User login
The Hospitalist only
Should You Report a Substance-Abusing Colleague to the State Licensing Board?

PRO
Hospitalists’ moral obligation is to protect the patient
In this era of historic budget deficits, wars, and political strife surrounding healthcare reform, one might ask if we can afford to spend valuable time and energy on the issue of reporting physicians who abuse substances.
At first glance, I certainly had skepticism about the subject, but then I dug deeper. To my surprise (and likely yours), studies indicate that physicians develop substance-abuse problems as often or more than the general population does.1 Recent reports detail horrific patient outcomes at the hands of health providers whose actions are compromised by drug use. With data showing the prevalence of substance abuse among physicians hovering around 10% to 12%, we must accept the reality that hospitalists are not exempt.2,3,4,5
As medical doctors, our promise to our patients is to provide care in an ethical manner. Even if we try to live in denial, most of us would agree that with great blessing (or power) comes great responsibility. So when the question of reporting a fellow hospitalist who is abusing substances was asked, my response was unequivocally yes.
In my opinion, this discussion can be limited to two overarching principles: First, we are compelled to put our patients first. As hospitalists, we are blessed to be caring for some of the most frail and vulnerable in our society. Fortunately, an overwhelming number of us do so with pride, skill, and integrity.
The task of providing high-quality care to an empowered patient population is difficult enough with us being physically, emotionally, and mentally exhausted. But to add substance abuse to this is just a complete and utter violation of our patients’ trust. We must agree that putting our patients’ well-being beyond reproach requires us to report any colleague who is compromised.
Second, delayed help for a colleague in trouble with substance-abuse issues could be fatal—and for more than just that single colleague. At some point, we are compelled to do more than just raise an eyebrow and shake our head. Usually at the time of discovery, months if not years of substance abuse already have gone by undetected. Deferring to the next person is just not an option. There is too much at stake. It is our moral duty to help our colleagues who are unable to realize the danger they are posing to themselves, the team, and, most importantly, the patients.
Certainly, physicians do not need another lecture about the perils of substance abuse. Whether discussing prescription drugs, alcohol, marijuana, cocaine, or the like, we all have witnessed the devastating effects of abuse. The fact is, any substance that alters our ability to perform our trusted duty must be avoided.
Colleagues, the algorithm is simple: Be vigilant, observe, confirm, and report. It is our moral and ethical imperative.
Dr. Pyke is chief medical officer of Medicus Consulting, LLC.

CON
Responsible, helpful action doesn’t always mean official involvement
Recognizing impairment in our colleagues is both difficult and ethically challenging. Despite national trends, medicine remains a largely self-regulated profession, and we have an ethical obligation to report impaired, incompetent, or unethical colleagues. Rarely are the indications for reporting or identifying a colleague clear.
As trained clinicians, we know the signs of substance abuse:6
- Frequent tardiness and absences;
- Unexplained disappearances during working hours;
- Inappropriate behavior;
- Affective lability or irritability;
- Interpersonal conflict;
- Avoidance of peers or supervisors;
- Keeping odd hours;
- Disorganized and forgetful;
- Incomplete charts and work performance;
- Heavy drinking at social functions;
- Unexplained changes in weight or energy level;
- Diminished personal hygiene;
- Slurred or rapid speech;
- Frequently dilated pupils or red, watery eyes and a runny nose;
- Defensiveness, anxiety, apathy, and manipulative behaviors; and
- Withdrawal from long-standing relationships.
Yet when it is a colleague, we are often in denial about their substance abuse. Certainly, simple seasonal allergies and allergy medications can cause a number of the above symptoms. We also are aware of and fear the potential impact of licensing board notification on a physician’s career. In fact, in a national survey of physicians, 45% of respondents who had encountered impaired or incompetent physicians had not reported them, even though 96% of those surveyed agreed that physicians should report impaired or incompetent colleagues.7
Similar to reporting child or elder abuse, you don’t want to be wrong.
At the same time, impaired physicians are disruptive. They negatively impact the lives of their patients, colleagues, and hospital staff.
It is possible to do both the responsible thing and not go directly to the licensing board. You are not responsible for diagnosing your colleagues, but rather recognizing possible impairment.
Check out the Federation of State Physician Health Programs’ website (www.fsphp.org) to identify a local physician health program. Call them and place a report of concern identifying your impaired colleague. While it’s possibly new to you, they have years of experience working with this situation. Trust these organizations, many of which are independent from licensing, to intervene responsibly and confidentially. They can evaluate your colleague and provide a treatment plan and monitoring, as needed. Their approach is rehabilitative rather than punitive, and they resist reporting to the medical board unless the physician-patient is noncompliant.
Physicians have better outcomes than the general population, with reported abstinence rates of 70% to 90% for those who complete treatment.8,9 Between 75% and 85% of physicians who complete rehabilitation and comply with close monitoring and follow-up care are able to return to work.9,10
There is hope for your impaired colleague. Contact your local physician health program.
Dr. Guerrasio is a hospitalist and director of resident and medical student remediation at the University of Colorado Denver.
References
- Hughes PH, Brandenburg N, Baldwin DC Jr., et al. Prevalence of substance use among US physicians. JAMA. 1992;267:2333-2339.
- Gold KB, Teitelbaum SA. Physicians impaired by substance abuse disorders. The Journal of Global Drug Policy and Practice website. Available at: http://www.globaldrugpolicy.org/2/2/3.php. Accessed June 27, 2011.
- Wolfgang AP. Substance abuse potential and job stress: a study of pharmacists, physicians, and nurses. J Pharm Mark Manage. 1989;3(4):97-110.
- Cicala RS. Substance abuse among physicians: What you need to know. Hosp Phys. 2003:39-46.
- Berge KH, Seppala MD, Schipper AM. Chemical dependency and the physician. Mayo Clin Proc. 2009;84(7):625-631.
- Bright RP, Krahn L. Impaired physicians: How to recognize, when to report, and where to refer. Curr Psy. 2010;9(6):11-20.
- Campbell EG, Regan S, Gruen RL, et al. Professionalism in medicine: results of a national survey of physicians. Ann Intern Med. 2007;147:795-802.
- Femino J, Nirenberg TD. Treatment outcome studies on physician impairment: a review of the literature. R I Med. 1994;77:345-350.
- Alpern F, Correnti CE, Dolan TE, Llufrio MC, Sill A. A survey of recovering Maryland physicians. Md Med J. 1992;41:301-303.
- Gallegos KV, Lubin BH, Bowers C, Blevins JW, Talbott GD, Wilson PO. Relapse and recovery: five to ten year follow-up study of chemically dependent physicians—the Georgia experience. Md Med J. 1992;41:315-319.
PRO
Hospitalists’ moral obligation is to protect the patient
In this era of historic budget deficits, wars, and political strife surrounding healthcare reform, one might ask if we can afford to spend valuable time and energy on the issue of reporting physicians who abuse substances.
At first glance, I certainly had skepticism about the subject, but then I dug deeper. To my surprise (and likely yours), studies indicate that physicians develop substance-abuse problems as often or more than the general population does.1 Recent reports detail horrific patient outcomes at the hands of health providers whose actions are compromised by drug use. With data showing the prevalence of substance abuse among physicians hovering around 10% to 12%, we must accept the reality that hospitalists are not exempt.2,3,4,5
As medical doctors, our promise to our patients is to provide care in an ethical manner. Even if we try to live in denial, most of us would agree that with great blessing (or power) comes great responsibility. So when the question of reporting a fellow hospitalist who is abusing substances was asked, my response was unequivocally yes.
In my opinion, this discussion can be limited to two overarching principles: First, we are compelled to put our patients first. As hospitalists, we are blessed to be caring for some of the most frail and vulnerable in our society. Fortunately, an overwhelming number of us do so with pride, skill, and integrity.
The task of providing high-quality care to an empowered patient population is difficult enough with us being physically, emotionally, and mentally exhausted. But to add substance abuse to this is just a complete and utter violation of our patients’ trust. We must agree that putting our patients’ well-being beyond reproach requires us to report any colleague who is compromised.
Second, delayed help for a colleague in trouble with substance-abuse issues could be fatal—and for more than just that single colleague. At some point, we are compelled to do more than just raise an eyebrow and shake our head. Usually at the time of discovery, months if not years of substance abuse already have gone by undetected. Deferring to the next person is just not an option. There is too much at stake. It is our moral duty to help our colleagues who are unable to realize the danger they are posing to themselves, the team, and, most importantly, the patients.
Certainly, physicians do not need another lecture about the perils of substance abuse. Whether discussing prescription drugs, alcohol, marijuana, cocaine, or the like, we all have witnessed the devastating effects of abuse. The fact is, any substance that alters our ability to perform our trusted duty must be avoided.
Colleagues, the algorithm is simple: Be vigilant, observe, confirm, and report. It is our moral and ethical imperative.
Dr. Pyke is chief medical officer of Medicus Consulting, LLC.
CON
Responsible, helpful action doesn’t always mean official involvement
Recognizing impairment in our colleagues is both difficult and ethically challenging. Despite national trends, medicine remains a largely self-regulated profession, and we have an ethical obligation to report impaired, incompetent, or unethical colleagues. Rarely are the indications for reporting or identifying a colleague clear.
As trained clinicians, we know the signs of substance abuse:6
- Frequent tardiness and absences;
- Unexplained disappearances during working hours;
- Inappropriate behavior;
- Affective lability or irritability;
- Interpersonal conflict;
- Avoidance of peers or supervisors;
- Keeping odd hours;
- Disorganized and forgetful;
- Incomplete charts and work performance;
- Heavy drinking at social functions;
- Unexplained changes in weight or energy level;
- Diminished personal hygiene;
- Slurred or rapid speech;
- Frequently dilated pupils or red, watery eyes and a runny nose;
- Defensiveness, anxiety, apathy, and manipulative behaviors; and
- Withdrawal from long-standing relationships.
Yet when it is a colleague, we are often in denial about their substance abuse. Certainly, simple seasonal allergies and allergy medications can cause a number of the above symptoms. We also are aware of and fear the potential impact of licensing board notification on a physician’s career. In fact, in a national survey of physicians, 45% of respondents who had encountered impaired or incompetent physicians had not reported them, even though 96% of those surveyed agreed that physicians should report impaired or incompetent colleagues.7
Similar to reporting child or elder abuse, you don’t want to be wrong.
At the same time, impaired physicians are disruptive. They negatively impact the lives of their patients, colleagues, and hospital staff.
It is possible to do both the responsible thing and not go directly to the licensing board. You are not responsible for diagnosing your colleagues, but rather recognizing possible impairment.
Check out the Federation of State Physician Health Programs’ website (www.fsphp.org) to identify a local physician health program. Call them and place a report of concern identifying your impaired colleague. While it’s possibly new to you, they have years of experience working with this situation. Trust these organizations, many of which are independent from licensing, to intervene responsibly and confidentially. They can evaluate your colleague and provide a treatment plan and monitoring, as needed. Their approach is rehabilitative rather than punitive, and they resist reporting to the medical board unless the physician-patient is noncompliant.
Physicians have better outcomes than the general population, with reported abstinence rates of 70% to 90% for those who complete treatment.8,9 Between 75% and 85% of physicians who complete rehabilitation and comply with close monitoring and follow-up care are able to return to work.9,10
There is hope for your impaired colleague. Contact your local physician health program.
Dr. Guerrasio is a hospitalist and director of resident and medical student remediation at the University of Colorado Denver.
References
- Hughes PH, Brandenburg N, Baldwin DC Jr., et al. Prevalence of substance use among US physicians. JAMA. 1992;267:2333-2339.
- Gold KB, Teitelbaum SA. Physicians impaired by substance abuse disorders. The Journal of Global Drug Policy and Practice website. Available at: http://www.globaldrugpolicy.org/2/2/3.php. Accessed June 27, 2011.
- Wolfgang AP. Substance abuse potential and job stress: a study of pharmacists, physicians, and nurses. J Pharm Mark Manage. 1989;3(4):97-110.
- Cicala RS. Substance abuse among physicians: What you need to know. Hosp Phys. 2003:39-46.
- Berge KH, Seppala MD, Schipper AM. Chemical dependency and the physician. Mayo Clin Proc. 2009;84(7):625-631.
- Bright RP, Krahn L. Impaired physicians: How to recognize, when to report, and where to refer. Curr Psy. 2010;9(6):11-20.
- Campbell EG, Regan S, Gruen RL, et al. Professionalism in medicine: results of a national survey of physicians. Ann Intern Med. 2007;147:795-802.
- Femino J, Nirenberg TD. Treatment outcome studies on physician impairment: a review of the literature. R I Med. 1994;77:345-350.
- Alpern F, Correnti CE, Dolan TE, Llufrio MC, Sill A. A survey of recovering Maryland physicians. Md Med J. 1992;41:301-303.
- Gallegos KV, Lubin BH, Bowers C, Blevins JW, Talbott GD, Wilson PO. Relapse and recovery: five to ten year follow-up study of chemically dependent physicians—the Georgia experience. Md Med J. 1992;41:315-319.
PRO
Hospitalists’ moral obligation is to protect the patient
In this era of historic budget deficits, wars, and political strife surrounding healthcare reform, one might ask if we can afford to spend valuable time and energy on the issue of reporting physicians who abuse substances.
At first glance, I certainly had skepticism about the subject, but then I dug deeper. To my surprise (and likely yours), studies indicate that physicians develop substance-abuse problems as often or more than the general population does.1 Recent reports detail horrific patient outcomes at the hands of health providers whose actions are compromised by drug use. With data showing the prevalence of substance abuse among physicians hovering around 10% to 12%, we must accept the reality that hospitalists are not exempt.2,3,4,5
As medical doctors, our promise to our patients is to provide care in an ethical manner. Even if we try to live in denial, most of us would agree that with great blessing (or power) comes great responsibility. So when the question of reporting a fellow hospitalist who is abusing substances was asked, my response was unequivocally yes.
In my opinion, this discussion can be limited to two overarching principles: First, we are compelled to put our patients first. As hospitalists, we are blessed to be caring for some of the most frail and vulnerable in our society. Fortunately, an overwhelming number of us do so with pride, skill, and integrity.
The task of providing high-quality care to an empowered patient population is difficult enough with us being physically, emotionally, and mentally exhausted. But to add substance abuse to this is just a complete and utter violation of our patients’ trust. We must agree that putting our patients’ well-being beyond reproach requires us to report any colleague who is compromised.
Second, delayed help for a colleague in trouble with substance-abuse issues could be fatal—and for more than just that single colleague. At some point, we are compelled to do more than just raise an eyebrow and shake our head. Usually at the time of discovery, months if not years of substance abuse already have gone by undetected. Deferring to the next person is just not an option. There is too much at stake. It is our moral duty to help our colleagues who are unable to realize the danger they are posing to themselves, the team, and, most importantly, the patients.
Certainly, physicians do not need another lecture about the perils of substance abuse. Whether discussing prescription drugs, alcohol, marijuana, cocaine, or the like, we all have witnessed the devastating effects of abuse. The fact is, any substance that alters our ability to perform our trusted duty must be avoided.
Colleagues, the algorithm is simple: Be vigilant, observe, confirm, and report. It is our moral and ethical imperative.
Dr. Pyke is chief medical officer of Medicus Consulting, LLC.
CON
Responsible, helpful action doesn’t always mean official involvement
Recognizing impairment in our colleagues is both difficult and ethically challenging. Despite national trends, medicine remains a largely self-regulated profession, and we have an ethical obligation to report impaired, incompetent, or unethical colleagues. Rarely are the indications for reporting or identifying a colleague clear.
As trained clinicians, we know the signs of substance abuse:6
- Frequent tardiness and absences;
- Unexplained disappearances during working hours;
- Inappropriate behavior;
- Affective lability or irritability;
- Interpersonal conflict;
- Avoidance of peers or supervisors;
- Keeping odd hours;
- Disorganized and forgetful;
- Incomplete charts and work performance;
- Heavy drinking at social functions;
- Unexplained changes in weight or energy level;
- Diminished personal hygiene;
- Slurred or rapid speech;
- Frequently dilated pupils or red, watery eyes and a runny nose;
- Defensiveness, anxiety, apathy, and manipulative behaviors; and
- Withdrawal from long-standing relationships.
Yet when it is a colleague, we are often in denial about their substance abuse. Certainly, simple seasonal allergies and allergy medications can cause a number of the above symptoms. We also are aware of and fear the potential impact of licensing board notification on a physician’s career. In fact, in a national survey of physicians, 45% of respondents who had encountered impaired or incompetent physicians had not reported them, even though 96% of those surveyed agreed that physicians should report impaired or incompetent colleagues.7
Similar to reporting child or elder abuse, you don’t want to be wrong.
At the same time, impaired physicians are disruptive. They negatively impact the lives of their patients, colleagues, and hospital staff.
It is possible to do both the responsible thing and not go directly to the licensing board. You are not responsible for diagnosing your colleagues, but rather recognizing possible impairment.
Check out the Federation of State Physician Health Programs’ website (www.fsphp.org) to identify a local physician health program. Call them and place a report of concern identifying your impaired colleague. While it’s possibly new to you, they have years of experience working with this situation. Trust these organizations, many of which are independent from licensing, to intervene responsibly and confidentially. They can evaluate your colleague and provide a treatment plan and monitoring, as needed. Their approach is rehabilitative rather than punitive, and they resist reporting to the medical board unless the physician-patient is noncompliant.
Physicians have better outcomes than the general population, with reported abstinence rates of 70% to 90% for those who complete treatment.8,9 Between 75% and 85% of physicians who complete rehabilitation and comply with close monitoring and follow-up care are able to return to work.9,10
There is hope for your impaired colleague. Contact your local physician health program.
Dr. Guerrasio is a hospitalist and director of resident and medical student remediation at the University of Colorado Denver.
References
- Hughes PH, Brandenburg N, Baldwin DC Jr., et al. Prevalence of substance use among US physicians. JAMA. 1992;267:2333-2339.
- Gold KB, Teitelbaum SA. Physicians impaired by substance abuse disorders. The Journal of Global Drug Policy and Practice website. Available at: http://www.globaldrugpolicy.org/2/2/3.php. Accessed June 27, 2011.
- Wolfgang AP. Substance abuse potential and job stress: a study of pharmacists, physicians, and nurses. J Pharm Mark Manage. 1989;3(4):97-110.
- Cicala RS. Substance abuse among physicians: What you need to know. Hosp Phys. 2003:39-46.
- Berge KH, Seppala MD, Schipper AM. Chemical dependency and the physician. Mayo Clin Proc. 2009;84(7):625-631.
- Bright RP, Krahn L. Impaired physicians: How to recognize, when to report, and where to refer. Curr Psy. 2010;9(6):11-20.
- Campbell EG, Regan S, Gruen RL, et al. Professionalism in medicine: results of a national survey of physicians. Ann Intern Med. 2007;147:795-802.
- Femino J, Nirenberg TD. Treatment outcome studies on physician impairment: a review of the literature. R I Med. 1994;77:345-350.
- Alpern F, Correnti CE, Dolan TE, Llufrio MC, Sill A. A survey of recovering Maryland physicians. Md Med J. 1992;41:301-303.
- Gallegos KV, Lubin BH, Bowers C, Blevins JW, Talbott GD, Wilson PO. Relapse and recovery: five to ten year follow-up study of chemically dependent physicians—the Georgia experience. Md Med J. 1992;41:315-319.
Conglomerate HM?
William Geers, MD, finished up his residency in 2007, then went to work for a close-knit emergency-medicine group of about 25 doctors in Daytona Beach, Fla.
“Everybody was pretty tight,” he says of his first job.
He had met his wife in residency in Daytona, but after a while, they figured it was time for a change. “We’d been in Daytona for about six years and were ready to go try someplace different,” Dr. Geers says. “Tallahassee seemed like a good match because that’s kind of right in between our families.”
He soon landed a hospitalist job at Capital Regional Medical Center, and he suddenly was a part of EmCare, one of the biggest corporations in the emergency-medicine field and, more recently, in the field of hospital medicine. EmCare provides doctors to about 400 hospitals nationwide.
Dr. Geers said the corporate affiliation didn’t factor into his decision, adding that he took more of a traditional approach when choosing a new job.
“At the time, this program was a little bit smaller, which I liked,” says Dr. Geers, who also looked at the city’s other hospital, Tallahassee Memorial. “I met some of the physicians over here. I liked them.”
But he has noticed perks.
“I think we have some advantages working with EmCare in that we do have a pretty big group that’s backing us,” he explains. “I feel a little more secure with issues like malpractice. If things like that ever come up, I really feel like I have a lot of support with EmCare.”
With the corporate presence on the rise in HM, more and more hospitalists are entering the ranks of large companies. Some are doing so straight out of residency. Some are giving up their private practices and selling them to corporations looking to expand.
Corporations that provide hospitalists to hospitals are getting ever bigger, using sophisticated infrastructure and economies of scale, they say, to make life easier for the people who work for them, allowing the hospitalists to focus on patient care. Their efficiencies are attractive to hospitals looking to simplify.
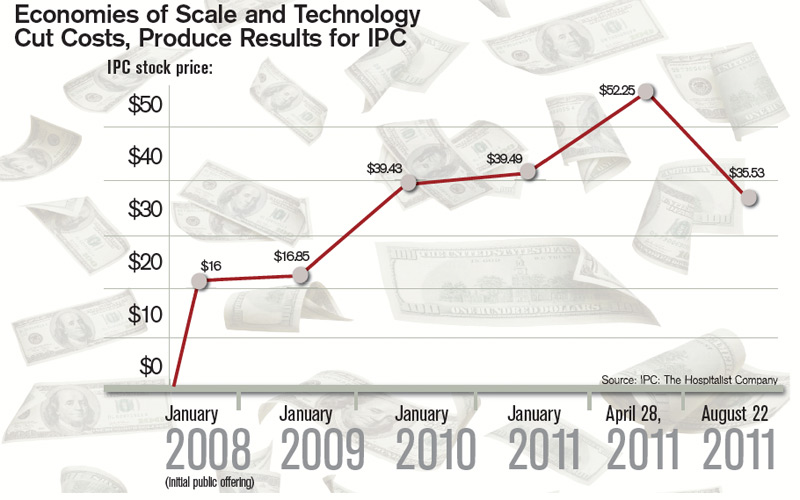
Three years ago, North Hollywood, Calif.-based IPC: The Hospitalist Company became a publicly traded company. Its stock price has more than doubled since then.
In July, Eagle Hospital Physicians acquired North Carolina-based PrimeDoc and its 100 doctors covering seven hospitals. Similar acquisitions by larger corporations have become almost weekly news.
And, probably most significantly, Cogent Healthcare recently completed a merger with Hospitalists Management Group, a union of two of the biggest hospitalist companies in the U.S. The new company, Cogent HMG, now includes a corps of 1,000 doctors, nurses, and physician assistants (PAs), with client hospitals in 28 states.
Cogent had clients that were medium to large in size, generally in more urban areas but scattered geographically. HMG mostly served small- to medium-sized hospitals with densities in certain regions. With the merger came a recognition that the larger a company becomes, the greater the opportunity for efficiency and better services, says Rusty Holman, MD, MHM, chief clinical officer of the new company.
“The real value out of bringing these two companies together is bringing the best of different worlds together, creating new products and services for hospitals that don’t exist today, and to be able to serve a broader customer base,” says Dr. Holman, a former SHM president. “It’s also to leverage some of the infrastructure that has been built over a greater number of programs and hospitals to gain efficiency and scale that way. So that is the primary focus of the integration today.”
Cogent HMG CEO Steve Houff, MD, says the merger will mean investment in clinical support, physician recruiting, and technology, and will benefit patients and hospital partners alike.
“Both Cogent and HMG have a track record for delivering improvements in clinical quality and patient satisfaction at each of the hospitals we serve. The plan is for that to continue on a broader scale,” he wrote in an email to The Hospitalist.

—R. Jeffrey Taylor, president, chief operating officer, IPC: The Hospitalist Company, North Hollywood, Calif.
The Good, the Bad, the Oligopoly
The average size of a hospitalist group in the U.S. is about 10 full-time equivalents, according to recent survey data from SHM and MGMA. With the swelling of the size of HM’s biggest corporate players comes the question of how far the coalescing will go: Will most patient care eventually be provided by only a few groups?
R. Jeffrey Taylor, IPC’s president and chief operating officer, says the mergers and acquisitions will continue, but he doesn’t see a day when there will be just a few titans ruling all.
“I do think there will be more consolidation going forward than there is now, but I don’t see a future in which there are, you know, two or three groups that completely dominate the landscape,” he says. “There’s always that concern that that’s going to happen in the hospital industry, or that’s going to happen with payors. And there are always new entrants.”

For all the movement toward bigger companies, “this is still an unconsolidated industry,” and new physician practices will always continue to be formed, he says.
“We’re the largest group, and we’re maybe 3 1/2 percent of all the hospitals in the country. I wouldn’t consider this, today, a terribly consolidated industry,” he adds. “I do think it will move in that direction. I just don’t think it will get all the way there, because of the sort of private, entrepreneurial, independent spirit that’s common among physicians.”
Mike Tarwater, a board member of the American Hospital Association, says private hospitalist providers will only be an alternative to—and not a replacement provider for—large, self-contained systems like the Carolinas Medical Center (CMC), for which he serves as CEO. The health system has a wide spectrum of facilities—from large, urban academic centers like the 874-bed medical center in Charlotte, N.C., to 52-bed Anson Community Hospital in Wadesboro, N.C., population 5,780.
“As a system, we have the wherewithal and the recruiting expertise, and, with 1,700 physician associates across the system, we’ve kind of got critical mass,” Tarwater says. “So we will be an alternative to that in our region.”
Frank Michota, MD, FHM, director of academic affairs in the Department of Hospital Medicine at The Cleveland Clinic, says that the extensive training programs of many of the larger hospitalist groups (e.g. Cogent Academy, IPC’s extensive onboarding process and leadership conferences) could be a very good thing for the field.
“I have always thought that companies like Cogent did a very nice job in orienting their hospitalists to the patient-care goals and the process variables that were being measured,” Dr. Michota says. “I think that by making an even larger group, they have the opportunity to continue to standardize the approach to hospital care so that one hospitalist equals one hospitalist equals one hospitalist. I think that’s a positive.”
The flip side, though, is that anything that might be done wrong would be magnified in such a system.
“I think that there are some dangers in how these large companies will incentivize their hospitalists,” he adds. “If they are consistent from hospitalist to hospitalist, but if there’s a perverse adverse effect from one of their financial incentives, it will be carried out across a lot of hospitals all at the same time. “But I think it’s a little early to tell what the impact of this might be. But, at least for right now, it’s actually a positive thing because it standardizes the hospitalist.”
Tarwater says that even when larger corporations buy smaller practices, familiarity tends to remain.
“Most of what I have seen are existing groups that join through merger or acquisition, and so we already have experience with the doctors, we already have long-standing relationships with the doctors,” he says. “I think any health system or hospital would be reticent to sign up with somebody that they’ve never heard of, that doesn’t have a track record, or that they don’t know already at least some of the players.” Hospitals looking to hire a private company have to exercise caution, particularly if the company is trying to break into a new region where it isn’t known.
“Those hospitals and healthcare systems just have to be really careful who they’re signing contracts with,” he said. “It’s no different than anything else we do. You just have to know who your partners are, and what drives them and where they stand on important issues.”
Executives say patient care is not at risk, even as consolidation continues. “With or without competition, we are relentlessly trying to improve our approach to patient care, our performance, and our hospital partnerships,” Cogent HMG’s Dr. Houff says.
Money Talks
It doesn’t appear that more hospitalist companies are planning to go public—at least for now.
The largest privately held company, Cogent HMG, is not planning an initial public offering anytime soon, Dr. Houff says. The company’s goal is to “continue investing in smart growth to capture more of the hospital medicine market, expand offerings to our existing hospital clients, and provide additional support to our clinical teams on the ground,” he says. “We have a strong capital partner to help us in that effort and are not looking at the public markets at this time.”
Taking on stockholders is a tricky business—one that requires careful planning and a willingness from practice leaders and administrators to relinquish some autonomy to outside interests. And then there are the financial requirements.
“They’ve really got to be able to produce some serious revenue in order for somebody to be willing to put some money into them,” says Mark Hamm, CEO of EmCare Inpatient Services.
The lure of working for a private hospitalist company promises to continue to be an attractive one. Some are drawn by the leadership possibilities—those who “aspire to be the true alpha doctor,” as IPC’s Taylor puts it. Others are drawn by the stability of a larger company.
There also is flexibility in location, Dr. Holman notes.
“Now, with Cogent HMG, [hospitalists] have even more choices in terms of relocating within the same company,” he says. “So they can keep all of the benefits, keep all of the knowledge and familiarity of the system and philosophy of care that we employ, and just be able to transfer.”
continued below...
Emergency-Medicine Companies Increasingly Venture into HM

Hollywood, Fla.-based Hospital Physician Partners (HPP) was an ED business when more opportunity came knocking: Hospitals started asking them to provide some hospitalists to go with their emergency-room doctors.
Today, HPP is firmly in the hospital medicine business. And all signs point toward more and more hospitals hiring companies to handle both emergency care and inpatient care.
“In many ways, we expanded our efforts into hospitalist medicine as a result of requests from our hospital partners where we are providing emergency, ER medicine,” said Ed Weinberg, HPP’s chief operating officer.
“Their needs were such that they asked us to provide hospital medicine services. So from that, it became clear that it was an area that was really growing.
And that is something we are pursuing as vigorously as we are emergency medicine.”
Handling both emergency care and hospital medicine can help with the transition of the patient from the emergency room to a bed upstairs, he says.
“The efficiency is being able to transition a patient from being in the emergency department as an inpatient very seamlessly,” he said. “That’s where our efficiencies are, because we have physicians working who are carrying out the same philosophy.”
Out of the company’s 120 contracts, 15 of them are in hospital medicine, but it’s growing quickly, he says.
At EmCare, traditionally an emergency-medicine company that is now getting into hospital medicine, there are about 400 emergency-medicine programs and more than 50 HM programs.
Mark Hamm, CEO of EmCare Inpatient Services, says that it can be much more cost-effective to contract with one company for both hospitalist and emergency-medicine services—which he said hospitals have found attractive.
Their arrangements range from completely separate emergency and hospital medicine staffs to small, rural hospitals where ER physicians also do rounds.
Some hospitals “just don’t have the money for a full-time hospitalist and don’t really need one,” Hamm says.
The patient transitions tend to go more smoothly when both types of care are provided by EmCare. When they’re not, there can be slowdowns.
“Our goal is to quickly and appropriately move patients through the system,” he says. “If we have a hospitalist provider that’s not really on the same page, that can create bottlenecks. . . . But it’s a blip.
“Our goal is to sit down, even if it’s not an EmCare hospitalist, to sit down with that director and say, ‘Hey, look, let’s be the leader here, let’s work together and appropriately expedite these patients.’ We do the same thing on the hospitalist side.”
Inpatient care promises to be a big part of their future business, most executives agree.
“Hospital medicine,” Weinberg says, “is growing by leaps and bounds.” —TC
Dr. Houff says the majority of newly recruited physicians are coming out of residency but that the company is attracting physicians in the middle of their careers, along with physicians having backgrounds beyond internal medicine.
In Tallahassee at Capital Regional, Dr. Geers says that he feels there is support from the company that can protect his job quality, with “a little bit more room to negotiate with the hospital if the hospital wants us to take on new responsibilities.
“Whereas if we worked directly for the hospital, I don’t think we’d have much say in the matter,” he says.
He also says he is happy with the predictable schedule; he’s responsible for 7 a.m. to 7 p.m. and nothing more.
“If you’re finished rounding and you’ve seen all your patients and tied up all your loose ends, you’re not always there till 7 p.m.,” he points out. “Sometimes you can leave a little early....Once 7 p.m. comes, you’re not going to get paged in the middle of the night.”
Thomas R. Collins is a freelance medical writer based in Florida.
Wall Street’s Rosy View of Hospital Medicine

When IPC: The Hospitalist Company went public in January 2008, its stock price was $16 a share. In late July of this year, it was hovering a tick below $50 a share.
It’s been an obvious financial success—a performance that speaks well of the hospitalist specialty as a whole, says analyst Kevin Campbell, who covers IPC for Avondale Partners.
“Investors like the industry,” Campbell explains. “They see the need for hospitalists....When investors look at that, they see the opportunity for continued growth.”
IPC’s management team, he adds, has done “an excellent job of growing both the revenues and the earnings.”
Revenues in 2008 were $251 million. This year, they’re projected to be $454 million, an increase of 80%.
Six of 10 analysts say the company is a “strong buy,” one says it’s a “buy,” and for three others, it’s a “hold,” according to research listed on the NASDAQ website.
One of the key reasons IPC has performed well, Campbell says, is that when it makes an acquisition, physicians whose practices are bought are not paid everything at once; a portion is paid out later. Because the payment is a factor of the company’s performance, that encourages the physicians to keep their newly acquired practices performing optimally.
That’s different from scenarios in which “doctors would take their big check and retire,” he says, “and the operations for the practice would decline significantly. This is one way that IPCM [the stock symbol] can ensure that that doesn’t happen.”
Campbell also says it probably is unlikely that there will be another public offering of a hospitalist company in the near future. “There’s not a lot of companies of scale,” he says. “You have to have some scale before you would consider going public.”
R. Jeffrey Taylor, IPC’s president and COO, says another public offering from a hospitalist company isn’t that far-fetched.
“I would not be at all surprised to see someone else follow that path,” he says. “Frankly, it will probably be a little easier for the second company to do it because we have helped educate people about the hospitalist model, and fortunately the company and the stock have performed well. So I think it would be an easier sell to the public market the second time around. And I expect that’s more likely than not in the next few years.” —TC
William Geers, MD, finished up his residency in 2007, then went to work for a close-knit emergency-medicine group of about 25 doctors in Daytona Beach, Fla.
“Everybody was pretty tight,” he says of his first job.
He had met his wife in residency in Daytona, but after a while, they figured it was time for a change. “We’d been in Daytona for about six years and were ready to go try someplace different,” Dr. Geers says. “Tallahassee seemed like a good match because that’s kind of right in between our families.”
He soon landed a hospitalist job at Capital Regional Medical Center, and he suddenly was a part of EmCare, one of the biggest corporations in the emergency-medicine field and, more recently, in the field of hospital medicine. EmCare provides doctors to about 400 hospitals nationwide.
Dr. Geers said the corporate affiliation didn’t factor into his decision, adding that he took more of a traditional approach when choosing a new job.
“At the time, this program was a little bit smaller, which I liked,” says Dr. Geers, who also looked at the city’s other hospital, Tallahassee Memorial. “I met some of the physicians over here. I liked them.”
But he has noticed perks.
“I think we have some advantages working with EmCare in that we do have a pretty big group that’s backing us,” he explains. “I feel a little more secure with issues like malpractice. If things like that ever come up, I really feel like I have a lot of support with EmCare.”
With the corporate presence on the rise in HM, more and more hospitalists are entering the ranks of large companies. Some are doing so straight out of residency. Some are giving up their private practices and selling them to corporations looking to expand.
Corporations that provide hospitalists to hospitals are getting ever bigger, using sophisticated infrastructure and economies of scale, they say, to make life easier for the people who work for them, allowing the hospitalists to focus on patient care. Their efficiencies are attractive to hospitals looking to simplify.
Three years ago, North Hollywood, Calif.-based IPC: The Hospitalist Company became a publicly traded company. Its stock price has more than doubled since then.
In July, Eagle Hospital Physicians acquired North Carolina-based PrimeDoc and its 100 doctors covering seven hospitals. Similar acquisitions by larger corporations have become almost weekly news.
And, probably most significantly, Cogent Healthcare recently completed a merger with Hospitalists Management Group, a union of two of the biggest hospitalist companies in the U.S. The new company, Cogent HMG, now includes a corps of 1,000 doctors, nurses, and physician assistants (PAs), with client hospitals in 28 states.
Cogent had clients that were medium to large in size, generally in more urban areas but scattered geographically. HMG mostly served small- to medium-sized hospitals with densities in certain regions. With the merger came a recognition that the larger a company becomes, the greater the opportunity for efficiency and better services, says Rusty Holman, MD, MHM, chief clinical officer of the new company.
“The real value out of bringing these two companies together is bringing the best of different worlds together, creating new products and services for hospitals that don’t exist today, and to be able to serve a broader customer base,” says Dr. Holman, a former SHM president. “It’s also to leverage some of the infrastructure that has been built over a greater number of programs and hospitals to gain efficiency and scale that way. So that is the primary focus of the integration today.”
Cogent HMG CEO Steve Houff, MD, says the merger will mean investment in clinical support, physician recruiting, and technology, and will benefit patients and hospital partners alike.
“Both Cogent and HMG have a track record for delivering improvements in clinical quality and patient satisfaction at each of the hospitals we serve. The plan is for that to continue on a broader scale,” he wrote in an email to The Hospitalist.
—R. Jeffrey Taylor, president, chief operating officer, IPC: The Hospitalist Company, North Hollywood, Calif.
The Good, the Bad, the Oligopoly
The average size of a hospitalist group in the U.S. is about 10 full-time equivalents, according to recent survey data from SHM and MGMA. With the swelling of the size of HM’s biggest corporate players comes the question of how far the coalescing will go: Will most patient care eventually be provided by only a few groups?
R. Jeffrey Taylor, IPC’s president and chief operating officer, says the mergers and acquisitions will continue, but he doesn’t see a day when there will be just a few titans ruling all.
“I do think there will be more consolidation going forward than there is now, but I don’t see a future in which there are, you know, two or three groups that completely dominate the landscape,” he says. “There’s always that concern that that’s going to happen in the hospital industry, or that’s going to happen with payors. And there are always new entrants.”
For all the movement toward bigger companies, “this is still an unconsolidated industry,” and new physician practices will always continue to be formed, he says.
“We’re the largest group, and we’re maybe 3 1/2 percent of all the hospitals in the country. I wouldn’t consider this, today, a terribly consolidated industry,” he adds. “I do think it will move in that direction. I just don’t think it will get all the way there, because of the sort of private, entrepreneurial, independent spirit that’s common among physicians.”
Mike Tarwater, a board member of the American Hospital Association, says private hospitalist providers will only be an alternative to—and not a replacement provider for—large, self-contained systems like the Carolinas Medical Center (CMC), for which he serves as CEO. The health system has a wide spectrum of facilities—from large, urban academic centers like the 874-bed medical center in Charlotte, N.C., to 52-bed Anson Community Hospital in Wadesboro, N.C., population 5,780.
“As a system, we have the wherewithal and the recruiting expertise, and, with 1,700 physician associates across the system, we’ve kind of got critical mass,” Tarwater says. “So we will be an alternative to that in our region.”
Frank Michota, MD, FHM, director of academic affairs in the Department of Hospital Medicine at The Cleveland Clinic, says that the extensive training programs of many of the larger hospitalist groups (e.g. Cogent Academy, IPC’s extensive onboarding process and leadership conferences) could be a very good thing for the field.
“I have always thought that companies like Cogent did a very nice job in orienting their hospitalists to the patient-care goals and the process variables that were being measured,” Dr. Michota says. “I think that by making an even larger group, they have the opportunity to continue to standardize the approach to hospital care so that one hospitalist equals one hospitalist equals one hospitalist. I think that’s a positive.”
The flip side, though, is that anything that might be done wrong would be magnified in such a system.
“I think that there are some dangers in how these large companies will incentivize their hospitalists,” he adds. “If they are consistent from hospitalist to hospitalist, but if there’s a perverse adverse effect from one of their financial incentives, it will be carried out across a lot of hospitals all at the same time. “But I think it’s a little early to tell what the impact of this might be. But, at least for right now, it’s actually a positive thing because it standardizes the hospitalist.”
Tarwater says that even when larger corporations buy smaller practices, familiarity tends to remain.
“Most of what I have seen are existing groups that join through merger or acquisition, and so we already have experience with the doctors, we already have long-standing relationships with the doctors,” he says. “I think any health system or hospital would be reticent to sign up with somebody that they’ve never heard of, that doesn’t have a track record, or that they don’t know already at least some of the players.” Hospitals looking to hire a private company have to exercise caution, particularly if the company is trying to break into a new region where it isn’t known.
“Those hospitals and healthcare systems just have to be really careful who they’re signing contracts with,” he said. “It’s no different than anything else we do. You just have to know who your partners are, and what drives them and where they stand on important issues.”
Executives say patient care is not at risk, even as consolidation continues. “With or without competition, we are relentlessly trying to improve our approach to patient care, our performance, and our hospital partnerships,” Cogent HMG’s Dr. Houff says.
Money Talks
It doesn’t appear that more hospitalist companies are planning to go public—at least for now.
The largest privately held company, Cogent HMG, is not planning an initial public offering anytime soon, Dr. Houff says. The company’s goal is to “continue investing in smart growth to capture more of the hospital medicine market, expand offerings to our existing hospital clients, and provide additional support to our clinical teams on the ground,” he says. “We have a strong capital partner to help us in that effort and are not looking at the public markets at this time.”
Taking on stockholders is a tricky business—one that requires careful planning and a willingness from practice leaders and administrators to relinquish some autonomy to outside interests. And then there are the financial requirements.
“They’ve really got to be able to produce some serious revenue in order for somebody to be willing to put some money into them,” says Mark Hamm, CEO of EmCare Inpatient Services.
The lure of working for a private hospitalist company promises to continue to be an attractive one. Some are drawn by the leadership possibilities—those who “aspire to be the true alpha doctor,” as IPC’s Taylor puts it. Others are drawn by the stability of a larger company.
There also is flexibility in location, Dr. Holman notes.
“Now, with Cogent HMG, [hospitalists] have even more choices in terms of relocating within the same company,” he says. “So they can keep all of the benefits, keep all of the knowledge and familiarity of the system and philosophy of care that we employ, and just be able to transfer.”
continued below...
Emergency-Medicine Companies Increasingly Venture into HM
Hollywood, Fla.-based Hospital Physician Partners (HPP) was an ED business when more opportunity came knocking: Hospitals started asking them to provide some hospitalists to go with their emergency-room doctors.
Today, HPP is firmly in the hospital medicine business. And all signs point toward more and more hospitals hiring companies to handle both emergency care and inpatient care.
“In many ways, we expanded our efforts into hospitalist medicine as a result of requests from our hospital partners where we are providing emergency, ER medicine,” said Ed Weinberg, HPP’s chief operating officer.
“Their needs were such that they asked us to provide hospital medicine services. So from that, it became clear that it was an area that was really growing.
And that is something we are pursuing as vigorously as we are emergency medicine.”
Handling both emergency care and hospital medicine can help with the transition of the patient from the emergency room to a bed upstairs, he says.
“The efficiency is being able to transition a patient from being in the emergency department as an inpatient very seamlessly,” he said. “That’s where our efficiencies are, because we have physicians working who are carrying out the same philosophy.”
Out of the company’s 120 contracts, 15 of them are in hospital medicine, but it’s growing quickly, he says.
At EmCare, traditionally an emergency-medicine company that is now getting into hospital medicine, there are about 400 emergency-medicine programs and more than 50 HM programs.
Mark Hamm, CEO of EmCare Inpatient Services, says that it can be much more cost-effective to contract with one company for both hospitalist and emergency-medicine services—which he said hospitals have found attractive.
Their arrangements range from completely separate emergency and hospital medicine staffs to small, rural hospitals where ER physicians also do rounds.
Some hospitals “just don’t have the money for a full-time hospitalist and don’t really need one,” Hamm says.
The patient transitions tend to go more smoothly when both types of care are provided by EmCare. When they’re not, there can be slowdowns.
“Our goal is to quickly and appropriately move patients through the system,” he says. “If we have a hospitalist provider that’s not really on the same page, that can create bottlenecks. . . . But it’s a blip.
“Our goal is to sit down, even if it’s not an EmCare hospitalist, to sit down with that director and say, ‘Hey, look, let’s be the leader here, let’s work together and appropriately expedite these patients.’ We do the same thing on the hospitalist side.”
Inpatient care promises to be a big part of their future business, most executives agree.
“Hospital medicine,” Weinberg says, “is growing by leaps and bounds.” —TC
Dr. Houff says the majority of newly recruited physicians are coming out of residency but that the company is attracting physicians in the middle of their careers, along with physicians having backgrounds beyond internal medicine.
In Tallahassee at Capital Regional, Dr. Geers says that he feels there is support from the company that can protect his job quality, with “a little bit more room to negotiate with the hospital if the hospital wants us to take on new responsibilities.
“Whereas if we worked directly for the hospital, I don’t think we’d have much say in the matter,” he says.
He also says he is happy with the predictable schedule; he’s responsible for 7 a.m. to 7 p.m. and nothing more.
“If you’re finished rounding and you’ve seen all your patients and tied up all your loose ends, you’re not always there till 7 p.m.,” he points out. “Sometimes you can leave a little early....Once 7 p.m. comes, you’re not going to get paged in the middle of the night.”
Thomas R. Collins is a freelance medical writer based in Florida.
Wall Street’s Rosy View of Hospital Medicine
When IPC: The Hospitalist Company went public in January 2008, its stock price was $16 a share. In late July of this year, it was hovering a tick below $50 a share.
It’s been an obvious financial success—a performance that speaks well of the hospitalist specialty as a whole, says analyst Kevin Campbell, who covers IPC for Avondale Partners.
“Investors like the industry,” Campbell explains. “They see the need for hospitalists....When investors look at that, they see the opportunity for continued growth.”
IPC’s management team, he adds, has done “an excellent job of growing both the revenues and the earnings.”
Revenues in 2008 were $251 million. This year, they’re projected to be $454 million, an increase of 80%.
Six of 10 analysts say the company is a “strong buy,” one says it’s a “buy,” and for three others, it’s a “hold,” according to research listed on the NASDAQ website.
One of the key reasons IPC has performed well, Campbell says, is that when it makes an acquisition, physicians whose practices are bought are not paid everything at once; a portion is paid out later. Because the payment is a factor of the company’s performance, that encourages the physicians to keep their newly acquired practices performing optimally.
That’s different from scenarios in which “doctors would take their big check and retire,” he says, “and the operations for the practice would decline significantly. This is one way that IPCM [the stock symbol] can ensure that that doesn’t happen.”
Campbell also says it probably is unlikely that there will be another public offering of a hospitalist company in the near future. “There’s not a lot of companies of scale,” he says. “You have to have some scale before you would consider going public.”
R. Jeffrey Taylor, IPC’s president and COO, says another public offering from a hospitalist company isn’t that far-fetched.
“I would not be at all surprised to see someone else follow that path,” he says. “Frankly, it will probably be a little easier for the second company to do it because we have helped educate people about the hospitalist model, and fortunately the company and the stock have performed well. So I think it would be an easier sell to the public market the second time around. And I expect that’s more likely than not in the next few years.” —TC
William Geers, MD, finished up his residency in 2007, then went to work for a close-knit emergency-medicine group of about 25 doctors in Daytona Beach, Fla.
“Everybody was pretty tight,” he says of his first job.
He had met his wife in residency in Daytona, but after a while, they figured it was time for a change. “We’d been in Daytona for about six years and were ready to go try someplace different,” Dr. Geers says. “Tallahassee seemed like a good match because that’s kind of right in between our families.”
He soon landed a hospitalist job at Capital Regional Medical Center, and he suddenly was a part of EmCare, one of the biggest corporations in the emergency-medicine field and, more recently, in the field of hospital medicine. EmCare provides doctors to about 400 hospitals nationwide.
Dr. Geers said the corporate affiliation didn’t factor into his decision, adding that he took more of a traditional approach when choosing a new job.
“At the time, this program was a little bit smaller, which I liked,” says Dr. Geers, who also looked at the city’s other hospital, Tallahassee Memorial. “I met some of the physicians over here. I liked them.”
But he has noticed perks.
“I think we have some advantages working with EmCare in that we do have a pretty big group that’s backing us,” he explains. “I feel a little more secure with issues like malpractice. If things like that ever come up, I really feel like I have a lot of support with EmCare.”
With the corporate presence on the rise in HM, more and more hospitalists are entering the ranks of large companies. Some are doing so straight out of residency. Some are giving up their private practices and selling them to corporations looking to expand.
Corporations that provide hospitalists to hospitals are getting ever bigger, using sophisticated infrastructure and economies of scale, they say, to make life easier for the people who work for them, allowing the hospitalists to focus on patient care. Their efficiencies are attractive to hospitals looking to simplify.
Three years ago, North Hollywood, Calif.-based IPC: The Hospitalist Company became a publicly traded company. Its stock price has more than doubled since then.
In July, Eagle Hospital Physicians acquired North Carolina-based PrimeDoc and its 100 doctors covering seven hospitals. Similar acquisitions by larger corporations have become almost weekly news.
And, probably most significantly, Cogent Healthcare recently completed a merger with Hospitalists Management Group, a union of two of the biggest hospitalist companies in the U.S. The new company, Cogent HMG, now includes a corps of 1,000 doctors, nurses, and physician assistants (PAs), with client hospitals in 28 states.
Cogent had clients that were medium to large in size, generally in more urban areas but scattered geographically. HMG mostly served small- to medium-sized hospitals with densities in certain regions. With the merger came a recognition that the larger a company becomes, the greater the opportunity for efficiency and better services, says Rusty Holman, MD, MHM, chief clinical officer of the new company.
“The real value out of bringing these two companies together is bringing the best of different worlds together, creating new products and services for hospitals that don’t exist today, and to be able to serve a broader customer base,” says Dr. Holman, a former SHM president. “It’s also to leverage some of the infrastructure that has been built over a greater number of programs and hospitals to gain efficiency and scale that way. So that is the primary focus of the integration today.”
Cogent HMG CEO Steve Houff, MD, says the merger will mean investment in clinical support, physician recruiting, and technology, and will benefit patients and hospital partners alike.
“Both Cogent and HMG have a track record for delivering improvements in clinical quality and patient satisfaction at each of the hospitals we serve. The plan is for that to continue on a broader scale,” he wrote in an email to The Hospitalist.
—R. Jeffrey Taylor, president, chief operating officer, IPC: The Hospitalist Company, North Hollywood, Calif.
The Good, the Bad, the Oligopoly
The average size of a hospitalist group in the U.S. is about 10 full-time equivalents, according to recent survey data from SHM and MGMA. With the swelling of the size of HM’s biggest corporate players comes the question of how far the coalescing will go: Will most patient care eventually be provided by only a few groups?
R. Jeffrey Taylor, IPC’s president and chief operating officer, says the mergers and acquisitions will continue, but he doesn’t see a day when there will be just a few titans ruling all.
“I do think there will be more consolidation going forward than there is now, but I don’t see a future in which there are, you know, two or three groups that completely dominate the landscape,” he says. “There’s always that concern that that’s going to happen in the hospital industry, or that’s going to happen with payors. And there are always new entrants.”
For all the movement toward bigger companies, “this is still an unconsolidated industry,” and new physician practices will always continue to be formed, he says.
“We’re the largest group, and we’re maybe 3 1/2 percent of all the hospitals in the country. I wouldn’t consider this, today, a terribly consolidated industry,” he adds. “I do think it will move in that direction. I just don’t think it will get all the way there, because of the sort of private, entrepreneurial, independent spirit that’s common among physicians.”
Mike Tarwater, a board member of the American Hospital Association, says private hospitalist providers will only be an alternative to—and not a replacement provider for—large, self-contained systems like the Carolinas Medical Center (CMC), for which he serves as CEO. The health system has a wide spectrum of facilities—from large, urban academic centers like the 874-bed medical center in Charlotte, N.C., to 52-bed Anson Community Hospital in Wadesboro, N.C., population 5,780.
“As a system, we have the wherewithal and the recruiting expertise, and, with 1,700 physician associates across the system, we’ve kind of got critical mass,” Tarwater says. “So we will be an alternative to that in our region.”
Frank Michota, MD, FHM, director of academic affairs in the Department of Hospital Medicine at The Cleveland Clinic, says that the extensive training programs of many of the larger hospitalist groups (e.g. Cogent Academy, IPC’s extensive onboarding process and leadership conferences) could be a very good thing for the field.
“I have always thought that companies like Cogent did a very nice job in orienting their hospitalists to the patient-care goals and the process variables that were being measured,” Dr. Michota says. “I think that by making an even larger group, they have the opportunity to continue to standardize the approach to hospital care so that one hospitalist equals one hospitalist equals one hospitalist. I think that’s a positive.”
The flip side, though, is that anything that might be done wrong would be magnified in such a system.
“I think that there are some dangers in how these large companies will incentivize their hospitalists,” he adds. “If they are consistent from hospitalist to hospitalist, but if there’s a perverse adverse effect from one of their financial incentives, it will be carried out across a lot of hospitals all at the same time. “But I think it’s a little early to tell what the impact of this might be. But, at least for right now, it’s actually a positive thing because it standardizes the hospitalist.”
Tarwater says that even when larger corporations buy smaller practices, familiarity tends to remain.
“Most of what I have seen are existing groups that join through merger or acquisition, and so we already have experience with the doctors, we already have long-standing relationships with the doctors,” he says. “I think any health system or hospital would be reticent to sign up with somebody that they’ve never heard of, that doesn’t have a track record, or that they don’t know already at least some of the players.” Hospitals looking to hire a private company have to exercise caution, particularly if the company is trying to break into a new region where it isn’t known.
“Those hospitals and healthcare systems just have to be really careful who they’re signing contracts with,” he said. “It’s no different than anything else we do. You just have to know who your partners are, and what drives them and where they stand on important issues.”
Executives say patient care is not at risk, even as consolidation continues. “With or without competition, we are relentlessly trying to improve our approach to patient care, our performance, and our hospital partnerships,” Cogent HMG’s Dr. Houff says.
Money Talks
It doesn’t appear that more hospitalist companies are planning to go public—at least for now.
The largest privately held company, Cogent HMG, is not planning an initial public offering anytime soon, Dr. Houff says. The company’s goal is to “continue investing in smart growth to capture more of the hospital medicine market, expand offerings to our existing hospital clients, and provide additional support to our clinical teams on the ground,” he says. “We have a strong capital partner to help us in that effort and are not looking at the public markets at this time.”
Taking on stockholders is a tricky business—one that requires careful planning and a willingness from practice leaders and administrators to relinquish some autonomy to outside interests. And then there are the financial requirements.
“They’ve really got to be able to produce some serious revenue in order for somebody to be willing to put some money into them,” says Mark Hamm, CEO of EmCare Inpatient Services.
The lure of working for a private hospitalist company promises to continue to be an attractive one. Some are drawn by the leadership possibilities—those who “aspire to be the true alpha doctor,” as IPC’s Taylor puts it. Others are drawn by the stability of a larger company.
There also is flexibility in location, Dr. Holman notes.
“Now, with Cogent HMG, [hospitalists] have even more choices in terms of relocating within the same company,” he says. “So they can keep all of the benefits, keep all of the knowledge and familiarity of the system and philosophy of care that we employ, and just be able to transfer.”
continued below...
Emergency-Medicine Companies Increasingly Venture into HM
Hollywood, Fla.-based Hospital Physician Partners (HPP) was an ED business when more opportunity came knocking: Hospitals started asking them to provide some hospitalists to go with their emergency-room doctors.
Today, HPP is firmly in the hospital medicine business. And all signs point toward more and more hospitals hiring companies to handle both emergency care and inpatient care.
“In many ways, we expanded our efforts into hospitalist medicine as a result of requests from our hospital partners where we are providing emergency, ER medicine,” said Ed Weinberg, HPP’s chief operating officer.
“Their needs were such that they asked us to provide hospital medicine services. So from that, it became clear that it was an area that was really growing.
And that is something we are pursuing as vigorously as we are emergency medicine.”
Handling both emergency care and hospital medicine can help with the transition of the patient from the emergency room to a bed upstairs, he says.
“The efficiency is being able to transition a patient from being in the emergency department as an inpatient very seamlessly,” he said. “That’s where our efficiencies are, because we have physicians working who are carrying out the same philosophy.”
Out of the company’s 120 contracts, 15 of them are in hospital medicine, but it’s growing quickly, he says.
At EmCare, traditionally an emergency-medicine company that is now getting into hospital medicine, there are about 400 emergency-medicine programs and more than 50 HM programs.
Mark Hamm, CEO of EmCare Inpatient Services, says that it can be much more cost-effective to contract with one company for both hospitalist and emergency-medicine services—which he said hospitals have found attractive.
Their arrangements range from completely separate emergency and hospital medicine staffs to small, rural hospitals where ER physicians also do rounds.
Some hospitals “just don’t have the money for a full-time hospitalist and don’t really need one,” Hamm says.
The patient transitions tend to go more smoothly when both types of care are provided by EmCare. When they’re not, there can be slowdowns.
“Our goal is to quickly and appropriately move patients through the system,” he says. “If we have a hospitalist provider that’s not really on the same page, that can create bottlenecks. . . . But it’s a blip.
“Our goal is to sit down, even if it’s not an EmCare hospitalist, to sit down with that director and say, ‘Hey, look, let’s be the leader here, let’s work together and appropriately expedite these patients.’ We do the same thing on the hospitalist side.”
Inpatient care promises to be a big part of their future business, most executives agree.
“Hospital medicine,” Weinberg says, “is growing by leaps and bounds.” —TC
Dr. Houff says the majority of newly recruited physicians are coming out of residency but that the company is attracting physicians in the middle of their careers, along with physicians having backgrounds beyond internal medicine.
In Tallahassee at Capital Regional, Dr. Geers says that he feels there is support from the company that can protect his job quality, with “a little bit more room to negotiate with the hospital if the hospital wants us to take on new responsibilities.
“Whereas if we worked directly for the hospital, I don’t think we’d have much say in the matter,” he says.
He also says he is happy with the predictable schedule; he’s responsible for 7 a.m. to 7 p.m. and nothing more.
“If you’re finished rounding and you’ve seen all your patients and tied up all your loose ends, you’re not always there till 7 p.m.,” he points out. “Sometimes you can leave a little early....Once 7 p.m. comes, you’re not going to get paged in the middle of the night.”
Thomas R. Collins is a freelance medical writer based in Florida.
Wall Street’s Rosy View of Hospital Medicine
When IPC: The Hospitalist Company went public in January 2008, its stock price was $16 a share. In late July of this year, it was hovering a tick below $50 a share.
It’s been an obvious financial success—a performance that speaks well of the hospitalist specialty as a whole, says analyst Kevin Campbell, who covers IPC for Avondale Partners.
“Investors like the industry,” Campbell explains. “They see the need for hospitalists....When investors look at that, they see the opportunity for continued growth.”
IPC’s management team, he adds, has done “an excellent job of growing both the revenues and the earnings.”
Revenues in 2008 were $251 million. This year, they’re projected to be $454 million, an increase of 80%.
Six of 10 analysts say the company is a “strong buy,” one says it’s a “buy,” and for three others, it’s a “hold,” according to research listed on the NASDAQ website.
One of the key reasons IPC has performed well, Campbell says, is that when it makes an acquisition, physicians whose practices are bought are not paid everything at once; a portion is paid out later. Because the payment is a factor of the company’s performance, that encourages the physicians to keep their newly acquired practices performing optimally.
That’s different from scenarios in which “doctors would take their big check and retire,” he says, “and the operations for the practice would decline significantly. This is one way that IPCM [the stock symbol] can ensure that that doesn’t happen.”
Campbell also says it probably is unlikely that there will be another public offering of a hospitalist company in the near future. “There’s not a lot of companies of scale,” he says. “You have to have some scale before you would consider going public.”
R. Jeffrey Taylor, IPC’s president and COO, says another public offering from a hospitalist company isn’t that far-fetched.
“I would not be at all surprised to see someone else follow that path,” he says. “Frankly, it will probably be a little easier for the second company to do it because we have helped educate people about the hospitalist model, and fortunately the company and the stock have performed well. So I think it would be an easier sell to the public market the second time around. And I expect that’s more likely than not in the next few years.” —TC
Modest Gains
Hospitalists are earning a little more, working a little harder, and are less likely to switch jobs or careers, according to the 2011 State of Hospital Medicine report. The annual report, based on data collected jointly by SHM and the Medical Group Management Association (MGMA), offers more than 10,000 compensation and productivity data points for all types of hospitalists, including, for the first time, an exclusive look at academic hospitalists.
As previously reported, median adult hospitalist compensation increased to $220,619, a 2.6% increase from the $215,000 figure reported last year. “I think that’s a reflection of the market and demand for hospitalists, and the value that hospitals and other healthcare payors see that hospitalists bring,” says William “Tex” Landis, MD, FHM, medical director of Wellspan Hospitalists in York, Pa., and chair of SHM’s Practice Analysis Committee.
The compensation increases for hospitalists reported in the SHM-MGMA survey mirror results in other recent surveys. The 2011 Medical Group Compensation and Financial Survey, produced by the American Medical Group Association, found the overall average increase in physician compensation was 2.4%. Primary-care physicians (PCPs) reported a 2.6% increase in 2010, while the “hospitalist-internal medicine” category saw one of the steepest increases at 6.29%, according to the report (www.amga.org).
According to the 2011 MedScape Physician Compensation Report, 27% of the more than 15,000 physicians surveyed said their income increased from 2009 to 2010, whereas 50% said they saw no change. About 23% reported a decline in income, the report showed (www.medscape.com/features/slideshow/compensation/2011/).
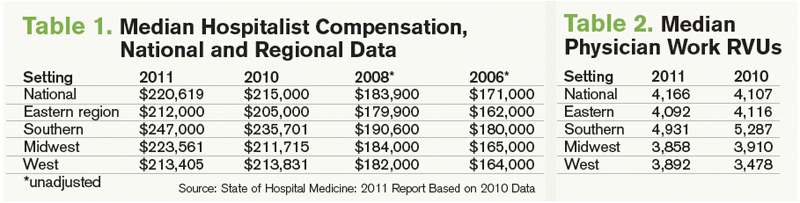
Continuing a decadelong trend, the SHM-MGMA report shows hospitalists in the South make the most (median compensation $247,000, up from $235,701 in 2010) and hospitalists in the East ($212,000, up from $205,000 in 2010) lag behind the other regions (see Table 1).

The Hospitalist spoke to five members of SHM’s Practice Analysis Committee (PAC) about the survey results, and each points to continued nationwide demand as the driver of increased compensation. However, the committee also cautions HM groups and directors to be leery of trending this data, as the report is based on a volunteer survey, the survey population changes year to year, and only two years of identical survey data are available.
“As hospital medicine continues to grow, the hospitals become so dependent on the services that the hospitalists provide,” says PAC member Scarlett Blue, RN-BC, MSN, NE-BC, CPHQ, vice president of quality and clinical development for Eagle Hospital Physicians. “[Hospitals] know HM is critical and…I think that hospitalists demonstrate tremendous value, which the hospitals and the management groups recognize.”
The 2011 report, available Sept. 14, compiled data about 4,633 hospitalists in 412 groups. Eighty-five percent of the respondents classified themselves as “adult” hospitalists, 5% as “pediatric” hospitalists, and 10% as both adult and pediatric. Of note, this is the first time SHM has produced compensation and productivity data in consecutive years. In addition to compensation, the survey provides drill-down capability on productivity and reimbursement metrics, along with specific data regarding night coverage arrangements (see “Survey Insights,”), financial support payments, physician turnover, and, for the first time, a look at nonphysician providers (NPPs) in HM practice (see “Nonphysician Provider Data Available for First Time,”).
continued below...
Nonphysician Provider Data Available for First Time

Hospitalist groups were asked about nurse practitioner (NP) and physician assistant (PA) employment, and 49% of HM groups reported having some type of nonphysician provider (NPP) on staff (see Figure 4). Those results, although not startling to some, should open the other half’s eyes, Dr. Landis says.
“Just looking to the future, I think most of us can see physician extenders¬⎯NPs and PAs⎯becoming more and more important in the delivery of hospital care,” he says. “We’re going to be looking to get more information about how that’s happening and what functions they’re performing and what resources, financially and otherwise, are required to help them be effective team members.”
Hawley says NPPs are a critical part of HM’s future but admits some hospitalists still are reluctant to work with NPPs because compensation and incentives are misaligned. “Oftentimes what a [physician] compensation plan will do is not provide for any work that is being done by the NPP,” she says. When physicians find out they also are being measured on patient satisfaction and other metrics, “then the NPP becomes very, very critical. So we’re seeing more and more acceptance. Our opinion, as a consulting group, is that there won’t be a [HM] program in this country that doesn’t somehow use nonphysician providers. There just aren’t enough hospitalists to go around.”
Dr. Landis says his committee is planning to collaborate with SHM’s Nonphysician Provider Committee to determine the best way to collect and disseminate NPP benchmarks. “That’s a future trend and everybody can see it,” he adds. “We have yet to solidify, though, how we’re going to measure and evaluate what’s going on there.” —JC
Hospitalist Productivity
Although hospitalists are earning more, the 2011 report also shows they are producing more work relative-value units (wRVUs) than ever before. The median physician wRVU rate annually for 2011 was 4,166, a 1.4% increase over the 2010 figure.
Hospitalists in the Eastern and Midwest regions reported relatively unchanged wRVUs when compared with 2010 figures. The Southern region, which outdistanced the other regions by more than 800 wRVUs per physician, reported a 6.7% decrease in wRVUs—4,931 in 2011 compared with 5,287 in 2010. On the flipside, the Western region showed a 11.9% increase per physician (see Table 2, left).
PAC committee members agree the wRVU variance between regions is difficult to explain, but most agree the slight year-over-year increase in productivity shows the specialty is stabilizing in terms of what productivity is expected from the average hospitalist.
“Maybe it is an indication that the field is maturing and we’re settling in at some data points that we can now potentially put some stock into,” says Beth E. Hawley, MBA, FACHE, senior vice president of The Cogent Group, a consulting division of Brentwood, Tenn.-based Cogent HMG. “Before, [the figures] changed dramatically from survey to survey; I think we’re seeing more stability now from last year to this year.

—Beth E. Hawley, MBA, FACHE, senior vice president, The Cogent Group, Brentwood, Tenn., SHM Practice Analysis Committee member
“It’s helpful to be able to sort [wRVUs] by employment model, by region, by large and small hospital. We can really get some better benchmarks, in terms of what should be the expectation.”
Chris Frost, MD, FHM, national medical director of hospital medicine services for HCA, says he remains somewhat hesitant to say HM is “settling into a number” for expected wRVUs, as he routinely hears from hospital administrators looking for “additional efficiencies that we can put in place to allow and position the hospitalists to be more productive” while maintaining a high quality care delivery model. He’s also puzzled by the geographic discrepancies. “I just have to scratch my head. I haven’t entirely figured that out yet,” he says.
That said, Dr. Frost agrees the wRVU benchmarks are the most useful in terms of “billable productivity. But I also would like to see—or believe—one of the reasons compensation is going up and the work RVU is flat is hospitalists are being recognized for their value in other arenas, as it relates to the transition from the fee-for-service to pay-for-value-type models, championing effective transitions of care, leading process improvement teams, etc. Those things can’t, or don’t, necessarily lend themselves well to a work RVU equivalent.”
The Buzz: Financial Support
First reported at HM11 in May, the survey shows hospitalist support payments increased more than 39%, to $136,403 per FTE hospitalist in 2011 from $98,253 in 2010. PAC members and other hospitalist experts in practice management attribute the startling increase in support payments to more accurate reporting. Others note that the rise in support payments could be attributed to the decline in collection of professional fees, a direct result of the economic downturn.
And, according to Dr. Landis, hospitals are more willing today to fund hospitalist services than ever before.
“I think [the rise in HM support] payments is because of the evolution of healthcare in the hospital as a whole,” he says. “Hospitals are looking to hospitalists to help them provide the care that that patients and families need, expect, and want. And we’re stepping up to the plate to do it, and they’re paying us to do it. I think that’s the story.
“If you want to tie that with why there’s $136,000 going per hospitalist, [it’s] because they want us there for that rapid-response team, and rapid-response teams don’t generate a lot of RVUs necessarily.”
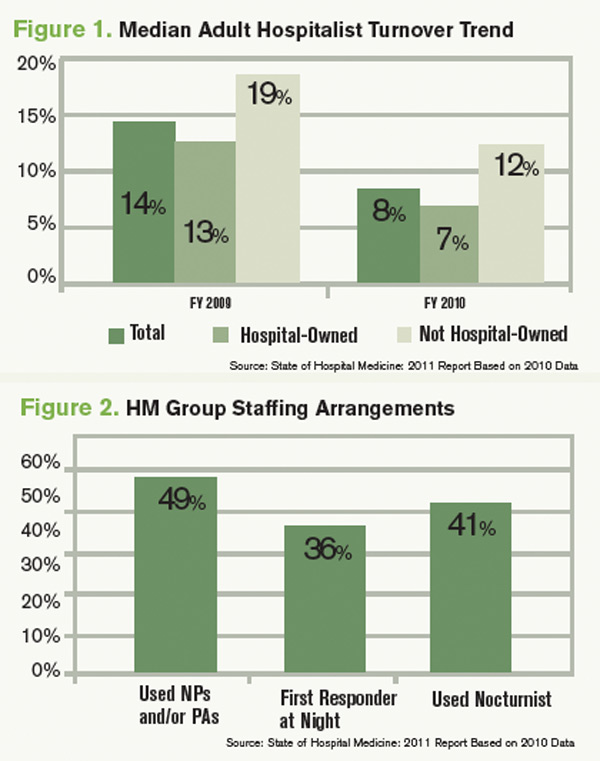
Hawley, the consultant, agrees the percentage increase in financial support is somewhat shocking, but she isn’t surprised by the median figure. She knows hospitals are asking more of HM groups, and all of those value-added, non-billable tasks and responsibilities come with a cost.
“It’s not totally surprising, but it’s a big leap,” she says. “I would say at least some of that has to be driven by the fact that we have hospitals and integrated delivery systems employing more and more of these physicians that responded to this survey, as well as physicians’ practices are perhaps becoming more educated as to what their finances are. There’s a better understanding of allocation of overhead, of billing fees, all of those things that go into a practice where … that may not have been as clear to folks when HM was a bit younger.”
Downward Trend: Hospitalist Turnover
In what some are calling a positive sign for the specialty, hospitalist turnover dropped to 8% in 2011, compared with a 14% turnover rate among hospitalist groups serving adults in 2010 (see Figure 1). Rates declined for both hospital-owned and non-hospital-owned groups, according to the report. Hawley, the consultant, says the decline in physician movement is “consistent” with what she sees in daily interactions with HM groups. Moreover, she considers that trend to be just as important as the overall decline in hospitalist turnover.
“[The survey indicates] more physicians are employed by a hospital or an integrated hospital system. With that, what we’re seeing on the consulting side is there are certain benefits with being employed by a hospital or healthcare system, in terms of retirement plans, things that [hospitalists] may not find as rich in a private practice or with a multispecialty group,” she says. When a hospitalist becomes employed with a hospital system, she hears them say, ‘This is where I want to live and raise my family.’ People choose this type of employment for a reason.”
That has been the experience of PAC member Tierza Stephan, MD, FACP, SFHM, who supervises more than 135 hospitalists as hospitalist district medical director for Minneapolis-based Allina Medical Clinic. Dr. Stephan currently has 15 openings at six of the eight HM groups she directs. Even so, she admits that her programs have been “blessed with low turnover.” The upshot: “We use that when we talk to the C-suite,” she says. “It’s way more costly to have one physician come in, train them, and then have them leave. The low turnover rate gets factored into the cost of what they’re paying.”
Dr. Frost says HM is becoming “less and less a stopover specialty,” as more physicians adopt HM as their career. Dr. Landis says that, although just two consecutive years of data are available, the decline in turnover rate is a good sign for the specialty.
“I think many of us suspect that as the hospitalist movement matures that there hopefully will be a stabilization of the turnover rate,” he says. “Hospitalists tend to be very portable, and when there’s a lot of open jobs and only a few hospitalists, there can be even more and more [turnover]. Typically, someone gets themselves into a situation, they feel that they’re overworked, underpaid, underappreciated, they’re going to look for another job, and those jobs are out there. As the market stabilizes, there will probably be less and less moving around.”
Interactive regional survey breakdowns
Jason Carris is editor of The Hospitalist.
Advice From a Numbers Guy

A self-described “numbers” guy, Troy Ahlstrom, MD, SFHM, agrees regional data is just as important as, if not more important than, the national numbers. He stresses knowing your market, your competitors, your hospital culture—and using that information along with the benchmarking data to formulate expectations for your group.
“Oftentimes you are measured against the guy next door,” says Dr. Ahlstrom, CFO of Traverse City-based Hospitalists of Northern Michigan. “You have to know the numbers, because [administrators] are going to know the numbers.”
Dr. Ahlstrom offers these tips for incorporating benchmarking data into your practice:
- Know your neighbors. “If you keep in mind your local needs, then you can look at the data and start to evaluate what parts are going to help you better formulate a practice that brings on the right people, does the right work, and continues to produce the amount of workload and compensation that makes sure they are happy in the future,” he says.
- Evaluate how applicable the data is. Pay attention to the total number of survey respondents in each category, and the standard deviation around the mean. “In other words, what is the central tendency of the data? You might find data in subsections that you find interesting, but it might not be data that has a central tendency,” he says. “Find data sets that are most applicable to your practice while assessing variations from the larger data sets. Consider how and why your practice might vary from the report as part of your evaluation.”
- Pick out trends and look at them in total. The key is to avoid looking at data points in isolation. “It’s important to look at trends in the data over time, and pick out where those trends are going to go,” he says.
- Involve your people. “I think that this data being available from the [provider] side and management side is a good thing,” Dr. Ahlstrom explains. “The more we are involved in understanding the trends in HM, the better we are going to plan where we are going in the future.”
—JC
Hospitalists are earning a little more, working a little harder, and are less likely to switch jobs or careers, according to the 2011 State of Hospital Medicine report. The annual report, based on data collected jointly by SHM and the Medical Group Management Association (MGMA), offers more than 10,000 compensation and productivity data points for all types of hospitalists, including, for the first time, an exclusive look at academic hospitalists.
As previously reported, median adult hospitalist compensation increased to $220,619, a 2.6% increase from the $215,000 figure reported last year. “I think that’s a reflection of the market and demand for hospitalists, and the value that hospitals and other healthcare payors see that hospitalists bring,” says William “Tex” Landis, MD, FHM, medical director of Wellspan Hospitalists in York, Pa., and chair of SHM’s Practice Analysis Committee.
The compensation increases for hospitalists reported in the SHM-MGMA survey mirror results in other recent surveys. The 2011 Medical Group Compensation and Financial Survey, produced by the American Medical Group Association, found the overall average increase in physician compensation was 2.4%. Primary-care physicians (PCPs) reported a 2.6% increase in 2010, while the “hospitalist-internal medicine” category saw one of the steepest increases at 6.29%, according to the report (www.amga.org).
According to the 2011 MedScape Physician Compensation Report, 27% of the more than 15,000 physicians surveyed said their income increased from 2009 to 2010, whereas 50% said they saw no change. About 23% reported a decline in income, the report showed (www.medscape.com/features/slideshow/compensation/2011/).
Continuing a decadelong trend, the SHM-MGMA report shows hospitalists in the South make the most (median compensation $247,000, up from $235,701 in 2010) and hospitalists in the East ($212,000, up from $205,000 in 2010) lag behind the other regions (see Table 1).
The Hospitalist spoke to five members of SHM’s Practice Analysis Committee (PAC) about the survey results, and each points to continued nationwide demand as the driver of increased compensation. However, the committee also cautions HM groups and directors to be leery of trending this data, as the report is based on a volunteer survey, the survey population changes year to year, and only two years of identical survey data are available.
“As hospital medicine continues to grow, the hospitals become so dependent on the services that the hospitalists provide,” says PAC member Scarlett Blue, RN-BC, MSN, NE-BC, CPHQ, vice president of quality and clinical development for Eagle Hospital Physicians. “[Hospitals] know HM is critical and…I think that hospitalists demonstrate tremendous value, which the hospitals and the management groups recognize.”
The 2011 report, available Sept. 14, compiled data about 4,633 hospitalists in 412 groups. Eighty-five percent of the respondents classified themselves as “adult” hospitalists, 5% as “pediatric” hospitalists, and 10% as both adult and pediatric. Of note, this is the first time SHM has produced compensation and productivity data in consecutive years. In addition to compensation, the survey provides drill-down capability on productivity and reimbursement metrics, along with specific data regarding night coverage arrangements (see “Survey Insights,”), financial support payments, physician turnover, and, for the first time, a look at nonphysician providers (NPPs) in HM practice (see “Nonphysician Provider Data Available for First Time,”).
continued below...
Nonphysician Provider Data Available for First Time
Hospitalist groups were asked about nurse practitioner (NP) and physician assistant (PA) employment, and 49% of HM groups reported having some type of nonphysician provider (NPP) on staff (see Figure 4). Those results, although not startling to some, should open the other half’s eyes, Dr. Landis says.
“Just looking to the future, I think most of us can see physician extenders¬⎯NPs and PAs⎯becoming more and more important in the delivery of hospital care,” he says. “We’re going to be looking to get more information about how that’s happening and what functions they’re performing and what resources, financially and otherwise, are required to help them be effective team members.”
Hawley says NPPs are a critical part of HM’s future but admits some hospitalists still are reluctant to work with NPPs because compensation and incentives are misaligned. “Oftentimes what a [physician] compensation plan will do is not provide for any work that is being done by the NPP,” she says. When physicians find out they also are being measured on patient satisfaction and other metrics, “then the NPP becomes very, very critical. So we’re seeing more and more acceptance. Our opinion, as a consulting group, is that there won’t be a [HM] program in this country that doesn’t somehow use nonphysician providers. There just aren’t enough hospitalists to go around.”
Dr. Landis says his committee is planning to collaborate with SHM’s Nonphysician Provider Committee to determine the best way to collect and disseminate NPP benchmarks. “That’s a future trend and everybody can see it,” he adds. “We have yet to solidify, though, how we’re going to measure and evaluate what’s going on there.” —JC
Hospitalist Productivity
Although hospitalists are earning more, the 2011 report also shows they are producing more work relative-value units (wRVUs) than ever before. The median physician wRVU rate annually for 2011 was 4,166, a 1.4% increase over the 2010 figure.
Hospitalists in the Eastern and Midwest regions reported relatively unchanged wRVUs when compared with 2010 figures. The Southern region, which outdistanced the other regions by more than 800 wRVUs per physician, reported a 6.7% decrease in wRVUs—4,931 in 2011 compared with 5,287 in 2010. On the flipside, the Western region showed a 11.9% increase per physician (see Table 2, left).
PAC committee members agree the wRVU variance between regions is difficult to explain, but most agree the slight year-over-year increase in productivity shows the specialty is stabilizing in terms of what productivity is expected from the average hospitalist.
“Maybe it is an indication that the field is maturing and we’re settling in at some data points that we can now potentially put some stock into,” says Beth E. Hawley, MBA, FACHE, senior vice president of The Cogent Group, a consulting division of Brentwood, Tenn.-based Cogent HMG. “Before, [the figures] changed dramatically from survey to survey; I think we’re seeing more stability now from last year to this year.
—Beth E. Hawley, MBA, FACHE, senior vice president, The Cogent Group, Brentwood, Tenn., SHM Practice Analysis Committee member
“It’s helpful to be able to sort [wRVUs] by employment model, by region, by large and small hospital. We can really get some better benchmarks, in terms of what should be the expectation.”
Chris Frost, MD, FHM, national medical director of hospital medicine services for HCA, says he remains somewhat hesitant to say HM is “settling into a number” for expected wRVUs, as he routinely hears from hospital administrators looking for “additional efficiencies that we can put in place to allow and position the hospitalists to be more productive” while maintaining a high quality care delivery model. He’s also puzzled by the geographic discrepancies. “I just have to scratch my head. I haven’t entirely figured that out yet,” he says.
That said, Dr. Frost agrees the wRVU benchmarks are the most useful in terms of “billable productivity. But I also would like to see—or believe—one of the reasons compensation is going up and the work RVU is flat is hospitalists are being recognized for their value in other arenas, as it relates to the transition from the fee-for-service to pay-for-value-type models, championing effective transitions of care, leading process improvement teams, etc. Those things can’t, or don’t, necessarily lend themselves well to a work RVU equivalent.”
The Buzz: Financial Support
First reported at HM11 in May, the survey shows hospitalist support payments increased more than 39%, to $136,403 per FTE hospitalist in 2011 from $98,253 in 2010. PAC members and other hospitalist experts in practice management attribute the startling increase in support payments to more accurate reporting. Others note that the rise in support payments could be attributed to the decline in collection of professional fees, a direct result of the economic downturn.
And, according to Dr. Landis, hospitals are more willing today to fund hospitalist services than ever before.
“I think [the rise in HM support] payments is because of the evolution of healthcare in the hospital as a whole,” he says. “Hospitals are looking to hospitalists to help them provide the care that that patients and families need, expect, and want. And we’re stepping up to the plate to do it, and they’re paying us to do it. I think that’s the story.
“If you want to tie that with why there’s $136,000 going per hospitalist, [it’s] because they want us there for that rapid-response team, and rapid-response teams don’t generate a lot of RVUs necessarily.”
Hawley, the consultant, agrees the percentage increase in financial support is somewhat shocking, but she isn’t surprised by the median figure. She knows hospitals are asking more of HM groups, and all of those value-added, non-billable tasks and responsibilities come with a cost.
“It’s not totally surprising, but it’s a big leap,” she says. “I would say at least some of that has to be driven by the fact that we have hospitals and integrated delivery systems employing more and more of these physicians that responded to this survey, as well as physicians’ practices are perhaps becoming more educated as to what their finances are. There’s a better understanding of allocation of overhead, of billing fees, all of those things that go into a practice where … that may not have been as clear to folks when HM was a bit younger.”
Downward Trend: Hospitalist Turnover
In what some are calling a positive sign for the specialty, hospitalist turnover dropped to 8% in 2011, compared with a 14% turnover rate among hospitalist groups serving adults in 2010 (see Figure 1). Rates declined for both hospital-owned and non-hospital-owned groups, according to the report. Hawley, the consultant, says the decline in physician movement is “consistent” with what she sees in daily interactions with HM groups. Moreover, she considers that trend to be just as important as the overall decline in hospitalist turnover.
“[The survey indicates] more physicians are employed by a hospital or an integrated hospital system. With that, what we’re seeing on the consulting side is there are certain benefits with being employed by a hospital or healthcare system, in terms of retirement plans, things that [hospitalists] may not find as rich in a private practice or with a multispecialty group,” she says. When a hospitalist becomes employed with a hospital system, she hears them say, ‘This is where I want to live and raise my family.’ People choose this type of employment for a reason.”
That has been the experience of PAC member Tierza Stephan, MD, FACP, SFHM, who supervises more than 135 hospitalists as hospitalist district medical director for Minneapolis-based Allina Medical Clinic. Dr. Stephan currently has 15 openings at six of the eight HM groups she directs. Even so, she admits that her programs have been “blessed with low turnover.” The upshot: “We use that when we talk to the C-suite,” she says. “It’s way more costly to have one physician come in, train them, and then have them leave. The low turnover rate gets factored into the cost of what they’re paying.”
Dr. Frost says HM is becoming “less and less a stopover specialty,” as more physicians adopt HM as their career. Dr. Landis says that, although just two consecutive years of data are available, the decline in turnover rate is a good sign for the specialty.
“I think many of us suspect that as the hospitalist movement matures that there hopefully will be a stabilization of the turnover rate,” he says. “Hospitalists tend to be very portable, and when there’s a lot of open jobs and only a few hospitalists, there can be even more and more [turnover]. Typically, someone gets themselves into a situation, they feel that they’re overworked, underpaid, underappreciated, they’re going to look for another job, and those jobs are out there. As the market stabilizes, there will probably be less and less moving around.”
Interactive regional survey breakdowns
Jason Carris is editor of The Hospitalist.
Advice From a Numbers Guy
A self-described “numbers” guy, Troy Ahlstrom, MD, SFHM, agrees regional data is just as important as, if not more important than, the national numbers. He stresses knowing your market, your competitors, your hospital culture—and using that information along with the benchmarking data to formulate expectations for your group.
“Oftentimes you are measured against the guy next door,” says Dr. Ahlstrom, CFO of Traverse City-based Hospitalists of Northern Michigan. “You have to know the numbers, because [administrators] are going to know the numbers.”
Dr. Ahlstrom offers these tips for incorporating benchmarking data into your practice:
- Know your neighbors. “If you keep in mind your local needs, then you can look at the data and start to evaluate what parts are going to help you better formulate a practice that brings on the right people, does the right work, and continues to produce the amount of workload and compensation that makes sure they are happy in the future,” he says.
- Evaluate how applicable the data is. Pay attention to the total number of survey respondents in each category, and the standard deviation around the mean. “In other words, what is the central tendency of the data? You might find data in subsections that you find interesting, but it might not be data that has a central tendency,” he says. “Find data sets that are most applicable to your practice while assessing variations from the larger data sets. Consider how and why your practice might vary from the report as part of your evaluation.”
- Pick out trends and look at them in total. The key is to avoid looking at data points in isolation. “It’s important to look at trends in the data over time, and pick out where those trends are going to go,” he says.
- Involve your people. “I think that this data being available from the [provider] side and management side is a good thing,” Dr. Ahlstrom explains. “The more we are involved in understanding the trends in HM, the better we are going to plan where we are going in the future.”
—JC
Hospitalists are earning a little more, working a little harder, and are less likely to switch jobs or careers, according to the 2011 State of Hospital Medicine report. The annual report, based on data collected jointly by SHM and the Medical Group Management Association (MGMA), offers more than 10,000 compensation and productivity data points for all types of hospitalists, including, for the first time, an exclusive look at academic hospitalists.
As previously reported, median adult hospitalist compensation increased to $220,619, a 2.6% increase from the $215,000 figure reported last year. “I think that’s a reflection of the market and demand for hospitalists, and the value that hospitals and other healthcare payors see that hospitalists bring,” says William “Tex” Landis, MD, FHM, medical director of Wellspan Hospitalists in York, Pa., and chair of SHM’s Practice Analysis Committee.
The compensation increases for hospitalists reported in the SHM-MGMA survey mirror results in other recent surveys. The 2011 Medical Group Compensation and Financial Survey, produced by the American Medical Group Association, found the overall average increase in physician compensation was 2.4%. Primary-care physicians (PCPs) reported a 2.6% increase in 2010, while the “hospitalist-internal medicine” category saw one of the steepest increases at 6.29%, according to the report (www.amga.org).
According to the 2011 MedScape Physician Compensation Report, 27% of the more than 15,000 physicians surveyed said their income increased from 2009 to 2010, whereas 50% said they saw no change. About 23% reported a decline in income, the report showed (www.medscape.com/features/slideshow/compensation/2011/).
Continuing a decadelong trend, the SHM-MGMA report shows hospitalists in the South make the most (median compensation $247,000, up from $235,701 in 2010) and hospitalists in the East ($212,000, up from $205,000 in 2010) lag behind the other regions (see Table 1).
The Hospitalist spoke to five members of SHM’s Practice Analysis Committee (PAC) about the survey results, and each points to continued nationwide demand as the driver of increased compensation. However, the committee also cautions HM groups and directors to be leery of trending this data, as the report is based on a volunteer survey, the survey population changes year to year, and only two years of identical survey data are available.
“As hospital medicine continues to grow, the hospitals become so dependent on the services that the hospitalists provide,” says PAC member Scarlett Blue, RN-BC, MSN, NE-BC, CPHQ, vice president of quality and clinical development for Eagle Hospital Physicians. “[Hospitals] know HM is critical and…I think that hospitalists demonstrate tremendous value, which the hospitals and the management groups recognize.”
The 2011 report, available Sept. 14, compiled data about 4,633 hospitalists in 412 groups. Eighty-five percent of the respondents classified themselves as “adult” hospitalists, 5% as “pediatric” hospitalists, and 10% as both adult and pediatric. Of note, this is the first time SHM has produced compensation and productivity data in consecutive years. In addition to compensation, the survey provides drill-down capability on productivity and reimbursement metrics, along with specific data regarding night coverage arrangements (see “Survey Insights,”), financial support payments, physician turnover, and, for the first time, a look at nonphysician providers (NPPs) in HM practice (see “Nonphysician Provider Data Available for First Time,”).
continued below...
Nonphysician Provider Data Available for First Time
Hospitalist groups were asked about nurse practitioner (NP) and physician assistant (PA) employment, and 49% of HM groups reported having some type of nonphysician provider (NPP) on staff (see Figure 4). Those results, although not startling to some, should open the other half’s eyes, Dr. Landis says.
“Just looking to the future, I think most of us can see physician extenders¬⎯NPs and PAs⎯becoming more and more important in the delivery of hospital care,” he says. “We’re going to be looking to get more information about how that’s happening and what functions they’re performing and what resources, financially and otherwise, are required to help them be effective team members.”
Hawley says NPPs are a critical part of HM’s future but admits some hospitalists still are reluctant to work with NPPs because compensation and incentives are misaligned. “Oftentimes what a [physician] compensation plan will do is not provide for any work that is being done by the NPP,” she says. When physicians find out they also are being measured on patient satisfaction and other metrics, “then the NPP becomes very, very critical. So we’re seeing more and more acceptance. Our opinion, as a consulting group, is that there won’t be a [HM] program in this country that doesn’t somehow use nonphysician providers. There just aren’t enough hospitalists to go around.”
Dr. Landis says his committee is planning to collaborate with SHM’s Nonphysician Provider Committee to determine the best way to collect and disseminate NPP benchmarks. “That’s a future trend and everybody can see it,” he adds. “We have yet to solidify, though, how we’re going to measure and evaluate what’s going on there.” —JC
Hospitalist Productivity
Although hospitalists are earning more, the 2011 report also shows they are producing more work relative-value units (wRVUs) than ever before. The median physician wRVU rate annually for 2011 was 4,166, a 1.4% increase over the 2010 figure.
Hospitalists in the Eastern and Midwest regions reported relatively unchanged wRVUs when compared with 2010 figures. The Southern region, which outdistanced the other regions by more than 800 wRVUs per physician, reported a 6.7% decrease in wRVUs—4,931 in 2011 compared with 5,287 in 2010. On the flipside, the Western region showed a 11.9% increase per physician (see Table 2, left).
PAC committee members agree the wRVU variance between regions is difficult to explain, but most agree the slight year-over-year increase in productivity shows the specialty is stabilizing in terms of what productivity is expected from the average hospitalist.
“Maybe it is an indication that the field is maturing and we’re settling in at some data points that we can now potentially put some stock into,” says Beth E. Hawley, MBA, FACHE, senior vice president of The Cogent Group, a consulting division of Brentwood, Tenn.-based Cogent HMG. “Before, [the figures] changed dramatically from survey to survey; I think we’re seeing more stability now from last year to this year.
—Beth E. Hawley, MBA, FACHE, senior vice president, The Cogent Group, Brentwood, Tenn., SHM Practice Analysis Committee member
“It’s helpful to be able to sort [wRVUs] by employment model, by region, by large and small hospital. We can really get some better benchmarks, in terms of what should be the expectation.”
Chris Frost, MD, FHM, national medical director of hospital medicine services for HCA, says he remains somewhat hesitant to say HM is “settling into a number” for expected wRVUs, as he routinely hears from hospital administrators looking for “additional efficiencies that we can put in place to allow and position the hospitalists to be more productive” while maintaining a high quality care delivery model. He’s also puzzled by the geographic discrepancies. “I just have to scratch my head. I haven’t entirely figured that out yet,” he says.
That said, Dr. Frost agrees the wRVU benchmarks are the most useful in terms of “billable productivity. But I also would like to see—or believe—one of the reasons compensation is going up and the work RVU is flat is hospitalists are being recognized for their value in other arenas, as it relates to the transition from the fee-for-service to pay-for-value-type models, championing effective transitions of care, leading process improvement teams, etc. Those things can’t, or don’t, necessarily lend themselves well to a work RVU equivalent.”
The Buzz: Financial Support
First reported at HM11 in May, the survey shows hospitalist support payments increased more than 39%, to $136,403 per FTE hospitalist in 2011 from $98,253 in 2010. PAC members and other hospitalist experts in practice management attribute the startling increase in support payments to more accurate reporting. Others note that the rise in support payments could be attributed to the decline in collection of professional fees, a direct result of the economic downturn.
And, according to Dr. Landis, hospitals are more willing today to fund hospitalist services than ever before.
“I think [the rise in HM support] payments is because of the evolution of healthcare in the hospital as a whole,” he says. “Hospitals are looking to hospitalists to help them provide the care that that patients and families need, expect, and want. And we’re stepping up to the plate to do it, and they’re paying us to do it. I think that’s the story.
“If you want to tie that with why there’s $136,000 going per hospitalist, [it’s] because they want us there for that rapid-response team, and rapid-response teams don’t generate a lot of RVUs necessarily.”
Hawley, the consultant, agrees the percentage increase in financial support is somewhat shocking, but she isn’t surprised by the median figure. She knows hospitals are asking more of HM groups, and all of those value-added, non-billable tasks and responsibilities come with a cost.
“It’s not totally surprising, but it’s a big leap,” she says. “I would say at least some of that has to be driven by the fact that we have hospitals and integrated delivery systems employing more and more of these physicians that responded to this survey, as well as physicians’ practices are perhaps becoming more educated as to what their finances are. There’s a better understanding of allocation of overhead, of billing fees, all of those things that go into a practice where … that may not have been as clear to folks when HM was a bit younger.”
Downward Trend: Hospitalist Turnover
In what some are calling a positive sign for the specialty, hospitalist turnover dropped to 8% in 2011, compared with a 14% turnover rate among hospitalist groups serving adults in 2010 (see Figure 1). Rates declined for both hospital-owned and non-hospital-owned groups, according to the report. Hawley, the consultant, says the decline in physician movement is “consistent” with what she sees in daily interactions with HM groups. Moreover, she considers that trend to be just as important as the overall decline in hospitalist turnover.
“[The survey indicates] more physicians are employed by a hospital or an integrated hospital system. With that, what we’re seeing on the consulting side is there are certain benefits with being employed by a hospital or healthcare system, in terms of retirement plans, things that [hospitalists] may not find as rich in a private practice or with a multispecialty group,” she says. When a hospitalist becomes employed with a hospital system, she hears them say, ‘This is where I want to live and raise my family.’ People choose this type of employment for a reason.”
That has been the experience of PAC member Tierza Stephan, MD, FACP, SFHM, who supervises more than 135 hospitalists as hospitalist district medical director for Minneapolis-based Allina Medical Clinic. Dr. Stephan currently has 15 openings at six of the eight HM groups she directs. Even so, she admits that her programs have been “blessed with low turnover.” The upshot: “We use that when we talk to the C-suite,” she says. “It’s way more costly to have one physician come in, train them, and then have them leave. The low turnover rate gets factored into the cost of what they’re paying.”
Dr. Frost says HM is becoming “less and less a stopover specialty,” as more physicians adopt HM as their career. Dr. Landis says that, although just two consecutive years of data are available, the decline in turnover rate is a good sign for the specialty.
“I think many of us suspect that as the hospitalist movement matures that there hopefully will be a stabilization of the turnover rate,” he says. “Hospitalists tend to be very portable, and when there’s a lot of open jobs and only a few hospitalists, there can be even more and more [turnover]. Typically, someone gets themselves into a situation, they feel that they’re overworked, underpaid, underappreciated, they’re going to look for another job, and those jobs are out there. As the market stabilizes, there will probably be less and less moving around.”
Interactive regional survey breakdowns
Jason Carris is editor of The Hospitalist.
Advice From a Numbers Guy
A self-described “numbers” guy, Troy Ahlstrom, MD, SFHM, agrees regional data is just as important as, if not more important than, the national numbers. He stresses knowing your market, your competitors, your hospital culture—and using that information along with the benchmarking data to formulate expectations for your group.
“Oftentimes you are measured against the guy next door,” says Dr. Ahlstrom, CFO of Traverse City-based Hospitalists of Northern Michigan. “You have to know the numbers, because [administrators] are going to know the numbers.”
Dr. Ahlstrom offers these tips for incorporating benchmarking data into your practice:
- Know your neighbors. “If you keep in mind your local needs, then you can look at the data and start to evaluate what parts are going to help you better formulate a practice that brings on the right people, does the right work, and continues to produce the amount of workload and compensation that makes sure they are happy in the future,” he says.
- Evaluate how applicable the data is. Pay attention to the total number of survey respondents in each category, and the standard deviation around the mean. “In other words, what is the central tendency of the data? You might find data in subsections that you find interesting, but it might not be data that has a central tendency,” he says. “Find data sets that are most applicable to your practice while assessing variations from the larger data sets. Consider how and why your practice might vary from the report as part of your evaluation.”
- Pick out trends and look at them in total. The key is to avoid looking at data points in isolation. “It’s important to look at trends in the data over time, and pick out where those trends are going to go,” he says.
- Involve your people. “I think that this data being available from the [provider] side and management side is a good thing,” Dr. Ahlstrom explains. “The more we are involved in understanding the trends in HM, the better we are going to plan where we are going in the future.”
—JC
The Bigger Picture

For those of you who were kind enough to pick up my column in The Hospitalist last month (see “A Critical First Step,” p. 56), you spent a few minutes reading my thoughts on the value of hospitalists. I mentioned the fact that the U.S. is moving rapidly toward a value-based system to purchase healthcare and that all healthcare providers, including hospitalists, will be increasingly judged on the value of care they deliver to their patients and the healthcare system. (Remember, value=quality÷cost.)
I believe that the hospitalist programs that are going to be the most successful are those that are able to continually measure their quality and costs, allowing them to make improvements. These are the groups that will understand their own performance well before others make their “value” judgments.
History Lesson
In his famous book “The Wealth of Nations,” 18th-century economist Adam Smith used the example of a pin factory to show how specialization improved human productivity. The process of producing a pin was broken down into many small tasks, each done by a different “specialist.” This resulted not only in increased efficiency, but also increased productivity. The factory was then able to reinvest the profits in even more efficient machinery, which was able to reduce labor costs. The lower cost for pins was a benefit, and it was spread across the entire population.
We have seen similar examples in American healthcare. In many American hospitals, the images of CT scans performed during nighttime hours are transmitted to India and other Asian countries where highly trained radiologists interpret the scans and transmit their interpretations back to the physicians caring for the patients. Like the pin factory workers, these radiologists are specialists with unique skills; they operate specialized machinery to make the system more efficient with resultant lower costs. At the level of the individual patient, this system means getting test results back in a more timely fashion. Increased quality and lower costs: These are high-value providers.
It should be obvious to us that hospitalists are “specialists.” While most hospitalists are trained as general internists, pediatricians, and family physicians, you and I are “specialists” who focus our efforts on the care of hospitalized patients. In the late 1990s, much was made of the fact that hospitalists were able to reduce hospital costs because of decreased length of stay (LOS) for patients, without any adverse effects on clinical outcomes. Today, hospitalists number more than 30,000 nationwide, and virtually all American hospitals with more than 200 beds have hospitalists.
Hospitals hired hospitalists in droves because they were perceived as “inpatient specialists” who were able to reduce the cost of healthcare delivery. Like lower pin costs, this economic benefit was spread across the entire population. Hospitalist “value” went up because of lower costs.
But an interesting thing changed over the past decade: It seems that fewer and fewer people are talking about hospitalists reducing LOS. They just expect it. LOS is raised as an issue only if it goes up. In many hospitals, the budget now takes into account the average LOS based on hospitalist care. (I suspect that in 18th-century Scotland, people also grew accustomed to the lower cost of pins, and grew to expect it, and the cost of pins was raised as an issue only if the price went up.)
But has anyone spoken to the hospitalists? Has anyone asked us about the benefits of our profession? Many of the hospitalists I meet mention “reduction of length of stay” as a main reason to have hospitalists. I think that response was appropriate more often than not over the past 15 years.
But today, ask any hospital administrator that same question, and what do you expect the answer to be? It should not be surprising to hospitalists that most hospitals expect much more from their hospitalist programs than “just reducing the length of stay.” These are the same hospitals that often support—to the tune of more than $100,000 per hospitalist full-time equivalent—your HM program. If your hospitalist program is anything like mine at Beth Israel Deaconess Medical Center in Boston, this represents millions of dollars to the hospitalist program budget.
Increased Pressures
The fact that hospitals’ expectations of hospitalists have changed should not come as a surprise. Americans’ expectations of hospitals have changed markedly over the past 15 years. In the 1990s, when hospital medicine was “born,” there was little mention of quality and patient satisfaction when it came to healthcare. Who would argue that improving quality and patient satisfaction is a bad thing?
Over the past decade, we’ve seen the development of Medicare core measures and the link between patient outcomes and Medicare reimbursement. Hospitals could not have achieved many of their performance improvements without their partnerships with hospitalists.
Hospitals are under increasing pressure to not only decrease costs, but also improve quality. It is understandable that they turn to the “inpatient specialists”—the hospitalists—to help them meet societal expectations. But as hospitalists, this puts pressure on us to continually improve our game—or face the consequences. A pin factory in Scotland can only survive if it produces higher-quality pins at a lower cost than its competitor.
Hospitals and our American healthcare system expect much more today from hospitalists, and they should; patients’ lives are at stake. It should not be a surprise that hospitalist programs that struggle are those that fail to meet expectations. Successful hospitalist programs, the ones that are able to demonstrate their “value,” do so well beyond knowing their patient’s average length of stay.
I am interested in learning about your efforts to demonstrate the “value” of your hospitalist group. Feel free to email me at [email protected].
Dr. Li is president of SHM.
For those of you who were kind enough to pick up my column in The Hospitalist last month (see “A Critical First Step,” p. 56), you spent a few minutes reading my thoughts on the value of hospitalists. I mentioned the fact that the U.S. is moving rapidly toward a value-based system to purchase healthcare and that all healthcare providers, including hospitalists, will be increasingly judged on the value of care they deliver to their patients and the healthcare system. (Remember, value=quality÷cost.)
I believe that the hospitalist programs that are going to be the most successful are those that are able to continually measure their quality and costs, allowing them to make improvements. These are the groups that will understand their own performance well before others make their “value” judgments.
History Lesson
In his famous book “The Wealth of Nations,” 18th-century economist Adam Smith used the example of a pin factory to show how specialization improved human productivity. The process of producing a pin was broken down into many small tasks, each done by a different “specialist.” This resulted not only in increased efficiency, but also increased productivity. The factory was then able to reinvest the profits in even more efficient machinery, which was able to reduce labor costs. The lower cost for pins was a benefit, and it was spread across the entire population.
We have seen similar examples in American healthcare. In many American hospitals, the images of CT scans performed during nighttime hours are transmitted to India and other Asian countries where highly trained radiologists interpret the scans and transmit their interpretations back to the physicians caring for the patients. Like the pin factory workers, these radiologists are specialists with unique skills; they operate specialized machinery to make the system more efficient with resultant lower costs. At the level of the individual patient, this system means getting test results back in a more timely fashion. Increased quality and lower costs: These are high-value providers.
It should be obvious to us that hospitalists are “specialists.” While most hospitalists are trained as general internists, pediatricians, and family physicians, you and I are “specialists” who focus our efforts on the care of hospitalized patients. In the late 1990s, much was made of the fact that hospitalists were able to reduce hospital costs because of decreased length of stay (LOS) for patients, without any adverse effects on clinical outcomes. Today, hospitalists number more than 30,000 nationwide, and virtually all American hospitals with more than 200 beds have hospitalists.
Hospitals hired hospitalists in droves because they were perceived as “inpatient specialists” who were able to reduce the cost of healthcare delivery. Like lower pin costs, this economic benefit was spread across the entire population. Hospitalist “value” went up because of lower costs.
But an interesting thing changed over the past decade: It seems that fewer and fewer people are talking about hospitalists reducing LOS. They just expect it. LOS is raised as an issue only if it goes up. In many hospitals, the budget now takes into account the average LOS based on hospitalist care. (I suspect that in 18th-century Scotland, people also grew accustomed to the lower cost of pins, and grew to expect it, and the cost of pins was raised as an issue only if the price went up.)
But has anyone spoken to the hospitalists? Has anyone asked us about the benefits of our profession? Many of the hospitalists I meet mention “reduction of length of stay” as a main reason to have hospitalists. I think that response was appropriate more often than not over the past 15 years.
But today, ask any hospital administrator that same question, and what do you expect the answer to be? It should not be surprising to hospitalists that most hospitals expect much more from their hospitalist programs than “just reducing the length of stay.” These are the same hospitals that often support—to the tune of more than $100,000 per hospitalist full-time equivalent—your HM program. If your hospitalist program is anything like mine at Beth Israel Deaconess Medical Center in Boston, this represents millions of dollars to the hospitalist program budget.
Increased Pressures
The fact that hospitals’ expectations of hospitalists have changed should not come as a surprise. Americans’ expectations of hospitals have changed markedly over the past 15 years. In the 1990s, when hospital medicine was “born,” there was little mention of quality and patient satisfaction when it came to healthcare. Who would argue that improving quality and patient satisfaction is a bad thing?
Over the past decade, we’ve seen the development of Medicare core measures and the link between patient outcomes and Medicare reimbursement. Hospitals could not have achieved many of their performance improvements without their partnerships with hospitalists.
Hospitals are under increasing pressure to not only decrease costs, but also improve quality. It is understandable that they turn to the “inpatient specialists”—the hospitalists—to help them meet societal expectations. But as hospitalists, this puts pressure on us to continually improve our game—or face the consequences. A pin factory in Scotland can only survive if it produces higher-quality pins at a lower cost than its competitor.
Hospitals and our American healthcare system expect much more today from hospitalists, and they should; patients’ lives are at stake. It should not be a surprise that hospitalist programs that struggle are those that fail to meet expectations. Successful hospitalist programs, the ones that are able to demonstrate their “value,” do so well beyond knowing their patient’s average length of stay.
I am interested in learning about your efforts to demonstrate the “value” of your hospitalist group. Feel free to email me at [email protected].
Dr. Li is president of SHM.
For those of you who were kind enough to pick up my column in The Hospitalist last month (see “A Critical First Step,” p. 56), you spent a few minutes reading my thoughts on the value of hospitalists. I mentioned the fact that the U.S. is moving rapidly toward a value-based system to purchase healthcare and that all healthcare providers, including hospitalists, will be increasingly judged on the value of care they deliver to their patients and the healthcare system. (Remember, value=quality÷cost.)
I believe that the hospitalist programs that are going to be the most successful are those that are able to continually measure their quality and costs, allowing them to make improvements. These are the groups that will understand their own performance well before others make their “value” judgments.
History Lesson
In his famous book “The Wealth of Nations,” 18th-century economist Adam Smith used the example of a pin factory to show how specialization improved human productivity. The process of producing a pin was broken down into many small tasks, each done by a different “specialist.” This resulted not only in increased efficiency, but also increased productivity. The factory was then able to reinvest the profits in even more efficient machinery, which was able to reduce labor costs. The lower cost for pins was a benefit, and it was spread across the entire population.
We have seen similar examples in American healthcare. In many American hospitals, the images of CT scans performed during nighttime hours are transmitted to India and other Asian countries where highly trained radiologists interpret the scans and transmit their interpretations back to the physicians caring for the patients. Like the pin factory workers, these radiologists are specialists with unique skills; they operate specialized machinery to make the system more efficient with resultant lower costs. At the level of the individual patient, this system means getting test results back in a more timely fashion. Increased quality and lower costs: These are high-value providers.
It should be obvious to us that hospitalists are “specialists.” While most hospitalists are trained as general internists, pediatricians, and family physicians, you and I are “specialists” who focus our efforts on the care of hospitalized patients. In the late 1990s, much was made of the fact that hospitalists were able to reduce hospital costs because of decreased length of stay (LOS) for patients, without any adverse effects on clinical outcomes. Today, hospitalists number more than 30,000 nationwide, and virtually all American hospitals with more than 200 beds have hospitalists.
Hospitals hired hospitalists in droves because they were perceived as “inpatient specialists” who were able to reduce the cost of healthcare delivery. Like lower pin costs, this economic benefit was spread across the entire population. Hospitalist “value” went up because of lower costs.
But an interesting thing changed over the past decade: It seems that fewer and fewer people are talking about hospitalists reducing LOS. They just expect it. LOS is raised as an issue only if it goes up. In many hospitals, the budget now takes into account the average LOS based on hospitalist care. (I suspect that in 18th-century Scotland, people also grew accustomed to the lower cost of pins, and grew to expect it, and the cost of pins was raised as an issue only if the price went up.)
But has anyone spoken to the hospitalists? Has anyone asked us about the benefits of our profession? Many of the hospitalists I meet mention “reduction of length of stay” as a main reason to have hospitalists. I think that response was appropriate more often than not over the past 15 years.
But today, ask any hospital administrator that same question, and what do you expect the answer to be? It should not be surprising to hospitalists that most hospitals expect much more from their hospitalist programs than “just reducing the length of stay.” These are the same hospitals that often support—to the tune of more than $100,000 per hospitalist full-time equivalent—your HM program. If your hospitalist program is anything like mine at Beth Israel Deaconess Medical Center in Boston, this represents millions of dollars to the hospitalist program budget.
Increased Pressures
The fact that hospitals’ expectations of hospitalists have changed should not come as a surprise. Americans’ expectations of hospitals have changed markedly over the past 15 years. In the 1990s, when hospital medicine was “born,” there was little mention of quality and patient satisfaction when it came to healthcare. Who would argue that improving quality and patient satisfaction is a bad thing?
Over the past decade, we’ve seen the development of Medicare core measures and the link between patient outcomes and Medicare reimbursement. Hospitals could not have achieved many of their performance improvements without their partnerships with hospitalists.
Hospitals are under increasing pressure to not only decrease costs, but also improve quality. It is understandable that they turn to the “inpatient specialists”—the hospitalists—to help them meet societal expectations. But as hospitalists, this puts pressure on us to continually improve our game—or face the consequences. A pin factory in Scotland can only survive if it produces higher-quality pins at a lower cost than its competitor.
Hospitals and our American healthcare system expect much more today from hospitalists, and they should; patients’ lives are at stake. It should not be a surprise that hospitalist programs that struggle are those that fail to meet expectations. Successful hospitalist programs, the ones that are able to demonstrate their “value,” do so well beyond knowing their patient’s average length of stay.
I am interested in learning about your efforts to demonstrate the “value” of your hospitalist group. Feel free to email me at [email protected].
Dr. Li is president of SHM.
Hospital-Focused Practice

As regular readers of The Hospitalist are aware, essentially every specialty in medicine is adopting the hospitalist model to some degree. After the “legacy” specialties of medicine and pediatrics, the model has more recently been embraced enthusiastically by neurologists, obstetricians, and general surgeons. But even fields like dermatology and ENT have put a hospitalist version of their specialties in place in at least a few places.
Did you know there is a Society for Dermatology Hospitalists? Did you know that the Neurohospitalist Society has its own journal? Did you know OB hospitalists have a really neat website, and the Society of OB/GYN Hospitalists is scheduled to have its first annual meeting in Boulder, Colo., Sept. 23-25?
It’ll make your head spin if you think about it too long. All of this raises a number of issues, including the need for more precise terminology to describe these fields and their practitioners.
The Need for Better Terminology
For example, now that we have neurohospitalists and psychiatric hospitalists, is it time to start attaching a modifier or prefix every time we use the word “hospitalist,” including when referring to “medical” hospitalists? I don’t think so. For the time being, I propose that when used alone, the word “hospitalist” still refers to a doctor who provides general medical care for adult inpatients. But I think any other use of the word does require a modifier, as in “peds hospitalist” or “GI hospitalist.”
(I think my view makes sense, but then, I’ve tried for years to ensure nocternist, with an E—NOCTernal intERNIST)—is the preferred spelling over nocternist, with a U. But Google returns nine hits for the former and 365,000 for the latter. Looks like I lost that one.)
Terminology for general and trauma surgeons is tricky. There is an emerging field of acute-care surgery, distinct from general surgery, which some argue passionately is nothing like a hospitalist model, and they tend to be offended if one uses the latter term. So, for now, we’ll need to use both “acute-care surgeon” and “surgical hospitalist” carefully. Although there are meaningful distinctions between acute-care surgery and a “standard” general surgery practice devoted to the hospital, there is an awful lot of overlap in the Venn diagrams of their expertise and what they do. But for now, it looks like we should expect both “acute-care surgeon” and “surgical hospitalist” to appear commonly, and the context will determine whether the terms could be used interchangeably.
While “obstetric hospitalist,” or “OB hospitalist,” is a perfectly useful term, I think it is great when laborist is substituted, at least in informal communication.
We still need a way to speak of all of these clinical roles (I don’t think we can properly call them specialties yet). I propose that we refer to all of them as specialties within the realm of “hospital-focused practice.” I’ve borrowed this term from the American Board of Internal Medicine’s Recognition of Focused Practice in Hospital Medicine, the new pathway to Maintenance of Certification.
And what about those doctors in each specialty who continue to practice in the traditional inpatient and outpatient model? Let’s call them “traditionalists.”
Hospital-Focused Practice
A rational vocabulary is only one of many significant issues raised by the growth of hospital-focused disciplines. In January, I participated in an SHM-convened, and AHA-supported, meeting of 11 practitioners who were hospitalists in neurology, obstetrics, general surgery, medicine, pediatrics, and ENT. (Sadly, the invited dermatology hospitalist couldn’t make it.) The meeting was filled with interest and sharing of lessons learned in each field. We discussed questions, and I have provided a very brief answer to each based on the conversation during the meeting and my own work with practices across many different specialties that have adopted the hospitalist model:
What are the reasons each specialty is turning to this model, and what is its prevalence? Hospitalists have appeared in a specialty largely to fill the void left by the traditionalists who no longer want to care for unattached patients admitted through the ED, or who want to leave the hospital altogether for a solely outpatient practice.
What are typical staffing models, night coverage arrangements, and provider career sustainability? These vary a lot by specialty, but laborists typically work 24-hour, in-house shifts. Surgical hospitalists usually work 12-hour shifts if they are in-house all the time, or 24-hour shifts if they take call from home. Neurohospitalists essentially always take call from home (did you even have to ask?).
Career longevity is still a matter of speculation, but the majority of those who have transitioned from traditional to hospitalist practice in their field are convinced they will have a longer career than if they hadn’t made the switch.
What are the effects of this practice model on clinical quality, patient outcomes, healthcare economics, and liability? It will be really difficult to get convincing research data on the quality effects of the hospitalist model in many fields. After more than 15 years in operation, research about the quality effects of the medical hospitalist model is not robust enough to satisfy some. But OB hospitalists may be the exception here. There is hope that their continuous, on-site presence will reduce complications from emergencies, and in doing so might reduce malpractice risk.
What is the prevalent financial model? The experience across a lot of healthcare settings to this point is that professional fee revenue alone usually is not enough to support a hospitalist practice model in any specialty. Just like medical and pediatric hospitalist models, the hospital in which the doctors practice usually provides additional financial support.
Hospitals usually are willing to do this because they are able to reallocate dollars spent paying for numerous specialty doctors to take ED call with poor performance, and instead use those dollars to support a hospitalist practice in that specialty that promises a better return on the investment.
Join us in November for a meeting to understand the implications of hospital-focused practice. Those of us at the January meeting of specialty hospitalists thought that it would be valuable to convene a much larger meeting to think about issues like those above and others. At the Nov. 4 meeting in Las Vegas, we plan to hear from such national figures as CMS’ chief medical officer, physicians practicing in a hospitalist model, and hospital and healthcare executives. The meeting will be structured to promote interaction and communication from attendees.
I hope to see you in Las Vegas. We have a lot to learn from one another.
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course codirector and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
As regular readers of The Hospitalist are aware, essentially every specialty in medicine is adopting the hospitalist model to some degree. After the “legacy” specialties of medicine and pediatrics, the model has more recently been embraced enthusiastically by neurologists, obstetricians, and general surgeons. But even fields like dermatology and ENT have put a hospitalist version of their specialties in place in at least a few places.
Did you know there is a Society for Dermatology Hospitalists? Did you know that the Neurohospitalist Society has its own journal? Did you know OB hospitalists have a really neat website, and the Society of OB/GYN Hospitalists is scheduled to have its first annual meeting in Boulder, Colo., Sept. 23-25?
It’ll make your head spin if you think about it too long. All of this raises a number of issues, including the need for more precise terminology to describe these fields and their practitioners.
The Need for Better Terminology
For example, now that we have neurohospitalists and psychiatric hospitalists, is it time to start attaching a modifier or prefix every time we use the word “hospitalist,” including when referring to “medical” hospitalists? I don’t think so. For the time being, I propose that when used alone, the word “hospitalist” still refers to a doctor who provides general medical care for adult inpatients. But I think any other use of the word does require a modifier, as in “peds hospitalist” or “GI hospitalist.”
(I think my view makes sense, but then, I’ve tried for years to ensure nocternist, with an E—NOCTernal intERNIST)—is the preferred spelling over nocternist, with a U. But Google returns nine hits for the former and 365,000 for the latter. Looks like I lost that one.)
Terminology for general and trauma surgeons is tricky. There is an emerging field of acute-care surgery, distinct from general surgery, which some argue passionately is nothing like a hospitalist model, and they tend to be offended if one uses the latter term. So, for now, we’ll need to use both “acute-care surgeon” and “surgical hospitalist” carefully. Although there are meaningful distinctions between acute-care surgery and a “standard” general surgery practice devoted to the hospital, there is an awful lot of overlap in the Venn diagrams of their expertise and what they do. But for now, it looks like we should expect both “acute-care surgeon” and “surgical hospitalist” to appear commonly, and the context will determine whether the terms could be used interchangeably.
While “obstetric hospitalist,” or “OB hospitalist,” is a perfectly useful term, I think it is great when laborist is substituted, at least in informal communication.
We still need a way to speak of all of these clinical roles (I don’t think we can properly call them specialties yet). I propose that we refer to all of them as specialties within the realm of “hospital-focused practice.” I’ve borrowed this term from the American Board of Internal Medicine’s Recognition of Focused Practice in Hospital Medicine, the new pathway to Maintenance of Certification.
And what about those doctors in each specialty who continue to practice in the traditional inpatient and outpatient model? Let’s call them “traditionalists.”
Hospital-Focused Practice
A rational vocabulary is only one of many significant issues raised by the growth of hospital-focused disciplines. In January, I participated in an SHM-convened, and AHA-supported, meeting of 11 practitioners who were hospitalists in neurology, obstetrics, general surgery, medicine, pediatrics, and ENT. (Sadly, the invited dermatology hospitalist couldn’t make it.) The meeting was filled with interest and sharing of lessons learned in each field. We discussed questions, and I have provided a very brief answer to each based on the conversation during the meeting and my own work with practices across many different specialties that have adopted the hospitalist model:
What are the reasons each specialty is turning to this model, and what is its prevalence? Hospitalists have appeared in a specialty largely to fill the void left by the traditionalists who no longer want to care for unattached patients admitted through the ED, or who want to leave the hospital altogether for a solely outpatient practice.
What are typical staffing models, night coverage arrangements, and provider career sustainability? These vary a lot by specialty, but laborists typically work 24-hour, in-house shifts. Surgical hospitalists usually work 12-hour shifts if they are in-house all the time, or 24-hour shifts if they take call from home. Neurohospitalists essentially always take call from home (did you even have to ask?).
Career longevity is still a matter of speculation, but the majority of those who have transitioned from traditional to hospitalist practice in their field are convinced they will have a longer career than if they hadn’t made the switch.
What are the effects of this practice model on clinical quality, patient outcomes, healthcare economics, and liability? It will be really difficult to get convincing research data on the quality effects of the hospitalist model in many fields. After more than 15 years in operation, research about the quality effects of the medical hospitalist model is not robust enough to satisfy some. But OB hospitalists may be the exception here. There is hope that their continuous, on-site presence will reduce complications from emergencies, and in doing so might reduce malpractice risk.
What is the prevalent financial model? The experience across a lot of healthcare settings to this point is that professional fee revenue alone usually is not enough to support a hospitalist practice model in any specialty. Just like medical and pediatric hospitalist models, the hospital in which the doctors practice usually provides additional financial support.
Hospitals usually are willing to do this because they are able to reallocate dollars spent paying for numerous specialty doctors to take ED call with poor performance, and instead use those dollars to support a hospitalist practice in that specialty that promises a better return on the investment.
Join us in November for a meeting to understand the implications of hospital-focused practice. Those of us at the January meeting of specialty hospitalists thought that it would be valuable to convene a much larger meeting to think about issues like those above and others. At the Nov. 4 meeting in Las Vegas, we plan to hear from such national figures as CMS’ chief medical officer, physicians practicing in a hospitalist model, and hospital and healthcare executives. The meeting will be structured to promote interaction and communication from attendees.
I hope to see you in Las Vegas. We have a lot to learn from one another.
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course codirector and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
As regular readers of The Hospitalist are aware, essentially every specialty in medicine is adopting the hospitalist model to some degree. After the “legacy” specialties of medicine and pediatrics, the model has more recently been embraced enthusiastically by neurologists, obstetricians, and general surgeons. But even fields like dermatology and ENT have put a hospitalist version of their specialties in place in at least a few places.
Did you know there is a Society for Dermatology Hospitalists? Did you know that the Neurohospitalist Society has its own journal? Did you know OB hospitalists have a really neat website, and the Society of OB/GYN Hospitalists is scheduled to have its first annual meeting in Boulder, Colo., Sept. 23-25?
It’ll make your head spin if you think about it too long. All of this raises a number of issues, including the need for more precise terminology to describe these fields and their practitioners.
The Need for Better Terminology
For example, now that we have neurohospitalists and psychiatric hospitalists, is it time to start attaching a modifier or prefix every time we use the word “hospitalist,” including when referring to “medical” hospitalists? I don’t think so. For the time being, I propose that when used alone, the word “hospitalist” still refers to a doctor who provides general medical care for adult inpatients. But I think any other use of the word does require a modifier, as in “peds hospitalist” or “GI hospitalist.”
(I think my view makes sense, but then, I’ve tried for years to ensure nocternist, with an E—NOCTernal intERNIST)—is the preferred spelling over nocternist, with a U. But Google returns nine hits for the former and 365,000 for the latter. Looks like I lost that one.)
Terminology for general and trauma surgeons is tricky. There is an emerging field of acute-care surgery, distinct from general surgery, which some argue passionately is nothing like a hospitalist model, and they tend to be offended if one uses the latter term. So, for now, we’ll need to use both “acute-care surgeon” and “surgical hospitalist” carefully. Although there are meaningful distinctions between acute-care surgery and a “standard” general surgery practice devoted to the hospital, there is an awful lot of overlap in the Venn diagrams of their expertise and what they do. But for now, it looks like we should expect both “acute-care surgeon” and “surgical hospitalist” to appear commonly, and the context will determine whether the terms could be used interchangeably.
While “obstetric hospitalist,” or “OB hospitalist,” is a perfectly useful term, I think it is great when laborist is substituted, at least in informal communication.
We still need a way to speak of all of these clinical roles (I don’t think we can properly call them specialties yet). I propose that we refer to all of them as specialties within the realm of “hospital-focused practice.” I’ve borrowed this term from the American Board of Internal Medicine’s Recognition of Focused Practice in Hospital Medicine, the new pathway to Maintenance of Certification.
And what about those doctors in each specialty who continue to practice in the traditional inpatient and outpatient model? Let’s call them “traditionalists.”
Hospital-Focused Practice
A rational vocabulary is only one of many significant issues raised by the growth of hospital-focused disciplines. In January, I participated in an SHM-convened, and AHA-supported, meeting of 11 practitioners who were hospitalists in neurology, obstetrics, general surgery, medicine, pediatrics, and ENT. (Sadly, the invited dermatology hospitalist couldn’t make it.) The meeting was filled with interest and sharing of lessons learned in each field. We discussed questions, and I have provided a very brief answer to each based on the conversation during the meeting and my own work with practices across many different specialties that have adopted the hospitalist model:
What are the reasons each specialty is turning to this model, and what is its prevalence? Hospitalists have appeared in a specialty largely to fill the void left by the traditionalists who no longer want to care for unattached patients admitted through the ED, or who want to leave the hospital altogether for a solely outpatient practice.
What are typical staffing models, night coverage arrangements, and provider career sustainability? These vary a lot by specialty, but laborists typically work 24-hour, in-house shifts. Surgical hospitalists usually work 12-hour shifts if they are in-house all the time, or 24-hour shifts if they take call from home. Neurohospitalists essentially always take call from home (did you even have to ask?).
Career longevity is still a matter of speculation, but the majority of those who have transitioned from traditional to hospitalist practice in their field are convinced they will have a longer career than if they hadn’t made the switch.
What are the effects of this practice model on clinical quality, patient outcomes, healthcare economics, and liability? It will be really difficult to get convincing research data on the quality effects of the hospitalist model in many fields. After more than 15 years in operation, research about the quality effects of the medical hospitalist model is not robust enough to satisfy some. But OB hospitalists may be the exception here. There is hope that their continuous, on-site presence will reduce complications from emergencies, and in doing so might reduce malpractice risk.
What is the prevalent financial model? The experience across a lot of healthcare settings to this point is that professional fee revenue alone usually is not enough to support a hospitalist practice model in any specialty. Just like medical and pediatric hospitalist models, the hospital in which the doctors practice usually provides additional financial support.
Hospitals usually are willing to do this because they are able to reallocate dollars spent paying for numerous specialty doctors to take ED call with poor performance, and instead use those dollars to support a hospitalist practice in that specialty that promises a better return on the investment.
Join us in November for a meeting to understand the implications of hospital-focused practice. Those of us at the January meeting of specialty hospitalists thought that it would be valuable to convene a much larger meeting to think about issues like those above and others. At the Nov. 4 meeting in Las Vegas, we plan to hear from such national figures as CMS’ chief medical officer, physicians practicing in a hospitalist model, and hospital and healthcare executives. The meeting will be structured to promote interaction and communication from attendees.
I hope to see you in Las Vegas. We have a lot to learn from one another.
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course codirector and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Dr. Hospitalist

What I am curious about are the current issues around using length of stay (LOS) or cost/case or the like as part of compensation packages. I have had discussions with several other folks, and I think I am getting the picture. However, it sounds like there has been some new interpretation of the laws around gainsharing, and that is what I am curious about.
K.S., Ohio
Dr. Hospitalist responds:
Tough question, and let me start by saying that I’m not a healthcare lawyer: This stuff is tricky. I’ll do my best to explain the current situation as I understand it, but I’m no expert on this.
So gainsharing, as generally defined in healthcare, is where a hospital and a group of physicians design a contract around services for which the two sides can share in any savings. Physicians are paid fee-for-service by Medicare, thus they are reimbursed per unit of work, with no incentive for cost control. Hospitals are paid on a per-case (or per-procedure) basis, so cost control means a lot to them: Because they get a set payment, any savings generated, they get to keep. Ideally, this means that better performance leads to more efficient care, less waste, and better outcomes. Unfortunately, that’s not always what happens, especially in the view of the federal government (you know, the guys who issue the bright orange jumpsuits for you to wear when you break the law).
Gainsharing has an interesting history as interpreted by the Office of the Inspector General (OIG) and the Centers for Medicare & Medicaid Services (CMS). Back in 1999, the OIG explicitly stopped any gainsharing models between physicians and hospitals based on concerns that these contracts might reduce the care provided to patients. The opinion was that there might be a “race to the bottom” in terms of cutting expenses (read: services).
Since then, there has been only incremental movement forward in the form of demonstration projects. One project looked at two very specific procedures: cardiac catheterization and coronary artery bypass grafting (CABG). The results showed that gainsharing could be beneficial to the hospital-physician relationship, and, more important, not harmful to the patient. There has since been some movement toward gainsharing, but only in the context of specific procedures, with very clear safeguards around it, including an independent auditor. Nothing to this point has suggested that a cost per case or adjusted LOS gainsharing agreement would pass muster with the OIG.
So, at this point in time, I would caution against any contract that contained explicit references connecting compensation to a change in hospital costs, such as reducing LOS or cost per case. The new accountable-care organization (ACO) model might be a different prism through which to view this, but it’s a world apart from an individual physician or hospitalist group contract (see “A Chilly Reception,” August 2011, p. 23).
For contractual compensation, I think that quality metrics can fill a need, and there are lots of ways to be creative here. You could set a target around something measurable (appropriate DVT prophylaxis is just one example) and tie dollars to that specific performance. The key is avoiding any language that would imply additional physician compensation for a reduction in patient services.
Might things change in the future? Your guess is as good as mine.
What I am curious about are the current issues around using length of stay (LOS) or cost/case or the like as part of compensation packages. I have had discussions with several other folks, and I think I am getting the picture. However, it sounds like there has been some new interpretation of the laws around gainsharing, and that is what I am curious about.
K.S., Ohio
Dr. Hospitalist responds:
Tough question, and let me start by saying that I’m not a healthcare lawyer: This stuff is tricky. I’ll do my best to explain the current situation as I understand it, but I’m no expert on this.
So gainsharing, as generally defined in healthcare, is where a hospital and a group of physicians design a contract around services for which the two sides can share in any savings. Physicians are paid fee-for-service by Medicare, thus they are reimbursed per unit of work, with no incentive for cost control. Hospitals are paid on a per-case (or per-procedure) basis, so cost control means a lot to them: Because they get a set payment, any savings generated, they get to keep. Ideally, this means that better performance leads to more efficient care, less waste, and better outcomes. Unfortunately, that’s not always what happens, especially in the view of the federal government (you know, the guys who issue the bright orange jumpsuits for you to wear when you break the law).
Gainsharing has an interesting history as interpreted by the Office of the Inspector General (OIG) and the Centers for Medicare & Medicaid Services (CMS). Back in 1999, the OIG explicitly stopped any gainsharing models between physicians and hospitals based on concerns that these contracts might reduce the care provided to patients. The opinion was that there might be a “race to the bottom” in terms of cutting expenses (read: services).
Since then, there has been only incremental movement forward in the form of demonstration projects. One project looked at two very specific procedures: cardiac catheterization and coronary artery bypass grafting (CABG). The results showed that gainsharing could be beneficial to the hospital-physician relationship, and, more important, not harmful to the patient. There has since been some movement toward gainsharing, but only in the context of specific procedures, with very clear safeguards around it, including an independent auditor. Nothing to this point has suggested that a cost per case or adjusted LOS gainsharing agreement would pass muster with the OIG.
So, at this point in time, I would caution against any contract that contained explicit references connecting compensation to a change in hospital costs, such as reducing LOS or cost per case. The new accountable-care organization (ACO) model might be a different prism through which to view this, but it’s a world apart from an individual physician or hospitalist group contract (see “A Chilly Reception,” August 2011, p. 23).
For contractual compensation, I think that quality metrics can fill a need, and there are lots of ways to be creative here. You could set a target around something measurable (appropriate DVT prophylaxis is just one example) and tie dollars to that specific performance. The key is avoiding any language that would imply additional physician compensation for a reduction in patient services.
Might things change in the future? Your guess is as good as mine.
What I am curious about are the current issues around using length of stay (LOS) or cost/case or the like as part of compensation packages. I have had discussions with several other folks, and I think I am getting the picture. However, it sounds like there has been some new interpretation of the laws around gainsharing, and that is what I am curious about.
K.S., Ohio
Dr. Hospitalist responds:
Tough question, and let me start by saying that I’m not a healthcare lawyer: This stuff is tricky. I’ll do my best to explain the current situation as I understand it, but I’m no expert on this.
So gainsharing, as generally defined in healthcare, is where a hospital and a group of physicians design a contract around services for which the two sides can share in any savings. Physicians are paid fee-for-service by Medicare, thus they are reimbursed per unit of work, with no incentive for cost control. Hospitals are paid on a per-case (or per-procedure) basis, so cost control means a lot to them: Because they get a set payment, any savings generated, they get to keep. Ideally, this means that better performance leads to more efficient care, less waste, and better outcomes. Unfortunately, that’s not always what happens, especially in the view of the federal government (you know, the guys who issue the bright orange jumpsuits for you to wear when you break the law).
Gainsharing has an interesting history as interpreted by the Office of the Inspector General (OIG) and the Centers for Medicare & Medicaid Services (CMS). Back in 1999, the OIG explicitly stopped any gainsharing models between physicians and hospitals based on concerns that these contracts might reduce the care provided to patients. The opinion was that there might be a “race to the bottom” in terms of cutting expenses (read: services).
Since then, there has been only incremental movement forward in the form of demonstration projects. One project looked at two very specific procedures: cardiac catheterization and coronary artery bypass grafting (CABG). The results showed that gainsharing could be beneficial to the hospital-physician relationship, and, more important, not harmful to the patient. There has since been some movement toward gainsharing, but only in the context of specific procedures, with very clear safeguards around it, including an independent auditor. Nothing to this point has suggested that a cost per case or adjusted LOS gainsharing agreement would pass muster with the OIG.
So, at this point in time, I would caution against any contract that contained explicit references connecting compensation to a change in hospital costs, such as reducing LOS or cost per case. The new accountable-care organization (ACO) model might be a different prism through which to view this, but it’s a world apart from an individual physician or hospitalist group contract (see “A Chilly Reception,” August 2011, p. 23).
For contractual compensation, I think that quality metrics can fill a need, and there are lots of ways to be creative here. You could set a target around something measurable (appropriate DVT prophylaxis is just one example) and tie dollars to that specific performance. The key is avoiding any language that would imply additional physician compensation for a reduction in patient services.
Might things change in the future? Your guess is as good as mine.
ONLINE EXCLUSIVE: Emergency Medicine Companies Venture into Hospital Medicine
Hollywood, Fla.-based Hospital Physician Partners (HPP) was an ED business when opportunity came knocking: Hospital administrators started asking, “Can you provide us with some hospitalists to go with our emergency-room doctors?”
Today, HPP is firmly in the HM business—and all signs point toward more hospitals hiring companies to handle both emergency care and inpatient care.
“In many ways, we expanded our efforts into hospitalist medicine as a result of requests from our hospital partners,” says Ed Weinberg, HPP’s chief operating officer. “Their needs were such that they asked us to provide hospital medicine services. So from that, it became clear that it was an area that was really growing. And that is something we are pursuing as vigorously as we are emergency medicine.”
HPP handling both emergency care and hospital medicine can help with the transition of patients from the ED to a hospital bed upstairs, he says.
“That’s where our efficiencies are, because we have physicians working who are carrying out the same philosophy,” he says.
Out of HPP’s 120 contracts, 15 are in hospital medicine. But the HM contract numbers are growing quickly, Weinberg notes.
EmCare has about 400 emergency-medicine programs and more than 50 HM programs, according to Mark Hamm, CEO of EmCare Inpatient Services. He says that it can be much more cost effective to contract with one company for both hospitalist and ED services, something hospitals find attractive.
EmCare service agreements range from completely separate emergency and HM staffs to small, rural hospitals where ED physicians also do rounds. Some hospitals “just don’t have the money for a full-time hospitalist and don’t really need one,” Hamm says.
The patient transitions tend to go more smoothly when both types of care are provided by EmCare, he adds. If they’re not, there can be slowdowns.
“Our goal is to quickly and appropriately move patients through the system,” he says. “If we have a hospitalist provider that’s not really on the same page, that can create bottlenecks. But it’s a blip. Our goal is to sit down, even if it’s not an EmCare hospitalist, to sit down with that director and say, ‘Hey look, let’s be the leader here, let’s work together and appropriately expedite these patients.’ We do the same thing on the hospitalist side.”
Inpatient care promises to be a big part of their future business, the executives agreed.
“Hospital medicine,” Weinberg says, “is growing by leaps and bounds.”
Hollywood, Fla.-based Hospital Physician Partners (HPP) was an ED business when opportunity came knocking: Hospital administrators started asking, “Can you provide us with some hospitalists to go with our emergency-room doctors?”
Today, HPP is firmly in the HM business—and all signs point toward more hospitals hiring companies to handle both emergency care and inpatient care.
“In many ways, we expanded our efforts into hospitalist medicine as a result of requests from our hospital partners,” says Ed Weinberg, HPP’s chief operating officer. “Their needs were such that they asked us to provide hospital medicine services. So from that, it became clear that it was an area that was really growing. And that is something we are pursuing as vigorously as we are emergency medicine.”
HPP handling both emergency care and hospital medicine can help with the transition of patients from the ED to a hospital bed upstairs, he says.
“That’s where our efficiencies are, because we have physicians working who are carrying out the same philosophy,” he says.
Out of HPP’s 120 contracts, 15 are in hospital medicine. But the HM contract numbers are growing quickly, Weinberg notes.
EmCare has about 400 emergency-medicine programs and more than 50 HM programs, according to Mark Hamm, CEO of EmCare Inpatient Services. He says that it can be much more cost effective to contract with one company for both hospitalist and ED services, something hospitals find attractive.
EmCare service agreements range from completely separate emergency and HM staffs to small, rural hospitals where ED physicians also do rounds. Some hospitals “just don’t have the money for a full-time hospitalist and don’t really need one,” Hamm says.
The patient transitions tend to go more smoothly when both types of care are provided by EmCare, he adds. If they’re not, there can be slowdowns.
“Our goal is to quickly and appropriately move patients through the system,” he says. “If we have a hospitalist provider that’s not really on the same page, that can create bottlenecks. But it’s a blip. Our goal is to sit down, even if it’s not an EmCare hospitalist, to sit down with that director and say, ‘Hey look, let’s be the leader here, let’s work together and appropriately expedite these patients.’ We do the same thing on the hospitalist side.”
Inpatient care promises to be a big part of their future business, the executives agreed.
“Hospital medicine,” Weinberg says, “is growing by leaps and bounds.”
Hollywood, Fla.-based Hospital Physician Partners (HPP) was an ED business when opportunity came knocking: Hospital administrators started asking, “Can you provide us with some hospitalists to go with our emergency-room doctors?”
Today, HPP is firmly in the HM business—and all signs point toward more hospitals hiring companies to handle both emergency care and inpatient care.
“In many ways, we expanded our efforts into hospitalist medicine as a result of requests from our hospital partners,” says Ed Weinberg, HPP’s chief operating officer. “Their needs were such that they asked us to provide hospital medicine services. So from that, it became clear that it was an area that was really growing. And that is something we are pursuing as vigorously as we are emergency medicine.”
HPP handling both emergency care and hospital medicine can help with the transition of patients from the ED to a hospital bed upstairs, he says.
“That’s where our efficiencies are, because we have physicians working who are carrying out the same philosophy,” he says.
Out of HPP’s 120 contracts, 15 are in hospital medicine. But the HM contract numbers are growing quickly, Weinberg notes.
EmCare has about 400 emergency-medicine programs and more than 50 HM programs, according to Mark Hamm, CEO of EmCare Inpatient Services. He says that it can be much more cost effective to contract with one company for both hospitalist and ED services, something hospitals find attractive.
EmCare service agreements range from completely separate emergency and HM staffs to small, rural hospitals where ED physicians also do rounds. Some hospitals “just don’t have the money for a full-time hospitalist and don’t really need one,” Hamm says.
The patient transitions tend to go more smoothly when both types of care are provided by EmCare, he adds. If they’re not, there can be slowdowns.
“Our goal is to quickly and appropriately move patients through the system,” he says. “If we have a hospitalist provider that’s not really on the same page, that can create bottlenecks. But it’s a blip. Our goal is to sit down, even if it’s not an EmCare hospitalist, to sit down with that director and say, ‘Hey look, let’s be the leader here, let’s work together and appropriately expedite these patients.’ We do the same thing on the hospitalist side.”
Inpatient care promises to be a big part of their future business, the executives agreed.
“Hospital medicine,” Weinberg says, “is growing by leaps and bounds.”
ONLINE EXCLUSIVE: Listen to Russell Holman and Ed Weinberg discuss companies' acquisition strategies
Power Through Afternoon Energy Slumps

Late-afternoon slowdowns are natural, explains Susan Swadener, PhD, RD, dietetic internship director and lecturer in the Food Science and Nutrition Department at California State University San Luis Obispo. "Your enzyme levels go down, which is part of your diurnal pattern to slow down the body's processes to get ready for the evening and sleep," she says.
Common-Sense Nutrition
To fight afternoon fatigue, adopt good nutritional habits throughout your day. It's essential to have a healthy breakfast in the morning, advises Dr. Swadener, who's also a registered dietitian in private practice. Make sure you eat lunch, too, with a balance of protein, carbohydrates, and fats.
Afternoon snacks are a good idea, especially if they incorporate some protein. Foods high in protein can increase norepinephrine and epinephrine production, which helps you stay alert. Some examples of quick and nutritious snacks: string cheese and an apple; sliced cheese or peanut butter on whole-wheat crackers; yogurt; a handful of almonds or walnuts; or trail mix.
And don't forget one of the most common directives to your patients: "Push the fluids." Have a glass of water or nonfat milk with your lunch, and make sure you keep your water bottle handy at your desk.
As for coffee, "you don't want to be drinking it constantly to keep your energy level up, because you'll just crash afterwards," Dr. Swadener says. If you don't abuse caffeine, one cup of coffee in the morning and one in the afternoon is found to be most effective in increasing your alertness.
Change It Up
Desk tasks can make you drowsy. Daniel Markovitz is president of TimeBack Management, which specializes in applying Lean manufacturing principles to increase personal productivity for healthcare workers. He's found—and research such as a 2003 study in Ergonomics and a 2007 National Institute for Occupational Safety and Health study in the American Journal of Industrial Medicine supports these conclusions—that taking mini-breaks and then returning to the task at hand can refresh you and make you more productive.
You also get energy by using it, so a brisk walk around the hospital or walking up and down a couple of flights of stairs can increase circulation and blood flow to the brain. "You don't even have to get up from your desk," Markovitz says. "Just by changing the nature of the work you're doing, it's refreshing to your brain." That might mean switching from dictation to administrative work, or from scheduling to research.
And remember the value of play, Markovitz advises. "We tend to discourage going on Facebook or playing a video game at work. But if you take a 15-minute break to do something that's pleasurable, that causes your brain to fire in different ways, that can be another helpful adaptation."
Gretchen Henkel is a freelance writer based in California.
Interactions are Engaging
You've just finished a brain-numbing administrative report, and you've got 10 minutes before your next task. Don't just fill that time with checking your email.
Corporate consultant Daniel Markovitz advises another tack: Walk down the hall to touch base with colleagues. "You don't have to get into an involved conversation about their QI project. Just ask them how it's going for them," he advises.
Breaking up a busy day with exercise or a social call can get you over the doldrums hump, he says, because "you're getting up and interacting with someone. At the same time, you're doing something that's really important for the hospital: You're strengthening those bonds and interrelationships with people.—GH
Late-afternoon slowdowns are natural, explains Susan Swadener, PhD, RD, dietetic internship director and lecturer in the Food Science and Nutrition Department at California State University San Luis Obispo. "Your enzyme levels go down, which is part of your diurnal pattern to slow down the body's processes to get ready for the evening and sleep," she says.
Common-Sense Nutrition
To fight afternoon fatigue, adopt good nutritional habits throughout your day. It's essential to have a healthy breakfast in the morning, advises Dr. Swadener, who's also a registered dietitian in private practice. Make sure you eat lunch, too, with a balance of protein, carbohydrates, and fats.
Afternoon snacks are a good idea, especially if they incorporate some protein. Foods high in protein can increase norepinephrine and epinephrine production, which helps you stay alert. Some examples of quick and nutritious snacks: string cheese and an apple; sliced cheese or peanut butter on whole-wheat crackers; yogurt; a handful of almonds or walnuts; or trail mix.
And don't forget one of the most common directives to your patients: "Push the fluids." Have a glass of water or nonfat milk with your lunch, and make sure you keep your water bottle handy at your desk.
As for coffee, "you don't want to be drinking it constantly to keep your energy level up, because you'll just crash afterwards," Dr. Swadener says. If you don't abuse caffeine, one cup of coffee in the morning and one in the afternoon is found to be most effective in increasing your alertness.
Change It Up
Desk tasks can make you drowsy. Daniel Markovitz is president of TimeBack Management, which specializes in applying Lean manufacturing principles to increase personal productivity for healthcare workers. He's found—and research such as a 2003 study in Ergonomics and a 2007 National Institute for Occupational Safety and Health study in the American Journal of Industrial Medicine supports these conclusions—that taking mini-breaks and then returning to the task at hand can refresh you and make you more productive.
You also get energy by using it, so a brisk walk around the hospital or walking up and down a couple of flights of stairs can increase circulation and blood flow to the brain. "You don't even have to get up from your desk," Markovitz says. "Just by changing the nature of the work you're doing, it's refreshing to your brain." That might mean switching from dictation to administrative work, or from scheduling to research.
And remember the value of play, Markovitz advises. "We tend to discourage going on Facebook or playing a video game at work. But if you take a 15-minute break to do something that's pleasurable, that causes your brain to fire in different ways, that can be another helpful adaptation."
Gretchen Henkel is a freelance writer based in California.
Interactions are Engaging
You've just finished a brain-numbing administrative report, and you've got 10 minutes before your next task. Don't just fill that time with checking your email.
Corporate consultant Daniel Markovitz advises another tack: Walk down the hall to touch base with colleagues. "You don't have to get into an involved conversation about their QI project. Just ask them how it's going for them," he advises.
Breaking up a busy day with exercise or a social call can get you over the doldrums hump, he says, because "you're getting up and interacting with someone. At the same time, you're doing something that's really important for the hospital: You're strengthening those bonds and interrelationships with people.—GH
Late-afternoon slowdowns are natural, explains Susan Swadener, PhD, RD, dietetic internship director and lecturer in the Food Science and Nutrition Department at California State University San Luis Obispo. "Your enzyme levels go down, which is part of your diurnal pattern to slow down the body's processes to get ready for the evening and sleep," she says.
Common-Sense Nutrition
To fight afternoon fatigue, adopt good nutritional habits throughout your day. It's essential to have a healthy breakfast in the morning, advises Dr. Swadener, who's also a registered dietitian in private practice. Make sure you eat lunch, too, with a balance of protein, carbohydrates, and fats.
Afternoon snacks are a good idea, especially if they incorporate some protein. Foods high in protein can increase norepinephrine and epinephrine production, which helps you stay alert. Some examples of quick and nutritious snacks: string cheese and an apple; sliced cheese or peanut butter on whole-wheat crackers; yogurt; a handful of almonds or walnuts; or trail mix.
And don't forget one of the most common directives to your patients: "Push the fluids." Have a glass of water or nonfat milk with your lunch, and make sure you keep your water bottle handy at your desk.
As for coffee, "you don't want to be drinking it constantly to keep your energy level up, because you'll just crash afterwards," Dr. Swadener says. If you don't abuse caffeine, one cup of coffee in the morning and one in the afternoon is found to be most effective in increasing your alertness.
Change It Up
Desk tasks can make you drowsy. Daniel Markovitz is president of TimeBack Management, which specializes in applying Lean manufacturing principles to increase personal productivity for healthcare workers. He's found—and research such as a 2003 study in Ergonomics and a 2007 National Institute for Occupational Safety and Health study in the American Journal of Industrial Medicine supports these conclusions—that taking mini-breaks and then returning to the task at hand can refresh you and make you more productive.
You also get energy by using it, so a brisk walk around the hospital or walking up and down a couple of flights of stairs can increase circulation and blood flow to the brain. "You don't even have to get up from your desk," Markovitz says. "Just by changing the nature of the work you're doing, it's refreshing to your brain." That might mean switching from dictation to administrative work, or from scheduling to research.
And remember the value of play, Markovitz advises. "We tend to discourage going on Facebook or playing a video game at work. But if you take a 15-minute break to do something that's pleasurable, that causes your brain to fire in different ways, that can be another helpful adaptation."
Gretchen Henkel is a freelance writer based in California.
Interactions are Engaging
You've just finished a brain-numbing administrative report, and you've got 10 minutes before your next task. Don't just fill that time with checking your email.
Corporate consultant Daniel Markovitz advises another tack: Walk down the hall to touch base with colleagues. "You don't have to get into an involved conversation about their QI project. Just ask them how it's going for them," he advises.
Breaking up a busy day with exercise or a social call can get you over the doldrums hump, he says, because "you're getting up and interacting with someone. At the same time, you're doing something that's really important for the hospital: You're strengthening those bonds and interrelationships with people.—GH
ONLINE EXCLUSIVE: Scheduling Rules of Thumb
John Krisa, MD, medical director of the hospitalist group at Albany Memorial Hospital in New York, pictures his HM group as an organic whole when he draws up the schedule. He tries to avoid a strict 50-50 parceling out of night and day shifts. The hospitalist group makes liberal use of per-diem hospitalists and moonlighters, and has a few nocturnists.
“The vast majority of the work at night is processing new admissions, so these tend to be single encounters. You want your full-time people there multiple consecutive days for continuity and to represent the face of your program,” he says.
But for the required, ’round-the-clock coverage, he and other group members are expected to pull their share of nights as well. “I was always more of a nighttime person, in terms of my body clock,” Dr. Krisa says, “but now that I have more daytime nonclinical duties [as regional site director for Cogent HMG], it’s been more of a challenge to juggle home responsibilities, night shifts, and multiple administrative meetings.”
There are some basic principles of sleep hygiene and lessons learned from industrial settings that are good to keep in mind, says Christopher P. Landrigan, MD, SFHM, MPH, associate professor of medicine and pediatrics at Harvard Medical School and director of the Sleep and Patient Safety Program at Brigham and Women’s Hospital in Boston. “It’s really incumbent upon hospitalist group leaders to recognize the hazards of scheduling people for too many nights in a row, which conveys a risk both to the patients and to the hospitalists themselves,” Dr. Landrigan says. “We know that if hospitalists are driving home after night shifts, particularly multiple night shifts, that they’re at risk for motor vehicle crashes and at risk of sticking themselves with needles and scalpels toward the tail end of their shifts. None of us want that.”
Dr. Landrigan advises hospitalist groups to be cognizant of the hazards and think about the schedule “proactively.”
John Krisa, MD, medical director of the hospitalist group at Albany Memorial Hospital in New York, pictures his HM group as an organic whole when he draws up the schedule. He tries to avoid a strict 50-50 parceling out of night and day shifts. The hospitalist group makes liberal use of per-diem hospitalists and moonlighters, and has a few nocturnists.
“The vast majority of the work at night is processing new admissions, so these tend to be single encounters. You want your full-time people there multiple consecutive days for continuity and to represent the face of your program,” he says.
But for the required, ’round-the-clock coverage, he and other group members are expected to pull their share of nights as well. “I was always more of a nighttime person, in terms of my body clock,” Dr. Krisa says, “but now that I have more daytime nonclinical duties [as regional site director for Cogent HMG], it’s been more of a challenge to juggle home responsibilities, night shifts, and multiple administrative meetings.”
There are some basic principles of sleep hygiene and lessons learned from industrial settings that are good to keep in mind, says Christopher P. Landrigan, MD, SFHM, MPH, associate professor of medicine and pediatrics at Harvard Medical School and director of the Sleep and Patient Safety Program at Brigham and Women’s Hospital in Boston. “It’s really incumbent upon hospitalist group leaders to recognize the hazards of scheduling people for too many nights in a row, which conveys a risk both to the patients and to the hospitalists themselves,” Dr. Landrigan says. “We know that if hospitalists are driving home after night shifts, particularly multiple night shifts, that they’re at risk for motor vehicle crashes and at risk of sticking themselves with needles and scalpels toward the tail end of their shifts. None of us want that.”
Dr. Landrigan advises hospitalist groups to be cognizant of the hazards and think about the schedule “proactively.”
John Krisa, MD, medical director of the hospitalist group at Albany Memorial Hospital in New York, pictures his HM group as an organic whole when he draws up the schedule. He tries to avoid a strict 50-50 parceling out of night and day shifts. The hospitalist group makes liberal use of per-diem hospitalists and moonlighters, and has a few nocturnists.
“The vast majority of the work at night is processing new admissions, so these tend to be single encounters. You want your full-time people there multiple consecutive days for continuity and to represent the face of your program,” he says.
But for the required, ’round-the-clock coverage, he and other group members are expected to pull their share of nights as well. “I was always more of a nighttime person, in terms of my body clock,” Dr. Krisa says, “but now that I have more daytime nonclinical duties [as regional site director for Cogent HMG], it’s been more of a challenge to juggle home responsibilities, night shifts, and multiple administrative meetings.”
There are some basic principles of sleep hygiene and lessons learned from industrial settings that are good to keep in mind, says Christopher P. Landrigan, MD, SFHM, MPH, associate professor of medicine and pediatrics at Harvard Medical School and director of the Sleep and Patient Safety Program at Brigham and Women’s Hospital in Boston. “It’s really incumbent upon hospitalist group leaders to recognize the hazards of scheduling people for too many nights in a row, which conveys a risk both to the patients and to the hospitalists themselves,” Dr. Landrigan says. “We know that if hospitalists are driving home after night shifts, particularly multiple night shifts, that they’re at risk for motor vehicle crashes and at risk of sticking themselves with needles and scalpels toward the tail end of their shifts. None of us want that.”
Dr. Landrigan advises hospitalist groups to be cognizant of the hazards and think about the schedule “proactively.”