User login
Getting a Grip on Occupational Hand Dermatitis: Key Considerations for Evaluation and Management
Getting a Grip on Occupational Hand Dermatitis: Key Considerations for Evaluation and Management
Hand dermatitis (HD) is a common dermatologic concern that can impair quality of life, work productivity, and daily functioning.1 Occupational HD is defined as hand eczema caused or worsened by workplace exposures. When caused by work, HD may lead to reduced productivity and even job loss. Subtypes of HD include irritant contact dermatitis (ICD), allergic contact dermatitis (ACD), protein contact dermatitis (PCD), atopic dermatitis (AD), hyperkeratotic HD, and dyshidrotic eczema.2,3
Often caused by wet work, ICD is the most common subtype, whereas PCD—which is caused by immediate hypersensitivity to protein—is less common and usually seen in food service workers.3,4 When HD does not improve with standard treatment, particularly in occupational cases, patch testing is prudent to evaluate for contact allergens. In this article, we review practical considerations for evaluation and management of occupational irritant and allergic HD, highlighting relevant exposures and pearls on workup and management.
Epidemiology of Hand Dermatitis
A 2021 systematic review and meta-analysis of European studies reported a 1-year HD prevalence of 9.1% and a lifetime prevalence of 14.5%.5 Hand dermatitis is most common in women; individuals aged 30 to 39 years; and those who are employed, underscoring the role of workplace exposure.6 High-risk occupations are those involving substantial wet work, such as hairdressers, beauticians, cleaners, and health care and construction workers.7 Individuals with a history of AD also are at high risk for HD.8
Hand Dermatitis Subtypes
Irritant Contact Dermatitis—Irritant contact dermatitis, the most common form of occupational HD, is caused by repeated exposure to irritants (eg, water, detergents, cleansers, and soaps) that disrupt the skin barrier.9 Occupations that involve wet work are a major risk factor, associated with a 56% higher likelihood of ICD.8 Wet work involves frequent handwashing, prolonged contact with liquids, or occlusive glove use.9 As a ubiquitous skin irritant, water can penetrate the stratum corneum, impair the skin barrier, and increase sensitization risk. The dorsal hands usually are affected by ICD due to the thinner stratum corneum in this area.9
Allergic Contact Dermatitis—Allergic contact dermatitis should be considered in cases of chronic, recurrent, or treatment-resistant disease. Clinical clues include dermatitis beyond irritant contact sites, recurrent pruritic and vesicular HD, and flares with occupational exposures or materials; however, it can be difficult to distinguish ACD from ICD on clinical presentation alone, as they have many overlapping features. When ACD is suspected, patch testing remains the gold standard for identifying allergens and guiding avoidance strategies, product alternatives, and workplace modifications.
Unique Occupational Considerations
Hairdressers—Hairdressers have an increased risk for HD due to wet work and exposure to sensitizers, with a pooled lifetime prevalence of 38.2% (including ICD, ACD, and occupational cases).10 Notably, frequent shampooing, rinsing, cutting wet hair, handwashing, and glove use increase the risk for ICD. Hairdressers also are exposed to allergens in hair products, including p-phenylenediamine, toluene-2,5-diamine, persulfate salts, glyceryl thioglycolate, preservatives, and fragrances. Occupational exposure to the preservative methylisothiazolinone is high among hairdressers, with a sensitization rate of 10.5% in HD cases.11
It has been reported that hyperkeratotic fissured eczema of the dorsal hands caused by wet work often indicates ICD, whereas pruritic dyshidrotic eczema involving the lateral fingers or palms suggests ACD; however, these conditions can share overlapping features.7 If ACD is suspected, broad patch testing with baseline and hairdresser series, along with specific chemicals that may be encountered in the workplace, is necessary. Management includes allergen avoidance, reduced wet work tasks, use of nitrile gloves with glove changes to mitigate occlusive effects, and skin barrier protection with emollients.
Health Care Workers—Health care workers are vulnerable to HD due to intensive hand hygiene, prolonged glove use, and allergen exposures, with a lifetime prevalence of self-reported HD of 33.4%.12 Common allergens among health care workers include rubber accelerators, most often from rubber gloves.13 Frequent handwashing and glove use can further impair the skin barrier, increasing irritant and sensitization risks.14 In contrast, alcohol-based hand sanitizers containing emollients are less irritating, with prior analyses showing no significant association with HD risk.15,16 Conversely, handwashing 8 to 10 times daily increased HD risk, with a relative risk of 1.51.15
Surgeons and proceduralists face unique risks for HD from preoperative scrubbing with products that can contain potential allergens such as chlorhexidine gluconate, chloroxylenol, povidone-iodine, fragrance, cocamide diethanolamine, lanolin, alkyl glucosides, sodium benzoate, sorbic acid, tocopherol, and propylene glycol.17,18 Subsequent occlusion under glove layers drives ICD and ACD risks, highlighting the importance of patch testing in affected individuals. While patch testing, exposure avoidance, and limited glove use can mitigate HD risk, frequent handwashing can contribute to refractory HD.
Food Service Workers—Food service workers have an increased risk for HD from allergens and irritants. In a retrospective study of patients with occupational food-related HD (N=372), 57% were diagnosed with ICD, 22% with PCD, and 1.8% with ACD.19 Skin barrier disruption from wet work, occlusion from glove use, and contact with food proteins increase HD risk, especially in bakers exposed to flours and grains, which can cause IgE–mediated PCD manifesting with contact urticaria. Protein contact dermatitis is confirmed by prick testing with suspected foods.20 Additionally, exposure to garlic can cause ICD and ACD due to sulfur-containing compounds, particularly allicin and diallyl disulfide.21,22 Pineapple also can trigger ICD associated with bromelain, a proteolytic enzyme that can break down the skin.23 Nickel exposure is another concern, as steel utensils and cookware can release nickel onto the skin of sensitized individuals.24 Rubber accelerator exposure from gloves also contributes to contact allergy and HD among food service workers; vinyl gloves usually are a good alternative in this setting.25 Management of food-related HD involves exposure avoidance, which may affect occupational viability
Construction Workers—Construction workers are at risk for occupational HD due to contact with irritants and sensitizers such as paints, adhesives, asphalt, cement, solvents, and gloves.26 A retrospective analysis of North American Contact Dermatitis Group data identified HD in 37.2% (253/681) of patch-tested construction workers. The most common occupational allergens include potassium dichromate, which can be present in cement and leather items; bisphenol A epoxy resin; cobalt chloride hexahydrate; and the rubber accelerators carba mix and thiuram mix.26 A thorough occupational history should assess materials handled, and patch testing should include common construction-related allergens to inform avoidance strategies. Workplace task modification can reduce exposure, as certain managerial roles in construction work may involve less contact with irritants and sensitizers.26
Nail Technicians—Nail technicians are at risk for HD, especially ACD from acrylate monomers used in nail gels, dips, and acrylics. In a 10-year analysis, around 87.5% (14/16) of nail technicians with contact allergy to methacrylate demonstrated hand involvement.27 Common acrylate monomers include 2-hydroxyethyl methacrylate, 2-hydroxypropyl methacrylate, and ethyl cyanoacrylate. 28 Evaluation requires a detailed occupational history, assessing HD onset relative to exposure, services performed, glove-use practices, and whether symptoms improve away from work. While gloves may appear to reduce exposure, a glove-penetration study showed that acrylate-containing nail products can penetrate commonly used disposable gloves from within seconds to approximately 20 minutes, depending on glove and product type.29 Among available options, nitrile gloves may provide dexterity and allergen avoidance when acrylate exposure is brief, with glove changes required every 15 to 30 minutes.30 Patch testing with 2-hydroxyethyl methacrylate and ethyl cyanoacrylate can identify nail acrylate allergy; however, avoidance can be challenging for nail technicians, as these products often are ubiquitous in their work.
Florists—Florists can develop HD from plant allergens and irritants, particularly tulipalin A and calcium oxalate, with a lifetime prevalence of 19.6%.31 Tulipalin A is a well-documented sensitizer causing ACD among florists exposed to tulip bulbs and other Alstroemeria flowers.32 The term tulip fingers actually was coined to describe ACD caused by tulip bulbs in the European tulip industry.33 Patch testing involves testing for tulipalin A, which may be commercially limited, or tulip plant materials; however, fresh tulips require open testing with small amounts due to higher allergen concentration.32 Additionally, the term daffodil itch describes a type of ICD caused by calcium oxalate crystals in daffodil bulbs and tulip sap.32,34 Diagnosis of plant-related HD requires an occupational history and targeted patch testing, while glove protection and exposure avoidance are essential for improvement.
Evaluation and Management
The workup for HD involves physical examination and medical history, including disease onset, course, and history of AD, along with occupational and exposure history to identify allergens and irritants. Understanding the patient’s tasks and responsibilities and workplace practices along with the materials they handle allows the dermatologist to anticipate relevant allergens for patch testing.
Patch testing should be comprehensive, as baseline screening series alone may miss between 26.3% and 50% of occupationally relevant allergens.35,36 Comprehensive patch testing also should include specialty series and supplemental allergens based on the patient’s clinical history and exposures. Specialty series may include hairdressing, bakery, cosmetics, dental, machinists, and adhesives.37 Gloves also warrant attention, as they may be overlooked as a sensitizer following repeated contact and occlusion. In persistent HD associated with glove use, patch testing should include a rubber accelerator series with relevant allergens, such as thiurams, carbamates, mercaptobenzothiazole, diphenylguanidine, and the patient’s own gloves.38 Latex allergy also should be considered, particularly in immediate-type reactions, and can be evaluated with latex-specific IgE testing.39
Management of HD relies on accurate diagnosis and allergen avoidance, which can be challenging in occupational settings. Structured tools, such as the American Contact Dermatitis Society’s Contact Allergen Management Program (https://www.contactderm.org/ resources/acds-camp), can help identify safe alternatives.
In occupational HD, risk assessment should identify occupational exposures and determine appropriate personal protective equipment while minimizing the risk for HD associated with such equipment. Protective gloves are advised to prevent contact with allergens and irritants. When glove use lasts more than 10 minutes, cotton glove liners may be worn to avoid occlusion and moisture retention.40 For wet work, vinyl gloves are recommended, with regular emollient use to support skin-barrier repair. Overall, gloves should be used when possible, changed regularly, and worn for limited periods of time to prevent ICD.
Work modification may be required to reduce exposure and flares, including task reassignment or substitution of materials containing allergens and irritants. Occupational HD may necessitate workplace accommodations, disability evaluation, medical leave, or even permanent job change. Dermatologists play a crucial role in the medical determination of work relatedness and functional impairment, guiding patients through occupational health, disability, and workers’ compensation when warranted.
Treatments for Occupational HD
Treatment of occupational HD depends on disease severity, chronicity, and avoidance of allergens and irritants in ACD, ICD, and PCD. Foundational management includes regular emollient use, which can even serve as monotherapy in mild occupational HD.40 Corticosteroids are the cornerstone of topical therapy, while calcineurin inhibitors can be used as a steroid-sparing option in milder disease.41 Off-label topical calcipotriol and AD-approved therapies crisaborole and ruxolitinib may be effective. For refractory disease after topical treatments, phototherapy can be considered.40 Biologic and targeted therapies also have emerged as potential treatments. Dupilumab is effective for atopic chronic HD and has demonstrated promise for nonatopic chronic HD.42 Recently, delgocitinib, a topical pan–Janus kinase inhibitor cream, showed clinical efficacy for chronic hand eczema and was approved by the US Food and Drug Administration.43 Off-label use of alternative systemic therapies, including acitretin, cyclosporine, methotrexate, and azathioprine, and other biologics and systemic Janus kinase inhibitors also may treat HD, but larger studies are lacking.40
Our Final Interpretation
Occupational HD is a common skin condition with multiple etiologies. It is important for clinicians to gather a thorough occupational and exposure history to narrow the differential diagnosis, inform patch testing, and guide effective management. In practice, successful treatment depends on screening for and diagnosis of workplace exposures driving disease.
- Agner T, Andersen KE, Brandao FM, et al. Hand eczema severity and quality of life: a cross-sectional, multicentre study of hand eczema patients. Contact Dermatitis. 2008;59:43-47. doi:10.1111 /j.1600-0536.2008.01362.x
- Agner T, Aalto-Korte K, Andersen KE, et al. Classification of hand eczema. J Eur Acad Dermatol Venereol. 2015;29:2417-2422. doi:10.1111 /jdv.13308
- Bissonnette R, Agner T, Molin S, et al. Hand eczema—part 1: epidemiology, pathogenesis, diagnosis, and work-up. J Am Acad Dermatol. 2025;93:1201-1210. doi:10.1016/j.jaad.2024.09.048
- Barbaud A. Mechanism and diagnosis of protein contact dermatitis. Curr Opin Allergy Clin Immunol. 2020;20:117-121. doi:10.1097/ACI.0000000000000621
- Quaade AS, Simonsen AB, Halling AS, et al. Prevalence, incidence, and severity of hand eczema in the general population - a systematic review and meta-analysis. Contact Dermatitis. 2021;84:361-374. doi:10.1111/cod.13804
- Apfelbacher C, Bewley A, Molin S, et al. Prevalence of chronic hand eczema in adults: a cross-sectional survey of over 60 000 respondents from the general population of Canada, France, Germany, Italy, Spain and the UK. Br J Dermatol. 2025;192:1047-1054. doi:10.1093 /bjd/ljaf020
- Weidinger S, Novak N. Hand eczema. Lancet. 2024;404:2476-2486. doi:10.1016/S0140-6736(24)01810-5
- Schütte MG, Tamminga SJ, de Groene GJ, et al. Work-related and personal risk factors for occupational contact dermatitis: a systematic review of the literature with meta-analysis. Contact Dermatitis. 2023;88:171-187. doi:10.1111/cod.14253
- Behroozy A, Keegel TG. Wet-work exposure: a main risk factor for occupational hand dermatitis. Saf Health Work. 2014;5:175-180. doi:10.1016/j.shaw.2014.08.001
- Havmose MS, Kezic S, Uter W, et al. Prevalence and incidence of hand eczema in hairdressers-a systematic review and meta-analysis of the published literature from 2000-2021. Contact Dermatitis. 2022;86:254-265. doi:10.1111/cod.14048
- Uter W, Hallmann S, Gefeller O, et al. Contact allergy to ingredients of hair cosmetics in female hairdressers and female consumers—an update based on IVDK data 2013–2020. Contact Dermatitis. 2023;89:161-170. doi:10.1111/cod.14363
- Yüksel YT, Symanzik C, Christensen MO, et al. Prevalence and incidence of hand eczema in healthcare workers: a systematic review and meta-analysis. Contact Dermatitis. 2024;90:331-342. doi:10.1111 /cod.14489
- Warshaw EM, Schram SE, Maibach HI, et al. Occupation-related contact dermatitis in North American health care workers referred for patch testing: cross-sectional data, 1998 to 2004. Dermatitis. 2008;19:261-274. doi:10.2310/6620.2008.07059
- Hamnerius N, Svedman C, Bergendorff O, et al. Wet work exposure and hand eczema among healthcare workers: a cross-sectional study. Br J Dermatol. 2018;178:452-461. doi:10.1111 /bjd.15813
- Loh EDW, Yew YW. Hand hygiene and hand eczema: a systematic review and meta-analysis. Contact Dermatitis. 2022;87:303-314. doi:10.1111/cod.14133
- Lotfinejad N, Peters A, Tartari E, et al. Hand hygiene in health care: 20 years of ongoing advances and perspectives. Lancet Infect Dis. 2021;21:e209-e221. doi:10.1016/S1473-3099(21)00383-2
- Schlarbaum JP, Hylwa SA. Allergic contact dermatitis to operating room scrubs and disinfectants. Dermat Contact Atopic Occup Drug. 2019;30:363-370. doi:10.1097/DER.0000000000000525
- Rodriguez-Homs LG, Atwater AR. Allergens in medical hand skin cleansers. Dermat Contact Atopic Occup Drug. 2019;30:336-341. doi:10.1097/DER.0000000000000504
- Vester L, Thyssen JP, Menné T, et al. Occupational food-related hand dermatoses seen over a 10-year period. Contact Dermatitis. 2012;66:264-270. doi:10.1111/j.1600-0536.2011.02048.x
- Pesonen M, Koskela K, Aalto-Korte K. Contact urticaria and protein contact dermatitis in the Finnish Register of Occupational Diseases in a period of 12 years. Contact Dermatitis. 2020;83:1-7. doi:10.1111/cod.13547
- McFadden JP, White JML, Basketter DA, et al. Reduced allergy rates in atopic eczema to contact allergens used in both skin products and foods: atopy and the “hapten-atopy hypothesis.” Contact Dermatitis. 2008;58:156-158. doi:10.1111/j.1600-0536.2007.01291.x
- Kao SH, Hsu CH, Su SN, et al. Identification and immunologic characterization of an allergen, alliin lyase, from garlic (Allium sativum). J Allergy Clin Immunol. 2004;113:161-168. doi:10.1016/j.jaci.2003.10.040
- Reddy VB, Lerner EA. Plant cysteine proteases that evoke itch activate protease-activated receptors. Br J Dermatol. 2010;163:532-535. doi:10.1111/j.1365-2133.2010.09862.x
- Silverberg NB, Pelletier JL, Jacob SE, et al; Section on Dermatology, Section on Allergy and Immunology. Nickel allergic contact dermatitis: identification, treatment, and prevention. Pediatrics. 2020;145:e20200628. doi:10.1542/peds.2020-0628
- Clément A, Ferrier le Bouëdec MC, Crépy MN, et al. Hand eczema in glove-wearing patients. Contact Dermatitis. 2023;89:143-152. doi:10.1111/cod.14357
- Reeder MJ, Idrogo-Lam A, Aravamuthan SR, et al. Occupational contact dermatitis in construction workers: a retrospective analysis of the North American Contact Dermatitis Group Data, 2001-2020. Dermat Contact Atopic Occup Drug. 2024;35:467-475. doi:10.1089/derm.2024.0018
- Fisch A, Hamnerius N, Isaksson M. Dermatitis and occupational (meth)acrylate contact allergy in nail technicians-a 10-year study. Contact Dermatitis. 2019;81:58-60. doi:10.1111/cod.13216
- Atwater AR, Reeder M. Trends in nail services may cause dermatitis: not your mother’s nail polish. Cutis. 2019;103:315-317.
- Suuronen K, Ylinen K, Heikkilä J, et al. Acrylates in artificial nails— results of product analyses and glove penetration studies. Contact Dermatitis. 2024;90:266-272. doi:10.1111/cod.14474
- Morgado F, Batista M, Gonçalo M. Short exposures and glove protection against (meth)acrylates in nail beauticians-thoughts on a rising concern. Contact Dermatitis. 2019;81:62-63. doi:10.1111 /cod.13222
- Paulsen E, Søgaard J, Andersen KE. Occupational dermatitis in Danish gardeners and greenhouse workers (I). prevalence and possible risk factors. Contact Dermatitis. 1997;37:263-270. doi:10.1111/j.1600-0536.1997.tb02462.x
- Fonacier L, Bernstein DI, Pacheco K, et al. Contact dermatitis: a practice parameter–update 2015. J Allergy Clin Immunol Pract. 2015; 3(3 suppl):S1-S39. doi:10.1016/j.jaip.2015.02.009
- Gette MT, Marks JE. Tulip fingers. Arch Dermatol. 1990;126:203-205.
- Bruynzeel DP. Bulb dermatitis. Dermatological problems in the flower bulb industries. Contact Dermatitis. 1997;37:70-77. doi:10.1111/j.1600-0536.1997.tb00042.x
- Nettis E, Marcandrea M, Colanardi MC, et al. Results of standard series patch testing in patients with occupational allergic contact dermatitis. Allergy. 2003;58:1304-1307. doi:10.1046/j.1398-9995.2003.00346.x
- Saripalli YV, Achen F, Belsito DV. The detection of clinically relevant contact allergens using a standard screening tray of twenty-three allergens. J Am Acad Dermatol. 2003;49:65-69. doi:10.1067/mjd.2003.489
- Warshaw EM, Buonomo M, DeKoven JG, et al. Importance of supplemental patch testing beyond a screening series for patients with dermatitis: the North American Contact Dermatitis Group experience. JAMA Dermatol. 2021;157:1456-1465. doi:10.1001/jamadermatol.2021.4314
- Geier J, Lessmann H, Mahler V, et al. Occupational contact allergy caused by rubber gloves--nothing has changed. Contact Dermatitis. 2012;67:149-156. doi:10.1111/j.1600-0536.2012.02139.x
- Toraason M, Sussman G, Biagini R, et al. Latex allergy in the workplace. Toxicol Sci Off J Soc Toxicol. 2000;58:5-14. doi:10.1093/toxsci/58.1.5
- Bissonnette R, Agner T, Taylor JS, et al. Hand eczema-part 2: prevention, management, and treatment. J Am Acad Dermatol. 2025;93:1213-1224. doi:10.1016/j.jaad.2024.09.049
- Schliemann S, Kelterer D, Bauer A, et al. Tacrolimus ointment in the treatment of occupationally induced chronic hand dermatitis. Contact Dermatitis. 2008;58:299-306. doi:10.1111/j.1600-0536.2007.01314.x
- Voorberg AN, Kamphuis E, Christoffers WA, et al. Efficacy and safety of dupilumab in patients with severe chronic hand eczema with inadequate response or intolerance to alitretinoin: a randomized, double-blind, placebo-controlled phase IIb proof-of-concept study. Br J Dermatol. 2023;189:400-409. doi:10.1093/bjd/ljad156
- Gooderham M, Molin S, Bissonnette R, et al. Long-term safety and efficacy of delgocitinib cream for up to 52 weeks in adults with chronic hand eczema: results of the phase 3 open-label extension DELTA 3 trial following the DELTA 1 and 2 trials. J Am Acad Dermatol. 2025;93:95-103. doi:10.1016/j.jaad.2025.03.008
Hand dermatitis (HD) is a common dermatologic concern that can impair quality of life, work productivity, and daily functioning.1 Occupational HD is defined as hand eczema caused or worsened by workplace exposures. When caused by work, HD may lead to reduced productivity and even job loss. Subtypes of HD include irritant contact dermatitis (ICD), allergic contact dermatitis (ACD), protein contact dermatitis (PCD), atopic dermatitis (AD), hyperkeratotic HD, and dyshidrotic eczema.2,3
Often caused by wet work, ICD is the most common subtype, whereas PCD—which is caused by immediate hypersensitivity to protein—is less common and usually seen in food service workers.3,4 When HD does not improve with standard treatment, particularly in occupational cases, patch testing is prudent to evaluate for contact allergens. In this article, we review practical considerations for evaluation and management of occupational irritant and allergic HD, highlighting relevant exposures and pearls on workup and management.
Epidemiology of Hand Dermatitis
A 2021 systematic review and meta-analysis of European studies reported a 1-year HD prevalence of 9.1% and a lifetime prevalence of 14.5%.5 Hand dermatitis is most common in women; individuals aged 30 to 39 years; and those who are employed, underscoring the role of workplace exposure.6 High-risk occupations are those involving substantial wet work, such as hairdressers, beauticians, cleaners, and health care and construction workers.7 Individuals with a history of AD also are at high risk for HD.8
Hand Dermatitis Subtypes
Irritant Contact Dermatitis—Irritant contact dermatitis, the most common form of occupational HD, is caused by repeated exposure to irritants (eg, water, detergents, cleansers, and soaps) that disrupt the skin barrier.9 Occupations that involve wet work are a major risk factor, associated with a 56% higher likelihood of ICD.8 Wet work involves frequent handwashing, prolonged contact with liquids, or occlusive glove use.9 As a ubiquitous skin irritant, water can penetrate the stratum corneum, impair the skin barrier, and increase sensitization risk. The dorsal hands usually are affected by ICD due to the thinner stratum corneum in this area.9
Allergic Contact Dermatitis—Allergic contact dermatitis should be considered in cases of chronic, recurrent, or treatment-resistant disease. Clinical clues include dermatitis beyond irritant contact sites, recurrent pruritic and vesicular HD, and flares with occupational exposures or materials; however, it can be difficult to distinguish ACD from ICD on clinical presentation alone, as they have many overlapping features. When ACD is suspected, patch testing remains the gold standard for identifying allergens and guiding avoidance strategies, product alternatives, and workplace modifications.
Unique Occupational Considerations
Hairdressers—Hairdressers have an increased risk for HD due to wet work and exposure to sensitizers, with a pooled lifetime prevalence of 38.2% (including ICD, ACD, and occupational cases).10 Notably, frequent shampooing, rinsing, cutting wet hair, handwashing, and glove use increase the risk for ICD. Hairdressers also are exposed to allergens in hair products, including p-phenylenediamine, toluene-2,5-diamine, persulfate salts, glyceryl thioglycolate, preservatives, and fragrances. Occupational exposure to the preservative methylisothiazolinone is high among hairdressers, with a sensitization rate of 10.5% in HD cases.11
It has been reported that hyperkeratotic fissured eczema of the dorsal hands caused by wet work often indicates ICD, whereas pruritic dyshidrotic eczema involving the lateral fingers or palms suggests ACD; however, these conditions can share overlapping features.7 If ACD is suspected, broad patch testing with baseline and hairdresser series, along with specific chemicals that may be encountered in the workplace, is necessary. Management includes allergen avoidance, reduced wet work tasks, use of nitrile gloves with glove changes to mitigate occlusive effects, and skin barrier protection with emollients.
Health Care Workers—Health care workers are vulnerable to HD due to intensive hand hygiene, prolonged glove use, and allergen exposures, with a lifetime prevalence of self-reported HD of 33.4%.12 Common allergens among health care workers include rubber accelerators, most often from rubber gloves.13 Frequent handwashing and glove use can further impair the skin barrier, increasing irritant and sensitization risks.14 In contrast, alcohol-based hand sanitizers containing emollients are less irritating, with prior analyses showing no significant association with HD risk.15,16 Conversely, handwashing 8 to 10 times daily increased HD risk, with a relative risk of 1.51.15
Surgeons and proceduralists face unique risks for HD from preoperative scrubbing with products that can contain potential allergens such as chlorhexidine gluconate, chloroxylenol, povidone-iodine, fragrance, cocamide diethanolamine, lanolin, alkyl glucosides, sodium benzoate, sorbic acid, tocopherol, and propylene glycol.17,18 Subsequent occlusion under glove layers drives ICD and ACD risks, highlighting the importance of patch testing in affected individuals. While patch testing, exposure avoidance, and limited glove use can mitigate HD risk, frequent handwashing can contribute to refractory HD.
Food Service Workers—Food service workers have an increased risk for HD from allergens and irritants. In a retrospective study of patients with occupational food-related HD (N=372), 57% were diagnosed with ICD, 22% with PCD, and 1.8% with ACD.19 Skin barrier disruption from wet work, occlusion from glove use, and contact with food proteins increase HD risk, especially in bakers exposed to flours and grains, which can cause IgE–mediated PCD manifesting with contact urticaria. Protein contact dermatitis is confirmed by prick testing with suspected foods.20 Additionally, exposure to garlic can cause ICD and ACD due to sulfur-containing compounds, particularly allicin and diallyl disulfide.21,22 Pineapple also can trigger ICD associated with bromelain, a proteolytic enzyme that can break down the skin.23 Nickel exposure is another concern, as steel utensils and cookware can release nickel onto the skin of sensitized individuals.24 Rubber accelerator exposure from gloves also contributes to contact allergy and HD among food service workers; vinyl gloves usually are a good alternative in this setting.25 Management of food-related HD involves exposure avoidance, which may affect occupational viability
Construction Workers—Construction workers are at risk for occupational HD due to contact with irritants and sensitizers such as paints, adhesives, asphalt, cement, solvents, and gloves.26 A retrospective analysis of North American Contact Dermatitis Group data identified HD in 37.2% (253/681) of patch-tested construction workers. The most common occupational allergens include potassium dichromate, which can be present in cement and leather items; bisphenol A epoxy resin; cobalt chloride hexahydrate; and the rubber accelerators carba mix and thiuram mix.26 A thorough occupational history should assess materials handled, and patch testing should include common construction-related allergens to inform avoidance strategies. Workplace task modification can reduce exposure, as certain managerial roles in construction work may involve less contact with irritants and sensitizers.26
Nail Technicians—Nail technicians are at risk for HD, especially ACD from acrylate monomers used in nail gels, dips, and acrylics. In a 10-year analysis, around 87.5% (14/16) of nail technicians with contact allergy to methacrylate demonstrated hand involvement.27 Common acrylate monomers include 2-hydroxyethyl methacrylate, 2-hydroxypropyl methacrylate, and ethyl cyanoacrylate. 28 Evaluation requires a detailed occupational history, assessing HD onset relative to exposure, services performed, glove-use practices, and whether symptoms improve away from work. While gloves may appear to reduce exposure, a glove-penetration study showed that acrylate-containing nail products can penetrate commonly used disposable gloves from within seconds to approximately 20 minutes, depending on glove and product type.29 Among available options, nitrile gloves may provide dexterity and allergen avoidance when acrylate exposure is brief, with glove changes required every 15 to 30 minutes.30 Patch testing with 2-hydroxyethyl methacrylate and ethyl cyanoacrylate can identify nail acrylate allergy; however, avoidance can be challenging for nail technicians, as these products often are ubiquitous in their work.
Florists—Florists can develop HD from plant allergens and irritants, particularly tulipalin A and calcium oxalate, with a lifetime prevalence of 19.6%.31 Tulipalin A is a well-documented sensitizer causing ACD among florists exposed to tulip bulbs and other Alstroemeria flowers.32 The term tulip fingers actually was coined to describe ACD caused by tulip bulbs in the European tulip industry.33 Patch testing involves testing for tulipalin A, which may be commercially limited, or tulip plant materials; however, fresh tulips require open testing with small amounts due to higher allergen concentration.32 Additionally, the term daffodil itch describes a type of ICD caused by calcium oxalate crystals in daffodil bulbs and tulip sap.32,34 Diagnosis of plant-related HD requires an occupational history and targeted patch testing, while glove protection and exposure avoidance are essential for improvement.
Evaluation and Management
The workup for HD involves physical examination and medical history, including disease onset, course, and history of AD, along with occupational and exposure history to identify allergens and irritants. Understanding the patient’s tasks and responsibilities and workplace practices along with the materials they handle allows the dermatologist to anticipate relevant allergens for patch testing.
Patch testing should be comprehensive, as baseline screening series alone may miss between 26.3% and 50% of occupationally relevant allergens.35,36 Comprehensive patch testing also should include specialty series and supplemental allergens based on the patient’s clinical history and exposures. Specialty series may include hairdressing, bakery, cosmetics, dental, machinists, and adhesives.37 Gloves also warrant attention, as they may be overlooked as a sensitizer following repeated contact and occlusion. In persistent HD associated with glove use, patch testing should include a rubber accelerator series with relevant allergens, such as thiurams, carbamates, mercaptobenzothiazole, diphenylguanidine, and the patient’s own gloves.38 Latex allergy also should be considered, particularly in immediate-type reactions, and can be evaluated with latex-specific IgE testing.39
Management of HD relies on accurate diagnosis and allergen avoidance, which can be challenging in occupational settings. Structured tools, such as the American Contact Dermatitis Society’s Contact Allergen Management Program (https://www.contactderm.org/ resources/acds-camp), can help identify safe alternatives.
In occupational HD, risk assessment should identify occupational exposures and determine appropriate personal protective equipment while minimizing the risk for HD associated with such equipment. Protective gloves are advised to prevent contact with allergens and irritants. When glove use lasts more than 10 minutes, cotton glove liners may be worn to avoid occlusion and moisture retention.40 For wet work, vinyl gloves are recommended, with regular emollient use to support skin-barrier repair. Overall, gloves should be used when possible, changed regularly, and worn for limited periods of time to prevent ICD.
Work modification may be required to reduce exposure and flares, including task reassignment or substitution of materials containing allergens and irritants. Occupational HD may necessitate workplace accommodations, disability evaluation, medical leave, or even permanent job change. Dermatologists play a crucial role in the medical determination of work relatedness and functional impairment, guiding patients through occupational health, disability, and workers’ compensation when warranted.
Treatments for Occupational HD
Treatment of occupational HD depends on disease severity, chronicity, and avoidance of allergens and irritants in ACD, ICD, and PCD. Foundational management includes regular emollient use, which can even serve as monotherapy in mild occupational HD.40 Corticosteroids are the cornerstone of topical therapy, while calcineurin inhibitors can be used as a steroid-sparing option in milder disease.41 Off-label topical calcipotriol and AD-approved therapies crisaborole and ruxolitinib may be effective. For refractory disease after topical treatments, phototherapy can be considered.40 Biologic and targeted therapies also have emerged as potential treatments. Dupilumab is effective for atopic chronic HD and has demonstrated promise for nonatopic chronic HD.42 Recently, delgocitinib, a topical pan–Janus kinase inhibitor cream, showed clinical efficacy for chronic hand eczema and was approved by the US Food and Drug Administration.43 Off-label use of alternative systemic therapies, including acitretin, cyclosporine, methotrexate, and azathioprine, and other biologics and systemic Janus kinase inhibitors also may treat HD, but larger studies are lacking.40
Our Final Interpretation
Occupational HD is a common skin condition with multiple etiologies. It is important for clinicians to gather a thorough occupational and exposure history to narrow the differential diagnosis, inform patch testing, and guide effective management. In practice, successful treatment depends on screening for and diagnosis of workplace exposures driving disease.
Hand dermatitis (HD) is a common dermatologic concern that can impair quality of life, work productivity, and daily functioning.1 Occupational HD is defined as hand eczema caused or worsened by workplace exposures. When caused by work, HD may lead to reduced productivity and even job loss. Subtypes of HD include irritant contact dermatitis (ICD), allergic contact dermatitis (ACD), protein contact dermatitis (PCD), atopic dermatitis (AD), hyperkeratotic HD, and dyshidrotic eczema.2,3
Often caused by wet work, ICD is the most common subtype, whereas PCD—which is caused by immediate hypersensitivity to protein—is less common and usually seen in food service workers.3,4 When HD does not improve with standard treatment, particularly in occupational cases, patch testing is prudent to evaluate for contact allergens. In this article, we review practical considerations for evaluation and management of occupational irritant and allergic HD, highlighting relevant exposures and pearls on workup and management.
Epidemiology of Hand Dermatitis
A 2021 systematic review and meta-analysis of European studies reported a 1-year HD prevalence of 9.1% and a lifetime prevalence of 14.5%.5 Hand dermatitis is most common in women; individuals aged 30 to 39 years; and those who are employed, underscoring the role of workplace exposure.6 High-risk occupations are those involving substantial wet work, such as hairdressers, beauticians, cleaners, and health care and construction workers.7 Individuals with a history of AD also are at high risk for HD.8
Hand Dermatitis Subtypes
Irritant Contact Dermatitis—Irritant contact dermatitis, the most common form of occupational HD, is caused by repeated exposure to irritants (eg, water, detergents, cleansers, and soaps) that disrupt the skin barrier.9 Occupations that involve wet work are a major risk factor, associated with a 56% higher likelihood of ICD.8 Wet work involves frequent handwashing, prolonged contact with liquids, or occlusive glove use.9 As a ubiquitous skin irritant, water can penetrate the stratum corneum, impair the skin barrier, and increase sensitization risk. The dorsal hands usually are affected by ICD due to the thinner stratum corneum in this area.9
Allergic Contact Dermatitis—Allergic contact dermatitis should be considered in cases of chronic, recurrent, or treatment-resistant disease. Clinical clues include dermatitis beyond irritant contact sites, recurrent pruritic and vesicular HD, and flares with occupational exposures or materials; however, it can be difficult to distinguish ACD from ICD on clinical presentation alone, as they have many overlapping features. When ACD is suspected, patch testing remains the gold standard for identifying allergens and guiding avoidance strategies, product alternatives, and workplace modifications.
Unique Occupational Considerations
Hairdressers—Hairdressers have an increased risk for HD due to wet work and exposure to sensitizers, with a pooled lifetime prevalence of 38.2% (including ICD, ACD, and occupational cases).10 Notably, frequent shampooing, rinsing, cutting wet hair, handwashing, and glove use increase the risk for ICD. Hairdressers also are exposed to allergens in hair products, including p-phenylenediamine, toluene-2,5-diamine, persulfate salts, glyceryl thioglycolate, preservatives, and fragrances. Occupational exposure to the preservative methylisothiazolinone is high among hairdressers, with a sensitization rate of 10.5% in HD cases.11
It has been reported that hyperkeratotic fissured eczema of the dorsal hands caused by wet work often indicates ICD, whereas pruritic dyshidrotic eczema involving the lateral fingers or palms suggests ACD; however, these conditions can share overlapping features.7 If ACD is suspected, broad patch testing with baseline and hairdresser series, along with specific chemicals that may be encountered in the workplace, is necessary. Management includes allergen avoidance, reduced wet work tasks, use of nitrile gloves with glove changes to mitigate occlusive effects, and skin barrier protection with emollients.
Health Care Workers—Health care workers are vulnerable to HD due to intensive hand hygiene, prolonged glove use, and allergen exposures, with a lifetime prevalence of self-reported HD of 33.4%.12 Common allergens among health care workers include rubber accelerators, most often from rubber gloves.13 Frequent handwashing and glove use can further impair the skin barrier, increasing irritant and sensitization risks.14 In contrast, alcohol-based hand sanitizers containing emollients are less irritating, with prior analyses showing no significant association with HD risk.15,16 Conversely, handwashing 8 to 10 times daily increased HD risk, with a relative risk of 1.51.15
Surgeons and proceduralists face unique risks for HD from preoperative scrubbing with products that can contain potential allergens such as chlorhexidine gluconate, chloroxylenol, povidone-iodine, fragrance, cocamide diethanolamine, lanolin, alkyl glucosides, sodium benzoate, sorbic acid, tocopherol, and propylene glycol.17,18 Subsequent occlusion under glove layers drives ICD and ACD risks, highlighting the importance of patch testing in affected individuals. While patch testing, exposure avoidance, and limited glove use can mitigate HD risk, frequent handwashing can contribute to refractory HD.
Food Service Workers—Food service workers have an increased risk for HD from allergens and irritants. In a retrospective study of patients with occupational food-related HD (N=372), 57% were diagnosed with ICD, 22% with PCD, and 1.8% with ACD.19 Skin barrier disruption from wet work, occlusion from glove use, and contact with food proteins increase HD risk, especially in bakers exposed to flours and grains, which can cause IgE–mediated PCD manifesting with contact urticaria. Protein contact dermatitis is confirmed by prick testing with suspected foods.20 Additionally, exposure to garlic can cause ICD and ACD due to sulfur-containing compounds, particularly allicin and diallyl disulfide.21,22 Pineapple also can trigger ICD associated with bromelain, a proteolytic enzyme that can break down the skin.23 Nickel exposure is another concern, as steel utensils and cookware can release nickel onto the skin of sensitized individuals.24 Rubber accelerator exposure from gloves also contributes to contact allergy and HD among food service workers; vinyl gloves usually are a good alternative in this setting.25 Management of food-related HD involves exposure avoidance, which may affect occupational viability
Construction Workers—Construction workers are at risk for occupational HD due to contact with irritants and sensitizers such as paints, adhesives, asphalt, cement, solvents, and gloves.26 A retrospective analysis of North American Contact Dermatitis Group data identified HD in 37.2% (253/681) of patch-tested construction workers. The most common occupational allergens include potassium dichromate, which can be present in cement and leather items; bisphenol A epoxy resin; cobalt chloride hexahydrate; and the rubber accelerators carba mix and thiuram mix.26 A thorough occupational history should assess materials handled, and patch testing should include common construction-related allergens to inform avoidance strategies. Workplace task modification can reduce exposure, as certain managerial roles in construction work may involve less contact with irritants and sensitizers.26
Nail Technicians—Nail technicians are at risk for HD, especially ACD from acrylate monomers used in nail gels, dips, and acrylics. In a 10-year analysis, around 87.5% (14/16) of nail technicians with contact allergy to methacrylate demonstrated hand involvement.27 Common acrylate monomers include 2-hydroxyethyl methacrylate, 2-hydroxypropyl methacrylate, and ethyl cyanoacrylate. 28 Evaluation requires a detailed occupational history, assessing HD onset relative to exposure, services performed, glove-use practices, and whether symptoms improve away from work. While gloves may appear to reduce exposure, a glove-penetration study showed that acrylate-containing nail products can penetrate commonly used disposable gloves from within seconds to approximately 20 minutes, depending on glove and product type.29 Among available options, nitrile gloves may provide dexterity and allergen avoidance when acrylate exposure is brief, with glove changes required every 15 to 30 minutes.30 Patch testing with 2-hydroxyethyl methacrylate and ethyl cyanoacrylate can identify nail acrylate allergy; however, avoidance can be challenging for nail technicians, as these products often are ubiquitous in their work.
Florists—Florists can develop HD from plant allergens and irritants, particularly tulipalin A and calcium oxalate, with a lifetime prevalence of 19.6%.31 Tulipalin A is a well-documented sensitizer causing ACD among florists exposed to tulip bulbs and other Alstroemeria flowers.32 The term tulip fingers actually was coined to describe ACD caused by tulip bulbs in the European tulip industry.33 Patch testing involves testing for tulipalin A, which may be commercially limited, or tulip plant materials; however, fresh tulips require open testing with small amounts due to higher allergen concentration.32 Additionally, the term daffodil itch describes a type of ICD caused by calcium oxalate crystals in daffodil bulbs and tulip sap.32,34 Diagnosis of plant-related HD requires an occupational history and targeted patch testing, while glove protection and exposure avoidance are essential for improvement.
Evaluation and Management
The workup for HD involves physical examination and medical history, including disease onset, course, and history of AD, along with occupational and exposure history to identify allergens and irritants. Understanding the patient’s tasks and responsibilities and workplace practices along with the materials they handle allows the dermatologist to anticipate relevant allergens for patch testing.
Patch testing should be comprehensive, as baseline screening series alone may miss between 26.3% and 50% of occupationally relevant allergens.35,36 Comprehensive patch testing also should include specialty series and supplemental allergens based on the patient’s clinical history and exposures. Specialty series may include hairdressing, bakery, cosmetics, dental, machinists, and adhesives.37 Gloves also warrant attention, as they may be overlooked as a sensitizer following repeated contact and occlusion. In persistent HD associated with glove use, patch testing should include a rubber accelerator series with relevant allergens, such as thiurams, carbamates, mercaptobenzothiazole, diphenylguanidine, and the patient’s own gloves.38 Latex allergy also should be considered, particularly in immediate-type reactions, and can be evaluated with latex-specific IgE testing.39
Management of HD relies on accurate diagnosis and allergen avoidance, which can be challenging in occupational settings. Structured tools, such as the American Contact Dermatitis Society’s Contact Allergen Management Program (https://www.contactderm.org/ resources/acds-camp), can help identify safe alternatives.
In occupational HD, risk assessment should identify occupational exposures and determine appropriate personal protective equipment while minimizing the risk for HD associated with such equipment. Protective gloves are advised to prevent contact with allergens and irritants. When glove use lasts more than 10 minutes, cotton glove liners may be worn to avoid occlusion and moisture retention.40 For wet work, vinyl gloves are recommended, with regular emollient use to support skin-barrier repair. Overall, gloves should be used when possible, changed regularly, and worn for limited periods of time to prevent ICD.
Work modification may be required to reduce exposure and flares, including task reassignment or substitution of materials containing allergens and irritants. Occupational HD may necessitate workplace accommodations, disability evaluation, medical leave, or even permanent job change. Dermatologists play a crucial role in the medical determination of work relatedness and functional impairment, guiding patients through occupational health, disability, and workers’ compensation when warranted.
Treatments for Occupational HD
Treatment of occupational HD depends on disease severity, chronicity, and avoidance of allergens and irritants in ACD, ICD, and PCD. Foundational management includes regular emollient use, which can even serve as monotherapy in mild occupational HD.40 Corticosteroids are the cornerstone of topical therapy, while calcineurin inhibitors can be used as a steroid-sparing option in milder disease.41 Off-label topical calcipotriol and AD-approved therapies crisaborole and ruxolitinib may be effective. For refractory disease after topical treatments, phototherapy can be considered.40 Biologic and targeted therapies also have emerged as potential treatments. Dupilumab is effective for atopic chronic HD and has demonstrated promise for nonatopic chronic HD.42 Recently, delgocitinib, a topical pan–Janus kinase inhibitor cream, showed clinical efficacy for chronic hand eczema and was approved by the US Food and Drug Administration.43 Off-label use of alternative systemic therapies, including acitretin, cyclosporine, methotrexate, and azathioprine, and other biologics and systemic Janus kinase inhibitors also may treat HD, but larger studies are lacking.40
Our Final Interpretation
Occupational HD is a common skin condition with multiple etiologies. It is important for clinicians to gather a thorough occupational and exposure history to narrow the differential diagnosis, inform patch testing, and guide effective management. In practice, successful treatment depends on screening for and diagnosis of workplace exposures driving disease.
- Agner T, Andersen KE, Brandao FM, et al. Hand eczema severity and quality of life: a cross-sectional, multicentre study of hand eczema patients. Contact Dermatitis. 2008;59:43-47. doi:10.1111 /j.1600-0536.2008.01362.x
- Agner T, Aalto-Korte K, Andersen KE, et al. Classification of hand eczema. J Eur Acad Dermatol Venereol. 2015;29:2417-2422. doi:10.1111 /jdv.13308
- Bissonnette R, Agner T, Molin S, et al. Hand eczema—part 1: epidemiology, pathogenesis, diagnosis, and work-up. J Am Acad Dermatol. 2025;93:1201-1210. doi:10.1016/j.jaad.2024.09.048
- Barbaud A. Mechanism and diagnosis of protein contact dermatitis. Curr Opin Allergy Clin Immunol. 2020;20:117-121. doi:10.1097/ACI.0000000000000621
- Quaade AS, Simonsen AB, Halling AS, et al. Prevalence, incidence, and severity of hand eczema in the general population - a systematic review and meta-analysis. Contact Dermatitis. 2021;84:361-374. doi:10.1111/cod.13804
- Apfelbacher C, Bewley A, Molin S, et al. Prevalence of chronic hand eczema in adults: a cross-sectional survey of over 60 000 respondents from the general population of Canada, France, Germany, Italy, Spain and the UK. Br J Dermatol. 2025;192:1047-1054. doi:10.1093 /bjd/ljaf020
- Weidinger S, Novak N. Hand eczema. Lancet. 2024;404:2476-2486. doi:10.1016/S0140-6736(24)01810-5
- Schütte MG, Tamminga SJ, de Groene GJ, et al. Work-related and personal risk factors for occupational contact dermatitis: a systematic review of the literature with meta-analysis. Contact Dermatitis. 2023;88:171-187. doi:10.1111/cod.14253
- Behroozy A, Keegel TG. Wet-work exposure: a main risk factor for occupational hand dermatitis. Saf Health Work. 2014;5:175-180. doi:10.1016/j.shaw.2014.08.001
- Havmose MS, Kezic S, Uter W, et al. Prevalence and incidence of hand eczema in hairdressers-a systematic review and meta-analysis of the published literature from 2000-2021. Contact Dermatitis. 2022;86:254-265. doi:10.1111/cod.14048
- Uter W, Hallmann S, Gefeller O, et al. Contact allergy to ingredients of hair cosmetics in female hairdressers and female consumers—an update based on IVDK data 2013–2020. Contact Dermatitis. 2023;89:161-170. doi:10.1111/cod.14363
- Yüksel YT, Symanzik C, Christensen MO, et al. Prevalence and incidence of hand eczema in healthcare workers: a systematic review and meta-analysis. Contact Dermatitis. 2024;90:331-342. doi:10.1111 /cod.14489
- Warshaw EM, Schram SE, Maibach HI, et al. Occupation-related contact dermatitis in North American health care workers referred for patch testing: cross-sectional data, 1998 to 2004. Dermatitis. 2008;19:261-274. doi:10.2310/6620.2008.07059
- Hamnerius N, Svedman C, Bergendorff O, et al. Wet work exposure and hand eczema among healthcare workers: a cross-sectional study. Br J Dermatol. 2018;178:452-461. doi:10.1111 /bjd.15813
- Loh EDW, Yew YW. Hand hygiene and hand eczema: a systematic review and meta-analysis. Contact Dermatitis. 2022;87:303-314. doi:10.1111/cod.14133
- Lotfinejad N, Peters A, Tartari E, et al. Hand hygiene in health care: 20 years of ongoing advances and perspectives. Lancet Infect Dis. 2021;21:e209-e221. doi:10.1016/S1473-3099(21)00383-2
- Schlarbaum JP, Hylwa SA. Allergic contact dermatitis to operating room scrubs and disinfectants. Dermat Contact Atopic Occup Drug. 2019;30:363-370. doi:10.1097/DER.0000000000000525
- Rodriguez-Homs LG, Atwater AR. Allergens in medical hand skin cleansers. Dermat Contact Atopic Occup Drug. 2019;30:336-341. doi:10.1097/DER.0000000000000504
- Vester L, Thyssen JP, Menné T, et al. Occupational food-related hand dermatoses seen over a 10-year period. Contact Dermatitis. 2012;66:264-270. doi:10.1111/j.1600-0536.2011.02048.x
- Pesonen M, Koskela K, Aalto-Korte K. Contact urticaria and protein contact dermatitis in the Finnish Register of Occupational Diseases in a period of 12 years. Contact Dermatitis. 2020;83:1-7. doi:10.1111/cod.13547
- McFadden JP, White JML, Basketter DA, et al. Reduced allergy rates in atopic eczema to contact allergens used in both skin products and foods: atopy and the “hapten-atopy hypothesis.” Contact Dermatitis. 2008;58:156-158. doi:10.1111/j.1600-0536.2007.01291.x
- Kao SH, Hsu CH, Su SN, et al. Identification and immunologic characterization of an allergen, alliin lyase, from garlic (Allium sativum). J Allergy Clin Immunol. 2004;113:161-168. doi:10.1016/j.jaci.2003.10.040
- Reddy VB, Lerner EA. Plant cysteine proteases that evoke itch activate protease-activated receptors. Br J Dermatol. 2010;163:532-535. doi:10.1111/j.1365-2133.2010.09862.x
- Silverberg NB, Pelletier JL, Jacob SE, et al; Section on Dermatology, Section on Allergy and Immunology. Nickel allergic contact dermatitis: identification, treatment, and prevention. Pediatrics. 2020;145:e20200628. doi:10.1542/peds.2020-0628
- Clément A, Ferrier le Bouëdec MC, Crépy MN, et al. Hand eczema in glove-wearing patients. Contact Dermatitis. 2023;89:143-152. doi:10.1111/cod.14357
- Reeder MJ, Idrogo-Lam A, Aravamuthan SR, et al. Occupational contact dermatitis in construction workers: a retrospective analysis of the North American Contact Dermatitis Group Data, 2001-2020. Dermat Contact Atopic Occup Drug. 2024;35:467-475. doi:10.1089/derm.2024.0018
- Fisch A, Hamnerius N, Isaksson M. Dermatitis and occupational (meth)acrylate contact allergy in nail technicians-a 10-year study. Contact Dermatitis. 2019;81:58-60. doi:10.1111/cod.13216
- Atwater AR, Reeder M. Trends in nail services may cause dermatitis: not your mother’s nail polish. Cutis. 2019;103:315-317.
- Suuronen K, Ylinen K, Heikkilä J, et al. Acrylates in artificial nails— results of product analyses and glove penetration studies. Contact Dermatitis. 2024;90:266-272. doi:10.1111/cod.14474
- Morgado F, Batista M, Gonçalo M. Short exposures and glove protection against (meth)acrylates in nail beauticians-thoughts on a rising concern. Contact Dermatitis. 2019;81:62-63. doi:10.1111 /cod.13222
- Paulsen E, Søgaard J, Andersen KE. Occupational dermatitis in Danish gardeners and greenhouse workers (I). prevalence and possible risk factors. Contact Dermatitis. 1997;37:263-270. doi:10.1111/j.1600-0536.1997.tb02462.x
- Fonacier L, Bernstein DI, Pacheco K, et al. Contact dermatitis: a practice parameter–update 2015. J Allergy Clin Immunol Pract. 2015; 3(3 suppl):S1-S39. doi:10.1016/j.jaip.2015.02.009
- Gette MT, Marks JE. Tulip fingers. Arch Dermatol. 1990;126:203-205.
- Bruynzeel DP. Bulb dermatitis. Dermatological problems in the flower bulb industries. Contact Dermatitis. 1997;37:70-77. doi:10.1111/j.1600-0536.1997.tb00042.x
- Nettis E, Marcandrea M, Colanardi MC, et al. Results of standard series patch testing in patients with occupational allergic contact dermatitis. Allergy. 2003;58:1304-1307. doi:10.1046/j.1398-9995.2003.00346.x
- Saripalli YV, Achen F, Belsito DV. The detection of clinically relevant contact allergens using a standard screening tray of twenty-three allergens. J Am Acad Dermatol. 2003;49:65-69. doi:10.1067/mjd.2003.489
- Warshaw EM, Buonomo M, DeKoven JG, et al. Importance of supplemental patch testing beyond a screening series for patients with dermatitis: the North American Contact Dermatitis Group experience. JAMA Dermatol. 2021;157:1456-1465. doi:10.1001/jamadermatol.2021.4314
- Geier J, Lessmann H, Mahler V, et al. Occupational contact allergy caused by rubber gloves--nothing has changed. Contact Dermatitis. 2012;67:149-156. doi:10.1111/j.1600-0536.2012.02139.x
- Toraason M, Sussman G, Biagini R, et al. Latex allergy in the workplace. Toxicol Sci Off J Soc Toxicol. 2000;58:5-14. doi:10.1093/toxsci/58.1.5
- Bissonnette R, Agner T, Taylor JS, et al. Hand eczema-part 2: prevention, management, and treatment. J Am Acad Dermatol. 2025;93:1213-1224. doi:10.1016/j.jaad.2024.09.049
- Schliemann S, Kelterer D, Bauer A, et al. Tacrolimus ointment in the treatment of occupationally induced chronic hand dermatitis. Contact Dermatitis. 2008;58:299-306. doi:10.1111/j.1600-0536.2007.01314.x
- Voorberg AN, Kamphuis E, Christoffers WA, et al. Efficacy and safety of dupilumab in patients with severe chronic hand eczema with inadequate response or intolerance to alitretinoin: a randomized, double-blind, placebo-controlled phase IIb proof-of-concept study. Br J Dermatol. 2023;189:400-409. doi:10.1093/bjd/ljad156
- Gooderham M, Molin S, Bissonnette R, et al. Long-term safety and efficacy of delgocitinib cream for up to 52 weeks in adults with chronic hand eczema: results of the phase 3 open-label extension DELTA 3 trial following the DELTA 1 and 2 trials. J Am Acad Dermatol. 2025;93:95-103. doi:10.1016/j.jaad.2025.03.008
- Agner T, Andersen KE, Brandao FM, et al. Hand eczema severity and quality of life: a cross-sectional, multicentre study of hand eczema patients. Contact Dermatitis. 2008;59:43-47. doi:10.1111 /j.1600-0536.2008.01362.x
- Agner T, Aalto-Korte K, Andersen KE, et al. Classification of hand eczema. J Eur Acad Dermatol Venereol. 2015;29:2417-2422. doi:10.1111 /jdv.13308
- Bissonnette R, Agner T, Molin S, et al. Hand eczema—part 1: epidemiology, pathogenesis, diagnosis, and work-up. J Am Acad Dermatol. 2025;93:1201-1210. doi:10.1016/j.jaad.2024.09.048
- Barbaud A. Mechanism and diagnosis of protein contact dermatitis. Curr Opin Allergy Clin Immunol. 2020;20:117-121. doi:10.1097/ACI.0000000000000621
- Quaade AS, Simonsen AB, Halling AS, et al. Prevalence, incidence, and severity of hand eczema in the general population - a systematic review and meta-analysis. Contact Dermatitis. 2021;84:361-374. doi:10.1111/cod.13804
- Apfelbacher C, Bewley A, Molin S, et al. Prevalence of chronic hand eczema in adults: a cross-sectional survey of over 60 000 respondents from the general population of Canada, France, Germany, Italy, Spain and the UK. Br J Dermatol. 2025;192:1047-1054. doi:10.1093 /bjd/ljaf020
- Weidinger S, Novak N. Hand eczema. Lancet. 2024;404:2476-2486. doi:10.1016/S0140-6736(24)01810-5
- Schütte MG, Tamminga SJ, de Groene GJ, et al. Work-related and personal risk factors for occupational contact dermatitis: a systematic review of the literature with meta-analysis. Contact Dermatitis. 2023;88:171-187. doi:10.1111/cod.14253
- Behroozy A, Keegel TG. Wet-work exposure: a main risk factor for occupational hand dermatitis. Saf Health Work. 2014;5:175-180. doi:10.1016/j.shaw.2014.08.001
- Havmose MS, Kezic S, Uter W, et al. Prevalence and incidence of hand eczema in hairdressers-a systematic review and meta-analysis of the published literature from 2000-2021. Contact Dermatitis. 2022;86:254-265. doi:10.1111/cod.14048
- Uter W, Hallmann S, Gefeller O, et al. Contact allergy to ingredients of hair cosmetics in female hairdressers and female consumers—an update based on IVDK data 2013–2020. Contact Dermatitis. 2023;89:161-170. doi:10.1111/cod.14363
- Yüksel YT, Symanzik C, Christensen MO, et al. Prevalence and incidence of hand eczema in healthcare workers: a systematic review and meta-analysis. Contact Dermatitis. 2024;90:331-342. doi:10.1111 /cod.14489
- Warshaw EM, Schram SE, Maibach HI, et al. Occupation-related contact dermatitis in North American health care workers referred for patch testing: cross-sectional data, 1998 to 2004. Dermatitis. 2008;19:261-274. doi:10.2310/6620.2008.07059
- Hamnerius N, Svedman C, Bergendorff O, et al. Wet work exposure and hand eczema among healthcare workers: a cross-sectional study. Br J Dermatol. 2018;178:452-461. doi:10.1111 /bjd.15813
- Loh EDW, Yew YW. Hand hygiene and hand eczema: a systematic review and meta-analysis. Contact Dermatitis. 2022;87:303-314. doi:10.1111/cod.14133
- Lotfinejad N, Peters A, Tartari E, et al. Hand hygiene in health care: 20 years of ongoing advances and perspectives. Lancet Infect Dis. 2021;21:e209-e221. doi:10.1016/S1473-3099(21)00383-2
- Schlarbaum JP, Hylwa SA. Allergic contact dermatitis to operating room scrubs and disinfectants. Dermat Contact Atopic Occup Drug. 2019;30:363-370. doi:10.1097/DER.0000000000000525
- Rodriguez-Homs LG, Atwater AR. Allergens in medical hand skin cleansers. Dermat Contact Atopic Occup Drug. 2019;30:336-341. doi:10.1097/DER.0000000000000504
- Vester L, Thyssen JP, Menné T, et al. Occupational food-related hand dermatoses seen over a 10-year period. Contact Dermatitis. 2012;66:264-270. doi:10.1111/j.1600-0536.2011.02048.x
- Pesonen M, Koskela K, Aalto-Korte K. Contact urticaria and protein contact dermatitis in the Finnish Register of Occupational Diseases in a period of 12 years. Contact Dermatitis. 2020;83:1-7. doi:10.1111/cod.13547
- McFadden JP, White JML, Basketter DA, et al. Reduced allergy rates in atopic eczema to contact allergens used in both skin products and foods: atopy and the “hapten-atopy hypothesis.” Contact Dermatitis. 2008;58:156-158. doi:10.1111/j.1600-0536.2007.01291.x
- Kao SH, Hsu CH, Su SN, et al. Identification and immunologic characterization of an allergen, alliin lyase, from garlic (Allium sativum). J Allergy Clin Immunol. 2004;113:161-168. doi:10.1016/j.jaci.2003.10.040
- Reddy VB, Lerner EA. Plant cysteine proteases that evoke itch activate protease-activated receptors. Br J Dermatol. 2010;163:532-535. doi:10.1111/j.1365-2133.2010.09862.x
- Silverberg NB, Pelletier JL, Jacob SE, et al; Section on Dermatology, Section on Allergy and Immunology. Nickel allergic contact dermatitis: identification, treatment, and prevention. Pediatrics. 2020;145:e20200628. doi:10.1542/peds.2020-0628
- Clément A, Ferrier le Bouëdec MC, Crépy MN, et al. Hand eczema in glove-wearing patients. Contact Dermatitis. 2023;89:143-152. doi:10.1111/cod.14357
- Reeder MJ, Idrogo-Lam A, Aravamuthan SR, et al. Occupational contact dermatitis in construction workers: a retrospective analysis of the North American Contact Dermatitis Group Data, 2001-2020. Dermat Contact Atopic Occup Drug. 2024;35:467-475. doi:10.1089/derm.2024.0018
- Fisch A, Hamnerius N, Isaksson M. Dermatitis and occupational (meth)acrylate contact allergy in nail technicians-a 10-year study. Contact Dermatitis. 2019;81:58-60. doi:10.1111/cod.13216
- Atwater AR, Reeder M. Trends in nail services may cause dermatitis: not your mother’s nail polish. Cutis. 2019;103:315-317.
- Suuronen K, Ylinen K, Heikkilä J, et al. Acrylates in artificial nails— results of product analyses and glove penetration studies. Contact Dermatitis. 2024;90:266-272. doi:10.1111/cod.14474
- Morgado F, Batista M, Gonçalo M. Short exposures and glove protection against (meth)acrylates in nail beauticians-thoughts on a rising concern. Contact Dermatitis. 2019;81:62-63. doi:10.1111 /cod.13222
- Paulsen E, Søgaard J, Andersen KE. Occupational dermatitis in Danish gardeners and greenhouse workers (I). prevalence and possible risk factors. Contact Dermatitis. 1997;37:263-270. doi:10.1111/j.1600-0536.1997.tb02462.x
- Fonacier L, Bernstein DI, Pacheco K, et al. Contact dermatitis: a practice parameter–update 2015. J Allergy Clin Immunol Pract. 2015; 3(3 suppl):S1-S39. doi:10.1016/j.jaip.2015.02.009
- Gette MT, Marks JE. Tulip fingers. Arch Dermatol. 1990;126:203-205.
- Bruynzeel DP. Bulb dermatitis. Dermatological problems in the flower bulb industries. Contact Dermatitis. 1997;37:70-77. doi:10.1111/j.1600-0536.1997.tb00042.x
- Nettis E, Marcandrea M, Colanardi MC, et al. Results of standard series patch testing in patients with occupational allergic contact dermatitis. Allergy. 2003;58:1304-1307. doi:10.1046/j.1398-9995.2003.00346.x
- Saripalli YV, Achen F, Belsito DV. The detection of clinically relevant contact allergens using a standard screening tray of twenty-three allergens. J Am Acad Dermatol. 2003;49:65-69. doi:10.1067/mjd.2003.489
- Warshaw EM, Buonomo M, DeKoven JG, et al. Importance of supplemental patch testing beyond a screening series for patients with dermatitis: the North American Contact Dermatitis Group experience. JAMA Dermatol. 2021;157:1456-1465. doi:10.1001/jamadermatol.2021.4314
- Geier J, Lessmann H, Mahler V, et al. Occupational contact allergy caused by rubber gloves--nothing has changed. Contact Dermatitis. 2012;67:149-156. doi:10.1111/j.1600-0536.2012.02139.x
- Toraason M, Sussman G, Biagini R, et al. Latex allergy in the workplace. Toxicol Sci Off J Soc Toxicol. 2000;58:5-14. doi:10.1093/toxsci/58.1.5
- Bissonnette R, Agner T, Taylor JS, et al. Hand eczema-part 2: prevention, management, and treatment. J Am Acad Dermatol. 2025;93:1213-1224. doi:10.1016/j.jaad.2024.09.049
- Schliemann S, Kelterer D, Bauer A, et al. Tacrolimus ointment in the treatment of occupationally induced chronic hand dermatitis. Contact Dermatitis. 2008;58:299-306. doi:10.1111/j.1600-0536.2007.01314.x
- Voorberg AN, Kamphuis E, Christoffers WA, et al. Efficacy and safety of dupilumab in patients with severe chronic hand eczema with inadequate response or intolerance to alitretinoin: a randomized, double-blind, placebo-controlled phase IIb proof-of-concept study. Br J Dermatol. 2023;189:400-409. doi:10.1093/bjd/ljad156
- Gooderham M, Molin S, Bissonnette R, et al. Long-term safety and efficacy of delgocitinib cream for up to 52 weeks in adults with chronic hand eczema: results of the phase 3 open-label extension DELTA 3 trial following the DELTA 1 and 2 trials. J Am Acad Dermatol. 2025;93:95-103. doi:10.1016/j.jaad.2025.03.008
Getting a Grip on Occupational Hand Dermatitis: Key Considerations for Evaluation and Management
Getting a Grip on Occupational Hand Dermatitis: Key Considerations for Evaluation and Management
PRACTICE POINTS
- Occupational hand dermatitis (HD) is a common multifactorial disease with a major impact on quality of life, worker safety, and productivity.
- High-risk occupations include those involving wet work, such as hairdressers, beauticians, cleaners, and health care and construction workers.
- A detailed occupational and exposure history is essential for managing occupational HD.

Alopecia and Pruritic Rash on the Forehead and Scalp
Alopecia and Pruritic Rash on the Forehead and Scalp
THE DIAGNOSIS: Folliculitis Decalvans
Biopsy results revealed a brisk perifollicular and intrafollicular mixed inflammatory infiltrate comprising lymphocytes, neutrophils, and plasma cells filling the upper dermis and encircling dilated hair follicles. Elastic stain (Verhoeff-van Gieson) demonstrated loss of elastic fibers in areas of scarring. Periodic acid–Schiff with diastase staining was negative for fungal elements, while Gram staining revealed colonies of bacterial cocci in the stratum corneum and within the hair follicles. Immunofluorescence was unremarkable, and culture revealed methicillin-sensitive Staphylococcus aureus, leading to a diagnosis of folliculitis decalvans (FD). The patient was treated with doxycycline 100 mg twice daily and received intralesional triamcinolone 2.5 mg/mL (total volume, 2 mL) every 6 weeks with considerable improvement in pustules, erythema, and scaling (Figure). While not yet in complete remission, our patient demonstrated short regrowing hairs in areas of incomplete scarring and focal remaining perifollicular erythema and scale along the midline frontal scalp 5 months after initial presentation.

Folliculitis decalvans is an uncommon subtype of cicatricial alopecia that may mimic other forms of alopecia. Cicatricial alopecia often is difficult to diagnose due to its overlapping clinical characteristics, but early diagnosis is essential for appropriate management and prevention of further permanent hair loss. Traditionally classified as a primary neutrophilic cicatricial alopecia, lymphocyte-predominant variants of FD now are recognized.1
Patients with FD typically present with patchy scarring alopecia at the vertex scalp that gradually expands and may demonstrate secondary features of follicular tufting and pustules.1-3 While the epidemiology of FD is poorly characterized, Vañó-Galván et al4 reported that FD accounted for 2.8% of all alopecia cases and 10.5% of cicatricial alopecia cases in a multicenter study of 2835 patients. The pathophysiology of FD still is under investigation but is thought to result from a dysregulated immune response to a chronic bacterial infection (eg, S aureus), with resulting neutrophilpredominant inflammation in early stages.1-3 Vañó-Galván et al4 reported that, among 35 patients with FD cultured for bacteria, 74% (26/35) returned positive results, 96% (25/26) of which grew S aureus.5
A systematic review of 20 studies that included 263 patients found rifampin and clindamycin to be the most common treatments for FD; however, there is insufficient evidence to determine if this treatment is the most effective.6 In our patient, clindamycin was avoided due to its propensity to negatively alter the gut microbiome long term.7 Other therapies such as oral tetracyclines, high-potency topical steroids, and intralesional triamcinolone also can be used to achieve disease remission.5,6 Other treatments such as isotretinoin, red-light photodynamic therapy, tacrolimus, and external beam radiation have been reported in the literature but vary in efficacy.6 Our patient improved on a regimen of topical benzoyl peroxide wash, oral doxycycline, and intralesional triamcinolone.
Notably, FD may share clinical features with other causes of cicatricial alopecia. In our patient, FD mimicked other entities including discoid lupus erythematosus, frontal fibrosing alopecia, dissecting cellulitis, and erosive pustular dermatosis (Table).1-14 Discoid lupus erythematosus manifests as round hypopigmented and hyperpigmented plaques with associated atrophy, perifollicular erythema, and follicular plugging. Frontal fibrosing alopecia is a primary lymphocytic scarring alopecia that manifests in a bandlike linear distribution over the frontal scalp and may involve the temporal scalp, posterior hairline, and/or eyebrows. Isolated hairs (known as lonely hairs) often are seen. Dissecting cellulitis is characterized by boggy nodules associated with alopecia on the scalp without notable epidermal change, although pustules and sinus tracts may develop.9 Erosive pustular dermatosis is a diagnosis of exclusion but often is seen in older adults with chronic sun damage and clinically manifests with eroded plaques with adherent crusts.10
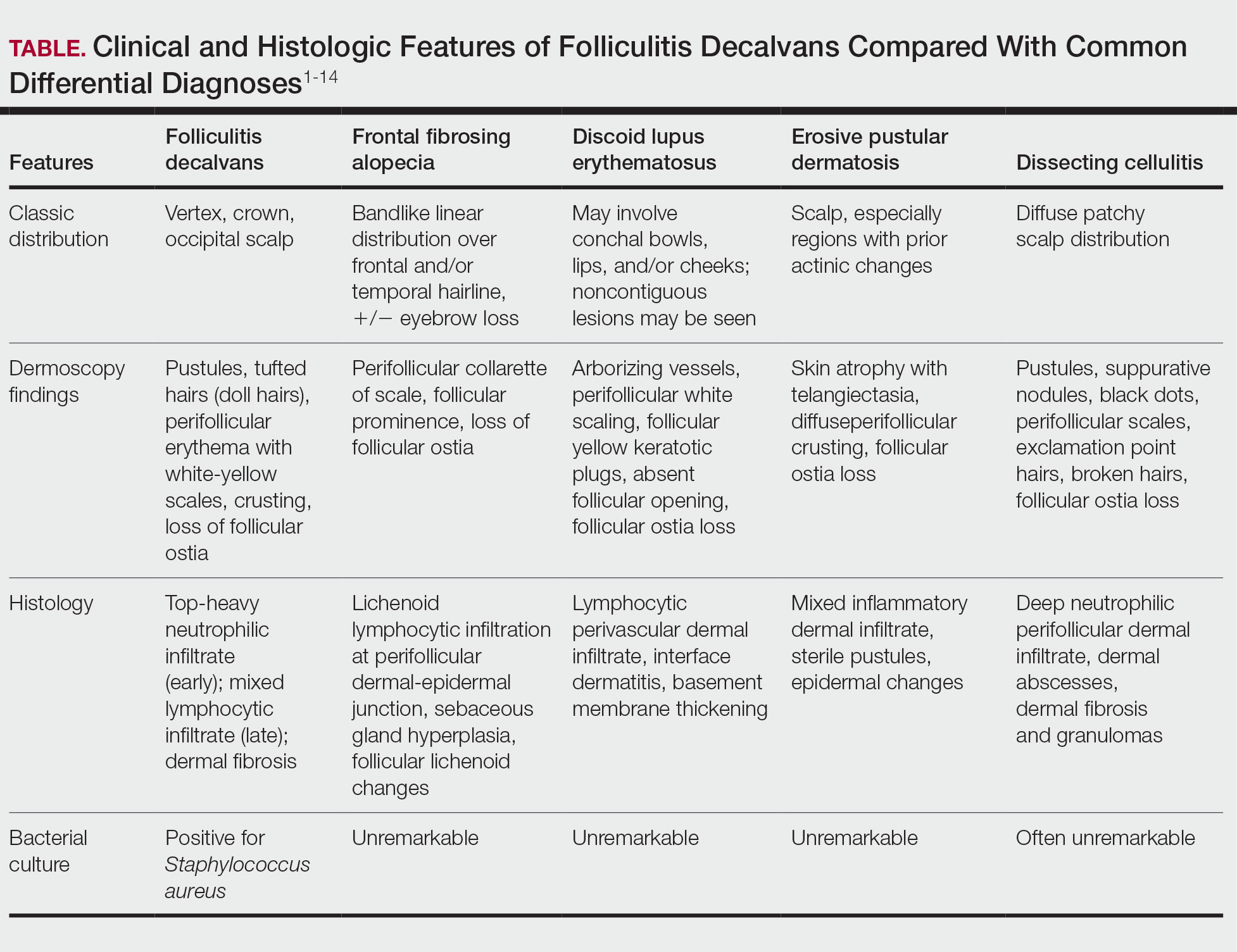
While our patient presented with several overlapping clinical features, including progressive hair loss along the frontal scalp in a bandlike pattern suspicious for frontal fibrosing alopecia as well as atrophic depigmented plaques with adherent peripheral scaling suspicious for discoid lupus erythematosus, the presence of pustules was an important clue. The biopsy demonstrating a mixed infiltrate inclusive of neutrophils confirmed the diagnosis of FD.
- Olsen EA, Bergfeld WF, Cotsarelis G, et al. Summary of North American Hair Research Society (NAHRS)-sponsored Workshop on Cicatricial Alopecia, Duke University Medical Center, February 10 and 11, 2001. J Am Acad Dermatol. 2003;48:103-110. doi:10.1067/mjd.2003.68
- Filbrandt R, Rufaut N, Jones L. Primary cicatricial alopecia: diagnosis and treatment. CMAJ. 2013;185:1579-1585. doi:10.1503/cmaj.111570
- Otberg N, Kang H, Alzolibani AA, et al. Folliculitis decalvans. Dermatol Ther. 2008;21:238-244. doi:10.1111/j.1529-8019.2008.00204.x
- Vañó-Galván S, Saceda-Corralo D, Blume-Peytavi U, et al. Frequency of the types of alopecia at twenty-two specialist hair clinics: a multicenter study. Skin Appendage Disord. 2019;5:309-315. doi:10.1159/000496708
- Vañó-Galván S, Molina-Ruiz AM, Fernández-Crehuet P, et al. Folliculitis decalvans: a multicentre review of 82 patients. J Eur Acad Dermatol Venereol. 2015;29:1750-1757. doi:10.1111/jdv.12993
- Rambhia PH, Conic RRZ, Murad A, et al. Updates in therapeutics for folliculitis decalvans: a systematic review with evidence-based analysis. J Am Acad Dermatol. 2019;80:794-801. doi:10.1016/j.jaad.2018.07.050
- Zimmermann P, Curtis N. The effect of antibiotics on the composition of the intestinal microbiota - a systematic review. J Infect. 2019;79:471-489. doi:10.1016/j.jinf.2019.10.008
- Kanti V, Röwert-Huber J, Vogt A, et al. Cicatricial alopecia. J Dtsch Dermatol Ges. 2018;16:435-461. doi:10.1111/ddg.13498
- Melo DF, Slaibi EB, Siqueira TMFM, et al. Trichoscopy findings in dissecting cellulitis. An Bras Dermatol. 2019;94:608-611. doi:10.1016/j.abd.2019.09.006
- Anzai A, Pirmez R, Vincenzi C, et al. Trichoscopy findings of frontal fibrosing alopecia on the eyebrows: a study of 151 cases. J Am Acad Dermatol. 2021;85:1130-1134. doi:10.1016/j.jaad.2019.12.023
- Starace M, Loi C, Bruni F, et al. Erosive pustular dermatosis of the scalp: clinical, trichoscopic, and histopathologic features of 20 cases. J Am Acad Dermatol. 2017;76:1109-1114. doi:10.1016/j.jaad.2016.12.016
- Rongioletti F, Christana K. Cicatricial (scarring) alopecias: an overview of pathogenesis, classification, diagnosis, and treatment. Am J Clin Dermatol. 2012;13:247-260. doi:10.2165/11596960-000000000-00000
- Badaoui A, Reygagne P, Cavelier-Balloy B, et al. Dissecting cellulitis of the scalp: a retrospective study of 51 patients and review of literature. Br J Dermatol. 2016;174:421-423. doi:10.1111/bjd.13999
- Michelerio A, Vassallo C, Fiandrino G, et al. Erosive pustular dermatosis of the scalp: a clinicopathologic study of fifty cases. Dermatopathology (Basel). 2021;8:450-462. doi:10.3390/dermatopathology8040048
THE DIAGNOSIS: Folliculitis Decalvans
Biopsy results revealed a brisk perifollicular and intrafollicular mixed inflammatory infiltrate comprising lymphocytes, neutrophils, and plasma cells filling the upper dermis and encircling dilated hair follicles. Elastic stain (Verhoeff-van Gieson) demonstrated loss of elastic fibers in areas of scarring. Periodic acid–Schiff with diastase staining was negative for fungal elements, while Gram staining revealed colonies of bacterial cocci in the stratum corneum and within the hair follicles. Immunofluorescence was unremarkable, and culture revealed methicillin-sensitive Staphylococcus aureus, leading to a diagnosis of folliculitis decalvans (FD). The patient was treated with doxycycline 100 mg twice daily and received intralesional triamcinolone 2.5 mg/mL (total volume, 2 mL) every 6 weeks with considerable improvement in pustules, erythema, and scaling (Figure). While not yet in complete remission, our patient demonstrated short regrowing hairs in areas of incomplete scarring and focal remaining perifollicular erythema and scale along the midline frontal scalp 5 months after initial presentation.
Folliculitis decalvans is an uncommon subtype of cicatricial alopecia that may mimic other forms of alopecia. Cicatricial alopecia often is difficult to diagnose due to its overlapping clinical characteristics, but early diagnosis is essential for appropriate management and prevention of further permanent hair loss. Traditionally classified as a primary neutrophilic cicatricial alopecia, lymphocyte-predominant variants of FD now are recognized.1
Patients with FD typically present with patchy scarring alopecia at the vertex scalp that gradually expands and may demonstrate secondary features of follicular tufting and pustules.1-3 While the epidemiology of FD is poorly characterized, Vañó-Galván et al4 reported that FD accounted for 2.8% of all alopecia cases and 10.5% of cicatricial alopecia cases in a multicenter study of 2835 patients. The pathophysiology of FD still is under investigation but is thought to result from a dysregulated immune response to a chronic bacterial infection (eg, S aureus), with resulting neutrophilpredominant inflammation in early stages.1-3 Vañó-Galván et al4 reported that, among 35 patients with FD cultured for bacteria, 74% (26/35) returned positive results, 96% (25/26) of which grew S aureus.5
A systematic review of 20 studies that included 263 patients found rifampin and clindamycin to be the most common treatments for FD; however, there is insufficient evidence to determine if this treatment is the most effective.6 In our patient, clindamycin was avoided due to its propensity to negatively alter the gut microbiome long term.7 Other therapies such as oral tetracyclines, high-potency topical steroids, and intralesional triamcinolone also can be used to achieve disease remission.5,6 Other treatments such as isotretinoin, red-light photodynamic therapy, tacrolimus, and external beam radiation have been reported in the literature but vary in efficacy.6 Our patient improved on a regimen of topical benzoyl peroxide wash, oral doxycycline, and intralesional triamcinolone.
Notably, FD may share clinical features with other causes of cicatricial alopecia. In our patient, FD mimicked other entities including discoid lupus erythematosus, frontal fibrosing alopecia, dissecting cellulitis, and erosive pustular dermatosis (Table).1-14 Discoid lupus erythematosus manifests as round hypopigmented and hyperpigmented plaques with associated atrophy, perifollicular erythema, and follicular plugging. Frontal fibrosing alopecia is a primary lymphocytic scarring alopecia that manifests in a bandlike linear distribution over the frontal scalp and may involve the temporal scalp, posterior hairline, and/or eyebrows. Isolated hairs (known as lonely hairs) often are seen. Dissecting cellulitis is characterized by boggy nodules associated with alopecia on the scalp without notable epidermal change, although pustules and sinus tracts may develop.9 Erosive pustular dermatosis is a diagnosis of exclusion but often is seen in older adults with chronic sun damage and clinically manifests with eroded plaques with adherent crusts.10
While our patient presented with several overlapping clinical features, including progressive hair loss along the frontal scalp in a bandlike pattern suspicious for frontal fibrosing alopecia as well as atrophic depigmented plaques with adherent peripheral scaling suspicious for discoid lupus erythematosus, the presence of pustules was an important clue. The biopsy demonstrating a mixed infiltrate inclusive of neutrophils confirmed the diagnosis of FD.
THE DIAGNOSIS: Folliculitis Decalvans
Biopsy results revealed a brisk perifollicular and intrafollicular mixed inflammatory infiltrate comprising lymphocytes, neutrophils, and plasma cells filling the upper dermis and encircling dilated hair follicles. Elastic stain (Verhoeff-van Gieson) demonstrated loss of elastic fibers in areas of scarring. Periodic acid–Schiff with diastase staining was negative for fungal elements, while Gram staining revealed colonies of bacterial cocci in the stratum corneum and within the hair follicles. Immunofluorescence was unremarkable, and culture revealed methicillin-sensitive Staphylococcus aureus, leading to a diagnosis of folliculitis decalvans (FD). The patient was treated with doxycycline 100 mg twice daily and received intralesional triamcinolone 2.5 mg/mL (total volume, 2 mL) every 6 weeks with considerable improvement in pustules, erythema, and scaling (Figure). While not yet in complete remission, our patient demonstrated short regrowing hairs in areas of incomplete scarring and focal remaining perifollicular erythema and scale along the midline frontal scalp 5 months after initial presentation.
Folliculitis decalvans is an uncommon subtype of cicatricial alopecia that may mimic other forms of alopecia. Cicatricial alopecia often is difficult to diagnose due to its overlapping clinical characteristics, but early diagnosis is essential for appropriate management and prevention of further permanent hair loss. Traditionally classified as a primary neutrophilic cicatricial alopecia, lymphocyte-predominant variants of FD now are recognized.1
Patients with FD typically present with patchy scarring alopecia at the vertex scalp that gradually expands and may demonstrate secondary features of follicular tufting and pustules.1-3 While the epidemiology of FD is poorly characterized, Vañó-Galván et al4 reported that FD accounted for 2.8% of all alopecia cases and 10.5% of cicatricial alopecia cases in a multicenter study of 2835 patients. The pathophysiology of FD still is under investigation but is thought to result from a dysregulated immune response to a chronic bacterial infection (eg, S aureus), with resulting neutrophilpredominant inflammation in early stages.1-3 Vañó-Galván et al4 reported that, among 35 patients with FD cultured for bacteria, 74% (26/35) returned positive results, 96% (25/26) of which grew S aureus.5
A systematic review of 20 studies that included 263 patients found rifampin and clindamycin to be the most common treatments for FD; however, there is insufficient evidence to determine if this treatment is the most effective.6 In our patient, clindamycin was avoided due to its propensity to negatively alter the gut microbiome long term.7 Other therapies such as oral tetracyclines, high-potency topical steroids, and intralesional triamcinolone also can be used to achieve disease remission.5,6 Other treatments such as isotretinoin, red-light photodynamic therapy, tacrolimus, and external beam radiation have been reported in the literature but vary in efficacy.6 Our patient improved on a regimen of topical benzoyl peroxide wash, oral doxycycline, and intralesional triamcinolone.
Notably, FD may share clinical features with other causes of cicatricial alopecia. In our patient, FD mimicked other entities including discoid lupus erythematosus, frontal fibrosing alopecia, dissecting cellulitis, and erosive pustular dermatosis (Table).1-14 Discoid lupus erythematosus manifests as round hypopigmented and hyperpigmented plaques with associated atrophy, perifollicular erythema, and follicular plugging. Frontal fibrosing alopecia is a primary lymphocytic scarring alopecia that manifests in a bandlike linear distribution over the frontal scalp and may involve the temporal scalp, posterior hairline, and/or eyebrows. Isolated hairs (known as lonely hairs) often are seen. Dissecting cellulitis is characterized by boggy nodules associated with alopecia on the scalp without notable epidermal change, although pustules and sinus tracts may develop.9 Erosive pustular dermatosis is a diagnosis of exclusion but often is seen in older adults with chronic sun damage and clinically manifests with eroded plaques with adherent crusts.10
While our patient presented with several overlapping clinical features, including progressive hair loss along the frontal scalp in a bandlike pattern suspicious for frontal fibrosing alopecia as well as atrophic depigmented plaques with adherent peripheral scaling suspicious for discoid lupus erythematosus, the presence of pustules was an important clue. The biopsy demonstrating a mixed infiltrate inclusive of neutrophils confirmed the diagnosis of FD.
- Olsen EA, Bergfeld WF, Cotsarelis G, et al. Summary of North American Hair Research Society (NAHRS)-sponsored Workshop on Cicatricial Alopecia, Duke University Medical Center, February 10 and 11, 2001. J Am Acad Dermatol. 2003;48:103-110. doi:10.1067/mjd.2003.68
- Filbrandt R, Rufaut N, Jones L. Primary cicatricial alopecia: diagnosis and treatment. CMAJ. 2013;185:1579-1585. doi:10.1503/cmaj.111570
- Otberg N, Kang H, Alzolibani AA, et al. Folliculitis decalvans. Dermatol Ther. 2008;21:238-244. doi:10.1111/j.1529-8019.2008.00204.x
- Vañó-Galván S, Saceda-Corralo D, Blume-Peytavi U, et al. Frequency of the types of alopecia at twenty-two specialist hair clinics: a multicenter study. Skin Appendage Disord. 2019;5:309-315. doi:10.1159/000496708
- Vañó-Galván S, Molina-Ruiz AM, Fernández-Crehuet P, et al. Folliculitis decalvans: a multicentre review of 82 patients. J Eur Acad Dermatol Venereol. 2015;29:1750-1757. doi:10.1111/jdv.12993
- Rambhia PH, Conic RRZ, Murad A, et al. Updates in therapeutics for folliculitis decalvans: a systematic review with evidence-based analysis. J Am Acad Dermatol. 2019;80:794-801. doi:10.1016/j.jaad.2018.07.050
- Zimmermann P, Curtis N. The effect of antibiotics on the composition of the intestinal microbiota - a systematic review. J Infect. 2019;79:471-489. doi:10.1016/j.jinf.2019.10.008
- Kanti V, Röwert-Huber J, Vogt A, et al. Cicatricial alopecia. J Dtsch Dermatol Ges. 2018;16:435-461. doi:10.1111/ddg.13498
- Melo DF, Slaibi EB, Siqueira TMFM, et al. Trichoscopy findings in dissecting cellulitis. An Bras Dermatol. 2019;94:608-611. doi:10.1016/j.abd.2019.09.006
- Anzai A, Pirmez R, Vincenzi C, et al. Trichoscopy findings of frontal fibrosing alopecia on the eyebrows: a study of 151 cases. J Am Acad Dermatol. 2021;85:1130-1134. doi:10.1016/j.jaad.2019.12.023
- Starace M, Loi C, Bruni F, et al. Erosive pustular dermatosis of the scalp: clinical, trichoscopic, and histopathologic features of 20 cases. J Am Acad Dermatol. 2017;76:1109-1114. doi:10.1016/j.jaad.2016.12.016
- Rongioletti F, Christana K. Cicatricial (scarring) alopecias: an overview of pathogenesis, classification, diagnosis, and treatment. Am J Clin Dermatol. 2012;13:247-260. doi:10.2165/11596960-000000000-00000
- Badaoui A, Reygagne P, Cavelier-Balloy B, et al. Dissecting cellulitis of the scalp: a retrospective study of 51 patients and review of literature. Br J Dermatol. 2016;174:421-423. doi:10.1111/bjd.13999
- Michelerio A, Vassallo C, Fiandrino G, et al. Erosive pustular dermatosis of the scalp: a clinicopathologic study of fifty cases. Dermatopathology (Basel). 2021;8:450-462. doi:10.3390/dermatopathology8040048
- Olsen EA, Bergfeld WF, Cotsarelis G, et al. Summary of North American Hair Research Society (NAHRS)-sponsored Workshop on Cicatricial Alopecia, Duke University Medical Center, February 10 and 11, 2001. J Am Acad Dermatol. 2003;48:103-110. doi:10.1067/mjd.2003.68
- Filbrandt R, Rufaut N, Jones L. Primary cicatricial alopecia: diagnosis and treatment. CMAJ. 2013;185:1579-1585. doi:10.1503/cmaj.111570
- Otberg N, Kang H, Alzolibani AA, et al. Folliculitis decalvans. Dermatol Ther. 2008;21:238-244. doi:10.1111/j.1529-8019.2008.00204.x
- Vañó-Galván S, Saceda-Corralo D, Blume-Peytavi U, et al. Frequency of the types of alopecia at twenty-two specialist hair clinics: a multicenter study. Skin Appendage Disord. 2019;5:309-315. doi:10.1159/000496708
- Vañó-Galván S, Molina-Ruiz AM, Fernández-Crehuet P, et al. Folliculitis decalvans: a multicentre review of 82 patients. J Eur Acad Dermatol Venereol. 2015;29:1750-1757. doi:10.1111/jdv.12993
- Rambhia PH, Conic RRZ, Murad A, et al. Updates in therapeutics for folliculitis decalvans: a systematic review with evidence-based analysis. J Am Acad Dermatol. 2019;80:794-801. doi:10.1016/j.jaad.2018.07.050
- Zimmermann P, Curtis N. The effect of antibiotics on the composition of the intestinal microbiota - a systematic review. J Infect. 2019;79:471-489. doi:10.1016/j.jinf.2019.10.008
- Kanti V, Röwert-Huber J, Vogt A, et al. Cicatricial alopecia. J Dtsch Dermatol Ges. 2018;16:435-461. doi:10.1111/ddg.13498
- Melo DF, Slaibi EB, Siqueira TMFM, et al. Trichoscopy findings in dissecting cellulitis. An Bras Dermatol. 2019;94:608-611. doi:10.1016/j.abd.2019.09.006
- Anzai A, Pirmez R, Vincenzi C, et al. Trichoscopy findings of frontal fibrosing alopecia on the eyebrows: a study of 151 cases. J Am Acad Dermatol. 2021;85:1130-1134. doi:10.1016/j.jaad.2019.12.023
- Starace M, Loi C, Bruni F, et al. Erosive pustular dermatosis of the scalp: clinical, trichoscopic, and histopathologic features of 20 cases. J Am Acad Dermatol. 2017;76:1109-1114. doi:10.1016/j.jaad.2016.12.016
- Rongioletti F, Christana K. Cicatricial (scarring) alopecias: an overview of pathogenesis, classification, diagnosis, and treatment. Am J Clin Dermatol. 2012;13:247-260. doi:10.2165/11596960-000000000-00000
- Badaoui A, Reygagne P, Cavelier-Balloy B, et al. Dissecting cellulitis of the scalp: a retrospective study of 51 patients and review of literature. Br J Dermatol. 2016;174:421-423. doi:10.1111/bjd.13999
- Michelerio A, Vassallo C, Fiandrino G, et al. Erosive pustular dermatosis of the scalp: a clinicopathologic study of fifty cases. Dermatopathology (Basel). 2021;8:450-462. doi:10.3390/dermatopathology8040048
Alopecia and Pruritic Rash on the Forehead and Scalp
Alopecia and Pruritic Rash on the Forehead and Scalp
A 52-year-old woman presented to the dermatology department with an intermittently pruritic rash in a bandlike distribution on the left upper forehead and the frontal and temporal scalp of 4 years’ duration. The rash initially was diagnosed as psoriasis at an outside facility. Treatment over the year prior to presentation included tildrakizumab-asmn; topical crisaborole 2%; and excimer laser, which was complicated by blistering. The patient reported no history of topical or injected steroid use in the involved areas. Physical examination at the current presentation revealed arcuate erythematous plaques with follicular prominence, perifollicular scaling, pustules, and lone hairs. There also were porcelain-white atrophic plaques with loss of follicular ostia that were most prominent over the temporal scalp. A biopsy of the left lateral forehead was performed.

