User login
Woman presents with cough and bronchorrhea
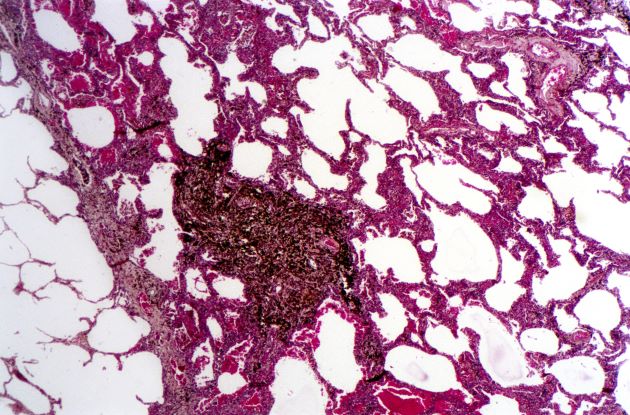
Bronchioalveolar cell carcinoma (BAC) is a variant of non–small cell lung cancer (NSCLC) that, in recent years, has received a new identity in some of the literature. Adenocarcinoma in situ (AIS) and minimally invasive adenocarcinoma (MIA) are relatively new entities that in some published literature have replaced the term BAC. The National Comprehensive Cancer Network recognizes these terms. AIS is defined as a localized adenocarcinoma of < 3 cm that exhibits a lepidic growth pattern, with neoplastic cells along the alveolar structures but without stromal, vascular, or pleural invasion. MIA refers to small, solitary adenocarcinomas < 3 cm with either pure lepidic growth or predominant lepidic growth with ≤ 5 mm of stromal invasion. BAC has unique epidemiologic, pathologic, and clinical features compared with other NSCLC subtypes. For example, although it is smoking-related, the relationship of BAC to smoking is less strong than with other types of NSCLC. About a third of patients with BAC are never-smokers.
There are also some unique radiographic features — its presentation may be confused with pneumonia or other inflammatory conditions in the lung, and only after a patient does not improve after a course of antibiotics should a diagnosis of BAC be considered. Unlike other types of lung cancer where chemotherapy may be the first plan of attack, surgery is often the first choice for treating BAC, particularly when there is no mediastinal node involvement (10%-25% of cases) or distal metastases (5% of cases). BAC usually harbors EGFR mutation. It is responsive to new targeted therapies for lung cancer, particularly osimertinib, afatinib, erlotinib, and gefitinib. Thus, people with BAC are good candidates for genetic testing.
Karl J. D'Silva, MD, Clinical Assistant Professor, Department of Medicine, Tufts University School of Medicine, Boston; Medical Director, Department of Oncology and Hematology, Lahey Hospital and Medical Center, Peabody, Massachusetts
Karl J. D'Silva, MD, has disclosed no relevant financial relationships.
Bronchioalveolar cell carcinoma (BAC) is a variant of non–small cell lung cancer (NSCLC) that, in recent years, has received a new identity in some of the literature. Adenocarcinoma in situ (AIS) and minimally invasive adenocarcinoma (MIA) are relatively new entities that in some published literature have replaced the term BAC. The National Comprehensive Cancer Network recognizes these terms. AIS is defined as a localized adenocarcinoma of < 3 cm that exhibits a lepidic growth pattern, with neoplastic cells along the alveolar structures but without stromal, vascular, or pleural invasion. MIA refers to small, solitary adenocarcinomas < 3 cm with either pure lepidic growth or predominant lepidic growth with ≤ 5 mm of stromal invasion. BAC has unique epidemiologic, pathologic, and clinical features compared with other NSCLC subtypes. For example, although it is smoking-related, the relationship of BAC to smoking is less strong than with other types of NSCLC. About a third of patients with BAC are never-smokers.
There are also some unique radiographic features — its presentation may be confused with pneumonia or other inflammatory conditions in the lung, and only after a patient does not improve after a course of antibiotics should a diagnosis of BAC be considered. Unlike other types of lung cancer where chemotherapy may be the first plan of attack, surgery is often the first choice for treating BAC, particularly when there is no mediastinal node involvement (10%-25% of cases) or distal metastases (5% of cases). BAC usually harbors EGFR mutation. It is responsive to new targeted therapies for lung cancer, particularly osimertinib, afatinib, erlotinib, and gefitinib. Thus, people with BAC are good candidates for genetic testing.
Karl J. D'Silva, MD, Clinical Assistant Professor, Department of Medicine, Tufts University School of Medicine, Boston; Medical Director, Department of Oncology and Hematology, Lahey Hospital and Medical Center, Peabody, Massachusetts
Karl J. D'Silva, MD, has disclosed no relevant financial relationships.
Bronchioalveolar cell carcinoma (BAC) is a variant of non–small cell lung cancer (NSCLC) that, in recent years, has received a new identity in some of the literature. Adenocarcinoma in situ (AIS) and minimally invasive adenocarcinoma (MIA) are relatively new entities that in some published literature have replaced the term BAC. The National Comprehensive Cancer Network recognizes these terms. AIS is defined as a localized adenocarcinoma of < 3 cm that exhibits a lepidic growth pattern, with neoplastic cells along the alveolar structures but without stromal, vascular, or pleural invasion. MIA refers to small, solitary adenocarcinomas < 3 cm with either pure lepidic growth or predominant lepidic growth with ≤ 5 mm of stromal invasion. BAC has unique epidemiologic, pathologic, and clinical features compared with other NSCLC subtypes. For example, although it is smoking-related, the relationship of BAC to smoking is less strong than with other types of NSCLC. About a third of patients with BAC are never-smokers.
There are also some unique radiographic features — its presentation may be confused with pneumonia or other inflammatory conditions in the lung, and only after a patient does not improve after a course of antibiotics should a diagnosis of BAC be considered. Unlike other types of lung cancer where chemotherapy may be the first plan of attack, surgery is often the first choice for treating BAC, particularly when there is no mediastinal node involvement (10%-25% of cases) or distal metastases (5% of cases). BAC usually harbors EGFR mutation. It is responsive to new targeted therapies for lung cancer, particularly osimertinib, afatinib, erlotinib, and gefitinib. Thus, people with BAC are good candidates for genetic testing.
Karl J. D'Silva, MD, Clinical Assistant Professor, Department of Medicine, Tufts University School of Medicine, Boston; Medical Director, Department of Oncology and Hematology, Lahey Hospital and Medical Center, Peabody, Massachusetts
Karl J. D'Silva, MD, has disclosed no relevant financial relationships.
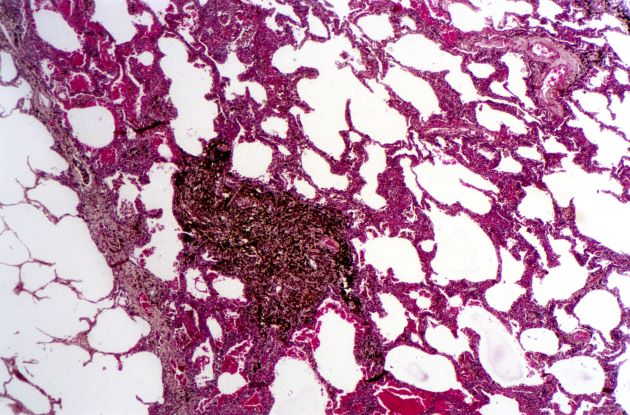
A 50-year-old woman, a never-smoker, presented with complaints of intermittent cough and shortness of breath for 3 months, associated with bronchorrhea (copious watery sputum production). She had lost 15 pounds in the past 2 months and had dyspnea on exertion for 1 month. Her pulse rate was 88/min, respiratory rate 18/min, and oxygen saturation 96% on room air. A chest x-ray (posteroanterior view) showed dense opacity in the right lower zone. Contrast-enhanced CT of the thorax showed diffuse ground-glass opacities around nodules and consolidation involving the apical and basal segments of the right lower lobe. Despite several courses of antimicrobials, bronchodilators, and IV corticosteroid therapy, the patient's condition worsened.
Breathing easier: The growing adoption of indwelling pleural catheters
Thoracic Oncology Network
Interventional Procedures Section
The management of recurrent pleural effusions is challenging. These devices have become an important treatment option in patients with malignant pleural effusions (MPE), particularly those with a nonexpandable lung (Feller-Kopman DJ, et al. Am J Respir Crit Care Med. 2018;198[7]:839) and when talc pleurodesis is unsuccessful in patients with an expandable lung (Dresler CM, et al. Chest. 2005;127[3]:909).
Over the last 5 years, studies evaluating the use of IPCs in treating nonmalignant pleural disease have proliferated. These studies have included and shown the successful treatment of pleural effusions due to end-stage renal disease, advanced heart failure (Walker SP, et al. Eur Respir J. 2022;59[2]:2101362), and cirrhosis, especially when a transjugular intrahepatic portosystemic shunt or liver transplant is not an option (Shojaee S, et al., Chest. 2019;155[3]:546). Compared with MPE, the rate of pleurodesis is generally lower and takes longer when an IPC is used to manage a nonmalignant pleural disease. Infection is the most common complication; most cases can be managed without catheter removal.
With many cited advantages, the IPC is an essential tool in the armamentarium of the chest physician and interventional radiologist. Indwelling pleural catheters have proven applications beyond MPE. When applied in a multidisciplinary fashion involving subspecialists and considering the patient’s goals, using an IPC can help achieve a crucial patient-centric goal in managing a recurrent nonmalignant pleural effusion.
Samiksha Gupta, MD
2nd Year Fellow
Sameer Kaushik Avasarala, MD
Section Member-at-Large
Thoracic Oncology Network
Interventional Procedures Section
The management of recurrent pleural effusions is challenging. These devices have become an important treatment option in patients with malignant pleural effusions (MPE), particularly those with a nonexpandable lung (Feller-Kopman DJ, et al. Am J Respir Crit Care Med. 2018;198[7]:839) and when talc pleurodesis is unsuccessful in patients with an expandable lung (Dresler CM, et al. Chest. 2005;127[3]:909).
Over the last 5 years, studies evaluating the use of IPCs in treating nonmalignant pleural disease have proliferated. These studies have included and shown the successful treatment of pleural effusions due to end-stage renal disease, advanced heart failure (Walker SP, et al. Eur Respir J. 2022;59[2]:2101362), and cirrhosis, especially when a transjugular intrahepatic portosystemic shunt or liver transplant is not an option (Shojaee S, et al., Chest. 2019;155[3]:546). Compared with MPE, the rate of pleurodesis is generally lower and takes longer when an IPC is used to manage a nonmalignant pleural disease. Infection is the most common complication; most cases can be managed without catheter removal.
With many cited advantages, the IPC is an essential tool in the armamentarium of the chest physician and interventional radiologist. Indwelling pleural catheters have proven applications beyond MPE. When applied in a multidisciplinary fashion involving subspecialists and considering the patient’s goals, using an IPC can help achieve a crucial patient-centric goal in managing a recurrent nonmalignant pleural effusion.
Samiksha Gupta, MD
2nd Year Fellow
Sameer Kaushik Avasarala, MD
Section Member-at-Large
Thoracic Oncology Network
Interventional Procedures Section
The management of recurrent pleural effusions is challenging. These devices have become an important treatment option in patients with malignant pleural effusions (MPE), particularly those with a nonexpandable lung (Feller-Kopman DJ, et al. Am J Respir Crit Care Med. 2018;198[7]:839) and when talc pleurodesis is unsuccessful in patients with an expandable lung (Dresler CM, et al. Chest. 2005;127[3]:909).
Over the last 5 years, studies evaluating the use of IPCs in treating nonmalignant pleural disease have proliferated. These studies have included and shown the successful treatment of pleural effusions due to end-stage renal disease, advanced heart failure (Walker SP, et al. Eur Respir J. 2022;59[2]:2101362), and cirrhosis, especially when a transjugular intrahepatic portosystemic shunt or liver transplant is not an option (Shojaee S, et al., Chest. 2019;155[3]:546). Compared with MPE, the rate of pleurodesis is generally lower and takes longer when an IPC is used to manage a nonmalignant pleural disease. Infection is the most common complication; most cases can be managed without catheter removal.
With many cited advantages, the IPC is an essential tool in the armamentarium of the chest physician and interventional radiologist. Indwelling pleural catheters have proven applications beyond MPE. When applied in a multidisciplinary fashion involving subspecialists and considering the patient’s goals, using an IPC can help achieve a crucial patient-centric goal in managing a recurrent nonmalignant pleural effusion.
Samiksha Gupta, MD
2nd Year Fellow
Sameer Kaushik Avasarala, MD
Section Member-at-Large
Standard-of-care therapy in lung cancer: Be open to new ideas
This transcript has been edited for clarity.
I’ll focus on some important topics related to decision-making and daily practice, and the practitioners’ thoughts from the meeting.
There’s no doubt that our outcomes are better for patients, but it’s much harder to make the best choice and I think there’s more pressure on us to make the best choice.
Topic one was the need for next-generation sequencing (NGS) testing. I’ll put it before you that every patient needs NGS testing at the time of diagnosis. It really shouldn’t be put off. How to do that is a topic for another day, but you need NGS testing.
Moving along with this, even when you’re thinking you’re going to go down the road of a checkpoint inhibitor with chemotherapy, the recent Food and Drug Administration approval for cemiplimab and chemotherapy says that you have to make sure that patients don’t have EGFR or ALK aberrations. Now, for cemiplimab, you have to make sure they don’t have ROS1 aberrations.
You need NGS testing to find those targets and give patients a targeted therapy. Even if you want to give a checkpoint inhibitor with or without chemotherapy, you need to have NGS testing.
Second, the way to get the most comprehensive analysis of targets for which there are therapeutic avenues is to do more comprehensive NGS testing, including both DNA and RNA. Not all the panels do this right now, and you really need that RNA-based testing to find all the fusions that are druggable by the current medications that we have.
Bottom line: NGS testing should be done for everybody, and you need to do the most comprehensive panel available both for DNA and RNA.
The next topic that there was great agreement on was the emergence of antibody-drug conjugates. I think everybody’s excited. All of them have shown evidence of benefit. There are varying degrees of side effects, and we’ll learn how to deal with those. They’re new drugs, they’re here, and they’re safe.
There are a couple of things to consider, though. Number one, these drugs do have chemotherapy and they have side effects from chemotherapy. I think the consensus is that when you treat patients with an antibody-drug conjugate, you need to give antiemetic regimens, at least for trastuzumab and the other deruxtecan drugs. You need to give a regimen for highly emetogenic chemotherapy as prophylactic antiemetics. I think that was a consensus thought.
Second, these drugs are making us rethink what it means to have the expression of the protein. I’m totally struck that for trastuzumab deruxtecan, patritumab deruxtecan, and datopotamab deruxtecan, the degree of protein expression is not particularly relevant, and these drugs can work in all patients. There have been cases clearly shown that datopotamab deruxtecan and patritumab deruxtecan both have benefit in patients with EGFR mutations after progression on osimertinib.
This idea of a need for overexpression, and maybe even the idea of testing, is being challenged now. These drugs seem to work as long as some protein is present. They don’t work in every patient, but they work in the vast majority. This thinking about overexpression with the antibody-drug conjugates is probably going to need to be reevaluated.
Last are some thoughts about our targeted therapies. Again, we have more targets. We have EGFR exon 20, for example, and more drugs for MET. I’d like to share a couple of thoughts on what the experts presented at the meeting.
First, although we have a bunch of new targeted agents for patients with EGFR-mutant cancers, probably the thing that’s going to change therapy now is adding chemotherapy to these agents. We may also use circulating tumor (ctDNA) to help guide us to identify which patients would be more likely to benefit from a chemotherapy with osimertinib. I see that as a trend and as a strategy that we’re likely to see move forward.
Another is in the ALK space. I know we’ve gotten very comfortable giving alectinib and brigatinib, but when you look at all the data, it points to lorlatinib perhaps being a better first-line therapy.
I think the experts thought lorlatinib would be a good drug. Yes, it has a different spectrum of side effects. The central nervous system (CNS) side effects are something we have to learn how to take care of; however, we can do that. Generally, with dose reduction, those side effects are manageable.
If you can get better outcomes in general and in patients with brain metastases, it may make some sense to displace our go-to first-line drugs, brigatinib and alectinib, with lorlatinib.
Changes in practice are happening now. There are drugs available. I urge oncologists to be open to rethinking what your standard of care is and also open to rethinking how these drugs work and to go with the data that we have.
We’re doing much better now, but the best is yet to come.
Mark G. Kris, MD, is chief of the thoracic oncology service and the William and Joy Ruane Chair in Thoracic Oncology at Memorial Sloan Kettering Cancer Center in New York City. His research interests include targeted therapies for lung cancer, multimodality therapy, the development of new anticancer drugs, and symptom management with a focus on preventing emesis. A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’ll focus on some important topics related to decision-making and daily practice, and the practitioners’ thoughts from the meeting.
There’s no doubt that our outcomes are better for patients, but it’s much harder to make the best choice and I think there’s more pressure on us to make the best choice.
Topic one was the need for next-generation sequencing (NGS) testing. I’ll put it before you that every patient needs NGS testing at the time of diagnosis. It really shouldn’t be put off. How to do that is a topic for another day, but you need NGS testing.
Moving along with this, even when you’re thinking you’re going to go down the road of a checkpoint inhibitor with chemotherapy, the recent Food and Drug Administration approval for cemiplimab and chemotherapy says that you have to make sure that patients don’t have EGFR or ALK aberrations. Now, for cemiplimab, you have to make sure they don’t have ROS1 aberrations.
You need NGS testing to find those targets and give patients a targeted therapy. Even if you want to give a checkpoint inhibitor with or without chemotherapy, you need to have NGS testing.
Second, the way to get the most comprehensive analysis of targets for which there are therapeutic avenues is to do more comprehensive NGS testing, including both DNA and RNA. Not all the panels do this right now, and you really need that RNA-based testing to find all the fusions that are druggable by the current medications that we have.
Bottom line: NGS testing should be done for everybody, and you need to do the most comprehensive panel available both for DNA and RNA.
The next topic that there was great agreement on was the emergence of antibody-drug conjugates. I think everybody’s excited. All of them have shown evidence of benefit. There are varying degrees of side effects, and we’ll learn how to deal with those. They’re new drugs, they’re here, and they’re safe.
There are a couple of things to consider, though. Number one, these drugs do have chemotherapy and they have side effects from chemotherapy. I think the consensus is that when you treat patients with an antibody-drug conjugate, you need to give antiemetic regimens, at least for trastuzumab and the other deruxtecan drugs. You need to give a regimen for highly emetogenic chemotherapy as prophylactic antiemetics. I think that was a consensus thought.
Second, these drugs are making us rethink what it means to have the expression of the protein. I’m totally struck that for trastuzumab deruxtecan, patritumab deruxtecan, and datopotamab deruxtecan, the degree of protein expression is not particularly relevant, and these drugs can work in all patients. There have been cases clearly shown that datopotamab deruxtecan and patritumab deruxtecan both have benefit in patients with EGFR mutations after progression on osimertinib.
This idea of a need for overexpression, and maybe even the idea of testing, is being challenged now. These drugs seem to work as long as some protein is present. They don’t work in every patient, but they work in the vast majority. This thinking about overexpression with the antibody-drug conjugates is probably going to need to be reevaluated.
Last are some thoughts about our targeted therapies. Again, we have more targets. We have EGFR exon 20, for example, and more drugs for MET. I’d like to share a couple of thoughts on what the experts presented at the meeting.
First, although we have a bunch of new targeted agents for patients with EGFR-mutant cancers, probably the thing that’s going to change therapy now is adding chemotherapy to these agents. We may also use circulating tumor (ctDNA) to help guide us to identify which patients would be more likely to benefit from a chemotherapy with osimertinib. I see that as a trend and as a strategy that we’re likely to see move forward.
Another is in the ALK space. I know we’ve gotten very comfortable giving alectinib and brigatinib, but when you look at all the data, it points to lorlatinib perhaps being a better first-line therapy.
I think the experts thought lorlatinib would be a good drug. Yes, it has a different spectrum of side effects. The central nervous system (CNS) side effects are something we have to learn how to take care of; however, we can do that. Generally, with dose reduction, those side effects are manageable.
If you can get better outcomes in general and in patients with brain metastases, it may make some sense to displace our go-to first-line drugs, brigatinib and alectinib, with lorlatinib.
Changes in practice are happening now. There are drugs available. I urge oncologists to be open to rethinking what your standard of care is and also open to rethinking how these drugs work and to go with the data that we have.
We’re doing much better now, but the best is yet to come.
Mark G. Kris, MD, is chief of the thoracic oncology service and the William and Joy Ruane Chair in Thoracic Oncology at Memorial Sloan Kettering Cancer Center in New York City. His research interests include targeted therapies for lung cancer, multimodality therapy, the development of new anticancer drugs, and symptom management with a focus on preventing emesis. A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’ll focus on some important topics related to decision-making and daily practice, and the practitioners’ thoughts from the meeting.
There’s no doubt that our outcomes are better for patients, but it’s much harder to make the best choice and I think there’s more pressure on us to make the best choice.
Topic one was the need for next-generation sequencing (NGS) testing. I’ll put it before you that every patient needs NGS testing at the time of diagnosis. It really shouldn’t be put off. How to do that is a topic for another day, but you need NGS testing.
Moving along with this, even when you’re thinking you’re going to go down the road of a checkpoint inhibitor with chemotherapy, the recent Food and Drug Administration approval for cemiplimab and chemotherapy says that you have to make sure that patients don’t have EGFR or ALK aberrations. Now, for cemiplimab, you have to make sure they don’t have ROS1 aberrations.
You need NGS testing to find those targets and give patients a targeted therapy. Even if you want to give a checkpoint inhibitor with or without chemotherapy, you need to have NGS testing.
Second, the way to get the most comprehensive analysis of targets for which there are therapeutic avenues is to do more comprehensive NGS testing, including both DNA and RNA. Not all the panels do this right now, and you really need that RNA-based testing to find all the fusions that are druggable by the current medications that we have.
Bottom line: NGS testing should be done for everybody, and you need to do the most comprehensive panel available both for DNA and RNA.
The next topic that there was great agreement on was the emergence of antibody-drug conjugates. I think everybody’s excited. All of them have shown evidence of benefit. There are varying degrees of side effects, and we’ll learn how to deal with those. They’re new drugs, they’re here, and they’re safe.
There are a couple of things to consider, though. Number one, these drugs do have chemotherapy and they have side effects from chemotherapy. I think the consensus is that when you treat patients with an antibody-drug conjugate, you need to give antiemetic regimens, at least for trastuzumab and the other deruxtecan drugs. You need to give a regimen for highly emetogenic chemotherapy as prophylactic antiemetics. I think that was a consensus thought.
Second, these drugs are making us rethink what it means to have the expression of the protein. I’m totally struck that for trastuzumab deruxtecan, patritumab deruxtecan, and datopotamab deruxtecan, the degree of protein expression is not particularly relevant, and these drugs can work in all patients. There have been cases clearly shown that datopotamab deruxtecan and patritumab deruxtecan both have benefit in patients with EGFR mutations after progression on osimertinib.
This idea of a need for overexpression, and maybe even the idea of testing, is being challenged now. These drugs seem to work as long as some protein is present. They don’t work in every patient, but they work in the vast majority. This thinking about overexpression with the antibody-drug conjugates is probably going to need to be reevaluated.
Last are some thoughts about our targeted therapies. Again, we have more targets. We have EGFR exon 20, for example, and more drugs for MET. I’d like to share a couple of thoughts on what the experts presented at the meeting.
First, although we have a bunch of new targeted agents for patients with EGFR-mutant cancers, probably the thing that’s going to change therapy now is adding chemotherapy to these agents. We may also use circulating tumor (ctDNA) to help guide us to identify which patients would be more likely to benefit from a chemotherapy with osimertinib. I see that as a trend and as a strategy that we’re likely to see move forward.
Another is in the ALK space. I know we’ve gotten very comfortable giving alectinib and brigatinib, but when you look at all the data, it points to lorlatinib perhaps being a better first-line therapy.
I think the experts thought lorlatinib would be a good drug. Yes, it has a different spectrum of side effects. The central nervous system (CNS) side effects are something we have to learn how to take care of; however, we can do that. Generally, with dose reduction, those side effects are manageable.
If you can get better outcomes in general and in patients with brain metastases, it may make some sense to displace our go-to first-line drugs, brigatinib and alectinib, with lorlatinib.
Changes in practice are happening now. There are drugs available. I urge oncologists to be open to rethinking what your standard of care is and also open to rethinking how these drugs work and to go with the data that we have.
We’re doing much better now, but the best is yet to come.
Mark G. Kris, MD, is chief of the thoracic oncology service and the William and Joy Ruane Chair in Thoracic Oncology at Memorial Sloan Kettering Cancer Center in New York City. His research interests include targeted therapies for lung cancer, multimodality therapy, the development of new anticancer drugs, and symptom management with a focus on preventing emesis. A version of this article first appeared on Medscape.com.
Myths about smoking, diet, alcohol, and cancer persist
FRANCE – Conducted every 5 years since 2005, the Cancer Survey documents the knowledge, perceptions, and way of life of the French people in relation to cancer. The researchers analyzed responses to telephone interviews of a representative sample of almost 5,000 individuals aged 15-85 years.
This study shows how thinking has changed over time and how difficult it is to alter preconceived notions.
Is cancer hereditary?
The report shows that 67.7% of respondents believe that cancer is a hereditary disease. Respondents were asked to explain their answer. “Data show that medical practices for cancer treatment substantiate this belief [that cancer is hereditary],” wrote the authors of the report.
“Indeed, health care professionals almost systematically ask questions about family history of breast cancer and, when a family member has been diagnosed with cancer, medical monitoring of other family members is often sought out, thus reinforcing the belief that cancer is hereditary,” they said.
Furthermore, there seems to be confusion regarding the role of genes in the development of cancer. A person can inherit cancer-predisposing genes, not cancer itself. The authors highlighted their concern that this confusion may “lead people to think that prevention measures are unnecessary because cancer is inherited.”
Misconceptions about smoking
About 41% of smokers think that the length of time one has been smoking is the biggest determining factor for developing cancer; 58.1% think the number of cigarettes smoked per day has a bigger impact.
Experts at InCA and SPF put the debate to rest, stating that prolonged exposure to carcinogenic substances is far more toxic. As for the danger threshold concerning the number of cigarettes smoked per day, respondents believed this to be 9.2 cigarettes per day, on average. They believed that the danger threshold for the number of years as an active smoker is 13.4, on average.
“The [survey] respondents clearly understand that smoking carries a risk, but many smokers think that light smoking or smoking for a short period of time doesn’t carry any risks.” Yet it is understood that even occasional tobacco consumption increases mortality.
This was not the only misconception regarding smoking and its relationship with cancer. About 34% of survey respondents agreed with the following statement: “Smoking doesn’t cause cancer unless you’re a heavy smoker and have smoked for a long time.” Furthermore, 43.3% agreed with the statement, “Pollution is more likely to cause cancer than smoking,” 54.6% think that “exercising cleans your lungs of tobacco,” and 61.6% think that “a smoker can prevent developing cancer caused by smoking if they know to quit on time.”
Overweight and obesity
Although diet and excess weight represent the third and fourth biggest avoidable cancer risk factors, after smoking and alcohol, only 30% of survey respondents knew of this link.
“Among the causes of cancer known and cited by respondents without prompting, excessive weight and obesity were mentioned only 100 times out of 12,558 responses,” highlighted the authors of the report. The explanation put forward by the authors is that discourse about diet has been more focused on diet as a protective health factor, especially in preventing cardiovascular diseases. “The link between cancer and diet is less prominent in the public space,” they noted.
Breastfeeding and cancer
About 63% of survey respondents, which for the first time included both women and men, believe that breastfeeding does not affect mothers’ risk of breast cancer, but this is a misconception. And almost 1 in 3 respondents said that breastfeeding provides health benefits for the mother.
Artificial UV rays
Exposure to UV rays, whether of natural or artificial origin, is a major risk factor for skin cancer. However, 1 in 5 people (20.9%) think that a session in a tanning bed is less harmful than sun exposure.
Daily stress
Regarding psychological factors linked to cancer, the authors noted that risk factors not supported by scientific evidence were, ironically, cited more often by respondents than proven risk factors. There is a real knowledge gap between scientific data and the beliefs of the French people. For example, “working at night” is largely not seen as a risk factor, but data show that it presents a clear risk. However, “not being able to express one’s feelings,” “having been weakened by traumatic experiences,” and “being exposed to the stress of modern life” are seen as risk factors of cancer, without any scientific evidence.
Cigarettes and e-cigarettes
About 53% of respondents agreed that “e-cigarettes are just as harmful or more harmful than traditional cigarettes.” Nicotine and the flavors in e-cigarettes are largely perceived as “very” or “extremely” harmful to the health of a person. However, the authors note that “no published study on nicotine substitutes has shown harmful effects on the health of a person, let alone determined it a risk factor for cancer. The nicotine doses in e-cigarettes are similar to traditional nicotine substitutes, and no cytotoxic effect of nicotine in its inhaled form has been found.” There seems to be confusion between dependence and risk of cancer.
Alcohol consumption
Eight of 10 respondents believe that “some people can drink a lot of alcohol all their life without ever getting cancer,” which goes against the scientific literature. The authors of the report state that the negative effects of alcohol on health seem poorly understood. Although alcohol is the second biggest cause of cancer, only a third of survey respondents cited it without having been prompted as one of the main causes of cancer. And 23.5% even think that “in terms of decreasing your risk of cancer, it’s better to drink a little wine than to drink no wine at all.”
This article was translated from the Medscape French edition. A version of this article appeared on Medscape.com.
FRANCE – Conducted every 5 years since 2005, the Cancer Survey documents the knowledge, perceptions, and way of life of the French people in relation to cancer. The researchers analyzed responses to telephone interviews of a representative sample of almost 5,000 individuals aged 15-85 years.
This study shows how thinking has changed over time and how difficult it is to alter preconceived notions.
Is cancer hereditary?
The report shows that 67.7% of respondents believe that cancer is a hereditary disease. Respondents were asked to explain their answer. “Data show that medical practices for cancer treatment substantiate this belief [that cancer is hereditary],” wrote the authors of the report.
“Indeed, health care professionals almost systematically ask questions about family history of breast cancer and, when a family member has been diagnosed with cancer, medical monitoring of other family members is often sought out, thus reinforcing the belief that cancer is hereditary,” they said.
Furthermore, there seems to be confusion regarding the role of genes in the development of cancer. A person can inherit cancer-predisposing genes, not cancer itself. The authors highlighted their concern that this confusion may “lead people to think that prevention measures are unnecessary because cancer is inherited.”
Misconceptions about smoking
About 41% of smokers think that the length of time one has been smoking is the biggest determining factor for developing cancer; 58.1% think the number of cigarettes smoked per day has a bigger impact.
Experts at InCA and SPF put the debate to rest, stating that prolonged exposure to carcinogenic substances is far more toxic. As for the danger threshold concerning the number of cigarettes smoked per day, respondents believed this to be 9.2 cigarettes per day, on average. They believed that the danger threshold for the number of years as an active smoker is 13.4, on average.
“The [survey] respondents clearly understand that smoking carries a risk, but many smokers think that light smoking or smoking for a short period of time doesn’t carry any risks.” Yet it is understood that even occasional tobacco consumption increases mortality.
This was not the only misconception regarding smoking and its relationship with cancer. About 34% of survey respondents agreed with the following statement: “Smoking doesn’t cause cancer unless you’re a heavy smoker and have smoked for a long time.” Furthermore, 43.3% agreed with the statement, “Pollution is more likely to cause cancer than smoking,” 54.6% think that “exercising cleans your lungs of tobacco,” and 61.6% think that “a smoker can prevent developing cancer caused by smoking if they know to quit on time.”
Overweight and obesity
Although diet and excess weight represent the third and fourth biggest avoidable cancer risk factors, after smoking and alcohol, only 30% of survey respondents knew of this link.
“Among the causes of cancer known and cited by respondents without prompting, excessive weight and obesity were mentioned only 100 times out of 12,558 responses,” highlighted the authors of the report. The explanation put forward by the authors is that discourse about diet has been more focused on diet as a protective health factor, especially in preventing cardiovascular diseases. “The link between cancer and diet is less prominent in the public space,” they noted.
Breastfeeding and cancer
About 63% of survey respondents, which for the first time included both women and men, believe that breastfeeding does not affect mothers’ risk of breast cancer, but this is a misconception. And almost 1 in 3 respondents said that breastfeeding provides health benefits for the mother.
Artificial UV rays
Exposure to UV rays, whether of natural or artificial origin, is a major risk factor for skin cancer. However, 1 in 5 people (20.9%) think that a session in a tanning bed is less harmful than sun exposure.
Daily stress
Regarding psychological factors linked to cancer, the authors noted that risk factors not supported by scientific evidence were, ironically, cited more often by respondents than proven risk factors. There is a real knowledge gap between scientific data and the beliefs of the French people. For example, “working at night” is largely not seen as a risk factor, but data show that it presents a clear risk. However, “not being able to express one’s feelings,” “having been weakened by traumatic experiences,” and “being exposed to the stress of modern life” are seen as risk factors of cancer, without any scientific evidence.
Cigarettes and e-cigarettes
About 53% of respondents agreed that “e-cigarettes are just as harmful or more harmful than traditional cigarettes.” Nicotine and the flavors in e-cigarettes are largely perceived as “very” or “extremely” harmful to the health of a person. However, the authors note that “no published study on nicotine substitutes has shown harmful effects on the health of a person, let alone determined it a risk factor for cancer. The nicotine doses in e-cigarettes are similar to traditional nicotine substitutes, and no cytotoxic effect of nicotine in its inhaled form has been found.” There seems to be confusion between dependence and risk of cancer.
Alcohol consumption
Eight of 10 respondents believe that “some people can drink a lot of alcohol all their life without ever getting cancer,” which goes against the scientific literature. The authors of the report state that the negative effects of alcohol on health seem poorly understood. Although alcohol is the second biggest cause of cancer, only a third of survey respondents cited it without having been prompted as one of the main causes of cancer. And 23.5% even think that “in terms of decreasing your risk of cancer, it’s better to drink a little wine than to drink no wine at all.”
This article was translated from the Medscape French edition. A version of this article appeared on Medscape.com.
FRANCE – Conducted every 5 years since 2005, the Cancer Survey documents the knowledge, perceptions, and way of life of the French people in relation to cancer. The researchers analyzed responses to telephone interviews of a representative sample of almost 5,000 individuals aged 15-85 years.
This study shows how thinking has changed over time and how difficult it is to alter preconceived notions.
Is cancer hereditary?
The report shows that 67.7% of respondents believe that cancer is a hereditary disease. Respondents were asked to explain their answer. “Data show that medical practices for cancer treatment substantiate this belief [that cancer is hereditary],” wrote the authors of the report.
“Indeed, health care professionals almost systematically ask questions about family history of breast cancer and, when a family member has been diagnosed with cancer, medical monitoring of other family members is often sought out, thus reinforcing the belief that cancer is hereditary,” they said.
Furthermore, there seems to be confusion regarding the role of genes in the development of cancer. A person can inherit cancer-predisposing genes, not cancer itself. The authors highlighted their concern that this confusion may “lead people to think that prevention measures are unnecessary because cancer is inherited.”
Misconceptions about smoking
About 41% of smokers think that the length of time one has been smoking is the biggest determining factor for developing cancer; 58.1% think the number of cigarettes smoked per day has a bigger impact.
Experts at InCA and SPF put the debate to rest, stating that prolonged exposure to carcinogenic substances is far more toxic. As for the danger threshold concerning the number of cigarettes smoked per day, respondents believed this to be 9.2 cigarettes per day, on average. They believed that the danger threshold for the number of years as an active smoker is 13.4, on average.
“The [survey] respondents clearly understand that smoking carries a risk, but many smokers think that light smoking or smoking for a short period of time doesn’t carry any risks.” Yet it is understood that even occasional tobacco consumption increases mortality.
This was not the only misconception regarding smoking and its relationship with cancer. About 34% of survey respondents agreed with the following statement: “Smoking doesn’t cause cancer unless you’re a heavy smoker and have smoked for a long time.” Furthermore, 43.3% agreed with the statement, “Pollution is more likely to cause cancer than smoking,” 54.6% think that “exercising cleans your lungs of tobacco,” and 61.6% think that “a smoker can prevent developing cancer caused by smoking if they know to quit on time.”
Overweight and obesity
Although diet and excess weight represent the third and fourth biggest avoidable cancer risk factors, after smoking and alcohol, only 30% of survey respondents knew of this link.
“Among the causes of cancer known and cited by respondents without prompting, excessive weight and obesity were mentioned only 100 times out of 12,558 responses,” highlighted the authors of the report. The explanation put forward by the authors is that discourse about diet has been more focused on diet as a protective health factor, especially in preventing cardiovascular diseases. “The link between cancer and diet is less prominent in the public space,” they noted.
Breastfeeding and cancer
About 63% of survey respondents, which for the first time included both women and men, believe that breastfeeding does not affect mothers’ risk of breast cancer, but this is a misconception. And almost 1 in 3 respondents said that breastfeeding provides health benefits for the mother.
Artificial UV rays
Exposure to UV rays, whether of natural or artificial origin, is a major risk factor for skin cancer. However, 1 in 5 people (20.9%) think that a session in a tanning bed is less harmful than sun exposure.
Daily stress
Regarding psychological factors linked to cancer, the authors noted that risk factors not supported by scientific evidence were, ironically, cited more often by respondents than proven risk factors. There is a real knowledge gap between scientific data and the beliefs of the French people. For example, “working at night” is largely not seen as a risk factor, but data show that it presents a clear risk. However, “not being able to express one’s feelings,” “having been weakened by traumatic experiences,” and “being exposed to the stress of modern life” are seen as risk factors of cancer, without any scientific evidence.
Cigarettes and e-cigarettes
About 53% of respondents agreed that “e-cigarettes are just as harmful or more harmful than traditional cigarettes.” Nicotine and the flavors in e-cigarettes are largely perceived as “very” or “extremely” harmful to the health of a person. However, the authors note that “no published study on nicotine substitutes has shown harmful effects on the health of a person, let alone determined it a risk factor for cancer. The nicotine doses in e-cigarettes are similar to traditional nicotine substitutes, and no cytotoxic effect of nicotine in its inhaled form has been found.” There seems to be confusion between dependence and risk of cancer.
Alcohol consumption
Eight of 10 respondents believe that “some people can drink a lot of alcohol all their life without ever getting cancer,” which goes against the scientific literature. The authors of the report state that the negative effects of alcohol on health seem poorly understood. Although alcohol is the second biggest cause of cancer, only a third of survey respondents cited it without having been prompted as one of the main causes of cancer. And 23.5% even think that “in terms of decreasing your risk of cancer, it’s better to drink a little wine than to drink no wine at all.”
This article was translated from the Medscape French edition. A version of this article appeared on Medscape.com.
Advanced imaging technology could help predict lung cancer progression after surgery
, according to new data.
The technology, known as highly multiplexed imaging mass cytometry (IMC), can provide cellular-level detail of the tumor immune microenvironment, which may allow clinicians to identify patients who need additional treatment, as well as those who don’t.
“It is well known that the frequency of certain cell populations within the tumor microenvironment correlates with clinical outcomes. These observations help us understand the biology underlying cancer progression,” senior author Logan Walsh, PhD, assistant professor of human genetics and the Rosalind Goodman Chair in Lung Cancer Research at McGill University’s Rosalind and Morris Goodman Cancer Institute, Montreal, said in an interview.
“We wanted to test whether using completely unbiased AI could find and use the spatial topography of the tumor microenvironment from IMC data to predict clinical outcomes,” he said. “It turns out the answer is yes! AI can predict clinical outcomes when combined with IMC with extremely high accuracy from a single 1-mm2 tumor core.”
The study was published on in Nature.
The immune landscape
Lung cancer is the leading cause of cancer-related death in Canada, surpassing breast, colon, and prostate cancer deaths combined, the study authors write.
Lung adenocarcinoma, a non–small cell lung cancer, is the most common subtype and is characterized by distinct cellular and molecular features. The tumor immune microenvironment influences disease progression and therapy response, the authors write. Understanding the spatial landscape of the microenvironment could provide insight into disease progression, therapeutic vulnerabilities, and biomarkers of response to existing treatments.
In a collaborative study, Dr. Walsh and colleagues from McGill University and Université Laval profiled the cellular composition and spatial organization of the tumor immune microenvironment in tumors from 416 patients with lung adenocarcinoma across five histologic patterns. They used IMC to assess at samples from the universities’ biobanks that patients had provided for research purposes.
The research team detected more than 1.6 million cells, which allowed spatial analysis of immune lineages and activation states with distinct clinical correlates, including survival. They used a supervised lineage assignment approach to classify 14 distinct immune cell populations, along with tumor cells and endothelial cells.
High-grade solid tumors had the greatest immune infiltrate (44.6%), compared with micropapillary (37%), acinar (39.7%), papillary (32.8%), and lepidic architectures (32.7%). Macrophages were the most frequent cell population in the tumor immune microenvironment, representing 12.3% of total cells and 34.1% of immune cells.
The prevalence of CD163+ macrophages was strongly correlated with FOXP3+ immunoregulatory T cells in the solid pattern. This relationship was less pronounced in low-grade lepidic and papillary architectures. This finding could suggest an interplay between macrophage and T-cell populations in the tumor immune microenvironment across lung adenocarcinoma patterns.
Using a deep neural network model, the researchers also analyzed the relationship between immune populations and clinical or pathologic variables by examining the frequency of individual cell types as a percentage of total cells in each image. Each image was cross-referenced with clinical data from patients, including sex, age, body mass index, smoking status, stage, progression, survival, and histologic subtype.
Overall, the researchers found that various clinical outcomes, including cancer progression, could be predicted with high accuracy using a single 1-mm2 tumor core. For instance, they could predict progression in stage IA and IB resected lung cancer with 95.9% accuracy.
Additional applications
“We were not surprised that AI was able to predict clinical outcomes, but we were surprised that it was able to do so with such high accuracy and precision,” said Dr. Walsh. “We were also surprised to learn that our predictions were equally accurate using only six-plex data, compared with 35-plex. This hinted to us that we could potentially scale down the number of markers to a practical number that would be amenable to technologies available in routine pathology labs.”
Dr. Walsh and colleagues are now validating the predictive tool using a lower-plex technology. In addition, they are investigating the immune landscapes of primary and metastatic brain tumors.
“This study is important, as it helps us to understand and appreciate the biological and mechanistic factors that may influence treatment outcomes. Our standard clinical predictors for predicting risk of recurrence and probability of response to therapy are not optimal,” Yee Ung, MD, an associate professor of radiation oncology at Sunnybrook Health Sciences Centre, Toronto, said in an interview.
Dr. Ung, who wasn’t involved with this study, has researched noninvasive hypoxia imaging and targeting in lung cancer. Ideally, he said, future studies should incorporate the use of noninvasive imaging predictive factors, in addition to the tumor immune microenvironment and clinical factors, to predict outcomes and provide personalized treatment.
“As we begin to investigate and understand more about cancer biology down to the cellular and molecular level, we need to strategically use AI methodologies in the processing and analysis of data,” he said.
The study was supported by the McGill Interdisciplinary Initiative in Infection and Immunity, the Brain Tumour Funders’ Collaborative, the Canadian Institutes of Health Research, and the Canadian Foundation for Innovation. Dr. Walsh and Dr. Ung have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, according to new data.
The technology, known as highly multiplexed imaging mass cytometry (IMC), can provide cellular-level detail of the tumor immune microenvironment, which may allow clinicians to identify patients who need additional treatment, as well as those who don’t.
“It is well known that the frequency of certain cell populations within the tumor microenvironment correlates with clinical outcomes. These observations help us understand the biology underlying cancer progression,” senior author Logan Walsh, PhD, assistant professor of human genetics and the Rosalind Goodman Chair in Lung Cancer Research at McGill University’s Rosalind and Morris Goodman Cancer Institute, Montreal, said in an interview.
“We wanted to test whether using completely unbiased AI could find and use the spatial topography of the tumor microenvironment from IMC data to predict clinical outcomes,” he said. “It turns out the answer is yes! AI can predict clinical outcomes when combined with IMC with extremely high accuracy from a single 1-mm2 tumor core.”
The study was published on in Nature.
The immune landscape
Lung cancer is the leading cause of cancer-related death in Canada, surpassing breast, colon, and prostate cancer deaths combined, the study authors write.
Lung adenocarcinoma, a non–small cell lung cancer, is the most common subtype and is characterized by distinct cellular and molecular features. The tumor immune microenvironment influences disease progression and therapy response, the authors write. Understanding the spatial landscape of the microenvironment could provide insight into disease progression, therapeutic vulnerabilities, and biomarkers of response to existing treatments.
In a collaborative study, Dr. Walsh and colleagues from McGill University and Université Laval profiled the cellular composition and spatial organization of the tumor immune microenvironment in tumors from 416 patients with lung adenocarcinoma across five histologic patterns. They used IMC to assess at samples from the universities’ biobanks that patients had provided for research purposes.
The research team detected more than 1.6 million cells, which allowed spatial analysis of immune lineages and activation states with distinct clinical correlates, including survival. They used a supervised lineage assignment approach to classify 14 distinct immune cell populations, along with tumor cells and endothelial cells.
High-grade solid tumors had the greatest immune infiltrate (44.6%), compared with micropapillary (37%), acinar (39.7%), papillary (32.8%), and lepidic architectures (32.7%). Macrophages were the most frequent cell population in the tumor immune microenvironment, representing 12.3% of total cells and 34.1% of immune cells.
The prevalence of CD163+ macrophages was strongly correlated with FOXP3+ immunoregulatory T cells in the solid pattern. This relationship was less pronounced in low-grade lepidic and papillary architectures. This finding could suggest an interplay between macrophage and T-cell populations in the tumor immune microenvironment across lung adenocarcinoma patterns.
Using a deep neural network model, the researchers also analyzed the relationship between immune populations and clinical or pathologic variables by examining the frequency of individual cell types as a percentage of total cells in each image. Each image was cross-referenced with clinical data from patients, including sex, age, body mass index, smoking status, stage, progression, survival, and histologic subtype.
Overall, the researchers found that various clinical outcomes, including cancer progression, could be predicted with high accuracy using a single 1-mm2 tumor core. For instance, they could predict progression in stage IA and IB resected lung cancer with 95.9% accuracy.
Additional applications
“We were not surprised that AI was able to predict clinical outcomes, but we were surprised that it was able to do so with such high accuracy and precision,” said Dr. Walsh. “We were also surprised to learn that our predictions were equally accurate using only six-plex data, compared with 35-plex. This hinted to us that we could potentially scale down the number of markers to a practical number that would be amenable to technologies available in routine pathology labs.”
Dr. Walsh and colleagues are now validating the predictive tool using a lower-plex technology. In addition, they are investigating the immune landscapes of primary and metastatic brain tumors.
“This study is important, as it helps us to understand and appreciate the biological and mechanistic factors that may influence treatment outcomes. Our standard clinical predictors for predicting risk of recurrence and probability of response to therapy are not optimal,” Yee Ung, MD, an associate professor of radiation oncology at Sunnybrook Health Sciences Centre, Toronto, said in an interview.
Dr. Ung, who wasn’t involved with this study, has researched noninvasive hypoxia imaging and targeting in lung cancer. Ideally, he said, future studies should incorporate the use of noninvasive imaging predictive factors, in addition to the tumor immune microenvironment and clinical factors, to predict outcomes and provide personalized treatment.
“As we begin to investigate and understand more about cancer biology down to the cellular and molecular level, we need to strategically use AI methodologies in the processing and analysis of data,” he said.
The study was supported by the McGill Interdisciplinary Initiative in Infection and Immunity, the Brain Tumour Funders’ Collaborative, the Canadian Institutes of Health Research, and the Canadian Foundation for Innovation. Dr. Walsh and Dr. Ung have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, according to new data.
The technology, known as highly multiplexed imaging mass cytometry (IMC), can provide cellular-level detail of the tumor immune microenvironment, which may allow clinicians to identify patients who need additional treatment, as well as those who don’t.
“It is well known that the frequency of certain cell populations within the tumor microenvironment correlates with clinical outcomes. These observations help us understand the biology underlying cancer progression,” senior author Logan Walsh, PhD, assistant professor of human genetics and the Rosalind Goodman Chair in Lung Cancer Research at McGill University’s Rosalind and Morris Goodman Cancer Institute, Montreal, said in an interview.
“We wanted to test whether using completely unbiased AI could find and use the spatial topography of the tumor microenvironment from IMC data to predict clinical outcomes,” he said. “It turns out the answer is yes! AI can predict clinical outcomes when combined with IMC with extremely high accuracy from a single 1-mm2 tumor core.”
The study was published on in Nature.
The immune landscape
Lung cancer is the leading cause of cancer-related death in Canada, surpassing breast, colon, and prostate cancer deaths combined, the study authors write.
Lung adenocarcinoma, a non–small cell lung cancer, is the most common subtype and is characterized by distinct cellular and molecular features. The tumor immune microenvironment influences disease progression and therapy response, the authors write. Understanding the spatial landscape of the microenvironment could provide insight into disease progression, therapeutic vulnerabilities, and biomarkers of response to existing treatments.
In a collaborative study, Dr. Walsh and colleagues from McGill University and Université Laval profiled the cellular composition and spatial organization of the tumor immune microenvironment in tumors from 416 patients with lung adenocarcinoma across five histologic patterns. They used IMC to assess at samples from the universities’ biobanks that patients had provided for research purposes.
The research team detected more than 1.6 million cells, which allowed spatial analysis of immune lineages and activation states with distinct clinical correlates, including survival. They used a supervised lineage assignment approach to classify 14 distinct immune cell populations, along with tumor cells and endothelial cells.
High-grade solid tumors had the greatest immune infiltrate (44.6%), compared with micropapillary (37%), acinar (39.7%), papillary (32.8%), and lepidic architectures (32.7%). Macrophages were the most frequent cell population in the tumor immune microenvironment, representing 12.3% of total cells and 34.1% of immune cells.
The prevalence of CD163+ macrophages was strongly correlated with FOXP3+ immunoregulatory T cells in the solid pattern. This relationship was less pronounced in low-grade lepidic and papillary architectures. This finding could suggest an interplay between macrophage and T-cell populations in the tumor immune microenvironment across lung adenocarcinoma patterns.
Using a deep neural network model, the researchers also analyzed the relationship between immune populations and clinical or pathologic variables by examining the frequency of individual cell types as a percentage of total cells in each image. Each image was cross-referenced with clinical data from patients, including sex, age, body mass index, smoking status, stage, progression, survival, and histologic subtype.
Overall, the researchers found that various clinical outcomes, including cancer progression, could be predicted with high accuracy using a single 1-mm2 tumor core. For instance, they could predict progression in stage IA and IB resected lung cancer with 95.9% accuracy.
Additional applications
“We were not surprised that AI was able to predict clinical outcomes, but we were surprised that it was able to do so with such high accuracy and precision,” said Dr. Walsh. “We were also surprised to learn that our predictions were equally accurate using only six-plex data, compared with 35-plex. This hinted to us that we could potentially scale down the number of markers to a practical number that would be amenable to technologies available in routine pathology labs.”
Dr. Walsh and colleagues are now validating the predictive tool using a lower-plex technology. In addition, they are investigating the immune landscapes of primary and metastatic brain tumors.
“This study is important, as it helps us to understand and appreciate the biological and mechanistic factors that may influence treatment outcomes. Our standard clinical predictors for predicting risk of recurrence and probability of response to therapy are not optimal,” Yee Ung, MD, an associate professor of radiation oncology at Sunnybrook Health Sciences Centre, Toronto, said in an interview.
Dr. Ung, who wasn’t involved with this study, has researched noninvasive hypoxia imaging and targeting in lung cancer. Ideally, he said, future studies should incorporate the use of noninvasive imaging predictive factors, in addition to the tumor immune microenvironment and clinical factors, to predict outcomes and provide personalized treatment.
“As we begin to investigate and understand more about cancer biology down to the cellular and molecular level, we need to strategically use AI methodologies in the processing and analysis of data,” he said.
The study was supported by the McGill Interdisciplinary Initiative in Infection and Immunity, the Brain Tumour Funders’ Collaborative, the Canadian Institutes of Health Research, and the Canadian Foundation for Innovation. Dr. Walsh and Dr. Ung have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM NATURE
Postop RT: Meaningful survival improvement in N2 lung cancer
This transcript has been edited for clarity.
I’m Mark Kris from Memorial Sloan Kettering, speaking today about a topic that’s become quite controversial, which is
Data from clinical trials and data from a SEER study showed approximately 7% improvement in overall survival in patients with N2 disease who received PORT. There has been a very clear demonstration of an improved local control rate in every trial that’s ever looked at PORT.
However, there was a randomized trial, the Lung ART trial, where patients were randomized to get PORT or not. PORT was delivered in a way that is not routinely used now. In that trial, the benefit of PORT was found in terms of local control, almost doubling control within the mediastinum.
The difference in overall survival was less than 12%. Again, I’m not surprised to see that because the improvement in overall survival is probably somewhere between 5% and 10%. They also found an excess of deaths, probably due to cardiac causes from the radiation in the radiation arm.
However, the trial used a type of radiation not used at this point – it used conformal, but now we would use 3D. And its ability at the time of the trial to estimate and lower cardiac risk was not what it is today. Owing to the design of the trial, it was not a significant difference and has largely been interpreted as saying that the PORT doesn’t work.
First, let’s please go to the guidelines. I’m going to the ASCO guidelines, which say that patients with mediastinal disease should not routinely get PORT, but they should be routinely referred to a radiation oncologist for consideration of PORT. I don’t think anything that’s been published so far changes that.
I think each case needs to be individualized and requires the specialty care of a radiation oncologist to weigh the pros and cons of PORT. It also depends upon the treatment plan. Can the heart be spared? Are there radiation techniques available that would eliminate or lessen heart exposure, such as using protons? The point is that PORT is still needed.
When we look at the trials of patients receiving adjuvant therapy – and I’m looking particularly at the ADAURA trial where patients received adjuvant osimertinib – the greatest number of failures now is in the chest. We have to look for good ways to cut down on failure in the chest. Unfortunately, failure in the chest means ultimately failure and lack of cure, and we have to do a better job at that. I think PORT can play a role there.
Please, when you have patients with N2 disease, after the completion of systemic therapies, think about the use of PORT and get the advice of a radiation oncologist to meet with the patient, review their clinical situation, and assess whether or not PORT could be useful for that patient.
That is following the NCCN guidelines, which were not changed on the basis of the Lung ART paper. I think we owe it to our patients to make sure that those who could benefit from this additional therapy receive it.
I’ll put it to you that radiation delivered in the most innovative way – taking very careful account of the effects on the heart – can improve local control. There’s no question about that. I think PORT has the ability to improve survival by a small amount – probably less than 12%, which I will agree the Lung ART trial showed – but still an important amount for patients with this condition.
Mark G. Kris, MD, is chief of the thoracic oncology service and the William and Joy Ruane Chair in Thoracic Oncology at Memorial Sloan Kettering Cancer Center in New York City. He reported conflicts of interest with Arial Pharmaceuticals, Pfizer, PUMA, and Roche/Genentech. A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’m Mark Kris from Memorial Sloan Kettering, speaking today about a topic that’s become quite controversial, which is
Data from clinical trials and data from a SEER study showed approximately 7% improvement in overall survival in patients with N2 disease who received PORT. There has been a very clear demonstration of an improved local control rate in every trial that’s ever looked at PORT.
However, there was a randomized trial, the Lung ART trial, where patients were randomized to get PORT or not. PORT was delivered in a way that is not routinely used now. In that trial, the benefit of PORT was found in terms of local control, almost doubling control within the mediastinum.
The difference in overall survival was less than 12%. Again, I’m not surprised to see that because the improvement in overall survival is probably somewhere between 5% and 10%. They also found an excess of deaths, probably due to cardiac causes from the radiation in the radiation arm.
However, the trial used a type of radiation not used at this point – it used conformal, but now we would use 3D. And its ability at the time of the trial to estimate and lower cardiac risk was not what it is today. Owing to the design of the trial, it was not a significant difference and has largely been interpreted as saying that the PORT doesn’t work.
First, let’s please go to the guidelines. I’m going to the ASCO guidelines, which say that patients with mediastinal disease should not routinely get PORT, but they should be routinely referred to a radiation oncologist for consideration of PORT. I don’t think anything that’s been published so far changes that.
I think each case needs to be individualized and requires the specialty care of a radiation oncologist to weigh the pros and cons of PORT. It also depends upon the treatment plan. Can the heart be spared? Are there radiation techniques available that would eliminate or lessen heart exposure, such as using protons? The point is that PORT is still needed.
When we look at the trials of patients receiving adjuvant therapy – and I’m looking particularly at the ADAURA trial where patients received adjuvant osimertinib – the greatest number of failures now is in the chest. We have to look for good ways to cut down on failure in the chest. Unfortunately, failure in the chest means ultimately failure and lack of cure, and we have to do a better job at that. I think PORT can play a role there.
Please, when you have patients with N2 disease, after the completion of systemic therapies, think about the use of PORT and get the advice of a radiation oncologist to meet with the patient, review their clinical situation, and assess whether or not PORT could be useful for that patient.
That is following the NCCN guidelines, which were not changed on the basis of the Lung ART paper. I think we owe it to our patients to make sure that those who could benefit from this additional therapy receive it.
I’ll put it to you that radiation delivered in the most innovative way – taking very careful account of the effects on the heart – can improve local control. There’s no question about that. I think PORT has the ability to improve survival by a small amount – probably less than 12%, which I will agree the Lung ART trial showed – but still an important amount for patients with this condition.
Mark G. Kris, MD, is chief of the thoracic oncology service and the William and Joy Ruane Chair in Thoracic Oncology at Memorial Sloan Kettering Cancer Center in New York City. He reported conflicts of interest with Arial Pharmaceuticals, Pfizer, PUMA, and Roche/Genentech. A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’m Mark Kris from Memorial Sloan Kettering, speaking today about a topic that’s become quite controversial, which is
Data from clinical trials and data from a SEER study showed approximately 7% improvement in overall survival in patients with N2 disease who received PORT. There has been a very clear demonstration of an improved local control rate in every trial that’s ever looked at PORT.
However, there was a randomized trial, the Lung ART trial, where patients were randomized to get PORT or not. PORT was delivered in a way that is not routinely used now. In that trial, the benefit of PORT was found in terms of local control, almost doubling control within the mediastinum.
The difference in overall survival was less than 12%. Again, I’m not surprised to see that because the improvement in overall survival is probably somewhere between 5% and 10%. They also found an excess of deaths, probably due to cardiac causes from the radiation in the radiation arm.
However, the trial used a type of radiation not used at this point – it used conformal, but now we would use 3D. And its ability at the time of the trial to estimate and lower cardiac risk was not what it is today. Owing to the design of the trial, it was not a significant difference and has largely been interpreted as saying that the PORT doesn’t work.
First, let’s please go to the guidelines. I’m going to the ASCO guidelines, which say that patients with mediastinal disease should not routinely get PORT, but they should be routinely referred to a radiation oncologist for consideration of PORT. I don’t think anything that’s been published so far changes that.
I think each case needs to be individualized and requires the specialty care of a radiation oncologist to weigh the pros and cons of PORT. It also depends upon the treatment plan. Can the heart be spared? Are there radiation techniques available that would eliminate or lessen heart exposure, such as using protons? The point is that PORT is still needed.
When we look at the trials of patients receiving adjuvant therapy – and I’m looking particularly at the ADAURA trial where patients received adjuvant osimertinib – the greatest number of failures now is in the chest. We have to look for good ways to cut down on failure in the chest. Unfortunately, failure in the chest means ultimately failure and lack of cure, and we have to do a better job at that. I think PORT can play a role there.
Please, when you have patients with N2 disease, after the completion of systemic therapies, think about the use of PORT and get the advice of a radiation oncologist to meet with the patient, review their clinical situation, and assess whether or not PORT could be useful for that patient.
That is following the NCCN guidelines, which were not changed on the basis of the Lung ART paper. I think we owe it to our patients to make sure that those who could benefit from this additional therapy receive it.
I’ll put it to you that radiation delivered in the most innovative way – taking very careful account of the effects on the heart – can improve local control. There’s no question about that. I think PORT has the ability to improve survival by a small amount – probably less than 12%, which I will agree the Lung ART trial showed – but still an important amount for patients with this condition.
Mark G. Kris, MD, is chief of the thoracic oncology service and the William and Joy Ruane Chair in Thoracic Oncology at Memorial Sloan Kettering Cancer Center in New York City. He reported conflicts of interest with Arial Pharmaceuticals, Pfizer, PUMA, and Roche/Genentech. A version of this article first appeared on Medscape.com.
Could your patients benefit? New trials in lung cancer
Untreated advanced non–small cell lung cancer (NSCLC). Adult patients with stage IIIB, IIIC, or IV disease without actionable genomic alterations can join a randomized, open-label, phase 3 study testing the survival advantage of datopotamab deruxtecan (Dato-DXd) (AstraZeneca/Daiichi Sankyo). Dato-DXd is one of a half dozen experimental antibody-drug conjugates that target TROP2, a transmembrane glycoprotein that is overexpressed in several solid tumors, including NSCLC. One group of participants will receive an intravenous (IV) infusion of Dato-DXd plus durvalumab (Imfinzi) for up to 4 years, and over the first 12 weeks, they will receive four rounds of IV carboplatin (Paraplatin). The other group will receive IV infusions of pembrolizumab (Keytruda) every 3 weeks plus a combination of standard IV chemotherapy appropriate for the patient’s histology (nonsquamous or squamous NSCLC). In the United States, centers in Arkansas, Nebraska, Ohio, and Texas started recruiting in December 2020; trial sites are planned in 16 other states and 23 other countries. The trialists plan to enroll 1,000 participants. Overall survival (OS) and progression-free survival (PFS) are the primary endpoints; quality of life (QoL) is not being tracked. More details at clinicaltrials.gov.
Untreated advanced or metastatic NSCLC. Adult patients in this clinical situation without actionable genomic alterations as well as those with a PD-L1 tumor proportion score (TPS) of < 50% are eligible to participate in a randomized, open-label, phase 3 trial of Dato-DXd in combination with pembrolizumab, with or without chemotherapy. One group of participants will receive IV Dato-DXd and pembrolizumab every 3 weeks. For the second group of patients, IV platinum chemotherapy will be added to the Dato-DXd and pembrolizumab for the first four rounds of treatment. The third group of individuals make up the comparator arm and will receive thrice-weekly IV pembrolizumab, pemetrexed (Alimta), plus platinum chemotherapy. All participants will be treated for approximately 2.5 years or until disease progression or death. The trial began recruiting 975 participants in Arizona, Florida, Maryland, and New Jersey, and in Japan in January 2023. The primary endpoints are OS and PFS; QoL will not be assessed. More details at clinicaltrials.gov.
Metastatic NSCLC. Individuals with this cancer who have a TPS of > 50% can also receive an antibody-drug conjugate targeting TROP2 in combination with pembrolizumab. This time, the product is sacituzumab govitecan (Trodelvy). The randomized, open-label phase 3 trial is testing whether the two drugs in combination improve survival and slow progression better than pembrolizumab alone. For approximately 2 years, one group of people in the trial will receive IV pembrolizumab every 3 weeks. The other group, in addition to the pembrolizumab, will receive IV sacituzumab govitecan weekly for 2 weeks then 1 week off until unacceptable toxicity, disease progression, withdrawal of consent, or death. Study sites in the states of Florida and Georgia, and in Australia, Taiwan, and Turkey, opened in February 2023 with the aim of recruiting 614 participants. Overall survival over 4 years and PFS are the primary outcomes. QoL is a secondary outcome. More details at clinicaltrials.gov.
Unresectable metastatic NSCLC. Individuals with this type of lung cancer are being recruited for a nonrandomized, phase 1/2 study to determine whether a combination of amivantamab (Rybrevant) and capmatinib (Tabrecta) is tolerable and more effective than either therapy alone. The two drugs inhibit different stages of mesenchymal-epithelial transition (MET), a step in cell development that is crucial for metastasis because it enhances cell mobility, invasion, and resistance to apoptosis. In the phase 1 study, participants will start with twice-daily tablets of capmatinib and IV amivantamab once weekly for 4 weeks then every 2 weeks. Doses will be adjusted on the basis of toxicities. In phase 2, a new group of participants will receive the refined doses for up to 2 years until progression or death. The study opened at the Oncology Institute of Hope and Innovation in Whittier, Calif., in December 2020 with the aim of recruiting 161 participants. Sites are gearing up in five more U.S. states and in Canada, Europe, and Asia. Objective response rate is the primary outcome of the phase 2 study, with OS and QoL as secondary endpoints. More details at clinicaltrials.gov.
Locally advanced or metastatic NSCLC with EGFR-exon-20 insertion mutations. Adults with this diagnosis who have not yet been treated and are not amenable to curative surgery or radiotherapy are sought for a randomized, open-label phase 3 trial testing whether investigational EGFR tyrosine-kinase inhibitor furmonertinib (from ArriVent) is more effective than chemotherapy for first-line treatment. Chemotherapy is currently standard of care in this indication with targeted therapies amivantamab-vmjw (Rybrevant) and mobocertinib succinate (Exkivity) as second-line options. Individuals in the trial will take daily tablets of furmonertinib or platinum-based IV chemotherapy for 32 months or until disease progression, whichever comes first. The study opened in December in sites across 15 U.S. states. Centers in a further nine states are gearing up, with the aim of enrolling a total of 375 people. The primary outcome is PFS. QoL and OS at 5 years are secondary outcomes. More details at clinicaltrials.gov.
NSCLC previously treated with at least one platinum chemotherapy and at least one targeted treatment. Adults aged 70 or younger with this type of lung cancer are eligible for a National Cancer Institute phase 2 investigation of autologous T-cell receptor (TCR) gene therapy. Unlike CAR T-cell therapy, which only reaches the 20% of cancer neoantigens that are expressed extracellularly, TCR technology can target the 80% of abnormal proteins that are expressed inside cancer cells. Participants will receive a single infusion of their own engineered T cells. They will attend follow-up visits every 3-6 months for 3 years, then join a long-term study in which they will be followed for 12 more years. The National Institutes of Health Clinical Center in Bethesda, Md., started recruiting for the trial’s 210 participants with one of a selection of solid cancers in February 2023. Response rate measured by objective tumor regression is the primary endpoint. OS and QoL will not be tracked. More details at clinicaltrials.gov.
All trial information is from the National Institutes of Health U.S. National Library of Medicine (online at clinicaltrials.gov).
A version of this article first appeared on Medscape.com.
Editor’s note: This article was changed on 24 February to remove an incorrect reference to osimertinib.
Untreated advanced non–small cell lung cancer (NSCLC). Adult patients with stage IIIB, IIIC, or IV disease without actionable genomic alterations can join a randomized, open-label, phase 3 study testing the survival advantage of datopotamab deruxtecan (Dato-DXd) (AstraZeneca/Daiichi Sankyo). Dato-DXd is one of a half dozen experimental antibody-drug conjugates that target TROP2, a transmembrane glycoprotein that is overexpressed in several solid tumors, including NSCLC. One group of participants will receive an intravenous (IV) infusion of Dato-DXd plus durvalumab (Imfinzi) for up to 4 years, and over the first 12 weeks, they will receive four rounds of IV carboplatin (Paraplatin). The other group will receive IV infusions of pembrolizumab (Keytruda) every 3 weeks plus a combination of standard IV chemotherapy appropriate for the patient’s histology (nonsquamous or squamous NSCLC). In the United States, centers in Arkansas, Nebraska, Ohio, and Texas started recruiting in December 2020; trial sites are planned in 16 other states and 23 other countries. The trialists plan to enroll 1,000 participants. Overall survival (OS) and progression-free survival (PFS) are the primary endpoints; quality of life (QoL) is not being tracked. More details at clinicaltrials.gov.
Untreated advanced or metastatic NSCLC. Adult patients in this clinical situation without actionable genomic alterations as well as those with a PD-L1 tumor proportion score (TPS) of < 50% are eligible to participate in a randomized, open-label, phase 3 trial of Dato-DXd in combination with pembrolizumab, with or without chemotherapy. One group of participants will receive IV Dato-DXd and pembrolizumab every 3 weeks. For the second group of patients, IV platinum chemotherapy will be added to the Dato-DXd and pembrolizumab for the first four rounds of treatment. The third group of individuals make up the comparator arm and will receive thrice-weekly IV pembrolizumab, pemetrexed (Alimta), plus platinum chemotherapy. All participants will be treated for approximately 2.5 years or until disease progression or death. The trial began recruiting 975 participants in Arizona, Florida, Maryland, and New Jersey, and in Japan in January 2023. The primary endpoints are OS and PFS; QoL will not be assessed. More details at clinicaltrials.gov.
Metastatic NSCLC. Individuals with this cancer who have a TPS of > 50% can also receive an antibody-drug conjugate targeting TROP2 in combination with pembrolizumab. This time, the product is sacituzumab govitecan (Trodelvy). The randomized, open-label phase 3 trial is testing whether the two drugs in combination improve survival and slow progression better than pembrolizumab alone. For approximately 2 years, one group of people in the trial will receive IV pembrolizumab every 3 weeks. The other group, in addition to the pembrolizumab, will receive IV sacituzumab govitecan weekly for 2 weeks then 1 week off until unacceptable toxicity, disease progression, withdrawal of consent, or death. Study sites in the states of Florida and Georgia, and in Australia, Taiwan, and Turkey, opened in February 2023 with the aim of recruiting 614 participants. Overall survival over 4 years and PFS are the primary outcomes. QoL is a secondary outcome. More details at clinicaltrials.gov.
Unresectable metastatic NSCLC. Individuals with this type of lung cancer are being recruited for a nonrandomized, phase 1/2 study to determine whether a combination of amivantamab (Rybrevant) and capmatinib (Tabrecta) is tolerable and more effective than either therapy alone. The two drugs inhibit different stages of mesenchymal-epithelial transition (MET), a step in cell development that is crucial for metastasis because it enhances cell mobility, invasion, and resistance to apoptosis. In the phase 1 study, participants will start with twice-daily tablets of capmatinib and IV amivantamab once weekly for 4 weeks then every 2 weeks. Doses will be adjusted on the basis of toxicities. In phase 2, a new group of participants will receive the refined doses for up to 2 years until progression or death. The study opened at the Oncology Institute of Hope and Innovation in Whittier, Calif., in December 2020 with the aim of recruiting 161 participants. Sites are gearing up in five more U.S. states and in Canada, Europe, and Asia. Objective response rate is the primary outcome of the phase 2 study, with OS and QoL as secondary endpoints. More details at clinicaltrials.gov.
Locally advanced or metastatic NSCLC with EGFR-exon-20 insertion mutations. Adults with this diagnosis who have not yet been treated and are not amenable to curative surgery or radiotherapy are sought for a randomized, open-label phase 3 trial testing whether investigational EGFR tyrosine-kinase inhibitor furmonertinib (from ArriVent) is more effective than chemotherapy for first-line treatment. Chemotherapy is currently standard of care in this indication with targeted therapies amivantamab-vmjw (Rybrevant) and mobocertinib succinate (Exkivity) as second-line options. Individuals in the trial will take daily tablets of furmonertinib or platinum-based IV chemotherapy for 32 months or until disease progression, whichever comes first. The study opened in December in sites across 15 U.S. states. Centers in a further nine states are gearing up, with the aim of enrolling a total of 375 people. The primary outcome is PFS. QoL and OS at 5 years are secondary outcomes. More details at clinicaltrials.gov.
NSCLC previously treated with at least one platinum chemotherapy and at least one targeted treatment. Adults aged 70 or younger with this type of lung cancer are eligible for a National Cancer Institute phase 2 investigation of autologous T-cell receptor (TCR) gene therapy. Unlike CAR T-cell therapy, which only reaches the 20% of cancer neoantigens that are expressed extracellularly, TCR technology can target the 80% of abnormal proteins that are expressed inside cancer cells. Participants will receive a single infusion of their own engineered T cells. They will attend follow-up visits every 3-6 months for 3 years, then join a long-term study in which they will be followed for 12 more years. The National Institutes of Health Clinical Center in Bethesda, Md., started recruiting for the trial’s 210 participants with one of a selection of solid cancers in February 2023. Response rate measured by objective tumor regression is the primary endpoint. OS and QoL will not be tracked. More details at clinicaltrials.gov.
All trial information is from the National Institutes of Health U.S. National Library of Medicine (online at clinicaltrials.gov).
A version of this article first appeared on Medscape.com.
Editor’s note: This article was changed on 24 February to remove an incorrect reference to osimertinib.
Untreated advanced non–small cell lung cancer (NSCLC). Adult patients with stage IIIB, IIIC, or IV disease without actionable genomic alterations can join a randomized, open-label, phase 3 study testing the survival advantage of datopotamab deruxtecan (Dato-DXd) (AstraZeneca/Daiichi Sankyo). Dato-DXd is one of a half dozen experimental antibody-drug conjugates that target TROP2, a transmembrane glycoprotein that is overexpressed in several solid tumors, including NSCLC. One group of participants will receive an intravenous (IV) infusion of Dato-DXd plus durvalumab (Imfinzi) for up to 4 years, and over the first 12 weeks, they will receive four rounds of IV carboplatin (Paraplatin). The other group will receive IV infusions of pembrolizumab (Keytruda) every 3 weeks plus a combination of standard IV chemotherapy appropriate for the patient’s histology (nonsquamous or squamous NSCLC). In the United States, centers in Arkansas, Nebraska, Ohio, and Texas started recruiting in December 2020; trial sites are planned in 16 other states and 23 other countries. The trialists plan to enroll 1,000 participants. Overall survival (OS) and progression-free survival (PFS) are the primary endpoints; quality of life (QoL) is not being tracked. More details at clinicaltrials.gov.
Untreated advanced or metastatic NSCLC. Adult patients in this clinical situation without actionable genomic alterations as well as those with a PD-L1 tumor proportion score (TPS) of < 50% are eligible to participate in a randomized, open-label, phase 3 trial of Dato-DXd in combination with pembrolizumab, with or without chemotherapy. One group of participants will receive IV Dato-DXd and pembrolizumab every 3 weeks. For the second group of patients, IV platinum chemotherapy will be added to the Dato-DXd and pembrolizumab for the first four rounds of treatment. The third group of individuals make up the comparator arm and will receive thrice-weekly IV pembrolizumab, pemetrexed (Alimta), plus platinum chemotherapy. All participants will be treated for approximately 2.5 years or until disease progression or death. The trial began recruiting 975 participants in Arizona, Florida, Maryland, and New Jersey, and in Japan in January 2023. The primary endpoints are OS and PFS; QoL will not be assessed. More details at clinicaltrials.gov.
Metastatic NSCLC. Individuals with this cancer who have a TPS of > 50% can also receive an antibody-drug conjugate targeting TROP2 in combination with pembrolizumab. This time, the product is sacituzumab govitecan (Trodelvy). The randomized, open-label phase 3 trial is testing whether the two drugs in combination improve survival and slow progression better than pembrolizumab alone. For approximately 2 years, one group of people in the trial will receive IV pembrolizumab every 3 weeks. The other group, in addition to the pembrolizumab, will receive IV sacituzumab govitecan weekly for 2 weeks then 1 week off until unacceptable toxicity, disease progression, withdrawal of consent, or death. Study sites in the states of Florida and Georgia, and in Australia, Taiwan, and Turkey, opened in February 2023 with the aim of recruiting 614 participants. Overall survival over 4 years and PFS are the primary outcomes. QoL is a secondary outcome. More details at clinicaltrials.gov.
Unresectable metastatic NSCLC. Individuals with this type of lung cancer are being recruited for a nonrandomized, phase 1/2 study to determine whether a combination of amivantamab (Rybrevant) and capmatinib (Tabrecta) is tolerable and more effective than either therapy alone. The two drugs inhibit different stages of mesenchymal-epithelial transition (MET), a step in cell development that is crucial for metastasis because it enhances cell mobility, invasion, and resistance to apoptosis. In the phase 1 study, participants will start with twice-daily tablets of capmatinib and IV amivantamab once weekly for 4 weeks then every 2 weeks. Doses will be adjusted on the basis of toxicities. In phase 2, a new group of participants will receive the refined doses for up to 2 years until progression or death. The study opened at the Oncology Institute of Hope and Innovation in Whittier, Calif., in December 2020 with the aim of recruiting 161 participants. Sites are gearing up in five more U.S. states and in Canada, Europe, and Asia. Objective response rate is the primary outcome of the phase 2 study, with OS and QoL as secondary endpoints. More details at clinicaltrials.gov.
Locally advanced or metastatic NSCLC with EGFR-exon-20 insertion mutations. Adults with this diagnosis who have not yet been treated and are not amenable to curative surgery or radiotherapy are sought for a randomized, open-label phase 3 trial testing whether investigational EGFR tyrosine-kinase inhibitor furmonertinib (from ArriVent) is more effective than chemotherapy for first-line treatment. Chemotherapy is currently standard of care in this indication with targeted therapies amivantamab-vmjw (Rybrevant) and mobocertinib succinate (Exkivity) as second-line options. Individuals in the trial will take daily tablets of furmonertinib or platinum-based IV chemotherapy for 32 months or until disease progression, whichever comes first. The study opened in December in sites across 15 U.S. states. Centers in a further nine states are gearing up, with the aim of enrolling a total of 375 people. The primary outcome is PFS. QoL and OS at 5 years are secondary outcomes. More details at clinicaltrials.gov.
NSCLC previously treated with at least one platinum chemotherapy and at least one targeted treatment. Adults aged 70 or younger with this type of lung cancer are eligible for a National Cancer Institute phase 2 investigation of autologous T-cell receptor (TCR) gene therapy. Unlike CAR T-cell therapy, which only reaches the 20% of cancer neoantigens that are expressed extracellularly, TCR technology can target the 80% of abnormal proteins that are expressed inside cancer cells. Participants will receive a single infusion of their own engineered T cells. They will attend follow-up visits every 3-6 months for 3 years, then join a long-term study in which they will be followed for 12 more years. The National Institutes of Health Clinical Center in Bethesda, Md., started recruiting for the trial’s 210 participants with one of a selection of solid cancers in February 2023. Response rate measured by objective tumor regression is the primary endpoint. OS and QoL will not be tracked. More details at clinicaltrials.gov.
All trial information is from the National Institutes of Health U.S. National Library of Medicine (online at clinicaltrials.gov).
A version of this article first appeared on Medscape.com.
Editor’s note: This article was changed on 24 February to remove an incorrect reference to osimertinib.
New cancer screen, same issues: Physicians confront Galleri test
In January 2022, Anthony Arenz, a 51-year-old living in Mesa, Ariz., breathed a small sigh of relief.
The Galleri blood test, which screens for 50 types of cancer, hadn’t detected any positive signs.
It would be welcome news to anyone but especially to a firefighter with a 9% greater risk of developing cancer and a 14% greater risk of dying from it than the average person. The Mesa unit had lost two servicemen to cancer in the past 3 years. Both were more than a decade younger than Mr. Arenz.
When the city of Mesa offered additional free screening – including a full-body MRI – to firefighters over 50, Mr. Arenz initially shrugged it off. With a negative Galleri test in hand, he didn’t want to spend more time dwelling on it.
Still, he began to feel a creeping guilt for skipping a test that many of his fallen colleagues hadn’t been offered. He tried to soothe his anxiety with research. A look through the company’s website didn’t set him at ease. According to Grail Bio, a test result of “no cancer signal detected” does not rule out cancer.
Mr. Arenz booked his free MRI.
The results left him heavy: stage I kidney cancer. The Galleri test had missed it.
Mr. Arenz received his free Galleri test through a cancer screening program funded by the city of Mesa. The program is housed at Vincere Cancer Center in Scottsdale, Ariz. Under the leadership of radiation oncologist and Vincere co-owner Vershalee Shukla, MD, the program currently screens first responders in more than 10 Arizona cities at no cost to them.
Vincere began using Galleri shortly after the test launched for consumers in June 2021. Since then, the first responder program has become the largest commercial user of the test in North America.
The Galleri test, which has not yet been approved by the Food and Drug Administration, is so new that few know what incorrect results look like in practice and how often they might occur.
After running the test on about 2,000 servicemen and servicewomen, Dr. Shukla can offer some insight about the test’s real-world value in a high-risk population.
“Cancer screening is a very complicated issue,” Dr. Shukla said in an interview. “Being honest, the tests are good but are not ready yet [for wider use].”
Mr. Arenz was not the only firefighter who got a surprise after taking a Galleri test.
In nearby Phoenix, 51-year-old firefighter Mike Curtis knew his risk for cancer was high, but he wasn’t that worried. Mr. Curtis had been running into fires since he was 17. His dad, also a firefighter, had died of cancer at age 58.
Mr. Curtis had taken the Vincere Cancer Center up on every free screening service since the program began in late 2018 – well before Dr. Shukla started using Galleri in 2021. His most recent lung CT was clear. But he underwent the Galleri test just to stay vigilant.
His result was a shock. The test detected signs of cancer.
Mr. Curtis decided to tell no one, not even his wife. He’d bear the bad news alone until he was certain.
Dr. Shukla, however, immediately doubted the blood test result. She expedited several follow-up tests. One week, a PET, and CT of the abdomen and pelvis later, her hunch was confirmed. The Galleri test result was wrong, Mr. Curtis did not have cancer.
The price of his peace of mind: an extensive workup with a $4,000 price tag. Fortunately, the bill was covered by the screening program.
Overall, in just over 18 months of using the blood test, Dr. Shukla has only encountered 1 other false positive out of about 2,000 Galleri results.
She also discovered two positive signals for cancer using Galleri that were confirmed with follow-up tests. One was a chordoma, a rare type of bone cancer, and the other was a squamous cell carcinoma of the head and neck. The Galleri test caught both remarkably early, in time for treatment.
For Dr. Shukla, however, false negatives were particularly “horrible.” Mr. Arenz’s was just 1 of 28 cancers that the blood test missed. And because 500 negative tests are yet to be validated, the 28 false negatives may be an underestimate.
In her experience, the binary test result – a simple positive or negative cancer signal – is an oversimplification of risk, she said. It “gives a false perception that you have cancer or you don’t,” although the test itself is not definitive.
Grail senior medical director Whitney Jones, MD, agreed that the test is not meant to be a stand-alone screening test for cancer. The purpose of the Galleri test is to “complement other screenings, not replace them,” Dr. Jones told this news organization.
According to an analysis of Galleri data and Dr. Shukla’s experience, the test’s specificity was over 99%. That means the test successfully minimizes false positives.
But the test’s sensitivity was much lower. From data from first responders, Dr. Shukla determined the sensitivity to be 6.7%. That means the test misses about 93 of every 100 cancers. According to Grail’s latest data from more than 6,300 people older than 50, the test’s sensitivity was 29%.
Specificity and sensitivity are metrics used to credential a test and establish confidence in its ability to detect the target disease. A test with high specificity can correctly identify patients who do not have the condition in question, while a test with high sensitivity can correctly identify patients who do have the disease. But there are trade-offs between sensitivity and specificity. One value is increased at the expense of the other.
It’s normal for a cancer screening test to prioritize specificity, according to Aparna Parikh, MD, an oncologist at Mass General Cancer Center in Boston. In a test like Galleri, which is meant to be an adjunct to other screening modalities, “at least we are seeing a good specificity, which is important, because we don’t want false positives, where the downstream impact on the patient can be high.”
Overall, Dr. Jones said, Grail Bio’s aim is to build a test that’s sensitive enough to catch the most dangerous cancers without inundating the healthcare system with false positives. In addition, Dr. Jones explained, sensitivity varies by cancer type. It tends to be lower for cancers for which other screening modalities are available, as well as for earlier-stage disease.
However, the Galleri sensitivity values are “a little bit scary,” said Ji-Hyun Lee, DrPH, professor of biostatistics at the University of Florida and director of the division of quantitative sciences at the University of Florida Health Cancer Center, both in Gainesville. Dr. Lee, who is not affiliated with Grail, reviewed the company’s publicly available data as well as Dr. Shukla’s data at the request of this news organization.
While there’s no definitive threshold for sensitivity, miss rates as high as 93% and 71% “provide little confidence in the [accuracy of the] test,” Dr. Lee said.
Positive and negative predictive values, however, are more clinically relevant measures of a screening test. These numbers indicate how likely it is that a patient’s results are true and therefore how worried they should be about a positive result and how much they should trust a negative result.
Galleri’s data in the over-50 population and Dr. Shukla’s in first responders suggest the test’s negative predictive value is very high – 98.6% and 98.1%, respectively – which means most people can trust a negative test result.
The positive predictive value, however, was less straightforward. In first responders, Dr. Shukla found that only half of positive Galleri tests were confirmed cases of cancer. And an analysis of Grail’s data found that only 38% of positive Galleri tests – 35 of 92 tests – represented a validated cancer diagnosis.
“In a clinical setting, positive predictive value is more usable for decision-making for the patient,” said Dr. Lee. “Positive predictive value isn’t always high, because everything doesn’t always transfer perfectly to the clinic.” But in the general population, if only 38% of patients with positive Galleri results truly have cancer, the test is “not quite useful to make a decision for the patient or the providers.”
Galleri may also be a costly prospect for patients, no matter the result, cautioned Electra Paskett, PhD, an epidemiologist and cancer screening expert at Ohio State University, Columbus. A positive Galleri test leads to a cascade of follow-up diagnostic tests, which payers may not cover. For a negative result, Galleri recommends that the patient undergo screening again in a year, at an annual cost of $950 plus the cost of any follow-up testing when Galleri does pick something up.
“If a provider wants to offer the Galleri test, all those things need to be made abundantly clear, in my opinion,” Dr. Paskett said.
Following the negative Galleri test, Mr. Arenz’s cancer didn’t slip through the cracks because he received other advanced imaging free of charge. But whether all doctors will go to such lengths to back up Galleri results, even for patients with negative results, is unknown.
A negative result can give patients “a huge false sense of security,” said Dr. Shukla. And if a test is positive, the workup isn’t simple. Chasing cancer, especially one that’s not really there, can be nerve-wracking and expensive.
The question, then, is why perform the Galleri test at all if results require so much validation?
Dr. Parikh explained that a high-risk group such as firefighters represents an ideal-use case for Galleri and other liquid biopsy tests. But she noted that she would be “wary of the ability of the system to manage this test en masse” were the test to be used more widely in the general population.
Dr. Shukla said it’s less about the results she’s getting today and more about making the test more effective for her patients in the future. First responders need a test such as this that can quickly identify multiple cancers. However, to improve the test, Grail needs more data from this high-risk population. That’s what she’s after.
Mr. Curtis doesn’t regret taking the Galleri test. The emotional toll of thinking he had cancer for a few days wasn’t too high a price, in his opinion. It’s part of cancer screening. But he acknowledged that it would have been a much more burdensome experience had he’d been financially responsible for the workup or if he hadn’t had Dr. Shukla to manage his case from start to finish.
Because it was free, Mr. Arenz doesn’t regret undergoing the Galleri test either. But he tells his coworkers to check the site, do their research, and get more screening.
“Any medical center that’s just doing this one test, you just have to be careful,” Dr. Shukla said. “It’s not that easy.”
A version of this article first appeared on Medscape.com.
In January 2022, Anthony Arenz, a 51-year-old living in Mesa, Ariz., breathed a small sigh of relief.
The Galleri blood test, which screens for 50 types of cancer, hadn’t detected any positive signs.
It would be welcome news to anyone but especially to a firefighter with a 9% greater risk of developing cancer and a 14% greater risk of dying from it than the average person. The Mesa unit had lost two servicemen to cancer in the past 3 years. Both were more than a decade younger than Mr. Arenz.
When the city of Mesa offered additional free screening – including a full-body MRI – to firefighters over 50, Mr. Arenz initially shrugged it off. With a negative Galleri test in hand, he didn’t want to spend more time dwelling on it.
Still, he began to feel a creeping guilt for skipping a test that many of his fallen colleagues hadn’t been offered. He tried to soothe his anxiety with research. A look through the company’s website didn’t set him at ease. According to Grail Bio, a test result of “no cancer signal detected” does not rule out cancer.
Mr. Arenz booked his free MRI.
The results left him heavy: stage I kidney cancer. The Galleri test had missed it.
Mr. Arenz received his free Galleri test through a cancer screening program funded by the city of Mesa. The program is housed at Vincere Cancer Center in Scottsdale, Ariz. Under the leadership of radiation oncologist and Vincere co-owner Vershalee Shukla, MD, the program currently screens first responders in more than 10 Arizona cities at no cost to them.
Vincere began using Galleri shortly after the test launched for consumers in June 2021. Since then, the first responder program has become the largest commercial user of the test in North America.
The Galleri test, which has not yet been approved by the Food and Drug Administration, is so new that few know what incorrect results look like in practice and how often they might occur.
After running the test on about 2,000 servicemen and servicewomen, Dr. Shukla can offer some insight about the test’s real-world value in a high-risk population.
“Cancer screening is a very complicated issue,” Dr. Shukla said in an interview. “Being honest, the tests are good but are not ready yet [for wider use].”
Mr. Arenz was not the only firefighter who got a surprise after taking a Galleri test.
In nearby Phoenix, 51-year-old firefighter Mike Curtis knew his risk for cancer was high, but he wasn’t that worried. Mr. Curtis had been running into fires since he was 17. His dad, also a firefighter, had died of cancer at age 58.
Mr. Curtis had taken the Vincere Cancer Center up on every free screening service since the program began in late 2018 – well before Dr. Shukla started using Galleri in 2021. His most recent lung CT was clear. But he underwent the Galleri test just to stay vigilant.
His result was a shock. The test detected signs of cancer.
Mr. Curtis decided to tell no one, not even his wife. He’d bear the bad news alone until he was certain.
Dr. Shukla, however, immediately doubted the blood test result. She expedited several follow-up tests. One week, a PET, and CT of the abdomen and pelvis later, her hunch was confirmed. The Galleri test result was wrong, Mr. Curtis did not have cancer.
The price of his peace of mind: an extensive workup with a $4,000 price tag. Fortunately, the bill was covered by the screening program.
Overall, in just over 18 months of using the blood test, Dr. Shukla has only encountered 1 other false positive out of about 2,000 Galleri results.
She also discovered two positive signals for cancer using Galleri that were confirmed with follow-up tests. One was a chordoma, a rare type of bone cancer, and the other was a squamous cell carcinoma of the head and neck. The Galleri test caught both remarkably early, in time for treatment.
For Dr. Shukla, however, false negatives were particularly “horrible.” Mr. Arenz’s was just 1 of 28 cancers that the blood test missed. And because 500 negative tests are yet to be validated, the 28 false negatives may be an underestimate.
In her experience, the binary test result – a simple positive or negative cancer signal – is an oversimplification of risk, she said. It “gives a false perception that you have cancer or you don’t,” although the test itself is not definitive.
Grail senior medical director Whitney Jones, MD, agreed that the test is not meant to be a stand-alone screening test for cancer. The purpose of the Galleri test is to “complement other screenings, not replace them,” Dr. Jones told this news organization.
According to an analysis of Galleri data and Dr. Shukla’s experience, the test’s specificity was over 99%. That means the test successfully minimizes false positives.
But the test’s sensitivity was much lower. From data from first responders, Dr. Shukla determined the sensitivity to be 6.7%. That means the test misses about 93 of every 100 cancers. According to Grail’s latest data from more than 6,300 people older than 50, the test’s sensitivity was 29%.
Specificity and sensitivity are metrics used to credential a test and establish confidence in its ability to detect the target disease. A test with high specificity can correctly identify patients who do not have the condition in question, while a test with high sensitivity can correctly identify patients who do have the disease. But there are trade-offs between sensitivity and specificity. One value is increased at the expense of the other.
It’s normal for a cancer screening test to prioritize specificity, according to Aparna Parikh, MD, an oncologist at Mass General Cancer Center in Boston. In a test like Galleri, which is meant to be an adjunct to other screening modalities, “at least we are seeing a good specificity, which is important, because we don’t want false positives, where the downstream impact on the patient can be high.”
Overall, Dr. Jones said, Grail Bio’s aim is to build a test that’s sensitive enough to catch the most dangerous cancers without inundating the healthcare system with false positives. In addition, Dr. Jones explained, sensitivity varies by cancer type. It tends to be lower for cancers for which other screening modalities are available, as well as for earlier-stage disease.
However, the Galleri sensitivity values are “a little bit scary,” said Ji-Hyun Lee, DrPH, professor of biostatistics at the University of Florida and director of the division of quantitative sciences at the University of Florida Health Cancer Center, both in Gainesville. Dr. Lee, who is not affiliated with Grail, reviewed the company’s publicly available data as well as Dr. Shukla’s data at the request of this news organization.
While there’s no definitive threshold for sensitivity, miss rates as high as 93% and 71% “provide little confidence in the [accuracy of the] test,” Dr. Lee said.
Positive and negative predictive values, however, are more clinically relevant measures of a screening test. These numbers indicate how likely it is that a patient’s results are true and therefore how worried they should be about a positive result and how much they should trust a negative result.
Galleri’s data in the over-50 population and Dr. Shukla’s in first responders suggest the test’s negative predictive value is very high – 98.6% and 98.1%, respectively – which means most people can trust a negative test result.
The positive predictive value, however, was less straightforward. In first responders, Dr. Shukla found that only half of positive Galleri tests were confirmed cases of cancer. And an analysis of Grail’s data found that only 38% of positive Galleri tests – 35 of 92 tests – represented a validated cancer diagnosis.
“In a clinical setting, positive predictive value is more usable for decision-making for the patient,” said Dr. Lee. “Positive predictive value isn’t always high, because everything doesn’t always transfer perfectly to the clinic.” But in the general population, if only 38% of patients with positive Galleri results truly have cancer, the test is “not quite useful to make a decision for the patient or the providers.”
Galleri may also be a costly prospect for patients, no matter the result, cautioned Electra Paskett, PhD, an epidemiologist and cancer screening expert at Ohio State University, Columbus. A positive Galleri test leads to a cascade of follow-up diagnostic tests, which payers may not cover. For a negative result, Galleri recommends that the patient undergo screening again in a year, at an annual cost of $950 plus the cost of any follow-up testing when Galleri does pick something up.
“If a provider wants to offer the Galleri test, all those things need to be made abundantly clear, in my opinion,” Dr. Paskett said.
Following the negative Galleri test, Mr. Arenz’s cancer didn’t slip through the cracks because he received other advanced imaging free of charge. But whether all doctors will go to such lengths to back up Galleri results, even for patients with negative results, is unknown.
A negative result can give patients “a huge false sense of security,” said Dr. Shukla. And if a test is positive, the workup isn’t simple. Chasing cancer, especially one that’s not really there, can be nerve-wracking and expensive.
The question, then, is why perform the Galleri test at all if results require so much validation?
Dr. Parikh explained that a high-risk group such as firefighters represents an ideal-use case for Galleri and other liquid biopsy tests. But she noted that she would be “wary of the ability of the system to manage this test en masse” were the test to be used more widely in the general population.
Dr. Shukla said it’s less about the results she’s getting today and more about making the test more effective for her patients in the future. First responders need a test such as this that can quickly identify multiple cancers. However, to improve the test, Grail needs more data from this high-risk population. That’s what she’s after.
Mr. Curtis doesn’t regret taking the Galleri test. The emotional toll of thinking he had cancer for a few days wasn’t too high a price, in his opinion. It’s part of cancer screening. But he acknowledged that it would have been a much more burdensome experience had he’d been financially responsible for the workup or if he hadn’t had Dr. Shukla to manage his case from start to finish.
Because it was free, Mr. Arenz doesn’t regret undergoing the Galleri test either. But he tells his coworkers to check the site, do their research, and get more screening.
“Any medical center that’s just doing this one test, you just have to be careful,” Dr. Shukla said. “It’s not that easy.”
A version of this article first appeared on Medscape.com.
In January 2022, Anthony Arenz, a 51-year-old living in Mesa, Ariz., breathed a small sigh of relief.
The Galleri blood test, which screens for 50 types of cancer, hadn’t detected any positive signs.
It would be welcome news to anyone but especially to a firefighter with a 9% greater risk of developing cancer and a 14% greater risk of dying from it than the average person. The Mesa unit had lost two servicemen to cancer in the past 3 years. Both were more than a decade younger than Mr. Arenz.
When the city of Mesa offered additional free screening – including a full-body MRI – to firefighters over 50, Mr. Arenz initially shrugged it off. With a negative Galleri test in hand, he didn’t want to spend more time dwelling on it.
Still, he began to feel a creeping guilt for skipping a test that many of his fallen colleagues hadn’t been offered. He tried to soothe his anxiety with research. A look through the company’s website didn’t set him at ease. According to Grail Bio, a test result of “no cancer signal detected” does not rule out cancer.
Mr. Arenz booked his free MRI.
The results left him heavy: stage I kidney cancer. The Galleri test had missed it.
Mr. Arenz received his free Galleri test through a cancer screening program funded by the city of Mesa. The program is housed at Vincere Cancer Center in Scottsdale, Ariz. Under the leadership of radiation oncologist and Vincere co-owner Vershalee Shukla, MD, the program currently screens first responders in more than 10 Arizona cities at no cost to them.
Vincere began using Galleri shortly after the test launched for consumers in June 2021. Since then, the first responder program has become the largest commercial user of the test in North America.
The Galleri test, which has not yet been approved by the Food and Drug Administration, is so new that few know what incorrect results look like in practice and how often they might occur.
After running the test on about 2,000 servicemen and servicewomen, Dr. Shukla can offer some insight about the test’s real-world value in a high-risk population.
“Cancer screening is a very complicated issue,” Dr. Shukla said in an interview. “Being honest, the tests are good but are not ready yet [for wider use].”
Mr. Arenz was not the only firefighter who got a surprise after taking a Galleri test.
In nearby Phoenix, 51-year-old firefighter Mike Curtis knew his risk for cancer was high, but he wasn’t that worried. Mr. Curtis had been running into fires since he was 17. His dad, also a firefighter, had died of cancer at age 58.
Mr. Curtis had taken the Vincere Cancer Center up on every free screening service since the program began in late 2018 – well before Dr. Shukla started using Galleri in 2021. His most recent lung CT was clear. But he underwent the Galleri test just to stay vigilant.
His result was a shock. The test detected signs of cancer.
Mr. Curtis decided to tell no one, not even his wife. He’d bear the bad news alone until he was certain.
Dr. Shukla, however, immediately doubted the blood test result. She expedited several follow-up tests. One week, a PET, and CT of the abdomen and pelvis later, her hunch was confirmed. The Galleri test result was wrong, Mr. Curtis did not have cancer.
The price of his peace of mind: an extensive workup with a $4,000 price tag. Fortunately, the bill was covered by the screening program.
Overall, in just over 18 months of using the blood test, Dr. Shukla has only encountered 1 other false positive out of about 2,000 Galleri results.
She also discovered two positive signals for cancer using Galleri that were confirmed with follow-up tests. One was a chordoma, a rare type of bone cancer, and the other was a squamous cell carcinoma of the head and neck. The Galleri test caught both remarkably early, in time for treatment.
For Dr. Shukla, however, false negatives were particularly “horrible.” Mr. Arenz’s was just 1 of 28 cancers that the blood test missed. And because 500 negative tests are yet to be validated, the 28 false negatives may be an underestimate.
In her experience, the binary test result – a simple positive or negative cancer signal – is an oversimplification of risk, she said. It “gives a false perception that you have cancer or you don’t,” although the test itself is not definitive.
Grail senior medical director Whitney Jones, MD, agreed that the test is not meant to be a stand-alone screening test for cancer. The purpose of the Galleri test is to “complement other screenings, not replace them,” Dr. Jones told this news organization.
According to an analysis of Galleri data and Dr. Shukla’s experience, the test’s specificity was over 99%. That means the test successfully minimizes false positives.
But the test’s sensitivity was much lower. From data from first responders, Dr. Shukla determined the sensitivity to be 6.7%. That means the test misses about 93 of every 100 cancers. According to Grail’s latest data from more than 6,300 people older than 50, the test’s sensitivity was 29%.
Specificity and sensitivity are metrics used to credential a test and establish confidence in its ability to detect the target disease. A test with high specificity can correctly identify patients who do not have the condition in question, while a test with high sensitivity can correctly identify patients who do have the disease. But there are trade-offs between sensitivity and specificity. One value is increased at the expense of the other.
It’s normal for a cancer screening test to prioritize specificity, according to Aparna Parikh, MD, an oncologist at Mass General Cancer Center in Boston. In a test like Galleri, which is meant to be an adjunct to other screening modalities, “at least we are seeing a good specificity, which is important, because we don’t want false positives, where the downstream impact on the patient can be high.”
Overall, Dr. Jones said, Grail Bio’s aim is to build a test that’s sensitive enough to catch the most dangerous cancers without inundating the healthcare system with false positives. In addition, Dr. Jones explained, sensitivity varies by cancer type. It tends to be lower for cancers for which other screening modalities are available, as well as for earlier-stage disease.
However, the Galleri sensitivity values are “a little bit scary,” said Ji-Hyun Lee, DrPH, professor of biostatistics at the University of Florida and director of the division of quantitative sciences at the University of Florida Health Cancer Center, both in Gainesville. Dr. Lee, who is not affiliated with Grail, reviewed the company’s publicly available data as well as Dr. Shukla’s data at the request of this news organization.
While there’s no definitive threshold for sensitivity, miss rates as high as 93% and 71% “provide little confidence in the [accuracy of the] test,” Dr. Lee said.
Positive and negative predictive values, however, are more clinically relevant measures of a screening test. These numbers indicate how likely it is that a patient’s results are true and therefore how worried they should be about a positive result and how much they should trust a negative result.
Galleri’s data in the over-50 population and Dr. Shukla’s in first responders suggest the test’s negative predictive value is very high – 98.6% and 98.1%, respectively – which means most people can trust a negative test result.
The positive predictive value, however, was less straightforward. In first responders, Dr. Shukla found that only half of positive Galleri tests were confirmed cases of cancer. And an analysis of Grail’s data found that only 38% of positive Galleri tests – 35 of 92 tests – represented a validated cancer diagnosis.
“In a clinical setting, positive predictive value is more usable for decision-making for the patient,” said Dr. Lee. “Positive predictive value isn’t always high, because everything doesn’t always transfer perfectly to the clinic.” But in the general population, if only 38% of patients with positive Galleri results truly have cancer, the test is “not quite useful to make a decision for the patient or the providers.”
Galleri may also be a costly prospect for patients, no matter the result, cautioned Electra Paskett, PhD, an epidemiologist and cancer screening expert at Ohio State University, Columbus. A positive Galleri test leads to a cascade of follow-up diagnostic tests, which payers may not cover. For a negative result, Galleri recommends that the patient undergo screening again in a year, at an annual cost of $950 plus the cost of any follow-up testing when Galleri does pick something up.
“If a provider wants to offer the Galleri test, all those things need to be made abundantly clear, in my opinion,” Dr. Paskett said.
Following the negative Galleri test, Mr. Arenz’s cancer didn’t slip through the cracks because he received other advanced imaging free of charge. But whether all doctors will go to such lengths to back up Galleri results, even for patients with negative results, is unknown.
A negative result can give patients “a huge false sense of security,” said Dr. Shukla. And if a test is positive, the workup isn’t simple. Chasing cancer, especially one that’s not really there, can be nerve-wracking and expensive.
The question, then, is why perform the Galleri test at all if results require so much validation?
Dr. Parikh explained that a high-risk group such as firefighters represents an ideal-use case for Galleri and other liquid biopsy tests. But she noted that she would be “wary of the ability of the system to manage this test en masse” were the test to be used more widely in the general population.
Dr. Shukla said it’s less about the results she’s getting today and more about making the test more effective for her patients in the future. First responders need a test such as this that can quickly identify multiple cancers. However, to improve the test, Grail needs more data from this high-risk population. That’s what she’s after.
Mr. Curtis doesn’t regret taking the Galleri test. The emotional toll of thinking he had cancer for a few days wasn’t too high a price, in his opinion. It’s part of cancer screening. But he acknowledged that it would have been a much more burdensome experience had he’d been financially responsible for the workup or if he hadn’t had Dr. Shukla to manage his case from start to finish.
Because it was free, Mr. Arenz doesn’t regret undergoing the Galleri test either. But he tells his coworkers to check the site, do their research, and get more screening.
“Any medical center that’s just doing this one test, you just have to be careful,” Dr. Shukla said. “It’s not that easy.”
A version of this article first appeared on Medscape.com.
Local therapies show promise for metastatic lung cancer
“Don’t close the barn door after the horse is gone,” the old proverb goes. In other words, there’s no sense in trying to prevent something when it’s already too late.
In many ways and for many years, this saying has applied to providing local therapies to treat cancers that have metastasized to distant sites. I learned this lesson early on from my mentors and have relayed it to countless patients with advanced cancer over the past several decades.
But a growing body of evidence, alongside promising new therapies, highlights more and more exceptions to this long-held belief.
This concept was outlined decades ago for oligometastatic disease and has since been studied in greater depth, and is even being applied in practice. Local therapy for colorectal cancer with limited liver-only metastases is now established as a path to potentially excellent long-term survival. And prospective randomized trials of local therapies for oligometastatic lung cancer or prostate cancer have also demonstrated improvements in clinical outcomes that should lead us to strongly consider integrating local therapy for appropriately selected patients.
In addition, early retrospective studies have provided a proof of principle that patients with solitary brain or adrenal metastases from non–small cell lung cancer (NSCLC) can do exceptionally well and even remain disease-free for many years after definitive local therapy to the primary tumor and oligometastatic disease. For example, a recent press release on the LUNAR trial reported an improvement in overall survival with tumor-treating fields (TTFs), a local therapy, compared with docetaxel as second-line therapy for patients with advanced NSCLC.
That said, the selection process for who receives local therapy remains subjective. In practice, I see patients who fall well outside of conventional oligometastatic parameters but who are directed to local therapy, commonly when systemic therapy is considered futile or prohibitively toxic.
At the same time, however, I also see many patients who would be appropriate candidates for local therapy for oligometastatic disease for whom this strategy is not pursued, perhaps because some oncologists remain dubious about the value of local therapy in this setting. And although we await the full data from the LUNAR trial, I would expect TTFs to face challenges in broad adoption because it is a novel platform with cumbersome practical application, particularly outside of larger centers.
But beyond the potential for TTFs to change management of previously treated advanced NSCLC, I think the findings are more significant because they represent a step, perhaps even a quantum leap, in the role that local therapy could play in improving survival in a broad, unselected population with advanced disease. That is a far more meaningful prospect than conferring benefits in well-selected patients with a narrow subtype of lung cancer. It will be important to determine whether certain subgroups from the LUNAR trial are driving this overall survival benefit.
Local therapy may even have value in the advanced cancer setting beyond oligometastatic disease. That potential is being explored in the SABR-COMET-10 trial, which randomly assigned 159 patients with 4-10 metastatic lesions from various cancers to stereotactic ablative body radiation with standard systemic therapy or the latter alone. With overall survival as the primary endpoint, this study could further revise our understanding of the use of local therapy for treating patients whose cancer biology does not fit the definition of oligometastatic disease.
Does this evolving landscape mean that we were wrong to minimize the role of local therapy?
I don’t think so. The risk/benefit of local therapy today is predicated on two key factors that were absent a few decades ago. First, local therapies such as stereotactic ablative body radiation, minimally invasive surgery, and TTFs now offer disease control with far less attendant toxicity than conventional external beam radiation therapy or open surgery. Second, newer systemic therapies that include targeted therapies and immunotherapy confer remarkably greater disease control for far more patients than does conventional chemotherapy alone.
It is this combination of local therapy’s excellent therapeutic index applied against a background of far better systemic disease control that makes the interplay of local and systemic treatments a newly relevant, open question.
We have yet to see the details of several pivotal trials, but I feel that we should be prepared to question some of the historic dogma in our field to achieve better outcomes not just for selected, narrow subgroups but for a broader population with different types of metastatic cancer.
Dr. West is clinical associate professor, department of medical oncology, City of Hope Comprehensive Cancer Care, Duarte, Calif. He disclosed ties with Ariad/Takeda, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Eli Lilly, Genentech/Roche, Merck, Pfizer, and Spectrum. A version of this article originally appeared on Medscape.com.
“Don’t close the barn door after the horse is gone,” the old proverb goes. In other words, there’s no sense in trying to prevent something when it’s already too late.
In many ways and for many years, this saying has applied to providing local therapies to treat cancers that have metastasized to distant sites. I learned this lesson early on from my mentors and have relayed it to countless patients with advanced cancer over the past several decades.
But a growing body of evidence, alongside promising new therapies, highlights more and more exceptions to this long-held belief.
This concept was outlined decades ago for oligometastatic disease and has since been studied in greater depth, and is even being applied in practice. Local therapy for colorectal cancer with limited liver-only metastases is now established as a path to potentially excellent long-term survival. And prospective randomized trials of local therapies for oligometastatic lung cancer or prostate cancer have also demonstrated improvements in clinical outcomes that should lead us to strongly consider integrating local therapy for appropriately selected patients.
In addition, early retrospective studies have provided a proof of principle that patients with solitary brain or adrenal metastases from non–small cell lung cancer (NSCLC) can do exceptionally well and even remain disease-free for many years after definitive local therapy to the primary tumor and oligometastatic disease. For example, a recent press release on the LUNAR trial reported an improvement in overall survival with tumor-treating fields (TTFs), a local therapy, compared with docetaxel as second-line therapy for patients with advanced NSCLC.
That said, the selection process for who receives local therapy remains subjective. In practice, I see patients who fall well outside of conventional oligometastatic parameters but who are directed to local therapy, commonly when systemic therapy is considered futile or prohibitively toxic.
At the same time, however, I also see many patients who would be appropriate candidates for local therapy for oligometastatic disease for whom this strategy is not pursued, perhaps because some oncologists remain dubious about the value of local therapy in this setting. And although we await the full data from the LUNAR trial, I would expect TTFs to face challenges in broad adoption because it is a novel platform with cumbersome practical application, particularly outside of larger centers.
But beyond the potential for TTFs to change management of previously treated advanced NSCLC, I think the findings are more significant because they represent a step, perhaps even a quantum leap, in the role that local therapy could play in improving survival in a broad, unselected population with advanced disease. That is a far more meaningful prospect than conferring benefits in well-selected patients with a narrow subtype of lung cancer. It will be important to determine whether certain subgroups from the LUNAR trial are driving this overall survival benefit.
Local therapy may even have value in the advanced cancer setting beyond oligometastatic disease. That potential is being explored in the SABR-COMET-10 trial, which randomly assigned 159 patients with 4-10 metastatic lesions from various cancers to stereotactic ablative body radiation with standard systemic therapy or the latter alone. With overall survival as the primary endpoint, this study could further revise our understanding of the use of local therapy for treating patients whose cancer biology does not fit the definition of oligometastatic disease.
Does this evolving landscape mean that we were wrong to minimize the role of local therapy?
I don’t think so. The risk/benefit of local therapy today is predicated on two key factors that were absent a few decades ago. First, local therapies such as stereotactic ablative body radiation, minimally invasive surgery, and TTFs now offer disease control with far less attendant toxicity than conventional external beam radiation therapy or open surgery. Second, newer systemic therapies that include targeted therapies and immunotherapy confer remarkably greater disease control for far more patients than does conventional chemotherapy alone.
It is this combination of local therapy’s excellent therapeutic index applied against a background of far better systemic disease control that makes the interplay of local and systemic treatments a newly relevant, open question.
We have yet to see the details of several pivotal trials, but I feel that we should be prepared to question some of the historic dogma in our field to achieve better outcomes not just for selected, narrow subgroups but for a broader population with different types of metastatic cancer.
Dr. West is clinical associate professor, department of medical oncology, City of Hope Comprehensive Cancer Care, Duarte, Calif. He disclosed ties with Ariad/Takeda, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Eli Lilly, Genentech/Roche, Merck, Pfizer, and Spectrum. A version of this article originally appeared on Medscape.com.
“Don’t close the barn door after the horse is gone,” the old proverb goes. In other words, there’s no sense in trying to prevent something when it’s already too late.
In many ways and for many years, this saying has applied to providing local therapies to treat cancers that have metastasized to distant sites. I learned this lesson early on from my mentors and have relayed it to countless patients with advanced cancer over the past several decades.
But a growing body of evidence, alongside promising new therapies, highlights more and more exceptions to this long-held belief.
This concept was outlined decades ago for oligometastatic disease and has since been studied in greater depth, and is even being applied in practice. Local therapy for colorectal cancer with limited liver-only metastases is now established as a path to potentially excellent long-term survival. And prospective randomized trials of local therapies for oligometastatic lung cancer or prostate cancer have also demonstrated improvements in clinical outcomes that should lead us to strongly consider integrating local therapy for appropriately selected patients.
In addition, early retrospective studies have provided a proof of principle that patients with solitary brain or adrenal metastases from non–small cell lung cancer (NSCLC) can do exceptionally well and even remain disease-free for many years after definitive local therapy to the primary tumor and oligometastatic disease. For example, a recent press release on the LUNAR trial reported an improvement in overall survival with tumor-treating fields (TTFs), a local therapy, compared with docetaxel as second-line therapy for patients with advanced NSCLC.
That said, the selection process for who receives local therapy remains subjective. In practice, I see patients who fall well outside of conventional oligometastatic parameters but who are directed to local therapy, commonly when systemic therapy is considered futile or prohibitively toxic.
At the same time, however, I also see many patients who would be appropriate candidates for local therapy for oligometastatic disease for whom this strategy is not pursued, perhaps because some oncologists remain dubious about the value of local therapy in this setting. And although we await the full data from the LUNAR trial, I would expect TTFs to face challenges in broad adoption because it is a novel platform with cumbersome practical application, particularly outside of larger centers.
But beyond the potential for TTFs to change management of previously treated advanced NSCLC, I think the findings are more significant because they represent a step, perhaps even a quantum leap, in the role that local therapy could play in improving survival in a broad, unselected population with advanced disease. That is a far more meaningful prospect than conferring benefits in well-selected patients with a narrow subtype of lung cancer. It will be important to determine whether certain subgroups from the LUNAR trial are driving this overall survival benefit.
Local therapy may even have value in the advanced cancer setting beyond oligometastatic disease. That potential is being explored in the SABR-COMET-10 trial, which randomly assigned 159 patients with 4-10 metastatic lesions from various cancers to stereotactic ablative body radiation with standard systemic therapy or the latter alone. With overall survival as the primary endpoint, this study could further revise our understanding of the use of local therapy for treating patients whose cancer biology does not fit the definition of oligometastatic disease.
Does this evolving landscape mean that we were wrong to minimize the role of local therapy?
I don’t think so. The risk/benefit of local therapy today is predicated on two key factors that were absent a few decades ago. First, local therapies such as stereotactic ablative body radiation, minimally invasive surgery, and TTFs now offer disease control with far less attendant toxicity than conventional external beam radiation therapy or open surgery. Second, newer systemic therapies that include targeted therapies and immunotherapy confer remarkably greater disease control for far more patients than does conventional chemotherapy alone.
It is this combination of local therapy’s excellent therapeutic index applied against a background of far better systemic disease control that makes the interplay of local and systemic treatments a newly relevant, open question.
We have yet to see the details of several pivotal trials, but I feel that we should be prepared to question some of the historic dogma in our field to achieve better outcomes not just for selected, narrow subgroups but for a broader population with different types of metastatic cancer.
Dr. West is clinical associate professor, department of medical oncology, City of Hope Comprehensive Cancer Care, Duarte, Calif. He disclosed ties with Ariad/Takeda, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Eli Lilly, Genentech/Roche, Merck, Pfizer, and Spectrum. A version of this article originally appeared on Medscape.com.
Less invasive NSCLC surgery does not compromise survival
suggest results from the CALGB 140503 trial, although strict patient selection remains key.
These new results contrast with those from a previous study from 1995, which found that local recurrence was three times higher and cancer mortality was twice as high with the less invasive procedure.
Those results from nearly 30 years ago established lobectomy as the standard of surgical care in this patient population, but since then advances in imaging and staging have allowed the detection of smaller and earlier tumors, which has “rekindled interest in sublobar resection,” the authors comment.
Hence, they conducted the new trial, which involved almost 700 U.S. patients with clinical T1aN0 NSCLC and a tumor size up to 2 cm, who were randomly assigned to lobar or sublobar tumor resection, and followed for 7 years.
The rates of both disease-free and overall survival were similar between the two groups, with no significant differences observed. There were also no substantial differences in rates of distant and locoregional recurrence.
In addition, there was a suggestion of less reduction in pulmonary function following the less invasive procedure.
“These findings affirm that sublobar resection ... is an effective management approach for this subgroup of patients with NSCLC,” says lead author Nasser Altorki, MD, Weill Cornell Medicine, NewYork–Presbyterian Hospital, New York.
“It is important that these results are interpreted strictly within the constraints of the eligibility criteria mandated by the trial, he emphasizes. “Specifically, the results are applicable only to a highly selected group of patients ... in whom the absence of metastases to hilar and mediastinal lymph nodes is pathologically confirmed.”
Nevertheless, Dr. Altorki said that “these results will become increasingly relevant as the proportion of patients with early-stage lung cancer increases with expanded implementation of lung cancer screening, and as the number of older persons with early-stage disease in whom sublobar resection may be the preferred surgical option increases.”
The study was published online in the New England Journal of Medicine.
In an accompanying editorial, Valerie W. Rusch, MD, Thoracic Service, Memorial Sloan Kettering Cancer Center, New York, agrees. “As CT screening becomes more widespread, this patient population will increase in clinical practice,” she explains.
However, Dr. Rusch also urges caution around patient selection, underlining that the results do not “provide a license for suboptimal surgical care.”
She says that “safeguards” such as the meticulous and strict patient criteria used in the trial “must be preserved in routine practice.”
“Thoracic surgeons will need to expand their expertise in sublobar resections, especially complex segmentectomies, and will need to collaborate closely with pathologists in assessing margins of resection, adequacy of lymph-node staging, and tumor characteristics that may predict recurrence.”
While emphasizing that lobectomy should still be performed when appropriate, Dr. Rusch nevertheless says: “The era of ‘precision’ surgery for NSCLC has arrived.”
Consistent with Japanese results
The investigators also point out that their findings are “consistent” with those of a recent Japanese study that compared lobectomy with anatomical segmentectomy, which found that the 5-year overall survival was 91.1% for lobectomy and 94.3% for segmentectomy.
The authors suggest that the difference in overall survival rates between the two trials might be due to anatomical segmentectomy being “considered by most surgeons to be more oncologically sound than wedge resection.”
In the current trial, wedge resection was allowed, however, “because it is the most frequently practiced method of sublobar resection in North America and Europe; thus, its inclusion would make the trial more representative of a ‘real world’ setting.”
Another important difference could be that more than 90% of the patients in the Japanese trial had adenocarcinoma, 45% with an associated ground-glass component, which is associated with better survival than a completely solid adenocarcinoma.
Dr. Rusch agrees that there are likely to be various factors related to the survival differences between the two trials, including patient selection, intraoperative management, and tumor characteristics.
“However, these two landmark trials are practice-changing because they establish sublobar resection as the standard of care for a select group of patients with NSCLC,” Dr. Rusch concluded.
Study details
Dr. Altorki and colleagues conducted the multicenter, international, randomized, noninferiority, phase 3 trial in patients with clinically staged T1aN0 NSCLC from 83 academic and community-based institutions in the United States, Canada, and Australia.
Patients were required to have a peripheral lung nodule with a solid component of up to 2 cm on preoperative CT, a tumor center in the outer third of the lung, and a tumor location amenable to sublobar resection, whether wedge or segment, or lobar resection, among other criteria.
In all, 697 patients were randomly assigned to undergo either lobar resection or sublobar resection, of whom 59.1% had wedge resection and 37.9% anatomical segmental resection. The median age was 67.9 years, and 57.4% were female. The vast majority (90%) were White.
After a median follow-up of 7 years, the 5-year disease-free survival was 63.6% with sublobar resection and 64.1% following lobar resection.
The team found that sublobar resection was not inferior to lobectomy for disease-free survival, at a hazard ratio for disease recurrence or death of 1.01 (90% confidence interval, 0.83-1.24), which adjusted to 0.99 after taking into account the site where the patient was treated.
The 5-year overall survival rate was 80.3% after sublobar resection, and 78.9% following lobar resection, at a hazard ratio for death of 0.95 (95% CI, 0.72-1.26).
The results were “generally consistent” when accounting for factors such as age group, sex, tumor location, histologic type, smoking history, tumor size, and ECOG performance status, the team says.
Turning to recurrence, they showed that, among 687 patients eligible for assessment, 30.4% of those in the sublobar resection group and 29.3% of those assigned to lobar resection experienced disease recurrence, with 13.4% and 10%, respectively, having locoregional recurrence.
An exploratory analysis indicated that 5-year recurrence-free survival was similar in the two groups, at 70.2% vs. 71.2% or a hazard ratio for recurrence of 1.05 (95% CI, 0.80-1.39). The cumulative incidence of death was also similar.
It was also notable that reduction in predictive forced expiratory volume in 1 second from baseline was lower with sublobar than lobar resection, at –4.0 vs. –6.0, as was the reduction in predicted forced vital capacity, at –3.0 vs. –5.0.
“Although this difference is arguably not clinically meaningful in this patient population with normal baseline pulmonary functions,” the team writes, “it may be more clinically relevant in patients with compromised pulmonary functions, or in those with lower-lobe disease in whom lobar resection may be associated with greater impairment of pulmonary function.”
Dr. Rusch suggests that “more sensitive or functional assessments” of pulmonary function might include “diffusion capacity and 6-minute walk tests,” although she noted that even short-term differences in pulmonary function “may affect perioperative and functional outcomes, especially for tumors in the lower lobe.”
The study was supported by the National Cancer Institute of the National Institutes of Health, including via grants to the Alliance for Clinical Trials in Oncology and the Canadian Cancer Trials Group, and supported in part by Covidien and Ethicon.
Dr. Altorki reports relationships with AstraZeneca, Genentech, Johnson & Johnson, and Regeneron. Dr. Rusch reports relationships with Cancer Research UK, Genentech, and the National Cancer Institute.
A version of this article first appeared on Medscape.com.
suggest results from the CALGB 140503 trial, although strict patient selection remains key.
These new results contrast with those from a previous study from 1995, which found that local recurrence was three times higher and cancer mortality was twice as high with the less invasive procedure.
Those results from nearly 30 years ago established lobectomy as the standard of surgical care in this patient population, but since then advances in imaging and staging have allowed the detection of smaller and earlier tumors, which has “rekindled interest in sublobar resection,” the authors comment.
Hence, they conducted the new trial, which involved almost 700 U.S. patients with clinical T1aN0 NSCLC and a tumor size up to 2 cm, who were randomly assigned to lobar or sublobar tumor resection, and followed for 7 years.
The rates of both disease-free and overall survival were similar between the two groups, with no significant differences observed. There were also no substantial differences in rates of distant and locoregional recurrence.
In addition, there was a suggestion of less reduction in pulmonary function following the less invasive procedure.
“These findings affirm that sublobar resection ... is an effective management approach for this subgroup of patients with NSCLC,” says lead author Nasser Altorki, MD, Weill Cornell Medicine, NewYork–Presbyterian Hospital, New York.
“It is important that these results are interpreted strictly within the constraints of the eligibility criteria mandated by the trial, he emphasizes. “Specifically, the results are applicable only to a highly selected group of patients ... in whom the absence of metastases to hilar and mediastinal lymph nodes is pathologically confirmed.”
Nevertheless, Dr. Altorki said that “these results will become increasingly relevant as the proportion of patients with early-stage lung cancer increases with expanded implementation of lung cancer screening, and as the number of older persons with early-stage disease in whom sublobar resection may be the preferred surgical option increases.”
The study was published online in the New England Journal of Medicine.
In an accompanying editorial, Valerie W. Rusch, MD, Thoracic Service, Memorial Sloan Kettering Cancer Center, New York, agrees. “As CT screening becomes more widespread, this patient population will increase in clinical practice,” she explains.
However, Dr. Rusch also urges caution around patient selection, underlining that the results do not “provide a license for suboptimal surgical care.”
She says that “safeguards” such as the meticulous and strict patient criteria used in the trial “must be preserved in routine practice.”
“Thoracic surgeons will need to expand their expertise in sublobar resections, especially complex segmentectomies, and will need to collaborate closely with pathologists in assessing margins of resection, adequacy of lymph-node staging, and tumor characteristics that may predict recurrence.”
While emphasizing that lobectomy should still be performed when appropriate, Dr. Rusch nevertheless says: “The era of ‘precision’ surgery for NSCLC has arrived.”
Consistent with Japanese results
The investigators also point out that their findings are “consistent” with those of a recent Japanese study that compared lobectomy with anatomical segmentectomy, which found that the 5-year overall survival was 91.1% for lobectomy and 94.3% for segmentectomy.
The authors suggest that the difference in overall survival rates between the two trials might be due to anatomical segmentectomy being “considered by most surgeons to be more oncologically sound than wedge resection.”
In the current trial, wedge resection was allowed, however, “because it is the most frequently practiced method of sublobar resection in North America and Europe; thus, its inclusion would make the trial more representative of a ‘real world’ setting.”
Another important difference could be that more than 90% of the patients in the Japanese trial had adenocarcinoma, 45% with an associated ground-glass component, which is associated with better survival than a completely solid adenocarcinoma.
Dr. Rusch agrees that there are likely to be various factors related to the survival differences between the two trials, including patient selection, intraoperative management, and tumor characteristics.
“However, these two landmark trials are practice-changing because they establish sublobar resection as the standard of care for a select group of patients with NSCLC,” Dr. Rusch concluded.
Study details
Dr. Altorki and colleagues conducted the multicenter, international, randomized, noninferiority, phase 3 trial in patients with clinically staged T1aN0 NSCLC from 83 academic and community-based institutions in the United States, Canada, and Australia.
Patients were required to have a peripheral lung nodule with a solid component of up to 2 cm on preoperative CT, a tumor center in the outer third of the lung, and a tumor location amenable to sublobar resection, whether wedge or segment, or lobar resection, among other criteria.
In all, 697 patients were randomly assigned to undergo either lobar resection or sublobar resection, of whom 59.1% had wedge resection and 37.9% anatomical segmental resection. The median age was 67.9 years, and 57.4% were female. The vast majority (90%) were White.
After a median follow-up of 7 years, the 5-year disease-free survival was 63.6% with sublobar resection and 64.1% following lobar resection.
The team found that sublobar resection was not inferior to lobectomy for disease-free survival, at a hazard ratio for disease recurrence or death of 1.01 (90% confidence interval, 0.83-1.24), which adjusted to 0.99 after taking into account the site where the patient was treated.
The 5-year overall survival rate was 80.3% after sublobar resection, and 78.9% following lobar resection, at a hazard ratio for death of 0.95 (95% CI, 0.72-1.26).
The results were “generally consistent” when accounting for factors such as age group, sex, tumor location, histologic type, smoking history, tumor size, and ECOG performance status, the team says.
Turning to recurrence, they showed that, among 687 patients eligible for assessment, 30.4% of those in the sublobar resection group and 29.3% of those assigned to lobar resection experienced disease recurrence, with 13.4% and 10%, respectively, having locoregional recurrence.
An exploratory analysis indicated that 5-year recurrence-free survival was similar in the two groups, at 70.2% vs. 71.2% or a hazard ratio for recurrence of 1.05 (95% CI, 0.80-1.39). The cumulative incidence of death was also similar.
It was also notable that reduction in predictive forced expiratory volume in 1 second from baseline was lower with sublobar than lobar resection, at –4.0 vs. –6.0, as was the reduction in predicted forced vital capacity, at –3.0 vs. –5.0.
“Although this difference is arguably not clinically meaningful in this patient population with normal baseline pulmonary functions,” the team writes, “it may be more clinically relevant in patients with compromised pulmonary functions, or in those with lower-lobe disease in whom lobar resection may be associated with greater impairment of pulmonary function.”
Dr. Rusch suggests that “more sensitive or functional assessments” of pulmonary function might include “diffusion capacity and 6-minute walk tests,” although she noted that even short-term differences in pulmonary function “may affect perioperative and functional outcomes, especially for tumors in the lower lobe.”
The study was supported by the National Cancer Institute of the National Institutes of Health, including via grants to the Alliance for Clinical Trials in Oncology and the Canadian Cancer Trials Group, and supported in part by Covidien and Ethicon.
Dr. Altorki reports relationships with AstraZeneca, Genentech, Johnson & Johnson, and Regeneron. Dr. Rusch reports relationships with Cancer Research UK, Genentech, and the National Cancer Institute.
A version of this article first appeared on Medscape.com.
suggest results from the CALGB 140503 trial, although strict patient selection remains key.
These new results contrast with those from a previous study from 1995, which found that local recurrence was three times higher and cancer mortality was twice as high with the less invasive procedure.
Those results from nearly 30 years ago established lobectomy as the standard of surgical care in this patient population, but since then advances in imaging and staging have allowed the detection of smaller and earlier tumors, which has “rekindled interest in sublobar resection,” the authors comment.
Hence, they conducted the new trial, which involved almost 700 U.S. patients with clinical T1aN0 NSCLC and a tumor size up to 2 cm, who were randomly assigned to lobar or sublobar tumor resection, and followed for 7 years.
The rates of both disease-free and overall survival were similar between the two groups, with no significant differences observed. There were also no substantial differences in rates of distant and locoregional recurrence.
In addition, there was a suggestion of less reduction in pulmonary function following the less invasive procedure.
“These findings affirm that sublobar resection ... is an effective management approach for this subgroup of patients with NSCLC,” says lead author Nasser Altorki, MD, Weill Cornell Medicine, NewYork–Presbyterian Hospital, New York.
“It is important that these results are interpreted strictly within the constraints of the eligibility criteria mandated by the trial, he emphasizes. “Specifically, the results are applicable only to a highly selected group of patients ... in whom the absence of metastases to hilar and mediastinal lymph nodes is pathologically confirmed.”
Nevertheless, Dr. Altorki said that “these results will become increasingly relevant as the proportion of patients with early-stage lung cancer increases with expanded implementation of lung cancer screening, and as the number of older persons with early-stage disease in whom sublobar resection may be the preferred surgical option increases.”
The study was published online in the New England Journal of Medicine.
In an accompanying editorial, Valerie W. Rusch, MD, Thoracic Service, Memorial Sloan Kettering Cancer Center, New York, agrees. “As CT screening becomes more widespread, this patient population will increase in clinical practice,” she explains.
However, Dr. Rusch also urges caution around patient selection, underlining that the results do not “provide a license for suboptimal surgical care.”
She says that “safeguards” such as the meticulous and strict patient criteria used in the trial “must be preserved in routine practice.”
“Thoracic surgeons will need to expand their expertise in sublobar resections, especially complex segmentectomies, and will need to collaborate closely with pathologists in assessing margins of resection, adequacy of lymph-node staging, and tumor characteristics that may predict recurrence.”
While emphasizing that lobectomy should still be performed when appropriate, Dr. Rusch nevertheless says: “The era of ‘precision’ surgery for NSCLC has arrived.”
Consistent with Japanese results
The investigators also point out that their findings are “consistent” with those of a recent Japanese study that compared lobectomy with anatomical segmentectomy, which found that the 5-year overall survival was 91.1% for lobectomy and 94.3% for segmentectomy.
The authors suggest that the difference in overall survival rates between the two trials might be due to anatomical segmentectomy being “considered by most surgeons to be more oncologically sound than wedge resection.”
In the current trial, wedge resection was allowed, however, “because it is the most frequently practiced method of sublobar resection in North America and Europe; thus, its inclusion would make the trial more representative of a ‘real world’ setting.”
Another important difference could be that more than 90% of the patients in the Japanese trial had adenocarcinoma, 45% with an associated ground-glass component, which is associated with better survival than a completely solid adenocarcinoma.
Dr. Rusch agrees that there are likely to be various factors related to the survival differences between the two trials, including patient selection, intraoperative management, and tumor characteristics.
“However, these two landmark trials are practice-changing because they establish sublobar resection as the standard of care for a select group of patients with NSCLC,” Dr. Rusch concluded.
Study details
Dr. Altorki and colleagues conducted the multicenter, international, randomized, noninferiority, phase 3 trial in patients with clinically staged T1aN0 NSCLC from 83 academic and community-based institutions in the United States, Canada, and Australia.
Patients were required to have a peripheral lung nodule with a solid component of up to 2 cm on preoperative CT, a tumor center in the outer third of the lung, and a tumor location amenable to sublobar resection, whether wedge or segment, or lobar resection, among other criteria.
In all, 697 patients were randomly assigned to undergo either lobar resection or sublobar resection, of whom 59.1% had wedge resection and 37.9% anatomical segmental resection. The median age was 67.9 years, and 57.4% were female. The vast majority (90%) were White.
After a median follow-up of 7 years, the 5-year disease-free survival was 63.6% with sublobar resection and 64.1% following lobar resection.
The team found that sublobar resection was not inferior to lobectomy for disease-free survival, at a hazard ratio for disease recurrence or death of 1.01 (90% confidence interval, 0.83-1.24), which adjusted to 0.99 after taking into account the site where the patient was treated.
The 5-year overall survival rate was 80.3% after sublobar resection, and 78.9% following lobar resection, at a hazard ratio for death of 0.95 (95% CI, 0.72-1.26).
The results were “generally consistent” when accounting for factors such as age group, sex, tumor location, histologic type, smoking history, tumor size, and ECOG performance status, the team says.
Turning to recurrence, they showed that, among 687 patients eligible for assessment, 30.4% of those in the sublobar resection group and 29.3% of those assigned to lobar resection experienced disease recurrence, with 13.4% and 10%, respectively, having locoregional recurrence.
An exploratory analysis indicated that 5-year recurrence-free survival was similar in the two groups, at 70.2% vs. 71.2% or a hazard ratio for recurrence of 1.05 (95% CI, 0.80-1.39). The cumulative incidence of death was also similar.
It was also notable that reduction in predictive forced expiratory volume in 1 second from baseline was lower with sublobar than lobar resection, at –4.0 vs. –6.0, as was the reduction in predicted forced vital capacity, at –3.0 vs. –5.0.
“Although this difference is arguably not clinically meaningful in this patient population with normal baseline pulmonary functions,” the team writes, “it may be more clinically relevant in patients with compromised pulmonary functions, or in those with lower-lobe disease in whom lobar resection may be associated with greater impairment of pulmonary function.”
Dr. Rusch suggests that “more sensitive or functional assessments” of pulmonary function might include “diffusion capacity and 6-minute walk tests,” although she noted that even short-term differences in pulmonary function “may affect perioperative and functional outcomes, especially for tumors in the lower lobe.”
The study was supported by the National Cancer Institute of the National Institutes of Health, including via grants to the Alliance for Clinical Trials in Oncology and the Canadian Cancer Trials Group, and supported in part by Covidien and Ethicon.
Dr. Altorki reports relationships with AstraZeneca, Genentech, Johnson & Johnson, and Regeneron. Dr. Rusch reports relationships with Cancer Research UK, Genentech, and the National Cancer Institute.
A version of this article first appeared on Medscape.com.
FROM NEW ENGLAND JOURNAL OF MEDICINE