User login
As a hospitalist who practices in a perioperative clinic, I probably spend more of my time with patients reviewing and discussing the medications they are taking than on any other single subject. Surgical patients—many of whom are elderly—commonly are on multiple medications, have renal or hepatic disease that can alter drug metabolism, and may not be adequately educated about their medication regimens.
Patient safety is the overriding concern behind perioperative medication management, consistent with the medication-related objectives in the Joint Commission’s 2009 National Patient Safety Goals.1 The increasing surgical burden that comes with an aging population, along with rising expectations for functional recovery, has likewise elevated the importance of perioperative medication management.
Despite these demands, there is scant evidence from randomized controlled trials to directly guide perioperative medication management. For this reason, recommendations in this area rely largely on other forms of evidence, including expert consensus, case reports, in vitro studies, recommendations from pharmaceutical companies, and other known data (pharmacokinetics, drug interactions with anesthetic agents, and effects of the agent on the primary disease and on perioperative risk).
This article reviews general principles of perioperative medication management and then presents four case vignettes to explore perioperative recommendations for a number of common medication classes. It is not intended as a comprehensive review of the perioperative management of all medications, as numerous classes (antiplatelets, beta-blockers, oral hypogycemic agents, insulin, statins) are discussed in detail elsewhere in this proceedings supplement.
GENERAL CONSIDERATIONS IN MEDICATION MANAGEMENT
A comprehensive medication history is fundamental
Effective perioperative management of medications requires an understanding of the patient and his or her comorbidities so that the risk of perioperative decompensation can be gauged. This understanding stems from a thorough medical history that includes a comprehensive medication history to provide a complete inventory of the following:
- All prescription medications
- All over-the-counter (OTC) agents (including nonsteroidal anti-inflammatory drugs [NSAIDs])
- All vitamins
- All herbal medications.
When to stop, when to resume?
Guidance on stopping and resuming medications in the perioperative period is relatively absent from the literature. General considerations include the following:
- The potential for withdrawal when stopping a medication
- The progression of disease with interruption of drug therapy
- The potential for interactions with anesthetic agents if the medication is continued.
Withdrawal potential
Abrupt discontinuation of some drugs may lead to unnecessary complications due to the potential for withdrawal. Common medications that have been associated with withdrawal symptoms are selective serotonin reuptake inhibitors (SSRIs), beta-blockers, clonidine, statins, and corticosteroids.2 A recent systematic literature review concluded that continuation of chronic corticosteroid therapy without supplemental (stress) doses of corticosteroids is appropriate unless patients have primary disease of the hypothalamic-pituitary-adrenal axis, in which case perioperative stress dosing is recommended to avoid acute adrenal insufficiency (addisonian crisis).3
Patients on chronic drugs are more likely to have complications
In a medication survey of 1,025 patients admitted to a general surgery unit, Kennedy et al reported that 49% of the patients were taking medications (other than vitamins) unrelated to their surgical procedure.4 Even while this percentage is considerably lower than what I observe in my practice, this study showed that medication use has important perioperative consequences4:
- The odds ratio for a postoperative complication was 2.7 (95% CI, 1.76–4.04) if patients were taking a drug unrelated to their surgery.
- The risk of a complication was particularly elevated if patients were taking cardiovascular drugs or agents that act on the central nervous system; if patients were on NPO (“nothing by mouth”) orders for more than 24 hours before surgery; and if the operation was more than 1 hour in duration. These findings could reflect destabilization of the disease processes for which the patients were taking chronic medications that required interruption.
Unintended discontinuation of chronic drugs
Stopping a chronic medication for a surgical procedure raises the possibility that its resumption could be overlooked, especially since medical errors are particularly common in the transition between health care settings following hospital discharge. A population-based cohort study among all elderly patients discharged from Ontario, Canada, hospitals over a 5½-year period found that 11.4% of patients undergoing elective surgery did not resume their indicated chronic warfarin therapy within 6 months after its presurgical discontinuation.5 Although 6-month rates of unintended failure to resume therapy were lower for statins (4%) and ophthalmic beta-blocker drops (8%),5 these findings underscore that drug discontinuation always carries a risk that therapy might not be resumed as indicated.
Additional considerations
Stress response to surgery. Decisions about perioperative drug therapy should always take into account the stress response to surgery and the challenge it presents to homeostasis in the face of increased sympathetic tone and release of pituitary hormones.
Unreliable absorption of oral medications. Surgery and the postoperative state can lead to unreliable absorption of oral drugs for any of a number of reasons: villous atrophy, diminished blood flow to the gut, edema, mucosal ischemia, diminished motility from postoperative ileus, and use of narcotics.6
Take-away general principles
The following principles can be applied to guide perioperative medication management in a general sense7:
- Continue medications with withdrawal potential
- Discontinue medications that increase surgical risk and are not essential for short-term quality of life
- Use clinical judgment when neither of the above two principles applies, but be mindful that many other medications are given in the narrow perioperative time window and that metabolism and elimination of chronic drugs may be altered.
CASE 1: A PATIENT ON A NONPRESCRIPTION NSAID FOR SEVERE ARTHRITIS
A 55-year-old man with severe osteoarthritis is scheduled for total hip arthroplasy in 2 days. He stopped his aspirin (325 mg/day) 1 week ago but continued taking ibuprofen 600 three times daily with food, explaining that “no one told me to stop.” His last dose was yesterday evening.
Question: What should you do?
A. Call the surgeon and cancel the surgery
B. Call the surgeon to notify, and tell the patient to stop the ibuprofen now
C. Check his bleeding time and proceed if normal
D. Just tell the patient to stop the ibuprofen now
E. Proceed to the operating room regardless of the ibuprofen dose
The best approach would be to notify the surgeon and tell the patient to stop the ibuprofen now. NSAIDs such as ibuprofen reversibly inhibit platelet cyclooxygenase (COX), diminish thromboxane A2 production, diminish platelet aggregation, and can increase bleeding time measurement and overall bleeding risk. They can induce renal failure in combination with other drugs, especially in the setting of hypotension.8,9 COX-2 inhibitors have less effect on platelet function but retain the potential for renal toxicity and also confer well-known cardiovascular risks.
In the past, NSAIDs were typically held for 7 days before surgery, but this practice was not supported with much evidence. In vitro assessment indicates that platelet function normalizes within 24 hours after cessation of regular ibuprofen or dexibuprofen in healthy individuals.10,11
Since NSAIDs vary in their effect on bleeding time, which does not correlate well with elimination half-life, a general recommendation is to stop most NSAIDs at least 3 days before surgery.
CASE 2: A PATIENT ON MULTIPLE CARDIOVASCULAR DRUGS
A 67-year-old man with dilated cardiomyopathy and an ejection fraction of 25% (well compensated) is scheduled for a laparoscopic cholecystectomy tomorrow. He is taking lisinopril (40 mg/day), irbesartan (150 mg/day), and furosemide (80 mg/day).
Question: What is your advice?
A. Call the surgeon and cancel the surgery
B. Call the surgeon to notify, and tell the patient to stop his medications now
C. Hold all of the above medications on the morning of surgery
D. Proceed to the operating room with the usual doses of his medications on the morning of surgery
The best approach is to withhold these medications on the morning of surgery.
Diuretics are typically held on the morning of surgery because of the potential for hypovolemia and electrolyte depletion.
Angiotensin-converting enzyme (ACE) inhibitors intensify the hypotensive effects of anesthesia induction. Because angiotensin II plays a key role in maintaining circulating volume in response to stressors, volume deficits can occur in ACE inhibitor-treated patients as angiotensin II cannot compensate for venous pooling of blood, resulting in diminished cardiac output and arterial hypotension. However, continued renin-angiotensin system suppression may protect regional circulation, as has been demonstrated by reduced release of cardiac enzymes with ACE inhibitor continuation (compared with interruption) in cardiac surgery patients. ACE inhibitors also have a renal protective effect, preserving glomerular filtration rate in patients undergoing aortic abdominal aneurysm repair or coronary artery bypass graft surgery. Hypotension with ACE inhibition is treatable with sympathomimetics, alpha-agonists, and intravenous fluids.12–15
If a patient’s ACE inhibitor is stopped, be prepared for rebound postoperative hypertension. The probability of postoperative atrial fibrillation is also increased with ACE inhibitor interruption.14 In patients with left ventricular dysfunction undergoing noncardiac vascular surgery, continued ACE inhibition is associated with reduced mortality.16 These data argue, at the very least, for prompt resumption of ACE inhibitors after surgery.
Angiotensin receptor blockers (ARBs) have largely the same clinical benefits as do ACE inhibitors. These agents also increase the risk of hypotension upon induction of anesthesia, and this hypotension is not as responsive to conventional vasopressors such as ephedrine and phenylephrine; a better response is achieved with vasopressin.15 In light of the long half-life of ARBs, current thinking is to withhold them 24 hours before surgery.
Rosenman et al recently published a meta-analysis of five studies assessing the effects of continuing or withholding ACE inhibitors and ARBs in the preoperative period.17 They found a statistically significant increase in the incidence of perioperative hypotension in patients in whom the drugs were continued compared with those in whom the drugs were withheld (relative risk = 1.50; 95% CI, 1.15–1.96), but there was no significant difference in the rate of perioperative MI between the two groups. Notably, the indication for ACE inhibitor or ARB use in all of the studies was hypertension, not heart failure.
My approach to the perioperative management of ACE inhibitors and ARBs is to withhold them on the morning of surgery (in the case of ARBs, 24 hours prior to surgery) if their only indication is for hypertension and if the patient’s blood pressure is well controlled. If the patient has another indication for these agents or has hypertension that is not well controlled, I am inclined to continue these agents but will first discuss the decision with the anesthesiologist.
CASE 3: A PATIENT TAKING HERBAL MEDICATIONS
A 68-year-old woman with a history of hypertension, osteoarthritis, and osteoporosis is scheduled for total hip replacement in 7 days. Her medications include atenolol, hydrochlorothiazide, and alendronate. She also reports taking some natural herbal medications. She does not recall their names initially but calls back with the names: ginkgo biloba for her memory and echinacea for her immune system.
Question: What are your recommendations?
A. Stop all medications now except atenolol and proceed to surgery
B. Stop the herbals now but take all other medications on the morning of surgery
C. Stop the herbals now and take only atenolol on the morning of surgery
D. Continue all medications now and take atenolol and the herbals on the morning of surgery
E. Cancel the surgery and call an herbalist for guidance
The best strategy is to stop the herbals now and tell her to take only atenolol (a beta-blocker) on the morning of surgery.
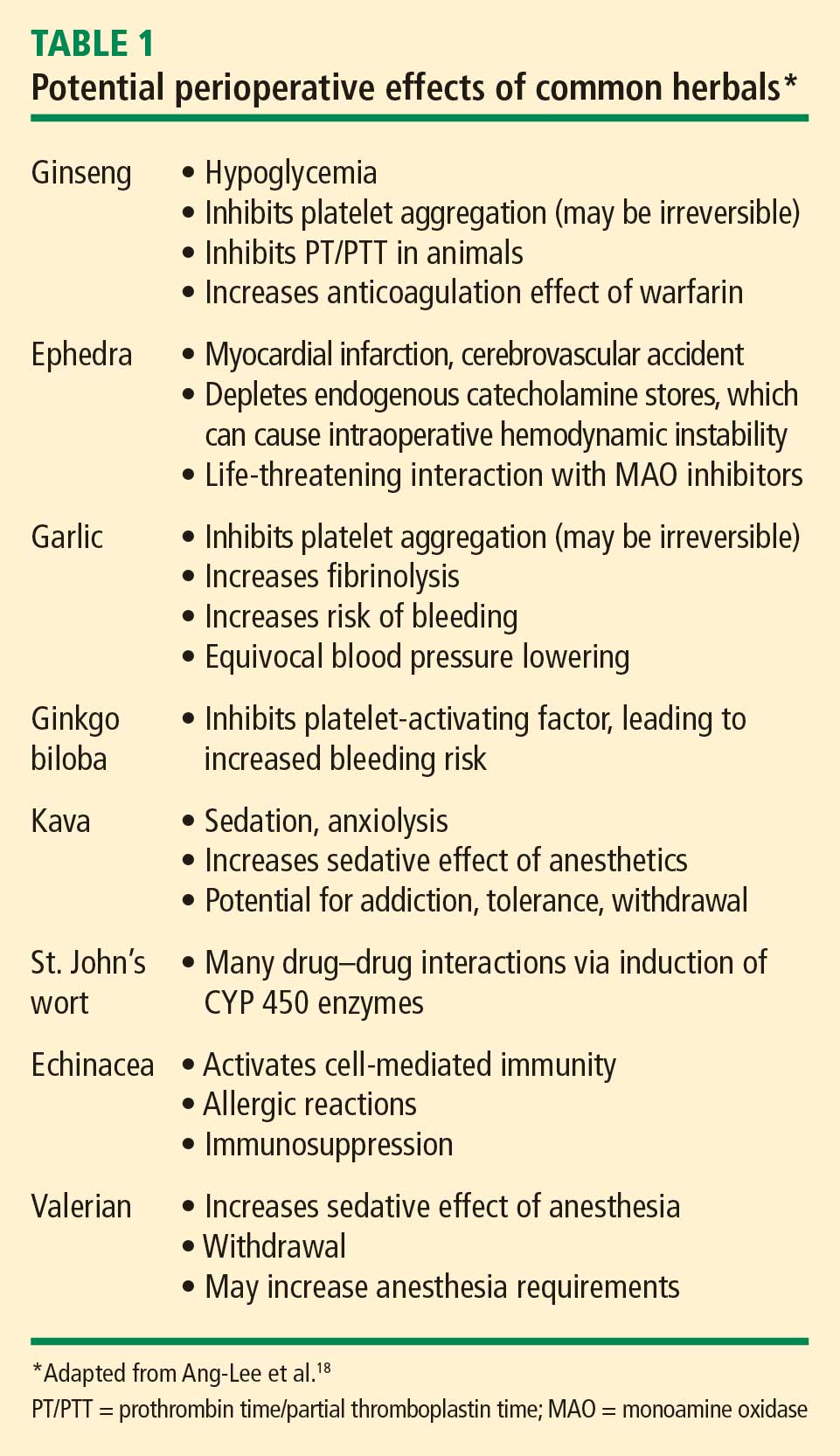
Because the US Food and Drug Administration (FDA) does not regulate herbal products, the contents of these products can vary widely. For example, an analysis using mass spectrometry of 50 commercial ginseng products from 11 countries found that the ginseng content varied from 0% (six preparations) to 9%.19 Catecholamine-type compounds were found in some of the products.19
Because of the uncertainty over their actual contents, herbal medications should be stopped at least 7 days prior to surgery. If a patient is still taking herbal supplements on the day before surgery, I typically alert the anesthesiologist and surgeon.
CASE 4: A PATIENT ON MULTIPLE PSYCHOTROPICS
A 38-year-old woman with a history of severe major depression is scheduled for a mastectomy for breast cancer the next day. Her medications include fluoxetine, lorazepam, and phenelzine, all of which she has been taking for many years.
Question: What is your course of action?
A. Call the surgeon and cancel the surgery
B. Call the surgeon and notify the day-of-surgery anesthesiologist that the patient is taking these agents
C. Stop all the medications now and proceed to the operating room
D. Request a psychiatric consult for an alternative drug regimen
E. Proceed and advise the patient to take all of these agents on the morning of surgery
My approach would be to notify the day-of-surgery anesthesiologist, specifically about the phenelzine, which is a monoamine oxidase (MAO) inhibitor (see below). The other two agents can be taken on the morning of surgery, although fluoxetine has a long half-life, so missing a dose should not be problematic, and lorazepam can be given intravenously if needed.
SSRIs, including fluoxetine, are generally safe perioperatively. Serotonin depletion from platelets, however, increases the risk of bleeding, especially gastrointestinal bleeding, when SSRIs are used with NSAIDs.20–22 A neurosurgical procedure may therefore be especially risky in patients who have not stopped their SSRI if they are also taking an NSAID or an herbal medication that may increase the risk of bleeding. The caveat to stopping SSRIs is the potential for a minor withdrawal syndrome.
Tricyclic antidepressants inhibit the reuptake of norepinephrine and serotonin and may increase the action of sympathomimetics. Although arrhythmias are thought to be a concern with tricyclics, there are no reported cases of association in the literature. In general, I advise continuing triclyclics perioperatively, especially in patients who are on high doses.
Benzodiazepines, including lorazepam, are safe to use perioperatively, and a potential for withdrawal symptoms (hypertension, agitation, delirium, seizures) argues against their discontinuation. Chronic benzodiazepine use may increase anesthetic requirements.
Antipsychotic agents, which include haloperidol, olanzapine, risperidone, and ziprasidone, have multiple routes of administration—intramuscular, oral, sublingual, and intravenous. These agents are generally safe to use in the perioperative period.
MAO inhibitors, including phenelzine, are no longer commonly used and are typically reserved for the treatment of refractory depression. But they merit attention, as their use can cause accumulation of biogenic amines in the central and autonomic nervous systems. There are two types of MAO reactions—excitatory and depressive. Excitatory reactions lead to serotonin syndrome. Depressive reactions induce inhibition of hepatic microsomal enzymes, leading to narcotic accumulation and increased sedation.23
MAO inhibitors are also of concern because of their many drug interactions. When used with indirect sympathomimetics such as ephedrine, they promote a massive release of stored norepinephrine, leading to severe hypertension. When used with opioids like meperidine and dextromethorphan, MAO inhibitors are associated with a serotonin syndrome characterized by agitation, headache, fever, seizures, coma, and death.
Discontinuing MAO inhibitors before the day of surgery is no longer universally recommended, due to the risk of precipitating an exacerbation of major depression. Safe anesthetic regimens in the setting of MAO inhibitors involve avoidance of meperidine (morphine and fentanyl are safe) and use of only direct-acting sympathomimetics.
CONCLUSIONS
A good medication history that includes herbal and OTC products is essential for safe induction of anesthesia and optimization of outcomes during and following surgery. In general, medications with the potential to induce withdrawal symptoms should be continued. The use of nonessential medications that can increase surgical risk should be discontinued. If neither of these conditions applies, consider the patient’s risk profile and the risk of the procedure when making perioperative management decisions. Be mindful of withdrawal syndromes and resume medications with the potential for such syndromes as soon as possible.
DISCUSSION
Comment from the audience: In regard to your comment that diuretics are typically held on the morning of surgery, my institution recently completed a randomized placebo-controlled trial (publication is pending) in which we studied the effect of continuing or not continuing furosemide preoperatively. We found no difference in the occurrence of intraoperative hypotension between the two groups. It will be interesting to see if these findings change practice over time.
Dr. Whinney: It’s good to know that hypotension is not a concern with furosemide, but the issue here is not just blood pressure but electrolyte abnormalities that could predispose to arrhythmias. The patients who concern me are those who haven’t been seen by a physician for a while and may be on high doses of furosemide. I would scrutinize such patients closely.
Question from the audience: We see a number of patients on methotrexate and other disease-modifying rheumatologic drugs. Can you comment on the perioperative management of these medications?
Dr. Whinney: Methotrexate has caused some anxiety over the risk of infection, but the literature does not support such concern.24 In fact, it appears that continuing methotrexate is probably advisable because the risk of decompensation of the disease may be worse than the potential infectious risks. The only caveat is the patient with renal insufficiency, in whom the recommendation is to withhold methotrexate for 2 weeks before surgery. While most rheumatologists favor withholding disease-modifying drugs perioperatively, a recent systematic review showed no increased risk of either total or infectious complications with use of immunomodulators including infliximab, azathioprine, and cyclosporine.25 It is still reasonable and prudent to discuss this issue with the patient’s rheumatologist. Hydroxychloroquine is safe to continue.
Comment from the audience: First, I would like to urge everyone to be mindful of medication-related indications for preoperative testing. There are many psychotropic drugs that prolong the QT interval and thus constitute an indication for a baseline electrocardiogram prior to surgery. Second, I believe there is a mythology in the perioperative community about the bleeding risk associated with omega-3 fatty acids and vitamin E. Can you comment on the bleeding risks associated with each?
Dr. Whinney: There are few data; the fear is based purely on the potential of these compounds to cause bleeding. Neither is beneficial for short-term quality of life or for chronic prevention, and there’s no withdrawal syndrome from either. So I generally withhold them, but if the patient is still taking them up to the day of surgery, it doesn’t merit postponing surgery. I generally let the surgeon or the nurse know, and it tends not to be a big deal.
Question from the audience: Do you stop herbal teas, energy drinks, and diet medications such as phentermine prior to surgery?
Dr. Whinney: You need to know which diet medications the patient is taking. The problem with many of the OTC products is that they may or may not be considered drugs, so they may not be approved by the FDA and thus you don’t know what the patient is actually taking. For the most part, a diet medication does not contribute to short-term quality of life. My aim is to get the patient through surgery as safely as possible, so if a patient is taking an agent with ingredients, known or unknown, with an interaction potential, then I will stop it.
The two types of diet agents are those that block the absorption of fat, which could interact with other oral agents given at the same time, and those that act via the gastrointestinal tract. I generally withhold the fat-absorption blockers the day before surgery. Phentermine has the potential for catecholinergic reactions or sympathomimetic actions. I would put it in the category of herbal-type medicines and withhold it for at least 7 days.
Question from the audience: Can you comment on combination drugs such as losartan/hydrochlorothiazide on the morning of surgery?
Dr. Whinney: The ARB losartan may have more physiologic benefit than the diuretic, so I would prescribe a single dose of losartan the morning of surgery if I had decided to continue this class of medication for uncontrolled hypertension or concern over heart failure decompensation. The same is true for a beta-blocker/diuretic combination product; I will prescribe the beta-blocker component individually and tell the patient to take it the morning of surgery.
Question from the audience: I’m confused by the recommendation to stop hydrochlorothiazide. It’s a far less potent diuretic than furosemide. Does the risk of stopping it, with resulting blood pressure elevation, outweigh the risk of a mild hypotensive response because of a mild diuretic effect? I’m aware of no data on the risk of stopping hydrochlorothiazide—are you?
Dr. Whinney: There are no data. Again, the recommendation is based on the physiology of the drug, as well as on expert consensus and opinion. Since anesthesia has a vasodilatory effect with a hypotensive response, it’s probably reasonable to hold hydrochlorothiazide if its only indication is for hypertension. That’s the logic behind the recommendation. If you continue it the day of surgery, it may not necessarily hurt, but we’re not certain.
Question from the audience: The implication from your third case study was that alendronate should be held. What’s the basis of that recommendation?
Dr. Whinney: First, the patient has to be upright for 30 minutes after taking alendronate, which could be a problem on the morning of surgery. Also, withholding it will not impair short-term quality of life; it’s a weekly medication, so the patient can take her next dose once she’s up and ambulatory.
Question from the audience: What do you for young women on oral contraceptives? I’m lucky if I see them within 7 days of surgery.
Dr. Whinney: You’re bringing up the concern with exogenous hormones and the risk of venous thromboembolism (VTE), a risk that clearly is increased with the hypercoagulable milieu of surgery. The recommendation is to stop hormone therapy 30 to 45 days prior to surgery in these patients. As you note, however, we don’t get the chance to see patients during that window of opportunity. So the question is whether stopping hormones within a shorter time period results in an incremental benefit. And that is not necessarily the case. These patients should be seen as being at risk for VTE and be given appropriate VTE prophylaxis. In fact, in the similar context of menopausal hormone therapy, a study among women undergoing orthopedic surgery showed that as long as they received appropriate VTE prophylaxis, there was no significant difference in VTE rates between the women whose hormone therapy was withheld versus those who continued it.26
Question from the audience: Are there concerns about withdrawal in patients with peripheral vascular disease treated with cilostazol or pentoxifylline?
Dr. Whinney: It’s not particularly well studied. Guidelines from the American College of Physicians suggest to hold these agents for elective surgeries.27 With respect to antiplatelet therapies, O’Riordan et al did a systematic review of 99 articles pertaining to antiplatelet agents in the perioperative period and concluded that aspirin should not be stopped in patients going for surgery.28 In vascular surgery, antiplatelet agents may help promote graft patency.
- National patient safety goals. The Joint Commission Web site. http://www.jointcommission.org/patientsafety/nationalpatientsafetygoals/. Accessed July 29, 2009.
- Papadopoulos S, Cook AM. You can withdraw from that? The effects of abrupt discontinuation of medications. Orthopedics 2006; 29:413–417.
- Marik PE, Varon J. Requirement of perioperative stress doses of corticosteroids: a systematic review of the literature. Arch Surg 2008; 143:1222–1226.
- Kennedy JM, van Rij AM, Spears GF, Pettigrew RA, Tucker IG. Polypharmacy in a general surgical unit and consequences of drug withdrawal. Br J Clin Pharmacol 2000; 49:353–362.
- Bell CM, Bajcar J, Bierman AS, Li P, Mamdani MM, Urbach DR. Potentially unintended discontinuation of long-term medication use after elective surgical procedures. Arch Intern Med 2006; 166:2525–2531.
- Pass SE, Simpson RW. Discontinuation and reinstitution of medications during the perioperative period. Am J Health Syst Pharm 2004; 61:899–912.
- Muluk V, Macpherson DS. Perioperative medication management. In: Rose BD, ed. UpToDate. Waltham, MA; 2008.
- Connelly CS, Panush RS. Should nonsteroidal anti-inflammatory drugs be stopped before elective surgery? Arch Intern Med 1991; 151:1963–1966.
- Robinson CM, Christie J, Malcolm-Smith N. Nonsteroidal antiinflammatory drugs, perioperative blood loss, and transfusion requirements in elective hip arthroplasty. J Arthroplasty 1993; 8:607–610.
- Goldenberg NA, Jacobson L, Manco-Johnson MJ. Brief communication: duration of platelet dysfunction after a 7-day course of ibuprofen. Ann Intern Med 2005; 142:506–509.
- González-Correa JA, Arrebola MM, Martín-Salido E, Muñoz-Marin J, de la Cuesta FS, De La Cruz JP. Effects of dexibuprofen on platelet function in humans: comparison with low-dose aspirin. Anesthesiology 2007; 106:218–225.
- Coriat P, Richer C, Douraki T, et al. Influence of chronic angiotensin-converting enzyme inhibition on anesthetic induction. Anesthesiology 1994; 81:299–307.
- Groban L, Butterworth J. Perioperative management of chronic heart failure. Anesth Analg 2006; 103:557–575.
- Mathew JP, Fontes ML, Tudor IC, et al. A multicenter risk index for atrial fibrillation after cardiac surgery. JAMA 2004; 291:1720–1729.
- Brabant SM, Bertrand M, Eyraud D, Darmon PL, Coriat P. The hemodynamic effects of anesthetic induction in vascular surgical patients chronically treated with angiotensin II receptor antagonists. Anesth Analg 1999; 89:1388–1392.
- Feringa HH, Bax JJ, Schouten O, Poldermans D. Protecting the heart with cardiac medication in patients with left ventricular dysfunction undergoing major noncardiac vascular surgery. Semin Cardiothorac Vasc Anesth 2006; 10:25–31.
- Rosenman DJ, McDonald FS, Ebbert JO, Erwin PJ, LaBella M, Montori VM. Clinical consequences of withholding versus administering renin-angiotensin-aldosterone system antagonists in the preoperative period. J Hosp Med 2008; 3:319–325.
- Ang-Lee MK, Moss J, Yuan CS. Herbal medicines and perioperative care. JAMA 2001; 286:208–216.
- Cui J, Garle M, Eneroth P, Björkhem I. What do commercial ginseng preparations contain? Lancet 1994; 344:134.
- Yuan Y, Tsoi K, Hunt RH. Selective serotonin reuptake inhibitors and risk of upper GI bleeding: confusion or confounding? Am J Med 2006; 119:719–727.
- de Abajo FJ, Montero D, Rodríguez LA, Madurga M. Antidepressants and risk of upper gastrointestinal bleeding. Basic Clin Pharmacol Toxicol 2006; 98:304–310.
- Serebruany VL. Selective serotonin reuptake inhibitors and increased bleeding risk: are we missing something? Am J Med 2006; 119:113–116.
- Stack CG, Rogers P, Linter SP. Monoamine oxidase inhibitors and anaesthesia: a review. Br J Anaesth 1988; 60:222–227.
- Grennan DM, Gray J, Loudon J, Fear S. Methotrexate and early postoperative complications in patients with rheumatoid arthritis undergoing elective orthopaedic surgery. Ann Rheum Dis 2001; 60:214–217.
- Subramanian V, Pollok RC, Kang JY, Kumar D. Systematic review of postoperative complications in patients with inflammatory bowel disease treated with immunomodulators. Br J Surg 2006; 93:793–799.
- Hurbanek JG, Jaffer AK, Morra N, Karafa M, Brotman DJ. Postmenopausal hormone replacement and venous thromboembolism following hip and knee arthroplasty. Thromb Haemost 2004; 92:337–343.
- Cohn SL. Perioperative medication management. American College of Physicians’ PIER (Physicians’ Information and Education Resource) Web site. http://pier.acponline.org/physicians/diseases/d835/diagnosis/d835-s3.html. Posted May 29, 2009. Accessed August 14, 2009.
- O’Riordan JM, Margey RJ, Blake G, O’Connell R. Antiplatelet agents in the perioperative period. Arch Surg 2009; 144:69–76.
As a hospitalist who practices in a perioperative clinic, I probably spend more of my time with patients reviewing and discussing the medications they are taking than on any other single subject. Surgical patients—many of whom are elderly—commonly are on multiple medications, have renal or hepatic disease that can alter drug metabolism, and may not be adequately educated about their medication regimens.
Patient safety is the overriding concern behind perioperative medication management, consistent with the medication-related objectives in the Joint Commission’s 2009 National Patient Safety Goals.1 The increasing surgical burden that comes with an aging population, along with rising expectations for functional recovery, has likewise elevated the importance of perioperative medication management.
Despite these demands, there is scant evidence from randomized controlled trials to directly guide perioperative medication management. For this reason, recommendations in this area rely largely on other forms of evidence, including expert consensus, case reports, in vitro studies, recommendations from pharmaceutical companies, and other known data (pharmacokinetics, drug interactions with anesthetic agents, and effects of the agent on the primary disease and on perioperative risk).
This article reviews general principles of perioperative medication management and then presents four case vignettes to explore perioperative recommendations for a number of common medication classes. It is not intended as a comprehensive review of the perioperative management of all medications, as numerous classes (antiplatelets, beta-blockers, oral hypogycemic agents, insulin, statins) are discussed in detail elsewhere in this proceedings supplement.
GENERAL CONSIDERATIONS IN MEDICATION MANAGEMENT
A comprehensive medication history is fundamental
Effective perioperative management of medications requires an understanding of the patient and his or her comorbidities so that the risk of perioperative decompensation can be gauged. This understanding stems from a thorough medical history that includes a comprehensive medication history to provide a complete inventory of the following:
- All prescription medications
- All over-the-counter (OTC) agents (including nonsteroidal anti-inflammatory drugs [NSAIDs])
- All vitamins
- All herbal medications.
When to stop, when to resume?
Guidance on stopping and resuming medications in the perioperative period is relatively absent from the literature. General considerations include the following:
- The potential for withdrawal when stopping a medication
- The progression of disease with interruption of drug therapy
- The potential for interactions with anesthetic agents if the medication is continued.
Withdrawal potential
Abrupt discontinuation of some drugs may lead to unnecessary complications due to the potential for withdrawal. Common medications that have been associated with withdrawal symptoms are selective serotonin reuptake inhibitors (SSRIs), beta-blockers, clonidine, statins, and corticosteroids.2 A recent systematic literature review concluded that continuation of chronic corticosteroid therapy without supplemental (stress) doses of corticosteroids is appropriate unless patients have primary disease of the hypothalamic-pituitary-adrenal axis, in which case perioperative stress dosing is recommended to avoid acute adrenal insufficiency (addisonian crisis).3
Patients on chronic drugs are more likely to have complications
In a medication survey of 1,025 patients admitted to a general surgery unit, Kennedy et al reported that 49% of the patients were taking medications (other than vitamins) unrelated to their surgical procedure.4 Even while this percentage is considerably lower than what I observe in my practice, this study showed that medication use has important perioperative consequences4:
- The odds ratio for a postoperative complication was 2.7 (95% CI, 1.76–4.04) if patients were taking a drug unrelated to their surgery.
- The risk of a complication was particularly elevated if patients were taking cardiovascular drugs or agents that act on the central nervous system; if patients were on NPO (“nothing by mouth”) orders for more than 24 hours before surgery; and if the operation was more than 1 hour in duration. These findings could reflect destabilization of the disease processes for which the patients were taking chronic medications that required interruption.
Unintended discontinuation of chronic drugs
Stopping a chronic medication for a surgical procedure raises the possibility that its resumption could be overlooked, especially since medical errors are particularly common in the transition between health care settings following hospital discharge. A population-based cohort study among all elderly patients discharged from Ontario, Canada, hospitals over a 5½-year period found that 11.4% of patients undergoing elective surgery did not resume their indicated chronic warfarin therapy within 6 months after its presurgical discontinuation.5 Although 6-month rates of unintended failure to resume therapy were lower for statins (4%) and ophthalmic beta-blocker drops (8%),5 these findings underscore that drug discontinuation always carries a risk that therapy might not be resumed as indicated.
Additional considerations
Stress response to surgery. Decisions about perioperative drug therapy should always take into account the stress response to surgery and the challenge it presents to homeostasis in the face of increased sympathetic tone and release of pituitary hormones.
Unreliable absorption of oral medications. Surgery and the postoperative state can lead to unreliable absorption of oral drugs for any of a number of reasons: villous atrophy, diminished blood flow to the gut, edema, mucosal ischemia, diminished motility from postoperative ileus, and use of narcotics.6
Take-away general principles
The following principles can be applied to guide perioperative medication management in a general sense7:
- Continue medications with withdrawal potential
- Discontinue medications that increase surgical risk and are not essential for short-term quality of life
- Use clinical judgment when neither of the above two principles applies, but be mindful that many other medications are given in the narrow perioperative time window and that metabolism and elimination of chronic drugs may be altered.
CASE 1: A PATIENT ON A NONPRESCRIPTION NSAID FOR SEVERE ARTHRITIS
A 55-year-old man with severe osteoarthritis is scheduled for total hip arthroplasy in 2 days. He stopped his aspirin (325 mg/day) 1 week ago but continued taking ibuprofen 600 three times daily with food, explaining that “no one told me to stop.” His last dose was yesterday evening.
Question: What should you do?
A. Call the surgeon and cancel the surgery
B. Call the surgeon to notify, and tell the patient to stop the ibuprofen now
C. Check his bleeding time and proceed if normal
D. Just tell the patient to stop the ibuprofen now
E. Proceed to the operating room regardless of the ibuprofen dose
The best approach would be to notify the surgeon and tell the patient to stop the ibuprofen now. NSAIDs such as ibuprofen reversibly inhibit platelet cyclooxygenase (COX), diminish thromboxane A2 production, diminish platelet aggregation, and can increase bleeding time measurement and overall bleeding risk. They can induce renal failure in combination with other drugs, especially in the setting of hypotension.8,9 COX-2 inhibitors have less effect on platelet function but retain the potential for renal toxicity and also confer well-known cardiovascular risks.
In the past, NSAIDs were typically held for 7 days before surgery, but this practice was not supported with much evidence. In vitro assessment indicates that platelet function normalizes within 24 hours after cessation of regular ibuprofen or dexibuprofen in healthy individuals.10,11
Since NSAIDs vary in their effect on bleeding time, which does not correlate well with elimination half-life, a general recommendation is to stop most NSAIDs at least 3 days before surgery.
CASE 2: A PATIENT ON MULTIPLE CARDIOVASCULAR DRUGS
A 67-year-old man with dilated cardiomyopathy and an ejection fraction of 25% (well compensated) is scheduled for a laparoscopic cholecystectomy tomorrow. He is taking lisinopril (40 mg/day), irbesartan (150 mg/day), and furosemide (80 mg/day).
Question: What is your advice?
A. Call the surgeon and cancel the surgery
B. Call the surgeon to notify, and tell the patient to stop his medications now
C. Hold all of the above medications on the morning of surgery
D. Proceed to the operating room with the usual doses of his medications on the morning of surgery
The best approach is to withhold these medications on the morning of surgery.
Diuretics are typically held on the morning of surgery because of the potential for hypovolemia and electrolyte depletion.
Angiotensin-converting enzyme (ACE) inhibitors intensify the hypotensive effects of anesthesia induction. Because angiotensin II plays a key role in maintaining circulating volume in response to stressors, volume deficits can occur in ACE inhibitor-treated patients as angiotensin II cannot compensate for venous pooling of blood, resulting in diminished cardiac output and arterial hypotension. However, continued renin-angiotensin system suppression may protect regional circulation, as has been demonstrated by reduced release of cardiac enzymes with ACE inhibitor continuation (compared with interruption) in cardiac surgery patients. ACE inhibitors also have a renal protective effect, preserving glomerular filtration rate in patients undergoing aortic abdominal aneurysm repair or coronary artery bypass graft surgery. Hypotension with ACE inhibition is treatable with sympathomimetics, alpha-agonists, and intravenous fluids.12–15
If a patient’s ACE inhibitor is stopped, be prepared for rebound postoperative hypertension. The probability of postoperative atrial fibrillation is also increased with ACE inhibitor interruption.14 In patients with left ventricular dysfunction undergoing noncardiac vascular surgery, continued ACE inhibition is associated with reduced mortality.16 These data argue, at the very least, for prompt resumption of ACE inhibitors after surgery.
Angiotensin receptor blockers (ARBs) have largely the same clinical benefits as do ACE inhibitors. These agents also increase the risk of hypotension upon induction of anesthesia, and this hypotension is not as responsive to conventional vasopressors such as ephedrine and phenylephrine; a better response is achieved with vasopressin.15 In light of the long half-life of ARBs, current thinking is to withhold them 24 hours before surgery.
Rosenman et al recently published a meta-analysis of five studies assessing the effects of continuing or withholding ACE inhibitors and ARBs in the preoperative period.17 They found a statistically significant increase in the incidence of perioperative hypotension in patients in whom the drugs were continued compared with those in whom the drugs were withheld (relative risk = 1.50; 95% CI, 1.15–1.96), but there was no significant difference in the rate of perioperative MI between the two groups. Notably, the indication for ACE inhibitor or ARB use in all of the studies was hypertension, not heart failure.
My approach to the perioperative management of ACE inhibitors and ARBs is to withhold them on the morning of surgery (in the case of ARBs, 24 hours prior to surgery) if their only indication is for hypertension and if the patient’s blood pressure is well controlled. If the patient has another indication for these agents or has hypertension that is not well controlled, I am inclined to continue these agents but will first discuss the decision with the anesthesiologist.
CASE 3: A PATIENT TAKING HERBAL MEDICATIONS
A 68-year-old woman with a history of hypertension, osteoarthritis, and osteoporosis is scheduled for total hip replacement in 7 days. Her medications include atenolol, hydrochlorothiazide, and alendronate. She also reports taking some natural herbal medications. She does not recall their names initially but calls back with the names: ginkgo biloba for her memory and echinacea for her immune system.
Question: What are your recommendations?
A. Stop all medications now except atenolol and proceed to surgery
B. Stop the herbals now but take all other medications on the morning of surgery
C. Stop the herbals now and take only atenolol on the morning of surgery
D. Continue all medications now and take atenolol and the herbals on the morning of surgery
E. Cancel the surgery and call an herbalist for guidance
The best strategy is to stop the herbals now and tell her to take only atenolol (a beta-blocker) on the morning of surgery.
Because the US Food and Drug Administration (FDA) does not regulate herbal products, the contents of these products can vary widely. For example, an analysis using mass spectrometry of 50 commercial ginseng products from 11 countries found that the ginseng content varied from 0% (six preparations) to 9%.19 Catecholamine-type compounds were found in some of the products.19
Because of the uncertainty over their actual contents, herbal medications should be stopped at least 7 days prior to surgery. If a patient is still taking herbal supplements on the day before surgery, I typically alert the anesthesiologist and surgeon.
CASE 4: A PATIENT ON MULTIPLE PSYCHOTROPICS
A 38-year-old woman with a history of severe major depression is scheduled for a mastectomy for breast cancer the next day. Her medications include fluoxetine, lorazepam, and phenelzine, all of which she has been taking for many years.
Question: What is your course of action?
A. Call the surgeon and cancel the surgery
B. Call the surgeon and notify the day-of-surgery anesthesiologist that the patient is taking these agents
C. Stop all the medications now and proceed to the operating room
D. Request a psychiatric consult for an alternative drug regimen
E. Proceed and advise the patient to take all of these agents on the morning of surgery
My approach would be to notify the day-of-surgery anesthesiologist, specifically about the phenelzine, which is a monoamine oxidase (MAO) inhibitor (see below). The other two agents can be taken on the morning of surgery, although fluoxetine has a long half-life, so missing a dose should not be problematic, and lorazepam can be given intravenously if needed.
SSRIs, including fluoxetine, are generally safe perioperatively. Serotonin depletion from platelets, however, increases the risk of bleeding, especially gastrointestinal bleeding, when SSRIs are used with NSAIDs.20–22 A neurosurgical procedure may therefore be especially risky in patients who have not stopped their SSRI if they are also taking an NSAID or an herbal medication that may increase the risk of bleeding. The caveat to stopping SSRIs is the potential for a minor withdrawal syndrome.
Tricyclic antidepressants inhibit the reuptake of norepinephrine and serotonin and may increase the action of sympathomimetics. Although arrhythmias are thought to be a concern with tricyclics, there are no reported cases of association in the literature. In general, I advise continuing triclyclics perioperatively, especially in patients who are on high doses.
Benzodiazepines, including lorazepam, are safe to use perioperatively, and a potential for withdrawal symptoms (hypertension, agitation, delirium, seizures) argues against their discontinuation. Chronic benzodiazepine use may increase anesthetic requirements.
Antipsychotic agents, which include haloperidol, olanzapine, risperidone, and ziprasidone, have multiple routes of administration—intramuscular, oral, sublingual, and intravenous. These agents are generally safe to use in the perioperative period.
MAO inhibitors, including phenelzine, are no longer commonly used and are typically reserved for the treatment of refractory depression. But they merit attention, as their use can cause accumulation of biogenic amines in the central and autonomic nervous systems. There are two types of MAO reactions—excitatory and depressive. Excitatory reactions lead to serotonin syndrome. Depressive reactions induce inhibition of hepatic microsomal enzymes, leading to narcotic accumulation and increased sedation.23
MAO inhibitors are also of concern because of their many drug interactions. When used with indirect sympathomimetics such as ephedrine, they promote a massive release of stored norepinephrine, leading to severe hypertension. When used with opioids like meperidine and dextromethorphan, MAO inhibitors are associated with a serotonin syndrome characterized by agitation, headache, fever, seizures, coma, and death.
Discontinuing MAO inhibitors before the day of surgery is no longer universally recommended, due to the risk of precipitating an exacerbation of major depression. Safe anesthetic regimens in the setting of MAO inhibitors involve avoidance of meperidine (morphine and fentanyl are safe) and use of only direct-acting sympathomimetics.
CONCLUSIONS
A good medication history that includes herbal and OTC products is essential for safe induction of anesthesia and optimization of outcomes during and following surgery. In general, medications with the potential to induce withdrawal symptoms should be continued. The use of nonessential medications that can increase surgical risk should be discontinued. If neither of these conditions applies, consider the patient’s risk profile and the risk of the procedure when making perioperative management decisions. Be mindful of withdrawal syndromes and resume medications with the potential for such syndromes as soon as possible.
DISCUSSION
Comment from the audience: In regard to your comment that diuretics are typically held on the morning of surgery, my institution recently completed a randomized placebo-controlled trial (publication is pending) in which we studied the effect of continuing or not continuing furosemide preoperatively. We found no difference in the occurrence of intraoperative hypotension between the two groups. It will be interesting to see if these findings change practice over time.
Dr. Whinney: It’s good to know that hypotension is not a concern with furosemide, but the issue here is not just blood pressure but electrolyte abnormalities that could predispose to arrhythmias. The patients who concern me are those who haven’t been seen by a physician for a while and may be on high doses of furosemide. I would scrutinize such patients closely.
Question from the audience: We see a number of patients on methotrexate and other disease-modifying rheumatologic drugs. Can you comment on the perioperative management of these medications?
Dr. Whinney: Methotrexate has caused some anxiety over the risk of infection, but the literature does not support such concern.24 In fact, it appears that continuing methotrexate is probably advisable because the risk of decompensation of the disease may be worse than the potential infectious risks. The only caveat is the patient with renal insufficiency, in whom the recommendation is to withhold methotrexate for 2 weeks before surgery. While most rheumatologists favor withholding disease-modifying drugs perioperatively, a recent systematic review showed no increased risk of either total or infectious complications with use of immunomodulators including infliximab, azathioprine, and cyclosporine.25 It is still reasonable and prudent to discuss this issue with the patient’s rheumatologist. Hydroxychloroquine is safe to continue.
Comment from the audience: First, I would like to urge everyone to be mindful of medication-related indications for preoperative testing. There are many psychotropic drugs that prolong the QT interval and thus constitute an indication for a baseline electrocardiogram prior to surgery. Second, I believe there is a mythology in the perioperative community about the bleeding risk associated with omega-3 fatty acids and vitamin E. Can you comment on the bleeding risks associated with each?
Dr. Whinney: There are few data; the fear is based purely on the potential of these compounds to cause bleeding. Neither is beneficial for short-term quality of life or for chronic prevention, and there’s no withdrawal syndrome from either. So I generally withhold them, but if the patient is still taking them up to the day of surgery, it doesn’t merit postponing surgery. I generally let the surgeon or the nurse know, and it tends not to be a big deal.
Question from the audience: Do you stop herbal teas, energy drinks, and diet medications such as phentermine prior to surgery?
Dr. Whinney: You need to know which diet medications the patient is taking. The problem with many of the OTC products is that they may or may not be considered drugs, so they may not be approved by the FDA and thus you don’t know what the patient is actually taking. For the most part, a diet medication does not contribute to short-term quality of life. My aim is to get the patient through surgery as safely as possible, so if a patient is taking an agent with ingredients, known or unknown, with an interaction potential, then I will stop it.
The two types of diet agents are those that block the absorption of fat, which could interact with other oral agents given at the same time, and those that act via the gastrointestinal tract. I generally withhold the fat-absorption blockers the day before surgery. Phentermine has the potential for catecholinergic reactions or sympathomimetic actions. I would put it in the category of herbal-type medicines and withhold it for at least 7 days.
Question from the audience: Can you comment on combination drugs such as losartan/hydrochlorothiazide on the morning of surgery?
Dr. Whinney: The ARB losartan may have more physiologic benefit than the diuretic, so I would prescribe a single dose of losartan the morning of surgery if I had decided to continue this class of medication for uncontrolled hypertension or concern over heart failure decompensation. The same is true for a beta-blocker/diuretic combination product; I will prescribe the beta-blocker component individually and tell the patient to take it the morning of surgery.
Question from the audience: I’m confused by the recommendation to stop hydrochlorothiazide. It’s a far less potent diuretic than furosemide. Does the risk of stopping it, with resulting blood pressure elevation, outweigh the risk of a mild hypotensive response because of a mild diuretic effect? I’m aware of no data on the risk of stopping hydrochlorothiazide—are you?
Dr. Whinney: There are no data. Again, the recommendation is based on the physiology of the drug, as well as on expert consensus and opinion. Since anesthesia has a vasodilatory effect with a hypotensive response, it’s probably reasonable to hold hydrochlorothiazide if its only indication is for hypertension. That’s the logic behind the recommendation. If you continue it the day of surgery, it may not necessarily hurt, but we’re not certain.
Question from the audience: The implication from your third case study was that alendronate should be held. What’s the basis of that recommendation?
Dr. Whinney: First, the patient has to be upright for 30 minutes after taking alendronate, which could be a problem on the morning of surgery. Also, withholding it will not impair short-term quality of life; it’s a weekly medication, so the patient can take her next dose once she’s up and ambulatory.
Question from the audience: What do you for young women on oral contraceptives? I’m lucky if I see them within 7 days of surgery.
Dr. Whinney: You’re bringing up the concern with exogenous hormones and the risk of venous thromboembolism (VTE), a risk that clearly is increased with the hypercoagulable milieu of surgery. The recommendation is to stop hormone therapy 30 to 45 days prior to surgery in these patients. As you note, however, we don’t get the chance to see patients during that window of opportunity. So the question is whether stopping hormones within a shorter time period results in an incremental benefit. And that is not necessarily the case. These patients should be seen as being at risk for VTE and be given appropriate VTE prophylaxis. In fact, in the similar context of menopausal hormone therapy, a study among women undergoing orthopedic surgery showed that as long as they received appropriate VTE prophylaxis, there was no significant difference in VTE rates between the women whose hormone therapy was withheld versus those who continued it.26
Question from the audience: Are there concerns about withdrawal in patients with peripheral vascular disease treated with cilostazol or pentoxifylline?
Dr. Whinney: It’s not particularly well studied. Guidelines from the American College of Physicians suggest to hold these agents for elective surgeries.27 With respect to antiplatelet therapies, O’Riordan et al did a systematic review of 99 articles pertaining to antiplatelet agents in the perioperative period and concluded that aspirin should not be stopped in patients going for surgery.28 In vascular surgery, antiplatelet agents may help promote graft patency.
As a hospitalist who practices in a perioperative clinic, I probably spend more of my time with patients reviewing and discussing the medications they are taking than on any other single subject. Surgical patients—many of whom are elderly—commonly are on multiple medications, have renal or hepatic disease that can alter drug metabolism, and may not be adequately educated about their medication regimens.
Patient safety is the overriding concern behind perioperative medication management, consistent with the medication-related objectives in the Joint Commission’s 2009 National Patient Safety Goals.1 The increasing surgical burden that comes with an aging population, along with rising expectations for functional recovery, has likewise elevated the importance of perioperative medication management.
Despite these demands, there is scant evidence from randomized controlled trials to directly guide perioperative medication management. For this reason, recommendations in this area rely largely on other forms of evidence, including expert consensus, case reports, in vitro studies, recommendations from pharmaceutical companies, and other known data (pharmacokinetics, drug interactions with anesthetic agents, and effects of the agent on the primary disease and on perioperative risk).
This article reviews general principles of perioperative medication management and then presents four case vignettes to explore perioperative recommendations for a number of common medication classes. It is not intended as a comprehensive review of the perioperative management of all medications, as numerous classes (antiplatelets, beta-blockers, oral hypogycemic agents, insulin, statins) are discussed in detail elsewhere in this proceedings supplement.
GENERAL CONSIDERATIONS IN MEDICATION MANAGEMENT
A comprehensive medication history is fundamental
Effective perioperative management of medications requires an understanding of the patient and his or her comorbidities so that the risk of perioperative decompensation can be gauged. This understanding stems from a thorough medical history that includes a comprehensive medication history to provide a complete inventory of the following:
- All prescription medications
- All over-the-counter (OTC) agents (including nonsteroidal anti-inflammatory drugs [NSAIDs])
- All vitamins
- All herbal medications.
When to stop, when to resume?
Guidance on stopping and resuming medications in the perioperative period is relatively absent from the literature. General considerations include the following:
- The potential for withdrawal when stopping a medication
- The progression of disease with interruption of drug therapy
- The potential for interactions with anesthetic agents if the medication is continued.
Withdrawal potential
Abrupt discontinuation of some drugs may lead to unnecessary complications due to the potential for withdrawal. Common medications that have been associated with withdrawal symptoms are selective serotonin reuptake inhibitors (SSRIs), beta-blockers, clonidine, statins, and corticosteroids.2 A recent systematic literature review concluded that continuation of chronic corticosteroid therapy without supplemental (stress) doses of corticosteroids is appropriate unless patients have primary disease of the hypothalamic-pituitary-adrenal axis, in which case perioperative stress dosing is recommended to avoid acute adrenal insufficiency (addisonian crisis).3
Patients on chronic drugs are more likely to have complications
In a medication survey of 1,025 patients admitted to a general surgery unit, Kennedy et al reported that 49% of the patients were taking medications (other than vitamins) unrelated to their surgical procedure.4 Even while this percentage is considerably lower than what I observe in my practice, this study showed that medication use has important perioperative consequences4:
- The odds ratio for a postoperative complication was 2.7 (95% CI, 1.76–4.04) if patients were taking a drug unrelated to their surgery.
- The risk of a complication was particularly elevated if patients were taking cardiovascular drugs or agents that act on the central nervous system; if patients were on NPO (“nothing by mouth”) orders for more than 24 hours before surgery; and if the operation was more than 1 hour in duration. These findings could reflect destabilization of the disease processes for which the patients were taking chronic medications that required interruption.
Unintended discontinuation of chronic drugs
Stopping a chronic medication for a surgical procedure raises the possibility that its resumption could be overlooked, especially since medical errors are particularly common in the transition between health care settings following hospital discharge. A population-based cohort study among all elderly patients discharged from Ontario, Canada, hospitals over a 5½-year period found that 11.4% of patients undergoing elective surgery did not resume their indicated chronic warfarin therapy within 6 months after its presurgical discontinuation.5 Although 6-month rates of unintended failure to resume therapy were lower for statins (4%) and ophthalmic beta-blocker drops (8%),5 these findings underscore that drug discontinuation always carries a risk that therapy might not be resumed as indicated.
Additional considerations
Stress response to surgery. Decisions about perioperative drug therapy should always take into account the stress response to surgery and the challenge it presents to homeostasis in the face of increased sympathetic tone and release of pituitary hormones.
Unreliable absorption of oral medications. Surgery and the postoperative state can lead to unreliable absorption of oral drugs for any of a number of reasons: villous atrophy, diminished blood flow to the gut, edema, mucosal ischemia, diminished motility from postoperative ileus, and use of narcotics.6
Take-away general principles
The following principles can be applied to guide perioperative medication management in a general sense7:
- Continue medications with withdrawal potential
- Discontinue medications that increase surgical risk and are not essential for short-term quality of life
- Use clinical judgment when neither of the above two principles applies, but be mindful that many other medications are given in the narrow perioperative time window and that metabolism and elimination of chronic drugs may be altered.
CASE 1: A PATIENT ON A NONPRESCRIPTION NSAID FOR SEVERE ARTHRITIS
A 55-year-old man with severe osteoarthritis is scheduled for total hip arthroplasy in 2 days. He stopped his aspirin (325 mg/day) 1 week ago but continued taking ibuprofen 600 three times daily with food, explaining that “no one told me to stop.” His last dose was yesterday evening.
Question: What should you do?
A. Call the surgeon and cancel the surgery
B. Call the surgeon to notify, and tell the patient to stop the ibuprofen now
C. Check his bleeding time and proceed if normal
D. Just tell the patient to stop the ibuprofen now
E. Proceed to the operating room regardless of the ibuprofen dose
The best approach would be to notify the surgeon and tell the patient to stop the ibuprofen now. NSAIDs such as ibuprofen reversibly inhibit platelet cyclooxygenase (COX), diminish thromboxane A2 production, diminish platelet aggregation, and can increase bleeding time measurement and overall bleeding risk. They can induce renal failure in combination with other drugs, especially in the setting of hypotension.8,9 COX-2 inhibitors have less effect on platelet function but retain the potential for renal toxicity and also confer well-known cardiovascular risks.
In the past, NSAIDs were typically held for 7 days before surgery, but this practice was not supported with much evidence. In vitro assessment indicates that platelet function normalizes within 24 hours after cessation of regular ibuprofen or dexibuprofen in healthy individuals.10,11
Since NSAIDs vary in their effect on bleeding time, which does not correlate well with elimination half-life, a general recommendation is to stop most NSAIDs at least 3 days before surgery.
CASE 2: A PATIENT ON MULTIPLE CARDIOVASCULAR DRUGS
A 67-year-old man with dilated cardiomyopathy and an ejection fraction of 25% (well compensated) is scheduled for a laparoscopic cholecystectomy tomorrow. He is taking lisinopril (40 mg/day), irbesartan (150 mg/day), and furosemide (80 mg/day).
Question: What is your advice?
A. Call the surgeon and cancel the surgery
B. Call the surgeon to notify, and tell the patient to stop his medications now
C. Hold all of the above medications on the morning of surgery
D. Proceed to the operating room with the usual doses of his medications on the morning of surgery
The best approach is to withhold these medications on the morning of surgery.
Diuretics are typically held on the morning of surgery because of the potential for hypovolemia and electrolyte depletion.
Angiotensin-converting enzyme (ACE) inhibitors intensify the hypotensive effects of anesthesia induction. Because angiotensin II plays a key role in maintaining circulating volume in response to stressors, volume deficits can occur in ACE inhibitor-treated patients as angiotensin II cannot compensate for venous pooling of blood, resulting in diminished cardiac output and arterial hypotension. However, continued renin-angiotensin system suppression may protect regional circulation, as has been demonstrated by reduced release of cardiac enzymes with ACE inhibitor continuation (compared with interruption) in cardiac surgery patients. ACE inhibitors also have a renal protective effect, preserving glomerular filtration rate in patients undergoing aortic abdominal aneurysm repair or coronary artery bypass graft surgery. Hypotension with ACE inhibition is treatable with sympathomimetics, alpha-agonists, and intravenous fluids.12–15
If a patient’s ACE inhibitor is stopped, be prepared for rebound postoperative hypertension. The probability of postoperative atrial fibrillation is also increased with ACE inhibitor interruption.14 In patients with left ventricular dysfunction undergoing noncardiac vascular surgery, continued ACE inhibition is associated with reduced mortality.16 These data argue, at the very least, for prompt resumption of ACE inhibitors after surgery.
Angiotensin receptor blockers (ARBs) have largely the same clinical benefits as do ACE inhibitors. These agents also increase the risk of hypotension upon induction of anesthesia, and this hypotension is not as responsive to conventional vasopressors such as ephedrine and phenylephrine; a better response is achieved with vasopressin.15 In light of the long half-life of ARBs, current thinking is to withhold them 24 hours before surgery.
Rosenman et al recently published a meta-analysis of five studies assessing the effects of continuing or withholding ACE inhibitors and ARBs in the preoperative period.17 They found a statistically significant increase in the incidence of perioperative hypotension in patients in whom the drugs were continued compared with those in whom the drugs were withheld (relative risk = 1.50; 95% CI, 1.15–1.96), but there was no significant difference in the rate of perioperative MI between the two groups. Notably, the indication for ACE inhibitor or ARB use in all of the studies was hypertension, not heart failure.
My approach to the perioperative management of ACE inhibitors and ARBs is to withhold them on the morning of surgery (in the case of ARBs, 24 hours prior to surgery) if their only indication is for hypertension and if the patient’s blood pressure is well controlled. If the patient has another indication for these agents or has hypertension that is not well controlled, I am inclined to continue these agents but will first discuss the decision with the anesthesiologist.
CASE 3: A PATIENT TAKING HERBAL MEDICATIONS
A 68-year-old woman with a history of hypertension, osteoarthritis, and osteoporosis is scheduled for total hip replacement in 7 days. Her medications include atenolol, hydrochlorothiazide, and alendronate. She also reports taking some natural herbal medications. She does not recall their names initially but calls back with the names: ginkgo biloba for her memory and echinacea for her immune system.
Question: What are your recommendations?
A. Stop all medications now except atenolol and proceed to surgery
B. Stop the herbals now but take all other medications on the morning of surgery
C. Stop the herbals now and take only atenolol on the morning of surgery
D. Continue all medications now and take atenolol and the herbals on the morning of surgery
E. Cancel the surgery and call an herbalist for guidance
The best strategy is to stop the herbals now and tell her to take only atenolol (a beta-blocker) on the morning of surgery.
Because the US Food and Drug Administration (FDA) does not regulate herbal products, the contents of these products can vary widely. For example, an analysis using mass spectrometry of 50 commercial ginseng products from 11 countries found that the ginseng content varied from 0% (six preparations) to 9%.19 Catecholamine-type compounds were found in some of the products.19
Because of the uncertainty over their actual contents, herbal medications should be stopped at least 7 days prior to surgery. If a patient is still taking herbal supplements on the day before surgery, I typically alert the anesthesiologist and surgeon.
CASE 4: A PATIENT ON MULTIPLE PSYCHOTROPICS
A 38-year-old woman with a history of severe major depression is scheduled for a mastectomy for breast cancer the next day. Her medications include fluoxetine, lorazepam, and phenelzine, all of which she has been taking for many years.
Question: What is your course of action?
A. Call the surgeon and cancel the surgery
B. Call the surgeon and notify the day-of-surgery anesthesiologist that the patient is taking these agents
C. Stop all the medications now and proceed to the operating room
D. Request a psychiatric consult for an alternative drug regimen
E. Proceed and advise the patient to take all of these agents on the morning of surgery
My approach would be to notify the day-of-surgery anesthesiologist, specifically about the phenelzine, which is a monoamine oxidase (MAO) inhibitor (see below). The other two agents can be taken on the morning of surgery, although fluoxetine has a long half-life, so missing a dose should not be problematic, and lorazepam can be given intravenously if needed.
SSRIs, including fluoxetine, are generally safe perioperatively. Serotonin depletion from platelets, however, increases the risk of bleeding, especially gastrointestinal bleeding, when SSRIs are used with NSAIDs.20–22 A neurosurgical procedure may therefore be especially risky in patients who have not stopped their SSRI if they are also taking an NSAID or an herbal medication that may increase the risk of bleeding. The caveat to stopping SSRIs is the potential for a minor withdrawal syndrome.
Tricyclic antidepressants inhibit the reuptake of norepinephrine and serotonin and may increase the action of sympathomimetics. Although arrhythmias are thought to be a concern with tricyclics, there are no reported cases of association in the literature. In general, I advise continuing triclyclics perioperatively, especially in patients who are on high doses.
Benzodiazepines, including lorazepam, are safe to use perioperatively, and a potential for withdrawal symptoms (hypertension, agitation, delirium, seizures) argues against their discontinuation. Chronic benzodiazepine use may increase anesthetic requirements.
Antipsychotic agents, which include haloperidol, olanzapine, risperidone, and ziprasidone, have multiple routes of administration—intramuscular, oral, sublingual, and intravenous. These agents are generally safe to use in the perioperative period.
MAO inhibitors, including phenelzine, are no longer commonly used and are typically reserved for the treatment of refractory depression. But they merit attention, as their use can cause accumulation of biogenic amines in the central and autonomic nervous systems. There are two types of MAO reactions—excitatory and depressive. Excitatory reactions lead to serotonin syndrome. Depressive reactions induce inhibition of hepatic microsomal enzymes, leading to narcotic accumulation and increased sedation.23
MAO inhibitors are also of concern because of their many drug interactions. When used with indirect sympathomimetics such as ephedrine, they promote a massive release of stored norepinephrine, leading to severe hypertension. When used with opioids like meperidine and dextromethorphan, MAO inhibitors are associated with a serotonin syndrome characterized by agitation, headache, fever, seizures, coma, and death.
Discontinuing MAO inhibitors before the day of surgery is no longer universally recommended, due to the risk of precipitating an exacerbation of major depression. Safe anesthetic regimens in the setting of MAO inhibitors involve avoidance of meperidine (morphine and fentanyl are safe) and use of only direct-acting sympathomimetics.
CONCLUSIONS
A good medication history that includes herbal and OTC products is essential for safe induction of anesthesia and optimization of outcomes during and following surgery. In general, medications with the potential to induce withdrawal symptoms should be continued. The use of nonessential medications that can increase surgical risk should be discontinued. If neither of these conditions applies, consider the patient’s risk profile and the risk of the procedure when making perioperative management decisions. Be mindful of withdrawal syndromes and resume medications with the potential for such syndromes as soon as possible.
DISCUSSION
Comment from the audience: In regard to your comment that diuretics are typically held on the morning of surgery, my institution recently completed a randomized placebo-controlled trial (publication is pending) in which we studied the effect of continuing or not continuing furosemide preoperatively. We found no difference in the occurrence of intraoperative hypotension between the two groups. It will be interesting to see if these findings change practice over time.
Dr. Whinney: It’s good to know that hypotension is not a concern with furosemide, but the issue here is not just blood pressure but electrolyte abnormalities that could predispose to arrhythmias. The patients who concern me are those who haven’t been seen by a physician for a while and may be on high doses of furosemide. I would scrutinize such patients closely.
Question from the audience: We see a number of patients on methotrexate and other disease-modifying rheumatologic drugs. Can you comment on the perioperative management of these medications?
Dr. Whinney: Methotrexate has caused some anxiety over the risk of infection, but the literature does not support such concern.24 In fact, it appears that continuing methotrexate is probably advisable because the risk of decompensation of the disease may be worse than the potential infectious risks. The only caveat is the patient with renal insufficiency, in whom the recommendation is to withhold methotrexate for 2 weeks before surgery. While most rheumatologists favor withholding disease-modifying drugs perioperatively, a recent systematic review showed no increased risk of either total or infectious complications with use of immunomodulators including infliximab, azathioprine, and cyclosporine.25 It is still reasonable and prudent to discuss this issue with the patient’s rheumatologist. Hydroxychloroquine is safe to continue.
Comment from the audience: First, I would like to urge everyone to be mindful of medication-related indications for preoperative testing. There are many psychotropic drugs that prolong the QT interval and thus constitute an indication for a baseline electrocardiogram prior to surgery. Second, I believe there is a mythology in the perioperative community about the bleeding risk associated with omega-3 fatty acids and vitamin E. Can you comment on the bleeding risks associated with each?
Dr. Whinney: There are few data; the fear is based purely on the potential of these compounds to cause bleeding. Neither is beneficial for short-term quality of life or for chronic prevention, and there’s no withdrawal syndrome from either. So I generally withhold them, but if the patient is still taking them up to the day of surgery, it doesn’t merit postponing surgery. I generally let the surgeon or the nurse know, and it tends not to be a big deal.
Question from the audience: Do you stop herbal teas, energy drinks, and diet medications such as phentermine prior to surgery?
Dr. Whinney: You need to know which diet medications the patient is taking. The problem with many of the OTC products is that they may or may not be considered drugs, so they may not be approved by the FDA and thus you don’t know what the patient is actually taking. For the most part, a diet medication does not contribute to short-term quality of life. My aim is to get the patient through surgery as safely as possible, so if a patient is taking an agent with ingredients, known or unknown, with an interaction potential, then I will stop it.
The two types of diet agents are those that block the absorption of fat, which could interact with other oral agents given at the same time, and those that act via the gastrointestinal tract. I generally withhold the fat-absorption blockers the day before surgery. Phentermine has the potential for catecholinergic reactions or sympathomimetic actions. I would put it in the category of herbal-type medicines and withhold it for at least 7 days.
Question from the audience: Can you comment on combination drugs such as losartan/hydrochlorothiazide on the morning of surgery?
Dr. Whinney: The ARB losartan may have more physiologic benefit than the diuretic, so I would prescribe a single dose of losartan the morning of surgery if I had decided to continue this class of medication for uncontrolled hypertension or concern over heart failure decompensation. The same is true for a beta-blocker/diuretic combination product; I will prescribe the beta-blocker component individually and tell the patient to take it the morning of surgery.
Question from the audience: I’m confused by the recommendation to stop hydrochlorothiazide. It’s a far less potent diuretic than furosemide. Does the risk of stopping it, with resulting blood pressure elevation, outweigh the risk of a mild hypotensive response because of a mild diuretic effect? I’m aware of no data on the risk of stopping hydrochlorothiazide—are you?
Dr. Whinney: There are no data. Again, the recommendation is based on the physiology of the drug, as well as on expert consensus and opinion. Since anesthesia has a vasodilatory effect with a hypotensive response, it’s probably reasonable to hold hydrochlorothiazide if its only indication is for hypertension. That’s the logic behind the recommendation. If you continue it the day of surgery, it may not necessarily hurt, but we’re not certain.
Question from the audience: The implication from your third case study was that alendronate should be held. What’s the basis of that recommendation?
Dr. Whinney: First, the patient has to be upright for 30 minutes after taking alendronate, which could be a problem on the morning of surgery. Also, withholding it will not impair short-term quality of life; it’s a weekly medication, so the patient can take her next dose once she’s up and ambulatory.
Question from the audience: What do you for young women on oral contraceptives? I’m lucky if I see them within 7 days of surgery.
Dr. Whinney: You’re bringing up the concern with exogenous hormones and the risk of venous thromboembolism (VTE), a risk that clearly is increased with the hypercoagulable milieu of surgery. The recommendation is to stop hormone therapy 30 to 45 days prior to surgery in these patients. As you note, however, we don’t get the chance to see patients during that window of opportunity. So the question is whether stopping hormones within a shorter time period results in an incremental benefit. And that is not necessarily the case. These patients should be seen as being at risk for VTE and be given appropriate VTE prophylaxis. In fact, in the similar context of menopausal hormone therapy, a study among women undergoing orthopedic surgery showed that as long as they received appropriate VTE prophylaxis, there was no significant difference in VTE rates between the women whose hormone therapy was withheld versus those who continued it.26
Question from the audience: Are there concerns about withdrawal in patients with peripheral vascular disease treated with cilostazol or pentoxifylline?
Dr. Whinney: It’s not particularly well studied. Guidelines from the American College of Physicians suggest to hold these agents for elective surgeries.27 With respect to antiplatelet therapies, O’Riordan et al did a systematic review of 99 articles pertaining to antiplatelet agents in the perioperative period and concluded that aspirin should not be stopped in patients going for surgery.28 In vascular surgery, antiplatelet agents may help promote graft patency.
- National patient safety goals. The Joint Commission Web site. http://www.jointcommission.org/patientsafety/nationalpatientsafetygoals/. Accessed July 29, 2009.
- Papadopoulos S, Cook AM. You can withdraw from that? The effects of abrupt discontinuation of medications. Orthopedics 2006; 29:413–417.
- Marik PE, Varon J. Requirement of perioperative stress doses of corticosteroids: a systematic review of the literature. Arch Surg 2008; 143:1222–1226.
- Kennedy JM, van Rij AM, Spears GF, Pettigrew RA, Tucker IG. Polypharmacy in a general surgical unit and consequences of drug withdrawal. Br J Clin Pharmacol 2000; 49:353–362.
- Bell CM, Bajcar J, Bierman AS, Li P, Mamdani MM, Urbach DR. Potentially unintended discontinuation of long-term medication use after elective surgical procedures. Arch Intern Med 2006; 166:2525–2531.
- Pass SE, Simpson RW. Discontinuation and reinstitution of medications during the perioperative period. Am J Health Syst Pharm 2004; 61:899–912.
- Muluk V, Macpherson DS. Perioperative medication management. In: Rose BD, ed. UpToDate. Waltham, MA; 2008.
- Connelly CS, Panush RS. Should nonsteroidal anti-inflammatory drugs be stopped before elective surgery? Arch Intern Med 1991; 151:1963–1966.
- Robinson CM, Christie J, Malcolm-Smith N. Nonsteroidal antiinflammatory drugs, perioperative blood loss, and transfusion requirements in elective hip arthroplasty. J Arthroplasty 1993; 8:607–610.
- Goldenberg NA, Jacobson L, Manco-Johnson MJ. Brief communication: duration of platelet dysfunction after a 7-day course of ibuprofen. Ann Intern Med 2005; 142:506–509.
- González-Correa JA, Arrebola MM, Martín-Salido E, Muñoz-Marin J, de la Cuesta FS, De La Cruz JP. Effects of dexibuprofen on platelet function in humans: comparison with low-dose aspirin. Anesthesiology 2007; 106:218–225.
- Coriat P, Richer C, Douraki T, et al. Influence of chronic angiotensin-converting enzyme inhibition on anesthetic induction. Anesthesiology 1994; 81:299–307.
- Groban L, Butterworth J. Perioperative management of chronic heart failure. Anesth Analg 2006; 103:557–575.
- Mathew JP, Fontes ML, Tudor IC, et al. A multicenter risk index for atrial fibrillation after cardiac surgery. JAMA 2004; 291:1720–1729.
- Brabant SM, Bertrand M, Eyraud D, Darmon PL, Coriat P. The hemodynamic effects of anesthetic induction in vascular surgical patients chronically treated with angiotensin II receptor antagonists. Anesth Analg 1999; 89:1388–1392.
- Feringa HH, Bax JJ, Schouten O, Poldermans D. Protecting the heart with cardiac medication in patients with left ventricular dysfunction undergoing major noncardiac vascular surgery. Semin Cardiothorac Vasc Anesth 2006; 10:25–31.
- Rosenman DJ, McDonald FS, Ebbert JO, Erwin PJ, LaBella M, Montori VM. Clinical consequences of withholding versus administering renin-angiotensin-aldosterone system antagonists in the preoperative period. J Hosp Med 2008; 3:319–325.
- Ang-Lee MK, Moss J, Yuan CS. Herbal medicines and perioperative care. JAMA 2001; 286:208–216.
- Cui J, Garle M, Eneroth P, Björkhem I. What do commercial ginseng preparations contain? Lancet 1994; 344:134.
- Yuan Y, Tsoi K, Hunt RH. Selective serotonin reuptake inhibitors and risk of upper GI bleeding: confusion or confounding? Am J Med 2006; 119:719–727.
- de Abajo FJ, Montero D, Rodríguez LA, Madurga M. Antidepressants and risk of upper gastrointestinal bleeding. Basic Clin Pharmacol Toxicol 2006; 98:304–310.
- Serebruany VL. Selective serotonin reuptake inhibitors and increased bleeding risk: are we missing something? Am J Med 2006; 119:113–116.
- Stack CG, Rogers P, Linter SP. Monoamine oxidase inhibitors and anaesthesia: a review. Br J Anaesth 1988; 60:222–227.
- Grennan DM, Gray J, Loudon J, Fear S. Methotrexate and early postoperative complications in patients with rheumatoid arthritis undergoing elective orthopaedic surgery. Ann Rheum Dis 2001; 60:214–217.
- Subramanian V, Pollok RC, Kang JY, Kumar D. Systematic review of postoperative complications in patients with inflammatory bowel disease treated with immunomodulators. Br J Surg 2006; 93:793–799.
- Hurbanek JG, Jaffer AK, Morra N, Karafa M, Brotman DJ. Postmenopausal hormone replacement and venous thromboembolism following hip and knee arthroplasty. Thromb Haemost 2004; 92:337–343.
- Cohn SL. Perioperative medication management. American College of Physicians’ PIER (Physicians’ Information and Education Resource) Web site. http://pier.acponline.org/physicians/diseases/d835/diagnosis/d835-s3.html. Posted May 29, 2009. Accessed August 14, 2009.
- O’Riordan JM, Margey RJ, Blake G, O’Connell R. Antiplatelet agents in the perioperative period. Arch Surg 2009; 144:69–76.
- National patient safety goals. The Joint Commission Web site. http://www.jointcommission.org/patientsafety/nationalpatientsafetygoals/. Accessed July 29, 2009.
- Papadopoulos S, Cook AM. You can withdraw from that? The effects of abrupt discontinuation of medications. Orthopedics 2006; 29:413–417.
- Marik PE, Varon J. Requirement of perioperative stress doses of corticosteroids: a systematic review of the literature. Arch Surg 2008; 143:1222–1226.
- Kennedy JM, van Rij AM, Spears GF, Pettigrew RA, Tucker IG. Polypharmacy in a general surgical unit and consequences of drug withdrawal. Br J Clin Pharmacol 2000; 49:353–362.
- Bell CM, Bajcar J, Bierman AS, Li P, Mamdani MM, Urbach DR. Potentially unintended discontinuation of long-term medication use after elective surgical procedures. Arch Intern Med 2006; 166:2525–2531.
- Pass SE, Simpson RW. Discontinuation and reinstitution of medications during the perioperative period. Am J Health Syst Pharm 2004; 61:899–912.
- Muluk V, Macpherson DS. Perioperative medication management. In: Rose BD, ed. UpToDate. Waltham, MA; 2008.
- Connelly CS, Panush RS. Should nonsteroidal anti-inflammatory drugs be stopped before elective surgery? Arch Intern Med 1991; 151:1963–1966.
- Robinson CM, Christie J, Malcolm-Smith N. Nonsteroidal antiinflammatory drugs, perioperative blood loss, and transfusion requirements in elective hip arthroplasty. J Arthroplasty 1993; 8:607–610.
- Goldenberg NA, Jacobson L, Manco-Johnson MJ. Brief communication: duration of platelet dysfunction after a 7-day course of ibuprofen. Ann Intern Med 2005; 142:506–509.
- González-Correa JA, Arrebola MM, Martín-Salido E, Muñoz-Marin J, de la Cuesta FS, De La Cruz JP. Effects of dexibuprofen on platelet function in humans: comparison with low-dose aspirin. Anesthesiology 2007; 106:218–225.
- Coriat P, Richer C, Douraki T, et al. Influence of chronic angiotensin-converting enzyme inhibition on anesthetic induction. Anesthesiology 1994; 81:299–307.
- Groban L, Butterworth J. Perioperative management of chronic heart failure. Anesth Analg 2006; 103:557–575.
- Mathew JP, Fontes ML, Tudor IC, et al. A multicenter risk index for atrial fibrillation after cardiac surgery. JAMA 2004; 291:1720–1729.
- Brabant SM, Bertrand M, Eyraud D, Darmon PL, Coriat P. The hemodynamic effects of anesthetic induction in vascular surgical patients chronically treated with angiotensin II receptor antagonists. Anesth Analg 1999; 89:1388–1392.
- Feringa HH, Bax JJ, Schouten O, Poldermans D. Protecting the heart with cardiac medication in patients with left ventricular dysfunction undergoing major noncardiac vascular surgery. Semin Cardiothorac Vasc Anesth 2006; 10:25–31.
- Rosenman DJ, McDonald FS, Ebbert JO, Erwin PJ, LaBella M, Montori VM. Clinical consequences of withholding versus administering renin-angiotensin-aldosterone system antagonists in the preoperative period. J Hosp Med 2008; 3:319–325.
- Ang-Lee MK, Moss J, Yuan CS. Herbal medicines and perioperative care. JAMA 2001; 286:208–216.
- Cui J, Garle M, Eneroth P, Björkhem I. What do commercial ginseng preparations contain? Lancet 1994; 344:134.
- Yuan Y, Tsoi K, Hunt RH. Selective serotonin reuptake inhibitors and risk of upper GI bleeding: confusion or confounding? Am J Med 2006; 119:719–727.
- de Abajo FJ, Montero D, Rodríguez LA, Madurga M. Antidepressants and risk of upper gastrointestinal bleeding. Basic Clin Pharmacol Toxicol 2006; 98:304–310.
- Serebruany VL. Selective serotonin reuptake inhibitors and increased bleeding risk: are we missing something? Am J Med 2006; 119:113–116.
- Stack CG, Rogers P, Linter SP. Monoamine oxidase inhibitors and anaesthesia: a review. Br J Anaesth 1988; 60:222–227.
- Grennan DM, Gray J, Loudon J, Fear S. Methotrexate and early postoperative complications in patients with rheumatoid arthritis undergoing elective orthopaedic surgery. Ann Rheum Dis 2001; 60:214–217.
- Subramanian V, Pollok RC, Kang JY, Kumar D. Systematic review of postoperative complications in patients with inflammatory bowel disease treated with immunomodulators. Br J Surg 2006; 93:793–799.
- Hurbanek JG, Jaffer AK, Morra N, Karafa M, Brotman DJ. Postmenopausal hormone replacement and venous thromboembolism following hip and knee arthroplasty. Thromb Haemost 2004; 92:337–343.
- Cohn SL. Perioperative medication management. American College of Physicians’ PIER (Physicians’ Information and Education Resource) Web site. http://pier.acponline.org/physicians/diseases/d835/diagnosis/d835-s3.html. Posted May 29, 2009. Accessed August 14, 2009.
- O’Riordan JM, Margey RJ, Blake G, O’Connell R. Antiplatelet agents in the perioperative period. Arch Surg 2009; 144:69–76.
KEY POINTS
- Common drugs that have been associated with withdrawal symptoms when discontinued preoperatively include selective serotonin reuptake inhibitors (SSRIs), beta-blockers, clonidine, statins, and corticosteroids.
- In general, most nonsteroidal anti-inflammatory drugs should be stopped at least 3 days before surgery.
- Although ACE inhibitors and angiotensin receptor blockers intensify the hypotensive effects of anesthesia, it may be prudent to continue them perioperatively unless their only indication is for hypertension and the patient’s blood pressure is well controlled.
- Herbal medications should be stopped at least 7 days before surgery, owing to the uncertainly over their actual contents.
- Among psychotropics, SSRIs, tricyclic antidepressants, benzodiazepines, and antipsychotics are generally safe to continue perioperatively.