User login
Asymptomatic Enlarging Lobulated Mass on the Lower Leg
Asymptomatic Enlarging Lobulated Mass on the Lower Leg
THE DIAGNOSIS: Dermatofibroma
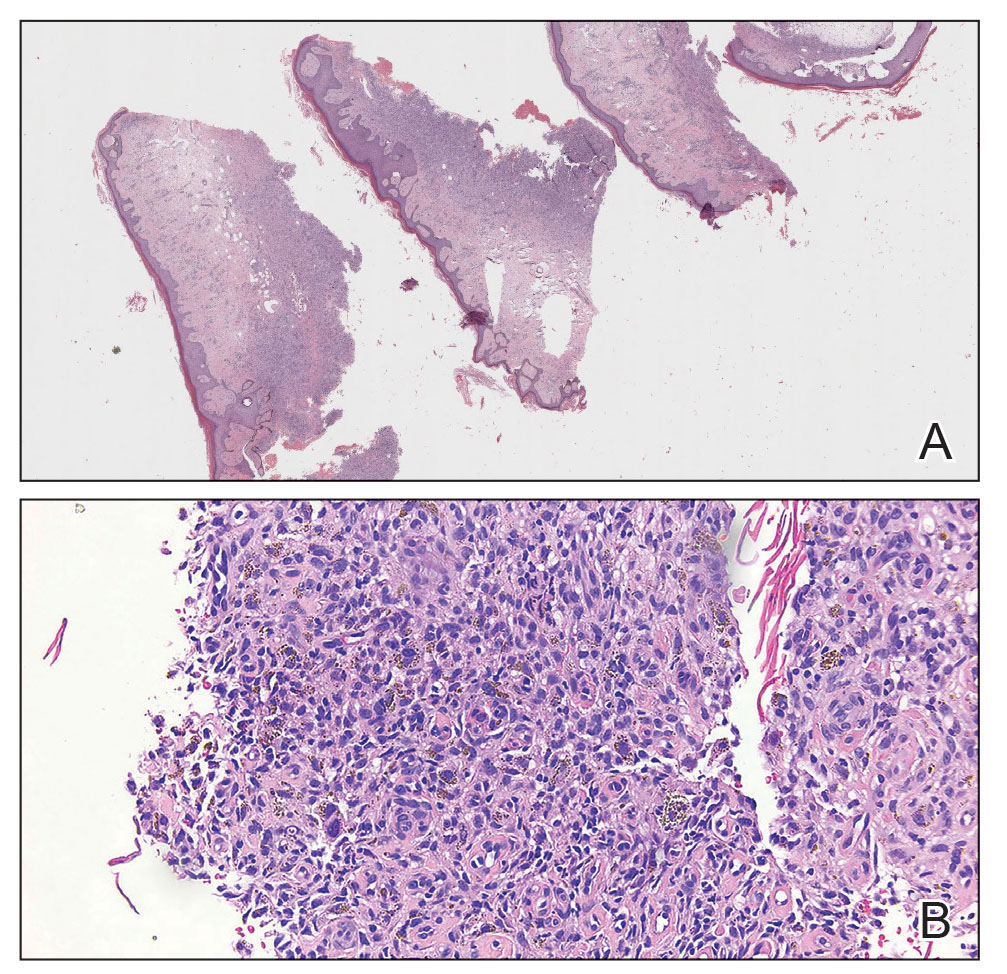
Histopathologic examination of the shave biopsy revealed fascicles of plump fibroblasts and histiocytes interposed between thick collagen bundles within the dermis, consistent with a diagnosis of dermatofibroma (DF). Dermatofibroma is a common benign skin tumor that classically manifests as brownish or reddish-brown firm papules or nodules that dimple when compressed. While the exact etiology of DF remains uncertain, it is believed to arise from a combined neoplastic and reactive fibroblastic proliferation process in response to stimuli, such as minor trauma or insect bites (as in our patient).1
On histopathology, the most common findings associated with DF are dermal proliferation of spindle-shaped fibroblasts arranged in a storiform or whorled pattern.2 In this patient, fascicles of plump fibroblasts and histiocytes were observed interspersed among thick collagen bundles within the dermis (Figure). Other histologic variants of DF include cellular, histiocytic, lipidized, angiomatous, aneurysmal, clear cell, monster cell, myxoid, keloidal, palisading, osteoclastic, and epithelioid.
On dermatoscopic examination, a pigment network is the most common feature, followed by a white scarlike patch, brown dots and globules, and vascular structures.2 Atypical DF variants can manifest with diverse clinical morphologies; one example is giant DF, which exceeds 5 cm and may exhibit an ulcerated or pedunculated appearance, as seen in our case.3 In such cases, a thorough clinical examination coupled with histopathologic analysis becomes paramount for accurate diagnosis.
Most cases of DF do not require intervention unless there are cosmetic concerns or the lesions are symptomatic. Surgical excision is a common and effective treatment method but results in scarring. Intralesional steroid injection and cryotherapy are less aggressive treatment options but have limited efficacy. Lasers, including carbon dioxide and pulsed dye lasers, are infrequently used; however, recurrence is possible with any treatment modality.4 Local recurrence is common, occurring in 26% to 50% of cases, particularly in atypical dermatofibroma variants after treatment.5 Recurrence is more likely with primary lesions larger than 1 cm.5
Several conditions share clinical features with DF, necessitating a thorough differential diagnosis. Dermatofibrosarcoma protuberans (DFSP) is a rare, locally aggressive, malignant tumor with a propensity for recurrence. It manifests as a slow-growing, red-brown, indurated plaque with irregular nodularity. Immunohistochemical staining can be used to differentiate DF from DFSP, with DF typically expressing factor XIIIa and lacking CD34, whereas DFSP exhibits CD34 positivity and lacks factor XIIIa expression.6 Another diagnosis in the differential is fibrosarcoma, a malignant tumor of fibroblasts that manifests as a painless, enlarging, poorly defined mass on the lower extremities. Histopathologic features include atypical fibroblasts and collagen with proliferation of atypical spindle-shaped cells.
Other benign lesions to consider include neurofibroma, which may manifest as a firm nodule but is derived from nerve tissue. Clinically, neurofibromas can be differentiated by their association with neurofibromatosis and softer texture. Cutaneous squamous cell carcinoma also should be considered, as it is a malignant proliferation of cutaneous epithelium that clinically manifests as a hyperkeratotic papule or plaque.5
- Hui P, J. Glusac E, Sinard JH, et al. Clonal analysis of cutaneous fibrous histiocytoma (dermatofibroma). J Cutan Pathol. 2002;29:385-389.
- Şenel E, Yuyucu Karabulut Y, Doğruer Şenel S. Clinical, histopathological, dermatoscopic and digital microscopic features of dermatofibroma: a retrospective analysis of 200 lesions. J Eur Acad Derm Venereol. 2015;29:1958-1966.
- Requena L, Fariña MC, Fuente C, et al. Giant dermatofibroma: a little-known clinical variant of dermatofibroma. J Am Acad Dermatol. 1994;30:714-718.
- Alonso-Castro L, Boixeda P, Segura-Palacios JM, et al. Dermatofibromas treated with pulsed dye laser: clinical and dermoscopic outcomes. J Cosmet Laser Ther. 2012;14:98-101.
- Gaufin M, Michaelis T, Duffy K. Cellular dermatofibroma: clinicopathologic review of 218 cases of cellular dermatofibroma to determine the clinical recurrence rate. Dermatol Surg. 2019;45:1359-1364.
- West KL, Cardona DM, Su Z, et al. Immunohistochemical markers in fibrohistiocytic lesions: factor XIIIa, CD34, S-100 and p75. Am J Dermatopathol. 2014;36:414-419.
THE DIAGNOSIS: Dermatofibroma
Histopathologic examination of the shave biopsy revealed fascicles of plump fibroblasts and histiocytes interposed between thick collagen bundles within the dermis, consistent with a diagnosis of dermatofibroma (DF). Dermatofibroma is a common benign skin tumor that classically manifests as brownish or reddish-brown firm papules or nodules that dimple when compressed. While the exact etiology of DF remains uncertain, it is believed to arise from a combined neoplastic and reactive fibroblastic proliferation process in response to stimuli, such as minor trauma or insect bites (as in our patient).1
On histopathology, the most common findings associated with DF are dermal proliferation of spindle-shaped fibroblasts arranged in a storiform or whorled pattern.2 In this patient, fascicles of plump fibroblasts and histiocytes were observed interspersed among thick collagen bundles within the dermis (Figure). Other histologic variants of DF include cellular, histiocytic, lipidized, angiomatous, aneurysmal, clear cell, monster cell, myxoid, keloidal, palisading, osteoclastic, and epithelioid.
On dermatoscopic examination, a pigment network is the most common feature, followed by a white scarlike patch, brown dots and globules, and vascular structures.2 Atypical DF variants can manifest with diverse clinical morphologies; one example is giant DF, which exceeds 5 cm and may exhibit an ulcerated or pedunculated appearance, as seen in our case.3 In such cases, a thorough clinical examination coupled with histopathologic analysis becomes paramount for accurate diagnosis.
Most cases of DF do not require intervention unless there are cosmetic concerns or the lesions are symptomatic. Surgical excision is a common and effective treatment method but results in scarring. Intralesional steroid injection and cryotherapy are less aggressive treatment options but have limited efficacy. Lasers, including carbon dioxide and pulsed dye lasers, are infrequently used; however, recurrence is possible with any treatment modality.4 Local recurrence is common, occurring in 26% to 50% of cases, particularly in atypical dermatofibroma variants after treatment.5 Recurrence is more likely with primary lesions larger than 1 cm.5
Several conditions share clinical features with DF, necessitating a thorough differential diagnosis. Dermatofibrosarcoma protuberans (DFSP) is a rare, locally aggressive, malignant tumor with a propensity for recurrence. It manifests as a slow-growing, red-brown, indurated plaque with irregular nodularity. Immunohistochemical staining can be used to differentiate DF from DFSP, with DF typically expressing factor XIIIa and lacking CD34, whereas DFSP exhibits CD34 positivity and lacks factor XIIIa expression.6 Another diagnosis in the differential is fibrosarcoma, a malignant tumor of fibroblasts that manifests as a painless, enlarging, poorly defined mass on the lower extremities. Histopathologic features include atypical fibroblasts and collagen with proliferation of atypical spindle-shaped cells.
Other benign lesions to consider include neurofibroma, which may manifest as a firm nodule but is derived from nerve tissue. Clinically, neurofibromas can be differentiated by their association with neurofibromatosis and softer texture. Cutaneous squamous cell carcinoma also should be considered, as it is a malignant proliferation of cutaneous epithelium that clinically manifests as a hyperkeratotic papule or plaque.5
THE DIAGNOSIS: Dermatofibroma
Histopathologic examination of the shave biopsy revealed fascicles of plump fibroblasts and histiocytes interposed between thick collagen bundles within the dermis, consistent with a diagnosis of dermatofibroma (DF). Dermatofibroma is a common benign skin tumor that classically manifests as brownish or reddish-brown firm papules or nodules that dimple when compressed. While the exact etiology of DF remains uncertain, it is believed to arise from a combined neoplastic and reactive fibroblastic proliferation process in response to stimuli, such as minor trauma or insect bites (as in our patient).1
On histopathology, the most common findings associated with DF are dermal proliferation of spindle-shaped fibroblasts arranged in a storiform or whorled pattern.2 In this patient, fascicles of plump fibroblasts and histiocytes were observed interspersed among thick collagen bundles within the dermis (Figure). Other histologic variants of DF include cellular, histiocytic, lipidized, angiomatous, aneurysmal, clear cell, monster cell, myxoid, keloidal, palisading, osteoclastic, and epithelioid.
On dermatoscopic examination, a pigment network is the most common feature, followed by a white scarlike patch, brown dots and globules, and vascular structures.2 Atypical DF variants can manifest with diverse clinical morphologies; one example is giant DF, which exceeds 5 cm and may exhibit an ulcerated or pedunculated appearance, as seen in our case.3 In such cases, a thorough clinical examination coupled with histopathologic analysis becomes paramount for accurate diagnosis.
Most cases of DF do not require intervention unless there are cosmetic concerns or the lesions are symptomatic. Surgical excision is a common and effective treatment method but results in scarring. Intralesional steroid injection and cryotherapy are less aggressive treatment options but have limited efficacy. Lasers, including carbon dioxide and pulsed dye lasers, are infrequently used; however, recurrence is possible with any treatment modality.4 Local recurrence is common, occurring in 26% to 50% of cases, particularly in atypical dermatofibroma variants after treatment.5 Recurrence is more likely with primary lesions larger than 1 cm.5
Several conditions share clinical features with DF, necessitating a thorough differential diagnosis. Dermatofibrosarcoma protuberans (DFSP) is a rare, locally aggressive, malignant tumor with a propensity for recurrence. It manifests as a slow-growing, red-brown, indurated plaque with irregular nodularity. Immunohistochemical staining can be used to differentiate DF from DFSP, with DF typically expressing factor XIIIa and lacking CD34, whereas DFSP exhibits CD34 positivity and lacks factor XIIIa expression.6 Another diagnosis in the differential is fibrosarcoma, a malignant tumor of fibroblasts that manifests as a painless, enlarging, poorly defined mass on the lower extremities. Histopathologic features include atypical fibroblasts and collagen with proliferation of atypical spindle-shaped cells.
Other benign lesions to consider include neurofibroma, which may manifest as a firm nodule but is derived from nerve tissue. Clinically, neurofibromas can be differentiated by their association with neurofibromatosis and softer texture. Cutaneous squamous cell carcinoma also should be considered, as it is a malignant proliferation of cutaneous epithelium that clinically manifests as a hyperkeratotic papule or plaque.5
- Hui P, J. Glusac E, Sinard JH, et al. Clonal analysis of cutaneous fibrous histiocytoma (dermatofibroma). J Cutan Pathol. 2002;29:385-389.
- Şenel E, Yuyucu Karabulut Y, Doğruer Şenel S. Clinical, histopathological, dermatoscopic and digital microscopic features of dermatofibroma: a retrospective analysis of 200 lesions. J Eur Acad Derm Venereol. 2015;29:1958-1966.
- Requena L, Fariña MC, Fuente C, et al. Giant dermatofibroma: a little-known clinical variant of dermatofibroma. J Am Acad Dermatol. 1994;30:714-718.
- Alonso-Castro L, Boixeda P, Segura-Palacios JM, et al. Dermatofibromas treated with pulsed dye laser: clinical and dermoscopic outcomes. J Cosmet Laser Ther. 2012;14:98-101.
- Gaufin M, Michaelis T, Duffy K. Cellular dermatofibroma: clinicopathologic review of 218 cases of cellular dermatofibroma to determine the clinical recurrence rate. Dermatol Surg. 2019;45:1359-1364.
- West KL, Cardona DM, Su Z, et al. Immunohistochemical markers in fibrohistiocytic lesions: factor XIIIa, CD34, S-100 and p75. Am J Dermatopathol. 2014;36:414-419.
- Hui P, J. Glusac E, Sinard JH, et al. Clonal analysis of cutaneous fibrous histiocytoma (dermatofibroma). J Cutan Pathol. 2002;29:385-389.
- Şenel E, Yuyucu Karabulut Y, Doğruer Şenel S. Clinical, histopathological, dermatoscopic and digital microscopic features of dermatofibroma: a retrospective analysis of 200 lesions. J Eur Acad Derm Venereol. 2015;29:1958-1966.
- Requena L, Fariña MC, Fuente C, et al. Giant dermatofibroma: a little-known clinical variant of dermatofibroma. J Am Acad Dermatol. 1994;30:714-718.
- Alonso-Castro L, Boixeda P, Segura-Palacios JM, et al. Dermatofibromas treated with pulsed dye laser: clinical and dermoscopic outcomes. J Cosmet Laser Ther. 2012;14:98-101.
- Gaufin M, Michaelis T, Duffy K. Cellular dermatofibroma: clinicopathologic review of 218 cases of cellular dermatofibroma to determine the clinical recurrence rate. Dermatol Surg. 2019;45:1359-1364.
- West KL, Cardona DM, Su Z, et al. Immunohistochemical markers in fibrohistiocytic lesions: factor XIIIa, CD34, S-100 and p75. Am J Dermatopathol. 2014;36:414-419.
Asymptomatic Enlarging Lobulated Mass on the Lower Leg
Asymptomatic Enlarging Lobulated Mass on the Lower Leg
A 69-year-old woman presented to the dermatology clinic with enlarging nodules on the bilateral lower legs of several years’ duration. Cutaneous examination of the legs revealed a brown, pedunculated, lobulated nodule on the lateral right lower leg measuring 5.0×1.9 cm. The patient reported that the lesion first appeared after a mosquito bite and then slowly grew over several years. A shave biopsy of the lesion was performed.


Training Lifeguards to Assist in Skin Cancer Prevention
Training Lifeguards to Assist in Skin Cancer Prevention
Lifeguards play a crucial role in ensuring water safety, but they also are uniquely positioned to promote skin cancer prevention and proper sunscreen use.1,2 There are several benefits and challenges to offering skin cancer prevention training for lifeguards.3 We examine the advantages of training, highlight the role lifeguards can play in larger public skin cancer prevention efforts, and address practical techniques for developing lifeguardfocused skin cancer education programs. By providing this knowledge to lifeguards, we can improve community health outcomes and encourage sun-safe behaviors in high-risk outdoor locations.
Benefits of Skin Cancer Prevention Training for Lifeguards
Research has shown that lifeguards are at an elevated risk for basal cell carcinoma, squamous cell carcinoma, and melanoma due to frequent prolonged occupational sun exposure.1,2,4-6 Therefore, comprehensive education on skin cancer prevention—including instruction on proper sunscreen application techniques and the importance of regular reapplication as well as how to recognize suspicious skin lesions—should be incorporated into lifeguard certification programs. One study evaluating the effectiveness of a skin cancer prevention program for lifeguards found that many of the participants lacked a thorough understanding of the different types of skin cancer.5 Another study found that lifeguards at pools in areas where societal norms supporting sun safety are stronger exhibited noticeably more sun protection practices, with regression estimates of 0.22 (95% CI, 0.17-0.26).7 Empowering lifeguards with valuable health knowledge during their regular training could potentially reduce their risk for skin cancer,4 as they may be more inclined to use sunscreen appropriately and reach out to a dermatologist for regular skin checks and evaluation of suspicious lesions.
Role of Lifeguards in Public Skin Cancer Prevention Efforts
Once trained on skin cancer prevention, lifeguards also can play a pivotal role in promoting sunscreen use among the public. Despite the widespread availability of high-quality sunscreens, many swimmers and beachgoers neglect to regularly apply or reapply sunscreen, especially on commonly exposed areas such as the back, shoulders, and face.8 Educating lifeguards on skin cancer prevention could enhance health outcomes by increasing early detection rates and promoting sun-safe behaviors among the general public.9 However, additional training requirements might increase the cost and time commitment for lifeguard certification, potentially leading to staffing shortages.3,7 There also is a risk of lifeguards overstepping their role and providing inaccurate medical advice, which could cause distress or even lead to liability issues.7 Balancing these factors will be crucial in developing effective and sustainable skin cancer prevention programs for lifeguards.
Implementing Lifeguard Skin Cancer Training
Implementing skin cancer prevention training programs for lifeguards requires strategic collaboration between dermatologists, and lifeguard training organizations to ensure that the participants receive consistent and comprehensive training.10 Additionally, public health campaigns can support these efforts by raising awareness about the importance of sun safety and regular skin checks.6 Tailored training modules/materials, ongoing technical assistance, and active, multicomponent approaches that account for both individual and environmental factors can increase program implementation in a variety of community settings.
Final Thoughts
Through effective education, lifeguards can potentially have a substantial impact on skin cancer prevention, both among lifeguards themselves and the general public. By promoting proper sunscreen use, lifeguards can help reduce the incidence and mortality associated with skin cancers. Future studies should focus on developing and implementing targeted education initiatives for lifeguards, fostering collaboration between relevant stakeholders, and raising public awareness about the importance of sun safety and early skin cancer detection. These efforts ultimately could lead to improved public health outcomes and reduced skin cancer rates, particularly in high-risk populations that frequently are exposed to UV radiation.
- Enos CW, Rey S, Slocum J, et al. Sun-protection behaviors among active members of the United States Lifesaving Association. J Clin Aesthet Dermatol. 2021;14:14-20.
- Verma K, Lewis DJ, Siddiqui FS, et al. Mohs micrographic surgery management of melanoma and melanoma in situ. StatPearls. Updated August 28, 2024. Accessed April 15, 2025. https://www.ncbi.nlm.nih.gov/books/NBK606123/
- Verma KK, Joshi TP, Lewis DJ, et al. Nail technicians as partners in early melanoma detection: bridging the knowledge gap. Arch Dermatol Res. 2024;316:586. doi:10.1007/s00403-024-03342-0
- Geller AC, Glanz K, Shigaki D, et al. Impact of skin cancer prevention on outdoor aquatics staff: the Pool Cool program in Hawaii and Massachusetts. Prev Med. 2001;33:155-161. doi:10.1006/pmed.2001.0870
- Hiemstra M, Glanz K, Nehl E. Changes in sunburn and tanning attitudes among lifeguards over a summer season. J Am Acad Dermatol. 2012;66:430-437. doi:10.1016/j.jaad.2010.11.050
- Verma KK, Ahmad N, Friedmann DP, et al. Melanoma in tattooed skin: diagnostic challenges and the potential for tattoo artists in early detection. Arch Dermatol Res. 2024;316:690. doi:10.1007/s00403-024-03415-0
- Hall DM, McCarty F, Elliott T, et al. Lifeguards’ sun protection habits and sunburns: association with sun-safe environments and skin cancer prevention program participation. Arch Dermatol. 2009;145:139-144. doi:10.1001/archdermatol.2008.553
- Emmons KM, Geller AC, Puleo E, et al. Skin cancer education and early detection at the beach: a randomized trial of dermatologist examination and biometric feedback. J Am Acad Dermatol. 2011;64:282-289. doi:10.1016/j.jaad.2010.01.040
- Rabin BA, Nehl E, Elliott T, et al. Individual and setting level predictors of the implementation of a skin cancer prevention program: a multilevel analysis. Implement Sci. 2010;5:40. doi:10.1186/1748-5908-5-40
- Walkosz BJ, Buller D, Buller M, et al. Sun safe workplaces: effect of an occupational skin cancer prevention program on employee sun safety practices. J Occup Environ Med. 2018;60:900-997. doi:10.1097 /JOM.0000000000001427
Lifeguards play a crucial role in ensuring water safety, but they also are uniquely positioned to promote skin cancer prevention and proper sunscreen use.1,2 There are several benefits and challenges to offering skin cancer prevention training for lifeguards.3 We examine the advantages of training, highlight the role lifeguards can play in larger public skin cancer prevention efforts, and address practical techniques for developing lifeguardfocused skin cancer education programs. By providing this knowledge to lifeguards, we can improve community health outcomes and encourage sun-safe behaviors in high-risk outdoor locations.
Benefits of Skin Cancer Prevention Training for Lifeguards
Research has shown that lifeguards are at an elevated risk for basal cell carcinoma, squamous cell carcinoma, and melanoma due to frequent prolonged occupational sun exposure.1,2,4-6 Therefore, comprehensive education on skin cancer prevention—including instruction on proper sunscreen application techniques and the importance of regular reapplication as well as how to recognize suspicious skin lesions—should be incorporated into lifeguard certification programs. One study evaluating the effectiveness of a skin cancer prevention program for lifeguards found that many of the participants lacked a thorough understanding of the different types of skin cancer.5 Another study found that lifeguards at pools in areas where societal norms supporting sun safety are stronger exhibited noticeably more sun protection practices, with regression estimates of 0.22 (95% CI, 0.17-0.26).7 Empowering lifeguards with valuable health knowledge during their regular training could potentially reduce their risk for skin cancer,4 as they may be more inclined to use sunscreen appropriately and reach out to a dermatologist for regular skin checks and evaluation of suspicious lesions.
Role of Lifeguards in Public Skin Cancer Prevention Efforts
Once trained on skin cancer prevention, lifeguards also can play a pivotal role in promoting sunscreen use among the public. Despite the widespread availability of high-quality sunscreens, many swimmers and beachgoers neglect to regularly apply or reapply sunscreen, especially on commonly exposed areas such as the back, shoulders, and face.8 Educating lifeguards on skin cancer prevention could enhance health outcomes by increasing early detection rates and promoting sun-safe behaviors among the general public.9 However, additional training requirements might increase the cost and time commitment for lifeguard certification, potentially leading to staffing shortages.3,7 There also is a risk of lifeguards overstepping their role and providing inaccurate medical advice, which could cause distress or even lead to liability issues.7 Balancing these factors will be crucial in developing effective and sustainable skin cancer prevention programs for lifeguards.
Implementing Lifeguard Skin Cancer Training
Implementing skin cancer prevention training programs for lifeguards requires strategic collaboration between dermatologists, and lifeguard training organizations to ensure that the participants receive consistent and comprehensive training.10 Additionally, public health campaigns can support these efforts by raising awareness about the importance of sun safety and regular skin checks.6 Tailored training modules/materials, ongoing technical assistance, and active, multicomponent approaches that account for both individual and environmental factors can increase program implementation in a variety of community settings.
Final Thoughts
Through effective education, lifeguards can potentially have a substantial impact on skin cancer prevention, both among lifeguards themselves and the general public. By promoting proper sunscreen use, lifeguards can help reduce the incidence and mortality associated with skin cancers. Future studies should focus on developing and implementing targeted education initiatives for lifeguards, fostering collaboration between relevant stakeholders, and raising public awareness about the importance of sun safety and early skin cancer detection. These efforts ultimately could lead to improved public health outcomes and reduced skin cancer rates, particularly in high-risk populations that frequently are exposed to UV radiation.
Lifeguards play a crucial role in ensuring water safety, but they also are uniquely positioned to promote skin cancer prevention and proper sunscreen use.1,2 There are several benefits and challenges to offering skin cancer prevention training for lifeguards.3 We examine the advantages of training, highlight the role lifeguards can play in larger public skin cancer prevention efforts, and address practical techniques for developing lifeguardfocused skin cancer education programs. By providing this knowledge to lifeguards, we can improve community health outcomes and encourage sun-safe behaviors in high-risk outdoor locations.
Benefits of Skin Cancer Prevention Training for Lifeguards
Research has shown that lifeguards are at an elevated risk for basal cell carcinoma, squamous cell carcinoma, and melanoma due to frequent prolonged occupational sun exposure.1,2,4-6 Therefore, comprehensive education on skin cancer prevention—including instruction on proper sunscreen application techniques and the importance of regular reapplication as well as how to recognize suspicious skin lesions—should be incorporated into lifeguard certification programs. One study evaluating the effectiveness of a skin cancer prevention program for lifeguards found that many of the participants lacked a thorough understanding of the different types of skin cancer.5 Another study found that lifeguards at pools in areas where societal norms supporting sun safety are stronger exhibited noticeably more sun protection practices, with regression estimates of 0.22 (95% CI, 0.17-0.26).7 Empowering lifeguards with valuable health knowledge during their regular training could potentially reduce their risk for skin cancer,4 as they may be more inclined to use sunscreen appropriately and reach out to a dermatologist for regular skin checks and evaluation of suspicious lesions.
Role of Lifeguards in Public Skin Cancer Prevention Efforts
Once trained on skin cancer prevention, lifeguards also can play a pivotal role in promoting sunscreen use among the public. Despite the widespread availability of high-quality sunscreens, many swimmers and beachgoers neglect to regularly apply or reapply sunscreen, especially on commonly exposed areas such as the back, shoulders, and face.8 Educating lifeguards on skin cancer prevention could enhance health outcomes by increasing early detection rates and promoting sun-safe behaviors among the general public.9 However, additional training requirements might increase the cost and time commitment for lifeguard certification, potentially leading to staffing shortages.3,7 There also is a risk of lifeguards overstepping their role and providing inaccurate medical advice, which could cause distress or even lead to liability issues.7 Balancing these factors will be crucial in developing effective and sustainable skin cancer prevention programs for lifeguards.
Implementing Lifeguard Skin Cancer Training
Implementing skin cancer prevention training programs for lifeguards requires strategic collaboration between dermatologists, and lifeguard training organizations to ensure that the participants receive consistent and comprehensive training.10 Additionally, public health campaigns can support these efforts by raising awareness about the importance of sun safety and regular skin checks.6 Tailored training modules/materials, ongoing technical assistance, and active, multicomponent approaches that account for both individual and environmental factors can increase program implementation in a variety of community settings.
Final Thoughts
Through effective education, lifeguards can potentially have a substantial impact on skin cancer prevention, both among lifeguards themselves and the general public. By promoting proper sunscreen use, lifeguards can help reduce the incidence and mortality associated with skin cancers. Future studies should focus on developing and implementing targeted education initiatives for lifeguards, fostering collaboration between relevant stakeholders, and raising public awareness about the importance of sun safety and early skin cancer detection. These efforts ultimately could lead to improved public health outcomes and reduced skin cancer rates, particularly in high-risk populations that frequently are exposed to UV radiation.
- Enos CW, Rey S, Slocum J, et al. Sun-protection behaviors among active members of the United States Lifesaving Association. J Clin Aesthet Dermatol. 2021;14:14-20.
- Verma K, Lewis DJ, Siddiqui FS, et al. Mohs micrographic surgery management of melanoma and melanoma in situ. StatPearls. Updated August 28, 2024. Accessed April 15, 2025. https://www.ncbi.nlm.nih.gov/books/NBK606123/
- Verma KK, Joshi TP, Lewis DJ, et al. Nail technicians as partners in early melanoma detection: bridging the knowledge gap. Arch Dermatol Res. 2024;316:586. doi:10.1007/s00403-024-03342-0
- Geller AC, Glanz K, Shigaki D, et al. Impact of skin cancer prevention on outdoor aquatics staff: the Pool Cool program in Hawaii and Massachusetts. Prev Med. 2001;33:155-161. doi:10.1006/pmed.2001.0870
- Hiemstra M, Glanz K, Nehl E. Changes in sunburn and tanning attitudes among lifeguards over a summer season. J Am Acad Dermatol. 2012;66:430-437. doi:10.1016/j.jaad.2010.11.050
- Verma KK, Ahmad N, Friedmann DP, et al. Melanoma in tattooed skin: diagnostic challenges and the potential for tattoo artists in early detection. Arch Dermatol Res. 2024;316:690. doi:10.1007/s00403-024-03415-0
- Hall DM, McCarty F, Elliott T, et al. Lifeguards’ sun protection habits and sunburns: association with sun-safe environments and skin cancer prevention program participation. Arch Dermatol. 2009;145:139-144. doi:10.1001/archdermatol.2008.553
- Emmons KM, Geller AC, Puleo E, et al. Skin cancer education and early detection at the beach: a randomized trial of dermatologist examination and biometric feedback. J Am Acad Dermatol. 2011;64:282-289. doi:10.1016/j.jaad.2010.01.040
- Rabin BA, Nehl E, Elliott T, et al. Individual and setting level predictors of the implementation of a skin cancer prevention program: a multilevel analysis. Implement Sci. 2010;5:40. doi:10.1186/1748-5908-5-40
- Walkosz BJ, Buller D, Buller M, et al. Sun safe workplaces: effect of an occupational skin cancer prevention program on employee sun safety practices. J Occup Environ Med. 2018;60:900-997. doi:10.1097 /JOM.0000000000001427
- Enos CW, Rey S, Slocum J, et al. Sun-protection behaviors among active members of the United States Lifesaving Association. J Clin Aesthet Dermatol. 2021;14:14-20.
- Verma K, Lewis DJ, Siddiqui FS, et al. Mohs micrographic surgery management of melanoma and melanoma in situ. StatPearls. Updated August 28, 2024. Accessed April 15, 2025. https://www.ncbi.nlm.nih.gov/books/NBK606123/
- Verma KK, Joshi TP, Lewis DJ, et al. Nail technicians as partners in early melanoma detection: bridging the knowledge gap. Arch Dermatol Res. 2024;316:586. doi:10.1007/s00403-024-03342-0
- Geller AC, Glanz K, Shigaki D, et al. Impact of skin cancer prevention on outdoor aquatics staff: the Pool Cool program in Hawaii and Massachusetts. Prev Med. 2001;33:155-161. doi:10.1006/pmed.2001.0870
- Hiemstra M, Glanz K, Nehl E. Changes in sunburn and tanning attitudes among lifeguards over a summer season. J Am Acad Dermatol. 2012;66:430-437. doi:10.1016/j.jaad.2010.11.050
- Verma KK, Ahmad N, Friedmann DP, et al. Melanoma in tattooed skin: diagnostic challenges and the potential for tattoo artists in early detection. Arch Dermatol Res. 2024;316:690. doi:10.1007/s00403-024-03415-0
- Hall DM, McCarty F, Elliott T, et al. Lifeguards’ sun protection habits and sunburns: association with sun-safe environments and skin cancer prevention program participation. Arch Dermatol. 2009;145:139-144. doi:10.1001/archdermatol.2008.553
- Emmons KM, Geller AC, Puleo E, et al. Skin cancer education and early detection at the beach: a randomized trial of dermatologist examination and biometric feedback. J Am Acad Dermatol. 2011;64:282-289. doi:10.1016/j.jaad.2010.01.040
- Rabin BA, Nehl E, Elliott T, et al. Individual and setting level predictors of the implementation of a skin cancer prevention program: a multilevel analysis. Implement Sci. 2010;5:40. doi:10.1186/1748-5908-5-40
- Walkosz BJ, Buller D, Buller M, et al. Sun safe workplaces: effect of an occupational skin cancer prevention program on employee sun safety practices. J Occup Environ Med. 2018;60:900-997. doi:10.1097 /JOM.0000000000001427
Training Lifeguards to Assist in Skin Cancer Prevention
Training Lifeguards to Assist in Skin Cancer Prevention
