User login
- To diagnose restless legs syndrome (RLS), start with the 4 “essential criteria”—(1) a powerful urge to move the legs that is (2) rest-induced, (3) improves with activity, and (4) worsens in the evening (C).
- Carefully screen for secondary causes of RLS, including renal failure, pregnancy, iron deficiency, and medications that can cause or exacerbate symptoms (A).
- Carbidopa/levodopa is the first-line treatment for patients with intermittent symptoms of RLS; dopamine agonists are recommended for those with daily or refractory symptoms (C).
Restless legs syndrome (RLS) has become increasingly familiar to Americans in recent years, as the medical literature, consumer ads, and lay press have focused on new findings and treatments. Yet much about this movement disorder remains a mystery.
Both the number of people with RLS and the proportion of RLS patients whose symptoms are frequent or severe are among the unknowns. Estimates of prevalence range from approximately 2% of the general population to 15% of adults.1-6
Diagnosing RLS remains complicated. Although 4 key features, or “essential criteria,” have been identified, there is no definitive clinical finding or laboratory test for this syndrome. And, because the symptoms of a number of other movement disorders resemble those of RLS, you need to be alert to other clinical features and distinguishing characteristics to confirm an RLS diagnosis.
The pathophysiology of RLS is certainly not clear-cut, either. Possible mechanisms involve overexcitation of the spinal cord by the brain stem, decreased dopamine signaling, and low iron levels.5-8 Low serum iron levels, and especially low central nervous system ferritin levels, have been closely correlated with the severity of RLS symptoms.5,9,10 Genetic links to RLS are also being studied, but have not yet been clearly established.2,7,10,11
What we do know is that the prevalence of RLS increases with age. In a National Sleep Foundation poll, nearly 25% of people older than 65 reported symptoms of RLS.12 In a more recent study of the elderly conducted under the auspices of the World Health Organization, 9.8% of participants met the criteria for RLS.13
An aging population means you’re likely to see an increasing number of patients with symptoms of RLS, which can range in severity from occasional discomfort to daily leg pain. This update will help you hone your diagnostic skills and provide the best possible care to patients who are affected.
Start with the URGE mnemonic
Initial diagnostic criteria for RLS were developed by the National Institutes of Health (NIH) in 2002 and revised by the International Restless Legs Syndrome Study Group (IRLSSG) in 2005.9 They begin with 4 essential criteria ( TABLE 1 ), easily remembered with this simple mnemonic:
- Urge to move the legs
Rest induced
Gets better with activity
Evening and night accentuation.
Here’s what to keep in mind about each.
Urge. Patients with RLS experience a powerful urge to move their legs, and often their arms or other body parts, as well. Some patients also experience discomfort in their legs,14,15 which arises from deep within the legs rather than from the surface—a characteristic that helps differentiate RLS from other movement disorders.3,6,16
Rest induced. Numerous studies have shown that RLS symptoms worsen during periods of physical and mental inactivity, and when patients are in a seated or lying position.3,5,15,16 The longer the rest period, the more severe the symptoms become. Mentally stimulating activities, such as playing video games or reading, are often enough to prevent the onset of symptoms, at least in the early stage of the disorder.3,5,15,16
Gets better with activity. While inactivity exacerbates RLS symptoms, activity typically brings complete or partial relief. Symptom relief can be the result of physical movement, a mentally stimulating activity, or even a change in temperature. Touching and rubbing the legs often helps, too, although this effect diminishes as RLS progresses.3,6,15,16
Evening accentuation. The severity of RLS symptoms tends to follow the same circadian pattern as body temperature—increasing in the evening and peaking between the hours of 11 PM and 3 AM, and making it difficult, if not impossible, for patients to experience hours of uninterrupted sleep.
TABLE 1
Diagnosing restless legs syndrome2,17,26,33
Essential diagnostic criteria (URGE mnemonic)
|
Supportive features
|
Associated features
|
| RLS, restless legs syndrome. |
Other clues to an RLS diagnosis
In addition to the essential criteria, the NIH and the IRLSSG developed a number of supportive and associated clinical features ( TABLE 1 ) that provide further help in differentiating RLS from conditions with similar symptoms.
Supportive clinical features
Although not every patient with RLS will have all (or possibly any) of the findings that are identified as supportive, their presence will lend support to an RLS diagnosis. These include:
- family history (1st-degree relative with RLS)
- improvement with dopaminergic therapy
- periodic leg movements during sleep (PLMS) in patients <50 years of age
- periodic leg movements while awake in patients of any age.17
In interpreting the second feature—dopaminergic therapy—it is important to note that while patient response often wanes over time, an initial response (often obtained by patient history, if the patient has ever been treated with a dopaminergic agent) has a sensitivity of 80% and a specificity of 100% for diagnosis of RLS.16 Keep in mind, too, that periodic leg movements—typically defined as jerking, repetitive motions—are present in many other disorders, and also tend to increase in elderly patients who do not have RLS.
Associated clinical features
Similarly, a diagnosis of RLS is not dependent on the presence of these findings. They’re noteworthy, however, because they’re experienced by many patients with RLS.16
A natural progression of RLS that follows an identifiable pattern is the first associated feature. The course of RLS varies, however, depending in part on the age of onset. Patients who develop RLS in young adulthood tend to have a slower progression, with long periods of remission, while RLS tends to progress more rapidly in those who develop the condition as older adults.15
Sleep disturbances. Leg movements typically result in frequent awakenings and increased sleep latency. Because of these disruptions, RLS patients often experience daytime somnolence and an inability to pay attention; they also have trouble performing daytime duties.
No abnormal findings. There are no physical exam or lab abnormalities associated with primary (idiopathic) RLS. The presence of abnormal findings should raise questions about the diagnosis, and cause clinicians to explore the possibility of a secondary cause.
CASE STUDY: Would you suspect RLS?
Grace (not her real name), a 54-year-old woman who underwent gastric bypass surgery several years ago, has come in today seeking help for chronic insomnia. She reports that she experiences uncomfortable sensations deep in her legs when she lies down at night. She says that she is able to get some relief from these sensations when she gets up and walks. She also notes that when she tries to lie still, she feels a need to move her legs.
Grace says that when she does fall asleep, she moves her legs so frequently that her husband has begun sleeping in a separate bed—symptoms that immediately arouse suspicion of RLS. If she were your patient, how would you support (or refute) the diagnosis, and how would you treat it?
Rule out conditions that mimic RLS
When evaluating patients like Grace with suspected RLS, it is crucial to be aware of conditions with similar symptoms—some of which may coexist. The differential diagnosis and spectrum of movement disorders that should be considered in patients with RLS symptoms are listed in TABLE 2. While some of the presenting symptoms overlap, keeping the essential criteria of RLS in mind may help in identifying distinguishing characteristics.
Neuropathic pain syndrome may occur at rest or during intense activity, for example, and peripheral vascular disease is provoked by activity, while RLS is brought on by rest.
Symptoms of neuroleptic-induced akathisia may occur day or night; in contrast, RLS typically follows a circadian rhythm.
Similarly, the urge to move the legs that patients with RLS experience is powerful, but the movement itself is voluntary. This feature distinguishes RLS from sleep starts (hypnagogic jerks), for example, which are involuntary movements.
TABLE 2
RLS: Distinguishing features and differential diagnosis6,26,33
| DIFFERENTIAL DIAGNOSIS | CHARACTERISTICS | DISTINGUISHING FEATURES OF RLS |
|---|---|---|
| Positional discomfort | Alleviated by change in body position without need for repetitive body movements. |
|
| Neuropathic pain syndrome | Pain may occur during periods of activity or rest. | |
| Peripheral vascular disease/claudications | Pain evoked by activity. | |
| Painful legs and moving toes syndrome | Continuous to semi-continuous involuntary movement of toes with associated pain in affected extremity. |
|
| Sleep starts (hypnagogic jerks) | Sudden, brief, involuntary jerks of arms or legs. | |
| Sleep-related cramps | Involve specific muscle groups and are relieved (or partially relieved) by stretching. |
|
| Neuroleptic-induced akathisia | Day- or nighttime motor restlessness that is generalized, immediately relieved with movement, and recurs immediately after the patient stops moving. | |
| Rheumatoid arthritis | Pain is chronic, not immediately relieved by moving the affected extremity, and characteristically associated with joint deformities. |
|
| RLS, restless legs syndrome. | ||
Review the need for iron replacement
The role that low levels of iron play in RLS is not entirely clear. One study found the median ferritin level in patients with RLS symptoms to be 33 mcg/L, compared with 59 mcg/L in those without symptoms.18 Another study showed patients with ferritin levels less than 50 mcg/L to have more severe RLS symptoms than those with levels greater than 50 mcg/L.19 Both iron and dopamine have been shown to have circadian rhythms similar to RLS, with their nadir correlating with the time of maximum severity of RLS symptoms. (Low levels of iron may be associated with either idiopathic or secondary RLS.)
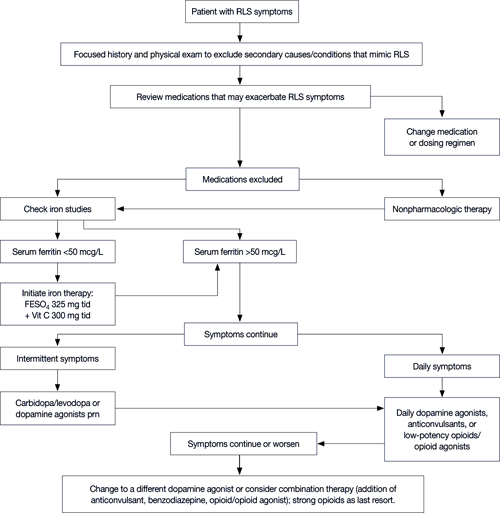
Consensus guidelines recommend against initiating iron replacement therapy without checking levels, as this could lead to iron overload.6 Any patient with a plasma ferritin concentration <50 mcg/L and RLS symptoms should be started on iron replacement therapy. The recommended dose of iron is 325 mg ferrous sulfate, taken with 300 mg vitamin C, 3 times a day. Vitamin C allows for better absorption of the iron.8
Monitor ferritin levels at 6-week intervals until they exceed 50 mcg/L, then check iron concentrations every few months. Iron replacement therapy can be decreased or discontinued, provided the ferritin remains at this level.17
Try these strategies for symptom relief
The goal in treating RLS is to decrease the severity and frequency of symptoms, leading to an improvement in sleep quality, a decrease in daytime somnolence, and an overall improvement in quality of life. Treatment guidelines, supported by the IRLSSG and the Medical Advisory Board of the Restless Legs Syndrome Foundation, are based on symptom frequency and severity—whether they are intermittent, daily, or refractory.3,9,17
The algorithm ( FIGURE ) provides recommendations for starting and escalating pharmacologic therapy. Nonpharmacologic treatments have not been studied in systematic trials; however, recommendations for their use are based on expert opinion, case series, or anecdotal reports. In patients who do not have severe symptoms, it makes sense to try simpler strategies first.
Review medications and diet. Many medications have been associated with RLS, either as a secondary cause or suspected of exacerbating symptoms. These include dopamine antagonists (neuroleptics, antiemetics); antidepressants, primarily tricyclics and selective serotonin reuptake inhibitors, lithium, and antipsychotics; antihistamines, including diphenhydramine and other over-the-counter cold and allergy remedies; calcium channel blockers; and diuretics.6,8,17
If a patient troubled by symptoms of RLS is taking any of these agents, consider changing the medication. If no suitable substitute is available, it may help to change the dosing schedule to earlier in the day—ideally no later than 3 PM.8,17 Advise patients, too, to avoid caffeine, tobacco, and alcohol, as well as any other food or beverage known to contain stimulants.
Encourage activity. Discuss the importance of exercise in the management of RLS symptoms. Encourage patients to routinely engage in physical activity and to pursue mentally stimulating activities such as reading, puzzles, or games.
Stress good sleep hygiene. Urge patients to follow a consistent sleep schedule, going to sleep and awakening at the same time each day; to use the bed only for rest or intimacy and avoid reading or watching TV in bed; and to establish a relaxing bedtime routine. Some patients have found that hot or cold baths before bed help to relieve symptoms; others report that massaging their legs or stretching leads to an improvement in symptoms.7,9,17
FIGURE
RLS: A treatment algorithm2,7,9,20
FESO4, ferrous sulfate; RLS, restless legs syndrome.
Pharmacologic options: Selecting the right one
In addition to iron replacement, there are 5 major types of RLS treatment:
- dopaminergic agents,
- dopamine agonists
- anticonvulsants,
- opioids,
- benzodiazepines.
Carbidopa/levodopa for intermittent symptoms
Most patients with RLS have a positive response to treatment with dopaminergic agents, at least initially, and for many years carbidopa/levodopa was the usual therapy for RLS. It remains a first-line treatment for patients with intermittent symptoms.
Early studies consistently showed that 70% to 80% of RLS patients treated with carbidopa/levodopa had a significant improvement in symptoms.20-22 But the studies were small, did not always include a placebo arm, and most were crossover trials, making it impossible to do a statistical comparison.5
Typical doses of carbidopa/levodopa as a treatment for RLS are 25/100 mg to 100/400 mg in divided doses, given before bedtime and again, if needed, in the middle of the sleep period.9 These doses are much lower than those used to treat Parkinsonism.
Common side effects of carbidopa/levodopa include nausea, headache, dry mouth, and daytime somnolence.2,21 An increased risk of melanoma has been seen in some studies of carbidopa/levodopa, but the evidence is inconclusive.23,24 Rebound (a worsening of symptom severity when the medication wears off) and augmentation (the development of more severe symptoms early in the day) have also been reported.
Tolerance to carbidopa/levodopa is infrequent among patients with RLS. One early study found that only 3 of 43 patients (7%) required an increase in dosage over time.21 The on/off phenomenon that occurs with this medication in the treatment of Parkinsonism is not mentioned in the literature in reference to RLS.
Because carbidopa/levodopa only provides relief for 4 to 6 hours, a second dose is often needed. If that second dose repeatedly disrupts the patient’s sleep, the recommended approach is to give 2 doses before bedtime—1 dose of regular carbidopa/levodopa and 1 dose of the controlled release form.6,9
Augmentation, the most serious problem associated with carbidopa/levodopa, occurs in 65% to 80% of RLS patients treated with this medication. It is more common in those with refractory symptoms and those taking higher doses, but can affect any RLS patient.
If augmentation develops, discontinue the carbidopa/levodopa and switch the patient to another agent. Augmentation reverses within a few weeks of stopping the medication and treatment can then be resumed, but be aware that the augmentation may reoccur.
Carbidopa/levodopa is a good choice for patients with intermittent RLS symptoms, despite the risks associated with this medication. Not only does it provide quick relief, but it can be used only on the days when symptoms occur.2,5,8
Dopamine agonists
The use of pramipexole or ropinirole as first-line treatment for people with daily or refractory symptoms of RLS is well supported by controlled studies.7,17,25 Dopamine agonists can also be used to treat patients with RLS with varying levels of severity,6 and are sometimes prescribed as the initial treatment for intermittent symptoms.
These newer agents have a longer half-life than carbidopa/levodopa, which eliminates the need for a second dose in the midst of the sleep cycle. They also have much lower rates of augmentation. Studies have been inconsistent with regard to the risk of augmentation associated with these drugs, however, with results ranging from a high of 33%7,26 to a low of 4%.27
Nausea, headache, fatigue, dizziness, orthostatic hypotension, and vomiting—the most common side effects of pramipexole and ropinirole—usually decrease in severity after 7 to 10 days of therapy. In a recent meta-analysis comparing dopamine agonists with placebo in RLS patients, the number needed to harm (NNH) was 77 and the number needed to treat (NNT) was 6.27
Pramipexole. Dosing is started at 0.125 mg at bedtime and slowly titrated up to minimize side effects. Most patients experience relief at an average dose of 0.375 mg, taken daily or intermittently for symptom relief. 6,17,27
Ropinirole. Dosing is started at 0.25 mg at bedtime (or at dinner and bedtime), and then slowly titrated up every few days to every week until a good response is obtained. Most patients respond to a dose between 1 and 2.5 mg/d.6,17,28
Tx alternatives: Anticonvulsants, opioids, and benzodiazepines
When patients are unable to tolerate—or do not respond adequately to—dopaminergic agents or dopamine agonists, anticonvulsants, opioids, or benzodiazepines may be effective alternatives, or adjunctive treatments. They may also be used in patients who have another disorder, such as chronic pain, for which these alternatives will be beneficial.
Anticonvulsants. Of the anticonvulsants studied in RLS patients, gabapentin has been shown to most effectively decrease symptoms.25 Use of the drug should be reserved for patients with daily symptoms or refractory RLS. Gabapentin also appears to be especially effective in patients who perceive their symptoms as painful, and in hemodialysis patients.2,17,28 The average effective daily dose of gabapentin for treatment of RLS is 1855 mg.6
A 2002 double-blind crossover trial found that after 6 weeks of therapy, 16 of 24 (66%) patients taking gabapentin had only mild RLS symptoms, compared with 8 of 24 (33%) of those taking placebo (NNT=3).14 The most common side effects were malaise, somnolence, dry mouth, and nausea (NNH=4). Of note, there was no significant difference in the incidence of side effects among those in the therapy group compared with the controls.
Gabapentin also has fewer side effects and drug interactions than other anticonvulsants. (Both carbamazepine and valproate have also been studied for the treatment of RLS symptoms, but at best, provided only modest improvements.)
Opioids have long been recognized as an effective treatment for RLS, but their use is limited by the potential for abuse.6 In a double-blind crossover trial, 10 of 11 patients preferred opioids over placebo, and significantly more rated their leg sensations as mild after 2 weeks of treatment with opioids (NNT=2). The most common side effects were constipation and sedation (NNH=3).17,29
Many patients obtain symptom relief from low-potency opioids such as codeine, taken at bedtime, and there appears to be a lower abuse potential when bedtime-only dosing is used. However, higher-potency opioids may be necessary for patients with refractory RLS.17
One study did show an increase in symptoms of sleep apnea in RLS patients treated with opioids. If you suspect sleep apnea in an RLS patient taking opioids, provide a referral for a polysomnography evaluation.30
Benzodiazepines. There is limited evidence to support the use of clonazepam in the treatment of RLS. Although a prospective controlled study found clonazepam to be no more effective than placebo in RLS treatment,31 clonazepam has been shown to be an effective treatment in patients with PLMS.32 Because of the association between these 2 movement disorders, clonazepam is considered an option to use alone or as adjunctive therapy in patients with RLS.2,7
CASE STUDY: Grace’s diagnosis and treatment
In addition to having the 4 essential criteria for RLS, Grace reported sleep disturbances and periodic leg movements—2 additional features that are common to RLS. She also had low serum iron levels; however, her iron deficiency was related to her gastric bypass, and she was unable to tolerate iron therapy. We started her on a low dose of pramipexole, and she had a significant—and rapid—improvement in symptoms. When we last saw her, she reported that she usually slept through the night and that her leg movements had diminished so much that her husband no longer found it necessary to sleep in a separate bed.
Correspondence
Darlene E. Moyer, MD, Scottsdale Healthcare Family Medicine Residency Program, University of Arizona School of Medicine, 7301 East 2nd Street, Suite 210, Scottsdale, AZ 85251; [email protected]
1. Karroum E, Konofal E, Arnulf I. Restless-legs syndrome. Rev Neurol. 2008;164:701-721.
2. Vergne-Salle P, Coyral D, Dufauret K, et al. Is restless legs syndrome underrecognized? Current management. Joint Bone Spine. 2006;73:369-373.
3. Fulda S, Wetter TC. Dopamine agonists for the treatment of restless legs syndrome. Expert Opin Pharmacother. 2005;6:2655-2666.
4. Allen RP, Walters AS, Montplaisir J, et al. Restless legs syndrome prevalence and impact: REST general population study. Arch Intern Med. 2005;165:1286-1292.
5. Conti C, de Oliveira MM, Andriolo RB, et al. Levodopa for idiopathic restless legs syndrome: evidence-based review. Mov Disord. 2007;22:1943-1951.
6. Restless Legs Syndrome Foundation. RLS Medical Bulletin. 2005. Available at: http://www.irlssg.org/RLSMB2005pf.pdf. Accessed July 9, 2009.
7. Ryan M, Slevin J. Restless legs syndrome. Am J Health Syst Pharm. 2006;63:1599-1612.
8. Oertel W, Trenkwalder C, Zucconi M, et al. State of the art in restless legs syndrome therapy: practice recommendations for treating restless legs syndrome. Mov Disord. 2007;22(suppl 18):S466-S475.
9. Thorpy M. New paradigms in the treatment of restless legs syndrome. Neurology. 2005;64(12 suppl 3):S28-S33.
10. Winkelman J. A better future for patients with restless legs syndrome. Am J Med. 2007;120(1 suppl 1):S28-S29.
11. Chahine L, Chemali Z. Restless legs syndrome: a review. CNS Spectr. 2006;11:511-520.
12. Johnson E. Omnibus Sleep in America poll. National Sleep Foundation. 1998.-
13. Rothdach AJ, Trenkwalder C, Haberstock J, et al. Prevalence and risk factors of RLS in an elderly population: the MEMO study. Neurology. 2000;54:1064-1068.
14. Garcia-Borreguero D. Time to REST: epidemiology and burden. Eur J Neurol. 2006;13(suppl 3):S15-S20.
15. Schapira A. RLS patients: who are they? Eur J Neurol. 2006;13(suppl 3):S2-S7.
16. Benes H, Walters AS, Allen RP, et al. Definition of restless legs syndrome, how to diagnose it, and how to differentiate it from RLS mimics. Mov Disord. 2007;22(suppl 18):S401-S408.
17. Hening W, Allen R, Tenzer P, et al. Restless legs syndrome: demographics, presentation and differential diagnosis. Geriatrics. 2007;62:26-29.
18. O’Keefe ST, Gavin K, Lavan JN. Iron status and restless legs in the elderly. Age Ageing. 1994;23:200-203.
19. Sun ER, Chen CA, Ho G, et al. Iron and the restless legs syndrome. Sleep. 1998;21:371-377.
20. Akpinar S. Restless legs syndrome treatment with dopaminergic drugs. Clin Neuropharmacol. 1987;10:69-79.
21. Becker P, Jamieson A, Brown D. Dopaminergic agents in restless legs syndrome and periodic limb movements of sleep: response and complications of extended treatment in 49 cases. Sleep. 1993;16:713-716.
22. Von Scheele C, Kempi V. Long-term effect of dopaminergic drugs in restless legs. A 2 year follow-up. Arch Neurol. 1990;47:1223-1224.
23. Bertoni JM, Arlette JP, Fernandez HH, et al. Epidemiologic association of Parkinson’s disease and melanoma. Mov Disord. 2006;21(suppl 15):S610.-
24. Fiala K, Whetteckey J, Manyam B. Malignant melanoma and levodopa in Parkinson’s disease: causality or coincidence? Parkinsonism Relat Disord. 2003;9:321-327.
25. Montagna P. The treatment of restless legs syndrome. Neurol Sci. 2007;28(suppl 1):S61-S66.
26. Kushida C. Clinical presentation, diagnosis and quality of life issues in restless legs syndrome. Am J Med. 2007;120(1 suppl 1):S4-S12.
27. Baker W, White C, Coleman C. Effect of nonergot dopamine agonists on symptoms of restless legs syndrome. Ann Fam Med. 2008;6:253-262.
28. Fulda S, Wetter T. Emerging drugs for restless legs syndrome. Expert Opin Emerg Drugs. 2005;10:527-552.
29. Walters A, Wagner M, Hening W, et al. Successful treatment of idiopathic restless legs syndrome in a randomized double-blind trial of oxycodone versus placebo. Sleep. 1993;16:327-332.
30. Walters A, Winkelman J, Trenkwalder C, et al. Long term follow-up on restless legs syndrome patients treated with opioids. Mov Disord. 2001;16:1105-1109.
31. Boghen D, Lamothe L, Elie R. The treatment of restless legs syndrome with clonazepam: a prospective controlled trial. Can J Neurol Sci. 1986;13:245-247.
32. Peled R, Lavie P. Double-blind evaluation of clonazepam on periodic leg movements in sleep. J Neurol Neurosurg Psychiatry. 1987;50:1679-1681.
33. Ferni-Strambi L. RLS-like symptoms: differential diagnosis by history and clinical assessment. Sleep Med. 2007;8(suppl 2):S3-S6.
- To diagnose restless legs syndrome (RLS), start with the 4 “essential criteria”—(1) a powerful urge to move the legs that is (2) rest-induced, (3) improves with activity, and (4) worsens in the evening (C).
- Carefully screen for secondary causes of RLS, including renal failure, pregnancy, iron deficiency, and medications that can cause or exacerbate symptoms (A).
- Carbidopa/levodopa is the first-line treatment for patients with intermittent symptoms of RLS; dopamine agonists are recommended for those with daily or refractory symptoms (C).
Restless legs syndrome (RLS) has become increasingly familiar to Americans in recent years, as the medical literature, consumer ads, and lay press have focused on new findings and treatments. Yet much about this movement disorder remains a mystery.
Both the number of people with RLS and the proportion of RLS patients whose symptoms are frequent or severe are among the unknowns. Estimates of prevalence range from approximately 2% of the general population to 15% of adults.1-6
Diagnosing RLS remains complicated. Although 4 key features, or “essential criteria,” have been identified, there is no definitive clinical finding or laboratory test for this syndrome. And, because the symptoms of a number of other movement disorders resemble those of RLS, you need to be alert to other clinical features and distinguishing characteristics to confirm an RLS diagnosis.
The pathophysiology of RLS is certainly not clear-cut, either. Possible mechanisms involve overexcitation of the spinal cord by the brain stem, decreased dopamine signaling, and low iron levels.5-8 Low serum iron levels, and especially low central nervous system ferritin levels, have been closely correlated with the severity of RLS symptoms.5,9,10 Genetic links to RLS are also being studied, but have not yet been clearly established.2,7,10,11
What we do know is that the prevalence of RLS increases with age. In a National Sleep Foundation poll, nearly 25% of people older than 65 reported symptoms of RLS.12 In a more recent study of the elderly conducted under the auspices of the World Health Organization, 9.8% of participants met the criteria for RLS.13
An aging population means you’re likely to see an increasing number of patients with symptoms of RLS, which can range in severity from occasional discomfort to daily leg pain. This update will help you hone your diagnostic skills and provide the best possible care to patients who are affected.
Start with the URGE mnemonic
Initial diagnostic criteria for RLS were developed by the National Institutes of Health (NIH) in 2002 and revised by the International Restless Legs Syndrome Study Group (IRLSSG) in 2005.9 They begin with 4 essential criteria ( TABLE 1 ), easily remembered with this simple mnemonic:
- Urge to move the legs
Rest induced
Gets better with activity
Evening and night accentuation.
Here’s what to keep in mind about each.
Urge. Patients with RLS experience a powerful urge to move their legs, and often their arms or other body parts, as well. Some patients also experience discomfort in their legs,14,15 which arises from deep within the legs rather than from the surface—a characteristic that helps differentiate RLS from other movement disorders.3,6,16
Rest induced. Numerous studies have shown that RLS symptoms worsen during periods of physical and mental inactivity, and when patients are in a seated or lying position.3,5,15,16 The longer the rest period, the more severe the symptoms become. Mentally stimulating activities, such as playing video games or reading, are often enough to prevent the onset of symptoms, at least in the early stage of the disorder.3,5,15,16
Gets better with activity. While inactivity exacerbates RLS symptoms, activity typically brings complete or partial relief. Symptom relief can be the result of physical movement, a mentally stimulating activity, or even a change in temperature. Touching and rubbing the legs often helps, too, although this effect diminishes as RLS progresses.3,6,15,16
Evening accentuation. The severity of RLS symptoms tends to follow the same circadian pattern as body temperature—increasing in the evening and peaking between the hours of 11 PM and 3 AM, and making it difficult, if not impossible, for patients to experience hours of uninterrupted sleep.
TABLE 1
Diagnosing restless legs syndrome2,17,26,33
Essential diagnostic criteria (URGE mnemonic)
|
Supportive features
|
Associated features
|
| RLS, restless legs syndrome. |
Other clues to an RLS diagnosis
In addition to the essential criteria, the NIH and the IRLSSG developed a number of supportive and associated clinical features ( TABLE 1 ) that provide further help in differentiating RLS from conditions with similar symptoms.
Supportive clinical features
Although not every patient with RLS will have all (or possibly any) of the findings that are identified as supportive, their presence will lend support to an RLS diagnosis. These include:
- family history (1st-degree relative with RLS)
- improvement with dopaminergic therapy
- periodic leg movements during sleep (PLMS) in patients <50 years of age
- periodic leg movements while awake in patients of any age.17
In interpreting the second feature—dopaminergic therapy—it is important to note that while patient response often wanes over time, an initial response (often obtained by patient history, if the patient has ever been treated with a dopaminergic agent) has a sensitivity of 80% and a specificity of 100% for diagnosis of RLS.16 Keep in mind, too, that periodic leg movements—typically defined as jerking, repetitive motions—are present in many other disorders, and also tend to increase in elderly patients who do not have RLS.
Associated clinical features
Similarly, a diagnosis of RLS is not dependent on the presence of these findings. They’re noteworthy, however, because they’re experienced by many patients with RLS.16
A natural progression of RLS that follows an identifiable pattern is the first associated feature. The course of RLS varies, however, depending in part on the age of onset. Patients who develop RLS in young adulthood tend to have a slower progression, with long periods of remission, while RLS tends to progress more rapidly in those who develop the condition as older adults.15
Sleep disturbances. Leg movements typically result in frequent awakenings and increased sleep latency. Because of these disruptions, RLS patients often experience daytime somnolence and an inability to pay attention; they also have trouble performing daytime duties.
No abnormal findings. There are no physical exam or lab abnormalities associated with primary (idiopathic) RLS. The presence of abnormal findings should raise questions about the diagnosis, and cause clinicians to explore the possibility of a secondary cause.
CASE STUDY: Would you suspect RLS?
Grace (not her real name), a 54-year-old woman who underwent gastric bypass surgery several years ago, has come in today seeking help for chronic insomnia. She reports that she experiences uncomfortable sensations deep in her legs when she lies down at night. She says that she is able to get some relief from these sensations when she gets up and walks. She also notes that when she tries to lie still, she feels a need to move her legs.
Grace says that when she does fall asleep, she moves her legs so frequently that her husband has begun sleeping in a separate bed—symptoms that immediately arouse suspicion of RLS. If she were your patient, how would you support (or refute) the diagnosis, and how would you treat it?
Rule out conditions that mimic RLS
When evaluating patients like Grace with suspected RLS, it is crucial to be aware of conditions with similar symptoms—some of which may coexist. The differential diagnosis and spectrum of movement disorders that should be considered in patients with RLS symptoms are listed in TABLE 2. While some of the presenting symptoms overlap, keeping the essential criteria of RLS in mind may help in identifying distinguishing characteristics.
Neuropathic pain syndrome may occur at rest or during intense activity, for example, and peripheral vascular disease is provoked by activity, while RLS is brought on by rest.
Symptoms of neuroleptic-induced akathisia may occur day or night; in contrast, RLS typically follows a circadian rhythm.
Similarly, the urge to move the legs that patients with RLS experience is powerful, but the movement itself is voluntary. This feature distinguishes RLS from sleep starts (hypnagogic jerks), for example, which are involuntary movements.
TABLE 2
RLS: Distinguishing features and differential diagnosis6,26,33
| DIFFERENTIAL DIAGNOSIS | CHARACTERISTICS | DISTINGUISHING FEATURES OF RLS |
|---|---|---|
| Positional discomfort | Alleviated by change in body position without need for repetitive body movements. |
|
| Neuropathic pain syndrome | Pain may occur during periods of activity or rest. | |
| Peripheral vascular disease/claudications | Pain evoked by activity. | |
| Painful legs and moving toes syndrome | Continuous to semi-continuous involuntary movement of toes with associated pain in affected extremity. |
|
| Sleep starts (hypnagogic jerks) | Sudden, brief, involuntary jerks of arms or legs. | |
| Sleep-related cramps | Involve specific muscle groups and are relieved (or partially relieved) by stretching. |
|
| Neuroleptic-induced akathisia | Day- or nighttime motor restlessness that is generalized, immediately relieved with movement, and recurs immediately after the patient stops moving. | |
| Rheumatoid arthritis | Pain is chronic, not immediately relieved by moving the affected extremity, and characteristically associated with joint deformities. |
|
| RLS, restless legs syndrome. | ||
Review the need for iron replacement
The role that low levels of iron play in RLS is not entirely clear. One study found the median ferritin level in patients with RLS symptoms to be 33 mcg/L, compared with 59 mcg/L in those without symptoms.18 Another study showed patients with ferritin levels less than 50 mcg/L to have more severe RLS symptoms than those with levels greater than 50 mcg/L.19 Both iron and dopamine have been shown to have circadian rhythms similar to RLS, with their nadir correlating with the time of maximum severity of RLS symptoms. (Low levels of iron may be associated with either idiopathic or secondary RLS.)
Consensus guidelines recommend against initiating iron replacement therapy without checking levels, as this could lead to iron overload.6 Any patient with a plasma ferritin concentration <50 mcg/L and RLS symptoms should be started on iron replacement therapy. The recommended dose of iron is 325 mg ferrous sulfate, taken with 300 mg vitamin C, 3 times a day. Vitamin C allows for better absorption of the iron.8
Monitor ferritin levels at 6-week intervals until they exceed 50 mcg/L, then check iron concentrations every few months. Iron replacement therapy can be decreased or discontinued, provided the ferritin remains at this level.17
Try these strategies for symptom relief
The goal in treating RLS is to decrease the severity and frequency of symptoms, leading to an improvement in sleep quality, a decrease in daytime somnolence, and an overall improvement in quality of life. Treatment guidelines, supported by the IRLSSG and the Medical Advisory Board of the Restless Legs Syndrome Foundation, are based on symptom frequency and severity—whether they are intermittent, daily, or refractory.3,9,17
The algorithm ( FIGURE ) provides recommendations for starting and escalating pharmacologic therapy. Nonpharmacologic treatments have not been studied in systematic trials; however, recommendations for their use are based on expert opinion, case series, or anecdotal reports. In patients who do not have severe symptoms, it makes sense to try simpler strategies first.
Review medications and diet. Many medications have been associated with RLS, either as a secondary cause or suspected of exacerbating symptoms. These include dopamine antagonists (neuroleptics, antiemetics); antidepressants, primarily tricyclics and selective serotonin reuptake inhibitors, lithium, and antipsychotics; antihistamines, including diphenhydramine and other over-the-counter cold and allergy remedies; calcium channel blockers; and diuretics.6,8,17
If a patient troubled by symptoms of RLS is taking any of these agents, consider changing the medication. If no suitable substitute is available, it may help to change the dosing schedule to earlier in the day—ideally no later than 3 PM.8,17 Advise patients, too, to avoid caffeine, tobacco, and alcohol, as well as any other food or beverage known to contain stimulants.
Encourage activity. Discuss the importance of exercise in the management of RLS symptoms. Encourage patients to routinely engage in physical activity and to pursue mentally stimulating activities such as reading, puzzles, or games.
Stress good sleep hygiene. Urge patients to follow a consistent sleep schedule, going to sleep and awakening at the same time each day; to use the bed only for rest or intimacy and avoid reading or watching TV in bed; and to establish a relaxing bedtime routine. Some patients have found that hot or cold baths before bed help to relieve symptoms; others report that massaging their legs or stretching leads to an improvement in symptoms.7,9,17
FIGURE
RLS: A treatment algorithm2,7,9,20
FESO4, ferrous sulfate; RLS, restless legs syndrome.
Pharmacologic options: Selecting the right one
In addition to iron replacement, there are 5 major types of RLS treatment:
- dopaminergic agents,
- dopamine agonists
- anticonvulsants,
- opioids,
- benzodiazepines.
Carbidopa/levodopa for intermittent symptoms
Most patients with RLS have a positive response to treatment with dopaminergic agents, at least initially, and for many years carbidopa/levodopa was the usual therapy for RLS. It remains a first-line treatment for patients with intermittent symptoms.
Early studies consistently showed that 70% to 80% of RLS patients treated with carbidopa/levodopa had a significant improvement in symptoms.20-22 But the studies were small, did not always include a placebo arm, and most were crossover trials, making it impossible to do a statistical comparison.5
Typical doses of carbidopa/levodopa as a treatment for RLS are 25/100 mg to 100/400 mg in divided doses, given before bedtime and again, if needed, in the middle of the sleep period.9 These doses are much lower than those used to treat Parkinsonism.
Common side effects of carbidopa/levodopa include nausea, headache, dry mouth, and daytime somnolence.2,21 An increased risk of melanoma has been seen in some studies of carbidopa/levodopa, but the evidence is inconclusive.23,24 Rebound (a worsening of symptom severity when the medication wears off) and augmentation (the development of more severe symptoms early in the day) have also been reported.
Tolerance to carbidopa/levodopa is infrequent among patients with RLS. One early study found that only 3 of 43 patients (7%) required an increase in dosage over time.21 The on/off phenomenon that occurs with this medication in the treatment of Parkinsonism is not mentioned in the literature in reference to RLS.
Because carbidopa/levodopa only provides relief for 4 to 6 hours, a second dose is often needed. If that second dose repeatedly disrupts the patient’s sleep, the recommended approach is to give 2 doses before bedtime—1 dose of regular carbidopa/levodopa and 1 dose of the controlled release form.6,9
Augmentation, the most serious problem associated with carbidopa/levodopa, occurs in 65% to 80% of RLS patients treated with this medication. It is more common in those with refractory symptoms and those taking higher doses, but can affect any RLS patient.
If augmentation develops, discontinue the carbidopa/levodopa and switch the patient to another agent. Augmentation reverses within a few weeks of stopping the medication and treatment can then be resumed, but be aware that the augmentation may reoccur.
Carbidopa/levodopa is a good choice for patients with intermittent RLS symptoms, despite the risks associated with this medication. Not only does it provide quick relief, but it can be used only on the days when symptoms occur.2,5,8
Dopamine agonists
The use of pramipexole or ropinirole as first-line treatment for people with daily or refractory symptoms of RLS is well supported by controlled studies.7,17,25 Dopamine agonists can also be used to treat patients with RLS with varying levels of severity,6 and are sometimes prescribed as the initial treatment for intermittent symptoms.
These newer agents have a longer half-life than carbidopa/levodopa, which eliminates the need for a second dose in the midst of the sleep cycle. They also have much lower rates of augmentation. Studies have been inconsistent with regard to the risk of augmentation associated with these drugs, however, with results ranging from a high of 33%7,26 to a low of 4%.27
Nausea, headache, fatigue, dizziness, orthostatic hypotension, and vomiting—the most common side effects of pramipexole and ropinirole—usually decrease in severity after 7 to 10 days of therapy. In a recent meta-analysis comparing dopamine agonists with placebo in RLS patients, the number needed to harm (NNH) was 77 and the number needed to treat (NNT) was 6.27
Pramipexole. Dosing is started at 0.125 mg at bedtime and slowly titrated up to minimize side effects. Most patients experience relief at an average dose of 0.375 mg, taken daily or intermittently for symptom relief. 6,17,27
Ropinirole. Dosing is started at 0.25 mg at bedtime (or at dinner and bedtime), and then slowly titrated up every few days to every week until a good response is obtained. Most patients respond to a dose between 1 and 2.5 mg/d.6,17,28
Tx alternatives: Anticonvulsants, opioids, and benzodiazepines
When patients are unable to tolerate—or do not respond adequately to—dopaminergic agents or dopamine agonists, anticonvulsants, opioids, or benzodiazepines may be effective alternatives, or adjunctive treatments. They may also be used in patients who have another disorder, such as chronic pain, for which these alternatives will be beneficial.
Anticonvulsants. Of the anticonvulsants studied in RLS patients, gabapentin has been shown to most effectively decrease symptoms.25 Use of the drug should be reserved for patients with daily symptoms or refractory RLS. Gabapentin also appears to be especially effective in patients who perceive their symptoms as painful, and in hemodialysis patients.2,17,28 The average effective daily dose of gabapentin for treatment of RLS is 1855 mg.6
A 2002 double-blind crossover trial found that after 6 weeks of therapy, 16 of 24 (66%) patients taking gabapentin had only mild RLS symptoms, compared with 8 of 24 (33%) of those taking placebo (NNT=3).14 The most common side effects were malaise, somnolence, dry mouth, and nausea (NNH=4). Of note, there was no significant difference in the incidence of side effects among those in the therapy group compared with the controls.
Gabapentin also has fewer side effects and drug interactions than other anticonvulsants. (Both carbamazepine and valproate have also been studied for the treatment of RLS symptoms, but at best, provided only modest improvements.)
Opioids have long been recognized as an effective treatment for RLS, but their use is limited by the potential for abuse.6 In a double-blind crossover trial, 10 of 11 patients preferred opioids over placebo, and significantly more rated their leg sensations as mild after 2 weeks of treatment with opioids (NNT=2). The most common side effects were constipation and sedation (NNH=3).17,29
Many patients obtain symptom relief from low-potency opioids such as codeine, taken at bedtime, and there appears to be a lower abuse potential when bedtime-only dosing is used. However, higher-potency opioids may be necessary for patients with refractory RLS.17
One study did show an increase in symptoms of sleep apnea in RLS patients treated with opioids. If you suspect sleep apnea in an RLS patient taking opioids, provide a referral for a polysomnography evaluation.30
Benzodiazepines. There is limited evidence to support the use of clonazepam in the treatment of RLS. Although a prospective controlled study found clonazepam to be no more effective than placebo in RLS treatment,31 clonazepam has been shown to be an effective treatment in patients with PLMS.32 Because of the association between these 2 movement disorders, clonazepam is considered an option to use alone or as adjunctive therapy in patients with RLS.2,7
CASE STUDY: Grace’s diagnosis and treatment
In addition to having the 4 essential criteria for RLS, Grace reported sleep disturbances and periodic leg movements—2 additional features that are common to RLS. She also had low serum iron levels; however, her iron deficiency was related to her gastric bypass, and she was unable to tolerate iron therapy. We started her on a low dose of pramipexole, and she had a significant—and rapid—improvement in symptoms. When we last saw her, she reported that she usually slept through the night and that her leg movements had diminished so much that her husband no longer found it necessary to sleep in a separate bed.
Correspondence
Darlene E. Moyer, MD, Scottsdale Healthcare Family Medicine Residency Program, University of Arizona School of Medicine, 7301 East 2nd Street, Suite 210, Scottsdale, AZ 85251; [email protected]
- To diagnose restless legs syndrome (RLS), start with the 4 “essential criteria”—(1) a powerful urge to move the legs that is (2) rest-induced, (3) improves with activity, and (4) worsens in the evening (C).
- Carefully screen for secondary causes of RLS, including renal failure, pregnancy, iron deficiency, and medications that can cause or exacerbate symptoms (A).
- Carbidopa/levodopa is the first-line treatment for patients with intermittent symptoms of RLS; dopamine agonists are recommended for those with daily or refractory symptoms (C).
Restless legs syndrome (RLS) has become increasingly familiar to Americans in recent years, as the medical literature, consumer ads, and lay press have focused on new findings and treatments. Yet much about this movement disorder remains a mystery.
Both the number of people with RLS and the proportion of RLS patients whose symptoms are frequent or severe are among the unknowns. Estimates of prevalence range from approximately 2% of the general population to 15% of adults.1-6
Diagnosing RLS remains complicated. Although 4 key features, or “essential criteria,” have been identified, there is no definitive clinical finding or laboratory test for this syndrome. And, because the symptoms of a number of other movement disorders resemble those of RLS, you need to be alert to other clinical features and distinguishing characteristics to confirm an RLS diagnosis.
The pathophysiology of RLS is certainly not clear-cut, either. Possible mechanisms involve overexcitation of the spinal cord by the brain stem, decreased dopamine signaling, and low iron levels.5-8 Low serum iron levels, and especially low central nervous system ferritin levels, have been closely correlated with the severity of RLS symptoms.5,9,10 Genetic links to RLS are also being studied, but have not yet been clearly established.2,7,10,11
What we do know is that the prevalence of RLS increases with age. In a National Sleep Foundation poll, nearly 25% of people older than 65 reported symptoms of RLS.12 In a more recent study of the elderly conducted under the auspices of the World Health Organization, 9.8% of participants met the criteria for RLS.13
An aging population means you’re likely to see an increasing number of patients with symptoms of RLS, which can range in severity from occasional discomfort to daily leg pain. This update will help you hone your diagnostic skills and provide the best possible care to patients who are affected.
Start with the URGE mnemonic
Initial diagnostic criteria for RLS were developed by the National Institutes of Health (NIH) in 2002 and revised by the International Restless Legs Syndrome Study Group (IRLSSG) in 2005.9 They begin with 4 essential criteria ( TABLE 1 ), easily remembered with this simple mnemonic:
- Urge to move the legs
Rest induced
Gets better with activity
Evening and night accentuation.
Here’s what to keep in mind about each.
Urge. Patients with RLS experience a powerful urge to move their legs, and often their arms or other body parts, as well. Some patients also experience discomfort in their legs,14,15 which arises from deep within the legs rather than from the surface—a characteristic that helps differentiate RLS from other movement disorders.3,6,16
Rest induced. Numerous studies have shown that RLS symptoms worsen during periods of physical and mental inactivity, and when patients are in a seated or lying position.3,5,15,16 The longer the rest period, the more severe the symptoms become. Mentally stimulating activities, such as playing video games or reading, are often enough to prevent the onset of symptoms, at least in the early stage of the disorder.3,5,15,16
Gets better with activity. While inactivity exacerbates RLS symptoms, activity typically brings complete or partial relief. Symptom relief can be the result of physical movement, a mentally stimulating activity, or even a change in temperature. Touching and rubbing the legs often helps, too, although this effect diminishes as RLS progresses.3,6,15,16
Evening accentuation. The severity of RLS symptoms tends to follow the same circadian pattern as body temperature—increasing in the evening and peaking between the hours of 11 PM and 3 AM, and making it difficult, if not impossible, for patients to experience hours of uninterrupted sleep.
TABLE 1
Diagnosing restless legs syndrome2,17,26,33
Essential diagnostic criteria (URGE mnemonic)
|
Supportive features
|
Associated features
|
| RLS, restless legs syndrome. |
Other clues to an RLS diagnosis
In addition to the essential criteria, the NIH and the IRLSSG developed a number of supportive and associated clinical features ( TABLE 1 ) that provide further help in differentiating RLS from conditions with similar symptoms.
Supportive clinical features
Although not every patient with RLS will have all (or possibly any) of the findings that are identified as supportive, their presence will lend support to an RLS diagnosis. These include:
- family history (1st-degree relative with RLS)
- improvement with dopaminergic therapy
- periodic leg movements during sleep (PLMS) in patients <50 years of age
- periodic leg movements while awake in patients of any age.17
In interpreting the second feature—dopaminergic therapy—it is important to note that while patient response often wanes over time, an initial response (often obtained by patient history, if the patient has ever been treated with a dopaminergic agent) has a sensitivity of 80% and a specificity of 100% for diagnosis of RLS.16 Keep in mind, too, that periodic leg movements—typically defined as jerking, repetitive motions—are present in many other disorders, and also tend to increase in elderly patients who do not have RLS.
Associated clinical features
Similarly, a diagnosis of RLS is not dependent on the presence of these findings. They’re noteworthy, however, because they’re experienced by many patients with RLS.16
A natural progression of RLS that follows an identifiable pattern is the first associated feature. The course of RLS varies, however, depending in part on the age of onset. Patients who develop RLS in young adulthood tend to have a slower progression, with long periods of remission, while RLS tends to progress more rapidly in those who develop the condition as older adults.15
Sleep disturbances. Leg movements typically result in frequent awakenings and increased sleep latency. Because of these disruptions, RLS patients often experience daytime somnolence and an inability to pay attention; they also have trouble performing daytime duties.
No abnormal findings. There are no physical exam or lab abnormalities associated with primary (idiopathic) RLS. The presence of abnormal findings should raise questions about the diagnosis, and cause clinicians to explore the possibility of a secondary cause.
CASE STUDY: Would you suspect RLS?
Grace (not her real name), a 54-year-old woman who underwent gastric bypass surgery several years ago, has come in today seeking help for chronic insomnia. She reports that she experiences uncomfortable sensations deep in her legs when she lies down at night. She says that she is able to get some relief from these sensations when she gets up and walks. She also notes that when she tries to lie still, she feels a need to move her legs.
Grace says that when she does fall asleep, she moves her legs so frequently that her husband has begun sleeping in a separate bed—symptoms that immediately arouse suspicion of RLS. If she were your patient, how would you support (or refute) the diagnosis, and how would you treat it?
Rule out conditions that mimic RLS
When evaluating patients like Grace with suspected RLS, it is crucial to be aware of conditions with similar symptoms—some of which may coexist. The differential diagnosis and spectrum of movement disorders that should be considered in patients with RLS symptoms are listed in TABLE 2. While some of the presenting symptoms overlap, keeping the essential criteria of RLS in mind may help in identifying distinguishing characteristics.
Neuropathic pain syndrome may occur at rest or during intense activity, for example, and peripheral vascular disease is provoked by activity, while RLS is brought on by rest.
Symptoms of neuroleptic-induced akathisia may occur day or night; in contrast, RLS typically follows a circadian rhythm.
Similarly, the urge to move the legs that patients with RLS experience is powerful, but the movement itself is voluntary. This feature distinguishes RLS from sleep starts (hypnagogic jerks), for example, which are involuntary movements.
TABLE 2
RLS: Distinguishing features and differential diagnosis6,26,33
| DIFFERENTIAL DIAGNOSIS | CHARACTERISTICS | DISTINGUISHING FEATURES OF RLS |
|---|---|---|
| Positional discomfort | Alleviated by change in body position without need for repetitive body movements. |
|
| Neuropathic pain syndrome | Pain may occur during periods of activity or rest. | |
| Peripheral vascular disease/claudications | Pain evoked by activity. | |
| Painful legs and moving toes syndrome | Continuous to semi-continuous involuntary movement of toes with associated pain in affected extremity. |
|
| Sleep starts (hypnagogic jerks) | Sudden, brief, involuntary jerks of arms or legs. | |
| Sleep-related cramps | Involve specific muscle groups and are relieved (or partially relieved) by stretching. |
|
| Neuroleptic-induced akathisia | Day- or nighttime motor restlessness that is generalized, immediately relieved with movement, and recurs immediately after the patient stops moving. | |
| Rheumatoid arthritis | Pain is chronic, not immediately relieved by moving the affected extremity, and characteristically associated with joint deformities. |
|
| RLS, restless legs syndrome. | ||
Review the need for iron replacement
The role that low levels of iron play in RLS is not entirely clear. One study found the median ferritin level in patients with RLS symptoms to be 33 mcg/L, compared with 59 mcg/L in those without symptoms.18 Another study showed patients with ferritin levels less than 50 mcg/L to have more severe RLS symptoms than those with levels greater than 50 mcg/L.19 Both iron and dopamine have been shown to have circadian rhythms similar to RLS, with their nadir correlating with the time of maximum severity of RLS symptoms. (Low levels of iron may be associated with either idiopathic or secondary RLS.)
Consensus guidelines recommend against initiating iron replacement therapy without checking levels, as this could lead to iron overload.6 Any patient with a plasma ferritin concentration <50 mcg/L and RLS symptoms should be started on iron replacement therapy. The recommended dose of iron is 325 mg ferrous sulfate, taken with 300 mg vitamin C, 3 times a day. Vitamin C allows for better absorption of the iron.8
Monitor ferritin levels at 6-week intervals until they exceed 50 mcg/L, then check iron concentrations every few months. Iron replacement therapy can be decreased or discontinued, provided the ferritin remains at this level.17
Try these strategies for symptom relief
The goal in treating RLS is to decrease the severity and frequency of symptoms, leading to an improvement in sleep quality, a decrease in daytime somnolence, and an overall improvement in quality of life. Treatment guidelines, supported by the IRLSSG and the Medical Advisory Board of the Restless Legs Syndrome Foundation, are based on symptom frequency and severity—whether they are intermittent, daily, or refractory.3,9,17
The algorithm ( FIGURE ) provides recommendations for starting and escalating pharmacologic therapy. Nonpharmacologic treatments have not been studied in systematic trials; however, recommendations for their use are based on expert opinion, case series, or anecdotal reports. In patients who do not have severe symptoms, it makes sense to try simpler strategies first.
Review medications and diet. Many medications have been associated with RLS, either as a secondary cause or suspected of exacerbating symptoms. These include dopamine antagonists (neuroleptics, antiemetics); antidepressants, primarily tricyclics and selective serotonin reuptake inhibitors, lithium, and antipsychotics; antihistamines, including diphenhydramine and other over-the-counter cold and allergy remedies; calcium channel blockers; and diuretics.6,8,17
If a patient troubled by symptoms of RLS is taking any of these agents, consider changing the medication. If no suitable substitute is available, it may help to change the dosing schedule to earlier in the day—ideally no later than 3 PM.8,17 Advise patients, too, to avoid caffeine, tobacco, and alcohol, as well as any other food or beverage known to contain stimulants.
Encourage activity. Discuss the importance of exercise in the management of RLS symptoms. Encourage patients to routinely engage in physical activity and to pursue mentally stimulating activities such as reading, puzzles, or games.
Stress good sleep hygiene. Urge patients to follow a consistent sleep schedule, going to sleep and awakening at the same time each day; to use the bed only for rest or intimacy and avoid reading or watching TV in bed; and to establish a relaxing bedtime routine. Some patients have found that hot or cold baths before bed help to relieve symptoms; others report that massaging their legs or stretching leads to an improvement in symptoms.7,9,17
FIGURE
RLS: A treatment algorithm2,7,9,20
FESO4, ferrous sulfate; RLS, restless legs syndrome.
Pharmacologic options: Selecting the right one
In addition to iron replacement, there are 5 major types of RLS treatment:
- dopaminergic agents,
- dopamine agonists
- anticonvulsants,
- opioids,
- benzodiazepines.
Carbidopa/levodopa for intermittent symptoms
Most patients with RLS have a positive response to treatment with dopaminergic agents, at least initially, and for many years carbidopa/levodopa was the usual therapy for RLS. It remains a first-line treatment for patients with intermittent symptoms.
Early studies consistently showed that 70% to 80% of RLS patients treated with carbidopa/levodopa had a significant improvement in symptoms.20-22 But the studies were small, did not always include a placebo arm, and most were crossover trials, making it impossible to do a statistical comparison.5
Typical doses of carbidopa/levodopa as a treatment for RLS are 25/100 mg to 100/400 mg in divided doses, given before bedtime and again, if needed, in the middle of the sleep period.9 These doses are much lower than those used to treat Parkinsonism.
Common side effects of carbidopa/levodopa include nausea, headache, dry mouth, and daytime somnolence.2,21 An increased risk of melanoma has been seen in some studies of carbidopa/levodopa, but the evidence is inconclusive.23,24 Rebound (a worsening of symptom severity when the medication wears off) and augmentation (the development of more severe symptoms early in the day) have also been reported.
Tolerance to carbidopa/levodopa is infrequent among patients with RLS. One early study found that only 3 of 43 patients (7%) required an increase in dosage over time.21 The on/off phenomenon that occurs with this medication in the treatment of Parkinsonism is not mentioned in the literature in reference to RLS.
Because carbidopa/levodopa only provides relief for 4 to 6 hours, a second dose is often needed. If that second dose repeatedly disrupts the patient’s sleep, the recommended approach is to give 2 doses before bedtime—1 dose of regular carbidopa/levodopa and 1 dose of the controlled release form.6,9
Augmentation, the most serious problem associated with carbidopa/levodopa, occurs in 65% to 80% of RLS patients treated with this medication. It is more common in those with refractory symptoms and those taking higher doses, but can affect any RLS patient.
If augmentation develops, discontinue the carbidopa/levodopa and switch the patient to another agent. Augmentation reverses within a few weeks of stopping the medication and treatment can then be resumed, but be aware that the augmentation may reoccur.
Carbidopa/levodopa is a good choice for patients with intermittent RLS symptoms, despite the risks associated with this medication. Not only does it provide quick relief, but it can be used only on the days when symptoms occur.2,5,8
Dopamine agonists
The use of pramipexole or ropinirole as first-line treatment for people with daily or refractory symptoms of RLS is well supported by controlled studies.7,17,25 Dopamine agonists can also be used to treat patients with RLS with varying levels of severity,6 and are sometimes prescribed as the initial treatment for intermittent symptoms.
These newer agents have a longer half-life than carbidopa/levodopa, which eliminates the need for a second dose in the midst of the sleep cycle. They also have much lower rates of augmentation. Studies have been inconsistent with regard to the risk of augmentation associated with these drugs, however, with results ranging from a high of 33%7,26 to a low of 4%.27
Nausea, headache, fatigue, dizziness, orthostatic hypotension, and vomiting—the most common side effects of pramipexole and ropinirole—usually decrease in severity after 7 to 10 days of therapy. In a recent meta-analysis comparing dopamine agonists with placebo in RLS patients, the number needed to harm (NNH) was 77 and the number needed to treat (NNT) was 6.27
Pramipexole. Dosing is started at 0.125 mg at bedtime and slowly titrated up to minimize side effects. Most patients experience relief at an average dose of 0.375 mg, taken daily or intermittently for symptom relief. 6,17,27
Ropinirole. Dosing is started at 0.25 mg at bedtime (or at dinner and bedtime), and then slowly titrated up every few days to every week until a good response is obtained. Most patients respond to a dose between 1 and 2.5 mg/d.6,17,28
Tx alternatives: Anticonvulsants, opioids, and benzodiazepines
When patients are unable to tolerate—or do not respond adequately to—dopaminergic agents or dopamine agonists, anticonvulsants, opioids, or benzodiazepines may be effective alternatives, or adjunctive treatments. They may also be used in patients who have another disorder, such as chronic pain, for which these alternatives will be beneficial.
Anticonvulsants. Of the anticonvulsants studied in RLS patients, gabapentin has been shown to most effectively decrease symptoms.25 Use of the drug should be reserved for patients with daily symptoms or refractory RLS. Gabapentin also appears to be especially effective in patients who perceive their symptoms as painful, and in hemodialysis patients.2,17,28 The average effective daily dose of gabapentin for treatment of RLS is 1855 mg.6
A 2002 double-blind crossover trial found that after 6 weeks of therapy, 16 of 24 (66%) patients taking gabapentin had only mild RLS symptoms, compared with 8 of 24 (33%) of those taking placebo (NNT=3).14 The most common side effects were malaise, somnolence, dry mouth, and nausea (NNH=4). Of note, there was no significant difference in the incidence of side effects among those in the therapy group compared with the controls.
Gabapentin also has fewer side effects and drug interactions than other anticonvulsants. (Both carbamazepine and valproate have also been studied for the treatment of RLS symptoms, but at best, provided only modest improvements.)
Opioids have long been recognized as an effective treatment for RLS, but their use is limited by the potential for abuse.6 In a double-blind crossover trial, 10 of 11 patients preferred opioids over placebo, and significantly more rated their leg sensations as mild after 2 weeks of treatment with opioids (NNT=2). The most common side effects were constipation and sedation (NNH=3).17,29
Many patients obtain symptom relief from low-potency opioids such as codeine, taken at bedtime, and there appears to be a lower abuse potential when bedtime-only dosing is used. However, higher-potency opioids may be necessary for patients with refractory RLS.17
One study did show an increase in symptoms of sleep apnea in RLS patients treated with opioids. If you suspect sleep apnea in an RLS patient taking opioids, provide a referral for a polysomnography evaluation.30
Benzodiazepines. There is limited evidence to support the use of clonazepam in the treatment of RLS. Although a prospective controlled study found clonazepam to be no more effective than placebo in RLS treatment,31 clonazepam has been shown to be an effective treatment in patients with PLMS.32 Because of the association between these 2 movement disorders, clonazepam is considered an option to use alone or as adjunctive therapy in patients with RLS.2,7
CASE STUDY: Grace’s diagnosis and treatment
In addition to having the 4 essential criteria for RLS, Grace reported sleep disturbances and periodic leg movements—2 additional features that are common to RLS. She also had low serum iron levels; however, her iron deficiency was related to her gastric bypass, and she was unable to tolerate iron therapy. We started her on a low dose of pramipexole, and she had a significant—and rapid—improvement in symptoms. When we last saw her, she reported that she usually slept through the night and that her leg movements had diminished so much that her husband no longer found it necessary to sleep in a separate bed.
Correspondence
Darlene E. Moyer, MD, Scottsdale Healthcare Family Medicine Residency Program, University of Arizona School of Medicine, 7301 East 2nd Street, Suite 210, Scottsdale, AZ 85251; [email protected]
1. Karroum E, Konofal E, Arnulf I. Restless-legs syndrome. Rev Neurol. 2008;164:701-721.
2. Vergne-Salle P, Coyral D, Dufauret K, et al. Is restless legs syndrome underrecognized? Current management. Joint Bone Spine. 2006;73:369-373.
3. Fulda S, Wetter TC. Dopamine agonists for the treatment of restless legs syndrome. Expert Opin Pharmacother. 2005;6:2655-2666.
4. Allen RP, Walters AS, Montplaisir J, et al. Restless legs syndrome prevalence and impact: REST general population study. Arch Intern Med. 2005;165:1286-1292.
5. Conti C, de Oliveira MM, Andriolo RB, et al. Levodopa for idiopathic restless legs syndrome: evidence-based review. Mov Disord. 2007;22:1943-1951.
6. Restless Legs Syndrome Foundation. RLS Medical Bulletin. 2005. Available at: http://www.irlssg.org/RLSMB2005pf.pdf. Accessed July 9, 2009.
7. Ryan M, Slevin J. Restless legs syndrome. Am J Health Syst Pharm. 2006;63:1599-1612.
8. Oertel W, Trenkwalder C, Zucconi M, et al. State of the art in restless legs syndrome therapy: practice recommendations for treating restless legs syndrome. Mov Disord. 2007;22(suppl 18):S466-S475.
9. Thorpy M. New paradigms in the treatment of restless legs syndrome. Neurology. 2005;64(12 suppl 3):S28-S33.
10. Winkelman J. A better future for patients with restless legs syndrome. Am J Med. 2007;120(1 suppl 1):S28-S29.
11. Chahine L, Chemali Z. Restless legs syndrome: a review. CNS Spectr. 2006;11:511-520.
12. Johnson E. Omnibus Sleep in America poll. National Sleep Foundation. 1998.-
13. Rothdach AJ, Trenkwalder C, Haberstock J, et al. Prevalence and risk factors of RLS in an elderly population: the MEMO study. Neurology. 2000;54:1064-1068.
14. Garcia-Borreguero D. Time to REST: epidemiology and burden. Eur J Neurol. 2006;13(suppl 3):S15-S20.
15. Schapira A. RLS patients: who are they? Eur J Neurol. 2006;13(suppl 3):S2-S7.
16. Benes H, Walters AS, Allen RP, et al. Definition of restless legs syndrome, how to diagnose it, and how to differentiate it from RLS mimics. Mov Disord. 2007;22(suppl 18):S401-S408.
17. Hening W, Allen R, Tenzer P, et al. Restless legs syndrome: demographics, presentation and differential diagnosis. Geriatrics. 2007;62:26-29.
18. O’Keefe ST, Gavin K, Lavan JN. Iron status and restless legs in the elderly. Age Ageing. 1994;23:200-203.
19. Sun ER, Chen CA, Ho G, et al. Iron and the restless legs syndrome. Sleep. 1998;21:371-377.
20. Akpinar S. Restless legs syndrome treatment with dopaminergic drugs. Clin Neuropharmacol. 1987;10:69-79.
21. Becker P, Jamieson A, Brown D. Dopaminergic agents in restless legs syndrome and periodic limb movements of sleep: response and complications of extended treatment in 49 cases. Sleep. 1993;16:713-716.
22. Von Scheele C, Kempi V. Long-term effect of dopaminergic drugs in restless legs. A 2 year follow-up. Arch Neurol. 1990;47:1223-1224.
23. Bertoni JM, Arlette JP, Fernandez HH, et al. Epidemiologic association of Parkinson’s disease and melanoma. Mov Disord. 2006;21(suppl 15):S610.-
24. Fiala K, Whetteckey J, Manyam B. Malignant melanoma and levodopa in Parkinson’s disease: causality or coincidence? Parkinsonism Relat Disord. 2003;9:321-327.
25. Montagna P. The treatment of restless legs syndrome. Neurol Sci. 2007;28(suppl 1):S61-S66.
26. Kushida C. Clinical presentation, diagnosis and quality of life issues in restless legs syndrome. Am J Med. 2007;120(1 suppl 1):S4-S12.
27. Baker W, White C, Coleman C. Effect of nonergot dopamine agonists on symptoms of restless legs syndrome. Ann Fam Med. 2008;6:253-262.
28. Fulda S, Wetter T. Emerging drugs for restless legs syndrome. Expert Opin Emerg Drugs. 2005;10:527-552.
29. Walters A, Wagner M, Hening W, et al. Successful treatment of idiopathic restless legs syndrome in a randomized double-blind trial of oxycodone versus placebo. Sleep. 1993;16:327-332.
30. Walters A, Winkelman J, Trenkwalder C, et al. Long term follow-up on restless legs syndrome patients treated with opioids. Mov Disord. 2001;16:1105-1109.
31. Boghen D, Lamothe L, Elie R. The treatment of restless legs syndrome with clonazepam: a prospective controlled trial. Can J Neurol Sci. 1986;13:245-247.
32. Peled R, Lavie P. Double-blind evaluation of clonazepam on periodic leg movements in sleep. J Neurol Neurosurg Psychiatry. 1987;50:1679-1681.
33. Ferni-Strambi L. RLS-like symptoms: differential diagnosis by history and clinical assessment. Sleep Med. 2007;8(suppl 2):S3-S6.
1. Karroum E, Konofal E, Arnulf I. Restless-legs syndrome. Rev Neurol. 2008;164:701-721.
2. Vergne-Salle P, Coyral D, Dufauret K, et al. Is restless legs syndrome underrecognized? Current management. Joint Bone Spine. 2006;73:369-373.
3. Fulda S, Wetter TC. Dopamine agonists for the treatment of restless legs syndrome. Expert Opin Pharmacother. 2005;6:2655-2666.
4. Allen RP, Walters AS, Montplaisir J, et al. Restless legs syndrome prevalence and impact: REST general population study. Arch Intern Med. 2005;165:1286-1292.
5. Conti C, de Oliveira MM, Andriolo RB, et al. Levodopa for idiopathic restless legs syndrome: evidence-based review. Mov Disord. 2007;22:1943-1951.
6. Restless Legs Syndrome Foundation. RLS Medical Bulletin. 2005. Available at: http://www.irlssg.org/RLSMB2005pf.pdf. Accessed July 9, 2009.
7. Ryan M, Slevin J. Restless legs syndrome. Am J Health Syst Pharm. 2006;63:1599-1612.
8. Oertel W, Trenkwalder C, Zucconi M, et al. State of the art in restless legs syndrome therapy: practice recommendations for treating restless legs syndrome. Mov Disord. 2007;22(suppl 18):S466-S475.
9. Thorpy M. New paradigms in the treatment of restless legs syndrome. Neurology. 2005;64(12 suppl 3):S28-S33.
10. Winkelman J. A better future for patients with restless legs syndrome. Am J Med. 2007;120(1 suppl 1):S28-S29.
11. Chahine L, Chemali Z. Restless legs syndrome: a review. CNS Spectr. 2006;11:511-520.
12. Johnson E. Omnibus Sleep in America poll. National Sleep Foundation. 1998.-
13. Rothdach AJ, Trenkwalder C, Haberstock J, et al. Prevalence and risk factors of RLS in an elderly population: the MEMO study. Neurology. 2000;54:1064-1068.
14. Garcia-Borreguero D. Time to REST: epidemiology and burden. Eur J Neurol. 2006;13(suppl 3):S15-S20.
15. Schapira A. RLS patients: who are they? Eur J Neurol. 2006;13(suppl 3):S2-S7.
16. Benes H, Walters AS, Allen RP, et al. Definition of restless legs syndrome, how to diagnose it, and how to differentiate it from RLS mimics. Mov Disord. 2007;22(suppl 18):S401-S408.
17. Hening W, Allen R, Tenzer P, et al. Restless legs syndrome: demographics, presentation and differential diagnosis. Geriatrics. 2007;62:26-29.
18. O’Keefe ST, Gavin K, Lavan JN. Iron status and restless legs in the elderly. Age Ageing. 1994;23:200-203.
19. Sun ER, Chen CA, Ho G, et al. Iron and the restless legs syndrome. Sleep. 1998;21:371-377.
20. Akpinar S. Restless legs syndrome treatment with dopaminergic drugs. Clin Neuropharmacol. 1987;10:69-79.
21. Becker P, Jamieson A, Brown D. Dopaminergic agents in restless legs syndrome and periodic limb movements of sleep: response and complications of extended treatment in 49 cases. Sleep. 1993;16:713-716.
22. Von Scheele C, Kempi V. Long-term effect of dopaminergic drugs in restless legs. A 2 year follow-up. Arch Neurol. 1990;47:1223-1224.
23. Bertoni JM, Arlette JP, Fernandez HH, et al. Epidemiologic association of Parkinson’s disease and melanoma. Mov Disord. 2006;21(suppl 15):S610.-
24. Fiala K, Whetteckey J, Manyam B. Malignant melanoma and levodopa in Parkinson’s disease: causality or coincidence? Parkinsonism Relat Disord. 2003;9:321-327.
25. Montagna P. The treatment of restless legs syndrome. Neurol Sci. 2007;28(suppl 1):S61-S66.
26. Kushida C. Clinical presentation, diagnosis and quality of life issues in restless legs syndrome. Am J Med. 2007;120(1 suppl 1):S4-S12.
27. Baker W, White C, Coleman C. Effect of nonergot dopamine agonists on symptoms of restless legs syndrome. Ann Fam Med. 2008;6:253-262.
28. Fulda S, Wetter T. Emerging drugs for restless legs syndrome. Expert Opin Emerg Drugs. 2005;10:527-552.
29. Walters A, Wagner M, Hening W, et al. Successful treatment of idiopathic restless legs syndrome in a randomized double-blind trial of oxycodone versus placebo. Sleep. 1993;16:327-332.
30. Walters A, Winkelman J, Trenkwalder C, et al. Long term follow-up on restless legs syndrome patients treated with opioids. Mov Disord. 2001;16:1105-1109.
31. Boghen D, Lamothe L, Elie R. The treatment of restless legs syndrome with clonazepam: a prospective controlled trial. Can J Neurol Sci. 1986;13:245-247.
32. Peled R, Lavie P. Double-blind evaluation of clonazepam on periodic leg movements in sleep. J Neurol Neurosurg Psychiatry. 1987;50:1679-1681.
33. Ferni-Strambi L. RLS-like symptoms: differential diagnosis by history and clinical assessment. Sleep Med. 2007;8(suppl 2):S3-S6.