User login
- Only symptomatic hemorrhoids require treatment. Most patients can be treated with conservative therapy alone or an office procedure.
- Anoscopy detects more lesions in the anorectal region than does flexible sigmoidoscopy. Visualization is best achieved with the slotted anoscope.
- Rubber band ligation is the preferred office procedure for treatment of grade I/II hemorrhoids that do not respond to medical therapy, and treatment of all grade III hemorrhoids.
Most cases of hemorrhoids can be managed in the primary care setting with simple measures and office procedures, including anoscopy. This paper reviews the advantages, disadvantages, and levels of evidence regarding specific treatments for different grades of hemorrhoids.
Prevalence
Prevalence varies from 4.4% in the general population to 36.4% in general practice.1 The annual rate of office visits for hemorrhoids is 12 for every 1000 patients in the United States2 ; its prevalence is similar between the sexes and increases with age until the seventh decade.3,4 Only a third of patients with symptomatic hemorrhoids seek medical help.4
Characteristics
Hemorrhoidal padding, which is critical to maintaining continence, accounts for approximately 15% to 20% of the anal resting pressure and supplies important sensory information that enables the differentiation between liquid, solid, and gas. When an individual coughs or performs a Valsalva maneuver, this vascular padding increases in area and volume, thereby enabling the anal canal to remain closed and avoid the loss of stools.
Hemorrhoids are associated with chronic straining secondary to constipation, diarrhea, tenesmus, or long periods trying to defecate, and are common during pregnancy and child-birth.5 The pathophysiology is not clearly understood, but current theories suggest that structural or vascular changes may be involved.
The mucocutaneous junction of the ano-rectum, or dentate line, divides hemorrhoids anatomically into internal (above the junction) and external (below). This anatomic “border” is of special clinical interest because external pain fibers end at this point, and most people have no sensation above this line.
Hemorrhoids originating above the junction, even if prolapsed, are still classified as internal hemorrhoids, and are divided into 4 categories depending on the grade of prolapse:
- Grade I—Protrudes into the anal canal but does not prolapse
- Grade II—Prolapses but reduces spontaneously
- Grade III—Prolapses and requires manual reduction
- Grade IV—Irreducible prolapse.
Hemorrhoids, especially if external, sometimes thrombose (Figure 1). Distention of overlying perianal skin and inflammation associated with the process of thrombosis can cause severe pain and discomfort.
FIGURE 1
Thrombosed hemorrhoids Anoscopy 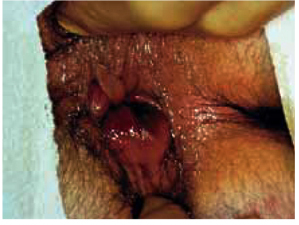
Thrombosis can be particularly painful due to distention of perianal skin and inflammation. Used with permission, National Procedures Institute, Midland, Mich.
Diagnosis
Symptoms
The most common symptoms of hemorrhoids are bleeding and prolapse. Less frequently, symptoms also include discomfort, pain, soiling, or itching.
Internal hemorrhoids are usually painless; bleeding or prolapse generally prompt a visit to the physician. Bleeding is described as bright red spotting on toilet tissue or as dripping in the toilet bowl and normally occurs at the end of defecation and separately from the stool.
External hemorrhoids may be asymptomatic, associated with discomfort, or a cause of acute pain in the event of a thrombosis. They generally do not bleed except in the case of a spontaneously resolved local thrombosis. Some individuals may have both types of hemorrhoids simultaneously (mixed).
The term hemorrhoids is commonly misused by patients to refer to any anal symptoms. Other diagnoses such as anal fissures, pruritus ani, abscess, fistula, and condyloma should be ruled out by examining the anus, the perianal region, and the anal canal. However, we have found no studies reporting on the accuracy of the medical history or the physical examination.
How to conduct a digital examination
The patient should be positioned in the left lateral decubitus position for the anorectal exam-ination.6 This position is more comfortable and less intimidating for the patient than the traditional head-down position, and it permits optimal visualization.
Digital palpation allows the entire circumference of the canal to be examined and rectal masses or tender points to be ruled out. Internal hem-orrhoids cannot be detected this way, however.6 The procedure, which must be done gently and with prior reassurance to the patient, is generally quite simple. Intense pain may prevent further examination and suggests the possibility of anal fissure or thrombosed external hemorrhoid.
Anoscopy: safe and essential office procedure
The most accurate method for examining the anal canal and distal rectum is anoscopy. Although several types of anoscopes are available, visualization is best achieved with the slotted anoscope (Figure 2).6 Once it has been inserted, the anoscope is gradually withdrawn while rotating right and left to allow inspection of the mucous membrane. Hemorrhoids appear as pink swellings of the mucosa. Ask the patient to strain during the examination to improve visualization.
Two prospective studies found that anoscopy detects a higher percentage of lesions in the anorectal region than does flexible sigmoidoscopy (99% vs 78%).7,8 It is the procedure of choice for evaluating rectal diseases.
In skilled hands, anoscopy is safe; complications are unusual, and it can be performed in a physician’s office on short notice and without bowel preparation. After appropriate training, primary care physicians can perform routine examinations safely and accurately.
FIGURE 2
Anoscopy
The slotted anoscope provides the best visualization. Used with permission, National Procedures Institute, Midland, Mich.
Office-Based Treatment
Primary care physicians can safely use simple treatment measures to manage most cases of symptomatic hemorrhoids (Figure 3). Only the more symptomatic patients require surgical intervention.
Patients should be made aware of the nature of the condition and the advantages and disadvantages of the different treatment options. The evidence regarding these treatments is summarized in the Table.
FIGURE 3
Management of adult patients with hemorrhoids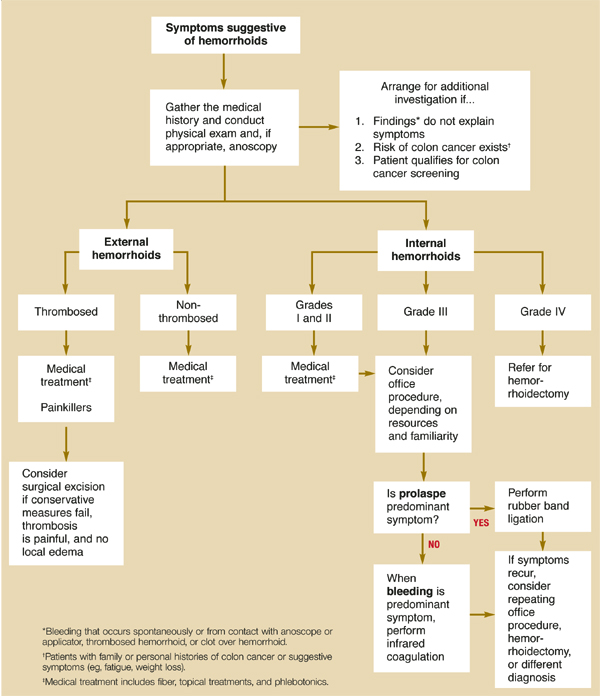
TABLE
Medical and surgical treatments for hemorrhoids
| Treatment | SOR* | Indication | Comments |
|---|---|---|---|
| Analgesics and anti-inflammatories2 | D | Grades I–IV and thrombosed external hemorrhoids | No trials comparing analgesics with anti-inflammatories |
| Topical treatments with corticosteroids or anesthetics3 | D | Grades I–III | No controlled trials with placebo are available, but patients report empiric benefit with their use; use only for brief periods |
| High-fiber diet or fiber supplements10-13 | B | Grades I–II | NNT=2.8 for reduction of rectal bleeding and 3.6 for pain relief23 |
| Office procedures23-25 | A | Grades I and II that do not respond to medical therapy, and grade III | Rubber band ligation was more effective and required fewer additional treatments for symptomatic recurrence than did infrared coagulation (NNT=9) and sclerotherapy (NNT=6.9); but rubber band ligation produced more complications than did infrared coagulation (pain: NNH=6) |
| Phlebotonics14-21 | B | Grades I–II | Moderate reduction of duration of bleeding during acute episodes of internal hemorrhoids; conflicting results for other outcomes (pain and prolapse) |
| Hemorrhoidectomy24 | A | Grades II–IV | Hemorrhoidectomy is more effective than office procedures, but it is more painful and presents more complications; office procedures are cheaper and require no time off from work |
| Stapling technique31-36 | A | Grades III–IV | Stapling technique is as effective as hemorrhoidectomy, is less painful, and requires less time off from work; more long-term data are needed37 |
| *For an explanation of strength of recommendation, see page 379. | |||
| SOR, strength of recommendation; NNT, number needed to treat; NNH, number needed to harm | |||
Benefits of lifestyle changes
The main purpose of lifestyle changes is to minimize prolonged straining during bowel movements, which is thought to contribute to the development of hemorrhoids. Such changes include increasing the amount of fiber in the diet, which is especially helpful for grade I and II internal hemorrhoids. Preventing constipation also helps alleviate more severe hemorrhoids and can help to prevent future episodes.10
Rectal bleeding can mask the diagnosis of cancer. The probability of colorectal cancer increases in the elderly, those with a family or personal history of colorectal cancer, and those with any other symptoms of colorectal cancer (fatigue, weight loss, palpable tumor, anemia). Patients at risk need a more thorough evaluation, including endoscopy, to rule out malignancy.9
It is important to document that observed hemorrhoids account for the bleeding episode (bleeding at the contact site with the anoscope or an applicator, thrombosed hemorrhoids, or a clot over the hemorrhoid).
Several clinical trials have reported the benefits of a high-fiber diet or fiber supplements compared with placebo in relieving pain, bleeding, and prolapse (strength of recommendation [SOR]: B).10-13 We found no studies comparing the different types of bulk laxatives.
Although the role of certain foods in the pathogenesis of hemorrhoids or their acute exacerbation is accepted empirically, this has not been proved. Also, no firm evidence to date shows that increasing physical exercise, limiting time on the commode, or improving local hygiene are beneficial. However, these measures are usually recommended because they have other health benefits or are thought to do no harm (SOR: D).
Medical therapy
No rigorous evidence exists to support the use of topical therapies, physical or pharmacologic (sitz baths, anesthetics, phlebotonics, corticoids, or ice). Most studies have employed poor methods, lacked placebo control, and addressed heterogeneous preparations with multiple associated components. It is therefore not possible to formulate firm recommendations.
Soothing agents. Popular topical soothing agents are often combined with corticosteroids or anesthetics and are available over the counter as creams or enemas. Many patients report some empirical benefit with their use, especially corticosteroids and anesthetics (SOR: D).3 Advise patients against prolonged use due to possible local allergic effects and sensitization of skin (SOR: D).
Phlebotonics. Several phlebotonics have been evaluated in the literature; diosmin is the best-studied agent, but it is not commercially available in the United States at this time. In studies of patients with acute attacks of internal hemorrhoids (grades I to II), the main perceived effect was reduced bleeding duration;14,15 the results were conflicting for other outcomes (mainly pain and prolapse)14-18 (SOR: B).
Other phlebotonics (the botanicals ginkgo biloba, troxerutin, and calcium dobesilate), when compared with placebo19,20 or diosmin,21 have shown similar effects (SOR: B). No studies thus far have evaluated the role of phlebotonics in thrombosis of external hemorrhoids.
Anti-inflammatories and analgesics. Most episodes of acute thrombosed external hemorrhoids improve spontaneously and therefore can be treated with symptomatic measures, including anti-inflammatory agents, analgesics, and stool softeners. Anti-inflammatories and analgesics can be effective during episodes of external and internal thromboses3 (SOR: D). Several clinical trials have reported benefits of fiber in relieving pain, bleeding, and prolapse
In a small randomized clinical trial, the addition of topical nifedipine (0.3%) to a lidocaine ointment (1.5%) was more effective than lidocaine alone in reducing pain and shortening resolution time.22
Surgical treatment
All office (nonoperative) and surgical procedures fix the sliding hemorrhoidal tissue back onto the muscle wall. The fixation takes place by directly promoting tissue fibrosis (eg, sclerotherapy or infrared coagulation) or by tissue destruction with subsequent fibrosis (eg, hemorrhoidectomy).
Office procedures. The most commonly used methods are rubber band ligation and infrared coagulation. Other methods include bipolar electrocoagulation, low-voltage direct current, sclerotherapy, laser therapy, and cryosurgery.
Two meta-analyses compared these nonoperative methods and concluded that rubber band ligation and infrared coagulation are the most effective. The first meta-analysis reported that ligation was more effective because it required fewer additional treatments for symptomatic recurrence than did coagulation (number needed to treat [NNT]=9) and sclerotherapy (NNT=6.9).23 However, ligation produced more complications than did coagulation (pain: number needed to harm=6) (SOR: A).
The second, more recent meta-analysis found ligation to have similar beneficial effect and a similar complication rate,24 although it was more painful. It appeared to be the therapy of choice for grades I to III (SOR: A). No difference was found between sclerotherapy and infrared coagulation for any outcome measure, but the authors of these meta-analyses commented that the overall quality of the studies was not high and their conclusions were therefore limited. One subsequent randomized clinical trial confirmed the advantages of rubber band ligation.25
In the event of a thrombosed hemorrhoid, whether to remove the clot promptly or wait for spontaneous resolution is controversial. We found no studies comparing these approaches. Excision should be performed when local measures fail, the thrombosis is painful, and there is no local edema (SOR: D).3
In the treatment of perianal thrombosis, one clinical trial found excision more effective than topically applied 0.2% glyceryl trinitrate or incision in reducing pain and the number of recurrences at 1 year (SOR: A).26 Residual hemorrhoidal tissue following an episode of acute thrombosis of external hemorrhoids also may cause symptoms, especially pruritus. These external anal tags can make it difficult to clean the anus and can be excised if symptoms warrant.
Surgery. Surgical treatment, though more invasive and expensive, is the most effective and definitive course for symptomatic hemorrhoids. The aim is to decrease blood flow to the anorectal ring and excise redundant hemorrhoidal tissue.
There are several techniques. In the United States, the Ferguson (closed) hemorrhoidectomy is preferred. The one used most commonly in Europe is the Milligan-Morgan technique (open). Both techniques have been shown to be similarly effective, although there is debate over healing time.27-30 Only a competently performed technique will produce satisfying results.
In their meta-analysis, MacRae and McLeod found that hemorrhoidectomy is more effective than all other treatment modalities, though complications such as pain and costs were greater (SOR: A).24
A new surgical procedure, the stapled hemorrhoidectomy, has been introduced as an alternative to the standard hemorrhoidectomy. Several randomized clinical trials have shown the procedure to be as effective, cause less pain, and require less time off from work compared with standard techniques (SOR: A).31-36 However, it is more expensive and requires advanced surgical skills. More long-term data are also needed.37
Anal stretch, or manual anal dilatation, has been reported to be effective in the treatment of hemorrhoids, but a high rate of incontinence after the procedure has led to abandonment of this technique.38,39 Antibiotic prophylaxis in colorectal surgery is highly recommended and has been shown to reduce infection and mortality (SOR: A).40
Surgery vs office procedures
Several clinical practice guidelines3,38 and meta-analyses23,24 have recommended office procedures for hemorrhoids of grades I through III. Although there is some discrepancy about the procedure of choice, rubber band ligation appears to be the most effective technique.
An evidence-based clinical practice guideline3 has recommended coagulation techniques for bleeding nonprolapsed hemorrhoids or those with a low grade of prolapse (grades I and II), and reserving rubber band ligation for hemorrhoids more severely prolapsed (grade III). The basis for this recommendation is that flat bleeding hemorrhoids may not provide enough tissue to grasp.
Surgical hemorrhoidectomy should be reserved for grade IV hemorrhoids and for grade III lesions that do not respond to other procedures.
This is an approximate rather than a rigid approach, and the final decision will depend on the physician’s technical training, the patient’s preferences, clinical circumstances, and local resources.
Prognosis: 90% require no surgery
Hemorrhoids are generally a chronic problem and tend to worsen with time. According to a retrospective cohort study, most patients will have several episodes during their lives; however, it can be considered a benign disorder, and approximately 90% of patients will not require surgery to alleviate their symptoms (SOR: B).41
It is worth noting that 26% of patients who require a hemorrhoidectomy may have a recurrence, and 11% will need further treatment.39 Similarly, approximately half of those who undergo office procedures may require further treatment or surgery in 5 to 10 years.42,43
ACKNOWLEDGMENTS
We thank E. Thompson for help in editing this manuscript and J. A. Ferrus and A. Hervas for their clinical comments. Dr Alonso-Coello holds a postgraduate research fellowship at the Instituto Carlos III, Spanish Ministry of Health, Spain.
Corresponding author
Pablo Alonso-Coello, MD, Ibero-american Cochrane Centre, Hospital de la Santa Creu i Sant Pau, Sant Antoni Mª Claret 171, 08041 Barcelona, Spain. E-mail: [email protected].
1. Hulme-Moir M, Bartolo DC. Hemorrhoids. Gastroenterol Clin North Am 2001;30:183-197.
2. Johanson JF, Sonnenberg A. Temporal changes in the occurrence of hemorrhoids in the United States and England. Dis Colon Rectum 1991;34:585-591.
3. Abramowitz L, Godeberge P, Staumont G, Soudan D. Clinical practice guidelines for the treatment of hemorrhoid disease [in French]. Gastroenterol Clin Biol 2001;25:674-702.
4. Johanson JF, Sonnenberg A. The prevalence of hemorrhoids and chronic constipation. An epidemiologic study. Gastroenterology 1990;98:380-386.
5. Beck DE. Hemorrhoidal disease. In: Beck DE, Wexner SD, eds. Fundamentals of Anorectal Surgery. 2nd ed. London: WB Saunders 1998;237-253.
6. Pfenninger JL, Zainea GG. Common anorectal conditions: part I. Symptoms and complaints. Am Fam Physician 2001;63:2391-2398.
7. Kelly SM, Sanowski RA, Foutch PG, Bellapravalu S, Haynes WC. A prospective comparison of anoscopy and fiber endoscopy in detecting anal lesions. J Clin Gastroenterol 1986;8:658-660.
8. Korkis AM, McDougall CJ. Rectal bleeding in patients less than 50 years of age. Dig Dis Sci 1995;40:1520-1523.
9. Wauters H, Van Casteren V, Buntinx F. Rectal bleeding and colorectal cancer in general practice: diagnostic study. BMJ 2000;321:998-999.
10. Moesgaard F, Nielsen ML, Hansen JB, Knudsen JT. High-fiber diet reduces bleeding and pain in patients with hemorrhoids: a double-blind trial of Vi-Siblin. Dis Colon Rectum 1982;25:454-456.
11. Broader JH, Gunn IF, Alexander-Williams J. Evaluation of a bulk-forming evacuant in the management of haemorrhoids. Br J Surg 1974;61:142-144.
12. Webster DJ, Gough DC, Craven JL. The use of bulk evacuant in patients with haemorrhoids. Br J Surg 1978;65:291-292.
13. Perez-Miranda M, Gomez-Cedenilla A, Leon-Colombo T, Pajares J, Mate-Jimenez J. Effect of fiber supplements on internal bleeding hemorrhoids. Hepatogastroenterology 1996;43:1504-1507.
14. Godeberge P. Daflon 500 mg in the treatment of hemorrhoidal disease: a demonstrated efficacy in comparison with placebo. Angiology 1994;45:574-578.
15. Ho YH, Tan M, Seow-Choen F. Micronized purified flavonidic fraction compared favorably with rubber band ligation and fiber alone in the management of bleeding hemorrhoids: randomized controlled trial. Dis Colon Rectum 2000;43:66-69.
16. Thanapongsathorn W, Vajrabukka T. Clinical trial of oral diosmin (Daflon) in the treatment of hemorrhoids. Dis Colon Rectum 1992;35:1085-1088.
17. Cospite M. Double-blind, placebo-controlled evaluation of clinical activity and safety of Daflon 500 mg in the treatment of acute hemorrhoids. Angiology 1994;45:566-573.
18. Misra MC, Parshad R. Randomized clinical trial of micronized flavonoids in the early control of bleeding from acute internal haemorrhoids. Br J Surg 2000;87:868-872.
19. Annoni F, Boccasanta P, Chiurazzi D, Mozzi E, Oberhauser V. Treatment of acute symptoms of hemorrhoid disease with high-dose oral O-(beta-hydroxyethyl)-rutosides [in Italian]. Minerva Med 1986;77:1663-1668
20. Mentes BB, Gorgul A, Tatlicioglu E, Ayoglu F, Unal S. Efficacy of calcium dobesilate in treating acute attacks of hemorrhoidal disease. Dis Colon Rectum 2001;44:1489-1495.
21. Debien P, Denis J. Traitements des signes fonctionnels de la maladie hèmorroïaigüe: essai multicentrique, randomisè, diosmine d’hèmisynthèse versus association extrait de Ginko biloba-heptaminol-troxèrutine. Med Chir Dig 1996;25:259-264.
22. Perrotti P, Antropoli C, Molino D, De Stefano G, Antropoli M. Conservative treatment of acute thrombosed external hemorrhoids with topical nifedipine. Dis Colon Rectum 2001;44:405-409.
23. Johanson JF, Rimm A. Optimal nonsurgical treatment of hemorrhoids: a comparative analysis of infrared coagulation, rubber band ligation, and injection sclerotherapy. Am J Gastroenterol 1992;87:1600-1606.
24. MacRae HM, McLeod RS. Comparison of hemorrhoidal treatment modalities. A meta-analysis. Dis Colon Rectum. 1995;38:687-694.
25. Poen AC, Felt-Bersma RJ, Cuesta MA, Deville W, Meuwissen SG. A randomized controlled trial of rubber band ligation versus infra-red coagulation in the treatment of internal haemorrhoids. Eur J Gastroenterol Hepatol 2000;12:535-539.
26. Cavcic J, Turcic J, Martinac P, Mestrovic T, Mladina R, Pezerovic-Panijan R. Comparison of topically applied 0.2% glyceryl trinitrate ointment, incision and excision in the treatment of perianal thrombosis. Dig Liver Dis 2001;33:335-340.
27. Ho YH, Seow-Choen F, Tan M, Leong AF. Randomized controlled trial of open and closed haemorrhoidectomy. Br J Surg 1997;84:1729-1730.
28. Carapeti EA, Kamm MA, McDonald PJ, Chadwick SJ, Phillips RK. Randomized trial of open versus closed day-case haemorrhoidectomy. Br J Surg 1999;86:612-613.
29. Arbman G, Krook H, Haapaniemi S. Closed vs. open hemorrhoidectomy—is there any difference? Dis Colon Rectum 2000;43:31-34.
30. Gencosmanoglu R, Sad O, Koc D, Inceoglu R. Hemorrhoidectomy: open or closed technique? A prospective, randomized clinical trial. Dis Colon Rectum 2002;45:70-75.
31. Mehigan BJ, Monson JR, Hartley JE. Stapling procedure for haemorrhoids versus Milligan-Morgan haemorrhoidectomy: randomised controlled trial. Lancet 2000;355:782-785.
32. Rowsell M, Bello M, Hemingway DM. Circumferential mucosectomy (stapled haemorrhoidectomy) versus conventional haemorrhoidectomy: randomised controlled trial. Lancet. 2000;355:779-781.
33. Khalil KH, O’Bichere A, Sellu D. Randomized clinical trial of sutured versus stapled closed haemorrhoidectomy. Br J Surg 2000;87:1352-1355.
34. Boccasanta P, Capretti PG, Venturi M, et al. Randomised controlled trial between stapled circumferential mucosectomy and conventional circular hemorrhoidectomy in advanced hemorrhoids with external mucosal prolapse. Am J Surg 2001;182:64-68.
35. Ganio E, Altomare DF, Gabrielli F, Milito G, Canuti S. Prospective randomized multicentre trial comparing stapled with open haemorrhoidectomy. Br J Surg 2001;88:669-674.
36. Shalaby R, Desoky A. Randomized clinical trial of stapled versus Milligan-Morgan haemorrhoidectomy. Br J Surg 2001;88:1049-1053.
37. Hetzer FH, Demartines N, Handschin AE, Clavien PA. Stapled vs excision hemorrhoidectomy: long-term results of a prospective randomized trial. Arch Surg 2002;137:337-340.
38. Standards Task Force of American Society of Colon and Rectal Surgeons Practice parameters for the treatment of hemorrhoids. Dis Colon Rectum 1993;36:1118-1120.
39. Konsten J, Baeten CG. Hemorrhoidectomy vs. Lord’s method: 17-year follow-up of a prospective, randomized trial. Dis Colon Rectum 2000;43:503-506.
40. Baum ML, Anish DS, Chalmers TC, Sacks HS, Smith H, Fagerstrom RM. A survey of clinical trials of antibiotic prophylaxis in colon surgery: evidence against further use of no-treatment controls. N Engl J Med 1981;305:795-799.
41. Bleday R, Pena JP, Rothenberger DA, Goldberg SM, Buls JG. Symptomatic hemorrhoids: current incidence and complications of operative therapy. Dis Colon Rectum 1992;35:477-481.
42. Wrobleski DE, Corman ML, Veidenheimer MC, Coller JA. Long-term evaluation of rubber ring ligation in hemorrhoidal disease. Dis Colon Rectum 1980;23:478-482.
43. Savioz D, Roche B, Glauser T, Dobrinov A, Ludwig C, Marti MC. Rubber band ligation of hemorrhoids: relapse as a function of time. Int J Colorectal Dis 1998;13:154-156.
- Only symptomatic hemorrhoids require treatment. Most patients can be treated with conservative therapy alone or an office procedure.
- Anoscopy detects more lesions in the anorectal region than does flexible sigmoidoscopy. Visualization is best achieved with the slotted anoscope.
- Rubber band ligation is the preferred office procedure for treatment of grade I/II hemorrhoids that do not respond to medical therapy, and treatment of all grade III hemorrhoids.
Most cases of hemorrhoids can be managed in the primary care setting with simple measures and office procedures, including anoscopy. This paper reviews the advantages, disadvantages, and levels of evidence regarding specific treatments for different grades of hemorrhoids.
Prevalence
Prevalence varies from 4.4% in the general population to 36.4% in general practice.1 The annual rate of office visits for hemorrhoids is 12 for every 1000 patients in the United States2 ; its prevalence is similar between the sexes and increases with age until the seventh decade.3,4 Only a third of patients with symptomatic hemorrhoids seek medical help.4
Characteristics
Hemorrhoidal padding, which is critical to maintaining continence, accounts for approximately 15% to 20% of the anal resting pressure and supplies important sensory information that enables the differentiation between liquid, solid, and gas. When an individual coughs or performs a Valsalva maneuver, this vascular padding increases in area and volume, thereby enabling the anal canal to remain closed and avoid the loss of stools.
Hemorrhoids are associated with chronic straining secondary to constipation, diarrhea, tenesmus, or long periods trying to defecate, and are common during pregnancy and child-birth.5 The pathophysiology is not clearly understood, but current theories suggest that structural or vascular changes may be involved.
The mucocutaneous junction of the ano-rectum, or dentate line, divides hemorrhoids anatomically into internal (above the junction) and external (below). This anatomic “border” is of special clinical interest because external pain fibers end at this point, and most people have no sensation above this line.
Hemorrhoids originating above the junction, even if prolapsed, are still classified as internal hemorrhoids, and are divided into 4 categories depending on the grade of prolapse:
- Grade I—Protrudes into the anal canal but does not prolapse
- Grade II—Prolapses but reduces spontaneously
- Grade III—Prolapses and requires manual reduction
- Grade IV—Irreducible prolapse.
Hemorrhoids, especially if external, sometimes thrombose (Figure 1). Distention of overlying perianal skin and inflammation associated with the process of thrombosis can cause severe pain and discomfort.
FIGURE 1
Thrombosed hemorrhoids Anoscopy
Thrombosis can be particularly painful due to distention of perianal skin and inflammation. Used with permission, National Procedures Institute, Midland, Mich.
Diagnosis
Symptoms
The most common symptoms of hemorrhoids are bleeding and prolapse. Less frequently, symptoms also include discomfort, pain, soiling, or itching.
Internal hemorrhoids are usually painless; bleeding or prolapse generally prompt a visit to the physician. Bleeding is described as bright red spotting on toilet tissue or as dripping in the toilet bowl and normally occurs at the end of defecation and separately from the stool.
External hemorrhoids may be asymptomatic, associated with discomfort, or a cause of acute pain in the event of a thrombosis. They generally do not bleed except in the case of a spontaneously resolved local thrombosis. Some individuals may have both types of hemorrhoids simultaneously (mixed).
The term hemorrhoids is commonly misused by patients to refer to any anal symptoms. Other diagnoses such as anal fissures, pruritus ani, abscess, fistula, and condyloma should be ruled out by examining the anus, the perianal region, and the anal canal. However, we have found no studies reporting on the accuracy of the medical history or the physical examination.
How to conduct a digital examination
The patient should be positioned in the left lateral decubitus position for the anorectal exam-ination.6 This position is more comfortable and less intimidating for the patient than the traditional head-down position, and it permits optimal visualization.
Digital palpation allows the entire circumference of the canal to be examined and rectal masses or tender points to be ruled out. Internal hem-orrhoids cannot be detected this way, however.6 The procedure, which must be done gently and with prior reassurance to the patient, is generally quite simple. Intense pain may prevent further examination and suggests the possibility of anal fissure or thrombosed external hemorrhoid.
Anoscopy: safe and essential office procedure
The most accurate method for examining the anal canal and distal rectum is anoscopy. Although several types of anoscopes are available, visualization is best achieved with the slotted anoscope (Figure 2).6 Once it has been inserted, the anoscope is gradually withdrawn while rotating right and left to allow inspection of the mucous membrane. Hemorrhoids appear as pink swellings of the mucosa. Ask the patient to strain during the examination to improve visualization.
Two prospective studies found that anoscopy detects a higher percentage of lesions in the anorectal region than does flexible sigmoidoscopy (99% vs 78%).7,8 It is the procedure of choice for evaluating rectal diseases.
In skilled hands, anoscopy is safe; complications are unusual, and it can be performed in a physician’s office on short notice and without bowel preparation. After appropriate training, primary care physicians can perform routine examinations safely and accurately.
FIGURE 2
Anoscopy
The slotted anoscope provides the best visualization. Used with permission, National Procedures Institute, Midland, Mich.
Office-Based Treatment
Primary care physicians can safely use simple treatment measures to manage most cases of symptomatic hemorrhoids (Figure 3). Only the more symptomatic patients require surgical intervention.
Patients should be made aware of the nature of the condition and the advantages and disadvantages of the different treatment options. The evidence regarding these treatments is summarized in the Table.
FIGURE 3
Management of adult patients with hemorrhoids
TABLE
Medical and surgical treatments for hemorrhoids
| Treatment | SOR* | Indication | Comments |
|---|---|---|---|
| Analgesics and anti-inflammatories2 | D | Grades I–IV and thrombosed external hemorrhoids | No trials comparing analgesics with anti-inflammatories |
| Topical treatments with corticosteroids or anesthetics3 | D | Grades I–III | No controlled trials with placebo are available, but patients report empiric benefit with their use; use only for brief periods |
| High-fiber diet or fiber supplements10-13 | B | Grades I–II | NNT=2.8 for reduction of rectal bleeding and 3.6 for pain relief23 |
| Office procedures23-25 | A | Grades I and II that do not respond to medical therapy, and grade III | Rubber band ligation was more effective and required fewer additional treatments for symptomatic recurrence than did infrared coagulation (NNT=9) and sclerotherapy (NNT=6.9); but rubber band ligation produced more complications than did infrared coagulation (pain: NNH=6) |
| Phlebotonics14-21 | B | Grades I–II | Moderate reduction of duration of bleeding during acute episodes of internal hemorrhoids; conflicting results for other outcomes (pain and prolapse) |
| Hemorrhoidectomy24 | A | Grades II–IV | Hemorrhoidectomy is more effective than office procedures, but it is more painful and presents more complications; office procedures are cheaper and require no time off from work |
| Stapling technique31-36 | A | Grades III–IV | Stapling technique is as effective as hemorrhoidectomy, is less painful, and requires less time off from work; more long-term data are needed37 |
| *For an explanation of strength of recommendation, see page 379. | |||
| SOR, strength of recommendation; NNT, number needed to treat; NNH, number needed to harm | |||
Benefits of lifestyle changes
The main purpose of lifestyle changes is to minimize prolonged straining during bowel movements, which is thought to contribute to the development of hemorrhoids. Such changes include increasing the amount of fiber in the diet, which is especially helpful for grade I and II internal hemorrhoids. Preventing constipation also helps alleviate more severe hemorrhoids and can help to prevent future episodes.10
Rectal bleeding can mask the diagnosis of cancer. The probability of colorectal cancer increases in the elderly, those with a family or personal history of colorectal cancer, and those with any other symptoms of colorectal cancer (fatigue, weight loss, palpable tumor, anemia). Patients at risk need a more thorough evaluation, including endoscopy, to rule out malignancy.9
It is important to document that observed hemorrhoids account for the bleeding episode (bleeding at the contact site with the anoscope or an applicator, thrombosed hemorrhoids, or a clot over the hemorrhoid).
Several clinical trials have reported the benefits of a high-fiber diet or fiber supplements compared with placebo in relieving pain, bleeding, and prolapse (strength of recommendation [SOR]: B).10-13 We found no studies comparing the different types of bulk laxatives.
Although the role of certain foods in the pathogenesis of hemorrhoids or their acute exacerbation is accepted empirically, this has not been proved. Also, no firm evidence to date shows that increasing physical exercise, limiting time on the commode, or improving local hygiene are beneficial. However, these measures are usually recommended because they have other health benefits or are thought to do no harm (SOR: D).
Medical therapy
No rigorous evidence exists to support the use of topical therapies, physical or pharmacologic (sitz baths, anesthetics, phlebotonics, corticoids, or ice). Most studies have employed poor methods, lacked placebo control, and addressed heterogeneous preparations with multiple associated components. It is therefore not possible to formulate firm recommendations.
Soothing agents. Popular topical soothing agents are often combined with corticosteroids or anesthetics and are available over the counter as creams or enemas. Many patients report some empirical benefit with their use, especially corticosteroids and anesthetics (SOR: D).3 Advise patients against prolonged use due to possible local allergic effects and sensitization of skin (SOR: D).
Phlebotonics. Several phlebotonics have been evaluated in the literature; diosmin is the best-studied agent, but it is not commercially available in the United States at this time. In studies of patients with acute attacks of internal hemorrhoids (grades I to II), the main perceived effect was reduced bleeding duration;14,15 the results were conflicting for other outcomes (mainly pain and prolapse)14-18 (SOR: B).
Other phlebotonics (the botanicals ginkgo biloba, troxerutin, and calcium dobesilate), when compared with placebo19,20 or diosmin,21 have shown similar effects (SOR: B). No studies thus far have evaluated the role of phlebotonics in thrombosis of external hemorrhoids.
Anti-inflammatories and analgesics. Most episodes of acute thrombosed external hemorrhoids improve spontaneously and therefore can be treated with symptomatic measures, including anti-inflammatory agents, analgesics, and stool softeners. Anti-inflammatories and analgesics can be effective during episodes of external and internal thromboses3 (SOR: D). Several clinical trials have reported benefits of fiber in relieving pain, bleeding, and prolapse
In a small randomized clinical trial, the addition of topical nifedipine (0.3%) to a lidocaine ointment (1.5%) was more effective than lidocaine alone in reducing pain and shortening resolution time.22
Surgical treatment
All office (nonoperative) and surgical procedures fix the sliding hemorrhoidal tissue back onto the muscle wall. The fixation takes place by directly promoting tissue fibrosis (eg, sclerotherapy or infrared coagulation) or by tissue destruction with subsequent fibrosis (eg, hemorrhoidectomy).
Office procedures. The most commonly used methods are rubber band ligation and infrared coagulation. Other methods include bipolar electrocoagulation, low-voltage direct current, sclerotherapy, laser therapy, and cryosurgery.
Two meta-analyses compared these nonoperative methods and concluded that rubber band ligation and infrared coagulation are the most effective. The first meta-analysis reported that ligation was more effective because it required fewer additional treatments for symptomatic recurrence than did coagulation (number needed to treat [NNT]=9) and sclerotherapy (NNT=6.9).23 However, ligation produced more complications than did coagulation (pain: number needed to harm=6) (SOR: A).
The second, more recent meta-analysis found ligation to have similar beneficial effect and a similar complication rate,24 although it was more painful. It appeared to be the therapy of choice for grades I to III (SOR: A). No difference was found between sclerotherapy and infrared coagulation for any outcome measure, but the authors of these meta-analyses commented that the overall quality of the studies was not high and their conclusions were therefore limited. One subsequent randomized clinical trial confirmed the advantages of rubber band ligation.25
In the event of a thrombosed hemorrhoid, whether to remove the clot promptly or wait for spontaneous resolution is controversial. We found no studies comparing these approaches. Excision should be performed when local measures fail, the thrombosis is painful, and there is no local edema (SOR: D).3
In the treatment of perianal thrombosis, one clinical trial found excision more effective than topically applied 0.2% glyceryl trinitrate or incision in reducing pain and the number of recurrences at 1 year (SOR: A).26 Residual hemorrhoidal tissue following an episode of acute thrombosis of external hemorrhoids also may cause symptoms, especially pruritus. These external anal tags can make it difficult to clean the anus and can be excised if symptoms warrant.
Surgery. Surgical treatment, though more invasive and expensive, is the most effective and definitive course for symptomatic hemorrhoids. The aim is to decrease blood flow to the anorectal ring and excise redundant hemorrhoidal tissue.
There are several techniques. In the United States, the Ferguson (closed) hemorrhoidectomy is preferred. The one used most commonly in Europe is the Milligan-Morgan technique (open). Both techniques have been shown to be similarly effective, although there is debate over healing time.27-30 Only a competently performed technique will produce satisfying results.
In their meta-analysis, MacRae and McLeod found that hemorrhoidectomy is more effective than all other treatment modalities, though complications such as pain and costs were greater (SOR: A).24
A new surgical procedure, the stapled hemorrhoidectomy, has been introduced as an alternative to the standard hemorrhoidectomy. Several randomized clinical trials have shown the procedure to be as effective, cause less pain, and require less time off from work compared with standard techniques (SOR: A).31-36 However, it is more expensive and requires advanced surgical skills. More long-term data are also needed.37
Anal stretch, or manual anal dilatation, has been reported to be effective in the treatment of hemorrhoids, but a high rate of incontinence after the procedure has led to abandonment of this technique.38,39 Antibiotic prophylaxis in colorectal surgery is highly recommended and has been shown to reduce infection and mortality (SOR: A).40
Surgery vs office procedures
Several clinical practice guidelines3,38 and meta-analyses23,24 have recommended office procedures for hemorrhoids of grades I through III. Although there is some discrepancy about the procedure of choice, rubber band ligation appears to be the most effective technique.
An evidence-based clinical practice guideline3 has recommended coagulation techniques for bleeding nonprolapsed hemorrhoids or those with a low grade of prolapse (grades I and II), and reserving rubber band ligation for hemorrhoids more severely prolapsed (grade III). The basis for this recommendation is that flat bleeding hemorrhoids may not provide enough tissue to grasp.
Surgical hemorrhoidectomy should be reserved for grade IV hemorrhoids and for grade III lesions that do not respond to other procedures.
This is an approximate rather than a rigid approach, and the final decision will depend on the physician’s technical training, the patient’s preferences, clinical circumstances, and local resources.
Prognosis: 90% require no surgery
Hemorrhoids are generally a chronic problem and tend to worsen with time. According to a retrospective cohort study, most patients will have several episodes during their lives; however, it can be considered a benign disorder, and approximately 90% of patients will not require surgery to alleviate their symptoms (SOR: B).41
It is worth noting that 26% of patients who require a hemorrhoidectomy may have a recurrence, and 11% will need further treatment.39 Similarly, approximately half of those who undergo office procedures may require further treatment or surgery in 5 to 10 years.42,43
ACKNOWLEDGMENTS
We thank E. Thompson for help in editing this manuscript and J. A. Ferrus and A. Hervas for their clinical comments. Dr Alonso-Coello holds a postgraduate research fellowship at the Instituto Carlos III, Spanish Ministry of Health, Spain.
Corresponding author
Pablo Alonso-Coello, MD, Ibero-american Cochrane Centre, Hospital de la Santa Creu i Sant Pau, Sant Antoni Mª Claret 171, 08041 Barcelona, Spain. E-mail: [email protected].
- Only symptomatic hemorrhoids require treatment. Most patients can be treated with conservative therapy alone or an office procedure.
- Anoscopy detects more lesions in the anorectal region than does flexible sigmoidoscopy. Visualization is best achieved with the slotted anoscope.
- Rubber band ligation is the preferred office procedure for treatment of grade I/II hemorrhoids that do not respond to medical therapy, and treatment of all grade III hemorrhoids.
Most cases of hemorrhoids can be managed in the primary care setting with simple measures and office procedures, including anoscopy. This paper reviews the advantages, disadvantages, and levels of evidence regarding specific treatments for different grades of hemorrhoids.
Prevalence
Prevalence varies from 4.4% in the general population to 36.4% in general practice.1 The annual rate of office visits for hemorrhoids is 12 for every 1000 patients in the United States2 ; its prevalence is similar between the sexes and increases with age until the seventh decade.3,4 Only a third of patients with symptomatic hemorrhoids seek medical help.4
Characteristics
Hemorrhoidal padding, which is critical to maintaining continence, accounts for approximately 15% to 20% of the anal resting pressure and supplies important sensory information that enables the differentiation between liquid, solid, and gas. When an individual coughs or performs a Valsalva maneuver, this vascular padding increases in area and volume, thereby enabling the anal canal to remain closed and avoid the loss of stools.
Hemorrhoids are associated with chronic straining secondary to constipation, diarrhea, tenesmus, or long periods trying to defecate, and are common during pregnancy and child-birth.5 The pathophysiology is not clearly understood, but current theories suggest that structural or vascular changes may be involved.
The mucocutaneous junction of the ano-rectum, or dentate line, divides hemorrhoids anatomically into internal (above the junction) and external (below). This anatomic “border” is of special clinical interest because external pain fibers end at this point, and most people have no sensation above this line.
Hemorrhoids originating above the junction, even if prolapsed, are still classified as internal hemorrhoids, and are divided into 4 categories depending on the grade of prolapse:
- Grade I—Protrudes into the anal canal but does not prolapse
- Grade II—Prolapses but reduces spontaneously
- Grade III—Prolapses and requires manual reduction
- Grade IV—Irreducible prolapse.
Hemorrhoids, especially if external, sometimes thrombose (Figure 1). Distention of overlying perianal skin and inflammation associated with the process of thrombosis can cause severe pain and discomfort.
FIGURE 1
Thrombosed hemorrhoids Anoscopy
Thrombosis can be particularly painful due to distention of perianal skin and inflammation. Used with permission, National Procedures Institute, Midland, Mich.
Diagnosis
Symptoms
The most common symptoms of hemorrhoids are bleeding and prolapse. Less frequently, symptoms also include discomfort, pain, soiling, or itching.
Internal hemorrhoids are usually painless; bleeding or prolapse generally prompt a visit to the physician. Bleeding is described as bright red spotting on toilet tissue or as dripping in the toilet bowl and normally occurs at the end of defecation and separately from the stool.
External hemorrhoids may be asymptomatic, associated with discomfort, or a cause of acute pain in the event of a thrombosis. They generally do not bleed except in the case of a spontaneously resolved local thrombosis. Some individuals may have both types of hemorrhoids simultaneously (mixed).
The term hemorrhoids is commonly misused by patients to refer to any anal symptoms. Other diagnoses such as anal fissures, pruritus ani, abscess, fistula, and condyloma should be ruled out by examining the anus, the perianal region, and the anal canal. However, we have found no studies reporting on the accuracy of the medical history or the physical examination.
How to conduct a digital examination
The patient should be positioned in the left lateral decubitus position for the anorectal exam-ination.6 This position is more comfortable and less intimidating for the patient than the traditional head-down position, and it permits optimal visualization.
Digital palpation allows the entire circumference of the canal to be examined and rectal masses or tender points to be ruled out. Internal hem-orrhoids cannot be detected this way, however.6 The procedure, which must be done gently and with prior reassurance to the patient, is generally quite simple. Intense pain may prevent further examination and suggests the possibility of anal fissure or thrombosed external hemorrhoid.
Anoscopy: safe and essential office procedure
The most accurate method for examining the anal canal and distal rectum is anoscopy. Although several types of anoscopes are available, visualization is best achieved with the slotted anoscope (Figure 2).6 Once it has been inserted, the anoscope is gradually withdrawn while rotating right and left to allow inspection of the mucous membrane. Hemorrhoids appear as pink swellings of the mucosa. Ask the patient to strain during the examination to improve visualization.
Two prospective studies found that anoscopy detects a higher percentage of lesions in the anorectal region than does flexible sigmoidoscopy (99% vs 78%).7,8 It is the procedure of choice for evaluating rectal diseases.
In skilled hands, anoscopy is safe; complications are unusual, and it can be performed in a physician’s office on short notice and without bowel preparation. After appropriate training, primary care physicians can perform routine examinations safely and accurately.
FIGURE 2
Anoscopy
The slotted anoscope provides the best visualization. Used with permission, National Procedures Institute, Midland, Mich.
Office-Based Treatment
Primary care physicians can safely use simple treatment measures to manage most cases of symptomatic hemorrhoids (Figure 3). Only the more symptomatic patients require surgical intervention.
Patients should be made aware of the nature of the condition and the advantages and disadvantages of the different treatment options. The evidence regarding these treatments is summarized in the Table.
FIGURE 3
Management of adult patients with hemorrhoids
TABLE
Medical and surgical treatments for hemorrhoids
| Treatment | SOR* | Indication | Comments |
|---|---|---|---|
| Analgesics and anti-inflammatories2 | D | Grades I–IV and thrombosed external hemorrhoids | No trials comparing analgesics with anti-inflammatories |
| Topical treatments with corticosteroids or anesthetics3 | D | Grades I–III | No controlled trials with placebo are available, but patients report empiric benefit with their use; use only for brief periods |
| High-fiber diet or fiber supplements10-13 | B | Grades I–II | NNT=2.8 for reduction of rectal bleeding and 3.6 for pain relief23 |
| Office procedures23-25 | A | Grades I and II that do not respond to medical therapy, and grade III | Rubber band ligation was more effective and required fewer additional treatments for symptomatic recurrence than did infrared coagulation (NNT=9) and sclerotherapy (NNT=6.9); but rubber band ligation produced more complications than did infrared coagulation (pain: NNH=6) |
| Phlebotonics14-21 | B | Grades I–II | Moderate reduction of duration of bleeding during acute episodes of internal hemorrhoids; conflicting results for other outcomes (pain and prolapse) |
| Hemorrhoidectomy24 | A | Grades II–IV | Hemorrhoidectomy is more effective than office procedures, but it is more painful and presents more complications; office procedures are cheaper and require no time off from work |
| Stapling technique31-36 | A | Grades III–IV | Stapling technique is as effective as hemorrhoidectomy, is less painful, and requires less time off from work; more long-term data are needed37 |
| *For an explanation of strength of recommendation, see page 379. | |||
| SOR, strength of recommendation; NNT, number needed to treat; NNH, number needed to harm | |||
Benefits of lifestyle changes
The main purpose of lifestyle changes is to minimize prolonged straining during bowel movements, which is thought to contribute to the development of hemorrhoids. Such changes include increasing the amount of fiber in the diet, which is especially helpful for grade I and II internal hemorrhoids. Preventing constipation also helps alleviate more severe hemorrhoids and can help to prevent future episodes.10
Rectal bleeding can mask the diagnosis of cancer. The probability of colorectal cancer increases in the elderly, those with a family or personal history of colorectal cancer, and those with any other symptoms of colorectal cancer (fatigue, weight loss, palpable tumor, anemia). Patients at risk need a more thorough evaluation, including endoscopy, to rule out malignancy.9
It is important to document that observed hemorrhoids account for the bleeding episode (bleeding at the contact site with the anoscope or an applicator, thrombosed hemorrhoids, or a clot over the hemorrhoid).
Several clinical trials have reported the benefits of a high-fiber diet or fiber supplements compared with placebo in relieving pain, bleeding, and prolapse (strength of recommendation [SOR]: B).10-13 We found no studies comparing the different types of bulk laxatives.
Although the role of certain foods in the pathogenesis of hemorrhoids or their acute exacerbation is accepted empirically, this has not been proved. Also, no firm evidence to date shows that increasing physical exercise, limiting time on the commode, or improving local hygiene are beneficial. However, these measures are usually recommended because they have other health benefits or are thought to do no harm (SOR: D).
Medical therapy
No rigorous evidence exists to support the use of topical therapies, physical or pharmacologic (sitz baths, anesthetics, phlebotonics, corticoids, or ice). Most studies have employed poor methods, lacked placebo control, and addressed heterogeneous preparations with multiple associated components. It is therefore not possible to formulate firm recommendations.
Soothing agents. Popular topical soothing agents are often combined with corticosteroids or anesthetics and are available over the counter as creams or enemas. Many patients report some empirical benefit with their use, especially corticosteroids and anesthetics (SOR: D).3 Advise patients against prolonged use due to possible local allergic effects and sensitization of skin (SOR: D).
Phlebotonics. Several phlebotonics have been evaluated in the literature; diosmin is the best-studied agent, but it is not commercially available in the United States at this time. In studies of patients with acute attacks of internal hemorrhoids (grades I to II), the main perceived effect was reduced bleeding duration;14,15 the results were conflicting for other outcomes (mainly pain and prolapse)14-18 (SOR: B).
Other phlebotonics (the botanicals ginkgo biloba, troxerutin, and calcium dobesilate), when compared with placebo19,20 or diosmin,21 have shown similar effects (SOR: B). No studies thus far have evaluated the role of phlebotonics in thrombosis of external hemorrhoids.
Anti-inflammatories and analgesics. Most episodes of acute thrombosed external hemorrhoids improve spontaneously and therefore can be treated with symptomatic measures, including anti-inflammatory agents, analgesics, and stool softeners. Anti-inflammatories and analgesics can be effective during episodes of external and internal thromboses3 (SOR: D). Several clinical trials have reported benefits of fiber in relieving pain, bleeding, and prolapse
In a small randomized clinical trial, the addition of topical nifedipine (0.3%) to a lidocaine ointment (1.5%) was more effective than lidocaine alone in reducing pain and shortening resolution time.22
Surgical treatment
All office (nonoperative) and surgical procedures fix the sliding hemorrhoidal tissue back onto the muscle wall. The fixation takes place by directly promoting tissue fibrosis (eg, sclerotherapy or infrared coagulation) or by tissue destruction with subsequent fibrosis (eg, hemorrhoidectomy).
Office procedures. The most commonly used methods are rubber band ligation and infrared coagulation. Other methods include bipolar electrocoagulation, low-voltage direct current, sclerotherapy, laser therapy, and cryosurgery.
Two meta-analyses compared these nonoperative methods and concluded that rubber band ligation and infrared coagulation are the most effective. The first meta-analysis reported that ligation was more effective because it required fewer additional treatments for symptomatic recurrence than did coagulation (number needed to treat [NNT]=9) and sclerotherapy (NNT=6.9).23 However, ligation produced more complications than did coagulation (pain: number needed to harm=6) (SOR: A).
The second, more recent meta-analysis found ligation to have similar beneficial effect and a similar complication rate,24 although it was more painful. It appeared to be the therapy of choice for grades I to III (SOR: A). No difference was found between sclerotherapy and infrared coagulation for any outcome measure, but the authors of these meta-analyses commented that the overall quality of the studies was not high and their conclusions were therefore limited. One subsequent randomized clinical trial confirmed the advantages of rubber band ligation.25
In the event of a thrombosed hemorrhoid, whether to remove the clot promptly or wait for spontaneous resolution is controversial. We found no studies comparing these approaches. Excision should be performed when local measures fail, the thrombosis is painful, and there is no local edema (SOR: D).3
In the treatment of perianal thrombosis, one clinical trial found excision more effective than topically applied 0.2% glyceryl trinitrate or incision in reducing pain and the number of recurrences at 1 year (SOR: A).26 Residual hemorrhoidal tissue following an episode of acute thrombosis of external hemorrhoids also may cause symptoms, especially pruritus. These external anal tags can make it difficult to clean the anus and can be excised if symptoms warrant.
Surgery. Surgical treatment, though more invasive and expensive, is the most effective and definitive course for symptomatic hemorrhoids. The aim is to decrease blood flow to the anorectal ring and excise redundant hemorrhoidal tissue.
There are several techniques. In the United States, the Ferguson (closed) hemorrhoidectomy is preferred. The one used most commonly in Europe is the Milligan-Morgan technique (open). Both techniques have been shown to be similarly effective, although there is debate over healing time.27-30 Only a competently performed technique will produce satisfying results.
In their meta-analysis, MacRae and McLeod found that hemorrhoidectomy is more effective than all other treatment modalities, though complications such as pain and costs were greater (SOR: A).24
A new surgical procedure, the stapled hemorrhoidectomy, has been introduced as an alternative to the standard hemorrhoidectomy. Several randomized clinical trials have shown the procedure to be as effective, cause less pain, and require less time off from work compared with standard techniques (SOR: A).31-36 However, it is more expensive and requires advanced surgical skills. More long-term data are also needed.37
Anal stretch, or manual anal dilatation, has been reported to be effective in the treatment of hemorrhoids, but a high rate of incontinence after the procedure has led to abandonment of this technique.38,39 Antibiotic prophylaxis in colorectal surgery is highly recommended and has been shown to reduce infection and mortality (SOR: A).40
Surgery vs office procedures
Several clinical practice guidelines3,38 and meta-analyses23,24 have recommended office procedures for hemorrhoids of grades I through III. Although there is some discrepancy about the procedure of choice, rubber band ligation appears to be the most effective technique.
An evidence-based clinical practice guideline3 has recommended coagulation techniques for bleeding nonprolapsed hemorrhoids or those with a low grade of prolapse (grades I and II), and reserving rubber band ligation for hemorrhoids more severely prolapsed (grade III). The basis for this recommendation is that flat bleeding hemorrhoids may not provide enough tissue to grasp.
Surgical hemorrhoidectomy should be reserved for grade IV hemorrhoids and for grade III lesions that do not respond to other procedures.
This is an approximate rather than a rigid approach, and the final decision will depend on the physician’s technical training, the patient’s preferences, clinical circumstances, and local resources.
Prognosis: 90% require no surgery
Hemorrhoids are generally a chronic problem and tend to worsen with time. According to a retrospective cohort study, most patients will have several episodes during their lives; however, it can be considered a benign disorder, and approximately 90% of patients will not require surgery to alleviate their symptoms (SOR: B).41
It is worth noting that 26% of patients who require a hemorrhoidectomy may have a recurrence, and 11% will need further treatment.39 Similarly, approximately half of those who undergo office procedures may require further treatment or surgery in 5 to 10 years.42,43
ACKNOWLEDGMENTS
We thank E. Thompson for help in editing this manuscript and J. A. Ferrus and A. Hervas for their clinical comments. Dr Alonso-Coello holds a postgraduate research fellowship at the Instituto Carlos III, Spanish Ministry of Health, Spain.
Corresponding author
Pablo Alonso-Coello, MD, Ibero-american Cochrane Centre, Hospital de la Santa Creu i Sant Pau, Sant Antoni Mª Claret 171, 08041 Barcelona, Spain. E-mail: [email protected].
1. Hulme-Moir M, Bartolo DC. Hemorrhoids. Gastroenterol Clin North Am 2001;30:183-197.
2. Johanson JF, Sonnenberg A. Temporal changes in the occurrence of hemorrhoids in the United States and England. Dis Colon Rectum 1991;34:585-591.
3. Abramowitz L, Godeberge P, Staumont G, Soudan D. Clinical practice guidelines for the treatment of hemorrhoid disease [in French]. Gastroenterol Clin Biol 2001;25:674-702.
4. Johanson JF, Sonnenberg A. The prevalence of hemorrhoids and chronic constipation. An epidemiologic study. Gastroenterology 1990;98:380-386.
5. Beck DE. Hemorrhoidal disease. In: Beck DE, Wexner SD, eds. Fundamentals of Anorectal Surgery. 2nd ed. London: WB Saunders 1998;237-253.
6. Pfenninger JL, Zainea GG. Common anorectal conditions: part I. Symptoms and complaints. Am Fam Physician 2001;63:2391-2398.
7. Kelly SM, Sanowski RA, Foutch PG, Bellapravalu S, Haynes WC. A prospective comparison of anoscopy and fiber endoscopy in detecting anal lesions. J Clin Gastroenterol 1986;8:658-660.
8. Korkis AM, McDougall CJ. Rectal bleeding in patients less than 50 years of age. Dig Dis Sci 1995;40:1520-1523.
9. Wauters H, Van Casteren V, Buntinx F. Rectal bleeding and colorectal cancer in general practice: diagnostic study. BMJ 2000;321:998-999.
10. Moesgaard F, Nielsen ML, Hansen JB, Knudsen JT. High-fiber diet reduces bleeding and pain in patients with hemorrhoids: a double-blind trial of Vi-Siblin. Dis Colon Rectum 1982;25:454-456.
11. Broader JH, Gunn IF, Alexander-Williams J. Evaluation of a bulk-forming evacuant in the management of haemorrhoids. Br J Surg 1974;61:142-144.
12. Webster DJ, Gough DC, Craven JL. The use of bulk evacuant in patients with haemorrhoids. Br J Surg 1978;65:291-292.
13. Perez-Miranda M, Gomez-Cedenilla A, Leon-Colombo T, Pajares J, Mate-Jimenez J. Effect of fiber supplements on internal bleeding hemorrhoids. Hepatogastroenterology 1996;43:1504-1507.
14. Godeberge P. Daflon 500 mg in the treatment of hemorrhoidal disease: a demonstrated efficacy in comparison with placebo. Angiology 1994;45:574-578.
15. Ho YH, Tan M, Seow-Choen F. Micronized purified flavonidic fraction compared favorably with rubber band ligation and fiber alone in the management of bleeding hemorrhoids: randomized controlled trial. Dis Colon Rectum 2000;43:66-69.
16. Thanapongsathorn W, Vajrabukka T. Clinical trial of oral diosmin (Daflon) in the treatment of hemorrhoids. Dis Colon Rectum 1992;35:1085-1088.
17. Cospite M. Double-blind, placebo-controlled evaluation of clinical activity and safety of Daflon 500 mg in the treatment of acute hemorrhoids. Angiology 1994;45:566-573.
18. Misra MC, Parshad R. Randomized clinical trial of micronized flavonoids in the early control of bleeding from acute internal haemorrhoids. Br J Surg 2000;87:868-872.
19. Annoni F, Boccasanta P, Chiurazzi D, Mozzi E, Oberhauser V. Treatment of acute symptoms of hemorrhoid disease with high-dose oral O-(beta-hydroxyethyl)-rutosides [in Italian]. Minerva Med 1986;77:1663-1668
20. Mentes BB, Gorgul A, Tatlicioglu E, Ayoglu F, Unal S. Efficacy of calcium dobesilate in treating acute attacks of hemorrhoidal disease. Dis Colon Rectum 2001;44:1489-1495.
21. Debien P, Denis J. Traitements des signes fonctionnels de la maladie hèmorroïaigüe: essai multicentrique, randomisè, diosmine d’hèmisynthèse versus association extrait de Ginko biloba-heptaminol-troxèrutine. Med Chir Dig 1996;25:259-264.
22. Perrotti P, Antropoli C, Molino D, De Stefano G, Antropoli M. Conservative treatment of acute thrombosed external hemorrhoids with topical nifedipine. Dis Colon Rectum 2001;44:405-409.
23. Johanson JF, Rimm A. Optimal nonsurgical treatment of hemorrhoids: a comparative analysis of infrared coagulation, rubber band ligation, and injection sclerotherapy. Am J Gastroenterol 1992;87:1600-1606.
24. MacRae HM, McLeod RS. Comparison of hemorrhoidal treatment modalities. A meta-analysis. Dis Colon Rectum. 1995;38:687-694.
25. Poen AC, Felt-Bersma RJ, Cuesta MA, Deville W, Meuwissen SG. A randomized controlled trial of rubber band ligation versus infra-red coagulation in the treatment of internal haemorrhoids. Eur J Gastroenterol Hepatol 2000;12:535-539.
26. Cavcic J, Turcic J, Martinac P, Mestrovic T, Mladina R, Pezerovic-Panijan R. Comparison of topically applied 0.2% glyceryl trinitrate ointment, incision and excision in the treatment of perianal thrombosis. Dig Liver Dis 2001;33:335-340.
27. Ho YH, Seow-Choen F, Tan M, Leong AF. Randomized controlled trial of open and closed haemorrhoidectomy. Br J Surg 1997;84:1729-1730.
28. Carapeti EA, Kamm MA, McDonald PJ, Chadwick SJ, Phillips RK. Randomized trial of open versus closed day-case haemorrhoidectomy. Br J Surg 1999;86:612-613.
29. Arbman G, Krook H, Haapaniemi S. Closed vs. open hemorrhoidectomy—is there any difference? Dis Colon Rectum 2000;43:31-34.
30. Gencosmanoglu R, Sad O, Koc D, Inceoglu R. Hemorrhoidectomy: open or closed technique? A prospective, randomized clinical trial. Dis Colon Rectum 2002;45:70-75.
31. Mehigan BJ, Monson JR, Hartley JE. Stapling procedure for haemorrhoids versus Milligan-Morgan haemorrhoidectomy: randomised controlled trial. Lancet 2000;355:782-785.
32. Rowsell M, Bello M, Hemingway DM. Circumferential mucosectomy (stapled haemorrhoidectomy) versus conventional haemorrhoidectomy: randomised controlled trial. Lancet. 2000;355:779-781.
33. Khalil KH, O’Bichere A, Sellu D. Randomized clinical trial of sutured versus stapled closed haemorrhoidectomy. Br J Surg 2000;87:1352-1355.
34. Boccasanta P, Capretti PG, Venturi M, et al. Randomised controlled trial between stapled circumferential mucosectomy and conventional circular hemorrhoidectomy in advanced hemorrhoids with external mucosal prolapse. Am J Surg 2001;182:64-68.
35. Ganio E, Altomare DF, Gabrielli F, Milito G, Canuti S. Prospective randomized multicentre trial comparing stapled with open haemorrhoidectomy. Br J Surg 2001;88:669-674.
36. Shalaby R, Desoky A. Randomized clinical trial of stapled versus Milligan-Morgan haemorrhoidectomy. Br J Surg 2001;88:1049-1053.
37. Hetzer FH, Demartines N, Handschin AE, Clavien PA. Stapled vs excision hemorrhoidectomy: long-term results of a prospective randomized trial. Arch Surg 2002;137:337-340.
38. Standards Task Force of American Society of Colon and Rectal Surgeons Practice parameters for the treatment of hemorrhoids. Dis Colon Rectum 1993;36:1118-1120.
39. Konsten J, Baeten CG. Hemorrhoidectomy vs. Lord’s method: 17-year follow-up of a prospective, randomized trial. Dis Colon Rectum 2000;43:503-506.
40. Baum ML, Anish DS, Chalmers TC, Sacks HS, Smith H, Fagerstrom RM. A survey of clinical trials of antibiotic prophylaxis in colon surgery: evidence against further use of no-treatment controls. N Engl J Med 1981;305:795-799.
41. Bleday R, Pena JP, Rothenberger DA, Goldberg SM, Buls JG. Symptomatic hemorrhoids: current incidence and complications of operative therapy. Dis Colon Rectum 1992;35:477-481.
42. Wrobleski DE, Corman ML, Veidenheimer MC, Coller JA. Long-term evaluation of rubber ring ligation in hemorrhoidal disease. Dis Colon Rectum 1980;23:478-482.
43. Savioz D, Roche B, Glauser T, Dobrinov A, Ludwig C, Marti MC. Rubber band ligation of hemorrhoids: relapse as a function of time. Int J Colorectal Dis 1998;13:154-156.
1. Hulme-Moir M, Bartolo DC. Hemorrhoids. Gastroenterol Clin North Am 2001;30:183-197.
2. Johanson JF, Sonnenberg A. Temporal changes in the occurrence of hemorrhoids in the United States and England. Dis Colon Rectum 1991;34:585-591.
3. Abramowitz L, Godeberge P, Staumont G, Soudan D. Clinical practice guidelines for the treatment of hemorrhoid disease [in French]. Gastroenterol Clin Biol 2001;25:674-702.
4. Johanson JF, Sonnenberg A. The prevalence of hemorrhoids and chronic constipation. An epidemiologic study. Gastroenterology 1990;98:380-386.
5. Beck DE. Hemorrhoidal disease. In: Beck DE, Wexner SD, eds. Fundamentals of Anorectal Surgery. 2nd ed. London: WB Saunders 1998;237-253.
6. Pfenninger JL, Zainea GG. Common anorectal conditions: part I. Symptoms and complaints. Am Fam Physician 2001;63:2391-2398.
7. Kelly SM, Sanowski RA, Foutch PG, Bellapravalu S, Haynes WC. A prospective comparison of anoscopy and fiber endoscopy in detecting anal lesions. J Clin Gastroenterol 1986;8:658-660.
8. Korkis AM, McDougall CJ. Rectal bleeding in patients less than 50 years of age. Dig Dis Sci 1995;40:1520-1523.
9. Wauters H, Van Casteren V, Buntinx F. Rectal bleeding and colorectal cancer in general practice: diagnostic study. BMJ 2000;321:998-999.
10. Moesgaard F, Nielsen ML, Hansen JB, Knudsen JT. High-fiber diet reduces bleeding and pain in patients with hemorrhoids: a double-blind trial of Vi-Siblin. Dis Colon Rectum 1982;25:454-456.
11. Broader JH, Gunn IF, Alexander-Williams J. Evaluation of a bulk-forming evacuant in the management of haemorrhoids. Br J Surg 1974;61:142-144.
12. Webster DJ, Gough DC, Craven JL. The use of bulk evacuant in patients with haemorrhoids. Br J Surg 1978;65:291-292.
13. Perez-Miranda M, Gomez-Cedenilla A, Leon-Colombo T, Pajares J, Mate-Jimenez J. Effect of fiber supplements on internal bleeding hemorrhoids. Hepatogastroenterology 1996;43:1504-1507.
14. Godeberge P. Daflon 500 mg in the treatment of hemorrhoidal disease: a demonstrated efficacy in comparison with placebo. Angiology 1994;45:574-578.
15. Ho YH, Tan M, Seow-Choen F. Micronized purified flavonidic fraction compared favorably with rubber band ligation and fiber alone in the management of bleeding hemorrhoids: randomized controlled trial. Dis Colon Rectum 2000;43:66-69.
16. Thanapongsathorn W, Vajrabukka T. Clinical trial of oral diosmin (Daflon) in the treatment of hemorrhoids. Dis Colon Rectum 1992;35:1085-1088.
17. Cospite M. Double-blind, placebo-controlled evaluation of clinical activity and safety of Daflon 500 mg in the treatment of acute hemorrhoids. Angiology 1994;45:566-573.
18. Misra MC, Parshad R. Randomized clinical trial of micronized flavonoids in the early control of bleeding from acute internal haemorrhoids. Br J Surg 2000;87:868-872.
19. Annoni F, Boccasanta P, Chiurazzi D, Mozzi E, Oberhauser V. Treatment of acute symptoms of hemorrhoid disease with high-dose oral O-(beta-hydroxyethyl)-rutosides [in Italian]. Minerva Med 1986;77:1663-1668
20. Mentes BB, Gorgul A, Tatlicioglu E, Ayoglu F, Unal S. Efficacy of calcium dobesilate in treating acute attacks of hemorrhoidal disease. Dis Colon Rectum 2001;44:1489-1495.
21. Debien P, Denis J. Traitements des signes fonctionnels de la maladie hèmorroïaigüe: essai multicentrique, randomisè, diosmine d’hèmisynthèse versus association extrait de Ginko biloba-heptaminol-troxèrutine. Med Chir Dig 1996;25:259-264.
22. Perrotti P, Antropoli C, Molino D, De Stefano G, Antropoli M. Conservative treatment of acute thrombosed external hemorrhoids with topical nifedipine. Dis Colon Rectum 2001;44:405-409.
23. Johanson JF, Rimm A. Optimal nonsurgical treatment of hemorrhoids: a comparative analysis of infrared coagulation, rubber band ligation, and injection sclerotherapy. Am J Gastroenterol 1992;87:1600-1606.
24. MacRae HM, McLeod RS. Comparison of hemorrhoidal treatment modalities. A meta-analysis. Dis Colon Rectum. 1995;38:687-694.
25. Poen AC, Felt-Bersma RJ, Cuesta MA, Deville W, Meuwissen SG. A randomized controlled trial of rubber band ligation versus infra-red coagulation in the treatment of internal haemorrhoids. Eur J Gastroenterol Hepatol 2000;12:535-539.
26. Cavcic J, Turcic J, Martinac P, Mestrovic T, Mladina R, Pezerovic-Panijan R. Comparison of topically applied 0.2% glyceryl trinitrate ointment, incision and excision in the treatment of perianal thrombosis. Dig Liver Dis 2001;33:335-340.
27. Ho YH, Seow-Choen F, Tan M, Leong AF. Randomized controlled trial of open and closed haemorrhoidectomy. Br J Surg 1997;84:1729-1730.
28. Carapeti EA, Kamm MA, McDonald PJ, Chadwick SJ, Phillips RK. Randomized trial of open versus closed day-case haemorrhoidectomy. Br J Surg 1999;86:612-613.
29. Arbman G, Krook H, Haapaniemi S. Closed vs. open hemorrhoidectomy—is there any difference? Dis Colon Rectum 2000;43:31-34.
30. Gencosmanoglu R, Sad O, Koc D, Inceoglu R. Hemorrhoidectomy: open or closed technique? A prospective, randomized clinical trial. Dis Colon Rectum 2002;45:70-75.
31. Mehigan BJ, Monson JR, Hartley JE. Stapling procedure for haemorrhoids versus Milligan-Morgan haemorrhoidectomy: randomised controlled trial. Lancet 2000;355:782-785.
32. Rowsell M, Bello M, Hemingway DM. Circumferential mucosectomy (stapled haemorrhoidectomy) versus conventional haemorrhoidectomy: randomised controlled trial. Lancet. 2000;355:779-781.
33. Khalil KH, O’Bichere A, Sellu D. Randomized clinical trial of sutured versus stapled closed haemorrhoidectomy. Br J Surg 2000;87:1352-1355.
34. Boccasanta P, Capretti PG, Venturi M, et al. Randomised controlled trial between stapled circumferential mucosectomy and conventional circular hemorrhoidectomy in advanced hemorrhoids with external mucosal prolapse. Am J Surg 2001;182:64-68.
35. Ganio E, Altomare DF, Gabrielli F, Milito G, Canuti S. Prospective randomized multicentre trial comparing stapled with open haemorrhoidectomy. Br J Surg 2001;88:669-674.
36. Shalaby R, Desoky A. Randomized clinical trial of stapled versus Milligan-Morgan haemorrhoidectomy. Br J Surg 2001;88:1049-1053.
37. Hetzer FH, Demartines N, Handschin AE, Clavien PA. Stapled vs excision hemorrhoidectomy: long-term results of a prospective randomized trial. Arch Surg 2002;137:337-340.
38. Standards Task Force of American Society of Colon and Rectal Surgeons Practice parameters for the treatment of hemorrhoids. Dis Colon Rectum 1993;36:1118-1120.
39. Konsten J, Baeten CG. Hemorrhoidectomy vs. Lord’s method: 17-year follow-up of a prospective, randomized trial. Dis Colon Rectum 2000;43:503-506.
40. Baum ML, Anish DS, Chalmers TC, Sacks HS, Smith H, Fagerstrom RM. A survey of clinical trials of antibiotic prophylaxis in colon surgery: evidence against further use of no-treatment controls. N Engl J Med 1981;305:795-799.
41. Bleday R, Pena JP, Rothenberger DA, Goldberg SM, Buls JG. Symptomatic hemorrhoids: current incidence and complications of operative therapy. Dis Colon Rectum 1992;35:477-481.
42. Wrobleski DE, Corman ML, Veidenheimer MC, Coller JA. Long-term evaluation of rubber ring ligation in hemorrhoidal disease. Dis Colon Rectum 1980;23:478-482.
43. Savioz D, Roche B, Glauser T, Dobrinov A, Ludwig C, Marti MC. Rubber band ligation of hemorrhoids: relapse as a function of time. Int J Colorectal Dis 1998;13:154-156.