User login

EDITOR’S NOTE: This month, we introduce a new column, “On the Horizon: Quality, Systems, Safety.” Herein, author Win Whitcomb, MD, MHM, one of SHM’s founders and medical director of healthcare quality at Baystate Medical Center in Springfield, Mass., will deliver his views on all things quality and monitor the major issues affecting hospitalists today. As a companion to Dr. Whitcomb’s perspectives, you’ll find “The View from the Center.” “The View” will on occasion provide readers with news and details of how SHM’s Center for Hospital Innovation and Improvement (“the center”) is addressing implementation of healthcare reform, planning programs to improve quality and safety of care, and influencing decisions that will affect hospital medicine for years to come.
Burke Kealey, MD, SFHM, SHM board member and medical director with HealthPartners in Minneapolis, once remarked, “The core measures program is one of the greatest gifts hospital medicine has been given.” Scoring high on the Centers for Medicare & Medicaid Services (CMS) core measures has been a no-brainer for many hospitalist programs over the years; this success has allowed hospitalists to distinguish themselves from traditional PCPs in the hospital.
Looking back, many of us saw the huge opportunity created by the core measures a decade ago. What could be so hard about writing for a flu shot or ordering an echocardiogram? We joined teams, and put systems in place to ensure high performance and, ahem, figured out how to jump through documentation hoops. (Who disputes that quality improvement is two parts better care, one part managing the medical record?)
The result? A bonanza for hospitalists (as overachievers) in the process measures known as the CMS core measures. Admittedly, some of us have struggled more than others in achieving high performance on some of the measures. For example, we couldn’t for the life of us figure out how to excel in “discharge instructions” for heart failure patients at my hospital because we stunk at medication reconciliation. And, being the team sport that QI is, some of these struggles have been beyond hospitalists’ influence.
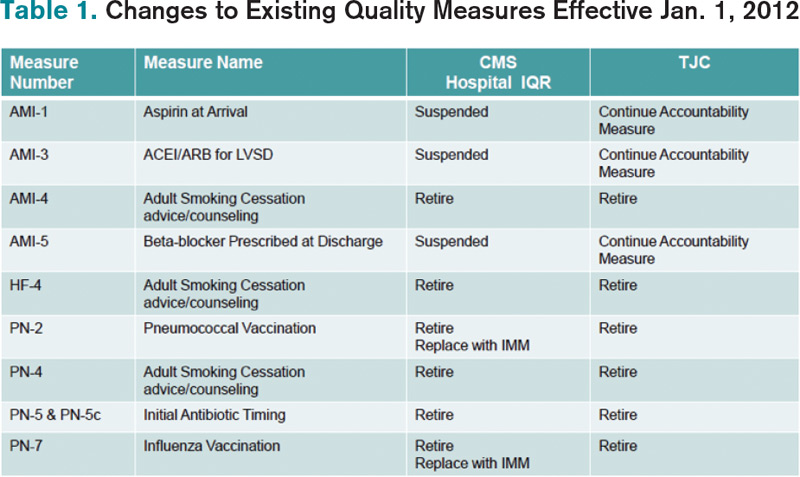
Well, times are changing, and a good number of core measures (the CMS Inpatient Quality Reporting, or IQR, Program) recently have been retired or suspended. Table 1 outlines the retired or suspended CMS measures; The Joint Commission is retiring many, but not all, of the same measures. To clarify, CMS uses Hospital IQR measures for reporting on the public website hospitalcompare.hhs.gov and, beginning in 2013, a subset will make up part of the value-based purchasing program (see “Value-Based Purchasing Raises the Stakes,” May 2011, p. 1, or visit www.hospitalmedicine.org/vbp). For the commission, the measures are used as part of the survey process for hospital accreditation.
Timeline
The changes described in Table 1 denote measures that will be retired or suspended from the FY14 Hospital IQR measure set, and were reflected in hospital discharges effective Jan. 1, 2012. In other words, the changes are reflected in CMS’ collection of data from hospitals as of this year.
A few words of explanation of the table terms: “AMI,” of course, stands for acute myocardial infarction, “HF” is heart failure, and “PN” is pneumonia.
“Retire” means just that. Let’s hope so, and not what Michael Jordan meant when calling it quits the first time to try out baseball.
“Suspended” means CMS is retaining the measure in the IQR program but is not collecting data until such time that evidence shows hospital performance has unacceptably declined. Win’s word: Hard to know exactly what that means. It scares me enough that my hospital will continue data collection for internal purposes and not take our eye off the ball regarding performance.
“IMM” is short for global immunization and means that influenza and pneumococcal vaccine administration will be tracked on all hospital patients, not just those with pneumonia, who meet the age and high-risk criteria. Win’s word: You read that correctly. All inpatients require these vaccinations if they meet the criteria.
“Accountability measures” became part of The Joint Commission’s accreditation process Jan. 1. According to the commission’s website, they refer to a subset of core measures resulting in “the greatest positive impact on patient outcomes when hospitals demonstrate improvement on them.” Each accountability measure must meet these four criteria:
RESEARCH: There is strong evidence that compliance with this process of care improves outcomes.
PROXIMITY: The process being measured is “close” to the outcome (i.e. relatively few steps between the process and outcome).
ACCURACY: The measure accurately reflects that the process actually has been provided. Win’s word: In = “aspirin on arrival” and “ACE/ARB for LVSD.” Out = “smoking cessation counseling.” For smoking cessation, who knows if this was actually provided or the box was simply checked?
ADVERSE EFFECTS: The measure minimizes adverse effects. Win’s word: The “initial antibiotic timing” measure probably reduced diagnostic accuracy of pneumonia. See ya.
The other core measures will remain in their current form for now. Going forward, the IQR program provides hospitalists new opportunities to shine. These went into effect Jan. 1:
- Admit decision time to ED departure for admitted patients;
- Median time from ED arrival to ED departure for admitted patients; and
- Catheter-associated UTI rates.
As with all the measures, working in teams will be essential to success in these new measures. So go out there and hit a few more home runs (or at least a base hit or two). The season is well underway.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder of SHM and an expert in quality improvement and hospitalist practice management. Write to him at [email protected].
EDITOR’S NOTE: This month, we introduce a new column, “On the Horizon: Quality, Systems, Safety.” Herein, author Win Whitcomb, MD, MHM, one of SHM’s founders and medical director of healthcare quality at Baystate Medical Center in Springfield, Mass., will deliver his views on all things quality and monitor the major issues affecting hospitalists today. As a companion to Dr. Whitcomb’s perspectives, you’ll find “The View from the Center.” “The View” will on occasion provide readers with news and details of how SHM’s Center for Hospital Innovation and Improvement (“the center”) is addressing implementation of healthcare reform, planning programs to improve quality and safety of care, and influencing decisions that will affect hospital medicine for years to come.
Burke Kealey, MD, SFHM, SHM board member and medical director with HealthPartners in Minneapolis, once remarked, “The core measures program is one of the greatest gifts hospital medicine has been given.” Scoring high on the Centers for Medicare & Medicaid Services (CMS) core measures has been a no-brainer for many hospitalist programs over the years; this success has allowed hospitalists to distinguish themselves from traditional PCPs in the hospital.
Looking back, many of us saw the huge opportunity created by the core measures a decade ago. What could be so hard about writing for a flu shot or ordering an echocardiogram? We joined teams, and put systems in place to ensure high performance and, ahem, figured out how to jump through documentation hoops. (Who disputes that quality improvement is two parts better care, one part managing the medical record?)
The result? A bonanza for hospitalists (as overachievers) in the process measures known as the CMS core measures. Admittedly, some of us have struggled more than others in achieving high performance on some of the measures. For example, we couldn’t for the life of us figure out how to excel in “discharge instructions” for heart failure patients at my hospital because we stunk at medication reconciliation. And, being the team sport that QI is, some of these struggles have been beyond hospitalists’ influence.
Well, times are changing, and a good number of core measures (the CMS Inpatient Quality Reporting, or IQR, Program) recently have been retired or suspended. Table 1 outlines the retired or suspended CMS measures; The Joint Commission is retiring many, but not all, of the same measures. To clarify, CMS uses Hospital IQR measures for reporting on the public website hospitalcompare.hhs.gov and, beginning in 2013, a subset will make up part of the value-based purchasing program (see “Value-Based Purchasing Raises the Stakes,” May 2011, p. 1, or visit www.hospitalmedicine.org/vbp). For the commission, the measures are used as part of the survey process for hospital accreditation.
Timeline
The changes described in Table 1 denote measures that will be retired or suspended from the FY14 Hospital IQR measure set, and were reflected in hospital discharges effective Jan. 1, 2012. In other words, the changes are reflected in CMS’ collection of data from hospitals as of this year.
A few words of explanation of the table terms: “AMI,” of course, stands for acute myocardial infarction, “HF” is heart failure, and “PN” is pneumonia.
“Retire” means just that. Let’s hope so, and not what Michael Jordan meant when calling it quits the first time to try out baseball.
“Suspended” means CMS is retaining the measure in the IQR program but is not collecting data until such time that evidence shows hospital performance has unacceptably declined. Win’s word: Hard to know exactly what that means. It scares me enough that my hospital will continue data collection for internal purposes and not take our eye off the ball regarding performance.
“IMM” is short for global immunization and means that influenza and pneumococcal vaccine administration will be tracked on all hospital patients, not just those with pneumonia, who meet the age and high-risk criteria. Win’s word: You read that correctly. All inpatients require these vaccinations if they meet the criteria.
“Accountability measures” became part of The Joint Commission’s accreditation process Jan. 1. According to the commission’s website, they refer to a subset of core measures resulting in “the greatest positive impact on patient outcomes when hospitals demonstrate improvement on them.” Each accountability measure must meet these four criteria:
RESEARCH: There is strong evidence that compliance with this process of care improves outcomes.
PROXIMITY: The process being measured is “close” to the outcome (i.e. relatively few steps between the process and outcome).
ACCURACY: The measure accurately reflects that the process actually has been provided. Win’s word: In = “aspirin on arrival” and “ACE/ARB for LVSD.” Out = “smoking cessation counseling.” For smoking cessation, who knows if this was actually provided or the box was simply checked?
ADVERSE EFFECTS: The measure minimizes adverse effects. Win’s word: The “initial antibiotic timing” measure probably reduced diagnostic accuracy of pneumonia. See ya.
The other core measures will remain in their current form for now. Going forward, the IQR program provides hospitalists new opportunities to shine. These went into effect Jan. 1:
- Admit decision time to ED departure for admitted patients;
- Median time from ED arrival to ED departure for admitted patients; and
- Catheter-associated UTI rates.
As with all the measures, working in teams will be essential to success in these new measures. So go out there and hit a few more home runs (or at least a base hit or two). The season is well underway.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder of SHM and an expert in quality improvement and hospitalist practice management. Write to him at [email protected].
EDITOR’S NOTE: This month, we introduce a new column, “On the Horizon: Quality, Systems, Safety.” Herein, author Win Whitcomb, MD, MHM, one of SHM’s founders and medical director of healthcare quality at Baystate Medical Center in Springfield, Mass., will deliver his views on all things quality and monitor the major issues affecting hospitalists today. As a companion to Dr. Whitcomb’s perspectives, you’ll find “The View from the Center.” “The View” will on occasion provide readers with news and details of how SHM’s Center for Hospital Innovation and Improvement (“the center”) is addressing implementation of healthcare reform, planning programs to improve quality and safety of care, and influencing decisions that will affect hospital medicine for years to come.
Burke Kealey, MD, SFHM, SHM board member and medical director with HealthPartners in Minneapolis, once remarked, “The core measures program is one of the greatest gifts hospital medicine has been given.” Scoring high on the Centers for Medicare & Medicaid Services (CMS) core measures has been a no-brainer for many hospitalist programs over the years; this success has allowed hospitalists to distinguish themselves from traditional PCPs in the hospital.
Looking back, many of us saw the huge opportunity created by the core measures a decade ago. What could be so hard about writing for a flu shot or ordering an echocardiogram? We joined teams, and put systems in place to ensure high performance and, ahem, figured out how to jump through documentation hoops. (Who disputes that quality improvement is two parts better care, one part managing the medical record?)
The result? A bonanza for hospitalists (as overachievers) in the process measures known as the CMS core measures. Admittedly, some of us have struggled more than others in achieving high performance on some of the measures. For example, we couldn’t for the life of us figure out how to excel in “discharge instructions” for heart failure patients at my hospital because we stunk at medication reconciliation. And, being the team sport that QI is, some of these struggles have been beyond hospitalists’ influence.
Well, times are changing, and a good number of core measures (the CMS Inpatient Quality Reporting, or IQR, Program) recently have been retired or suspended. Table 1 outlines the retired or suspended CMS measures; The Joint Commission is retiring many, but not all, of the same measures. To clarify, CMS uses Hospital IQR measures for reporting on the public website hospitalcompare.hhs.gov and, beginning in 2013, a subset will make up part of the value-based purchasing program (see “Value-Based Purchasing Raises the Stakes,” May 2011, p. 1, or visit www.hospitalmedicine.org/vbp). For the commission, the measures are used as part of the survey process for hospital accreditation.
Timeline
The changes described in Table 1 denote measures that will be retired or suspended from the FY14 Hospital IQR measure set, and were reflected in hospital discharges effective Jan. 1, 2012. In other words, the changes are reflected in CMS’ collection of data from hospitals as of this year.
A few words of explanation of the table terms: “AMI,” of course, stands for acute myocardial infarction, “HF” is heart failure, and “PN” is pneumonia.
“Retire” means just that. Let’s hope so, and not what Michael Jordan meant when calling it quits the first time to try out baseball.
“Suspended” means CMS is retaining the measure in the IQR program but is not collecting data until such time that evidence shows hospital performance has unacceptably declined. Win’s word: Hard to know exactly what that means. It scares me enough that my hospital will continue data collection for internal purposes and not take our eye off the ball regarding performance.
“IMM” is short for global immunization and means that influenza and pneumococcal vaccine administration will be tracked on all hospital patients, not just those with pneumonia, who meet the age and high-risk criteria. Win’s word: You read that correctly. All inpatients require these vaccinations if they meet the criteria.
“Accountability measures” became part of The Joint Commission’s accreditation process Jan. 1. According to the commission’s website, they refer to a subset of core measures resulting in “the greatest positive impact on patient outcomes when hospitals demonstrate improvement on them.” Each accountability measure must meet these four criteria:
RESEARCH: There is strong evidence that compliance with this process of care improves outcomes.
PROXIMITY: The process being measured is “close” to the outcome (i.e. relatively few steps between the process and outcome).
ACCURACY: The measure accurately reflects that the process actually has been provided. Win’s word: In = “aspirin on arrival” and “ACE/ARB for LVSD.” Out = “smoking cessation counseling.” For smoking cessation, who knows if this was actually provided or the box was simply checked?
ADVERSE EFFECTS: The measure minimizes adverse effects. Win’s word: The “initial antibiotic timing” measure probably reduced diagnostic accuracy of pneumonia. See ya.
The other core measures will remain in their current form for now. Going forward, the IQR program provides hospitalists new opportunities to shine. These went into effect Jan. 1:
- Admit decision time to ED departure for admitted patients;
- Median time from ED arrival to ED departure for admitted patients; and
- Catheter-associated UTI rates.
As with all the measures, working in teams will be essential to success in these new measures. So go out there and hit a few more home runs (or at least a base hit or two). The season is well underway.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder of SHM and an expert in quality improvement and hospitalist practice management. Write to him at [email protected].