User login
Mid-October flulike illness cases higher than past 5 years
Outpatient visits for influenzalike illness (ILI), which includes influenza, SARS-CoV-2, and RSV, were higher after 3 weeks than for any of the previous five flu seasons: 3.3% of visits reported through the CDC’s Outpatient Influenza-like Illness Surveillance Network involved ILI as of Oct. 22. The highest comparable rate in the previous 5 years was the 1.9% recorded in late October of 2021, shortly after the definition of ILI was changed to also include illnesses other than influenza.
This season’s higher flu activity is in contrast to the previous two, which were unusually mild. The change, however, is not unexpected, as William Schaffner, MD, an infectious disease expert and professor of preventive medicine at Vanderbilt University, recently told CNN.
“Here we are in the middle of October – not the middle of November – we’re already seeing scattered influenza cases, even hospitalized influenza cases, around the country,” he said. “So we know that this virus is now spreading out in the community already. It’s gathering speed already. It looks to me to be about a month early.”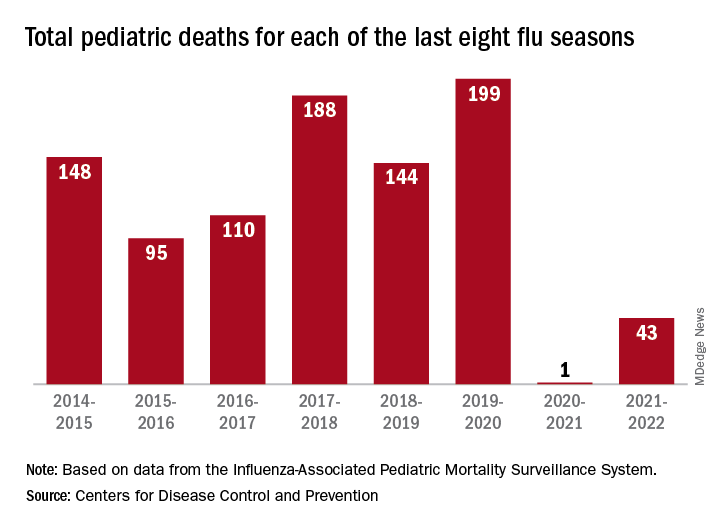
One indication of the mildness of the previous two flu seasons was the number of deaths, both pediatric and overall. Influenza-associated pediatric deaths had averaged about 110 per season over the previous eight seasons, compared with just 1 for 2020-2021 and 43 in 2021-2022. Overall flu deaths never reached 1% of all weekly deaths for either season, well below baseline levels for the flu, which range from 5.5% to 6.8%, CDC data show.
Other indicators of early severity
This season’s early rise in viral activity also can be seen in hospitalizations. The cumulative rate of flu-related admissions was 1.5 per 100,000 population as of Oct. 22, higher than the rate observed in the comparable week of previous seasons going back to 2010-2011, according to the CDC’s Influenza Hospitalization Surveillance Network.
A look at state reports of ILI outpatient visit rates shows that the District of Columbia and South Carolina are already in the very high range of the CDC’s severity scale, while 11 states are in the high range. Again going back to 2010-2011, no jurisdiction has ever been in the very high range this early in the season, based on data from the Outpatient Influenza-like Illness Surveillance Network.
Outpatient visits for influenzalike illness (ILI), which includes influenza, SARS-CoV-2, and RSV, were higher after 3 weeks than for any of the previous five flu seasons: 3.3% of visits reported through the CDC’s Outpatient Influenza-like Illness Surveillance Network involved ILI as of Oct. 22. The highest comparable rate in the previous 5 years was the 1.9% recorded in late October of 2021, shortly after the definition of ILI was changed to also include illnesses other than influenza.
This season’s higher flu activity is in contrast to the previous two, which were unusually mild. The change, however, is not unexpected, as William Schaffner, MD, an infectious disease expert and professor of preventive medicine at Vanderbilt University, recently told CNN.
“Here we are in the middle of October – not the middle of November – we’re already seeing scattered influenza cases, even hospitalized influenza cases, around the country,” he said. “So we know that this virus is now spreading out in the community already. It’s gathering speed already. It looks to me to be about a month early.”
One indication of the mildness of the previous two flu seasons was the number of deaths, both pediatric and overall. Influenza-associated pediatric deaths had averaged about 110 per season over the previous eight seasons, compared with just 1 for 2020-2021 and 43 in 2021-2022. Overall flu deaths never reached 1% of all weekly deaths for either season, well below baseline levels for the flu, which range from 5.5% to 6.8%, CDC data show.
Other indicators of early severity
This season’s early rise in viral activity also can be seen in hospitalizations. The cumulative rate of flu-related admissions was 1.5 per 100,000 population as of Oct. 22, higher than the rate observed in the comparable week of previous seasons going back to 2010-2011, according to the CDC’s Influenza Hospitalization Surveillance Network.
A look at state reports of ILI outpatient visit rates shows that the District of Columbia and South Carolina are already in the very high range of the CDC’s severity scale, while 11 states are in the high range. Again going back to 2010-2011, no jurisdiction has ever been in the very high range this early in the season, based on data from the Outpatient Influenza-like Illness Surveillance Network.
Outpatient visits for influenzalike illness (ILI), which includes influenza, SARS-CoV-2, and RSV, were higher after 3 weeks than for any of the previous five flu seasons: 3.3% of visits reported through the CDC’s Outpatient Influenza-like Illness Surveillance Network involved ILI as of Oct. 22. The highest comparable rate in the previous 5 years was the 1.9% recorded in late October of 2021, shortly after the definition of ILI was changed to also include illnesses other than influenza.
This season’s higher flu activity is in contrast to the previous two, which were unusually mild. The change, however, is not unexpected, as William Schaffner, MD, an infectious disease expert and professor of preventive medicine at Vanderbilt University, recently told CNN.
“Here we are in the middle of October – not the middle of November – we’re already seeing scattered influenza cases, even hospitalized influenza cases, around the country,” he said. “So we know that this virus is now spreading out in the community already. It’s gathering speed already. It looks to me to be about a month early.”
One indication of the mildness of the previous two flu seasons was the number of deaths, both pediatric and overall. Influenza-associated pediatric deaths had averaged about 110 per season over the previous eight seasons, compared with just 1 for 2020-2021 and 43 in 2021-2022. Overall flu deaths never reached 1% of all weekly deaths for either season, well below baseline levels for the flu, which range from 5.5% to 6.8%, CDC data show.
Other indicators of early severity
This season’s early rise in viral activity also can be seen in hospitalizations. The cumulative rate of flu-related admissions was 1.5 per 100,000 population as of Oct. 22, higher than the rate observed in the comparable week of previous seasons going back to 2010-2011, according to the CDC’s Influenza Hospitalization Surveillance Network.
A look at state reports of ILI outpatient visit rates shows that the District of Columbia and South Carolina are already in the very high range of the CDC’s severity scale, while 11 states are in the high range. Again going back to 2010-2011, no jurisdiction has ever been in the very high range this early in the season, based on data from the Outpatient Influenza-like Illness Surveillance Network.
Metabolites may distinguish severe subtypes of PAH
, based on data from approximately 1,500 individuals.
The overall prognosis and therapeutic response for patients with pulmonary arterial hypertension associated with systemic sclerosis (SSc-PAH) tends to be worse than for patients with other types of PAH, such as idiopathic pulmonary arterial hypertension (IPAH), but the impact of different metabolite profiles among subtypes of disease has not been explored, wrote Mona Alotaibi, MD, of the University of California, San Diego, and colleagues.
“Recently, metabolic dysregulation has been proposed as a key mechanism by which IPAH and SSc-PAH differ and could control such disparities,” they noted. Clarifying the molecular mechanisms of SSc-PAH could inform management and treatment, they added.
In a study published in the journal Chest, the researchers sought to identify a bioactive lipid signature unique to SSc-PAH. They identified 400 patients with SSc-PAH and 1,082 with IPAH. An additional 100 patients with scleroderma but no PH and 44 patients with scleroderma who had PH were included for external validation. The mean ages of the patients with IPAH and SSc-PAH in the discovery and validation cohorts ranged from approximately 51 to 65 years; more than 75% of patients across the groups were women.
The researchers tested more than 700 bioactive lipid metabolites using liquid chromatography/mass spectrometry. They found five metabolites that distinguished SSc-PAH and IPAH that were significantly associated with markers of disease severity: 17-beta estradiol, novel Eic, nervonic acid, fatty acid esters of hydroxy fatty acids, and prostaglandin F2 alpha (PGF 2 alpha).
The biomarkers were increased in SSc-PAH patients compared to patients with SSC alone, which suggests that the biomarkers are related to PAH and not to scleroderma alone, the researchers noted.
In particular, nervonic acid was associated with worse functional capacity, in SSc-PAH patients, as were higher levels of 17-beta estradiol and prostaglandin F2 alpha. Also, 17-beta estradiol was associated with lower cardiac impairment (CI) and stroke volume index (SVI) in SSc-PAH patients, but higher SVI in IPAH patients. PGF 2 alpha was associated with lower CI and SVI and higher pulmonary vascular resistance in SSc-PAH and IPAH combined.
The study findings were limited by several factors including the inability to adjust for all potential confounders between IPAH and SSc-PAH, and the fact that a clear causal relationship could not be determined, the researchers noted. Inadequate statistical power to analyze SSc-PAH data was another limitation, and studies with detailed scleroderma phenotypes are needed to validate the results, they said.
However, the current study provides insight on the metabolic differences in SSc-PAH and the potential impact on disease pathology that may inform diagnosis, prognosis, and treatment strategies for SSc-PAH patients, they concluded.
The study was supported by the National Institutes of Health. Several individual investigators received support from organizations including the American Heart Association and the Chest Foundation, and from companies including Livanova, Equillium, Corvus, Bayer, and Actelion, but the authors had no relevant financial conflicts to disclose.
, based on data from approximately 1,500 individuals.
The overall prognosis and therapeutic response for patients with pulmonary arterial hypertension associated with systemic sclerosis (SSc-PAH) tends to be worse than for patients with other types of PAH, such as idiopathic pulmonary arterial hypertension (IPAH), but the impact of different metabolite profiles among subtypes of disease has not been explored, wrote Mona Alotaibi, MD, of the University of California, San Diego, and colleagues.
“Recently, metabolic dysregulation has been proposed as a key mechanism by which IPAH and SSc-PAH differ and could control such disparities,” they noted. Clarifying the molecular mechanisms of SSc-PAH could inform management and treatment, they added.
In a study published in the journal Chest, the researchers sought to identify a bioactive lipid signature unique to SSc-PAH. They identified 400 patients with SSc-PAH and 1,082 with IPAH. An additional 100 patients with scleroderma but no PH and 44 patients with scleroderma who had PH were included for external validation. The mean ages of the patients with IPAH and SSc-PAH in the discovery and validation cohorts ranged from approximately 51 to 65 years; more than 75% of patients across the groups were women.
The researchers tested more than 700 bioactive lipid metabolites using liquid chromatography/mass spectrometry. They found five metabolites that distinguished SSc-PAH and IPAH that were significantly associated with markers of disease severity: 17-beta estradiol, novel Eic, nervonic acid, fatty acid esters of hydroxy fatty acids, and prostaglandin F2 alpha (PGF 2 alpha).
The biomarkers were increased in SSc-PAH patients compared to patients with SSC alone, which suggests that the biomarkers are related to PAH and not to scleroderma alone, the researchers noted.
In particular, nervonic acid was associated with worse functional capacity, in SSc-PAH patients, as were higher levels of 17-beta estradiol and prostaglandin F2 alpha. Also, 17-beta estradiol was associated with lower cardiac impairment (CI) and stroke volume index (SVI) in SSc-PAH patients, but higher SVI in IPAH patients. PGF 2 alpha was associated with lower CI and SVI and higher pulmonary vascular resistance in SSc-PAH and IPAH combined.
The study findings were limited by several factors including the inability to adjust for all potential confounders between IPAH and SSc-PAH, and the fact that a clear causal relationship could not be determined, the researchers noted. Inadequate statistical power to analyze SSc-PAH data was another limitation, and studies with detailed scleroderma phenotypes are needed to validate the results, they said.
However, the current study provides insight on the metabolic differences in SSc-PAH and the potential impact on disease pathology that may inform diagnosis, prognosis, and treatment strategies for SSc-PAH patients, they concluded.
The study was supported by the National Institutes of Health. Several individual investigators received support from organizations including the American Heart Association and the Chest Foundation, and from companies including Livanova, Equillium, Corvus, Bayer, and Actelion, but the authors had no relevant financial conflicts to disclose.
, based on data from approximately 1,500 individuals.
The overall prognosis and therapeutic response for patients with pulmonary arterial hypertension associated with systemic sclerosis (SSc-PAH) tends to be worse than for patients with other types of PAH, such as idiopathic pulmonary arterial hypertension (IPAH), but the impact of different metabolite profiles among subtypes of disease has not been explored, wrote Mona Alotaibi, MD, of the University of California, San Diego, and colleagues.
“Recently, metabolic dysregulation has been proposed as a key mechanism by which IPAH and SSc-PAH differ and could control such disparities,” they noted. Clarifying the molecular mechanisms of SSc-PAH could inform management and treatment, they added.
In a study published in the journal Chest, the researchers sought to identify a bioactive lipid signature unique to SSc-PAH. They identified 400 patients with SSc-PAH and 1,082 with IPAH. An additional 100 patients with scleroderma but no PH and 44 patients with scleroderma who had PH were included for external validation. The mean ages of the patients with IPAH and SSc-PAH in the discovery and validation cohorts ranged from approximately 51 to 65 years; more than 75% of patients across the groups were women.
The researchers tested more than 700 bioactive lipid metabolites using liquid chromatography/mass spectrometry. They found five metabolites that distinguished SSc-PAH and IPAH that were significantly associated with markers of disease severity: 17-beta estradiol, novel Eic, nervonic acid, fatty acid esters of hydroxy fatty acids, and prostaglandin F2 alpha (PGF 2 alpha).
The biomarkers were increased in SSc-PAH patients compared to patients with SSC alone, which suggests that the biomarkers are related to PAH and not to scleroderma alone, the researchers noted.
In particular, nervonic acid was associated with worse functional capacity, in SSc-PAH patients, as were higher levels of 17-beta estradiol and prostaglandin F2 alpha. Also, 17-beta estradiol was associated with lower cardiac impairment (CI) and stroke volume index (SVI) in SSc-PAH patients, but higher SVI in IPAH patients. PGF 2 alpha was associated with lower CI and SVI and higher pulmonary vascular resistance in SSc-PAH and IPAH combined.
The study findings were limited by several factors including the inability to adjust for all potential confounders between IPAH and SSc-PAH, and the fact that a clear causal relationship could not be determined, the researchers noted. Inadequate statistical power to analyze SSc-PAH data was another limitation, and studies with detailed scleroderma phenotypes are needed to validate the results, they said.
However, the current study provides insight on the metabolic differences in SSc-PAH and the potential impact on disease pathology that may inform diagnosis, prognosis, and treatment strategies for SSc-PAH patients, they concluded.
The study was supported by the National Institutes of Health. Several individual investigators received support from organizations including the American Heart Association and the Chest Foundation, and from companies including Livanova, Equillium, Corvus, Bayer, and Actelion, but the authors had no relevant financial conflicts to disclose.
FROM CHEST
What’s the best age to stop smoking? Study offers clue
Researchers also quantified the benefit of quitting for those older than 35. The added risk of death associated with smoking was reduced by 90% for those who quit before age 45 and 66% for those who quit at ages 45 to 64.
“The distal nature of the health consequences for young smokers is a challenge for professionals trying to motivate quitting in younger age groups. Without a proximal goal, it is tempting for smokers to abandon a quit attempt with cognitions such as ‘I don’t really need to do it just now,’ ” John P. Pierce, PhD, director for Population Sciences at UC-San Diego’s Moores Cancer Center, wrote in a commentary.
Current smokers were twice as likely to die from any cause during the study, compared with the group researchers called “never smokers,” who were defined as smoking fewer than 100 lifetime cigarettes.
Published in JAMA Network Open, the study involved 551,388 U.S. participants using information collected by the CDC from 1997 to 2018. Researchers collected data for specific causes of death of participants through the end of 2019.
The results echo past findings but also established whether demographic factors such as a smoker’s race and gender impact the benefits of quitting. (In many areas of health research, a person’s race or gender is associated with varying risks.)
The researchers found that the benefits of quitting smoking in reducing risk of death are comparable across demographic groups.
“Among former smokers in each racial and ethnic group, whether male or female, quitting was associated with reductions of approximately 80% of the excess mortality associated with continued smoking,” the authors stated. “These associations were generally consistent for deaths from cancer, cardiovascular disease, and lower respiratory disease.”
The findings are also important for guiding stop-smoking efforts because while smoking nationwide has decreased, the reduction has varied across demographic groups.
“Monitoring the association of smoking with mortality by race, ethnicity, and sex is critical to understanding how the U.S. tobacco epidemic continues to evolve over time and who is most affected by the changes,” the authors stated. “Despite continued decreases in U.S. smoking prevalence in recent decades, progress has not been equal across demographic groups. Recent progress in raising the quit ratio among U.S. ever-smokers overall has been modest, and the quit ratio has been consistently lower among Black and Hispanic ever-smokers than among non-Hispanic White ever-smokers.”
A version of this article first appeared on WebMD.com.
This article was updated 10/27/22.
Researchers also quantified the benefit of quitting for those older than 35. The added risk of death associated with smoking was reduced by 90% for those who quit before age 45 and 66% for those who quit at ages 45 to 64.
“The distal nature of the health consequences for young smokers is a challenge for professionals trying to motivate quitting in younger age groups. Without a proximal goal, it is tempting for smokers to abandon a quit attempt with cognitions such as ‘I don’t really need to do it just now,’ ” John P. Pierce, PhD, director for Population Sciences at UC-San Diego’s Moores Cancer Center, wrote in a commentary.
Current smokers were twice as likely to die from any cause during the study, compared with the group researchers called “never smokers,” who were defined as smoking fewer than 100 lifetime cigarettes.
Published in JAMA Network Open, the study involved 551,388 U.S. participants using information collected by the CDC from 1997 to 2018. Researchers collected data for specific causes of death of participants through the end of 2019.
The results echo past findings but also established whether demographic factors such as a smoker’s race and gender impact the benefits of quitting. (In many areas of health research, a person’s race or gender is associated with varying risks.)
The researchers found that the benefits of quitting smoking in reducing risk of death are comparable across demographic groups.
“Among former smokers in each racial and ethnic group, whether male or female, quitting was associated with reductions of approximately 80% of the excess mortality associated with continued smoking,” the authors stated. “These associations were generally consistent for deaths from cancer, cardiovascular disease, and lower respiratory disease.”
The findings are also important for guiding stop-smoking efforts because while smoking nationwide has decreased, the reduction has varied across demographic groups.
“Monitoring the association of smoking with mortality by race, ethnicity, and sex is critical to understanding how the U.S. tobacco epidemic continues to evolve over time and who is most affected by the changes,” the authors stated. “Despite continued decreases in U.S. smoking prevalence in recent decades, progress has not been equal across demographic groups. Recent progress in raising the quit ratio among U.S. ever-smokers overall has been modest, and the quit ratio has been consistently lower among Black and Hispanic ever-smokers than among non-Hispanic White ever-smokers.”
A version of this article first appeared on WebMD.com.
This article was updated 10/27/22.
Researchers also quantified the benefit of quitting for those older than 35. The added risk of death associated with smoking was reduced by 90% for those who quit before age 45 and 66% for those who quit at ages 45 to 64.
“The distal nature of the health consequences for young smokers is a challenge for professionals trying to motivate quitting in younger age groups. Without a proximal goal, it is tempting for smokers to abandon a quit attempt with cognitions such as ‘I don’t really need to do it just now,’ ” John P. Pierce, PhD, director for Population Sciences at UC-San Diego’s Moores Cancer Center, wrote in a commentary.
Current smokers were twice as likely to die from any cause during the study, compared with the group researchers called “never smokers,” who were defined as smoking fewer than 100 lifetime cigarettes.
Published in JAMA Network Open, the study involved 551,388 U.S. participants using information collected by the CDC from 1997 to 2018. Researchers collected data for specific causes of death of participants through the end of 2019.
The results echo past findings but also established whether demographic factors such as a smoker’s race and gender impact the benefits of quitting. (In many areas of health research, a person’s race or gender is associated with varying risks.)
The researchers found that the benefits of quitting smoking in reducing risk of death are comparable across demographic groups.
“Among former smokers in each racial and ethnic group, whether male or female, quitting was associated with reductions of approximately 80% of the excess mortality associated with continued smoking,” the authors stated. “These associations were generally consistent for deaths from cancer, cardiovascular disease, and lower respiratory disease.”
The findings are also important for guiding stop-smoking efforts because while smoking nationwide has decreased, the reduction has varied across demographic groups.
“Monitoring the association of smoking with mortality by race, ethnicity, and sex is critical to understanding how the U.S. tobacco epidemic continues to evolve over time and who is most affected by the changes,” the authors stated. “Despite continued decreases in U.S. smoking prevalence in recent decades, progress has not been equal across demographic groups. Recent progress in raising the quit ratio among U.S. ever-smokers overall has been modest, and the quit ratio has been consistently lower among Black and Hispanic ever-smokers than among non-Hispanic White ever-smokers.”
A version of this article first appeared on WebMD.com.
This article was updated 10/27/22.
FROM JAMA NETWORK OPEN
Shopping voucher incentives ‘doubles smoking quit rate in pregnancy’
Offering shopping vouchers to pregnant women as an incentive to quit smoking showed promising results, a study found, despite most participants relapsing after giving birth.
Rewarding pregnant women with up to £400 to spend on Main Street, in addition to usual support, more than doubled the proportion who were still smoke-free late in their pregnancy, and could save the National Health Service money in the long term, according to the research, published in the BMJ, led by the University of Glasgow and the University of York, England.
Although the proportion of women in the United Kingdom who smoke during pregnancy has halved over the past 20 years, those who still do are more reluctant to engage with cessation services.
Interventions using financial incentives were pioneered in the United States, but there is a lack of evidence for how effective they might be in the United Kingdom.
Vouchers linked to passing saliva tests
The phase 3 Cessation in Pregnancy Incentives Trial was based on an earlier feasibility study in Glasgow and involved 941 pregnant women aged 16 or older, with a mean age of 27.9 years when they were recruited, from seven stop-smoking services in Scotland, Northern Ireland, and England between January 2018 and April 2020. Participants self-reported that they smoked at least one cigarette a week.
The cohort was randomised into two groups: a control group who received usual stop smoking support that included the offer of counselling by trained workers combined with free nicotine-replacement therapy, and an intervention group who were given the same interventional support plus targets to receive LoveToShop vouchers.
Although vouchers to the value of £400 were on offer, earning them depended on successfully reaching four milestones. They received a first £50 voucher for engaging with stop-smoking services and setting a quit date and further vouchers for being declared smoke-free by biochemical verification at specific time points in the pregnancy.
Factors including the mother’s age, years of smoking, income, use of nicotine-replacement therapy and e-cigarettes, timing of birth, and birth weight were taken into account.
The study found that 71% of the participants in the incentive group engaged with stop-smoking services and set a quit date, compared with 64% in the control group. By late pregnancy, 126 participants (27%) of the 471 in the intervention group were smoke-free, compared with 58 (12%) of the 470 in the control group.
Most women in the trial went back to smoking
However, abstinence rates measured 6 months after giving birth were low in both groups: 6% in the intervention group vs. 4% in the control group.
The researchers also reported no significant differences in birth weight between the two groups.
Overall, the birth weight of babies from 443 intervention participants and 450 controls showed no significant difference between groups (average 3.18 kg vs. 3.13 kg).
The researchers did find a clinically important but not significant 10% increase in birth weight in the subset of participants who adhered with their treatment allocation, but they said further analysis is needed to better understand the relevance of this finding.
Severity of preterm birth was similar between groups, and all serious adverse events, such as miscarriages and stillbirths, were considered unrelated to the intervention.
The researchers acknowledged some limitations to their investigation, including that only 23% of women screened by stop-smoking services were enrolled, and that almost all participants were White. Also, the onset of COVID-19 disrupted some of the trial processes.
However, they concluded that their trial “supports implementation advocated in NICE [National Institute for Health and Care Excellence] guidelines by showing an effective, cost-effective, and generalisable pragmatic bolt-on U.K. format for incentive payments” to reduce smoking rates in pregnancy.
In a linked editorial, Daniel Kotz from the Heinrich Heine University, Düsseldorf, Germany, and Jasper Been from University Medical Center, Rotterdam, the Netherlands, pointed out that “partners of most pregnant women who smoke are also smokers,” which needed to be addressed. However, they wrote: “The medical community now has good evidence supporting effective tools, such as financial incentives, to reduce the health burden associated with tobacco smoking during pregnancy. These tools should be implemented wherever possible to protect and improve the health of women, their children, and their families.”
The trial was funded by Cancer Research UK; Chief Scientist Office, Scottish Government; HSC Public Health Agency Northern Ireland; Health and Social Care R&D Division NI Opportunity-Led Research Award; Chest Heart and Stroke Northern Ireland; Scottish Cot Death Trust; and Lullaby Trust 272. The authors declare no competing interests.
A version of this article first appeared on MedscapeUK.
Offering shopping vouchers to pregnant women as an incentive to quit smoking showed promising results, a study found, despite most participants relapsing after giving birth.
Rewarding pregnant women with up to £400 to spend on Main Street, in addition to usual support, more than doubled the proportion who were still smoke-free late in their pregnancy, and could save the National Health Service money in the long term, according to the research, published in the BMJ, led by the University of Glasgow and the University of York, England.
Although the proportion of women in the United Kingdom who smoke during pregnancy has halved over the past 20 years, those who still do are more reluctant to engage with cessation services.
Interventions using financial incentives were pioneered in the United States, but there is a lack of evidence for how effective they might be in the United Kingdom.
Vouchers linked to passing saliva tests
The phase 3 Cessation in Pregnancy Incentives Trial was based on an earlier feasibility study in Glasgow and involved 941 pregnant women aged 16 or older, with a mean age of 27.9 years when they were recruited, from seven stop-smoking services in Scotland, Northern Ireland, and England between January 2018 and April 2020. Participants self-reported that they smoked at least one cigarette a week.
The cohort was randomised into two groups: a control group who received usual stop smoking support that included the offer of counselling by trained workers combined with free nicotine-replacement therapy, and an intervention group who were given the same interventional support plus targets to receive LoveToShop vouchers.
Although vouchers to the value of £400 were on offer, earning them depended on successfully reaching four milestones. They received a first £50 voucher for engaging with stop-smoking services and setting a quit date and further vouchers for being declared smoke-free by biochemical verification at specific time points in the pregnancy.
Factors including the mother’s age, years of smoking, income, use of nicotine-replacement therapy and e-cigarettes, timing of birth, and birth weight were taken into account.
The study found that 71% of the participants in the incentive group engaged with stop-smoking services and set a quit date, compared with 64% in the control group. By late pregnancy, 126 participants (27%) of the 471 in the intervention group were smoke-free, compared with 58 (12%) of the 470 in the control group.
Most women in the trial went back to smoking
However, abstinence rates measured 6 months after giving birth were low in both groups: 6% in the intervention group vs. 4% in the control group.
The researchers also reported no significant differences in birth weight between the two groups.
Overall, the birth weight of babies from 443 intervention participants and 450 controls showed no significant difference between groups (average 3.18 kg vs. 3.13 kg).
The researchers did find a clinically important but not significant 10% increase in birth weight in the subset of participants who adhered with their treatment allocation, but they said further analysis is needed to better understand the relevance of this finding.
Severity of preterm birth was similar between groups, and all serious adverse events, such as miscarriages and stillbirths, were considered unrelated to the intervention.
The researchers acknowledged some limitations to their investigation, including that only 23% of women screened by stop-smoking services were enrolled, and that almost all participants were White. Also, the onset of COVID-19 disrupted some of the trial processes.
However, they concluded that their trial “supports implementation advocated in NICE [National Institute for Health and Care Excellence] guidelines by showing an effective, cost-effective, and generalisable pragmatic bolt-on U.K. format for incentive payments” to reduce smoking rates in pregnancy.
In a linked editorial, Daniel Kotz from the Heinrich Heine University, Düsseldorf, Germany, and Jasper Been from University Medical Center, Rotterdam, the Netherlands, pointed out that “partners of most pregnant women who smoke are also smokers,” which needed to be addressed. However, they wrote: “The medical community now has good evidence supporting effective tools, such as financial incentives, to reduce the health burden associated with tobacco smoking during pregnancy. These tools should be implemented wherever possible to protect and improve the health of women, their children, and their families.”
The trial was funded by Cancer Research UK; Chief Scientist Office, Scottish Government; HSC Public Health Agency Northern Ireland; Health and Social Care R&D Division NI Opportunity-Led Research Award; Chest Heart and Stroke Northern Ireland; Scottish Cot Death Trust; and Lullaby Trust 272. The authors declare no competing interests.
A version of this article first appeared on MedscapeUK.
Offering shopping vouchers to pregnant women as an incentive to quit smoking showed promising results, a study found, despite most participants relapsing after giving birth.
Rewarding pregnant women with up to £400 to spend on Main Street, in addition to usual support, more than doubled the proportion who were still smoke-free late in their pregnancy, and could save the National Health Service money in the long term, according to the research, published in the BMJ, led by the University of Glasgow and the University of York, England.
Although the proportion of women in the United Kingdom who smoke during pregnancy has halved over the past 20 years, those who still do are more reluctant to engage with cessation services.
Interventions using financial incentives were pioneered in the United States, but there is a lack of evidence for how effective they might be in the United Kingdom.
Vouchers linked to passing saliva tests
The phase 3 Cessation in Pregnancy Incentives Trial was based on an earlier feasibility study in Glasgow and involved 941 pregnant women aged 16 or older, with a mean age of 27.9 years when they were recruited, from seven stop-smoking services in Scotland, Northern Ireland, and England between January 2018 and April 2020. Participants self-reported that they smoked at least one cigarette a week.
The cohort was randomised into two groups: a control group who received usual stop smoking support that included the offer of counselling by trained workers combined with free nicotine-replacement therapy, and an intervention group who were given the same interventional support plus targets to receive LoveToShop vouchers.
Although vouchers to the value of £400 were on offer, earning them depended on successfully reaching four milestones. They received a first £50 voucher for engaging with stop-smoking services and setting a quit date and further vouchers for being declared smoke-free by biochemical verification at specific time points in the pregnancy.
Factors including the mother’s age, years of smoking, income, use of nicotine-replacement therapy and e-cigarettes, timing of birth, and birth weight were taken into account.
The study found that 71% of the participants in the incentive group engaged with stop-smoking services and set a quit date, compared with 64% in the control group. By late pregnancy, 126 participants (27%) of the 471 in the intervention group were smoke-free, compared with 58 (12%) of the 470 in the control group.
Most women in the trial went back to smoking
However, abstinence rates measured 6 months after giving birth were low in both groups: 6% in the intervention group vs. 4% in the control group.
The researchers also reported no significant differences in birth weight between the two groups.
Overall, the birth weight of babies from 443 intervention participants and 450 controls showed no significant difference between groups (average 3.18 kg vs. 3.13 kg).
The researchers did find a clinically important but not significant 10% increase in birth weight in the subset of participants who adhered with their treatment allocation, but they said further analysis is needed to better understand the relevance of this finding.
Severity of preterm birth was similar between groups, and all serious adverse events, such as miscarriages and stillbirths, were considered unrelated to the intervention.
The researchers acknowledged some limitations to their investigation, including that only 23% of women screened by stop-smoking services were enrolled, and that almost all participants were White. Also, the onset of COVID-19 disrupted some of the trial processes.
However, they concluded that their trial “supports implementation advocated in NICE [National Institute for Health and Care Excellence] guidelines by showing an effective, cost-effective, and generalisable pragmatic bolt-on U.K. format for incentive payments” to reduce smoking rates in pregnancy.
In a linked editorial, Daniel Kotz from the Heinrich Heine University, Düsseldorf, Germany, and Jasper Been from University Medical Center, Rotterdam, the Netherlands, pointed out that “partners of most pregnant women who smoke are also smokers,” which needed to be addressed. However, they wrote: “The medical community now has good evidence supporting effective tools, such as financial incentives, to reduce the health burden associated with tobacco smoking during pregnancy. These tools should be implemented wherever possible to protect and improve the health of women, their children, and their families.”
The trial was funded by Cancer Research UK; Chief Scientist Office, Scottish Government; HSC Public Health Agency Northern Ireland; Health and Social Care R&D Division NI Opportunity-Led Research Award; Chest Heart and Stroke Northern Ireland; Scottish Cot Death Trust; and Lullaby Trust 272. The authors declare no competing interests.
A version of this article first appeared on MedscapeUK.
FROM BMJ
Global Initiative for Chronic Obstructive Lung Disease guidelines 2022: Management and treatment
In the United States and around the globe, chronic obstructive pulmonary disease (COPD) remains one of the leading causes of death. In addition to new diagnostic guidelines, the Global Initiative for Chronic Obstructive Lung Disease 2022 Report, or GOLD report, sets forth recommendations for management and treatment.
According to the GOLD report, initial management of COPD should aim at reducing exposure to risk factors such as smoking or other chemical exposures. In addition to medications, stable COPD patients should be evaluated for inhaler technique, adherence to prescribed therapies, smoking status, and continued exposure to other risk factors. Also, physical activity should be advised and pulmonary rehabilitation should be considered. Spirometry should be performed annually.

These guidelines offer very practical advice but often are difficult to implement in clinical practice. Everyone knows smoking is harmful and quitting provides huge health benefits, not only regarding COPD. However, nicotine is very addictive, and most smokers cannot just quit. Many need smoking cessation aids and counseling. Additionally, some smokers just don’t want to quit. Regarding workplace exposures, it often is not easy for someone just to change their job. Many are afraid to speak because they are afraid of losing their jobs. Everyone, not just patients with COPD, can benefit from increased physical activity, and all doctors know how difficult it is to motivate patients to do this.
The decision to initiate medications should be based on an individual patient’s symptoms and risk of exacerbations. In general, long-acting bronchodilators, including long-acting beta agonists (LABA) and long-acting muscarinic antagonists (LAMA), are preferred except when immediate relief of dyspnea is needed, and then short-acting bronchodilators should be used. Either a single long-acting or dual long-acting bronchodilator can be initiated. If a patient continues to have dyspnea on a single long-acting bronchodilator, treatment should be switched to a dual therapy.
In general, inhaled corticosteroids (ICS) are not recommended for stable COPD patients. If a patient has exacerbations despite appropriate treatment with LABAs, an ICS may be added to the LABA, the GOLD guidelines say. Oral corticosteroids are not recommended for long-term use. PDE4 inhibitors should be considered in patents with severe to very severe airflow obstruction, chronic bronchitis, and exacerbations. Macrolide antibiotics, especially azithromycin, can be considered in acute exacerbations. There is no evidence to support the use of antitussives and mucolytics are advised in only certain patients. Inhaled bronchodilators are advised over oral ones and theophylline is recommended when long-acting bronchodilators are unavailable or unaffordable.
In clinical practice, I see many patients treated based on symptomatology with spirometry testing not being done. This may help control many symptoms, but unless my patient has an accurate diagnosis, I won’t know if my patient is receiving the correct treatment.
It is important to keep in mind that COPD is a progressive disease and without appropriate treatment and monitoring, it will just get worse, and this is most likely to be irreversible.
Medications and treatment goals for patients with COPD
Patients with alpha-1 antitrypsin deficiency may benefit from the addition of alpha-1 antitrypsin augmentation therapy, the new guidelines say. In patients with severe disease experiencing dyspnea, oral and parental opioids can be considered. Medications that are used to treat primary pulmonary hypertension are not advised to treat pulmonary hypertension secondary to COPD.
The treatment goals of COPD should be to decrease severity of symptoms, reduce the occurrence of exacerbations, and improve exercise tolerance. Peripheral eosinophil counts can be used to guide the use of ICS to prevent exacerbations. However, the best predictor of exacerbations is previous exacerbations. Frequent exacerbations are defined as two or more annually. Additionally, deteriorating airflow is correlated with increased risk of exacerbations, hospitalizations, and death. Forced expiratory volume in 1 second (FEV1) alone lacks precision to predict exacerbations or death.
Vaccines and pulmonary rehabilitation recommended
The Centers for Disease Control and Prevention and World Health Organization recommend several vaccines for stable patients with COPD. Influenza vaccine was shown to reduce serious complications in COPD patients. Pneumococcal vaccines (PCV13 and PPSV23) reduced the likelihood of COPD exacerbations. The COVID-19 vaccine also has been effective at reducing hospitalizations, in particular ICU admissions, and death in patients with COPD. The CDC also recommends TdaP and Zoster vaccines.
An acute exacerbation of COPD occurs when a patient experiences worsening of respiratory symptoms that requires additional treatment, according to the updated GOLD guidelines. They are usually associated with increased airway inflammation, mucous productions, and trapping of gases. They are often triggered by viral infections, but bacterial and environment factors play a role as well. Less commonly, fungi such as Aspergillus can be observed as well. COPD exacerbations contribute to overall progression of the disease.
In patients with hypoxemia, supplemental oxygen should be titrated to a target O2 saturation of 88%-92%. It is important to follow blood gases to be sure adequate oxygenation is taking place while at the same time avoiding carbon dioxide retention and/or worsening acidosis. In patients with severe exacerbations whose dyspnea does not respond to initial emergency therapy, ICU admission is warranted. Other factors indicating the need for ICU admission include mental status changes, persistent or worsening hypoxemia, severe or worsening respiratory acidosis, the need for mechanical ventilation, and hemodynamic instability. Following an acute exacerbation, steps to prevent further exacerbations should be initiated.
Systemic glucocorticoids are indicated during acute exacerbations. They have been shown to hasten recovery time and improve functioning of the lungs as well as oxygenation. It is recommended to give prednisone 40 mg per day for 5 days. Antibiotics should be used in exacerbations if patients have dyspnea, sputum production, and purulence of the sputum or require mechanical ventilation. The choice of which antibiotic to use should be based on local bacterial resistance.
Pulmonary rehabilitation is an important component of COPD management. It incorporates exercise, education, and self-management aimed to change behavior and improve conditioning. The benefits of rehab have been shown to be considerable. The optimal length is 6-8 weeks. Palliative and end-of-life care are also very important factors to consider when treating COPD patients, according to the GOLD guidelines.
COPD is a very common disease and cause of mortality seen by family physicians. The GOLD report is an extensive document providing very clear guidelines and evidence to support these guidelines in every level of the treatment of COPD patients. As primary care doctors, we are often the first to treat patients with COPD and it is important to know the latest guidelines.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at [email protected].
In the United States and around the globe, chronic obstructive pulmonary disease (COPD) remains one of the leading causes of death. In addition to new diagnostic guidelines, the Global Initiative for Chronic Obstructive Lung Disease 2022 Report, or GOLD report, sets forth recommendations for management and treatment.
According to the GOLD report, initial management of COPD should aim at reducing exposure to risk factors such as smoking or other chemical exposures. In addition to medications, stable COPD patients should be evaluated for inhaler technique, adherence to prescribed therapies, smoking status, and continued exposure to other risk factors. Also, physical activity should be advised and pulmonary rehabilitation should be considered. Spirometry should be performed annually.
These guidelines offer very practical advice but often are difficult to implement in clinical practice. Everyone knows smoking is harmful and quitting provides huge health benefits, not only regarding COPD. However, nicotine is very addictive, and most smokers cannot just quit. Many need smoking cessation aids and counseling. Additionally, some smokers just don’t want to quit. Regarding workplace exposures, it often is not easy for someone just to change their job. Many are afraid to speak because they are afraid of losing their jobs. Everyone, not just patients with COPD, can benefit from increased physical activity, and all doctors know how difficult it is to motivate patients to do this.
The decision to initiate medications should be based on an individual patient’s symptoms and risk of exacerbations. In general, long-acting bronchodilators, including long-acting beta agonists (LABA) and long-acting muscarinic antagonists (LAMA), are preferred except when immediate relief of dyspnea is needed, and then short-acting bronchodilators should be used. Either a single long-acting or dual long-acting bronchodilator can be initiated. If a patient continues to have dyspnea on a single long-acting bronchodilator, treatment should be switched to a dual therapy.
In general, inhaled corticosteroids (ICS) are not recommended for stable COPD patients. If a patient has exacerbations despite appropriate treatment with LABAs, an ICS may be added to the LABA, the GOLD guidelines say. Oral corticosteroids are not recommended for long-term use. PDE4 inhibitors should be considered in patents with severe to very severe airflow obstruction, chronic bronchitis, and exacerbations. Macrolide antibiotics, especially azithromycin, can be considered in acute exacerbations. There is no evidence to support the use of antitussives and mucolytics are advised in only certain patients. Inhaled bronchodilators are advised over oral ones and theophylline is recommended when long-acting bronchodilators are unavailable or unaffordable.
In clinical practice, I see many patients treated based on symptomatology with spirometry testing not being done. This may help control many symptoms, but unless my patient has an accurate diagnosis, I won’t know if my patient is receiving the correct treatment.
It is important to keep in mind that COPD is a progressive disease and without appropriate treatment and monitoring, it will just get worse, and this is most likely to be irreversible.
Medications and treatment goals for patients with COPD
Patients with alpha-1 antitrypsin deficiency may benefit from the addition of alpha-1 antitrypsin augmentation therapy, the new guidelines say. In patients with severe disease experiencing dyspnea, oral and parental opioids can be considered. Medications that are used to treat primary pulmonary hypertension are not advised to treat pulmonary hypertension secondary to COPD.
The treatment goals of COPD should be to decrease severity of symptoms, reduce the occurrence of exacerbations, and improve exercise tolerance. Peripheral eosinophil counts can be used to guide the use of ICS to prevent exacerbations. However, the best predictor of exacerbations is previous exacerbations. Frequent exacerbations are defined as two or more annually. Additionally, deteriorating airflow is correlated with increased risk of exacerbations, hospitalizations, and death. Forced expiratory volume in 1 second (FEV1) alone lacks precision to predict exacerbations or death.
Vaccines and pulmonary rehabilitation recommended
The Centers for Disease Control and Prevention and World Health Organization recommend several vaccines for stable patients with COPD. Influenza vaccine was shown to reduce serious complications in COPD patients. Pneumococcal vaccines (PCV13 and PPSV23) reduced the likelihood of COPD exacerbations. The COVID-19 vaccine also has been effective at reducing hospitalizations, in particular ICU admissions, and death in patients with COPD. The CDC also recommends TdaP and Zoster vaccines.
An acute exacerbation of COPD occurs when a patient experiences worsening of respiratory symptoms that requires additional treatment, according to the updated GOLD guidelines. They are usually associated with increased airway inflammation, mucous productions, and trapping of gases. They are often triggered by viral infections, but bacterial and environment factors play a role as well. Less commonly, fungi such as Aspergillus can be observed as well. COPD exacerbations contribute to overall progression of the disease.
In patients with hypoxemia, supplemental oxygen should be titrated to a target O2 saturation of 88%-92%. It is important to follow blood gases to be sure adequate oxygenation is taking place while at the same time avoiding carbon dioxide retention and/or worsening acidosis. In patients with severe exacerbations whose dyspnea does not respond to initial emergency therapy, ICU admission is warranted. Other factors indicating the need for ICU admission include mental status changes, persistent or worsening hypoxemia, severe or worsening respiratory acidosis, the need for mechanical ventilation, and hemodynamic instability. Following an acute exacerbation, steps to prevent further exacerbations should be initiated.
Systemic glucocorticoids are indicated during acute exacerbations. They have been shown to hasten recovery time and improve functioning of the lungs as well as oxygenation. It is recommended to give prednisone 40 mg per day for 5 days. Antibiotics should be used in exacerbations if patients have dyspnea, sputum production, and purulence of the sputum or require mechanical ventilation. The choice of which antibiotic to use should be based on local bacterial resistance.
Pulmonary rehabilitation is an important component of COPD management. It incorporates exercise, education, and self-management aimed to change behavior and improve conditioning. The benefits of rehab have been shown to be considerable. The optimal length is 6-8 weeks. Palliative and end-of-life care are also very important factors to consider when treating COPD patients, according to the GOLD guidelines.
COPD is a very common disease and cause of mortality seen by family physicians. The GOLD report is an extensive document providing very clear guidelines and evidence to support these guidelines in every level of the treatment of COPD patients. As primary care doctors, we are often the first to treat patients with COPD and it is important to know the latest guidelines.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at [email protected].
In the United States and around the globe, chronic obstructive pulmonary disease (COPD) remains one of the leading causes of death. In addition to new diagnostic guidelines, the Global Initiative for Chronic Obstructive Lung Disease 2022 Report, or GOLD report, sets forth recommendations for management and treatment.
According to the GOLD report, initial management of COPD should aim at reducing exposure to risk factors such as smoking or other chemical exposures. In addition to medications, stable COPD patients should be evaluated for inhaler technique, adherence to prescribed therapies, smoking status, and continued exposure to other risk factors. Also, physical activity should be advised and pulmonary rehabilitation should be considered. Spirometry should be performed annually.
These guidelines offer very practical advice but often are difficult to implement in clinical practice. Everyone knows smoking is harmful and quitting provides huge health benefits, not only regarding COPD. However, nicotine is very addictive, and most smokers cannot just quit. Many need smoking cessation aids and counseling. Additionally, some smokers just don’t want to quit. Regarding workplace exposures, it often is not easy for someone just to change their job. Many are afraid to speak because they are afraid of losing their jobs. Everyone, not just patients with COPD, can benefit from increased physical activity, and all doctors know how difficult it is to motivate patients to do this.
The decision to initiate medications should be based on an individual patient’s symptoms and risk of exacerbations. In general, long-acting bronchodilators, including long-acting beta agonists (LABA) and long-acting muscarinic antagonists (LAMA), are preferred except when immediate relief of dyspnea is needed, and then short-acting bronchodilators should be used. Either a single long-acting or dual long-acting bronchodilator can be initiated. If a patient continues to have dyspnea on a single long-acting bronchodilator, treatment should be switched to a dual therapy.
In general, inhaled corticosteroids (ICS) are not recommended for stable COPD patients. If a patient has exacerbations despite appropriate treatment with LABAs, an ICS may be added to the LABA, the GOLD guidelines say. Oral corticosteroids are not recommended for long-term use. PDE4 inhibitors should be considered in patents with severe to very severe airflow obstruction, chronic bronchitis, and exacerbations. Macrolide antibiotics, especially azithromycin, can be considered in acute exacerbations. There is no evidence to support the use of antitussives and mucolytics are advised in only certain patients. Inhaled bronchodilators are advised over oral ones and theophylline is recommended when long-acting bronchodilators are unavailable or unaffordable.
In clinical practice, I see many patients treated based on symptomatology with spirometry testing not being done. This may help control many symptoms, but unless my patient has an accurate diagnosis, I won’t know if my patient is receiving the correct treatment.
It is important to keep in mind that COPD is a progressive disease and without appropriate treatment and monitoring, it will just get worse, and this is most likely to be irreversible.
Medications and treatment goals for patients with COPD
Patients with alpha-1 antitrypsin deficiency may benefit from the addition of alpha-1 antitrypsin augmentation therapy, the new guidelines say. In patients with severe disease experiencing dyspnea, oral and parental opioids can be considered. Medications that are used to treat primary pulmonary hypertension are not advised to treat pulmonary hypertension secondary to COPD.
The treatment goals of COPD should be to decrease severity of symptoms, reduce the occurrence of exacerbations, and improve exercise tolerance. Peripheral eosinophil counts can be used to guide the use of ICS to prevent exacerbations. However, the best predictor of exacerbations is previous exacerbations. Frequent exacerbations are defined as two or more annually. Additionally, deteriorating airflow is correlated with increased risk of exacerbations, hospitalizations, and death. Forced expiratory volume in 1 second (FEV1) alone lacks precision to predict exacerbations or death.
Vaccines and pulmonary rehabilitation recommended
The Centers for Disease Control and Prevention and World Health Organization recommend several vaccines for stable patients with COPD. Influenza vaccine was shown to reduce serious complications in COPD patients. Pneumococcal vaccines (PCV13 and PPSV23) reduced the likelihood of COPD exacerbations. The COVID-19 vaccine also has been effective at reducing hospitalizations, in particular ICU admissions, and death in patients with COPD. The CDC also recommends TdaP and Zoster vaccines.
An acute exacerbation of COPD occurs when a patient experiences worsening of respiratory symptoms that requires additional treatment, according to the updated GOLD guidelines. They are usually associated with increased airway inflammation, mucous productions, and trapping of gases. They are often triggered by viral infections, but bacterial and environment factors play a role as well. Less commonly, fungi such as Aspergillus can be observed as well. COPD exacerbations contribute to overall progression of the disease.
In patients with hypoxemia, supplemental oxygen should be titrated to a target O2 saturation of 88%-92%. It is important to follow blood gases to be sure adequate oxygenation is taking place while at the same time avoiding carbon dioxide retention and/or worsening acidosis. In patients with severe exacerbations whose dyspnea does not respond to initial emergency therapy, ICU admission is warranted. Other factors indicating the need for ICU admission include mental status changes, persistent or worsening hypoxemia, severe or worsening respiratory acidosis, the need for mechanical ventilation, and hemodynamic instability. Following an acute exacerbation, steps to prevent further exacerbations should be initiated.
Systemic glucocorticoids are indicated during acute exacerbations. They have been shown to hasten recovery time and improve functioning of the lungs as well as oxygenation. It is recommended to give prednisone 40 mg per day for 5 days. Antibiotics should be used in exacerbations if patients have dyspnea, sputum production, and purulence of the sputum or require mechanical ventilation. The choice of which antibiotic to use should be based on local bacterial resistance.
Pulmonary rehabilitation is an important component of COPD management. It incorporates exercise, education, and self-management aimed to change behavior and improve conditioning. The benefits of rehab have been shown to be considerable. The optimal length is 6-8 weeks. Palliative and end-of-life care are also very important factors to consider when treating COPD patients, according to the GOLD guidelines.
COPD is a very common disease and cause of mortality seen by family physicians. The GOLD report is an extensive document providing very clear guidelines and evidence to support these guidelines in every level of the treatment of COPD patients. As primary care doctors, we are often the first to treat patients with COPD and it is important to know the latest guidelines.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at [email protected].
Asthma ED visits predict failed housing inspections
, according to a new study presented at the annual meeting of the American College of Emergency Physicians.
While links between asthma and low-quality housing prone to harboring allergens have been well-documented, the current study takes the extra step of looking at housing down to the level of individual land parcels and suggests that asthma hospital visits can be used to identify hazardous housing earlier.
“Emergency department visits for asthma provide a leading indicator that can be used by health departments or housing authorities to direct housing inspections and remediation of poor housing conditions, track improvements in housing quality, measure housing department performance, support resident grievances, and inform funding allocation decisions,” said the study’s lead researcher, Elizabeth Samuels, MD, who is assistant professor of epidemiology and emergency medicine at Brown University, Providence, R.I.
Researchers retrospectively looked at cases of children and adults in the Greater New Haven area of Connecticut seen at the Yale New Haven Hospital ED for asthma-related problems between March 2013 and August 2017. The region has the fifth-highest prevalence of asthma in the United States, the researchers point out, due to its air quality, pollens, and quality of its housing. More than half of residences were built before 1,940, compared with about 13% nationally. Patient addresses were matched with HUD inspection records.
The review encompassed 11,429 ED visits by 6,366 individuals; 54% were insured by Medicaid, and 42% were Black. Controlling for patient and neighborhood data, researchers found that increased asthma ED visits at the parcel level were associated with decreased HUD inspection scores to a highly significant degree (P < .001).
They also found that there was a relationship in terms of timing between asthma ED visits and inspection scores: asthma ED visits increased more than 1 year before a failed HUD inspection. They also found that asthma ED visits were not elevated at housing units that passed inspection. Using asthma ED visits to predict failed housing inspections produced a specificity rate of 92.3% in an adjusted model, Dr. Samuels noted.
“This approach represents a novel method of early identification of dangerous housing conditions, which could aid in the prevention of asthma-related morbidity and mortality,” Dr. Samuels said.
The investigators noted that, of the parcels with the top three incidence rates of asthma ED visits, “all of them have been closed or demolished.”
In addition to limiting exposure of patients with asthma to the allergens of mold, mice and rats, and cockroaches, improving poor-quality housing earlier could help asthma by reducing stress, she said.
“There is also an increasing evidence base that psychosocial stress increases the risk of asthma attacks, and it’s therefore possible that living in poor housing conditions – often highly stressful situations – drives exacerbation risk via this pathway,” she said. “Synergistic effects between these pathways are also possible or even likely.”
Neeta Thakur, MD, associate professor of medicine at the University of California, San Francisco, who researches asthma, said the findings could lead to a strategy for improving poor-quality housing more quickly. As it is, inspections are too infrequent, often prompted by resident complaints.
“Once the complaints get to a certain threshold, then there might be an inspection that happens, and if there is a periodic review of the buildings, they often happen few and far between,” she said. “We could actually use some of the information that we’re already getting from something like ED visits and see if there is a pattern.”
An important follow-up would be to see whether asthma outcomes improve after housing deficiencies are addressed and whether the predictive capacity of ED visits occurs in other places.
“Would you then see a decline in the ED visit rates from individuals living in those buildings?” Dr. Thakur said. “It’s important to find a leading indicator, but you want to be sure that that leading indicator is useful as something that can be intervened upon.”
Dr. Samuels and Dr. Thakur have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, according to a new study presented at the annual meeting of the American College of Emergency Physicians.
While links between asthma and low-quality housing prone to harboring allergens have been well-documented, the current study takes the extra step of looking at housing down to the level of individual land parcels and suggests that asthma hospital visits can be used to identify hazardous housing earlier.
“Emergency department visits for asthma provide a leading indicator that can be used by health departments or housing authorities to direct housing inspections and remediation of poor housing conditions, track improvements in housing quality, measure housing department performance, support resident grievances, and inform funding allocation decisions,” said the study’s lead researcher, Elizabeth Samuels, MD, who is assistant professor of epidemiology and emergency medicine at Brown University, Providence, R.I.
Researchers retrospectively looked at cases of children and adults in the Greater New Haven area of Connecticut seen at the Yale New Haven Hospital ED for asthma-related problems between March 2013 and August 2017. The region has the fifth-highest prevalence of asthma in the United States, the researchers point out, due to its air quality, pollens, and quality of its housing. More than half of residences were built before 1,940, compared with about 13% nationally. Patient addresses were matched with HUD inspection records.
The review encompassed 11,429 ED visits by 6,366 individuals; 54% were insured by Medicaid, and 42% were Black. Controlling for patient and neighborhood data, researchers found that increased asthma ED visits at the parcel level were associated with decreased HUD inspection scores to a highly significant degree (P < .001).
They also found that there was a relationship in terms of timing between asthma ED visits and inspection scores: asthma ED visits increased more than 1 year before a failed HUD inspection. They also found that asthma ED visits were not elevated at housing units that passed inspection. Using asthma ED visits to predict failed housing inspections produced a specificity rate of 92.3% in an adjusted model, Dr. Samuels noted.
“This approach represents a novel method of early identification of dangerous housing conditions, which could aid in the prevention of asthma-related morbidity and mortality,” Dr. Samuels said.
The investigators noted that, of the parcels with the top three incidence rates of asthma ED visits, “all of them have been closed or demolished.”
In addition to limiting exposure of patients with asthma to the allergens of mold, mice and rats, and cockroaches, improving poor-quality housing earlier could help asthma by reducing stress, she said.
“There is also an increasing evidence base that psychosocial stress increases the risk of asthma attacks, and it’s therefore possible that living in poor housing conditions – often highly stressful situations – drives exacerbation risk via this pathway,” she said. “Synergistic effects between these pathways are also possible or even likely.”
Neeta Thakur, MD, associate professor of medicine at the University of California, San Francisco, who researches asthma, said the findings could lead to a strategy for improving poor-quality housing more quickly. As it is, inspections are too infrequent, often prompted by resident complaints.
“Once the complaints get to a certain threshold, then there might be an inspection that happens, and if there is a periodic review of the buildings, they often happen few and far between,” she said. “We could actually use some of the information that we’re already getting from something like ED visits and see if there is a pattern.”
An important follow-up would be to see whether asthma outcomes improve after housing deficiencies are addressed and whether the predictive capacity of ED visits occurs in other places.
“Would you then see a decline in the ED visit rates from individuals living in those buildings?” Dr. Thakur said. “It’s important to find a leading indicator, but you want to be sure that that leading indicator is useful as something that can be intervened upon.”
Dr. Samuels and Dr. Thakur have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, according to a new study presented at the annual meeting of the American College of Emergency Physicians.
While links between asthma and low-quality housing prone to harboring allergens have been well-documented, the current study takes the extra step of looking at housing down to the level of individual land parcels and suggests that asthma hospital visits can be used to identify hazardous housing earlier.
“Emergency department visits for asthma provide a leading indicator that can be used by health departments or housing authorities to direct housing inspections and remediation of poor housing conditions, track improvements in housing quality, measure housing department performance, support resident grievances, and inform funding allocation decisions,” said the study’s lead researcher, Elizabeth Samuels, MD, who is assistant professor of epidemiology and emergency medicine at Brown University, Providence, R.I.
Researchers retrospectively looked at cases of children and adults in the Greater New Haven area of Connecticut seen at the Yale New Haven Hospital ED for asthma-related problems between March 2013 and August 2017. The region has the fifth-highest prevalence of asthma in the United States, the researchers point out, due to its air quality, pollens, and quality of its housing. More than half of residences were built before 1,940, compared with about 13% nationally. Patient addresses were matched with HUD inspection records.
The review encompassed 11,429 ED visits by 6,366 individuals; 54% were insured by Medicaid, and 42% were Black. Controlling for patient and neighborhood data, researchers found that increased asthma ED visits at the parcel level were associated with decreased HUD inspection scores to a highly significant degree (P < .001).
They also found that there was a relationship in terms of timing between asthma ED visits and inspection scores: asthma ED visits increased more than 1 year before a failed HUD inspection. They also found that asthma ED visits were not elevated at housing units that passed inspection. Using asthma ED visits to predict failed housing inspections produced a specificity rate of 92.3% in an adjusted model, Dr. Samuels noted.
“This approach represents a novel method of early identification of dangerous housing conditions, which could aid in the prevention of asthma-related morbidity and mortality,” Dr. Samuels said.
The investigators noted that, of the parcels with the top three incidence rates of asthma ED visits, “all of them have been closed or demolished.”
In addition to limiting exposure of patients with asthma to the allergens of mold, mice and rats, and cockroaches, improving poor-quality housing earlier could help asthma by reducing stress, she said.
“There is also an increasing evidence base that psychosocial stress increases the risk of asthma attacks, and it’s therefore possible that living in poor housing conditions – often highly stressful situations – drives exacerbation risk via this pathway,” she said. “Synergistic effects between these pathways are also possible or even likely.”
Neeta Thakur, MD, associate professor of medicine at the University of California, San Francisco, who researches asthma, said the findings could lead to a strategy for improving poor-quality housing more quickly. As it is, inspections are too infrequent, often prompted by resident complaints.
“Once the complaints get to a certain threshold, then there might be an inspection that happens, and if there is a periodic review of the buildings, they often happen few and far between,” she said. “We could actually use some of the information that we’re already getting from something like ED visits and see if there is a pattern.”
An important follow-up would be to see whether asthma outcomes improve after housing deficiencies are addressed and whether the predictive capacity of ED visits occurs in other places.
“Would you then see a decline in the ED visit rates from individuals living in those buildings?” Dr. Thakur said. “It’s important to find a leading indicator, but you want to be sure that that leading indicator is useful as something that can be intervened upon.”
Dr. Samuels and Dr. Thakur have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ACEP 2022
Mucus unplugged
Just uttering the word “mucus” is often sufficient to elicit amusement from those within earshot, but to patients with chronic inflammatory airway diseases, mucus is no laughing matter.
, which are then moved by cilia out of the airways for expulsion through coughing.
But in cystic fibrosis (CF), for example, mucus hypersecretion can be deadly. The underlying pathology of CF – a mutation in the CFTR gene, which codes for the protein CF transmembrane conductance regulator – leads to buildup in the lungs of abnormally viscous and sticky mucus, resulting in frequent, severe infections (particularly with Pseudomonas aeruginosa), progressive lung damage, and prior to the development of effective disease management, significantly premature death.
Mucus hypersecretion is also a feature of chronic obstructive pulmonary disease (COPD), noted Victor Kim, MD, from Temple University, Philadelphia, Christopher M. Evans, PhD, from the University of Colorado at Denver, Aurora, and Burton F. Dickey, MD, from the University of Texas MD Anderson Cancer Center, Houston.
In COPD, “mucus dysfunction arises from several mechanisms, including excess production due to inflammation, decreased elimination due to impaired ciliary clearance and reduced cough efficiency, and excessive concentration due to smoke-induced dysfunction of transepithelial anion transport resembling CF,” they wrote in an editorial published in the American Journal of Respiratory and Critical Care Medicine.
In patients with idiopathic pulmonary fibrosis, a polymorphism in the enhancer region of MUC5B, a gene that encodes for mucin glycoproteins, results in a 20-fold overexpression of the gene and prominent mucus production that has been shown to parallel lung inflammation and decline in forced vital capacity (FVC).
In patients with asthma, up-regulation of MUC5AC and stimulated mucus secretion conspire to obstruct airways, which can in extreme cases lead to death.
‘Short shrift’
Yet until recently, the role of mucus hypersecretion in diseases such as COPD has been largely overlooked, or as Dr. Kim and colleagues put it, “airway mucus often receives short shrift from clinicians.”
“It’s a pretty hot topic in pulmonary medicine today because it has been so neglected for so long,” Dr. Dickey said in an interview with CHEST Physician. “As clinicians we haven’t had a way to identify who needs treatment, which is ridiculous, because many of the people who expectorate a lot, like those with chronic bronchitis, don’t actually have small airway obstruction, and conversely, a lot of asthmatics, who have very serious small airway obstruction, don’t expectorate, so you can’t really tell from symptoms.”
What has changed in recent years is the use of chest CT to image muco-obstructive pathology, commonly called “mucus plugging” in the peripheral airways of patients with COPD and asthma.
“In the last decade or so, we’ve seen the emergence in obstructive lung diseases such as asthma and COPD the use of more objective measures on CT scans, including the problem of mucus plugging, which is unfortunately very common,” Dr. Kim said in an interview.
The discovery of the extent and severity of mucus in obstructive lung diseases has led to new strategies to combat mucus overconcentration, such as hydration, mucolytics, and an intriguing investigational approach to decrease calcium-induced hypersecretion with designer peptides.
Mighty mucins
Under normal physiologic conditions mucus is composed largely of water (97%) and salts (2%), with the remainder consisting of entrapped globular proteins (0.7%) and mucins (0.3%), Dr. Dickey explains.
Yet those meager mucins pack a real punch, with the ability to absorb 300 times their mass of water after secretion, creating mucus of optimal consistency and viscoelasticity.
“Personally, I’ve never understood – maybe I should have paid more attention in physics – how a compound can absorb 300-fold its mass, but it does,” he said.
In a recent review article in the journal Clinical and Translational Medicine, Dr. Dickey and colleagues described how good mucus can go bad.
“[H]igh levels of mucin production from inflammatory stimulation (termed ‘mucous metaplasia’), followed by rapid release (together, termed ‘mucus hypersecretion’), can plug airways due to mucus volume expansion. In addition, if available lumenal liquid is insufficient, concentrated mucus of excessive viscoelasticity and adhesivity can cause mucus stasis,” they wrote.
Therapeutic strategies
In patients with CF, CFTR modulator therapy has markedly reduced but not eliminated the need for some patients to have mucolytic therapy, which may include dornase alfa, a recombinant human deoxyribonuclease that reduces the viscosity of lung secretions, hypertonic saline inhaled twice daily (for patients 12 and older), mannitol, and physical manipulations to help patients clear mucus. The manipulations can include both manual percussion and the use of devices for high-frequency chest wall oscillation.
Unlike in CF, where treating the underlying genetic pathology can help to resolve the thick, sticky mucus problems and thereby significantly reduce risk of infections and progressive lung damage, treatment of mucus metaplasia or hypersecretion in other diseases is aimed at symptomatic relief; it is still unclear whether symptomatic improvement of mucus overproduction would correlate with other disease-related outcomes, Dr. Kim and Dr. Dickey noted.
Potential therapeutic strategies to reduce excess mucus in the lungs include the use of mucolytic agents to thin secretions for more effective expulsion, decreasing mucus production through the use of an interleukin-13 (IL-13) inhibitor such as the anti-asthma agent dupilumab (Dupixent), and a novel strategy, still in the experimental phase, aimed at “disrupting the fusion of mucin storage granules with the cell membrane, thereby blocking secretion,” wrote Irina Gitlin, PhD, and John Fahy, MD, from the University of California, San Francisco, in Nature.
They were referring to research by Dr. Dickey and colleagues described in the same issue of Nature focusing on the inhibition of calcium-triggered mucus secretion by the use of hydrocarbon-stapled peptides, short chains of amino acids stabilized with a chemical bridge to a hydrocarbon molecule.
Knocking secretion down, but not out
The work has centered on decreasing overproduction of mucins with a focus on the signals for mucin production, including IL-13 and interleukin-1 beta, and on the signals for rapid release of mucins, including adenosine 5’-triphosphate (ATP), best known as an intracellular energy-storage module.
“But ATP is also steadily released by ciliated cells in response to the shear stress of tidal breathing, and it tells the neighboring secretory cells to slowly and steadily release mucin. But if the ciliated cells get stressed by any of a number of mechanisms, it can release a lot of ATP, and then the secretory cell can explosively release essentially all of its mucin content,” Dr. Dickey explained.
Other important signals for rapid release of mucins are acetylcholine and histamine, and all three of these agonists – ATP, acetylcholine, and histamine – cause a rise in intracellular calcium, which triggers calcium sensors that then lead to calcium-triggered membrane fusion and secretion.
Working as a postdoc in the Dickey laboratory, Dr. Evans had previously shown that deleting MUC5B in mice led to early development of serious lung abnormalities, some of which were fatal, indicating that MUC5B, a gene that is highly preserved in evolution, is essential for respiratory health.
This observation was later supported by a study of a family with a pattern of hereditary mucin deficiency caused by a homozygous loss-of-function mutation in MUC5B. The main subject in this study was an adult woman with unexplained bronchiectasis, impaired pulmonary function, and repeated Staphylococcus aureus infections. Her sibling, who also had the biallelic mutation, had extensive sinus disease with nasal polyps. Other siblings who were heterozygous for the mutation were asymptomatic but had mild functional lung impairment.
The trick for the investigators, then, was to figure out how to reduce stimulated release of stored mucins while still preserving normal release of mucins to allow for ciliary clearance of mucus, and Dr. Dickey and colleagues appear to have accomplished this, at least in mice.
They first validated as a potential therapeutic target a protein labeled synaptotagmin-2 (Syt2). Syt2 is a calcium sensor that is an essential part of the system that triggers calcium-triggered secretion. In a model for allergic asthma, mice with Syt2 deleted from airway epithelia had marked reductions in both stimulated mucin secretion and in mucus occlusion in airway lumens, but remained otherwise healthy with normal lung function.
Working with structural biologist Axel Brunger, PhD, from Stanford (Calif.) University, Dr. Dickey and coinvestigators developed and validated a peptide that could specifically inhibit Syt2, and found that it mimicked the action of the Syt2 deletion, preventing mucus occlusion in the allergic asthma model without adversely effecting normal production.
Not ready for prime time
Dr. Dickey and colleagues are now working to translate the therapy into a form that can be used in humans, most likely as an aerosol that could be used for acute treatment of patients with mucus plugging from asthma and COPD, and also as a therapy for patients with chronic disease.
“In the chronic situation, what we would hope to do is identify patients with muco-obstructive lung disease – asthma, COPD, cystic fibrosis – who have airway mucus obstruction and then use the inhaled peptide on a regular basis as one part of a program to try to prevent this chronic mucus occlusion,” Dr. Dickey said.
As Dr. Gitlin and Dr. Fahy wrote in their editorial, “by confirming that it is possible to block calcium-regulated mucin secretion, Lai and colleagues have shown the potential of such an approach as a new therapeutic strategy for lung illnesses associated with mucus pathology, including diseases such as asthma and COPD, for which there is a large unmet medical need.”
The study by Dr. Dickey and colleagues was supported by grants from the German Research Foundation, National Institutes of Health and the Cystic Fibrosis Foundation. Dr. Dickey disclosed consulting for Arrowhead Pharmaceuticals. Dr. Kim disclosed personal fees from Medscape and others. Dr. Evans reported no relevant disclosures. Dr. Fahy and Dr. Gitlin are named inventors on patents for mucolytic drugs, and shareholders in Aer Therapeutics.
Just uttering the word “mucus” is often sufficient to elicit amusement from those within earshot, but to patients with chronic inflammatory airway diseases, mucus is no laughing matter.
, which are then moved by cilia out of the airways for expulsion through coughing.
But in cystic fibrosis (CF), for example, mucus hypersecretion can be deadly. The underlying pathology of CF – a mutation in the CFTR gene, which codes for the protein CF transmembrane conductance regulator – leads to buildup in the lungs of abnormally viscous and sticky mucus, resulting in frequent, severe infections (particularly with Pseudomonas aeruginosa), progressive lung damage, and prior to the development of effective disease management, significantly premature death.
Mucus hypersecretion is also a feature of chronic obstructive pulmonary disease (COPD), noted Victor Kim, MD, from Temple University, Philadelphia, Christopher M. Evans, PhD, from the University of Colorado at Denver, Aurora, and Burton F. Dickey, MD, from the University of Texas MD Anderson Cancer Center, Houston.
In COPD, “mucus dysfunction arises from several mechanisms, including excess production due to inflammation, decreased elimination due to impaired ciliary clearance and reduced cough efficiency, and excessive concentration due to smoke-induced dysfunction of transepithelial anion transport resembling CF,” they wrote in an editorial published in the American Journal of Respiratory and Critical Care Medicine.
In patients with idiopathic pulmonary fibrosis, a polymorphism in the enhancer region of MUC5B, a gene that encodes for mucin glycoproteins, results in a 20-fold overexpression of the gene and prominent mucus production that has been shown to parallel lung inflammation and decline in forced vital capacity (FVC).
In patients with asthma, up-regulation of MUC5AC and stimulated mucus secretion conspire to obstruct airways, which can in extreme cases lead to death.
‘Short shrift’
Yet until recently, the role of mucus hypersecretion in diseases such as COPD has been largely overlooked, or as Dr. Kim and colleagues put it, “airway mucus often receives short shrift from clinicians.”
“It’s a pretty hot topic in pulmonary medicine today because it has been so neglected for so long,” Dr. Dickey said in an interview with CHEST Physician. “As clinicians we haven’t had a way to identify who needs treatment, which is ridiculous, because many of the people who expectorate a lot, like those with chronic bronchitis, don’t actually have small airway obstruction, and conversely, a lot of asthmatics, who have very serious small airway obstruction, don’t expectorate, so you can’t really tell from symptoms.”
What has changed in recent years is the use of chest CT to image muco-obstructive pathology, commonly called “mucus plugging” in the peripheral airways of patients with COPD and asthma.
“In the last decade or so, we’ve seen the emergence in obstructive lung diseases such as asthma and COPD the use of more objective measures on CT scans, including the problem of mucus plugging, which is unfortunately very common,” Dr. Kim said in an interview.
The discovery of the extent and severity of mucus in obstructive lung diseases has led to new strategies to combat mucus overconcentration, such as hydration, mucolytics, and an intriguing investigational approach to decrease calcium-induced hypersecretion with designer peptides.
Mighty mucins
Under normal physiologic conditions mucus is composed largely of water (97%) and salts (2%), with the remainder consisting of entrapped globular proteins (0.7%) and mucins (0.3%), Dr. Dickey explains.
Yet those meager mucins pack a real punch, with the ability to absorb 300 times their mass of water after secretion, creating mucus of optimal consistency and viscoelasticity.
“Personally, I’ve never understood – maybe I should have paid more attention in physics – how a compound can absorb 300-fold its mass, but it does,” he said.
In a recent review article in the journal Clinical and Translational Medicine, Dr. Dickey and colleagues described how good mucus can go bad.
“[H]igh levels of mucin production from inflammatory stimulation (termed ‘mucous metaplasia’), followed by rapid release (together, termed ‘mucus hypersecretion’), can plug airways due to mucus volume expansion. In addition, if available lumenal liquid is insufficient, concentrated mucus of excessive viscoelasticity and adhesivity can cause mucus stasis,” they wrote.
Therapeutic strategies
In patients with CF, CFTR modulator therapy has markedly reduced but not eliminated the need for some patients to have mucolytic therapy, which may include dornase alfa, a recombinant human deoxyribonuclease that reduces the viscosity of lung secretions, hypertonic saline inhaled twice daily (for patients 12 and older), mannitol, and physical manipulations to help patients clear mucus. The manipulations can include both manual percussion and the use of devices for high-frequency chest wall oscillation.
Unlike in CF, where treating the underlying genetic pathology can help to resolve the thick, sticky mucus problems and thereby significantly reduce risk of infections and progressive lung damage, treatment of mucus metaplasia or hypersecretion in other diseases is aimed at symptomatic relief; it is still unclear whether symptomatic improvement of mucus overproduction would correlate with other disease-related outcomes, Dr. Kim and Dr. Dickey noted.
Potential therapeutic strategies to reduce excess mucus in the lungs include the use of mucolytic agents to thin secretions for more effective expulsion, decreasing mucus production through the use of an interleukin-13 (IL-13) inhibitor such as the anti-asthma agent dupilumab (Dupixent), and a novel strategy, still in the experimental phase, aimed at “disrupting the fusion of mucin storage granules with the cell membrane, thereby blocking secretion,” wrote Irina Gitlin, PhD, and John Fahy, MD, from the University of California, San Francisco, in Nature.
They were referring to research by Dr. Dickey and colleagues described in the same issue of Nature focusing on the inhibition of calcium-triggered mucus secretion by the use of hydrocarbon-stapled peptides, short chains of amino acids stabilized with a chemical bridge to a hydrocarbon molecule.
Knocking secretion down, but not out
The work has centered on decreasing overproduction of mucins with a focus on the signals for mucin production, including IL-13 and interleukin-1 beta, and on the signals for rapid release of mucins, including adenosine 5’-triphosphate (ATP), best known as an intracellular energy-storage module.
“But ATP is also steadily released by ciliated cells in response to the shear stress of tidal breathing, and it tells the neighboring secretory cells to slowly and steadily release mucin. But if the ciliated cells get stressed by any of a number of mechanisms, it can release a lot of ATP, and then the secretory cell can explosively release essentially all of its mucin content,” Dr. Dickey explained.
Other important signals for rapid release of mucins are acetylcholine and histamine, and all three of these agonists – ATP, acetylcholine, and histamine – cause a rise in intracellular calcium, which triggers calcium sensors that then lead to calcium-triggered membrane fusion and secretion.
Working as a postdoc in the Dickey laboratory, Dr. Evans had previously shown that deleting MUC5B in mice led to early development of serious lung abnormalities, some of which were fatal, indicating that MUC5B, a gene that is highly preserved in evolution, is essential for respiratory health.
This observation was later supported by a study of a family with a pattern of hereditary mucin deficiency caused by a homozygous loss-of-function mutation in MUC5B. The main subject in this study was an adult woman with unexplained bronchiectasis, impaired pulmonary function, and repeated Staphylococcus aureus infections. Her sibling, who also had the biallelic mutation, had extensive sinus disease with nasal polyps. Other siblings who were heterozygous for the mutation were asymptomatic but had mild functional lung impairment.
The trick for the investigators, then, was to figure out how to reduce stimulated release of stored mucins while still preserving normal release of mucins to allow for ciliary clearance of mucus, and Dr. Dickey and colleagues appear to have accomplished this, at least in mice.
They first validated as a potential therapeutic target a protein labeled synaptotagmin-2 (Syt2). Syt2 is a calcium sensor that is an essential part of the system that triggers calcium-triggered secretion. In a model for allergic asthma, mice with Syt2 deleted from airway epithelia had marked reductions in both stimulated mucin secretion and in mucus occlusion in airway lumens, but remained otherwise healthy with normal lung function.
Working with structural biologist Axel Brunger, PhD, from Stanford (Calif.) University, Dr. Dickey and coinvestigators developed and validated a peptide that could specifically inhibit Syt2, and found that it mimicked the action of the Syt2 deletion, preventing mucus occlusion in the allergic asthma model without adversely effecting normal production.
Not ready for prime time
Dr. Dickey and colleagues are now working to translate the therapy into a form that can be used in humans, most likely as an aerosol that could be used for acute treatment of patients with mucus plugging from asthma and COPD, and also as a therapy for patients with chronic disease.
“In the chronic situation, what we would hope to do is identify patients with muco-obstructive lung disease – asthma, COPD, cystic fibrosis – who have airway mucus obstruction and then use the inhaled peptide on a regular basis as one part of a program to try to prevent this chronic mucus occlusion,” Dr. Dickey said.
As Dr. Gitlin and Dr. Fahy wrote in their editorial, “by confirming that it is possible to block calcium-regulated mucin secretion, Lai and colleagues have shown the potential of such an approach as a new therapeutic strategy for lung illnesses associated with mucus pathology, including diseases such as asthma and COPD, for which there is a large unmet medical need.”
The study by Dr. Dickey and colleagues was supported by grants from the German Research Foundation, National Institutes of Health and the Cystic Fibrosis Foundation. Dr. Dickey disclosed consulting for Arrowhead Pharmaceuticals. Dr. Kim disclosed personal fees from Medscape and others. Dr. Evans reported no relevant disclosures. Dr. Fahy and Dr. Gitlin are named inventors on patents for mucolytic drugs, and shareholders in Aer Therapeutics.
Just uttering the word “mucus” is often sufficient to elicit amusement from those within earshot, but to patients with chronic inflammatory airway diseases, mucus is no laughing matter.
, which are then moved by cilia out of the airways for expulsion through coughing.
But in cystic fibrosis (CF), for example, mucus hypersecretion can be deadly. The underlying pathology of CF – a mutation in the CFTR gene, which codes for the protein CF transmembrane conductance regulator – leads to buildup in the lungs of abnormally viscous and sticky mucus, resulting in frequent, severe infections (particularly with Pseudomonas aeruginosa), progressive lung damage, and prior to the development of effective disease management, significantly premature death.
Mucus hypersecretion is also a feature of chronic obstructive pulmonary disease (COPD), noted Victor Kim, MD, from Temple University, Philadelphia, Christopher M. Evans, PhD, from the University of Colorado at Denver, Aurora, and Burton F. Dickey, MD, from the University of Texas MD Anderson Cancer Center, Houston.
In COPD, “mucus dysfunction arises from several mechanisms, including excess production due to inflammation, decreased elimination due to impaired ciliary clearance and reduced cough efficiency, and excessive concentration due to smoke-induced dysfunction of transepithelial anion transport resembling CF,” they wrote in an editorial published in the American Journal of Respiratory and Critical Care Medicine.
In patients with idiopathic pulmonary fibrosis, a polymorphism in the enhancer region of MUC5B, a gene that encodes for mucin glycoproteins, results in a 20-fold overexpression of the gene and prominent mucus production that has been shown to parallel lung inflammation and decline in forced vital capacity (FVC).
In patients with asthma, up-regulation of MUC5AC and stimulated mucus secretion conspire to obstruct airways, which can in extreme cases lead to death.
‘Short shrift’
Yet until recently, the role of mucus hypersecretion in diseases such as COPD has been largely overlooked, or as Dr. Kim and colleagues put it, “airway mucus often receives short shrift from clinicians.”
“It’s a pretty hot topic in pulmonary medicine today because it has been so neglected for so long,” Dr. Dickey said in an interview with CHEST Physician. “As clinicians we haven’t had a way to identify who needs treatment, which is ridiculous, because many of the people who expectorate a lot, like those with chronic bronchitis, don’t actually have small airway obstruction, and conversely, a lot of asthmatics, who have very serious small airway obstruction, don’t expectorate, so you can’t really tell from symptoms.”
What has changed in recent years is the use of chest CT to image muco-obstructive pathology, commonly called “mucus plugging” in the peripheral airways of patients with COPD and asthma.
“In the last decade or so, we’ve seen the emergence in obstructive lung diseases such as asthma and COPD the use of more objective measures on CT scans, including the problem of mucus plugging, which is unfortunately very common,” Dr. Kim said in an interview.
The discovery of the extent and severity of mucus in obstructive lung diseases has led to new strategies to combat mucus overconcentration, such as hydration, mucolytics, and an intriguing investigational approach to decrease calcium-induced hypersecretion with designer peptides.
Mighty mucins
Under normal physiologic conditions mucus is composed largely of water (97%) and salts (2%), with the remainder consisting of entrapped globular proteins (0.7%) and mucins (0.3%), Dr. Dickey explains.
Yet those meager mucins pack a real punch, with the ability to absorb 300 times their mass of water after secretion, creating mucus of optimal consistency and viscoelasticity.
“Personally, I’ve never understood – maybe I should have paid more attention in physics – how a compound can absorb 300-fold its mass, but it does,” he said.
In a recent review article in the journal Clinical and Translational Medicine, Dr. Dickey and colleagues described how good mucus can go bad.
“[H]igh levels of mucin production from inflammatory stimulation (termed ‘mucous metaplasia’), followed by rapid release (together, termed ‘mucus hypersecretion’), can plug airways due to mucus volume expansion. In addition, if available lumenal liquid is insufficient, concentrated mucus of excessive viscoelasticity and adhesivity can cause mucus stasis,” they wrote.
Therapeutic strategies
In patients with CF, CFTR modulator therapy has markedly reduced but not eliminated the need for some patients to have mucolytic therapy, which may include dornase alfa, a recombinant human deoxyribonuclease that reduces the viscosity of lung secretions, hypertonic saline inhaled twice daily (for patients 12 and older), mannitol, and physical manipulations to help patients clear mucus. The manipulations can include both manual percussion and the use of devices for high-frequency chest wall oscillation.
Unlike in CF, where treating the underlying genetic pathology can help to resolve the thick, sticky mucus problems and thereby significantly reduce risk of infections and progressive lung damage, treatment of mucus metaplasia or hypersecretion in other diseases is aimed at symptomatic relief; it is still unclear whether symptomatic improvement of mucus overproduction would correlate with other disease-related outcomes, Dr. Kim and Dr. Dickey noted.
Potential therapeutic strategies to reduce excess mucus in the lungs include the use of mucolytic agents to thin secretions for more effective expulsion, decreasing mucus production through the use of an interleukin-13 (IL-13) inhibitor such as the anti-asthma agent dupilumab (Dupixent), and a novel strategy, still in the experimental phase, aimed at “disrupting the fusion of mucin storage granules with the cell membrane, thereby blocking secretion,” wrote Irina Gitlin, PhD, and John Fahy, MD, from the University of California, San Francisco, in Nature.
They were referring to research by Dr. Dickey and colleagues described in the same issue of Nature focusing on the inhibition of calcium-triggered mucus secretion by the use of hydrocarbon-stapled peptides, short chains of amino acids stabilized with a chemical bridge to a hydrocarbon molecule.
Knocking secretion down, but not out
The work has centered on decreasing overproduction of mucins with a focus on the signals for mucin production, including IL-13 and interleukin-1 beta, and on the signals for rapid release of mucins, including adenosine 5’-triphosphate (ATP), best known as an intracellular energy-storage module.
“But ATP is also steadily released by ciliated cells in response to the shear stress of tidal breathing, and it tells the neighboring secretory cells to slowly and steadily release mucin. But if the ciliated cells get stressed by any of a number of mechanisms, it can release a lot of ATP, and then the secretory cell can explosively release essentially all of its mucin content,” Dr. Dickey explained.
Other important signals for rapid release of mucins are acetylcholine and histamine, and all three of these agonists – ATP, acetylcholine, and histamine – cause a rise in intracellular calcium, which triggers calcium sensors that then lead to calcium-triggered membrane fusion and secretion.
Working as a postdoc in the Dickey laboratory, Dr. Evans had previously shown that deleting MUC5B in mice led to early development of serious lung abnormalities, some of which were fatal, indicating that MUC5B, a gene that is highly preserved in evolution, is essential for respiratory health.
This observation was later supported by a study of a family with a pattern of hereditary mucin deficiency caused by a homozygous loss-of-function mutation in MUC5B. The main subject in this study was an adult woman with unexplained bronchiectasis, impaired pulmonary function, and repeated Staphylococcus aureus infections. Her sibling, who also had the biallelic mutation, had extensive sinus disease with nasal polyps. Other siblings who were heterozygous for the mutation were asymptomatic but had mild functional lung impairment.
The trick for the investigators, then, was to figure out how to reduce stimulated release of stored mucins while still preserving normal release of mucins to allow for ciliary clearance of mucus, and Dr. Dickey and colleagues appear to have accomplished this, at least in mice.
They first validated as a potential therapeutic target a protein labeled synaptotagmin-2 (Syt2). Syt2 is a calcium sensor that is an essential part of the system that triggers calcium-triggered secretion. In a model for allergic asthma, mice with Syt2 deleted from airway epithelia had marked reductions in both stimulated mucin secretion and in mucus occlusion in airway lumens, but remained otherwise healthy with normal lung function.
Working with structural biologist Axel Brunger, PhD, from Stanford (Calif.) University, Dr. Dickey and coinvestigators developed and validated a peptide that could specifically inhibit Syt2, and found that it mimicked the action of the Syt2 deletion, preventing mucus occlusion in the allergic asthma model without adversely effecting normal production.
Not ready for prime time
Dr. Dickey and colleagues are now working to translate the therapy into a form that can be used in humans, most likely as an aerosol that could be used for acute treatment of patients with mucus plugging from asthma and COPD, and also as a therapy for patients with chronic disease.
“In the chronic situation, what we would hope to do is identify patients with muco-obstructive lung disease – asthma, COPD, cystic fibrosis – who have airway mucus obstruction and then use the inhaled peptide on a regular basis as one part of a program to try to prevent this chronic mucus occlusion,” Dr. Dickey said.
As Dr. Gitlin and Dr. Fahy wrote in their editorial, “by confirming that it is possible to block calcium-regulated mucin secretion, Lai and colleagues have shown the potential of such an approach as a new therapeutic strategy for lung illnesses associated with mucus pathology, including diseases such as asthma and COPD, for which there is a large unmet medical need.”
The study by Dr. Dickey and colleagues was supported by grants from the German Research Foundation, National Institutes of Health and the Cystic Fibrosis Foundation. Dr. Dickey disclosed consulting for Arrowhead Pharmaceuticals. Dr. Kim disclosed personal fees from Medscape and others. Dr. Evans reported no relevant disclosures. Dr. Fahy and Dr. Gitlin are named inventors on patents for mucolytic drugs, and shareholders in Aer Therapeutics.
VTE prophylaxis overused in low-risk hospitalized patients
A majority of hospitalized patients at low risk for venous thromboembolism were unnecessarily treated with medication, based on data from more than 400 individuals.
Prevention of venous thromboembolism (VTE) is important, and current guidelines from the American College of Chest Physicians suggest that patients with high or moderate risk for VTE be treated with mechanical prophylaxis, and that pharmacological prophylaxis is not recommended for patients at high risk for bleeding, said Hui Chong Lau, MD, in a presentation at the annual meeting of the American College of Chest Physicians (CHEST).
However, the nature of VTE prophylaxis using a risk assessment score has not been explored, said Dr. Lau, a third-year resident in internal medicine at Crozer-Chester Medical Center, Upland, Penn.
Low-molecular-weight heparin (LWMH) and intermittent pneumatic compression are often used to reduce VTE risk during hospitalization, but for patients with low VTE risk, prophylaxis is not necessarily recommended, he said. In fact, overuse of chemical prophylaxis in low-risk patients can increase bleeding risk and contribute to patient discomfort in the form of additional needle sticks while hospitalized, Dr. Lau said in the presentation.
“We wanted to see how well physicians in the hospital used a risk assessment model to stratify patients,” and how well the patients were assigned to the correct prophylaxis, he explained.
Dr. Lau and colleagues reviewed data from 469 adult patients hospitalized at a single medical center who were hospitalized between January 2021 and June 2021. The researchers retrospectively performed risk assessment using the Padua prediction score. A score of less than 4 was considered low risk for VTE, and a score of 4 or higher was considered high risk.
In the study population, 180 patients were identified as low risk and 289 were considered high risk.
Based on the Padua score, 95% of the patients at high risk were on the correct prophylaxis, Dr. Lau said.
A total of 193 high-risk patients were on heparin. However, many of these patients had good kidney function, and could have been treated with enoxaparin instead; “this would have spared them two needle sticks per day,” Dr. Lau noted.
Of the 180 low-risk patients, 168 (93.3%) were on chemical prophylaxis, and should have been on mechanical prophylaxis, he said. Only 10 patients (5%) who were considered low risk were placed on mechanical prophylaxis.
Overall, 3.6% of all patients who received chemical VTE prophylaxis developed bleeding.
The results were limited by the retrospective design and use of data from a single center. However, the findings emphasize the need for better attention to VTE risk when considering prophylaxis, said Dr. Lau. “We have to have risk assessment every day,” during a hospital stay, and adjust treatment accordingly, he said.
he concluded.
Additional research is needed to better understand the potential consequences of overusing chemical VTE, including not only bleeding risk, but also financial costs and patient discomfort, he said.
The study received no outside funding. The researchers had no financial conflicts to disclose.
A majority of hospitalized patients at low risk for venous thromboembolism were unnecessarily treated with medication, based on data from more than 400 individuals.
Prevention of venous thromboembolism (VTE) is important, and current guidelines from the American College of Chest Physicians suggest that patients with high or moderate risk for VTE be treated with mechanical prophylaxis, and that pharmacological prophylaxis is not recommended for patients at high risk for bleeding, said Hui Chong Lau, MD, in a presentation at the annual meeting of the American College of Chest Physicians (CHEST).
However, the nature of VTE prophylaxis using a risk assessment score has not been explored, said Dr. Lau, a third-year resident in internal medicine at Crozer-Chester Medical Center, Upland, Penn.
Low-molecular-weight heparin (LWMH) and intermittent pneumatic compression are often used to reduce VTE risk during hospitalization, but for patients with low VTE risk, prophylaxis is not necessarily recommended, he said. In fact, overuse of chemical prophylaxis in low-risk patients can increase bleeding risk and contribute to patient discomfort in the form of additional needle sticks while hospitalized, Dr. Lau said in the presentation.
“We wanted to see how well physicians in the hospital used a risk assessment model to stratify patients,” and how well the patients were assigned to the correct prophylaxis, he explained.
Dr. Lau and colleagues reviewed data from 469 adult patients hospitalized at a single medical center who were hospitalized between January 2021 and June 2021. The researchers retrospectively performed risk assessment using the Padua prediction score. A score of less than 4 was considered low risk for VTE, and a score of 4 or higher was considered high risk.
In the study population, 180 patients were identified as low risk and 289 were considered high risk.
Based on the Padua score, 95% of the patients at high risk were on the correct prophylaxis, Dr. Lau said.
A total of 193 high-risk patients were on heparin. However, many of these patients had good kidney function, and could have been treated with enoxaparin instead; “this would have spared them two needle sticks per day,” Dr. Lau noted.
Of the 180 low-risk patients, 168 (93.3%) were on chemical prophylaxis, and should have been on mechanical prophylaxis, he said. Only 10 patients (5%) who were considered low risk were placed on mechanical prophylaxis.
Overall, 3.6% of all patients who received chemical VTE prophylaxis developed bleeding.
The results were limited by the retrospective design and use of data from a single center. However, the findings emphasize the need for better attention to VTE risk when considering prophylaxis, said Dr. Lau. “We have to have risk assessment every day,” during a hospital stay, and adjust treatment accordingly, he said.
he concluded.
Additional research is needed to better understand the potential consequences of overusing chemical VTE, including not only bleeding risk, but also financial costs and patient discomfort, he said.
The study received no outside funding. The researchers had no financial conflicts to disclose.
A majority of hospitalized patients at low risk for venous thromboembolism were unnecessarily treated with medication, based on data from more than 400 individuals.
Prevention of venous thromboembolism (VTE) is important, and current guidelines from the American College of Chest Physicians suggest that patients with high or moderate risk for VTE be treated with mechanical prophylaxis, and that pharmacological prophylaxis is not recommended for patients at high risk for bleeding, said Hui Chong Lau, MD, in a presentation at the annual meeting of the American College of Chest Physicians (CHEST).
However, the nature of VTE prophylaxis using a risk assessment score has not been explored, said Dr. Lau, a third-year resident in internal medicine at Crozer-Chester Medical Center, Upland, Penn.
Low-molecular-weight heparin (LWMH) and intermittent pneumatic compression are often used to reduce VTE risk during hospitalization, but for patients with low VTE risk, prophylaxis is not necessarily recommended, he said. In fact, overuse of chemical prophylaxis in low-risk patients can increase bleeding risk and contribute to patient discomfort in the form of additional needle sticks while hospitalized, Dr. Lau said in the presentation.
“We wanted to see how well physicians in the hospital used a risk assessment model to stratify patients,” and how well the patients were assigned to the correct prophylaxis, he explained.
Dr. Lau and colleagues reviewed data from 469 adult patients hospitalized at a single medical center who were hospitalized between January 2021 and June 2021. The researchers retrospectively performed risk assessment using the Padua prediction score. A score of less than 4 was considered low risk for VTE, and a score of 4 or higher was considered high risk.
In the study population, 180 patients were identified as low risk and 289 were considered high risk.
Based on the Padua score, 95% of the patients at high risk were on the correct prophylaxis, Dr. Lau said.
A total of 193 high-risk patients were on heparin. However, many of these patients had good kidney function, and could have been treated with enoxaparin instead; “this would have spared them two needle sticks per day,” Dr. Lau noted.
Of the 180 low-risk patients, 168 (93.3%) were on chemical prophylaxis, and should have been on mechanical prophylaxis, he said. Only 10 patients (5%) who were considered low risk were placed on mechanical prophylaxis.
Overall, 3.6% of all patients who received chemical VTE prophylaxis developed bleeding.
The results were limited by the retrospective design and use of data from a single center. However, the findings emphasize the need for better attention to VTE risk when considering prophylaxis, said Dr. Lau. “We have to have risk assessment every day,” during a hospital stay, and adjust treatment accordingly, he said.
he concluded.
Additional research is needed to better understand the potential consequences of overusing chemical VTE, including not only bleeding risk, but also financial costs and patient discomfort, he said.
The study received no outside funding. The researchers had no financial conflicts to disclose.
FROM CHEST 2022
Large trial of home-based COPD rehab shows positive results
NASHVILLE – The first multicenter randomized controlled trial of a home-based rehabilitation program for patients with chronic obstructive pulmonary disease (COPD) showed highly positive results, according to findings presented at the annual meeting of the American College of Chest Physicians (CHEST).
At the end of 12 weeks, those randomly assigned to the intervention had a significant and clinically meaningful improvement in all domains of the Chronic Respiratory Questionnaire (CRQ), including activity levels and emotional well-being, reported Roberto P. Benzo, MD, a consultant in the division of pulmonary and critical care medicine, Mayo Clinic, Rochester, Minn.
Presenting soon-to-be-published data, Dr. Benzo said that the intervention is based on a tablet-based app. The tablet is programmed to upload data captured from an activity monitor and pulse oximeter. Along with documentation of app usage, this information can then be downloaded for the remote coach to review with the patient.
The primary outcome of the randomized study were the physical and emotional domains of the CRQ quality of life, but a long list of secondary outcomes – including physical activity, symptoms of depression, sleep quality, and health care utilization, such as emergency room visits – was also analyzed.
In addition to the significant benefit on the primary outcomes, the home-based rehabilitation program relative to a wait list for intervention was associated with benefit or a trend for benefit on essentially every outcome measured. Health care utilization was a possible exception, but even then, the absolute number of visits was lower in the treatment arm.
“With a study period of only 12 weeks, we were limited to our ability to show a difference in emergency room visits,” said Dr. Benzo, who also noted that the study was conducted during the COVID-19 pandemic, when hospital visits were already occurring at a lower than usual rate. Based on the other findings, he suspects that a reduction in health care utilization could also be shown in more typical circumstances, particularly with a longer follow-up.
In the study, 375 patients with COPD were randomly assigned to a home health care regimen delivered by an app with remote coaching or to a wait list and usual care. The median age was 69 years. Fifty-nine percent were women. The median FEV1 at enrollment was 45% of predicted.
The patients were able to access their own data to monitor their progress at any time, not just at the time of coaching, but contact with the remote coach occurred on a weekly basis. Patients rated their level of energy, how they felt generally, and their progress toward daily goals, which was also captured on the app and could be discussed with the coach during the review of the previous week’s activity.
At 12 weeks, the favorable 0.54-point change (P < .001) and 0.51 change (P < .001) in the physical and emotional summary scores, respectively, met the criteria for a clinically meaningful change, Dr. Benzo reported. There were also significantly favorable changes from baseline and relative to controls in CRQ domains of self-management, sleep quality, and depression (all P ≤ .01).
Other data collected are supportive. For example, Dr. Benzo reported that those in the rehabilitation group took 624 more steps on average per day than those in the control group. The experimental group also spent nearly an hour more performing moderate or greater levels of activity.
“The app promotes behavioral change,” said Dr. Benzo, who said that this “completely home-based model” of rehabilitation is likely to be cost-effective given the relatively low costs of remote coaching and reasonable costs of the activity monitor, tablet, and other equipment.
Importantly, home-based rehabilitation is a billable practice under currently available CPT codes, according to Dr. Benzo, who believes this approach is not only effective but “feasible and practical.”
Two clinicians active in the care of patients with COPD believe this approach could fulfill an unmet need if further validated. Andrew Berman, MD, professor of medicine, New Jersey Medical School, Newark, thinks the premise is sound.
“Digital competency is still a big issue as is access to adequate quality Internet, but this could be a very useful approach for many individuals, and it avoids visits to a center, which could be a big advantage for patients,” Dr. Berman said.
Abebaw M. Johannes, PhD, a professor of physical therapy at Azusa Pacific University, Azusa, Calif., agreed. He said that home-based remote coaching could be a way of overcoming the current hurdles of participating in institutional-based programs
“This is clearly an unmet need in COPD,” he said.
The development of more effective and patient-friendly programs is what was driving this research, according to Dr. Benzo. He cited data suggesting that only about 30% of patients with COPD are participating in rehabilitation programs once discharged from the hospital despite the evidence that they can improve quality of life. For many of these patients, a home-based program might be the answer.
Dr. Benzo, Dr. Berman, and Dr. Johannes reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
NASHVILLE – The first multicenter randomized controlled trial of a home-based rehabilitation program for patients with chronic obstructive pulmonary disease (COPD) showed highly positive results, according to findings presented at the annual meeting of the American College of Chest Physicians (CHEST).
At the end of 12 weeks, those randomly assigned to the intervention had a significant and clinically meaningful improvement in all domains of the Chronic Respiratory Questionnaire (CRQ), including activity levels and emotional well-being, reported Roberto P. Benzo, MD, a consultant in the division of pulmonary and critical care medicine, Mayo Clinic, Rochester, Minn.
Presenting soon-to-be-published data, Dr. Benzo said that the intervention is based on a tablet-based app. The tablet is programmed to upload data captured from an activity monitor and pulse oximeter. Along with documentation of app usage, this information can then be downloaded for the remote coach to review with the patient.
The primary outcome of the randomized study were the physical and emotional domains of the CRQ quality of life, but a long list of secondary outcomes – including physical activity, symptoms of depression, sleep quality, and health care utilization, such as emergency room visits – was also analyzed.
In addition to the significant benefit on the primary outcomes, the home-based rehabilitation program relative to a wait list for intervention was associated with benefit or a trend for benefit on essentially every outcome measured. Health care utilization was a possible exception, but even then, the absolute number of visits was lower in the treatment arm.
“With a study period of only 12 weeks, we were limited to our ability to show a difference in emergency room visits,” said Dr. Benzo, who also noted that the study was conducted during the COVID-19 pandemic, when hospital visits were already occurring at a lower than usual rate. Based on the other findings, he suspects that a reduction in health care utilization could also be shown in more typical circumstances, particularly with a longer follow-up.
In the study, 375 patients with COPD were randomly assigned to a home health care regimen delivered by an app with remote coaching or to a wait list and usual care. The median age was 69 years. Fifty-nine percent were women. The median FEV1 at enrollment was 45% of predicted.
The patients were able to access their own data to monitor their progress at any time, not just at the time of coaching, but contact with the remote coach occurred on a weekly basis. Patients rated their level of energy, how they felt generally, and their progress toward daily goals, which was also captured on the app and could be discussed with the coach during the review of the previous week’s activity.
At 12 weeks, the favorable 0.54-point change (P < .001) and 0.51 change (P < .001) in the physical and emotional summary scores, respectively, met the criteria for a clinically meaningful change, Dr. Benzo reported. There were also significantly favorable changes from baseline and relative to controls in CRQ domains of self-management, sleep quality, and depression (all P ≤ .01).
Other data collected are supportive. For example, Dr. Benzo reported that those in the rehabilitation group took 624 more steps on average per day than those in the control group. The experimental group also spent nearly an hour more performing moderate or greater levels of activity.
“The app promotes behavioral change,” said Dr. Benzo, who said that this “completely home-based model” of rehabilitation is likely to be cost-effective given the relatively low costs of remote coaching and reasonable costs of the activity monitor, tablet, and other equipment.
Importantly, home-based rehabilitation is a billable practice under currently available CPT codes, according to Dr. Benzo, who believes this approach is not only effective but “feasible and practical.”
Two clinicians active in the care of patients with COPD believe this approach could fulfill an unmet need if further validated. Andrew Berman, MD, professor of medicine, New Jersey Medical School, Newark, thinks the premise is sound.
“Digital competency is still a big issue as is access to adequate quality Internet, but this could be a very useful approach for many individuals, and it avoids visits to a center, which could be a big advantage for patients,” Dr. Berman said.
Abebaw M. Johannes, PhD, a professor of physical therapy at Azusa Pacific University, Azusa, Calif., agreed. He said that home-based remote coaching could be a way of overcoming the current hurdles of participating in institutional-based programs
“This is clearly an unmet need in COPD,” he said.
The development of more effective and patient-friendly programs is what was driving this research, according to Dr. Benzo. He cited data suggesting that only about 30% of patients with COPD are participating in rehabilitation programs once discharged from the hospital despite the evidence that they can improve quality of life. For many of these patients, a home-based program might be the answer.
Dr. Benzo, Dr. Berman, and Dr. Johannes reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
NASHVILLE – The first multicenter randomized controlled trial of a home-based rehabilitation program for patients with chronic obstructive pulmonary disease (COPD) showed highly positive results, according to findings presented at the annual meeting of the American College of Chest Physicians (CHEST).
At the end of 12 weeks, those randomly assigned to the intervention had a significant and clinically meaningful improvement in all domains of the Chronic Respiratory Questionnaire (CRQ), including activity levels and emotional well-being, reported Roberto P. Benzo, MD, a consultant in the division of pulmonary and critical care medicine, Mayo Clinic, Rochester, Minn.
Presenting soon-to-be-published data, Dr. Benzo said that the intervention is based on a tablet-based app. The tablet is programmed to upload data captured from an activity monitor and pulse oximeter. Along with documentation of app usage, this information can then be downloaded for the remote coach to review with the patient.
The primary outcome of the randomized study were the physical and emotional domains of the CRQ quality of life, but a long list of secondary outcomes – including physical activity, symptoms of depression, sleep quality, and health care utilization, such as emergency room visits – was also analyzed.
In addition to the significant benefit on the primary outcomes, the home-based rehabilitation program relative to a wait list for intervention was associated with benefit or a trend for benefit on essentially every outcome measured. Health care utilization was a possible exception, but even then, the absolute number of visits was lower in the treatment arm.
“With a study period of only 12 weeks, we were limited to our ability to show a difference in emergency room visits,” said Dr. Benzo, who also noted that the study was conducted during the COVID-19 pandemic, when hospital visits were already occurring at a lower than usual rate. Based on the other findings, he suspects that a reduction in health care utilization could also be shown in more typical circumstances, particularly with a longer follow-up.
In the study, 375 patients with COPD were randomly assigned to a home health care regimen delivered by an app with remote coaching or to a wait list and usual care. The median age was 69 years. Fifty-nine percent were women. The median FEV1 at enrollment was 45% of predicted.
The patients were able to access their own data to monitor their progress at any time, not just at the time of coaching, but contact with the remote coach occurred on a weekly basis. Patients rated their level of energy, how they felt generally, and their progress toward daily goals, which was also captured on the app and could be discussed with the coach during the review of the previous week’s activity.
At 12 weeks, the favorable 0.54-point change (P < .001) and 0.51 change (P < .001) in the physical and emotional summary scores, respectively, met the criteria for a clinically meaningful change, Dr. Benzo reported. There were also significantly favorable changes from baseline and relative to controls in CRQ domains of self-management, sleep quality, and depression (all P ≤ .01).
Other data collected are supportive. For example, Dr. Benzo reported that those in the rehabilitation group took 624 more steps on average per day than those in the control group. The experimental group also spent nearly an hour more performing moderate or greater levels of activity.
“The app promotes behavioral change,” said Dr. Benzo, who said that this “completely home-based model” of rehabilitation is likely to be cost-effective given the relatively low costs of remote coaching and reasonable costs of the activity monitor, tablet, and other equipment.
Importantly, home-based rehabilitation is a billable practice under currently available CPT codes, according to Dr. Benzo, who believes this approach is not only effective but “feasible and practical.”
Two clinicians active in the care of patients with COPD believe this approach could fulfill an unmet need if further validated. Andrew Berman, MD, professor of medicine, New Jersey Medical School, Newark, thinks the premise is sound.
“Digital competency is still a big issue as is access to adequate quality Internet, but this could be a very useful approach for many individuals, and it avoids visits to a center, which could be a big advantage for patients,” Dr. Berman said.
Abebaw M. Johannes, PhD, a professor of physical therapy at Azusa Pacific University, Azusa, Calif., agreed. He said that home-based remote coaching could be a way of overcoming the current hurdles of participating in institutional-based programs
“This is clearly an unmet need in COPD,” he said.
The development of more effective and patient-friendly programs is what was driving this research, according to Dr. Benzo. He cited data suggesting that only about 30% of patients with COPD are participating in rehabilitation programs once discharged from the hospital despite the evidence that they can improve quality of life. For many of these patients, a home-based program might be the answer.
Dr. Benzo, Dr. Berman, and Dr. Johannes reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CHEST 2022
You and the skeptical patient: Who’s the doctor here?
“I spoke to him on many occasions about the dangers of COVID, but he just didn’t believe me,” said Dr. Hood, an internist in Lexington, Ky. “He just didn’t give me enough time to help him. He waited to let me know he was ill with COVID and took days to pick up the medicine. Unfortunately, he then passed away.”
The rise of the skeptical patient
It can be extremely frustrating for doctors when patients question or disbelieve their physician’s medical advice and explanations. And many physicians resent the amount of time they spend trying to explain or make their case, especially during a busy day. But patients’ skepticism about the validity of some treatments seems to be increasing.
“Patients are now more likely to have their own medical explanation for their complaint than they used to, and that can be bad for their health,” Dr. Hood said.
Dr. Hood sees medical cynicism as part of Americans’ growing distrust of experts, leveraged by easy access to the internet. “When people Google, they tend to look for support of their opinions, rather than arrive at a fully educated decision.”
Only about half of patients believe their physicians “provide fair and accurate treatment information all or most of the time,” according to a 2019 survey by the Pew Research Center.
Patients’ distrust has become more obvious during the COVID-19 pandemic, said John Schumann, MD, an internist with Oak Street Health, a practice with more than 500 physicians and other providers in 20 states, treating almost exclusively Medicare patients.
“The skeptics became more entrenched during the pandemic,” said Dr. Schumann, who is based in Tulsa, Okla. “They may think the COVID vaccines were approved too quickly, or believe the pandemic itself is a hoax.”
“There’s a lot of antiscience rhetoric now,” Dr. Schumann added. “I’d say about half of my patients are comfortable with science-based decisions and the other half are not.”
What are patients mistrustful about?
Patients’ suspicions of certain therapies began long before the pandemic. In dermatology, for example, some patients refuse to take topical steroids, said Steven R. Feldman, MD, a dermatologist in Winston-Salem, N.C.
“Their distrust is usually based on anecdotal stories they read about,” he noted. “Patients in other specialties are dead set against vaccinations.”
In addition to refusing treatments and inoculations, some patients ask for questionable regimens mentioned in the news. “Some patients have demanded hydroxychloroquine or Noromectin, drugs that are unproven in the treatment of COVID,” Dr. Schumann said. “We refuse to prescribe them.”
Dr. Hood said patients’ reluctance to follow medical advice can often be based on cost. “I have a patient who was more willing to save $20 than to save his life. But when the progression of his test results fit my predictions, he became more willing to take treatments. I had to wait for the opportune moment to convince him.”
Many naysayer patients keep their views to themselves, and physicians may be unaware that the patients are stonewalling. A 2006 study estimated that about 10%-16% of primary care patients actively resist medical authority.
Dr. Schumann cited patients who don’t want to hear an upsetting diagnosis. “Some patients might refuse to take a biopsy to see if they have cancer because they don’t want to know,” he said. “In many cases, they simply won’t get the biopsy and won’t tell the doctor that they didn’t.”
Sometimes skeptics’ arguments have merit
Some patients’ concerns can be valid, such as when they refuse to go on statins, said Zain Hakeem, DO, a physician in Austin, Tex.
“In some cases, I feel that statins are not necessary,” he said. “The science on statins for primary prevention is not strong, although they should be used for exceedingly high-risk patients.”
Certain patients, especially those with chronic conditions, do a great deal of research, using legitimate sources on the Web, and their research is well supported.
However, these patients can be overconfident in their conclusions. Several studies have shown that with just a little experience, people can replace beginners’ caution with a false sense of competence.
For example, “Patients may not weigh the risks correctly,” Dr. Hakeem said. “They can be more concerned about the risk of having their colon perforated during a colonoscopy, while the risk of cancer if they don’t have a colonoscopy is much higher.”
Some highly successful people may be more likely to trust their own medical instincts. When Steve Jobs, the founder of Apple, was diagnosed with pancreatic cancer in 2003, he put off surgery for 9 months while he tried to cure his disease with a vegan diet, acupuncture, herbs, bowel cleansings, and other remedies he read about. He died in 2011. Some experts believe that delay hastened his death.
Of course, not all physicians’ diagnoses or treatments are correct. One study indicated doctors’ diagnostic error rate could be as high as 15%. And just as patients can be overconfident in their conclusions, so can doctors. Another study found that physicians’ stated confidence in their diagnosis was only slightly affected by the inaccuracy of that diagnosis or the difficulty of the case.
Best ways to deal with cynical patients
Patients’ skepticism can frustrate doctors, reduce the efficiency of care delivery, and interfere with recovery. What can doctors do to deal with these problems?
1. Build the patient’s trust in you. “Getting patients to adhere to your advice involves making sure they feel they have a caring doctor whom they trust,” Dr. Feldman said.
“I want to show patients that I am entirely focused on them,” he added. “For example, I may rush to the door of the exam room from my last appointment, but I open the door very slowly and deliberately, because I want the patient to see that I won’t hurry with them.”
2. Spend time with the patient. Familiarity builds trust. Dr. Schumann said doctors at Oak Street Health see their patients an average of six to eight times a year, an unusually high number. “The more patients see their physicians, the more likely they are to trust them.”
3. Keep up to date. “I make sure I’m up to date with the literature, and I try to present a truthful message,” Dr. Hood said. “For instance, my research showed that inflammation played a strong role in developing complications from COVID, so I wrote a detailed treatment protocol aimed at the inflammation and the immune response, which has been very effective.”
4. Confront patients tactfully. Patients who do research on the Web don’t want to be scolded, Dr. Feldman said. In fact, he praises them, even if he doesn’t agree with their findings. “I might say: ‘What a relief to finally find patients who’ve taken the time to educate themselves before coming here.’ ”
Dr. Feldman is careful not to dispute patients’ conclusions. “Debating the issues is not an effective approach to get patients to trust you. The last thing you want to tell a patient is: ‘Listen to me! I’m an expert.’ People just dig in.”
However, it does help to give patients feedback. “I’m a big fan of patients arguing with me,” Dr. Hakeem said. “It means you can straighten out misunderstandings and improve decision-making.”
5. Explain your reasoning. “You need to communicate clearly and show them your thinking,” Dr. Hood said. “For instance, I’ll explain why a patient has a strong risk for heart attack.”
6. Acknowledge uncertainties. “The doctor may present the science as far more certain than it is,” Dr. Hakeem said. “If you don’t acknowledge the uncertainties, you could break the patient’s trust in you.”
7. Don’t use a lot of numbers. “Data is not a good tool to convince patients,” Dr. Feldman said. “The human brain isn’t designed to work that way.”
If you want to use numbers to show clinical risk, Dr. Hakeem advisd using natural frequencies, such as 10 out of 10,000, which is less confusing to the patient than the equivalent percentage of 0.1%.
It can be helpful to refer to familiar concepts. One way to understand a risk is to compare it with risks in daily life, such as the dangers of driving or falling in the shower, Dr. Hakeem added.
Dr. Feldman often refers to another person’s experience when presenting his medical advice. “I might say to the patient: ‘You remind me of another patient I had. They were sitting in the same chair you’re sitting in. They did really well on this drug, and I think it’s probably the best choice for you, too.’ ”
8. Adopt shared decision-making. This approach involves empowering the patient to become an equal partner in medical decisions. The patient is given information through portals and is encouraged to do research. Critics, however, say that most patients don’t want this degree of empowerment and would rather depend on the doctor’s advice.
Conclusion
It’s often impossible to get through to a skeptical patient, which can be disheartening for doctors. “Physicians want to do what is best for the patient, so when the patient doesn’t listen, they may take it personally,” Dr. Hood said. “But you always have to remember, the patient is the one with disease, and it’s up to the patient to open the door.”
Still, some skeptical patients ultimately change their minds. Dr. Schumann said patients who initially declined the COVID vaccine eventually decided to get it. “It often took them more than a year. but it’s never too late.”
A version of this article first appeared on Medscape.com.
“I spoke to him on many occasions about the dangers of COVID, but he just didn’t believe me,” said Dr. Hood, an internist in Lexington, Ky. “He just didn’t give me enough time to help him. He waited to let me know he was ill with COVID and took days to pick up the medicine. Unfortunately, he then passed away.”
The rise of the skeptical patient
It can be extremely frustrating for doctors when patients question or disbelieve their physician’s medical advice and explanations. And many physicians resent the amount of time they spend trying to explain or make their case, especially during a busy day. But patients’ skepticism about the validity of some treatments seems to be increasing.
“Patients are now more likely to have their own medical explanation for their complaint than they used to, and that can be bad for their health,” Dr. Hood said.
Dr. Hood sees medical cynicism as part of Americans’ growing distrust of experts, leveraged by easy access to the internet. “When people Google, they tend to look for support of their opinions, rather than arrive at a fully educated decision.”
Only about half of patients believe their physicians “provide fair and accurate treatment information all or most of the time,” according to a 2019 survey by the Pew Research Center.
Patients’ distrust has become more obvious during the COVID-19 pandemic, said John Schumann, MD, an internist with Oak Street Health, a practice with more than 500 physicians and other providers in 20 states, treating almost exclusively Medicare patients.
“The skeptics became more entrenched during the pandemic,” said Dr. Schumann, who is based in Tulsa, Okla. “They may think the COVID vaccines were approved too quickly, or believe the pandemic itself is a hoax.”
“There’s a lot of antiscience rhetoric now,” Dr. Schumann added. “I’d say about half of my patients are comfortable with science-based decisions and the other half are not.”
What are patients mistrustful about?
Patients’ suspicions of certain therapies began long before the pandemic. In dermatology, for example, some patients refuse to take topical steroids, said Steven R. Feldman, MD, a dermatologist in Winston-Salem, N.C.
“Their distrust is usually based on anecdotal stories they read about,” he noted. “Patients in other specialties are dead set against vaccinations.”
In addition to refusing treatments and inoculations, some patients ask for questionable regimens mentioned in the news. “Some patients have demanded hydroxychloroquine or Noromectin, drugs that are unproven in the treatment of COVID,” Dr. Schumann said. “We refuse to prescribe them.”
Dr. Hood said patients’ reluctance to follow medical advice can often be based on cost. “I have a patient who was more willing to save $20 than to save his life. But when the progression of his test results fit my predictions, he became more willing to take treatments. I had to wait for the opportune moment to convince him.”
Many naysayer patients keep their views to themselves, and physicians may be unaware that the patients are stonewalling. A 2006 study estimated that about 10%-16% of primary care patients actively resist medical authority.
Dr. Schumann cited patients who don’t want to hear an upsetting diagnosis. “Some patients might refuse to take a biopsy to see if they have cancer because they don’t want to know,” he said. “In many cases, they simply won’t get the biopsy and won’t tell the doctor that they didn’t.”
Sometimes skeptics’ arguments have merit
Some patients’ concerns can be valid, such as when they refuse to go on statins, said Zain Hakeem, DO, a physician in Austin, Tex.
“In some cases, I feel that statins are not necessary,” he said. “The science on statins for primary prevention is not strong, although they should be used for exceedingly high-risk patients.”
Certain patients, especially those with chronic conditions, do a great deal of research, using legitimate sources on the Web, and their research is well supported.
However, these patients can be overconfident in their conclusions. Several studies have shown that with just a little experience, people can replace beginners’ caution with a false sense of competence.
For example, “Patients may not weigh the risks correctly,” Dr. Hakeem said. “They can be more concerned about the risk of having their colon perforated during a colonoscopy, while the risk of cancer if they don’t have a colonoscopy is much higher.”
Some highly successful people may be more likely to trust their own medical instincts. When Steve Jobs, the founder of Apple, was diagnosed with pancreatic cancer in 2003, he put off surgery for 9 months while he tried to cure his disease with a vegan diet, acupuncture, herbs, bowel cleansings, and other remedies he read about. He died in 2011. Some experts believe that delay hastened his death.
Of course, not all physicians’ diagnoses or treatments are correct. One study indicated doctors’ diagnostic error rate could be as high as 15%. And just as patients can be overconfident in their conclusions, so can doctors. Another study found that physicians’ stated confidence in their diagnosis was only slightly affected by the inaccuracy of that diagnosis or the difficulty of the case.
Best ways to deal with cynical patients
Patients’ skepticism can frustrate doctors, reduce the efficiency of care delivery, and interfere with recovery. What can doctors do to deal with these problems?
1. Build the patient’s trust in you. “Getting patients to adhere to your advice involves making sure they feel they have a caring doctor whom they trust,” Dr. Feldman said.
“I want to show patients that I am entirely focused on them,” he added. “For example, I may rush to the door of the exam room from my last appointment, but I open the door very slowly and deliberately, because I want the patient to see that I won’t hurry with them.”
2. Spend time with the patient. Familiarity builds trust. Dr. Schumann said doctors at Oak Street Health see their patients an average of six to eight times a year, an unusually high number. “The more patients see their physicians, the more likely they are to trust them.”
3. Keep up to date. “I make sure I’m up to date with the literature, and I try to present a truthful message,” Dr. Hood said. “For instance, my research showed that inflammation played a strong role in developing complications from COVID, so I wrote a detailed treatment protocol aimed at the inflammation and the immune response, which has been very effective.”
4. Confront patients tactfully. Patients who do research on the Web don’t want to be scolded, Dr. Feldman said. In fact, he praises them, even if he doesn’t agree with their findings. “I might say: ‘What a relief to finally find patients who’ve taken the time to educate themselves before coming here.’ ”
Dr. Feldman is careful not to dispute patients’ conclusions. “Debating the issues is not an effective approach to get patients to trust you. The last thing you want to tell a patient is: ‘Listen to me! I’m an expert.’ People just dig in.”
However, it does help to give patients feedback. “I’m a big fan of patients arguing with me,” Dr. Hakeem said. “It means you can straighten out misunderstandings and improve decision-making.”
5. Explain your reasoning. “You need to communicate clearly and show them your thinking,” Dr. Hood said. “For instance, I’ll explain why a patient has a strong risk for heart attack.”
6. Acknowledge uncertainties. “The doctor may present the science as far more certain than it is,” Dr. Hakeem said. “If you don’t acknowledge the uncertainties, you could break the patient’s trust in you.”
7. Don’t use a lot of numbers. “Data is not a good tool to convince patients,” Dr. Feldman said. “The human brain isn’t designed to work that way.”
If you want to use numbers to show clinical risk, Dr. Hakeem advisd using natural frequencies, such as 10 out of 10,000, which is less confusing to the patient than the equivalent percentage of 0.1%.
It can be helpful to refer to familiar concepts. One way to understand a risk is to compare it with risks in daily life, such as the dangers of driving or falling in the shower, Dr. Hakeem added.
Dr. Feldman often refers to another person’s experience when presenting his medical advice. “I might say to the patient: ‘You remind me of another patient I had. They were sitting in the same chair you’re sitting in. They did really well on this drug, and I think it’s probably the best choice for you, too.’ ”
8. Adopt shared decision-making. This approach involves empowering the patient to become an equal partner in medical decisions. The patient is given information through portals and is encouraged to do research. Critics, however, say that most patients don’t want this degree of empowerment and would rather depend on the doctor’s advice.
Conclusion
It’s often impossible to get through to a skeptical patient, which can be disheartening for doctors. “Physicians want to do what is best for the patient, so when the patient doesn’t listen, they may take it personally,” Dr. Hood said. “But you always have to remember, the patient is the one with disease, and it’s up to the patient to open the door.”
Still, some skeptical patients ultimately change their minds. Dr. Schumann said patients who initially declined the COVID vaccine eventually decided to get it. “It often took them more than a year. but it’s never too late.”
A version of this article first appeared on Medscape.com.
“I spoke to him on many occasions about the dangers of COVID, but he just didn’t believe me,” said Dr. Hood, an internist in Lexington, Ky. “He just didn’t give me enough time to help him. He waited to let me know he was ill with COVID and took days to pick up the medicine. Unfortunately, he then passed away.”
The rise of the skeptical patient
It can be extremely frustrating for doctors when patients question or disbelieve their physician’s medical advice and explanations. And many physicians resent the amount of time they spend trying to explain or make their case, especially during a busy day. But patients’ skepticism about the validity of some treatments seems to be increasing.
“Patients are now more likely to have their own medical explanation for their complaint than they used to, and that can be bad for their health,” Dr. Hood said.
Dr. Hood sees medical cynicism as part of Americans’ growing distrust of experts, leveraged by easy access to the internet. “When people Google, they tend to look for support of their opinions, rather than arrive at a fully educated decision.”
Only about half of patients believe their physicians “provide fair and accurate treatment information all or most of the time,” according to a 2019 survey by the Pew Research Center.
Patients’ distrust has become more obvious during the COVID-19 pandemic, said John Schumann, MD, an internist with Oak Street Health, a practice with more than 500 physicians and other providers in 20 states, treating almost exclusively Medicare patients.
“The skeptics became more entrenched during the pandemic,” said Dr. Schumann, who is based in Tulsa, Okla. “They may think the COVID vaccines were approved too quickly, or believe the pandemic itself is a hoax.”
“There’s a lot of antiscience rhetoric now,” Dr. Schumann added. “I’d say about half of my patients are comfortable with science-based decisions and the other half are not.”
What are patients mistrustful about?
Patients’ suspicions of certain therapies began long before the pandemic. In dermatology, for example, some patients refuse to take topical steroids, said Steven R. Feldman, MD, a dermatologist in Winston-Salem, N.C.
“Their distrust is usually based on anecdotal stories they read about,” he noted. “Patients in other specialties are dead set against vaccinations.”
In addition to refusing treatments and inoculations, some patients ask for questionable regimens mentioned in the news. “Some patients have demanded hydroxychloroquine or Noromectin, drugs that are unproven in the treatment of COVID,” Dr. Schumann said. “We refuse to prescribe them.”
Dr. Hood said patients’ reluctance to follow medical advice can often be based on cost. “I have a patient who was more willing to save $20 than to save his life. But when the progression of his test results fit my predictions, he became more willing to take treatments. I had to wait for the opportune moment to convince him.”
Many naysayer patients keep their views to themselves, and physicians may be unaware that the patients are stonewalling. A 2006 study estimated that about 10%-16% of primary care patients actively resist medical authority.
Dr. Schumann cited patients who don’t want to hear an upsetting diagnosis. “Some patients might refuse to take a biopsy to see if they have cancer because they don’t want to know,” he said. “In many cases, they simply won’t get the biopsy and won’t tell the doctor that they didn’t.”
Sometimes skeptics’ arguments have merit
Some patients’ concerns can be valid, such as when they refuse to go on statins, said Zain Hakeem, DO, a physician in Austin, Tex.
“In some cases, I feel that statins are not necessary,” he said. “The science on statins for primary prevention is not strong, although they should be used for exceedingly high-risk patients.”
Certain patients, especially those with chronic conditions, do a great deal of research, using legitimate sources on the Web, and their research is well supported.
However, these patients can be overconfident in their conclusions. Several studies have shown that with just a little experience, people can replace beginners’ caution with a false sense of competence.
For example, “Patients may not weigh the risks correctly,” Dr. Hakeem said. “They can be more concerned about the risk of having their colon perforated during a colonoscopy, while the risk of cancer if they don’t have a colonoscopy is much higher.”
Some highly successful people may be more likely to trust their own medical instincts. When Steve Jobs, the founder of Apple, was diagnosed with pancreatic cancer in 2003, he put off surgery for 9 months while he tried to cure his disease with a vegan diet, acupuncture, herbs, bowel cleansings, and other remedies he read about. He died in 2011. Some experts believe that delay hastened his death.
Of course, not all physicians’ diagnoses or treatments are correct. One study indicated doctors’ diagnostic error rate could be as high as 15%. And just as patients can be overconfident in their conclusions, so can doctors. Another study found that physicians’ stated confidence in their diagnosis was only slightly affected by the inaccuracy of that diagnosis or the difficulty of the case.
Best ways to deal with cynical patients
Patients’ skepticism can frustrate doctors, reduce the efficiency of care delivery, and interfere with recovery. What can doctors do to deal with these problems?
1. Build the patient’s trust in you. “Getting patients to adhere to your advice involves making sure they feel they have a caring doctor whom they trust,” Dr. Feldman said.
“I want to show patients that I am entirely focused on them,” he added. “For example, I may rush to the door of the exam room from my last appointment, but I open the door very slowly and deliberately, because I want the patient to see that I won’t hurry with them.”
2. Spend time with the patient. Familiarity builds trust. Dr. Schumann said doctors at Oak Street Health see their patients an average of six to eight times a year, an unusually high number. “The more patients see their physicians, the more likely they are to trust them.”
3. Keep up to date. “I make sure I’m up to date with the literature, and I try to present a truthful message,” Dr. Hood said. “For instance, my research showed that inflammation played a strong role in developing complications from COVID, so I wrote a detailed treatment protocol aimed at the inflammation and the immune response, which has been very effective.”
4. Confront patients tactfully. Patients who do research on the Web don’t want to be scolded, Dr. Feldman said. In fact, he praises them, even if he doesn’t agree with their findings. “I might say: ‘What a relief to finally find patients who’ve taken the time to educate themselves before coming here.’ ”
Dr. Feldman is careful not to dispute patients’ conclusions. “Debating the issues is not an effective approach to get patients to trust you. The last thing you want to tell a patient is: ‘Listen to me! I’m an expert.’ People just dig in.”
However, it does help to give patients feedback. “I’m a big fan of patients arguing with me,” Dr. Hakeem said. “It means you can straighten out misunderstandings and improve decision-making.”
5. Explain your reasoning. “You need to communicate clearly and show them your thinking,” Dr. Hood said. “For instance, I’ll explain why a patient has a strong risk for heart attack.”
6. Acknowledge uncertainties. “The doctor may present the science as far more certain than it is,” Dr. Hakeem said. “If you don’t acknowledge the uncertainties, you could break the patient’s trust in you.”
7. Don’t use a lot of numbers. “Data is not a good tool to convince patients,” Dr. Feldman said. “The human brain isn’t designed to work that way.”
If you want to use numbers to show clinical risk, Dr. Hakeem advisd using natural frequencies, such as 10 out of 10,000, which is less confusing to the patient than the equivalent percentage of 0.1%.
It can be helpful to refer to familiar concepts. One way to understand a risk is to compare it with risks in daily life, such as the dangers of driving or falling in the shower, Dr. Hakeem added.
Dr. Feldman often refers to another person’s experience when presenting his medical advice. “I might say to the patient: ‘You remind me of another patient I had. They were sitting in the same chair you’re sitting in. They did really well on this drug, and I think it’s probably the best choice for you, too.’ ”
8. Adopt shared decision-making. This approach involves empowering the patient to become an equal partner in medical decisions. The patient is given information through portals and is encouraged to do research. Critics, however, say that most patients don’t want this degree of empowerment and would rather depend on the doctor’s advice.
Conclusion
It’s often impossible to get through to a skeptical patient, which can be disheartening for doctors. “Physicians want to do what is best for the patient, so when the patient doesn’t listen, they may take it personally,” Dr. Hood said. “But you always have to remember, the patient is the one with disease, and it’s up to the patient to open the door.”
Still, some skeptical patients ultimately change their minds. Dr. Schumann said patients who initially declined the COVID vaccine eventually decided to get it. “It often took them more than a year. but it’s never too late.”
A version of this article first appeared on Medscape.com.