User login
Is air filtration the best public health intervention against respiratory viruses?
This transcript has been edited for clarity.
When it comes to the public health fight against respiratory viruses – COVID, flu, RSV, and so on – it has always struck me as strange how staunchly basically any intervention is opposed. Masking was, of course, the prototypical entrenched warfare of opposing ideologies, with advocates pointing to studies suggesting the efficacy of masking to prevent transmission and advocating for broad masking recommendations, and detractors citing studies that suggested masks were ineffective and characterizing masking policies as fascist overreach. I’ll admit that I was always perplexed by this a bit, as that particular intervention seemed so benign – a bit annoying, I guess, but not crazy.
I have come to appreciate what I call status quo bias, which is the tendency to reject any policy, advice, or intervention that would force you, as an individual, to change your usual behavior. We just don’t like to do that. It has made me think that the most successful public health interventions might be the ones that take the individual out of the loop. And air quality control seems an ideal fit here. Here is a potential intervention where you, the individual, have to do precisely nothing. The status quo is preserved. We just, you know, have cleaner indoor air.
But even the suggestion of air treatment systems as a bulwark against respiratory virus transmission has been met with not just skepticism but cynicism, and perhaps even defeatism. It seems that there are those out there who think there really is nothing we can do. Sickness is interpreted in a Calvinistic framework: You become ill because it is your pre-destiny. But maybe air treatment could actually work. It seems like it might, if a new paper from PLOS One is to be believed.
What we’re talking about is a study titled “Bipolar Ionization Rapidly Inactivates Real-World, Airborne Concentrations of Infective Respiratory Viruses” – a highly controlled, laboratory-based analysis of a bipolar ionization system which seems to rapidly reduce viral counts in the air.
The proposed mechanism of action is pretty simple. The ionization system – which, don’t worry, has been shown not to produce ozone – spits out positively and negatively charged particles, which float around the test chamber, designed to look like a pretty standard room that you might find in an office or a school.
Virus is then injected into the chamber through an aerosolization machine, to achieve concentrations on the order of what you might get standing within 6 feet or so of someone actively infected with COVID while they are breathing and talking.
The idea is that those ions stick to the virus particles, similar to how a balloon sticks to the wall after you rub it on your hair, and that tends to cause them to clump together and settle on surfaces more rapidly, and thus get farther away from their ports of entry to the human system: nose, mouth, and eyes. But the ions may also interfere with viruses’ ability to bind to cellular receptors, even in the air.
To quantify viral infectivity, the researchers used a biological system. Basically, you take air samples and expose a petri dish of cells to them and see how many cells die. Fewer cells dying, less infective. Under control conditions, you can see that virus infectivity does decrease over time. Time zero here is the end of a SARS-CoV-2 aerosolization.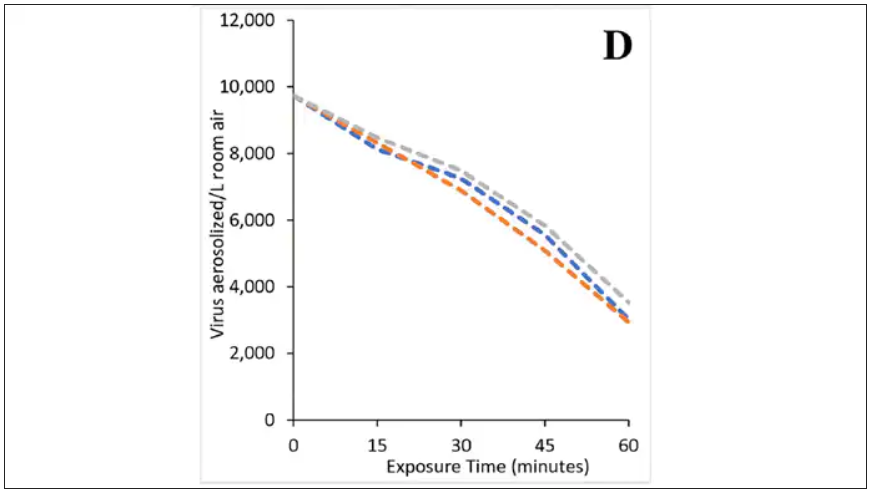
This may simply reflect the fact that virus particles settle out of the air. But As you can see, within about an hour, you have almost no infective virus detectable. That’s fairly impressive.
Now, I’m not saying that this is a panacea, but it is certainly worth considering the use of technologies like these if we are going to revamp the infrastructure of our offices and schools. And, of course, it would be nice to see this tested in a rigorous clinical trial with actual infected people, not cells, as the outcome. But I continue to be encouraged by interventions like this which, to be honest, ask very little of us as individuals. Maybe it’s time we accept the things, or people, that we cannot change.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. He reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
When it comes to the public health fight against respiratory viruses – COVID, flu, RSV, and so on – it has always struck me as strange how staunchly basically any intervention is opposed. Masking was, of course, the prototypical entrenched warfare of opposing ideologies, with advocates pointing to studies suggesting the efficacy of masking to prevent transmission and advocating for broad masking recommendations, and detractors citing studies that suggested masks were ineffective and characterizing masking policies as fascist overreach. I’ll admit that I was always perplexed by this a bit, as that particular intervention seemed so benign – a bit annoying, I guess, but not crazy.
I have come to appreciate what I call status quo bias, which is the tendency to reject any policy, advice, or intervention that would force you, as an individual, to change your usual behavior. We just don’t like to do that. It has made me think that the most successful public health interventions might be the ones that take the individual out of the loop. And air quality control seems an ideal fit here. Here is a potential intervention where you, the individual, have to do precisely nothing. The status quo is preserved. We just, you know, have cleaner indoor air.
But even the suggestion of air treatment systems as a bulwark against respiratory virus transmission has been met with not just skepticism but cynicism, and perhaps even defeatism. It seems that there are those out there who think there really is nothing we can do. Sickness is interpreted in a Calvinistic framework: You become ill because it is your pre-destiny. But maybe air treatment could actually work. It seems like it might, if a new paper from PLOS One is to be believed.
What we’re talking about is a study titled “Bipolar Ionization Rapidly Inactivates Real-World, Airborne Concentrations of Infective Respiratory Viruses” – a highly controlled, laboratory-based analysis of a bipolar ionization system which seems to rapidly reduce viral counts in the air.
The proposed mechanism of action is pretty simple. The ionization system – which, don’t worry, has been shown not to produce ozone – spits out positively and negatively charged particles, which float around the test chamber, designed to look like a pretty standard room that you might find in an office or a school.
Virus is then injected into the chamber through an aerosolization machine, to achieve concentrations on the order of what you might get standing within 6 feet or so of someone actively infected with COVID while they are breathing and talking.
The idea is that those ions stick to the virus particles, similar to how a balloon sticks to the wall after you rub it on your hair, and that tends to cause them to clump together and settle on surfaces more rapidly, and thus get farther away from their ports of entry to the human system: nose, mouth, and eyes. But the ions may also interfere with viruses’ ability to bind to cellular receptors, even in the air.
To quantify viral infectivity, the researchers used a biological system. Basically, you take air samples and expose a petri dish of cells to them and see how many cells die. Fewer cells dying, less infective. Under control conditions, you can see that virus infectivity does decrease over time. Time zero here is the end of a SARS-CoV-2 aerosolization.
This may simply reflect the fact that virus particles settle out of the air. But As you can see, within about an hour, you have almost no infective virus detectable. That’s fairly impressive.
Now, I’m not saying that this is a panacea, but it is certainly worth considering the use of technologies like these if we are going to revamp the infrastructure of our offices and schools. And, of course, it would be nice to see this tested in a rigorous clinical trial with actual infected people, not cells, as the outcome. But I continue to be encouraged by interventions like this which, to be honest, ask very little of us as individuals. Maybe it’s time we accept the things, or people, that we cannot change.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. He reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
When it comes to the public health fight against respiratory viruses – COVID, flu, RSV, and so on – it has always struck me as strange how staunchly basically any intervention is opposed. Masking was, of course, the prototypical entrenched warfare of opposing ideologies, with advocates pointing to studies suggesting the efficacy of masking to prevent transmission and advocating for broad masking recommendations, and detractors citing studies that suggested masks were ineffective and characterizing masking policies as fascist overreach. I’ll admit that I was always perplexed by this a bit, as that particular intervention seemed so benign – a bit annoying, I guess, but not crazy.
I have come to appreciate what I call status quo bias, which is the tendency to reject any policy, advice, or intervention that would force you, as an individual, to change your usual behavior. We just don’t like to do that. It has made me think that the most successful public health interventions might be the ones that take the individual out of the loop. And air quality control seems an ideal fit here. Here is a potential intervention where you, the individual, have to do precisely nothing. The status quo is preserved. We just, you know, have cleaner indoor air.
But even the suggestion of air treatment systems as a bulwark against respiratory virus transmission has been met with not just skepticism but cynicism, and perhaps even defeatism. It seems that there are those out there who think there really is nothing we can do. Sickness is interpreted in a Calvinistic framework: You become ill because it is your pre-destiny. But maybe air treatment could actually work. It seems like it might, if a new paper from PLOS One is to be believed.
What we’re talking about is a study titled “Bipolar Ionization Rapidly Inactivates Real-World, Airborne Concentrations of Infective Respiratory Viruses” – a highly controlled, laboratory-based analysis of a bipolar ionization system which seems to rapidly reduce viral counts in the air.
The proposed mechanism of action is pretty simple. The ionization system – which, don’t worry, has been shown not to produce ozone – spits out positively and negatively charged particles, which float around the test chamber, designed to look like a pretty standard room that you might find in an office or a school.
Virus is then injected into the chamber through an aerosolization machine, to achieve concentrations on the order of what you might get standing within 6 feet or so of someone actively infected with COVID while they are breathing and talking.
The idea is that those ions stick to the virus particles, similar to how a balloon sticks to the wall after you rub it on your hair, and that tends to cause them to clump together and settle on surfaces more rapidly, and thus get farther away from their ports of entry to the human system: nose, mouth, and eyes. But the ions may also interfere with viruses’ ability to bind to cellular receptors, even in the air.
To quantify viral infectivity, the researchers used a biological system. Basically, you take air samples and expose a petri dish of cells to them and see how many cells die. Fewer cells dying, less infective. Under control conditions, you can see that virus infectivity does decrease over time. Time zero here is the end of a SARS-CoV-2 aerosolization.
This may simply reflect the fact that virus particles settle out of the air. But As you can see, within about an hour, you have almost no infective virus detectable. That’s fairly impressive.
Now, I’m not saying that this is a panacea, but it is certainly worth considering the use of technologies like these if we are going to revamp the infrastructure of our offices and schools. And, of course, it would be nice to see this tested in a rigorous clinical trial with actual infected people, not cells, as the outcome. But I continue to be encouraged by interventions like this which, to be honest, ask very little of us as individuals. Maybe it’s time we accept the things, or people, that we cannot change.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. He reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Low-dose methotrexate carries higher risk for older patients with CKD
TOPLINE:
The use of low-dose methotrexate among older adults with chronic kidney disease (CKD) was associated with a significantly increased risk at 90 days for serious adverse events requiring a hospital visit, compared with starting treatment with hydroxychloroquine.
METHODOLOGY:
- In a retrospective, population-based cohort study conducted in Ontario, researchers used linked administrative healthcare data to identify adults aged 66 years and older with CKD who were not undergoing dialysis and were new to medication; CKD was defined as an estimated glomerular filtration rate (eGFR) of less than 60 mL/min per 1.73 m2.
- The study population included 2,309 individuals who began treatment with low-dose methotrexate (5-35 mg/week); they were matched with 2,309 individuals who began treatment with hydroxychloroquine (200-400 mg/day). The median age was 76 years, 69% were women, and rheumatoid arthritis was the most common diagnosis (56%).
- The primary outcome was the risk of a hospital visit at 90 days for a composite of serious adverse events that included myelosuppression, sepsis, pneumotoxic effects, or hepatoxic effects.
TAKEAWAY:
- Overall, 3.55% of methotrexate patients and 1.73% of hydroxychloroquine patients met the primary outcome (risk ratio, 2.05); these events occurred at a median of 49 days and 43 days after starting the medications for the two groups, respectively.
- In an analysis by eGFR category, the risk of serious adverse events at 90 days increased among patients with eGFR levels less than 45 mL/min per 1.73 m2 (RR, 2.79).
- In a secondary comparison, the 90-day risk of serious adverse events was higher among methotrexate patients who began treatment with doses of 15-35 mg/week in comparison with those whose initial doses were 5 to less than 15 mg/week.
IN PRACTICE:
“Patients with CKD starting low-dose methotrexate should have active surveillance, including blood tests and chest radiographs performed regularly to monitor for signs of myelosuppression, infection, hepatotoxic effects, and pneumotoxic effects,” the researchers wrote.
SOURCE:
The lead author on the study was Flory T. Muanda, MD, of Western University, London, Ont. The study was published online in JAMA Network Open.
LIMITATIONS:
The observational design and lack of data on patients’ adherence to medications were among the limiting factors, as were the focus on older adults with CKD and the lack of assessment of the risk-benefit ratio of low-dose methotrexate.
DISCLOSURES:
The study was supported by the Institute for Clinical Evaluative Sciences. Dr. Muanda had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
TOPLINE:
The use of low-dose methotrexate among older adults with chronic kidney disease (CKD) was associated with a significantly increased risk at 90 days for serious adverse events requiring a hospital visit, compared with starting treatment with hydroxychloroquine.
METHODOLOGY:
- In a retrospective, population-based cohort study conducted in Ontario, researchers used linked administrative healthcare data to identify adults aged 66 years and older with CKD who were not undergoing dialysis and were new to medication; CKD was defined as an estimated glomerular filtration rate (eGFR) of less than 60 mL/min per 1.73 m2.
- The study population included 2,309 individuals who began treatment with low-dose methotrexate (5-35 mg/week); they were matched with 2,309 individuals who began treatment with hydroxychloroquine (200-400 mg/day). The median age was 76 years, 69% were women, and rheumatoid arthritis was the most common diagnosis (56%).
- The primary outcome was the risk of a hospital visit at 90 days for a composite of serious adverse events that included myelosuppression, sepsis, pneumotoxic effects, or hepatoxic effects.
TAKEAWAY:
- Overall, 3.55% of methotrexate patients and 1.73% of hydroxychloroquine patients met the primary outcome (risk ratio, 2.05); these events occurred at a median of 49 days and 43 days after starting the medications for the two groups, respectively.
- In an analysis by eGFR category, the risk of serious adverse events at 90 days increased among patients with eGFR levels less than 45 mL/min per 1.73 m2 (RR, 2.79).
- In a secondary comparison, the 90-day risk of serious adverse events was higher among methotrexate patients who began treatment with doses of 15-35 mg/week in comparison with those whose initial doses were 5 to less than 15 mg/week.
IN PRACTICE:
“Patients with CKD starting low-dose methotrexate should have active surveillance, including blood tests and chest radiographs performed regularly to monitor for signs of myelosuppression, infection, hepatotoxic effects, and pneumotoxic effects,” the researchers wrote.
SOURCE:
The lead author on the study was Flory T. Muanda, MD, of Western University, London, Ont. The study was published online in JAMA Network Open.
LIMITATIONS:
The observational design and lack of data on patients’ adherence to medications were among the limiting factors, as were the focus on older adults with CKD and the lack of assessment of the risk-benefit ratio of low-dose methotrexate.
DISCLOSURES:
The study was supported by the Institute for Clinical Evaluative Sciences. Dr. Muanda had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
TOPLINE:
The use of low-dose methotrexate among older adults with chronic kidney disease (CKD) was associated with a significantly increased risk at 90 days for serious adverse events requiring a hospital visit, compared with starting treatment with hydroxychloroquine.
METHODOLOGY:
- In a retrospective, population-based cohort study conducted in Ontario, researchers used linked administrative healthcare data to identify adults aged 66 years and older with CKD who were not undergoing dialysis and were new to medication; CKD was defined as an estimated glomerular filtration rate (eGFR) of less than 60 mL/min per 1.73 m2.
- The study population included 2,309 individuals who began treatment with low-dose methotrexate (5-35 mg/week); they were matched with 2,309 individuals who began treatment with hydroxychloroquine (200-400 mg/day). The median age was 76 years, 69% were women, and rheumatoid arthritis was the most common diagnosis (56%).
- The primary outcome was the risk of a hospital visit at 90 days for a composite of serious adverse events that included myelosuppression, sepsis, pneumotoxic effects, or hepatoxic effects.
TAKEAWAY:
- Overall, 3.55% of methotrexate patients and 1.73% of hydroxychloroquine patients met the primary outcome (risk ratio, 2.05); these events occurred at a median of 49 days and 43 days after starting the medications for the two groups, respectively.
- In an analysis by eGFR category, the risk of serious adverse events at 90 days increased among patients with eGFR levels less than 45 mL/min per 1.73 m2 (RR, 2.79).
- In a secondary comparison, the 90-day risk of serious adverse events was higher among methotrexate patients who began treatment with doses of 15-35 mg/week in comparison with those whose initial doses were 5 to less than 15 mg/week.
IN PRACTICE:
“Patients with CKD starting low-dose methotrexate should have active surveillance, including blood tests and chest radiographs performed regularly to monitor for signs of myelosuppression, infection, hepatotoxic effects, and pneumotoxic effects,” the researchers wrote.
SOURCE:
The lead author on the study was Flory T. Muanda, MD, of Western University, London, Ont. The study was published online in JAMA Network Open.
LIMITATIONS:
The observational design and lack of data on patients’ adherence to medications were among the limiting factors, as were the focus on older adults with CKD and the lack of assessment of the risk-benefit ratio of low-dose methotrexate.
DISCLOSURES:
The study was supported by the Institute for Clinical Evaluative Sciences. Dr. Muanda had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
Nail psoriasis in Black patients often overlooked
NEW YORK – From clinical trials to textbooks, , even when the skin disease has already been diagnosed, according to Shari R. Lipner, MD.
In a recently published review of 45 randomized controlled trials of therapies for nail psoriasis, almost all included information about the gender of the patients enrolled, but only about 35% reported race and/or ethnicity, Dr. Lipner, associate professor of dermatology, Weill Cornell Medical College, New York, said at the Skin of Color Update 2023. The proportion climbed to 59% in trials that included at least one study site in the United States, although representation of non-White patients in studies conducted in the United States was not proportional to the population (13.4% vs. 39.9%), said Dr. Lipner, senior author of the review .
Black patients largely unrepresented in photos
When an Internet search was conducted for images of nail psoriasis, the proportion of images fell as the number of the Fitzpatrick scale increased. Fitzpatrick skin types 1 or 2 represented 70% of the images, skin types 3 to 4 represented about 27%, leaving just 3% represented by darker skin types, Dr. Lipner said.

“Unfortunately, things are not much better if you look at the dermatology and nail-specific textbooks. In fact, the percentages we see are almost identical,” said Dr. Lipner, noting that her review of images suggested that only about 3% of images in textbooks are of Fitzpatrick skin types 5 or 6, an obstacle for clinicians learning to recognize nail involvement in skin of color patients with psoriasis.
“We have written a couple of papers on this topic, including a call to action” in a letter to the editor in the Journal of the American Academy of Dermatology, Dr. Lipner noted. “To ensure access to safe and effective treatments for all patient populations,” she and her coauthor wrote, “we advocate the prioritized enrollment of racial and ethnic minority groups in psoriasis, PsA [psoriatic arthritis], and NP [nail psoriasis] clinical trials.”
Data from the 2009-2010 U.S. National Health and Nutrition Examination Survey (NHANES) confirms that psoriasis is less common in Blacks (1.9%) and Hispanics (1.6%) than Whites (3.6%). But these lower numbers still translate into substantial numbers nationally. Of those with psoriasis, the lifetime incidence of nail involvement has been variously estimated between 80% and 90%, Dr. Lipner said.
In about 10% of patients with psoriasis, nail involvement is isolated, occurring in the absence of skin lesions, a proportion that appears to be similar in Blacks and Whites according to Dr. Lipner.
Patient characteristics similar by race
In a study conducted at her own center, many of the characteristics of psoriasis were similar when those with a Fitzpatrick skin type 4 or higher were compared to those of 3 or lower. This included male-female distribution, smoking history, and presence of accompanying psoriatic arthritis. There was one discrepancy between lighter and darker skin.
“The big difference was that it took almost 3 years longer [on average] for darker skin to be diagnosed, and there was worse severity of disease,” Dr. Lipner said.
Like cutaneous manifestations of psoriasis, there are differences in appearance in the nail, many of which are simply produced by how skin color alters the appearance, such as the brownish hue of erythema in darker versus lighter skin. Dr. Lipner also noted that many of the features, such as keratosis, can be more severe in patients with darker skin types, but this is likely because of the delay in diagnosis.
The problem with overlooking nail psoriasis in patients of any skin color is the significant and independent adverse impact imposed by nail disease on quality of life, she added. She recounted the case of a 22-year-old Black patient whose nail psoriasis was overlooked even as she was being treated for her skin lesions.
“The diagnosis of nail psoriasis was missed for 3 years,” said Dr. Lipner, noting that the nail involvement was not trivial. “She had trouble doing her daily activities of life, but also, she was very embarrassed by her nails, not surprisingly.”
The problem of underrepresentation of Blacks in photos depicting nail diseases is not going unnoticed.
“Recently, there has been a concerted effort on the part of authors and editors to include more images of skin of color patients in published articles and textbooks,” said Jane S. Bellet, MD, professor of dermatology, Duke University, Durham, N.C.
An expert in nail disorders, particularly in children, Dr. Bellet said in an interview that this trend “must continue and increase in volume.” She said that the need for more images of nail disease in skin of color is not restricted to textbooks but includes “other learning materials, such as online atlases.”
Dr. Lipner and Dr. Bellet reported no potential conflicts of interest relative to this topic.
NEW YORK – From clinical trials to textbooks, , even when the skin disease has already been diagnosed, according to Shari R. Lipner, MD.
In a recently published review of 45 randomized controlled trials of therapies for nail psoriasis, almost all included information about the gender of the patients enrolled, but only about 35% reported race and/or ethnicity, Dr. Lipner, associate professor of dermatology, Weill Cornell Medical College, New York, said at the Skin of Color Update 2023. The proportion climbed to 59% in trials that included at least one study site in the United States, although representation of non-White patients in studies conducted in the United States was not proportional to the population (13.4% vs. 39.9%), said Dr. Lipner, senior author of the review .
Black patients largely unrepresented in photos
When an Internet search was conducted for images of nail psoriasis, the proportion of images fell as the number of the Fitzpatrick scale increased. Fitzpatrick skin types 1 or 2 represented 70% of the images, skin types 3 to 4 represented about 27%, leaving just 3% represented by darker skin types, Dr. Lipner said.
“Unfortunately, things are not much better if you look at the dermatology and nail-specific textbooks. In fact, the percentages we see are almost identical,” said Dr. Lipner, noting that her review of images suggested that only about 3% of images in textbooks are of Fitzpatrick skin types 5 or 6, an obstacle for clinicians learning to recognize nail involvement in skin of color patients with psoriasis.
“We have written a couple of papers on this topic, including a call to action” in a letter to the editor in the Journal of the American Academy of Dermatology, Dr. Lipner noted. “To ensure access to safe and effective treatments for all patient populations,” she and her coauthor wrote, “we advocate the prioritized enrollment of racial and ethnic minority groups in psoriasis, PsA [psoriatic arthritis], and NP [nail psoriasis] clinical trials.”
Data from the 2009-2010 U.S. National Health and Nutrition Examination Survey (NHANES) confirms that psoriasis is less common in Blacks (1.9%) and Hispanics (1.6%) than Whites (3.6%). But these lower numbers still translate into substantial numbers nationally. Of those with psoriasis, the lifetime incidence of nail involvement has been variously estimated between 80% and 90%, Dr. Lipner said.
In about 10% of patients with psoriasis, nail involvement is isolated, occurring in the absence of skin lesions, a proportion that appears to be similar in Blacks and Whites according to Dr. Lipner.
Patient characteristics similar by race
In a study conducted at her own center, many of the characteristics of psoriasis were similar when those with a Fitzpatrick skin type 4 or higher were compared to those of 3 or lower. This included male-female distribution, smoking history, and presence of accompanying psoriatic arthritis. There was one discrepancy between lighter and darker skin.
“The big difference was that it took almost 3 years longer [on average] for darker skin to be diagnosed, and there was worse severity of disease,” Dr. Lipner said.
Like cutaneous manifestations of psoriasis, there are differences in appearance in the nail, many of which are simply produced by how skin color alters the appearance, such as the brownish hue of erythema in darker versus lighter skin. Dr. Lipner also noted that many of the features, such as keratosis, can be more severe in patients with darker skin types, but this is likely because of the delay in diagnosis.
The problem with overlooking nail psoriasis in patients of any skin color is the significant and independent adverse impact imposed by nail disease on quality of life, she added. She recounted the case of a 22-year-old Black patient whose nail psoriasis was overlooked even as she was being treated for her skin lesions.
“The diagnosis of nail psoriasis was missed for 3 years,” said Dr. Lipner, noting that the nail involvement was not trivial. “She had trouble doing her daily activities of life, but also, she was very embarrassed by her nails, not surprisingly.”
The problem of underrepresentation of Blacks in photos depicting nail diseases is not going unnoticed.
“Recently, there has been a concerted effort on the part of authors and editors to include more images of skin of color patients in published articles and textbooks,” said Jane S. Bellet, MD, professor of dermatology, Duke University, Durham, N.C.
An expert in nail disorders, particularly in children, Dr. Bellet said in an interview that this trend “must continue and increase in volume.” She said that the need for more images of nail disease in skin of color is not restricted to textbooks but includes “other learning materials, such as online atlases.”
Dr. Lipner and Dr. Bellet reported no potential conflicts of interest relative to this topic.
NEW YORK – From clinical trials to textbooks, , even when the skin disease has already been diagnosed, according to Shari R. Lipner, MD.
In a recently published review of 45 randomized controlled trials of therapies for nail psoriasis, almost all included information about the gender of the patients enrolled, but only about 35% reported race and/or ethnicity, Dr. Lipner, associate professor of dermatology, Weill Cornell Medical College, New York, said at the Skin of Color Update 2023. The proportion climbed to 59% in trials that included at least one study site in the United States, although representation of non-White patients in studies conducted in the United States was not proportional to the population (13.4% vs. 39.9%), said Dr. Lipner, senior author of the review .
Black patients largely unrepresented in photos
When an Internet search was conducted for images of nail psoriasis, the proportion of images fell as the number of the Fitzpatrick scale increased. Fitzpatrick skin types 1 or 2 represented 70% of the images, skin types 3 to 4 represented about 27%, leaving just 3% represented by darker skin types, Dr. Lipner said.
“Unfortunately, things are not much better if you look at the dermatology and nail-specific textbooks. In fact, the percentages we see are almost identical,” said Dr. Lipner, noting that her review of images suggested that only about 3% of images in textbooks are of Fitzpatrick skin types 5 or 6, an obstacle for clinicians learning to recognize nail involvement in skin of color patients with psoriasis.
“We have written a couple of papers on this topic, including a call to action” in a letter to the editor in the Journal of the American Academy of Dermatology, Dr. Lipner noted. “To ensure access to safe and effective treatments for all patient populations,” she and her coauthor wrote, “we advocate the prioritized enrollment of racial and ethnic minority groups in psoriasis, PsA [psoriatic arthritis], and NP [nail psoriasis] clinical trials.”
Data from the 2009-2010 U.S. National Health and Nutrition Examination Survey (NHANES) confirms that psoriasis is less common in Blacks (1.9%) and Hispanics (1.6%) than Whites (3.6%). But these lower numbers still translate into substantial numbers nationally. Of those with psoriasis, the lifetime incidence of nail involvement has been variously estimated between 80% and 90%, Dr. Lipner said.
In about 10% of patients with psoriasis, nail involvement is isolated, occurring in the absence of skin lesions, a proportion that appears to be similar in Blacks and Whites according to Dr. Lipner.
Patient characteristics similar by race
In a study conducted at her own center, many of the characteristics of psoriasis were similar when those with a Fitzpatrick skin type 4 or higher were compared to those of 3 or lower. This included male-female distribution, smoking history, and presence of accompanying psoriatic arthritis. There was one discrepancy between lighter and darker skin.
“The big difference was that it took almost 3 years longer [on average] for darker skin to be diagnosed, and there was worse severity of disease,” Dr. Lipner said.
Like cutaneous manifestations of psoriasis, there are differences in appearance in the nail, many of which are simply produced by how skin color alters the appearance, such as the brownish hue of erythema in darker versus lighter skin. Dr. Lipner also noted that many of the features, such as keratosis, can be more severe in patients with darker skin types, but this is likely because of the delay in diagnosis.
The problem with overlooking nail psoriasis in patients of any skin color is the significant and independent adverse impact imposed by nail disease on quality of life, she added. She recounted the case of a 22-year-old Black patient whose nail psoriasis was overlooked even as she was being treated for her skin lesions.
“The diagnosis of nail psoriasis was missed for 3 years,” said Dr. Lipner, noting that the nail involvement was not trivial. “She had trouble doing her daily activities of life, but also, she was very embarrassed by her nails, not surprisingly.”
The problem of underrepresentation of Blacks in photos depicting nail diseases is not going unnoticed.
“Recently, there has been a concerted effort on the part of authors and editors to include more images of skin of color patients in published articles and textbooks,” said Jane S. Bellet, MD, professor of dermatology, Duke University, Durham, N.C.
An expert in nail disorders, particularly in children, Dr. Bellet said in an interview that this trend “must continue and increase in volume.” She said that the need for more images of nail disease in skin of color is not restricted to textbooks but includes “other learning materials, such as online atlases.”
Dr. Lipner and Dr. Bellet reported no potential conflicts of interest relative to this topic.
AT SOC 2023
Long-term use of ADHD meds and CVD risk: New data
results of a large Swedish nested case-control study suggest.
The increased risk was evident only for hypertension and arterial disease, was dose dependent, and was higher for stimulant than nonstimulant ADHD medications.
“Clinicians should be vigilant in monitoring signs and symptoms of cardiovascular diseases, particularly among those receiving higher doses,” Zheng Chang, PhD, principal researcher, department of medical epidemiology and biostatistics, Karolinska Institutet, Stockholm, said in an interview.
“Treatment decisions, as always, should be based on careful weighing of potential benefits and risks at individual patient level, rather than simple one-size-fits-all recommendations,” Dr. Chang added.
The study was published online in JAMA Psychiatry
Filling in the research gaps
The use of medications to treat ADHD has increased markedly over the past decades in both children and adults. The potential risk for CVD associated with long-term ADHD medication use remains unclear. Most “longitudinal” studies that have looked at the association have an average follow-up time of no more than 2 years, the authors note.
In contrast, the Swedish study assessed the association between cumulative use of ADHD medication in children and adults followed for up to 14 years and also looked at whether associations differ across types of medication and dosages, types of CVD, gender, and age.
Among 278,027 individuals aged 6-64 years diagnosed with ADHD or dispensed ADHD medication, 10,388 with CVD were identified and matched to 51,672 controls without CVD.
Longer cumulative duration of ADHD medication use was associated with a statistically significant increased risk for CVD, compared with no use.
When the risk for specific CVDs was examined, long-term use of ADHD medication (compared with no use) was associated with an increased risk for hypertension and arterial disease but not arrhythmias, heart failure, ischemic heart disease, thromboembolic disease, or cerebrovascular disease.
For hypertension, the adjusted odds ratio was 1.72 (95% confidence interval, 1.51-1.97) for 3 to ≤ 5 years and 1.80 (95% CI, 1.55-2.08) for > 5 years of medication use. For arterial disease, the AOR was 1.65 (95% CI, 1.11-2.45) for 3 to ≤ 5 years and 1.49 (95% CI, 0.96-2.32) for > 5 years of use.
Stimulants confer greatest risk
Across the 14-year follow-up period, each additional year of ADHD medication use was associated with an average 4% increased CVD risk, with a larger 8% increased risk in the first 3 years of cumulative use, followed by stable risk over the remaining follow-up.
Similar risks were observed in children and adults, as well as in females and males.
When focusing on specific ADHD medications, compared with no use, long-term use of the stimulant methylphenidate was associated with an increased risk for CVD (AOR, 1.20 [95% CI, 1.10-1.31] for 3 to ≤ 5 years and 1.19 [95% CI, 1.08-1.31] for > 5 years).
The same was true for long-term use of the stimulant lisdexamfetamine (AOR, 1.23 [95% CI, 1.05-1.44] for 2 to ≤ 3 years and 1.17 [95% CI, 0.98-1.40] for > 3 years).
In contrast, use of the nonstimulant atomoxetine was associated with elevated CVD risk only for the first year of use (AOR, 1.07; 95% CI, 1.01-1.13).
The increased risk for CVD occurred only above certain average daily doses: 45 mg for methylphenidate and lisdexamfetamine, 22.5 mg for amphetamines, and 120 mg for atomoxetine.
The authors note that, although they accounted for a wide range of potential confounding variables, considering the observational nature of the study and the possibility of residual confounding, they could not prove causality.
‘Tricky trade-offs’
The coauthors of an editorial in JAMA Psychiatry (2023 Nov 22. doi: 10.1001/jamapsychiatry.2023.4126) note that the study “should remind us that clinical decision-making is often based on tricky trade-offs that should be considered at the individual patient level.”
Given that hypertension is the leading cause of CV morbidity and mortality worldwide, the increased likelihood of hypertension with long-term use of ADHD medications “cannot be disregarded,” write Samuele Cortese, MD, PhD, and Cristiano Fava, MD, PhD, with University of Southampton (England).
“These findings are especially relevant given the reported association between ADHD and physical conditions, such as obesity, which further contribute to increased cardiovascular risk,” they add.
Dr. Cortese and Dr. Fava say that the increased CV risk – averaging 4% per year and stabilizing after 3 years of treatment – “should be carefully weighed against the established benefits, on a case-by-case basis.”
“Importantly,” they write, “large real-world self-controlled studies have shown that individuals with ADHD experience significantly fewer unintentional physical injuries, motor vehicle crashes, substance use disorders, and criminal acts, as well as improved academic functioning, during periods when they are taking, compared with periods when they are not taking, methylphenidate.”
The risk-benefit ratio, however, may be lower in people with preexisting heart conditions. However, more evidence and precise recommendations are needed in relation to the treatment of individuals with ADHD and preexisting CV conditions, the editorial writers say.
This study was supported by grants from the Swedish Research Council for Health, Working Life, and Welfare and the European Union’s Horizon 2020 research and innovation program. The authors and editorial writers have no relevant conflicts of interest.
A version of this article appeared on Medscape.com.
results of a large Swedish nested case-control study suggest.
The increased risk was evident only for hypertension and arterial disease, was dose dependent, and was higher for stimulant than nonstimulant ADHD medications.
“Clinicians should be vigilant in monitoring signs and symptoms of cardiovascular diseases, particularly among those receiving higher doses,” Zheng Chang, PhD, principal researcher, department of medical epidemiology and biostatistics, Karolinska Institutet, Stockholm, said in an interview.
“Treatment decisions, as always, should be based on careful weighing of potential benefits and risks at individual patient level, rather than simple one-size-fits-all recommendations,” Dr. Chang added.
The study was published online in JAMA Psychiatry
Filling in the research gaps
The use of medications to treat ADHD has increased markedly over the past decades in both children and adults. The potential risk for CVD associated with long-term ADHD medication use remains unclear. Most “longitudinal” studies that have looked at the association have an average follow-up time of no more than 2 years, the authors note.
In contrast, the Swedish study assessed the association between cumulative use of ADHD medication in children and adults followed for up to 14 years and also looked at whether associations differ across types of medication and dosages, types of CVD, gender, and age.
Among 278,027 individuals aged 6-64 years diagnosed with ADHD or dispensed ADHD medication, 10,388 with CVD were identified and matched to 51,672 controls without CVD.
Longer cumulative duration of ADHD medication use was associated with a statistically significant increased risk for CVD, compared with no use.
When the risk for specific CVDs was examined, long-term use of ADHD medication (compared with no use) was associated with an increased risk for hypertension and arterial disease but not arrhythmias, heart failure, ischemic heart disease, thromboembolic disease, or cerebrovascular disease.
For hypertension, the adjusted odds ratio was 1.72 (95% confidence interval, 1.51-1.97) for 3 to ≤ 5 years and 1.80 (95% CI, 1.55-2.08) for > 5 years of medication use. For arterial disease, the AOR was 1.65 (95% CI, 1.11-2.45) for 3 to ≤ 5 years and 1.49 (95% CI, 0.96-2.32) for > 5 years of use.
Stimulants confer greatest risk
Across the 14-year follow-up period, each additional year of ADHD medication use was associated with an average 4% increased CVD risk, with a larger 8% increased risk in the first 3 years of cumulative use, followed by stable risk over the remaining follow-up.
Similar risks were observed in children and adults, as well as in females and males.
When focusing on specific ADHD medications, compared with no use, long-term use of the stimulant methylphenidate was associated with an increased risk for CVD (AOR, 1.20 [95% CI, 1.10-1.31] for 3 to ≤ 5 years and 1.19 [95% CI, 1.08-1.31] for > 5 years).
The same was true for long-term use of the stimulant lisdexamfetamine (AOR, 1.23 [95% CI, 1.05-1.44] for 2 to ≤ 3 years and 1.17 [95% CI, 0.98-1.40] for > 3 years).
In contrast, use of the nonstimulant atomoxetine was associated with elevated CVD risk only for the first year of use (AOR, 1.07; 95% CI, 1.01-1.13).
The increased risk for CVD occurred only above certain average daily doses: 45 mg for methylphenidate and lisdexamfetamine, 22.5 mg for amphetamines, and 120 mg for atomoxetine.
The authors note that, although they accounted for a wide range of potential confounding variables, considering the observational nature of the study and the possibility of residual confounding, they could not prove causality.
‘Tricky trade-offs’
The coauthors of an editorial in JAMA Psychiatry (2023 Nov 22. doi: 10.1001/jamapsychiatry.2023.4126) note that the study “should remind us that clinical decision-making is often based on tricky trade-offs that should be considered at the individual patient level.”
Given that hypertension is the leading cause of CV morbidity and mortality worldwide, the increased likelihood of hypertension with long-term use of ADHD medications “cannot be disregarded,” write Samuele Cortese, MD, PhD, and Cristiano Fava, MD, PhD, with University of Southampton (England).
“These findings are especially relevant given the reported association between ADHD and physical conditions, such as obesity, which further contribute to increased cardiovascular risk,” they add.
Dr. Cortese and Dr. Fava say that the increased CV risk – averaging 4% per year and stabilizing after 3 years of treatment – “should be carefully weighed against the established benefits, on a case-by-case basis.”
“Importantly,” they write, “large real-world self-controlled studies have shown that individuals with ADHD experience significantly fewer unintentional physical injuries, motor vehicle crashes, substance use disorders, and criminal acts, as well as improved academic functioning, during periods when they are taking, compared with periods when they are not taking, methylphenidate.”
The risk-benefit ratio, however, may be lower in people with preexisting heart conditions. However, more evidence and precise recommendations are needed in relation to the treatment of individuals with ADHD and preexisting CV conditions, the editorial writers say.
This study was supported by grants from the Swedish Research Council for Health, Working Life, and Welfare and the European Union’s Horizon 2020 research and innovation program. The authors and editorial writers have no relevant conflicts of interest.
A version of this article appeared on Medscape.com.
results of a large Swedish nested case-control study suggest.
The increased risk was evident only for hypertension and arterial disease, was dose dependent, and was higher for stimulant than nonstimulant ADHD medications.
“Clinicians should be vigilant in monitoring signs and symptoms of cardiovascular diseases, particularly among those receiving higher doses,” Zheng Chang, PhD, principal researcher, department of medical epidemiology and biostatistics, Karolinska Institutet, Stockholm, said in an interview.
“Treatment decisions, as always, should be based on careful weighing of potential benefits and risks at individual patient level, rather than simple one-size-fits-all recommendations,” Dr. Chang added.
The study was published online in JAMA Psychiatry
Filling in the research gaps
The use of medications to treat ADHD has increased markedly over the past decades in both children and adults. The potential risk for CVD associated with long-term ADHD medication use remains unclear. Most “longitudinal” studies that have looked at the association have an average follow-up time of no more than 2 years, the authors note.
In contrast, the Swedish study assessed the association between cumulative use of ADHD medication in children and adults followed for up to 14 years and also looked at whether associations differ across types of medication and dosages, types of CVD, gender, and age.
Among 278,027 individuals aged 6-64 years diagnosed with ADHD or dispensed ADHD medication, 10,388 with CVD were identified and matched to 51,672 controls without CVD.
Longer cumulative duration of ADHD medication use was associated with a statistically significant increased risk for CVD, compared with no use.
When the risk for specific CVDs was examined, long-term use of ADHD medication (compared with no use) was associated with an increased risk for hypertension and arterial disease but not arrhythmias, heart failure, ischemic heart disease, thromboembolic disease, or cerebrovascular disease.
For hypertension, the adjusted odds ratio was 1.72 (95% confidence interval, 1.51-1.97) for 3 to ≤ 5 years and 1.80 (95% CI, 1.55-2.08) for > 5 years of medication use. For arterial disease, the AOR was 1.65 (95% CI, 1.11-2.45) for 3 to ≤ 5 years and 1.49 (95% CI, 0.96-2.32) for > 5 years of use.
Stimulants confer greatest risk
Across the 14-year follow-up period, each additional year of ADHD medication use was associated with an average 4% increased CVD risk, with a larger 8% increased risk in the first 3 years of cumulative use, followed by stable risk over the remaining follow-up.
Similar risks were observed in children and adults, as well as in females and males.
When focusing on specific ADHD medications, compared with no use, long-term use of the stimulant methylphenidate was associated with an increased risk for CVD (AOR, 1.20 [95% CI, 1.10-1.31] for 3 to ≤ 5 years and 1.19 [95% CI, 1.08-1.31] for > 5 years).
The same was true for long-term use of the stimulant lisdexamfetamine (AOR, 1.23 [95% CI, 1.05-1.44] for 2 to ≤ 3 years and 1.17 [95% CI, 0.98-1.40] for > 3 years).
In contrast, use of the nonstimulant atomoxetine was associated with elevated CVD risk only for the first year of use (AOR, 1.07; 95% CI, 1.01-1.13).
The increased risk for CVD occurred only above certain average daily doses: 45 mg for methylphenidate and lisdexamfetamine, 22.5 mg for amphetamines, and 120 mg for atomoxetine.
The authors note that, although they accounted for a wide range of potential confounding variables, considering the observational nature of the study and the possibility of residual confounding, they could not prove causality.
‘Tricky trade-offs’
The coauthors of an editorial in JAMA Psychiatry (2023 Nov 22. doi: 10.1001/jamapsychiatry.2023.4126) note that the study “should remind us that clinical decision-making is often based on tricky trade-offs that should be considered at the individual patient level.”
Given that hypertension is the leading cause of CV morbidity and mortality worldwide, the increased likelihood of hypertension with long-term use of ADHD medications “cannot be disregarded,” write Samuele Cortese, MD, PhD, and Cristiano Fava, MD, PhD, with University of Southampton (England).
“These findings are especially relevant given the reported association between ADHD and physical conditions, such as obesity, which further contribute to increased cardiovascular risk,” they add.
Dr. Cortese and Dr. Fava say that the increased CV risk – averaging 4% per year and stabilizing after 3 years of treatment – “should be carefully weighed against the established benefits, on a case-by-case basis.”
“Importantly,” they write, “large real-world self-controlled studies have shown that individuals with ADHD experience significantly fewer unintentional physical injuries, motor vehicle crashes, substance use disorders, and criminal acts, as well as improved academic functioning, during periods when they are taking, compared with periods when they are not taking, methylphenidate.”
The risk-benefit ratio, however, may be lower in people with preexisting heart conditions. However, more evidence and precise recommendations are needed in relation to the treatment of individuals with ADHD and preexisting CV conditions, the editorial writers say.
This study was supported by grants from the Swedish Research Council for Health, Working Life, and Welfare and the European Union’s Horizon 2020 research and innovation program. The authors and editorial writers have no relevant conflicts of interest.
A version of this article appeared on Medscape.com.
FROM JAMA PSYCHIATRY
Physicians: Don’t ignore sexuality in your dying patients
I have a long history of being interested in conversations that others avoid. In medical school, I felt that we didn’t talk enough about death, so I organized a lecture series on end-of-life care for my fellow students. Now, as a sexual medicine specialist, I have other conversations from which many medical providers shy away. So, buckle up!
A key question in palliative care is: How do you want to live the life you have left? And where does the wide range of human pleasures fit in? In her book The Pleasure Zone, sex therapist Stella Resnick describes eight kinds of pleasure:
- pain relief
- play, humor, movement, and sound
- mental
- emotional
- sensual
- spiritual
- primal (just being)
- sexual
At the end of life, both medically and culturally, we pay attention to many of these pleasures. But sexuality is often ignored.
Sexuality – which can be defined as the experience of oneself as a sexual being – may include how sex is experienced in relationships or with oneself, sexual orientation, body image, gender expression and identity, as well as sexual satisfaction and pleasure. People may have different priorities at different times regarding their sexuality, but sexuality is a key aspect of feeling fully alive and human across the lifespan. At the end of life, sexuality, sexual expression, and physical connection may play even more important roles than previously.
‘I just want to be able to have sex with my husband again’
Z was a 75-year-old woman who came to me for help with vaginal stenosis. Her cancer treatments were not going well. I asked her one of my typical questions: “What does sex mean to you?”
Sexual pleasure was “glue” – a critical way for her to connect with her sense of self and with her husband, a man of few words. She described transcendent experiences with partnered sex during her life. Finally, she explained, she was saddened by the idea of not experiencing that again before she died.
As medical providers, we don’t all need to be sex experts, but our patients should be able to have open and shame-free conversations with us about these issues at all stages of life. Up to 86% of palliative care patients want the chance to discuss their sexual concerns with a skilled clinician, and many consider this issue important to their psychological well-being. And yet, 91% reported that sexuality had not been addressed in their care.
In a Canadian study of 10 palliative care patients (and their partners), all but one felt that their medical providers should initiate conversations about sexuality and the effect of illness on sexual experience. They felt that this communication should be an integral component of care. The one person who disagreed said it was appropriate for clinicians to ask patients whether they wanted to talk about sexuality.
Before this study, sexuality had been discussed with only one participant. Here’s the magic part: Several of the patients reported that the study itself was therapeutic. This is my clinical experience as well. More often than not, open and shame-free clinical discussions about sexuality led to patients reflecting: “I’ve never been able to say this to another person, and now I feel so much better.”
One study of palliative care nurses found that while the nurses acknowledged the importance of addressing sexuality, their way of addressing sexuality followed cultural myths and norms or relied on their own experience rather than knowledge-based guidelines. Why? One explanation could be that clinicians raised and educated in North America probably did not get adequate training on this topic. We need to do better.
Second, cultural concepts that equate sexuality with healthy and able bodies who are partnered, young, cisgender, and heterosexual make it hard to conceive of how to relate sexuality to other bodies. We’ve been steeped in the biases of our culture.
Some medical providers avoid the topic because they feel vulnerable, fearful that a conversation about sexuality with a patient will reveal something about themselves. Others may simply deny the possibility that sexual function changes in the face of serious illness or that this could be a priority for their patients. Of course, we have a million other things to talk about – I get it.
Views on sex and sexuality affect how clinicians approach these conversations as well. A study of palliative care professionals described themes among those who did and did not address the topic. The professionals who did not discuss sexuality endorsed a narrow definition of sex based on genital sexual acts between two partners, usually heterosexual. Among these clinicians, when the issue came up, patients had raised the topic. They talked about sex using jokes and euphemisms (“are you still enjoying ‘good moments’ with your partner?”), perhaps to ease their own discomfort.
On the other hand, professionals who more frequently discussed sexuality with their patients endorsed a more holistic concept of sexuality: including genital and nongenital contact as well as nonphysical components like verbal communication and emotions. These clinicians found sexuality applicable to all individuals across the lifespan. They were more likely to initiate discussions about the effect of medications or illness on sexual function and address the need for equipment, such as a larger hospital bed.
I’m hoping that you might one day find yourself in the second group. Our patients at the end of life need our help in accessing the full range of pleasure in their lives. We need better medical education on how to help with sexual concerns when they arise (an article for another day), but we can start right now by simply initiating open, shame-free sexual health conversations. This is often the most important therapeutic intervention.
Dr. Kranz, Clinical Assistant Professor of Obstetrics/Gynecology and Family Medicine, University of Rochester (N.Y.) Medical Center, has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
I have a long history of being interested in conversations that others avoid. In medical school, I felt that we didn’t talk enough about death, so I organized a lecture series on end-of-life care for my fellow students. Now, as a sexual medicine specialist, I have other conversations from which many medical providers shy away. So, buckle up!
A key question in palliative care is: How do you want to live the life you have left? And where does the wide range of human pleasures fit in? In her book The Pleasure Zone, sex therapist Stella Resnick describes eight kinds of pleasure:
- pain relief
- play, humor, movement, and sound
- mental
- emotional
- sensual
- spiritual
- primal (just being)
- sexual
At the end of life, both medically and culturally, we pay attention to many of these pleasures. But sexuality is often ignored.
Sexuality – which can be defined as the experience of oneself as a sexual being – may include how sex is experienced in relationships or with oneself, sexual orientation, body image, gender expression and identity, as well as sexual satisfaction and pleasure. People may have different priorities at different times regarding their sexuality, but sexuality is a key aspect of feeling fully alive and human across the lifespan. At the end of life, sexuality, sexual expression, and physical connection may play even more important roles than previously.
‘I just want to be able to have sex with my husband again’
Z was a 75-year-old woman who came to me for help with vaginal stenosis. Her cancer treatments were not going well. I asked her one of my typical questions: “What does sex mean to you?”
Sexual pleasure was “glue” – a critical way for her to connect with her sense of self and with her husband, a man of few words. She described transcendent experiences with partnered sex during her life. Finally, she explained, she was saddened by the idea of not experiencing that again before she died.
As medical providers, we don’t all need to be sex experts, but our patients should be able to have open and shame-free conversations with us about these issues at all stages of life. Up to 86% of palliative care patients want the chance to discuss their sexual concerns with a skilled clinician, and many consider this issue important to their psychological well-being. And yet, 91% reported that sexuality had not been addressed in their care.
In a Canadian study of 10 palliative care patients (and their partners), all but one felt that their medical providers should initiate conversations about sexuality and the effect of illness on sexual experience. They felt that this communication should be an integral component of care. The one person who disagreed said it was appropriate for clinicians to ask patients whether they wanted to talk about sexuality.
Before this study, sexuality had been discussed with only one participant. Here’s the magic part: Several of the patients reported that the study itself was therapeutic. This is my clinical experience as well. More often than not, open and shame-free clinical discussions about sexuality led to patients reflecting: “I’ve never been able to say this to another person, and now I feel so much better.”
One study of palliative care nurses found that while the nurses acknowledged the importance of addressing sexuality, their way of addressing sexuality followed cultural myths and norms or relied on their own experience rather than knowledge-based guidelines. Why? One explanation could be that clinicians raised and educated in North America probably did not get adequate training on this topic. We need to do better.
Second, cultural concepts that equate sexuality with healthy and able bodies who are partnered, young, cisgender, and heterosexual make it hard to conceive of how to relate sexuality to other bodies. We’ve been steeped in the biases of our culture.
Some medical providers avoid the topic because they feel vulnerable, fearful that a conversation about sexuality with a patient will reveal something about themselves. Others may simply deny the possibility that sexual function changes in the face of serious illness or that this could be a priority for their patients. Of course, we have a million other things to talk about – I get it.
Views on sex and sexuality affect how clinicians approach these conversations as well. A study of palliative care professionals described themes among those who did and did not address the topic. The professionals who did not discuss sexuality endorsed a narrow definition of sex based on genital sexual acts between two partners, usually heterosexual. Among these clinicians, when the issue came up, patients had raised the topic. They talked about sex using jokes and euphemisms (“are you still enjoying ‘good moments’ with your partner?”), perhaps to ease their own discomfort.
On the other hand, professionals who more frequently discussed sexuality with their patients endorsed a more holistic concept of sexuality: including genital and nongenital contact as well as nonphysical components like verbal communication and emotions. These clinicians found sexuality applicable to all individuals across the lifespan. They were more likely to initiate discussions about the effect of medications or illness on sexual function and address the need for equipment, such as a larger hospital bed.
I’m hoping that you might one day find yourself in the second group. Our patients at the end of life need our help in accessing the full range of pleasure in their lives. We need better medical education on how to help with sexual concerns when they arise (an article for another day), but we can start right now by simply initiating open, shame-free sexual health conversations. This is often the most important therapeutic intervention.
Dr. Kranz, Clinical Assistant Professor of Obstetrics/Gynecology and Family Medicine, University of Rochester (N.Y.) Medical Center, has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
I have a long history of being interested in conversations that others avoid. In medical school, I felt that we didn’t talk enough about death, so I organized a lecture series on end-of-life care for my fellow students. Now, as a sexual medicine specialist, I have other conversations from which many medical providers shy away. So, buckle up!
A key question in palliative care is: How do you want to live the life you have left? And where does the wide range of human pleasures fit in? In her book The Pleasure Zone, sex therapist Stella Resnick describes eight kinds of pleasure:
- pain relief
- play, humor, movement, and sound
- mental
- emotional
- sensual
- spiritual
- primal (just being)
- sexual
At the end of life, both medically and culturally, we pay attention to many of these pleasures. But sexuality is often ignored.
Sexuality – which can be defined as the experience of oneself as a sexual being – may include how sex is experienced in relationships or with oneself, sexual orientation, body image, gender expression and identity, as well as sexual satisfaction and pleasure. People may have different priorities at different times regarding their sexuality, but sexuality is a key aspect of feeling fully alive and human across the lifespan. At the end of life, sexuality, sexual expression, and physical connection may play even more important roles than previously.
‘I just want to be able to have sex with my husband again’
Z was a 75-year-old woman who came to me for help with vaginal stenosis. Her cancer treatments were not going well. I asked her one of my typical questions: “What does sex mean to you?”
Sexual pleasure was “glue” – a critical way for her to connect with her sense of self and with her husband, a man of few words. She described transcendent experiences with partnered sex during her life. Finally, she explained, she was saddened by the idea of not experiencing that again before she died.
As medical providers, we don’t all need to be sex experts, but our patients should be able to have open and shame-free conversations with us about these issues at all stages of life. Up to 86% of palliative care patients want the chance to discuss their sexual concerns with a skilled clinician, and many consider this issue important to their psychological well-being. And yet, 91% reported that sexuality had not been addressed in their care.
In a Canadian study of 10 palliative care patients (and their partners), all but one felt that their medical providers should initiate conversations about sexuality and the effect of illness on sexual experience. They felt that this communication should be an integral component of care. The one person who disagreed said it was appropriate for clinicians to ask patients whether they wanted to talk about sexuality.
Before this study, sexuality had been discussed with only one participant. Here’s the magic part: Several of the patients reported that the study itself was therapeutic. This is my clinical experience as well. More often than not, open and shame-free clinical discussions about sexuality led to patients reflecting: “I’ve never been able to say this to another person, and now I feel so much better.”
One study of palliative care nurses found that while the nurses acknowledged the importance of addressing sexuality, their way of addressing sexuality followed cultural myths and norms or relied on their own experience rather than knowledge-based guidelines. Why? One explanation could be that clinicians raised and educated in North America probably did not get adequate training on this topic. We need to do better.
Second, cultural concepts that equate sexuality with healthy and able bodies who are partnered, young, cisgender, and heterosexual make it hard to conceive of how to relate sexuality to other bodies. We’ve been steeped in the biases of our culture.
Some medical providers avoid the topic because they feel vulnerable, fearful that a conversation about sexuality with a patient will reveal something about themselves. Others may simply deny the possibility that sexual function changes in the face of serious illness or that this could be a priority for their patients. Of course, we have a million other things to talk about – I get it.
Views on sex and sexuality affect how clinicians approach these conversations as well. A study of palliative care professionals described themes among those who did and did not address the topic. The professionals who did not discuss sexuality endorsed a narrow definition of sex based on genital sexual acts between two partners, usually heterosexual. Among these clinicians, when the issue came up, patients had raised the topic. They talked about sex using jokes and euphemisms (“are you still enjoying ‘good moments’ with your partner?”), perhaps to ease their own discomfort.
On the other hand, professionals who more frequently discussed sexuality with their patients endorsed a more holistic concept of sexuality: including genital and nongenital contact as well as nonphysical components like verbal communication and emotions. These clinicians found sexuality applicable to all individuals across the lifespan. They were more likely to initiate discussions about the effect of medications or illness on sexual function and address the need for equipment, such as a larger hospital bed.
I’m hoping that you might one day find yourself in the second group. Our patients at the end of life need our help in accessing the full range of pleasure in their lives. We need better medical education on how to help with sexual concerns when they arise (an article for another day), but we can start right now by simply initiating open, shame-free sexual health conversations. This is often the most important therapeutic intervention.
Dr. Kranz, Clinical Assistant Professor of Obstetrics/Gynecology and Family Medicine, University of Rochester (N.Y.) Medical Center, has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Commentary: Examining DMARD Use in PsA, December 2023

Limiting radiographic progression is an important long-term goal of treatment of PsA. In a post hoc analysis that included 449 biologic-naive patients with PsA from the DISCOVER-2 trial who received 100 mg guselkumab every 4 or 8 weeks, Mease and colleagues demonstrated that a greater improvement in the Disease Activity Index for PsA (DAPSA) scores as early as week 8 and the achievement of DAPSA low disease activity at week 8 were associated with a significantly lower progression of radiographic joint damage (total PsA-modified van der Heijde-Sharp score) through week 100. Thus, patients who respond well early have better long-term outcomes.
The safety of targeted therapies is always of concern and is inadequately addressed by individual clinical trials. Meta-analyses may provide further insights. In a network meta-analysis of 94 randomized controlled trials that included a total of 54,369 patients with PsA or psoriasis who were treated with 14 biologics, five small molecules, or placebo, Chiu and colleagues found that for patients with psoriasis, infliximab, deucravacitinib, and bimekizumab had the highest risks for infection. In patients with PsA, bimekizumab, apremilast, and 30 mg upadacitinib led to a significantly higher risk for infection compared with placebo, and 30 mg upadacitinib also increasing the risk for serious infection compared with placebo. The risk for infection in patients with PsA did not increase with most bDMARD and targeted synthetic DMARD (tsDMARD), except bimekizumab, apremilast, and 30 mg upadacitinib.
There is increasing recognition of the difficulty in managing patients with refractory PsA. One approach to such difficult-to-treat disease is dual targeted therapy (DTT). However, the safety of these combinations is of major concern. There is currently an ongoing clinical trial comparing a combination of guselkumab and golimumab vs guselkumab alone for treatment-resistant PsA. In the meantime, Valero-Martinez and colleagues have reported results from an observational, retrospective, cross-sectional study that included patients with refractory PsA (n = 14) or spondyloarthritis (n = 22) who simultaneously received two bDMARD or tsDMARD with different therapeutic targets. The most commonly used combinations were a tumor necrosis factor (TNF) inhibitor plus an interleukin (IL)-12/23 pathway inhibitor, followed by a TNF inhibitor plus an IL-17 inhibitor. They found that at a median exposure of 14.86 months, the DTT retention rate in patients with PsA was 42.8%, with 40.0% and 53.3% of patients achieving remission or low activity and major clinical improvements, respectively. Treatment discontinuation due to adverse events was reported in one patient with PsA and multiple comorbidities. Thus, DTT led to satisfactory clinical improvements and no serious adverse events in patients with refractory PsA. The results of larger observational and randomized trials are awaited.
Limiting radiographic progression is an important long-term goal of treatment of PsA. In a post hoc analysis that included 449 biologic-naive patients with PsA from the DISCOVER-2 trial who received 100 mg guselkumab every 4 or 8 weeks, Mease and colleagues demonstrated that a greater improvement in the Disease Activity Index for PsA (DAPSA) scores as early as week 8 and the achievement of DAPSA low disease activity at week 8 were associated with a significantly lower progression of radiographic joint damage (total PsA-modified van der Heijde-Sharp score) through week 100. Thus, patients who respond well early have better long-term outcomes.
The safety of targeted therapies is always of concern and is inadequately addressed by individual clinical trials. Meta-analyses may provide further insights. In a network meta-analysis of 94 randomized controlled trials that included a total of 54,369 patients with PsA or psoriasis who were treated with 14 biologics, five small molecules, or placebo, Chiu and colleagues found that for patients with psoriasis, infliximab, deucravacitinib, and bimekizumab had the highest risks for infection. In patients with PsA, bimekizumab, apremilast, and 30 mg upadacitinib led to a significantly higher risk for infection compared with placebo, and 30 mg upadacitinib also increasing the risk for serious infection compared with placebo. The risk for infection in patients with PsA did not increase with most bDMARD and targeted synthetic DMARD (tsDMARD), except bimekizumab, apremilast, and 30 mg upadacitinib.
There is increasing recognition of the difficulty in managing patients with refractory PsA. One approach to such difficult-to-treat disease is dual targeted therapy (DTT). However, the safety of these combinations is of major concern. There is currently an ongoing clinical trial comparing a combination of guselkumab and golimumab vs guselkumab alone for treatment-resistant PsA. In the meantime, Valero-Martinez and colleagues have reported results from an observational, retrospective, cross-sectional study that included patients with refractory PsA (n = 14) or spondyloarthritis (n = 22) who simultaneously received two bDMARD or tsDMARD with different therapeutic targets. The most commonly used combinations were a tumor necrosis factor (TNF) inhibitor plus an interleukin (IL)-12/23 pathway inhibitor, followed by a TNF inhibitor plus an IL-17 inhibitor. They found that at a median exposure of 14.86 months, the DTT retention rate in patients with PsA was 42.8%, with 40.0% and 53.3% of patients achieving remission or low activity and major clinical improvements, respectively. Treatment discontinuation due to adverse events was reported in one patient with PsA and multiple comorbidities. Thus, DTT led to satisfactory clinical improvements and no serious adverse events in patients with refractory PsA. The results of larger observational and randomized trials are awaited.
Limiting radiographic progression is an important long-term goal of treatment of PsA. In a post hoc analysis that included 449 biologic-naive patients with PsA from the DISCOVER-2 trial who received 100 mg guselkumab every 4 or 8 weeks, Mease and colleagues demonstrated that a greater improvement in the Disease Activity Index for PsA (DAPSA) scores as early as week 8 and the achievement of DAPSA low disease activity at week 8 were associated with a significantly lower progression of radiographic joint damage (total PsA-modified van der Heijde-Sharp score) through week 100. Thus, patients who respond well early have better long-term outcomes.
The safety of targeted therapies is always of concern and is inadequately addressed by individual clinical trials. Meta-analyses may provide further insights. In a network meta-analysis of 94 randomized controlled trials that included a total of 54,369 patients with PsA or psoriasis who were treated with 14 biologics, five small molecules, or placebo, Chiu and colleagues found that for patients with psoriasis, infliximab, deucravacitinib, and bimekizumab had the highest risks for infection. In patients with PsA, bimekizumab, apremilast, and 30 mg upadacitinib led to a significantly higher risk for infection compared with placebo, and 30 mg upadacitinib also increasing the risk for serious infection compared with placebo. The risk for infection in patients with PsA did not increase with most bDMARD and targeted synthetic DMARD (tsDMARD), except bimekizumab, apremilast, and 30 mg upadacitinib.
There is increasing recognition of the difficulty in managing patients with refractory PsA. One approach to such difficult-to-treat disease is dual targeted therapy (DTT). However, the safety of these combinations is of major concern. There is currently an ongoing clinical trial comparing a combination of guselkumab and golimumab vs guselkumab alone for treatment-resistant PsA. In the meantime, Valero-Martinez and colleagues have reported results from an observational, retrospective, cross-sectional study that included patients with refractory PsA (n = 14) or spondyloarthritis (n = 22) who simultaneously received two bDMARD or tsDMARD with different therapeutic targets. The most commonly used combinations were a tumor necrosis factor (TNF) inhibitor plus an interleukin (IL)-12/23 pathway inhibitor, followed by a TNF inhibitor plus an IL-17 inhibitor. They found that at a median exposure of 14.86 months, the DTT retention rate in patients with PsA was 42.8%, with 40.0% and 53.3% of patients achieving remission or low activity and major clinical improvements, respectively. Treatment discontinuation due to adverse events was reported in one patient with PsA and multiple comorbidities. Thus, DTT led to satisfactory clinical improvements and no serious adverse events in patients with refractory PsA. The results of larger observational and randomized trials are awaited.
Not all exercise is beneficial: The physical activity paradox explained
In the pursuit of optimal health, regular physical activity (PA) is recommended to protect against dementia, cardiovascular disease (CVD), cancer, and other noncommunicable diseases. A significant body of research suggests the benefits of PA are positively correlated with higher frequency and intensity – with more often deemed better. This research has spawned a focus on increasing step counts and investing in standing desks and other interventions aimed at keeping people active.
But , but they also actually experience an increased risk for the very conditions that PA is intended to prevent.
A study published recently in The Lancet Regional Health – Europe used registry data from more than 7,000 adults in Norway, following them from age 33 to 65 years, to assess PA trajectories and risks for later-life mild cognitive impairment (MCI) and dementia at age 70 or older.
“Incorporating a life-course perspective gives a broader picture of how participants’ occupational histories relate to cognitive impairment later in life,” principal investigator Vegard Skirbekk, PhD, Columbia University Mailman School of Public Health, New York, said in an interview. Other studies typically have assessed occupational PA at a single time point, often close to the end of an individual’s career, and largely relied on self-report, he said.
Study participants worked in more than 300 different occupations. General physical activities performed on the included jobs required “considerable” use of arms and legs and moving the whole body, such as climbing, lifting, balancing, walking, stooping, and handling of materials.
Dr. Skirbekk and colleagues grouped participants into four PA trajectories over the 44-year study period: stable low, increasing then decreasing, stable intermediate, and stable high.
A total of 902 individuals were diagnosed with dementia and 2,407 with MCI at age 70 years or older. After adjustment, risks for MCI and dementia were 15.5% for those with higher occupational PA scores in the latter part of their working life and 9% for those with lower physical demands. The researchers concluded that “consistently working in an occupation with intermediate or high occupational PA was linked to an increased risk of cognitive impairment.”
The findings support those of the Copenhagen Male Study. Published in 2020, this longitudinal study compared leisure-time and occupational PA among more than 4,000 men in Denmark aged 40-59 at baseline in 1970-1971 and followed them until they turned 60. After adjustment, participants with high occupational PA had a 55% greater risk of developing dementia compared with those doing sedentary work.
Good vs. bad PA
“[T]he WHO [World Health Organization] guide to preventing dementia and disease on the whole mentions physical activity as an important factor. But our study suggests that it must be a ‘good’ form of physical activity, which hard physical work is not,” said Kirsten Nabe-Nielsen, PhD, lead author of this study
Beyond dementia, another recent study adds to a wealth of data on associations between occupational PA and cardiovascular risks. The cross-sectional analysis of U.S. data from the National Institute for Occupational Safety and Health showed that odds of CVD were higher when participants were “always” performing total occupational activity (odds ratio [OR], 1.99), occupational exertion (OR, 2.15), or occupational standing and walking around (OR, 1.84) compared with “never” engaging in these activities.
The contrasting effects of leisure-time vs. occupational PA constitute the “physical activity paradox” hypothesis. Starting in 2011, multiple studies by Andreas Holtermann, PhD, of the National Research Centre for the Working Environment lend support to the PA paradox theory, as do subsequent studies by others.
Although only “marginally considered” until a few years ago, recent large cohort studies seem to confirm the paradox, Pier Luigi Temporelli, MD wrote in a recent editorial.
In separate interviews, Dr. Skirbekk and lead author Tyler Quinn, PhD, MS, West Virginia University, Morgantown, pointed to the PA paradox as an explanation for their own recent findings, suggesting that the mechanisms that underlie it probably are responsible for the associated deleterious effects of occupational PA on the brain and heart, and even mortality.
“It’s well established that PA in your leisure time can be positive, but in the workplace, the results are quite the opposite,” Dr. Skirbekk said. “The specific mechanisms for why occupational PA is associated with elevated dementia risk are still not well understood and we need more knowledge. But we know that higher occupational physical demands have been linked to smaller hippocampal volume and poorer memory performance.”
Furthermore, he said, individuals working in jobs with high demands, both psychological and physical, combined with low job control perform more poorly on cognitive testing later in life.
“We looked mainly at professions where people have heavy workloads and you have much less autonomy, such as nursing assistants, office cleaners, childcare workers, and other personal care workers,” he said. “You cannot sit. You have somebody relying on you. It’s not all pleasure, and it can be very hard. That’s where we find the associations.”
Lack of autonomy
Specific characteristics indirectly associated with high occupational PA jobs – low cognitive stimuli, lifestyle factors, and socioeconomic influences – as well as factors directly related to high occupational PA, such as long hours, repetitive tasks, low levels of control, and stress, could also adversely affect cognitive trajectories, Dr. Skirbekk explained.
“By contrast, leisure-time physical activities tend to be of much shorter duration; are associated with socialization, play, [and] positive emotions; and [include] the opportunity to take breaks or shift to other types of activities if one prefers,” he said. “It may also be that too little or too much PA could be adversely related to cognitive outcomes – hence moderate activity levels, for example 10,000 steps a day, are still likely beneficial for cognitive functioning.”
Dr. Quinn said most of the CVD risk linked to occupational PA has to do with long periods of exertion such as lifting and carrying objects. While occupational standing and walking all day are also linked to CVD risk, they’re not as risky as lifting and carrying, he said.
Like Dr. Skirbekk, Dr. Quinn noted that individuals can take a break from leisure-time PA when they are tired, but occupational PA doesn’t have that same autonomy to allow for recovery.
“So, in many cases, individuals are not getting the recovery their body needs to actually experience PA benefits, because those benefits come during rest,” Dr. Quinn said.
“We’ve shown that PA at work raises acute cardiovascular responses, which are related to cardiovascular risk. For example, 24-hour and waking heart rate and diastolic blood pressure, as well as nonwork diastolic blood pressure, all were significantly higher on workdays versus non-workdays,” he said.
Dr. Quinn also said that psychological stress at work amplifies risk. “A person who does PA at work and is stressed is likely to be at greater risk than someone who has a physically active job but doesn’t have psychological stress combined with it.”
Research gaps
However, Dr. Skirbekk noted that there are strategies that can reduce the risk for MCI and dementia despite high levels of occupational PA. “It is often difficult to change professions, and even if you do, it won’t immediately affect cognition. But altering one’s lifestyle is likely to have effects on cognitive development across the life cycle.
“Many clinicians say they always advise lifestyle changes, but nothing happens. But it makes sense to emphasize that these changes – stopping smoking, eating well, getting proper sleep, etc. – affect not only cardiovascular risk but also cognition. And I think clinicians should also take a patient’s occupation into account during any evaluation,” Dr. Skirbekk noted.
Dr. Quinn said it isn’t realistic to expect workers to come up with solutions to the PA paradox because many don’t have the autonomy to be able to mitigate their occupational risk.
“I think administrative controls and policy changes eventually will be the levers of change. We’re not quite there yet, but those are the types of things we should do when we’re trying to reduce loads in some way, or reduce the time that people spend doing certain tasks we know are potentially bad,” he said.
However, not everyone agrees that occupational PA doesn’t confer the same benefits of leisure-time PA, at least with respect to cardiovascular risk. For example, the Prospective Urban Rural Epidemiology (PURE) study, which includes a cohort of 130,000 people from 17 high-income, middle-income, and low-income countries, concluded that both higher recreational and nonrecreational PA were associated with a lower risk for mortality and CVD events.
What additional research is needed to clarify the effects of occupational and leisure-time activity and to address conflicting findings?
“Even studies coming out now regarding the effects of occupational PA have mainly used older data,” Dr. Skirbekk noted. “Labor markets and job demands have changed over time. There are different types of tasks and skills required now than there were 20 or 40 years ago. And of course, working from home is a recent phenomenon that’s happened on a large scale and might affect daily routines, sleep patterns, and also cognition. We need a better understanding of what the consequences might be.”
Health inequity issue
More research is also necessary to understand the social determinants of cognitive decline, impairment, and dementia, he said. “Many of the studies we see today are based on self-report of what someone has done in the past, which is particularly problematic for individuals who are impaired or who give interviews with others, which can induce biases.”
Dr. Quinn suggests that PA guidelines may need to differentiate between occupational and leisure-time PA to better reflect current research findings.
Meanwhile, Dr. Skirbekk and Dr. Quinn both point to the toll that occupational PA takes on the brain and body in lower-income workers as an important health equity issue.
“Our national guidelines for PA include occupational activity,” said Dr. Quinn. “But it’s clear that a lot of people who are getting a lot of occupational PA, particularly socioeconomic and racial/ethnic minorities, are not benefiting from it.”
Dr. Holtermann, who has arguably done the most research to date on the PA paradox, noted in a recent editorial that the majority of workers with high occupational PA have a low socioeconomic position and therefore “improving our understanding of the underlying mechanisms behind the PA health paradox and identifying new intervention targets along those pathways will be an important step to reduce socioeconomic health inequalities across the globe.”
A version of this article first appeared on Medscape.com.
In the pursuit of optimal health, regular physical activity (PA) is recommended to protect against dementia, cardiovascular disease (CVD), cancer, and other noncommunicable diseases. A significant body of research suggests the benefits of PA are positively correlated with higher frequency and intensity – with more often deemed better. This research has spawned a focus on increasing step counts and investing in standing desks and other interventions aimed at keeping people active.
But , but they also actually experience an increased risk for the very conditions that PA is intended to prevent.
A study published recently in The Lancet Regional Health – Europe used registry data from more than 7,000 adults in Norway, following them from age 33 to 65 years, to assess PA trajectories and risks for later-life mild cognitive impairment (MCI) and dementia at age 70 or older.
“Incorporating a life-course perspective gives a broader picture of how participants’ occupational histories relate to cognitive impairment later in life,” principal investigator Vegard Skirbekk, PhD, Columbia University Mailman School of Public Health, New York, said in an interview. Other studies typically have assessed occupational PA at a single time point, often close to the end of an individual’s career, and largely relied on self-report, he said.
Study participants worked in more than 300 different occupations. General physical activities performed on the included jobs required “considerable” use of arms and legs and moving the whole body, such as climbing, lifting, balancing, walking, stooping, and handling of materials.
Dr. Skirbekk and colleagues grouped participants into four PA trajectories over the 44-year study period: stable low, increasing then decreasing, stable intermediate, and stable high.
A total of 902 individuals were diagnosed with dementia and 2,407 with MCI at age 70 years or older. After adjustment, risks for MCI and dementia were 15.5% for those with higher occupational PA scores in the latter part of their working life and 9% for those with lower physical demands. The researchers concluded that “consistently working in an occupation with intermediate or high occupational PA was linked to an increased risk of cognitive impairment.”
The findings support those of the Copenhagen Male Study. Published in 2020, this longitudinal study compared leisure-time and occupational PA among more than 4,000 men in Denmark aged 40-59 at baseline in 1970-1971 and followed them until they turned 60. After adjustment, participants with high occupational PA had a 55% greater risk of developing dementia compared with those doing sedentary work.
Good vs. bad PA
“[T]he WHO [World Health Organization] guide to preventing dementia and disease on the whole mentions physical activity as an important factor. But our study suggests that it must be a ‘good’ form of physical activity, which hard physical work is not,” said Kirsten Nabe-Nielsen, PhD, lead author of this study
Beyond dementia, another recent study adds to a wealth of data on associations between occupational PA and cardiovascular risks. The cross-sectional analysis of U.S. data from the National Institute for Occupational Safety and Health showed that odds of CVD were higher when participants were “always” performing total occupational activity (odds ratio [OR], 1.99), occupational exertion (OR, 2.15), or occupational standing and walking around (OR, 1.84) compared with “never” engaging in these activities.
The contrasting effects of leisure-time vs. occupational PA constitute the “physical activity paradox” hypothesis. Starting in 2011, multiple studies by Andreas Holtermann, PhD, of the National Research Centre for the Working Environment lend support to the PA paradox theory, as do subsequent studies by others.
Although only “marginally considered” until a few years ago, recent large cohort studies seem to confirm the paradox, Pier Luigi Temporelli, MD wrote in a recent editorial.
In separate interviews, Dr. Skirbekk and lead author Tyler Quinn, PhD, MS, West Virginia University, Morgantown, pointed to the PA paradox as an explanation for their own recent findings, suggesting that the mechanisms that underlie it probably are responsible for the associated deleterious effects of occupational PA on the brain and heart, and even mortality.
“It’s well established that PA in your leisure time can be positive, but in the workplace, the results are quite the opposite,” Dr. Skirbekk said. “The specific mechanisms for why occupational PA is associated with elevated dementia risk are still not well understood and we need more knowledge. But we know that higher occupational physical demands have been linked to smaller hippocampal volume and poorer memory performance.”
Furthermore, he said, individuals working in jobs with high demands, both psychological and physical, combined with low job control perform more poorly on cognitive testing later in life.
“We looked mainly at professions where people have heavy workloads and you have much less autonomy, such as nursing assistants, office cleaners, childcare workers, and other personal care workers,” he said. “You cannot sit. You have somebody relying on you. It’s not all pleasure, and it can be very hard. That’s where we find the associations.”
Lack of autonomy
Specific characteristics indirectly associated with high occupational PA jobs – low cognitive stimuli, lifestyle factors, and socioeconomic influences – as well as factors directly related to high occupational PA, such as long hours, repetitive tasks, low levels of control, and stress, could also adversely affect cognitive trajectories, Dr. Skirbekk explained.
“By contrast, leisure-time physical activities tend to be of much shorter duration; are associated with socialization, play, [and] positive emotions; and [include] the opportunity to take breaks or shift to other types of activities if one prefers,” he said. “It may also be that too little or too much PA could be adversely related to cognitive outcomes – hence moderate activity levels, for example 10,000 steps a day, are still likely beneficial for cognitive functioning.”
Dr. Quinn said most of the CVD risk linked to occupational PA has to do with long periods of exertion such as lifting and carrying objects. While occupational standing and walking all day are also linked to CVD risk, they’re not as risky as lifting and carrying, he said.
Like Dr. Skirbekk, Dr. Quinn noted that individuals can take a break from leisure-time PA when they are tired, but occupational PA doesn’t have that same autonomy to allow for recovery.
“So, in many cases, individuals are not getting the recovery their body needs to actually experience PA benefits, because those benefits come during rest,” Dr. Quinn said.
“We’ve shown that PA at work raises acute cardiovascular responses, which are related to cardiovascular risk. For example, 24-hour and waking heart rate and diastolic blood pressure, as well as nonwork diastolic blood pressure, all were significantly higher on workdays versus non-workdays,” he said.
Dr. Quinn also said that psychological stress at work amplifies risk. “A person who does PA at work and is stressed is likely to be at greater risk than someone who has a physically active job but doesn’t have psychological stress combined with it.”
Research gaps
However, Dr. Skirbekk noted that there are strategies that can reduce the risk for MCI and dementia despite high levels of occupational PA. “It is often difficult to change professions, and even if you do, it won’t immediately affect cognition. But altering one’s lifestyle is likely to have effects on cognitive development across the life cycle.
“Many clinicians say they always advise lifestyle changes, but nothing happens. But it makes sense to emphasize that these changes – stopping smoking, eating well, getting proper sleep, etc. – affect not only cardiovascular risk but also cognition. And I think clinicians should also take a patient’s occupation into account during any evaluation,” Dr. Skirbekk noted.
Dr. Quinn said it isn’t realistic to expect workers to come up with solutions to the PA paradox because many don’t have the autonomy to be able to mitigate their occupational risk.
“I think administrative controls and policy changes eventually will be the levers of change. We’re not quite there yet, but those are the types of things we should do when we’re trying to reduce loads in some way, or reduce the time that people spend doing certain tasks we know are potentially bad,” he said.
However, not everyone agrees that occupational PA doesn’t confer the same benefits of leisure-time PA, at least with respect to cardiovascular risk. For example, the Prospective Urban Rural Epidemiology (PURE) study, which includes a cohort of 130,000 people from 17 high-income, middle-income, and low-income countries, concluded that both higher recreational and nonrecreational PA were associated with a lower risk for mortality and CVD events.
What additional research is needed to clarify the effects of occupational and leisure-time activity and to address conflicting findings?
“Even studies coming out now regarding the effects of occupational PA have mainly used older data,” Dr. Skirbekk noted. “Labor markets and job demands have changed over time. There are different types of tasks and skills required now than there were 20 or 40 years ago. And of course, working from home is a recent phenomenon that’s happened on a large scale and might affect daily routines, sleep patterns, and also cognition. We need a better understanding of what the consequences might be.”
Health inequity issue
More research is also necessary to understand the social determinants of cognitive decline, impairment, and dementia, he said. “Many of the studies we see today are based on self-report of what someone has done in the past, which is particularly problematic for individuals who are impaired or who give interviews with others, which can induce biases.”
Dr. Quinn suggests that PA guidelines may need to differentiate between occupational and leisure-time PA to better reflect current research findings.
Meanwhile, Dr. Skirbekk and Dr. Quinn both point to the toll that occupational PA takes on the brain and body in lower-income workers as an important health equity issue.
“Our national guidelines for PA include occupational activity,” said Dr. Quinn. “But it’s clear that a lot of people who are getting a lot of occupational PA, particularly socioeconomic and racial/ethnic minorities, are not benefiting from it.”
Dr. Holtermann, who has arguably done the most research to date on the PA paradox, noted in a recent editorial that the majority of workers with high occupational PA have a low socioeconomic position and therefore “improving our understanding of the underlying mechanisms behind the PA health paradox and identifying new intervention targets along those pathways will be an important step to reduce socioeconomic health inequalities across the globe.”
A version of this article first appeared on Medscape.com.
In the pursuit of optimal health, regular physical activity (PA) is recommended to protect against dementia, cardiovascular disease (CVD), cancer, and other noncommunicable diseases. A significant body of research suggests the benefits of PA are positively correlated with higher frequency and intensity – with more often deemed better. This research has spawned a focus on increasing step counts and investing in standing desks and other interventions aimed at keeping people active.
But , but they also actually experience an increased risk for the very conditions that PA is intended to prevent.
A study published recently in The Lancet Regional Health – Europe used registry data from more than 7,000 adults in Norway, following them from age 33 to 65 years, to assess PA trajectories and risks for later-life mild cognitive impairment (MCI) and dementia at age 70 or older.
“Incorporating a life-course perspective gives a broader picture of how participants’ occupational histories relate to cognitive impairment later in life,” principal investigator Vegard Skirbekk, PhD, Columbia University Mailman School of Public Health, New York, said in an interview. Other studies typically have assessed occupational PA at a single time point, often close to the end of an individual’s career, and largely relied on self-report, he said.
Study participants worked in more than 300 different occupations. General physical activities performed on the included jobs required “considerable” use of arms and legs and moving the whole body, such as climbing, lifting, balancing, walking, stooping, and handling of materials.
Dr. Skirbekk and colleagues grouped participants into four PA trajectories over the 44-year study period: stable low, increasing then decreasing, stable intermediate, and stable high.
A total of 902 individuals were diagnosed with dementia and 2,407 with MCI at age 70 years or older. After adjustment, risks for MCI and dementia were 15.5% for those with higher occupational PA scores in the latter part of their working life and 9% for those with lower physical demands. The researchers concluded that “consistently working in an occupation with intermediate or high occupational PA was linked to an increased risk of cognitive impairment.”
The findings support those of the Copenhagen Male Study. Published in 2020, this longitudinal study compared leisure-time and occupational PA among more than 4,000 men in Denmark aged 40-59 at baseline in 1970-1971 and followed them until they turned 60. After adjustment, participants with high occupational PA had a 55% greater risk of developing dementia compared with those doing sedentary work.
Good vs. bad PA
“[T]he WHO [World Health Organization] guide to preventing dementia and disease on the whole mentions physical activity as an important factor. But our study suggests that it must be a ‘good’ form of physical activity, which hard physical work is not,” said Kirsten Nabe-Nielsen, PhD, lead author of this study
Beyond dementia, another recent study adds to a wealth of data on associations between occupational PA and cardiovascular risks. The cross-sectional analysis of U.S. data from the National Institute for Occupational Safety and Health showed that odds of CVD were higher when participants were “always” performing total occupational activity (odds ratio [OR], 1.99), occupational exertion (OR, 2.15), or occupational standing and walking around (OR, 1.84) compared with “never” engaging in these activities.
The contrasting effects of leisure-time vs. occupational PA constitute the “physical activity paradox” hypothesis. Starting in 2011, multiple studies by Andreas Holtermann, PhD, of the National Research Centre for the Working Environment lend support to the PA paradox theory, as do subsequent studies by others.
Although only “marginally considered” until a few years ago, recent large cohort studies seem to confirm the paradox, Pier Luigi Temporelli, MD wrote in a recent editorial.
In separate interviews, Dr. Skirbekk and lead author Tyler Quinn, PhD, MS, West Virginia University, Morgantown, pointed to the PA paradox as an explanation for their own recent findings, suggesting that the mechanisms that underlie it probably are responsible for the associated deleterious effects of occupational PA on the brain and heart, and even mortality.
“It’s well established that PA in your leisure time can be positive, but in the workplace, the results are quite the opposite,” Dr. Skirbekk said. “The specific mechanisms for why occupational PA is associated with elevated dementia risk are still not well understood and we need more knowledge. But we know that higher occupational physical demands have been linked to smaller hippocampal volume and poorer memory performance.”
Furthermore, he said, individuals working in jobs with high demands, both psychological and physical, combined with low job control perform more poorly on cognitive testing later in life.
“We looked mainly at professions where people have heavy workloads and you have much less autonomy, such as nursing assistants, office cleaners, childcare workers, and other personal care workers,” he said. “You cannot sit. You have somebody relying on you. It’s not all pleasure, and it can be very hard. That’s where we find the associations.”
Lack of autonomy
Specific characteristics indirectly associated with high occupational PA jobs – low cognitive stimuli, lifestyle factors, and socioeconomic influences – as well as factors directly related to high occupational PA, such as long hours, repetitive tasks, low levels of control, and stress, could also adversely affect cognitive trajectories, Dr. Skirbekk explained.
“By contrast, leisure-time physical activities tend to be of much shorter duration; are associated with socialization, play, [and] positive emotions; and [include] the opportunity to take breaks or shift to other types of activities if one prefers,” he said. “It may also be that too little or too much PA could be adversely related to cognitive outcomes – hence moderate activity levels, for example 10,000 steps a day, are still likely beneficial for cognitive functioning.”
Dr. Quinn said most of the CVD risk linked to occupational PA has to do with long periods of exertion such as lifting and carrying objects. While occupational standing and walking all day are also linked to CVD risk, they’re not as risky as lifting and carrying, he said.
Like Dr. Skirbekk, Dr. Quinn noted that individuals can take a break from leisure-time PA when they are tired, but occupational PA doesn’t have that same autonomy to allow for recovery.
“So, in many cases, individuals are not getting the recovery their body needs to actually experience PA benefits, because those benefits come during rest,” Dr. Quinn said.
“We’ve shown that PA at work raises acute cardiovascular responses, which are related to cardiovascular risk. For example, 24-hour and waking heart rate and diastolic blood pressure, as well as nonwork diastolic blood pressure, all were significantly higher on workdays versus non-workdays,” he said.
Dr. Quinn also said that psychological stress at work amplifies risk. “A person who does PA at work and is stressed is likely to be at greater risk than someone who has a physically active job but doesn’t have psychological stress combined with it.”
Research gaps
However, Dr. Skirbekk noted that there are strategies that can reduce the risk for MCI and dementia despite high levels of occupational PA. “It is often difficult to change professions, and even if you do, it won’t immediately affect cognition. But altering one’s lifestyle is likely to have effects on cognitive development across the life cycle.
“Many clinicians say they always advise lifestyle changes, but nothing happens. But it makes sense to emphasize that these changes – stopping smoking, eating well, getting proper sleep, etc. – affect not only cardiovascular risk but also cognition. And I think clinicians should also take a patient’s occupation into account during any evaluation,” Dr. Skirbekk noted.
Dr. Quinn said it isn’t realistic to expect workers to come up with solutions to the PA paradox because many don’t have the autonomy to be able to mitigate their occupational risk.
“I think administrative controls and policy changes eventually will be the levers of change. We’re not quite there yet, but those are the types of things we should do when we’re trying to reduce loads in some way, or reduce the time that people spend doing certain tasks we know are potentially bad,” he said.
However, not everyone agrees that occupational PA doesn’t confer the same benefits of leisure-time PA, at least with respect to cardiovascular risk. For example, the Prospective Urban Rural Epidemiology (PURE) study, which includes a cohort of 130,000 people from 17 high-income, middle-income, and low-income countries, concluded that both higher recreational and nonrecreational PA were associated with a lower risk for mortality and CVD events.
What additional research is needed to clarify the effects of occupational and leisure-time activity and to address conflicting findings?
“Even studies coming out now regarding the effects of occupational PA have mainly used older data,” Dr. Skirbekk noted. “Labor markets and job demands have changed over time. There are different types of tasks and skills required now than there were 20 or 40 years ago. And of course, working from home is a recent phenomenon that’s happened on a large scale and might affect daily routines, sleep patterns, and also cognition. We need a better understanding of what the consequences might be.”
Health inequity issue
More research is also necessary to understand the social determinants of cognitive decline, impairment, and dementia, he said. “Many of the studies we see today are based on self-report of what someone has done in the past, which is particularly problematic for individuals who are impaired or who give interviews with others, which can induce biases.”
Dr. Quinn suggests that PA guidelines may need to differentiate between occupational and leisure-time PA to better reflect current research findings.
Meanwhile, Dr. Skirbekk and Dr. Quinn both point to the toll that occupational PA takes on the brain and body in lower-income workers as an important health equity issue.
“Our national guidelines for PA include occupational activity,” said Dr. Quinn. “But it’s clear that a lot of people who are getting a lot of occupational PA, particularly socioeconomic and racial/ethnic minorities, are not benefiting from it.”
Dr. Holtermann, who has arguably done the most research to date on the PA paradox, noted in a recent editorial that the majority of workers with high occupational PA have a low socioeconomic position and therefore “improving our understanding of the underlying mechanisms behind the PA health paradox and identifying new intervention targets along those pathways will be an important step to reduce socioeconomic health inequalities across the globe.”
A version of this article first appeared on Medscape.com.
The Lancet Regional Health – Europe
Chronic pain in the United States: New data
data from the Centers for Disease Control and Prevention show.
Results from the annual National Health Interview Survey (NHIS) show that over-the-counter (OTC) pain relievers were the most commonly used pharmacologic treatment and exercise was the most common choice among nonpharmacologic options.
The results also revealed that prescription opioid use for chronic pain decreased from 15.2% in 2019 to 13.5% in 2020. However, there was no corresponding increase in nonpharmacologic therapies, despite current CDC guidelines that recommend maximizing the use of medication alternatives.
“Public health efforts may reduce health inequities by increasing access to pain management therapies so that all persons with chronic pain can receive safe and effective care,” S. Michaela Rikard, PhD, and colleagues wrote.
The findings were published online in a research letter in Annals of Internal Medicine.
Among 31,500 survey respondents, 7,400 indicated that they had pain on most days or every day for the past 3 months.
The survey collected data on self-reported opioid prescriptions in the past 3 months, as well as prescription and nonprescription opiate use during the same time period.
Among adult respondents, 60% used a combination of pharmacologic and nonpharmacologic treatments for pain and almost 27% used medications alone. Older adults, those with low incomes, uninsured individuals, and those living in the South were among those least likely to turn to nonpharmacologic treatment for pain.
After exercise, complementary therapies were the most commonly used nonpharmacologic options, including massage, meditation, or guided imagery, and spinal manipulation or other forms of chiropractic care.
For those taking medications, 76% self-reported using OTC pain relievers for pain, followed by prescription nonopioids (31%) and prescription opioids (13.5%).
Of those who used both pharmacologic and nonpharmacologic therapies, about half reported nonopioid and nonpharmacologic therapy use and 8% reported combined use of opioids, nonopioids, and nonpharmacologic therapy.
After adjustment for multiple factors, investigators found those who were older, had public insurance, or had more severe pain were more likely to use prescription opioids. They also reported severe pain (22%), but 4% reported only mild pain.
Study limitations included generalizability only to noninstitutionalized civilian adults, potential recall bias, and cross-sectional results that do not include patient or treatment history.
“Despite its limitations, this study identifies opportunities to improve guideline-concordant use of pharmacologic and nonpharmacologic therapies among adults with chronic pain,” the authors wrote.
There was no specific funding source for the study. The authors have reported no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
data from the Centers for Disease Control and Prevention show.
Results from the annual National Health Interview Survey (NHIS) show that over-the-counter (OTC) pain relievers were the most commonly used pharmacologic treatment and exercise was the most common choice among nonpharmacologic options.
The results also revealed that prescription opioid use for chronic pain decreased from 15.2% in 2019 to 13.5% in 2020. However, there was no corresponding increase in nonpharmacologic therapies, despite current CDC guidelines that recommend maximizing the use of medication alternatives.
“Public health efforts may reduce health inequities by increasing access to pain management therapies so that all persons with chronic pain can receive safe and effective care,” S. Michaela Rikard, PhD, and colleagues wrote.
The findings were published online in a research letter in Annals of Internal Medicine.
Among 31,500 survey respondents, 7,400 indicated that they had pain on most days or every day for the past 3 months.
The survey collected data on self-reported opioid prescriptions in the past 3 months, as well as prescription and nonprescription opiate use during the same time period.
Among adult respondents, 60% used a combination of pharmacologic and nonpharmacologic treatments for pain and almost 27% used medications alone. Older adults, those with low incomes, uninsured individuals, and those living in the South were among those least likely to turn to nonpharmacologic treatment for pain.
After exercise, complementary therapies were the most commonly used nonpharmacologic options, including massage, meditation, or guided imagery, and spinal manipulation or other forms of chiropractic care.
For those taking medications, 76% self-reported using OTC pain relievers for pain, followed by prescription nonopioids (31%) and prescription opioids (13.5%).
Of those who used both pharmacologic and nonpharmacologic therapies, about half reported nonopioid and nonpharmacologic therapy use and 8% reported combined use of opioids, nonopioids, and nonpharmacologic therapy.
After adjustment for multiple factors, investigators found those who were older, had public insurance, or had more severe pain were more likely to use prescription opioids. They also reported severe pain (22%), but 4% reported only mild pain.
Study limitations included generalizability only to noninstitutionalized civilian adults, potential recall bias, and cross-sectional results that do not include patient or treatment history.
“Despite its limitations, this study identifies opportunities to improve guideline-concordant use of pharmacologic and nonpharmacologic therapies among adults with chronic pain,” the authors wrote.
There was no specific funding source for the study. The authors have reported no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
data from the Centers for Disease Control and Prevention show.
Results from the annual National Health Interview Survey (NHIS) show that over-the-counter (OTC) pain relievers were the most commonly used pharmacologic treatment and exercise was the most common choice among nonpharmacologic options.
The results also revealed that prescription opioid use for chronic pain decreased from 15.2% in 2019 to 13.5% in 2020. However, there was no corresponding increase in nonpharmacologic therapies, despite current CDC guidelines that recommend maximizing the use of medication alternatives.
“Public health efforts may reduce health inequities by increasing access to pain management therapies so that all persons with chronic pain can receive safe and effective care,” S. Michaela Rikard, PhD, and colleagues wrote.
The findings were published online in a research letter in Annals of Internal Medicine.
Among 31,500 survey respondents, 7,400 indicated that they had pain on most days or every day for the past 3 months.
The survey collected data on self-reported opioid prescriptions in the past 3 months, as well as prescription and nonprescription opiate use during the same time period.
Among adult respondents, 60% used a combination of pharmacologic and nonpharmacologic treatments for pain and almost 27% used medications alone. Older adults, those with low incomes, uninsured individuals, and those living in the South were among those least likely to turn to nonpharmacologic treatment for pain.
After exercise, complementary therapies were the most commonly used nonpharmacologic options, including massage, meditation, or guided imagery, and spinal manipulation or other forms of chiropractic care.
For those taking medications, 76% self-reported using OTC pain relievers for pain, followed by prescription nonopioids (31%) and prescription opioids (13.5%).
Of those who used both pharmacologic and nonpharmacologic therapies, about half reported nonopioid and nonpharmacologic therapy use and 8% reported combined use of opioids, nonopioids, and nonpharmacologic therapy.
After adjustment for multiple factors, investigators found those who were older, had public insurance, or had more severe pain were more likely to use prescription opioids. They also reported severe pain (22%), but 4% reported only mild pain.
Study limitations included generalizability only to noninstitutionalized civilian adults, potential recall bias, and cross-sectional results that do not include patient or treatment history.
“Despite its limitations, this study identifies opportunities to improve guideline-concordant use of pharmacologic and nonpharmacologic therapies among adults with chronic pain,” the authors wrote.
There was no specific funding source for the study. The authors have reported no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
FROM ANNALS OF INTERNAL MEDICINE
Alzheimer’s blood test coming within 5 years, UK group pledges
Alzheimer’s Research UK, the Alzheimer’s Society, and the National Institute for Health and Care Research (NIHR) are collaborating and leading AD researchers to bring a diagnostic blood test to the UK’s National Health Service (NHS).
“Dementia affects around 900,000 people in the UK today, and that number is expected to rise to 1.4 million by 2040. It is the UK’s biggest killer,” Fiona Carragher, with the Alzheimer’s Society, said during a media briefing announcing the project.
Yet, many people face a very long wait of up to 2-4 years to get a dementia diagnosis, and many cases remain undiagnosed, she noted.
A chief reason is lack of access to specialized diagnostic testing. Currently, only 2% of people in the United Kingdom have access to advanced diagnostic tests such as PET scans and lumbar punctures owing to limited availability.
“Getting an early and accurate diagnosis is the pivotal first step to getting help today and unlocking hope for the future” and blood biomarkers provide a “real opportunity to disrupt the diagnostic paradigm,” Ms. Carragher said. It also offers greater opportunities to participate in research and clinical trials, she added.
Attitude shift
Susan Kohlhaas, PhD, with Alzheimer’s Research UK, noted that attitudes toward dementia diagnosis have changed in the past few years. The days when people may have not wanted to know if they have dementia are gone.
Data from the latest wave of the Alzheimer’s Research UK Dementia Attitudes Monitor survey show that 9 in 10 people would seek a diagnosis from their provider. “That’s been driven by awareness of treatments and things that people can proactively do to try and slow disease progression,” Dr. Kohlhaas said.
“As new treatments for dementia become available there will to be a surge in people seeking a diagnosis. At the moment, we don’t have adequate infrastructure to cope with that demand,” Dr. Kohlhaas added.
She noted that blood tests are starting to show their potential as an effective part of the diagnosis and are widely used in research.
“In some cases, they are similar in sensitivity to gold-standard PET scans and lumbar punctures, and they’re less expensive and potentially more scalable on the NHS. What we need to do over the next several years is to understand how they fit into the clinical pathway,” Dr. Kohlhaas said.
The project will involve working with leading dementia researchers to pilot the implementation of potential blood tests in the NHS that can give an early and accurate diagnose of dementia.
The project, which kicks off in January 2024, will receive £5 million ($6.13 million) awarded by the UK Postcode Dream Fund. Specific details regarding the leadership team, participating centers, and specific blood biomarker tests to be trialed will be announced then.
Ms. Carragher and Dr. Kohlhaas reported no relevant financial conflicts of interest.
A version of this article appeared on Medscape.com.
Alzheimer’s Research UK, the Alzheimer’s Society, and the National Institute for Health and Care Research (NIHR) are collaborating and leading AD researchers to bring a diagnostic blood test to the UK’s National Health Service (NHS).
“Dementia affects around 900,000 people in the UK today, and that number is expected to rise to 1.4 million by 2040. It is the UK’s biggest killer,” Fiona Carragher, with the Alzheimer’s Society, said during a media briefing announcing the project.
Yet, many people face a very long wait of up to 2-4 years to get a dementia diagnosis, and many cases remain undiagnosed, she noted.
A chief reason is lack of access to specialized diagnostic testing. Currently, only 2% of people in the United Kingdom have access to advanced diagnostic tests such as PET scans and lumbar punctures owing to limited availability.
“Getting an early and accurate diagnosis is the pivotal first step to getting help today and unlocking hope for the future” and blood biomarkers provide a “real opportunity to disrupt the diagnostic paradigm,” Ms. Carragher said. It also offers greater opportunities to participate in research and clinical trials, she added.
Attitude shift
Susan Kohlhaas, PhD, with Alzheimer’s Research UK, noted that attitudes toward dementia diagnosis have changed in the past few years. The days when people may have not wanted to know if they have dementia are gone.
Data from the latest wave of the Alzheimer’s Research UK Dementia Attitudes Monitor survey show that 9 in 10 people would seek a diagnosis from their provider. “That’s been driven by awareness of treatments and things that people can proactively do to try and slow disease progression,” Dr. Kohlhaas said.
“As new treatments for dementia become available there will to be a surge in people seeking a diagnosis. At the moment, we don’t have adequate infrastructure to cope with that demand,” Dr. Kohlhaas added.
She noted that blood tests are starting to show their potential as an effective part of the diagnosis and are widely used in research.
“In some cases, they are similar in sensitivity to gold-standard PET scans and lumbar punctures, and they’re less expensive and potentially more scalable on the NHS. What we need to do over the next several years is to understand how they fit into the clinical pathway,” Dr. Kohlhaas said.
The project will involve working with leading dementia researchers to pilot the implementation of potential blood tests in the NHS that can give an early and accurate diagnose of dementia.
The project, which kicks off in January 2024, will receive £5 million ($6.13 million) awarded by the UK Postcode Dream Fund. Specific details regarding the leadership team, participating centers, and specific blood biomarker tests to be trialed will be announced then.
Ms. Carragher and Dr. Kohlhaas reported no relevant financial conflicts of interest.
A version of this article appeared on Medscape.com.
Alzheimer’s Research UK, the Alzheimer’s Society, and the National Institute for Health and Care Research (NIHR) are collaborating and leading AD researchers to bring a diagnostic blood test to the UK’s National Health Service (NHS).
“Dementia affects around 900,000 people in the UK today, and that number is expected to rise to 1.4 million by 2040. It is the UK’s biggest killer,” Fiona Carragher, with the Alzheimer’s Society, said during a media briefing announcing the project.
Yet, many people face a very long wait of up to 2-4 years to get a dementia diagnosis, and many cases remain undiagnosed, she noted.
A chief reason is lack of access to specialized diagnostic testing. Currently, only 2% of people in the United Kingdom have access to advanced diagnostic tests such as PET scans and lumbar punctures owing to limited availability.
“Getting an early and accurate diagnosis is the pivotal first step to getting help today and unlocking hope for the future” and blood biomarkers provide a “real opportunity to disrupt the diagnostic paradigm,” Ms. Carragher said. It also offers greater opportunities to participate in research and clinical trials, she added.
Attitude shift
Susan Kohlhaas, PhD, with Alzheimer’s Research UK, noted that attitudes toward dementia diagnosis have changed in the past few years. The days when people may have not wanted to know if they have dementia are gone.
Data from the latest wave of the Alzheimer’s Research UK Dementia Attitudes Monitor survey show that 9 in 10 people would seek a diagnosis from their provider. “That’s been driven by awareness of treatments and things that people can proactively do to try and slow disease progression,” Dr. Kohlhaas said.
“As new treatments for dementia become available there will to be a surge in people seeking a diagnosis. At the moment, we don’t have adequate infrastructure to cope with that demand,” Dr. Kohlhaas added.
She noted that blood tests are starting to show their potential as an effective part of the diagnosis and are widely used in research.
“In some cases, they are similar in sensitivity to gold-standard PET scans and lumbar punctures, and they’re less expensive and potentially more scalable on the NHS. What we need to do over the next several years is to understand how they fit into the clinical pathway,” Dr. Kohlhaas said.
The project will involve working with leading dementia researchers to pilot the implementation of potential blood tests in the NHS that can give an early and accurate diagnose of dementia.
The project, which kicks off in January 2024, will receive £5 million ($6.13 million) awarded by the UK Postcode Dream Fund. Specific details regarding the leadership team, participating centers, and specific blood biomarker tests to be trialed will be announced then.
Ms. Carragher and Dr. Kohlhaas reported no relevant financial conflicts of interest.
A version of this article appeared on Medscape.com.
Military service linked to Alzheimer’s neuropathology
TOPLINE:
METHODOLOGY:
- The study included 597 male decedents who donated their brains to one of two Alzheimer’s Disease Research Center (ADRC) brain bank programs between 1986 and 2018.
- Researchers conducted public data tracing for historical information on military history, which included searching online commercial genealogical databases and paper archives.
- They evaluated tau tangles (using a B score of neurofibrillary tangle deposition in four stages: B0 [not present], B1 [transentorhinal stages], B2 [limbic stages], and B3 [isocortical stages]) and amyloid plaque pathology (using a C score that classifies neuritic amyloid plaque into four categories: no plaques, sparse, moderate, or frequent).
- The study involved three B score comparisons (1, 2, 3 vs. 0; 2, 3 vs. 0, 1; and 3 vs. 0, 1, 2) and two C score comparisons (sparse, moderate, or frequent vs. no plaques, and moderate or frequent vs. no plaque or sparse).
TAKEAWAY:
- Public record tracing determined that 60% of the sample of male decedents had a history of military service; the median year of birth was 1923 and the median year of death was 2007.
- After adjustment for age and year of death, those with a military service history had a 26% increased risk for a higher neuritic amyloid plaque C score compared with those without such history (odds ratio [OR], 1.26; 95% confidence interval [CI], 1.06-1.49), an increase that applied for both relevant comparisons.
- A history of military service was also associated with a 10% greater adjusted odds of a higher neurofibrillary tangle B score (OR, 1.10; 95% CI, 1.08-1.12), with the increase applying to all three comparisons.
- A sensitivity analysis that included both the male decedents and 556 female decedents (increasing the overall sample to 1,153) and was adjusted for sex in addition to age and year of death showed similar results to the male-only sample estimations for both B and C score comparisons.
IN PRACTICE:
Understanding how military service affects AD biological processes is “essential” from a research perspective, the investigators noted. These new findings “emphasize that targeted AD therapies in the veteran population are urgently needed.”
SOURCE:
The study was conducted by W. Ryan Powell, Center for Health Disparities Research and Department of Medicine, Geriatrics Division, University of Wisconsin School of Medicine and Public Health, and colleagues. It was published online in Alzheimer’s & Dementia.
LIMITATIONS:
Selection bias in brain donation is likely because ADRC cohorts are recruitment based. The study was unable to rigorously identify factors that may explain why individuals with military service are at greater risk of having amyloid and tau neuropathology (including the interplay between environmental and genetic risk factors such as apolipoprotein E status).
DISCLOSURES:
The study was supported by the National Institute on Aging. The authors reported no disclosures.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- The study included 597 male decedents who donated their brains to one of two Alzheimer’s Disease Research Center (ADRC) brain bank programs between 1986 and 2018.
- Researchers conducted public data tracing for historical information on military history, which included searching online commercial genealogical databases and paper archives.
- They evaluated tau tangles (using a B score of neurofibrillary tangle deposition in four stages: B0 [not present], B1 [transentorhinal stages], B2 [limbic stages], and B3 [isocortical stages]) and amyloid plaque pathology (using a C score that classifies neuritic amyloid plaque into four categories: no plaques, sparse, moderate, or frequent).
- The study involved three B score comparisons (1, 2, 3 vs. 0; 2, 3 vs. 0, 1; and 3 vs. 0, 1, 2) and two C score comparisons (sparse, moderate, or frequent vs. no plaques, and moderate or frequent vs. no plaque or sparse).
TAKEAWAY:
- Public record tracing determined that 60% of the sample of male decedents had a history of military service; the median year of birth was 1923 and the median year of death was 2007.
- After adjustment for age and year of death, those with a military service history had a 26% increased risk for a higher neuritic amyloid plaque C score compared with those without such history (odds ratio [OR], 1.26; 95% confidence interval [CI], 1.06-1.49), an increase that applied for both relevant comparisons.
- A history of military service was also associated with a 10% greater adjusted odds of a higher neurofibrillary tangle B score (OR, 1.10; 95% CI, 1.08-1.12), with the increase applying to all three comparisons.
- A sensitivity analysis that included both the male decedents and 556 female decedents (increasing the overall sample to 1,153) and was adjusted for sex in addition to age and year of death showed similar results to the male-only sample estimations for both B and C score comparisons.
IN PRACTICE:
Understanding how military service affects AD biological processes is “essential” from a research perspective, the investigators noted. These new findings “emphasize that targeted AD therapies in the veteran population are urgently needed.”
SOURCE:
The study was conducted by W. Ryan Powell, Center for Health Disparities Research and Department of Medicine, Geriatrics Division, University of Wisconsin School of Medicine and Public Health, and colleagues. It was published online in Alzheimer’s & Dementia.
LIMITATIONS:
Selection bias in brain donation is likely because ADRC cohorts are recruitment based. The study was unable to rigorously identify factors that may explain why individuals with military service are at greater risk of having amyloid and tau neuropathology (including the interplay between environmental and genetic risk factors such as apolipoprotein E status).
DISCLOSURES:
The study was supported by the National Institute on Aging. The authors reported no disclosures.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- The study included 597 male decedents who donated their brains to one of two Alzheimer’s Disease Research Center (ADRC) brain bank programs between 1986 and 2018.
- Researchers conducted public data tracing for historical information on military history, which included searching online commercial genealogical databases and paper archives.
- They evaluated tau tangles (using a B score of neurofibrillary tangle deposition in four stages: B0 [not present], B1 [transentorhinal stages], B2 [limbic stages], and B3 [isocortical stages]) and amyloid plaque pathology (using a C score that classifies neuritic amyloid plaque into four categories: no plaques, sparse, moderate, or frequent).
- The study involved three B score comparisons (1, 2, 3 vs. 0; 2, 3 vs. 0, 1; and 3 vs. 0, 1, 2) and two C score comparisons (sparse, moderate, or frequent vs. no plaques, and moderate or frequent vs. no plaque or sparse).
TAKEAWAY:
- Public record tracing determined that 60% of the sample of male decedents had a history of military service; the median year of birth was 1923 and the median year of death was 2007.
- After adjustment for age and year of death, those with a military service history had a 26% increased risk for a higher neuritic amyloid plaque C score compared with those without such history (odds ratio [OR], 1.26; 95% confidence interval [CI], 1.06-1.49), an increase that applied for both relevant comparisons.
- A history of military service was also associated with a 10% greater adjusted odds of a higher neurofibrillary tangle B score (OR, 1.10; 95% CI, 1.08-1.12), with the increase applying to all three comparisons.
- A sensitivity analysis that included both the male decedents and 556 female decedents (increasing the overall sample to 1,153) and was adjusted for sex in addition to age and year of death showed similar results to the male-only sample estimations for both B and C score comparisons.
IN PRACTICE:
Understanding how military service affects AD biological processes is “essential” from a research perspective, the investigators noted. These new findings “emphasize that targeted AD therapies in the veteran population are urgently needed.”
SOURCE:
The study was conducted by W. Ryan Powell, Center for Health Disparities Research and Department of Medicine, Geriatrics Division, University of Wisconsin School of Medicine and Public Health, and colleagues. It was published online in Alzheimer’s & Dementia.
LIMITATIONS:
Selection bias in brain donation is likely because ADRC cohorts are recruitment based. The study was unable to rigorously identify factors that may explain why individuals with military service are at greater risk of having amyloid and tau neuropathology (including the interplay between environmental and genetic risk factors such as apolipoprotein E status).
DISCLOSURES:
The study was supported by the National Institute on Aging. The authors reported no disclosures.
A version of this article appeared on Medscape.com.