User login
Treating depression to remission: Target recovery, and give patients back their lives
Remission is considered the standard of treatment for major depression,1-4 but many patients fall short of this goal:
- 25% to 50% of those who respond to treatment have residual symptoms5
- 60% to 70% respond to treatment, but only 20% to 40% achieve remission.6
We offer practical, evidence-based suggestions and resources to help you take more of your patients beyond response to remission and then to recovery (Table 1).7,8
Table 1
Outcomes in depression: Defining the 4 ‘R’s
| Outcome | Definition | Comment |
|---|---|---|
| Response | Clinically significant reduction of symptoms | 50% reduction in symptoms on psychometric scales may leave severely depressed patients with disabling symptoms |
| Remission | Depression resolves completely or nearly completely, with return to baseline function | Score of ≤7 on the HRSD used in many studies; ACNP Task Force defines remission by 9 core depression symptoms in DSM-IV-TR |
| Recovery | Remission lasts for extended time; signifies end of a major depressive episode | ACNP Task Force defines recovery as 4 months of remission |
| Relapse | Return to full symptoms during remission but before recovery; signifies re-emergence of current depressive episode | Residual symptoms during response or remission greatly increase chances of relapse |
| HRSD: Hamilton Rating Scale for Depression | ||
| ACNP: American College of Neuropsychopharmacology | ||
| DSM-IV-TR: Diagnostic and statistical manual of mental disorders, 4th ed., text rev. | ||
| Source: References 7, 8 | ||
Case report: missing the target
Ms. M, age 32, develops depressive symptoms after taking on several new projects in her work as an accountant. At first she notices difficulty falling asleep at night and that she seems tired all day. Typically efficient and neat, she finds herself absently staring at her computer screen while a messy pile of unfinished paperwork accumulates on her desk.
She begins chastising herself for falling behind, yet she feels she will never catch up. When she unexpectedly bursts out sobbing in a board meeting, she knows she needs help.
Ms. M reports that she has been taking fluoxetine, 20 mg/d, for 4 weeks as her primary care physician prescribed, with no improvement. She has no history of depression or other psychiatric illness, is taking no other medication, and has no medical illnesses. Her brother has a history of bipolar disorder.
Initial diagnostic workup includes laboratory tests such as thyroid stimulating hormone, vitamin B12, and folate. All values are within normal limits. Her Hamilton Rating Scale for Depression (HRSD) score is 17, indicating moderate depression.
The psychiatrist increases fluoxetine to 40 mg/d, and after about 3 weeks Ms. M starts feeling better. Her hopelessness lifts, she is more engaged, and her sleep improves, yet she continues to feel sluggish and dazed. Her financial reports contain uncharacteristic errors, and her pace is noticeably slow. Twice her supervisor approaches her about substandard work, then a week later warns that she will lose her job unless she improves.
Barriers to remission. Patient, provider, and health care system barriers prevent patients with major depression from achieving remission (Table 2).3 Patients may feel better with antidepressant therapy but do not recognize and report residual depressive symptoms, such as Ms. M’s fatigue and substandard job performance.
Clinicians also play a role in depression undertreatment. For example, in a study of 239 patients with ≥ 5 depression symptoms,9 28% did not receive treatment consistent with depression management guidelines.
Fava et al10 suggested the following reasons for depression undertreatment: “… clinicians have partial therapeutic targets, neglect residual symptoms, and equate therapeutic response with full remission.” Others have found that physicians may underdose medications or fail to plan treatment in clear phases.11
Table 2
Barriers to remission during depression treatment
| Who and what | Behavior and system problems |
|---|---|
| Patients | Nonadherence to treatment, underreporting of symptoms, satisfaction with suboptimal outcomes, failure to recognize depressive symptoms, underestimating depression severity, limited access to care, reluctance to see a mental health specialist |
| Providers | Medication under-dosing, inadequate treatment duration, inaccurate diagnosis, failure to recognize residual symptoms, limited training in interpersonal skills, inadequate time to evaluate and treat depression, failure to consider psychotherapeutic approaches |
| Health care systems | Limited therapeutic choices, limited number of mental health care visits, restricted access to providers |
| Source: Reference 3 | |
Relapse risk
Increased risk of relapse is perhaps the greatest cost of undertreated major depression. Patients with residual subsyndromal depressive symptoms relapse five times faster than patients in full remission.12
Residual symptoms may be a more powerful relapse predictor than number of past depressive episodes:13
- Chronic mood symptoms for ≥ 2 years double the relapse risk.14
- 50% to 80% of patients in partial remission relapse.15
In a study of patients in recovery from a major depressive episode, 76% (13 of 17) with residual symptoms relapsed within 15 months, compared with 25% (10 of 40) who completely recovered.16
Illness course. After a first major depressive episode, 26 patients with residual subsyndromal symptoms showed a more-severe, chronic illness compared with 70 asymptomatic patients:
- those with residual symptoms had more depression recurrences, with faster relapse and shorter intervals when they felt well
- subsequent depressive episodes occurred >3 times sooner
- well intervals between depressive episodes were 7 times shorter.17
The authors noted that “patients recovering from major depressive episodes with residual subsyndromal depression experience very rapid episode relapse and have strikingly more chronic future courses of illness that are characterized by early and more frequent episode relapses and recurrences.”18 Each major depression recurrence increases the risk of a successive episode.13,19,20
Treatment resistance. Over time, incomplete remission may contribute to treatment resistance,21 although this theory remains untested.
Social health costs
Residual depressive symptoms and impaired psychosocial, interpersonal, and occupational functioning are strongly correlated. In a study of patients who recovered from a major depressive episode, those with residual symptoms scored significantly worse on markers of social performance, relationships, and occupational functioning.6
Psychosocial costs. Compared with the general population, persons with subsyndromal depression have poorer health status and job functioning (as did Ms. M), and greater familial discord, financial strain, irritability, restricted activity, and number of days in bed.22 In 635 patients with chronic depression treated for 12 weeks with imipramine or sertraline:
- nonresponders scored lowest in psychosocial functioning
- responders scored in a mid-range
- remitters scored highest—as well or nearly as well as healthy controls did.23
Occupational costs. Depression leads to workplace absenteeism—twice the rate of nondepressed workers—and less effectiveness. Depressed persons are seven times more likely to be unemployed, employed part-time, or in jobs below their education levels, compared with community samples.24
Medical costs of depressed persons average twice those of the nondepressed,25 and depressed persons use three times as many health care services.26 Depression may increase the risk of:
- cardiac morbidity and mortality
- poor glycemic control in diabetic patients
- HIV progression
- cerebrovascular events
- and overall mortality.
Depression is associated with worse outcomes after myocardial infarction and among nursing home patients, stroke patients, and those with cancer or HIV infection.21
How to improve remission rates
To improve remission rates, we recommend that you follow a rational treatment progression and observe established guidelines, as described in the follow-up report on Ms. M:
Case continued: Part way there. Back at the psychiatrist’s office for 30-day medication monitoring, Ms. M reports that increasing her antidepressant has worked—no more crying in meetings or feeling down on herself. She even sleeps better. Her HRSD score is now 10, indicating improvement, though with some residual symptoms.
When the psychiatrist asks about her job performance, Ms. M is surprised to learn that her fatigue and disorganized thoughts might be lingering features of depression. She said she thought she just wasn’t trying hard enough.
Following practice guidelines,27 the psychiatrist increases fluoxetine to 60 mg/d. This higher dosage remains less than the maximum recommended 80 mg/d, and Ms. M has shown partial improvement with fluoxetine.
Patients being treated for depression need adequate follow-up to ensure they are improving. As with Ms. M, encourage patients to describe residual symptoms and functional domains that remain suboptimal. Educate them about the importance of taking antidepressants as prescribed ( Box). If poor response continues, address possible nonadherence.
Use objective assessments. Global, haphazard, or subjective assessments of patient progress can miss important ongoing depressive symptoms. We recommend using patient- or clinician-rated symptom scales to rapidly identify and monitor residual symptoms ( Table 3).
You may wish to design your own questionnaires to elicit easily missed data or symptoms particular to a certain treatment—such as common side effects of the medication a patient is taking. Nurses or other providers in a busy practice can help assess patients between or before doctor visits.
Keep in mind that the common practice of defining treatment response as a 50% reduction in HRSD scores7,8 leaves many patients with residual depressive symptoms. For example, an HRSD score reduction from 32 to 16 would signify treatment response, but this patient would remain quite depressed.
- Full remission from depression is the treatment goal, and any lesser outcome requires further attention
- Finding the proper medication may require trial and error, and several weeks may pass before a drug’s therapeutic effect occurs
- Continuing to take the medication as prescribed is important to achieving remission
- Medication may have predictable side effects
Table 3
Useful scales to identify and monitor depressive symptoms
| Scale | Administration | Features |
|---|---|---|
| Hamilton Rating Scale for Depression (21- or 17-item HRSD versions) | 15 to 20 minutes, clinician-rated | Focuses on somatic symptoms, excellent reliability, often used to evaluate response to medications |
| Beck Depression Inventory (BDI versions I or II) | 5 to 10 minutes, self-administered | Focuses on behavioral and cognitive elements (somatic symptoms added to BDI-II), good for measuring depression severity, not for depression screening |
| Zung Self-Rating Depression Scale | 5 to 10 minutes, self-administered | Good for screening, not studied as extensively as Hamilton and Beck scales |
| Montgomery-Asberg Depression Rating Scale | 5 to 10 minutes, clinician-rated | 10 items, often used in research |
A Stepwise approach
An expert panel recommends a stepwise approach for patients who respond inadequately to initial antidepressant therapy (Algorithm).27
Re-evaluate the diagnosis. Patients with bipolar disorder or comorbid medical or psychiatric disorders may need medications other than antidepressants. Address concomitant substance abuse, which may interfere with depression treatment. Also exclude or appropriately treat depressive symptoms associated with general medical conditions, such as hypothyroidism.
Optimize dosages. Consider increasing medication dosages as needed until limited by side effects or the drug’s safety profile. Before exceeding an FDA-recommended dosage (Table 4), obtain the patient’s informed consent and document this discussion in the chart.
Consider augmenting or switching. For patients who continue to show partial response, consider combining the initial medication with another antidepressant or augment with another agent, such as lithium, stimulants, thyroid hormone, or even atypical antipsychotics. For patients with no response to optimal dosages of the initial medication after 3 to 4 weeks, try switching to another antidepressant—not necessarily in a different class. One switch within the same class is reasonable.
Some authors emphasize the choice of antidepressant in attaining remission. Although no antidepressant is clearly more efficacious than another, those with fewer side effects (such as selective serotonin reuptake inhibitors vs. tricyclics) may improve adherence.
Numerous trials have shown higher remission rates with serotonin/norepinephrine reuptake inhibitors such as venlafaxine or duloxetine than with other antidepressants.28-30 This evidence is not universally accepted, however.31 Depressive illness probably has a heterogeneous biology, and with greater understanding we may eventually tailor treatment to individual patients’ needs.
Consider psychotherapy or ECT. Patients who do not achieve remission with medication may be candidates for combined treatment with psychotherapy or electroconvulsive therapy (ECT). Life issues—such as family or work stressors—may need to be addressed along with depressive symptoms.
Algorithm A stepwise approach to remission when antidepressant therapy falls short
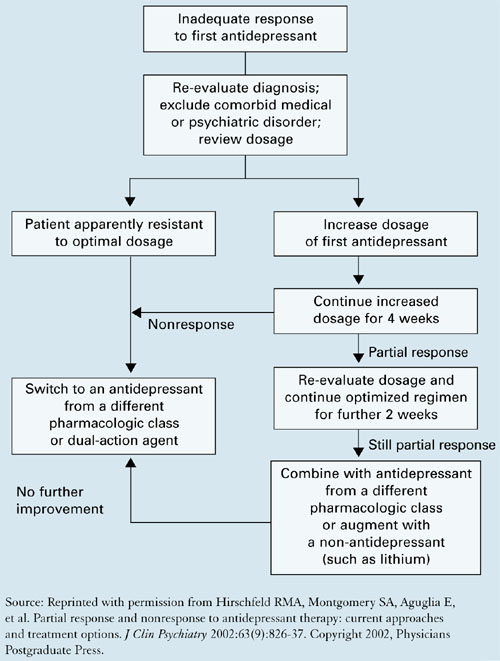
Table 4
Using common antidepressants for adults with major depression
| FDA-approved maximum dosage* | |||
|---|---|---|---|
| Antidepressant mg/d | mg/d | (mg/kg/d) | Common side effects at maximum dosage* |
| SSRIs | |||
| Citalopram | 80 | (1.0) | Nausea, dry mouth, somnolence |
| Escitalopram | 20 | Nausea, delayed ejaculation, insomnia | |
| Fluoxetine | 80 | (1.33) | Nausea, headache, insomnia |
| Paroxetine | 50 | (0.83) | Nausea, somnolence, headache |
| Sertraline | 200 | (3.33) | Nausea, headache, insomnia |
| SNRIs | |||
| Duloxetine | 120 | Nausea, dry mouth, fatigue | |
| Venlafaxine | 375 | (6.25) | Nausea, somnolence, dry mouth |
| Tricyclics | |||
| Amitriptyline | 300 | (5.0) | Drowsiness, dry mouth, dizziness |
| Desipramine | 300 | (5.0) | Same as above |
| Imipramine | 300 | Same as above | |
| Nortriptyline | 200 | (1.67) | Same as above |
| Others | |||
| Bupropion | 450 | (7.5) | Insomnia, dry mouth, headache |
| Mirtazapine | 45 | (0.75) | Somnolence, dry mouth, increased appetite |
| SSRIs: selective serotonin reuptake inhibitors | |||
| SNRIs: serotonin-norepinephrine reuptake inhibitors | |||
| * Informed consent discussion and documentation is recommended for dosages that exceed FDA-approved maximums. | |||
| Sources: Food and Drug Administration, and Kaplan HI, Sadock B. Kaplan & Sadock’s synopsis of psychiatry (9th ed). Philadelphia: Lippincott Williams & Wilkins, 2002. | |||
Case: monitoring after remission
Ms. M feels back to normal 2 weeks after starting fluoxetine at 60 mg/d. She experienced some transient nausea and headache at this dosage but did not stop the medication because her psychiatrist had told her these side effects might occur.
Ms. M also agrees to short-term psychotherapy to address self-esteem issues that may have contributed to her depressive episode. She soon files the mountain of papers on her desk and corrects erroneous financial statements she has made. Her supervisor is relieved—and so is she.
The psychiatrist schedules monthly medication monitoring and plans to gradually reduce the fluoxetine dosage if depressive symptoms remain in remission for 6 months. Because Ms. M had no past depressive episodes, the medication trial may not need to be extended past 6 months.
Related resources
- McManamy J. McMan’s Depression and Bipolar Web. Treating to remission. http://www.mcmanweb.com/article-181.htm.
- American Psychiatric Association. Practice guideline for the treatment of patients with major depressive disorder (2nd ed.). http://www.psych.org/psych_pract/treatg/pg/Depression2e.book.cfm.
- Stahl S. Essential psychopharmacology: Neuroscientific basis and practical applications (2nd ed.). Cambridge, UK: Cambridge University Presss, 2004, chapters 5-7.
Drug brand names
- Amitriptyline • Elavil, Endep
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Desipramine • Norpramin
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Imipramine • Tofranil
- Mirtazapine • Remeron
- Nortriptyline • Pamelor
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosures
Dr. Van Rhoads reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Gelenberg receives research grants from Pfizer Inc. and Novartis Pharmaceuticals Corp. He is a consultant or a speaker for Eli Lilly and Co., Pfizer Inc., Bristol-Myers Squibb Co., AstraZeneca Pharmaceuticals, Wyeth, GlaxoSmithKline, and Cyberonics.
1. Agency for Health Care Policy and Research. Clinical practice guideline, number 5: Depression in primary care: vol. 2. Treatment of major depression. AHCPR publication 93-0551. Rockville, MD: US Department of Health and Human Services, 1993.
2. American Psychiatric Association. Practice guideline for the treatment of patients with major depressive disorder. Am J Psychiatry 2000;157(suppl 4):1-45.
3. Hirschfeld RM, Keller MB, Panico BS, et al. The National Depressive and Manic-Depressive Association consensus statement on the undertreatment of depression. JAMA 1997;277:333-40.
4. Crismon ML, Trivedi M, Pigott TA, et al. The Texas Medication Algorithm Project: Report of the Texas Consensus Conference Panel on medication treatment of major depressive disorder. J Clin Psychiatry 1999;60:142-56.
5. Nierenberg AA, Keefe BR, Leslie VA, et al. Residual symptoms in depressed patients who respond acutely to fluoxetine. J Clin Psychiatry 1999;60:221-5.
6. Kennedy N, Paykel ES. Residual symptoms at remission from depression: impact on long-term outcome. J Affect Disord 2004;80(2-3):135-44.
7. Rush AJ, Kraemer HC, Sackeim HA, et al. Report by the ACNP Task Force on Response and Remission in Major Depressive Disorder. Submitted for publication.
8. Keller M. Past, present, and future directions for defining optimal treatment outcome in depression: remission and beyond. JAMA 2003;289(23):3152-60.
9. Nutting P, Rost K, Diceinson M, et al. Barriers to initiating depression treatment in primary care practice. J Gen Intern Med 2002;17:103-11.
10. Fava GA, Rafanelli C, Grandi S, et al. Letter to the editor. Arch Gen Psychiatry 1999;56:765.-
11. Ramana R, Paykel ES, Cooper Z, et al. Remission and relapse in major depression: a two year prospective follow-up study. Psychol Med 1995;25(6):1171-80.
12. Judd LL, Akiskal HS, Maser JD, et al. Major depressive disorder: a prospective study of residual subthreshold depressive symptoms as a predictor of rapid relapse. J Affect Disord 1999;50:97-108.
13. Pintor L, Gastó G, Navarro V, et al. Relapse of major depression after complete and partial remission during a 2-year follow-up. J Affect Disord 2003;73:237-44.
14. Lin E, Katon W, Von Korff M, et al. Relapse of depression in primary care: rate and clinical predictors. Arch Fam Med 1998;7(5):443-9.
15. Cornwall P, Scott J. Partial remission in depressive disorders. Acta Psychiatr Scand 1997;95(4):265-71.
16. Paykel ES, Ramana R, Cooper Z, et al. Residual symptoms after partial remission: an important outcome in depression. Psychol Med 1995;25(6):1171-80.
17. Judd LL, Paulus MJ, Schettler PJ, et al. Does incomplete recovery from first lifetime major depressive episode herald a chronic course of illness? Am J Psychiatry 2000;157(9):1501-4.
18. Judd LL, Paulus MP, Zeller P. The role of residual subthreshold depressive symptoms in early episode relapse in unipolar major depressive disorder. Arch Gen Psychiatry 1999;56(8):764-5.
19. Solomon DA, Keller MB, Leon AC, et al. Multiple recurrences of major depressive disorder. Am J Psychiatry 2000;157(2):229-33.
20. Kennedy N, Paykel ES. Residual symptoms at remission from depression: impact on long-term outcome. J Affect Disord 2004;80(2-3):135-44.
21. Zajecka JM. Treating depression to remission. J Clin Psychiatry 2003;64(suppl 15):7-12.
22. Judd LL, Paulus MP, Wells KB, Rapaport MH. Socioeconomic burden of subsyndromal depressive symptoms and major depressionin a sample of the general population. Am J Psychiatry 1996;153(11):1411-7.
23. Miller IW, Keitner GI, Schatzberg AF, et al. The treatment of chronic depression, part 3: psychosocial functioning before and after treatment with sertraline or imipramine. J Clin Psychiatry 1998;59(11):608-19.
24. Druss B, Schlesinger M, Allen H. Depressive symptoms, satisfaction with health care, and 2-year work outcomes in an employed population. Am J Psychiatry 2001;158(5):731-4.
25. Simon G, Ormel J, VonKorff M, et al. Health care costs associated with depressive and anxiety disorders in primary care. Am J Psychiatry 1995;152(3):352-7.
26. Katon W, Schulberg H. Epidemiology of depression in primary care. Gen Hosp Psychiatry 1992;14(4):237-47.
27. Hirschfeld RMA, Montgomery SA, Aguglia E, et al. Partial response and nonresponse to antidepressant therapy: current approaches and treatment options. J Clin Psychiatry 2002;63(9):826-37.
28. Thase ME, Entsuah AR, Rudolph RL. Remission rates during treatment with venlafaxine or selective serotonin reuptake inhibitors. Br J Psychiatry 2001;178:234-41.
29. Kelsey J, Entsuah R. Venlafaxine offers significant therapeutic benefits over existing SSRI treatments irrespective of the patient’s depressive duration (poster presentation). Montreal: Collegium Internationale Neuropsychopharmacologicum, June 2002.
30. Thase ME. Effectiveness of antidepressants: comparative remission rates. J Clin Psychiatry 2003;64(suppl 2):3-7.
31. Shelton C. Long-term management of major depressive disorder: are differences among antidepressant treatments meaningful? J Clin Psychiatry 2004;65(suppl 17):29-33.
Remission is considered the standard of treatment for major depression,1-4 but many patients fall short of this goal:
- 25% to 50% of those who respond to treatment have residual symptoms5
- 60% to 70% respond to treatment, but only 20% to 40% achieve remission.6
We offer practical, evidence-based suggestions and resources to help you take more of your patients beyond response to remission and then to recovery (Table 1).7,8
Table 1
Outcomes in depression: Defining the 4 ‘R’s
| Outcome | Definition | Comment |
|---|---|---|
| Response | Clinically significant reduction of symptoms | 50% reduction in symptoms on psychometric scales may leave severely depressed patients with disabling symptoms |
| Remission | Depression resolves completely or nearly completely, with return to baseline function | Score of ≤7 on the HRSD used in many studies; ACNP Task Force defines remission by 9 core depression symptoms in DSM-IV-TR |
| Recovery | Remission lasts for extended time; signifies end of a major depressive episode | ACNP Task Force defines recovery as 4 months of remission |
| Relapse | Return to full symptoms during remission but before recovery; signifies re-emergence of current depressive episode | Residual symptoms during response or remission greatly increase chances of relapse |
| HRSD: Hamilton Rating Scale for Depression | ||
| ACNP: American College of Neuropsychopharmacology | ||
| DSM-IV-TR: Diagnostic and statistical manual of mental disorders, 4th ed., text rev. | ||
| Source: References 7, 8 | ||
Case report: missing the target
Ms. M, age 32, develops depressive symptoms after taking on several new projects in her work as an accountant. At first she notices difficulty falling asleep at night and that she seems tired all day. Typically efficient and neat, she finds herself absently staring at her computer screen while a messy pile of unfinished paperwork accumulates on her desk.
She begins chastising herself for falling behind, yet she feels she will never catch up. When she unexpectedly bursts out sobbing in a board meeting, she knows she needs help.
Ms. M reports that she has been taking fluoxetine, 20 mg/d, for 4 weeks as her primary care physician prescribed, with no improvement. She has no history of depression or other psychiatric illness, is taking no other medication, and has no medical illnesses. Her brother has a history of bipolar disorder.
Initial diagnostic workup includes laboratory tests such as thyroid stimulating hormone, vitamin B12, and folate. All values are within normal limits. Her Hamilton Rating Scale for Depression (HRSD) score is 17, indicating moderate depression.
The psychiatrist increases fluoxetine to 40 mg/d, and after about 3 weeks Ms. M starts feeling better. Her hopelessness lifts, she is more engaged, and her sleep improves, yet she continues to feel sluggish and dazed. Her financial reports contain uncharacteristic errors, and her pace is noticeably slow. Twice her supervisor approaches her about substandard work, then a week later warns that she will lose her job unless she improves.
Barriers to remission. Patient, provider, and health care system barriers prevent patients with major depression from achieving remission (Table 2).3 Patients may feel better with antidepressant therapy but do not recognize and report residual depressive symptoms, such as Ms. M’s fatigue and substandard job performance.
Clinicians also play a role in depression undertreatment. For example, in a study of 239 patients with ≥ 5 depression symptoms,9 28% did not receive treatment consistent with depression management guidelines.
Fava et al10 suggested the following reasons for depression undertreatment: “… clinicians have partial therapeutic targets, neglect residual symptoms, and equate therapeutic response with full remission.” Others have found that physicians may underdose medications or fail to plan treatment in clear phases.11
Table 2
Barriers to remission during depression treatment
| Who and what | Behavior and system problems |
|---|---|
| Patients | Nonadherence to treatment, underreporting of symptoms, satisfaction with suboptimal outcomes, failure to recognize depressive symptoms, underestimating depression severity, limited access to care, reluctance to see a mental health specialist |
| Providers | Medication under-dosing, inadequate treatment duration, inaccurate diagnosis, failure to recognize residual symptoms, limited training in interpersonal skills, inadequate time to evaluate and treat depression, failure to consider psychotherapeutic approaches |
| Health care systems | Limited therapeutic choices, limited number of mental health care visits, restricted access to providers |
| Source: Reference 3 | |
Relapse risk
Increased risk of relapse is perhaps the greatest cost of undertreated major depression. Patients with residual subsyndromal depressive symptoms relapse five times faster than patients in full remission.12
Residual symptoms may be a more powerful relapse predictor than number of past depressive episodes:13
- Chronic mood symptoms for ≥ 2 years double the relapse risk.14
- 50% to 80% of patients in partial remission relapse.15
In a study of patients in recovery from a major depressive episode, 76% (13 of 17) with residual symptoms relapsed within 15 months, compared with 25% (10 of 40) who completely recovered.16
Illness course. After a first major depressive episode, 26 patients with residual subsyndromal symptoms showed a more-severe, chronic illness compared with 70 asymptomatic patients:
- those with residual symptoms had more depression recurrences, with faster relapse and shorter intervals when they felt well
- subsequent depressive episodes occurred >3 times sooner
- well intervals between depressive episodes were 7 times shorter.17
The authors noted that “patients recovering from major depressive episodes with residual subsyndromal depression experience very rapid episode relapse and have strikingly more chronic future courses of illness that are characterized by early and more frequent episode relapses and recurrences.”18 Each major depression recurrence increases the risk of a successive episode.13,19,20
Treatment resistance. Over time, incomplete remission may contribute to treatment resistance,21 although this theory remains untested.
Social health costs
Residual depressive symptoms and impaired psychosocial, interpersonal, and occupational functioning are strongly correlated. In a study of patients who recovered from a major depressive episode, those with residual symptoms scored significantly worse on markers of social performance, relationships, and occupational functioning.6
Psychosocial costs. Compared with the general population, persons with subsyndromal depression have poorer health status and job functioning (as did Ms. M), and greater familial discord, financial strain, irritability, restricted activity, and number of days in bed.22 In 635 patients with chronic depression treated for 12 weeks with imipramine or sertraline:
- nonresponders scored lowest in psychosocial functioning
- responders scored in a mid-range
- remitters scored highest—as well or nearly as well as healthy controls did.23
Occupational costs. Depression leads to workplace absenteeism—twice the rate of nondepressed workers—and less effectiveness. Depressed persons are seven times more likely to be unemployed, employed part-time, or in jobs below their education levels, compared with community samples.24
Medical costs of depressed persons average twice those of the nondepressed,25 and depressed persons use three times as many health care services.26 Depression may increase the risk of:
- cardiac morbidity and mortality
- poor glycemic control in diabetic patients
- HIV progression
- cerebrovascular events
- and overall mortality.
Depression is associated with worse outcomes after myocardial infarction and among nursing home patients, stroke patients, and those with cancer or HIV infection.21
How to improve remission rates
To improve remission rates, we recommend that you follow a rational treatment progression and observe established guidelines, as described in the follow-up report on Ms. M:
Case continued: Part way there. Back at the psychiatrist’s office for 30-day medication monitoring, Ms. M reports that increasing her antidepressant has worked—no more crying in meetings or feeling down on herself. She even sleeps better. Her HRSD score is now 10, indicating improvement, though with some residual symptoms.
When the psychiatrist asks about her job performance, Ms. M is surprised to learn that her fatigue and disorganized thoughts might be lingering features of depression. She said she thought she just wasn’t trying hard enough.
Following practice guidelines,27 the psychiatrist increases fluoxetine to 60 mg/d. This higher dosage remains less than the maximum recommended 80 mg/d, and Ms. M has shown partial improvement with fluoxetine.
Patients being treated for depression need adequate follow-up to ensure they are improving. As with Ms. M, encourage patients to describe residual symptoms and functional domains that remain suboptimal. Educate them about the importance of taking antidepressants as prescribed ( Box). If poor response continues, address possible nonadherence.
Use objective assessments. Global, haphazard, or subjective assessments of patient progress can miss important ongoing depressive symptoms. We recommend using patient- or clinician-rated symptom scales to rapidly identify and monitor residual symptoms ( Table 3).
You may wish to design your own questionnaires to elicit easily missed data or symptoms particular to a certain treatment—such as common side effects of the medication a patient is taking. Nurses or other providers in a busy practice can help assess patients between or before doctor visits.
Keep in mind that the common practice of defining treatment response as a 50% reduction in HRSD scores7,8 leaves many patients with residual depressive symptoms. For example, an HRSD score reduction from 32 to 16 would signify treatment response, but this patient would remain quite depressed.
- Full remission from depression is the treatment goal, and any lesser outcome requires further attention
- Finding the proper medication may require trial and error, and several weeks may pass before a drug’s therapeutic effect occurs
- Continuing to take the medication as prescribed is important to achieving remission
- Medication may have predictable side effects
Table 3
Useful scales to identify and monitor depressive symptoms
| Scale | Administration | Features |
|---|---|---|
| Hamilton Rating Scale for Depression (21- or 17-item HRSD versions) | 15 to 20 minutes, clinician-rated | Focuses on somatic symptoms, excellent reliability, often used to evaluate response to medications |
| Beck Depression Inventory (BDI versions I or II) | 5 to 10 minutes, self-administered | Focuses on behavioral and cognitive elements (somatic symptoms added to BDI-II), good for measuring depression severity, not for depression screening |
| Zung Self-Rating Depression Scale | 5 to 10 minutes, self-administered | Good for screening, not studied as extensively as Hamilton and Beck scales |
| Montgomery-Asberg Depression Rating Scale | 5 to 10 minutes, clinician-rated | 10 items, often used in research |
A Stepwise approach
An expert panel recommends a stepwise approach for patients who respond inadequately to initial antidepressant therapy (Algorithm).27
Re-evaluate the diagnosis. Patients with bipolar disorder or comorbid medical or psychiatric disorders may need medications other than antidepressants. Address concomitant substance abuse, which may interfere with depression treatment. Also exclude or appropriately treat depressive symptoms associated with general medical conditions, such as hypothyroidism.
Optimize dosages. Consider increasing medication dosages as needed until limited by side effects or the drug’s safety profile. Before exceeding an FDA-recommended dosage (Table 4), obtain the patient’s informed consent and document this discussion in the chart.
Consider augmenting or switching. For patients who continue to show partial response, consider combining the initial medication with another antidepressant or augment with another agent, such as lithium, stimulants, thyroid hormone, or even atypical antipsychotics. For patients with no response to optimal dosages of the initial medication after 3 to 4 weeks, try switching to another antidepressant—not necessarily in a different class. One switch within the same class is reasonable.
Some authors emphasize the choice of antidepressant in attaining remission. Although no antidepressant is clearly more efficacious than another, those with fewer side effects (such as selective serotonin reuptake inhibitors vs. tricyclics) may improve adherence.
Numerous trials have shown higher remission rates with serotonin/norepinephrine reuptake inhibitors such as venlafaxine or duloxetine than with other antidepressants.28-30 This evidence is not universally accepted, however.31 Depressive illness probably has a heterogeneous biology, and with greater understanding we may eventually tailor treatment to individual patients’ needs.
Consider psychotherapy or ECT. Patients who do not achieve remission with medication may be candidates for combined treatment with psychotherapy or electroconvulsive therapy (ECT). Life issues—such as family or work stressors—may need to be addressed along with depressive symptoms.
Algorithm A stepwise approach to remission when antidepressant therapy falls short
Table 4
Using common antidepressants for adults with major depression
| FDA-approved maximum dosage* | |||
|---|---|---|---|
| Antidepressant mg/d | mg/d | (mg/kg/d) | Common side effects at maximum dosage* |
| SSRIs | |||
| Citalopram | 80 | (1.0) | Nausea, dry mouth, somnolence |
| Escitalopram | 20 | Nausea, delayed ejaculation, insomnia | |
| Fluoxetine | 80 | (1.33) | Nausea, headache, insomnia |
| Paroxetine | 50 | (0.83) | Nausea, somnolence, headache |
| Sertraline | 200 | (3.33) | Nausea, headache, insomnia |
| SNRIs | |||
| Duloxetine | 120 | Nausea, dry mouth, fatigue | |
| Venlafaxine | 375 | (6.25) | Nausea, somnolence, dry mouth |
| Tricyclics | |||
| Amitriptyline | 300 | (5.0) | Drowsiness, dry mouth, dizziness |
| Desipramine | 300 | (5.0) | Same as above |
| Imipramine | 300 | Same as above | |
| Nortriptyline | 200 | (1.67) | Same as above |
| Others | |||
| Bupropion | 450 | (7.5) | Insomnia, dry mouth, headache |
| Mirtazapine | 45 | (0.75) | Somnolence, dry mouth, increased appetite |
| SSRIs: selective serotonin reuptake inhibitors | |||
| SNRIs: serotonin-norepinephrine reuptake inhibitors | |||
| * Informed consent discussion and documentation is recommended for dosages that exceed FDA-approved maximums. | |||
| Sources: Food and Drug Administration, and Kaplan HI, Sadock B. Kaplan & Sadock’s synopsis of psychiatry (9th ed). Philadelphia: Lippincott Williams & Wilkins, 2002. | |||
Case: monitoring after remission
Ms. M feels back to normal 2 weeks after starting fluoxetine at 60 mg/d. She experienced some transient nausea and headache at this dosage but did not stop the medication because her psychiatrist had told her these side effects might occur.
Ms. M also agrees to short-term psychotherapy to address self-esteem issues that may have contributed to her depressive episode. She soon files the mountain of papers on her desk and corrects erroneous financial statements she has made. Her supervisor is relieved—and so is she.
The psychiatrist schedules monthly medication monitoring and plans to gradually reduce the fluoxetine dosage if depressive symptoms remain in remission for 6 months. Because Ms. M had no past depressive episodes, the medication trial may not need to be extended past 6 months.
Related resources
- McManamy J. McMan’s Depression and Bipolar Web. Treating to remission. http://www.mcmanweb.com/article-181.htm.
- American Psychiatric Association. Practice guideline for the treatment of patients with major depressive disorder (2nd ed.). http://www.psych.org/psych_pract/treatg/pg/Depression2e.book.cfm.
- Stahl S. Essential psychopharmacology: Neuroscientific basis and practical applications (2nd ed.). Cambridge, UK: Cambridge University Presss, 2004, chapters 5-7.
Drug brand names
- Amitriptyline • Elavil, Endep
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Desipramine • Norpramin
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Imipramine • Tofranil
- Mirtazapine • Remeron
- Nortriptyline • Pamelor
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosures
Dr. Van Rhoads reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Gelenberg receives research grants from Pfizer Inc. and Novartis Pharmaceuticals Corp. He is a consultant or a speaker for Eli Lilly and Co., Pfizer Inc., Bristol-Myers Squibb Co., AstraZeneca Pharmaceuticals, Wyeth, GlaxoSmithKline, and Cyberonics.
Remission is considered the standard of treatment for major depression,1-4 but many patients fall short of this goal:
- 25% to 50% of those who respond to treatment have residual symptoms5
- 60% to 70% respond to treatment, but only 20% to 40% achieve remission.6
We offer practical, evidence-based suggestions and resources to help you take more of your patients beyond response to remission and then to recovery (Table 1).7,8
Table 1
Outcomes in depression: Defining the 4 ‘R’s
| Outcome | Definition | Comment |
|---|---|---|
| Response | Clinically significant reduction of symptoms | 50% reduction in symptoms on psychometric scales may leave severely depressed patients with disabling symptoms |
| Remission | Depression resolves completely or nearly completely, with return to baseline function | Score of ≤7 on the HRSD used in many studies; ACNP Task Force defines remission by 9 core depression symptoms in DSM-IV-TR |
| Recovery | Remission lasts for extended time; signifies end of a major depressive episode | ACNP Task Force defines recovery as 4 months of remission |
| Relapse | Return to full symptoms during remission but before recovery; signifies re-emergence of current depressive episode | Residual symptoms during response or remission greatly increase chances of relapse |
| HRSD: Hamilton Rating Scale for Depression | ||
| ACNP: American College of Neuropsychopharmacology | ||
| DSM-IV-TR: Diagnostic and statistical manual of mental disorders, 4th ed., text rev. | ||
| Source: References 7, 8 | ||
Case report: missing the target
Ms. M, age 32, develops depressive symptoms after taking on several new projects in her work as an accountant. At first she notices difficulty falling asleep at night and that she seems tired all day. Typically efficient and neat, she finds herself absently staring at her computer screen while a messy pile of unfinished paperwork accumulates on her desk.
She begins chastising herself for falling behind, yet she feels she will never catch up. When she unexpectedly bursts out sobbing in a board meeting, she knows she needs help.
Ms. M reports that she has been taking fluoxetine, 20 mg/d, for 4 weeks as her primary care physician prescribed, with no improvement. She has no history of depression or other psychiatric illness, is taking no other medication, and has no medical illnesses. Her brother has a history of bipolar disorder.
Initial diagnostic workup includes laboratory tests such as thyroid stimulating hormone, vitamin B12, and folate. All values are within normal limits. Her Hamilton Rating Scale for Depression (HRSD) score is 17, indicating moderate depression.
The psychiatrist increases fluoxetine to 40 mg/d, and after about 3 weeks Ms. M starts feeling better. Her hopelessness lifts, she is more engaged, and her sleep improves, yet she continues to feel sluggish and dazed. Her financial reports contain uncharacteristic errors, and her pace is noticeably slow. Twice her supervisor approaches her about substandard work, then a week later warns that she will lose her job unless she improves.
Barriers to remission. Patient, provider, and health care system barriers prevent patients with major depression from achieving remission (Table 2).3 Patients may feel better with antidepressant therapy but do not recognize and report residual depressive symptoms, such as Ms. M’s fatigue and substandard job performance.
Clinicians also play a role in depression undertreatment. For example, in a study of 239 patients with ≥ 5 depression symptoms,9 28% did not receive treatment consistent with depression management guidelines.
Fava et al10 suggested the following reasons for depression undertreatment: “… clinicians have partial therapeutic targets, neglect residual symptoms, and equate therapeutic response with full remission.” Others have found that physicians may underdose medications or fail to plan treatment in clear phases.11
Table 2
Barriers to remission during depression treatment
| Who and what | Behavior and system problems |
|---|---|
| Patients | Nonadherence to treatment, underreporting of symptoms, satisfaction with suboptimal outcomes, failure to recognize depressive symptoms, underestimating depression severity, limited access to care, reluctance to see a mental health specialist |
| Providers | Medication under-dosing, inadequate treatment duration, inaccurate diagnosis, failure to recognize residual symptoms, limited training in interpersonal skills, inadequate time to evaluate and treat depression, failure to consider psychotherapeutic approaches |
| Health care systems | Limited therapeutic choices, limited number of mental health care visits, restricted access to providers |
| Source: Reference 3 | |
Relapse risk
Increased risk of relapse is perhaps the greatest cost of undertreated major depression. Patients with residual subsyndromal depressive symptoms relapse five times faster than patients in full remission.12
Residual symptoms may be a more powerful relapse predictor than number of past depressive episodes:13
- Chronic mood symptoms for ≥ 2 years double the relapse risk.14
- 50% to 80% of patients in partial remission relapse.15
In a study of patients in recovery from a major depressive episode, 76% (13 of 17) with residual symptoms relapsed within 15 months, compared with 25% (10 of 40) who completely recovered.16
Illness course. After a first major depressive episode, 26 patients with residual subsyndromal symptoms showed a more-severe, chronic illness compared with 70 asymptomatic patients:
- those with residual symptoms had more depression recurrences, with faster relapse and shorter intervals when they felt well
- subsequent depressive episodes occurred >3 times sooner
- well intervals between depressive episodes were 7 times shorter.17
The authors noted that “patients recovering from major depressive episodes with residual subsyndromal depression experience very rapid episode relapse and have strikingly more chronic future courses of illness that are characterized by early and more frequent episode relapses and recurrences.”18 Each major depression recurrence increases the risk of a successive episode.13,19,20
Treatment resistance. Over time, incomplete remission may contribute to treatment resistance,21 although this theory remains untested.
Social health costs
Residual depressive symptoms and impaired psychosocial, interpersonal, and occupational functioning are strongly correlated. In a study of patients who recovered from a major depressive episode, those with residual symptoms scored significantly worse on markers of social performance, relationships, and occupational functioning.6
Psychosocial costs. Compared with the general population, persons with subsyndromal depression have poorer health status and job functioning (as did Ms. M), and greater familial discord, financial strain, irritability, restricted activity, and number of days in bed.22 In 635 patients with chronic depression treated for 12 weeks with imipramine or sertraline:
- nonresponders scored lowest in psychosocial functioning
- responders scored in a mid-range
- remitters scored highest—as well or nearly as well as healthy controls did.23
Occupational costs. Depression leads to workplace absenteeism—twice the rate of nondepressed workers—and less effectiveness. Depressed persons are seven times more likely to be unemployed, employed part-time, or in jobs below their education levels, compared with community samples.24
Medical costs of depressed persons average twice those of the nondepressed,25 and depressed persons use three times as many health care services.26 Depression may increase the risk of:
- cardiac morbidity and mortality
- poor glycemic control in diabetic patients
- HIV progression
- cerebrovascular events
- and overall mortality.
Depression is associated with worse outcomes after myocardial infarction and among nursing home patients, stroke patients, and those with cancer or HIV infection.21
How to improve remission rates
To improve remission rates, we recommend that you follow a rational treatment progression and observe established guidelines, as described in the follow-up report on Ms. M:
Case continued: Part way there. Back at the psychiatrist’s office for 30-day medication monitoring, Ms. M reports that increasing her antidepressant has worked—no more crying in meetings or feeling down on herself. She even sleeps better. Her HRSD score is now 10, indicating improvement, though with some residual symptoms.
When the psychiatrist asks about her job performance, Ms. M is surprised to learn that her fatigue and disorganized thoughts might be lingering features of depression. She said she thought she just wasn’t trying hard enough.
Following practice guidelines,27 the psychiatrist increases fluoxetine to 60 mg/d. This higher dosage remains less than the maximum recommended 80 mg/d, and Ms. M has shown partial improvement with fluoxetine.
Patients being treated for depression need adequate follow-up to ensure they are improving. As with Ms. M, encourage patients to describe residual symptoms and functional domains that remain suboptimal. Educate them about the importance of taking antidepressants as prescribed ( Box). If poor response continues, address possible nonadherence.
Use objective assessments. Global, haphazard, or subjective assessments of patient progress can miss important ongoing depressive symptoms. We recommend using patient- or clinician-rated symptom scales to rapidly identify and monitor residual symptoms ( Table 3).
You may wish to design your own questionnaires to elicit easily missed data or symptoms particular to a certain treatment—such as common side effects of the medication a patient is taking. Nurses or other providers in a busy practice can help assess patients between or before doctor visits.
Keep in mind that the common practice of defining treatment response as a 50% reduction in HRSD scores7,8 leaves many patients with residual depressive symptoms. For example, an HRSD score reduction from 32 to 16 would signify treatment response, but this patient would remain quite depressed.
- Full remission from depression is the treatment goal, and any lesser outcome requires further attention
- Finding the proper medication may require trial and error, and several weeks may pass before a drug’s therapeutic effect occurs
- Continuing to take the medication as prescribed is important to achieving remission
- Medication may have predictable side effects
Table 3
Useful scales to identify and monitor depressive symptoms
| Scale | Administration | Features |
|---|---|---|
| Hamilton Rating Scale for Depression (21- or 17-item HRSD versions) | 15 to 20 minutes, clinician-rated | Focuses on somatic symptoms, excellent reliability, often used to evaluate response to medications |
| Beck Depression Inventory (BDI versions I or II) | 5 to 10 minutes, self-administered | Focuses on behavioral and cognitive elements (somatic symptoms added to BDI-II), good for measuring depression severity, not for depression screening |
| Zung Self-Rating Depression Scale | 5 to 10 minutes, self-administered | Good for screening, not studied as extensively as Hamilton and Beck scales |
| Montgomery-Asberg Depression Rating Scale | 5 to 10 minutes, clinician-rated | 10 items, often used in research |
A Stepwise approach
An expert panel recommends a stepwise approach for patients who respond inadequately to initial antidepressant therapy (Algorithm).27
Re-evaluate the diagnosis. Patients with bipolar disorder or comorbid medical or psychiatric disorders may need medications other than antidepressants. Address concomitant substance abuse, which may interfere with depression treatment. Also exclude or appropriately treat depressive symptoms associated with general medical conditions, such as hypothyroidism.
Optimize dosages. Consider increasing medication dosages as needed until limited by side effects or the drug’s safety profile. Before exceeding an FDA-recommended dosage (Table 4), obtain the patient’s informed consent and document this discussion in the chart.
Consider augmenting or switching. For patients who continue to show partial response, consider combining the initial medication with another antidepressant or augment with another agent, such as lithium, stimulants, thyroid hormone, or even atypical antipsychotics. For patients with no response to optimal dosages of the initial medication after 3 to 4 weeks, try switching to another antidepressant—not necessarily in a different class. One switch within the same class is reasonable.
Some authors emphasize the choice of antidepressant in attaining remission. Although no antidepressant is clearly more efficacious than another, those with fewer side effects (such as selective serotonin reuptake inhibitors vs. tricyclics) may improve adherence.
Numerous trials have shown higher remission rates with serotonin/norepinephrine reuptake inhibitors such as venlafaxine or duloxetine than with other antidepressants.28-30 This evidence is not universally accepted, however.31 Depressive illness probably has a heterogeneous biology, and with greater understanding we may eventually tailor treatment to individual patients’ needs.
Consider psychotherapy or ECT. Patients who do not achieve remission with medication may be candidates for combined treatment with psychotherapy or electroconvulsive therapy (ECT). Life issues—such as family or work stressors—may need to be addressed along with depressive symptoms.
Algorithm A stepwise approach to remission when antidepressant therapy falls short
Table 4
Using common antidepressants for adults with major depression
| FDA-approved maximum dosage* | |||
|---|---|---|---|
| Antidepressant mg/d | mg/d | (mg/kg/d) | Common side effects at maximum dosage* |
| SSRIs | |||
| Citalopram | 80 | (1.0) | Nausea, dry mouth, somnolence |
| Escitalopram | 20 | Nausea, delayed ejaculation, insomnia | |
| Fluoxetine | 80 | (1.33) | Nausea, headache, insomnia |
| Paroxetine | 50 | (0.83) | Nausea, somnolence, headache |
| Sertraline | 200 | (3.33) | Nausea, headache, insomnia |
| SNRIs | |||
| Duloxetine | 120 | Nausea, dry mouth, fatigue | |
| Venlafaxine | 375 | (6.25) | Nausea, somnolence, dry mouth |
| Tricyclics | |||
| Amitriptyline | 300 | (5.0) | Drowsiness, dry mouth, dizziness |
| Desipramine | 300 | (5.0) | Same as above |
| Imipramine | 300 | Same as above | |
| Nortriptyline | 200 | (1.67) | Same as above |
| Others | |||
| Bupropion | 450 | (7.5) | Insomnia, dry mouth, headache |
| Mirtazapine | 45 | (0.75) | Somnolence, dry mouth, increased appetite |
| SSRIs: selective serotonin reuptake inhibitors | |||
| SNRIs: serotonin-norepinephrine reuptake inhibitors | |||
| * Informed consent discussion and documentation is recommended for dosages that exceed FDA-approved maximums. | |||
| Sources: Food and Drug Administration, and Kaplan HI, Sadock B. Kaplan & Sadock’s synopsis of psychiatry (9th ed). Philadelphia: Lippincott Williams & Wilkins, 2002. | |||
Case: monitoring after remission
Ms. M feels back to normal 2 weeks after starting fluoxetine at 60 mg/d. She experienced some transient nausea and headache at this dosage but did not stop the medication because her psychiatrist had told her these side effects might occur.
Ms. M also agrees to short-term psychotherapy to address self-esteem issues that may have contributed to her depressive episode. She soon files the mountain of papers on her desk and corrects erroneous financial statements she has made. Her supervisor is relieved—and so is she.
The psychiatrist schedules monthly medication monitoring and plans to gradually reduce the fluoxetine dosage if depressive symptoms remain in remission for 6 months. Because Ms. M had no past depressive episodes, the medication trial may not need to be extended past 6 months.
Related resources
- McManamy J. McMan’s Depression and Bipolar Web. Treating to remission. http://www.mcmanweb.com/article-181.htm.
- American Psychiatric Association. Practice guideline for the treatment of patients with major depressive disorder (2nd ed.). http://www.psych.org/psych_pract/treatg/pg/Depression2e.book.cfm.
- Stahl S. Essential psychopharmacology: Neuroscientific basis and practical applications (2nd ed.). Cambridge, UK: Cambridge University Presss, 2004, chapters 5-7.
Drug brand names
- Amitriptyline • Elavil, Endep
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Desipramine • Norpramin
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Imipramine • Tofranil
- Mirtazapine • Remeron
- Nortriptyline • Pamelor
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosures
Dr. Van Rhoads reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Gelenberg receives research grants from Pfizer Inc. and Novartis Pharmaceuticals Corp. He is a consultant or a speaker for Eli Lilly and Co., Pfizer Inc., Bristol-Myers Squibb Co., AstraZeneca Pharmaceuticals, Wyeth, GlaxoSmithKline, and Cyberonics.
1. Agency for Health Care Policy and Research. Clinical practice guideline, number 5: Depression in primary care: vol. 2. Treatment of major depression. AHCPR publication 93-0551. Rockville, MD: US Department of Health and Human Services, 1993.
2. American Psychiatric Association. Practice guideline for the treatment of patients with major depressive disorder. Am J Psychiatry 2000;157(suppl 4):1-45.
3. Hirschfeld RM, Keller MB, Panico BS, et al. The National Depressive and Manic-Depressive Association consensus statement on the undertreatment of depression. JAMA 1997;277:333-40.
4. Crismon ML, Trivedi M, Pigott TA, et al. The Texas Medication Algorithm Project: Report of the Texas Consensus Conference Panel on medication treatment of major depressive disorder. J Clin Psychiatry 1999;60:142-56.
5. Nierenberg AA, Keefe BR, Leslie VA, et al. Residual symptoms in depressed patients who respond acutely to fluoxetine. J Clin Psychiatry 1999;60:221-5.
6. Kennedy N, Paykel ES. Residual symptoms at remission from depression: impact on long-term outcome. J Affect Disord 2004;80(2-3):135-44.
7. Rush AJ, Kraemer HC, Sackeim HA, et al. Report by the ACNP Task Force on Response and Remission in Major Depressive Disorder. Submitted for publication.
8. Keller M. Past, present, and future directions for defining optimal treatment outcome in depression: remission and beyond. JAMA 2003;289(23):3152-60.
9. Nutting P, Rost K, Diceinson M, et al. Barriers to initiating depression treatment in primary care practice. J Gen Intern Med 2002;17:103-11.
10. Fava GA, Rafanelli C, Grandi S, et al. Letter to the editor. Arch Gen Psychiatry 1999;56:765.-
11. Ramana R, Paykel ES, Cooper Z, et al. Remission and relapse in major depression: a two year prospective follow-up study. Psychol Med 1995;25(6):1171-80.
12. Judd LL, Akiskal HS, Maser JD, et al. Major depressive disorder: a prospective study of residual subthreshold depressive symptoms as a predictor of rapid relapse. J Affect Disord 1999;50:97-108.
13. Pintor L, Gastó G, Navarro V, et al. Relapse of major depression after complete and partial remission during a 2-year follow-up. J Affect Disord 2003;73:237-44.
14. Lin E, Katon W, Von Korff M, et al. Relapse of depression in primary care: rate and clinical predictors. Arch Fam Med 1998;7(5):443-9.
15. Cornwall P, Scott J. Partial remission in depressive disorders. Acta Psychiatr Scand 1997;95(4):265-71.
16. Paykel ES, Ramana R, Cooper Z, et al. Residual symptoms after partial remission: an important outcome in depression. Psychol Med 1995;25(6):1171-80.
17. Judd LL, Paulus MJ, Schettler PJ, et al. Does incomplete recovery from first lifetime major depressive episode herald a chronic course of illness? Am J Psychiatry 2000;157(9):1501-4.
18. Judd LL, Paulus MP, Zeller P. The role of residual subthreshold depressive symptoms in early episode relapse in unipolar major depressive disorder. Arch Gen Psychiatry 1999;56(8):764-5.
19. Solomon DA, Keller MB, Leon AC, et al. Multiple recurrences of major depressive disorder. Am J Psychiatry 2000;157(2):229-33.
20. Kennedy N, Paykel ES. Residual symptoms at remission from depression: impact on long-term outcome. J Affect Disord 2004;80(2-3):135-44.
21. Zajecka JM. Treating depression to remission. J Clin Psychiatry 2003;64(suppl 15):7-12.
22. Judd LL, Paulus MP, Wells KB, Rapaport MH. Socioeconomic burden of subsyndromal depressive symptoms and major depressionin a sample of the general population. Am J Psychiatry 1996;153(11):1411-7.
23. Miller IW, Keitner GI, Schatzberg AF, et al. The treatment of chronic depression, part 3: psychosocial functioning before and after treatment with sertraline or imipramine. J Clin Psychiatry 1998;59(11):608-19.
24. Druss B, Schlesinger M, Allen H. Depressive symptoms, satisfaction with health care, and 2-year work outcomes in an employed population. Am J Psychiatry 2001;158(5):731-4.
25. Simon G, Ormel J, VonKorff M, et al. Health care costs associated with depressive and anxiety disorders in primary care. Am J Psychiatry 1995;152(3):352-7.
26. Katon W, Schulberg H. Epidemiology of depression in primary care. Gen Hosp Psychiatry 1992;14(4):237-47.
27. Hirschfeld RMA, Montgomery SA, Aguglia E, et al. Partial response and nonresponse to antidepressant therapy: current approaches and treatment options. J Clin Psychiatry 2002;63(9):826-37.
28. Thase ME, Entsuah AR, Rudolph RL. Remission rates during treatment with venlafaxine or selective serotonin reuptake inhibitors. Br J Psychiatry 2001;178:234-41.
29. Kelsey J, Entsuah R. Venlafaxine offers significant therapeutic benefits over existing SSRI treatments irrespective of the patient’s depressive duration (poster presentation). Montreal: Collegium Internationale Neuropsychopharmacologicum, June 2002.
30. Thase ME. Effectiveness of antidepressants: comparative remission rates. J Clin Psychiatry 2003;64(suppl 2):3-7.
31. Shelton C. Long-term management of major depressive disorder: are differences among antidepressant treatments meaningful? J Clin Psychiatry 2004;65(suppl 17):29-33.
1. Agency for Health Care Policy and Research. Clinical practice guideline, number 5: Depression in primary care: vol. 2. Treatment of major depression. AHCPR publication 93-0551. Rockville, MD: US Department of Health and Human Services, 1993.
2. American Psychiatric Association. Practice guideline for the treatment of patients with major depressive disorder. Am J Psychiatry 2000;157(suppl 4):1-45.
3. Hirschfeld RM, Keller MB, Panico BS, et al. The National Depressive and Manic-Depressive Association consensus statement on the undertreatment of depression. JAMA 1997;277:333-40.
4. Crismon ML, Trivedi M, Pigott TA, et al. The Texas Medication Algorithm Project: Report of the Texas Consensus Conference Panel on medication treatment of major depressive disorder. J Clin Psychiatry 1999;60:142-56.
5. Nierenberg AA, Keefe BR, Leslie VA, et al. Residual symptoms in depressed patients who respond acutely to fluoxetine. J Clin Psychiatry 1999;60:221-5.
6. Kennedy N, Paykel ES. Residual symptoms at remission from depression: impact on long-term outcome. J Affect Disord 2004;80(2-3):135-44.
7. Rush AJ, Kraemer HC, Sackeim HA, et al. Report by the ACNP Task Force on Response and Remission in Major Depressive Disorder. Submitted for publication.
8. Keller M. Past, present, and future directions for defining optimal treatment outcome in depression: remission and beyond. JAMA 2003;289(23):3152-60.
9. Nutting P, Rost K, Diceinson M, et al. Barriers to initiating depression treatment in primary care practice. J Gen Intern Med 2002;17:103-11.
10. Fava GA, Rafanelli C, Grandi S, et al. Letter to the editor. Arch Gen Psychiatry 1999;56:765.-
11. Ramana R, Paykel ES, Cooper Z, et al. Remission and relapse in major depression: a two year prospective follow-up study. Psychol Med 1995;25(6):1171-80.
12. Judd LL, Akiskal HS, Maser JD, et al. Major depressive disorder: a prospective study of residual subthreshold depressive symptoms as a predictor of rapid relapse. J Affect Disord 1999;50:97-108.
13. Pintor L, Gastó G, Navarro V, et al. Relapse of major depression after complete and partial remission during a 2-year follow-up. J Affect Disord 2003;73:237-44.
14. Lin E, Katon W, Von Korff M, et al. Relapse of depression in primary care: rate and clinical predictors. Arch Fam Med 1998;7(5):443-9.
15. Cornwall P, Scott J. Partial remission in depressive disorders. Acta Psychiatr Scand 1997;95(4):265-71.
16. Paykel ES, Ramana R, Cooper Z, et al. Residual symptoms after partial remission: an important outcome in depression. Psychol Med 1995;25(6):1171-80.
17. Judd LL, Paulus MJ, Schettler PJ, et al. Does incomplete recovery from first lifetime major depressive episode herald a chronic course of illness? Am J Psychiatry 2000;157(9):1501-4.
18. Judd LL, Paulus MP, Zeller P. The role of residual subthreshold depressive symptoms in early episode relapse in unipolar major depressive disorder. Arch Gen Psychiatry 1999;56(8):764-5.
19. Solomon DA, Keller MB, Leon AC, et al. Multiple recurrences of major depressive disorder. Am J Psychiatry 2000;157(2):229-33.
20. Kennedy N, Paykel ES. Residual symptoms at remission from depression: impact on long-term outcome. J Affect Disord 2004;80(2-3):135-44.
21. Zajecka JM. Treating depression to remission. J Clin Psychiatry 2003;64(suppl 15):7-12.
22. Judd LL, Paulus MP, Wells KB, Rapaport MH. Socioeconomic burden of subsyndromal depressive symptoms and major depressionin a sample of the general population. Am J Psychiatry 1996;153(11):1411-7.
23. Miller IW, Keitner GI, Schatzberg AF, et al. The treatment of chronic depression, part 3: psychosocial functioning before and after treatment with sertraline or imipramine. J Clin Psychiatry 1998;59(11):608-19.
24. Druss B, Schlesinger M, Allen H. Depressive symptoms, satisfaction with health care, and 2-year work outcomes in an employed population. Am J Psychiatry 2001;158(5):731-4.
25. Simon G, Ormel J, VonKorff M, et al. Health care costs associated with depressive and anxiety disorders in primary care. Am J Psychiatry 1995;152(3):352-7.
26. Katon W, Schulberg H. Epidemiology of depression in primary care. Gen Hosp Psychiatry 1992;14(4):237-47.
27. Hirschfeld RMA, Montgomery SA, Aguglia E, et al. Partial response and nonresponse to antidepressant therapy: current approaches and treatment options. J Clin Psychiatry 2002;63(9):826-37.
28. Thase ME, Entsuah AR, Rudolph RL. Remission rates during treatment with venlafaxine or selective serotonin reuptake inhibitors. Br J Psychiatry 2001;178:234-41.
29. Kelsey J, Entsuah R. Venlafaxine offers significant therapeutic benefits over existing SSRI treatments irrespective of the patient’s depressive duration (poster presentation). Montreal: Collegium Internationale Neuropsychopharmacologicum, June 2002.
30. Thase ME. Effectiveness of antidepressants: comparative remission rates. J Clin Psychiatry 2003;64(suppl 2):3-7.
31. Shelton C. Long-term management of major depressive disorder: are differences among antidepressant treatments meaningful? J Clin Psychiatry 2004;65(suppl 17):29-33.