User login
In 1958, shortly after the first descriptions of granulomatosis with polyangiitis, or GPA (Wegener’s granulomatosis), the 1-year mortality was 18%,1 mainly due to renal failure. Physicians tried to combat the disease using various immunosuppressive drugs (nitrogen mustard and, in later years, azathioprine and methotrexate), but measurable success came only after investigators introduced cyclophosphamide (CYC) in combination with the glucocorticoid prednisone.2
A key 1992 study showed that the CYC/prednisone combination markedly improved the disease status in 91% of patients,3 with 75% achieving complete remission. The treatment came at a price, however, with almost all patients suffering serious morbidity or side effects. The results also highlighted concerns about potential malignancies caused by prolonged use of CYC and glucocorticoids. Those concerns motivated the European Vasculitis Study Group in the late 1980s and early 1990s to design and validate testing for antineutrophil cytoplasmic antibody (ANCA)–associated vasculitides (AAV) and pursue consensus regarding treatment.4
ALTERNATIVES TO STANDARD THERAPY
The accepted therapeutic strategy for GPA is to first induce remission using high doses of CYC and then prevent relapse with longer-term, less toxic therapeutic alternatives. These less toxic therapies include newer agents as well as new methods of delivery, particularly for patients with nonsevere forms of disease.
Methotrexate—effective for early treatment
Methotrexate showed early promise in several nonrandomized trials of patients with nonsevere disease. In one such study, de Groot et al subclassified 100 patients at diagnosis according to the extent and severity of the disease.5 Patients were then randomized to receive either standard oral CYC or methotrexate, each combined with prednisolone. Remission rates (90% to 94%) were comparable regardless of whether patients received CYC or methotrexate, although patients with more severe disease who were taking methotrexate took longer to achieve remission. At the same time, relapse rates were higher for methotrexate-taking patients (70%) compared with the CYC group (47%). Thus, while methotrexate could replace CYC for initial treatment of early AAV, CYC had a greater influence on subsequent relapse rates, particularly in patients with more severe forms of disease.
Pulse cyclophosphamide—a new method
Investigators tested pulse delivery of CYC compared with oral daily administration as a means of reducing the CYC dose. An analysis of 14 relatively small studies showed that pulse CYC had the same survival and renal failure rates as continuous therapy.6
One such trial, the CYC Daily Oral Versus Pulsed (CYCLOPS) trial, involved 149 patients with generalized disease (nephritis, GPA, and microscopic polyangiitis [MPA]) who were administered either an intravenous (IV) pulse or a daily oral CYC regimen.7 The pulse CYC neither shortened patients’ time to remission nor increased the proportion of patients who achieved it. Patients receiving pulse CYC suffered one-third the rate of leukopenia experienced by patients who received the oral regimen. Since infection is a source of mortality in vasculitis, this finding is an important consideration when balancing the benefits of day-to-day control offered by oral administration against the safety of at-risk patients such as the elderly.
This treatment strategy may be relevant for patients with renal impairment. It was once thought that patients with renal failure after receiving CYC had more aggressive disease and therefore needed higher dosages. Investigators who studied the impact of renal insufficiency and hemodialysis on the pharmacokinetics of CYC found that clearance of CYC is impaired in patients with reduced renal function.8 Thus, when renal function is suppressed, the CYC dosage should be reduced rather than increased.
Mycophenolate mofetil—efficacy not yet confirmed
Another alternative to CYC, mycophenolate mofetil (MMF), has gained much attention, although its effectiveness is not yet certain. Pilot data show that 13 of 17 patients with MPA achieved remission after 6 months of treatment with MMF.9 Meanwhile, the so-called MYCYC trial, in which patients with newly diagnosed AAV receive either the CYCLOPS regimen or MMF, is under way.10
Deoxyspergualin—remission not sustained
A nonstandard drug that warrants attention is deoxyspergualin (now called gusperimus), licensed in Japan for 15 years. In a prospective, open-label trial of 45 patients with relapsing or refractory GPA, investigators showed that 95% achieved partial remission and 45% full remission, although remission was not sustained when therapy was stopped.11 Because the drug must be administered daily for 21 days by subcutaneous injection, deoxyspergualin is not easy to use. It may represent an alternative, however, because it permitted prednisolone dosage reduction.
EVALUATING RISK AND CHOOSING THERAPIES
CONSIDERATIONS IN CHOOSING REMISSION THERAPY
Overall, when planning remission therapy and its duration, clinicians must balance the efficacy of CYC and glucocorticoids against their toxicity. Close monitoring and the patient’s capacity to adhere to instructions are two critical issues. Other important considerations include the risk and consequences of relapse, which vary in different circumstances, and the association of cancer with CYC therapy.
Relapse risk is variable
Certain patients are at higher risk of relapse than others. Patients with GPA or proteinase-3-ANCA–positive disease are at higher relapse risk than those who have MPA. ANCA-positive disease in remission or rising ANCA markers both increase the risk of relapse. Ear, nose, throat, and lung diseases increase the likelihood of relapse. Patients with GPA who are Staphylococcus aureus carriers have increased risk. Serum creatinine levels of 2.0 to 3.0 mg/dL at the end of induction therapy should arouse concern about renal relapse.
Most relapses affect the ear, nose, and throat system and do not threaten vital organs. Relapse does not increase the risk of end-stage renal disease or death.
Consider mortality and cancer data
Although the strongest predictor of early death is infection, advanced age and renal impairment also predict death. Chronic kidney disease stage at entry and glomerular filtration rate significantly predict mortality.21 More than 36 g CYC (equivalent to 9 to 12 months of standard oral therapy) increases the risk of bladder cancer 10-fold and myeloid leukemia 60-fold, but the cancer risk is time-dependent; malignancy requires 12 years on average to emerge.22
CONCLUSION
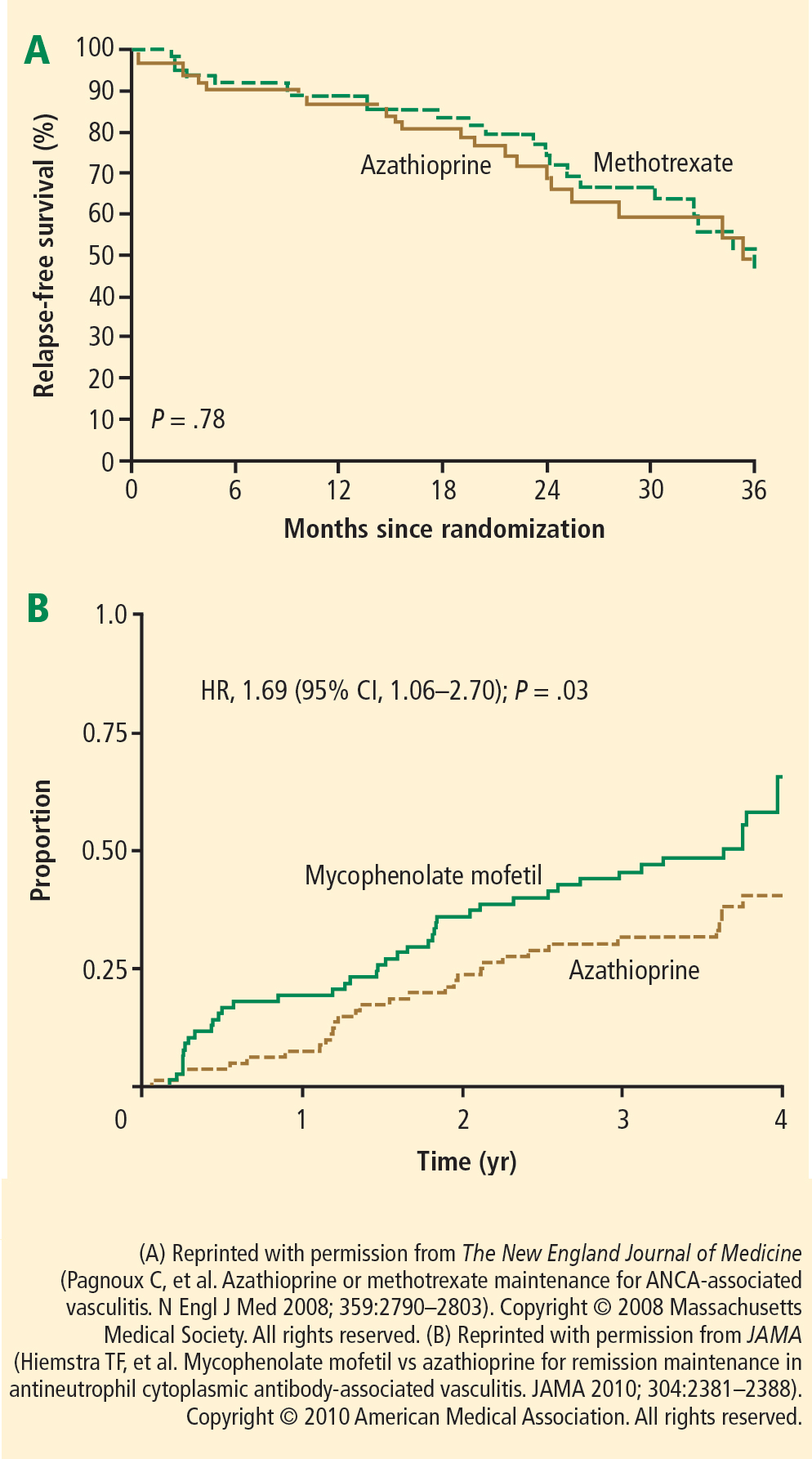
Cyclophosphamide in combination with glucocorticoids remains the standard therapy for GPA and related vasculitides, despite the risk of significant treatment-related comorbidities. Several strategies can be employed to reduce exposure, such as sequential withdrawal of CYC and IV administration. The optimization of glucocorticoid dosing will be a major research focus in the next decade. Newer agents may improve the maintenance of remission; for example, azathioprine and methotrexate show equal efficacy and safety, while MMF is less effective. When planning remission maintenance therapy, the relapse risk should be considered carefully because it varies among clinical scenarios. Other factors in the decision include the consequences for the patient, monitoring requirements, and the patient’s ability to understand and adhere to instructions.
- Walton EW. Giant-cell granuloma of the respiratory tract (Wegener’s granulomatosis). Br Med J 1958; 2:265–270.
- Novack SN, Pearson CM. Cyclophosphamide therapy in Wegener’s granulomatosis. N Engl J Med 1971; 284:938–942.
- Hoffman GS, Kerr GS, Leavitt RY, et al. Wegener granulomatosis: an analysis of 158 patients. Ann Intern Med 1992; 116:488–498.
- Rasmussen N, Jayne DRW, Abramowicz D, et al. European therapeutic trials in ANCA-associated systemic vasculitis: disease scoring, consensus regimens and proposed clinical trials. Clin Exp Immunol 1995; 101 (suppl 1):29–34.
- de Groot K, Rasmussen N, Bacon PA, et al. Randomized trial of cyclophosphamide versus methotrexate for induction of remission in early systemic antineutrophil cytoplasmic antibody-associated vasculitis. Arthritis Rheum 2005; 52:2461–2469.
- de Groot K, Adu D, Savage COS; for EUVAS (European Vasculitis Study Group). The value of pulse cyclophosphamide in ANCA-associated vasculitis: meta-analysis and critical review. Nephrol Dial Transplant 2001; 16:2018–2027.
- de Groot K, Harper L, Jayne DRW, et al. Pulse versus daily oral cyclophosphamide for induction of remission in antineutrophil cytoplasmic antibody-associated vasculitis: a randomized trial. Ann Intern Med 2009; 150:670–680.
- Haubitz M, Bohnenstengel F, Brunkhorst R, Schwab M, Hofmann U, Busse D. Cyclophosphamide pharmacokinetics and dose requirements in patients with renal insufficiency. Kidney Int 2002; 61:1495–1501.
- Silva F, Specks U, Kalra S, et al. Mycophenolate mofetil for induction and maintenance of remission in microscopic polyangiitis with mild to moderate renal involvement: a prospective, open-label pilot trial [published online ahead of print January 21, 2010]. Clin J Am Soc Nephrol 2010; 5:445–453. doi: 10.2215/CJN.06010809
- MYCYC clinical trial protocol. The European Vasculitis Society Web site. http://www.vasculitis.org. Updated April 12, 2011. Accessed June 13, 2012.
- Flossmann O, Baslund B, Bruchfeld A, et al. Deoxyspergualin in relapsing and refractory Wegener’s granulomatosis [published online ahead of print August 19, 2008]. Ann Rheum Dis 2009; 68:1125–1130. doi: 10.1136/ard.2008.092429
- Mukhtyar C, Guillevin L, Cid MC, et al; for the European Vasculitis Study Group. EULAR recommendations for the management of primary small and medium vessel vasculitis [published online ahead of print April 15, 2008]. Ann Rheum Dis 2009; 68:310–317. doi: 10.1136/ard.2008.088096
- Mukhtyar C, Guillevin L, Cid MC, et al; for the European Vasculitis Study Group. EULAR recommendations for the management of large vessel vasculitis [published online ahead of print April 15, 2008]. Ann Rheum Dis 2009; 68:318–323. doi: 10.1136/ard.2008.088351
- Hellmich B, Flossmann O, Gross WL, et al; on behalf of the European Vasculitis Study Group. EULAR recommendations for conducting clinical studies and/or clinical trials in systemic vasculitis: focus on anti-neutrophil cytoplasm antibody-associated vasculitis [published online ahead of print December 14, 2006]. Ann Rheum Dis 2007; 66:605–617. doi: 10.1136/ard.2006.062711
- Jayne D, Rasmussen N, Andrassy K, et al; for the European Vasculitis Study Group. A randomized trial of maintenance therapy for vasculitis associated with antineutrophil cytoplasmic autoantibodies. N Engl J Med 2003; 349:36–44.
- Pagnoux C, Mahr A, Hamidou MA, et al; for the French Vasculitis Study Group. Azathioprine or methotrexate maintenance for ANCA-associated vasculitis. N Engl J Med 2008; 359:2790–2803.
- Hiemstra TF, Walsh M, Mahr A, et al; for the European Vasculitis Study Group (EUVAS). Mycophenolate mofetil vs azathioprine for remission maintenance in antineutrophil cytoplasmic antibodyassociated vasculitis: a randomized controlled trial [published online ahead of print November 8, 2010]. JAMA 2010; 304:2381–2388. doi: 10.1001/jama.2010.1658
- Metzler C, Miehle N, Manger K, et al; for the German Network of Rheumatic Diseases. Elevated relapse rate under oral methotrexate versus leflunomide for maintenance of remission in Wegener’s granulomatosis [published online ahead of print May 22, 2007]. Rheumatology 2007; 46:1087–1091. doi: 10.1093/rheumatology/kem029
- Walsh M, Merkel PA, Mahr A, Jayne D. Effects of duration of glucocorticoid therapy on relapse rate in antineutrophil cytoplasmic antibody-associated vasculitis: a meta-analysis. Arthritis Care Res (Hoboken) 2010; 62:1166–1173.
- Vanková Z, Ríhová Z, Jancová E, Rysavá R, Merta M, Tesar V. Optimizing the therapeutic strategies in ANCA-associated vasculitis— single centre experience with international randomized trials. Prague Med Rep 2006; 107:199–212.
- Flossmann O, Berden A, de Groot K, et al; for the European Vasculitis Study Group. Long-term patient survival in ANCA-associated vasculitis [published online ahead of print November 24, 2010]. Ann Rheum Dis 2011; 70:488–494. doi: 10.1136/ard.2010.137778
- Faurschou M, Sorensen IJ, Mellemkjaer L, et al. Malignancies in Wegener’s granulomatosis: incidence and relation to cyclophosphamide therapy in a cohort of 293 patients [published online ahead of print October 15, 2007]. J Rheumatol 2008; 35:100–105.
In 1958, shortly after the first descriptions of granulomatosis with polyangiitis, or GPA (Wegener’s granulomatosis), the 1-year mortality was 18%,1 mainly due to renal failure. Physicians tried to combat the disease using various immunosuppressive drugs (nitrogen mustard and, in later years, azathioprine and methotrexate), but measurable success came only after investigators introduced cyclophosphamide (CYC) in combination with the glucocorticoid prednisone.2
A key 1992 study showed that the CYC/prednisone combination markedly improved the disease status in 91% of patients,3 with 75% achieving complete remission. The treatment came at a price, however, with almost all patients suffering serious morbidity or side effects. The results also highlighted concerns about potential malignancies caused by prolonged use of CYC and glucocorticoids. Those concerns motivated the European Vasculitis Study Group in the late 1980s and early 1990s to design and validate testing for antineutrophil cytoplasmic antibody (ANCA)–associated vasculitides (AAV) and pursue consensus regarding treatment.4
ALTERNATIVES TO STANDARD THERAPY
The accepted therapeutic strategy for GPA is to first induce remission using high doses of CYC and then prevent relapse with longer-term, less toxic therapeutic alternatives. These less toxic therapies include newer agents as well as new methods of delivery, particularly for patients with nonsevere forms of disease.
Methotrexate—effective for early treatment
Methotrexate showed early promise in several nonrandomized trials of patients with nonsevere disease. In one such study, de Groot et al subclassified 100 patients at diagnosis according to the extent and severity of the disease.5 Patients were then randomized to receive either standard oral CYC or methotrexate, each combined with prednisolone. Remission rates (90% to 94%) were comparable regardless of whether patients received CYC or methotrexate, although patients with more severe disease who were taking methotrexate took longer to achieve remission. At the same time, relapse rates were higher for methotrexate-taking patients (70%) compared with the CYC group (47%). Thus, while methotrexate could replace CYC for initial treatment of early AAV, CYC had a greater influence on subsequent relapse rates, particularly in patients with more severe forms of disease.
Pulse cyclophosphamide—a new method
Investigators tested pulse delivery of CYC compared with oral daily administration as a means of reducing the CYC dose. An analysis of 14 relatively small studies showed that pulse CYC had the same survival and renal failure rates as continuous therapy.6
One such trial, the CYC Daily Oral Versus Pulsed (CYCLOPS) trial, involved 149 patients with generalized disease (nephritis, GPA, and microscopic polyangiitis [MPA]) who were administered either an intravenous (IV) pulse or a daily oral CYC regimen.7 The pulse CYC neither shortened patients’ time to remission nor increased the proportion of patients who achieved it. Patients receiving pulse CYC suffered one-third the rate of leukopenia experienced by patients who received the oral regimen. Since infection is a source of mortality in vasculitis, this finding is an important consideration when balancing the benefits of day-to-day control offered by oral administration against the safety of at-risk patients such as the elderly.
This treatment strategy may be relevant for patients with renal impairment. It was once thought that patients with renal failure after receiving CYC had more aggressive disease and therefore needed higher dosages. Investigators who studied the impact of renal insufficiency and hemodialysis on the pharmacokinetics of CYC found that clearance of CYC is impaired in patients with reduced renal function.8 Thus, when renal function is suppressed, the CYC dosage should be reduced rather than increased.
Mycophenolate mofetil—efficacy not yet confirmed
Another alternative to CYC, mycophenolate mofetil (MMF), has gained much attention, although its effectiveness is not yet certain. Pilot data show that 13 of 17 patients with MPA achieved remission after 6 months of treatment with MMF.9 Meanwhile, the so-called MYCYC trial, in which patients with newly diagnosed AAV receive either the CYCLOPS regimen or MMF, is under way.10
Deoxyspergualin—remission not sustained
A nonstandard drug that warrants attention is deoxyspergualin (now called gusperimus), licensed in Japan for 15 years. In a prospective, open-label trial of 45 patients with relapsing or refractory GPA, investigators showed that 95% achieved partial remission and 45% full remission, although remission was not sustained when therapy was stopped.11 Because the drug must be administered daily for 21 days by subcutaneous injection, deoxyspergualin is not easy to use. It may represent an alternative, however, because it permitted prednisolone dosage reduction.
EVALUATING RISK AND CHOOSING THERAPIES
CONSIDERATIONS IN CHOOSING REMISSION THERAPY
Overall, when planning remission therapy and its duration, clinicians must balance the efficacy of CYC and glucocorticoids against their toxicity. Close monitoring and the patient’s capacity to adhere to instructions are two critical issues. Other important considerations include the risk and consequences of relapse, which vary in different circumstances, and the association of cancer with CYC therapy.
Relapse risk is variable
Certain patients are at higher risk of relapse than others. Patients with GPA or proteinase-3-ANCA–positive disease are at higher relapse risk than those who have MPA. ANCA-positive disease in remission or rising ANCA markers both increase the risk of relapse. Ear, nose, throat, and lung diseases increase the likelihood of relapse. Patients with GPA who are Staphylococcus aureus carriers have increased risk. Serum creatinine levels of 2.0 to 3.0 mg/dL at the end of induction therapy should arouse concern about renal relapse.
Most relapses affect the ear, nose, and throat system and do not threaten vital organs. Relapse does not increase the risk of end-stage renal disease or death.
Consider mortality and cancer data
Although the strongest predictor of early death is infection, advanced age and renal impairment also predict death. Chronic kidney disease stage at entry and glomerular filtration rate significantly predict mortality.21 More than 36 g CYC (equivalent to 9 to 12 months of standard oral therapy) increases the risk of bladder cancer 10-fold and myeloid leukemia 60-fold, but the cancer risk is time-dependent; malignancy requires 12 years on average to emerge.22
CONCLUSION
Cyclophosphamide in combination with glucocorticoids remains the standard therapy for GPA and related vasculitides, despite the risk of significant treatment-related comorbidities. Several strategies can be employed to reduce exposure, such as sequential withdrawal of CYC and IV administration. The optimization of glucocorticoid dosing will be a major research focus in the next decade. Newer agents may improve the maintenance of remission; for example, azathioprine and methotrexate show equal efficacy and safety, while MMF is less effective. When planning remission maintenance therapy, the relapse risk should be considered carefully because it varies among clinical scenarios. Other factors in the decision include the consequences for the patient, monitoring requirements, and the patient’s ability to understand and adhere to instructions.
In 1958, shortly after the first descriptions of granulomatosis with polyangiitis, or GPA (Wegener’s granulomatosis), the 1-year mortality was 18%,1 mainly due to renal failure. Physicians tried to combat the disease using various immunosuppressive drugs (nitrogen mustard and, in later years, azathioprine and methotrexate), but measurable success came only after investigators introduced cyclophosphamide (CYC) in combination with the glucocorticoid prednisone.2
A key 1992 study showed that the CYC/prednisone combination markedly improved the disease status in 91% of patients,3 with 75% achieving complete remission. The treatment came at a price, however, with almost all patients suffering serious morbidity or side effects. The results also highlighted concerns about potential malignancies caused by prolonged use of CYC and glucocorticoids. Those concerns motivated the European Vasculitis Study Group in the late 1980s and early 1990s to design and validate testing for antineutrophil cytoplasmic antibody (ANCA)–associated vasculitides (AAV) and pursue consensus regarding treatment.4
ALTERNATIVES TO STANDARD THERAPY
The accepted therapeutic strategy for GPA is to first induce remission using high doses of CYC and then prevent relapse with longer-term, less toxic therapeutic alternatives. These less toxic therapies include newer agents as well as new methods of delivery, particularly for patients with nonsevere forms of disease.
Methotrexate—effective for early treatment
Methotrexate showed early promise in several nonrandomized trials of patients with nonsevere disease. In one such study, de Groot et al subclassified 100 patients at diagnosis according to the extent and severity of the disease.5 Patients were then randomized to receive either standard oral CYC or methotrexate, each combined with prednisolone. Remission rates (90% to 94%) were comparable regardless of whether patients received CYC or methotrexate, although patients with more severe disease who were taking methotrexate took longer to achieve remission. At the same time, relapse rates were higher for methotrexate-taking patients (70%) compared with the CYC group (47%). Thus, while methotrexate could replace CYC for initial treatment of early AAV, CYC had a greater influence on subsequent relapse rates, particularly in patients with more severe forms of disease.
Pulse cyclophosphamide—a new method
Investigators tested pulse delivery of CYC compared with oral daily administration as a means of reducing the CYC dose. An analysis of 14 relatively small studies showed that pulse CYC had the same survival and renal failure rates as continuous therapy.6
One such trial, the CYC Daily Oral Versus Pulsed (CYCLOPS) trial, involved 149 patients with generalized disease (nephritis, GPA, and microscopic polyangiitis [MPA]) who were administered either an intravenous (IV) pulse or a daily oral CYC regimen.7 The pulse CYC neither shortened patients’ time to remission nor increased the proportion of patients who achieved it. Patients receiving pulse CYC suffered one-third the rate of leukopenia experienced by patients who received the oral regimen. Since infection is a source of mortality in vasculitis, this finding is an important consideration when balancing the benefits of day-to-day control offered by oral administration against the safety of at-risk patients such as the elderly.
This treatment strategy may be relevant for patients with renal impairment. It was once thought that patients with renal failure after receiving CYC had more aggressive disease and therefore needed higher dosages. Investigators who studied the impact of renal insufficiency and hemodialysis on the pharmacokinetics of CYC found that clearance of CYC is impaired in patients with reduced renal function.8 Thus, when renal function is suppressed, the CYC dosage should be reduced rather than increased.
Mycophenolate mofetil—efficacy not yet confirmed
Another alternative to CYC, mycophenolate mofetil (MMF), has gained much attention, although its effectiveness is not yet certain. Pilot data show that 13 of 17 patients with MPA achieved remission after 6 months of treatment with MMF.9 Meanwhile, the so-called MYCYC trial, in which patients with newly diagnosed AAV receive either the CYCLOPS regimen or MMF, is under way.10
Deoxyspergualin—remission not sustained
A nonstandard drug that warrants attention is deoxyspergualin (now called gusperimus), licensed in Japan for 15 years. In a prospective, open-label trial of 45 patients with relapsing or refractory GPA, investigators showed that 95% achieved partial remission and 45% full remission, although remission was not sustained when therapy was stopped.11 Because the drug must be administered daily for 21 days by subcutaneous injection, deoxyspergualin is not easy to use. It may represent an alternative, however, because it permitted prednisolone dosage reduction.
EVALUATING RISK AND CHOOSING THERAPIES
CONSIDERATIONS IN CHOOSING REMISSION THERAPY
Overall, when planning remission therapy and its duration, clinicians must balance the efficacy of CYC and glucocorticoids against their toxicity. Close monitoring and the patient’s capacity to adhere to instructions are two critical issues. Other important considerations include the risk and consequences of relapse, which vary in different circumstances, and the association of cancer with CYC therapy.
Relapse risk is variable
Certain patients are at higher risk of relapse than others. Patients with GPA or proteinase-3-ANCA–positive disease are at higher relapse risk than those who have MPA. ANCA-positive disease in remission or rising ANCA markers both increase the risk of relapse. Ear, nose, throat, and lung diseases increase the likelihood of relapse. Patients with GPA who are Staphylococcus aureus carriers have increased risk. Serum creatinine levels of 2.0 to 3.0 mg/dL at the end of induction therapy should arouse concern about renal relapse.
Most relapses affect the ear, nose, and throat system and do not threaten vital organs. Relapse does not increase the risk of end-stage renal disease or death.
Consider mortality and cancer data
Although the strongest predictor of early death is infection, advanced age and renal impairment also predict death. Chronic kidney disease stage at entry and glomerular filtration rate significantly predict mortality.21 More than 36 g CYC (equivalent to 9 to 12 months of standard oral therapy) increases the risk of bladder cancer 10-fold and myeloid leukemia 60-fold, but the cancer risk is time-dependent; malignancy requires 12 years on average to emerge.22
CONCLUSION
Cyclophosphamide in combination with glucocorticoids remains the standard therapy for GPA and related vasculitides, despite the risk of significant treatment-related comorbidities. Several strategies can be employed to reduce exposure, such as sequential withdrawal of CYC and IV administration. The optimization of glucocorticoid dosing will be a major research focus in the next decade. Newer agents may improve the maintenance of remission; for example, azathioprine and methotrexate show equal efficacy and safety, while MMF is less effective. When planning remission maintenance therapy, the relapse risk should be considered carefully because it varies among clinical scenarios. Other factors in the decision include the consequences for the patient, monitoring requirements, and the patient’s ability to understand and adhere to instructions.
- Walton EW. Giant-cell granuloma of the respiratory tract (Wegener’s granulomatosis). Br Med J 1958; 2:265–270.
- Novack SN, Pearson CM. Cyclophosphamide therapy in Wegener’s granulomatosis. N Engl J Med 1971; 284:938–942.
- Hoffman GS, Kerr GS, Leavitt RY, et al. Wegener granulomatosis: an analysis of 158 patients. Ann Intern Med 1992; 116:488–498.
- Rasmussen N, Jayne DRW, Abramowicz D, et al. European therapeutic trials in ANCA-associated systemic vasculitis: disease scoring, consensus regimens and proposed clinical trials. Clin Exp Immunol 1995; 101 (suppl 1):29–34.
- de Groot K, Rasmussen N, Bacon PA, et al. Randomized trial of cyclophosphamide versus methotrexate for induction of remission in early systemic antineutrophil cytoplasmic antibody-associated vasculitis. Arthritis Rheum 2005; 52:2461–2469.
- de Groot K, Adu D, Savage COS; for EUVAS (European Vasculitis Study Group). The value of pulse cyclophosphamide in ANCA-associated vasculitis: meta-analysis and critical review. Nephrol Dial Transplant 2001; 16:2018–2027.
- de Groot K, Harper L, Jayne DRW, et al. Pulse versus daily oral cyclophosphamide for induction of remission in antineutrophil cytoplasmic antibody-associated vasculitis: a randomized trial. Ann Intern Med 2009; 150:670–680.
- Haubitz M, Bohnenstengel F, Brunkhorst R, Schwab M, Hofmann U, Busse D. Cyclophosphamide pharmacokinetics and dose requirements in patients with renal insufficiency. Kidney Int 2002; 61:1495–1501.
- Silva F, Specks U, Kalra S, et al. Mycophenolate mofetil for induction and maintenance of remission in microscopic polyangiitis with mild to moderate renal involvement: a prospective, open-label pilot trial [published online ahead of print January 21, 2010]. Clin J Am Soc Nephrol 2010; 5:445–453. doi: 10.2215/CJN.06010809
- MYCYC clinical trial protocol. The European Vasculitis Society Web site. http://www.vasculitis.org. Updated April 12, 2011. Accessed June 13, 2012.
- Flossmann O, Baslund B, Bruchfeld A, et al. Deoxyspergualin in relapsing and refractory Wegener’s granulomatosis [published online ahead of print August 19, 2008]. Ann Rheum Dis 2009; 68:1125–1130. doi: 10.1136/ard.2008.092429
- Mukhtyar C, Guillevin L, Cid MC, et al; for the European Vasculitis Study Group. EULAR recommendations for the management of primary small and medium vessel vasculitis [published online ahead of print April 15, 2008]. Ann Rheum Dis 2009; 68:310–317. doi: 10.1136/ard.2008.088096
- Mukhtyar C, Guillevin L, Cid MC, et al; for the European Vasculitis Study Group. EULAR recommendations for the management of large vessel vasculitis [published online ahead of print April 15, 2008]. Ann Rheum Dis 2009; 68:318–323. doi: 10.1136/ard.2008.088351
- Hellmich B, Flossmann O, Gross WL, et al; on behalf of the European Vasculitis Study Group. EULAR recommendations for conducting clinical studies and/or clinical trials in systemic vasculitis: focus on anti-neutrophil cytoplasm antibody-associated vasculitis [published online ahead of print December 14, 2006]. Ann Rheum Dis 2007; 66:605–617. doi: 10.1136/ard.2006.062711
- Jayne D, Rasmussen N, Andrassy K, et al; for the European Vasculitis Study Group. A randomized trial of maintenance therapy for vasculitis associated with antineutrophil cytoplasmic autoantibodies. N Engl J Med 2003; 349:36–44.
- Pagnoux C, Mahr A, Hamidou MA, et al; for the French Vasculitis Study Group. Azathioprine or methotrexate maintenance for ANCA-associated vasculitis. N Engl J Med 2008; 359:2790–2803.
- Hiemstra TF, Walsh M, Mahr A, et al; for the European Vasculitis Study Group (EUVAS). Mycophenolate mofetil vs azathioprine for remission maintenance in antineutrophil cytoplasmic antibodyassociated vasculitis: a randomized controlled trial [published online ahead of print November 8, 2010]. JAMA 2010; 304:2381–2388. doi: 10.1001/jama.2010.1658
- Metzler C, Miehle N, Manger K, et al; for the German Network of Rheumatic Diseases. Elevated relapse rate under oral methotrexate versus leflunomide for maintenance of remission in Wegener’s granulomatosis [published online ahead of print May 22, 2007]. Rheumatology 2007; 46:1087–1091. doi: 10.1093/rheumatology/kem029
- Walsh M, Merkel PA, Mahr A, Jayne D. Effects of duration of glucocorticoid therapy on relapse rate in antineutrophil cytoplasmic antibody-associated vasculitis: a meta-analysis. Arthritis Care Res (Hoboken) 2010; 62:1166–1173.
- Vanková Z, Ríhová Z, Jancová E, Rysavá R, Merta M, Tesar V. Optimizing the therapeutic strategies in ANCA-associated vasculitis— single centre experience with international randomized trials. Prague Med Rep 2006; 107:199–212.
- Flossmann O, Berden A, de Groot K, et al; for the European Vasculitis Study Group. Long-term patient survival in ANCA-associated vasculitis [published online ahead of print November 24, 2010]. Ann Rheum Dis 2011; 70:488–494. doi: 10.1136/ard.2010.137778
- Faurschou M, Sorensen IJ, Mellemkjaer L, et al. Malignancies in Wegener’s granulomatosis: incidence and relation to cyclophosphamide therapy in a cohort of 293 patients [published online ahead of print October 15, 2007]. J Rheumatol 2008; 35:100–105.
- Walton EW. Giant-cell granuloma of the respiratory tract (Wegener’s granulomatosis). Br Med J 1958; 2:265–270.
- Novack SN, Pearson CM. Cyclophosphamide therapy in Wegener’s granulomatosis. N Engl J Med 1971; 284:938–942.
- Hoffman GS, Kerr GS, Leavitt RY, et al. Wegener granulomatosis: an analysis of 158 patients. Ann Intern Med 1992; 116:488–498.
- Rasmussen N, Jayne DRW, Abramowicz D, et al. European therapeutic trials in ANCA-associated systemic vasculitis: disease scoring, consensus regimens and proposed clinical trials. Clin Exp Immunol 1995; 101 (suppl 1):29–34.
- de Groot K, Rasmussen N, Bacon PA, et al. Randomized trial of cyclophosphamide versus methotrexate for induction of remission in early systemic antineutrophil cytoplasmic antibody-associated vasculitis. Arthritis Rheum 2005; 52:2461–2469.
- de Groot K, Adu D, Savage COS; for EUVAS (European Vasculitis Study Group). The value of pulse cyclophosphamide in ANCA-associated vasculitis: meta-analysis and critical review. Nephrol Dial Transplant 2001; 16:2018–2027.
- de Groot K, Harper L, Jayne DRW, et al. Pulse versus daily oral cyclophosphamide for induction of remission in antineutrophil cytoplasmic antibody-associated vasculitis: a randomized trial. Ann Intern Med 2009; 150:670–680.
- Haubitz M, Bohnenstengel F, Brunkhorst R, Schwab M, Hofmann U, Busse D. Cyclophosphamide pharmacokinetics and dose requirements in patients with renal insufficiency. Kidney Int 2002; 61:1495–1501.
- Silva F, Specks U, Kalra S, et al. Mycophenolate mofetil for induction and maintenance of remission in microscopic polyangiitis with mild to moderate renal involvement: a prospective, open-label pilot trial [published online ahead of print January 21, 2010]. Clin J Am Soc Nephrol 2010; 5:445–453. doi: 10.2215/CJN.06010809
- MYCYC clinical trial protocol. The European Vasculitis Society Web site. http://www.vasculitis.org. Updated April 12, 2011. Accessed June 13, 2012.
- Flossmann O, Baslund B, Bruchfeld A, et al. Deoxyspergualin in relapsing and refractory Wegener’s granulomatosis [published online ahead of print August 19, 2008]. Ann Rheum Dis 2009; 68:1125–1130. doi: 10.1136/ard.2008.092429
- Mukhtyar C, Guillevin L, Cid MC, et al; for the European Vasculitis Study Group. EULAR recommendations for the management of primary small and medium vessel vasculitis [published online ahead of print April 15, 2008]. Ann Rheum Dis 2009; 68:310–317. doi: 10.1136/ard.2008.088096
- Mukhtyar C, Guillevin L, Cid MC, et al; for the European Vasculitis Study Group. EULAR recommendations for the management of large vessel vasculitis [published online ahead of print April 15, 2008]. Ann Rheum Dis 2009; 68:318–323. doi: 10.1136/ard.2008.088351
- Hellmich B, Flossmann O, Gross WL, et al; on behalf of the European Vasculitis Study Group. EULAR recommendations for conducting clinical studies and/or clinical trials in systemic vasculitis: focus on anti-neutrophil cytoplasm antibody-associated vasculitis [published online ahead of print December 14, 2006]. Ann Rheum Dis 2007; 66:605–617. doi: 10.1136/ard.2006.062711
- Jayne D, Rasmussen N, Andrassy K, et al; for the European Vasculitis Study Group. A randomized trial of maintenance therapy for vasculitis associated with antineutrophil cytoplasmic autoantibodies. N Engl J Med 2003; 349:36–44.
- Pagnoux C, Mahr A, Hamidou MA, et al; for the French Vasculitis Study Group. Azathioprine or methotrexate maintenance for ANCA-associated vasculitis. N Engl J Med 2008; 359:2790–2803.
- Hiemstra TF, Walsh M, Mahr A, et al; for the European Vasculitis Study Group (EUVAS). Mycophenolate mofetil vs azathioprine for remission maintenance in antineutrophil cytoplasmic antibodyassociated vasculitis: a randomized controlled trial [published online ahead of print November 8, 2010]. JAMA 2010; 304:2381–2388. doi: 10.1001/jama.2010.1658
- Metzler C, Miehle N, Manger K, et al; for the German Network of Rheumatic Diseases. Elevated relapse rate under oral methotrexate versus leflunomide for maintenance of remission in Wegener’s granulomatosis [published online ahead of print May 22, 2007]. Rheumatology 2007; 46:1087–1091. doi: 10.1093/rheumatology/kem029
- Walsh M, Merkel PA, Mahr A, Jayne D. Effects of duration of glucocorticoid therapy on relapse rate in antineutrophil cytoplasmic antibody-associated vasculitis: a meta-analysis. Arthritis Care Res (Hoboken) 2010; 62:1166–1173.
- Vanková Z, Ríhová Z, Jancová E, Rysavá R, Merta M, Tesar V. Optimizing the therapeutic strategies in ANCA-associated vasculitis— single centre experience with international randomized trials. Prague Med Rep 2006; 107:199–212.
- Flossmann O, Berden A, de Groot K, et al; for the European Vasculitis Study Group. Long-term patient survival in ANCA-associated vasculitis [published online ahead of print November 24, 2010]. Ann Rheum Dis 2011; 70:488–494. doi: 10.1136/ard.2010.137778
- Faurschou M, Sorensen IJ, Mellemkjaer L, et al. Malignancies in Wegener’s granulomatosis: incidence and relation to cyclophosphamide therapy in a cohort of 293 patients [published online ahead of print October 15, 2007]. J Rheumatol 2008; 35:100–105.