User login
It’s that time of year again … the time when hospitals around the country are being notified of their 30-day readmission penalties from the Centers for Medicare and Medicaid Services (CMS). Now in the fourth year of the program, many hospitals have come to dread the announcement of how much they are being penalized each year.1
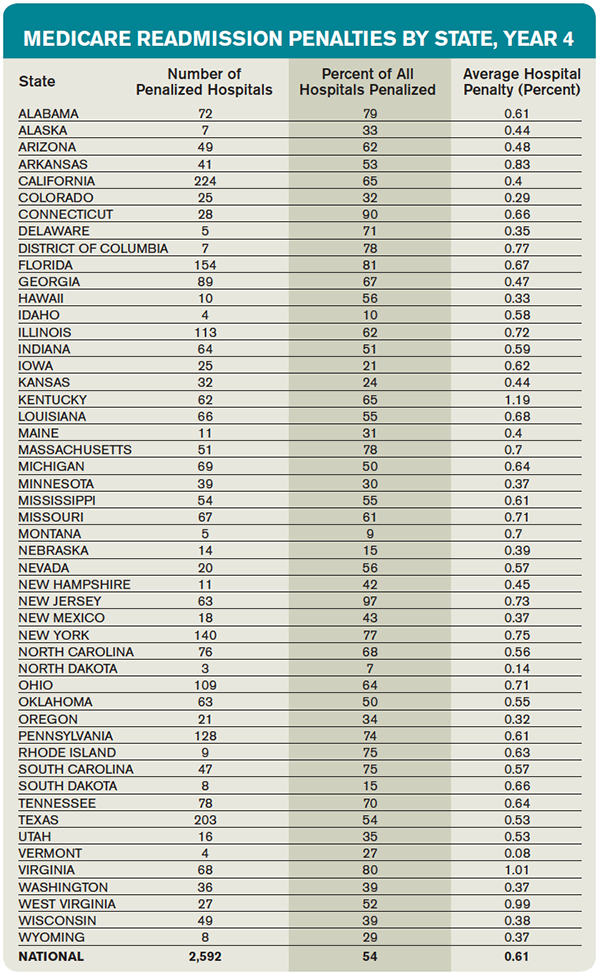
This year, the readmission reduction program will decrease Medicare payments within a total of 2,592 U.S. hospitals, for a combined total of $420 million. This year’s program included readmissions from July 2011 to June 2014; the program uses a three-year rolling average for its calculations.2
The readmission program, which initially was implemented through the Affordable Care Act in 2012, aimed to penalize hospitals with higher than expected 30-day readmission rates on select conditions (currently heart attack, heart failure, pneumonia, COPD, and hip/knee replacements). Medicare estimates that it spends $17 billion a year in avoidable readmissions, which prompted the initial support for the program. For each condition, CMS calculates expected readmission rates (based on risk adjustment models that include age, severity of illness, and comorbid conditions) and observed rates, and then calculates an “excess readmission ratio” for each hospital. Based on the overall ratio, the hospital is penalized up to 3% of its Medicare payments for all inpatient stays for that fiscal year. Each year, CMS reassesses the readmission rates for hospitals and readjusts the magnitude of the penalty. The purpose of the program is to incent hospitals to invest in discharge planning and care coordination efforts and do everything possible to avoid readmissions.1
Who Gets Penalized?
This year, most eligible hospitals were penalized to some extent, and all but 209 of the hospitals that were penalized last year were penalized again.
The average Medicare payment reduction will be 0.61% per patient stay.
A total of 506 hospitals will lose at least 1% of their Medicare payments, and 38 hospitals will receive the maximum 3% penalty.
Unfortunately, safety net hospitals were about 60% more likely than other hospitals to have been penalized in all three years of the program. In addition, hospitals with the lowest profit margins were 36% more likely to be penalized than those with higher margins.
Some states were disproportionately affected, with at least three-quarters of hospitals affected in Alabama, Connecticut, Florida, Massachusetts, New Jersey, New York, Rhode Island, South Carolina, Virginia, and the District of Columbia. States that fared the best were Idaho, Iowa, Kansas, Montana, Nebraska, North Dakota, and South Dakota.
Most of the 2,232 hospitals that avoided a penalty were spared because they were exempted from the program (Veterans Affairs hospitals, children’s hospitals, critical access hospitals, or those with too few Medicare patients), not because of exceptional performance.
Does the Program Work?
Despite criticism, there is no doubt that this program has forced hospitals to pay keen attention to transitions of care and avoidable readmissions. And it does appear to be an effective strategy for CMS to achieve its goals; there has been an overall decrease in 30-day readmission rates among Medicare recipients since the program began, in all types of hospitals.
Compared to 2012, there were 100,000 fewer readmissions among Medicare beneficiaries in the U.S. in 2013. As such, there is no evidence that the program will be discontinued, although it will hopefully be altered in some key aspects.3
What the Future Holds
The program has been criticized on many fronts. For one, it recalculates a three-year rolling average each year, which makes it incredibly difficult to “wash out” older (poor) performance and get off the penalty list.
In addition, critics have pointed out that the program fails to take into account the socioeconomic background of patients when assessing readmission penalties. Many argue that social determinants of readmissions that are beyond the immediate control of a hospital system can have a huge impact on readmission rates.
The National Quality Forum is examining the impact of these factors on readmissions, but this evaluation likely will take years.
In the meantime, the Hospital Readmissions Program Accuracy and Accountability Act of 2014 has been introduced as a bill that would require CMS to factor socioeconomic status into the equation when determining readmission penalties.
What All This Means for Hospitalists
All of us working within the confines of the current program can do a few things to improve our understanding and our hospitals’ performance:
- If your hospital is one that incurred a penalty, know that most “eligible” hospitals also incurred a penalty.
- Look at how your hospital fared within your state and find out if you are above or below average in the amount.3
- Continue to focus on exemplary care transition protocols, policies, and programs within your hospital system, because the penalties are unlikely to go away and are very likely to expand over time.
- Support any advocacy efforts toward improving risk adjustment methodologies for readmissions; all hospitals are likely to benefit from more accurate risk adjustments.

References
- Centers for Medicare and Medicaid Services. Readmissions reduction program. Accessed October 3, 2015.
- Rau J. Half of nation’s hospitals fail again to escape Medicare’s readmissions penalties. August 3, 2015. Accessed October 3, 2015.
- Medpac. The hospital readmission penalty: how well is it working?. Accessed October 3, 2015.
It’s that time of year again … the time when hospitals around the country are being notified of their 30-day readmission penalties from the Centers for Medicare and Medicaid Services (CMS). Now in the fourth year of the program, many hospitals have come to dread the announcement of how much they are being penalized each year.1
This year, the readmission reduction program will decrease Medicare payments within a total of 2,592 U.S. hospitals, for a combined total of $420 million. This year’s program included readmissions from July 2011 to June 2014; the program uses a three-year rolling average for its calculations.2
The readmission program, which initially was implemented through the Affordable Care Act in 2012, aimed to penalize hospitals with higher than expected 30-day readmission rates on select conditions (currently heart attack, heart failure, pneumonia, COPD, and hip/knee replacements). Medicare estimates that it spends $17 billion a year in avoidable readmissions, which prompted the initial support for the program. For each condition, CMS calculates expected readmission rates (based on risk adjustment models that include age, severity of illness, and comorbid conditions) and observed rates, and then calculates an “excess readmission ratio” for each hospital. Based on the overall ratio, the hospital is penalized up to 3% of its Medicare payments for all inpatient stays for that fiscal year. Each year, CMS reassesses the readmission rates for hospitals and readjusts the magnitude of the penalty. The purpose of the program is to incent hospitals to invest in discharge planning and care coordination efforts and do everything possible to avoid readmissions.1
Who Gets Penalized?
This year, most eligible hospitals were penalized to some extent, and all but 209 of the hospitals that were penalized last year were penalized again.
The average Medicare payment reduction will be 0.61% per patient stay.
A total of 506 hospitals will lose at least 1% of their Medicare payments, and 38 hospitals will receive the maximum 3% penalty.
Unfortunately, safety net hospitals were about 60% more likely than other hospitals to have been penalized in all three years of the program. In addition, hospitals with the lowest profit margins were 36% more likely to be penalized than those with higher margins.
Some states were disproportionately affected, with at least three-quarters of hospitals affected in Alabama, Connecticut, Florida, Massachusetts, New Jersey, New York, Rhode Island, South Carolina, Virginia, and the District of Columbia. States that fared the best were Idaho, Iowa, Kansas, Montana, Nebraska, North Dakota, and South Dakota.
Most of the 2,232 hospitals that avoided a penalty were spared because they were exempted from the program (Veterans Affairs hospitals, children’s hospitals, critical access hospitals, or those with too few Medicare patients), not because of exceptional performance.
Does the Program Work?
Despite criticism, there is no doubt that this program has forced hospitals to pay keen attention to transitions of care and avoidable readmissions. And it does appear to be an effective strategy for CMS to achieve its goals; there has been an overall decrease in 30-day readmission rates among Medicare recipients since the program began, in all types of hospitals.
Compared to 2012, there were 100,000 fewer readmissions among Medicare beneficiaries in the U.S. in 2013. As such, there is no evidence that the program will be discontinued, although it will hopefully be altered in some key aspects.3
What the Future Holds
The program has been criticized on many fronts. For one, it recalculates a three-year rolling average each year, which makes it incredibly difficult to “wash out” older (poor) performance and get off the penalty list.
In addition, critics have pointed out that the program fails to take into account the socioeconomic background of patients when assessing readmission penalties. Many argue that social determinants of readmissions that are beyond the immediate control of a hospital system can have a huge impact on readmission rates.
The National Quality Forum is examining the impact of these factors on readmissions, but this evaluation likely will take years.
In the meantime, the Hospital Readmissions Program Accuracy and Accountability Act of 2014 has been introduced as a bill that would require CMS to factor socioeconomic status into the equation when determining readmission penalties.
What All This Means for Hospitalists
All of us working within the confines of the current program can do a few things to improve our understanding and our hospitals’ performance:
- If your hospital is one that incurred a penalty, know that most “eligible” hospitals also incurred a penalty.
- Look at how your hospital fared within your state and find out if you are above or below average in the amount.3
- Continue to focus on exemplary care transition protocols, policies, and programs within your hospital system, because the penalties are unlikely to go away and are very likely to expand over time.
- Support any advocacy efforts toward improving risk adjustment methodologies for readmissions; all hospitals are likely to benefit from more accurate risk adjustments.
References
- Centers for Medicare and Medicaid Services. Readmissions reduction program. Accessed October 3, 2015.
- Rau J. Half of nation’s hospitals fail again to escape Medicare’s readmissions penalties. August 3, 2015. Accessed October 3, 2015.
- Medpac. The hospital readmission penalty: how well is it working?. Accessed October 3, 2015.
It’s that time of year again … the time when hospitals around the country are being notified of their 30-day readmission penalties from the Centers for Medicare and Medicaid Services (CMS). Now in the fourth year of the program, many hospitals have come to dread the announcement of how much they are being penalized each year.1
This year, the readmission reduction program will decrease Medicare payments within a total of 2,592 U.S. hospitals, for a combined total of $420 million. This year’s program included readmissions from July 2011 to June 2014; the program uses a three-year rolling average for its calculations.2
The readmission program, which initially was implemented through the Affordable Care Act in 2012, aimed to penalize hospitals with higher than expected 30-day readmission rates on select conditions (currently heart attack, heart failure, pneumonia, COPD, and hip/knee replacements). Medicare estimates that it spends $17 billion a year in avoidable readmissions, which prompted the initial support for the program. For each condition, CMS calculates expected readmission rates (based on risk adjustment models that include age, severity of illness, and comorbid conditions) and observed rates, and then calculates an “excess readmission ratio” for each hospital. Based on the overall ratio, the hospital is penalized up to 3% of its Medicare payments for all inpatient stays for that fiscal year. Each year, CMS reassesses the readmission rates for hospitals and readjusts the magnitude of the penalty. The purpose of the program is to incent hospitals to invest in discharge planning and care coordination efforts and do everything possible to avoid readmissions.1
Who Gets Penalized?
This year, most eligible hospitals were penalized to some extent, and all but 209 of the hospitals that were penalized last year were penalized again.
The average Medicare payment reduction will be 0.61% per patient stay.
A total of 506 hospitals will lose at least 1% of their Medicare payments, and 38 hospitals will receive the maximum 3% penalty.
Unfortunately, safety net hospitals were about 60% more likely than other hospitals to have been penalized in all three years of the program. In addition, hospitals with the lowest profit margins were 36% more likely to be penalized than those with higher margins.
Some states were disproportionately affected, with at least three-quarters of hospitals affected in Alabama, Connecticut, Florida, Massachusetts, New Jersey, New York, Rhode Island, South Carolina, Virginia, and the District of Columbia. States that fared the best were Idaho, Iowa, Kansas, Montana, Nebraska, North Dakota, and South Dakota.
Most of the 2,232 hospitals that avoided a penalty were spared because they were exempted from the program (Veterans Affairs hospitals, children’s hospitals, critical access hospitals, or those with too few Medicare patients), not because of exceptional performance.
Does the Program Work?
Despite criticism, there is no doubt that this program has forced hospitals to pay keen attention to transitions of care and avoidable readmissions. And it does appear to be an effective strategy for CMS to achieve its goals; there has been an overall decrease in 30-day readmission rates among Medicare recipients since the program began, in all types of hospitals.
Compared to 2012, there were 100,000 fewer readmissions among Medicare beneficiaries in the U.S. in 2013. As such, there is no evidence that the program will be discontinued, although it will hopefully be altered in some key aspects.3
What the Future Holds
The program has been criticized on many fronts. For one, it recalculates a three-year rolling average each year, which makes it incredibly difficult to “wash out” older (poor) performance and get off the penalty list.
In addition, critics have pointed out that the program fails to take into account the socioeconomic background of patients when assessing readmission penalties. Many argue that social determinants of readmissions that are beyond the immediate control of a hospital system can have a huge impact on readmission rates.
The National Quality Forum is examining the impact of these factors on readmissions, but this evaluation likely will take years.
In the meantime, the Hospital Readmissions Program Accuracy and Accountability Act of 2014 has been introduced as a bill that would require CMS to factor socioeconomic status into the equation when determining readmission penalties.
What All This Means for Hospitalists
All of us working within the confines of the current program can do a few things to improve our understanding and our hospitals’ performance:
- If your hospital is one that incurred a penalty, know that most “eligible” hospitals also incurred a penalty.
- Look at how your hospital fared within your state and find out if you are above or below average in the amount.3
- Continue to focus on exemplary care transition protocols, policies, and programs within your hospital system, because the penalties are unlikely to go away and are very likely to expand over time.
- Support any advocacy efforts toward improving risk adjustment methodologies for readmissions; all hospitals are likely to benefit from more accurate risk adjustments.
References
- Centers for Medicare and Medicaid Services. Readmissions reduction program. Accessed October 3, 2015.
- Rau J. Half of nation’s hospitals fail again to escape Medicare’s readmissions penalties. August 3, 2015. Accessed October 3, 2015.
- Medpac. The hospital readmission penalty: how well is it working?. Accessed October 3, 2015.