey. Am J Psychiatry 1998;155:486-92.
5. Grant BF, Dawson DA. Age at onset of alcohol use and its association with DSM-IV alcohol abuse/dependence: results from the National Longitudinal Alcohol Epidemiological Survey. J Subst Abuse 1997;9:103-10.
6. Tarter RE, Laird SB, Bukstein O, Kaminer Y. Validation of the adolescent drug use screening inventory: preliminary findings. Psychol Addict Behav 1992;6:322-6.
7. Rahdert E (ed). The adolescent assessment/referral system manual. DHHS pub. no. (ADM) 91-1735. Rockville, MD: U.S. Department of Health and Human Services, 1991.
8. Kaminer Y, Bukstein OG, Tarter RE. The teen addiction severity index (T-ASI): rationale and reliability. Int J Addict 1991;26:219-26.
9. Meyers K, McLellan AT, Jaeger JL, Pettinati A. The development of the Comprehensive Addiction Severity Index for Adolescents (CASI-A): an interview for assessing multiple problems of adolescents. J Subst Abuse Treat 1995;12:181-93.
10. Deas DV, Roberts JS, Randall CL, Anton RF. Adolescent Obsessive-Compulsive Drinking Scale (A-OCDS): an assessment tool for problem drinking. J Natl Med Assoc 2001;93:92-103.
11. Deas D, Randall CL, Thomas S. The utility of the Deas-Marijuana Obsessive-Compulsive Scale (Deas-MOCS) in an inpatient adolescent substance abusing sample. Drug Alcohol Depend 2002;66(June):S43.-
12. Deas-Nesmith D, Campbell S, Brady KT. Substance use disorders in an adolescent inpatient psychiatric population. JAMA 1998;90:233-8.
13. Clark DB, Lesnick L, Hegedus AM. Traumas and other adverse life events in adolescents with alcohol abuse and dependence. Am Acad Child Adolesc Psychiatry 1997;36:1744-51.
14. Kilpatrick DG, Acierno R, Saunders B, et al. Risk factors for adolescent substance abuse and dependence: data from a national sample. J Consult Clin Psychol 2000;68:19-30.
15. Rose RJ. A developmental behavioral-genetic perspective on alcoholism risk. Alcohol Health Res World 1998;22:131-43.
16. Swadi H. Individual risk factors for adolescent substance use. Drug Alcohol Depend 1999;55:209-24.
17. Azrin N, McMahon P, Donohue B, et al. Behavior therapy for drug abuse: a controlled treatment outcome study. Behav Res Ther 1994;32:857-66.
18. Kaminer Y, Burleson JA, Goldberger R. Cognitive-behavioral coping skills and psychoeducation therapies for adolescent substance abuse. J Nerv Ment Dis 2002;190:737-45.
19. Liddle H, Dakof G. Efficacy of family therapy for drug abuse: promising but not definitive. J Marital Fam Ther 1995;21:511-43.
20. Waldron HB. Adolescent substance abuse and family therapy outcome: a review of randomized trials. Adv Clin Child Psychol 1997;19:199-234.
21. Henggeler SW, Melton LA. Effects of multisystemic therapy on drug use and abuse in serious juvenile offenders: a progress report from two outcome studies. Family Dynamics of Addiction Quarterly 1991;1:40-51.
22. Jaffe S. Step workbook for adolescent chemical dependency recovery. Washington, DC: American Academy of Child and Adolescent Psychiatry, 1990.
23. Deas DV, Randall C, Roberts J, Anton R. A double-blind, placebo-controlled trial of sertraline in depressed adolescent alcoholics: a pilot study. Human Psychopharmacology Clinical and Experimental 2000;15:461-9.
24. Geller B, Cooper T, Sun K, et al. Double-blind and placebo-controlled study of lithium for adolescent bipolar disorders with secondary substance dependency. J Am Acad Child Adolesc Psychiatry 1998;37:171-8.