User login
Directed questions:
1. What are the two main subtypes of pulmonary sequestration?
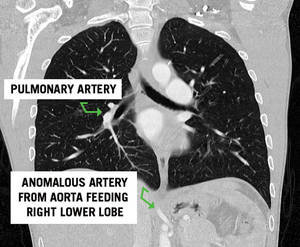
2. This patient had a normal appearing lung field on CT scan. What subtype of pulmonary sequestration does this represent?
3. What is the vascular anatomy that defines the difference between the two subtypes of sequestration?
4. In which lobes are sequestrations most commonly found?
5. Which subtype is associated with congenital anomalies?
6. What therapy would you recommend to this patient?
7. Is there a role for the resection of an incidentally found, asymptomatic sequestration?
Answers and discussion on page 4.
Clinical Challenge: Kety Points
--Definition:
- Portion of lung parenchyma with absence of normal bronchial communication with the tracheobronchial tree and systemic arterial blood supply.
--Two types:
- Extralobar: mass of lung tissue separate from normal lung with its own pleural investment. Venous drainage and arterial supply are systemic, not pulmonary in origin
- Intralobar: mass of abnormal lung tissue intimately related with normal lung parenchyma with systemic arterial supply but normal pulmonary venous drainage
--Common presentation:
- recurrent, chronic pulmonary infections
--Arterial blood supply is always systemic
- Most commonly, arising from the descending thoracic or abdominal aorta
--Most commonly located in the lower lobe but extralobar sequestrations have been reported below the diaphragm as well
--Treatment:
- Elective surgical resection
- May need urgent/emergent resection if significant hemoptysis or intrathoracic hemorrhage
- Intralobar sequestrations often require lobectomy while extralobar resections can often be dissected free from normal lung parenchyma
Selected References and Additional Resources:
Bratu, I. The multiple facets of pulmonary sequestration. J Pediatric Surgery. 35(5):784-790, 2001.
Mendeloff, EN. Sequestrations, Congenital Cystic Adenomatoid Malformations, and Congenital Lobar Emphysema. J
Thoracic and Cardiovascular Surgery. 16:209-214, 2004.
Hamanaka, H. Surgical Treatment of infected intralobar pulmonary sequestration: a collective review of patients older than 50 years reported in the literature. Ann Thoracic and Cardiovascular Surgery. 13(5):331, 2007.
Stanton, M. Systemic review and meta-analysis of the postnatal management of congenital cystic lung lesions. J Pediatric Surg. 44(5): 1027, 2009.
Yamanaka, A. Anomalous systemic arterial supply to normal basal segments of the left lower lobe. Ann Thoracic Surgery. 68(2): 332-8, 1999.
TSDAWeekly Curriculum - "Congenital Lung Anomalies" http://www.tsda.org/documents/PDF/Weekly%20Curricula/E-mail%20Archive/06.10.10.pdf
Answers to the Clinical Challenge
1. Intralobar and extralobar pulmonary sequestrations.
2. Pryce type I sequestration classifies a rare subtype characterized by anomalous systemic arterial supply to a normal segment of lung
3. Both intralobar and extralobar sequestrations are characterized by systemic arterial inflow, most commonly from the aorta. Intralobar sequestrations have pulmonary venous return. In contrast, extralobar sequestrations have systemic venous drainage, most commonly via the azygous or hemiazygous venous system.
4. Pulmonary sequestrations are most commonly found in the lower lobe, left side more common than right. Uncommonly, extralobar sequestrations can be found outside of the chest cavity with reports of lesions below the diaphragm.
5. Over half of patients with extralobar sequestrations have associated congenital anomalies. Common anomalies include congenital diaphragmatic hernia, pericardial defects, other bronchopulmonary foregut malformations and total anomalous pulmonary venous return. Congenital anomalies are uncommon with intralobar sequestrations.
6. Resection of the sequestration with directed ligation of the arterial feeding vessel.
7. Asymptomatic sequestrations should be resected due to the potential for developing infection or hemorrhage, including aneurysm formation and rupture of the aberrant arterial vasculature. There are reports that suggest resection for symptomatic disease, especially infection, is associated with a higher morbidity than resection for asymptomatic disease.
Directed questions:
1. What are the two main subtypes of pulmonary sequestration?
2. This patient had a normal appearing lung field on CT scan. What subtype of pulmonary sequestration does this represent?
3. What is the vascular anatomy that defines the difference between the two subtypes of sequestration?
4. In which lobes are sequestrations most commonly found?
5. Which subtype is associated with congenital anomalies?
6. What therapy would you recommend to this patient?
7. Is there a role for the resection of an incidentally found, asymptomatic sequestration?
Answers and discussion on page 4.
Clinical Challenge: Kety Points
--Definition:
- Portion of lung parenchyma with absence of normal bronchial communication with the tracheobronchial tree and systemic arterial blood supply.
--Two types:
- Extralobar: mass of lung tissue separate from normal lung with its own pleural investment. Venous drainage and arterial supply are systemic, not pulmonary in origin
- Intralobar: mass of abnormal lung tissue intimately related with normal lung parenchyma with systemic arterial supply but normal pulmonary venous drainage
--Common presentation:
- recurrent, chronic pulmonary infections
--Arterial blood supply is always systemic
- Most commonly, arising from the descending thoracic or abdominal aorta
--Most commonly located in the lower lobe but extralobar sequestrations have been reported below the diaphragm as well
--Treatment:
- Elective surgical resection
- May need urgent/emergent resection if significant hemoptysis or intrathoracic hemorrhage
- Intralobar sequestrations often require lobectomy while extralobar resections can often be dissected free from normal lung parenchyma
Selected References and Additional Resources:
Bratu, I. The multiple facets of pulmonary sequestration. J Pediatric Surgery. 35(5):784-790, 2001.
Mendeloff, EN. Sequestrations, Congenital Cystic Adenomatoid Malformations, and Congenital Lobar Emphysema. J
Thoracic and Cardiovascular Surgery. 16:209-214, 2004.
Hamanaka, H. Surgical Treatment of infected intralobar pulmonary sequestration: a collective review of patients older than 50 years reported in the literature. Ann Thoracic and Cardiovascular Surgery. 13(5):331, 2007.
Stanton, M. Systemic review and meta-analysis of the postnatal management of congenital cystic lung lesions. J Pediatric Surg. 44(5): 1027, 2009.
Yamanaka, A. Anomalous systemic arterial supply to normal basal segments of the left lower lobe. Ann Thoracic Surgery. 68(2): 332-8, 1999.
TSDAWeekly Curriculum - "Congenital Lung Anomalies" http://www.tsda.org/documents/PDF/Weekly%20Curricula/E-mail%20Archive/06.10.10.pdf
Answers to the Clinical Challenge
1. Intralobar and extralobar pulmonary sequestrations.
2. Pryce type I sequestration classifies a rare subtype characterized by anomalous systemic arterial supply to a normal segment of lung
3. Both intralobar and extralobar sequestrations are characterized by systemic arterial inflow, most commonly from the aorta. Intralobar sequestrations have pulmonary venous return. In contrast, extralobar sequestrations have systemic venous drainage, most commonly via the azygous or hemiazygous venous system.
4. Pulmonary sequestrations are most commonly found in the lower lobe, left side more common than right. Uncommonly, extralobar sequestrations can be found outside of the chest cavity with reports of lesions below the diaphragm.
5. Over half of patients with extralobar sequestrations have associated congenital anomalies. Common anomalies include congenital diaphragmatic hernia, pericardial defects, other bronchopulmonary foregut malformations and total anomalous pulmonary venous return. Congenital anomalies are uncommon with intralobar sequestrations.
6. Resection of the sequestration with directed ligation of the arterial feeding vessel.
7. Asymptomatic sequestrations should be resected due to the potential for developing infection or hemorrhage, including aneurysm formation and rupture of the aberrant arterial vasculature. There are reports that suggest resection for symptomatic disease, especially infection, is associated with a higher morbidity than resection for asymptomatic disease.
Directed questions:
1. What are the two main subtypes of pulmonary sequestration?
2. This patient had a normal appearing lung field on CT scan. What subtype of pulmonary sequestration does this represent?
3. What is the vascular anatomy that defines the difference between the two subtypes of sequestration?
4. In which lobes are sequestrations most commonly found?
5. Which subtype is associated with congenital anomalies?
6. What therapy would you recommend to this patient?
7. Is there a role for the resection of an incidentally found, asymptomatic sequestration?
Answers and discussion on page 4.
Clinical Challenge: Kety Points
--Definition:
- Portion of lung parenchyma with absence of normal bronchial communication with the tracheobronchial tree and systemic arterial blood supply.
--Two types:
- Extralobar: mass of lung tissue separate from normal lung with its own pleural investment. Venous drainage and arterial supply are systemic, not pulmonary in origin
- Intralobar: mass of abnormal lung tissue intimately related with normal lung parenchyma with systemic arterial supply but normal pulmonary venous drainage
--Common presentation:
- recurrent, chronic pulmonary infections
--Arterial blood supply is always systemic
- Most commonly, arising from the descending thoracic or abdominal aorta
--Most commonly located in the lower lobe but extralobar sequestrations have been reported below the diaphragm as well
--Treatment:
- Elective surgical resection
- May need urgent/emergent resection if significant hemoptysis or intrathoracic hemorrhage
- Intralobar sequestrations often require lobectomy while extralobar resections can often be dissected free from normal lung parenchyma
Selected References and Additional Resources:
Bratu, I. The multiple facets of pulmonary sequestration. J Pediatric Surgery. 35(5):784-790, 2001.
Mendeloff, EN. Sequestrations, Congenital Cystic Adenomatoid Malformations, and Congenital Lobar Emphysema. J
Thoracic and Cardiovascular Surgery. 16:209-214, 2004.
Hamanaka, H. Surgical Treatment of infected intralobar pulmonary sequestration: a collective review of patients older than 50 years reported in the literature. Ann Thoracic and Cardiovascular Surgery. 13(5):331, 2007.
Stanton, M. Systemic review and meta-analysis of the postnatal management of congenital cystic lung lesions. J Pediatric Surg. 44(5): 1027, 2009.
Yamanaka, A. Anomalous systemic arterial supply to normal basal segments of the left lower lobe. Ann Thoracic Surgery. 68(2): 332-8, 1999.
TSDAWeekly Curriculum - "Congenital Lung Anomalies" http://www.tsda.org/documents/PDF/Weekly%20Curricula/E-mail%20Archive/06.10.10.pdf
Answers to the Clinical Challenge
1. Intralobar and extralobar pulmonary sequestrations.
2. Pryce type I sequestration classifies a rare subtype characterized by anomalous systemic arterial supply to a normal segment of lung
3. Both intralobar and extralobar sequestrations are characterized by systemic arterial inflow, most commonly from the aorta. Intralobar sequestrations have pulmonary venous return. In contrast, extralobar sequestrations have systemic venous drainage, most commonly via the azygous or hemiazygous venous system.
4. Pulmonary sequestrations are most commonly found in the lower lobe, left side more common than right. Uncommonly, extralobar sequestrations can be found outside of the chest cavity with reports of lesions below the diaphragm.
5. Over half of patients with extralobar sequestrations have associated congenital anomalies. Common anomalies include congenital diaphragmatic hernia, pericardial defects, other bronchopulmonary foregut malformations and total anomalous pulmonary venous return. Congenital anomalies are uncommon with intralobar sequestrations.
6. Resection of the sequestration with directed ligation of the arterial feeding vessel.
7. Asymptomatic sequestrations should be resected due to the potential for developing infection or hemorrhage, including aneurysm formation and rupture of the aberrant arterial vasculature. There are reports that suggest resection for symptomatic disease, especially infection, is associated with a higher morbidity than resection for asymptomatic disease.