User login
Yes, team-based care appears to lower systolic blood pressure (SBP) by 5 to 11 mm Hg and diastolic blood pressure (DBP) by 2 to 6 mm Hg in patients with hypertension and improve lipid control in patients with diabetes (strength of recommendation: C, disease-oriented outcomes).
Team-based care lowers BP in hypertensive patients
A systematic review evaluated 80 trials (total N not defined), which included randomized controlled trials (RCTs) and quasi-experimental trials, to compare blood pressure control in hypertensive patients who received team-based care with that of patients who received usual care.1
Team-based care was defined as adding new staff or changing the roles of existing staff to provide process support and share responsibility for hypertension care with a primary care provider. Examples included using staff to help with medication management, active patient follow-up, adherence, and self-management support. The mean duration of the interventions was 12 months.
The intervention group showed greater reductions in SBP (44 trials; 5.4 mm Hg; interquartile interval [IQI]=2.0-7.2) and DBP (38 trials; 1.8 mm Hg; IQI=0.7-3.2) compared with usual care.
Free medication, care involving nurses, pharmacists lead to lower BP
Another meta-analysis examined 37 RCTs (total N not provided) comparing blood pressure control in hypertensive patients who received team-based care with patients who received usual care.2 The meta-analysis divided the studies by specific types of team-based interventions and analyzed the effect of each type on blood pressure control. It also analyzed studies based on what kind of health care professionals were involved in the intervention.
The largest absolute changes in both SBP and DBP were observed with the following interventions, compared with the control group: free medication (3 trials; SBP reduction (SBPR)=−11 mm Hg; interquartile range [IQR]=−15 to −9.1; DBP reduction [DBPR]=−6.4 mm Hg; IQR=−8.7 to −3.9); pharmacist recommending medication to physician (15 trials; SBPR=−9.3 mm Hg; IQR=−15 to −5.0; DBPR=−3.6 mm Hg; IQR=−7.0 to −1.0); education about BP medications (23 trials; SBPR=−8.8 mm Hg; IQR=−12 to −4.3; DBPR=−3.6 mm Hg; IQR=−7.0 to −1.0); and pharmacist-performed intervention (22 trials; SBPR=−8.4 mm Hg; IQR=−12 to −4; DBPR=−3.3 mm Hg; IQR=−6.9 to −0.90).
Patients who underwent team-based care interventions had greater SBP control (defined as <140, or <130 in patients with diabetes mellitus or chronic kidney disease) than the control group in trials involving nurses (8 trials; odds ratio [OR]=1.7; 95% confidence interval [CI], 1.5-1.9), trials conducted in community pharmacies (5 trials; OR=2.9; 95% CI, 1.8-4.6), and trials incorporating pharmacists into primary care clinics (9 trials; OR=2.2; 95% CI, 1.8-2.7).
Team-based care improves lipid control
An RCT of 6963 patients with type 2 diabetes mellitus in 9 clinics examined the proportion of patients receiving team-based care that achieved a target low-density lipoprotein (LDL) of ≤100 mg/dL compared with patients receiving usual care.3
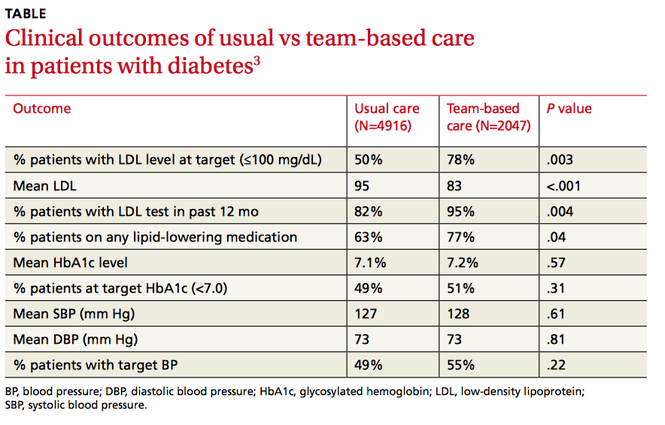
Clinics were randomized to participate in team-based care (defined as a physician-pharmacist team in which the pharmacist reviewed the medical charts of patients with elevated LDL and then developed individualized, evidence-based treatment recommendations) or usual care, which involved access to a disease management program providing automated quality reporting, benchmarking, and care opportunity decision support.
Over 2 years, the team-based care model had significantly more patients with a lower LDL, more patients at LDL goal, and more patients on lipid-lowering medication (TABLE3).
1. Proia KK, Thota AB, Njie GJ, et al. Team-based care and improved blood pressure control: a community guide systematic review. Am J Prev Med. 2014;47:86-99.
2. Carter BL, Rogers M, Daly J, et al. The potency of team-based care interventions for hypertension: a meta-analysis. Arch Intern Med. 2009;169:1748-1755.
3. Pape GA, Hunt JS, Butler KL, et al. Team-based care approach to cholesterol management in diabetes mellitus. Arch Intern Med. 2011;171:1480-1486.
Yes, team-based care appears to lower systolic blood pressure (SBP) by 5 to 11 mm Hg and diastolic blood pressure (DBP) by 2 to 6 mm Hg in patients with hypertension and improve lipid control in patients with diabetes (strength of recommendation: C, disease-oriented outcomes).
Team-based care lowers BP in hypertensive patients
A systematic review evaluated 80 trials (total N not defined), which included randomized controlled trials (RCTs) and quasi-experimental trials, to compare blood pressure control in hypertensive patients who received team-based care with that of patients who received usual care.1
Team-based care was defined as adding new staff or changing the roles of existing staff to provide process support and share responsibility for hypertension care with a primary care provider. Examples included using staff to help with medication management, active patient follow-up, adherence, and self-management support. The mean duration of the interventions was 12 months.
The intervention group showed greater reductions in SBP (44 trials; 5.4 mm Hg; interquartile interval [IQI]=2.0-7.2) and DBP (38 trials; 1.8 mm Hg; IQI=0.7-3.2) compared with usual care.
Free medication, care involving nurses, pharmacists lead to lower BP
Another meta-analysis examined 37 RCTs (total N not provided) comparing blood pressure control in hypertensive patients who received team-based care with patients who received usual care.2 The meta-analysis divided the studies by specific types of team-based interventions and analyzed the effect of each type on blood pressure control. It also analyzed studies based on what kind of health care professionals were involved in the intervention.
The largest absolute changes in both SBP and DBP were observed with the following interventions, compared with the control group: free medication (3 trials; SBP reduction (SBPR)=−11 mm Hg; interquartile range [IQR]=−15 to −9.1; DBP reduction [DBPR]=−6.4 mm Hg; IQR=−8.7 to −3.9); pharmacist recommending medication to physician (15 trials; SBPR=−9.3 mm Hg; IQR=−15 to −5.0; DBPR=−3.6 mm Hg; IQR=−7.0 to −1.0); education about BP medications (23 trials; SBPR=−8.8 mm Hg; IQR=−12 to −4.3; DBPR=−3.6 mm Hg; IQR=−7.0 to −1.0); and pharmacist-performed intervention (22 trials; SBPR=−8.4 mm Hg; IQR=−12 to −4; DBPR=−3.3 mm Hg; IQR=−6.9 to −0.90).
Patients who underwent team-based care interventions had greater SBP control (defined as <140, or <130 in patients with diabetes mellitus or chronic kidney disease) than the control group in trials involving nurses (8 trials; odds ratio [OR]=1.7; 95% confidence interval [CI], 1.5-1.9), trials conducted in community pharmacies (5 trials; OR=2.9; 95% CI, 1.8-4.6), and trials incorporating pharmacists into primary care clinics (9 trials; OR=2.2; 95% CI, 1.8-2.7).
Team-based care improves lipid control
An RCT of 6963 patients with type 2 diabetes mellitus in 9 clinics examined the proportion of patients receiving team-based care that achieved a target low-density lipoprotein (LDL) of ≤100 mg/dL compared with patients receiving usual care.3
Clinics were randomized to participate in team-based care (defined as a physician-pharmacist team in which the pharmacist reviewed the medical charts of patients with elevated LDL and then developed individualized, evidence-based treatment recommendations) or usual care, which involved access to a disease management program providing automated quality reporting, benchmarking, and care opportunity decision support.
Over 2 years, the team-based care model had significantly more patients with a lower LDL, more patients at LDL goal, and more patients on lipid-lowering medication (TABLE3).
Yes, team-based care appears to lower systolic blood pressure (SBP) by 5 to 11 mm Hg and diastolic blood pressure (DBP) by 2 to 6 mm Hg in patients with hypertension and improve lipid control in patients with diabetes (strength of recommendation: C, disease-oriented outcomes).
Team-based care lowers BP in hypertensive patients
A systematic review evaluated 80 trials (total N not defined), which included randomized controlled trials (RCTs) and quasi-experimental trials, to compare blood pressure control in hypertensive patients who received team-based care with that of patients who received usual care.1
Team-based care was defined as adding new staff or changing the roles of existing staff to provide process support and share responsibility for hypertension care with a primary care provider. Examples included using staff to help with medication management, active patient follow-up, adherence, and self-management support. The mean duration of the interventions was 12 months.
The intervention group showed greater reductions in SBP (44 trials; 5.4 mm Hg; interquartile interval [IQI]=2.0-7.2) and DBP (38 trials; 1.8 mm Hg; IQI=0.7-3.2) compared with usual care.
Free medication, care involving nurses, pharmacists lead to lower BP
Another meta-analysis examined 37 RCTs (total N not provided) comparing blood pressure control in hypertensive patients who received team-based care with patients who received usual care.2 The meta-analysis divided the studies by specific types of team-based interventions and analyzed the effect of each type on blood pressure control. It also analyzed studies based on what kind of health care professionals were involved in the intervention.
The largest absolute changes in both SBP and DBP were observed with the following interventions, compared with the control group: free medication (3 trials; SBP reduction (SBPR)=−11 mm Hg; interquartile range [IQR]=−15 to −9.1; DBP reduction [DBPR]=−6.4 mm Hg; IQR=−8.7 to −3.9); pharmacist recommending medication to physician (15 trials; SBPR=−9.3 mm Hg; IQR=−15 to −5.0; DBPR=−3.6 mm Hg; IQR=−7.0 to −1.0); education about BP medications (23 trials; SBPR=−8.8 mm Hg; IQR=−12 to −4.3; DBPR=−3.6 mm Hg; IQR=−7.0 to −1.0); and pharmacist-performed intervention (22 trials; SBPR=−8.4 mm Hg; IQR=−12 to −4; DBPR=−3.3 mm Hg; IQR=−6.9 to −0.90).
Patients who underwent team-based care interventions had greater SBP control (defined as <140, or <130 in patients with diabetes mellitus or chronic kidney disease) than the control group in trials involving nurses (8 trials; odds ratio [OR]=1.7; 95% confidence interval [CI], 1.5-1.9), trials conducted in community pharmacies (5 trials; OR=2.9; 95% CI, 1.8-4.6), and trials incorporating pharmacists into primary care clinics (9 trials; OR=2.2; 95% CI, 1.8-2.7).
Team-based care improves lipid control
An RCT of 6963 patients with type 2 diabetes mellitus in 9 clinics examined the proportion of patients receiving team-based care that achieved a target low-density lipoprotein (LDL) of ≤100 mg/dL compared with patients receiving usual care.3
Clinics were randomized to participate in team-based care (defined as a physician-pharmacist team in which the pharmacist reviewed the medical charts of patients with elevated LDL and then developed individualized, evidence-based treatment recommendations) or usual care, which involved access to a disease management program providing automated quality reporting, benchmarking, and care opportunity decision support.
Over 2 years, the team-based care model had significantly more patients with a lower LDL, more patients at LDL goal, and more patients on lipid-lowering medication (TABLE3).
1. Proia KK, Thota AB, Njie GJ, et al. Team-based care and improved blood pressure control: a community guide systematic review. Am J Prev Med. 2014;47:86-99.
2. Carter BL, Rogers M, Daly J, et al. The potency of team-based care interventions for hypertension: a meta-analysis. Arch Intern Med. 2009;169:1748-1755.
3. Pape GA, Hunt JS, Butler KL, et al. Team-based care approach to cholesterol management in diabetes mellitus. Arch Intern Med. 2011;171:1480-1486.
1. Proia KK, Thota AB, Njie GJ, et al. Team-based care and improved blood pressure control: a community guide systematic review. Am J Prev Med. 2014;47:86-99.
2. Carter BL, Rogers M, Daly J, et al. The potency of team-based care interventions for hypertension: a meta-analysis. Arch Intern Med. 2009;169:1748-1755.
3. Pape GA, Hunt JS, Butler KL, et al. Team-based care approach to cholesterol management in diabetes mellitus. Arch Intern Med. 2011;171:1480-1486.
Evidence-based answers from the Family Physicians Inquiries Network