User login
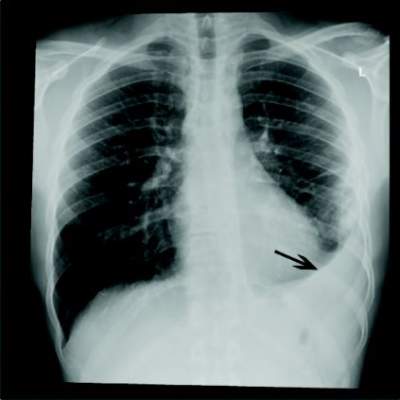
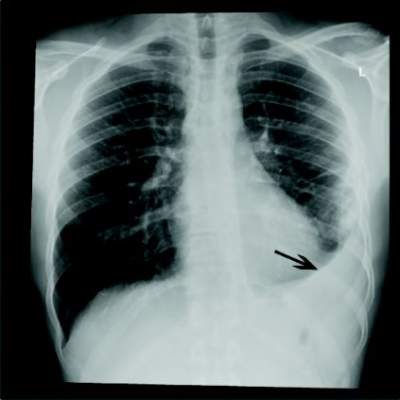
AMSTERDAM – Adding a macrolide to beta-lactam antibiotic treatment didn’t improve outcomes in HIV-infected patients with community-acquired bacterial pneumonia, according to the results of a Brazilian study.
Dr. Claudia Figueiredo Mello of the Instituto de Infectologia Emílio Ribas, São Paolo, said her study found no difference in in-hospital mortality between treatment with a beta-lactam alone, and treatment with the combination of a beta-lactam and a macrolide. Indeed, length of hospital stay was exactly the same. Dr. Mello reported the study results at the European Society of Clinical Microbiology and Infectious Diseases annual congress.
The study involved 228 patients with longstanding HIV infections and community-acquired bacterial pneumonia who were randomized to two treatment regimens. Protocol 1 was the standard treatment of 1 g ceftriaxone intravenously every 12 hours plus placebo for a minimum of 7 days. Protocol 2 was the same ceftriaxone treatment with the addition of azithromycin 500 mg/day or clarithromycin 500 mg every 12 hours.
Patients were a mean of 40 years old, with a median HIV duration of 12 years. Only about 20% were on regular highly active antiretroviral therapy (HAART); this was reflected in the low proportion of patients with a viral load of less than 50 copies/mL (about 16%), Dr. Mello said.
The median CD4 T-cell count varied widely in patients, but in half it was below 50 cells/mm3. Comorbidities were common in the cohort (30%); the most common were hypertension (12%) and liver disease (10%). Many patients used tobacco (41%), and illicit drug use was also common (about a third).
Most patients (60%) were risk class I-III on the Pneumonia Severity Index. Risk class III occurred in 20%, and the remainder were risk class IV and V.
In the intention-to-treat analysis, in-hospital mortality was 11% in the beta-lactam–only group and 15% in the combination therapy group – not a significant difference. The time to reach clinical stability was 5 days in each group, and the hospital length of stay, 14 days in each group.
Dr. Mello said she and her colleagues would continue to examine the data to determine if a specific subgroup might benefit from combination therapy, as extant data do suggest that adding a macrolide to beta-lactam treatment improves outcomes in a general population. She could not speculate as to why combination therapy didn’t appear to confer additional benefit on this cohort of patients living with HIV.
She had no financial disclosures.
AMSTERDAM – Adding a macrolide to beta-lactam antibiotic treatment didn’t improve outcomes in HIV-infected patients with community-acquired bacterial pneumonia, according to the results of a Brazilian study.
Dr. Claudia Figueiredo Mello of the Instituto de Infectologia Emílio Ribas, São Paolo, said her study found no difference in in-hospital mortality between treatment with a beta-lactam alone, and treatment with the combination of a beta-lactam and a macrolide. Indeed, length of hospital stay was exactly the same. Dr. Mello reported the study results at the European Society of Clinical Microbiology and Infectious Diseases annual congress.
The study involved 228 patients with longstanding HIV infections and community-acquired bacterial pneumonia who were randomized to two treatment regimens. Protocol 1 was the standard treatment of 1 g ceftriaxone intravenously every 12 hours plus placebo for a minimum of 7 days. Protocol 2 was the same ceftriaxone treatment with the addition of azithromycin 500 mg/day or clarithromycin 500 mg every 12 hours.
Patients were a mean of 40 years old, with a median HIV duration of 12 years. Only about 20% were on regular highly active antiretroviral therapy (HAART); this was reflected in the low proportion of patients with a viral load of less than 50 copies/mL (about 16%), Dr. Mello said.
The median CD4 T-cell count varied widely in patients, but in half it was below 50 cells/mm3. Comorbidities were common in the cohort (30%); the most common were hypertension (12%) and liver disease (10%). Many patients used tobacco (41%), and illicit drug use was also common (about a third).
Most patients (60%) were risk class I-III on the Pneumonia Severity Index. Risk class III occurred in 20%, and the remainder were risk class IV and V.
In the intention-to-treat analysis, in-hospital mortality was 11% in the beta-lactam–only group and 15% in the combination therapy group – not a significant difference. The time to reach clinical stability was 5 days in each group, and the hospital length of stay, 14 days in each group.
Dr. Mello said she and her colleagues would continue to examine the data to determine if a specific subgroup might benefit from combination therapy, as extant data do suggest that adding a macrolide to beta-lactam treatment improves outcomes in a general population. She could not speculate as to why combination therapy didn’t appear to confer additional benefit on this cohort of patients living with HIV.
She had no financial disclosures.
AMSTERDAM – Adding a macrolide to beta-lactam antibiotic treatment didn’t improve outcomes in HIV-infected patients with community-acquired bacterial pneumonia, according to the results of a Brazilian study.
Dr. Claudia Figueiredo Mello of the Instituto de Infectologia Emílio Ribas, São Paolo, said her study found no difference in in-hospital mortality between treatment with a beta-lactam alone, and treatment with the combination of a beta-lactam and a macrolide. Indeed, length of hospital stay was exactly the same. Dr. Mello reported the study results at the European Society of Clinical Microbiology and Infectious Diseases annual congress.
The study involved 228 patients with longstanding HIV infections and community-acquired bacterial pneumonia who were randomized to two treatment regimens. Protocol 1 was the standard treatment of 1 g ceftriaxone intravenously every 12 hours plus placebo for a minimum of 7 days. Protocol 2 was the same ceftriaxone treatment with the addition of azithromycin 500 mg/day or clarithromycin 500 mg every 12 hours.
Patients were a mean of 40 years old, with a median HIV duration of 12 years. Only about 20% were on regular highly active antiretroviral therapy (HAART); this was reflected in the low proportion of patients with a viral load of less than 50 copies/mL (about 16%), Dr. Mello said.
The median CD4 T-cell count varied widely in patients, but in half it was below 50 cells/mm3. Comorbidities were common in the cohort (30%); the most common were hypertension (12%) and liver disease (10%). Many patients used tobacco (41%), and illicit drug use was also common (about a third).
Most patients (60%) were risk class I-III on the Pneumonia Severity Index. Risk class III occurred in 20%, and the remainder were risk class IV and V.
In the intention-to-treat analysis, in-hospital mortality was 11% in the beta-lactam–only group and 15% in the combination therapy group – not a significant difference. The time to reach clinical stability was 5 days in each group, and the hospital length of stay, 14 days in each group.
Dr. Mello said she and her colleagues would continue to examine the data to determine if a specific subgroup might benefit from combination therapy, as extant data do suggest that adding a macrolide to beta-lactam treatment improves outcomes in a general population. She could not speculate as to why combination therapy didn’t appear to confer additional benefit on this cohort of patients living with HIV.
She had no financial disclosures.
AT ECCMID 2016
Key clinical point: Adding a macrolide to beta-lactam antibiotic treatment didn’t improve outcomes in HIV-positive patients with community-acquired pneumonia.
Major finding: In-hospital mortality was 11% in the combination group and 15% in the beta-lactam–only group.
Data source: A randomized, controlled trial comprising 228 patients.
Disclosures: Dr. Mello had no financial obligations.