User login
Discuss this article at www.facebook.com/CurrentPsychiatry
You are treating Mr. P, age 34, for schizoaffective disorder. He smokes 1 pack of cigarettes per day and has smoked for approximately 17 years. He has tried to stop but never has been able to quit for more than a few weeks. He reveals whenever he tries to quit, he starts feeling extremely lethargic and “depressed” and resumes smoking to prevent these symptoms from worsening. However, Mr. P expresses some interest in trying to quit again and asks whether any medications could prevent him from becoming depressed while he tries to quit.
Cigarette smoking is overrepresented and undertreated among individuals with psychiatric illness, in part because of the largely unfounded belief held by some patients and clinicians that smoking cessation might worsen psychiatric symptoms. In this article, we argue this challenge can be overcome and psychiatrists and other mental health professionals can and should help their patients reap the innumerable benefits of quitting smoking. We discuss:
- the short- and long-term effects of smoking cessation
- evidence-based treatment guidelines for working with motivated and unmotivated smokers
- unique issues that may arise when treating smokers who have psychiatric disorders.
Quitting: Profound benefits
Quitting smoking has substantial benefits beginning within minutes after taking the last puff. Some of the benefits that occur within the first few days of quitting include:
- decreased blood pressure and pulse rate
- improved circulation
- improved ability to smell and taste
- easier breathing.
Longer-term smoking abstinence drastically reduces risk of heart attack, stroke, cancer, respiratory disease, and a host of other illnesses that affect—and kill—individuals with psychiatric disorders several decades earlier than their counterparts in the general population.1 There also are financial benefits to quitting; using the 2009 national average of $5.33 per pack, a 1-pack-per-day smoker who quits would save >$150 per month, which accounts for only the direct cost of cigarettes.2
Although the beneficial effects of quitting smoking are profound and far-reaching, in the short-term they are counterbalanced by nicotine withdrawal symptoms—including restlessness, irritability, depressed mood, concentration problems, and increased appetite/weight gain—that are formidable distractions from the positive aspects of quitting. Additionally, nicotine withdrawal symptoms tend to be more severe in smokers who have a psychiatric disorder.3 Fortunately, there are effective, evidence-based methods of reducing withdrawal symptoms and helping smokers cope with these and other challenges of quitting.
Combined treatment is best
Current treatment guidelines4 suggest all smokers should be offered pharmacotherapy and counseling to aid quitting because this combined approach has the highest success rate (Algorithm). Table 1 4 provides information about dosing, efficacy, and side effect profile of each of the 7 FDA-approved medications for smoking cessation. Using any of the approved medications at least doubles the odds of successful quitting compared with placebo.4 These pharmacotherapies can reduce or prevent nicotine withdrawal symptoms and—at least in the case of bupropion and varenicline—decrease reinforcement from smoking, thereby lowering the likelihood a lapse (ie, smoking ≥1 cigarettes without returning to regular smoking) will develop into a full-blown relapse (ie, return to regular smoking).
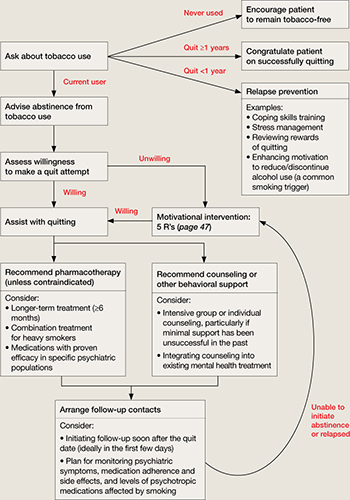
Algorithm: Tobacco cessation treatment for psychiatric patients
Source: Adapted from reference 4 Medication selection depends on many factors, including:
- the patient’s psychiatric illness
- her/his prior response to smoking cessation pharmacotherapies
- concomitant psychiatric medications
- patient preference.5
Placebo-controlled trials of smoking cessation aids in psychiatrically ill patients are limited, but several studies of smokers with a history of major depression indicate treatment with bupropion SR or nortriptyline is effective.6 Similarly, although relapse rates generally are higher in patients with schizophrenia compared with non-mentally ill smokers, nicotine replacement therapy and bupropion SR are more effective than placebo in patients with this disorder.7,8 When we prescribe these treatments, we tend to extend the duration of treatment beyond those described in Table 1 ,4 and to use combined treatments (eg, a transdermal patch with a shorter-acting gum or lozenge preparation) to better target the marked withdrawal symptoms more severely nicotine-dependent patients frequently experience.
Table 1
First-line pharmacotherapies for smoking cessation
| Medication | Standard dosage | Efficacy (OR, % abstinent at 6 mos. [with 95% CI]) | Contraindications (C) and precautions (P) | Common side effects |
|---|---|---|---|---|
| Non-nicotine medications | ||||
| Bupropion | Days 1-3: 150 mg/d Days 4-8: 150 mg bid Continue for 7-12 weeks at 150 mg bid | 2.0 (1.8-2.2), 24% (22%-26%) | C: Eating disorders, seizure history, taking bupropion, MAOI in past 2 weeks P: Pregnancy, cardiovascular disease, warning for emergent psychiatric symptoms | Insomnia, dry mouth |
| Varenicline | Days 1-3: 0.5 mg/d Days 4-7: 0.5 mg bid Day 8+: 1 mg bid Continue 11 weeks at 1 mg bid; up to 6 months for maintenance | 3.1 (2.5-3.8), 33% (29%-38%) | P: Warning for emergent psychiatric symptoms | Nausea, sleep problems, abnormal dreams |
| Nicotine replacement therapies | ||||
| Nicotine gum | 1 piece every 1-2 hours for 6-12 weeks <20 cigarettes/d: 2 mg gum ≥20 cigarettes/d: 4 mg gum | 1.5 (1.2-1.7), 19% (17%-22%) | P: Pregnancy, recent myocardial infarction, serious arrhythmia, unstable angina | Mouth soreness, hiccups, dyspepsia |
| Nicotine inhaler | 6-16 cartridges/d, up to 6 months | 2.1 (1.5-2.9), 25% (19%-32%) | Same as above | Mouth/throat irritation, coughing, rhinitis |
| Nicotine lozenge | 9-20 lozenges/d, up to 12 weeks Smoke ≤30 minutes after waking: 4 mg lozenge Smoke >30 minutes after waking: 2 mg lozenge | 2.0 (1.6-2.5)a | Same as above | Nausea, hiccups, heartburn |
| Nicotine nasal spray | 1-2 doses/hour, 8-40 doses/d for 3-6 months | 2.3 (1.7-3.0), 27% (22%-33%) | C: Severe reactive airway disease P: Same as above | Nasal irritation, higher risk of dependency |
| Nicotine patch | 1 patch/d, step-down dosing over 8 weeks Weeks 1-4: 21 mg patch Weeks 5-6: 14 mg patch Weeks 7-8: 7 mg patch | 1.9 (1.7-2.2) 23% (21%-26%) | P: Same as above | Skin reactions, sleep problems, abnormal dreams |
| aStead LF, Perera R, Bullen C, et al. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev. 2008;1:CD000146. bid: twice a day; CI: confidence interval; MAOI: monoamine oxidase inhibitor; OR: odds ratio Source: Adapted from reference 4 | ||||
Counseling. All smokers should be provided with brief interventions consistent with the 5 A’s—Ask, Advise, Assess, Assist, and Arrange (Table 2).4 For smokers who are not motivated to quit, the recommended approach follows the principles of the 5 R’s—Relevance, Risks, Rewards, Roadblocks, and Repetition (Table 3).4 Smokers who are motivated to quit and willing to participate in more intensive treatment may be offered face-to-face individual or group counseling (depending upon availability) or referred to a telephone quit line (see Related Resources). Intensive treatments such as these typically provide social support and assistance overcoming barriers to cessation and developing skills to initiate and maintain abstinence (eg, coping with a lapse or handling cravings, identifying and avoiding high-risk situations for smoking). As a general rule, greater intensity of counseling is associated with a greater likelihood of quitting.4
Table 2
The 5 A’s of tobacco treatment
| Intervention | Example | |
|---|---|---|
| Ask | Systematically inquire about tobacco use | “Do you currently use, or have you ever used, tobacco products?” |
| Advise | Counsel all tobacco users to quit in a clear, strong, and personalized manner | “I think it is very important for you quit smoking to keep your breathing problems from getting any worse” |
| Assess | Determine the tobacco user’s willingness to make a quit attempt | “What do you think? Are you ready to quit?” |
| Assist | Offer or refer to treatment/support (if ready to quit; if not ready, see Table 3 for recommended interventions) | “I’m here to help you with this. Let me start by letting you know about the many options available to help you quit” |
| Arrange | Plan for follow-up contacts (at least 1, preferably within 1 week of the quit date) | “I would like to give you a call within the next week to see how you did with your quit date. Would that be OK with you?” |
| Source: Adapted from reference 4 | ||
Table 3
The 5 R’s: Principles of interventions for smokers not ready to quit
| Principle | Example | |
|---|---|---|
| Relevance | Why is quitting smoking personally relevant? | “You’ve told me your kids sometimes make comments to you about quitting smoking. How does that affect you?” |
| Risks | What are the negative consequences of smoking? | “What don’t you like about smoking? What problems have you had from smoking?” |
| Rewards | What are the benefits of quitting smoking? | “Can you think of anything that would be good about quitting? Tell me about that” |
| Roadblocks | What are the barriers to quitting? | “What worries do you have about trying to quit? What happened the last time you tried to quit smoking?” |
| Repetition | Message repeated at every visit | “I know we have talked about quitting smoking before, but things may have changed since then. I also think that this is such an important issue we should keep it on the table for discussion. What do you think?” |
| Source: Adapted from reference 4 | ||
Q&A about treatment
How effective are smoking cessation interventions for individuals with psychiatric disorders? Several studies have demonstrated, on any given quit attempt, smokers with psychiatric or substance use disorders can be as successful as smokers without these disorders.9-11 In fact, quit rates as high as approximately 70% for end-of-treatment11 and 30% for 6-month follow-up10 have been reported. Of course, effectiveness varies by type and intensity of treatment as well as by individual characteristics of the smoker. Smokers with psychiatric disorders may fare better with more intensive interventions than briefer ones,12,13 and factors such as high levels of nicotine dependence and exposure to smoking environments—both of which are characteristic of smokers with serious mental illness—can negatively impact treatment outcomes.4
Should the nature of the psychiatric disorder(s) guide decisions about the optimal pharmacotherapy or counseling approach? There have been numerous attempts to investigate the effectiveness of targeted interventions for particular subgroups of smokers with psychiatric disorders, including:
- studies of the efficacy of the antidepressants bupropion14 and nortriptyline15 as well as cognitive-behavioral therapy-based mood management counseling16 for depressed smokers
- integrative treatment approaches for smokers with posttraumatic stress disorder (PTSD)17
- group counseling designed specifically for smokers with schizophrenia.18,19
Although more research is needed and there have been some promising early results (eg, McFall et al17), current literature does not provide consistent evidence supporting treatment matching solely on the basis of the psychiatric disorder. Rather, patient preference, safety considerations (eg, use of medications in children/adolescents, pregnant women), medication side effect profiles, prior experience with the treatment approach, and cost/availability of treatment should guide development of the treatment plan. When results from placebo-controlled trials are available for subgroups of patients (eg, those with a history of major depression), consider this information when selecting a pharmacologic smoking cessation aid.
What is the risk of psychiatric symptoms worsening as a result of quitting smoking? Little research on this topic is available because more often than not, smokers with psychiatric disorders are excluded from tobacco treatment studies. However, research examining psychiatric status changes among recent quitters with schizophrenia,20,21 depression,22,23 PTSD,17 and substance use disorders24 suggests smoking cessation does not worsen symptoms of these disorders, and may be associated with symptom improvement.17 Nonetheless, driven largely by anecdotal evidence, the misconception that smoking cessation worsens psychiatric symptoms remains a substantial barrier to treatment.
Mr. P’s case is an example of how not probing about the nature of psychiatric complaints can be problematic. Mr. P reported what on first glance appeared to be a worsening of psychiatric symptoms starting when he stopped smoking and resolved when he resumed smoking. However, without gathering additional information about these events, we cannot conclude stopping smoking caused his psychiatric symptoms to worsen. Other potential explanations include nicotine withdrawal symptoms, side effects of smoking cessation medications, an increase in levels of psychotropic medications for which metabolism is affected by tobacco smoke, or the natural course of his mood disorder. The timing of the onset and offset of symptoms seems to argue against Mr. P’s symptoms reflecting the natural course of his mood disorder, but the other 3 explanations remain plausible.
It is important to distinguish whether Mr. P’s worsening symptoms are consistent with a depressive episode or whether they are a manifestation of the transient dysphoria that accompanies nicotine withdrawal. Assessing the severity and persistence of the mood disturbance as well as the timing of onset could help make this determination. Nicotine withdrawal symptoms typically emerge within 24 hours of quitting or significantly reducing smoking and tend to peak within approximately 1 week. Thus, depressive symptoms that develop after weeks or months of abstinence would be less consistent with nicotine withdrawal. Additionally, the lethargy Mr. P reported may be a symptom of depression, or it may stem from a cessation-induced increase in antipsychotic serum levels. Because tobacco smoke increases the metabolism of several antipsychotics and antidepressants—including olanzapine, clozapine, haloperidol, and fluoxetine25—stopping smoking may increase medication levels and side effects. To rule out medication side effects as a cause of post-cessation mood changes, the psychiatrist should ask Mr. P about which smoking cessation pharmacotherapies (if any) he was using and which psychotropic medications he was taking. Unfortunately, such a detailed history is not always taken, and patient-generated theories of smoking cessation causing worsening psychiatric symptoms often are taken at face value.
When should smokers with psychiatric disorders be encouraged to quit? Are there times when smoking cessation should be discouraged? Tobacco treatment guidelines4 recommend advising users to quit at every clinical encounter, but there has been some debate about the timing of tobacco treatment for smokers with psychiatric disorders. There is minimal research to guide such treatment decisions. However, even if quit attempts are more successful during times of symptomatic stability—and there is no conclusive evidence to indicate they are—waiting for perfect mental health before initiating smoking cessation treatment is unnecessary and ill-advised. In some situations, such as when a patient has experienced an acute increase in psychiatric symptoms or when psychotropics are being titrated, a short-term postponement of quitting may be reasonable. However, discouraging smokers from trying to quit when they express readiness to try should be done sparingly, because it is uncertain how long that window of opportunity will be open, and the consequences of missed opportunities can be fatal.
- National Tobacco Quitline. 1-800-QUIT-NOW. www.smokefree.gov.
- University of California, San Francisco, Schools of Pharmacy and Medicine. Rx for Change (free online training program for clinicians). http://rxforchange.ucsf.edu.
- National Association of State Mental Health Program Directors. Tobacco-free living in psychiatric settings: a best-practices toolkit promoting wellness and recovery. www.nasmhpd.org/general_files/publications/NASMHPD.toolkitfinalupdated90707.pdf.
Drug Brand Names
- Bupropion • Wellbutrin, Zyban
- Clozapine • Clozaril
- Fluoxetine • Prozac
- Haloperidol • Haldol
- Nortriptyline • Aventyl, Pamelor
- Olanzapine • Zyprexa
- Varenicline • Chantix
Disclosures
Dr. Heffner was supported by National Institute on Drug Abuse grant#026517. She is a consultant to Pfizer Inc.
Dr. Anthenelli is supported by National Institute on Alcohol Abuse and Alcoholism grant#AA19720 and by the Department of Veterans Affairs. He is a consultant to GlaxoSmithKline and Pfizer Inc.
The Tri-State Tobacco and Alcohol Research Center receives research support from Eli Lilly and Company, Nabi Biopharmaceuticals, Pfizer Inc., and sanofi-aventis.
1. Colton CW, Manderscheid RW. Congruencies in increased mortality rates years of potential life lost, and causes of death among public mental health clients in eight states. Prev Chronic Dis. 2006;3(2):A42.-
2. Centers for Disease Control and Prevention. Trends in state and federal cigarette tax and retail price—1970-2009. 2010. Available at: http://www.cdc.gov/tobacco/data_statistics/tables/economics/trends. Accessed June 28 2011.
3. Xian H, Scherrer JF, Eisen SA, et al. Nicotine dependence subtypes: association with smoking history, diagnostic criteria and psychiatric disorders in 5440 regular smokers from the Vietnam Era Twin Registry. Addict Behav. 2007;32(1):137-147.
4. Fiore MC, Jaén CR, Baker TB, et al. A clinical practice guideline for treating tobacco use and dependence: 2008 update. A U. S. Public Health Service report. Am J Prev Med. 2008;35(2):158-176.
5. Anthenelli RM. How–and why–to help psychiatric patients stop smoking. Current Psychiatry. 2005;4(1):77-87.
6. Hughes JR, Stead LF, Lancaster T. Antidepressants for smoking cessation. Cochrane Database Syst Rev. 2007;1:CD000031.-
7. Williams JM, Foulds J. Successful tobacco dependence treatment in schizophrenia. Am J Psychiatry. 2007;164(2):222-227.
8. George TP, Vessicchio JC, Termine A, et al. A placebo controlled trial of bupropion for smoking cessation in schizophrenia. Biol Psychiatry. 2002;52(1):53-61.
9. Hughes JR, Kalman D. Do smokers with alcohol problems have more difficulty quitting? Drug Alcohol Depend. 2006;82(2):91-102.
10. McClure JB, Swan GE, Catz SL, et al. Smoking outcome by psychiatric history after behavioral and varenicline treatment. J Subst Abuse Treat. 2010;38(4):394-402.
11. Stapleton JA, Watson L, Spirling LI, et al. Varenicline in the routine treatment of tobacco dependence: a pre-post comparison with nicotine replacement therapy and an evaluation in those with mental illness. Addiction. 2008;103(1):146-154.
12. Hall SM, Muñoz RF, Reus VI. Cognitive-behavioral intervention increases abstinence rates for depressive-history smokers. J Consult Clin Psychol. 1994;62(1):141-146.
13. Hall SM, Muñoz RF, Reus VI, et al. Mood management and nicotine gum in smoking treatment: a therapeutic contact and placebo-controlled study. J Consult Clin Psychol. 1996;64(5):1003-1009.
14. Evins AE, Culhane MA, Alpert JE, et al. A controlled trial of bupropion added to nicotine patch and behavioral therapy for smoking cessation in adults with unipolar depressive disorders. J Clin Psychopharmacol. 2008;28(6):660-666.
15. Hall SM, Reus VI, Muñoz RF, et al. Nortriptyline and cognitive-behavioral therapy in the treatment of cigarette smoking. Arch Gen Psychiatry. 1998;55(8):683-690.
16. Brown RA, Kahler CW, Niaura R, et al. Cognitive-behavioral treatment for depression in smoking cessation. J Consult Clin Psychol. 2001;69(3):471-480.
17. McFall M, Saxon AJ, Malte CA, et al. Integrating tobacco cessation into mental health care for posttraumatic stress disorder: a randomized controlled trial. JAMA. 2010;304(22):2485-2493.
18. George TP, Ziedonis DM, Feingold A, et al. Nicotine transdermal patch and atypical antipsychotic medications for smoking cessation in schizophrenia. Am J Psychiatry. 2000;157(11):1835-1842.
19. Williams JM, Steinberg ML, Zimmermann MH, et al. Comparison of two intensities of tobacco dependence counseling in schizophrenia and schizoaffective disorder. J Subst Abuse Treat. 2010;38(4):384-393.
20. Evins AE, Cather C, Culhane MA, et al. A 12-week double-blind, placebo-controlled study of bupropion sr added to high-dose dual nicotine replacement therapy for smoking cessation or reduction in schizophrenia. J Clin Psychopharmacol. 2007;27(4):380-386.
21. Weinberger AH, Hitsman B, Papandonatos GD, et al. Predictors of abstinence and changes in psychiatric symptoms in a pooled sample of smokers with schizophrenia receiving combination pharmacotherapy and behavioral therapy for smoking cessation. J Clin Psychopharmacol. 2009;29(6):601-603.
22. Prochaska JJ, Hall SM, Tsoh JY, et al. Treating tobacco dependence in clinically depressed smokers: effect of smoking cessation on mental health functioning. Am J Public Health. 2008;98(3):446-448.
23. Tsoh JY, Humfleet GL, Muñoz RF, et al. Development of major depression after treatment for smoking cessation. Am J Psychiatry. 2000;157(3):368-374.
24. Prochaska JJ, Delucchi K, Hall SM. A meta-analysis of smoking cessation interventions with individuals in substance abuse treatment or recovery. J Consult Clin Psychol. 2004;72(6):1144-1156.
25. Zevin S, Benowitz NL. Drug interactions with tobacco smoking. An update. Clin Pharmacokinet. 1999;36(6):425-438.
Discuss this article at www.facebook.com/CurrentPsychiatry
You are treating Mr. P, age 34, for schizoaffective disorder. He smokes 1 pack of cigarettes per day and has smoked for approximately 17 years. He has tried to stop but never has been able to quit for more than a few weeks. He reveals whenever he tries to quit, he starts feeling extremely lethargic and “depressed” and resumes smoking to prevent these symptoms from worsening. However, Mr. P expresses some interest in trying to quit again and asks whether any medications could prevent him from becoming depressed while he tries to quit.
Cigarette smoking is overrepresented and undertreated among individuals with psychiatric illness, in part because of the largely unfounded belief held by some patients and clinicians that smoking cessation might worsen psychiatric symptoms. In this article, we argue this challenge can be overcome and psychiatrists and other mental health professionals can and should help their patients reap the innumerable benefits of quitting smoking. We discuss:
- the short- and long-term effects of smoking cessation
- evidence-based treatment guidelines for working with motivated and unmotivated smokers
- unique issues that may arise when treating smokers who have psychiatric disorders.
Quitting: Profound benefits
Quitting smoking has substantial benefits beginning within minutes after taking the last puff. Some of the benefits that occur within the first few days of quitting include:
- decreased blood pressure and pulse rate
- improved circulation
- improved ability to smell and taste
- easier breathing.
Longer-term smoking abstinence drastically reduces risk of heart attack, stroke, cancer, respiratory disease, and a host of other illnesses that affect—and kill—individuals with psychiatric disorders several decades earlier than their counterparts in the general population.1 There also are financial benefits to quitting; using the 2009 national average of $5.33 per pack, a 1-pack-per-day smoker who quits would save >$150 per month, which accounts for only the direct cost of cigarettes.2
Although the beneficial effects of quitting smoking are profound and far-reaching, in the short-term they are counterbalanced by nicotine withdrawal symptoms—including restlessness, irritability, depressed mood, concentration problems, and increased appetite/weight gain—that are formidable distractions from the positive aspects of quitting. Additionally, nicotine withdrawal symptoms tend to be more severe in smokers who have a psychiatric disorder.3 Fortunately, there are effective, evidence-based methods of reducing withdrawal symptoms and helping smokers cope with these and other challenges of quitting.
Combined treatment is best
Current treatment guidelines4 suggest all smokers should be offered pharmacotherapy and counseling to aid quitting because this combined approach has the highest success rate (Algorithm). Table 1 4 provides information about dosing, efficacy, and side effect profile of each of the 7 FDA-approved medications for smoking cessation. Using any of the approved medications at least doubles the odds of successful quitting compared with placebo.4 These pharmacotherapies can reduce or prevent nicotine withdrawal symptoms and—at least in the case of bupropion and varenicline—decrease reinforcement from smoking, thereby lowering the likelihood a lapse (ie, smoking ≥1 cigarettes without returning to regular smoking) will develop into a full-blown relapse (ie, return to regular smoking).
Algorithm: Tobacco cessation treatment for psychiatric patients
Source: Adapted from reference 4 Medication selection depends on many factors, including:
- the patient’s psychiatric illness
- her/his prior response to smoking cessation pharmacotherapies
- concomitant psychiatric medications
- patient preference.5
Placebo-controlled trials of smoking cessation aids in psychiatrically ill patients are limited, but several studies of smokers with a history of major depression indicate treatment with bupropion SR or nortriptyline is effective.6 Similarly, although relapse rates generally are higher in patients with schizophrenia compared with non-mentally ill smokers, nicotine replacement therapy and bupropion SR are more effective than placebo in patients with this disorder.7,8 When we prescribe these treatments, we tend to extend the duration of treatment beyond those described in Table 1 ,4 and to use combined treatments (eg, a transdermal patch with a shorter-acting gum or lozenge preparation) to better target the marked withdrawal symptoms more severely nicotine-dependent patients frequently experience.
Table 1
First-line pharmacotherapies for smoking cessation
| Medication | Standard dosage | Efficacy (OR, % abstinent at 6 mos. [with 95% CI]) | Contraindications (C) and precautions (P) | Common side effects |
|---|---|---|---|---|
| Non-nicotine medications | ||||
| Bupropion | Days 1-3: 150 mg/d Days 4-8: 150 mg bid Continue for 7-12 weeks at 150 mg bid | 2.0 (1.8-2.2), 24% (22%-26%) | C: Eating disorders, seizure history, taking bupropion, MAOI in past 2 weeks P: Pregnancy, cardiovascular disease, warning for emergent psychiatric symptoms | Insomnia, dry mouth |
| Varenicline | Days 1-3: 0.5 mg/d Days 4-7: 0.5 mg bid Day 8+: 1 mg bid Continue 11 weeks at 1 mg bid; up to 6 months for maintenance | 3.1 (2.5-3.8), 33% (29%-38%) | P: Warning for emergent psychiatric symptoms | Nausea, sleep problems, abnormal dreams |
| Nicotine replacement therapies | ||||
| Nicotine gum | 1 piece every 1-2 hours for 6-12 weeks <20 cigarettes/d: 2 mg gum ≥20 cigarettes/d: 4 mg gum | 1.5 (1.2-1.7), 19% (17%-22%) | P: Pregnancy, recent myocardial infarction, serious arrhythmia, unstable angina | Mouth soreness, hiccups, dyspepsia |
| Nicotine inhaler | 6-16 cartridges/d, up to 6 months | 2.1 (1.5-2.9), 25% (19%-32%) | Same as above | Mouth/throat irritation, coughing, rhinitis |
| Nicotine lozenge | 9-20 lozenges/d, up to 12 weeks Smoke ≤30 minutes after waking: 4 mg lozenge Smoke >30 minutes after waking: 2 mg lozenge | 2.0 (1.6-2.5)a | Same as above | Nausea, hiccups, heartburn |
| Nicotine nasal spray | 1-2 doses/hour, 8-40 doses/d for 3-6 months | 2.3 (1.7-3.0), 27% (22%-33%) | C: Severe reactive airway disease P: Same as above | Nasal irritation, higher risk of dependency |
| Nicotine patch | 1 patch/d, step-down dosing over 8 weeks Weeks 1-4: 21 mg patch Weeks 5-6: 14 mg patch Weeks 7-8: 7 mg patch | 1.9 (1.7-2.2) 23% (21%-26%) | P: Same as above | Skin reactions, sleep problems, abnormal dreams |
| aStead LF, Perera R, Bullen C, et al. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev. 2008;1:CD000146. bid: twice a day; CI: confidence interval; MAOI: monoamine oxidase inhibitor; OR: odds ratio Source: Adapted from reference 4 | ||||
Counseling. All smokers should be provided with brief interventions consistent with the 5 A’s—Ask, Advise, Assess, Assist, and Arrange (Table 2).4 For smokers who are not motivated to quit, the recommended approach follows the principles of the 5 R’s—Relevance, Risks, Rewards, Roadblocks, and Repetition (Table 3).4 Smokers who are motivated to quit and willing to participate in more intensive treatment may be offered face-to-face individual or group counseling (depending upon availability) or referred to a telephone quit line (see Related Resources). Intensive treatments such as these typically provide social support and assistance overcoming barriers to cessation and developing skills to initiate and maintain abstinence (eg, coping with a lapse or handling cravings, identifying and avoiding high-risk situations for smoking). As a general rule, greater intensity of counseling is associated with a greater likelihood of quitting.4
Table 2
The 5 A’s of tobacco treatment
| Intervention | Example | |
|---|---|---|
| Ask | Systematically inquire about tobacco use | “Do you currently use, or have you ever used, tobacco products?” |
| Advise | Counsel all tobacco users to quit in a clear, strong, and personalized manner | “I think it is very important for you quit smoking to keep your breathing problems from getting any worse” |
| Assess | Determine the tobacco user’s willingness to make a quit attempt | “What do you think? Are you ready to quit?” |
| Assist | Offer or refer to treatment/support (if ready to quit; if not ready, see Table 3 for recommended interventions) | “I’m here to help you with this. Let me start by letting you know about the many options available to help you quit” |
| Arrange | Plan for follow-up contacts (at least 1, preferably within 1 week of the quit date) | “I would like to give you a call within the next week to see how you did with your quit date. Would that be OK with you?” |
| Source: Adapted from reference 4 | ||
Table 3
The 5 R’s: Principles of interventions for smokers not ready to quit
| Principle | Example | |
|---|---|---|
| Relevance | Why is quitting smoking personally relevant? | “You’ve told me your kids sometimes make comments to you about quitting smoking. How does that affect you?” |
| Risks | What are the negative consequences of smoking? | “What don’t you like about smoking? What problems have you had from smoking?” |
| Rewards | What are the benefits of quitting smoking? | “Can you think of anything that would be good about quitting? Tell me about that” |
| Roadblocks | What are the barriers to quitting? | “What worries do you have about trying to quit? What happened the last time you tried to quit smoking?” |
| Repetition | Message repeated at every visit | “I know we have talked about quitting smoking before, but things may have changed since then. I also think that this is such an important issue we should keep it on the table for discussion. What do you think?” |
| Source: Adapted from reference 4 | ||
Q&A about treatment
How effective are smoking cessation interventions for individuals with psychiatric disorders? Several studies have demonstrated, on any given quit attempt, smokers with psychiatric or substance use disorders can be as successful as smokers without these disorders.9-11 In fact, quit rates as high as approximately 70% for end-of-treatment11 and 30% for 6-month follow-up10 have been reported. Of course, effectiveness varies by type and intensity of treatment as well as by individual characteristics of the smoker. Smokers with psychiatric disorders may fare better with more intensive interventions than briefer ones,12,13 and factors such as high levels of nicotine dependence and exposure to smoking environments—both of which are characteristic of smokers with serious mental illness—can negatively impact treatment outcomes.4
Should the nature of the psychiatric disorder(s) guide decisions about the optimal pharmacotherapy or counseling approach? There have been numerous attempts to investigate the effectiveness of targeted interventions for particular subgroups of smokers with psychiatric disorders, including:
- studies of the efficacy of the antidepressants bupropion14 and nortriptyline15 as well as cognitive-behavioral therapy-based mood management counseling16 for depressed smokers
- integrative treatment approaches for smokers with posttraumatic stress disorder (PTSD)17
- group counseling designed specifically for smokers with schizophrenia.18,19
Although more research is needed and there have been some promising early results (eg, McFall et al17), current literature does not provide consistent evidence supporting treatment matching solely on the basis of the psychiatric disorder. Rather, patient preference, safety considerations (eg, use of medications in children/adolescents, pregnant women), medication side effect profiles, prior experience with the treatment approach, and cost/availability of treatment should guide development of the treatment plan. When results from placebo-controlled trials are available for subgroups of patients (eg, those with a history of major depression), consider this information when selecting a pharmacologic smoking cessation aid.
What is the risk of psychiatric symptoms worsening as a result of quitting smoking? Little research on this topic is available because more often than not, smokers with psychiatric disorders are excluded from tobacco treatment studies. However, research examining psychiatric status changes among recent quitters with schizophrenia,20,21 depression,22,23 PTSD,17 and substance use disorders24 suggests smoking cessation does not worsen symptoms of these disorders, and may be associated with symptom improvement.17 Nonetheless, driven largely by anecdotal evidence, the misconception that smoking cessation worsens psychiatric symptoms remains a substantial barrier to treatment.
Mr. P’s case is an example of how not probing about the nature of psychiatric complaints can be problematic. Mr. P reported what on first glance appeared to be a worsening of psychiatric symptoms starting when he stopped smoking and resolved when he resumed smoking. However, without gathering additional information about these events, we cannot conclude stopping smoking caused his psychiatric symptoms to worsen. Other potential explanations include nicotine withdrawal symptoms, side effects of smoking cessation medications, an increase in levels of psychotropic medications for which metabolism is affected by tobacco smoke, or the natural course of his mood disorder. The timing of the onset and offset of symptoms seems to argue against Mr. P’s symptoms reflecting the natural course of his mood disorder, but the other 3 explanations remain plausible.
It is important to distinguish whether Mr. P’s worsening symptoms are consistent with a depressive episode or whether they are a manifestation of the transient dysphoria that accompanies nicotine withdrawal. Assessing the severity and persistence of the mood disturbance as well as the timing of onset could help make this determination. Nicotine withdrawal symptoms typically emerge within 24 hours of quitting or significantly reducing smoking and tend to peak within approximately 1 week. Thus, depressive symptoms that develop after weeks or months of abstinence would be less consistent with nicotine withdrawal. Additionally, the lethargy Mr. P reported may be a symptom of depression, or it may stem from a cessation-induced increase in antipsychotic serum levels. Because tobacco smoke increases the metabolism of several antipsychotics and antidepressants—including olanzapine, clozapine, haloperidol, and fluoxetine25—stopping smoking may increase medication levels and side effects. To rule out medication side effects as a cause of post-cessation mood changes, the psychiatrist should ask Mr. P about which smoking cessation pharmacotherapies (if any) he was using and which psychotropic medications he was taking. Unfortunately, such a detailed history is not always taken, and patient-generated theories of smoking cessation causing worsening psychiatric symptoms often are taken at face value.
When should smokers with psychiatric disorders be encouraged to quit? Are there times when smoking cessation should be discouraged? Tobacco treatment guidelines4 recommend advising users to quit at every clinical encounter, but there has been some debate about the timing of tobacco treatment for smokers with psychiatric disorders. There is minimal research to guide such treatment decisions. However, even if quit attempts are more successful during times of symptomatic stability—and there is no conclusive evidence to indicate they are—waiting for perfect mental health before initiating smoking cessation treatment is unnecessary and ill-advised. In some situations, such as when a patient has experienced an acute increase in psychiatric symptoms or when psychotropics are being titrated, a short-term postponement of quitting may be reasonable. However, discouraging smokers from trying to quit when they express readiness to try should be done sparingly, because it is uncertain how long that window of opportunity will be open, and the consequences of missed opportunities can be fatal.
- National Tobacco Quitline. 1-800-QUIT-NOW. www.smokefree.gov.
- University of California, San Francisco, Schools of Pharmacy and Medicine. Rx for Change (free online training program for clinicians). http://rxforchange.ucsf.edu.
- National Association of State Mental Health Program Directors. Tobacco-free living in psychiatric settings: a best-practices toolkit promoting wellness and recovery. www.nasmhpd.org/general_files/publications/NASMHPD.toolkitfinalupdated90707.pdf.
Drug Brand Names
- Bupropion • Wellbutrin, Zyban
- Clozapine • Clozaril
- Fluoxetine • Prozac
- Haloperidol • Haldol
- Nortriptyline • Aventyl, Pamelor
- Olanzapine • Zyprexa
- Varenicline • Chantix
Disclosures
Dr. Heffner was supported by National Institute on Drug Abuse grant#026517. She is a consultant to Pfizer Inc.
Dr. Anthenelli is supported by National Institute on Alcohol Abuse and Alcoholism grant#AA19720 and by the Department of Veterans Affairs. He is a consultant to GlaxoSmithKline and Pfizer Inc.
The Tri-State Tobacco and Alcohol Research Center receives research support from Eli Lilly and Company, Nabi Biopharmaceuticals, Pfizer Inc., and sanofi-aventis.
Discuss this article at www.facebook.com/CurrentPsychiatry
You are treating Mr. P, age 34, for schizoaffective disorder. He smokes 1 pack of cigarettes per day and has smoked for approximately 17 years. He has tried to stop but never has been able to quit for more than a few weeks. He reveals whenever he tries to quit, he starts feeling extremely lethargic and “depressed” and resumes smoking to prevent these symptoms from worsening. However, Mr. P expresses some interest in trying to quit again and asks whether any medications could prevent him from becoming depressed while he tries to quit.
Cigarette smoking is overrepresented and undertreated among individuals with psychiatric illness, in part because of the largely unfounded belief held by some patients and clinicians that smoking cessation might worsen psychiatric symptoms. In this article, we argue this challenge can be overcome and psychiatrists and other mental health professionals can and should help their patients reap the innumerable benefits of quitting smoking. We discuss:
- the short- and long-term effects of smoking cessation
- evidence-based treatment guidelines for working with motivated and unmotivated smokers
- unique issues that may arise when treating smokers who have psychiatric disorders.
Quitting: Profound benefits
Quitting smoking has substantial benefits beginning within minutes after taking the last puff. Some of the benefits that occur within the first few days of quitting include:
- decreased blood pressure and pulse rate
- improved circulation
- improved ability to smell and taste
- easier breathing.
Longer-term smoking abstinence drastically reduces risk of heart attack, stroke, cancer, respiratory disease, and a host of other illnesses that affect—and kill—individuals with psychiatric disorders several decades earlier than their counterparts in the general population.1 There also are financial benefits to quitting; using the 2009 national average of $5.33 per pack, a 1-pack-per-day smoker who quits would save >$150 per month, which accounts for only the direct cost of cigarettes.2
Although the beneficial effects of quitting smoking are profound and far-reaching, in the short-term they are counterbalanced by nicotine withdrawal symptoms—including restlessness, irritability, depressed mood, concentration problems, and increased appetite/weight gain—that are formidable distractions from the positive aspects of quitting. Additionally, nicotine withdrawal symptoms tend to be more severe in smokers who have a psychiatric disorder.3 Fortunately, there are effective, evidence-based methods of reducing withdrawal symptoms and helping smokers cope with these and other challenges of quitting.
Combined treatment is best
Current treatment guidelines4 suggest all smokers should be offered pharmacotherapy and counseling to aid quitting because this combined approach has the highest success rate (Algorithm). Table 1 4 provides information about dosing, efficacy, and side effect profile of each of the 7 FDA-approved medications for smoking cessation. Using any of the approved medications at least doubles the odds of successful quitting compared with placebo.4 These pharmacotherapies can reduce or prevent nicotine withdrawal symptoms and—at least in the case of bupropion and varenicline—decrease reinforcement from smoking, thereby lowering the likelihood a lapse (ie, smoking ≥1 cigarettes without returning to regular smoking) will develop into a full-blown relapse (ie, return to regular smoking).
Algorithm: Tobacco cessation treatment for psychiatric patients
Source: Adapted from reference 4 Medication selection depends on many factors, including:
- the patient’s psychiatric illness
- her/his prior response to smoking cessation pharmacotherapies
- concomitant psychiatric medications
- patient preference.5
Placebo-controlled trials of smoking cessation aids in psychiatrically ill patients are limited, but several studies of smokers with a history of major depression indicate treatment with bupropion SR or nortriptyline is effective.6 Similarly, although relapse rates generally are higher in patients with schizophrenia compared with non-mentally ill smokers, nicotine replacement therapy and bupropion SR are more effective than placebo in patients with this disorder.7,8 When we prescribe these treatments, we tend to extend the duration of treatment beyond those described in Table 1 ,4 and to use combined treatments (eg, a transdermal patch with a shorter-acting gum or lozenge preparation) to better target the marked withdrawal symptoms more severely nicotine-dependent patients frequently experience.
Table 1
First-line pharmacotherapies for smoking cessation
| Medication | Standard dosage | Efficacy (OR, % abstinent at 6 mos. [with 95% CI]) | Contraindications (C) and precautions (P) | Common side effects |
|---|---|---|---|---|
| Non-nicotine medications | ||||
| Bupropion | Days 1-3: 150 mg/d Days 4-8: 150 mg bid Continue for 7-12 weeks at 150 mg bid | 2.0 (1.8-2.2), 24% (22%-26%) | C: Eating disorders, seizure history, taking bupropion, MAOI in past 2 weeks P: Pregnancy, cardiovascular disease, warning for emergent psychiatric symptoms | Insomnia, dry mouth |
| Varenicline | Days 1-3: 0.5 mg/d Days 4-7: 0.5 mg bid Day 8+: 1 mg bid Continue 11 weeks at 1 mg bid; up to 6 months for maintenance | 3.1 (2.5-3.8), 33% (29%-38%) | P: Warning for emergent psychiatric symptoms | Nausea, sleep problems, abnormal dreams |
| Nicotine replacement therapies | ||||
| Nicotine gum | 1 piece every 1-2 hours for 6-12 weeks <20 cigarettes/d: 2 mg gum ≥20 cigarettes/d: 4 mg gum | 1.5 (1.2-1.7), 19% (17%-22%) | P: Pregnancy, recent myocardial infarction, serious arrhythmia, unstable angina | Mouth soreness, hiccups, dyspepsia |
| Nicotine inhaler | 6-16 cartridges/d, up to 6 months | 2.1 (1.5-2.9), 25% (19%-32%) | Same as above | Mouth/throat irritation, coughing, rhinitis |
| Nicotine lozenge | 9-20 lozenges/d, up to 12 weeks Smoke ≤30 minutes after waking: 4 mg lozenge Smoke >30 minutes after waking: 2 mg lozenge | 2.0 (1.6-2.5)a | Same as above | Nausea, hiccups, heartburn |
| Nicotine nasal spray | 1-2 doses/hour, 8-40 doses/d for 3-6 months | 2.3 (1.7-3.0), 27% (22%-33%) | C: Severe reactive airway disease P: Same as above | Nasal irritation, higher risk of dependency |
| Nicotine patch | 1 patch/d, step-down dosing over 8 weeks Weeks 1-4: 21 mg patch Weeks 5-6: 14 mg patch Weeks 7-8: 7 mg patch | 1.9 (1.7-2.2) 23% (21%-26%) | P: Same as above | Skin reactions, sleep problems, abnormal dreams |
| aStead LF, Perera R, Bullen C, et al. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev. 2008;1:CD000146. bid: twice a day; CI: confidence interval; MAOI: monoamine oxidase inhibitor; OR: odds ratio Source: Adapted from reference 4 | ||||
Counseling. All smokers should be provided with brief interventions consistent with the 5 A’s—Ask, Advise, Assess, Assist, and Arrange (Table 2).4 For smokers who are not motivated to quit, the recommended approach follows the principles of the 5 R’s—Relevance, Risks, Rewards, Roadblocks, and Repetition (Table 3).4 Smokers who are motivated to quit and willing to participate in more intensive treatment may be offered face-to-face individual or group counseling (depending upon availability) or referred to a telephone quit line (see Related Resources). Intensive treatments such as these typically provide social support and assistance overcoming barriers to cessation and developing skills to initiate and maintain abstinence (eg, coping with a lapse or handling cravings, identifying and avoiding high-risk situations for smoking). As a general rule, greater intensity of counseling is associated with a greater likelihood of quitting.4
Table 2
The 5 A’s of tobacco treatment
| Intervention | Example | |
|---|---|---|
| Ask | Systematically inquire about tobacco use | “Do you currently use, or have you ever used, tobacco products?” |
| Advise | Counsel all tobacco users to quit in a clear, strong, and personalized manner | “I think it is very important for you quit smoking to keep your breathing problems from getting any worse” |
| Assess | Determine the tobacco user’s willingness to make a quit attempt | “What do you think? Are you ready to quit?” |
| Assist | Offer or refer to treatment/support (if ready to quit; if not ready, see Table 3 for recommended interventions) | “I’m here to help you with this. Let me start by letting you know about the many options available to help you quit” |
| Arrange | Plan for follow-up contacts (at least 1, preferably within 1 week of the quit date) | “I would like to give you a call within the next week to see how you did with your quit date. Would that be OK with you?” |
| Source: Adapted from reference 4 | ||
Table 3
The 5 R’s: Principles of interventions for smokers not ready to quit
| Principle | Example | |
|---|---|---|
| Relevance | Why is quitting smoking personally relevant? | “You’ve told me your kids sometimes make comments to you about quitting smoking. How does that affect you?” |
| Risks | What are the negative consequences of smoking? | “What don’t you like about smoking? What problems have you had from smoking?” |
| Rewards | What are the benefits of quitting smoking? | “Can you think of anything that would be good about quitting? Tell me about that” |
| Roadblocks | What are the barriers to quitting? | “What worries do you have about trying to quit? What happened the last time you tried to quit smoking?” |
| Repetition | Message repeated at every visit | “I know we have talked about quitting smoking before, but things may have changed since then. I also think that this is such an important issue we should keep it on the table for discussion. What do you think?” |
| Source: Adapted from reference 4 | ||
Q&A about treatment
How effective are smoking cessation interventions for individuals with psychiatric disorders? Several studies have demonstrated, on any given quit attempt, smokers with psychiatric or substance use disorders can be as successful as smokers without these disorders.9-11 In fact, quit rates as high as approximately 70% for end-of-treatment11 and 30% for 6-month follow-up10 have been reported. Of course, effectiveness varies by type and intensity of treatment as well as by individual characteristics of the smoker. Smokers with psychiatric disorders may fare better with more intensive interventions than briefer ones,12,13 and factors such as high levels of nicotine dependence and exposure to smoking environments—both of which are characteristic of smokers with serious mental illness—can negatively impact treatment outcomes.4
Should the nature of the psychiatric disorder(s) guide decisions about the optimal pharmacotherapy or counseling approach? There have been numerous attempts to investigate the effectiveness of targeted interventions for particular subgroups of smokers with psychiatric disorders, including:
- studies of the efficacy of the antidepressants bupropion14 and nortriptyline15 as well as cognitive-behavioral therapy-based mood management counseling16 for depressed smokers
- integrative treatment approaches for smokers with posttraumatic stress disorder (PTSD)17
- group counseling designed specifically for smokers with schizophrenia.18,19
Although more research is needed and there have been some promising early results (eg, McFall et al17), current literature does not provide consistent evidence supporting treatment matching solely on the basis of the psychiatric disorder. Rather, patient preference, safety considerations (eg, use of medications in children/adolescents, pregnant women), medication side effect profiles, prior experience with the treatment approach, and cost/availability of treatment should guide development of the treatment plan. When results from placebo-controlled trials are available for subgroups of patients (eg, those with a history of major depression), consider this information when selecting a pharmacologic smoking cessation aid.
What is the risk of psychiatric symptoms worsening as a result of quitting smoking? Little research on this topic is available because more often than not, smokers with psychiatric disorders are excluded from tobacco treatment studies. However, research examining psychiatric status changes among recent quitters with schizophrenia,20,21 depression,22,23 PTSD,17 and substance use disorders24 suggests smoking cessation does not worsen symptoms of these disorders, and may be associated with symptom improvement.17 Nonetheless, driven largely by anecdotal evidence, the misconception that smoking cessation worsens psychiatric symptoms remains a substantial barrier to treatment.
Mr. P’s case is an example of how not probing about the nature of psychiatric complaints can be problematic. Mr. P reported what on first glance appeared to be a worsening of psychiatric symptoms starting when he stopped smoking and resolved when he resumed smoking. However, without gathering additional information about these events, we cannot conclude stopping smoking caused his psychiatric symptoms to worsen. Other potential explanations include nicotine withdrawal symptoms, side effects of smoking cessation medications, an increase in levels of psychotropic medications for which metabolism is affected by tobacco smoke, or the natural course of his mood disorder. The timing of the onset and offset of symptoms seems to argue against Mr. P’s symptoms reflecting the natural course of his mood disorder, but the other 3 explanations remain plausible.
It is important to distinguish whether Mr. P’s worsening symptoms are consistent with a depressive episode or whether they are a manifestation of the transient dysphoria that accompanies nicotine withdrawal. Assessing the severity and persistence of the mood disturbance as well as the timing of onset could help make this determination. Nicotine withdrawal symptoms typically emerge within 24 hours of quitting or significantly reducing smoking and tend to peak within approximately 1 week. Thus, depressive symptoms that develop after weeks or months of abstinence would be less consistent with nicotine withdrawal. Additionally, the lethargy Mr. P reported may be a symptom of depression, or it may stem from a cessation-induced increase in antipsychotic serum levels. Because tobacco smoke increases the metabolism of several antipsychotics and antidepressants—including olanzapine, clozapine, haloperidol, and fluoxetine25—stopping smoking may increase medication levels and side effects. To rule out medication side effects as a cause of post-cessation mood changes, the psychiatrist should ask Mr. P about which smoking cessation pharmacotherapies (if any) he was using and which psychotropic medications he was taking. Unfortunately, such a detailed history is not always taken, and patient-generated theories of smoking cessation causing worsening psychiatric symptoms often are taken at face value.
When should smokers with psychiatric disorders be encouraged to quit? Are there times when smoking cessation should be discouraged? Tobacco treatment guidelines4 recommend advising users to quit at every clinical encounter, but there has been some debate about the timing of tobacco treatment for smokers with psychiatric disorders. There is minimal research to guide such treatment decisions. However, even if quit attempts are more successful during times of symptomatic stability—and there is no conclusive evidence to indicate they are—waiting for perfect mental health before initiating smoking cessation treatment is unnecessary and ill-advised. In some situations, such as when a patient has experienced an acute increase in psychiatric symptoms or when psychotropics are being titrated, a short-term postponement of quitting may be reasonable. However, discouraging smokers from trying to quit when they express readiness to try should be done sparingly, because it is uncertain how long that window of opportunity will be open, and the consequences of missed opportunities can be fatal.
- National Tobacco Quitline. 1-800-QUIT-NOW. www.smokefree.gov.
- University of California, San Francisco, Schools of Pharmacy and Medicine. Rx for Change (free online training program for clinicians). http://rxforchange.ucsf.edu.
- National Association of State Mental Health Program Directors. Tobacco-free living in psychiatric settings: a best-practices toolkit promoting wellness and recovery. www.nasmhpd.org/general_files/publications/NASMHPD.toolkitfinalupdated90707.pdf.
Drug Brand Names
- Bupropion • Wellbutrin, Zyban
- Clozapine • Clozaril
- Fluoxetine • Prozac
- Haloperidol • Haldol
- Nortriptyline • Aventyl, Pamelor
- Olanzapine • Zyprexa
- Varenicline • Chantix
Disclosures
Dr. Heffner was supported by National Institute on Drug Abuse grant#026517. She is a consultant to Pfizer Inc.
Dr. Anthenelli is supported by National Institute on Alcohol Abuse and Alcoholism grant#AA19720 and by the Department of Veterans Affairs. He is a consultant to GlaxoSmithKline and Pfizer Inc.
The Tri-State Tobacco and Alcohol Research Center receives research support from Eli Lilly and Company, Nabi Biopharmaceuticals, Pfizer Inc., and sanofi-aventis.
1. Colton CW, Manderscheid RW. Congruencies in increased mortality rates years of potential life lost, and causes of death among public mental health clients in eight states. Prev Chronic Dis. 2006;3(2):A42.-
2. Centers for Disease Control and Prevention. Trends in state and federal cigarette tax and retail price—1970-2009. 2010. Available at: http://www.cdc.gov/tobacco/data_statistics/tables/economics/trends. Accessed June 28 2011.
3. Xian H, Scherrer JF, Eisen SA, et al. Nicotine dependence subtypes: association with smoking history, diagnostic criteria and psychiatric disorders in 5440 regular smokers from the Vietnam Era Twin Registry. Addict Behav. 2007;32(1):137-147.
4. Fiore MC, Jaén CR, Baker TB, et al. A clinical practice guideline for treating tobacco use and dependence: 2008 update. A U. S. Public Health Service report. Am J Prev Med. 2008;35(2):158-176.
5. Anthenelli RM. How–and why–to help psychiatric patients stop smoking. Current Psychiatry. 2005;4(1):77-87.
6. Hughes JR, Stead LF, Lancaster T. Antidepressants for smoking cessation. Cochrane Database Syst Rev. 2007;1:CD000031.-
7. Williams JM, Foulds J. Successful tobacco dependence treatment in schizophrenia. Am J Psychiatry. 2007;164(2):222-227.
8. George TP, Vessicchio JC, Termine A, et al. A placebo controlled trial of bupropion for smoking cessation in schizophrenia. Biol Psychiatry. 2002;52(1):53-61.
9. Hughes JR, Kalman D. Do smokers with alcohol problems have more difficulty quitting? Drug Alcohol Depend. 2006;82(2):91-102.
10. McClure JB, Swan GE, Catz SL, et al. Smoking outcome by psychiatric history after behavioral and varenicline treatment. J Subst Abuse Treat. 2010;38(4):394-402.
11. Stapleton JA, Watson L, Spirling LI, et al. Varenicline in the routine treatment of tobacco dependence: a pre-post comparison with nicotine replacement therapy and an evaluation in those with mental illness. Addiction. 2008;103(1):146-154.
12. Hall SM, Muñoz RF, Reus VI. Cognitive-behavioral intervention increases abstinence rates for depressive-history smokers. J Consult Clin Psychol. 1994;62(1):141-146.
13. Hall SM, Muñoz RF, Reus VI, et al. Mood management and nicotine gum in smoking treatment: a therapeutic contact and placebo-controlled study. J Consult Clin Psychol. 1996;64(5):1003-1009.
14. Evins AE, Culhane MA, Alpert JE, et al. A controlled trial of bupropion added to nicotine patch and behavioral therapy for smoking cessation in adults with unipolar depressive disorders. J Clin Psychopharmacol. 2008;28(6):660-666.
15. Hall SM, Reus VI, Muñoz RF, et al. Nortriptyline and cognitive-behavioral therapy in the treatment of cigarette smoking. Arch Gen Psychiatry. 1998;55(8):683-690.
16. Brown RA, Kahler CW, Niaura R, et al. Cognitive-behavioral treatment for depression in smoking cessation. J Consult Clin Psychol. 2001;69(3):471-480.
17. McFall M, Saxon AJ, Malte CA, et al. Integrating tobacco cessation into mental health care for posttraumatic stress disorder: a randomized controlled trial. JAMA. 2010;304(22):2485-2493.
18. George TP, Ziedonis DM, Feingold A, et al. Nicotine transdermal patch and atypical antipsychotic medications for smoking cessation in schizophrenia. Am J Psychiatry. 2000;157(11):1835-1842.
19. Williams JM, Steinberg ML, Zimmermann MH, et al. Comparison of two intensities of tobacco dependence counseling in schizophrenia and schizoaffective disorder. J Subst Abuse Treat. 2010;38(4):384-393.
20. Evins AE, Cather C, Culhane MA, et al. A 12-week double-blind, placebo-controlled study of bupropion sr added to high-dose dual nicotine replacement therapy for smoking cessation or reduction in schizophrenia. J Clin Psychopharmacol. 2007;27(4):380-386.
21. Weinberger AH, Hitsman B, Papandonatos GD, et al. Predictors of abstinence and changes in psychiatric symptoms in a pooled sample of smokers with schizophrenia receiving combination pharmacotherapy and behavioral therapy for smoking cessation. J Clin Psychopharmacol. 2009;29(6):601-603.
22. Prochaska JJ, Hall SM, Tsoh JY, et al. Treating tobacco dependence in clinically depressed smokers: effect of smoking cessation on mental health functioning. Am J Public Health. 2008;98(3):446-448.
23. Tsoh JY, Humfleet GL, Muñoz RF, et al. Development of major depression after treatment for smoking cessation. Am J Psychiatry. 2000;157(3):368-374.
24. Prochaska JJ, Delucchi K, Hall SM. A meta-analysis of smoking cessation interventions with individuals in substance abuse treatment or recovery. J Consult Clin Psychol. 2004;72(6):1144-1156.
25. Zevin S, Benowitz NL. Drug interactions with tobacco smoking. An update. Clin Pharmacokinet. 1999;36(6):425-438.
1. Colton CW, Manderscheid RW. Congruencies in increased mortality rates years of potential life lost, and causes of death among public mental health clients in eight states. Prev Chronic Dis. 2006;3(2):A42.-
2. Centers for Disease Control and Prevention. Trends in state and federal cigarette tax and retail price—1970-2009. 2010. Available at: http://www.cdc.gov/tobacco/data_statistics/tables/economics/trends. Accessed June 28 2011.
3. Xian H, Scherrer JF, Eisen SA, et al. Nicotine dependence subtypes: association with smoking history, diagnostic criteria and psychiatric disorders in 5440 regular smokers from the Vietnam Era Twin Registry. Addict Behav. 2007;32(1):137-147.
4. Fiore MC, Jaén CR, Baker TB, et al. A clinical practice guideline for treating tobacco use and dependence: 2008 update. A U. S. Public Health Service report. Am J Prev Med. 2008;35(2):158-176.
5. Anthenelli RM. How–and why–to help psychiatric patients stop smoking. Current Psychiatry. 2005;4(1):77-87.
6. Hughes JR, Stead LF, Lancaster T. Antidepressants for smoking cessation. Cochrane Database Syst Rev. 2007;1:CD000031.-
7. Williams JM, Foulds J. Successful tobacco dependence treatment in schizophrenia. Am J Psychiatry. 2007;164(2):222-227.
8. George TP, Vessicchio JC, Termine A, et al. A placebo controlled trial of bupropion for smoking cessation in schizophrenia. Biol Psychiatry. 2002;52(1):53-61.
9. Hughes JR, Kalman D. Do smokers with alcohol problems have more difficulty quitting? Drug Alcohol Depend. 2006;82(2):91-102.
10. McClure JB, Swan GE, Catz SL, et al. Smoking outcome by psychiatric history after behavioral and varenicline treatment. J Subst Abuse Treat. 2010;38(4):394-402.
11. Stapleton JA, Watson L, Spirling LI, et al. Varenicline in the routine treatment of tobacco dependence: a pre-post comparison with nicotine replacement therapy and an evaluation in those with mental illness. Addiction. 2008;103(1):146-154.
12. Hall SM, Muñoz RF, Reus VI. Cognitive-behavioral intervention increases abstinence rates for depressive-history smokers. J Consult Clin Psychol. 1994;62(1):141-146.
13. Hall SM, Muñoz RF, Reus VI, et al. Mood management and nicotine gum in smoking treatment: a therapeutic contact and placebo-controlled study. J Consult Clin Psychol. 1996;64(5):1003-1009.
14. Evins AE, Culhane MA, Alpert JE, et al. A controlled trial of bupropion added to nicotine patch and behavioral therapy for smoking cessation in adults with unipolar depressive disorders. J Clin Psychopharmacol. 2008;28(6):660-666.
15. Hall SM, Reus VI, Muñoz RF, et al. Nortriptyline and cognitive-behavioral therapy in the treatment of cigarette smoking. Arch Gen Psychiatry. 1998;55(8):683-690.
16. Brown RA, Kahler CW, Niaura R, et al. Cognitive-behavioral treatment for depression in smoking cessation. J Consult Clin Psychol. 2001;69(3):471-480.
17. McFall M, Saxon AJ, Malte CA, et al. Integrating tobacco cessation into mental health care for posttraumatic stress disorder: a randomized controlled trial. JAMA. 2010;304(22):2485-2493.
18. George TP, Ziedonis DM, Feingold A, et al. Nicotine transdermal patch and atypical antipsychotic medications for smoking cessation in schizophrenia. Am J Psychiatry. 2000;157(11):1835-1842.
19. Williams JM, Steinberg ML, Zimmermann MH, et al. Comparison of two intensities of tobacco dependence counseling in schizophrenia and schizoaffective disorder. J Subst Abuse Treat. 2010;38(4):384-393.
20. Evins AE, Cather C, Culhane MA, et al. A 12-week double-blind, placebo-controlled study of bupropion sr added to high-dose dual nicotine replacement therapy for smoking cessation or reduction in schizophrenia. J Clin Psychopharmacol. 2007;27(4):380-386.
21. Weinberger AH, Hitsman B, Papandonatos GD, et al. Predictors of abstinence and changes in psychiatric symptoms in a pooled sample of smokers with schizophrenia receiving combination pharmacotherapy and behavioral therapy for smoking cessation. J Clin Psychopharmacol. 2009;29(6):601-603.
22. Prochaska JJ, Hall SM, Tsoh JY, et al. Treating tobacco dependence in clinically depressed smokers: effect of smoking cessation on mental health functioning. Am J Public Health. 2008;98(3):446-448.
23. Tsoh JY, Humfleet GL, Muñoz RF, et al. Development of major depression after treatment for smoking cessation. Am J Psychiatry. 2000;157(3):368-374.
24. Prochaska JJ, Delucchi K, Hall SM. A meta-analysis of smoking cessation interventions with individuals in substance abuse treatment or recovery. J Consult Clin Psychol. 2004;72(6):1144-1156.
25. Zevin S, Benowitz NL. Drug interactions with tobacco smoking. An update. Clin Pharmacokinet. 1999;36(6):425-438.