User login
In January, I attended the AMA’s Relative Value Update Committee (RUC) as an observer. As many of you are aware, the Centers for Medicare and Medicaid Services has requested a systematic review of the physician work and practice expenses for more than 100 endoscopic procedures performed by gastroenterologists. Several very dedicated physicians and staff from the AGA and the American Society for Gastrointestinal Endoscopy (ASGE) are heavily involved with this process, which will take several years to complete. Their dedication and passion for the process is truly impressive.
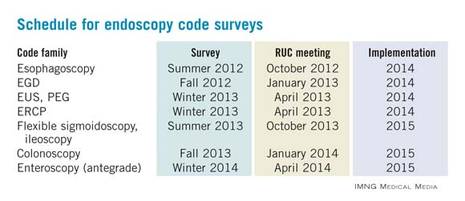
The schedule for the endoscopy codes to be surveyed is as follows:
Almost 20 years ago, when Medicare transitioned to a physician payment system based on the Resource Based-Relative Value Scale (RBRVS), the American Medical Association formulated a multispecialty committee, known as the RUC. The RUC carefully reviews survey data presented by specialty societies and develops recommendations for consideration by CMS. The RUC’s cycle for developing recommendations is closely coordinated with both the Current Procedural Terminology (CPT) Editorial Panel’s schedule for annual code revisions and the CMS schedule for annual updates in the Medicare Physician Payment Schedule.
The survey process asks physicians to assess the time, intensity, complexity, and the medical decision making to perform a procedure. Surveys are obtained from a random sample of practicing physicians. The surveyed physician is asked to value the pre-, intra- and postservice work of a given service, using the total work of a reference procedure for comparison.
The survey asks physicians to estimate the following in detail:
• Intraservice time of the procedure.
• Work of the service, compared with the work of a specialty standard.
• Times of preoperative tasks including preprocedure evaluation, positioning, and scrub, dress, and wait time.
• Times of immediate postoperative services, including monitoring the patient.
Once the surveys are completed, the societies analyze the data and prepare recommendations to ensure that the time, effort, and complexity of your work is accurately estimated in the hierarchy of the other codes in both the GI family and the rest of the fee schedule. Responding to a survey is critical, for the more people who respond to the survey, the better are the data that the societies can present to the RUC.
Over the fall of 2012, the EGD (esophagogastroduodenoscopy) codes were surveyed. During the holidays, the data were aggregated and analyzed. An expert panel was convened by the AGA, ASGE, and the Society of American Gastrointestinal and Endoscopic Surgeons to review the data and to prepare recommendations for the RUC. This is where I became involved in the process. The physicians and staff met throughout the month of January, with more than 25 hours of telephone and in-person meetings and almost another 70 hours of behind-the-scenes work to prepare for the RUC meeting.
As you can see, the physicians and staff were challenged with multiple major issues. The RUC meeting is not a vacation to an exotic location. The meeting took place in an airport hotel located between two freeways where there was nothing to do except work. From the time we arrived on Wednesday afternoon until the meeting ended on Saturday evening, our RUC advisers and staff were constantly in meetings 12-16 hours each day. During the meetings, the societies met with teams of physicians from the RUC who analyze the survey data. Ultimately, the societies make a facilitated recommendation to the RUC regarding the physician work, practice expense, and professional liability that ranks procedures within a family (for example, the EGD codes) against procedures in similar families (for example, the esophagoscopy codes), and to procedures outside of gastroenterology (for example, evaluation and management services, radiology, surgery, cardiology, etc.).
The wealth of knowledge that is possessed by our RUC advisers is much more than one can master in the course of these meetings. Our physicians and staff are very passionate about the process and have mastered a knowledge base that has required significant time and much effort to understand. This group of dedicated individuals should be commended on the tremendous amount of work they perform on behalf of our specialty. We all owe them much for their service.
We will await the final review by CMS, who will publish their first set of recommendations when the final rule is released this November. In the meantime, if you receive a request to participate in an RUC survey, make sure you do so.
In January, I attended the AMA’s Relative Value Update Committee (RUC) as an observer. As many of you are aware, the Centers for Medicare and Medicaid Services has requested a systematic review of the physician work and practice expenses for more than 100 endoscopic procedures performed by gastroenterologists. Several very dedicated physicians and staff from the AGA and the American Society for Gastrointestinal Endoscopy (ASGE) are heavily involved with this process, which will take several years to complete. Their dedication and passion for the process is truly impressive.
The schedule for the endoscopy codes to be surveyed is as follows:
Almost 20 years ago, when Medicare transitioned to a physician payment system based on the Resource Based-Relative Value Scale (RBRVS), the American Medical Association formulated a multispecialty committee, known as the RUC. The RUC carefully reviews survey data presented by specialty societies and develops recommendations for consideration by CMS. The RUC’s cycle for developing recommendations is closely coordinated with both the Current Procedural Terminology (CPT) Editorial Panel’s schedule for annual code revisions and the CMS schedule for annual updates in the Medicare Physician Payment Schedule.
The survey process asks physicians to assess the time, intensity, complexity, and the medical decision making to perform a procedure. Surveys are obtained from a random sample of practicing physicians. The surveyed physician is asked to value the pre-, intra- and postservice work of a given service, using the total work of a reference procedure for comparison.
The survey asks physicians to estimate the following in detail:
• Intraservice time of the procedure.
• Work of the service, compared with the work of a specialty standard.
• Times of preoperative tasks including preprocedure evaluation, positioning, and scrub, dress, and wait time.
• Times of immediate postoperative services, including monitoring the patient.
Once the surveys are completed, the societies analyze the data and prepare recommendations to ensure that the time, effort, and complexity of your work is accurately estimated in the hierarchy of the other codes in both the GI family and the rest of the fee schedule. Responding to a survey is critical, for the more people who respond to the survey, the better are the data that the societies can present to the RUC.
Over the fall of 2012, the EGD (esophagogastroduodenoscopy) codes were surveyed. During the holidays, the data were aggregated and analyzed. An expert panel was convened by the AGA, ASGE, and the Society of American Gastrointestinal and Endoscopic Surgeons to review the data and to prepare recommendations for the RUC. This is where I became involved in the process. The physicians and staff met throughout the month of January, with more than 25 hours of telephone and in-person meetings and almost another 70 hours of behind-the-scenes work to prepare for the RUC meeting.
As you can see, the physicians and staff were challenged with multiple major issues. The RUC meeting is not a vacation to an exotic location. The meeting took place in an airport hotel located between two freeways where there was nothing to do except work. From the time we arrived on Wednesday afternoon until the meeting ended on Saturday evening, our RUC advisers and staff were constantly in meetings 12-16 hours each day. During the meetings, the societies met with teams of physicians from the RUC who analyze the survey data. Ultimately, the societies make a facilitated recommendation to the RUC regarding the physician work, practice expense, and professional liability that ranks procedures within a family (for example, the EGD codes) against procedures in similar families (for example, the esophagoscopy codes), and to procedures outside of gastroenterology (for example, evaluation and management services, radiology, surgery, cardiology, etc.).
The wealth of knowledge that is possessed by our RUC advisers is much more than one can master in the course of these meetings. Our physicians and staff are very passionate about the process and have mastered a knowledge base that has required significant time and much effort to understand. This group of dedicated individuals should be commended on the tremendous amount of work they perform on behalf of our specialty. We all owe them much for their service.
We will await the final review by CMS, who will publish their first set of recommendations when the final rule is released this November. In the meantime, if you receive a request to participate in an RUC survey, make sure you do so.
In January, I attended the AMA’s Relative Value Update Committee (RUC) as an observer. As many of you are aware, the Centers for Medicare and Medicaid Services has requested a systematic review of the physician work and practice expenses for more than 100 endoscopic procedures performed by gastroenterologists. Several very dedicated physicians and staff from the AGA and the American Society for Gastrointestinal Endoscopy (ASGE) are heavily involved with this process, which will take several years to complete. Their dedication and passion for the process is truly impressive.
The schedule for the endoscopy codes to be surveyed is as follows:
Almost 20 years ago, when Medicare transitioned to a physician payment system based on the Resource Based-Relative Value Scale (RBRVS), the American Medical Association formulated a multispecialty committee, known as the RUC. The RUC carefully reviews survey data presented by specialty societies and develops recommendations for consideration by CMS. The RUC’s cycle for developing recommendations is closely coordinated with both the Current Procedural Terminology (CPT) Editorial Panel’s schedule for annual code revisions and the CMS schedule for annual updates in the Medicare Physician Payment Schedule.
The survey process asks physicians to assess the time, intensity, complexity, and the medical decision making to perform a procedure. Surveys are obtained from a random sample of practicing physicians. The surveyed physician is asked to value the pre-, intra- and postservice work of a given service, using the total work of a reference procedure for comparison.
The survey asks physicians to estimate the following in detail:
• Intraservice time of the procedure.
• Work of the service, compared with the work of a specialty standard.
• Times of preoperative tasks including preprocedure evaluation, positioning, and scrub, dress, and wait time.
• Times of immediate postoperative services, including monitoring the patient.
Once the surveys are completed, the societies analyze the data and prepare recommendations to ensure that the time, effort, and complexity of your work is accurately estimated in the hierarchy of the other codes in both the GI family and the rest of the fee schedule. Responding to a survey is critical, for the more people who respond to the survey, the better are the data that the societies can present to the RUC.
Over the fall of 2012, the EGD (esophagogastroduodenoscopy) codes were surveyed. During the holidays, the data were aggregated and analyzed. An expert panel was convened by the AGA, ASGE, and the Society of American Gastrointestinal and Endoscopic Surgeons to review the data and to prepare recommendations for the RUC. This is where I became involved in the process. The physicians and staff met throughout the month of January, with more than 25 hours of telephone and in-person meetings and almost another 70 hours of behind-the-scenes work to prepare for the RUC meeting.
As you can see, the physicians and staff were challenged with multiple major issues. The RUC meeting is not a vacation to an exotic location. The meeting took place in an airport hotel located between two freeways where there was nothing to do except work. From the time we arrived on Wednesday afternoon until the meeting ended on Saturday evening, our RUC advisers and staff were constantly in meetings 12-16 hours each day. During the meetings, the societies met with teams of physicians from the RUC who analyze the survey data. Ultimately, the societies make a facilitated recommendation to the RUC regarding the physician work, practice expense, and professional liability that ranks procedures within a family (for example, the EGD codes) against procedures in similar families (for example, the esophagoscopy codes), and to procedures outside of gastroenterology (for example, evaluation and management services, radiology, surgery, cardiology, etc.).
The wealth of knowledge that is possessed by our RUC advisers is much more than one can master in the course of these meetings. Our physicians and staff are very passionate about the process and have mastered a knowledge base that has required significant time and much effort to understand. This group of dedicated individuals should be commended on the tremendous amount of work they perform on behalf of our specialty. We all owe them much for their service.
We will await the final review by CMS, who will publish their first set of recommendations when the final rule is released this November. In the meantime, if you receive a request to participate in an RUC survey, make sure you do so.