User login
Performance anxiety: How to ease stage fright
The violin is slippery in my grasp. I hear the thud of my foot tapping, but the tempo feels wrong. I’m aware of my chest pounding, a lump in my throat, and heat rising from my face. Everyone is watching me, waiting for me to make a mistake.
Why can’t I stop my hand from trembling? I can only watch as the bow jumps noisily across the strings. I should have practiced more. My mind goes blank, and I miss the page turn.
Silence. I blink, and the lights blind me as the applause comes, thankfully, and I exhale and run off the stage as the curtain closes.
Well-known performing artists—Sir Laurence Olivier, Kim Basinger, Peter O’Toole, Richard Burton, Barbra Streisand, and Luciano Pavarotti —have described bouts with acute stage fright. Performance anxiety can occur with acting, singing, or playing a musical instrument, and with nonartistic performances such as public speaking, oral examinations, competing in sporting events, sexual activity, using public restrooms, or being watched while doing a task such as surgery, eating, or writing.2
Like social phobia, performance anxiety probably develops in accomplished artists and not-so-famous individuals because of a mélange of genetic factors, innate temperament, parental influences, conditioning events, and cognitive influences.3
NORMAL VS. ABNORMAL FEAR
Performance anxiety is characterized by persisting, distressful apprehension about—or actual impairment of—performance skills to a degree unwarranted by the individual’s aptitude, training, and preparation.1 Not all performance anxiety qualifies as a mental disorder; for example, though 85% of the population experiences discomfort about public speaking,4 this anxiety does not impair most people’s ability to function.
Mild to moderate anxiety is normal and motivating in performances.5 However, anxiety’s effect on performance does not follow a bell-shaped curve, wherein moderate anxiety promotes optimal performance.6 Instead, a catastrophic model is more accurate: increasing anxiety is helpful until a certain threshold is reached, then performance plunges.7
Diagnostic criteria. DSM-IV-TR describes performance anxiety as a form of social phobia (or social anxiety disorder) characterized by marked and persistent fear of social or performance situations in which embarrassment or humiliation might occur. Approximately 13% of adults experience social phobia,8 and about 2% suffer from severe discrete performance anxiety.9
Performance anxiety does not completely overlap with social phobia, however. Test-taking anxiety and writer’s block, which can occur in a nonpublic context, do not fit neatly into the social phobia category.2 Thus, some performance anxiety forms are better grouped as another type of anxiety disorder, such as specific phobia (Figure).
Figure Performance anxiety features overlap with other anxieties
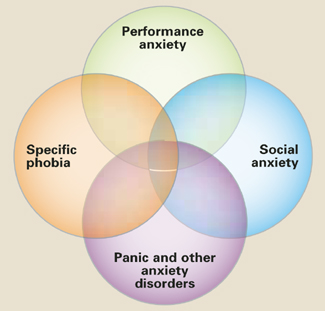
Performance anxiety is not easy to categorize. It is situational anxiety that occurs in a public context and overlaps with but does not entirely match diagnostic criteria for specific phobia, social anxiety, or panic disorder and generalized anxiety.
DIFFERENTIAL DIAGNOSIS
Social anxiety? Ask the patient about all situations that provoke anxiety to differentiate between:
- discrete performance anxiety (1 or 2 performance situations that provoke anxiety)
- and generalized social anxiety (3 or more situations that provoke anxiety).9
Individuals with “trait” anxiety may exhibit innate shyness and are considered to have generalized social phobia. Those with “state” anxiety experience anxiety in specific situations or circumstances and are more aptly described as having discrete performance anxiety.10 Whereas persons with social phobia may avoid the feared activity without inner conflict, those with performance anxiety are committed to performing the activity and are distressed when unable to perform.9
Specific phobia? A specific phobia is a circumscribed fear of a specific object, situation, or activity from which a grim outcome is feared. Specific phobia usually has no performance aspect or fear of embarrassment or failure.
Some clinicians consider certain performance anxieties—such as writer’s block, test-taking anxiety, paruresis, and even fear about sexual performance—to be specific phobias. Because performance anxieties and phobias share some cognitive and behavioral components, their treatments are similar and use of medication is controversial.
General medical condition? Perform or refer the patient for a thorough medical evaluation before you diagnose performance anxiety, as endocrine, cardiovascular, respiratory, and circulatory abnormalities can mimic or exacerbate anxiety disorders. Also consider substance abuse or withdrawal as possible causes of anxiety.
PATIENT EVALUATION
Family history. Individuals with social anxiety often report a family history of generalized social anxiety, panic disorder, or major depressive disorder.3 Similar findings seem plausible for persons with discrete performance anxiety, although comparable family history data have not been reported.
Cognitive symptoms. Four cognitive distortions are common in persons with social phobia (Table 1).11 These negative thoughts are presumably the same for performance anxiety, at least when it is a sub-type of social phobia.
Somatic symptoms. Persons with performance anxiety tend to have heightened awareness of hyperadrenergic arousal symptoms (Table 2), sometimes in all body systems. Symptoms may resemble those of a panic attack.
Behavioral symptoms. Behavioral symptoms include stuttering, mumbling, trembling voice, yawning, biting nails or lips, gritting jaw, poor eye contact, shuffling or tapping feet, unnatural or rigid postures or movements, warming up too fast or too slowly, wearing excessive makeup, or smiling abnormally. A performer may forget to carry out a routine task such as blinking, moistening lips, or turning a page of music.
These behaviors may perpetuate and reinforce anxiety by eliciting negative reactions from an audience and fulfilling the performer’s pessimistic expectations. The therapist can identify these maladaptive behaviors and target them for treatment.
Table 1
4 cognitive distortions that underlie performance anxiety
|
Table 2
Somatic symptoms of performance anxiety
| Bodily system | Symptoms |
|---|---|
| Autonomic | Blushing, diaphoresis, dry mouth |
| GI, urologic | Urinary or bowel urgency, GI discomfort |
| Cardiovascular | Tachycardia, palpitations |
| Neuromuscular | Muscle tension, tremor, paralysis |
PSYCHIATRIC COMORBIDITY
About one-third of individuals with performance anxiety have psychiatric comorbidities.9 Most common are other anxiety disorders, specifically the generalized form of social phobia, generalized anxiety disorder, panic disorder, or specific phobia.12 Mood disorders are less common. We also recommend monitoring for eating disorders because some performing artists are driven to maintain high physical appearance standards.
Personality disorder comorbidities with performance anxiety have not been studied. Some experts believe that avoidant personality and social phobia are the same conditions expressed to varying degrees on a continuum.13 Other personality disorders to consider include schizoid, paranoid, and obsessive-compulsive personalities.
Alcohol and substance use disorders are highly comorbid with performance anxiety. Alcohol use decreases public speaking anxiety,14 and approximately 6% of orchestral musicians use alcohol before a performance.15 For comparison, approximately 16% of patients who present for treatment of generalized anxiety disorder abuse alcohol, often as an attempt to self-medicate.16
TREATMENT PLANNING
Just as performance anxiety’s diagnostic classification may vary, so may treatment. Pharmacologic interventions and psychotherapy for social and specific phobias are similar. Some clinicians favor a multimodal approach addressing behavior, affect, sensation, imagery, cognition, interpersonal relationships, and biological factors.9
The performing arts community is competitive, and individuals may have differing standards about what treatments are acceptable. Some may view using medications as “cheating” or an admission of professional failure. A performer may feel medication gives an unfair advantage, that respect would be lost if others found out, or that taking medication before performing is similar to steroid use by athletes.17,18
Medication vs. psychotherapy. Medication can help diminish anxiety’s physical symptoms, but certain psychotherapies rely on these somatic symptoms for effective treatment and extinguishing of responses. Concurrent use of medications and psychotherapy for social phobia is common in everyday practice, although some studies find the combination no more effective than either treatment alone.11 Symptoms appear less likely to return after cognitive-behavioral therapy (CBT) ends than after medication is discontinued.16
Discuss treatment options with the patient. A patient who feels unable to perform without medication may develop psychological dependency. Conversely, a patient may not be able to afford the full course of psychotherapy needed for positive results. For performing artists, longer visits that incorporate medication management with psychotherapy may be more successful than brief, symptom-targeted visits.
MEDICATION MANAGEMENT
All medication use for performance anxiety is off-label. The most common choices are short-acting agents such as beta blockers or benzodiazepines (Table 3).
Table 3
Medications used to treat performance anxiety*
| Medication | Typical dosage | Possible side effects |
|---|---|---|
| Beta blockers | Medical: sedation, fatigue, dizziness, ataxia, nausea, sexual dysfunction Psychiatric:insomnia, nightmares, depression Contraindications: heart failure, bradycardia, breathing difficulties, hypotension | |
| Propranolol | 10 to 40 mg | |
| Nadolol | 20 to 120 mg | |
| Atenolol | 50 to 100 mg | |
| Benzodiazepines | Performance decrement, amnesia, sedation, discontinuation symptoms, tolerance, abuse potential | |
| Clonazepam | 0.25 to 0.5 mg | |
| Lorazepam | 0.5 to 1 mg | |
| * Off-label use; taken as-needed approximately 1 hour before performance | ||
Beta blockers can relieve autonomic and somatic symptoms such as tachycardia, tremor, and stuttering when used in low doses as needed for mild to moderate circumscribed performance anxiety.16,19 Propranolol, 10 mg about 1 hour before the performance, is most often prescribed.
Before prescribing a beta blocker, evaluate the patient’s medical history and cardiovascular status, including blood pressure and pulse. Have the patient try a test dose before the first live performance to check for side effects and tolerability (Table 3).16,19
Benzodiazepines have been used to treat social anxiety, but controlled studies have not reliably addressed their efficacy in performance anxiety. Advise the patient to abstain from alcohol when taking these medications (Table 3).
PSYCHOTHERAPY OPTIONS
CBT with components of exposure and retraining can ameliorate performance anxiety.10,20
Many performers forgo normal childhood social experiences to hone their talents, at times sacrificing sound coping skills.17 CBT’s goal is to help them reduce negative biases and restructure cognitive processes to function better at whatever task is at hand. This involves teaching them to:
- recognize pessimistic thoughts that occur before, during, and after performances
- challenge the accuracy of these thoughts
- replace them with rational, helpful thoughts based on the assimilated information.11
Exposure therapy can help individuals face feared activities so that counter-conditioning through habituation and extinction can safely occur. Useful strategies include imagination, role play, confrontation, videotaping, and homework assignments.11
Experiencing anxiety is a component of exposure therapy. Thus, some clinicians avoid using concomitant medication that might decrease anxiety’s physical symptoms and interfere with the exposure process.21
Relaxation training can help the patient recognize and respond to autonomic and physical arousal during a performance.11 For example, progressive muscle relaxation can be practiced first in session and then as homework.
Social skills training can help patients identify and change anxiety behaviors that cause negative audience reactions. Tools to help direct the patient towards more appropriate behaviors include modeling, behavior rehearsal, corrective feedback, social reinforcement, and homework assignments such as videotaping performances.11 For public speaking anxiety, vocal and physical skills training10 and computerized virtual reality courses can help.4
Interpersonal therapy may be useful, based on the premise that performance anxiety occurs within a social and interpersonal context.22
Related resources
- Toastmasters for public speaking. http://www.toastmasters.com
- Anxiety Disorders Association of America. http://www.adaa.org
- Social Anxiety Association. http://www.socialphobia.org
Drug brand names
- Atenolol • Tenormin
- Clonazepam • Klonopin
- Lorazepam • Ativan
- Nadolol • Corgard
- Propranolol • Inderal
Disclosure
Dr. Kelly reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Saveanu receives research support from Pfizer Inc. and is a consultant and speaker for Pfizer Inc. and GlaxoSmithKline.
1. Salmon PG. A psychological perspective on musical performance anxiety: a review of the literature. Med Prob Perform Artists 1900;51(1):2-11.
2. Beatty M. Situational and predispositional correlates of public speaking anxiety. Commun Ed 1998;37:28-39.
3. Ollendick TH, Hirshfeld-Becker DR. The developmental psychopathology of social anxiety disorder. Biol Psychiatry 2002;51(1):44-58.
4. Harris SR, Kemmerling RL, North MM. Brief virtual reality therapy for public speaking anxiety. Cyberpsychol Behav 2002;5(6):543-50.
5. Rafferty BD, Smith RE, Ptacek JT. Facilitating and debilitating trait anxiety, situational anxiety, and coping with an anticipated stressor: a process analysis. J Pers Soc Psychol 1997;72:892-906.
6. Yerkes RM, Dodson JD. The relation of strength of stimulus to rapidity of habit formation. J Comp Neurol Psychol 1908;18:459-482.
7. Hardy L, Parfitt G. A catastrophic model of anxiety and performance. Br J Psychol 1991;82:163-78.
8. Kessler RC, McGonagle KA, Zhao S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: results from the National Comorbidity Survey. Arch Gen Psychiatry 1994;51(1):8-19.
9. Powell D. Treating individuals with debilitating performance anxiety: an introduction. J Clin Psychol 2004;60(8):801-8.
10. Merritt L, Richards A, Davis P. Performance anxiety: loss of the spoken edge. J Voice 2001;15(2):257-69.
11. Heimberg RG. Cognitive-behavioral therapy for social anxiety disorder: current status and future directions. Biol Psychiatry 2002;51:101-8.
12. Brown TA, Barlow DH. Comorbidities among anxiety disorders: implications for treatment and DSM-IV. J Consult Clin Psychol 1992;60(6):835-44.
13. Schneier FR, Johnson J, Hornig CD, et al. Social phobia: comorbidity and morbidity in an epidemiologic sample. Arch Gen Psychiatry 1992;49:282-8.
14. Abrams K, Kushner M, Medina K, Voight A. Self-administration of alcohol before and after a public speaking challenge by individuals with social phobias. Psychol Addict Behav 2002;16(1):121-8.
15. Maran AGD. Performing arts medicine. Br J Sports Med 1998;32(1):5.-
16. Bruce TJ, Saeed SA. Social anxiety disorder: a common, underrecognized mental disorder. Am Fam Physician 1999;60(8):2311-22.
17. Ostwald PF, Baron BC, Byl NM, Wilson FR. Performing arts medicine. West J Med 1994;160:48-52.
18. Slomka J. Playing with propranolol. Hastings Cent Rep 1992;22(4):13-18.
19. Blanco C, Antia SX, Liebowitz MR. Pharmacotherapy of social anxiety disorder. Biol Psychiatry 2002;51:109-20.
20. Rodebaugh TL, Chambless DL. Cognitive therapy for performance anxiety. J Clin Psychol 2004;60(8):809-20.
21. Birk L. Pharmacotherapy for performance anxiety disorders: occasionally useful but typically contraindicated. J Clin Psychol: In Session 2004;60(8):867-79.
22. Lipsitz JD, Markowitz JC, Cherry S, Fyer AJ. Open trial of interpersonal psychotherapy for the treatment of social phobia. Am J Psychiatry 1999;156(11):1814-6.
The violin is slippery in my grasp. I hear the thud of my foot tapping, but the tempo feels wrong. I’m aware of my chest pounding, a lump in my throat, and heat rising from my face. Everyone is watching me, waiting for me to make a mistake.
Why can’t I stop my hand from trembling? I can only watch as the bow jumps noisily across the strings. I should have practiced more. My mind goes blank, and I miss the page turn.
Silence. I blink, and the lights blind me as the applause comes, thankfully, and I exhale and run off the stage as the curtain closes.
Well-known performing artists—Sir Laurence Olivier, Kim Basinger, Peter O’Toole, Richard Burton, Barbra Streisand, and Luciano Pavarotti —have described bouts with acute stage fright. Performance anxiety can occur with acting, singing, or playing a musical instrument, and with nonartistic performances such as public speaking, oral examinations, competing in sporting events, sexual activity, using public restrooms, or being watched while doing a task such as surgery, eating, or writing.2
Like social phobia, performance anxiety probably develops in accomplished artists and not-so-famous individuals because of a mélange of genetic factors, innate temperament, parental influences, conditioning events, and cognitive influences.3
NORMAL VS. ABNORMAL FEAR
Performance anxiety is characterized by persisting, distressful apprehension about—or actual impairment of—performance skills to a degree unwarranted by the individual’s aptitude, training, and preparation.1 Not all performance anxiety qualifies as a mental disorder; for example, though 85% of the population experiences discomfort about public speaking,4 this anxiety does not impair most people’s ability to function.
Mild to moderate anxiety is normal and motivating in performances.5 However, anxiety’s effect on performance does not follow a bell-shaped curve, wherein moderate anxiety promotes optimal performance.6 Instead, a catastrophic model is more accurate: increasing anxiety is helpful until a certain threshold is reached, then performance plunges.7
Diagnostic criteria. DSM-IV-TR describes performance anxiety as a form of social phobia (or social anxiety disorder) characterized by marked and persistent fear of social or performance situations in which embarrassment or humiliation might occur. Approximately 13% of adults experience social phobia,8 and about 2% suffer from severe discrete performance anxiety.9
Performance anxiety does not completely overlap with social phobia, however. Test-taking anxiety and writer’s block, which can occur in a nonpublic context, do not fit neatly into the social phobia category.2 Thus, some performance anxiety forms are better grouped as another type of anxiety disorder, such as specific phobia (Figure).
Figure Performance anxiety features overlap with other anxieties
Performance anxiety is not easy to categorize. It is situational anxiety that occurs in a public context and overlaps with but does not entirely match diagnostic criteria for specific phobia, social anxiety, or panic disorder and generalized anxiety.
DIFFERENTIAL DIAGNOSIS
Social anxiety? Ask the patient about all situations that provoke anxiety to differentiate between:
- discrete performance anxiety (1 or 2 performance situations that provoke anxiety)
- and generalized social anxiety (3 or more situations that provoke anxiety).9
Individuals with “trait” anxiety may exhibit innate shyness and are considered to have generalized social phobia. Those with “state” anxiety experience anxiety in specific situations or circumstances and are more aptly described as having discrete performance anxiety.10 Whereas persons with social phobia may avoid the feared activity without inner conflict, those with performance anxiety are committed to performing the activity and are distressed when unable to perform.9
Specific phobia? A specific phobia is a circumscribed fear of a specific object, situation, or activity from which a grim outcome is feared. Specific phobia usually has no performance aspect or fear of embarrassment or failure.
Some clinicians consider certain performance anxieties—such as writer’s block, test-taking anxiety, paruresis, and even fear about sexual performance—to be specific phobias. Because performance anxieties and phobias share some cognitive and behavioral components, their treatments are similar and use of medication is controversial.
General medical condition? Perform or refer the patient for a thorough medical evaluation before you diagnose performance anxiety, as endocrine, cardiovascular, respiratory, and circulatory abnormalities can mimic or exacerbate anxiety disorders. Also consider substance abuse or withdrawal as possible causes of anxiety.
PATIENT EVALUATION
Family history. Individuals with social anxiety often report a family history of generalized social anxiety, panic disorder, or major depressive disorder.3 Similar findings seem plausible for persons with discrete performance anxiety, although comparable family history data have not been reported.
Cognitive symptoms. Four cognitive distortions are common in persons with social phobia (Table 1).11 These negative thoughts are presumably the same for performance anxiety, at least when it is a sub-type of social phobia.
Somatic symptoms. Persons with performance anxiety tend to have heightened awareness of hyperadrenergic arousal symptoms (Table 2), sometimes in all body systems. Symptoms may resemble those of a panic attack.
Behavioral symptoms. Behavioral symptoms include stuttering, mumbling, trembling voice, yawning, biting nails or lips, gritting jaw, poor eye contact, shuffling or tapping feet, unnatural or rigid postures or movements, warming up too fast or too slowly, wearing excessive makeup, or smiling abnormally. A performer may forget to carry out a routine task such as blinking, moistening lips, or turning a page of music.
These behaviors may perpetuate and reinforce anxiety by eliciting negative reactions from an audience and fulfilling the performer’s pessimistic expectations. The therapist can identify these maladaptive behaviors and target them for treatment.
Table 1
4 cognitive distortions that underlie performance anxiety
|
Table 2
Somatic symptoms of performance anxiety
| Bodily system | Symptoms |
|---|---|
| Autonomic | Blushing, diaphoresis, dry mouth |
| GI, urologic | Urinary or bowel urgency, GI discomfort |
| Cardiovascular | Tachycardia, palpitations |
| Neuromuscular | Muscle tension, tremor, paralysis |
PSYCHIATRIC COMORBIDITY
About one-third of individuals with performance anxiety have psychiatric comorbidities.9 Most common are other anxiety disorders, specifically the generalized form of social phobia, generalized anxiety disorder, panic disorder, or specific phobia.12 Mood disorders are less common. We also recommend monitoring for eating disorders because some performing artists are driven to maintain high physical appearance standards.
Personality disorder comorbidities with performance anxiety have not been studied. Some experts believe that avoidant personality and social phobia are the same conditions expressed to varying degrees on a continuum.13 Other personality disorders to consider include schizoid, paranoid, and obsessive-compulsive personalities.
Alcohol and substance use disorders are highly comorbid with performance anxiety. Alcohol use decreases public speaking anxiety,14 and approximately 6% of orchestral musicians use alcohol before a performance.15 For comparison, approximately 16% of patients who present for treatment of generalized anxiety disorder abuse alcohol, often as an attempt to self-medicate.16
TREATMENT PLANNING
Just as performance anxiety’s diagnostic classification may vary, so may treatment. Pharmacologic interventions and psychotherapy for social and specific phobias are similar. Some clinicians favor a multimodal approach addressing behavior, affect, sensation, imagery, cognition, interpersonal relationships, and biological factors.9
The performing arts community is competitive, and individuals may have differing standards about what treatments are acceptable. Some may view using medications as “cheating” or an admission of professional failure. A performer may feel medication gives an unfair advantage, that respect would be lost if others found out, or that taking medication before performing is similar to steroid use by athletes.17,18
Medication vs. psychotherapy. Medication can help diminish anxiety’s physical symptoms, but certain psychotherapies rely on these somatic symptoms for effective treatment and extinguishing of responses. Concurrent use of medications and psychotherapy for social phobia is common in everyday practice, although some studies find the combination no more effective than either treatment alone.11 Symptoms appear less likely to return after cognitive-behavioral therapy (CBT) ends than after medication is discontinued.16
Discuss treatment options with the patient. A patient who feels unable to perform without medication may develop psychological dependency. Conversely, a patient may not be able to afford the full course of psychotherapy needed for positive results. For performing artists, longer visits that incorporate medication management with psychotherapy may be more successful than brief, symptom-targeted visits.
MEDICATION MANAGEMENT
All medication use for performance anxiety is off-label. The most common choices are short-acting agents such as beta blockers or benzodiazepines (Table 3).
Table 3
Medications used to treat performance anxiety*
| Medication | Typical dosage | Possible side effects |
|---|---|---|
| Beta blockers | Medical: sedation, fatigue, dizziness, ataxia, nausea, sexual dysfunction Psychiatric:insomnia, nightmares, depression Contraindications: heart failure, bradycardia, breathing difficulties, hypotension | |
| Propranolol | 10 to 40 mg | |
| Nadolol | 20 to 120 mg | |
| Atenolol | 50 to 100 mg | |
| Benzodiazepines | Performance decrement, amnesia, sedation, discontinuation symptoms, tolerance, abuse potential | |
| Clonazepam | 0.25 to 0.5 mg | |
| Lorazepam | 0.5 to 1 mg | |
| * Off-label use; taken as-needed approximately 1 hour before performance | ||
Beta blockers can relieve autonomic and somatic symptoms such as tachycardia, tremor, and stuttering when used in low doses as needed for mild to moderate circumscribed performance anxiety.16,19 Propranolol, 10 mg about 1 hour before the performance, is most often prescribed.
Before prescribing a beta blocker, evaluate the patient’s medical history and cardiovascular status, including blood pressure and pulse. Have the patient try a test dose before the first live performance to check for side effects and tolerability (Table 3).16,19
Benzodiazepines have been used to treat social anxiety, but controlled studies have not reliably addressed their efficacy in performance anxiety. Advise the patient to abstain from alcohol when taking these medications (Table 3).
PSYCHOTHERAPY OPTIONS
CBT with components of exposure and retraining can ameliorate performance anxiety.10,20
Many performers forgo normal childhood social experiences to hone their talents, at times sacrificing sound coping skills.17 CBT’s goal is to help them reduce negative biases and restructure cognitive processes to function better at whatever task is at hand. This involves teaching them to:
- recognize pessimistic thoughts that occur before, during, and after performances
- challenge the accuracy of these thoughts
- replace them with rational, helpful thoughts based on the assimilated information.11
Exposure therapy can help individuals face feared activities so that counter-conditioning through habituation and extinction can safely occur. Useful strategies include imagination, role play, confrontation, videotaping, and homework assignments.11
Experiencing anxiety is a component of exposure therapy. Thus, some clinicians avoid using concomitant medication that might decrease anxiety’s physical symptoms and interfere with the exposure process.21
Relaxation training can help the patient recognize and respond to autonomic and physical arousal during a performance.11 For example, progressive muscle relaxation can be practiced first in session and then as homework.
Social skills training can help patients identify and change anxiety behaviors that cause negative audience reactions. Tools to help direct the patient towards more appropriate behaviors include modeling, behavior rehearsal, corrective feedback, social reinforcement, and homework assignments such as videotaping performances.11 For public speaking anxiety, vocal and physical skills training10 and computerized virtual reality courses can help.4
Interpersonal therapy may be useful, based on the premise that performance anxiety occurs within a social and interpersonal context.22
Related resources
- Toastmasters for public speaking. http://www.toastmasters.com
- Anxiety Disorders Association of America. http://www.adaa.org
- Social Anxiety Association. http://www.socialphobia.org
Drug brand names
- Atenolol • Tenormin
- Clonazepam • Klonopin
- Lorazepam • Ativan
- Nadolol • Corgard
- Propranolol • Inderal
Disclosure
Dr. Kelly reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Saveanu receives research support from Pfizer Inc. and is a consultant and speaker for Pfizer Inc. and GlaxoSmithKline.
The violin is slippery in my grasp. I hear the thud of my foot tapping, but the tempo feels wrong. I’m aware of my chest pounding, a lump in my throat, and heat rising from my face. Everyone is watching me, waiting for me to make a mistake.
Why can’t I stop my hand from trembling? I can only watch as the bow jumps noisily across the strings. I should have practiced more. My mind goes blank, and I miss the page turn.
Silence. I blink, and the lights blind me as the applause comes, thankfully, and I exhale and run off the stage as the curtain closes.
Well-known performing artists—Sir Laurence Olivier, Kim Basinger, Peter O’Toole, Richard Burton, Barbra Streisand, and Luciano Pavarotti —have described bouts with acute stage fright. Performance anxiety can occur with acting, singing, or playing a musical instrument, and with nonartistic performances such as public speaking, oral examinations, competing in sporting events, sexual activity, using public restrooms, or being watched while doing a task such as surgery, eating, or writing.2
Like social phobia, performance anxiety probably develops in accomplished artists and not-so-famous individuals because of a mélange of genetic factors, innate temperament, parental influences, conditioning events, and cognitive influences.3
NORMAL VS. ABNORMAL FEAR
Performance anxiety is characterized by persisting, distressful apprehension about—or actual impairment of—performance skills to a degree unwarranted by the individual’s aptitude, training, and preparation.1 Not all performance anxiety qualifies as a mental disorder; for example, though 85% of the population experiences discomfort about public speaking,4 this anxiety does not impair most people’s ability to function.
Mild to moderate anxiety is normal and motivating in performances.5 However, anxiety’s effect on performance does not follow a bell-shaped curve, wherein moderate anxiety promotes optimal performance.6 Instead, a catastrophic model is more accurate: increasing anxiety is helpful until a certain threshold is reached, then performance plunges.7
Diagnostic criteria. DSM-IV-TR describes performance anxiety as a form of social phobia (or social anxiety disorder) characterized by marked and persistent fear of social or performance situations in which embarrassment or humiliation might occur. Approximately 13% of adults experience social phobia,8 and about 2% suffer from severe discrete performance anxiety.9
Performance anxiety does not completely overlap with social phobia, however. Test-taking anxiety and writer’s block, which can occur in a nonpublic context, do not fit neatly into the social phobia category.2 Thus, some performance anxiety forms are better grouped as another type of anxiety disorder, such as specific phobia (Figure).
Figure Performance anxiety features overlap with other anxieties
Performance anxiety is not easy to categorize. It is situational anxiety that occurs in a public context and overlaps with but does not entirely match diagnostic criteria for specific phobia, social anxiety, or panic disorder and generalized anxiety.
DIFFERENTIAL DIAGNOSIS
Social anxiety? Ask the patient about all situations that provoke anxiety to differentiate between:
- discrete performance anxiety (1 or 2 performance situations that provoke anxiety)
- and generalized social anxiety (3 or more situations that provoke anxiety).9
Individuals with “trait” anxiety may exhibit innate shyness and are considered to have generalized social phobia. Those with “state” anxiety experience anxiety in specific situations or circumstances and are more aptly described as having discrete performance anxiety.10 Whereas persons with social phobia may avoid the feared activity without inner conflict, those with performance anxiety are committed to performing the activity and are distressed when unable to perform.9
Specific phobia? A specific phobia is a circumscribed fear of a specific object, situation, or activity from which a grim outcome is feared. Specific phobia usually has no performance aspect or fear of embarrassment or failure.
Some clinicians consider certain performance anxieties—such as writer’s block, test-taking anxiety, paruresis, and even fear about sexual performance—to be specific phobias. Because performance anxieties and phobias share some cognitive and behavioral components, their treatments are similar and use of medication is controversial.
General medical condition? Perform or refer the patient for a thorough medical evaluation before you diagnose performance anxiety, as endocrine, cardiovascular, respiratory, and circulatory abnormalities can mimic or exacerbate anxiety disorders. Also consider substance abuse or withdrawal as possible causes of anxiety.
PATIENT EVALUATION
Family history. Individuals with social anxiety often report a family history of generalized social anxiety, panic disorder, or major depressive disorder.3 Similar findings seem plausible for persons with discrete performance anxiety, although comparable family history data have not been reported.
Cognitive symptoms. Four cognitive distortions are common in persons with social phobia (Table 1).11 These negative thoughts are presumably the same for performance anxiety, at least when it is a sub-type of social phobia.
Somatic symptoms. Persons with performance anxiety tend to have heightened awareness of hyperadrenergic arousal symptoms (Table 2), sometimes in all body systems. Symptoms may resemble those of a panic attack.
Behavioral symptoms. Behavioral symptoms include stuttering, mumbling, trembling voice, yawning, biting nails or lips, gritting jaw, poor eye contact, shuffling or tapping feet, unnatural or rigid postures or movements, warming up too fast or too slowly, wearing excessive makeup, or smiling abnormally. A performer may forget to carry out a routine task such as blinking, moistening lips, or turning a page of music.
These behaviors may perpetuate and reinforce anxiety by eliciting negative reactions from an audience and fulfilling the performer’s pessimistic expectations. The therapist can identify these maladaptive behaviors and target them for treatment.
Table 1
4 cognitive distortions that underlie performance anxiety
|
Table 2
Somatic symptoms of performance anxiety
| Bodily system | Symptoms |
|---|---|
| Autonomic | Blushing, diaphoresis, dry mouth |
| GI, urologic | Urinary or bowel urgency, GI discomfort |
| Cardiovascular | Tachycardia, palpitations |
| Neuromuscular | Muscle tension, tremor, paralysis |
PSYCHIATRIC COMORBIDITY
About one-third of individuals with performance anxiety have psychiatric comorbidities.9 Most common are other anxiety disorders, specifically the generalized form of social phobia, generalized anxiety disorder, panic disorder, or specific phobia.12 Mood disorders are less common. We also recommend monitoring for eating disorders because some performing artists are driven to maintain high physical appearance standards.
Personality disorder comorbidities with performance anxiety have not been studied. Some experts believe that avoidant personality and social phobia are the same conditions expressed to varying degrees on a continuum.13 Other personality disorders to consider include schizoid, paranoid, and obsessive-compulsive personalities.
Alcohol and substance use disorders are highly comorbid with performance anxiety. Alcohol use decreases public speaking anxiety,14 and approximately 6% of orchestral musicians use alcohol before a performance.15 For comparison, approximately 16% of patients who present for treatment of generalized anxiety disorder abuse alcohol, often as an attempt to self-medicate.16
TREATMENT PLANNING
Just as performance anxiety’s diagnostic classification may vary, so may treatment. Pharmacologic interventions and psychotherapy for social and specific phobias are similar. Some clinicians favor a multimodal approach addressing behavior, affect, sensation, imagery, cognition, interpersonal relationships, and biological factors.9
The performing arts community is competitive, and individuals may have differing standards about what treatments are acceptable. Some may view using medications as “cheating” or an admission of professional failure. A performer may feel medication gives an unfair advantage, that respect would be lost if others found out, or that taking medication before performing is similar to steroid use by athletes.17,18
Medication vs. psychotherapy. Medication can help diminish anxiety’s physical symptoms, but certain psychotherapies rely on these somatic symptoms for effective treatment and extinguishing of responses. Concurrent use of medications and psychotherapy for social phobia is common in everyday practice, although some studies find the combination no more effective than either treatment alone.11 Symptoms appear less likely to return after cognitive-behavioral therapy (CBT) ends than after medication is discontinued.16
Discuss treatment options with the patient. A patient who feels unable to perform without medication may develop psychological dependency. Conversely, a patient may not be able to afford the full course of psychotherapy needed for positive results. For performing artists, longer visits that incorporate medication management with psychotherapy may be more successful than brief, symptom-targeted visits.
MEDICATION MANAGEMENT
All medication use for performance anxiety is off-label. The most common choices are short-acting agents such as beta blockers or benzodiazepines (Table 3).
Table 3
Medications used to treat performance anxiety*
| Medication | Typical dosage | Possible side effects |
|---|---|---|
| Beta blockers | Medical: sedation, fatigue, dizziness, ataxia, nausea, sexual dysfunction Psychiatric:insomnia, nightmares, depression Contraindications: heart failure, bradycardia, breathing difficulties, hypotension | |
| Propranolol | 10 to 40 mg | |
| Nadolol | 20 to 120 mg | |
| Atenolol | 50 to 100 mg | |
| Benzodiazepines | Performance decrement, amnesia, sedation, discontinuation symptoms, tolerance, abuse potential | |
| Clonazepam | 0.25 to 0.5 mg | |
| Lorazepam | 0.5 to 1 mg | |
| * Off-label use; taken as-needed approximately 1 hour before performance | ||
Beta blockers can relieve autonomic and somatic symptoms such as tachycardia, tremor, and stuttering when used in low doses as needed for mild to moderate circumscribed performance anxiety.16,19 Propranolol, 10 mg about 1 hour before the performance, is most often prescribed.
Before prescribing a beta blocker, evaluate the patient’s medical history and cardiovascular status, including blood pressure and pulse. Have the patient try a test dose before the first live performance to check for side effects and tolerability (Table 3).16,19
Benzodiazepines have been used to treat social anxiety, but controlled studies have not reliably addressed their efficacy in performance anxiety. Advise the patient to abstain from alcohol when taking these medications (Table 3).
PSYCHOTHERAPY OPTIONS
CBT with components of exposure and retraining can ameliorate performance anxiety.10,20
Many performers forgo normal childhood social experiences to hone their talents, at times sacrificing sound coping skills.17 CBT’s goal is to help them reduce negative biases and restructure cognitive processes to function better at whatever task is at hand. This involves teaching them to:
- recognize pessimistic thoughts that occur before, during, and after performances
- challenge the accuracy of these thoughts
- replace them with rational, helpful thoughts based on the assimilated information.11
Exposure therapy can help individuals face feared activities so that counter-conditioning through habituation and extinction can safely occur. Useful strategies include imagination, role play, confrontation, videotaping, and homework assignments.11
Experiencing anxiety is a component of exposure therapy. Thus, some clinicians avoid using concomitant medication that might decrease anxiety’s physical symptoms and interfere with the exposure process.21
Relaxation training can help the patient recognize and respond to autonomic and physical arousal during a performance.11 For example, progressive muscle relaxation can be practiced first in session and then as homework.
Social skills training can help patients identify and change anxiety behaviors that cause negative audience reactions. Tools to help direct the patient towards more appropriate behaviors include modeling, behavior rehearsal, corrective feedback, social reinforcement, and homework assignments such as videotaping performances.11 For public speaking anxiety, vocal and physical skills training10 and computerized virtual reality courses can help.4
Interpersonal therapy may be useful, based on the premise that performance anxiety occurs within a social and interpersonal context.22
Related resources
- Toastmasters for public speaking. http://www.toastmasters.com
- Anxiety Disorders Association of America. http://www.adaa.org
- Social Anxiety Association. http://www.socialphobia.org
Drug brand names
- Atenolol • Tenormin
- Clonazepam • Klonopin
- Lorazepam • Ativan
- Nadolol • Corgard
- Propranolol • Inderal
Disclosure
Dr. Kelly reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Saveanu receives research support from Pfizer Inc. and is a consultant and speaker for Pfizer Inc. and GlaxoSmithKline.
1. Salmon PG. A psychological perspective on musical performance anxiety: a review of the literature. Med Prob Perform Artists 1900;51(1):2-11.
2. Beatty M. Situational and predispositional correlates of public speaking anxiety. Commun Ed 1998;37:28-39.
3. Ollendick TH, Hirshfeld-Becker DR. The developmental psychopathology of social anxiety disorder. Biol Psychiatry 2002;51(1):44-58.
4. Harris SR, Kemmerling RL, North MM. Brief virtual reality therapy for public speaking anxiety. Cyberpsychol Behav 2002;5(6):543-50.
5. Rafferty BD, Smith RE, Ptacek JT. Facilitating and debilitating trait anxiety, situational anxiety, and coping with an anticipated stressor: a process analysis. J Pers Soc Psychol 1997;72:892-906.
6. Yerkes RM, Dodson JD. The relation of strength of stimulus to rapidity of habit formation. J Comp Neurol Psychol 1908;18:459-482.
7. Hardy L, Parfitt G. A catastrophic model of anxiety and performance. Br J Psychol 1991;82:163-78.
8. Kessler RC, McGonagle KA, Zhao S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: results from the National Comorbidity Survey. Arch Gen Psychiatry 1994;51(1):8-19.
9. Powell D. Treating individuals with debilitating performance anxiety: an introduction. J Clin Psychol 2004;60(8):801-8.
10. Merritt L, Richards A, Davis P. Performance anxiety: loss of the spoken edge. J Voice 2001;15(2):257-69.
11. Heimberg RG. Cognitive-behavioral therapy for social anxiety disorder: current status and future directions. Biol Psychiatry 2002;51:101-8.
12. Brown TA, Barlow DH. Comorbidities among anxiety disorders: implications for treatment and DSM-IV. J Consult Clin Psychol 1992;60(6):835-44.
13. Schneier FR, Johnson J, Hornig CD, et al. Social phobia: comorbidity and morbidity in an epidemiologic sample. Arch Gen Psychiatry 1992;49:282-8.
14. Abrams K, Kushner M, Medina K, Voight A. Self-administration of alcohol before and after a public speaking challenge by individuals with social phobias. Psychol Addict Behav 2002;16(1):121-8.
15. Maran AGD. Performing arts medicine. Br J Sports Med 1998;32(1):5.-
16. Bruce TJ, Saeed SA. Social anxiety disorder: a common, underrecognized mental disorder. Am Fam Physician 1999;60(8):2311-22.
17. Ostwald PF, Baron BC, Byl NM, Wilson FR. Performing arts medicine. West J Med 1994;160:48-52.
18. Slomka J. Playing with propranolol. Hastings Cent Rep 1992;22(4):13-18.
19. Blanco C, Antia SX, Liebowitz MR. Pharmacotherapy of social anxiety disorder. Biol Psychiatry 2002;51:109-20.
20. Rodebaugh TL, Chambless DL. Cognitive therapy for performance anxiety. J Clin Psychol 2004;60(8):809-20.
21. Birk L. Pharmacotherapy for performance anxiety disorders: occasionally useful but typically contraindicated. J Clin Psychol: In Session 2004;60(8):867-79.
22. Lipsitz JD, Markowitz JC, Cherry S, Fyer AJ. Open trial of interpersonal psychotherapy for the treatment of social phobia. Am J Psychiatry 1999;156(11):1814-6.
1. Salmon PG. A psychological perspective on musical performance anxiety: a review of the literature. Med Prob Perform Artists 1900;51(1):2-11.
2. Beatty M. Situational and predispositional correlates of public speaking anxiety. Commun Ed 1998;37:28-39.
3. Ollendick TH, Hirshfeld-Becker DR. The developmental psychopathology of social anxiety disorder. Biol Psychiatry 2002;51(1):44-58.
4. Harris SR, Kemmerling RL, North MM. Brief virtual reality therapy for public speaking anxiety. Cyberpsychol Behav 2002;5(6):543-50.
5. Rafferty BD, Smith RE, Ptacek JT. Facilitating and debilitating trait anxiety, situational anxiety, and coping with an anticipated stressor: a process analysis. J Pers Soc Psychol 1997;72:892-906.
6. Yerkes RM, Dodson JD. The relation of strength of stimulus to rapidity of habit formation. J Comp Neurol Psychol 1908;18:459-482.
7. Hardy L, Parfitt G. A catastrophic model of anxiety and performance. Br J Psychol 1991;82:163-78.
8. Kessler RC, McGonagle KA, Zhao S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: results from the National Comorbidity Survey. Arch Gen Psychiatry 1994;51(1):8-19.
9. Powell D. Treating individuals with debilitating performance anxiety: an introduction. J Clin Psychol 2004;60(8):801-8.
10. Merritt L, Richards A, Davis P. Performance anxiety: loss of the spoken edge. J Voice 2001;15(2):257-69.
11. Heimberg RG. Cognitive-behavioral therapy for social anxiety disorder: current status and future directions. Biol Psychiatry 2002;51:101-8.
12. Brown TA, Barlow DH. Comorbidities among anxiety disorders: implications for treatment and DSM-IV. J Consult Clin Psychol 1992;60(6):835-44.
13. Schneier FR, Johnson J, Hornig CD, et al. Social phobia: comorbidity and morbidity in an epidemiologic sample. Arch Gen Psychiatry 1992;49:282-8.
14. Abrams K, Kushner M, Medina K, Voight A. Self-administration of alcohol before and after a public speaking challenge by individuals with social phobias. Psychol Addict Behav 2002;16(1):121-8.
15. Maran AGD. Performing arts medicine. Br J Sports Med 1998;32(1):5.-
16. Bruce TJ, Saeed SA. Social anxiety disorder: a common, underrecognized mental disorder. Am Fam Physician 1999;60(8):2311-22.
17. Ostwald PF, Baron BC, Byl NM, Wilson FR. Performing arts medicine. West J Med 1994;160:48-52.
18. Slomka J. Playing with propranolol. Hastings Cent Rep 1992;22(4):13-18.
19. Blanco C, Antia SX, Liebowitz MR. Pharmacotherapy of social anxiety disorder. Biol Psychiatry 2002;51:109-20.
20. Rodebaugh TL, Chambless DL. Cognitive therapy for performance anxiety. J Clin Psychol 2004;60(8):809-20.
21. Birk L. Pharmacotherapy for performance anxiety disorders: occasionally useful but typically contraindicated. J Clin Psychol: In Session 2004;60(8):867-79.
22. Lipsitz JD, Markowitz JC, Cherry S, Fyer AJ. Open trial of interpersonal psychotherapy for the treatment of social phobia. Am J Psychiatry 1999;156(11):1814-6.