User login
HIV screening: Latest testing guidelines
• Patients with mental illness are at elevated risk for HIV infection.
• Fourth-generation (p24) HIV testing allows accurate, office-based screening during the period of highest infectivity.
• Psychiatrists may be uniquely able to discuss and alter patients’ high-risk behaviors related to HIV transmission and treatment.
Substance use and high-risk sexual behaviors are common among persons with severe mental illness and make them vulnerable to human immunodeficiency virus (HIV) infection.1-3 The prevalence of HIV is 3 times higher among these patients compared with individuals who are not mentally ill. This article reviews risk factors for HIV transmission, HIV screening recommendations, and current testing options, including the fourth-generation HIV test.
According to the World Health Organization, in 2009:
- 33 million people were infected with HIV
- there were 2.6 million new infections
- 1.8 million people died from causes related to acquired immune deficiency syndrome (AIDS).4
In the United States, approximately 1 million people are living with HIV; 55, 000 new cases were diagnosed in North America in 2009.5 The demographics of those infected with HIV in the United States have changed substantially. Most newly infected individuals are African American, and younger adults have higher rates of new infections.6 With the introduction of standardized antiviral medication combinations and federal programs to provide universal access to medications in the mid 1990s, the number of AIDS cases and mortality dropped, but there have not been similar gains in the past decade.6
In countries With access to antiviral medications, medical advances in HIV treatment have transformed an infection with a high mortality rate into a chronic illness. However, the rate of new cases has not changed significantly in the past 10 years. Early detection and treatment initiation reduces high-risk behavior and subsequent transmission in patients with HIV. Evidence suggests that detecting HIV in the acute phase of the illness, when the viral load is high, reduces HIV transmission.1,5,6
HIV screening
HIV screening should be part of routine psychiatric practice, especially in community and forensic settings. We recommend that all psychiatrists understand HIV screening guidelines from the Centers for Disease Control and Prevention (CDC)7 and the American College of Physicians (ACP).8 The CDC (2006)7 and ACP (2009)8 guidelines recommend HIV screening for:
- all patients age 13 to 64, unless the prevalence of undiagnosed HIV infection in your patients has been documented to be <0. 1%7
- all patients seeking treatment for sexually transmitted diseases, including each visit for a new complaint7
- all pregnant women7
- any patient who received a blood transfusion between 1978 and 1985.8
Rescreening frequency is determined on an individual basis, taking into consideration the patient’s risk of contracting HIV. The ACP guidelines recommend using rapid tests when available.8 Although the false positive rates are higher with rapid tests, the benefits of early detection and reducing transmission outweigh the cost of confirming positive tests.8
The fourth-generation test
The gold standard for HIV screening is the enzyme-linked immunosorbent assay antibody test followed by a western blot.8 This has a high sensitivity and specificity but there is a window of time between infection and detectable antibodies in serum during which patients have high virus levels (Figure).9 The combined antibody and antigen p24 test is a fourth-generation screening tool that detects HIV in the acute phase of the illness without requiring expensive ribonucleic acid viral tests.10 The fourth-generation test’s capacity to detect infection during the antibody-negative window when infectivity is highest may help decrease HIV transmission.11
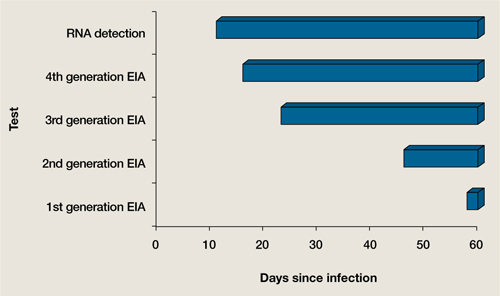
Figure When can HIV tests detect the virus?
EIA: enzyme immunoassay; HIV: human immunodeficiency virus; RNA: ribonucleic acid
Source: Adapted from reference 9
Psychiatrists’ role
Because psychiatrists routinely interact with patients who have an increased risk of HIV, they may be uniquely qualified to help these individuals. Psychiatrists often are comfortable discussing patients’ sexual and substance use history, which allows them to uncover and effectively address high-risk behaviors with appropriate testing and counseling. If testing confirms HIV infection, psychiatrists also can discuss altering high-risk behaviors (Table),1,2 which has significant implications not only for patients, but also for public health.
Table
HIV transmission risk factors
| Intravenous drug use |
| Nonintravenous cocaine use |
| Sex without barrier protection, especially in patients with multiple partners |
| Sex trade or sex work |
| HIV: human immunodeficiency virus |
| Source: References 1,2 |
Related Resource
- Centers for Disease Control and Prevention. HIV/AIDS. www.cdc.gov/hiv.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Rosenberg SD, Goodman LA, Osher FC, et al. Prevalence of HIV, hepatitis B, and hepatitis C in people with severe mental illness. Am J Health. 2001;91:31-37.
2. Quinn TC, Glasser D, Cannon RO, et al. Human immunodeficiency virus infection among patients attending clinics for sexually transmitted diseases. N Eng J Med. 1988;318:197-203.
3. Erickson B, Wasserheit JN, Rompalo AM, et al. Routine voluntary HIV screening in STD clinic clients: characterization of infected clients. Sex Transm Dis. 1990;17:194-199.
4. World Health Organization. Global summary of the AIDS epidemic. Available at: http://www.who.int/hiv/data/2009_global_summary.png. Accessed February 10 2011.
5. Hall HI, Song R, Rhodes P, et al. Estimation of HIV incidence in the United States. JAMA. 2008;300:520-529.
6. Glynn MK, Lee LM, McKenna MT. The status of national HIV case surveillance United States 2006. Public Health Rep. 2007;122(suppl 1):63-71.
7. Branson BM, Handsfield HH, Lampe MA, et al. and the Centers for Disease Control and Prevention. Revised recommendations for HIV testing of adults adolescents, and pregnant women in health-care settings. MMWR Recomm Rep. 2006;55(RR-14):1-17; quiz CE1-CE4.
8. Qaseem A, Snow V, Shekelle P, et al. and the Clinical Efficacy Assessment Subcommittee American College of Physicians. Screening for HIV in health care settings: a guidance statement from the American College of Physicians and HIV Medicine Association. Ann Intern Med. 2009;150:125-131.
9. Branson BM. The future of HIV testing. J Acquir Immune Defic Syndr. 2010;55:S102-S105.
10. Eshleman S, Khaki L, Laeyendecker O, et al. Detection of individuals with acute HIV-1 infection using the ARCHITECT HIV Ag/Ab combo assay. J Acquir Immune Defic Syndr. 2009;52:121-124.
11. Pandori MW, Hackett J, Jr, Louie B, et al. Assessment of the ability of a fourth-generation immunoassay for human immunodeficiency virus (HIV) antibody and p24 antigen to detect both acute and recent HIV infections in a high-risk setting. J Clin Microbiol. 2009;47:2639-2642.
John Onate, MD
Dr. Onate is Health Sciences Assistant Clinical Professor, Department of Psychiatry and Behavioral Sciences
Travis Fisher, MD
Dr. Fisher is Fellow, Department of Psychosomatic Medicine, University of California Davis Medical Center, Sacramento, CA.
Robert M. McCarron, DO
Series Editor
John Onate, MD
Dr. Onate is Health Sciences Assistant Clinical Professor, Department of Psychiatry and Behavioral Sciences
Travis Fisher, MD
Dr. Fisher is Fellow, Department of Psychosomatic Medicine, University of California Davis Medical Center, Sacramento, CA.
Robert M. McCarron, DO
Series Editor
John Onate, MD
Dr. Onate is Health Sciences Assistant Clinical Professor, Department of Psychiatry and Behavioral Sciences
Travis Fisher, MD
Dr. Fisher is Fellow, Department of Psychosomatic Medicine, University of California Davis Medical Center, Sacramento, CA.
Robert M. McCarron, DO
Series Editor
• Patients with mental illness are at elevated risk for HIV infection.
• Fourth-generation (p24) HIV testing allows accurate, office-based screening during the period of highest infectivity.
• Psychiatrists may be uniquely able to discuss and alter patients’ high-risk behaviors related to HIV transmission and treatment.
Substance use and high-risk sexual behaviors are common among persons with severe mental illness and make them vulnerable to human immunodeficiency virus (HIV) infection.1-3 The prevalence of HIV is 3 times higher among these patients compared with individuals who are not mentally ill. This article reviews risk factors for HIV transmission, HIV screening recommendations, and current testing options, including the fourth-generation HIV test.
According to the World Health Organization, in 2009:
- 33 million people were infected with HIV
- there were 2.6 million new infections
- 1.8 million people died from causes related to acquired immune deficiency syndrome (AIDS).4
In the United States, approximately 1 million people are living with HIV; 55, 000 new cases were diagnosed in North America in 2009.5 The demographics of those infected with HIV in the United States have changed substantially. Most newly infected individuals are African American, and younger adults have higher rates of new infections.6 With the introduction of standardized antiviral medication combinations and federal programs to provide universal access to medications in the mid 1990s, the number of AIDS cases and mortality dropped, but there have not been similar gains in the past decade.6
In countries With access to antiviral medications, medical advances in HIV treatment have transformed an infection with a high mortality rate into a chronic illness. However, the rate of new cases has not changed significantly in the past 10 years. Early detection and treatment initiation reduces high-risk behavior and subsequent transmission in patients with HIV. Evidence suggests that detecting HIV in the acute phase of the illness, when the viral load is high, reduces HIV transmission.1,5,6
HIV screening
HIV screening should be part of routine psychiatric practice, especially in community and forensic settings. We recommend that all psychiatrists understand HIV screening guidelines from the Centers for Disease Control and Prevention (CDC)7 and the American College of Physicians (ACP).8 The CDC (2006)7 and ACP (2009)8 guidelines recommend HIV screening for:
- all patients age 13 to 64, unless the prevalence of undiagnosed HIV infection in your patients has been documented to be <0. 1%7
- all patients seeking treatment for sexually transmitted diseases, including each visit for a new complaint7
- all pregnant women7
- any patient who received a blood transfusion between 1978 and 1985.8
Rescreening frequency is determined on an individual basis, taking into consideration the patient’s risk of contracting HIV. The ACP guidelines recommend using rapid tests when available.8 Although the false positive rates are higher with rapid tests, the benefits of early detection and reducing transmission outweigh the cost of confirming positive tests.8
The fourth-generation test
The gold standard for HIV screening is the enzyme-linked immunosorbent assay antibody test followed by a western blot.8 This has a high sensitivity and specificity but there is a window of time between infection and detectable antibodies in serum during which patients have high virus levels (Figure).9 The combined antibody and antigen p24 test is a fourth-generation screening tool that detects HIV in the acute phase of the illness without requiring expensive ribonucleic acid viral tests.10 The fourth-generation test’s capacity to detect infection during the antibody-negative window when infectivity is highest may help decrease HIV transmission.11
Figure When can HIV tests detect the virus?
EIA: enzyme immunoassay; HIV: human immunodeficiency virus; RNA: ribonucleic acid
Source: Adapted from reference 9
Psychiatrists’ role
Because psychiatrists routinely interact with patients who have an increased risk of HIV, they may be uniquely qualified to help these individuals. Psychiatrists often are comfortable discussing patients’ sexual and substance use history, which allows them to uncover and effectively address high-risk behaviors with appropriate testing and counseling. If testing confirms HIV infection, psychiatrists also can discuss altering high-risk behaviors (Table),1,2 which has significant implications not only for patients, but also for public health.
Table
HIV transmission risk factors
| Intravenous drug use |
| Nonintravenous cocaine use |
| Sex without barrier protection, especially in patients with multiple partners |
| Sex trade or sex work |
| HIV: human immunodeficiency virus |
| Source: References 1,2 |
Related Resource
- Centers for Disease Control and Prevention. HIV/AIDS. www.cdc.gov/hiv.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
• Patients with mental illness are at elevated risk for HIV infection.
• Fourth-generation (p24) HIV testing allows accurate, office-based screening during the period of highest infectivity.
• Psychiatrists may be uniquely able to discuss and alter patients’ high-risk behaviors related to HIV transmission and treatment.
Substance use and high-risk sexual behaviors are common among persons with severe mental illness and make them vulnerable to human immunodeficiency virus (HIV) infection.1-3 The prevalence of HIV is 3 times higher among these patients compared with individuals who are not mentally ill. This article reviews risk factors for HIV transmission, HIV screening recommendations, and current testing options, including the fourth-generation HIV test.
According to the World Health Organization, in 2009:
- 33 million people were infected with HIV
- there were 2.6 million new infections
- 1.8 million people died from causes related to acquired immune deficiency syndrome (AIDS).4
In the United States, approximately 1 million people are living with HIV; 55, 000 new cases were diagnosed in North America in 2009.5 The demographics of those infected with HIV in the United States have changed substantially. Most newly infected individuals are African American, and younger adults have higher rates of new infections.6 With the introduction of standardized antiviral medication combinations and federal programs to provide universal access to medications in the mid 1990s, the number of AIDS cases and mortality dropped, but there have not been similar gains in the past decade.6
In countries With access to antiviral medications, medical advances in HIV treatment have transformed an infection with a high mortality rate into a chronic illness. However, the rate of new cases has not changed significantly in the past 10 years. Early detection and treatment initiation reduces high-risk behavior and subsequent transmission in patients with HIV. Evidence suggests that detecting HIV in the acute phase of the illness, when the viral load is high, reduces HIV transmission.1,5,6
HIV screening
HIV screening should be part of routine psychiatric practice, especially in community and forensic settings. We recommend that all psychiatrists understand HIV screening guidelines from the Centers for Disease Control and Prevention (CDC)7 and the American College of Physicians (ACP).8 The CDC (2006)7 and ACP (2009)8 guidelines recommend HIV screening for:
- all patients age 13 to 64, unless the prevalence of undiagnosed HIV infection in your patients has been documented to be <0. 1%7
- all patients seeking treatment for sexually transmitted diseases, including each visit for a new complaint7
- all pregnant women7
- any patient who received a blood transfusion between 1978 and 1985.8
Rescreening frequency is determined on an individual basis, taking into consideration the patient’s risk of contracting HIV. The ACP guidelines recommend using rapid tests when available.8 Although the false positive rates are higher with rapid tests, the benefits of early detection and reducing transmission outweigh the cost of confirming positive tests.8
The fourth-generation test
The gold standard for HIV screening is the enzyme-linked immunosorbent assay antibody test followed by a western blot.8 This has a high sensitivity and specificity but there is a window of time between infection and detectable antibodies in serum during which patients have high virus levels (Figure).9 The combined antibody and antigen p24 test is a fourth-generation screening tool that detects HIV in the acute phase of the illness without requiring expensive ribonucleic acid viral tests.10 The fourth-generation test’s capacity to detect infection during the antibody-negative window when infectivity is highest may help decrease HIV transmission.11
Figure When can HIV tests detect the virus?
EIA: enzyme immunoassay; HIV: human immunodeficiency virus; RNA: ribonucleic acid
Source: Adapted from reference 9
Psychiatrists’ role
Because psychiatrists routinely interact with patients who have an increased risk of HIV, they may be uniquely qualified to help these individuals. Psychiatrists often are comfortable discussing patients’ sexual and substance use history, which allows them to uncover and effectively address high-risk behaviors with appropriate testing and counseling. If testing confirms HIV infection, psychiatrists also can discuss altering high-risk behaviors (Table),1,2 which has significant implications not only for patients, but also for public health.
Table
HIV transmission risk factors
| Intravenous drug use |
| Nonintravenous cocaine use |
| Sex without barrier protection, especially in patients with multiple partners |
| Sex trade or sex work |
| HIV: human immunodeficiency virus |
| Source: References 1,2 |
Related Resource
- Centers for Disease Control and Prevention. HIV/AIDS. www.cdc.gov/hiv.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Rosenberg SD, Goodman LA, Osher FC, et al. Prevalence of HIV, hepatitis B, and hepatitis C in people with severe mental illness. Am J Health. 2001;91:31-37.
2. Quinn TC, Glasser D, Cannon RO, et al. Human immunodeficiency virus infection among patients attending clinics for sexually transmitted diseases. N Eng J Med. 1988;318:197-203.
3. Erickson B, Wasserheit JN, Rompalo AM, et al. Routine voluntary HIV screening in STD clinic clients: characterization of infected clients. Sex Transm Dis. 1990;17:194-199.
4. World Health Organization. Global summary of the AIDS epidemic. Available at: http://www.who.int/hiv/data/2009_global_summary.png. Accessed February 10 2011.
5. Hall HI, Song R, Rhodes P, et al. Estimation of HIV incidence in the United States. JAMA. 2008;300:520-529.
6. Glynn MK, Lee LM, McKenna MT. The status of national HIV case surveillance United States 2006. Public Health Rep. 2007;122(suppl 1):63-71.
7. Branson BM, Handsfield HH, Lampe MA, et al. and the Centers for Disease Control and Prevention. Revised recommendations for HIV testing of adults adolescents, and pregnant women in health-care settings. MMWR Recomm Rep. 2006;55(RR-14):1-17; quiz CE1-CE4.
8. Qaseem A, Snow V, Shekelle P, et al. and the Clinical Efficacy Assessment Subcommittee American College of Physicians. Screening for HIV in health care settings: a guidance statement from the American College of Physicians and HIV Medicine Association. Ann Intern Med. 2009;150:125-131.
9. Branson BM. The future of HIV testing. J Acquir Immune Defic Syndr. 2010;55:S102-S105.
10. Eshleman S, Khaki L, Laeyendecker O, et al. Detection of individuals with acute HIV-1 infection using the ARCHITECT HIV Ag/Ab combo assay. J Acquir Immune Defic Syndr. 2009;52:121-124.
11. Pandori MW, Hackett J, Jr, Louie B, et al. Assessment of the ability of a fourth-generation immunoassay for human immunodeficiency virus (HIV) antibody and p24 antigen to detect both acute and recent HIV infections in a high-risk setting. J Clin Microbiol. 2009;47:2639-2642.
1. Rosenberg SD, Goodman LA, Osher FC, et al. Prevalence of HIV, hepatitis B, and hepatitis C in people with severe mental illness. Am J Health. 2001;91:31-37.
2. Quinn TC, Glasser D, Cannon RO, et al. Human immunodeficiency virus infection among patients attending clinics for sexually transmitted diseases. N Eng J Med. 1988;318:197-203.
3. Erickson B, Wasserheit JN, Rompalo AM, et al. Routine voluntary HIV screening in STD clinic clients: characterization of infected clients. Sex Transm Dis. 1990;17:194-199.
4. World Health Organization. Global summary of the AIDS epidemic. Available at: http://www.who.int/hiv/data/2009_global_summary.png. Accessed February 10 2011.
5. Hall HI, Song R, Rhodes P, et al. Estimation of HIV incidence in the United States. JAMA. 2008;300:520-529.
6. Glynn MK, Lee LM, McKenna MT. The status of national HIV case surveillance United States 2006. Public Health Rep. 2007;122(suppl 1):63-71.
7. Branson BM, Handsfield HH, Lampe MA, et al. and the Centers for Disease Control and Prevention. Revised recommendations for HIV testing of adults adolescents, and pregnant women in health-care settings. MMWR Recomm Rep. 2006;55(RR-14):1-17; quiz CE1-CE4.
8. Qaseem A, Snow V, Shekelle P, et al. and the Clinical Efficacy Assessment Subcommittee American College of Physicians. Screening for HIV in health care settings: a guidance statement from the American College of Physicians and HIV Medicine Association. Ann Intern Med. 2009;150:125-131.
9. Branson BM. The future of HIV testing. J Acquir Immune Defic Syndr. 2010;55:S102-S105.
10. Eshleman S, Khaki L, Laeyendecker O, et al. Detection of individuals with acute HIV-1 infection using the ARCHITECT HIV Ag/Ab combo assay. J Acquir Immune Defic Syndr. 2009;52:121-124.
11. Pandori MW, Hackett J, Jr, Louie B, et al. Assessment of the ability of a fourth-generation immunoassay for human immunodeficiency virus (HIV) antibody and p24 antigen to detect both acute and recent HIV infections in a high-risk setting. J Clin Microbiol. 2009;47:2639-2642.