User login
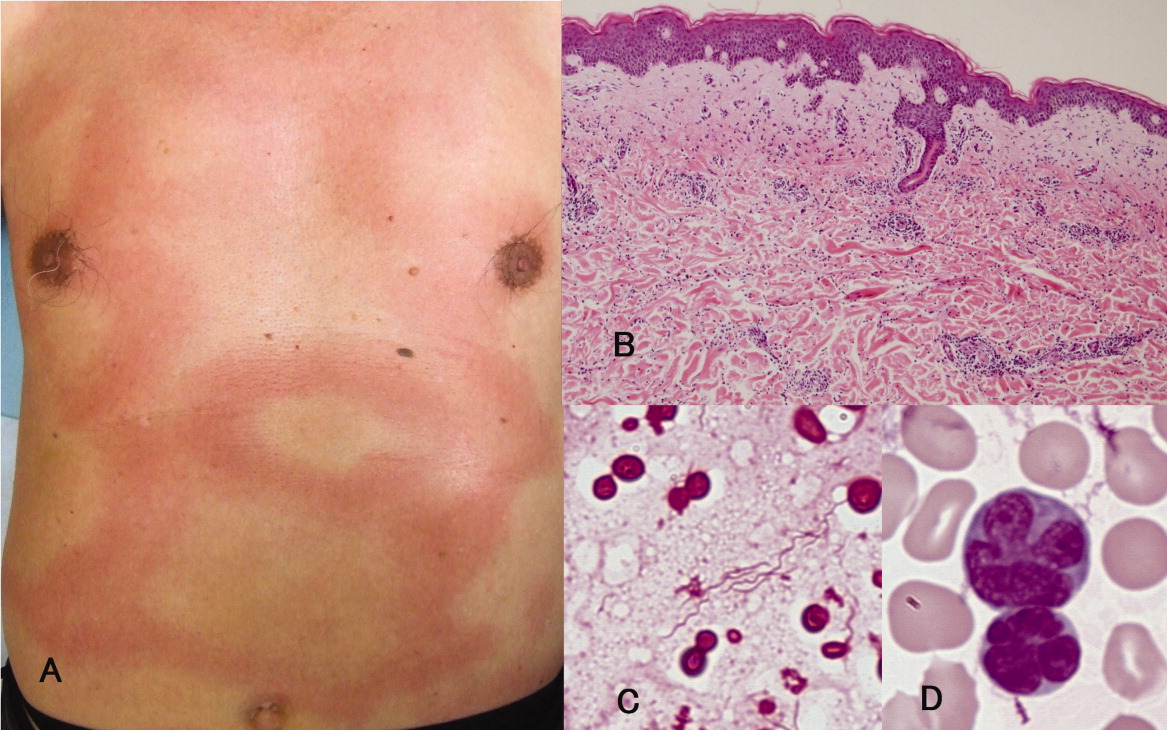
A previously healthy 66‐year‐old man was admitted with a 4‐day history of high fever and an extensive, nonpruritic, nonmigratory, erythematous rash with areas of induration over his torso (Figure 1A). Biopsy of the rash, which spontaneously subsided within 8 days, revealed only nonspecific superficial and deep perivascular lymphocytic infiltration, without vasculitis, granulomas, or immunohistochemical evidence of malignant cells (Figure 1B). Blood cultures grew spiral‐shaped Gram‐negative rods (Figure 1C), which were identified as Helicobacter cinaedi by polymerase chain reaction (PCR). H. cinaedi is a rare pathogen that is reported to cause bacteremia in immunocompromised hosts. Peripheral blood showed more than 2000/L of lymphocytes with prominent hyperlobulated flower‐like nuclei (Figure 1D), which were CD4+/CD8 and CD25+ by flow cytometry. Human T‐lymphotropic virus 1 (HTLV‐1) antibody was positive, highlighting the fact that the patient's mother was from southern Kyushu, Japan, where HTLV‐1 is endemic. Diagnosis of adult T‐cell leukemia was confirmed by southern blot hybridization analysis. We believe that this case makes an important addition to the library of annular or gyrate erythemas, which can be secondary to bacteremia, leukemia, or both.

A previously healthy 66‐year‐old man was admitted with a 4‐day history of high fever and an extensive, nonpruritic, nonmigratory, erythematous rash with areas of induration over his torso (Figure 1A). Biopsy of the rash, which spontaneously subsided within 8 days, revealed only nonspecific superficial and deep perivascular lymphocytic infiltration, without vasculitis, granulomas, or immunohistochemical evidence of malignant cells (Figure 1B). Blood cultures grew spiral‐shaped Gram‐negative rods (Figure 1C), which were identified as Helicobacter cinaedi by polymerase chain reaction (PCR). H. cinaedi is a rare pathogen that is reported to cause bacteremia in immunocompromised hosts. Peripheral blood showed more than 2000/L of lymphocytes with prominent hyperlobulated flower‐like nuclei (Figure 1D), which were CD4+/CD8 and CD25+ by flow cytometry. Human T‐lymphotropic virus 1 (HTLV‐1) antibody was positive, highlighting the fact that the patient's mother was from southern Kyushu, Japan, where HTLV‐1 is endemic. Diagnosis of adult T‐cell leukemia was confirmed by southern blot hybridization analysis. We believe that this case makes an important addition to the library of annular or gyrate erythemas, which can be secondary to bacteremia, leukemia, or both.
A previously healthy 66‐year‐old man was admitted with a 4‐day history of high fever and an extensive, nonpruritic, nonmigratory, erythematous rash with areas of induration over his torso (Figure 1A). Biopsy of the rash, which spontaneously subsided within 8 days, revealed only nonspecific superficial and deep perivascular lymphocytic infiltration, without vasculitis, granulomas, or immunohistochemical evidence of malignant cells (Figure 1B). Blood cultures grew spiral‐shaped Gram‐negative rods (Figure 1C), which were identified as Helicobacter cinaedi by polymerase chain reaction (PCR). H. cinaedi is a rare pathogen that is reported to cause bacteremia in immunocompromised hosts. Peripheral blood showed more than 2000/L of lymphocytes with prominent hyperlobulated flower‐like nuclei (Figure 1D), which were CD4+/CD8 and CD25+ by flow cytometry. Human T‐lymphotropic virus 1 (HTLV‐1) antibody was positive, highlighting the fact that the patient's mother was from southern Kyushu, Japan, where HTLV‐1 is endemic. Diagnosis of adult T‐cell leukemia was confirmed by southern blot hybridization analysis. We believe that this case makes an important addition to the library of annular or gyrate erythemas, which can be secondary to bacteremia, leukemia, or both.