User login
Sammy, age 7, is referred to you by his pediatrician because of a 4-week history of frequent eye blinking. His parents say he blinks a lot when bored but very little when playing baseball. They recall that he also has intermittently sniffed and nodded his head over the last 12 months. Neither Sammy nor his friends seem to be bothered by the blinking. Except for the tics, Sammy’s physical and mental status exams are normal.
Since preschool, Sammy’s teachers have complained that his backpack and desk are always a mess. Sammy is well-meaning but forgetful in his chores at home. A paternal uncle has head-turning movements, counts his steps, and becomes distressed if books on his shelf are not in alphabetical order.
Tics, such as strong eye blinks or repetitive shoulder shrugs, can distress a child or his/her parents, but the conditions associated with tic disorders often are more problematic than the tic disorder itself. High rates of comorbid conditions are recognized in persons with Tourette syndrome, including:
- obsessive-compulsive disorder (OCD) in >80%1
- attention-deficit/hyperactivity disorder (ADHD) in ≤70%2
- anxiety disorders in 30%3
- rage, aggression, learning disabilities, and autism less commonly.
The strategy we recommend for managing tic disorders includes assessing tic severity, educating the family about the illness, determining whether a comorbid condition is present, and managing these conditions appropriately. Above all, we emphasize a risk-benefit analysis guided by the Hippocratic principle of “do no harm.”
Characteristics of tic disorders
You diagnose Sammy with Tourette syndrome because he meets DSM-IV-TR criteria of at least 2 motor tics and 1 vocal tic that have persisted for 1 year without more than a 3-month hiatus, with tic onset before age 18. Because tics may resemble other movement disorders, you rule out stereotypies, dystonia, chorea, ballism, and myoclonus (Table 1). You explain to his parents that Sammy’s condition is a heritable, neurobehavioral disorder that typically begins in childhood and is associated in families with OCD, ADHD, and autism spectrum disorders.
His parents ask about the difference between tics and other movements. You explain that eye-blinking tics—like other motor tics—appear as sudden, repetitive, stereotyped, nonrhythmic movements that involve discrete muscle groups. (View a video of a patient with tics.) Simple motor tics are focal movements involving 1 group of muscles, whereas complex tics are sequential patterns of movement that involve >1 muscle group or resemble purposeful movements (Table 2).
Table 1
Features of 5 movement disorders that may resemble tics
| Tics | Stereotypies | Dystonia | Chorea | Ballism | Myoclonus |
|---|---|---|---|---|---|
| Sudden, repetitive, stereotyped, nonrhythmic movements or sounds | Patterned, nonpurposeful movement | Cocontraction of agonist and antagonist muscles, causing an abnormal twisting posture | Continuous, flowing, nonrhythmic, nonpurposeful movement | Forceful, flinging, large amplitude choreic movement | Sudden, quick, shock-like movement |
| Usually start after age 3 | Usually start before age 3 and resolve by adolescence | More common in adults | — | — | — |
| Decrease when focused; increase when stressed, anxious, fatigued, or bored | Occur when the child is excited | Worsens during motor tasks | Worsens during motor tasks | Worsens during motor tasks | — |
| Comorbid conditions include OCD and ADHD | Common in children with mental retardation or autism | — | Can occur after streptococcal infection | Can occur after streptococcal infection | — |
| Preceded by a premonitory urge or sensation | Possibly preceded by an urge | Not preceded by an urge | Not preceded by an urge | Not preceded by an urge | Not preceded by an urge |
| Temporarily suppressible | Suppressible | Not suppressible | Partially suppressible; can incorporate into semi-purposeful movements | Partially suppressible | Not suppressible |
| ADHD: attention-deficit/hyperactivity disorder; OCD: obsessive-compulsive disorder | |||||
Table 2
Characteristics of simple and complex motor and vocal tics*
| Simple tics | Complex tics |
|---|---|
| Eye blinking or eye rolling Nose, mouth, tongue, or facial grimaces (nose twitch, nasal flaring, chewing lip, teeth grinding, sticking out tongue, mouth stretching, lip licking) Head jerks or movements (neck stretching, touching chin to shoulder) Shoulder jerks/movements (shoulder shrugging, jerking a shoulder) Arm or hand movements (flexing or extending arms or fingers) Coughing Throat clearing, grunting Sniffing, snorting, shouting Humming | Jumping Spinning Touching objects or people Throwing objects Repeating others’ action (echopraxia) Obscene gestures (copropraxia) Repeating one’s own words (palilalia) Repeating what someone else said (echolalia) Obscene, inappropriate words (coprolalia) |
| *Simple tics are focal movements involving 1 group of muscles; complex tics are sequential patterns of movement that involve >1 muscle group or resemble purposeful movements | |
Older children frequently describe a premonitory urge prior to the tic. Patients typically can suppress tics for a transient period of time, although during tic suppression they usually feel restless and anticipate performing their tic. The ultimate performance of the tic brings relief. Tic suppression also occurs during focused activity. Emotional stress, fatigue, illness, or boredom can exacerbate tics.
To begin monitoring Sammy’s clinical course, you administer 3 assessment tools described inTable 3. You explain to Sammy’s parents that these tests will be repeated yearly or when tics worsen. However, you tell his parents that these scores alone will not determine present or future clinical decisions, including treatments. You also recommend that they connect with support groups on the Tourette Syndrome Association (TSA) Web site.
CASE CONTINUED: Changes over time
Sammy’s parents appreciate your explanation and say they will share information from the TSA Web site with Sammy’s principal, teachers, and classmates. The family agrees to return in 6 months or sooner if the tics worsen.
By age 8, Sammy develops multiple tics: facial grimacing, looking upwards, punching movements, whistling, and throat clearing. He is slightly bothered by these tics, and his friends have asked him about them. He tells them he has Tourette syndrome, and that usually ends the questioning. He returns for a follow-up visit because his parents notice a dramatic increase in his tics after Sammy’s father loses his job.
Treatment options
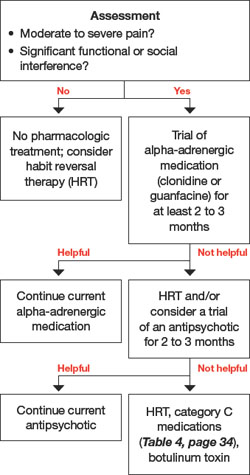
When deciding to treat a child’s tics, the first step is to determine whether to pursue a nonpharmacologic or pharmacologic approach (Algorithm). To tailor an approach most suited for an individual child, discuss with the family their feelings about therapy and medications. This information—along with tic severity—will help determine a treatment plan.
Behavior therapy and medication are management strategies; neither can cure a tic disorder. The most conservative approach to tic treatment is to:
- provide the child and family with basic guidelines for managing tics
- help alleviate environmental stress and other potential triggers.
Algorithm: Recommended treatment of tics in children and adolescents
CASE CONTINUED: A first intervention
You discuss treatment options with Sammy’s family, and they view medication as a last resort. Sammy does not seem to be bothered by his tics, and his parents do not wish to start him on daily medications. Given this situation, habit reversal therapy (HRT) is appropriate for Sammy because he is old enough to participate in HRT to reduce his tics.
HRT is an effective nonpharmacologic approach to help children with tics.4 Its 3 components are:
- awareness training
- competing response training
- social support.5
This simplified version of the original HRT can be completed in eight 1-hour sessions. Good candidates are patients who are cognitively mature enough to understand the therapy’s goals and compliant with frequent clinic visits. They also must practice the strategies at home.
It should not be difficult for psychiatrists to learn HRT—or refer to therapists who are willing to learn it—with the available instructional manual.
CASE CONTINUED: Practicing alternatives
You ask Sammy to imitate his tics. After helping him become more aware of his tics, you encourage him to develop a more socially appropriate movement to engage in whenever he feels the urge to punch. Sammy chooses to clench his fist in his pocket. He also learns to breathe in whenever he has an urge to whistle. you advise Sammy’s parents to reward his efforts to suppress the tics. He practices the strategies daily.
At age 12, Sammy returns to your office. He has begun to have frequent neck-jerking tics, which cause neck pain and daily headaches. He also is slapping his thigh and having frequent vocal tics characterized by loud shrieking. The vocal tics are disruptive in class, even though Sammy sits toward the back of the room. Sammy’s classmates tease him, and he is very frustrated.
Medication approach
The decision to start a medication for tics is complex. Scores from the YGTSS, PUTS, and GTS-QOL scales (Table 3) provide only a partial clinical picture. This decision should be reached after a detailed discussion with the family about benefits and risks of medications and ensuring that everyone’s expectations are reasonable.
A variety of medications are available to treat patients with tics (Table 4). No medication can completely eliminate tics, however, and many have substantial side effects. Before initiating medical treatment, consider 3 questions:
- Is moderate or severe pain involved?
- Is there significant functional interference?
- Is there significant social disruption despite efforts to optimize the social environment for the child?
Sammy’s frequent neck-jerking tics now cause chronic daily headaches, and his shrieking vocal tics are interfering with classroom activities, so we recommended a 3-month trial of guanfacine following the dosing schedule in Table 4.
Table 3
3 scales for assessing tic severity and impact on functioning
| Instrument | Purpose | Description | Design | Administration frequency |
|---|---|---|---|---|
| Yale Global Tic Severity Scale (YGTSS) | Assess tic severity | Review of motor and vocal tics. Rate number, frequency, intensity, complexity, and interference on a 5-point scale | Clinician-rated | Annual and as needed for increased tics |
| Premonitory Urge for Tics Scale (PUTS) | Detect the presence of unpleasant sensations that precedes tics | 10 questions | Self-report | Annual and as needed for increased tics |
| Gilles de la Tourette Syndrome Quality of Life Scale (GTS-QOL) | Measure quality of life | 27 questions, 4 subscales: psychological, physical, obsessional, and cognitive | Self-report | Annual and as needed for increased tics |
Table 4
Medications with evidence of tic-suppressing effects*
| Category A evidence | ||
|---|---|---|
| Medication | Starting dose | Target dose |
| Haloperidol | 0.25 to 0.5 mg/d | 1 to 4 mg/d |
| Pimozide | 0.5 to 1 mg/d | 2 to 8 mg/d |
| Risperidone | 0.25 to 0.5 mg/d | 1 to 3 mg/d |
| Category B evidence | ||
| Medication | Starting dose | Target dose |
| Fluphenazine | 0.5 to 1 mg/d | 1.5 to 10 mg/d |
| Ziprasidone | 5 to 10 mg/d | 10 to 80 mg/d |
| Clonidine | 0.025 to 0.05 mg/d | 0.1 to 0.3 mg/d |
| Guanfacine | 0.5 to 1 mg/d | 1 to 3 mg/d |
| Botulinum toxin | 30 to 300 units | |
| Category C evidence | ||
| Medication | Starting dose | Target dose |
| Olanzapine | 2.5 to 5 mg/d | 2.5 to 12.5 mg/d |
| Tetrabenazine | 25 mg/d | 37.5 to 150 mg/d |
| Baclofen | 10 mg/d | 40 to 60 mg/d |
| Nicotine patch | 7 mg/d | 7 to 21 mg/d |
| Mecamylamine | 2.5 mg/d | 2.5 to 7.5 mg/d |
| Flutamide | 250 mg/d | 750 mg/d |
| *Category A: supported by ≥2 placebo-controlled trials; category B: supported by 1 placebo-controlled trial; category C: supported by open-label study | ||
| Source: Reference 6 | ||
The first-line pharmacologic agent for tic suppression generally is an alpha-adrenergic medication, unless the tics are severe.6
Clonidine and guanfacine usually are started at low doses and increased gradually. Although not as effective as neuroleptics, alpha-adrenergics have a lower potential for side effects and are easier to use because no laboratory tests need to be monitored. Adverse effects associated with alpha-adrenergic medications include sedation, dry mouth, dizziness, headache, and rebound hypertension if discontinued abruptly.
If tics are causing pain, some clinicians prefer conservative measures such as heat or ice, massage, analgesics, relaxation therapy, and reassurance.
Second-line agents include typical and atypical antipsychotics. Haloperidol and pimozide have shown efficacy in reducing tics in placebo- controlled studies,7,8 as have risperidone (in 4 randomized controlled trials [RCTs]) and ziprasidone (in 1 RCT).9,10 The emergence of serious side effects is a risk for both typical and atypical antipsychotics (Table 5).
Table 5
Potential adverse effects of antipsychotic treatment in children*
| Adverse effect | Examples |
|---|---|
| Sedation | — |
| Acute dystonic reactions | Oculogyric crisis, torticollis |
| Appetite changes | Weight gain |
| Endocrine abnormalities | Amenorrhea, diabetes, galactorrhea, gynecomastia, hyperprolactinemia |
| Cognitive effects | Impaired concentration |
| Akathisia | Difficulty sitting still |
| ECG changes | Prolonged QT interval |
| Parkinsonism | Tremor, bradykinesia, rigidity, postural instability |
| Tardive syndrome | Orofacial dyskinesia, chorea, dystonia, myoclonus, tics |
| Neuroleptic malignant syndrome | Potentially fatal; consists of muscular rigidity, fever, autonomic dysfunction, labile blood pressure, sweating, urinary incontinence, fluctuating level of consciousness, leukocytosis, elevated serum creatine kinase |
| *Potential adverse effects are listed from most to least likely to occur | |
As part of your informed consent discussion, weigh the risk of side effects against the benefits of treatment. Point out to patients and their families that they can expect to see a decrease in tic frequency, but symptoms will not necessarily disappear with any medication. We tell our patients that with antipsychotics the best we can hope for is to reduce tic frequency by approximately one-half.6
When treating tics, start with 1 medication. However, if the tics are severe enough to require more than 1 medication, check for drug interactions.
Third-line agents. Agents that have not been tested in placebo-controlled trials can be considered third line; these are listed as category C (supported by open-label studies) in Table 4. Botulinum toxin injection has been found to be effective for motor and vocal tics.11,12 Botulinum toxin and implantation of deep brain stimulators13 are invasive options and generally are reserved for severe, treatment-resistant tics.
CASE CONTINUED: Managing antipsychotics
After trying guanfacine for 12 weeks, Sammy notices no tic reduction. His parents consent to a low dose of risperidone. you review with them the American Psychiatric Association (APA)/American Diabetes Association (ADA) guidelines14 for managing metabolic problems in patients treated with atypical antipsychotics.
As instructed in the APA/ADA guidelines, obtain baseline measurements and monitor for metabolic effects of antipsychotic therapy over time (Table 6). Sammy starts risperidone at 0.5 mg once daily. After 2 weeks, he notices a decrease in his tics. At the 3-month visit after starting risperidone, he is happy with his risperidone dose and does not want to increase it. He has gained 3 pounds, and you instruct him to eat a well-balanced diet and exercise routinely. At the 6-month visit, his tics are minimal and his weight has stabilized.
Table 6
Children receiving antipsychotics: monitoring recommendations
| Clinical information | Frequency |
|---|---|
| Family history | Initial visit |
| Weight | Baseline, monthly |
| Height | Baseline, monthly |
| BMI | Baseline, monthly |
| Waist circumference | Baseline, annually |
| Blood pressure | Baseline, 3 months after treatment starts, and annually thereafter |
| Fasting lipid profile | Baseline, every 3 months initially, then every 6 months thereafter |
| Fasting serum glucose | Baseline, every 3 months, then every 6 months thereafter |
| BMI: body mass index | |
| Source: References 14,16 | |
You recommend that Sammy remain on risperidone for another 3 months of stability and then begin to taper this medication. You review the risks and benefits of long-term treatment with risperidone, pointing out that it may lead to abnormal movements upon withdrawal, and explain that you typically do not treat children with antipsychotics for more than one year continuously.
CASE CONTINUED: Comorbid symptoms
Since starting 7th grade, Sammy has worried excessively about making mistakes. He spends 6 hours each night on homework, which he often does not turn in because of anxiety about not getting answers perfectly right. Classmates notice that Sammy taps the door 3 times when he comes into the classroom and that he steps over the black tiles in the hallway.
Consider the presence and impact of comorbid OCD or ADHD, which can impair children’s quality of life more than tics themselves.15 Assessment scales can help you make a diagnosis and monitor treatment.
If you suspect OCD, the clinician-rated Children’s Yale Brown Obsessive Compulsive Scale is the gold standard for describing the phenomenology and measuring symptom severity. Additional scales to measure symptoms’ impact on family life include the Leyton Obsessional Inventory—child version, Family Accommodation Scale for OCD, and Child OCD Impact Scale.
ADHD scales include the Conners Parent Rating Scale—Revised, Conners Teacher Rating Scale—Revised, Swanson, Nolan, and Pelham, or the Vanderbilt ADHD Diagnostic Parent and Teacher Rating Scales. Because ADHD symptoms must be present in more than 1 environment to meet diagnostic criteria, ask parents and teachers to complete the Conners or Vanderbilt scales.
In children who present with a tic disorder plus a comorbid condition, prioritize treatment by determining which symptoms interfere with the child’s ability to function at school, at home, and in the social arena. Children who require treatment for >1 disorder often are referred initially for cognitive-behavioral therapy for OCD symptoms while receiving pharmacologic treatment for ADHD and/or Tourette syndrome. When necessary, it is usually safe to combine antipsychotics, stimulants, and selective serotonin reuptake inhibitors, although medication interactions should be reviewed in each specific case.
Related resources
- Woods DW. Managing Tourette syndrome: a behavioral intervention for children and adults. Therapist guide. New York, NY: Oxford University Press; 2008.
- Tourette Syndrome Association. www.tsa-usa.org.
- International OCD Foundation. www.ocfoundation.org.
Drug brand names
- Baclofen • Lioresal
- Botulinum toxin • Botox, Myobloc
- Clomipramine • Anafranil
- Clonidine • Catapres
- Guanfacine • Tenex
- Fluphenazine • Prolixin
- Flutamide • Eulexin
- Haloperidol • Haldol
- Mecamylamine • Inversine
- Nicotine patch • NicoDerm
- Olanzapine • Zyprexa
- Pimozide • Orap
- Risperidone • Risperdal
- Tetrabenazine • Xenazine
- Ziprasidone • Geodon
Disclosures
Dr. Harris has received research support from the Translational Research Initiative at Cincinnati Children’s Hospital Medical Center.
Dr. Wu reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Robertson M. Tourette syndrome, associated conditions and the complexities of treatment. Brain. 2000;123(3):425-462.
2. Freeman R. For the Tourette Syndrome International Database Consortium. Tic disorders and ADHD: answers from a worldwide clinical dataset on Tourette syndrome. Eur Child Adolesc Psychiatry. 2007;16(suppl 1):15-23.
3. Stefl M. Mental health needs associated with Tourette syndrome. Am J Public Health. 1984;74:1310-1313.
4. Deckersbach T, Rauch S, Buhlmann U, et al. Habit reversal versus supportive psychotherapy in Tourette’s disorder: a randomized controlled trial and predictors of treatment response. Behav Res Ther. 2006;44:1079-1090.
5. Woods DW, Miltenberger RG. Habit reversal: a review of applications and variations. J Behav Ther Exp Psychiatry. 1995;26:123-131.
6. Scahill L, Erenberg G, Berlin C, et al. Contemporary assessment and pharmacotherapy of Tourette syndrome. NeuroRx. 2006;3(2):192-206.
7. Shapiro E, Shapiro A, Fulop G, et al. Controlled study of haloperidol, pimozide, and placebo for the treatment of Gilles de la Tourette’s syndrome. 1989;46:722-730.
8. Sallee F, Nesbitt L, Jackson C, et al. Relative efficacy of haloperidol and pimozide in children and adolescents with Tourette’s disorder. Am J Psychiatry. 1997;154:1057-1062.
9. Scahill L, Leckman J, Schultz R, et al. A placebo-controlled trial of risperidone in Tourette syndrome. Neurology. 2003;60:1130-1135.
10. Sallee F, Kurlan R, Goetz C, et al. Ziprasidone treatment of children and adolescents with Tourette’s syndrome: a pilot study. J Am Acad Child Adolesc Psychiatry. 2000;39(3):292-299.
11. Marras C, Andrews D, Sime E, et al. Botulinum toxin for simple motor tics: a randomized, double-blind, controlled clinical trial. Neurology. 2001;56(5):605-610.
12. Porta M, Maggioni G, Ottaviani F, et al. Treatment of phonic tics in patients with Tourette’s syndrome using botulinum toxin type A. Neurol Sci. 2004;24(6):420-423.
13. Porta M, Sevello D, Sassi M, et al. Issues related to deep brain stimulation for treatment-refractory Tourette’s syndrome. Eur Neurol. 2009;62(5):264-273.
14. American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists, North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. J Clin Psychiatry. 2004;65:1335-1342.
15. Bernard BA, Stebbins GT, Siegel S, et al. Determinants of quality of life in children with Gilles de la Tourette syndrome. Mov Disord. 2009;24(7):1070-1073.
16. Understanding the risks of antipsychotic treatment in young people. Advice for managing side effects in children and teenagers. Harv Ment Health Lett. 2009;25(9):1-3.
Sammy, age 7, is referred to you by his pediatrician because of a 4-week history of frequent eye blinking. His parents say he blinks a lot when bored but very little when playing baseball. They recall that he also has intermittently sniffed and nodded his head over the last 12 months. Neither Sammy nor his friends seem to be bothered by the blinking. Except for the tics, Sammy’s physical and mental status exams are normal.
Since preschool, Sammy’s teachers have complained that his backpack and desk are always a mess. Sammy is well-meaning but forgetful in his chores at home. A paternal uncle has head-turning movements, counts his steps, and becomes distressed if books on his shelf are not in alphabetical order.
Tics, such as strong eye blinks or repetitive shoulder shrugs, can distress a child or his/her parents, but the conditions associated with tic disorders often are more problematic than the tic disorder itself. High rates of comorbid conditions are recognized in persons with Tourette syndrome, including:
- obsessive-compulsive disorder (OCD) in >80%1
- attention-deficit/hyperactivity disorder (ADHD) in ≤70%2
- anxiety disorders in 30%3
- rage, aggression, learning disabilities, and autism less commonly.
The strategy we recommend for managing tic disorders includes assessing tic severity, educating the family about the illness, determining whether a comorbid condition is present, and managing these conditions appropriately. Above all, we emphasize a risk-benefit analysis guided by the Hippocratic principle of “do no harm.”
Characteristics of tic disorders
You diagnose Sammy with Tourette syndrome because he meets DSM-IV-TR criteria of at least 2 motor tics and 1 vocal tic that have persisted for 1 year without more than a 3-month hiatus, with tic onset before age 18. Because tics may resemble other movement disorders, you rule out stereotypies, dystonia, chorea, ballism, and myoclonus (Table 1). You explain to his parents that Sammy’s condition is a heritable, neurobehavioral disorder that typically begins in childhood and is associated in families with OCD, ADHD, and autism spectrum disorders.
His parents ask about the difference between tics and other movements. You explain that eye-blinking tics—like other motor tics—appear as sudden, repetitive, stereotyped, nonrhythmic movements that involve discrete muscle groups. (View a video of a patient with tics.) Simple motor tics are focal movements involving 1 group of muscles, whereas complex tics are sequential patterns of movement that involve >1 muscle group or resemble purposeful movements (Table 2).
Table 1
Features of 5 movement disorders that may resemble tics
| Tics | Stereotypies | Dystonia | Chorea | Ballism | Myoclonus |
|---|---|---|---|---|---|
| Sudden, repetitive, stereotyped, nonrhythmic movements or sounds | Patterned, nonpurposeful movement | Cocontraction of agonist and antagonist muscles, causing an abnormal twisting posture | Continuous, flowing, nonrhythmic, nonpurposeful movement | Forceful, flinging, large amplitude choreic movement | Sudden, quick, shock-like movement |
| Usually start after age 3 | Usually start before age 3 and resolve by adolescence | More common in adults | — | — | — |
| Decrease when focused; increase when stressed, anxious, fatigued, or bored | Occur when the child is excited | Worsens during motor tasks | Worsens during motor tasks | Worsens during motor tasks | — |
| Comorbid conditions include OCD and ADHD | Common in children with mental retardation or autism | — | Can occur after streptococcal infection | Can occur after streptococcal infection | — |
| Preceded by a premonitory urge or sensation | Possibly preceded by an urge | Not preceded by an urge | Not preceded by an urge | Not preceded by an urge | Not preceded by an urge |
| Temporarily suppressible | Suppressible | Not suppressible | Partially suppressible; can incorporate into semi-purposeful movements | Partially suppressible | Not suppressible |
| ADHD: attention-deficit/hyperactivity disorder; OCD: obsessive-compulsive disorder | |||||
Table 2
Characteristics of simple and complex motor and vocal tics*
| Simple tics | Complex tics |
|---|---|
| Eye blinking or eye rolling Nose, mouth, tongue, or facial grimaces (nose twitch, nasal flaring, chewing lip, teeth grinding, sticking out tongue, mouth stretching, lip licking) Head jerks or movements (neck stretching, touching chin to shoulder) Shoulder jerks/movements (shoulder shrugging, jerking a shoulder) Arm or hand movements (flexing or extending arms or fingers) Coughing Throat clearing, grunting Sniffing, snorting, shouting Humming | Jumping Spinning Touching objects or people Throwing objects Repeating others’ action (echopraxia) Obscene gestures (copropraxia) Repeating one’s own words (palilalia) Repeating what someone else said (echolalia) Obscene, inappropriate words (coprolalia) |
| *Simple tics are focal movements involving 1 group of muscles; complex tics are sequential patterns of movement that involve >1 muscle group or resemble purposeful movements | |
Older children frequently describe a premonitory urge prior to the tic. Patients typically can suppress tics for a transient period of time, although during tic suppression they usually feel restless and anticipate performing their tic. The ultimate performance of the tic brings relief. Tic suppression also occurs during focused activity. Emotional stress, fatigue, illness, or boredom can exacerbate tics.
To begin monitoring Sammy’s clinical course, you administer 3 assessment tools described inTable 3. You explain to Sammy’s parents that these tests will be repeated yearly or when tics worsen. However, you tell his parents that these scores alone will not determine present or future clinical decisions, including treatments. You also recommend that they connect with support groups on the Tourette Syndrome Association (TSA) Web site.
CASE CONTINUED: Changes over time
Sammy’s parents appreciate your explanation and say they will share information from the TSA Web site with Sammy’s principal, teachers, and classmates. The family agrees to return in 6 months or sooner if the tics worsen.
By age 8, Sammy develops multiple tics: facial grimacing, looking upwards, punching movements, whistling, and throat clearing. He is slightly bothered by these tics, and his friends have asked him about them. He tells them he has Tourette syndrome, and that usually ends the questioning. He returns for a follow-up visit because his parents notice a dramatic increase in his tics after Sammy’s father loses his job.
Treatment options
When deciding to treat a child’s tics, the first step is to determine whether to pursue a nonpharmacologic or pharmacologic approach (Algorithm). To tailor an approach most suited for an individual child, discuss with the family their feelings about therapy and medications. This information—along with tic severity—will help determine a treatment plan.
Behavior therapy and medication are management strategies; neither can cure a tic disorder. The most conservative approach to tic treatment is to:
- provide the child and family with basic guidelines for managing tics
- help alleviate environmental stress and other potential triggers.
Algorithm: Recommended treatment of tics in children and adolescents
CASE CONTINUED: A first intervention
You discuss treatment options with Sammy’s family, and they view medication as a last resort. Sammy does not seem to be bothered by his tics, and his parents do not wish to start him on daily medications. Given this situation, habit reversal therapy (HRT) is appropriate for Sammy because he is old enough to participate in HRT to reduce his tics.
HRT is an effective nonpharmacologic approach to help children with tics.4 Its 3 components are:
- awareness training
- competing response training
- social support.5
This simplified version of the original HRT can be completed in eight 1-hour sessions. Good candidates are patients who are cognitively mature enough to understand the therapy’s goals and compliant with frequent clinic visits. They also must practice the strategies at home.
It should not be difficult for psychiatrists to learn HRT—or refer to therapists who are willing to learn it—with the available instructional manual.
CASE CONTINUED: Practicing alternatives
You ask Sammy to imitate his tics. After helping him become more aware of his tics, you encourage him to develop a more socially appropriate movement to engage in whenever he feels the urge to punch. Sammy chooses to clench his fist in his pocket. He also learns to breathe in whenever he has an urge to whistle. you advise Sammy’s parents to reward his efforts to suppress the tics. He practices the strategies daily.
At age 12, Sammy returns to your office. He has begun to have frequent neck-jerking tics, which cause neck pain and daily headaches. He also is slapping his thigh and having frequent vocal tics characterized by loud shrieking. The vocal tics are disruptive in class, even though Sammy sits toward the back of the room. Sammy’s classmates tease him, and he is very frustrated.
Medication approach
The decision to start a medication for tics is complex. Scores from the YGTSS, PUTS, and GTS-QOL scales (Table 3) provide only a partial clinical picture. This decision should be reached after a detailed discussion with the family about benefits and risks of medications and ensuring that everyone’s expectations are reasonable.
A variety of medications are available to treat patients with tics (Table 4). No medication can completely eliminate tics, however, and many have substantial side effects. Before initiating medical treatment, consider 3 questions:
- Is moderate or severe pain involved?
- Is there significant functional interference?
- Is there significant social disruption despite efforts to optimize the social environment for the child?
Sammy’s frequent neck-jerking tics now cause chronic daily headaches, and his shrieking vocal tics are interfering with classroom activities, so we recommended a 3-month trial of guanfacine following the dosing schedule in Table 4.
Table 3
3 scales for assessing tic severity and impact on functioning
| Instrument | Purpose | Description | Design | Administration frequency |
|---|---|---|---|---|
| Yale Global Tic Severity Scale (YGTSS) | Assess tic severity | Review of motor and vocal tics. Rate number, frequency, intensity, complexity, and interference on a 5-point scale | Clinician-rated | Annual and as needed for increased tics |
| Premonitory Urge for Tics Scale (PUTS) | Detect the presence of unpleasant sensations that precedes tics | 10 questions | Self-report | Annual and as needed for increased tics |
| Gilles de la Tourette Syndrome Quality of Life Scale (GTS-QOL) | Measure quality of life | 27 questions, 4 subscales: psychological, physical, obsessional, and cognitive | Self-report | Annual and as needed for increased tics |
Table 4
Medications with evidence of tic-suppressing effects*
| Category A evidence | ||
|---|---|---|
| Medication | Starting dose | Target dose |
| Haloperidol | 0.25 to 0.5 mg/d | 1 to 4 mg/d |
| Pimozide | 0.5 to 1 mg/d | 2 to 8 mg/d |
| Risperidone | 0.25 to 0.5 mg/d | 1 to 3 mg/d |
| Category B evidence | ||
| Medication | Starting dose | Target dose |
| Fluphenazine | 0.5 to 1 mg/d | 1.5 to 10 mg/d |
| Ziprasidone | 5 to 10 mg/d | 10 to 80 mg/d |
| Clonidine | 0.025 to 0.05 mg/d | 0.1 to 0.3 mg/d |
| Guanfacine | 0.5 to 1 mg/d | 1 to 3 mg/d |
| Botulinum toxin | 30 to 300 units | |
| Category C evidence | ||
| Medication | Starting dose | Target dose |
| Olanzapine | 2.5 to 5 mg/d | 2.5 to 12.5 mg/d |
| Tetrabenazine | 25 mg/d | 37.5 to 150 mg/d |
| Baclofen | 10 mg/d | 40 to 60 mg/d |
| Nicotine patch | 7 mg/d | 7 to 21 mg/d |
| Mecamylamine | 2.5 mg/d | 2.5 to 7.5 mg/d |
| Flutamide | 250 mg/d | 750 mg/d |
| *Category A: supported by ≥2 placebo-controlled trials; category B: supported by 1 placebo-controlled trial; category C: supported by open-label study | ||
| Source: Reference 6 | ||
The first-line pharmacologic agent for tic suppression generally is an alpha-adrenergic medication, unless the tics are severe.6
Clonidine and guanfacine usually are started at low doses and increased gradually. Although not as effective as neuroleptics, alpha-adrenergics have a lower potential for side effects and are easier to use because no laboratory tests need to be monitored. Adverse effects associated with alpha-adrenergic medications include sedation, dry mouth, dizziness, headache, and rebound hypertension if discontinued abruptly.
If tics are causing pain, some clinicians prefer conservative measures such as heat or ice, massage, analgesics, relaxation therapy, and reassurance.
Second-line agents include typical and atypical antipsychotics. Haloperidol and pimozide have shown efficacy in reducing tics in placebo- controlled studies,7,8 as have risperidone (in 4 randomized controlled trials [RCTs]) and ziprasidone (in 1 RCT).9,10 The emergence of serious side effects is a risk for both typical and atypical antipsychotics (Table 5).
Table 5
Potential adverse effects of antipsychotic treatment in children*
| Adverse effect | Examples |
|---|---|
| Sedation | — |
| Acute dystonic reactions | Oculogyric crisis, torticollis |
| Appetite changes | Weight gain |
| Endocrine abnormalities | Amenorrhea, diabetes, galactorrhea, gynecomastia, hyperprolactinemia |
| Cognitive effects | Impaired concentration |
| Akathisia | Difficulty sitting still |
| ECG changes | Prolonged QT interval |
| Parkinsonism | Tremor, bradykinesia, rigidity, postural instability |
| Tardive syndrome | Orofacial dyskinesia, chorea, dystonia, myoclonus, tics |
| Neuroleptic malignant syndrome | Potentially fatal; consists of muscular rigidity, fever, autonomic dysfunction, labile blood pressure, sweating, urinary incontinence, fluctuating level of consciousness, leukocytosis, elevated serum creatine kinase |
| *Potential adverse effects are listed from most to least likely to occur | |
As part of your informed consent discussion, weigh the risk of side effects against the benefits of treatment. Point out to patients and their families that they can expect to see a decrease in tic frequency, but symptoms will not necessarily disappear with any medication. We tell our patients that with antipsychotics the best we can hope for is to reduce tic frequency by approximately one-half.6
When treating tics, start with 1 medication. However, if the tics are severe enough to require more than 1 medication, check for drug interactions.
Third-line agents. Agents that have not been tested in placebo-controlled trials can be considered third line; these are listed as category C (supported by open-label studies) in Table 4. Botulinum toxin injection has been found to be effective for motor and vocal tics.11,12 Botulinum toxin and implantation of deep brain stimulators13 are invasive options and generally are reserved for severe, treatment-resistant tics.
CASE CONTINUED: Managing antipsychotics
After trying guanfacine for 12 weeks, Sammy notices no tic reduction. His parents consent to a low dose of risperidone. you review with them the American Psychiatric Association (APA)/American Diabetes Association (ADA) guidelines14 for managing metabolic problems in patients treated with atypical antipsychotics.
As instructed in the APA/ADA guidelines, obtain baseline measurements and monitor for metabolic effects of antipsychotic therapy over time (Table 6). Sammy starts risperidone at 0.5 mg once daily. After 2 weeks, he notices a decrease in his tics. At the 3-month visit after starting risperidone, he is happy with his risperidone dose and does not want to increase it. He has gained 3 pounds, and you instruct him to eat a well-balanced diet and exercise routinely. At the 6-month visit, his tics are minimal and his weight has stabilized.
Table 6
Children receiving antipsychotics: monitoring recommendations
| Clinical information | Frequency |
|---|---|
| Family history | Initial visit |
| Weight | Baseline, monthly |
| Height | Baseline, monthly |
| BMI | Baseline, monthly |
| Waist circumference | Baseline, annually |
| Blood pressure | Baseline, 3 months after treatment starts, and annually thereafter |
| Fasting lipid profile | Baseline, every 3 months initially, then every 6 months thereafter |
| Fasting serum glucose | Baseline, every 3 months, then every 6 months thereafter |
| BMI: body mass index | |
| Source: References 14,16 | |
You recommend that Sammy remain on risperidone for another 3 months of stability and then begin to taper this medication. You review the risks and benefits of long-term treatment with risperidone, pointing out that it may lead to abnormal movements upon withdrawal, and explain that you typically do not treat children with antipsychotics for more than one year continuously.
CASE CONTINUED: Comorbid symptoms
Since starting 7th grade, Sammy has worried excessively about making mistakes. He spends 6 hours each night on homework, which he often does not turn in because of anxiety about not getting answers perfectly right. Classmates notice that Sammy taps the door 3 times when he comes into the classroom and that he steps over the black tiles in the hallway.
Consider the presence and impact of comorbid OCD or ADHD, which can impair children’s quality of life more than tics themselves.15 Assessment scales can help you make a diagnosis and monitor treatment.
If you suspect OCD, the clinician-rated Children’s Yale Brown Obsessive Compulsive Scale is the gold standard for describing the phenomenology and measuring symptom severity. Additional scales to measure symptoms’ impact on family life include the Leyton Obsessional Inventory—child version, Family Accommodation Scale for OCD, and Child OCD Impact Scale.
ADHD scales include the Conners Parent Rating Scale—Revised, Conners Teacher Rating Scale—Revised, Swanson, Nolan, and Pelham, or the Vanderbilt ADHD Diagnostic Parent and Teacher Rating Scales. Because ADHD symptoms must be present in more than 1 environment to meet diagnostic criteria, ask parents and teachers to complete the Conners or Vanderbilt scales.
In children who present with a tic disorder plus a comorbid condition, prioritize treatment by determining which symptoms interfere with the child’s ability to function at school, at home, and in the social arena. Children who require treatment for >1 disorder often are referred initially for cognitive-behavioral therapy for OCD symptoms while receiving pharmacologic treatment for ADHD and/or Tourette syndrome. When necessary, it is usually safe to combine antipsychotics, stimulants, and selective serotonin reuptake inhibitors, although medication interactions should be reviewed in each specific case.
Related resources
- Woods DW. Managing Tourette syndrome: a behavioral intervention for children and adults. Therapist guide. New York, NY: Oxford University Press; 2008.
- Tourette Syndrome Association. www.tsa-usa.org.
- International OCD Foundation. www.ocfoundation.org.
Drug brand names
- Baclofen • Lioresal
- Botulinum toxin • Botox, Myobloc
- Clomipramine • Anafranil
- Clonidine • Catapres
- Guanfacine • Tenex
- Fluphenazine • Prolixin
- Flutamide • Eulexin
- Haloperidol • Haldol
- Mecamylamine • Inversine
- Nicotine patch • NicoDerm
- Olanzapine • Zyprexa
- Pimozide • Orap
- Risperidone • Risperdal
- Tetrabenazine • Xenazine
- Ziprasidone • Geodon
Disclosures
Dr. Harris has received research support from the Translational Research Initiative at Cincinnati Children’s Hospital Medical Center.
Dr. Wu reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Sammy, age 7, is referred to you by his pediatrician because of a 4-week history of frequent eye blinking. His parents say he blinks a lot when bored but very little when playing baseball. They recall that he also has intermittently sniffed and nodded his head over the last 12 months. Neither Sammy nor his friends seem to be bothered by the blinking. Except for the tics, Sammy’s physical and mental status exams are normal.
Since preschool, Sammy’s teachers have complained that his backpack and desk are always a mess. Sammy is well-meaning but forgetful in his chores at home. A paternal uncle has head-turning movements, counts his steps, and becomes distressed if books on his shelf are not in alphabetical order.
Tics, such as strong eye blinks or repetitive shoulder shrugs, can distress a child or his/her parents, but the conditions associated with tic disorders often are more problematic than the tic disorder itself. High rates of comorbid conditions are recognized in persons with Tourette syndrome, including:
- obsessive-compulsive disorder (OCD) in >80%1
- attention-deficit/hyperactivity disorder (ADHD) in ≤70%2
- anxiety disorders in 30%3
- rage, aggression, learning disabilities, and autism less commonly.
The strategy we recommend for managing tic disorders includes assessing tic severity, educating the family about the illness, determining whether a comorbid condition is present, and managing these conditions appropriately. Above all, we emphasize a risk-benefit analysis guided by the Hippocratic principle of “do no harm.”
Characteristics of tic disorders
You diagnose Sammy with Tourette syndrome because he meets DSM-IV-TR criteria of at least 2 motor tics and 1 vocal tic that have persisted for 1 year without more than a 3-month hiatus, with tic onset before age 18. Because tics may resemble other movement disorders, you rule out stereotypies, dystonia, chorea, ballism, and myoclonus (Table 1). You explain to his parents that Sammy’s condition is a heritable, neurobehavioral disorder that typically begins in childhood and is associated in families with OCD, ADHD, and autism spectrum disorders.
His parents ask about the difference between tics and other movements. You explain that eye-blinking tics—like other motor tics—appear as sudden, repetitive, stereotyped, nonrhythmic movements that involve discrete muscle groups. (View a video of a patient with tics.) Simple motor tics are focal movements involving 1 group of muscles, whereas complex tics are sequential patterns of movement that involve >1 muscle group or resemble purposeful movements (Table 2).
Table 1
Features of 5 movement disorders that may resemble tics
| Tics | Stereotypies | Dystonia | Chorea | Ballism | Myoclonus |
|---|---|---|---|---|---|
| Sudden, repetitive, stereotyped, nonrhythmic movements or sounds | Patterned, nonpurposeful movement | Cocontraction of agonist and antagonist muscles, causing an abnormal twisting posture | Continuous, flowing, nonrhythmic, nonpurposeful movement | Forceful, flinging, large amplitude choreic movement | Sudden, quick, shock-like movement |
| Usually start after age 3 | Usually start before age 3 and resolve by adolescence | More common in adults | — | — | — |
| Decrease when focused; increase when stressed, anxious, fatigued, or bored | Occur when the child is excited | Worsens during motor tasks | Worsens during motor tasks | Worsens during motor tasks | — |
| Comorbid conditions include OCD and ADHD | Common in children with mental retardation or autism | — | Can occur after streptococcal infection | Can occur after streptococcal infection | — |
| Preceded by a premonitory urge or sensation | Possibly preceded by an urge | Not preceded by an urge | Not preceded by an urge | Not preceded by an urge | Not preceded by an urge |
| Temporarily suppressible | Suppressible | Not suppressible | Partially suppressible; can incorporate into semi-purposeful movements | Partially suppressible | Not suppressible |
| ADHD: attention-deficit/hyperactivity disorder; OCD: obsessive-compulsive disorder | |||||
Table 2
Characteristics of simple and complex motor and vocal tics*
| Simple tics | Complex tics |
|---|---|
| Eye blinking or eye rolling Nose, mouth, tongue, or facial grimaces (nose twitch, nasal flaring, chewing lip, teeth grinding, sticking out tongue, mouth stretching, lip licking) Head jerks or movements (neck stretching, touching chin to shoulder) Shoulder jerks/movements (shoulder shrugging, jerking a shoulder) Arm or hand movements (flexing or extending arms or fingers) Coughing Throat clearing, grunting Sniffing, snorting, shouting Humming | Jumping Spinning Touching objects or people Throwing objects Repeating others’ action (echopraxia) Obscene gestures (copropraxia) Repeating one’s own words (palilalia) Repeating what someone else said (echolalia) Obscene, inappropriate words (coprolalia) |
| *Simple tics are focal movements involving 1 group of muscles; complex tics are sequential patterns of movement that involve >1 muscle group or resemble purposeful movements | |
Older children frequently describe a premonitory urge prior to the tic. Patients typically can suppress tics for a transient period of time, although during tic suppression they usually feel restless and anticipate performing their tic. The ultimate performance of the tic brings relief. Tic suppression also occurs during focused activity. Emotional stress, fatigue, illness, or boredom can exacerbate tics.
To begin monitoring Sammy’s clinical course, you administer 3 assessment tools described inTable 3. You explain to Sammy’s parents that these tests will be repeated yearly or when tics worsen. However, you tell his parents that these scores alone will not determine present or future clinical decisions, including treatments. You also recommend that they connect with support groups on the Tourette Syndrome Association (TSA) Web site.
CASE CONTINUED: Changes over time
Sammy’s parents appreciate your explanation and say they will share information from the TSA Web site with Sammy’s principal, teachers, and classmates. The family agrees to return in 6 months or sooner if the tics worsen.
By age 8, Sammy develops multiple tics: facial grimacing, looking upwards, punching movements, whistling, and throat clearing. He is slightly bothered by these tics, and his friends have asked him about them. He tells them he has Tourette syndrome, and that usually ends the questioning. He returns for a follow-up visit because his parents notice a dramatic increase in his tics after Sammy’s father loses his job.
Treatment options
When deciding to treat a child’s tics, the first step is to determine whether to pursue a nonpharmacologic or pharmacologic approach (Algorithm). To tailor an approach most suited for an individual child, discuss with the family their feelings about therapy and medications. This information—along with tic severity—will help determine a treatment plan.
Behavior therapy and medication are management strategies; neither can cure a tic disorder. The most conservative approach to tic treatment is to:
- provide the child and family with basic guidelines for managing tics
- help alleviate environmental stress and other potential triggers.
Algorithm: Recommended treatment of tics in children and adolescents
CASE CONTINUED: A first intervention
You discuss treatment options with Sammy’s family, and they view medication as a last resort. Sammy does not seem to be bothered by his tics, and his parents do not wish to start him on daily medications. Given this situation, habit reversal therapy (HRT) is appropriate for Sammy because he is old enough to participate in HRT to reduce his tics.
HRT is an effective nonpharmacologic approach to help children with tics.4 Its 3 components are:
- awareness training
- competing response training
- social support.5
This simplified version of the original HRT can be completed in eight 1-hour sessions. Good candidates are patients who are cognitively mature enough to understand the therapy’s goals and compliant with frequent clinic visits. They also must practice the strategies at home.
It should not be difficult for psychiatrists to learn HRT—or refer to therapists who are willing to learn it—with the available instructional manual.
CASE CONTINUED: Practicing alternatives
You ask Sammy to imitate his tics. After helping him become more aware of his tics, you encourage him to develop a more socially appropriate movement to engage in whenever he feels the urge to punch. Sammy chooses to clench his fist in his pocket. He also learns to breathe in whenever he has an urge to whistle. you advise Sammy’s parents to reward his efforts to suppress the tics. He practices the strategies daily.
At age 12, Sammy returns to your office. He has begun to have frequent neck-jerking tics, which cause neck pain and daily headaches. He also is slapping his thigh and having frequent vocal tics characterized by loud shrieking. The vocal tics are disruptive in class, even though Sammy sits toward the back of the room. Sammy’s classmates tease him, and he is very frustrated.
Medication approach
The decision to start a medication for tics is complex. Scores from the YGTSS, PUTS, and GTS-QOL scales (Table 3) provide only a partial clinical picture. This decision should be reached after a detailed discussion with the family about benefits and risks of medications and ensuring that everyone’s expectations are reasonable.
A variety of medications are available to treat patients with tics (Table 4). No medication can completely eliminate tics, however, and many have substantial side effects. Before initiating medical treatment, consider 3 questions:
- Is moderate or severe pain involved?
- Is there significant functional interference?
- Is there significant social disruption despite efforts to optimize the social environment for the child?
Sammy’s frequent neck-jerking tics now cause chronic daily headaches, and his shrieking vocal tics are interfering with classroom activities, so we recommended a 3-month trial of guanfacine following the dosing schedule in Table 4.
Table 3
3 scales for assessing tic severity and impact on functioning
| Instrument | Purpose | Description | Design | Administration frequency |
|---|---|---|---|---|
| Yale Global Tic Severity Scale (YGTSS) | Assess tic severity | Review of motor and vocal tics. Rate number, frequency, intensity, complexity, and interference on a 5-point scale | Clinician-rated | Annual and as needed for increased tics |
| Premonitory Urge for Tics Scale (PUTS) | Detect the presence of unpleasant sensations that precedes tics | 10 questions | Self-report | Annual and as needed for increased tics |
| Gilles de la Tourette Syndrome Quality of Life Scale (GTS-QOL) | Measure quality of life | 27 questions, 4 subscales: psychological, physical, obsessional, and cognitive | Self-report | Annual and as needed for increased tics |
Table 4
Medications with evidence of tic-suppressing effects*
| Category A evidence | ||
|---|---|---|
| Medication | Starting dose | Target dose |
| Haloperidol | 0.25 to 0.5 mg/d | 1 to 4 mg/d |
| Pimozide | 0.5 to 1 mg/d | 2 to 8 mg/d |
| Risperidone | 0.25 to 0.5 mg/d | 1 to 3 mg/d |
| Category B evidence | ||
| Medication | Starting dose | Target dose |
| Fluphenazine | 0.5 to 1 mg/d | 1.5 to 10 mg/d |
| Ziprasidone | 5 to 10 mg/d | 10 to 80 mg/d |
| Clonidine | 0.025 to 0.05 mg/d | 0.1 to 0.3 mg/d |
| Guanfacine | 0.5 to 1 mg/d | 1 to 3 mg/d |
| Botulinum toxin | 30 to 300 units | |
| Category C evidence | ||
| Medication | Starting dose | Target dose |
| Olanzapine | 2.5 to 5 mg/d | 2.5 to 12.5 mg/d |
| Tetrabenazine | 25 mg/d | 37.5 to 150 mg/d |
| Baclofen | 10 mg/d | 40 to 60 mg/d |
| Nicotine patch | 7 mg/d | 7 to 21 mg/d |
| Mecamylamine | 2.5 mg/d | 2.5 to 7.5 mg/d |
| Flutamide | 250 mg/d | 750 mg/d |
| *Category A: supported by ≥2 placebo-controlled trials; category B: supported by 1 placebo-controlled trial; category C: supported by open-label study | ||
| Source: Reference 6 | ||
The first-line pharmacologic agent for tic suppression generally is an alpha-adrenergic medication, unless the tics are severe.6
Clonidine and guanfacine usually are started at low doses and increased gradually. Although not as effective as neuroleptics, alpha-adrenergics have a lower potential for side effects and are easier to use because no laboratory tests need to be monitored. Adverse effects associated with alpha-adrenergic medications include sedation, dry mouth, dizziness, headache, and rebound hypertension if discontinued abruptly.
If tics are causing pain, some clinicians prefer conservative measures such as heat or ice, massage, analgesics, relaxation therapy, and reassurance.
Second-line agents include typical and atypical antipsychotics. Haloperidol and pimozide have shown efficacy in reducing tics in placebo- controlled studies,7,8 as have risperidone (in 4 randomized controlled trials [RCTs]) and ziprasidone (in 1 RCT).9,10 The emergence of serious side effects is a risk for both typical and atypical antipsychotics (Table 5).
Table 5
Potential adverse effects of antipsychotic treatment in children*
| Adverse effect | Examples |
|---|---|
| Sedation | — |
| Acute dystonic reactions | Oculogyric crisis, torticollis |
| Appetite changes | Weight gain |
| Endocrine abnormalities | Amenorrhea, diabetes, galactorrhea, gynecomastia, hyperprolactinemia |
| Cognitive effects | Impaired concentration |
| Akathisia | Difficulty sitting still |
| ECG changes | Prolonged QT interval |
| Parkinsonism | Tremor, bradykinesia, rigidity, postural instability |
| Tardive syndrome | Orofacial dyskinesia, chorea, dystonia, myoclonus, tics |
| Neuroleptic malignant syndrome | Potentially fatal; consists of muscular rigidity, fever, autonomic dysfunction, labile blood pressure, sweating, urinary incontinence, fluctuating level of consciousness, leukocytosis, elevated serum creatine kinase |
| *Potential adverse effects are listed from most to least likely to occur | |
As part of your informed consent discussion, weigh the risk of side effects against the benefits of treatment. Point out to patients and their families that they can expect to see a decrease in tic frequency, but symptoms will not necessarily disappear with any medication. We tell our patients that with antipsychotics the best we can hope for is to reduce tic frequency by approximately one-half.6
When treating tics, start with 1 medication. However, if the tics are severe enough to require more than 1 medication, check for drug interactions.
Third-line agents. Agents that have not been tested in placebo-controlled trials can be considered third line; these are listed as category C (supported by open-label studies) in Table 4. Botulinum toxin injection has been found to be effective for motor and vocal tics.11,12 Botulinum toxin and implantation of deep brain stimulators13 are invasive options and generally are reserved for severe, treatment-resistant tics.
CASE CONTINUED: Managing antipsychotics
After trying guanfacine for 12 weeks, Sammy notices no tic reduction. His parents consent to a low dose of risperidone. you review with them the American Psychiatric Association (APA)/American Diabetes Association (ADA) guidelines14 for managing metabolic problems in patients treated with atypical antipsychotics.
As instructed in the APA/ADA guidelines, obtain baseline measurements and monitor for metabolic effects of antipsychotic therapy over time (Table 6). Sammy starts risperidone at 0.5 mg once daily. After 2 weeks, he notices a decrease in his tics. At the 3-month visit after starting risperidone, he is happy with his risperidone dose and does not want to increase it. He has gained 3 pounds, and you instruct him to eat a well-balanced diet and exercise routinely. At the 6-month visit, his tics are minimal and his weight has stabilized.
Table 6
Children receiving antipsychotics: monitoring recommendations
| Clinical information | Frequency |
|---|---|
| Family history | Initial visit |
| Weight | Baseline, monthly |
| Height | Baseline, monthly |
| BMI | Baseline, monthly |
| Waist circumference | Baseline, annually |
| Blood pressure | Baseline, 3 months after treatment starts, and annually thereafter |
| Fasting lipid profile | Baseline, every 3 months initially, then every 6 months thereafter |
| Fasting serum glucose | Baseline, every 3 months, then every 6 months thereafter |
| BMI: body mass index | |
| Source: References 14,16 | |
You recommend that Sammy remain on risperidone for another 3 months of stability and then begin to taper this medication. You review the risks and benefits of long-term treatment with risperidone, pointing out that it may lead to abnormal movements upon withdrawal, and explain that you typically do not treat children with antipsychotics for more than one year continuously.
CASE CONTINUED: Comorbid symptoms
Since starting 7th grade, Sammy has worried excessively about making mistakes. He spends 6 hours each night on homework, which he often does not turn in because of anxiety about not getting answers perfectly right. Classmates notice that Sammy taps the door 3 times when he comes into the classroom and that he steps over the black tiles in the hallway.
Consider the presence and impact of comorbid OCD or ADHD, which can impair children’s quality of life more than tics themselves.15 Assessment scales can help you make a diagnosis and monitor treatment.
If you suspect OCD, the clinician-rated Children’s Yale Brown Obsessive Compulsive Scale is the gold standard for describing the phenomenology and measuring symptom severity. Additional scales to measure symptoms’ impact on family life include the Leyton Obsessional Inventory—child version, Family Accommodation Scale for OCD, and Child OCD Impact Scale.
ADHD scales include the Conners Parent Rating Scale—Revised, Conners Teacher Rating Scale—Revised, Swanson, Nolan, and Pelham, or the Vanderbilt ADHD Diagnostic Parent and Teacher Rating Scales. Because ADHD symptoms must be present in more than 1 environment to meet diagnostic criteria, ask parents and teachers to complete the Conners or Vanderbilt scales.
In children who present with a tic disorder plus a comorbid condition, prioritize treatment by determining which symptoms interfere with the child’s ability to function at school, at home, and in the social arena. Children who require treatment for >1 disorder often are referred initially for cognitive-behavioral therapy for OCD symptoms while receiving pharmacologic treatment for ADHD and/or Tourette syndrome. When necessary, it is usually safe to combine antipsychotics, stimulants, and selective serotonin reuptake inhibitors, although medication interactions should be reviewed in each specific case.
Related resources
- Woods DW. Managing Tourette syndrome: a behavioral intervention for children and adults. Therapist guide. New York, NY: Oxford University Press; 2008.
- Tourette Syndrome Association. www.tsa-usa.org.
- International OCD Foundation. www.ocfoundation.org.
Drug brand names
- Baclofen • Lioresal
- Botulinum toxin • Botox, Myobloc
- Clomipramine • Anafranil
- Clonidine • Catapres
- Guanfacine • Tenex
- Fluphenazine • Prolixin
- Flutamide • Eulexin
- Haloperidol • Haldol
- Mecamylamine • Inversine
- Nicotine patch • NicoDerm
- Olanzapine • Zyprexa
- Pimozide • Orap
- Risperidone • Risperdal
- Tetrabenazine • Xenazine
- Ziprasidone • Geodon
Disclosures
Dr. Harris has received research support from the Translational Research Initiative at Cincinnati Children’s Hospital Medical Center.
Dr. Wu reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Robertson M. Tourette syndrome, associated conditions and the complexities of treatment. Brain. 2000;123(3):425-462.
2. Freeman R. For the Tourette Syndrome International Database Consortium. Tic disorders and ADHD: answers from a worldwide clinical dataset on Tourette syndrome. Eur Child Adolesc Psychiatry. 2007;16(suppl 1):15-23.
3. Stefl M. Mental health needs associated with Tourette syndrome. Am J Public Health. 1984;74:1310-1313.
4. Deckersbach T, Rauch S, Buhlmann U, et al. Habit reversal versus supportive psychotherapy in Tourette’s disorder: a randomized controlled trial and predictors of treatment response. Behav Res Ther. 2006;44:1079-1090.
5. Woods DW, Miltenberger RG. Habit reversal: a review of applications and variations. J Behav Ther Exp Psychiatry. 1995;26:123-131.
6. Scahill L, Erenberg G, Berlin C, et al. Contemporary assessment and pharmacotherapy of Tourette syndrome. NeuroRx. 2006;3(2):192-206.
7. Shapiro E, Shapiro A, Fulop G, et al. Controlled study of haloperidol, pimozide, and placebo for the treatment of Gilles de la Tourette’s syndrome. 1989;46:722-730.
8. Sallee F, Nesbitt L, Jackson C, et al. Relative efficacy of haloperidol and pimozide in children and adolescents with Tourette’s disorder. Am J Psychiatry. 1997;154:1057-1062.
9. Scahill L, Leckman J, Schultz R, et al. A placebo-controlled trial of risperidone in Tourette syndrome. Neurology. 2003;60:1130-1135.
10. Sallee F, Kurlan R, Goetz C, et al. Ziprasidone treatment of children and adolescents with Tourette’s syndrome: a pilot study. J Am Acad Child Adolesc Psychiatry. 2000;39(3):292-299.
11. Marras C, Andrews D, Sime E, et al. Botulinum toxin for simple motor tics: a randomized, double-blind, controlled clinical trial. Neurology. 2001;56(5):605-610.
12. Porta M, Maggioni G, Ottaviani F, et al. Treatment of phonic tics in patients with Tourette’s syndrome using botulinum toxin type A. Neurol Sci. 2004;24(6):420-423.
13. Porta M, Sevello D, Sassi M, et al. Issues related to deep brain stimulation for treatment-refractory Tourette’s syndrome. Eur Neurol. 2009;62(5):264-273.
14. American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists, North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. J Clin Psychiatry. 2004;65:1335-1342.
15. Bernard BA, Stebbins GT, Siegel S, et al. Determinants of quality of life in children with Gilles de la Tourette syndrome. Mov Disord. 2009;24(7):1070-1073.
16. Understanding the risks of antipsychotic treatment in young people. Advice for managing side effects in children and teenagers. Harv Ment Health Lett. 2009;25(9):1-3.
1. Robertson M. Tourette syndrome, associated conditions and the complexities of treatment. Brain. 2000;123(3):425-462.
2. Freeman R. For the Tourette Syndrome International Database Consortium. Tic disorders and ADHD: answers from a worldwide clinical dataset on Tourette syndrome. Eur Child Adolesc Psychiatry. 2007;16(suppl 1):15-23.
3. Stefl M. Mental health needs associated with Tourette syndrome. Am J Public Health. 1984;74:1310-1313.
4. Deckersbach T, Rauch S, Buhlmann U, et al. Habit reversal versus supportive psychotherapy in Tourette’s disorder: a randomized controlled trial and predictors of treatment response. Behav Res Ther. 2006;44:1079-1090.
5. Woods DW, Miltenberger RG. Habit reversal: a review of applications and variations. J Behav Ther Exp Psychiatry. 1995;26:123-131.
6. Scahill L, Erenberg G, Berlin C, et al. Contemporary assessment and pharmacotherapy of Tourette syndrome. NeuroRx. 2006;3(2):192-206.
7. Shapiro E, Shapiro A, Fulop G, et al. Controlled study of haloperidol, pimozide, and placebo for the treatment of Gilles de la Tourette’s syndrome. 1989;46:722-730.
8. Sallee F, Nesbitt L, Jackson C, et al. Relative efficacy of haloperidol and pimozide in children and adolescents with Tourette’s disorder. Am J Psychiatry. 1997;154:1057-1062.
9. Scahill L, Leckman J, Schultz R, et al. A placebo-controlled trial of risperidone in Tourette syndrome. Neurology. 2003;60:1130-1135.
10. Sallee F, Kurlan R, Goetz C, et al. Ziprasidone treatment of children and adolescents with Tourette’s syndrome: a pilot study. J Am Acad Child Adolesc Psychiatry. 2000;39(3):292-299.
11. Marras C, Andrews D, Sime E, et al. Botulinum toxin for simple motor tics: a randomized, double-blind, controlled clinical trial. Neurology. 2001;56(5):605-610.
12. Porta M, Maggioni G, Ottaviani F, et al. Treatment of phonic tics in patients with Tourette’s syndrome using botulinum toxin type A. Neurol Sci. 2004;24(6):420-423.
13. Porta M, Sevello D, Sassi M, et al. Issues related to deep brain stimulation for treatment-refractory Tourette’s syndrome. Eur Neurol. 2009;62(5):264-273.
14. American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists, North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. J Clin Psychiatry. 2004;65:1335-1342.
15. Bernard BA, Stebbins GT, Siegel S, et al. Determinants of quality of life in children with Gilles de la Tourette syndrome. Mov Disord. 2009;24(7):1070-1073.
16. Understanding the risks of antipsychotic treatment in young people. Advice for managing side effects in children and teenagers. Harv Ment Health Lett. 2009;25(9):1-3.