User login
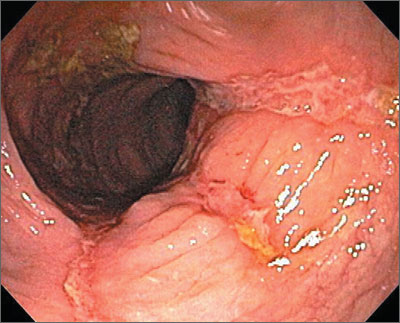
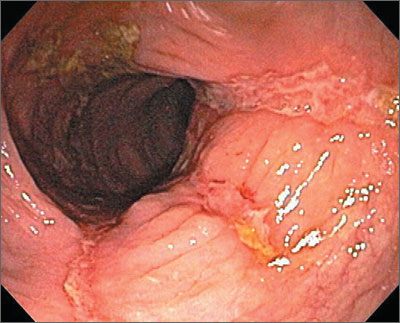
The colonoscopy revealed deep longitudinal ulcers and normal-appearing tissue in between—indicative of Crohn’s disease. The biopsies clinched the diagnosis, as the tissue in between the ulcers was normal. (Crohn’s disease often skips areas, whereas ulcerative colitis is diffuse.)
Symptoms in patients with Crohn’s disease depend on the location of the disease. Patients become symptomatic when lesions are extensive or distal (eg, colitis), systemic inflammatory reaction is present, or when disease is complicated by stricture, abscess, or fistula. Gross blood and mucus in the stool are less frequent than in ulcerative colitis and systemic symptoms, extracolonic features, pain, perineal disease, and obstruction are more common. There is no relationship between symptoms and anatomic damage.
Treatment for mild to moderate disease includes: oral aminosalicylates (ASAs), topical mesalamine, or topical steroids. An oral 5-ASA agent can be a prodrug (eg, sulfasalazine, 2-6 g/day), a drug with a pH-dependent coating (eg, Asacol, 2.4-4.8 g/day), or a slow-release agent (Pentasa, 2-4 g/day).
Patients with Crohn’s disease are also treated with nutritional therapy. Treatment for mild to moderate active ileocolic Crohn’s disease includes oral budesonide or prednisone if distal colonic disease is present. For patients who do not tolerate steroids or in cases where steroids are ineffective, biologic therapy with infliximab, adalimumab, or certolizumab pegol is appropriate. Methotrexate (up to 25 mg/week) is also effective. Patients with weight loss or strictures may benefit from early introduction of a biologic or immunomodulator therapy.
In this case, the gastroenterologist initially treated the patient with oral prednisone. He subsequently talked with her about other systemic therapies.
Photo courtesy of Marvin Derezin, MD. Text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Smith M. Inflammatory bowel disease. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:405-413.
To learn more about the Color Atlas of Family Medicine, see: http://www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking this link: http://usatinemedia.com/
The colonoscopy revealed deep longitudinal ulcers and normal-appearing tissue in between—indicative of Crohn’s disease. The biopsies clinched the diagnosis, as the tissue in between the ulcers was normal. (Crohn’s disease often skips areas, whereas ulcerative colitis is diffuse.)
Symptoms in patients with Crohn’s disease depend on the location of the disease. Patients become symptomatic when lesions are extensive or distal (eg, colitis), systemic inflammatory reaction is present, or when disease is complicated by stricture, abscess, or fistula. Gross blood and mucus in the stool are less frequent than in ulcerative colitis and systemic symptoms, extracolonic features, pain, perineal disease, and obstruction are more common. There is no relationship between symptoms and anatomic damage.
Treatment for mild to moderate disease includes: oral aminosalicylates (ASAs), topical mesalamine, or topical steroids. An oral 5-ASA agent can be a prodrug (eg, sulfasalazine, 2-6 g/day), a drug with a pH-dependent coating (eg, Asacol, 2.4-4.8 g/day), or a slow-release agent (Pentasa, 2-4 g/day).
Patients with Crohn’s disease are also treated with nutritional therapy. Treatment for mild to moderate active ileocolic Crohn’s disease includes oral budesonide or prednisone if distal colonic disease is present. For patients who do not tolerate steroids or in cases where steroids are ineffective, biologic therapy with infliximab, adalimumab, or certolizumab pegol is appropriate. Methotrexate (up to 25 mg/week) is also effective. Patients with weight loss or strictures may benefit from early introduction of a biologic or immunomodulator therapy.
In this case, the gastroenterologist initially treated the patient with oral prednisone. He subsequently talked with her about other systemic therapies.
Photo courtesy of Marvin Derezin, MD. Text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Smith M. Inflammatory bowel disease. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:405-413.
To learn more about the Color Atlas of Family Medicine, see: http://www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking this link: http://usatinemedia.com/
The colonoscopy revealed deep longitudinal ulcers and normal-appearing tissue in between—indicative of Crohn’s disease. The biopsies clinched the diagnosis, as the tissue in between the ulcers was normal. (Crohn’s disease often skips areas, whereas ulcerative colitis is diffuse.)
Symptoms in patients with Crohn’s disease depend on the location of the disease. Patients become symptomatic when lesions are extensive or distal (eg, colitis), systemic inflammatory reaction is present, or when disease is complicated by stricture, abscess, or fistula. Gross blood and mucus in the stool are less frequent than in ulcerative colitis and systemic symptoms, extracolonic features, pain, perineal disease, and obstruction are more common. There is no relationship between symptoms and anatomic damage.
Treatment for mild to moderate disease includes: oral aminosalicylates (ASAs), topical mesalamine, or topical steroids. An oral 5-ASA agent can be a prodrug (eg, sulfasalazine, 2-6 g/day), a drug with a pH-dependent coating (eg, Asacol, 2.4-4.8 g/day), or a slow-release agent (Pentasa, 2-4 g/day).
Patients with Crohn’s disease are also treated with nutritional therapy. Treatment for mild to moderate active ileocolic Crohn’s disease includes oral budesonide or prednisone if distal colonic disease is present. For patients who do not tolerate steroids or in cases where steroids are ineffective, biologic therapy with infliximab, adalimumab, or certolizumab pegol is appropriate. Methotrexate (up to 25 mg/week) is also effective. Patients with weight loss or strictures may benefit from early introduction of a biologic or immunomodulator therapy.
In this case, the gastroenterologist initially treated the patient with oral prednisone. He subsequently talked with her about other systemic therapies.
Photo courtesy of Marvin Derezin, MD. Text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Smith M. Inflammatory bowel disease. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:405-413.
To learn more about the Color Atlas of Family Medicine, see: http://www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking this link: http://usatinemedia.com/