User login
Meeting the Needs of Those Who Have Served: The Role of VHA Specialized Mental Health Centers of Excellence
Meeting the Needs of Those Who Have Served: The Role of VHA Specialized Mental Health Centers of Excellence
Accessible and effective mental health services are a vital component of the Veterans Health Administration (VHA) mission to provide exceptional care that improves veterans’ health and well-being. Veterans are seeking mental health care at the VHA at significantly higher rates than in previous years. From 2009 through 2024, the number of veterans who received direct mental health care from the VHA increased 78%.1 The proportion of veterans enrolled in the VHA who also received direct mental health care expanded from 23% of total enrollees in 2009 to 33% in 2024. The increase in VHA mental health care delivery is also reflected in the number of outpatient mental health care and treatment visits at the VHA, which increased from 12.7 million to 21.5 million over the same period.
The Sergeant First Class (SFC) Heath Robinson Honoring Our Promise to Address Comprehensive Toxics (PACT) Act of 2022 expanded eligibility for VHA services, including mental health care and counseling, to new cohorts of toxic-exposed veterans. From 2022 to 2024, > 680,000 veterans enrolled in VHA care, and 45% of those were PACT Act-eligible cohorts.2 Research highlighted the high prevalence of physical and psychiatric comorbidities in toxic-exposed veterans.3 As such, the VHA may face greater demand for direct mental health care with these newly eligible cohorts of veterans.
Veterans often have mental health conditions (eg, depression, posttraumatic stress disorder [PTSD]), substance use disorders (SUDs), unique military experiences (eg, deployments), and injuries and illnesses (eg, traumatic brain injury [TBI]) that increase the complexity of their clinical presentation. The varied nature of these mental health conditions, as well as veterans’ unique military-related experiences, necessitates specialized centers focused on distinct high-priority areas of mental health in the VHA.
A series of public laws charged the US Department of Veterans Affairs (VA) with developing specialized mental health Centers of Excellence (CoEs) focused on high-priority areas of veteran mental health. The first of these laws, Public Law 98- 528, established the National Center for PTSD (NCPTSD), which opened in 1989.4 In 1996, Congress established specialized mental health CoEs known as Mental Illness Research, Education, and Clinical Centers (MIRECCs) across the VHA.5 To address the unique needs of post-9/11 veterans, 3 additional specialized centers were established in 2005.6 Finally, under the authority of the Secretary of the VA, specialized mental health CoEs were established to focus on SUD and integrated health care.
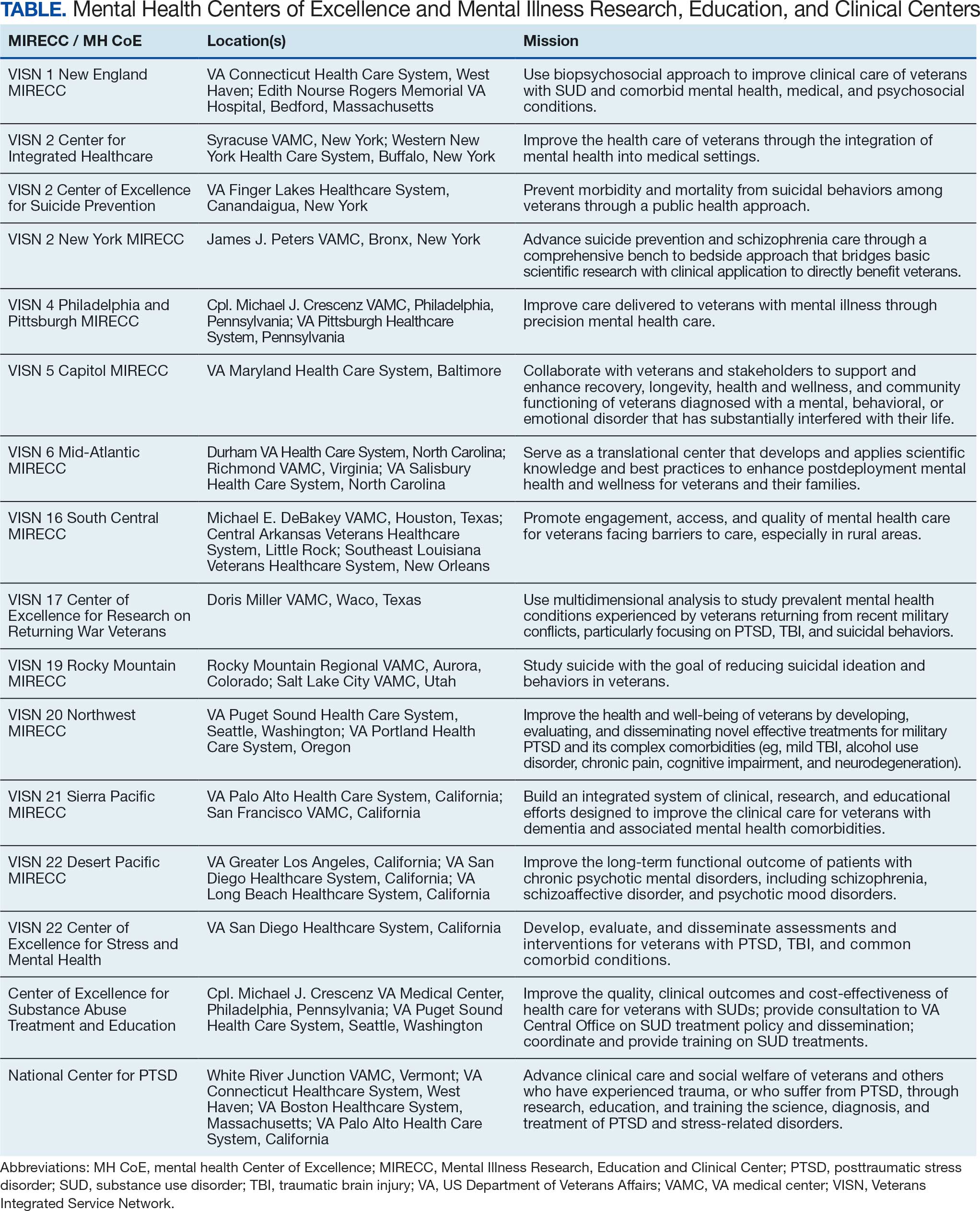
There are 17 geographically diverse mental health CoEs and MIRECCs across the VA (Table). CoEs are embedded in VA medical centers (VAMCs) with strong medical school academic affiliations. Organizational oversight of the CoEs is provided by the VA Office of Mental Health and Office of Suicide Prevention, respectively. As part of the oversight process, CoEs submit annual reports detailing their advancements in research, education and training, and clinical activities, as well as participate in a peer-reviewed renewal process.
These specialized centers are united in a shared tripartite mission to generate new knowledge about the causes and treatments of mental health conditions, to educate and train VHA clinicians and personnel, and to develop and implement innovative clinical programs within the VHA. This combined focus on research, education, and improved clinical care reduces the time from discovery to implementation and improves the health and well-being of veterans.
Examples of this acceleration translation from scientific discovery to clinical practice are evident throughout mental health CoEs. The NCPTSD is a leader in research on PTSD and traumatic stress. Its work led to the development of national training programs for VHA clinicians, facilitating the broad dissemination of efficacious PTSD treatments across the enterprise.7 Researchers at the Veterans Integrated Service Network (VISN) 21 Sierra Pacific MIRECC identified depression as a significant risk factor for dementia and subsequently launched the first multisite trial of repetitive transcranial magnetic stimulation (rTMS) in the VHA in 2012 (CSP #556: the effectiveness of rTMS in depressed VA patients).8 This project laid the groundwork for the national clinical rTMS program launched in 2017, which is now clinically available at 60 VAMCs. In the largest pragmatic randomized clinical trial of its kind, the VISN 4 Philadelphia and Pittsburgh MIRECC found that pharmacogenomic testing significantly reduced the number of prescription medications with predicted drug-gene interactions and improved clinical outcomes among veterans with depression.9
Mental health CoEs are also leaders in suicide prevention, a top clinical priority for the VHA. The VISN 2 New York MIRECC developed Project Life Force, a safety planning skills group for veterans with suicidal ideation, now implemented across 10 VAMCs, including telehealth hubs, outpatient settings, and veteran peer programs.10 The VISN 2 CoE for Suicide Prevention and VISN 19 Rocky Mountain MIRECC coordinate key suicide prevention services for VA, including the analysis of suicide surveillance data; evaluation of national VA suicide prevention initiatives; the support of veterans, families, and clinicians; and enhanced access to evidence-based treatments for at-risk veterans.
Mental health CoEs are a key operational partner in VHA treatment of SUDs. The CoEs in Substance Addiction Treatment and Education (CESATEs) are national resources dedicated to improving the quality, clinical outcomes, and cost-effectiveness of VHA SUD treatment. CESATEs developed and implemented a national rollout of an effective treatment for stimulant use disorders, training staff at > 120 VA programs. The VISN 1 Mid-Atlantic MIRECC’s focus on SUD and comorbid/co-occurring mental health conditions has highlighted the significant prevalence of these conditions and the impact they have on treatment response.11
Serious mental illness (SMI) (eg, schizophrenia, schizoaffective disorder) impacts up to 5% of veterans.12 VISN 22 Desert Pacific MIRECC has developed interventions to improve the lives of veterans with SMI. Its research established supported employment as an effective intervention to improve outcomes in veterans with psychotic disorders and supported its implementation in the VHA.13 Peer specialists are a cornerstone in the VHA commitment to recovery-oriented services for veterans with SMI. VISN 5 Capitol MIRECC has long championed research, clinical training, and educational activities that contributed to the effective deployment of peer specialists across the VHA enterprise.
Veterans have unique military-related experiences (eg, deployment, traumatic stress, transition to civilian status) and injuries and illnesses (eg, TBI, posttraumatic headaches) that significantly impact their mental health and quality of life.
The period between active duty and transition to civilian status is a critical time in a veteran’s life. The VISN 17 CoE Veteran Sponsorship Initiative connects veterans with VA care within 30 days postdischarge, with the option of additional support in the community. The VISN 22 CoE for Stress and Mental Health (CESAMH) develops, evaluates, and disseminates diagnostics and treatments for veterans affected by traumatic events and brain injuries, with a unique focus on supporting their whole health needs. The VISN 6 Mid-Atlantic MIRECC leads the ongoing VISN-6 Post-Deployment Mental Health (PDMH) study, the largest biorepository of post-9/11 veterans. PDMH has greatly expanded the understanding of the unique needs of post-9/11 veterans, with > 100 peer-reviewed publications to date. Veterans with mild TBI frequently experience chronic posttraumatic headaches that can be disabling and nonresponsive to treatment. The VISN 20 Northwest MIRECC demonstrated that prazosin, a repurposed, low-cost, widely available, nonaddictive medication, can safely and effectively reduce the frequency of these headaches and improve functional impairment in veterans and active-duty service members.14
Increased and enhanced access to effective mental health treatment is a priority for VA. In 2007, the VA launched the National Primary Care Mental Health Integration program, which integrated mental health services into primary care settings. The Center for Integrated Healthcare (CIH) has supported the VA in these efforts. In 2024, CIH trained > 5000 health care staff on high-fidelity integration of behavioral health and medical care. VA has also focused on increasing access to mental health services via expanded telehealth offerings. The VISN 16 MIRECC, with its unique focus on increasing access to care for rural veterans via distance-based and digital health technology, supported the VA Offices of Mental Health and Connected Care to virtualize mental health care and promote adoption and sustained use of VA Video Connect across the enterprise.
Specialized MH CoEs are uniquely equipped to support the VHA in providing training and education to VA clinicians, veterans, care partners and family members, and the community on high-priority mental health topics. Education is a core component of the MH CoEs tripartite mission. As such, MH CoEs offer national trainings, conferences, consultation services, clinical demonstration projects, development of clinical dashboards and toolkits, and public awareness campaigns. Researchers, educators, and clinicians at the CoEs frequently serve as subject matter experts on topics aligned with their respective missions. Several national rollout programs that disseminated evidence-based treatments for mental health conditions to the field (eg, cognitive behavioral therapy for depression, cognitive behavioral therapy for insomnia, and prolonged exposure) were developed at specialized CoEs.
The VHA provides advanced training, residencies, and fellowships to > 120,000 trainees annually. Many of these trainees choose to remain at the VA. Seven of 10 VHA psychologists and 6 of 10 VHA physicians trained within the VHA prior to their employment.15 The MH CoEs and MIRECCs play an important role in preparing these trainees for VHA mental health careers. These centers are funded to provide advanced postdoctoral training to physicians as well as allied health professionals in clinical and counseling psychology, social work, pharmacy, and nursing. Training is not limited to postdoctoral fellows: graduate students, residents, and interns from affiliated accredited training programs may rotate through mental health CoEs each academic year.
Conclusions
For > 30 years, mental health CoEs have brought thousands of veterans advanced treatments for their mental health needs and helped reduce death by suicide. The centers have a bright future ahead, harnessing advances in artificial intelligence and genomics to permit the matching of the individual veterans to the treatment most likely to benefit them. Precision medicine, as espoused by the Hannon Act, will not only encourage the efficient use of health care resources but also rapidly reduce pain in veterans with mental health and SUDs.
- Congressionally Mandated Report: Report on Transparency in Mental Health Care Services. US Dept of Veterans Affairs; December 2022. Accessed December 5, 2025. https://www.govinfo.gov/content/pkg/CMR-VA1-00181657/pdf/CMR-VA1-00181657.pdf
- Beckman AL, Jacobs J, Elnahal SM. The PACT Act—expanding coverage and access for veterans. JAMA. 2024;332:1423-1424. doi:10.1001/jama.2024.16013
- Morse JL, Acheson DT, Almklov E, et al. Associations among environmental exposures and physical and psychiatric symptoms in a care-seeking sample of U.S. military veterans. Mil Med. 2024;189:e1397-e1402. doi:10.1093/milmed/usae035
- Veterans’ Health Care Act of 1984, 38 USC §98-528 (1984). Accessed March 27, 2026. https://www.congress.gov/bill/98th-congress/house-bill/5618/text
- Veterans’ Health Care Eligibility Reform Act of 1996, 38 USC §104-262 (1996). Accessed March 27, 2026. https://www.congress.gov/bill/104th-congress/house-bill/3118/text
- Military Quality of Life and Veterans Affairs Appropriations Act, 2006. Pub L No. 109-114, 119 Stat. 2372. Accessed March 27, 2026. https://www.congress.gov/bill/109th-congress/house-bill/2528/text
- Karlin BE, Ruzek JI, Chard KM, et al. Dissemination of evidence‐based psychological treatments for posttraumatic stress disorder in the Veterans Health Administration. J Trauma Stress. 2010;23:663-673. doi:10.1002/jts.20588
- Byers AL, Covinsky KE, Barnes DE, et al. Dysthymia and depression increase risk of dementia and mortality among older veterans. Am J Geriatr Psychiatry. 2012;20:664-672. doi:10.1097/JGP.0b013e31822001c1
- Oslin DW, Lynch KG, Shih MC, et al. Effect of pharmacogenomic testing for drug-gene interactions on medication selection and remission of symptoms in major depressive disorder: the PRIME Care randomized clinical trial. JAMA. 2022;328:151-161. doi:10.1001/jama.2022.9805
- Goodman M, Brown GK, Galfalvy HC, et al. Group (“Project Life Force”) versus individual suicide safety planning: a randomized clinical trial. Contemp Clin Trials Commun. 2020;17:100520. doi:10.1016/j.conctc.2020.100520
- Na PJ, Ralevski E, Jegede O, et al. Depression and/or PTSD comorbidity affects response to antidepressants in those with alcohol use disorder. Front Psychiatry. 2022;12:768318. doi:10.3389/fpsyt.2021.768318
- McCarthy JF, Blow FC, Valenstein M, et al. Veterans Affairs Health System and mental health treatment retention among patients with serious mental illness: evaluating accessibility and availability barriers. Health Serv Res. 2007;42:1042-1060. doi:10.1111/j.1475-6773.2006.00642.x
- Glynn SM, Marder SR, Noordsy DL, et al. An RCT evaluating the effects of skills training and medication type on work outcomes among patients with schizophrenia. Psychiatr Serv. 2016;67:500-506. doi:10.1176/appips201500171
- Mayer CL, Savage PJ, Engle CK, et al. Randomized controlled pilot trial of prazosin for prophylaxis of posttraumatic headaches in active-duty service members and veterans. Headache. 2023;63:751-762. doi:10.1111/head.14529
- Hill C. Medical education at VA: it’s all about the veterans. VA News. August 18, 2021. Accessed December 5, 2025. https://news.va.gov/93370/medical-education-at-va-its-all-about-the-veterans/
Accessible and effective mental health services are a vital component of the Veterans Health Administration (VHA) mission to provide exceptional care that improves veterans’ health and well-being. Veterans are seeking mental health care at the VHA at significantly higher rates than in previous years. From 2009 through 2024, the number of veterans who received direct mental health care from the VHA increased 78%.1 The proportion of veterans enrolled in the VHA who also received direct mental health care expanded from 23% of total enrollees in 2009 to 33% in 2024. The increase in VHA mental health care delivery is also reflected in the number of outpatient mental health care and treatment visits at the VHA, which increased from 12.7 million to 21.5 million over the same period.
The Sergeant First Class (SFC) Heath Robinson Honoring Our Promise to Address Comprehensive Toxics (PACT) Act of 2022 expanded eligibility for VHA services, including mental health care and counseling, to new cohorts of toxic-exposed veterans. From 2022 to 2024, > 680,000 veterans enrolled in VHA care, and 45% of those were PACT Act-eligible cohorts.2 Research highlighted the high prevalence of physical and psychiatric comorbidities in toxic-exposed veterans.3 As such, the VHA may face greater demand for direct mental health care with these newly eligible cohorts of veterans.
Veterans often have mental health conditions (eg, depression, posttraumatic stress disorder [PTSD]), substance use disorders (SUDs), unique military experiences (eg, deployments), and injuries and illnesses (eg, traumatic brain injury [TBI]) that increase the complexity of their clinical presentation. The varied nature of these mental health conditions, as well as veterans’ unique military-related experiences, necessitates specialized centers focused on distinct high-priority areas of mental health in the VHA.
A series of public laws charged the US Department of Veterans Affairs (VA) with developing specialized mental health Centers of Excellence (CoEs) focused on high-priority areas of veteran mental health. The first of these laws, Public Law 98- 528, established the National Center for PTSD (NCPTSD), which opened in 1989.4 In 1996, Congress established specialized mental health CoEs known as Mental Illness Research, Education, and Clinical Centers (MIRECCs) across the VHA.5 To address the unique needs of post-9/11 veterans, 3 additional specialized centers were established in 2005.6 Finally, under the authority of the Secretary of the VA, specialized mental health CoEs were established to focus on SUD and integrated health care.
There are 17 geographically diverse mental health CoEs and MIRECCs across the VA (Table). CoEs are embedded in VA medical centers (VAMCs) with strong medical school academic affiliations. Organizational oversight of the CoEs is provided by the VA Office of Mental Health and Office of Suicide Prevention, respectively. As part of the oversight process, CoEs submit annual reports detailing their advancements in research, education and training, and clinical activities, as well as participate in a peer-reviewed renewal process.
These specialized centers are united in a shared tripartite mission to generate new knowledge about the causes and treatments of mental health conditions, to educate and train VHA clinicians and personnel, and to develop and implement innovative clinical programs within the VHA. This combined focus on research, education, and improved clinical care reduces the time from discovery to implementation and improves the health and well-being of veterans.
Examples of this acceleration translation from scientific discovery to clinical practice are evident throughout mental health CoEs. The NCPTSD is a leader in research on PTSD and traumatic stress. Its work led to the development of national training programs for VHA clinicians, facilitating the broad dissemination of efficacious PTSD treatments across the enterprise.7 Researchers at the Veterans Integrated Service Network (VISN) 21 Sierra Pacific MIRECC identified depression as a significant risk factor for dementia and subsequently launched the first multisite trial of repetitive transcranial magnetic stimulation (rTMS) in the VHA in 2012 (CSP #556: the effectiveness of rTMS in depressed VA patients).8 This project laid the groundwork for the national clinical rTMS program launched in 2017, which is now clinically available at 60 VAMCs. In the largest pragmatic randomized clinical trial of its kind, the VISN 4 Philadelphia and Pittsburgh MIRECC found that pharmacogenomic testing significantly reduced the number of prescription medications with predicted drug-gene interactions and improved clinical outcomes among veterans with depression.9
Mental health CoEs are also leaders in suicide prevention, a top clinical priority for the VHA. The VISN 2 New York MIRECC developed Project Life Force, a safety planning skills group for veterans with suicidal ideation, now implemented across 10 VAMCs, including telehealth hubs, outpatient settings, and veteran peer programs.10 The VISN 2 CoE for Suicide Prevention and VISN 19 Rocky Mountain MIRECC coordinate key suicide prevention services for VA, including the analysis of suicide surveillance data; evaluation of national VA suicide prevention initiatives; the support of veterans, families, and clinicians; and enhanced access to evidence-based treatments for at-risk veterans.
Mental health CoEs are a key operational partner in VHA treatment of SUDs. The CoEs in Substance Addiction Treatment and Education (CESATEs) are national resources dedicated to improving the quality, clinical outcomes, and cost-effectiveness of VHA SUD treatment. CESATEs developed and implemented a national rollout of an effective treatment for stimulant use disorders, training staff at > 120 VA programs. The VISN 1 Mid-Atlantic MIRECC’s focus on SUD and comorbid/co-occurring mental health conditions has highlighted the significant prevalence of these conditions and the impact they have on treatment response.11
Serious mental illness (SMI) (eg, schizophrenia, schizoaffective disorder) impacts up to 5% of veterans.12 VISN 22 Desert Pacific MIRECC has developed interventions to improve the lives of veterans with SMI. Its research established supported employment as an effective intervention to improve outcomes in veterans with psychotic disorders and supported its implementation in the VHA.13 Peer specialists are a cornerstone in the VHA commitment to recovery-oriented services for veterans with SMI. VISN 5 Capitol MIRECC has long championed research, clinical training, and educational activities that contributed to the effective deployment of peer specialists across the VHA enterprise.
Veterans have unique military-related experiences (eg, deployment, traumatic stress, transition to civilian status) and injuries and illnesses (eg, TBI, posttraumatic headaches) that significantly impact their mental health and quality of life.
The period between active duty and transition to civilian status is a critical time in a veteran’s life. The VISN 17 CoE Veteran Sponsorship Initiative connects veterans with VA care within 30 days postdischarge, with the option of additional support in the community. The VISN 22 CoE for Stress and Mental Health (CESAMH) develops, evaluates, and disseminates diagnostics and treatments for veterans affected by traumatic events and brain injuries, with a unique focus on supporting their whole health needs. The VISN 6 Mid-Atlantic MIRECC leads the ongoing VISN-6 Post-Deployment Mental Health (PDMH) study, the largest biorepository of post-9/11 veterans. PDMH has greatly expanded the understanding of the unique needs of post-9/11 veterans, with > 100 peer-reviewed publications to date. Veterans with mild TBI frequently experience chronic posttraumatic headaches that can be disabling and nonresponsive to treatment. The VISN 20 Northwest MIRECC demonstrated that prazosin, a repurposed, low-cost, widely available, nonaddictive medication, can safely and effectively reduce the frequency of these headaches and improve functional impairment in veterans and active-duty service members.14
Increased and enhanced access to effective mental health treatment is a priority for VA. In 2007, the VA launched the National Primary Care Mental Health Integration program, which integrated mental health services into primary care settings. The Center for Integrated Healthcare (CIH) has supported the VA in these efforts. In 2024, CIH trained > 5000 health care staff on high-fidelity integration of behavioral health and medical care. VA has also focused on increasing access to mental health services via expanded telehealth offerings. The VISN 16 MIRECC, with its unique focus on increasing access to care for rural veterans via distance-based and digital health technology, supported the VA Offices of Mental Health and Connected Care to virtualize mental health care and promote adoption and sustained use of VA Video Connect across the enterprise.
Specialized MH CoEs are uniquely equipped to support the VHA in providing training and education to VA clinicians, veterans, care partners and family members, and the community on high-priority mental health topics. Education is a core component of the MH CoEs tripartite mission. As such, MH CoEs offer national trainings, conferences, consultation services, clinical demonstration projects, development of clinical dashboards and toolkits, and public awareness campaigns. Researchers, educators, and clinicians at the CoEs frequently serve as subject matter experts on topics aligned with their respective missions. Several national rollout programs that disseminated evidence-based treatments for mental health conditions to the field (eg, cognitive behavioral therapy for depression, cognitive behavioral therapy for insomnia, and prolonged exposure) were developed at specialized CoEs.
The VHA provides advanced training, residencies, and fellowships to > 120,000 trainees annually. Many of these trainees choose to remain at the VA. Seven of 10 VHA psychologists and 6 of 10 VHA physicians trained within the VHA prior to their employment.15 The MH CoEs and MIRECCs play an important role in preparing these trainees for VHA mental health careers. These centers are funded to provide advanced postdoctoral training to physicians as well as allied health professionals in clinical and counseling psychology, social work, pharmacy, and nursing. Training is not limited to postdoctoral fellows: graduate students, residents, and interns from affiliated accredited training programs may rotate through mental health CoEs each academic year.
Conclusions
For > 30 years, mental health CoEs have brought thousands of veterans advanced treatments for their mental health needs and helped reduce death by suicide. The centers have a bright future ahead, harnessing advances in artificial intelligence and genomics to permit the matching of the individual veterans to the treatment most likely to benefit them. Precision medicine, as espoused by the Hannon Act, will not only encourage the efficient use of health care resources but also rapidly reduce pain in veterans with mental health and SUDs.
Accessible and effective mental health services are a vital component of the Veterans Health Administration (VHA) mission to provide exceptional care that improves veterans’ health and well-being. Veterans are seeking mental health care at the VHA at significantly higher rates than in previous years. From 2009 through 2024, the number of veterans who received direct mental health care from the VHA increased 78%.1 The proportion of veterans enrolled in the VHA who also received direct mental health care expanded from 23% of total enrollees in 2009 to 33% in 2024. The increase in VHA mental health care delivery is also reflected in the number of outpatient mental health care and treatment visits at the VHA, which increased from 12.7 million to 21.5 million over the same period.
The Sergeant First Class (SFC) Heath Robinson Honoring Our Promise to Address Comprehensive Toxics (PACT) Act of 2022 expanded eligibility for VHA services, including mental health care and counseling, to new cohorts of toxic-exposed veterans. From 2022 to 2024, > 680,000 veterans enrolled in VHA care, and 45% of those were PACT Act-eligible cohorts.2 Research highlighted the high prevalence of physical and psychiatric comorbidities in toxic-exposed veterans.3 As such, the VHA may face greater demand for direct mental health care with these newly eligible cohorts of veterans.
Veterans often have mental health conditions (eg, depression, posttraumatic stress disorder [PTSD]), substance use disorders (SUDs), unique military experiences (eg, deployments), and injuries and illnesses (eg, traumatic brain injury [TBI]) that increase the complexity of their clinical presentation. The varied nature of these mental health conditions, as well as veterans’ unique military-related experiences, necessitates specialized centers focused on distinct high-priority areas of mental health in the VHA.
A series of public laws charged the US Department of Veterans Affairs (VA) with developing specialized mental health Centers of Excellence (CoEs) focused on high-priority areas of veteran mental health. The first of these laws, Public Law 98- 528, established the National Center for PTSD (NCPTSD), which opened in 1989.4 In 1996, Congress established specialized mental health CoEs known as Mental Illness Research, Education, and Clinical Centers (MIRECCs) across the VHA.5 To address the unique needs of post-9/11 veterans, 3 additional specialized centers were established in 2005.6 Finally, under the authority of the Secretary of the VA, specialized mental health CoEs were established to focus on SUD and integrated health care.
There are 17 geographically diverse mental health CoEs and MIRECCs across the VA (Table). CoEs are embedded in VA medical centers (VAMCs) with strong medical school academic affiliations. Organizational oversight of the CoEs is provided by the VA Office of Mental Health and Office of Suicide Prevention, respectively. As part of the oversight process, CoEs submit annual reports detailing their advancements in research, education and training, and clinical activities, as well as participate in a peer-reviewed renewal process.
These specialized centers are united in a shared tripartite mission to generate new knowledge about the causes and treatments of mental health conditions, to educate and train VHA clinicians and personnel, and to develop and implement innovative clinical programs within the VHA. This combined focus on research, education, and improved clinical care reduces the time from discovery to implementation and improves the health and well-being of veterans.
Examples of this acceleration translation from scientific discovery to clinical practice are evident throughout mental health CoEs. The NCPTSD is a leader in research on PTSD and traumatic stress. Its work led to the development of national training programs for VHA clinicians, facilitating the broad dissemination of efficacious PTSD treatments across the enterprise.7 Researchers at the Veterans Integrated Service Network (VISN) 21 Sierra Pacific MIRECC identified depression as a significant risk factor for dementia and subsequently launched the first multisite trial of repetitive transcranial magnetic stimulation (rTMS) in the VHA in 2012 (CSP #556: the effectiveness of rTMS in depressed VA patients).8 This project laid the groundwork for the national clinical rTMS program launched in 2017, which is now clinically available at 60 VAMCs. In the largest pragmatic randomized clinical trial of its kind, the VISN 4 Philadelphia and Pittsburgh MIRECC found that pharmacogenomic testing significantly reduced the number of prescription medications with predicted drug-gene interactions and improved clinical outcomes among veterans with depression.9
Mental health CoEs are also leaders in suicide prevention, a top clinical priority for the VHA. The VISN 2 New York MIRECC developed Project Life Force, a safety planning skills group for veterans with suicidal ideation, now implemented across 10 VAMCs, including telehealth hubs, outpatient settings, and veteran peer programs.10 The VISN 2 CoE for Suicide Prevention and VISN 19 Rocky Mountain MIRECC coordinate key suicide prevention services for VA, including the analysis of suicide surveillance data; evaluation of national VA suicide prevention initiatives; the support of veterans, families, and clinicians; and enhanced access to evidence-based treatments for at-risk veterans.
Mental health CoEs are a key operational partner in VHA treatment of SUDs. The CoEs in Substance Addiction Treatment and Education (CESATEs) are national resources dedicated to improving the quality, clinical outcomes, and cost-effectiveness of VHA SUD treatment. CESATEs developed and implemented a national rollout of an effective treatment for stimulant use disorders, training staff at > 120 VA programs. The VISN 1 Mid-Atlantic MIRECC’s focus on SUD and comorbid/co-occurring mental health conditions has highlighted the significant prevalence of these conditions and the impact they have on treatment response.11
Serious mental illness (SMI) (eg, schizophrenia, schizoaffective disorder) impacts up to 5% of veterans.12 VISN 22 Desert Pacific MIRECC has developed interventions to improve the lives of veterans with SMI. Its research established supported employment as an effective intervention to improve outcomes in veterans with psychotic disorders and supported its implementation in the VHA.13 Peer specialists are a cornerstone in the VHA commitment to recovery-oriented services for veterans with SMI. VISN 5 Capitol MIRECC has long championed research, clinical training, and educational activities that contributed to the effective deployment of peer specialists across the VHA enterprise.
Veterans have unique military-related experiences (eg, deployment, traumatic stress, transition to civilian status) and injuries and illnesses (eg, TBI, posttraumatic headaches) that significantly impact their mental health and quality of life.
The period between active duty and transition to civilian status is a critical time in a veteran’s life. The VISN 17 CoE Veteran Sponsorship Initiative connects veterans with VA care within 30 days postdischarge, with the option of additional support in the community. The VISN 22 CoE for Stress and Mental Health (CESAMH) develops, evaluates, and disseminates diagnostics and treatments for veterans affected by traumatic events and brain injuries, with a unique focus on supporting their whole health needs. The VISN 6 Mid-Atlantic MIRECC leads the ongoing VISN-6 Post-Deployment Mental Health (PDMH) study, the largest biorepository of post-9/11 veterans. PDMH has greatly expanded the understanding of the unique needs of post-9/11 veterans, with > 100 peer-reviewed publications to date. Veterans with mild TBI frequently experience chronic posttraumatic headaches that can be disabling and nonresponsive to treatment. The VISN 20 Northwest MIRECC demonstrated that prazosin, a repurposed, low-cost, widely available, nonaddictive medication, can safely and effectively reduce the frequency of these headaches and improve functional impairment in veterans and active-duty service members.14
Increased and enhanced access to effective mental health treatment is a priority for VA. In 2007, the VA launched the National Primary Care Mental Health Integration program, which integrated mental health services into primary care settings. The Center for Integrated Healthcare (CIH) has supported the VA in these efforts. In 2024, CIH trained > 5000 health care staff on high-fidelity integration of behavioral health and medical care. VA has also focused on increasing access to mental health services via expanded telehealth offerings. The VISN 16 MIRECC, with its unique focus on increasing access to care for rural veterans via distance-based and digital health technology, supported the VA Offices of Mental Health and Connected Care to virtualize mental health care and promote adoption and sustained use of VA Video Connect across the enterprise.
Specialized MH CoEs are uniquely equipped to support the VHA in providing training and education to VA clinicians, veterans, care partners and family members, and the community on high-priority mental health topics. Education is a core component of the MH CoEs tripartite mission. As such, MH CoEs offer national trainings, conferences, consultation services, clinical demonstration projects, development of clinical dashboards and toolkits, and public awareness campaigns. Researchers, educators, and clinicians at the CoEs frequently serve as subject matter experts on topics aligned with their respective missions. Several national rollout programs that disseminated evidence-based treatments for mental health conditions to the field (eg, cognitive behavioral therapy for depression, cognitive behavioral therapy for insomnia, and prolonged exposure) were developed at specialized CoEs.
The VHA provides advanced training, residencies, and fellowships to > 120,000 trainees annually. Many of these trainees choose to remain at the VA. Seven of 10 VHA psychologists and 6 of 10 VHA physicians trained within the VHA prior to their employment.15 The MH CoEs and MIRECCs play an important role in preparing these trainees for VHA mental health careers. These centers are funded to provide advanced postdoctoral training to physicians as well as allied health professionals in clinical and counseling psychology, social work, pharmacy, and nursing. Training is not limited to postdoctoral fellows: graduate students, residents, and interns from affiliated accredited training programs may rotate through mental health CoEs each academic year.
Conclusions
For > 30 years, mental health CoEs have brought thousands of veterans advanced treatments for their mental health needs and helped reduce death by suicide. The centers have a bright future ahead, harnessing advances in artificial intelligence and genomics to permit the matching of the individual veterans to the treatment most likely to benefit them. Precision medicine, as espoused by the Hannon Act, will not only encourage the efficient use of health care resources but also rapidly reduce pain in veterans with mental health and SUDs.
- Congressionally Mandated Report: Report on Transparency in Mental Health Care Services. US Dept of Veterans Affairs; December 2022. Accessed December 5, 2025. https://www.govinfo.gov/content/pkg/CMR-VA1-00181657/pdf/CMR-VA1-00181657.pdf
- Beckman AL, Jacobs J, Elnahal SM. The PACT Act—expanding coverage and access for veterans. JAMA. 2024;332:1423-1424. doi:10.1001/jama.2024.16013
- Morse JL, Acheson DT, Almklov E, et al. Associations among environmental exposures and physical and psychiatric symptoms in a care-seeking sample of U.S. military veterans. Mil Med. 2024;189:e1397-e1402. doi:10.1093/milmed/usae035
- Veterans’ Health Care Act of 1984, 38 USC §98-528 (1984). Accessed March 27, 2026. https://www.congress.gov/bill/98th-congress/house-bill/5618/text
- Veterans’ Health Care Eligibility Reform Act of 1996, 38 USC §104-262 (1996). Accessed March 27, 2026. https://www.congress.gov/bill/104th-congress/house-bill/3118/text
- Military Quality of Life and Veterans Affairs Appropriations Act, 2006. Pub L No. 109-114, 119 Stat. 2372. Accessed March 27, 2026. https://www.congress.gov/bill/109th-congress/house-bill/2528/text
- Karlin BE, Ruzek JI, Chard KM, et al. Dissemination of evidence‐based psychological treatments for posttraumatic stress disorder in the Veterans Health Administration. J Trauma Stress. 2010;23:663-673. doi:10.1002/jts.20588
- Byers AL, Covinsky KE, Barnes DE, et al. Dysthymia and depression increase risk of dementia and mortality among older veterans. Am J Geriatr Psychiatry. 2012;20:664-672. doi:10.1097/JGP.0b013e31822001c1
- Oslin DW, Lynch KG, Shih MC, et al. Effect of pharmacogenomic testing for drug-gene interactions on medication selection and remission of symptoms in major depressive disorder: the PRIME Care randomized clinical trial. JAMA. 2022;328:151-161. doi:10.1001/jama.2022.9805
- Goodman M, Brown GK, Galfalvy HC, et al. Group (“Project Life Force”) versus individual suicide safety planning: a randomized clinical trial. Contemp Clin Trials Commun. 2020;17:100520. doi:10.1016/j.conctc.2020.100520
- Na PJ, Ralevski E, Jegede O, et al. Depression and/or PTSD comorbidity affects response to antidepressants in those with alcohol use disorder. Front Psychiatry. 2022;12:768318. doi:10.3389/fpsyt.2021.768318
- McCarthy JF, Blow FC, Valenstein M, et al. Veterans Affairs Health System and mental health treatment retention among patients with serious mental illness: evaluating accessibility and availability barriers. Health Serv Res. 2007;42:1042-1060. doi:10.1111/j.1475-6773.2006.00642.x
- Glynn SM, Marder SR, Noordsy DL, et al. An RCT evaluating the effects of skills training and medication type on work outcomes among patients with schizophrenia. Psychiatr Serv. 2016;67:500-506. doi:10.1176/appips201500171
- Mayer CL, Savage PJ, Engle CK, et al. Randomized controlled pilot trial of prazosin for prophylaxis of posttraumatic headaches in active-duty service members and veterans. Headache. 2023;63:751-762. doi:10.1111/head.14529
- Hill C. Medical education at VA: it’s all about the veterans. VA News. August 18, 2021. Accessed December 5, 2025. https://news.va.gov/93370/medical-education-at-va-its-all-about-the-veterans/
- Congressionally Mandated Report: Report on Transparency in Mental Health Care Services. US Dept of Veterans Affairs; December 2022. Accessed December 5, 2025. https://www.govinfo.gov/content/pkg/CMR-VA1-00181657/pdf/CMR-VA1-00181657.pdf
- Beckman AL, Jacobs J, Elnahal SM. The PACT Act—expanding coverage and access for veterans. JAMA. 2024;332:1423-1424. doi:10.1001/jama.2024.16013
- Morse JL, Acheson DT, Almklov E, et al. Associations among environmental exposures and physical and psychiatric symptoms in a care-seeking sample of U.S. military veterans. Mil Med. 2024;189:e1397-e1402. doi:10.1093/milmed/usae035
- Veterans’ Health Care Act of 1984, 38 USC §98-528 (1984). Accessed March 27, 2026. https://www.congress.gov/bill/98th-congress/house-bill/5618/text
- Veterans’ Health Care Eligibility Reform Act of 1996, 38 USC §104-262 (1996). Accessed March 27, 2026. https://www.congress.gov/bill/104th-congress/house-bill/3118/text
- Military Quality of Life and Veterans Affairs Appropriations Act, 2006. Pub L No. 109-114, 119 Stat. 2372. Accessed March 27, 2026. https://www.congress.gov/bill/109th-congress/house-bill/2528/text
- Karlin BE, Ruzek JI, Chard KM, et al. Dissemination of evidence‐based psychological treatments for posttraumatic stress disorder in the Veterans Health Administration. J Trauma Stress. 2010;23:663-673. doi:10.1002/jts.20588
- Byers AL, Covinsky KE, Barnes DE, et al. Dysthymia and depression increase risk of dementia and mortality among older veterans. Am J Geriatr Psychiatry. 2012;20:664-672. doi:10.1097/JGP.0b013e31822001c1
- Oslin DW, Lynch KG, Shih MC, et al. Effect of pharmacogenomic testing for drug-gene interactions on medication selection and remission of symptoms in major depressive disorder: the PRIME Care randomized clinical trial. JAMA. 2022;328:151-161. doi:10.1001/jama.2022.9805
- Goodman M, Brown GK, Galfalvy HC, et al. Group (“Project Life Force”) versus individual suicide safety planning: a randomized clinical trial. Contemp Clin Trials Commun. 2020;17:100520. doi:10.1016/j.conctc.2020.100520
- Na PJ, Ralevski E, Jegede O, et al. Depression and/or PTSD comorbidity affects response to antidepressants in those with alcohol use disorder. Front Psychiatry. 2022;12:768318. doi:10.3389/fpsyt.2021.768318
- McCarthy JF, Blow FC, Valenstein M, et al. Veterans Affairs Health System and mental health treatment retention among patients with serious mental illness: evaluating accessibility and availability barriers. Health Serv Res. 2007;42:1042-1060. doi:10.1111/j.1475-6773.2006.00642.x
- Glynn SM, Marder SR, Noordsy DL, et al. An RCT evaluating the effects of skills training and medication type on work outcomes among patients with schizophrenia. Psychiatr Serv. 2016;67:500-506. doi:10.1176/appips201500171
- Mayer CL, Savage PJ, Engle CK, et al. Randomized controlled pilot trial of prazosin for prophylaxis of posttraumatic headaches in active-duty service members and veterans. Headache. 2023;63:751-762. doi:10.1111/head.14529
- Hill C. Medical education at VA: it’s all about the veterans. VA News. August 18, 2021. Accessed December 5, 2025. https://news.va.gov/93370/medical-education-at-va-its-all-about-the-veterans/
Meeting the Needs of Those Who Have Served: The Role of VHA Specialized Mental Health Centers of Excellence
Meeting the Needs of Those Who Have Served: The Role of VHA Specialized Mental Health Centers of Excellence
Accelerated Unified Protocol for Transdiagnostic Treatment of Anxiety Disorders in a VHA System
Accelerated Unified Protocol for Transdiagnostic Treatment of Anxiety Disorders in a VHA System
Cognitive behavioral therapy (CBT) is supported as an effective treatment for depression by clinical practice guidelines from the US Department of Veterans Affairs (VA) and US Department of Defense.1-3 Despite research supporting the use of evidence-based CBT for anxiety, mood, and emotional disorders, patient access to these interventions is limited.4 One barrier to CBT for anxiety, mood, and emotional disorders is the traditional use of single-disorder protocols (SDPs) to separately treat each disorder (eg, major depression, generalized anxiety disorder, panic disorder).
Use of SDPs places a high burden on clinicians, requiring them to learn and competently implement multiple different manualized interventions for each anxiety, mood, or emotional disorder encountered in practice.4 It is common for individuals who present with an anxiety, mood, or emotional disorder to experience co-occurring disorders.5 Traditional SDP-based CBT may require multiple SDPs to address co-occurring disorders, extending time in treatment and increasing training burden. There is evidence that even when an SDP is used, co-occurring difficulties may decrease in intensity.6 Thus, evidence-based CBT for 1 presenting concern may positively affect co-occurring difficulties that are not the primary treatment target.6
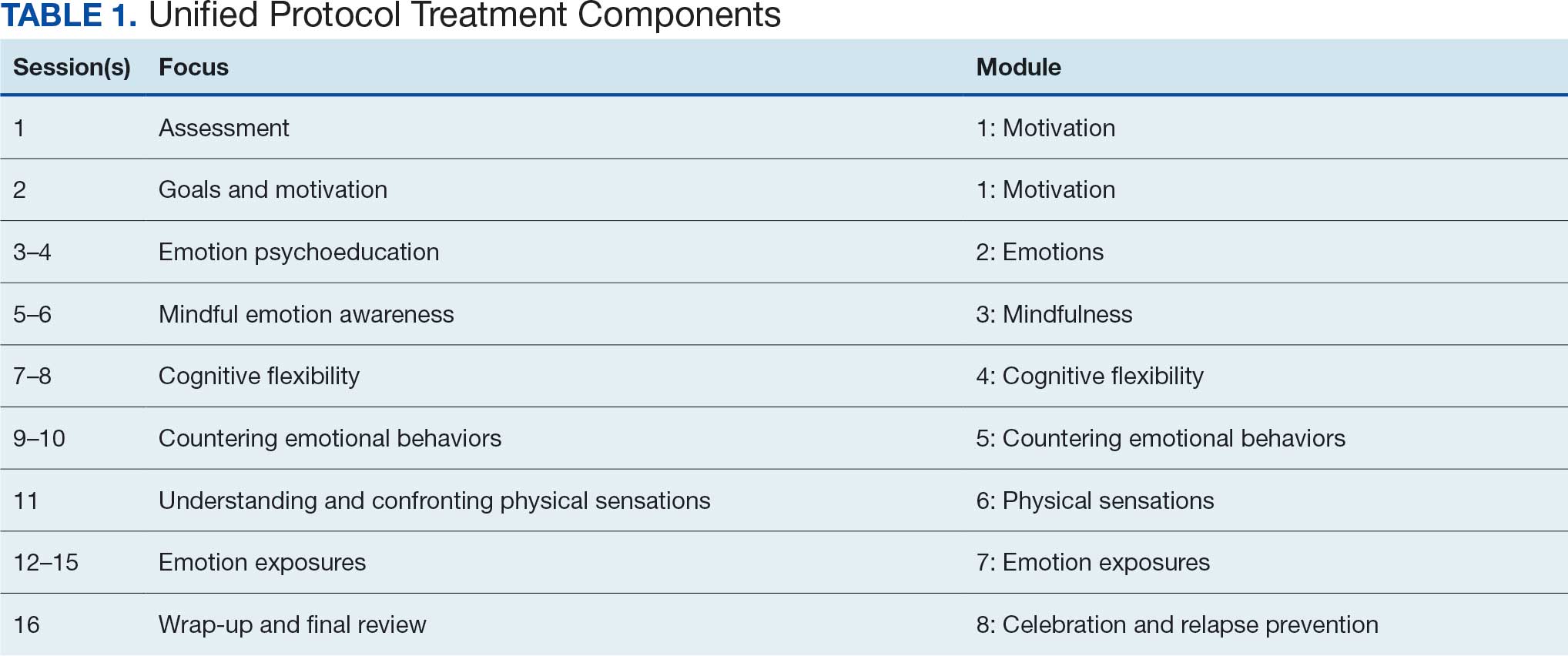
Unified Protocol (UP) is a transdiagnostic CBT intervention for anxiety and mood disorders. UP targets emotional experiences (eg, negative affect and emotional distress) that are present in multiple anxiety, depression, and emotional disorders. UP is organized into 8 modules and uses interventions present in other CBT SDPs, such as teaching objective assessment methods to clients, motivational enhancement and goal setting, emotion psychoeducation, mindful awareness, cognitive reframing, and exposure principles as mechanisms of change (Table 1).4 UP is an ideal intervention for addressing a number of anxiety, mood, and emotional disorders as well as addressing cooccurring disorders within the same course of treatment.
UP has been compared to SDPs; studies illustrate that UP is equivalent to SDPs at the end of treatment and at 6 months posttreatment.4,7 Additionally, patients who received UP experienced symptom reduction for multiple co-occurring disorders.7 Furthermore, patients were less likely to drop out of UP when compared with SDPs.4
Studies have reported positive impacts on affective disorders with UP. A 2019 meta-analysis found significant reductions in depression and anxiety-related disorders.8 Additionally, UP has been shown to be effective when delivered in person and via telehealth.9,10 UP has also been successfully used in veterans.11 While traditional models of UP (1-2 sessions weekly) have a lower dropout rate than SDPs, UP and CBT dropout rates still leave room for improvement.12-14 Specifically, rates of attrition from SDP CBT and transdiagnostic CBT protocols range from 9% to 35%, and dropout reduces the likelihood of attaining a full therapeutic dose of any course of CBT. Notably, accelerated delivery of CBT (ie, ≥ 3 sessions/wk) has been shown to reduce risk of dropout.14,15
Veterans are at increased risk for suicide, and anxiety and mood disorders are associated with increased risk of suicide attempt and death.16,17 Very few veterans who could benefit from high-quality CBT interventions, whether SDP or UP, are able to access them. Only 6.3% of veterans received ≥1 session of an evidence-based CBT SDP for posttraumatic stress disorder (PTSD) at 6 clinics evaluated in 2010.18
We identified 2 strategies to increase access to and completion of an evidence-based CBT course. First, the use of transdiagnostic UP instead of SDPs reduced burden on therapists and allowed them to address presenting and co-occurring disorders within the same course of care. Second, the use of an accelerated model of service delivery reduced dropout risk. Training clinicians to deliver UP is efficient and cost-effective, considering clinicians use core strategies that can be tailored and flexibly applied to a range of emotional difficulties. Thus, implementing UP may decrease barriers to receiving an optimal dose of an evidence-based CBT delivered with fidelity in a time- and cost-efficient manner.4 Two studies have found no evidence of differences in outcomes between UP and SDPs, suggesting that training and supervising clinicians in a single transdiagnostic UP intervention may prepare them to treat heterogeneous and co-occurring anxiety, mood, and emotional disorders with less burden than learning multiple SDPs.7,19
Delivering UP in an accelerated or massed format (≥4 sessions/wk) instead of the traditional spaced model (1 session/wk) has empirical support but has not been widely implemented. This approach, sometimes referred to as a UP-intensive outpatient program (UP-IOP) or UP-intensive outpatient track (UP-IOT), has been shown to be feasible, acceptable, and effective, with increased completion rates compared with traditional UP delivery (1-2 sessions/wk).20-22
Ragsdale et al describe a 2-week IOP with multiple treatment tracks, including a general track.20 The general track includes massed UP and additional standard services, including case management, wellness services, family services, and a single session effective behaviors group. Additional augmentation services are available when clinically indicated (eg, repetitive transcranial magnetic stimulation, transcranial direct current stimulation, psychoeducation, motivational interviewing, relapse prevention). In other words, this was an UP-IOP.20
Thompson-Brenner et al described a successful implementation of massed UP applied in intensive treatment settings, such as residential and day-hospital programs, for eating disorders. Patients reported improvements in 3 UP targets: experiential avoidance, mindfulness, and anxiety.21 Watkins et al evaluated a 2-week IOP using CBT for comorbid substance use and mental health disorders, including prolonged exposure, UP, and relapse prevention for substance use disorders. Participants were post-9/11 veterans and activeduty personnel. Results indicated that UP reduced PTSD and depressive symptoms following treatment. Furthermore, the retention rate (91%) was higher than retention in outpatient treatment (39%-65%), supporting the IOP model as a strategy to reduce dropout.22
Massed psychotherapy has been extended to IOP programs for PTSD treatment within the Veterans Health Administration (VHA). Yamokoski et al found that patients who completed an IOP that included massed CBT for PTSD had high retention, high satisfaction, and significant reduction in self-reported co-occurring depression symptoms. The authors also found that this model of care could be implemented and sustained within a VHA facility using minimal staffing resources.23
The UP-IOP models described by Ragsdale et al and Watkins et al included massed UP as the primary evidence-based practice (EBP) with adjunctive groups (eg, wellness and educational groups and access to complementary interventions such as mindfulness and yoga); they found that adding these groups increased retention and patient- reported satisfaction (ie, UP-IOP).20,22 The addition of wellness education alongside a primary EBP aligns with the VHA focus on whole health well-being and wellness. This includes understanding factors that motivate a patient toward health and well-being, providing health education, and offering access to complementary interventions such as mindfulness.24
Dryden et al described the whole health transformation within VHA as a proactive approach to addressing both employee and patient wellness. Their research found that the whole health model promoted wellbeing in patients and staff and these improvements were sustained during the COVID-19 pandemic. Dryden et al also noted that virtual technologies facilitated continued whole health implementation.25
The literature illustrates that (1) massed UP can be delivered with complementary education and wellness offerings that may increase retention and satisfaction by enriching treatment (eg, delivering UP-IOP); (2) whole health, including wellness education and complementary interventions (eg, mindfulness, motivational enhancement), promotes well-being in patients and clinicians; and (3) whole health education and complementary interventions can be delivered virtually.
IVET
Health Care Need
Veterans Affairs Pacific Islands Health Care System (VAPIHCS) provides medical services to veterans in the Hawaiian Islands, American Samoa, Guam, and Saipan spanning nearly 4000 miles across the Pacific Ocean. Prior to implementation of this program, veterans who received care at VAPIHCS had little to no access to UP in outpatient settings and no access to UP in residential settings. Access to UP depended on the presence of a therapist trained in UP within a given clinic and was geographically limited to the location of the UP-trained therapist. The limited outpatient access to UP was restricted to the traditional UP delivery model (eg, about 1 session/wk); thus, there was no access to accelerated UP for veterans served at VAPIHCS. In the fiscal year prior to implementation of the massed UP program, > 1000 VAPIHCS veterans had been diagnosed with obsessive-compulsive related disorder or anxiety. A massed-UP program with weekly rolling admissions would support access to UP for more veterans over 12 months, and the virtual treatment modality would reduce barriers for diverse and underserved veterans, making care more equitable and inclusive.
Successful implementation and sustainment of an EBP prompted the establishment of this UP program. In 2022, VAPIHCS launched the Intensive Virtual Evidence- Based Psychotherapy Team (iVET) for treatment of PTSD. This clinic and associated EBP project demonstrated that massed (≥3 individual sessions/wk) of prolonged exposure (PE) therapy, delivered virtually to a geographically diverse veteran population with PTSD, resulted in significant reductions in PTSD, depression, and anxiety symptoms and substance use risk factors, with very high retention rates. The iVET for PTSD program was feasible, acceptable, and effective, with veterans reporting significant improvement in quality of life and high satisfaction with their mental health services.15 Given the known benefits of transdiagnostic UP treatment (vs SDPs), the need for accelerated UP, and success with accelerated PE, our goal was to spread the EBP of massed (≥3 sessions/ wk) virtual psychotherapy to other presenting problems (eg, anxiety disorders with or without co-occurring unipolar depression) using transdiagnostic UP.
Program Description
The program implemented within outpatient mental health services at VAPIHCS was iVET for the treatment of anxiety with or without co-occurring depression. The program model consists of an accelerated course of UP and whole health education provided via VA Video Connect (VVC), the VA video telehealth platform. iVET is a 2- to 4-week program and consists of 3 parts: (1) massed individual UP for transdiagnostic treatment of anxiety and co-occurring depression, (2) group whole health and wellness classes, and (3) individual health coaching to address personal wellness goals. Programming is offered over 10-hour days to increase access across multiple time zones, especially to allow participation from Guam and Saipan.
When a patient is referred to iVET, the first contact is a video (or telephone) appointment with a registered nurse (RN) for a screening session. The screening session is designed to provide education about the program (including interventions, time commitment, and resources required for participation). Following education, the RN completes a safety screening, including screening for suicidal ideation and risk, as well as intimate partner violence risk. If urgent safety concerns are present, a licensed social worker or psychologist joins the screening to complete further risk assessment and address any safety concerns.
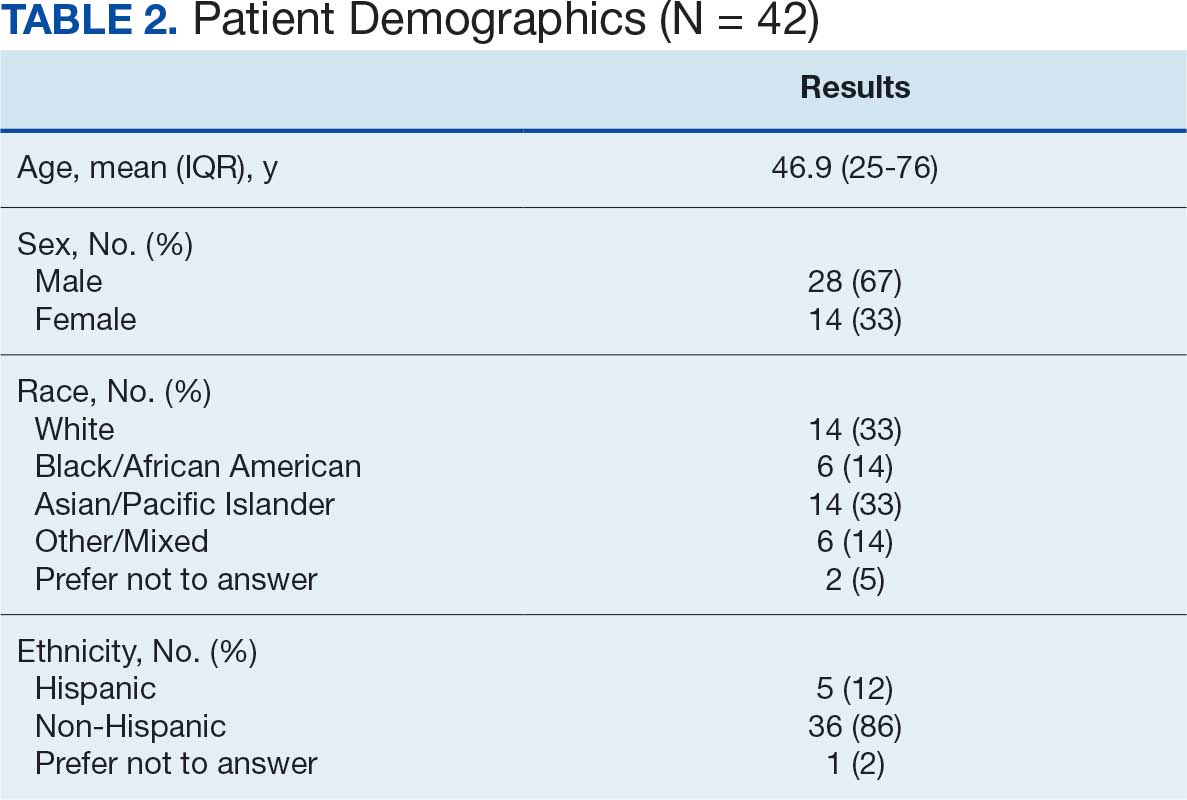
Following screening, patients are scheduled for a VVC telehealth intake with a licensed therapist (social worker or psychologist) to complete a diagnostic interview. Patients are sent a secure link to complete a measurement-based care (MBC) battery of self-report measures, including assessments of demographics, anxiety symptoms, depression symptoms, substance use, psychological flexibility, quality of life, and satisfaction with mental health care. The results of the diagnostic interview and self-report measures are discussed with the patient during the intake session to plan next steps and support shared decision-making. This initial VVC intake not only allows for fit assessment but also serves to troubleshoot technical difficulties with the virtual platforms.
Notably, there are minimal exclusion criteria for participation in iVET. These include active unmanaged psychosis or manic symptoms, recent suicidal crises (attempt within 8 weeks), active nonsuicidal self-injury (within 8 weeks), and moderate to severe cognitive impairment. Following intake, patients are scheduled to begin their course of care with iVET. Upon completion of intake, patients receive program materials for individual and group classes and are told they will receive email links for all VVC telehealth appointments. Patients are admitted to the iVET on a rolling basis, thereby increasing access compared with closed group and/or cohort models of care.
Patients receiving iVET attend 2 to 4 telehealth appointments daily and complete exercises between sessions. The primary iVET for Anxiety program EBP intervention is a massed or accelerated individual course of UP, which includes 8 primary components: assessment, goals and motivation, understanding emotions, mindful emotion awareness, cognitive flexibility, countering emotional behaviors, understanding and confronting physical sensations, and emotional exposures. UP is delivered in 4 to 8 individual sessions weekly (60-90 minutes each), allowing completion of the full UP protocol with fidelity in 2 to 4 weeks. In addition to primary EBP intervention, patients participate in 4 group sessions weekly (50 minutes each) of a whole health and wellness education class and have access to 1 individual health coaching session weekly (30- 60 minutes) to set wellness goals and receive coaching. During iVET, patients are invited to complete MBC batteries of self-report measures assessing anxiety symptoms, depression symptoms, substance use, psychological flexibility, quality of life, and satisfaction with mental health care at sessions 1, 5, 9, 13, and the final UP session. Following discharge from the iVET, patients are offered 1-, 3-, and 6-month individual postdischarge check-up sessions with a therapist, during which they are invited to complete MBC measures and review relapse prevention and maintenance of treatment gains. Likewise, patients are offered 1-, 3-, and 6-month individual postdischarge check-up sessions with an RN focused on maintaining wellness gains.
The iVET for Anxiety staff has 3 therapists (psychologists or social workers) and 1 RN. Additionally, the iVET for Anxiety is supported by a program manager and a program support assistant who support 2 programs total (the iVET for Anxiety plus another mental health program). The primary cost of the program is staff salary. Additional resources included computer equipment for staff and supplies (eg, printed materials for patients and office supplies). Due to the virtual environment of care, iVET staff telework and do not require physical space within VAPIHCS.
Outcomes
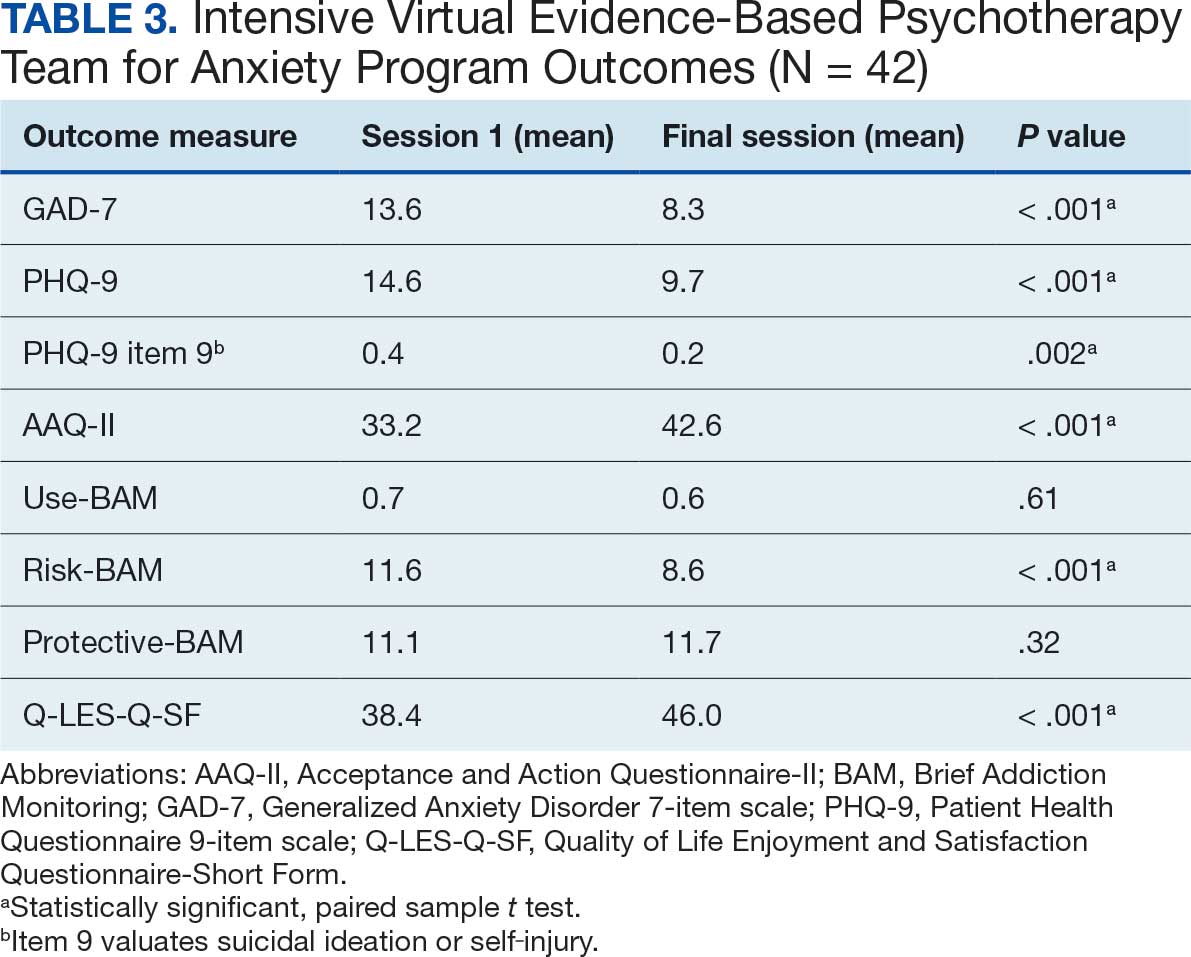
Veterans receiving iVET for Anxiety are invited to complete MBC multiple times, including pretreatment, during UP treatment (sessions 1, 5, 9, 13, and the final session), and posttreatment (1, 3, and 6 months). MBC measures include self-reported demographics; a 2-item measure of satisfaction with mental health services; the Acceptance and Action Questionnaire II,26 the Brief Addiction Monitor-Intensive Outpatient Program, 27 the Generalized Anxiety Disorder-7,28 the Patient Health Questionnaire (PHQ-9),29 and the Quality of Life Enjoyment and Satisfaction Questionnaire-Short Form.30
Forty-two veterans completed the iVET for Anxiety program, with a retention rate of 87.5% completing . 16 sessions of massed UP (Table 2). Veterans reported reduced anxiety (P < .001), depression (P < .001), and substance use risk (P < .001). Veterans experienced improved acceptance of emotional experiences (P < .001) and quality of life (P < .001), based on paired sample t tests comparing session 1 vs final session scores on the self-reported measures. Veterans also reported high satisfaction with mental health care in iVET for Anxiety.
Veterans experienced reduced thoughts of death or suicidal ideation (SI) based on responses to item 9 of PHQ-9. When SI was categorically analyzed (presence vs absence) using PHQ-9 item 9, there was an association observed between absence of SI and completion of a course of massed UP that does not appear to be due to chance, (X2 [1, N = 42) = 3.94; P = .047). In addition, veterans who completed the program showed a significant decrease in SI severity measured continuously (range, 0-3) on PHQ-9 item 9 (P < .05) (Table 3).
Future Directions
The aim of this program is to see sustained patient outcomes as iVET continues to serve more veterans. Another line of inquiry is longer- term follow-up, given that long-term follow- up was not addressed in this project. We also hope that the accelerated model of care can be applied to treatment of other presenting concerns (eg, relationship difficulties, insomnia). Expansion of accelerated mental health treatment into other federal and nonfederal health care settings is another area worthy of future inquiry. Exploration of staff satisfaction and burnout related to providing accelerated UP is another important future direction. Relatedly, assessment of the staff burden to learn 1 transdiagnostic EBP vs learning multiple SDPs is another future direction. Likewise, exploration of institutional benefits of investment in transdiagnostic training, supervision, and consultation for UP vs multiple SDPs may be important. These areas could also result in insightful, beneficial evidence of the effectiveness of massed UP to add to the existing literature.
Conclusions
UP for transdiagnostic treatment of anxiety, depressive, and emotional disorders has demonstrated reduced suffering and improved functioning and is supported by multiple clinical practice guidelines.1-4 Federal practitioners are positioned to improve access to this intervention, thereby reducing pain and improving lives. Indeed, it is crucial to envision a future state in which access to UP for a range of anxiety and depressive disorders is improved and broad, retention rates are dramatically improved, and clinicians providing UP do not experience the high burden and burnout associated with needing to learn and implement a variety of SDPs. Development of these programs, or similar tracks within existing programs, that provide massed or accelerated UP for transdiagnostic treatment of a range of anxiety and depressive disorders with virtual delivery options, is imperative to advance improved care for patients and clinicians.
Federal health care settings treating patients with anxiety and depression, such as those within the US Department of Defense, Indian Health Services, Bureau of Prisons, and VHA, are positioned to implement programs like iVET. Moreover, at the institutional level, investment in training and supervision in the transdiagnostic UP as opposed to multiple SDPs warrants consideration. We believe this model of care has great merit and foresee a future where all patients seeking treatment for anxiety and depression have the option to complete an accelerated or massed course of transdiagnostic care with UP if they so desire. Our experiences with iVET illustrate the feasibility, acceptability, and sustainability of such programs without requiring substantial staffing and financial resources.
- US Department of Veterans Affairs, US Department of Defense. VA/DoD clinical practice guideline for the management of major depressive disorder. Version 4. 2022. Accessed February 1, 2026. https://www.healthquality.va.gov/guidelines/MH/mdd/VADoDMDDCPGFinal508.pdf
- American Psychological Association. Clinical practice guideline for the treatment of depression across three age cohorts. February 2019. Accessed February 4, 2026. https://www.apa.org/depression-guideline/guideline.pdf
- Katzman MA, Bleau P, Blier P, et al. Canadian clinical practice guidelines for the management of anxiety, posttraumatic stress and obsessive compulsive disorders. BMC Psychiatry. 2014;14:S1. doi:10.1186/1471-244X-14-S1-S1
- Barlow DH, Farchione TJ, Bullis JR, et al. The unified protocol for transdiagnostic treatment of emotional disorders compared with diagnosis-specific protocols for anxiety disorders: a randomized clinical trial. JAMA Psychiatry. 2017;74:875-884. doi:10.1001/jamapsychiatry.2017.2164
- Calkins AW, et al. Comorbidity of anxiety and depression. In: Ressler KJ, Pine DS, Rothbaum BO, eds. Anxiety Disorders, Primer On. Oxford Academic; 2015. https://doi.org/10.1093/med/9780199395125.003.0021
- Manber R, Edinger JD, Gress JL, et al. Cognitive behavioral therapy for insomnia enhances depression outcome in patients with comorbid major depressive disorder and insomnia. Sleep. 2008;31:489-495. doi:10.1093/sleep/31.4.489
- Steele SJ, Farchione TJ, Cassiello-Robbins C, et al. Efficacy of the Unified Protocol for transdiagnostic treatment of comorbid psychopathology accompanying emotional disorders compared to treatments targeting single disorders. J Psychiatr Res. 2018;104:211-216. doi:10.1016/j.jpsychires.2018.08.005
- Sakiris N, Berle D. A systematic review and meta-analysis of the Unified Protocol as a transdiagnostic emotion regulation based intervention. Clin Psychol Rev. 2019;72:101751. doi:10.1016/j.cpr.2019.101751
- Cassiello-Robbins C, Rosenthal MZ, Ammirati RJ. Delivering transdiagnostic treatment over telehealth during the COVID-19 pandemic: application of the unified protocol. Cogn Behav Pract. 2021;28:555-572. doi:10.1016/j.cbpra.2021.04.007
- Meyer EC, Coe E, Pennington ML, et al. The unified protocol for transdiagnostic treatment of emotional disorders delivered to firefighters via videoconferencing: pilot outcomes highlighting improvements in alcohol use disorder and posttraumatic stress disorder symptoms. Cogn Behav Pract. 2024;31:215-229. doi:10.1016/j.cbpra.2022.08.004
- Varkovitzky RL, Sherrill AM, Reger GM. Effectiveness of the unified protocol for transdiagnostic treatment of emotional disorders among veterans with posttraumatic stress disorder: a pilot study. Behav Modif. 2018;42:210-230. doi:10.1177/0145445517724539
- Oliveira JT, Sousa I, Ribeiro AP, et al. Premature termination of the unified protocol for the transdiagnostic treatment of emotional disorders: The role of ambivalence towards change. Clin Psychol Psychother. 2022;29:1089-1100. doi:10.1002/cpp.2694
- Schaeuffele C, Homeyer S, Perea L, et al. The unified protocol as an internet-based intervention for emotional disorders: Randomized controlled trial. PLoS One. 2022;17:e0270178. doi:10.1371/journal.pone.0270178
- Bentley KH, Cohen ZD, Kim T, et al. The nature, timing, and symptom trajectories of dropout from transdiagnostic and single-diagnosis cognitive-behavioral therapy for anxiety disorders. Behav Ther. 2021;52:1364-1376. doi:10.1016/j.beth.2021.03.007
- Aosved AC, Brown TB, Bell JC, et al. Accelerated prolonged exposure therapy for posttraumatic stress disorder in a Veterans Health Administration system. Fed Pract. 2025;42:S6-S11. doi:10.12788/fp.0568
- Nepon J, Belik SL, Bolton J, et al. The relationship between anxiety disorders and suicide attempts: findings from the National Epidemiologic Survey on Alcohol and Related Conditions. Depress Anxiety. 2010;27:791-798. doi:10.1002/da.20674
- Shiner B, D’Avolio LW, Nguyen TM, et al. Measuring use of evidence based psychotherapy for posttraumatic stress disorder. Adm Policy Ment Health. 2013;40:311-318. doi:10.1007/s10488-012-0421-0
- Nichter B, Stein MB, Monteith LL, et al. Risk factors for suicide attempts among U.S. military veterans: A 7-year population-based, longitudinal cohort study. Suicide Life Threat Behav. 2022;52:303-316. doi:10.1111/sltb.12822
- McHugh RK, Barlow DH. The dissemination and implementation of evidence-based psychological treatments. A review of current efforts. Am Psychol. 2010;65:73-84. doi:10.1037/a0018121
- Ragsdale KA, Nichols AA, Mehta M, et al. Comorbid treatment of traumatic brain injury and mental health disorders. NeuroRehabilitation. 2024;55:375-384. doi:10.3233/NRE-230235
- Thompson-Brenner H, Brooks GE, Boswell JF, et al. Evidence-based implementation practices applied to the intensive treatment of eating disorders: summary of research and illustration of principles using a case example. Clin Psychol Sci Pract. 2018;25:e12221. doi:10.1111/cpsp.12221
- Watkins LE, Patton SC, Drexler K, et al. Clinical effectiveness of an intensive outpatient program for integrated treatment of comorbid substance abuse and mental health disorders. Cog Behav Pract. 2023;30:354-366.
- Yamokoski C, Flores H, Facemire V, et al. Feasibility of an intensive outpatient treatment program for post-traumatic stress disorder within the veterans health care administration. Psychol Serv. 2023;20:506-515. doi:10.1037/ser0000628
- Gaudet T, Kligler B. Whole health in the whole system of the Veterans Administration: how will we know we have reached this future state?. J Altern Complement Med. 2019;25:S7-S11. doi:10.1089/acm.2018.29061.gau
- Dryden EM, Bolton RE, Bokhour BG, et al. Leaning into whole health: sustaining system transformation while supporting patients and employees during COVID-19. Glob Adv Health Med. 2021;10:21649561211021047. doi:10.1177/21649561211021047
- Bond FW, Hayes SC, Baer RA, et al. Preliminary psychometric properties of the Acceptance and Action Questionnaire-II: a revised measure of psychological inflexibility and experiential avoidance. Behav Ther. 2011;42:676-688. doi:10.1016/j.beth.2011.03.007
- Cacciola JS, Alterman AI, Dephilippis D, et al. Development and initial evaluation of the Brief Addiction Monitor (BAM). J Subst Abuse Treat. 2013;44:256-263. doi:10.1016/j.jsat.2012.07.013
- Spitzer RL, Kroenke K, Williams JB, et al. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166:1092-1097. doi:10.1001/archinte.166.10.1092
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606-613. doi:10.1046/j.1525-1497.2001.016009606.x
- Stevanovic D. Quality of life enjoyment and satisfaction questionnaire-short form for quality of life assessments in clinical practice: a psychometric study. J Psychiatr Ment Health Nurs. 2011;18:744-750. doi:10.1111/j.1365-2850.2011.01735.x
Cognitive behavioral therapy (CBT) is supported as an effective treatment for depression by clinical practice guidelines from the US Department of Veterans Affairs (VA) and US Department of Defense.1-3 Despite research supporting the use of evidence-based CBT for anxiety, mood, and emotional disorders, patient access to these interventions is limited.4 One barrier to CBT for anxiety, mood, and emotional disorders is the traditional use of single-disorder protocols (SDPs) to separately treat each disorder (eg, major depression, generalized anxiety disorder, panic disorder).
Use of SDPs places a high burden on clinicians, requiring them to learn and competently implement multiple different manualized interventions for each anxiety, mood, or emotional disorder encountered in practice.4 It is common for individuals who present with an anxiety, mood, or emotional disorder to experience co-occurring disorders.5 Traditional SDP-based CBT may require multiple SDPs to address co-occurring disorders, extending time in treatment and increasing training burden. There is evidence that even when an SDP is used, co-occurring difficulties may decrease in intensity.6 Thus, evidence-based CBT for 1 presenting concern may positively affect co-occurring difficulties that are not the primary treatment target.6
Unified Protocol (UP) is a transdiagnostic CBT intervention for anxiety and mood disorders. UP targets emotional experiences (eg, negative affect and emotional distress) that are present in multiple anxiety, depression, and emotional disorders. UP is organized into 8 modules and uses interventions present in other CBT SDPs, such as teaching objective assessment methods to clients, motivational enhancement and goal setting, emotion psychoeducation, mindful awareness, cognitive reframing, and exposure principles as mechanisms of change (Table 1).4 UP is an ideal intervention for addressing a number of anxiety, mood, and emotional disorders as well as addressing cooccurring disorders within the same course of treatment.
UP has been compared to SDPs; studies illustrate that UP is equivalent to SDPs at the end of treatment and at 6 months posttreatment.4,7 Additionally, patients who received UP experienced symptom reduction for multiple co-occurring disorders.7 Furthermore, patients were less likely to drop out of UP when compared with SDPs.4
Studies have reported positive impacts on affective disorders with UP. A 2019 meta-analysis found significant reductions in depression and anxiety-related disorders.8 Additionally, UP has been shown to be effective when delivered in person and via telehealth.9,10 UP has also been successfully used in veterans.11 While traditional models of UP (1-2 sessions weekly) have a lower dropout rate than SDPs, UP and CBT dropout rates still leave room for improvement.12-14 Specifically, rates of attrition from SDP CBT and transdiagnostic CBT protocols range from 9% to 35%, and dropout reduces the likelihood of attaining a full therapeutic dose of any course of CBT. Notably, accelerated delivery of CBT (ie, ≥ 3 sessions/wk) has been shown to reduce risk of dropout.14,15
Veterans are at increased risk for suicide, and anxiety and mood disorders are associated with increased risk of suicide attempt and death.16,17 Very few veterans who could benefit from high-quality CBT interventions, whether SDP or UP, are able to access them. Only 6.3% of veterans received ≥1 session of an evidence-based CBT SDP for posttraumatic stress disorder (PTSD) at 6 clinics evaluated in 2010.18
We identified 2 strategies to increase access to and completion of an evidence-based CBT course. First, the use of transdiagnostic UP instead of SDPs reduced burden on therapists and allowed them to address presenting and co-occurring disorders within the same course of care. Second, the use of an accelerated model of service delivery reduced dropout risk. Training clinicians to deliver UP is efficient and cost-effective, considering clinicians use core strategies that can be tailored and flexibly applied to a range of emotional difficulties. Thus, implementing UP may decrease barriers to receiving an optimal dose of an evidence-based CBT delivered with fidelity in a time- and cost-efficient manner.4 Two studies have found no evidence of differences in outcomes between UP and SDPs, suggesting that training and supervising clinicians in a single transdiagnostic UP intervention may prepare them to treat heterogeneous and co-occurring anxiety, mood, and emotional disorders with less burden than learning multiple SDPs.7,19
Delivering UP in an accelerated or massed format (≥4 sessions/wk) instead of the traditional spaced model (1 session/wk) has empirical support but has not been widely implemented. This approach, sometimes referred to as a UP-intensive outpatient program (UP-IOP) or UP-intensive outpatient track (UP-IOT), has been shown to be feasible, acceptable, and effective, with increased completion rates compared with traditional UP delivery (1-2 sessions/wk).20-22
Ragsdale et al describe a 2-week IOP with multiple treatment tracks, including a general track.20 The general track includes massed UP and additional standard services, including case management, wellness services, family services, and a single session effective behaviors group. Additional augmentation services are available when clinically indicated (eg, repetitive transcranial magnetic stimulation, transcranial direct current stimulation, psychoeducation, motivational interviewing, relapse prevention). In other words, this was an UP-IOP.20
Thompson-Brenner et al described a successful implementation of massed UP applied in intensive treatment settings, such as residential and day-hospital programs, for eating disorders. Patients reported improvements in 3 UP targets: experiential avoidance, mindfulness, and anxiety.21 Watkins et al evaluated a 2-week IOP using CBT for comorbid substance use and mental health disorders, including prolonged exposure, UP, and relapse prevention for substance use disorders. Participants were post-9/11 veterans and activeduty personnel. Results indicated that UP reduced PTSD and depressive symptoms following treatment. Furthermore, the retention rate (91%) was higher than retention in outpatient treatment (39%-65%), supporting the IOP model as a strategy to reduce dropout.22
Massed psychotherapy has been extended to IOP programs for PTSD treatment within the Veterans Health Administration (VHA). Yamokoski et al found that patients who completed an IOP that included massed CBT for PTSD had high retention, high satisfaction, and significant reduction in self-reported co-occurring depression symptoms. The authors also found that this model of care could be implemented and sustained within a VHA facility using minimal staffing resources.23
The UP-IOP models described by Ragsdale et al and Watkins et al included massed UP as the primary evidence-based practice (EBP) with adjunctive groups (eg, wellness and educational groups and access to complementary interventions such as mindfulness and yoga); they found that adding these groups increased retention and patient- reported satisfaction (ie, UP-IOP).20,22 The addition of wellness education alongside a primary EBP aligns with the VHA focus on whole health well-being and wellness. This includes understanding factors that motivate a patient toward health and well-being, providing health education, and offering access to complementary interventions such as mindfulness.24
Dryden et al described the whole health transformation within VHA as a proactive approach to addressing both employee and patient wellness. Their research found that the whole health model promoted wellbeing in patients and staff and these improvements were sustained during the COVID-19 pandemic. Dryden et al also noted that virtual technologies facilitated continued whole health implementation.25
The literature illustrates that (1) massed UP can be delivered with complementary education and wellness offerings that may increase retention and satisfaction by enriching treatment (eg, delivering UP-IOP); (2) whole health, including wellness education and complementary interventions (eg, mindfulness, motivational enhancement), promotes well-being in patients and clinicians; and (3) whole health education and complementary interventions can be delivered virtually.
IVET
Health Care Need
Veterans Affairs Pacific Islands Health Care System (VAPIHCS) provides medical services to veterans in the Hawaiian Islands, American Samoa, Guam, and Saipan spanning nearly 4000 miles across the Pacific Ocean. Prior to implementation of this program, veterans who received care at VAPIHCS had little to no access to UP in outpatient settings and no access to UP in residential settings. Access to UP depended on the presence of a therapist trained in UP within a given clinic and was geographically limited to the location of the UP-trained therapist. The limited outpatient access to UP was restricted to the traditional UP delivery model (eg, about 1 session/wk); thus, there was no access to accelerated UP for veterans served at VAPIHCS. In the fiscal year prior to implementation of the massed UP program, > 1000 VAPIHCS veterans had been diagnosed with obsessive-compulsive related disorder or anxiety. A massed-UP program with weekly rolling admissions would support access to UP for more veterans over 12 months, and the virtual treatment modality would reduce barriers for diverse and underserved veterans, making care more equitable and inclusive.
Successful implementation and sustainment of an EBP prompted the establishment of this UP program. In 2022, VAPIHCS launched the Intensive Virtual Evidence- Based Psychotherapy Team (iVET) for treatment of PTSD. This clinic and associated EBP project demonstrated that massed (≥3 individual sessions/wk) of prolonged exposure (PE) therapy, delivered virtually to a geographically diverse veteran population with PTSD, resulted in significant reductions in PTSD, depression, and anxiety symptoms and substance use risk factors, with very high retention rates. The iVET for PTSD program was feasible, acceptable, and effective, with veterans reporting significant improvement in quality of life and high satisfaction with their mental health services.15 Given the known benefits of transdiagnostic UP treatment (vs SDPs), the need for accelerated UP, and success with accelerated PE, our goal was to spread the EBP of massed (≥3 sessions/ wk) virtual psychotherapy to other presenting problems (eg, anxiety disorders with or without co-occurring unipolar depression) using transdiagnostic UP.
Program Description
The program implemented within outpatient mental health services at VAPIHCS was iVET for the treatment of anxiety with or without co-occurring depression. The program model consists of an accelerated course of UP and whole health education provided via VA Video Connect (VVC), the VA video telehealth platform. iVET is a 2- to 4-week program and consists of 3 parts: (1) massed individual UP for transdiagnostic treatment of anxiety and co-occurring depression, (2) group whole health and wellness classes, and (3) individual health coaching to address personal wellness goals. Programming is offered over 10-hour days to increase access across multiple time zones, especially to allow participation from Guam and Saipan.
When a patient is referred to iVET, the first contact is a video (or telephone) appointment with a registered nurse (RN) for a screening session. The screening session is designed to provide education about the program (including interventions, time commitment, and resources required for participation). Following education, the RN completes a safety screening, including screening for suicidal ideation and risk, as well as intimate partner violence risk. If urgent safety concerns are present, a licensed social worker or psychologist joins the screening to complete further risk assessment and address any safety concerns.
Following screening, patients are scheduled for a VVC telehealth intake with a licensed therapist (social worker or psychologist) to complete a diagnostic interview. Patients are sent a secure link to complete a measurement-based care (MBC) battery of self-report measures, including assessments of demographics, anxiety symptoms, depression symptoms, substance use, psychological flexibility, quality of life, and satisfaction with mental health care. The results of the diagnostic interview and self-report measures are discussed with the patient during the intake session to plan next steps and support shared decision-making. This initial VVC intake not only allows for fit assessment but also serves to troubleshoot technical difficulties with the virtual platforms.
Notably, there are minimal exclusion criteria for participation in iVET. These include active unmanaged psychosis or manic symptoms, recent suicidal crises (attempt within 8 weeks), active nonsuicidal self-injury (within 8 weeks), and moderate to severe cognitive impairment. Following intake, patients are scheduled to begin their course of care with iVET. Upon completion of intake, patients receive program materials for individual and group classes and are told they will receive email links for all VVC telehealth appointments. Patients are admitted to the iVET on a rolling basis, thereby increasing access compared with closed group and/or cohort models of care.
Patients receiving iVET attend 2 to 4 telehealth appointments daily and complete exercises between sessions. The primary iVET for Anxiety program EBP intervention is a massed or accelerated individual course of UP, which includes 8 primary components: assessment, goals and motivation, understanding emotions, mindful emotion awareness, cognitive flexibility, countering emotional behaviors, understanding and confronting physical sensations, and emotional exposures. UP is delivered in 4 to 8 individual sessions weekly (60-90 minutes each), allowing completion of the full UP protocol with fidelity in 2 to 4 weeks. In addition to primary EBP intervention, patients participate in 4 group sessions weekly (50 minutes each) of a whole health and wellness education class and have access to 1 individual health coaching session weekly (30- 60 minutes) to set wellness goals and receive coaching. During iVET, patients are invited to complete MBC batteries of self-report measures assessing anxiety symptoms, depression symptoms, substance use, psychological flexibility, quality of life, and satisfaction with mental health care at sessions 1, 5, 9, 13, and the final UP session. Following discharge from the iVET, patients are offered 1-, 3-, and 6-month individual postdischarge check-up sessions with a therapist, during which they are invited to complete MBC measures and review relapse prevention and maintenance of treatment gains. Likewise, patients are offered 1-, 3-, and 6-month individual postdischarge check-up sessions with an RN focused on maintaining wellness gains.
The iVET for Anxiety staff has 3 therapists (psychologists or social workers) and 1 RN. Additionally, the iVET for Anxiety is supported by a program manager and a program support assistant who support 2 programs total (the iVET for Anxiety plus another mental health program). The primary cost of the program is staff salary. Additional resources included computer equipment for staff and supplies (eg, printed materials for patients and office supplies). Due to the virtual environment of care, iVET staff telework and do not require physical space within VAPIHCS.
Outcomes
Veterans receiving iVET for Anxiety are invited to complete MBC multiple times, including pretreatment, during UP treatment (sessions 1, 5, 9, 13, and the final session), and posttreatment (1, 3, and 6 months). MBC measures include self-reported demographics; a 2-item measure of satisfaction with mental health services; the Acceptance and Action Questionnaire II,26 the Brief Addiction Monitor-Intensive Outpatient Program, 27 the Generalized Anxiety Disorder-7,28 the Patient Health Questionnaire (PHQ-9),29 and the Quality of Life Enjoyment and Satisfaction Questionnaire-Short Form.30
Forty-two veterans completed the iVET for Anxiety program, with a retention rate of 87.5% completing . 16 sessions of massed UP (Table 2). Veterans reported reduced anxiety (P < .001), depression (P < .001), and substance use risk (P < .001). Veterans experienced improved acceptance of emotional experiences (P < .001) and quality of life (P < .001), based on paired sample t tests comparing session 1 vs final session scores on the self-reported measures. Veterans also reported high satisfaction with mental health care in iVET for Anxiety.
Veterans experienced reduced thoughts of death or suicidal ideation (SI) based on responses to item 9 of PHQ-9. When SI was categorically analyzed (presence vs absence) using PHQ-9 item 9, there was an association observed between absence of SI and completion of a course of massed UP that does not appear to be due to chance, (X2 [1, N = 42) = 3.94; P = .047). In addition, veterans who completed the program showed a significant decrease in SI severity measured continuously (range, 0-3) on PHQ-9 item 9 (P < .05) (Table 3).
Future Directions
The aim of this program is to see sustained patient outcomes as iVET continues to serve more veterans. Another line of inquiry is longer- term follow-up, given that long-term follow- up was not addressed in this project. We also hope that the accelerated model of care can be applied to treatment of other presenting concerns (eg, relationship difficulties, insomnia). Expansion of accelerated mental health treatment into other federal and nonfederal health care settings is another area worthy of future inquiry. Exploration of staff satisfaction and burnout related to providing accelerated UP is another important future direction. Relatedly, assessment of the staff burden to learn 1 transdiagnostic EBP vs learning multiple SDPs is another future direction. Likewise, exploration of institutional benefits of investment in transdiagnostic training, supervision, and consultation for UP vs multiple SDPs may be important. These areas could also result in insightful, beneficial evidence of the effectiveness of massed UP to add to the existing literature.
Conclusions
UP for transdiagnostic treatment of anxiety, depressive, and emotional disorders has demonstrated reduced suffering and improved functioning and is supported by multiple clinical practice guidelines.1-4 Federal practitioners are positioned to improve access to this intervention, thereby reducing pain and improving lives. Indeed, it is crucial to envision a future state in which access to UP for a range of anxiety and depressive disorders is improved and broad, retention rates are dramatically improved, and clinicians providing UP do not experience the high burden and burnout associated with needing to learn and implement a variety of SDPs. Development of these programs, or similar tracks within existing programs, that provide massed or accelerated UP for transdiagnostic treatment of a range of anxiety and depressive disorders with virtual delivery options, is imperative to advance improved care for patients and clinicians.
Federal health care settings treating patients with anxiety and depression, such as those within the US Department of Defense, Indian Health Services, Bureau of Prisons, and VHA, are positioned to implement programs like iVET. Moreover, at the institutional level, investment in training and supervision in the transdiagnostic UP as opposed to multiple SDPs warrants consideration. We believe this model of care has great merit and foresee a future where all patients seeking treatment for anxiety and depression have the option to complete an accelerated or massed course of transdiagnostic care with UP if they so desire. Our experiences with iVET illustrate the feasibility, acceptability, and sustainability of such programs without requiring substantial staffing and financial resources.
Cognitive behavioral therapy (CBT) is supported as an effective treatment for depression by clinical practice guidelines from the US Department of Veterans Affairs (VA) and US Department of Defense.1-3 Despite research supporting the use of evidence-based CBT for anxiety, mood, and emotional disorders, patient access to these interventions is limited.4 One barrier to CBT for anxiety, mood, and emotional disorders is the traditional use of single-disorder protocols (SDPs) to separately treat each disorder (eg, major depression, generalized anxiety disorder, panic disorder).
Use of SDPs places a high burden on clinicians, requiring them to learn and competently implement multiple different manualized interventions for each anxiety, mood, or emotional disorder encountered in practice.4 It is common for individuals who present with an anxiety, mood, or emotional disorder to experience co-occurring disorders.5 Traditional SDP-based CBT may require multiple SDPs to address co-occurring disorders, extending time in treatment and increasing training burden. There is evidence that even when an SDP is used, co-occurring difficulties may decrease in intensity.6 Thus, evidence-based CBT for 1 presenting concern may positively affect co-occurring difficulties that are not the primary treatment target.6
Unified Protocol (UP) is a transdiagnostic CBT intervention for anxiety and mood disorders. UP targets emotional experiences (eg, negative affect and emotional distress) that are present in multiple anxiety, depression, and emotional disorders. UP is organized into 8 modules and uses interventions present in other CBT SDPs, such as teaching objective assessment methods to clients, motivational enhancement and goal setting, emotion psychoeducation, mindful awareness, cognitive reframing, and exposure principles as mechanisms of change (Table 1).4 UP is an ideal intervention for addressing a number of anxiety, mood, and emotional disorders as well as addressing cooccurring disorders within the same course of treatment.
UP has been compared to SDPs; studies illustrate that UP is equivalent to SDPs at the end of treatment and at 6 months posttreatment.4,7 Additionally, patients who received UP experienced symptom reduction for multiple co-occurring disorders.7 Furthermore, patients were less likely to drop out of UP when compared with SDPs.4
Studies have reported positive impacts on affective disorders with UP. A 2019 meta-analysis found significant reductions in depression and anxiety-related disorders.8 Additionally, UP has been shown to be effective when delivered in person and via telehealth.9,10 UP has also been successfully used in veterans.11 While traditional models of UP (1-2 sessions weekly) have a lower dropout rate than SDPs, UP and CBT dropout rates still leave room for improvement.12-14 Specifically, rates of attrition from SDP CBT and transdiagnostic CBT protocols range from 9% to 35%, and dropout reduces the likelihood of attaining a full therapeutic dose of any course of CBT. Notably, accelerated delivery of CBT (ie, ≥ 3 sessions/wk) has been shown to reduce risk of dropout.14,15
Veterans are at increased risk for suicide, and anxiety and mood disorders are associated with increased risk of suicide attempt and death.16,17 Very few veterans who could benefit from high-quality CBT interventions, whether SDP or UP, are able to access them. Only 6.3% of veterans received ≥1 session of an evidence-based CBT SDP for posttraumatic stress disorder (PTSD) at 6 clinics evaluated in 2010.18
We identified 2 strategies to increase access to and completion of an evidence-based CBT course. First, the use of transdiagnostic UP instead of SDPs reduced burden on therapists and allowed them to address presenting and co-occurring disorders within the same course of care. Second, the use of an accelerated model of service delivery reduced dropout risk. Training clinicians to deliver UP is efficient and cost-effective, considering clinicians use core strategies that can be tailored and flexibly applied to a range of emotional difficulties. Thus, implementing UP may decrease barriers to receiving an optimal dose of an evidence-based CBT delivered with fidelity in a time- and cost-efficient manner.4 Two studies have found no evidence of differences in outcomes between UP and SDPs, suggesting that training and supervising clinicians in a single transdiagnostic UP intervention may prepare them to treat heterogeneous and co-occurring anxiety, mood, and emotional disorders with less burden than learning multiple SDPs.7,19
Delivering UP in an accelerated or massed format (≥4 sessions/wk) instead of the traditional spaced model (1 session/wk) has empirical support but has not been widely implemented. This approach, sometimes referred to as a UP-intensive outpatient program (UP-IOP) or UP-intensive outpatient track (UP-IOT), has been shown to be feasible, acceptable, and effective, with increased completion rates compared with traditional UP delivery (1-2 sessions/wk).20-22
Ragsdale et al describe a 2-week IOP with multiple treatment tracks, including a general track.20 The general track includes massed UP and additional standard services, including case management, wellness services, family services, and a single session effective behaviors group. Additional augmentation services are available when clinically indicated (eg, repetitive transcranial magnetic stimulation, transcranial direct current stimulation, psychoeducation, motivational interviewing, relapse prevention). In other words, this was an UP-IOP.20
Thompson-Brenner et al described a successful implementation of massed UP applied in intensive treatment settings, such as residential and day-hospital programs, for eating disorders. Patients reported improvements in 3 UP targets: experiential avoidance, mindfulness, and anxiety.21 Watkins et al evaluated a 2-week IOP using CBT for comorbid substance use and mental health disorders, including prolonged exposure, UP, and relapse prevention for substance use disorders. Participants were post-9/11 veterans and activeduty personnel. Results indicated that UP reduced PTSD and depressive symptoms following treatment. Furthermore, the retention rate (91%) was higher than retention in outpatient treatment (39%-65%), supporting the IOP model as a strategy to reduce dropout.22
Massed psychotherapy has been extended to IOP programs for PTSD treatment within the Veterans Health Administration (VHA). Yamokoski et al found that patients who completed an IOP that included massed CBT for PTSD had high retention, high satisfaction, and significant reduction in self-reported co-occurring depression symptoms. The authors also found that this model of care could be implemented and sustained within a VHA facility using minimal staffing resources.23
The UP-IOP models described by Ragsdale et al and Watkins et al included massed UP as the primary evidence-based practice (EBP) with adjunctive groups (eg, wellness and educational groups and access to complementary interventions such as mindfulness and yoga); they found that adding these groups increased retention and patient- reported satisfaction (ie, UP-IOP).20,22 The addition of wellness education alongside a primary EBP aligns with the VHA focus on whole health well-being and wellness. This includes understanding factors that motivate a patient toward health and well-being, providing health education, and offering access to complementary interventions such as mindfulness.24
Dryden et al described the whole health transformation within VHA as a proactive approach to addressing both employee and patient wellness. Their research found that the whole health model promoted wellbeing in patients and staff and these improvements were sustained during the COVID-19 pandemic. Dryden et al also noted that virtual technologies facilitated continued whole health implementation.25
The literature illustrates that (1) massed UP can be delivered with complementary education and wellness offerings that may increase retention and satisfaction by enriching treatment (eg, delivering UP-IOP); (2) whole health, including wellness education and complementary interventions (eg, mindfulness, motivational enhancement), promotes well-being in patients and clinicians; and (3) whole health education and complementary interventions can be delivered virtually.
IVET
Health Care Need
Veterans Affairs Pacific Islands Health Care System (VAPIHCS) provides medical services to veterans in the Hawaiian Islands, American Samoa, Guam, and Saipan spanning nearly 4000 miles across the Pacific Ocean. Prior to implementation of this program, veterans who received care at VAPIHCS had little to no access to UP in outpatient settings and no access to UP in residential settings. Access to UP depended on the presence of a therapist trained in UP within a given clinic and was geographically limited to the location of the UP-trained therapist. The limited outpatient access to UP was restricted to the traditional UP delivery model (eg, about 1 session/wk); thus, there was no access to accelerated UP for veterans served at VAPIHCS. In the fiscal year prior to implementation of the massed UP program, > 1000 VAPIHCS veterans had been diagnosed with obsessive-compulsive related disorder or anxiety. A massed-UP program with weekly rolling admissions would support access to UP for more veterans over 12 months, and the virtual treatment modality would reduce barriers for diverse and underserved veterans, making care more equitable and inclusive.
Successful implementation and sustainment of an EBP prompted the establishment of this UP program. In 2022, VAPIHCS launched the Intensive Virtual Evidence- Based Psychotherapy Team (iVET) for treatment of PTSD. This clinic and associated EBP project demonstrated that massed (≥3 individual sessions/wk) of prolonged exposure (PE) therapy, delivered virtually to a geographically diverse veteran population with PTSD, resulted in significant reductions in PTSD, depression, and anxiety symptoms and substance use risk factors, with very high retention rates. The iVET for PTSD program was feasible, acceptable, and effective, with veterans reporting significant improvement in quality of life and high satisfaction with their mental health services.15 Given the known benefits of transdiagnostic UP treatment (vs SDPs), the need for accelerated UP, and success with accelerated PE, our goal was to spread the EBP of massed (≥3 sessions/ wk) virtual psychotherapy to other presenting problems (eg, anxiety disorders with or without co-occurring unipolar depression) using transdiagnostic UP.
Program Description
The program implemented within outpatient mental health services at VAPIHCS was iVET for the treatment of anxiety with or without co-occurring depression. The program model consists of an accelerated course of UP and whole health education provided via VA Video Connect (VVC), the VA video telehealth platform. iVET is a 2- to 4-week program and consists of 3 parts: (1) massed individual UP for transdiagnostic treatment of anxiety and co-occurring depression, (2) group whole health and wellness classes, and (3) individual health coaching to address personal wellness goals. Programming is offered over 10-hour days to increase access across multiple time zones, especially to allow participation from Guam and Saipan.
When a patient is referred to iVET, the first contact is a video (or telephone) appointment with a registered nurse (RN) for a screening session. The screening session is designed to provide education about the program (including interventions, time commitment, and resources required for participation). Following education, the RN completes a safety screening, including screening for suicidal ideation and risk, as well as intimate partner violence risk. If urgent safety concerns are present, a licensed social worker or psychologist joins the screening to complete further risk assessment and address any safety concerns.
Following screening, patients are scheduled for a VVC telehealth intake with a licensed therapist (social worker or psychologist) to complete a diagnostic interview. Patients are sent a secure link to complete a measurement-based care (MBC) battery of self-report measures, including assessments of demographics, anxiety symptoms, depression symptoms, substance use, psychological flexibility, quality of life, and satisfaction with mental health care. The results of the diagnostic interview and self-report measures are discussed with the patient during the intake session to plan next steps and support shared decision-making. This initial VVC intake not only allows for fit assessment but also serves to troubleshoot technical difficulties with the virtual platforms.
Notably, there are minimal exclusion criteria for participation in iVET. These include active unmanaged psychosis or manic symptoms, recent suicidal crises (attempt within 8 weeks), active nonsuicidal self-injury (within 8 weeks), and moderate to severe cognitive impairment. Following intake, patients are scheduled to begin their course of care with iVET. Upon completion of intake, patients receive program materials for individual and group classes and are told they will receive email links for all VVC telehealth appointments. Patients are admitted to the iVET on a rolling basis, thereby increasing access compared with closed group and/or cohort models of care.
Patients receiving iVET attend 2 to 4 telehealth appointments daily and complete exercises between sessions. The primary iVET for Anxiety program EBP intervention is a massed or accelerated individual course of UP, which includes 8 primary components: assessment, goals and motivation, understanding emotions, mindful emotion awareness, cognitive flexibility, countering emotional behaviors, understanding and confronting physical sensations, and emotional exposures. UP is delivered in 4 to 8 individual sessions weekly (60-90 minutes each), allowing completion of the full UP protocol with fidelity in 2 to 4 weeks. In addition to primary EBP intervention, patients participate in 4 group sessions weekly (50 minutes each) of a whole health and wellness education class and have access to 1 individual health coaching session weekly (30- 60 minutes) to set wellness goals and receive coaching. During iVET, patients are invited to complete MBC batteries of self-report measures assessing anxiety symptoms, depression symptoms, substance use, psychological flexibility, quality of life, and satisfaction with mental health care at sessions 1, 5, 9, 13, and the final UP session. Following discharge from the iVET, patients are offered 1-, 3-, and 6-month individual postdischarge check-up sessions with a therapist, during which they are invited to complete MBC measures and review relapse prevention and maintenance of treatment gains. Likewise, patients are offered 1-, 3-, and 6-month individual postdischarge check-up sessions with an RN focused on maintaining wellness gains.
The iVET for Anxiety staff has 3 therapists (psychologists or social workers) and 1 RN. Additionally, the iVET for Anxiety is supported by a program manager and a program support assistant who support 2 programs total (the iVET for Anxiety plus another mental health program). The primary cost of the program is staff salary. Additional resources included computer equipment for staff and supplies (eg, printed materials for patients and office supplies). Due to the virtual environment of care, iVET staff telework and do not require physical space within VAPIHCS.
Outcomes
Veterans receiving iVET for Anxiety are invited to complete MBC multiple times, including pretreatment, during UP treatment (sessions 1, 5, 9, 13, and the final session), and posttreatment (1, 3, and 6 months). MBC measures include self-reported demographics; a 2-item measure of satisfaction with mental health services; the Acceptance and Action Questionnaire II,26 the Brief Addiction Monitor-Intensive Outpatient Program, 27 the Generalized Anxiety Disorder-7,28 the Patient Health Questionnaire (PHQ-9),29 and the Quality of Life Enjoyment and Satisfaction Questionnaire-Short Form.30
Forty-two veterans completed the iVET for Anxiety program, with a retention rate of 87.5% completing . 16 sessions of massed UP (Table 2). Veterans reported reduced anxiety (P < .001), depression (P < .001), and substance use risk (P < .001). Veterans experienced improved acceptance of emotional experiences (P < .001) and quality of life (P < .001), based on paired sample t tests comparing session 1 vs final session scores on the self-reported measures. Veterans also reported high satisfaction with mental health care in iVET for Anxiety.
Veterans experienced reduced thoughts of death or suicidal ideation (SI) based on responses to item 9 of PHQ-9. When SI was categorically analyzed (presence vs absence) using PHQ-9 item 9, there was an association observed between absence of SI and completion of a course of massed UP that does not appear to be due to chance, (X2 [1, N = 42) = 3.94; P = .047). In addition, veterans who completed the program showed a significant decrease in SI severity measured continuously (range, 0-3) on PHQ-9 item 9 (P < .05) (Table 3).
Future Directions
The aim of this program is to see sustained patient outcomes as iVET continues to serve more veterans. Another line of inquiry is longer- term follow-up, given that long-term follow- up was not addressed in this project. We also hope that the accelerated model of care can be applied to treatment of other presenting concerns (eg, relationship difficulties, insomnia). Expansion of accelerated mental health treatment into other federal and nonfederal health care settings is another area worthy of future inquiry. Exploration of staff satisfaction and burnout related to providing accelerated UP is another important future direction. Relatedly, assessment of the staff burden to learn 1 transdiagnostic EBP vs learning multiple SDPs is another future direction. Likewise, exploration of institutional benefits of investment in transdiagnostic training, supervision, and consultation for UP vs multiple SDPs may be important. These areas could also result in insightful, beneficial evidence of the effectiveness of massed UP to add to the existing literature.
Conclusions
UP for transdiagnostic treatment of anxiety, depressive, and emotional disorders has demonstrated reduced suffering and improved functioning and is supported by multiple clinical practice guidelines.1-4 Federal practitioners are positioned to improve access to this intervention, thereby reducing pain and improving lives. Indeed, it is crucial to envision a future state in which access to UP for a range of anxiety and depressive disorders is improved and broad, retention rates are dramatically improved, and clinicians providing UP do not experience the high burden and burnout associated with needing to learn and implement a variety of SDPs. Development of these programs, or similar tracks within existing programs, that provide massed or accelerated UP for transdiagnostic treatment of a range of anxiety and depressive disorders with virtual delivery options, is imperative to advance improved care for patients and clinicians.
Federal health care settings treating patients with anxiety and depression, such as those within the US Department of Defense, Indian Health Services, Bureau of Prisons, and VHA, are positioned to implement programs like iVET. Moreover, at the institutional level, investment in training and supervision in the transdiagnostic UP as opposed to multiple SDPs warrants consideration. We believe this model of care has great merit and foresee a future where all patients seeking treatment for anxiety and depression have the option to complete an accelerated or massed course of transdiagnostic care with UP if they so desire. Our experiences with iVET illustrate the feasibility, acceptability, and sustainability of such programs without requiring substantial staffing and financial resources.
- US Department of Veterans Affairs, US Department of Defense. VA/DoD clinical practice guideline for the management of major depressive disorder. Version 4. 2022. Accessed February 1, 2026. https://www.healthquality.va.gov/guidelines/MH/mdd/VADoDMDDCPGFinal508.pdf
- American Psychological Association. Clinical practice guideline for the treatment of depression across three age cohorts. February 2019. Accessed February 4, 2026. https://www.apa.org/depression-guideline/guideline.pdf
- Katzman MA, Bleau P, Blier P, et al. Canadian clinical practice guidelines for the management of anxiety, posttraumatic stress and obsessive compulsive disorders. BMC Psychiatry. 2014;14:S1. doi:10.1186/1471-244X-14-S1-S1
- Barlow DH, Farchione TJ, Bullis JR, et al. The unified protocol for transdiagnostic treatment of emotional disorders compared with diagnosis-specific protocols for anxiety disorders: a randomized clinical trial. JAMA Psychiatry. 2017;74:875-884. doi:10.1001/jamapsychiatry.2017.2164
- Calkins AW, et al. Comorbidity of anxiety and depression. In: Ressler KJ, Pine DS, Rothbaum BO, eds. Anxiety Disorders, Primer On. Oxford Academic; 2015. https://doi.org/10.1093/med/9780199395125.003.0021
- Manber R, Edinger JD, Gress JL, et al. Cognitive behavioral therapy for insomnia enhances depression outcome in patients with comorbid major depressive disorder and insomnia. Sleep. 2008;31:489-495. doi:10.1093/sleep/31.4.489
- Steele SJ, Farchione TJ, Cassiello-Robbins C, et al. Efficacy of the Unified Protocol for transdiagnostic treatment of comorbid psychopathology accompanying emotional disorders compared to treatments targeting single disorders. J Psychiatr Res. 2018;104:211-216. doi:10.1016/j.jpsychires.2018.08.005
- Sakiris N, Berle D. A systematic review and meta-analysis of the Unified Protocol as a transdiagnostic emotion regulation based intervention. Clin Psychol Rev. 2019;72:101751. doi:10.1016/j.cpr.2019.101751
- Cassiello-Robbins C, Rosenthal MZ, Ammirati RJ. Delivering transdiagnostic treatment over telehealth during the COVID-19 pandemic: application of the unified protocol. Cogn Behav Pract. 2021;28:555-572. doi:10.1016/j.cbpra.2021.04.007
- Meyer EC, Coe E, Pennington ML, et al. The unified protocol for transdiagnostic treatment of emotional disorders delivered to firefighters via videoconferencing: pilot outcomes highlighting improvements in alcohol use disorder and posttraumatic stress disorder symptoms. Cogn Behav Pract. 2024;31:215-229. doi:10.1016/j.cbpra.2022.08.004
- Varkovitzky RL, Sherrill AM, Reger GM. Effectiveness of the unified protocol for transdiagnostic treatment of emotional disorders among veterans with posttraumatic stress disorder: a pilot study. Behav Modif. 2018;42:210-230. doi:10.1177/0145445517724539
- Oliveira JT, Sousa I, Ribeiro AP, et al. Premature termination of the unified protocol for the transdiagnostic treatment of emotional disorders: The role of ambivalence towards change. Clin Psychol Psychother. 2022;29:1089-1100. doi:10.1002/cpp.2694
- Schaeuffele C, Homeyer S, Perea L, et al. The unified protocol as an internet-based intervention for emotional disorders: Randomized controlled trial. PLoS One. 2022;17:e0270178. doi:10.1371/journal.pone.0270178
- Bentley KH, Cohen ZD, Kim T, et al. The nature, timing, and symptom trajectories of dropout from transdiagnostic and single-diagnosis cognitive-behavioral therapy for anxiety disorders. Behav Ther. 2021;52:1364-1376. doi:10.1016/j.beth.2021.03.007
- Aosved AC, Brown TB, Bell JC, et al. Accelerated prolonged exposure therapy for posttraumatic stress disorder in a Veterans Health Administration system. Fed Pract. 2025;42:S6-S11. doi:10.12788/fp.0568
- Nepon J, Belik SL, Bolton J, et al. The relationship between anxiety disorders and suicide attempts: findings from the National Epidemiologic Survey on Alcohol and Related Conditions. Depress Anxiety. 2010;27:791-798. doi:10.1002/da.20674
- Shiner B, D’Avolio LW, Nguyen TM, et al. Measuring use of evidence based psychotherapy for posttraumatic stress disorder. Adm Policy Ment Health. 2013;40:311-318. doi:10.1007/s10488-012-0421-0
- Nichter B, Stein MB, Monteith LL, et al. Risk factors for suicide attempts among U.S. military veterans: A 7-year population-based, longitudinal cohort study. Suicide Life Threat Behav. 2022;52:303-316. doi:10.1111/sltb.12822
- McHugh RK, Barlow DH. The dissemination and implementation of evidence-based psychological treatments. A review of current efforts. Am Psychol. 2010;65:73-84. doi:10.1037/a0018121
- Ragsdale KA, Nichols AA, Mehta M, et al. Comorbid treatment of traumatic brain injury and mental health disorders. NeuroRehabilitation. 2024;55:375-384. doi:10.3233/NRE-230235
- Thompson-Brenner H, Brooks GE, Boswell JF, et al. Evidence-based implementation practices applied to the intensive treatment of eating disorders: summary of research and illustration of principles using a case example. Clin Psychol Sci Pract. 2018;25:e12221. doi:10.1111/cpsp.12221
- Watkins LE, Patton SC, Drexler K, et al. Clinical effectiveness of an intensive outpatient program for integrated treatment of comorbid substance abuse and mental health disorders. Cog Behav Pract. 2023;30:354-366.
- Yamokoski C, Flores H, Facemire V, et al. Feasibility of an intensive outpatient treatment program for post-traumatic stress disorder within the veterans health care administration. Psychol Serv. 2023;20:506-515. doi:10.1037/ser0000628
- Gaudet T, Kligler B. Whole health in the whole system of the Veterans Administration: how will we know we have reached this future state?. J Altern Complement Med. 2019;25:S7-S11. doi:10.1089/acm.2018.29061.gau
- Dryden EM, Bolton RE, Bokhour BG, et al. Leaning into whole health: sustaining system transformation while supporting patients and employees during COVID-19. Glob Adv Health Med. 2021;10:21649561211021047. doi:10.1177/21649561211021047
- Bond FW, Hayes SC, Baer RA, et al. Preliminary psychometric properties of the Acceptance and Action Questionnaire-II: a revised measure of psychological inflexibility and experiential avoidance. Behav Ther. 2011;42:676-688. doi:10.1016/j.beth.2011.03.007
- Cacciola JS, Alterman AI, Dephilippis D, et al. Development and initial evaluation of the Brief Addiction Monitor (BAM). J Subst Abuse Treat. 2013;44:256-263. doi:10.1016/j.jsat.2012.07.013
- Spitzer RL, Kroenke K, Williams JB, et al. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166:1092-1097. doi:10.1001/archinte.166.10.1092
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606-613. doi:10.1046/j.1525-1497.2001.016009606.x
- Stevanovic D. Quality of life enjoyment and satisfaction questionnaire-short form for quality of life assessments in clinical practice: a psychometric study. J Psychiatr Ment Health Nurs. 2011;18:744-750. doi:10.1111/j.1365-2850.2011.01735.x
- US Department of Veterans Affairs, US Department of Defense. VA/DoD clinical practice guideline for the management of major depressive disorder. Version 4. 2022. Accessed February 1, 2026. https://www.healthquality.va.gov/guidelines/MH/mdd/VADoDMDDCPGFinal508.pdf
- American Psychological Association. Clinical practice guideline for the treatment of depression across three age cohorts. February 2019. Accessed February 4, 2026. https://www.apa.org/depression-guideline/guideline.pdf
- Katzman MA, Bleau P, Blier P, et al. Canadian clinical practice guidelines for the management of anxiety, posttraumatic stress and obsessive compulsive disorders. BMC Psychiatry. 2014;14:S1. doi:10.1186/1471-244X-14-S1-S1
- Barlow DH, Farchione TJ, Bullis JR, et al. The unified protocol for transdiagnostic treatment of emotional disorders compared with diagnosis-specific protocols for anxiety disorders: a randomized clinical trial. JAMA Psychiatry. 2017;74:875-884. doi:10.1001/jamapsychiatry.2017.2164
- Calkins AW, et al. Comorbidity of anxiety and depression. In: Ressler KJ, Pine DS, Rothbaum BO, eds. Anxiety Disorders, Primer On. Oxford Academic; 2015. https://doi.org/10.1093/med/9780199395125.003.0021
- Manber R, Edinger JD, Gress JL, et al. Cognitive behavioral therapy for insomnia enhances depression outcome in patients with comorbid major depressive disorder and insomnia. Sleep. 2008;31:489-495. doi:10.1093/sleep/31.4.489
- Steele SJ, Farchione TJ, Cassiello-Robbins C, et al. Efficacy of the Unified Protocol for transdiagnostic treatment of comorbid psychopathology accompanying emotional disorders compared to treatments targeting single disorders. J Psychiatr Res. 2018;104:211-216. doi:10.1016/j.jpsychires.2018.08.005
- Sakiris N, Berle D. A systematic review and meta-analysis of the Unified Protocol as a transdiagnostic emotion regulation based intervention. Clin Psychol Rev. 2019;72:101751. doi:10.1016/j.cpr.2019.101751
- Cassiello-Robbins C, Rosenthal MZ, Ammirati RJ. Delivering transdiagnostic treatment over telehealth during the COVID-19 pandemic: application of the unified protocol. Cogn Behav Pract. 2021;28:555-572. doi:10.1016/j.cbpra.2021.04.007
- Meyer EC, Coe E, Pennington ML, et al. The unified protocol for transdiagnostic treatment of emotional disorders delivered to firefighters via videoconferencing: pilot outcomes highlighting improvements in alcohol use disorder and posttraumatic stress disorder symptoms. Cogn Behav Pract. 2024;31:215-229. doi:10.1016/j.cbpra.2022.08.004
- Varkovitzky RL, Sherrill AM, Reger GM. Effectiveness of the unified protocol for transdiagnostic treatment of emotional disorders among veterans with posttraumatic stress disorder: a pilot study. Behav Modif. 2018;42:210-230. doi:10.1177/0145445517724539
- Oliveira JT, Sousa I, Ribeiro AP, et al. Premature termination of the unified protocol for the transdiagnostic treatment of emotional disorders: The role of ambivalence towards change. Clin Psychol Psychother. 2022;29:1089-1100. doi:10.1002/cpp.2694
- Schaeuffele C, Homeyer S, Perea L, et al. The unified protocol as an internet-based intervention for emotional disorders: Randomized controlled trial. PLoS One. 2022;17:e0270178. doi:10.1371/journal.pone.0270178
- Bentley KH, Cohen ZD, Kim T, et al. The nature, timing, and symptom trajectories of dropout from transdiagnostic and single-diagnosis cognitive-behavioral therapy for anxiety disorders. Behav Ther. 2021;52:1364-1376. doi:10.1016/j.beth.2021.03.007
- Aosved AC, Brown TB, Bell JC, et al. Accelerated prolonged exposure therapy for posttraumatic stress disorder in a Veterans Health Administration system. Fed Pract. 2025;42:S6-S11. doi:10.12788/fp.0568
- Nepon J, Belik SL, Bolton J, et al. The relationship between anxiety disorders and suicide attempts: findings from the National Epidemiologic Survey on Alcohol and Related Conditions. Depress Anxiety. 2010;27:791-798. doi:10.1002/da.20674
- Shiner B, D’Avolio LW, Nguyen TM, et al. Measuring use of evidence based psychotherapy for posttraumatic stress disorder. Adm Policy Ment Health. 2013;40:311-318. doi:10.1007/s10488-012-0421-0
- Nichter B, Stein MB, Monteith LL, et al. Risk factors for suicide attempts among U.S. military veterans: A 7-year population-based, longitudinal cohort study. Suicide Life Threat Behav. 2022;52:303-316. doi:10.1111/sltb.12822
- McHugh RK, Barlow DH. The dissemination and implementation of evidence-based psychological treatments. A review of current efforts. Am Psychol. 2010;65:73-84. doi:10.1037/a0018121
- Ragsdale KA, Nichols AA, Mehta M, et al. Comorbid treatment of traumatic brain injury and mental health disorders. NeuroRehabilitation. 2024;55:375-384. doi:10.3233/NRE-230235
- Thompson-Brenner H, Brooks GE, Boswell JF, et al. Evidence-based implementation practices applied to the intensive treatment of eating disorders: summary of research and illustration of principles using a case example. Clin Psychol Sci Pract. 2018;25:e12221. doi:10.1111/cpsp.12221
- Watkins LE, Patton SC, Drexler K, et al. Clinical effectiveness of an intensive outpatient program for integrated treatment of comorbid substance abuse and mental health disorders. Cog Behav Pract. 2023;30:354-366.
- Yamokoski C, Flores H, Facemire V, et al. Feasibility of an intensive outpatient treatment program for post-traumatic stress disorder within the veterans health care administration. Psychol Serv. 2023;20:506-515. doi:10.1037/ser0000628
- Gaudet T, Kligler B. Whole health in the whole system of the Veterans Administration: how will we know we have reached this future state?. J Altern Complement Med. 2019;25:S7-S11. doi:10.1089/acm.2018.29061.gau
- Dryden EM, Bolton RE, Bokhour BG, et al. Leaning into whole health: sustaining system transformation while supporting patients and employees during COVID-19. Glob Adv Health Med. 2021;10:21649561211021047. doi:10.1177/21649561211021047
- Bond FW, Hayes SC, Baer RA, et al. Preliminary psychometric properties of the Acceptance and Action Questionnaire-II: a revised measure of psychological inflexibility and experiential avoidance. Behav Ther. 2011;42:676-688. doi:10.1016/j.beth.2011.03.007
- Cacciola JS, Alterman AI, Dephilippis D, et al. Development and initial evaluation of the Brief Addiction Monitor (BAM). J Subst Abuse Treat. 2013;44:256-263. doi:10.1016/j.jsat.2012.07.013
- Spitzer RL, Kroenke K, Williams JB, et al. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166:1092-1097. doi:10.1001/archinte.166.10.1092
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606-613. doi:10.1046/j.1525-1497.2001.016009606.x
- Stevanovic D. Quality of life enjoyment and satisfaction questionnaire-short form for quality of life assessments in clinical practice: a psychometric study. J Psychiatr Ment Health Nurs. 2011;18:744-750. doi:10.1111/j.1365-2850.2011.01735.x
Accelerated Unified Protocol for Transdiagnostic Treatment of Anxiety Disorders in a VHA System
Accelerated Unified Protocol for Transdiagnostic Treatment of Anxiety Disorders in a VHA System
Young Adults With Suicidal Ideation: Who Reaches Out by Texting for Help and Why Do Others Hold Back?
Young Adults With Suicidal Ideation: Who Reaches Out by Texting for Help and Why Do Others Hold Back?
TOPLINE:
Among young adults with suicidal ideation, factors associated with the use of crisis text services were female sex, minoritized sexual orientation, engagement with a mental health provider, and prior hospitalizations. Participants who never texted crisis lines faced barriers such as doubts about effectiveness and embarrassment.
METHODOLOGY:
- Researchers conducted a cross-sectional survey study in Oregon from August to December 2023 to identify characteristics linked to the use of crisis text services and barriers to use in young adults aged 18-24 years with suicidal ideation and financial stress.
- Overall, 118 participants were recruited through community partners and social media advertisements; 76% of them identified having a minoritized gender or sexual orientation.
- Participants completed an online survey with 38 closed-ended and two open-ended items, including questions about hospitalizations for suicidal thoughts, suicide attempts, mental health provider status, service use, decision-making factors for contacting crisis lines, and barriers preventing the use of the service.
- Differences in demographic and health care characteristics between those who had ever texted crisis lines and those who had never were examined.
TAKEAWAY:
- When asked about disclosing suicidal ideation, participants most frequently told no one (69%), told a friend/boyfriend/girlfriend (64%), and texted/chatted with a crisis line (47%).
- Female sex (P = .019) and having a minoritized sexual orientation (P = .048) were significantly associated with the use of crisis text services, whereas minoritized gender status, race, and urbanicity showed no significant association. Having a mental health provider correlated with the use of crisis text services (P = .010), as did prior hospitalization for suicidal ideation or suicide attempt (P = .003).
- Participants who had ever texted crisis lines (n = 55) most often reported using crisis text services because they had no one else to talk to (78%), felt like a burden to others (71%), and preferred anonymity (65%).
- Among 63 participants who never texted crisis lines, 84% had heard of crisis text services but chose not to use them; key reasons for not texting included believing it would not help (46%), embarrassment (41%), and preferring to solve the problem independently (35%).
IN PRACTICE:
"[The study findings] highlight that unique outreach efforts may be necessary to engage young adults reluctant to seek support," the authors wrote, further suggesting that "local and national lines could benefit from improved conversational quality within CTS [crisis text services], possibly including enhanced training for counselors to increase the personalization of counseling and sensitivity to texters' situations."
SOURCE:
The study was led by Kate LaForge, PhD, MPH, of the Center to Improve Veteran Involvement in Care at the VA Portland Healthcare System in Portland, Oregon. It was published online on March 13, 2026, in the Journal of Adolescent Health.
LIMITATIONS:
The cross-sectional design did not allow for determining causal relationships between healthcare characteristics and the use of the crisis text service. Relying on self-reported data may have introduced recall bias. The severity of suicidal ideation was not measured, and the sample size was small.
DISCLOSURES:
The research was supported by the Office of Academic Affiliations and the Office of Research and Development Health Systems Research Service, US Department of Veterans Affairs. Some authors reported being supported by various sources, including the Agency for Healthcare Research & Quality, National Institute on Drug Abuse, or Department of Veterans Affairs Health Systems Research, and one of them reported being a paid consultant for Google Health. The authors declared having no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Among young adults with suicidal ideation, factors associated with the use of crisis text services were female sex, minoritized sexual orientation, engagement with a mental health provider, and prior hospitalizations. Participants who never texted crisis lines faced barriers such as doubts about effectiveness and embarrassment.
METHODOLOGY:
- Researchers conducted a cross-sectional survey study in Oregon from August to December 2023 to identify characteristics linked to the use of crisis text services and barriers to use in young adults aged 18-24 years with suicidal ideation and financial stress.
- Overall, 118 participants were recruited through community partners and social media advertisements; 76% of them identified having a minoritized gender or sexual orientation.
- Participants completed an online survey with 38 closed-ended and two open-ended items, including questions about hospitalizations for suicidal thoughts, suicide attempts, mental health provider status, service use, decision-making factors for contacting crisis lines, and barriers preventing the use of the service.
- Differences in demographic and health care characteristics between those who had ever texted crisis lines and those who had never were examined.
TAKEAWAY:
- When asked about disclosing suicidal ideation, participants most frequently told no one (69%), told a friend/boyfriend/girlfriend (64%), and texted/chatted with a crisis line (47%).
- Female sex (P = .019) and having a minoritized sexual orientation (P = .048) were significantly associated with the use of crisis text services, whereas minoritized gender status, race, and urbanicity showed no significant association. Having a mental health provider correlated with the use of crisis text services (P = .010), as did prior hospitalization for suicidal ideation or suicide attempt (P = .003).
- Participants who had ever texted crisis lines (n = 55) most often reported using crisis text services because they had no one else to talk to (78%), felt like a burden to others (71%), and preferred anonymity (65%).
- Among 63 participants who never texted crisis lines, 84% had heard of crisis text services but chose not to use them; key reasons for not texting included believing it would not help (46%), embarrassment (41%), and preferring to solve the problem independently (35%).
IN PRACTICE:
"[The study findings] highlight that unique outreach efforts may be necessary to engage young adults reluctant to seek support," the authors wrote, further suggesting that "local and national lines could benefit from improved conversational quality within CTS [crisis text services], possibly including enhanced training for counselors to increase the personalization of counseling and sensitivity to texters' situations."
SOURCE:
The study was led by Kate LaForge, PhD, MPH, of the Center to Improve Veteran Involvement in Care at the VA Portland Healthcare System in Portland, Oregon. It was published online on March 13, 2026, in the Journal of Adolescent Health.
LIMITATIONS:
The cross-sectional design did not allow for determining causal relationships between healthcare characteristics and the use of the crisis text service. Relying on self-reported data may have introduced recall bias. The severity of suicidal ideation was not measured, and the sample size was small.
DISCLOSURES:
The research was supported by the Office of Academic Affiliations and the Office of Research and Development Health Systems Research Service, US Department of Veterans Affairs. Some authors reported being supported by various sources, including the Agency for Healthcare Research & Quality, National Institute on Drug Abuse, or Department of Veterans Affairs Health Systems Research, and one of them reported being a paid consultant for Google Health. The authors declared having no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Among young adults with suicidal ideation, factors associated with the use of crisis text services were female sex, minoritized sexual orientation, engagement with a mental health provider, and prior hospitalizations. Participants who never texted crisis lines faced barriers such as doubts about effectiveness and embarrassment.
METHODOLOGY:
- Researchers conducted a cross-sectional survey study in Oregon from August to December 2023 to identify characteristics linked to the use of crisis text services and barriers to use in young adults aged 18-24 years with suicidal ideation and financial stress.
- Overall, 118 participants were recruited through community partners and social media advertisements; 76% of them identified having a minoritized gender or sexual orientation.
- Participants completed an online survey with 38 closed-ended and two open-ended items, including questions about hospitalizations for suicidal thoughts, suicide attempts, mental health provider status, service use, decision-making factors for contacting crisis lines, and barriers preventing the use of the service.
- Differences in demographic and health care characteristics between those who had ever texted crisis lines and those who had never were examined.
TAKEAWAY:
- When asked about disclosing suicidal ideation, participants most frequently told no one (69%), told a friend/boyfriend/girlfriend (64%), and texted/chatted with a crisis line (47%).
- Female sex (P = .019) and having a minoritized sexual orientation (P = .048) were significantly associated with the use of crisis text services, whereas minoritized gender status, race, and urbanicity showed no significant association. Having a mental health provider correlated with the use of crisis text services (P = .010), as did prior hospitalization for suicidal ideation or suicide attempt (P = .003).
- Participants who had ever texted crisis lines (n = 55) most often reported using crisis text services because they had no one else to talk to (78%), felt like a burden to others (71%), and preferred anonymity (65%).
- Among 63 participants who never texted crisis lines, 84% had heard of crisis text services but chose not to use them; key reasons for not texting included believing it would not help (46%), embarrassment (41%), and preferring to solve the problem independently (35%).
IN PRACTICE:
"[The study findings] highlight that unique outreach efforts may be necessary to engage young adults reluctant to seek support," the authors wrote, further suggesting that "local and national lines could benefit from improved conversational quality within CTS [crisis text services], possibly including enhanced training for counselors to increase the personalization of counseling and sensitivity to texters' situations."
SOURCE:
The study was led by Kate LaForge, PhD, MPH, of the Center to Improve Veteran Involvement in Care at the VA Portland Healthcare System in Portland, Oregon. It was published online on March 13, 2026, in the Journal of Adolescent Health.
LIMITATIONS:
The cross-sectional design did not allow for determining causal relationships between healthcare characteristics and the use of the crisis text service. Relying on self-reported data may have introduced recall bias. The severity of suicidal ideation was not measured, and the sample size was small.
DISCLOSURES:
The research was supported by the Office of Academic Affiliations and the Office of Research and Development Health Systems Research Service, US Department of Veterans Affairs. Some authors reported being supported by various sources, including the Agency for Healthcare Research & Quality, National Institute on Drug Abuse, or Department of Veterans Affairs Health Systems Research, and one of them reported being a paid consultant for Google Health. The authors declared having no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
Young Adults With Suicidal Ideation: Who Reaches Out by Texting for Help and Why Do Others Hold Back?
Young Adults With Suicidal Ideation: Who Reaches Out by Texting for Help and Why Do Others Hold Back?
Drone Warfare May Raise New Mental Health Concerns
Drone Warfare May Raise New Mental Health Concerns
At the 24th edition of the L’Encéphale Congress, a psychiatry conference held in Paris, France, speakers discussed how the growing use of drones has become a defining feature of modern warfare and how these technologies may affect the mental health of both combatants and civilian populations. The topic was addressed during a session on war psychiatry.
The growing integration of drones into military operations is transforming the conduct of modern warfare and raising new concerns about the mental health effects on soldiers and civilian populations.
“In the age of drones, a new era of warfare has begun,” said Marie Dominique Colas, MD, a psychiatrist, and general practitioner at Military Teaching Hospital Sainte Anne in Toulon, France, speaking during a session on war.
The conflict following the Russian invasion of Ukraine illustrates this change. Drones are now widely used across multiple tactical levels for reconnaissance, surveillance, and attacks. According to Colas, this is the first high-intensity conflict in which these systems have been deployed on a large scale, primarily to destroy targets and cause casualties, rather than to eliminate specific identified individuals, which had been more typical in earlier operations in the Sahel or Afghanistan.
Combat Experience
The characteristics of drones, particularly their observation capabilities and ease of operation, have been gamechangers on the battlefield.
“The widespread use of drones has changed the subjective experience of combat,” said Emeric Saguin, MD, a psychiatrist in the Department of Psychiatry at the Begin Military Teaching Hospital, Saint-Mandé, France.
These miniaturized, stealthy, and often undetectable weapons have made battlefields increasingly transparent. “In Ukraine, enemy observation is almost constant for several kilometers behind the front line, creating a persistent sense of vulnerability and limiting medical care to basic first aid provided by fellow soldiers,” said Saguin.
The nature of these attacks has changed. “Gunshot wounds have become almost anecdotal. In Ukraine, more than 90% of attacks are caused by artillery and drones,” he added. Therefore, mental health specialists are increasingly examining how the constant threat posed by these weapons may affect psychological functioning, both individually and within groups.
Psychological Effects
Beyond their destructive capacity, drones are estimated to account for approximately 50% of casualties, and they can affect the morale of both opposing forces and civilian populations. Therefore, these precision weapons act as powerful tools for psychological attrition.
Clinically, “what predominates is not so much the traumatic impact of an isolated event as the repetition of exposures and the lack of recovery, leading to cumulative fatigue,” Saguin said. In his view, the clinical patterns observed are “less the result of a single shock than of a process of cumulative erosion.”
A key question raised by specialists is whether the widespread use of drones could lead to new clinical forms of war-related psychological disorders among drone operators.
Although drone operators remain physically distant from combat zones, they are not immune to the psychological effects of warfare. “Nearly half of drone operators show signs of psychological distress, primarily anxiety, which can affect both professional functioning and family life,” said Cécile Gorin, a senior psychiatrist at the Hôpital d’Instruction des Armées Sainte-Anne in Toulon, France. Greater vulnerability to emotional disengagement, posttraumatic stress disorder (PTSD), and burnout among drone operators has been linked to specific working conditions, including prolonged periods of intense vigilance, repeated exposure to detailed combat footage, and direct involvement in lethal decision-making.
“Exposure to images of destruction, particularly when civilians are affected by bombings, is a major risk factor for developing PTSD among these operators,” Gorin stated. A study analyzing drone operators found that 45.7% presented at least one psychological symptom, such as alcohol consumption, sleep disturbances, or anxiety. PTSD was identified with 2.9% of participants. However, according to the available literature, the prevalence of PTSD among drone operators may range from 5% to 10%, lower than among combatants deployed on the ground, where rates can reach up to 35%, Gorin noted.
The repeated and large-scale use of drones, including swarms and single-use devices, affects both civilians and combatants. This persistent threat can disrupt daily life and economic activity while creating a climate of constant uncertainty.
“The permanent, diffuse, and inescapable threat alters temporal and spatial reference points and fosters isolation,” Gorin explained. Prolonged exposure to such conditions can contribute to collective trauma, characterized by generalized anxiety, depressive episodes, erosion of social ties, and declining trust in institutions responsible for maintaining security.
Civilian populations living under continuous drone surveillance may also change their behavior patterns. Studies conducted among Afghan populations during wartime have described a phenomenon of self-objectification linked to constant surveillance and unpredictable strikes. In the context of chronic psychological insecurity, civilians gradually modified their behavior, particularly in social settings, avoiding gatherings, and adjusting daily activities to reduce the risk of being perceived as a threat.
Although the available data remain limited, similar patterns have emerged in Ukraine. A recent study on parents of Ukrainian children exposed to war conditions reported increased anxiety in 35% of respondents and sadness in 25%, along with behavioral problems and attention difficulties in approximately 25% of children.
This story was translated from Medscape’s French edition.
A version of this article first appeared on Medscape.com.
At the 24th edition of the L’Encéphale Congress, a psychiatry conference held in Paris, France, speakers discussed how the growing use of drones has become a defining feature of modern warfare and how these technologies may affect the mental health of both combatants and civilian populations. The topic was addressed during a session on war psychiatry.
The growing integration of drones into military operations is transforming the conduct of modern warfare and raising new concerns about the mental health effects on soldiers and civilian populations.
“In the age of drones, a new era of warfare has begun,” said Marie Dominique Colas, MD, a psychiatrist, and general practitioner at Military Teaching Hospital Sainte Anne in Toulon, France, speaking during a session on war.
The conflict following the Russian invasion of Ukraine illustrates this change. Drones are now widely used across multiple tactical levels for reconnaissance, surveillance, and attacks. According to Colas, this is the first high-intensity conflict in which these systems have been deployed on a large scale, primarily to destroy targets and cause casualties, rather than to eliminate specific identified individuals, which had been more typical in earlier operations in the Sahel or Afghanistan.
Combat Experience
The characteristics of drones, particularly their observation capabilities and ease of operation, have been gamechangers on the battlefield.
“The widespread use of drones has changed the subjective experience of combat,” said Emeric Saguin, MD, a psychiatrist in the Department of Psychiatry at the Begin Military Teaching Hospital, Saint-Mandé, France.
These miniaturized, stealthy, and often undetectable weapons have made battlefields increasingly transparent. “In Ukraine, enemy observation is almost constant for several kilometers behind the front line, creating a persistent sense of vulnerability and limiting medical care to basic first aid provided by fellow soldiers,” said Saguin.
The nature of these attacks has changed. “Gunshot wounds have become almost anecdotal. In Ukraine, more than 90% of attacks are caused by artillery and drones,” he added. Therefore, mental health specialists are increasingly examining how the constant threat posed by these weapons may affect psychological functioning, both individually and within groups.
Psychological Effects
Beyond their destructive capacity, drones are estimated to account for approximately 50% of casualties, and they can affect the morale of both opposing forces and civilian populations. Therefore, these precision weapons act as powerful tools for psychological attrition.
Clinically, “what predominates is not so much the traumatic impact of an isolated event as the repetition of exposures and the lack of recovery, leading to cumulative fatigue,” Saguin said. In his view, the clinical patterns observed are “less the result of a single shock than of a process of cumulative erosion.”
A key question raised by specialists is whether the widespread use of drones could lead to new clinical forms of war-related psychological disorders among drone operators.
Although drone operators remain physically distant from combat zones, they are not immune to the psychological effects of warfare. “Nearly half of drone operators show signs of psychological distress, primarily anxiety, which can affect both professional functioning and family life,” said Cécile Gorin, a senior psychiatrist at the Hôpital d’Instruction des Armées Sainte-Anne in Toulon, France. Greater vulnerability to emotional disengagement, posttraumatic stress disorder (PTSD), and burnout among drone operators has been linked to specific working conditions, including prolonged periods of intense vigilance, repeated exposure to detailed combat footage, and direct involvement in lethal decision-making.
“Exposure to images of destruction, particularly when civilians are affected by bombings, is a major risk factor for developing PTSD among these operators,” Gorin stated. A study analyzing drone operators found that 45.7% presented at least one psychological symptom, such as alcohol consumption, sleep disturbances, or anxiety. PTSD was identified with 2.9% of participants. However, according to the available literature, the prevalence of PTSD among drone operators may range from 5% to 10%, lower than among combatants deployed on the ground, where rates can reach up to 35%, Gorin noted.
The repeated and large-scale use of drones, including swarms and single-use devices, affects both civilians and combatants. This persistent threat can disrupt daily life and economic activity while creating a climate of constant uncertainty.
“The permanent, diffuse, and inescapable threat alters temporal and spatial reference points and fosters isolation,” Gorin explained. Prolonged exposure to such conditions can contribute to collective trauma, characterized by generalized anxiety, depressive episodes, erosion of social ties, and declining trust in institutions responsible for maintaining security.
Civilian populations living under continuous drone surveillance may also change their behavior patterns. Studies conducted among Afghan populations during wartime have described a phenomenon of self-objectification linked to constant surveillance and unpredictable strikes. In the context of chronic psychological insecurity, civilians gradually modified their behavior, particularly in social settings, avoiding gatherings, and adjusting daily activities to reduce the risk of being perceived as a threat.
Although the available data remain limited, similar patterns have emerged in Ukraine. A recent study on parents of Ukrainian children exposed to war conditions reported increased anxiety in 35% of respondents and sadness in 25%, along with behavioral problems and attention difficulties in approximately 25% of children.
This story was translated from Medscape’s French edition.
A version of this article first appeared on Medscape.com.
At the 24th edition of the L’Encéphale Congress, a psychiatry conference held in Paris, France, speakers discussed how the growing use of drones has become a defining feature of modern warfare and how these technologies may affect the mental health of both combatants and civilian populations. The topic was addressed during a session on war psychiatry.
The growing integration of drones into military operations is transforming the conduct of modern warfare and raising new concerns about the mental health effects on soldiers and civilian populations.
“In the age of drones, a new era of warfare has begun,” said Marie Dominique Colas, MD, a psychiatrist, and general practitioner at Military Teaching Hospital Sainte Anne in Toulon, France, speaking during a session on war.
The conflict following the Russian invasion of Ukraine illustrates this change. Drones are now widely used across multiple tactical levels for reconnaissance, surveillance, and attacks. According to Colas, this is the first high-intensity conflict in which these systems have been deployed on a large scale, primarily to destroy targets and cause casualties, rather than to eliminate specific identified individuals, which had been more typical in earlier operations in the Sahel or Afghanistan.
Combat Experience
The characteristics of drones, particularly their observation capabilities and ease of operation, have been gamechangers on the battlefield.
“The widespread use of drones has changed the subjective experience of combat,” said Emeric Saguin, MD, a psychiatrist in the Department of Psychiatry at the Begin Military Teaching Hospital, Saint-Mandé, France.
These miniaturized, stealthy, and often undetectable weapons have made battlefields increasingly transparent. “In Ukraine, enemy observation is almost constant for several kilometers behind the front line, creating a persistent sense of vulnerability and limiting medical care to basic first aid provided by fellow soldiers,” said Saguin.
The nature of these attacks has changed. “Gunshot wounds have become almost anecdotal. In Ukraine, more than 90% of attacks are caused by artillery and drones,” he added. Therefore, mental health specialists are increasingly examining how the constant threat posed by these weapons may affect psychological functioning, both individually and within groups.
Psychological Effects
Beyond their destructive capacity, drones are estimated to account for approximately 50% of casualties, and they can affect the morale of both opposing forces and civilian populations. Therefore, these precision weapons act as powerful tools for psychological attrition.
Clinically, “what predominates is not so much the traumatic impact of an isolated event as the repetition of exposures and the lack of recovery, leading to cumulative fatigue,” Saguin said. In his view, the clinical patterns observed are “less the result of a single shock than of a process of cumulative erosion.”
A key question raised by specialists is whether the widespread use of drones could lead to new clinical forms of war-related psychological disorders among drone operators.
Although drone operators remain physically distant from combat zones, they are not immune to the psychological effects of warfare. “Nearly half of drone operators show signs of psychological distress, primarily anxiety, which can affect both professional functioning and family life,” said Cécile Gorin, a senior psychiatrist at the Hôpital d’Instruction des Armées Sainte-Anne in Toulon, France. Greater vulnerability to emotional disengagement, posttraumatic stress disorder (PTSD), and burnout among drone operators has been linked to specific working conditions, including prolonged periods of intense vigilance, repeated exposure to detailed combat footage, and direct involvement in lethal decision-making.
“Exposure to images of destruction, particularly when civilians are affected by bombings, is a major risk factor for developing PTSD among these operators,” Gorin stated. A study analyzing drone operators found that 45.7% presented at least one psychological symptom, such as alcohol consumption, sleep disturbances, or anxiety. PTSD was identified with 2.9% of participants. However, according to the available literature, the prevalence of PTSD among drone operators may range from 5% to 10%, lower than among combatants deployed on the ground, where rates can reach up to 35%, Gorin noted.
The repeated and large-scale use of drones, including swarms and single-use devices, affects both civilians and combatants. This persistent threat can disrupt daily life and economic activity while creating a climate of constant uncertainty.
“The permanent, diffuse, and inescapable threat alters temporal and spatial reference points and fosters isolation,” Gorin explained. Prolonged exposure to such conditions can contribute to collective trauma, characterized by generalized anxiety, depressive episodes, erosion of social ties, and declining trust in institutions responsible for maintaining security.
Civilian populations living under continuous drone surveillance may also change their behavior patterns. Studies conducted among Afghan populations during wartime have described a phenomenon of self-objectification linked to constant surveillance and unpredictable strikes. In the context of chronic psychological insecurity, civilians gradually modified their behavior, particularly in social settings, avoiding gatherings, and adjusting daily activities to reduce the risk of being perceived as a threat.
Although the available data remain limited, similar patterns have emerged in Ukraine. A recent study on parents of Ukrainian children exposed to war conditions reported increased anxiety in 35% of respondents and sadness in 25%, along with behavioral problems and attention difficulties in approximately 25% of children.
This story was translated from Medscape’s French edition.
A version of this article first appeared on Medscape.com.
Drone Warfare May Raise New Mental Health Concerns
Drone Warfare May Raise New Mental Health Concerns
Mental Health Prescribers’ Perceptions of Patients With Substance Use Disorders and Harm Reduction Services
Mental Health Prescribers’ Perceptions of Patients With Substance Use Disorders and Harm Reduction Services
The Public Health and Welfare Act of 1988 prohibited the use of federal funds to “provide individuals with hypodermic needles or syringes so that such individuals may use illegal drugs.”1 Although the Act included the caveat that the US Surgeon General may determine that “a demonstration needle exchange program would be effective in reducing drug abuse,” and thus federal funds could be used, the legislation prohibited federal, state, and local agencies from funding syringe services programs (SSPs). SSPs use various harm reduction tools to improve public safety and reduce the potential harmful consequences of risky behaviors, similar to how using a seat belt while driving reduces the risk of injury or death.2 SSPs are rooted in evidence-based practices, and several studies, according to the Centers for Disease Control and Prevention, have found that people who use drugs (PWUDs) who use community-based SSPs are 5 times more likely to enter treatment than those who do not use these programs. Additionally, these programs have shown an estimated 50% reduction in HIV and hepatitis C infections.3
Amid a 2015 HIV outbreak in Indiana among individuals sharing needles for injection drug use, Congress passed an omnibus spending bill that partially lifted the federal funding restriction. Federal funds now may be used for operational costs that support SSPs but may not be used to purchase syringes themselves.4
Following the 2015 legislation, federal agencies began implementing SSPs. The Veterans Health Administration (VHA) established SSPs at 3 medical centers in 2017.5 Veterans who participated in the programs were able to access supplies (eg, syringes, fentanyl test strips, wound care kits, and condoms) through donations to US Department of Veterans Affairs (VA) medical centers (VAMCs). The success of these programs laid the foundation for the VHA to implement SSPs nationally. VHA SSPs provided access to naloxone (an opioid overdose reversal medication), fentanyl test strips, condoms, sterile syringe distribution, testing for blood-borne viruses, HIV pre-exposure prophylaxis, as well as educational materials and resources, and low-barrier access to drug treatment (eg, medications for opioid use disorder [OUD]).
In 2020, the Biden Administration outlined 7 drug policy priorities, which included enhancing evidence-based harm reduction efforts. 6 This policy also discussed mandates for federal agencies to remove barriers to federal funding for purchasing syringes and other harm reduction supplies. The VHA responded to the policy by publishing guidance that recommended VAMCs develop and/or ensure veterans have access to harm reduction services in the community, where state law is not legally more stringent.7
In 2025 the Trump administration Statement of Drug Policy Priorities encouraged local jurisdictions to increase the availability of drug test strips and naloxone.8 These significant policy shifts moved SSPs from being housed mostly in local public health departments and community-based organizations to also being available at health care facilities. 9 VAMCs have unique opportunities to provide universal health care that includes both prevention services and other medical management to PWUD.
One study assessed staff perceptions of PWUD at a VAMC in preparation for a training program about harm reduction. The results indicated an overall positive staff perception of PWUD, although only the Drug and Drug Problems Perceptions Questionnaire (DDPPQ) was administered, which assessed comfort of working with this population and not explicitly the use of harm reduction.10 Another study interviewed clinical pharmacists, primary care clinicians, social workers, and directors of addiction and mental health services to determine barriers and facilitators (ie, potential opportunities to promote change) to implementing harm reduction at the VHA. The study identified barriers to be a lack of knowledge, time, and comfort, while suggesting opportunities for improvement were engagement of champions, communication and educational strategies, and adaptation of existing infrastructure.11
While these findings are insightful for the VHA to disseminate a harm reduction program, there remains a gap in assessing staff willingness to provide harm reduction services. Evidence on harm reduction services among veterans is limited and more research is needed to better understand the role of these services and acceptance among enrolled veterans and VHA staff. Specifically, more research is needed on health care practitioners’ (HCPs) perceptions of harm reduction use.
Mental health care practitioners frequently treat patients with substance use disorders (SUDs), making them an ideal initial cohort to assess willingness to provide harm reduction to this population. By analyzing mental HCPs’ perceptions, additional interventions could be identified, implemented, and evaluated to improve their willingness to provide harm reduction tools.
This project focused on mental health clinicians with prescribing privileges: physicians (allopathic and osteopathic physicians), nurse practitioners, physician assistants, and clinical pharmacist practitioners. Mental health prescribers were selected because they are uniquely positioned at the intersection of prevention and treatment in drug use. Furthermore, mental health prescribers at the VAMCs included in this study are usually the primary point of entry to SUD clinics. This mixed-methods study used an anonymous online survey and voluntary postsurvey discussions with mental health care prescribers to elaborate on their beliefs and attitudes, providing deeper insight into their responses regarding harm reduction.
Methods
This project was conducted by the Veterans Integrated Services Network (VISN) 5 academic detailing team. VISN 5 serves veterans from economically and demographically diverse areas in Maryland; Washington, DC; West Virginia; and portions of Virginia, Pennsylvania, Ohio, and Kentucky. VAMCs in Baltimore, Maryland, and Washington, DC, serve a largely urban population while the 4 West Virginia facilities in Martinsburg, Huntington, Beckley, and Clarksburg, serve a largely rural population. West Virginia has been the epicenter of the opioid crisis and consistently has the highest drug overdose deaths per capita in the United States.12 Among cities, Baltimore, Maryland, has the highest number of drug overdose deaths per capita with 174.1 per 100,000 people.12,13
At the time of this project, the 6 VISN 5 VAMCs had established overdose education and naloxone distribution (OEND) programs. Although OEND programs have existed since 2013, VISN 5 SSPs and harm reduction services that provided fentanyl test strips were only available at the Martinsburg, Beckley, and Huntington VAMCs. All 6 VAMCs had substance use treatment programs with a variety of inpatient and outpatient mental health services. The Washington, DC and Baltimore VAMCs had opioid treatment programs that provided methadone maintenance.
The VISN 5 academic detailing team consists of 7 clinical pharmacists. These academic detailers plan annual systematic interventions to provide medical knowledge translation services on health-related campaigns. Academic detailers are trained in change management and motivational interviewing. They uniquely facilitate conversations with HCPs on various topics or campaigns, aiming for quality improvement and behavioral change through positive relationships and sharing resources.14 Academic detailing conversations and relationships with HCPs involve assessing and understanding HCP behaviors, including barriers and readiness to change to align with the goal of improving patient outcomes. Academic detailing has improved practice behaviors around providing OEND in VHA.15
To prepare for a harm reduction campaign, the academic detailers sought to gain insight from target VISN 5 mental health prescribers. Figure 1 outlines the project timeline, which started with emails inviting mental health prescribers to complete an anonymous online survey. Academic detailers from each site emailed mental health prescribers who completed the survey to determine interest in expanding on survey findings. Mental health prescribers who completed the survey could participate in a postsurvey discussion.

Surveys
Between January 29, 2024, and February 22, 2024, the academic detailers emailed facility mental health prescribers (N = 156) a link to an anonymous 15-question survey. The email informed recipients of the survey’s purpose: to gain a better understanding of prescriber perceptions of veterans with SUD and harm reduction programs and their willingness to provide harm reduction tools, to better determine interventions that could be implemented.
The survey collected prescriber demographic data and their perceptions of PWUD and harm reduction tools and education. Survey questions were extrapolated from validated surveys (eg, DDPPQ) and survey-based implicit association test.16,17 The survey used multiple choice and 5-point Likert scale questions. Mental health prescribers were asked about their role at the VHA, years in practice, medical center affiliation, type of SUDs treated (eg, opioid, stimulant, alcohol, cannabis, or other), and whether they had previously met with academic detailers about harm reduction.
Respondents read statements about patients with or without SUD and provided Likert scale responses describing their regard, level of comfort, and preferences. The survey included Likert scale questions about respondents’ comfort in providing harm reduction education and supplies. Respondents also noted whether they believed harm reduction reduced substance use, harm reduction tools encourage people with SUD to continue using drugs, and whether HCPs can impact clinical change.
Postsurvey interviews with predetermined questions were conducted in-person or via video conference with ≥ 1 prescriber at each VAMC by an academic detailer. The postsurvey discussion offered an opportunity for respondents to further elaborate and describe previous experiences and current beliefs that may affect their attitudes toward people with SUD and their views on harm reduction. Participants received no compensation for survey completion or interviews.
Analysis
The Washington VAMC Institutional Review Board reviewed and approved this project as quality improvement with potential publication. No inferential statistics were calculated. Survey participant demographics were reported using frequencies and proportions reported for categorical variables. Notes from follow-up interviews were analyzed using the Prosci Awareness, Desire, Knowledge, Ability, and Reinforcement (ADKAR) Model for Change Management.18 This framework is used by academic detailers to determine a prescriber’s stage of change, which helps select the appropriate resources to move the clinician along a change framework. Completed postsurvey interview sheets, including notes written by the academic detailer, were analyzed by the project lead (NJ) who reviewed each interview sheet and analysis with the academic detailer who led the discussion.
Results
Sixty-six respondents completed the online survey (42% response rate), and 7 mental health prescribers participated in a postsurvey discussion. Thirty-one participants (47%) were physicians and 17 (26%) were in practice for > 20 years. Response rates reflected the size of mental health staff at each VAMC at the time of the survey: 17 respondents (26%) worked at each of the Martinsburg and Baltimore VAMCs, with fewer at the other VAMCs (Table 1). Alcohol use disorder was the most commonly reported SUD treated (n = 62; 33%), followed by cannabis use disorder (n = 40; 21%), OUD (n = 38; 20%), and stimulant use disorder (n = 37; 20%).
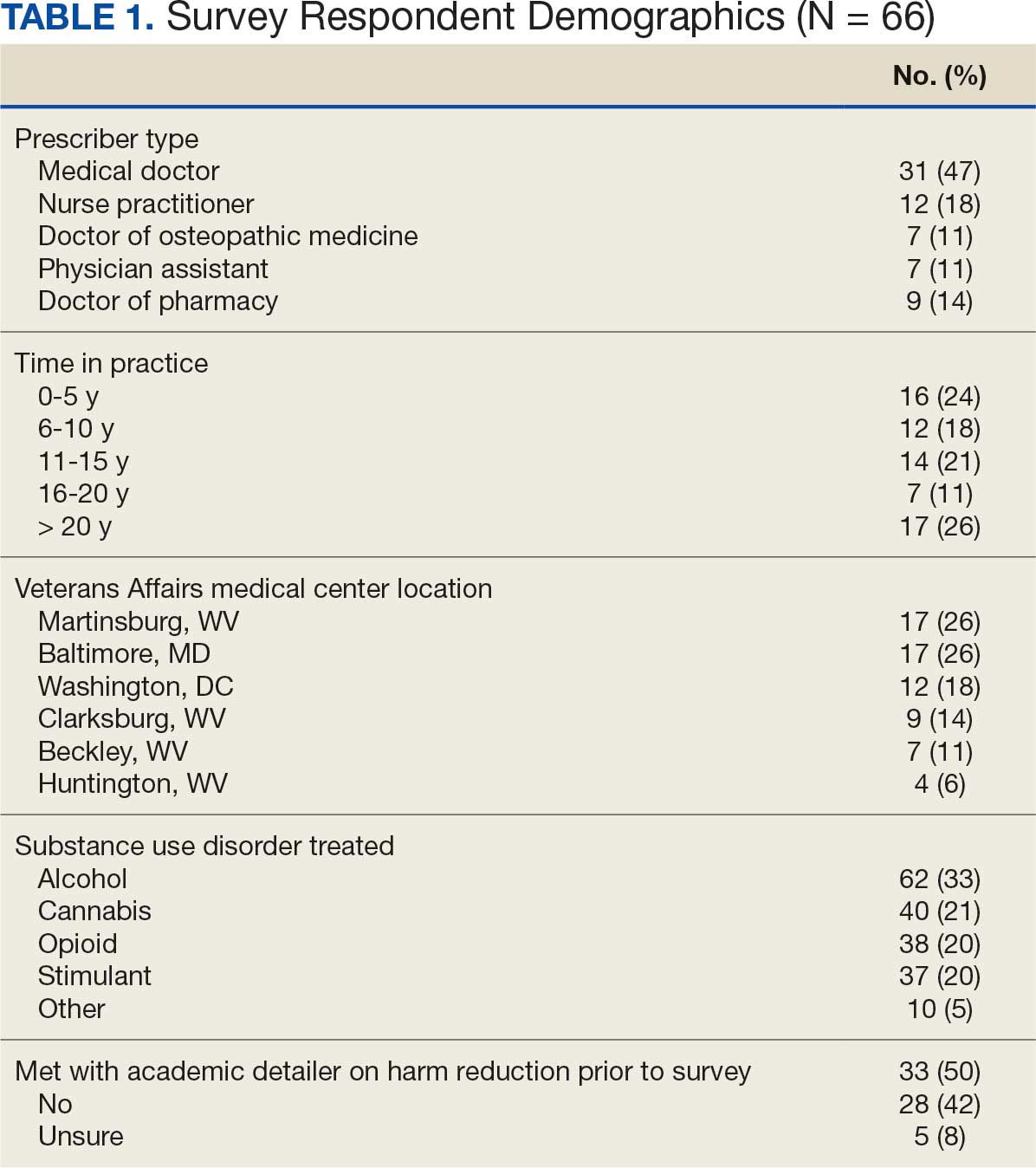
Respondents felt comfortable and confident educating patients on ways to reduce harm related to substance use (91%; mean [SD], 4.24 [0.84]). Most prescribers surveyed (97%; mean [SD], 1.59 [0.68]) disagreed or strongly disagreed that harm reduction encourages patients with SUD to continue using drugs, and all prescribers surveyed disagreed that there is nothing they can do to encourage harm reduction. Survey results were mixed for personal comfort in working with people with SUD vs people without SUD (Figure 2). Respondents were most willing to provide naloxone (95%; mean [SD], 4.71 [0.78]), compared to fentanyl test strips (61%; mean [SD], 3.61 [1.41]) or syringes (39%; mean [SD], 3.18 [1.39]). Respondents were neutral or least willing to provide syringes (Figure 3).
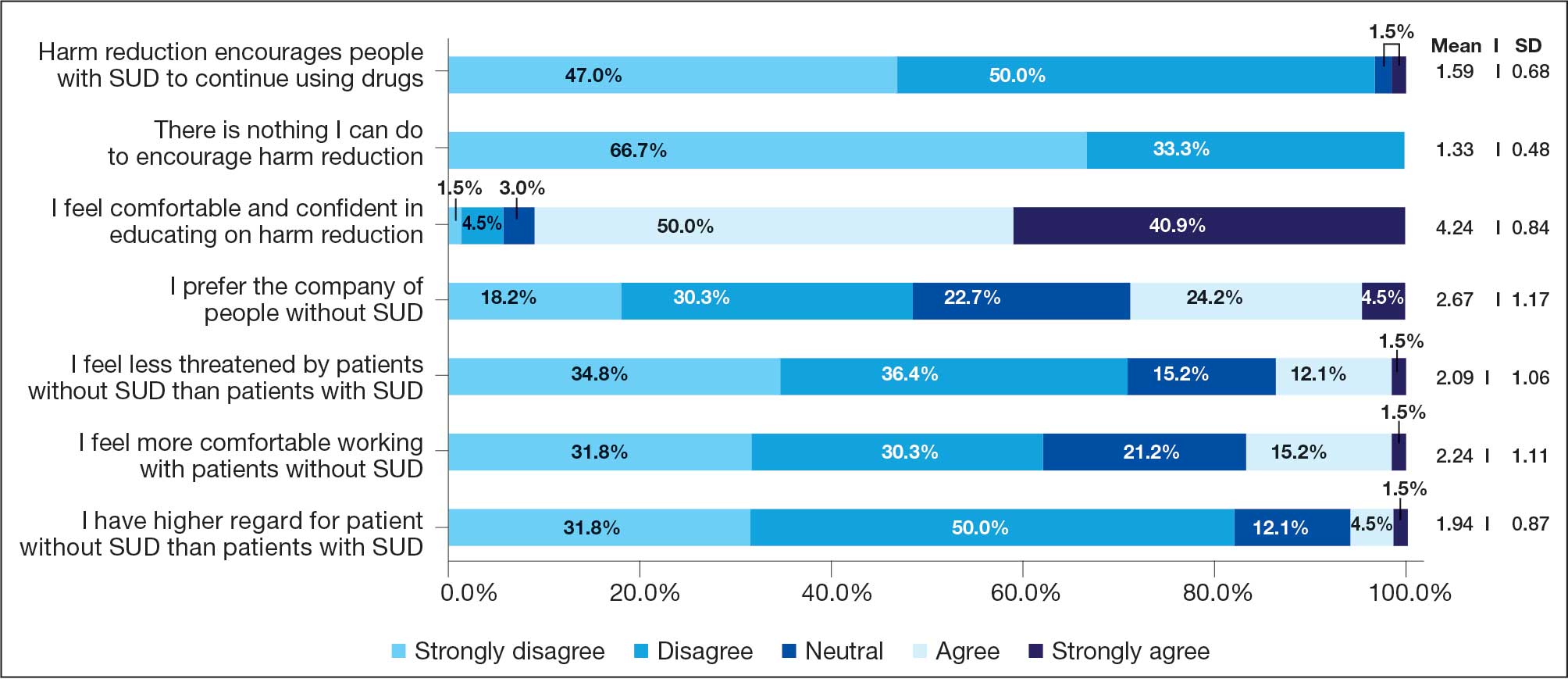
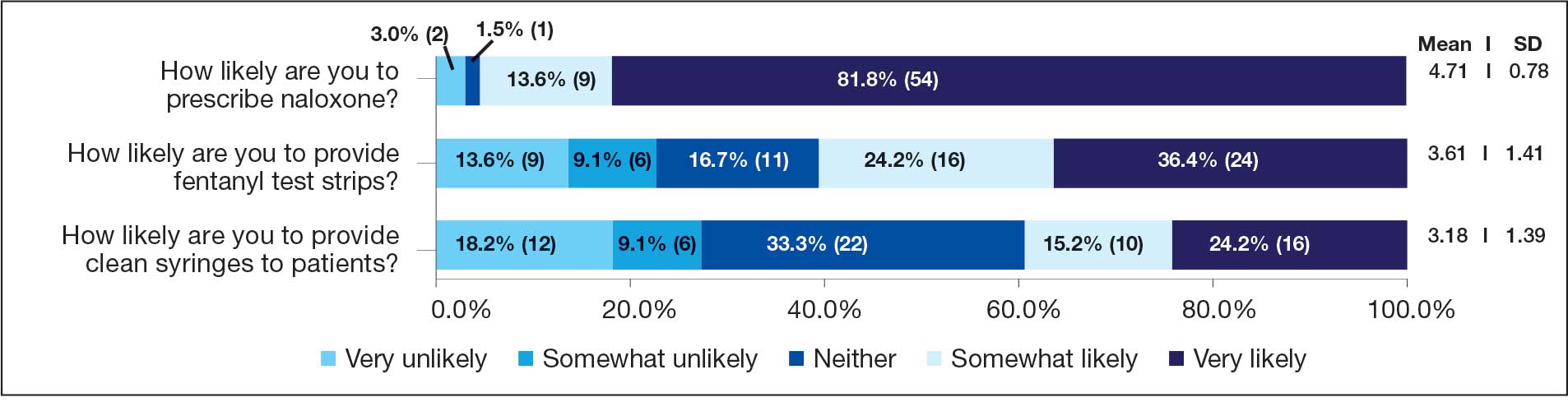
Seven postsurvey interviews were completed between academic detailers and mental health clinicians across the 6 VAMCs. Respondents included 1 physician assistant, 1 nurse practitioner, 1 pharmacist, and 4 physicians. Notes were analyzed using the ADKAR Change Competency Model to organize clinician stages of change (Table 2).
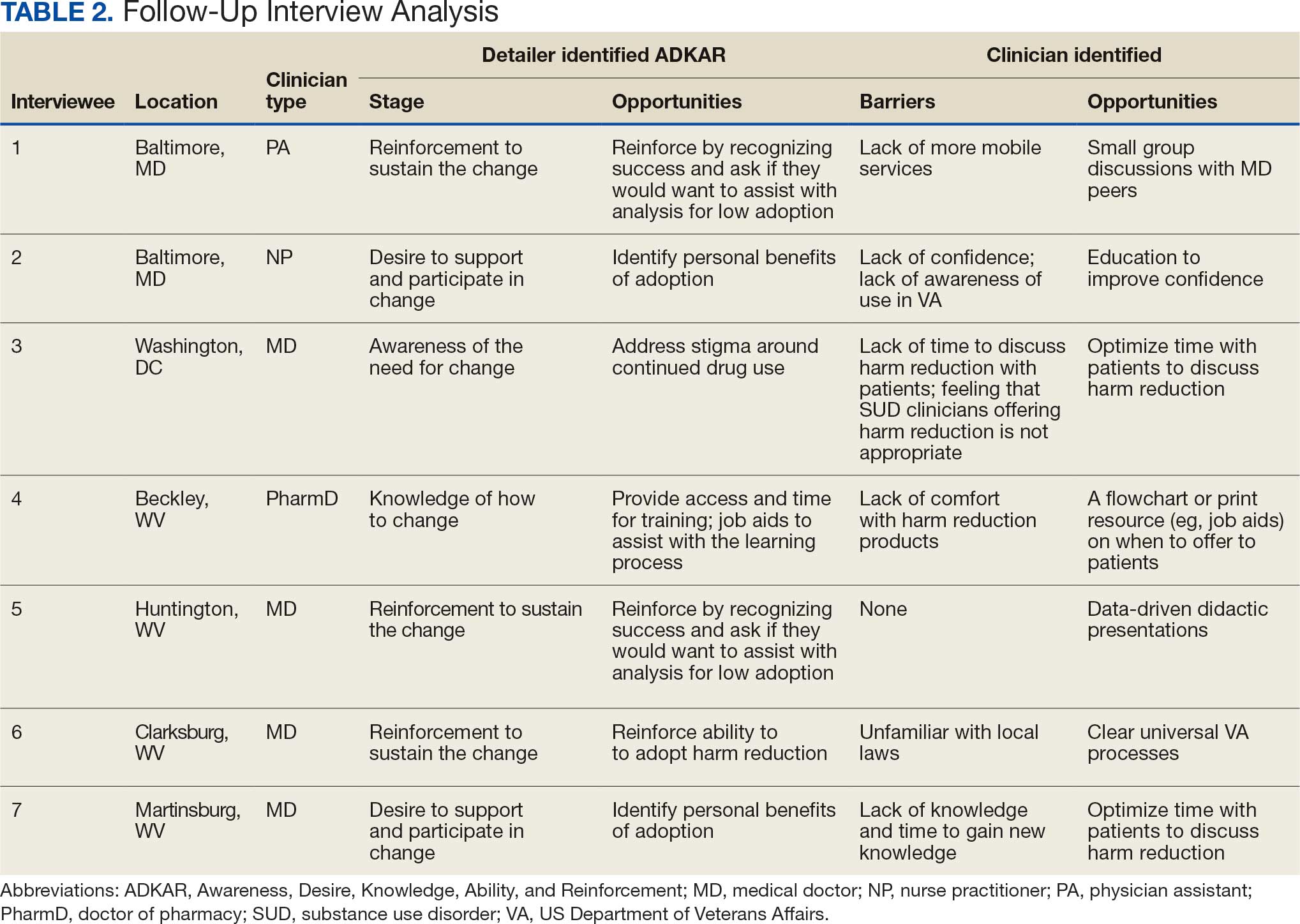
Barriers identified by interviewees included lack of mobile services, lack of confidence and awareness of the availability of harm reduction at their respective medical center, lack of time to discuss harm reduction, negative sentiments toward providing SUD-related harm reduction, discomfort with harm reduction products, and lack of knowledge and time to learn about harm reduction services. Opportunities identified to drive change in practice included additional time allotted during patient appointments, educational discussions and presentations to increase knowledge of and comfort with harm reduction tools, a clear clinical patient care workflow and process for harm reduction services, and reinforcement strategies to recognize success.
Discussion
This project investigated mental health prescribers’ perceptions of harm reduction at VAMCs in West Virginia, Maryland, and Washington, DC. While previous studies have demonstrated the efficacy of harm reduction tools, there is a lack of research on HCPs willingness to use these resources. This study suggests that while most respondents feel confident in and see the value of offering harm reduction resources to patients, a disparity exists between which resources HCPs are more likely to use and factors that would further enhance their ability to integrate harm reduction into practice. The follow-up interviews provided additional insight into the survey results.
Most respondents met the awareness and desire stage and moved to the knowledge, ability, or reinforcement ADKAR stage. It would be reasonable to extrapolate that most of the respondents felt comfortable with and were very likely to offer certain harm reduction tools. In the ADKAR interview analysis, the most common factors needed to drive change included having more time during patient appointments, additional education, clear processes for harm reduction services, and reinforcement strategies to sustain change. Respondents noted that harm reduction discussions took extra time in their already limited appointments with patients, which may have limited time for discussions surrounding all other mental health concerns. These discussions often necessitate in-depth conversations to accurately understand the patients’ needs. Given HCP time constraints, they may view harm reduction as lower in urgency and priority relative to other concerns. While most respondents were in the reinforcement phase, it is important to note the ADKAR model is fluid, and therefore an HCP could move forward or backward. This movement can be noted in the postsurvey interviews where, for example, prescriber 6 was determined to be in the reinforcement stage since they had already discussed harm reduction with patients. However, prescriber 6 also noted a barrier of unfamiliarity with local laws, which could shift them to the ADKAR knowledge stage.
Respondents noted that education through didactic sessions could lead to better incorporation of harm reduction into patient care. While harm reduction has evidence supporting its effectiveness, the respondents noted willingness to discuss harm reduction when treatment fails or the patient refuses treatment or referrals. Respondents expressed mixed opinions on use of harm reduction tools among patients with SUDs as some prescribers viewed harm reduction as part of a treatment plan and others viewed a return to drug use as a failure of treatment. Furthermore, respondents expressed hesitancy surrounding certain harm reduction tools, such as fentanyl test strips or syringes, and perceived these supplies as intended for medical use rather than harm reduction. HCPs may feel uncomfortable offering these supplies for drug use, despite their use for reducing risk.
Most responses were received from VAMCs with large mental health substance use programs. Respondents at larger, urban facilities (Washington, DC, and Baltimore, Maryland) expressed more hesitancy around using harm reduction tools despite having more harm reduction resources available compared to smaller or rural sites. These results align with previous studies that found no difference in prescribers providing medications for OUD in rural and urban VAMCs, showing urban sites, despite more resources, are not more willing to provide harm reduction or other addiction services.19 This evidence might indicate that urban sites may not use available resources (eg, methadone clinics) or that rural sites can provide just as robust medications for OUD care as urban sites.
Follow-up interview analysis indicated that HCPs lack knowledge of certain harm reduction tools. One-on-one peer discussions, like academic detailing, can facilitate discussions around a prescriber’s role in harm reduction, address gaps in knowledge by sharing what is available at the facilities for harm reduction, and suggest conversation points to help prescribers start harm reduction discussions with patients unwilling to begin treatment. Additionally, academic detailing can connect prescribers to available resources in the community to provide pragmatic approaches and suggestions. A clear and consistent treatment process may reduce barriers by reassuring prescribers they have support and by providing consistent directions so that prescribers do not waste time.
Reinforcement is important for sustaining change. VAMCs could consider positive feedback and other evidence-based reinforcement strategies (eg, social recognition, continuing education) to communicate that these changes are noticed and appreciated.20 Late adopters may also be influenced by seeing positive feedback and results for peers. Systematic changes can be the catalyst for and sustain individual change.
Shifting perceptions and adopting change may be challenging, especially for SUD, which can be highly stigmatized. Promotion of successful change should be multifaceted and include both system and individual approaches. VHA systemic changes that could contribute to positive change include provision of time and access to SUD treatment training, a clear and sustainable treatment process, and reinforcement by recognizing success. In addition, facility leadership could provide support through dedicated time and resources during the workday for SUD treatment and harm reduction training. Support could empower HCPs and convey leadership support for harm reduction. This dedicated time could be used for didactic lecture sessions or individual meetings with academic detailers who can tailor discussions to the prescriber’s practice.
Strengths and Limitations
This survey included prescribers from a range of mental health care practice settings (eg, inpatient, outpatient clinic, rural, urban) and varied years of experience. This variety resulted in diverse perspectives and knowledge bases. Postsurvey interviews allowed academic detailers to gain deeper insight into answers in the survey, which can guide future interventions. Postsurvey interviews and application of the ADKAR model provided additional viewpoints on harm reduction.
A limitation of this project is the absence of an assessment of respondents’ harm reduction knowledge accuracy. Although respondents reported confidence in discussing harm reduction with patients, the survey did not assess whether their knowledge was accurate. Additionally, the survey did not ask about the availability of syringes and test strips at the prescribers’ VAMC, which could explain discrepancies in responses between naloxone and other forms of harm reduction (drug test strips and syringes were not available to all HCPs in the VISN). This lack of availability may have skewed responses. West Virginia SSPs, for example, were closed following legislative changes, which may contribute to stigma.21
Not all respondents were asked to do a follow-up interview, which limited the perspectives included in this study. Each site had ≥ 1 follow-up interview to limit the academic detailer’s workload. The initial survey included the phrase clean syringe, which can be stigmatizing and insinuate that PWUD are not clean. The preferred term would have been sterile syringe.22
Conclusions
This survey of mental health prescribers found that most respondents are comfortable treating patients with SUD and confident in educating patients on harm reduction. Additionally, most respondents were more willing to provide naloxone vs fentanyl test strips or sterile syringes. A lack of time and awareness was the most frequently cited barrier to harm reduction services. As the VHA continues to expand access to harm reduction programs, which have proven to increase treatment rates and reduce disease, it will be imperative for HCPs, including mental health prescribers, to recognize the benefit of these programs for veterans with SUD. Future interventions should be designed and evaluated in collaboration with all HCPs and patients. This project determined ways to promote change for prescribers, but it will be important for further research to continue those conversations and incorporate patient perspectives.
- Use of funds to supply hypodermic needles or syringes for illegal drug use; prohibition, 42 USC § 300ee-5 (1988). Accessed January 5, 2026. https://www.law.cornell.edu /uscode/text/42/300ee-5
- OD2A Case Study: Harm Reduction. Centers for Disease Control and Prevention. June 9, 2025. Accessed January 5, 2026. https://www.cdc.gov/overdose-prevention/php /od2a/harm-reduction.html
- Strengthening Syringe Services Programs (SSPs). Centers for Disease Control and Prevention. March 20, 2024. Accessed January 5, 2026. https://www.cdc.gov/hepatitis -syringe-services/php/about/index.html
- Weinmeyer R. Needle exchange programs’ status in US politics. AMA J Ethics. 2016;18:252-257. doi:10.1001/journalofethics.2016.18.3.hlaw1-1603
- Rife-Pennington T, Dinges E, Ho MQ. Implementing syringe services programs within the Veterans Health Administration: facility experiences and next steps. J Am Pharm Assoc (2003). 2023;63:234-240. doi:10.1016/j.japh.2022.10.019
- The Biden-Harris Administration’s Statement of Drug Policy Priorities for Year One. Executive Office of the President, Office of National Drug Control Policy. April 1, 2021. Accessed January 5, 2026. https://bidenwhitehouse.archives.gov/wp-content/uploads/2021/03/BidenHarris -Statement-of-Drug-Policy-Priorities-April-1.pdf
- HIV - for veterans and the public syringe services programs. US Department of Veterans Affairs. Updated August 16, 2021. Accessed January 5, 2026. https://www.hiv .va.gov/patient/ssp.asp
- Trump Administration’s Statement of Drug Policy Priorities. White House. April 1, 2025. Accessed January 7, 2026. https://www.whitehouse.gov/wp-content /uploads/2025/04/2025-Trump-Administration-Drug-Policy -Priorities.pdf
- Health Centers and Syringe Services Programs. National Health Care for the Homeless Council. May 2023. Accessed January 5, 2026. https://nhchc.org/wp-content /uploads/2023/06/Health-Centers-SSPs-Final.pdf
- Lynch RD, Biederman DJ, Silva S, Demasi K. A syringe service program within a federal system: foundations for implementation. J Addict Nurs. 2021;32:152-158. doi:10.1097/JAN.0000000000000402
- Harvey LH, Sliwinski SK, Flike K, et al. The integration of harm reduction services in the Veterans Health Administration (VHA): a qualitative analysis of barriers and facilitators. J Addict Dis. 2024;42:326-334. doi:10.1080/10550887.2023.2210021
- Drug Overdose Death Rates. National Center for Drug Abuse Statistics. Accessed January 5, 2026. https:// drugabusestatistics.org/drug-overdose-deaths
- Ng G. New database shows Baltimore greatly devastated by opioid epidemic. Updated August 21, 2023. Accessed January 5, 2026. https://www.wbaltv.com/article/opioid -epidemic-database-baltimore-deaths/44869671
- Introductory Guide to Academic Detailing. National Resource Center for Academic Detailing. 2017. Accessed January 5, 2026. https://www.narcad.org /uploads/5/7/9/5/57955981/introductory_guide_to_ad.pdf
- Zhang J. Can educational outreach improve experts’ decision making? Evidence from a national opioid academic detailing program. SSRN. 2023;4297398. doi:10.2139/ssrn.4297398
- Watson H, Maclaren W, Kerr S. Staff attitudes towards working with drug users: development of the Drug Problems Perceptions Questionnaire. Addiction. 2007;102:206- 215. doi:10.1111/j.1360-0443.2006.01686.x
- Dahl RA, Vakkalanka JP, Harland KK, Radke J. Investigating healthcare provider bias toward patients who use drugs using a survey-based implicit association test: pilot study. J Addict Med. 2022;16:557-562. doi:10.1097/ADM.0000000000000970
- Hiatt JM, Creasey TJ. Change Management: The People Side of Change. Prosci Learning Center Publications; 2012.
- Wyse JJ, Shull S, Lindner S, et al. Access to medications for opioid use disorder in rural versus urban Veterans Health Administration facilities. J Gen Intern Med. 2023;38:1871-1876. doi:10.1007/s11606-023-08027-4
- Mostofian F, Ruban C, Simunovic N, Bhandari M. Changing physician behavior: what works?. Am J Manag Care. 2015;21(1):75-84.
- Bergdorf-Smith K, Bridge Initiative for S&T Policy, Leadership, and Communications. Syringe Service Programs and HIV Prevention in West Virginia. West Virginia University. February 5, 2024. Accessed January 5, 2026. https:// scitechpolicy.wvu.edu/science-and-technology-notes -articles/2024/02/05/syringe-service-programs-and-hiv -prevention-in-west-virginia
- Brunsdon N. Stop saying ‘clean’. Injecting Advice. February 7, 2011. Accessed January 5, 2026. https:// injectingadvice.com/stop-saying-clean/
The Public Health and Welfare Act of 1988 prohibited the use of federal funds to “provide individuals with hypodermic needles or syringes so that such individuals may use illegal drugs.”1 Although the Act included the caveat that the US Surgeon General may determine that “a demonstration needle exchange program would be effective in reducing drug abuse,” and thus federal funds could be used, the legislation prohibited federal, state, and local agencies from funding syringe services programs (SSPs). SSPs use various harm reduction tools to improve public safety and reduce the potential harmful consequences of risky behaviors, similar to how using a seat belt while driving reduces the risk of injury or death.2 SSPs are rooted in evidence-based practices, and several studies, according to the Centers for Disease Control and Prevention, have found that people who use drugs (PWUDs) who use community-based SSPs are 5 times more likely to enter treatment than those who do not use these programs. Additionally, these programs have shown an estimated 50% reduction in HIV and hepatitis C infections.3
Amid a 2015 HIV outbreak in Indiana among individuals sharing needles for injection drug use, Congress passed an omnibus spending bill that partially lifted the federal funding restriction. Federal funds now may be used for operational costs that support SSPs but may not be used to purchase syringes themselves.4
Following the 2015 legislation, federal agencies began implementing SSPs. The Veterans Health Administration (VHA) established SSPs at 3 medical centers in 2017.5 Veterans who participated in the programs were able to access supplies (eg, syringes, fentanyl test strips, wound care kits, and condoms) through donations to US Department of Veterans Affairs (VA) medical centers (VAMCs). The success of these programs laid the foundation for the VHA to implement SSPs nationally. VHA SSPs provided access to naloxone (an opioid overdose reversal medication), fentanyl test strips, condoms, sterile syringe distribution, testing for blood-borne viruses, HIV pre-exposure prophylaxis, as well as educational materials and resources, and low-barrier access to drug treatment (eg, medications for opioid use disorder [OUD]).
In 2020, the Biden Administration outlined 7 drug policy priorities, which included enhancing evidence-based harm reduction efforts. 6 This policy also discussed mandates for federal agencies to remove barriers to federal funding for purchasing syringes and other harm reduction supplies. The VHA responded to the policy by publishing guidance that recommended VAMCs develop and/or ensure veterans have access to harm reduction services in the community, where state law is not legally more stringent.7
In 2025 the Trump administration Statement of Drug Policy Priorities encouraged local jurisdictions to increase the availability of drug test strips and naloxone.8 These significant policy shifts moved SSPs from being housed mostly in local public health departments and community-based organizations to also being available at health care facilities. 9 VAMCs have unique opportunities to provide universal health care that includes both prevention services and other medical management to PWUD.
One study assessed staff perceptions of PWUD at a VAMC in preparation for a training program about harm reduction. The results indicated an overall positive staff perception of PWUD, although only the Drug and Drug Problems Perceptions Questionnaire (DDPPQ) was administered, which assessed comfort of working with this population and not explicitly the use of harm reduction.10 Another study interviewed clinical pharmacists, primary care clinicians, social workers, and directors of addiction and mental health services to determine barriers and facilitators (ie, potential opportunities to promote change) to implementing harm reduction at the VHA. The study identified barriers to be a lack of knowledge, time, and comfort, while suggesting opportunities for improvement were engagement of champions, communication and educational strategies, and adaptation of existing infrastructure.11
While these findings are insightful for the VHA to disseminate a harm reduction program, there remains a gap in assessing staff willingness to provide harm reduction services. Evidence on harm reduction services among veterans is limited and more research is needed to better understand the role of these services and acceptance among enrolled veterans and VHA staff. Specifically, more research is needed on health care practitioners’ (HCPs) perceptions of harm reduction use.
Mental health care practitioners frequently treat patients with substance use disorders (SUDs), making them an ideal initial cohort to assess willingness to provide harm reduction to this population. By analyzing mental HCPs’ perceptions, additional interventions could be identified, implemented, and evaluated to improve their willingness to provide harm reduction tools.
This project focused on mental health clinicians with prescribing privileges: physicians (allopathic and osteopathic physicians), nurse practitioners, physician assistants, and clinical pharmacist practitioners. Mental health prescribers were selected because they are uniquely positioned at the intersection of prevention and treatment in drug use. Furthermore, mental health prescribers at the VAMCs included in this study are usually the primary point of entry to SUD clinics. This mixed-methods study used an anonymous online survey and voluntary postsurvey discussions with mental health care prescribers to elaborate on their beliefs and attitudes, providing deeper insight into their responses regarding harm reduction.
Methods
This project was conducted by the Veterans Integrated Services Network (VISN) 5 academic detailing team. VISN 5 serves veterans from economically and demographically diverse areas in Maryland; Washington, DC; West Virginia; and portions of Virginia, Pennsylvania, Ohio, and Kentucky. VAMCs in Baltimore, Maryland, and Washington, DC, serve a largely urban population while the 4 West Virginia facilities in Martinsburg, Huntington, Beckley, and Clarksburg, serve a largely rural population. West Virginia has been the epicenter of the opioid crisis and consistently has the highest drug overdose deaths per capita in the United States.12 Among cities, Baltimore, Maryland, has the highest number of drug overdose deaths per capita with 174.1 per 100,000 people.12,13
At the time of this project, the 6 VISN 5 VAMCs had established overdose education and naloxone distribution (OEND) programs. Although OEND programs have existed since 2013, VISN 5 SSPs and harm reduction services that provided fentanyl test strips were only available at the Martinsburg, Beckley, and Huntington VAMCs. All 6 VAMCs had substance use treatment programs with a variety of inpatient and outpatient mental health services. The Washington, DC and Baltimore VAMCs had opioid treatment programs that provided methadone maintenance.
The VISN 5 academic detailing team consists of 7 clinical pharmacists. These academic detailers plan annual systematic interventions to provide medical knowledge translation services on health-related campaigns. Academic detailers are trained in change management and motivational interviewing. They uniquely facilitate conversations with HCPs on various topics or campaigns, aiming for quality improvement and behavioral change through positive relationships and sharing resources.14 Academic detailing conversations and relationships with HCPs involve assessing and understanding HCP behaviors, including barriers and readiness to change to align with the goal of improving patient outcomes. Academic detailing has improved practice behaviors around providing OEND in VHA.15
To prepare for a harm reduction campaign, the academic detailers sought to gain insight from target VISN 5 mental health prescribers. Figure 1 outlines the project timeline, which started with emails inviting mental health prescribers to complete an anonymous online survey. Academic detailers from each site emailed mental health prescribers who completed the survey to determine interest in expanding on survey findings. Mental health prescribers who completed the survey could participate in a postsurvey discussion.
Surveys
Between January 29, 2024, and February 22, 2024, the academic detailers emailed facility mental health prescribers (N = 156) a link to an anonymous 15-question survey. The email informed recipients of the survey’s purpose: to gain a better understanding of prescriber perceptions of veterans with SUD and harm reduction programs and their willingness to provide harm reduction tools, to better determine interventions that could be implemented.
The survey collected prescriber demographic data and their perceptions of PWUD and harm reduction tools and education. Survey questions were extrapolated from validated surveys (eg, DDPPQ) and survey-based implicit association test.16,17 The survey used multiple choice and 5-point Likert scale questions. Mental health prescribers were asked about their role at the VHA, years in practice, medical center affiliation, type of SUDs treated (eg, opioid, stimulant, alcohol, cannabis, or other), and whether they had previously met with academic detailers about harm reduction.
Respondents read statements about patients with or without SUD and provided Likert scale responses describing their regard, level of comfort, and preferences. The survey included Likert scale questions about respondents’ comfort in providing harm reduction education and supplies. Respondents also noted whether they believed harm reduction reduced substance use, harm reduction tools encourage people with SUD to continue using drugs, and whether HCPs can impact clinical change.
Postsurvey interviews with predetermined questions were conducted in-person or via video conference with ≥ 1 prescriber at each VAMC by an academic detailer. The postsurvey discussion offered an opportunity for respondents to further elaborate and describe previous experiences and current beliefs that may affect their attitudes toward people with SUD and their views on harm reduction. Participants received no compensation for survey completion or interviews.
Analysis
The Washington VAMC Institutional Review Board reviewed and approved this project as quality improvement with potential publication. No inferential statistics were calculated. Survey participant demographics were reported using frequencies and proportions reported for categorical variables. Notes from follow-up interviews were analyzed using the Prosci Awareness, Desire, Knowledge, Ability, and Reinforcement (ADKAR) Model for Change Management.18 This framework is used by academic detailers to determine a prescriber’s stage of change, which helps select the appropriate resources to move the clinician along a change framework. Completed postsurvey interview sheets, including notes written by the academic detailer, were analyzed by the project lead (NJ) who reviewed each interview sheet and analysis with the academic detailer who led the discussion.
Results
Sixty-six respondents completed the online survey (42% response rate), and 7 mental health prescribers participated in a postsurvey discussion. Thirty-one participants (47%) were physicians and 17 (26%) were in practice for > 20 years. Response rates reflected the size of mental health staff at each VAMC at the time of the survey: 17 respondents (26%) worked at each of the Martinsburg and Baltimore VAMCs, with fewer at the other VAMCs (Table 1). Alcohol use disorder was the most commonly reported SUD treated (n = 62; 33%), followed by cannabis use disorder (n = 40; 21%), OUD (n = 38; 20%), and stimulant use disorder (n = 37; 20%).
Respondents felt comfortable and confident educating patients on ways to reduce harm related to substance use (91%; mean [SD], 4.24 [0.84]). Most prescribers surveyed (97%; mean [SD], 1.59 [0.68]) disagreed or strongly disagreed that harm reduction encourages patients with SUD to continue using drugs, and all prescribers surveyed disagreed that there is nothing they can do to encourage harm reduction. Survey results were mixed for personal comfort in working with people with SUD vs people without SUD (Figure 2). Respondents were most willing to provide naloxone (95%; mean [SD], 4.71 [0.78]), compared to fentanyl test strips (61%; mean [SD], 3.61 [1.41]) or syringes (39%; mean [SD], 3.18 [1.39]). Respondents were neutral or least willing to provide syringes (Figure 3).
Seven postsurvey interviews were completed between academic detailers and mental health clinicians across the 6 VAMCs. Respondents included 1 physician assistant, 1 nurse practitioner, 1 pharmacist, and 4 physicians. Notes were analyzed using the ADKAR Change Competency Model to organize clinician stages of change (Table 2).
Barriers identified by interviewees included lack of mobile services, lack of confidence and awareness of the availability of harm reduction at their respective medical center, lack of time to discuss harm reduction, negative sentiments toward providing SUD-related harm reduction, discomfort with harm reduction products, and lack of knowledge and time to learn about harm reduction services. Opportunities identified to drive change in practice included additional time allotted during patient appointments, educational discussions and presentations to increase knowledge of and comfort with harm reduction tools, a clear clinical patient care workflow and process for harm reduction services, and reinforcement strategies to recognize success.
Discussion
This project investigated mental health prescribers’ perceptions of harm reduction at VAMCs in West Virginia, Maryland, and Washington, DC. While previous studies have demonstrated the efficacy of harm reduction tools, there is a lack of research on HCPs willingness to use these resources. This study suggests that while most respondents feel confident in and see the value of offering harm reduction resources to patients, a disparity exists between which resources HCPs are more likely to use and factors that would further enhance their ability to integrate harm reduction into practice. The follow-up interviews provided additional insight into the survey results.
Most respondents met the awareness and desire stage and moved to the knowledge, ability, or reinforcement ADKAR stage. It would be reasonable to extrapolate that most of the respondents felt comfortable with and were very likely to offer certain harm reduction tools. In the ADKAR interview analysis, the most common factors needed to drive change included having more time during patient appointments, additional education, clear processes for harm reduction services, and reinforcement strategies to sustain change. Respondents noted that harm reduction discussions took extra time in their already limited appointments with patients, which may have limited time for discussions surrounding all other mental health concerns. These discussions often necessitate in-depth conversations to accurately understand the patients’ needs. Given HCP time constraints, they may view harm reduction as lower in urgency and priority relative to other concerns. While most respondents were in the reinforcement phase, it is important to note the ADKAR model is fluid, and therefore an HCP could move forward or backward. This movement can be noted in the postsurvey interviews where, for example, prescriber 6 was determined to be in the reinforcement stage since they had already discussed harm reduction with patients. However, prescriber 6 also noted a barrier of unfamiliarity with local laws, which could shift them to the ADKAR knowledge stage.
Respondents noted that education through didactic sessions could lead to better incorporation of harm reduction into patient care. While harm reduction has evidence supporting its effectiveness, the respondents noted willingness to discuss harm reduction when treatment fails or the patient refuses treatment or referrals. Respondents expressed mixed opinions on use of harm reduction tools among patients with SUDs as some prescribers viewed harm reduction as part of a treatment plan and others viewed a return to drug use as a failure of treatment. Furthermore, respondents expressed hesitancy surrounding certain harm reduction tools, such as fentanyl test strips or syringes, and perceived these supplies as intended for medical use rather than harm reduction. HCPs may feel uncomfortable offering these supplies for drug use, despite their use for reducing risk.
Most responses were received from VAMCs with large mental health substance use programs. Respondents at larger, urban facilities (Washington, DC, and Baltimore, Maryland) expressed more hesitancy around using harm reduction tools despite having more harm reduction resources available compared to smaller or rural sites. These results align with previous studies that found no difference in prescribers providing medications for OUD in rural and urban VAMCs, showing urban sites, despite more resources, are not more willing to provide harm reduction or other addiction services.19 This evidence might indicate that urban sites may not use available resources (eg, methadone clinics) or that rural sites can provide just as robust medications for OUD care as urban sites.
Follow-up interview analysis indicated that HCPs lack knowledge of certain harm reduction tools. One-on-one peer discussions, like academic detailing, can facilitate discussions around a prescriber’s role in harm reduction, address gaps in knowledge by sharing what is available at the facilities for harm reduction, and suggest conversation points to help prescribers start harm reduction discussions with patients unwilling to begin treatment. Additionally, academic detailing can connect prescribers to available resources in the community to provide pragmatic approaches and suggestions. A clear and consistent treatment process may reduce barriers by reassuring prescribers they have support and by providing consistent directions so that prescribers do not waste time.
Reinforcement is important for sustaining change. VAMCs could consider positive feedback and other evidence-based reinforcement strategies (eg, social recognition, continuing education) to communicate that these changes are noticed and appreciated.20 Late adopters may also be influenced by seeing positive feedback and results for peers. Systematic changes can be the catalyst for and sustain individual change.
Shifting perceptions and adopting change may be challenging, especially for SUD, which can be highly stigmatized. Promotion of successful change should be multifaceted and include both system and individual approaches. VHA systemic changes that could contribute to positive change include provision of time and access to SUD treatment training, a clear and sustainable treatment process, and reinforcement by recognizing success. In addition, facility leadership could provide support through dedicated time and resources during the workday for SUD treatment and harm reduction training. Support could empower HCPs and convey leadership support for harm reduction. This dedicated time could be used for didactic lecture sessions or individual meetings with academic detailers who can tailor discussions to the prescriber’s practice.
Strengths and Limitations
This survey included prescribers from a range of mental health care practice settings (eg, inpatient, outpatient clinic, rural, urban) and varied years of experience. This variety resulted in diverse perspectives and knowledge bases. Postsurvey interviews allowed academic detailers to gain deeper insight into answers in the survey, which can guide future interventions. Postsurvey interviews and application of the ADKAR model provided additional viewpoints on harm reduction.
A limitation of this project is the absence of an assessment of respondents’ harm reduction knowledge accuracy. Although respondents reported confidence in discussing harm reduction with patients, the survey did not assess whether their knowledge was accurate. Additionally, the survey did not ask about the availability of syringes and test strips at the prescribers’ VAMC, which could explain discrepancies in responses between naloxone and other forms of harm reduction (drug test strips and syringes were not available to all HCPs in the VISN). This lack of availability may have skewed responses. West Virginia SSPs, for example, were closed following legislative changes, which may contribute to stigma.21
Not all respondents were asked to do a follow-up interview, which limited the perspectives included in this study. Each site had ≥ 1 follow-up interview to limit the academic detailer’s workload. The initial survey included the phrase clean syringe, which can be stigmatizing and insinuate that PWUD are not clean. The preferred term would have been sterile syringe.22
Conclusions
This survey of mental health prescribers found that most respondents are comfortable treating patients with SUD and confident in educating patients on harm reduction. Additionally, most respondents were more willing to provide naloxone vs fentanyl test strips or sterile syringes. A lack of time and awareness was the most frequently cited barrier to harm reduction services. As the VHA continues to expand access to harm reduction programs, which have proven to increase treatment rates and reduce disease, it will be imperative for HCPs, including mental health prescribers, to recognize the benefit of these programs for veterans with SUD. Future interventions should be designed and evaluated in collaboration with all HCPs and patients. This project determined ways to promote change for prescribers, but it will be important for further research to continue those conversations and incorporate patient perspectives.
The Public Health and Welfare Act of 1988 prohibited the use of federal funds to “provide individuals with hypodermic needles or syringes so that such individuals may use illegal drugs.”1 Although the Act included the caveat that the US Surgeon General may determine that “a demonstration needle exchange program would be effective in reducing drug abuse,” and thus federal funds could be used, the legislation prohibited federal, state, and local agencies from funding syringe services programs (SSPs). SSPs use various harm reduction tools to improve public safety and reduce the potential harmful consequences of risky behaviors, similar to how using a seat belt while driving reduces the risk of injury or death.2 SSPs are rooted in evidence-based practices, and several studies, according to the Centers for Disease Control and Prevention, have found that people who use drugs (PWUDs) who use community-based SSPs are 5 times more likely to enter treatment than those who do not use these programs. Additionally, these programs have shown an estimated 50% reduction in HIV and hepatitis C infections.3
Amid a 2015 HIV outbreak in Indiana among individuals sharing needles for injection drug use, Congress passed an omnibus spending bill that partially lifted the federal funding restriction. Federal funds now may be used for operational costs that support SSPs but may not be used to purchase syringes themselves.4
Following the 2015 legislation, federal agencies began implementing SSPs. The Veterans Health Administration (VHA) established SSPs at 3 medical centers in 2017.5 Veterans who participated in the programs were able to access supplies (eg, syringes, fentanyl test strips, wound care kits, and condoms) through donations to US Department of Veterans Affairs (VA) medical centers (VAMCs). The success of these programs laid the foundation for the VHA to implement SSPs nationally. VHA SSPs provided access to naloxone (an opioid overdose reversal medication), fentanyl test strips, condoms, sterile syringe distribution, testing for blood-borne viruses, HIV pre-exposure prophylaxis, as well as educational materials and resources, and low-barrier access to drug treatment (eg, medications for opioid use disorder [OUD]).
In 2020, the Biden Administration outlined 7 drug policy priorities, which included enhancing evidence-based harm reduction efforts. 6 This policy also discussed mandates for federal agencies to remove barriers to federal funding for purchasing syringes and other harm reduction supplies. The VHA responded to the policy by publishing guidance that recommended VAMCs develop and/or ensure veterans have access to harm reduction services in the community, where state law is not legally more stringent.7
In 2025 the Trump administration Statement of Drug Policy Priorities encouraged local jurisdictions to increase the availability of drug test strips and naloxone.8 These significant policy shifts moved SSPs from being housed mostly in local public health departments and community-based organizations to also being available at health care facilities. 9 VAMCs have unique opportunities to provide universal health care that includes both prevention services and other medical management to PWUD.
One study assessed staff perceptions of PWUD at a VAMC in preparation for a training program about harm reduction. The results indicated an overall positive staff perception of PWUD, although only the Drug and Drug Problems Perceptions Questionnaire (DDPPQ) was administered, which assessed comfort of working with this population and not explicitly the use of harm reduction.10 Another study interviewed clinical pharmacists, primary care clinicians, social workers, and directors of addiction and mental health services to determine barriers and facilitators (ie, potential opportunities to promote change) to implementing harm reduction at the VHA. The study identified barriers to be a lack of knowledge, time, and comfort, while suggesting opportunities for improvement were engagement of champions, communication and educational strategies, and adaptation of existing infrastructure.11
While these findings are insightful for the VHA to disseminate a harm reduction program, there remains a gap in assessing staff willingness to provide harm reduction services. Evidence on harm reduction services among veterans is limited and more research is needed to better understand the role of these services and acceptance among enrolled veterans and VHA staff. Specifically, more research is needed on health care practitioners’ (HCPs) perceptions of harm reduction use.
Mental health care practitioners frequently treat patients with substance use disorders (SUDs), making them an ideal initial cohort to assess willingness to provide harm reduction to this population. By analyzing mental HCPs’ perceptions, additional interventions could be identified, implemented, and evaluated to improve their willingness to provide harm reduction tools.
This project focused on mental health clinicians with prescribing privileges: physicians (allopathic and osteopathic physicians), nurse practitioners, physician assistants, and clinical pharmacist practitioners. Mental health prescribers were selected because they are uniquely positioned at the intersection of prevention and treatment in drug use. Furthermore, mental health prescribers at the VAMCs included in this study are usually the primary point of entry to SUD clinics. This mixed-methods study used an anonymous online survey and voluntary postsurvey discussions with mental health care prescribers to elaborate on their beliefs and attitudes, providing deeper insight into their responses regarding harm reduction.
Methods
This project was conducted by the Veterans Integrated Services Network (VISN) 5 academic detailing team. VISN 5 serves veterans from economically and demographically diverse areas in Maryland; Washington, DC; West Virginia; and portions of Virginia, Pennsylvania, Ohio, and Kentucky. VAMCs in Baltimore, Maryland, and Washington, DC, serve a largely urban population while the 4 West Virginia facilities in Martinsburg, Huntington, Beckley, and Clarksburg, serve a largely rural population. West Virginia has been the epicenter of the opioid crisis and consistently has the highest drug overdose deaths per capita in the United States.12 Among cities, Baltimore, Maryland, has the highest number of drug overdose deaths per capita with 174.1 per 100,000 people.12,13
At the time of this project, the 6 VISN 5 VAMCs had established overdose education and naloxone distribution (OEND) programs. Although OEND programs have existed since 2013, VISN 5 SSPs and harm reduction services that provided fentanyl test strips were only available at the Martinsburg, Beckley, and Huntington VAMCs. All 6 VAMCs had substance use treatment programs with a variety of inpatient and outpatient mental health services. The Washington, DC and Baltimore VAMCs had opioid treatment programs that provided methadone maintenance.
The VISN 5 academic detailing team consists of 7 clinical pharmacists. These academic detailers plan annual systematic interventions to provide medical knowledge translation services on health-related campaigns. Academic detailers are trained in change management and motivational interviewing. They uniquely facilitate conversations with HCPs on various topics or campaigns, aiming for quality improvement and behavioral change through positive relationships and sharing resources.14 Academic detailing conversations and relationships with HCPs involve assessing and understanding HCP behaviors, including barriers and readiness to change to align with the goal of improving patient outcomes. Academic detailing has improved practice behaviors around providing OEND in VHA.15
To prepare for a harm reduction campaign, the academic detailers sought to gain insight from target VISN 5 mental health prescribers. Figure 1 outlines the project timeline, which started with emails inviting mental health prescribers to complete an anonymous online survey. Academic detailers from each site emailed mental health prescribers who completed the survey to determine interest in expanding on survey findings. Mental health prescribers who completed the survey could participate in a postsurvey discussion.
Surveys
Between January 29, 2024, and February 22, 2024, the academic detailers emailed facility mental health prescribers (N = 156) a link to an anonymous 15-question survey. The email informed recipients of the survey’s purpose: to gain a better understanding of prescriber perceptions of veterans with SUD and harm reduction programs and their willingness to provide harm reduction tools, to better determine interventions that could be implemented.
The survey collected prescriber demographic data and their perceptions of PWUD and harm reduction tools and education. Survey questions were extrapolated from validated surveys (eg, DDPPQ) and survey-based implicit association test.16,17 The survey used multiple choice and 5-point Likert scale questions. Mental health prescribers were asked about their role at the VHA, years in practice, medical center affiliation, type of SUDs treated (eg, opioid, stimulant, alcohol, cannabis, or other), and whether they had previously met with academic detailers about harm reduction.
Respondents read statements about patients with or without SUD and provided Likert scale responses describing their regard, level of comfort, and preferences. The survey included Likert scale questions about respondents’ comfort in providing harm reduction education and supplies. Respondents also noted whether they believed harm reduction reduced substance use, harm reduction tools encourage people with SUD to continue using drugs, and whether HCPs can impact clinical change.
Postsurvey interviews with predetermined questions were conducted in-person or via video conference with ≥ 1 prescriber at each VAMC by an academic detailer. The postsurvey discussion offered an opportunity for respondents to further elaborate and describe previous experiences and current beliefs that may affect their attitudes toward people with SUD and their views on harm reduction. Participants received no compensation for survey completion or interviews.
Analysis
The Washington VAMC Institutional Review Board reviewed and approved this project as quality improvement with potential publication. No inferential statistics were calculated. Survey participant demographics were reported using frequencies and proportions reported for categorical variables. Notes from follow-up interviews were analyzed using the Prosci Awareness, Desire, Knowledge, Ability, and Reinforcement (ADKAR) Model for Change Management.18 This framework is used by academic detailers to determine a prescriber’s stage of change, which helps select the appropriate resources to move the clinician along a change framework. Completed postsurvey interview sheets, including notes written by the academic detailer, were analyzed by the project lead (NJ) who reviewed each interview sheet and analysis with the academic detailer who led the discussion.
Results
Sixty-six respondents completed the online survey (42% response rate), and 7 mental health prescribers participated in a postsurvey discussion. Thirty-one participants (47%) were physicians and 17 (26%) were in practice for > 20 years. Response rates reflected the size of mental health staff at each VAMC at the time of the survey: 17 respondents (26%) worked at each of the Martinsburg and Baltimore VAMCs, with fewer at the other VAMCs (Table 1). Alcohol use disorder was the most commonly reported SUD treated (n = 62; 33%), followed by cannabis use disorder (n = 40; 21%), OUD (n = 38; 20%), and stimulant use disorder (n = 37; 20%).
Respondents felt comfortable and confident educating patients on ways to reduce harm related to substance use (91%; mean [SD], 4.24 [0.84]). Most prescribers surveyed (97%; mean [SD], 1.59 [0.68]) disagreed or strongly disagreed that harm reduction encourages patients with SUD to continue using drugs, and all prescribers surveyed disagreed that there is nothing they can do to encourage harm reduction. Survey results were mixed for personal comfort in working with people with SUD vs people without SUD (Figure 2). Respondents were most willing to provide naloxone (95%; mean [SD], 4.71 [0.78]), compared to fentanyl test strips (61%; mean [SD], 3.61 [1.41]) or syringes (39%; mean [SD], 3.18 [1.39]). Respondents were neutral or least willing to provide syringes (Figure 3).
Seven postsurvey interviews were completed between academic detailers and mental health clinicians across the 6 VAMCs. Respondents included 1 physician assistant, 1 nurse practitioner, 1 pharmacist, and 4 physicians. Notes were analyzed using the ADKAR Change Competency Model to organize clinician stages of change (Table 2).
Barriers identified by interviewees included lack of mobile services, lack of confidence and awareness of the availability of harm reduction at their respective medical center, lack of time to discuss harm reduction, negative sentiments toward providing SUD-related harm reduction, discomfort with harm reduction products, and lack of knowledge and time to learn about harm reduction services. Opportunities identified to drive change in practice included additional time allotted during patient appointments, educational discussions and presentations to increase knowledge of and comfort with harm reduction tools, a clear clinical patient care workflow and process for harm reduction services, and reinforcement strategies to recognize success.
Discussion
This project investigated mental health prescribers’ perceptions of harm reduction at VAMCs in West Virginia, Maryland, and Washington, DC. While previous studies have demonstrated the efficacy of harm reduction tools, there is a lack of research on HCPs willingness to use these resources. This study suggests that while most respondents feel confident in and see the value of offering harm reduction resources to patients, a disparity exists between which resources HCPs are more likely to use and factors that would further enhance their ability to integrate harm reduction into practice. The follow-up interviews provided additional insight into the survey results.
Most respondents met the awareness and desire stage and moved to the knowledge, ability, or reinforcement ADKAR stage. It would be reasonable to extrapolate that most of the respondents felt comfortable with and were very likely to offer certain harm reduction tools. In the ADKAR interview analysis, the most common factors needed to drive change included having more time during patient appointments, additional education, clear processes for harm reduction services, and reinforcement strategies to sustain change. Respondents noted that harm reduction discussions took extra time in their already limited appointments with patients, which may have limited time for discussions surrounding all other mental health concerns. These discussions often necessitate in-depth conversations to accurately understand the patients’ needs. Given HCP time constraints, they may view harm reduction as lower in urgency and priority relative to other concerns. While most respondents were in the reinforcement phase, it is important to note the ADKAR model is fluid, and therefore an HCP could move forward or backward. This movement can be noted in the postsurvey interviews where, for example, prescriber 6 was determined to be in the reinforcement stage since they had already discussed harm reduction with patients. However, prescriber 6 also noted a barrier of unfamiliarity with local laws, which could shift them to the ADKAR knowledge stage.
Respondents noted that education through didactic sessions could lead to better incorporation of harm reduction into patient care. While harm reduction has evidence supporting its effectiveness, the respondents noted willingness to discuss harm reduction when treatment fails or the patient refuses treatment or referrals. Respondents expressed mixed opinions on use of harm reduction tools among patients with SUDs as some prescribers viewed harm reduction as part of a treatment plan and others viewed a return to drug use as a failure of treatment. Furthermore, respondents expressed hesitancy surrounding certain harm reduction tools, such as fentanyl test strips or syringes, and perceived these supplies as intended for medical use rather than harm reduction. HCPs may feel uncomfortable offering these supplies for drug use, despite their use for reducing risk.
Most responses were received from VAMCs with large mental health substance use programs. Respondents at larger, urban facilities (Washington, DC, and Baltimore, Maryland) expressed more hesitancy around using harm reduction tools despite having more harm reduction resources available compared to smaller or rural sites. These results align with previous studies that found no difference in prescribers providing medications for OUD in rural and urban VAMCs, showing urban sites, despite more resources, are not more willing to provide harm reduction or other addiction services.19 This evidence might indicate that urban sites may not use available resources (eg, methadone clinics) or that rural sites can provide just as robust medications for OUD care as urban sites.
Follow-up interview analysis indicated that HCPs lack knowledge of certain harm reduction tools. One-on-one peer discussions, like academic detailing, can facilitate discussions around a prescriber’s role in harm reduction, address gaps in knowledge by sharing what is available at the facilities for harm reduction, and suggest conversation points to help prescribers start harm reduction discussions with patients unwilling to begin treatment. Additionally, academic detailing can connect prescribers to available resources in the community to provide pragmatic approaches and suggestions. A clear and consistent treatment process may reduce barriers by reassuring prescribers they have support and by providing consistent directions so that prescribers do not waste time.
Reinforcement is important for sustaining change. VAMCs could consider positive feedback and other evidence-based reinforcement strategies (eg, social recognition, continuing education) to communicate that these changes are noticed and appreciated.20 Late adopters may also be influenced by seeing positive feedback and results for peers. Systematic changes can be the catalyst for and sustain individual change.
Shifting perceptions and adopting change may be challenging, especially for SUD, which can be highly stigmatized. Promotion of successful change should be multifaceted and include both system and individual approaches. VHA systemic changes that could contribute to positive change include provision of time and access to SUD treatment training, a clear and sustainable treatment process, and reinforcement by recognizing success. In addition, facility leadership could provide support through dedicated time and resources during the workday for SUD treatment and harm reduction training. Support could empower HCPs and convey leadership support for harm reduction. This dedicated time could be used for didactic lecture sessions or individual meetings with academic detailers who can tailor discussions to the prescriber’s practice.
Strengths and Limitations
This survey included prescribers from a range of mental health care practice settings (eg, inpatient, outpatient clinic, rural, urban) and varied years of experience. This variety resulted in diverse perspectives and knowledge bases. Postsurvey interviews allowed academic detailers to gain deeper insight into answers in the survey, which can guide future interventions. Postsurvey interviews and application of the ADKAR model provided additional viewpoints on harm reduction.
A limitation of this project is the absence of an assessment of respondents’ harm reduction knowledge accuracy. Although respondents reported confidence in discussing harm reduction with patients, the survey did not assess whether their knowledge was accurate. Additionally, the survey did not ask about the availability of syringes and test strips at the prescribers’ VAMC, which could explain discrepancies in responses between naloxone and other forms of harm reduction (drug test strips and syringes were not available to all HCPs in the VISN). This lack of availability may have skewed responses. West Virginia SSPs, for example, were closed following legislative changes, which may contribute to stigma.21
Not all respondents were asked to do a follow-up interview, which limited the perspectives included in this study. Each site had ≥ 1 follow-up interview to limit the academic detailer’s workload. The initial survey included the phrase clean syringe, which can be stigmatizing and insinuate that PWUD are not clean. The preferred term would have been sterile syringe.22
Conclusions
This survey of mental health prescribers found that most respondents are comfortable treating patients with SUD and confident in educating patients on harm reduction. Additionally, most respondents were more willing to provide naloxone vs fentanyl test strips or sterile syringes. A lack of time and awareness was the most frequently cited barrier to harm reduction services. As the VHA continues to expand access to harm reduction programs, which have proven to increase treatment rates and reduce disease, it will be imperative for HCPs, including mental health prescribers, to recognize the benefit of these programs for veterans with SUD. Future interventions should be designed and evaluated in collaboration with all HCPs and patients. This project determined ways to promote change for prescribers, but it will be important for further research to continue those conversations and incorporate patient perspectives.
- Use of funds to supply hypodermic needles or syringes for illegal drug use; prohibition, 42 USC § 300ee-5 (1988). Accessed January 5, 2026. https://www.law.cornell.edu /uscode/text/42/300ee-5
- OD2A Case Study: Harm Reduction. Centers for Disease Control and Prevention. June 9, 2025. Accessed January 5, 2026. https://www.cdc.gov/overdose-prevention/php /od2a/harm-reduction.html
- Strengthening Syringe Services Programs (SSPs). Centers for Disease Control and Prevention. March 20, 2024. Accessed January 5, 2026. https://www.cdc.gov/hepatitis -syringe-services/php/about/index.html
- Weinmeyer R. Needle exchange programs’ status in US politics. AMA J Ethics. 2016;18:252-257. doi:10.1001/journalofethics.2016.18.3.hlaw1-1603
- Rife-Pennington T, Dinges E, Ho MQ. Implementing syringe services programs within the Veterans Health Administration: facility experiences and next steps. J Am Pharm Assoc (2003). 2023;63:234-240. doi:10.1016/j.japh.2022.10.019
- The Biden-Harris Administration’s Statement of Drug Policy Priorities for Year One. Executive Office of the President, Office of National Drug Control Policy. April 1, 2021. Accessed January 5, 2026. https://bidenwhitehouse.archives.gov/wp-content/uploads/2021/03/BidenHarris -Statement-of-Drug-Policy-Priorities-April-1.pdf
- HIV - for veterans and the public syringe services programs. US Department of Veterans Affairs. Updated August 16, 2021. Accessed January 5, 2026. https://www.hiv .va.gov/patient/ssp.asp
- Trump Administration’s Statement of Drug Policy Priorities. White House. April 1, 2025. Accessed January 7, 2026. https://www.whitehouse.gov/wp-content /uploads/2025/04/2025-Trump-Administration-Drug-Policy -Priorities.pdf
- Health Centers and Syringe Services Programs. National Health Care for the Homeless Council. May 2023. Accessed January 5, 2026. https://nhchc.org/wp-content /uploads/2023/06/Health-Centers-SSPs-Final.pdf
- Lynch RD, Biederman DJ, Silva S, Demasi K. A syringe service program within a federal system: foundations for implementation. J Addict Nurs. 2021;32:152-158. doi:10.1097/JAN.0000000000000402
- Harvey LH, Sliwinski SK, Flike K, et al. The integration of harm reduction services in the Veterans Health Administration (VHA): a qualitative analysis of barriers and facilitators. J Addict Dis. 2024;42:326-334. doi:10.1080/10550887.2023.2210021
- Drug Overdose Death Rates. National Center for Drug Abuse Statistics. Accessed January 5, 2026. https:// drugabusestatistics.org/drug-overdose-deaths
- Ng G. New database shows Baltimore greatly devastated by opioid epidemic. Updated August 21, 2023. Accessed January 5, 2026. https://www.wbaltv.com/article/opioid -epidemic-database-baltimore-deaths/44869671
- Introductory Guide to Academic Detailing. National Resource Center for Academic Detailing. 2017. Accessed January 5, 2026. https://www.narcad.org /uploads/5/7/9/5/57955981/introductory_guide_to_ad.pdf
- Zhang J. Can educational outreach improve experts’ decision making? Evidence from a national opioid academic detailing program. SSRN. 2023;4297398. doi:10.2139/ssrn.4297398
- Watson H, Maclaren W, Kerr S. Staff attitudes towards working with drug users: development of the Drug Problems Perceptions Questionnaire. Addiction. 2007;102:206- 215. doi:10.1111/j.1360-0443.2006.01686.x
- Dahl RA, Vakkalanka JP, Harland KK, Radke J. Investigating healthcare provider bias toward patients who use drugs using a survey-based implicit association test: pilot study. J Addict Med. 2022;16:557-562. doi:10.1097/ADM.0000000000000970
- Hiatt JM, Creasey TJ. Change Management: The People Side of Change. Prosci Learning Center Publications; 2012.
- Wyse JJ, Shull S, Lindner S, et al. Access to medications for opioid use disorder in rural versus urban Veterans Health Administration facilities. J Gen Intern Med. 2023;38:1871-1876. doi:10.1007/s11606-023-08027-4
- Mostofian F, Ruban C, Simunovic N, Bhandari M. Changing physician behavior: what works?. Am J Manag Care. 2015;21(1):75-84.
- Bergdorf-Smith K, Bridge Initiative for S&T Policy, Leadership, and Communications. Syringe Service Programs and HIV Prevention in West Virginia. West Virginia University. February 5, 2024. Accessed January 5, 2026. https:// scitechpolicy.wvu.edu/science-and-technology-notes -articles/2024/02/05/syringe-service-programs-and-hiv -prevention-in-west-virginia
- Brunsdon N. Stop saying ‘clean’. Injecting Advice. February 7, 2011. Accessed January 5, 2026. https:// injectingadvice.com/stop-saying-clean/
- Use of funds to supply hypodermic needles or syringes for illegal drug use; prohibition, 42 USC § 300ee-5 (1988). Accessed January 5, 2026. https://www.law.cornell.edu /uscode/text/42/300ee-5
- OD2A Case Study: Harm Reduction. Centers for Disease Control and Prevention. June 9, 2025. Accessed January 5, 2026. https://www.cdc.gov/overdose-prevention/php /od2a/harm-reduction.html
- Strengthening Syringe Services Programs (SSPs). Centers for Disease Control and Prevention. March 20, 2024. Accessed January 5, 2026. https://www.cdc.gov/hepatitis -syringe-services/php/about/index.html
- Weinmeyer R. Needle exchange programs’ status in US politics. AMA J Ethics. 2016;18:252-257. doi:10.1001/journalofethics.2016.18.3.hlaw1-1603
- Rife-Pennington T, Dinges E, Ho MQ. Implementing syringe services programs within the Veterans Health Administration: facility experiences and next steps. J Am Pharm Assoc (2003). 2023;63:234-240. doi:10.1016/j.japh.2022.10.019
- The Biden-Harris Administration’s Statement of Drug Policy Priorities for Year One. Executive Office of the President, Office of National Drug Control Policy. April 1, 2021. Accessed January 5, 2026. https://bidenwhitehouse.archives.gov/wp-content/uploads/2021/03/BidenHarris -Statement-of-Drug-Policy-Priorities-April-1.pdf
- HIV - for veterans and the public syringe services programs. US Department of Veterans Affairs. Updated August 16, 2021. Accessed January 5, 2026. https://www.hiv .va.gov/patient/ssp.asp
- Trump Administration’s Statement of Drug Policy Priorities. White House. April 1, 2025. Accessed January 7, 2026. https://www.whitehouse.gov/wp-content /uploads/2025/04/2025-Trump-Administration-Drug-Policy -Priorities.pdf
- Health Centers and Syringe Services Programs. National Health Care for the Homeless Council. May 2023. Accessed January 5, 2026. https://nhchc.org/wp-content /uploads/2023/06/Health-Centers-SSPs-Final.pdf
- Lynch RD, Biederman DJ, Silva S, Demasi K. A syringe service program within a federal system: foundations for implementation. J Addict Nurs. 2021;32:152-158. doi:10.1097/JAN.0000000000000402
- Harvey LH, Sliwinski SK, Flike K, et al. The integration of harm reduction services in the Veterans Health Administration (VHA): a qualitative analysis of barriers and facilitators. J Addict Dis. 2024;42:326-334. doi:10.1080/10550887.2023.2210021
- Drug Overdose Death Rates. National Center for Drug Abuse Statistics. Accessed January 5, 2026. https:// drugabusestatistics.org/drug-overdose-deaths
- Ng G. New database shows Baltimore greatly devastated by opioid epidemic. Updated August 21, 2023. Accessed January 5, 2026. https://www.wbaltv.com/article/opioid -epidemic-database-baltimore-deaths/44869671
- Introductory Guide to Academic Detailing. National Resource Center for Academic Detailing. 2017. Accessed January 5, 2026. https://www.narcad.org /uploads/5/7/9/5/57955981/introductory_guide_to_ad.pdf
- Zhang J. Can educational outreach improve experts’ decision making? Evidence from a national opioid academic detailing program. SSRN. 2023;4297398. doi:10.2139/ssrn.4297398
- Watson H, Maclaren W, Kerr S. Staff attitudes towards working with drug users: development of the Drug Problems Perceptions Questionnaire. Addiction. 2007;102:206- 215. doi:10.1111/j.1360-0443.2006.01686.x
- Dahl RA, Vakkalanka JP, Harland KK, Radke J. Investigating healthcare provider bias toward patients who use drugs using a survey-based implicit association test: pilot study. J Addict Med. 2022;16:557-562. doi:10.1097/ADM.0000000000000970
- Hiatt JM, Creasey TJ. Change Management: The People Side of Change. Prosci Learning Center Publications; 2012.
- Wyse JJ, Shull S, Lindner S, et al. Access to medications for opioid use disorder in rural versus urban Veterans Health Administration facilities. J Gen Intern Med. 2023;38:1871-1876. doi:10.1007/s11606-023-08027-4
- Mostofian F, Ruban C, Simunovic N, Bhandari M. Changing physician behavior: what works?. Am J Manag Care. 2015;21(1):75-84.
- Bergdorf-Smith K, Bridge Initiative for S&T Policy, Leadership, and Communications. Syringe Service Programs and HIV Prevention in West Virginia. West Virginia University. February 5, 2024. Accessed January 5, 2026. https:// scitechpolicy.wvu.edu/science-and-technology-notes -articles/2024/02/05/syringe-service-programs-and-hiv -prevention-in-west-virginia
- Brunsdon N. Stop saying ‘clean’. Injecting Advice. February 7, 2011. Accessed January 5, 2026. https:// injectingadvice.com/stop-saying-clean/
Mental Health Prescribers’ Perceptions of Patients With Substance Use Disorders and Harm Reduction Services
Mental Health Prescribers’ Perceptions of Patients With Substance Use Disorders and Harm Reduction Services
Does Cannabis Really Help PTSD? New Data Cast Doubt
Does Cannabis Really Help PTSD? New Data Cast Doubt
New research challenges the assumption that long-term cannabis use improves symptoms or functioning in posttraumatic stress disorder (PTSD).
On the contrary, researchers found that abstaining from cannabis for 3 months was associated with significantly greater reductions in PTSD symptoms in adults with PTSD and comorbid cannabis use disorder (CUD).
The data suggest that continued cannabis use could limit recovery in some domains — underscoring the need to routinely assess cannabis use during PTSD treatment and to educate patients on the potential consequences of continued use, the researchers said.
The study was published online February 18 in the Journal of Clinical Psychiatry.
Helpful or Harmful?
PTSD is a debilitating psychiatric condition marked by intrusive memories, avoidance, negative changes in mood and cognition, and hyperarousal. Many patients turn to cannabis to ease symptoms. In one recent study, roughly 28% of individuals with PTSD reported past-year cannabis use and 9% met criteria for CUD.
Although some studies have suggested PTSD symptom reduction with cannabis or cannabinoid-based treatments, others have identified potential risks, such as disrupted fear-extinction learning and worse clinical and treatment outcomes.
A recent systematic review found mixed evidence overall, with six studies suggesting benefits, five reporting worsening of symptoms, and three showing no significant impact of cannabis use in the setting of PTSD.
Led by Ahmed Hassan, MD, University of Toronto, Ontario, the researchers recruited adults aged 18-65 years with confirmed PTSD and CUD through the Centre for Addiction and Mental Health in Toronto and asked them to discontinue cannabis for 12 weeks.
Abstinence was defined as a urine 11-nor-9-carboxy-tetrahydrocannabinol level of 50 ng/mL or lower with no self-reported use, verified at multiple timepoints. Participants received escalating cash incentives for remaining abstinent at weeks 4, 8, and 12.
Eleven (52%) of the 21 participants who completed the 12-week protocol achieved biochemically verified abstinence, while 10 did not.
Those who achieved abstinence reported significantly greater reductions in total PTSD symptom severity and symptom count compared to those who did not.
Total severity scores on the Clinician-Administered PTSD Scale for DSM-5 dropped from 36.2 at baseline to 10.5 at week 12 among abstainers vs 34.6 to 21.8 among those who did not maintain abstinence (P = .001).
A similar pattern emerged for total symptom count, with abstinent participants dropping from 14.3 symptoms at baseline to 4.1 at week 12, compared to a decrease from 13.5 to 8.9 among nonabstainers.
Notably, the investigators observed that individuals who remained abstinent showed greater reductions in several core symptom clusters, including avoidance, negative alterations in mood, cognition, and hyperarousal — domains that are often cited as targets for cannabis-based self-medication among individuals with PTSD.
“However, in this comorbid PTSD and CUD sample, sustained cannabis abstinence was associated with symptom improvement, thereby challenging assumptions about its clinical utility in this population,” they wrote.
Interestingly, they added that there were no differential effects on reexperiencing symptoms such as flashbacks, intrusive memories, and nightmares. Both abstinent and nonabstinent participants reported similar improvements in reexperiencing, suggesting that factors unrelated to cannabis use may have contributed to symptom change or insufficient power, the authors said.
The researchers called for larger randomized trials to “replicate and extend” these preliminary findings and to investigate mechanisms through which abstinence may relate to symptom changes in PTSD with CUD.
The study had no commercial funding. The authors had no relevant disclosures.
A version of this article first appeared on Medscape.com.
New research challenges the assumption that long-term cannabis use improves symptoms or functioning in posttraumatic stress disorder (PTSD).
On the contrary, researchers found that abstaining from cannabis for 3 months was associated with significantly greater reductions in PTSD symptoms in adults with PTSD and comorbid cannabis use disorder (CUD).
The data suggest that continued cannabis use could limit recovery in some domains — underscoring the need to routinely assess cannabis use during PTSD treatment and to educate patients on the potential consequences of continued use, the researchers said.
The study was published online February 18 in the Journal of Clinical Psychiatry.
Helpful or Harmful?
PTSD is a debilitating psychiatric condition marked by intrusive memories, avoidance, negative changes in mood and cognition, and hyperarousal. Many patients turn to cannabis to ease symptoms. In one recent study, roughly 28% of individuals with PTSD reported past-year cannabis use and 9% met criteria for CUD.
Although some studies have suggested PTSD symptom reduction with cannabis or cannabinoid-based treatments, others have identified potential risks, such as disrupted fear-extinction learning and worse clinical and treatment outcomes.
A recent systematic review found mixed evidence overall, with six studies suggesting benefits, five reporting worsening of symptoms, and three showing no significant impact of cannabis use in the setting of PTSD.
Led by Ahmed Hassan, MD, University of Toronto, Ontario, the researchers recruited adults aged 18-65 years with confirmed PTSD and CUD through the Centre for Addiction and Mental Health in Toronto and asked them to discontinue cannabis for 12 weeks.
Abstinence was defined as a urine 11-nor-9-carboxy-tetrahydrocannabinol level of 50 ng/mL or lower with no self-reported use, verified at multiple timepoints. Participants received escalating cash incentives for remaining abstinent at weeks 4, 8, and 12.
Eleven (52%) of the 21 participants who completed the 12-week protocol achieved biochemically verified abstinence, while 10 did not.
Those who achieved abstinence reported significantly greater reductions in total PTSD symptom severity and symptom count compared to those who did not.
Total severity scores on the Clinician-Administered PTSD Scale for DSM-5 dropped from 36.2 at baseline to 10.5 at week 12 among abstainers vs 34.6 to 21.8 among those who did not maintain abstinence (P = .001).
A similar pattern emerged for total symptom count, with abstinent participants dropping from 14.3 symptoms at baseline to 4.1 at week 12, compared to a decrease from 13.5 to 8.9 among nonabstainers.
Notably, the investigators observed that individuals who remained abstinent showed greater reductions in several core symptom clusters, including avoidance, negative alterations in mood, cognition, and hyperarousal — domains that are often cited as targets for cannabis-based self-medication among individuals with PTSD.
“However, in this comorbid PTSD and CUD sample, sustained cannabis abstinence was associated with symptom improvement, thereby challenging assumptions about its clinical utility in this population,” they wrote.
Interestingly, they added that there were no differential effects on reexperiencing symptoms such as flashbacks, intrusive memories, and nightmares. Both abstinent and nonabstinent participants reported similar improvements in reexperiencing, suggesting that factors unrelated to cannabis use may have contributed to symptom change or insufficient power, the authors said.
The researchers called for larger randomized trials to “replicate and extend” these preliminary findings and to investigate mechanisms through which abstinence may relate to symptom changes in PTSD with CUD.
The study had no commercial funding. The authors had no relevant disclosures.
A version of this article first appeared on Medscape.com.
New research challenges the assumption that long-term cannabis use improves symptoms or functioning in posttraumatic stress disorder (PTSD).
On the contrary, researchers found that abstaining from cannabis for 3 months was associated with significantly greater reductions in PTSD symptoms in adults with PTSD and comorbid cannabis use disorder (CUD).
The data suggest that continued cannabis use could limit recovery in some domains — underscoring the need to routinely assess cannabis use during PTSD treatment and to educate patients on the potential consequences of continued use, the researchers said.
The study was published online February 18 in the Journal of Clinical Psychiatry.
Helpful or Harmful?
PTSD is a debilitating psychiatric condition marked by intrusive memories, avoidance, negative changes in mood and cognition, and hyperarousal. Many patients turn to cannabis to ease symptoms. In one recent study, roughly 28% of individuals with PTSD reported past-year cannabis use and 9% met criteria for CUD.
Although some studies have suggested PTSD symptom reduction with cannabis or cannabinoid-based treatments, others have identified potential risks, such as disrupted fear-extinction learning and worse clinical and treatment outcomes.
A recent systematic review found mixed evidence overall, with six studies suggesting benefits, five reporting worsening of symptoms, and three showing no significant impact of cannabis use in the setting of PTSD.
Led by Ahmed Hassan, MD, University of Toronto, Ontario, the researchers recruited adults aged 18-65 years with confirmed PTSD and CUD through the Centre for Addiction and Mental Health in Toronto and asked them to discontinue cannabis for 12 weeks.
Abstinence was defined as a urine 11-nor-9-carboxy-tetrahydrocannabinol level of 50 ng/mL or lower with no self-reported use, verified at multiple timepoints. Participants received escalating cash incentives for remaining abstinent at weeks 4, 8, and 12.
Eleven (52%) of the 21 participants who completed the 12-week protocol achieved biochemically verified abstinence, while 10 did not.
Those who achieved abstinence reported significantly greater reductions in total PTSD symptom severity and symptom count compared to those who did not.
Total severity scores on the Clinician-Administered PTSD Scale for DSM-5 dropped from 36.2 at baseline to 10.5 at week 12 among abstainers vs 34.6 to 21.8 among those who did not maintain abstinence (P = .001).
A similar pattern emerged for total symptom count, with abstinent participants dropping from 14.3 symptoms at baseline to 4.1 at week 12, compared to a decrease from 13.5 to 8.9 among nonabstainers.
Notably, the investigators observed that individuals who remained abstinent showed greater reductions in several core symptom clusters, including avoidance, negative alterations in mood, cognition, and hyperarousal — domains that are often cited as targets for cannabis-based self-medication among individuals with PTSD.
“However, in this comorbid PTSD and CUD sample, sustained cannabis abstinence was associated with symptom improvement, thereby challenging assumptions about its clinical utility in this population,” they wrote.
Interestingly, they added that there were no differential effects on reexperiencing symptoms such as flashbacks, intrusive memories, and nightmares. Both abstinent and nonabstinent participants reported similar improvements in reexperiencing, suggesting that factors unrelated to cannabis use may have contributed to symptom change or insufficient power, the authors said.
The researchers called for larger randomized trials to “replicate and extend” these preliminary findings and to investigate mechanisms through which abstinence may relate to symptom changes in PTSD with CUD.
The study had no commercial funding. The authors had no relevant disclosures.
A version of this article first appeared on Medscape.com.
Does Cannabis Really Help PTSD? New Data Cast Doubt
Does Cannabis Really Help PTSD? New Data Cast Doubt
Mortality Data Reveals How US Service Members and Veterans Died in 21st Century
US service members and veterans were less likely to die than the general population from most causes of death over a 17-year period, a population-based, prospective analysis found. But there was a glaring exception: suicide by firearm.
Among 201,618 subjects tracked from 2001 to 2018 by the Millennium Cohort Study, the overall death rate was less than half that of a comparable group of US adults (standardized mortality ratios [SMR], 0.44), reported Edward J. Boyko, MD, MPH, staff physician with the Veterans Affairs (VA) Puget Sound Health Care System and professor of medicine at the University of Washington, Seattle, and colleagues in BMC Public Health. However, suicides by firearm—while rare—were more common overall (SMR, 1.42), among military men only (SMR, 1.33), and among military women only (SMR, 2.83) than civilians.
The findings about the overall death rate may reflect the better health of those who join the military and have access to health care during and after service, Boyko told Federal Practitioner. The suicide data may reflect higher access to firearms, he said, although “more research is needed to identify what types of military exposures or physical and mental health predictors are associated with increased mortality risk due to suicide.”
The ongoing Millennium Cohort Study began in 2001 to track the health of military personnel over time. The study has spawned > 180 reports “used to inform and guide policy, guidelines, and health promotion efforts within the military and VA,” Boyko said. “As the Millennium Cohort Study approaches its 25-year anniversary, it seemed like an ideal time to assess mortality, especially cause-specific mortality, as a way to measure the impact of military service on long-term health.”
The analysis tracks 4 panels of subjects enrolled at various times between 2001 and 2013. Of the 201,619 participants, 3018 (1.5%) died by 2018. Of the 198,01 nondeceased participants, 69.2% were male; 8.1% were born before 1960, 16.1% were born from 1960 to 1969, 24.4% were born from 1970 to 1979, and 51.5% were born in or after 1980. The racial/ethnic makeup was 72.7% non-Hispanic White, 12.2% non-Hispanic Black, 7.9% Hispanic, and 7.1% other. Two-thirds (66.4%) were active duty, and 33.6% were in the Reserve or National Guard.
Of the 3018 deceased participants, 81.2% were male. In terms of birth year, 32.4% were born before 1960, 22.1% were born from 1960 to 1969, 18.2% were born from 1970 to 1979, and 27.3% were born in or after 1980. The racial/ethnic makeup was 77.7% non-Hispanic White, 11.9% non-Hispanic Black, 5.5% Hispanic, and 4.9% other. About half (51.0%) were active duty, and 49.0% were in the Reserve or National Guard.
Most deaths were due to natural causes (57.0%), followed by accident (20.1%), suicide (17.1%), operations of war (3.0%), homicide (2.1%), and other causes (1.2%). The new report noted that the Millennium Cohort Study and other research have identified a “healthy soldier effect, in which military populations tend to be healthier than the general US population.”
Boyko explained that “the fitness requirements for joining the military may favor the selection of healthier individuals from the general population. Another benefit of military service is free access to health care, especially among those on active duty, as well as eligibility for VA health care and other benefits after leaving service. This would allow for greater access to preventive care and treatments, as well as routine screening for health conditions such as cancer, diabetes, or cardiovascular disease.”
Overall suicide rates were higher among female subjects than among civilians (SMR, 1.65), but no statistically significant difference was seen in men (SMR, 0.96) or across all participants (SMR, 1.03). Regarding the large gaps in firearm suicide rates in military subjects vs civilians, Boyko said, “accessibility and familiarity with firearms, a highly lethal means of suicide, may be driving the elevated risk of suicide by firearms … prior research has found that unsecure firearms storage—such as unlocked, loaded firearms—increases the risk of suicide by firearms.”
Rachel Sayko Adams, PhD, MPH, a research associate professor with the Department of Health Law, Policy and Management at Boston University School of Public Health, is familiar with the study findings. Adams, a principal investigator at the VA Rocky Mountain Mental Illness Research, Education and Clinical Center for Suicide Prevention, told Federal Practitioner that “efforts to further develop suicide prevention programs that consider the unique needs and preferences of female service members and veterans are critical to prevent future suicide mortality in this population.”
Adams added: “Just because service members and veterans have a lower all-cause mortality rate compared to the general US population, we should not assume that they are universally low risk or that we can reduce our public health prevention efforts targeting this population.”
Boyko highlighted KeepItSecure.net, which “helps veterans and service members protect themselves and their families by making it easier to store firearms securely during stressful or high-risk periods.” The site offers practical, judgment-free guidance with powerful storytelling and public outreach, with clear, actionable steps—such as using a cable gun lock or lockbox—to lower suicide risk long before a crisis occurs. The VA, Boyko said, provides free cable gun locks nationwide.
The Millennium Cohort Study is funded by the Department of Veterans Affairs and Department of Defense Military Operational Medicine Research Program and Defense Health Program. The report authors and Adams have no disclosures.
US service members and veterans were less likely to die than the general population from most causes of death over a 17-year period, a population-based, prospective analysis found. But there was a glaring exception: suicide by firearm.
Among 201,618 subjects tracked from 2001 to 2018 by the Millennium Cohort Study, the overall death rate was less than half that of a comparable group of US adults (standardized mortality ratios [SMR], 0.44), reported Edward J. Boyko, MD, MPH, staff physician with the Veterans Affairs (VA) Puget Sound Health Care System and professor of medicine at the University of Washington, Seattle, and colleagues in BMC Public Health. However, suicides by firearm—while rare—were more common overall (SMR, 1.42), among military men only (SMR, 1.33), and among military women only (SMR, 2.83) than civilians.
The findings about the overall death rate may reflect the better health of those who join the military and have access to health care during and after service, Boyko told Federal Practitioner. The suicide data may reflect higher access to firearms, he said, although “more research is needed to identify what types of military exposures or physical and mental health predictors are associated with increased mortality risk due to suicide.”
The ongoing Millennium Cohort Study began in 2001 to track the health of military personnel over time. The study has spawned > 180 reports “used to inform and guide policy, guidelines, and health promotion efforts within the military and VA,” Boyko said. “As the Millennium Cohort Study approaches its 25-year anniversary, it seemed like an ideal time to assess mortality, especially cause-specific mortality, as a way to measure the impact of military service on long-term health.”
The analysis tracks 4 panels of subjects enrolled at various times between 2001 and 2013. Of the 201,619 participants, 3018 (1.5%) died by 2018. Of the 198,01 nondeceased participants, 69.2% were male; 8.1% were born before 1960, 16.1% were born from 1960 to 1969, 24.4% were born from 1970 to 1979, and 51.5% were born in or after 1980. The racial/ethnic makeup was 72.7% non-Hispanic White, 12.2% non-Hispanic Black, 7.9% Hispanic, and 7.1% other. Two-thirds (66.4%) were active duty, and 33.6% were in the Reserve or National Guard.
Of the 3018 deceased participants, 81.2% were male. In terms of birth year, 32.4% were born before 1960, 22.1% were born from 1960 to 1969, 18.2% were born from 1970 to 1979, and 27.3% were born in or after 1980. The racial/ethnic makeup was 77.7% non-Hispanic White, 11.9% non-Hispanic Black, 5.5% Hispanic, and 4.9% other. About half (51.0%) were active duty, and 49.0% were in the Reserve or National Guard.
Most deaths were due to natural causes (57.0%), followed by accident (20.1%), suicide (17.1%), operations of war (3.0%), homicide (2.1%), and other causes (1.2%). The new report noted that the Millennium Cohort Study and other research have identified a “healthy soldier effect, in which military populations tend to be healthier than the general US population.”
Boyko explained that “the fitness requirements for joining the military may favor the selection of healthier individuals from the general population. Another benefit of military service is free access to health care, especially among those on active duty, as well as eligibility for VA health care and other benefits after leaving service. This would allow for greater access to preventive care and treatments, as well as routine screening for health conditions such as cancer, diabetes, or cardiovascular disease.”
Overall suicide rates were higher among female subjects than among civilians (SMR, 1.65), but no statistically significant difference was seen in men (SMR, 0.96) or across all participants (SMR, 1.03). Regarding the large gaps in firearm suicide rates in military subjects vs civilians, Boyko said, “accessibility and familiarity with firearms, a highly lethal means of suicide, may be driving the elevated risk of suicide by firearms … prior research has found that unsecure firearms storage—such as unlocked, loaded firearms—increases the risk of suicide by firearms.”
Rachel Sayko Adams, PhD, MPH, a research associate professor with the Department of Health Law, Policy and Management at Boston University School of Public Health, is familiar with the study findings. Adams, a principal investigator at the VA Rocky Mountain Mental Illness Research, Education and Clinical Center for Suicide Prevention, told Federal Practitioner that “efforts to further develop suicide prevention programs that consider the unique needs and preferences of female service members and veterans are critical to prevent future suicide mortality in this population.”
Adams added: “Just because service members and veterans have a lower all-cause mortality rate compared to the general US population, we should not assume that they are universally low risk or that we can reduce our public health prevention efforts targeting this population.”
Boyko highlighted KeepItSecure.net, which “helps veterans and service members protect themselves and their families by making it easier to store firearms securely during stressful or high-risk periods.” The site offers practical, judgment-free guidance with powerful storytelling and public outreach, with clear, actionable steps—such as using a cable gun lock or lockbox—to lower suicide risk long before a crisis occurs. The VA, Boyko said, provides free cable gun locks nationwide.
The Millennium Cohort Study is funded by the Department of Veterans Affairs and Department of Defense Military Operational Medicine Research Program and Defense Health Program. The report authors and Adams have no disclosures.
US service members and veterans were less likely to die than the general population from most causes of death over a 17-year period, a population-based, prospective analysis found. But there was a glaring exception: suicide by firearm.
Among 201,618 subjects tracked from 2001 to 2018 by the Millennium Cohort Study, the overall death rate was less than half that of a comparable group of US adults (standardized mortality ratios [SMR], 0.44), reported Edward J. Boyko, MD, MPH, staff physician with the Veterans Affairs (VA) Puget Sound Health Care System and professor of medicine at the University of Washington, Seattle, and colleagues in BMC Public Health. However, suicides by firearm—while rare—were more common overall (SMR, 1.42), among military men only (SMR, 1.33), and among military women only (SMR, 2.83) than civilians.
The findings about the overall death rate may reflect the better health of those who join the military and have access to health care during and after service, Boyko told Federal Practitioner. The suicide data may reflect higher access to firearms, he said, although “more research is needed to identify what types of military exposures or physical and mental health predictors are associated with increased mortality risk due to suicide.”
The ongoing Millennium Cohort Study began in 2001 to track the health of military personnel over time. The study has spawned > 180 reports “used to inform and guide policy, guidelines, and health promotion efforts within the military and VA,” Boyko said. “As the Millennium Cohort Study approaches its 25-year anniversary, it seemed like an ideal time to assess mortality, especially cause-specific mortality, as a way to measure the impact of military service on long-term health.”
The analysis tracks 4 panels of subjects enrolled at various times between 2001 and 2013. Of the 201,619 participants, 3018 (1.5%) died by 2018. Of the 198,01 nondeceased participants, 69.2% were male; 8.1% were born before 1960, 16.1% were born from 1960 to 1969, 24.4% were born from 1970 to 1979, and 51.5% were born in or after 1980. The racial/ethnic makeup was 72.7% non-Hispanic White, 12.2% non-Hispanic Black, 7.9% Hispanic, and 7.1% other. Two-thirds (66.4%) were active duty, and 33.6% were in the Reserve or National Guard.
Of the 3018 deceased participants, 81.2% were male. In terms of birth year, 32.4% were born before 1960, 22.1% were born from 1960 to 1969, 18.2% were born from 1970 to 1979, and 27.3% were born in or after 1980. The racial/ethnic makeup was 77.7% non-Hispanic White, 11.9% non-Hispanic Black, 5.5% Hispanic, and 4.9% other. About half (51.0%) were active duty, and 49.0% were in the Reserve or National Guard.
Most deaths were due to natural causes (57.0%), followed by accident (20.1%), suicide (17.1%), operations of war (3.0%), homicide (2.1%), and other causes (1.2%). The new report noted that the Millennium Cohort Study and other research have identified a “healthy soldier effect, in which military populations tend to be healthier than the general US population.”
Boyko explained that “the fitness requirements for joining the military may favor the selection of healthier individuals from the general population. Another benefit of military service is free access to health care, especially among those on active duty, as well as eligibility for VA health care and other benefits after leaving service. This would allow for greater access to preventive care and treatments, as well as routine screening for health conditions such as cancer, diabetes, or cardiovascular disease.”
Overall suicide rates were higher among female subjects than among civilians (SMR, 1.65), but no statistically significant difference was seen in men (SMR, 0.96) or across all participants (SMR, 1.03). Regarding the large gaps in firearm suicide rates in military subjects vs civilians, Boyko said, “accessibility and familiarity with firearms, a highly lethal means of suicide, may be driving the elevated risk of suicide by firearms … prior research has found that unsecure firearms storage—such as unlocked, loaded firearms—increases the risk of suicide by firearms.”
Rachel Sayko Adams, PhD, MPH, a research associate professor with the Department of Health Law, Policy and Management at Boston University School of Public Health, is familiar with the study findings. Adams, a principal investigator at the VA Rocky Mountain Mental Illness Research, Education and Clinical Center for Suicide Prevention, told Federal Practitioner that “efforts to further develop suicide prevention programs that consider the unique needs and preferences of female service members and veterans are critical to prevent future suicide mortality in this population.”
Adams added: “Just because service members and veterans have a lower all-cause mortality rate compared to the general US population, we should not assume that they are universally low risk or that we can reduce our public health prevention efforts targeting this population.”
Boyko highlighted KeepItSecure.net, which “helps veterans and service members protect themselves and their families by making it easier to store firearms securely during stressful or high-risk periods.” The site offers practical, judgment-free guidance with powerful storytelling and public outreach, with clear, actionable steps—such as using a cable gun lock or lockbox—to lower suicide risk long before a crisis occurs. The VA, Boyko said, provides free cable gun locks nationwide.
The Millennium Cohort Study is funded by the Department of Veterans Affairs and Department of Defense Military Operational Medicine Research Program and Defense Health Program. The report authors and Adams have no disclosures.
Veteran Suicide Rate Declines Slightly, VA Report Shows
Veteran Suicide Rate Declines Slightly, VA Report Shows
Fewer veterans died by suicide in 2023 than 2022, according to the recently released 2025 National Veteran Suicide Prevention Annual Report from the US Department of Veterans Affairs (VA).
More than half of suicides, the Veterans Health Administration (VHA) found, were driven by pain (52.3%) or sleep problems (51.5%). Increased health problems were factors in 43.1% of cases, particularly traumatic brain injury (TBI) and cancer diagnosis. The suicide rate was 77.6 per 100,000 for veterans with a recent diagnosis of TBI, 94.3% higher than the rate of individuals without such a diagnosis. The suicide rate following a cancer diagnosis was 10.3% higher than for other veterans in VHA care—emphasizing the need, according to the VHA, to continue to expand efforts to integrate suicide prevention resources across all areas serving high-risk veteran groups.
VA has published the National Veteran Suicide Prevention report annually since 2016, with its release typically occurring in December. Release of the 2025 report was delayed until February 2026. The VA attributed the delay, however, due to the federal government shutdown from October 1 to November 12, 2025. At a January 2026 Senate Veterans’ Affairs Committee hearing, VA Secretary Doug Collins denied that there was an effort to halt its release.
Veteran deaths by suicide have often been called an epidemic, with the suicide rate having risen faster for veterans than it has for nonveterans since 2005. Veterans are 1.5 times more likely to die by suicide, a statistic that led Collins, veteran advocates, and members of Congress to identify veteran suicide prevention as a top priority.
The report indicates that the number of veteran suicides per year has remained relatively constant in the 6 most recent years of available data: 6738 in 2018, 6510 in 2019, 6347 in 2020, 6429 in 2021, 6442 in 2022, and 6398 in 2023. The fewest veteran suicides in the last 25 years happened both in 2001 and 2004 (6021), while the most (6738) came in 2018.
Although the overall veteran population has declined over time, more veterans are enrolling in VHA care, increasing from 3.8 million in 2001 to 6.1 million in 2023. However, the VHA found that 61% of veterans who died by suicide in 2023 were not receiving VHA care in the final year of their life.
The suicide rate among veterans in VHA care with mental health or substance use disorder diagnoses fell 34.7%, highlighting “the importance of both strengthening VA’s direct care system and expanding outreach and suicide prevention efforts for veterans who are not engaged in VHA health care,” Sen. Richard Blumenthal (D-CT), Ranking Member on the Senate Veterans’ Affairs Committee, said in a Feb. 5 statement about the report.
Aligning with previous VA data, the report presented information suggesting VHA services such as the Veterans Crisis Line (VCL) may reduce veteran suicide rates. Twelve months after the first contact with the VCL, the suicide rate for veterans in VHA care in 2022 was 16.1% lower than for those in 2021.
More than 2800 local and state coalitions are “actively working to meet community needs, expand available resources, and raise awareness” about suicide risks and prevention, the report says. The Staff Sergeant Parker Gordon Fox Suicide Prevention Grants Program, for example, provides community-based services for veterans, service members, and their families.
“Veteran suicide has been a scourge on our nation for far too long,” Collins said in a press release. “Most veterans who die by suicide were not in recent VA care, so making it easier for those who have worn the uniform to access the VA benefits they have earned is key.”
Fewer veterans died by suicide in 2023 than 2022, according to the recently released 2025 National Veteran Suicide Prevention Annual Report from the US Department of Veterans Affairs (VA).
More than half of suicides, the Veterans Health Administration (VHA) found, were driven by pain (52.3%) or sleep problems (51.5%). Increased health problems were factors in 43.1% of cases, particularly traumatic brain injury (TBI) and cancer diagnosis. The suicide rate was 77.6 per 100,000 for veterans with a recent diagnosis of TBI, 94.3% higher than the rate of individuals without such a diagnosis. The suicide rate following a cancer diagnosis was 10.3% higher than for other veterans in VHA care—emphasizing the need, according to the VHA, to continue to expand efforts to integrate suicide prevention resources across all areas serving high-risk veteran groups.
VA has published the National Veteran Suicide Prevention report annually since 2016, with its release typically occurring in December. Release of the 2025 report was delayed until February 2026. The VA attributed the delay, however, due to the federal government shutdown from October 1 to November 12, 2025. At a January 2026 Senate Veterans’ Affairs Committee hearing, VA Secretary Doug Collins denied that there was an effort to halt its release.
Veteran deaths by suicide have often been called an epidemic, with the suicide rate having risen faster for veterans than it has for nonveterans since 2005. Veterans are 1.5 times more likely to die by suicide, a statistic that led Collins, veteran advocates, and members of Congress to identify veteran suicide prevention as a top priority.
The report indicates that the number of veteran suicides per year has remained relatively constant in the 6 most recent years of available data: 6738 in 2018, 6510 in 2019, 6347 in 2020, 6429 in 2021, 6442 in 2022, and 6398 in 2023. The fewest veteran suicides in the last 25 years happened both in 2001 and 2004 (6021), while the most (6738) came in 2018.
Although the overall veteran population has declined over time, more veterans are enrolling in VHA care, increasing from 3.8 million in 2001 to 6.1 million in 2023. However, the VHA found that 61% of veterans who died by suicide in 2023 were not receiving VHA care in the final year of their life.
The suicide rate among veterans in VHA care with mental health or substance use disorder diagnoses fell 34.7%, highlighting “the importance of both strengthening VA’s direct care system and expanding outreach and suicide prevention efforts for veterans who are not engaged in VHA health care,” Sen. Richard Blumenthal (D-CT), Ranking Member on the Senate Veterans’ Affairs Committee, said in a Feb. 5 statement about the report.
Aligning with previous VA data, the report presented information suggesting VHA services such as the Veterans Crisis Line (VCL) may reduce veteran suicide rates. Twelve months after the first contact with the VCL, the suicide rate for veterans in VHA care in 2022 was 16.1% lower than for those in 2021.
More than 2800 local and state coalitions are “actively working to meet community needs, expand available resources, and raise awareness” about suicide risks and prevention, the report says. The Staff Sergeant Parker Gordon Fox Suicide Prevention Grants Program, for example, provides community-based services for veterans, service members, and their families.
“Veteran suicide has been a scourge on our nation for far too long,” Collins said in a press release. “Most veterans who die by suicide were not in recent VA care, so making it easier for those who have worn the uniform to access the VA benefits they have earned is key.”
Fewer veterans died by suicide in 2023 than 2022, according to the recently released 2025 National Veteran Suicide Prevention Annual Report from the US Department of Veterans Affairs (VA).
More than half of suicides, the Veterans Health Administration (VHA) found, were driven by pain (52.3%) or sleep problems (51.5%). Increased health problems were factors in 43.1% of cases, particularly traumatic brain injury (TBI) and cancer diagnosis. The suicide rate was 77.6 per 100,000 for veterans with a recent diagnosis of TBI, 94.3% higher than the rate of individuals without such a diagnosis. The suicide rate following a cancer diagnosis was 10.3% higher than for other veterans in VHA care—emphasizing the need, according to the VHA, to continue to expand efforts to integrate suicide prevention resources across all areas serving high-risk veteran groups.
VA has published the National Veteran Suicide Prevention report annually since 2016, with its release typically occurring in December. Release of the 2025 report was delayed until February 2026. The VA attributed the delay, however, due to the federal government shutdown from October 1 to November 12, 2025. At a January 2026 Senate Veterans’ Affairs Committee hearing, VA Secretary Doug Collins denied that there was an effort to halt its release.
Veteran deaths by suicide have often been called an epidemic, with the suicide rate having risen faster for veterans than it has for nonveterans since 2005. Veterans are 1.5 times more likely to die by suicide, a statistic that led Collins, veteran advocates, and members of Congress to identify veteran suicide prevention as a top priority.
The report indicates that the number of veteran suicides per year has remained relatively constant in the 6 most recent years of available data: 6738 in 2018, 6510 in 2019, 6347 in 2020, 6429 in 2021, 6442 in 2022, and 6398 in 2023. The fewest veteran suicides in the last 25 years happened both in 2001 and 2004 (6021), while the most (6738) came in 2018.
Although the overall veteran population has declined over time, more veterans are enrolling in VHA care, increasing from 3.8 million in 2001 to 6.1 million in 2023. However, the VHA found that 61% of veterans who died by suicide in 2023 were not receiving VHA care in the final year of their life.
The suicide rate among veterans in VHA care with mental health or substance use disorder diagnoses fell 34.7%, highlighting “the importance of both strengthening VA’s direct care system and expanding outreach and suicide prevention efforts for veterans who are not engaged in VHA health care,” Sen. Richard Blumenthal (D-CT), Ranking Member on the Senate Veterans’ Affairs Committee, said in a Feb. 5 statement about the report.
Aligning with previous VA data, the report presented information suggesting VHA services such as the Veterans Crisis Line (VCL) may reduce veteran suicide rates. Twelve months after the first contact with the VCL, the suicide rate for veterans in VHA care in 2022 was 16.1% lower than for those in 2021.
More than 2800 local and state coalitions are “actively working to meet community needs, expand available resources, and raise awareness” about suicide risks and prevention, the report says. The Staff Sergeant Parker Gordon Fox Suicide Prevention Grants Program, for example, provides community-based services for veterans, service members, and their families.
“Veteran suicide has been a scourge on our nation for far too long,” Collins said in a press release. “Most veterans who die by suicide were not in recent VA care, so making it easier for those who have worn the uniform to access the VA benefits they have earned is key.”
Veteran Suicide Rate Declines Slightly, VA Report Shows
Veteran Suicide Rate Declines Slightly, VA Report Shows
Fibromyalgia-PTSD Link Shows Bidirectional Relationship With Exposure to Combat Environments
Fibromyalgia-PTSD Link Shows Bidirectional Relationship With Exposure to Combat Environments
Spending time in a war zone can lead to chronic mental and physical pain. Now, research points to a link between two common disorders that can leave service members struggling.
Published in the journal Arthritis Care & Research, a longitudinal cohort study of 1761 US military service members found that those who had posttraumatic stress disorder (PTSD) before deployment were nearly 3times more likely to develop fibromyalgia after returning home (odds ratio, 2.96; 95% CI, 2.08-4.22). Those with fibromyalgia before deployment had more than threefold greater likelihood of developing PTSD after deployment (odds ratio, 3.12; 95% CI, 1.63-5.95).
This is the largest prospective study to date linking the stress of combat deployment to the onset of fibromyalgia.
“We had the advantage of observing a large population before and after exposure to an environment that often involves significant stress,” said lead study author Jay Higgs, MD, a retired rheumatologist with Brooke Army Medical Center and the University of Texas Health Science Center at San Antonio.
Here’s what the team found and why it matters.
Significant Increase in Fibromyalgia After Development
Service members were checked for fibromyalgia using the 2011 questionnaire modification of the 2010 American College of Rheumatology preliminary diagnostic criteria for fibromyalgia. They were assessed for PTSD using the PTSD Checklist Stressor-Specific Version.
Before deployment, service members had similar rates of fibromyalgia as the general population: 2.2% in men and 2.0% in women. After deployment, fibromyalgia rates increased significantly to 8.0% in men and 11.1% in women.
While fibromyalgia tends to be underreported in men, the findings suggest it should not be overlooked in this population. “Our results are consistent with the notion that there should be no gender bias when considering the possibility of fibromyalgia in an individual patient,” Higgs said.
Before deployment, 20.7% of men and 18.3% of women had PTSD symptoms. After deployment, the PTSD rate increased slightly to 22.7% in men and 25.5% in women.
The Link Between Fibromyalgia and PTSD
The researchers said the results suggest that PTSD and fibromyalgia might be linked through central nervous system mechanisms such as central sensitization, elevated hypothalamic-pituitary-adrenal axis activity, elevated cortisol, and proinflammatory cytokines. However, shared causation, associated risk factors, selection bias, or alternative mechanisms within the central and peripheral neuroendocrine and cytokine systems could also be part of the story.
“What we do not know is how much of what we see clinically represents central nervous system pathology, peripheral problems, or a combination of the 2,” Higgs said. “Neurotransmission in the central nervous system is highly complex, and may not only involve specific structures, but a web of communications between them.”
Loci in the midbrain appear especially important, he said.
Elizabeth Hoge, MD, professor and director of the Anxiety Disorders Research Program at Georgetown University School of Medicine, Washington, DC, said that patients with PTSD often have pain, headaches, sleep disturbances, and other symptoms that are part of the picture of fibromyalgia. It’s plausible that pain syndromes could be manifestations of PTSD or groupings of symptoms that suggest a subtype.
“Pain is one way that people experience distress, and we know that in PTSD, sometimes the trauma memories are encoded too strongly, more stressful and more alarming to the body system,” she said.
When patients have symptoms such as chronic pain, headaches, fatigue, or cognitive brain fog, clinicians should remember to ask about trauma exposure, Hoge said. You might be the first to broach the subject.
“I’ve certainly seen patients in clinic who never get asked about the exposure to trauma, including sexual trauma, so sometimes that can be the first pathway to helping people feel better is just to have their trauma recognized,” Hoge said.
If a patient has experienced or witnessed violence, consider a referral to a psychiatrist or psychologist to evaluate them for PTSD. Higgs said he collaborated closely with a psychologist to complement his treatment plans for active duty and retired military service members and families.
The US Department of Veterans Affairs and the Department of Defense (DoD) recommend trauma-focused psychotherapy as the first line of treatment for PTSD. This form of therapy deliberately focuses on bringing trauma memories into the open, Hoge said.
“When a person talks about their trauma, and it comes into direct consciousness, somehow it’s malleable, and so when it goes back down into the memory banks, it’s changed somewhat,” she said.
This study was supported by the DoD through awards from the US Army Medical Research and Materiel Command, Congressionally Directed Medical Research Programs, and Psychological Health and Traumatic Brain Injury Research Program. The funding organizations played no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Higgs’s comments are his own and do not necessarily reflect the official policy or position of the Defense Health Agency, Brooke Army Medical Center, Carl R. Darnall Army Medical Center, the DoD, the Department of Veterans Affairs, or any agencies under the US government. Hoge had no relevant disclosures.
A version of this article first appeared on Medscape.com.
Spending time in a war zone can lead to chronic mental and physical pain. Now, research points to a link between two common disorders that can leave service members struggling.
Published in the journal Arthritis Care & Research, a longitudinal cohort study of 1761 US military service members found that those who had posttraumatic stress disorder (PTSD) before deployment were nearly 3times more likely to develop fibromyalgia after returning home (odds ratio, 2.96; 95% CI, 2.08-4.22). Those with fibromyalgia before deployment had more than threefold greater likelihood of developing PTSD after deployment (odds ratio, 3.12; 95% CI, 1.63-5.95).
This is the largest prospective study to date linking the stress of combat deployment to the onset of fibromyalgia.
“We had the advantage of observing a large population before and after exposure to an environment that often involves significant stress,” said lead study author Jay Higgs, MD, a retired rheumatologist with Brooke Army Medical Center and the University of Texas Health Science Center at San Antonio.
Here’s what the team found and why it matters.
Significant Increase in Fibromyalgia After Development
Service members were checked for fibromyalgia using the 2011 questionnaire modification of the 2010 American College of Rheumatology preliminary diagnostic criteria for fibromyalgia. They were assessed for PTSD using the PTSD Checklist Stressor-Specific Version.
Before deployment, service members had similar rates of fibromyalgia as the general population: 2.2% in men and 2.0% in women. After deployment, fibromyalgia rates increased significantly to 8.0% in men and 11.1% in women.
While fibromyalgia tends to be underreported in men, the findings suggest it should not be overlooked in this population. “Our results are consistent with the notion that there should be no gender bias when considering the possibility of fibromyalgia in an individual patient,” Higgs said.
Before deployment, 20.7% of men and 18.3% of women had PTSD symptoms. After deployment, the PTSD rate increased slightly to 22.7% in men and 25.5% in women.
The Link Between Fibromyalgia and PTSD
The researchers said the results suggest that PTSD and fibromyalgia might be linked through central nervous system mechanisms such as central sensitization, elevated hypothalamic-pituitary-adrenal axis activity, elevated cortisol, and proinflammatory cytokines. However, shared causation, associated risk factors, selection bias, or alternative mechanisms within the central and peripheral neuroendocrine and cytokine systems could also be part of the story.
“What we do not know is how much of what we see clinically represents central nervous system pathology, peripheral problems, or a combination of the 2,” Higgs said. “Neurotransmission in the central nervous system is highly complex, and may not only involve specific structures, but a web of communications between them.”
Loci in the midbrain appear especially important, he said.
Elizabeth Hoge, MD, professor and director of the Anxiety Disorders Research Program at Georgetown University School of Medicine, Washington, DC, said that patients with PTSD often have pain, headaches, sleep disturbances, and other symptoms that are part of the picture of fibromyalgia. It’s plausible that pain syndromes could be manifestations of PTSD or groupings of symptoms that suggest a subtype.
“Pain is one way that people experience distress, and we know that in PTSD, sometimes the trauma memories are encoded too strongly, more stressful and more alarming to the body system,” she said.
When patients have symptoms such as chronic pain, headaches, fatigue, or cognitive brain fog, clinicians should remember to ask about trauma exposure, Hoge said. You might be the first to broach the subject.
“I’ve certainly seen patients in clinic who never get asked about the exposure to trauma, including sexual trauma, so sometimes that can be the first pathway to helping people feel better is just to have their trauma recognized,” Hoge said.
If a patient has experienced or witnessed violence, consider a referral to a psychiatrist or psychologist to evaluate them for PTSD. Higgs said he collaborated closely with a psychologist to complement his treatment plans for active duty and retired military service members and families.
The US Department of Veterans Affairs and the Department of Defense (DoD) recommend trauma-focused psychotherapy as the first line of treatment for PTSD. This form of therapy deliberately focuses on bringing trauma memories into the open, Hoge said.
“When a person talks about their trauma, and it comes into direct consciousness, somehow it’s malleable, and so when it goes back down into the memory banks, it’s changed somewhat,” she said.
This study was supported by the DoD through awards from the US Army Medical Research and Materiel Command, Congressionally Directed Medical Research Programs, and Psychological Health and Traumatic Brain Injury Research Program. The funding organizations played no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Higgs’s comments are his own and do not necessarily reflect the official policy or position of the Defense Health Agency, Brooke Army Medical Center, Carl R. Darnall Army Medical Center, the DoD, the Department of Veterans Affairs, or any agencies under the US government. Hoge had no relevant disclosures.
A version of this article first appeared on Medscape.com.
Spending time in a war zone can lead to chronic mental and physical pain. Now, research points to a link between two common disorders that can leave service members struggling.
Published in the journal Arthritis Care & Research, a longitudinal cohort study of 1761 US military service members found that those who had posttraumatic stress disorder (PTSD) before deployment were nearly 3times more likely to develop fibromyalgia after returning home (odds ratio, 2.96; 95% CI, 2.08-4.22). Those with fibromyalgia before deployment had more than threefold greater likelihood of developing PTSD after deployment (odds ratio, 3.12; 95% CI, 1.63-5.95).
This is the largest prospective study to date linking the stress of combat deployment to the onset of fibromyalgia.
“We had the advantage of observing a large population before and after exposure to an environment that often involves significant stress,” said lead study author Jay Higgs, MD, a retired rheumatologist with Brooke Army Medical Center and the University of Texas Health Science Center at San Antonio.
Here’s what the team found and why it matters.
Significant Increase in Fibromyalgia After Development
Service members were checked for fibromyalgia using the 2011 questionnaire modification of the 2010 American College of Rheumatology preliminary diagnostic criteria for fibromyalgia. They were assessed for PTSD using the PTSD Checklist Stressor-Specific Version.
Before deployment, service members had similar rates of fibromyalgia as the general population: 2.2% in men and 2.0% in women. After deployment, fibromyalgia rates increased significantly to 8.0% in men and 11.1% in women.
While fibromyalgia tends to be underreported in men, the findings suggest it should not be overlooked in this population. “Our results are consistent with the notion that there should be no gender bias when considering the possibility of fibromyalgia in an individual patient,” Higgs said.
Before deployment, 20.7% of men and 18.3% of women had PTSD symptoms. After deployment, the PTSD rate increased slightly to 22.7% in men and 25.5% in women.
The Link Between Fibromyalgia and PTSD
The researchers said the results suggest that PTSD and fibromyalgia might be linked through central nervous system mechanisms such as central sensitization, elevated hypothalamic-pituitary-adrenal axis activity, elevated cortisol, and proinflammatory cytokines. However, shared causation, associated risk factors, selection bias, or alternative mechanisms within the central and peripheral neuroendocrine and cytokine systems could also be part of the story.
“What we do not know is how much of what we see clinically represents central nervous system pathology, peripheral problems, or a combination of the 2,” Higgs said. “Neurotransmission in the central nervous system is highly complex, and may not only involve specific structures, but a web of communications between them.”
Loci in the midbrain appear especially important, he said.
Elizabeth Hoge, MD, professor and director of the Anxiety Disorders Research Program at Georgetown University School of Medicine, Washington, DC, said that patients with PTSD often have pain, headaches, sleep disturbances, and other symptoms that are part of the picture of fibromyalgia. It’s plausible that pain syndromes could be manifestations of PTSD or groupings of symptoms that suggest a subtype.
“Pain is one way that people experience distress, and we know that in PTSD, sometimes the trauma memories are encoded too strongly, more stressful and more alarming to the body system,” she said.
When patients have symptoms such as chronic pain, headaches, fatigue, or cognitive brain fog, clinicians should remember to ask about trauma exposure, Hoge said. You might be the first to broach the subject.
“I’ve certainly seen patients in clinic who never get asked about the exposure to trauma, including sexual trauma, so sometimes that can be the first pathway to helping people feel better is just to have their trauma recognized,” Hoge said.
If a patient has experienced or witnessed violence, consider a referral to a psychiatrist or psychologist to evaluate them for PTSD. Higgs said he collaborated closely with a psychologist to complement his treatment plans for active duty and retired military service members and families.
The US Department of Veterans Affairs and the Department of Defense (DoD) recommend trauma-focused psychotherapy as the first line of treatment for PTSD. This form of therapy deliberately focuses on bringing trauma memories into the open, Hoge said.
“When a person talks about their trauma, and it comes into direct consciousness, somehow it’s malleable, and so when it goes back down into the memory banks, it’s changed somewhat,” she said.
This study was supported by the DoD through awards from the US Army Medical Research and Materiel Command, Congressionally Directed Medical Research Programs, and Psychological Health and Traumatic Brain Injury Research Program. The funding organizations played no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Higgs’s comments are his own and do not necessarily reflect the official policy or position of the Defense Health Agency, Brooke Army Medical Center, Carl R. Darnall Army Medical Center, the DoD, the Department of Veterans Affairs, or any agencies under the US government. Hoge had no relevant disclosures.
A version of this article first appeared on Medscape.com.
Fibromyalgia-PTSD Link Shows Bidirectional Relationship With Exposure to Combat Environments
Fibromyalgia-PTSD Link Shows Bidirectional Relationship With Exposure to Combat Environments
Social Challenges Linked to More Suicidality in Vets
Veterans experiencing unstable housing, financial strain, and with poor access to health care have a higher risk of suicidal thoughts and behaviors, according to findings in a new study, leading researchers to call for additional screening to identify those in jeopardy.
Each incremental increase in social disadvantage was tied to increases in the likelihood of recent suicidal thoughts (odds ratio [OR], 2.14), future suicidal intent (OR, 2.21), and lifetime suicide attempt (OR, 1.78) in a weighted analysis. The self-reported data was published as a cross-sectional study by Pietrzak et al in the December 2025 issue of JAMA Psychiatry.
Veterans whose social plights ranked in the worst 5% were > 20 times more likely to report suicidal thoughts and behaviors than those in the top 5%. Especially striking were the magnitudes of the associations and their persistence after adjustment for psychiatric conditions and other suicide risk factors, lead author Robert H. Pietrzak, PhD, MPH said in an interview with Federal Practitioner.
“This finding highlights how extreme cumulative disadvantage can be overwhelming,” Pietrzak said. “It suggests that suicide risk among veterans increases dramatically when multiple social stressors cluster together. Rather than any single hardship driving risk, it is the cumulative impact of social disadvantage that appears most strongly linked to elevated suicide risk.”
As Pietrzak explained, veterans account for < 7% of total US adults but about 14% of suicide deaths. “Several factors may contribute to this difference, including higher exposure to trauma, elevated rates of psychiatric conditions, challenges with reintegration into civilian life, and structural barriers to care,” Pietrzak said. “Increasingly, social and economic stressors are also recognized by experts and researchers as critical contributors to suicide risk.”
Social determinants of health (SDOH) such as unemployment and lack of access to health care have also been linked to suicide risk, he said.
“Less well understood is how multiple adverse social conditions interact and accumulate to compound suicide risk,” Pietrzak said.
The new study sought to determine the impact of SDOH as a whole, not just in isolation. The study analyzed SDOH in 5 areas—education access and quality, economic conditions, health care access and quality, neighborhood and built environment, and social and community context—via the National Health and Resilience in Veterans Study, which surveyed 4069 veterans. The participants had weighted demographics of mean age 62.2 years; 90.2% were male; and 78.1% White, 11.2% Black, 6.6% Hispanic, 4.2% other.
Past-year suicidal ideation was most highly linked to psychosocial difficulties (OR, 1.58; 95% CI, 1.43-1.75). Future suicidal intent was most highly linked to residing in a mobile home, recreational vehicle, or van (OR, 1.60; 95% CI, 1.24-2.07) in addition to psychosocial difficulties (OR, 1.45; 95% CI, 1.18-1.80). Lifetime suicidal attempt was most highly linked to history of homelessness (OR, 1.37; 95% CI, 1.22-1.55; all P < .001).
“The results of our study underscore the importance of routine, standardized screening for cumulative social disadvantage within VA and community care settings that serve veterans,” Pietrzak said.
He added that findings make it clear that “suicide prevention extends beyond mental health care. Improving the social conditions in which veterans live, work, and age is not only good public policy. It may save lives.”
Mark S. Kaplan, DrPH, a research professor of Social Welfare at the University of California at Los Angeles Luskin School of Public Affairs is familiar with the study findings and said they highlight the need to “approach the question of suicide in much wider terms as opposed to reducing it to psychiatric traits.”
J. John Mann, MD, a professor of translational neuroscience in psychiatry and radiology who studies suicide at Columbia University, New York City, said the study’s findings illustrate that clinicians must do more to understand the lives of patients outside the examination room. He predicted that more screening for social determinants of health will “enrich the amount of information that the clinician will have and lead to a more comprehensive clinical care plan.”
The US Department of Veterans Affairs supported the study. Pietrzak has no disclosures. Other study authors report various disclosures.
Veterans experiencing unstable housing, financial strain, and with poor access to health care have a higher risk of suicidal thoughts and behaviors, according to findings in a new study, leading researchers to call for additional screening to identify those in jeopardy.
Each incremental increase in social disadvantage was tied to increases in the likelihood of recent suicidal thoughts (odds ratio [OR], 2.14), future suicidal intent (OR, 2.21), and lifetime suicide attempt (OR, 1.78) in a weighted analysis. The self-reported data was published as a cross-sectional study by Pietrzak et al in the December 2025 issue of JAMA Psychiatry.
Veterans whose social plights ranked in the worst 5% were > 20 times more likely to report suicidal thoughts and behaviors than those in the top 5%. Especially striking were the magnitudes of the associations and their persistence after adjustment for psychiatric conditions and other suicide risk factors, lead author Robert H. Pietrzak, PhD, MPH said in an interview with Federal Practitioner.
“This finding highlights how extreme cumulative disadvantage can be overwhelming,” Pietrzak said. “It suggests that suicide risk among veterans increases dramatically when multiple social stressors cluster together. Rather than any single hardship driving risk, it is the cumulative impact of social disadvantage that appears most strongly linked to elevated suicide risk.”
As Pietrzak explained, veterans account for < 7% of total US adults but about 14% of suicide deaths. “Several factors may contribute to this difference, including higher exposure to trauma, elevated rates of psychiatric conditions, challenges with reintegration into civilian life, and structural barriers to care,” Pietrzak said. “Increasingly, social and economic stressors are also recognized by experts and researchers as critical contributors to suicide risk.”
Social determinants of health (SDOH) such as unemployment and lack of access to health care have also been linked to suicide risk, he said.
“Less well understood is how multiple adverse social conditions interact and accumulate to compound suicide risk,” Pietrzak said.
The new study sought to determine the impact of SDOH as a whole, not just in isolation. The study analyzed SDOH in 5 areas—education access and quality, economic conditions, health care access and quality, neighborhood and built environment, and social and community context—via the National Health and Resilience in Veterans Study, which surveyed 4069 veterans. The participants had weighted demographics of mean age 62.2 years; 90.2% were male; and 78.1% White, 11.2% Black, 6.6% Hispanic, 4.2% other.
Past-year suicidal ideation was most highly linked to psychosocial difficulties (OR, 1.58; 95% CI, 1.43-1.75). Future suicidal intent was most highly linked to residing in a mobile home, recreational vehicle, or van (OR, 1.60; 95% CI, 1.24-2.07) in addition to psychosocial difficulties (OR, 1.45; 95% CI, 1.18-1.80). Lifetime suicidal attempt was most highly linked to history of homelessness (OR, 1.37; 95% CI, 1.22-1.55; all P < .001).
“The results of our study underscore the importance of routine, standardized screening for cumulative social disadvantage within VA and community care settings that serve veterans,” Pietrzak said.
He added that findings make it clear that “suicide prevention extends beyond mental health care. Improving the social conditions in which veterans live, work, and age is not only good public policy. It may save lives.”
Mark S. Kaplan, DrPH, a research professor of Social Welfare at the University of California at Los Angeles Luskin School of Public Affairs is familiar with the study findings and said they highlight the need to “approach the question of suicide in much wider terms as opposed to reducing it to psychiatric traits.”
J. John Mann, MD, a professor of translational neuroscience in psychiatry and radiology who studies suicide at Columbia University, New York City, said the study’s findings illustrate that clinicians must do more to understand the lives of patients outside the examination room. He predicted that more screening for social determinants of health will “enrich the amount of information that the clinician will have and lead to a more comprehensive clinical care plan.”
The US Department of Veterans Affairs supported the study. Pietrzak has no disclosures. Other study authors report various disclosures.
Veterans experiencing unstable housing, financial strain, and with poor access to health care have a higher risk of suicidal thoughts and behaviors, according to findings in a new study, leading researchers to call for additional screening to identify those in jeopardy.
Each incremental increase in social disadvantage was tied to increases in the likelihood of recent suicidal thoughts (odds ratio [OR], 2.14), future suicidal intent (OR, 2.21), and lifetime suicide attempt (OR, 1.78) in a weighted analysis. The self-reported data was published as a cross-sectional study by Pietrzak et al in the December 2025 issue of JAMA Psychiatry.
Veterans whose social plights ranked in the worst 5% were > 20 times more likely to report suicidal thoughts and behaviors than those in the top 5%. Especially striking were the magnitudes of the associations and their persistence after adjustment for psychiatric conditions and other suicide risk factors, lead author Robert H. Pietrzak, PhD, MPH said in an interview with Federal Practitioner.
“This finding highlights how extreme cumulative disadvantage can be overwhelming,” Pietrzak said. “It suggests that suicide risk among veterans increases dramatically when multiple social stressors cluster together. Rather than any single hardship driving risk, it is the cumulative impact of social disadvantage that appears most strongly linked to elevated suicide risk.”
As Pietrzak explained, veterans account for < 7% of total US adults but about 14% of suicide deaths. “Several factors may contribute to this difference, including higher exposure to trauma, elevated rates of psychiatric conditions, challenges with reintegration into civilian life, and structural barriers to care,” Pietrzak said. “Increasingly, social and economic stressors are also recognized by experts and researchers as critical contributors to suicide risk.”
Social determinants of health (SDOH) such as unemployment and lack of access to health care have also been linked to suicide risk, he said.
“Less well understood is how multiple adverse social conditions interact and accumulate to compound suicide risk,” Pietrzak said.
The new study sought to determine the impact of SDOH as a whole, not just in isolation. The study analyzed SDOH in 5 areas—education access and quality, economic conditions, health care access and quality, neighborhood and built environment, and social and community context—via the National Health and Resilience in Veterans Study, which surveyed 4069 veterans. The participants had weighted demographics of mean age 62.2 years; 90.2% were male; and 78.1% White, 11.2% Black, 6.6% Hispanic, 4.2% other.
Past-year suicidal ideation was most highly linked to psychosocial difficulties (OR, 1.58; 95% CI, 1.43-1.75). Future suicidal intent was most highly linked to residing in a mobile home, recreational vehicle, or van (OR, 1.60; 95% CI, 1.24-2.07) in addition to psychosocial difficulties (OR, 1.45; 95% CI, 1.18-1.80). Lifetime suicidal attempt was most highly linked to history of homelessness (OR, 1.37; 95% CI, 1.22-1.55; all P < .001).
“The results of our study underscore the importance of routine, standardized screening for cumulative social disadvantage within VA and community care settings that serve veterans,” Pietrzak said.
He added that findings make it clear that “suicide prevention extends beyond mental health care. Improving the social conditions in which veterans live, work, and age is not only good public policy. It may save lives.”
Mark S. Kaplan, DrPH, a research professor of Social Welfare at the University of California at Los Angeles Luskin School of Public Affairs is familiar with the study findings and said they highlight the need to “approach the question of suicide in much wider terms as opposed to reducing it to psychiatric traits.”
J. John Mann, MD, a professor of translational neuroscience in psychiatry and radiology who studies suicide at Columbia University, New York City, said the study’s findings illustrate that clinicians must do more to understand the lives of patients outside the examination room. He predicted that more screening for social determinants of health will “enrich the amount of information that the clinician will have and lead to a more comprehensive clinical care plan.”
The US Department of Veterans Affairs supported the study. Pietrzak has no disclosures. Other study authors report various disclosures.