User login
A 57-year-old woman with a history of breast cancer comes to your office complaining of pain and swelling on the left side of her neck. She has recently had a mastectomy and chemotherapy; her port was removed in the past week. She has no chills, cough, dyspnea, palpitations, chest pain, nausea, weight gain, edema, or urinary complaints. She is, however, experiencing mild, general fatigue and a “scratchy throat”; otherwise there are no systemic symptoms. She is worried that her “cancer has come back.”
A:
Other medical history
- Hypothyroidism and hypertension
- History of deep venous thrombosis (DVT) attributed to her cancer; was on warfarin but “held” last week for her port removal surgery.
- Remote history of cholecystectomy
- No known drug allergies
- No history of myocardial infarction, congestive heart failure, stroke, or diabetes
- No recent international travel
- Current medications: anastrozole, hydrochlorothiazide, levothyroxine, calcium, warfarin, epoetin alfa, and acetaminophen
Family and social history
- Family history is significant for coronary artery disease late in life in her parents
- No family history of cancer, blood dyscrasia, or immunocompromise
- Formerly a smoker, only recently quit
- Moderate caffeine intake (coffee)
- Employed as a banker
Physical examination
- Temperature 99.7°F, pulse 92, respirations 20, blood pressure 122/74 mm Hg, weight 130 lbs
- Alert, oriented, no distress, full affect
- PERRLA (pupils equal, round, reactive to light and accommodation), extraocular motions intact, cranial nerves II–XII intact, mucous membranes moist, pharynx clear, no carotid bruits, minimal cervical adenopathy
- There is a tender, ill-defined mass on the left side of the neck, extending from angle of the mandible to the clavicle behind which it disappears
- Heart regular without murmurs or enlargement
- Lungs clear to auscultation in all fields
- Operative site on the left anterior thorax (port removal) is clean, dry, nonerythematous, healing well
- Abdomen is soft, nontender, nondistended, no organomegaly, normal bowel sounds
- Extremities show no significant edema or venous distention
A:
Lab results
- White bloods cell count elevated at 13 (3.9–10.9), 76% neutrophils with no bands
- Mild anemia of 11.3 (11.7–16.0)
- International normalized ratio (INR)= 0.94
- Blood cultures are pending
- Rapid strep test is negative
Next step: Order imaging studies
This particular presentation prompts you to order a computed tomography (CT) scan of her neck and chest, looking for a specific pathology (FIGURE 1).
When the scan is complete, the radiologist calls and confirms that there is occlusion of the left internal jugular vein, brachiocephalic vein, and a portion of the left subclavian vein with thrombosis.
A second CT of the chest again reveals the thrombosed veins, but there are no filling defects suggestive of pulmonary emboli or peripheral infiltrates or cavitary lesions suggestive of septic emboli (FIGURE 2).
The details. Thrombosis of the left internal jugular vein extends from the jugular siphon to the left subclavian vein. A portion of the left subclavian vein and probably the left brachiocephalic vein are also thrombosed. Numerous collaterals appear in the neck base. The left internal jugular vein measures 2.0 cm in diameter; the right measures 1.5 × 1.1 cm. There is also mild wall thickening of the internal jugular vein and infiltration of the surrounding fat—suggestive of septic thrombosis. No soft-tissue abscess is seen in the neck. The right internal jugular vein is normal. No definite thrombus is seen in the left jugular siphon or sigmoid sinus.
The parapharyngeal spaces are symmetric, though the infiltration of the fat around the left internal jugular vein is causing soft-tissue swelling and possibly mild tracheal deviation. The airway is not compromised. The superior mediastinum is grossly unremarkable. The upper lungs are clear.
A:
You vaguely recall that jugular thrombophlebitis is associated with some syndrome, so you turn to UpToDate and do a search on “jugular thrombophlebitis.”
There you learn that Lemierre’s syndrome, also known as necrobacillosis, is septic thrombophlebitis of the jugular vein. It most commonly develops following pharyngitis, and has been associated with dental microbes.1,2
Similar syndromes of suppurative thrombophlebitis may also occur in peripheral veins, associated with intravenous catheterization (especially PICC lines3), the superior and inferior vena cava, always associated with central lines,4 and the ovarian veins.5
FIGURE 1 Thrombosed veins
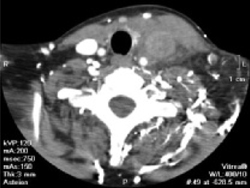
CT image with IV contrast of the base of the neck showing thrombosed veins.
FIGURE 2 Collateral circulation

This 3D reconstruction of CT images shows the extensive collateral circulation on the left, compared with the right.
You caught it early
Suppurative thrombophlebitis. This problem often presents with fever and rigorous chills. Swelling and tenderness is noted over the affected vein in about half the cases. Obviously, though, inspection and palpation of the vena cava is challenging and such signs do not apply when these vessels are involved.
Respiratory distress due to septic pulmonary emboli and secondary pneumonia is common. Metastatic abscess formation at other sites, such as joint and bone, have been reported.1,6
You realize that most patients with suppurative thrombophlebitis present in a much more toxic state than yours did. Perhaps you caught it early. She certainly has risk factors, including her recent pharyngitis and central venous catheterization. The prominent collateral circulation raises the possibility that this may have developed subacutely, following a more indolent course than is generally reported.
The organisms responsible for suppurative thrombophlebitis depend on the infection’s site of origin. Most of the time in the peripheral veins or vena cava, Staphylococcus, a member of normal skin flora, is the pathogen. Streptococcus, Enterobacteriaceae, Candida, and even cytomegalovirus have been documented.4,7,8 Jugular septic thrombophlebitis draws from the oral flora, with the most common causative agent being the anaerobic Fusobacterium.
A thrombus provides an excellent source of nutrients for the microbes, which colonize it and establish what is essentially a biofilm. These complex microbial architectures are extraordinarily resistant to antibiotic therapy, especially when compared with plantonic bacteria.9 Not only does the thrombus facilitate the infection, but the bacteria facilitate thrombus formation by promoting platelet aggregation.10
A:
Chemotherapy is only one of the many circumstances in which central venous access is required. Central venous access devices (CVADs) are also used for administration of antibiotics, hydration, total parenteral nutrition, or long-term blood sampling.
The central lines that most family physicians learned to insert during residency are only one of a dizzying array of CVADs in use. The triple-lumen lines are inserted transcutaneously by the resident into either the jugular or subclavian veins and are good for short-to-medium duration therapies. They require diligent care to prevent occlusion or infection, including daily flushing.
For longer-duration therapies, tunneled catheters may be placed, typically by surgical consultants. These are less prone to bleeding or infection but still require diligent attention and regular flushing. Some models do permit weekly flushing.
Peripherally-inserted central venous catheters (PICCs) may be used for up to a year. Generally inserted by nursing staff, they are still fairly high-maintenance and require daily flushes.

Representative venous access devices. Clockwise from upper left: triple lumen catheter, tunneled catheter, subcutaneous port, PICC.
Your patient had a subcutaneous CVAD, which is often called a “port.” It is surgically implanted, not unlike a pacemaker, and is ideal for long-term use, especially when required access is intermittent. It requires flushing only monthly (weekly when being accessed).
Medication or surgery?
Because of its resistance to antibiotic treatment, peripheral venous suppurative thrombophlebitis is a surgical disease, not unlike an abscess, and requires excision or incision and drainage of the affected vessel. Antibiotics alone are inadequate. Excision of thrombophlebitis of the central veins affected is not feasible (though thrombectomies are occasionally undertaken). In this case, prolonged antibiotic therapy is indicated.
Anticoagulation may also be considered, though no strong evidence supports that addition. Given the effect of Fusobacterium on platelet aggregation, aspirin might be expected to provide benefit. In vitro studies show inhibition of this aggregation with aspirin,10 but no clinical studies or even case reports indicate improved outcomes with its use.
A hospital stay
Prolonged antibiotics
You admit the patient to the hospital with a presumptive diagnosis of Lemierre’s syndrome and begin piperacillin/tazobactam intravenously, covering both Fusobacterium and Staphlococcus. You also opt to begin heparin and resume her warfarin, more for her history of DVT than because of documented benefit of anticoagulation in the management of suppurative thrombophlebitis.
An awareness of potential complications is vital before undertaking any medical intervention. Although it would be unusual for a family physician to place a port, insertion of central venous lines is a commonly performed procedure that shares many of the same risks. fortunately, septic thrombophlebitis is a rare complication; unfortunately, a variety of other complications may occur. These include hemorrhage, venous thrombosis (uninfected), extravascular hematoma, local or systemic infection, pneumo- hydro- hemo- or chylo-thorax, air embolus, catheter fragment embolus, nerve injury, arteriovenous fistula, and cardiac arrhythmias or tamponade. The likelihood of complications from this procedure can be diminished by strict adherence to aseptic technique, and a thorough knowledge of the surrounding anatomy. Contraindications include distorted anatomy, suspected superior vena cava injury, compromise (such as pneumothorax on the side contralateral to the planned insertion site), infection or full-thickness burns at the planned insertion site, and coagulopathy.
—Mark Huntington, MD
Anticoagulation
Over the course of her hospital stay, she spikes a fever (≥100°F) every 24 hours for the first 5 days, after which the peak temperatures slowly drop to normal. She reaches therapeutic levels on warfarin and the heparin is discontinued. At no point do any respiratory symptoms develop. Aerobic blood cultures show no growth; to your chagrin, you find out that anaerobic cultures were not obtained. After 8 days, the patient’s neck is no longer tender, the swelling has gone down, she’s adequately anticoagulated, has been afebrile for 48 hours, and is extremely eager to go home.
She is discharged with a prescription of amoxicillin/clavulanate 3 times daily for 4 weeks, as the literature suggests that most Fusobacterium are sensitive to this agent.11 She is instructed to return if any recurrent fevers, chest pain, or respiratory symptoms develop. At a routine follow-up appointment in a month, she remains asymptomatic.
1. Sinave CP, Hardy GJ, Fardy PW. The lemierre Syndrome: suppurative thrombophlebitis of the internal jugular vein secondary to oropharyngeal infection. Medicine (Baltimore) 1989;68:85-94.
2. Ely EW, Stump TE, Hudspeth AS, Haponik EF. Thoracic complications of dental surgical procedures: hazards of the dental drill. Am J Med 1993;95:456-465.
3. Andres DR, Urban AW, Acher CW, Maki DG. Septic thrombosis of the basilic, axillary, and subclavian veins caused by a peripherally inserted central venous catheter. Am J Med 1998;105:446-450.
4. Strinden WD, Helgerson RB, Maki DG. Candida septic thrombosis of the great central veins associated with central catheters. Clinical features and management. Ann Surg 1985;202:653-658.
5. Garcia J, Aboujaoude R, Apuzzio J, Alvares JR. Septic pelvic thrombophlebitis: diagnosis and management. Infect Dis Obstetr Gynecol 2006;2006:1-4.
6. Pruitt BA, Jr, McManus WF, Kim SH, Treat RC. Diagnosis and treatment of cannula-related intravenous sepsis in burn patients. Ann Surg 1980;191:546-554.
7. Baker CC, Petersen SR, Sheldon GF. Septic phlebitis: a neglected disease. Am J Surg 1979;138:97-103.
8. Peterson P, Stahl-Bayliss CM. Cytomegalovirus thrombophlebitis after successful DHPG therapy [letter]. Ann Intern Med 1987;106:632-633.
9. Parsek MR, Singh PK. Bacterial biofilms: an emerging link to disease pathogenesis. Ann Rev Microbiol 2003;57:677-701.
10. Forrester LJ, Campbell BJ, Berg JN, Barrett JT. Aggregation of platelets by Fusobacterium necrophorum. J Clin Micro 1985;22:245-249.
11. Kuriyama T, Karasawa T, Nakagawa K, Yamamoto E, Nakamura S. Incidence of beta-lactamase production and antimicrobial susceptibility of anaerobic gram-negative rods isolated from pus specimens of orofacial odontogenic infections. Oral Microbiol Immunol 2001;16:10-15.
CORRESPONDENCE: Mark K. Huntington, MD, PhD, Center for Family Medicine, 1115 East 20th Street, Sioux Falls, SD 57105. E-mail: [email protected]
A 57-year-old woman with a history of breast cancer comes to your office complaining of pain and swelling on the left side of her neck. She has recently had a mastectomy and chemotherapy; her port was removed in the past week. She has no chills, cough, dyspnea, palpitations, chest pain, nausea, weight gain, edema, or urinary complaints. She is, however, experiencing mild, general fatigue and a “scratchy throat”; otherwise there are no systemic symptoms. She is worried that her “cancer has come back.”
A:
Other medical history
- Hypothyroidism and hypertension
- History of deep venous thrombosis (DVT) attributed to her cancer; was on warfarin but “held” last week for her port removal surgery.
- Remote history of cholecystectomy
- No known drug allergies
- No history of myocardial infarction, congestive heart failure, stroke, or diabetes
- No recent international travel
- Current medications: anastrozole, hydrochlorothiazide, levothyroxine, calcium, warfarin, epoetin alfa, and acetaminophen
Family and social history
- Family history is significant for coronary artery disease late in life in her parents
- No family history of cancer, blood dyscrasia, or immunocompromise
- Formerly a smoker, only recently quit
- Moderate caffeine intake (coffee)
- Employed as a banker
Physical examination
- Temperature 99.7°F, pulse 92, respirations 20, blood pressure 122/74 mm Hg, weight 130 lbs
- Alert, oriented, no distress, full affect
- PERRLA (pupils equal, round, reactive to light and accommodation), extraocular motions intact, cranial nerves II–XII intact, mucous membranes moist, pharynx clear, no carotid bruits, minimal cervical adenopathy
- There is a tender, ill-defined mass on the left side of the neck, extending from angle of the mandible to the clavicle behind which it disappears
- Heart regular without murmurs or enlargement
- Lungs clear to auscultation in all fields
- Operative site on the left anterior thorax (port removal) is clean, dry, nonerythematous, healing well
- Abdomen is soft, nontender, nondistended, no organomegaly, normal bowel sounds
- Extremities show no significant edema or venous distention
A:
Lab results
- White bloods cell count elevated at 13 (3.9–10.9), 76% neutrophils with no bands
- Mild anemia of 11.3 (11.7–16.0)
- International normalized ratio (INR)= 0.94
- Blood cultures are pending
- Rapid strep test is negative
Next step: Order imaging studies
This particular presentation prompts you to order a computed tomography (CT) scan of her neck and chest, looking for a specific pathology (FIGURE 1).
When the scan is complete, the radiologist calls and confirms that there is occlusion of the left internal jugular vein, brachiocephalic vein, and a portion of the left subclavian vein with thrombosis.
A second CT of the chest again reveals the thrombosed veins, but there are no filling defects suggestive of pulmonary emboli or peripheral infiltrates or cavitary lesions suggestive of septic emboli (FIGURE 2).
The details. Thrombosis of the left internal jugular vein extends from the jugular siphon to the left subclavian vein. A portion of the left subclavian vein and probably the left brachiocephalic vein are also thrombosed. Numerous collaterals appear in the neck base. The left internal jugular vein measures 2.0 cm in diameter; the right measures 1.5 × 1.1 cm. There is also mild wall thickening of the internal jugular vein and infiltration of the surrounding fat—suggestive of septic thrombosis. No soft-tissue abscess is seen in the neck. The right internal jugular vein is normal. No definite thrombus is seen in the left jugular siphon or sigmoid sinus.
The parapharyngeal spaces are symmetric, though the infiltration of the fat around the left internal jugular vein is causing soft-tissue swelling and possibly mild tracheal deviation. The airway is not compromised. The superior mediastinum is grossly unremarkable. The upper lungs are clear.
A:
You vaguely recall that jugular thrombophlebitis is associated with some syndrome, so you turn to UpToDate and do a search on “jugular thrombophlebitis.”
There you learn that Lemierre’s syndrome, also known as necrobacillosis, is septic thrombophlebitis of the jugular vein. It most commonly develops following pharyngitis, and has been associated with dental microbes.1,2
Similar syndromes of suppurative thrombophlebitis may also occur in peripheral veins, associated with intravenous catheterization (especially PICC lines3), the superior and inferior vena cava, always associated with central lines,4 and the ovarian veins.5
FIGURE 1 Thrombosed veins
CT image with IV contrast of the base of the neck showing thrombosed veins.
FIGURE 2 Collateral circulation
This 3D reconstruction of CT images shows the extensive collateral circulation on the left, compared with the right.
You caught it early
Suppurative thrombophlebitis. This problem often presents with fever and rigorous chills. Swelling and tenderness is noted over the affected vein in about half the cases. Obviously, though, inspection and palpation of the vena cava is challenging and such signs do not apply when these vessels are involved.
Respiratory distress due to septic pulmonary emboli and secondary pneumonia is common. Metastatic abscess formation at other sites, such as joint and bone, have been reported.1,6
You realize that most patients with suppurative thrombophlebitis present in a much more toxic state than yours did. Perhaps you caught it early. She certainly has risk factors, including her recent pharyngitis and central venous catheterization. The prominent collateral circulation raises the possibility that this may have developed subacutely, following a more indolent course than is generally reported.
The organisms responsible for suppurative thrombophlebitis depend on the infection’s site of origin. Most of the time in the peripheral veins or vena cava, Staphylococcus, a member of normal skin flora, is the pathogen. Streptococcus, Enterobacteriaceae, Candida, and even cytomegalovirus have been documented.4,7,8 Jugular septic thrombophlebitis draws from the oral flora, with the most common causative agent being the anaerobic Fusobacterium.
A thrombus provides an excellent source of nutrients for the microbes, which colonize it and establish what is essentially a biofilm. These complex microbial architectures are extraordinarily resistant to antibiotic therapy, especially when compared with plantonic bacteria.9 Not only does the thrombus facilitate the infection, but the bacteria facilitate thrombus formation by promoting platelet aggregation.10
A:
Chemotherapy is only one of the many circumstances in which central venous access is required. Central venous access devices (CVADs) are also used for administration of antibiotics, hydration, total parenteral nutrition, or long-term blood sampling.
The central lines that most family physicians learned to insert during residency are only one of a dizzying array of CVADs in use. The triple-lumen lines are inserted transcutaneously by the resident into either the jugular or subclavian veins and are good for short-to-medium duration therapies. They require diligent care to prevent occlusion or infection, including daily flushing.
For longer-duration therapies, tunneled catheters may be placed, typically by surgical consultants. These are less prone to bleeding or infection but still require diligent attention and regular flushing. Some models do permit weekly flushing.
Peripherally-inserted central venous catheters (PICCs) may be used for up to a year. Generally inserted by nursing staff, they are still fairly high-maintenance and require daily flushes.
Representative venous access devices. Clockwise from upper left: triple lumen catheter, tunneled catheter, subcutaneous port, PICC.
Your patient had a subcutaneous CVAD, which is often called a “port.” It is surgically implanted, not unlike a pacemaker, and is ideal for long-term use, especially when required access is intermittent. It requires flushing only monthly (weekly when being accessed).
Medication or surgery?
Because of its resistance to antibiotic treatment, peripheral venous suppurative thrombophlebitis is a surgical disease, not unlike an abscess, and requires excision or incision and drainage of the affected vessel. Antibiotics alone are inadequate. Excision of thrombophlebitis of the central veins affected is not feasible (though thrombectomies are occasionally undertaken). In this case, prolonged antibiotic therapy is indicated.
Anticoagulation may also be considered, though no strong evidence supports that addition. Given the effect of Fusobacterium on platelet aggregation, aspirin might be expected to provide benefit. In vitro studies show inhibition of this aggregation with aspirin,10 but no clinical studies or even case reports indicate improved outcomes with its use.
A hospital stay
Prolonged antibiotics
You admit the patient to the hospital with a presumptive diagnosis of Lemierre’s syndrome and begin piperacillin/tazobactam intravenously, covering both Fusobacterium and Staphlococcus. You also opt to begin heparin and resume her warfarin, more for her history of DVT than because of documented benefit of anticoagulation in the management of suppurative thrombophlebitis.
An awareness of potential complications is vital before undertaking any medical intervention. Although it would be unusual for a family physician to place a port, insertion of central venous lines is a commonly performed procedure that shares many of the same risks. fortunately, septic thrombophlebitis is a rare complication; unfortunately, a variety of other complications may occur. These include hemorrhage, venous thrombosis (uninfected), extravascular hematoma, local or systemic infection, pneumo- hydro- hemo- or chylo-thorax, air embolus, catheter fragment embolus, nerve injury, arteriovenous fistula, and cardiac arrhythmias or tamponade. The likelihood of complications from this procedure can be diminished by strict adherence to aseptic technique, and a thorough knowledge of the surrounding anatomy. Contraindications include distorted anatomy, suspected superior vena cava injury, compromise (such as pneumothorax on the side contralateral to the planned insertion site), infection or full-thickness burns at the planned insertion site, and coagulopathy.
—Mark Huntington, MD
Anticoagulation
Over the course of her hospital stay, she spikes a fever (≥100°F) every 24 hours for the first 5 days, after which the peak temperatures slowly drop to normal. She reaches therapeutic levels on warfarin and the heparin is discontinued. At no point do any respiratory symptoms develop. Aerobic blood cultures show no growth; to your chagrin, you find out that anaerobic cultures were not obtained. After 8 days, the patient’s neck is no longer tender, the swelling has gone down, she’s adequately anticoagulated, has been afebrile for 48 hours, and is extremely eager to go home.
She is discharged with a prescription of amoxicillin/clavulanate 3 times daily for 4 weeks, as the literature suggests that most Fusobacterium are sensitive to this agent.11 She is instructed to return if any recurrent fevers, chest pain, or respiratory symptoms develop. At a routine follow-up appointment in a month, she remains asymptomatic.
A 57-year-old woman with a history of breast cancer comes to your office complaining of pain and swelling on the left side of her neck. She has recently had a mastectomy and chemotherapy; her port was removed in the past week. She has no chills, cough, dyspnea, palpitations, chest pain, nausea, weight gain, edema, or urinary complaints. She is, however, experiencing mild, general fatigue and a “scratchy throat”; otherwise there are no systemic symptoms. She is worried that her “cancer has come back.”
A:
Other medical history
- Hypothyroidism and hypertension
- History of deep venous thrombosis (DVT) attributed to her cancer; was on warfarin but “held” last week for her port removal surgery.
- Remote history of cholecystectomy
- No known drug allergies
- No history of myocardial infarction, congestive heart failure, stroke, or diabetes
- No recent international travel
- Current medications: anastrozole, hydrochlorothiazide, levothyroxine, calcium, warfarin, epoetin alfa, and acetaminophen
Family and social history
- Family history is significant for coronary artery disease late in life in her parents
- No family history of cancer, blood dyscrasia, or immunocompromise
- Formerly a smoker, only recently quit
- Moderate caffeine intake (coffee)
- Employed as a banker
Physical examination
- Temperature 99.7°F, pulse 92, respirations 20, blood pressure 122/74 mm Hg, weight 130 lbs
- Alert, oriented, no distress, full affect
- PERRLA (pupils equal, round, reactive to light and accommodation), extraocular motions intact, cranial nerves II–XII intact, mucous membranes moist, pharynx clear, no carotid bruits, minimal cervical adenopathy
- There is a tender, ill-defined mass on the left side of the neck, extending from angle of the mandible to the clavicle behind which it disappears
- Heart regular without murmurs or enlargement
- Lungs clear to auscultation in all fields
- Operative site on the left anterior thorax (port removal) is clean, dry, nonerythematous, healing well
- Abdomen is soft, nontender, nondistended, no organomegaly, normal bowel sounds
- Extremities show no significant edema or venous distention
A:
Lab results
- White bloods cell count elevated at 13 (3.9–10.9), 76% neutrophils with no bands
- Mild anemia of 11.3 (11.7–16.0)
- International normalized ratio (INR)= 0.94
- Blood cultures are pending
- Rapid strep test is negative
Next step: Order imaging studies
This particular presentation prompts you to order a computed tomography (CT) scan of her neck and chest, looking for a specific pathology (FIGURE 1).
When the scan is complete, the radiologist calls and confirms that there is occlusion of the left internal jugular vein, brachiocephalic vein, and a portion of the left subclavian vein with thrombosis.
A second CT of the chest again reveals the thrombosed veins, but there are no filling defects suggestive of pulmonary emboli or peripheral infiltrates or cavitary lesions suggestive of septic emboli (FIGURE 2).
The details. Thrombosis of the left internal jugular vein extends from the jugular siphon to the left subclavian vein. A portion of the left subclavian vein and probably the left brachiocephalic vein are also thrombosed. Numerous collaterals appear in the neck base. The left internal jugular vein measures 2.0 cm in diameter; the right measures 1.5 × 1.1 cm. There is also mild wall thickening of the internal jugular vein and infiltration of the surrounding fat—suggestive of septic thrombosis. No soft-tissue abscess is seen in the neck. The right internal jugular vein is normal. No definite thrombus is seen in the left jugular siphon or sigmoid sinus.
The parapharyngeal spaces are symmetric, though the infiltration of the fat around the left internal jugular vein is causing soft-tissue swelling and possibly mild tracheal deviation. The airway is not compromised. The superior mediastinum is grossly unremarkable. The upper lungs are clear.
A:
You vaguely recall that jugular thrombophlebitis is associated with some syndrome, so you turn to UpToDate and do a search on “jugular thrombophlebitis.”
There you learn that Lemierre’s syndrome, also known as necrobacillosis, is septic thrombophlebitis of the jugular vein. It most commonly develops following pharyngitis, and has been associated with dental microbes.1,2
Similar syndromes of suppurative thrombophlebitis may also occur in peripheral veins, associated with intravenous catheterization (especially PICC lines3), the superior and inferior vena cava, always associated with central lines,4 and the ovarian veins.5
FIGURE 1 Thrombosed veins
CT image with IV contrast of the base of the neck showing thrombosed veins.
FIGURE 2 Collateral circulation
This 3D reconstruction of CT images shows the extensive collateral circulation on the left, compared with the right.
You caught it early
Suppurative thrombophlebitis. This problem often presents with fever and rigorous chills. Swelling and tenderness is noted over the affected vein in about half the cases. Obviously, though, inspection and palpation of the vena cava is challenging and such signs do not apply when these vessels are involved.
Respiratory distress due to septic pulmonary emboli and secondary pneumonia is common. Metastatic abscess formation at other sites, such as joint and bone, have been reported.1,6
You realize that most patients with suppurative thrombophlebitis present in a much more toxic state than yours did. Perhaps you caught it early. She certainly has risk factors, including her recent pharyngitis and central venous catheterization. The prominent collateral circulation raises the possibility that this may have developed subacutely, following a more indolent course than is generally reported.
The organisms responsible for suppurative thrombophlebitis depend on the infection’s site of origin. Most of the time in the peripheral veins or vena cava, Staphylococcus, a member of normal skin flora, is the pathogen. Streptococcus, Enterobacteriaceae, Candida, and even cytomegalovirus have been documented.4,7,8 Jugular septic thrombophlebitis draws from the oral flora, with the most common causative agent being the anaerobic Fusobacterium.
A thrombus provides an excellent source of nutrients for the microbes, which colonize it and establish what is essentially a biofilm. These complex microbial architectures are extraordinarily resistant to antibiotic therapy, especially when compared with plantonic bacteria.9 Not only does the thrombus facilitate the infection, but the bacteria facilitate thrombus formation by promoting platelet aggregation.10
A:
Chemotherapy is only one of the many circumstances in which central venous access is required. Central venous access devices (CVADs) are also used for administration of antibiotics, hydration, total parenteral nutrition, or long-term blood sampling.
The central lines that most family physicians learned to insert during residency are only one of a dizzying array of CVADs in use. The triple-lumen lines are inserted transcutaneously by the resident into either the jugular or subclavian veins and are good for short-to-medium duration therapies. They require diligent care to prevent occlusion or infection, including daily flushing.
For longer-duration therapies, tunneled catheters may be placed, typically by surgical consultants. These are less prone to bleeding or infection but still require diligent attention and regular flushing. Some models do permit weekly flushing.
Peripherally-inserted central venous catheters (PICCs) may be used for up to a year. Generally inserted by nursing staff, they are still fairly high-maintenance and require daily flushes.
Representative venous access devices. Clockwise from upper left: triple lumen catheter, tunneled catheter, subcutaneous port, PICC.
Your patient had a subcutaneous CVAD, which is often called a “port.” It is surgically implanted, not unlike a pacemaker, and is ideal for long-term use, especially when required access is intermittent. It requires flushing only monthly (weekly when being accessed).
Medication or surgery?
Because of its resistance to antibiotic treatment, peripheral venous suppurative thrombophlebitis is a surgical disease, not unlike an abscess, and requires excision or incision and drainage of the affected vessel. Antibiotics alone are inadequate. Excision of thrombophlebitis of the central veins affected is not feasible (though thrombectomies are occasionally undertaken). In this case, prolonged antibiotic therapy is indicated.
Anticoagulation may also be considered, though no strong evidence supports that addition. Given the effect of Fusobacterium on platelet aggregation, aspirin might be expected to provide benefit. In vitro studies show inhibition of this aggregation with aspirin,10 but no clinical studies or even case reports indicate improved outcomes with its use.
A hospital stay
Prolonged antibiotics
You admit the patient to the hospital with a presumptive diagnosis of Lemierre’s syndrome and begin piperacillin/tazobactam intravenously, covering both Fusobacterium and Staphlococcus. You also opt to begin heparin and resume her warfarin, more for her history of DVT than because of documented benefit of anticoagulation in the management of suppurative thrombophlebitis.
An awareness of potential complications is vital before undertaking any medical intervention. Although it would be unusual for a family physician to place a port, insertion of central venous lines is a commonly performed procedure that shares many of the same risks. fortunately, septic thrombophlebitis is a rare complication; unfortunately, a variety of other complications may occur. These include hemorrhage, venous thrombosis (uninfected), extravascular hematoma, local or systemic infection, pneumo- hydro- hemo- or chylo-thorax, air embolus, catheter fragment embolus, nerve injury, arteriovenous fistula, and cardiac arrhythmias or tamponade. The likelihood of complications from this procedure can be diminished by strict adherence to aseptic technique, and a thorough knowledge of the surrounding anatomy. Contraindications include distorted anatomy, suspected superior vena cava injury, compromise (such as pneumothorax on the side contralateral to the planned insertion site), infection or full-thickness burns at the planned insertion site, and coagulopathy.
—Mark Huntington, MD
Anticoagulation
Over the course of her hospital stay, she spikes a fever (≥100°F) every 24 hours for the first 5 days, after which the peak temperatures slowly drop to normal. She reaches therapeutic levels on warfarin and the heparin is discontinued. At no point do any respiratory symptoms develop. Aerobic blood cultures show no growth; to your chagrin, you find out that anaerobic cultures were not obtained. After 8 days, the patient’s neck is no longer tender, the swelling has gone down, she’s adequately anticoagulated, has been afebrile for 48 hours, and is extremely eager to go home.
She is discharged with a prescription of amoxicillin/clavulanate 3 times daily for 4 weeks, as the literature suggests that most Fusobacterium are sensitive to this agent.11 She is instructed to return if any recurrent fevers, chest pain, or respiratory symptoms develop. At a routine follow-up appointment in a month, she remains asymptomatic.
1. Sinave CP, Hardy GJ, Fardy PW. The lemierre Syndrome: suppurative thrombophlebitis of the internal jugular vein secondary to oropharyngeal infection. Medicine (Baltimore) 1989;68:85-94.
2. Ely EW, Stump TE, Hudspeth AS, Haponik EF. Thoracic complications of dental surgical procedures: hazards of the dental drill. Am J Med 1993;95:456-465.
3. Andres DR, Urban AW, Acher CW, Maki DG. Septic thrombosis of the basilic, axillary, and subclavian veins caused by a peripherally inserted central venous catheter. Am J Med 1998;105:446-450.
4. Strinden WD, Helgerson RB, Maki DG. Candida septic thrombosis of the great central veins associated with central catheters. Clinical features and management. Ann Surg 1985;202:653-658.
5. Garcia J, Aboujaoude R, Apuzzio J, Alvares JR. Septic pelvic thrombophlebitis: diagnosis and management. Infect Dis Obstetr Gynecol 2006;2006:1-4.
6. Pruitt BA, Jr, McManus WF, Kim SH, Treat RC. Diagnosis and treatment of cannula-related intravenous sepsis in burn patients. Ann Surg 1980;191:546-554.
7. Baker CC, Petersen SR, Sheldon GF. Septic phlebitis: a neglected disease. Am J Surg 1979;138:97-103.
8. Peterson P, Stahl-Bayliss CM. Cytomegalovirus thrombophlebitis after successful DHPG therapy [letter]. Ann Intern Med 1987;106:632-633.
9. Parsek MR, Singh PK. Bacterial biofilms: an emerging link to disease pathogenesis. Ann Rev Microbiol 2003;57:677-701.
10. Forrester LJ, Campbell BJ, Berg JN, Barrett JT. Aggregation of platelets by Fusobacterium necrophorum. J Clin Micro 1985;22:245-249.
11. Kuriyama T, Karasawa T, Nakagawa K, Yamamoto E, Nakamura S. Incidence of beta-lactamase production and antimicrobial susceptibility of anaerobic gram-negative rods isolated from pus specimens of orofacial odontogenic infections. Oral Microbiol Immunol 2001;16:10-15.
CORRESPONDENCE: Mark K. Huntington, MD, PhD, Center for Family Medicine, 1115 East 20th Street, Sioux Falls, SD 57105. E-mail: [email protected]
1. Sinave CP, Hardy GJ, Fardy PW. The lemierre Syndrome: suppurative thrombophlebitis of the internal jugular vein secondary to oropharyngeal infection. Medicine (Baltimore) 1989;68:85-94.
2. Ely EW, Stump TE, Hudspeth AS, Haponik EF. Thoracic complications of dental surgical procedures: hazards of the dental drill. Am J Med 1993;95:456-465.
3. Andres DR, Urban AW, Acher CW, Maki DG. Septic thrombosis of the basilic, axillary, and subclavian veins caused by a peripherally inserted central venous catheter. Am J Med 1998;105:446-450.
4. Strinden WD, Helgerson RB, Maki DG. Candida septic thrombosis of the great central veins associated with central catheters. Clinical features and management. Ann Surg 1985;202:653-658.
5. Garcia J, Aboujaoude R, Apuzzio J, Alvares JR. Septic pelvic thrombophlebitis: diagnosis and management. Infect Dis Obstetr Gynecol 2006;2006:1-4.
6. Pruitt BA, Jr, McManus WF, Kim SH, Treat RC. Diagnosis and treatment of cannula-related intravenous sepsis in burn patients. Ann Surg 1980;191:546-554.
7. Baker CC, Petersen SR, Sheldon GF. Septic phlebitis: a neglected disease. Am J Surg 1979;138:97-103.
8. Peterson P, Stahl-Bayliss CM. Cytomegalovirus thrombophlebitis after successful DHPG therapy [letter]. Ann Intern Med 1987;106:632-633.
9. Parsek MR, Singh PK. Bacterial biofilms: an emerging link to disease pathogenesis. Ann Rev Microbiol 2003;57:677-701.
10. Forrester LJ, Campbell BJ, Berg JN, Barrett JT. Aggregation of platelets by Fusobacterium necrophorum. J Clin Micro 1985;22:245-249.
11. Kuriyama T, Karasawa T, Nakagawa K, Yamamoto E, Nakamura S. Incidence of beta-lactamase production and antimicrobial susceptibility of anaerobic gram-negative rods isolated from pus specimens of orofacial odontogenic infections. Oral Microbiol Immunol 2001;16:10-15.
CORRESPONDENCE: Mark K. Huntington, MD, PhD, Center for Family Medicine, 1115 East 20th Street, Sioux Falls, SD 57105. E-mail: [email protected]