User login
Jason Carris is director, Digital Media and Strategy, Society Partners, at Frontline Medical Communications. He previously worked in the newspaper industry as a writer and editor. He resides in Central New Jersey with his wife and three children. Email him at [email protected].
Researchers Earn First SHM Junior Faculty Development Awards
NATIONAL HARBOR, Md. — Kirsten Kangelaris, MD, and Evan Fieldston, MD, MBA, MSHP, were presented $50,000 Junior Faculty Development Awards this morning at HM10. The first-year awards are part of SHM’s commitment to helping the “generation of new knowledge,” said Scott Flanders, SHM’s outgoing president.
Dr. Kangelaris, a fellow in internal medicine at the University of California at San Francisco, focuses her research on continued clinical and biologic genetic risk-prediction algorithms that will improve the triage and early-management strategies for hospitalized patients with inflammatory illness.
Dr. Fieldston, an assistant professor in pediatrics at the University of Pennsylvania School of Medicine and Children’s Hospital of Philadelphia, plans to use his award to examine the association between dynamic aspects of workload, workforce, and quality of care at children’s hospitals.
SHM also handed out its annual Awards of Excellence and announced winners from the Research, Innovation, and Clinical Vignette (PDF) competition. Judges scored more than 400 posters; some of the winning project teams included medical students.
“I am particularly proud to see that we had medical students as award winners,” said Flanders, chief of the hospital medicine division at the University of Michigan Health System in Ann Arbor. “That gives me great hope for the future of HM.”
Awards of Excellence
- Clinical Excellence: Jennifer Myers (pictured), MD, FHM, patient safety officer at the Hospital of the University of Pennsylvania;
- Excellence in Research: Margaret Fang, MD, MPH, FHM, assistant professor of medicine at the University of California at San Francisco;
- Outstanding Service in Hospital Medicine: Mitchell Wilson, MD, SFHM, corporate medical director for Eagle Hospital Physicians;
- Excellence in Teaching: Amir Jaffer, associate professor of medicine, chief of the hospital medicine division in the Department of Medicine at the University of Miami (Fla.); and
- Excellence in Teamwork in Quality Improvement: Emory Healthcare’s VTE Prevention Team.
Research, Innovation, and Clinical Vignettes winners
- Research: Will Southern, MD, MS, and Julia Arnsten, MD, MPH, Montefiore Medical Center, Bronx, N.Y.: “Increased Mortality and Readmission Among Patients Discharged against Medical Advice.”
- Innovation Poster: Aaron Farberg, BS, Andrew Lin, BS, Latoya Kuhn, MPH, Scott Flanders, MD, SFHM, Christopher Kim, MD, MBA, University of Michigan Medical School, “Dear Doctor: A Tool to Facilitate Patient-Centered Care and Enhance Communication.”
- Adult Vignette: Jennie Wei, MD, and Patrick Kneeland, MD, University of California at San Francisco, “A Case of Skin Ulcers and Neutropenia: Definitely Not a Helminth Problem.”
- Pediatric Vignette: Harry Hoar, MD, Baystate Children’s Hospitalist, Springfield, Mass., “A Teen with Varices: An Uncommon Presentation of a Familiar Disease.”
NATIONAL HARBOR, Md. — Kirsten Kangelaris, MD, and Evan Fieldston, MD, MBA, MSHP, were presented $50,000 Junior Faculty Development Awards this morning at HM10. The first-year awards are part of SHM’s commitment to helping the “generation of new knowledge,” said Scott Flanders, SHM’s outgoing president.
Dr. Kangelaris, a fellow in internal medicine at the University of California at San Francisco, focuses her research on continued clinical and biologic genetic risk-prediction algorithms that will improve the triage and early-management strategies for hospitalized patients with inflammatory illness.
Dr. Fieldston, an assistant professor in pediatrics at the University of Pennsylvania School of Medicine and Children’s Hospital of Philadelphia, plans to use his award to examine the association between dynamic aspects of workload, workforce, and quality of care at children’s hospitals.
SHM also handed out its annual Awards of Excellence and announced winners from the Research, Innovation, and Clinical Vignette (PDF) competition. Judges scored more than 400 posters; some of the winning project teams included medical students.
“I am particularly proud to see that we had medical students as award winners,” said Flanders, chief of the hospital medicine division at the University of Michigan Health System in Ann Arbor. “That gives me great hope for the future of HM.”
Awards of Excellence
- Clinical Excellence: Jennifer Myers (pictured), MD, FHM, patient safety officer at the Hospital of the University of Pennsylvania;
- Excellence in Research: Margaret Fang, MD, MPH, FHM, assistant professor of medicine at the University of California at San Francisco;
- Outstanding Service in Hospital Medicine: Mitchell Wilson, MD, SFHM, corporate medical director for Eagle Hospital Physicians;
- Excellence in Teaching: Amir Jaffer, associate professor of medicine, chief of the hospital medicine division in the Department of Medicine at the University of Miami (Fla.); and
- Excellence in Teamwork in Quality Improvement: Emory Healthcare’s VTE Prevention Team.
Research, Innovation, and Clinical Vignettes winners
- Research: Will Southern, MD, MS, and Julia Arnsten, MD, MPH, Montefiore Medical Center, Bronx, N.Y.: “Increased Mortality and Readmission Among Patients Discharged against Medical Advice.”
- Innovation Poster: Aaron Farberg, BS, Andrew Lin, BS, Latoya Kuhn, MPH, Scott Flanders, MD, SFHM, Christopher Kim, MD, MBA, University of Michigan Medical School, “Dear Doctor: A Tool to Facilitate Patient-Centered Care and Enhance Communication.”
- Adult Vignette: Jennie Wei, MD, and Patrick Kneeland, MD, University of California at San Francisco, “A Case of Skin Ulcers and Neutropenia: Definitely Not a Helminth Problem.”
- Pediatric Vignette: Harry Hoar, MD, Baystate Children’s Hospitalist, Springfield, Mass., “A Teen with Varices: An Uncommon Presentation of a Familiar Disease.”
NATIONAL HARBOR, Md. — Kirsten Kangelaris, MD, and Evan Fieldston, MD, MBA, MSHP, were presented $50,000 Junior Faculty Development Awards this morning at HM10. The first-year awards are part of SHM’s commitment to helping the “generation of new knowledge,” said Scott Flanders, SHM’s outgoing president.
Dr. Kangelaris, a fellow in internal medicine at the University of California at San Francisco, focuses her research on continued clinical and biologic genetic risk-prediction algorithms that will improve the triage and early-management strategies for hospitalized patients with inflammatory illness.
Dr. Fieldston, an assistant professor in pediatrics at the University of Pennsylvania School of Medicine and Children’s Hospital of Philadelphia, plans to use his award to examine the association between dynamic aspects of workload, workforce, and quality of care at children’s hospitals.
SHM also handed out its annual Awards of Excellence and announced winners from the Research, Innovation, and Clinical Vignette (PDF) competition. Judges scored more than 400 posters; some of the winning project teams included medical students.
“I am particularly proud to see that we had medical students as award winners,” said Flanders, chief of the hospital medicine division at the University of Michigan Health System in Ann Arbor. “That gives me great hope for the future of HM.”
Awards of Excellence
- Clinical Excellence: Jennifer Myers (pictured), MD, FHM, patient safety officer at the Hospital of the University of Pennsylvania;
- Excellence in Research: Margaret Fang, MD, MPH, FHM, assistant professor of medicine at the University of California at San Francisco;
- Outstanding Service in Hospital Medicine: Mitchell Wilson, MD, SFHM, corporate medical director for Eagle Hospital Physicians;
- Excellence in Teaching: Amir Jaffer, associate professor of medicine, chief of the hospital medicine division in the Department of Medicine at the University of Miami (Fla.); and
- Excellence in Teamwork in Quality Improvement: Emory Healthcare’s VTE Prevention Team.
Research, Innovation, and Clinical Vignettes winners
- Research: Will Southern, MD, MS, and Julia Arnsten, MD, MPH, Montefiore Medical Center, Bronx, N.Y.: “Increased Mortality and Readmission Among Patients Discharged against Medical Advice.”
- Innovation Poster: Aaron Farberg, BS, Andrew Lin, BS, Latoya Kuhn, MPH, Scott Flanders, MD, SFHM, Christopher Kim, MD, MBA, University of Michigan Medical School, “Dear Doctor: A Tool to Facilitate Patient-Centered Care and Enhance Communication.”
- Adult Vignette: Jennie Wei, MD, and Patrick Kneeland, MD, University of California at San Francisco, “A Case of Skin Ulcers and Neutropenia: Definitely Not a Helminth Problem.”
- Pediatric Vignette: Harry Hoar, MD, Baystate Children’s Hospitalist, Springfield, Mass., “A Teen with Varices: An Uncommon Presentation of a Familiar Disease.”
First, Do No Harm
NATIONAL HARBOR, Md. — Paul Levy doesn’t take well to the idea that things just happen in a hospital, whether it’s a central-line infection, a patient fall, or an accommodation for excellence.
Levy, president and CEO of Beth Israel Deaconess Medical Center in Boston, insists that improvement be a central tenet of his institution—and the only way to improve things is to monitor them first to establish a baseline.
Many of the roughly 2,500 hospitalists gathered for HM10 here might have expected Levy to talk about the recently passed healthcare reform package. Surprisingly, he instead told them to “ignore the healthcare reform bill" during this morning’s keynote address.
“Ignore all the fuss about it," he said. "Focus instead on the underlying values that you each have individually, and that you have collectively, as to why you became docs in the first place.”
Levy, who is not a physician, has quickly made a name as a leading voice in quality and transparency discussions, particularly via his popular blog. This morning, he told thousands of hospitalists that while change can be difficult, “we are doing too much harm in our hospitals.” He encouraged hospitalists to take charge of quality programs and point out processes and systems that could be improved.
And while he didn’t discount the federal mandate to provide increased access to medical care, he noted that the future delivery of care will improve as a function of thoughtful analysis and dedicated work, not because of new budgeting rules.
“It won’t be because we changed the payment regime,” Levy boasted. “It will be because you did the job.”
NATIONAL HARBOR, Md. — Paul Levy doesn’t take well to the idea that things just happen in a hospital, whether it’s a central-line infection, a patient fall, or an accommodation for excellence.
Levy, president and CEO of Beth Israel Deaconess Medical Center in Boston, insists that improvement be a central tenet of his institution—and the only way to improve things is to monitor them first to establish a baseline.
Many of the roughly 2,500 hospitalists gathered for HM10 here might have expected Levy to talk about the recently passed healthcare reform package. Surprisingly, he instead told them to “ignore the healthcare reform bill" during this morning’s keynote address.
“Ignore all the fuss about it," he said. "Focus instead on the underlying values that you each have individually, and that you have collectively, as to why you became docs in the first place.”
Levy, who is not a physician, has quickly made a name as a leading voice in quality and transparency discussions, particularly via his popular blog. This morning, he told thousands of hospitalists that while change can be difficult, “we are doing too much harm in our hospitals.” He encouraged hospitalists to take charge of quality programs and point out processes and systems that could be improved.
And while he didn’t discount the federal mandate to provide increased access to medical care, he noted that the future delivery of care will improve as a function of thoughtful analysis and dedicated work, not because of new budgeting rules.
“It won’t be because we changed the payment regime,” Levy boasted. “It will be because you did the job.”
NATIONAL HARBOR, Md. — Paul Levy doesn’t take well to the idea that things just happen in a hospital, whether it’s a central-line infection, a patient fall, or an accommodation for excellence.
Levy, president and CEO of Beth Israel Deaconess Medical Center in Boston, insists that improvement be a central tenet of his institution—and the only way to improve things is to monitor them first to establish a baseline.
Many of the roughly 2,500 hospitalists gathered for HM10 here might have expected Levy to talk about the recently passed healthcare reform package. Surprisingly, he instead told them to “ignore the healthcare reform bill" during this morning’s keynote address.
“Ignore all the fuss about it," he said. "Focus instead on the underlying values that you each have individually, and that you have collectively, as to why you became docs in the first place.”
Levy, who is not a physician, has quickly made a name as a leading voice in quality and transparency discussions, particularly via his popular blog. This morning, he told thousands of hospitalists that while change can be difficult, “we are doing too much harm in our hospitals.” He encouraged hospitalists to take charge of quality programs and point out processes and systems that could be improved.
And while he didn’t discount the federal mandate to provide increased access to medical care, he noted that the future delivery of care will improve as a function of thoughtful analysis and dedicated work, not because of new budgeting rules.
“It won’t be because we changed the payment regime,” Levy boasted. “It will be because you did the job.”
New Knowledge Paramount to HM10 Attendees
For an early-career hospitalist like Michele DeKorte, MD, HM10 offers a plethora of opportunities for practical knowledge and bushels of take-home points. “This is my first time, and I’m excited to be here,” Dr. DeKorte said moments after registering for HM10 at the Gaylord National Resort and Convention Center just outside Washington, D.C.
Dr. DeKorte, who has worked as a hospitalist at the University of California at San Diego since 2008, is one of a record 2,500 hospitalists registered for SHM’s annual meeting. She and hundreds of other hospitalists were taking part in Thursday’s lineup of pre-courses.
“I’m doing the procedures pre-course [Essential Procedures for the Hospitalist A Hands-on Experience] in the afternoon. I like procedures, so I think it will be fun,” she said, noting she will focus on the clinical track throughout the four-day event, which features more than 90 educational sessions. “It’s more interesting to me at this stage of the game. I want to have a better idea of how people are practicing HM around the country.”
Catherine Fitzgerald, DO, has worked as a hospitalist since 2005 and is attending her first annual meeting. For two years, she worked in an administrative role with CPMG at St. Joseph’s Memorial Hospital in Denver, and she plans to attend a smattering of practice-management sessions. “I also sit on our heart-failure committee at St. Joseph’s, so I have signed up for the session ‘How to Prevent Heart Failure Readmissions.’” she explained. “The meeting sessions are good reviews of things you already know, and interspersed in the discussions usually are these little pearls of new knowledge for your practice.”
In addition to aiming to improve her HM practice, Dr. Fitzgerald is excited to be in the nation’s capital with loved ones. Dr. Fitzgerald’s mother and 6-year-old son are scheduled to visit the White House.
“I’ll be at the conference all day, but that’s OK,” she said, with a hint of jealousy. “It was snowing in Denver, and we had to de-ice the plane last night. It’s 80 and sunny here, so this is beautiful.”
One of Dr. DeKorte’s colleagues at UCSD, Diana Childers, MD, was filling up the tank of knowledge in the “Documentation and Coding for Hospitalists” pre-course. Dr. Childers is one of the UCSD group’s billing experts, and Dr. DeKorte was looking forward to picking her brain.
“It’s still overwhelming to me,” Dr. DeKorte says. “I’m hoping she’ll pass along the nuggets, the gems of billing and coding.”
For an early-career hospitalist like Michele DeKorte, MD, HM10 offers a plethora of opportunities for practical knowledge and bushels of take-home points. “This is my first time, and I’m excited to be here,” Dr. DeKorte said moments after registering for HM10 at the Gaylord National Resort and Convention Center just outside Washington, D.C.
Dr. DeKorte, who has worked as a hospitalist at the University of California at San Diego since 2008, is one of a record 2,500 hospitalists registered for SHM’s annual meeting. She and hundreds of other hospitalists were taking part in Thursday’s lineup of pre-courses.
“I’m doing the procedures pre-course [Essential Procedures for the Hospitalist A Hands-on Experience] in the afternoon. I like procedures, so I think it will be fun,” she said, noting she will focus on the clinical track throughout the four-day event, which features more than 90 educational sessions. “It’s more interesting to me at this stage of the game. I want to have a better idea of how people are practicing HM around the country.”
Catherine Fitzgerald, DO, has worked as a hospitalist since 2005 and is attending her first annual meeting. For two years, she worked in an administrative role with CPMG at St. Joseph’s Memorial Hospital in Denver, and she plans to attend a smattering of practice-management sessions. “I also sit on our heart-failure committee at St. Joseph’s, so I have signed up for the session ‘How to Prevent Heart Failure Readmissions.’” she explained. “The meeting sessions are good reviews of things you already know, and interspersed in the discussions usually are these little pearls of new knowledge for your practice.”
In addition to aiming to improve her HM practice, Dr. Fitzgerald is excited to be in the nation’s capital with loved ones. Dr. Fitzgerald’s mother and 6-year-old son are scheduled to visit the White House.
“I’ll be at the conference all day, but that’s OK,” she said, with a hint of jealousy. “It was snowing in Denver, and we had to de-ice the plane last night. It’s 80 and sunny here, so this is beautiful.”
One of Dr. DeKorte’s colleagues at UCSD, Diana Childers, MD, was filling up the tank of knowledge in the “Documentation and Coding for Hospitalists” pre-course. Dr. Childers is one of the UCSD group’s billing experts, and Dr. DeKorte was looking forward to picking her brain.
“It’s still overwhelming to me,” Dr. DeKorte says. “I’m hoping she’ll pass along the nuggets, the gems of billing and coding.”
For an early-career hospitalist like Michele DeKorte, MD, HM10 offers a plethora of opportunities for practical knowledge and bushels of take-home points. “This is my first time, and I’m excited to be here,” Dr. DeKorte said moments after registering for HM10 at the Gaylord National Resort and Convention Center just outside Washington, D.C.
Dr. DeKorte, who has worked as a hospitalist at the University of California at San Diego since 2008, is one of a record 2,500 hospitalists registered for SHM’s annual meeting. She and hundreds of other hospitalists were taking part in Thursday’s lineup of pre-courses.
“I’m doing the procedures pre-course [Essential Procedures for the Hospitalist A Hands-on Experience] in the afternoon. I like procedures, so I think it will be fun,” she said, noting she will focus on the clinical track throughout the four-day event, which features more than 90 educational sessions. “It’s more interesting to me at this stage of the game. I want to have a better idea of how people are practicing HM around the country.”
Catherine Fitzgerald, DO, has worked as a hospitalist since 2005 and is attending her first annual meeting. For two years, she worked in an administrative role with CPMG at St. Joseph’s Memorial Hospital in Denver, and she plans to attend a smattering of practice-management sessions. “I also sit on our heart-failure committee at St. Joseph’s, so I have signed up for the session ‘How to Prevent Heart Failure Readmissions.’” she explained. “The meeting sessions are good reviews of things you already know, and interspersed in the discussions usually are these little pearls of new knowledge for your practice.”
In addition to aiming to improve her HM practice, Dr. Fitzgerald is excited to be in the nation’s capital with loved ones. Dr. Fitzgerald’s mother and 6-year-old son are scheduled to visit the White House.
“I’ll be at the conference all day, but that’s OK,” she said, with a hint of jealousy. “It was snowing in Denver, and we had to de-ice the plane last night. It’s 80 and sunny here, so this is beautiful.”
One of Dr. DeKorte’s colleagues at UCSD, Diana Childers, MD, was filling up the tank of knowledge in the “Documentation and Coding for Hospitalists” pre-course. Dr. Childers is one of the UCSD group’s billing experts, and Dr. DeKorte was looking forward to picking her brain.
“It’s still overwhelming to me,” Dr. DeKorte says. “I’m hoping she’ll pass along the nuggets, the gems of billing and coding.”
Hospitalists in Haiti
Hours after the devastating earthquake that shook the Haitian capital of Port-au-Prince, University of Miami Miller School of Medicine physicians, nurses, and administrators were drawing up plans to aid in the relief effort. One day after the quake, a tent hospital was erected at the airport, and dozens of providers were on the ground caring for the wounded, orphaned, and visibly shaken.
Hospitalists Amir Jaffer, MD, FHM, and Lisa Luly-Rivera, MD (photo, at right), recently returned from a five-day medical relief mission. They worked with surgeons and coordinated with nursing staff to ensure patients were properly hydrated and had the right pain medications. The staff also managed patients’ medical conditions and nutrition. Dr. Jaffer, an associate professor and the division chief of hospital medicine at the Miller School of Medicine, oversaw the transfer of 138 patients from a makeshift hospital to the new tent hospital, which opened Jan. 20 and offers spacious wards, a pathology lab, and two operating rooms.
“Most of the patients had a fracture, amputation, infected wound, or a spinal cord injury,” Dr. Jaffer says. “The conditions were dire when we landed. The role of the hospitalists was managing care. We also were involved in triaging patients who were being transferred.”
On Jan. 22, nearly 10 days after the quake, the university opened an imaging center radiology lab. “Some of the patients were splinted and needed X-ray,” Dr. Jaffer says, adding that more than 100 films were completed the first day. “Some patients were being brought in to us a week later who had fractures that had not been cared for.”
One of the poorest countries in the world, Haiti’s lack of infrastructure is wreaking havoc on rescue and relief efforts. The people are afraid to return to their homes, “and they have no place to go,” Dr. Jaffer says.
The 25 hospitalists in the HM group at the University of Miami Miller School of Medicine are planning five-day rotations to Haiti. The hospital needs translators, nurses, and internal-medicine specialists to cover the shifts of providers traveling to Haiti. If you’re interested in helping out, send an e-mail to the university. If you’d like to assist relief efforts in Haiti, make a donation to the American Red Cross.
Hours after the devastating earthquake that shook the Haitian capital of Port-au-Prince, University of Miami Miller School of Medicine physicians, nurses, and administrators were drawing up plans to aid in the relief effort. One day after the quake, a tent hospital was erected at the airport, and dozens of providers were on the ground caring for the wounded, orphaned, and visibly shaken.
Hospitalists Amir Jaffer, MD, FHM, and Lisa Luly-Rivera, MD (photo, at right), recently returned from a five-day medical relief mission. They worked with surgeons and coordinated with nursing staff to ensure patients were properly hydrated and had the right pain medications. The staff also managed patients’ medical conditions and nutrition. Dr. Jaffer, an associate professor and the division chief of hospital medicine at the Miller School of Medicine, oversaw the transfer of 138 patients from a makeshift hospital to the new tent hospital, which opened Jan. 20 and offers spacious wards, a pathology lab, and two operating rooms.
“Most of the patients had a fracture, amputation, infected wound, or a spinal cord injury,” Dr. Jaffer says. “The conditions were dire when we landed. The role of the hospitalists was managing care. We also were involved in triaging patients who were being transferred.”
On Jan. 22, nearly 10 days after the quake, the university opened an imaging center radiology lab. “Some of the patients were splinted and needed X-ray,” Dr. Jaffer says, adding that more than 100 films were completed the first day. “Some patients were being brought in to us a week later who had fractures that had not been cared for.”
One of the poorest countries in the world, Haiti’s lack of infrastructure is wreaking havoc on rescue and relief efforts. The people are afraid to return to their homes, “and they have no place to go,” Dr. Jaffer says.
The 25 hospitalists in the HM group at the University of Miami Miller School of Medicine are planning five-day rotations to Haiti. The hospital needs translators, nurses, and internal-medicine specialists to cover the shifts of providers traveling to Haiti. If you’re interested in helping out, send an e-mail to the university. If you’d like to assist relief efforts in Haiti, make a donation to the American Red Cross.
Hours after the devastating earthquake that shook the Haitian capital of Port-au-Prince, University of Miami Miller School of Medicine physicians, nurses, and administrators were drawing up plans to aid in the relief effort. One day after the quake, a tent hospital was erected at the airport, and dozens of providers were on the ground caring for the wounded, orphaned, and visibly shaken.
Hospitalists Amir Jaffer, MD, FHM, and Lisa Luly-Rivera, MD (photo, at right), recently returned from a five-day medical relief mission. They worked with surgeons and coordinated with nursing staff to ensure patients were properly hydrated and had the right pain medications. The staff also managed patients’ medical conditions and nutrition. Dr. Jaffer, an associate professor and the division chief of hospital medicine at the Miller School of Medicine, oversaw the transfer of 138 patients from a makeshift hospital to the new tent hospital, which opened Jan. 20 and offers spacious wards, a pathology lab, and two operating rooms.
“Most of the patients had a fracture, amputation, infected wound, or a spinal cord injury,” Dr. Jaffer says. “The conditions were dire when we landed. The role of the hospitalists was managing care. We also were involved in triaging patients who were being transferred.”
On Jan. 22, nearly 10 days after the quake, the university opened an imaging center radiology lab. “Some of the patients were splinted and needed X-ray,” Dr. Jaffer says, adding that more than 100 films were completed the first day. “Some patients were being brought in to us a week later who had fractures that had not been cared for.”
One of the poorest countries in the world, Haiti’s lack of infrastructure is wreaking havoc on rescue and relief efforts. The people are afraid to return to their homes, “and they have no place to go,” Dr. Jaffer says.
The 25 hospitalists in the HM group at the University of Miami Miller School of Medicine are planning five-day rotations to Haiti. The hospital needs translators, nurses, and internal-medicine specialists to cover the shifts of providers traveling to Haiti. If you’re interested in helping out, send an e-mail to the university. If you’d like to assist relief efforts in Haiti, make a donation to the American Red Cross.
HM Growth: Phase 2

The growth of our medical specialty is old news. Yes, we now number about 30,000; yes, we now manage the medical care of 50% of hospitalized Medicare patients; yes, hospitalists are in two-thirds of U.S. hospitals. I could go on and on. But recently, I have observed a different type of growth altogether. It is the growth of stability.
In the recent history of HM, the focus was on the increasing number of hospitals that had hospitalists, the growth of SHM’s membership, the growth of our annual meeting, and the ever-increasing number of doctors who, at least when surveyed, called themselves hospitalists. It all looked so impressive.
Many of you know, however, that when you lifted up the hood of our field, it was not always as it seemed. HM actually was a bit unstable. Some doctors who called themselves hospitalists were, in reality, biding time until they moved on to a “real job” or went off to do a fellowship. Multiple groups competed for patients within any given hospital, and also competed for doctors. There were numerous jobs available for any given hospitalist, and, as a result, some groups had substantial turnover despite growth in numbers. In these programs, the group photo from one year to the next had an entirely new set of faces.
Instability did not just affect rank-and-file hospitalists; it also existed within programmatic leadership and entire programs. Annually in many hospitals, the hospitalists had to convince administration that the hospital needed hospitalists and that they were worthy of support. Unfortunately, it was not always successful, so some programs vanished.
Five years ago in Michigan, we were working to create a multihospital safety consortium. We had several participating institutions, all with hospitalist programs. One day, my secretary complained that every time she sent an e-mail to the consortium listserv, a handful would bounce back and indicate a handful of e-mail addresses no longer were in service, or note that an individual had “left the program.” Some of them were HM program directors. Follow-up calls showed that the program had a new director or had folded. In some cases, however, they were just too busy figuring out how to survive instead of focus on safety issues.
Fortunately, that all appears to be changing.
From Unknown to Accepted to Counted On
I have seen the change in my own institution. We, of course, continue to negotiate with hospital administration, but it is no longer about whether we should continue the program or not. Negotiations now center on line items in the budget, how much space we need, where we anticipate future growth, and what quality and safety initiatives we’re working on.
I like to think that the HM program is important infrastructure. Just as you can’t imagine a hospital without an ED or an ICU, the same holds true for the HM program.
Perhaps an even better analogy could be found in technologic innovation. Back when Al Gore invented the Internet, having an Internet connection at home was viewed as a luxury. Now, it nearly is a necessity. Just like HM programs! (OK, maybe that was a stretch.)
There also is stability within the faculty ranks. Many of our faculty have been here for years and plan to stay. Turnover has decreased dramatically. This is not unique to our program, but anecdotally is happening everywhere. In fact, we are in the process of launching additional multihospital HM-based safety projects and collaboratives. And when I reach out to programs to ask them to participate, the directors of these programs are the same ones when I last checked. If they have moved on, it has been to assume a local leadership role. The group photos also show all the same old faces, plus a few new ones. There really has been some stabilization in the field.
New Paradigm Here to Stay
The factors behind this newfound stability are numerous. Among them is the recognized importance of a well-managed HM program. In many institutions, the alternatives to hospitalists (primary-care physicians, surgeons managing all post-operative care, specialists admitting their own patients, etc.) have left the building. There is no going back, and there is no “plan B” if HM programs fold.
The recognition by prospective hospitalists—residents and students—that HM is a viable career path has increased interest in the field, and, in turn, has given many programs more choices among qualified applicants. Hospitalists currently employed in a reasonably functioning program are less likely to jump ship every year looking for something slightly better. And I expect the current economic climate has been a factor as well. As hospitals see operating margins erode, plans for infrastructure growth are delayed, funding for new programs shrinks, and hospitalist groups are asked to do more with less. In other words, they are not hiring as many new hospitalists.
In some sense, the perceived slowing in the growth of hospitalists might be concerning. I see it a different way. Slowing growth in overall numbers allows programs and the field to stabilize a bit, and this growth in stability creates enormous opportunity. Programs formerly struggling to survive can begin to innovate. We’ve seen that in Michigan, as the interest among hospitalist programs that want to participate in QI collaborations has grown. And when we hear what some programs are working on, it’s an impressive list of high-impact projects.
Hospitalists are taking ownership of care transitions, prevention of hospital-acquired complications, and disease-based QI initiatives centered on patients with heart failure, COPD, and diabetes.
Nationally, we have seen hospitalist programs coming together to successfully compete for federal research grants or foundation support targeting important national healthcare priorities. If the current healthcare reform legislation passes, it will better position HM to lead the transformation of healthcare in U.S. hospitals.
My big hope is that 10 to 20 years from now, HM is better known for its second phase of growth. Right now, we are more famous for our rapid growth and, to some extent, our impact on efficiency of care. Efficiency clearly is important; dollars saved from waste can be better put to use improving quality. But I want the field to be judged by our ability to innovate, improve the quality of hospital-care delivery, and to generate new knowledge that advances the care of all patients. Those accomplishments will have a more lasting impact on healthcare.
The stabilization of HM is making all of this possible. Our population expects and deserves great things from the nation’s fastest-growing “specialty,” and I am optimistic we will not let them down. TH
Dr. Flanders is president of SHM.
The growth of our medical specialty is old news. Yes, we now number about 30,000; yes, we now manage the medical care of 50% of hospitalized Medicare patients; yes, hospitalists are in two-thirds of U.S. hospitals. I could go on and on. But recently, I have observed a different type of growth altogether. It is the growth of stability.
In the recent history of HM, the focus was on the increasing number of hospitals that had hospitalists, the growth of SHM’s membership, the growth of our annual meeting, and the ever-increasing number of doctors who, at least when surveyed, called themselves hospitalists. It all looked so impressive.
Many of you know, however, that when you lifted up the hood of our field, it was not always as it seemed. HM actually was a bit unstable. Some doctors who called themselves hospitalists were, in reality, biding time until they moved on to a “real job” or went off to do a fellowship. Multiple groups competed for patients within any given hospital, and also competed for doctors. There were numerous jobs available for any given hospitalist, and, as a result, some groups had substantial turnover despite growth in numbers. In these programs, the group photo from one year to the next had an entirely new set of faces.
Instability did not just affect rank-and-file hospitalists; it also existed within programmatic leadership and entire programs. Annually in many hospitals, the hospitalists had to convince administration that the hospital needed hospitalists and that they were worthy of support. Unfortunately, it was not always successful, so some programs vanished.
Five years ago in Michigan, we were working to create a multihospital safety consortium. We had several participating institutions, all with hospitalist programs. One day, my secretary complained that every time she sent an e-mail to the consortium listserv, a handful would bounce back and indicate a handful of e-mail addresses no longer were in service, or note that an individual had “left the program.” Some of them were HM program directors. Follow-up calls showed that the program had a new director or had folded. In some cases, however, they were just too busy figuring out how to survive instead of focus on safety issues.
Fortunately, that all appears to be changing.
From Unknown to Accepted to Counted On
I have seen the change in my own institution. We, of course, continue to negotiate with hospital administration, but it is no longer about whether we should continue the program or not. Negotiations now center on line items in the budget, how much space we need, where we anticipate future growth, and what quality and safety initiatives we’re working on.
I like to think that the HM program is important infrastructure. Just as you can’t imagine a hospital without an ED or an ICU, the same holds true for the HM program.
Perhaps an even better analogy could be found in technologic innovation. Back when Al Gore invented the Internet, having an Internet connection at home was viewed as a luxury. Now, it nearly is a necessity. Just like HM programs! (OK, maybe that was a stretch.)
There also is stability within the faculty ranks. Many of our faculty have been here for years and plan to stay. Turnover has decreased dramatically. This is not unique to our program, but anecdotally is happening everywhere. In fact, we are in the process of launching additional multihospital HM-based safety projects and collaboratives. And when I reach out to programs to ask them to participate, the directors of these programs are the same ones when I last checked. If they have moved on, it has been to assume a local leadership role. The group photos also show all the same old faces, plus a few new ones. There really has been some stabilization in the field.
New Paradigm Here to Stay
The factors behind this newfound stability are numerous. Among them is the recognized importance of a well-managed HM program. In many institutions, the alternatives to hospitalists (primary-care physicians, surgeons managing all post-operative care, specialists admitting their own patients, etc.) have left the building. There is no going back, and there is no “plan B” if HM programs fold.
The recognition by prospective hospitalists—residents and students—that HM is a viable career path has increased interest in the field, and, in turn, has given many programs more choices among qualified applicants. Hospitalists currently employed in a reasonably functioning program are less likely to jump ship every year looking for something slightly better. And I expect the current economic climate has been a factor as well. As hospitals see operating margins erode, plans for infrastructure growth are delayed, funding for new programs shrinks, and hospitalist groups are asked to do more with less. In other words, they are not hiring as many new hospitalists.
In some sense, the perceived slowing in the growth of hospitalists might be concerning. I see it a different way. Slowing growth in overall numbers allows programs and the field to stabilize a bit, and this growth in stability creates enormous opportunity. Programs formerly struggling to survive can begin to innovate. We’ve seen that in Michigan, as the interest among hospitalist programs that want to participate in QI collaborations has grown. And when we hear what some programs are working on, it’s an impressive list of high-impact projects.
Hospitalists are taking ownership of care transitions, prevention of hospital-acquired complications, and disease-based QI initiatives centered on patients with heart failure, COPD, and diabetes.
Nationally, we have seen hospitalist programs coming together to successfully compete for federal research grants or foundation support targeting important national healthcare priorities. If the current healthcare reform legislation passes, it will better position HM to lead the transformation of healthcare in U.S. hospitals.
My big hope is that 10 to 20 years from now, HM is better known for its second phase of growth. Right now, we are more famous for our rapid growth and, to some extent, our impact on efficiency of care. Efficiency clearly is important; dollars saved from waste can be better put to use improving quality. But I want the field to be judged by our ability to innovate, improve the quality of hospital-care delivery, and to generate new knowledge that advances the care of all patients. Those accomplishments will have a more lasting impact on healthcare.
The stabilization of HM is making all of this possible. Our population expects and deserves great things from the nation’s fastest-growing “specialty,” and I am optimistic we will not let them down. TH
Dr. Flanders is president of SHM.
The growth of our medical specialty is old news. Yes, we now number about 30,000; yes, we now manage the medical care of 50% of hospitalized Medicare patients; yes, hospitalists are in two-thirds of U.S. hospitals. I could go on and on. But recently, I have observed a different type of growth altogether. It is the growth of stability.
In the recent history of HM, the focus was on the increasing number of hospitals that had hospitalists, the growth of SHM’s membership, the growth of our annual meeting, and the ever-increasing number of doctors who, at least when surveyed, called themselves hospitalists. It all looked so impressive.
Many of you know, however, that when you lifted up the hood of our field, it was not always as it seemed. HM actually was a bit unstable. Some doctors who called themselves hospitalists were, in reality, biding time until they moved on to a “real job” or went off to do a fellowship. Multiple groups competed for patients within any given hospital, and also competed for doctors. There were numerous jobs available for any given hospitalist, and, as a result, some groups had substantial turnover despite growth in numbers. In these programs, the group photo from one year to the next had an entirely new set of faces.
Instability did not just affect rank-and-file hospitalists; it also existed within programmatic leadership and entire programs. Annually in many hospitals, the hospitalists had to convince administration that the hospital needed hospitalists and that they were worthy of support. Unfortunately, it was not always successful, so some programs vanished.
Five years ago in Michigan, we were working to create a multihospital safety consortium. We had several participating institutions, all with hospitalist programs. One day, my secretary complained that every time she sent an e-mail to the consortium listserv, a handful would bounce back and indicate a handful of e-mail addresses no longer were in service, or note that an individual had “left the program.” Some of them were HM program directors. Follow-up calls showed that the program had a new director or had folded. In some cases, however, they were just too busy figuring out how to survive instead of focus on safety issues.
Fortunately, that all appears to be changing.
From Unknown to Accepted to Counted On
I have seen the change in my own institution. We, of course, continue to negotiate with hospital administration, but it is no longer about whether we should continue the program or not. Negotiations now center on line items in the budget, how much space we need, where we anticipate future growth, and what quality and safety initiatives we’re working on.
I like to think that the HM program is important infrastructure. Just as you can’t imagine a hospital without an ED or an ICU, the same holds true for the HM program.
Perhaps an even better analogy could be found in technologic innovation. Back when Al Gore invented the Internet, having an Internet connection at home was viewed as a luxury. Now, it nearly is a necessity. Just like HM programs! (OK, maybe that was a stretch.)
There also is stability within the faculty ranks. Many of our faculty have been here for years and plan to stay. Turnover has decreased dramatically. This is not unique to our program, but anecdotally is happening everywhere. In fact, we are in the process of launching additional multihospital HM-based safety projects and collaboratives. And when I reach out to programs to ask them to participate, the directors of these programs are the same ones when I last checked. If they have moved on, it has been to assume a local leadership role. The group photos also show all the same old faces, plus a few new ones. There really has been some stabilization in the field.
New Paradigm Here to Stay
The factors behind this newfound stability are numerous. Among them is the recognized importance of a well-managed HM program. In many institutions, the alternatives to hospitalists (primary-care physicians, surgeons managing all post-operative care, specialists admitting their own patients, etc.) have left the building. There is no going back, and there is no “plan B” if HM programs fold.
The recognition by prospective hospitalists—residents and students—that HM is a viable career path has increased interest in the field, and, in turn, has given many programs more choices among qualified applicants. Hospitalists currently employed in a reasonably functioning program are less likely to jump ship every year looking for something slightly better. And I expect the current economic climate has been a factor as well. As hospitals see operating margins erode, plans for infrastructure growth are delayed, funding for new programs shrinks, and hospitalist groups are asked to do more with less. In other words, they are not hiring as many new hospitalists.
In some sense, the perceived slowing in the growth of hospitalists might be concerning. I see it a different way. Slowing growth in overall numbers allows programs and the field to stabilize a bit, and this growth in stability creates enormous opportunity. Programs formerly struggling to survive can begin to innovate. We’ve seen that in Michigan, as the interest among hospitalist programs that want to participate in QI collaborations has grown. And when we hear what some programs are working on, it’s an impressive list of high-impact projects.
Hospitalists are taking ownership of care transitions, prevention of hospital-acquired complications, and disease-based QI initiatives centered on patients with heart failure, COPD, and diabetes.
Nationally, we have seen hospitalist programs coming together to successfully compete for federal research grants or foundation support targeting important national healthcare priorities. If the current healthcare reform legislation passes, it will better position HM to lead the transformation of healthcare in U.S. hospitals.
My big hope is that 10 to 20 years from now, HM is better known for its second phase of growth. Right now, we are more famous for our rapid growth and, to some extent, our impact on efficiency of care. Efficiency clearly is important; dollars saved from waste can be better put to use improving quality. But I want the field to be judged by our ability to innovate, improve the quality of hospital-care delivery, and to generate new knowledge that advances the care of all patients. Those accomplishments will have a more lasting impact on healthcare.
The stabilization of HM is making all of this possible. Our population expects and deserves great things from the nation’s fastest-growing “specialty,” and I am optimistic we will not let them down. TH
Dr. Flanders is president of SHM.
Academics Energized
Frank Marquez, MD, wasn't told he was going to the Academic Hospitalist Academy (AHA) until a couple of days before the start of the four-day training program in Atlanta. Short notice aside, Dr. Marquez was elated he was able to attend.
"There are a lot of practical tips. For me, the biggest thing is the academy has shown me that I have to stop being passive and start being proactive. I need to take an active role, serve on committees," says Dr. Marquez, a third-year academic hospitalist at St. Joseph's Hospital and Medical Center in Phoenix. "I think that's going to help my career."
Dr. Marquez, who leads a five-person team of residents, interns, and medical students, was one of nearly 80 early-career physicians—the average attendee had two years of HM experience—who attended AHA. The inaugural event was co-sponsored by SHM, the Society of General Internal Medicine and the Associate Chiefs of General Internal Medicine. The program featured top-flight HM faculty, but Dr. Marquez especially enjoyed the emphasis on small-group workshops and interactive teaching.
"When we first took our jobs as hospitalists, no one took the time to explain to us how to be an effective leader, mentor people, implement change," he says. "Here you have an opportunity to learn that and to participate. It’s not a lecture; it’s not intimidating. You can speak up."
Frank Marquez, MD, wasn't told he was going to the Academic Hospitalist Academy (AHA) until a couple of days before the start of the four-day training program in Atlanta. Short notice aside, Dr. Marquez was elated he was able to attend.
"There are a lot of practical tips. For me, the biggest thing is the academy has shown me that I have to stop being passive and start being proactive. I need to take an active role, serve on committees," says Dr. Marquez, a third-year academic hospitalist at St. Joseph's Hospital and Medical Center in Phoenix. "I think that's going to help my career."
Dr. Marquez, who leads a five-person team of residents, interns, and medical students, was one of nearly 80 early-career physicians—the average attendee had two years of HM experience—who attended AHA. The inaugural event was co-sponsored by SHM, the Society of General Internal Medicine and the Associate Chiefs of General Internal Medicine. The program featured top-flight HM faculty, but Dr. Marquez especially enjoyed the emphasis on small-group workshops and interactive teaching.
"When we first took our jobs as hospitalists, no one took the time to explain to us how to be an effective leader, mentor people, implement change," he says. "Here you have an opportunity to learn that and to participate. It’s not a lecture; it’s not intimidating. You can speak up."
Frank Marquez, MD, wasn't told he was going to the Academic Hospitalist Academy (AHA) until a couple of days before the start of the four-day training program in Atlanta. Short notice aside, Dr. Marquez was elated he was able to attend.
"There are a lot of practical tips. For me, the biggest thing is the academy has shown me that I have to stop being passive and start being proactive. I need to take an active role, serve on committees," says Dr. Marquez, a third-year academic hospitalist at St. Joseph's Hospital and Medical Center in Phoenix. "I think that's going to help my career."
Dr. Marquez, who leads a five-person team of residents, interns, and medical students, was one of nearly 80 early-career physicians—the average attendee had two years of HM experience—who attended AHA. The inaugural event was co-sponsored by SHM, the Society of General Internal Medicine and the Associate Chiefs of General Internal Medicine. The program featured top-flight HM faculty, but Dr. Marquez especially enjoyed the emphasis on small-group workshops and interactive teaching.
"When we first took our jobs as hospitalists, no one took the time to explain to us how to be an effective leader, mentor people, implement change," he says. "Here you have an opportunity to learn that and to participate. It’s not a lecture; it’s not intimidating. You can speak up."
A-Plus Achievement
Timing is everything. Christopher Columbus, Abraham Lincoln, Harry Truman … each benefited from perfect timing and, in turn, helped change the course of history.
HM has had great timing, too. With numbers now estimated at more than 30,000 hospitalists nationwide, HM is systematically changing the way patients are cared for in the hospital. The maturation process is equally evident. In less than two decades, HM has organized annual meetings, developed educational programs, established a peer-reviewed journal, and published core competencies.
The next step in the evolutionary process: the Recognition of Focused Practice (RFP) in Hospital Medicine through the American Board of Internal Medicine’s (ABIM) maintenance of certification (MOC) program. Registration for the RFP in HM should be available by May 2010, with the first MOC in fall 2010.
“The timing is perfect. It’s appropriate,” says Robert Wachter, MD, FHM, chief of the hospital medicine
division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco, a former SHM president, and author of the blog Wachter’s World. “We knew we needed to ripen and mature. It’s like watching your child growing up: their first steps, first day of school, graduating high school. This has a lot of the same feeling. This is one more statement that the field is real, here to stay, and vitally important to medicine.”
The new pathway to board recertification is as meaningful to HM’s founding fathers as it will be to the next generation of hospitalists. It represents validation to physicians who have chosen a career in HM, and it offers early-career physicians a specialized path to recertification. Moreover, hospitalists agree the RFP in HM provides accountability to the profession and patients.
“Hospitalists must be able to exhibit clinical competence in the areas of patient safety, quality, and clinical care transitions,” says Jeff Wiese, MD, FACP, FHM, associate dean of Graduate Medical Education and professor of medicine at Tulane University in New Orleans, SHM president-elect, and chair of the ABIM Hospital Medicine Maintenance of Certification Question Writing Committee. “Everything is driving at those issues. Individuals who go through the four parts of this certification will be able to say to their patients, with confidence, that one, they are a competent internist knowledgeable in hospital-based care, and two, they are an expert in patient safety, quality, and transitions of care.”
ABIM, for its part, expects to learn from this “new paradigm,” says Eric Holmbloe, MD, ABIM’s senior vice president and chief medical officer.
“The major change is the ability to implement the concept of a focused practice. It’s the first time, and it does recognize that the world has changed,” Dr. Holmbloe says, noting his group is “working feverishly” to complete the examination and build the online infrastructure needed for testing. “For those individuals whose [certificates] expire in 2010 or 2011, this is a viable pathway for recertification.”
Satisfaction Guaranteed
Ask any long-in-the-tooth hospitalist what the RFP in HM means to them, and more often than not the answer centers on professional self-regulation and career validation. Few will argue the specialty has, at times, suffered from an identity crisis. Sans fellowships, specialized training, or a particular organ to hang their hat on, HM physicians have labored to carve their niche and gain a seat at the specialist’s table.
The RFP in HM, many hospitalists envision, solves a number of those acceptance-related issues (see “Certified Special,” p. 53). Most importantly, it identifies physicians who have chosen to make HM their career.
“Hospitalists have always struggled, especially in academic settings,” says Scott Flanders, MD, FHM, SHM president, associate professor and director of the hospitalist program at the University of Michigan Health System in Ann Arbor. “I think this is a major, major moment for the field. It validates the field, and the belief that HM is a positive [for medicine].”
The new designation likely has greater meaning to older HM physicians, those who remember the early days of society formation (i.e., the National Association of Inpatient Physicians) and annual meeting attendance in the hundreds, not thousands.
“With the older docs, validation is particularly meaningful,” says Dr. Wachter, who, along with Lee Goldman, MD, first coined the term “hospitalist” in a 1996 article in the New England Journal of Medicine.1 “Paradoxically, most of the older physicians don’t have to take this test.”
That might be true, but only a small percentage of the 30,000-plus hospitalists in the U.S. are grandfathered into time-unlimited IM certificates. ABIM began time-limited certificates in 1990. The average hospitalist is 40, according to SHM’s “2007-2008 Bi-Annual Survey on the State of the Hospital Medicine Movement.”
John Nelson, MD, doesn’t have to recertify, but the co-founder of SHM is planning to be among the first to take the test. “It’s the first way hospitalists will be able to show their competence,” says Dr. Nelson, FACP, FHM, past president of SHM, and a principal in the national practice management firm Nelson Flores Hospital Medicine Consultants. A regular contributor to The Hospitalist, Dr. Nelson says the RFP in HM “will help people take our field more seriously.”
Inclusive of IM
The RFP in HM pathway is not a way to distance hospitalists from their internal medicine (IM) training and certification. Nearly 85% of hospitalists are IM-trained, according to SHM’s 2007-2008 bi-annual survey, and clinical competence as an internist will be a requisite for recertification through the new ABIM test.
“HM is borne of internal medicine … and has evolved to something unique. Therefore, your credentials should reflect that uniqueness,” says Larry Wellikson, MD, FHM, CEO of SHM. “This [process] is going to make the whole maintenance of certification process more relevant to hospitalists. This is recognition that hospitalists should be accountable for learning new things after they complete their formal training—things not emphasized in training like patient safety, quality, and care transitions.”
The language used on ABIM’s Web site to announce the new testing program furthers the message: “ABIM is developing a program to assess, set standards for, and recognize the proficiency of general internists who focus their practice in the care of hospitalized patients. The board’s decision to advance this program is consistent with its primary role of certifying internal-medicine physicians who meet the profession’s standards for focused practice in internal medicine.”
In addition to quality, patient safety, and transitions, “accountability to the patient” is a popular catchphrase used by members of the committee dedicated to writing the new certification test. Licensure and certification provide public accountability to patients, colleagues, and stakeholders, says Dr. Wiese. What differentiates career hospitalists from those making a pit stop during an alternate career path is increased accessibility to patients, expertise in patient safety and quality initiatives, and knowledge of clinical care transitions, he explains.
“Everything is driving at those issues,” he says. “From the beginning, there has been no agenda to change residency training. Any information contrary is a complete myth. Principle No. 1 is that you have to be competent internist. This new [MOC process] is much closer to an MBA.”
How hospitalists who are recertifying through the RFP in HM will refer to themselves remains up for debate. Although some physicians might say they are “board-certified in hospital medicine,” Dr. Wachter hopes hospitalists will use the phrase “board-certified in internal medicine with a recognized focused practice in hospital medicine.” “I hope to think our physicians will still say ‘IM,’ ” he says. “The goal here is not to sever ties with IM. That is a concern.”
Dr. Wiese, who, along with Dr. Wachter and other members of the test-writing committee, was required to complete the IM maintenance of certification (MOC), envisions a four-part process (see “Board Certification, With a Healthy Dose of HM,” p. 31) that challenges hospitalists in the core competencies of hospital-based practice.
“The [IM] recertification was the one test in my career that made me a better physician. I think this HM examination is going to be the same way,” Dr. Wiese says. “I want hospitalists to say, ‘When I go back to take care of my patients, they’ll be better off for it.’ ”
Target Audience
Dr. Flanders has about 40 hospitalists in his HM group at the University of Michigan. Although he recertified in IM in 2006, he knows many of his hospitalists are itching to take ABIM’s new HM-focused test. “They will be thrilled. They have all said to me that we can’t get this done fast enough,” he says, noting three or four of his hospitalists probably will recertify through the new test in fall 2010. “Our field is young; I suspect there are a lot of hospitalists out there who are within the 10-year window for recertification. I plan to do it at my next MOC … and that date could be moved up the way things are going.”
Dr. Wachter agrees the RFP in HM is an “attractive” option to hospitalists, especially those whose recertification is looming in the next two or three years. This MOC, he explains, “offers a pathway that is more in sync with the medicine [they are practicing] day in and day out.”
ABIM plans to have comprehensive information about the process available on its Web site (www.abim.org) this month and online registration available in May 2010 (see “FAQs,” left). While the test-writing committee finishes its tasks, Dr. Holmbloe says, ABIM’s systems department is working to build the online infrastructure. The first RFP in HM tests should go live in fall 2010.
“For those individuals [whose certificates] expire in 2010 or 2011, this is a viable pathway for recertification. If HM is their passion, this is for them,” Dr. Holmbloe says. “The major change, from ABIM’s perspective, is the ability to implement the concept of a focused practice. It’s the first time, a new paradigm. This does recognize that the world has changed.”
Crash Course
Every physician, sometime in his or her career, has crammed for a test. ABIM, however, recommends physicians start this process two or three years before their certificate expires. That timetable might work for some hospitalists, not so much for others. In any event, Dr. Flanders says hospitalists can count on SHM to help them prepare for the HM-specific examination.
“SHM has to help develop the tools and resources hospitalists will need to successfully prepare for and pass this test,” he says. He expects educational resources and self-assessment modules will be available on SHM’s Web site (www.hospitalmedicine.org) and at HM10, April 8-11 in Washington, D.C.
Dr. Wellikson says MOC preparedness “should match [SHM’s] educational projects,” and his staff “will continue to develop” tools and resources to assist hospitalists. He also recognizes the moment: the notch on HM’s evolutionary timeline where a once-fledgling group of inpatient physicians helped chart a new course for American medicine.
“Obviously, 10 years ago was too early. Now there are 30,000 hospitalists. Many of them are making HM a career. It’s evolving as a discipline,” Dr. Wellikson says. “We’ve moved beyond the idea of HM to the reality of HM.” TH
Jason Carris is editor of The Hospitalist.
Reference
- Wachter RM, Goldman L. The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996;335(7):514-517.
Image Source: PORCOREX/ISTOCKPHOTO.COM
Timing is everything. Christopher Columbus, Abraham Lincoln, Harry Truman … each benefited from perfect timing and, in turn, helped change the course of history.
HM has had great timing, too. With numbers now estimated at more than 30,000 hospitalists nationwide, HM is systematically changing the way patients are cared for in the hospital. The maturation process is equally evident. In less than two decades, HM has organized annual meetings, developed educational programs, established a peer-reviewed journal, and published core competencies.
The next step in the evolutionary process: the Recognition of Focused Practice (RFP) in Hospital Medicine through the American Board of Internal Medicine’s (ABIM) maintenance of certification (MOC) program. Registration for the RFP in HM should be available by May 2010, with the first MOC in fall 2010.
“The timing is perfect. It’s appropriate,” says Robert Wachter, MD, FHM, chief of the hospital medicine
division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco, a former SHM president, and author of the blog Wachter’s World. “We knew we needed to ripen and mature. It’s like watching your child growing up: their first steps, first day of school, graduating high school. This has a lot of the same feeling. This is one more statement that the field is real, here to stay, and vitally important to medicine.”
The new pathway to board recertification is as meaningful to HM’s founding fathers as it will be to the next generation of hospitalists. It represents validation to physicians who have chosen a career in HM, and it offers early-career physicians a specialized path to recertification. Moreover, hospitalists agree the RFP in HM provides accountability to the profession and patients.
“Hospitalists must be able to exhibit clinical competence in the areas of patient safety, quality, and clinical care transitions,” says Jeff Wiese, MD, FACP, FHM, associate dean of Graduate Medical Education and professor of medicine at Tulane University in New Orleans, SHM president-elect, and chair of the ABIM Hospital Medicine Maintenance of Certification Question Writing Committee. “Everything is driving at those issues. Individuals who go through the four parts of this certification will be able to say to their patients, with confidence, that one, they are a competent internist knowledgeable in hospital-based care, and two, they are an expert in patient safety, quality, and transitions of care.”
ABIM, for its part, expects to learn from this “new paradigm,” says Eric Holmbloe, MD, ABIM’s senior vice president and chief medical officer.
“The major change is the ability to implement the concept of a focused practice. It’s the first time, and it does recognize that the world has changed,” Dr. Holmbloe says, noting his group is “working feverishly” to complete the examination and build the online infrastructure needed for testing. “For those individuals whose [certificates] expire in 2010 or 2011, this is a viable pathway for recertification.”
Satisfaction Guaranteed
Ask any long-in-the-tooth hospitalist what the RFP in HM means to them, and more often than not the answer centers on professional self-regulation and career validation. Few will argue the specialty has, at times, suffered from an identity crisis. Sans fellowships, specialized training, or a particular organ to hang their hat on, HM physicians have labored to carve their niche and gain a seat at the specialist’s table.
The RFP in HM, many hospitalists envision, solves a number of those acceptance-related issues (see “Certified Special,” p. 53). Most importantly, it identifies physicians who have chosen to make HM their career.
“Hospitalists have always struggled, especially in academic settings,” says Scott Flanders, MD, FHM, SHM president, associate professor and director of the hospitalist program at the University of Michigan Health System in Ann Arbor. “I think this is a major, major moment for the field. It validates the field, and the belief that HM is a positive [for medicine].”
The new designation likely has greater meaning to older HM physicians, those who remember the early days of society formation (i.e., the National Association of Inpatient Physicians) and annual meeting attendance in the hundreds, not thousands.
“With the older docs, validation is particularly meaningful,” says Dr. Wachter, who, along with Lee Goldman, MD, first coined the term “hospitalist” in a 1996 article in the New England Journal of Medicine.1 “Paradoxically, most of the older physicians don’t have to take this test.”
That might be true, but only a small percentage of the 30,000-plus hospitalists in the U.S. are grandfathered into time-unlimited IM certificates. ABIM began time-limited certificates in 1990. The average hospitalist is 40, according to SHM’s “2007-2008 Bi-Annual Survey on the State of the Hospital Medicine Movement.”
John Nelson, MD, doesn’t have to recertify, but the co-founder of SHM is planning to be among the first to take the test. “It’s the first way hospitalists will be able to show their competence,” says Dr. Nelson, FACP, FHM, past president of SHM, and a principal in the national practice management firm Nelson Flores Hospital Medicine Consultants. A regular contributor to The Hospitalist, Dr. Nelson says the RFP in HM “will help people take our field more seriously.”
Inclusive of IM
The RFP in HM pathway is not a way to distance hospitalists from their internal medicine (IM) training and certification. Nearly 85% of hospitalists are IM-trained, according to SHM’s 2007-2008 bi-annual survey, and clinical competence as an internist will be a requisite for recertification through the new ABIM test.
“HM is borne of internal medicine … and has evolved to something unique. Therefore, your credentials should reflect that uniqueness,” says Larry Wellikson, MD, FHM, CEO of SHM. “This [process] is going to make the whole maintenance of certification process more relevant to hospitalists. This is recognition that hospitalists should be accountable for learning new things after they complete their formal training—things not emphasized in training like patient safety, quality, and care transitions.”
The language used on ABIM’s Web site to announce the new testing program furthers the message: “ABIM is developing a program to assess, set standards for, and recognize the proficiency of general internists who focus their practice in the care of hospitalized patients. The board’s decision to advance this program is consistent with its primary role of certifying internal-medicine physicians who meet the profession’s standards for focused practice in internal medicine.”
In addition to quality, patient safety, and transitions, “accountability to the patient” is a popular catchphrase used by members of the committee dedicated to writing the new certification test. Licensure and certification provide public accountability to patients, colleagues, and stakeholders, says Dr. Wiese. What differentiates career hospitalists from those making a pit stop during an alternate career path is increased accessibility to patients, expertise in patient safety and quality initiatives, and knowledge of clinical care transitions, he explains.
“Everything is driving at those issues,” he says. “From the beginning, there has been no agenda to change residency training. Any information contrary is a complete myth. Principle No. 1 is that you have to be competent internist. This new [MOC process] is much closer to an MBA.”
How hospitalists who are recertifying through the RFP in HM will refer to themselves remains up for debate. Although some physicians might say they are “board-certified in hospital medicine,” Dr. Wachter hopes hospitalists will use the phrase “board-certified in internal medicine with a recognized focused practice in hospital medicine.” “I hope to think our physicians will still say ‘IM,’ ” he says. “The goal here is not to sever ties with IM. That is a concern.”
Dr. Wiese, who, along with Dr. Wachter and other members of the test-writing committee, was required to complete the IM maintenance of certification (MOC), envisions a four-part process (see “Board Certification, With a Healthy Dose of HM,” p. 31) that challenges hospitalists in the core competencies of hospital-based practice.
“The [IM] recertification was the one test in my career that made me a better physician. I think this HM examination is going to be the same way,” Dr. Wiese says. “I want hospitalists to say, ‘When I go back to take care of my patients, they’ll be better off for it.’ ”
Target Audience
Dr. Flanders has about 40 hospitalists in his HM group at the University of Michigan. Although he recertified in IM in 2006, he knows many of his hospitalists are itching to take ABIM’s new HM-focused test. “They will be thrilled. They have all said to me that we can’t get this done fast enough,” he says, noting three or four of his hospitalists probably will recertify through the new test in fall 2010. “Our field is young; I suspect there are a lot of hospitalists out there who are within the 10-year window for recertification. I plan to do it at my next MOC … and that date could be moved up the way things are going.”
Dr. Wachter agrees the RFP in HM is an “attractive” option to hospitalists, especially those whose recertification is looming in the next two or three years. This MOC, he explains, “offers a pathway that is more in sync with the medicine [they are practicing] day in and day out.”
ABIM plans to have comprehensive information about the process available on its Web site (www.abim.org) this month and online registration available in May 2010 (see “FAQs,” left). While the test-writing committee finishes its tasks, Dr. Holmbloe says, ABIM’s systems department is working to build the online infrastructure. The first RFP in HM tests should go live in fall 2010.
“For those individuals [whose certificates] expire in 2010 or 2011, this is a viable pathway for recertification. If HM is their passion, this is for them,” Dr. Holmbloe says. “The major change, from ABIM’s perspective, is the ability to implement the concept of a focused practice. It’s the first time, a new paradigm. This does recognize that the world has changed.”
Crash Course
Every physician, sometime in his or her career, has crammed for a test. ABIM, however, recommends physicians start this process two or three years before their certificate expires. That timetable might work for some hospitalists, not so much for others. In any event, Dr. Flanders says hospitalists can count on SHM to help them prepare for the HM-specific examination.
“SHM has to help develop the tools and resources hospitalists will need to successfully prepare for and pass this test,” he says. He expects educational resources and self-assessment modules will be available on SHM’s Web site (www.hospitalmedicine.org) and at HM10, April 8-11 in Washington, D.C.
Dr. Wellikson says MOC preparedness “should match [SHM’s] educational projects,” and his staff “will continue to develop” tools and resources to assist hospitalists. He also recognizes the moment: the notch on HM’s evolutionary timeline where a once-fledgling group of inpatient physicians helped chart a new course for American medicine.
“Obviously, 10 years ago was too early. Now there are 30,000 hospitalists. Many of them are making HM a career. It’s evolving as a discipline,” Dr. Wellikson says. “We’ve moved beyond the idea of HM to the reality of HM.” TH
Jason Carris is editor of The Hospitalist.
Reference
- Wachter RM, Goldman L. The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996;335(7):514-517.
Image Source: PORCOREX/ISTOCKPHOTO.COM
Timing is everything. Christopher Columbus, Abraham Lincoln, Harry Truman … each benefited from perfect timing and, in turn, helped change the course of history.
HM has had great timing, too. With numbers now estimated at more than 30,000 hospitalists nationwide, HM is systematically changing the way patients are cared for in the hospital. The maturation process is equally evident. In less than two decades, HM has organized annual meetings, developed educational programs, established a peer-reviewed journal, and published core competencies.
The next step in the evolutionary process: the Recognition of Focused Practice (RFP) in Hospital Medicine through the American Board of Internal Medicine’s (ABIM) maintenance of certification (MOC) program. Registration for the RFP in HM should be available by May 2010, with the first MOC in fall 2010.
“The timing is perfect. It’s appropriate,” says Robert Wachter, MD, FHM, chief of the hospital medicine
division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco, a former SHM president, and author of the blog Wachter’s World. “We knew we needed to ripen and mature. It’s like watching your child growing up: their first steps, first day of school, graduating high school. This has a lot of the same feeling. This is one more statement that the field is real, here to stay, and vitally important to medicine.”
The new pathway to board recertification is as meaningful to HM’s founding fathers as it will be to the next generation of hospitalists. It represents validation to physicians who have chosen a career in HM, and it offers early-career physicians a specialized path to recertification. Moreover, hospitalists agree the RFP in HM provides accountability to the profession and patients.
“Hospitalists must be able to exhibit clinical competence in the areas of patient safety, quality, and clinical care transitions,” says Jeff Wiese, MD, FACP, FHM, associate dean of Graduate Medical Education and professor of medicine at Tulane University in New Orleans, SHM president-elect, and chair of the ABIM Hospital Medicine Maintenance of Certification Question Writing Committee. “Everything is driving at those issues. Individuals who go through the four parts of this certification will be able to say to their patients, with confidence, that one, they are a competent internist knowledgeable in hospital-based care, and two, they are an expert in patient safety, quality, and transitions of care.”
ABIM, for its part, expects to learn from this “new paradigm,” says Eric Holmbloe, MD, ABIM’s senior vice president and chief medical officer.
“The major change is the ability to implement the concept of a focused practice. It’s the first time, and it does recognize that the world has changed,” Dr. Holmbloe says, noting his group is “working feverishly” to complete the examination and build the online infrastructure needed for testing. “For those individuals whose [certificates] expire in 2010 or 2011, this is a viable pathway for recertification.”
Satisfaction Guaranteed
Ask any long-in-the-tooth hospitalist what the RFP in HM means to them, and more often than not the answer centers on professional self-regulation and career validation. Few will argue the specialty has, at times, suffered from an identity crisis. Sans fellowships, specialized training, or a particular organ to hang their hat on, HM physicians have labored to carve their niche and gain a seat at the specialist’s table.
The RFP in HM, many hospitalists envision, solves a number of those acceptance-related issues (see “Certified Special,” p. 53). Most importantly, it identifies physicians who have chosen to make HM their career.
“Hospitalists have always struggled, especially in academic settings,” says Scott Flanders, MD, FHM, SHM president, associate professor and director of the hospitalist program at the University of Michigan Health System in Ann Arbor. “I think this is a major, major moment for the field. It validates the field, and the belief that HM is a positive [for medicine].”
The new designation likely has greater meaning to older HM physicians, those who remember the early days of society formation (i.e., the National Association of Inpatient Physicians) and annual meeting attendance in the hundreds, not thousands.
“With the older docs, validation is particularly meaningful,” says Dr. Wachter, who, along with Lee Goldman, MD, first coined the term “hospitalist” in a 1996 article in the New England Journal of Medicine.1 “Paradoxically, most of the older physicians don’t have to take this test.”
That might be true, but only a small percentage of the 30,000-plus hospitalists in the U.S. are grandfathered into time-unlimited IM certificates. ABIM began time-limited certificates in 1990. The average hospitalist is 40, according to SHM’s “2007-2008 Bi-Annual Survey on the State of the Hospital Medicine Movement.”
John Nelson, MD, doesn’t have to recertify, but the co-founder of SHM is planning to be among the first to take the test. “It’s the first way hospitalists will be able to show their competence,” says Dr. Nelson, FACP, FHM, past president of SHM, and a principal in the national practice management firm Nelson Flores Hospital Medicine Consultants. A regular contributor to The Hospitalist, Dr. Nelson says the RFP in HM “will help people take our field more seriously.”
Inclusive of IM
The RFP in HM pathway is not a way to distance hospitalists from their internal medicine (IM) training and certification. Nearly 85% of hospitalists are IM-trained, according to SHM’s 2007-2008 bi-annual survey, and clinical competence as an internist will be a requisite for recertification through the new ABIM test.
“HM is borne of internal medicine … and has evolved to something unique. Therefore, your credentials should reflect that uniqueness,” says Larry Wellikson, MD, FHM, CEO of SHM. “This [process] is going to make the whole maintenance of certification process more relevant to hospitalists. This is recognition that hospitalists should be accountable for learning new things after they complete their formal training—things not emphasized in training like patient safety, quality, and care transitions.”
The language used on ABIM’s Web site to announce the new testing program furthers the message: “ABIM is developing a program to assess, set standards for, and recognize the proficiency of general internists who focus their practice in the care of hospitalized patients. The board’s decision to advance this program is consistent with its primary role of certifying internal-medicine physicians who meet the profession’s standards for focused practice in internal medicine.”
In addition to quality, patient safety, and transitions, “accountability to the patient” is a popular catchphrase used by members of the committee dedicated to writing the new certification test. Licensure and certification provide public accountability to patients, colleagues, and stakeholders, says Dr. Wiese. What differentiates career hospitalists from those making a pit stop during an alternate career path is increased accessibility to patients, expertise in patient safety and quality initiatives, and knowledge of clinical care transitions, he explains.
“Everything is driving at those issues,” he says. “From the beginning, there has been no agenda to change residency training. Any information contrary is a complete myth. Principle No. 1 is that you have to be competent internist. This new [MOC process] is much closer to an MBA.”
How hospitalists who are recertifying through the RFP in HM will refer to themselves remains up for debate. Although some physicians might say they are “board-certified in hospital medicine,” Dr. Wachter hopes hospitalists will use the phrase “board-certified in internal medicine with a recognized focused practice in hospital medicine.” “I hope to think our physicians will still say ‘IM,’ ” he says. “The goal here is not to sever ties with IM. That is a concern.”
Dr. Wiese, who, along with Dr. Wachter and other members of the test-writing committee, was required to complete the IM maintenance of certification (MOC), envisions a four-part process (see “Board Certification, With a Healthy Dose of HM,” p. 31) that challenges hospitalists in the core competencies of hospital-based practice.
“The [IM] recertification was the one test in my career that made me a better physician. I think this HM examination is going to be the same way,” Dr. Wiese says. “I want hospitalists to say, ‘When I go back to take care of my patients, they’ll be better off for it.’ ”
Target Audience
Dr. Flanders has about 40 hospitalists in his HM group at the University of Michigan. Although he recertified in IM in 2006, he knows many of his hospitalists are itching to take ABIM’s new HM-focused test. “They will be thrilled. They have all said to me that we can’t get this done fast enough,” he says, noting three or four of his hospitalists probably will recertify through the new test in fall 2010. “Our field is young; I suspect there are a lot of hospitalists out there who are within the 10-year window for recertification. I plan to do it at my next MOC … and that date could be moved up the way things are going.”
Dr. Wachter agrees the RFP in HM is an “attractive” option to hospitalists, especially those whose recertification is looming in the next two or three years. This MOC, he explains, “offers a pathway that is more in sync with the medicine [they are practicing] day in and day out.”
ABIM plans to have comprehensive information about the process available on its Web site (www.abim.org) this month and online registration available in May 2010 (see “FAQs,” left). While the test-writing committee finishes its tasks, Dr. Holmbloe says, ABIM’s systems department is working to build the online infrastructure. The first RFP in HM tests should go live in fall 2010.
“For those individuals [whose certificates] expire in 2010 or 2011, this is a viable pathway for recertification. If HM is their passion, this is for them,” Dr. Holmbloe says. “The major change, from ABIM’s perspective, is the ability to implement the concept of a focused practice. It’s the first time, a new paradigm. This does recognize that the world has changed.”
Crash Course
Every physician, sometime in his or her career, has crammed for a test. ABIM, however, recommends physicians start this process two or three years before their certificate expires. That timetable might work for some hospitalists, not so much for others. In any event, Dr. Flanders says hospitalists can count on SHM to help them prepare for the HM-specific examination.
“SHM has to help develop the tools and resources hospitalists will need to successfully prepare for and pass this test,” he says. He expects educational resources and self-assessment modules will be available on SHM’s Web site (www.hospitalmedicine.org) and at HM10, April 8-11 in Washington, D.C.
Dr. Wellikson says MOC preparedness “should match [SHM’s] educational projects,” and his staff “will continue to develop” tools and resources to assist hospitalists. He also recognizes the moment: the notch on HM’s evolutionary timeline where a once-fledgling group of inpatient physicians helped chart a new course for American medicine.
“Obviously, 10 years ago was too early. Now there are 30,000 hospitalists. Many of them are making HM a career. It’s evolving as a discipline,” Dr. Wellikson says. “We’ve moved beyond the idea of HM to the reality of HM.” TH
Jason Carris is editor of The Hospitalist.
Reference
- Wachter RM, Goldman L. The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996;335(7):514-517.
Image Source: PORCOREX/ISTOCKPHOTO.COM
HM's Watershed Moment
John Nelson, MD, FACP, FHM, hasn't taken a medical test in more than 20 years. So when news began to spread last week that the American Board of Internal Medicine (ABIM) soon will be offering a Recognition of Focused Practice (RFP) in Hospital Medicine certification, he started to get a little nervous.
"I will lose sleep the week before I take this test," says Dr. Nelson, co-founder and past president of SHM, and a principal in the practice management firm Nelson Flores Hospital Medicine Consultants. "This exam will help identify those who see this as a career. … Boy, there is nothing like a test to demonstrate professional centeredness."
The exam, likely to be available in the fall of 2010, will identify physicians who have "maintained their internal medicine certification focused in hospital medicine," according to the ABIM Web site.
"For those individuals [whose certificate] will be expiring in 2010 or 2011, this is a viable pathway for re-certification," says Eric Holmbloe, MD, senior vice president and chief medical officer at ABIM. "Interested diplomats should be able to begin the application process in early 2010. We are feverishly working to complete the test and build the technology infrastructure. We should have more information available in about six weeks."
HM pioneers like Dr. Nelson consider the RFP designation a validation of decades-long efforts to carve a niche in medicine. The test will symbolize dedication to the specialty and provide HM physicians with professional self-regulation.
Scott Flanders, MD, FHM, president of SHM, terms the announcement a "watershed moment" for the field.
"I think this is a major, major moment for HM," says Dr. Flanders, who practices at the University of Michigan Medical Center in Ann Arbor. "We've been looking at this for a long time. This validates the field, and the belief that HM is a positive [for the field of medicine]."
Dr. Nelson couldn't agree more. "This test is the first way hospitalists will be able to show their competence," he says. "I think it's a great opportunity. This will help people take our field more seriously."
John Nelson, MD, FACP, FHM, hasn't taken a medical test in more than 20 years. So when news began to spread last week that the American Board of Internal Medicine (ABIM) soon will be offering a Recognition of Focused Practice (RFP) in Hospital Medicine certification, he started to get a little nervous.
"I will lose sleep the week before I take this test," says Dr. Nelson, co-founder and past president of SHM, and a principal in the practice management firm Nelson Flores Hospital Medicine Consultants. "This exam will help identify those who see this as a career. … Boy, there is nothing like a test to demonstrate professional centeredness."
The exam, likely to be available in the fall of 2010, will identify physicians who have "maintained their internal medicine certification focused in hospital medicine," according to the ABIM Web site.
"For those individuals [whose certificate] will be expiring in 2010 or 2011, this is a viable pathway for re-certification," says Eric Holmbloe, MD, senior vice president and chief medical officer at ABIM. "Interested diplomats should be able to begin the application process in early 2010. We are feverishly working to complete the test and build the technology infrastructure. We should have more information available in about six weeks."
HM pioneers like Dr. Nelson consider the RFP designation a validation of decades-long efforts to carve a niche in medicine. The test will symbolize dedication to the specialty and provide HM physicians with professional self-regulation.
Scott Flanders, MD, FHM, president of SHM, terms the announcement a "watershed moment" for the field.
"I think this is a major, major moment for HM," says Dr. Flanders, who practices at the University of Michigan Medical Center in Ann Arbor. "We've been looking at this for a long time. This validates the field, and the belief that HM is a positive [for the field of medicine]."
Dr. Nelson couldn't agree more. "This test is the first way hospitalists will be able to show their competence," he says. "I think it's a great opportunity. This will help people take our field more seriously."
John Nelson, MD, FACP, FHM, hasn't taken a medical test in more than 20 years. So when news began to spread last week that the American Board of Internal Medicine (ABIM) soon will be offering a Recognition of Focused Practice (RFP) in Hospital Medicine certification, he started to get a little nervous.
"I will lose sleep the week before I take this test," says Dr. Nelson, co-founder and past president of SHM, and a principal in the practice management firm Nelson Flores Hospital Medicine Consultants. "This exam will help identify those who see this as a career. … Boy, there is nothing like a test to demonstrate professional centeredness."
The exam, likely to be available in the fall of 2010, will identify physicians who have "maintained their internal medicine certification focused in hospital medicine," according to the ABIM Web site.
"For those individuals [whose certificate] will be expiring in 2010 or 2011, this is a viable pathway for re-certification," says Eric Holmbloe, MD, senior vice president and chief medical officer at ABIM. "Interested diplomats should be able to begin the application process in early 2010. We are feverishly working to complete the test and build the technology infrastructure. We should have more information available in about six weeks."
HM pioneers like Dr. Nelson consider the RFP designation a validation of decades-long efforts to carve a niche in medicine. The test will symbolize dedication to the specialty and provide HM physicians with professional self-regulation.
Scott Flanders, MD, FHM, president of SHM, terms the announcement a "watershed moment" for the field.
"I think this is a major, major moment for HM," says Dr. Flanders, who practices at the University of Michigan Medical Center in Ann Arbor. "We've been looking at this for a long time. This validates the field, and the belief that HM is a positive [for the field of medicine]."
Dr. Nelson couldn't agree more. "This test is the first way hospitalists will be able to show their competence," he says. "I think it's a great opportunity. This will help people take our field more seriously."
JHM Names Baudendistel CME Editor

Some physicians have an interest in teaching; some are really good at it, and some make a career out of it. For Thomas Baudendistel, MD, FACP, teaching comes second nature and, as one of his former colleagues says, is a definition of who he is.
It’s those qualities, his experience in both academic and community hospital settings, and a passion for innovation that Dr. Baudendistel, the internal-medicine residency program director for Kaiser Permanente in Oakland, Calif., hopes to infuse as CME editor of the Journal of Hospital Medicine (JHM).
He was appointed to the new position in June. The first issue containing article-level CME, the answers to which will be submitted online, is scheduled to appear in the October issue.
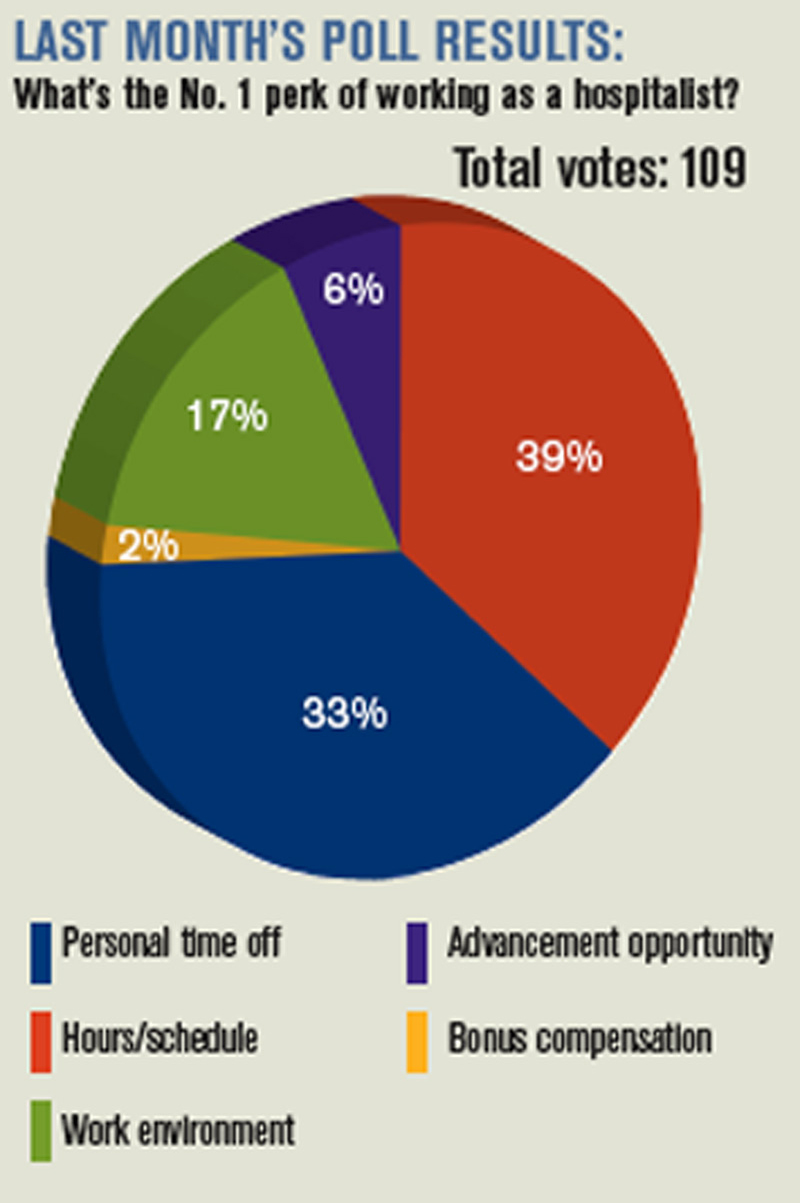
“Tom is a superlative educator. He has defined himself that way. He has a passion for it and a talent for it,” says Brian J. Harte, MD, FHM, chair of the department of hospital medicine at The Cleveland Clinic and a deputy editor of JHM.
Dr. Harte, who first met Dr. Baudendistel in 1996 during his residency at the University of California at San Francisco, says his former mentor “can take a submission, drill down to the most important teaching point, and challenge the readership.”
Dr. Baudendistel admits teaching is why he “gets out of bed in the morning.” He says he wants to take advantage of the young, tech-savvy nature of most HM physicians.
“JHM has been an innovative journal. I see the CME piece as being equally innovative,” says Dr. Baudendistel, who served four years as a JHM associate editor. “I’d like to move [CME] past the pencil-and-paper phase.” TH
Some physicians have an interest in teaching; some are really good at it, and some make a career out of it. For Thomas Baudendistel, MD, FACP, teaching comes second nature and, as one of his former colleagues says, is a definition of who he is.
It’s those qualities, his experience in both academic and community hospital settings, and a passion for innovation that Dr. Baudendistel, the internal-medicine residency program director for Kaiser Permanente in Oakland, Calif., hopes to infuse as CME editor of the Journal of Hospital Medicine (JHM).
He was appointed to the new position in June. The first issue containing article-level CME, the answers to which will be submitted online, is scheduled to appear in the October issue.
“Tom is a superlative educator. He has defined himself that way. He has a passion for it and a talent for it,” says Brian J. Harte, MD, FHM, chair of the department of hospital medicine at The Cleveland Clinic and a deputy editor of JHM.
Dr. Harte, who first met Dr. Baudendistel in 1996 during his residency at the University of California at San Francisco, says his former mentor “can take a submission, drill down to the most important teaching point, and challenge the readership.”
Dr. Baudendistel admits teaching is why he “gets out of bed in the morning.” He says he wants to take advantage of the young, tech-savvy nature of most HM physicians.
“JHM has been an innovative journal. I see the CME piece as being equally innovative,” says Dr. Baudendistel, who served four years as a JHM associate editor. “I’d like to move [CME] past the pencil-and-paper phase.” TH
Some physicians have an interest in teaching; some are really good at it, and some make a career out of it. For Thomas Baudendistel, MD, FACP, teaching comes second nature and, as one of his former colleagues says, is a definition of who he is.
It’s those qualities, his experience in both academic and community hospital settings, and a passion for innovation that Dr. Baudendistel, the internal-medicine residency program director for Kaiser Permanente in Oakland, Calif., hopes to infuse as CME editor of the Journal of Hospital Medicine (JHM).
He was appointed to the new position in June. The first issue containing article-level CME, the answers to which will be submitted online, is scheduled to appear in the October issue.
“Tom is a superlative educator. He has defined himself that way. He has a passion for it and a talent for it,” says Brian J. Harte, MD, FHM, chair of the department of hospital medicine at The Cleveland Clinic and a deputy editor of JHM.
Dr. Harte, who first met Dr. Baudendistel in 1996 during his residency at the University of California at San Francisco, says his former mentor “can take a submission, drill down to the most important teaching point, and challenge the readership.”
Dr. Baudendistel admits teaching is why he “gets out of bed in the morning.” He says he wants to take advantage of the young, tech-savvy nature of most HM physicians.
“JHM has been an innovative journal. I see the CME piece as being equally innovative,” says Dr. Baudendistel, who served four years as a JHM associate editor. “I’d like to move [CME] past the pencil-and-paper phase.” TH
Leadership Lessons
In more than 30 years as a healthcare industry consultant, Jack Silversin, DMD, DrPH, has watched as hospitals have evolved into complex organizations that emphasize efficiency, teamwork, and cost-effectiveness—three things absent from most medical training programs, he says.
“Doctors have been trained to be autonomous, but the new organizational structure is to be collective,” says Dr. Silversin, CEO of the Boston-based consulting firm Amicus Inc.
The changes doctors and HM groups are being asked to make are challenging their way of life and their work, Dr. Silversin says, and leading a group of independent-thinking hospitalists is no easy task.
“It’s a very challenging thing to be a leader. … It’s having the confidence and mind-set to engage people and make decisions,” says Dr. Silversin, who plans to address such issues during his daylong seminar at SHM’s Leadership Academy Sept. 14-17 in Miami.
Part of an expert faculty that teaches skills and concepts on beginner and advanced tracks, Dr. Silversin says Leadership Academy attendees learn how to define their roles and how to present their expectations to their groups.
“You go back to your hospital and see things in a different light,” he says. “You need to have the answers, but you need to balance that with relationships.”
The next Leadership Academy is Jan. 25-28 in Scottsdale, Ariz. For complete faculty bios and more information on participating, visit SHM’s events Web site.
In more than 30 years as a healthcare industry consultant, Jack Silversin, DMD, DrPH, has watched as hospitals have evolved into complex organizations that emphasize efficiency, teamwork, and cost-effectiveness—three things absent from most medical training programs, he says.
“Doctors have been trained to be autonomous, but the new organizational structure is to be collective,” says Dr. Silversin, CEO of the Boston-based consulting firm Amicus Inc.
The changes doctors and HM groups are being asked to make are challenging their way of life and their work, Dr. Silversin says, and leading a group of independent-thinking hospitalists is no easy task.
“It’s a very challenging thing to be a leader. … It’s having the confidence and mind-set to engage people and make decisions,” says Dr. Silversin, who plans to address such issues during his daylong seminar at SHM’s Leadership Academy Sept. 14-17 in Miami.
Part of an expert faculty that teaches skills and concepts on beginner and advanced tracks, Dr. Silversin says Leadership Academy attendees learn how to define their roles and how to present their expectations to their groups.
“You go back to your hospital and see things in a different light,” he says. “You need to have the answers, but you need to balance that with relationships.”
The next Leadership Academy is Jan. 25-28 in Scottsdale, Ariz. For complete faculty bios and more information on participating, visit SHM’s events Web site.
In more than 30 years as a healthcare industry consultant, Jack Silversin, DMD, DrPH, has watched as hospitals have evolved into complex organizations that emphasize efficiency, teamwork, and cost-effectiveness—three things absent from most medical training programs, he says.
“Doctors have been trained to be autonomous, but the new organizational structure is to be collective,” says Dr. Silversin, CEO of the Boston-based consulting firm Amicus Inc.
The changes doctors and HM groups are being asked to make are challenging their way of life and their work, Dr. Silversin says, and leading a group of independent-thinking hospitalists is no easy task.
“It’s a very challenging thing to be a leader. … It’s having the confidence and mind-set to engage people and make decisions,” says Dr. Silversin, who plans to address such issues during his daylong seminar at SHM’s Leadership Academy Sept. 14-17 in Miami.
Part of an expert faculty that teaches skills and concepts on beginner and advanced tracks, Dr. Silversin says Leadership Academy attendees learn how to define their roles and how to present their expectations to their groups.
“You go back to your hospital and see things in a different light,” he says. “You need to have the answers, but you need to balance that with relationships.”
The next Leadership Academy is Jan. 25-28 in Scottsdale, Ariz. For complete faculty bios and more information on participating, visit SHM’s events Web site.