User login
The Hospitalist only
Power Struggles

Many hospitalist practices are started by “traditionalists”: primary-care physicians (PCPs) active in the outpatient and hospital settings. The practice typically grows due in large part to the leadership of the founders. Ultimately, the practice is made up of both the founders and a cadre of part- or full-time hospitalists who don’t work in the outpatient setting. And sometimes they have different incentives and ideas about how the practice should operate.
When these individuals disagree, which group should break the tie—the founding “hybrid” or “rotating” doctors who work part time on the hospitalist service or the doctors who work only as hospitalists?
This is a reasonably common issue for “medical” hospitalist groups, and in many cases is becoming an issue for groups in other specialties that adopt the hospitalist model, such as surgical hospitalists, laborists, etc.
A Common Scenario
Let me illustrate this issue with a composite of several former consulting clients. Let’s say this is a hospitalist practice that serves a 250-bed community hospital. One large private internal medicine group adopted a “rotating hospitalist” model there in the late 1990s. One of the internists provided the daytime hospital coverage for all the group’s patients one week out of every six. Their hospital volume grew quickly. They were asked to take on responsibility for admitting an increasing portion of the unassigned patients, provide care for patients referred by other PCPs who wanted to drop out of hospital work, and increasingly were asked to consult on patients admitted by surgeons.
When faced with this situation, many PCP groups decided to exit the hospital themselves and turn that work over to hospitalists. This group stuck it out. At first, the one doctor in the group covering the hospital each week kept up with the growing volume by simply working harder and longer every day. Eventually, the group sought financial help from the hospital to hire hospitalists who didn’t have outpatient responsibilities.
Years passed, and this PCP group transitioned to employment by the hospital, just like the full-time hospitalists. And by this time, the hospitalist practice was seen as distinct from the original PCP group. About 80% of the staffing was provided by hospitalists who didn’t work in the outpatient setting, the remainder by PCPs who essentially founded the practice. The PCPs chose to continue providing hospital care, both because they found it professionally satisfying and their compensation formula made it attractive for generating production in the hospital.
Tensions arose between the hospitalists and the “hybrids.” The hybrids refused to work night shifts and generally were unable to fill in for unplanned absences by the hospitalists. And because of the PCPs’ compensation formula, and possibly the work ethic of more senior doctors, they favored managing larger patient volumes and decreasing weekend staffing significantly to allow more weekends off in total for everyone. The hospitalists had other ideas about these things, and they were unhappy that the PCPs would have first say about when they could work hospital shifts, thereby decreasing the hospitalists’ scheduling flexibility.
The hospitalists were all within a few years of their residency training, and most of the PCPs were midcareer. This created a social divide, making it that much more difficult for the two groups to work through the issues. While the hybrid doctors saw the hospitalists as good clinicians, and vice versa, each group said: “The other guys are difficult to work with. They don’t understand what it is like for us.”
Need for Paradigm Shift
At many sites, the doctors and their administrative counterparts get stuck in a stalemate and have the same, unhappy conversations repeatedly. These conversations are really gripe sessions more than anything else.
I think the best solution is for everyone to acknowledge the valuable contribution of the hybrid doctors in founding and leading the hospitalist practice through years of growth, but also to begin seeing the hospitalist practice as being owned and governed primarily by the hospitalists who do most of the work. For most issues in which the two factions can’t agree, the hospitalists should have the tie-breaking vote.
While this approach reduces the autonomy of the hybrid doctors to make operational decisions, it doesn’t mean they have zero influence. In fact, the practice usually has a critical need for the hybrid doctors to continue providing some of the staffing. This usually means that the practice will need to ensure it puts together a package of compensation and available shifts on the schedule to ensure the hybrids want to remain active in the practice.
In most cases, all involved should ensure that those hybrid doctors who want to remain active in the hospital, and perform well in the hospitalist practice, should have the opportunity to do so indefinitely.
Compensation Methods for Hybrids
Even if the hybrids and hospitalists are able to harmoniously agree on things like work schedules, the hybrid doctors often have compensation schemes such that when working in the hospital, they have different financial incentives from the hospitalists. (I’m using “hybrid” to describe physicians who work in both inpatient and outpatient settings, usually more time in the office practice.) A common situation is that the production (i.e. wRVUs) generated in the hospital counts toward their office productivity. So the hybrids and the hospitalists will have different ideas about how hard they want to work.
The solution here is to divorce the office and hospital compensation schemes. There should be no connection between the compensation in the two settings, and both should be designed to ensure a competitive amount of money and performance incentives appropriate for that setting. Such methods usually mean that a day of work in the office will result in a different-sized paycheck than what comes with a day of work in the hospital.
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm. He is course codirector and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Many hospitalist practices are started by “traditionalists”: primary-care physicians (PCPs) active in the outpatient and hospital settings. The practice typically grows due in large part to the leadership of the founders. Ultimately, the practice is made up of both the founders and a cadre of part- or full-time hospitalists who don’t work in the outpatient setting. And sometimes they have different incentives and ideas about how the practice should operate.
When these individuals disagree, which group should break the tie—the founding “hybrid” or “rotating” doctors who work part time on the hospitalist service or the doctors who work only as hospitalists?
This is a reasonably common issue for “medical” hospitalist groups, and in many cases is becoming an issue for groups in other specialties that adopt the hospitalist model, such as surgical hospitalists, laborists, etc.
A Common Scenario
Let me illustrate this issue with a composite of several former consulting clients. Let’s say this is a hospitalist practice that serves a 250-bed community hospital. One large private internal medicine group adopted a “rotating hospitalist” model there in the late 1990s. One of the internists provided the daytime hospital coverage for all the group’s patients one week out of every six. Their hospital volume grew quickly. They were asked to take on responsibility for admitting an increasing portion of the unassigned patients, provide care for patients referred by other PCPs who wanted to drop out of hospital work, and increasingly were asked to consult on patients admitted by surgeons.
When faced with this situation, many PCP groups decided to exit the hospital themselves and turn that work over to hospitalists. This group stuck it out. At first, the one doctor in the group covering the hospital each week kept up with the growing volume by simply working harder and longer every day. Eventually, the group sought financial help from the hospital to hire hospitalists who didn’t have outpatient responsibilities.
Years passed, and this PCP group transitioned to employment by the hospital, just like the full-time hospitalists. And by this time, the hospitalist practice was seen as distinct from the original PCP group. About 80% of the staffing was provided by hospitalists who didn’t work in the outpatient setting, the remainder by PCPs who essentially founded the practice. The PCPs chose to continue providing hospital care, both because they found it professionally satisfying and their compensation formula made it attractive for generating production in the hospital.
Tensions arose between the hospitalists and the “hybrids.” The hybrids refused to work night shifts and generally were unable to fill in for unplanned absences by the hospitalists. And because of the PCPs’ compensation formula, and possibly the work ethic of more senior doctors, they favored managing larger patient volumes and decreasing weekend staffing significantly to allow more weekends off in total for everyone. The hospitalists had other ideas about these things, and they were unhappy that the PCPs would have first say about when they could work hospital shifts, thereby decreasing the hospitalists’ scheduling flexibility.
The hospitalists were all within a few years of their residency training, and most of the PCPs were midcareer. This created a social divide, making it that much more difficult for the two groups to work through the issues. While the hybrid doctors saw the hospitalists as good clinicians, and vice versa, each group said: “The other guys are difficult to work with. They don’t understand what it is like for us.”
Need for Paradigm Shift
At many sites, the doctors and their administrative counterparts get stuck in a stalemate and have the same, unhappy conversations repeatedly. These conversations are really gripe sessions more than anything else.
I think the best solution is for everyone to acknowledge the valuable contribution of the hybrid doctors in founding and leading the hospitalist practice through years of growth, but also to begin seeing the hospitalist practice as being owned and governed primarily by the hospitalists who do most of the work. For most issues in which the two factions can’t agree, the hospitalists should have the tie-breaking vote.
While this approach reduces the autonomy of the hybrid doctors to make operational decisions, it doesn’t mean they have zero influence. In fact, the practice usually has a critical need for the hybrid doctors to continue providing some of the staffing. This usually means that the practice will need to ensure it puts together a package of compensation and available shifts on the schedule to ensure the hybrids want to remain active in the practice.
In most cases, all involved should ensure that those hybrid doctors who want to remain active in the hospital, and perform well in the hospitalist practice, should have the opportunity to do so indefinitely.
Compensation Methods for Hybrids
Even if the hybrids and hospitalists are able to harmoniously agree on things like work schedules, the hybrid doctors often have compensation schemes such that when working in the hospital, they have different financial incentives from the hospitalists. (I’m using “hybrid” to describe physicians who work in both inpatient and outpatient settings, usually more time in the office practice.) A common situation is that the production (i.e. wRVUs) generated in the hospital counts toward their office productivity. So the hybrids and the hospitalists will have different ideas about how hard they want to work.
The solution here is to divorce the office and hospital compensation schemes. There should be no connection between the compensation in the two settings, and both should be designed to ensure a competitive amount of money and performance incentives appropriate for that setting. Such methods usually mean that a day of work in the office will result in a different-sized paycheck than what comes with a day of work in the hospital.
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm. He is course codirector and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Many hospitalist practices are started by “traditionalists”: primary-care physicians (PCPs) active in the outpatient and hospital settings. The practice typically grows due in large part to the leadership of the founders. Ultimately, the practice is made up of both the founders and a cadre of part- or full-time hospitalists who don’t work in the outpatient setting. And sometimes they have different incentives and ideas about how the practice should operate.
When these individuals disagree, which group should break the tie—the founding “hybrid” or “rotating” doctors who work part time on the hospitalist service or the doctors who work only as hospitalists?
This is a reasonably common issue for “medical” hospitalist groups, and in many cases is becoming an issue for groups in other specialties that adopt the hospitalist model, such as surgical hospitalists, laborists, etc.
A Common Scenario
Let me illustrate this issue with a composite of several former consulting clients. Let’s say this is a hospitalist practice that serves a 250-bed community hospital. One large private internal medicine group adopted a “rotating hospitalist” model there in the late 1990s. One of the internists provided the daytime hospital coverage for all the group’s patients one week out of every six. Their hospital volume grew quickly. They were asked to take on responsibility for admitting an increasing portion of the unassigned patients, provide care for patients referred by other PCPs who wanted to drop out of hospital work, and increasingly were asked to consult on patients admitted by surgeons.
When faced with this situation, many PCP groups decided to exit the hospital themselves and turn that work over to hospitalists. This group stuck it out. At first, the one doctor in the group covering the hospital each week kept up with the growing volume by simply working harder and longer every day. Eventually, the group sought financial help from the hospital to hire hospitalists who didn’t have outpatient responsibilities.
Years passed, and this PCP group transitioned to employment by the hospital, just like the full-time hospitalists. And by this time, the hospitalist practice was seen as distinct from the original PCP group. About 80% of the staffing was provided by hospitalists who didn’t work in the outpatient setting, the remainder by PCPs who essentially founded the practice. The PCPs chose to continue providing hospital care, both because they found it professionally satisfying and their compensation formula made it attractive for generating production in the hospital.
Tensions arose between the hospitalists and the “hybrids.” The hybrids refused to work night shifts and generally were unable to fill in for unplanned absences by the hospitalists. And because of the PCPs’ compensation formula, and possibly the work ethic of more senior doctors, they favored managing larger patient volumes and decreasing weekend staffing significantly to allow more weekends off in total for everyone. The hospitalists had other ideas about these things, and they were unhappy that the PCPs would have first say about when they could work hospital shifts, thereby decreasing the hospitalists’ scheduling flexibility.
The hospitalists were all within a few years of their residency training, and most of the PCPs were midcareer. This created a social divide, making it that much more difficult for the two groups to work through the issues. While the hybrid doctors saw the hospitalists as good clinicians, and vice versa, each group said: “The other guys are difficult to work with. They don’t understand what it is like for us.”
Need for Paradigm Shift
At many sites, the doctors and their administrative counterparts get stuck in a stalemate and have the same, unhappy conversations repeatedly. These conversations are really gripe sessions more than anything else.
I think the best solution is for everyone to acknowledge the valuable contribution of the hybrid doctors in founding and leading the hospitalist practice through years of growth, but also to begin seeing the hospitalist practice as being owned and governed primarily by the hospitalists who do most of the work. For most issues in which the two factions can’t agree, the hospitalists should have the tie-breaking vote.
While this approach reduces the autonomy of the hybrid doctors to make operational decisions, it doesn’t mean they have zero influence. In fact, the practice usually has a critical need for the hybrid doctors to continue providing some of the staffing. This usually means that the practice will need to ensure it puts together a package of compensation and available shifts on the schedule to ensure the hybrids want to remain active in the practice.
In most cases, all involved should ensure that those hybrid doctors who want to remain active in the hospital, and perform well in the hospitalist practice, should have the opportunity to do so indefinitely.
Compensation Methods for Hybrids
Even if the hybrids and hospitalists are able to harmoniously agree on things like work schedules, the hybrid doctors often have compensation schemes such that when working in the hospital, they have different financial incentives from the hospitalists. (I’m using “hybrid” to describe physicians who work in both inpatient and outpatient settings, usually more time in the office practice.) A common situation is that the production (i.e. wRVUs) generated in the hospital counts toward their office productivity. So the hybrids and the hospitalists will have different ideas about how hard they want to work.
The solution here is to divorce the office and hospital compensation schemes. There should be no connection between the compensation in the two settings, and both should be designed to ensure a competitive amount of money and performance incentives appropriate for that setting. Such methods usually mean that a day of work in the office will result in a different-sized paycheck than what comes with a day of work in the hospital.
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm. He is course codirector and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Maternity Management
Editor's Note: Second in a two-part series
Lest anyone forget, it is essential to support workers having children for one reason—the continuation of the human species, says Rachel Lovins, MD, SFHM, who directs the hospitalist program at Waterbury Hospital in Waterbury, Conn. For HM program directors, that means following pregnancy labor laws. But it also should involve reasonably accommodating hospitalists who are balancing their new baby’s needs with the demands of their profession, says Dr. Lovins and other HM leaders.
"As there are more women in medicine, everybody needs to be more aware of this issue. We don’t want to make good talent feel uncomfortable with the process of taking maternity leave and reducing time," says Michelle Marks, DO, FAAP, SFHM, director of the Center for Pediatric Hospital Medicine at the Cleveland Clinic.
All HM program directors need to be aware of such federal laws as the Pregnancy Discrimination Act and the Family and Medical Leave Act (www.eeoc.gov/laws/types/pregnancy.cfm), as well as the corresponding laws of the state in which they work. Directors can contact their human resources (HR) department for assistance.
"Calling them upfront will save a lot of headaches later on," says Jasen Gundersen, MD, MBA, CPE, SFHM, chief medical officer of the hospital medicine division in Fort Lauderdale, Fla., for Knoxville, Tenn.-based TeamHealth.
Here are some other recommendations on how HM directors can best manage pregnancy issues affecting their team:
The "R" in Relationship
There are many reasons why the director of a hospitalist group should develop a good relationship with the providers in their group, but one of them is that a hospitalist is more likely to tell her director sooner rather than later that she is pregnant, Dr. Marks says.
"Knowing your staff well and knowing them personally helps a lot, too, because you can gauge where they are going personally, as far as marriage, children, that type of thing," she adds.
The earlier a group leader knows a staff member is pregnant, the more time they have to plan for maternity leave. And the better the plan, the easier the leave is on the entire group, says Dr. Gundersen.
Generally, finding out that a physician is pregnant within three to five months of conception provides enough time to make adequate arrangements for coverage, Drs. Marks and Lovins note.

The Conversation
Before scheduling a meeting to discuss maternity leave and plans for returning to work with the hospitalist, the group leader should call HR to see if such a conversation is permissible, says Dr. Marks. A better approach might be to wait until the hospitalist broaches the subject.
"So many times the hospitalist will ask for counseling as far as what are her options of coming back," Dr. Marks says. "That opens the door for an open discussion."
Once the conversation starts, the group leader should gauge the length of maternity leave, her plans for coming back full time or part time, and the anticipated scheduling limitations or childcare considerations, Dr. Gundersen says.
"That’s not to say the pregnant woman can really predict all the time what’s going to happen," says Kerry Weiner, MD, MPH, chief clinical officer for North Hollywood, Calif.-based IPC: The Hospitalist Company, Inc. "Obviously, it’s a medical condition that can change and everyone understands that. It’s getting a feel of what you can actually know at the time."
If it’s the HM director’s intent to call the physician while she is on leave to see how she and the baby are doing and how the maternity leave is going, that should be discussed during the conversation, Dr. Gundersen says.
"If you establish upfront that you are going to make that phone call, I think that’s fine to do," he explains. "If you’re calling constantly and pressuring the person, I don’t think that that’s kosher at all."

—Rachel Lovins, MD, SFHM, director, hospitalist program, Waterbury (Conn.) Hospital
The Coverage Plan
Most maternity leaves are from eight to 12 weeks, although the length varies by HM program and individual. It is essential to have your group’s coverage plan outlined well in advance of the maternity leave.
In a private-practice model in which hospitalists work weekdays and have a call-coverage schedule for nights and weekends, a group leader can spread the extra work among the other hospitalists in the group because there are more hospitalists working during the day when patient census is higher, Dr. Weiner says.
Shifting the workload in other schedule models isn’t always as easy. "In the seven-day-on, seven-day-off model, because of that maximum patient-to-doctor ratio, I don’t think there’s any way to do it without hiring help," Dr. Lovins says. "It’s important to recruit per diems all the time. When you’re in a bind is the worst time to do it."
To limit the disruption to patient care and operations quality, the goal when using outside hospitalists is to contract with physicians who have worked with the group before and who know the community, hospital, systems, and patients, Dr. Weiner says.
For HM groups that use a flexible schedule, maternity coverage plans aren’t really needed, says Reuben Tovar, MD, chairman of Hospital Internists of Austin, a physician-owned and -managed hospitalist practice in Texas.
"We’re not salary, so that changes the dynamic completely. People who work more make more, and people who work less make less," he explains. "We are much more liberal about time off, because if a person is taking off to do what is important to them, like taking care of a child, then the rest of us feel better about doing extra work."
—Michelle Marks, DO, FAAP, SFHM, director, Center for Pediatric Hospital Medicine, Cleveland Clinic
Things Change
Plans discussed at the outset with a pregnant hospitalist can change after the child is born, HM group directors caution.
"Particularly for the first child, people say, ‘I’ll come back full blast. Don’t worry about it.’ And they figure out how hard all that is in the first couple of weeks, and then I get a different answer," Dr. Tovar says. "I think the whole mom/wife/doctor thing is tough. I recognize how hard that is. Even though I am not in that role, I can see it."
Dr. Gundersen suggests group directors have a backup plan, in case the maternity leave lasts longer than expected or the transition back to work is delayed. "It really prevents you from putting pressure on the physician," he says.
If a hospitalist who had planned to come back full time decides that she wants to work less, a director should check with HR to see what the process would entail.
"Generally, we have to negotiate a time frame for when they can drop down" to part-time hours, Dr. Marks says. "It usually takes three to four months for me to be able to adjust staffing to make it work."
Back to Work
Physicians can return from maternity leave in a reduced role, but they very rarely drop out of medicine entirely, Dr. Marks says.
"[They] have put in a lot of time to get where they are," she says. "Plus, women in medicine are usually high achievers and very interested in their careers."
Yet hospitalist leaders should recognize that returning to work after having a baby is stressful. It will take some time for the returning hospitalist to develop a rhythm between her duties as a mother and a doctor.
Directors can review the hospitalist’s nonclinical roles, help with priorities, and perhaps reassign some of the responsibilities to colleagues, Dr. Marks says. With more women breastfeeding, it is important to provide a convenient space with a door that locks for women to breast-pump at work, she and the other directors say.
"The best thing in the world is to have colleagues that you trust and can rely on," Dr. Lovins says. "That way, people can help each other out in emergencies, like if someone has to take their kid to the doctor. That’s the kind of program I want to have and would want to be part of."
Lisa Ryan is a freelance writer based in New Jersey.
Editor's Note: Second in a two-part series
Lest anyone forget, it is essential to support workers having children for one reason—the continuation of the human species, says Rachel Lovins, MD, SFHM, who directs the hospitalist program at Waterbury Hospital in Waterbury, Conn. For HM program directors, that means following pregnancy labor laws. But it also should involve reasonably accommodating hospitalists who are balancing their new baby’s needs with the demands of their profession, says Dr. Lovins and other HM leaders.
"As there are more women in medicine, everybody needs to be more aware of this issue. We don’t want to make good talent feel uncomfortable with the process of taking maternity leave and reducing time," says Michelle Marks, DO, FAAP, SFHM, director of the Center for Pediatric Hospital Medicine at the Cleveland Clinic.
All HM program directors need to be aware of such federal laws as the Pregnancy Discrimination Act and the Family and Medical Leave Act (www.eeoc.gov/laws/types/pregnancy.cfm), as well as the corresponding laws of the state in which they work. Directors can contact their human resources (HR) department for assistance.
"Calling them upfront will save a lot of headaches later on," says Jasen Gundersen, MD, MBA, CPE, SFHM, chief medical officer of the hospital medicine division in Fort Lauderdale, Fla., for Knoxville, Tenn.-based TeamHealth.
Here are some other recommendations on how HM directors can best manage pregnancy issues affecting their team:
The "R" in Relationship
There are many reasons why the director of a hospitalist group should develop a good relationship with the providers in their group, but one of them is that a hospitalist is more likely to tell her director sooner rather than later that she is pregnant, Dr. Marks says.
"Knowing your staff well and knowing them personally helps a lot, too, because you can gauge where they are going personally, as far as marriage, children, that type of thing," she adds.
The earlier a group leader knows a staff member is pregnant, the more time they have to plan for maternity leave. And the better the plan, the easier the leave is on the entire group, says Dr. Gundersen.
Generally, finding out that a physician is pregnant within three to five months of conception provides enough time to make adequate arrangements for coverage, Drs. Marks and Lovins note.
The Conversation
Before scheduling a meeting to discuss maternity leave and plans for returning to work with the hospitalist, the group leader should call HR to see if such a conversation is permissible, says Dr. Marks. A better approach might be to wait until the hospitalist broaches the subject.
"So many times the hospitalist will ask for counseling as far as what are her options of coming back," Dr. Marks says. "That opens the door for an open discussion."
Once the conversation starts, the group leader should gauge the length of maternity leave, her plans for coming back full time or part time, and the anticipated scheduling limitations or childcare considerations, Dr. Gundersen says.
"That’s not to say the pregnant woman can really predict all the time what’s going to happen," says Kerry Weiner, MD, MPH, chief clinical officer for North Hollywood, Calif.-based IPC: The Hospitalist Company, Inc. "Obviously, it’s a medical condition that can change and everyone understands that. It’s getting a feel of what you can actually know at the time."
If it’s the HM director’s intent to call the physician while she is on leave to see how she and the baby are doing and how the maternity leave is going, that should be discussed during the conversation, Dr. Gundersen says.
"If you establish upfront that you are going to make that phone call, I think that’s fine to do," he explains. "If you’re calling constantly and pressuring the person, I don’t think that that’s kosher at all."
—Rachel Lovins, MD, SFHM, director, hospitalist program, Waterbury (Conn.) Hospital
The Coverage Plan
Most maternity leaves are from eight to 12 weeks, although the length varies by HM program and individual. It is essential to have your group’s coverage plan outlined well in advance of the maternity leave.
In a private-practice model in which hospitalists work weekdays and have a call-coverage schedule for nights and weekends, a group leader can spread the extra work among the other hospitalists in the group because there are more hospitalists working during the day when patient census is higher, Dr. Weiner says.
Shifting the workload in other schedule models isn’t always as easy. "In the seven-day-on, seven-day-off model, because of that maximum patient-to-doctor ratio, I don’t think there’s any way to do it without hiring help," Dr. Lovins says. "It’s important to recruit per diems all the time. When you’re in a bind is the worst time to do it."
To limit the disruption to patient care and operations quality, the goal when using outside hospitalists is to contract with physicians who have worked with the group before and who know the community, hospital, systems, and patients, Dr. Weiner says.
For HM groups that use a flexible schedule, maternity coverage plans aren’t really needed, says Reuben Tovar, MD, chairman of Hospital Internists of Austin, a physician-owned and -managed hospitalist practice in Texas.
"We’re not salary, so that changes the dynamic completely. People who work more make more, and people who work less make less," he explains. "We are much more liberal about time off, because if a person is taking off to do what is important to them, like taking care of a child, then the rest of us feel better about doing extra work."
—Michelle Marks, DO, FAAP, SFHM, director, Center for Pediatric Hospital Medicine, Cleveland Clinic
Things Change
Plans discussed at the outset with a pregnant hospitalist can change after the child is born, HM group directors caution.
"Particularly for the first child, people say, ‘I’ll come back full blast. Don’t worry about it.’ And they figure out how hard all that is in the first couple of weeks, and then I get a different answer," Dr. Tovar says. "I think the whole mom/wife/doctor thing is tough. I recognize how hard that is. Even though I am not in that role, I can see it."
Dr. Gundersen suggests group directors have a backup plan, in case the maternity leave lasts longer than expected or the transition back to work is delayed. "It really prevents you from putting pressure on the physician," he says.
If a hospitalist who had planned to come back full time decides that she wants to work less, a director should check with HR to see what the process would entail.
"Generally, we have to negotiate a time frame for when they can drop down" to part-time hours, Dr. Marks says. "It usually takes three to four months for me to be able to adjust staffing to make it work."
Back to Work
Physicians can return from maternity leave in a reduced role, but they very rarely drop out of medicine entirely, Dr. Marks says.
"[They] have put in a lot of time to get where they are," she says. "Plus, women in medicine are usually high achievers and very interested in their careers."
Yet hospitalist leaders should recognize that returning to work after having a baby is stressful. It will take some time for the returning hospitalist to develop a rhythm between her duties as a mother and a doctor.
Directors can review the hospitalist’s nonclinical roles, help with priorities, and perhaps reassign some of the responsibilities to colleagues, Dr. Marks says. With more women breastfeeding, it is important to provide a convenient space with a door that locks for women to breast-pump at work, she and the other directors say.
"The best thing in the world is to have colleagues that you trust and can rely on," Dr. Lovins says. "That way, people can help each other out in emergencies, like if someone has to take their kid to the doctor. That’s the kind of program I want to have and would want to be part of."
Lisa Ryan is a freelance writer based in New Jersey.
Editor's Note: Second in a two-part series
Lest anyone forget, it is essential to support workers having children for one reason—the continuation of the human species, says Rachel Lovins, MD, SFHM, who directs the hospitalist program at Waterbury Hospital in Waterbury, Conn. For HM program directors, that means following pregnancy labor laws. But it also should involve reasonably accommodating hospitalists who are balancing their new baby’s needs with the demands of their profession, says Dr. Lovins and other HM leaders.
"As there are more women in medicine, everybody needs to be more aware of this issue. We don’t want to make good talent feel uncomfortable with the process of taking maternity leave and reducing time," says Michelle Marks, DO, FAAP, SFHM, director of the Center for Pediatric Hospital Medicine at the Cleveland Clinic.
All HM program directors need to be aware of such federal laws as the Pregnancy Discrimination Act and the Family and Medical Leave Act (www.eeoc.gov/laws/types/pregnancy.cfm), as well as the corresponding laws of the state in which they work. Directors can contact their human resources (HR) department for assistance.
"Calling them upfront will save a lot of headaches later on," says Jasen Gundersen, MD, MBA, CPE, SFHM, chief medical officer of the hospital medicine division in Fort Lauderdale, Fla., for Knoxville, Tenn.-based TeamHealth.
Here are some other recommendations on how HM directors can best manage pregnancy issues affecting their team:
The "R" in Relationship
There are many reasons why the director of a hospitalist group should develop a good relationship with the providers in their group, but one of them is that a hospitalist is more likely to tell her director sooner rather than later that she is pregnant, Dr. Marks says.
"Knowing your staff well and knowing them personally helps a lot, too, because you can gauge where they are going personally, as far as marriage, children, that type of thing," she adds.
The earlier a group leader knows a staff member is pregnant, the more time they have to plan for maternity leave. And the better the plan, the easier the leave is on the entire group, says Dr. Gundersen.
Generally, finding out that a physician is pregnant within three to five months of conception provides enough time to make adequate arrangements for coverage, Drs. Marks and Lovins note.
The Conversation
Before scheduling a meeting to discuss maternity leave and plans for returning to work with the hospitalist, the group leader should call HR to see if such a conversation is permissible, says Dr. Marks. A better approach might be to wait until the hospitalist broaches the subject.
"So many times the hospitalist will ask for counseling as far as what are her options of coming back," Dr. Marks says. "That opens the door for an open discussion."
Once the conversation starts, the group leader should gauge the length of maternity leave, her plans for coming back full time or part time, and the anticipated scheduling limitations or childcare considerations, Dr. Gundersen says.
"That’s not to say the pregnant woman can really predict all the time what’s going to happen," says Kerry Weiner, MD, MPH, chief clinical officer for North Hollywood, Calif.-based IPC: The Hospitalist Company, Inc. "Obviously, it’s a medical condition that can change and everyone understands that. It’s getting a feel of what you can actually know at the time."
If it’s the HM director’s intent to call the physician while she is on leave to see how she and the baby are doing and how the maternity leave is going, that should be discussed during the conversation, Dr. Gundersen says.
"If you establish upfront that you are going to make that phone call, I think that’s fine to do," he explains. "If you’re calling constantly and pressuring the person, I don’t think that that’s kosher at all."
—Rachel Lovins, MD, SFHM, director, hospitalist program, Waterbury (Conn.) Hospital
The Coverage Plan
Most maternity leaves are from eight to 12 weeks, although the length varies by HM program and individual. It is essential to have your group’s coverage plan outlined well in advance of the maternity leave.
In a private-practice model in which hospitalists work weekdays and have a call-coverage schedule for nights and weekends, a group leader can spread the extra work among the other hospitalists in the group because there are more hospitalists working during the day when patient census is higher, Dr. Weiner says.
Shifting the workload in other schedule models isn’t always as easy. "In the seven-day-on, seven-day-off model, because of that maximum patient-to-doctor ratio, I don’t think there’s any way to do it without hiring help," Dr. Lovins says. "It’s important to recruit per diems all the time. When you’re in a bind is the worst time to do it."
To limit the disruption to patient care and operations quality, the goal when using outside hospitalists is to contract with physicians who have worked with the group before and who know the community, hospital, systems, and patients, Dr. Weiner says.
For HM groups that use a flexible schedule, maternity coverage plans aren’t really needed, says Reuben Tovar, MD, chairman of Hospital Internists of Austin, a physician-owned and -managed hospitalist practice in Texas.
"We’re not salary, so that changes the dynamic completely. People who work more make more, and people who work less make less," he explains. "We are much more liberal about time off, because if a person is taking off to do what is important to them, like taking care of a child, then the rest of us feel better about doing extra work."
—Michelle Marks, DO, FAAP, SFHM, director, Center for Pediatric Hospital Medicine, Cleveland Clinic
Things Change
Plans discussed at the outset with a pregnant hospitalist can change after the child is born, HM group directors caution.
"Particularly for the first child, people say, ‘I’ll come back full blast. Don’t worry about it.’ And they figure out how hard all that is in the first couple of weeks, and then I get a different answer," Dr. Tovar says. "I think the whole mom/wife/doctor thing is tough. I recognize how hard that is. Even though I am not in that role, I can see it."
Dr. Gundersen suggests group directors have a backup plan, in case the maternity leave lasts longer than expected or the transition back to work is delayed. "It really prevents you from putting pressure on the physician," he says.
If a hospitalist who had planned to come back full time decides that she wants to work less, a director should check with HR to see what the process would entail.
"Generally, we have to negotiate a time frame for when they can drop down" to part-time hours, Dr. Marks says. "It usually takes three to four months for me to be able to adjust staffing to make it work."
Back to Work
Physicians can return from maternity leave in a reduced role, but they very rarely drop out of medicine entirely, Dr. Marks says.
"[They] have put in a lot of time to get where they are," she says. "Plus, women in medicine are usually high achievers and very interested in their careers."
Yet hospitalist leaders should recognize that returning to work after having a baby is stressful. It will take some time for the returning hospitalist to develop a rhythm between her duties as a mother and a doctor.
Directors can review the hospitalist’s nonclinical roles, help with priorities, and perhaps reassign some of the responsibilities to colleagues, Dr. Marks says. With more women breastfeeding, it is important to provide a convenient space with a door that locks for women to breast-pump at work, she and the other directors say.
"The best thing in the world is to have colleagues that you trust and can rely on," Dr. Lovins says. "That way, people can help each other out in emergencies, like if someone has to take their kid to the doctor. That’s the kind of program I want to have and would want to be part of."
Lisa Ryan is a freelance writer based in New Jersey.
ONLINE EXCLUSIVE: Listen to program directors discuss managing a group when a hospitalist is out on maternity leave
Click here to listen to Dr. Weiner
Click here to listen to Dr. Marks
Click here to listen to Dr. Weiner
Click here to listen to Dr. Marks
Click here to listen to Dr. Weiner
Click here to listen to Dr. Marks
How High Can Your Support Payments Go?
Last December, St. Peter’s Hospital, a 122-bed acute-care facility in Helena, Mont., crossed a symbolic line in the decade-long evolution of the financial payments that hospitals have provided to HM groups to make up the gap that exists between the expenses of running a hospitalist service and the professional fees that generate its revenue.
Hospital administrators asked the outpatient providers at the Helena Physicians’ Clinic to pay nearly $400,000 per year to support the in-house HM service at St. Peter’s, according to a series of stories in the local paper, the Helena Independent Record. The fee was never instituted and, in fact, some Helena patients and physicians have questioned whether the high-stakes payment was part of a broader campaign for the hospital to take over the clinic, a process that culminated in March with the hospital’s purchase of the clinic’s building.
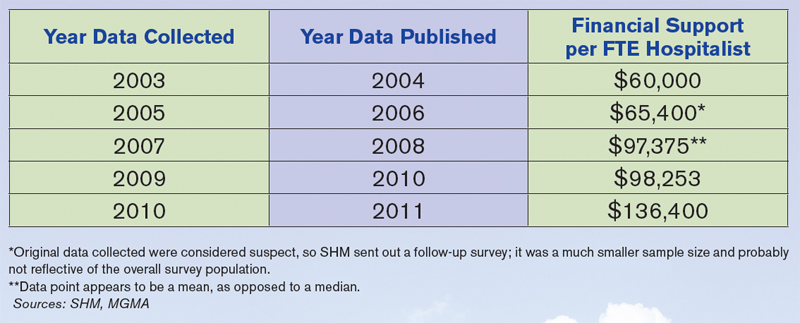
Still, the Montana case focused a spotlight on the doughnut hole of HM ledger sheets: hospital subsidies. More than 80% of HM groups took financial support from their host institutions in fiscal year 2010, according to new data from SHM and the Medical Group Management Association (MGMA), which will be released in September. And the amount of that support has more than doubled, from $60,000 per full-time equivalent (FTE) in 2003-2004 to $136,400 per FTE in the latest data, according to a presentation at HM11 in May.
HM leaders agree the growth is unsustainable, particularly in the new world of healthcare reform, but they also concur that satisfaction with the benefits a hospitalist service offers make it unlikely other institutions will implement a fee-for-service system similar to that of St. Peter’s (see “Pay to Play?,” p. 38). As hospital administrators struggle to dole out pieces of their ever-shrinking financial pie, hospitalists also agree that they will find it more and more difficult to ask their C-suite for continually larger payments (see Figure 1, “Growth in Hospitalist Financial Support,” p. 37). Even when portrayed as “investments” in physicians that provide more than clinical care (e.g. hospitalists assuming leadership roles on hospital committees and pushing quality-improvement initiatives), a hospital’s bottom line can only afford so much.
“It’s not sustainable,” says Burke Kealey, MD, SFHM, medical director of hospital specialties at HealthPartners in Minneapolis and an SHM board member. “I think hospitals are pretty much tapped out by and large.
“What we’ve been seeing is practices have been able to ramp up their productivity, but people have also found other revenue streams, be it perioperative clinics, be it trying to find direct subsidies from specialty practices, be it educational funds for teaching. … We’re kind of entering a time when payment reform of some sort is going to have to come into play.”
History Lesson
Support payments have been around since HM’s earliest days, Dr. Kealey says. From the outset, it was difficult for most practices to cover their own salaries and expenses with reimbursement to the charges that make up the bulk of the field’s billing opportunities. “The economics of the situation are such that it is pretty difficult for a hospitalist to cover their own salary with the standard E/M codes,” he adds.
Hospitals, though, quickly realized that hospitalist practices were a valuable presence and created a payment stream to help offset the difference.
John Laverty, DHA, vice president of hospital-based physicians at HCA Physician Services in Nashville, Tenn., says four main factors drive the need for the hospitalist subsidy:
- Physician productivity. How many patients can a practice see on a daily or a monthly basis? Most averages teeter between 15 and 20 patients per day, often less in academic models. There is a mathematical point at which a group can generate enough revenue to cover costs, but many HM leaders say that comes at the cost of quality care delivery and physician satisfaction.
- Nonclinical/non-revenue-generating activities performed by hospitalists. HM groups usually are involved in QI and patient-safety initiatives, which, while important, are not necessarily captured by billing codes. Some HM contracts call for compensation tied to those activities, but many still do not, leaving groups with a gap to cover.
- Payor mix. A particularly difficult mix with high charity care and uninsured patients can lower the average net collected revenue per visit. There also is the choice between being a Medicaid participating provider or a nonparticipating provider with managed-care payors. So-called “non-par” providers typically have the ability to negotiate higher rates.
- Expenses. “How rich is your benefit package for your physicians?” Laverty asks. “Do you provide a retirement plan? Health, dental and vision? … Do you pay for CME?”
Dr. Kealey says it’s not “impossible” to cover all of a hospitalist’s costs through professional fees; however, “it usually requires a hospitalist be in an area with a very good payor mix or a hospital of very high efficiency, where they can see lots of patients. And often, there might be a setup where they aren’t covering unproductive times or tasks.”
Another Point of View
Not everyone thinks the subsidy is a fait accompli. Jeff Taylor, president and chief operating officer of IPC: The Hospitalist Co., a national physician group practice based in North Hollywood, Calif., says subsidies do not need to be a factor in a practice’s bottom line. Taylor says that IPC generates just 5% of its revenues from subsidies, with the remaining 95% financed by professional fees.
He attributes much of that to the work schedule, particularly the popular model of seven days on clinical duty followed by seven days off. He says that model has led to increased practice costs that then require financial support from their hospital. The schedule’s popularity is fueled by the balance it offers physicians between their work and personal lives, Taylor says, but it also means that practitioners working under it lose two weeks a month of billing opportunities.
He’s right about the popularity, as more than 70% of hospitalist groups use a shift-based staffing model, according to the State of Hospital Medicine: 2010 Report Based on 2009 Data. The number of HM groups employing call-based and hybrid coverage (some shift, some call) is 30%.

—Todd Nelson, MBA, technical director, Healthcare Financial Management Association, Chicago
“There is nothing else inherent in hospital medicine that makes this expensive, other than scheduling,” Taylor says. “Absent a very difficult payor mix, it’s the scheduling and the number of days worked that drives the cost. … We have been saying that for years, but we haven’t seen much of a waver yet. Once hospitals realize—some of them are starting to get it—that it’s the underlying work schedule that drives cost, they’re not going to continue to do it.”
Todd Nelson, MBA, a technical director at the Healthcare Financial Management Association in Chicago, agrees that the upward trajectory of hospital support payments will have to end, likely in concert with the expected payment reform of the next five years. But, he adds, the mere fact that hospital administrators have allowed the payments to double suggests that they view the support as an investment. In return for that money, though, C-suite members should contract for and then demand adherence to performance measures, he notes.
“Many specialties say, ‘We’re valuable; help us out,’ ” says Nelson, a former chief financial officer at Grinnell Regional Medical Center in Iowa. “In the hospital world, you can’t just ‘help out.’ They need to be providing a service you’re paying them for.”
SHM President Joseph Li, MD, SFHM, associate professor of medicine at Harvard Medical School and director of the hospital medicine division at Beth Israel Deaconess Medical Center in Boston, could not agree more. “The way I view monies that are sent to a group for nonclinical work is exactly that,” he says. “It’s compensation for nonclinical work. Subsidy, to me, seems to mean that despite whatever you’re doing, you need some more to pay because you can’t make your ends meet. That’s not true. What that figure is, for my group and for the vast majority of groups in this country, is really compensation for nonclinical efforts.”
HM groups should take it upon themselves to discuss their value contribution with their chief financial officer, as many in that position view hospitalist services as a “cost center” rather than as a means to the end of better financial performance for the institution as a whole, says Beth Hawley, senior vice president with Brentwood, Tenn.-based Cogent HMG.
“You need to look at it from the viewpoint of your CFO,” she says. “It is really important to educate your CFO on the myriad ways that your hospitalist program can create value for the hospital.”

—Jeff Taylor, president, COO, IPC: The Hospitalist Co., North Hollywood, Calif.
Hospitalist John Bulger, DO, FACP, FHM, of Geisinger Medical Center in Danville, Pa., says such education should highlight the intangible values of HM services, but it also needs to include firm, eye-opening data points. Put another way: “Have true ROI [return on investment], not soft ROI,” he says.
Dr. Bulger suggests pointing out that what some call a subsidy, he views as simply a payment, no different from the lump-sum check a hospital or healthcare system might cut for the group running its ED, or the check it writes for a cardiology specialty.
“There’s a subsidy for all those groups, but it’s never been looked at as a subsidy,” he adds. “But from a business perspective, it’s the same thing.”
The Future of Support
The relative value, justification, and existence of the support aside, the question remains: What is its future?
“Subsidies are not going to go away, because you can’t recruit and retain physicians in this environment for the most part without them,” says Troy Ahlstrom, MD, SFHM, CFO of Hospitalists of Northern Michigan, a hospitalist-owned and -managed group based in Traverse City. “Especially not when physicians coming out of residency have a desire to maintain a reasonable work and personal life, with fewer shifts where possible, fewer patients per shift. And they also have income goals that they have to maintain with that because they’re coming out of training with larger debt loads than ever before. That’s the tricky part for CMS and the federal government moving forward.”
Nelson, however, says that the future of support will be tied to payment reform, as bundled payments, value-based purchasing (VBP), and other initiatives to reduce overall healthcare spending are implemented. He said HM and other specialties should keep in mind that the point of reform is less overall spending, which translates to less support for everyone.
“When the pie shrinks, the table manners change,” he adds. “People are going to have to figure out how to slice that pie.”
Accountable-care organizations (ACOs) could be one answer. An ACO is a type of healthcare delivery model being piloted by the Centers for Medicare & Medicaid Services (CMS), in which a group of providers band together to coordinate the care of beneficiaries (see “Quality over Quantity,” December 2009, p. 23). Reimbursement is shared by the group and is tied to the quality of care provided. Nelson says the model could significantly cut the need for support, as HM groups are allowed to share in the upside created by the ACO.
The program is set to go live Jan. 1, 2012, but a leading hospitalist already has questioned whether the proposed rules provide enough capitated risk and, therefore, whether the incentive is enough to spur adoption of the model and the potential support reductions it would bring.
“You can certainly start by taking a lower amount of risk, just upside risk,” Cogent HMG chief medical officer Ron Greeno, MD, FCCP, SFHM, told The Hospitalist eWire in April, when the proposed rules were issued. “But your plan should be not to stay there. Your plan should be to take more and more risk as soon as you can, as soon as you’re capable.”
Nelson says that the support can continue in some form or fashion in the new models as long as the hospital and its practitioners are integrated and looking to achieve the same goal.
“The reality is, from the hospital perspective, you need to make sure you’re getting some value,” he says. “What are they buying in exchange for that [payment]?” TH
Richard Quinn is a freelance writer based in New Jersey.
Pay to Play?

When St. Peter’s Hospital in Helena, Mont., proposed charging an outpatient clinic nearly $400,000 a year to use its in-house HM group, it prompted a new question from the hospitalist field: Will hospitals begin charging a fee for HM services?
The near-universal answer from hospitalists is no.
“At the end of the day, what the hospital wants is to keep peace in the valley and drive volume,” says John Laverty, DHA, vice president of hospital-based physicians at HCA Physician Services in Nashville, Tenn. “Any way that they encourage volume by going out and adding subscribing physicians, or docs that want to turn their patients over to hospitalists, I can’t see a hospital charging a fee for that service. Obviously, they’re cutting their nose off because they’re going to limit [referrals].”
Hospitalists have heard about institutions attempting to institute a fee, but pushback from stakeholders usually makes the paradigm unworkable.
Hospitals usually value their relationships with primary-care physicians (PCPs) too much to alienate them, says hospitalist John Bulger, DO, FACP, FHM, of Geisinger Medical Center in Danville, Pa. This is particularly so, he says, when PCPs point out that should they object to paying such a fee to use HM services, many of their patients would end up in a hospital regardless of referrals.
In that context, the attempt by St. Peter’s to charge a fee is the perfect example of the failed premise: The idea was raised but never executed.
“PCPs love hospitalists,” Dr. Bulger says. “But part of the reason they love HM is it’s free.”—RQ
Last December, St. Peter’s Hospital, a 122-bed acute-care facility in Helena, Mont., crossed a symbolic line in the decade-long evolution of the financial payments that hospitals have provided to HM groups to make up the gap that exists between the expenses of running a hospitalist service and the professional fees that generate its revenue.
Hospital administrators asked the outpatient providers at the Helena Physicians’ Clinic to pay nearly $400,000 per year to support the in-house HM service at St. Peter’s, according to a series of stories in the local paper, the Helena Independent Record. The fee was never instituted and, in fact, some Helena patients and physicians have questioned whether the high-stakes payment was part of a broader campaign for the hospital to take over the clinic, a process that culminated in March with the hospital’s purchase of the clinic’s building.
Still, the Montana case focused a spotlight on the doughnut hole of HM ledger sheets: hospital subsidies. More than 80% of HM groups took financial support from their host institutions in fiscal year 2010, according to new data from SHM and the Medical Group Management Association (MGMA), which will be released in September. And the amount of that support has more than doubled, from $60,000 per full-time equivalent (FTE) in 2003-2004 to $136,400 per FTE in the latest data, according to a presentation at HM11 in May.
HM leaders agree the growth is unsustainable, particularly in the new world of healthcare reform, but they also concur that satisfaction with the benefits a hospitalist service offers make it unlikely other institutions will implement a fee-for-service system similar to that of St. Peter’s (see “Pay to Play?,” p. 38). As hospital administrators struggle to dole out pieces of their ever-shrinking financial pie, hospitalists also agree that they will find it more and more difficult to ask their C-suite for continually larger payments (see Figure 1, “Growth in Hospitalist Financial Support,” p. 37). Even when portrayed as “investments” in physicians that provide more than clinical care (e.g. hospitalists assuming leadership roles on hospital committees and pushing quality-improvement initiatives), a hospital’s bottom line can only afford so much.
“It’s not sustainable,” says Burke Kealey, MD, SFHM, medical director of hospital specialties at HealthPartners in Minneapolis and an SHM board member. “I think hospitals are pretty much tapped out by and large.
“What we’ve been seeing is practices have been able to ramp up their productivity, but people have also found other revenue streams, be it perioperative clinics, be it trying to find direct subsidies from specialty practices, be it educational funds for teaching. … We’re kind of entering a time when payment reform of some sort is going to have to come into play.”
History Lesson
Support payments have been around since HM’s earliest days, Dr. Kealey says. From the outset, it was difficult for most practices to cover their own salaries and expenses with reimbursement to the charges that make up the bulk of the field’s billing opportunities. “The economics of the situation are such that it is pretty difficult for a hospitalist to cover their own salary with the standard E/M codes,” he adds.
Hospitals, though, quickly realized that hospitalist practices were a valuable presence and created a payment stream to help offset the difference.
John Laverty, DHA, vice president of hospital-based physicians at HCA Physician Services in Nashville, Tenn., says four main factors drive the need for the hospitalist subsidy:
- Physician productivity. How many patients can a practice see on a daily or a monthly basis? Most averages teeter between 15 and 20 patients per day, often less in academic models. There is a mathematical point at which a group can generate enough revenue to cover costs, but many HM leaders say that comes at the cost of quality care delivery and physician satisfaction.
- Nonclinical/non-revenue-generating activities performed by hospitalists. HM groups usually are involved in QI and patient-safety initiatives, which, while important, are not necessarily captured by billing codes. Some HM contracts call for compensation tied to those activities, but many still do not, leaving groups with a gap to cover.
- Payor mix. A particularly difficult mix with high charity care and uninsured patients can lower the average net collected revenue per visit. There also is the choice between being a Medicaid participating provider or a nonparticipating provider with managed-care payors. So-called “non-par” providers typically have the ability to negotiate higher rates.
- Expenses. “How rich is your benefit package for your physicians?” Laverty asks. “Do you provide a retirement plan? Health, dental and vision? … Do you pay for CME?”
Dr. Kealey says it’s not “impossible” to cover all of a hospitalist’s costs through professional fees; however, “it usually requires a hospitalist be in an area with a very good payor mix or a hospital of very high efficiency, where they can see lots of patients. And often, there might be a setup where they aren’t covering unproductive times or tasks.”
Another Point of View
Not everyone thinks the subsidy is a fait accompli. Jeff Taylor, president and chief operating officer of IPC: The Hospitalist Co., a national physician group practice based in North Hollywood, Calif., says subsidies do not need to be a factor in a practice’s bottom line. Taylor says that IPC generates just 5% of its revenues from subsidies, with the remaining 95% financed by professional fees.
He attributes much of that to the work schedule, particularly the popular model of seven days on clinical duty followed by seven days off. He says that model has led to increased practice costs that then require financial support from their hospital. The schedule’s popularity is fueled by the balance it offers physicians between their work and personal lives, Taylor says, but it also means that practitioners working under it lose two weeks a month of billing opportunities.
He’s right about the popularity, as more than 70% of hospitalist groups use a shift-based staffing model, according to the State of Hospital Medicine: 2010 Report Based on 2009 Data. The number of HM groups employing call-based and hybrid coverage (some shift, some call) is 30%.
—Todd Nelson, MBA, technical director, Healthcare Financial Management Association, Chicago
“There is nothing else inherent in hospital medicine that makes this expensive, other than scheduling,” Taylor says. “Absent a very difficult payor mix, it’s the scheduling and the number of days worked that drives the cost. … We have been saying that for years, but we haven’t seen much of a waver yet. Once hospitals realize—some of them are starting to get it—that it’s the underlying work schedule that drives cost, they’re not going to continue to do it.”
Todd Nelson, MBA, a technical director at the Healthcare Financial Management Association in Chicago, agrees that the upward trajectory of hospital support payments will have to end, likely in concert with the expected payment reform of the next five years. But, he adds, the mere fact that hospital administrators have allowed the payments to double suggests that they view the support as an investment. In return for that money, though, C-suite members should contract for and then demand adherence to performance measures, he notes.
“Many specialties say, ‘We’re valuable; help us out,’ ” says Nelson, a former chief financial officer at Grinnell Regional Medical Center in Iowa. “In the hospital world, you can’t just ‘help out.’ They need to be providing a service you’re paying them for.”
SHM President Joseph Li, MD, SFHM, associate professor of medicine at Harvard Medical School and director of the hospital medicine division at Beth Israel Deaconess Medical Center in Boston, could not agree more. “The way I view monies that are sent to a group for nonclinical work is exactly that,” he says. “It’s compensation for nonclinical work. Subsidy, to me, seems to mean that despite whatever you’re doing, you need some more to pay because you can’t make your ends meet. That’s not true. What that figure is, for my group and for the vast majority of groups in this country, is really compensation for nonclinical efforts.”
HM groups should take it upon themselves to discuss their value contribution with their chief financial officer, as many in that position view hospitalist services as a “cost center” rather than as a means to the end of better financial performance for the institution as a whole, says Beth Hawley, senior vice president with Brentwood, Tenn.-based Cogent HMG.
“You need to look at it from the viewpoint of your CFO,” she says. “It is really important to educate your CFO on the myriad ways that your hospitalist program can create value for the hospital.”
—Jeff Taylor, president, COO, IPC: The Hospitalist Co., North Hollywood, Calif.
Hospitalist John Bulger, DO, FACP, FHM, of Geisinger Medical Center in Danville, Pa., says such education should highlight the intangible values of HM services, but it also needs to include firm, eye-opening data points. Put another way: “Have true ROI [return on investment], not soft ROI,” he says.
Dr. Bulger suggests pointing out that what some call a subsidy, he views as simply a payment, no different from the lump-sum check a hospital or healthcare system might cut for the group running its ED, or the check it writes for a cardiology specialty.
“There’s a subsidy for all those groups, but it’s never been looked at as a subsidy,” he adds. “But from a business perspective, it’s the same thing.”
The Future of Support
The relative value, justification, and existence of the support aside, the question remains: What is its future?
“Subsidies are not going to go away, because you can’t recruit and retain physicians in this environment for the most part without them,” says Troy Ahlstrom, MD, SFHM, CFO of Hospitalists of Northern Michigan, a hospitalist-owned and -managed group based in Traverse City. “Especially not when physicians coming out of residency have a desire to maintain a reasonable work and personal life, with fewer shifts where possible, fewer patients per shift. And they also have income goals that they have to maintain with that because they’re coming out of training with larger debt loads than ever before. That’s the tricky part for CMS and the federal government moving forward.”
Nelson, however, says that the future of support will be tied to payment reform, as bundled payments, value-based purchasing (VBP), and other initiatives to reduce overall healthcare spending are implemented. He said HM and other specialties should keep in mind that the point of reform is less overall spending, which translates to less support for everyone.
“When the pie shrinks, the table manners change,” he adds. “People are going to have to figure out how to slice that pie.”
Accountable-care organizations (ACOs) could be one answer. An ACO is a type of healthcare delivery model being piloted by the Centers for Medicare & Medicaid Services (CMS), in which a group of providers band together to coordinate the care of beneficiaries (see “Quality over Quantity,” December 2009, p. 23). Reimbursement is shared by the group and is tied to the quality of care provided. Nelson says the model could significantly cut the need for support, as HM groups are allowed to share in the upside created by the ACO.
The program is set to go live Jan. 1, 2012, but a leading hospitalist already has questioned whether the proposed rules provide enough capitated risk and, therefore, whether the incentive is enough to spur adoption of the model and the potential support reductions it would bring.
“You can certainly start by taking a lower amount of risk, just upside risk,” Cogent HMG chief medical officer Ron Greeno, MD, FCCP, SFHM, told The Hospitalist eWire in April, when the proposed rules were issued. “But your plan should be not to stay there. Your plan should be to take more and more risk as soon as you can, as soon as you’re capable.”
Nelson says that the support can continue in some form or fashion in the new models as long as the hospital and its practitioners are integrated and looking to achieve the same goal.
“The reality is, from the hospital perspective, you need to make sure you’re getting some value,” he says. “What are they buying in exchange for that [payment]?” TH
Richard Quinn is a freelance writer based in New Jersey.
Pay to Play?
When St. Peter’s Hospital in Helena, Mont., proposed charging an outpatient clinic nearly $400,000 a year to use its in-house HM group, it prompted a new question from the hospitalist field: Will hospitals begin charging a fee for HM services?
The near-universal answer from hospitalists is no.
“At the end of the day, what the hospital wants is to keep peace in the valley and drive volume,” says John Laverty, DHA, vice president of hospital-based physicians at HCA Physician Services in Nashville, Tenn. “Any way that they encourage volume by going out and adding subscribing physicians, or docs that want to turn their patients over to hospitalists, I can’t see a hospital charging a fee for that service. Obviously, they’re cutting their nose off because they’re going to limit [referrals].”
Hospitalists have heard about institutions attempting to institute a fee, but pushback from stakeholders usually makes the paradigm unworkable.
Hospitals usually value their relationships with primary-care physicians (PCPs) too much to alienate them, says hospitalist John Bulger, DO, FACP, FHM, of Geisinger Medical Center in Danville, Pa. This is particularly so, he says, when PCPs point out that should they object to paying such a fee to use HM services, many of their patients would end up in a hospital regardless of referrals.
In that context, the attempt by St. Peter’s to charge a fee is the perfect example of the failed premise: The idea was raised but never executed.
“PCPs love hospitalists,” Dr. Bulger says. “But part of the reason they love HM is it’s free.”—RQ
Last December, St. Peter’s Hospital, a 122-bed acute-care facility in Helena, Mont., crossed a symbolic line in the decade-long evolution of the financial payments that hospitals have provided to HM groups to make up the gap that exists between the expenses of running a hospitalist service and the professional fees that generate its revenue.
Hospital administrators asked the outpatient providers at the Helena Physicians’ Clinic to pay nearly $400,000 per year to support the in-house HM service at St. Peter’s, according to a series of stories in the local paper, the Helena Independent Record. The fee was never instituted and, in fact, some Helena patients and physicians have questioned whether the high-stakes payment was part of a broader campaign for the hospital to take over the clinic, a process that culminated in March with the hospital’s purchase of the clinic’s building.
Still, the Montana case focused a spotlight on the doughnut hole of HM ledger sheets: hospital subsidies. More than 80% of HM groups took financial support from their host institutions in fiscal year 2010, according to new data from SHM and the Medical Group Management Association (MGMA), which will be released in September. And the amount of that support has more than doubled, from $60,000 per full-time equivalent (FTE) in 2003-2004 to $136,400 per FTE in the latest data, according to a presentation at HM11 in May.
HM leaders agree the growth is unsustainable, particularly in the new world of healthcare reform, but they also concur that satisfaction with the benefits a hospitalist service offers make it unlikely other institutions will implement a fee-for-service system similar to that of St. Peter’s (see “Pay to Play?,” p. 38). As hospital administrators struggle to dole out pieces of their ever-shrinking financial pie, hospitalists also agree that they will find it more and more difficult to ask their C-suite for continually larger payments (see Figure 1, “Growth in Hospitalist Financial Support,” p. 37). Even when portrayed as “investments” in physicians that provide more than clinical care (e.g. hospitalists assuming leadership roles on hospital committees and pushing quality-improvement initiatives), a hospital’s bottom line can only afford so much.
“It’s not sustainable,” says Burke Kealey, MD, SFHM, medical director of hospital specialties at HealthPartners in Minneapolis and an SHM board member. “I think hospitals are pretty much tapped out by and large.
“What we’ve been seeing is practices have been able to ramp up their productivity, but people have also found other revenue streams, be it perioperative clinics, be it trying to find direct subsidies from specialty practices, be it educational funds for teaching. … We’re kind of entering a time when payment reform of some sort is going to have to come into play.”
History Lesson
Support payments have been around since HM’s earliest days, Dr. Kealey says. From the outset, it was difficult for most practices to cover their own salaries and expenses with reimbursement to the charges that make up the bulk of the field’s billing opportunities. “The economics of the situation are such that it is pretty difficult for a hospitalist to cover their own salary with the standard E/M codes,” he adds.
Hospitals, though, quickly realized that hospitalist practices were a valuable presence and created a payment stream to help offset the difference.
John Laverty, DHA, vice president of hospital-based physicians at HCA Physician Services in Nashville, Tenn., says four main factors drive the need for the hospitalist subsidy:
- Physician productivity. How many patients can a practice see on a daily or a monthly basis? Most averages teeter between 15 and 20 patients per day, often less in academic models. There is a mathematical point at which a group can generate enough revenue to cover costs, but many HM leaders say that comes at the cost of quality care delivery and physician satisfaction.
- Nonclinical/non-revenue-generating activities performed by hospitalists. HM groups usually are involved in QI and patient-safety initiatives, which, while important, are not necessarily captured by billing codes. Some HM contracts call for compensation tied to those activities, but many still do not, leaving groups with a gap to cover.
- Payor mix. A particularly difficult mix with high charity care and uninsured patients can lower the average net collected revenue per visit. There also is the choice between being a Medicaid participating provider or a nonparticipating provider with managed-care payors. So-called “non-par” providers typically have the ability to negotiate higher rates.
- Expenses. “How rich is your benefit package for your physicians?” Laverty asks. “Do you provide a retirement plan? Health, dental and vision? … Do you pay for CME?”
Dr. Kealey says it’s not “impossible” to cover all of a hospitalist’s costs through professional fees; however, “it usually requires a hospitalist be in an area with a very good payor mix or a hospital of very high efficiency, where they can see lots of patients. And often, there might be a setup where they aren’t covering unproductive times or tasks.”
Another Point of View
Not everyone thinks the subsidy is a fait accompli. Jeff Taylor, president and chief operating officer of IPC: The Hospitalist Co., a national physician group practice based in North Hollywood, Calif., says subsidies do not need to be a factor in a practice’s bottom line. Taylor says that IPC generates just 5% of its revenues from subsidies, with the remaining 95% financed by professional fees.
He attributes much of that to the work schedule, particularly the popular model of seven days on clinical duty followed by seven days off. He says that model has led to increased practice costs that then require financial support from their hospital. The schedule’s popularity is fueled by the balance it offers physicians between their work and personal lives, Taylor says, but it also means that practitioners working under it lose two weeks a month of billing opportunities.
He’s right about the popularity, as more than 70% of hospitalist groups use a shift-based staffing model, according to the State of Hospital Medicine: 2010 Report Based on 2009 Data. The number of HM groups employing call-based and hybrid coverage (some shift, some call) is 30%.
—Todd Nelson, MBA, technical director, Healthcare Financial Management Association, Chicago
“There is nothing else inherent in hospital medicine that makes this expensive, other than scheduling,” Taylor says. “Absent a very difficult payor mix, it’s the scheduling and the number of days worked that drives the cost. … We have been saying that for years, but we haven’t seen much of a waver yet. Once hospitals realize—some of them are starting to get it—that it’s the underlying work schedule that drives cost, they’re not going to continue to do it.”
Todd Nelson, MBA, a technical director at the Healthcare Financial Management Association in Chicago, agrees that the upward trajectory of hospital support payments will have to end, likely in concert with the expected payment reform of the next five years. But, he adds, the mere fact that hospital administrators have allowed the payments to double suggests that they view the support as an investment. In return for that money, though, C-suite members should contract for and then demand adherence to performance measures, he notes.
“Many specialties say, ‘We’re valuable; help us out,’ ” says Nelson, a former chief financial officer at Grinnell Regional Medical Center in Iowa. “In the hospital world, you can’t just ‘help out.’ They need to be providing a service you’re paying them for.”
SHM President Joseph Li, MD, SFHM, associate professor of medicine at Harvard Medical School and director of the hospital medicine division at Beth Israel Deaconess Medical Center in Boston, could not agree more. “The way I view monies that are sent to a group for nonclinical work is exactly that,” he says. “It’s compensation for nonclinical work. Subsidy, to me, seems to mean that despite whatever you’re doing, you need some more to pay because you can’t make your ends meet. That’s not true. What that figure is, for my group and for the vast majority of groups in this country, is really compensation for nonclinical efforts.”
HM groups should take it upon themselves to discuss their value contribution with their chief financial officer, as many in that position view hospitalist services as a “cost center” rather than as a means to the end of better financial performance for the institution as a whole, says Beth Hawley, senior vice president with Brentwood, Tenn.-based Cogent HMG.
“You need to look at it from the viewpoint of your CFO,” she says. “It is really important to educate your CFO on the myriad ways that your hospitalist program can create value for the hospital.”
—Jeff Taylor, president, COO, IPC: The Hospitalist Co., North Hollywood, Calif.
Hospitalist John Bulger, DO, FACP, FHM, of Geisinger Medical Center in Danville, Pa., says such education should highlight the intangible values of HM services, but it also needs to include firm, eye-opening data points. Put another way: “Have true ROI [return on investment], not soft ROI,” he says.
Dr. Bulger suggests pointing out that what some call a subsidy, he views as simply a payment, no different from the lump-sum check a hospital or healthcare system might cut for the group running its ED, or the check it writes for a cardiology specialty.
“There’s a subsidy for all those groups, but it’s never been looked at as a subsidy,” he adds. “But from a business perspective, it’s the same thing.”
The Future of Support
The relative value, justification, and existence of the support aside, the question remains: What is its future?
“Subsidies are not going to go away, because you can’t recruit and retain physicians in this environment for the most part without them,” says Troy Ahlstrom, MD, SFHM, CFO of Hospitalists of Northern Michigan, a hospitalist-owned and -managed group based in Traverse City. “Especially not when physicians coming out of residency have a desire to maintain a reasonable work and personal life, with fewer shifts where possible, fewer patients per shift. And they also have income goals that they have to maintain with that because they’re coming out of training with larger debt loads than ever before. That’s the tricky part for CMS and the federal government moving forward.”
Nelson, however, says that the future of support will be tied to payment reform, as bundled payments, value-based purchasing (VBP), and other initiatives to reduce overall healthcare spending are implemented. He said HM and other specialties should keep in mind that the point of reform is less overall spending, which translates to less support for everyone.
“When the pie shrinks, the table manners change,” he adds. “People are going to have to figure out how to slice that pie.”
Accountable-care organizations (ACOs) could be one answer. An ACO is a type of healthcare delivery model being piloted by the Centers for Medicare & Medicaid Services (CMS), in which a group of providers band together to coordinate the care of beneficiaries (see “Quality over Quantity,” December 2009, p. 23). Reimbursement is shared by the group and is tied to the quality of care provided. Nelson says the model could significantly cut the need for support, as HM groups are allowed to share in the upside created by the ACO.
The program is set to go live Jan. 1, 2012, but a leading hospitalist already has questioned whether the proposed rules provide enough capitated risk and, therefore, whether the incentive is enough to spur adoption of the model and the potential support reductions it would bring.
“You can certainly start by taking a lower amount of risk, just upside risk,” Cogent HMG chief medical officer Ron Greeno, MD, FCCP, SFHM, told The Hospitalist eWire in April, when the proposed rules were issued. “But your plan should be not to stay there. Your plan should be to take more and more risk as soon as you can, as soon as you’re capable.”
Nelson says that the support can continue in some form or fashion in the new models as long as the hospital and its practitioners are integrated and looking to achieve the same goal.
“The reality is, from the hospital perspective, you need to make sure you’re getting some value,” he says. “What are they buying in exchange for that [payment]?” TH
Richard Quinn is a freelance writer based in New Jersey.
Pay to Play?
When St. Peter’s Hospital in Helena, Mont., proposed charging an outpatient clinic nearly $400,000 a year to use its in-house HM group, it prompted a new question from the hospitalist field: Will hospitals begin charging a fee for HM services?
The near-universal answer from hospitalists is no.
“At the end of the day, what the hospital wants is to keep peace in the valley and drive volume,” says John Laverty, DHA, vice president of hospital-based physicians at HCA Physician Services in Nashville, Tenn. “Any way that they encourage volume by going out and adding subscribing physicians, or docs that want to turn their patients over to hospitalists, I can’t see a hospital charging a fee for that service. Obviously, they’re cutting their nose off because they’re going to limit [referrals].”
Hospitalists have heard about institutions attempting to institute a fee, but pushback from stakeholders usually makes the paradigm unworkable.
Hospitals usually value their relationships with primary-care physicians (PCPs) too much to alienate them, says hospitalist John Bulger, DO, FACP, FHM, of Geisinger Medical Center in Danville, Pa. This is particularly so, he says, when PCPs point out that should they object to paying such a fee to use HM services, many of their patients would end up in a hospital regardless of referrals.
In that context, the attempt by St. Peter’s to charge a fee is the perfect example of the failed premise: The idea was raised but never executed.
“PCPs love hospitalists,” Dr. Bulger says. “But part of the reason they love HM is it’s free.”—RQ
Red Flags within Documentation for Hospitalists
With the number of clinical hospitalists still growing, more patients are under HM care, which puts hospitalists at higher risk for lawsuits. The goal for a hospitalist should be to take care of their patients, but at the same point make a defensible medical record. Plaintiffs’ attorneys look for potential red flags in the medical record. Potential red flags could be illegibility, omissions of date and time, criticism of other healthcare providers, vague terminology, abbreviations, delayed entries, inconsistencies between healthcare providers, corrections, and opinions about the patient.
The medical record is a legal document that is required by law and regulatory bodies. It serves as a communication vehicle for healthcare providers; it tells the patient’s story as well as the care that has been received. It is used for implementing quality-improvement initiatives, determining appropriate level of care, and research and education. It also is the most credible evidence in a legal proceeding. Inaccurate or incomplete documentation can mean serious trouble.
The most common documentation error is illegible handwriting. It is well known throughout medicine that if it’s not documented, it has not been done. At the same time, what is not readable has not been done. Electronic health records (EHR) have minimized this problem; however, EHR is not universally available, and documentation could include both electronic and handwritten entries.
Common sense dictates that all records should be legible, but it is surprising the number of progress notes that are illegible. Physicians are encouraged to write in black ink, so that the notes are capable of being photocopied. Some colored inks can run when they become wet. Also, all entries should include the full date, time, and the name of the physician, as well as their title and designation, which should be printed alongside their signatures.
Correction fluid must not be used in any patient records. Corrections should be made with a single line drawn through them, initialed, dated, and timed, so the error can still be read. All entries should be in a chronological order, with no spaces between the entries. Extra words should not be squeezed onto a line; a line must be drawn through any empty space at the end of an entry. Ditto marks should never be used. Use of glue is not permitted in the medical record, unless some special pages have tabs to allow sheets to be attached to the notes.
No paper should be removed from the clinical file, other than for purposes of photocopying, and those should be returned immediately. Each page of the documentation should be sequentially numbered; if the pages are kept in separate sections, make sure that is clear. Each progress note should have three unique patient identifiers: patient name, date of birth, and a record number. Most hospitals use sticker systems or printable progress notes, which have taken care of this problem.
Notes from various specialties, including nursing records, should be documented in the patient chart. If any of these include discussions held outside of normal working hours, those entry notes should clearly state the time and location of the discussions and state that the entry is made retrospectively.
Leaving space to accommodate late documentation never is a good idea. If the space is too small and subsequent documentation is squeezed in, an attorney could allege that the squeeze documentation was added to cover something up. If the space is too large, the blank space remains unaccounted for. When a late entry is made several days later, it should include a rationale for the delay. Unexplained late entries, along with erased or obliterated entries, are serious red flags.
The clinical content of a progress note should state in full a legible and understandable history. This should include a full assessment, including the positive and negative findings, interventions, and outcomes, as well as initial and ongoing assessments by each provider. Legible instructions should be included for all treatment therapies and medications. These records should be factual, consistent, and accurate.
When physicians disagree among themselves, criticism of that should not be on the record. In fact, this variance should be documented in the chart and the provider making this decision should clearly document the processes that led to the decision.
It is unwise to include abbreviations. In cases where abbreviations are necessary, they should be spelled out fully the first time. Institutional policies should be followed for appropriate abbreviations. Jargon, meaningless phrases, irrelevant speculation, and offensive or subjective statements should not be written. Labels to describe a patient as obnoxious, belligerent, or rude can lead to serious allegations. In fact, direct quotes should be applied on the record. The patient’s refusal of treatment should be documented, including the patient’s stated reason for refusal, if provided, and any action taken by the provider, as well as patient education and notifying the patient and their family. Patients who refuse to accept treatment recommendations might bear partial responsibility for a subsequent injury, which is known as “contributory negligence.”
Vague terminology should be avoided (e.g. “Cl urine” could mean colored urine, clear urine, or cloudy urine) as it can be subject to interpretation. Institutional policies should be followed for reporting incident reports. Peer-review processes should be noted; however, do not indicate in the chart that an incident report has been filed or an event report has been completed. This can serve as a red flag and could give the plaintiff’s attorney the right to access the record.
Documentation red flags should be addressed on a daily basis. Progress notes should be catered not only to providing an accurate record of the physicians’ thought process, but as an assessment of the patient, keeping in mind that if this case is called into court three or four years later, the record will speak for itself.
Deepak Pahuja, MD, FACP,
hospitalist, director of CME,
Erie Physician Network Hospitalists,
St. Vincent Health Center, Erie, Pa.,
CEO, Aerolib Healthcare Solutions LLC;
Priyanka Chadha, MD,
cofounder, Aerolib Healthcare Solutions LLC
DRG Accuracy Increases Medicare Reimbursement, Reduces Risks
Clinical documentation integrity (CDI) programs started in the 1990s. Most of the programs were experimental pilots that assessed the impact on physician documentation and quality.
In 2007, the Centers for Medicare & Medicaid Services (CMS) implemented the Medicare Severity Diagnosis Related Group (DRG). The focus of the DRG system was severity of illness and mortality rates. Indicators such as present on admission (POA) and hospital-acquired condition (HCA) were added the next year to identify conditions noted when a patient was admitted into the hospital.
Currently, the purpose of the CDI program is to optimize the DRG by capturing conditions through clear, concise documentation and coding. Accuracy in reporting DRG assignments will increase Medicare reimbursement and reduce compliance risks. CDI program popularity has grown because of careful consideration of the benefits of implementation.
Are we ready for the change? Launching a CDI program is not an easy task. It takes courage, tenacity, patience, and a great plan. The success of a CDI program depends on one key element: buy-in by physicians at your facility. Yes, physicians. Physician resistance is high for two key reasons: time and education.
A physician’s focus primarily has been the care of the patient, with time allowed to clarify their working or discharge diagnosis and maintaining their patients in the hospital setting. That’s where a clinical documentation specialist (CDS) comes in. At Civista Medical Center in Maryland, color-coded worksheets are printed and attached to the patient’s medical record. The purpose of the worksheet is to trigger the physician to write specific documentation.
Education! Education! It cannot be stressed enough. Healthcare is a team effort. To achieve accurate and concise documentation, physicians must be educated about the importance of documentation. Nonspecific documentation leads to nonspecific coding of the medical record. Therefore, the true severity of illness, mortality rate, and intensity of service goes uncaptured. The lack of specificity in documentation affects the quality of patient care, compliance risk, data integrity, and reimbursement.
The implementation of a CDI program can be successful by enlisting internal support at your facility, including administration, physicians, and such ancillary staff members as case management. A clear, concise plan that includes physicians every step of the way will be imperative.
Consider the many avenues you might have to implement your query system, either by paper or electronically. If the coding department does not own the concurrent CDI query process, make sure they are involved in the process of establishing the program. In addition, provide feedback to various facility departments about the impact the CDI program is having on quality, integrity, and reimbursement. Include an ongoing program to educate the physicians on ICD 9-CM, as well as the forthcoming ICD 10, for a smoother transition.
Karen Stanley, RN, MBA,
White Plains, Md.
With the number of clinical hospitalists still growing, more patients are under HM care, which puts hospitalists at higher risk for lawsuits. The goal for a hospitalist should be to take care of their patients, but at the same point make a defensible medical record. Plaintiffs’ attorneys look for potential red flags in the medical record. Potential red flags could be illegibility, omissions of date and time, criticism of other healthcare providers, vague terminology, abbreviations, delayed entries, inconsistencies between healthcare providers, corrections, and opinions about the patient.
The medical record is a legal document that is required by law and regulatory bodies. It serves as a communication vehicle for healthcare providers; it tells the patient’s story as well as the care that has been received. It is used for implementing quality-improvement initiatives, determining appropriate level of care, and research and education. It also is the most credible evidence in a legal proceeding. Inaccurate or incomplete documentation can mean serious trouble.
The most common documentation error is illegible handwriting. It is well known throughout medicine that if it’s not documented, it has not been done. At the same time, what is not readable has not been done. Electronic health records (EHR) have minimized this problem; however, EHR is not universally available, and documentation could include both electronic and handwritten entries.
Common sense dictates that all records should be legible, but it is surprising the number of progress notes that are illegible. Physicians are encouraged to write in black ink, so that the notes are capable of being photocopied. Some colored inks can run when they become wet. Also, all entries should include the full date, time, and the name of the physician, as well as their title and designation, which should be printed alongside their signatures.
Correction fluid must not be used in any patient records. Corrections should be made with a single line drawn through them, initialed, dated, and timed, so the error can still be read. All entries should be in a chronological order, with no spaces between the entries. Extra words should not be squeezed onto a line; a line must be drawn through any empty space at the end of an entry. Ditto marks should never be used. Use of glue is not permitted in the medical record, unless some special pages have tabs to allow sheets to be attached to the notes.
No paper should be removed from the clinical file, other than for purposes of photocopying, and those should be returned immediately. Each page of the documentation should be sequentially numbered; if the pages are kept in separate sections, make sure that is clear. Each progress note should have three unique patient identifiers: patient name, date of birth, and a record number. Most hospitals use sticker systems or printable progress notes, which have taken care of this problem.
Notes from various specialties, including nursing records, should be documented in the patient chart. If any of these include discussions held outside of normal working hours, those entry notes should clearly state the time and location of the discussions and state that the entry is made retrospectively.
Leaving space to accommodate late documentation never is a good idea. If the space is too small and subsequent documentation is squeezed in, an attorney could allege that the squeeze documentation was added to cover something up. If the space is too large, the blank space remains unaccounted for. When a late entry is made several days later, it should include a rationale for the delay. Unexplained late entries, along with erased or obliterated entries, are serious red flags.
The clinical content of a progress note should state in full a legible and understandable history. This should include a full assessment, including the positive and negative findings, interventions, and outcomes, as well as initial and ongoing assessments by each provider. Legible instructions should be included for all treatment therapies and medications. These records should be factual, consistent, and accurate.
When physicians disagree among themselves, criticism of that should not be on the record. In fact, this variance should be documented in the chart and the provider making this decision should clearly document the processes that led to the decision.
It is unwise to include abbreviations. In cases where abbreviations are necessary, they should be spelled out fully the first time. Institutional policies should be followed for appropriate abbreviations. Jargon, meaningless phrases, irrelevant speculation, and offensive or subjective statements should not be written. Labels to describe a patient as obnoxious, belligerent, or rude can lead to serious allegations. In fact, direct quotes should be applied on the record. The patient’s refusal of treatment should be documented, including the patient’s stated reason for refusal, if provided, and any action taken by the provider, as well as patient education and notifying the patient and their family. Patients who refuse to accept treatment recommendations might bear partial responsibility for a subsequent injury, which is known as “contributory negligence.”
Vague terminology should be avoided (e.g. “Cl urine” could mean colored urine, clear urine, or cloudy urine) as it can be subject to interpretation. Institutional policies should be followed for reporting incident reports. Peer-review processes should be noted; however, do not indicate in the chart that an incident report has been filed or an event report has been completed. This can serve as a red flag and could give the plaintiff’s attorney the right to access the record.
Documentation red flags should be addressed on a daily basis. Progress notes should be catered not only to providing an accurate record of the physicians’ thought process, but as an assessment of the patient, keeping in mind that if this case is called into court three or four years later, the record will speak for itself.
Deepak Pahuja, MD, FACP,
hospitalist, director of CME,
Erie Physician Network Hospitalists,
St. Vincent Health Center, Erie, Pa.,
CEO, Aerolib Healthcare Solutions LLC;
Priyanka Chadha, MD,
cofounder, Aerolib Healthcare Solutions LLC
DRG Accuracy Increases Medicare Reimbursement, Reduces Risks
Clinical documentation integrity (CDI) programs started in the 1990s. Most of the programs were experimental pilots that assessed the impact on physician documentation and quality.
In 2007, the Centers for Medicare & Medicaid Services (CMS) implemented the Medicare Severity Diagnosis Related Group (DRG). The focus of the DRG system was severity of illness and mortality rates. Indicators such as present on admission (POA) and hospital-acquired condition (HCA) were added the next year to identify conditions noted when a patient was admitted into the hospital.
Currently, the purpose of the CDI program is to optimize the DRG by capturing conditions through clear, concise documentation and coding. Accuracy in reporting DRG assignments will increase Medicare reimbursement and reduce compliance risks. CDI program popularity has grown because of careful consideration of the benefits of implementation.
Are we ready for the change? Launching a CDI program is not an easy task. It takes courage, tenacity, patience, and a great plan. The success of a CDI program depends on one key element: buy-in by physicians at your facility. Yes, physicians. Physician resistance is high for two key reasons: time and education.
A physician’s focus primarily has been the care of the patient, with time allowed to clarify their working or discharge diagnosis and maintaining their patients in the hospital setting. That’s where a clinical documentation specialist (CDS) comes in. At Civista Medical Center in Maryland, color-coded worksheets are printed and attached to the patient’s medical record. The purpose of the worksheet is to trigger the physician to write specific documentation.
Education! Education! It cannot be stressed enough. Healthcare is a team effort. To achieve accurate and concise documentation, physicians must be educated about the importance of documentation. Nonspecific documentation leads to nonspecific coding of the medical record. Therefore, the true severity of illness, mortality rate, and intensity of service goes uncaptured. The lack of specificity in documentation affects the quality of patient care, compliance risk, data integrity, and reimbursement.
The implementation of a CDI program can be successful by enlisting internal support at your facility, including administration, physicians, and such ancillary staff members as case management. A clear, concise plan that includes physicians every step of the way will be imperative.
Consider the many avenues you might have to implement your query system, either by paper or electronically. If the coding department does not own the concurrent CDI query process, make sure they are involved in the process of establishing the program. In addition, provide feedback to various facility departments about the impact the CDI program is having on quality, integrity, and reimbursement. Include an ongoing program to educate the physicians on ICD 9-CM, as well as the forthcoming ICD 10, for a smoother transition.
Karen Stanley, RN, MBA,
White Plains, Md.
With the number of clinical hospitalists still growing, more patients are under HM care, which puts hospitalists at higher risk for lawsuits. The goal for a hospitalist should be to take care of their patients, but at the same point make a defensible medical record. Plaintiffs’ attorneys look for potential red flags in the medical record. Potential red flags could be illegibility, omissions of date and time, criticism of other healthcare providers, vague terminology, abbreviations, delayed entries, inconsistencies between healthcare providers, corrections, and opinions about the patient.
The medical record is a legal document that is required by law and regulatory bodies. It serves as a communication vehicle for healthcare providers; it tells the patient’s story as well as the care that has been received. It is used for implementing quality-improvement initiatives, determining appropriate level of care, and research and education. It also is the most credible evidence in a legal proceeding. Inaccurate or incomplete documentation can mean serious trouble.
The most common documentation error is illegible handwriting. It is well known throughout medicine that if it’s not documented, it has not been done. At the same time, what is not readable has not been done. Electronic health records (EHR) have minimized this problem; however, EHR is not universally available, and documentation could include both electronic and handwritten entries.
Common sense dictates that all records should be legible, but it is surprising the number of progress notes that are illegible. Physicians are encouraged to write in black ink, so that the notes are capable of being photocopied. Some colored inks can run when they become wet. Also, all entries should include the full date, time, and the name of the physician, as well as their title and designation, which should be printed alongside their signatures.
Correction fluid must not be used in any patient records. Corrections should be made with a single line drawn through them, initialed, dated, and timed, so the error can still be read. All entries should be in a chronological order, with no spaces between the entries. Extra words should not be squeezed onto a line; a line must be drawn through any empty space at the end of an entry. Ditto marks should never be used. Use of glue is not permitted in the medical record, unless some special pages have tabs to allow sheets to be attached to the notes.
No paper should be removed from the clinical file, other than for purposes of photocopying, and those should be returned immediately. Each page of the documentation should be sequentially numbered; if the pages are kept in separate sections, make sure that is clear. Each progress note should have three unique patient identifiers: patient name, date of birth, and a record number. Most hospitals use sticker systems or printable progress notes, which have taken care of this problem.
Notes from various specialties, including nursing records, should be documented in the patient chart. If any of these include discussions held outside of normal working hours, those entry notes should clearly state the time and location of the discussions and state that the entry is made retrospectively.
Leaving space to accommodate late documentation never is a good idea. If the space is too small and subsequent documentation is squeezed in, an attorney could allege that the squeeze documentation was added to cover something up. If the space is too large, the blank space remains unaccounted for. When a late entry is made several days later, it should include a rationale for the delay. Unexplained late entries, along with erased or obliterated entries, are serious red flags.
The clinical content of a progress note should state in full a legible and understandable history. This should include a full assessment, including the positive and negative findings, interventions, and outcomes, as well as initial and ongoing assessments by each provider. Legible instructions should be included for all treatment therapies and medications. These records should be factual, consistent, and accurate.
When physicians disagree among themselves, criticism of that should not be on the record. In fact, this variance should be documented in the chart and the provider making this decision should clearly document the processes that led to the decision.
It is unwise to include abbreviations. In cases where abbreviations are necessary, they should be spelled out fully the first time. Institutional policies should be followed for appropriate abbreviations. Jargon, meaningless phrases, irrelevant speculation, and offensive or subjective statements should not be written. Labels to describe a patient as obnoxious, belligerent, or rude can lead to serious allegations. In fact, direct quotes should be applied on the record. The patient’s refusal of treatment should be documented, including the patient’s stated reason for refusal, if provided, and any action taken by the provider, as well as patient education and notifying the patient and their family. Patients who refuse to accept treatment recommendations might bear partial responsibility for a subsequent injury, which is known as “contributory negligence.”
Vague terminology should be avoided (e.g. “Cl urine” could mean colored urine, clear urine, or cloudy urine) as it can be subject to interpretation. Institutional policies should be followed for reporting incident reports. Peer-review processes should be noted; however, do not indicate in the chart that an incident report has been filed or an event report has been completed. This can serve as a red flag and could give the plaintiff’s attorney the right to access the record.
Documentation red flags should be addressed on a daily basis. Progress notes should be catered not only to providing an accurate record of the physicians’ thought process, but as an assessment of the patient, keeping in mind that if this case is called into court three or four years later, the record will speak for itself.
Deepak Pahuja, MD, FACP,
hospitalist, director of CME,
Erie Physician Network Hospitalists,
St. Vincent Health Center, Erie, Pa.,
CEO, Aerolib Healthcare Solutions LLC;
Priyanka Chadha, MD,
cofounder, Aerolib Healthcare Solutions LLC
DRG Accuracy Increases Medicare Reimbursement, Reduces Risks
Clinical documentation integrity (CDI) programs started in the 1990s. Most of the programs were experimental pilots that assessed the impact on physician documentation and quality.
In 2007, the Centers for Medicare & Medicaid Services (CMS) implemented the Medicare Severity Diagnosis Related Group (DRG). The focus of the DRG system was severity of illness and mortality rates. Indicators such as present on admission (POA) and hospital-acquired condition (HCA) were added the next year to identify conditions noted when a patient was admitted into the hospital.
Currently, the purpose of the CDI program is to optimize the DRG by capturing conditions through clear, concise documentation and coding. Accuracy in reporting DRG assignments will increase Medicare reimbursement and reduce compliance risks. CDI program popularity has grown because of careful consideration of the benefits of implementation.
Are we ready for the change? Launching a CDI program is not an easy task. It takes courage, tenacity, patience, and a great plan. The success of a CDI program depends on one key element: buy-in by physicians at your facility. Yes, physicians. Physician resistance is high for two key reasons: time and education.
A physician’s focus primarily has been the care of the patient, with time allowed to clarify their working or discharge diagnosis and maintaining their patients in the hospital setting. That’s where a clinical documentation specialist (CDS) comes in. At Civista Medical Center in Maryland, color-coded worksheets are printed and attached to the patient’s medical record. The purpose of the worksheet is to trigger the physician to write specific documentation.
Education! Education! It cannot be stressed enough. Healthcare is a team effort. To achieve accurate and concise documentation, physicians must be educated about the importance of documentation. Nonspecific documentation leads to nonspecific coding of the medical record. Therefore, the true severity of illness, mortality rate, and intensity of service goes uncaptured. The lack of specificity in documentation affects the quality of patient care, compliance risk, data integrity, and reimbursement.
The implementation of a CDI program can be successful by enlisting internal support at your facility, including administration, physicians, and such ancillary staff members as case management. A clear, concise plan that includes physicians every step of the way will be imperative.
Consider the many avenues you might have to implement your query system, either by paper or electronically. If the coding department does not own the concurrent CDI query process, make sure they are involved in the process of establishing the program. In addition, provide feedback to various facility departments about the impact the CDI program is having on quality, integrity, and reimbursement. Include an ongoing program to educate the physicians on ICD 9-CM, as well as the forthcoming ICD 10, for a smoother transition.
Karen Stanley, RN, MBA,
White Plains, Md.
ONLINE EXCLUSIVE: Hospitalists discuss the time-honored tradition of hospital payments to HM groups
Into the Night
The halls are quiet, the lights dimmed, the incessant ringing of telephones has fallen silent, patients slumber in their rooms, nurses sit and chart, waiting for the inevitable patient call light to glow once again. Then it happens: the overhead announcement that slices through the night like a knife.
“Code blue, code blue!”
As the code team scurries to the room, they start the protocols. However, they are waiting for someone—the conductor of the symphony, if you will. Who will answer the call? Who will whisk down the hall to take the podium? Will that patient’s primary-care physician (PCP) come? The cardiologist, maybe the pulmonologist?
No, there is one person who walks the halls at night when all others are asleep (even the ED doctors, though awake, are consumed by crowded emergency rooms and cannot help). This person is the nocturnist.
What is a nocturnist, you ask? Well, among the many titles, job descriptions, and opportunities that being a hospitalist can entail, being a nocturnist is the one that shines in the dark of night when everyone else is fast asleep. A nocturnist is a hospitalist who works the night shift. As a resident, you might have nightmares about the many nights you’ve worked, the assembly line of patients, procedures, and cross-cover calls you’ve processed.
Nocturnists are the lone wolves of the night. They wear many hats and encounter a milieu of incessant admissions, more cross-cover calls than you can swing at, more grumpy, sleepy consultant phone exchanges than you would like, and endure the chronic fatigue of a person 20 years older than their actual age. But deep down in the muck of it all, there is something about the night shift that keeps a nocturnist coming back night after night.
Nocturnist in Charge
Working as a nocturnist is the last, purest form of practicing medicine. This position affords you the perfect opportunity to get back to the patient-doctor relationship because you are not rounding on other patients, juggling staff meetings, or battling a slew of other staff pining for your patient (i.e. case workers, physical therapists, consultants, etc.). Therefore, you can spend an adequate amount of time getting to know your patient without feeling rushed.
As far as admissions are concerned, there still are those days when you feel you need more hours in a day and two extra hands to take on the flood, but as the physician in charge, you have the ability to better triage these patients and defer to a specialist if needed. It’s not like those residency days of admitting whatever they call you for.
In addition, you have the opportunity to really hone your medical skills and procedural skills, because you are the specialist at 3 a.m. There will be times when you have to make decisions without the luxury of an immediate consultation; that has its pros and cons, but it definitely makes for an exciting Friday night. Consequently, you usually are the first point of contact for the nursing staff at night, so you have the ability to formulate relationships with nurses like no other physician can, because you are there with them, side by side, handling all the emergent (and often nonemergent) cross-cover calls. The nurses learn to trust you and you them, and there is a sense of camaraderie that forms from that trust.
Night-Shift Benefits
If you are still not convinced that the nocturnist world is for you—though you will be able to spend more time and have a more meaningful relationship with patients, nursing staff, and be the hero to every consultant and PCP you allow to sleep through the night—then I must reveal that the real cherry on top is actually green. Since you are working the least desired shift in your HM group, you are somewhat of a rock star. No one wants you to be unhappy, because they really want you to keep working the night shift. It’s evident by the fact that most nocturnists are paid a 10% to 20% shift differential, according to Payscale.com. In layman’s terms, you get paid more money than everyone else.
Another benefit is that nocturnist shifts range from eight to 12 hours; some even allow you to take call from home, so you can find a position that fits your schedule. The average number of monthly shifts usually is fewer than those working the day shift (10 to 14 shifts compared with 14 to 18 shifts) on average.
Depending on what type of hospital you choose (rural or urban, community or academic), you can have a wide range of nightly responsibilities. Some nocturnists perform as many procedures as they like; others choose to perform no procedures. Patient caps might exist on the number of patients you can admit during a shift. And working as a nocturnist can afford you a terrific lifestyle, because there is an a la carte menu of hospitalist groups, shifts, and practice lifestyles to choose from. And everybody in HM knows that everyone is looking for a nocturnist, so the availability of job offers is never a problem.
Nevertheless, with more money and choices comes more responsibility. As a nocturnist, you have to be flexible and creative in order to stay informed, as you will find it challenging to make all the staff meetings. Ask your group to schedule important group meetings early, so that you can stay after your shift and attend. Sometimes you just have to dig in and stay for those later meetings, if need be. (Sleeping in the call room until your next shift makes you somewhat of a martyr.) And remind your medical director to email you any important information you might have missed.
Even though you won’t be around during the day, you must stay abreast of quality initiatives (CHF, AMI, etc.). Beware of charting requirements, which can change from day to day.
If you are looking for an exciting way of life, and the ability to practice pure medicine after residency, you might want to get “into the night” and consider an HM career as a nocturnist. TH
Dr. Cunningham has been a hospitalist since 2004 and a nocturnist the past three years at Hamilton Medical Center, a community hospital in Dalton, Ga., and locum tenens in the Tennessee area.
The halls are quiet, the lights dimmed, the incessant ringing of telephones has fallen silent, patients slumber in their rooms, nurses sit and chart, waiting for the inevitable patient call light to glow once again. Then it happens: the overhead announcement that slices through the night like a knife.
“Code blue, code blue!”
As the code team scurries to the room, they start the protocols. However, they are waiting for someone—the conductor of the symphony, if you will. Who will answer the call? Who will whisk down the hall to take the podium? Will that patient’s primary-care physician (PCP) come? The cardiologist, maybe the pulmonologist?
No, there is one person who walks the halls at night when all others are asleep (even the ED doctors, though awake, are consumed by crowded emergency rooms and cannot help). This person is the nocturnist.
What is a nocturnist, you ask? Well, among the many titles, job descriptions, and opportunities that being a hospitalist can entail, being a nocturnist is the one that shines in the dark of night when everyone else is fast asleep. A nocturnist is a hospitalist who works the night shift. As a resident, you might have nightmares about the many nights you’ve worked, the assembly line of patients, procedures, and cross-cover calls you’ve processed.
Nocturnists are the lone wolves of the night. They wear many hats and encounter a milieu of incessant admissions, more cross-cover calls than you can swing at, more grumpy, sleepy consultant phone exchanges than you would like, and endure the chronic fatigue of a person 20 years older than their actual age. But deep down in the muck of it all, there is something about the night shift that keeps a nocturnist coming back night after night.
Nocturnist in Charge
Working as a nocturnist is the last, purest form of practicing medicine. This position affords you the perfect opportunity to get back to the patient-doctor relationship because you are not rounding on other patients, juggling staff meetings, or battling a slew of other staff pining for your patient (i.e. case workers, physical therapists, consultants, etc.). Therefore, you can spend an adequate amount of time getting to know your patient without feeling rushed.
As far as admissions are concerned, there still are those days when you feel you need more hours in a day and two extra hands to take on the flood, but as the physician in charge, you have the ability to better triage these patients and defer to a specialist if needed. It’s not like those residency days of admitting whatever they call you for.
In addition, you have the opportunity to really hone your medical skills and procedural skills, because you are the specialist at 3 a.m. There will be times when you have to make decisions without the luxury of an immediate consultation; that has its pros and cons, but it definitely makes for an exciting Friday night. Consequently, you usually are the first point of contact for the nursing staff at night, so you have the ability to formulate relationships with nurses like no other physician can, because you are there with them, side by side, handling all the emergent (and often nonemergent) cross-cover calls. The nurses learn to trust you and you them, and there is a sense of camaraderie that forms from that trust.
Night-Shift Benefits
If you are still not convinced that the nocturnist world is for you—though you will be able to spend more time and have a more meaningful relationship with patients, nursing staff, and be the hero to every consultant and PCP you allow to sleep through the night—then I must reveal that the real cherry on top is actually green. Since you are working the least desired shift in your HM group, you are somewhat of a rock star. No one wants you to be unhappy, because they really want you to keep working the night shift. It’s evident by the fact that most nocturnists are paid a 10% to 20% shift differential, according to Payscale.com. In layman’s terms, you get paid more money than everyone else.
Another benefit is that nocturnist shifts range from eight to 12 hours; some even allow you to take call from home, so you can find a position that fits your schedule. The average number of monthly shifts usually is fewer than those working the day shift (10 to 14 shifts compared with 14 to 18 shifts) on average.
Depending on what type of hospital you choose (rural or urban, community or academic), you can have a wide range of nightly responsibilities. Some nocturnists perform as many procedures as they like; others choose to perform no procedures. Patient caps might exist on the number of patients you can admit during a shift. And working as a nocturnist can afford you a terrific lifestyle, because there is an a la carte menu of hospitalist groups, shifts, and practice lifestyles to choose from. And everybody in HM knows that everyone is looking for a nocturnist, so the availability of job offers is never a problem.
Nevertheless, with more money and choices comes more responsibility. As a nocturnist, you have to be flexible and creative in order to stay informed, as you will find it challenging to make all the staff meetings. Ask your group to schedule important group meetings early, so that you can stay after your shift and attend. Sometimes you just have to dig in and stay for those later meetings, if need be. (Sleeping in the call room until your next shift makes you somewhat of a martyr.) And remind your medical director to email you any important information you might have missed.
Even though you won’t be around during the day, you must stay abreast of quality initiatives (CHF, AMI, etc.). Beware of charting requirements, which can change from day to day.
If you are looking for an exciting way of life, and the ability to practice pure medicine after residency, you might want to get “into the night” and consider an HM career as a nocturnist. TH
Dr. Cunningham has been a hospitalist since 2004 and a nocturnist the past three years at Hamilton Medical Center, a community hospital in Dalton, Ga., and locum tenens in the Tennessee area.
The halls are quiet, the lights dimmed, the incessant ringing of telephones has fallen silent, patients slumber in their rooms, nurses sit and chart, waiting for the inevitable patient call light to glow once again. Then it happens: the overhead announcement that slices through the night like a knife.
“Code blue, code blue!”
As the code team scurries to the room, they start the protocols. However, they are waiting for someone—the conductor of the symphony, if you will. Who will answer the call? Who will whisk down the hall to take the podium? Will that patient’s primary-care physician (PCP) come? The cardiologist, maybe the pulmonologist?
No, there is one person who walks the halls at night when all others are asleep (even the ED doctors, though awake, are consumed by crowded emergency rooms and cannot help). This person is the nocturnist.
What is a nocturnist, you ask? Well, among the many titles, job descriptions, and opportunities that being a hospitalist can entail, being a nocturnist is the one that shines in the dark of night when everyone else is fast asleep. A nocturnist is a hospitalist who works the night shift. As a resident, you might have nightmares about the many nights you’ve worked, the assembly line of patients, procedures, and cross-cover calls you’ve processed.
Nocturnists are the lone wolves of the night. They wear many hats and encounter a milieu of incessant admissions, more cross-cover calls than you can swing at, more grumpy, sleepy consultant phone exchanges than you would like, and endure the chronic fatigue of a person 20 years older than their actual age. But deep down in the muck of it all, there is something about the night shift that keeps a nocturnist coming back night after night.
Nocturnist in Charge
Working as a nocturnist is the last, purest form of practicing medicine. This position affords you the perfect opportunity to get back to the patient-doctor relationship because you are not rounding on other patients, juggling staff meetings, or battling a slew of other staff pining for your patient (i.e. case workers, physical therapists, consultants, etc.). Therefore, you can spend an adequate amount of time getting to know your patient without feeling rushed.
As far as admissions are concerned, there still are those days when you feel you need more hours in a day and two extra hands to take on the flood, but as the physician in charge, you have the ability to better triage these patients and defer to a specialist if needed. It’s not like those residency days of admitting whatever they call you for.
In addition, you have the opportunity to really hone your medical skills and procedural skills, because you are the specialist at 3 a.m. There will be times when you have to make decisions without the luxury of an immediate consultation; that has its pros and cons, but it definitely makes for an exciting Friday night. Consequently, you usually are the first point of contact for the nursing staff at night, so you have the ability to formulate relationships with nurses like no other physician can, because you are there with them, side by side, handling all the emergent (and often nonemergent) cross-cover calls. The nurses learn to trust you and you them, and there is a sense of camaraderie that forms from that trust.
Night-Shift Benefits
If you are still not convinced that the nocturnist world is for you—though you will be able to spend more time and have a more meaningful relationship with patients, nursing staff, and be the hero to every consultant and PCP you allow to sleep through the night—then I must reveal that the real cherry on top is actually green. Since you are working the least desired shift in your HM group, you are somewhat of a rock star. No one wants you to be unhappy, because they really want you to keep working the night shift. It’s evident by the fact that most nocturnists are paid a 10% to 20% shift differential, according to Payscale.com. In layman’s terms, you get paid more money than everyone else.
Another benefit is that nocturnist shifts range from eight to 12 hours; some even allow you to take call from home, so you can find a position that fits your schedule. The average number of monthly shifts usually is fewer than those working the day shift (10 to 14 shifts compared with 14 to 18 shifts) on average.
Depending on what type of hospital you choose (rural or urban, community or academic), you can have a wide range of nightly responsibilities. Some nocturnists perform as many procedures as they like; others choose to perform no procedures. Patient caps might exist on the number of patients you can admit during a shift. And working as a nocturnist can afford you a terrific lifestyle, because there is an a la carte menu of hospitalist groups, shifts, and practice lifestyles to choose from. And everybody in HM knows that everyone is looking for a nocturnist, so the availability of job offers is never a problem.
Nevertheless, with more money and choices comes more responsibility. As a nocturnist, you have to be flexible and creative in order to stay informed, as you will find it challenging to make all the staff meetings. Ask your group to schedule important group meetings early, so that you can stay after your shift and attend. Sometimes you just have to dig in and stay for those later meetings, if need be. (Sleeping in the call room until your next shift makes you somewhat of a martyr.) And remind your medical director to email you any important information you might have missed.
Even though you won’t be around during the day, you must stay abreast of quality initiatives (CHF, AMI, etc.). Beware of charting requirements, which can change from day to day.
If you are looking for an exciting way of life, and the ability to practice pure medicine after residency, you might want to get “into the night” and consider an HM career as a nocturnist. TH
Dr. Cunningham has been a hospitalist since 2004 and a nocturnist the past three years at Hamilton Medical Center, a community hospital in Dalton, Ga., and locum tenens in the Tennessee area.
Academic Institutions
Hospitalists work in many types of facilities, including academic centers that utilize residents (including interns) in healthcare delivery. Medical and surgical services furnished by a resident within the scope of the training program are covered as provider services and paid by Medicare through direct Graduate Medical Education (GME) and Indirect Medical Education (IME) payments; the services of the resident may not be billed or paid for using the Medicare Physician Fee Schedule.
Similarly, the teaching physician is not paid for the resident’s work. The teaching physician is paid for their participation in patient care. In other words, payment is provided to the teaching physician for services that are:
- Furnished by a physician who is not a resident; or
- Furnished by a resident with a teaching physician physically present during the critical or key portion(s) of the service.
Teaching physicians participate in evaluation and management (E/M) services with residents in several ways. Consider the following teaching physician scenarios:
Scenario 1: “Stand-Alone” Service
The resident sees a patient in the morning. The teaching physician independently sees the patient later that same day, performing all required elements to support their own bill (e.g. 99233: subsequent hospital care, per day, which requires at least two of these three key components: a detailed interval history, a detailed examination, or high-complexity medical decision-making). When documenting, the teaching physician can write their own note with or without any of the residents’ information. The attending note “stands alone” in support of the reported visit level. Alternatively, the teaching physician might “link to” the resident note, instead of personally redocumenting the entire service.
Appropriate documentation includes teaching physician notation of the provided critical or key portion(s) of the service and the involvement in patient management. The visit level is based upon the combined documentation, both teaching physician and resident.
Using Medicare-approved linkage statements will ensure compliance with teaching physician rules. Examples:
- “I performed a history and physical examination of the patient and discussed his management with the resident. I reviewed the resident’s note and agree with the documented findings and plan of care.”
- “I saw and evaluated the patient. I agree with the findings and the plan of care as documented in the resident’s note.”
- “I saw and examined the patient. I agree with the resident’s note, except the heart murmur is louder, so I will obtain an echo to evaluate.”
Each of the above linkage statements is acceptable, and “more is always better.” The last example best identifies the teaching physician’s involvement in patient management and best supports other regulatory goals and quality initiatives of the current healthcare environment.
Scenario 2: “Supervised” Service
The resident and the teaching physician see the patient at the same time. The teaching physician supervises the resident’s performance of the required service elements or personally performs elements separate from those completed by the resident. Despite personal supervision, the attending still must document their presence during the encounter, performance of the critical or key portion(s) of the service, and involvement in patient management. The visit level is based upon the combined documentation.
Medicare-accepted teaching physician statements associated with this scenario include:
- “I was present with the resident during the history and exam. I discussed the case with the resident and agree with the findings and plan as documented in the resident’s note.”
- “I saw the patient with the resident and agree with the resident’s findings and plan.”
These generalized statements will be accepted for billing under teaching physician rules. However, documenting patient-specific elements of the assessment and plan unequivocally demonstrates teaching- physician involvement in patient care and the quality of care provided.
Scenario 3: The “Shared” Service
The resident performs a portion or all of the required service elements without teaching-physician presence and documents this service. The teaching physician then independently performs only the critical or key portion(s) of the service and, as appropriate, discusses the case with the resident. As in the other scenarios, the attending documents the presence and performance of the critical or key portion(s) of the service, as well as involvement in patient management. The teaching physician selects the visit level based upon the combined documentation of the teaching physician and resident.
Such Medicare-approved statements for use by teaching physicians under this scenario include:
- “I saw and evaluated the patient. I reviewed the resident’s note and agree, except that picture is more consistent with pericarditis than myocardial ischemia. Will begin NSAIDs.”
- “I saw and evaluated the patient. Discussed with resident and agree with resident’s findings and plan as documented in the resident’s note.”
- “See resident’s note for details. I saw and evaluated the patient and agree with the resident’s finding and plans as written.”
- “I saw and evaluated the patient. Agree with resident’s note, but lower extremities are weaker, now 3/5; MRI of L/S spine today.”
Regardless of the timing between the attending and the resident encounter represented in each scenario, the teaching physician cannot “link to” a resident note that has not been written. More specifically, if the resident’s note has not been documented at the time the teaching physician writes their note, the teaching physician can’t link to the resident’s note or consider it for billing purposes.
Time-Based Exception
Time-based E/M services (e.g. critical-care services, discharge-day management, prolonged care, etc.) do not follow the same guideline as the standard E/M services, which are selected upon the level of history, exam, and decision-making. Only the billing provider’s time counts toward the reported visit level. This means that the teaching physician must be present for the entire period of time for which the claim is made. Documentation should identify the teaching physician’s total visit time (spent on the unit/floor for inpatient services), including face-to-face time with the patient. Time spent by the resident without the presence of the teaching physician does not count toward the teaching physician’s reported time. Additionally, time spent “teaching” the resident cannot be attributed to the teaching physician’s visit time.
Student Notes
Per Medicare guidelines, students (medical, nurse practitioner, etc.) can document services in the medical record. However, the teaching physician can only refer to medical student documentation associated with the review of systems and/or past/family/social history. The teaching physician cannot refer to a student’s documentation of physical exam findings or medical decision-making.
If the medical student documents E/M services, the teaching physician must verify and redocument the history of present illness, as well as perform and redocument the physical exam and medical decision-making activities of the service. The teaching physician then selects the visit level and documents service. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Guidelines for Teaching Physicians, Interns, Residents. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/MLNProducts/downloads/gdelinesteachgresfctsht.pdf. Accessed May 6, 2011.
- Medicare Claims Processing Manual: Chapter 12, Section 100. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 6, 2011.
- Medicare Benefit Policy Manual: Chapter 15, Section 30.2. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/Downloads/bp102c15.pdf. Accessed May 6, 2011.
- Manaker, S. Teaching Physician Regulations. In: Coding for Chest Medicine 2008. Northbrook, IL: American College of Chest Physicians, 2008; 279-285.
- Pohlig, C. Evaluation & Management Services: An Overview. In: Coding for Chest Medicine 2011. Northbrook, IL: American College of Chest Physicians, 2010; 323-330.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2011.
Hospitalists work in many types of facilities, including academic centers that utilize residents (including interns) in healthcare delivery. Medical and surgical services furnished by a resident within the scope of the training program are covered as provider services and paid by Medicare through direct Graduate Medical Education (GME) and Indirect Medical Education (IME) payments; the services of the resident may not be billed or paid for using the Medicare Physician Fee Schedule.
Similarly, the teaching physician is not paid for the resident’s work. The teaching physician is paid for their participation in patient care. In other words, payment is provided to the teaching physician for services that are:
- Furnished by a physician who is not a resident; or
- Furnished by a resident with a teaching physician physically present during the critical or key portion(s) of the service.
Teaching physicians participate in evaluation and management (E/M) services with residents in several ways. Consider the following teaching physician scenarios:
Scenario 1: “Stand-Alone” Service
The resident sees a patient in the morning. The teaching physician independently sees the patient later that same day, performing all required elements to support their own bill (e.g. 99233: subsequent hospital care, per day, which requires at least two of these three key components: a detailed interval history, a detailed examination, or high-complexity medical decision-making). When documenting, the teaching physician can write their own note with or without any of the residents’ information. The attending note “stands alone” in support of the reported visit level. Alternatively, the teaching physician might “link to” the resident note, instead of personally redocumenting the entire service.
Appropriate documentation includes teaching physician notation of the provided critical or key portion(s) of the service and the involvement in patient management. The visit level is based upon the combined documentation, both teaching physician and resident.
Using Medicare-approved linkage statements will ensure compliance with teaching physician rules. Examples:
- “I performed a history and physical examination of the patient and discussed his management with the resident. I reviewed the resident’s note and agree with the documented findings and plan of care.”
- “I saw and evaluated the patient. I agree with the findings and the plan of care as documented in the resident’s note.”
- “I saw and examined the patient. I agree with the resident’s note, except the heart murmur is louder, so I will obtain an echo to evaluate.”
Each of the above linkage statements is acceptable, and “more is always better.” The last example best identifies the teaching physician’s involvement in patient management and best supports other regulatory goals and quality initiatives of the current healthcare environment.
Scenario 2: “Supervised” Service
The resident and the teaching physician see the patient at the same time. The teaching physician supervises the resident’s performance of the required service elements or personally performs elements separate from those completed by the resident. Despite personal supervision, the attending still must document their presence during the encounter, performance of the critical or key portion(s) of the service, and involvement in patient management. The visit level is based upon the combined documentation.
Medicare-accepted teaching physician statements associated with this scenario include:
- “I was present with the resident during the history and exam. I discussed the case with the resident and agree with the findings and plan as documented in the resident’s note.”
- “I saw the patient with the resident and agree with the resident’s findings and plan.”
These generalized statements will be accepted for billing under teaching physician rules. However, documenting patient-specific elements of the assessment and plan unequivocally demonstrates teaching- physician involvement in patient care and the quality of care provided.
Scenario 3: The “Shared” Service
The resident performs a portion or all of the required service elements without teaching-physician presence and documents this service. The teaching physician then independently performs only the critical or key portion(s) of the service and, as appropriate, discusses the case with the resident. As in the other scenarios, the attending documents the presence and performance of the critical or key portion(s) of the service, as well as involvement in patient management. The teaching physician selects the visit level based upon the combined documentation of the teaching physician and resident.
Such Medicare-approved statements for use by teaching physicians under this scenario include:
- “I saw and evaluated the patient. I reviewed the resident’s note and agree, except that picture is more consistent with pericarditis than myocardial ischemia. Will begin NSAIDs.”
- “I saw and evaluated the patient. Discussed with resident and agree with resident’s findings and plan as documented in the resident’s note.”
- “See resident’s note for details. I saw and evaluated the patient and agree with the resident’s finding and plans as written.”
- “I saw and evaluated the patient. Agree with resident’s note, but lower extremities are weaker, now 3/5; MRI of L/S spine today.”
Regardless of the timing between the attending and the resident encounter represented in each scenario, the teaching physician cannot “link to” a resident note that has not been written. More specifically, if the resident’s note has not been documented at the time the teaching physician writes their note, the teaching physician can’t link to the resident’s note or consider it for billing purposes.
Time-Based Exception
Time-based E/M services (e.g. critical-care services, discharge-day management, prolonged care, etc.) do not follow the same guideline as the standard E/M services, which are selected upon the level of history, exam, and decision-making. Only the billing provider’s time counts toward the reported visit level. This means that the teaching physician must be present for the entire period of time for which the claim is made. Documentation should identify the teaching physician’s total visit time (spent on the unit/floor for inpatient services), including face-to-face time with the patient. Time spent by the resident without the presence of the teaching physician does not count toward the teaching physician’s reported time. Additionally, time spent “teaching” the resident cannot be attributed to the teaching physician’s visit time.
Student Notes
Per Medicare guidelines, students (medical, nurse practitioner, etc.) can document services in the medical record. However, the teaching physician can only refer to medical student documentation associated with the review of systems and/or past/family/social history. The teaching physician cannot refer to a student’s documentation of physical exam findings or medical decision-making.
If the medical student documents E/M services, the teaching physician must verify and redocument the history of present illness, as well as perform and redocument the physical exam and medical decision-making activities of the service. The teaching physician then selects the visit level and documents service. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Guidelines for Teaching Physicians, Interns, Residents. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/MLNProducts/downloads/gdelinesteachgresfctsht.pdf. Accessed May 6, 2011.
- Medicare Claims Processing Manual: Chapter 12, Section 100. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 6, 2011.
- Medicare Benefit Policy Manual: Chapter 15, Section 30.2. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/Downloads/bp102c15.pdf. Accessed May 6, 2011.
- Manaker, S. Teaching Physician Regulations. In: Coding for Chest Medicine 2008. Northbrook, IL: American College of Chest Physicians, 2008; 279-285.
- Pohlig, C. Evaluation & Management Services: An Overview. In: Coding for Chest Medicine 2011. Northbrook, IL: American College of Chest Physicians, 2010; 323-330.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2011.
Hospitalists work in many types of facilities, including academic centers that utilize residents (including interns) in healthcare delivery. Medical and surgical services furnished by a resident within the scope of the training program are covered as provider services and paid by Medicare through direct Graduate Medical Education (GME) and Indirect Medical Education (IME) payments; the services of the resident may not be billed or paid for using the Medicare Physician Fee Schedule.
Similarly, the teaching physician is not paid for the resident’s work. The teaching physician is paid for their participation in patient care. In other words, payment is provided to the teaching physician for services that are:
- Furnished by a physician who is not a resident; or
- Furnished by a resident with a teaching physician physically present during the critical or key portion(s) of the service.
Teaching physicians participate in evaluation and management (E/M) services with residents in several ways. Consider the following teaching physician scenarios:
Scenario 1: “Stand-Alone” Service
The resident sees a patient in the morning. The teaching physician independently sees the patient later that same day, performing all required elements to support their own bill (e.g. 99233: subsequent hospital care, per day, which requires at least two of these three key components: a detailed interval history, a detailed examination, or high-complexity medical decision-making). When documenting, the teaching physician can write their own note with or without any of the residents’ information. The attending note “stands alone” in support of the reported visit level. Alternatively, the teaching physician might “link to” the resident note, instead of personally redocumenting the entire service.
Appropriate documentation includes teaching physician notation of the provided critical or key portion(s) of the service and the involvement in patient management. The visit level is based upon the combined documentation, both teaching physician and resident.
Using Medicare-approved linkage statements will ensure compliance with teaching physician rules. Examples:
- “I performed a history and physical examination of the patient and discussed his management with the resident. I reviewed the resident’s note and agree with the documented findings and plan of care.”
- “I saw and evaluated the patient. I agree with the findings and the plan of care as documented in the resident’s note.”
- “I saw and examined the patient. I agree with the resident’s note, except the heart murmur is louder, so I will obtain an echo to evaluate.”
Each of the above linkage statements is acceptable, and “more is always better.” The last example best identifies the teaching physician’s involvement in patient management and best supports other regulatory goals and quality initiatives of the current healthcare environment.
Scenario 2: “Supervised” Service
The resident and the teaching physician see the patient at the same time. The teaching physician supervises the resident’s performance of the required service elements or personally performs elements separate from those completed by the resident. Despite personal supervision, the attending still must document their presence during the encounter, performance of the critical or key portion(s) of the service, and involvement in patient management. The visit level is based upon the combined documentation.
Medicare-accepted teaching physician statements associated with this scenario include:
- “I was present with the resident during the history and exam. I discussed the case with the resident and agree with the findings and plan as documented in the resident’s note.”
- “I saw the patient with the resident and agree with the resident’s findings and plan.”
These generalized statements will be accepted for billing under teaching physician rules. However, documenting patient-specific elements of the assessment and plan unequivocally demonstrates teaching- physician involvement in patient care and the quality of care provided.
Scenario 3: The “Shared” Service
The resident performs a portion or all of the required service elements without teaching-physician presence and documents this service. The teaching physician then independently performs only the critical or key portion(s) of the service and, as appropriate, discusses the case with the resident. As in the other scenarios, the attending documents the presence and performance of the critical or key portion(s) of the service, as well as involvement in patient management. The teaching physician selects the visit level based upon the combined documentation of the teaching physician and resident.
Such Medicare-approved statements for use by teaching physicians under this scenario include:
- “I saw and evaluated the patient. I reviewed the resident’s note and agree, except that picture is more consistent with pericarditis than myocardial ischemia. Will begin NSAIDs.”
- “I saw and evaluated the patient. Discussed with resident and agree with resident’s findings and plan as documented in the resident’s note.”
- “See resident’s note for details. I saw and evaluated the patient and agree with the resident’s finding and plans as written.”
- “I saw and evaluated the patient. Agree with resident’s note, but lower extremities are weaker, now 3/5; MRI of L/S spine today.”
Regardless of the timing between the attending and the resident encounter represented in each scenario, the teaching physician cannot “link to” a resident note that has not been written. More specifically, if the resident’s note has not been documented at the time the teaching physician writes their note, the teaching physician can’t link to the resident’s note or consider it for billing purposes.
Time-Based Exception
Time-based E/M services (e.g. critical-care services, discharge-day management, prolonged care, etc.) do not follow the same guideline as the standard E/M services, which are selected upon the level of history, exam, and decision-making. Only the billing provider’s time counts toward the reported visit level. This means that the teaching physician must be present for the entire period of time for which the claim is made. Documentation should identify the teaching physician’s total visit time (spent on the unit/floor for inpatient services), including face-to-face time with the patient. Time spent by the resident without the presence of the teaching physician does not count toward the teaching physician’s reported time. Additionally, time spent “teaching” the resident cannot be attributed to the teaching physician’s visit time.
Student Notes
Per Medicare guidelines, students (medical, nurse practitioner, etc.) can document services in the medical record. However, the teaching physician can only refer to medical student documentation associated with the review of systems and/or past/family/social history. The teaching physician cannot refer to a student’s documentation of physical exam findings or medical decision-making.
If the medical student documents E/M services, the teaching physician must verify and redocument the history of present illness, as well as perform and redocument the physical exam and medical decision-making activities of the service. The teaching physician then selects the visit level and documents service. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Guidelines for Teaching Physicians, Interns, Residents. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/MLNProducts/downloads/gdelinesteachgresfctsht.pdf. Accessed May 6, 2011.
- Medicare Claims Processing Manual: Chapter 12, Section 100. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 6, 2011.
- Medicare Benefit Policy Manual: Chapter 15, Section 30.2. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/Downloads/bp102c15.pdf. Accessed May 6, 2011.
- Manaker, S. Teaching Physician Regulations. In: Coding for Chest Medicine 2008. Northbrook, IL: American College of Chest Physicians, 2008; 279-285.
- Pohlig, C. Evaluation & Management Services: An Overview. In: Coding for Chest Medicine 2011. Northbrook, IL: American College of Chest Physicians, 2010; 323-330.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2011.
Subsidy or Payment?

Question: Before hospitalists, who cared for hospitalized patients?
Answer: Generalists—in other words, internists, family physicians, pediatricians.
Q: How much did that system cost hospitals?
A: Nothing, or very little. In some cases, support dollars were available for weekend, night, or uninsured patient coverage, but by and large this system cost hospitals little. Physicians admitted their patients to the hospital because the alternatives (sending a hypoxic pneumonia patient home from clinic, turning out the office lights and hoping the patient survived the night, or bringing the patient home with them) offered uncomfortable ethical, malpractice, or alimony consequences. So doctors admitted these patients to the hospital and visited them daily.
Q: The average amount of support per hospitalist is $131,564, or about $1.7 million per HM group seeing adult patients. The bulk of those dollars come from the hospital. If we assume that the people running hospitals are smart, then why would those smart businesspeople pay $1.7 million for something they used to get for free?
A: Because there is something they get in return for that money. Or, perhaps, something they think they are getting in return for those dollars.
Q: What?
A: I often go through this exercise with the residents in our hospitalist training program when we discuss the drivers of the HM movement. I usually discuss the reasons why a hospital should fund these groups; it always seems like such a no-brainer to me.
Enter a recent news item from Montana. The story from the Helena Independent Record (see “Unsustainable Growth?” p. 1) noted that a multispecialty group practice in Helena announced they were no longer admitting their patients to a local hospital in protest over a new hospital policy to charge the clinic practice. The fee was to defray some of the costs of the HM program. A hospital representative was quoted as saying “physicians are responsible for obtaining hospital coverage for their own patients, not the hospital.”
I can’t really argue with the logic of that statement. Surely a clinic has responsibility to ensure that their patients get cared for while they are inpatients. If an internist is going to see a patient in the clinic and admit them to the hospital, shouldn’t an internist then see the patient in the hospital?
If I’m a hospital CEO, the answer is no.
To retrench a bit, yes, I’d want a board-certified internal-medicine (or pediatric or family medicine) physician to see the hospitalized patient. But in the process, I wouldn’t want them to only practice internal medicine. That was the model hospitals had 25 years ago—a model that cost them very little, a model that they played a large part in exterminating. The fact that most hospitals are willing to pay millions or more per year to not have that system tells me that they don’t want that system.
Q: So, what do hospitals want?
A: Hospitalists, not internists in the hospital.
What’s the difference? Well, it’s a perception issue. Many, if not most, believe that all it takes to be a great hospitalist is to show up for your shift, provide great care to your 15 patients, and go home. That is, the job is defined by the clinical effort—the internist part. Although there is tremendous benefit to this and I recognize its importance (and let’s not forget the weekend, night, and holiday coverage), this sells us short and puts our financial stability in peril.
To be great, to best help our patients, to give our hospitals what they want and need, we have to evolve from “internists in the hospital” to hospitalists. Hospitalists are defined not by our clinical effort but rather by our nonclinical effort. This is what hospitals are paying $1.7 million per year for. They had the internist in the hospital model and chose to pay more—they chose the hospitalist model.
To be a great hospitalist group means embracing the nonclinical work that envelops the clinical practice—the process and quality improvement (QI). That is, fundamentally changing the unsafe systems that surround our patients. Making them safer, more efficient and of higher quality.
This takes time.
Time = Money
It takes time to implement a QI project to reduce central line infections in the ICU. Or to develop and implement a VTE prophylaxis order set or an insulin or heparin drip protocol. Or to work closely with nursing to reduce falls on a medical unit. It takes time to be at the pneumonia core measures meeting every Monday at 7 a.m. and the hospital credentialing committee meeting every other Friday at 3 p.m. It also takes time to implement a new electronic health record or roll out the new LEAN project to reduce ED wait times.
This takes time, effort, and bandwidth—the kind that can’t be shoehorned into the average clinical day. This is work that needs to be done primarily during nonclinical hours. It’s the kind of work that defines HM as a field; the kind of work that increasingly determines your hospital’s bottom line; the kind of work that has tremendous value; the kind of work that requires remuneration.
In paying for the hospitalist model, your hospital is paying for the clinical (internist) and nonclinical (hospitalist) work you do. The $1.7 million per year is not a subsidy they pay to keep you in business. It’s the price they must pay to compensate your group for all the nonclinical work you do around quality, safety, efficiency, and leadership.
Q: But what if my group isn’t doing these kinds of things?
A: Then your hospital funding is at risk. The Montana story addresses just such a scenario. Clearly the hospital C-suite in this instance only valued (or was presented with) clinical work. Therefore, they felt that others should subsidize the hospitalist salaries—in this case, the clinic. I don’t know the particulars of this case but deduce this because it would be ludicrous to expect the clinic to pay for the part of the hospitalists’ time spent improving the hospital’s systems of care.
Writing the Final Chapter
At the core of the HM funding model is the concept of subsidy versus compensation. If we are only providing clinical care, then the offset dollars from the hospital to support our salaries is functionally a subsidy—a dollar amount to make up for our collections shortfall. However, if it is support for the nonclinical work we are doing, then it is compensation.
As the story of hospitalist funding is written, the report from Montana should serve as a cautionary tale. Hospital financial pressures likely will focus more scrutiny on the hospitalist financial support model. And as this story plays out, HM groups will be expected to bring more to the table than patient care.
Those that do will live happily ever after.
Those that don’t will be forced to answer the tough question: What’s the difference between an internist in the hospital and a hospitalist? If the answer is nothing, that story will have a decidedly and predictably less happy ending. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Question: Before hospitalists, who cared for hospitalized patients?
Answer: Generalists—in other words, internists, family physicians, pediatricians.
Q: How much did that system cost hospitals?
A: Nothing, or very little. In some cases, support dollars were available for weekend, night, or uninsured patient coverage, but by and large this system cost hospitals little. Physicians admitted their patients to the hospital because the alternatives (sending a hypoxic pneumonia patient home from clinic, turning out the office lights and hoping the patient survived the night, or bringing the patient home with them) offered uncomfortable ethical, malpractice, or alimony consequences. So doctors admitted these patients to the hospital and visited them daily.
Q: The average amount of support per hospitalist is $131,564, or about $1.7 million per HM group seeing adult patients. The bulk of those dollars come from the hospital. If we assume that the people running hospitals are smart, then why would those smart businesspeople pay $1.7 million for something they used to get for free?
A: Because there is something they get in return for that money. Or, perhaps, something they think they are getting in return for those dollars.
Q: What?
A: I often go through this exercise with the residents in our hospitalist training program when we discuss the drivers of the HM movement. I usually discuss the reasons why a hospital should fund these groups; it always seems like such a no-brainer to me.
Enter a recent news item from Montana. The story from the Helena Independent Record (see “Unsustainable Growth?” p. 1) noted that a multispecialty group practice in Helena announced they were no longer admitting their patients to a local hospital in protest over a new hospital policy to charge the clinic practice. The fee was to defray some of the costs of the HM program. A hospital representative was quoted as saying “physicians are responsible for obtaining hospital coverage for their own patients, not the hospital.”
I can’t really argue with the logic of that statement. Surely a clinic has responsibility to ensure that their patients get cared for while they are inpatients. If an internist is going to see a patient in the clinic and admit them to the hospital, shouldn’t an internist then see the patient in the hospital?
If I’m a hospital CEO, the answer is no.
To retrench a bit, yes, I’d want a board-certified internal-medicine (or pediatric or family medicine) physician to see the hospitalized patient. But in the process, I wouldn’t want them to only practice internal medicine. That was the model hospitals had 25 years ago—a model that cost them very little, a model that they played a large part in exterminating. The fact that most hospitals are willing to pay millions or more per year to not have that system tells me that they don’t want that system.
Q: So, what do hospitals want?
A: Hospitalists, not internists in the hospital.
What’s the difference? Well, it’s a perception issue. Many, if not most, believe that all it takes to be a great hospitalist is to show up for your shift, provide great care to your 15 patients, and go home. That is, the job is defined by the clinical effort—the internist part. Although there is tremendous benefit to this and I recognize its importance (and let’s not forget the weekend, night, and holiday coverage), this sells us short and puts our financial stability in peril.
To be great, to best help our patients, to give our hospitals what they want and need, we have to evolve from “internists in the hospital” to hospitalists. Hospitalists are defined not by our clinical effort but rather by our nonclinical effort. This is what hospitals are paying $1.7 million per year for. They had the internist in the hospital model and chose to pay more—they chose the hospitalist model.
To be a great hospitalist group means embracing the nonclinical work that envelops the clinical practice—the process and quality improvement (QI). That is, fundamentally changing the unsafe systems that surround our patients. Making them safer, more efficient and of higher quality.
This takes time.
Time = Money
It takes time to implement a QI project to reduce central line infections in the ICU. Or to develop and implement a VTE prophylaxis order set or an insulin or heparin drip protocol. Or to work closely with nursing to reduce falls on a medical unit. It takes time to be at the pneumonia core measures meeting every Monday at 7 a.m. and the hospital credentialing committee meeting every other Friday at 3 p.m. It also takes time to implement a new electronic health record or roll out the new LEAN project to reduce ED wait times.
This takes time, effort, and bandwidth—the kind that can’t be shoehorned into the average clinical day. This is work that needs to be done primarily during nonclinical hours. It’s the kind of work that defines HM as a field; the kind of work that increasingly determines your hospital’s bottom line; the kind of work that has tremendous value; the kind of work that requires remuneration.
In paying for the hospitalist model, your hospital is paying for the clinical (internist) and nonclinical (hospitalist) work you do. The $1.7 million per year is not a subsidy they pay to keep you in business. It’s the price they must pay to compensate your group for all the nonclinical work you do around quality, safety, efficiency, and leadership.
Q: But what if my group isn’t doing these kinds of things?
A: Then your hospital funding is at risk. The Montana story addresses just such a scenario. Clearly the hospital C-suite in this instance only valued (or was presented with) clinical work. Therefore, they felt that others should subsidize the hospitalist salaries—in this case, the clinic. I don’t know the particulars of this case but deduce this because it would be ludicrous to expect the clinic to pay for the part of the hospitalists’ time spent improving the hospital’s systems of care.
Writing the Final Chapter
At the core of the HM funding model is the concept of subsidy versus compensation. If we are only providing clinical care, then the offset dollars from the hospital to support our salaries is functionally a subsidy—a dollar amount to make up for our collections shortfall. However, if it is support for the nonclinical work we are doing, then it is compensation.
As the story of hospitalist funding is written, the report from Montana should serve as a cautionary tale. Hospital financial pressures likely will focus more scrutiny on the hospitalist financial support model. And as this story plays out, HM groups will be expected to bring more to the table than patient care.
Those that do will live happily ever after.
Those that don’t will be forced to answer the tough question: What’s the difference between an internist in the hospital and a hospitalist? If the answer is nothing, that story will have a decidedly and predictably less happy ending. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Question: Before hospitalists, who cared for hospitalized patients?
Answer: Generalists—in other words, internists, family physicians, pediatricians.
Q: How much did that system cost hospitals?
A: Nothing, or very little. In some cases, support dollars were available for weekend, night, or uninsured patient coverage, but by and large this system cost hospitals little. Physicians admitted their patients to the hospital because the alternatives (sending a hypoxic pneumonia patient home from clinic, turning out the office lights and hoping the patient survived the night, or bringing the patient home with them) offered uncomfortable ethical, malpractice, or alimony consequences. So doctors admitted these patients to the hospital and visited them daily.
Q: The average amount of support per hospitalist is $131,564, or about $1.7 million per HM group seeing adult patients. The bulk of those dollars come from the hospital. If we assume that the people running hospitals are smart, then why would those smart businesspeople pay $1.7 million for something they used to get for free?
A: Because there is something they get in return for that money. Or, perhaps, something they think they are getting in return for those dollars.
Q: What?
A: I often go through this exercise with the residents in our hospitalist training program when we discuss the drivers of the HM movement. I usually discuss the reasons why a hospital should fund these groups; it always seems like such a no-brainer to me.
Enter a recent news item from Montana. The story from the Helena Independent Record (see “Unsustainable Growth?” p. 1) noted that a multispecialty group practice in Helena announced they were no longer admitting their patients to a local hospital in protest over a new hospital policy to charge the clinic practice. The fee was to defray some of the costs of the HM program. A hospital representative was quoted as saying “physicians are responsible for obtaining hospital coverage for their own patients, not the hospital.”
I can’t really argue with the logic of that statement. Surely a clinic has responsibility to ensure that their patients get cared for while they are inpatients. If an internist is going to see a patient in the clinic and admit them to the hospital, shouldn’t an internist then see the patient in the hospital?
If I’m a hospital CEO, the answer is no.
To retrench a bit, yes, I’d want a board-certified internal-medicine (or pediatric or family medicine) physician to see the hospitalized patient. But in the process, I wouldn’t want them to only practice internal medicine. That was the model hospitals had 25 years ago—a model that cost them very little, a model that they played a large part in exterminating. The fact that most hospitals are willing to pay millions or more per year to not have that system tells me that they don’t want that system.
Q: So, what do hospitals want?
A: Hospitalists, not internists in the hospital.
What’s the difference? Well, it’s a perception issue. Many, if not most, believe that all it takes to be a great hospitalist is to show up for your shift, provide great care to your 15 patients, and go home. That is, the job is defined by the clinical effort—the internist part. Although there is tremendous benefit to this and I recognize its importance (and let’s not forget the weekend, night, and holiday coverage), this sells us short and puts our financial stability in peril.
To be great, to best help our patients, to give our hospitals what they want and need, we have to evolve from “internists in the hospital” to hospitalists. Hospitalists are defined not by our clinical effort but rather by our nonclinical effort. This is what hospitals are paying $1.7 million per year for. They had the internist in the hospital model and chose to pay more—they chose the hospitalist model.
To be a great hospitalist group means embracing the nonclinical work that envelops the clinical practice—the process and quality improvement (QI). That is, fundamentally changing the unsafe systems that surround our patients. Making them safer, more efficient and of higher quality.
This takes time.
Time = Money
It takes time to implement a QI project to reduce central line infections in the ICU. Or to develop and implement a VTE prophylaxis order set or an insulin or heparin drip protocol. Or to work closely with nursing to reduce falls on a medical unit. It takes time to be at the pneumonia core measures meeting every Monday at 7 a.m. and the hospital credentialing committee meeting every other Friday at 3 p.m. It also takes time to implement a new electronic health record or roll out the new LEAN project to reduce ED wait times.
This takes time, effort, and bandwidth—the kind that can’t be shoehorned into the average clinical day. This is work that needs to be done primarily during nonclinical hours. It’s the kind of work that defines HM as a field; the kind of work that increasingly determines your hospital’s bottom line; the kind of work that has tremendous value; the kind of work that requires remuneration.
In paying for the hospitalist model, your hospital is paying for the clinical (internist) and nonclinical (hospitalist) work you do. The $1.7 million per year is not a subsidy they pay to keep you in business. It’s the price they must pay to compensate your group for all the nonclinical work you do around quality, safety, efficiency, and leadership.
Q: But what if my group isn’t doing these kinds of things?
A: Then your hospital funding is at risk. The Montana story addresses just such a scenario. Clearly the hospital C-suite in this instance only valued (or was presented with) clinical work. Therefore, they felt that others should subsidize the hospitalist salaries—in this case, the clinic. I don’t know the particulars of this case but deduce this because it would be ludicrous to expect the clinic to pay for the part of the hospitalists’ time spent improving the hospital’s systems of care.
Writing the Final Chapter
At the core of the HM funding model is the concept of subsidy versus compensation. If we are only providing clinical care, then the offset dollars from the hospital to support our salaries is functionally a subsidy—a dollar amount to make up for our collections shortfall. However, if it is support for the nonclinical work we are doing, then it is compensation.
As the story of hospitalist funding is written, the report from Montana should serve as a cautionary tale. Hospital financial pressures likely will focus more scrutiny on the hospitalist financial support model. And as this story plays out, HM groups will be expected to bring more to the table than patient care.
Those that do will live happily ever after.
Those that don’t will be forced to answer the tough question: What’s the difference between an internist in the hospital and a hospitalist? If the answer is nothing, that story will have a decidedly and predictably less happy ending. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
New Developments
HM11 and the publication of the SHM-MGMA survey on hospitalist productivity and compensation occur every summer, and they always provide lots of new information to get me thinking. Two things stand out this year: Hospitalist demand remains high, and hospitals are paying a lot to have hospitalist services.
Supply and Demand
Along with SHM President Joe Li and Rob Bessler, who is CEO of Sound Physicians, I had the pleasure of presenting a preview of some data from the latest SHM-MGMA survey at the annual meeting May 11 in Dallas. During the session, I asked the large crowd of hospitalists how many were from practices that are actively recruiting additional hospitalists. About 40% of the hands went up.
If 40% of HM groups are actively recruiting, some for more than one open position, that’s a lot of recruiting. But it is dramatically less than the response I got when I asked the same question just three years ago at HM08 in San Diego. At that meeting, nearly every hand in the room went up, indicating everybody was recruiting (see “We’re Hiring,” July 2008, p. 62).
Of course, my show-of-hands survey of attendees at SHM meetings is not a perfect method to assess hospitalist supply and demand. But I think the dramatic change in responses from 2008 to 2011 is meaningful; it also matches what I’m seeing in the marketplace. I hear repeatedly that the years of rapid growth in hospitalist staffing have ended in many or most major metropolitan areas. For example, in places like Seattle (where I practice), Minneapolis, and Boston, there are far fewer open positions now than just two years ago, and most are to replace a departing doctor rather than to increase the overall staffing level.
But the far more numerous smaller markets are still recruiting aggressively in an effort to increase the overall staffing of the practice (and not just replace departing doctors). And changes in resident work-hour limitations are requiring teaching hospitals to increase hospitalist staffing to offset the reduction in resident availability. But it’s possible that if the larger markets are indeed becoming somewhat saturated with hospitalists, then there will be a trickledown effect, which should make more candidates available everywhere.
What will be the side effects if indeed the supply of hospitalists catches up to the demand, or even exceeds demand, in some places? It is easy to imagine that greater competition among candidates might mean that practices are increasingly able to hire the more talented and committed doctors, which should improve the overall performance of hospitalist practices.
Although I don’t have proof, I think this phenomenon has been in play in the field of emergency medicine for many years. When I was a resident in the 1980s, ED doctors typically were not the best and brightest at their hospitals. But the way I see it, the field began to attract better candidates, and as ED residencies and practices began to “fill up,” they could be more selective in new hires. Therefore, the average talent of the average ED doctor went up.
I think the average hospitalist today is pretty talented, but I also think it could get even better if the supply of hospitalists exceeds demand. I just hope I continue to make the cut!
If typical market forces are operative for hospitalists (far from a guarantee in any healthcare enterprise), then an oversupply of hospitalists could mean a flattening of the historical trend in hospitalist incomes. To this point, in our relatively young field, incomes have risen faster than can be explained solely by inflation or increases in hospitalist productivity. A relative shortage of hospitalists might be one of the main forces pushing incomes up, and it might go away.
We’ll see.
Hospital Support Trends Up
The most remarkable number in the 2011 SHM-MGMA survey is the financial support provided to practices per FTE hospitalist annually. This support nearly always comes from a hospital, and is often colloquially, and misleadingly, referred to as the “subsidy.”
In 2001, hospital support was about $65,000 per FTE. In the 2008 and 2010 surveys, the median financial support per FTE was $97,000 and $98,000, respectively. But it jumped to $136,403 this year. That is a really huge jump in one year. (Note: The surveys changed from biannual to annual in 2010, and the new SHM-MGMA survey uses a different financial support question/methodology and has a different respondent pool than the previous SHM surveys.)
Some of the increased dollars probably went to pay rising hospitalist compensation, which rose about 3% over the prior year without any significant increase in productivity. But that 3% salary increase translates to only about $5,000 (median compensation rose from roughly $215,000 to $220,000), and could be explained in part by such factors as removing academicians from this data set. (Starting in 2010, academic hospitalists are surveyed and reported separately, so aren’t included here.) So I don’t think the change in hospitalist incomes seen in this survey has much to do with the dramatic, near-40% increase in financial support.
The survey showed that hospitalist productivity hasn’t declined, so the other most likely culprit is declining professional fee collections, which might be due to an increasing portion of hospitalized patients who are uninsured or underinsured. Many hospitals report that their “payor mix” has worsened since the economic crisis of the last few years. And because hospitals typically hold the risk for the financial performance of their hospitalists, then if the latter see more uninsured patients and collect less in professional fees, the hospital will make up the difference. This phenomenon might explain much of the increased financial support.
But I’m not satisfied that a worsening payor mix explains everything. For example, if this were the most significant reason for increasing financial support, I think we would have seen this effect in the prior survey. Why did it “hit” so suddenly in this year alone?
We will get more information about collection rates when the second part of the survey is published in September. For example, we’ll be able to compare the dollars collected per encounter or per wRVU in the current survey to the prior one. If there was a significant drop, then it will require only a little math to see how much overall collections dropped per FTE and see if it is similar to the rise in financial support provided.
Of course, it will be very informative to see what the financial support turns out to be in the next survey (check back in late spring 2012). Will it stay around $136,000 per FTE or be something very different? TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
HM11 and the publication of the SHM-MGMA survey on hospitalist productivity and compensation occur every summer, and they always provide lots of new information to get me thinking. Two things stand out this year: Hospitalist demand remains high, and hospitals are paying a lot to have hospitalist services.
Supply and Demand
Along with SHM President Joe Li and Rob Bessler, who is CEO of Sound Physicians, I had the pleasure of presenting a preview of some data from the latest SHM-MGMA survey at the annual meeting May 11 in Dallas. During the session, I asked the large crowd of hospitalists how many were from practices that are actively recruiting additional hospitalists. About 40% of the hands went up.
If 40% of HM groups are actively recruiting, some for more than one open position, that’s a lot of recruiting. But it is dramatically less than the response I got when I asked the same question just three years ago at HM08 in San Diego. At that meeting, nearly every hand in the room went up, indicating everybody was recruiting (see “We’re Hiring,” July 2008, p. 62).
Of course, my show-of-hands survey of attendees at SHM meetings is not a perfect method to assess hospitalist supply and demand. But I think the dramatic change in responses from 2008 to 2011 is meaningful; it also matches what I’m seeing in the marketplace. I hear repeatedly that the years of rapid growth in hospitalist staffing have ended in many or most major metropolitan areas. For example, in places like Seattle (where I practice), Minneapolis, and Boston, there are far fewer open positions now than just two years ago, and most are to replace a departing doctor rather than to increase the overall staffing level.
But the far more numerous smaller markets are still recruiting aggressively in an effort to increase the overall staffing of the practice (and not just replace departing doctors). And changes in resident work-hour limitations are requiring teaching hospitals to increase hospitalist staffing to offset the reduction in resident availability. But it’s possible that if the larger markets are indeed becoming somewhat saturated with hospitalists, then there will be a trickledown effect, which should make more candidates available everywhere.
What will be the side effects if indeed the supply of hospitalists catches up to the demand, or even exceeds demand, in some places? It is easy to imagine that greater competition among candidates might mean that practices are increasingly able to hire the more talented and committed doctors, which should improve the overall performance of hospitalist practices.
Although I don’t have proof, I think this phenomenon has been in play in the field of emergency medicine for many years. When I was a resident in the 1980s, ED doctors typically were not the best and brightest at their hospitals. But the way I see it, the field began to attract better candidates, and as ED residencies and practices began to “fill up,” they could be more selective in new hires. Therefore, the average talent of the average ED doctor went up.
I think the average hospitalist today is pretty talented, but I also think it could get even better if the supply of hospitalists exceeds demand. I just hope I continue to make the cut!
If typical market forces are operative for hospitalists (far from a guarantee in any healthcare enterprise), then an oversupply of hospitalists could mean a flattening of the historical trend in hospitalist incomes. To this point, in our relatively young field, incomes have risen faster than can be explained solely by inflation or increases in hospitalist productivity. A relative shortage of hospitalists might be one of the main forces pushing incomes up, and it might go away.
We’ll see.
Hospital Support Trends Up
The most remarkable number in the 2011 SHM-MGMA survey is the financial support provided to practices per FTE hospitalist annually. This support nearly always comes from a hospital, and is often colloquially, and misleadingly, referred to as the “subsidy.”
In 2001, hospital support was about $65,000 per FTE. In the 2008 and 2010 surveys, the median financial support per FTE was $97,000 and $98,000, respectively. But it jumped to $136,403 this year. That is a really huge jump in one year. (Note: The surveys changed from biannual to annual in 2010, and the new SHM-MGMA survey uses a different financial support question/methodology and has a different respondent pool than the previous SHM surveys.)
Some of the increased dollars probably went to pay rising hospitalist compensation, which rose about 3% over the prior year without any significant increase in productivity. But that 3% salary increase translates to only about $5,000 (median compensation rose from roughly $215,000 to $220,000), and could be explained in part by such factors as removing academicians from this data set. (Starting in 2010, academic hospitalists are surveyed and reported separately, so aren’t included here.) So I don’t think the change in hospitalist incomes seen in this survey has much to do with the dramatic, near-40% increase in financial support.
The survey showed that hospitalist productivity hasn’t declined, so the other most likely culprit is declining professional fee collections, which might be due to an increasing portion of hospitalized patients who are uninsured or underinsured. Many hospitals report that their “payor mix” has worsened since the economic crisis of the last few years. And because hospitals typically hold the risk for the financial performance of their hospitalists, then if the latter see more uninsured patients and collect less in professional fees, the hospital will make up the difference. This phenomenon might explain much of the increased financial support.
But I’m not satisfied that a worsening payor mix explains everything. For example, if this were the most significant reason for increasing financial support, I think we would have seen this effect in the prior survey. Why did it “hit” so suddenly in this year alone?
We will get more information about collection rates when the second part of the survey is published in September. For example, we’ll be able to compare the dollars collected per encounter or per wRVU in the current survey to the prior one. If there was a significant drop, then it will require only a little math to see how much overall collections dropped per FTE and see if it is similar to the rise in financial support provided.
Of course, it will be very informative to see what the financial support turns out to be in the next survey (check back in late spring 2012). Will it stay around $136,000 per FTE or be something very different? TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
HM11 and the publication of the SHM-MGMA survey on hospitalist productivity and compensation occur every summer, and they always provide lots of new information to get me thinking. Two things stand out this year: Hospitalist demand remains high, and hospitals are paying a lot to have hospitalist services.
Supply and Demand
Along with SHM President Joe Li and Rob Bessler, who is CEO of Sound Physicians, I had the pleasure of presenting a preview of some data from the latest SHM-MGMA survey at the annual meeting May 11 in Dallas. During the session, I asked the large crowd of hospitalists how many were from practices that are actively recruiting additional hospitalists. About 40% of the hands went up.
If 40% of HM groups are actively recruiting, some for more than one open position, that’s a lot of recruiting. But it is dramatically less than the response I got when I asked the same question just three years ago at HM08 in San Diego. At that meeting, nearly every hand in the room went up, indicating everybody was recruiting (see “We’re Hiring,” July 2008, p. 62).
Of course, my show-of-hands survey of attendees at SHM meetings is not a perfect method to assess hospitalist supply and demand. But I think the dramatic change in responses from 2008 to 2011 is meaningful; it also matches what I’m seeing in the marketplace. I hear repeatedly that the years of rapid growth in hospitalist staffing have ended in many or most major metropolitan areas. For example, in places like Seattle (where I practice), Minneapolis, and Boston, there are far fewer open positions now than just two years ago, and most are to replace a departing doctor rather than to increase the overall staffing level.
But the far more numerous smaller markets are still recruiting aggressively in an effort to increase the overall staffing of the practice (and not just replace departing doctors). And changes in resident work-hour limitations are requiring teaching hospitals to increase hospitalist staffing to offset the reduction in resident availability. But it’s possible that if the larger markets are indeed becoming somewhat saturated with hospitalists, then there will be a trickledown effect, which should make more candidates available everywhere.
What will be the side effects if indeed the supply of hospitalists catches up to the demand, or even exceeds demand, in some places? It is easy to imagine that greater competition among candidates might mean that practices are increasingly able to hire the more talented and committed doctors, which should improve the overall performance of hospitalist practices.
Although I don’t have proof, I think this phenomenon has been in play in the field of emergency medicine for many years. When I was a resident in the 1980s, ED doctors typically were not the best and brightest at their hospitals. But the way I see it, the field began to attract better candidates, and as ED residencies and practices began to “fill up,” they could be more selective in new hires. Therefore, the average talent of the average ED doctor went up.
I think the average hospitalist today is pretty talented, but I also think it could get even better if the supply of hospitalists exceeds demand. I just hope I continue to make the cut!
If typical market forces are operative for hospitalists (far from a guarantee in any healthcare enterprise), then an oversupply of hospitalists could mean a flattening of the historical trend in hospitalist incomes. To this point, in our relatively young field, incomes have risen faster than can be explained solely by inflation or increases in hospitalist productivity. A relative shortage of hospitalists might be one of the main forces pushing incomes up, and it might go away.
We’ll see.
Hospital Support Trends Up
The most remarkable number in the 2011 SHM-MGMA survey is the financial support provided to practices per FTE hospitalist annually. This support nearly always comes from a hospital, and is often colloquially, and misleadingly, referred to as the “subsidy.”
In 2001, hospital support was about $65,000 per FTE. In the 2008 and 2010 surveys, the median financial support per FTE was $97,000 and $98,000, respectively. But it jumped to $136,403 this year. That is a really huge jump in one year. (Note: The surveys changed from biannual to annual in 2010, and the new SHM-MGMA survey uses a different financial support question/methodology and has a different respondent pool than the previous SHM surveys.)
Some of the increased dollars probably went to pay rising hospitalist compensation, which rose about 3% over the prior year without any significant increase in productivity. But that 3% salary increase translates to only about $5,000 (median compensation rose from roughly $215,000 to $220,000), and could be explained in part by such factors as removing academicians from this data set. (Starting in 2010, academic hospitalists are surveyed and reported separately, so aren’t included here.) So I don’t think the change in hospitalist incomes seen in this survey has much to do with the dramatic, near-40% increase in financial support.
The survey showed that hospitalist productivity hasn’t declined, so the other most likely culprit is declining professional fee collections, which might be due to an increasing portion of hospitalized patients who are uninsured or underinsured. Many hospitals report that their “payor mix” has worsened since the economic crisis of the last few years. And because hospitals typically hold the risk for the financial performance of their hospitalists, then if the latter see more uninsured patients and collect less in professional fees, the hospital will make up the difference. This phenomenon might explain much of the increased financial support.
But I’m not satisfied that a worsening payor mix explains everything. For example, if this were the most significant reason for increasing financial support, I think we would have seen this effect in the prior survey. Why did it “hit” so suddenly in this year alone?
We will get more information about collection rates when the second part of the survey is published in September. For example, we’ll be able to compare the dollars collected per encounter or per wRVU in the current survey to the prior one. If there was a significant drop, then it will require only a little math to see how much overall collections dropped per FTE and see if it is similar to the rise in financial support provided.
Of course, it will be very informative to see what the financial support turns out to be in the next survey (check back in late spring 2012). Will it stay around $136,000 per FTE or be something very different? TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.