User login
The Hospitalist only
Fishing for a Diagnosis

A63-year-old female with a history of hypertension and nicotine dependence presented with acute substernal chest pain. The patient reported that the pain was a dull pressure, 5/10 in severity, which radiated into her neck and left arm and was associated with dyspnea.
The patient was on atenolol for hypertension. She reported a 30-year smoking history. A physical exam revealed an anxious, hypertensive (180/95), tachycardic (123 bpm) female. Findings on cardiovascular exam were otherwise unremarkable. Electrocardiogram revealed a 2-3 mm ST-segment elevation in leads V2-V6. Laboratory tests revealed an elevated troponin T level (0.32 ng/mL [nl < 0.03 ng/mL]) and an elevated creatinine kinase-MB fraction (8.2 ng/mL [nl < 6.2 ng/mL]).
Using the above information, the diagnosis of an ST-segment elevation MI was made. The patient went in for urgent cardiac catheterization, which revealed normal coronary anatomy. A left ventriculogram demonstrated moderate hypokinesis of the apical segment and a left ventricular ejection fraction of 34%. TH

What is the most likely cause of the patient’s ECG changes, elevated cardiac biomarkers, and reduced left ventricular function?
- Left ventricular aneurysm
- ST-segment elevation myocardial infarction
- Left ventricular apical ballooning syndrome
- Myocarditis
- Amyloidosis
Discussion
The answer is C: left ventricular apical ballooning syndrome. Transient left ventricular apical ballooning syndrome is a recently described cardiac condition that mimics the clinical presentation of atherosclerotic acute coronary syndrome. Also known as Takotsubo cardiomyopathy, after a round-bottomed, narrow-necked Japanese fishing pot used for trapping octopus, transient left ventricular apical ballooning syndrome was first described in Japan by Dote and colleagues more than a decade ago.1
Typical findings include patients with ischemia-like chest pain and dyspnea, ST-segment elevation and evolutionary T-wave inversion noted on ECG, mildly elevated levels of cardiac biomarkers, and transient apical wall motion abnormalities. These findings occur in the absence of obstructive coronary atherosclerosis. The condition is predominantly seen in postmenopausal women, and most episodes occur after an event causing physical or emotional stress.
The etiology of this condition is widely debated. Many feel that an exaggerated sympathetic response is the critical mechanism of this syndrome. One study has shown that patients with this syndrome had supraphysiologic levels of plasma catecholamines and stress-related neuropeptides.
Treatment is mainly supportive once ST-segment elevation myocardial infarction has been ruled out with a coronary angiogram. Beta-blocker therapy may be appropriate due to presumed catecholamine surge. Short-term cardiac monitoring is also prudent to evaluate for dysrhythmia. Finally, anticoagulation may be considered to prevent mural thrombosis formation.
The prognosis for patients with transient left ventricular apical ballooning syndrome is favorable, with most patients regaining normal systolic ventricular function within several months, and recurrence is rare. Follow-up echocardiographic evaluation is commonly conducted to ensure adequate resolution of systolic left ventricular dysfunction.
Universal diagnostic criteria for transient left ventricular apical ballooning syndrome have not been established. One diagnostic algorithm recently published includes four criteria: 1) transient regional wall motion abnormalities of the left ventricular apical and midventricular segments; 2) absence of obstructive coronary disease or plaque rupture; 3) new ST-segment elevation and/or T-wave inversion; and 4) absence of an obvious alternative cause (e.g., recent head trauma, extensive intracranial bleeding, myocarditis, pheochromocytoma, hypertrophic cardiomyopathy). To make the diagnosis of transient left ventricular apical ballooning syndrome, all four criteria must be met.
As awareness of transient left ventricular apical ballooning syndrome increases, and as evaluation of left ventricular function becomes standard, this diagnosis is becoming more common. In patients presenting with ST-segment elevation and suspected acute coronary syndromes, one must keep apical ballooning syndrome in the differential. Prompt recognition and aggressive supportive treatment are indicated, and recovery of systolic function can be expected. TH
References
- Dote K, Sato H, Tateishi H, et al. Myocardial stunning due to simultaneous multivessel coronary spasms: a review of 5 cases [in Japanese]. J Cardiol. 1991;21(2):203-214.
A63-year-old female with a history of hypertension and nicotine dependence presented with acute substernal chest pain. The patient reported that the pain was a dull pressure, 5/10 in severity, which radiated into her neck and left arm and was associated with dyspnea.
The patient was on atenolol for hypertension. She reported a 30-year smoking history. A physical exam revealed an anxious, hypertensive (180/95), tachycardic (123 bpm) female. Findings on cardiovascular exam were otherwise unremarkable. Electrocardiogram revealed a 2-3 mm ST-segment elevation in leads V2-V6. Laboratory tests revealed an elevated troponin T level (0.32 ng/mL [nl < 0.03 ng/mL]) and an elevated creatinine kinase-MB fraction (8.2 ng/mL [nl < 6.2 ng/mL]).
Using the above information, the diagnosis of an ST-segment elevation MI was made. The patient went in for urgent cardiac catheterization, which revealed normal coronary anatomy. A left ventriculogram demonstrated moderate hypokinesis of the apical segment and a left ventricular ejection fraction of 34%. TH
What is the most likely cause of the patient’s ECG changes, elevated cardiac biomarkers, and reduced left ventricular function?
- Left ventricular aneurysm
- ST-segment elevation myocardial infarction
- Left ventricular apical ballooning syndrome
- Myocarditis
- Amyloidosis
Discussion
The answer is C: left ventricular apical ballooning syndrome. Transient left ventricular apical ballooning syndrome is a recently described cardiac condition that mimics the clinical presentation of atherosclerotic acute coronary syndrome. Also known as Takotsubo cardiomyopathy, after a round-bottomed, narrow-necked Japanese fishing pot used for trapping octopus, transient left ventricular apical ballooning syndrome was first described in Japan by Dote and colleagues more than a decade ago.1
Typical findings include patients with ischemia-like chest pain and dyspnea, ST-segment elevation and evolutionary T-wave inversion noted on ECG, mildly elevated levels of cardiac biomarkers, and transient apical wall motion abnormalities. These findings occur in the absence of obstructive coronary atherosclerosis. The condition is predominantly seen in postmenopausal women, and most episodes occur after an event causing physical or emotional stress.
The etiology of this condition is widely debated. Many feel that an exaggerated sympathetic response is the critical mechanism of this syndrome. One study has shown that patients with this syndrome had supraphysiologic levels of plasma catecholamines and stress-related neuropeptides.
Treatment is mainly supportive once ST-segment elevation myocardial infarction has been ruled out with a coronary angiogram. Beta-blocker therapy may be appropriate due to presumed catecholamine surge. Short-term cardiac monitoring is also prudent to evaluate for dysrhythmia. Finally, anticoagulation may be considered to prevent mural thrombosis formation.
The prognosis for patients with transient left ventricular apical ballooning syndrome is favorable, with most patients regaining normal systolic ventricular function within several months, and recurrence is rare. Follow-up echocardiographic evaluation is commonly conducted to ensure adequate resolution of systolic left ventricular dysfunction.
Universal diagnostic criteria for transient left ventricular apical ballooning syndrome have not been established. One diagnostic algorithm recently published includes four criteria: 1) transient regional wall motion abnormalities of the left ventricular apical and midventricular segments; 2) absence of obstructive coronary disease or plaque rupture; 3) new ST-segment elevation and/or T-wave inversion; and 4) absence of an obvious alternative cause (e.g., recent head trauma, extensive intracranial bleeding, myocarditis, pheochromocytoma, hypertrophic cardiomyopathy). To make the diagnosis of transient left ventricular apical ballooning syndrome, all four criteria must be met.
As awareness of transient left ventricular apical ballooning syndrome increases, and as evaluation of left ventricular function becomes standard, this diagnosis is becoming more common. In patients presenting with ST-segment elevation and suspected acute coronary syndromes, one must keep apical ballooning syndrome in the differential. Prompt recognition and aggressive supportive treatment are indicated, and recovery of systolic function can be expected. TH
References
- Dote K, Sato H, Tateishi H, et al. Myocardial stunning due to simultaneous multivessel coronary spasms: a review of 5 cases [in Japanese]. J Cardiol. 1991;21(2):203-214.
A63-year-old female with a history of hypertension and nicotine dependence presented with acute substernal chest pain. The patient reported that the pain was a dull pressure, 5/10 in severity, which radiated into her neck and left arm and was associated with dyspnea.
The patient was on atenolol for hypertension. She reported a 30-year smoking history. A physical exam revealed an anxious, hypertensive (180/95), tachycardic (123 bpm) female. Findings on cardiovascular exam were otherwise unremarkable. Electrocardiogram revealed a 2-3 mm ST-segment elevation in leads V2-V6. Laboratory tests revealed an elevated troponin T level (0.32 ng/mL [nl < 0.03 ng/mL]) and an elevated creatinine kinase-MB fraction (8.2 ng/mL [nl < 6.2 ng/mL]).
Using the above information, the diagnosis of an ST-segment elevation MI was made. The patient went in for urgent cardiac catheterization, which revealed normal coronary anatomy. A left ventriculogram demonstrated moderate hypokinesis of the apical segment and a left ventricular ejection fraction of 34%. TH
What is the most likely cause of the patient’s ECG changes, elevated cardiac biomarkers, and reduced left ventricular function?
- Left ventricular aneurysm
- ST-segment elevation myocardial infarction
- Left ventricular apical ballooning syndrome
- Myocarditis
- Amyloidosis
Discussion
The answer is C: left ventricular apical ballooning syndrome. Transient left ventricular apical ballooning syndrome is a recently described cardiac condition that mimics the clinical presentation of atherosclerotic acute coronary syndrome. Also known as Takotsubo cardiomyopathy, after a round-bottomed, narrow-necked Japanese fishing pot used for trapping octopus, transient left ventricular apical ballooning syndrome was first described in Japan by Dote and colleagues more than a decade ago.1
Typical findings include patients with ischemia-like chest pain and dyspnea, ST-segment elevation and evolutionary T-wave inversion noted on ECG, mildly elevated levels of cardiac biomarkers, and transient apical wall motion abnormalities. These findings occur in the absence of obstructive coronary atherosclerosis. The condition is predominantly seen in postmenopausal women, and most episodes occur after an event causing physical or emotional stress.
The etiology of this condition is widely debated. Many feel that an exaggerated sympathetic response is the critical mechanism of this syndrome. One study has shown that patients with this syndrome had supraphysiologic levels of plasma catecholamines and stress-related neuropeptides.
Treatment is mainly supportive once ST-segment elevation myocardial infarction has been ruled out with a coronary angiogram. Beta-blocker therapy may be appropriate due to presumed catecholamine surge. Short-term cardiac monitoring is also prudent to evaluate for dysrhythmia. Finally, anticoagulation may be considered to prevent mural thrombosis formation.
The prognosis for patients with transient left ventricular apical ballooning syndrome is favorable, with most patients regaining normal systolic ventricular function within several months, and recurrence is rare. Follow-up echocardiographic evaluation is commonly conducted to ensure adequate resolution of systolic left ventricular dysfunction.
Universal diagnostic criteria for transient left ventricular apical ballooning syndrome have not been established. One diagnostic algorithm recently published includes four criteria: 1) transient regional wall motion abnormalities of the left ventricular apical and midventricular segments; 2) absence of obstructive coronary disease or plaque rupture; 3) new ST-segment elevation and/or T-wave inversion; and 4) absence of an obvious alternative cause (e.g., recent head trauma, extensive intracranial bleeding, myocarditis, pheochromocytoma, hypertrophic cardiomyopathy). To make the diagnosis of transient left ventricular apical ballooning syndrome, all four criteria must be met.
As awareness of transient left ventricular apical ballooning syndrome increases, and as evaluation of left ventricular function becomes standard, this diagnosis is becoming more common. In patients presenting with ST-segment elevation and suspected acute coronary syndromes, one must keep apical ballooning syndrome in the differential. Prompt recognition and aggressive supportive treatment are indicated, and recovery of systolic function can be expected. TH
References
- Dote K, Sato H, Tateishi H, et al. Myocardial stunning due to simultaneous multivessel coronary spasms: a review of 5 cases [in Japanese]. J Cardiol. 1991;21(2):203-214.
SHM Heart Failure Research Program Awardees
Heart failure (HF) afflicts almost 5 million individuals in the United States and ranks among the most costly inpatient conditions, with hospital costs for 2004 estimated between $14 and $20 billion. Approximately 25% of heart failure patients are readmitted within 30 days of hospital discharge, and more than 50% of elderly patients with HF are readmitted to the hospital within six months. SHM believes that hospitalists are well positioned to improve adherence to published guidelines for the care of congestive HF and are ideal candidates for developing and studying strategies for providing safer, more effective care for patients hospitalized with HF.
In May 2005, SHM disseminated a request for applications for the Heart Failure Research Program. The program, which was made possible by an unrestricted educational grant from Scios, Inc. (a biopharmaceutical company), offered two-year grants to support prospective evaluations of hospitalist-led initiatives designed to improve quality of care for patients hospitalized with HF. A 15-member scientific review group, chaired by Andrew Auerbach, MD, and convened in conjunction with the SHM Research Committee and the SHM Executive Board, reviewed the 18 submitted applications and selected two excellent studies for funding.
The Cardiology Quality of Care Study is a collaborative effort between the sections of General Internal Medicine and Cardiology and the University of Chicago Hospitals. Under the direction of principal investigator Chad Whelan, MD, the study team will evaluate a cost-effective system of improving compliance with the well-validated Centers for Medicare and Medicaid Services (CMS) quality indicators for HF. Trained research assistants will perform chart reviews on all hospitalized patients with HF. If a chart review reveals that certain CMS measures have not been met, the research assistant will send a notification e-mail to the clinical team to alert them that a potentially indicated therapy has not been implemented. Follow-up telephone interviews with patients and post-discharge hospital chart abstractions will be used to evaluate the effectiveness of the intervention. The process may be an effective and inexpensive method for hospitals across the country to use to improve compliance with evidence-based, guideline-supported quality of care measures.
The second study, Improving Quality and Efficiency of Heart Failure Care at Hospital Discharge, is being conducted at the Cleveland Clinic Foundation under the direction of Dr. Christopher Phillips. This single-center, randomized, controlled trial will study changes in 30-day readmission rates resulting from an educational intervention designed to enhance self-care behavior in patients discharged with a primary diagnosis of HF. An RN cardiovascular specialist will contact patients weekly by phone for four weeks after hospital discharge. The calls will focus on identifying and correcting deficits in knowledge, motivation, and behavior with respect to HF self-care. Study findings may improve our understanding of patients’ ability to translate HF education and counseling into motivation to adhere to recommended HF self-care behaviors during the post-discharge period. Improved insight into these processes will inform efforts aimed at optimizing the transition from acute hospital care to home, a process that is a major determinant of early readmission.
Both studies are evaluating novel, practical, reproducible means of improving HF care. We look forward to seeing the results. TH
Heart failure (HF) afflicts almost 5 million individuals in the United States and ranks among the most costly inpatient conditions, with hospital costs for 2004 estimated between $14 and $20 billion. Approximately 25% of heart failure patients are readmitted within 30 days of hospital discharge, and more than 50% of elderly patients with HF are readmitted to the hospital within six months. SHM believes that hospitalists are well positioned to improve adherence to published guidelines for the care of congestive HF and are ideal candidates for developing and studying strategies for providing safer, more effective care for patients hospitalized with HF.
In May 2005, SHM disseminated a request for applications for the Heart Failure Research Program. The program, which was made possible by an unrestricted educational grant from Scios, Inc. (a biopharmaceutical company), offered two-year grants to support prospective evaluations of hospitalist-led initiatives designed to improve quality of care for patients hospitalized with HF. A 15-member scientific review group, chaired by Andrew Auerbach, MD, and convened in conjunction with the SHM Research Committee and the SHM Executive Board, reviewed the 18 submitted applications and selected two excellent studies for funding.
The Cardiology Quality of Care Study is a collaborative effort between the sections of General Internal Medicine and Cardiology and the University of Chicago Hospitals. Under the direction of principal investigator Chad Whelan, MD, the study team will evaluate a cost-effective system of improving compliance with the well-validated Centers for Medicare and Medicaid Services (CMS) quality indicators for HF. Trained research assistants will perform chart reviews on all hospitalized patients with HF. If a chart review reveals that certain CMS measures have not been met, the research assistant will send a notification e-mail to the clinical team to alert them that a potentially indicated therapy has not been implemented. Follow-up telephone interviews with patients and post-discharge hospital chart abstractions will be used to evaluate the effectiveness of the intervention. The process may be an effective and inexpensive method for hospitals across the country to use to improve compliance with evidence-based, guideline-supported quality of care measures.
The second study, Improving Quality and Efficiency of Heart Failure Care at Hospital Discharge, is being conducted at the Cleveland Clinic Foundation under the direction of Dr. Christopher Phillips. This single-center, randomized, controlled trial will study changes in 30-day readmission rates resulting from an educational intervention designed to enhance self-care behavior in patients discharged with a primary diagnosis of HF. An RN cardiovascular specialist will contact patients weekly by phone for four weeks after hospital discharge. The calls will focus on identifying and correcting deficits in knowledge, motivation, and behavior with respect to HF self-care. Study findings may improve our understanding of patients’ ability to translate HF education and counseling into motivation to adhere to recommended HF self-care behaviors during the post-discharge period. Improved insight into these processes will inform efforts aimed at optimizing the transition from acute hospital care to home, a process that is a major determinant of early readmission.
Both studies are evaluating novel, practical, reproducible means of improving HF care. We look forward to seeing the results. TH
Heart failure (HF) afflicts almost 5 million individuals in the United States and ranks among the most costly inpatient conditions, with hospital costs for 2004 estimated between $14 and $20 billion. Approximately 25% of heart failure patients are readmitted within 30 days of hospital discharge, and more than 50% of elderly patients with HF are readmitted to the hospital within six months. SHM believes that hospitalists are well positioned to improve adherence to published guidelines for the care of congestive HF and are ideal candidates for developing and studying strategies for providing safer, more effective care for patients hospitalized with HF.
In May 2005, SHM disseminated a request for applications for the Heart Failure Research Program. The program, which was made possible by an unrestricted educational grant from Scios, Inc. (a biopharmaceutical company), offered two-year grants to support prospective evaluations of hospitalist-led initiatives designed to improve quality of care for patients hospitalized with HF. A 15-member scientific review group, chaired by Andrew Auerbach, MD, and convened in conjunction with the SHM Research Committee and the SHM Executive Board, reviewed the 18 submitted applications and selected two excellent studies for funding.
The Cardiology Quality of Care Study is a collaborative effort between the sections of General Internal Medicine and Cardiology and the University of Chicago Hospitals. Under the direction of principal investigator Chad Whelan, MD, the study team will evaluate a cost-effective system of improving compliance with the well-validated Centers for Medicare and Medicaid Services (CMS) quality indicators for HF. Trained research assistants will perform chart reviews on all hospitalized patients with HF. If a chart review reveals that certain CMS measures have not been met, the research assistant will send a notification e-mail to the clinical team to alert them that a potentially indicated therapy has not been implemented. Follow-up telephone interviews with patients and post-discharge hospital chart abstractions will be used to evaluate the effectiveness of the intervention. The process may be an effective and inexpensive method for hospitals across the country to use to improve compliance with evidence-based, guideline-supported quality of care measures.
The second study, Improving Quality and Efficiency of Heart Failure Care at Hospital Discharge, is being conducted at the Cleveland Clinic Foundation under the direction of Dr. Christopher Phillips. This single-center, randomized, controlled trial will study changes in 30-day readmission rates resulting from an educational intervention designed to enhance self-care behavior in patients discharged with a primary diagnosis of HF. An RN cardiovascular specialist will contact patients weekly by phone for four weeks after hospital discharge. The calls will focus on identifying and correcting deficits in knowledge, motivation, and behavior with respect to HF self-care. Study findings may improve our understanding of patients’ ability to translate HF education and counseling into motivation to adhere to recommended HF self-care behaviors during the post-discharge period. Improved insight into these processes will inform efforts aimed at optimizing the transition from acute hospital care to home, a process that is a major determinant of early readmission.
Both studies are evaluating novel, practical, reproducible means of improving HF care. We look forward to seeing the results. TH
Advocacy Efforts Continue in Support of Proposed E&M Increases
SHM intensified its advocacy efforts over the past several months in support of proposed changes to the Medicare physician fee schedule that would significantly increase payments to hospitalists for many services next year, if adopted by the Centers for Medicare and Medicaid Services (CMS). In June, CMS proposed to make the largest increase in the work relative value units (RVUs) assigned to evaluation and management (E/M) services since Medicare implemented the physician fee schedule in 1992. E/M codes, which represent the time and effort that physicians spend to evaluate patient conditions, have long been viewed as undervalued. Since the release of the proposed rule, SHM has voiced its strong support for CMS’ proposed changes. (See “Calculating the Future of Medicare Payments,” Oct., p. 1).
In an August 18 letter, SHM joined the American College of Physicians (ACP) and 12 other physician groups in urging CMS Administrator Mark McClellan, MD, to include in the final rule the proposed increases in the RVUs assigned to office and hospital visits, and consultations. The groups applauded CMS’ decision to accept the recommendations made by the AMA Relative Value Scale Update Committee (RUC) regarding the evaluation and management codes under the five-year review. “We support the decision to include them in this proposed rule and we strongly urge CMS to include the same proposed work relative value units (RVUs) in the final rule,” the letter stated.
The RUC was careful to ensure that these codes went through the standard survey process and that the data supporting the changes was very strong. The letter emphasized: “The RUC approval of these recommendations, which requires support from at least two-thirds of the RUC members, indicates wide recognition of the work changes in evaluation and management in the 10 years since CMS last reviewed the codes. During our investigation into the increased intensity of evaluation and management services and throughout the RUC process for determining accurate, current work RVUs, we became increasingly aware that enormous changes in patient and physician practice characteristics necessitated these changes.”
In addition, the letter urged CMS to make the required budget neutrality adjustments that result from the five-year review to the conversion factor rather than by an adjustment to the work RVUs. CMS is required by law to offset increases in costs with a mandatory adjustment to keep 2007 expenditures roughly equal to their 2006 level. In the proposed rule, the agency recommended cutting work RVUs by 10% in order to achieve budget neutrality.
SHM joined the AMA and more than 70 other physician organizations in a separate letter. That letter asked CMS not to apply a 10% cut to the work component of the fee schedule, but instead to make an adjustment to the Medicare conversion factor.
“Applying budget neutrality to the work RVUs to offset the improvements in E/M and other services is a step backward and we strongly urge CMS to instead apply any necessary adjustments to the conversion factor,” the organizations said in an August 21 letter to CMS.
When the agency reduced the work RVUs in the past, it created confusion among private insurers, the letter said. Since 1998, similar reductions have been applied to the conversion factor. “CMS does not explain why it proposes to alter this long utilized method and move backward to an approach that the agency itself remarked was inappropriate.”
SHM and the physician community have also lobbied Congress to block a 5.1% cut in the Medicare physician fee schedule that will take effect on January 1, 2007, unless lawmakers take action this fall.
For more news on the five-year review, the 2007 update, and other issues, visit the advocacy and policy section of the SHM Web site at www.hospitalmedicine.org.
Allendorf is senior advisor of Advocacy and Government Affairs for SHM.
SHM intensified its advocacy efforts over the past several months in support of proposed changes to the Medicare physician fee schedule that would significantly increase payments to hospitalists for many services next year, if adopted by the Centers for Medicare and Medicaid Services (CMS). In June, CMS proposed to make the largest increase in the work relative value units (RVUs) assigned to evaluation and management (E/M) services since Medicare implemented the physician fee schedule in 1992. E/M codes, which represent the time and effort that physicians spend to evaluate patient conditions, have long been viewed as undervalued. Since the release of the proposed rule, SHM has voiced its strong support for CMS’ proposed changes. (See “Calculating the Future of Medicare Payments,” Oct., p. 1).
In an August 18 letter, SHM joined the American College of Physicians (ACP) and 12 other physician groups in urging CMS Administrator Mark McClellan, MD, to include in the final rule the proposed increases in the RVUs assigned to office and hospital visits, and consultations. The groups applauded CMS’ decision to accept the recommendations made by the AMA Relative Value Scale Update Committee (RUC) regarding the evaluation and management codes under the five-year review. “We support the decision to include them in this proposed rule and we strongly urge CMS to include the same proposed work relative value units (RVUs) in the final rule,” the letter stated.
The RUC was careful to ensure that these codes went through the standard survey process and that the data supporting the changes was very strong. The letter emphasized: “The RUC approval of these recommendations, which requires support from at least two-thirds of the RUC members, indicates wide recognition of the work changes in evaluation and management in the 10 years since CMS last reviewed the codes. During our investigation into the increased intensity of evaluation and management services and throughout the RUC process for determining accurate, current work RVUs, we became increasingly aware that enormous changes in patient and physician practice characteristics necessitated these changes.”
In addition, the letter urged CMS to make the required budget neutrality adjustments that result from the five-year review to the conversion factor rather than by an adjustment to the work RVUs. CMS is required by law to offset increases in costs with a mandatory adjustment to keep 2007 expenditures roughly equal to their 2006 level. In the proposed rule, the agency recommended cutting work RVUs by 10% in order to achieve budget neutrality.
SHM joined the AMA and more than 70 other physician organizations in a separate letter. That letter asked CMS not to apply a 10% cut to the work component of the fee schedule, but instead to make an adjustment to the Medicare conversion factor.
“Applying budget neutrality to the work RVUs to offset the improvements in E/M and other services is a step backward and we strongly urge CMS to instead apply any necessary adjustments to the conversion factor,” the organizations said in an August 21 letter to CMS.
When the agency reduced the work RVUs in the past, it created confusion among private insurers, the letter said. Since 1998, similar reductions have been applied to the conversion factor. “CMS does not explain why it proposes to alter this long utilized method and move backward to an approach that the agency itself remarked was inappropriate.”
SHM and the physician community have also lobbied Congress to block a 5.1% cut in the Medicare physician fee schedule that will take effect on January 1, 2007, unless lawmakers take action this fall.
For more news on the five-year review, the 2007 update, and other issues, visit the advocacy and policy section of the SHM Web site at www.hospitalmedicine.org.
Allendorf is senior advisor of Advocacy and Government Affairs for SHM.
SHM intensified its advocacy efforts over the past several months in support of proposed changes to the Medicare physician fee schedule that would significantly increase payments to hospitalists for many services next year, if adopted by the Centers for Medicare and Medicaid Services (CMS). In June, CMS proposed to make the largest increase in the work relative value units (RVUs) assigned to evaluation and management (E/M) services since Medicare implemented the physician fee schedule in 1992. E/M codes, which represent the time and effort that physicians spend to evaluate patient conditions, have long been viewed as undervalued. Since the release of the proposed rule, SHM has voiced its strong support for CMS’ proposed changes. (See “Calculating the Future of Medicare Payments,” Oct., p. 1).
In an August 18 letter, SHM joined the American College of Physicians (ACP) and 12 other physician groups in urging CMS Administrator Mark McClellan, MD, to include in the final rule the proposed increases in the RVUs assigned to office and hospital visits, and consultations. The groups applauded CMS’ decision to accept the recommendations made by the AMA Relative Value Scale Update Committee (RUC) regarding the evaluation and management codes under the five-year review. “We support the decision to include them in this proposed rule and we strongly urge CMS to include the same proposed work relative value units (RVUs) in the final rule,” the letter stated.
The RUC was careful to ensure that these codes went through the standard survey process and that the data supporting the changes was very strong. The letter emphasized: “The RUC approval of these recommendations, which requires support from at least two-thirds of the RUC members, indicates wide recognition of the work changes in evaluation and management in the 10 years since CMS last reviewed the codes. During our investigation into the increased intensity of evaluation and management services and throughout the RUC process for determining accurate, current work RVUs, we became increasingly aware that enormous changes in patient and physician practice characteristics necessitated these changes.”
In addition, the letter urged CMS to make the required budget neutrality adjustments that result from the five-year review to the conversion factor rather than by an adjustment to the work RVUs. CMS is required by law to offset increases in costs with a mandatory adjustment to keep 2007 expenditures roughly equal to their 2006 level. In the proposed rule, the agency recommended cutting work RVUs by 10% in order to achieve budget neutrality.
SHM joined the AMA and more than 70 other physician organizations in a separate letter. That letter asked CMS not to apply a 10% cut to the work component of the fee schedule, but instead to make an adjustment to the Medicare conversion factor.
“Applying budget neutrality to the work RVUs to offset the improvements in E/M and other services is a step backward and we strongly urge CMS to instead apply any necessary adjustments to the conversion factor,” the organizations said in an August 21 letter to CMS.
When the agency reduced the work RVUs in the past, it created confusion among private insurers, the letter said. Since 1998, similar reductions have been applied to the conversion factor. “CMS does not explain why it proposes to alter this long utilized method and move backward to an approach that the agency itself remarked was inappropriate.”
SHM and the physician community have also lobbied Congress to block a 5.1% cut in the Medicare physician fee schedule that will take effect on January 1, 2007, unless lawmakers take action this fall.
For more news on the five-year review, the 2007 update, and other issues, visit the advocacy and policy section of the SHM Web site at www.hospitalmedicine.org.
Allendorf is senior advisor of Advocacy and Government Affairs for SHM.
Membership and Marketing Initiatives

I joined SHM earlier this year to work with SHM’s Membership and Marketing staff. My role at SHM is to manage our growing organization’s communications. So what does that mean in real terms? Most importantly, we have been tasked with understanding what is important to our members and what value SHM membership needs to provide to you. We’re also working to build a strong foundation for the SHM brand, so keep an eye out for an updated, consistent look to our communications—both online and off.
Feedback from our members and the hospital medicine community at large is vital to us. Samuel Johnson (1709-1764), an often-quoted English writer, once said, “The next best thing to knowing something is knowing where to find it.” One common thread among those I have talked to over the past few months has been concern that although our Web site is comprehensive, finding specific information can be challenging. Quickly making the Web site user-friendly became a priority and, along with our resident Web design guru Bruce Hansen, we have created a navigation system designed to get you to our site’s most popular information in the fewest number of clicks.
Looking for a link to the Journal of Hospital Medicine pages? The Hospitalist Web site? Our new Career Center? Or our Resource Rooms? Look no further than the top of our homepage (www.hospitalmedicine.org). Our new clickable banner will get you where you need to go in no time.
In a few short clicks, you can read pages from the Journal, including expert articles by leading practitioners on current and future trends in hospital medicine. Surf over to The Hospitalist Web site for the latest issue of our monthly newsmagazine. Have a story idea or want to contact the editor? You can do it all on The Hospitalist Web site.
Find your first or next hospitalist job at our new SHM Career Center. This one-of-a-kind forum for those looking for jobs and those with positions to fill helps you to avoid the excess of other career sites by focusing on our specific industry. Our Resource Rooms provide you with access to expert advice and information on every aspect of your practice. We’ve got the tools you need, and our Resource Rooms are the toolbox.
Of course, we hope you won’t forget the rest of our Web site: Look for the latest in advocacy and policy updates, our online discussion communities, and breaking news in the field of hospital medicine.
We hope you will set aside a few minutes each month to review our revamped SHM eNewsletter. Kudos again to Bruce for its ultra-sleek, contemporary design, which both pleases the eye and improves the readability of the articles. Research has shown us that most people read our articles online, as opposed to printing them out and reading them, so look for larger fonts and a clean layout.
We’ve introduced many new columns that will become a regular part of the SHM eNewsletter, including our Career Center Job of the Month, Clinical News, Advocacy News, upcoming articles from The Hospitalist—and more. We are also proud to introduce our featured product of the month from our newly launched SHM Store. Looking for a way to show your hospitalist pride? Why not grab one of our SHM polo shirts, scrub tops, or a baseball cap? The SHM store also features educational products. Looking for an extra copy of The Core Competencies or the ““Bi-Annual Survey on the State of the Hospital Medicine Movement”? You’ll find them, along with nearly 100 other items, at the SHM Store.
These are just a few of the changes we have made to transform SHM into your organization. Keep watching, and you will find that SHM, ground central for the hospital medicine movement, is the best place to turn for anything and everything relating to hospital medicine.
If you should have any questions or comments, our doors and ears are always open and ready to welcome you. Feel free to give us a call at (800) 843-3360.
Stay tuned for next month’s SHM staff member report from Tina Budnitz, SHM’s senior advisor for quality initiatives.
Sanders is the marketing manager for SHM.

SHM CHAPTER REPORTS
Lake Erie
SHM’s Lake Erie Chapter met at Morton’s Steakhouse in Cleveland on August 9. The guest speaker was Ron J. Kattoo, MD, associate director of intensive care at Henry Ford Hospital and Health System in Detroit. Dr. Kattoo spoke about the management options for healthcare and ventilator-associated pneumonia, followed by a discussion about the role of hospitalists in the management of this severe condition. The meeting was sponsored by Pfizer Pharmaceutical Company. For more information on the Lake Erie Chapter of SHM, please contact Christopher Whinney, MD, at [email protected].
Long Island
SHM’s Long Island (N.Y.) Chapter held a meeting on August 24 at Burton & Doyle Steakhouse in East Great Neck, N.Y. A presentation titled “Sleep Disorders: How They Affect Patients and Providers” was given by Sonia Ancoli-Israel, PhD, a University of California at San Diego School of Medicine professor of psychiatry. At the conclusion of the presentation, Dr. Ancoli-Israel fielded questions.
I joined SHM earlier this year to work with SHM’s Membership and Marketing staff. My role at SHM is to manage our growing organization’s communications. So what does that mean in real terms? Most importantly, we have been tasked with understanding what is important to our members and what value SHM membership needs to provide to you. We’re also working to build a strong foundation for the SHM brand, so keep an eye out for an updated, consistent look to our communications—both online and off.
Feedback from our members and the hospital medicine community at large is vital to us. Samuel Johnson (1709-1764), an often-quoted English writer, once said, “The next best thing to knowing something is knowing where to find it.” One common thread among those I have talked to over the past few months has been concern that although our Web site is comprehensive, finding specific information can be challenging. Quickly making the Web site user-friendly became a priority and, along with our resident Web design guru Bruce Hansen, we have created a navigation system designed to get you to our site’s most popular information in the fewest number of clicks.
Looking for a link to the Journal of Hospital Medicine pages? The Hospitalist Web site? Our new Career Center? Or our Resource Rooms? Look no further than the top of our homepage (www.hospitalmedicine.org). Our new clickable banner will get you where you need to go in no time.
In a few short clicks, you can read pages from the Journal, including expert articles by leading practitioners on current and future trends in hospital medicine. Surf over to The Hospitalist Web site for the latest issue of our monthly newsmagazine. Have a story idea or want to contact the editor? You can do it all on The Hospitalist Web site.
Find your first or next hospitalist job at our new SHM Career Center. This one-of-a-kind forum for those looking for jobs and those with positions to fill helps you to avoid the excess of other career sites by focusing on our specific industry. Our Resource Rooms provide you with access to expert advice and information on every aspect of your practice. We’ve got the tools you need, and our Resource Rooms are the toolbox.
Of course, we hope you won’t forget the rest of our Web site: Look for the latest in advocacy and policy updates, our online discussion communities, and breaking news in the field of hospital medicine.
We hope you will set aside a few minutes each month to review our revamped SHM eNewsletter. Kudos again to Bruce for its ultra-sleek, contemporary design, which both pleases the eye and improves the readability of the articles. Research has shown us that most people read our articles online, as opposed to printing them out and reading them, so look for larger fonts and a clean layout.
We’ve introduced many new columns that will become a regular part of the SHM eNewsletter, including our Career Center Job of the Month, Clinical News, Advocacy News, upcoming articles from The Hospitalist—and more. We are also proud to introduce our featured product of the month from our newly launched SHM Store. Looking for a way to show your hospitalist pride? Why not grab one of our SHM polo shirts, scrub tops, or a baseball cap? The SHM store also features educational products. Looking for an extra copy of The Core Competencies or the ““Bi-Annual Survey on the State of the Hospital Medicine Movement”? You’ll find them, along with nearly 100 other items, at the SHM Store.
These are just a few of the changes we have made to transform SHM into your organization. Keep watching, and you will find that SHM, ground central for the hospital medicine movement, is the best place to turn for anything and everything relating to hospital medicine.
If you should have any questions or comments, our doors and ears are always open and ready to welcome you. Feel free to give us a call at (800) 843-3360.
Stay tuned for next month’s SHM staff member report from Tina Budnitz, SHM’s senior advisor for quality initiatives.
Sanders is the marketing manager for SHM.
SHM CHAPTER REPORTS
Lake Erie
SHM’s Lake Erie Chapter met at Morton’s Steakhouse in Cleveland on August 9. The guest speaker was Ron J. Kattoo, MD, associate director of intensive care at Henry Ford Hospital and Health System in Detroit. Dr. Kattoo spoke about the management options for healthcare and ventilator-associated pneumonia, followed by a discussion about the role of hospitalists in the management of this severe condition. The meeting was sponsored by Pfizer Pharmaceutical Company. For more information on the Lake Erie Chapter of SHM, please contact Christopher Whinney, MD, at [email protected].
Long Island
SHM’s Long Island (N.Y.) Chapter held a meeting on August 24 at Burton & Doyle Steakhouse in East Great Neck, N.Y. A presentation titled “Sleep Disorders: How They Affect Patients and Providers” was given by Sonia Ancoli-Israel, PhD, a University of California at San Diego School of Medicine professor of psychiatry. At the conclusion of the presentation, Dr. Ancoli-Israel fielded questions.
I joined SHM earlier this year to work with SHM’s Membership and Marketing staff. My role at SHM is to manage our growing organization’s communications. So what does that mean in real terms? Most importantly, we have been tasked with understanding what is important to our members and what value SHM membership needs to provide to you. We’re also working to build a strong foundation for the SHM brand, so keep an eye out for an updated, consistent look to our communications—both online and off.
Feedback from our members and the hospital medicine community at large is vital to us. Samuel Johnson (1709-1764), an often-quoted English writer, once said, “The next best thing to knowing something is knowing where to find it.” One common thread among those I have talked to over the past few months has been concern that although our Web site is comprehensive, finding specific information can be challenging. Quickly making the Web site user-friendly became a priority and, along with our resident Web design guru Bruce Hansen, we have created a navigation system designed to get you to our site’s most popular information in the fewest number of clicks.
Looking for a link to the Journal of Hospital Medicine pages? The Hospitalist Web site? Our new Career Center? Or our Resource Rooms? Look no further than the top of our homepage (www.hospitalmedicine.org). Our new clickable banner will get you where you need to go in no time.
In a few short clicks, you can read pages from the Journal, including expert articles by leading practitioners on current and future trends in hospital medicine. Surf over to The Hospitalist Web site for the latest issue of our monthly newsmagazine. Have a story idea or want to contact the editor? You can do it all on The Hospitalist Web site.
Find your first or next hospitalist job at our new SHM Career Center. This one-of-a-kind forum for those looking for jobs and those with positions to fill helps you to avoid the excess of other career sites by focusing on our specific industry. Our Resource Rooms provide you with access to expert advice and information on every aspect of your practice. We’ve got the tools you need, and our Resource Rooms are the toolbox.
Of course, we hope you won’t forget the rest of our Web site: Look for the latest in advocacy and policy updates, our online discussion communities, and breaking news in the field of hospital medicine.
We hope you will set aside a few minutes each month to review our revamped SHM eNewsletter. Kudos again to Bruce for its ultra-sleek, contemporary design, which both pleases the eye and improves the readability of the articles. Research has shown us that most people read our articles online, as opposed to printing them out and reading them, so look for larger fonts and a clean layout.
We’ve introduced many new columns that will become a regular part of the SHM eNewsletter, including our Career Center Job of the Month, Clinical News, Advocacy News, upcoming articles from The Hospitalist—and more. We are also proud to introduce our featured product of the month from our newly launched SHM Store. Looking for a way to show your hospitalist pride? Why not grab one of our SHM polo shirts, scrub tops, or a baseball cap? The SHM store also features educational products. Looking for an extra copy of The Core Competencies or the ““Bi-Annual Survey on the State of the Hospital Medicine Movement”? You’ll find them, along with nearly 100 other items, at the SHM Store.
These are just a few of the changes we have made to transform SHM into your organization. Keep watching, and you will find that SHM, ground central for the hospital medicine movement, is the best place to turn for anything and everything relating to hospital medicine.
If you should have any questions or comments, our doors and ears are always open and ready to welcome you. Feel free to give us a call at (800) 843-3360.
Stay tuned for next month’s SHM staff member report from Tina Budnitz, SHM’s senior advisor for quality initiatives.
Sanders is the marketing manager for SHM.
SHM CHAPTER REPORTS
Lake Erie
SHM’s Lake Erie Chapter met at Morton’s Steakhouse in Cleveland on August 9. The guest speaker was Ron J. Kattoo, MD, associate director of intensive care at Henry Ford Hospital and Health System in Detroit. Dr. Kattoo spoke about the management options for healthcare and ventilator-associated pneumonia, followed by a discussion about the role of hospitalists in the management of this severe condition. The meeting was sponsored by Pfizer Pharmaceutical Company. For more information on the Lake Erie Chapter of SHM, please contact Christopher Whinney, MD, at [email protected].
Long Island
SHM’s Long Island (N.Y.) Chapter held a meeting on August 24 at Burton & Doyle Steakhouse in East Great Neck, N.Y. A presentation titled “Sleep Disorders: How They Affect Patients and Providers” was given by Sonia Ancoli-Israel, PhD, a University of California at San Diego School of Medicine professor of psychiatry. At the conclusion of the presentation, Dr. Ancoli-Israel fielded questions.
The Hammer and the Anvil

In the not-too-distant future, a multiphysician hospitalist group is a participant in a pay-for-performance (P4P) program. Dr. Buchmann, the group’s lead hospitalist, is confronted by his hospital’s administration and informed that his doctors are performing below regional benchmarks for standards of care for community-acquired pneumonia, and, in fact, the hospital as a whole is below the mean performance levels.
The hospital threatens to break its contract with Dr. Buchmann’s group despite his response that his group sees a far more complex population than these standards can account for—and besides, his group has implemented a number of important quality initiatives in other diseases that are not part of the P4P program.
Several of the group’s hospitalists state that they will stop seeing indigent patients and will no longer take referrals for high-risk patients. Another partner feels it is unethical to continue treating pneumonia patients at the hospital without informing them of these quality findings and at least offering the option of transfer to a facility with better scores. Dr. Buchmann finds all these propositions unsettling.
While these physicians’ responses may sound extreme, the behavior of physicians caught between the hammer of financial survival and the anvil of professional ethics is unpredictable. Medicare and other payers have been implementing P4P plans as the latest attempt to stimulate quality reform. There are dozens of P4P-based programs operating in the United States, and the financial implications are daunting. Further, P4P is taking hold despite a relative paucity of research regarding its effectiveness in improving outcomes.
The underlying rationale of P4P is the use of economic incentives to stimulate changes in provider behavior. Recent work from the RAND Corporation suggests that as much as one-half of healthcare is not based on “accepted” best practices.1 And with increasing attention on the role of errors in medical practice, any effort to improve care seems, on its surface, laudable.
In general, key elements of P4P programs include a set of performance measures, the collection of data, comparison of provider data with benchmarks, and rewards for physicians who meet or exceed those targets. The interface between economic and financial incentives requires physicians to ensure that their behavior is in line with ethical and professional standards. While journals of medicine, law, and business contain many articles devoted to the policy and market implications of P4P, there is surprisingly little discussion in the literature regarding the potential ethical challenges that physicians may face in these programs.
For hospitalists (and other physicians), P4P may present several troubling ethical issues. Because the current scope of P4P is limited to a few diseases, widespread implementation might lead to relative neglect of patients with other illnesses. Higher-risk patients might be avoided, and individual patient concerns might become subjugated to population performance measures. Hospitalists could face the additional conflict of being accountable to (and/or dependent upon) hospitals, which feel P4P pressures of their own. A final issue is the question of whether shared decision-making and patient-centered care mandate disclosure of non-public quality data to patients.
The American Medical Association (AMA) has a policy that specifically addresses P4P.2 Its “Pay-for-Performance Principles and Guidelines” call for physician participation in P4P to be voluntary and to allow physicians to access their ratings for potential appeal prior to wider release. The policy insists that quality of care be paramount over cost savings and that the physician-patient relationship be preserved. Of course, P4P programs may not share the AMA’s ethical concerns and are not bound to consider them.
Of particular concern—for both inpatient and outpatient physicians—is the fate of high-risk and unassigned patients. According to SHM’s 2005-2006 “Bi-Annual Survey on the State of the Hospital Medicine Movement” (www.hospital medicine.org), 96% of hospitalists are involved in the care of unassigned patients, and, in general, one of the strengths of hospital-based physicians should be their relative familiarity with the acute problems of patients who are older and of those with concomitant morbidities. Yet these are precisely the patient groups that are not well served by typical P4P measurements.
The potential for P4P incentives to create disparities in patient care among different patient groups and diseases is one of the prime concerns in the Council on Ethical and Judicial Affairs’ recent opinion for the AMA on P4P programs.3 The care of older patients, for instance, because of their own choices and due to frequency of comorbidities, may well come up short in performance measures designed for individuals who have a single disease.
This is not just a policy problem because P4P is not only unlikely to adequately address the ethical concerns of equitable care to these groups, it could exacerbate the vulnerability of these populations by creating a disincentive to provide care.4 A recent publication describing reports of cardiac surgeons turning away high-risk patients after “CABG report cards” became publicly available suggests that when given the option at least some physicians may indeed change their behavior when quality information is being collected and reported.5 Ironically, a system that incentivizes doctors to avoid the highest-risk patients could worsen—rather than improve—the overall quality of care.
Hospitalists may not be as sensitive to these pressures as surgeons or outpatient physicians, especially given the hospitalist’s limited flexibility in “choosing” patients. Care of unassigned patients may be a contractual obligation for which a hospitalist is paid by the hospital (which may face its own pressures in this area). And lower-risk referrals from outpatient physicians may “compensate” for the occasional complex patient.
Hospitalists are generally “need-based” practitioners who legally and ethically may not have the option to refuse care without risking patient abandonment. Yet the fact that hospitalists take on such patients may make their performance scores inferior to even non-hospital-based doctors—a difficult position to be in if one’s group receives payments from the hospital with an expectation of superior performance. Hospitalists in particular must consider whether or not insurance companies and the Centers for Medicare and Medicaid Services (CMS) could really accommodate all possible confounders in a risk-adjustment model to offset the nature of their patients. While the ethical choice might be for hospitalists simply to refuse to participate in P4P, citing multiple conflicts of interest, there is no clear indication regarding how “optional” these programs will be as they become increasingly prevalent, presenting yet another ethical issue.
Further, Medicare’s current P4P system for hospitals is directed at just five conditions, only two of which (congestive heart failure and pneumonia) are likely to fall within a hospitalist’s realm. But the list of common diagnoses under the hospitalist’s umbrella is, of course, much larger, including thromboembolism, pyelonephritis, COPD, cirrhosis, and sepsis. The data that exists for compliance with recommended care for some of these conditions (e.g., COPD) suggests that there may be substantial variability.6
But if hospitals base their support for hospitalist programs on their performance within a few CMS diagnoses, the effect on care for and development of appropriate guidelines and resources toward many other conditions may suffer. Already, hospital discharge forms are pre-printed with checkboxes for an angiotensin-converting enzyme (ACE) inhibitor prescription for congestive heart failure and counseling for smoking cessation. The (unethical) implication is that some diagnoses are more valuable than others, and that physician energies may be inequitably distributed—whether consciously or not. It is difficult to see how P4P could encompass standards for every patient condition, or how hospitals and providers could avoid focusing resources on those conditions that are more closely scrutinized by their payers.
Another issue arises if patient autonomy dictates that a treatment plan has to deviate from established guidelines; in such a case, hospitalists and other physicians may be forced to provide a care plan that is entirely reasonable from a medical standpoint but counts against them when compared with a benchmark. Ethical principles dictate that patient care be given priority, but unless consideration is made within the scoring system, performance measures that do not accommodate the ethical mandates to respect patient wishes or physician judgment are substantial pitfalls in the pursuit of better quality.7,8
One last issue concerns the question of whether or not providers have an obligation to disclose quality data to patients in the context of shared decision-making. This is a murky subject that involves determining the boundaries between the best means of pursuing quality improvement and the ethics of patient advocacy. The AMA’s Code of Medical Ethics states, “Patients should receive guidance from their physicians as to the optimal course of action,” and the issue of competence and responsibility to the care of the individual patient is the focus of several of the Principles of Medical Ethics. However, there is practically nothing published regarding the ethics, implications, or results of such disclosure, presumably because the availability of large amounts of quality-based data is such a new phenomenon and the considerations of such disclosure are so uncomfortable for many physicians.
Of course, some information—“CABG report cards,” for instance—is publicly available, but the evidence that patients actually utilize this information to a significant extent or that quality has improved due to its use is mixed.5 The question of whether an obligation exists to disclose non-public information when a provider knows that there is a question about performance relative to a benchmark or comparative peer group is uncharted water, ethically speaking; the issue is further complicated by the fact that appraisal of quality is far from a perfect science. It may be that the benefits of P4P result primarily from transparency, rather than from financial incentives. If so, disclosure may be the major component of quality reform, giving further weight to this question.
The ethical problems raised by P4P are underappreciated and inadequately discussed in the literature, particularly for how rapidly and rampantly these programs are being piloted and implemented. Although the AMA has taken a fairly clear and reasonable stance on the appropriate considerations for P4P programs, it is not clear that payers are incorporating all these concerns. A substantial number of hospitalist groups receive payments from medical groups or hospitals, which in turn are already involved in P4P for some diagnoses.
All hospitalists should read and familiarize themselves with these guidelines and carefully assess the implications of forthcoming P4P proposals for their own practices and patients. On a larger scale, SHM and its membership should strongly consider taking the lead in defining appropriate processes and outcomes for hospital care that incorporate these ethical concerns and allow for meaningful conclusions regarding both quality of care and opportunities for improvement.
Dr. Harte works at the Cleveland Clinic, and Dr. Rajput works at the Robert Wood Johnson Medical School, Camden, N.J. The authors wish to thank Tom Baudendistel and Donald Krause for their review and suggestions.
References
- Asch SM, Kerr EA, Keesey J, et al. Who is at greatest risk for receiving poor-quality health care? N Engl J Med. 2006 Mar 16;354:1147-1156.
- American Medical Association. Pay-for-performance principles and guidelines. Accessible at: www.ama-assn.org/meetings/public/annual05/bot5a05.doc. Last accessed September 13, 2006.
- American Medical Association. CEJA 3-1-05 Report, July 2006. Available at: www.ama-assn.org/ama/pub/category/4325.html. Last accessed September 13, 2006.
- Morreim EH. Result-based compensation in health care: a good, but limited, idea. J Law Med Ethics. 2001 Summer;29(2):174-181.
- Werner RM, Asch DA. The unintended consequences of publicly reporting quality information. JAMA. 2005 Mar 9;293:1239-1244.
- Lindenauer PK, Pekow P, Gao S, et al. Quality of care for patients hospitalized for acute exacerbations of chronic obstructive pulmonary disease. Ann Intern Med. 2006;144(12):894-903.
- Walter LC, Davidowitz NP, Heineken PA, et al. Pitfalls of converting practice guidelines into quality measures: lessons learned from a VA performance measure. JAMA. 2004 May 26;291(20):2466-2470.
- Boyd CM, Darer J, Boult C, et al. Clinical practice guidelines and quality of care for older patients with multiple comorbid diseases: implications for pay for performance. JAMA. 2005 Aug 10;294(6):716-724.
In the not-too-distant future, a multiphysician hospitalist group is a participant in a pay-for-performance (P4P) program. Dr. Buchmann, the group’s lead hospitalist, is confronted by his hospital’s administration and informed that his doctors are performing below regional benchmarks for standards of care for community-acquired pneumonia, and, in fact, the hospital as a whole is below the mean performance levels.
The hospital threatens to break its contract with Dr. Buchmann’s group despite his response that his group sees a far more complex population than these standards can account for—and besides, his group has implemented a number of important quality initiatives in other diseases that are not part of the P4P program.
Several of the group’s hospitalists state that they will stop seeing indigent patients and will no longer take referrals for high-risk patients. Another partner feels it is unethical to continue treating pneumonia patients at the hospital without informing them of these quality findings and at least offering the option of transfer to a facility with better scores. Dr. Buchmann finds all these propositions unsettling.
While these physicians’ responses may sound extreme, the behavior of physicians caught between the hammer of financial survival and the anvil of professional ethics is unpredictable. Medicare and other payers have been implementing P4P plans as the latest attempt to stimulate quality reform. There are dozens of P4P-based programs operating in the United States, and the financial implications are daunting. Further, P4P is taking hold despite a relative paucity of research regarding its effectiveness in improving outcomes.
The underlying rationale of P4P is the use of economic incentives to stimulate changes in provider behavior. Recent work from the RAND Corporation suggests that as much as one-half of healthcare is not based on “accepted” best practices.1 And with increasing attention on the role of errors in medical practice, any effort to improve care seems, on its surface, laudable.
In general, key elements of P4P programs include a set of performance measures, the collection of data, comparison of provider data with benchmarks, and rewards for physicians who meet or exceed those targets. The interface between economic and financial incentives requires physicians to ensure that their behavior is in line with ethical and professional standards. While journals of medicine, law, and business contain many articles devoted to the policy and market implications of P4P, there is surprisingly little discussion in the literature regarding the potential ethical challenges that physicians may face in these programs.
For hospitalists (and other physicians), P4P may present several troubling ethical issues. Because the current scope of P4P is limited to a few diseases, widespread implementation might lead to relative neglect of patients with other illnesses. Higher-risk patients might be avoided, and individual patient concerns might become subjugated to population performance measures. Hospitalists could face the additional conflict of being accountable to (and/or dependent upon) hospitals, which feel P4P pressures of their own. A final issue is the question of whether shared decision-making and patient-centered care mandate disclosure of non-public quality data to patients.
The American Medical Association (AMA) has a policy that specifically addresses P4P.2 Its “Pay-for-Performance Principles and Guidelines” call for physician participation in P4P to be voluntary and to allow physicians to access their ratings for potential appeal prior to wider release. The policy insists that quality of care be paramount over cost savings and that the physician-patient relationship be preserved. Of course, P4P programs may not share the AMA’s ethical concerns and are not bound to consider them.
Of particular concern—for both inpatient and outpatient physicians—is the fate of high-risk and unassigned patients. According to SHM’s 2005-2006 “Bi-Annual Survey on the State of the Hospital Medicine Movement” (www.hospital medicine.org), 96% of hospitalists are involved in the care of unassigned patients, and, in general, one of the strengths of hospital-based physicians should be their relative familiarity with the acute problems of patients who are older and of those with concomitant morbidities. Yet these are precisely the patient groups that are not well served by typical P4P measurements.
The potential for P4P incentives to create disparities in patient care among different patient groups and diseases is one of the prime concerns in the Council on Ethical and Judicial Affairs’ recent opinion for the AMA on P4P programs.3 The care of older patients, for instance, because of their own choices and due to frequency of comorbidities, may well come up short in performance measures designed for individuals who have a single disease.
This is not just a policy problem because P4P is not only unlikely to adequately address the ethical concerns of equitable care to these groups, it could exacerbate the vulnerability of these populations by creating a disincentive to provide care.4 A recent publication describing reports of cardiac surgeons turning away high-risk patients after “CABG report cards” became publicly available suggests that when given the option at least some physicians may indeed change their behavior when quality information is being collected and reported.5 Ironically, a system that incentivizes doctors to avoid the highest-risk patients could worsen—rather than improve—the overall quality of care.
Hospitalists may not be as sensitive to these pressures as surgeons or outpatient physicians, especially given the hospitalist’s limited flexibility in “choosing” patients. Care of unassigned patients may be a contractual obligation for which a hospitalist is paid by the hospital (which may face its own pressures in this area). And lower-risk referrals from outpatient physicians may “compensate” for the occasional complex patient.
Hospitalists are generally “need-based” practitioners who legally and ethically may not have the option to refuse care without risking patient abandonment. Yet the fact that hospitalists take on such patients may make their performance scores inferior to even non-hospital-based doctors—a difficult position to be in if one’s group receives payments from the hospital with an expectation of superior performance. Hospitalists in particular must consider whether or not insurance companies and the Centers for Medicare and Medicaid Services (CMS) could really accommodate all possible confounders in a risk-adjustment model to offset the nature of their patients. While the ethical choice might be for hospitalists simply to refuse to participate in P4P, citing multiple conflicts of interest, there is no clear indication regarding how “optional” these programs will be as they become increasingly prevalent, presenting yet another ethical issue.
Further, Medicare’s current P4P system for hospitals is directed at just five conditions, only two of which (congestive heart failure and pneumonia) are likely to fall within a hospitalist’s realm. But the list of common diagnoses under the hospitalist’s umbrella is, of course, much larger, including thromboembolism, pyelonephritis, COPD, cirrhosis, and sepsis. The data that exists for compliance with recommended care for some of these conditions (e.g., COPD) suggests that there may be substantial variability.6
But if hospitals base their support for hospitalist programs on their performance within a few CMS diagnoses, the effect on care for and development of appropriate guidelines and resources toward many other conditions may suffer. Already, hospital discharge forms are pre-printed with checkboxes for an angiotensin-converting enzyme (ACE) inhibitor prescription for congestive heart failure and counseling for smoking cessation. The (unethical) implication is that some diagnoses are more valuable than others, and that physician energies may be inequitably distributed—whether consciously or not. It is difficult to see how P4P could encompass standards for every patient condition, or how hospitals and providers could avoid focusing resources on those conditions that are more closely scrutinized by their payers.
Another issue arises if patient autonomy dictates that a treatment plan has to deviate from established guidelines; in such a case, hospitalists and other physicians may be forced to provide a care plan that is entirely reasonable from a medical standpoint but counts against them when compared with a benchmark. Ethical principles dictate that patient care be given priority, but unless consideration is made within the scoring system, performance measures that do not accommodate the ethical mandates to respect patient wishes or physician judgment are substantial pitfalls in the pursuit of better quality.7,8
One last issue concerns the question of whether or not providers have an obligation to disclose quality data to patients in the context of shared decision-making. This is a murky subject that involves determining the boundaries between the best means of pursuing quality improvement and the ethics of patient advocacy. The AMA’s Code of Medical Ethics states, “Patients should receive guidance from their physicians as to the optimal course of action,” and the issue of competence and responsibility to the care of the individual patient is the focus of several of the Principles of Medical Ethics. However, there is practically nothing published regarding the ethics, implications, or results of such disclosure, presumably because the availability of large amounts of quality-based data is such a new phenomenon and the considerations of such disclosure are so uncomfortable for many physicians.
Of course, some information—“CABG report cards,” for instance—is publicly available, but the evidence that patients actually utilize this information to a significant extent or that quality has improved due to its use is mixed.5 The question of whether an obligation exists to disclose non-public information when a provider knows that there is a question about performance relative to a benchmark or comparative peer group is uncharted water, ethically speaking; the issue is further complicated by the fact that appraisal of quality is far from a perfect science. It may be that the benefits of P4P result primarily from transparency, rather than from financial incentives. If so, disclosure may be the major component of quality reform, giving further weight to this question.
The ethical problems raised by P4P are underappreciated and inadequately discussed in the literature, particularly for how rapidly and rampantly these programs are being piloted and implemented. Although the AMA has taken a fairly clear and reasonable stance on the appropriate considerations for P4P programs, it is not clear that payers are incorporating all these concerns. A substantial number of hospitalist groups receive payments from medical groups or hospitals, which in turn are already involved in P4P for some diagnoses.
All hospitalists should read and familiarize themselves with these guidelines and carefully assess the implications of forthcoming P4P proposals for their own practices and patients. On a larger scale, SHM and its membership should strongly consider taking the lead in defining appropriate processes and outcomes for hospital care that incorporate these ethical concerns and allow for meaningful conclusions regarding both quality of care and opportunities for improvement.
Dr. Harte works at the Cleveland Clinic, and Dr. Rajput works at the Robert Wood Johnson Medical School, Camden, N.J. The authors wish to thank Tom Baudendistel and Donald Krause for their review and suggestions.
References
- Asch SM, Kerr EA, Keesey J, et al. Who is at greatest risk for receiving poor-quality health care? N Engl J Med. 2006 Mar 16;354:1147-1156.
- American Medical Association. Pay-for-performance principles and guidelines. Accessible at: www.ama-assn.org/meetings/public/annual05/bot5a05.doc. Last accessed September 13, 2006.
- American Medical Association. CEJA 3-1-05 Report, July 2006. Available at: www.ama-assn.org/ama/pub/category/4325.html. Last accessed September 13, 2006.
- Morreim EH. Result-based compensation in health care: a good, but limited, idea. J Law Med Ethics. 2001 Summer;29(2):174-181.
- Werner RM, Asch DA. The unintended consequences of publicly reporting quality information. JAMA. 2005 Mar 9;293:1239-1244.
- Lindenauer PK, Pekow P, Gao S, et al. Quality of care for patients hospitalized for acute exacerbations of chronic obstructive pulmonary disease. Ann Intern Med. 2006;144(12):894-903.
- Walter LC, Davidowitz NP, Heineken PA, et al. Pitfalls of converting practice guidelines into quality measures: lessons learned from a VA performance measure. JAMA. 2004 May 26;291(20):2466-2470.
- Boyd CM, Darer J, Boult C, et al. Clinical practice guidelines and quality of care for older patients with multiple comorbid diseases: implications for pay for performance. JAMA. 2005 Aug 10;294(6):716-724.
In the not-too-distant future, a multiphysician hospitalist group is a participant in a pay-for-performance (P4P) program. Dr. Buchmann, the group’s lead hospitalist, is confronted by his hospital’s administration and informed that his doctors are performing below regional benchmarks for standards of care for community-acquired pneumonia, and, in fact, the hospital as a whole is below the mean performance levels.
The hospital threatens to break its contract with Dr. Buchmann’s group despite his response that his group sees a far more complex population than these standards can account for—and besides, his group has implemented a number of important quality initiatives in other diseases that are not part of the P4P program.
Several of the group’s hospitalists state that they will stop seeing indigent patients and will no longer take referrals for high-risk patients. Another partner feels it is unethical to continue treating pneumonia patients at the hospital without informing them of these quality findings and at least offering the option of transfer to a facility with better scores. Dr. Buchmann finds all these propositions unsettling.
While these physicians’ responses may sound extreme, the behavior of physicians caught between the hammer of financial survival and the anvil of professional ethics is unpredictable. Medicare and other payers have been implementing P4P plans as the latest attempt to stimulate quality reform. There are dozens of P4P-based programs operating in the United States, and the financial implications are daunting. Further, P4P is taking hold despite a relative paucity of research regarding its effectiveness in improving outcomes.
The underlying rationale of P4P is the use of economic incentives to stimulate changes in provider behavior. Recent work from the RAND Corporation suggests that as much as one-half of healthcare is not based on “accepted” best practices.1 And with increasing attention on the role of errors in medical practice, any effort to improve care seems, on its surface, laudable.
In general, key elements of P4P programs include a set of performance measures, the collection of data, comparison of provider data with benchmarks, and rewards for physicians who meet or exceed those targets. The interface between economic and financial incentives requires physicians to ensure that their behavior is in line with ethical and professional standards. While journals of medicine, law, and business contain many articles devoted to the policy and market implications of P4P, there is surprisingly little discussion in the literature regarding the potential ethical challenges that physicians may face in these programs.
For hospitalists (and other physicians), P4P may present several troubling ethical issues. Because the current scope of P4P is limited to a few diseases, widespread implementation might lead to relative neglect of patients with other illnesses. Higher-risk patients might be avoided, and individual patient concerns might become subjugated to population performance measures. Hospitalists could face the additional conflict of being accountable to (and/or dependent upon) hospitals, which feel P4P pressures of their own. A final issue is the question of whether shared decision-making and patient-centered care mandate disclosure of non-public quality data to patients.
The American Medical Association (AMA) has a policy that specifically addresses P4P.2 Its “Pay-for-Performance Principles and Guidelines” call for physician participation in P4P to be voluntary and to allow physicians to access their ratings for potential appeal prior to wider release. The policy insists that quality of care be paramount over cost savings and that the physician-patient relationship be preserved. Of course, P4P programs may not share the AMA’s ethical concerns and are not bound to consider them.
Of particular concern—for both inpatient and outpatient physicians—is the fate of high-risk and unassigned patients. According to SHM’s 2005-2006 “Bi-Annual Survey on the State of the Hospital Medicine Movement” (www.hospital medicine.org), 96% of hospitalists are involved in the care of unassigned patients, and, in general, one of the strengths of hospital-based physicians should be their relative familiarity with the acute problems of patients who are older and of those with concomitant morbidities. Yet these are precisely the patient groups that are not well served by typical P4P measurements.
The potential for P4P incentives to create disparities in patient care among different patient groups and diseases is one of the prime concerns in the Council on Ethical and Judicial Affairs’ recent opinion for the AMA on P4P programs.3 The care of older patients, for instance, because of their own choices and due to frequency of comorbidities, may well come up short in performance measures designed for individuals who have a single disease.
This is not just a policy problem because P4P is not only unlikely to adequately address the ethical concerns of equitable care to these groups, it could exacerbate the vulnerability of these populations by creating a disincentive to provide care.4 A recent publication describing reports of cardiac surgeons turning away high-risk patients after “CABG report cards” became publicly available suggests that when given the option at least some physicians may indeed change their behavior when quality information is being collected and reported.5 Ironically, a system that incentivizes doctors to avoid the highest-risk patients could worsen—rather than improve—the overall quality of care.
Hospitalists may not be as sensitive to these pressures as surgeons or outpatient physicians, especially given the hospitalist’s limited flexibility in “choosing” patients. Care of unassigned patients may be a contractual obligation for which a hospitalist is paid by the hospital (which may face its own pressures in this area). And lower-risk referrals from outpatient physicians may “compensate” for the occasional complex patient.
Hospitalists are generally “need-based” practitioners who legally and ethically may not have the option to refuse care without risking patient abandonment. Yet the fact that hospitalists take on such patients may make their performance scores inferior to even non-hospital-based doctors—a difficult position to be in if one’s group receives payments from the hospital with an expectation of superior performance. Hospitalists in particular must consider whether or not insurance companies and the Centers for Medicare and Medicaid Services (CMS) could really accommodate all possible confounders in a risk-adjustment model to offset the nature of their patients. While the ethical choice might be for hospitalists simply to refuse to participate in P4P, citing multiple conflicts of interest, there is no clear indication regarding how “optional” these programs will be as they become increasingly prevalent, presenting yet another ethical issue.
Further, Medicare’s current P4P system for hospitals is directed at just five conditions, only two of which (congestive heart failure and pneumonia) are likely to fall within a hospitalist’s realm. But the list of common diagnoses under the hospitalist’s umbrella is, of course, much larger, including thromboembolism, pyelonephritis, COPD, cirrhosis, and sepsis. The data that exists for compliance with recommended care for some of these conditions (e.g., COPD) suggests that there may be substantial variability.6
But if hospitals base their support for hospitalist programs on their performance within a few CMS diagnoses, the effect on care for and development of appropriate guidelines and resources toward many other conditions may suffer. Already, hospital discharge forms are pre-printed with checkboxes for an angiotensin-converting enzyme (ACE) inhibitor prescription for congestive heart failure and counseling for smoking cessation. The (unethical) implication is that some diagnoses are more valuable than others, and that physician energies may be inequitably distributed—whether consciously or not. It is difficult to see how P4P could encompass standards for every patient condition, or how hospitals and providers could avoid focusing resources on those conditions that are more closely scrutinized by their payers.
Another issue arises if patient autonomy dictates that a treatment plan has to deviate from established guidelines; in such a case, hospitalists and other physicians may be forced to provide a care plan that is entirely reasonable from a medical standpoint but counts against them when compared with a benchmark. Ethical principles dictate that patient care be given priority, but unless consideration is made within the scoring system, performance measures that do not accommodate the ethical mandates to respect patient wishes or physician judgment are substantial pitfalls in the pursuit of better quality.7,8
One last issue concerns the question of whether or not providers have an obligation to disclose quality data to patients in the context of shared decision-making. This is a murky subject that involves determining the boundaries between the best means of pursuing quality improvement and the ethics of patient advocacy. The AMA’s Code of Medical Ethics states, “Patients should receive guidance from their physicians as to the optimal course of action,” and the issue of competence and responsibility to the care of the individual patient is the focus of several of the Principles of Medical Ethics. However, there is practically nothing published regarding the ethics, implications, or results of such disclosure, presumably because the availability of large amounts of quality-based data is such a new phenomenon and the considerations of such disclosure are so uncomfortable for many physicians.
Of course, some information—“CABG report cards,” for instance—is publicly available, but the evidence that patients actually utilize this information to a significant extent or that quality has improved due to its use is mixed.5 The question of whether an obligation exists to disclose non-public information when a provider knows that there is a question about performance relative to a benchmark or comparative peer group is uncharted water, ethically speaking; the issue is further complicated by the fact that appraisal of quality is far from a perfect science. It may be that the benefits of P4P result primarily from transparency, rather than from financial incentives. If so, disclosure may be the major component of quality reform, giving further weight to this question.
The ethical problems raised by P4P are underappreciated and inadequately discussed in the literature, particularly for how rapidly and rampantly these programs are being piloted and implemented. Although the AMA has taken a fairly clear and reasonable stance on the appropriate considerations for P4P programs, it is not clear that payers are incorporating all these concerns. A substantial number of hospitalist groups receive payments from medical groups or hospitals, which in turn are already involved in P4P for some diagnoses.
All hospitalists should read and familiarize themselves with these guidelines and carefully assess the implications of forthcoming P4P proposals for their own practices and patients. On a larger scale, SHM and its membership should strongly consider taking the lead in defining appropriate processes and outcomes for hospital care that incorporate these ethical concerns and allow for meaningful conclusions regarding both quality of care and opportunities for improvement.
Dr. Harte works at the Cleveland Clinic, and Dr. Rajput works at the Robert Wood Johnson Medical School, Camden, N.J. The authors wish to thank Tom Baudendistel and Donald Krause for their review and suggestions.
References
- Asch SM, Kerr EA, Keesey J, et al. Who is at greatest risk for receiving poor-quality health care? N Engl J Med. 2006 Mar 16;354:1147-1156.
- American Medical Association. Pay-for-performance principles and guidelines. Accessible at: www.ama-assn.org/meetings/public/annual05/bot5a05.doc. Last accessed September 13, 2006.
- American Medical Association. CEJA 3-1-05 Report, July 2006. Available at: www.ama-assn.org/ama/pub/category/4325.html. Last accessed September 13, 2006.
- Morreim EH. Result-based compensation in health care: a good, but limited, idea. J Law Med Ethics. 2001 Summer;29(2):174-181.
- Werner RM, Asch DA. The unintended consequences of publicly reporting quality information. JAMA. 2005 Mar 9;293:1239-1244.
- Lindenauer PK, Pekow P, Gao S, et al. Quality of care for patients hospitalized for acute exacerbations of chronic obstructive pulmonary disease. Ann Intern Med. 2006;144(12):894-903.
- Walter LC, Davidowitz NP, Heineken PA, et al. Pitfalls of converting practice guidelines into quality measures: lessons learned from a VA performance measure. JAMA. 2004 May 26;291(20):2466-2470.
- Boyd CM, Darer J, Boult C, et al. Clinical practice guidelines and quality of care for older patients with multiple comorbid diseases: implications for pay for performance. JAMA. 2005 Aug 10;294(6):716-724.
Doctors of the American Frontier

Discussions of the mid-19th century American physician often conjure up images of the surgeons of the Civil War who tirelessly plied their trade during battle: “During the rest of the night and early morning, he [amputated] arms below the elbow and legs below the knee in less than five minutes. The deep incision … the sweeping cut … pull back the soft parts to expose the bone … saw swiftly.”1
However, in the same period but some thousand miles west, frontier physicians faced similar battle wounds sustained in campaigns against American Indians, as well as a myriad of other duties. Some frontier physicians met these challenges with remarkable ingenuity, while others resorted to treatments later deemed quackery. They often practiced alone in the wilderness without a hospital or colleagues for support.
The first and most obvious task of a military physician on the frontier was to attend to soldiers wounded during battle. The first hurdle was reaching the soldier. In 1874, Surgeon George Miller Sternberg faced daunting challenges in aiding seriously wounded soldiers of General Oliver Otis Howard’s company after a melee with Chief Joseph’s Nez Percé tribe. As dark settled across Clearwater River, Idaho, “Surgeon George Miller Sternberg and an aide crawled out onto the battlefield looking for the wounded. They crept so close to the enemy that they could hear the Indians talking.”1 Dr. Sternberg worked tirelessly throughout the night ligating pulsing arteries and soothing the suffering soldiers with whatever means he had, from opium balls to whiskey. During the course of the evening, an American Indian sentinel spotted Dr. Sternberg’s lantern and shot it out, forcing Dr. Sternberg to continue his treatment in darkness.
In other conflicts, the frontier physician often found himself an active participant in a battle. In the Battle of the Lava Beds fought in Oregon in 1873, Dr. George Martin Kober received a gunshot wound in the arm during the course of the battle. Despite his wound he continued to “treat the wounded before he allowed Dr. Skinner to come to his relief.”1
In the Battle of Bates Creek, fought in the summer of 1874, Dr. Thomas Maghee “was the object of the direct fire of an Indian. Until, laying down his instruments for a moment, he took his carbine and killed the Indian and then returned quietly to his work.”1
When the battle concluded and the soldiers returned to camp, the physicians began to wage a fierce war with disease. Among the plagues that stalked the camps: cholera, scurvy, yellow fever, tuberculosis, and typhoid fever. On one occasion in 1874 cholera struck in the heat of the summer at Fort Riley in Kansas. The pestilence devastated the fort by swiftly taking the lives of dozens of soldiers and compelling a hundred more to desert the fort in fear. One ignorant physician attempted in vain to combat the disease by “burning barrels of pine tar beneath the open windows of the fort hospital.”1
Eventually, Dr. Sternberg conquered the outbreak by implementing a strict disinfection and isolation campaign. In the battle against scurvy, military physicians noted that the typical diet of “meat, white bread, soda biscuits, syrup, lard, and black coffee” was insufficient and often attempted to plant and harvest their own supply of vegetables to treat the vitamin C-deficient soldiers.1
The frontier physician’s duties often expanded outside of the realms of medicine because “by order of the Secretary of War they also studied weather, geography, plants, fauna, Indian customs, and antiquities.”1 In fulfilling these duties, physicians made remarkable contributions to the preservation of the history of the American West, such as Dr. James Kimball’s purchase of the autobiography of Sitting Bull. Indeed, life as a military physician on the American frontier tested the courage, durability, and ingenuity of the early American doctor. TH
John Bois is a second-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.
Reference
- Dunlop R. Doctors of the American Frontier. Garden City, New York: Doubleday & Company; 1965: 73.
Discussions of the mid-19th century American physician often conjure up images of the surgeons of the Civil War who tirelessly plied their trade during battle: “During the rest of the night and early morning, he [amputated] arms below the elbow and legs below the knee in less than five minutes. The deep incision … the sweeping cut … pull back the soft parts to expose the bone … saw swiftly.”1
However, in the same period but some thousand miles west, frontier physicians faced similar battle wounds sustained in campaigns against American Indians, as well as a myriad of other duties. Some frontier physicians met these challenges with remarkable ingenuity, while others resorted to treatments later deemed quackery. They often practiced alone in the wilderness without a hospital or colleagues for support.
The first and most obvious task of a military physician on the frontier was to attend to soldiers wounded during battle. The first hurdle was reaching the soldier. In 1874, Surgeon George Miller Sternberg faced daunting challenges in aiding seriously wounded soldiers of General Oliver Otis Howard’s company after a melee with Chief Joseph’s Nez Percé tribe. As dark settled across Clearwater River, Idaho, “Surgeon George Miller Sternberg and an aide crawled out onto the battlefield looking for the wounded. They crept so close to the enemy that they could hear the Indians talking.”1 Dr. Sternberg worked tirelessly throughout the night ligating pulsing arteries and soothing the suffering soldiers with whatever means he had, from opium balls to whiskey. During the course of the evening, an American Indian sentinel spotted Dr. Sternberg’s lantern and shot it out, forcing Dr. Sternberg to continue his treatment in darkness.
In other conflicts, the frontier physician often found himself an active participant in a battle. In the Battle of the Lava Beds fought in Oregon in 1873, Dr. George Martin Kober received a gunshot wound in the arm during the course of the battle. Despite his wound he continued to “treat the wounded before he allowed Dr. Skinner to come to his relief.”1
In the Battle of Bates Creek, fought in the summer of 1874, Dr. Thomas Maghee “was the object of the direct fire of an Indian. Until, laying down his instruments for a moment, he took his carbine and killed the Indian and then returned quietly to his work.”1
When the battle concluded and the soldiers returned to camp, the physicians began to wage a fierce war with disease. Among the plagues that stalked the camps: cholera, scurvy, yellow fever, tuberculosis, and typhoid fever. On one occasion in 1874 cholera struck in the heat of the summer at Fort Riley in Kansas. The pestilence devastated the fort by swiftly taking the lives of dozens of soldiers and compelling a hundred more to desert the fort in fear. One ignorant physician attempted in vain to combat the disease by “burning barrels of pine tar beneath the open windows of the fort hospital.”1
Eventually, Dr. Sternberg conquered the outbreak by implementing a strict disinfection and isolation campaign. In the battle against scurvy, military physicians noted that the typical diet of “meat, white bread, soda biscuits, syrup, lard, and black coffee” was insufficient and often attempted to plant and harvest their own supply of vegetables to treat the vitamin C-deficient soldiers.1
The frontier physician’s duties often expanded outside of the realms of medicine because “by order of the Secretary of War they also studied weather, geography, plants, fauna, Indian customs, and antiquities.”1 In fulfilling these duties, physicians made remarkable contributions to the preservation of the history of the American West, such as Dr. James Kimball’s purchase of the autobiography of Sitting Bull. Indeed, life as a military physician on the American frontier tested the courage, durability, and ingenuity of the early American doctor. TH
John Bois is a second-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.
Reference
- Dunlop R. Doctors of the American Frontier. Garden City, New York: Doubleday & Company; 1965: 73.
Discussions of the mid-19th century American physician often conjure up images of the surgeons of the Civil War who tirelessly plied their trade during battle: “During the rest of the night and early morning, he [amputated] arms below the elbow and legs below the knee in less than five minutes. The deep incision … the sweeping cut … pull back the soft parts to expose the bone … saw swiftly.”1
However, in the same period but some thousand miles west, frontier physicians faced similar battle wounds sustained in campaigns against American Indians, as well as a myriad of other duties. Some frontier physicians met these challenges with remarkable ingenuity, while others resorted to treatments later deemed quackery. They often practiced alone in the wilderness without a hospital or colleagues for support.
The first and most obvious task of a military physician on the frontier was to attend to soldiers wounded during battle. The first hurdle was reaching the soldier. In 1874, Surgeon George Miller Sternberg faced daunting challenges in aiding seriously wounded soldiers of General Oliver Otis Howard’s company after a melee with Chief Joseph’s Nez Percé tribe. As dark settled across Clearwater River, Idaho, “Surgeon George Miller Sternberg and an aide crawled out onto the battlefield looking for the wounded. They crept so close to the enemy that they could hear the Indians talking.”1 Dr. Sternberg worked tirelessly throughout the night ligating pulsing arteries and soothing the suffering soldiers with whatever means he had, from opium balls to whiskey. During the course of the evening, an American Indian sentinel spotted Dr. Sternberg’s lantern and shot it out, forcing Dr. Sternberg to continue his treatment in darkness.
In other conflicts, the frontier physician often found himself an active participant in a battle. In the Battle of the Lava Beds fought in Oregon in 1873, Dr. George Martin Kober received a gunshot wound in the arm during the course of the battle. Despite his wound he continued to “treat the wounded before he allowed Dr. Skinner to come to his relief.”1
In the Battle of Bates Creek, fought in the summer of 1874, Dr. Thomas Maghee “was the object of the direct fire of an Indian. Until, laying down his instruments for a moment, he took his carbine and killed the Indian and then returned quietly to his work.”1
When the battle concluded and the soldiers returned to camp, the physicians began to wage a fierce war with disease. Among the plagues that stalked the camps: cholera, scurvy, yellow fever, tuberculosis, and typhoid fever. On one occasion in 1874 cholera struck in the heat of the summer at Fort Riley in Kansas. The pestilence devastated the fort by swiftly taking the lives of dozens of soldiers and compelling a hundred more to desert the fort in fear. One ignorant physician attempted in vain to combat the disease by “burning barrels of pine tar beneath the open windows of the fort hospital.”1
Eventually, Dr. Sternberg conquered the outbreak by implementing a strict disinfection and isolation campaign. In the battle against scurvy, military physicians noted that the typical diet of “meat, white bread, soda biscuits, syrup, lard, and black coffee” was insufficient and often attempted to plant and harvest their own supply of vegetables to treat the vitamin C-deficient soldiers.1
The frontier physician’s duties often expanded outside of the realms of medicine because “by order of the Secretary of War they also studied weather, geography, plants, fauna, Indian customs, and antiquities.”1 In fulfilling these duties, physicians made remarkable contributions to the preservation of the history of the American West, such as Dr. James Kimball’s purchase of the autobiography of Sitting Bull. Indeed, life as a military physician on the American frontier tested the courage, durability, and ingenuity of the early American doctor. TH
John Bois is a second-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.
Reference
- Dunlop R. Doctors of the American Frontier. Garden City, New York: Doubleday & Company; 1965: 73.
Rash Judgement
A 38-year-old, healthy, incarcerated, African-American man presented with a one-and-a-half year history of an eruption in his axillae. The patient stated that the “rash” worsened with sweating but the lesions were otherwise asymptomatic.
Corticosteroid creams, antifungal creams, and oral antibiotics had not led to any improvement. The eruption progressed to involve his trunk, arms, and face. The skin exam showed hyperpigmented, firm plaques with erythematous papules in the axillae. The plaques were also present on the chest, back, and upper extremities. Verrucous papules were noted on the flexural areas of upper extremities as well as tan colored plaques at the lateral canthi of eyes. (See Figures 1-3 this page.)
CBC and serum electrolytes were normal. Lipid panel showed a cholesterol of 593 mg/dL, triglycerides 106 mg/dL, high density lipoprotein of 37 g/dL, low density lipoprotein of 535 mg/dL, and very low density lipoprotein of 21 mg/dL. A biopsy from the axilla and the umbilical area were sent for histologic examination. (See Figure 4 this page.)



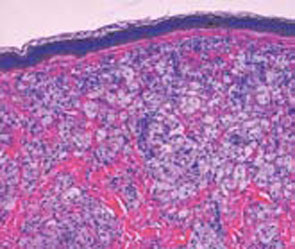
What is this patient’s most likely diagnosis?
- Sarcoidosis
- Disseminated xanthomas
- Xanthoma disseminatum
- Erythema elevatum diutinum
- Necrobiosis lipoidica
Discussion
The answer is B: disseminated xanthomas. Punch biopsy from the axilla and shave biopsy from the periumbilical area both revealed localized infiltrates of lipid containing macrophages.
Xanthomas develop due to accumulation of lipid-filled macrophages and suggest an underlying disorder of lipid metabolism. Morbidity and mortality are primarily related to atherosclerosis (e.g., coronary artery disease) and pancreatitis, which occur secondarily to the increased lipid levels rather than the xanthoma itself.
In general, four clinical types of xanthomas exist: tendinous, planar, tuberous, and eruptive. A particular diagnosis cannot necessarily be made on the basis of clinical signs; however, certain types of xanthomas are more characteristic of specific hyperlipidemias. Eruptive xanthomas are found in the setting of primary or secondary hypertriglyeridemia. Tuberous xanthomas have both elevated serum cholesterol and triglycerides. This patient had plane xanthomas and xanthelasma and was especially notable for intertriginous plane xanthomas, which can be pathognomonic for homozygous familial hypercholesterolemia.
This patient’s histology from both the periumbilical area and the axilla depict the characteristic presence of vacuolated macrophages (foamy macrophages) to confirm the diagnosis as disseminated xanthoma.1-3 Sarcoidosis is a chronic idiopathic disorder characterized by noncaseating granulomas that can affect any organ system. Cutaneous sarcoidosis typically presents as asymptomatic, red-brown macules and papules affecting the face, periorbital areas, nasolabial folds, and/or extensor surfaces. Typical sarcoid lesions are characterized by the presence of circumscribed granulomas of epithelioid cells with little or no necrosis. The granulomas are characteristically referred to as “naked” due to the sparse lymphocytic infiltrate at the margins.
This patient’s histologic exam did not reveal any granulomas and localized infiltrates of lipid containing macrophages make the diagnosis of cutaneous sarcoidosis unlikely.4,5
Necrobiosis lipoidica (NL) is a cutaneous disorder that is often, but not always, associated with diabetes mellitus. NL is a disorder of collagen degeneration with a granulomatous response, thickening of blood vessel walls, and fat deposition. Patients usually present with asymptomatic shiny patches that slowly enlarge over months to years. The patient’s main complaint is the unsightly cosmetic appearance of the lesions.
Skin lesions of classic NL begin as 1- to 3-mm well-circumscribed papules or nodules that expand with an active border to become waxy, atrophic, round plaques centrally. Initially, these plaques are red-brown in color but progressively become more yellow and atrophic in appearance. Most cases of NL occur on the pretibial area, but cases have been reported on the face, scalp, trunk, and upper extremities where the diagnosis is more likely to be missed.
Although this patient’s mother had diabetes, his fasting blood glucose was well within normal limits (71 mg/dL). Histologically NL displays sclerotic collagen and obliteration of the bundle pattern, with interstitial and palisaded granulomas that involve the subcutaneous tissue and dermis. Fat containing foam cells are often present.
Although our patient’s biopsy showed fat containing foam cells, it did not have the interstitial granulomas or the sclerotic collagen. In addition, the lack of diabetes makes this diagnosis less likely.6,7
Erythema elevatum diutinum (EED) is a rare type of leukocytoclastic vasculitis characterized by red, purple, brown, or yellow papules, plaques, or nodules. These lesions are usually distributed on the extensor surfaces of the body. The lesions are usually asymptomatic but can be associated occasionally with joint pain. Clinical studies show a preference for the extensor surfaces of the hands, the wrists, the elbows, the ankles, the Achilles’ tendons, the fingers, and the toes. The buttocks, the face, and the ears as well as the palms, the soles, the legs, the forearms, and the genitals may be involved; however, the trunk is usually spared. EED is a type of necrotizing vasculitis.
In its early stages, there are no specific histologic findings that can be used to single out the diagnosis of EED from other leukocytoclastic diseases. Although the distribution and lack of symptomatology in EED is reminiscent of our patient, this patient’s lesions were more often found in the flexural areas rather than extensors. In addition, there was no necrotizing vasculitis on histology, which precludes this rare diagnosis of EED.8
Xanthoma disseminatum (XD) is a rare, benign, proliferative disorder in children and young adults characterized by xanthomatous lesions especially in the flexural folds and eyelids. Although it sounds like a disorder of lipid metabolism, it is actually a histiocytic disorder that is not associated with lipoprotein abnormalities and patients are normolipemic. Histologically, it shows mononuclear phagocyte proliferation with Touton giant cells and CD68 positivity on immunophenotyping. It is unlikely that this patient has XD despite the appropriate clinical presentation because histologically all that is found are foam cells. In addition, the patient had a definite lipoprotein abnormality while XD patients are normolipemic.9 TH
References
- Cruz PD, East C, Bergstresser P. Dermal, subcutaneous, and tendon xanthomas: diagnostic markers for specific lipoprotein disorders. J Am Acad Dermatol 1988 Jul;19(1 pt 1):95-111.
- Massengale WT, Nesbitt LT. Xanthomas. In: Bolognia JL, Jorrizo JL, Rapini RP, eds. Dermatology. Vol. 2. London: Mosby; 2003:1447-1454.
- Parker F. Xanthomas and hyperlipidemias. J Am Acad Dermatol. 1985 Jul;13 (1):1-30.
- Young RJ, 3rd, Gilson RT, Yanase D, et al. Cutaneous sarcoidosis. Int J Dermatol. 2001;40:249-253.
- English JC, Patel PJ, Greer KE. Sarcoidosis. J Am Acad Dermatol. 2001;44:725-743: quiz 744-746.
- Fitzpatrick TB, Johnson R, Wolff K, et al. Genetic, metabolic, endocrine and nutritional diseases. Color Atlas and Synopsis of Clinical Dermatology, Common and Serious Diseases. New York: McGraw-Hill; 2001:415-416.
- Lowitt MH, Dover JS. Necrobiosis lipoidica. J Am Acad Dermatol. 1991; 25:735-748.
- Yiannias JA, el-Azhary RA, Gibson LE. Erythema elevatum diutinum: a clinical and histopathologic study of 13 patients. J Am Acad Dermatol 1992 Jan;26(1):38-44.
- Alexander AS, Turner R, Uniate L, et al. Xanthoma disseminatum: a case report and literature review. Br J Radiol 2005 Feb;78(926):153-157.
A 38-year-old, healthy, incarcerated, African-American man presented with a one-and-a-half year history of an eruption in his axillae. The patient stated that the “rash” worsened with sweating but the lesions were otherwise asymptomatic.
Corticosteroid creams, antifungal creams, and oral antibiotics had not led to any improvement. The eruption progressed to involve his trunk, arms, and face. The skin exam showed hyperpigmented, firm plaques with erythematous papules in the axillae. The plaques were also present on the chest, back, and upper extremities. Verrucous papules were noted on the flexural areas of upper extremities as well as tan colored plaques at the lateral canthi of eyes. (See Figures 1-3 this page.)
CBC and serum electrolytes were normal. Lipid panel showed a cholesterol of 593 mg/dL, triglycerides 106 mg/dL, high density lipoprotein of 37 g/dL, low density lipoprotein of 535 mg/dL, and very low density lipoprotein of 21 mg/dL. A biopsy from the axilla and the umbilical area were sent for histologic examination. (See Figure 4 this page.)
What is this patient’s most likely diagnosis?
- Sarcoidosis
- Disseminated xanthomas
- Xanthoma disseminatum
- Erythema elevatum diutinum
- Necrobiosis lipoidica
Discussion
The answer is B: disseminated xanthomas. Punch biopsy from the axilla and shave biopsy from the periumbilical area both revealed localized infiltrates of lipid containing macrophages.
Xanthomas develop due to accumulation of lipid-filled macrophages and suggest an underlying disorder of lipid metabolism. Morbidity and mortality are primarily related to atherosclerosis (e.g., coronary artery disease) and pancreatitis, which occur secondarily to the increased lipid levels rather than the xanthoma itself.
In general, four clinical types of xanthomas exist: tendinous, planar, tuberous, and eruptive. A particular diagnosis cannot necessarily be made on the basis of clinical signs; however, certain types of xanthomas are more characteristic of specific hyperlipidemias. Eruptive xanthomas are found in the setting of primary or secondary hypertriglyeridemia. Tuberous xanthomas have both elevated serum cholesterol and triglycerides. This patient had plane xanthomas and xanthelasma and was especially notable for intertriginous plane xanthomas, which can be pathognomonic for homozygous familial hypercholesterolemia.
This patient’s histology from both the periumbilical area and the axilla depict the characteristic presence of vacuolated macrophages (foamy macrophages) to confirm the diagnosis as disseminated xanthoma.1-3 Sarcoidosis is a chronic idiopathic disorder characterized by noncaseating granulomas that can affect any organ system. Cutaneous sarcoidosis typically presents as asymptomatic, red-brown macules and papules affecting the face, periorbital areas, nasolabial folds, and/or extensor surfaces. Typical sarcoid lesions are characterized by the presence of circumscribed granulomas of epithelioid cells with little or no necrosis. The granulomas are characteristically referred to as “naked” due to the sparse lymphocytic infiltrate at the margins.
This patient’s histologic exam did not reveal any granulomas and localized infiltrates of lipid containing macrophages make the diagnosis of cutaneous sarcoidosis unlikely.4,5
Necrobiosis lipoidica (NL) is a cutaneous disorder that is often, but not always, associated with diabetes mellitus. NL is a disorder of collagen degeneration with a granulomatous response, thickening of blood vessel walls, and fat deposition. Patients usually present with asymptomatic shiny patches that slowly enlarge over months to years. The patient’s main complaint is the unsightly cosmetic appearance of the lesions.
Skin lesions of classic NL begin as 1- to 3-mm well-circumscribed papules or nodules that expand with an active border to become waxy, atrophic, round plaques centrally. Initially, these plaques are red-brown in color but progressively become more yellow and atrophic in appearance. Most cases of NL occur on the pretibial area, but cases have been reported on the face, scalp, trunk, and upper extremities where the diagnosis is more likely to be missed.
Although this patient’s mother had diabetes, his fasting blood glucose was well within normal limits (71 mg/dL). Histologically NL displays sclerotic collagen and obliteration of the bundle pattern, with interstitial and palisaded granulomas that involve the subcutaneous tissue and dermis. Fat containing foam cells are often present.
Although our patient’s biopsy showed fat containing foam cells, it did not have the interstitial granulomas or the sclerotic collagen. In addition, the lack of diabetes makes this diagnosis less likely.6,7
Erythema elevatum diutinum (EED) is a rare type of leukocytoclastic vasculitis characterized by red, purple, brown, or yellow papules, plaques, or nodules. These lesions are usually distributed on the extensor surfaces of the body. The lesions are usually asymptomatic but can be associated occasionally with joint pain. Clinical studies show a preference for the extensor surfaces of the hands, the wrists, the elbows, the ankles, the Achilles’ tendons, the fingers, and the toes. The buttocks, the face, and the ears as well as the palms, the soles, the legs, the forearms, and the genitals may be involved; however, the trunk is usually spared. EED is a type of necrotizing vasculitis.
In its early stages, there are no specific histologic findings that can be used to single out the diagnosis of EED from other leukocytoclastic diseases. Although the distribution and lack of symptomatology in EED is reminiscent of our patient, this patient’s lesions were more often found in the flexural areas rather than extensors. In addition, there was no necrotizing vasculitis on histology, which precludes this rare diagnosis of EED.8
Xanthoma disseminatum (XD) is a rare, benign, proliferative disorder in children and young adults characterized by xanthomatous lesions especially in the flexural folds and eyelids. Although it sounds like a disorder of lipid metabolism, it is actually a histiocytic disorder that is not associated with lipoprotein abnormalities and patients are normolipemic. Histologically, it shows mononuclear phagocyte proliferation with Touton giant cells and CD68 positivity on immunophenotyping. It is unlikely that this patient has XD despite the appropriate clinical presentation because histologically all that is found are foam cells. In addition, the patient had a definite lipoprotein abnormality while XD patients are normolipemic.9 TH
References
- Cruz PD, East C, Bergstresser P. Dermal, subcutaneous, and tendon xanthomas: diagnostic markers for specific lipoprotein disorders. J Am Acad Dermatol 1988 Jul;19(1 pt 1):95-111.
- Massengale WT, Nesbitt LT. Xanthomas. In: Bolognia JL, Jorrizo JL, Rapini RP, eds. Dermatology. Vol. 2. London: Mosby; 2003:1447-1454.
- Parker F. Xanthomas and hyperlipidemias. J Am Acad Dermatol. 1985 Jul;13 (1):1-30.
- Young RJ, 3rd, Gilson RT, Yanase D, et al. Cutaneous sarcoidosis. Int J Dermatol. 2001;40:249-253.
- English JC, Patel PJ, Greer KE. Sarcoidosis. J Am Acad Dermatol. 2001;44:725-743: quiz 744-746.
- Fitzpatrick TB, Johnson R, Wolff K, et al. Genetic, metabolic, endocrine and nutritional diseases. Color Atlas and Synopsis of Clinical Dermatology, Common and Serious Diseases. New York: McGraw-Hill; 2001:415-416.
- Lowitt MH, Dover JS. Necrobiosis lipoidica. J Am Acad Dermatol. 1991; 25:735-748.
- Yiannias JA, el-Azhary RA, Gibson LE. Erythema elevatum diutinum: a clinical and histopathologic study of 13 patients. J Am Acad Dermatol 1992 Jan;26(1):38-44.
- Alexander AS, Turner R, Uniate L, et al. Xanthoma disseminatum: a case report and literature review. Br J Radiol 2005 Feb;78(926):153-157.
A 38-year-old, healthy, incarcerated, African-American man presented with a one-and-a-half year history of an eruption in his axillae. The patient stated that the “rash” worsened with sweating but the lesions were otherwise asymptomatic.
Corticosteroid creams, antifungal creams, and oral antibiotics had not led to any improvement. The eruption progressed to involve his trunk, arms, and face. The skin exam showed hyperpigmented, firm plaques with erythematous papules in the axillae. The plaques were also present on the chest, back, and upper extremities. Verrucous papules were noted on the flexural areas of upper extremities as well as tan colored plaques at the lateral canthi of eyes. (See Figures 1-3 this page.)
CBC and serum electrolytes were normal. Lipid panel showed a cholesterol of 593 mg/dL, triglycerides 106 mg/dL, high density lipoprotein of 37 g/dL, low density lipoprotein of 535 mg/dL, and very low density lipoprotein of 21 mg/dL. A biopsy from the axilla and the umbilical area were sent for histologic examination. (See Figure 4 this page.)
What is this patient’s most likely diagnosis?
- Sarcoidosis
- Disseminated xanthomas
- Xanthoma disseminatum
- Erythema elevatum diutinum
- Necrobiosis lipoidica
Discussion
The answer is B: disseminated xanthomas. Punch biopsy from the axilla and shave biopsy from the periumbilical area both revealed localized infiltrates of lipid containing macrophages.
Xanthomas develop due to accumulation of lipid-filled macrophages and suggest an underlying disorder of lipid metabolism. Morbidity and mortality are primarily related to atherosclerosis (e.g., coronary artery disease) and pancreatitis, which occur secondarily to the increased lipid levels rather than the xanthoma itself.
In general, four clinical types of xanthomas exist: tendinous, planar, tuberous, and eruptive. A particular diagnosis cannot necessarily be made on the basis of clinical signs; however, certain types of xanthomas are more characteristic of specific hyperlipidemias. Eruptive xanthomas are found in the setting of primary or secondary hypertriglyeridemia. Tuberous xanthomas have both elevated serum cholesterol and triglycerides. This patient had plane xanthomas and xanthelasma and was especially notable for intertriginous plane xanthomas, which can be pathognomonic for homozygous familial hypercholesterolemia.
This patient’s histology from both the periumbilical area and the axilla depict the characteristic presence of vacuolated macrophages (foamy macrophages) to confirm the diagnosis as disseminated xanthoma.1-3 Sarcoidosis is a chronic idiopathic disorder characterized by noncaseating granulomas that can affect any organ system. Cutaneous sarcoidosis typically presents as asymptomatic, red-brown macules and papules affecting the face, periorbital areas, nasolabial folds, and/or extensor surfaces. Typical sarcoid lesions are characterized by the presence of circumscribed granulomas of epithelioid cells with little or no necrosis. The granulomas are characteristically referred to as “naked” due to the sparse lymphocytic infiltrate at the margins.
This patient’s histologic exam did not reveal any granulomas and localized infiltrates of lipid containing macrophages make the diagnosis of cutaneous sarcoidosis unlikely.4,5
Necrobiosis lipoidica (NL) is a cutaneous disorder that is often, but not always, associated with diabetes mellitus. NL is a disorder of collagen degeneration with a granulomatous response, thickening of blood vessel walls, and fat deposition. Patients usually present with asymptomatic shiny patches that slowly enlarge over months to years. The patient’s main complaint is the unsightly cosmetic appearance of the lesions.
Skin lesions of classic NL begin as 1- to 3-mm well-circumscribed papules or nodules that expand with an active border to become waxy, atrophic, round plaques centrally. Initially, these plaques are red-brown in color but progressively become more yellow and atrophic in appearance. Most cases of NL occur on the pretibial area, but cases have been reported on the face, scalp, trunk, and upper extremities where the diagnosis is more likely to be missed.
Although this patient’s mother had diabetes, his fasting blood glucose was well within normal limits (71 mg/dL). Histologically NL displays sclerotic collagen and obliteration of the bundle pattern, with interstitial and palisaded granulomas that involve the subcutaneous tissue and dermis. Fat containing foam cells are often present.
Although our patient’s biopsy showed fat containing foam cells, it did not have the interstitial granulomas or the sclerotic collagen. In addition, the lack of diabetes makes this diagnosis less likely.6,7
Erythema elevatum diutinum (EED) is a rare type of leukocytoclastic vasculitis characterized by red, purple, brown, or yellow papules, plaques, or nodules. These lesions are usually distributed on the extensor surfaces of the body. The lesions are usually asymptomatic but can be associated occasionally with joint pain. Clinical studies show a preference for the extensor surfaces of the hands, the wrists, the elbows, the ankles, the Achilles’ tendons, the fingers, and the toes. The buttocks, the face, and the ears as well as the palms, the soles, the legs, the forearms, and the genitals may be involved; however, the trunk is usually spared. EED is a type of necrotizing vasculitis.
In its early stages, there are no specific histologic findings that can be used to single out the diagnosis of EED from other leukocytoclastic diseases. Although the distribution and lack of symptomatology in EED is reminiscent of our patient, this patient’s lesions were more often found in the flexural areas rather than extensors. In addition, there was no necrotizing vasculitis on histology, which precludes this rare diagnosis of EED.8
Xanthoma disseminatum (XD) is a rare, benign, proliferative disorder in children and young adults characterized by xanthomatous lesions especially in the flexural folds and eyelids. Although it sounds like a disorder of lipid metabolism, it is actually a histiocytic disorder that is not associated with lipoprotein abnormalities and patients are normolipemic. Histologically, it shows mononuclear phagocyte proliferation with Touton giant cells and CD68 positivity on immunophenotyping. It is unlikely that this patient has XD despite the appropriate clinical presentation because histologically all that is found are foam cells. In addition, the patient had a definite lipoprotein abnormality while XD patients are normolipemic.9 TH
References
- Cruz PD, East C, Bergstresser P. Dermal, subcutaneous, and tendon xanthomas: diagnostic markers for specific lipoprotein disorders. J Am Acad Dermatol 1988 Jul;19(1 pt 1):95-111.
- Massengale WT, Nesbitt LT. Xanthomas. In: Bolognia JL, Jorrizo JL, Rapini RP, eds. Dermatology. Vol. 2. London: Mosby; 2003:1447-1454.
- Parker F. Xanthomas and hyperlipidemias. J Am Acad Dermatol. 1985 Jul;13 (1):1-30.
- Young RJ, 3rd, Gilson RT, Yanase D, et al. Cutaneous sarcoidosis. Int J Dermatol. 2001;40:249-253.
- English JC, Patel PJ, Greer KE. Sarcoidosis. J Am Acad Dermatol. 2001;44:725-743: quiz 744-746.
- Fitzpatrick TB, Johnson R, Wolff K, et al. Genetic, metabolic, endocrine and nutritional diseases. Color Atlas and Synopsis of Clinical Dermatology, Common and Serious Diseases. New York: McGraw-Hill; 2001:415-416.
- Lowitt MH, Dover JS. Necrobiosis lipoidica. J Am Acad Dermatol. 1991; 25:735-748.
- Yiannias JA, el-Azhary RA, Gibson LE. Erythema elevatum diutinum: a clinical and histopathologic study of 13 patients. J Am Acad Dermatol 1992 Jan;26(1):38-44.
- Alexander AS, Turner R, Uniate L, et al. Xanthoma disseminatum: a case report and literature review. Br J Radiol 2005 Feb;78(926):153-157.
Shift Perspectives
The shifts worked by a hospital medicine group can reflect its values or simply ensure adequate coverage. Either way, the shifts your group assigns can play a significant role in recruiting new hospitalists and retaining those you have. And there may be more scheduling options than you have considered.
The Most Attractive Shift Debunked
Many new hospitalists seek as much time off as possible, and there are plenty of groups catering to that desire. “Most physicians prefer time off, and seven on, seven off is attractive in recruiting new people to your practice—but it strikes me as a poisonous way to work,” says John Nelson, MD, co-founder of SHM, medical director of the hospitalist practice at Overlake Hospital in Bellevue, Wash., and author of the “Practice Management” column in The Hospitalist. Dr. Nelson acts as a consultant to hospitalist practices around the country and has written articles and given presentations on the topic of scheduling for hospital medicine groups.
Dr. Nelson understands the attractions of working seven on, seven off—particularly for young physicians. “Even seven on is not as bad as being an intern; it’s easier than they were used to in their residency,” he says. “But I worry this schedule might increase burnout and resentment of work. It’s asystole/diastole lifestyle and may not be a healthy way to organize your life or your career.”
An Alternative Scheduling Idea
Dr. Nelson has his own unique ideas of how a group’s shift assignments should work to ensure better coverage and keep hospitalists happy. His ideas are not just theories—his own group lives and works by a flexible arrangement.
Their schedule is partly dictated by a desire to keep the physicians happy and healthy. “I believe a constant mix of work and the rest of your life is best,” says Dr. Nelson. “You shouldn’t have to put the rest of your life into the seven days that you’re off.”
So Dr. Nelson’s practice allows considerable flexibility to each physician, but ensures that any given workday is shorter than 12 hours. “I think it’s better not to have a rigidly repeating schedule,” he explains.
Dr. Nelson’s group uses pagers to ensure a hospitalist is always available during coverage hours, but they don’t adhere to a strict schedule. “So many groups work specified shifts, whether it’s 10 or 12 hours, and I think there’s a better idea,” he says. “If everyone has to punch a clock, it interferes with flexibility. I would not tell doctors when to start or stop.”
Of course, as a group, someone has to be available for emergencies all the time, and physicians may need to start daily rounds to write most discharge orders by a certain time. “I have a pager on by 7 a.m., but nothing says I have to be in the hospital by 7 a.m.,” says Dr. Nelson. “It’s often in my interest to start rounding earlier than 7 a.m. so that I can finish earlier or have time for a break later in the day.”
Greater Flexibility = Better Coverage
Another benefit to moving to shorter, more flexible days is ensuring adequate coverage. “Rigidly defined shifts almost never precisely match the day’s workload,” points out Dr. Nelson. Therefore, his practice boosts staffing to cover busy periods. “My recommendation is to intentionally overstaff for the average day’s workload. When it’s busy, everyone can pitch in and work an extra one or two hours.”
If it’s not busy, one or more doctors may leave early. “This is nimble and responsive to the day-to-day workload,” says Dr. Nelson.
To move from a seven on, seven off schedule to this model, Dr. Nelson recommends that every doctor in the practice work 30 to 40 more days annually. A seven on, seven off schedule would have a physician work 182.5 days per year; if you decrease the hours per day and boost the number of working days to 220 a year, your physicians will be working the same number of hours, but in shorter days—even if the practice workload stays the same and each individual doctor’s annual productivity stays the same.
“It’s more realistic to work more days when they’re not so grueling,” says Dr. Nelson. “Plus, you have a built-in capacity to meet a sudden increase in workload. Imagine an eight-man group, where four doctors each work 12-hour shifts. Now imagine that instead of four, you get a fifth doctor to show up every day. [You can get this fifth doctor without adding staff if each doctor works more days annually.] When a day is unpredictably busy, the physicians won’t be absolutely overwhelmed. If it’s not busy, you can send someone home early. You get a lot more flexibility.”
For a hospital medicine group, implementing a flexible schedule such as this generally requires payment for production, which ties individual physicians into the economic health of their group. Compensation matches workload, allowing individual physicians to work to their values—more money or more free time.
“I think it’s better to pay on production,” says Dr. Nelson. “That way each person has the opportunity to choose. If one values money, he can volunteer to stay and work more and make more money. Each works to their own sweet spot, whereas a seven on, seven off schedule with rigidly defined shifts forces everyone to do the same thing.”
Physicians working on a flexible schedule still need to get their work finished each day, but they have more autonomy in how and when they get it done. “Doctors who work fast can go home early; physicians can decide for themselves the right balance for spending time each patient,” says Dr. Nelson. “As long as they understand there are economic consequences … and act with reasonableness. In our group, we get the work done. There’s no official start or stop time. Each of us chooses an individual work style. There are boundaries; the work needs to be done. There are costs as well, but I believe this system is healthy and liberating.” TH
Jane Jerrard regularly writes “Career Development.”
The shifts worked by a hospital medicine group can reflect its values or simply ensure adequate coverage. Either way, the shifts your group assigns can play a significant role in recruiting new hospitalists and retaining those you have. And there may be more scheduling options than you have considered.
The Most Attractive Shift Debunked
Many new hospitalists seek as much time off as possible, and there are plenty of groups catering to that desire. “Most physicians prefer time off, and seven on, seven off is attractive in recruiting new people to your practice—but it strikes me as a poisonous way to work,” says John Nelson, MD, co-founder of SHM, medical director of the hospitalist practice at Overlake Hospital in Bellevue, Wash., and author of the “Practice Management” column in The Hospitalist. Dr. Nelson acts as a consultant to hospitalist practices around the country and has written articles and given presentations on the topic of scheduling for hospital medicine groups.
Dr. Nelson understands the attractions of working seven on, seven off—particularly for young physicians. “Even seven on is not as bad as being an intern; it’s easier than they were used to in their residency,” he says. “But I worry this schedule might increase burnout and resentment of work. It’s asystole/diastole lifestyle and may not be a healthy way to organize your life or your career.”
An Alternative Scheduling Idea
Dr. Nelson has his own unique ideas of how a group’s shift assignments should work to ensure better coverage and keep hospitalists happy. His ideas are not just theories—his own group lives and works by a flexible arrangement.
Their schedule is partly dictated by a desire to keep the physicians happy and healthy. “I believe a constant mix of work and the rest of your life is best,” says Dr. Nelson. “You shouldn’t have to put the rest of your life into the seven days that you’re off.”
So Dr. Nelson’s practice allows considerable flexibility to each physician, but ensures that any given workday is shorter than 12 hours. “I think it’s better not to have a rigidly repeating schedule,” he explains.
Dr. Nelson’s group uses pagers to ensure a hospitalist is always available during coverage hours, but they don’t adhere to a strict schedule. “So many groups work specified shifts, whether it’s 10 or 12 hours, and I think there’s a better idea,” he says. “If everyone has to punch a clock, it interferes with flexibility. I would not tell doctors when to start or stop.”
Of course, as a group, someone has to be available for emergencies all the time, and physicians may need to start daily rounds to write most discharge orders by a certain time. “I have a pager on by 7 a.m., but nothing says I have to be in the hospital by 7 a.m.,” says Dr. Nelson. “It’s often in my interest to start rounding earlier than 7 a.m. so that I can finish earlier or have time for a break later in the day.”
Greater Flexibility = Better Coverage
Another benefit to moving to shorter, more flexible days is ensuring adequate coverage. “Rigidly defined shifts almost never precisely match the day’s workload,” points out Dr. Nelson. Therefore, his practice boosts staffing to cover busy periods. “My recommendation is to intentionally overstaff for the average day’s workload. When it’s busy, everyone can pitch in and work an extra one or two hours.”
If it’s not busy, one or more doctors may leave early. “This is nimble and responsive to the day-to-day workload,” says Dr. Nelson.
To move from a seven on, seven off schedule to this model, Dr. Nelson recommends that every doctor in the practice work 30 to 40 more days annually. A seven on, seven off schedule would have a physician work 182.5 days per year; if you decrease the hours per day and boost the number of working days to 220 a year, your physicians will be working the same number of hours, but in shorter days—even if the practice workload stays the same and each individual doctor’s annual productivity stays the same.
“It’s more realistic to work more days when they’re not so grueling,” says Dr. Nelson. “Plus, you have a built-in capacity to meet a sudden increase in workload. Imagine an eight-man group, where four doctors each work 12-hour shifts. Now imagine that instead of four, you get a fifth doctor to show up every day. [You can get this fifth doctor without adding staff if each doctor works more days annually.] When a day is unpredictably busy, the physicians won’t be absolutely overwhelmed. If it’s not busy, you can send someone home early. You get a lot more flexibility.”
For a hospital medicine group, implementing a flexible schedule such as this generally requires payment for production, which ties individual physicians into the economic health of their group. Compensation matches workload, allowing individual physicians to work to their values—more money or more free time.
“I think it’s better to pay on production,” says Dr. Nelson. “That way each person has the opportunity to choose. If one values money, he can volunteer to stay and work more and make more money. Each works to their own sweet spot, whereas a seven on, seven off schedule with rigidly defined shifts forces everyone to do the same thing.”
Physicians working on a flexible schedule still need to get their work finished each day, but they have more autonomy in how and when they get it done. “Doctors who work fast can go home early; physicians can decide for themselves the right balance for spending time each patient,” says Dr. Nelson. “As long as they understand there are economic consequences … and act with reasonableness. In our group, we get the work done. There’s no official start or stop time. Each of us chooses an individual work style. There are boundaries; the work needs to be done. There are costs as well, but I believe this system is healthy and liberating.” TH
Jane Jerrard regularly writes “Career Development.”
The shifts worked by a hospital medicine group can reflect its values or simply ensure adequate coverage. Either way, the shifts your group assigns can play a significant role in recruiting new hospitalists and retaining those you have. And there may be more scheduling options than you have considered.
The Most Attractive Shift Debunked
Many new hospitalists seek as much time off as possible, and there are plenty of groups catering to that desire. “Most physicians prefer time off, and seven on, seven off is attractive in recruiting new people to your practice—but it strikes me as a poisonous way to work,” says John Nelson, MD, co-founder of SHM, medical director of the hospitalist practice at Overlake Hospital in Bellevue, Wash., and author of the “Practice Management” column in The Hospitalist. Dr. Nelson acts as a consultant to hospitalist practices around the country and has written articles and given presentations on the topic of scheduling for hospital medicine groups.
Dr. Nelson understands the attractions of working seven on, seven off—particularly for young physicians. “Even seven on is not as bad as being an intern; it’s easier than they were used to in their residency,” he says. “But I worry this schedule might increase burnout and resentment of work. It’s asystole/diastole lifestyle and may not be a healthy way to organize your life or your career.”
An Alternative Scheduling Idea
Dr. Nelson has his own unique ideas of how a group’s shift assignments should work to ensure better coverage and keep hospitalists happy. His ideas are not just theories—his own group lives and works by a flexible arrangement.
Their schedule is partly dictated by a desire to keep the physicians happy and healthy. “I believe a constant mix of work and the rest of your life is best,” says Dr. Nelson. “You shouldn’t have to put the rest of your life into the seven days that you’re off.”
So Dr. Nelson’s practice allows considerable flexibility to each physician, but ensures that any given workday is shorter than 12 hours. “I think it’s better not to have a rigidly repeating schedule,” he explains.
Dr. Nelson’s group uses pagers to ensure a hospitalist is always available during coverage hours, but they don’t adhere to a strict schedule. “So many groups work specified shifts, whether it’s 10 or 12 hours, and I think there’s a better idea,” he says. “If everyone has to punch a clock, it interferes with flexibility. I would not tell doctors when to start or stop.”
Of course, as a group, someone has to be available for emergencies all the time, and physicians may need to start daily rounds to write most discharge orders by a certain time. “I have a pager on by 7 a.m., but nothing says I have to be in the hospital by 7 a.m.,” says Dr. Nelson. “It’s often in my interest to start rounding earlier than 7 a.m. so that I can finish earlier or have time for a break later in the day.”
Greater Flexibility = Better Coverage
Another benefit to moving to shorter, more flexible days is ensuring adequate coverage. “Rigidly defined shifts almost never precisely match the day’s workload,” points out Dr. Nelson. Therefore, his practice boosts staffing to cover busy periods. “My recommendation is to intentionally overstaff for the average day’s workload. When it’s busy, everyone can pitch in and work an extra one or two hours.”
If it’s not busy, one or more doctors may leave early. “This is nimble and responsive to the day-to-day workload,” says Dr. Nelson.
To move from a seven on, seven off schedule to this model, Dr. Nelson recommends that every doctor in the practice work 30 to 40 more days annually. A seven on, seven off schedule would have a physician work 182.5 days per year; if you decrease the hours per day and boost the number of working days to 220 a year, your physicians will be working the same number of hours, but in shorter days—even if the practice workload stays the same and each individual doctor’s annual productivity stays the same.
“It’s more realistic to work more days when they’re not so grueling,” says Dr. Nelson. “Plus, you have a built-in capacity to meet a sudden increase in workload. Imagine an eight-man group, where four doctors each work 12-hour shifts. Now imagine that instead of four, you get a fifth doctor to show up every day. [You can get this fifth doctor without adding staff if each doctor works more days annually.] When a day is unpredictably busy, the physicians won’t be absolutely overwhelmed. If it’s not busy, you can send someone home early. You get a lot more flexibility.”
For a hospital medicine group, implementing a flexible schedule such as this generally requires payment for production, which ties individual physicians into the economic health of their group. Compensation matches workload, allowing individual physicians to work to their values—more money or more free time.
“I think it’s better to pay on production,” says Dr. Nelson. “That way each person has the opportunity to choose. If one values money, he can volunteer to stay and work more and make more money. Each works to their own sweet spot, whereas a seven on, seven off schedule with rigidly defined shifts forces everyone to do the same thing.”
Physicians working on a flexible schedule still need to get their work finished each day, but they have more autonomy in how and when they get it done. “Doctors who work fast can go home early; physicians can decide for themselves the right balance for spending time each patient,” says Dr. Nelson. “As long as they understand there are economic consequences … and act with reasonableness. In our group, we get the work done. There’s no official start or stop time. Each of us chooses an individual work style. There are boundaries; the work needs to be done. There are costs as well, but I believe this system is healthy and liberating.” TH
Jane Jerrard regularly writes “Career Development.”
SHM Surveys Revisited
The Benchmarks Committee has had a busy 2006 so far. Many thanks to the 400-plus hospital medicine groups that completed the 2005-06 SHM survey, “The Authoritative Source on the State of Hospital Medicine,” as well as those of you who participated in the follow-up survey to clarify questions around additional revenue or supplements to program income.
We had some behind-the-scenes work on the survey. After the first pass of data analysis, it became clear that there was something amiss with the responses pertaining to the supplemental income questions. Only 47% of programs reported that they received additional income from hospitals or other sources. This seemed incompatible with what we know about current payment rates for fee-for-service work. A quick discussion took place among the committee and we decided to resurvey the group with more precise questions on exactly how finances flow into a program. As you have seen, the additional results bore out our suspicions. With the revised survey tool, 97% of the programs (when re-queried) reported receiving income above and beyond fees from direct patient care.
It was a Herculean task of digesting and formatting the data into usable form. SHM Senior Vice President Joe Miller deserves many thanks for poring through the data and creating something that all of you can use to better your programs.
Now, a few words about the recent annual meeting in Washington, DC: The work of the Benchmarks Committee was highlighted by SHM CEO Larry Wellikson, MD, in a plenary session on the first day of the meeting. An insightful panel discussion followed in which panel members Bob Wachter, MD (representing academic hospital medicine), Mary Jo Gorman, MD (corporate hospital medicine), and John Nelson, MD (community hospital medicine) gave some insightful commentary on the results of the survey and then fielded questions from the audience.
In between sessions at the conference, the committee held its annual face-to-face meeting and discussed plans for the year.
Under the guidance and editorial excellence of committee member Leslie Flores, the Benchmarks Committee continues to make strong progress with the dashboard project. As you may recall, this project will document and describe 10 commonly used dashboard metrics, including sample reports. There are plans for this material to be published as a supplement to The Hospitalist later this year.
The committee discussed the type of surveys conducted by SHM. A recommendation came out of our meeting to change from large-scale, all-encompassing, biannual surveys to smaller annual surveys. The annual survey would alternate its focus every other year between evaluating individuals’ productivity and compensation, and the characteristics of hospital medicine groups. Each survey would also have the flexibility to address specific timely questions that might focus on a specific research or hot topic of the day. The goal is to get our first trial survey out by the end of 2006, which would focus on group characteristics.
Lastly, a big thank you to our outgoing chairperson, Teresa Jones. Her hard work and organizational skills are going to be a tough act to follow.
Dr. Kealey is chair of SHM’s Benchmarks Committee
Advocacy Day Educates Lawmakers about Hospital Medicine
By Eric Siegal, MD
As reported in the SHM Meeting Reporter (see July The Hospitalist, supplement 1), SHM’s first Legislative Advocacy Day was an overwhelming success. More than 70 members from 29 states visited Capitol Hill on May 3 to educate lawmakers and their staffs about hospital medicine and SHM’s proposals to improve the quality of care in our nation’s hospitals.
Advocacy Day participants attended a morning briefing that covered procedural tips on how to have a successful meeting and the health issues currently before Congress—and SHM’s positions—before leaving for previously scheduled appointments on Capitol Hill.
Once there, hospitalists took time to educate legislators and their staff members about the fastest growing medical specialty in the United States, and then turned to SHM’s recommendations for improving the quality, safety, and cost-effectiveness of inpatient medical care.
Among the issues discussed with lawmakers: the need for more funding for the Agency for Healthcare Research and Quality (AHRQ); SHM support for federal initiatives to measure resource use and improve quality, including a CMS demonstration project to assess the contributions of hospital medicine programs to improve patient care and more efficient management of hospital resources; and the importance of gainsharing demonstration projects that focus on inpatient medical services such as those provided by hospital medicine programs.
More than 130 appointments were scheduled with House and Senate offices, many with members of Congress who sit on the key health committees with jurisdiction over Medicare as well as on committees responsible for determining funding levels for the National Institutes of Health, the CDC, and the Agency for Healthcare Research and Quality.
SHM encourages those of you who participated in Advocacy Day to thank the lawmakers and staff with whom you visited (view the sample thank-you letter and instructions online at www.hospitalmedicine.org under “Advocacy & Policy”).
Advocacy Day opened doors to congressional offices; follow-up from SHM members will keep hospital medicine’s issues before lawmakers as they vote on legislation of importance to our specialty. The more SHM members interact with members of Congress and their staff, the louder our voices and the more effective our messages. Advocacy Day is just the beginning of regular contact by hospitalists with their elected representatives in Washington.
A New Way to Get Everything SHM
SHM has launched the SHM Store, a new Internet-based marketplace that will redefine the way SHM educational products and apparel are distributed. The online store will be a convenient option for hectic lifestyles because it will be open 24 hours a day and can be accessed from anywhere there is an Internet connection.
The SHM Store is user-friendly and allows you to easily and quickly purchase the quality products and apparel that you have come to expect from SHM. Apparel and accessories include men’s and women’s wind jackets, golf shirts, scrub tops, baseball caps, and lapel pins—all with the SHM logo.
You’ll also find the most up-to-date educational materials from SHM. The 2005-2006 results of the SHM survey, “The Authoritative Source on the State of Hospital Medicine,” can be ordered in CD and print format. The Practice Management Course CD with binder is also available. This combination package includes all of the materials distributed at an onsite presentation of the course. And, last but not least, get your very own copy or additional copies of The Core Competencies in Hospital Medicine: A Framework For Curriculum Development.
The ordering process is simple. Access the SHM Store at www.hospitalmedicine.org/shmstore or navigate from www.hospitalmedicine.org and click on SHM Store. The store allows you to browse available products and descriptions. When you see something you want, select the quantity you’d like to purchase and add the items to your shopping cart. Once you have completed your shopping trip, click “Check Out.” A confirmation of your transaction will be sent to your e-mail inbox and your products will be shipped to your attention.
It’s that easy. Make sure you go online to browse the new SHM Store. If you have any questions or would like to learn more about the SHM Store, contact SHM at CustomerService@hospitalmedicine. org.
SHM, Health Groups Urge House to Boost Discretionary Funding
SHM joined more than 800 health, education, and labor organizations in writing a May 8 letter to the House leadership. Organized by the Coalition for Health Funding and the Committee on Education Funding, the letter calls on Congress to add $7 billion to the budget in discretionary funding for health, education, and labor programs. It asks lawmakers to ensure that the final allocation for the House and Senate Labor, Health and Human Services, Education Appropriations Subcommittees reflects a $7 billion increase above the President’s request for these critically important programs in FY 2007.
“While our organizations represent a wide array of domestic priorities,” the letter states, “we are united in our effort to advance the bipartisan goal of adding $7 billion in discretionary funding for health, education, labor enforcement, job training, and social services programs as the budget process moves forward. On behalf of our millions of constituents, we strongly urge you to provide at least $7 billion in additional federal support to restore funding levels to FY 2005. This is essential to sustain the well-being and prosperity of our nation.”
Agencies whose funding could be boosted by the additional spending called for in the coalition letter include the Agency for Healthcare Research and Quality, the National Institutes of Health, and the Centers for Disease Control and Prevention.
For full coverage of May 2006 advocacy and policy news, visit www.hospitalmedicine.org. TH
Dr. Siegal is chair of SHM’s Public Policy Committee.
SHM: BEHIND THE SCENES
Education and Quality Initiatives: SHM’s Heart and Soul
By Geri Barnes

This month’s SHM staff article highlights the department responsible for SHM’s education and quality initiatives. While my fellow senior managers may disagree, I believe that we are the heart and soul of SHM in meeting members’ needs. So important is this organizational focus that the Education Committee, chaired by Preetha Basaviah, MD, has its own mission, which parallels and provides detail to the organizational mission of promoting excellence in the practice of hospital medicine. And the Hospital Quality and Patient Safety Committee, chaired by Mahalakshmi Halasyamani, MD, is one of the most dynamic and prolific of SHM’s committees.
We know that members join SHM for the opportunity to effect change and network with colleagues. Equally strong is the quest for educational resources that will facilitate their efforts in improving quality inpatient care. SHM’s education plan focuses and organizes our energy on developing those resources.
SHM’s resources come in many forms. The most visible is our annual meeting. By all accounts, the 2006 annual meeting was extremely successful. It was our largest meeting to date, with almost 1,200 attendees, 99% of whom were members. That number represents more than 21% of our total membership. I wonder how many other organizations can boast of such a high percentage of member attendance at their annual meeting. The attendees actively participated in the educational sessions and the Research, Innovations, and Clinical Vignettes poster session, visited the exhibits, and networked during breaks and social events. To enhance the educational experience, we created a password-protected Web site where registrants could access the handouts for sessions they planned to attend. Because of the value of these materials, we are currently determining ways to utilize the handouts to expand our educational resources.
For several years, SHM has presented the Leadership Academy and “Best Practices in Managing a Hospital Medicine Program” course. These courses are so popular that they have become a mainstay of SHM educational programs and are offered on an annual basis. In September we will present the first Level II Leadership Academy designed to build upon and expand Leadership Academy I. Additionally, “Fundamentals in Billing and Coding” a pre-course to the University of California San Francisco “Management of the Hospitalized Patient” course will be offered in October for the first time. This outgrowth of the Best Practices course was identified as a need by attendees and other members. We anticipate that we will continue to offer these important programs for many years to come.
While we reach a significant number of hospitalists and other healthcare providers through our annual meeting and other face-to-face meetings, we reach many more through other educational and quality improvement efforts. Hospitalists, in their unique role as providers responsible for the general medical care of hospitalized patients, find themselves filling roles as key players and drivers of institutional quality improvement. To aid them in this effort, we’ve developed Web-based resource rooms designed to facilitate the implementation of a quality improvement program for specific disease state/clinical condition, including antimicrobial resistance, stroke, venous thromboembolism, and heart failure. Resource rooms on glycemic control and discharge planning are currently under development.
For most resource rooms, the key is the QI Workbook, a resource built on proven principles of quality improvement, personal experiences, and evidence-based medicine. Resources in addition to the workbook include slide sets that can be used in training sessions, “Teaching Pearls,” patient education resources, and clinical tools in the form of algorithms, order sets, and discharge planning sheets. Most of the resource rooms have online CME programs and each room has a well-developed bibliography.
What will likely prove to be SHM’s most far-reaching resource is The Core Competencies in Hospital Medicine: A Framework For Curriculum Development. Published earlier this year as a supplement to the Journal of Hospital Medicine, the Core Competencies provides a structure for professional and curricular development based on a shared understanding of the essential knowledge, skills, and attitudes expected of physicians working as hospitalists. While the target audience is the directors of hospitalist programs and fellowships and residency programs (and medical school internal medicine clerkships), imagine the number of people reached when the Core Competencies touch hospitalist students across the board. Additionally, the Core Competencies are the focal point for every educational and quality improvement initiative that we undertake. This document will continue to drive the content of each annual meeting, provide direction for the organization, and help us prioritize the development of resources rooms and other educational and quality improvement resources.
SHM is lucky to have partners who understand the importance of hospitalists as key members of the multidisciplinary team and the army that will lead the charge in implementing protocols to improve patient care. From foundations and sister associations, to government and industry, we partner with organizations that appreciate the role that hospitalists play in improving the healthcare system. The partnerships have led to the development of toolkits, resource rooms, CME modules, and other important resources. New initiatives soon to be launched are mentored implementation programs and demonstration projects that will provide us with increased knowledge of how our resources are used and identify areas in which they can be improved.
What is required on a staff level to make this happen? A commitment to do whatever it takes to get the job done. Six of us are equally dedicated to leading, managing, and supporting these efforts. In addition to me, staff members Tina Budnitz, Erica Pearson, Joy Wittnebert, Lillian Higgins, and Theresa Jones chart new ground and are actively engaged in a dynamic learning process on a daily basis. But it is our members and experts that drive this process, and we are grateful for their patience and guidance.
The Education and Quality Initiatives staff members do not work in a vacuum in the national office. We have the support and brainpower of the rest of the staff, with whom we collaborate daily. Membership and marketing, information technology, and business operations staff all play a role in our success.
What makes the national office run as a well-oiled machine? Next month you’ll hear from Steve Poitras, director, Business Operations, who is instrumental in making that happen.
Barnes is director, Education & Quality Initiatives, for SHM.
The Benchmarks Committee has had a busy 2006 so far. Many thanks to the 400-plus hospital medicine groups that completed the 2005-06 SHM survey, “The Authoritative Source on the State of Hospital Medicine,” as well as those of you who participated in the follow-up survey to clarify questions around additional revenue or supplements to program income.
We had some behind-the-scenes work on the survey. After the first pass of data analysis, it became clear that there was something amiss with the responses pertaining to the supplemental income questions. Only 47% of programs reported that they received additional income from hospitals or other sources. This seemed incompatible with what we know about current payment rates for fee-for-service work. A quick discussion took place among the committee and we decided to resurvey the group with more precise questions on exactly how finances flow into a program. As you have seen, the additional results bore out our suspicions. With the revised survey tool, 97% of the programs (when re-queried) reported receiving income above and beyond fees from direct patient care.
It was a Herculean task of digesting and formatting the data into usable form. SHM Senior Vice President Joe Miller deserves many thanks for poring through the data and creating something that all of you can use to better your programs.
Now, a few words about the recent annual meeting in Washington, DC: The work of the Benchmarks Committee was highlighted by SHM CEO Larry Wellikson, MD, in a plenary session on the first day of the meeting. An insightful panel discussion followed in which panel members Bob Wachter, MD (representing academic hospital medicine), Mary Jo Gorman, MD (corporate hospital medicine), and John Nelson, MD (community hospital medicine) gave some insightful commentary on the results of the survey and then fielded questions from the audience.
In between sessions at the conference, the committee held its annual face-to-face meeting and discussed plans for the year.
Under the guidance and editorial excellence of committee member Leslie Flores, the Benchmarks Committee continues to make strong progress with the dashboard project. As you may recall, this project will document and describe 10 commonly used dashboard metrics, including sample reports. There are plans for this material to be published as a supplement to The Hospitalist later this year.
The committee discussed the type of surveys conducted by SHM. A recommendation came out of our meeting to change from large-scale, all-encompassing, biannual surveys to smaller annual surveys. The annual survey would alternate its focus every other year between evaluating individuals’ productivity and compensation, and the characteristics of hospital medicine groups. Each survey would also have the flexibility to address specific timely questions that might focus on a specific research or hot topic of the day. The goal is to get our first trial survey out by the end of 2006, which would focus on group characteristics.
Lastly, a big thank you to our outgoing chairperson, Teresa Jones. Her hard work and organizational skills are going to be a tough act to follow.
Dr. Kealey is chair of SHM’s Benchmarks Committee
Advocacy Day Educates Lawmakers about Hospital Medicine
By Eric Siegal, MD
As reported in the SHM Meeting Reporter (see July The Hospitalist, supplement 1), SHM’s first Legislative Advocacy Day was an overwhelming success. More than 70 members from 29 states visited Capitol Hill on May 3 to educate lawmakers and their staffs about hospital medicine and SHM’s proposals to improve the quality of care in our nation’s hospitals.
Advocacy Day participants attended a morning briefing that covered procedural tips on how to have a successful meeting and the health issues currently before Congress—and SHM’s positions—before leaving for previously scheduled appointments on Capitol Hill.
Once there, hospitalists took time to educate legislators and their staff members about the fastest growing medical specialty in the United States, and then turned to SHM’s recommendations for improving the quality, safety, and cost-effectiveness of inpatient medical care.
Among the issues discussed with lawmakers: the need for more funding for the Agency for Healthcare Research and Quality (AHRQ); SHM support for federal initiatives to measure resource use and improve quality, including a CMS demonstration project to assess the contributions of hospital medicine programs to improve patient care and more efficient management of hospital resources; and the importance of gainsharing demonstration projects that focus on inpatient medical services such as those provided by hospital medicine programs.
More than 130 appointments were scheduled with House and Senate offices, many with members of Congress who sit on the key health committees with jurisdiction over Medicare as well as on committees responsible for determining funding levels for the National Institutes of Health, the CDC, and the Agency for Healthcare Research and Quality.
SHM encourages those of you who participated in Advocacy Day to thank the lawmakers and staff with whom you visited (view the sample thank-you letter and instructions online at www.hospitalmedicine.org under “Advocacy & Policy”).
Advocacy Day opened doors to congressional offices; follow-up from SHM members will keep hospital medicine’s issues before lawmakers as they vote on legislation of importance to our specialty. The more SHM members interact with members of Congress and their staff, the louder our voices and the more effective our messages. Advocacy Day is just the beginning of regular contact by hospitalists with their elected representatives in Washington.
A New Way to Get Everything SHM
SHM has launched the SHM Store, a new Internet-based marketplace that will redefine the way SHM educational products and apparel are distributed. The online store will be a convenient option for hectic lifestyles because it will be open 24 hours a day and can be accessed from anywhere there is an Internet connection.
The SHM Store is user-friendly and allows you to easily and quickly purchase the quality products and apparel that you have come to expect from SHM. Apparel and accessories include men’s and women’s wind jackets, golf shirts, scrub tops, baseball caps, and lapel pins—all with the SHM logo.
You’ll also find the most up-to-date educational materials from SHM. The 2005-2006 results of the SHM survey, “The Authoritative Source on the State of Hospital Medicine,” can be ordered in CD and print format. The Practice Management Course CD with binder is also available. This combination package includes all of the materials distributed at an onsite presentation of the course. And, last but not least, get your very own copy or additional copies of The Core Competencies in Hospital Medicine: A Framework For Curriculum Development.
The ordering process is simple. Access the SHM Store at www.hospitalmedicine.org/shmstore or navigate from www.hospitalmedicine.org and click on SHM Store. The store allows you to browse available products and descriptions. When you see something you want, select the quantity you’d like to purchase and add the items to your shopping cart. Once you have completed your shopping trip, click “Check Out.” A confirmation of your transaction will be sent to your e-mail inbox and your products will be shipped to your attention.
It’s that easy. Make sure you go online to browse the new SHM Store. If you have any questions or would like to learn more about the SHM Store, contact SHM at CustomerService@hospitalmedicine. org.
SHM, Health Groups Urge House to Boost Discretionary Funding
SHM joined more than 800 health, education, and labor organizations in writing a May 8 letter to the House leadership. Organized by the Coalition for Health Funding and the Committee on Education Funding, the letter calls on Congress to add $7 billion to the budget in discretionary funding for health, education, and labor programs. It asks lawmakers to ensure that the final allocation for the House and Senate Labor, Health and Human Services, Education Appropriations Subcommittees reflects a $7 billion increase above the President’s request for these critically important programs in FY 2007.
“While our organizations represent a wide array of domestic priorities,” the letter states, “we are united in our effort to advance the bipartisan goal of adding $7 billion in discretionary funding for health, education, labor enforcement, job training, and social services programs as the budget process moves forward. On behalf of our millions of constituents, we strongly urge you to provide at least $7 billion in additional federal support to restore funding levels to FY 2005. This is essential to sustain the well-being and prosperity of our nation.”
Agencies whose funding could be boosted by the additional spending called for in the coalition letter include the Agency for Healthcare Research and Quality, the National Institutes of Health, and the Centers for Disease Control and Prevention.
For full coverage of May 2006 advocacy and policy news, visit www.hospitalmedicine.org. TH
Dr. Siegal is chair of SHM’s Public Policy Committee.
SHM: BEHIND THE SCENES
Education and Quality Initiatives: SHM’s Heart and Soul
By Geri Barnes
This month’s SHM staff article highlights the department responsible for SHM’s education and quality initiatives. While my fellow senior managers may disagree, I believe that we are the heart and soul of SHM in meeting members’ needs. So important is this organizational focus that the Education Committee, chaired by Preetha Basaviah, MD, has its own mission, which parallels and provides detail to the organizational mission of promoting excellence in the practice of hospital medicine. And the Hospital Quality and Patient Safety Committee, chaired by Mahalakshmi Halasyamani, MD, is one of the most dynamic and prolific of SHM’s committees.
We know that members join SHM for the opportunity to effect change and network with colleagues. Equally strong is the quest for educational resources that will facilitate their efforts in improving quality inpatient care. SHM’s education plan focuses and organizes our energy on developing those resources.
SHM’s resources come in many forms. The most visible is our annual meeting. By all accounts, the 2006 annual meeting was extremely successful. It was our largest meeting to date, with almost 1,200 attendees, 99% of whom were members. That number represents more than 21% of our total membership. I wonder how many other organizations can boast of such a high percentage of member attendance at their annual meeting. The attendees actively participated in the educational sessions and the Research, Innovations, and Clinical Vignettes poster session, visited the exhibits, and networked during breaks and social events. To enhance the educational experience, we created a password-protected Web site where registrants could access the handouts for sessions they planned to attend. Because of the value of these materials, we are currently determining ways to utilize the handouts to expand our educational resources.
For several years, SHM has presented the Leadership Academy and “Best Practices in Managing a Hospital Medicine Program” course. These courses are so popular that they have become a mainstay of SHM educational programs and are offered on an annual basis. In September we will present the first Level II Leadership Academy designed to build upon and expand Leadership Academy I. Additionally, “Fundamentals in Billing and Coding” a pre-course to the University of California San Francisco “Management of the Hospitalized Patient” course will be offered in October for the first time. This outgrowth of the Best Practices course was identified as a need by attendees and other members. We anticipate that we will continue to offer these important programs for many years to come.
While we reach a significant number of hospitalists and other healthcare providers through our annual meeting and other face-to-face meetings, we reach many more through other educational and quality improvement efforts. Hospitalists, in their unique role as providers responsible for the general medical care of hospitalized patients, find themselves filling roles as key players and drivers of institutional quality improvement. To aid them in this effort, we’ve developed Web-based resource rooms designed to facilitate the implementation of a quality improvement program for specific disease state/clinical condition, including antimicrobial resistance, stroke, venous thromboembolism, and heart failure. Resource rooms on glycemic control and discharge planning are currently under development.
For most resource rooms, the key is the QI Workbook, a resource built on proven principles of quality improvement, personal experiences, and evidence-based medicine. Resources in addition to the workbook include slide sets that can be used in training sessions, “Teaching Pearls,” patient education resources, and clinical tools in the form of algorithms, order sets, and discharge planning sheets. Most of the resource rooms have online CME programs and each room has a well-developed bibliography.
What will likely prove to be SHM’s most far-reaching resource is The Core Competencies in Hospital Medicine: A Framework For Curriculum Development. Published earlier this year as a supplement to the Journal of Hospital Medicine, the Core Competencies provides a structure for professional and curricular development based on a shared understanding of the essential knowledge, skills, and attitudes expected of physicians working as hospitalists. While the target audience is the directors of hospitalist programs and fellowships and residency programs (and medical school internal medicine clerkships), imagine the number of people reached when the Core Competencies touch hospitalist students across the board. Additionally, the Core Competencies are the focal point for every educational and quality improvement initiative that we undertake. This document will continue to drive the content of each annual meeting, provide direction for the organization, and help us prioritize the development of resources rooms and other educational and quality improvement resources.
SHM is lucky to have partners who understand the importance of hospitalists as key members of the multidisciplinary team and the army that will lead the charge in implementing protocols to improve patient care. From foundations and sister associations, to government and industry, we partner with organizations that appreciate the role that hospitalists play in improving the healthcare system. The partnerships have led to the development of toolkits, resource rooms, CME modules, and other important resources. New initiatives soon to be launched are mentored implementation programs and demonstration projects that will provide us with increased knowledge of how our resources are used and identify areas in which they can be improved.
What is required on a staff level to make this happen? A commitment to do whatever it takes to get the job done. Six of us are equally dedicated to leading, managing, and supporting these efforts. In addition to me, staff members Tina Budnitz, Erica Pearson, Joy Wittnebert, Lillian Higgins, and Theresa Jones chart new ground and are actively engaged in a dynamic learning process on a daily basis. But it is our members and experts that drive this process, and we are grateful for their patience and guidance.
The Education and Quality Initiatives staff members do not work in a vacuum in the national office. We have the support and brainpower of the rest of the staff, with whom we collaborate daily. Membership and marketing, information technology, and business operations staff all play a role in our success.
What makes the national office run as a well-oiled machine? Next month you’ll hear from Steve Poitras, director, Business Operations, who is instrumental in making that happen.
Barnes is director, Education & Quality Initiatives, for SHM.
The Benchmarks Committee has had a busy 2006 so far. Many thanks to the 400-plus hospital medicine groups that completed the 2005-06 SHM survey, “The Authoritative Source on the State of Hospital Medicine,” as well as those of you who participated in the follow-up survey to clarify questions around additional revenue or supplements to program income.
We had some behind-the-scenes work on the survey. After the first pass of data analysis, it became clear that there was something amiss with the responses pertaining to the supplemental income questions. Only 47% of programs reported that they received additional income from hospitals or other sources. This seemed incompatible with what we know about current payment rates for fee-for-service work. A quick discussion took place among the committee and we decided to resurvey the group with more precise questions on exactly how finances flow into a program. As you have seen, the additional results bore out our suspicions. With the revised survey tool, 97% of the programs (when re-queried) reported receiving income above and beyond fees from direct patient care.
It was a Herculean task of digesting and formatting the data into usable form. SHM Senior Vice President Joe Miller deserves many thanks for poring through the data and creating something that all of you can use to better your programs.
Now, a few words about the recent annual meeting in Washington, DC: The work of the Benchmarks Committee was highlighted by SHM CEO Larry Wellikson, MD, in a plenary session on the first day of the meeting. An insightful panel discussion followed in which panel members Bob Wachter, MD (representing academic hospital medicine), Mary Jo Gorman, MD (corporate hospital medicine), and John Nelson, MD (community hospital medicine) gave some insightful commentary on the results of the survey and then fielded questions from the audience.
In between sessions at the conference, the committee held its annual face-to-face meeting and discussed plans for the year.
Under the guidance and editorial excellence of committee member Leslie Flores, the Benchmarks Committee continues to make strong progress with the dashboard project. As you may recall, this project will document and describe 10 commonly used dashboard metrics, including sample reports. There are plans for this material to be published as a supplement to The Hospitalist later this year.
The committee discussed the type of surveys conducted by SHM. A recommendation came out of our meeting to change from large-scale, all-encompassing, biannual surveys to smaller annual surveys. The annual survey would alternate its focus every other year between evaluating individuals’ productivity and compensation, and the characteristics of hospital medicine groups. Each survey would also have the flexibility to address specific timely questions that might focus on a specific research or hot topic of the day. The goal is to get our first trial survey out by the end of 2006, which would focus on group characteristics.
Lastly, a big thank you to our outgoing chairperson, Teresa Jones. Her hard work and organizational skills are going to be a tough act to follow.
Dr. Kealey is chair of SHM’s Benchmarks Committee
Advocacy Day Educates Lawmakers about Hospital Medicine
By Eric Siegal, MD
As reported in the SHM Meeting Reporter (see July The Hospitalist, supplement 1), SHM’s first Legislative Advocacy Day was an overwhelming success. More than 70 members from 29 states visited Capitol Hill on May 3 to educate lawmakers and their staffs about hospital medicine and SHM’s proposals to improve the quality of care in our nation’s hospitals.
Advocacy Day participants attended a morning briefing that covered procedural tips on how to have a successful meeting and the health issues currently before Congress—and SHM’s positions—before leaving for previously scheduled appointments on Capitol Hill.
Once there, hospitalists took time to educate legislators and their staff members about the fastest growing medical specialty in the United States, and then turned to SHM’s recommendations for improving the quality, safety, and cost-effectiveness of inpatient medical care.
Among the issues discussed with lawmakers: the need for more funding for the Agency for Healthcare Research and Quality (AHRQ); SHM support for federal initiatives to measure resource use and improve quality, including a CMS demonstration project to assess the contributions of hospital medicine programs to improve patient care and more efficient management of hospital resources; and the importance of gainsharing demonstration projects that focus on inpatient medical services such as those provided by hospital medicine programs.
More than 130 appointments were scheduled with House and Senate offices, many with members of Congress who sit on the key health committees with jurisdiction over Medicare as well as on committees responsible for determining funding levels for the National Institutes of Health, the CDC, and the Agency for Healthcare Research and Quality.
SHM encourages those of you who participated in Advocacy Day to thank the lawmakers and staff with whom you visited (view the sample thank-you letter and instructions online at www.hospitalmedicine.org under “Advocacy & Policy”).
Advocacy Day opened doors to congressional offices; follow-up from SHM members will keep hospital medicine’s issues before lawmakers as they vote on legislation of importance to our specialty. The more SHM members interact with members of Congress and their staff, the louder our voices and the more effective our messages. Advocacy Day is just the beginning of regular contact by hospitalists with their elected representatives in Washington.
A New Way to Get Everything SHM
SHM has launched the SHM Store, a new Internet-based marketplace that will redefine the way SHM educational products and apparel are distributed. The online store will be a convenient option for hectic lifestyles because it will be open 24 hours a day and can be accessed from anywhere there is an Internet connection.
The SHM Store is user-friendly and allows you to easily and quickly purchase the quality products and apparel that you have come to expect from SHM. Apparel and accessories include men’s and women’s wind jackets, golf shirts, scrub tops, baseball caps, and lapel pins—all with the SHM logo.
You’ll also find the most up-to-date educational materials from SHM. The 2005-2006 results of the SHM survey, “The Authoritative Source on the State of Hospital Medicine,” can be ordered in CD and print format. The Practice Management Course CD with binder is also available. This combination package includes all of the materials distributed at an onsite presentation of the course. And, last but not least, get your very own copy or additional copies of The Core Competencies in Hospital Medicine: A Framework For Curriculum Development.
The ordering process is simple. Access the SHM Store at www.hospitalmedicine.org/shmstore or navigate from www.hospitalmedicine.org and click on SHM Store. The store allows you to browse available products and descriptions. When you see something you want, select the quantity you’d like to purchase and add the items to your shopping cart. Once you have completed your shopping trip, click “Check Out.” A confirmation of your transaction will be sent to your e-mail inbox and your products will be shipped to your attention.
It’s that easy. Make sure you go online to browse the new SHM Store. If you have any questions or would like to learn more about the SHM Store, contact SHM at CustomerService@hospitalmedicine. org.
SHM, Health Groups Urge House to Boost Discretionary Funding
SHM joined more than 800 health, education, and labor organizations in writing a May 8 letter to the House leadership. Organized by the Coalition for Health Funding and the Committee on Education Funding, the letter calls on Congress to add $7 billion to the budget in discretionary funding for health, education, and labor programs. It asks lawmakers to ensure that the final allocation for the House and Senate Labor, Health and Human Services, Education Appropriations Subcommittees reflects a $7 billion increase above the President’s request for these critically important programs in FY 2007.
“While our organizations represent a wide array of domestic priorities,” the letter states, “we are united in our effort to advance the bipartisan goal of adding $7 billion in discretionary funding for health, education, labor enforcement, job training, and social services programs as the budget process moves forward. On behalf of our millions of constituents, we strongly urge you to provide at least $7 billion in additional federal support to restore funding levels to FY 2005. This is essential to sustain the well-being and prosperity of our nation.”
Agencies whose funding could be boosted by the additional spending called for in the coalition letter include the Agency for Healthcare Research and Quality, the National Institutes of Health, and the Centers for Disease Control and Prevention.
For full coverage of May 2006 advocacy and policy news, visit www.hospitalmedicine.org. TH
Dr. Siegal is chair of SHM’s Public Policy Committee.
SHM: BEHIND THE SCENES
Education and Quality Initiatives: SHM’s Heart and Soul
By Geri Barnes
This month’s SHM staff article highlights the department responsible for SHM’s education and quality initiatives. While my fellow senior managers may disagree, I believe that we are the heart and soul of SHM in meeting members’ needs. So important is this organizational focus that the Education Committee, chaired by Preetha Basaviah, MD, has its own mission, which parallels and provides detail to the organizational mission of promoting excellence in the practice of hospital medicine. And the Hospital Quality and Patient Safety Committee, chaired by Mahalakshmi Halasyamani, MD, is one of the most dynamic and prolific of SHM’s committees.
We know that members join SHM for the opportunity to effect change and network with colleagues. Equally strong is the quest for educational resources that will facilitate their efforts in improving quality inpatient care. SHM’s education plan focuses and organizes our energy on developing those resources.
SHM’s resources come in many forms. The most visible is our annual meeting. By all accounts, the 2006 annual meeting was extremely successful. It was our largest meeting to date, with almost 1,200 attendees, 99% of whom were members. That number represents more than 21% of our total membership. I wonder how many other organizations can boast of such a high percentage of member attendance at their annual meeting. The attendees actively participated in the educational sessions and the Research, Innovations, and Clinical Vignettes poster session, visited the exhibits, and networked during breaks and social events. To enhance the educational experience, we created a password-protected Web site where registrants could access the handouts for sessions they planned to attend. Because of the value of these materials, we are currently determining ways to utilize the handouts to expand our educational resources.
For several years, SHM has presented the Leadership Academy and “Best Practices in Managing a Hospital Medicine Program” course. These courses are so popular that they have become a mainstay of SHM educational programs and are offered on an annual basis. In September we will present the first Level II Leadership Academy designed to build upon and expand Leadership Academy I. Additionally, “Fundamentals in Billing and Coding” a pre-course to the University of California San Francisco “Management of the Hospitalized Patient” course will be offered in October for the first time. This outgrowth of the Best Practices course was identified as a need by attendees and other members. We anticipate that we will continue to offer these important programs for many years to come.
While we reach a significant number of hospitalists and other healthcare providers through our annual meeting and other face-to-face meetings, we reach many more through other educational and quality improvement efforts. Hospitalists, in their unique role as providers responsible for the general medical care of hospitalized patients, find themselves filling roles as key players and drivers of institutional quality improvement. To aid them in this effort, we’ve developed Web-based resource rooms designed to facilitate the implementation of a quality improvement program for specific disease state/clinical condition, including antimicrobial resistance, stroke, venous thromboembolism, and heart failure. Resource rooms on glycemic control and discharge planning are currently under development.
For most resource rooms, the key is the QI Workbook, a resource built on proven principles of quality improvement, personal experiences, and evidence-based medicine. Resources in addition to the workbook include slide sets that can be used in training sessions, “Teaching Pearls,” patient education resources, and clinical tools in the form of algorithms, order sets, and discharge planning sheets. Most of the resource rooms have online CME programs and each room has a well-developed bibliography.
What will likely prove to be SHM’s most far-reaching resource is The Core Competencies in Hospital Medicine: A Framework For Curriculum Development. Published earlier this year as a supplement to the Journal of Hospital Medicine, the Core Competencies provides a structure for professional and curricular development based on a shared understanding of the essential knowledge, skills, and attitudes expected of physicians working as hospitalists. While the target audience is the directors of hospitalist programs and fellowships and residency programs (and medical school internal medicine clerkships), imagine the number of people reached when the Core Competencies touch hospitalist students across the board. Additionally, the Core Competencies are the focal point for every educational and quality improvement initiative that we undertake. This document will continue to drive the content of each annual meeting, provide direction for the organization, and help us prioritize the development of resources rooms and other educational and quality improvement resources.
SHM is lucky to have partners who understand the importance of hospitalists as key members of the multidisciplinary team and the army that will lead the charge in implementing protocols to improve patient care. From foundations and sister associations, to government and industry, we partner with organizations that appreciate the role that hospitalists play in improving the healthcare system. The partnerships have led to the development of toolkits, resource rooms, CME modules, and other important resources. New initiatives soon to be launched are mentored implementation programs and demonstration projects that will provide us with increased knowledge of how our resources are used and identify areas in which they can be improved.
What is required on a staff level to make this happen? A commitment to do whatever it takes to get the job done. Six of us are equally dedicated to leading, managing, and supporting these efforts. In addition to me, staff members Tina Budnitz, Erica Pearson, Joy Wittnebert, Lillian Higgins, and Theresa Jones chart new ground and are actively engaged in a dynamic learning process on a daily basis. But it is our members and experts that drive this process, and we are grateful for their patience and guidance.
The Education and Quality Initiatives staff members do not work in a vacuum in the national office. We have the support and brainpower of the rest of the staff, with whom we collaborate daily. Membership and marketing, information technology, and business operations staff all play a role in our success.
What makes the national office run as a well-oiled machine? Next month you’ll hear from Steve Poitras, director, Business Operations, who is instrumental in making that happen.
Barnes is director, Education & Quality Initiatives, for SHM.
Virus Alerts
CDC Urges Awareness of Measles in Americans Returning from Germany
By Alfred Valles, resident, internal medicine, Mayo Clinic College of Medicine
The Centers for Disease Control and Prevention (CDC) has issued an alert urging American travelers to remain aware of the possibility of measles exposure. Many Americans have traveled to and from Germany for the World Cup soccer championship games. Three of the twelve hosting cities—Cologne, Dortmund, and Gelsenkirchen—are of particular concern, given the recent measles outbreaks that have been reported in those cities and their surrounding areas.
Since January 1 of this year, some 1,200 cases have been identified in or near these cities. American travelers were undoubtedly among the large crowds of people gathered to pay homage to their favorite sport, and many others will visit Germany on vacation or business, making transmission of this respiratory droplet-born pathogen a very real threat.
The CDC recommends the following precautions:
- Travelers who plan to go to Germany should check their immunization records and visit their doctors if they are not immune to measles or are not sure they are.
- People returning from Germany, especially those who went to see the World Cup, should see a healthcare provider if they develop the symptoms of measles, including a fever, a raised rash that begins on the face and spreads to the arms and legs, a cough, red eyes, or a runny nose.
- People with these symptoms should limit their contact with others.
- Clinicians seeing patients with these symptoms should inquire about travel history and immunization status.
This warning is not to be taken lightly. Approximately two of every 1,000 patients infected with measles will die of the disease. Complications such as encephalitis are of particular concern for those who are malnourished or immunosuppressed.
Remember, live virus measles vaccine given within 72 hours of exposure may prevent the disease, while immune globulin given up to six days after exposure may prevent complications of measles in those who are at risk, including pregnant women, people with weak immune systems, and children.
The World cup can be dangerous, even for non-players. For more information about the measles outbreak and travel precautions, visit www.cdc.gov.
Lymphocytic Choriomeningitis Virus: Facts and Prevention
By the Special Pathogens Branch, CDC
In May 2005, the CDC investigated a cluster of lymphocytic choriomeningitis virus (LCMV) illnesses in four solid organ transplant recipients from a common donor, three of whom died. The source of the LCMV was traced to a hamster that had recently been acquired by a member of the donor’s household. It was subsequently determined that several LCMV-infected pet rodents had originated from a single distributor, who may have distributed other infected rodents to pet stores in the northeastern and midwestern United States.1 However, the risk of contracting LCMV from rodent exposure is not limited only to this outbreak, nor is the danger confined only to patients undergoing organ transplant.
Clinicians need to be familiar with LCMV because of its potential to cause meningitis, its teratogenicity, and the risk that it may bring about serious disease in immunocompromised individuals.
LCMV is normally carried by wild house mice, but can be transmitted to laboratory and pet rodents at breeding facilities, in pet stores, and in homes. Humans become infected in one of the following ways:
- Through direct contact with the secretions or excretions of infected rodents;
- By inhalation of dust or droplets containing LCMV from rodents;
- As a result of transplacental spread from an infected pregnant woman to her fetus; and
- By receipt of an organ transplant from an infected donor.2
Among those tested, about 5% have shown serologic evidence of previous infection with LCMV.3,4 In healthy adults, LCMV is typically a nonspecific viral syndrome sometimes followed by aseptic meningitis or other neurologic signs. Patients with weakened immune systems can suffer severe, possibly fatal systemic illness.2,5 Maternal infection with LCMV during pregnancy can result in spontaneous abortion or early neonatal death, as well as in defects similar to those of other congenital infections such as toxoplasmosis and cytomegalovirus (“TORCH” infections).6-10 The proportion of developmental defects caused by LCMV is not known.
Clinicians should consider LCMV in the differential diagnosis of patients with aseptic meningitis; in cases of fetal demise or congenital defects, including congenital hydrocephalus, chorioretinitis, blindness, or mental retardation; or in recent transplant recipients who present with signs of post-transplant infection. A detailed rodent exposure history should be taken. Contact your state health department or Special Pathogens Branch, CDC (404-639-1510), for information about testing for LCMV.
Currently, there is no specific treatment for LCMV infection other than supportive care. Ribavirin inhibits LCMV multiplication in laboratory experiments but has not been tested in clinical trials.
Clinicians should counsel their patients about the risks of contracting LCMV from laboratory, pet, and wild rodents. Wild mice in the home should be controlled and removed promptly. Immunocompromised individuals and women who are pregnant or planning to become pregnant should avoid any contact with wild or pet rodents, their excretions, and their nesting materials. While a woman is pregnant, pet rodents should be housed outside the home or in a separate part of the home where other individuals can care for the pets and clean their cages. Counseling a woman already exposed to rodents during pregnancy can be challenging; for assistance, contact your state health department.
Further information about LCMV infection and its prevention, including management and prevention of rodent infestation in the home, is available from Special Pathogens Branch, CDC, at www.cdc.gov/ncidod/dvrd/spb/mnpages/dispages/lcmv.htm. For more information about diseases commonly carried by rodents, please visit www.cdc.gov/rodents. TH
References
- Centers for Disease Control and Prevention. Update: interim guidance for minimizing risk for human lymphocytic choriomeningitis virus infection associated with pet rodents. MMWR. Aug 19, 2005;54(32):799-801.
- Fischer SA, Graham MB, Kuehnert MJ, et al. Transmission of lymphocytic choriomeningitis virus by organ transplantation. N Engl J Med. 2006;354(21):2235-2249.
- Childs JE, Glass GE, Ksiazek TG, et al. Human-rodent contact and infection with lymphocytic choriomeningitis and Seoul viruses in an inner-city population. Am J Trop Med Hyg. 1991 Feb;44(2):117–121.
- Park JY, Peters CJ, Rollin PE, et al. Age distribution of lymphocytic choriomeningitis virus serum antibody in Birmingham, Alabama: evidence of a decreased risk of infection. Am J Trop Med Hyg. 1997 Jul;57(1):37–41.
- Horton J, Hotchin JE, Olson KB, et al. The effects of MP virus infection in lymphoma. Cancer Res. 1971 Aug;31(8):1066–1068.
- Barton LL, Mets MB. Congenital lymphocytic choriomeningitis virus infection: decade of rediscovery. Clin Infect Dis. 2001 Aug 1;33(3):370–374.
- Barton LL, Mets MB, Beauchamp CL. Lymphocytic choriomeningitis virus: emerging fetal teratogen. Am J Obstet Gynecol. 2002 Dec ;187(6):1715–1716.
- Wright R, Johnson D, Neumann M, et al. Congenital lymphocytic choriomeningitis virus syndrome: a disease that mimics congenital toxoplasmosis or cytomegalovirus infection. Pediatrics. 1997 Jul;100(1):E9.
- Ford-Jones EL, Ryan G . Implications for the fetus of maternal infections in pregnancy. In: Cohen J, Powderly WG, eds. Infectious Diseases, 2nd ed. New York, NY: Mosby; 2004: 709–723.
- Greenhow TL, Weintrub PS. Your diagnosis, please. Neonate with hydrocephalus. Pediatr Infect Dis J. 2003 Dec;22(12):1099, 1111–1112.
CDC Urges Awareness of Measles in Americans Returning from Germany
By Alfred Valles, resident, internal medicine, Mayo Clinic College of Medicine
The Centers for Disease Control and Prevention (CDC) has issued an alert urging American travelers to remain aware of the possibility of measles exposure. Many Americans have traveled to and from Germany for the World Cup soccer championship games. Three of the twelve hosting cities—Cologne, Dortmund, and Gelsenkirchen—are of particular concern, given the recent measles outbreaks that have been reported in those cities and their surrounding areas.
Since January 1 of this year, some 1,200 cases have been identified in or near these cities. American travelers were undoubtedly among the large crowds of people gathered to pay homage to their favorite sport, and many others will visit Germany on vacation or business, making transmission of this respiratory droplet-born pathogen a very real threat.
The CDC recommends the following precautions:
- Travelers who plan to go to Germany should check their immunization records and visit their doctors if they are not immune to measles or are not sure they are.
- People returning from Germany, especially those who went to see the World Cup, should see a healthcare provider if they develop the symptoms of measles, including a fever, a raised rash that begins on the face and spreads to the arms and legs, a cough, red eyes, or a runny nose.
- People with these symptoms should limit their contact with others.
- Clinicians seeing patients with these symptoms should inquire about travel history and immunization status.
This warning is not to be taken lightly. Approximately two of every 1,000 patients infected with measles will die of the disease. Complications such as encephalitis are of particular concern for those who are malnourished or immunosuppressed.
Remember, live virus measles vaccine given within 72 hours of exposure may prevent the disease, while immune globulin given up to six days after exposure may prevent complications of measles in those who are at risk, including pregnant women, people with weak immune systems, and children.
The World cup can be dangerous, even for non-players. For more information about the measles outbreak and travel precautions, visit www.cdc.gov.
Lymphocytic Choriomeningitis Virus: Facts and Prevention
By the Special Pathogens Branch, CDC
In May 2005, the CDC investigated a cluster of lymphocytic choriomeningitis virus (LCMV) illnesses in four solid organ transplant recipients from a common donor, three of whom died. The source of the LCMV was traced to a hamster that had recently been acquired by a member of the donor’s household. It was subsequently determined that several LCMV-infected pet rodents had originated from a single distributor, who may have distributed other infected rodents to pet stores in the northeastern and midwestern United States.1 However, the risk of contracting LCMV from rodent exposure is not limited only to this outbreak, nor is the danger confined only to patients undergoing organ transplant.
Clinicians need to be familiar with LCMV because of its potential to cause meningitis, its teratogenicity, and the risk that it may bring about serious disease in immunocompromised individuals.
LCMV is normally carried by wild house mice, but can be transmitted to laboratory and pet rodents at breeding facilities, in pet stores, and in homes. Humans become infected in one of the following ways:
- Through direct contact with the secretions or excretions of infected rodents;
- By inhalation of dust or droplets containing LCMV from rodents;
- As a result of transplacental spread from an infected pregnant woman to her fetus; and
- By receipt of an organ transplant from an infected donor.2
Among those tested, about 5% have shown serologic evidence of previous infection with LCMV.3,4 In healthy adults, LCMV is typically a nonspecific viral syndrome sometimes followed by aseptic meningitis or other neurologic signs. Patients with weakened immune systems can suffer severe, possibly fatal systemic illness.2,5 Maternal infection with LCMV during pregnancy can result in spontaneous abortion or early neonatal death, as well as in defects similar to those of other congenital infections such as toxoplasmosis and cytomegalovirus (“TORCH” infections).6-10 The proportion of developmental defects caused by LCMV is not known.
Clinicians should consider LCMV in the differential diagnosis of patients with aseptic meningitis; in cases of fetal demise or congenital defects, including congenital hydrocephalus, chorioretinitis, blindness, or mental retardation; or in recent transplant recipients who present with signs of post-transplant infection. A detailed rodent exposure history should be taken. Contact your state health department or Special Pathogens Branch, CDC (404-639-1510), for information about testing for LCMV.
Currently, there is no specific treatment for LCMV infection other than supportive care. Ribavirin inhibits LCMV multiplication in laboratory experiments but has not been tested in clinical trials.
Clinicians should counsel their patients about the risks of contracting LCMV from laboratory, pet, and wild rodents. Wild mice in the home should be controlled and removed promptly. Immunocompromised individuals and women who are pregnant or planning to become pregnant should avoid any contact with wild or pet rodents, their excretions, and their nesting materials. While a woman is pregnant, pet rodents should be housed outside the home or in a separate part of the home where other individuals can care for the pets and clean their cages. Counseling a woman already exposed to rodents during pregnancy can be challenging; for assistance, contact your state health department.
Further information about LCMV infection and its prevention, including management and prevention of rodent infestation in the home, is available from Special Pathogens Branch, CDC, at www.cdc.gov/ncidod/dvrd/spb/mnpages/dispages/lcmv.htm. For more information about diseases commonly carried by rodents, please visit www.cdc.gov/rodents. TH
References
- Centers for Disease Control and Prevention. Update: interim guidance for minimizing risk for human lymphocytic choriomeningitis virus infection associated with pet rodents. MMWR. Aug 19, 2005;54(32):799-801.
- Fischer SA, Graham MB, Kuehnert MJ, et al. Transmission of lymphocytic choriomeningitis virus by organ transplantation. N Engl J Med. 2006;354(21):2235-2249.
- Childs JE, Glass GE, Ksiazek TG, et al. Human-rodent contact and infection with lymphocytic choriomeningitis and Seoul viruses in an inner-city population. Am J Trop Med Hyg. 1991 Feb;44(2):117–121.
- Park JY, Peters CJ, Rollin PE, et al. Age distribution of lymphocytic choriomeningitis virus serum antibody in Birmingham, Alabama: evidence of a decreased risk of infection. Am J Trop Med Hyg. 1997 Jul;57(1):37–41.
- Horton J, Hotchin JE, Olson KB, et al. The effects of MP virus infection in lymphoma. Cancer Res. 1971 Aug;31(8):1066–1068.
- Barton LL, Mets MB. Congenital lymphocytic choriomeningitis virus infection: decade of rediscovery. Clin Infect Dis. 2001 Aug 1;33(3):370–374.
- Barton LL, Mets MB, Beauchamp CL. Lymphocytic choriomeningitis virus: emerging fetal teratogen. Am J Obstet Gynecol. 2002 Dec ;187(6):1715–1716.
- Wright R, Johnson D, Neumann M, et al. Congenital lymphocytic choriomeningitis virus syndrome: a disease that mimics congenital toxoplasmosis or cytomegalovirus infection. Pediatrics. 1997 Jul;100(1):E9.
- Ford-Jones EL, Ryan G . Implications for the fetus of maternal infections in pregnancy. In: Cohen J, Powderly WG, eds. Infectious Diseases, 2nd ed. New York, NY: Mosby; 2004: 709–723.
- Greenhow TL, Weintrub PS. Your diagnosis, please. Neonate with hydrocephalus. Pediatr Infect Dis J. 2003 Dec;22(12):1099, 1111–1112.
CDC Urges Awareness of Measles in Americans Returning from Germany
By Alfred Valles, resident, internal medicine, Mayo Clinic College of Medicine
The Centers for Disease Control and Prevention (CDC) has issued an alert urging American travelers to remain aware of the possibility of measles exposure. Many Americans have traveled to and from Germany for the World Cup soccer championship games. Three of the twelve hosting cities—Cologne, Dortmund, and Gelsenkirchen—are of particular concern, given the recent measles outbreaks that have been reported in those cities and their surrounding areas.
Since January 1 of this year, some 1,200 cases have been identified in or near these cities. American travelers were undoubtedly among the large crowds of people gathered to pay homage to their favorite sport, and many others will visit Germany on vacation or business, making transmission of this respiratory droplet-born pathogen a very real threat.
The CDC recommends the following precautions:
- Travelers who plan to go to Germany should check their immunization records and visit their doctors if they are not immune to measles or are not sure they are.
- People returning from Germany, especially those who went to see the World Cup, should see a healthcare provider if they develop the symptoms of measles, including a fever, a raised rash that begins on the face and spreads to the arms and legs, a cough, red eyes, or a runny nose.
- People with these symptoms should limit their contact with others.
- Clinicians seeing patients with these symptoms should inquire about travel history and immunization status.
This warning is not to be taken lightly. Approximately two of every 1,000 patients infected with measles will die of the disease. Complications such as encephalitis are of particular concern for those who are malnourished or immunosuppressed.
Remember, live virus measles vaccine given within 72 hours of exposure may prevent the disease, while immune globulin given up to six days after exposure may prevent complications of measles in those who are at risk, including pregnant women, people with weak immune systems, and children.
The World cup can be dangerous, even for non-players. For more information about the measles outbreak and travel precautions, visit www.cdc.gov.
Lymphocytic Choriomeningitis Virus: Facts and Prevention
By the Special Pathogens Branch, CDC
In May 2005, the CDC investigated a cluster of lymphocytic choriomeningitis virus (LCMV) illnesses in four solid organ transplant recipients from a common donor, three of whom died. The source of the LCMV was traced to a hamster that had recently been acquired by a member of the donor’s household. It was subsequently determined that several LCMV-infected pet rodents had originated from a single distributor, who may have distributed other infected rodents to pet stores in the northeastern and midwestern United States.1 However, the risk of contracting LCMV from rodent exposure is not limited only to this outbreak, nor is the danger confined only to patients undergoing organ transplant.
Clinicians need to be familiar with LCMV because of its potential to cause meningitis, its teratogenicity, and the risk that it may bring about serious disease in immunocompromised individuals.
LCMV is normally carried by wild house mice, but can be transmitted to laboratory and pet rodents at breeding facilities, in pet stores, and in homes. Humans become infected in one of the following ways:
- Through direct contact with the secretions or excretions of infected rodents;
- By inhalation of dust or droplets containing LCMV from rodents;
- As a result of transplacental spread from an infected pregnant woman to her fetus; and
- By receipt of an organ transplant from an infected donor.2
Among those tested, about 5% have shown serologic evidence of previous infection with LCMV.3,4 In healthy adults, LCMV is typically a nonspecific viral syndrome sometimes followed by aseptic meningitis or other neurologic signs. Patients with weakened immune systems can suffer severe, possibly fatal systemic illness.2,5 Maternal infection with LCMV during pregnancy can result in spontaneous abortion or early neonatal death, as well as in defects similar to those of other congenital infections such as toxoplasmosis and cytomegalovirus (“TORCH” infections).6-10 The proportion of developmental defects caused by LCMV is not known.
Clinicians should consider LCMV in the differential diagnosis of patients with aseptic meningitis; in cases of fetal demise or congenital defects, including congenital hydrocephalus, chorioretinitis, blindness, or mental retardation; or in recent transplant recipients who present with signs of post-transplant infection. A detailed rodent exposure history should be taken. Contact your state health department or Special Pathogens Branch, CDC (404-639-1510), for information about testing for LCMV.
Currently, there is no specific treatment for LCMV infection other than supportive care. Ribavirin inhibits LCMV multiplication in laboratory experiments but has not been tested in clinical trials.
Clinicians should counsel their patients about the risks of contracting LCMV from laboratory, pet, and wild rodents. Wild mice in the home should be controlled and removed promptly. Immunocompromised individuals and women who are pregnant or planning to become pregnant should avoid any contact with wild or pet rodents, their excretions, and their nesting materials. While a woman is pregnant, pet rodents should be housed outside the home or in a separate part of the home where other individuals can care for the pets and clean their cages. Counseling a woman already exposed to rodents during pregnancy can be challenging; for assistance, contact your state health department.
Further information about LCMV infection and its prevention, including management and prevention of rodent infestation in the home, is available from Special Pathogens Branch, CDC, at www.cdc.gov/ncidod/dvrd/spb/mnpages/dispages/lcmv.htm. For more information about diseases commonly carried by rodents, please visit www.cdc.gov/rodents. TH
References
- Centers for Disease Control and Prevention. Update: interim guidance for minimizing risk for human lymphocytic choriomeningitis virus infection associated with pet rodents. MMWR. Aug 19, 2005;54(32):799-801.
- Fischer SA, Graham MB, Kuehnert MJ, et al. Transmission of lymphocytic choriomeningitis virus by organ transplantation. N Engl J Med. 2006;354(21):2235-2249.
- Childs JE, Glass GE, Ksiazek TG, et al. Human-rodent contact and infection with lymphocytic choriomeningitis and Seoul viruses in an inner-city population. Am J Trop Med Hyg. 1991 Feb;44(2):117–121.
- Park JY, Peters CJ, Rollin PE, et al. Age distribution of lymphocytic choriomeningitis virus serum antibody in Birmingham, Alabama: evidence of a decreased risk of infection. Am J Trop Med Hyg. 1997 Jul;57(1):37–41.
- Horton J, Hotchin JE, Olson KB, et al. The effects of MP virus infection in lymphoma. Cancer Res. 1971 Aug;31(8):1066–1068.
- Barton LL, Mets MB. Congenital lymphocytic choriomeningitis virus infection: decade of rediscovery. Clin Infect Dis. 2001 Aug 1;33(3):370–374.
- Barton LL, Mets MB, Beauchamp CL. Lymphocytic choriomeningitis virus: emerging fetal teratogen. Am J Obstet Gynecol. 2002 Dec ;187(6):1715–1716.
- Wright R, Johnson D, Neumann M, et al. Congenital lymphocytic choriomeningitis virus syndrome: a disease that mimics congenital toxoplasmosis or cytomegalovirus infection. Pediatrics. 1997 Jul;100(1):E9.
- Ford-Jones EL, Ryan G . Implications for the fetus of maternal infections in pregnancy. In: Cohen J, Powderly WG, eds. Infectious Diseases, 2nd ed. New York, NY: Mosby; 2004: 709–723.
- Greenhow TL, Weintrub PS. Your diagnosis, please. Neonate with hydrocephalus. Pediatr Infect Dis J. 2003 Dec;22(12):1099, 1111–1112.