User login
Cutaneous Reactions to Triatomine (Kissing Bug) Bites and the Risk for Chagas Disease
Cutaneous Reactions to Triatomine (Kissing Bug) Bites and the Risk for Chagas Disease
Triatome bugs cause painful bites and serve as vectors for Chagas disease. In this article, we will address diagnosis and vector identification.
Key Morphologic Features
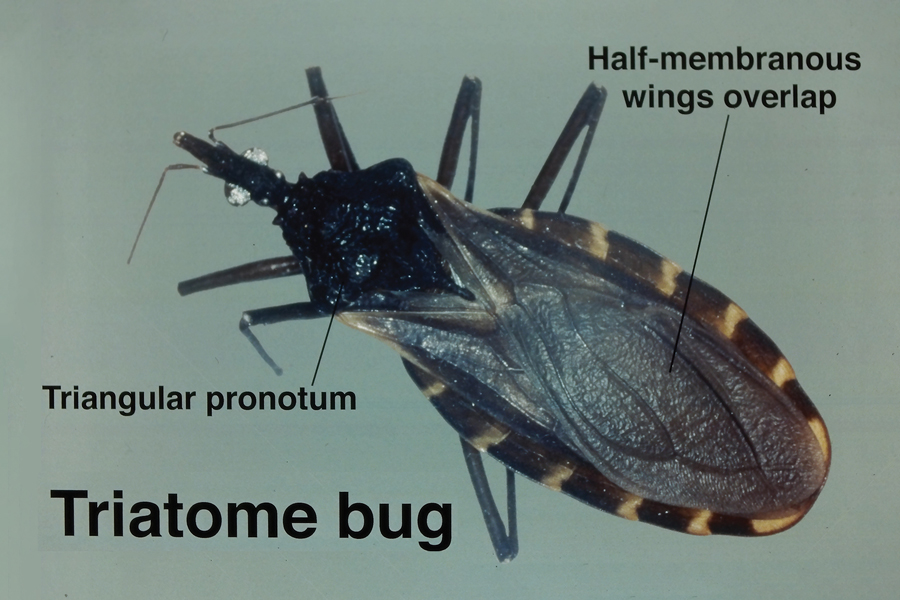
Insects from the subfamily Triatominae are identifiable by their long legs and a shieldlike abdomen behind a platelike pronotum that covers the thorax. Their half-membranous wings overlap, covering the central abdomen but leaving the lateral portions visible. Tigerlike stripes are characteristically prominent on the visible portions of the lateral abdomen. The stalklike head has an articulated beaklike mouth that can be retracted and used to deliver a powerful bite (Figure 1).
Feeding Mechanisms and Host Reactions
Triatome bugs are blood-feeding arthropods that hide in cracks and crevices in domestic structures by day and feed at night. They are shy feeders, and laboratory colonies have been known to die rather than feed in daylight. They are particularly common in thatched or wattle-and-daub dwellings, where they can be present in great numbers and descend on sleeping inhabitants at night. Triatome bugs require regular blood meals throughout the 5 developmental nymph stages in order to undergo successful molting.
In the wild, triatome bugs feed on a range of animals with little specificity, but in domestic settings they feed largely on humans. Thermosensors in the antennae help them locate blood vessels under the skin, which they penetrate easily due to their long mouthparts. Like other blood-sucking arthropods, they release an anticoagulant that facilitates continuous blood flow while feeding, which accounts for many of the cutaneous reactions observed after the host sustains a triatomine bite.1
Triatomine bugs have trouble feeding through clothing and seek out exposed skin, particularly the eyelids, producing the characteristic unilateral eyelid swelling known as the Romaña sign. Other bite reactions include purpura; macular erythema; and vesiculobullous, papular, and urticarial lesions (Figure 2).2 Associated lymphangitis or lymphadenopathy may be noted, and anaphylaxis has been reported. Similar to those of cockroaches, triatome antigens have been associated with atopic dermatitis and asthma.3

Chagas Disease Risk and Transmission
Triatomine reduviids are the primary vector of Chagas disease, and the geographic range of both continues to expand, particularly in North America. The disease remains endemic in Latin America, with the highest incidence now reported in Brazil.4 An estimated 240,000 to 350,000 individuals in the United States are infected, primarily immigrants from Mexico, Central America, and South America; approximately 30% of those infected will develop cardiac and/or gastrointestinal complications.4 If left untreated, Chagas disease leads to autonomic ganglion destruction and subsequent gastrointestinal and cardiac complications, including megacolon, dilated cardiomyopathy, and heart failure.5
Trypanosoma cruzi, the microorganism responsible for Chagas disease, is spread to humans through triatomine fecal matter scratched into the bite wound.6 Triatomine bugs have a highly developed gastrocolic reflex and defecate liberally as they feed. Fecal volume is heavily dependent on species and sex, with fifth-stage female nymphs producing the highest volume of excrement and thereby acting as particularly adept disease vectors.6 Triatoma infestans and members of the genus Mepraia are key vectors of T cruzi.1 In areas of South America where populations of T infestans are controlled through public health measures, Mepraia emerge as a largely uncontrolled disease vector.1,7 While endemic to the southern United States and South America, T cruzi has spread to much of North America and Europe by way of Triatominae as naturalized or invasive species.8
There are 3 phases of Chagas disease: acute, indeterminate, and chronic. A chagoma is a localized erythematous swelling at the site of the bite. The acute phase often lacks systemic symptoms but may include fever, myalgia, and headache. The intermediate phase may include fatigue and recurrent fevers. The most serious manifestations occur in the chronic phase and include cardiomyopathy with signs of congestive heart failure, irregular heartbeat, cardiac arrest, abdominal pain, constipation, and dysphagia.
Deforestation has been identified as a driving factor in the spread of Chagas disease, as the disease vectors shift from wilderness areas and animal hosts to inhabited areas where humans are the most readily available food source. Triatome bugs in areas experiencing higher levels of development or forest harvesting are forced into human-populated areas. As a result, instances of Chagas disease are on the rise in these communities.7 Salvador, Bahia, Brazil, has been identified as one such target of increased vector presence due to heavy deforestation, and the hottest months were identified as having the greatest threat of vector exposure.9 Brazil became the leading geographic area for the disease partly because of heavy loss of forested land.10
Vector Control and Prevention Strategies
Elimination of cracks and crevices in walls; replacement of wattle and daub with stucco, plaster, and other solid building materials; and the use of insecticides with durability in the environment have been used to reduce triatome bug infestation in homes. However, highly persistent insecticides carry greater environmental risk and may drive resistance as declining concentrations select for resistant arthropods. Repellents have less environmental impact and play an important role in vector control. Citronella essential oil has been observed to repel several species of triatome bugs that are common in Arizona; specifically, the component alcohols geraniol and citronellol were found to be effective at inhibiting triatome feeding.11
Early detection of Chagas disease is essential, as end-stage cardiomyopathy and megacolon are difficult to treat. Newly developed multiantigen testing has shown promising results, suggesting a potential for more accurate testing for Chagas disease.8 Geospatial tracking and mapping of T cruzi vectors now are employed to track seasonal vector changes and disease patterns.9 Researchers also have developed a dedicated dichotomous key for the identification of triatome bugs endemic in Brazil with the hope of better identification and mapping of disease vector presence and density.10 The key consists of a series of statements with 2 choices in each step. It uses observable features of the arthropod to lead users to the correct identification.
Final Thoughts
Identification of triatome bugs can help with public health efforts to control the spread of disease. Patients with unilateral eyelid swelling should be evaluated for possible bedbug or triatome exposure.
- Egaña C, Pinto R, Vergara F, et al. Fluctuations in Trypanosoma cruzi discrete typing unit composition in two naturally infected triatomines: Mepraia gajardoi and M. spinolai after laboratory feeding. Acta Trop. 2016;160:9-14. Erratum in: Acta Trop. 2016;162:248. doi:10.1016/j.actatropica.2016.04.008
- Moffitt JE, Venarske D, Goddard J, et al. Allergic reactions to Triatoma bites. Ann Allergy Asthma Immunol. 2003;91:122-128.
- Alonso A, Potenza M, Mouchián K, et al. Proteinase and gelatinolytic properties of a Triatoma infestans extract. Allergol Immunopathol (Madr). 2004;32:223-227.
- Hochberg NS, Montgomery SP. Chagas disease. Ann Intern Med. 2023;176:ITC17-ITC32. doi:10.7326/AITC202302210
- Pless M, Juranek D, Kozarsky P, et al. The epidemiology of Chagas’ disease in a hyperendemic area of Cochabamba, Bolivia: a clinical study including electrocardiography, seroreactivity to Trypanosoma cruzi, xenodiagnosis, and domiciliary triatomine distribution. Am J Trop Med Hyg. 1992;47:539-546.
- Piesman J, Sherlock IA. Factors controlling the volume of feces produced by triatomine vectors of Chagas’ disease. Acta Trop. 1983;40:351-358.
- Steverding D. The history of Chagas disease. Parasit Vectors. 2014;10:317.
- Granjon E, Dichtel-Danjoy ML, Saba E, et al. Development of a novel multiplex immunoassay multi-cruzi for the serological confirmation of Chagas disease. PLoS Negl Trop Dis. 2016;10:e0004596.
- Santana Kde S, Bavia ME, Lima AD, et al. Spatial distribution of triatomines (Reduviidae: Triatominae) in urban areas of the city of Salvador, Bahia, Brazil. Geospat Health. 2011;5:199-203.
- de Mello DV, Nhapulo EF, Cesaretto LP, et al. Dichotomous keys based on cytogenetic data for triatomines reported in Brazilian regions with outbreaks of orally transmitted Chagas disease (Pernambuco and Rio Grande Do Norte). Trop Med Infect Dis. 2023;8:196.
- Zamora D, Klotz SA, Meister EA, et al. Repellency of the components of the essential oil, citronella, to Triatoma rubida, Triatoma protracta, and Triatoma recurva (Hemiptera: Reduviidae: Triatominae). J Med Entomol. 2015;52:719-721.
Triatome bugs cause painful bites and serve as vectors for Chagas disease. In this article, we will address diagnosis and vector identification.
Key Morphologic Features
Insects from the subfamily Triatominae are identifiable by their long legs and a shieldlike abdomen behind a platelike pronotum that covers the thorax. Their half-membranous wings overlap, covering the central abdomen but leaving the lateral portions visible. Tigerlike stripes are characteristically prominent on the visible portions of the lateral abdomen. The stalklike head has an articulated beaklike mouth that can be retracted and used to deliver a powerful bite (Figure 1).
Feeding Mechanisms and Host Reactions
Triatome bugs are blood-feeding arthropods that hide in cracks and crevices in domestic structures by day and feed at night. They are shy feeders, and laboratory colonies have been known to die rather than feed in daylight. They are particularly common in thatched or wattle-and-daub dwellings, where they can be present in great numbers and descend on sleeping inhabitants at night. Triatome bugs require regular blood meals throughout the 5 developmental nymph stages in order to undergo successful molting.
In the wild, triatome bugs feed on a range of animals with little specificity, but in domestic settings they feed largely on humans. Thermosensors in the antennae help them locate blood vessels under the skin, which they penetrate easily due to their long mouthparts. Like other blood-sucking arthropods, they release an anticoagulant that facilitates continuous blood flow while feeding, which accounts for many of the cutaneous reactions observed after the host sustains a triatomine bite.1
Triatomine bugs have trouble feeding through clothing and seek out exposed skin, particularly the eyelids, producing the characteristic unilateral eyelid swelling known as the Romaña sign. Other bite reactions include purpura; macular erythema; and vesiculobullous, papular, and urticarial lesions (Figure 2).2 Associated lymphangitis or lymphadenopathy may be noted, and anaphylaxis has been reported. Similar to those of cockroaches, triatome antigens have been associated with atopic dermatitis and asthma.3
Chagas Disease Risk and Transmission
Triatomine reduviids are the primary vector of Chagas disease, and the geographic range of both continues to expand, particularly in North America. The disease remains endemic in Latin America, with the highest incidence now reported in Brazil.4 An estimated 240,000 to 350,000 individuals in the United States are infected, primarily immigrants from Mexico, Central America, and South America; approximately 30% of those infected will develop cardiac and/or gastrointestinal complications.4 If left untreated, Chagas disease leads to autonomic ganglion destruction and subsequent gastrointestinal and cardiac complications, including megacolon, dilated cardiomyopathy, and heart failure.5
Trypanosoma cruzi, the microorganism responsible for Chagas disease, is spread to humans through triatomine fecal matter scratched into the bite wound.6 Triatomine bugs have a highly developed gastrocolic reflex and defecate liberally as they feed. Fecal volume is heavily dependent on species and sex, with fifth-stage female nymphs producing the highest volume of excrement and thereby acting as particularly adept disease vectors.6 Triatoma infestans and members of the genus Mepraia are key vectors of T cruzi.1 In areas of South America where populations of T infestans are controlled through public health measures, Mepraia emerge as a largely uncontrolled disease vector.1,7 While endemic to the southern United States and South America, T cruzi has spread to much of North America and Europe by way of Triatominae as naturalized or invasive species.8
There are 3 phases of Chagas disease: acute, indeterminate, and chronic. A chagoma is a localized erythematous swelling at the site of the bite. The acute phase often lacks systemic symptoms but may include fever, myalgia, and headache. The intermediate phase may include fatigue and recurrent fevers. The most serious manifestations occur in the chronic phase and include cardiomyopathy with signs of congestive heart failure, irregular heartbeat, cardiac arrest, abdominal pain, constipation, and dysphagia.
Deforestation has been identified as a driving factor in the spread of Chagas disease, as the disease vectors shift from wilderness areas and animal hosts to inhabited areas where humans are the most readily available food source. Triatome bugs in areas experiencing higher levels of development or forest harvesting are forced into human-populated areas. As a result, instances of Chagas disease are on the rise in these communities.7 Salvador, Bahia, Brazil, has been identified as one such target of increased vector presence due to heavy deforestation, and the hottest months were identified as having the greatest threat of vector exposure.9 Brazil became the leading geographic area for the disease partly because of heavy loss of forested land.10
Vector Control and Prevention Strategies
Elimination of cracks and crevices in walls; replacement of wattle and daub with stucco, plaster, and other solid building materials; and the use of insecticides with durability in the environment have been used to reduce triatome bug infestation in homes. However, highly persistent insecticides carry greater environmental risk and may drive resistance as declining concentrations select for resistant arthropods. Repellents have less environmental impact and play an important role in vector control. Citronella essential oil has been observed to repel several species of triatome bugs that are common in Arizona; specifically, the component alcohols geraniol and citronellol were found to be effective at inhibiting triatome feeding.11
Early detection of Chagas disease is essential, as end-stage cardiomyopathy and megacolon are difficult to treat. Newly developed multiantigen testing has shown promising results, suggesting a potential for more accurate testing for Chagas disease.8 Geospatial tracking and mapping of T cruzi vectors now are employed to track seasonal vector changes and disease patterns.9 Researchers also have developed a dedicated dichotomous key for the identification of triatome bugs endemic in Brazil with the hope of better identification and mapping of disease vector presence and density.10 The key consists of a series of statements with 2 choices in each step. It uses observable features of the arthropod to lead users to the correct identification.
Final Thoughts
Identification of triatome bugs can help with public health efforts to control the spread of disease. Patients with unilateral eyelid swelling should be evaluated for possible bedbug or triatome exposure.
Triatome bugs cause painful bites and serve as vectors for Chagas disease. In this article, we will address diagnosis and vector identification.
Key Morphologic Features
Insects from the subfamily Triatominae are identifiable by their long legs and a shieldlike abdomen behind a platelike pronotum that covers the thorax. Their half-membranous wings overlap, covering the central abdomen but leaving the lateral portions visible. Tigerlike stripes are characteristically prominent on the visible portions of the lateral abdomen. The stalklike head has an articulated beaklike mouth that can be retracted and used to deliver a powerful bite (Figure 1).
Feeding Mechanisms and Host Reactions
Triatome bugs are blood-feeding arthropods that hide in cracks and crevices in domestic structures by day and feed at night. They are shy feeders, and laboratory colonies have been known to die rather than feed in daylight. They are particularly common in thatched or wattle-and-daub dwellings, where they can be present in great numbers and descend on sleeping inhabitants at night. Triatome bugs require regular blood meals throughout the 5 developmental nymph stages in order to undergo successful molting.
In the wild, triatome bugs feed on a range of animals with little specificity, but in domestic settings they feed largely on humans. Thermosensors in the antennae help them locate blood vessels under the skin, which they penetrate easily due to their long mouthparts. Like other blood-sucking arthropods, they release an anticoagulant that facilitates continuous blood flow while feeding, which accounts for many of the cutaneous reactions observed after the host sustains a triatomine bite.1
Triatomine bugs have trouble feeding through clothing and seek out exposed skin, particularly the eyelids, producing the characteristic unilateral eyelid swelling known as the Romaña sign. Other bite reactions include purpura; macular erythema; and vesiculobullous, papular, and urticarial lesions (Figure 2).2 Associated lymphangitis or lymphadenopathy may be noted, and anaphylaxis has been reported. Similar to those of cockroaches, triatome antigens have been associated with atopic dermatitis and asthma.3
Chagas Disease Risk and Transmission
Triatomine reduviids are the primary vector of Chagas disease, and the geographic range of both continues to expand, particularly in North America. The disease remains endemic in Latin America, with the highest incidence now reported in Brazil.4 An estimated 240,000 to 350,000 individuals in the United States are infected, primarily immigrants from Mexico, Central America, and South America; approximately 30% of those infected will develop cardiac and/or gastrointestinal complications.4 If left untreated, Chagas disease leads to autonomic ganglion destruction and subsequent gastrointestinal and cardiac complications, including megacolon, dilated cardiomyopathy, and heart failure.5
Trypanosoma cruzi, the microorganism responsible for Chagas disease, is spread to humans through triatomine fecal matter scratched into the bite wound.6 Triatomine bugs have a highly developed gastrocolic reflex and defecate liberally as they feed. Fecal volume is heavily dependent on species and sex, with fifth-stage female nymphs producing the highest volume of excrement and thereby acting as particularly adept disease vectors.6 Triatoma infestans and members of the genus Mepraia are key vectors of T cruzi.1 In areas of South America where populations of T infestans are controlled through public health measures, Mepraia emerge as a largely uncontrolled disease vector.1,7 While endemic to the southern United States and South America, T cruzi has spread to much of North America and Europe by way of Triatominae as naturalized or invasive species.8
There are 3 phases of Chagas disease: acute, indeterminate, and chronic. A chagoma is a localized erythematous swelling at the site of the bite. The acute phase often lacks systemic symptoms but may include fever, myalgia, and headache. The intermediate phase may include fatigue and recurrent fevers. The most serious manifestations occur in the chronic phase and include cardiomyopathy with signs of congestive heart failure, irregular heartbeat, cardiac arrest, abdominal pain, constipation, and dysphagia.
Deforestation has been identified as a driving factor in the spread of Chagas disease, as the disease vectors shift from wilderness areas and animal hosts to inhabited areas where humans are the most readily available food source. Triatome bugs in areas experiencing higher levels of development or forest harvesting are forced into human-populated areas. As a result, instances of Chagas disease are on the rise in these communities.7 Salvador, Bahia, Brazil, has been identified as one such target of increased vector presence due to heavy deforestation, and the hottest months were identified as having the greatest threat of vector exposure.9 Brazil became the leading geographic area for the disease partly because of heavy loss of forested land.10
Vector Control and Prevention Strategies
Elimination of cracks and crevices in walls; replacement of wattle and daub with stucco, plaster, and other solid building materials; and the use of insecticides with durability in the environment have been used to reduce triatome bug infestation in homes. However, highly persistent insecticides carry greater environmental risk and may drive resistance as declining concentrations select for resistant arthropods. Repellents have less environmental impact and play an important role in vector control. Citronella essential oil has been observed to repel several species of triatome bugs that are common in Arizona; specifically, the component alcohols geraniol and citronellol were found to be effective at inhibiting triatome feeding.11
Early detection of Chagas disease is essential, as end-stage cardiomyopathy and megacolon are difficult to treat. Newly developed multiantigen testing has shown promising results, suggesting a potential for more accurate testing for Chagas disease.8 Geospatial tracking and mapping of T cruzi vectors now are employed to track seasonal vector changes and disease patterns.9 Researchers also have developed a dedicated dichotomous key for the identification of triatome bugs endemic in Brazil with the hope of better identification and mapping of disease vector presence and density.10 The key consists of a series of statements with 2 choices in each step. It uses observable features of the arthropod to lead users to the correct identification.
Final Thoughts
Identification of triatome bugs can help with public health efforts to control the spread of disease. Patients with unilateral eyelid swelling should be evaluated for possible bedbug or triatome exposure.
- Egaña C, Pinto R, Vergara F, et al. Fluctuations in Trypanosoma cruzi discrete typing unit composition in two naturally infected triatomines: Mepraia gajardoi and M. spinolai after laboratory feeding. Acta Trop. 2016;160:9-14. Erratum in: Acta Trop. 2016;162:248. doi:10.1016/j.actatropica.2016.04.008
- Moffitt JE, Venarske D, Goddard J, et al. Allergic reactions to Triatoma bites. Ann Allergy Asthma Immunol. 2003;91:122-128.
- Alonso A, Potenza M, Mouchián K, et al. Proteinase and gelatinolytic properties of a Triatoma infestans extract. Allergol Immunopathol (Madr). 2004;32:223-227.
- Hochberg NS, Montgomery SP. Chagas disease. Ann Intern Med. 2023;176:ITC17-ITC32. doi:10.7326/AITC202302210
- Pless M, Juranek D, Kozarsky P, et al. The epidemiology of Chagas’ disease in a hyperendemic area of Cochabamba, Bolivia: a clinical study including electrocardiography, seroreactivity to Trypanosoma cruzi, xenodiagnosis, and domiciliary triatomine distribution. Am J Trop Med Hyg. 1992;47:539-546.
- Piesman J, Sherlock IA. Factors controlling the volume of feces produced by triatomine vectors of Chagas’ disease. Acta Trop. 1983;40:351-358.
- Steverding D. The history of Chagas disease. Parasit Vectors. 2014;10:317.
- Granjon E, Dichtel-Danjoy ML, Saba E, et al. Development of a novel multiplex immunoassay multi-cruzi for the serological confirmation of Chagas disease. PLoS Negl Trop Dis. 2016;10:e0004596.
- Santana Kde S, Bavia ME, Lima AD, et al. Spatial distribution of triatomines (Reduviidae: Triatominae) in urban areas of the city of Salvador, Bahia, Brazil. Geospat Health. 2011;5:199-203.
- de Mello DV, Nhapulo EF, Cesaretto LP, et al. Dichotomous keys based on cytogenetic data for triatomines reported in Brazilian regions with outbreaks of orally transmitted Chagas disease (Pernambuco and Rio Grande Do Norte). Trop Med Infect Dis. 2023;8:196.
- Zamora D, Klotz SA, Meister EA, et al. Repellency of the components of the essential oil, citronella, to Triatoma rubida, Triatoma protracta, and Triatoma recurva (Hemiptera: Reduviidae: Triatominae). J Med Entomol. 2015;52:719-721.
- Egaña C, Pinto R, Vergara F, et al. Fluctuations in Trypanosoma cruzi discrete typing unit composition in two naturally infected triatomines: Mepraia gajardoi and M. spinolai after laboratory feeding. Acta Trop. 2016;160:9-14. Erratum in: Acta Trop. 2016;162:248. doi:10.1016/j.actatropica.2016.04.008
- Moffitt JE, Venarske D, Goddard J, et al. Allergic reactions to Triatoma bites. Ann Allergy Asthma Immunol. 2003;91:122-128.
- Alonso A, Potenza M, Mouchián K, et al. Proteinase and gelatinolytic properties of a Triatoma infestans extract. Allergol Immunopathol (Madr). 2004;32:223-227.
- Hochberg NS, Montgomery SP. Chagas disease. Ann Intern Med. 2023;176:ITC17-ITC32. doi:10.7326/AITC202302210
- Pless M, Juranek D, Kozarsky P, et al. The epidemiology of Chagas’ disease in a hyperendemic area of Cochabamba, Bolivia: a clinical study including electrocardiography, seroreactivity to Trypanosoma cruzi, xenodiagnosis, and domiciliary triatomine distribution. Am J Trop Med Hyg. 1992;47:539-546.
- Piesman J, Sherlock IA. Factors controlling the volume of feces produced by triatomine vectors of Chagas’ disease. Acta Trop. 1983;40:351-358.
- Steverding D. The history of Chagas disease. Parasit Vectors. 2014;10:317.
- Granjon E, Dichtel-Danjoy ML, Saba E, et al. Development of a novel multiplex immunoassay multi-cruzi for the serological confirmation of Chagas disease. PLoS Negl Trop Dis. 2016;10:e0004596.
- Santana Kde S, Bavia ME, Lima AD, et al. Spatial distribution of triatomines (Reduviidae: Triatominae) in urban areas of the city of Salvador, Bahia, Brazil. Geospat Health. 2011;5:199-203.
- de Mello DV, Nhapulo EF, Cesaretto LP, et al. Dichotomous keys based on cytogenetic data for triatomines reported in Brazilian regions with outbreaks of orally transmitted Chagas disease (Pernambuco and Rio Grande Do Norte). Trop Med Infect Dis. 2023;8:196.
- Zamora D, Klotz SA, Meister EA, et al. Repellency of the components of the essential oil, citronella, to Triatoma rubida, Triatoma protracta, and Triatoma recurva (Hemiptera: Reduviidae: Triatominae). J Med Entomol. 2015;52:719-721.
Cutaneous Reactions to Triatomine (Kissing Bug) Bites and the Risk for Chagas Disease
Cutaneous Reactions to Triatomine (Kissing Bug) Bites and the Risk for Chagas Disease
Practice Points
- Triatomine bugs, commonly known as kissing bugs, are widespread, especially in warmer climates, and their geographic range is expanding.
- The Romaña sign, characterized by unilateral swelling of the eyelid, is common in triatomine bites.
- Triatomine bugs are the primary vector for transmission of the parasite Trypanosoma cruzi, the causative agent of Chagas disease.
- In recent years, T cruzi has been detected in triatomine reduviids in suburban areas of the southwestern United States.

Pigmented Mass on the Shoulder
The Diagnosis: Pigmented Dermatofibrosarcoma Protuberans
Pigmented dermatofibrosarcoma protuberans (PDFSP), also known as Bednar tumor, is an uncommon variant of dermatofibrosarcoma protuberans (DFSP). Pigmented dermatofibrosarcoma protuberans constitutes 1% to 5% of all DFSP cases and most commonly is seen in nonwhite adults in the fourth decade of life, with occasional cases seen in pediatric patients, including some congenital cases. Typical sites of involvement include the shoulders, trunk, arms, legs, head, and neck.1,2 It also has been reported at sites of prior immunization, trauma, and insect bites.3
Histopathologic examination of our patient's shoulder nodule revealed an infiltrative neoplasm in the dermis and subcutaneous tissue composed of spindled cells with a storiform pattern and foci of scattered elongated dendritic pigmented cells. A narrow grenz zone separated the tumor from the epidermis, and characteristic honeycomb infiltration by tumor cells was noted in the subcutaneous fat. The nuclei were bland and monomorphous with areas of neuroid differentiation containing whorls and nerve cord-like structures (quiz image). The tumor cells were diffusely CD34 and vimentin positive, while S-100, SOX-10, neurofilament, smooth muscle actin, desmin, epithelial membrane antigen, and cytokeratins were negative. The immunophenotype excluded the possibility of neurogenic, pericytic, myofibroblastic, and myoid differentiation.
Wang and Yang4 previously reported a case of PDFSP with prominent meningothelial-like whorls focally resembling extracranial meningioma; however, the tumor cells were CD34 positive and epithelial membrane antigen negative, weighing against a diagnosis of meningioma. Most cases of PDFSP demonstrate the COL1A1-PDGFB (collagen type I α; 1/platelet-derived growth factor B-chain) fusion protein caused by the translocation t(17;22)(q22;q13), as in classic DFSP.5
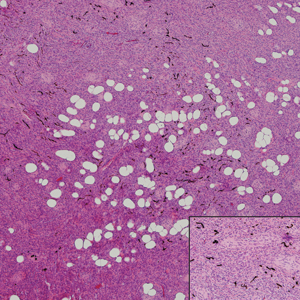
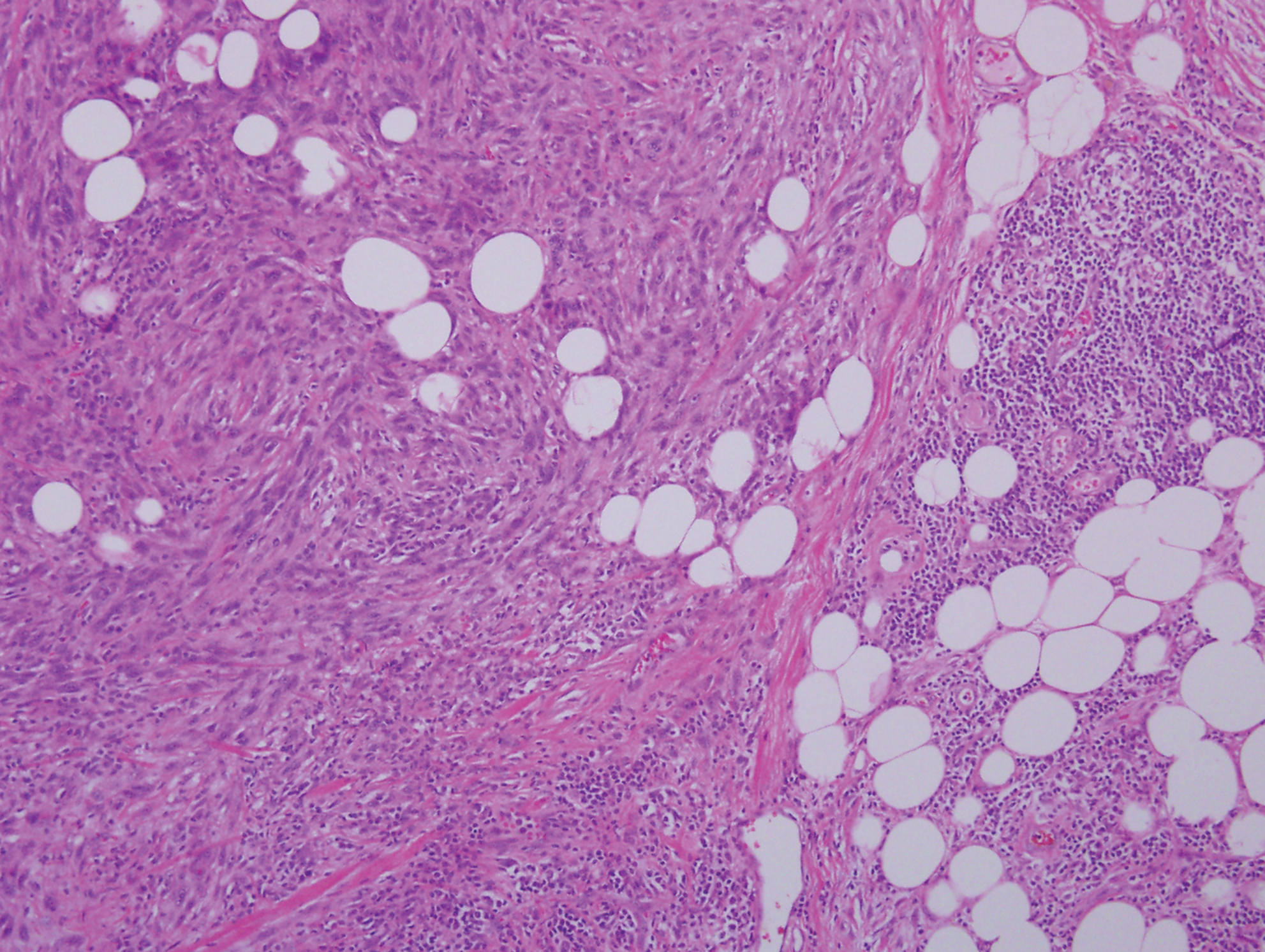
Cellular blue nevus (CBN) is a benign melanocytic neoplasm that can present at any age and often occurs on the buttocks and in the sacrococcygeal region. Clinically, CBN presents as a firm, bluish black to bluish gray, dome-shaped nodule. The size varies from a few millimeters to several centimeters.6,7 Histologically, CBN is located completely in the dermis, extending along the adnexae into the subcutaneous tissue with a dumbbell-shaped outline (Figure 1).6-8 The tumor demonstrates oval epithelioid melanocytes with vesicular nuclei and prominent nucleoli. Immunohistochemically, tumor cells stain positively for melanocytic markers such as S-100, SOX-10, MART-1, and human melanoma black 45. CD34 expression rarely is reported in a subset of CBN.9
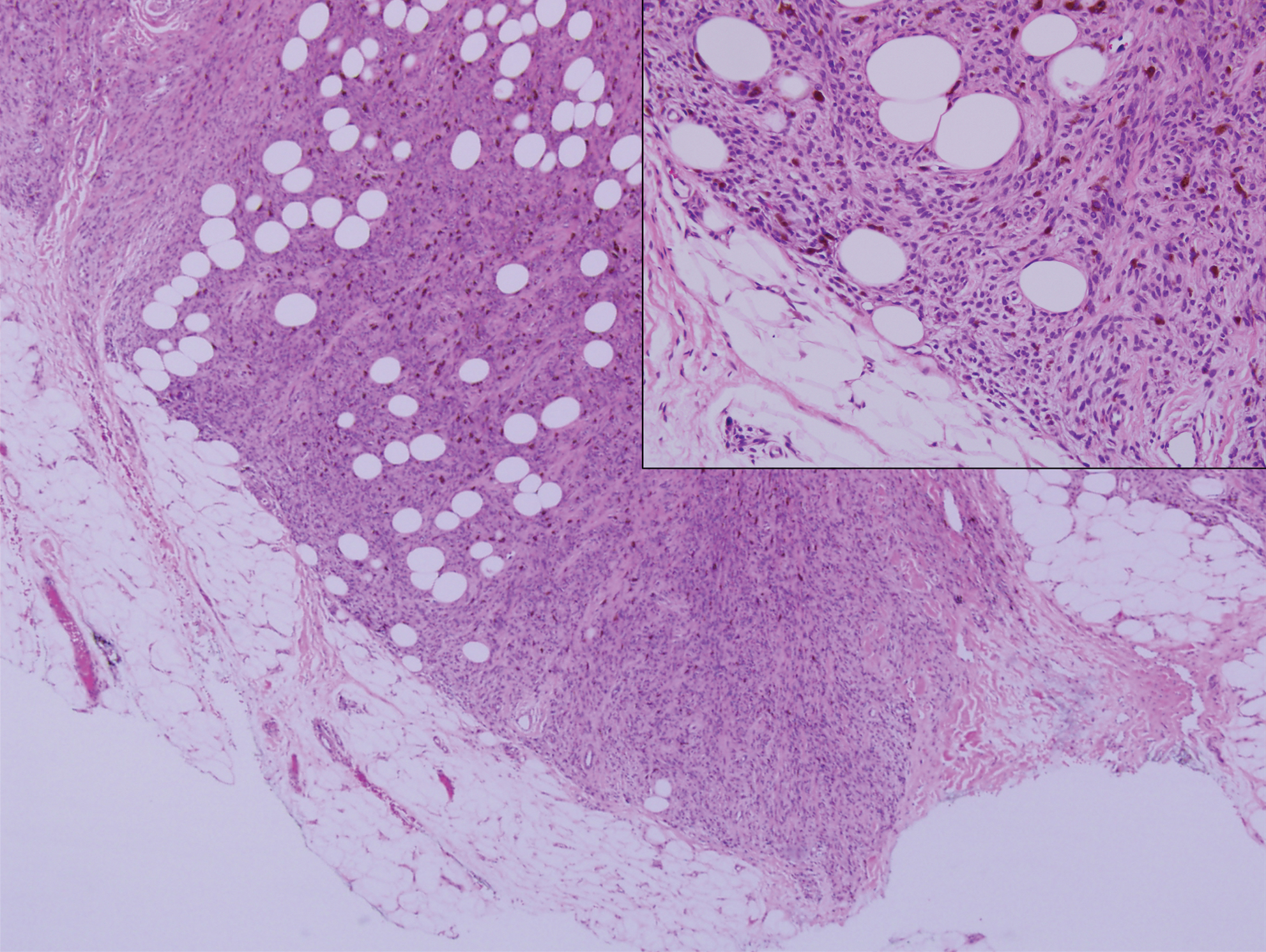
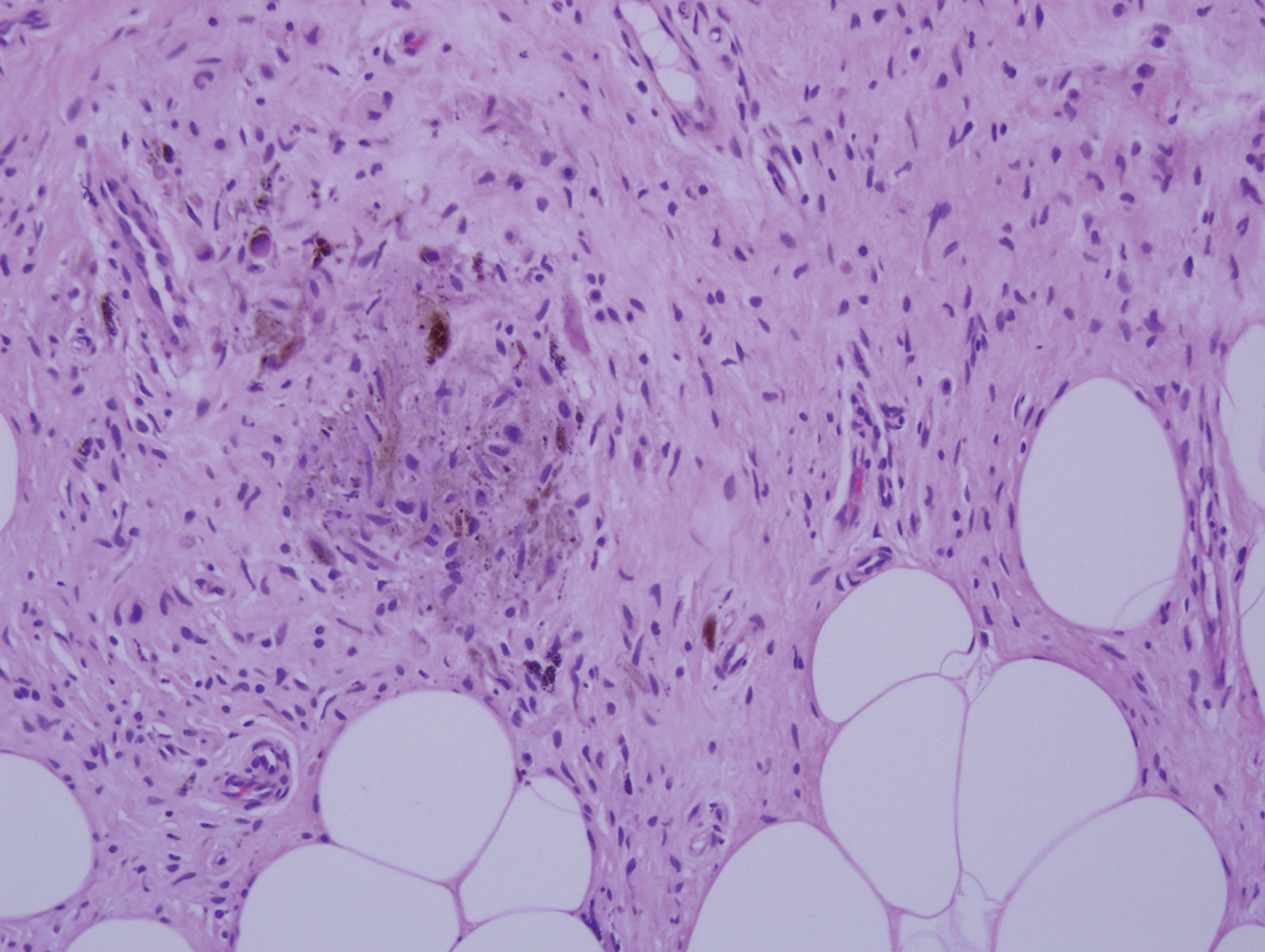
Pigmented neurofibroma is a rare variant of neurofibroma that produces melanin pigment and has a strong association with neurofibromatosis.10 It occurs most frequently in dark-skinned populations (Fitzpatrick skin types IV-VI). The most common location is the head and neck region.11,12 Histologically, pigmented neurofibroma resembles a diffuse neurofibroma admixed with melanin-producing cells (Figure 2).12 Immunostaining shows positivity for S-100 in both pigmented and Schwann cells; however, the pigmented cells stain positively for human melanoma black 45, Melan-A, and tyrosinase.10 CD34 can be fingerprint positive in neurofibroma, but a distinction from DFSP can be made by S-100 and SOX-10 immunostaining.13
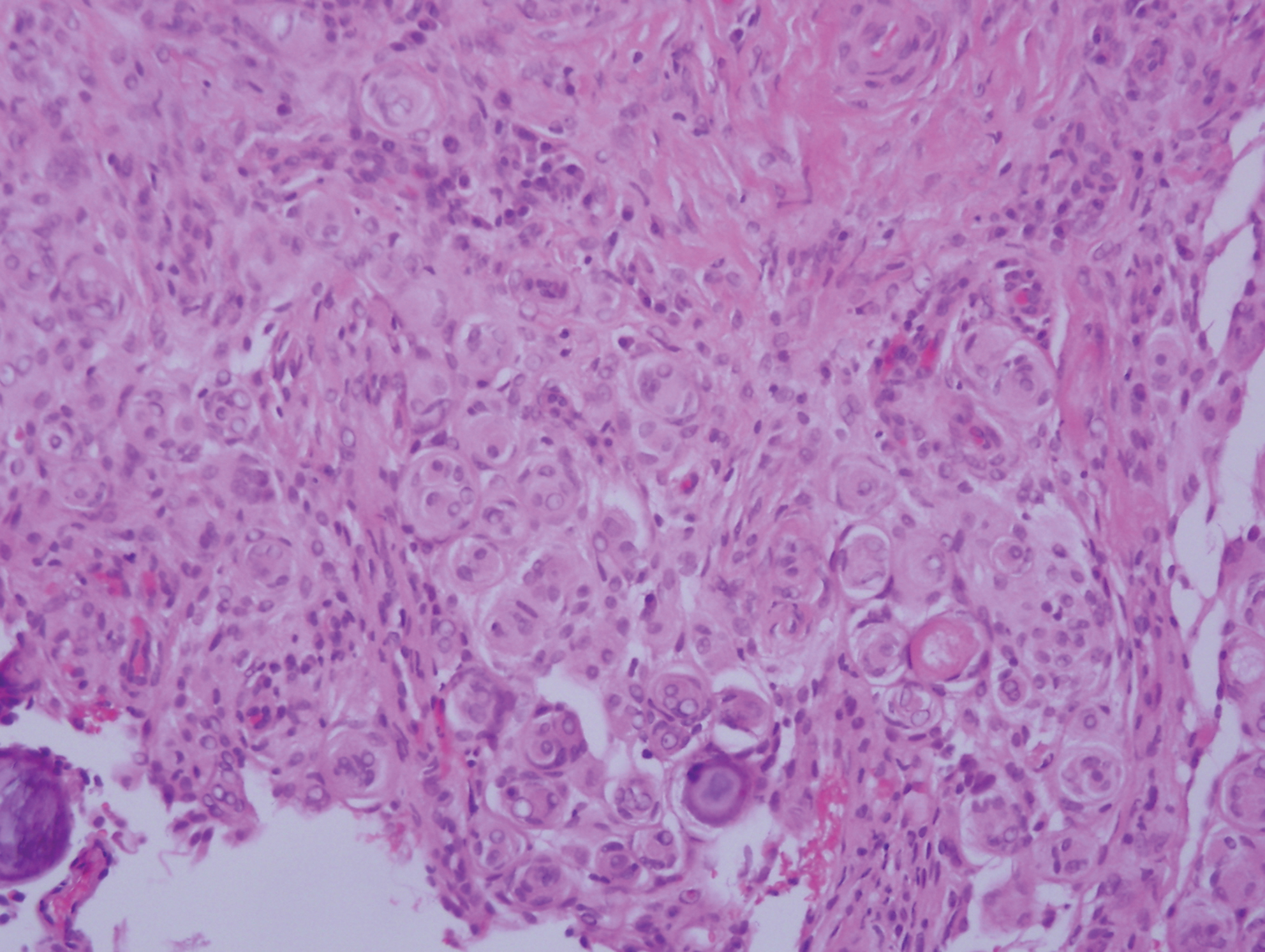
Desmoplastic melanoma (DM) is an uncommon variant of malignant melanoma and has a higher tendency for persistent local growth and less frequent metastases than other variants of melanoma. It has a predilection for chronically sun-exposed areas such as the head and neck and occurs later in life. Clinically, DM appears as nonspecific, often amelanotic nodules or plaques or as scarlike lesions.14 Histologically, DM can be classified as mixed or pure based on the degree of desmoplasia and cellularity. A paucicellular proliferation of malignant spindled melanocytes within a densely fibrotic stroma with lymphoid nodules in the dermis is characteristic (Figure 3); perineural involvement is common.14,15 The most reliable confirmative stains are S-100 and SOX-10.16
Cutaneous meningioma is a rare tumor and could be subtyped into 3 groups. Type I is primary cutaneous meningioma and usually is present at birth on the scalp and paravertebral regions with a relatively good prognosis. Type II is ectopic soft-tissue meningioma that extends into the skin from around the sensory organs on the face. Type III is local invasion or true metastasis from a central nervous system meningioma. Types II and III develop later in life and the prognosis is poor.17,18 Clinically, lesions present as firm subcutaneous nodules or swellings. Cutaneous meningioma has several histopathologic variants. The classic presentation reveals concentric wrapping of tumor cells with round-oval nuclei containing delicate chromatin. Psammoma bodies are a common finding (Figure 4). Immunohistochemically, tumor cells are diffusely positive for epithelial membrane antigen and vimentin.18,19
- Amonkar GP, Rupani A, Shah A, et al. Bednar tumor: an uncommon entity. Dermatopathology (Basel). 2016;3:36-38.
- El Hachem M, Diociaiuti A, Latella E, et al. Congenital myxoid and pigmented dermatofibrosarcoma protuberans: a case report. Pediatr Dermatol. 2013;30:E74-E77.
- Anon-Requena MJ, Pico-Valimana M, Munoz-Arias G. Bednar tumor (pigmented dermatofibrosarcoma protuberans). Actas Dermosifiliogr. 2016;107:618-620.
- Wang J, Yang W. Pigmented dermatofibrosarcoma protuberans with prominent meningothelial-like whorls. J Cutan Pathol. 2008;35(suppl 1):65-69.
- Zardawi IM, Kattampallil J, Rode J. An unusual pigmented skin tumour. Bednar tumour, dorsum of left foot (pigmented dermatofibrosarcoma protuberans). Pathology. 2004;36:358-361.
- Sugianto JZ, Ralston JS, Metcalf JS, et al. Blue nevus and "malignant blue nevus": a concise review. Semin Diagn Pathol. 2016;33:219-224.
- Zembowicz A. Blue nevi and related tumors. Clin Lab Med. 2017;37:401-415.
- Zembowicz A, Granter SR, McKee PH, et al. Amelanotic cellular blue nevus: a hypopigmented variant of the cellular blue nevus: clinicopathologic analysis of 20 cases. Am J Surg Pathol. 2002;26:1493-1500.
- Smith K, Germain M, Williams J, et al. CD34-positive cellular blue nevi. J Cutan Pathol. 2001;28:145-150.
- Inaba M, Yamamoto T, Minami R, et al. Pigmented neurofibroma: report of two cases and literature review. Pathol Int. 2001;51:565-569.
- Fetsch JF, Michal M, Miettinen M. Pigmented (melanotic) neurofibroma: a clinicopathologic and immunohistochemical analysis of 19 lesions from 17 patients. Am J Surg Pathol. 2000;24:331-343.
- Motoi T, Ishida T, Kawato A, et al. Pigmented neurofibroma: review of Japanese patients with an analysis of melanogenesis demonstrating coexpression of c-met protooncogene and microphthalmia-associated transcription factor. Hum Pathol. 2005;36:871-877.
- Yeh I, McCalmont TH. Distinguishing neurofibroma from desmoplastic melanoma: the value of the CD34 fingerprint. J Cutan Pathol. 2011;38:625-630.
- Chen LL, Jaimes N, Barker CA, et al. Desmoplastic melanoma: a review. J Am Acad Dermatol. 2013;68:825-833.
- Busam KJ. Desmoplastic melanoma. Clin Lab Med. 2011;31:321-330.
- Schleich C, Ferringer T. Desmoplastic melanoma. Cutis. 2015;96:306, 313-314, 335.
- Lopez DA, Silvers DN, Helwig EB. Cutaneous meningiomas--a clinicopathologic study. Cancer. 1974;34:728-744.
- Miedema JR, Zedek D. Cutaneous meningioma. Arch Pathol Lab Med. 2012;136:208-211.
- Bhanusali DG, Heath C, Gur D, et al. Metastatic meningioma of the scalp. Cutis. 2018;101:386-389.
The Diagnosis: Pigmented Dermatofibrosarcoma Protuberans
Pigmented dermatofibrosarcoma protuberans (PDFSP), also known as Bednar tumor, is an uncommon variant of dermatofibrosarcoma protuberans (DFSP). Pigmented dermatofibrosarcoma protuberans constitutes 1% to 5% of all DFSP cases and most commonly is seen in nonwhite adults in the fourth decade of life, with occasional cases seen in pediatric patients, including some congenital cases. Typical sites of involvement include the shoulders, trunk, arms, legs, head, and neck.1,2 It also has been reported at sites of prior immunization, trauma, and insect bites.3
Histopathologic examination of our patient's shoulder nodule revealed an infiltrative neoplasm in the dermis and subcutaneous tissue composed of spindled cells with a storiform pattern and foci of scattered elongated dendritic pigmented cells. A narrow grenz zone separated the tumor from the epidermis, and characteristic honeycomb infiltration by tumor cells was noted in the subcutaneous fat. The nuclei were bland and monomorphous with areas of neuroid differentiation containing whorls and nerve cord-like structures (quiz image). The tumor cells were diffusely CD34 and vimentin positive, while S-100, SOX-10, neurofilament, smooth muscle actin, desmin, epithelial membrane antigen, and cytokeratins were negative. The immunophenotype excluded the possibility of neurogenic, pericytic, myofibroblastic, and myoid differentiation.
Wang and Yang4 previously reported a case of PDFSP with prominent meningothelial-like whorls focally resembling extracranial meningioma; however, the tumor cells were CD34 positive and epithelial membrane antigen negative, weighing against a diagnosis of meningioma. Most cases of PDFSP demonstrate the COL1A1-PDGFB (collagen type I α; 1/platelet-derived growth factor B-chain) fusion protein caused by the translocation t(17;22)(q22;q13), as in classic DFSP.5
Cellular blue nevus (CBN) is a benign melanocytic neoplasm that can present at any age and often occurs on the buttocks and in the sacrococcygeal region. Clinically, CBN presents as a firm, bluish black to bluish gray, dome-shaped nodule. The size varies from a few millimeters to several centimeters.6,7 Histologically, CBN is located completely in the dermis, extending along the adnexae into the subcutaneous tissue with a dumbbell-shaped outline (Figure 1).6-8 The tumor demonstrates oval epithelioid melanocytes with vesicular nuclei and prominent nucleoli. Immunohistochemically, tumor cells stain positively for melanocytic markers such as S-100, SOX-10, MART-1, and human melanoma black 45. CD34 expression rarely is reported in a subset of CBN.9
Pigmented neurofibroma is a rare variant of neurofibroma that produces melanin pigment and has a strong association with neurofibromatosis.10 It occurs most frequently in dark-skinned populations (Fitzpatrick skin types IV-VI). The most common location is the head and neck region.11,12 Histologically, pigmented neurofibroma resembles a diffuse neurofibroma admixed with melanin-producing cells (Figure 2).12 Immunostaining shows positivity for S-100 in both pigmented and Schwann cells; however, the pigmented cells stain positively for human melanoma black 45, Melan-A, and tyrosinase.10 CD34 can be fingerprint positive in neurofibroma, but a distinction from DFSP can be made by S-100 and SOX-10 immunostaining.13
Desmoplastic melanoma (DM) is an uncommon variant of malignant melanoma and has a higher tendency for persistent local growth and less frequent metastases than other variants of melanoma. It has a predilection for chronically sun-exposed areas such as the head and neck and occurs later in life. Clinically, DM appears as nonspecific, often amelanotic nodules or plaques or as scarlike lesions.14 Histologically, DM can be classified as mixed or pure based on the degree of desmoplasia and cellularity. A paucicellular proliferation of malignant spindled melanocytes within a densely fibrotic stroma with lymphoid nodules in the dermis is characteristic (Figure 3); perineural involvement is common.14,15 The most reliable confirmative stains are S-100 and SOX-10.16
Cutaneous meningioma is a rare tumor and could be subtyped into 3 groups. Type I is primary cutaneous meningioma and usually is present at birth on the scalp and paravertebral regions with a relatively good prognosis. Type II is ectopic soft-tissue meningioma that extends into the skin from around the sensory organs on the face. Type III is local invasion or true metastasis from a central nervous system meningioma. Types II and III develop later in life and the prognosis is poor.17,18 Clinically, lesions present as firm subcutaneous nodules or swellings. Cutaneous meningioma has several histopathologic variants. The classic presentation reveals concentric wrapping of tumor cells with round-oval nuclei containing delicate chromatin. Psammoma bodies are a common finding (Figure 4). Immunohistochemically, tumor cells are diffusely positive for epithelial membrane antigen and vimentin.18,19
The Diagnosis: Pigmented Dermatofibrosarcoma Protuberans
Pigmented dermatofibrosarcoma protuberans (PDFSP), also known as Bednar tumor, is an uncommon variant of dermatofibrosarcoma protuberans (DFSP). Pigmented dermatofibrosarcoma protuberans constitutes 1% to 5% of all DFSP cases and most commonly is seen in nonwhite adults in the fourth decade of life, with occasional cases seen in pediatric patients, including some congenital cases. Typical sites of involvement include the shoulders, trunk, arms, legs, head, and neck.1,2 It also has been reported at sites of prior immunization, trauma, and insect bites.3
Histopathologic examination of our patient's shoulder nodule revealed an infiltrative neoplasm in the dermis and subcutaneous tissue composed of spindled cells with a storiform pattern and foci of scattered elongated dendritic pigmented cells. A narrow grenz zone separated the tumor from the epidermis, and characteristic honeycomb infiltration by tumor cells was noted in the subcutaneous fat. The nuclei were bland and monomorphous with areas of neuroid differentiation containing whorls and nerve cord-like structures (quiz image). The tumor cells were diffusely CD34 and vimentin positive, while S-100, SOX-10, neurofilament, smooth muscle actin, desmin, epithelial membrane antigen, and cytokeratins were negative. The immunophenotype excluded the possibility of neurogenic, pericytic, myofibroblastic, and myoid differentiation.
Wang and Yang4 previously reported a case of PDFSP with prominent meningothelial-like whorls focally resembling extracranial meningioma; however, the tumor cells were CD34 positive and epithelial membrane antigen negative, weighing against a diagnosis of meningioma. Most cases of PDFSP demonstrate the COL1A1-PDGFB (collagen type I α; 1/platelet-derived growth factor B-chain) fusion protein caused by the translocation t(17;22)(q22;q13), as in classic DFSP.5
Cellular blue nevus (CBN) is a benign melanocytic neoplasm that can present at any age and often occurs on the buttocks and in the sacrococcygeal region. Clinically, CBN presents as a firm, bluish black to bluish gray, dome-shaped nodule. The size varies from a few millimeters to several centimeters.6,7 Histologically, CBN is located completely in the dermis, extending along the adnexae into the subcutaneous tissue with a dumbbell-shaped outline (Figure 1).6-8 The tumor demonstrates oval epithelioid melanocytes with vesicular nuclei and prominent nucleoli. Immunohistochemically, tumor cells stain positively for melanocytic markers such as S-100, SOX-10, MART-1, and human melanoma black 45. CD34 expression rarely is reported in a subset of CBN.9
Pigmented neurofibroma is a rare variant of neurofibroma that produces melanin pigment and has a strong association with neurofibromatosis.10 It occurs most frequently in dark-skinned populations (Fitzpatrick skin types IV-VI). The most common location is the head and neck region.11,12 Histologically, pigmented neurofibroma resembles a diffuse neurofibroma admixed with melanin-producing cells (Figure 2).12 Immunostaining shows positivity for S-100 in both pigmented and Schwann cells; however, the pigmented cells stain positively for human melanoma black 45, Melan-A, and tyrosinase.10 CD34 can be fingerprint positive in neurofibroma, but a distinction from DFSP can be made by S-100 and SOX-10 immunostaining.13
Desmoplastic melanoma (DM) is an uncommon variant of malignant melanoma and has a higher tendency for persistent local growth and less frequent metastases than other variants of melanoma. It has a predilection for chronically sun-exposed areas such as the head and neck and occurs later in life. Clinically, DM appears as nonspecific, often amelanotic nodules or plaques or as scarlike lesions.14 Histologically, DM can be classified as mixed or pure based on the degree of desmoplasia and cellularity. A paucicellular proliferation of malignant spindled melanocytes within a densely fibrotic stroma with lymphoid nodules in the dermis is characteristic (Figure 3); perineural involvement is common.14,15 The most reliable confirmative stains are S-100 and SOX-10.16
Cutaneous meningioma is a rare tumor and could be subtyped into 3 groups. Type I is primary cutaneous meningioma and usually is present at birth on the scalp and paravertebral regions with a relatively good prognosis. Type II is ectopic soft-tissue meningioma that extends into the skin from around the sensory organs on the face. Type III is local invasion or true metastasis from a central nervous system meningioma. Types II and III develop later in life and the prognosis is poor.17,18 Clinically, lesions present as firm subcutaneous nodules or swellings. Cutaneous meningioma has several histopathologic variants. The classic presentation reveals concentric wrapping of tumor cells with round-oval nuclei containing delicate chromatin. Psammoma bodies are a common finding (Figure 4). Immunohistochemically, tumor cells are diffusely positive for epithelial membrane antigen and vimentin.18,19
- Amonkar GP, Rupani A, Shah A, et al. Bednar tumor: an uncommon entity. Dermatopathology (Basel). 2016;3:36-38.
- El Hachem M, Diociaiuti A, Latella E, et al. Congenital myxoid and pigmented dermatofibrosarcoma protuberans: a case report. Pediatr Dermatol. 2013;30:E74-E77.
- Anon-Requena MJ, Pico-Valimana M, Munoz-Arias G. Bednar tumor (pigmented dermatofibrosarcoma protuberans). Actas Dermosifiliogr. 2016;107:618-620.
- Wang J, Yang W. Pigmented dermatofibrosarcoma protuberans with prominent meningothelial-like whorls. J Cutan Pathol. 2008;35(suppl 1):65-69.
- Zardawi IM, Kattampallil J, Rode J. An unusual pigmented skin tumour. Bednar tumour, dorsum of left foot (pigmented dermatofibrosarcoma protuberans). Pathology. 2004;36:358-361.
- Sugianto JZ, Ralston JS, Metcalf JS, et al. Blue nevus and "malignant blue nevus": a concise review. Semin Diagn Pathol. 2016;33:219-224.
- Zembowicz A. Blue nevi and related tumors. Clin Lab Med. 2017;37:401-415.
- Zembowicz A, Granter SR, McKee PH, et al. Amelanotic cellular blue nevus: a hypopigmented variant of the cellular blue nevus: clinicopathologic analysis of 20 cases. Am J Surg Pathol. 2002;26:1493-1500.
- Smith K, Germain M, Williams J, et al. CD34-positive cellular blue nevi. J Cutan Pathol. 2001;28:145-150.
- Inaba M, Yamamoto T, Minami R, et al. Pigmented neurofibroma: report of two cases and literature review. Pathol Int. 2001;51:565-569.
- Fetsch JF, Michal M, Miettinen M. Pigmented (melanotic) neurofibroma: a clinicopathologic and immunohistochemical analysis of 19 lesions from 17 patients. Am J Surg Pathol. 2000;24:331-343.
- Motoi T, Ishida T, Kawato A, et al. Pigmented neurofibroma: review of Japanese patients with an analysis of melanogenesis demonstrating coexpression of c-met protooncogene and microphthalmia-associated transcription factor. Hum Pathol. 2005;36:871-877.
- Yeh I, McCalmont TH. Distinguishing neurofibroma from desmoplastic melanoma: the value of the CD34 fingerprint. J Cutan Pathol. 2011;38:625-630.
- Chen LL, Jaimes N, Barker CA, et al. Desmoplastic melanoma: a review. J Am Acad Dermatol. 2013;68:825-833.
- Busam KJ. Desmoplastic melanoma. Clin Lab Med. 2011;31:321-330.
- Schleich C, Ferringer T. Desmoplastic melanoma. Cutis. 2015;96:306, 313-314, 335.
- Lopez DA, Silvers DN, Helwig EB. Cutaneous meningiomas--a clinicopathologic study. Cancer. 1974;34:728-744.
- Miedema JR, Zedek D. Cutaneous meningioma. Arch Pathol Lab Med. 2012;136:208-211.
- Bhanusali DG, Heath C, Gur D, et al. Metastatic meningioma of the scalp. Cutis. 2018;101:386-389.
- Amonkar GP, Rupani A, Shah A, et al. Bednar tumor: an uncommon entity. Dermatopathology (Basel). 2016;3:36-38.
- El Hachem M, Diociaiuti A, Latella E, et al. Congenital myxoid and pigmented dermatofibrosarcoma protuberans: a case report. Pediatr Dermatol. 2013;30:E74-E77.
- Anon-Requena MJ, Pico-Valimana M, Munoz-Arias G. Bednar tumor (pigmented dermatofibrosarcoma protuberans). Actas Dermosifiliogr. 2016;107:618-620.
- Wang J, Yang W. Pigmented dermatofibrosarcoma protuberans with prominent meningothelial-like whorls. J Cutan Pathol. 2008;35(suppl 1):65-69.
- Zardawi IM, Kattampallil J, Rode J. An unusual pigmented skin tumour. Bednar tumour, dorsum of left foot (pigmented dermatofibrosarcoma protuberans). Pathology. 2004;36:358-361.
- Sugianto JZ, Ralston JS, Metcalf JS, et al. Blue nevus and "malignant blue nevus": a concise review. Semin Diagn Pathol. 2016;33:219-224.
- Zembowicz A. Blue nevi and related tumors. Clin Lab Med. 2017;37:401-415.
- Zembowicz A, Granter SR, McKee PH, et al. Amelanotic cellular blue nevus: a hypopigmented variant of the cellular blue nevus: clinicopathologic analysis of 20 cases. Am J Surg Pathol. 2002;26:1493-1500.
- Smith K, Germain M, Williams J, et al. CD34-positive cellular blue nevi. J Cutan Pathol. 2001;28:145-150.
- Inaba M, Yamamoto T, Minami R, et al. Pigmented neurofibroma: report of two cases and literature review. Pathol Int. 2001;51:565-569.
- Fetsch JF, Michal M, Miettinen M. Pigmented (melanotic) neurofibroma: a clinicopathologic and immunohistochemical analysis of 19 lesions from 17 patients. Am J Surg Pathol. 2000;24:331-343.
- Motoi T, Ishida T, Kawato A, et al. Pigmented neurofibroma: review of Japanese patients with an analysis of melanogenesis demonstrating coexpression of c-met protooncogene and microphthalmia-associated transcription factor. Hum Pathol. 2005;36:871-877.
- Yeh I, McCalmont TH. Distinguishing neurofibroma from desmoplastic melanoma: the value of the CD34 fingerprint. J Cutan Pathol. 2011;38:625-630.
- Chen LL, Jaimes N, Barker CA, et al. Desmoplastic melanoma: a review. J Am Acad Dermatol. 2013;68:825-833.
- Busam KJ. Desmoplastic melanoma. Clin Lab Med. 2011;31:321-330.
- Schleich C, Ferringer T. Desmoplastic melanoma. Cutis. 2015;96:306, 313-314, 335.
- Lopez DA, Silvers DN, Helwig EB. Cutaneous meningiomas--a clinicopathologic study. Cancer. 1974;34:728-744.
- Miedema JR, Zedek D. Cutaneous meningioma. Arch Pathol Lab Med. 2012;136:208-211.
- Bhanusali DG, Heath C, Gur D, et al. Metastatic meningioma of the scalp. Cutis. 2018;101:386-389.

A 37-year-old woman presented with an asymptomatic, indurated, pigmented, subcutaneous nodule on the right shoulder of more than 3 years' duration. The lesion had gradually increased in size with no associated symptoms. The patient had a history of endometrial adenocarcinoma and papillary thyroid carcinoma, which had been treated by hysterectomy-oophorectomy and right thyroidectomy, respectively. She had no other notable systemic abnormalities, and there was no family history of genetic disease or cancer. Physical examination demonstrated a 1.2×1.8-cm nontender, pigmented, subcutaneous nodule with a rough surface and indistinct borders. An excisional biopsy was performed.