User login
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM's "Best Practices in Managing a Hospital Medicine Program" course. Write to him at [email protected].
John Nelson: Peformance Key to Federal Value-Based Payment Modifier Plan

For years, your hospital was paid additional money by Medicare to report its performance on such things as core measures. Medicare then shared that information with the public via www.hospitalcompare.hhs.gov. Even if the hospital never gave Pneumovax when indicated, it was paid more simply for reporting that fact. (Fortunately, there were lots of reasons hospitals wanted to perform well.)
The days of hospitals being paid more simply for reporting ended a long time ago. Now performance, e.g., how often Pneumovax was given when indicated, influences payment. That is, things have transitioned from pay-for-reporting to a pay-for-performance program called hospital value-based purchasing (VBP).
I hope that at least one member of your hospitalist group is keeping up with hospital VBP. It got a lot of attention in the fall because it was the first time Medicare Part A payments to hospitals were adjusted based on performance on some core measures and patient satisfaction domains, as well as readmission rates for congestive heart failure (CHF), acute myocardial infarction (AMI), and pneumonia patients. The dollars at stake and performance metrics change will change every year, so plan to pay attention to hospital VBP on an ongoing basis.
Physicians’ Turn
Medicare payment to physicians is evolving along the same trajectory as hospitals. For several years, doctors have had the option to voluntarily participate in the Physician Quality Reporting System (PQRS). As long as a doctor reported quality performance on a sufficient portion of certain patient types, Medicare would provide a “bonus” at the end of the year. From 2012 through 2014, the “bonus” is 0.5% of that doctor’s total allowable Medicare charges. For example, if that doctor generated $150,000 of Medicare allowable charges over the calendar year, the additional payment for successful reporting PQRS would be $750 (0.5% of $150,000).
Although $750 is only a tiny fraction of collections, the right charge-capture system can make it pretty easy to achieve. And an extra payment of $750 sure is better than the 1.5% penalty for not participating; that program starts in 2015 and increases to a 2% penalty in 2016. If you are still not participating successfully in PQRS in 2015, the reimbursement for that $150,000 in charges will be reduced by $2,250 (1.5% of $150,000). So I strongly recommend that you begin reporting in 2013 so that you have time to work out the kinks well ahead of 2015. Don’t delay, but don’t panic, either, because you can still succeed in 2013 even if you don’t start capturing or reporting PQRS data until late winter or early spring.
At some point in the next year or so, data from as early as January 2013 for doctors reporting through PQRS will be made public on the Centers for Medicare & Medicaid’s (CMS) physician compare website: www.medicare.gov/find-a-doctor/provider-search.aspx. For example, should you choose to report the portion of stroke patients for whom you prescribed DVT prophylaxis, the public will be able to see your data.
The Next Wave of Physician Pay for Performance
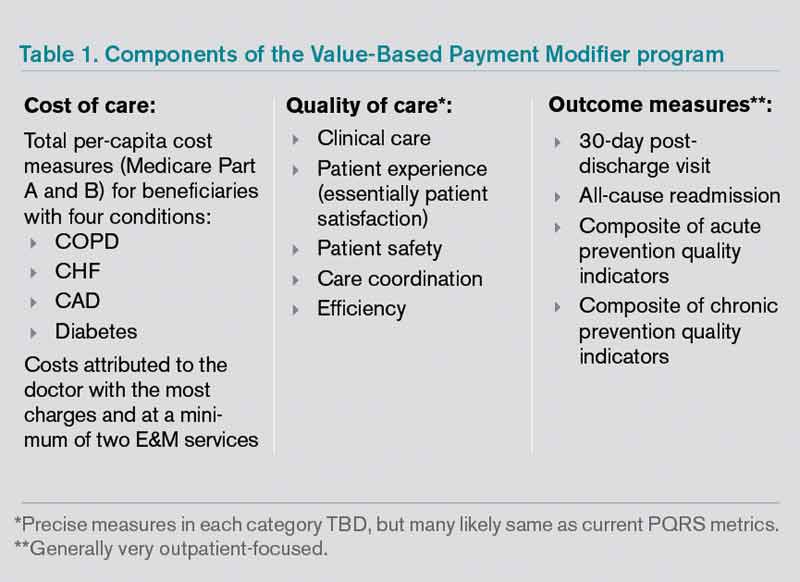
As the name implies, PQRS is a program based on reporting. Now CMS is adding the Value-Based Payment Modifier (VBPM) program, in which performance determines payments (see Table 1). It incorporates quality measures from PQRS, but is for now a separate program. It is very similar in name and structure to the hospital VBP program mentioned above, but incorporates cost of care data as well as quality performance. So it is really about value and not just quality performance (hence the name).
For providers in groups of more than 100 that bill under the same tax ID number (they don’t have to be in the same specialty), VBPM will first influence Part B Medicare reimbursement for physician services in 2015. It will expand to include all providers in 2017.
But don’t think you have until 2015 or 2017 to learn about all of this. There is a two-year lag, so payments in 2015 are based on performance in 2013 and 2017 payments presumably will be based on 2015 performance. In the fall of 2013, CMS plans to provide group-level (not individual) performance reports to all doctors in groups of 100 or more under the same tax ID number. These performance reports are known as quality resource use reports (QRURs). QRURs were trialed on physicians in a few states who received reports in 2012 based on 2011 performance, but in 2013, reports based on 2012 performance will be distributed to all doctors who practice in groups of 100 or more.
The calculation to determine whether a doctor is due additional payment for good performance (more accurately, good value) is awfully complicated. But providers have a choice to make. They can choose to:
- Not report data and accept a 1% penalty (likely to increase in successive years and in addition to the penalty for not reporting PQRS data, for a total penalty of 2.5%);
- Report data but not compete for financial upside or downside; or
- Compete for additional payments (amount to be determined) and risk a penalty of 0.5% or 1% for poor performance.
Look for more details about the VBPM program in future columns and other articles in The Hospitalist. There are a number of good online resources, including a CMS presentation titled “CMS Proposals for the Physician Value-Based Payment Modifier under the Medicare Physician Fee Schedule.” Type “Value-Based Payment Modifier” and “CMS” into any search engine to locate the video.
Parting Recommendations
Just about every hospitalist group should:
- Designate someone in your group to keep up with evolving pay-for-performance programs. It doesn’t have to be an MD, but you do need someone local that can guide your group through it. Consider becoming the most expert physician at your hospital on this topic.
- Start reporting through PQRS in 2013 if you haven’t already.
- Support SHM’s efforts to provide feedback to CMS to ensure that the metrics are meaningful for the type of care we provide.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
Author’s note: For helping to explain all this pay-for-performance stuff, I once again owe thanks to Dr. Pat Torcson, a hospitalist in Covington, La., and member of SHM’s Public Policy Committee. He does an amazing job of keeping up with the evolving pay-for-performance programs, advocating on behalf of hospitalists and the patients we serve, and graciously answers my tedious questions with thoughtful and informative replies. He is a really pleasant guy and a terrific asset to SHM and hospital medicine.
For years, your hospital was paid additional money by Medicare to report its performance on such things as core measures. Medicare then shared that information with the public via www.hospitalcompare.hhs.gov. Even if the hospital never gave Pneumovax when indicated, it was paid more simply for reporting that fact. (Fortunately, there were lots of reasons hospitals wanted to perform well.)
The days of hospitals being paid more simply for reporting ended a long time ago. Now performance, e.g., how often Pneumovax was given when indicated, influences payment. That is, things have transitioned from pay-for-reporting to a pay-for-performance program called hospital value-based purchasing (VBP).
I hope that at least one member of your hospitalist group is keeping up with hospital VBP. It got a lot of attention in the fall because it was the first time Medicare Part A payments to hospitals were adjusted based on performance on some core measures and patient satisfaction domains, as well as readmission rates for congestive heart failure (CHF), acute myocardial infarction (AMI), and pneumonia patients. The dollars at stake and performance metrics change will change every year, so plan to pay attention to hospital VBP on an ongoing basis.
Physicians’ Turn
Medicare payment to physicians is evolving along the same trajectory as hospitals. For several years, doctors have had the option to voluntarily participate in the Physician Quality Reporting System (PQRS). As long as a doctor reported quality performance on a sufficient portion of certain patient types, Medicare would provide a “bonus” at the end of the year. From 2012 through 2014, the “bonus” is 0.5% of that doctor’s total allowable Medicare charges. For example, if that doctor generated $150,000 of Medicare allowable charges over the calendar year, the additional payment for successful reporting PQRS would be $750 (0.5% of $150,000).
Although $750 is only a tiny fraction of collections, the right charge-capture system can make it pretty easy to achieve. And an extra payment of $750 sure is better than the 1.5% penalty for not participating; that program starts in 2015 and increases to a 2% penalty in 2016. If you are still not participating successfully in PQRS in 2015, the reimbursement for that $150,000 in charges will be reduced by $2,250 (1.5% of $150,000). So I strongly recommend that you begin reporting in 2013 so that you have time to work out the kinks well ahead of 2015. Don’t delay, but don’t panic, either, because you can still succeed in 2013 even if you don’t start capturing or reporting PQRS data until late winter or early spring.
At some point in the next year or so, data from as early as January 2013 for doctors reporting through PQRS will be made public on the Centers for Medicare & Medicaid’s (CMS) physician compare website: www.medicare.gov/find-a-doctor/provider-search.aspx. For example, should you choose to report the portion of stroke patients for whom you prescribed DVT prophylaxis, the public will be able to see your data.
The Next Wave of Physician Pay for Performance
As the name implies, PQRS is a program based on reporting. Now CMS is adding the Value-Based Payment Modifier (VBPM) program, in which performance determines payments (see Table 1). It incorporates quality measures from PQRS, but is for now a separate program. It is very similar in name and structure to the hospital VBP program mentioned above, but incorporates cost of care data as well as quality performance. So it is really about value and not just quality performance (hence the name).
For providers in groups of more than 100 that bill under the same tax ID number (they don’t have to be in the same specialty), VBPM will first influence Part B Medicare reimbursement for physician services in 2015. It will expand to include all providers in 2017.
But don’t think you have until 2015 or 2017 to learn about all of this. There is a two-year lag, so payments in 2015 are based on performance in 2013 and 2017 payments presumably will be based on 2015 performance. In the fall of 2013, CMS plans to provide group-level (not individual) performance reports to all doctors in groups of 100 or more under the same tax ID number. These performance reports are known as quality resource use reports (QRURs). QRURs were trialed on physicians in a few states who received reports in 2012 based on 2011 performance, but in 2013, reports based on 2012 performance will be distributed to all doctors who practice in groups of 100 or more.
The calculation to determine whether a doctor is due additional payment for good performance (more accurately, good value) is awfully complicated. But providers have a choice to make. They can choose to:
- Not report data and accept a 1% penalty (likely to increase in successive years and in addition to the penalty for not reporting PQRS data, for a total penalty of 2.5%);
- Report data but not compete for financial upside or downside; or
- Compete for additional payments (amount to be determined) and risk a penalty of 0.5% or 1% for poor performance.
Look for more details about the VBPM program in future columns and other articles in The Hospitalist. There are a number of good online resources, including a CMS presentation titled “CMS Proposals for the Physician Value-Based Payment Modifier under the Medicare Physician Fee Schedule.” Type “Value-Based Payment Modifier” and “CMS” into any search engine to locate the video.
Parting Recommendations
Just about every hospitalist group should:
- Designate someone in your group to keep up with evolving pay-for-performance programs. It doesn’t have to be an MD, but you do need someone local that can guide your group through it. Consider becoming the most expert physician at your hospital on this topic.
- Start reporting through PQRS in 2013 if you haven’t already.
- Support SHM’s efforts to provide feedback to CMS to ensure that the metrics are meaningful for the type of care we provide.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
Author’s note: For helping to explain all this pay-for-performance stuff, I once again owe thanks to Dr. Pat Torcson, a hospitalist in Covington, La., and member of SHM’s Public Policy Committee. He does an amazing job of keeping up with the evolving pay-for-performance programs, advocating on behalf of hospitalists and the patients we serve, and graciously answers my tedious questions with thoughtful and informative replies. He is a really pleasant guy and a terrific asset to SHM and hospital medicine.
For years, your hospital was paid additional money by Medicare to report its performance on such things as core measures. Medicare then shared that information with the public via www.hospitalcompare.hhs.gov. Even if the hospital never gave Pneumovax when indicated, it was paid more simply for reporting that fact. (Fortunately, there were lots of reasons hospitals wanted to perform well.)
The days of hospitals being paid more simply for reporting ended a long time ago. Now performance, e.g., how often Pneumovax was given when indicated, influences payment. That is, things have transitioned from pay-for-reporting to a pay-for-performance program called hospital value-based purchasing (VBP).
I hope that at least one member of your hospitalist group is keeping up with hospital VBP. It got a lot of attention in the fall because it was the first time Medicare Part A payments to hospitals were adjusted based on performance on some core measures and patient satisfaction domains, as well as readmission rates for congestive heart failure (CHF), acute myocardial infarction (AMI), and pneumonia patients. The dollars at stake and performance metrics change will change every year, so plan to pay attention to hospital VBP on an ongoing basis.
Physicians’ Turn
Medicare payment to physicians is evolving along the same trajectory as hospitals. For several years, doctors have had the option to voluntarily participate in the Physician Quality Reporting System (PQRS). As long as a doctor reported quality performance on a sufficient portion of certain patient types, Medicare would provide a “bonus” at the end of the year. From 2012 through 2014, the “bonus” is 0.5% of that doctor’s total allowable Medicare charges. For example, if that doctor generated $150,000 of Medicare allowable charges over the calendar year, the additional payment for successful reporting PQRS would be $750 (0.5% of $150,000).
Although $750 is only a tiny fraction of collections, the right charge-capture system can make it pretty easy to achieve. And an extra payment of $750 sure is better than the 1.5% penalty for not participating; that program starts in 2015 and increases to a 2% penalty in 2016. If you are still not participating successfully in PQRS in 2015, the reimbursement for that $150,000 in charges will be reduced by $2,250 (1.5% of $150,000). So I strongly recommend that you begin reporting in 2013 so that you have time to work out the kinks well ahead of 2015. Don’t delay, but don’t panic, either, because you can still succeed in 2013 even if you don’t start capturing or reporting PQRS data until late winter or early spring.
At some point in the next year or so, data from as early as January 2013 for doctors reporting through PQRS will be made public on the Centers for Medicare & Medicaid’s (CMS) physician compare website: www.medicare.gov/find-a-doctor/provider-search.aspx. For example, should you choose to report the portion of stroke patients for whom you prescribed DVT prophylaxis, the public will be able to see your data.
The Next Wave of Physician Pay for Performance
As the name implies, PQRS is a program based on reporting. Now CMS is adding the Value-Based Payment Modifier (VBPM) program, in which performance determines payments (see Table 1). It incorporates quality measures from PQRS, but is for now a separate program. It is very similar in name and structure to the hospital VBP program mentioned above, but incorporates cost of care data as well as quality performance. So it is really about value and not just quality performance (hence the name).
For providers in groups of more than 100 that bill under the same tax ID number (they don’t have to be in the same specialty), VBPM will first influence Part B Medicare reimbursement for physician services in 2015. It will expand to include all providers in 2017.
But don’t think you have until 2015 or 2017 to learn about all of this. There is a two-year lag, so payments in 2015 are based on performance in 2013 and 2017 payments presumably will be based on 2015 performance. In the fall of 2013, CMS plans to provide group-level (not individual) performance reports to all doctors in groups of 100 or more under the same tax ID number. These performance reports are known as quality resource use reports (QRURs). QRURs were trialed on physicians in a few states who received reports in 2012 based on 2011 performance, but in 2013, reports based on 2012 performance will be distributed to all doctors who practice in groups of 100 or more.
The calculation to determine whether a doctor is due additional payment for good performance (more accurately, good value) is awfully complicated. But providers have a choice to make. They can choose to:
- Not report data and accept a 1% penalty (likely to increase in successive years and in addition to the penalty for not reporting PQRS data, for a total penalty of 2.5%);
- Report data but not compete for financial upside or downside; or
- Compete for additional payments (amount to be determined) and risk a penalty of 0.5% or 1% for poor performance.
Look for more details about the VBPM program in future columns and other articles in The Hospitalist. There are a number of good online resources, including a CMS presentation titled “CMS Proposals for the Physician Value-Based Payment Modifier under the Medicare Physician Fee Schedule.” Type “Value-Based Payment Modifier” and “CMS” into any search engine to locate the video.
Parting Recommendations
Just about every hospitalist group should:
- Designate someone in your group to keep up with evolving pay-for-performance programs. It doesn’t have to be an MD, but you do need someone local that can guide your group through it. Consider becoming the most expert physician at your hospital on this topic.
- Start reporting through PQRS in 2013 if you haven’t already.
- Support SHM’s efforts to provide feedback to CMS to ensure that the metrics are meaningful for the type of care we provide.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
Author’s note: For helping to explain all this pay-for-performance stuff, I once again owe thanks to Dr. Pat Torcson, a hospitalist in Covington, La., and member of SHM’s Public Policy Committee. He does an amazing job of keeping up with the evolving pay-for-performance programs, advocating on behalf of hospitalists and the patients we serve, and graciously answers my tedious questions with thoughtful and informative replies. He is a really pleasant guy and a terrific asset to SHM and hospital medicine.
John Nelson: Learning CPT Coding and Documentation Tricky for Hospitalists

There is a lot to learn when it comes to proper coding and the documentation requirements that go with it. It can even be tricky for a new residency grad to keep the difference in CPT and ICD-9 coding straight, to say nothing of the difference between documentation requirements for physician reimbursement versus hospital reimbursement. This column addresses only physician CPT coding (I’ll save documentation to support hospital billing for another column).
Although I believe that devoting the large number of brain cells required to keep this stuff straight gets in the way of maintaining necessary clinical knowledge, physicians have no real choice but to do it. (One could argue that having a professional coder read charts to determine proper CPT codes relieves a doctor of the burden of documentation and coding headaches. But this is only partially true. The doctor still needs to ensure that the documentation accurately reflects what was done for the coder to be able to select the appropriate codes, so he still needs to know a lot about this topic.)
All providers have a duty to reasonably ensure that submitted claims (bills) are true and accurate. Failing to document and code correctly risks anything from you or your employer having to return money, potentially with a penalty and interest, to being accused of criminal fraud.
Medicare and other payors generally categorize inaccurate claims as follows:
- Erroneous claims include inadvertent mistakes, innocent errors, or even negligence but still require payments associated with the error to be returned.
- Fraudulent claims are ones judged to be intentionally or recklessly false, and are subject to administrative or civil penalties, such as fines.
- Claims associated with criminal intent to defraud are subject to criminal penalties, which could include jail time.
While I haven’t heard of any hospitalists being accused of fraud, I know of several who have undergone audits and been required to return money. Whether your employer would refund the money or you would have to write a personal check to refund the money depends on your employment situation. For example, in most cases, the hospital would be liable to make the repayment for hospitalists it employs. If you’re an independent contractor, there is a good chance you could be stuck making the repayment yourself.
Trend: Increased Use of Higher-Level Codes
You might have missed it, but there was a recent study of Medicare Part B claims data from 2001 to 2010 showing that “physicians increased their billing of higher-level E/M codes in all types of E/M services.”1 For example, the report showed a steady decrease in use of the 99231 code, the lowest of the three subsequent inpatient hospital care codes, and an increase in the highest level code, 99233 (see Figure 1, below).
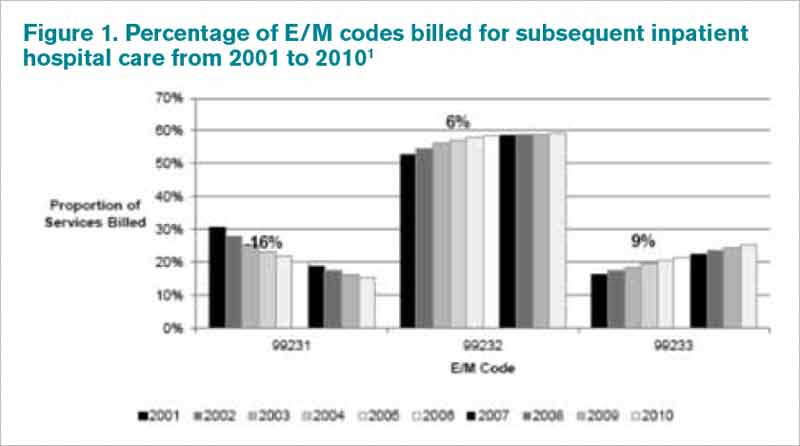
I can think of two reasons hospitalists might be increasing the use of higher codes. One, less-sick patients just aren’t seen in the hospital as often as they used to be, so the remaining patients require more intensive services, which could lead to the appropriate use of higher-level codes. Two, doctors have over the past 10 to 15 years invested more energy in learning appropriate documentation and coding, which might have led to correcting historical overuse of lower-level codes.
Did I tell you who conducted the study showing increased use of higher-level codes? It was the federal Office of Inspector General (OIG), which is responsible for preventing and detecting fraud and waste. Although the OIG might agree that the sicker patients and correction of historical undercoding might explain some of the trend, it’s a pretty safe bet they’re also concerned that a significant portion is inappropriate or fraudulent. Some portion of it probably is.
“CMS concurred with [OIG’s] recommendations to (1) continue to educate physicians on proper billing for E/M services and (2) encourage its contractor to review physicians’ billing for E/M services. CMS partially concurred with [OIG’s] third recommendation, to review physicians who bill higher-level E/M codes for appropriate action,” the OIG report noted.1
Plan for Education, Compliance
My sense is that most hospitalists employed by a large entity, such as a hospital or large medical group, have access to a certified coder to perform documentation and coding audits, as well as educational feedback when needed. If your practice doesn’t have access to a certified coder, you should consider photocopying some chart notes (e.g. 10 notes from each of your docs) and send them to an outside coder for an audit. Though they are very valuable, audits usually are not enough to ensure good performance.
In my March 2007 column, I described a reasonably simple chart audit allowing each doctor to compare his or her CPT coding pattern to everyone else in the group. You can compare your own coding to national coding patterns via SHM’s 2012 State of Hospital Medicine Report (www.hospitalmedicine.org/survey) or data from the CMS website, and the Medical Group Management Association (MGMA) will have data in future surveys. Such comparisons might help uncover unusual patterns that are worthy of a closer look.
Other strategies to promote proper documentation and coding include online educational programs, such as:
- SHM’s CODE-H webinars (www.hospitalmedicine.org/codeh), which are available on demand for a fee;
- American Association of Professional Coders Evaluation and Management Online Training (http://www.aapc.com/training/evaluation-management-coding-training.aspx); and
- The American Health Information Management Association’s (AHIMA) Coding Basics Program (www.ahima.org/continuinged/campus/courseinfo/cb.aspx).
If you prefer, an Internet search can turn up in-person courses to learn documentation and coding. Additionally, your in-house or external coding auditors can provide training.
To address tricky issues that come up only occasionally, several in our practice have compiled a “coding manual” by distilling guidance from our certified coders and compliance people on issues as they came up. Some issues would stump all of us, and we’d have to go to the Internet for help. All hospitalists are provided with a copy of the manual during orientation, and an electronic copy is available on the hospital’s Intranet. Topics addressed in the manual include things like how to bill the first inpatient day when a patient has changed from observation status, how to bill initial consult visits for various payors (an issue since Medicare eliminated consult codes a few years ago), how to bill when a patient is seen and discharged from the ED, etc.
Lastly, I suggest someone in your group talk with your hospital’s compliance department about its own coding and billing compliance plan. This could lead to ideas or help develop a compliance plan for your group.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
Reference
There is a lot to learn when it comes to proper coding and the documentation requirements that go with it. It can even be tricky for a new residency grad to keep the difference in CPT and ICD-9 coding straight, to say nothing of the difference between documentation requirements for physician reimbursement versus hospital reimbursement. This column addresses only physician CPT coding (I’ll save documentation to support hospital billing for another column).
Although I believe that devoting the large number of brain cells required to keep this stuff straight gets in the way of maintaining necessary clinical knowledge, physicians have no real choice but to do it. (One could argue that having a professional coder read charts to determine proper CPT codes relieves a doctor of the burden of documentation and coding headaches. But this is only partially true. The doctor still needs to ensure that the documentation accurately reflects what was done for the coder to be able to select the appropriate codes, so he still needs to know a lot about this topic.)
All providers have a duty to reasonably ensure that submitted claims (bills) are true and accurate. Failing to document and code correctly risks anything from you or your employer having to return money, potentially with a penalty and interest, to being accused of criminal fraud.
Medicare and other payors generally categorize inaccurate claims as follows:
- Erroneous claims include inadvertent mistakes, innocent errors, or even negligence but still require payments associated with the error to be returned.
- Fraudulent claims are ones judged to be intentionally or recklessly false, and are subject to administrative or civil penalties, such as fines.
- Claims associated with criminal intent to defraud are subject to criminal penalties, which could include jail time.
While I haven’t heard of any hospitalists being accused of fraud, I know of several who have undergone audits and been required to return money. Whether your employer would refund the money or you would have to write a personal check to refund the money depends on your employment situation. For example, in most cases, the hospital would be liable to make the repayment for hospitalists it employs. If you’re an independent contractor, there is a good chance you could be stuck making the repayment yourself.
Trend: Increased Use of Higher-Level Codes
You might have missed it, but there was a recent study of Medicare Part B claims data from 2001 to 2010 showing that “physicians increased their billing of higher-level E/M codes in all types of E/M services.”1 For example, the report showed a steady decrease in use of the 99231 code, the lowest of the three subsequent inpatient hospital care codes, and an increase in the highest level code, 99233 (see Figure 1, below).
I can think of two reasons hospitalists might be increasing the use of higher codes. One, less-sick patients just aren’t seen in the hospital as often as they used to be, so the remaining patients require more intensive services, which could lead to the appropriate use of higher-level codes. Two, doctors have over the past 10 to 15 years invested more energy in learning appropriate documentation and coding, which might have led to correcting historical overuse of lower-level codes.
Did I tell you who conducted the study showing increased use of higher-level codes? It was the federal Office of Inspector General (OIG), which is responsible for preventing and detecting fraud and waste. Although the OIG might agree that the sicker patients and correction of historical undercoding might explain some of the trend, it’s a pretty safe bet they’re also concerned that a significant portion is inappropriate or fraudulent. Some portion of it probably is.
“CMS concurred with [OIG’s] recommendations to (1) continue to educate physicians on proper billing for E/M services and (2) encourage its contractor to review physicians’ billing for E/M services. CMS partially concurred with [OIG’s] third recommendation, to review physicians who bill higher-level E/M codes for appropriate action,” the OIG report noted.1
Plan for Education, Compliance
My sense is that most hospitalists employed by a large entity, such as a hospital or large medical group, have access to a certified coder to perform documentation and coding audits, as well as educational feedback when needed. If your practice doesn’t have access to a certified coder, you should consider photocopying some chart notes (e.g. 10 notes from each of your docs) and send them to an outside coder for an audit. Though they are very valuable, audits usually are not enough to ensure good performance.
In my March 2007 column, I described a reasonably simple chart audit allowing each doctor to compare his or her CPT coding pattern to everyone else in the group. You can compare your own coding to national coding patterns via SHM’s 2012 State of Hospital Medicine Report (www.hospitalmedicine.org/survey) or data from the CMS website, and the Medical Group Management Association (MGMA) will have data in future surveys. Such comparisons might help uncover unusual patterns that are worthy of a closer look.
Other strategies to promote proper documentation and coding include online educational programs, such as:
- SHM’s CODE-H webinars (www.hospitalmedicine.org/codeh), which are available on demand for a fee;
- American Association of Professional Coders Evaluation and Management Online Training (http://www.aapc.com/training/evaluation-management-coding-training.aspx); and
- The American Health Information Management Association’s (AHIMA) Coding Basics Program (www.ahima.org/continuinged/campus/courseinfo/cb.aspx).
If you prefer, an Internet search can turn up in-person courses to learn documentation and coding. Additionally, your in-house or external coding auditors can provide training.
To address tricky issues that come up only occasionally, several in our practice have compiled a “coding manual” by distilling guidance from our certified coders and compliance people on issues as they came up. Some issues would stump all of us, and we’d have to go to the Internet for help. All hospitalists are provided with a copy of the manual during orientation, and an electronic copy is available on the hospital’s Intranet. Topics addressed in the manual include things like how to bill the first inpatient day when a patient has changed from observation status, how to bill initial consult visits for various payors (an issue since Medicare eliminated consult codes a few years ago), how to bill when a patient is seen and discharged from the ED, etc.
Lastly, I suggest someone in your group talk with your hospital’s compliance department about its own coding and billing compliance plan. This could lead to ideas or help develop a compliance plan for your group.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
Reference
There is a lot to learn when it comes to proper coding and the documentation requirements that go with it. It can even be tricky for a new residency grad to keep the difference in CPT and ICD-9 coding straight, to say nothing of the difference between documentation requirements for physician reimbursement versus hospital reimbursement. This column addresses only physician CPT coding (I’ll save documentation to support hospital billing for another column).
Although I believe that devoting the large number of brain cells required to keep this stuff straight gets in the way of maintaining necessary clinical knowledge, physicians have no real choice but to do it. (One could argue that having a professional coder read charts to determine proper CPT codes relieves a doctor of the burden of documentation and coding headaches. But this is only partially true. The doctor still needs to ensure that the documentation accurately reflects what was done for the coder to be able to select the appropriate codes, so he still needs to know a lot about this topic.)
All providers have a duty to reasonably ensure that submitted claims (bills) are true and accurate. Failing to document and code correctly risks anything from you or your employer having to return money, potentially with a penalty and interest, to being accused of criminal fraud.
Medicare and other payors generally categorize inaccurate claims as follows:
- Erroneous claims include inadvertent mistakes, innocent errors, or even negligence but still require payments associated with the error to be returned.
- Fraudulent claims are ones judged to be intentionally or recklessly false, and are subject to administrative or civil penalties, such as fines.
- Claims associated with criminal intent to defraud are subject to criminal penalties, which could include jail time.
While I haven’t heard of any hospitalists being accused of fraud, I know of several who have undergone audits and been required to return money. Whether your employer would refund the money or you would have to write a personal check to refund the money depends on your employment situation. For example, in most cases, the hospital would be liable to make the repayment for hospitalists it employs. If you’re an independent contractor, there is a good chance you could be stuck making the repayment yourself.
Trend: Increased Use of Higher-Level Codes
You might have missed it, but there was a recent study of Medicare Part B claims data from 2001 to 2010 showing that “physicians increased their billing of higher-level E/M codes in all types of E/M services.”1 For example, the report showed a steady decrease in use of the 99231 code, the lowest of the three subsequent inpatient hospital care codes, and an increase in the highest level code, 99233 (see Figure 1, below).
I can think of two reasons hospitalists might be increasing the use of higher codes. One, less-sick patients just aren’t seen in the hospital as often as they used to be, so the remaining patients require more intensive services, which could lead to the appropriate use of higher-level codes. Two, doctors have over the past 10 to 15 years invested more energy in learning appropriate documentation and coding, which might have led to correcting historical overuse of lower-level codes.
Did I tell you who conducted the study showing increased use of higher-level codes? It was the federal Office of Inspector General (OIG), which is responsible for preventing and detecting fraud and waste. Although the OIG might agree that the sicker patients and correction of historical undercoding might explain some of the trend, it’s a pretty safe bet they’re also concerned that a significant portion is inappropriate or fraudulent. Some portion of it probably is.
“CMS concurred with [OIG’s] recommendations to (1) continue to educate physicians on proper billing for E/M services and (2) encourage its contractor to review physicians’ billing for E/M services. CMS partially concurred with [OIG’s] third recommendation, to review physicians who bill higher-level E/M codes for appropriate action,” the OIG report noted.1
Plan for Education, Compliance
My sense is that most hospitalists employed by a large entity, such as a hospital or large medical group, have access to a certified coder to perform documentation and coding audits, as well as educational feedback when needed. If your practice doesn’t have access to a certified coder, you should consider photocopying some chart notes (e.g. 10 notes from each of your docs) and send them to an outside coder for an audit. Though they are very valuable, audits usually are not enough to ensure good performance.
In my March 2007 column, I described a reasonably simple chart audit allowing each doctor to compare his or her CPT coding pattern to everyone else in the group. You can compare your own coding to national coding patterns via SHM’s 2012 State of Hospital Medicine Report (www.hospitalmedicine.org/survey) or data from the CMS website, and the Medical Group Management Association (MGMA) will have data in future surveys. Such comparisons might help uncover unusual patterns that are worthy of a closer look.
Other strategies to promote proper documentation and coding include online educational programs, such as:
- SHM’s CODE-H webinars (www.hospitalmedicine.org/codeh), which are available on demand for a fee;
- American Association of Professional Coders Evaluation and Management Online Training (http://www.aapc.com/training/evaluation-management-coding-training.aspx); and
- The American Health Information Management Association’s (AHIMA) Coding Basics Program (www.ahima.org/continuinged/campus/courseinfo/cb.aspx).
If you prefer, an Internet search can turn up in-person courses to learn documentation and coding. Additionally, your in-house or external coding auditors can provide training.
To address tricky issues that come up only occasionally, several in our practice have compiled a “coding manual” by distilling guidance from our certified coders and compliance people on issues as they came up. Some issues would stump all of us, and we’d have to go to the Internet for help. All hospitalists are provided with a copy of the manual during orientation, and an electronic copy is available on the hospital’s Intranet. Topics addressed in the manual include things like how to bill the first inpatient day when a patient has changed from observation status, how to bill initial consult visits for various payors (an issue since Medicare eliminated consult codes a few years ago), how to bill when a patient is seen and discharged from the ED, etc.
Lastly, I suggest someone in your group talk with your hospital’s compliance department about its own coding and billing compliance plan. This could lead to ideas or help develop a compliance plan for your group.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
Reference
John Nelson: Post-Discharge Calls

There are lots of places to learn methods to improve patient satisfaction, including my thoughts from the January 2009 issue. Run an Internet search on “improve patient satisfaction” to get a huge number of articles, many of which have useful information and inspiration.
If you’re in a high-functioning hospitalist group, you’ve already read a lot on the topic, listened to presentations by someone at your hospital and elsewhere, and reliably reported and analyzed satisfaction survey results including HCAHPS questions and others. Maybe you’ve even engaged a consultant to help.
You might already have in place a number of strategies, such as reliably providing a business card with your photo, always sitting down in the patient’s room, asking “Is there anything else I can do?” before ending your time with a patient, etc. You’re doing all these things and more, but perhaps you’ve barely moved the needle on your satisfaction scores.
Despite your efforts, I bet your hospitalist group’s aggregate score is among the lowest of any physician group at your hospital.
You’re not alone.
What can you do about this?
High-Value Strategy: Phoning Patients after Discharge
I’m lucky enough to practice with some of the smartest, most professional, and most personable hospitalists you could ever meet. Yet our satisfaction scores are among the lowest for physicians at our hospital. Despite all of the improvement strategies we put in place over the last few years, our scores have barely budged. But that all changed once we instituted a formal program of phoning patients after discharge. That produced the largest uptick in our scores we’ve ever seen.
I can’t guarantee that our results are generalizable. But I have all the anecdotal information I need to be willing to invest the resources to make the calls. They improve scores. Likely more than any other single strategy. And they seem to have a positive effect on all survey questions, from how well the doctor explained things (nearly always the lowest of the HCAHPS scores for hospitalists) to the patient’s opinion of the hospital food.
Though initially resistant to expending the time and energy to make the calls, most in our group have said that they regularly feel really gratified by the response they get from patients or families. I think it is much better if a hospitalist who cared for the patient makes the calls, and I suspect (I have no proof) that calls made by a nurse or clerk are much less effective at improving patient satisfaction. And the call can serve as a valuable clinical encounter to briefly troubleshoot a problem or review a test result that was pending at discharge.
Simple Strategies
- More than 80% of these calls should last less than three minutes. Most patients or family members will report things are going OK and thank you profusely for the call. “No doctor has ever called before,” many will say. “Can we get you the next time Mom is hospitalized?”
- You could reduce the number of calls needed if you limit them to patients eligible for a survey; this typically is only about half of a hospitalist’s patient census. For example, patients on observation status and those discharged somewhere other than to home (e.g. to a skilled-nursing facility) are not eligible for a survey.
- It’s usually best not to tell a patient or family to expect the call. Surprising them makes them more delighted when you do call, and a patient told to expect a call but doesn’t get one will be less satisfied than if never told to expect it. Best if no one at the hospital knows you’re making the calls, because someone might brag about you and tell the patient to expect the call.
- For patients seen by several hospitalists, decide ahead of time which doctor makes the call. The doctor who discharged the patient is probably the simplest protocol.
- Develop a system to track patients who have been discharged. Every morning, we get a printout of all patients discharged the prior day. We try to call all patients the day after discharge to ensure that we reach them before they’ve had a chance to complete a satisfaction survey and before the discharging doctor rotates off.
- Develop a protocol to document the calls. Calls that lead to any new advice or therapies (e.g. see your primary-care physician sooner than planned) must be documented in the medical record, e.g., by dictating an addendum to the discharge summary. Don’t let the system get too complicated or keep you from making the calls.
- Use your judgment about whether to call the patient or just call a family member directly; it’s often better to do the latter.
- If you reach a voicemail (about 50% of the calls I make), leave a message and don’t keep calling back to reach a person.
Sample Scripts
Here are some simple scripts to use for post-discharge calls. If you reach the patient or family member:
- “This is Dr. X from Superior Hospital. I was just thinking about you/your mother/your father and wanted to know how things have gone since you/she/he left the hospital.”
- Ask about something related to the reason for their stay. “How is your appetite?” or “You haven’t had any more fever, have you?” or “Have you made your appointment with Dr. PCP yet?”
- “I hope things go really well for you, but if you ever need the hospital again, we’d be happy to care for you at Superior Hospital.”
If you get a voicemail:
- “This is Dr. X from Superior Hospital. I’ve been thinking about you/your mother/father since you/she/he left the hospital, and I am calling just to check on how things are going.” (For HIPPA reasons, don’t use the patient’s name when leaving a voicemail.)
- Mention some medical concern specific to the patient, e.g., “Your culture test turned out OK and I hope you’ve been able to get the antibiotic I prescribed.”
- “You don’t need to call me back, but if you have questions or want to provide an update, I can be reached at 555-123-4567.” (It’s very important to include this last sentence and a number where you can be reached. If omitted, many patients/families will think you must have called to convey something really important and will be distressed until able to reach you.)
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course.
There are lots of places to learn methods to improve patient satisfaction, including my thoughts from the January 2009 issue. Run an Internet search on “improve patient satisfaction” to get a huge number of articles, many of which have useful information and inspiration.
If you’re in a high-functioning hospitalist group, you’ve already read a lot on the topic, listened to presentations by someone at your hospital and elsewhere, and reliably reported and analyzed satisfaction survey results including HCAHPS questions and others. Maybe you’ve even engaged a consultant to help.
You might already have in place a number of strategies, such as reliably providing a business card with your photo, always sitting down in the patient’s room, asking “Is there anything else I can do?” before ending your time with a patient, etc. You’re doing all these things and more, but perhaps you’ve barely moved the needle on your satisfaction scores.
Despite your efforts, I bet your hospitalist group’s aggregate score is among the lowest of any physician group at your hospital.
You’re not alone.
What can you do about this?
High-Value Strategy: Phoning Patients after Discharge
I’m lucky enough to practice with some of the smartest, most professional, and most personable hospitalists you could ever meet. Yet our satisfaction scores are among the lowest for physicians at our hospital. Despite all of the improvement strategies we put in place over the last few years, our scores have barely budged. But that all changed once we instituted a formal program of phoning patients after discharge. That produced the largest uptick in our scores we’ve ever seen.
I can’t guarantee that our results are generalizable. But I have all the anecdotal information I need to be willing to invest the resources to make the calls. They improve scores. Likely more than any other single strategy. And they seem to have a positive effect on all survey questions, from how well the doctor explained things (nearly always the lowest of the HCAHPS scores for hospitalists) to the patient’s opinion of the hospital food.
Though initially resistant to expending the time and energy to make the calls, most in our group have said that they regularly feel really gratified by the response they get from patients or families. I think it is much better if a hospitalist who cared for the patient makes the calls, and I suspect (I have no proof) that calls made by a nurse or clerk are much less effective at improving patient satisfaction. And the call can serve as a valuable clinical encounter to briefly troubleshoot a problem or review a test result that was pending at discharge.
Simple Strategies
- More than 80% of these calls should last less than three minutes. Most patients or family members will report things are going OK and thank you profusely for the call. “No doctor has ever called before,” many will say. “Can we get you the next time Mom is hospitalized?”
- You could reduce the number of calls needed if you limit them to patients eligible for a survey; this typically is only about half of a hospitalist’s patient census. For example, patients on observation status and those discharged somewhere other than to home (e.g. to a skilled-nursing facility) are not eligible for a survey.
- It’s usually best not to tell a patient or family to expect the call. Surprising them makes them more delighted when you do call, and a patient told to expect a call but doesn’t get one will be less satisfied than if never told to expect it. Best if no one at the hospital knows you’re making the calls, because someone might brag about you and tell the patient to expect the call.
- For patients seen by several hospitalists, decide ahead of time which doctor makes the call. The doctor who discharged the patient is probably the simplest protocol.
- Develop a system to track patients who have been discharged. Every morning, we get a printout of all patients discharged the prior day. We try to call all patients the day after discharge to ensure that we reach them before they’ve had a chance to complete a satisfaction survey and before the discharging doctor rotates off.
- Develop a protocol to document the calls. Calls that lead to any new advice or therapies (e.g. see your primary-care physician sooner than planned) must be documented in the medical record, e.g., by dictating an addendum to the discharge summary. Don’t let the system get too complicated or keep you from making the calls.
- Use your judgment about whether to call the patient or just call a family member directly; it’s often better to do the latter.
- If you reach a voicemail (about 50% of the calls I make), leave a message and don’t keep calling back to reach a person.
Sample Scripts
Here are some simple scripts to use for post-discharge calls. If you reach the patient or family member:
- “This is Dr. X from Superior Hospital. I was just thinking about you/your mother/your father and wanted to know how things have gone since you/she/he left the hospital.”
- Ask about something related to the reason for their stay. “How is your appetite?” or “You haven’t had any more fever, have you?” or “Have you made your appointment with Dr. PCP yet?”
- “I hope things go really well for you, but if you ever need the hospital again, we’d be happy to care for you at Superior Hospital.”
If you get a voicemail:
- “This is Dr. X from Superior Hospital. I’ve been thinking about you/your mother/father since you/she/he left the hospital, and I am calling just to check on how things are going.” (For HIPPA reasons, don’t use the patient’s name when leaving a voicemail.)
- Mention some medical concern specific to the patient, e.g., “Your culture test turned out OK and I hope you’ve been able to get the antibiotic I prescribed.”
- “You don’t need to call me back, but if you have questions or want to provide an update, I can be reached at 555-123-4567.” (It’s very important to include this last sentence and a number where you can be reached. If omitted, many patients/families will think you must have called to convey something really important and will be distressed until able to reach you.)
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course.
There are lots of places to learn methods to improve patient satisfaction, including my thoughts from the January 2009 issue. Run an Internet search on “improve patient satisfaction” to get a huge number of articles, many of which have useful information and inspiration.
If you’re in a high-functioning hospitalist group, you’ve already read a lot on the topic, listened to presentations by someone at your hospital and elsewhere, and reliably reported and analyzed satisfaction survey results including HCAHPS questions and others. Maybe you’ve even engaged a consultant to help.
You might already have in place a number of strategies, such as reliably providing a business card with your photo, always sitting down in the patient’s room, asking “Is there anything else I can do?” before ending your time with a patient, etc. You’re doing all these things and more, but perhaps you’ve barely moved the needle on your satisfaction scores.
Despite your efforts, I bet your hospitalist group’s aggregate score is among the lowest of any physician group at your hospital.
You’re not alone.
What can you do about this?
High-Value Strategy: Phoning Patients after Discharge
I’m lucky enough to practice with some of the smartest, most professional, and most personable hospitalists you could ever meet. Yet our satisfaction scores are among the lowest for physicians at our hospital. Despite all of the improvement strategies we put in place over the last few years, our scores have barely budged. But that all changed once we instituted a formal program of phoning patients after discharge. That produced the largest uptick in our scores we’ve ever seen.
I can’t guarantee that our results are generalizable. But I have all the anecdotal information I need to be willing to invest the resources to make the calls. They improve scores. Likely more than any other single strategy. And they seem to have a positive effect on all survey questions, from how well the doctor explained things (nearly always the lowest of the HCAHPS scores for hospitalists) to the patient’s opinion of the hospital food.
Though initially resistant to expending the time and energy to make the calls, most in our group have said that they regularly feel really gratified by the response they get from patients or families. I think it is much better if a hospitalist who cared for the patient makes the calls, and I suspect (I have no proof) that calls made by a nurse or clerk are much less effective at improving patient satisfaction. And the call can serve as a valuable clinical encounter to briefly troubleshoot a problem or review a test result that was pending at discharge.
Simple Strategies
- More than 80% of these calls should last less than three minutes. Most patients or family members will report things are going OK and thank you profusely for the call. “No doctor has ever called before,” many will say. “Can we get you the next time Mom is hospitalized?”
- You could reduce the number of calls needed if you limit them to patients eligible for a survey; this typically is only about half of a hospitalist’s patient census. For example, patients on observation status and those discharged somewhere other than to home (e.g. to a skilled-nursing facility) are not eligible for a survey.
- It’s usually best not to tell a patient or family to expect the call. Surprising them makes them more delighted when you do call, and a patient told to expect a call but doesn’t get one will be less satisfied than if never told to expect it. Best if no one at the hospital knows you’re making the calls, because someone might brag about you and tell the patient to expect the call.
- For patients seen by several hospitalists, decide ahead of time which doctor makes the call. The doctor who discharged the patient is probably the simplest protocol.
- Develop a system to track patients who have been discharged. Every morning, we get a printout of all patients discharged the prior day. We try to call all patients the day after discharge to ensure that we reach them before they’ve had a chance to complete a satisfaction survey and before the discharging doctor rotates off.
- Develop a protocol to document the calls. Calls that lead to any new advice or therapies (e.g. see your primary-care physician sooner than planned) must be documented in the medical record, e.g., by dictating an addendum to the discharge summary. Don’t let the system get too complicated or keep you from making the calls.
- Use your judgment about whether to call the patient or just call a family member directly; it’s often better to do the latter.
- If you reach a voicemail (about 50% of the calls I make), leave a message and don’t keep calling back to reach a person.
Sample Scripts
Here are some simple scripts to use for post-discharge calls. If you reach the patient or family member:
- “This is Dr. X from Superior Hospital. I was just thinking about you/your mother/your father and wanted to know how things have gone since you/she/he left the hospital.”
- Ask about something related to the reason for their stay. “How is your appetite?” or “You haven’t had any more fever, have you?” or “Have you made your appointment with Dr. PCP yet?”
- “I hope things go really well for you, but if you ever need the hospital again, we’d be happy to care for you at Superior Hospital.”
If you get a voicemail:
- “This is Dr. X from Superior Hospital. I’ve been thinking about you/your mother/father since you/she/he left the hospital, and I am calling just to check on how things are going.” (For HIPPA reasons, don’t use the patient’s name when leaving a voicemail.)
- Mention some medical concern specific to the patient, e.g., “Your culture test turned out OK and I hope you’ve been able to get the antibiotic I prescribed.”
- “You don’t need to call me back, but if you have questions or want to provide an update, I can be reached at 555-123-4567.” (It’s very important to include this last sentence and a number where you can be reached. If omitted, many patients/families will think you must have called to convey something really important and will be distressed until able to reach you.)
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course.
John Nelson: Admit Resolution

Editor’s note: Second in a two-part series.
I used last month’s column to frame the issue of disagreement between doctors over who should admit a particular patient, as well as discuss the value of good social connections to reduce the chance that divergent opinions lead to outright conflict. This month, I’ll review another worthwhile strategy—one that could be a definitive solution to these disagreements but often falls short of that goal in practice.
Service Agreements, or “Compacts,” between Physician Groups
If, at your hospital, there are reasonably frequent cases of divergent opinions regarding whether an ED admission or transfer from elsewhere should be admitted by a hospitalist or doctor in another specialty, why not meet in advance to decide this? Many hospitalist groups have held meetings with doctors in other specialties and now have a collection of agreements outlining scenarios, such as:
- ESRD patients: Hospitalist admits for non-dialysis issues (pneumonia, diabetic issues, etc.); nephrologist admits for urgent dialysis issues (K+>6.3, pH<7.3, etc.).
- Cardiology: Hospitalist admits CHF and non-ST elevation chest pain; cardiologist admits STEMI.
- General surgery: Hospitalist admits ileus, pseudo obstruction, and SBO due to adhesions; general surgery admits bowel obstruction in “virgin abdomen,” volvulus, and any obstruction thought to require urgent surgery.
To be clear, I’m not suggesting the above guidelines are evidence-based or are the right ones for your institution. I just made these up, so yours might differ significantly. I just want to provide a sense of the kinds of issues these agreements typically cover. The comanagement section of the SHM website has several documents regarding hospitalist-orthopedic service agreements.
The Negotiation Process
It’s tempting for the lead hospitalist to just have a hallway chat with a spokesperson from the other specialty, then email a draft agreement, exchange a few messages until both parties are satisfied, then email a copy of the final document to all the doctors in both groups. This might work for some simple service agreements, but for any area with significant ambiguity or disagreements (or potential for disagreements), one or more in-person meetings are usually necessary. Ideally, several doctors in both groups will attend these meetings.
Much work could be done in advance of the first meeting, including surveying other practices to see how they decide which group admits the same kinds of patents, gathering any relevant published research, and possibly drafting a “straw man” proposed agreement. When meeting in person, the doctors will have a chance to explain their points of view, needs, and concerns, and gain a greater appreciation of the way “the other guy” sees things. An important purpose of the in-person meeting is to “look the other guy in the eye” to know if he or she really is committed to following through.
Remember that written agreements like these might become an issue in malpractice suits, so you might want to have them reviewed first by risk managers. You might also write them as guidelines rather than rigid protocols that don’t allow variations.
Maximize Effectiveness
Ideally, every doctor involved in the agreement should document their approval with a signature and date. My experience is that this doesn’t happen at most places, but if there is concern about whether everyone will comply, signing the document will probably help at least a little.
The completed agreements should be provided to all doctors in both groups, the ED, affected hospital nursing units, and others. Any new doctor should get a copy of all such agreements that might be relevant. And, most important, it should be made available electronically so that it is easy to find at any time. Some agreements cover uncommon events, and the doctors on duty might not remember what the agreement said and will need ready access to it.
Most service agreements should be reviewed and updated every two or three years or as needed. If there is confusion or controversy around a particular agreement, or if disagreements about which doctor does the admission are common despite the agreement, then an in-person meeting between the physician groups should be scheduled to revise or update it.
Keep Your Fingers Crossed
If it sounds like a lot of work to develop and maintain these agreements, it is. But they’re worth every bit of that work if they reduce confusion or discord. Sadly, for several reasons, they rarely prove so effective.
One doctor might think the agreement applies, but the other doctor says this patient is an exception and the agreement doesn’t apply. It is impossible to write an agreement that addresses all possible scenarios, so a doctor can argue that any particular patient falls outside the agreement because of things like comorbidities, which service admitted the patient last time (many agreements will have defined “bounce back” intervals), which primary-care physician (PCP) the patient sees, etc.
Even if there is no dispute about whether the agreement covers a particular patient, many doctors simply don’t feel obligated to uphold the agreement. Such a doctor might tell the ED doctor: “Yep, I signed the agreement, but only as a way to get the meeting over with. I was never in favor of it and just can’t admit the patient. Call the other guy to admit.” So in spite of all the work done to create a reasonable agreement, some doctors might feel entitled to ignore it when it suits them.
Compliance Is Critical
Sadly, my take is that despite the tremendous hoped-for benefits that service agreements might provide, poor compliance means they rarely achieve their potential. Even so, they are usually worth the time and effort to create them if it leads doctors in the two specialties to schedule time away from patient care to listen to the other group’s point of view and discuss how best to handle particular types of patients. In some cases, it will be the first time the two groups of doctors have set aside time to talk about the work they do together; that alone can have significant value.
Tom Lorence, MD, a Kaiser hospitalist in Portland, Ore., who is chief of hospital medicine for Northwest Permanente, developed more than 20 service agreements with many different specialties at his institution. He has found that they are worth the effort, and that they helped allay hospitalists’ feeling of being “dumped on.”
He also told me a rule that probably applies to all such agreements in any setting: The tie goes to the hospitalist—that is, when there is reasonable uncertainty or disagreement about which group should admit a patient, it is nearly always the hospitalist who will do so.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course.
Editor’s note: Second in a two-part series.
I used last month’s column to frame the issue of disagreement between doctors over who should admit a particular patient, as well as discuss the value of good social connections to reduce the chance that divergent opinions lead to outright conflict. This month, I’ll review another worthwhile strategy—one that could be a definitive solution to these disagreements but often falls short of that goal in practice.
Service Agreements, or “Compacts,” between Physician Groups
If, at your hospital, there are reasonably frequent cases of divergent opinions regarding whether an ED admission or transfer from elsewhere should be admitted by a hospitalist or doctor in another specialty, why not meet in advance to decide this? Many hospitalist groups have held meetings with doctors in other specialties and now have a collection of agreements outlining scenarios, such as:
- ESRD patients: Hospitalist admits for non-dialysis issues (pneumonia, diabetic issues, etc.); nephrologist admits for urgent dialysis issues (K+>6.3, pH<7.3, etc.).
- Cardiology: Hospitalist admits CHF and non-ST elevation chest pain; cardiologist admits STEMI.
- General surgery: Hospitalist admits ileus, pseudo obstruction, and SBO due to adhesions; general surgery admits bowel obstruction in “virgin abdomen,” volvulus, and any obstruction thought to require urgent surgery.
To be clear, I’m not suggesting the above guidelines are evidence-based or are the right ones for your institution. I just made these up, so yours might differ significantly. I just want to provide a sense of the kinds of issues these agreements typically cover. The comanagement section of the SHM website has several documents regarding hospitalist-orthopedic service agreements.
The Negotiation Process
It’s tempting for the lead hospitalist to just have a hallway chat with a spokesperson from the other specialty, then email a draft agreement, exchange a few messages until both parties are satisfied, then email a copy of the final document to all the doctors in both groups. This might work for some simple service agreements, but for any area with significant ambiguity or disagreements (or potential for disagreements), one or more in-person meetings are usually necessary. Ideally, several doctors in both groups will attend these meetings.
Much work could be done in advance of the first meeting, including surveying other practices to see how they decide which group admits the same kinds of patents, gathering any relevant published research, and possibly drafting a “straw man” proposed agreement. When meeting in person, the doctors will have a chance to explain their points of view, needs, and concerns, and gain a greater appreciation of the way “the other guy” sees things. An important purpose of the in-person meeting is to “look the other guy in the eye” to know if he or she really is committed to following through.
Remember that written agreements like these might become an issue in malpractice suits, so you might want to have them reviewed first by risk managers. You might also write them as guidelines rather than rigid protocols that don’t allow variations.
Maximize Effectiveness
Ideally, every doctor involved in the agreement should document their approval with a signature and date. My experience is that this doesn’t happen at most places, but if there is concern about whether everyone will comply, signing the document will probably help at least a little.
The completed agreements should be provided to all doctors in both groups, the ED, affected hospital nursing units, and others. Any new doctor should get a copy of all such agreements that might be relevant. And, most important, it should be made available electronically so that it is easy to find at any time. Some agreements cover uncommon events, and the doctors on duty might not remember what the agreement said and will need ready access to it.
Most service agreements should be reviewed and updated every two or three years or as needed. If there is confusion or controversy around a particular agreement, or if disagreements about which doctor does the admission are common despite the agreement, then an in-person meeting between the physician groups should be scheduled to revise or update it.
Keep Your Fingers Crossed
If it sounds like a lot of work to develop and maintain these agreements, it is. But they’re worth every bit of that work if they reduce confusion or discord. Sadly, for several reasons, they rarely prove so effective.
One doctor might think the agreement applies, but the other doctor says this patient is an exception and the agreement doesn’t apply. It is impossible to write an agreement that addresses all possible scenarios, so a doctor can argue that any particular patient falls outside the agreement because of things like comorbidities, which service admitted the patient last time (many agreements will have defined “bounce back” intervals), which primary-care physician (PCP) the patient sees, etc.
Even if there is no dispute about whether the agreement covers a particular patient, many doctors simply don’t feel obligated to uphold the agreement. Such a doctor might tell the ED doctor: “Yep, I signed the agreement, but only as a way to get the meeting over with. I was never in favor of it and just can’t admit the patient. Call the other guy to admit.” So in spite of all the work done to create a reasonable agreement, some doctors might feel entitled to ignore it when it suits them.
Compliance Is Critical
Sadly, my take is that despite the tremendous hoped-for benefits that service agreements might provide, poor compliance means they rarely achieve their potential. Even so, they are usually worth the time and effort to create them if it leads doctors in the two specialties to schedule time away from patient care to listen to the other group’s point of view and discuss how best to handle particular types of patients. In some cases, it will be the first time the two groups of doctors have set aside time to talk about the work they do together; that alone can have significant value.
Tom Lorence, MD, a Kaiser hospitalist in Portland, Ore., who is chief of hospital medicine for Northwest Permanente, developed more than 20 service agreements with many different specialties at his institution. He has found that they are worth the effort, and that they helped allay hospitalists’ feeling of being “dumped on.”
He also told me a rule that probably applies to all such agreements in any setting: The tie goes to the hospitalist—that is, when there is reasonable uncertainty or disagreement about which group should admit a patient, it is nearly always the hospitalist who will do so.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course.
Editor’s note: Second in a two-part series.
I used last month’s column to frame the issue of disagreement between doctors over who should admit a particular patient, as well as discuss the value of good social connections to reduce the chance that divergent opinions lead to outright conflict. This month, I’ll review another worthwhile strategy—one that could be a definitive solution to these disagreements but often falls short of that goal in practice.
Service Agreements, or “Compacts,” between Physician Groups
If, at your hospital, there are reasonably frequent cases of divergent opinions regarding whether an ED admission or transfer from elsewhere should be admitted by a hospitalist or doctor in another specialty, why not meet in advance to decide this? Many hospitalist groups have held meetings with doctors in other specialties and now have a collection of agreements outlining scenarios, such as:
- ESRD patients: Hospitalist admits for non-dialysis issues (pneumonia, diabetic issues, etc.); nephrologist admits for urgent dialysis issues (K+>6.3, pH<7.3, etc.).
- Cardiology: Hospitalist admits CHF and non-ST elevation chest pain; cardiologist admits STEMI.
- General surgery: Hospitalist admits ileus, pseudo obstruction, and SBO due to adhesions; general surgery admits bowel obstruction in “virgin abdomen,” volvulus, and any obstruction thought to require urgent surgery.
To be clear, I’m not suggesting the above guidelines are evidence-based or are the right ones for your institution. I just made these up, so yours might differ significantly. I just want to provide a sense of the kinds of issues these agreements typically cover. The comanagement section of the SHM website has several documents regarding hospitalist-orthopedic service agreements.
The Negotiation Process
It’s tempting for the lead hospitalist to just have a hallway chat with a spokesperson from the other specialty, then email a draft agreement, exchange a few messages until both parties are satisfied, then email a copy of the final document to all the doctors in both groups. This might work for some simple service agreements, but for any area with significant ambiguity or disagreements (or potential for disagreements), one or more in-person meetings are usually necessary. Ideally, several doctors in both groups will attend these meetings.
Much work could be done in advance of the first meeting, including surveying other practices to see how they decide which group admits the same kinds of patents, gathering any relevant published research, and possibly drafting a “straw man” proposed agreement. When meeting in person, the doctors will have a chance to explain their points of view, needs, and concerns, and gain a greater appreciation of the way “the other guy” sees things. An important purpose of the in-person meeting is to “look the other guy in the eye” to know if he or she really is committed to following through.
Remember that written agreements like these might become an issue in malpractice suits, so you might want to have them reviewed first by risk managers. You might also write them as guidelines rather than rigid protocols that don’t allow variations.
Maximize Effectiveness
Ideally, every doctor involved in the agreement should document their approval with a signature and date. My experience is that this doesn’t happen at most places, but if there is concern about whether everyone will comply, signing the document will probably help at least a little.
The completed agreements should be provided to all doctors in both groups, the ED, affected hospital nursing units, and others. Any new doctor should get a copy of all such agreements that might be relevant. And, most important, it should be made available electronically so that it is easy to find at any time. Some agreements cover uncommon events, and the doctors on duty might not remember what the agreement said and will need ready access to it.
Most service agreements should be reviewed and updated every two or three years or as needed. If there is confusion or controversy around a particular agreement, or if disagreements about which doctor does the admission are common despite the agreement, then an in-person meeting between the physician groups should be scheduled to revise or update it.
Keep Your Fingers Crossed
If it sounds like a lot of work to develop and maintain these agreements, it is. But they’re worth every bit of that work if they reduce confusion or discord. Sadly, for several reasons, they rarely prove so effective.
One doctor might think the agreement applies, but the other doctor says this patient is an exception and the agreement doesn’t apply. It is impossible to write an agreement that addresses all possible scenarios, so a doctor can argue that any particular patient falls outside the agreement because of things like comorbidities, which service admitted the patient last time (many agreements will have defined “bounce back” intervals), which primary-care physician (PCP) the patient sees, etc.
Even if there is no dispute about whether the agreement covers a particular patient, many doctors simply don’t feel obligated to uphold the agreement. Such a doctor might tell the ED doctor: “Yep, I signed the agreement, but only as a way to get the meeting over with. I was never in favor of it and just can’t admit the patient. Call the other guy to admit.” So in spite of all the work done to create a reasonable agreement, some doctors might feel entitled to ignore it when it suits them.
Compliance Is Critical
Sadly, my take is that despite the tremendous hoped-for benefits that service agreements might provide, poor compliance means they rarely achieve their potential. Even so, they are usually worth the time and effort to create them if it leads doctors in the two specialties to schedule time away from patient care to listen to the other group’s point of view and discuss how best to handle particular types of patients. In some cases, it will be the first time the two groups of doctors have set aside time to talk about the work they do together; that alone can have significant value.
Tom Lorence, MD, a Kaiser hospitalist in Portland, Ore., who is chief of hospital medicine for Northwest Permanente, developed more than 20 service agreements with many different specialties at his institution. He has found that they are worth the effort, and that they helped allay hospitalists’ feeling of being “dumped on.”
He also told me a rule that probably applies to all such agreements in any setting: The tie goes to the hospitalist—that is, when there is reasonable uncertainty or disagreement about which group should admit a patient, it is nearly always the hospitalist who will do so.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course.
John Nelson: Conflict Resolution

Editor’s note: First of a two-part series.
Think about the last time you found yourself in the middle of a contentious conversation with another doctor about whether a patient should be admitted by you, the hospitalist, or by a doctor in another specialty. Such conversations can sometimes move quickly from respectful disagreement to posturing, drawing lines in the sand, or worse.
Respectful conversations between doctors with differing opinions about the best plan of care for patients are valuable. But disagreements that lead doctors to talk at rather than with each other risk creating quality-of-care issues for the patient, demoralize other hospital staff, and can result in lasting harm to the relationship between the doctors involved. I’d bet the frequency of such disputes could serve as a reliable predictor of overall quality of care, and might correlate with cost of care. Doctors in all specialties should work diligently to reduce the chance that such conversations lead to conflict and stress.
Middle Manager
This conflict arises most often when an ED doctor is calling about a patient needing admission; the way communication between ED doctors and other physicians happens nearly everywhere is one reason the problem is so difficult to eradicate. (To be clear, I’m not faulting ED doctors for causing this problem; I think they usually try very hard to prevent it.)
Because the ED doctor is often in the middle of the chain of communication (disagreement), those whom the ED doctor is asking to admit the patient often are emboldened to take more unreasonable or extreme positions. It is a lot easier for Dr. Perry to make a case to the ED doctors that Dr. Mercury should admit a patient than to present the same rationale to Dr. Mercury himself. In many cases, the ED doctors can make the problem go away, or at least extricate themselves from the disagreement, by insisting that Dr. Perry and Dr. Mercury speak directly to each other.
Of course, things can sometimes go so badly that they refuse to speak directly with one another and force the ED doctor to settle the dispute a power given to the ED doctor by the medical staff bylaws at nearly every hospital. Or maybe they do speak directly and that leads to greater conflict (i.e. shouting or an abrupt hang-up).
Improved Social Connections
Most hospitals I’ve worked with seem to feature harmonious and collegial relationships between the ED doctors, hospitalists, and other specialties. But for some, divisive conflict crops up frequently. A first step for those hospitals laden with conflict could be to deliberately work to improve the social connections between the physician groups that often disagree. I’m not Pollyannaish; sometimes relationships are beyond repair, or one of the doctors involved might have a character disorder that requires more significant interventions.
A few years ago, I visited a place where years of conflict between ED doctors and hospitalists had led to remarkably adversarial relationships. Both of the lead physicians for the ED doctors and hospitalists were pleasant, professional, and highly regarded by others. Nonetheless, they both were fed up with the ongoing conflict and found themselves in such an adversarial relationship that I worried the next nighttime dispute could come to blows (literally). With a combination of support and pressure from hospital leaders and physician peers, they committed to a series of dinner meetings, just the two of them. They agreed to meet monthly, away from the hospital, and for the first few meetings avoid any conversation about work-related issues. The point was for them to build social connections so that they could find new ways of communicating, thus regain respect for the character of the other.
Some months later, I heard from the lead hospitalist, who said that the meetings had proven very valuable and things had improved dramatically between the department heads. He also said they were working together to improve the way their whole groups interacted. This wouldn’t work so well everywhere, and would have failed if not for the good character of both the doctors. But I’m struck by how infrequently the formation of social ties is included in any plan to reduce physician conflict. It is valuable, regardless of which specialties the doctors work in.
Hospitals have figured this out. Most provide a doctor’s lounge where meals might be served to provide a place for socialization. Some arrange periodic retreats for physician and hospital leaders to spend a weekend in a nice setting (with some time devoted to business and ample time for recreation and socialization). Expensive “perks” like these probably pay dividends in improving culture and reducing conflict. They also might soon be a thing of the past due to cost pressures. If so, we should all think deliberately about other ways hospitals can preserve and enhance the social fabric of what is becoming a more segregated medical staff as doctors narrow their sites of care and specialty focus.
The Universal Admitter
The most effective way to eliminate disagreements in admission decisions is to have the hospitalist admit all of them—that is, make the hospitalist a universal admitter.
Some hospitalist groups are nearly universal admitters already. No, they aren’t admitting all patients, including women in labor and some others. But they do admit and serve as attending for patients with hip fractures and other trauma and surgical issues, scheduled chemotherapy patients, etc.
I’ll save of my comments about the appropriateness of hospitalists as universal admitters for a future column. But I think that it is overkill to move to that model solely to address disagreements regarding which group admits a patient.
Service Agreements
Another way to reduce conflict over which physician group will serve as admitting/attending physician is to develop service agreements, or “compacts,” between different specialties. The idea is to create a set of clear, written guidelines or rules that determine which group admits the patient. For example, should the hospitalist or the surgeon admit?
ED doctors usually are delighted when the hospitalists and surgeons have met to create such an agreement. It could mean the end of disputes about who admits the patient. But does it?
I’ll discuss these agreements further in next month’s column, including elements that should be addressed, how to maximize compliance with them, and why they almost always fall short of realizing their hoped-for potential.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course.
Editor’s note: First of a two-part series.
Think about the last time you found yourself in the middle of a contentious conversation with another doctor about whether a patient should be admitted by you, the hospitalist, or by a doctor in another specialty. Such conversations can sometimes move quickly from respectful disagreement to posturing, drawing lines in the sand, or worse.
Respectful conversations between doctors with differing opinions about the best plan of care for patients are valuable. But disagreements that lead doctors to talk at rather than with each other risk creating quality-of-care issues for the patient, demoralize other hospital staff, and can result in lasting harm to the relationship between the doctors involved. I’d bet the frequency of such disputes could serve as a reliable predictor of overall quality of care, and might correlate with cost of care. Doctors in all specialties should work diligently to reduce the chance that such conversations lead to conflict and stress.
Middle Manager
This conflict arises most often when an ED doctor is calling about a patient needing admission; the way communication between ED doctors and other physicians happens nearly everywhere is one reason the problem is so difficult to eradicate. (To be clear, I’m not faulting ED doctors for causing this problem; I think they usually try very hard to prevent it.)
Because the ED doctor is often in the middle of the chain of communication (disagreement), those whom the ED doctor is asking to admit the patient often are emboldened to take more unreasonable or extreme positions. It is a lot easier for Dr. Perry to make a case to the ED doctors that Dr. Mercury should admit a patient than to present the same rationale to Dr. Mercury himself. In many cases, the ED doctors can make the problem go away, or at least extricate themselves from the disagreement, by insisting that Dr. Perry and Dr. Mercury speak directly to each other.
Of course, things can sometimes go so badly that they refuse to speak directly with one another and force the ED doctor to settle the dispute a power given to the ED doctor by the medical staff bylaws at nearly every hospital. Or maybe they do speak directly and that leads to greater conflict (i.e. shouting or an abrupt hang-up).
Improved Social Connections
Most hospitals I’ve worked with seem to feature harmonious and collegial relationships between the ED doctors, hospitalists, and other specialties. But for some, divisive conflict crops up frequently. A first step for those hospitals laden with conflict could be to deliberately work to improve the social connections between the physician groups that often disagree. I’m not Pollyannaish; sometimes relationships are beyond repair, or one of the doctors involved might have a character disorder that requires more significant interventions.
A few years ago, I visited a place where years of conflict between ED doctors and hospitalists had led to remarkably adversarial relationships. Both of the lead physicians for the ED doctors and hospitalists were pleasant, professional, and highly regarded by others. Nonetheless, they both were fed up with the ongoing conflict and found themselves in such an adversarial relationship that I worried the next nighttime dispute could come to blows (literally). With a combination of support and pressure from hospital leaders and physician peers, they committed to a series of dinner meetings, just the two of them. They agreed to meet monthly, away from the hospital, and for the first few meetings avoid any conversation about work-related issues. The point was for them to build social connections so that they could find new ways of communicating, thus regain respect for the character of the other.
Some months later, I heard from the lead hospitalist, who said that the meetings had proven very valuable and things had improved dramatically between the department heads. He also said they were working together to improve the way their whole groups interacted. This wouldn’t work so well everywhere, and would have failed if not for the good character of both the doctors. But I’m struck by how infrequently the formation of social ties is included in any plan to reduce physician conflict. It is valuable, regardless of which specialties the doctors work in.
Hospitals have figured this out. Most provide a doctor’s lounge where meals might be served to provide a place for socialization. Some arrange periodic retreats for physician and hospital leaders to spend a weekend in a nice setting (with some time devoted to business and ample time for recreation and socialization). Expensive “perks” like these probably pay dividends in improving culture and reducing conflict. They also might soon be a thing of the past due to cost pressures. If so, we should all think deliberately about other ways hospitals can preserve and enhance the social fabric of what is becoming a more segregated medical staff as doctors narrow their sites of care and specialty focus.
The Universal Admitter
The most effective way to eliminate disagreements in admission decisions is to have the hospitalist admit all of them—that is, make the hospitalist a universal admitter.
Some hospitalist groups are nearly universal admitters already. No, they aren’t admitting all patients, including women in labor and some others. But they do admit and serve as attending for patients with hip fractures and other trauma and surgical issues, scheduled chemotherapy patients, etc.
I’ll save of my comments about the appropriateness of hospitalists as universal admitters for a future column. But I think that it is overkill to move to that model solely to address disagreements regarding which group admits a patient.
Service Agreements
Another way to reduce conflict over which physician group will serve as admitting/attending physician is to develop service agreements, or “compacts,” between different specialties. The idea is to create a set of clear, written guidelines or rules that determine which group admits the patient. For example, should the hospitalist or the surgeon admit?
ED doctors usually are delighted when the hospitalists and surgeons have met to create such an agreement. It could mean the end of disputes about who admits the patient. But does it?
I’ll discuss these agreements further in next month’s column, including elements that should be addressed, how to maximize compliance with them, and why they almost always fall short of realizing their hoped-for potential.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course.
Editor’s note: First of a two-part series.
Think about the last time you found yourself in the middle of a contentious conversation with another doctor about whether a patient should be admitted by you, the hospitalist, or by a doctor in another specialty. Such conversations can sometimes move quickly from respectful disagreement to posturing, drawing lines in the sand, or worse.
Respectful conversations between doctors with differing opinions about the best plan of care for patients are valuable. But disagreements that lead doctors to talk at rather than with each other risk creating quality-of-care issues for the patient, demoralize other hospital staff, and can result in lasting harm to the relationship between the doctors involved. I’d bet the frequency of such disputes could serve as a reliable predictor of overall quality of care, and might correlate with cost of care. Doctors in all specialties should work diligently to reduce the chance that such conversations lead to conflict and stress.
Middle Manager
This conflict arises most often when an ED doctor is calling about a patient needing admission; the way communication between ED doctors and other physicians happens nearly everywhere is one reason the problem is so difficult to eradicate. (To be clear, I’m not faulting ED doctors for causing this problem; I think they usually try very hard to prevent it.)
Because the ED doctor is often in the middle of the chain of communication (disagreement), those whom the ED doctor is asking to admit the patient often are emboldened to take more unreasonable or extreme positions. It is a lot easier for Dr. Perry to make a case to the ED doctors that Dr. Mercury should admit a patient than to present the same rationale to Dr. Mercury himself. In many cases, the ED doctors can make the problem go away, or at least extricate themselves from the disagreement, by insisting that Dr. Perry and Dr. Mercury speak directly to each other.
Of course, things can sometimes go so badly that they refuse to speak directly with one another and force the ED doctor to settle the dispute a power given to the ED doctor by the medical staff bylaws at nearly every hospital. Or maybe they do speak directly and that leads to greater conflict (i.e. shouting or an abrupt hang-up).
Improved Social Connections
Most hospitals I’ve worked with seem to feature harmonious and collegial relationships between the ED doctors, hospitalists, and other specialties. But for some, divisive conflict crops up frequently. A first step for those hospitals laden with conflict could be to deliberately work to improve the social connections between the physician groups that often disagree. I’m not Pollyannaish; sometimes relationships are beyond repair, or one of the doctors involved might have a character disorder that requires more significant interventions.
A few years ago, I visited a place where years of conflict between ED doctors and hospitalists had led to remarkably adversarial relationships. Both of the lead physicians for the ED doctors and hospitalists were pleasant, professional, and highly regarded by others. Nonetheless, they both were fed up with the ongoing conflict and found themselves in such an adversarial relationship that I worried the next nighttime dispute could come to blows (literally). With a combination of support and pressure from hospital leaders and physician peers, they committed to a series of dinner meetings, just the two of them. They agreed to meet monthly, away from the hospital, and for the first few meetings avoid any conversation about work-related issues. The point was for them to build social connections so that they could find new ways of communicating, thus regain respect for the character of the other.
Some months later, I heard from the lead hospitalist, who said that the meetings had proven very valuable and things had improved dramatically between the department heads. He also said they were working together to improve the way their whole groups interacted. This wouldn’t work so well everywhere, and would have failed if not for the good character of both the doctors. But I’m struck by how infrequently the formation of social ties is included in any plan to reduce physician conflict. It is valuable, regardless of which specialties the doctors work in.
Hospitals have figured this out. Most provide a doctor’s lounge where meals might be served to provide a place for socialization. Some arrange periodic retreats for physician and hospital leaders to spend a weekend in a nice setting (with some time devoted to business and ample time for recreation and socialization). Expensive “perks” like these probably pay dividends in improving culture and reducing conflict. They also might soon be a thing of the past due to cost pressures. If so, we should all think deliberately about other ways hospitals can preserve and enhance the social fabric of what is becoming a more segregated medical staff as doctors narrow their sites of care and specialty focus.
The Universal Admitter
The most effective way to eliminate disagreements in admission decisions is to have the hospitalist admit all of them—that is, make the hospitalist a universal admitter.
Some hospitalist groups are nearly universal admitters already. No, they aren’t admitting all patients, including women in labor and some others. But they do admit and serve as attending for patients with hip fractures and other trauma and surgical issues, scheduled chemotherapy patients, etc.
I’ll save of my comments about the appropriateness of hospitalists as universal admitters for a future column. But I think that it is overkill to move to that model solely to address disagreements regarding which group admits a patient.
Service Agreements
Another way to reduce conflict over which physician group will serve as admitting/attending physician is to develop service agreements, or “compacts,” between different specialties. The idea is to create a set of clear, written guidelines or rules that determine which group admits the patient. For example, should the hospitalist or the surgeon admit?
ED doctors usually are delighted when the hospitalists and surgeons have met to create such an agreement. It could mean the end of disputes about who admits the patient. But does it?
I’ll discuss these agreements further in next month’s column, including elements that should be addressed, how to maximize compliance with them, and why they almost always fall short of realizing their hoped-for potential.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course.
John Nelson: Recognition, Promotion, Development Critical to Group Success

Well-designed forms of non-monetary compensation can have a greater impact on a hospitalist than providing a reward in dollars. This is true for any employee in any enterprise. It can have a greater impact than dollars in making a doctor feel appreciated and committed to the work of the organization. For example, a $100 gift certificate at a nice local restaurant can have a lot more impact and value than adding an extra $100 to the next paycheck.
A hospitalist’s salary and typical benefits (e.g. health insurance and retirement plan) must be attractive and competitive in the marketplace (obviously), but they are typically seen as entitlements, so they aren’t very effective at improving retention or motivating a doctor to perform well. Various forms of non-monetary compensation can be an effective way to achieve these things.
I should say that as I’m using the term here, non-monetary compensation includes things provided in some form other than dollars. But many forms—such as a restaurant gift certificate or tickets to a baseball game—likely will cost the practice something to provide. They also could be taxable to the doctor (i.e. should be reported on a W-2 statement), and Stark laws apply.
When discussing a citizenship bonus in my November 2011 column (see “Good Citizenship,” p. 53), I mentioned Daniel Pink’s book Drive: The Surprising Truth About What Motivates Us. In it, he argues that “Carrots and sticks are so last-century. We need to upgrade to autonomy, mastery, and purpose.” I’ll discuss forms of non-monetary compensation that fall into a modified version of Pink’s three upgrade categories.
Recognition
When is the last time a hospitalist leader or hospital executive sent a handwritten note of thanks and recognition to a hospitalist? It costs nothing, and it can be brief. Variations on this theme include awarding a plaque or trophy at a group meeting, or having an annual social event, such as a holiday party, that includes expressions of praise and gratitude for accomplishments in front of all the hospitalists and their significant others.
SHM past president Joseph Ming Wah Li, MD, SFHM, presides over his group’s annual “Hospy Awards,” a name inspired by ESPN’s ESPY Awards. Nurses, case managers, and residents vote for different awards and are asked to provide written comments about the doctor they’re voting for. Joe reads comments about both the winners and other hospitalists. The group has several additional social events each year, and photos from these are posted on the Internet.
Some hospital CEOs or other leaders periodically invite hospitalists to their homes for a dinner as a way of recognizing their work, as well as to build relationships and connectedness.
I was co-presenter in a session at HM12 in San Diego. Attendees had several terrific suggestions, including:
- Sending a note to the hospitalist’s significant other, rather than the hospitalist herself, expressing thanks for sharing her with us. Doing so is a way of acknowledging the good work of the hospitalist and the potential sacrifice of his or her family behind it. A short note of thanks with a restaurant gift certificate, so that hospitalist and a significant other can have dinner out paid for by the practice, seems like a great idea.
- Another idea that on the surface seems pretty silly, but likely has real value, is to identify a “superhero hospitalist” at some or all monthly group meetings. The group leader who brought it up does this by superimposing a photo of the doctor’s head onto a picture of a superhero like Superman and projects it during the meeting while saying something about the good work done to earn it. While silly, it has created some interest within the group regarding who the next winner will be and which superhero the honoree will be.
Promotion
Promoting a doctor into a position with greater responsibility, and perhaps a little (OK, maybe very little) prestige can be a valuable form of non-monetary compensation. A promotion could be as small as electing a doctor to serve on the hospitalist group’s own advisory committee, or representing the group at the hospital’s medical executive committee or other leadership group. More significant promotions could be having the hospitalist serve as medical director for case management or a clinical activity, such as palliative care; these positions often include additional monetary compensation.
SHM offers recognition in the form of fellowship and the opportunity for promotion to Senior Fellow in Hospital Medicine and Master of Hospital Medicine status. This can be seen as a promotion.
Professional Development
I think it is pretty tough to work an entire career devoted solely to patient care in any field, not just hospitalist practice. In June 2011 (see “Good Advice, Bad Advice,” p. 46), I wrote about the value of every hospitalist having at least a few additional professional interests and activities. A practice can encourage development of new interests and career roles, and make some available as a reward and recognition for good performance. Examples include sending your superstar doctors to SHM’s Leadership Academy, or even enroll them in a course to expand their clinical skill set, such as a procedures course or one that teaches interpretation of carotid ultrasounds or echocardiograms. An institution might find it worthwhile to reward the right doctor by paying their tuition at an executive MHA or MBA program.
It is all too easy to think that salary and benefits are the only rewards—i.e., compensation—that matter. Yet, in addition to money, all of us seek rewards in recognition, promotion, and professional development, and every practice should think deliberately about whether there are valuable opportunities in these categories.
I’d love to hear from anyone who has put in place novel and effective non-monetary compensation.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course.
Well-designed forms of non-monetary compensation can have a greater impact on a hospitalist than providing a reward in dollars. This is true for any employee in any enterprise. It can have a greater impact than dollars in making a doctor feel appreciated and committed to the work of the organization. For example, a $100 gift certificate at a nice local restaurant can have a lot more impact and value than adding an extra $100 to the next paycheck.
A hospitalist’s salary and typical benefits (e.g. health insurance and retirement plan) must be attractive and competitive in the marketplace (obviously), but they are typically seen as entitlements, so they aren’t very effective at improving retention or motivating a doctor to perform well. Various forms of non-monetary compensation can be an effective way to achieve these things.
I should say that as I’m using the term here, non-monetary compensation includes things provided in some form other than dollars. But many forms—such as a restaurant gift certificate or tickets to a baseball game—likely will cost the practice something to provide. They also could be taxable to the doctor (i.e. should be reported on a W-2 statement), and Stark laws apply.
When discussing a citizenship bonus in my November 2011 column (see “Good Citizenship,” p. 53), I mentioned Daniel Pink’s book Drive: The Surprising Truth About What Motivates Us. In it, he argues that “Carrots and sticks are so last-century. We need to upgrade to autonomy, mastery, and purpose.” I’ll discuss forms of non-monetary compensation that fall into a modified version of Pink’s three upgrade categories.
Recognition
When is the last time a hospitalist leader or hospital executive sent a handwritten note of thanks and recognition to a hospitalist? It costs nothing, and it can be brief. Variations on this theme include awarding a plaque or trophy at a group meeting, or having an annual social event, such as a holiday party, that includes expressions of praise and gratitude for accomplishments in front of all the hospitalists and their significant others.
SHM past president Joseph Ming Wah Li, MD, SFHM, presides over his group’s annual “Hospy Awards,” a name inspired by ESPN’s ESPY Awards. Nurses, case managers, and residents vote for different awards and are asked to provide written comments about the doctor they’re voting for. Joe reads comments about both the winners and other hospitalists. The group has several additional social events each year, and photos from these are posted on the Internet.
Some hospital CEOs or other leaders periodically invite hospitalists to their homes for a dinner as a way of recognizing their work, as well as to build relationships and connectedness.
I was co-presenter in a session at HM12 in San Diego. Attendees had several terrific suggestions, including:
- Sending a note to the hospitalist’s significant other, rather than the hospitalist herself, expressing thanks for sharing her with us. Doing so is a way of acknowledging the good work of the hospitalist and the potential sacrifice of his or her family behind it. A short note of thanks with a restaurant gift certificate, so that hospitalist and a significant other can have dinner out paid for by the practice, seems like a great idea.
- Another idea that on the surface seems pretty silly, but likely has real value, is to identify a “superhero hospitalist” at some or all monthly group meetings. The group leader who brought it up does this by superimposing a photo of the doctor’s head onto a picture of a superhero like Superman and projects it during the meeting while saying something about the good work done to earn it. While silly, it has created some interest within the group regarding who the next winner will be and which superhero the honoree will be.
Promotion
Promoting a doctor into a position with greater responsibility, and perhaps a little (OK, maybe very little) prestige can be a valuable form of non-monetary compensation. A promotion could be as small as electing a doctor to serve on the hospitalist group’s own advisory committee, or representing the group at the hospital’s medical executive committee or other leadership group. More significant promotions could be having the hospitalist serve as medical director for case management or a clinical activity, such as palliative care; these positions often include additional monetary compensation.
SHM offers recognition in the form of fellowship and the opportunity for promotion to Senior Fellow in Hospital Medicine and Master of Hospital Medicine status. This can be seen as a promotion.
Professional Development
I think it is pretty tough to work an entire career devoted solely to patient care in any field, not just hospitalist practice. In June 2011 (see “Good Advice, Bad Advice,” p. 46), I wrote about the value of every hospitalist having at least a few additional professional interests and activities. A practice can encourage development of new interests and career roles, and make some available as a reward and recognition for good performance. Examples include sending your superstar doctors to SHM’s Leadership Academy, or even enroll them in a course to expand their clinical skill set, such as a procedures course or one that teaches interpretation of carotid ultrasounds or echocardiograms. An institution might find it worthwhile to reward the right doctor by paying their tuition at an executive MHA or MBA program.
It is all too easy to think that salary and benefits are the only rewards—i.e., compensation—that matter. Yet, in addition to money, all of us seek rewards in recognition, promotion, and professional development, and every practice should think deliberately about whether there are valuable opportunities in these categories.
I’d love to hear from anyone who has put in place novel and effective non-monetary compensation.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course.
Well-designed forms of non-monetary compensation can have a greater impact on a hospitalist than providing a reward in dollars. This is true for any employee in any enterprise. It can have a greater impact than dollars in making a doctor feel appreciated and committed to the work of the organization. For example, a $100 gift certificate at a nice local restaurant can have a lot more impact and value than adding an extra $100 to the next paycheck.
A hospitalist’s salary and typical benefits (e.g. health insurance and retirement plan) must be attractive and competitive in the marketplace (obviously), but they are typically seen as entitlements, so they aren’t very effective at improving retention or motivating a doctor to perform well. Various forms of non-monetary compensation can be an effective way to achieve these things.
I should say that as I’m using the term here, non-monetary compensation includes things provided in some form other than dollars. But many forms—such as a restaurant gift certificate or tickets to a baseball game—likely will cost the practice something to provide. They also could be taxable to the doctor (i.e. should be reported on a W-2 statement), and Stark laws apply.
When discussing a citizenship bonus in my November 2011 column (see “Good Citizenship,” p. 53), I mentioned Daniel Pink’s book Drive: The Surprising Truth About What Motivates Us. In it, he argues that “Carrots and sticks are so last-century. We need to upgrade to autonomy, mastery, and purpose.” I’ll discuss forms of non-monetary compensation that fall into a modified version of Pink’s three upgrade categories.
Recognition
When is the last time a hospitalist leader or hospital executive sent a handwritten note of thanks and recognition to a hospitalist? It costs nothing, and it can be brief. Variations on this theme include awarding a plaque or trophy at a group meeting, or having an annual social event, such as a holiday party, that includes expressions of praise and gratitude for accomplishments in front of all the hospitalists and their significant others.
SHM past president Joseph Ming Wah Li, MD, SFHM, presides over his group’s annual “Hospy Awards,” a name inspired by ESPN’s ESPY Awards. Nurses, case managers, and residents vote for different awards and are asked to provide written comments about the doctor they’re voting for. Joe reads comments about both the winners and other hospitalists. The group has several additional social events each year, and photos from these are posted on the Internet.
Some hospital CEOs or other leaders periodically invite hospitalists to their homes for a dinner as a way of recognizing their work, as well as to build relationships and connectedness.
I was co-presenter in a session at HM12 in San Diego. Attendees had several terrific suggestions, including:
- Sending a note to the hospitalist’s significant other, rather than the hospitalist herself, expressing thanks for sharing her with us. Doing so is a way of acknowledging the good work of the hospitalist and the potential sacrifice of his or her family behind it. A short note of thanks with a restaurant gift certificate, so that hospitalist and a significant other can have dinner out paid for by the practice, seems like a great idea.
- Another idea that on the surface seems pretty silly, but likely has real value, is to identify a “superhero hospitalist” at some or all monthly group meetings. The group leader who brought it up does this by superimposing a photo of the doctor’s head onto a picture of a superhero like Superman and projects it during the meeting while saying something about the good work done to earn it. While silly, it has created some interest within the group regarding who the next winner will be and which superhero the honoree will be.
Promotion
Promoting a doctor into a position with greater responsibility, and perhaps a little (OK, maybe very little) prestige can be a valuable form of non-monetary compensation. A promotion could be as small as electing a doctor to serve on the hospitalist group’s own advisory committee, or representing the group at the hospital’s medical executive committee or other leadership group. More significant promotions could be having the hospitalist serve as medical director for case management or a clinical activity, such as palliative care; these positions often include additional monetary compensation.
SHM offers recognition in the form of fellowship and the opportunity for promotion to Senior Fellow in Hospital Medicine and Master of Hospital Medicine status. This can be seen as a promotion.
Professional Development
I think it is pretty tough to work an entire career devoted solely to patient care in any field, not just hospitalist practice. In June 2011 (see “Good Advice, Bad Advice,” p. 46), I wrote about the value of every hospitalist having at least a few additional professional interests and activities. A practice can encourage development of new interests and career roles, and make some available as a reward and recognition for good performance. Examples include sending your superstar doctors to SHM’s Leadership Academy, or even enroll them in a course to expand their clinical skill set, such as a procedures course or one that teaches interpretation of carotid ultrasounds or echocardiograms. An institution might find it worthwhile to reward the right doctor by paying their tuition at an executive MHA or MBA program.
It is all too easy to think that salary and benefits are the only rewards—i.e., compensation—that matter. Yet, in addition to money, all of us seek rewards in recognition, promotion, and professional development, and every practice should think deliberately about whether there are valuable opportunities in these categories.
I’d love to hear from anyone who has put in place novel and effective non-monetary compensation.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course.
John Nelson: Your Hospital Should Use Scripts to Describe Hospitalists to Patients

My anecdotal experience (no scientific research data) has convinced me that nearly every patient has some or all of the following questions or concerns when admitted by a hospitalist for the first time:
- Why is my usual doctor (PCP) not going to be in charge of my hospital care?
- Is the hospitalist a “real” doctor or someone in training, and whatdoes my regular doctor think of the hospitalist?
- Does the arrival of the hospitalist mean my long-term relationship with my PCP has been severed and I’ll see the hospitalist for all care (inpatient and outpatient) from now on?
- How will the hospitalist know my medical history, and will she communicate with my PCP?
Ideally, all communication about the hospitalist as an individual and the whole system of hospitalist care should help answer these questions and reassure the patient. Sadly, many people at the hospital unwittingly do the opposite.
Unintentional Undermining of Patient Confidence
Despite good intentions, doctors and nurses at the hospital often describe hospitalists to patients in a way that undermines the patients’ satisfaction and confidence in the hospitalist. They may say something like: Your doctor (PCP) doesn’t come to the hospital anymore and we have these doctors who are here all the time called hospitalists. I’ll ask one of them to see you.
To a patient, this might sound like he’s getting just any old doctor who happens to be around with nothing to do, rather than someone who specializes in the care of hospital patients and comes highly recommended by his PCP. The patient is left wondering why their “regular doctor” isn’t in charge of the hospital care, and often suspects the PCP has terminated their relationship or has been forced to refer by an insurance company when, in fact, the PCP chose to refer. Misunderstandings like these are a recipe for less satisfied and less confident patients.
Most hospitalist groups have a brochure explaining their practice, which addresses all of these points. (A simple Internet search for “hospitalist brochure patient information” or similar terms will reveal a number of good samples.) However, some patients never get a copy, and many won’t read it. So just having a brochure isn’t enough; there needs to be a way to ensure that all verbal communication serves to enlighten and reassure the patient.
Scripts for Nurses and Non-Hospitalist Physicians
Nurses and non-hospitalist doctors might not realize they’re sowing seeds of unhappiness in how they describe the hospitalist. Targeted education usually is necessary and can provide them with a new way of talking about the hospitalist. In most cases, it will be most effective to provide them with a script to use. For example, they could say: Your doctor has decided to focus her practice on the office to be more available to you there. As a result, she has decided to refer you to Dr. Bonamassa, a doctor who specializes in the care of hospitalized patients with problems like yours. Dr. Bonamassa will communicate with your primary doctor, and you should plan to follow up with her when you are discharged.
Or:
Your doctor has asked Dr. Trucks to take care of you while you are in the hospital. He is a specialist in the care of hospitalized patients and works with a team of doctors who are in the hospital 24 hours a day. Dr. Trucks will be your main doctor while you are in the hospital.
The Two Most Valuable Things For A Patient To Hear Are...
- That their PCP is in favor of the referral to a hospitalist, and that the patient’s relationship with the PCP will remain intact. Many patients worry that the arrival of the hospitalist means they won’t see their PCP ever again. Hence, the value in mentioning the patient will follow up with their usual PCP after discharge.
- That the hospitalist is a doctor devoted to the care of hospitalized patients, or a specialist in hospital care, rather than just a doctor who happens to be available.
My experience is that some PCPs worry that their patients might think less of them if they don’t provide hospital care. So despite good intentions, these PCPs’ words, demeanor, or body language could communicate unhappiness in, or something other than enthusiasm for, the hospitalist. The PCP may tell the patient something like, “I’m sending you to the hospital where you’ll be seen by a hospitalist, but I’ll be involved or overseeing everything.” This might be said with the intention of reassuring the patient, but it has the effect of undermining the patient’s confidence in the hospitalist. Such PCPs would benefit from adopting a better script.
It takes a reasonable amount of encouragement and cajoling to get others to adopt a script like I’ve suggested above, and requires periodic remedial education to ensure it isn’t abandoned in favor of old habits. But it is worth the effort.
Ensure Others Know the Hospitalist’s Name
Using the above scripts will have limited value if others don’t have a way of knowing the name of the hospitalist who will actually see the patient. If a worried family walks out of a room and asks the nurse, “Who is taking care of my father?” it is a lot better for the nurse to respond with the hospitalist’s name rather than “Your father is on the gold service, and the gold team doctor will be around later. I’m not sure which doctor has the gold service today.”
Try to ensure that everyone at the hospital knows which hospitalist is caring for every patient every day.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course
.
My anecdotal experience (no scientific research data) has convinced me that nearly every patient has some or all of the following questions or concerns when admitted by a hospitalist for the first time:
- Why is my usual doctor (PCP) not going to be in charge of my hospital care?
- Is the hospitalist a “real” doctor or someone in training, and whatdoes my regular doctor think of the hospitalist?
- Does the arrival of the hospitalist mean my long-term relationship with my PCP has been severed and I’ll see the hospitalist for all care (inpatient and outpatient) from now on?
- How will the hospitalist know my medical history, and will she communicate with my PCP?
Ideally, all communication about the hospitalist as an individual and the whole system of hospitalist care should help answer these questions and reassure the patient. Sadly, many people at the hospital unwittingly do the opposite.
Unintentional Undermining of Patient Confidence
Despite good intentions, doctors and nurses at the hospital often describe hospitalists to patients in a way that undermines the patients’ satisfaction and confidence in the hospitalist. They may say something like: Your doctor (PCP) doesn’t come to the hospital anymore and we have these doctors who are here all the time called hospitalists. I’ll ask one of them to see you.
To a patient, this might sound like he’s getting just any old doctor who happens to be around with nothing to do, rather than someone who specializes in the care of hospital patients and comes highly recommended by his PCP. The patient is left wondering why their “regular doctor” isn’t in charge of the hospital care, and often suspects the PCP has terminated their relationship or has been forced to refer by an insurance company when, in fact, the PCP chose to refer. Misunderstandings like these are a recipe for less satisfied and less confident patients.
Most hospitalist groups have a brochure explaining their practice, which addresses all of these points. (A simple Internet search for “hospitalist brochure patient information” or similar terms will reveal a number of good samples.) However, some patients never get a copy, and many won’t read it. So just having a brochure isn’t enough; there needs to be a way to ensure that all verbal communication serves to enlighten and reassure the patient.
Scripts for Nurses and Non-Hospitalist Physicians
Nurses and non-hospitalist doctors might not realize they’re sowing seeds of unhappiness in how they describe the hospitalist. Targeted education usually is necessary and can provide them with a new way of talking about the hospitalist. In most cases, it will be most effective to provide them with a script to use. For example, they could say: Your doctor has decided to focus her practice on the office to be more available to you there. As a result, she has decided to refer you to Dr. Bonamassa, a doctor who specializes in the care of hospitalized patients with problems like yours. Dr. Bonamassa will communicate with your primary doctor, and you should plan to follow up with her when you are discharged.
Or:
Your doctor has asked Dr. Trucks to take care of you while you are in the hospital. He is a specialist in the care of hospitalized patients and works with a team of doctors who are in the hospital 24 hours a day. Dr. Trucks will be your main doctor while you are in the hospital.
The Two Most Valuable Things For A Patient To Hear Are...
- That their PCP is in favor of the referral to a hospitalist, and that the patient’s relationship with the PCP will remain intact. Many patients worry that the arrival of the hospitalist means they won’t see their PCP ever again. Hence, the value in mentioning the patient will follow up with their usual PCP after discharge.
- That the hospitalist is a doctor devoted to the care of hospitalized patients, or a specialist in hospital care, rather than just a doctor who happens to be available.
My experience is that some PCPs worry that their patients might think less of them if they don’t provide hospital care. So despite good intentions, these PCPs’ words, demeanor, or body language could communicate unhappiness in, or something other than enthusiasm for, the hospitalist. The PCP may tell the patient something like, “I’m sending you to the hospital where you’ll be seen by a hospitalist, but I’ll be involved or overseeing everything.” This might be said with the intention of reassuring the patient, but it has the effect of undermining the patient’s confidence in the hospitalist. Such PCPs would benefit from adopting a better script.
It takes a reasonable amount of encouragement and cajoling to get others to adopt a script like I’ve suggested above, and requires periodic remedial education to ensure it isn’t abandoned in favor of old habits. But it is worth the effort.
Ensure Others Know the Hospitalist’s Name
Using the above scripts will have limited value if others don’t have a way of knowing the name of the hospitalist who will actually see the patient. If a worried family walks out of a room and asks the nurse, “Who is taking care of my father?” it is a lot better for the nurse to respond with the hospitalist’s name rather than “Your father is on the gold service, and the gold team doctor will be around later. I’m not sure which doctor has the gold service today.”
Try to ensure that everyone at the hospital knows which hospitalist is caring for every patient every day.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course
.
My anecdotal experience (no scientific research data) has convinced me that nearly every patient has some or all of the following questions or concerns when admitted by a hospitalist for the first time:
- Why is my usual doctor (PCP) not going to be in charge of my hospital care?
- Is the hospitalist a “real” doctor or someone in training, and whatdoes my regular doctor think of the hospitalist?
- Does the arrival of the hospitalist mean my long-term relationship with my PCP has been severed and I’ll see the hospitalist for all care (inpatient and outpatient) from now on?
- How will the hospitalist know my medical history, and will she communicate with my PCP?
Ideally, all communication about the hospitalist as an individual and the whole system of hospitalist care should help answer these questions and reassure the patient. Sadly, many people at the hospital unwittingly do the opposite.
Unintentional Undermining of Patient Confidence
Despite good intentions, doctors and nurses at the hospital often describe hospitalists to patients in a way that undermines the patients’ satisfaction and confidence in the hospitalist. They may say something like: Your doctor (PCP) doesn’t come to the hospital anymore and we have these doctors who are here all the time called hospitalists. I’ll ask one of them to see you.
To a patient, this might sound like he’s getting just any old doctor who happens to be around with nothing to do, rather than someone who specializes in the care of hospital patients and comes highly recommended by his PCP. The patient is left wondering why their “regular doctor” isn’t in charge of the hospital care, and often suspects the PCP has terminated their relationship or has been forced to refer by an insurance company when, in fact, the PCP chose to refer. Misunderstandings like these are a recipe for less satisfied and less confident patients.
Most hospitalist groups have a brochure explaining their practice, which addresses all of these points. (A simple Internet search for “hospitalist brochure patient information” or similar terms will reveal a number of good samples.) However, some patients never get a copy, and many won’t read it. So just having a brochure isn’t enough; there needs to be a way to ensure that all verbal communication serves to enlighten and reassure the patient.
Scripts for Nurses and Non-Hospitalist Physicians
Nurses and non-hospitalist doctors might not realize they’re sowing seeds of unhappiness in how they describe the hospitalist. Targeted education usually is necessary and can provide them with a new way of talking about the hospitalist. In most cases, it will be most effective to provide them with a script to use. For example, they could say: Your doctor has decided to focus her practice on the office to be more available to you there. As a result, she has decided to refer you to Dr. Bonamassa, a doctor who specializes in the care of hospitalized patients with problems like yours. Dr. Bonamassa will communicate with your primary doctor, and you should plan to follow up with her when you are discharged.
Or:
Your doctor has asked Dr. Trucks to take care of you while you are in the hospital. He is a specialist in the care of hospitalized patients and works with a team of doctors who are in the hospital 24 hours a day. Dr. Trucks will be your main doctor while you are in the hospital.
The Two Most Valuable Things For A Patient To Hear Are...
- That their PCP is in favor of the referral to a hospitalist, and that the patient’s relationship with the PCP will remain intact. Many patients worry that the arrival of the hospitalist means they won’t see their PCP ever again. Hence, the value in mentioning the patient will follow up with their usual PCP after discharge.
- That the hospitalist is a doctor devoted to the care of hospitalized patients, or a specialist in hospital care, rather than just a doctor who happens to be available.
My experience is that some PCPs worry that their patients might think less of them if they don’t provide hospital care. So despite good intentions, these PCPs’ words, demeanor, or body language could communicate unhappiness in, or something other than enthusiasm for, the hospitalist. The PCP may tell the patient something like, “I’m sending you to the hospital where you’ll be seen by a hospitalist, but I’ll be involved or overseeing everything.” This might be said with the intention of reassuring the patient, but it has the effect of undermining the patient’s confidence in the hospitalist. Such PCPs would benefit from adopting a better script.
It takes a reasonable amount of encouragement and cajoling to get others to adopt a script like I’ve suggested above, and requires periodic remedial education to ensure it isn’t abandoned in favor of old habits. But it is worth the effort.
Ensure Others Know the Hospitalist’s Name
Using the above scripts will have limited value if others don’t have a way of knowing the name of the hospitalist who will actually see the patient. If a worried family walks out of a room and asks the nurse, “Who is taking care of my father?” it is a lot better for the nurse to respond with the hospitalist’s name rather than “Your father is on the gold service, and the gold team doctor will be around later. I’m not sure which doctor has the gold service today.”
Try to ensure that everyone at the hospital knows which hospitalist is caring for every patient every day.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course
.
JOHN NELSON: Morning Discharges and Length of Stay

Last month, I discussed ED, or “front end,” throughput. This month I will focus on what can be thought of as the two components of “back end” throughput: effective management of length of stay (LOS) and patient discharge in the morning rather than late in the day.
How many times have you heard a well-intentioned administrator ask: “We can’t get patients from the ED to ward more quickly unless we can discharge patients earlier in the day to make beds available. So please round on your potential discharges and get the D/C order written early”?
Easier said than done. But not impossible, if you’re willing to make some adjustments in how you organize your work.
Strategies Re-examined
I provided a list of strategies in my April 2009 column (see “Early-Day Discharge Strategies,” p. 48), and in May 2010 I described in greater detail two ideas that can help with early-morning discharge. The easiest of these is to increase the portion of patients who discharge early in the day. To do this, hospitalists should write in the order section of the chart (not just the progress notes where it can be missed by nursing staff) an order like “possible disch tomorrow” or “Probably discharge Thurs or Fri.” That will help hospital staff anticipate and prepare for discharge, and there is little cost if the patient isn’t ready on the day forecast.
More difficult, but more effective, is fully preparing a patient’s discharge a day ahead of time. I do this on about half or more of my patients and, despite having no rigorous data to prove it, I’m convinced that it makes for better discharges and transitions, and it’s a real stress-reliever for me. My mornings are much less hectic, as I rarely have to devote 30-60 minutes to a discharge while other patients are waiting to be rounded on. And it helps me uncover loose ends like the need to get additional chest imaging to evaluate a possible lung lesion early enough that I can order the additional test without delaying discharge (it can be done the night before).
Note that when billing the discharge visit only, the time spent on the day of discharge counts as billable time. So preparing everything the day before will mean that nearly all discharges will be billed at the lower level: 99238 rather than 99239. You will have to decide for yourself whether losing the ability to bill some discharges at the higher level is worth it. Most hospitals probably will be willing to make up the lost professional fee revenue if it led to a meaningful improvement in the portion of patients with discharge orders early in the day.
One CMS administrator told my consulting partner, Leslie Flores, that discharge summaries can’t be dictated on a day prior to discharge because they have to include all information related to the hospital stay, including any relevant information from the night before discharge. The administrator said that CMS would view this as a surgeon dictating an operative report before performing the operation. (Are there surgeons who are actually doing that?) I think care is better when I do a discharge summary unhurried and with few interruptions in the evening before discharge rather than the busy morning of the discharge day. And I can always add an addendum (and often do) at the time of actual discharge. So you might want to ask your hospital compliance expert about dictating a D/C summary the day before discharge.
A Tricky Proposition
It is pretty easy for administrators to think that the time of day a discharge order is written is nearly always up to the doctor and how they organize their day. To them, it might seem reasonable to expect more than 50% of discharge orders to be written before 10 a.m. or earlier. But wait … it is more complicated than that.
The same administrators care a lot about LOS, which is most commonly reported in days but can also be measured in hours. So the time of day a discharge order is written, arguably the most important determinant of when a patient will vacate a room, is a determinant of LOS. If we’re really managing LOS optimally, we should discharge a patient at the first moment it is clinically appropriate, which means discharging at any hour of the day or night. (Of course, no one is proposing that we discharge and expect patients to vacate rooms in the middle of the night. Yet.)
But that would mean only a small portion of patients would end up with early-morning discharge orders. So excellent LOS management and a high portion of discharge orders written early in the day are incompatible. Setting the target percentage of early-a.m. discharge orders too high probably will increase LOS and defeat the original objective.
Benefits and Costs of Improved Throughput
Let’s say you’re sold on the value of improving throughput. It should lead to improved efficiency and financial performance for your hospital. I suspect it will improve quality and reduce iatrogenesis for some patients, but risk more readmissions and quality lapses or errors for others. And as every department tries to improve their own throughput, there will be a tendency to push problems off on others. For example, it is easy to improve ED throughput if the ED doctor just does a lot less evaluation and sends patients upstairs without much of a workup. Example: “The patient has fever and low sats, so I know he’s going to be admitted. Why should I keep him in the ED to do a workup?”
In fact, I think we should move away from using the ED as a triage unit and send some patients directly from ED triage to the inpatient unit. But we’ll need to put in place systems that make that safe and ensure good care. I don’t think any hospital has such systems in place now.
Let’s say that by 2013 most hospitals have dramatically improved their throughput, have short ED admit decision time to ED departure, and many patients are discharged and vacate their rooms early in the day. And let’s say we’ve been able to do that while maintaining or improving quality of care (we must!). We’ll then have happy patients and hospital administrators, and can bring up this improved performance when negotiating for hospital financial support for our practice. Everyone is happy, right?
Well, won’t this increase marginal or unnecessary admissions and readmissions, and lead to overall increased hospital utilization? After all, if it becomes really quick and easy to admit a patient to the hospital, won’t we do it more often? I think we will, but would never propose that we maintain poor throughput to keep a lid on costs and inappropriate utilization. But we’d better come up with other ways, or improved throughput will just be one more factor contributing to escalating healthcare costs.
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm.
Last month, I discussed ED, or “front end,” throughput. This month I will focus on what can be thought of as the two components of “back end” throughput: effective management of length of stay (LOS) and patient discharge in the morning rather than late in the day.
How many times have you heard a well-intentioned administrator ask: “We can’t get patients from the ED to ward more quickly unless we can discharge patients earlier in the day to make beds available. So please round on your potential discharges and get the D/C order written early”?
Easier said than done. But not impossible, if you’re willing to make some adjustments in how you organize your work.
Strategies Re-examined
I provided a list of strategies in my April 2009 column (see “Early-Day Discharge Strategies,” p. 48), and in May 2010 I described in greater detail two ideas that can help with early-morning discharge. The easiest of these is to increase the portion of patients who discharge early in the day. To do this, hospitalists should write in the order section of the chart (not just the progress notes where it can be missed by nursing staff) an order like “possible disch tomorrow” or “Probably discharge Thurs or Fri.” That will help hospital staff anticipate and prepare for discharge, and there is little cost if the patient isn’t ready on the day forecast.
More difficult, but more effective, is fully preparing a patient’s discharge a day ahead of time. I do this on about half or more of my patients and, despite having no rigorous data to prove it, I’m convinced that it makes for better discharges and transitions, and it’s a real stress-reliever for me. My mornings are much less hectic, as I rarely have to devote 30-60 minutes to a discharge while other patients are waiting to be rounded on. And it helps me uncover loose ends like the need to get additional chest imaging to evaluate a possible lung lesion early enough that I can order the additional test without delaying discharge (it can be done the night before).
Note that when billing the discharge visit only, the time spent on the day of discharge counts as billable time. So preparing everything the day before will mean that nearly all discharges will be billed at the lower level: 99238 rather than 99239. You will have to decide for yourself whether losing the ability to bill some discharges at the higher level is worth it. Most hospitals probably will be willing to make up the lost professional fee revenue if it led to a meaningful improvement in the portion of patients with discharge orders early in the day.
One CMS administrator told my consulting partner, Leslie Flores, that discharge summaries can’t be dictated on a day prior to discharge because they have to include all information related to the hospital stay, including any relevant information from the night before discharge. The administrator said that CMS would view this as a surgeon dictating an operative report before performing the operation. (Are there surgeons who are actually doing that?) I think care is better when I do a discharge summary unhurried and with few interruptions in the evening before discharge rather than the busy morning of the discharge day. And I can always add an addendum (and often do) at the time of actual discharge. So you might want to ask your hospital compliance expert about dictating a D/C summary the day before discharge.
A Tricky Proposition
It is pretty easy for administrators to think that the time of day a discharge order is written is nearly always up to the doctor and how they organize their day. To them, it might seem reasonable to expect more than 50% of discharge orders to be written before 10 a.m. or earlier. But wait … it is more complicated than that.
The same administrators care a lot about LOS, which is most commonly reported in days but can also be measured in hours. So the time of day a discharge order is written, arguably the most important determinant of when a patient will vacate a room, is a determinant of LOS. If we’re really managing LOS optimally, we should discharge a patient at the first moment it is clinically appropriate, which means discharging at any hour of the day or night. (Of course, no one is proposing that we discharge and expect patients to vacate rooms in the middle of the night. Yet.)
But that would mean only a small portion of patients would end up with early-morning discharge orders. So excellent LOS management and a high portion of discharge orders written early in the day are incompatible. Setting the target percentage of early-a.m. discharge orders too high probably will increase LOS and defeat the original objective.
Benefits and Costs of Improved Throughput
Let’s say you’re sold on the value of improving throughput. It should lead to improved efficiency and financial performance for your hospital. I suspect it will improve quality and reduce iatrogenesis for some patients, but risk more readmissions and quality lapses or errors for others. And as every department tries to improve their own throughput, there will be a tendency to push problems off on others. For example, it is easy to improve ED throughput if the ED doctor just does a lot less evaluation and sends patients upstairs without much of a workup. Example: “The patient has fever and low sats, so I know he’s going to be admitted. Why should I keep him in the ED to do a workup?”
In fact, I think we should move away from using the ED as a triage unit and send some patients directly from ED triage to the inpatient unit. But we’ll need to put in place systems that make that safe and ensure good care. I don’t think any hospital has such systems in place now.
Let’s say that by 2013 most hospitals have dramatically improved their throughput, have short ED admit decision time to ED departure, and many patients are discharged and vacate their rooms early in the day. And let’s say we’ve been able to do that while maintaining or improving quality of care (we must!). We’ll then have happy patients and hospital administrators, and can bring up this improved performance when negotiating for hospital financial support for our practice. Everyone is happy, right?
Well, won’t this increase marginal or unnecessary admissions and readmissions, and lead to overall increased hospital utilization? After all, if it becomes really quick and easy to admit a patient to the hospital, won’t we do it more often? I think we will, but would never propose that we maintain poor throughput to keep a lid on costs and inappropriate utilization. But we’d better come up with other ways, or improved throughput will just be one more factor contributing to escalating healthcare costs.
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm.
Last month, I discussed ED, or “front end,” throughput. This month I will focus on what can be thought of as the two components of “back end” throughput: effective management of length of stay (LOS) and patient discharge in the morning rather than late in the day.
How many times have you heard a well-intentioned administrator ask: “We can’t get patients from the ED to ward more quickly unless we can discharge patients earlier in the day to make beds available. So please round on your potential discharges and get the D/C order written early”?
Easier said than done. But not impossible, if you’re willing to make some adjustments in how you organize your work.
Strategies Re-examined
I provided a list of strategies in my April 2009 column (see “Early-Day Discharge Strategies,” p. 48), and in May 2010 I described in greater detail two ideas that can help with early-morning discharge. The easiest of these is to increase the portion of patients who discharge early in the day. To do this, hospitalists should write in the order section of the chart (not just the progress notes where it can be missed by nursing staff) an order like “possible disch tomorrow” or “Probably discharge Thurs or Fri.” That will help hospital staff anticipate and prepare for discharge, and there is little cost if the patient isn’t ready on the day forecast.
More difficult, but more effective, is fully preparing a patient’s discharge a day ahead of time. I do this on about half or more of my patients and, despite having no rigorous data to prove it, I’m convinced that it makes for better discharges and transitions, and it’s a real stress-reliever for me. My mornings are much less hectic, as I rarely have to devote 30-60 minutes to a discharge while other patients are waiting to be rounded on. And it helps me uncover loose ends like the need to get additional chest imaging to evaluate a possible lung lesion early enough that I can order the additional test without delaying discharge (it can be done the night before).
Note that when billing the discharge visit only, the time spent on the day of discharge counts as billable time. So preparing everything the day before will mean that nearly all discharges will be billed at the lower level: 99238 rather than 99239. You will have to decide for yourself whether losing the ability to bill some discharges at the higher level is worth it. Most hospitals probably will be willing to make up the lost professional fee revenue if it led to a meaningful improvement in the portion of patients with discharge orders early in the day.
One CMS administrator told my consulting partner, Leslie Flores, that discharge summaries can’t be dictated on a day prior to discharge because they have to include all information related to the hospital stay, including any relevant information from the night before discharge. The administrator said that CMS would view this as a surgeon dictating an operative report before performing the operation. (Are there surgeons who are actually doing that?) I think care is better when I do a discharge summary unhurried and with few interruptions in the evening before discharge rather than the busy morning of the discharge day. And I can always add an addendum (and often do) at the time of actual discharge. So you might want to ask your hospital compliance expert about dictating a D/C summary the day before discharge.
A Tricky Proposition
It is pretty easy for administrators to think that the time of day a discharge order is written is nearly always up to the doctor and how they organize their day. To them, it might seem reasonable to expect more than 50% of discharge orders to be written before 10 a.m. or earlier. But wait … it is more complicated than that.
The same administrators care a lot about LOS, which is most commonly reported in days but can also be measured in hours. So the time of day a discharge order is written, arguably the most important determinant of when a patient will vacate a room, is a determinant of LOS. If we’re really managing LOS optimally, we should discharge a patient at the first moment it is clinically appropriate, which means discharging at any hour of the day or night. (Of course, no one is proposing that we discharge and expect patients to vacate rooms in the middle of the night. Yet.)
But that would mean only a small portion of patients would end up with early-morning discharge orders. So excellent LOS management and a high portion of discharge orders written early in the day are incompatible. Setting the target percentage of early-a.m. discharge orders too high probably will increase LOS and defeat the original objective.
Benefits and Costs of Improved Throughput
Let’s say you’re sold on the value of improving throughput. It should lead to improved efficiency and financial performance for your hospital. I suspect it will improve quality and reduce iatrogenesis for some patients, but risk more readmissions and quality lapses or errors for others. And as every department tries to improve their own throughput, there will be a tendency to push problems off on others. For example, it is easy to improve ED throughput if the ED doctor just does a lot less evaluation and sends patients upstairs without much of a workup. Example: “The patient has fever and low sats, so I know he’s going to be admitted. Why should I keep him in the ED to do a workup?”
In fact, I think we should move away from using the ED as a triage unit and send some patients directly from ED triage to the inpatient unit. But we’ll need to put in place systems that make that safe and ensure good care. I don’t think any hospital has such systems in place now.
Let’s say that by 2013 most hospitals have dramatically improved their throughput, have short ED admit decision time to ED departure, and many patients are discharged and vacate their rooms early in the day. And let’s say we’ve been able to do that while maintaining or improving quality of care (we must!). We’ll then have happy patients and hospital administrators, and can bring up this improved performance when negotiating for hospital financial support for our practice. Everyone is happy, right?
Well, won’t this increase marginal or unnecessary admissions and readmissions, and lead to overall increased hospital utilization? After all, if it becomes really quick and easy to admit a patient to the hospital, won’t we do it more often? I think we will, but would never propose that we maintain poor throughput to keep a lid on costs and inappropriate utilization. But we’d better come up with other ways, or improved throughput will just be one more factor contributing to escalating healthcare costs.
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm.
John Nelson: ED Patient Throughput Is New Core Measure

To understand one reason why your hospital cares so much about patient throughput and discharging patients before noon, think of tables in a restaurant. A restaurant has a limited number of tables, and the more quickly they serve customers, the sooner they’re able to seat a new party. So by improving their throughput, they can serve more customers and increase profitability without having to add tables.
Of course, the more a restaurant pushes to increase throughput, the more it risks a decrease in the satisfaction of its customers. Too much focus on throughput could annoy customers so much that it puts them out of business (Seinfeld’s Soup Nazi is one notable exception).
Yet hospitals are likely to increase their customers’ satisfaction by improving “front-end” throughput from the ED to the inpatient unit. In fact, CMS added two new core measures (known as inpatient quality reporting, or IQR) that hospitals began reporting on Jan. 1:
- Median time from ED arrival to ED departure for admitted patients, and
- Admit decision time to ED departure for admitted patients.
You already knew about these, right? Although they don’t directly influence Medicare payments to your hospital now, there is a pretty good chance they could become part of the Hospital Value-Based Purchasing program in the future. So expect administrative leaders at your hospital to continue pestering you about ED throughput with even greater intensity.
I confess that improving throughput feels like one of the most difficult things for me to do, and I sweat when in meetings about it. Yet I know intellectually that we can do better. After all, it wasn’t that long ago that a patient could expect to wait hours to see an ED doctor, and shortening the wait seemed an impossible task. But EDs everywhere have done just that, and now lots of them post the current ED wait time (typically less than 10 or 15 minutes!) on the Internet or billboards. So if they can do it, then I’m sure hospitalists can, too.
I wrote about hospital throughput in my April 2009 and May 2010 columns, and included some strategies you might want to try. Here are a few more directed at ED-to-inpatient ward throughput.
The One-Admitter Approach
Most practices have no option other than a single admitter at night, but if your one admitter during daytime hours reliably gets behind, then you should have “rounders” help with admitting duties. While this is stressful for the rounder, and could sometimes delay the rounder’s ability to discharge patients early (more on that later), in most cases, the benefit will be worth the cost. In fact, I think the best arrangement is for all, or nearly all, daytime hospitalists to share admissions every day.
Remember, this approach will eliminate the admitter-to-rounder handoff from Day One to Day Two, resulting in a net increase in efficiency (and probably patient satisfaction). Plus, reduction handoff errors should decrease, because only one doctor, rather than two, will have to get to know the new patient.
Eliminate Impediments
Some hospitalists with inefficient work habits have an opportunity to become more efficient at taking a history and reviewing records, along with other steps in the admission process, without risking poor quality. But most are reasonably efficient at those tasks already and shouldn’t make them the focus of throughput efforts.
That said, most, or nearly all, hospitalists could shorten the time from when the ED pages on a new admission to when we appear in the ED to see the patient.
Here is one scenario that gives rise to the type of delay I’m talking about. The ED doctor pages a triage hospitalist, and the two finally speak directly 10 minutes later. After a five-minute conversation, the triage doctor pages the hospitalist who will actually admit the patient, waits 10 minutes for the return call, relays the information (possibly leaving out or misrepresenting some of what the ED doc said), and the admitting hospitalist heads to the ED 15 minutes later. Each person in this scenario acted reasonably promptly, but the clock starts with the first ED page. The hospitalist is already at 45 minutes when they arrive to see the patient!
You need to minimize “daisy chain” communication between the ED doctor and the hospitalist who will actually see the patient. In the scenario above, I think it would be best to eliminate the triage doctor entirely (see my December 2008 column for ideas about how to do this) so that the hospitalist who will actually admit the patient learns of the new referral quickly and speaks directly with the ED doctor.
Another reason for a poor “page from ED to hospitalist at patient’s bedside” time is that the admitting hospitalist just doesn’t make it a priority to get to the ED quickly. They might decide to round on two or three more patients before working on the new admission. Of course, we must triage and sometimes delay getting to the ED while attending to an unstable floor patient, but not too often, in my experience.
I’m not suggesting that others adopt my habit: I typically don’t call the ED back at all. Instead, I just head to the ED immediately after being paged, and usually arrive in less time than I would have spent on hold waiting for the ED doc to come to the phone.
When presented with several ED patients to admit at the same time or tied up with a critical patient on the floor, getting to the ED quickly isn’t possible.
Write Admission or “Holding” Orders and Move the Patient to His/Her Room
This is frustrating for the admitting hospitalist, because among other problems, families often leave when the patient moves to the inpatient ward, and additional tests likely will take longer to complete from the floor rather than ED. And while it is hard to quantify, I think this practice increases the risk of errors—though some studies have shown that long ED stays are associated with worse outcomes for the patient, too.
One of the marquee principles of ED medicine has historically been “ED doctors should never write admission orders.” Even so, I sense that this view is shifting, and many now see this as clinically reasonable, and in some cases necessary, to ensure good performance. Our ED docs have agreed to do this if there is concern that the hospitalist can’t finish writing orders within an hour of first being paged about the patient. Ask me in a year and I’ll let you know just how this is going.
And, of course, another option is for the admitting hospitalist to provide admission orders or “holding” orders by phone. I think this is safe for many patients, as long as it is followed by a bedside admission visit by the hospitalist before too long.
Next month: What about throughput at the discharge end of the hospital stay? And yes, improving throughput risks quality of care, yet we have to do it while maintaining or improving quality.
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm.
To understand one reason why your hospital cares so much about patient throughput and discharging patients before noon, think of tables in a restaurant. A restaurant has a limited number of tables, and the more quickly they serve customers, the sooner they’re able to seat a new party. So by improving their throughput, they can serve more customers and increase profitability without having to add tables.
Of course, the more a restaurant pushes to increase throughput, the more it risks a decrease in the satisfaction of its customers. Too much focus on throughput could annoy customers so much that it puts them out of business (Seinfeld’s Soup Nazi is one notable exception).
Yet hospitals are likely to increase their customers’ satisfaction by improving “front-end” throughput from the ED to the inpatient unit. In fact, CMS added two new core measures (known as inpatient quality reporting, or IQR) that hospitals began reporting on Jan. 1:
- Median time from ED arrival to ED departure for admitted patients, and
- Admit decision time to ED departure for admitted patients.
You already knew about these, right? Although they don’t directly influence Medicare payments to your hospital now, there is a pretty good chance they could become part of the Hospital Value-Based Purchasing program in the future. So expect administrative leaders at your hospital to continue pestering you about ED throughput with even greater intensity.
I confess that improving throughput feels like one of the most difficult things for me to do, and I sweat when in meetings about it. Yet I know intellectually that we can do better. After all, it wasn’t that long ago that a patient could expect to wait hours to see an ED doctor, and shortening the wait seemed an impossible task. But EDs everywhere have done just that, and now lots of them post the current ED wait time (typically less than 10 or 15 minutes!) on the Internet or billboards. So if they can do it, then I’m sure hospitalists can, too.
I wrote about hospital throughput in my April 2009 and May 2010 columns, and included some strategies you might want to try. Here are a few more directed at ED-to-inpatient ward throughput.
The One-Admitter Approach
Most practices have no option other than a single admitter at night, but if your one admitter during daytime hours reliably gets behind, then you should have “rounders” help with admitting duties. While this is stressful for the rounder, and could sometimes delay the rounder’s ability to discharge patients early (more on that later), in most cases, the benefit will be worth the cost. In fact, I think the best arrangement is for all, or nearly all, daytime hospitalists to share admissions every day.
Remember, this approach will eliminate the admitter-to-rounder handoff from Day One to Day Two, resulting in a net increase in efficiency (and probably patient satisfaction). Plus, reduction handoff errors should decrease, because only one doctor, rather than two, will have to get to know the new patient.
Eliminate Impediments
Some hospitalists with inefficient work habits have an opportunity to become more efficient at taking a history and reviewing records, along with other steps in the admission process, without risking poor quality. But most are reasonably efficient at those tasks already and shouldn’t make them the focus of throughput efforts.
That said, most, or nearly all, hospitalists could shorten the time from when the ED pages on a new admission to when we appear in the ED to see the patient.
Here is one scenario that gives rise to the type of delay I’m talking about. The ED doctor pages a triage hospitalist, and the two finally speak directly 10 minutes later. After a five-minute conversation, the triage doctor pages the hospitalist who will actually admit the patient, waits 10 minutes for the return call, relays the information (possibly leaving out or misrepresenting some of what the ED doc said), and the admitting hospitalist heads to the ED 15 minutes later. Each person in this scenario acted reasonably promptly, but the clock starts with the first ED page. The hospitalist is already at 45 minutes when they arrive to see the patient!
You need to minimize “daisy chain” communication between the ED doctor and the hospitalist who will actually see the patient. In the scenario above, I think it would be best to eliminate the triage doctor entirely (see my December 2008 column for ideas about how to do this) so that the hospitalist who will actually admit the patient learns of the new referral quickly and speaks directly with the ED doctor.
Another reason for a poor “page from ED to hospitalist at patient’s bedside” time is that the admitting hospitalist just doesn’t make it a priority to get to the ED quickly. They might decide to round on two or three more patients before working on the new admission. Of course, we must triage and sometimes delay getting to the ED while attending to an unstable floor patient, but not too often, in my experience.
I’m not suggesting that others adopt my habit: I typically don’t call the ED back at all. Instead, I just head to the ED immediately after being paged, and usually arrive in less time than I would have spent on hold waiting for the ED doc to come to the phone.
When presented with several ED patients to admit at the same time or tied up with a critical patient on the floor, getting to the ED quickly isn’t possible.
Write Admission or “Holding” Orders and Move the Patient to His/Her Room
This is frustrating for the admitting hospitalist, because among other problems, families often leave when the patient moves to the inpatient ward, and additional tests likely will take longer to complete from the floor rather than ED. And while it is hard to quantify, I think this practice increases the risk of errors—though some studies have shown that long ED stays are associated with worse outcomes for the patient, too.
One of the marquee principles of ED medicine has historically been “ED doctors should never write admission orders.” Even so, I sense that this view is shifting, and many now see this as clinically reasonable, and in some cases necessary, to ensure good performance. Our ED docs have agreed to do this if there is concern that the hospitalist can’t finish writing orders within an hour of first being paged about the patient. Ask me in a year and I’ll let you know just how this is going.
And, of course, another option is for the admitting hospitalist to provide admission orders or “holding” orders by phone. I think this is safe for many patients, as long as it is followed by a bedside admission visit by the hospitalist before too long.
Next month: What about throughput at the discharge end of the hospital stay? And yes, improving throughput risks quality of care, yet we have to do it while maintaining or improving quality.
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm.
To understand one reason why your hospital cares so much about patient throughput and discharging patients before noon, think of tables in a restaurant. A restaurant has a limited number of tables, and the more quickly they serve customers, the sooner they’re able to seat a new party. So by improving their throughput, they can serve more customers and increase profitability without having to add tables.
Of course, the more a restaurant pushes to increase throughput, the more it risks a decrease in the satisfaction of its customers. Too much focus on throughput could annoy customers so much that it puts them out of business (Seinfeld’s Soup Nazi is one notable exception).
Yet hospitals are likely to increase their customers’ satisfaction by improving “front-end” throughput from the ED to the inpatient unit. In fact, CMS added two new core measures (known as inpatient quality reporting, or IQR) that hospitals began reporting on Jan. 1:
- Median time from ED arrival to ED departure for admitted patients, and
- Admit decision time to ED departure for admitted patients.
You already knew about these, right? Although they don’t directly influence Medicare payments to your hospital now, there is a pretty good chance they could become part of the Hospital Value-Based Purchasing program in the future. So expect administrative leaders at your hospital to continue pestering you about ED throughput with even greater intensity.
I confess that improving throughput feels like one of the most difficult things for me to do, and I sweat when in meetings about it. Yet I know intellectually that we can do better. After all, it wasn’t that long ago that a patient could expect to wait hours to see an ED doctor, and shortening the wait seemed an impossible task. But EDs everywhere have done just that, and now lots of them post the current ED wait time (typically less than 10 or 15 minutes!) on the Internet or billboards. So if they can do it, then I’m sure hospitalists can, too.
I wrote about hospital throughput in my April 2009 and May 2010 columns, and included some strategies you might want to try. Here are a few more directed at ED-to-inpatient ward throughput.
The One-Admitter Approach
Most practices have no option other than a single admitter at night, but if your one admitter during daytime hours reliably gets behind, then you should have “rounders” help with admitting duties. While this is stressful for the rounder, and could sometimes delay the rounder’s ability to discharge patients early (more on that later), in most cases, the benefit will be worth the cost. In fact, I think the best arrangement is for all, or nearly all, daytime hospitalists to share admissions every day.
Remember, this approach will eliminate the admitter-to-rounder handoff from Day One to Day Two, resulting in a net increase in efficiency (and probably patient satisfaction). Plus, reduction handoff errors should decrease, because only one doctor, rather than two, will have to get to know the new patient.
Eliminate Impediments
Some hospitalists with inefficient work habits have an opportunity to become more efficient at taking a history and reviewing records, along with other steps in the admission process, without risking poor quality. But most are reasonably efficient at those tasks already and shouldn’t make them the focus of throughput efforts.
That said, most, or nearly all, hospitalists could shorten the time from when the ED pages on a new admission to when we appear in the ED to see the patient.
Here is one scenario that gives rise to the type of delay I’m talking about. The ED doctor pages a triage hospitalist, and the two finally speak directly 10 minutes later. After a five-minute conversation, the triage doctor pages the hospitalist who will actually admit the patient, waits 10 minutes for the return call, relays the information (possibly leaving out or misrepresenting some of what the ED doc said), and the admitting hospitalist heads to the ED 15 minutes later. Each person in this scenario acted reasonably promptly, but the clock starts with the first ED page. The hospitalist is already at 45 minutes when they arrive to see the patient!
You need to minimize “daisy chain” communication between the ED doctor and the hospitalist who will actually see the patient. In the scenario above, I think it would be best to eliminate the triage doctor entirely (see my December 2008 column for ideas about how to do this) so that the hospitalist who will actually admit the patient learns of the new referral quickly and speaks directly with the ED doctor.
Another reason for a poor “page from ED to hospitalist at patient’s bedside” time is that the admitting hospitalist just doesn’t make it a priority to get to the ED quickly. They might decide to round on two or three more patients before working on the new admission. Of course, we must triage and sometimes delay getting to the ED while attending to an unstable floor patient, but not too often, in my experience.
I’m not suggesting that others adopt my habit: I typically don’t call the ED back at all. Instead, I just head to the ED immediately after being paged, and usually arrive in less time than I would have spent on hold waiting for the ED doc to come to the phone.
When presented with several ED patients to admit at the same time or tied up with a critical patient on the floor, getting to the ED quickly isn’t possible.
Write Admission or “Holding” Orders and Move the Patient to His/Her Room
This is frustrating for the admitting hospitalist, because among other problems, families often leave when the patient moves to the inpatient ward, and additional tests likely will take longer to complete from the floor rather than ED. And while it is hard to quantify, I think this practice increases the risk of errors—though some studies have shown that long ED stays are associated with worse outcomes for the patient, too.
One of the marquee principles of ED medicine has historically been “ED doctors should never write admission orders.” Even so, I sense that this view is shifting, and many now see this as clinically reasonable, and in some cases necessary, to ensure good performance. Our ED docs have agreed to do this if there is concern that the hospitalist can’t finish writing orders within an hour of first being paged about the patient. Ask me in a year and I’ll let you know just how this is going.
And, of course, another option is for the admitting hospitalist to provide admission orders or “holding” orders by phone. I think this is safe for many patients, as long as it is followed by a bedside admission visit by the hospitalist before too long.
Next month: What about throughput at the discharge end of the hospital stay? And yes, improving throughput risks quality of care, yet we have to do it while maintaining or improving quality.
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm.
Hospital Value-Based Purchasing

Like all healthcare payors, Medicare has for some time tried to change from being a passive payor of services to a purchaser of value. There might be a lot of ways to do that, but one easy to conceptualize method is for Medicare to pay different amounts for a given service (i.e. a hospital stay for congestive heart failure) based on the quality of that service. Of course, the details of how to measure quality and implement such a program become terribly complex in a hurry.
Hospital value-based purchasing (HVBP), one of the provisions health reform, is one of the Centers for Medicare & Medicaid Services’ (CMS) first large-scale attempts to do just that.
CMS’ goals for this program include improving clinical quality, encouraging more patient-centered care, encouraging hospitals and clinicians to work together to improve quality of care, and empowering consumers to make value-based decisions about their healthcare (see “Value-Based Purchasing Raises the Stakes,” May 2011).
You already were aware that baseline measurements of quality performance for your hospital were collected from July 2009 through March 2010, right? And data collected from July 2010 through March 2011 serves as the first “Performance Period” to determine payment that will begin in October 2012. (If you are not aware, visit www.hospitalcompare.hhs.gov to see the performance your hospital is currently reporting. All the providers in your hospitalist group should be familiar with the data; another good site is www.whynotthebest.org. But keep in mind there is a significant delay in getting the data to display on these sites. In many cases, the data they display today is from nearly a year prior.)
Some Generalizations
HVBP has a number of features that are typical of new reimbursement programs:
- It is budget-neutral for Medicare. In other words, some hospitals will perform well and realize reimbursement increases; some hospitals will not perform well and will see reduced reimbursement.
- It builds on previous programs. HVBP essentially moves performance on core measures and HCAHPS surveys, all of which have been in place several years, from being publically reported to serving as metrics that influence reimbursement.
- The dollar amounts involved grow each year.
- Expect the program to evolve continuously. For example, the number and type of quality metrics on which the program is based will increase each year.
How It Works
Medicare will start withholding a portion of diagnosis-related group (DRG) payments to hospitals, starting with 1% initially and increasing by 0.25% annually, so that 2% is withheld in 2017. Keep in mind that amount is withheld from all DRG payments to a hospital, not just those related to the diagnoses that are part of the HVBP program.
Based on performance on core measures and patient satisfaction, hospitals have a chance to earn additional compensation that could be more or less than the initial 2% withholding. Additional performance measures will be added every year or so.
There are two ways a hospital can earn some of this performance-based compensation based on its “Total Performance Score.” Expressed in the language of Little League baseball, a hospital needs to be either a most valuable player—an MVP—or a most improved player.
The MVP pathway, known as “achievement,” is to grade hospitals on a curve established from the data collected for all hospitals the prior year. Those at the high end of the curve are paid more than the amount that was withheld from them (so they are “net winners”); those at the bottom of the curve are paid nothing (“net losers,” as they lost the chance to earn back any of the amount withheld).
The most improved pathway, cleverly called “improvement,” is for a hospital to improve its performance over its previous baseline, even if it fails to attain a high score relative to others. Measurement of the first baseline year ran from July 2010 through March 2011, and will be used as the reference point for performance from July 2011 through March 2012.
The precise amount of the payment for either of the two methods above is based on a sliding scale rather than an all-or-none threshold. SHM’s website (www.hospitalmedicine.org/hvbp) has an example of this calculation. A simple way to think of it is that a hospital won’t have to do a lot to earn back some portion of the amount withheld, but it has to hit a home run to earn back more than that.
The Dollars at Risk
It is worth thinking about the most a hospital could lose or gain under HVBP. Let’s take an example of a hospital that is paid $50 million annually by Medicare across all DRGs (this would be a pretty small hospital). In 2013, Medicare will pay that hospital only $49.5 million; that is, it will withhold 1% ($500,000) as part of the HVBP program. After the hospital’s Total Performance Score is computed, Medicare might pay more to the hospital in the form of an “add on” to the hospital’s typical DRG payments. If performance stinks or is worse than most hospitals and does not improve significantly over its own baseline, Medicare might not pay a nickel more. But for respectable performance, it might be paid 80% of the amount withheld—$400,000, in this example. So this hypothetical hospital would end up being a “net loser” of $100,000. By 2017, when 2% is withheld, the dollars at risk would be double.
From a practical perspective, the amount by which reimbursement will go up or down for most hospitals will be significantly less than the total withhold amount for most hospitals, so it probably won’t be enough to result in financial disaster or great profits. (Your hospital CFO may dispute this conclusion and you should listen to them.) But because a new “grading curve” is established each year, a score that puts a hospital in a financially attractive category one year might not look so good the next year. Therefore, a hospital whose performance stands still will likely become a net loser within a year or two.
Even if you were to conclude that the potential financial upside isn’t compelling enough to devote a lot of energy to perform well, the fact that most of the measures really do matter to our patients, and that this information is publicly reported, means every hospital should do whatever it takes to perform well. I suspect that patients and employers, as well as all types of payors, will pay more and more attention to your hospital’s performance and overall hospital volume affected in locales where patients have a choice of more than one hospital.
Learn More
I’ve provided only a very general HVBP overview here. Most hospitalist groups should identify at least one person who develops meaningful expertise in this program and other components of healthcare reform (i.e. bundled payments, penalties for excess readmissions, and penalties for hospital-acquired conditions). SHM is a terrific educational resource for these things and has a very informative HVBP toolkit available via its website.
Thanks to Drs. Win Whitcomb and Pat Torcson for helping to explain all this stuff to me. They and others at SHM do a great job of staying on top of things like healthcare reform.
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Like all healthcare payors, Medicare has for some time tried to change from being a passive payor of services to a purchaser of value. There might be a lot of ways to do that, but one easy to conceptualize method is for Medicare to pay different amounts for a given service (i.e. a hospital stay for congestive heart failure) based on the quality of that service. Of course, the details of how to measure quality and implement such a program become terribly complex in a hurry.
Hospital value-based purchasing (HVBP), one of the provisions health reform, is one of the Centers for Medicare & Medicaid Services’ (CMS) first large-scale attempts to do just that.
CMS’ goals for this program include improving clinical quality, encouraging more patient-centered care, encouraging hospitals and clinicians to work together to improve quality of care, and empowering consumers to make value-based decisions about their healthcare (see “Value-Based Purchasing Raises the Stakes,” May 2011).
You already were aware that baseline measurements of quality performance for your hospital were collected from July 2009 through March 2010, right? And data collected from July 2010 through March 2011 serves as the first “Performance Period” to determine payment that will begin in October 2012. (If you are not aware, visit www.hospitalcompare.hhs.gov to see the performance your hospital is currently reporting. All the providers in your hospitalist group should be familiar with the data; another good site is www.whynotthebest.org. But keep in mind there is a significant delay in getting the data to display on these sites. In many cases, the data they display today is from nearly a year prior.)
Some Generalizations
HVBP has a number of features that are typical of new reimbursement programs:
- It is budget-neutral for Medicare. In other words, some hospitals will perform well and realize reimbursement increases; some hospitals will not perform well and will see reduced reimbursement.
- It builds on previous programs. HVBP essentially moves performance on core measures and HCAHPS surveys, all of which have been in place several years, from being publically reported to serving as metrics that influence reimbursement.
- The dollar amounts involved grow each year.
- Expect the program to evolve continuously. For example, the number and type of quality metrics on which the program is based will increase each year.
How It Works
Medicare will start withholding a portion of diagnosis-related group (DRG) payments to hospitals, starting with 1% initially and increasing by 0.25% annually, so that 2% is withheld in 2017. Keep in mind that amount is withheld from all DRG payments to a hospital, not just those related to the diagnoses that are part of the HVBP program.
Based on performance on core measures and patient satisfaction, hospitals have a chance to earn additional compensation that could be more or less than the initial 2% withholding. Additional performance measures will be added every year or so.
There are two ways a hospital can earn some of this performance-based compensation based on its “Total Performance Score.” Expressed in the language of Little League baseball, a hospital needs to be either a most valuable player—an MVP—or a most improved player.
The MVP pathway, known as “achievement,” is to grade hospitals on a curve established from the data collected for all hospitals the prior year. Those at the high end of the curve are paid more than the amount that was withheld from them (so they are “net winners”); those at the bottom of the curve are paid nothing (“net losers,” as they lost the chance to earn back any of the amount withheld).
The most improved pathway, cleverly called “improvement,” is for a hospital to improve its performance over its previous baseline, even if it fails to attain a high score relative to others. Measurement of the first baseline year ran from July 2010 through March 2011, and will be used as the reference point for performance from July 2011 through March 2012.
The precise amount of the payment for either of the two methods above is based on a sliding scale rather than an all-or-none threshold. SHM’s website (www.hospitalmedicine.org/hvbp) has an example of this calculation. A simple way to think of it is that a hospital won’t have to do a lot to earn back some portion of the amount withheld, but it has to hit a home run to earn back more than that.
The Dollars at Risk
It is worth thinking about the most a hospital could lose or gain under HVBP. Let’s take an example of a hospital that is paid $50 million annually by Medicare across all DRGs (this would be a pretty small hospital). In 2013, Medicare will pay that hospital only $49.5 million; that is, it will withhold 1% ($500,000) as part of the HVBP program. After the hospital’s Total Performance Score is computed, Medicare might pay more to the hospital in the form of an “add on” to the hospital’s typical DRG payments. If performance stinks or is worse than most hospitals and does not improve significantly over its own baseline, Medicare might not pay a nickel more. But for respectable performance, it might be paid 80% of the amount withheld—$400,000, in this example. So this hypothetical hospital would end up being a “net loser” of $100,000. By 2017, when 2% is withheld, the dollars at risk would be double.
From a practical perspective, the amount by which reimbursement will go up or down for most hospitals will be significantly less than the total withhold amount for most hospitals, so it probably won’t be enough to result in financial disaster or great profits. (Your hospital CFO may dispute this conclusion and you should listen to them.) But because a new “grading curve” is established each year, a score that puts a hospital in a financially attractive category one year might not look so good the next year. Therefore, a hospital whose performance stands still will likely become a net loser within a year or two.
Even if you were to conclude that the potential financial upside isn’t compelling enough to devote a lot of energy to perform well, the fact that most of the measures really do matter to our patients, and that this information is publicly reported, means every hospital should do whatever it takes to perform well. I suspect that patients and employers, as well as all types of payors, will pay more and more attention to your hospital’s performance and overall hospital volume affected in locales where patients have a choice of more than one hospital.
Learn More
I’ve provided only a very general HVBP overview here. Most hospitalist groups should identify at least one person who develops meaningful expertise in this program and other components of healthcare reform (i.e. bundled payments, penalties for excess readmissions, and penalties for hospital-acquired conditions). SHM is a terrific educational resource for these things and has a very informative HVBP toolkit available via its website.
Thanks to Drs. Win Whitcomb and Pat Torcson for helping to explain all this stuff to me. They and others at SHM do a great job of staying on top of things like healthcare reform.
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Like all healthcare payors, Medicare has for some time tried to change from being a passive payor of services to a purchaser of value. There might be a lot of ways to do that, but one easy to conceptualize method is for Medicare to pay different amounts for a given service (i.e. a hospital stay for congestive heart failure) based on the quality of that service. Of course, the details of how to measure quality and implement such a program become terribly complex in a hurry.
Hospital value-based purchasing (HVBP), one of the provisions health reform, is one of the Centers for Medicare & Medicaid Services’ (CMS) first large-scale attempts to do just that.
CMS’ goals for this program include improving clinical quality, encouraging more patient-centered care, encouraging hospitals and clinicians to work together to improve quality of care, and empowering consumers to make value-based decisions about their healthcare (see “Value-Based Purchasing Raises the Stakes,” May 2011).
You already were aware that baseline measurements of quality performance for your hospital were collected from July 2009 through March 2010, right? And data collected from July 2010 through March 2011 serves as the first “Performance Period” to determine payment that will begin in October 2012. (If you are not aware, visit www.hospitalcompare.hhs.gov to see the performance your hospital is currently reporting. All the providers in your hospitalist group should be familiar with the data; another good site is www.whynotthebest.org. But keep in mind there is a significant delay in getting the data to display on these sites. In many cases, the data they display today is from nearly a year prior.)
Some Generalizations
HVBP has a number of features that are typical of new reimbursement programs:
- It is budget-neutral for Medicare. In other words, some hospitals will perform well and realize reimbursement increases; some hospitals will not perform well and will see reduced reimbursement.
- It builds on previous programs. HVBP essentially moves performance on core measures and HCAHPS surveys, all of which have been in place several years, from being publically reported to serving as metrics that influence reimbursement.
- The dollar amounts involved grow each year.
- Expect the program to evolve continuously. For example, the number and type of quality metrics on which the program is based will increase each year.
How It Works
Medicare will start withholding a portion of diagnosis-related group (DRG) payments to hospitals, starting with 1% initially and increasing by 0.25% annually, so that 2% is withheld in 2017. Keep in mind that amount is withheld from all DRG payments to a hospital, not just those related to the diagnoses that are part of the HVBP program.
Based on performance on core measures and patient satisfaction, hospitals have a chance to earn additional compensation that could be more or less than the initial 2% withholding. Additional performance measures will be added every year or so.
There are two ways a hospital can earn some of this performance-based compensation based on its “Total Performance Score.” Expressed in the language of Little League baseball, a hospital needs to be either a most valuable player—an MVP—or a most improved player.
The MVP pathway, known as “achievement,” is to grade hospitals on a curve established from the data collected for all hospitals the prior year. Those at the high end of the curve are paid more than the amount that was withheld from them (so they are “net winners”); those at the bottom of the curve are paid nothing (“net losers,” as they lost the chance to earn back any of the amount withheld).
The most improved pathway, cleverly called “improvement,” is for a hospital to improve its performance over its previous baseline, even if it fails to attain a high score relative to others. Measurement of the first baseline year ran from July 2010 through March 2011, and will be used as the reference point for performance from July 2011 through March 2012.
The precise amount of the payment for either of the two methods above is based on a sliding scale rather than an all-or-none threshold. SHM’s website (www.hospitalmedicine.org/hvbp) has an example of this calculation. A simple way to think of it is that a hospital won’t have to do a lot to earn back some portion of the amount withheld, but it has to hit a home run to earn back more than that.
The Dollars at Risk
It is worth thinking about the most a hospital could lose or gain under HVBP. Let’s take an example of a hospital that is paid $50 million annually by Medicare across all DRGs (this would be a pretty small hospital). In 2013, Medicare will pay that hospital only $49.5 million; that is, it will withhold 1% ($500,000) as part of the HVBP program. After the hospital’s Total Performance Score is computed, Medicare might pay more to the hospital in the form of an “add on” to the hospital’s typical DRG payments. If performance stinks or is worse than most hospitals and does not improve significantly over its own baseline, Medicare might not pay a nickel more. But for respectable performance, it might be paid 80% of the amount withheld—$400,000, in this example. So this hypothetical hospital would end up being a “net loser” of $100,000. By 2017, when 2% is withheld, the dollars at risk would be double.
From a practical perspective, the amount by which reimbursement will go up or down for most hospitals will be significantly less than the total withhold amount for most hospitals, so it probably won’t be enough to result in financial disaster or great profits. (Your hospital CFO may dispute this conclusion and you should listen to them.) But because a new “grading curve” is established each year, a score that puts a hospital in a financially attractive category one year might not look so good the next year. Therefore, a hospital whose performance stands still will likely become a net loser within a year or two.
Even if you were to conclude that the potential financial upside isn’t compelling enough to devote a lot of energy to perform well, the fact that most of the measures really do matter to our patients, and that this information is publicly reported, means every hospital should do whatever it takes to perform well. I suspect that patients and employers, as well as all types of payors, will pay more and more attention to your hospital’s performance and overall hospital volume affected in locales where patients have a choice of more than one hospital.
Learn More
I’ve provided only a very general HVBP overview here. Most hospitalist groups should identify at least one person who develops meaningful expertise in this program and other components of healthcare reform (i.e. bundled payments, penalties for excess readmissions, and penalties for hospital-acquired conditions). SHM is a terrific educational resource for these things and has a very informative HVBP toolkit available via its website.
Thanks to Drs. Win Whitcomb and Pat Torcson for helping to explain all this stuff to me. They and others at SHM do a great job of staying on top of things like healthcare reform.
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.